HEARTBURN AND CHOKING – IS IT ALL DUE TO REFLUX? Peggy Marcon Hospital for Sick Children Northern Ontario Pediatric Conference

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

HEARTBURN AND CHOKING – IS IT ALL DUE TO REFLUX?
Peggy MarconHospital for Sick ChildrenNorthern Ontario Pediatric Conference

Declaration
I have nothing to declare.

Physiology Lesson
TLESRGastric Emptying
Meal Size and Content

Definitions
Regurgitation: sudden effortless exteriorisation of a variable quantity of liquid derived from the stomach or esophagus into the mouth or the pharynx
Vomiting: generally preceded by nausea and associated with abdominal muscle contractions, resulting in involuntary forceful emission of gastric contents into the mouth
Rumination: The voluntary return of food to the oropharynx. The food is then either re-swallowed or spit out.

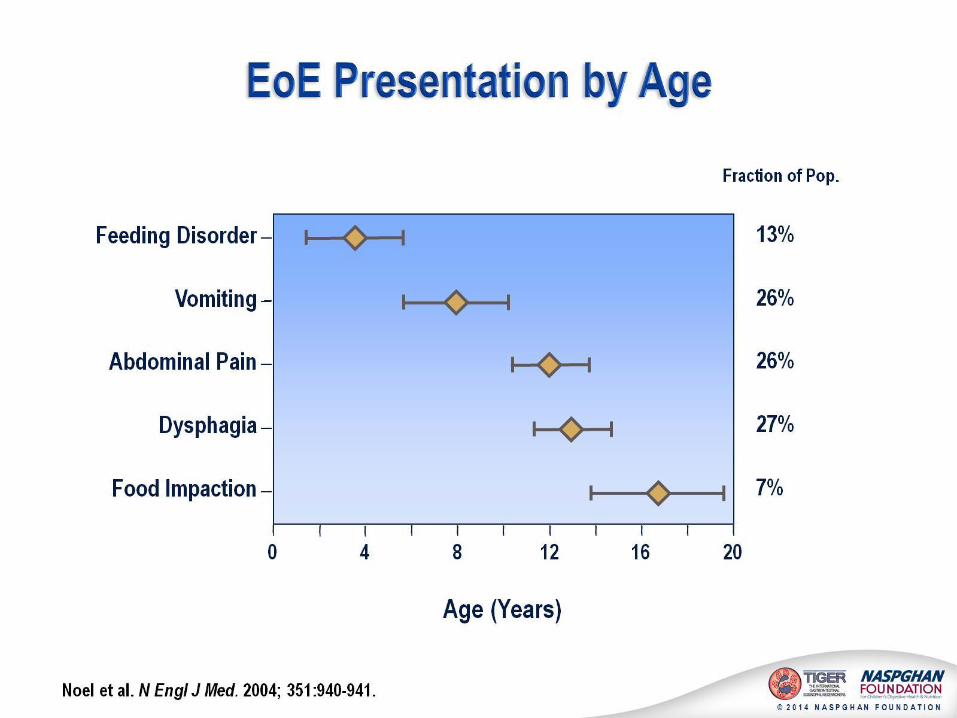
Case 1
A very concerned mother brings her 4-week-old boy to your office
Uncomplicated pregnancy and birth weight 4,150 g
Breast feeding
Regurgitates a lot
No other health issues
Especially no eczema / constipation / diarrhea


It gets worse before it gets better!

Treatment for Simple GERD in Infancy
Review feeding practice
No smoking
Reassurance
Position


Nutritional Therapy
Breast feeding / Breast milk Formula change – protein intolerance syndrome
Thicken formula
THERE IS A HUGE OVERLAP WITH “CLASSIC’ INFANT GERD AND PROTEIN INTOLERANCE!
**Thickening agents / Commercial thickened formula should not** be used indiscriminately in healthy thriving infants.
*Orenstein Pediatr 1987;110:181-186 *Vandenplas Clin Pediatr 1987;26:66-68 *Wenzl Pediatrics 2003;111:e355-59 *Aggett JPGN 2002;34:496-498

Clinical Presentation:Warning signs in Infants
Irritability**
Feeding Resistance**
Failure to Thrive
Hemetemesis
Anemia**
Posturing (Sandifer’sSyndrome).
**Protein Intolerance / Allergy?
Recurrent pneumonia
Wheezing and asthma
Apnea
Stridor and recurrent croup

Treatment for Complicated GERD in Infancy
Acid Blockade H2 Blockers
PPI
Prokinetics Metaclopramide: now contraindicated in infants
Domperidone: suggest baseline and dose increases ECG
Nutritional Rehabilitation
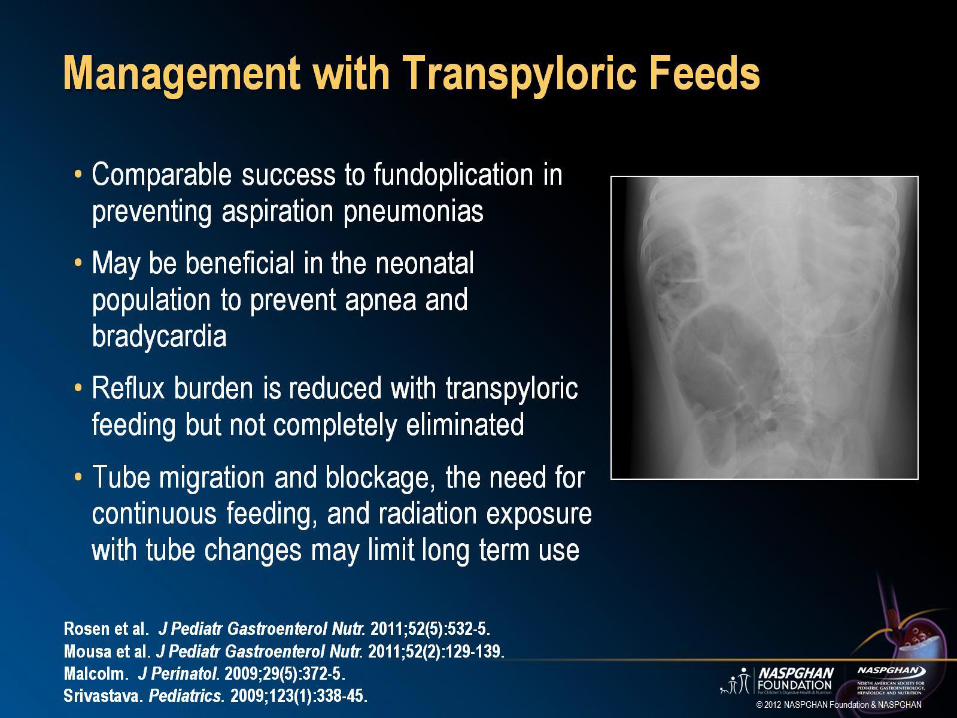
Tube supplementation
Surgery



Clinical Presentation of GERD
In infants and children with oromotorproblems simple regurgitation
can be life threatening problem!

COULD IT BE THE FOOD THAT IS THE PROBLEM?

GER:
• Regurgitation > vomiting
• Irritability shortly after feed
• Arching
• Rumination**
• Feeding difficulties**
• Bowel movements: usually normal
CMPA
• Vomiting > regurgitation• Irritability: 30 m to 2 h • Rumination**• Feeding difficulties**• Gas ++• No problem during feedings• Diarrhea (mucousy stools) or
severe constipation• Rectal bleeding• Atopic dermatitis• Eosinophilia, thrombocytosis,
mild hypoalbuminemia

“Allergic Disease” in the Breast fed baby
Unclear if there is a role for restricted maternal diet during pregnancy.
For infants with atopy, colitis or possibly GERD and severe constipation you may want to restrict mother’s diet.
Breast Milk Fortifers are CM based.

Feeding behavior
Infants with simple GERD* / n=63 / control = 93 4% of infants had resistance to oral feeding severe enough to
require a tube.
Children’s Eating Behavior Inventory
Feeding and mealtime problems at 1 year f/u.
8% case vs. 0% control: ‘my child takes more than an hour to eat.”
14% case parents vs. 4% control parents: “I get upset when I think of our meals.”
Nelson Pediatrics 1998;102:E67. * Some of these may have had prointolerance

After Infancy

2nd case
A 12 year old boy comes to see you because he has been experiencing stomach aches and on questioning waterbrash. Otherwise he is well – what advice to you give?


GERD: at increased risk
Prematurity
Neurologic disease
Hypotonia / Myopathies
Chronic Lung Disease ?Asthma
Cystic Fibrosis
Congenital Esophageal Anomalies / Foregut anomalies
Increased Abdominal pressure
Chromosomal Anomalies
Syndromes
Collagen Vascular Disease
Drugs
Obesity
Hiatus Hernia (especially congenital)

Simple heartburn
Try conservative measures
Review medication and supplement use
No second hand smoke
Trial of PPI or H2 Blocker for 8 weeks
Adolescence –
NO smoking including marijuana and E Cigs
Check how much alcohol use
If they had change infant formula to a non dairy based formula you might stop dairy products.
Rumination
Effortless “regurgitation” that is
either swallowed back or spit out
20 or 30 times a day
Often bothers the parents more than the child unless happening at school
May be “learned” from an organic problem that may still be on going or has resolved.
Always needs behavioral intervention
RISK: ASD, Neurologic impairment,
TIC, anxiety and depression



Prevalence of GERD Symptoms in Children
Nelson SP et al. Arch Pediatr Adolesc Med 2000;154:150-54
1.8%
7.2%
2.3%
5.2%5.0%
8.2%
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
Heartburn Epigastric pain Regurgitation
% o
f ch
ild
ren
Reported by the parents (children age 3-9 years) (n=566)
Reported by children (age 10-17 years)
(n=615)

Erosive esophagitis
In Children with GERD symptoms without co morbidities for whom an endoscopy is indicated: 34.6%
In Neurologically impaired children: 30-70%
In GER Infants and children without c morbidities :: < 5%
Respiratory manifestations: 20%
In children with GERD symptoms :
Asthma 13.2%;
Pneumonia 6.3%
ENT manifestations: 6.9%
In children with GERD symptoms :
Sinusitis 4.2%;
Laryngitis 0.7%; otitis media 2%
Epidemiology of Reflux Complications in Children
El-Serag HB et al. Am J Gastroenterol 2002;97:1635-39
El-Serag HB et al. Gastroenterology 2001;121:1294-99.

Evaluation for GERD:
Upper gastrointestinal barium study (UGI) To look for anatomical problems
+ SB series if indicated
+ “marshmallow” for solid food dysphagia
Videofluoroscopic Feeding Study If have concerns re oromotor coordination
Nuclear Medicine Studies
24 hour Intraesophageal pH study “Gold” standard
Maybe Impedance
Upper gastrointestinal endoscopy A “must” for solid food dysphagia

Management of GERD
Lifestyle
Nutrition / Diet changes
Medication
Surgery

Indications for Treatment in Children
Mild esophagitis:• 8 weeks PPI full dose treatment.
• PPIs on demand or Step-down strategy (H2RA on-demand)
• If relapse or PPI dependent: surgery?
Severe esophagitis, stricture, Barrett, neurological impairment:• 8 weeks PPI full dose treatment.
• Maintenance therapy w/ PPI or
Asthma + GER:• PPI full dose treatment for at least 6 months
• Evaluation
• If improvement : Maintenance therapy? Surgery?
Rudolph CD et al. JPGN 2001;32:S1-31
Khoshoo V et al. Chest 2003;123:1008-13.

Treatment
PPI Rules
1 to 3 mg/kg
Up to Adult dosing
Rate of metabolism is genetic: slow, middle and fast.
Faster and better response than H2
? H2 better in infant EoE
Omeprazole dissolved for gtubes
Prevacid FasTAb Not covered ODB
Ranitidine
5 - 10 mg/kg/day tid
(300mg divided bid)
Tachyphylaxis

Recent “suggested” issues with PPIs ↑Community acquired pneumonia
↑Upper respiratory Infection
↑C. difficle infection
↑ Risk of fractures
Decreased Mg+

Pharmacotherapy: Promotility
Prokinetic *Cisapride
0.8 mg/kg/day qid (10-20mg qid) ECG
**Domperidone 1.2-2.4 mg/kg/day (30mg/day) ECG
Metoclopramide No use under 1 year e Smaller dosing: 0.5 mg/kg/day)

Treatment for GERD: On the Net!
Quote “Apple Cedar Vinegar is a
Natural remedy for acid reflux”
Even Dr. Oz says – but
No good studies published – but there is a chewing gum with this that might help!
It may be the licorice in the gum!
Melatonin may help

Step Down Approach
Shown in adults to be clinically and economically better
PPI
H2 Blocker

Outcome?
Various studies suggest GERD may go away and other say stay long-term in children and adolescents.
Risk of developing Esophageal Cancer in someone with Barrett’s esophagus is 1%.
Current “rewriting” what to do with adults Some groups are at increased risk of
Barrett’s and Esophageal Cancer: TEF / Some Syndromes / Erosive esophagitis

Case 2
He returns after two months still complaining of heartburn and now occasionally has difficulty getting some foods down? BBQ chicken stuck last weekend.
What advice to you give now?1. Increase the dose of the PPI
2. Add antacids
3. Referral for further investigation
4. Relaxation therapy

EoE Explosion Incidence of EoE varied from 0.7 to 10/100,000 per
person-year
Prevalence ranged from 0.2 to 43/100,000.
Based on review of 25 studies J Pediatr Gastroenterol Nutr. 2013 Jul;57(1):72-80. Incidence and prevalence of eosinophilic esophagitis in children
Male
Females
This is from a study looking at the rise inboth EoE and Celiac Disease

EoE
EoE is a clinicopathologic disorder diagnosed by clinicians taking into consideration both clinical and pathologic information without either of these parameters interpreted in isolation and defined by the following criteria:
Esophageal symptoms
≥ 15 eosinophils/hpf
Isolated to esophagus, persists after PPI trial
Secondary causes excluded
(responds to dietary or steroid therapy) Am J Gastroenterology 2013; 108:679-692
Epidemiology
Infancy thru adolescence and now
well reported in adulthood.
Male > Female.
2/3 history of atopy
Reported in families (father / son)
PPI responsive and non responsive


Remedios Gastrointestinal Endoscopy 2006;63:3-12.
Classic EoE
Barium study most often NORMAL
Tram tracking and trachealization

Diagnosing it: defined by # of eosinophils in the biopsy
Oren
stein GER Eosinophilic esophagitisNormal esophagus
Other Investgations
May or may not have a peripheral eosinophilia(50%).
Hemoglobin and serum albumin are often normal. IgE may or may not be elevated. RAST testing has generally NOT been helpful. Patch testing may be helpful. Barium swallow often read as normal.

Other causes of esophageal eosinophilia EGE
PPI-responsive esophageal eosinophilia*
Celiac disease
Crohn’s disease
Infection (be careful – may predispose to infection)
Hypereosinophilic syndrome
Achalasia
Drug hypersensitivity
Vasculitis
Pemphigus
Connective tissue diseases
Graft vs. host disease

EE treatment
Local steroids
Systemic Steroids
Diet (elemental vs. elimination)
Mast cell stabilizers
Anti-IL 5 antibodies




Steroids and EE
Topical corticosteroids
Fluticasone swallowed in divided doses:
Children: 440 – 880ug/d x 6-8weeks
Adolescents/adult: 880 – 1760ug/d x 6-8 weeks No spacer
No food or drink for at least 30 minutes after ingesting the dose
x 4 weeks then taper over 6 weeks
Budesonide children: 1-2mg daily x 3-4 months
adults*: 2-12mg daily x 2-6 weeks
Mix with Splenda®

Easier said then done!
Changing His Diet

Diet Therapy
Elemental (formula based) Very effective: 86 to 95% remission Hugh effect of QofL if used longterm Aim to then go thru food reintroduction
Skin prick and history guided 78% had significant clinical and histological remission. Soy, wheat, chicken, and beef most frequently identified
6 Food Elimination Cow’s milk protein, soy, wheat, egg, peanut/tree nut, and fish/shellfish were the only
foods excluded 74% of children and adults had significant clinical and histological
4 Food Elimination Dairy products, wheat, egg, and legumes 54% remission with additional 31% when changed to 6 food
In all cases Dairy is a big issue
Eo
E: M
aintan
ce Th
erapy 2
015



And where do adolescents fit?

Food choices?Best plan is a dietitian
Eo
E: M
aintan
ce Th
erapy 2
015
Fro
m: S
pe
rge
lJM
, Sh
uke
rM
. Nu
trition
al m
an
ag
em
en
t of
eo
sin
op
hilic
eso
ph
ag
itis. G
astro
inte
stE
nd
osc
Clin
No
rth
Am
2008;1
8:1
79–194.
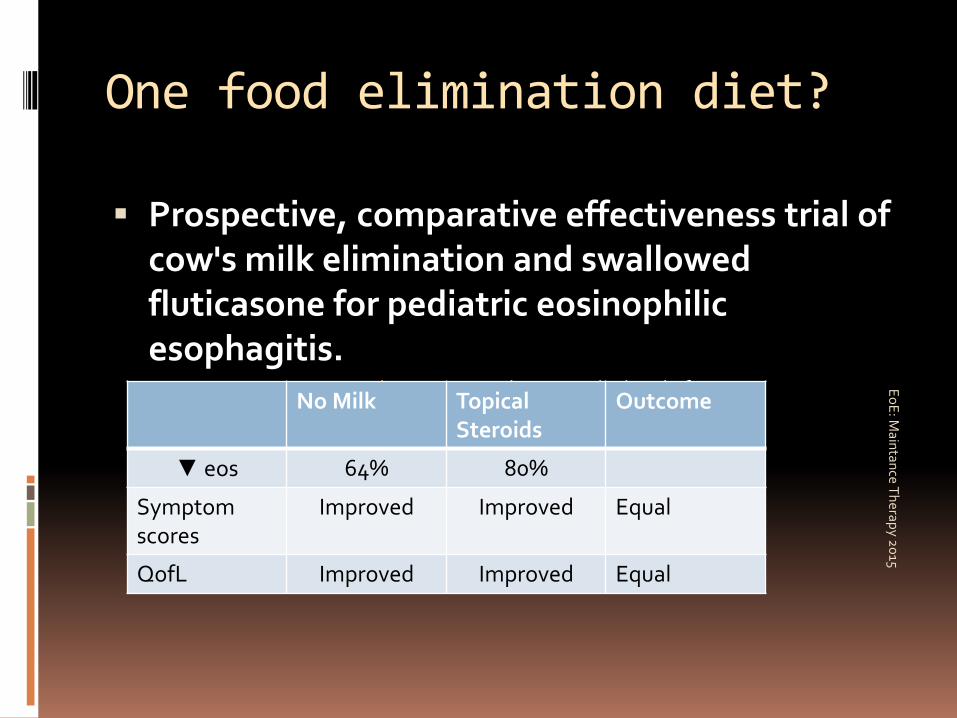
One food elimination diet?
Prospective, comparative effectiveness trial of cow's milk elimination and swallowed fluticasone for pediatric eosinophilicesophagitis.
Dis Esophagus. 2015 Feb 26. [Epub ahead of print] Eo
E: M
aintan
ce Th
erapy 2
015
No Milk Topical Steroids
Outcome
▼ eos 64% 80%
Symptomscores
Improved Improved Equal
QofL Improved Improved Equal

Maintenance Therapy
All of these patients want to know
what to do so they feel well
and can eat “normally”.
Do I do Dietary Therapy?
Do I do Drug Therapy?
Role of Dilation?
Or some combination of the above?
Eo
E: M
aintan
ce Th
erapy 2
015

Easier way to follow food reintroduction? Esophageal String Test
Furuta GT et al. The oesophageal string test: a novel, minimally invasive method measures mucosal inflammation in eosinophilic oesophagitis. Gut 2013;62:1395–1405.
Cytosponge Katzka DA, Geno DM, Ravi A, et al. Accuracy, safety, and tolerability of tissue
collection by cytosponge vs endoscocpy for evaluation of eosinophilic esophagitis. Clin Gastroenterol Hepatol 2015 Jan;13(1):77-83
Eo
E: M
aintan
ce Th
erapy 2
015

Allergist?
All the reviews recommend seeing an Allergist to look for IgE mediated allergies that may be contributing to issues.
Remember the actual mechanism(s) of disease are unknown and foods not picked up on skin prick testing can be significant issues
Most places find Patch testing not helpful
RAST testing has been unhelpful
Eo
E: M
aintan
ce Th
erapy 2
015

Etiology
J Gastrointestin Liver Dis. 2013 Jun;22(2):205-8. De-novo onset of eosinophilic
esophagitis after large volume allergen exposures.
Lawn mower Moldy house Renovation
My patient – cleaning the grain silo out with his father!

Other Pharmacological Treatments Mast cell stabilizers
Case series suggest that liquid preparation of Cromolyn offers benefits
Leukotrienes inhibitors (Montelukast) One study showed clinical improvement but no impact on
esophageal eosinophilia.
Ketotifen Useful for Eosinophilic gastroenteritis and colitis
Not clear if useful for “classic” EE
Role of PPIs not clear. Does it worsen allergic issues?

Maintenance Therapy in EoE
Disease waxes and wanes
Best long term options not clear
Choices are
Pharmacotherapy
Diet Therapy
Combination of above
Role of dilation in combination with PPI?
Long term compliance is also an issue!
Eo
E: M
aintan
ce Th
erapy 2
015

GERD Guidelines
Guidelines for the Evaluation and
Treatment of Gastroesophageal Reflux
in Infants and Children
Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) J Pediatr Gastroenterol Nutr 2009;49:498-547
www.naspghan.org
http://www.gikids.org/
Downloadable handouts for patients and parents at this site including coloring books!

Guidelines EoE
Am J Gastroenterol 2013; 108:679–692
ESPGHAN: Journal of Pediatric Gastroenterology & Nutrition: January 2014 - Volume 58 - Issue 1 -p 107–118
NASPGHAN in Gastroenterology 2007;133:1342–1363
Related Documents











