.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

.

والجراحي لباطني ا التمريض والجراحي مدرس لباطني ا التمريض مدرس
الحرجة الحرجة والحالت والحالت
التمريض التمريض كلية طنطا – كلية طنطا – جامعة جامعة
HerniaHernia
العبدجيهانديونسحكيم

Definition:
hernia is the protrusion of an organ,
tissue or the part of an organ
through the wall of the cavity that
normally contains it.
Hernia

Weakness of the abdominal muscles.
Increase intra abdominal pressure.
Weakness of containing membranes
or muscles is usually congenital, or
increases with age or due to any risk
factors.
Causes of hernia

Risk Factors
Stretching of muscles during pregnancy.Obese people.Chronic constipation and straining during a bowel movement or urination.Chronic hard coughing Improper heavy weight l i f t ing.

Tight clothing and incorrect posture.
Or because of scars from previous surgery.
Many conditions increase intra-abdominal
pressure, (ascites, COPD, benign prostatic
hypertrophy)
Also, if muscles are weakened due to poor
nutrition, smoking, and overexertion.

1-Hernia may be congenital or acquired:
congenital hernias: occur prenatal or in the
first year of life, and are caused by a
congenital defect.
Acquired hernias: develop later on in life.
2- Hernia may be complete or incomplete: for
example, the stomach may partially or
completely herniate into the chest.
Classification of hernia

3- Hernia may be internal or external:
external ones herniate to the outside
world, whereas internal hernias
protrude from their normal
compartment to another.

4. Hernia may be Reducible or Irreducible:
• Reducible hernia: is one which can be
pushed back into the abdomen by putting
manual pressure to it.
• Irreducible hernia: is one which cannot be
pushed back into the abdomen by applying
manual pressure.

Defect or weakness in the muscular wall may
be congenital, acquired weakness or caused
by trauma.
Increased the intraabdominal pressure as a
result of any risk factors that discussed
before.
As a results of weakness of the abdominal
wall and increased pressure, the abdominal
contents can protrude causing herniation
Pathophysiology of hernia:

When the contents of the hernial sac can be
replaced into the abdominal cavity by
manipulation, the hernia is said to be
reducible.
Irreducible and incarcerated hernia refers to
hernias that cannot be replaced by
manipulation.
When the pressure from the hernial ring cuts
off the blood supply to the herniated
segment of the bowel, it becomes
strangulated.

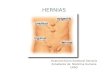
Hernias can be classified according to their
anatomical location into:
• Abdominal hernias and diaphragmatic hernias.
(1) Inguinal hernia:
• An inguinal hernia is a protrusion of abdominal
cavity contents through the inguinal canal.
Types of hernia:

• -There are two types of inguinal hernia, direct
and indirect.
1-Direct inguinal hernias:
- This hernia passes through the abdominal
Wall in an area of muscular weakness not
through a canal.
- It occur medial to the inferior epigastric
vessels when abdominal contents herniate
through a weak spot in the part of the
posterior wall of the inguinal canal.

2-Indirect inguinal hernias: occur when
abdominal contents protrude through the
deep inguinal ring, lateral to the inferior
epigastric vessels.
• In female, the opening of the superficial
inguinal ring is smaller than that of the male.
As a result, the possibility for hernias
through the inguinal canal in males is
common because they have a larger opening
and a much weaker wall for the intestines to
protrude through it.
•

(2) Femoral hernia:• Femoral hernias occur just below the
inguinal ligament, when abdominal contents
pass into the weak area at the posterior wall
of the femoral canal.
• They can be hard to distinguish from the
inguinal type. Femoral hernias are most
common in women, especially those who are
pregnant or obese.

(3) Umbilical hernia:• It is protrusion of intra abdominal contents
through a weakness at the site of passage of the umbilical cord through the abdominal wall.
• These hernias often resolve spontaneously.
• Umbilical hernias in adults are acquired, and are more frequent in obese or pregnant women. There are three types of umbilical hernia:

1- Para umbilical hernia: a type of
umbilical hernia occurring in adults. It
develop around the area of the
umbilicus.
2- Congenital umbilical hernia
3- Acquired umbilical hernia

(4) Incisional hernia:
• In an incisional hernia, the intestine
pushes through the abdominal wall at
the site of previous abdominal surgery.
• This type is most common in elderly or
overweight people who are inactive
after abdominal surgery.
•

(5) Hiatus hernia:
Diaphragmatic hernia results when part
of the stomach or intestine protrudes
into the chest cavity through a defect in
the diaphragm.
Hiatus hernias may be sliding or rolling

• Sliding hernia: in which the gastroesophageal
junction and upper part of the stomach slides through the defect into the chest.
• Non-sliding : the junction remains fixed while another portion of the stomach moves up through the defect.
• Non-sliding hernias can be dangerous as they may allow the stomach to rotate and obstruct.
• Repair is usually advised.

• Patient with Sliding hernia have
manifestations of reflux and
complications of hemorrhage,
obstruction and strangulation can occur.
• Patient with rolling hernia does not have
manifestations of reflux as the
gastrointestinal sphincter is intact.

• Pathophysiology of haital hernia:
• The diaphragm is a large dome-shaped muscle that separates the chest cavity from the abdomen.
• Normally, the esophagus passes into the stomach through an opening in the diaphragm called the
hiatus.
• Hiatus hernias occur when the muscle tissue
surrounding this opening becomes weak, and the upper part of the stomach bulges up through the
diaphragm into the chest cavity.
• Also, pressure on the stomach may contribute to the
formation of hiatus hernia.

(6) Epigastric hernia:
It is a protrusion of the epigastric
contents through the abdominal wall.
The protrusion occurs between the
linea Alba and the lower part of the rib
cage in the midline of the abdomen.

1) Bulging and painless swelling at first.
2) Pain: Pain may be:
• Localized Pain: Pain may occur as a result of
irritation of or damage to area or nerves as a result
of the hernia and its contents pushing into or pinching the nerves.
• Generalized Pain: If the contents of the hernia
become trapped or incarcerated, the intestine's
blood supply may become compromised or shut off.
Clinical manifestation of hernia:

• Referred Pain:
• If the hernia irritates, inflames, the pain
felt from the hernia may not be at the site
of the hernia, but rather at the area to
which these nerves are traveling.
• For example, pain from an Inguinal Hernia
may be felt as discomfort in the back,
upper leg and /or hip area.

3) Nausea and vomiting:
• When intestine becomes trapped within
the hernia, the normal flow of food
through the intestine becomes blocked.
This creates a progressive back-up
within the intestine and may result in
nausea and vomiting.

4) Constipation:
• If the intestine is blocked within the hernia,
and normal flow of food contents and feces
is blocked, the patient may develop
constipation.
5) Urinary Symptoms:
• If the bladder becomes irritated within a
hernia (usually an Inguinal Hernia). Urinary
symptoms such as frequency, urinary
burning, frequent infections, and bladder
stones may all occur

Heartburn: occur 30 to 60 minutes after
meals
Difficulty in swallowing
Fatigue
Felling of fullness after eating
Difficulty of breathing
Chest pain
Clinical manifestation specific to hiatus hernia

1) Medical treatment:
• Hernias that are not strangulated can be
mechanically reduced.
• Truss (firm pad) held by a belt to keep the
hernia in place or reduced.
• The patient is taught to apply the truss daily.
• Instruct the patient to inspect the skin under
the truss for any manifestation of skin
breakdown.
Treatment

• If patient has preexisting medical conditions that
make surgery unsafe, doctor may not repair hernia
but will watch it closely.
• Some hernias have very large openings in the
abdominal wall, and closing the opening is
complicated because of their large size. These kinds
of hernias may be treated without surgery, using
abdominal binders.
• Some doctors feel that the hernias with large
openings have a low risk of strangulation.
• An attempt to (push back) the hernia will generally
be made, often after giving medicine for pain and
muscle relaxation

2) Surgical treatment:
1) A hernia repair is performed using a
small incision directly over the
weakened area. The intestine is then
returned to the perineal cavity, the
hernial sac excised and the muscle
closed tightly over the area.
2) Hernias in the inguinal region are
usually repaired under spinal or local
anesthesia.

3) Some repair is difficult because there is
insufficient muscle to keep the intestines in
place. So steel mesh grafts are used to
reinforce the area of herniation
4) Clients with difficult repairs are usually
hospitalized for 1 to 2 days to receive
prophylactic antibiotics.
5) If the intestinal contents of the hernia had
the blood supply cut off, the development of
dead (gangrenous) bowel is possible in as
little as six hours.

• The nurse encourages the patient to void
immediately after surgery, because urinary
retention is a common problem.
• Give prescribed medication as ordered.
• The patient should be returned to general
diet as soon as he tolerates food.
• Encourage post operative ambulation as
soon as possible to prevent complications of
immobility.
• Instruct the patient to avoid any risk factors
that facilitate hernial recurrence.
Post operative care

Management of haital hernia:
• Provide small frequent diets that can
pass easily through the esophagus.
• Advise the patient not to sleep for 1
hour after eating to prevent reflux.

• Paraesophageal hernia (Rolling haital hernia) may
require emergency surgery to correct twisting of the
stomach.
Postoperative Outcome:• Patients undergoing elective surgical repair may be
able to go home the same day. However, emergency
repair carries a greater morbidity and mortality rate
and this is directly proportional to the degree of
bowel compromise. Other co-existing medical
conditions also influence outcome.

Complication of hernia:
1. Strangulation: pressure and compromise
blood supply causing venous congestion
ischemia, and later necrosis and gangrene
may occur.
2. Obstruction: for example, when a part of the
bowel herniates, bowel contents can no
longer pass the obstruction. This results in
cramps, vomiting, ileus, and absence of
defecation.
3. Dysfunction: the herniated organ itself, or
surrounding organs, start to malfunction
Related Documents