Evidence‐Based Management of Femoroacetabular Impingement Syndrome TPTA Annual Conference – Arlington, TX October 23, 2015 Ed Mulligan, PT, DPT, OCS, SCS, ATC UT Southwestern School of Health Professions 1 Evidence-Based Management of Femoroacetabular Impingement Syndrome Presenters Ed Mulligan, PT, DPT, OCS, SCS, ATC Associate Professor; Residency Programs Director UT Southwestern Medical Center School of Health Professions Department of Physical Therapy - Dallas, TX UT Southwestern Medical Center – Dallas, TX Orthopedic, Neurological, and Sports Residency Programs Presentation Objectives 1. Define and differentially diagnose acetabular labral pathology and describe the epidemiology and risk factors associated with femoroacetabular impingement 2. Conduct a comprehensive subjective history and objective examination to manage intra‐articular hip pathology 3. Describe the intervention strategy, sequence, and points of emphasis for the non‐operative and post‐surgical management of labral pathology and athletic pubalgia 4. Select and utilize appropriate self‐report outcome tools for athletic hip problems and implement return to sports activities and criteria Disclosure Statement Neither I, Edward P. Mulligan, nor any family member(s), have any relevant financial relationships to be discussed, directly or indirectly, referred to or illustrated with or without recognition within the presentation Diagnosis Outcome Measures Intervention Conservative and Post‐Op Prognosis Return to Activity Examination History – Systems Review – Physical Exam ‐ Imaging Evaluation Presentation Agenda The Elements of Patient/Client Management Leading to Optimal Outcomes

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 1
Evidence-Based Management of Femoroacetabular Impingement Syndrome Presenters
Ed Mulligan, PT, DPT, OCS, SCS, ATC Associate Professor; Residency Programs Director
UT Southwestern Medical Center School of Health Professions Department of Physical Therapy - Dallas, TX
UT Southwestern Medical Center – Dallas, TXOrthopedic, Neurological, and Sports Residency Programs Presentation Objectives
1. Define and differentially diagnose acetabular labral pathology and describe the epidemiology and risk factors associated with femoroacetabular impingement
2. Conduct a comprehensive subjective history and objective examination to manage intra‐articular hip pathology
3. Describe the intervention strategy, sequence, and points of emphasis for the non‐operative and post‐surgical management of labral pathology and athletic pubalgia
4. Select and utilize appropriate self‐report outcome tools for athletic hip problems and implement return to sports activities and criteria
Disclosure Statement
Neither I, Edward P. Mulligan, nor any family member(s), have any relevant financial relationships to be discussed, directly or indirectly, referred to or illustrated with or without recognition within the presentation
DiagnosisOutcome Measures
InterventionConservative and Post‐Op
Prognosis
Return to Activity
ExaminationHistory – Systems Review –Physical Exam ‐ Imaging
Evaluation
Presentation AgendaThe Elements of Patient/Client Management Leading to Optimal Outcomes
Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 2
Femoroacetabular Impingement
Abnormal, pathological femoral acetabular contact or shearing that occurs within a normal ROM secondary to bony deformities or spatial malorientation that eventually manifests as symptomatic
15-year trend in publications on FAI
1 2 3 4 1018 20
38 40
81
99
142
173
251236
FAI is an intra-articular, non-arthritic hip pathology
Possible anatomical variants that may predispose to injury
– Femoral neck anomalies– Structural instability– Femoral or acetabular torsion/version
Resultant Symptomatic Pathologies
– Acetabular labral tears– Osteochondral lesions– Loose bodies– Ligamentum teres tears
Variants and pathologies are not mutually exclusive
Common Injuries
Acetabular (fibrocartilaginous rim) Labral Tears– radial flap (most common), radial fibrillated, longitudinal
peripheral, and abnormally mobile (partially detached)
Osteochondral Lesions– focal loss of cartilage on the articular surfaces
Ruptured Ligamentum Teres– strong intrinsic ligament stabilizer that resists hip joint
subluxation particularly when the hip is externally rotated in flexion or internally rotated in extension
Loose Bodies– small fragments of bone or cartilage within the joint from
osteochondritis or synovial chondromotosis
Mechanisms of Injury
Traumatic
– Twisting/Pivoting (golf, gymnastics, hockey, baseball, etc)
most often hip extension and ER
– Repetitive Hyperflexion (soccer, diving, running, etc)
Structural/Congenital Predisposition
– Femoral Acetabular Impingement (FAI)
Cam – large femoral head
Pincer – abnormal acetabulum with over coverage
– Capsular Laxity (congenital vs. acquired)
Down’s or Ehlers‐Danlos Syndrome
– Acetabular dysplasia
Structural Variants

Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 3
Imaging
Standard x‐ray views– AP– Frog‐Leg Lateral View
MRA/MRI– Much better SN for labral pathology with MRA than MRI (90 vs. 30%)
Major Radiographic Findings in FAI
How do the radiographic findings correlate with the physical exam
Dunn Viewlateral, cross-table, frog-leg Radiographic Findings
Cam Impingement – femoral head/neck profile exceeds the radius curvature of the acetabulum
– Alpha angle > 55‐60° No absolute cut‐off value
only an indicator of the size of the bony anomaly
A high alpha angle in an asymptomatic patient should be be considered an incidental finding
– Head‐neck offset ratio < 0.14(more in a minute)
Alpha Angle
On axial oblique MRI sequence, angle formed by a line parallel to the femoral neck axis and line from center of the femoral head to the transition of the femoral head into the femoral neck (neck radius exceeds head radius)
Abnormal > 55‐60° indicates cam deformity
Cam abnormal contact between femoral head/neck and acetabular margin
Prevalent in asymptomatic patients indicating that activity level is an important variable and that diagnosis is based on the clinical exam – not the image

Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 4
Cam = “Pistol Grip Deformity” abnormal contact between femoral head/neck and acetabular margin
Cam
– Asphericity of the femoral head creating a prominent bump on the anterosuperior head‐neck junction (pistol grip)
Can be secondary to epiphyseal injury or SCFE
wave sign
Resultant Pathology abnormal contact between femoral head/neck and acetabular margin
Cartilage in area of asphericity is delaminated from the bony acetabulum
• Convex bump (yellow arrowheads) at anterior femoral head-neck junction• Area of chondral loss (red arrows) present on the acetabular side of the joint• Subtle subchondral degenerative changes (red arrowhead) located on the
corresponding femoral side of the joint
Cam femoroacetabular impingement varieties
Head-Neck Offset RatioFemoral Morphology SummaryAlpha Angle and Head/Neck Offset
< 9 mm offset is considered abnormal
Dunn View
CAM Lesionvideographic explanation of pathological process Pincer Impingement
Increased Acetabular Depth
– Coxa profunda (lateral center‐edge angle > 35°)
– Fossa acetabuli is medial to Kohler’s line (deepsocket)
– Acetabular protrusion
– Femoral head is medial to Kohler’s (ilioischial) line
red line = ilioischial (Kohler’s) line

Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 5
Center Edge Angle (coxa profunda)
angle formed by a vertical line and a line connecting the femoral head center with the lateral edge of the acetabulum
Abnormal > 39° indicating pincer deformity
Radiographic Findings
• Acetabular Retroversion
― Crossover sign (indicating anterosuperior over coverage)
― Posterior acetabular rim does not lie lateral to the anterior wall on AP view
Crossover Signacetabular overcoverage secondary to retroversion
AP X-ray demonstrating bilateral acetabular retroversion as determined by crossover of the anterior and posterior acetabular walls (dotted lines)
Acetabular Version Anomalies Summary
Acetabular retroversion – anterior overcoverage of femoral head; posterior undercoverage
– Early contact with anterosuperior labrum when hip is internally rotated and flexed
Acetabular anteversion – posterior overcoverage of femoral head; anterior undercoverage
– Early contact with anterosuperior labrum when hip is externally rotated and extended
Clinical Recognition of Transverse Plane Hip Structure
AntevertedRetroverted• Femoral Anteversion
– torsion angle > 15°– toeing in
Femoral Retroversion– torsion angle < 8°– toeing out
NormalCraig’s Test and/or proportional hip ROM to identify presence
Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 6
Femoral Version Impact
Decreased femoral torsion allowing impingement in IR
Increased femoral torsion allowing impingement in ER
NORMAL
anterior head/neck junction closer to anterior acetabular rim
posterior head/neck junction closer to posterior acetabular rim
Structural Instability
Extraphysiologic motion of traumatic, atraumatic, or microtraumatic origin
– Shallow acetabulum
– Excessive femoral torsion or acetabular version
– Dysplasia (congenital or developmental)
More common in females than males
Sex Prevalence in FAI ImagingMixed Cam-Pincer on A/P and Lateral Frog Leg
20-30 yo
30-40 yo
Diagnostic Imaging Reminder
Morphology Pathology Cam/Pincer are structural findings but do not
automatically cause pathology
– Only implies that shape could allow abnormal contact particularly with repetitive loading
Evaluation of the Hip subjective history
Age and Sex
– Hip injuries tend to be age specific
Chief Complaint
Functional Disabilities
Patient's Goal‐Expectation(s)
“… Stop squirming, Mr. Silcox. The sooner we fill out these forms, the sooner we’ll find out exactly what’s wrong with you.”

Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 7
Hip InjuriesDifferential Diagnosis based on Age
AGE
0‐2 Development Dysplasia
4‐8 Legg‐Calves‐Perthes
9‐15 SCFE; Apophysitis
14‐25 Overuse Injuries – Strains, Sports Hernia, Stress Fractures
20‐40 Labral Pathology*
35‐55 GTPS; Snapping Hips
55+ DJD and Hip Fractures
Acetabular Labral Mechanism of Injury
Degenerative in older patients
Traumatic or overuse in youth
Increased risk if dysplastic or structural anomalies
Acetabular Labral Tears
Epidemiology
– Usually presents in 20s to 40s
– 20% of athletes with chronic or unresolved groin pain; 55% of adults with undiagnosed mechanical hip pain
– deep, intermittent groin pain with “mechanical” presentation during or after activity
– Most common area is anterior‐superior labrum (in U.S.)
Anterosuperior Posterosuperior Anteroinferior Posteroinferior
Acetabular labral lesion locations in order of frequency
subjective history
FAI hip pain location– Typically in the anterior or medial groin area
• Lateral pain is trochanteric or L4 referred
• Posterior may be SIJ, piriformis, or L5‐S1 referred
• Hip pain can also extend down the thigh towards the knee (pseudoradiculopathy)
C sign – classic representation of FAI-related pathology
Absence of groin pain helps rule out FAI because of its high sensitivity (0.96‐1.00)Byrd JW, N Am J Sports Phys Ther, 2007Keeney et al, Clin Ortho Relat Res, 2004,McCarthy et al, Orthopedics, 1995

Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 8
Acetabular Labral Symptom Presentation
Pain Location– 92% groin;
59% lateral hip; 52% anterior thigh/medial knee; 38% buttock area
– 85%+ have sharp pain with activity and painful mechanical lockingBurnett RS, J Bone Joint Surg, 2006
Clicking/Catching– 100% specificity/85% sensitivity
Narvani, Knee Surg Sport Traumatol Arthrosc, 2003
Symptoms Seem Activity Dependent
Pain Characteristics % Involvement
Sharp 73
Ache 73
Burn 25
Numb 10
Constant 46
Intermittent 42
Rest 35
Prevents Sleep 42
Wakes from Sleep 19
Aggravating Factors % Involvement
Activity related 71
Running 69
Pivoting 63
Walking 58
Sitting 65
Standing 44Clohisy JC, Clin Orthop Relat Res, 2009
Typical Onset and Nature of Complaint
65% insidious vs. 35% specific incident
65% have “mechanical” symptom
Mechanical Feature % Involvement
Pop 46
Snap 44
Catch (Crackle) 33
Lock 29
Subluxation/Instability 19Clohisy JC, Clin Orthop Relat Res, 2009
Cam Related Postural and Activity Related Complaints/Exacerbations
Prolonged Sitting (low chairs or driving)
– should get up and move every 5‐10 minutes
Activities that require repetitive, end‐range hip flexion
– uphill running
– stair ascent
– sprinting
– kicking
– recumbent cycling
Getting in/out of car
Pincer Related Postural and Activity Related Complaints/Exacerbations
Repeated hip hyperextension
– downhill walking
Weight bearing pivoting
– particularly towards side of involvement
Intercourse positionsLeft side
involvement
Right side involvement

Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 9
Activity Related Complaints
Walking-Stairs ADLs
ADL – Functional Activity
Limp at any time 73%
Limb Severity Slight Moderate Severe/Need Assistance
57% 14% 2%
Limited in Walking distance 37%
Distance Limitation > 6 blocks > 2 blocks Limited to indoors
22% 12% 2%
Require Use of Bannister on Stairs 39%
Clohisy JC, Clin Orthop Relat Res, 2009
Activity Related Complaints
Sitting/Dressing Tolerance
ADL – Functional Activity
Sitting Tolerance
Time One hour > 30 minutes < 30 minutes
37% 20% 43%
Donning shoes and socks 35%
Difficulty Difficult Unable
31%% 4%
Clohisy JC, Clin Orthop Relat Res, 2009
Subjective Self-Report Outcome Measures
Region Specific
HOS*
HAGOS
iHOT‐33
LEFS
Dimension Specific
• FABQ
• TKS
• GROC
Disease/Condition Specific• WOMAC – Osteoarthritis
• Oxford and Harris Hip Scores – Post‐op
* Note: The HOS was specifically developed to assess young patients with labral pathology
Q of L
PSFS
• SF‐36
• SF‐12
Self-report Outcome Tool Clinimetrics
Reliability – “repeatedly consistent”
– ICC > 0.75 is “good”
Validity – measures what it intends to measure
– Construct: quantitative assessment of relationship to a similar variable
– Pearson (r) > 0.40 is a “strong” correlation
Responsiveness – ability to detect a change over time when meaningful change has occurred
– MCD ‐ statistically reliable change of the tool
– MCID ‐minimal clinical change perceived as important
– SEM ‐ standard deviation of the distribution sample
HOS
Hip, ADL and Sports subscales
On the ADL subscale, the items related to sitting and putting on socks and shoes are not scored
17 items scored from 0‐4 with a max total of 68
Must answer at least 14 of 19
Sports subscale is optional and has max of 36 points
Highly reliable (ICC > 0.9)
MCID – 9 pt. ADL and 6 pt. sports subscale
Copenhagen Hip and Groin Outcome Score (HAGOS)
Newer region specific outcome measure tool designed for active younger to middle age patients with hip/groin pain
100 point questionnaire with 6 subscales of function
Construct Validity ‐ r = 0.37‐0.73
Test‐retest reliability ‐ ICC = 0.82‐0.92
MCID ± 5.2 on any of the 6 subscales
Thorborg et al, Br J Sports Med, 2014
Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 10
International Hip Outcome Tool-33 iHOT-33
Region specific 100 point VAS questionnaire for young active patients
Construct validity
― r = 0.81
Test‐retest reliability
― ICC = 0.78
MCID ± 6 Mohatadi et al, Arthroscopy, 2012
International Hip Outcome Tool-12 iHOT-12
Excellent agreement with iHOT‐33
Equivalent sensitivity to change
Automated versions available at:
http://www.nsmoc.com/pdf/ihot.pdf
http://www.scottfaucettmd.com/ihot/
Griffin DR et al, Arthroscopy, 2012
Lower Extremity Functional Scale (LEFS) Lower Extremity Functional Scale (LEFS)
Self report of functional ability via region specific 20‐item Likert scale questionnaire
Construct validity (r = 0.64‐0.80)
Reliable test‐retest measure (ICC = 0.80‐0.94)
SEM: 5 point margin of error
MCID ± 9
Low ceiling effect
Widely used in research and clinically
Binkley et al, Phys Ther, 1999
PSFS Patient Specific Functional Scale
3 self‐selected functional items rated on 0‐10 scale from unable to fully able to perform
Sum of 3 scores/3
MCD = 3 points single item; 2 points on average
MCID based on GROC satisfaction
– Small + change = ~ 1 point
– Medium + change = ~ 2 points
– Large + change = ~ 3 points
Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 11
Outcome Tool Clinimetric Summary
Thorborg K, Tijssen M, Habets B, Bartels EM, Roos EM, Kemp J, Crossley KM, Hölmich P. Patient‐Reported Outcome (PRO) questionnaires for young to middle‐aged adults with hip and groin disability: a systematic review of the clinimetric evidence. Br J Sports Med. 2015 Jun;49(12):812. doi: 10.1136/bjsports‐2014‐094224. Epub 2015 Jan 13.
Differential Diagnoses
Hip Dysplasia (age)
Lumbogenic Origin (posture/trunk motion)
Snapping Hip (symptom location/quality)
Trochanteric bursitis (age, sex, symptom location)
Piriformis Syndrome (symptom location/quality)
Sports Hernia (symptom location and provocation)
Osteoarthritis (age, stiffness)
Stress fracture (age, activity level)
Objective Examination You can see a lot by looking …
• Posture
― Sagittal, A/P, and transverse planes
• Limb Length Discrepancies
― No known correlation between limb length and FAI structural abnormalities on long or short limb
Patel SH, ISHA Annual Meeting, 2014
Hip ROM/Flexibility Assessment
Thomas Test –One/Two Joint Hip Flexors
PiriformisHip Rotators
AdductorsHamstringsOber Test –TFL/ITB
Quads/Rectus Femoris
Contrast may be important
Hip Rotations in Flexion and Extension
Contrast amounts of internal and external hip rotation in positions of flexion and extension
Cam lesions tend to limit mobility in flexion but not extension
Could also simply differentiate capsular and muscular mobility about the hip
Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 12
Hip Joint ROM
MOTION Normal ROM
Flexion (end feel) 0‐120°
Extension 0‐20°
Abduction 0‐45°
Adduction 0‐30°
External Rotation 0‐45°
Internal Rotation (end feel) 0‐45°
Common activities that may require substitution motions secondary to Cam deformities
Tie Your Shoes 120˚ flexion
Sit in Chair 110˚ flexion
Fig 4 Sit 120˚ flexion/20˚ Abd/ER
Put Pants On 90˚ flexion
FAI Physical Exam: Motion Summary
Terminal Motions Lost
– Limited IR (< 20°) when hip is flexed to 90°
Kubiak‐Langer M et al, Clin Orthop Relat Res, 2007
– Hip elevation maneuvers often limited (flexion and abduction)
– Obligatory hip external rotation with end‐range hip flexion (Drehmann’s sign)
Abnormal Arthrokinematics Excessive anterior femoral glide during ASLR
Because of the articular congruity there should be minimal glide of the femoral head in the acetabulum during sagittal plane motion
If anterosuperior glide is detected with familiar groin pain it may indicate overactive TFL and labral provocation
– Concordant sign may be relieved by allowing slight hip abduction and ER during the maneuvers
This is a theoretical, unproven construct
Harris‐ Hayes, Sahrmann, & Van Dillen, 2009; Van Dillen et al., 2000
Palpable anterior glide during SLR or passive hip/knee flexion
Improper Recruitment in Hip Extension
Encourage participation of the gluteals in extension
Excessive anterior motion of the trochanter may indicate hip IR and inadequate firing of the gluteals or overdependence upon the hamstrings
Train for the hamstrings and gluteals to turn on simultaneously to see if that minimizes or eliminates anterior hip pain
Lewis and Sahrmann suggest that hamstrings may cause anterior glide while gluteals will prevent forward migration of the femoral head in the acetabulum
Lewis CL et al, J Biomech, 2007; Clin Biomech, 2009; J Athl Train, 2009
FAI Movement Dysfunctions
subjects tend to avoid hip flexion and provide movement in spine rather than flexing the hip –avoiding lordotic positions

Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 13
Quadruped Rock Assessment
Hip flexion posterior capsule tightness may be suspected with quadruped ischial height asymmetry (or lateral shift away from tight side).
Hip Manual Muscle Testing
Hip Flexors–Iliopsoas vs. TFL
Hip Rotators Internal vs. External
Hip Extensors-Gluteus Maximus
Hip Abductors –Gluteus Medius
Hip Adductors
Impact of strength deficits
Significant strength deficits (8‐9%) in hip flexion and abduction were common (40‐50%)and correlated (r = 0.37) with loss of function
Hip Muscular Endurance Test
Symmetry in hold times or number of metronome paced repetitions without compensatory substitutions
FAI Special TestsHip Area PainClassification-Based Treatment
Lumbopelvic
HipLog Roll
Intra-articularTraumatic
ImpingementFADIR
Hypermobility
Hypomobility
Pediatric
Extra-articular:Strains – Tendinopathy –
Bursitis
Pelvic
Lumbosacral
R/O with lumbar mobility and repeated movements and SIJ provocation testing
R/O log roll, scouring, and FABER‐FADIR maneuvers
R/I with symptom location/palpation

Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 14
Differential Diagnosis
Extra‐articular
– Internal/external snapping hips
– Greater Trochanter Pain Syndrome
Pelvic‐Hip Mimickers
– Rectus abdominis strains
– Athletic pubalgia/sports hernia
– Adductor tendinosis
– Genitourinary nerve entrapment
Differentiating Athletic Pubalgia
Retrospective case series found 86% of subjects undergoing surgery for sports hernia had radiographic evidence of FAI
Econompoulos, Sports Health, 2014
Prospective case series showing 94% of athletes with recalcitrant adductor pain had radiographic signs of FAI
Weir A, Brit J Sports Med, 2011
Identyifying Athletic Pubalgia
Reiman MP, Brit J Sports Med, 2013
Log Roll TestDifferentiate Intra from extra-articular involvement
Gently rolling the femur into IR/ER ROM (femoral head rolls on stationary acetabulum)
Moving the femoral head in relation to the acetabulum doesn’t significantly challenge myotendinous or nervous structures
+ test rules in intra‐articular hip pathology however a negative test is not sensitive enough to rule out an intra‐articular hip problem
Byrd et al, 2007
reliability = 0.61
Martin RR, J Orthop Sports Phys Ther, 2008
Scouring (Quadrant Test)
Circumduction, rotation and/or ab‐adduction of the hip joint while in 90‐140°of flexion concurrent with long axis compression along the femur
clears for hip OA and may aggravate labral pathology in quadrants of involvement
…however, single study that evaluated diagnostic accuracy for IA hip pain found
SN = 50; SP = 29; +LR = 0.70; ‐LR – 1.4
Maslowski E, et al, PM R, 2010
Femoroacetabular/Labral Pathology Tests
Anterior Hip Impingement Test Methodologies
– F‐ADD‐IR
– F‐IR
– F‐IR with axial compression
– F‐ADD with axial compression

Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 15
Anterior Labral Test
Flexion-ABduction-External Rotation Flexion-ADduction-Internal Rotation
Femoral Acetabular Impingement Position
Highly SN (> .80‐.99) but very poor SP(.08 ‐ .43) in pooled analysis for FAITijjsen M, et al, Arthrscopy, 2012 and Reiman M, Br J Sports Med, 2015
Femoroacetabular/Labral Pathology Tests
Lateral Rim Hip Impingement
– Flexion, ABduction, and External Rotation of hip (Patrick’s sign) by placing distal lateral leg on the opposite anterior distal thigh
– extremity should fall parallel to the table with‐ out an increase in SIJ or anterior groin discomfort
– High SN (.80 in pooled analysis) but poor SP (.18 ‐ .24) for FAI
Tijjsen M, et al, Arthroscopy, 2012
• Also may indicate adductor/hip flexor injury, osteitis pubis, sports hernia, or SIJ pathology
Posteroinferior Impingement TestParvizi J et al, J Amer Acad Ortho Surg, 2007
External rotation in supine with hips at edge of table to allow maximal extension
Positive test is reproduction of familiar deep groin pain
Unknown diagnostic accuracy
Clinical-Radiographic Correlation
Physical Exam Findings Radiographic Findings Interpretation
FADIR with IR
Acetabular Index > 0°Anterosuperior acetabular overcoverage
Lateral Center Edge Angle > 39° Acetabular retroversion
Alpha Angle > 50° Anterosuperior cam
FABER with EREdge of anterior acetabular wall well medial to posterior wall
Acetabular anteversion
FADIR/FABER with IR/ER
Medial acetabular wall touches or passes ilioischial (Kohler’s) line
Acetabular profunda
Medial femoral head passes the ilioischial (Kohler’s) line
Acetabular protrusio
Clinical-Radiographic Correlation
Physical Exam Findings Radiographic Findings Interpretation
Apprehension and
ER/IRFemoral head extrusion index > 25°Lateral Center Edge Angle < 25°
Global undercoverage
Apprehension with ER
Edge of anterior acetabular wall well medial to posterior wall
Acetabular anteversion
Apprehension with IR
Crossover sign Acetabular retroversion
Stinchfield TestResisted SLR
General test of hip intra‐articular pain/irritation by resisted a straight leg raise
SN = 0.59
SP = 0.32
Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 16
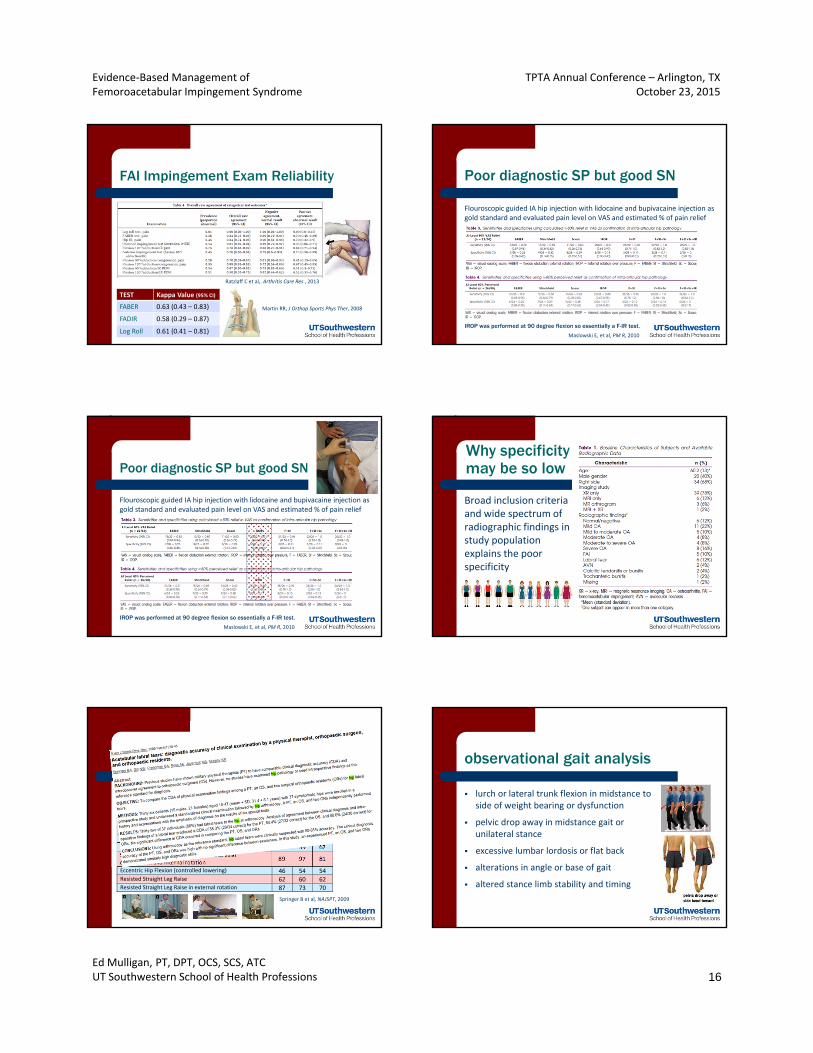
FAI Impingement Exam Reliability
Ratzlaff C et al,. Arthritis Care Res , 2013
TEST Kappa Value (95% CI)
FABER 0.63 (0.43 – 0.83)
FADIR 0.58 (0.29 – 0.87)
Log Roll 0.61 (0.41 – 0.81)
Martin RR, J Orthop Sports Phys Ther, 2008
IROP was performed at 90 degree flexion so essentially a F-IR test.
Maslowski E, et al, PM R, 2010
Flouroscopic guided IA hip injection with lidocaine and bupivacaine injection as gold standard and evaluated pain level on VAS and estimated % of pain relief
Poor diagnostic SP but good SN
IROP was performed at 90 degree flexion so essentially a F-IR test.
Maslowski E, et al, PM R, 2010
Flouroscopic guided IA hip injection with lidocaine and bupivacaine injection as gold standard and evaluated pain level on VAS and estimated % of pain relief
Poor diagnostic SP but good SNWhy specificity may be so low
Broad inclusion criteria and wide spectrum of radiographic findings in study population explains the poor specificity
PT n = 34
OS n = 32
OR n = 30
McCarthy Sign: Passive hip flexion to extension in external rotation
84 76 68
McCarthy Sign: Passive hip flexion to extension in internal rotation
78 89 84
Fitzgerald Anterior Labrum: FLEX‐ABD‐ER to EXT‐ADD‐IR 89 62 76 Fitzgerald Posterior Labrum; FLEX‐ADD‐IR to EXT‐ABD‐IR 87 39 62 Scouring in full flexion with simultaneous axial compression and internal rotation
89 97 81
Eccentric Hip Flexion (controlled lowering) 46 54 54 Resisted Straight Leg Raise 62 60 62 Resisted Straight Leg Raise in external rotation 87 73 70
Additional Labral Examination Techniques
% of positive findings for Physical Therapist (PT), Orthopedic Surgeon (OS), and Orthopedic Residents (OR)
Springer B et al, NAJSPT, 2009
observational gait analysis
lurch or lateral trunk flexion in midstance to side of weight bearing or dysfunction
pelvic drop away in midstance gait or unilateral stance
excessive lumbar lordosis or flat back
alterations in angle or base of gait
altered stance limb stability and timing
Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 17
Trendelenburg Sign
Glut Med Tendinopathy– reliable test with SN of 73%
using MRI evidence of torn tendon as reference standard
Bird PA et al, Arthritis Rheum. 2001
Osteoarthritis– SN = 55; SP = 70
– +LR = 1.8; ‐LR = 0.82Reiman MP et al, Br J Sports Med, 2015
Functional Movement Screen (FMS™)www.functionalmovement.com
Each test scored on a 0‐3 scale
0 – too painful to complete
1 – significant deviations
2 – limited abilities or notable movement deviations
3 – normal (no compensations or limitations)
Highly reliable and very specific but poorly sensitive in predicting sports injury
Full Squat In‐line LungeHurdle Step Active Leg Raise Trunk Stability Push Up
Quadruped Rotational Reach
Behind Back Reach
FAI Intervention
• FAI• Hip dyplasia • Acetabular labral tears • Chondral injuries• Loose bodies
60% (3 of 5) experimental studies reported favorable outcomes for non‐op treatment
65% (31 of 48) review articles felt non‐op treatment was appropriate with activity modification and various forms of exercise therapy being cited most frequently– Increase strength, motor control, mobility, and flexibility of hip and
trunk muscles
– Avoid motion extremes and teach activity and technique modifications
Non-Operative Management Case Series
Case series demonstrating con‐servative success in 4 subjects
Phase I:― modalities; core stabilization
Phase II: ― manual therapy and hip strengthening
Phase III:― unstable surface dynamic, activity‐specific training
Yazbek PM, et al, May 2011 issue
Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 18
My Perspective/Experience Managing Hip Pain
Grade I/II Mobilization
Electrotherapeutic Modalities
LLLT
Needling/Acupressure
Evidence for Dry Needling
reduce trigger point hypersensitivity
Dry Needling RCT
Neither dry needling or placebo needling of gluteals altered straight leg raise or hip internal rotation ROM
Both techniques showed short‐term reduction in pain but no difference between actual and sham interventions
Activity Modifications
Caution and/or avoidance with:
resisted hip flexion– symptomatic SLRs or sitting knee lifts
end range activities
lunges
weight‐bearing rotations
prolonged sitting
bent‐knee sit ups
cycling (particularly low seat)
Manual Therapyto improve joint mobility
Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 19
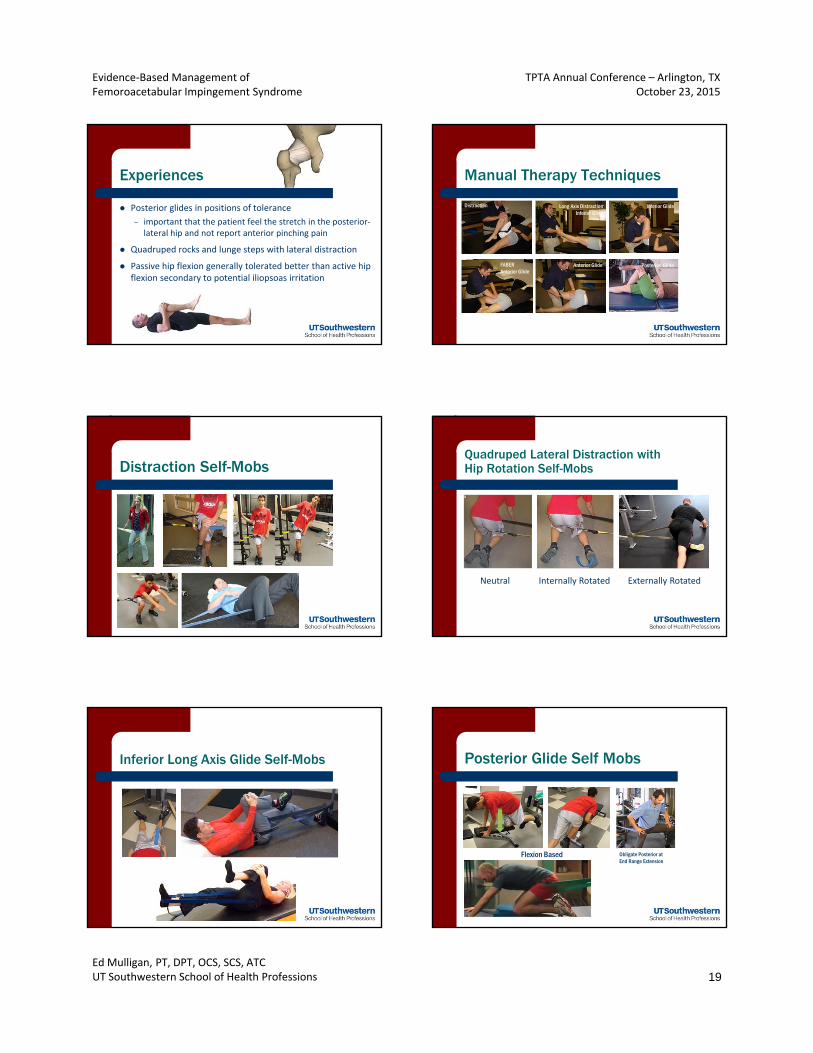
Experiences
Posterior glides in positions of tolerance
– important that the patient feel the stretch in the posterior‐lateral hip and not report anterior pinching pain
Quadruped rocks and lunge steps with lateral distraction
Passive hip flexion generally tolerated better than active hip flexion secondary to potential iliopsoas irritation
Manual Therapy Techniques
Distraction
Posterior GlideAnterior GlideFABER Anterior Glide
Inferior GlideLong Axis DistractionInferior Glide
Distraction Self-MobsQuadruped Lateral Distraction with Hip Rotation Self-Mobs
Neutral Internally Rotated Externally Rotated
Inferior Long Axis Glide Self-Mobs Posterior Glide Self Mobs
Flexion Based Obligate Posterior at End Range Extension
Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 20
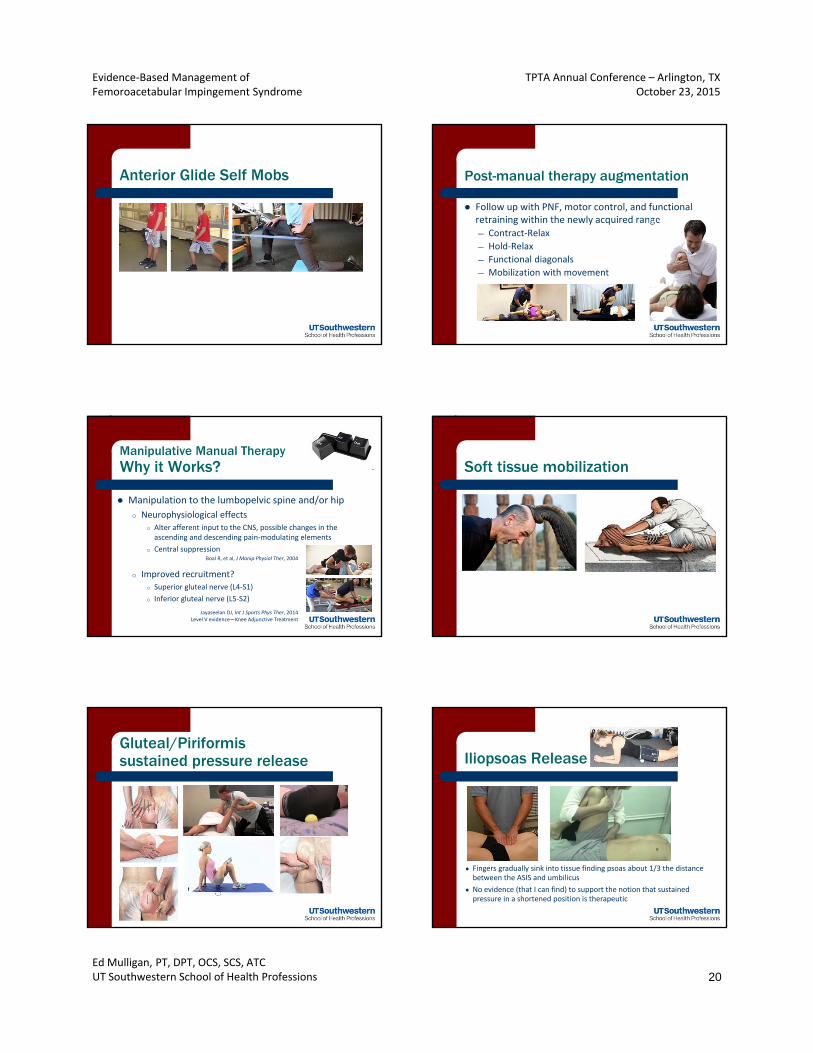
Anterior Glide Self Mobs Post-manual therapy augmentation
Follow up with PNF, motor control, and functional retraining within the newly acquired range— Contract‐Relax
— Hold‐Relax
— Functional diagonals
— Mobilization with movement
Manipulative Manual TherapyWhy it Works?
Manipulation to the lumbopelvic spine and/or hip
o Neurophysiological effects
o Alter afferent input to the CNS, possible changes in the ascending and descending pain‐modulating elements
o Central suppression
o Improved recruitment?
o Superior gluteal nerve (L4‐S1)
o Inferior gluteal nerve (L5‐S2)
Boal R, et al, J Manip Physiol Ther, 2004
Jayaseelan DJ, Int J Sports Phys Ther, 2014Level V evidence—Knee Adjunctive Treatment
Soft tissue mobilization
Gluteal/Piriformis sustained pressure release Iliopsoas Release
● Fingers gradually sink into tissue finding psoas about 1/3 the distance between the ASIS and umbilicus
● No evidence (that I can find) to support the notion that sustained pressure in a shortened position is therapeutic
Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 21
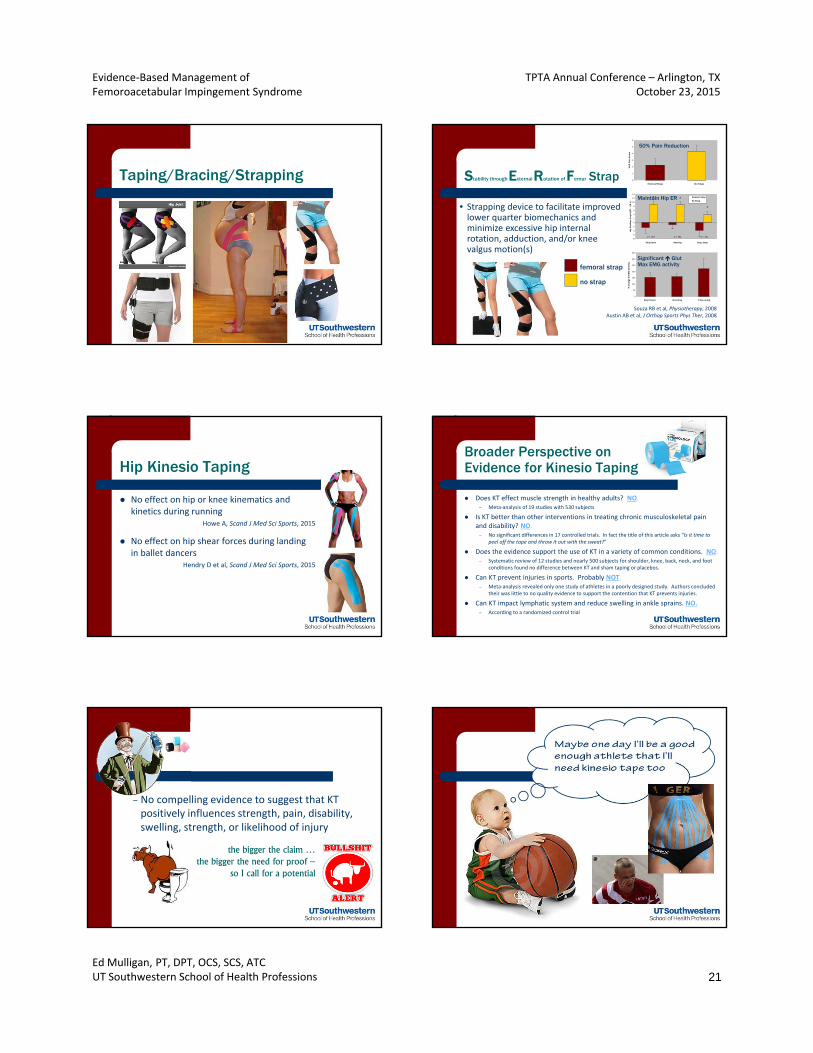
Taping/Bracing/Strapping
0
50
100
150
200
250
300
350
Step Down Running Drop Jump
% c
han
ge in
EM
G a
cti
vity)
-8
-6
-4
-2
0
2
4
6
8
10
12
14
Step Down Running Drop Jump
Hip
Ro
tati
on
An
gle
(E
R -
/ I
R +
)
Femoral Strap
No Strap
*
* *
p = .003 p = .001 p = .011
0
1
2
3
4
5
6
Femoral Strap No Strap
VA
S P
ain
Sco
re
50% Pain Reduction
Maintain Hip ER
Significant Glut Max EMG activity
• Strapping device to facilitate improved lower quarter biomechanics and minimize excessive hip internal rotation, adduction, and/or knee valgus motion(s)
femoral strap
no strap
Stability through External Rotation of Femur Strap
Souza RB et al, Physiotherapy, 2008Austin AB et al, J Orthop Sports Phys Ther, 2008
Hip Kinesio Taping
No effect on hip or knee kinematics and kinetics during running
Howe A, Scand J Med Sci Sports, 2015
No effect on hip shear forces during landing in ballet dancers
Hendry D et al, Scand J Med Sci Sports, 2015
Broader Perspective on Evidence for Kinesio Taping
Does KT effect muscle strength in healthy adults? NO.– Meta‐analysis of 19 studies with 530 subjects
Is KT better than other interventions in treating chronic musculoskeletal pain and disability? NO.– No significant differences in 17 controlled trials. In fact the title of this article asks “Is it time to
peel off the tape and throw it out with the sweat?”
Does the evidence support the use of KT in a variety of common conditions. NO.– Systematic review of 12 studies and nearly 500 subjects for shoulder, knee, back, neck, and foot
conditions found no difference between KT and sham taping or placebos.
Can KT prevent injuries in sports. Probably NOT.– Meta‐analysis revealed only one study of athletes in a poorly designed study. Authors concluded
their was little to no quality evidence to support the contention that KT prevents injuries.
Can KT impact lymphatic system and reduce swelling in ankle sprains. NO.– According to a randomized control trial
the bigger the claim … the bigger the need for proof –
so I call for a potential
– No compelling evidence to suggest that KT positively influences strength, pain, disability, swelling, strength, or likelihood of injury
Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 22
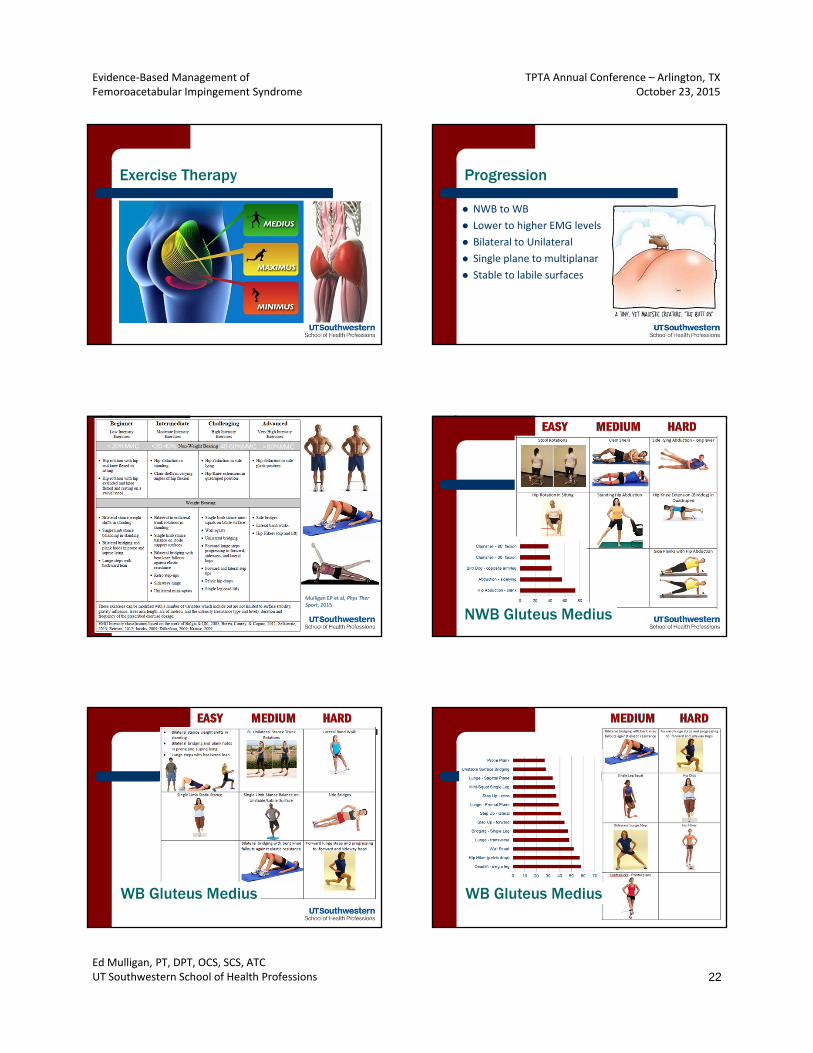
Exercise Therapy Progression
NWB to WB
Lower to higher EMG levels
Bilateral to Unilateral
Single plane to multiplanar
Stable to labile surfaces
< 20% MVIC <20-40% 40-60% MVIC > 60% MVIC
Mulligan EP et al, Phys Ther Sport, 2015
NWB Gluteus Medius
WB Gluteus Medius WB Gluteus Medius

Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 23
Hip Extension Exercises
Gluteal training lacks high quality evidence for efficacy as well
particularly for specific types of exercise training or exercise selection for specific type of pathology
Possible Rehab Complications
Hip flexor/adductor tendonitis
Joint irritation/edema
Faulty movement patterns
Lumbopelvic pain
Usual Cause
– joint overload – aggressive return to ADLs
Alter-G Treadmill Training
• Decreased GRF allows for safe acceleration of functional activity
• Improved gait without minimal alterations in normal mechanics
Cutuk A et al, J Appl Physiol, 1985
No research to support to this intervention perspective but it does seem to make intuitive sense
Similar or Concurrent Presentations
Athletic Pubalgia Internal Snapping Hip

Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 24
Sports Hernia
Athletic pubalgia without a true herniation– Weakening of the abdominal wall in the area of the inguinal canal– Possible entrapment of the genitofemoral nerve
Pain with twisting/turning in single limb stance; resisted adduction; sit‐ups
+ Rocker Test
Valsalva type maneuver may be provocative – forcible exhalation against a closed airway
Rest or surgical repair with emphasis on restoration of abdominal strength, adductor flexibility, and a gradual resumption of activity
Sports HerniaProposed Treatment Algorithm
YES YES
NONOIs initial pain rating >7?
Is hip rotation or abduction ROM limited?
Strength and Stability Training
Pain Control: activity mods, PROM, soft tissue techniques, nitro patches
ROM Training
Hegedus EJ et al, Phys Ther Sport, 2013Ellsworth AA et al, Int J Sports Phys Ther, 2014Kachingwe AF et al, J Ortho Sports Phys Ther, 2008
Internal Snapping Hip
Audible “snap” deep in anterior groin area with movement
Internal
– Iliopsoas tendon crossing iliopectineal eminence when uncrossing the legs from a flexed, abducted, externally rotated position
– Ludloff sign – active SLR from sitting in chair where RF is actively insufficient
Snapping Hip Treatment
Address identified impairments
Correct LLD
Strengthen weak gluteal muscles
Train core trunk stability
Hip Mobilization
Stretch tight muscles
– ITB (external) and Iliopsoas (internal)
Tolerance for Conservative Treatment
Failed conservative intervention over 4‐6 weeks is probably a good indicator that arthroscopic hip surgery should be considered
Surgical Intervention

Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 25
Post-Op Rehabilitation Considerations
PWB for first 2‐4 weeks dependent upon resection vs. repair
Careful of end range motions during the first couple of weeks
Expect full PROM in 2‐6 weeks
Isometrics can begin 2nd post‐op day; AROM in most planes at about 2 weeks
Weight bearing PREs can began as tolerated when non‐antalgic FWB gait
Summary of Weight-Bearing Status/Progression, CPM, and Orthoses Recommendations
Debridement, excision, removal, etc
Repairs, …plasties, etc Microfracture
Weight‐BearingImmediate post‐op WBAT
Flat‐foot PWB
Flat‐Foot (< 20 lbs) PWB
WB Progression FWB by 1‐2 wks 2‐4 weeks 6‐8 weeks
CPM UtilizationCPM or self ranging on bike optional
50% yes4‐8 hours/day for 2‐4 wks
Braces/Orthoses No33% yes to limit unwanted sagittal or transverse plane end range
based on systematic review from 14 studies ‐ Grzybowski JS et al, Frontiers Surg, 2015www.bryankellymd.com
“Excise” Protocol
Phase I ‐ Acute Phase II ‐ Subacute Phase III ‐ Return to Sport
Time 0‐2 to 4 weeks 4‐8 weeks 8 weeks +
ROM Bike freewheelingLog Rolls/Stool rotationsPROM
Hip MobilizationsLE Stretching
Dynamic StretchingProprioceptive work
Exercise Isometrics → IsotonicsPelvic TiltsSupine Bridging
Glute Med ProgressionGlute Max ProgressionTreadmill Progression
Elliptical
“Repair” Protocol
Phase I ‐ Acute Phase II ‐ Subacute Phase III ‐ Return to Sport
Time 0‐4 weeks 4‐12 weeks 12 weeks +
ROM Bike freewheeling/CPMLog Rolls/Stool RotationsPROM – limit extension/ER
AROM (minimal mobs)LE Stretching
Dynamic StretchingProprioceptive work
Exercise Isometrics → Isotonics (no flexion)Pelvic TiltsSupine Bridging
Glute Med ProgressionGlute Max ProgressionTreadmill Progression
Elliptical
Precautions and Progression Criteria
Phase I – Acute0‐4 weeks
Phase II – Subacute4‐12 weeks
Phase III ‐ Return to Sport12+ weeks
Progression Criteria
Normal gait70‐80% PROMControllable symptoms
Pain‐free ADLsSymmetric ROMCORE control/stability
AvoidanceSLRsPassive end range activities: (F/E; IR/ER; Ab/Add)
Ballistic stretching
PrecautionsIliopsoas irritationSynovitisGTPS
Careful with walking progressions
based on systematic review from 14 studies ‐ Grzybowski JS et al, Frontiers Surg, 2015www.bryankellymd.com
Good resource for post-op guidelines
www.bryankellymd.com

Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 26
Functional Testing for the Hip So, what do we do?
Shift from impairment‐based rehab to performance‐based rehab driven by results of functional assessment when:
• healing time is adequate
• NPRS levels are controlled
• ROM and motor control goals are achieved
• gait mechanics have normalized
Best-evidence is Expert Opinion Progression Criteria
Return to Sport Phases
– Step Down Mechanics
– Plank Test Performance
– Self‐Report Outcomes (HOS)
– Isokinetic Torque Symmetry
– Functional Tests
Y‐Balance, Hop Tests, Tuck Jumps
Wahoff M et al, Int J Sports Phys Ther, 2014
Vail Hip Sports Test
Wahoff M, Clin Sports Med, 2011
Selected FMS Tests
15/18 minimum to RTS
Evidence‐Based Management of Femoroacetabular Impingement Syndrome
TPTA Annual Conference – Arlington, TXOctober 23, 2015
Ed Mulligan, PT, DPT, OCS, SCS, ATCUT Southwestern School of Health Professions 27
Return to Sport
Systematic review of 18 case series (moderate to high
quality) involving almost 1000 hips of professional, collegiate, high school, and recreational athletes
– mean age: 28 (15‐41)
– 76% male
87% return to sport
82% at same level of competition
Casartelli NC et al, Br J Sports Med, 2015
Return to Sport Guidelines
Low impact loading and deep squatting exercises generally begin at 3 months with return to sport at 4‐6 months
McDonald JE et al, Arthroscopy, 2013
McCormick F et al, Arthroscopy, 2012
Stafford GH et al, Hip Int, 2011
Byrd JW et al, Arthroscopy, 2011
Horisberger M et al, Arthroscopy, 2010
Outcomes
Study LOE Subjects Study design Intervention Primary outcome
McDonald 3Elite athletes
Case‐control Microfracture RTS: 77% in microfracture vs. 84% in non‐microfracture (p > 0.05)
Krych 1 Females RCTLabral repair vs. debridement
• Better HOS (ADL, sport) in repair group (p < 0.05 for both)
• Better subjective outcome in repair group (p < 0.05)
McCormick 3labral tears
Case‐controlLabral repair vs. debridement
• Presence of OA at arthroscopy predicts worse outcome
• Age >40 years predicts worse outcomes
Philippon 4FAI11–16
Case seriesFAI ‐ labral treatment
• Significant improvement in mHHS at 3 yrs• 13% (all girls) need repeat arthroscopy for adhesions
Malviya 4FAI, 14–75
Case seriesFAI ‐ labral treatment
• Significant (p < 0.05) improvement in QoL• 74% of patients happy with results
Grzybowski et al, Front Surg, 2015
Outcomes
Study LOE Subjects Study design Intervention Primary outcome
Byrd 4 FAI Case seriesFAI and labral treatment
Significant (p < 0.001) improvement in mHHS at 2 years
Nho 4High‐level athletes, FAI
Case seriesFAI and labral treatment
• Significant improvements in mHHS and HOS at 2 years
• 79% return to sports at mean 9.4 months
Philippon 4FAI, 38–44
Case seriesFAI and labral treatment
• Significant improvements in mHHS at 2 years
Streich 4Labral tears, no FAI
Case series Labral treatment
• Significant improvements in Larson hip score and mHHS
• Presence of acetabular chondral defect worse prognosis
Stafford 4FAI, chondral defect
Case seriesMicrofracture with cartilage repair
Significant (p < 0.001) improvement in mHHS at 2 years
Grzybowski et al, Front Surg, 2015
Interpretation
Address all defects (microfracture and repair as needed)
Worse outcomes if older or osteoarthritic
Significantly better at 2 years according to self‐report
Good chance for RTS in athletic subjects
Related Documents











