Radiation Oncology Case Rounds 21 ST MAY 2015

Hippocampal sparing whole brain radiation therapy- Making a case!
Aug 10, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Radiation Oncology Case Rounds
21ST MAY 2015

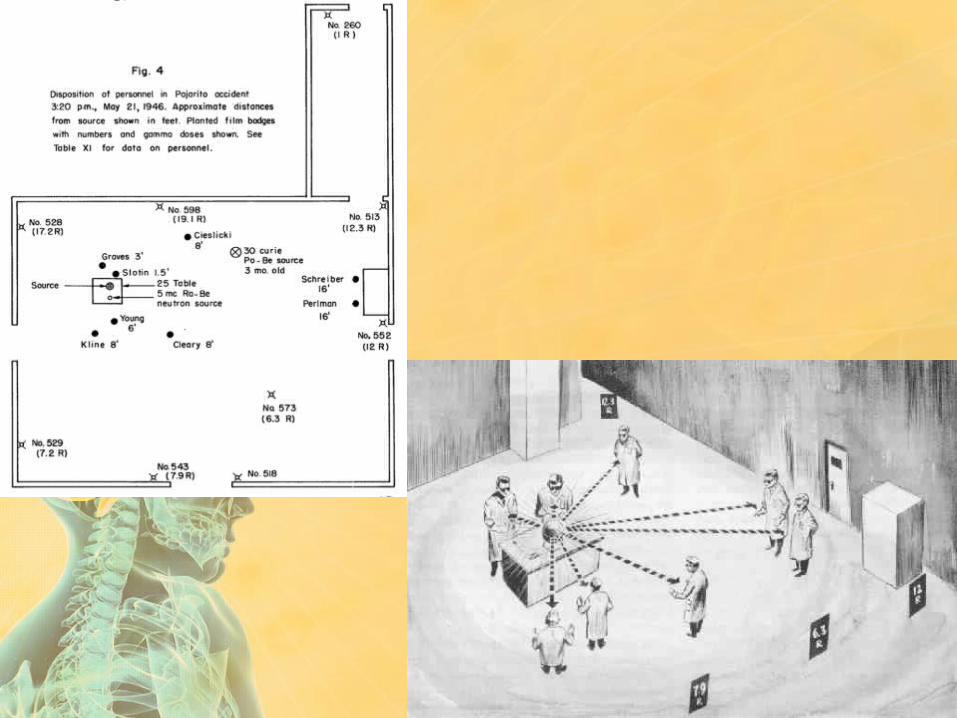
• Physicist and chemist• Winnipeg, Manitoba, Canada• 2nd person to die of criticality
accident (Manhattan Project)• Proposed dollar unit of reactivity• Louis Slotin
May 21st 1946

IN THE MEDIA

TICKLING THE DRAGON’S TAIL

IN THE MEDIA

BACK TO BUSINESS

HA-WBRT (Hippocampal Avoidance WBRT)
Judy Morrow


“Everything I do is slow. I walk, talk, and think slowly… I still have no short-term memory…
Much of the time I can't even remember the names of relatives and close friends… I am always confused…
Because I look normal and often sound normal, people assume I am normal. But I'm not…
I get depressed a lot knowing that I will never have my competence back.”
-Sontag Foundation Distinguished Scientists Awards ceremony speech at the Society for Neuro-Oncology Meeting, Toronto,
Canada, November 20, 2004
- Susan Sontag (full time homemaker and mother / Cancer & brain radiation survivor )

• Whole-brain radiotherapy (WBRT) is the most widely used treatment option for patients with multiple brain metastases
• Benefits• rapid palliation of neurologic symptoms • improved local control as an adjuvant to
resection or radiosurgery. • prolongs time to neurocognitive function (NCF)
decline.( deterioration in NCF preceded self-reported quality of life decline by up to 153 days)
WBRT

• Before 1970, the human brain was
thought to be radioresistant;
• the acute central nervous system
(CNS) syndrome occurs after single
doses of ≥30 Gy, and white matter
necrosis can occur at fractionated
doses of ≥60 Gy
CNS Toxicity

• Radiation necrosis of the brain typically occurs 3 months to several years after radiotherapy (median 1–2 years)
• Emami et al • 5% risk of radionecrosis at 5 years
with a dose of 60 Gy to one-third of the brain with standard fractionation
• Quantec : For standard fractionation, the incidence of radionecrosis appears to be • <3% for a dose of <60 Gy. • 5% with a dose of 72 Gy • 10% with a dose of 90 Gy. However
But that’s not what we are talking about!!

• Early neurocognitive decline, within the first 1-4 months, which primarily reflects memory.
• Long-term serious and permanent adverse effects, including cognitive deterioration in other domains and cerebellar dysfunction
• As many as11% of long-term brain metastases survivors (>12 months) treated with WBRT develop severe dementia, especially with the use of larger dose-per-fraction schedules
Neuro-cognitive toxicity in WBRT

• According to the principle of double effect, • “sometimes it is permissible to
cause a harm as a side effect (or “double effect”) of bringing about a good result even though it would not be permissible to cause such a harm as a means to bringing about the same good end.”
Doctrine of Double Effect
St. Thomas Aquinas; Summa Theologica (II-II, Qu.
64, Art.7)

• radiation-induced injury to
proliferating neuronal progenitor cells
in the subgranular zone of the
hippocampi
PATHOGENESIS

• Approximately 100 000 patients
per year in the United States with
primary and metastatic brain tumor
survive long enough (>6 months) to
develop radiation-induced brain
injury
Is this a big deal in these stage IV patients?

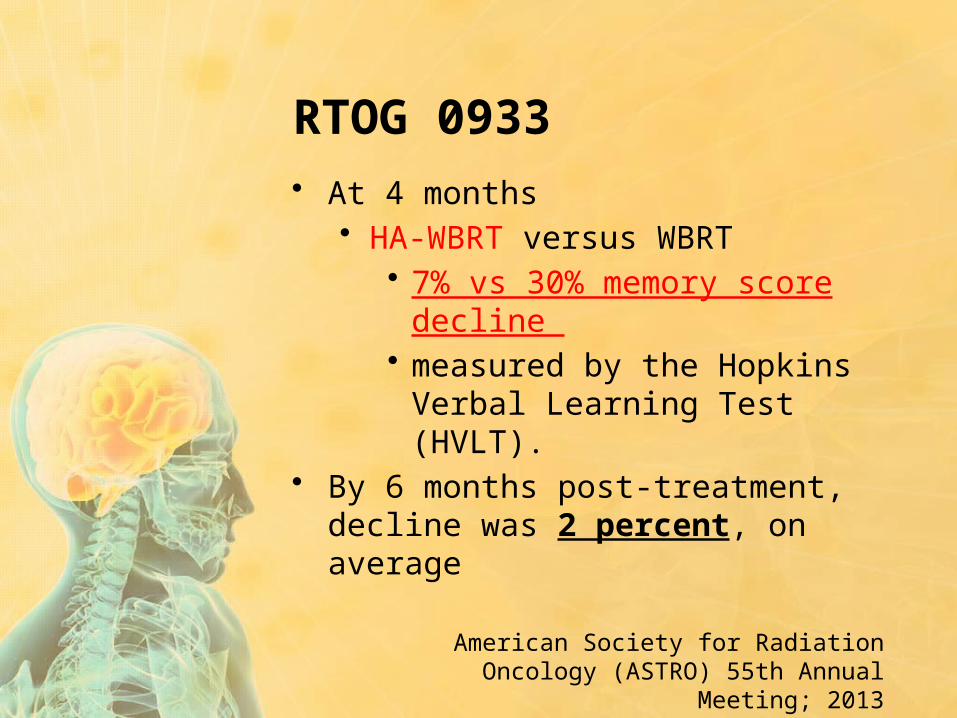
• At 4 months• HA-WBRT versus WBRT
• 7% vs 30% memory score decline
• measured by the Hopkins Verbal Learning Test (HVLT).
• By 6 months post-treatment, decline was 2 percent, on average
RTOG 0933
American Society for Radiation Oncology (ASTRO) 55th Annual Meeting; 2013

HIPPOCAMPAL CONTOURING

HIPPOCAMPAL CONTOURING

My interest

• MRI:• 3D-SPGR axial MRI scan of the head with standard axial and coronal
FLAIR, axial T2-weighted and gadolinium contrast-enhanced T1-weighted sequence acquisitions .
• 1.25mm slice thickness is preferred to contour the hippocampus accurately. Slice thickness of 1.5mm or less is permitted.
• Obtain in supine position; immobilization devices used for CT simulation and daily radiation treatments not necessary.
• CT Simulation:• Non-contrast treatment-planning CT scan of the entire head region.
• 1.25-1.5mm slice thickness is preferred for accurate hippocampal sparing planning. Slice thickness of 2.5mm or less is permitted.
• Immobilize patient in supine position using an immobilization device such as an Aquaplast mask over the head. Treat patients in the immobilization device.
• MRI-CT Fusion:• Fuse the 3D-SPGR MRI and the treatment-planning CT.
SIM INFO (0933)


HA-WBRT IMRTPlanning
PTV D2% ≤ 37.5 GyD98% ≥ 25 Gy
Hippocampus D100% ≤ 9 GyMaximum dose ≤ 16 Gy
Optic Nervesand Chiasm
Maximum dose ≤ 37.5 Gy
0933 dose constraints

IS THS FOR ALL BRAIN METS PATIENTS??
HOW DO WE SELECT THE PATIENTS FOR SUCH APPROACH??

Recursive Partitioning Analysis (RPA)
RPA Stages For Brain Metastases
Stage Characteristics Median Survival (mo)
IKPS >=70, age <65, primary
controlled, no other extracranial mets
7.1
II all others 4.2
III KPS <70 2.3

GPA Criteria For Brain Metastases
Variable 0 Points0.5
Points1 Point 2 Points 3 Points 4 Points
NSCLC/SCLC
Age >60 50-59 <50 - - -
KPS <70 70-80 90-100 - - -
No. Cranial Mets
>3 2-3 1 - - -
Extra-cranial Mets
Present - Absent - - -
Renal/Melanoma
KPS <70 - 70-80 90-100 - -
No. Cranial Mets
>3 - 2-3 1 - -
Breast/GIKPS <70 - 70 80 90 100
Median OS Survival (months)
GPA Score
NSCLC
SCLC Melanoma
Renal cell
Breast GI
0-1 3.0 2.8 3.4 3.3 6.1 3.1
1.5-2.5 6.5 5.3 4.7 7.3 9.4 4.4
3.0 11.3 9.6 8.8 11.3 16.9 6.9
3.5-4.0 14.8 17.0 13.2 14.8 18.7 13.5
Overall 7.0 4.9 6.7 9.6 11.9 5.4

Which tumor types??
• RTOG 0933• other than small cell lung cancer
and germ cell malignancy

• 58 y/o nurse & smoker• c/o headache, nausea, mental status
changes• CT showed 3 metastasis : radiologic
diagnosis• No other site of primary on CT T/A/P• no other etiology suspected
CASE SUMMARY

CECT

MRI BRAIN
• No other site of primary detected on staging CT scan. No pathology!
• Awaiting PET CT for staging

1. WBRT (of course!)
2. WBRT + VMAT Boost
?? Double effect / risk of toxicity
OPTIONS

RPA Stages For Brain Metastases
Stage Characteristics Median Survival (mo)
IKPS >=70, age <65, primary
controlled, no other extracranial mets
7.1
II all others 4.2
III KPS <70 2.3

GPA Criteria For Brain Metastases
Variable 0 Points0.5
Points1 Point 2 Points 3 Points 4 Points
NSCLC/SCLC
Age >60 50-59 <50 - - -
KPS <70 70-80 90-100 - - -
No. Cranial Mets
>3 2-3 1 - - -
Extra-cranial Mets
Present - Absent - - -
Renal/Melanoma
KPS <70 - 70-80 90-100 - -
No. Cranial Mets
>3 - 2-3 1 - -
Breast/GIKPS <70 - 70 80 90 100
Median OS Survival (months)
GPA Score
NSCLC
SCLC Melanoma
Renal cell
Breast GI
0-1 3.0 2.8 3.4 3.3 6.1 3.1
1.5-2.5 6.5 5.3 4.7 7.3 9.4 4.4
3.0 11.3 9.6 8.8 11.3 16.9 6.9
3.5-4.0 14.8 17.0 13.2 14.8 18.7 13.5
Overall 7.0 4.9 6.7 9.6 11.9 5.4



• Patients ≤50 years old • SRS alone
• median survival of 13.6 months• SRS plus WBRT
• 8.2 months for patients ≤50 who were treated.
• Patients >50 years old had a median survival of 10.1 months when treated with SRS alone, and 8.6 months for those who received SRS plus WBRT.


THANK YOU FOR YOUR PATIENCE!
Related Documents