American Journal of Transplantation 2007; 7: 423–433 Blackwell Munksgaard C 2006 The Authors Journal compilation C 2006 The American Society of Transplantation and the American Society of Transplant Surgeons doi: 10.1111/j.1600-6143.2006.01625.x Heightened Expression of the Cytotoxicity Receptor NKG2D Correlates with Acute and Chronic Nephropathy After Kidney Transplantation M. Seiler a , I. Brabcova b , O. Viklicky b , P. Hribova b , C. Rosenberger c , J. Pratschke d , A. Lodererova b , M. Matz a , C. Sch ¨ onemann e , P. Reinke c , H.-D. Volk a and K. Kotsch a, ∗ a Institute of Medical Immunology, Universit¨ atsmedizin Charit ´ e, Campus Mitte, Berlin, Germany b Transplant Laboratory, Transplantcentre, Institute for Clinical and Experimental Medicine, Prague, Czech Republic c Department of Nephrology and Intensive Care, Universit ¨ atsmedizin Charit ´ e, Campus Virchow, Berlin, Germany d Department of Visceral and Transplantation Surgery, Universit ¨ atsmedizin Charit ´ e, Campus Virchow, Berlin, Germany e Institute of Transfusion Medicine, HLA Laboratory, Universit ¨ atsmedizin Charit ´ e, Campus Virchow, Berlin, Germany ∗ Corresponding author: Katja Kotsch, [email protected] The activating cytotoxicity receptor NKG2D binds to stress-regulated molecules encoded by the major his- tocompatibility complex class I chain-related (MIC) and UL-16-binding protein (ULBP)/retinoic acid early tran- script (RAET) gene family. To assess whether acute allograft rejection leads to an induction of these inducible ligands and their receptor NKG2D, we ex- amined the mRNA profiles in kidney transplant biop- sies. Expression levels were correlated with the inci- dence of acute rejection (aRx) episodes and chronic allograft nephropathy (CAN) proven by histology. Whereas MICA, ULBP1/3 and RAET1-E did not display heightened gene expression, elevated levels of NKG2D mRNA could be associated with aRx (p < 0.001). Im- munohistology of kidney biopsies diagnosed with aRx revealed NKG2D + cells in tubulointerstitial areas pos- itive for CD8 + cells. Most importantly, elevated lev- els of NKG2D mRNA were associated with restricted long-term graft function assessed by the glomerular filtration rate at 6, 12 and 18 months posttransplanta- tion. Induced NKG2D mRNA expression was still ob- servable in biopsies diagnosed with CAN (p < 0.001), demonstrating a higher sensitivity and specificity com- pared to CD3, granzyme B and granulysin mRNA mea- surement. Significant elevated levels of NKG2D mRNA M. Seiler and I. Brabcova contributed equally to the manuscript. could be further detected in urine sediment prior to aRx, suggesting this receptor as a new candidate marker for the diagnosis of acute and chronic allograft rejection. Key words: Acute rejection, cytotoxicity receptor, graft function, kidney transplantation Received 20 February 2006, revised 30 August 2006 and accepted for publication 6 October 2006 Introduction Kidney transplantation is the treatment of choice for pa- tients with end-stage renal diseases. Despite the applica- tion of modern immunosuppressive therapies and consid- ering histocompatibility (HLA), acute rejection (aRx) is still a serious and frequent complication during the early post- transplant period. Moreover, chronic allograft nephropa- thy (CAN), leading to progressive allograft dysfunction, re- mains additionally an obstacle for the long-term allograft survival (1). In the recent past, major contributions have been made to identify the molecular signature within the rejecting allograft. Because acute allograft rejection is char- acterized by the infiltration of activated T cells, the ex- pression of characteristic T-cell markers is evident in renal biopsies obtained from patients who underwent transplant rejection (2,3). Furthermore, as activated donor-specific cytotoxic T lymphocytes (CTLs) infiltrate rejecting trans- plants, the expression analysis of cytotoxic molecules in renal biopsies has been shown to be associated with aRx (4–6). In the context of early noninvasive diagnosis espe- cially the urine attracts increasing attention because of its potential diagnostic and pathophysiologic biomarker infor- mation (7–11). The polymorphic major histocompatibility complex (MHC) class I chain-related proteins A and B (MICA/B) are cell- surface molecules which are constitutively expressed in the gastrointestinal epithelium (12). In response to cellu- lar stress such as heat shock or inflammation these so- called MICA/B proteins have been further detected on the cell surface of epithelial, endothelial and fibroblast cells (12,13). Although MICA is not expressed on resting lym- phocytes, Molinero et al. demonstrated that these antigens could be further induced on activated T cells (14,15). Sev- eral reports illustrated that MIC antigens might play a role in autoimmunity, tumor and virus recognition (16,17) and 423

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
American Journal of Transplantation 2007; 7: 423–433Blackwell Munksgaard
C© 2006 The AuthorsJournal compilation C© 2006 The American Society of
Transplantation and the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2006.01625.x
Heightened Expression of the Cytotoxicity ReceptorNKG2D Correlates with Acute and ChronicNephropathy After Kidney Transplantation
M. Seilera, I. Brabcovab, O. Viklickyb, P. Hribovab,
C. Rosenbergerc, J. Pratschked, A. Lodererovab,
M. Matza, C. Schonemanne, P. Reinkec,
H.-D. Volka and K. Kotscha,∗
aInstitute of Medical Immunology, UniversitatsmedizinCharite, Campus Mitte, Berlin, GermanybTransplant Laboratory, Transplantcentre, Institute forClinical and Experimental Medicine, Prague, CzechRepubliccDepartment of Nephrology and Intensive Care,Universitatsmedizin Charite, Campus Virchow, Berlin,GermanydDepartment of Visceral and Transplantation Surgery,Universitatsmedizin Charite, Campus Virchow, Berlin,GermanyeInstitute of Transfusion Medicine, HLA Laboratory,Universitatsmedizin Charite, Campus Virchow, Berlin,Germany∗Corresponding author: Katja Kotsch,[email protected]
The activating cytotoxicity receptor NKG2D binds tostress-regulated molecules encoded by the major his-tocompatibility complex class I chain-related (MIC) andUL-16-binding protein (ULBP)/retinoic acid early tran-script (RAET) gene family. To assess whether acuteallograft rejection leads to an induction of theseinducible ligands and their receptor NKG2D, we ex-amined the mRNA profiles in kidney transplant biop-sies. Expression levels were correlated with the inci-dence of acute rejection (aRx) episodes and chronicallograft nephropathy (CAN) proven by histology.Whereas MICA, ULBP1/3 and RAET1-E did not displayheightened gene expression, elevated levels of NKG2DmRNA could be associated with aRx (p < 0.001). Im-munohistology of kidney biopsies diagnosed with aRxrevealed NKG2D+ cells in tubulointerstitial areas pos-itive for CD8+ cells. Most importantly, elevated lev-els of NKG2D mRNA were associated with restrictedlong-term graft function assessed by the glomerularfiltration rate at 6, 12 and 18 months posttransplanta-tion. Induced NKG2D mRNA expression was still ob-servable in biopsies diagnosed with CAN (p < 0.001),demonstrating a higher sensitivity and specificity com-pared to CD3, granzyme B and granulysin mRNA mea-surement. Significant elevated levels of NKG2D mRNA
M. Seiler and I. Brabcova contributed equally to the manuscript.
could be further detected in urine sediment prior toaRx, suggesting this receptor as a new candidatemarker for the diagnosis of acute and chronic allograftrejection.
Key words: Acute rejection, cytotoxicity receptor,graft function, kidney transplantation
Received 20 February 2006, revised 30 August 2006 andaccepted for publication 6 October 2006
Introduction
Kidney transplantation is the treatment of choice for pa-tients with end-stage renal diseases. Despite the applica-tion of modern immunosuppressive therapies and consid-ering histocompatibility (HLA), acute rejection (aRx) is stilla serious and frequent complication during the early post-transplant period. Moreover, chronic allograft nephropa-thy (CAN), leading to progressive allograft dysfunction, re-mains additionally an obstacle for the long-term allograftsurvival (1). In the recent past, major contributions havebeen made to identify the molecular signature within therejecting allograft. Because acute allograft rejection is char-acterized by the infiltration of activated T cells, the ex-pression of characteristic T-cell markers is evident in renalbiopsies obtained from patients who underwent transplantrejection (2,3). Furthermore, as activated donor-specificcytotoxic T lymphocytes (CTLs) infiltrate rejecting trans-plants, the expression analysis of cytotoxic molecules inrenal biopsies has been shown to be associated with aRx(4–6). In the context of early noninvasive diagnosis espe-cially the urine attracts increasing attention because of itspotential diagnostic and pathophysiologic biomarker infor-mation (7–11).
The polymorphic major histocompatibility complex (MHC)class I chain-related proteins A and B (MICA/B) are cell-surface molecules which are constitutively expressed inthe gastrointestinal epithelium (12). In response to cellu-lar stress such as heat shock or inflammation these so-called MICA/B proteins have been further detected on thecell surface of epithelial, endothelial and fibroblast cells(12,13). Although MICA is not expressed on resting lym-phocytes, Molinero et al. demonstrated that these antigenscould be further induced on activated T cells (14,15). Sev-eral reports illustrated that MIC antigens might play a rolein autoimmunity, tumor and virus recognition (16,17) and
423

Seiler et al.
recent publications suggested an association between theexpression of MIC proteins and solid organ transplant re-jection. In this context, Zwirner et al. proved the existenceof MICA-specific antibodies in sera of kidney transplantedpatients who rejected their allografts in the presence orabsence of HLA class I and II antibodies (18). Furthermore,renal and pancreatic grafts with the evidence for bothacute and chronic rejection have been shown to expressMIC proteins (19). Among molecules belonging to theUL-16-binding protein (ULBP; ULBP1-3) family or retinoicacid early transcript-1 cluster (RAET1; ULBP4/RAET1E andRAET1G) (20) MIC antigens are the natural ligands of theactivating natural killer cell (NK) receptor NKG2D which isa homodimeric C-type lectin-like receptor that triggers NKcells and costimulates c d T cells, CD8+ ab T cells anda subset of potentially autoreactive CD4+ T cells (21). Incolocalization with the transmembrane signaling adapterprotein DAP10, NKG2D leads to cell-mediated cytotoxic-ity of NK cells and causes cytokine production includingMIP-1b, tumor necrosis factor (TNF)a and interferon (IFN)c(22).
We investigated whether aRx leads to messenger RNA(mRNA) induction of MICA in kidney biopsies as a di-rect consequence of cellular stress. Thus this moleculemight serve as additional candidate biomarker for the de-tection of inflammatory changes within the graft. To as-certain whether additional NKG2D ligands are induced dur-ing allograft rejection, we further included the mRNA anal-ysis of ULBP1, ULBP3 and RAET1-E. We hypothesizedthat an induction of these ligands might lead to an en-hanced triggering of their activating cytotoxicity recep-tor NKG2D. Our data could not support previous reportson MICA expression in renal allografts (19). Furthermorewe could not detect elevated mRNA expression levelsof alternative ligands. In contrast we observed a strongmRNA induction of NKG2D during renal allograft rejec-tion which could be verified by immunohistology in kid-ney biopsies. Significant levels of NKG2D transcripts werestill detectable in biopsies derived from patients diagnosedwith CAN demonstrating a higher sensitivity and specificitycompared to CD3 mRNA measurement as a marker ofT-cell infiltration or granzyme B and granulysin mRNA anal-ysis as indicators of cytotoxic effector function. Moreover,heightened NKG2D mRNA expression could be already de-tected in urine sediment of rejecting patients prior to aRxdiagnosis.
Table 1: Demographics for patients analyzed for mRNA expression in kidney biopsies
Banff’ 97 (grade)Male/ Mean age 1st Re Brain dead/ Cold ischemia Time of biopsy post HLA-Female (years) Tx Tx Living (hours) Tx (months) ATN (days) mismatch A/B/DR BL I II III
aRx (n = 31) 19/12 44 ± 20 29 2 23/8 12.5 ± 7.6 2.5 ± 2.8 3 ± 3 7 8 16 –cRx (n = 37) 20/17 49 ± 37 30 7 36/1 20.6 ± 5.5 46.8 ± 32.4 3 ± 3ATN (n = 10) 5/5 58 ± 11 8 2 10/– 21.3 ± 5.6 7.6 ± 6.1 3 ± 2nRx (n = 31) 21/10 49 ± 20 30 1 23/8 11.5 ± 7.8 9.2 ± 6.1 3 ± 2
Tx = transplantation; aRx = acute rejection; cRx = chronic rejection; ATN = acute tubular necrosis; nRx = no rejection.
Patients and Methods
Subjects
In a collaborative study, we selected 109 adult kidney transplant recipi-ents who had undergone kidney transplantation between June 1993 andSeptember 2004 from the Transplantcentre of the Institute for Clinical andExperimental Medicine, Prague, Czech Republic. Renal graft biopsy wasperformed due to kidney graft function deterioration. Maintenance immuno-suppression consisted of triple-drug therapy regimen based on either cy-closporine A or tacrolimus, mycophenolate mofetil or azathioprine and ta-pered steroids. Biopsy-proven aRx was treated with methylprednisoloneand in the case of resistance by anti-CD3 mAb. All biopsies were taken us-ing a 14G tru-cut needle (Uni-Cut Nadeln, Angiomed, Germany) controlledby ultrasound (Toshiba, Power Vision 6000, Japan). Biopsies were obtainedbased on protocol surveillance criteria or as clinically indicated. Small por-tions of cortical or juxtamedulary zone renal tissue were immediately frozenin liquid nitrogen and stored at −80◦C. Histological findings were classifiedaccording to the Banff ’97 criteria (23) and carried out under the super-vision of one experienced nephropathologist. Thirty-one biopsy samplesfrom renal transplant recipients revealed acute cellular-mediated (Banff I, II)or borderline rejection. Another 37 biopsy samples were classified as CANand 10 biopsy samples as acute tubular necrosis (ATN). Thirty-one protocolbiopsies derived from patients with stable renal function served as controls.The study was approved by the Ethics Committee of the Institute of Clinicaland Experimental Medicine in Prague and all patients agreed to participateand signed an informed consent (Table 1).
Urinary samples and RNA isolation
For the analysis of mRNA expression profiles in urine sediment 52 kidneytransplanted recipients who developed an aRx episode within the first 3postoperative months were selected from our study cohort from the De-partments of Surgery and Nephrology, Virchow-Clinic, UniversitatsmedizinCharite, Germany between October 2002 and May 2004 and were analyzedretrospectively. Urine specimens from patients with the diagnosis of ATN(n = 8), urinary tract infection (UTI; n = 10) and cytomegalovirus (CMV)infection (n = 5) were also included in the analysis. Forty-two renal trans-planted patients with stable graft function served as controls. Immunosup-pression consisted of methylprednisolone and tacrolimus ± mycophenolatemofetil and most patients additionally received anti-IL-2R mAb induction.Histology was classified according to the Banff ’97 criteria and confirmedaRx episodes were treated with methylprednisolone bolus or OKT3 mAb(Table 2). Urinary samples of 100 mL were collected three times/week/patient during hospitalization and twice/month from outpatients. Urine wascentrifuged at 10 000 rpm and 4◦C for 15 min. Pellets were washed in 1 mLphosphate-buffered saline (PBS) and centrifuged at 14 000 rpm for 7 minat 4◦C. Supernatants were discarded and total RNA was isolated from thepellet using the RNeasy® Mini Kit (Qiagen, Hilden, Germany).
Quantification of mRNA gene expression
Complementary DNA synthesis and real-time reverse transcription-polymerase chain reaction (RT-PCR) of nonamplified mRNA were performed
424 American Journal of Transplantation 2007; 7: 423–433
NKG2D Expression During Acute and Chronic Allograft Nephropathy
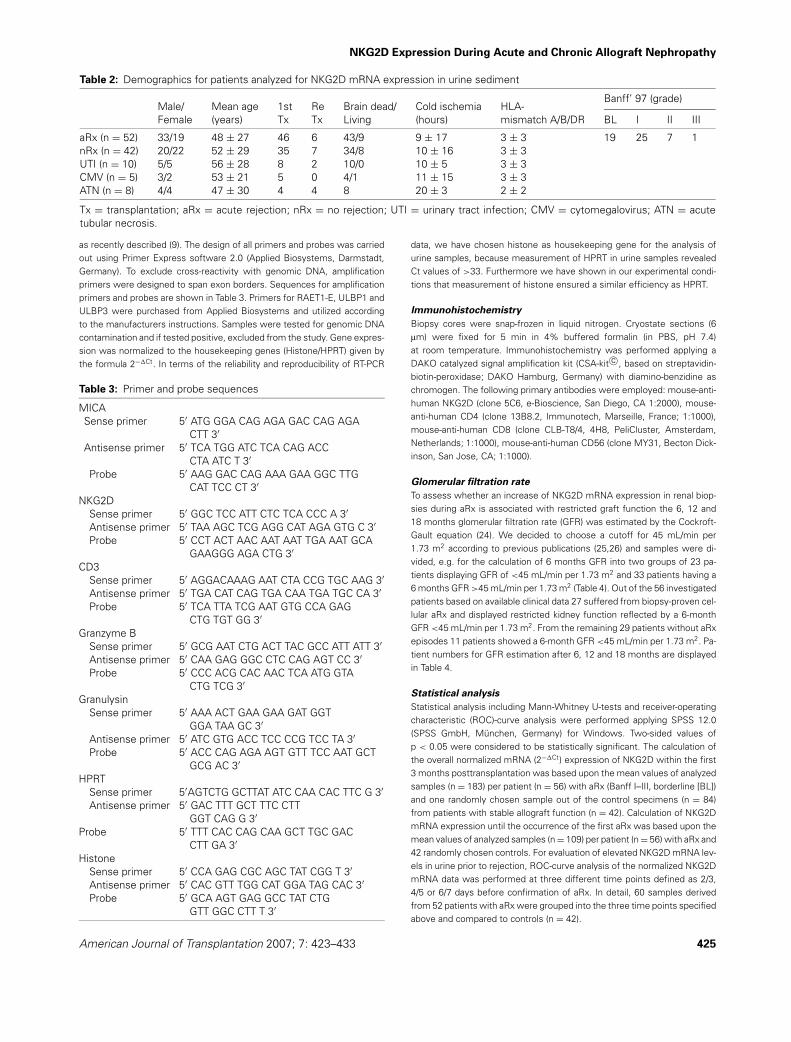
Table 2: Demographics for patients analyzed for NKG2D mRNA expression in urine sediment
Banff’ 97 (grade)Male/ Mean age 1st Re Brain dead/ Cold ischemia HLA-Female (years) Tx Tx Living (hours) mismatch A/B/DR BL I II III
aRx (n = 52) 33/19 48 ± 27 46 6 43/9 9 ± 17 3 ± 3 19 25 7 1nRx (n = 42) 20/22 52 ± 29 35 7 34/8 10 ± 16 3 ± 3UTI (n = 10) 5/5 56 ± 28 8 2 10/0 10 ± 5 3 ± 3CMV (n = 5) 3/2 53 ± 21 5 0 4/1 11 ± 15 3 ± 3ATN (n = 8) 4/4 47 ± 30 4 4 8 20 ± 3 2 ± 2
Tx = transplantation; aRx = acute rejection; nRx = no rejection; UTI = urinary tract infection; CMV = cytomegalovirus; ATN = acutetubular necrosis.
as recently described (9). The design of all primers and probes was carriedout using Primer Express software 2.0 (Applied Biosystems, Darmstadt,Germany). To exclude cross-reactivity with genomic DNA, amplificationprimers were designed to span exon borders. Sequences for amplificationprimers and probes are shown in Table 3. Primers for RAET1-E, ULBP1 andULBP3 were purchased from Applied Biosystems and utilized accordingto the manufacturers instructions. Samples were tested for genomic DNAcontamination and if tested positive, excluded from the study. Gene expres-sion was normalized to the housekeeping genes (Histone/HPRT) given bythe formula 2−�Ct. In terms of the reliability and reproducibility of RT-PCR
Table 3: Primer and probe sequences
MICASense primer 5′ ATG GGA CAG AGA GAC CAG AGA
CTT 3′Antisense primer 5′ TCA TGG ATC TCA CAG ACC
CTA ATC T 3′Probe 5′ AAG GAC CAG AAA GAA GGC TTG
CAT TCC CT 3′NKG2D
Sense primer 5′ GGC TCC ATT CTC TCA CCC A 3′Antisense primer 5′ TAA AGC TCG AGG CAT AGA GTG C 3′Probe 5′ CCT ACT AAC AAT AAT TGA AAT GCA
GAAGGG AGA CTG 3′CD3
Sense primer 5′ AGGACAAAG AAT CTA CCG TGC AAG 3′Antisense primer 5′ TGA CAT CAG TGA CAA TGA TGC CA 3′Probe 5′ TCA TTA TCG AAT GTG CCA GAG
CTG TGT GG 3′Granzyme B
Sense primer 5′ GCG AAT CTG ACT TAC GCC ATT ATT 3′Antisense primer 5′ CAA GAG GGC CTC CAG AGT CC 3′Probe 5′ CCC ACG CAC AAC TCA ATG GTA
CTG TCG 3′Granulysin
Sense primer 5′ AAA ACT GAA GAA GAT GGTGGA TAA GC 3′
Antisense primer 5′ ATC GTG ACC TCC CCG TCC TA 3′Probe 5′ ACC CAG AGA AGT GTT TCC AAT GCT
GCG AC 3′HPRT
Sense primer 5′AGTCTG GCTTAT ATC CAA CAC TTC G 3′Antisense primer 5′ GAC TTT GCT TTC CTT
GGT CAG G 3′Probe 5′ TTT CAC CAG CAA GCT TGC GAC
CTT GA 3′Histone
Sense primer 5′ CCA GAG CGC AGC TAT CGG T 3′Antisense primer 5′ CAC GTT TGG CAT GGA TAG CAC 3′Probe 5′ GCA AGT GAG GCC TAT CTG
GTT GGC CTT T 3′
data, we have chosen histone as housekeeping gene for the analysis ofurine samples, because measurement of HPRT in urine samples revealedCt values of >33. Furthermore we have shown in our experimental condi-tions that measurement of histone ensured a similar efficiency as HPRT.
Immunohistochemistry
Biopsy cores were snap-frozen in liquid nitrogen. Cryostate sections (6lm) were fixed for 5 min in 4% buffered formalin (in PBS, pH 7.4)at room temperature. Immunohistochemistry was performed applying aDAKO catalyzed signal amplification kit (CSA-kit c©, based on streptavidin-biotin-peroxidase; DAKO Hamburg, Germany) with diamino-benzidine aschromogen. The following primary antibodies were employed: mouse-anti-human NKG2D (clone 5C6, e-Bioscience, San Diego, CA 1:2000), mouse-anti-human CD4 (clone 13B8.2, Immunotech, Marseille, France; 1:1000),mouse-anti-human CD8 (clone CLB-T8/4, 4H8, PeliCluster, Amsterdam,Netherlands; 1:1000), mouse-anti-human CD56 (clone MY31, Becton Dick-inson, San Jose, CA; 1:1000).
Glomerular filtration rate
To assess whether an increase of NKG2D mRNA expression in renal biop-sies during aRx is associated with restricted graft function the 6, 12 and18 months glomerular filtration rate (GFR) was estimated by the Cockroft-Gault equation (24). We decided to choose a cutoff for 45 mL/min per1.73 m2 according to previous publications (25,26) and samples were di-vided, e.g. for the calculation of 6 months GFR into two groups of 23 pa-tients displaying GFR of <45 mL/min per 1.73 m2 and 33 patients having a6 months GFR >45 mL/min per 1.73 m2 (Table 4). Out of the 56 investigatedpatients based on available clinical data 27 suffered from biopsy-proven cel-lular aRx and displayed restricted kidney function reflected by a 6-monthGFR <45 mL/min per 1.73 m2. From the remaining 29 patients without aRxepisodes 11 patients showed a 6-month GFR <45 mL/min per 1.73 m2. Pa-tient numbers for GFR estimation after 6, 12 and 18 months are displayedin Table 4.
Statistical analysis
Statistical analysis including Mann-Whitney U-tests and receiver-operatingcharacteristic (ROC)-curve analysis were performed applying SPSS 12.0(SPSS GmbH, Munchen, Germany) for Windows. Two-sided values ofp < 0.05 were considered to be statistically significant. The calculation ofthe overall normalized mRNA (2−�Ct) expression of NKG2D within the first3 months posttransplantation was based upon the mean values of analyzedsamples (n = 183) per patient (n = 56) with aRx (Banff I–III, borderline [BL])and one randomly chosen sample out of the control specimens (n = 84)from patients with stable allograft function (n = 42). Calculation of NKG2DmRNA expression until the occurrence of the first aRx was based upon themean values of analyzed samples (n = 109) per patient (n = 56) with aRx and42 randomly chosen controls. For evaluation of elevated NKG2D mRNA lev-els in urine prior to rejection, ROC-curve analysis of the normalized NKG2DmRNA data was performed at three different time points defined as 2/3,4/5 or 6/7 days before confirmation of aRx. In detail, 60 samples derivedfrom 52 patients with aRx were grouped into the three time points specifiedabove and compared to controls (n = 42).
American Journal of Transplantation 2007; 7: 423–433 425
Seiler et al.
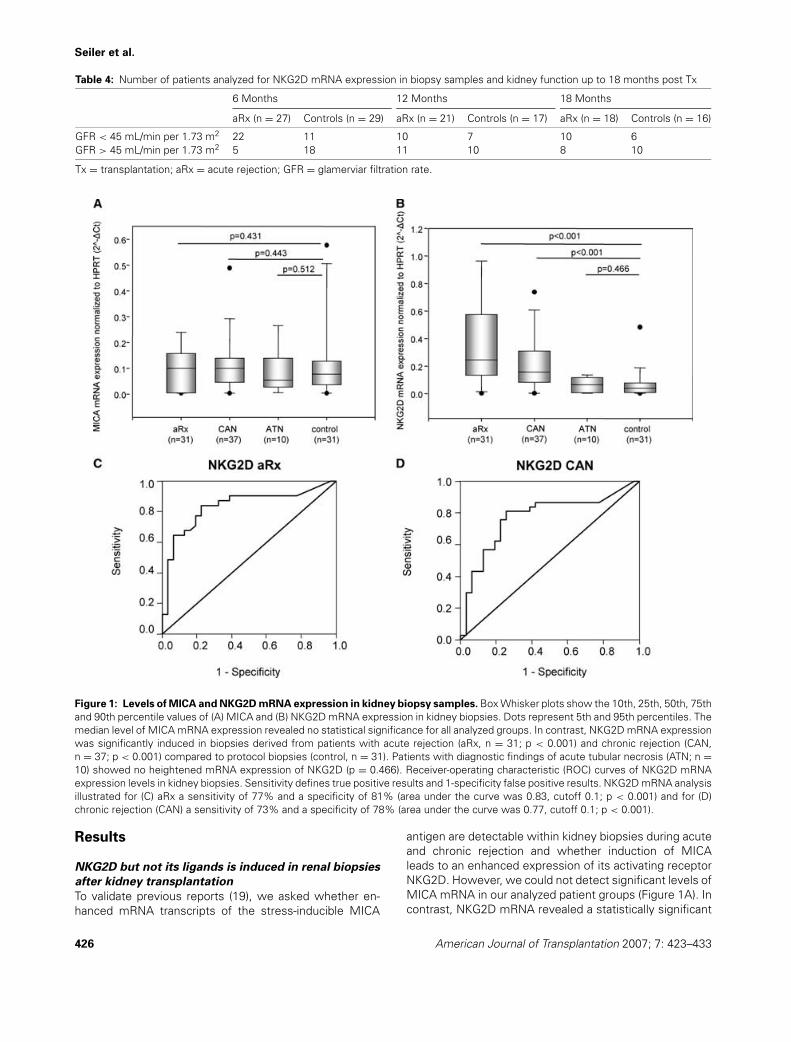
Table 4: Number of patients analyzed for NKG2D mRNA expression in biopsy samples and kidney function up to 18 months post Tx
6 Months 12 Months 18 Months
aRx (n = 27) Controls (n = 29) aRx (n = 21) Controls (n = 17) aRx (n = 18) Controls (n = 16)
GFR < 45 mL/min per 1.73 m2 22 11 10 7 10 6GFR > 45 mL/min per 1.73 m2 5 18 11 10 8 10
Tx = transplantation; aRx = acute rejection; GFR = glamerviar filtration rate.
Figure 1: Levels of MICA and NKG2D mRNA expression in kidney biopsy samples. Box Whisker plots show the 10th, 25th, 50th, 75thand 90th percentile values of (A) MICA and (B) NKG2D mRNA expression in kidney biopsies. Dots represent 5th and 95th percentiles. Themedian level of MICA mRNA expression revealed no statistical significance for all analyzed groups. In contrast, NKG2D mRNA expressionwas significantly induced in biopsies derived from patients with acute rejection (aRx, n = 31; p < 0.001) and chronic rejection (CAN,n = 37; p < 0.001) compared to protocol biopsies (control, n = 31). Patients with diagnostic findings of acute tubular necrosis (ATN; n =10) showed no heightened mRNA expression of NKG2D (p = 0.466). Receiver-operating characteristic (ROC) curves of NKG2D mRNAexpression levels in kidney biopsies. Sensitivity defines true positive results and 1-specificity false positive results. NKG2D mRNA analysisillustrated for (C) aRx a sensitivity of 77% and a specificity of 81% (area under the curve was 0.83, cutoff 0.1; p < 0.001) and for (D)chronic rejection (CAN) a sensitivity of 73% and a specificity of 78% (area under the curve was 0.77, cutoff 0.1; p < 0.001).
Results
NKG2D but not its ligands is induced in renal biopsies
after kidney transplantation
To validate previous reports (19), we asked whether en-hanced mRNA transcripts of the stress-inducible MICA
antigen are detectable within kidney biopsies during acuteand chronic rejection and whether induction of MICAleads to an enhanced expression of its activating receptorNKG2D. However, we could not detect significant levels ofMICA mRNA in our analyzed patient groups (Figure 1A). Incontrast, NKG2D mRNA revealed a statistically significant
426 American Journal of Transplantation 2007; 7: 423–433
NKG2D Expression During Acute and Chronic Allograft Nephropathy
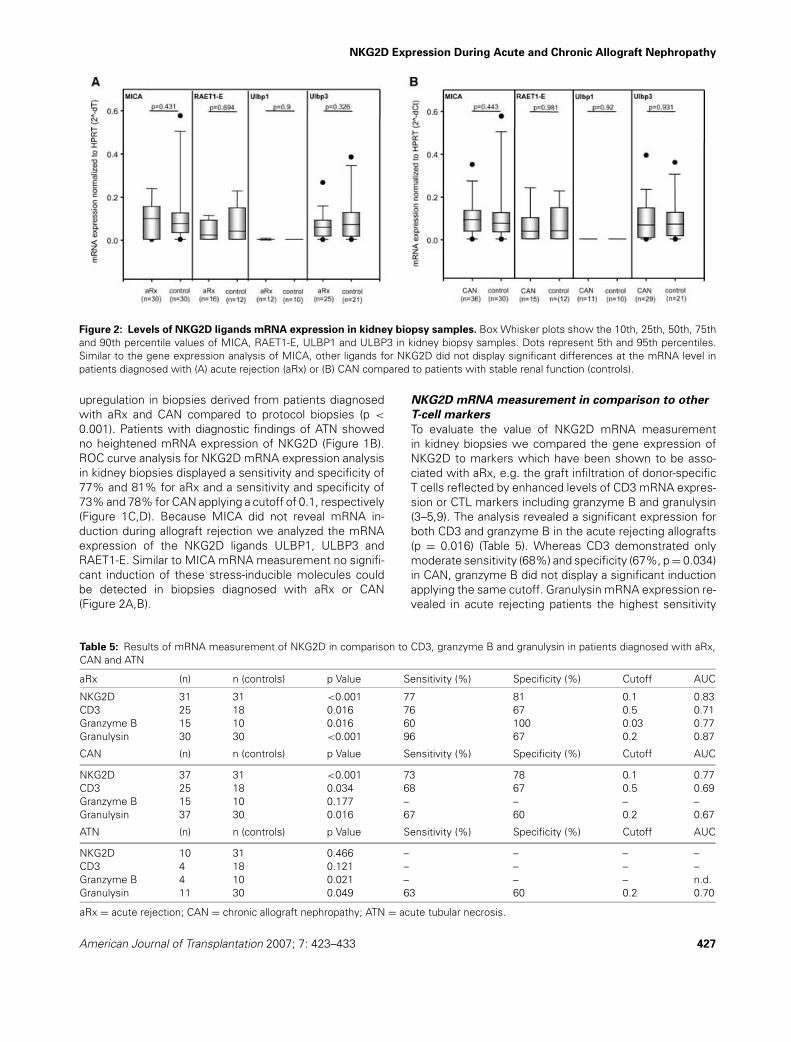
Figure 2: Levels of NKG2D ligands mRNA expression in kidney biopsy samples. Box Whisker plots show the 10th, 25th, 50th, 75thand 90th percentile values of MICA, RAET1-E, ULBP1 and ULBP3 in kidney biopsy samples. Dots represent 5th and 95th percentiles.Similar to the gene expression analysis of MICA, other ligands for NKG2D did not display significant differences at the mRNA level inpatients diagnosed with (A) acute rejection (aRx) or (B) CAN compared to patients with stable renal function (controls).
upregulation in biopsies derived from patients diagnosedwith aRx and CAN compared to protocol biopsies (p <
0.001). Patients with diagnostic findings of ATN showedno heightened mRNA expression of NKG2D (Figure 1B).ROC curve analysis for NKG2D mRNA expression analysisin kidney biopsies displayed a sensitivity and specificity of77% and 81% for aRx and a sensitivity and specificity of73% and 78% for CAN applying a cutoff of 0.1, respectively(Figure 1C,D). Because MICA did not reveal mRNA in-duction during allograft rejection we analyzed the mRNAexpression of the NKG2D ligands ULBP1, ULBP3 andRAET1-E. Similar to MICA mRNA measurement no signifi-cant induction of these stress-inducible molecules couldbe detected in biopsies diagnosed with aRx or CAN(Figure 2A,B).
Table 5: Results of mRNA measurement of NKG2D in comparison to CD3, granzyme B and granulysin in patients diagnosed with aRx,CAN and ATN
aRx (n) n (controls) p Value Sensitivity (%) Specificity (%) Cutoff AUC
NKG2D 31 31 <0.001 77 81 0.1 0.83CD3 25 18 0.016 76 67 0.5 0.71Granzyme B 15 10 0.016 60 100 0.03 0.77Granulysin 30 30 <0.001 96 67 0.2 0.87
CAN (n) n (controls) p Value Sensitivity (%) Specificity (%) Cutoff AUC
NKG2D 37 31 <0.001 73 78 0.1 0.77CD3 25 18 0.034 68 67 0.5 0.69Granzyme B 15 10 0.177 – – – –Granulysin 37 30 0.016 67 60 0.2 0.67
ATN (n) n (controls) p Value Sensitivity (%) Specificity (%) Cutoff AUC
NKG2D 10 31 0.466 – – – –CD3 4 18 0.121 – – – –Granzyme B 4 10 0.021 – – – n.d.Granulysin 11 30 0.049 63 60 0.2 0.70
aRx = acute rejection; CAN = chronic allograft nephropathy; ATN = acute tubular necrosis.
NKG2D mRNA measurement in comparison to other
T-cell markers
To evaluate the value of NKG2D mRNA measurementin kidney biopsies we compared the gene expression ofNKG2D to markers which have been shown to be asso-ciated with aRx, e.g. the graft infiltration of donor-specificT cells reflected by enhanced levels of CD3 mRNA expres-sion or CTL markers including granzyme B and granulysin(3–5,9). The analysis revealed a significant expression forboth CD3 and granzyme B in the acute rejecting allografts(p = 0.016) (Table 5). Whereas CD3 demonstrated onlymoderate sensitivity (68%) and specificity (67%, p = 0.034)in CAN, granzyme B did not display a significant inductionapplying the same cutoff. Granulysin mRNA expression re-vealed in acute rejecting patients the highest sensitivity
American Journal of Transplantation 2007; 7: 423–433 427
Seiler et al.
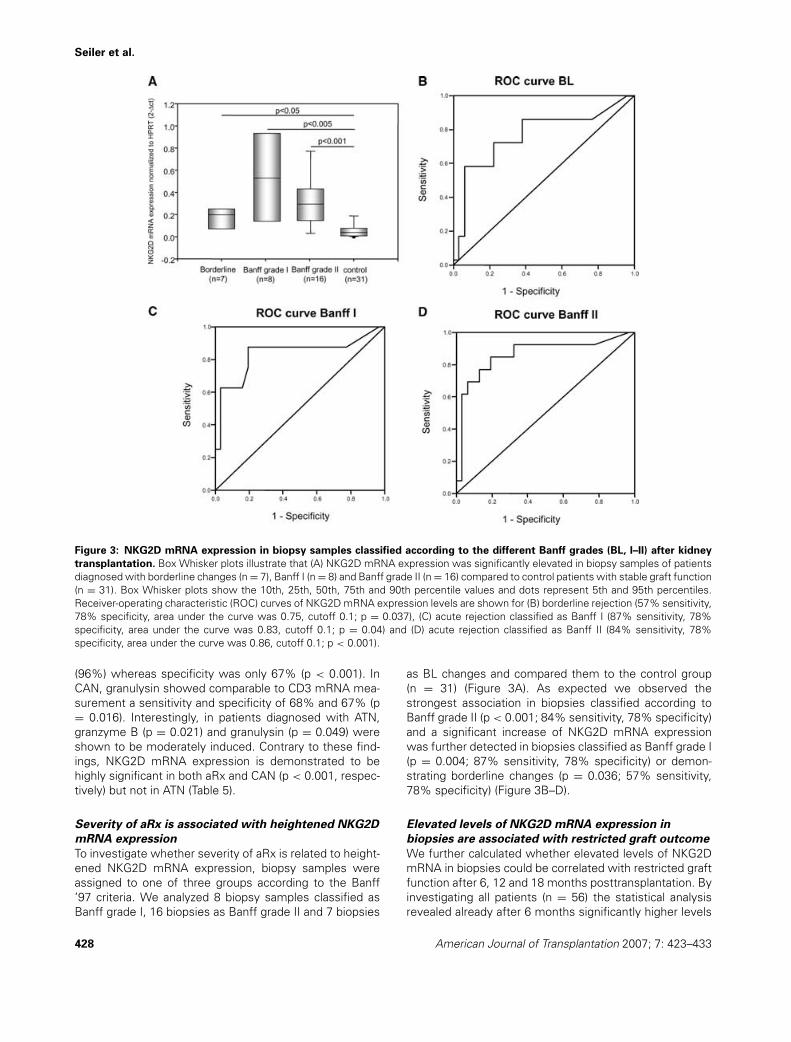
Figure 3: NKG2D mRNA expression in biopsy samples classified according to the different Banff grades (BL, I–II) after kidney
transplantation. Box Whisker plots illustrate that (A) NKG2D mRNA expression was significantly elevated in biopsy samples of patientsdiagnosed with borderline changes (n = 7), Banff I (n = 8) and Banff grade II (n = 16) compared to control patients with stable graft function(n = 31). Box Whisker plots show the 10th, 25th, 50th, 75th and 90th percentile values and dots represent 5th and 95th percentiles.Receiver-operating characteristic (ROC) curves of NKG2D mRNA expression levels are shown for (B) borderline rejection (57% sensitivity,78% specificity, area under the curve was 0.75, cutoff 0.1; p = 0.037), (C) acute rejection classified as Banff I (87% sensitivity, 78%specificity, area under the curve was 0.83, cutoff 0.1; p = 0.04) and (D) acute rejection classified as Banff II (84% sensitivity, 78%specificity, area under the curve was 0.86, cutoff 0.1; p < 0.001).
(96%) whereas specificity was only 67% (p < 0.001). InCAN, granulysin showed comparable to CD3 mRNA mea-surement a sensitivity and specificity of 68% and 67% (p= 0.016). Interestingly, in patients diagnosed with ATN,granzyme B (p = 0.021) and granulysin (p = 0.049) wereshown to be moderately induced. Contrary to these find-ings, NKG2D mRNA expression is demonstrated to behighly significant in both aRx and CAN (p < 0.001, respec-tively) but not in ATN (Table 5).
Severity of aRx is associated with heightened NKG2D
mRNA expression
To investigate whether severity of aRx is related to height-ened NKG2D mRNA expression, biopsy samples wereassigned to one of three groups according to the Banff’97 criteria. We analyzed 8 biopsy samples classified asBanff grade I, 16 biopsies as Banff grade II and 7 biopsies
as BL changes and compared them to the control group(n = 31) (Figure 3A). As expected we observed thestrongest association in biopsies classified according toBanff grade II (p < 0.001; 84% sensitivity, 78% specificity)and a significant increase of NKG2D mRNA expressionwas further detected in biopsies classified as Banff grade I(p = 0.004; 87% sensitivity, 78% specificity) or demon-strating borderline changes (p = 0.036; 57% sensitivity,78% specificity) (Figure 3B–D).
Elevated levels of NKG2D mRNA expression in
biopsies are associated with restricted graft outcome
We further calculated whether elevated levels of NKG2DmRNA in biopsies could be correlated with restricted graftfunction after 6, 12 and 18 months posttransplantation. Byinvestigating all patients (n = 56) the statistical analysisrevealed already after 6 months significantly higher levels
428 American Journal of Transplantation 2007; 7: 423–433
NKG2D Expression During Acute and Chronic Allograft Nephropathy
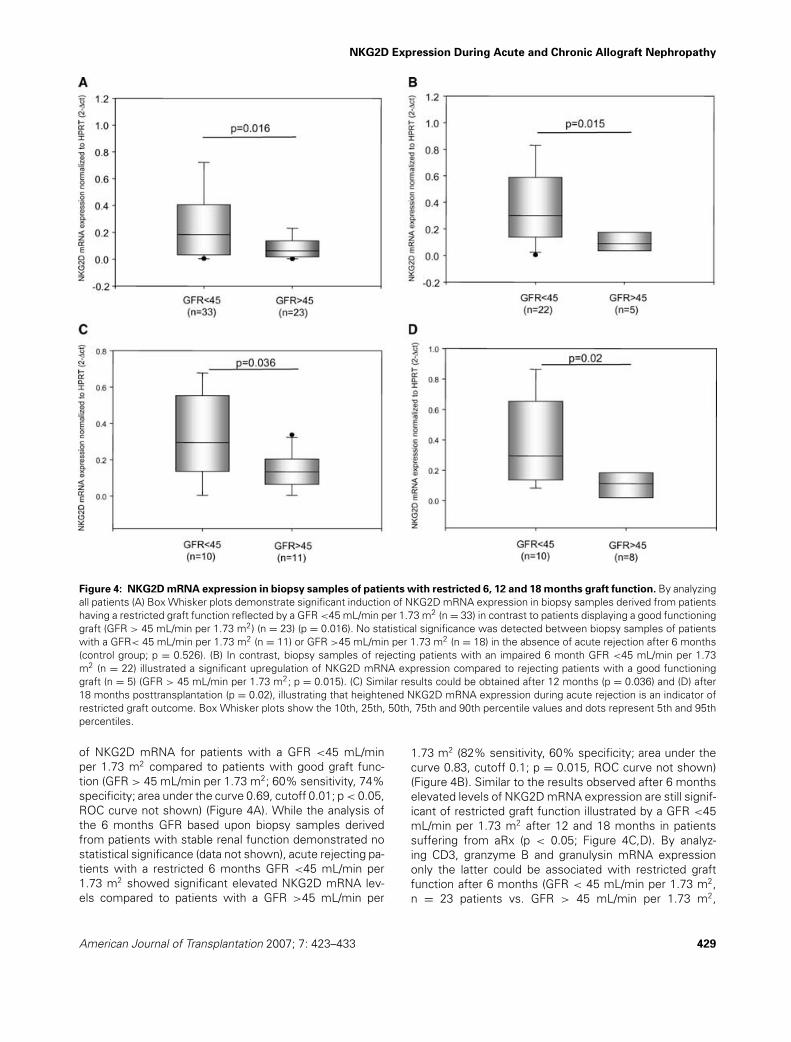
Figure 4: NKG2D mRNA expression in biopsy samples of patients with restricted 6, 12 and 18 months graft function. By analyzingall patients (A) Box Whisker plots demonstrate significant induction of NKG2D mRNA expression in biopsy samples derived from patientshaving a restricted graft function reflected by a GFR <45 mL/min per 1.73 m2 (n = 33) in contrast to patients displaying a good functioninggraft (GFR > 45 mL/min per 1.73 m2) (n = 23) (p = 0.016). No statistical significance was detected between biopsy samples of patientswith a GFR< 45 mL/min per 1.73 m2 (n = 11) or GFR >45 mL/min per 1.73 m2 (n = 18) in the absence of acute rejection after 6 months(control group; p = 0.526). (B) In contrast, biopsy samples of rejecting patients with an impaired 6 month GFR <45 mL/min per 1.73m2 (n = 22) illustrated a significant upregulation of NKG2D mRNA expression compared to rejecting patients with a good functioninggraft (n = 5) (GFR > 45 mL/min per 1.73 m2; p = 0.015). (C) Similar results could be obtained after 12 months (p = 0.036) and (D) after18 months posttransplantation (p = 0.02), illustrating that heightened NKG2D mRNA expression during acute rejection is an indicator ofrestricted graft outcome. Box Whisker plots show the 10th, 25th, 50th, 75th and 90th percentile values and dots represent 5th and 95thpercentiles.
of NKG2D mRNA for patients with a GFR <45 mL/minper 1.73 m2 compared to patients with good graft func-tion (GFR > 45 mL/min per 1.73 m2; 60% sensitivity, 74%specificity; area under the curve 0.69, cutoff 0.01; p < 0.05,ROC curve not shown) (Figure 4A). While the analysis ofthe 6 months GFR based upon biopsy samples derivedfrom patients with stable renal function demonstrated nostatistical significance (data not shown), acute rejecting pa-tients with a restricted 6 months GFR <45 mL/min per1.73 m2 showed significant elevated NKG2D mRNA lev-els compared to patients with a GFR >45 mL/min per
1.73 m2 (82% sensitivity, 60% specificity; area under thecurve 0.83, cutoff 0.1; p = 0.015, ROC curve not shown)(Figure 4B). Similar to the results observed after 6 monthselevated levels of NKG2D mRNA expression are still signif-icant of restricted graft function illustrated by a GFR <45mL/min per 1.73 m2 after 12 and 18 months in patientssuffering from aRx (p < 0.05; Figure 4C,D). By analyz-ing CD3, granzyme B and granulysin mRNA expressiononly the latter could be associated with restricted graftfunction after 6 months (GFR < 45 mL/min per 1.73 m2,n = 23 patients vs. GFR > 45 mL/min per 1.73 m2,
American Journal of Transplantation 2007; 7: 423–433 429
Seiler et al.
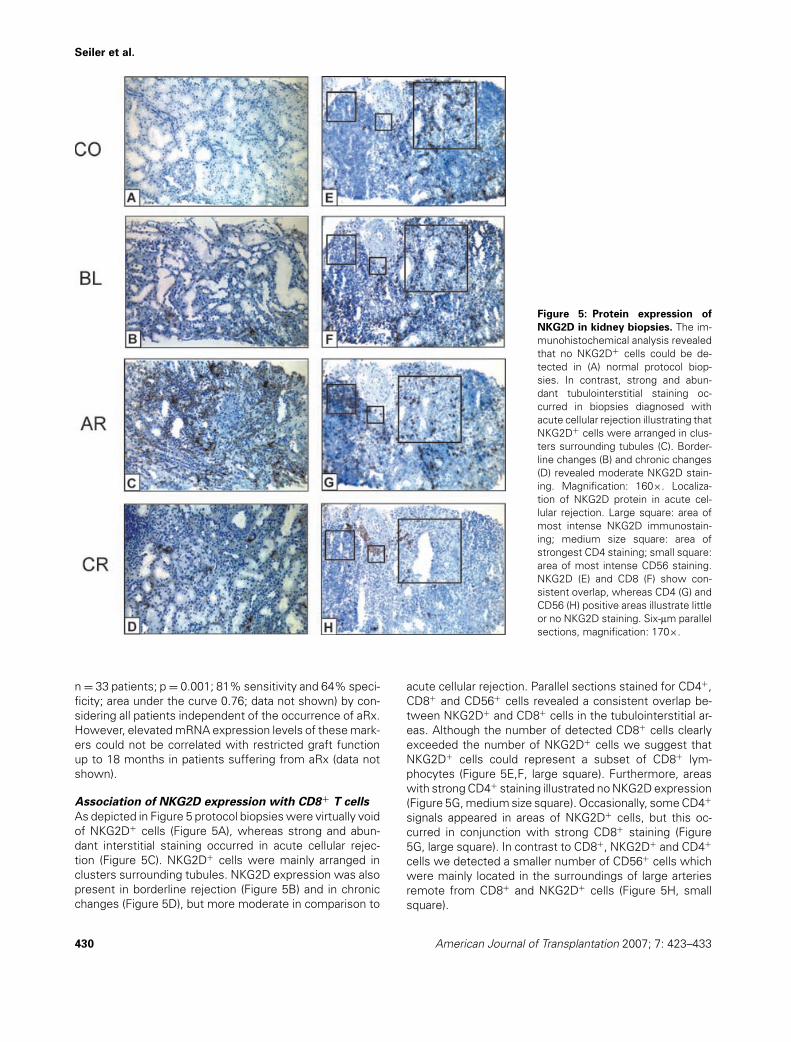
Figure 5: Protein expression of
NKG2D in kidney biopsies. The im-munohistochemical analysis revealedthat no NKG2D+ cells could be de-tected in (A) normal protocol biop-sies. In contrast, strong and abun-dant tubulointerstitial staining oc-curred in biopsies diagnosed withacute cellular rejection illustrating thatNKG2D+ cells were arranged in clus-ters surrounding tubules (C). Border-line changes (B) and chronic changes(D) revealed moderate NKG2D stain-ing. Magnification: 160×. Localiza-tion of NKG2D protein in acute cel-lular rejection. Large square: area ofmost intense NKG2D immunostain-ing; medium size square: area ofstrongest CD4 staining; small square:area of most intense CD56 staining.NKG2D (E) and CD8 (F) show con-sistent overlap, whereas CD4 (G) andCD56 (H) positive areas illustrate littleor no NKG2D staining. Six-lm parallelsections, magnification: 170×.
n = 33 patients; p = 0.001; 81% sensitivity and 64% speci-ficity; area under the curve 0.76; data not shown) by con-sidering all patients independent of the occurrence of aRx.However, elevated mRNA expression levels of these mark-ers could not be correlated with restricted graft functionup to 18 months in patients suffering from aRx (data notshown).
Association of NKG2D expression with CD8+ T cells
As depicted in Figure 5 protocol biopsies were virtually voidof NKG2D+ cells (Figure 5A), whereas strong and abun-dant interstitial staining occurred in acute cellular rejec-tion (Figure 5C). NKG2D+ cells were mainly arranged inclusters surrounding tubules. NKG2D expression was alsopresent in borderline rejection (Figure 5B) and in chronicchanges (Figure 5D), but more moderate in comparison to
acute cellular rejection. Parallel sections stained for CD4+,CD8+ and CD56+ cells revealed a consistent overlap be-tween NKG2D+ and CD8+ cells in the tubulointerstitial ar-eas. Although the number of detected CD8+ cells clearlyexceeded the number of NKG2D+ cells we suggest thatNKG2D+ cells could represent a subset of CD8+ lym-phocytes (Figure 5E,F, large square). Furthermore, areaswith strong CD4+ staining illustrated no NKG2D expression(Figure 5G, medium size square). Occasionally, some CD4+
signals appeared in areas of NKG2D+ cells, but this oc-curred in conjunction with strong CD8+ staining (Figure5G, large square). In contrast to CD8+, NKG2D+ and CD4+
cells we detected a smaller number of CD56+ cells whichwere mainly located in the surroundings of large arteriesremote from CD8+ and NKG2D+ cells (Figure 5H, smallsquare).
430 American Journal of Transplantation 2007; 7: 423–433
NKG2D Expression During Acute and Chronic Allograft Nephropathy
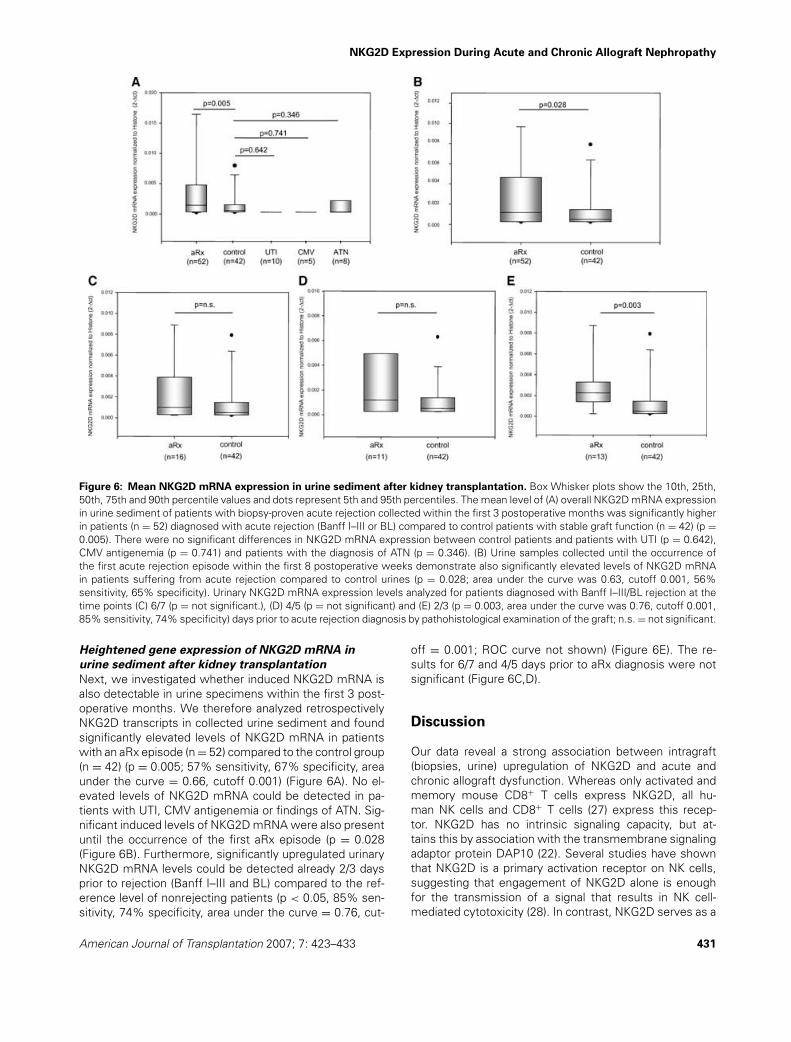
Figure 6: Mean NKG2D mRNA expression in urine sediment after kidney transplantation. Box Whisker plots show the 10th, 25th,50th, 75th and 90th percentile values and dots represent 5th and 95th percentiles. The mean level of (A) overall NKG2D mRNA expressionin urine sediment of patients with biopsy-proven acute rejection collected within the first 3 postoperative months was significantly higherin patients (n = 52) diagnosed with acute rejection (Banff I–III or BL) compared to control patients with stable graft function (n = 42) (p =0.005). There were no significant differences in NKG2D mRNA expression between control patients and patients with UTI (p = 0.642),CMV antigenemia (p = 0.741) and patients with the diagnosis of ATN (p = 0.346). (B) Urine samples collected until the occurrence ofthe first acute rejection episode within the first 8 postoperative weeks demonstrate also significantly elevated levels of NKG2D mRNAin patients suffering from acute rejection compared to control urines (p = 0.028; area under the curve was 0.63, cutoff 0.001, 56%sensitivity, 65% specificity). Urinary NKG2D mRNA expression levels analyzed for patients diagnosed with Banff I–III/BL rejection at thetime points (C) 6/7 (p = not significant.), (D) 4/5 (p = not significant) and (E) 2/3 (p = 0.003, area under the curve was 0.76, cutoff 0.001,85% sensitivity, 74% specificity) days prior to acute rejection diagnosis by pathohistological examination of the graft; n.s. = not significant.
Heightened gene expression of NKG2D mRNA in
urine sediment after kidney transplantation
Next, we investigated whether induced NKG2D mRNA isalso detectable in urine specimens within the first 3 post-operative months. We therefore analyzed retrospectivelyNKG2D transcripts in collected urine sediment and foundsignificantly elevated levels of NKG2D mRNA in patientswith an aRx episode (n = 52) compared to the control group(n = 42) (p = 0.005; 57% sensitivity, 67% specificity, areaunder the curve = 0.66, cutoff 0.001) (Figure 6A). No el-evated levels of NKG2D mRNA could be detected in pa-tients with UTI, CMV antigenemia or findings of ATN. Sig-nificant induced levels of NKG2D mRNA were also presentuntil the occurrence of the first aRx episode (p = 0.028(Figure 6B). Furthermore, significantly upregulated urinaryNKG2D mRNA levels could be detected already 2/3 daysprior to rejection (Banff I–III and BL) compared to the ref-erence level of nonrejecting patients (p < 0.05, 85% sen-sitivity, 74% specificity, area under the curve = 0.76, cut-
off = 0.001; ROC curve not shown) (Figure 6E). The re-sults for 6/7 and 4/5 days prior to aRx diagnosis were notsignificant (Figure 6C,D).
Discussion
Our data reveal a strong association between intragraft(biopsies, urine) upregulation of NKG2D and acute andchronic allograft dysfunction. Whereas only activated andmemory mouse CD8+ T cells express NKG2D, all hu-man NK cells and CD8+ T cells (27) express this recep-tor. NKG2D has no intrinsic signaling capacity, but at-tains this by association with the transmembrane signalingadaptor protein DAP10 (22). Several studies have shownthat NKG2D is a primary activation receptor on NK cells,suggesting that engagement of NKG2D alone is enoughfor the transmission of a signal that results in NK cell-mediated cytotoxicity (28). In contrast, NKG2D serves as a
American Journal of Transplantation 2007; 7: 423–433 431

Seiler et al.
costimulatory receptor for T-cell receptor (TCR)-mediatedsignals in naive CD8+ T cells in a manner similar to CD28(16,29). These results gained by Maasho et al. (29) showthat the engagement of NKG2D along with the TCR favorsthe development of Th1 over Th2 cells. Furthermore, theirresults illustrate that NKG2D costimulated human naiveCD8+ T cells are more functional, because they respondbetter to homeostatic cytokines compared to cells thathave been only TCR stimulated. Expression and functionof NKG2D is selectively upregulated by IL-15, which hasbeen shown to be induced during aRx and resistant tocalcineurin inhibitor action (3,30,31). NKG2D engagementmay markedly enhance T-cell activation under conditionsof suboptimal TCR engagement for a variety of effectorfunctions.
Multiple ligands have been described for human NKG2Dincluding MIC, UL16-binding (ULBP)/RAET1 proteins. Asnew candidates for transplant-related antibodies, severalpublications focused on MICA genes (18,19,32,33). Unlikeprevious reports we could not detect elevated mRNA ex-pression levels of MICA and alternative NKG2D ligands in-cluding ULBP1, ULBP3 and RAET1-E in kidney biopsiesderived from patients undergoing aRx or CAN but we ob-served heightened gene expression of NKG2D (Figures1A–D and 2A,B). This gene expression pattern was as-sociated with the severity of aRx already significantly de-tectable in biopsies with borderline changes but displayingthe highest sensitivity and specificity in biopsies classifiedaccording to Banff grade II (p < 0.001) (Figure 3A–D). Thefindings by Roberts et al. (28) suggest that NKG2D and MICmay contribute to tissue destruction under immunopatho-logical conditions in the presence of IL-15. Whereas naiveCD8+ T cells encountering Ag-loaded dendritic cells (DC)in lymph nodes use the CD28/B7 costimulatory pathway,effector CTL in the tissue microenvironment might be con-trolled by an alternative costimulatory mechanism basedupon the induction of the nonclassical MHC-like moleculesMIC. Our immunohistological analysis revealed a strong in-filtration of CD8+ T cells during aRx. NKG2D+ cells weredetected in tubulointerstitial areas positive for CD8+ cellsand not for CD56+ cells suggesting a coexpression ofNKG2D by graft infiltrating CTLs and not with NK cells(Figure 5E,F). Because we could not detect significantgene expression of the natural ligands these data suggestthat detected levels of NKG2D mRNA reflect enhancedgraft infiltration of CTLs rather an induction by its ligands.Most importantly, presence of NKG2D+ cells could be ver-ified in kidney biopsies diagnosed with CAN at the mRNA(Figure 1B,D) and protein level (Figure 5D) indicating a con-tribution of NKG2D+ cells to chronic allograft destruction.However, a functional proof whether NKG2D receptor ex-pression leads to enhanced T-cell activation of CD8+ cellsduring acute and chronic allograft rejection remains to beclarified and needs further investigations.
It is supported by several reports on CD8+ effector geneexpression by T cells in peripheral blood or urine of renal al-
lograft recipients that CD8+ effector populations are poten-tial key contributors to renal allograft rejection (3–7,9,34).Although we measured comparable to NKG2D mRNA lev-els granulysin mRNA in the same kidney biopsies duringaRx (p < 0.001; Table 4), gene expression of this cytotoxicmolecule displayed only restricted significance during CANcompared to NKG2D (p = 0.016 for granulysin vs. p < 0.001for NKG2D). Similar results were gained for analyzing CD3and granzyme B. Thus, NKG2D mRNA expression does notnecessarily correlates with cytotoxic effector function. Incontrast to granulysin and granzyme B we could not detectinduced NKG2D mRNA expression in diagnostic findingsof ATN. Therefore it would be of great interest to evaluatethis marker in forthcoming and prospective studies as asuitable candidate for aRx screening approaches in otherkidney transplantation-associated complications includingdrug toxicity or delayed graft function.
We assumed that elevated NKG2D mRNA expression inkidney biopsies correlates with an impaired graft outcomeand could demonstrate that patients having elevated lev-els of NKG2D mRNA expression during aRx suffer from re-stricted graft function already after 6 months (Figure 4A,B).Similar observations could be made after 12 and 18 months(Figure 4C,D). NKG2D gene expression was even elevatedin urinary sediment of a second study population suffer-ing from aRx within the first 3 postoperative months com-pared to patients with stable renal function (p = 0.005)(Figure 6A). This gene expression was confirmed by inves-tigating urinary samples until the occurrence of the firstaRx episode. Moreover, NKG2D mRNA transcripts havealready been detectable 2/3 days prior to aRx diagnosis(Figure 6E). Although it has been illustrated by McNerneyet al. that targeting of NKG2D fails to prevent acute al-lograft rejection in CD28 deficient mice (35), we suggestthat our current findings regarding elevated expression ofNKG2D in biopsies and urine during acute kidney allograftrejection implies this molecule as an additionally informa-tive biomarker of transplant outcome. Because it has beenlately demonstrated that NKG2D is not only expressed byNK cells but also by interferon-producing killer DC (36,37)we propose this marker as an interesting target for inter-vening therapeutic approaches in the future.
Acknowledgments
The authors thank Annelie Dernier, Katerina Hyklova and MichaelaProkopova for excellent technological assistance and Nathalie Durkopp forcareful reading of the manuscript. Katja Kotsch was supported by a grantfrom the Else-Kroner Fresenius Foundation. Part of the study was supportedby a grant from the Institute for Clinical and Experimental Medicine IKEM(MZO 00023001).
References
1. Joosten SA, Sijpkens YW, van Kooten C, Paul LC. Chronic re-nal allograft rejection: Pathophysiologic considerations. Kidney Int2005; 68: 1–13.
2. Strehlau J, Pavlakis M, Lipman M et al. Quantitative detection
432 American Journal of Transplantation 2007; 7: 423–433

NKG2D Expression During Acute and Chronic Allograft Nephropathy
of immune activation transcripts as a diagnostic tool in kidneytransplantation. Proc Natl Acad Sci USA 1997; 94: 695–700.
3. Pavlakis M, Lipman M, Strom TB. Intragraft T cell receptor tran-script expression in human renal allografts. J Am Soc Nephrol1995; 6: 281–285.
4. Vasconcellos LM, Schachter AD, Zheng XX et al. Cytotoxic lym-phocyte gene expression in peripheral blood leukocytes correlateswith rejecting renal allografts. Transplantation 1998; 66: 562–566.
5. Lipman ML, Stevens AC, Strom TB. Heightened intragraft CTLgene expression in acutely rejecting renal allografts. J Immunol1994; 152: 5120–5127.
6. Lipman ML, Stevens AC, Bleackley RC et al. The strong corre-lation of cytotoxic T lymphocyte-specific serine protease genetranscripts with renal allograft rejection. Transplantation 1992; 53:73–79.
7. Li B, Hartono C, Ding R et al. Noninvasive diagnosis of renal-allograft rejection by measurement of messenger RNA for per-forin and granzyme B in urine. N Engl J Med 2001; 344: 947–954.
8. Tatapudi RR, Muthukumar T, Dadhania D et al. Noninvasivedetection of renal allograft inflammation by measurements ofmRNA for IP-10 and CXCR3 in urine. Kidney Int 2004; 65: 2390–2397.
9. Kotsch K, Mashreghi MF, Bold G et al. Enhanced granulysin mRNAexpression in urinary sediment in early and delayed acute renalallograft rejection. Transplantation 2004; 77: 1866–1875.
10. Mas VR, Maluf DG, Archer KJ et al. Study of mRNA growth fac-tors in urinary cells of kidney transplant recipients as predictorsof chronic allograft nephropathy. Transplantation 2005; 80: 1686–1691.
11. Muthukumar T, Dadhania D, Ding R et al. Messenger RNA forFOXP3 in the urine of renal-allograft recipients. N Engl J Med2005; 353: 2342–2351.
12. Groh V, Bahram S, Bauer S, Herman A, Beauchamp M, SpiesT. Cell stress-regulated human major histocompatibility complexclass I gene expressed in gastrointestinal epithelium. Proc NatlAcad Sci USA 1996; 93: 12445–12450.
13. Hamerman JA, Ogasawara K, Lanier LL. Cutting edge: Toll-likereceptor signaling in macrophages induces ligands for the NKG2Dreceptor. J Immunol 2004; 172: 2001–2005.
14. Molinero LL, Fuertes MB, Rabinovich GA, Fainboim L, ZwirnerNW. Activation-induced expression of MICA on T lymphocytesinvolves engagement of CD3 and CD28. J Leukoc Biol 2002; 71:791–797.
15. Molinero LL, Fuertes MB, Girart MV et al. NF-kappa B regulatesexpression of the MHC class I-related chain A gene in activated Tlymphocytes. J Immunol 2004; 173: 5583.
16. Groh V, Rhinehart R, Randolph-Habecker J, Topp MS, Riddell SR,Spies T. Costimulation of CD8alphabeta T cells by NKG2D viaengagement by MIC induced on virus-infected cells. Nat Immunol2001; 2: 255–262.
17. Groh V, Rhinehart R, Secrist H, Bauer S, Grabstein KH, SpiesT. Broad tumor-associated expression and recognition by tumor-derived gamma delta T cells of MICA and MICB. Proc Natl AcadSci USA 1999; 96: 6879–6889.
18. Zwirner NW, Marcos CY, Mirbaha F, Zou Y, Stastny P. Identifi-cation of MICA as a new polymorphic alloantigen recognized byantibodies in sera of organ transplant recipients. Hum Immunol2000; 61: 917–924.
19. Hankey KG, Drachenberg CB, Papadimitriou JC et al. MIC expres-sion in renal and pancreatic allografts. Transplantation 2002; 73:304–306.
20. Bacon L, Eagle RA, Meyer M, Easom N, Young NT, Trowsdale J.Two human ULBP/RAET1 molecules with transmembrane regionsare ligands for NKG2D. J Immunol 2004; 173: 1078.
21. Bauer S, Groh V, Wu J et al. Activation of NK cells and T cells byNKG2D, a receptor for stress-inducible MICA. Science 1999; 285:727–729.
22. Wu J, Song Y, Bakker AB et al. An activating immunoreceptorcomplex formed by NKG2D and DAP10. Science 1999; 285: 730–732.
23. Racusen LC, Solez K, Colvin RB et al. The Banff 97 workingclassification of renal allograft pathology. Kidney Int 1999; 55:713–723.
24. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. Amore accurate method to estimate glomerular filtration rate fromserum creatinine: A new prediction equation. Modification of Dietin Renal Disease Study Group. Ann Intern Med 1999; 130: 461–470.
25. Kasiske BL, Gaston RS, Gourishankar S et al. Long-term dete-rioration of kidney allograft function. Am J Transplant 2005; 5:1405–1414.
26. Gourishankar S, Hunsicker LG, Jhangri GS, Cockfield SM, HalloranPF. The stability of the glomerular filtration rate after renal trans-plantation is improving. J Am Soc Nephrol 2003; 14: 2387–2394.
27. Raulet DH. Roles of the NKG2D immunoreceptor and its ligands.Nat Rev Immunol 2003; 3: 781–790.
28. Jamieson AM, Diefenbach A, McMahon CW, Xiong N, Carlyle JR,Raulet DH. The role of the NKG2D immunoreceptor in immunecell activation and natural killing. Immunity 2002; 17: 19–29.
29. Maasho K, Opoku-Anane J, Marusina AI, Coligan JE, Borrego F.NKG2D is a costimulatory receptor for human naive CD8+ T cells.J Immunol 2005; 174: 4480–4484.
30. Roberts AI, Lee L, Schwarz E et al. NKG2D receptors inducedby IL-15 costimulate CD28-negative effector CTL in the tissuemicroenvironment. J Immunol 2001; 167: 5527–5530.
31. Pavlakis M, Strehlau J, Lipman M, Shapiro M, Maslinski W, StromTB. Intragraft IL-15 transcripts are increased in human renal allo-graft rejection. Transplantation 1996; 62: 543–545.
32. Sumitran-Holgersson S, Wilczek HE, Holgersson J, SoderstromK. Identification of the nonclassical HLA molecules, mica, as tar-gets for humoral immunity associated with irreversible rejectionof kidney allografts. Transplantation 2002; 74: 268–277.
33. Mizutani K, Terasaki P, Rosen A et al. Serial ten-year follow-up ofHLA and MICA antibody production prior to kidney graft failure.Am J Transplant 2005; 5: 2265–2272.
34. Sarwal MM, Jani A, Chang S et al. Granulysin expression is amarker for acute rejection and steroid resistance in human renaltransplantation. Hum Immunol 2001; 62: 21–31.
35. McNerney ME, Lee KM, Zhou P et al. Role of natural killer cellsubsets in cardiac allograft rejection. Am J Transplant 2006; 6:505–513.
36. Taieb J, Chaput N, Menard C et al. A novel dendritic cell subsetinvolved in tumor immunosurveillance. Nat Med 2006; 12: 214–219. Epub January 29, 2006.
37. Chan CW, Crafton E, Fan HN et al. Interferon-producing killer den-dritic cells provide a link between innate and adaptive immunity.Nat Med 2006; 12: 207–213. Epub January 29, 2006.
American Journal of Transplantation 2007; 7: 423–433 433
Related Documents











