Higher risk for dehydration th an adults Babies have Sx great er surface area than adults Longer Gl tract Metabolic needs are faster need for water - excretion in GI tract heat production I mmature kidneys - babies cannot dilute or concentrate urine unitL

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Higher risk for dehydration than adults
Babies have Sx greater surface area than adults
Longer Gl tract
Metabolic needs are faster
need for water
- excretion in GI tract
heat production
Immature kidneys
- babies cannot dilute or concentrate urine
unitL

Occurs whenever the total output of fluid exceeds the total ontake, regardless of underlyong cause
TYPES 1. Isot on ic · <•sonatrem•c}
Electrclyte anCI water defiCitS are present1n approx•matelv balanced proport•on
Plasma Na = WNL (130·150)
Hypoton ic • (hypanatrem•c)
Electrolyte def•c•t exceeds the water def•c•t Plasma Na =- less than 130 mEQ /liter
3. Hypertonic · (hypernatrem1c)
Waler loss '" excess of electrolyte loss Plasma Na = greater than 150 mEq /liter
Weight loss-Infants 3%·SO:o 6%·9%
We1ght loss ch••<~ren J~·" ·~% 6·::.:.-a~.~
Pulse Normal Slightly
Ke:sp1rettory rate Normal Sl•ght tachy~mca
Blood pressure Normal Normal to orthostatiC
B~hav•or Normal trntilble
Thirst Slight N od crate
r.,ucous membranes ,.lorrnal Dry
Tears Present Decreased
Anterior font.wc! Nornml r~orrrMI to sunken
ExrcrniJI Jugular Vtsib!e Not vis1blc
~ktn Cap refill Cap refill ] 4 sec; ~] !;eC Skill turgor
Urtne spectflr gravity .;;: 1.020 > 1.020; ollgurin
• Hydrate
• Strict I &O; daily weight
• Pulse oximeter
• Monitor capillary refi ll
• Measure and weigh diapers
10% or greater
10":,-:,
Very
ltyperpnea
Orthostatic to shock
ttyperlrntable to lethruglc
Intense
Parched
Absent, sunken eyes
Sunken
Not visible
Very delayed t(lp refill ( >4 sec); tencmg
Ollgmla or ;muriL~
• Counting stools or weighing if liquid
• Check t ongue for fissures
0 Calculate child's weight in kg
Allow 100 ml/kg for first 10 kg body weight
Allow 50 ml/kg for second 10 kg body weight
• Allow 20 ml/kg for remaining body weight
Child weighs 32 kg
• l OOmL x 10 for first 10 kg of body weight = 1000 mL
• 50mL x 10 for second 10 kg of body weight = 500 ml
• 20ml x 12 for remaining body weight = 240 mL
• 1000 + 500 + 240 = 1740 ml/ 24 hr
Child weighs 8.5 kg
• lOOmL x 8.5 for first 10 kg of body weight = 850mL
• No further calculations
• 850 ml /24 hr
1. Emergency Phase for severe dehydration • Restore circu lat ion rapid ly (except in
hypertonic)
• OS 1/4NS
• Checking for behaviors indicating hydration status
• Urine Specific Gravity
• WN L 1.010 t o 1.020
• Severely dehydrat ed > 1.024
2. Repletion Phase • Restore body fluids to volume
that will permit adequate circu lation and good renal function
• IV solut ion given slower than in emergent phase.
• K+ is added to IV when rena l function is established.
• May add Na Bicarb if acidotic
MODEL FOR ORAL REHYDRATION • Rehydration solution should consist of 75-90 mEq of Na per liter (not sports drinks). Give 40 to SO ml/kg of rehydration solution over 4 hours. May need maintenance therapy (not to exceed 150 ml/kg/day of ORS).
Late Recovery Phase • Concerned with realimentation
NO BRAT diet- Begin normal diet within reason.

88-90% of all diarrhea is caused by rota virus
Increase in November to May
Temporary lactose intolerance- don't give cow based milk. Breast milk OK.
Resulting acidosis • Loss of bicarbonate - metabolic acidosis • Impaired renal function • Accumulation of lactic acid • Ketosis
Put in isolation (until stool cultures back)
I & 0
Daily weights
Stoo l Cultures
History
0 Been out of the country?
Pediatric Nutrition

Food Guide
=---=---- -------
~~~i:~'="~~~-:
Food Plate Guidelines
MyPiate
Classification of Anemias
• Etiology and physiology: - RBC and/or Hgb depletion
• Morphology : - Characteristic changes in RBC
size, shape, and/or color

Effects of Anemia on ,__............,· culatD__t:_v. S_')Lstecu _____ __.~
• Hemodilution • Decreased peripheral resistance • Increased cardiac circulation and
turbulence: - Ma y h av e mur mur - May lead to cardiac failure Bi_rF'1
• Cyanosis ElSI -~ ..... - 6!!!1
·~ • Growth retardation
Caused by inadequate supply of dietary iron
Factors (Infants )
• Fetal iron stores are good for 5-6 months; preemies 2-3 months
• Anemia when feed only milk after 6 mo.
Gene rally preventable : ·Iron-fortified cereals and formulas for infants; cereal after 6 months
·Adolescents at risk due to rapid growth and poor eating habits
If Prolonged • Cognitive, behaviora l problems • Fatigue • Enlarged heart
Treatment
• Hgb at least 11. Treatment usually @ least 6 mo. · Give iron with vitamin C (except infants), through straw or syringe • Brush teeth, wipe gums • Check stools
• If severe, rece1ve IM (I mferon) • Iron can cause GI problems

Failure to Thrive
Refers to a state of inadequate growth from inability to obtain and/or use calories required for growth
It is a symptom, not a disease
No universal defin ition. Book calls this "Avoidant/Restrictive Food I ntake Disorder"
o Weight and sometimes height that fa ll below the S'h percentile for the chi ld's age or fa lls off normal growth curve.
Must take into account cu ltu ral differences in build; plot on HT/WT chart
.. "

0 Organic FTT (OFTT)
• Result of a physical cause (CHD,neuro prob, chronic UTI)
• Accounts for less than half of all FTTs
• Must be ruled out by physical assessment
Non-Organic FTT (NFTT)
Definable cause that is unrelated to disease
Psycho social factors
Poor parenting skills/lack of knowledge
Poverty, health beliefs, inadequate nutritional knowledge, family stress, feeding resistance, insufficient breast milk
• Disturbance in mother/child attachment
Idiopathic or Mixed FTT
• Unexplained, but usually accounted with NFTT
Plot on curve
Dietary history
Physical Examination
~_, Cha racteristics of FTT Child • Avoids eye contact (shows lack of bonding)
• Intense watchfulness
• Avoidance of contact - stiff or floppy
• Repetitive self-stimulating behaviors
(rocking, head banging)

Characteristics of FTT Child (cont) Disturbed affect (irritability, apathy or extreme compliance) " • -·-
Sleep disturbances r.- ~ - \
Lack of age-appropriate stranger anxiety
Lack of appropriate preferences for parents
Slow in social behavior - smiling
Dietary "quirks" - turn away from food, regurgitation, etc.
Characteristic Behavior of Caregiver Substance abusers
Inadequate support systems
Poor parenting practices - lack of commitment to parenting
No bonding due to lack of contact
Making negative comments
No name given to baby
Therapeutic Management Goal is reversing the malnutrition - may need hospitalization or close home health monitoring
Structuring the environment for positive psychosocial interactions
Multidisciplinary team to work with family
Prognosis - Uncerta in, related to cause & controlling factors
ASSESSMENT, TEACHING, ROLE MODEL

GI Problems of I nfancy
.~ FIG. 24-5 t-iypenroph•c pylouc s1f.:no5<~s A, EnlAfgcd musr.ui:Jr area neat1y Obl1leraTe!. pylortc cnannel B, Longrlu<1UI:l' ~urgtc.al O•v•~•on or musclt: d()Wfl to sut,mucnsa eslablt stu~s a-dl~(luil t f: passag,'!wfly
Constriction of pyloric s phincter with ob structio n of gastric outle t
" Signs and Symptom s
Projectile vomiting; non bilious
Baby is always hungry
J Signs of dehydration - Acid-base imbalance
Ph increases
Creatinine and BUN increase
Stools decrease
Visible peristaltic waves - see going left to right
Palpable - feels like an olive usually RUQ

Diagnosis - Upper GI or Ultrasound (preferred)
Treatment - Surgery after F & E imbalances corrected.
Minor procedure
Post op vomiting common - keep IV until sure tolerating feeds. >one vomiting concerning.
Begin feedings 4-6 hr; 24 hrs give formula, BM rigflt away.
HOB in high fowlers
Burp frequently
Pyloric Stenosis
• Nursing care - Meet fluid and electrolyte
needs. - Minimize weight loss. - Promote rest and comfort. - Prevent infection . - Provide supportive care. - Discharge planning and home
care t eaching.
Pyloric Stenosis
• Nursing care - Meet fluid and e lectrolyte
needs. - Minimize weight loss. - Promote r est and comfort. - Prevent infection. - Provide supportive care. - Discharge planning and home
care t eaching.

Failed separation of the esophagus and trachea by the forth week of
gestation
FIG. 24-4 A-E, Fr.~e mo~l common ~s of "soph.:tgt>al atreSia and llacheoesophagc~t ft5Ulo)
Cl inical Manifestations • Excessive sal ivation and drooling
· Three C's of tracheoesophageal fistu la
·Coughing
-Choking
-Cyanosis
· Apnea ---·-• Increased respiratory distress after feeding
• Abdominal distent ion
Nursing Implications
• Immediately NPO
• HOB up to prevent reflux
· Suction frequently
• Begin antibiotiCS immediately
• Keep g-tube unclamped to vent
Post-op
• Monitor for respiratory distress
• G- tube feed ings
• Tracheomalasia may be seen
Pathophysiology
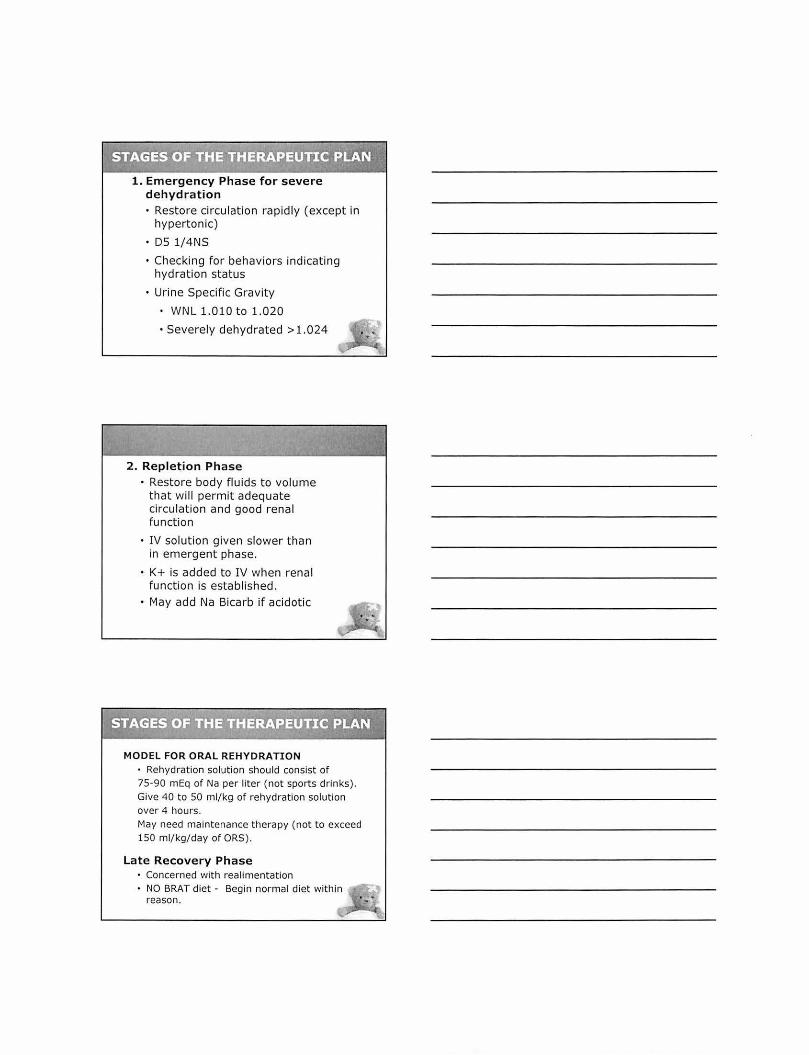
• Absence of autonomic parasympathetic ganglion cells in one section of the colon
• Problem in embryonic development
• Results in lack of propulsive movements (penstalsis)
• Accumulation of int. contents and distention of the bowel proximal to the defect causes a large or megacolon
Pathophysiology ( cont)
• Also internal rectal sphincter not relaxed - > prevent evacuation of solids, liquids, gas
• Most common site is rectosigmo id colon
• Intestinal distention and ischemia from distention of bowel wall cause enterocolitis-leading cause of death

Clin ical Manifestations Vary according to age
Newborn · Not pass mecon1um withm24-48 hours • Reluctance to drink • B1le sta1ned vom1tus • Abdom1nal d1stent1on if not treated- resp distress and shock
Infancy · FTI • Constipation • D1arrhea and vom1t111g (fever, sometimes with explosive, bloody, watery diarrhea signify enterocolitis)
Clin ical Manifestations (cont)
Childhood
· Chron ic sym ptoms of constipat ion - pass r ibbon -like, foul smelling stools
• Abdominal distention; feca l mass palpable
• Visible peristalsis
• Poorly nourished and anemic
Diagnostic Evaluation · Newborn- fails to pass meconium
• Later childhood and mfancy- h1story. rectum free or feces, sphincter t1ght, leakage or liquids, gas and foul. pale stool, chronic constipation. poor feeding poor we1ght gain
• Sometimes megacolon won't develop unt1l 3-4 weeks or months after b1rth
• Need rectal biopsy for definitive diagnosis.

Therapeutic Management •Treated surg1cally. Usually 2 stage repair- Remove aganghomc section of colon and do colostomy. At approx . 20 lbs,{ in 2 mo to 1 year) will do sphincterotomy and pull-down of functional bowel and close colostomy.
•Currently, if d1agnosed in neonatal penod, wi ll do a 1 stage repa1r. Resect aganglionic sect1on and pull down colon and anastomose to rectum {no colostomy) .
·May do laproscop1cally through anus. Good resul t s; no maJOr abdominal surgery; less hospital stay; !l~ colostomy care; completion of treatment at ea ~ • age •
Nursing Considerations
Preoperative
· Depends on condition of child and age . If malnounshed- will need h1gh cal, h1gh protein, low f1ber d1et and ISOtonic enemas, unt il cond1t1on improves and can Withstand surgery.
• Preop wil l have NG Golytely, anl1b10t1CS and rectal 1rngat1ons. Dally abdominal Circumference.
· Psychological preparatiOn for colostomy
• NPO, IV; abdom1nal dressmgs, penanal dsgs; may have NG tube; ostomy care
Ft9ura 25-7 ~ ••fl'ln! has •ever at g.~stro.at~tln•l p~oblems and requw~ ottom~C"s fQf
re~d~tl{J' and t01 dr!\mage of I <leal n ah:nal Note the app~<uMce of the
• I t
Most frequent cause of intestinal obstruction during infancy
SO% occurs less than 1 year (most 3 mo to 12 mo)
Most others occur before 2 nd year (Some books say 3 yrs)
3 X more in males
Cause unknown. May have a viral origin. More in cystic fibrosis and Celiac's Disease
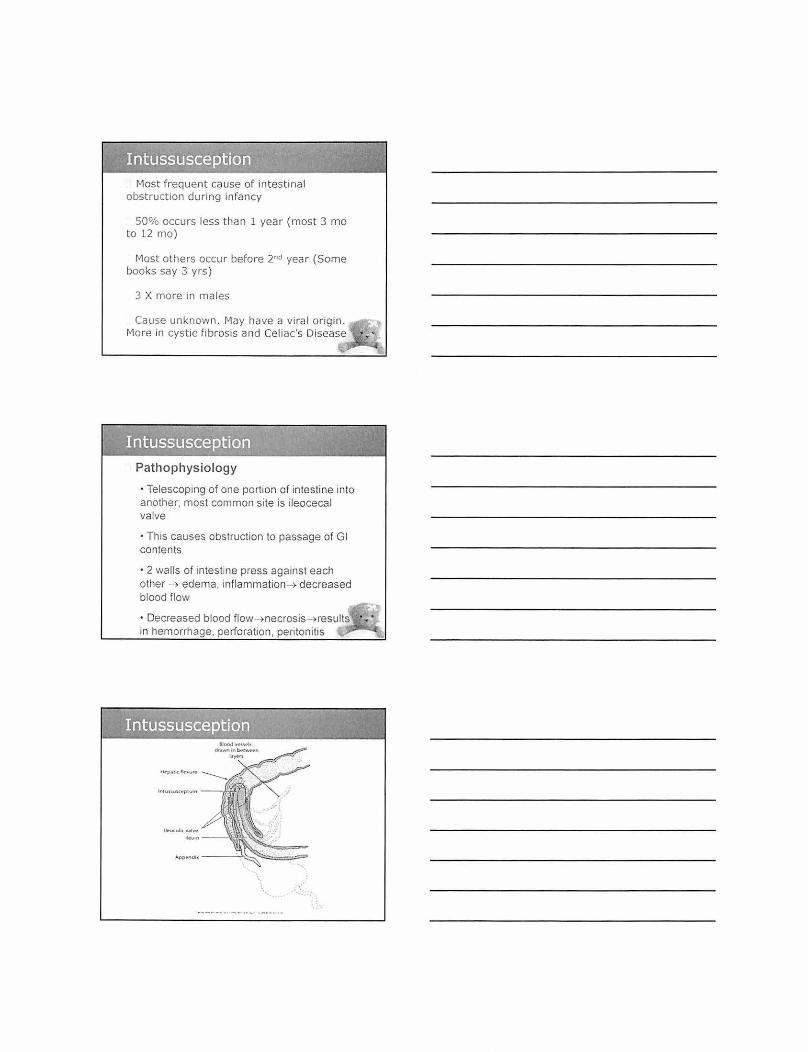
Pathophys iology
• Telescoping of one portion of intestine into another; most common site is ileocecal valve
• Th1s causes obstruction to passage of Gl contents
• 2 walls of intestine press against each other -~ edema, inflammation- > decreased blood flow
• Decreased blood flow- >necrosis- >results in hemorrhage, perforation, peritonitis

Clinical Manifestations
• Sudden acute pain w1th interva ls where child is normal
• Vom1t1ng; may pass 1 normal stool
• Stools become red-currantjelly (blood, mucous, and stool)
• Abdomen tender and d1stended
• Sausage shaped mass 1n rt upper quadrant
· Dance's sign- lower rt quadrant feels emptybowel distal to obstruction less involved; free of contents
• Chron1c p1cture may appear as d1arrhea, vom1t1ng, constipation and periodic colic
Diagnost ic evaluation ·Rectal exam
Therapeutic management
• Nonsurg1cal hydrostatic reduction. Successful 75% of t1me. If not; manual reduction and resection any non-v1able mtestine
· Barium enema- barium becoming less used.
·Use water soluble contrast or saline under ultrasound or pneumon1c insufflatiOn with a1r or 02.
Nursing Care
• Prepare parents- teach using glove with water
• Pre-op- watch for passage of normal stool. Report immediately- could mean intussuscept ion resolved
• After hydrostatic reduction- chance of recurrence within 36 hour.
• Observe stool patterns
· Child kept in hospital???? Observe 12-24 hour s at least

GE reflux is the passive transfer of gastric contents into esophagus
Affects 1 in 300 to 1000 children
Caused by inappropriate relaxation of lower esophageal sphincter
Could be problem with CNS or developmentally exaggerated enteric refl ex
High risk- children with TEF or other esophagea l repair, neurological disorders, scoliosis, asthma, CF
Clinical Manifestat ions
• Most common is passive regurgitation or emesis
• Poor weight gain, anemia, irritability, gagging and choking, apnea, recu rrent pneumonias, heme-positive emesis or stools
• Esophagitis from acid ic gastric contentsanemia, discomfort, poor weight gain
• Multiple respiratory abnormalities

Diagnostic Eva luation
• Need a history of feeding habits
• Stool for blood, growt h assessment
• Esophageal PH monitoring and UGI
• Endoscopy to assess for esophagitis with biopsy if needed.
Therapeutic Management
• Controversy over thickened formula"
• Position - upright with HOB elevated, not in car seat or infant carrier.
• Pharmacological treatment
·No PP!s in infants (Prevacid, Pri losec)
• Antacids or H2 blockers - Tagament, Zant ac, Pepcid (reduce acid in gastric contents)
· Prokinetic meds - Reglan, Urechol ine, erythromicin may refl ux
· To keep elevated may need harness, wedge, elevated mattress
· Th1cken feed1ng - 1 tsp to 1 tbsp of nee cereal per oz of formula. May need special nipple. ~1ay need gavage feed1ngs.
• G1ve paCifier - Increase suck1ng helps clear food from esophagus; keep qu1et after feeding
· If severe complications (ALTE's; apnea) wi ll do N1ssen fundopllcation. Also pyloroplasty; g-tube
· Prognos1s good for most. Most cured by 18 mo
• In severe cases- esophag1t1s; esophageal stnctures; recurrent respiratory distress; aspiration pneumonia

A
c
Gastroesophageal Reflux
• Nursing care - Support nutritional intake. - Promote interventions to
reduce complications. - Support the family. - Monitor weight daily and plot
growth on chart. - Observe for respi r atory
distress. - Keep airway clear of emesis. - Education .
Nlntn Fundopl lc~Uon

Diagnosis
• Obvious at birth
• Unilateral or bilateral
• Assessing a cleft palate
- Need thorough assessment of the mouth
- Put glove on and palpate for a cleft
- Suspect if infant is having trouble sucking
Treatm ent
• Repair lip first, then palate
• Z-shaped suture line
- protected by logan bow or butterfly suture
- don't put them on their stomachs
- restrain arms and elbows
• Perform before faulty speech; before teeth

Long-term problems
o Speech, hearing 1mpa~rments o Otitis med1a, problems with teeth
Nursing Implications Preop o Feeding
- keep head upnght
- watch closely when they eat
- large soft mpples
- encourage sucking 0 frequent bur p1ng
- can breastfeed
Post-op Care after palate repair
• No tongue blades
· No straws
No oral temperatures
No forks; wide bowl spoon
Discharge on soft diet
Rinse mouth after feeding
May have problems breathing

Musculoskeletal Problems of Infancy
Pre I uxation - (Acetabular Dysplasia)
Shallow acetabulum • Delay in acetabular development • No dislocation of subluxation
Subluxation Incomplete dislocation; a dislocatable hip Femur in contact with acetabulum - not displaced due to a stretch ligamentum
teres and capsule
Dislocation Femoral head loses contact with acetabulum and is displaced posteriorly and superiorly
......

F•guru 29-G Common Stgm or dcvtlopmcntal d,.splat.~tl of the hlp (DOH) Tho Asymmetry of cjtl1tl'll and thgh sU'IIolds IS easy to -sec tn thts ctllld 'WI1h DOH
Galeazzi sign (A) • Asymmetry of gluteal and .--, -~
thigh folds with shortening of i::J ( ) the thigh 3 . · \ /- ,
Ortolani t est (B) .83~' 1 :J • Limited hip abduction, as see,;:;:{) W
in flexion ) • ...t.J J Allissign(C) '1(!) 1-;7
Apparent shortening of the 1 ! 1 1 ;;
femur, as indicated by the .., ... ·v 'w'
level of the knees in flexion ~
'1 Barrow test co> -r . r · ::.r1 ll Opposite of Ortolani. Adduct '-"' I()' /
hips one at a time. ~, 1 Trendelenburg sign (E) ~ q,4-:'_ ·r., • Pelvis tilts downward Instead D ~ W E t.!
of upwards when weight is ......... ___ .. beared on affected hip
Clinical Manifestations I nfant
Shortening of limb on affected side
Restricted abduction of hip on affected side
unequal gluteal folds (infant prone)
Posit ive Ortolani, Barlow tests, Allis sign (under 3 months).
Positive ultrasound before 4 months. Positive xrays after 4 months.

Clinical Manifestations
Older I nfant and Child
Affected leg shorter than the other
Telescoping or piston mobility of the joint
Trendelenburg sign
Greater t rochanter prominent and appearing above a line from anterosuperior iliac spine to tuberosity of ischium
Marked lordosis (bilateral d islocations)
Waddling gait (bilateral dislocations)
Pavlik Harness
Th~ mOil! Gommon lrc.;Ument 101 DOH tn a ch~d wtdtH 3 month& 1t1 A Pl\llttk harncs~ A thf1 &hotlkt be wom urKlet the llftrnes.s to pr~vent skirt atnt.tbon (!1 was omitted IOf danty ut th~ photogr~ph)
Treatment
Bryant's traction
- Loosens ligaments and muscles, easier to treat dislocation
• Surgery and Spica cast
Neurological Problems of Infancy
Hydrocephalus, Spina Biflda, Down Syndrome
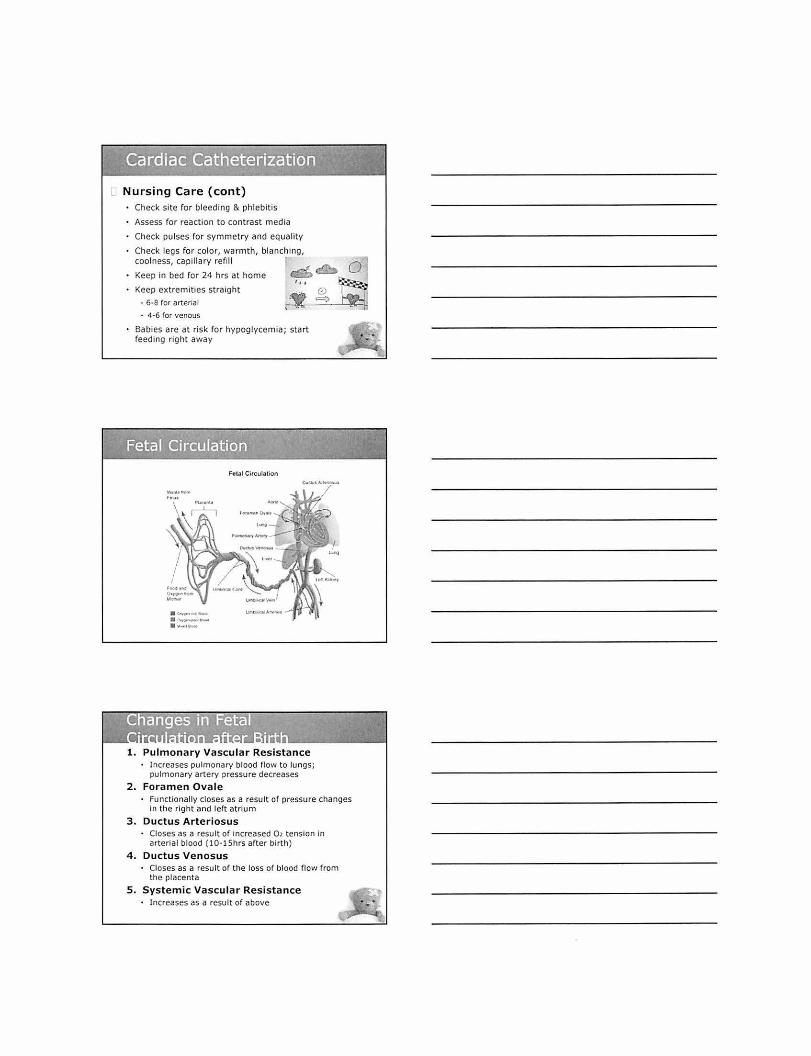
Non
~~::~ro::::::;,:~:.:·:.::,' •,JF.~-., I
through the ventricular -system
Communicating/ Non ~
Obstructive '~' ~--,,. \ ........ , .. Impaired absorption of CSF ~: cc~o~';,~;~';.~ within the subarachnoid space
Malfunction of the arachnoid villi
e l\.or .. .-
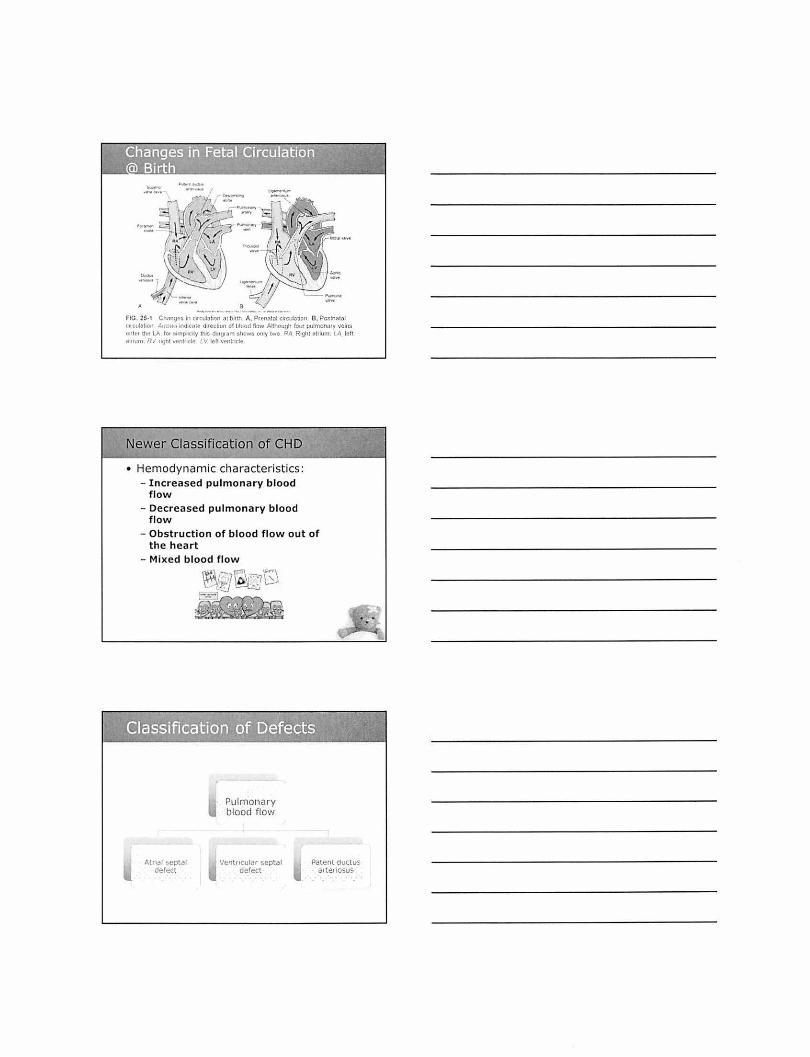
Clinical Manifestations Infancy (early) - Abnormally rapid head growth - Bulging fontanels (especially anterior) - Dilated scalp veins - Separated sutures - Cracked-pot sound - Thinning of skull bones
Infancy ( later) - Frontal enlargement, or bossing - Depressed eyes - Sun setting eyes - Pupils sluggish, unequal response to light
Setting-Sun Sign

Clinical Manifestations ( cont) I nfancy (g eneral)
- Irritability - Lethargy - Cries when picked up - Early infantile reflex acts may persist - Normally expected responses fail to appear
May display: • Changes In LOC - Opisthotonos (often extreme) - Lower extremity spasticity ·Vomiting
Advanced cases: - Olfficulty in sucking and feeding • Shrill, brief, high-pitched cry
D Clinical Manifestations (cont) Childhood
- Headache on awakening; improvement following emesis or upright posture
- Papilledema
- Strabismus;diplopia
- Ataxia· Unsteady gait
- Ir r itability
- Lethargy
- Apathy
-Confusion
- Incoherence
-Vomiting
Treatment Remove obstruction surgically
~ Shunt -Spinal fluid drained into peritoneal cavity, right
atrium, pleural spaces or subga leal space (between skull and scalp).
• Need shunt revisions throughout their life
Complications Infection or malfunction - 1-2 months after placement highest risk for
infection - Mechanical difficulties; kinking, plugging, or
separation or migration of the t ubing - Mechanical obstruction: tissue or exudate

Nursing Care Pre-op • Head circumference
• Assess change in LOC
Post-op Position on non-operative side
Keep nat (after 1" shunt )
Check any drainage for glucose
Pa in control but no sedation
Shunt revision - HOB up
Observe for ICP and infect ion
NPO for 24-48 hr
Teach parents signs of !CP
Due to failure of the neural tube to close during embryonic development
Spina bifida occulta
• Defect that 1s not VISible externally
Meningocele
• Encases men1nges and sp1nal fiUid but no neural elements
Meningomyelocele
• Contams men1nges, sp1na l flu1d, and nerves
Clinical Manifestations
Spina bifida occulta
-J~~ . \ '\. \ 1\ .. \ ' )
• Frequently no observable manifestations • May be associated with one or more
cutaneous manifestations: - Skin depression or dimple - Port-wine nevi, ang iomas - Dark tufts of hair - Soft, subcutaneous lipomas
• May have neuromuscular d istu rbances: - Progressive d istu rbances of galt with foot
weakness - Bowel and bladder sphincter disturbances

[l Clinica l Manifesta t ions
Spina bifida cystica Sensory disturbances usually parallel to motor
dysfunction Below second lumbar vertebra:
- Flaccid, partial paralysis or lower extremities
urine - Lack or bowel control - Rectal prolapse
Below third sacral vertebra:
Posit ion on their abdomen
Low trendelenburg (unless hydrocephalus)
Assess for hydrocephalus
Monitor sac
No diapers
1 No covers
Moist NS dressing over sac; change q2hr
Feeding - place in prone and nipple while
head is turn to the side

Latex Allergy
• Spina bifida patients at high risk for latex allergy due to repeated exposure to latex products from multiple surgeries and repeated urinary catheterizations.
• Range from urticaria, wheezing, rash, to anaphylaxis.
• Reactions tend to increase in severity when latex comes in contact with mucous membranes, wet skin, bloodstream, or airway.
• Cross-reactions with foods: banana, avocado, kiwi, chestnuts.
Down Syndrome
• Also called trisomy 21 - Extra chromosome 21 in 92°/o
to 95% -Translocation of chromosome
21 in 3°/o to 6% - Mosaicism in 1% to 3%
Down Syndrome (cont.)
• Et iology unknown-likely multiple causes
• Most common chromosome abnormality - 1 in 800 to 1000 live births
• Most common genetic cause of MR

Down Syndrome (cont.)
• Maternal age - Age 30: incidence
approximately 1 in 950 - Age 40 : incidence
approximately 1 in 100 - In about 5°/o of cases extra
chromosome is from father - Most infants with Down
syndrome have mothers younger than 35 years old
Down Syndrome: Manifestations
• Head, face, eyes, musculoskeletal • Chest, neck, abdomen • Genitalia, skin • Hands, feet • Heart
DS Congenital Anomalies
• 40% to 45% heart defects • Renal, Hirschsprung, TE fistu la • Altered immune function • Skeletal defects
- Atlantoaxial instability

Down Syndrome IQ
• Wide variation from severely retarded to low-average intelligence
• Generally mild to moderate MR
• Poor feed ing • Tachypnea, tachycardia • Failure to thrive, poor weight
gain, act iv ity intolerance • Developmental delays • Positive prenatal hist ory • Positive family history of
congenital cardiac disease

CHD
• Incidence: 5-8 per 1000 live b irths - About 2-3 of these are
symptomatic in first year of life - Major cause of death in first
year of life (after prematurity) - Most common anomaly is
ventricular septal defect - 28% of kids w ith CHD have
another recognized anomaly
Cardiac catheterization used to diagnose and treat some heart conditions and measure:
02 saturation of blood in chambers and great vessels
Pressure changes
Changes in CO or stroke volume
Detect anatomic abnormalities
Nursing Care Prepare child and parent
Explain according to developmental level
- what they see, hear, and feel
- don't say inject "dye" into arm
NPO 4 -6 hr (with babies 4 hr)
Assess vital signs q!Smin x 4; t hen qlhr
Check pulse distal to the site
Take apical pulse for 1 minute
- dysrhythmias common
Nursing Care (cont) Check site for bleeding & phlebitis
Assess for reaction to contrast m edia
Check pulses for symmetry and eQuality
Check legs for color, warmth, blanching, coolness, capillary refill
Keep in bed for 24 hrs at home
Keep extremities straight
• 6·8 for arterial
- 4-6 ror venous
Babies are at risk for hypoglycemia; start feeding r ight away
·~· ·. .... ~ ....... ·\L·•f•-
Feto~l Circulation
1 . Pulmonary Vascular Resistance • Increases pulmonary blood flow to lungs;
pulmonary artery pressure decreases
2. Foramen Ovale • Functionally closes as a result of pressure changes
In the right and left atrium
3 . Ductus Arter iosus • Closes as a result of increased 0> tension in
arterial blood (10- l Shrs after birth )
4. Ductus Venosus • Closes as a result of the loss of blood flow from
the placenta
5 . Systemic Vascular Resistance • Increases as a result of above
............. )
a --· ... -·- ...... _, . - ... -~ FlO. 25 ·1 Ch:m<;'!$ 10 CIICtlln!JOn ot blfth A. P renatal Cltctllatlon. B. Postnal£11 <11Ct~t~hon Arm • .,,-; ~ndiC~It d11e•:b<1n of tJJood f11m. AJihous.Jh f:>tll pulm()nary ver•s entc:• ttwlA lor sunpllc•ly tht!i dr;tS}fam shows ordy tvm RA Rtght otoum LA 111ft ~t l uum R'l nght ventncle l.V 1e l1 \ll"rtlnde
Newer Classification of CHD
• Hemodynamic characteristics: - Increased pulmonary blood
flow - Decreased pulmonary blood
flow - Obstruction of blood flow out of
the heart - Mixed blood flow
Atnal septal derect
~,:-,]0,=- ""'\ \:--{!j I~ b) --- ] .
Pulmonary blood flow
.
Ventncular septal derect
Patent ductus arteriosus

Increased Pulmonary ~QO~~~~------~~ • Abnormal connection between
two sides of heart - Either the septum or the great
vessels
• Increased blood volume on right side of heart
• Increased pulmonary blood flow • Decreased systemic blood flow
Failure of Ductus Arterious to close after birth
Left to right shunt- Increased pulmonary blood flow
Clinical Manifestations Machine type murmur
• Widened pulse pressure
Complications • CHF
T rea tment
Cardiomegaly Bounding pulse Tachycardia
• May wait until 1-2 yrs of age (ligation) • Preemie - Indomethacin or Ibuproferon to close • 6 mo - 1 yr put coils in ductus • 1-2 yrs clip on duct us arteriosus
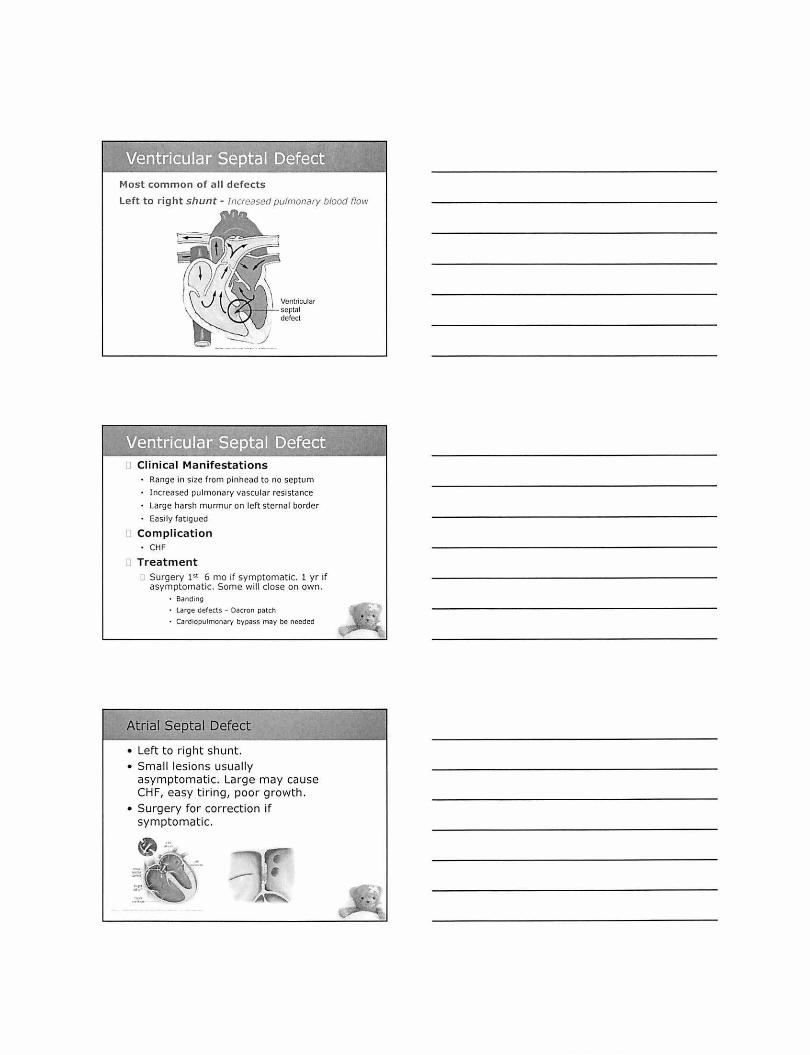
Most common of a ll def ect s
Lef t to r ight shunt- Increased pulmonary blood flow
Ventricular ~+--t-:....septot
defect
[' Clinical Manifestations Range in size from pi nhead to no septum
Increased pulmonary vascular resistance
Large harsh murmur on left sternal border
Easily fatigued
Complication • CHF
Treatment Surgery 1st 6 mo if symptomatic. 1 yr if asymptomat ic. Some will close on own.
· Banding
• Large defects - Dacron patch • Cardiopulmonary bypass m ay be needed
Atrial Septal Defect
• Left to right shunt. • Small lesions usually
asymptomatic. Large may cause CHF, easy t iring, poor growth.
• Surgery for correction if symptomatic.

Pulmonary blood flow
Tetralogy of Fallot
4 Defects:
Pulmonic Stenosis
Overriding Aorta
Ventricular Septal Defect
Rignt Ventncular Hypertrophy
Right to left shunt-
0 Pulmonary Blood Flow
Cyanotic
Pulmontc Stenosts
htttJ'S://www.youtube.com/watch?v:ycPivAibR4A
Infants are very cyanotic
Poor feeding
Babies have tet spells
Children have increased hypoxia that cause clubbing, squatting, and poor growth
Tachypnea & dyspnea
Complication Polycythemia
• Cerebral vascular disease

Initial Treatm ent
Put In knee-chest pos1t1on
• 100% 02 by mask
• Morphine
Surgical Treatment
Palliative shunt (temporary) II surgery needs to be delayed.
• May result in pulmonary artery distortion
Complete repair - closure or the VSD and resection or the Infundibular stenosis, with placement or a pericardia! patch to enlarge the right ventricular outnow tract
Symptomatic surgery at 3·4 mo of aoe
• Asymptomatic performed at 1·2 years
Narrowing at entrance to pulmonary artery
Righ t to l eft shunt- Obstruction to blood flow ftom ventttcles
PuJmonw:. IIOnostS --f1f-''-+· /\
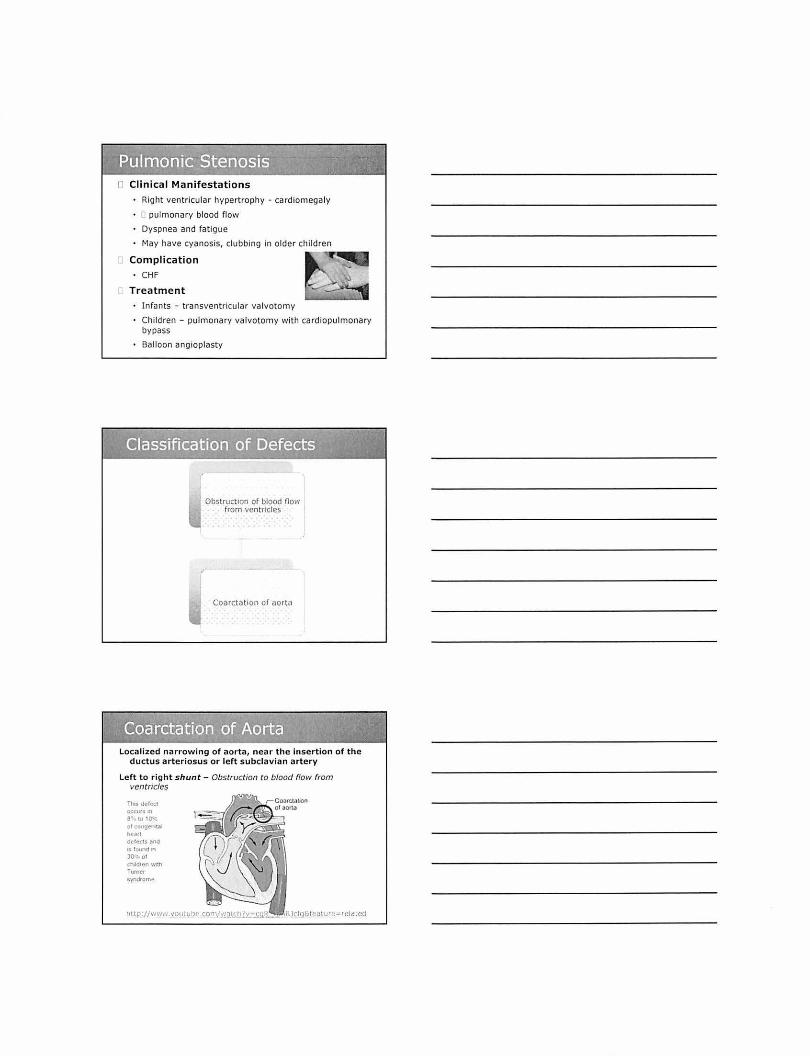
r' Clinical Manifestations
Right ventricular hypertrophy - cardiomegaly
, pulmonary blood flow
Dyspnea and fatigue
May have cyanosis, clubbing in older children
Complication a-"""rll_ ..
• CHF
Treatment
Infants - transventricular valvotomy
Children - pulmonary valvotomy with cardiopulmonary bypass
Balloon angioplasty
Obstruction of blood flow from ventricles
Coarctat1on or aorta
Localized narrowing of aorta, near t he Insertion of the ductus arteriosus or left subclavian artery
Left to right shunt- Obstruction to blood flow from ventricles
TlMS dcl"'ct 0((111' -l'"
S" 1!1 10·--: ol cOf~et ~t.l h,.N I
ddeCU l'lnd tS IO\Wldlf'l 30~ ot
t"hhldren With Turner syndrome
RJclqC.f~aw r e-= r elatecJ

Coarctation of t he Aorta (COA)
- Clinical manifestations • Many children are asymptomatic and grow normally. • Reduced blood now through the descending aorta causes
lower blood pressure in legs and higher blood pressure in arms, neck, and head.
- Brachial and radial pulses are typically bounding, but femoral and leg pulses are weak or absent.
- Older children may complain of weakness and pain In the legs after exercise.
• Infants with moderate constnction are pare. - May have poor feeding, avoidant/restrictive food
intake disorder (failure to thnve), and Increased respiratory effort
- May develop CHF • Newborns with severe constriction may have cyanosis in
the lower extremities, heart failure, and shock as the ductus arteriosus closes.
- Renal failure and necrotizing enterocolitis may develop.
Coarctation of the Aorta (COA)
- Clin ica l m an ifest a ti on s • On auscultation, 52 is heard as a
loud single sound. -A systolic ejection murmur may be
heard at the upper right and middle or lower left sternal border.
• A thrill may be palpated in the suprasternal notch.
1 OUT Of EVERY 100 BABIES ut ... I'I'IU~"'"IIO!Io.~llllln lil"'trllai"Y••""'ul~ _,..,_
Coarctation of the Aorta (COA)
- Diagnost ic tests • The chest radiograph may reveal
cardiomegaly, pulmonary venous congestion, and indentation of the descending aorta.
-Dilation of the ascending aorta may be seen.
• Rib notching is rarely seen before 5 years of age.
• MRI is preferred for imaging to see the aortic arch, site of coarctation, and collateral circulation.
- ECG may be normal or show left ventricular hypertrophy.
• Echocardiogram shows the size of the aorta and functioning of the aortic valve and left ventricle.

Coarctation of the Aorta (COA)
- Clinical therapy • In symptomatic newborns, PGE 1
is given to reopen the ductus arteriosus and promote blood flow to the kidneys and lower extremities.
• Treatment to prevent CHF may be initiated with inotropic medications (digoxin), diuretics, and oxygen.
• Surgical resection is often preferred to bal loon dilation during cardiac catheterization to reduce the risk for recoarctation .
Coarctation of the Aorta (COA)
- Clinical therapy • Balloon dilation with stent
placement may be performed for sick newborns who will eventually need surgical repair and stent removal.
• Balloon angioplasty may be performed if coarctation recurs.
Coarctation of the Aorta (COA)
-Prognosis • Balloon di lation and surgical
resection are palliative because coarctation may recur with either procedure.
• Lifelong follow-up is necessary. • Persistent hypertension occurs in
some children.
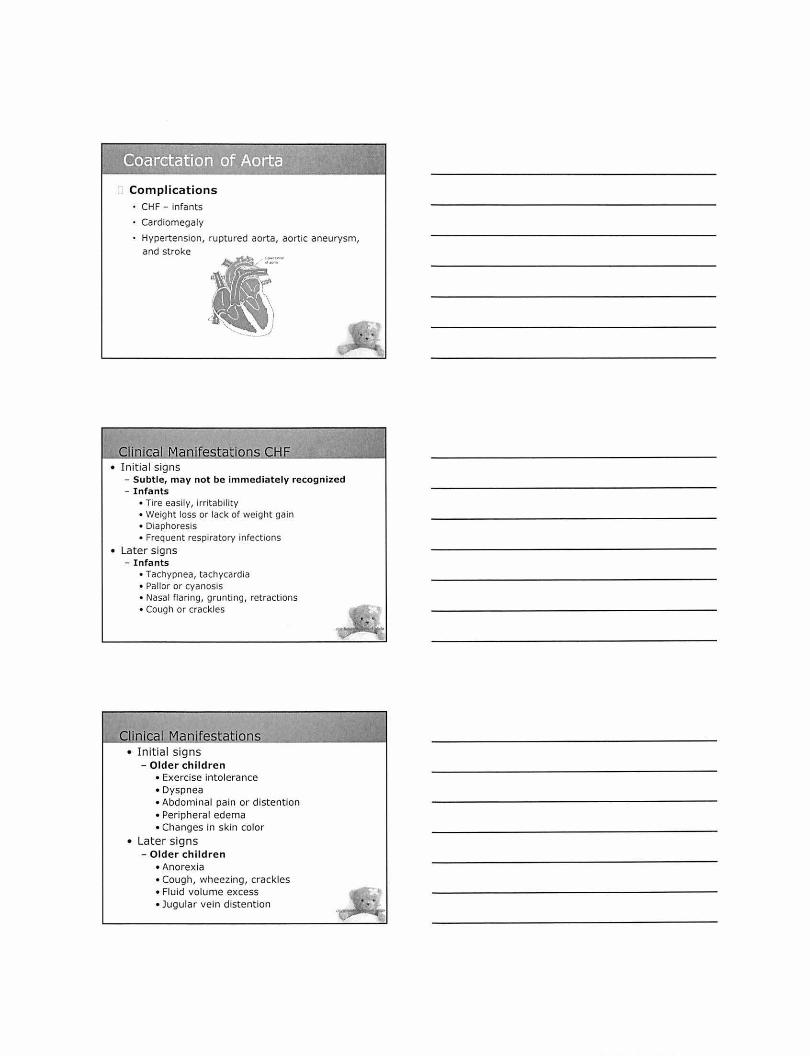
Complications CHF- infants
Cardiomegaly
Hypertension, ruptured aorta, aortic aneurysm, and stroke
.. .
• Initial signs - Subtle, may not be immediately recognized - Infants
• Tire easily, irritability • Weight loss or lack of weight gain • Diaphoresis • Frequent respiratory infections
• Later signs - Infants
• Tachypnea, tachycardia • Pallor or cyanosis • Nasal flaring, grunting, retractions • Cough or crackles
Clinical1:1aoifestatlons • Initia l signs
- Older children • Exercise intolerance • Dyspnea • Abdominal pain or distention • Peripheral edema • Changes in skin color
• Later signs - Older children
• Anorexia • Cough, wheezing, crackles • Fluid volume excess • Jugular vein distention
"""' -·

CiKI? Clin ica l Mani fest ations
., ,, Tachycardta Tachypnea Weight oa.n
Sweatmg (tnappropnate) Dyspnea Hepatomegaly
Unnary Output Retracttons (Infan ts) Pen pheral edema
Fat•gue Flanng nares Asctt tes
Weakness Exe .. clse intolerance Neck vein dlstent•on
Restlessness Orthopnea
Anorexia Cough, hoarseness
Pale, cool extremtt•es Cyanosts
Weak penpheral pulse Vlheezmg
Decreased blocx:J pressure Grunttng
Gallop rhythm
Cardtomegaly
Nursing Management of CHF
• Assessment of child and famil y • Promote oxygenation • Cardiovascular function • Administration of medications • Growth and development • Family planning • Family education for home care
- Therapeutic Management
Digoxin
- Increases force of contraction, decreases heart rate, slows conduction through AV node, enhances diuresis.
CJ Check pulse - babies< 100 bpm don't give
U Give at regular Intervals
'"' Give slowly, directing to the side of the mouth
Do not m•x wah foods or other nuids
- Toxicity : vomiting and bradycardia
Elixir 50 mcg/ml; never give more than 1 ml
Ace Inhibitors - Promotes vascular relaxation and reduced
peripheral vascular resistance. - Captoprll, Vasotec, Enaloprll - Always check bp - Assess for hyperkalemia
Diuretics - Check potassium labs; If potassium ~, digoxin
absorpt ion ; if potassium [ , digoxin absorption 0 - laslx, aldactone
Neutral thermal environment
Treat infections
HOB up - reduce breathing efforts
environmental stimuli to provide rest
Feed q 3hrs; give 112 hr to eat
Diuretics - strict I &0 and daily weight
Kawasaki Syndrome
• Acute febri le, systemic vascular inflammatory disorder that affects small and midsize arteries, including the coronary arteries
• Leading cause of acquired heart disease in chi ldren
• Etiology - Unknow n -Thought to be an infectious 1
trigger in genetically predisposed children

Kawasaki Disease
• 75% of cases in child ren <5 yrs • Three phases:
- Acute : sudden high fever, unresponsive to antipyretics and antibiotics
- Subacute: end of fever through end of all KD clinical signs
-Convalescent: clinical signs resolved, but laboratory values not returned to normal; completed with normal values (6-8 weeks)
Diagnosis - based on cl1nical and lab find1ngs - fever for 5 or more days and musl have 4 out of 5 symptoms.
• Brlateral conJunclrvrtls (111JeCted)
• Erythema of the lips strawberry tongue
• Erythema or tt1e palms and soles peelrng o111ands and feet
• Polymorphous rash
• Cervrcallympha<lenopathy (one lymph node > 1 5 em)
tp fw..w.- youluhe conllw.llch?•,:.PTTor9xW0;:8&feoture-lcl<.llad
Kawasaki Disease
• Treatment -Intravenous immunoglobulin
- 1" 10 days of illness; single large transfusion over 10- 12 hrs
- Ideally first 72 hours
-Aspirin • Anti-inflammatory dose initially • Antiplatelet dose after fever
decreases • Aspirin 80-100mg/kg/q6hr; after
fever 3-Smg/kg/day for antiplatelet effect

Kawasaki Disease
• Treatment - Monitor for coronary artery
aneurysms. • Occur in 5% of those treated
with intravenous gammaglobulin (IVIG)
• Small aneurysms may resolve spont aneously.
• Stenosed corona ry arteries may require bypass operation.
(. .........._ .1." . -v..... · ; }' ._.,..
~' :
:1 Risk for myocardial infarction Symptoms of MI in children 0 Abdom inal pain 0 Vomiting 0 Restlessness o Inconsolable 0 Crying 0 Pallor to shock
Nursing Interventions
Monitor cardiac status 1&0 Daily weights Mouth care Clear liquids, soft diet Promote rest Loose clothing Warm tub (arthritis) Teach parents to defer immunizations for 12 months Administer medications Promote comfort Home teaching

Pediatric Respiratory Problems of Infancy
SIDS, RSV
Sudden une•plaoned death of a baby under one year of age who seemed othel\vose healloy
Death rema1ns unoxpla•ned after rev•ew1ng med1cal no story onvesllgatong the death scene. performong an autopsy
Etoology unknown
Cannot be predocled or prevented.
90% SIDS dealhs occur by 6 months of age.
Assocoated woth sleep
Most SIDS deaths occur on onfants bel\<een 2 and 4 months of age
Higher percentage of males
Increased incidents in the winter
Greater incidence in African-Americans, Native Americans, and Hispanics
Lower socio-economic class Pre-term infants
Low Apgar score
Birth order (increased r isk with increased birth order)
Lower incidence in breast-feed infants
Maternal factors - young age, smoking, poor prenatal care, substance abuse

Sudden Infant Death 5 d o e (SIDS),_ ___ ~---1 • Parent educat ion related to
prevention - Back to sleep, prone to play - Avoid loose bedding, toys,
pillows - Discourage co-sleeping (Sleep
in same room for 6 months) - Use of pacifier recommended
-~~;:;~:::.~:~~~~·@
o Death of a child Allow the parents to spend unlimited time with their baby Follow up to see how parents coping Referrals - SIDS associations
0 Common grief response Denial
Anger
Hysteria
Withdrawal
Intense gui lt No visible response
Mourning period may take 1 year or forever
O<::cuucnc:o or SIDS risk faC1ors according to Infant age
--~·~""~ ..... . - ... JI.Uil,KliJD¥ ..... li>llu'l>"lrD~-"'-" ....,__,_ Xlllt .... U.,l ,.,:·~·;,'lo't)

Brief Resolved Unexplained Event
• Clinicians should use the term BRUE, rather than the term ALTE (apparent llre·Lhreatening event) to describe an event occurring In an Infant aged < 1 year when the observer reportS a sudden, brief, and now resolved episode of ~ 1 or the following:
• ' Cyanosis or pallor. • Absent, decreased, or Irregular breathing. • Marked change In tone (hyper· or
hypotonia). Altered level or responsiveness.
BRUE - Brief Resolved Unexplained Event
Infant experiencing a BRUE may exhibit - Apnea
- Change in color or muscle tone - Choking, gagging, or coughing
The BRUE requires significant intervention Infants who experience a BRUE may be discharged with home apnea monitors (controversial) Parents are taught how to administer CPR
AAP Statement
• o There is no need to admit patients to t he hospita l for monitor ing and no need to get blood work, chest x-rays, EEGs, stud ies for GERD, prescribe t herapy for GERD, or init iate home monit oring . (for low risk infants)

Bronchiolitis
• Respiratory syncytial virus (RSV) and other v iruses are main cause.
• Symptoms - Nasal symptoms -Cough - Fever -Wheezing - Tachypnea - Retractions - Decreased activity level - Decreased oral intake - Deh dration
Newbom
Adult
(~ I I v
4mm
1 mm --4{;i; swelling t)
2mm
-=--
( ( liiifrd ( ~ ~mm~~ ~swelli ng ~
f.Jrw:.•v Oi<tmctc1
@l,·:•r4olt
diameter of airway diameter of airway \ .. • ~
~~
0 Between ages 2- 12 months; rare after 2 years Clinical Manifestation
Bronchioles become inflamed & swollen; lumina filled with exudates Prolonged expiratory phase Obstruction in small air passages; patchy areas of atelectasis Dyspnea, irritability, tachypnea, nasal flaring, substernal intercostal retraction Fine rales and crackles Wheezing Emphysema with barrel chest

Diagnosis Nasal secretions
• ELISA (enzyme-linked immunosorbent assay)
Treatment Rest 0 2therapy Fluids (npo if tachypnea) Pulse ox Respiratory therapy - albuterol Corticosteriods (controversial) Suction
Treatment (cont) Ribavirin (very controversial)
- 18-20hr/day for 7 days
- in isolation under hood
- teratogenetic drug
Synergist (palivizumab)
- preemie with chronic lung disease
- $1400/shot once a month
RSV immune globulin
- neutralizes antibodies against RSV
Related Documents











