Hepatic Energy Metabolism and the Differential Protective Effects of Sevoflurane and Isoflurane Anesthesia in a Rat Hepatic Ischemia-Reperfusion Injury Model Nurdan Bedirli, MD* Ebru Ofluoglu, PhD† Mustafa Kerem, MD‡ Gulten Utebey, MD* Murat Alper, MD§ Demet Yilmazer, MD§ Abdulkadir Bedirli, MD‡ Onur Ozlu, MD* Hatice Pasaoglu, MD† BACKGROUND: We investigated the effects of isoflurane and sevoflurane in a warm liver ischemia-reperfusion (IR) model on cytokines, hepatic tissue blood flow (HTBF), energy content, and liver structure. METHODS: Seventy-two Wistar rats were randomly assigned into 1 of 3 groups: Control group, no volatile anesthetics; sevoflurane group, 2% sevoflurane; isoflu- rane group, 1.5% isoflurane. Thirty minutes after the start of volatile anesthetics, rats were subjected to 45 min hepatic ischemia and 2 and 4 h of reperfusion. Rats were killed at the end of ischemia, 2 and 4 h of reperfusion. Aspartate aminotrans- ferase and alanine aminotransferase, HTBF, malondialdehyde, tumor necrosis factor (TNF)-, interleukin (IL)-1, energy charge, and histologic examination were used to evaluate the extent of liver injury. RESULTS: Serum alanine aminotransferase and aspartate aminotransferase levels were similar in control and isoflurane groups while there was a significant decrease in the sevoflurane group in the postischemic period (P 0.01). HTBF was remarkably better in the sevoflurane group than in the isoflurane group and worse in the control group. Tissue malondialdehyde levels were significantly low in the sevoflurane group compared with the isoflurane group at 2 h of reperfusion (P 0.05) and reached its maximum value in the postischemic period in the control group. After ischemia, 2 and 4 h of reperfusion, tumor necrosis factor- and interleukin-1 values were lowest in the sevoflurane group and highest in the control group but it was not statistically significant (P 0.05). In the sevoflurane group, hepatic adenosine triphosphate and energy charge were significantly high at all measurement times. At the postischemic period, energy charge was lower compared with the sevoflurane and isoflurane groups. The degree of hepatocyte injury was small in the sevoflurane group. CONCLUSIONS: Clinically relevant concentrations of sevoflurane given before, dur- ing, and after hepatic ischemia protected the liver against IR injury, whereas the effects of isoflurane on hepatic IR injury were not notable. (Anesth Analg 2008;106:830 –7) Intraoperative temporary interruption of liver blood flow sometimes occurs during surgical procedures. This hepatic ischemia and subsequent reperfusion can lead to liver dysfunction or severe hepatic failure, depending on the severity and duration of the isch- emia. The balance between hepatic oxygen supply through hepatic tissue blood flow (HTBF) and oxygen consumption by hepatocytes is an essential factor in hepatic metabolism. 1 The reduction of HTBF may impair hepatic energy metabolism. Ischemia causes functional and structural damage to liver cells. 2 The status of energy metabolism is one of the more impor- tant functional disorders for predicting the viability of the ischemic organ. Reperfusion after ischemic injury triggers activation of several transcription factors, including nuclear factors, which, in turn, alter the transcription of multiple genes associated with inflam- matory response, including intercellular adhesion molecule-1, interleukin (IL)-1, IL-8, and tumor necro- sis factor (TNF)-. 3 Kupffer cell activation is a central hepatic pathophysiologic mechanism of the reperfu- sion injury. Activated Kupffer cells release reactive oxygen species, which leads to the generation of end-products of lipid peroxidation, such as malondi- aldehyde (MDA). 4 Inhaled anesthetics, besides their anesthetic effects, have significant nonanesthetic physiologic effects. For some years, data have been accumulating from in vivo From the *Department of Anesthesiology, Diskapi Training and Research Hospital; Departments of †Biochemistry and ‡General Sur- gery, Gazi University Medical School; and §Department of Pathology, Diskapi Training and Research Hospital, Ankara, Turkey. Accepted for publication November 1, 2007. Address correspondence and reprint requests to Nurdan Bedirli, MD, Mesa Koru Sit. Fulya Blok, 85/39, 06810, Cayyolu, Ankara, Turkey. Address e-mail to [email protected]. Copyright © 2008 International Anesthesia Research Society DOI: 10.1213/ane.0b013e3181616fc9 Vol. 106, No. 3, March 2008 830

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Hepatic Energy Metabolism and the DifferentialProtective Effects of Sevoflurane and IsofluraneAnesthesia in a Rat Hepatic Ischemia-ReperfusionInjury Model
Nurdan Bedirli, MD*
Ebru Ofluoglu, PhD†
Mustafa Kerem, MD‡
Gulten Utebey, MD*
Murat Alper, MD§
Demet Yilmazer, MD§
Abdulkadir Bedirli, MD‡
Onur Ozlu, MD*
Hatice Pasaoglu, MD†
BACKGROUND: We investigated the effects of isoflurane and sevoflurane in a warmliver ischemia-reperfusion (IR) model on cytokines, hepatic tissue blood flow(HTBF), energy content, and liver structure.METHODS: Seventy-two Wistar rats were randomly assigned into 1 of 3 groups:Control group, no volatile anesthetics; sevoflurane group, 2% sevoflurane; isoflu-rane group, 1.5% isoflurane. Thirty minutes after the start of volatile anesthetics,rats were subjected to 45 min hepatic ischemia and 2 and 4 h of reperfusion. Ratswere killed at the end of ischemia, 2 and 4 h of reperfusion. Aspartate aminotrans-ferase and alanine aminotransferase, HTBF, malondialdehyde, tumor necrosisfactor (TNF)-�, interleukin (IL)-1�, energy charge, and histologic examination wereused to evaluate the extent of liver injury.RESULTS: Serum alanine aminotransferase and aspartate aminotransferase levelswere similar in control and isoflurane groups while there was a significant decreasein the sevoflurane group in the postischemic period (P � 0.01). HTBF wasremarkably better in the sevoflurane group than in the isoflurane group and worsein the control group. Tissue malondialdehyde levels were significantly low in thesevoflurane group compared with the isoflurane group at 2 h of reperfusion (P �0.05) and reached its maximum value in the postischemic period in the controlgroup. After ischemia, 2 and 4 h of reperfusion, tumor necrosis factor-� andinterleukin-1� values were lowest in the sevoflurane group and highest in thecontrol group but it was not statistically significant (P � 0.05). In the sevofluranegroup, hepatic adenosine triphosphate and energy charge were significantly highat all measurement times. At the postischemic period, energy charge was lowercompared with the sevoflurane and isoflurane groups. The degree of hepatocyteinjury was small in the sevoflurane group.CONCLUSIONS: Clinically relevant concentrations of sevoflurane given before, dur-ing, and after hepatic ischemia protected the liver against IR injury, whereas theeffects of isoflurane on hepatic IR injury were not notable.(Anesth Analg 2008;106:830–7)
Intraoperative temporary interruption of liver bloodflow sometimes occurs during surgical procedures.This hepatic ischemia and subsequent reperfusion canlead to liver dysfunction or severe hepatic failure,depending on the severity and duration of the isch-emia. The balance between hepatic oxygen supplythrough hepatic tissue blood flow (HTBF) and oxygenconsumption by hepatocytes is an essential factor inhepatic metabolism.1 The reduction of HTBF may
impair hepatic energy metabolism. Ischemia causesfunctional and structural damage to liver cells.2 Thestatus of energy metabolism is one of the more impor-tant functional disorders for predicting the viability ofthe ischemic organ. Reperfusion after ischemic injurytriggers activation of several transcription factors,including nuclear factors, which, in turn, alter thetranscription of multiple genes associated with inflam-matory response, including intercellular adhesionmolecule-1, interleukin (IL)-1�, IL-8, and tumor necro-sis factor (TNF)-�.3 Kupffer cell activation is a centralhepatic pathophysiologic mechanism of the reperfu-sion injury. Activated Kupffer cells release reactiveoxygen species, which leads to the generation ofend-products of lipid peroxidation, such as malondi-aldehyde (MDA).4
Inhaled anesthetics, besides their anesthetic effects,have significant nonanesthetic physiologic effects. Forsome years, data have been accumulating from in vivo
From the *Department of Anesthesiology, Diskapi Training andResearch Hospital; Departments of †Biochemistry and ‡General Sur-gery, Gazi University Medical School; and §Department of Pathology,Diskapi Training and Research Hospital, Ankara, Turkey.
Accepted for publication November 1, 2007.Address correspondence and reprint requests to Nurdan Bedirli,
MD, Mesa Koru Sit. Fulya Blok, 85/39, 06810, Cayyolu, Ankara,Turkey. Address e-mail to [email protected].
Copyright © 2008 International Anesthesia Research SocietyDOI: 10.1213/ane.0b013e3181616fc9
Vol. 106, No. 3, March 2008830

and in vitro experiments suggesting that inhaled an-esthetics, such as sevoflurane and isoflurane, exertprotective effects against ischemia-reperfusion (IR)injury in various organs.5–9 Previous studies haveshown that these anesthetics could protect against IRinjury of the heart,10 brain,11 and liver.12 Specifically,pretreatment with volatile anesthetics before cardiacischemia protects against IR injury.10,13 The mecha-nisms of organ protection by volatile anesthetics areunclear; however, several studies have suggested thatinhaled anesthetics protect the heart via activation ofadenosine triphosphate-dependent potassium (K�
ATP) channels.14 Other studies suggest that inhaledanesthetics protect against IR injury in the heart15 andlung6 via antiinflammatory effects.
The aim of this study was to investigate theeffects of administration of isoflurane and sevoflu-rane before ischemia in a rat model of warm liver IRon systemic cytokine levels, HTBF, energy charge,and liver histology.
METHODSThe experimental protocols were conducted with
the approval of the Animal Research Committee atGazi University, Ankara. All animals were maintainedin accordance with the recommendations of the Na-tional Institutes of Health Guidelines for the Care andUse of Laboratory Animals.
Animals and Experimental DesignSeventy-two male Wistar rats weighing 280–315 g
were housed at 22°C with a 12-h light–dark cycle andfree access to food and water. The rats were randomlydivided into three groups, control (n � 24; no vola-tiles), sevoflurane (n � 24; 2% sevoflurane), andisoflurane (n � 24; 1.5% isoflurane). The rats wereanesthetized by IM injection of 50 mg/kg ketaminehydrochloride (Ketalar, Parke Davis, Berlin, Germany)and 0.01 mg atropine. All rats were placed on anelectric heating pad under a warming light. Electriccardiography was monitored. After ketamine injec-tion, within approximately 5 min, tracheostomy wasperformed with a 16-gauge cannula, intratracheal in-tubation was established, and the lungs were venti-lated with volatile anesthetics without muscle relaxants.The right femoral artery was cannulated to monitormean arterial blood pressure (MABP) and for bloodgas analysis. Hydration was maintained by hourlyintraperitoneal injection of 5 mL saline solution. Bothvolatile anesthetics were carried in 100% oxygen andthe flow of oxygen gas was set at 4 L/min with theanesthesia apparatus.
Surgical ProcedureThe rats were placed on the operating table in a
supine position with a baseline period of inhalation ofanesthesia (30 min), during which there was no sur-gical intervention. After this period, with local anes-thesia achieved using 1% lidocaine, a midline abdominal
incision was made. The liver was exposed and allstructures in the portal triad (hepatic artery, portalvein, and bile duct) to the left lateral and median liverlobes were interrupted (Fig. 1A) for 45 min with avascular clip (Harvard Apparatus, Inc., Hollinston,MA). This method of partial hepatic ischemia pre-vented mesenteric venous congestion by permittingportal decompression through the right and caudatelobes. A laser Doppler miniprobe was placed on theleft lateral lobe to monitor HTBF (Fig. 1B). After 45min of ischemia, the clip was removed to allow 4 h ofreperfusion.
Rats in the sevoflurane and isoflurane groups wereexposed to 2% sevoflurane (Abbott Laboratories,Queenborough, UK) and 1.5% isoflurane (Abbott Lab-oratories), respectively, with an agent-specific vapor-izer until the end of reperfusion. From each group,eight rats were killed at the end of ischemia, 2 and 4 hof reperfusion. Blood samples were withdrawn for themeasurement of liver enzymes aspartate aminotrans-ferase (AST) and alanine aminotransferase (ALT),TNF-�, IL-1�, and liver samples from the left lateraland median hepatic lobes (segment II–IV) were col-lected for the measurement of MDA concentration,
Figure 1. A, Liver partial ischemia. Schematic representation.B, A laser Doppler miniprobe was placed on the left laterallobe to monitor blood flow.
Vol. 106, No. 3, March 2008 © 2008 International Anesthesia Research Society 831

ATP, adenosine S�-diphosphate (ADP), adenosine 5�-monophosphate (AMP) content, and histologic exami-nation. All surgical procedures were maintained withvolatile anesthetic administration.
HTBFHTBF was measured with a laser Doppler flowme-
ter (Periflux 5000, Perimed, Sweden) before ischemia,at 5, 15, and 45 min after initiation of ischemia, and at5, 15, 30, and 60 min after reperfusion. At each timepoint, a mean of three values obtained at three differ-ent lobes was calculated. HTBF was expressed as apercentage of the preischemic value.
Biochemical DeterminationsSerum AST and ALT activities were measured on
the Aeroset autoanalyzer (Abbott Laboratories) andreported in units per liter.
TNF-� and IL-1� ImmunoassaySerum TNF-� and IL-1� levels were detected in a
96-well microtitre plate by using a commercialenzyme-linked immunosorbent assay kit (BioSourceInternational, Inc., Camarillo, CA) according to themanufacturer’s guidelines. All samples were tested induplicate. The plate was read on ELx800 automatedmicroplate reader (Bio-Tek Instruments, Inc., Winooski,VT) at 450 nm. The concentrations of TNF-� and IL-1�were calculated from a standard curve and expressedin picogram per milliliter (pg/mL). The lower limit ofdetection for enzyme-linked immunosorbent assaywas 8–16 pg/mL.
MDA MeasurementThe extent of lipid peroxidation in the liver was
determined by measuring MDA, an end-product ofliver peroxidation. Tissue sampled from the liver washomogenized with a Virsonic 100 (Virtis CompanyInc., Gardiner, NY) ultrasonic homogenizer. TissueMDA levels were measured according to the methodof Ohkawa et al.16 Briefly, 0.1 mL of homogenate wasmixed with 0.1 mL of 8.1% sodium dodecyl sulfate,0.75%, 0.8% thiobarbituric acid, and 0.3 mL of distilledwater and kept in a boiling water bath for 60 min.After cooling, 0.5 mL of distilled water and 2.5 mL15/1 (v/v) n-butanol/pyridine was added. After cen-trifugation at 4000 rpm, the absorbance of the super-natant at 532 nm was measured with spectrophotometry(Shimadzu Corp., Tokyo, Japan) using a calibrationcurve obtained from MDA standard. Protein concen-trations of supernatant were measured using Brad-ford’s method.17 MDA activity was expressed as nanomoleper gram protein.
Determination of Tissue ATP, ADP, AMP, andEnergy Charge
For the measurement of tissue ATP, ADP, and AMPconcentrations, we used high-performance liquidchromatography. The tissues were homogenized in 1mL cold 0.6 N perchloric acid and homogenates placed
on ice for 1 h, followed by neutralization with 450 �L ofK2HPO4 (1M), centrifugation for 15 min at 10,000g at4°C, and filtration through a 0.2 �m syringe filter.Supernatants were stored at �80°C until analysis. ATP,ADP, and AMP were measured at a wavelength of 254nm on a Agilent 1100 series (Agilent Technologies Inc.,Palo Alto, CA), using Allsphere ODS-2, C-18 5 �mreverse-phase column with a mobile phase of 160 mMKH2PO4 with 100 mM KCl at pH 6.5.18 ATP and itscatabolites were expressed as micromole per gram liver.Tissue energy charge was calculated as ([ATP] � 0.5[ADP])/([ATP] � [ADP] � [AMP]).19
Histological Assessment Liver I/R InjuryHistological assessment was performed by a re-
searcher blinded to the study groups. For morphometricassessment of reperfusion injury and polymorpho-nuclear neutrophil (PMN) adhesion, excised liver speci-mens were fixed in 10% formalin and embedded inparaffin. Six-micrometer thick hematoxylin- and eosin-stained sections were evaluated at �200 magnificationby a point-counting method for severity of hepatic injuryusing an ordinal scale as follows: grade 0, minimal or noevidence of injury; grade 1, mild injury consisting ofcytoplasmic vacuolation and focal nuclear pyknosis;grade 2, moderate to severe injury with extensivenuclear pyknosis, cytoplasmic hypereosinophilia, andloss of intercellular borders; and grade 3, severe necrosiswith disintegration of hepatic cords, hemorrhage, andPMN infiltration.
Statistical AnalysisAll values were expressed as the mean � sd. Data
were compared by analysis of variance with post hocanalysis using Newman–Keuls test. When a differ-ence was found, specific differences were identifiedby using Kruskal–Wallis test. Statistical evaluationwas performed by using SPSS 10.0 software (SPSS,Chicago, IL). Values of P � 0.05 were accepted assignificant.
RESULTSThroughout the experiment, the heart rate ranged
from 370 to 480 bpm and the MABP ranged from 95 to160 mm Hg in all groups. There were no significantdifferences in heart rate and MABP among groups (Fig.2). The Paco2 levels were also compared and no differ-ences were found within the three groups (Fig. 3).
HTBF before and after IR was measured by using alaser Doppler flowmeter. Blood flow decreased imme-diately after ischemia and did not change duringreperfusion; it remained significantly lower in thevehicle-treated group at 5, 15, 30, and 60 min afterreperfusion was initiated, compared with that beforeischemia. In contrast, with sevoflurane, the impairedHTBF almost completely recovered after IR: recoverywas 98% at 15 min and 102% at 60 min after reperfu-sion. Isoflurane did not affect the reduction of HTBFinduced by IR (Fig. 4).
832 Sevoflurane, Isoflurane in Hepatic Ischemia ANESTHESIA & ANALGESIA
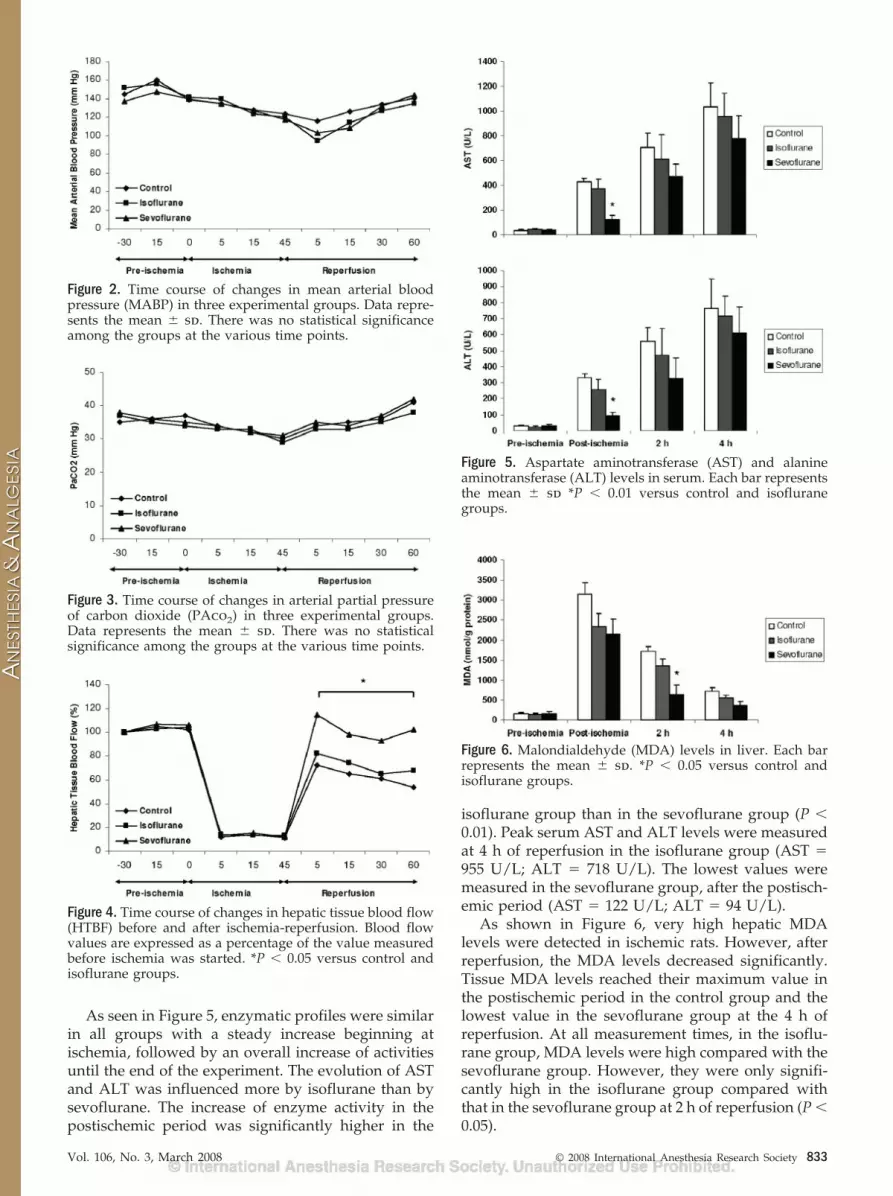
As seen in Figure 5, enzymatic profiles were similarin all groups with a steady increase beginning atischemia, followed by an overall increase of activitiesuntil the end of the experiment. The evolution of ASTand ALT was influenced more by isoflurane than bysevoflurane. The increase of enzyme activity in thepostischemic period was significantly higher in the
isoflurane group than in the sevoflurane group (P �0.01). Peak serum AST and ALT levels were measuredat 4 h of reperfusion in the isoflurane group (AST �955 U/L; ALT � 718 U/L). The lowest values weremeasured in the sevoflurane group, after the postisch-emic period (AST � 122 U/L; ALT � 94 U/L).
As shown in Figure 6, very high hepatic MDAlevels were detected in ischemic rats. However, afterreperfusion, the MDA levels decreased significantly.Tissue MDA levels reached their maximum value inthe postischemic period in the control group and thelowest value in the sevoflurane group at the 4 h ofreperfusion. At all measurement times, in the isoflu-rane group, MDA levels were high compared with thesevoflurane group. However, they were only signifi-cantly high in the isoflurane group compared withthat in the sevoflurane group at 2 h of reperfusion (P �0.05).
Figure 2. Time course of changes in mean arterial bloodpressure (MABP) in three experimental groups. Data repre-sents the mean � sd. There was no statistical significanceamong the groups at the various time points.
Figure 3. Time course of changes in arterial partial pressureof carbon dioxide (PAco2) in three experimental groups.Data represents the mean � sd. There was no statisticalsignificance among the groups at the various time points.
Figure 4. Time course of changes in hepatic tissue blood flow(HTBF) before and after ischemia-reperfusion. Blood flowvalues are expressed as a percentage of the value measuredbefore ischemia was started. *P � 0.05 versus control andisoflurane groups.
Figure 5. Aspartate aminotransferase (AST) and alanineaminotransferase (ALT) levels in serum. Each bar representsthe mean � sd *P � 0.01 versus control and isofluranegroups.
Figure 6. Malondialdehyde (MDA) levels in liver. Each barrepresents the mean � sd. *P � 0.05 versus control andisoflurane groups.
Vol. 106, No. 3, March 2008 © 2008 International Anesthesia Research Society 833

TNF-� concentrations after ischemia, 2 and 4 h ofreperfusion are displayed in Figure 7. TNF-� wasglobally higher in the isoflurane group but no signifi-cant difference was observed among the groups (P �0.05). TNF-� levels reached their highest value at 2 hof reperfusion in the isoflurane group. Similarly, in-creased IL-1� expression was detected in the isoflu-rane group and reached its highest level at 2 h ofreperfusion.
Changes in adenine nucleotide contents in ischemicliver are shown in Table 1. The ATP levels in the liverwere low after ischemia, whereas a concomitant tran-sient increase in the AMP level was observed. At 4 hafter reperfusion, the hepatic ATP levels were higherthan in the postischemic period. The hepatic energycharge was significantly lower in the isoflurane groupthan in the sevoflurane group at all measurementtimes. The energy charge was low after ischemia;however, it increased 4 h after reperfusion.
Liver biopsy specimens were obtained after isch-emia, 2 and 4 h of reperfusion for morphometricassessment of liver injury. After 45 min of warmischemia, both isoflurane and sevoflurane administra-tion resulted in a reduction grade of hepatocyte injurycompared with the control group, this reduction wasalso higher in the sevoflurane group but the differencewas not significant (Fig. 8). None of the rats had a highdegree of hepatocyte necrosis (grade 3). After 2 h ofreperfusion, the sevoflurane group (13%, grade 2)showed markedly reduced hepatocytic degenerationcompared with the isoflurane group (38%, grade 2)and control group (50%, grade 2). After 4 h of reper-fusion, the percentage of grade 3 necrosis in liversfrom the sevoflurane, isoflurane, and control groupswere 13%, 13%, and 25%, respectively (Table 2).
DISCUSSIONThe development of strategies to counteract the
manifestation of IR injury of the liver is a majorchallenge in liver surgery. Ischemic preconditioningrefers to a phenomenon in which tissues are renderedresistant to the deleterious effects of IR by previousexposure to brief periods of vascular occlusion. Theprotective effect of ischemic preconditioning was first
Table 1. Changes in Adenosine 5�-Triphosphate (ATP), Adenosine 5�-Diphosphate (ADP), Adenosine 5�-Monophosphate (AMP), andEnergy Charge in Livers
Preischemia Postischemia
Reperfusion
2 h 4 hATP (�mol/g liver)
Control 7.18 � 1.23 2.16 � 0.48 3.36 � 0.76 4.12 � 1.18Isoflurane 7.53 � 1.34 2.55 � 0.69 3.63 � 0.78 4.92 � 0.95Sevoflurane 7.22 � 1.07 2.74 � 0.90* 4.19 � 1.22* 5.56 � 1.20*
ADP (�mol/g liver)Control 2.69 � 0.75 2.16 � 0.28 1.82 � 0.17 1.86 � 0.18Isoflurane 2.49 � 0.81 2.21 � 0.63 2.02 � 0.19 1.75 � 0.36Sevoflurane 2.51 � 0.68 1.83 � 0.33 2.16 � 0.23 2.36 � 0.43
AMP (�mol/g liver)Control 4.28 � 0.97 7.65 � 2.12 6.93 � 2.27 6.40 � 1.53Isoflurane 4.43 � 1.02 5.23 � 1.16 4.12 � 1.25 3.36 � 1.22Sevoflurane 4.20 � 1.10 4.14 � 1.66 3.39 � 1.30 2.63 � 1.22
Energy chargeControl 0.60 � 0.05 0.28 � 0.04 0.34 � 0.04 0.41 � 0.03Isoflurane 0.61 � 0.06 0.39 � 0.09 0.49 � 0.07 0.61 � 0.10Sevoflurane 0.61 � 0.08 0.43 � 0.10* 0.54 � 0.09* 0.65 � 0.08*
Data are expressed as mean � SD.* P � 0.05 versus control and isoflurane groups.
Figure 7. Serum tumor necrosis factor (TNF)-� and interleu-kin (IL)-1� concentrations in rats postischemia, 2 and 4 hafter reperfusion. Each bar represents the mean � sd.
834 Sevoflurane, Isoflurane in Hepatic Ischemia ANESTHESIA & ANALGESIA

described in myocardium,20 but a considerable num-ber of studies have documented that ischemic precon-ditioning is also a powerful tool to increase ischemictolerance in the liver.21,22 Evidence has shown theprotective effects of volatile anesthetic pretreatmentagainst IR injury in the heart similar to the phenom-enon of ischemic preconditioning.10 Both isofluraneand sevoflurane have been reported to mimic isch-emia preconditioning effects in the heart, suggestingthat the preischemic administration of these anesthet-ics may be protective against liver IR injury.23 Inisolated perfused rat liver, isoflurane, sevoflurane,and halothane reduced IR injury when administered
during the reperfusion phase; however, they did notreduce injury when administered only during isch-emia.24 Heindl et al.5 showed that both sevofluraneand isoflurane reduced the adhesion of PMNs in thereperfused coronary system, and thereby helped topreserve cardiac function; the effects of these twodrugs were not significantly different from each other.However, Preckel et al. suggested that sevofluranehad more prominent protective effects than isofluraneon myocardial reperfusion injury.25 In addition tothese studies, to clarify the significance of hepatictissue perfusion for the protective effects of sevoflu-rane and isoflurane, we evaluated HTBF and hepaticenergy metabolism before, during and after hepaticischemia and reperfusion. To use a clinically relevantamount of anesthetics, the rats inhaled 2% sevofluraneor 1.5% isoflurane (approximately 1 MAC). We havedemonstrated that only sevoflurane provided signifi-cant hepatic protection against IR injury. Although itis not appropriate to directly apply these data tohumans, the administration of sevoflurane rather thanisoflurane for general anesthesia for hepatic surgerymight be considered.
In humans, about 2%–4% of sevoflurane undergoeshepatic metabolism, compared with 0.1%–0.2% ofisoflurane. Indeed, hepatic injury from the metabolismof sevoflurane may result. Thus, conventional wisdomhas suggested that isoflurane is less likely to result inhepatic injury, as it better preserves the balance ofhepatic oxygen supply and demand. However, in criticalsituations, such as IR, hemorrhage, and cirrhosis, theeffects of anesthetics might be changed. Nishiyama etal.26 compared sevoflurane and isoflurane in cirrhoticpatients and found that patients anesthetized withisoflurane had more enzymatic evidence of hepatocellu-lar damage than patients anesthetized with sevoflurane.Nevertheless, no patients in that study developed he-patic failure. All increases in liver enzymes were smalland of questionable clinical relevance.
Figure 8. Liver sections of rats in control and isofluranegroups after 4 h reperfusion showed cytoplasmic hypereosi-nophilia, loss of intercellular borders and extensive nuclearpyknosis (A and B). On the contrary, livers of sevoflurane-pretreated rats showed mild injury consisting of cytoplasmicvacuolation and focal nuclear pyknosis (C) (hematoxylinand eosin, �400).
Table 2. Histopathologic Liver Changes
Time afteroperation
Severity of hepatic injury
G0 G1 G2 G3
PostischemiaControl 1 4 3Isoflurane 1 6 1Sevoflurane 2 6
2 h reperfusionControl 3 4 1Isoflurane 5 3Sevoflurane 7* 1**
4 h reperfusionControl 2 4 2Isoflurane 3 4 1Sevoflurane 5* 2 1
Data are expressed as mean � SD.* P � 0.05 versus control group.** P � 0.05 versus control and isoflurane groups.
Vol. 106, No. 3, March 2008 © 2008 International Anesthesia Research Society 835

The hepatic inflammatory response to IR comprisesof two distinct phases. In the acute phase, the ischemicinsult induces oxidant stress within the liver resultingin Kupffer cells activation and oxidant-mediated in-jury to hepatocytes.3 The activation of Kupffer cellsresults in their production of the early response cyto-kines TNF-� and IL-1�. These potent proinflammatorycytokines are generally thought to have similar over-lapping functions. Accordingly, administration ofdrugs that reduce the effects of TNF-� has resulted inamelioration of liver IR injury. Previous studies dem-onstrated that some volatile anesthetics has antiin-flammatory properties.27,28 Liu et al.6 reported thatsevoflurane administered at 1 MAC before ischemiainhibited an increase in TNF-� during IR-inducedinjury in isolated rat lungs. In this regard, sevofluranesuppressed the proinflammatory effects of TNF-�under conditions of renal IR.29 Although it was notsignificant, we observed more than 40% decrease inboth TNF-� and IL-1� release after reperfusion inanimals treated with sevoflurane, compared with con-trols; these results correlated with decreased lipidperoxidation, as demonstrated by lower content ofliver MDA.
Studies showed that the increase of blood flow inthe liver can contribute to a good prognosis in liverdisease when the liver has been injured ischemically.1
When oxygen supply to hepatocytes becomes insuffi-cient as result of reduced or absent blood flow, there isinhibition of the mitochondrial oxidative phosphory-lation, with the subsequent reduction in ATP synthesis.30
Depletion of cellular ATP store induces alterations intransmembrane ion transport by inhibition of theATP-dependent Na�/K� ATPase, leading to sodiumand chloride influx changes, intracellular sodium ac-cumulation, secondary alterations in cellular calciumhomeostasis, and particularly, cell swelling and death.31
Subsequent reperfusion results in plasma membraneinjury due to the production of superoxide radicals.An excessive acute inflammatory response, whichtakes place promptly after blood flow restoration, hasbeen recognized as the key mechanism of liver injuryduring the reperfusion period. Therefore, it is impor-tant to control the hepatic microcirculatory state afterischemic insult to the liver. We measured HTBF todetermine whether volatile anesthetic pretreatmentimproves hepatic microcirculation and attenuates IRinjury of the liver. Isoflurane did not affect the reduc-tion of HTBF induced by IR. In contrast, with sevoflu-rane, the impaired HTBF almost completely recoveredafter IR.
The hepatic ATP concentration has been used ex-tensively in several studies as an indicator of liverfunction.21 A marked decrease of hepatic ATP levelwas observed in nontreated ischemic livers, confirm-ing that oxidative phosphorylation is rapidly andseriously affected by ischemia.28 Sevoflurane partiallyrestored the ATP content in the liver, regardless ofwhether the time after reperfusion was 2 or 4 h. In this
study, the increased ATP level and tissue blood flowwas a clear indication of increased cell viability andimproved microcirculatory perfusion. It is generallyaccepted that there is an ischemic period during whichthe tissue is vulnerable to reperfusion injury. In thisstudy, sevoflurane treatment attenuated parenchymalhepatocyte injury with respect to ATP concentration inliver homogenates. These data suggest that sevoflu-rane treatment can alleviate IR-related injury of theliver.
In our study, organ protection was indicated by adecrease in plasma liver enzymes during the postisch-emic period, increased HTBF during the reperfusionperiod, decreased tissue MDA levels at 2 h of reper-fusion. Increased hepatic ATP and energy levels alsodecreased hepatocyte injury in the sevoflurane group.The maintenance of microvascular perfusion afterhepatic ischemia plays a crucial role in prevention ofliver injury. As shown by Chun et al.,32 early restora-tion of liver blood flow after ischemia is of particularimportance to prevent hepatocellular death. Weshowed that HTBF almost completely recovered afterIR in the sevoflurane group. Although the longest timepoint presented by this study is 4 h (which does notnecessarily constitute long-term protection or anychange in ischemic outcome) by evaluation of micro-circulatory alterations, estimating tissue MDA andATP content in liver homogenates, measuring proin-flammatory cytokine level, and histologic evaluation,we concluded that treatment with sevoflurane mayameliorate IR injury of the liver.
REFERENCES
1. Miller CD, Fitch W, Thomson IA. Effect of isoflurane on thecanine hepatic circulation and hepatic oxygen balance. Br JAnaesth 1990;65:698–703
2. Mittnacht S Jr, Farber JL. Reversal of ischemic mitochondrialdysfunction. J Biol Chem 1981;256:3199–206
3. Jaeschke H. Mechanisms of liver injury. II. Mechanisms ofneutrophil-induced liver cell injury during hepatic ischemia-reperfusion and other acute inflammatory conditions. Am JPhysiol Gastrointest Liver Physiol 2006;290:G1083–G1088
4. Toledo-Pereyra LH, Suzuki S. Neutrophils, cytokines, and ad-hesion molecules in hepatic ischemia and reperfusion injury.J Am Coll Surg 1994;179:758–62
5. Heindl B, Reichle FM, Zahler S, Conzen PF, Becker BF. Sevoflu-rane and isoflurane protect the reperfused guinea pig heart byreducing postischemic adhesion of polymorphonuclear neutro-phils. Anesthesiology 1999;91:521–30
6. Liu R, Ishibe Y, Ueda M. Isoflurane-sevoflurane administrationbefore ischemia attenuates ischemia-reperfusion-induced injuryin isolated rat lungs. Anesthesiology 2000;92:833–40
7. Schlack W, Preckel B, Stunneck D, Thamer V. Effects of halo-thane, enflurane, isoflurane, sevoflurane and desflurane onmyocardial reperfusion injury in the isolated rat heart. Br JAnaesth 1998;81:913–9
8. Pape M, Englelhard K, Eberspacher E, Hollweck R, KellermannK, Zintner S, Hutzler P, Werner C. The long-term effect ofsevoflurane on neuronal cell damage and expression of apopto-tic factors after cerebral ischemia and reperfusion in rats. AnesthAnalg 2006;103:173–9
9. Samuta T, Becker GL, Pohorecki R, Armstrong K, Landers DF.Effects of isoflurane dose, duration of anoxia, and reoxygen-ation on isoflurane’s preservation of energy balance in anoxicisolated hepatocytes. Anesth Analg 1993;77:38–43
836 Sevoflurane, Isoflurane in Hepatic Ischemia ANESTHESIA & ANALGESIA

10. Cope DK, Impastato WK, Cohen MV, Downey JM. Volatileanesthetics protect the ischemic rabbit myocardium from infarc-tion. Anesthesiology 1997;86:699–709
11. Patel PM, Drummond JC, Cole DJ, Kelly PJ, Watson M. Isoflu-rane and pentobarbital reduce the frequency of transient isch-emic depolarizations during focal ischemia in rats. AnesthAnalg 1998;86:773–80
12. Kon S, Imai M, Inaba H. Isoflurane attenautes early neutrophil-independent hypoxia-reoxygenation injuries in the reperfusedliver in fasted rats. Anesthesiology 1997;86:128–36
13. Novalija E, Fujita S, Kampine JP, Stowe DW. Sevofluranemimics ischemic preconditioning effects on coronary flowand nitric oxide release in isolated hearts. Anesthesiology1999;91:701–12
14. Masui K, Kashimoto S, Furuya A, Oguchi T. Isoflurane andsevoflurane during reperfusion prevent recovery from isch-aemia in mitochondrial KATP channel blocker pretreated hearts.Eur J Anaesthesiol 2006;23:123–9
15. Kowalski C, Zahler S, Becker BF, Flaucher A, Conzen PF,Gerlach E, Peter K. Halothane, isoflurane, and sevofluranereduce postischemic adhesion of neutrophils in the coranarysystem. Anesthesiology 1997;86:188–95
16. Ohkawa H, Ohishi N, Yagi K. Assay for lipid peroxides inanimal tissues by thiobarbituric acid reaction. Anal Biochem1979;95:351–8
17. Bradford MM. A rapid and sensitive method for the quantita-tion of microgram quantities of protein utilizing the principle ofprotein-dye binding. Anal Biochem 1976;72:248–54
18. Kerem M, Bedirli A, Ofluoglu E, Deniz K, Turkozkan N,Pasaoglu H, Sakrak O. Ischemic preconditioning improves liverregeneration by sustaining energy metabolism after partialhepatectomy under ischemia in rats. Liver Int 2006;26:994–9
19. Szabo C, Saunders C, O’Connor M, Salzman AL. Peroxynitritecauses energy depletion and increases permeability via activa-tion of poly (ADP-ribose) synthetase in pulmonary epithelialcells. Am J Respir Cell Mol Biol 1997;16:105–9
20. Murray CE, Jennings RB, Reimer KA. Preconditioning withischemia: a delay of lethal cell injury in ischemic myocardium.Circulation 1986;74:1124–36
21. Yoshizumi T, Yanaga K, Soejima Y, Maeda T, Uchiyama H,Sugimachi K. Amelioration of liver injury by ischaemic precon-ditioning. Br J Surg 1998;85:1636–40
22. Lee WY, Lee SM. Ischemic preconditioning protects post-ischemic oxidative damage to mitochondria in rat liver. Shock2005;24:370–5
23. Zaugg M, Lucchinetti E, Spahn DR, Pasch T, Schaub MC.Volatile anesthetics mimic cardiac preconditioning by primingthe activation of mitochondrial K(ATP) channels via multiplesignaling pathways. Anesthesiology 2002;97:4–14
24. Imai M, Kon S, Inaba H. Effects of halotane, isoflurane andsevoflurane on ischemia-reperfusion injury in perfused liver offasted rats. Acta Anasthesiol Scand 1996;40:1242–8
25. Preckel B, Schlack W, Comfere T, Obal D, Barthel H, Thamer V.Effects of enflurane, isoflurane, sevoflurane and desflurane onreperfusion injury after regional myocardial ischaemia in therabbit heart in vivo. Br J Anaesth 1998;81:905–12
26. Nishiyama T, Fujimoto T, Hanaoka K. A comparison of liverfunction after hepatectomy in cirrhotic patients betweensevoflurane and isoflurane in anesthesia with nitrous oxide andepidural block. Anesth Analg 2004;98:990–3
27. Allaouchiche B, Debon R, Goudable J, Chassard D, Duflo F.Oxidative stress status during exposure to propofol, sevofluraneand desflurane. Anesth Analg 2001;93:981–5
28. Mitsuhata H, Shimizu R, Yokoyama MM. Suppressive effectsof volatile anesthetics on cytokine release in human periph-eral blood mononuclear cells. Int J Immunopharmacol1995;17:529 – 4
29. Lee HT, Kim M, Jan M, Emala CW. Anti-inflammatory andantinecrotic effects of the volatile anesthetic sevoflurane inkidney proximal tubule cells. Am J Physiol Renal Physiol2006;291:67–78
30. Kurokawa T, Kobayashi H, Nonami T, Harada A, Nakao A,Takagi H. Mitochondrial glutathione redox and energy produc-ing function during liver ischemia and reperfusion. J Surg Res1996;66:1–5
31. Belzer FO, Southard JH. Principles of solid-organ preservationby cold storage. Transplantation 1988;45:673–6
32. Chun K, Zhang J, Biewer J, Ferguson D, Clemens MG. Micro-circilatory failure determines lethal hepatocyte injury inishemic/reperfused rat livers. Shock 1994;1:3–9
Vol. 106, No. 3, March 2008 © 2008 International Anesthesia Research Society 837
Related Documents











