Prof. U. C. SAMAL MD, FICC, FACC, FIACM, FIAE, FISE, FISC, FAPVS Ex- Prof. Cardiology & Ex-HOD Medicine Patna Medical College, Patna, Bihar Past President, Indian College of Cardiology Permanent & Chief Trustee, ICC-Heart Failure Foundation National Convener Heart Failure Sub Specialty, CSI 1 HEART FAILURE

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Prof. U. C. SAMALMD, FICC, FACC, FIACM, FIAE, FISE, FISC, FAPVSEx- Prof. Cardiology & Ex-HOD Medicine Patna Medical College, Patna, BiharPast President, Indian College of CardiologyPermanent & Chief Trustee, ICC-Heart Failure FoundationNational Convener Heart Failure Sub Specialty, CSIExecutive Member (National), Cardiological Society of IndiaPresident, CSI Bihar / Vice President, API Bihar 1
HEART FAILURE

Heart failure -- Epidemiology
Prevalence • > 2% - 3% overall; 10% - 20% at > 70 yrs• European society of cardiology countries : > 15 milion patients with heart failure and increasing
Burden • Primary cause of 5% of hospital admissions• Present in 10% of hospitalized patients• 2% of national health expenditure [60% - 70% of cost due to heart failure hospitalization]• 40% of patients admitted to hospital with heart failure are dead or readmitted within 1 yr
Mcmurray J J Et Al Eur Heart J 2013; 33 [14]: 1787-1847
Dickstein K Et Al Eur Heart J 2006; 29: 2388-2442
Fina
l Pat
hway
s Di
seas
e

Total Population of India - 1.16 Billion (2009 Est)

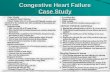
Classification of Heart FailureACCF/AHA Stages of HF NYHA Functional Classification
A At high risk for HF but without structural heart disease or symptoms of HF.
None
B Structural heart disease but without signs or symptoms of HF.
I No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF.
C Structural heart disease with prior or current symptoms of HF.
I No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF.
II Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in symptoms of HF.
III Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes symptoms of HF.
IV Unable to carry on any physical activity without symptoms of HF, or symptoms of HF at rest.
D Refractory HF requiring specialized interventions.

Stages, Phenotypes and Treatment of HF
STAGE AAt high risk for HF but without structural heart
disease or symptoms of HF
STAGE BStructural heart disease
but without signs or symptoms of HF
THERAPYGoals· Control symptoms· Improve HRQOL· Prevent hospitalization· Prevent mortality
Strategies· Identification of comorbidities
Treatment· Diuresis to relieve symptoms
of congestion· Follow guideline driven
indications for comorbidities, e.g., HTN, AF, CAD, DM
· Revascularization or valvular surgery as appropriate
STAGE CStructural heart disease
with prior or current symptoms of HF
THERAPYGoals· Control symptoms· Patient education· Prevent hospitalization· Prevent mortality
Drugs for routine use· Diuretics for fluid retention· ACEI or ARB· Beta blockers· Aldosterone antagonists
Drugs for use in selected patients· Hydralazine/isosorbide dinitrate· ACEI and ARB· Digoxin
In selected patients· CRT· ICD· Revascularization or valvular
surgery as appropriate
STAGE DRefractory HF
THERAPYGoals· Prevent HF symptoms· Prevent further cardiac
remodeling
Drugs· ACEI or ARB as
appropriate · Beta blockers as
appropriate
In selected patients· ICD· Revascularization or
valvular surgery as appropriate
e.g., Patients with:· Known structural heart disease and· HF signs and symptoms
HFpEF HFrEF
THERAPYGoals· Heart healthy lifestyle· Prevent vascular,
coronary disease· Prevent LV structural
abnormalities
Drugs· ACEI or ARB in
appropriate patients for vascular disease or DM
· Statins as appropriate
THERAPYGoals· Control symptoms· Improve HRQOL· Reduce hospital
readmissions· Establish patient’s end-
of-life goals
Options· Advanced care
measures· Heart transplant· Chronic inotropes· Temporary or permanent
MCS· Experimental surgery or
drugs· Palliative care and
hospice· ICD deactivation
Refractory symptoms of HF at rest, despite GDMT
At Risk for Heart Failure Heart Failure
e.g., Patients with:· Marked HF symptoms at
rest · Recurrent hospitalizations
despite GDMT
e.g., Patients with:· Previous MI· LV remodeling including
LVH and low EF· Asymptomatic valvular
disease
e.g., Patients with:· HTN· Atherosclerotic disease· DM· Obesity· Metabolic syndrome orPatients· Using cardiotoxins· With family history of
cardiomyopathy
Development of symptoms of HF
Structural heart disease
2013 ACCF/AHA Guideline for the Management of Heart Failure


• diuretics• ultrafiltration
Vasodilators • nitroglycerin• nesiritide• nitroprusside
INOTROPES • dobutamine• dopamine• levosimendan• nitroprusside
Fluid retention or redistribution ? Pulmoedema??
“dry out”
“warm up & “dry out”
Assessment of hemodynamic profile : therapeutic implications
Adapted from Stevenson L W, Eur Heart j
7
SIGNS/SYMPTOMS CONGESTION:DYSPNOEA/( EXERTION /REST)ORTHOPNEA PNHJV DISTENSIONRALES (uncommon in chronic cases)LOUD P2 INCREASING S3PEDAL OEDEMAABDOMINOJUGULAR REFLUXASCITESVALSALVA SQUARE WAVE
POSSIBLE EVIDENCE OF LOW PERFUSION:SLEEPY / OBTUNDEDCOOL EXTREMITIESNARROW PULSE PRESSUREHYPOTENSION WITH ACE INHIBITORLOW SERUM SODIUMAKI / RENAL DYSFUNCTIONELEVATED LFTsPULSUS ALTERNANS
67%
28%5%
67%
28%5%
ACE-I / ARB/ BB/ MRA MM/ MN


Linking Short- term intervention with long-term benefit:What is needed?
Better understanding of Acute Heart Failure pathophysiology
MORTALITY
• Myocardial injury [Tn release]
• Renal dysfunction [CRS]
• Liver dysfunction
PREVENTION OF END-ORGAN DAMAGE
Congestion Viable but
dysfunctional myocardium
Neurohormonal & inflammatory
activationMechanisms which
can be targetedMetabolic
factors
Hemodynamic deterioration
[↑LVFP,↓ CO, ↓ PERFUSION]
Vascular resistance /stiffness ↑
ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012 Reviewed by Ponikowski

Diagnosis of HF in untreated patients with symptoms suggestive of HF using natriuretic peptides
Clinical examinationECG, Chest X-rayEchocardiography
Natriuretic peptides
BNP < 100pg/mlNT-proBNP <
400pg/ml
BNP < 100-400 pg/mlNT-proBNP 400-2000
pg/ml
BNP > 400 pg/mlNT-proBNP > 2000
pg/ml
Chronic HF likely Uncertain diagnosis Chronic HF likely

“HF management ‘guided’ by natriuretic peptides would be superior to standard HF therapy alone.”
11
van Kimmenade, R. R. & Januzzi, J. L. Jr. Clin. Chem. 58, 127–138 (2012).

12
Clinical Value of diagnostic testing modality : BNP/ NT-BNP
Adapted and reprinted with permission from Januzzi JL,Camargo CA, Anwarudding S ,et al. The N-terminal Pro-BNP investigation of Dyspnea in the Emergency Department (PRIDE) Study. Am J Cardiol 2005;95:948-954

Effect of cardiac and extra cardiac parameters on BNP and NT-proBNP
Raised in Cardiac Factors
Lower Ejection Fraction, Larger Left ventricular mass, Atrial size, Atrial fibrillation, Coronary heart disease , Valvular heart disease, Acute coronary
syndrome, Cor pulmonale (acute/ chronic), COLD (right heart strain)
Extra Cardiac factorsAge, Female gender, Low glomerular filtration, Hematocrit low, Hyperthyroidism,
Cushing syndrome. Liver cirrhosis with ascites, paraneoplastic syndrome, Subarachnoidal bleeding, Sepsis, Rheumatic diseases, Stroke
Reduced in Extra Cardiac factors
Obesity,ACE-I/ARB, Diuretics, Hypothyroidsm, Primary hyperaldosteronism
Biomarkers in medicine 3.5 (Oct 2009) p46513

14
“For example, over the past 2 decades, the once-held view of chronic HF as a syndrome of disordered hemodynamics and fluid balance caused by alterations in the structure of the heart has been succeeded by a view of the disease that involves molecular pathways in disarray. Chronic HF is now seen as a systemic illness that involves interplay between myocardial factors, systemic inflammation, renal dysfunction, and neurohormonal activation. Our assessment and treatment of patients with chronic HF has, thus, progressed from a focus on improving hemodynamics to measuring and modifying the maladaptive molecular processes that contribute to progression of disease”
Braunwald, E. N. Engl. J. Med. 358, 2148–2159 (2008).

NeurohormonesNorepinephrine
ReninAngiotensin II
CopeptinEndothelin
Vascular systemHomocysteine
Adhesion molecules(ICAM, P-selectin)
EndothelinAdiponectin
C-type natriuretic peptide
InflammationC-reactive protein
sST2Tumor necrosis factor
FAS (APO-1)GDF-15
Pentraxin 3AdipokinesCytokines
ProcalcitoninOsteoprotegerin
Myocardial stressNatriureticpeptides
Mid-regional pro-adrenomedullin
NeuregulinsST2
Myocardial injuryCardiac troponins
High sensitivity cardiac troponinsMyosin light-chain kinase 1
Heart-type fatty acid binding proteinPentraxin 3
Matrix and cellularremodelingGalectin-3
sST2GDF-15MMPsTIMPs
Collagen propeptidesOsteopontin
Cardio-renal syndromeCreatinineCystatin C
NGALß-Trace protein
Oxidative stressOxidized LDL
MyeloperoxidaseUrinary biopyrrins
Urinary and plasma isoprostanes
Plasma malondialdehyde
HF as a systemic illness.
15Nature Review Cardiology Vol.9 June 12 pg 349

“HF-CBS-SRS”Quantitative results in~ 15 minutes! EDTA Whole Blood , No Centrifugation
Anywhere, anytime, in time
Point of Care System for rapid, accurate results• Easy• Portable• Reliable Results in about minutes
Fluorescence Sandwich immunoassay
Test Normal RangeCKMB ng/mL (0.0 - 4.3)
MYO ng/mL (0.0 – 107)TNI ng/mL (0.00 - 0.40)BNP pg/mL (0.00 - 100)
DDIM ng/mL (0.0 - 400)
NGAL* ng/mL (0-149)
PANEL OF SOB TRIAGE/ AMI/ AKI
15
6 Biomarkers 750 +750 bucks
* Galectin3/BNP+NGAL being uploaded to the test platform
16

SOB TRIAGE METER PLATFORM
Parameters Normal Range
Cost(Rs.) Timing
CKMB 0.0-4.3SOB
PANEL
Rs. 750
10-15 MinMYO 0.0-107
TNI 0.00-0.40
BNP 0.00-100
DDIM 0.1-400
NAGAL 0-149 Rs. 850 15 Min

Triage® Meter: Three Simple Steps
1. Add whole blood to Test Device
2. Insert Test Device into Meter
3. Read results

Intelligent Nephelometry TechnologySmart Card CalibrationEconomic 10 Parameter Assay Panelser- friendly 3 Step Assay ProcedureNo Sample dilution
Test Normal Range
ASO I/mL (50 - 1000)
CRP mg/L (0.5 - 320)
RF I/mL (10-120)
HbA1c % (3-13%)
IgE I/mL (1-1000)
MICROALBMIN mg/L (5-200)
Lp(a) Mg/dl (1-100)
CYSTATIN C mg/L (0.0-10)
FERRITIN I/mL (1-1000)
D-DIMER ng/mL
REPORT OF MISPA PANEL SERUM / URINE
“HF-CBS-SRS” MeasuresACR
&Routine rine Parameters
• 95% Correlation with conventional immunoturbidimetric test• Analyze spot rine sample• Works on batteries or power cable• Provides Printed report
“15/23 Minutes Exercise”
10 Biomarkers 1000 Bucks
19

Agappe Mispa carries ISO 13485:2003 and CE marking; GMP and FDA compliant ISO 9001: 2008 certified

1st Ht Consult

Parameters Pack size Test Range Normal Range Price TimingASO 30 Test 50-1000 IU/ml 0-200 IU/ml 62 5 Min
CRP 30 Test 0.5-250 mg/L 0.000-6.000mg/L 51 5Min
RF 30 TEST 10-120 IU/ml 0.000-20.000/IU/ml 46 6 min
CYSTATIN C 30 TEST 0.1-10 mg/L 0.000-1.149 mg/L 161 6 min
HbA1C 30 TEST 3-13% 4.000-6.000 % 160 7 min
D-DIMER 30 TEST 0-400 ng/mL 0.000-400 ng/ml 160 7 min
IgE 30 TEST 0-1000 IU/mL 0.000-400 IU/mL 180 6 min
FERRITIN 30 TEST 0-1000 ng/mL 0.000-230 ng/mL 200 6 min
Lp(a) 30 TEST 1-100 mg/dL 0-30 mg/dL 180 7 min
MICROALBUMIN 30 TEST 5-200 mg/L 0.000-25.000 mg/L 101 5 min
Intelligent Double Chanel Nephlometry Technology

Possible future strategies for biomarker-guided therapies in chronic HF. 2013-14 Optimism :
Ahmad T et al Nat. Rev. Cardiol.9,347-359(2012)
23

Cumulative benefits of medical therapy on mortality. Adapted, with permission, from Fonarow GC, et al. Potential impact of optimal implementation of evidence-based heart failure therapies on mortality. Am Heart J 2011;161:1024-30.
Heart Failure Therapies
Beta-blocker Beta-blocker + ACEI/ARB
Beta-blocker + ACEI/ARB+ ICD
Beta-blocker + ACEI/ARB+ ICD+ HF education
Beta-blocker + ACEI/ARB+ ICD+ HF education+ anticoagulation for AF
Beta-blocker + ACEI/ARB+ ICD+ HF education+ anticoagulation for AF +CRT
Chan
ge in
Odd
s of
24-
Mon
th M
orta
lity
(%)
-39%[-28% to -49%]
P < 0.0001
-63%[-54% to -71%]
P < 0.0001 -76%[-68% to -81%]
P < 0.0001-81%
[-75% to -86%]P < 0.0001
-83%[-77% to -88%]
P < 0.0001
-81%[-72% to -87%]
P < 0.0001

Number needed to treat for mortality
25
Guideline recommended therapy
Relative risk reduction in mortality
Number needed to treat for mortality
Number needed to treat for mortality [ standardized to 36 mths]
Relative risk reduction in HF hospitalisations
ACEI / ARB 17% 22 over 42 mths 26 31%
Beta blocker 34% 28 over 12 mths 9 41%
Aldosterone antagonist
30% 9 over 24 months 6 35%
Hydralazine / nitrate
43% 25 over 10 mths 7 33%
CRT 36% 12 over 24 mths 8 52%
ICD 23% 14 over 60 mths 23 NA
Reproduced with permission from Fonarow GC et al Am Heart j 2011; 161: 1024-30

Milton Packer 2008 JCF
• … Yet, despite substantial advances in our understanding and management of heart failure, we have had
• few successes and many failures.
• Nearly 1,000 new drugs and devices have been developed for the treatment of heart failure duringthe past 20 years, but only 9 have received regulatory approval and are being used in the clinical setting.
• Most of our efforts to correct fluid retention, stimulate the inotropic state of the heart, and modulate neurohormonal systems have not predictably improved the condition of patients with HF…

“Poly Client Challenge”• Poly co-morbidities• Poly – pharmacy• Poly - side effects• Poly – healthcare providers• Poly - clinics• Poly-labs / investigation
• POLY – CONFUSION…….END RESULT You must have patience to find
little pink hope!!!
Yes , a Pandora’s box !
but
Heart Failure Care is always rewarding


29

30

HF----
We are all equals but some are better equalsHeart Failurists are less equal

32

33

Related Documents