DISORDERS OF PERFUSION Dr. Jyothi Reshma S Tutor Dept of Pathology HYPEREMIA, CONGESTION, HEMORRHAGE HEMODYNAMICS - 2

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PowerPoint Presentation
DISORDERS OF PERFUSIONDr. Jyothi Reshma STutorDept of PathologyHYPEREMIA, CONGESTION, HEMORRHAGE
HEMODYNAMICS - 2
ACTIVE HYPEREMIA Active hyperemia : increased supply of blood from the arterial system
Physiologic response to increased functional demand
Eg: heart and skeletal muscle during exercise, inflammation
Neurogenic and hormonal influences
Reactive hyperemia - temporary interruption of blood supply (ischemia) - histamine
PASSIVE HYPEREMIAPassive hyperemia or congestion : impaired exit of blood through venous pathways
Increased hydrostatic pressure - edema.
Lack of blood flow - chronic hypoxia - ischemic tissue injury and scarring.
Capillary rupture - small hemorrhages - catabolism of extravasated red cells - hemosiderin-laden macrophages - Chronic venous congestion (CVC)
Consequences of Impaired Venous OutflowIncreased intravascular pressure StasisHAEMORRHAGENECROSISCONGESTIONOEDEMAHYPOXIAFIBROSISCapillary ruptureAcuteChronic
CVC LUNGEnlarged, heavyFibrosis + iron = firm brown lung - brown induration
CVC LUNG
Alveolar congestionIntra-alveolar hemorrhageHemosiderin-laden macrophages in the lung - congestive heart failure heart failure cells
LIVER - ORGANIZATION
CVC LIVER
Distension - central vein and sinusoids Centrilobular area is at the distal end of the hepatic blood supply - ischemic necrosis
Periportal hepatocytes - better oxygenated because of proximity to hepatic arterioles fatty change.
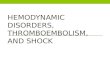
CVC LIVER NUTMEG LIVER
Dark foci of centrilobular congestion surrounded by paler zones of unaffected peripheral portions of the lobules
CVC LIVER M/S
Centrilobular hemorrhage
Hemosiderin-laden macrophages
Hepatocytedropout and necrosis
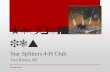
CVC SPLEENGross : enlarged and tense
M/s: Diffuse splenic fibrosis - iron-containing, fibrotic and calcified foci of old hemorrhage Gamna-Gandy bodies
Excessive functional activityhypersplenism - hematologic abnormalities - thrombocytopenia
13
CVC SPLEEN
Gamna-Gandy bodies
SUMMARYGROSSMICROSCOPY
EnlargedReddish blue - cyanosedC/s : oozing of bloodFirm : fibrosisCapsule : thickened
Capillary (sinusoids) : dilated , congested bloodSepta : thickenedFibrotic bandsHemosiderin laden macrophages : special names (lung, spleen)
PATHOGENESIS
HEMORRHAGE
Escape of blood from the vasculature into surrounding tissues, a hollow organ or body cavity, or to the outsideETIOLOGY, TYPES, CONSEQUENCES
HEMATOMALocalized hemorrhage - within a tissue or organ
PETECHIAE
Pinpoint hemorrhages - 1cmPurple green yellow (progressive oxidation of bilirubin released from the hemoglobin of degraded erythrocytes)
Hemothorax, hemopericardium, hemarthrosis, hemoperitoneum
COMPREHENSION QUESTIONSA 40-year-old woman dies after a long history of an illness characterized by dyspnea, orthopnea, hepatomegaly, distended neck veins, and peripheral edema. The cut surface of the liver as it appears at autopsy is shown in the first panel. The second panel shows the microscopic appearance of the liver. What is the most likely cause of these findings?
A 36-year-old man dies during cardiac surgery. He had a history of long-standing rheumatic heart disease with mitral stenosis. At autopsy, the pathologist reports findings consistent with mitral stenosis and noted the presence of heart failure cells. This finding results from
(A) activation of the coagulation cascade.(B) chronic passive congestion of the lungs.(C) hypoxic myocardial injury.(D) myocardial hyperemia.
EXAMPLE OF
ECCHYMOSIS
THANKYOU
Related Documents