Endometriotic lesions can penetrate the retroperi- toneal space and constitute a specific entity known as deeply infiltrating endometriosis (DIE). 1 The patho- genesis of DIE is the subject of much debate. Some authors consider that implantation takes place subse- quent to menstrual reflux followed by retroperitoneal penetration. 1–3 Others believe it is more likely meta- plasia 4 of the peritoneal serosa 5 or mullerian rem- nants. 6 Histologic study of DIE lesions has been much discussed. 7,8 Certain authors believe that the lesions, whether located on the bladder 8,9 or rectovaginal sep- tum, 6 are nodules of adenomyosis. We performed a his- tologic study of deep endometriosis lesions observed on the uterosacral ligaments (USL), which is the most frequent location for DIE. 10 Materials and Methods We carried out a retrospective study of 149 patients who underwent resection of one or both USL because of endometriosis. All women experienced painful functional symptoms (dysmennorrhea, deep dyspareunia, noncyclic chronic pelvic pain) with a strong suspicion of DIE infiltrating the USL. This 519 November 2002, Vol. 9, No. 4 The Journal of the American Association of Gynecologic Laparoscopists From the Service Central d’Anatomie et Cytologie Pathologiques (Drs. Bonte and Vacher-Lavenu) and Service de Chirurgie Gynecologique, Clinique Universitaire Baudelocque (Drs. Chapron, Vieira, Fauconnier, Barakat, and Dubuisson), Assistance Publique-Hopitaux de Paris, CHU Cochin Port-Royal; and Service de Gynecologie Obstetrique, Assistance Publique-Hopitaux de Paris, Hopital Rothschild (Dr. Fritel), Paris, France. Address reprint requests to Charles Chapron, M.D., Service de Chirurgie Gynécologique, Clinique Universitaire Baudelocque, Cochin Port-Royal, 123 Boulevard Port-Royal, 75014 Paris, France; fax 33 1 58 4118 70. Accepted for publication May 6, 2002. Abstract Study Objective. To describe the histologic appearance of deep endometriosis infiltrating the uterosacral ligaments (USL). Design. Retrospective analysis (Canadian Task Force classification II-2). Setting. University-affiliated hospital. Patients. One hundred forty-nine women with pain due to endometriosis. Intervention. Resection of one or both USL. Measurements and Main Results. One hundred seventy-two USL were examined by histology after unilateral resec- tion in 126 patients (84.6%) and bilateral resection in 23 (15.4%). Two-thirds of women (122, 70.9%) had a clas- sic appearance of endometriosis. Lesions of myoproliferative endometriosis with a histologic appearance of so-called adenomyotic nodules were observed in 25 (14.5%). Associated fibrosis was most frequent in patients with positive compared with negative histology (85, 69.7% vs 18, 36.0%). Conclusion. Anatomicopathologic lesions of deep endometriosis infiltrating the USL are heterogeneous. Adeno- myotic nodules are not frequently observed. (J Am Assoc Gynecol Laparosc 9(4):519–524, 2002) Histologic Appearance of Endometriosis Infiltrating Uterosacral Ligaments in Women with Painful Symptoms Hélène Bonte, M.D., Charles Chapron, M.D., Marco Vieira, M.D., Arnaud Fauconnier, M.D., Habib Barakat, M.D., Xavier Fritel, M.D., Marie-Cécile Vacher-Lavenu, M.D., Ph.D., and Jean-Bernard Dubuisson, M.D.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Endometriotic lesions can penetrate the retroperi-toneal space and constitute a specific entity known asdeeply infiltrating endometriosis (DIE).1 The patho-genesis of DIE is the subject of much debate. Someauthors consider that implantation takes place subse-quent to menstrual reflux followed by retroperitonealpenetration.1–3 Others believe it is more likely meta-plasia4 of the peritoneal serosa5 or mullerian rem-nants.6 Histologic study of DIE lesions has been muchdiscussed.7,8 Certain authors believe that the lesions,whether located on the bladder8,9 or rectovaginal sep-tum,6 are nodules of adenomyosis. We performed a his-
tologic study of deep endometriosis lesions observedon the uterosacral ligaments (USL), which is the mostfrequent location for DIE.10
Materials and Methods
We carried out a retrospective study of 149patients who underwent resection of one or both USLbecause of endometriosis. All women experiencedpainful functional symptoms (dysmennorrhea, deepdyspareunia, noncyclic chronic pelvic pain) with astrong suspicion of DIE infiltrating the USL. This
519
November 2002, Vol. 9, No. 4 The Journal of the American Association of Gynecologic Laparoscopists
From the Service Central d’Anatomie et Cytologie Pathologiques (Drs. Bonte and Vacher-Lavenu) and Service de Chirurgie Gynecologique, CliniqueUniversitaire Baudelocque (Drs. Chapron, Vieira, Fauconnier, Barakat, and Dubuisson), Assistance Publique-Hopitaux de Paris, CHU Cochin Port-Royal;and Service de Gynecologie Obstetrique, Assistance Publique-Hopitaux de Paris, Hopital Rothschild (Dr. Fritel), Paris, France.
Address reprint requests to Charles Chapron, M.D., Service de Chirurgie Gynécologique, Clinique Universitaire Baudelocque, Cochin Port-Royal, 123Boulevard Port-Royal, 75014 Paris, France; fax 33 1 58 4118 70.
Accepted for publication May 6, 2002.
Abstract
Study Objective.To describe the histologic appearance of deep endometriosis infiltrating the uterosacral ligaments(USL).Design. Retrospective analysis (Canadian Task Force classification II-2).Setting. University-affiliated hospital.Patients. One hundred forty-nine women with pain due to endometriosis.Intervention. Resection of one or both USL.Measurements and Main Results. One hundred seventy-two USL were examined by histology after unilateral resec-tion in 126 patients (84.6%) and bilateral resection in 23 (15.4%). Two-thirds of women (122, 70.9%) had a clas-sic appearance of endometriosis. Lesions of myoproliferative endometriosis with a histologic appearance ofso-called adenomyotic nodules were observed in 25 (14.5%). Associated fibrosis was most frequent in patientswith positive compared with negative histology (85, 69.7% vs 18, 36.0%).Conclusion. Anatomicopathologic lesions of deep endometriosis infiltrating the USL are heterogeneous. Adeno-myotic nodules are not frequently observed.
(J Am Assoc Gynecol Laparosc 9(4):519–524, 2002)
Histologic Appearance of EndometriosisInfiltrating Uterosacral Ligaments in Women with Painful SymptomsHélène Bonte, M.D., Charles Chapron, M.D., Marco Vieira, M.D., Arnaud Fauconnier, M.D., Habib Barakat, M.D., Xavier Fritel, M.D., Marie-Cécile Vacher-Lavenu, M.D., Ph.D., and Jean-Bernard Dubuisson, M.D.

suspicion was based on clinical11,12 (painful nodule,painful induration for which palpation during a vagi-nal touch caused recurrence of pain) and/or laparo-scopic findings (asymmetry of USL, visible nodule onUSL). All laparoscopies were performed by techniquedescribed elsewhere.13
Samples were fixed with 10% formol and set inparaffin. Seried 4-µm sections were cut and coloredwith hematoxylin-eosin-saffron and examined histo-logically. Endometriosis was defined as endometrialtissue (endometrial gland, simple endometrial epithe-lium with stroma) located ectopically with no con-nection with endometrium.14 A systematic search wasmade for the presence of hemosiderin deposits, fibro-sis, and smooth muscle hyperplasia in contact with theendometriosis implants. All slides were reexamined bya pathologist experienced in gynecologic pathology(HB).
Results
One hundred seventy-two USL were examined inthese 149 patients who all had histologically provedendometriosis. Resection was unilateral in 126 patients(84.6%) and bilateral in 23 (15.4%).
Considerable differences were found on histo-logic examination. In 122 cases (70.9%) typical endo-metriosis lesions were observed on the USL (Figure1). Associated lesions were as follows: fibrosis in 103(59.9%; Figure 2); smooth muscle hyperplasia result-
ing in an appearance of pseudo-adenomyoma in 25(14.5%; Figure 3); and hemosiderin deposits in 45(26.2%). In 29.1% of cases (50 USL) histologic analy-sis was negative for endometriosis. Fibrosis was mostoften observed in women with positive as opposed tonegative histology (85, 69.7% vs 18, 36.0%).
The epithelial surface layer over endometrioticimplants was simple, and in most cases cubocylindricor endotheliform. Associated chorion was most oftenfibrous. Sometimes endometriotic implants locatedwithin connective-muscular tissue of USL were in
520
Histologic Appearance of Endometriosis Infiltrating Uterosacral Ligaments Bonte et al
FIGURE 1. Uterosacral ligament with scanty endometrial-type stroma and glandular epithelium (arrow). (Hematoxylin-eosin-saffron; magnification 250×).
FIGURE 2. Fibrosis (arrow) of uterosacral ligament with fociof endometriosis. (Hematoxylin-eosin-saffron; magnification100×).
FIGURE 3. Endometriotic glands and stroma surrounded byhyperplastic smooth muscle fibers (arrow). (Hematoxylin-eosin-saffron; magnification 100×).
contact with big networks of nerve tissue (Figure 4).Endometriotic tissue in adipose tissues was observedin only one case (Figure 5). Assessment of fibrosis wasmade difficult by the quantity of artifacts due to elec-trocoagulation, which resulted in connective tissuetaking on a homogeneous hyalin appearance (Figure6). When smooth muscle hyperplasia was present, itwas always moderate and limited to discreet hyper-plasia of smooth muscle bundles directly in contact
with endometrial glands. In these 25 cases endometri-otic lesions had an appearance of so-called adeno-myotic nodules. Histologic analysis was reliable,insofar as reexamination by a pathologist experiencedin gynecologic pathology always confirmed the ini-tial diagnosis.
Discussion
Our results show the appearance of classic endo-metriosis on USL in a little over two of three patients(122, 70.9%). Myoproliferative endometriosis lesionswith the appearance of adenomyotic nodules wereobserved in only 14.5% (25). Fibrosis was found inover half of patients (103, 59.9%). This histologicdiagnosis is reproducible since in our experience it wasnever modified after reexamination of the slides. Theseresults are in agreement with published findings15
(Table 1). In cases of DIE affecting the USL, the ade-nomyotic nodule is not the most frequent histologicappearance. These heterogeneous results confirm thatdeep endometriosis is present in lesions varying fromfibrosis to adenomyosis.16 With hindsight, the fact thatfibrosis was more often associated with histologiclyproved endometriosis should encourage the patholo-gist to multiply the rates of cross sections for patientswith fibrosis but without histologicly confirmed endo-metriosis so as not to overlook a mild form of the
521
November 2002, Vol. 9, No. 4 The Journal of the American Association of Gynecologic Laparoscopists
FIGURE 4. Nerve sheet (arrow) surrounded by endometrio-sis. (Hematoxylin-eosin-saffron; magnification 100×).
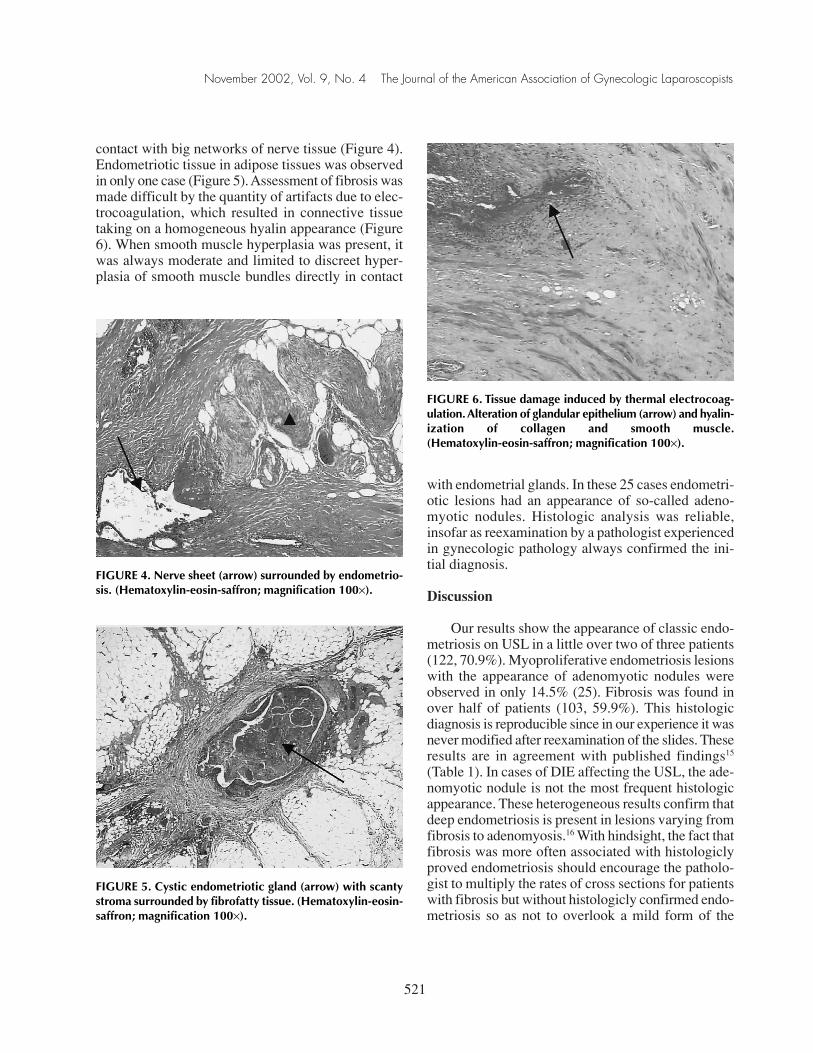
FIGURE 6. Tissue damage induced by thermal electrocoag-ulation. Alteration of glandular epithelium (arrow) and hyalin-ization of collagen and smooth muscle.(Hematoxylin-eosin-saffron; magnification 100×).
FIGURE 5. Cystic endometriotic gland (arrow) with scantystroma surrounded by fibrofatty tissue. (Hematoxylin-eosin-saffron; magnification 100×).

disease. It is essential to take fibrosis into considera-tion because it contributes to pain in the context ofDIE.
Histologic studies show that there are nerve struc-tures on the USL17,18 and that entrapment of nervestructures by fibrotic tissue could represent etiopath-ogenic mechanisms of pelvic pain.19 Other authors15
also reported that negative histologic results are pos-sible. This should not call the diagnosis into question,because histologic appearance depends on a numberof factors, notably hormone treatment before operationand the length of time lesions have been in existence,because they evolve progressively toward sclerosis,with glands and stroma becoming less numerous.Fibrosis associated with deep endometriosis is thereason why symptoms may persist even though endo-metriosis may not be active.20 The same hypothe-sis explains why laparoscopic resection of USL torelieve dysmenorrhea and deep dyspareunia is just as
effective whether histologic results are positive ornegative.21
Histologic results appear to differ according to thelocation of the DIE lesions. In cases of DIE infiltrat-ing the rectovaginal septum,6,15 adenomyotic nodulesseem to be found far more frequently than whenlesions are located on the USL. Similarly, the rate ofnegative histologic results seems to be far lower incases of infiltration of the rectovaginal septum thanwhen DIE affects the USL (Table 2). Thus, on the basisof these results the histologic appearance of DIE isneither unique nor synonymous with adenomyoticnodules.
Several studies suggested that peritoneal liquidplays a part in the pathogenesis of endometriosis.22–24
If this is true it is logical to consider that the liquid’sinfluence on endometriosis lesions varies according tothe depth of lesions. Concentrations of steroid hor-mones and notably progesterone are much higher inperitoneal fluid than in plasma for at least 1 weekafter ovulation.25 This high concentration of proges-terone could have an inhibiting effect on the devel-opment of endometriotic lesions. Thus the deeper thelesions (rectovaginal septum) the less they would beexposed to inhibiting action of peritoneal liquid.10 Dueto obliteration of the pouch of Douglas that is mostoften present,3 lesions infiltrating the upper third of theposterior surface of the vagina26 (considered by someauthors as rectovaginal septum) are deprived of theinhibiting effects of peritoneal liquid, which couldexplain the very low rate of negative histologic results.Given that retroperitoneal lesions located on the USLare more superficial, they would thus be far moreexposed to the influence of the fluid.
522
Histologic Appearance of Endometriosis Infiltrating Uterosacral Ligaments Bonte et al
TABLE 1. Histologic Appearance of Endometriosis DeeplyInfiltrating Uterosacral Ligaments
Histologically Positiveno. (%) Histologically
No. of With Without Negative,Patients MPL MPL no. (%)
2815 7 (25.0)a 15 (53.6)a 6 (21.4)a
172b 25 (14.5)a 97 (56.4)a 50 (29.1)a
MPL = myoproliferative lesion of endometriosis(adenomyoma nodule).aNS, Fisher’s exact test.bPresent study.
TABLE 2. Histologic Appearance of Endometriosis According to Location of Deeply Infiltrating Lesions
HistologicallyHistologically Positive, no. (%) Negative,
Number of Patients Location With MPL Without MPL no. (%)
1115 RVS 10a (91) 0b (0) 1a (9)2815 USL 7a (25) 15b (54) 6a (21)2316 RVS 231a (100) — —172c USL 25a (14) 97b (57) 50a (29)
MPL = myoproliferative lesions of endometriosis (adenomyoma nodule); USL = uterosacral ligaments; RVS = rectovaginalseptum.ap <0.0001, χ2 test.bp = 0.0014, χ2 test.cPresent study.

Our histologic results show that where the USLare concerned, the appearance is classic endometriosisin two of three patients. The histologic appearance ofadenomyotic nodules is present in only 14.5% ofpatients.
References
1. Koninckx PR, Meuleman C, Demeyere S, et al:Suggestive evidence that pelvic endometriosis is a pro-gressive disease, whereas deeply infiltrating endome-triosis is associated with pelvic pain. Fertil Steril55:759–65, 1991
2. Sampson JA: Peritoneal endometriosis due to premen-strual dissemination of endometrial tissue into the peri-toneal cavity. Am J Obstet Gynecol 14:422–469, 1927
3. Vercellini P, Aimi G, Panazza S, et al: Deep endo-metriosis conundrum: Evidence in favor of a peritonealorigin. Fertil Steril 73:1043–1046, 2000
4. Meyer R: Uber den stand der frage der adenomyositisund adenomyoma in algemeinen und insbesondere uberadenomyositis und adenomyometritis sarcomatosa.Zentrlbl Gynäkol 43:745–750, 1919
5. Gruenwald P: Origin of endometriosis from mesen-chyme of the coelomic walls. Am J Obstst Gynecol44:470–474, 1942
6. Donnez J, Nisolle M, Casanas-Roux F, et al: Recto-vaginal septum, endometriosis or adenomyosis: Lapa-roscopic management in a series of 231 patients. HumReprod 10:630–635, 1995
7. Donnez J, Nisolle M, Smoes P, et al: Peritoneal endo-metriosis and “endometriotic” nodules of the recto-vaginal septum are two different entities. Fertil Steril66:362–368, 1996
8. Fedele L, Piazzola E, Rafelli R, et al: Bladder endo-metriosis: Deep infiltrating endometriosis or adeno-myosis? Fertil Steril 69:972–975, 1998
9. Donnez J, Spada F, Squifflet J, et al: Bladder endome-triosis must be considered as bladder adenomyosis. Fer-til Steril 74:1175–1181, 2000
10. Cornillie FJ, Oosterlynck D, Lauweryns JM, et al:Deeply infiltrating pelvic endometriosis: Histology andclinical significance. Fertil Steril 53:978–983, 1990
11. Chapron C, Dubuisson JB, Pansini V, et al: Routine clin-ical examination is not sufficient for diagnosing andlocating deeply infiltrating endometriosis. J Am AssocGynecol Laparosc 9(2):115–119, 2002
12. Koninckx P, Meuleman C, Oosterlynck D, et al: Diag-nosis of deep endometriosis by clinical examinationduring menstruation and plasma CA-125 concentra-tion. Fertil Steril 65:280–287, 1996
13. Chapron C, Dubuisson JB: Laparoscopic treatment ofdeep endometriosis located on the uterosacral liga-ments. Hum Reprod 11:868–873, 1996
14. Clement PB: Diseases of the peritoneum. In Blaustein’sPathology of the Female Genital Tract. Edited by RJKurman, MT Mazur. New York, Spinger-Verlag, 1994,p 647
15. Nieminen U: Studies on the vascular pattern of ectopicendometrium with special reference to cyclic changes.Acta Obstet Gynecol Scand 41(suppl 3):9–81, 1962
16. Brosens IA: New principles in the management of endo-metriosis. Acta Obstet Gynecol Scand Suppl 159:18–21,1994
17. Campbell RM, Arbor A: The anatomy and histology ofthe sacrouterine ligaments. Am J Obstet Gynecol59:1–12, 1950
18. Southoul JH, Anthonioz P, Bertrand J: Les modificationsde structures des ligaments utéro-sacrés après la nais-sance et dans l’enfance. A la recherche d’une signifi-cation fonctionnelle de ces formations. J Gynecol ObstetBiol Reprod 1:299–308, 1972
19. Anaf V, Simon P, El Nakadi I, et al: Relationshipbetween endometriotic foci and nerves in rectovaginalendometriosis nodules. Hum Reprod 15:1744–1750,2000
20. Coronado C, Franklin RR, Lotze EC, et al: Surgicaltreatment of symptomatic colorectal endometriosis.Fertil Steril 53:411–416, 1990
21. Chapron C, Dubuisson JB, Tardif D, et al: Retroperi-toneal endometriosis and pelvic pain: Results of lapa-roscopic uterosacral ligament resection according tothe rAFS classification and histopathologic results.J Gynecol Surg 14:51–58, 1998
22. Koninckx PR, Kennedy SH, Barlow DH: Pathogenesisof endometriosis: The role of peritoneal fluid. GynecolObstet Invest 47(suppl 1):23–24, 1999
23. Ramey JW, Archer DF: Peritoneal fluid: Its relevanceto the development of endometriosis. Fertil Steril60:1–14, 1993
24. Oral E, Olive DL, Arici A: The peritoneal environmentin endometriosis. Hum Reprod Update 2:385–398, 1997
523
November 2002, Vol. 9, No. 4 The Journal of the American Association of Gynecologic Laparoscopists

25. Koninckx PR, Heyns W, Verhoeven G, et al: Bio-chemical characterization of peritoneal fluid in womenduring the menstrual cycle. J Clin Endocrinol Metab51:1239–1244, 1980
26. Martin DC, Batt RE: Retrocervical, rectovaginal pouch,and rectovaginal septum endometriosis. J Am AssocGynecol Laparosc 8:12–17, 2001
524
Histologic Appearance of Endometriosis Infiltrating Uterosacral Ligaments Bonte et al
Related Documents











