Chapter 24: Hallux Valgus & Related Disorders Goals of HAV Surgery Anatomical Facts of the 1st MPJ Predisposing Factors Biomechanics Etiology of HAV Deformity Types Radiological Measurements for HAV Physical Examination Preoperative Considerations Arthroplasty Procedures Capsule-Tendon Balancing Procedures Implant Arthroplasty Procedures Arthrodesing Procedures Proximal Phalangeal Osteotomies Distal Metatarsal Osteotomies Proximal Metatarsal Osteotomies Shaft Osteotomies Combination Procedures Other Procedures Hallux Rigidus and Limitus Hallux Varus Hallux Hammertoe Diff. Diagnosis of Pain in the Sesamoid Area Complications of HAV Surgery HAV Procedure Chart and Their Indications

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Chapter 24: Hallux Valgus & Related DisordersGoals of HAV SurgeryAnatomical Facts of the 1st MPJPredisposing FactorsBiomechanicsEtiology of HAVDeformity TypesRadiological Measurements for HAV Physical Examination Preoperative Considerations Arthroplasty Procedures Capsule-Tendon Balancing Procedures Implant Arthroplasty Procedures Arthrodesing Procedures Proximal Phalangeal Osteotomies Distal Metatarsal Osteotomies Proximal Metatarsal Osteotomies Shaft OsteotomiesCombination Procedures Other ProceduresHallux Rigidus and Limitus Hallux VarusHallux HammertoeDiff. Diagnosis of Pain in the Sesamoid Area Complications of HAV SurgeryHAV Procedure Chart and Their Indications

HALLUX VALGUS AND RELATEDDISORDERS
Goals of Hallux Valgus Surgery1. Pain free joint2. IM angle less than 100
3. Congruent joint4. Good range of motion5. Sesamoids in good position (TSP 3 or less) 6. Cosmetic result acceptable
Anatomical Facts of the 1st M.P. J.1. The articular surface of the base of the proximal phalanx is larger plantarly than dorsally.
2. The medullary canal of the proximal phalanx Is dorsal to middle of the proximal articular surface; this is due to the concave nature of the plantar curvature.
3. The bony prominence on the dorsum of the proximal phalanx is for the EHB.
4. 1st metatarsal has cristae on the plantars
5. The nutrient foramen on the lateral aspect of the shaft is 2.7cm from the M.PJ.urface of the head to separate the sesamoids.
6. The epiphysis is on the base, so head osteotomies are permissible on children; but watch the nutrient artery.
7. The ligaments of the 1 st MPJ are:a. Medial collateral: intracapsularb. Lateral collateral :intracapsularc. Tibial plantar sesamoidald. Fibular plantar sesamoidale. Tibial sesamoidal: intracapsularf. Fibular sesamoidal: intracapsularg. Inter-sesamoidal: intracapsularh. Deep transverse metatarsali. Capsule8. The capsule itself:a. The sesamoids are invested in the capsule through which the FHB runs b. The capsule blends with the periosteum and may be removed easily from the base with an elevatorc. The capsule is strongly attached to the metatarsal head d. There are medial and lateral collateral ligaments9. EHL attaches through the hood ligament and lifts the proximal

phalanx into extention (the EHB is under the hood ligament).
10. The hood ligament attaches the dorsal to plantar structures
11. The capsularis is actually a branch of the tibialis anterior
12. The only structure that never changes is the interosseous ligament
13. The bunion bump Is the abnormal position of the cartilaginous surface
14. Blood Supply to the 1st MTP and 1st metatarsal are via the 1st dorsal and plantar metatarsal arteries and the superficial branch of the medial plantar artery
Predisposing Factors1. Biomechanical
a. Primarily genetic in natureb. Acquired factors
2. Arthritica. RAb. Psoriatic arthritis
3. Neuromuscular a. Cerebral palsy
4. Traumatic (primarily hallux limitus and hallux rigidus)
5. Genetic:a. Down's syndromeb. Ehler-Danlos syndrome c. Marfan's syndrome
Biomechanics1. The first metatarsal dorsiflexes due to hypermobility and when dorsiflexed it also inverts (the 1st ray axis is medial/proximal/dorsal to plantar/lateral/distal).
2. A
foot with a low axis to the transverse plane gets a small amount of abduction/adduction of the first ray as does a rectus foot. This type will develop more of a dorsal bunion. The metatarsus adductus foot with a higher 1st ray axis gets a more medial bunion.
3. As the 1st metatarsal dorsiflexes and inverts, the hallux which is held to the ground by muscle power, is everting and dorsiflexing as well as subluxing laterally due to adduction of the first metatarsal.
4. Due to poor weight bearing of the 1st metatarsal, the second gets transfer lesions and the 1st develops a dorso-medial metatarsal head hypertrophy to form a bunion.
5. This is an acquired condition due to abnormal pronation in an adducted foot type or inflammatory disease of the joint which changes mechanics and muscle direction around the joint due to edema.
6. There must be a propulsive phase of gait for HAV to develop.
7. A hypermobile 1st ray is the primary cause due to a pronatory force and weakening of the peroneus longus.
NOTE* There is almost no transverse plane motion due to the horizontal positioning of the axis

8. Pronatory problems may develop from neuromuscular pathology, but a neuromuscular problem may not show bunion development even with pronation due to poor propulsion.
9. The loss of the normal tibial sesamoid position or excision of the tibial sesamoid will hasten the development of HAV.
10. Factors that affect the rate of progression of HAV are: a. The amount of pronation during propulsionb. The amount of adduction of the forefootc. The amount of calcaneal eversion (a flatter STJ axis increases eversion and hastens HAV development)d. The amount of STJ and MTJ subluxatione. The presence of inflammation of the 1 st MTPJf. The angle and base of gaitg. The stride length (amount of time in propulsion) h. Obesityi. Terrainh. Poor fitting shoe gear
11. If you see HAV prior to age 3-4 suspect an anatomical anomaly or neuromuscular problem (there is no active propulsion In this age group)
12. The hallux is prevented from following the metatarsal head due to the need for ground purchase, therefore, at the 1st MTPJ torque is formed to sublux the joint. A normal 1st MTPJ does not have frontal plane motion, so as the metatarsal dorsiflexes and inverts, the stable hallux dorsiflexes and everts, and subluxation begins.
13. The hallux loses stability at weightbearing due to the hypermobile base, causing the lesser mets to carry more of the load.
14. Lateral subluxation of the hallux occurs due to weakening of the peroneus longus and dorsiflexion of the metatarsal with the transverse head of the adductor pulling on the hallux and enhancing its lateral migration.
15. The sesamoids migrate laterally to change the abductory forces on the hallux. This causes bony adaptation on the plantar metatarsal head so that the crista is gradually worn away, to allow further lateral shift of the sesamoids.
16. Bony adapation shows medial deposition and lateral absorption of the metatarsal head.
17. The metatarsal head develops a groove (sagittal groove) where the phalanx now articulates. This allows for normal

plantar/dorsiflexion inthe plantar part of the metatarsal head, but on the dorsal part you get abduction and eversion due to the new bony adaptation.
18. As metatarsus adductus increases, HAV develops. The angulation in the met-cuneiform joint helps this progression.
19. If the bunion develops lateral pressure on the lesser toes look for: a. Onychocryptosis of the fibular nail groove of the hallux b. Interdigital soft cornc. Hammertoes and underlapping digits.
20. A stable hallux against the second digit causes the retrograde muscle contraction to cause the 1st ray to adduct, therefore, the IM angle Increases (this causes the met-cuneiform split).
21. As long as you have a propulsive gait the HAV worsens. It stops when you have a plodding type of gait.
22. After a long time of dorsiflexion of the 1st ray, there is an adaptation of the 1st ray into a position of elevatus that is somewhat rigid.
23. The medial branch of the superficial peroneal nerve may develop neuritis due to trauma.
24. Rheumatoid complications that help the development of HAV are: a. Intra-articular swelling causes the long tendons to migrate laterally b. Intrinsic muscle spasm causes the sesamoids to migrate laterally c. Pain of the lesser metatarsals may cause excess pronation to get the weight off the painful area
Etiology of Hallux Abducto Valgus1. Excessive pronation during stance phase results ina. Hypermobile 1st ray due to loss of proper P. longus mechanicsi. Results in dorsiflexion/varus of the 1st MTPJ and mild adduction of the metatarsalii. A stretching and loosening of the medial sesamoid ligaments and adaptive tightening of the fibular sesamoid ligament (also some lateral subluxation of the hallux)(GRADE 1)iii. Valgus hallux due to continuation of 1st metatarsal medially and abnormal lateral tracking of the sesamoidiv. Crista starts to erode and transverse adductor helps pull hallux over along with increased ground reaction force from hypermobile first rayv. Abductor hallucis becomes displaced plantarly, as the crista continues to erode and the sesamoids move laterally to change the mechanical advantage
of the adductor hallucis and flexor hallucis brevis to decrease the stability of the halluxvi. The hallux moves laterally and buttresses the second toe (GRADE 2) vii. The IM angle becomes increased due to the retrograde force from the abductor hallucis position (GRADE 3)
viii. The PASA increases adaptively, the crista erodes more as the joint pain increases and the lateral metatarsal head degenerates
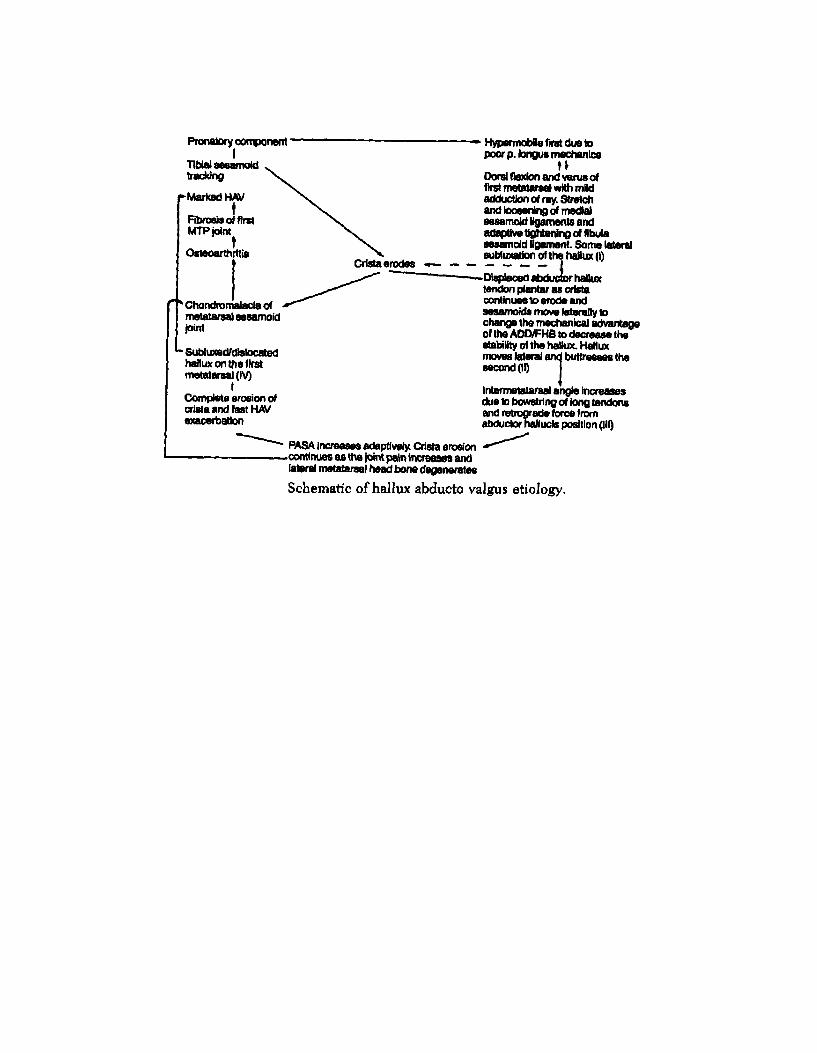
ix. Eventually there is complete erosion of the crista and fast exacerbation of the HAV deformityx. The hallux becomes subluxed and dislocated on the 1st metatarsal (GRADE 4)xi. Marked HAV deformity
b. Tibial sesamoid tracking problems i. Crista erodes
ii. Chondromalaciaiii. Osteoarthritisiv. Fibrosis of the 1st MTPJv. Marked HAV deformity
NOTE* The longer it takes to change from one stage to the next, the less severe the resultant deformity will be
NOTE* When the crista erodes you can transfer the adductor hallucis to the tibial sesamoidal ligament to hold the sesamoids in the proper position

1. Structural Deformity (bony): A deformity in which there is osseous change in either the PASA the DASA or both (so either the PASA or DASA are abnormal). The structural deformity has as its characteristics the congruous joint. The HA deformity is also equal to the summation of the PASA and the DASA.
2. Positional Deformity (soft tissue): There is an abnormality in the HA angle. The PASA and DASA are normal. The joint is either deviated or

subluxed. The summation of the PASA and DASA are less than the HA angle.3. Combined Deformity: Has elements of both structural and positional deformities. Either the PASA or the DASA or both are abnormal, and when added together they do not equal the HA angle. The joint is either deviated or subluxed.
Radiological Measurements For HAV1. Hallux abductus interphalangeal angle = normal 0-10°i. When abnormal, a structural abductus deformity of either the head of the proximal phalanx or the distal phalanx base or both may be present. However, the abnormality is most often seen at the head of the proximal phalanx, and regardless of the site is corrected via osteotomies. Valgus rotations falsely affect the HAI
2. Hallux abductus angle= normal 15°i. Significance: This measurement is the prime method of quantifying the abductus in a HAV condition. Can be either structural, positional, or combined
3. Distal articular set angle= normal 0-10°i. Significance: DASA is a structural component of HA. When abnormalities are detected with this measurement, osteotomies of the hallux proximal phalanx are indicated
4. Proximal articular set angle= normal 7.5°i. Significance: PASA represents a structural component of hallux abductus, and is an attempt to quantify the structural adaptation of the 1st MTPJ
5. 1st Metatarsal Declination Angle = normal 15-20°i. Significance: Gives information regarding sagittal plane position
6. Joint position: The 1st MTPJ is either parallel, deviated or subluxed
NOTE* Structural deformities may exist at levels other than the 1st metatarsophalangeal joint and contribute to the metatarsophalangeal deformity
NOTE* The HA angle is a combination of PASA+DASA+JOINT DEVIATION
NOTE* Situations exist where PASA of 12° is normal.Functional vs. Dysfunctional PASA:PASA remains functional so long as PASA is less than the IM angle or Dysfunctional PASA= PASA - IMTherefore, if the PASA exceeds the IM angle, the PASA should be corrected by at least the number of degrees difference between the two angles. In cases that require correction of the IM angle by base/shaft procedures, the anticipated postoperative IM angle must be determined.

7. Metatarsus primus adductus angle (intermetatarsal angle)= normal 8-12° in the rectus foot and 8-10° In the adductus footi. Significance: When the angle is abnormally increased the condition may be termed metatarsus primus adductus. The MA angle may determine the significance of the IM angle. Adducted foot types require correction of the IM at a lesser angle, therefore, the adducted foot type will require a base/shaft procedure at lower degrees than a rectus foot type.
8. Metatarsus adductus angle (MA)= normal under 15°i. Significance: The MA determines the significance of other measurements (IM, HA, and PASA). MA is influential in the choice of procedures. MA feet tend to develop HAV more rapidly than rectus feet
9. Metatarsal protrusion distance (MPD)= normal +2 mm. to -2 mm.i. Significance: An excessively long metatarsal may be the etiologic factor in hallux limitus or HAV, and an excessively short metatarsal can cause 2nd metatarsalgia. Procedures should be selected that avoid shortening the MPD or if unavoidable combine with a plantarflexing procedure
10. Tibial sesamoid position= normal 1-31. Significance: TSP documents the stage of progression of HAV. The plantar-axial view is best to determine the exact position of the sesamoids with regard to their position in their respective grooves
11. First metatarsal base gapping= normal Is less than a 2mm gap
Physical Examination1. The foot of the patient is evaluated on a weightbearing and on anonweightbearing attitude:a. Weightbearing:i. EHL contracture ii. Hallux purchaseiii. Hallux position with regard to resting calcaneal stanceposition/neutral calcaneal stance positioniv. Radiographic analysis (including mineralization, osteophytes, andcysts)b. Nonweightbearing:i. 1st ray ROMii. Manual reduction of IMiii. 1 st MTPJ ROM, quality of motion, and axis of motion iv. Location of painv. Location of bunionvi. Hallux position relative to 2nd toe vii. Callusesviii. EHL contracture (rare)ix. Associated deformities (2nd hammertoe, etc.)x. Trackbound (position the toe in a rectus position and dorsiflex and plantarflex- there is inability for adequate ROM with resultant pain)

2. A complete vascular, neurologic, dermatological, and biomechanical examination should additionally be performed.
Preoperative Considerations (planning)1. Decide upon the right choice of procedure based upon radiological and clinical assessment2. Remember that capsulotomies will not correct a structural deformity3. Use a template in preoperative planning if you are unsure4. Use fixation method which you are most comfortable with and that will provide the best stability5. Try to minimize complications with proper execution of procedure and normal postoperative recovery period6. Review the risks and consequences thoroughly with the patient
Arthroplasty Procedures1. Kellera. Indicationsi. HAV with degenerative joint diseaseii. Second and third degree hallux rigidus
iii. Geriatric bunionb. Advantagesi. Relief of painii. Establish/restore 1st MTPJ ROM iii. IM reduction of 3-5° iv. Minimal rehabilitation v. Early return to shoesc. Disadvantagesi. Short halluxii. Loss of purchaseiii. Sesamoid retraction iv. Altered gait
Note* Second degree hallux rigidus a. Established arthrosis b. Painful ROMc. Loss of central articular cartilaged. Proliferation and enlargement of peripheral osteophytes e. Ankylosis
Third degree hallux rigidusa. Complete disappearance of the joint space b. Ankylosis of the MTPJ c. Sign (cant hypertrophy of the joint d. Irregular hypertrophic osteophytes
v. Limited ROMvi. Limited IM reductiond. Complicationsi. Hallux extensus ii. Loss of purchaseiii. Retraction of the hallux with loss-of joint spaceiv. Metatarsalgia/stress fracture 2nd metatarsal and/or 3rd metatarsalv. Edema/telescoping of the hallux basee. Modificationsi. Reattachment of the flexor brevis ii. EHL lengthening iii. Purse-stringing the capsule iv. Capsular flapv. K-wire splintingvi. Implant arthroplastyvii. Anchor the FHL to the sesamoids and the base of the proximalphalanx
2. Hueter: Complete resection of the 1 st metatarsal head, usually performed as part of the Hoffman-Clayton
3. Mayo: Resection of one-quarter inch of the 1 st metatarsal head and medial eminence.
4. Stone: Remodeling of the 1st metatarsal head. An oblique plane resection of the head, leaving a three-quarter inch space at the 1st MTPJ
5. Regnauld: Resection of a portion of the base of the proximal phalanx with the fashioning of a "hat-shaped". inverted, or "cork shaped" autogenous graft. This procedure besides shortening a long proximal phalanx and increasing ROM in the presence of DJD, will also correct a mildly abnormal DASA, mildly abnormal HIA by angling the surface of the base of the proximal phalanx.
6. Valenti "V" Resection:a. Indicationsi. Hallux valgusii. Hallux limitus in the elderlyiii. Nonactive patientiv. Hallux rigidus in cases of implant salvageb. Surgical technique: A "V" shaped osteotomy at the head of the 1st metatarsal and the base of the proximal phalanx (a 45° angular resection of the metatarsal and phalanx) on the dorsal and plantar aspect. A dorsal U-shaped capsular flap perserves intrinsic attachments at the base of the proximal phalanx. EHL lengtheningc. Advantages:i. Restoration of ROMii. Preservation of hallux purchase

iii. Immediate weightbearing
Capsule-Tendon Balance Procedures1. McBride: Originally described with an incision lateral to the EHL, excision of fibular sesamoid, medial eminence removed, adductor tendon transferred to the lateral side of the metatarsal head, and the medial capsule and adductor tendon shortened (several modifications to date)a. Criteria: Structural deformities of the 1st ray should not be present unless corrected by other proceduresi. Normal HIAii. Normal DASAiii. Normal PASAiv. Normal IM anglev. Hypertrophied medial eminencevi. Deviated to subluxed 1st MTPJvii. Deviation of sesamoids >4 (fibular sesamoid may be arthritic) viii. Increased HA angleb. Surgical technique:i. A 6 cm. dorsolinear incision parallel and medial to the ii. Inverted "L" capsulotomyiii. Medial eminence removeddrilling with .045 k-wire to produce fibrocartilageiv. If erosions in the cartilage are found then perform subchondralv. Removal of the fibular sesamoid only if it is acting as a deforming force and an adductor transfer is not being done (just freeing the attachments is not enough)vi. Release OR transfer of the Adductor tendon The tendon is pulled over the 1st metatarsal neck and sutured into the
medial capsule. This repositions the sesamoids The tendon is tied into the metatarsal neck and into the medial capsule
(this helps close the IM anglevii. Cut EHB
b. Contraindications:i. Structural deformities ii. Hallux rigidusiii. DJDc. Complications:i. Stiff jointii. Undercorrection of the deformity iii. Hallux varus
2. Silver:a. Indications:i. Hypertrophied medial eminence ii. Mild HA angle
NOTE Do not cut the adductor and remove the fibular sesamoid, you will predispose to a hallux varus

iii. No other structural abnormalitiesb. Surgical technique: Removal of the medial eminencec. Complications:i. Stiff jointii. Increase on HA angle following surgery due to cutting of medial stabilizing structures
3. Hiss: Like the Silver, plus the abductor hallucis is repositioned on the medial aspect of the 1st MTPJ (trying to balance the abductory component)
Implant Arthroplasties
1. Hemi implant:a., Criteria:i. Joint painii. Adequate bone stock of the proximal phalanxiii. Normal IM angle unless reduced by another procedureiv. Normal articular cartilage of the head of the 1st metatarsal (no DJD) v. Adequate capsular tissue to allow for implant coverageb. Complications:i. Implant instability: Pistoning can occur from removal of too much bone as well as axial rotation of the implantii. Implant failure: Mechanical stress can produce microfragmentation with migration of the silicone particles into the lymphatic system. With this there will be obvious loss of function and possible deformity. Not so with titanium implants
Implants utilized for the 1st MTPJ are static spacers which relieve pain, allow for limited painless motion, and give some internal stability to the joint.Ideally, biocompatibility requires the implant to be: Chemically inert or free from biodegradation and sterile capable of withstanding stresses imposed upon it Durable or possess an integrity of structure without modification of its
physical properties because of the biological environment Non-irritation, eliciting only a benign local tissue responseGeneral indications for 1 st MTPJ implant arthroplasty: Hallux valgus with subluxation and painful limited ROM End stage hallux rigidus Revisional surgery Rheumatoid arthritis Painful DJD Gouty arthrosis/arthritis Osteochondral fractures Intra-articular fracturesGeneral contraindications for Implant arthroplasty: infection Salvagable joint

iii. Foreign body reaction: lymphadenopathy which is reminiscent of metastatic Ca clinicallyiv. Osteochondritis dessicans: From excessive stripping of the periosteum and resultant avasular necrosisv. Detritic synovitis reaction: The surgical area will become red and swollen with a chronic low grade pain. Once infection is ruled out the patient can be treated with NSAIDS or remove the implant device (less chance of this with titanium implants)vi. Infection: Implant must be removed and not replaced for at least 6 months to 1 year. If gram negative infection was present, implant should not be replaced for longer period of time if at allvii. Pistoning of the implant into cancellous bone (if implant chosen is too small)viii. Chronic edemac. Contraindications:1. DJD of the 1st metatarsal head contraindicates a hemi implant ii. Severe osteoporosis of the involved bones iii. Inability to correct a high IM angleiv. History of a prior joint infection within the last 6 months v. History of allergic reaction to implant material
2. Hemi-angled Implant (Well): for accommodation up to 15° lateral deviation of the 1st metatarsal articular surface
a. Criteria: As above plusi. Abnormal PASAii. Revisional surgery for hallux varus (reverse the implant) b. Complications: As above
3. Total Swanson Implant: Manufactured by Dow-Corning Wright, comes in 7 anatomical sizes plus the addition of titanium grommets. A central hinge in a "U" configuration allows for dorsiflexion. An intramedullary stem on both sides of the implant stabilizes the implant within the medullary canals. There is no angulation of the stems in the sagittal or transverse plane. There is a short stem version available in 6 sizes
NOTE* This device eliminates the "lateral gap sign" as seen with the standard hemi-implant, which is. the nonarticulation between hemi- implant and lateral metatarsal articular surface

a. Criteria: As above plus
i. Good bone stock of the 1 st metatarsal headii. Degenerative changes of the 1 st metatarsal head iii. Abnormally low metatarsal declination angle
b. Complications: As abovec. Contraindications: As above
4. Total Lawrence Implant: Manufactured by Sutter Biomedical and is marketed In 4 sizes. The proximal stem is angled 150 dorsally in the sagittal plane to allow for normal 1 st metatarsal declination, without sacrificing excursion of the implant to compensate for this. It is designed for a ROM of 85° of dorsiflexion

a. Criteria: As above plusi. Normal 15° declination angle b. Complications: As above c. Contraindications: As above
5. Total LaPorta Implant: Manufactured by Sutter Biomedical, comes in right, left, and neutral, referring to the deviation of the stems on the transverse plane. The right and left implant show a 100 angulation (lateralward) on the transverse plane. It is designed for a ROM of 60° a. Criteria: As above plusi. Normal 150 declination angle or use a neutral LaPorta implant for an abnormally low metatarsal declination angle.ii. Can be used for a mildly elevated IM angle without performing a procedure to reduce it, due to the 100 transverse plane abduction built into the proximal stemb. Complications: As abovec. Contraindications: As above
6. Total Bioaction Implant: Newer two-piece device made of high density polyethelene, cobalt steel and titanium.a. Criteria: As per total Swanson implantb. Complications: As abovec. Contraindications: As above
7. Kinetic Great Toe Implant: Two piece titanium/cobalt chromium implant with an anatomic dorsal flange providing an anatomic range
of motiona. Criteria: as aboveb. Complications: as abovec. Contraindications: as above
Arthrodesis1. McKeever Type (fusion of the 1st m.p.j.): Originally described as a peg-in-hole 1st mpj fusion.a. Criteria:i. Flail toeii. Failed implant arthroplastyIii. Arthritis/goutiv Severe hallux valgus deformityv. Loss of extensor and/or flexor functionvi. Intra-articular fractures with post-traumatic arthritis vii. Previously failed bunion proceduresviii. Failed Keller arthroplasty procedureix. Prior infection/septic arthritisx. Hallux limitus/rigidusxi. Rheumatoid arthritisxii. Charcot joint/osteoarthropathyxiii. latrogenic hallux varusxiv. Tumorb. Ideal position of fusioni. Slight dorsiflexion (5-10° from the ground supporting surface)ii. Slight abduction (parallel to the 2nd toe) or 10-15° on the transverse planeiii. No frontal plane valgus or varus rotation
c. Surgical technique:
NOTE* This device also may be used to replace previous implants that have failed. This system offers implants that are anatomically and biomechanically accurate, with instrumentation that is precise to aid in its installation.The system consists of four phalangeal components which articulate with all six metatarsal (three left/three right) components. The metatarsal component is made from cobalt chromium (CoCr) which is the same material used for the femoral component of the total knee inn plant. The phalangeal component is made form titanium alloy as the backing to a high molecular weight polyethylene bearing surface
NOTE* It is mandatory that all patients after receiving the implant arthroplasty be advised that prior to any invasive procedure (medical/ dental) that the patient be given prophylactic antibiotics, as is the case with all implanted prosthetic devices
NOTE* Position will vary depending on activity, lifestyle, and shoe gear

i. Cartilage denudingii. Metatarsal head resection ( as part of pan-metatarsal head resection) iii. With bone grafting (i.e. failure of implant cases) d. Possible ancillary procedures:i. Tibial or fibular sesamoidectomyii. IPJ arthrodesis (most common)iii. Relocation and arthrodesis of the lesser toes iv. Possible metatarsal osteotomies v. Possible Hoffman-Clayton vi. EHL lengtheningvii. Excision of ipj sesamoid viii. CBWO/ Lapidus/ OBWOe. Fixation types:i. Insertion of crossed .045 k-wiresii. Monofilament 28 gauge wire loops iii. 4.0 cancellous screwiv. 3.5 Cortical screw in a lag technique v. 2.7 mm. screw in a lag technique vi. Herbert screwf. Advantages:i. Preserves adductor, short flexor, and EDB ms. functionii. Improved cosmetic appearanceiii. Improved stabilityiv. Improved overall balance and gait vi. Improved position of lesser toesvii. Restores and maintains weightbearing function to the 1st rayviii. May be converted to Keller or implant arthroplastyix. Relief of painx. Simultaneous reduction of IM angle xi. Recurrence of the deformity is unlikelyg. Disadvantages:i. May promote arthritic changes at the ipjii. Optimum position may be difficult to achieve as it is technicallydifficult to performiii. May require autogenous graft iv. May limit shoe gear v. May result in gait alterations v. Difficulty in kneelingh. Complications:i. IPJ arthritis of the halluxii. Delayed union/non-union/malunion/pseudoarthrosisiii. Fractureiv. Onychocryptosisv. Medioplantar calluses vi. Hallux flexus vii. Impaired gait viii. Balance problemsix. Possible subluxation of toes 2 and 3 x. Improper positioning

2. Lapidus Type (fusion of the 1st metatarsal-cuneiform joint): a. Anatomy:i. The joint is arthrodial with its own synovial membraneii. The medial cuneiform distal articular surface is reniform in shape with a convex medial border and concave lateral borderiii. The surface is elongated in the vertical direction with an inferior and medial inclinationiv. The proximal articular surface of the 1st metatarsal is reniform with upper and lower partsv. There is a variable articulation between the 2nd metatarsal at itsproximal medial aspect and the first metatarsal at its proximal lateral aspect vi. Dorsal and plantar 1st metatarsal-1st cuneiform ligaments are present vii. There are no interosseous ligaments between the base of metatarsals1 and 2viii. There is a strong interosseous ligament between the 1st and 2nd cuneiform and between the 1st and 2nd cuneiform and 2nd metatarsalix. Tibialis anterior tendon inserts at the proximal junction of the medial and inferior surfaces of the 1st metatarsalx. Peroneus longus tendon inserts at the proximal junction of the lateral and inferior surfaces of the first metatarsalb. Indications:i. Extreme hypermobility associated with HAVii. Correction of sagittal plane deformityiii. Correction of severe metatarsus primus adductus associated with a hypermobile or structurally medially deviated M-T-C joint iv. Repair of fracture or dislocationv. Hypermobile flatfoot with medial column sagc. Surgical technique: Via a dorsal longitudinal incision medial to the EHL tendon, with capsular incision dorsal linear or transverse. Articular cartilage is resected from the joint surfaces. The metatarsal is then adducted and slightly plantarflexed and then fixated appropriately with a compression screw, staple or k-wires. A BK NWB cast is applied until radiographic signs of fusion and stability are seen. Originally, Lapidus fused the 1st and 2nd metatarsal bases, but this is rarely necessary. Modifications of this procedure includei. Transfixation of the 1st to 2nd metatarsals with a threaded k-wire ii. Fusion of the 1st to 2nd metatarsal base with bone graft obtained from the medial exostosis of the metatarsal head
NOTE* There exist 3 surgical alternatives for extreme hypermobility cases:a. Cartilage abrasion and subchondral perforation, manual reduction, temporary fixation followed by bone screw fixationb. Joint wedge resection, minimal bone resection, lateral plantar wedge with bone-screw fixation and -stress receiving graftc. Joint resection, minimal bone removal with temporary reduction of the lengthening by means of allogeneic bone, double screw fixation, and occasional temporary plates.With each, there must be at least two points of fixation

d. Complications:i. Prolonged healing timeii. Malalignment in the frontal, sagittal or transverse planesiii. Severence of the vascular structures in the proximal intermetatarsal spaceiv. Non-union and pseudoarthrosis
Proximal Phalangeat OsteotomiesThe Akin-type procedures are generally combined with other types of bunion procedures to correct deformities around the 1st MTPJ, however, the cylindrical Akin is often used independently to shorten a long proximal phalanx1. Proximal Akin: It is a medial closing wedge osteotomy at the metaphysis of the proximal phalanx. Is used to correct a high DASA. There should be adequate bone stock and adequate length of the proximal phalanx. The IM and HA angles will be unaffected. The lateral hinge is kept intact and the osteotomy should be fixated.
2. Distal Akin: It is a medial closing wedge osteotomy of the distal part of the proximal phalanx used to correct a high HI angle. IM angle unaffected. a. Indications:i. Pressure of the hallux on the 2nd digitii. Epiphysis may be openiii. Good bone stockiv. HIA > 100
v. Adequate length of proximal phalanxvi. DASA is normalvii. Congruous 1st mpj unless corrected by another procedure b. Disadvantages:i. Long healing phaseii. Fixation needediii. Elimination of propulsive phase of gait for 3-6 weeks c. Complications:i. Poor correctionii. Pain postop due to poor fixationiii. Non-unioniv. Short halluxv. Hallux elevatus from FHL damage
3. Cylindrical Akin: Removal of cylindrical section to shorten a long proximal phalanx. The proximal osteotomy is one and one-half cm. from the base of the proximal phalanx, and the second osteotomy is made distally to the first cut.
4. IPJ fusion: Used to correct a hallux hammertoe or injury to the ipj. Must have good ROM of the 1st MTPJ.
5. Kessel-Bonney: A dorsal wedge osteotomy of the base of the proximal phalanx, used for hallux limitus. This extends pre-existing joint motion more

dorsally.a. Advantages:i. Allows the hallux to be in a dorsal position at the propulsive phase of gaitii. Allows for immediate ambulationb. Disadvantages:i. Requires an osteotomy with fixationii. Does not really increase overall 1 st MTPJ ROM iii. Often creates a lack of toe purchaseiv. Does not correct the underlying etiology of the deformityv. Requires elimination of the propulsive phase of gait for 3-6 weeks


Distal Metatarsal Osteotomies
1. Austin:a. Criteriai. Normal to mildly abnormal PASAii. Increased IM angle (max 14°/depends on other factors)
iii. Normal metatarsal declinationb. Surgical technique: V osteotomy with 60° angular cuts, originallydescribed with no fixation, but commonly fixation devices utilized.c. Advantagesi. Reduces the IM angleii. Performed in cancellous boneiii. Stable in the sagittal plane allowing early ambulationiv. Avoids the sesamoidsd. Disadvantagesi. Technically challenging (easier with Reece osteotomy guide)ii. Dislocation potentiale. Complicationsi. Dislocation of capital fragment ii. Intra-articular fracture iii. Aseptic necrosis
The major criteria for all distal osteotomies of the 1st metatarsal head are adequate bone density, adequate ROM, and arthritis-free joint. The potential complication for all distal 1st metatarsal osteotomies is avascular necrosis.
NOTE* 1 mm in lateral shift of the capital fragment equals a reduction of 1° of IM angle.
NOTE* One can safely shy the metatarsal head laterally one-third of the width of the bone. So if the metatarsal head measures 21 mm. across, you can safely shy the bone 7 mm. and thereby close the IM angle 7° (since the wider the bone the more lateral shifting you can perform)

2. Austin/Kalish modification: As above but with a smaller angular cut to allow for longer dorsal wing for placement of 2-2.7mm screws or one 3.5 mm screw
3. Austin/Youngswick modification: a. Criteriai. Normal to slightly abnormal PASAii. Increase IM angle (mild) iii. Metatarsus elevatus iv. Limited ROMb. Operative technique: Similar to other Austin procedures except withremoval of rectangular wedge from dorsal arm of the 600 angle of the V.Additionally the wedge can be placed in the plantar arm of the V cut foradditional plantarflexion of the capital fragment.c. Advantagesi. Plantarflexesii. Shortens- relaxes the tension around the joint, thereby increasingROMiii. Stable if fixatediv. Done in cancellous boned. Disadvantagesi. Potential displacement ii. Difficult to perform iii. Needs fixationiv. Should be non-weight bearing 4-6 weekse. Complicationsi. Intra-articular fracture ii. Excessive shortening iii. Dorsal displacement iv. Metatarsalgia
4. Austin/Bicorrectional modification:a. Criteriai. Abnormal PASAii. Increased IM angle
NOTE* It has been reported in the literature that an unusual sequel of this procedure has been for the capital fragment to pop out of the wound and fall on the operating room floor. The suggested protocol for this is to: a. Pick up the fragment with a sterile forceps and place in a basin containing 1 liter of sterile saline + 1 cc. Neosporin G. U. irrigant + 1:100, 000 Bacitracin for 5 minutes.b. Then transfer to another basin with the same type of solution for another 5 minutes.c. Then transfer to a third basin containing the same solution and swirl for an additional 1 minute and replace back into the foot with fixation. d. Advise the patient of the occurrence.e. Prophylaxis with 1 gm IV Cefadyl at 8, 16, and 24 hours postoperatively.
iii. Normal metatarsal declinationb. Operative technique: Same as traditional Austin except another cut is made which is thicker medially so as to remove a trapezoidal wedge of bone from the dorso-medial metatarsal head. When! the capital fragment is shifted laterally and impacted the IM and PASA is subsequently reduced. c. Advantages:i. Same as the Austin plusii. Reduces the PASAd. Disadvantagesi. Technically challenging (more so than the traditional Austin) ii. Dislocation potentiale. Complicationsi. Same as the traditional Austin
5. Reverdin:a. Criteriai. Increased PASA ii. Normal IM angleiii. Normal metatarsal declinationb. Advantages:i. Reduces the PASAii. Performed in cancellous bone iii. Fixation optional iv. Good visualizationc. Disadvantages:i. Potential sesamoid traumaii. No IM angle reduction or sagittal plane reductiond. Complications: DJD
6. Reverdin-Green (distal "L" osteotomy): This is identical to the Reverdin except with an additional plantar osteotomy cut made parallel to the weight-bearing surface to protect the sesamoids
7. Reverdin-Laird: Adds transposition of the metatarsal head to the Reverdin-Green procedure, with reduction of the IM angle
8. Reverdin-Todd: Combined with the Reverdin-Green and Reverdin-Laird, this modification adds correction of the sagittal plane deformity of the 1st metatarsal
9. Hohmann: Its modifications are the Mitchell and the DRATO a. Criteria: Sagittal and transverse plane deformities i. Increased PASAii. Increased IM angleiii. Elevatusb. Precautions: Cannot be used for frontal plane deformities, in the presence of degeneration of the crista or any DJD c. Advantages:

i. Reduces PASAii. Reduces IM angleiii. Plantarflexesd. Disadvantages:i. Highly unstableii. Needs 2 point' fixationiii. Cast requirediv. Extracapsularv. Performed in cortical bonevi. Does not remove the medial eminence e. Complications:i. Dislocationii. Delayed or non-unioniii. Metatarsus elevatus
10. Mitchell: A step down transpositional/angulation osteotomy at the metatarsal necka. Criteria:i. Normal PASAii. Moderate increase in IM angleiii. Positive metatarsal protrusioniv. Metatarsal elevatusb. Advantages:i. Reduces the IM angleii. Removes the medial eminenceiii. Plantarflexes the met headiv. Avoids the sesamoidsv. More stable than the Hohmannc. Disadvantages:i. No PASA correctionii. Shortens the metatarsaliii. Performed in cortical boneiv. Dislocation potential
11. DRATO:a. Criteria:i. Abnormal PASAii. Mild increase of IM angleiii. Valgus rotation of the metatarsal headiv. Sagittal plane deviation of 1st metatarsal head articular cartilage (facing either plantarward or dorsalward)b. Advantages: It addresses 4 deformities in one procedure (PASA, sagittal plane 1st met head, valgus rotation, and IM angle) c. Disadvantages:i. Very difficult to performii. Done in cortical boneiii. Cast/ NWB 6-8 weeksd. Complications: Same as with other procedures of this type
12. Waterman: Distal metaphyseal dorsal wedge osteotomy that raises the declination of the metatarsal head. Utilized for hallux limitus. a. Disadvantages:i. Does not actually increase the 1st MTPJ ROMii. Can create a lack of hallux toe purchaseiii. Does not correct the underlying etiologyiv. Requires removal of the propulsive phase of gait for 3-6 weeks postop.
13. Wilson: An oblique displacement osteotomy that shortens the 1st metatarsal and decreases the IM angle.
14. Peabody: Similar to the Reverdin except performed more proximally.
15. Lambrinudi: A plantarfiexory osteotomy of the 1st metatarsal. Reserved for the younger active individual without severe joint disease with hallux limitus complaints.
Proximal Metatarsal Osteotomies:
1.
Trethoan (opening base wedge): Used when the metatarsal is relatively short. Must utilize a bone graft (best to fixate with a staple to avoid compression of the bone graft).
2. Louisan-Balacescu (closing base wedge): A transverse closing base wedge osteotomy. Fixated with a staple. osteoclasp, K-wires, or monofilament wire. Complications have been elevatus of the metatarsal, non-unions, and delayed unions. The Juvara modifications allows for AO fixation.
3. Juvara Type A: Oblique base/shaft osteotomy from medial-proximal to lateral-distal, a wedge of bone removed to close the IM angle, medial hinge is kept intact, and screw fixation utilized.
4. Juvara Type B: As in type A, a wedge is removed for IM angle reduction, also the hinge is broken after screw insertion for sagittal plane rotation.
5. Juvara Type C: No wedge is removed but the hinge is broken, so that sagittal plane rotation is possible and axial transposition is possible
These procedures are used when the true IM angle should be reduced (greater than or equal to 140 in the rectus foot) and/or when a sagittal plane deformity of the first ray needs to be corrected. These procedures are performed transversely across the metatarsal, perpendicular to the long axis, and 1-1.5cm distal to the met-cuneiform joint.
NOTE* For screw fixation the osteotomy cut is performed obliquely and must be at least twice as long as the width of the metatarsal shaft

(lengthening or shortening).
6. Arcuate (Weinstock): A proximal dome shaped osteotomy that reduces a high IM angle and sagittal plane deformity. No cortical hinge is left intact. Its benefit is that it avoids shortening the metatarsal. Its drawback is that it is
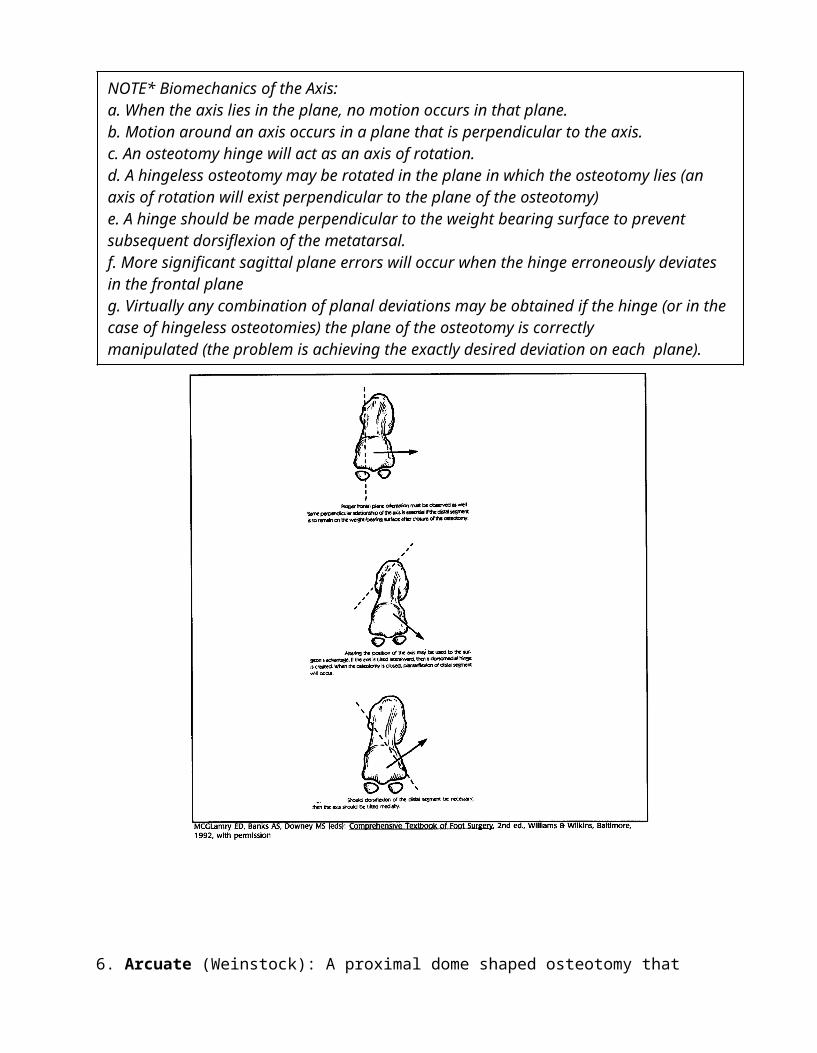
NOTE* Biomechanics of the Axis:a. When the axis lies in the plane, no motion occurs in that plane.b. Motion around an axis occurs in a plane that is perpendicular to the axis. c. An osteotomy hinge will act as an axis of rotation.d. A hingeless osteotomy may be rotated in the plane in which the osteotomy lies (an axis of rotation will exist perpendicular to the plane of the osteotomy) e. A hinge should be made perpendicular to the weight bearing surface to prevent subsequent dorsiflexion of the metatarsal.f. More significant sagittal plane errors will occur when the hinge erroneously deviates in the frontal planeg. Virtually any combination of planal deviations may be obtained if the hinge (or in the case of hingeless osteotomies) the plane of the osteotomy is correctlymanipulated (the problem is achieving the exactly desired deviation on each plane).
unstable and occasionally difficult to fixate.
7. Van Ness: Plantar closing base wedge osteotomy for reduction of metatarsal elevatus. K-wire fixation utilized.
Shaft Procedures 1. Offset V (Vogler): a. Criteria:i. IM angle of 17-18°ii. PASA between 8-30°
iii. Minimal to no joint painiv. No excessive DJDb. Operative technique: A long V osteotomy that extends almost to the met-cuneiform joint enabling reduction of the IM angle and PASA. The apex of the
NOTE* Fixation studies of proximal metatarsal osteotomies revealed:a. Dorsal loop: failed at 1 lb pressureb. Dorsal loop with .062 k-wire: failed at 3.5 lb pressure c. Right angle loops: failed at 6 lb pressure d. Crossed. 062 k- wires: failed at 6 lb pressure e. 4 mm. cancellous screw: failed at 8 lb pressure f. 3.5 mm. cortical screw: failed at 9.5 lb pressureg. Two 2.7 mm. cortical screws: failed at 10 lb pressure (gives better and more even compression)h. Right angle loops with .062 k-wires: failed at 10 lbs pressure
NOTE* It has been reported that there is an average reduction in IM angle of 9.1° and PASA of 7.99°

V is more proximal than the standard Austin (done at the metaphyseal-diaphyseal junction) with the angle measured at 35°. The dorsal arm is longer extending between midshaft and the proximal one-third of the metatarsal. Fixation is achieved with 1 K-wire or 2.7 mm. screw.b. Complications: As per most osteotomies of this type
2. Scarf:a. Criteria:i. Increased IM angleii. Increased PASAb. Operative technique: A long Z osteotomy that reduces the IM angle andthe PASA. Modifications of this procedure include:i. A medially based incisionii. The length of the horizontal osteotomy is in direct proportion to thewidth of the IM angleiii. The direction of the osteotomy has been modified such that approx.two-thirds of the width of bone is dorsal to the osteotomy, proximally,and one third is plantar, in order to prevent stress fractures from occurringc. Advantages:i. The long plantar fragment possesses stability in two planesii. Lends itself to AO fixation (tension band effect)d. Disadvantages:i. Difficult to performii. Possible vascular compromise iii. Performed in diaphyseal bonee. Complications:i. Aseptic necrosis
3. Mau (Gudas modification for screw fixation): An oblique shaft osteotomy from plantar-proximal to dorsal-distal. Indicated for IM angle reduction.
4. Ludloff (Engelman modification for screw fixation): An oblique shaft osteotomy from dorsal-proximal to plantar-distal
Combination Procedures1. Stamm (opening base wedge + Keller) 2. Logroscino (closing wedge + Reverdin)
Other Procedures1. Cotton (1st cuneiform opening wedge osteotomy): a. Criteria:i. Metatarsus primus adductusii. Pronounced obliquity of the 1st met-cuneiform joint iii. Whenever a double osteotomy is indicatedb. Contraindications:i. Excessive bony bridging at the opposing surfaces of the osteotomyc. Operative technique: A wedge is removed from the 1st cuneiform. The cut is made parallel to the joint and does not enter the met-cuneiform joint

plantarly, and is placed tibial to the intercuneiform joint at the bases of the 1st and second metatarsals. The 1st cuneiform osteotomy is then performed on the distal 1/3 of the bone. The more distal the osteotomy the more effect it has on the joint direction. The graft comes from the medial eminence and is fashioned prior to removal of the cuneiform wedge.
d.
Complications:i. Inadequate reduction of the deformityii. Malalignment of the osteotomyiii. latrogenic tenotomy of the FHLiv. Metatarsus primus elevatuse. Advantages:i. This procedure can be added if the distal metaphyseal osteotomy proves to be inadequate to repair the deformityii. Postoperative recovery is far easier than a closing base wedge or Lapidusiii. No cast is required and partial weight bearing can begin several days postoperativelyiv. Allows surgery in the presence of a short 1st metatarsal as this procedure lengthens the 1st ray
2. Cheilectomy: Removal of osteophytes from the 1st MTPJ
Hallux Rigidus and Hallux Limitus1. Etiology:a. Dorsiflexed 1st metatarsal secondary to abnormal pronation and hypermobility of the 1st ray.b. Dorsiflexed 1st metatarsal secondary to muscle imbalance affecting the 1st ray.c. Dorsiflexed 1st metatarsal secondary to sagittal plane structural malalignment of the 1st metatarsal.d. Abnormally long 1st metatarsal.e. Prolonged 1st MTPJ immobilization.f. Arthritic conditions of the 1st MTPJ either traumatic or metabolicg. latrogenic secondary to previous foot surgery affecting the 1st ray.
NOTE* Dissection of the 1st cuneiform must be done carefully to avoid avascular necrosis of this bone
2. Preoperative Symptoms:a. Spasms or tendonitis of the EHL.b. Inability to move the hallux normally and or pain on motion.c. Inability to wear high heeled shoes.d. Painful hyperkeratotic lesion under the IPJ of the hallux. e. Painful hallux nail plate.f. Enlargement over the dorsal aspect of the 1st MTPJ 3. Preoperative signs:a. Dorsal bunion with or without skin irritation. b. Limited or absent 1st MTPJ motion c. Hallux extention distal to the IPJ d. Deformation of the hallux nail platee. Weakness of the peroneus longus and/or hyperactivity of the anteriortibial ms.f. Crepitation and/or pain with 1st MTPJ ROM.4. Preoperative radiographic signs:
a. Dorsal osteophytic proliferationb. Dorsiflexed 1st metatarsal relative to talar bisection c. Narrowing of the 1st MPJ joint space d. Flattening of the 1st metatarsal head e. Arthritic changes of the 1st MPJf. Subchondral sclerosis
5. Biomechanical considerations: One must determine if there is a functional component that is producing the deformity, as a functional limitus is a common finding in the patient with significant uncontrolled pronation producing hypermobility of the 1st ray. To determine this examine the patient in a relaxed vs. neutral calcaneal stance position. A functional limitus only occurs in the relaxed position.
6. Conservative treatment: a. Orthosesb. Metatarsal barc. Rocker-bottom shoes
7. Surgical treatment- Joint preservation techniques:a. Soft tissue release: Should be followed by immediate ROM excercisesi. Release of fibrosis on the dorsal aspect of the jointii. Release of the dorsal capsuleiii. Release of the medial capsule if previously overcorrectediv. Release of the plantar adhesions between the sesamoid apparatus and the plantar aspect of the metatarsal head
b. Cheilectomy: The osseous proliferation around the joint is excised i. Advantages: Easily performed Reduces the dorsal enlargement Allows for increase in ROM in many cases Creates minimal postoperative disability Allows for immediate postop propulsive phase ambulation ii. Disadvantages: Potential for capsulodesis Does not correct the underlying etiology

c. Kessel-Bonney osteotomy:i. Advantages: Allows the hallux to be in a dorsal position at the propulsive phase of gait Allows for immediate postoperative ambulationii. Disadvantages: Requires an osteotomy with no fixation Does not actually increase the overall ROM Often creates a lack of hallux purchase Does not correct the underlying etiology Requires the elimination of the propulsive phase of gait for 3-6 weeks
postop
d. Mitchell-type osteotomy: This produces shortening and plantarflexion of the metatarsal headi. Advantages: Allows for correction of an abnormally long metatarsal Allows for mild plantarflexion of the 1st metatarsal Increases overall 1st MTPJ motion by relaxing tension around the joint
produced by a long metatarsal Allows for mild correction of an abnormal IM angle Does not interfere with an open epiphysisii. Disadvantages:
Requires an osteotomy with fixation Allows only minimal plantarflexion of the head Requires non-weightbearing for 4-6 weeks postop
e. Watermann osteotomy:i. Advantages: Allows the hallux to become more dorsal without using any additional joint
motionii. Disadvantages: Does not correct the underlying etiology of the deformity Can create a lack of toe purchase, and requires the elimination of the
propulsive phase of gait for 3-6 weeks postop
f. Austin-Youngswick osteotomy: This procedure produces a shortening and plantarflexion of the headi. Advantages: Allows for correction of an abnormally long 1st metatarsal Allows for mild plantarflexion correction Relaxes tension around the joint via the shortening Allows for immediate postoperative ambulation Can be utilized to correct abnormal IM angle Does not interfere with an open epiphysisii. Disadvantages: Requires an osteotomy Allows only minimal plantarflexion Requires elimination of the propulsive phase of gait for 3-6 weeks postop
g. Plantarflexory wedge osteotomy (Van Ness): A wedge of bone is removed from the plantar aspect of the 1st metatarsal base i. Advantages: Allows for true correction of a structurally dorsiflexed 1st metatarsal Increases overall 1st MPJ ROMii. Disadvantages: Requires non-weightbearing with immobilization for 6 weeks postop Does not allow for easy repositioning of the 1st ray intraoperatively if too
much bone is resected
h. Juvara type C osteotomy:i. Advantages: Allows for true correction of a structurally dorsiflexed 1st metatarsal Increases overall 1st MTPJ ROM Does not require removal of a bony wedge Can be modified for reduction of an high IM angle Allows for easy intraoperative repositioning of the 1st metatarsal on the
sagittal planeii. Disadvantages: Requires non-weightbearing with immobilization for 6 weeks postop Requires the use of two cortical screws for fixation8. Surgical treatment- Joint destructive procedures:

a. Keller arthroplastyi. Advantages: Elimination of joint pain Allows for increase ROM Easily performed Allows for immediate propulsive-type gaitii. Disadvantages: Destroys the joint Creates instability of the 1st ray Does not correct the underlying etiology Creates lesser metatarsalgia
b. Arthroplasty with joint prosthesis:
c. Arthroplasty with joint prosthesis and proximal plantarflexory osteotomy
d. Arthrodesis:i. Advantages: Eliminates joint pain Creates significant internal stability of the 1st rayii. Disadvantages: Eliminates all motion of the 1st MTPJ Requires fixation for 6-8 weeks with immobilization Restricts the type of shoes which can be worn postoperatively depending
upon hallux position in the sagittal plane
Hallux Varus1. Etiology:a. Congenital and often accompanied by other congenital abnormalities b. Most commonly latrogenic following surgical treatment of HAV i. Excessive resection of the medial eminenceii. Excision of the fibular sesamoid and release of the adductor tendon iii. Overcorrection of the IM angleiv. Overtightening of the medial capsulev. Overcorrection of the PASA
2. Preoperative Symptoms of latrogenic Hallux Varus:a. Inability to wear conventional shoe gear comfortably b. Pain along the medial aspect of the halluxc. Pain along the medial side of the arch (ms. contracture) d. Pain may be present at the MPJ with or without shoes
3. Preoperative Signs of latrogenic Hallux Varus: a. Presence of an adducted positioned hallux b. Contracture of the hallux IPJ (sometimes)c. Contracture of the EHL (sometimes)
NOTE* Capsulitis of the 2nd MPJ may be the only initial complaint

d. Contracture of the abductor hallucis (sometimes)e. Pain and crepitation may be present at the 1st MTPJ f. Hallux limitus may be present at the 1st MTPJ
4. Preoperative Radiographic Signs:a. The hallux will be in an adducted position at the 1st MTPJ b. The IM angle will usually be reducedc. The head of the 1st metatarsal may be staked d. The fibular sesamoid may be absente. The evidence of a previous osteotomy on the 1st metatarsal may be seenf. A negative PASA may be presentg. Arthritic changes may be present at the 1st MTPJ h. Arthritic changes may be present at the hallux IPJ
5. Operative Considerations:a. The deformity should be corrected as soon as possible to prevent DJD of the jointb. There is no one surgical procedure. The causative factor(s) must be determined and corrected along with any secondary changes that had developed, by selecting the proper procedures (i.e. reverse Austin, reverse Akin, reverse hemi-angulated implant , soft tissue balancing, arthrodesis, and Keller/total implant arthroplasty)
Hallux Hammertoe (etiology)1. Cavus foot (extensor substitution) 2. Removal of the sesamoids3. Detachment of the flexor tendons 4. Overzealous HAV surgery 5. Plantar hallux IPJ sesamoid
Differential Diagnosis of Pain in the SesamoidArea1. Joplin's neuroma2. Sesamoiditis3. Osteochondritis of the sesamoids4. Ruptured bipartite sesamoid5. DJD with an eroded crista6. Hypertrophic sesamoid7. Fractured sesamoid8. Tumor of the sesamoid (a giant cell tumor has been reported)
Complications of HAV Surgery (General)1. Staking the metatarsal head and producing hallux varus 2. Hallux hammertoe3. Longitudinal fracture when removing the exostosis
NOTE* Most bipartite sesamoids are tibial, 75% are unilateral, and ossification of the sesamoids occurs at age 8-10 years

4. Sesamoiditis from invasion of the met-sesamoid articulation by tumor 5. Fracture of the articular cartilage of the MTPJ6. Unstable osteotomy7. Non or delayed union8. Damage to the neurovascular structures9. Elevatus and iatrogenic hallux rigidus10. Over or undercorrection11. Osteoporosis from disuse12. Infection13. Problems with the fixation devices14. Hallux limitus/rigidus15. Avascular necrosis

Chart of Procedures and Their IndicationsAbbreviations:
HI= Hallux InterphalangeusIM= Intermetatarsal Angle DASA= Distal Articular Set Angle MP= Metatarsal ProtrusionPASA= Proximal Articular Set Angle SES= Sesamoid Position HA= Hallux Abductus AngleD/PF= Motion of the 1st ray (dorsi/plantarflexion) JNT= Condition of the 1st m.p. joint TYPE= Type of ProcedureN= Normal I= Increased D= Decrease G= Good P= PositionalS=StructuralA= Arthritic
Related Documents











