Heart and Soul - Cardiology Day Seminar Saturday 20 March 2021, Pacific Bay Resort, Coffs Harbour AVA NSW Northern Regions Saturday 20 March 2021 8.30am - 9.00am Delegate Registration 9.00am - 10.00am Diagnosis and management of congestive heart failure - Dr Rita Singh 10.00am - 11.00am Why won't Fluffy stop coughing? Heart failure vs respiratory disease in dogs - Dr Rita Singh 11.00am - 11.30am Morning Tea 11.30am - 12.00pm Approach to the dyspnoeic cat - Dr Katherine Briscoe 12.00pm - 12.30pm Update on feline upper respiratory infections - Dr Katherine Briscoe 12.30pm - 1.30pm Lunch 1.30pm - 2.30pm The ECG: it's not as hard as you think! - Dr Rita Singh 2.30pm - 3.30pm Workshop spon- sored by Jurox Workshop A: i. Practice your skills - ECG interpretation - Dr Rita Singh ii. Supporting your clients - Resting respiratory rate monitoring - Sponsored by Jurox Workshop B: i. Practice your skills - Blood pressure monitoring and supporting your patients - Dr Katherine Briscoe ii. Supporting your patients – Selecting sedation and anaesthesia agents for the cardiac patient - Sponsored by Jurox 3.30pm - 4.00pm Afternoon Tea 4.00pm - 5.00pm Workshop spon- sored by Jurox Workshop A: i. Practice your skills - Blood pressure monitoring and supporting your patients - Dr Katherine Briscoe ii. Supporting your patients – Selecting sedation and anaesthesia agents for the cardiac patient - Sponsored by Jurox Workshop B: i. Practice your skills - ECG interpretation - Dr Rita Singh ii. Supporting your clients - Resting respiratory rate monitoring - Sponsored by Jurox Seminar program

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Heart and Soul - Cardiology Day SeminarSaturday 20 March 2021, Pacific Bay Resort, Coffs Harbour
AVA NSW Northern Regions
Saturday 20 March 2021
8.30am - 9.00am Delegate Registration
9.00am - 10.00am Diagnosis and management of congestive heart failure - Dr Rita Singh
10.00am - 11.00amWhy won't Fluffy stop coughing? Heart failure vs respiratory disease in dogs - Dr Rita Singh
11.00am - 11.30am Morning Tea
11.30am - 12.00pm Approach to the dyspnoeic cat - Dr Katherine Briscoe
12.00pm - 12.30pm Update on feline upper respiratory infections - Dr Katherine Briscoe
12.30pm - 1.30pm Lunch
1.30pm - 2.30pm The ECG: it's not as hard as you think! - Dr Rita Singh
2.30pm - 3.30pm Workshop spon-
sored by Jurox
Workshop A: i. Practice your skills - ECG interpretation - Dr Rita Singh
ii. Supporting your clients - Resting respiratory rate monitoring - Sponsored by Jurox
Workshop B:
i. Practice your skills - Blood pressure monitoring and supporting your patients - Dr Katherine Briscoe
ii. Supporting your patients – Selecting sedation and anaesthesia agents for the cardiac patient - Sponsored by Jurox
3.30pm - 4.00pm Afternoon Tea
4.00pm - 5.00pmWorkshop spon-
sored by Jurox
Workshop A:
i. Practice your skills - Blood pressure monitoring and supporting your patients - Dr Katherine Briscoe
ii. Supporting your patients – Selecting sedation and anaesthesia agents for the cardiac patient - Sponsored by Jurox
Workshop B:
i. Practice your skills - ECG interpretation - Dr Rita Singh
ii. Supporting your clients - Resting respiratory rate monitoring - Sponsored by Jurox
Seminar program
Meet the speakers

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
Diagnosis and Management of Congestive Heart Failure: Tips, Pitfalls and Perils
Dr Rita Singh BSc, BVMS, DipVetClinStud, FANZCVS, Dip ACVIM (Cardiology) Veterinary Cardiac Referrals
[email protected] www.vetcardioreferrals.com
Most definitions of heart failure as applicable to veterinary patients are flawed as they are extrapolated from human medicine. These include such statements as “a state in which the heart fails to maintain adequate circulation for the needs of the body despite satisfactory venous pressure,” or “a clinical syndrome characterized by exertional symptoms and caused by heart disease.” These are human definitions, which usually relate to systolic dysfunction. The critical event in the progression from heart disease to heart failure is activation of neurohormonal abnormalities (i.e. the sympathetic nervous system and renin-angiotensin-aldosterone system). Such signs as exertional symptoms are difficult to recognize in domestic pets, particularly cats, whom spend 90% of their day sleeping. In veterinary patients’ congestion is usually the first recognised symptom. Hence, a more appropriate definition is “impaired cardiac function leading to elevated venous and capillary pressures causing organs to become congested”.
Causes of heart failure
While there are many diseases that can result in congestive heart failure in our patients, this presentation will focus on the three most common causes: myxomatous mitral valve degeneration (MMVD), dilated cardiomyopathy (DCM) and, in cats, hypertrophic cardiomyopathy (HCM).
Pathophysiology
In MMVD, the cause of >95% of heart failure in older small breed dogs, degeneration of the mitral valve results in regurgitation. The initial event is hemodynamic (valve regurgitation). With each contraction, more of the stroke volume is recycled so there is a greater volume of blood per heartbeat. The result is an increase in preload. In order for the heart to deal with this there is eccentric (longitudinal) hypertrophy, which increases chamber size without increasing wall thickness. The result is enhanced early diastolic filling and decreased left ventricular stiffness. The outcome is an improved diastolic function. However, the increased left ventricular chamber size increases wall stress.
DCM should be considered in any large breed dog with a left apical systolic heart murmur. DCM refers to myocardial failure of unknown or inherited cause. The myocardial failure initially results in an increased end systolic and, eventually an increased end diastolic volume. Poor systolic pressure generation causes the ejection fraction to decrease resulting in self-induced volume overload and increased wall stress. The stroke volume and cardiac output are impaired. Generalized muscle fatigue occurs due to poor cardiac output.
In cats, the most common cause of heart failure is HCM. In this disease left ventricular concentric hypertrophy (wall thickening) results in a reduction in the size of the left ventricular lumen and a consequent inability to fill normally. The ultimate result is a diastolic failure (inability to fill). The eventual outcome being increased venous pressure and pulmonary congestion due to imperfect left atrial emptying and filling of the left ventricle.

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
In all these diseases, regardless of whether the initiating factor is volume overload from MMVD, systolic failure from DCM or diastolic failure from HCM the outcome, if the disease is severe enough, may be reduced cardiac output. Baroreceptors in the aortic arch and carotid sinus’s detect this reduced cardiac output and stimulate the sympathetic nervous system (SNS). The SNS stimulates the cardiac beta-receptors resulting in an increased heart rate and contractility and systemic arteriolar constriction, which normalize haemodynamics. However, it is well known that chronic SNS stimulation results in down regulation of cardiac beta-1 receptors. In chronic heart failure, approximately 50% of the cardiac beta-1 receptors can no longer be stimulated. The increased heart rate and contractility diminishes, and another mechanism is required to maintain cardiac output. This is renal compensation. The combination of decreased blood pressure, beta-1 stimulation, decreased renal perfusion and decreased sodium
reabsorption stimulates the renal release of renin via the renin-angiotensin-aldosterone system (RAAS). Via multiple actions, renin causes fluid retention and increases blood volume, the aim being to increase cardiac output. In an animal that has a normal blood volume, the result is volume overload and, eventual congestion. It is important to be aware that all of these described changes i.e. stimulation of SNS, stimulation of the RAAS, fluid retention and congestive heart failure usually only occur with severe heart disease. In MMVD or HCM severe disease usually refers to a markedly enlarged left atrium. The exceptions to this rule are acute chordae rupture in MMVD in which case there will be severe respiratory signs and a suddenly loud murmur. The left atrium is suddenly exposed to a large pressure increase, often before it has had a chance to enlarge. Cats with mild HCM that have been fluid overloaded or severely stressed can develop cardiomegaly and heart failure despite previously having no evidence of left atrial enlargement. In DCM there is usually severe systolic dysfunction. Congestive heart failure is not likely if the fractional shortening is > 15%. If on echocardiography, there is cardiac disease, but it appears mild, one needs to consider other causes for the respiratory signs or fatigue. Once in heart failure the average survival for dogs with MMVD is 12 months, for DCM is 8 months (Dobermans 4 months) and for HCM 18 months. Diagnostic tests Don’t forget the importance of an accurate and thorough physical exam prior to performing diagnostic tests. Most animals in congestive heart failure will have a combination of a heart murmur, tachycardia and tachypnoea. Keep in mind that a cough on its own is no longer considered a sign of congestive failure. These animals are usually dyspneac as well (sleeping respiratory rate of > 40 breaths/minute). In MMVD, dogs with congestive heart failure have severe disease and the grade of murmur usually correlates with this. Hence, the murmur should be loud (at least a grade IV/VI). In this disease, it is well documented that the severity of the disease correlates with the murmur in small breed dogs at the lower end of the spectrum i.e. a grade I-II murmur is going to be mild disease while grades III-VI murmurs can be more severe disease or can still be mild disease. This does not apply to large breed dogs that get systolic dysfunction earlier or may have DCM in which case the murmur is often soft even with severe disease. Cats are a whole other ball game. They can have severe heart disease and no murmur or a murmur and no heart disease. If a patient has the above clinical signs and is severely dyspneac, you are justified to commence oxygen and frusemide prior to thoracic radiographs and echocardiogram. Be sure to get a baseline body weight, as this will be closely monitored as the heart failure therapy intensifies. Most patients will need to lose 7-10% their body weight to come out of heart failure. A blood kidney profile and urinalysis prior to treatment (if possible) is also

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
useful. Frusemide will interfere with both these parameters, and, if abnormal later, it makes it difficult to know if there is underlying kidney disease or if it was the frusemide that caused the abnormalities. Good quality, inspiratory thoracic radiographs are required to make a diagnosis of congestive heart failure, to assess its severity and to stage the cardiac disease via an estimation of left atrial size. They are also useful to assess for comorbidities such as chronic airway disease, tracheal collapse, pneumonia, parasitic infestations or neoplasia. Echocardiography is useful in MMVD to confirm the severity of cardiac enlargement, to look for concurrent pulmonary hypertension, to assess for chordae rupture and, with very severe disease to look for pericardial effusion that may indicate left atrial tear. Echocardiography is recommended in any large breed dog with a heart murmur, as DCM is usually associated with a worse prognosis than MMVD and there may be a treatable underlying cause. In cats, echocardiography is usually required to establish a diagnosis, as cardiac size in this species can be difficult to interpret on thoracic radiographs. Cats can have physiologic murmurs without structural cardiac disease. Echocardiography is also helpful to look for evidence of thrombus formation and to assess the severity or presence of end stage disease, which may warrant additional cardiac medications. Treatment Dogs with Stage A or Stage B1 MMVD are not given any treatment. Monitoring only is recommend for these stages. Dogs with Stage B2 MMVD are commenced on pimobendan 0.25mg/kg q 12 hrs. Dogs with DCM are also started on pimobendan prior to heart failure. Cats with HCM are not usually given treatment prior to heart failure unless they have systolic anterior motion of the mitral valve causing severe left ventricular outflow tract obstruction (aortic pressure gradient > 75 mmHg). Once in heart failure, combinations of diuretics, angiotensin converting enzyme inhibitors (ACEi), vasodilators, positive inotropes and antiarrhythmics are used. Frusemide is the only drug in the ‘triple therapy’ group of cardiac drugs that will actively remove pulmonary oedema and is the most essential of the drugs when treating congestive heart failure. There are many routes and published doses. I usually give 1-3 mg/kg q 8-12 hr in mild-moderate heart failure and 4 mg/kg q 8 hr in severe or refractory chronic heart failure. In severe acute congestive heart failure (RR > 80 breaths/minute) oxygen therapy and intravenous frusemide 4mg/kg hourly as a bolus or CRI is required till the respiratory rate is < 60 breaths/minute. The dose then needs to be reduced to avoid dehydration and electrolyte abnormalities. Frusemide has very few side effects but can cause dehydration and azotaemia if not used judiciously. Vasodilation is useful in congestive heart failure and there are many drugs that can achieve this. Vasodilation refers to dilation of the venous or arteriolar system. The aim of venodilation is redistribution of blood volume and increased venous capacity. Drugs that achieve this include angiotensin converting enzyme inhibitors (ACEi), pimobendan and nitroglycerin. Arteriolar dilation helps congestive heart failure by decreasing systemic vascular resistance, decreasing mitral regurgitation and improving forward flow. Drugs that achieve this include ACEi, hydralazine, amlodipine, pimobendan and sodium nitroprusside. Positive inotropes are used to improve cardiac contractility. In severe acute heart failure with poor cardiac output dobutamine may be lifesaving. Dobutamine is a synthetic analogue of dopamine. It causes beta-1 stimulation with less beta-2 and alpha stimulation. The outcome is an increased heart rate and contractility with less effect on

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
vasculature. Pimobendan increases the binding affinity of calcium to cardiac troponin C and inhibits cardiac phosphodiesterase III. This reduces the breakdown of cAMP, which increases cardiac beta-1 stimulation. The combined effect is improved myocardial contractility and relaxation as well as vasodilation. Pimobendan is also available in an intravenous form (as an IV bolus) for use in the acute setting. Other diuretics, which are used in the later stages of heart failure, include spironolactone and hydrochlorothiazide. Spironolactone is an aldosterone antagonist. There is a well-established link between increased aldosterone and cardiac fibrosis. Spironolactone is usually combined with frusemide to limit hypokalaemia and aid diuresis. A final diuretic is the thiazide diuretic hydrochlorothiazide. The thiazide diuretics can cause potent diuresis when combined with high dose frusemide and spironolactone so care must be taken when dosing (start very low) and monitor renal parameters and electrolytes carefully. The diuretic torsemide is hopefully soon to hit our shores. Torsemide is loop diuretic with a similar mechanism of action to frusemide. Like frusemide, it inhibits sodium and chloride reabsorption in the proximal ascending limb of the loop of Henle by interfering with the Cl-binding site of the Na+/K+/Cl- cotransporter. Torsemide is more potent than frusemide and its diuretic effects persist for longer. It also appears to cause less potassium excretion in the dog. As it is 10X more potent than frusemide, the starting dose is 0.1-0.2mg/kg bid or 10% that of the current frusemide dose being used. As it has a longer mechanism of action, dosing frequency can also be reduced. Torsemide is used in place of furosemide (not in addition to). Treatment protocols The following protocols are how I treat the various stages of heart failure. Bear in mind however that each patient is an individual whose treatment needs to be tailored appropriately and that each cardiologist will differ slightly in his or her approach. Dogs with mild to moderate congestive heart failure usually present with tachycardia and tachypnoea with resting respiratory rates of around 40-60 breaths/minute. There should be severe regurgitation if heart failure is due to MMVD or severe systolic dysfunction if it is due to DCM. Thoracic radiographs will confirm cardiomegaly with mild-moderate pulmonary infiltrates. Treatment is always indicated in these patients with frusemide, an ACEi and pimobendan. Dogs in severe fulminant heart failure are a medical emergency. They present markedly dyspnoeic and hypoxemic. They may be coughing up white or blood tinged froth. The respiratory rates can range from 60 to over 100 breaths/minute. These patients need to be handled gently and diagnostic tests withheld until they are stable. I treat these patients immediately with oxygen and intravenous frusemide at doses of 4-6mg/kg/hr or as a continuous rate infusion at 2-3 mg/kg/hr. In situations of suspected poor cardiac output, intravenous dobutamine or pimobendan is helpful. If the patient does not appear to be stabilizing quickly consider arteriolar dilation with intravenous sodium nitroprusside (blood pressure monitoring is essential). In some situations, anaesthesia and intermittent positive pressure ventilation is lifesaving. Chronic refractory congestive heart failure refers to dogs that are generally stable but have severe heart disease and their resting respiratory rate remains greater than 40 breaths/minute despite appropriate therapy with frusemide, an ACEi and pimobendan. In this situation, providing the patient is not markedly azotaemic, I will gradually maximise frusemide to a dose of 4mg/kg q 8 hours. Spironolactone and hydrochlorothiazide are

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
gradually added in addition to antiarrhythmics if needed. Once it becomes available in Australia, torsemide as a substitute for frusemide, has been shown to be helpful. In the final stages, arteriolar dilation to improve forward flow with drugs such as hydralazine or amlodipine may buy some time. In some countries, surgery is an option for dogs with MMVD. It is the treatment of choice in humans with valvular disease with valve repair being preferable to replacement due to the lifelong potential for thrombosis with replacement. Repair is difficult in dogs with very few trained veterinarians worldwide, the need for cardiopulmonary bypass, high cost and high mortality. Treatment in cats In the asymptomatic cat with HCM no treatment is currently shown to slow the progression of the disease. The exception to this is the cat with systolic anterior motion of the mitral valve and significant left ventricular outflow tact obstruction in which case a beta blocker (atenolol) is recommended. Once the cat is in heart failure, I commence frusemide at a dose 1-2 mg/kg bid-tid with an ACEi. If there is significant pleural effusion thoracocentesis can be lifesaving. In severe end stage disease, systolic dysfunction and poor cardiac output can occur. In the severe acute setting, dobutamine may be required with oral pimobendan long term. If it is deemed there is a potential for thromboembolism clopidogrel is now favoured over asprin and warfarin. References 1) Kittleson MK, Kienle R. Small Animal Cardiovascular Medicine. St Loius: Mosby Inc; 1998. 2) Beijerink N, Campbell F, Gavaghan B, Singh R, Woolley R. A Guide to the Diagnosis of Canine Congestive Heart Failure due to Myxomatous Mitral Valve Disease. Published online via Vetforum, Boehringer Ingelheim 2015. 3) Keene B, Atkins C, Bonagura J, et al. ACVIM Consensus Guidelines for the Diagnosis and Treatment of Myxomatous Mitral Valve Disease in Dogs. J Vet Intern Med, March 2019 (early view). 4) Summerfield N, Boswood A, O’Grady M, et al. Efficacy of Pimobendan in the Preventation of Congestive Heart Failure or Sudden Death in Doberman Pinschers with Preclinical Dilated Cardiomyopathy (the PROTECT study). J Vet Intern Med, 2012, 26(6), 1337-1349.

Singh, R – Why won’t Fluffy stop coughing? Heart failure vs respiratory disease in dogs Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
Why Won’t Fluffy Stop Coughing? Heart Failure vs Respiratory Disease in Dogs
Dr Rita Singh BSc, BVMS, DipVetClinStud, FANZCVS, Dip ACVIM (Cardiology)
Veterinary Cardiac Referrals [email protected]
www.vetcardioreferrals.com
The coughing dog presents a diagnostic and therapeutic dilemma to the veterinarian. This is particularly true in middle aged to older small breed dogs that often have myxomatous mitral valve degeneration (MMVD) causing a heart murmur. This type of dog is also prone to developing respiratory disease and the cough in these dogs may be related to different pathophysiologic mechanisms including chronic bronchitis, tracheal collapse, pneumonia, parasitic infestation, neoplasia or pulmonary oedema due to congestive heart failure (CHF).
In the presence of severe left atrial enlargement without CHF the cough is also commonly attributed to airway compression by a large left atrium. In humans, an enlarged left atrium combined with increased pulmonary artery pressure is reported to lead to compression of the left main stem bronchus and results in aggressive therapeutics aimed at reducing left atrial size. Studies addressing this treatment in canines is lacking.
In order to determine if such a dog is in heart failure some important questions much first be considered. Firstly, a dog in congestive heart failure must have severe heart disease. The murmur should be loud in heart failure due to degenerative valvular disease (at least a grade IV/VI). If the murmur is a grade III or less in this signalment of dog, one needs to strongly consider other causes for the respiratory signs and refrain from using frusemide until further diagnostics can be performed. In heart failure, the sympathetic nervous system is stimulated. This is to increase heart rate and contractility in the failing heart in order to maintain organ perfusion. Hence these dogs are usually tachycardic with heart rates > 120 bpm. A loud murmur combined with tachycardia provides positive clinical evidence of congestive heart failure. These dogs will usually also have an increased resting respiratory rate. In early congestion, this may be hard to determine as these dogs often present stressed and panting to the hospital. Once allowed to settle or if sent home for owner monitoring, the sleeping respiratory rate, if in CHF, is usually > 30 breaths/minute.
Any patient presenting with respiratory signs should have thoracic radiographs taken. Even more so in the older small breed dog with a murmur and cough. As previously discussed, there are many causes for cough and, if the murmur is soft or the dog is not tachycardic, one must be sure they are correct if starting treatment for CHF. It is also important to realize that cough alone is no longer considered a reliable sign of congestive heart failure. It has long been recognized that other species such as humans, horses and cats, don’t exhibit coughing as a clinical sign of congestive heart failure.
Coughing is an important physiologic function in mammalian species. It is present to expel harmful substances such as foreign bodies, mucous and debris and to preserve normal health of the respiratory tract. Cough can be evoked by stimulation of cough receptors located in the larynx, trachea or bronchi. Irritation of the smaller bronchi, bronchioles and alveoli does not elicit a cough due to an absence of cough receptors

Singh, R – Why won’t Fluffy stop coughing? Heart failure vs respiratory disease in dogs Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
in these locations. In addition, luminal flow in the lower respiratory tract would be too low to generate enough force to clear airway mucous and debris. Hence, pulmonary oedema would not be expected to cause a cough, unless fluid accumulation is severe enough to build up within the airways. This produces a soft moist cough but is also associated with an increased respiratory rate.
Congestive Heart Failure Diagnosing a coughing dog with early congestive heart failure can be difficult. A consensus statement was formulated by Australian Veterinary Cardiology Advisory Board and Boehringer Ingelheim, to aid veterinarians when faced with such a patient.
Consensus Statement for the Diagnosis of Congestive Heart Failure due to Myxomatous Mitral Valve Degeneration (MMVD):
1) The dog is older than 7 yrs and < 15kg
2) The murmur is loud (Grade IV/VI or more)
3) The dog is tachycardic (HR >120 bpm) and sinus arrhythmia is absent
4) The dog is dyspneac at rest (sleeping RR > 30 breaths/minute)
If the dog satisfies these criteria, it is reasonable to commence immediate treatment with frusemide and obtain confirmatory radiographs once stable. Also note that cough on its own in a dog that is not tachycardic and has a normal sleeping respiratory rate is not consistent with congestive heart failure and thoracic radiographs are recommended in this instance rather than a treatment trial with frusemide. Any dog that is dyspneac, regardless of the presence or absence of a murmur requires thoracic radiographs. Good quality thoracic radiographs are essential for the diagnosis, assessing severity and monitoring of heart disease. One can stage the severity of the disease via assessment of left atrial size. Vertebral left atrial size is the preferred method of assessing cardiomegaly causing left heart failure in dogs with MMVD and is my preferred method over vertebral heart score. Thoracic radiographs help one assess if the cough is due to pulmonary oedema. They allow for the possible assessment of chronic airway disease via examination for regions of airway collapse and evidence of thickened airways (bronchial pattern). Thoracic radiographs also help to rule out neoplasia, pneumonia or significant heart worm disease as potential causes of the cough.
Chronic Airway Disease Tracheobronchomalacia (TBM) refers to weakness of the tracheal or bronchial walls caused either by softening of the supporting cartilaginous rings, redundancy of the connective tissue of the dorsal tracheal membrane (due to reduction and atrophy of elastic fibers) or both. It is a diagnosis made through visual identification of a >50% reduction in luminal diameter of the airway during bronchoscopy in humans or a >25% reduction at rest in dogs. In humans, TBM may be primary (congenital) or acquired (secondary). The etiology of TBM in dogs is unknown but may be due to congenital cartilage weakness, an acquired syndrome, or a combination of weakness of the cartilage and chronic inflammation.
During my residency, we investigated the syndrome of coughing in the older small breed dog with a murmur. We aimed to investigate if there was any relationship between a large left atrium and airway collapse. Small breed dogs with a chronic

Singh, R – Why won’t Fluffy stop coughing? Heart failure vs respiratory disease in dogs Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
cough of >3 months where screened for inclusion in the study. Study dogs included those with MMVD, moderate to severe left atrial enlargement, were not in congestive heart failure but whom had a chronic persistent cough. If congestive heart failure had been diagnosed but was controlled with diuretics, angiotensin converting enzyme inhibitors and pimobendan as deemed necessary by the primary clinician and the cough persisted, dogs were considered eligible for the study. The control group included age and weight matched dogs with a chronic cough, with or without MMVD but with no or only mild left atrial enlargement. Dogs had full blood work, thoracic radiographs, fluoroscopy, echocardiography and bronchoscopy with bronchoalveolar lavage performed.
Airway collapse was detected in both groups at all sites. All dogs in both groups had severe collapse of the left cranial lobar bronchus. The second most commonly affected airways were the right middle and left caudal lobar bronchi. There was no significant difference in the distribution of airway collapse between groups. Bronchoscopy revealed gross evidence of airway inflammation in all dogs in each group. Cytology of bronchoalveolar lavage fluid confirmed inflammation in all dogs in both groups, with either suppurative, lymphocytic or mixed inflammation being present.
In this small study, we did not detect a correlation between the presence or absence of left atrial enlargement and airway collapse. There was no significant difference in the distribution of airway collapse between dogs with a severely enlarged left atrium and those with negligible left atrial enlargement with most dogs regardless of group having severe collapse of the left cranial, left caudal and right middle lobar bronchi. All dogs, regardless of group assignment, had airway inflammation. This is an important finding to consider when treating these patients as non-specific suppression of cough is contraindicated in the presence of airway inflammation.
I now approach the coughing small breed dog with a murmur secondary to myxomatous mitral valve degeneration in a stepwise approach. If echocardiography, clinical findings and radiographic findings are not suggestive of CHF, neoplasia, pneumonia, heart worm disease or severe inflammatory disease, I commence a course of doxycycline 5mg/kg bid and theophylline (sustained release) 10 mg/kg bid for 3 weeks. Bronchoscopy is also recommended. I ask the owner to call me in 10 days with an update on the percentage improvement in the cough. I aim for an objective number e.g. 60%. If there is a 70% or > improvement, this treatment can be continued indefinitely for as long as it is effective. Usually the positive effect wanes over time. I find around 50% of dogs have a 70-90% improvement on this treatment alone and this can sometimes last for 6 months up to 2 yrs. If bronchoscopy was done and there was significant inflammation, prednisolone is commenced with gradual switching over to inhaled corticosteroids. This will also be recommended if bronchoscopy was not done but the cough remains significant. Only once I am happy that inflammation is controlled will I add in cough suppressants such as codeine.
References 1) Singh MK, Johnson LR, Kittleson MD et al. Bronchomalacia in Dogs with
Myxomatous Mitral Valve Degeneration. J Vet Intern Med 2012;26: 312-319
2) Ferrasin L, Crews L, Biller KE et al. Risk Factors for Coughing in Dogs with Naturally Acquired Myxomatous Mitral Valve Disease. J Vet Intern Med 2013; 27:286-292

Singh, R – Why won’t Fluffy stop coughing? Heart failure vs respiratory disease in dogs Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
3) Johnson LR, Singh MK, Pollard RE. Agreement Among Radiographs, Fluoroscopy and Bronchoscopy in Documentation of Airway Collapse in Dogs. J Vet Intern Med 2015; 29:1619-1626
4) Malcom EL, Visser LC, Phillips KL, Johnson LR. Diagnostic Value of Vertebral Left Atrial Size as Determined from Thoracic Radiographs for Assessment of Left Atrial Size in Dogs with Myxomatous Mitral Valve Disease. JAVMA 2018; 253: 1038-1045
Briscoe, K – Approach to the dyspnoeic cat Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
Approach to the Dyspnoeic Cat
Dr Katherine Briscoe Pacific Vetcare, Coffs Harbour
320 Harbour Drive Coffs Harbour NSW 2450
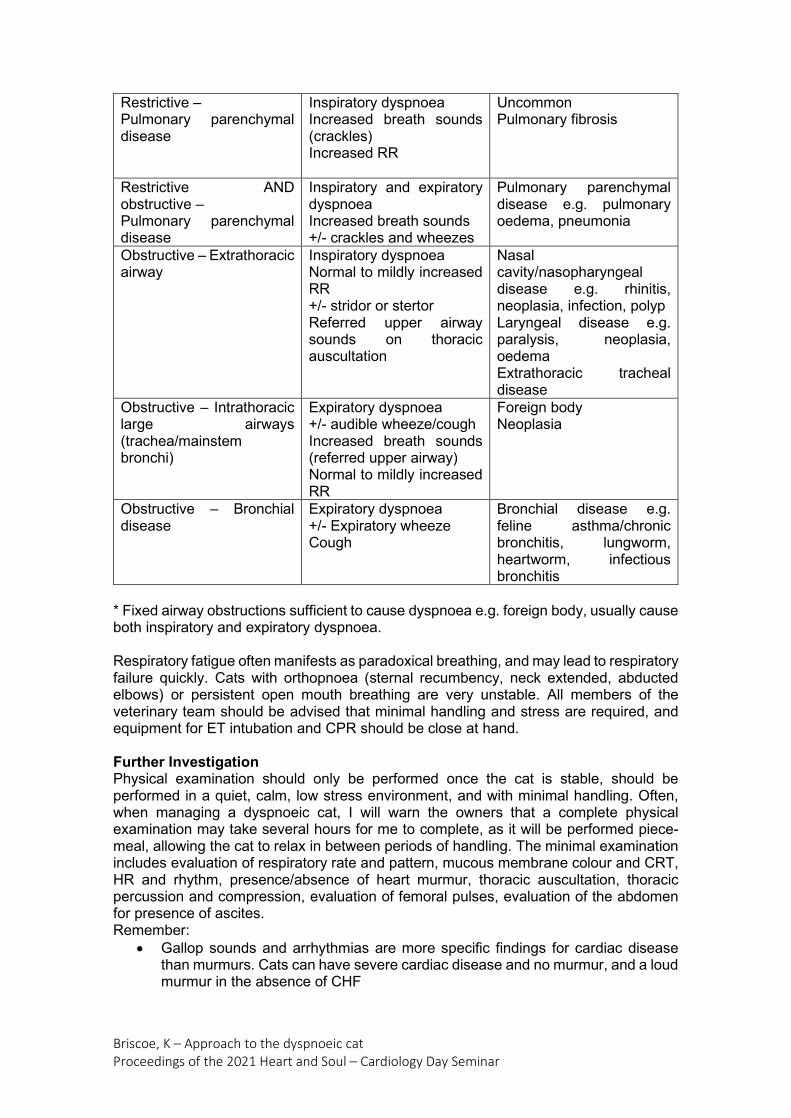
Cats in respiratory distress present unique challenges, requiring a careful approach to diagnosis and therapy. The cat is often very unstable and may easily decompensate with even minimal handling after arrival. Thus, initial handling and interventions should be kept to a minimum. Initial Stabilisation Initial management of the dyspnoeic cat should keep in mind the unstable nature of the patient, and the risk of decompensation. The single most important therapy that should be provided is oxygen via an oxygen cage/box or flow-by. If the cat tolerates oxygen by face mask, then this can also be used however most dyspnoeic cats resent this therapy and they should not be restrained to facilitate this process. Most dyspnoeic cats will benefit from light sedation, often butorphanol 0.2-0.4mg/kg SC/IM. Acepromazine (0.002-0.005mg/kg) or alfaxan (5mg/kg IM) can also be used but care should be taken to avoid sedation which will adversely affect the cardiovascular system, as CHF may be the cause of dyspnoea. In my experience, butorphanol alone is adequate to provide sedation in most dyspnoeic cats. In order to prevent decompensation, and allow the rapid management of the patient, obtaining a detailed history may have to be delayed, or alternatively a brief history and consent for treatment may be obtained by a nurse. An estimate should be provided, and consent obtained for physical examination, supplemental oxygen, radiographs and/or ultrasound, thoracocentesis, hospitalisation and drug therapy. Placement of an intravenous catheter and collection of blood samples should not be performed until after the patient is stabilised. Whilst delivering oxygen therapy, the respiratory pattern of the patient should be carefully observed. The type of respiratory pattern can often give clues as to what the underlying cause of dyspnoea may be. Restrictive respiratory disorders are due to diseases that restrict lung expansion including diseases of the pulmonary parenchyma, chest wall, pleural cavity, diaphragm, peritoneal cavity and peripheral nerves. An increased respiratory rate and decreased inspiratory volume minimises respiratory effort in non-compliant lungs. Obstructive respiratory disorders are due to airway obstruction, either extrathoracic or intrathoracic. They may be endomural (e.g. mucous, foreign body), mural (e.g. bronchospasm) or extramural (e.g. neoplasia). Respiratory Pattern Features Differential diagnoses Restrictive – Pleural space disease Thoracic wall/diaphragm disease
Rapid, shallow breathing Increased RR Decreased inspiratory volume Normal to reduced breath sounds Inspiratory dyspnoea
Pleural space disease: pleural effusion, pneumothorax, pleural mass Thoracic wall/diaphragm disease: thoracic wall trauma/pain, diaphragmatic hernia
Briscoe, K – Approach to the dyspnoeic cat Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
Restrictive – Pulmonary parenchymal disease
Inspiratory dyspnoea Increased breath sounds (crackles) Increased RR
Uncommon Pulmonary fibrosis
Restrictive AND obstructive – Pulmonary parenchymal disease
Inspiratory and expiratory dyspnoea Increased breath sounds +/- crackles and wheezes
Pulmonary parenchymal disease e.g. pulmonary oedema, pneumonia
Obstructive – Extrathoracic airway
Inspiratory dyspnoea Normal to mildly increased RR +/- stridor or stertor Referred upper airway sounds on thoracic auscultation
Nasal cavity/nasopharyngeal disease e.g. rhinitis, neoplasia, infection, polyp Laryngeal disease e.g. paralysis, neoplasia, oedema Extrathoracic tracheal disease
Obstructive – Intrathoracic large airways (trachea/mainstem bronchi)
Expiratory dyspnoea +/- audible wheeze/cough Increased breath sounds (referred upper airway) Normal to mildly increased RR
Foreign body Neoplasia
Obstructive – Bronchial disease
Expiratory dyspnoea +/- Expiratory wheeze Cough
Bronchial disease e.g. feline asthma/chronic bronchitis, lungworm, heartworm, infectious bronchitis
* Fixed airway obstructions sufficient to cause dyspnoea e.g. foreign body, usually cause both inspiratory and expiratory dyspnoea. Respiratory fatigue often manifests as paradoxical breathing, and may lead to respiratory failure quickly. Cats with orthopnoea (sternal recumbency, neck extended, abducted elbows) or persistent open mouth breathing are very unstable. All members of the veterinary team should be advised that minimal handling and stress are required, and equipment for ET intubation and CPR should be close at hand. Further Investigation Physical examination should only be performed once the cat is stable, should be performed in a quiet, calm, low stress environment, and with minimal handling. Often, when managing a dyspnoeic cat, I will warn the owners that a complete physical examination may take several hours for me to complete, as it will be performed piece-meal, allowing the cat to relax in between periods of handling. The minimal examination includes evaluation of respiratory rate and pattern, mucous membrane colour and CRT, HR and rhythm, presence/absence of heart murmur, thoracic auscultation, thoracic percussion and compression, evaluation of femoral pulses, evaluation of the abdomen for presence of ascites. Remember:
• Gallop sounds and arrhythmias are more specific findings for cardiac disease than murmurs. Cats can have severe cardiac disease and no murmur, and a loud murmur in the absence of CHF
Briscoe, K – Approach to the dyspnoeic cat Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
• Pleural effusion is often associated with reduced lung sounds and reduced compression of the sternal portion of the thorax
• Pneumothorax are often associated with absent lung sounds and hyperresonant percussion dorsally
• Chronic bronchitis/asthma is associated with loud, coarse crackles and inspiratory or expiratory wheezes
• Pulmonary oedema may be associated with soft, subtle crackles Thoracic radiographs can be very stressful for a dyspnoeic cat. Care should be taken to avoid decompensation. It should only be performed following stabilisation. A single DV radiograph is less stressful to the patient than performing lateral radiographs and can provide information on the presence/absence of pleural effusion, pneumothorax, cardiomegaly and pulmonary parenchymal disease. Thoracic radiography is usually reserved for situations where thoracic ultrasound is unavailable and a tentative diagnosis cannot be achieved based on observation of respiratory pattern and physical examination. Thoracic ultrasonography can be used to evaluate for the presence of pleural fluid, pneumothorax, and pulmonary oedema, and can be performed with minimal disruption to the patient. It is performed with the patient in sternal recumbency. Thoracocentesis may be both diagnostic and therapeutic, and may provide rapid benefit to the patient with pleural fluid. Equipment needed includes a butterfly needle (18-20g), a three-way stop cock, and a syringe (10ml or 20ml). The patient is pre-oxygenated, the thorax is clipped and surgically prepared. The needle is placed in the 7-9th ICS, in a dorsal location if pneumothorax is suspected, ventrally if pleural effusion is suspected. Once inserted the needle is flattened against the thoracic wall to avoid trauma to the lungs. The caudal border to the ribs is avoided as this is where the vessels and nerves are located. A sample of pleural effusion should be kept in an EDTA and serum tube for fluid analysis, cytology and culture, and an air-dried sample should also be made. As much fluid as possible is drained. Empiric Therapy Following initial evaluation, stabilisation, physical examination, and diagnostic imaging it is usually possible to rule out pleural space disease. If pleural space disease is excluded, the most likely differential diagnoses include CHF, lower airway disease (e.g. feline bronchial disease), and neoplasia. Empiric therapy may be necessary to stabilise the patient further to allow further diagnostic investigations such as complete thoracic radiographs or echocardiography. An obstructive breathing pattern is suggestive of pulmonary parenchymal disease. A treatment trial might include bronchodilator therapy (inhaled salbutamol or injectable terbutaline 0.01mg/kg IV, IM, SC) and an anti-inflammatory dose of corticosteroids (dexamethasone 0.125-0.5mg/kg IM, IV). A restrictive or paradoxical respiratory pattern and/or a pleural effusion that is a modified transudate may be caused by cardiac disease or neoplasia. The easier of these to exclude through treatment trial is congestive heart failure. Cardiac disease would be highly suspected in a cat with an arrhythmia or gallop sound. In this case, a focused assessment of left atrial size may be performed, or measurement of NT-proBNP in pleural effusion or blood may be performed. Empiric therapy for CHF includes frusemide 2-4mg/kg IV, IM, SC. References available on request
Briscoe, K – Update on feline upper respiratory infections Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
Feline Upper Respiratory Tract Infection: An Update
Dr Katherine Briscoe Pacific Vetcare, Coffs Harbour
320 Harbour Drive Coffs Harbour NSW 2450
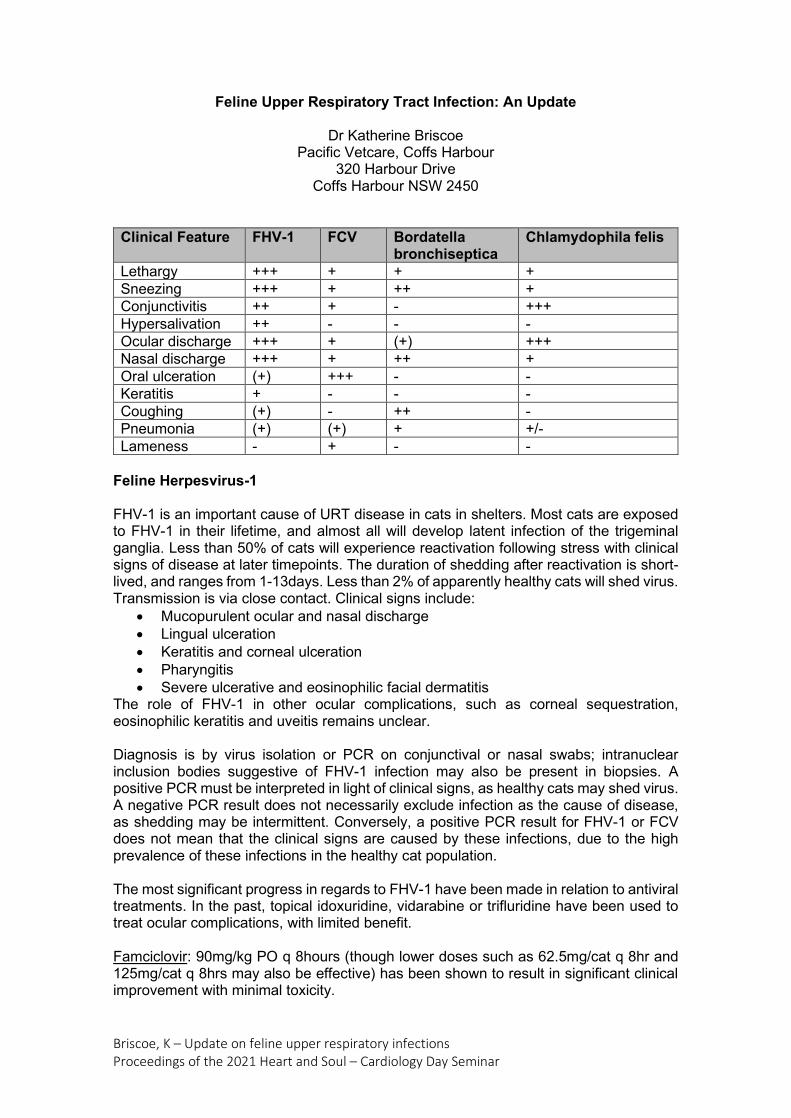
Clinical Feature FHV-1 FCV Bordatella
bronchiseptica Chlamydophila felis
Lethargy +++ + + + Sneezing +++ + ++ + Conjunctivitis ++ + - +++ Hypersalivation ++ - - - Ocular discharge +++ + (+) +++ Nasal discharge +++ + ++ + Oral ulceration (+) +++ - - Keratitis + - - - Coughing (+) - ++ - Pneumonia (+) (+) + +/- Lameness - + - -
Feline Herpesvirus-1 FHV-1 is an important cause of URT disease in cats in shelters. Most cats are exposed to FHV-1 in their lifetime, and almost all will develop latent infection of the trigeminal ganglia. Less than 50% of cats will experience reactivation following stress with clinical signs of disease at later timepoints. The duration of shedding after reactivation is short-lived, and ranges from 1-13days. Less than 2% of apparently healthy cats will shed virus. Transmission is via close contact. Clinical signs include:
• Mucopurulent ocular and nasal discharge • Lingual ulceration • Keratitis and corneal ulceration • Pharyngitis • Severe ulcerative and eosinophilic facial dermatitis
The role of FHV-1 in other ocular complications, such as corneal sequestration, eosinophilic keratitis and uveitis remains unclear. Diagnosis is by virus isolation or PCR on conjunctival or nasal swabs; intranuclear inclusion bodies suggestive of FHV-1 infection may also be present in biopsies. A positive PCR must be interpreted in light of clinical signs, as healthy cats may shed virus. A negative PCR result does not necessarily exclude infection as the cause of disease, as shedding may be intermittent. Conversely, a positive PCR result for FHV-1 or FCV does not mean that the clinical signs are caused by these infections, due to the high prevalence of these infections in the healthy cat population. The most significant progress in regards to FHV-1 have been made in relation to antiviral treatments. In the past, topical idoxuridine, vidarabine or trifluridine have been used to treat ocular complications, with limited benefit. Famciclovir: 90mg/kg PO q 8hours (though lower doses such as 62.5mg/cat q 8hr and 125mg/cat q 8hrs may also be effective) has been shown to result in significant clinical improvement with minimal toxicity.

Briscoe, K – Update on feline upper respiratory infections Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
Cidofovir: A topical ophthalmic preparation of 0.5% cidofovir applied q 12 hours has been shown to be effective in managing the ocular manifestations of disease. Oral lysine: is no longer thought to be of benefit. Studies in shelter cats has indicated that oral lysine may actually have a detrimental effect. Recombinant interferon: Human recombinant IFN-a and recombinant feline IFN-w, which inhibit FHV-1 replication in vitro, have been administered parenterally, topically (for keratitis) and orally to cats with FHV-1 infection. Controlled clinical studies that demonstrate benefit in large number of cats are lacking. Feline Calicivirus Feline calicivirus (FCV) like other RNA viruses undergoes rapid mutation, increasing the diversity over time. Infected cats may have persistent oropharyngeal infection (>1 month in duration) in the absence of obvious clinical signs. The virus persists for a long time in the environment, thus fomites are an important means of disease transmission. FCV has been most strongly associated with erosive or ulcerative lesions which can occur on the nasal planum, tongue, kips and occasionally conjunctiva, and heal over a period of 2-3 weeks. Persistent FCV infection is associated with chronic ulceroproliferative and lymphoplasmacytic gingivostomatitis. Diagnosis of FCV is by virus isolation or PCR on conjunctival, nasal or oropharyngeal swabs. Up to 20% of healthy cats may shed FCV, thus the significance of a positive result may be unclear. Treatment is supportive. Virulent Systemic Calicivirus: Highly virulent strains of FCV have been isolated from outbreaks of severe systemic febrile illness in cats in the USA and Europe known as virulent systemic disease (VSD), with mortality rates around 50%. Current vaccines against FCV do not appear to be effective against VSD. Kittens tend to be less severely affected than adult, vaccinated cats. Infections spread rapidly during outbreaks, including through fomites to pet cats of hospital employees, however in the outbreaks reported so far infection has been limited to affected clinics or shelters. That is, infection has not spread within the wider community. Outbreaks have resolved within approximately 2 months once appropriate control measures are employed. Distinctive clinical signs of VSD include signs typical of FCV infection (anorexia, oral ulceration, nasal or ocular discharge; often severe), fever, peripheral oedema, crusting and ulceration of the nose, lips, pinnae, periocular skin and distal limb. Other features which may be present include alopecia, reluctance to walk, icterus, severe respiratory distress secondary to pulmonary oedema or pleural effusion, pancreatitis, epistaxis and haematochezia. Lymphoplasmacytic Gingivostomatitis: Caudal stomatitis in cats infected with FCV is often refractory to medical treatment alone, and may require extraction of the teeth in the vicinity of the lesions, treatment with antimicrobial drugs and the use of antiseptic mouth washes. Approximately 10% of cats will fail to improve with extraction of affected teeth and may require long term with immunosuppressive therapy (prednisolone or cyclosporine). Recombinant IFN- w administered either SC or orally may also result in significant clinical important. Chlamydophila Felis Chlamydophila felis primarily causes acute and chronic conjunctivitis in cats, almost always associated with clinical signs of URT disease. It is transmitted by direct contact between cats. An age-related immunity to C.felis results in cats younger than 1-2 years

Briscoe, K – Update on feline upper respiratory infections Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
of age being most susceptible to infection. Treatment should include the use of doxycycline for a minimum of 3 weeks, and all cats within the household should be treated. Bordatella Bronchiseptica Strains of B.bronchiseptica which infect dogs can also infect cats. Prevalence of infection increases in cats housed in groups, with the greatest proportion of infected cats seen in shelter and breeding environments, and large multi-cat households. B.bronchiseptica can be isolated from healthy cats but is more often isolated from cats with respiratory disease. The organism is inhaled, attaches to respiratory cilia, evades the immune system and secretes toxins that damage the respiratory epithelium. Shedding may continue intermittently for several months after infection. Diagnosis is through bacterial culture or PCR of nasal or oropharyngeal swabs, BAL fluid, or respiratory tissue. Co-infection with viral pathogens is common. Doxycycline is the initial drug of choice for treatment, however ideally antimicrobial therapy is based on results of culture and sensitivity. Kittens are particularly susceptible to severe clinical disease i.e. pneumonia, thus early treatment is particularly important. Pneumonia may develop rapidly following infection. Mycoplasma spp Mycoplasma spp (M.gatae, M.felis, M.feliminutum) may be isolated from both healthy cats and those with URT disease, thus the role of this pathogen in upper respiratory tract disease is unclear. It is generally accepted that Mycoplasma spp may be involved in conjunctivitis and URT disease in some cats, and are an important cause of lower respiratory tract infection in cats. It is unclear whether they are primary or secondary pathogens. Mycoplasmas have been detected by culture or PCR in up to 15-22% of cats with LRT disease, and have been reported to cause bronchopneumonia, focal pulmonary abscessation and pyothorax. Detection of Mycoplasmas by PCR or culture needs to be interpreted in light of clinical signs and BAL cytology/culture. The presence of squamous epithelial cells and light mixed bacterial growth suggests URT contamination, whilst the funding of numerous inflammatory cells and absence of mixed bacterial growth suggests a pathogenic role for mycoplasmas. Mycoplasmas are typically susceptible to doxycycline, though fluoroquinolones may also be used. Prolonged periods of treatment (up to 6weeks) may be necessary for LRT disease. References available on request

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
The ECG: It’s Not as Hard as You Think
Dr Rita Singh BSc BVMS DipVetClinStud DipACVIM (Cardiology) Veterinary Cardiac Referrals
[email protected] www.vetcardioreferrals.com
The Electrical System of the Heart
The heart is composed of muscle fibres with a coordinated conduction system. The conduction system consists of the sinoatrial node, the internodal atrial pathways (the anterior internodal tract, the middle internodal tract, the posterior internodal tract and Bachmans bundle), the atrioventricular node, the bundle of His, the right and left bundle branches (which then divide into anterior and posterior fascicles) and the Purkinje system.
The electrical system of the heart.
Early investigators discovered that the beating heart was stimulated to do so by electrical processes and found that body fluids are good conductors of electricity. It was then Willem Einthoven whom introduced the labels P, Q, R, S, and T for the various deflections.
The ECG is simply a recording of the wave of electrical activity as it spreads through the heart. This is the mean wave of depolarization for a mass of individual cells. When a muscle fibre is stimulated, a wave of depolarization passes over the cell. The ECG will record an upward deflection if the depolarization wave flows towards the positive electrode of the ECG and a downward deflection if it flows toward the negative electrode of the ECG.
The standard bipolar leads are leads I, II and III. These standard limb leads show the activity of the heart from two directions.
Lead I depicts the wave of depolarization in the direction from the right arm to the left arm. The right arm is the negative pole and the left arm the positive pole.

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
Lead II depicts the wave of depolarization in the direction from the right arm to the left leg, which is the base orientation of the heart. The right arm in the negative pole, the left leg the positive pole.
Lead III depicts the wave of depolarization from the left arm to the left leg. The left arm is the negative pole, the left leg the positive pole.
Augmented limb leads: These use the same electrodes as used to record the standard bipolar leads, but they are now recording in different combinations. Thus, cardiac electrical activity can be studied from 3 new angles.
Lead aVR simply depicts the electrical activity from the right arm to a point between the left arm and left leg.
Lead aVL depicts the electrical activity from the left arm to a point between the right arm and left leg.
Lead aVF depicts the electrical activity from the head to the tail.
These augmented limb leads in combination with the bipolar leads make up the standard 6 lead ECG and are useful for determining the mean electrical axis or position of the heart and for confirming information obtained from other leads.
Configurations of the standard and augmented limb leads. C/o Tilley. Essentials of Canine and Feline Electrocardiography
Indications for an ECG:

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
The ECG is a most useful tool in two major areas: diagnosis of cardiac arrhythmias and providing information on the status of the myocardium. Some important indications include evaluation of:
Tachycardia, bradycardia or arrhythmia heard on auscultation
Acute onset dyspnea
Shock
Fainting or seizures
Cardiac monitoring during or after surgery
Preoperatively in older animals
Cardiac murmurs
Cardiomegaly found on thoracic radiographs
Cyanosis
Evaluating the effect of cardiac drugs such as digoxin, quinidine, calcium channel blockers and beta blockers
For monitoring location of needle during pericardiocentesis
For evaluating systemic disease that can effect the heart (eg GDV, pyometra, uraemia, pancreatitis)
For evaluating the effect of electrolyte disturbances, especially those of potassium, on the myocardium
Limitations of the ECG: The ECG needs to be interpreted with the clinical picture
It tells us nothing about function of heart
It may not tell us prognosis
It only gives information on the myocardium
The division between normal and abnormal is broad
There is wide variation in dogs
It is essential to be aware of the limitations of the ECG and resist the tendency to read too much into it.
When reading an ECG, always consider:
Interpreting it as part of the entire clinical picture.
The ECG tells nothing about the mechanical status of the heart i.e., an animal with severe cardiomegaly and CHF can have a normal ECG.
It can’t always evaluate prognosis.
It doesn’t record pathology of heart valves, coronary arteries, endocardium or pericardium. It only gives us information on the myocardium.
The division between normal and abnormal must be considered as a broad zone rather than a sharp line. Don’t read too much into borderline changes.

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
Wide variations in body conformation and breeds of dogs may alter the accepted standards of measurement.
The ECG must be recorded properly. It must be complete with a stable baseline in order to be accurately interpreted.
Placing the ECG
When attaching an ECG, the right hind leg is the ground.
It is essential to restrain the animal in right lateral recumbency EVERYTIME. This is for 2 reasons: A standing, moving, trembling animal just produces to much baseline artifact (no matter how still you think it is standing). The second reason is that the reference ranges for measurement of complexes are derived from the dog or cat in right lateral recumbency.
The only exception to this rule is in the markedly dyspneac animal. In this situation an immediate ECG is usually not a major priority. If it is deemed that an ECG is really needed, then the position the patient is most comfortable in will suffice. A more accurate ECG can be recorded again when the animal is stable.
The animal needs to be placed on a non-conductive surface. A metal table is not good. It will need to be covered with a rubber mat.
The ECG clips can be placed anywhere on the limb. Place them where there is a good amount of loose skin and to minimize trembling/ panting artifact as much as possible i.e., don’t place the clip above the elbow or stifle on a dog that is panting heavily as the chest movement will produce to much artifact. Go as distal on the limb as possible. Wet the skin with alcohol or electrode coupling gel to ensure good contact.
The Approach to the ECG
I approach all ECGs in the same way. Following a routine every time helps minimise jumping to conclusions and mistakes being made. I always use the same stepwise approach:
What is the heart rate?
Is the rhythm regular or irregular?
Are there p waves for each QRS complex and vice versa?
Are all QRS complexes narrow and upright in leads I, II, III and aVF or it there a variation on this? If so, characterize this further

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
This is how I characterize and report on EVERY ECG.
In the ECG above, the paper speed is 25mm/s so the time between lines at the bottom of the page is 1 sec. I would report it as follows: The heart rate was 220 bpm and regular (count number of complexes in 3 sec then multiply by 20 to make beats/minute). There were p waves for each QRS complex and vice versa. QRS complexes are narrow and upright consistent with supraventricular origin. Diagnosis: sinus tachycardia.
Common Artifacts
It is important to remember that the ECG is a mechanical recording. Hence, any number of technical or mechanical problems can occur. These problems will be superimposed on the cardiac complexes and may interfere with interpretation. Hence, it is important to be aware of the common artifacts.
Electrical interference: This appears as a regular sequence of 60 sharp up and down waves/second, hence, the common name 60 cycle interference. If severe, the ECG cannot be interpreted so the cause needs to be found and eliminated. Possible sources include:
• Lack of proper grounding of the power cord to a 3-prong wall outlet. This will ground the ECG automatically while a 2-prong power cord won’t. • Reapplying the electrode clips making sure all are securely attached to skin and that clips are only dampened (not saturated) with alcohol. • Make sure clips are clean and securely attached to the cables • Pull the plug on all other electrical equipment close by and turn off fluorescent lights. • Make sure the animals legs are held apart so the clips aren’t touching each other • Make sure the holder is not touching any clips • If a metal table is being used with a rubber mat, make sure no part of the animal or leads is touching the metal
Inadequate clip contact After reapplication

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
60 cycle interference
Muscle tremor: This can be due to simple muscle tremoring, panting or purring. Sometimes it may be impossible to get rid of this artifact, but this will need to be taken into account when trying to interpret the EGG. Try to make sure the dog or cat is as comfortable as possible. Gentle blowing into the face may help stop a cat from purring. Having the owner in the room, placing a hand on the chest or reapplying the electrodes to make them as comfortable as possible. Reducing the amplitude to ½ sensitivity may help reduce the artifact enough to make the ECG more interpretable. Occasionally mild sedation may be needed but, again, this needs to be taken into account when interpreting the ECG.
Wandering baseline: This is usually due to respiratory or general movement. It will usually resolve itself as the patient settles. Again, make sure the patient is as calm and comfortable as possible.
Purring artefact
Panting artefact
Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
Common Arrhythmias
SINUS ARRHYTHMIA
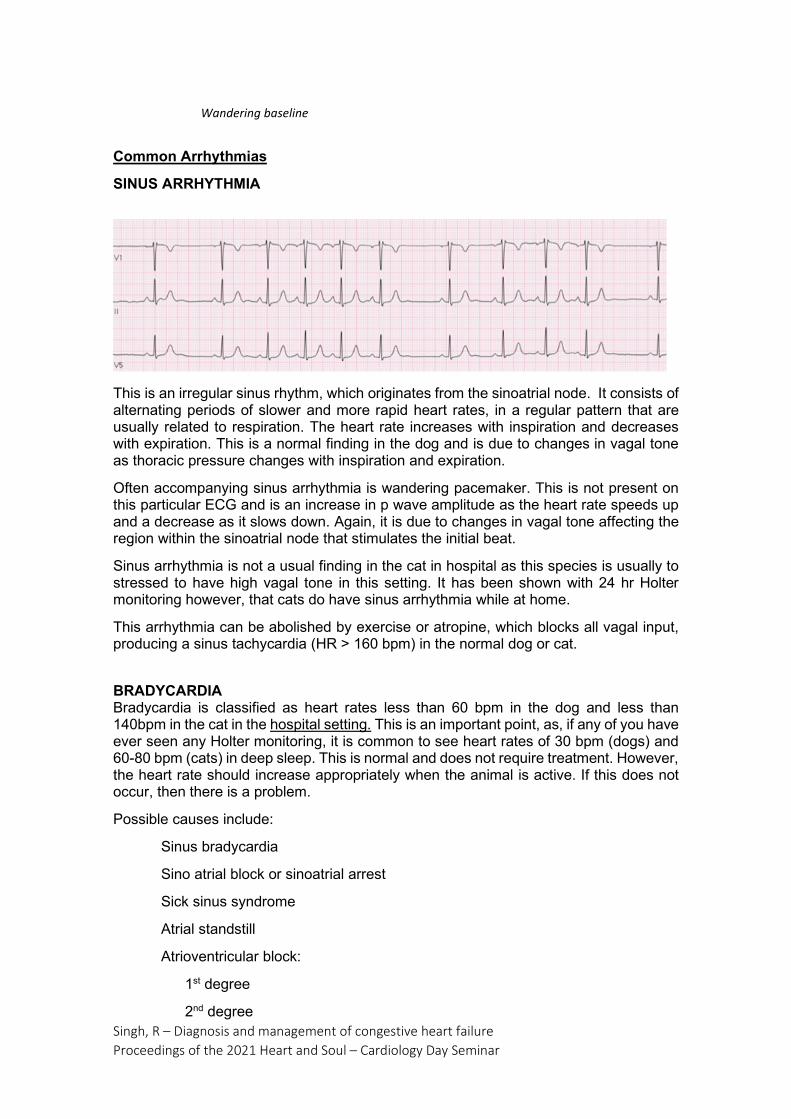
This is an irregular sinus rhythm, which originates from the sinoatrial node. It consists of alternating periods of slower and more rapid heart rates, in a regular pattern that are usually related to respiration. The heart rate increases with inspiration and decreases with expiration. This is a normal finding in the dog and is due to changes in vagal tone as thoracic pressure changes with inspiration and expiration.
Often accompanying sinus arrhythmia is wandering pacemaker. This is not present on this particular ECG and is an increase in p wave amplitude as the heart rate speeds up and a decrease as it slows down. Again, it is due to changes in vagal tone affecting the region within the sinoatrial node that stimulates the initial beat.
Sinus arrhythmia is not a usual finding in the cat in hospital as this species is usually to stressed to have high vagal tone in this setting. It has been shown with 24 hr Holter monitoring however, that cats do have sinus arrhythmia while at home.
This arrhythmia can be abolished by exercise or atropine, which blocks all vagal input, producing a sinus tachycardia (HR > 160 bpm) in the normal dog or cat.
BRADYCARDIA Bradycardia is classified as heart rates less than 60 bpm in the dog and less than 140bpm in the cat in the hospital setting. This is an important point, as, if any of you have ever seen any Holter monitoring, it is common to see heart rates of 30 bpm (dogs) and 60-80 bpm (cats) in deep sleep. This is normal and does not require treatment. However, the heart rate should increase appropriately when the animal is active. If this does not occur, then there is a problem.
Possible causes include:
Sinus bradycardia
Sino atrial block or sinoatrial arrest
Sick sinus syndrome
Atrial standstill
Atrioventricular block:
1st degree
2nd degree
Wandering baseline

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
3rd degree
SINUS BRADYCARDIA
Sinus bradycardia is a normal sinus rhythm that is considered slower that appropriate for the situation. It can be due to:
Increased parasympathetic tone (i.e. high vagal tone). Causes include ocular disease, gastrointestinal abnormalities, chronic respiratory disease, systemic disease and central nervous system disease. Quite commonly, in the otherwise healthy animal, despite extensive searching, I fail to identify the cause.
Athletic animal
General anaesthesia
Impending cardiac arrest
Hypothermia
Severe hypothyroidism
Sick sinus syndrome
Drugs (digoxin, beta blockers, Ca++ blockers) e.g. in cats on beta blockers, I expect and aim for a heart rate of around 140 bpm.
Early hyperkalaemia
Treatment is rarely required, usually one needs to treat the underling cause.
If severe, atropine may be required while the underlying cause is being found and treated
SINOATRIAL BLOCK/SINOATRIAL ARREST
Sinus arrest is failure of impulses to be formed in the sinoatrial (SA) node due to depressed automaticity in the node. SA block looks similar to sinus arrest but the transmission of the regularly formed impulse from the node is blocked from entering the atrial myocardium. Differentiating between the two can be difficult. The rhythm is regularly irregular and may look like an exaggerated sinus arrhythmia with pauses

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
showing complete absence of P-QRS-T complexes. The pauses are twice or greater than 2x the normal R-R interval. If the pauses are an exact series of the normal RR interval (i.e. 2x) then this suggests SA block over SA arrest. If the pauses are long enough, a junctional or ventricular escape may occur
This arrhythmia is again, often due to high vagal tone. If this is the case, it will be abolished by atropine. Pathologic causes include conditions of the atria such as dilation, fibrosis, neoplasia or sick sinus syndrome. These generally will have no or a partial response to atropine.
SICK SINUS SYNDROME Sick sinus syndrome is due to disease (usually fibrosis) of the SA node. While it is commonly referred to as sick sinus syndrome, it is not uncommon in advanced cases to see disease of lower conduction pathways (eg AV node, bundle of His, right and left bundle branches) concurrently. This disease commonly results in a bradycardia, with long periods of sinus block or sinus arrest. In the ECG below, the 2 second pause has been broken by a ventricular escape beat (30 beats/minute).
Sick sinus syndrome in an 11 yo Miniature Schnauzer
This syndrome is also known as ‘tachycardia/ bradycardia’ syndrome due to periods of bradycardia interspersed with runs of atrial premature contractions or supraventricular tachycardia. I have rarely seen this form of the disease. Usually it presents purely as a bradycardia.
When trying to differentiate if this type of an ECG is due to high vagal tone or sick sinus syndrome, an atropine response test is done. When using atropine in the cardiac (rather than anaesthetic) setting use the maximum dose of 0.04mg/kg (IV or SC). We want to know FOR SURE if atropine is or isn’t going to work so it makes no sense to go with a lower dose. I usually do the dose SC then recheck the ECG 30 minutes later. If doing it IV, keep the ECG on the patient and continue to check it for 5 minutes looking for a response. A complete response is a heart rate > 160 bpm (dog) with a regular, sinus tachycardia. Anything less than this could be termed a partial response or if there is no change at all, no response.
If this has no effect then isoproterenol (a pure beta agonist), dopamine, dobutamine or cardiac pacing may be required. Due to disease of the SA node, SSS is often poorly responsive to atropine. If the animal is clinical (e.g. having weakness or syncopal episodes), some time may be bought with anticholinergic or symphathomimetic drugs such as propantheline bromide, terbutaline or theophylline. However, if there has been

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
some initial response, this usually wanes over time with permanent pacemaker implantation the only definitive treatment.
1ST DEGREE ATRIOVENTRICULAR BLOCK A delay or interruption in conduction of the supraventricular impulse through the atrioventricular (AV) junction and bundle of His is termed AV block. There are 3 types of AV block: 1st degree, 2nd degree and 3rd degree.
In 1st degree AV block the p wave and QRS complex look normal but there is a delay in conduction through the AV node or bundle of His. A P-R interval > 0.13s (dog) and > 0.09s (cat) is considered to be 1st degree AV block. The most common cause of 1st degree AV block is high vagal tone in which case the abnormality should be abolished by atropine (0.04mg/kg SC). If atropine does not abolish the block, early AV nodal/ Bundle of His degeneration is likely, and this may progress onto a higher grade of AV block.
Drugs that effect conduction through the AV node can cause 1st degree AV block and include digoxin, calcium channel blockers, beta blockers, and class 1a antiarrhythmics (quinidine and procainamide). Hyperkalaemia is another cause.
1st degree AV block in a dog. This ECG is recorded at 25 mm/s. The P-R interval is 6 boxes = 0.24s (normal < 0.13s).
2ND DEGREE AV BLOCK
2nd degree AV block is characterized by intermittent failure of the p waves to conduct through to the ventricles. One or more p waves are not followed by a QRS complex. There are 3 types of 2nd degree AV block: Mobitz type I (Wenckebach), Mobitz type II and high grade.
Mobitz type I (Wenckebach) is characterized by a progressively elongating p-R interval until a p wave is blocked (see ECG above). This form of 2nd degree AV block is most commonly caused by high vagal tone and, again, should abolish with atropine (check out the video on YouTube: ‘Diagnosis Wenckebach’. It is a good way to remember this!).
Mobitz type II: In this form of 2nd degree AV block the p-R interval stays consistent but a QRS complex will be dropped intermittently. This form is more likely to be due to AV nodal disease such as degeneration, fibrosis, inflammation or ischemia and, hence, is less likely to respond to atropine.
Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
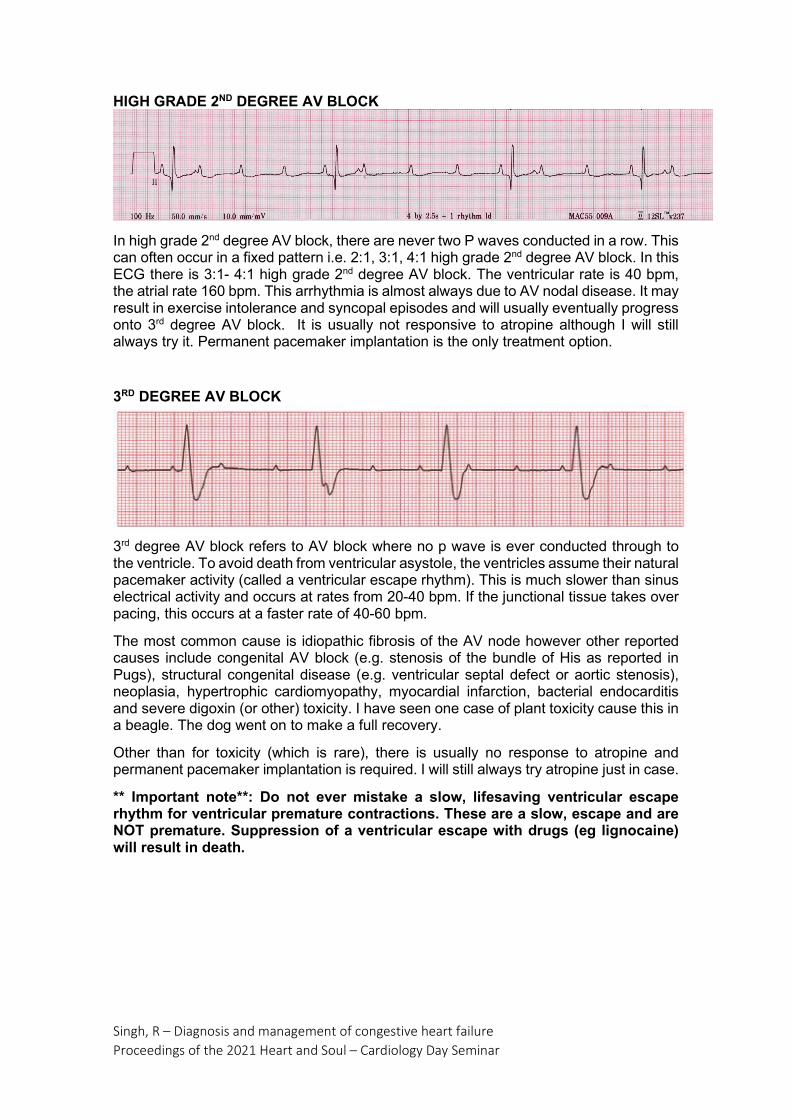
HIGH GRADE 2ND DEGREE AV BLOCK
In high grade 2nd degree AV block, there are never two P waves conducted in a row. This can often occur in a fixed pattern i.e. 2:1, 3:1, 4:1 high grade 2nd degree AV block. In this ECG there is 3:1- 4:1 high grade 2nd degree AV block. The ventricular rate is 40 bpm, the atrial rate 160 bpm. This arrhythmia is almost always due to AV nodal disease. It may result in exercise intolerance and syncopal episodes and will usually eventually progress onto 3rd degree AV block. It is usually not responsive to atropine although I will still always try it. Permanent pacemaker implantation is the only treatment option.
3RD DEGREE AV BLOCK
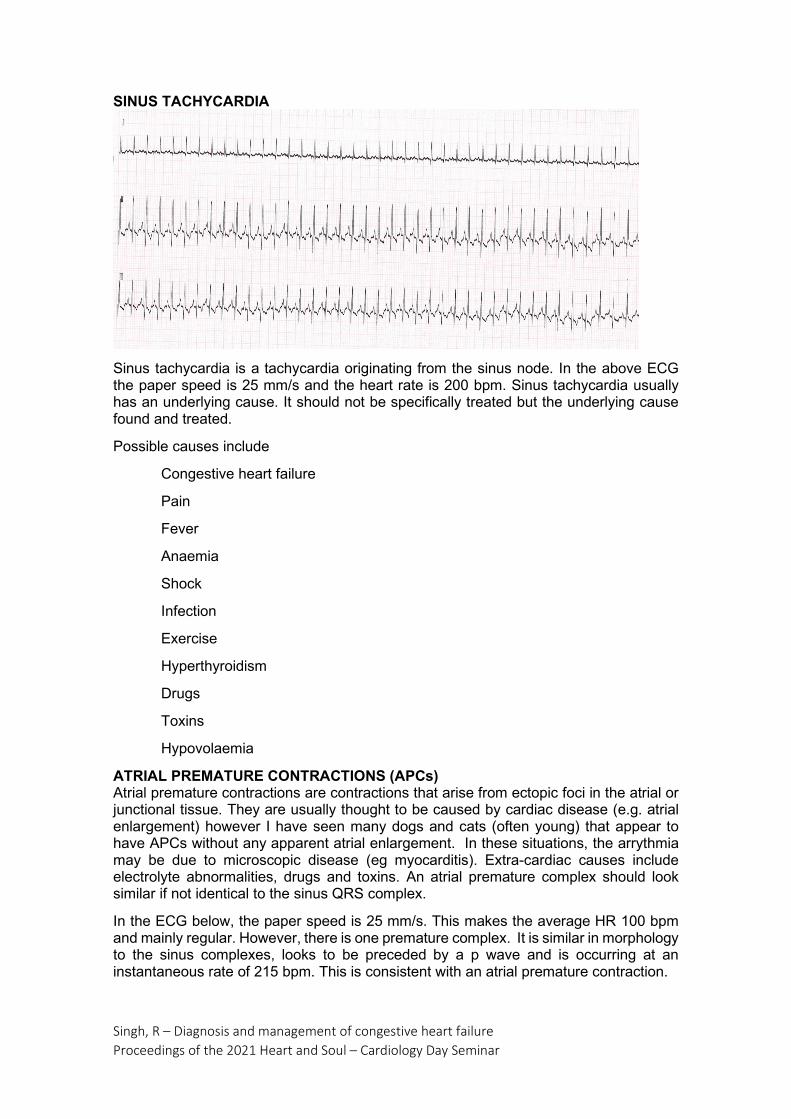
3rd degree AV block refers to AV block where no p wave is ever conducted through to the ventricle. To avoid death from ventricular asystole, the ventricles assume their natural pacemaker activity (called a ventricular escape rhythm). This is much slower than sinus electrical activity and occurs at rates from 20-40 bpm. If the junctional tissue takes over pacing, this occurs at a faster rate of 40-60 bpm.
The most common cause is idiopathic fibrosis of the AV node however other reported causes include congenital AV block (e.g. stenosis of the bundle of His as reported in Pugs), structural congenital disease (e.g. ventricular septal defect or aortic stenosis), neoplasia, hypertrophic cardiomyopathy, myocardial infarction, bacterial endocarditis and severe digoxin (or other) toxicity. I have seen one case of plant toxicity cause this in a beagle. The dog went on to make a full recovery.
Other than for toxicity (which is rare), there is usually no response to atropine and permanent pacemaker implantation is required. I will still always try atropine just in case.
** Important note**: Do not ever mistake a slow, lifesaving ventricular escape rhythm for ventricular premature contractions. These are a slow, escape and are NOT premature. Suppression of a ventricular escape with drugs (eg lignocaine) will result in death.

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
ATRIAL STANDSTILL
Persistant atrial standstill in an 8 yo English Spinger Spaniel. There is a complete absence of p waves. The heart rate is 40 bpm and QRS complexes are wide and bizarre consistent with a ventricular escape.
Atrial standstill is characterized by a complete absence of p waves and by a regular escape rhythm. This can be junctional or ventricular. Atrial standstill may be temporary, persistent or terminal. The most common cause of temporary atrial standstill in dogs and cats is severe hyperkalaemia. This is really a sinoventricular rhythm as intracardiac catheterization studies show that the SA node is more refractory to the effects of hyperkalaemia. Hence, the SA node is still firing off, and the impulses are transmitted via the internodal pathways to the ventricles. The atria are unable to contract as the atrial myocardium itself can’t be activated. Another, but less common cause these days is digoxin toxicity.
Persistent atrial standstill has been most commonly reported in the English Springer Spaniel due to an atrial myopathy. These dogs develop markedly enlarged, paper-thin atria. It can also occur in conjunction with systemic neuromuscular disorders such as Duchenne muscular dystrophy. The condition is not responsive to anticholinergic or sympathomimetic drugs. The only treatment is permanent pacemaker implantation however long-term survival can still be poor due to progressive atrial enlargement eventually resulting in congestive heart failure.
TACHYCARDIA Heart rates persistently greater than 150 bpm in the dog and 240 bpm cat are considered abnormal. The word ‘persistent’ is important here. At times of stress and during exercise, the heart rate can go as high as 240 bpm in the dog. This is only able to occur in short bursts however and is not able to be sustained for long periods of time.
Possible cause of tachycardia in dogs and cats include:
Sinus tachycardia
Supraventricular tachycardia
Atrial flutter
Atrial fibrillation
Ventricular tachycardia
Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
SINUS TACHYCARDIA
Sinus tachycardia is a tachycardia originating from the sinus node. In the above ECG the paper speed is 25 mm/s and the heart rate is 200 bpm. Sinus tachycardia usually has an underlying cause. It should not be specifically treated but the underlying cause found and treated.
Possible causes include
Congestive heart failure
Pain
Fever
Anaemia
Shock
Infection
Exercise
Hyperthyroidism
Drugs
Toxins
Hypovolaemia
ATRIAL PREMATURE CONTRACTIONS (APCs) Atrial premature contractions are contractions that arise from ectopic foci in the atrial or junctional tissue. They are usually thought to be caused by cardiac disease (e.g. atrial enlargement) however I have seen many dogs and cats (often young) that appear to have APCs without any apparent atrial enlargement. In these situations, the arrythmia may be due to microscopic disease (eg myocarditis). Extra-cardiac causes include electrolyte abnormalities, drugs and toxins. An atrial premature complex should look similar if not identical to the sinus QRS complex.
In the ECG below, the paper speed is 25 mm/s. This makes the average HR 100 bpm and mainly regular. However, there is one premature complex. It is similar in morphology to the sinus complexes, looks to be preceded by a p wave and is occurring at an instantaneous rate of 215 bpm. This is consistent with an atrial premature contraction.

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
Generally, single APCs don’t require treatment unless they are very frequent. My drug of choice is diltiazem.
SUPRAVENTRICULAR TACHYCARDIA (SVT)
Supraventricular tachycardia (SVT) is a rapid regular rhythm originating at an atrial or junctional focus. As for single APCs, the complexes in SVT should be similar to if not identical to sinus complexes. This arrhythmia is usually going to be due to cardiac disease such as atrial enlargement or a microscopic abnormality.
There are two main mechanisms for which SVT occurs:
An ectopic focus (enhanced automaticity). This is an abnormal focus of electrical activity in the atrial tissue, which is intermittently firing off.
A re-entrant pathway. This is due to an accessory pathway, which is conducting electrical activity.
On the ECG below, the paper speed is 50 mm/s. This makes the heart rate 320 bpm and regular. QRS complexes appear a little wide but on measurement are 0.04 (normal width). P waves are not able to be seen as the rate is to fast and they are buried in the T waves. This is consistent with a supraventricular tachycardia.
Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
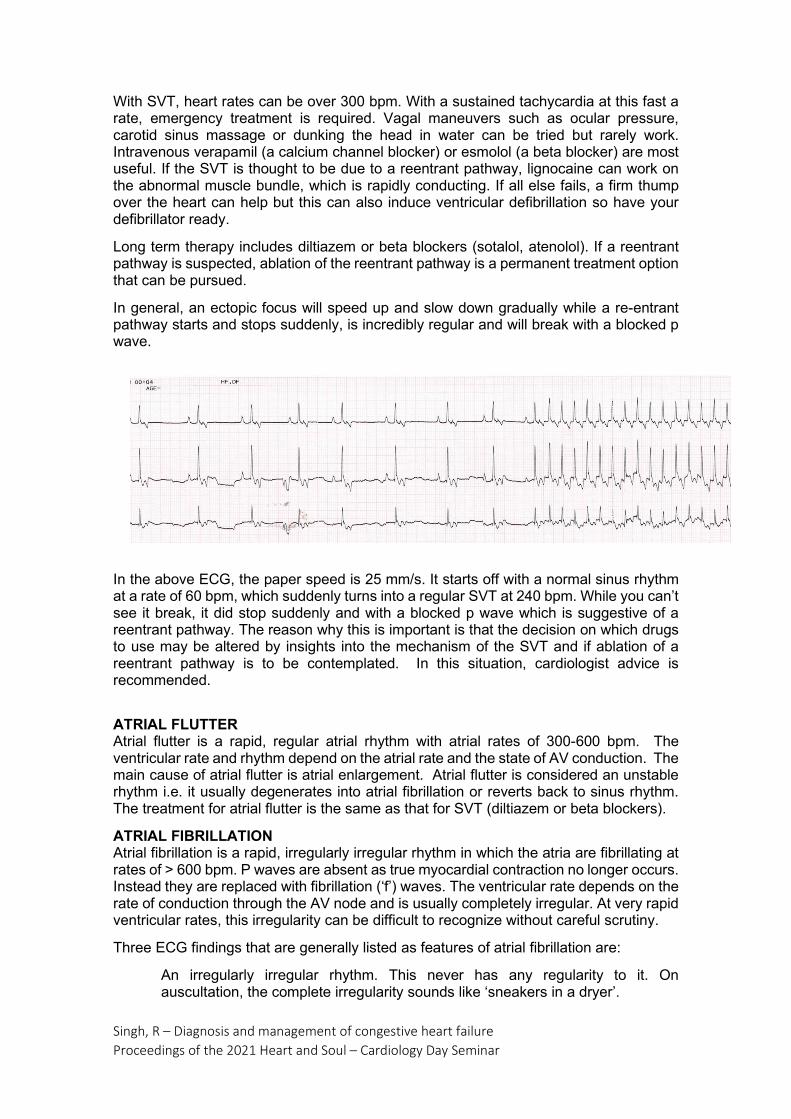
With SVT, heart rates can be over 300 bpm. With a sustained tachycardia at this fast a rate, emergency treatment is required. Vagal maneuvers such as ocular pressure, carotid sinus massage or dunking the head in water can be tried but rarely work. Intravenous verapamil (a calcium channel blocker) or esmolol (a beta blocker) are most useful. If the SVT is thought to be due to a reentrant pathway, lignocaine can work on the abnormal muscle bundle, which is rapidly conducting. If all else fails, a firm thump over the heart can help but this can also induce ventricular defibrillation so have your defibrillator ready.
Long term therapy includes diltiazem or beta blockers (sotalol, atenolol). If a reentrant pathway is suspected, ablation of the reentrant pathway is a permanent treatment option that can be pursued.
In general, an ectopic focus will speed up and slow down gradually while a re-entrant pathway starts and stops suddenly, is incredibly regular and will break with a blocked p wave.
In the above ECG, the paper speed is 25 mm/s. It starts off with a normal sinus rhythm at a rate of 60 bpm, which suddenly turns into a regular SVT at 240 bpm. While you can’t see it break, it did stop suddenly and with a blocked p wave which is suggestive of a reentrant pathway. The reason why this is important is that the decision on which drugs to use may be altered by insights into the mechanism of the SVT and if ablation of a reentrant pathway is to be contemplated. In this situation, cardiologist advice is recommended.
ATRIAL FLUTTER Atrial flutter is a rapid, regular atrial rhythm with atrial rates of 300-600 bpm. The ventricular rate and rhythm depend on the atrial rate and the state of AV conduction. The main cause of atrial flutter is atrial enlargement. Atrial flutter is considered an unstable rhythm i.e. it usually degenerates into atrial fibrillation or reverts back to sinus rhythm. The treatment for atrial flutter is the same as that for SVT (diltiazem or beta blockers).
ATRIAL FIBRILLATION Atrial fibrillation is a rapid, irregularly irregular rhythm in which the atria are fibrillating at rates of > 600 bpm. P waves are absent as true myocardial contraction no longer occurs. Instead they are replaced with fibrillation (‘f’) waves. The ventricular rate depends on the rate of conduction through the AV node and is usually completely irregular. At very rapid ventricular rates, this irregularity can be difficult to recognize without careful scrutiny.
Three ECG findings that are generally listed as features of atrial fibrillation are:
An irregularly irregular rhythm. This never has any regularity to it. On auscultation, the complete irregularity sounds like ‘sneakers in a dryer’.

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
Absent p waves
Rapid rhythm
Of these three features, the only one that holds true every time is the irregularly irregular rhythm. P waves are absent but, as you saw previously, you often can’t see p waves in a rapid supraventricular tachycardia. While the majority of atrial fibrillation ventricular rates are rapid, horses and some giant breed dogs can have atrial fibrillation with slow ventricular response rates.
In this ECG the paper speed is 50 mm/s making the heart rate 220 bpm and irregularly irregular. P waves are not visible. The diagnosis is atrial fibrillation. With this patient, QRS complexes are wide (0.08s). This is likely due to left ventricular enlargement.
Atrial fibrillation usually occurs due to a severely diseased atrial myocardium. People, horses and some giant breeds of dog, can develop ‘lone atrial fibrillation’. This is atrial fibrillation without an obviously enlarged or diseased atrium. In dogs and cats with atrial fibrillation due to a large left atrium, the main aim is to slow the ventricular rate (rate control) not convert back to sinus rhythm (rhythm control). Slowing the ventricular response rate is achieved by drugs that slow conduction through the AV node (calcium channel blockers, beta blockers or digoxin). My drug of choice in dogs is diltiazem and in cats is atenolol.
Electrical cardioversion is the delivery of a specifically timed electrical shock to the heart in order to restore sinus rhythm. This is most useful in animals without a diseased myocardium (horses and giant breed dogs).
VENTRICULAR PREMATURE CONTRACTIONS (VPCs) Ventricular premature contractions are premature impulses that arise from below the AV node, in the ventricular tissue. As these impulses do not travel through the specialized conduction tissue of the heart but through ordinary cardiac muscle, the transmission of electrical activity is slower resulting in the typical ‘wide and bizarre’ configuration that is classic for these complexes.
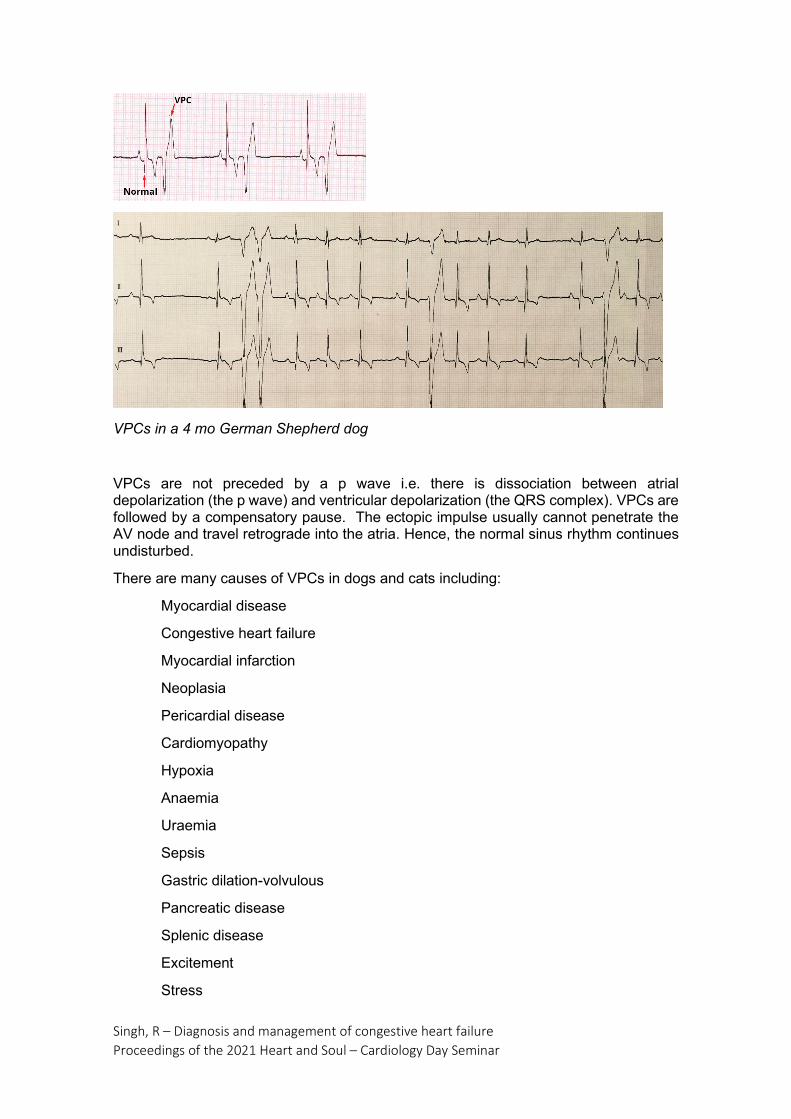
Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
VPCs in a 4 mo German Shepherd dog
VPCs are not preceded by a p wave i.e. there is dissociation between atrial depolarization (the p wave) and ventricular depolarization (the QRS complex). VPCs are followed by a compensatory pause. The ectopic impulse usually cannot penetrate the AV node and travel retrograde into the atria. Hence, the normal sinus rhythm continues undisturbed.
There are many causes of VPCs in dogs and cats including:
Myocardial disease
Congestive heart failure
Myocardial infarction
Neoplasia
Pericardial disease
Cardiomyopathy
Hypoxia
Anaemia
Uraemia
Sepsis
Gastric dilation-volvulous
Pancreatic disease
Splenic disease
Excitement
Stress
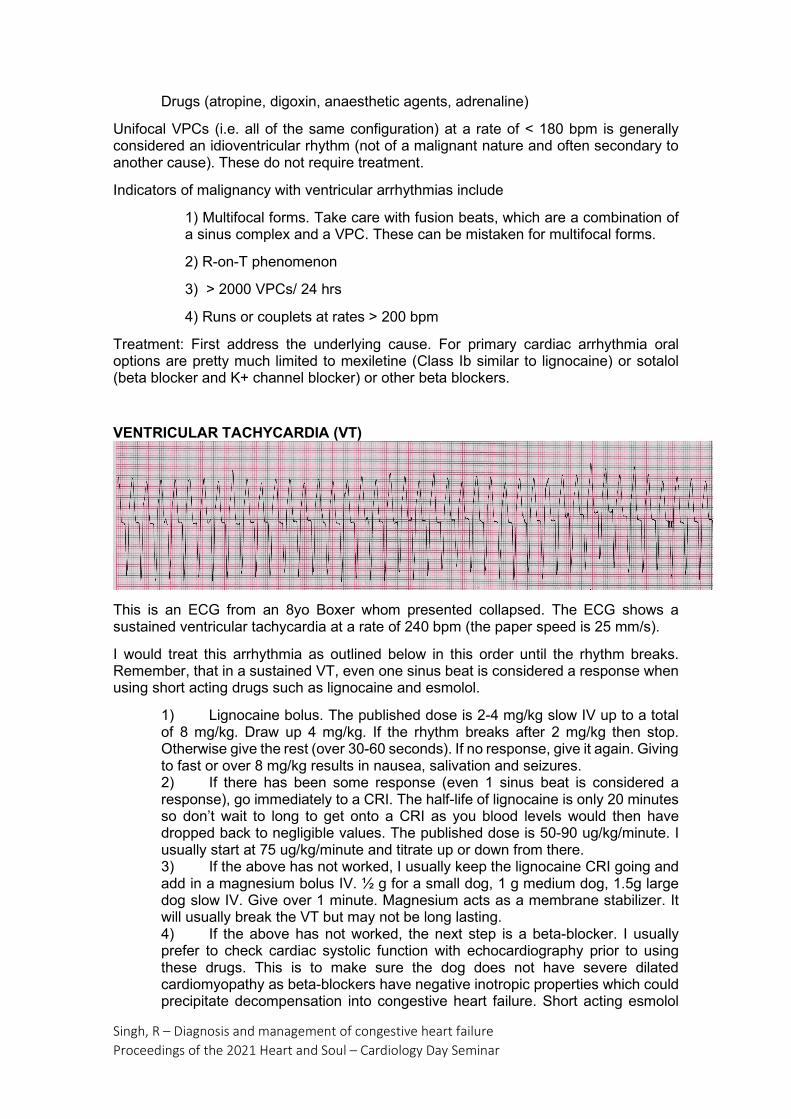
Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
Drugs (atropine, digoxin, anaesthetic agents, adrenaline)
Unifocal VPCs (i.e. all of the same configuration) at a rate of < 180 bpm is generally considered an idioventricular rhythm (not of a malignant nature and often secondary to another cause). These do not require treatment.
Indicators of malignancy with ventricular arrhythmias include
1) Multifocal forms. Take care with fusion beats, which are a combination of a sinus complex and a VPC. These can be mistaken for multifocal forms.
2) R-on-T phenomenon
3) > 2000 VPCs/ 24 hrs
4) Runs or couplets at rates > 200 bpm
Treatment: First address the underlying cause. For primary cardiac arrhythmia oral options are pretty much limited to mexiletine (Class Ib similar to lignocaine) or sotalol (beta blocker and K+ channel blocker) or other beta blockers.
VENTRICULAR TACHYCARDIA (VT)
This is an ECG from an 8yo Boxer whom presented collapsed. The ECG shows a sustained ventricular tachycardia at a rate of 240 bpm (the paper speed is 25 mm/s).
I would treat this arrhythmia as outlined below in this order until the rhythm breaks. Remember, that in a sustained VT, even one sinus beat is considered a response when using short acting drugs such as lignocaine and esmolol.
1) Lignocaine bolus. The published dose is 2-4 mg/kg slow IV up to a total of 8 mg/kg. Draw up 4 mg/kg. If the rhythm breaks after 2 mg/kg then stop. Otherwise give the rest (over 30-60 seconds). If no response, give it again. Giving to fast or over 8 mg/kg results in nausea, salivation and seizures. 2) If there has been some response (even 1 sinus beat is considered a response), go immediately to a CRI. The half-life of lignocaine is only 20 minutes so don’t wait to long to get onto a CRI as you blood levels would then have dropped back to negligible values. The published dose is 50-90 ug/kg/minute. I usually start at 75 ug/kg/minute and titrate up or down from there. 3) If the above has not worked, I usually keep the lignocaine CRI going and add in a magnesium bolus IV. ½ g for a small dog, 1 g medium dog, 1.5g large dog slow IV. Give over 1 minute. Magnesium acts as a membrane stabilizer. It will usually break the VT but may not be long lasting. 4) If the above has not worked, the next step is a beta-blocker. I usually prefer to check cardiac systolic function with echocardiography prior to using these drugs. This is to make sure the dog does not have severe dilated cardiomyopathy as beta-blockers have negative inotropic properties which could precipitate decompensation into congestive heart failure. Short acting esmolol

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
(T1/2 9 minute) or oral sotalol are the two choices. In the emergency situation where echocardiographic assessment of systolic function is not possible, esmolol is the safer drug due to the short half-life. As I can check an echocardiogram first, I generally give oral sotalol on top of the previous two drugs as I have had good success with this. 5) If none of this has worked. I stop the previous drugs and give IV amiodarone. Amiodarone has good efficacy for VT but there are many side effects including hypotensive shock (possibly due to a reaction in the vector of the drug), cutaneous and membranous flushing and possible long-term hepatic and pulmonary side effects. IV prednisolone and antihistamines are given prior. 6) The final step if none of the above has worked is electrical cardioversion. This is generally only used if it is felt the animal is in dire straights and cardiac arrest may imminent.
SMALL QRS COMPLEXES AND ELECTRICAL ALTERNANS
The amplitude of the QRS complex has wide normal limits depending on the age and breed of the dog. An amplitude of < 0.5mV is considered small for most dogs. Cats normally have small QRS complexes so this would be difficult to recognize in a cat. The amplitude of QRS complexes can be affected by many factors other than cardiac disease. For example, the distance of the heart from the recording electrode leads has a major effect on the amplitude of the QRS. This distance can be influenced by many factors including the size of the chest, obesity, the presence of thoracic masses or pleural effusion. Another non-cardiac cause of small QRS complexes is hypothyroidism.
The most common cardiac disease associated with small QRS complexes is pericardial effusion. This may be seen in combination with electrical alternans. This is an alternating variation in amplitude of the QRS complexes and is almost pathognomic for pericardial effusion. It is thought to occur because of the heart swinging back and forth in the pericardial effusion.
Electrical alternans in a 10 yo Border Collie with pericardial effusion
Right Bundle Branch Block

Singh, R – Diagnosis and management of congestive heart failure Proceedings of the 2021 Heart and Soul – Cardiology Day Seminar
In this ECG, at first glance the arrhythmia looks like a run of ventricular premature contractions. However, on a closer look, there are p waves with a regular and normal P-R interval prior to each QRS complex. This tells us that each complex has originated from the sinoatrial node (not the ventricles) and that a delay in conduction is what is causing them to be wide and bizarre. As the complexes have deep S waves in the 3 visible leads, this is most consistent with right bundle branch block. This is a delay or block of conduction in the right bundle branch of the hearts electrical system.
The conduction system consists of the sinoatrial node, the internodal atrial pathways, the AV node, the bundle of His, the right and left bundle branches (which then divide into anterior and posterior fascicles) and the Purkinje system. In complete RBBB, no electrical activity passes down the right bundle branch. The right ventricle is stimulated by electrical activity that passes from myocyte-myocyte from the left ventricle. As the electrical activity doesn’t pass through the rapidly conducting electrical pathways, impulse conduction to the right ventricle is much slower, hence the complexes become wide and bizarre (similar to a VPC).
References:
1. Small Animal Cardiovascular Medicine. Kittleson and Kienle. Mosby Inc. 1998. Textbook of Canine and Feline Cardiology. Fox, Sisson, Moise. W.B Saunders Co. 1999.
2. Essentials of Canine and Feline Electrocardiography. Tilley L.P. Mosby Co. 1979
Related Documents











