HEPATITIS AND ITS COMPLICATIONS PRESENTERS: OTAALO BRIAN BYONANUWE SIMON

Hepatitis and its complications
Aug 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

HEPATITIS AND ITS COMPLICATIONS
PRESENTERS: OTAALO BRIANBYONANUWE SIMON

Outline
• Definition• Classification • Clinical features• Specific causes of hepatitis • Hepatitis B & Complications

Hepatitis
• Defn- inflammation of the liver
Classification• Duration : acute hepatitis vs chronic hepatitis• Aetiology: Viral, drug induced, autoimmune
Causes
Acute hepatitis• Viral hepatitis• Non-viral infection• Alcohol• Toxins• Drugs• Autoimmune
Chronic hepatitis• Viral hepatitis• Alcohol• Drugs• Non-alcoholic steatohepatitis• Autoimmune
Clinical features
Acute hepatitis• Fatigue, anorexia, nausea, and vomiting• Jaundice • Severe cases may progress to acute liver failure

Cont…
Chronic hepatitis• Peripheral stigmata of chronic liver disease- clubbing, leukonychia, palmar erythema, Dupuytren’s contracture - Paucity of axillary or pubic hair- Spider naevi, jaundice ,parotic enlargement- Gynaecomastia - Ascites - Testicular atrophy
Viral Hepatitis

Hepatitis A virus (HAV)• Spread by fecal-oral route• Incubation: 2-6wksSymptoms• Prodomal- fever, malaise, anorexia, nausea, arthralgia• Jaundice +/- hepatomegaly, splenomegalyTests- AST & ALT rise 22-40 days after exposure - IgM rises after day 25, IgG remains detectable for lifeTreatment- supportivePrevention- immunizationPrognosis- usually selflimiting, chronic liver disease doesn’t occur
Hepatitis C virus (HCV)
• Caused by RNA flavirus• Spread through blood Risk factors• IV drug misuse (95% in UK)• Needle stick injury (3%)• Vertical transmission (3%)• Iatrogenic parenteral transmission

HCV cont…
Clinical presentation• Early infection is often mild/ asymptomatic• in asymptomatic pple, its usually identified when screened for• Patients are usually identified with chronic liver disease• 80% develop chronic inf, 20-30% progress to cirrhosisTests• Anti-HCV antibodies• Comfirmed by HCV RNA in an antibody positive person

HCV cont…
Treatment• Aim is to eradicate infection• Combination therapy of PEGylated interferon alpha & ribavirin• Rivabirin – given as an oral drug-main side effects (S.Es) – hemolytic anaemia & teratogenicity• PEGinterferon alpha – give subcutaneously once everywk- S.Es- flu like symptoms, irritability & depressionLiver transplant- in complications of cirrhosis
Hepatitis D virus (HDV)
• Incomplete RNA virus • Only exists with HBV, therefore spread with HBV• Signs: increased risk of acute hepatic failure and cirrhosis• Tests: Anti-D antibody

Drug Induced Hepatitis
• The liver is the primary site of drug metabolismRisk Factors• Occupational xposure, herbsCommon drugs• Paracetamol overdose• Pyrazinzmide,Isoniazid, rifampicin• AZT, NVP• Halothane Treatment: withdraw offending drug
Autoimmune Hepatitis(AIH)
• Liver disease characterized by suppressor T cell defects with autoantibodies directed against hepatocyte surface antigens
• Predominantly affects women, in their 2nd & 3rd decades classification• Type I- affects adults or children(bi modial distributuion) - Anti smooth muscle antibodies(ASMA) +ve in 80% - antinuclear antibodies (ANA) +ve in 10 - Hypergammaglobulinaemia (IgG)
AIH cont…….
• Type II – Affects mainly girls & young women - more commonly progresses to cirrhosis - anti liver/kidney microsomal type 1 (LKM1) antibodies• Type III – affects adults & clinically distinguishable from type1 - antibodies against soluble liver antigen or liver –pancrease AgClinical Features• 25% present with acute hepatitis & signs of autoimmune disease-fever,malaise, urticarial rash, glomerulonephritis
Cont..
• Signs of chronic liver disease• Complications- cirrhosisTests• Abnormal LFT ( increased AST,ALT,birilubin,ALP)• Hyperalbuminaemia (esp IgG)• +ve autoantibodies (ANA,SMA, LKM1 or SLA)• Anaemia, reduced WCC & platelets – hypersplenism• Liver biopsy
Cont..
• Diagnosis depends on excluding other diseasesManagement• Immunosuppression therapy- prednisolone 30mg/d for a month, decrease by 5mg a month - Maintanance dose 5-10mg/d for a month - Azathioprine (50-100mg/d) may b used as asteroid sparing agent• Liver transplant- in decompensated cirrhosis - failure to respond to medical therapy• Prognosis- 10yr survival approx. 80%

The virusSmall(42nm), double stranded, DNA virusAlso called Dane particleHepadnaviridaeInfects only humansGenetic variations A-HRx implicationsGlobal distribution

• Double shelled, inner core and outer envelope

TransmissionVertical transmission(90%), from mother to child in the perinatal period, is the most common cause of infection world-wide and carries the highest risk.
Others;• Injection drug use • Infected unscreened blood products•Tattoos/acupuncture needles •Sexual (homosexual and heterosexual)

Risk groups
• Iv drug users and their sexual partners• Health workers• Hemophiliacs and their cares• The sexualy promiscuous
Natural hx
• Predominantly affect hepatocytes• Causes both acute and chronic disease• Incubation period 1-6mts• There’s an initial immunitolerant phase• An immunological torelance then occurs with elvn in hep
transaminases, liver damage• Cirrhosis if the response sustained over many yrs

Mechanism
• Liver injury believed to be immunologically mediated• Mediated by cytotoxic t cells• Specific cytokines produced by the T cells• These damage hepatocytes

C/features: Acute infn
• Often asymptomatic• Non specific symptoms eg fatigue, anorexia, nausea, abd
pain, low grade fevers• Typically lasts 2-4mts• Infants, cn <5yrs and iss adults more likely asymptomatic• In aduots with healthy immune system; ~95% self ltd• <5% adults progress to to chronic infection• A small no (1%)develop AHF, may die or require urgent
liver transplant.

C/f: chronic inf• Considered chronic if >6/12• Risk inversely related to age, abt 90% of infected infant,
30% <5YRS, <5% older pple• NB; a serum sickness-like immunological syndrome may be
seen.• urticaria or a maculopapular rash• polyarthritis affecting small joints occurring in up to 25% of
cases in the prodromal period. • Extrahepatic immune complex-mediated conditions such
as an arteritis or glomerulonephritis are occasionally seen
Dx
• Serology-HBsAg, HBsAb, HBcAb.• LFTs• Viral load/HBV PCR• Monitoring response to therapy• Identifying patients with pre coremutants• Specific genotypes can be identified-B&C more aggressive!
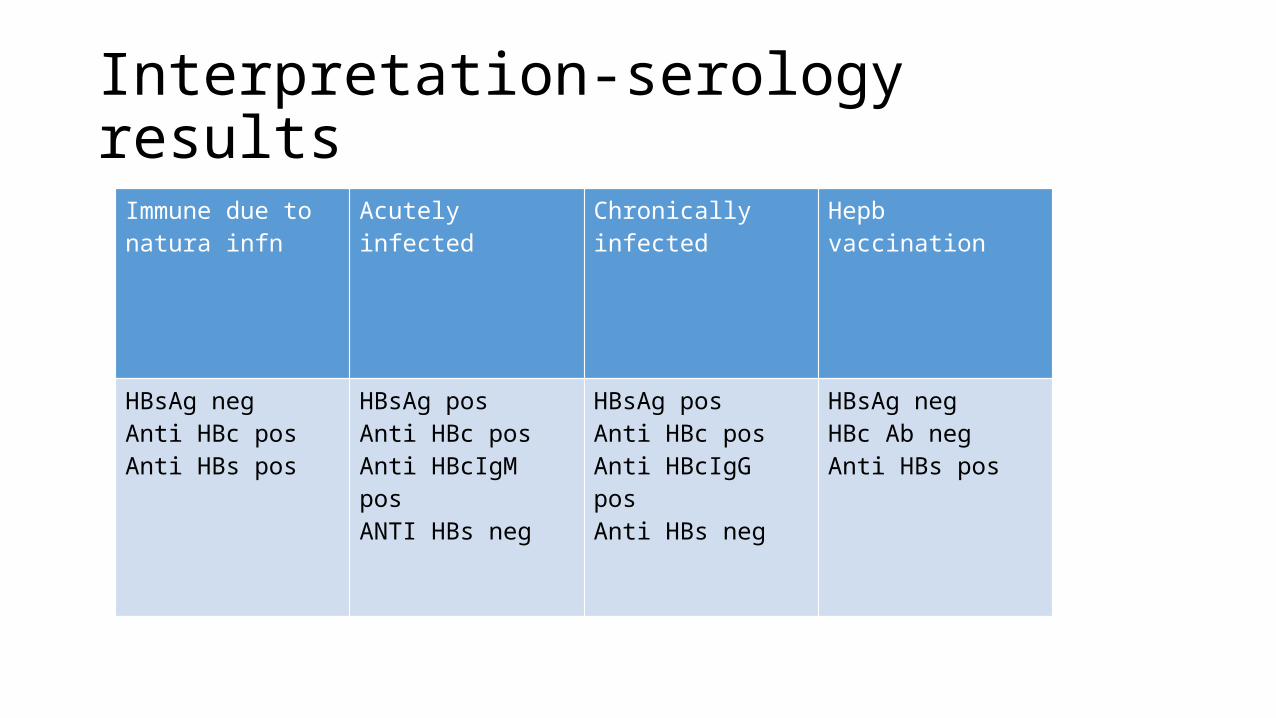
Interpretation-serology resultsImmune due to natura infn
Acutely infected Chronically infected Hepb vaccination
HBsAg negAnti HBc posAnti HBs pos
HBsAg posAnti HBc posAnti HBcIgM posANTI HBs neg
HBsAg posAnti HBc posAnti HBcIgG posAnti HBs neg
HBsAg negHBc Ab negAnti HBs pos

Rx; acute
• Supportive• Avoid alcohol

Who shd be treated?
·Chronic HBV infection: HBsAg+ > 6 months
·Evidence of virus replication: serum HBV DNA >105 copies/ml
·Evidence of liver damage: elevated ALT and/or chronic hepatitis on biopsy
Rx; chronic• Indicatation: high viral load in presence of active hep as
may be demonstrated by:• Elevated transaminases and/or• Histological evidence of inflammn• Goals: • Reduce infllammn • Prevent liver failure • Reduce risk of cirrhosis and complications by suppressing
HBV replication
• Inj. Pegylated interferon alfa 2a 180mcg/wk X 48/52• Or other antiviral(oral) e.g• Adevofir 10mg/day• Lamivudine 100mg/day • Tenofovir 300mg/day• Others recommended telbivudine, entecavir.• Add 2nd antiviral if HBV DNA stil detactable wthin 6-12mts• Monitor renal function
Complications
• Fulminant HF• Cirrhosis and its complications• Extrahepatic dse• Etc
CIRRHOSIS • end stage of chronic liver disease characterised by: • destruction of the normal hepatic archtecture by fibrous
septa • that encompass regenerative nodules of hepatocytes
The liver architecture is diffusely abnormal this interferes with liver blood flow and function. This derangement produces the clinical features of portal
hypertension and impaired liver cell function.
There’s…
• Parenchymal injury and consequent fibrosis are diffuse, extending throughout the liver.
• Irreversible fibrosis• Nodularity • Vascular architecture is reorganised by the parenchymal
damage and scarring formation of abnormal interconnections between vascular inflow and hepatic vein outflow channels.
Causes• Alcohol• Chronic viral hepatitis (B or C) Non-alcoholic fatty liver disease• ImmunePrimary sclerosing cholangitisAutoimmune liver disease • BiliaryPrimary biliary cirrhosisCystic fibrosis • GeneticHaemochromatosisα1-antitrypsin deficiencyWilson's disease • Cryptogenic (unknown

Pathogenesis • Chronic injury to the liver---inflammation--necrosis and,
eventually, fibrosis. • Fibrosis initiated by activation of stellate cells. • Kupffer cells seem to have a role in their activation, but
hepatocytes and other cells are probably involved. • Stellate cells are activated by many cytokines.

Cont…
• In the early stage of activation the stellate cells become swollen with upregulation of receptors for proliferative and fibrogenic cytokines, such as PDGF, and possibly transforming growth factor β1 (TGF-β1).
• In the space of Disse, the normal matrix is replaced by collagens, predominantly types 1 and 3, and fibronectin.
• Subendothelial fibrosis leads to loss of the endothelial fenestrations, and this impairs liver function.
• increase in tissue inhibitors of metalloproteinases (TIMPs), wc inhibit Collagenases (matrix metalloproteinases, MMP) that wd o/wise degrade this collagen.
Two types of cirrhosis have been described
• Micronodular cirrhosis. Xterised by small nodules, abt 1mm in diameter( less than 3 mm) in size and the liver is involved uniformly. Often in alcohol cirhhosis, biliaryb tract dse
• Macronodular cirrhosis. Large nodules are of variable size. often seen following previous hepatitis, such as HBV infection.
• A mixed picture with small and large nodules is sometimes seen.
Clinical features • vary greatly• may be entirely asymptomatic; in life it may be found
incidentally at surgery or may be associated with minimal features such as isolated hepatomegaly.
• Frequent complaints include weakness, fatigue, muscle cramps, weight loss and non-specific digestive symptoms such as anorexia, nausea, vomiting and upper abdominal discomfort.
• Otherwise, clinical features are due mainly to hepatic insufficiency and portal hypertension
Cont…• Hepatomegaly (although liver may also be small) • Jaundice • Ascites • Circulatory changes
• Spider telangiectasia, palmar erythema, cyanosis • Endocrine changes
• Loss of libido, hair loss • Men: gynaecomastia, testicular atrophy, impotence • Women: breast atrophy, irregular menses,
amenorrhoea
Cont…• Haemorrhagic tendency • Bruises, purpura, epistaxis, menorrhagia • Portal hypertension • Splenomegaly, collateral vessels, variceal bleeding, fetor
hepaticus • Hepatic (portosystemic) encephalopathy • Other features • Pigmentation, digital clubbing

Investigations• Labs• LFTs- normal, or increasd biliru, AST, ALT, ALK PHOSPH AND
GGT. • LATER with loss of synthetic fuction, look for decreased
albn.• Decreased WCC, and platelates indicatete hypersplensm• Find the cause; ferritin, iron/total ironbinding capacity,
hepatitis serology, immunoglobulins, ceruloplasmin, etc• U/s may show small livr or hepatomega, splenom, ascites,
focal liver lesions etc.• Ascitic tap—MC+S, NEUTRO>250/mm3 indicate SBP.• Liver bx-----confirms dx.

ComplicationsVARICES• Varices• Anemia• Renal failure• Infection• Coagulopathy• Encephalopathy• Sepsis
Mx• General measures• Nutritional counsellg• Alcohol abstinence• Regular u/s +/- alfa fetoprotein 3-6mts.• Manage complications
PORTAL HYPERTENSION • Characterised by prolonged elevation of the portal venous
pressure (normally 2-5 mmHg). • Patients developing clinical features or complications of
portal hypertension usually have portal venous pressures above 12 mmHg.
• Can be classified according to the site of obstruction: • prehepatic • intrahepatic - due to distortion of the liver architecture,
can be presinusoidal (e.g. in schistosomiasis) or postsinusoidal (e.g. in cirrhosis)
Cont…
• posthepatic - due to venous blockage outside the liver (rare). • As portal pressure rises above12 mmHg, the compliant venous system
dilates and collaterals occur within the systemic venous system. • Main sites of collaterals are at gastro-oesophageal junction and
rectum.
CausesPrehepatic:-obstructive thrombosis, narrowing of portal vein before it branches within the liver.- massive splenomegally may shunt excessive blood into the splenic vein. Posthepatic causes:- severe right-sided heart failure- constrictive pericarditis- hepatic vein outflow obstruction Intrahepatic causes:- cirrhosis (most dominant)- schistosomiasis- massive fatty change- diffuse fibrosis eg. Sarcoidosis. eg granulomatous disease- milliary tuberculosis.
Pathophysio…• Portal hypertension in cirrhosis results from
- increased resistance to portal flow at the level of the sinusoids. - compression of central veins by perivenular fibrosis• This increased resistance leads to portal hypertension and
opening of portosystemic anastomoses

Consequences
• Ascites• Formation of porto-systemic shunts• Congestive splenomegaly• Congestive gastropathy• Hepatic encephalopathy

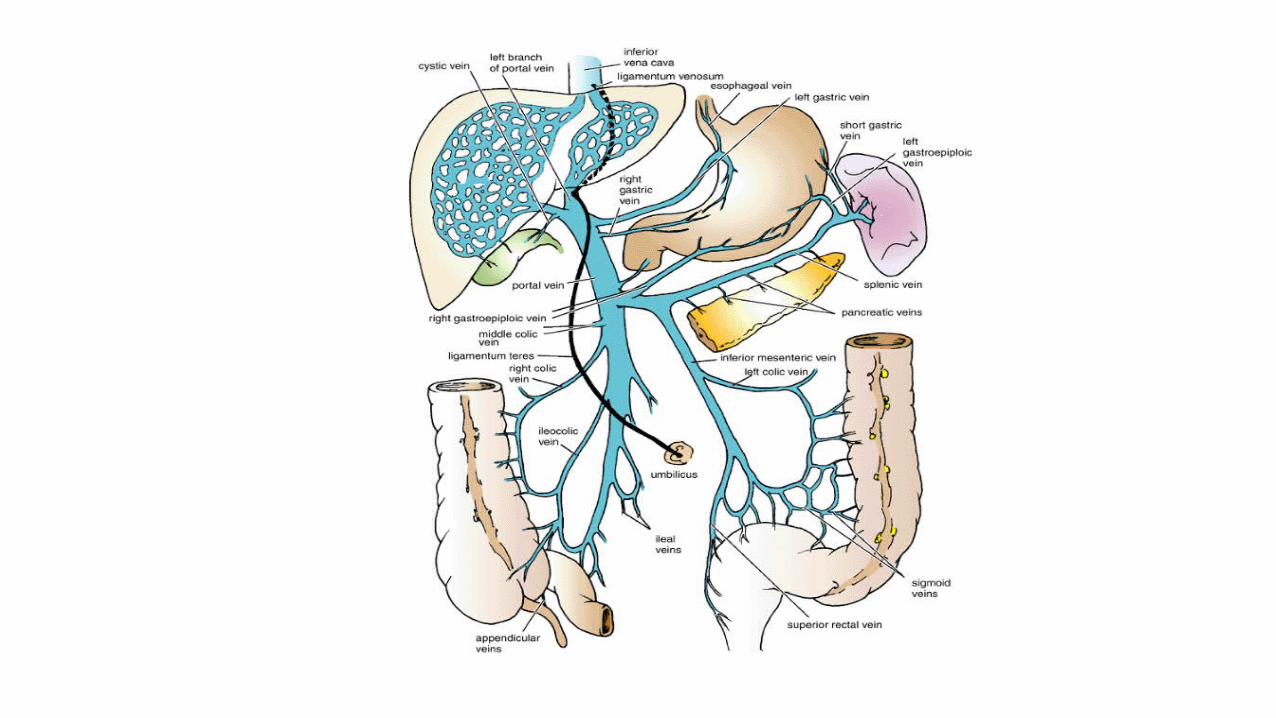
VARICEAL BEEDING• important to appreciate the portal systemic shuntsWith the rise in portal system pressure, bypasses develop
wherever systemic and portal circulation share common capillary beds:
i. Veins around and within rectum ( hemorrhoids)• Superior rectal vein Vs middle and inferior rectal veinsii. Cardio-esophageal junction (esophago-gastric varices)• Left gastric Vs azygosiii. Retroperitoneum and falciform ligament of the liver involving the periumbilical and abnominal wall collaterals) caput medusa• Paraumbilical Vs left branch of portal vein

Important…• ~90% of cirrhosis patients develop esophageal varices• ~1/3 bleed• Bleeding more likely in• Large varices• Red signs • Severe liver dse• Drugs capable of causing mucosal erosions eg NSAIDS
better avoided. can ppt bleedg.

Mx:
• active bleeding, • prevent rebleeding, • prophylaxix to prevent 1st hemorrhage.
Cont…Acute variceal bleedingABC, iv access, samples gping&xmatch,hb, pt/INRetc,
resuscitate-restore circuln wth blood and plasma.Urgent endoscopy, even in known case; 20% not varices
but other lesions-acute gastric erosionsLocal measures-used to control acute v. bleedg• Endoscopic Band ligation or sclerotherapy-most widely used initial Rx, stops variceal bleeding in 80% .

Cont…• Balloon tamponade• Oesophageal transection• Pharmacological treatment • Terlipressin is the current drug of choice and releases the
vasoconstrictor, vasopressin, over several hours in amounts sufficient to reduce the portal pressure without producing systemic effects.
dose: 2 mg i.v. 6-hrly until bleeding stops, then 1 mg 6-hrlyxfurther 24 hrs.
Cont…• Octreotide, the synthetic form of somatostatin, 50 μg iv,
followed by an infusion of 50 μg hourly. • TIPSS and shunt surgery(transjugular intrahepatic
portosystemic stent shunting ) • used for acute bleeding not responding to sclerotherapy or
banding.• Asscociated high (50%) mortality or more, now virtually
never used for treating active variceal bleeding.
Prevention of recurrent bleeding
• Recurrent bleeding is the rule rather than the exception in patients who have previously bled from oesophageal varices, and treatment to prevent this is needed.
Band ligation • Varices occluded with a tight rubber band. The occluded
varix subsequently sloughs with variceal obliteration. • repeated every 1-2 weeks until the varices are obliterated. • Regular follow-up endoscopy required to identify and treat
any recurrence of varices. • generally more effective than sclerotherapy, has fewer side-
effects and is now the treatment of choice.
Cont…
• Sclerotherapy • varices are injected with a sclerosing agent, been largely
abandoned in pref to banding ligation. • !transient chest or abd pain, fever, dysphagia, occasionally
oes. perforation. Oesophageal strictures may also develop.
Cont…• TIPSS • Stent placed between the portal vein and the hepatic vein
in the liver to provide a portosystemic shunt and therefore reduce portal pressure.

Cont…• β-blockers • Propranolol (80-160 mg/day) or nadolol• Reduces portal venous pressure in portal hypertension and
have been used to prevent recurrent variceal bleeding
CONGESTIVE GASTROPATHY
• chronic gastric congestion due to Long-standing portal hypertension
• Endoscopy-multiple areas of punctate erythema. • Rarely, similar lesions occur more distally in the GIT. • may become eroded, causing bleeding from multiple sites. • Acute bleeding can occur, but repeated minor bleeding causing
iron-deficiency anaemia is more common. • Anaemia may be prevented by oral iron supplements. • Reduction of the portal pressure using propranolol 80-160
mg/day is the best initial Rx. • If ineffective, TIPSS can be undertaken.

…….end
Related Documents