HEMATOLOGY; ALTERATIONS OF BLOOD CELL AND LYMPHOID FUNCTION

HEMATOLOGY; ALTERATIONS OF BLOOD CELL AND LYMPHOID FUNCTION.
Dec 19, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

HEMATOLOGY; ALTERATIONS OF BLOOD CELL AND LYMPHOID FUNCTION
Blood• Plasma
– Complex, aqueous
– Organic, inorganic molecules
• Plasma proteins
– Greatest weight in total plasma
– Important plasma proteins:
• Albumins
• Globulins
• Clotting factors

Blood – cont’d• Other components
– Formed elements (blood cells)
• Erythrocytes (= red blood cells = rbc’s)
• Leukocytes (= white blood cells = wbc’s)
• Lymphocytes (= B and T cells)
• Thrombocytes (= platelets)
• Development (= hematopoiesis)
– Common stem cell
• Mitosis signaled by biochem’s released from the body
• Differentiate needed blood cell
• Hematopoiesis/cell breakdown continuous

Erythrocytes (= Red Blood Cells = RBC’s)
• Development = erythropoiesis
– Erythropoietin
• Renal hormone
• Rel’d when kidney senses decr’d blood oxygen
red bone marrow
• Signals differentiation of common stem cell rbc’s

RBC’s – cont’d
• Rbc cytoplasm contains
– Hemoglobin
– Other proteins, electrolytes
– Not many (if any) organelles
• No nucleus
• Doesn’t replicate on own in bloodstream
– Where do more rbc’s come from?
RBC’s – cont’d
• Hemoglobin (Hb) – carries O2 and CO2 within rbc’s
– Composition
• Four protein chains (= globin)
• Complex organic molecule embedded in each globin chain (= heme)
• Iron (Fe) atom held in globin
– “Binds” oxygen
– Body’s synth of Hb requires
• Sufficient Fe and amino acids
• Vitamins folate (or folic acid) and B12


RBC’s – cont’d• Hb – cont’d
– Rbc/Hb breakdown
• Healthy rbc’s live 120 days
– Approx. 174 million rbc’s break down per minute
– In liver and spleen
• Hb released, broken down following rbc breakdown
– Globin amino acids; recycled new proteins
– Fe – stored or recycled
– Heme converted bilirubin
» Bilirubin either stored or recycled, or
» Further converted in liver to bile
Abnormalities of RBC’s
• Anemias
Clinical symptoms:
• Fatigue
• Dyspnea
• Syncope
• Angina
• Tachycardia
• Organ dysfunctions

Anemias – cont’d
• Macrocytic/megaloblastic – large rbc’s
– Commonly due to deficiency of Vit B12 or folate
– Pernicious anemia - typical
• Possible causes
– Congenital –deficiency in protein nec to absorb B12 from small intestine
– Adult onset – one example: autoimmune dysfunction destruction of gastric mucosa
• Develops slowly
• Fatal if untreated

Anemias – cont’d
• Microcytic –abnormally small rbc’s w/ decr’d Hb
– Possible causes: disorders of
• Fe metabolism
• Globin synthesis
• Heme synthesis

Anemias – cont’d• Microcytic – cont’d
– Iron deficiency anemia – typical
• Common causes
– Insufficient Fe intake
– Chronic blood loss (even 2-4 mL/day)
» Men – gastrointestinal bleeding
» Women – profuse menstruation, pregnancy
• Other causes
– Drugs gastrointestinal bleeding
– Eating disorders insufficient Fe

Anemias – cont’d
• Microcytic – cont’d
– Treatment
• Eliminate blood loss
• Replace Fe
• Normocytic
– Aplastic anemia - typical
• Bone marrow dysfunction underdeveloped, defective, absent marrow or stem cells
Anemias – cont’d• Normocytic – cont’d
– Aplastic anemia – cont’d
• Possible causes of bone marrow dysfunction:
– Cancer cells in marrow
– Autoimmune response
– Renal failure
– Exposure to radiation, drugs, toxins harming bone marrow
• Clinical symptoms – those typical of anemias
• Treatment
– Treat underlying disorder
– Blood transfusions to increase [Hb]
– Bone marrow transplant

Abnormalities of RBC’s – cont’d
• Myeloproliferative disorders
– Polycythemia = excessive proliferation of rbc’s
• Secondary is most common
– Physiological response to hypoxia
– Seen in
» Smokers
» Those w/ congestive heart failure
» Those w/ cardiopulmonary diseases

Polycythemia – cont’d• Leads to
– Incr’d blood volume, viscosity
– Congestion of liver, spleen
– Clotting; thrombus formation
• Clinical
– Headache, dizziness, weakness
– Increased blood pressure
– Itching/sweating
• Treatment
– Reduce blood volume (= phlebotomy) to reduce rbc #
– Control symptoms
– Prevent thrombosis
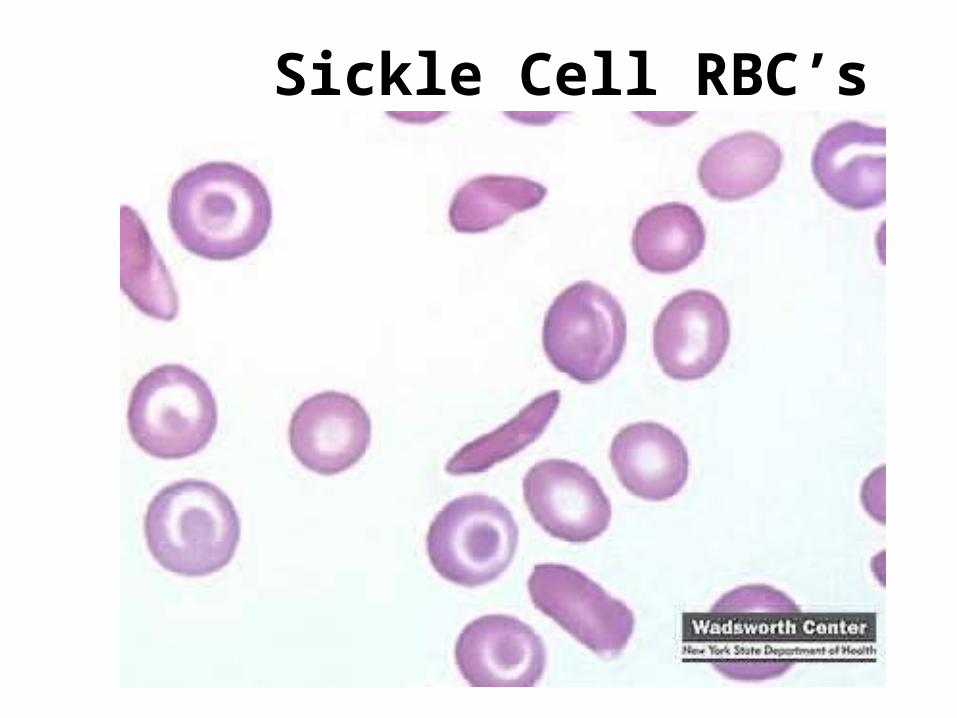
Sickle Cell RBC’s

Leukocytes (= White Blood Cells = wbc’s)
• Granulocytes – granules in cytoplasm
– Granules contain
• Enzymes to kill invading cells, break down cell debris
• Other biochem’s that signal, mediate inflammatory response
– Cell types (mostly phagocytic)
• Neutrophils
• Eosinophils
• Basophils

Leukocytes (= White Blood Cells = wbc’s)
• Agranulocytes – no granules in cytoplasm
– Also impt phagocytes, release biochem signals
– Cell types
• Monocytes
• Macrophages

Leukocytes (= White Blood Cells = wbc’s)
• Origination
– Same red bone marrow stem cells as rbc’s (and platelets and lymphocytes)
– Granulocytes mature in marrow
• Lifetime hours to days
– Agranulocytes mature in blood
• Live about 2-3 months

Leukocytes (= White Blood Cells = wbc’s)
• Production incr’s when
– Infection
– Presence of steroids
– Decr’d reserve leukocyte pool in bone marrow

Leukocytes (= White Blood Cells = wbc’s)
• Abnormalities
– Leukocytosis = incr’d # wbc’s
• May be a normal response
– When??
• OR may signify a disease state
– When??
– Leukopenia = decr’d # wbc’s
• Always pathological
Leukemias -- malignant disorders of blood cells
• Single cell may undergo transformation to dysfunctional cell, then proliferates to dysfunctional clones
– Not nec faster prolif’n, but do displace normal cells
• Result: dysfunct’l cells accumulate, compete w/ proliferation of normal blood cells within bone marrow Overcrowding of bone marrow decr’d
production of normal, functioning blood cells

Leukemias -- cont’d
• Probably risk env. factors + genetic predisposition
– Risk factors
• Some disorders of bone marrow, other organs; can progress to acute leukemias
• Some viruses
• Ionizing radiation in large doses
• Drugs
• Genetic - sibling occurrence
Leukemias -- cont’d
• Classified as acute/chronic; myeloid/lymphoid
– Acute leukemias
• Characteristics
– Abrupt onset
– Rapid progression
– Severe symptoms
– Histology: incr’d # immature blood cells
• Survival rate
Leukemias -- cont’d
– Acute leukemias – cont’d
• Clinical
– Signs/symptoms related to bone marrow depression
» Fatigue
» Bleeding
» Fever
» Anorexia/weight loss
» Enlargement of liver/spleen

Leukemias -- cont’d
– Acute leukemias – cont’d
• Clinical – cont’d
» Neurologic effects (headache, vomiting, facial palsy, blurred vision
• Early detection difficult
• Treatment
– Chemotherapy
– Immunotherapy
– Marrow transplants

Leukemias -- cont’d
– Chronic leukemias
• Characteristics
– Predominant cell mature but abnormal function
– Gradual onset
– Relatively longer survival time
• Chronic lymphocytic one example
– B cells fail to mature to active plasma cells
– Ig’s not produced, plasma cell # decr’d
– Most signification
» Incr’d infections
» Incr’d autoimmune response

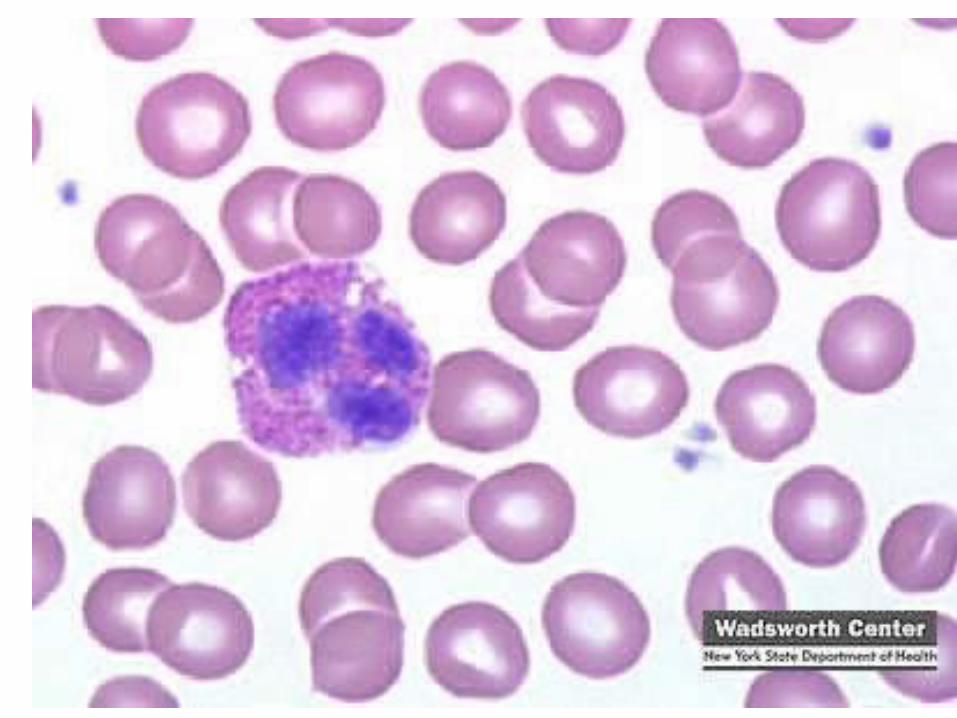
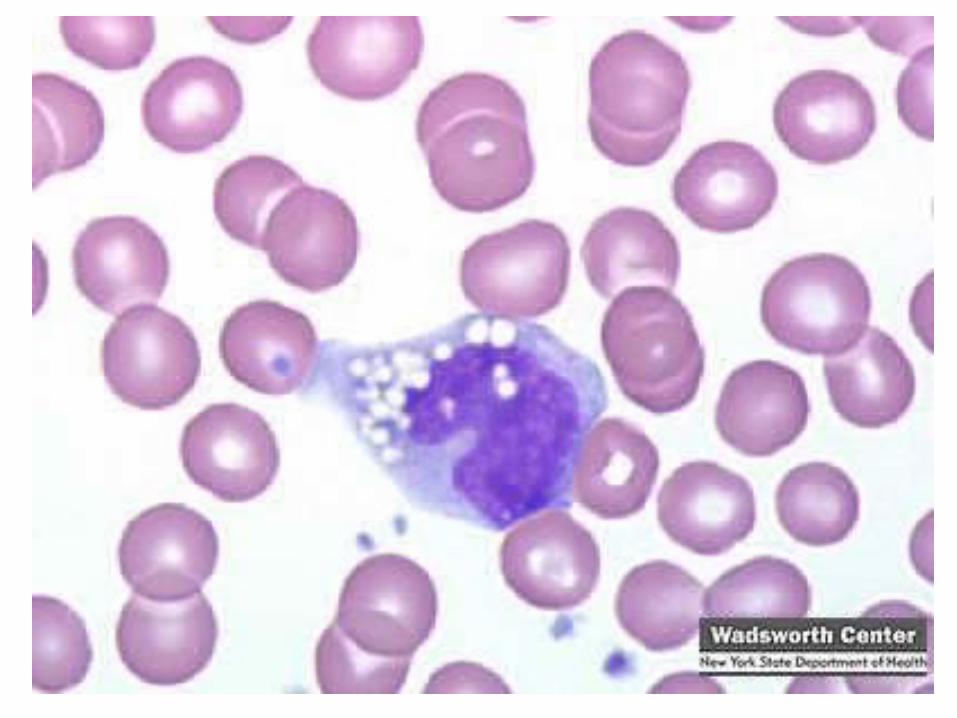
Chronic lymphocytic leukemia (CLL) Lymphocyte (small, mature-looking)
Acute lymphocytic leukemia (ALL) Two lymphoblasts, one neutrophil
Lymphomas• Often in secondary lymph tissue
– Lymph nodes, spleen, tonsils, intestinal lymphatic tissue
– Not in blood-borne cells, so “solid tumor”
• Hodgkin’s - distinctive abnormal chromosomes
– Cause unknown. May be
• Genetic
• Transmissible agent
• Other (strange) risk factors include: tonsillectomy/appendectomy; wood working (?)

Lymphomas – cont’d
• Hodgkin’s – cont’d
– Clinical
• Painless swelling or lump in neck
• Intermittent fever
• Weakness, weight loss
• Obstruction/pressure can lead to secondary involvement of
– Lung
– Spinal cord/neurons
– Skin

Lymphomas – cont’d
• Hodgkin’s – cont’d
– Early detection difficult
– Treatment
• Chemotherapy
• Radiation
• Prognosis good with early treatment

Lymphomas – cont’d
• Non-Hodgkin’s
– Cause unknown
– See B-cell and T-cell abnormalities
– Clinical
• Lymph node enlargement (gradual, painless)
• Extra-nodal areas can be affected
– Treatment
• Bone marrow transplant
• Prognosis good if growth is restricted to lymph node

Thrombocytes = Platelets
• Characteristics
– Prod’d by fragmentation of megakaryocyte
– Life span ~ 3 days
– Many held in spleen
• Coagulation (= hemostasis): Converts fluid blood to a nonflowing gel
– Long protein threads (fibrin) formed, come together to form blood clot


Thrombocytes – cont’d• Coagulation – cont’d
– Many proteins/enzymes/factors nec for clotting “cascade”
– Platelets bind at site of clot then activated
Nec biochem changes at clot site successful clot formed
• Disorders of platelets
– Thrombocytopenia
• Decr’d # platelets, due to
• Decr’d prod’n platelets, seen w/
– Tumors
– Drugs/toxins
– Other
Thrombocytes – cont’d– Thrombocytopenia causes – cont’d
• OR incr’d clearance of platelets, seen with
– Splenomegaly
– Tumors
– Infections
– Immune disorders
– Clotting factor disorders
• Clotting factors can’t work to make a successful clot
• May be
– Genetic
» Hemophilia
» VonWillebrand’s disease
Thrombocytes – cont’d– Clotting factor disorders – cont’d
• May be
– Acquired
» Liver disease (where some clotting factors prod’d)
– Drugs/toxins
– Inappropriate clotting
• Body has anticlotting mechanism (also necessary)
– Keeps clots from being too large, blocking vessel
– Keeps unneeded clots from forming
– Important in vascular disorders
Related Documents











