Hepatitis C: an epidemiological review M. I. Memon 1 and M. A. Memon 2 1 Department of Community Health, Guild NHS Trust, Honorary Lecturer Lancashire Post Graduate Medical School, Preston and Professor of Ethnicity and Community Health, Bolton Institute, Bolton, and 2 Department of Surgery, Queen’s Medical Centre, Nottingham, UK Received March 2001; accepted for publication July 2001 EPIDEMIOLOGY OF HEPATITIS C VIRUS Hepatitis C virus (HCV), a positive strand RNA virus which is related to flavi and pestiviruses family, was first identified in the USA in 1989 as a major causative agent of post trans- fusion non-A, non-B hepatitis [1]. According to WHO esti- mates, approximately 3% of the world population, or about 170 million people, may be infected with hepatitis C virus [2,3]. In the USA, antibodies to HCV are encountered in between 0.1% to 1.8% of the general population (Table 1). In healthy volunteer blood donors the incidence of HCV in the USA varies between 0.17% to 1.4% and in the UK is 0.35% (Table 2). However in other parts of the world the incidence HCV infection both in the general population and blood donors may be much higher (Tables 1 and 2). Although the annual incidence of newly acquired HCV has declined substantially in the USA, from 180 000 to 30 000 in the past decade, there still remains a large reservoir of chronically infected Americans (estimated to be 3.9 million) who can serve as a source of transmission to others and who are at risk of severe consequences of chronic liver disease [4]. HCV infections leads to acute hepatitis in 20% of cases and chronic hepatitis in 50% of cases, 20% of who develop cir- rhosis [5,6]. There is also a strong relationship between HCV and hepatocellular carcinoma [7,8]. HCV is transmitted primarily by exposure to infected blood. However, in up to 50% of cases no recognizable transmission factor/route could be identified [9]. Therefore, a number of other routes of transmission such as sexual or household exposure to an infected contact are postulated but not widely accepted. This is because conflicting data has emerged regarding the presence of HCV in body fluids other than blood. Some authors have found total absence of the virus in sperm, saliva, vaginal secretions and other body fluids [9]. However, others have documented the presence of HCV-specific antigens in semen of infected individuals [10,11]. Risk factors for HCV infection include intravenous drug abuse, haemodialysis, transfusion of blood products, tattooing, high sexual behaviour, exposure to healthcare and organ transplants from HCV-positive donors and use of blood contaminated straws for cocaine snorting [12,13]. As far back as 1981, two separate American studies showed that there was increased risk of acquiring post-transfusion non-A, non-B infection (PTH-NANB) following blood trans- fusion if the donors have elevated ALT levels compared with normal ALT levels [14–16]. Furthermore the exclusion of blood donors with antibodies to the hepatitis B core antigen was found to prevent another 20–30% of the PTH-NANB, Abbreviations: HCC, hepatocellular carcinoma; HCV, hepatitis C virus; PTH-NANB, post-transfusion non-A, non-B infection. Correspondence: Professor M. I. Memon, Oakwood, Whitehall Road, Darwen, Lancashire BB3 2LH, UK. E-mail: [email protected] Journal of Viral Hepatitis, 2002, 9, 84–100 Ó 2002 Blackwell Science Ltd SUMMARY. The aim of the study was to analyse the current literature regarding the mode of transmission of HCV and its global prevalence in different groups of people. A systematic review of the literature on the epidemiology of hepatitis C from 1991 to 2000 using computerized bibliographic data- bases which include Medline, Current Content and Embase. The prevalence of hepatitis C virus (HCV) varies tremen- dously in different parts of the world, with the highest inci- dence in the Eastern parts of the globe compared with the Western parts. Furthermore, certain groups of individuals such as intravenous drug users are at increased risk of ac- quiring this disease irrespective of the geographical location. Although the main route of transmission is via contamin- ated blood, curiously enough in up to 50% of the cases no recognizable transmission factor/route could be identified. Therefore, a number of other routes of transmission such as sexual or household exposure to infected contacts have been investigated with conflicting results. Hepatitis C in- fection is an important public health issue globally. Better understanding of routes of transmission will help to combat the spread of disease. In order to prevent a world wide epidemic of this disease, urgent measures are required to (i) develop a strategy to inform and educate the public re- garding this disease and (ii) expedite the efforts to develop a vaccine. Keywords: epidemiology, etiology, hepatitis C, prevention and control, risk factors, statistics and numerical data.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Hepatitis C: an epidemiological reviewM. I. Memon1 and M. A. Memon2 1Department of Community Health, Guild NHS Trust, Honorary Lecturer Lancashire Post
Graduate Medical School, Preston and Professor of Ethnicity and Community Health, Bolton Institute, Bolton, and 2Department of Surgery, Queen's
Medical Centre, Nottingham, UK
Received March 2001; accepted for publication July 2001
EPIDEMIOLOGY OF HEPATITIS C VIRUS
Hepatitis C virus (HCV), a positive strand RNA virus which is
related to ¯avi and pestiviruses family, was ®rst identi®ed in
the USA in 1989 as a major causative agent of post trans-
fusion non-A, non-B hepatitis [1]. According to WHO esti-
mates, approximately 3% of the world population, or about
170 million people, may be infected with hepatitis C virus
[2,3]. In the USA, antibodies to HCV are encountered in
between 0.1% to 1.8% of the general population (Table 1).
In healthy volunteer blood donors the incidence of HCV in
the USA varies between 0.17% to 1.4% and in the UK is
0.35% (Table 2). However in other parts of the world the
incidence HCV infection both in the general population and
blood donors may be much higher (Tables 1 and 2).
Although the annual incidence of newly acquired HCV has
declined substantially in the USA, from 180 000 to 30 000
in the past decade, there still remains a large reservoir of
chronically infected Americans (estimated to be 3.9 million)
who can serve as a source of transmission to others and who
are at risk of severe consequences of chronic liver disease [4].
HCV infections leads to acute hepatitis in 20% of cases and
chronic hepatitis in 50% of cases, 20% of who develop cir-
rhosis [5,6]. There is also a strong relationship between HCV
and hepatocellular carcinoma [7,8].
HCV is transmitted primarily by exposure to infected
blood. However, in up to 50% of cases no recognizable
transmission factor/route could be identi®ed [9]. Therefore, a
number of other routes of transmission such as sexual or
household exposure to an infected contact are postulated but
not widely accepted. This is because con¯icting data has
emerged regarding the presence of HCV in body ¯uids other
than blood. Some authors have found total absence of the
virus in sperm, saliva, vaginal secretions and other body
¯uids [9]. However, others have documented the presence of
HCV-speci®c antigens in semen of infected individuals
[10,11]. Risk factors for HCV infection include intravenous
drug abuse, haemodialysis, transfusion of blood products,
tattooing, high sexual behaviour, exposure to healthcare
and organ transplants from HCV-positive donors and use of
blood contaminated straws for cocaine snorting [12,13].
As far back as 1981, two separate American studies showed
that there was increased risk of acquiring post-transfusion
non-A, non-B infection (PTH-NANB) following blood trans-
fusion if the donors have elevated ALT levels compared with
normal ALT levels [14±16]. Furthermore the exclusion of
blood donors with antibodies to the hepatitis B core antigen
was found to prevent another 20±30% of the PTH-NANB,
Abbreviations: HCC, hepatocellular carcinoma; HCV, hepatitis C
virus; PTH-NANB, post-transfusion non-A, non-B infection.
Correspondence: Professor M. I. Memon, Oakwood, Whitehall
Road, Darwen, Lancashire BB3 2LH, UK.
E-mail: [email protected]
Journal of Viral Hepatitis, 2002, 9, 84±100
Ó 2002 Blackwell Science Ltd
SUMMARY. The aim of the study was to analyse the current
literature regarding the mode of transmission of HCV and its
global prevalence in different groups of people. A systematic
review of the literature on the epidemiology of hepatitis C
from 1991 to 2000 using computerized bibliographic data-
bases which include Medline, Current Content and Embase.
The prevalence of hepatitis C virus (HCV) varies tremen-
dously in different parts of the world, with the highest inci-
dence in the Eastern parts of the globe compared with the
Western parts. Furthermore, certain groups of individuals
such as intravenous drug users are at increased risk of ac-
quiring this disease irrespective of the geographical location.
Although the main route of transmission is via contamin-
ated blood, curiously enough in up to 50% of the cases no
recognizable transmission factor/route could be identi®ed.
Therefore, a number of other routes of transmission such as
sexual or household exposure to infected contacts have
been investigated with con¯icting results. Hepatitis C in-
fection is an important public health issue globally. Better
understanding of routes of transmission will help to combat
the spread of disease. In order to prevent a world wide
epidemic of this disease, urgent measures are required to (i)
develop a strategy to inform and educate the public re-
garding this disease and (ii) expedite the efforts to develop a
vaccine.
Keywords: epidemiology, etiology, hepatitis C, prevention
and control, risk factors, statistics and numerical data.
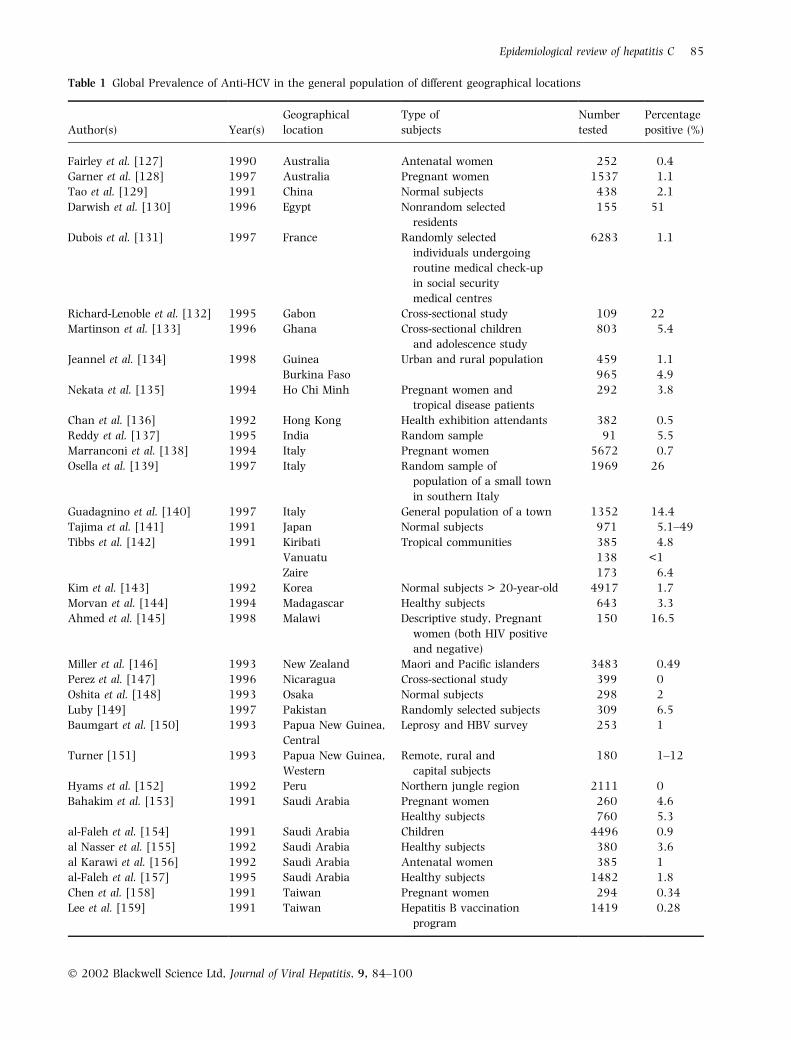
Table 1 Global Prevalence of Anti-HCV in the general population of different geographical locations
Author(s) Year(s)
Geographical
location
Type of
subjects
Number
tested
Percentage
positive (%)
Fairley et al. [127] 1990 Australia Antenatal women 252 0.4
Garner et al. [128] 1997 Australia Pregnant women 1537 1.1
Tao et al. [129] 1991 China Normal subjects 438 2.1
Darwish et al. [130] 1996 Egypt Nonrandom selected
residents
155 51
Dubois et al. [131] 1997 France Randomly selected
individuals undergoing
routine medical check-up
in social security
medical centres
6283 1.1
Richard-Lenoble et al. [132] 1995 Gabon Cross-sectional study 109 22
Martinson et al. [133] 1996 Ghana Cross-sectional children
and adolescence study
803 5.4
Jeannel et al. [134] 1998 Guinea Urban and rural population 459 1.1
Burkina Faso 965 4.9
Nekata et al. [135] 1994 Ho Chi Minh Pregnant women and
tropical disease patients
292 3.8
Chan et al. [136] 1992 Hong Kong Health exhibition attendants 382 0.5
Reddy et al. [137] 1995 India Random sample 91 5.5
Marranconi et al. [138] 1994 Italy Pregnant women 5672 0.7
Osella et al. [139] 1997 Italy Random sample of
population of a small town
in southern Italy
1969 26
Guadagnino et al. [140] 1997 Italy General population of a town 1352 14.4
Tajima et al. [141] 1991 Japan Normal subjects 971 5.1±49
Tibbs et al. [142] 1991 Kiribati Tropical communities 385 4.8
Vanuatu 138 <1
Zaire 173 6.4
Kim et al. [143] 1992 Korea Normal subjects > 20-year-old 4917 1.7
Morvan et al. [144] 1994 Madagascar Healthy subjects 643 3.3
Ahmed et al. [145] 1998 Malawi Descriptive study, Pregnant
women (both HIV positive
and negative)
150 16.5
Miller et al. [146] 1993 New Zealand Maori and Paci®c islanders 3483 0.49
Perez et al. [147] 1996 Nicaragua Cross-sectional study 399 0
Oshita et al. [148] 1993 Osaka Normal subjects 298 2
Luby [149] 1997 Pakistan Randomly selected subjects 309 6.5
Baumgart et al. [150] 1993 Papua New Guinea,
Central
Leprosy and HBV survey 253 1
Turner [151] 1993 Papua New Guinea,
Western
Remote, rural and
capital subjects
180 1±12
Hyams et al. [152] 1992 Peru Northern jungle region 2111 0
Bahakim et al. [153] 1991 Saudi Arabia Pregnant women 260 4.6
Healthy subjects 760 5.3
al-Faleh et al. [154] 1991 Saudi Arabia Children 4496 0.9
al Nasser et al. [155] 1992 Saudi Arabia Healthy subjects 380 3.6
al Karawi et al. [156] 1992 Saudi Arabia Antenatal women 385 1
al-Faleh et al. [157] 1995 Saudi Arabia Healthy subjects 1482 1.8
Chen et al. [158] 1991 Taiwan Pregnant women 294 0.34
Lee et al. [159] 1991 Taiwan Hepatitis B vaccination
program
1419 0.28
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
Epidemiological review of hepatitis C 85
though this was not con®rmed by other European studies
[16±18]. The screening of donors for ALT and anti-HBc for
prevention of PTH-NANB was termed surrogate testing.
Before 1986, the incidence of post-transfusion HCV ran-
ged from 5% to 13% which declined to between 1.5% to 9%
from 1986 to 1990 [19±25]. Since 1990, when anti-HCV
screening of blood donors became mandatory, the incidence
of post-transfusion HCV declined to < 1% but not completely
eliminated. This is because the ®rst generation ELISA may
not become positive for months after infection with HCV
[26]. Furthermore, seronegative HCV carriers were respon-
sible for 10±15% of HCV transmission [26]. The new gen-
eration of various tests will further reduce the risk of
transfusion-transmitted HCV as they are able to detect a
number of additional antigens and are more sensitive.
It has been suggested that HCV can down-regulate the
pace of replication in order to escape viral clearance by the
host immune system, yet can still exist in a quiescent or low
replicative state within hepatocytes which in part is
responsible for the high degree of viral persistence in HCV
infection [26]. HCV displays a high mutation rate like many
RNA viruses which (i) provides protection against immu-
nological detection and destruction which leads to its per-
sistence, ¯are up and transmission of disease; (ii) can lead to
unreliability of antibody tests; (iii) higher reinfection rate due
to incomplete immunity; (iv) variable clinical expression;
(v) variable and unpredictable response to treatment; and,
lastly, (vi) dif®culty in development of a reliable vaccine
[27±29].
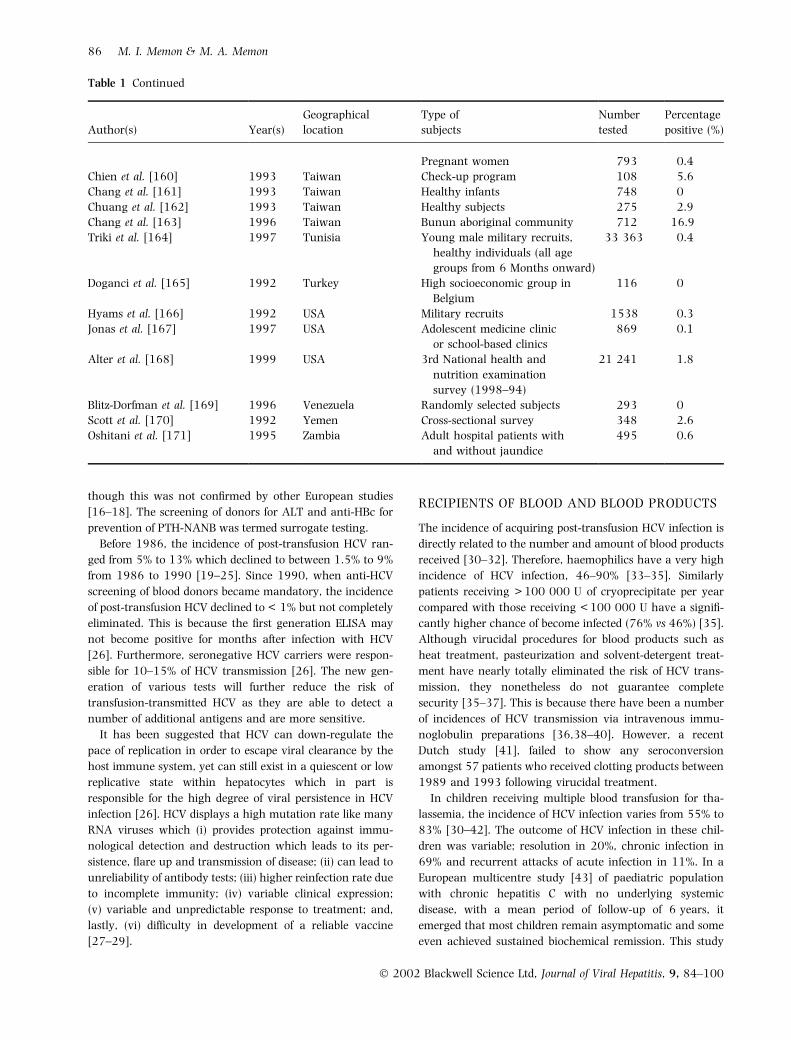
RECIPIENTS OF BLOOD AND BLOOD PRODUCTS
The incidence of acquiring post-transfusion HCV infection is
directly related to the number and amount of blood products
received [30±32]. Therefore, haemophilics have a very high
incidence of HCV infection, 46±90% [33±35]. Similarly
patients receiving > 100 000 U of cryoprecipitate per year
compared with those receiving < 100 000 U have a signi®-
cantly higher chance of become infected (76% vs 46%) [35].
Although virucidal procedures for blood products such as
heat treatment, pasteurization and solvent-detergent treat-
ment have nearly totally eliminated the risk of HCV trans-
mission, they nonetheless do not guarantee complete
security [35±37]. This is because there have been a number
of incidences of HCV transmission via intravenous immu-
noglobulin preparations [36,38±40]. However, a recent
Dutch study [41], failed to show any seroconversion
amongst 57 patients who received clotting products between
1989 and 1993 following virucidal treatment.
In children receiving multiple blood transfusion for tha-
lassemia, the incidence of HCV infection varies from 55% to
83% [30±42]. The outcome of HCV infection in these chil-
dren was variable; resolution in 20%, chronic infection in
69% and recurrent attacks of acute infection in 11%. In a
European multicentre study [43] of paediatric population
with chronic hepatitis C with no underlying systemic
disease, with a mean period of follow-up of 6 years, it
emerged that most children remain asymptomatic and some
even achieved sustained biochemical remission. This study
Table 1 Continued
Author(s) Year(s)
Geographical
location
Type of
subjects
Number
tested
Percentage
positive (%)
Pregnant women 793 0.4
Chien et al. [160] 1993 Taiwan Check-up program 108 5.6
Chang et al. [161] 1993 Taiwan Healthy infants 748 0
Chuang et al. [162] 1993 Taiwan Healthy subjects 275 2.9
Chang et al. [163] 1996 Taiwan Bunun aboriginal community 712 16.9
Triki et al. [164] 1997 Tunisia Young male military recruits,
healthy individuals (all age
groups from 6 Months onward)
33 363 0.4
Doganci et al. [165] 1992 Turkey High socioeconomic group in
Belgium
116 0
Hyams et al. [166] 1992 USA Military recruits 1538 0.3
Jonas et al. [167] 1997 USA Adolescent medicine clinic
or school-based clinics
869 0.1
Alter et al. [168] 1999 USA 3rd National health and
nutrition examination
survey (1998±94)
21 241 1.8
Blitz-Dorfman et al. [169] 1996 Venezuela Randomly selected subjects 293 0
Scott et al. [170] 1992 Yemen Cross-sectional survey 348 2.6
Oshitani et al. [171] 1995 Zambia Adult hospital patients with
and without jaundice
495 0.6
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
86 M. I. Memon & M. A. Memon
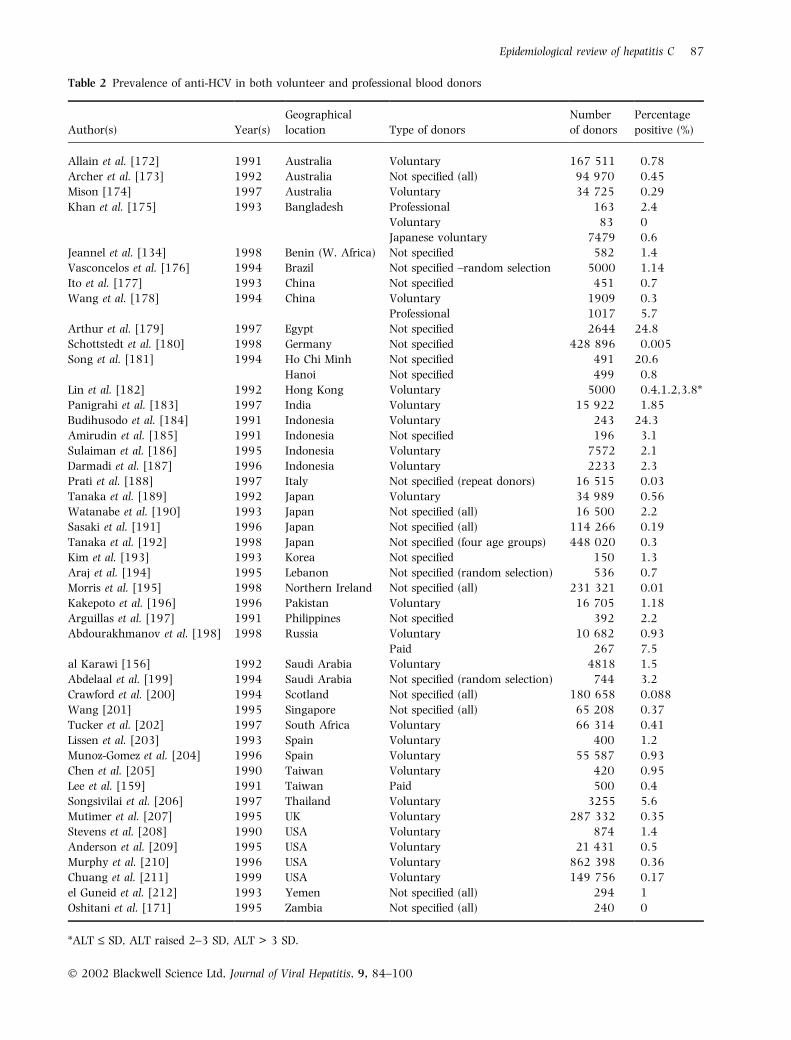
Table 2 Prevalence of anti-HCV in both volunteer and professional blood donors
Author(s) Year(s)
Geographical
location Type of donors
Number
of donors
Percentage
positive (%)
Allain et al. [172] 1991 Australia Voluntary 167 511 0.78
Archer et al. [173] 1992 Australia Not speci®ed (all) 94 970 0.45
Mison [174] 1997 Australia Voluntary 34 725 0.29
Khan et al. [175] 1993 Bangladesh Professional 163 2.4
Voluntary 83 0
Japanese voluntary 7479 0.6
Jeannel et al. [134] 1998 Benin (W. Africa) Not speci®ed 582 1.4
Vasconcelos et al. [176] 1994 Brazil Not speci®ed ±random selection 5000 1.14
Ito et al. [177] 1993 China Not speci®ed 451 0.7
Wang et al. [178] 1994 China Voluntary 1909 0.3
Professional 1017 5.7
Arthur et al. [179] 1997 Egypt Not speci®ed 2644 24.8
Schottstedt et al. [180] 1998 Germany Not speci®ed 428 896 0.005
Song et al. [181] 1994 Ho Chi Minh Not speci®ed 491 20.6
Hanoi Not speci®ed 499 0.8
Lin et al. [182] 1992 Hong Kong Voluntary 5000 0.4,1.2,3.8*
Panigrahi et al. [183] 1997 India Voluntary 15 922 1.85
Budihusodo et al. [184] 1991 Indonesia Voluntary 243 24.3
Amirudin et al. [185] 1991 Indonesia Not speci®ed 196 3.1
Sulaiman et al. [186] 1995 Indonesia Voluntary 7572 2.1
Darmadi et al. [187] 1996 Indonesia Voluntary 2233 2.3
Prati et al. [188] 1997 Italy Not speci®ed (repeat donors) 16 515 0.03
Tanaka et al. [189] 1992 Japan Voluntary 34 989 0.56
Watanabe et al. [190] 1993 Japan Not speci®ed (all) 16 500 2.2
Sasaki et al. [191] 1996 Japan Not speci®ed (all) 114 266 0.19
Tanaka et al. [192] 1998 Japan Not speci®ed (four age groups) 448 020 0.3
Kim et al. [193] 1993 Korea Not speci®ed 150 1.3
Araj et al. [194] 1995 Lebanon Not speci®ed (random selection) 536 0.7
Morris et al. [195] 1998 Northern Ireland Not speci®ed (all) 231 321 0.01
Kakepoto et al. [196] 1996 Pakistan Voluntary 16 705 1.18
Arguillas et al. [197] 1991 Philippines Not speci®ed 392 2.2
Abdourakhmanov et al. [198] 1998 Russia Voluntary 10 682 0.93
Paid 267 7.5
al Karawi [156] 1992 Saudi Arabia Voluntary 4818 1.5
Abdelaal et al. [199] 1994 Saudi Arabia Not speci®ed (random selection) 744 3.2
Crawford et al. [200] 1994 Scotland Not speci®ed (all) 180 658 0.088
Wang [201] 1995 Singapore Not speci®ed (all) 65 208 0.37
Tucker et al. [202] 1997 South Africa Voluntary 66 314 0.41
Lissen et al. [203] 1993 Spain Voluntary 400 1.2
Munoz-Gomez et al. [204] 1996 Spain Voluntary 55 587 0.93
Chen et al. [205] 1990 Taiwan Voluntary 420 0.95
Lee et al. [159] 1991 Taiwan Paid 500 0.4
Songsivilai et al. [206] 1997 Thailand Voluntary 3255 5.6
Mutimer et al. [207] 1995 UK Voluntary 287 332 0.35
Stevens et al. [208] 1990 USA Voluntary 874 1.4
Anderson et al. [209] 1995 USA Voluntary 21 431 0.5
Murphy et al. [210] 1996 USA Voluntary 862 398 0.36
Chuang et al. [211] 1999 USA Voluntary 149 756 0.17
el Guneid et al. [212] 1993 Yemen Not speci®ed (all) 294 1
Oshitani et al. [171] 1995 Zambia Not speci®ed (all) 240 0
*ALT £ SD, ALT raised 2±3 SD, ALT > 3 SD.
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
Epidemiological review of hepatitis C 87

concluded on the basis of repeated liver biopsies, that severe
hepatitis and cirrhosis are infrequently encountered with
chronic hepatitis C infection in children and adolescence.
The risk of developing hepatic decompensation in HCV
patients in the presence of coinfection with HIV is 21 times
higher compared with those who are HIV negative [44,45].
OTHER IATROGENIC ROUTESOF TRANSMISSION
There is increased prevalence of HCV infections amongst
certain groups of patients which include: (i) long-term can-
cer survivors (20%); (ii) bone marrow transplant recipients
(29%); (iii) renal dialysis patients (15±20%); (iv) renal
transplant patients ± which is directly related to the fre-
quency and duration of haemodialysis received prior to their
transplant [29,32,46±54]. However, the prevalence of HCV
infection differs greatly between different countries and even
between different dialysis centres in the same country, the
highest has been reported from Brazil (82%) and the lowest
from Europe (4%) [55]. There is a direct correlation with the
duration of dialysis and number of blood transfusions
received and the incidence of acquiring HCV infection [55].
Other possible mechanisms of transmission include sharing
dialysis machines between HCV positive and negative
patients [56,57] and nosocomial transmission by the dialysis
staff [58±61]. It is clear from various studies that rigorously
applied universal infection precautions during dialysis by the
staff signi®cantly decrease the nosocomial transmission of
HCV infections [55,59,60,62,63]. The nosocomial trans-
mission has also been documented from a cardiac surgeon
(to ®ve patients), via anaesthetic tubing, and via syringes for
intravenous catheter ¯ushing [64±66].
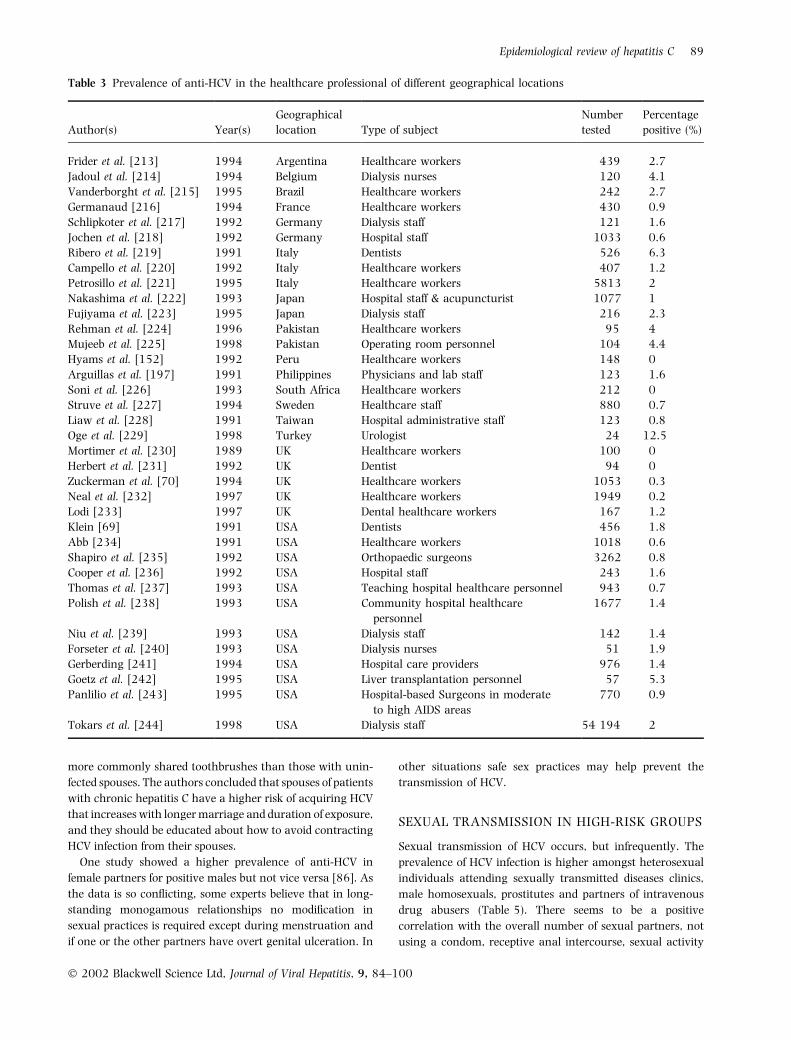
RISK TO HEALTHCARE PROFESSIONALS
Healthcare professionals dealing with blood and blood
products are at a greater risk of contracting HCV via need
stick injury. The risk of acquiring HCV infection following a
single needle stick injury with contaminated blood is low as
determined by anti-HCV seroconversion using second gen-
eration assay and PCR [67±69]. High risk groups include
surgeons, obstetricians, haemodialysis nurses/technicians,
oral surgeons, emergency department workers and intensive
care workers (Table 3). The risk factors include: (i) type of
needle, i.e. hollow vs solid; (ii) the frequency of occupational
blood contacts; (iii) the type of patients, i.e. acute infection vs
chronic carriers; and (iv) prevalence of HCV amongst
patients. Three European studies [70±72] failed to show any
HCV seroconversion in healthcare workers following anti-
HCV positive needle prick injuries following at least
10 months of follow-up. In contrast, two Japanese pros-
pective studies revealed a seroconversion rate of between
3.3% and 5.6% amongst 90 and 56 healthcare workers,
respectively, following needle-stick injury [73,74]. Use of
blunt needles, use of double gloving in high-risk patients, use
of protective goggles and passing of sharp instruments via a
tray rather than directly are important precautionary
measures in minimizing iatrogenic transmission of HCV. It is
clear from the various studies that the risk of occupational
risk of HCV transmission does exist and preventive measures
as outlined above are currently the mainstay of healthcare
workers against HCV infection.
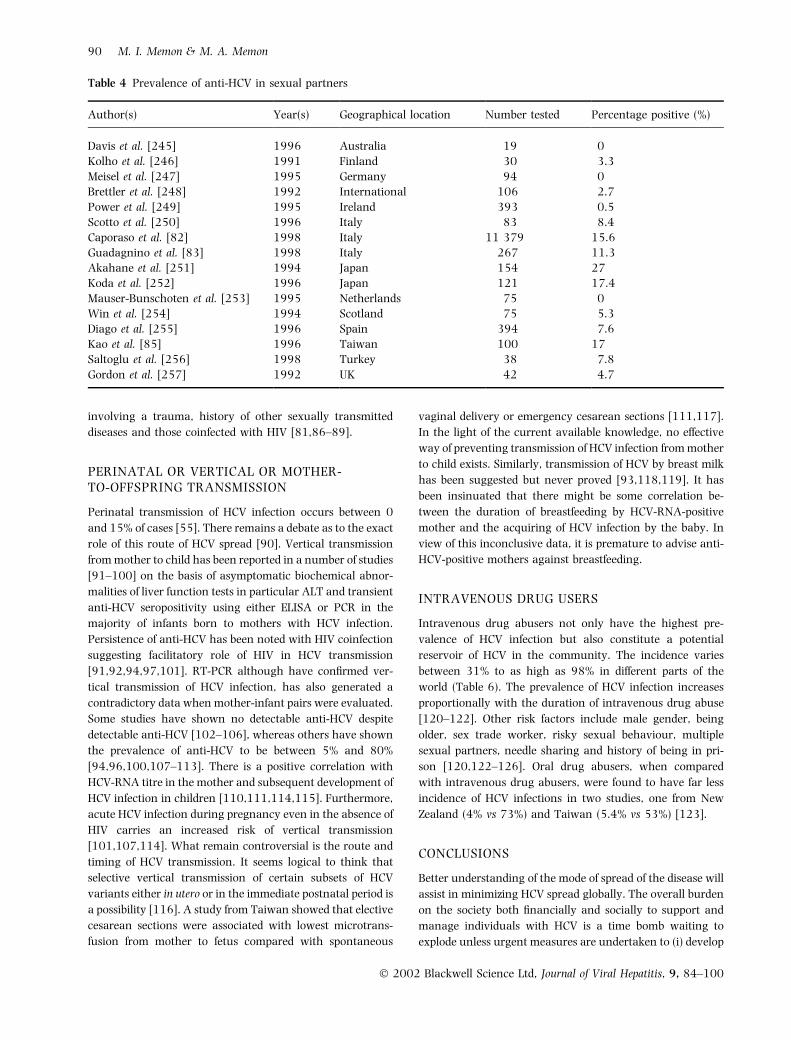
INTRAFAMILIAL TRANSMISSION
There is some evidence that intrafamilial spread of HCV also
occur as seropositivity for anti-HCV is 5±10-fold in individ-
uals living with an HCV-positive patient compared with
general population (Table 4). A number of studies [75±80]
totalling 335 patients, found the prevalence of HCV infection
in household (nonsexual) contacts to be between 0% to 11%
(average 3.6%). Children are less effected than spouses. The
nonsexual household transmission of HCV is speculative and
include sharing of toothbrushes, dental appliances, razors
and nail-grooming equipment.
The low rates of transmission may be due to low serum
titre of virus in HCV carriers during HCV infection [81].
However, no conclusive data exists as to the threshold
concentration of HCV required to transmit infection [29].
The prevalence of anti-HCV among the sexual and
household contacts of chronic hepatitis C patients ranges
between 0% to 27% (Table 4). Caporaso et al. [82] published
one of the largest studies evaluating the intrafamilial spread
of HCV among 1370 household contacts of 585 HCV pos-
itive subjects (index cases). By using third generation ELISA
and PCR techniques they found the incidence of anti-HCV to
be 7.3% (15.6% spouses, 3.2% in other relatives). After
adjusting for various confounders, the study failed to show
any correlation between spouses vs other relatives and
length of marriage and acquiring HCV infection. The
authors concluded that sexual transmission does not seem to
play a role in the intrafamilial spread of HCV infection. In
contrast to this study Guadagnino et al. [83] showed that
spouses who had been married to the index cases longer
than 20 years had a 7.5-fold risk of HCV seropositivity as
compared with those married less than 20 years. They
concluded that sexual contact plays an independent role in
the spread of HCV infection in the family setting.
A study from Japan [84] found spouses with anti-HCV-
positive partners to be twice as likely to have anti-HCV than
spouses with anti-HCV-negative partners. However, 50% of
the couples presented discordant HCV genotypes. The authors
concluded that the clustering of HCV infection among speci®c
couples within this endemic population may not be attribut-
able to heterosexual transmission. In contrast a study from
Taiwan [85] showed direct correlation with the duration of
marriage (> 20 years vs < 20 years) and duration of actual
exposure to the index patients but not with serum HCV titres.
The infected couples had more frequent sexual contacts and
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
88 M. I. Memon & M. A. Memon
more commonly shared toothbrushes than those with unin-
fected spouses. The authors concluded that spouses of patients
with chronic hepatitis C have a higher risk of acquiring HCV
that increases with longer marriage and duration of exposure,
and they should be educated about how to avoid contracting
HCV infection from their spouses.
One study showed a higher prevalence of anti-HCV in
female partners for positive males but not vice versa [86]. As
the data is so con¯icting, some experts believe that in long-
standing monogamous relationships no modi®cation in
sexual practices is required except during menstruation and
if one or the other partners have overt genital ulceration. In
other situations safe sex practices may help prevent the
transmission of HCV.
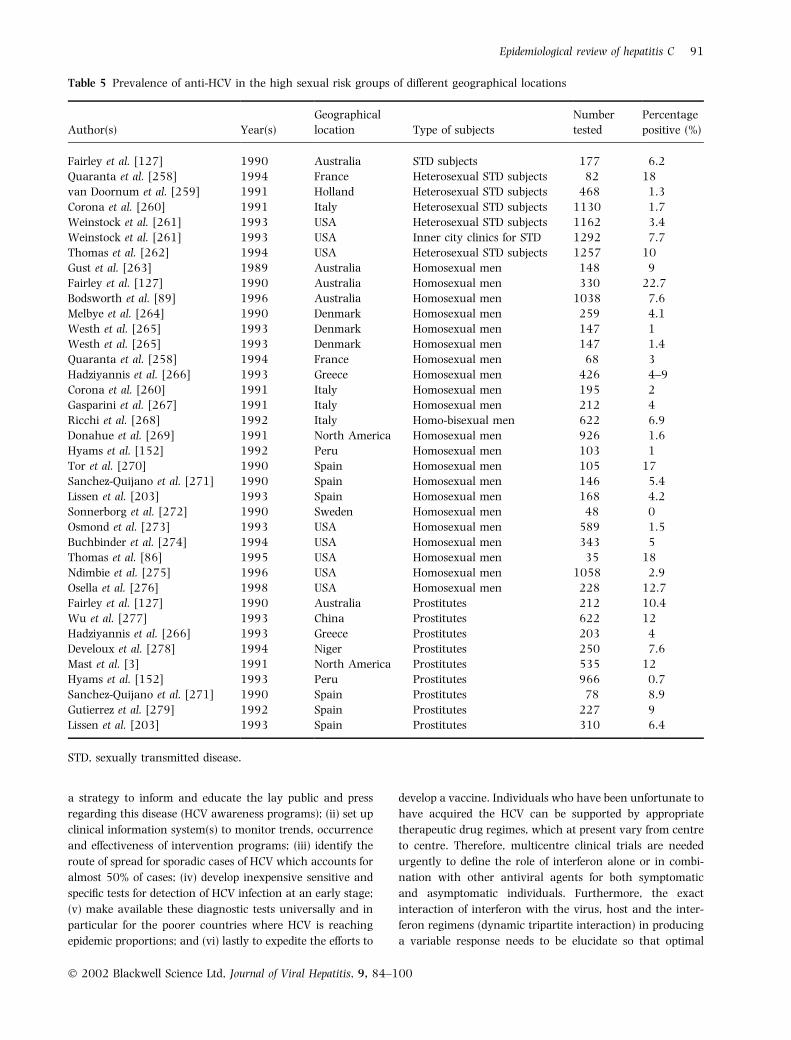
SEXUAL TRANSMISSION IN HIGH-RISK GROUPS
Sexual transmission of HCV occurs, but infrequently. The
prevalence of HCV infection is higher amongst heterosexual
individuals attending sexually transmitted diseases clinics,
male homosexuals, prostitutes and partners of intravenous
drug abusers (Table 5). There seems to be a positive
correlation with the overall number of sexual partners, not
using a condom, receptive anal intercourse, sexual activity
Table 3 Prevalence of anti-HCV in the healthcare professional of different geographical locations
Author(s) Year(s)
Geographical
location Type of subject
Number
tested
Percentage
positive (%)
Frider et al. [213] 1994 Argentina Healthcare workers 439 2.7
Jadoul et al. [214] 1994 Belgium Dialysis nurses 120 4.1
Vanderborght et al. [215] 1995 Brazil Healthcare workers 242 2.7
Germanaud [216] 1994 France Healthcare workers 430 0.9
Schlipkoter et al. [217] 1992 Germany Dialysis staff 121 1.6
Jochen et al. [218] 1992 Germany Hospital staff 1033 0.6
Ribero et al. [219] 1991 Italy Dentists 526 6.3
Campello et al. [220] 1992 Italy Healthcare workers 407 1.2
Petrosillo et al. [221] 1995 Italy Healthcare workers 5813 2
Nakashima et al. [222] 1993 Japan Hospital staff & acupuncturist 1077 1
Fujiyama et al. [223] 1995 Japan Dialysis staff 216 2.3
Rehman et al. [224] 1996 Pakistan Healthcare workers 95 4
Mujeeb et al. [225] 1998 Pakistan Operating room personnel 104 4.4
Hyams et al. [152] 1992 Peru Healthcare workers 148 0
Arguillas et al. [197] 1991 Philippines Physicians and lab staff 123 1.6
Soni et al. [226] 1993 South Africa Healthcare workers 212 0
Struve et al. [227] 1994 Sweden Healthcare staff 880 0.7
Liaw et al. [228] 1991 Taiwan Hospital administrative staff 123 0.8
Oge et al. [229] 1998 Turkey Urologist 24 12.5
Mortimer et al. [230] 1989 UK Healthcare workers 100 0
Herbert et al. [231] 1992 UK Dentist 94 0
Zuckerman et al. [70] 1994 UK Healthcare workers 1053 0.3
Neal et al. [232] 1997 UK Healthcare workers 1949 0.2
Lodi [233] 1997 UK Dental healthcare workers 167 1.2
Klein [69] 1991 USA Dentists 456 1.8
Abb [234] 1991 USA Healthcare workers 1018 0.6
Shapiro et al. [235] 1992 USA Orthopaedic surgeons 3262 0.8
Cooper et al. [236] 1992 USA Hospital staff 243 1.6
Thomas et al. [237] 1993 USA Teaching hospital healthcare personnel 943 0.7
Polish et al. [238] 1993 USA Community hospital healthcare
personnel
1677 1.4
Niu et al. [239] 1993 USA Dialysis staff 142 1.4
Forseter et al. [240] 1993 USA Dialysis nurses 51 1.9
Gerberding [241] 1994 USA Hospital care providers 976 1.4
Goetz et al. [242] 1995 USA Liver transplantation personnel 57 5.3
Panlilio et al. [243] 1995 USA Hospital-based Surgeons in moderate
to high AIDS areas
770 0.9
Tokars et al. [244] 1998 USA Dialysis staff 54 194 2
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
Epidemiological review of hepatitis C 89
involving a trauma, history of other sexually transmitted
diseases and those coinfected with HIV [81,86±89].
PERINATAL OR VERTICAL OR MOTHER-TO-OFFSPRING TRANSMISSION
Perinatal transmission of HCV infection occurs between 0
and 15% of cases [55]. There remains a debate as to the exact
role of this route of HCV spread [90]. Vertical transmission
from mother to child has been reported in a number of studies
[91±100] on the basis of asymptomatic biochemical abnor-
malities of liver function tests in particular ALT and transient
anti-HCV seropositivity using either ELISA or PCR in the
majority of infants born to mothers with HCV infection.
Persistence of anti-HCV has been noted with HIV coinfection
suggesting facilitatory role of HIV in HCV transmission
[91,92,94,97,101]. RT-PCR although have con®rmed ver-
tical transmission of HCV infection, has also generated a
contradictory data when mother-infant pairs were evaluated.
Some studies have shown no detectable anti-HCV despite
detectable anti-HCV [102±106], whereas others have shown
the prevalence of anti-HCV to be between 5% and 80%
[94,96,100,107±113]. There is a positive correlation with
HCV-RNA titre in the mother and subsequent development of
HCV infection in children [110,111,114,115]. Furthermore,
acute HCV infection during pregnancy even in the absence of
HIV carries an increased risk of vertical transmission
[101,107,114]. What remain controversial is the route and
timing of HCV transmission. It seems logical to think that
selective vertical transmission of certain subsets of HCV
variants either in utero or in the immediate postnatal period is
a possibility [116]. A study from Taiwan showed that elective
cesarean sections were associated with lowest microtrans-
fusion from mother to fetus compared with spontaneous
vaginal delivery or emergency cesarean sections [111,117].
In the light of the current available knowledge, no effective
way of preventing transmission of HCV infection from mother
to child exists. Similarly, transmission of HCV by breast milk
has been suggested but never proved [93,118,119]. It has
been insinuated that there might be some correlation be-
tween the duration of breastfeeding by HCV-RNA-positive
mother and the acquiring of HCV infection by the baby. In
view of this inconclusive data, it is premature to advise anti-
HCV-positive mothers against breastfeeding.
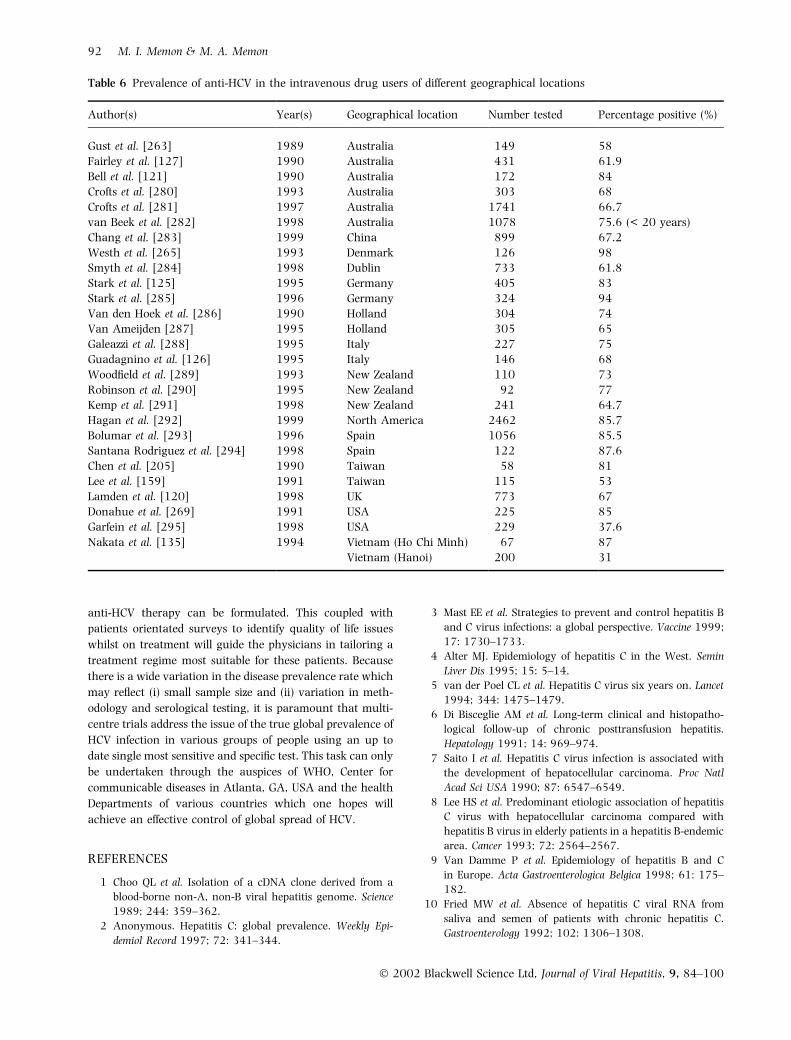
INTRAVENOUS DRUG USERS
Intravenous drug abusers not only have the highest pre-
valence of HCV infection but also constitute a potential
reservoir of HCV in the community. The incidence varies
between 31% to as high as 98% in different parts of the
world (Table 6). The prevalence of HCV infection increases
proportionally with the duration of intravenous drug abuse
[120±122]. Other risk factors include male gender, being
older, sex trade worker, risky sexual behaviour, multiple
sexual partners, needle sharing and history of being in pri-
son [120,122±126]. Oral drug abusers, when compared
with intravenous drug abusers, were found to have far less
incidence of HCV infections in two studies, one from New
Zealand (4% vs 73%) and Taiwan (5.4% vs 53%) [123].
CONCLUSIONS
Better understanding of the mode of spread of the disease will
assist in minimizing HCV spread globally. The overall burden
on the society both ®nancially and socially to support and
manage individuals with HCV is a time bomb waiting to
explode unless urgent measures are undertaken to (i) develop
Table 4 Prevalence of anti-HCV in sexual partners
Author(s) Year(s) Geographical location Number tested Percentage positive (%)
Davis et al. [245] 1996 Australia 19 0
Kolho et al. [246] 1991 Finland 30 3.3
Meisel et al. [247] 1995 Germany 94 0
Brettler et al. [248] 1992 International 106 2.7
Power et al. [249] 1995 Ireland 393 0.5
Scotto et al. [250] 1996 Italy 83 8.4
Caporaso et al. [82] 1998 Italy 11 379 15.6
Guadagnino et al. [83] 1998 Italy 267 11.3
Akahane et al. [251] 1994 Japan 154 27
Koda et al. [252] 1996 Japan 121 17.4
Mauser-Bunschoten et al. [253] 1995 Netherlands 75 0
Win et al. [254] 1994 Scotland 75 5.3
Diago et al. [255] 1996 Spain 394 7.6
Kao et al. [85] 1996 Taiwan 100 17
Saltoglu et al. [256] 1998 Turkey 38 7.8
Gordon et al. [257] 1992 UK 42 4.7
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
90 M. I. Memon & M. A. Memon
a strategy to inform and educate the lay public and press
regarding this disease (HCV awareness programs); (ii) set up
clinical information system(s) to monitor trends, occurrence
and effectiveness of intervention programs; (iii) identify the
route of spread for sporadic cases of HCV which accounts for
almost 50% of cases; (iv) develop inexpensive sensitive and
speci®c tests for detection of HCV infection at an early stage;
(v) make available these diagnostic tests universally and in
particular for the poorer countries where HCV is reaching
epidemic proportions; and (vi) lastly to expedite the efforts to
develop a vaccine. Individuals who have been unfortunate to
have acquired the HCV can be supported by appropriate
therapeutic drug regimes, which at present vary from centre
to centre. Therefore, multicentre clinical trials are needed
urgently to de®ne the role of interferon alone or in combi-
nation with other antiviral agents for both symptomatic
and asymptomatic individuals. Furthermore, the exact
interaction of interferon with the virus, host and the inter-
feron regimens (dynamic tripartite interaction) in producing
a variable response needs to be elucidate so that optimal
Table 5 Prevalence of anti-HCV in the high sexual risk groups of different geographical locations
Author(s) Year(s)
Geographical
location Type of subjects
Number
tested
Percentage
positive (%)
Fairley et al. [127] 1990 Australia STD subjects 177 6.2
Quaranta et al. [258] 1994 France Heterosexual STD subjects 82 18
van Doornum et al. [259] 1991 Holland Heterosexual STD subjects 468 1.3
Corona et al. [260] 1991 Italy Heterosexual STD subjects 1130 1.7
Weinstock et al. [261] 1993 USA Heterosexual STD subjects 1162 3.4
Weinstock et al. [261] 1993 USA Inner city clinics for STD 1292 7.7
Thomas et al. [262] 1994 USA Heterosexual STD subjects 1257 10
Gust et al. [263] 1989 Australia Homosexual men 148 9
Fairley et al. [127] 1990 Australia Homosexual men 330 22.7
Bodsworth et al. [89] 1996 Australia Homosexual men 1038 7.6
Melbye et al. [264] 1990 Denmark Homosexual men 259 4.1
Westh et al. [265] 1993 Denmark Homosexual men 147 1
Westh et al. [265] 1993 Denmark Homosexual men 147 1.4
Quaranta et al. [258] 1994 France Homosexual men 68 3
Hadziyannis et al. [266] 1993 Greece Homosexual men 426 4±9
Corona et al. [260] 1991 Italy Homosexual men 195 2
Gasparini et al. [267] 1991 Italy Homosexual men 212 4
Ricchi et al. [268] 1992 Italy Homo-bisexual men 622 6.9
Donahue et al. [269] 1991 North America Homosexual men 926 1.6
Hyams et al. [152] 1992 Peru Homosexual men 103 1
Tor et al. [270] 1990 Spain Homosexual men 105 17
Sanchez-Quijano et al. [271] 1990 Spain Homosexual men 146 5.4
Lissen et al. [203] 1993 Spain Homosexual men 168 4.2
Sonnerborg et al. [272] 1990 Sweden Homosexual men 48 0
Osmond et al. [273] 1993 USA Homosexual men 589 1.5
Buchbinder et al. [274] 1994 USA Homosexual men 343 5
Thomas et al. [86] 1995 USA Homosexual men 35 18
Ndimbie et al. [275] 1996 USA Homosexual men 1058 2.9
Osella et al. [276] 1998 USA Homosexual men 228 12.7
Fairley et al. [127] 1990 Australia Prostitutes 212 10.4
Wu et al. [277] 1993 China Prostitutes 622 12
Hadziyannis et al. [266] 1993 Greece Prostitutes 203 4
Develoux et al. [278] 1994 Niger Prostitutes 250 7.6
Mast et al. [3] 1991 North America Prostitutes 535 12
Hyams et al. [152] 1993 Peru Prostitutes 966 0.7
Sanchez-Quijano et al. [271] 1990 Spain Prostitutes 78 8.9
Gutierrez et al. [279] 1992 Spain Prostitutes 227 9
Lissen et al. [203] 1993 Spain Prostitutes 310 6.4
STD, sexually transmitted disease.
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
Epidemiological review of hepatitis C 91
anti-HCV therapy can be formulated. This coupled with
patients orientated surveys to identify quality of life issues
whilst on treatment will guide the physicians in tailoring a
treatment regime most suitable for these patients. Because
there is a wide variation in the disease prevalence rate which
may re¯ect (i) small sample size and (ii) variation in meth-
odology and serological testing, it is paramount that multi-
centre trials address the issue of the true global prevalence of
HCV infection in various groups of people using an up to
date single most sensitive and speci®c test. This task can only
be undertaken through the auspices of WHO, Center for
communicable diseases in Atlanta, GA, USA and the health
Departments of various countries which one hopes will
achieve an effective control of global spread of HCV.
REFERENCES
1 Choo QL et al. Isolation of a cDNA clone derived from a
blood-borne non-A, non-B viral hepatitis genome. Science
1989; 244: 359±362.
2 Anonymous. Hepatitis C: global prevalence. Weekly Epi-
demiol Record 1997; 72: 341±344.
3 Mast EE et al. Strategies to prevent and control hepatitis B
and C virus infections: a global perspective. Vaccine 1999;
17: 1730±1733.
4 Alter MJ. Epidemiology of hepatitis C in the West. Semin
Liver Dis 1995; 15: 5±14.
5 van der Poel CL et al. Hepatitis C virus six years on. Lancet
1994; 344: 1475±1479.
6 Di Bisceglie AM et al. Long-term clinical and histopatho-
logical follow-up of chronic posttransfusion hepatitis.
Hepatology 1991; 14: 969±974.
7 Saito I et al. Hepatitis C virus infection is associated with
the development of hepatocellular carcinoma. Proc Natl
Acad Sci USA 1990; 87: 6547±6549.
8 Lee HS et al. Predominant etiologic association of hepatitis
C virus with hepatocellular carcinoma compared with
hepatitis B virus in elderly patients in a hepatitis B-endemic
area. Cancer 1993; 72: 2564±2567.
9 Van Damme P et al. Epidemiology of hepatitis B and C
in Europe. Acta Gastroenterologica Belgica 1998; 61: 175±
182.
10 Fried MW et al. Absence of hepatitis C viral RNA from
saliva and semen of patients with chronic hepatitis C.
Gastroenterology 1992; 102: 1306±1308.
Table 6 Prevalence of anti-HCV in the intravenous drug users of different geographical locations
Author(s) Year(s) Geographical location Number tested Percentage positive (%)
Gust et al. [263] 1989 Australia 149 58
Fairley et al. [127] 1990 Australia 431 61.9
Bell et al. [121] 1990 Australia 172 84
Crofts et al. [280] 1993 Australia 303 68
Crofts et al. [281] 1997 Australia 1741 66.7
van Beek et al. [282] 1998 Australia 1078 75.6 (< 20 years)
Chang et al. [283] 1999 China 899 67.2
Westh et al. [265] 1993 Denmark 126 98
Smyth et al. [284] 1998 Dublin 733 61.8
Stark et al. [125] 1995 Germany 405 83
Stark et al. [285] 1996 Germany 324 94
Van den Hoek et al. [286] 1990 Holland 304 74
Van Ameijden [287] 1995 Holland 305 65
Galeazzi et al. [288] 1995 Italy 227 75
Guadagnino et al. [126] 1995 Italy 146 68
Wood®eld et al. [289] 1993 New Zealand 110 73
Robinson et al. [290] 1995 New Zealand 92 77
Kemp et al. [291] 1998 New Zealand 241 64.7
Hagan et al. [292] 1999 North America 2462 85.7
Bolumar et al. [293] 1996 Spain 1056 85.5
Santana Rodriguez et al. [294] 1998 Spain 122 87.6
Chen et al. [205] 1990 Taiwan 58 81
Lee et al. [159] 1991 Taiwan 115 53
Lamden et al. [120] 1998 UK 773 67
Donahue et al. [269] 1991 USA 225 85
Garfein et al. [295] 1998 USA 229 37.6
Nakata et al. [135] 1994 Vietnam (Ho Chi Minh) 67 87
Vietnam (Hanoi) 200 31
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
92 M. I. Memon & M. A. Memon
11 Kotwal GJ et al. Detection of hepatitis C virus-speci®c
antigens in semen from non-A, non-B hepatitis patients.
Dig Dis Sci 1992; 37: 641±644.
12 Sharara AI et al. Hepatitis C. Ann Intern Med 1996; 125:
658±668.
13 Conry-Cantilena C et al. Routes of infection, viremia, and
liver disease in blood donors found to have hepatitis C virus
infection. N Engl J Med 1996; 334: 1691±1696.
14 Alter HJ et al. Donor transaminase and recipient hepatitis.
Impact on blood transfusion services. JAMA 1981; 246:
630±634.
15 Aach RD et al. Serum alanine aminotransferase of donors
in relation to the risk of non-A,non-B hepatitis in recipi-
ents: the transfusion-transmitted viruses study. N Engl
J Med 1981; 304: 989±994.
16 Widell A et al. Relation between donor transaminase and
recipient hepatitis non-A, non-B in Sweden. Vox Sang
1988; 54: 154±159.
17 Reesink HW et al. HCV and blood transfusion. Arch Virol
Suppl 1992; 4: 241±243.
18 Aymard JP et al. Post-transfusion non-A, non-B hepatitis
after cardiac surgery. Prospective analysis of donor blood
anti-HBc antibody as a predictive indicator of the occur-
rence of non-A, non-B hepatitis in recipients. Vox Sang
1986; 51: 236±238.
19 Esteban JI et al. Evaluation of antibodies to hepatitis C virus
in a study of transfusion-associated hepatitis. N Engl J Med
1990; 323: 1107±1112.
20 Aach RD et al. Hepatitis C virus infection in post-transfu-
sion hepatitis. An analysis with ®rst- and second-genera-
tion assays. N Engl J Med 1991; 325: 1325±1329.
21 Barrera JM et al. Incidence of non-A, non-B hepatitis after
screening blood donors for antibodies to hepatitis C virus and
surrogate markers. Ann Intern Med 1991; 115: 596±600.
22 Elia GF et al. Incidence of anti-hepatitis C virus antibodies
in non-A, non-B post-transfusion hepatitis in an area of
northern Italy. Infection 1991; 19: 336±339.
23 Mattsson L et al. Seroconversion to hepatitis C virus anti-
bodies in patients with acute posttransfusion non-A, non-B
hepatitis in Sweden. Infection 1991; 19: 309±312.
24 Jullien AM et al. Impact of screening donor blood for
alanine aminotransferase and antibody to hepatitis B core
antigen on the risk of hepatitis C virus transmission. Eur J
Clin Microbiol Infect Dis 1993; 12: 668±672.
25 Donahue JG et al. The declining risk of post-transfusion
hepatitis C virus infection. N Engl J Med 1992; 327:
369±373.
26 Farci P et al. A long-term study of hepatitis C virus repli-
cation in non-A, non-B hepatitis. N Engl J Med 1991; 325:
98±104.
27 Houghton M et al. Molecular biology of the hepatitis C
viruses: implications for diagnosis, development and con-
trol of viral disease. Hepatology 1991; 14: 381±388.
28 Bukh J et al. Sequence analysis of the core gene of 14
hepatitis C virus genotypes. Proc Natl Acad Sci USA 1994;
91: 8239±8243.
29 Nowicki MJ et al. The hepatitis C virus: identi®cation, epi-
demiology, and clinical controversies. J Pediatr Gastro-
enterol Nutrition 1995; 20: 248±274.
30 Lai ME et al. Evaluation of antibodies to hepatitis C virus in
a long-term prospective study of posttransfusion hepatitis
among thalassemic children: comparison between ®rst-
and second-generation assay. J Pediatr Gastroenterol
Nutrition 1993; 16: 458±464.
31 Khalifa AS et al. Prevalence of hepatitis C viral antibody in
transfused and nontransfused Egyptian children. Am J Trop
Med Hyg 1993; 49: 316±321.
32 Fink FM et al. Association of hepatitis C virus infection
with chronic liver disease in paediatric cancer patients. Eur
J Pediatr 1993; 152: 490±492.
33 Kanesaki T et al. Hepatitis C virus infection in children
with hemophilia: characterization of antibody response to
four different antigens and relationship of antibody
response, viremia, and hepatic dysfunction. J Pediatr 1993;
123: 381±387.
34 Eyster ME et al. Natural history of hepatitis C virus infec-
tion in multitransfused hemophiliacs: effect of coinfection
with human immunode®ciency virus. The Multicenter
Hemophilia Cohort Study. J Acquir Immune De®c Syndr
1993; 6: 602±610.
35 Makris M et al. Hepatitis C antibody and chronic liver
disease in haemophilia. Lancet 1990; 335: 1117±1119.
36 Pawlotsky JM et al. Chronic hepatitis C after high-dose
intravenous immunoglobulin. Transfusion 1994; 34: 86±87.
37 Maisonneuve P et al. Antibody to hepatitis C (anti C 100±3)
in French hemophiliacs. Nouvelle Revue Francaise D Hema-
tologie 1991; 33: 263±266.
38 Yu MW et al. Hepatitis C transmission associated with intra-
venous immunoglobulins. Lancet 1995; 345: 1173±1174.
39 Schneider LC et al. Intravenous immunoglobulin and
hepatitis C virus: the Boston episode. Clin Ther 1996; 18
(suppl B): 108±109.
40 Bresee JS et al. Hepatitis C virus infection associated with
administration of intravenous immune globulin. A cohort
study. JAMA 1996; 276: 1563±1567.
41 Mauser-Bunschoten EP et al. Hepatitis C infection and
viremia in Dutch hemophilia patients. J Med Virol 1995;
45: 241±246.
42 Resti M et al. Prevalence of hepatitis C virus antibody in
beta-thalassemic polytransfused children in a long-term
follow-up. Vox Sang 1991; 60: 246±247.
43 Bortolotti F et al. Posttransfusion and community-acquired
hepatitis C in childhood. J Pediatr Gastroenterol Nutr 1994;
18: 279±283.
44 Tagariello G et al. Hepatitis C virus genotypes and severity
of chronic liver disease in haemophiliacs. Br J Haematol
1995; 91: 708±713.
45 Makris M et al. The natural history of chronic hepatitis C in
haemophiliacs. Br J Haematol 1996; 94: 746±752.
46 Locasciulli A et al. Hepatitis C virus serum markers and
liver disease in children with leukemia during and after
chemotherapy. Blood 1993; 82: 2564±2567.
47 Ribas A et al. How important is hepatitis C virus (HCV)-
infection in persons with acute leukemia? Leukemia Res
1997; 21: 785±788.
48 Cesaro S et al. Chronic hepatitis C virus infection after
treatment for pediatric malignancy. Blood 1997; 90:
1315±1320.
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
Epidemiological review of hepatitis C 93
49 Locasciulli A et al. Hepatitis C virus infection and liver fail-
ure in patients undergoing allogeneic bone marrow trans-
plantation. Bone Marrow Transplant 1995; 16: 407±411.
50 Diego JM et al. Hepatitis C in dialysis and transplantation.
Curr Opin Nephrol Hypertens 1996; 5: 497±503.
51 Fabrizi F et al. Detection of de novo hepatitis C virus
infection by polymerase chain reaction in hemodialysis
patients. Am J Nephrol 1999; 19: 383±388.
52 Izopet J et al. Molecular evidence for nosocomial trans-
mission of hepatitis C virus in a French hemodialysis unit.
J Med Virol 1999; 58: 139±144.
53 Sandhu J et al. Hepatitis C prevalence and risk factors in
the northern Alberta dialysis population. Am J Epidemiol
1999; 150: 58±66.
54 Lettau LA. The A, B, C, D, and E of viral hepatitis: spelling
out the risks for healthcare workers. Infect Control Hosp
Epidemiol 1992; 13: 77±81.
55 van der Poel CL et al. Hepatitis C virus: epidemiology,
transmission and prevention. Curr Stud Hematol Blood
Transfus 1998: 208±236
56 Pru CE et al. Hepatitis C transmission through dialysis
machines. ASAIO J 1994; 40: M889±91.
57 McLaughlin KJ et al. Nosocomial transmission of hepatitis
C virus within a British dialysis centre. Nephrol Dialysis
Transplant 1997; 12: 304±309.
58 Irish DN et al. Identi®cation of hepatitis C virus serocon-
version resulting from nosocomial transmission on a hae-
modialysis unit: implications for infection control and
laboratory screening. J Med Virol 1999; 59: 135±140.
59 Okuda K et al. Mode of hepatitis C infection not associated
with blood transfusion among chronic hemodialysis
patients. J Hepatol 1995; 23: 28±31.
60 Fabrizi F et al. Incidence of seroconversion for hepatitis C
virus in chronic haemodialysis patients: a prospective
study. Nephrol Dialysis Transplant 1994; 9: 1611±1615.
61 Schneeberger PM et al. Infection control of hepatitis C in
Dutch dialysis centres [news]. Nephrol Dialysis Transplant
1998; 13: 3037±3040.
62 Huraib S et al. High prevalence of and risk factors for
hepatitis C in haemodialysis patients in Saudi Arabia: a
need for new dialysis strategies. Nephrol Dialysis Transplant
1995; 10: 470±474.
63 Gilli P et al. Prevention of hepatitis C virus in dialysis units.
Nephron 1995; 70: 301±306.
64 Esteban JI et al. Transmission of hepatitis C virus by a
cardiac surgeon. N Engl J Med 1996; 334: 555±560.
65 Schvarcz R et al. Nosocomial transmission of hepatitis C
virus. Infection 1997; 25: 74±77.
66 Allander T et al. Frequent patient-to-patient transmission
of hepatitis C virus in a haematology ward. Lancet 1995;
345: 603±607.
67 Mitsui T et al. Hepatitis C virus infection in medical per-
sonnel after needlestick accident. Hepatology 1992; 16:
1109±1114.
68 Kelen GD et al. Hepatitis B and hepatitis C in emergency
department patients. N Engl J Med 1992; 326: 1399±1404.
69 Klein RS et al. Occupational risk for hepatitis C virus
infection among New York City dentists. Lancet 1991; 338:
1539±1542.
70 Zuckerman J et al. Prevalence of hepatitis C antibodies
in clinical health-care workers. Lancet 1994; 343:
1618±1620.
71 Petrosillo N et al. Prevalence of hepatitis C antibodies in
health-care workers. Italian Study Group on Blood-borne
Occupational Risk in Dialysis [letter; comment]. Lancet
1994; 344: 339±340.
72 Hernandez ME et al. Risk of needle-stick injuries in the
transmission of hepatitis C virus in hospital personnel.
J Hepatol 1992; 16: 56±58.
73 Sodeyama T et al. Detection of hepatitis C virus markers
and hepatitis C virus genomic-RNA after needlestick acci-
dents. Arch Intern Med 1993; 153: 1565±1572.
74 Arai Y et al. A prospective study of hepatitis C virus infec-
tion after needlestick accidents. Liver 1996; 16: 331±334.
75 Everhart JE et al. Risk for non-A, non-B (type C) hepatitis
through sexual or household contact with chronic carriers.
Ann Intern Med 1990; 112: 544±545.
76 Deny P et al. Low rate of hepatitis C virus (HCV) trans-
mission within the family. J Hepatol 1992; 14: 409±410.
77 Mondello P et al. Anti-HCV antibodies in household con-
tacts of patients with cirrhosis of the liver ± preliminary
results. Infection 1992; 20: 51±52.
78 Bellobuono A et al. Intrafamilial spread of hepatitis C virus.
Transfusion 1991; 31: 475.
79 Scaraggi FA et al. Intrafamilial and sexual transmission of
hepatitis C virus [letter; comment]. Lancet 1993; 342:
1300±1302.
80 Camarero C et al. Horizontal transmission of hepatitis C
virus in households of infected children. J Pediatr 1993;
123: 98±99.
81 Esteban JI et al. Hepatitis C virus antibodies among risk
groups in Spain. Lancet 1989; 2: 294±297.
82 Caporaso N et al. Spread of hepatitis C virus infection
within families. Investigators of an Italian Multicenter
Group. J Viral Hepat 1998; 5: 67±72.
83 Guadagnino V et al. Hepatitis C virus infection in family
setting. Eur J Epidemiol 1998; 14: 229±232.
84 Tanaka K et al. Heterosexual transmission of hepatitis C
virus among married couples in southwestern Japan. Int J
Cancer 1997; 72: 50±55.
85 Kao JH et al. Transmission of hepatitis C virus between
spouses: the important role of exposure duration. Am J
Gastroenterol 1996; 91: 2087±2090.
86 Thomas DL et al. Sexual transmission of hepatitis C virus
among patients attending sexually transmitted diseases
clinics in Baltimore ± an analysis of 309 sex partnerships.
J Infect Dis 1995; 171: 768±775.
87 Hess G et al. Hepatitis C virus and sexual transmission.
Lancet 1989; 2: 987.
88 Tedder RS et al. Hepatitis C virus: evidence for sexual
transmission. BMJ 1991; 302: 1299±1302.
89 Bodsworth NJ et al. Hepatitis C virus infection in a large
cohort of homosexually active men: independent associa-
tions with HIV-1 infection and injecting drug use but not
sexual behaviour. Genitourin Med 1996; 72: 118±122.
90 Koff RS. The low ef®ciency of maternal-neonatal trans-
mission of hepatitis C virus: how certain are we? [Editorial
comment] Ann Intern Med 1992; 117: 967±969.
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
94 M. I. Memon & M. A. Memon
91 Weintrub PS et al. Hepatitis C virus infection in infants
whose mothers took street drugs intravenously. J Pediatr
1991; 119: 869±874.
92 Giovannini M et al. Maternal-infant transmission of hepa-
titis C virus and HIV infections: a possible interaction.
Lancet 1990; 335: 1166.
93 Wejstal R et al. Mother to infant transmission of hepatitis C
virus infection. J Med Virol 1990; 30: 178±180.
94 Wejstal R et al. Mother-to-infant transmission of hepatitis
C virus. Ann Intern Med 1992; 117: 887±890.
95 Novati R et al. Mother-to-child transmission of hepatitis C
virus detected by nested polymerase chain reaction. J Infect
Dis 1992; 165: 720±723.
96 Thaler MM et al. Vertical transmission of hepatitis C virus.
Lancet 1991; 338: 17±18.
97 Paccagnini S et al. Perinatal transmission and manifesta-
tion of hepatitis C virus infection in a high risk population.
Pediatr Infect Dis J 1995; 14: 195±199.
98 Tanzi E et al. Is HCV transmitted by the vertical/perinatal
route? Arch Virol Suppl 1993; 8: 229±234.
99 Aizaki H et al. Mother-to-child transmission of a hepatitis C
virus variant with an insertional mutation in its hyper-
variable region. J Hepatol 1996; 25: 608±613.
100 Matsubara T et al. Mother-to-infant transmission of hepa-
titis C virus: a prospective study. Eur J Pediatr 1995; 154:
973±978.
101 Maggiore G et al. Vertical transmission of hepatitis C [let-
ter; comment]. Lancet 1995; 345: 1122.
102 Uehara S et al. The incidence of vertical transmission of
hepatitis C virus. Tohoku J Exp Med 1993; 171: 195±202.
103 Marcellin P et al. Prevalence of hepatitis C virus infection
in asymptomatic anti-HIV1 negative pregnant women and
their children. Dig Dis Sci 1993; 38: 2151±2155.
104 Roudot-Thoraval F et al. Lack of mother-to-infant trans-
mission of hepatitis C virus in human immunode®ciency
virus-seronegative women: a prospective study with
hepatitis C virus RNA testing. Hepatology 1993; 17:
772±777.
105 Reinus JF et al. Failure to detect vertical transmission of
hepatitis C virus. Ann Intern Med 1992; 117: 881±886.
106 Fischler B et al. Vertical transmission of hepatitis C virus
infection. Scand J Infect Dis 1996; 28: 353±356.
107 Sabatino G et al. Vertical transmission of hepatitis C virus:
an epidemiological study on 2,980 pregnant women in
Italy. Eur J Epidemiol 1996; 12: 443±447.
108 Kuroki T et al. Vertical transmission of hepatitis C virus
(HCV) detected by HCV-RNA analysis. Gut 1993; 34:
S52±53.
109 Lam JP et al. Infrequent vertical transmission of hepatitis C
virus. J Infect Dis 1993; 167: 572±576.
110 Ohto H et al. Transmission of hepatitis C virus from
mothers to infants. The Vertical Transmission of Hepatitis
C Virus Collaborative Study Group. N Engl J Med 1994;
330: 744±750.
111 Lin HH et al. Possible role of high-titer maternal viremia in
perinatal transmission of hepatitis C virus. J Infect Dis
1994; 169: 638±641.
112 Ni YH et al. Temporal pro®le of hepatitis C virus antibody
and genome in infants born to mothers infected with
hepatitis C virus but without human immunode®ciency
virus coinfection. J Hepatol 1994; 20: 641±645.
113 Gonzalez A et al. Ef®cacy of screening donors for antibodies
to the hepatitis C virus to prevent transfusion-associated
hepatitis: ®nal report of a prospective trial. Hepatology
1995; 22: 439±445.
114 Resti M et al. Mother to child transmission of hepatitis C
virus: prospective study of risk factors and timing of
infection in children born to women seronegative for
HIV-1. Tuscany Study Group on Hepatitis C Virus Infec-
tion. BMJ 1998; 317: 437±441.
115 Zanetti AR et al. A prospective study on mother-to-infant
transmission of hepatitis C virus. Intervirology 1998; 41:
208±212.
116 Weiner AJ et al. A unique, predominant hepatitis C virus
variant found in an infant born to a mother with multiple
variants. J Virol 1993; 67: 4365±4368.
117 Lin HH et al. Least microtransfusion from mother to fetus
in elective cesarean delivery. Obstet Gynecol 1996; 87:
244±248.
118 Nagata I et al. Mother-to-infant transmission of hepatitis C
virus. J Pediatr 1992; 120: 432±434.
119 Ogasawara S et al. Hepatitis C virus RNA in saliva and
breastmilk of hepatitis C carrier mothers. Lancet 1993;
341: 561.
120 Lamden KH et al. Hepatitis B and hepatitis C virus infec-
tions: risk factors among drug users in Northwest England.
J Infect 1998; 37: 260±269.
121 Bell J et al. Hepatitis C virus in intravenous drug users. Med
J Aust 1990; 153: 274±276.
122 Medin C et al. Seroconversion to hepatitis C virus in
dialysis patients: a retrospective and prospective study.
Nephron 1993; 65: 40±45.
123 Mansell CJ et al. Epidemiology of hepatitis C in the East.
Semin Liver Dis 1995; 15: 15±32.
124 Chang CJ et al. Seroepidemiology of hepatitis C virus
infection among drug abusers in southern Taiwan. J For-
mosan Med Assoc 1998; 97: 826±829.
125 Stark K et al. Prevalence and determinants of anti-HCV
seropositivity and of HCV genotype among intravenous
drug users in Berlin. Scand J Infect Dis 1995; 27: 331±337.
126 Guadagnino V et al. Relevance of intravenous cocaine use
in relation to prevalence of HIV, hepatitis B and C virus
markers among intravenous drug abusers in southern
Italy. J Clin Lab Immunol 1995; 47: 1±9.
127 Fairley CK et al. Epidemiology and hepatitis C virus in
Victoria. Med J Aust 1990; 153: 271±273.
128 Garner JJ et al. Prevalence of hepatitis C infection in
pregnant women in South Australia. Med J Aust 1997;
167: 470±472.
129 Tao QM et al. Seroepidemiology of HCV and HBV infection
in northern China. Gastroenterol Japon 1991; 26 (Suppl. 3):
156±158.
130 Darwish MA et al. High seroprevalence of hepatitis A, B, C,
and E viruses in residents in an Egyptian village in The Nile
Delta: a pilot study. Am J Trop Med Hyg 1996; 54:
554±558.
131 Dubois F et al. Hepatitis C in a French population-
based survey, 1994 seroprevalence, frequency of viremia,
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
Epidemiological review of hepatitis C 95
genotype distribution, and risk factors. The Collaborative
Study Group. Hepatology 1997; 25: 1490±1496.
132 Richard-Lenoble D et al. Hepatitis B, C, D, and E markers in
rural equatorial African villages (Gabon). Am J Trop Med
Hyg 1995; 53: 338±341.
133 Martinson FE et al. Seroepidemiological survey of hepatitis
B and C virus infections in Ghanaian children. J Med Virol
1996; 48: 278±283.
134 Jeannel D et al. Evidence for high genetic diversity and
long-term endemicity of hepatitis C virus genotypes 1 and
2 in West Africa. J Med Virol 1998; 55: 92±97.
135 Nakata S et al. Hepatitis C and B virus infections
in populations at low or high risk in Ho Chi Minh and
Hanoi. Vietnam J Gastroenterol Hepatol 1994; 9: 416±
419.
136 Chan GC et al. Prevalence of hepatitis C infection in Hong
Kong. J Gastroenterol Hepatol 1992; 7: 117±120.
137 Reddy PH et al. Hepatitis virus markers in the Baiga tribal
population of Madhya Pradesh, India. Trans R Soc Trop Med
Hyg 1995; 89: 620.
138 Marranconi F et al. Prevalence of anti-HCV and risk factors
for hepatitis C virus infection in healthy pregnant women.
Infection 1994; 22: 333±337.
139 Osella AR et al. Epidemiology of hepatitis C virus infection
in an area of Southern Italy. J Hepatol 1997; 27: 30±35.
140 Guadagnino V et al. Prevalence, risk factors, and genotype
distribution of hepatitis C virus infection in the general
population: a community-based survey in southern Italy.
Hepatology 1997; 26: 1006±1011.
141 Tajima K et al. Natural horizontal transmission of HCV
in microepidemic town in Japan. Lancet 1991; 337:
1410±1411.
142 Tibbs CJ et al. Prevalence of hepatitis C in tropical com-
munities: the importance of con®rmatory assays. J Med
Virol 1991; 34: 143±147.
143 Kim YS et al. Prevalence of hepatitis C virus antibody
among Korean adults. J Korean Med Sci 1992; 7: 333±336.
144 Morvan JM et al. Anti-HCV antibody prevalence among an
asymptomatic population living in two villages in
Madagascar. Trans R Soc Trop Med Hyg 1994; 88: 657.
145 Ahmed SD et al. Seroprevalence of hepatitis B and C and
HIV in Malawian pregnant women. J Infect 1998; 37:
248±251.
146 Miller J et al. The epidemiology and control of hepatitis C in
New Zealand. Commun Dis NZ 1993; 93: 33±41 (Abstract).
147 Perez OM et al. Prevalence of antibodies to hepatitis A, B,
C, and E viruses in a healthy population in Leon. Nicaragua
Am J Trop Med Hyg 1996; 55: 17±21.
148 Oshita M et al. Prevalence of hepatitis C virus in family
members of patients with hepatitis C. J Med Virol 1993; 41:
251±255.
149 Luby SP et al. The relationship between therapeutic injec-
tions and high prevalence of hepatitis C infection in
Ha®zabad. Pakistan Epidemiol Infect 1997; 119: 349±356.
150 Baumgart KW et al. Hepatitis C virus in the central prov-
ince of Papua New Guinea [letter; comment]. Med J Aust
1993; 159: 284±285.
151 Turner PF. Hepatitis C virus in the Western Province of
Papua New Guinea. Med J Aust 1993; 158: 140.
152 Hyams KC et al. Seroprevalence of hepatitis C antibody in
Peru. J Med Virol 1992; 37: 127±131.
153 Bahakim H et al. Hepatitis C virus antibodies in high-risk
Saudi groups. Vox Sang 1991; 60: 162±164.
154 al-Faleh FZ et al. Prevalence of antibody to hepatitis C virus
among Saudi Arabian children: a community-based study.
Hepatology 1991; 14: 215±218.
155 al Nasser MN et al. Seropositivity to hepatitis C virus in
Saudi haemodialysis patients. Vox Sang 1992; 62: 94±97.
156 al Karawi MA et al. Hepatitis C virus infection in chronic
liver disease and hepatocellular carcinoma in Saudi Ara-
bia. J Gastroenterol Hepatol 1992; 7: 237±239.
157 al-Faleh FZ et al. Pro®le of hepatitis C virus and the possible
modes of transmission of the virus in the Gizan area of
Saudi Arabia: a community-based study. Ann Trop Med
Parasitol 1995; 89: 431±437.
158 Chen DS et al. Hepatitis C virus infection in Taiwan. Gas-
troenterol Japon 1991; 26 (Suppl. 3): 164±166.
159 Lee SD et al. Seroepidemiology of hepatitis C virus infection
in Taiwan. Hepatology 1991; 13: 830±833.
160 Chien RN et al. Low prevalences of HBV and HCV infection
in patients with primary biliary cirrhosis in Taiwan: a case
control study. J Gastroenterol Hepatol 1993; 8: 574±576.
161 Chang MH et al. Minimal role of hepatitis C virus infection
in childhood liver diseases in an area hyperendemic for
hepatitis B infection. J Med Virol 1993; 40: 322±325.
162 Chuang WL et al. The role of hepatitis C virus in chronic
hepatitis B virus infection. Gastroenterol Japon 1993; 28
(Suppl. 5): 23±27.
163 Chang SJ et al. Risk factors of hepatitis C virus infection in
a Taiwanese aboriginal community. Kao-Hsiung I Hsueh Ko
Hsueh Tsa Chih [Kaohsiung J Med Sci] 1996; 12: 241±247.
164 Triki H et al. Seroepidemiology of hepatitis B, C and delta
viruses in Tunisia. Trans R Soc Trop Med Hyg 1997; 91:
11±14.
165 Doganci L et al. Prevalence of hepatitis A, B and C in
Turkey. Eur J Clin Microbiol Infect Dis 1992; 11: 661±662.
166 Hyams KC et al. Seroprevalence of hepatitis A, B, and C in
a United States military recruit population. Military Med
1992; 157: 579±582.
167 Jonas MM et al. Low prevalence of antibody to hepatitis C
virus in an urban adolescent population. J Pediatr 1997;
131: 314±316.
168 Alter MJ et al. The prevalence of hepatitis C virus infection
in the United States, 1988 through 1994. N Engl J Med
1999; 341: 556±562.
169 Blitz-Dorfman L et al. Serological survey of markers of
infection with viral hepatitis among the Yukpa Amerindi-
ans from western Venezuela. Ann Trop Med Parasitol 1996;
90: 655±657.
170 Scott DA et al. The epidemiology of hepatitis C virus anti-
body in Yemen. Am J Trop Med Hyg 1992; 46: 63±68.
171 Oshitani H et al. Low prevalence of hepatitis C virus
infection in Lusaka. Zambia Trans R Soc Trop Med Hygiene
1995; 89: 380.
172 Allain JP et al. Prediction of hepatitis C virus infectivity
in seropositive Australian blood donors by supplemental
immunoassays and detection of viral RNA. Blood 1991;
78: 2462±2468.
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
96 M. I. Memon & M. A. Memon
173 Archer GT et al. Prevalence of hepatitis C virus antibod-
ies in Sydney blood donors. Med J Aust 1992; 157:
225±227.
174 Mison LM et al. Prevalence of hepatitis C virus and geno-
type distribution in an Australian volunteer blood donor
population. Transfusion 1997; 37: 73±78.
175 Khan M et al. Comparison of seroepidemiology of hepatitis
C in blood donors between Bangladesh and Japan. Gas-
troenterol Japon 1993; 28 (suppl 5): 28±31.
176 Vasconcelos HC et al. Hepatitis B and C prevalences among
blood donors in the south region of Brazil. Memorias Do
Instituto Oswaldo Cruz 1994; 89: 503±507.
177 Ito S et al. Epidemiological characteristics of the incidence
of hepatitis C virus (C100±3) antibodies in patients with
liver diseases in the inshore area of the Yangtze River.
J Gastroenterol Hepatol 1993; 8: 232±237.
178 Wang Y et al. Hepatitis C virus RNA and antibodies among
blood donors in Beijing. J Hepatol 1994; 21: 634±640.
179 Arthur RR et al. Hepatitis C antibody prevalence in blood
donors in different governorates in Egypt. Trans R Soc Trop
Med Hyg 1997; 91: 271±274.
180 Schottstedt V et al. PCR for HBV, HCV and HIV-1 experi-
ences and ®rst results from a routine screening programme
in a large blood transfusion service. Biologicals 1998; 26:
101±104.
181 Song P et al. Markers of hepatitis C and B virus infections
among blood donors in Ho Chi Minh City and Hanoi.
Vietnam Clin Diagnostic Lab Immunol 1994; 1: 413±418.
182 Lin CK et al. A study of hepatitis C virus antibodies and
serum alanine amino transferase in blood donors in Hong
Kong Chinese. Vox Sang 1992; 62: 98±101.
183 Panigrahi AK et al. Magnitude of hepatitis C virus infection
in India: prevalence in healthy blood donors, acute and
chronic liver diseases. J Med Virol 1997; 51: 167±174.
184 Budihusodo U et al. Seroepidemiology of HBV and HCV
infection in Jakarta, Indonesia. Gastroenterol Japon 1991;
26 (Suppl. 3): 196±201.
185 Amirudin R et al. Hepatitis B and C virus infection in Ujung
Pandang, Indonesia. Gastroenterol Japon 1991; 26 (Suppl.
3): 184±188.
186 Sulaiman HA et al. Prevalence of hepatitis B and C viruses
in healthy Indonesian blood donors. Trans R Soc Trop Med
Hyg 1995; 89: 167±170.
187 Darmadi S et al. Hepatitis C virus infection-associated
markers in sera from blood donors in Surabaya. Indonesia
Microbiol Immunol 1996; 40: 401±405.
188 Prati D et al. The incidence and risk factors of community-
acquired hepatitis C in a cohort of Italian blood donors.
Hepatology 1997; 25: 702±704.
189 Tanaka E et al. Prevalence of antibody to hepatitis C virus
in Japanese schoolchildren: comparison with adult blood
donors. Am J Trop Med Hyg 1992; 46: 460±464.
190 Watanabe J et al. Predictive value of screening tests for
persistent hepatitis C virus infection evidenced by viraemia.
Japanese experience. Vox Sang 1993; 65: 199±203.
191 Sasaki F et al. Very low incidence rates of community-
acquired hepatitis C virus infection in company employees,
long-term inpatients, and blood donors in Japan. J Epi-
demiol 1996; 6: 198±203.
192 Tanaka H et al. The risk of hepatitis C virus infection
among blood donors in Osaka. Japan J Epidemiol 1998; 8:
292±296.
193 Kim BS et al. Prevalence of hepatitis C virus related to liver
diseases in Korea. Gastroenterol Japon 1993; 28 (Suppl. 5):
17±22.
194 Araj GF et al. Hepatitis C virus: prevalence in Lebanese
blood donors and brief overview of the disease. J Med
Libanais ± Lebanese Med Journal 1995; 43: 11±16.
195 Morris K et al. Completed hepatitis C lookback in Northern
Ireland. Transfusion Med 1997; 7: 269±275.
196 Kakepoto GN et al. Epidemiology of blood-borne viruses: a
study of healthy blood donors in Southern Pakistan.
Southeast Asian J Trop Med Public Health 1996; 27:
703±706.
197 Arguillas MO et al. Seroepidemiology of hepatitis C virus
infection in the Philippines: a preliminary study and
comparison with hepatitis B virus infection among blood
donors, medical personnel, and patient groups in Davao.
Philippines Gastroenterol Japon 1991; 26 (Suppl. 3):
170±175.
198 Abdourakhmanov DT et al. Epidemiological and clinical
aspects of hepatitis C virus infection in the Russian
Republic of Daghestan. Eur J Epidemiol 1998; 14: 549±553.
199 Abdelaal M et al. Epidemiology of hepatitis C virus: a study
of male blood donors in Saudi Arabia. Transfusion 1994;
34: 135±137.
200 Crawford RJ et al. Prevalence and epidemiological char-
acteristics of hepatitis C in Scottish blood donors. Trans-
fusion Med 1994; 4: 121±124.
201 Wang JE. A study on the epidemiology of hepatitis C
infection among blood donors in Singapore. J Public Health
Med 1995; 17: 387±391.
202 Tucker TJ et al. Hepatitis C virus infection rate in volunteer
blood donors from the Western Cape ± comparison of
screening tests and PCR. South African Med J 1997; 87:
603±605.
203 Lissen E et al. Hepatitis C virus infection among sexually
promiscuous groups and the heterosexual partners of
hepatitis C virus infected index cases. Eur J Clin Microbiol
Infect Dis 1993; 12: 827±831.
204 Munoz-Gomez R et al. Hepatitis C virus infection in Span-
ish volunteer blood donors: HCV RNA analysis and liver
disease. Eur J Gastroenterol Hepatol 1996; 8: 273±277.
205 Chen DS et al. Hepatitis C virus infection in an area
hyperendemic for hepatitis B and chronic liver disease: the
Taiwan experience. J Infect Dis 1990; 162: 817±822.
206 Songsivilai S et al. High prevalence of hepatitis C infection
among blood donors in northeastern Thailand. Am J Trop
Med Hyg 1997; 57: 66±69.
207 Mutimer DJ et al. Hepatitis C virus infection in the
asymptomatic British blood donor. J Viral Hepat 1995; 2:
47±53.
208 Stevens CE et al. Epidemiology of hepatitis C virus. A pre-
liminary study in volunteer blood donors. JAMA 1990;
263: 49±53.
209 Anderson SC et al. Comparison of two second-generation
anti-hepatitis C virus ELISA on 21431 US blood donor
samples. J Viral Hepat 1995; 2: 55±61.
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
Epidemiological review of hepatitis C 97
210 Murphy EL et al. Demographic determinants of hepatitis C
virus seroprevalence among blood donors. JAMA 1996;
275: 995±1000.
211 Chuang TY et al. Porphyria cutanea tarda and hepatitis C
virus: a case-control study and meta-analysis of the lit-
erature. J Am Acad Dermatol 1999; 41: 31±36.
212 el Guneid AM et al. Prevalence of hepatitis B, C, and D
virus markers in Yemeni patients with chronic liver dis-
ease. J Med Virol 1993; 40: 330±333.
213 Frider B et al. Prevalence of hepatitis C in health care
workers investigated by 2nd generation enzyme-linked and
line immunoassays. Acta Gastroenterol Latinoamericana
1994; 24: 71±75.
214 Jadoul M et al. Prevalence of hepatitis C antibodies in health-
care workers [letter; comment]. Lancet 1994; 344: 339.
215 Vanderborght BO et al. High prevalence of hepatitis C
infection among Brazilian hemodialysis patients in Rio de
Janeiro: a one-year follow-up study. Revista Do Instituto
Med Trop Sao Paulo 1995; 37: 75±79.
216 Germanaud J et al. The occupational risk of hepatitis C
infection among hospital employees. Am J Public Health
1994; 84: 122.
217 Schlipkoter U et al. Transmission of hepatitis C virus (HCV)
from a haemodialysis patient to a medical staff member.
Scand J Infect Dis 1990; 22: 757±758.
218 Jochen AB. Occupationally acquired hepatitis C virus
infection [letter; comment]. Lancet 1992; 339: 304.
219 Ribero ML et al. Prevalence of HCV antibody among Italian
dental practitioners. Third Int Symp HCV, Strasbourg, 96
(Abstract), 1991.
220 Campello C et al. Prevalence of HCV antibodies in health-
care workers from northern Italy. Infection 1992; 20:
224±226.
221 Petrosillo N et al. Hepatitis B virus, hepatitis C virus and
human immunode®ciency virus infection in health care
workers: a multiple regression analysis of risk factors.
J Hosp Infect 1995; 30: 273±281.
222 Nakashima K et al. Low prevalence of hepatitis C virus
infection among hospital staff and acupuncturists in
Kyushu. Japan J Infect 1993; 26: 17±25.
223 Fujiyama S et al. Changes in prevalence of anti-HCV
antibodies associated with preventive measures among
hemodialysis patients and dialysis staff. Hepato-Gastroen-
terology 1995; 42: 162±165.
224 Rehman K et al. Prevalence of seromarkers of HBV and
HCV in health care personnel and apparently healthy
blood donors. JPMA ± J Pakistan Med Assoc 1996; 46:
152±154.
225 Mujeeb SA et al. Frequency of parenteral exposure and
seroprevalence of HBV, HCV, and HIV among operation
room personnel. J Hosp Infect 1998; 38: 133±137.
226 Soni PN et al. Hepatitis C virus antibodies among risk
groups in a South African area endemic for hepatitis B
virus. J Med Virol 1993; 40: 65±68.
227 Struve J et al. Prevalence of antibodies against hepatitis C
virus infection among health care workers in Stockholm.
Scand J Gastroenterol 1994; 29: 360±362.
228 Liaw YF et al. Hepatitis C virus infection in patients with
chronic liver diseases in an endemic area for hepatitis B
virus infection. Gastroenterol Japon 1991; 26 (suppl 3):
167±169.
229 Oge O et al. Occupational risk of hepatitis B and C infec-
tions in urologists. Urol Intis 1998; 61: 206±209.
230 Mortimer PP et al. Hepatitis C virus antibody. Lancet 1989;
2: 798.
231 Herbert AM et al. Occupationally acquired hepatitis C virus
infection. Lancet 1992; 339: 305.
232 Neal KR et al. Prevalence of hepatitis C antibodies among
healthcare workers of two teaching hospitals. Who is at
risk? BMJ 1997; 314: 179±180.
233 Lodi G et al. Prevalence of HCV infection in health care
workers of a UK dental hospital. Br Dental J 1997; 183:
329±332.
234 Abb J. Prevalence of hepatitis C virus antibodies in hospital
personnel. Zentralblatt Fur Bakteriologie 1991; 274:
543±547.
235 Shapiro CN et al. Use of the hepatitis-B vaccine and infec-
tion with hepatitis B and C among orthopaedic surgeons.
The American Academy of Orthopaedic Surgeons Sero-
survey Study Committee. J Bone Joint Surg Am 1996; 78:
1791±1800.
236 Cooper BW et al. Seroprevalence of antibodies to hepatitis
C virus in high-risk hospital personnel. Infect Control Hosp
Epidemiol 1992; 13: 82±85.
237 Thomas DL et al. Viral hepatitis in health care personnel at
The Johns Hopkins Hospital. The seroprevalence of and
risk factors for hepatitis B virus and hepatitis C virus
infection. Arch Intern Med 1993; 153: 1705±1712.
238 Polish LB et al. Risk factors for hepatitis C virus infection
among health care personnel in a community hospital. Am
J Infect Control 1993; 21: 196±200.
239 Niu MT et al. Multicenter study of hepatitis C virus infec-
tion in chronic hemodialysis patients and hemodialysis
center staff members. Am J Kidney Dis 1993; 22: 568±573.
240 Forseter G et al. Hepatitis C in the health care setting. II.
Seroprevalence among hemodialysis staff and patients in
suburban New York City. Am J Infect Control 1993; 21: 5±8.
241 Gerberding JL. Incidence and prevalence of human
immunode®ciency virus, hepatitis B virus, hepatitis C
virus, and cytomegalovirus among health care personnel
at risk for blood exposure: ®nal report from a longitudinal
study. J Infect Dis 1994; 170: 1410±1417.
242 Goetz AM et al. Prevalence of hepatitis C infection in health
care workers af®liated with a liver transplant center.
Transplantation 1995; 59: 990±994.
243 Panlilio AL et al. Serosurvey of human immunode®ciency
virus, hepatitis B virus, and hepatitis C virus infection
among hospital-based surgeons. Serosurvey Study Group.
J Am College Surgeons 1995; 180: 16±24.
244 Tokars JI et al. National surveillance of dialysis associated
diseases in the United States. 1995 ASAIO J 1998; 44:
98±107.
245 Davis AR et al. Hepatitis C virus transmission to hetero-
sexual partner: bedroom or bathroom hazard? Med J Aust
1996; 164: 126.
246 Kolho E et al. Transmission of hepatitis C virus to sexual
partners of seropositive patients with bleeding disorders: a
rare event. Scand J Infect Dis 1991; 23: 667±670.
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
98 M. I. Memon & M. A. Memon
247 Meisel H et al. Transmission of hepatitis C virus to children
and husbands by women infected with contaminated anti-
D immunoglobulin. Lancet 1995; 345: 1209±1211.
248 Brettler DB et al. The low risk of hepatitis C virus trans-
mission among sexual partners of hepatitis C-infected
hemophilic males: an international, multicenter study.
Blood 1992; 80: 540±543.
249 Power JP et al. Hepatitis C infection from anti-D immuno-
globulin [letter; comment]. Lancet 1995; 346: 372±373.
250 Scotto G et al. Sexual transmission of hepatitis C virus
infection. Eur J Epidemiol 1996; 12: 241±244.
251 Akahane Y et al. Hepatitis C virus infection in spouses of
patients with type C chronic liver disease. Ann Intern Med
1994; 120: 748±752.
252 Koda T et al. Hepatitis C transmission between spouses.
J Gastroenterol Hepatol 1996; 11: 1001±1005.
253 Mauser-Bunschoten EP et al. Transmission of hepatitis C
virus to spouses [letter; comment]. Ann Intern Med 1995;
122: 154±155.
254 Win N et al. The low risk of hepatitis C virus transmission
among sexual partners of con®rmed HCV-positive blood
donors. Transfusion Med 1994; 4: 243±244.
255 Diago M et al. Intrafamily transmission of hepatitis C virus:
sexual and non-sexual contacts. J Hepatol 1996; 25:
125±128.
256 Saltoglu N et al. Sexual and non-sexual intrafamilial
spread of hepatitis C virus: intrafamilial transmission of
HCV. Eur J Epidemiol 1998; 14: 225±228.
257 Gordon SC et al. Lack of evidence for the heterosexual
transmission of hepatitis C. Am J Gastroenterol 1992; 87:
1849±1851.
258 Quaranta JF et al. Prevalence of antibody to hepatitis C
virus (HCV) in HIV-1-infected patients (nice SEROCO
cohort). J Med Virol 1994; 42: 29±32.
259 van Doornum GJ et al. Prevalence of hepatitis C virus
infections among heterosexuals with multiple partners.
J Med Virol 1991; 35: 22±27.
260 Corona R et al. Heterosexual and homosexual transmission
of hepatitis C virus: relation with hepatitis B virus and
human immunode®ciency virus type 1. Epidemiol Infect
1991; 107: 667±672.
261 Weinstock HS et al. Hepatitis C virus infection among
patients attending a clinic for sexually transmitted diseases.
JAMA 1993; 269: 392±394.
262 Thomas DL et al. Hepatitis C, hepatitis B, and human
immunode®ciency virus infections among non-intraven-
ous drug-using patients attending clinics for sexually
transmitted diseases. J Infect Dis 1994; 169: 990±995.
263 Gust I et al. Prevalence of infection with hepatitis C virus in
Australia. Med J Aust 1989; 151: 719±18.
264 Melbye M et al. Sexual transmission of hepatitis C virus:
cohort study 1981±9 among European homosexual men.
BMJ 1990; 301: 210±212.
265 Westh H et al. Hepatitis C virus antibodies in homosexual
men and intravenous drug users in Denmark. Infection
1993; 21: 115±117.
266 Hadziyannis SJ et al. Hepatitis C virus infection in Greece
and its role in chronic liver disease and hepatocellular
carcinoma. J Hepatol 1993; 17 (suppl 3): S72±7.
267 Gasparini V et al. Hepatitis C virus infection in homosexual
men: a seroepidemiological study in gay clubs in north-
east Italy. Eur J Epidemiol 1991; 7: 665±669.
268 Ricchi E et al. Anti-hepatitis C virus antibodies amongst
Italian homo-bisexual males. Eur J Epidemiol 1992; 8:
804±807.
269 Donahue JG et al. Antibody to hepatitis C virus among
cardiac surgery patients, homosexual men, and intraven-
ous drug users in Baltimore. Maryland Am J Epidemiol
1991; 134: 1206±1211.
270 Tor J et al. Sexual transmission of hepatitis C virus and its
relation with hepatitis B virus and HIV. BMJ 1990; 301:
1130±1133.
271 Sanchez-Quijano A et al. Hepatitis C virus infection in
sexually promiscuous groups. Eur J Clin Microbiol Infect Dis
1990; 9: 610±612.
272 Sonnerborg A et al. Hepatitis C virus infection in individ-
uals with or without human immunode®ciency virus type
1 infection. Infection 1990; 18: 347±351.
273 Osmond DH et al. Comparison of risk factors for hepatitis C
and hepatitis B virus infection in homosexual men. J Infect
Dis 1993; 167: 66±71.
274 Buchbinder SP et al. Hepatitis C virus infection in sexually
active homosexual men. J Infect 1994; 29: 263±269.
275 Ndimbie OK et al. Hepatitis C virus infection in a male
homosexual cohort: risk factor analysis. Genitourin Med
1996; 72: 213±216.
276 Osella AR et al. Hepatitis B and C virus sexual transmission
among homosexual men. Am J Gastroenterol 1998; 93:
49±52.
277 Wu JC et al. Prevalence, infectivity, and risk factor analysis
of hepatitis C virus infection in prostitutes. J Med Virol
1993; 39: 312±317.
278 Develoux M et al. Hepatitis C virus antibodies in prostitutes
in Niger. Trans R Soc Trop Med Hyg 1994; 88: 536.
279 Gutierrez P et al. Prevalence of anti-hepatitis C virus anti-
bodies in positive FTA-ABS non-drug abusing female
prostitutes in Spain. Sex Transm Dis 1992; 19: 39±40.
280 Crofts N et al. Hepatitis C virus infection among a cohort of
Victorian injecting drug users. Med J Aust 1993; 159:
237±241.
281 Crofts N et al. Methadone maintenance and hepatitis C
virus infection among injecting drug users. Addiction 1997;
92: 999±1005.
282 van Beek I et al. Infection with HIV and hepatitis C virus
among injecting drug users in a prevention setting: retro-
spective cohort study. BMJ 1998; 317: 433±437.
283 Chang CJ et al. Hepatitis C virus infection among short-
term intravenous drug users in southern Taiwan. Eur
J Epidemiol 1999; 15: 597±601.
284 Smyth BP et al. Bloodborne viral infection in Irish injecting
drug users. Addiction 1998; 93: 1649±1656.
285 Stark K et al. Frontloading: a risk factor for HIV and
hepatitis C virus infection among injecting drug users in
Berlin. AIDS 1996; 10: 311±317.
286 Van den Hoek JA et al. Prevalence, incidence, and risk
factors of hepatitis C virus infection among drug users in
Amsterdam. J Infect Dis 1990; 162: 823±826.
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
Epidemiological review of hepatitis C 99

287 Van Ameijden EJ et al. A longitudinal study on the inci-
dence and transmission patterns of HIV, HBV and HCV
infection among drug users in Amsterdam. Eur J Epidemiol
1993; 9: 255±262.
288 Galeazzi B et al. Hepatitis C virus infection in Italian
intravenous drug users: epidemiological and clinical
aspects. Liver 1995; 15: 209±212.
289 Wood®eld DG et al. Hepatitis C virus infections in
oral and injectable drug users. NZ Med J 1993; 106:
332±334.
290 Robinson GM et al. Hepatitis C prevalence and needle/
syringe sharing behaviours in recent onset injecting drug
users. NZ Med J 1995; 108: 103±105.
291 Kemp et al. Injecting behaviours and prevalence of hepa-
titis B, C and D markers in New Zealand injecting drug user
populations. NZ Med J 1998; 111: 50±53.
292 Hagan H et al. Syringe exchange and risk of infection
with hepatitis B and C viruses. Am J Epidemiol 1999; 149:
203±213.
293 Bolumar F et al. Prevalence of antibiotics to hepatitis C in a
population of intravenous drug users in Valencia, Spain.
1990±92. Int J Epidemiol 1996; 25: 204±209.
294 Santana Rodriguez OE et al. Prevalence of serologic
markers of HBV, HDV, HCV and HIV in non-injection drug
users compared to injection drug users in Gran Canaria,
Spain. Eur J Epidemiol 1998; 14: 555±561.
295 Garfein RS et al. Prevalence and incidence of hepatitis C
virus infection among young adult injection drug users.
JAIDS 1998; 18 (suppl 1): S11±9.
Ó 2002 Blackwell Science Ltd, Journal of Viral Hepatitis, 9, 84±100
100 M. I. Memon & M. A. Memon
Related Documents











