High prevalence of occult hepatitis B virus infection in children born to HBsAg-positive mothers despite prophylaxis with hepatitis B vaccination and HBIG Sajad Shahmoradi 1 , Yousef Yahyapour 2 , Mahmood Mahmoodi 3 , Seyed Moayed Alavian 4 , Zeinab Fazeli 1 , Seyed Mohammad Jazayeri 1,⇑ 1 Hepatitis B Molecular Laboratory, Department of Virology, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran; 2 Babol University of Medical Sciences, Infectious Diseases and Tropical Medicine Research Center, Babol, Iran; 3 Department of Epidemiology and Biostatistics, School of Public Health, Tehran University of Medical Sciences (TUMS), Tehran, Iran; 4 Baqiyatallah University of Medical Sciences, Baqiyatallah Research Center for Gastroenterology and Liver Disease, Tehran, Iran See Editorial, pages 484–485 Background & Aims: Occult hepatitis B virus (HBV) infection is a well-recognized clinical entity characterized by the detection of HBV DNA in serum and/or liver in the absence of detectable hep- atitis B surface antigen (HBsAg). The frequency of the diagnosis depends on the relative sensitivity of both HBsAg and HBV DNA assays. We aimed at determining the prevalence of occult HBV infec- tion in a high risk group of children who developed HBV infection despite immunoprophylaxis. Methods: The sera of 75 children born to HBsAg-positive mothers previously immunized by HBIG and prophylaxic vaccine regimen were assayed for HBV DNA by real-time PCR. Subsequently, the samples were tested using a sensitive standard PCR, with an inde- pendent set of primers for all HBV genes, and analyzed by direct sequencing. Results: HBV DNA was detected in 21/75 (28%) children, and ran- ged between 77 and 9240 copies/ml. All were positive for anti- HBs. Five (24%) children were found to be positive for anti-HBc, while anti-HBc-only positive individuals were not observed. Eight isolates (38%) did not carry any mutation. Thirteen infected children (62%) had at least one mutation in regions known to be involved in functional and/or immune epitope activity. Ten had G145R mutations. Conclusions: HBV occult infection seems to be relatively fre- quent in immunized children born to HBsAg-positive mothers. HBsAg negativity is not sufficient to completely exclude HBV DNA presence. These findings emphasize the importance of con- sidering occult HBV infection in hypo-endemic areas. Ó 2012 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved. Introduction WHO aims at controlling hepatitis B virus (HBV) worldwide, to decrease the incidence of HBV-related chronic liver disease, cirrhosis, and hepatocellular carcinoma, by integrating hepatitis B vaccination into routine infant (and possibly adolescent) immu- nization programs. Hepatitis B vaccination is safe and effective, although breakthrough infections occasionally occur in vaccinees [1–3]. The appearance of anti-HBs neutralizing antibodies is usually associated with patient recovery. These antibodies are directed against the HBV envelope, the major S protein (HBsAg), which contains the highly conserved ‘‘a’’ determinant. HBV mutants with amino acid substitutions, within the ‘‘a’’ determi- nant of HBsAg, have been identified, which can potentially escape vaccine-induced immunity [4–6]. As documented in a number of reports, the HBsAg with such variants could not be detected in some assays (diagnostic-escape) [7–9]. In spite of the increasing use of HBV vaccine, which has had overwhelming positive influ- ence on the prevention of HBV infection, it has no effect on those mutants; re-infection despite vaccine/HBIG prophylaxis may be caused by inadequate neutralization against HBV or the emer- gence of viral immune escape variants of HBV carrying mutations in the ‘‘a’’ determinant [10–12]. Occult HBV infection (OBI) is defined as ‘‘detection of HBV DNA by PCR among HBsAg negative patients’’ and is classified into seropositive and seronegative infections depending on positivity for anti-core (HBc) and anti-HBs antibodies [13,14]. However, the presence of a serologic profile of anti-HBc/anti- HBs does not exclude OBI, and detectable HBV DNA has also been reported in those patients who are negative for both serologic markers [15,16]. The diagnosis of OBI requires a sen- sitive HBV DNA PCR assay because the level of HBV DNA in the sera of these patients is usually less than 10 4 copies/ml [17,18]. Journal of Hepatology 2012 vol. 57 j 515–521 Keywords: Occult hepatitis B infection; HBsAg vaccine; Escape mutants; HBsAg mutant assays. Received 26 October 2011; received in revised form 5 April 2012; accepted 11 April 2012; available online 19 May 2012 q DOI of original article: http://dx.doi.org/10.1016/j.jhep.2012.06.003. ⇑ Corresponding author. Address: Hepatitis B Molecular Laboratory, Department of Virology, School of Public Health, Tehran University of Medical Sciences, PO Box: 15155 6446, Tehran, Iran. Tel./fax: +98 21 8899 2660. E-mail address: [email protected] (S.M. Jazayeri). Research Article

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Research Article
High prevalence of occult hepatitis B virus infection in childrenborn to HBsAg-positive mothers despite prophylaxis with hepatitis
B vaccination and HBIG
Sajad Shahmoradi1, Yousef Yahyapour2, Mahmood Mahmoodi3, Seyed Moayed Alavian4,Zeinab Fazeli1, Seyed Mohammad Jazayeri1,⇑
1Hepatitis B Molecular Laboratory, Department of Virology, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran;2Babol University of Medical Sciences, Infectious Diseases and Tropical Medicine Research Center, Babol, Iran;
3Department of Epidemiology and Biostatistics, School of Public Health, Tehran University of Medical Sciences (TUMS), Tehran, Iran;4Baqiyatallah University of Medical Sciences, Baqiyatallah Research Center for Gastroenterology and Liver Disease, Tehran, Iran
See Editorial, pages 484–485
Background & Aims: Occult hepatitis B virus (HBV) infection is a � 2012 European Association for the Study of the Liver. Published
well-recognized clinical entity characterized by the detection ofHBV DNA in serum and/or liver in the absence of detectable hep-atitis B surface antigen (HBsAg). The frequency of the diagnosisdepends on the relative sensitivity of both HBsAg and HBV DNAassays.We aimed at determining the prevalence of occult HBV infec-tion in a high risk group of children who developed HBV infectiondespite immunoprophylaxis.Methods: The sera of 75 children born to HBsAg-positive motherspreviously immunized by HBIG and prophylaxic vaccine regimenwere assayed for HBV DNA by real-time PCR. Subsequently, thesamples were tested using a sensitive standard PCR, with an inde-pendent set of primers for all HBV genes, and analyzed by directsequencing.Results: HBV DNA was detected in 21/75 (28%) children, and ran-ged between 77 and 9240 copies/ml. All were positive for anti-HBs. Five (24%) children were found to be positive for anti-HBc,while anti-HBc-only positive individuals were not observed.Eight isolates (38%) did not carry any mutation. Thirteen infectedchildren (62%) had at least one mutation in regions known to beinvolved in functional and/or immune epitope activity. Ten hadG145R mutations.Conclusions: HBV occult infection seems to be relatively fre-quent in immunized children born to HBsAg-positive mothers.HBsAg negativity is not sufficient to completely exclude HBVDNA presence. These findings emphasize the importance of con-sidering occult HBV infection in hypo-endemic areas.
Journal of Hepatology 20
Keywords: Occult hepatitis B infection; HBsAg vaccine; Escape mutants; HBsAgmutant assays.Received 26 October 2011; received in revised form 5 April 2012; accepted 11 April2012; available online 19 May 2012q DOI of original article: http://dx.doi.org/10.1016/j.jhep.2012.06.003.⇑ Corresponding author. Address: Hepatitis B Molecular Laboratory, Departmentof Virology, School of Public Health, Tehran University of Medical Sciences, POBox: 15155 6446, Tehran, Iran. Tel./fax: +98 21 8899 2660.E-mail address: [email protected] (S.M. Jazayeri).
by Elsevier B.V. All rights reserved.
Introduction
WHO aims at controlling hepatitis B virus (HBV) worldwide, todecrease the incidence of HBV-related chronic liver disease,cirrhosis, and hepatocellular carcinoma, by integrating hepatitisB vaccination into routine infant (and possibly adolescent) immu-nization programs. Hepatitis B vaccination is safe and effective,although breakthrough infections occasionally occur in vaccinees[1–3]. The appearance of anti-HBs neutralizing antibodies isusually associated with patient recovery. These antibodies aredirected against the HBV envelope, the major S protein (HBsAg),which contains the highly conserved ‘‘a’’ determinant. HBVmutants with amino acid substitutions, within the ‘‘a’’ determi-nant of HBsAg, have been identified, which can potentially escapevaccine-induced immunity [4–6]. As documented in a number ofreports, the HBsAg with such variants could not be detected insome assays (diagnostic-escape) [7–9]. In spite of the increasinguse of HBV vaccine, which has had overwhelming positive influ-ence on the prevention of HBV infection, it has no effect on thosemutants; re-infection despite vaccine/HBIG prophylaxis may becaused by inadequate neutralization against HBV or the emer-gence of viral immune escape variants of HBV carrying mutationsin the ‘‘a’’ determinant [10–12].
Occult HBV infection (OBI) is defined as ‘‘detection of HBVDNA by PCR among HBsAg negative patients’’ and is classifiedinto seropositive and seronegative infections depending onpositivity for anti-core (HBc) and anti-HBs antibodies [13,14].However, the presence of a serologic profile of anti-HBc/anti-HBs does not exclude OBI, and detectable HBV DNA has alsobeen reported in those patients who are negative for bothserologic markers [15,16]. The diagnosis of OBI requires a sen-sitive HBV DNA PCR assay because the level of HBV DNA inthe sera of these patients is usually less than 104 copies/ml[17,18].
12 vol. 57 j 515–521

Table 1. Oligonucleotide primers used for PCR and sequencing. Base positions numbered from the EcoRI site.
Primer Gene Sequence 5’ 3’ of oligonucleotides Location 5’ 3’ Sense/anti-sense
P1 Complete genome 5’-CCGGAAAGCTTGAGCTCTTCTTTTTCACCTCTGCCTAATCA-3’ 1821-1841 sense P2 Complete genome 5’-CCGGAAAGCTTGAGCTCTTCAAAAAGTTGCATGGTGCTGG-3’ 1806-1825 antisense S1 Surface 5’-CCTGCTGGTGGCTCCAGTTC-3’ 56-75 sense S2 Surface 5’-CCACAATTCKTTGACATACTTTCCA-3’ ( K = G/T) 1003-979 antisense S6 Surface 5’-GCACACGGAATTCCGAGGACTGGGGACCCTG-3’ 113-146 sense S7 Surface 5’-GACACCAAGCTTGGTTAGGGTTTAAATGTATACC-3’ 857-823 antisense X1 X 5’-TGCCAAGTGTTTGCTGACGC-3’ 1176-1195 sense X2 X 5’-AAGGAAAGAAGTCAGAAGG-3’ 1960-1978 antisense PS1 Pre-S 5’-TCAGAATTCTCACCATATTCTTGGGAACAA-3’ 2817-2839 sense PS2 Pre 5’-CACTAGTAAACTGAGCCA-3’ 668-687 antisense PS3 Pre 5’-AGTAAGCTTAGAAGATGAGGCATAGCAGC-3’ 415-434 antisense C1 Core/pre-core 5’-CGGGATCCGAGGAGTTGGGGGAGGAGTT-3’ 1726-1754 sense C3 Core/pre-core 5’-GATCTATGTATTAGGAGGCTG-3’ 1763-1783 sense C4 Core/pre-core 5’-CCTTATGAGTCCAAGGAATA-3’ 2478-2459 antisense
Research Article
Although the mechanism and clinical implications have notyet been clearly elucidated, OBI has its own risks of disease trans-mission and may contribute to acute exacerbation and develop-ment of HBV-associated diseases such as hepatitis, cirrhosis,and hepatocellular carcinoma (HCC) [19–21].
The prevalence of HBV in Iran varies between 1.7% and 2.5% inthe general population [22–24]. HBV vaccination has beenincluded in the extended program of immunization (EPI) in Iransince 1993 [25]. A current study indicates that 98% of the targetpopulation has received a full dose of the HBV vaccination [26].Furthermore, an adequate immunity (anti-HBs >10 mIU/ml) hasbeen reported in 69–90.9% of children who received a full doseof vaccine [27–30]. However, the children born to HBsAg-positivemothers immunized with the vaccine alone (no HBIG) and a com-bination of vaccine/HBIG had an overall response rates of 86%[31] and 82.1%, respectively [32].
The aim of this study was to investigate the prevalence ofpotential OBI in a population at high risk of infection whoreceived HBIG and full coverage of prophylaxis vaccine regimen.In the present study, the HBV proteins of those infected individ-uals were analyzed to identify the mutation patterns that mightbe related to the pathogenesis of OBI in vaccinated children.
Materials and methods
Study population
This retrospective study included the revision of 31,241 child birth files fromAmol region, North of Iran; in the study group, 130 mothers (0.42%) wereHBsAg-positive. Seventy-five children born to HBsAg-positive mothers, whowere subsequently immunized against HBV using a dose of HBIG (Hyper HEPB, USA) and three standard injections of vaccine (Pasteur Institute, Iran) at zero,one and six-month intervals, were traced. The first dose of vaccine and HBIGwas received within 72 h of birth. Blood samples were drawn from the subjectsat least 2 months after the third dose (8 months old) up to 128 months of age.In this study, all subjects were HBsAg negative regardless of their HBs antibodytiters. All parents signed an informed consent and provided the child’s vaccina-tion history based on a booklet provided by the local Ethics Committee, BabolUniversity of Medical Sciences. All patients were negative for antibodies against
516 Journal of Hepatology 201
hepatitis C, hepatitis D and human immunodeficiency virus. The occult hepati-tis B infection (OBI) was defined as HBsAg negativity but HBV DNA positivity,by real time PCR, regardless of positivity for either/or anti-HBc and anti-HBsantibodies.
Sera
A blood sample was drawn from all enrolled subjects, sera were taken and storedat �80 �C. The serological markers of hepatitis B (HBsAg and anti-HBc/anti-HBs)were assayed using ELISA (BIOKIT, Barcelona, Spain). A further serological inves-tigation on the above-mentioned characteristics was carried out by a second sero-logical survey (Acon, CA, USA).
DNA extraction
HBV DNA was extracted from a 200-ll aliquot of serum from prevaccination andsix-month post-vaccination samples using a Purelink™ 96 Viral RNA/DNA kits(Invitrogen, Ca, USA) and an automated extractor (X-tractor Gene™, Corbett, Syd-ney, Australia), according to manufacturer’s instructions. The lysate was preparedby adding 25 ll of proteinase K to each sample, followed by 200 ll of lysis buffer.Then samples were incubated at 56 �C for 15 min. After a brief centrifugation,250 ll 96–100% ethanol was added to each well, and samples were incubatedfor five min at room temperature. Then, the lysate was transferred into a 96-wellfilter plate. Five hundred ll of wash buffer with ethanol was added to each well,and after several vacuum procedures at different times and depletion of wastematerials, 150 ll RNase-free water was added to each well. The eluted DNAwas stored at �80 �C.
Polymerase chain reaction
HBV DNA was initially determined in all samples by real time PCR (Fast-TrackDiagnostics, Luxembourg). Then, all positive samples, regardless of their viral loadlevels, were selected for PCR reactions with a single set of primers P1 and P2,using the Gunther et al.’s methodology [33], (Table 1).
The method used by Gunther et al. for the amplification of the full-length gen-ome worked only in four samples, and repeatedly failed with the rest of them. Forthose samples in which the amplification failed, several nested, semi-nested andsingle-step PCRs were carried out. The PCR mix was the same for all reactions andconsisted of lx PCR buffer, 1.5 mM MgCl2, 0.2 mM dNTPs, 1.5 U of a highly sensi-tive Taq DNA polymerase HotStart Taq PCR (Qiagen, Hilden, Germany), 0.25 mMof the first and 0.5 mM of the second round primers (Table 1); 5 ll of extractedHBV DNA for the first round, and 1 ll of the first round PCR-amplified productwere used as templates for the second round PCR reaction. The thermal profilesused for all reactions were similar to those described previously [34,35], with
2 vol. 57 j 515–521
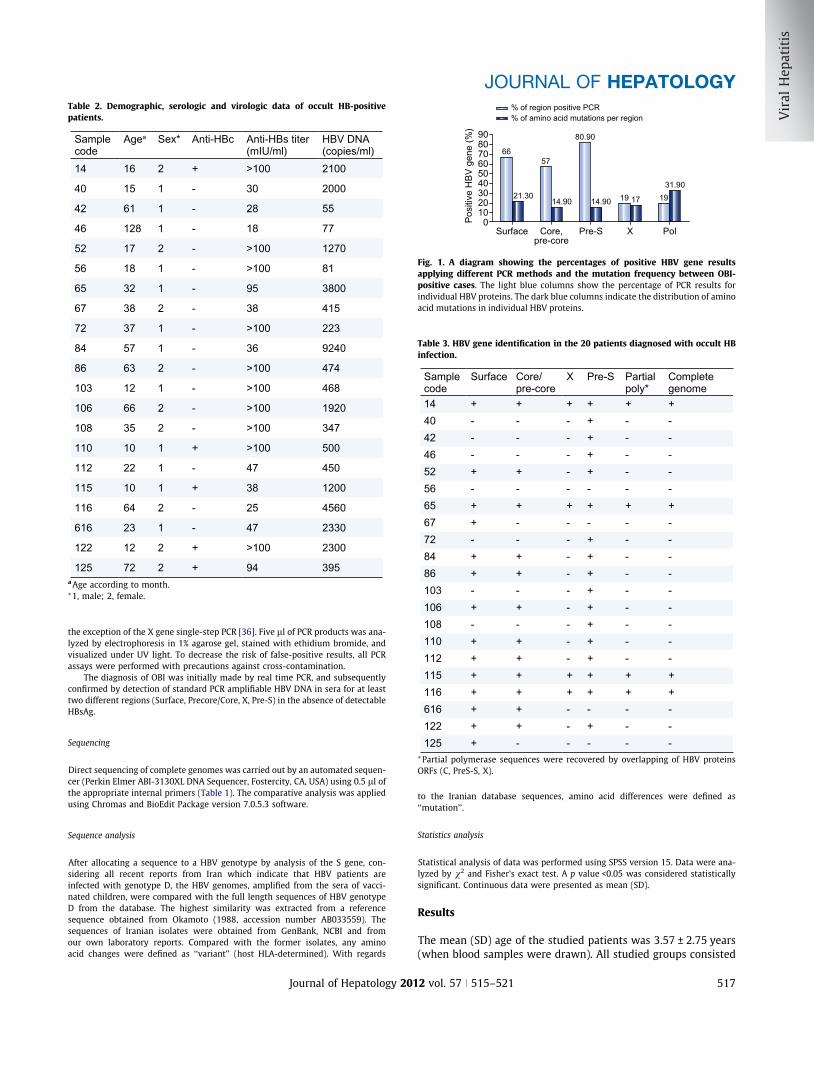
Table 2. Demographic, serologic and virologic data of occult HB-positivepatients.
Sample code
Agea Sex* Anti-HBc Anti-HBs titer (mIU/ml)
HBV DNA (copies/ml)
14 16 2 + >100 2100
40 15 1 - 30 2000
42 61 1 - 28 55
46 128 1 - 18 77
52 17 2 - >100 1270
56 18 1 - >100 81
65 32 1 - 95 3800
67 38 2 - 38 415
72 37 1 - >100 223
84 57 1 - 36 9240
86 63 2 - >100 474
103 12 1 - >100 468
106 66 2 - >100 1920
108 35 2 - >100 347
110 10 1 + >100 500
112 22 1 - 47 450
115 10 1 + 38 1200
116 64 2 - 25 4560
616 23 1 - 47 2330
122 12 2 + >100 2300
125 72 2 + 94 395a Age according to month.⁄1, male; 2, female.
Table 3. HBV gene identification in the 20 patients diagnosed with occult HBinfection.
Sample code
Surface Core/pre-core
X Pre-S Partial poly*
Complete genome
14 + + + + + +40 - - - + - -42 - - - + - -46 - - - + - -52 + + - + - -56 - - - - - -65 + + + + + +67 + - - - - -72 - - - + - -84 + + - + - -86 + + - + - -103 - - - + - -106 + + - + - -108 - - - + - -110 + + - + - -112 + + - + - -115 + + + + + +116 + + + + + +616 + + - - - -
Posi
tive
HBV
gen
e (%
) 9080706050403020100
Surface Core,pre-core
Pre-S X Pol
% of region positive PCR% of amino acid mutations per region
6657
19 17 19
80.90
31.90
14.9014.9021.30
ig. 1. A diagram showing the percentages of positive HBV gene resultspplying different PCR methods and the mutation frequency between OBI-ositive cases. The light blue columns show the percentage of PCR results fordividual HBV proteins. The dark blue columns indicate the distribution of amino
acid mutations in individual HBV proteins.
JOURNAL OF HEPATOLOGY
the exception of the X gene single-step PCR [36]. Five ll of PCR products was ana-lyzed by electrophoresis in 1% agarose gel, stained with ethidium bromide, andvisualized under UV light. To decrease the risk of false-positive results, all PCRassays were performed with precautions against cross-contamination.
The diagnosis of OBI was initially made by real time PCR, and subsequentlyconfirmed by detection of standard PCR amplifiable HBV DNA in sera for at leasttwo different regions (Surface, Precore/Core, X, Pre-S) in the absence of detectableHBsAg.
122 + + - + - -125 + - - - - -⁄Partial polymerase sequences were recovered by overlapping of HBV proteinsORFs (C, PreS-S, X).
Sequencing
Direct sequencing of complete genomes was carried out by an automated sequen-cer (Perkin Elmer ABI-3130XL DNA Sequencer, Fostercity, CA, USA) using 0.5 ll ofthe appropriate internal primers (Table 1). The comparative analysis was appliedusing Chromas and BioEdit Package version 7.0.5.3 software.
Sequence analysis
After allocating a sequence to a HBV genotype by analysis of the S gene, con-sidering all recent reports from Iran which indicate that HBV patients areinfected with genotype D, the HBV genomes, amplified from the sera of vacci-nated children, were compared with the full length sequences of HBV genotypeD from the database. The highest similarity was extracted from a referencesequence obtained from Okamoto (1988, accession number AB033559). Thesequences of Iranian isolates were obtained from GenBank, NCBI and fromour own laboratory reports. Compared with the former isolates, any aminoacid changes were defined as ‘‘variant’’ (host HLA-determined). With regards
Journal of Hepatology 201
Fapin
to the Iranian database sequences, amino acid differences were defined as‘‘mutation’’.
Statistics analysis
Statistical analysis of data was performed using SPSS version 15. Data were ana-lyzed by v2 and Fisher’s exact test. A p value <0.05 was considered statisticallysignificant. Continuous data were presented as mean (SD).
Results
The mean (SD) age of the studied patients was 3.57 ± 2.75 years(when blood samples were drawn). All studied groups consisted
2 vol. 57 j 515–521 517

Table 4. Amino acid changes in different proteins of HBV in OBI-positive cases.
Sample code Surface Core/pre-core X Pol Pre-S14 V21A, Q87R A251S65 G145R V21A, Q87R S240G, T266A, R499Q67 G145R72 V39A, P41H84 G145R86 G145R106 G145R R167K112 G145R E64K, P163L, R165S V39A, P41H115 E64K, P163L, R165S V21A, Q87R L28F, D30V, S240G, T266A, S782P, R841K P15R116 G145R V21A, Q87R S240G, T266A, R499Q, S782P, R841K616 G145R122 G145R V39A, P41H125 G145RTotal substitutions
10 7 8 15 7
Research Article
of 37 (49%) boys and 38 (51%) girls and were negative for HBsAg.
Serologic markers
Among the 75 children screened, 9 (12%) were positive for anti-HBc and anti-HBs, 55 (73%) were positive only for anti-HBs, and11 (15%) had no serologic markers of HBV (data not shown).The presence of OBI was detected in 21 (28%) immunized chil-dren who were positive for anti-HBs (i.e. >10 mIU/ml) (Table 2).Age, gender, serological and virological data of 21 children thatwere positive for OBI are presented in Table 2.
Serology markers
No significant association was found between mean age and gen-der of OBI-positive (n = 21) and negative (n = 54) groups (data notshown). Both groups were negative for anti-HBc alone. Five (24%)out of 21 OBI-positive and four (7%) out of 54 OBI-negative chil-dren were found positive for both anti-HBc and anti-HBs (datanot shown). Sixteen (76%) of 21 and 39 (72%) of 54 cases had iso-lated anti-HBs in HBV DNA positive and negative groups, respec-tively. Ten (48%) of 21 OBI-positive children had an anti-HBs titer>100 IU/ml (Table 2). There were no significant associationsamong the HBV serologic markers between the two groups (datanot shown). Seven (9.3%) out of 75 mothers were HBeAg positive.There was no correlation between HBeAg and anti-HBe positivemothers in terms of demography, serology and viral kinetics(results not shown).
Real time/standard PCR results
HBV viral loads ranged between 77 and 9240 (mean: 1629)copies/ml (Table 2). There were no significant associationsbetween the different levels of viral load and the presence ofanti-HBc, as well as the titers of anti-HBs (data not shown).
Among the 75 collected samples, 21 had detectable HBV DNAusing real time PCR. The positivity of all samples (except No 56)was confirmed by standard PCRs at least for one site of the HBV
518 Journal of Hepatology 201
genome. Using PCR, 14 (67%; 95% CI: 43.03–85.41%), 12 (57%; 95%CI: 34.02–78.18%), 4 (19%; 95% CI: 5.45–41.91%) and 17 (81%; 95%CI: 58.09–94.55%) patients were found positive for surface, core/pre-core, X and pre-S regions, respectively (Table 3). Thus, themost specific region used in our method was the pre-S gene.Overall, four (19%) samples were positive for all four regions (fullgenome), seven (33%) for three regions, one (5%) for two regionsand eight (38%) for one region (Fig 1). A strong association wasfound between viral load levels of >1000 copies/ml and positiveresults of standard PCR (p = 0.001). In particular, positive casesfor all four HBV genomic regions were examined using the Gun-ther’s methodology and the viral load ranged from 1200 to4560 copies/ml (Table 2).
Direct sequencing/genotyping
According to the positive PCR results, the full length HBV gen-omes from 4 patients were successfully recovered and each ofthe six HBV regions was analyzed using bidirectional sequencing(Table 3). A partially sequenced polymerase gene was recoveredwith the standard strategy, covering the overlapping poly-ORFwith other HBV ORFs, by using appropriate internal primers(Table 1). All patients were infected with HBV genotype D, sub-type ayw2, thus, the HBV genome extracted from vaccinated chil-dren was compared to the recognized HBV full length sequencesof genotype D from the database.
Mutation analysis
A nucleotide consensus sequence was deduced from each sam-ple by aligning the corresponding sequences representative ofthe most frequent nucleotide found at each position in differentCaucasians. Each consensus sequence was combined with thecorresponding sequence obtained from the database in orderto generate a HBV genome sequence for Iranian OBI-positivesamples. The consensus nucleotide sequences and the derivedamino acid sequences from the four OBI-positive samples werecompared with full genome reference sequences of HBV
2 vol. 57 j 515–521

JOURNAL OF HEPATOLOGY
genotype D strains retrieved from HBsAg-positive Iranianindividuals.Altogether, 74 and 47 mutations were identified at the nucle-otide and amino acid levels, respectively. Fig. 1 shows the per-centages of individual protein amino acid substitutions; 21.30%,14.90%, 14.90%, 17% and 31.90% of amino acid substitutions werefound in surface, pre-S, core/pre-core, X, and polymeraseproteins, respectively. As shown in Table 4, within the envelopeprotein, 10 out of 14 available surface proteins from OBI-positiveisolates (71%) contained the G145R mutation in the ‘‘a’’ determi-nant. The association between presence of G145R and HBV DNAlevels was significant; 60% of patients who carried G145Rpresented with a viral load >1900 copies/ml (p = 0.012).
In isolates 72, 122 and 115, a double V39A and P41H mutationwas found in the pre-S protein. Complete and partial poly-geneanalysis of the polymerase protein showed that no viral straincarried the M204I/V substitution inside the conserved YMDDmotif of the reverse transcriptase (RT) domain. S240G andT266A (both in the spacer domain) were found in sequences65, 115 and 116. R499Q (amino acid 150 of RT, A-B interdomain)was found in isolates 65 and 116. Thus, no amino acid mutationwithin the RT domain, shown to affect HBV replication efficiency,was found in any of the HBV strains from our patients. Finally,S782P and R841K (both located in the RNase domain) were foundin isolates 115 and 116 (Table 4).
Two patients (112 and 115) carried a triple mutation, E64K,P163L and R165S, in the core protein. Isolate 106 carriedR167K. No pre-core mutation, including A1896G, was found inany isolate. In the X region, a double mutation (V21A, Q87R)was found in four isolates (14, 65, 115 and 116). No basal corepromoter (BCP) mutation was found in any sequence (Table 4).
Samples 112, 115 and 116 had the highest number of muta-tions: 6, 12 and 8, respectively (Table 4). These three isolateshad in common only low levels of anti-HBs antibody (<50 mIU/ml).
All over the sequenced regions, an average frequency of 5.69and 3.61 substitutions occurred at the nucleotide and amino acidlevels, respectively. Thirteen of 21 patients (62%) had at least onemutation; eight (38%) did not have any mutation at the nucleo-tide and amino acid levels in the studied regions. Overall, datafor the sequence regions mainly showed a dS/dN (synonymous/non-synonymous) ratio (27/47) of 0.57, indicating ‘‘sequenceinstability’’ or ‘‘positive selection.’’ The highest and lowest dS/dN ratios were generally observed within the pre-S (2.75) andcore (0)/surface (0) regions, respectively.
Discussion
Occult HBV is present worldwide, and varies significantlybetween geographic regions and populations [13,37,38]. OBIhas received increasing attention in recent years because itappears to accelerate the progression of liver fibrosis and cirrho-sis, ultimately leading to HCC [19–21]. OBI has also been reportedin vaccinated children from Taiwan [39] and Singapore [40].However, our study is the first report on the prevalence of OBIamong a selected high-risk group of children born to HBsAg-posi-tive mothers, particularly from a region with low to intermediateprevalence of HBV [22].
In the present cross-sectional study, serum samples of 75HBsAg negative children who received a full prophylactic cover-
Journal of Hepatology 201
age (vaccine and HBIG) against HBV were examined for the pres-ence of HBV DNA. Furthermore, we analyzed the availablesequences of HBV genome isolated from patients with OBI andcompared them with the wild type HBV genome prevalent inIran. Twenty-eight percent of patients harbored OBI in the pres-ence of adequate levels of anti-HBs, of whom only four showedserological evidence of past HBV exposure (anti-HBc positivity).
HBV sequences obtained from the analysis of sera of HBsAgseronegative carriers, showed a plethora of mutations (pointmutations, deletions and splicing alternatives) associated withOBI [41–43], however, it is unclear whether these mutationsare a cause or a consequence of OBI. Ten (71%) of 14 HBV sur-face-positive isolates carried G145R, which confirmed the previ-ous reports concerning the presence of vaccine-escaped mutantsin children despite full immunization against HBV [10–12].
Due to the vaccine-induced escape phenomenon, the relation-ship between the anti-HBs antibody level and specific epitopes atthe HBV surface must be taken into account. This phenomenonmay result from at least five conditions. First, individuals pro-tected by HBV vaccines had low immune system response capac-ities (in early childhood); as shown in our study, 11 of 21 (52%)HBV DNA-infected children had anti-HBs levels <100 IU/ml. Sec-ond, the blood of newborn babies was contaminated with HBVparticles in uterus during the delivery, consequently the HBV vac-cines were ineffective (no mutations were observed in eightpatients). Third, children were infected with HBV mutants orsimultaneously infected with the wild type and mutant HBV;since we did not carry out any molecular cloning, the third con-dition could not be documented in the present study. It is possi-ble that a minor amount of wild type HBV co-exists with thevariant as a quasi-species, but this population cannot be detectedby sequencing analysis. Therefore, the true proportion of patientscarrying HBsAg variants should be higher than what observed inthis study. Fourth, mutations within the surface gene of the HBVgenome are one of the factors contributing to the loss of HBsAgdetection by immunoassay (diagnostic-escape mutants) [7–9].These ‘‘a’’ determinant variants may not be detected by conven-tional HBsAg screening tests. G145R has also been shown to exhi-bit various degrees of altered binding of HBsAg in differentcommercial assays [44,45]. Fifth, low expression levels of HBsAgdue to a low viral load might be enough for viral assembly, butbelow the sensitivity threshold of standard detection tests. Asshown in our study, low levels of HBV DNA, rather than geneticvariability in the major hydrophilic region (MHR), were more fre-quently found among OBI; all isolates showed an amount of DNA<104 copies/ml.
In other studies, however, failure to detect HBsAg in OBIpatients was not fully explained by S gene mutations [46,47].Mutations outside the surface protein may also influence theHBV replication capacity. These mutants have also been reportedto be less ‘‘replication fit’’ in comparison with the wild type virus[48,49], providing a plausible explanation for the low HBV DNAlevels. Furthermore, in the present study, we found multiplemutations outside the surface protein located within the core,pre-S, X, and polymerase with known functional and/or immuneepitope reactivity. Two isolates (112 and 115) carried a triplemutation: E64K, P163L and R165S in the core protein. Isolate106 carried R167K. Positions 163–167 are located within the C-terminal portion of the core protein (aa 150–183), which isknown to interact with pre-genomic RNA for the assembly of rep-lication-competent HBV nucleocapsids and/or the phosphoryla-
2 vol. 57 j 515–521 519

Research Article
tion of the core protein [50,51]. Moreover, it has been observedthat two isolates (115 and 116) carried mutations (S782P,R841K) in the coding region of RNase H, which block the synthe-sis of mature HBV DNA caused by the abnormal persistence of theRNA:DNA heteroduplex generated during reverse transcription[52]. Moreover, it has been shown that residues 782 and 841were located within the polymerase region of MHC classII-restricted peptides [53]. Pre-S2 double mutations V39A, P41H,(found in three isolate) and P15R (in isolate 115) have beenlocated within epitopes known to stimulate T cells and B cells,respectively [39]. In four isolates, the combination of V21A andQ87R in the X region located within the two HLA-A0201-restricted CD8 T cell epitopes was identified [54]. Altogether, all13 patients had at least one amino acid mutation interfering witheither the functional and/or the immune epitope activity.Nonetheless, accumulating evidence indicates that, in mostcases, the genomic heterogeneity of the virus does not accountfor the occult status [37,40,42]. Eight OBI-positive cases did nothave any mutation at all (in this study, some parts of HBV weremissed in a certain number of patients).
Most studies suggested that detection of ‘‘anti-HBc antibodyalone’’ could reflect unrecognized OBI [55,56]. On the other hand,in the study group, comparable to earlier studies [12,57], OBI wasnot associated with the presence of the anti-HBc antibody alone;and 16 (76%) patients with OBI were negative for anti-HBc, a phe-nomenon that has also been described earlier [13]. The possibilityof false negative results for anti-HBc IgG should be considered inthis study. In summary, a proportion of subjects with OBI wereapparently negative for anti-HBc IgG while they were not trulynegative due to the result of the low antibody titer.
The patients group consisted of asymptomatic children whoacquired infection from their mother either vertically (duringbirth) or horizontally (after birth) in their early childhood. Theymust be followed carefully, as OBI is known to be linked tovarious liver diseases, including acute hepatitis and HCCdevelopment.
In conclusion, it is suggested that HBsAg negativity is not suf-ficient to completely exclude HBV DNA carriers. OBI seems to berelatively frequent in immunized children born to HBsAg-positivemothers. This finding might be more frequent in HBV endemicareas such as South and East Asia. This study highlights the factthat anti-HBc, anti-HBs and HBsAg may not be effective toolsfor the diagnosis of HBV infection in this high-risk population,and we need to screen vaccine/HBIG escape mutants. These find-ings emphasize the need for OBI monitoring. Further studies onthe clinical significance of OBI, alternative immunization regi-mens (e.g. administration of boosters), or more effective HBV vac-cines (a third generation or HBV DNA vaccines) are required.
Conflict of interest
The authors who have taken part in this study declared that theydo not have anything to disclose regarding funding or conflict ofinterest with respect to this manuscript.
References
[1] Cooreman MP, van Roosmalen MH, te Morsche R, Sunnen CM, de Ven EM,Jansen JB, et al. Characterization of the reactivity pattern of murinemonoclonal antibodies against wild type hepatitis B surface antigen to
520 Journal of Hepatology 201
G145R and other naturally occurring ‘‘a’’ loop escape mutations. Hepatology1999;30:1287–1292.
[2] Carman WF, Zanetti AR, Karayiannis P, Waters J, Manzillo G, Tanzi E, et al.Vaccine-induced escape mutant of hepatitis B virus. Lancet1990;336:325–329.
[3] Zuckerman AJ. Effect of hepatitis B virus mutants on efficacy of vaccination.Lancet 2000;355:1382–1384.
[4] Ijaz S, Torre F, Tedder RS, Williams R, Naoumov NV. Novel immunoassay forthe detection of hepatitis B surface ‘escape’ mutants and its application inliver transplant recipients. J Med Virol 2001;63:210–216.
[5] Yamamoto K, Horikita M, Tsuda F, Itoh K, Akahane Y, Yotsumoto S, et al.Naturally occurring escape mutants of hepatitis B virus with variousmutations in the S gene in carriers seropositive for antibody to hepatitis Bsurface antigen. J Virol 1994;68:2671–2676.
[6] Carman WF, Korula J, Wallace L, MacPhee R, Mimms L, Decker R. Fulminantreactivation of hepatitis B due to envelope protein mutant that escapeddetection by monoclonal HBsAg ELISA. Lancet 1995;345:1406–1407.
[7] Ireland JH, O’Donnell B, Basuni AA, Kean JD, Wallace LA, Lau GK, et al.Reactivity of 13 in vitro expressed hepatitis B surface antigen variants in 7commercial diagnostic assays. Hepatology 2000;31:1176–1182.
[8] Weber B. Diagnostic impact of the genetic variability of the hepatitis B virussurface antigen gene. J Med Virol 2006;78 (Suppl. 1):S59–S65.
[9] Hollinger FB, Hepatitis B. Virus genetic diversity and its impact on diagnosticassays. J Viral Hepat 2007;14 (Suppl. 1):11–15.
[10] Carman WF. The clinical significance of surface antigen variants of hepatitisB virus. J Viral Hepat 1997;4 (Suppl. 1):11–20.
[11] Protzer-Knolle U, Naumann U, Bartenschlager R, Berg T, Hopf U, Meyer zumBuschenfelde KH, et al. Hepatitis B virus with antigenically altered hepatitisB surface antigen is selected by high-dose hepatitis B immune globulin afterliver transplantation. Hepatology 1998;27:254–263.
[12] Okamoto H, Yano K, Nozaki Y, Matsui A, Miyazaki H, Yamamoto K, et al.Mutations within the S gene of hepatitis B virus transmitted from mothers tobabies immunized with hepatitis B immune globulin and vaccine. PediatrRes 1992;32:264–268.
[13] Brechot C, Thiers V, Kremsdorf D, Nalpas B, Pol S, Paterlini-Brechot P.Persistent hepatitis B virus infection in subjects without hepatitis B surfaceantigen: clinically significant or purely ‘‘occult’’? Hepatology 2001;34:194–203.
[14] Hollinger FB, Habibollahi P, Daneshmand A, Alavian SM. Occult hepatitis Binfection in chronic hemodialysis patients: current concepts and strategy.Hepat Mon 2010;10:199–204.
[15] Giannini E, Ceppa P, Botta F, Fasoli A, Romagnoli P, Ansaldi F, et al. Previoushepatitis B virus infection is associated with worse disease stage and occulthepatitis B virus infection has low prevalence and pathogenicity in hepatitisC virus-positive patients. Liver Int 2003;23:12–18.
[16] Cacciola I, Pollicino T, Squadrito G, Cerenzia G, Orlando ME, Raimondo G.Occult hepatitis B virus infection in patients with chronic hepatitis C liverdisease. N Engl J Med 1999;341:22–26.
[17] Hu KQ. Occult hepatitis B virus infection and its clinical implications. J ViralHepat 2002;9:243–257.
[18] Fabris P, Brown D, Tositti G, Bozzola L, Giordani MT, Bevilacqua P, et al.Occult hepatitis B virus infection does not affect liver histology or responseto therapy with interferon alpha and ribavirin in intravenous drug userswith chronic hepatitis C. J Clin Virol 2004;29:160–166.
[19] Pollicino T, Squadrito G, Cerenzia G, Cacciola I, Raffa G, Craxi A, et al.Hepatitis B virus maintains its pro-oncogenic properties in the case of occultHBV infection. Gastroenterology 2004;126:102–110.
[20] Chan HL, Tsang SW, Leung NW, Tse CH, Hui Y, Tam JS, et al. Occult HBVinfection in cryptogenic liver cirrhosis in an area with high prevalence ofHBV infection. Am J Gastroenterol 2002;97:1211–1215.
[21] Liu CJ, Chen DS, Chen PJ. Epidemiology of HBV infection in Asian blooddonors: emphasis on occult HBV infection and the role of NAT. J Clin Virol2006;36 (Suppl. 1):S33–S44.
[22] Alavian SM, Hajariazdeh B, Ahmadzad Asl M, Kabir A, Bagheri Lankarani K.Hepatitis B virus infection in Iran: a systematic review. Hepat Mon2008;8:281–294.
[23] Hajiani E, Hashemi S, Masjedizadeh A. Seroepidemiology of hepatitis B virusinfection in Khuzestan Province, Southwest of Iran. Hepat Mon2009;9:34–38.
[24] Nokhodian Z, Kassaian N, Ataei B, Javadi AA, Shoaei P, Farajzadegan Z, et al.Hepatitis B markers in Isfahan, Central Iran: a population-based study.Hepat Mon 2009;9:12–16.
[25] Alavian SM. Ministry of Health in Iran is serious about controlling hepatitisB. Hepat Mon 2007;7:3–5.
2 vol. 57 j 515–521

JOURNAL OF HEPATOLOGY
[26] Alavian SM, Gooya MM, Hajarizadeh B, Esteghamati AR, Moeinzadeh AM,Haghazali M, et al. Mass vaccination campaign against hepatitis B inadolescents in Iran: estimating coverage using administrative data. HepatMon 2009;9:189–195.
[27] Moradi A, Khodabakhshi B, Roshandel G, Kalavi K, Besharat S, Semnani S.Response to the hepatitis B virus vaccine in Iranian infants. Hepat Mon2009;9:229–231.
[28] Hosseini SM, Ranjbar R, Abolghasemi H, Turkaman M. Evaluation of the levelof HBV antibody titer after HBV vaccination among children in Tehran, Iran.Hepat Mon 2009;9:150–153.
[29] Kabir A, Alavian SM, Ahanchi N, Malekzadeh R. Combined passive and activeimmunoprophylaxis for preventing perinatal transmission of the hepatitis Bvirus in infants born to HBsAg-positive mothers in comparison with vaccinealone. Hepatol Res 2006;36:265–271.
[30] Hashemi SA, Moghadami M, Lankarani KB, Alborzi A, Mahboudi A. Theefficacy of hepatitis B vaccination among school age children in SouthernIran. Iran Red Cres Med J 2010;12:45–48.
[31] Adibi P, Ghassemian R, Alavian SM, Ranjbar M, Mohammadalizadeh AH,Nematizadeh F, et al. Effectiveness of hepatitis B vaccination in children ofchronic hepatitis B mothers. Saudi Med J 2004;25:1414–1418.
[32] Yahyapour Y, Karimi M, Hashemzadeh O, Jazayeri SM, Saadatmand Z,Mahmoodi M. Seromarkers of hepatitis B virus in children of HBs Ag positivemothers. J Gorgan Univ Med Sci 2009;11:43–48, [in Persian].
[33] Gunther S, Li BC, Miska S, Kruger DH, Meisel H, Will H. A novel method forefficient amplification of whole hepatitis B virus genomes permits rapidfunctional analysis and reveals deletion mutants in immunosuppressedpatients. J Virol 1995;69:5437–5444.
[34] Jazayeri M, Basuni AA, Sran N, Gish R, Cooksley G, Locarnini S, et al. HBV coresequence. definition of genotype-specific variability and correlation withgeographical origin. J Viral Hepat 2004;11:488–501.
[35] Goodarzi Z, Malekzadeh R, Montazeri G, Alavian SM, Qurbanalizadgan M,Daram M, et al. Phylogenetic analysis of HBV based on PreS region in Iranianhepatocellular carcinoma patients. Hepat Mon 2007;7:201–205.
[36] Liu XH, Lin J, Zhang SH, Zhang SM, Feitelson MA, Gao HJ, et al. COOH-terminal deletion of HBx gene is a frequent event in HBV-associatedhepatocellular carcinoma. World J Gastroenterol 2008;14:1346–1352.
[37] Chemin I, Trepo C. Clinical impact of occult HBV infections. J Clin Virol2005;34 (Suppl. 1):S15–S21.
[38] Raimondo G, Pollicino T, Cacciola I, Squadrito G. Occult hepatitis B virusinfection. J Hepatol 2007;46:160–170.
[39] Mu SC, Lin YM, Jow GM, Chen BF. Occult hepatitis B virus infection inhepatitis B vaccinated children in Taiwan. J Hepatol 2009;50:264–272.
[40] Chen WN, Oon CJ. Hepatitis B virus surface antigen (HBsAg) mutants inSingapore adults and vaccinated children with high anti-hepatitis Bvirus antibody levels but negative for HBsAg. J Clin Microbiol2000;38:2793–2794.
[41] Chaudhuri V, Tayal R, Nayak B, Acharya SK, Panda SK. Occult hepatitis B virusinfection in chronic liver disease: full-length genome and analysis of mutantsurface promoter. Gastroenterology 2004;127:1356–1371.
[42] Pollicino T, Raffa G, Costantino L, Lisa A, Campello C, Squadrito G, et al.Molecular and functional analysis of occult hepatitis B virus isolates frompatients with hepatocellular carcinoma. Hepatology 2007;45:277–285.
Journal of Hepatology 201
[43] Cabrerizo M, Bartolome J, Caramelo C, Barril G, Carreno V. Molecular analysisof hepatitis B virus DNA in serum and peripheral blood mononuclear cellsfrom hepatitis B surface antigen-negative cases. Hepatology2000;32:116–123.
[44] Weber B, Melchior W, Gehrke R, Doerr HW, Berger A, Rabenau H. Hepatitis Bvirus markers in anti-HBc only positive individuals. J Med Virol2001;64:312–319.
[45] El Chaar M, Candotti D, Crowther RA, Allain JP. Impact of hepatitis B virussurface protein mutations on the diagnosis of occult hepatitis B virusinfection. Hepatology 2010;52:1600–1610.
[46] Banerjee A, Chandra PK, Datta S, Biswas A, Bhattacharya P, Chakraborty S,et al. Frequency and significance of hepatitis B virus surface gene variantcirculating among ‘antiHBc only’ individuals in Eastern India. J Clin Virol2007;40:312–317.
[47] Brojer E, Grabarczyk P, Liszewski G, Mikulska M, Allain JP, Letowska M.Characterization of HBV DNA+/HBsAg� blood donors in Poland identified bytriplex NAT. Hepatology 2006;44:1666–1674.
[48] Pollicino T, Belloni L, Raffa G, Pediconi N, Squadrito G, Raimondo G, et al.Hepatitis B virus replication is regulated by the acetylation status ofhepatitis B virus cccDNA-bound H3 and H4 histones. Gastroenterology2006;130:823–837.
[49] Sheldon J, Rodes B, Zoulim F, Bartholomeusz A, Soriano V. Mutationsaffecting the replication capacity of the hepatitis B virus. J Viral Hepat2006;13:427–434.
[50] Nassal M. The arginine-rich domain of the hepatitis B virus core proteinis required for pregenome encapsidation and productive viral positive-strand DNA synthesis but not for virus assembly. J Virol1992;66:4107–4116.
[51] Kann M, Gerlich WH. Effect of core protein phosphorylation by proteinkinase C on encapsidation of RNA within core particles of hepatitis B virus. JVirol 1994;68:7993–8000.
[52] Chen Y, Robinson WS, Marion PL. Selected mutations of the duck hepatitis Bvirus P gene RNase H domain affect both RNA packaging and priming ofminus-strand DNA synthesis. J Virol 1994;68:5232–5238.
[53] Mizukoshi E, Sidney J, Livingston B, Ghany M, Hoofnagle JH, Sette A, et al.Cellular immune responses to the hepatitis B virus polymerase. J Immunol2004;173:5863–5871.
[54] Ding FX, Wang F, Lu YM, Li K, Wang KH, He XW, et al. Multiepitope peptide-loaded virus-like particles as a vaccine against hepatitis B virus-relatedhepatocellular carcinoma. Hepatology 2009;49:1492–1502.
[55] Fukuda R, Ishimura N, Niigaki M, Hamamoto S, Satoh S, Tanaka S, et al.Serologically silent hepatitis B virus coinfection in patients with hepatitis Cvirus-associated chronic liver disease: clinical and virological significance. JMed Virol 1999;58:201–207.
[56] Jilg W, Sieger E, Zachoval R, Schatzl H. Individuals with antibodies againsthepatitis B core antigen as the only serological marker for hepatitis Binfection: high percentage of carriers of hepatitis B and C virus. J Hepatol1995;23:14–20.
[57] Waters JA, Kennedy M, Voet P, Hauser P, Petre J, Carman W, et al. Loss of thecommon ‘‘A’’ determinant of hepatitis B surface antigen by a vaccine-induced escape mutant. J Clin Invest 1992;90:2543–2547.
2 vol. 57 j 515–521 521
Related Documents











