Pharmacology: Hematology Heme Pharm I: Platelet Drugs & EPO...................................................................................................................................... 2 Heme Pharm II: Heparins, Coumarins, Thrombolytics, Procoagulants ................................................................................... 5

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Pharmacology: Hematology Heme Pharm I: Platelet Drugs & EPO ...................................................................................................................................... 2
Heme Pharm II: Heparins, Coumarins, Thrombolytics, Procoagulants ................................................................................... 5

Heme Pharm I: Platelet Drugs & EPO
Note that platelet inhibitors are used PROPHYLACTICALLY ONLY (they have NO EFFECT on a formed thrombus)
Aspirin (acetyl salicylic acid): the antiplatelet drug supreme! Safe, cheap, effective
aspirin Mechanism of Action: antiplatelet agent (and anti-inflammatory too).
Covalently inhibits cyclooxygenase (which produces thromboxane A2 in platelets) Effects:
inhibits thromboxane-A2-mediated platelet aggregation & vasoconstriction (aspirin --> vasodilation).
Inhibition is long-lived (platelets don't synthesize new protein; have to wait for new platelets to be made) Administration:
Dose to inhibit platelet cyclooxygenase (160mg) is less than dose for anti-inflammatory / antipyretic effects.
More than 320mg is counterproductive (can block formation of PGI2 / prostacyclin, a natural inhibitor of platelet aggregation)
Other: Safe, effective, and really cost-effective (cheap!)
Dipyridamole
dipyridamole Mechanism of Action: antiplatelet agent with dual mechanisms, both leading to increased cAMP:
inhibits cyclic nucleotide phosphodiesterase
inhibits nucleoside transport/uptake (stimulates adenylate cyclase) Effects: increased intracellular cAMP inhibits platelet aggregation. (also has vasodilator properties) Indications: combination treatment for prophylaxis of thrombosis / embolization Administration: only proven effective in combination (warfarin or aspirin); does not prevent embolization / thrombus by itself Toxicity: headache & hypotension (esp. in high doses More than 320mg is counterproductive (can block formation of PGI2 / prostacyclin, a natural inhibitor of platelet aggregation) Other: Safe, effective, and really cost-effective (cheap!)

Platelet Glycoprotein IIb/IIIa antagonists GP IIb/IIIa: receptor for fibrinogen; plays role in platelet activation ( platelet aggregation, adherence)
3 kinds (antibody, small peptide, small molecule; don’t have to memorize names)
All cause bleeding but DON’T appear to cause increased intercranial bleeding
VERY EXPENSIVE ($1500-$2000/course) but may actually save money (prevent re-stenosis post-angioplasty, prevent need for repeat angioplasty / CABG)
mAb: abciximab
mAb IIb/IIIa antagonist (abciximab)
Mechanism of Action: antiplatelet agent. Blocks GPIIb/IIIa-mediated platelet aggregation Indications: only anti-platelet mAB shown to have anti-thrombotic activity in humans Administration:
Always given with heparin & aspirin.
Rapidly cleared (10m half life); give as large bolus then slow infusion (18-24h).
Half-life of recovery of aggregation is 24h (Fabs remain on platelets & can redistribute to GPIIb/IIIa on new platelets).
Toxicity:
bleeding (2x vs heparin+aspirin alone)
pseudothrombocytopenia (Ab-mediated platelet clumping) Resistance: anti-murine antibodies (6.5% after 1 dose, very important - avoid giving a second time!) Other:
chimeric (mouse variable, human constant regions); only Fab portion used.
Could use platelet transfusion to reverse side-effects if needed.
small peptide: eptifibatide
small peptide IIb/IIIa antagonist (eptifibatide)
Mechanism of Action: antiplatelet agent. Blocks GPIIb/IIIa-mediated platelet aggregation by blocking fibrinogen, vWF, vitronectin binding to IIb/IIIa Effects: mimics AA sequences important for GPIIb/IIIa binding: (KGD mediates fibrinogen binding; RGD mediates vWF binding) Indications: anti-thrombotic Administration:
Given with aspirin + heparin.
More slowly cleared than abciximab; still given as rapid large bolus + slow infusion for up to 72 hrs.
Rapidly reversible effects (mediated by drug clearance from plasma). Toxicity: bleeding (marginally increased vs heparin+aspirin alone), not immunogenic Other: Elimitated via proteolysis to AA & urinary elimination of unchanged drug
small molecule: tirofiban
small molecule IIb/IIIa antagonist (tirofiban)
Mechanism of Action: antiplatelet agent.
Blocks GPIIb/IIIa-mediated platelet aggregation by inhibiting fibrinogen binding to GPIIb/IIIa Effects: binds reversibly to IIb/IIIa receptor Indications: anti-thrombotic Administration: Give as large bolus then slow infusion (up to 108h). Toxicity: bleeding (2x vs heparin+aspirin alone) Other: Renal clearance (2h half-life); effects rapidly reversible (mediated by plasma clearance)

ADP Antagonists Looking for better / more expensive aspirin
Clopidogrel - “Plavix”, 2nd to market but maybe less toxic?
ticlopidine clopidogrel
Mechanism of Action: antiplatelet agents; inhibit ADP-induced platelet aggregation Effects:
Bind irreversibly to low-affinity ADP receptors (non-competitive)
Block ADP-mediated release of platelet alpha granules / dense granules
Inhibit fibrinogen binding to activated platelets
indirectly block activation of platelet glycoprotein IIb/IIIa receptor Indications: Slightly better at preventing stroke in pts with TIAs than aspirin; can help prevent coronary thrombosis Administration: long-lived effects (ADP receptor blocked for life span of platelet; need to synthesize new ones: 7-10d) Toxicity:
neutropenia (severe but reversible, ticlopidine 1%, clopidogrel 0.1%)
bleeding, diarrhea, thrombocytopenia (TTP) Other:
CYP450 substrates - activity requires conversion to active metabolite (complicates treatment, as activity varies from pt to pt);
inhibit CYP 2C9.
Clopidogrel = Plavix; thought to be less toxic than ticlopidine.
Much more expensive than aspirin
Erythropoietin (EPO)
erythropoietin (EPO) Mechanism of Action: promotes erythropoiesis (hormone) Effects:
1. binds EPO receptor on erythroid precursor cells 2. causes conformational change & activates Jak-STAT pathway (Jak-2 TK p-lates receptor,
recruits STAT-5, which gets p-lated & goes to nucleus as transcription factor) 3. induces red cell maturation gene expression. 4. Actually primarily BLOCKS APOPTOSIS of erythroid precursor cells.
Indications:
anemia (chronic renal failure, cancer, AIDS)
perioperatively (reduce transfusion)
illicit (blood doping by athletes) Administration: IV/sub-q, usually start at 80-120 U/kg 3x/wk; sustained effect after its disappearance Toxicity:
aggravates hypertension
potential increase in thrombosis risk
theoretical neoplasm risk (cell growth factor - now a black box warming) Other: 193-AA protein, 1st 23 AA cleaved off, then heavily glycosylated (recombinant form used)
Heme Pharm II: Heparins, Coumarins, Thrombolytics, Procoagulants
Coagulation System Review Intrinsic Extrinsic
Activated by Phospholipids, particulate matter (kaolin) – “intrinsic” to plasma
Tissue Factor, phospholipids (thromboplastin) – “extrinsic” to vessel lumen
Test Activated partial thromboplastin time (APTT) – used for heparin monitoring
Prothrombin time (PT) – used for warfarin monitoring
Endogenous mechanisms to prevent/control thrombosis
Prostacyclin(PGI2): inhibits platelet aggregation
Antithrombin: specific protease inhibitor (like α1 antitrypsin); interferes with various factors (suicide substrate for serine proteases)
Heparan sulfate: endothelial cell surface proteoglycan, like heparin boosts antithrombin
Protein C: + protein S, VaVi and VIIIa VIIIi
Indications for anticoagulant tx
Prevention:
Heparins & coumarins prevent thrombus formation in lots of settings
Antiplatelets for long-term prevention (esp. coronary / cerebral artery disease)
Treatment: Heparin (acute) and coumarin (chronic) therapy
Prevent further thrombus formation
Don’t act on already existing thrombi Used for: Arterial & venous thrombosis; artificial heart valve
thrombi, thrombi assoc. with atrial fibrillation
Dissolution: Thrombolytics (“clot busters”)
Actively dissolve pathologic thrombi
Used for: coronary arteries, peripheral arteries, large veins, venous caths
Don’t prevent thrombus formation: follow with short-term anticoagulation (heparin, sometimes warfarin)
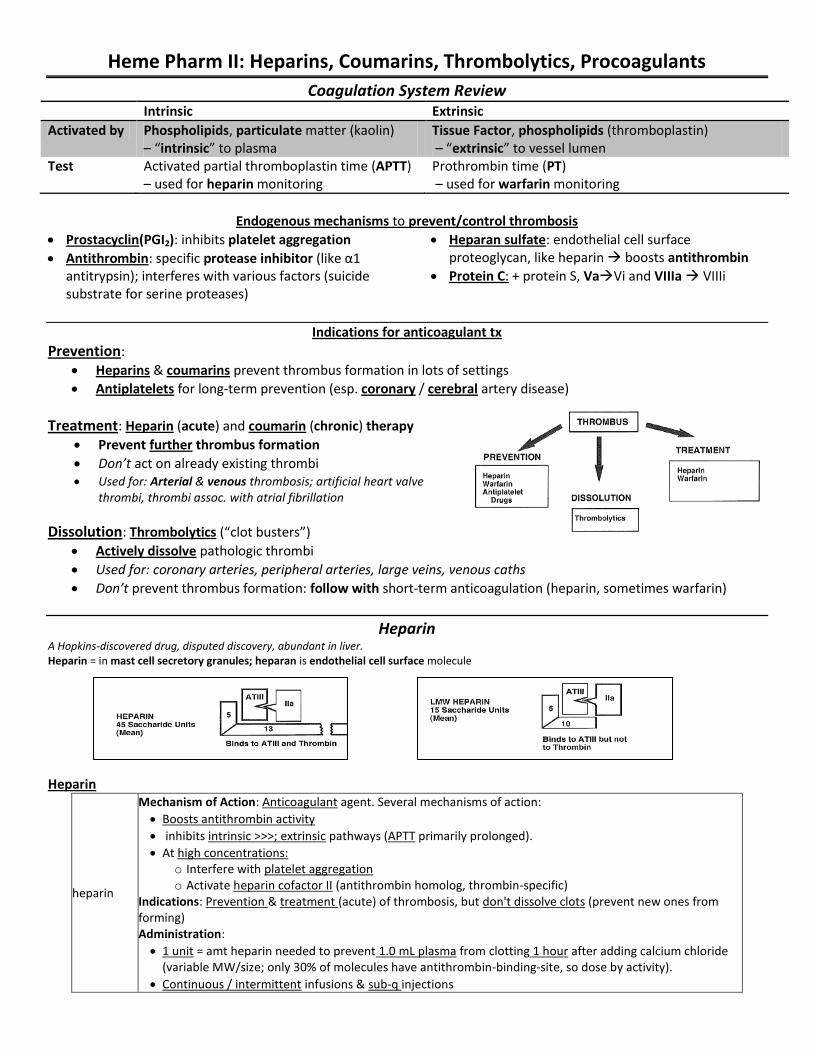
Heparin A Hopkins-discovered drug, disputed discovery, abundant in liver. Heparin = in mast cell secretory granules; heparan is endothelial cell surface molecule
Heparin
heparin
Mechanism of Action: Anticoagulant agent. Several mechanisms of action:
Boosts antithrombin activity
inhibits intrinsic >>>; extrinsic pathways (APTT primarily prolonged).
At high concentrations: o Interfere with platelet aggregation o Activate heparin cofactor II (antithrombin homolog, thrombin-specific)
Indications: Prevention & treatment (acute) of thrombosis, but don't dissolve clots (prevent new ones from forming) Administration:
1 unit = amt heparin needed to prevent 1.0 mL plasma from clotting 1 hour after adding calcium chloride (variable MW/size; only 30% of molecules have antithrombin-binding-site, so dose by activity).
Continuous / intermittent infusions & sub-q injections

Toxicity:
Bleeding (often inadequte therapeutic monitoring, more common in elderly, worry about intercranial bleeding.
Thrombocytopenia (mild is common; severe less frequently & 7-14d post tx initiation, always reversible with discontinuation)
Paradoxical thrombosis / white clot syndrome (uncommon), reversible alopecia
OSTEOPOROSIS (very important, lots of elderly pts) Reversal of toxicity:
STOP THERAPY
Can give protamine (positively charged low molecular weight proteins from fish sperm; give equimolar amount to titrate out heparin, only if life-threatening b/c can induce hypotension/anaphylaxis/hypercoagulation.
Diabetics who take insulin with protamine are more prone to anaphylaxis: may already have anti-protamine Ab)
Pharmacokinetics: complex & unusual.
Vd: confined to plasma (high MW, neg charge)
not orally bioavailable
clearance is NON-LINEAR (dose-dependent), cleared via RES, longer infusions can diminish clearance
therapeutic monitoring needed to reach target APTT (1.5-2x)
Other: naturally occuring, polymer of D-glucosamine/D-glucoronic acid. Found in mast cell secretory granules but natural function unknown; sulfation/molecular weight variable; prepared from bovine lung/porcine intestinal mucosa
LMW Heparin
Low molecular weight heparins (enoxaparin, dalteparin, ardeparin) & LMW hepanoid (danaproid)
Mechanism of Action: Anticoagulant agent. inhibit Factor Xa but not thrombin.
still bind to antithrombin III
do not prolong APTT but work as well clinically.
Indications: Prevention & treatment (acute) of thrombosis, but don't dissolve clots (prevent new ones forming).
At least as good as preventing DVT as heparin; probably equivalent in treating DVT Administration: Dosed in mg instead of units; give sub-q. Toxicity: Bleeding (same as heparin); thrombocytopenia (maybe less frequently) Pharmacokinetics: less frequent dosing than heparin (reduced binding to plasma proteins / platelets /
cells; increased bioavailability, longer half-life, dose-proportional / more normal PK, not non-linear like heparin) Other: Preparation: depolymerization & size fractionation of HMW heparins; mixed species. Way more expensive but popular (no therapeutic monitoring, given sub-q, a little easier to manage).
Coumarin Anticoagulants Discovered in cattle; produced as rotenticide (still used as rat poison) by Wisconsin Alumni Research Foundation (=WARFarin), suicide attempts
INR = international normalized ratio = PTpatient
PTreference
ISI
Enhanced oral anticoagulant activity ↓ vitamin K absorption Antibiotics, mineral oil, cholestyramine
Displacement from plasma proteins Sailicylates, clofibrate, chloral hydrate
Inhibition of biotransformation Allopurinal, metronidazole, chloramphenicol
Inhibition of platelet aggregation Aspirin, dipyridamole
Decreased clotting factor production Quinidine
Depressed oral anticoagulant activity Metabolizing enzyme induction Barbituates, glutethimide, griseofulvin
Increased clotting factor production Vitamin K, oral contraceptives

Coumarins (warfarin sodium / coumadin, dicumarol, etc.)
Mechanism of Action: Anticoagulant agent. Blocks reduction of Vit K by vitamin K reductases Effects: Vitamin K required for factor II, VII, IX, X (and proteins C&S) to have gamma-carboxylated glutamic acid residues, which help bind Ca++ and PLs on platelets to enhance clotting.
1. decreases synthesis of vitamin K-dependent factors (30-50%) 2. factors produced only have 10-40% of normal biologic activity
Indications: Prevention & treatment (chronic) of thrombosis, but don't dissolve clots (prevent new ones from forming) Administration:
therapeutic monitoring with PT (1.2-1.5x normal); INR widely used now.
LONG HALF LIFE + INVOLVEMENT OF CLOTTING FACTORS = LONG TIME TO STEADY STATE. Adjust dose only q48-72h and escalate conservatively
Resistance: occurs but is rare Toxicity & Reversal: less toxicity with lower levels of anticoagulation (and equal efficacy).
Bleeding: reverse with: o FFP to replace coagulation factors (first line for acute bleeding) or o Vitamin K in high doses (some reductases can bypass if enough vit K around; takes longer -
24h, have to wait for synthesis of new factors; effect lasts for days so use only if serious, might have to substitute heparin for 7-10d after high-dose vitamin K)
Skin necrosis: from Protein C inhibition necrotic infarction, watch out for protein C-deficient pts.
Alopecia
TERATOGENICITY: esp 1st trimester, nasal hypoplasia / stippled epiphyseal calcifications / abortion / neonatal hemorrhage. STRICTLY CONTRAINDICATED IN PREGNANCY (heparin safer).
Drug interactions: VERY IMPORTANT. See chart above Pharmacokinetics:
Nearly complete absorption,
99% bound to plasma protein (albumin),
metabolism to inactive metabolites by hydroxylation (hepatic) is variable in population, genetically determined; half-life of ~40h.
Time course of antithrombotic effect is different than plasma concentration (circulating half-lives of factors, which have to be re-synthesized: II > IX/X > VII for half-life, so VII recovered first and thrombin last)
Other: Has an asymmetric carbon (racemic mixture, the enantiomers have different potency / metabolism)
Thrombolytics Fibrinolytic system: zymogen cascade; breaks down fibrin (remodel/trim thrombus)
plasmin (activated from plasminogen via plasminogen activator) is key actor o binds fibrin via amino terminus (high lysine affinity) o α2-antiplasmin also binds to plasmin at this site; so plasmin bound to fibrin escapes α2AP inhibition
“lytic state” - Too much plasmin digests physiologic thrombi; consumes plasma coag factors o increases hemorrhage risk o usually prevented by localization of plasminogen activator to endothelial cells & presence of α2AP in circulation
Tissue plasminogen activator (tPA): released in response to hemodynamic indicators of thrombus formation
o Short half-life (3m); inactivated by circulating inhibitor (plasminogen activator inhibitor-1), preventing lytic state o Controls can be overwhelmed by large doses of systemic thrombolytic drugs

Streptokinase: from β-hemolytic strep streptokinase Mechanism of Action: Thrombolytic agent. Not a kinase / protease but binds to plasminogen, induces
conformational change, results in cleavage of arg-val bond & activation of enzyme (plasmin) Indications: clot buster (helps digest pre-existing thrombi) Administration: Need large loading dose to absorb pre-existing Abs; used to give intracoronary but probably not much better. Get it in FAST! Toxicity: Bleeding, allergic reactions, anaphylaxis, fever. VERY ANTIGENIC (don't give more than q6-12m) Pharmacokinetics: Half life of about 80m after Abs absorbed Other: All adults have pre-existing anti-SK antibodies (exposure to strep)
Urokinase
urokinase Mechanism of Action: Thrombolytic agent. Cleaves plasminogen to plasmin directly at arg-val bond (like TPA) Effects: activity not localized at clot (can cause systemic fibrinolysis) Indications: clot buster (helps digest pre-existing thrombi) Toxicity: Bleeding, allergic reactions (less frequent than with streptokinase: skin rash, fever, bronchospasm) Pharmacokinetics: Metabolized by liver, half life 15m Other: Kind of like an early version of TPA
Recombinant Tissue Plasminogen Activator
rtPA Mechanism of Action: Thrombolytic agent. Recombinant serine protease; Effects: Much tighter binding to fibrin-bound plasminogen than circulating free plasminogen (tPA has lysine binding sites at amino terminus) so more active against bound plasminogen (less systemic activity, more localized); can overwhelm control mechanism (serum concentrations 30-300x higher than physiologic [tPA]) Indications: clot buster (helps digest pre-existing thrombi) Administration: IV bolus + short infusion (short half life, bleeding complications) Toxicity: despite localization, can induce lytic state. Bleeding (more in elderly, intercranial is serious).
Unique to rtPA: 1. Damages endothelial cell membranes \ increases circulating vWF; 2. mid-moderate thrombocytopenia (10% cases)
Pharmacokinetics: Metabolized by liver, identical halflife to tPA (3m) Other: Most common thrombolytic agent in clinical use
Comparison of thrombolytics Efficacy:
All better than heparin for resolving pathologic thrombi
More mature thrombus = less successful thrombolysis
USE WITHIN 6h OF ACUTE MI o rTPA faster onset than SK but outcome equivalent
UK/rTPA have higher success than SK for thrombi in peripheral veins, arteries, indwelling caths Toxicity: all have risk of bleeding, rTPA > SK for intercranial hemorrhage, data mixed on UK vs rtPA/SK Bottom line: very similar, cost is big issue (consider SK 1st for low cost but don’t use repeatedly: antigenic)
t1/2 (m) Antigenic Cost
SK 80 Yes $200-250 UK 15 No $1,000-$1,500 rtPA 3 No $2,000-$2,500
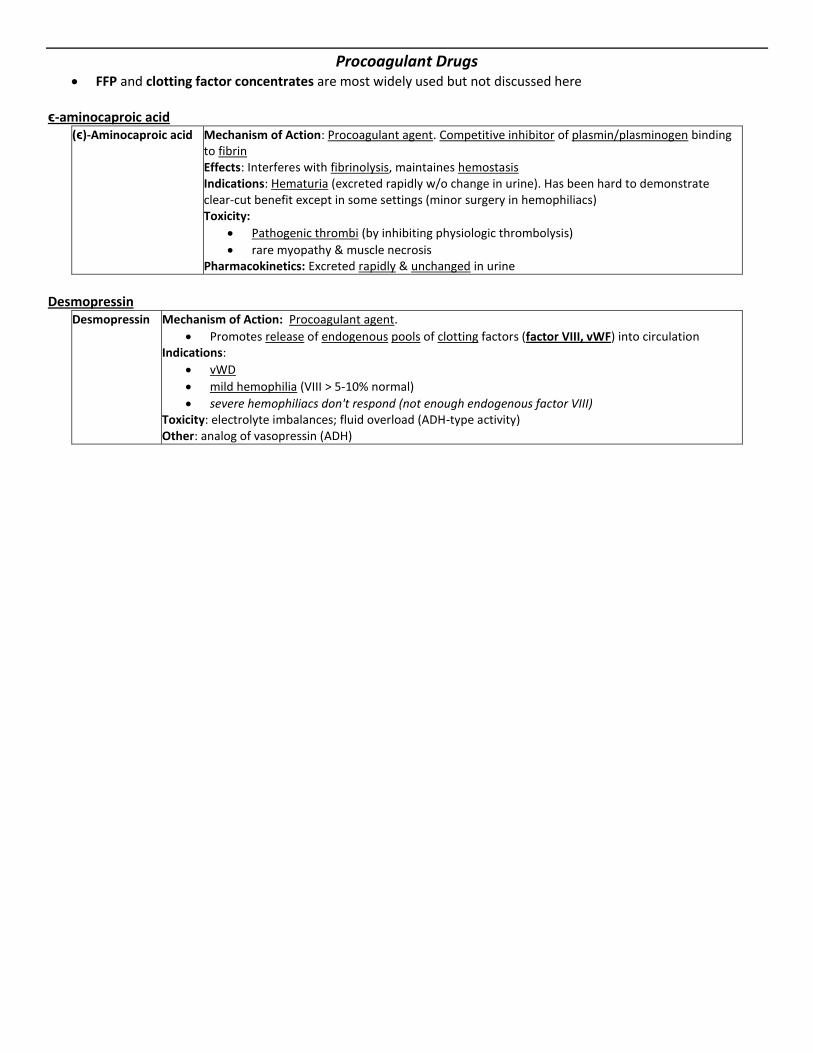
Procoagulant Drugs FFP and clotting factor concentrates are most widely used but not discussed here
ϵ-aminocaproic acid
(ϵ)-Aminocaproic acid Mechanism of Action: Procoagulant agent. Competitive inhibitor of plasmin/plasminogen binding to fibrin Effects: Interferes with fibrinolysis, maintaines hemostasis Indications: Hematuria (excreted rapidly w/o change in urine). Has been hard to demonstrate clear-cut benefit except in some settings (minor surgery in hemophiliacs) Toxicity:
Pathogenic thrombi (by inhibiting physiologic thrombolysis)
rare myopathy & muscle necrosis Pharmacokinetics: Excreted rapidly & unchanged in urine
Desmopressin
Desmopressin Mechanism of Action: Procoagulant agent.
Promotes release of endogenous pools of clotting factors (factor VIII, vWF) into circulation Indications:
vWD
mild hemophilia (VIII > 5-10% normal)
severe hemophiliacs don't respond (not enough endogenous factor VIII) Toxicity: electrolyte imbalances; fluid overload (ADH-type activity) Other: analog of vasopressin (ADH)
Related Documents