Page 22 D I A B ETES War Against New Mental Health Section Providing Our Kids with Healthier Snacks Page 9 Page 10 Page 18 Mom’s Dilemma - Work or Stay at Home Genetics Based Treatment A Mental Health Magazine February 2012 A Mental Health Magazine MIND, BODY SOUL & A Publication of Supplement to the Jewish Press Periodical Publication Supplement to the Jewish Press Periodical Publication SEE INSIDE A Publication of February 2012 SPECIAL Subscription Offer See Page 21 Margaret Tietz NURSING & REHABILITATION CENTER See Page 31

health_living_jewish_press
Mar 22, 2016
Design and layout is produced by the company DESIGN-ER ([email protected])
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Page 22DIABETESWar Against
New MentalHealth Section
Providing OurKids with
Healthier Snacks
Page 9
Page 10
Page 18
Mom’s Dilemma -Work or Stay
at Home
Genetics BasedTreatment
A Mental Health Magazine
February 2012
A Mental Health Magazine
MIND,BODY
SOUL&
A Publication of
Supplement to the Jewish Press
Periodical PublicationSupplement to the Jewish Press
Periodical Publication
SEE INSIDE
A Publication of
February 2012
SPECIAL Subscription Offer
See Page 21Margaret TietzNURSING & REHABILITATION CENTER See PageSee Page 31
2
946 McDonald Avenue Brooklyn, NY 11218T. (718) 705-5800 F. (718) 682-0055
[email protected] www.edisonhhc.com
FREENo Obligation Consultation
718.705.5800
ED ISONHOME HEALTH CARE
Having trouble navigating today’s complex world of Home Health Care? Confused about your options and unsure how to make the best decisions? You need a different kind of Home Health Care provider. You need someone that will make the entire process easy to understand, answer all your questions and guide you through every step in a simple and clear manner that leaves you with a feeling of confidence and peace of mind. You need Edison Home Health Care.
f Personalized home care for the elderly and disabledf Skilled, compassionate professionalsf Medical, nursing, therapeutic and social supportf Private Pay and Long Term Care Insurance specialistsf Low introductory ratesf FREE Medicaid planning Provided by:
ADVE
RTIS
ING
BY: H
OOPL
A! 7
18-6
77-7
710
Your HomecareOptions Shouldn’tBe a Mystery to You.
HOMECAREPL ANNINGSOLUTION S

3
Ask Zahler®
Have Questions? The signature Zahler® advice is available free of charge via
the Ask Zahler® nutrition line:
1-877-ASK-ZAHLER® (NYC: 1-212-444-9936)Every vitamin developed by Zahler® goes through
rigorous testing and is manufactured and bottled in a state-of-the-art GMP, NNFA & NSF® certified facility.
THIS WINTER SEASON, INFLUENZA STANDS NO CHANCE.
BE PROTECTED
FROM VIRAL AND BACTERIAL
INFECTIONSALL WINTER
LONG
Includes 985mg of Elderberry
Extract
ABBREVIATE YOUR COLD.
Take Zahler® Abreve™ at the
first sign of cold or flu symptoms.
Zahler® Abreve™ advanced Cold & Flu formula is a powerful blend of herbs and nutrients that stops oncoming colds in their tracks. Plus, it contains nearly 1000mg of elderberry extract, which boosts the overall immune system and has been proven even more effective than Tamiflu® in reducing the severity and length of the flu.
4

FEBRUARY 2012
55
H&
L B
RIE
FS
From the Editors
Welcome to the new, expanded version of Health & Living. In its updated format, we can now provide you with new features
covering a broader range of topics, including men’s and women’s health, diet and exercise guidance, technology-related issues, a product showcase, a community profile and much more.
Count on Health & Living to continue bringing you articles with information that will help you and the members of your family to live a healthier and more enjoyable life.
In addition, we are pleased to present our ex-panded mental health section, Mind, Body and Soul.
Here are some of the more compelling topics covered in this issue of Health & Living.
We offer potentially lifesaving information about one of the fastest growing health problems of our times, the epidemic of diabetes.
We explore the moral issues confronting end of life choices, and the proper role of our doctors and rabbis in helping us to make the right decisions.
We offer parents practical advice about guard-ing the health of their children by putting sensible limits on the snacks they eat. We also give tips to parents on finding ways to bolster the self esteem of all of their children, while recognizing that each of them is unique, and ways to bring more happi-ness (simcha) into their homes.
For seniors, we provide an introduction to the newest and most popular gadgets of our day, the smartphone and the tablet computer, and explain the various ways they can make their lives easier and more convenient. We also offer medical sci-ence’s latest advice on warding off the onset of Al-zheimer’s disease.
We examine the secrets to long life known as the ‘Okinawa Diet and Lifestyle,’ which has been modeled after the residents of the Japanese island of Okinawa.
We take a look at the latest in lifesaving de-vices, the portable defibrillator, as well as ways to preserve our hearing from the din of digital devices which are becoming so ubiquitous.
Finally, in our Doctor’s Desk column, we examine the topic of how we as patients can understand and minimize the risk of life-threatening medical errors.
All of these new features and sections are de-signed to provide you with more of the information you want and need. Please send us your feedback and opinions about the new Health & Living, and topics which you would like us to cover in future issues.
Health & Living Digest . . . . . . . . . . . . . . . . . . . . . . . . . . .7
Issues
End of Life . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
Genetic Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
Raising Our Children
Kids Snack Attack . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Twins Multiplying . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Sunshine Vitamin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Kids’ Self-Esteem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Exercise and Academia. . . . . . . . . . . . . . . . . . . . . . . . . 15
Redefining Autism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Unvaccinated Children . . . . . . . . . . . . . . . . . . . . . . . . . 17
Women’s Health
Working Moms vs. Stay at Home Moms . . . . . . . . 18
New Clues Found in Lupus . . . . . . . . . . . . . . . . . . . . . 19
Fighting Breast Cancer with Cholesterol Drug . . 20
Komen Controversy with Planned Parenthood . 20
Golden Years
Diabetes: The Silent Killer. . . . . . . . . . . . . . . . . . . . . . . 22
Cataracts. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Parkinson’s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Antioxidants and Longevity . . . . . . . . . . . . . . . . . . . . 28
Seniors and Technology. . . . . . . . . . . . . . . . . . . . . . . . 29
Preventing Alzheimer’s. . . . . . . . . . . . . . . . . . . . . . . . . 30
■ Contents ■
A Mental Health Magazine
February 2012
A Mental Health Magazine
MIND,BODY
SOUL&
A Publication of
In Collaboration With:
see center of publication
End of LifeIt has become the ‘in’ practice in medicine
today for patients and their families to consider end of life choices when treatment has become too daunting. Medical journals cite that more doctors are encouraging this practice since they opt out of medical intervention themselves. As Jews though, we must consider the Torah and our Rabbi’s input as our ul-timate medical authority.
Kids Snack AttackSnack is under attack in America. Mayor
Bloomberg and even First Lady Michelle Obama are on a mission to eliminate unhealthy snacks from our schools’ lunches, vending machines and even grocery lists. American kids snack three times a day on chips, candy and other junk foods which now account for more than 27 percent of children's daily caloric intake, ac-cording to a recent study.
Diabetes: The Silent KillerDiabetes is a phenomenon of modern living.
It is largely the result of eating an unhealthy diet combined with a sedentary lifestyle. As a result, diabetes is nearly four times as common today as all types of cancer combined, and it causes more deaths each year than breast and prostate cancer combined. More than 25 million Ameri-cans already have diabetes, and more than double that number have blood sugar numbers high enough to classify them as suffering from pre-diabetes. That means that they are likely to develop the full blown Type 2 diabetes in the near future if they do not make the necessary changes in their diet and lifestyles to prevent it.
8
10
22

FEBRUARY 2012
66
H&
L B
RIE
FS
Is published by the Jewish PressPublishing since 1960
Supplement PublisherMoshe Klass
Senior EditorYaakov Kornreich
Associate Editor
Tzivia Emmer
Copy EditorIta Yankovich
Features Editor
Leah Rothstein
Children EditorDana Ledereich
Sales Director
Heshy Korenblit
Advertising SalesArthur Klass
David Hoppenwasser
Advertising CoordinatorShaindy Urman
Design Michael Kurov
Health & Living, in its sole discretion, reserves the
right to decline any submitted advertisement or to
discontinue publication of any advertisement previ-
ously accepted. The acceptance of advertising by
Health & Living does not constitute endorsement
of the services, products, or information advertised.
For subscription requests, advertising rates, gen-
eral inquiries, calendar information and schedules
contact Health & Living at 718-330-1100 ext. 352.
You may also write to: Health & Living c/o The Jew-
ish Press, 4915 16th Avenue, Brooklyn, NY 11204-
1115 or e-mail [email protected].
SUBMISSION
INFORMATION
Health & Living invites readers to submit Letters to
the Editor. Letters will be selected for publication at
the sole discretion of the editor, and may be edited
for size and content. Submissions become the
property of The Jewish Press.
Please e-mail your Letter to the Editor to HYPERLINK
"mailto:[email protected]"
Healthy Living
Okinawa Lifestyle . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
Truth about Juice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Trim and Fit – A Workout for All. . . . . . . . . . . . . . . . . 34
Flavorful Dishes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Natural Healing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
Controlling Back Pain . . . . . . . . . . . . . . . . . . . . . . . . . . 36
Raw Food Diet . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Health & Living Tech
Hair Replacement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
Demystifying Defibrillators . . . . . . . . . . . . . . . . . . . . . 39
Protecting Your Hearing. . . . . . . . . . . . . . . . . . . . . . . . 40
Health & Living Showcase . . . . . . . . . . . . . . . . . . . 42-43
Profile
Organizational Profile . . . . . . . . . . . . . . . . . . . . . . . . . . 44
Medical Profile . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
Community Profile Bulletin. . . . . . . . . . . . . . . . . . . . . 46
Community Calendar . . . . . . . . . . . . . . . . . . . . . . . . . . 47
Service Directory. . . . . . . . . . . . . . . . . . . . . . . 48-49
Picking the Right Pharmacy & Pharmacy Directory . . . . . . . . . . . . . . . . . . . . . . . . . . 48
From the Doctor’s Desk. . . . . . . . . . . . . . . . . . 50
■ Contents ■Okinawa Lifestyle
While many of us are searching for the se-cret to the fountain of youth, the residents of Okinawa, in Japan, have all the answers. Their lifestyle now called “The Okinawan Diet” shows that their longevity is the product of a health-ful diet, coupled with exercise and a productive social atmosphere.
Hair ReplacementMajority of men experience some form of
hair loss by the time they are 50. Years ago, men had few viable options for disguising hair loss, but today thanks to technological advance-ment, men have the option of being proactive beyond applying Rogaine and can consider op-tions such as: hair restoration surgery, scalp flap, and scalp reduction.
From the Doctor’s DeskA Medical director of a Pediatric ER explains
how medical errors occur in hospitals and what patients and relatives can do to minimize their occurrence.
32
38
50
FEBRUARY 2012
77
H&
L B
RIE
FS
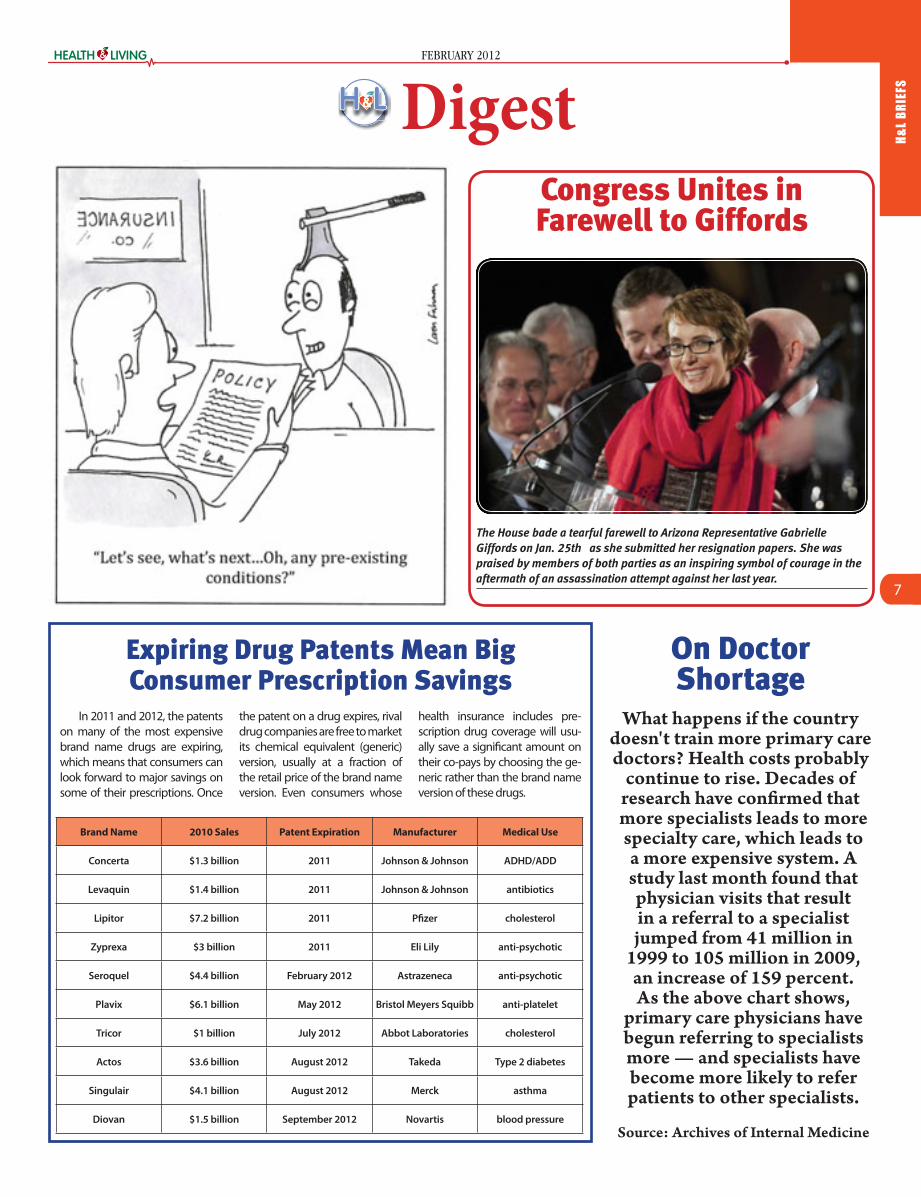
Expiring Drug Patents Mean Big Consumer Prescription Savings
In 2011 and 2012, the patents on many of the most expensive brand name drugs are expiring, which means that consumers can look forward to major savings on some of their prescriptions. Once
the patent on a drug expires, rival drug companies are free to market its chemical equivalent (generic) version, usually at a fraction of the retail price of the brand name version. Even consumers whose
health insurance includes pre-scription drug coverage will usu-ally save a significant amount on their co-pays by choosing the ge-neric rather than the brand name version of these drugs.
The House bade a tearful farewell to Arizona Representative Gabrielle
Giffords on Jan. 25th as she submitted her resignation papers. She was
praised by members of both parties as an inspiring symbol of courage in the
aftermath of an assassination attempt against her last year.
Congress Unites in Farewell to Giffords
On Doctor Shortage
What happens if the country doesn't train more primary care doctors? Health costs probably
continue to rise. Decades of research have confirmed that more specialists leads to more specialty care, which leads to a more expensive system. A study last month found that physician visits that result in a referral to a specialist jumped from 41 million in
1999 to 105 million in 2009, an increase of 159 percent. As the above chart shows,
primary care physicians have begun referring to specialists more — and specialists have become more likely to refer patients to other specialists.
Source: Archives of Internal Medicine
Digest
Brand Name 2010 Sales Patent Expiration Manufacturer Medical Use
Concerta $1.3 billion 2011 Johnson & Johnson ADHD/ADD
Levaquin $1.4 billion 2011 Johnson & Johnson antibiotics
Lipitor $7.2 billion 2011 Pfizer cholesterol
Zyprexa $3 billion 2011 Eli Lily anti-psychotic
Seroquel $4.4 billion February 2012 Astrazeneca anti-psychotic
Plavix $6.1 billion May 2012 Bristol Meyers Squibb anti-platelet
Tricor $1 billion July 2012 Abbot Laboratories cholesterol
Actos $3.6 billion August 2012 Takeda Type 2 diabetes
Singulair $4.1 billion August 2012 Merck asthma
Diovan $1.5 billion September 2012 Novartis blood pressure

FEBRUARY 2012
88
ISS
UES “End of Life” Choices:
Reading Between the LinesBy Barbara A. Olevitch
There is now a new popular literary genre - well-written, seemingly-thoughtful essays encouraging
patients and families with serious ill-nesses to choose less medical care. An example is the recent article called “How Doctors Die: It’s Not Like the Rest of Us, But It Should Be” by Dr. Ken Murray, posted on the Zocalo Public Square Blog. It suggests that most doctors are choosing not to have ag-gressive care at the end of their lives and that the rest of us should follow their example.
In America right now, the role of the doctor is to offer medical care and the role of the patient is to de-cide whether or not to accept it. By arguing that we should all do as doc-tors do, Dr. Murray seems to be sug-gesting that the doctor can play both roles.
Do doctors truly choose less care, and if they do, is there really any rea-son why we should imitate them?
Dr. Murray’s article doesn’t really prove that doctors are choosing less care. He offers his impression, but no statistical evidence to back it up.
I found some counterexamples in a book by another doctor, The Anato-my of Hope by Jerome Groopman.
Dr. Groopman tells about an ill colleague, George Griffin, who was diagnosed with a usually fatal stom-ach cancer. In spite of the fact that his fellow doctors were against it, Griffin insisted on “combining high doses of chemotherapy with intensive ra-diation.” Then he had surgery and another round of chemotherapy and radiation, despite severe, painful side effects.
After describing Griffin in a terribly weakened condition, Dr. Groopman surprises the reader with an amazing scene that occurred 13 years later. Griffin is still alive and Dr. Groopman meets with him to ask him about his decision to take all those treatments that weren’t expected to cure him.
Griffin said that he knew everyone disagreed with his decision to take treatment.
“I knew all the arguments made in cases like mine. Treatment would cause unnecessary suffering - for me and for my family. Add in that it throws away society’s money on a doomed person . . .I find these argu-
ments patronizing . . .I, of course, had a crystal-clear understanding of my chances. And it was my right to choose what I did.
“Even if I didn’t prevail . . .I deeply wanted to live, so I had to fight. Then I could tell myself that I had tried, that I had done everything possible. There would be no regrets.”
Dr. Groopman also tells the story of Richard Keyes, another doctor with
a serious tumor. He had surgery but resisted the idea of taking radiation therapy afterwards.
Keyes eloquently expressed his skepticism, “I won’t be strung along...What - get dragged down to radiation every day, come back feeling sick as a dog? ...And when that’s over, everyone can say that they tried their best and then tuck me in my coffin with a clear conscience.”
But his physician, Dr. Andrews, was not inhibited by the fact that Keyes was a medical expert. He offered him arguments to accept the treatment. He emphasized to him that although cure was not likely, it could occur.
Keyes, despite his eloquently ex-pressed skepticism, went through with the radiation therapy, and al-though it was difficult, it did work. He was cured.
Another counterexample is partic-ularly striking because it concerned a palliative care doctor. Anemona Har-tocollis wrote in the New York Times on April 4, 2010 about Dr. Desiree Pardi.
Hartocollis wrote, “While she and her colleagues had been trained to talk about accepting death, and mak-ing it as comfortable as possible, she wanted to try treatments even if they
were painful and offered only a 2 per-cent chance of survival. When the usual cycles of chemotherapy failed to slow the cancer, she found a doctor who would bombard her with more.”
Even if Dr. Murray is right in claim-ing that more doctors choose to avoid aggressive care, does this necessarily mean that we should emulate them? Could such a bias against aggressive treatment be a result not of the su-
perior knowledge they gained from their practice but, rather, of the pres-sures that they endure or of their over-exposure to the stress of treatment? Must we accept Dr. Murray’s implica-tion that doctors rejecting aggressive treatment for themselves are mak-ing rational decisions on the basis of their superior knowledge? Perhaps it would be more accurate to view them as ordinary human beings whose ill-ness is even harder to bear because of their background.
There is a popular saying, “Doctors make the worst patients.”
There is much evidence that doc-tors do experience a high level of stress in their occupation.
Dr. Pauline W. Chen wrote in the New York Times on October 7, 2010 that “for several decades now, studies have consistently shown that physi-cians have higher rates of suicide than the general population - 40 percent higher for male doctors and a stag-gering 130 percent higher for female doctors.”
There are all sorts of theories that seek to explain the elevated rates of depression and suicide among medi-cal students and doctors, but the most important point for our discussion
is how depression affects decision-making. When someone is depressed, even the ordinary pressures of life seem too much. A depressed patient may find it too much trouble to get dressed or comb his hair, much less undergo a difficult course of chemo-therapy!
It is a normal part of medicine to take note of a patient’s depression and to treat it if necessary. But when the patient is a doctor himself and he expresses his desire to quit, those around him may be too awed by his medical expertise and his dignified bearing to realize that he needs en-couragement, and, that in fact he may, because of his experiences, need even more help than the average patient.
The biggest trouble with Dr. Mur-ray’s essay is that it implies that there is one right path and that it is always better to choose less care. This tends to minimize the real dilemma in mak-ing such decisions, namely the uncer-tainty of the outcome.
In Judaism, we believe that every moment of life is precious and that it is meritorious to maintain hope. The doctor is our helper but not our ut-most authority who we must imitate. We think that while the doctor can help the patient find out what care is available, it is the role of the Rabbi to help the patient decide which care should be accepted. Even in the case of a dying patient whose Rabbi has ruled that the patient is not obligated to accept a certain treatment because of its limited effect and the suffering involved, we still believe that it would be wrong to make the patient feel that he is being foolish or selfish if he chooses to continue fighting against his illness.
There is no denying that in today’s American culture, it is the “in” thing to talk about discontinuing medical care. But as Jews, we have to maintain our own cultural atmosphere and talk to each other in ways that acknowledge the unpredictability of life and death, which are in Hashem’s hands. We must not discourage our ill loved ones or bias their important decision-making by allowing them to be drawn into the fashionable pessimism of the culture that surrounds us.
Barbara A. Olevitch, Ph.D., is a clinical psy-
chologist living in St. Louis, Missouri, and
author of Life is a Treasure: The Jewish Way of
Coping with Illness (Targum Press).
In Judaism, we believe that every moment
of life is precious and that it is meritorious
to maintain hope. The doctor is our helper but
not our ultimate authority who we must imitate.
FEBRUARY 2012
99
ISS
UESMedicine’s Newest Tool
in Genetic AnalysisBy Yaakov Kornreich
Less than a decade after scientists first se-quenced the first complete human genome — the DNA’s genetic instructions for making
all the body's cells — the bioscience industry is working to offer doctors and hospitals the ability to analyze a person’s entire genome and to in-terpret its medical significance at a low enough cost to make it a routine medical diagnostic test.
The DNA scanning technology has already been mastered, and the main challenge now is to develop software that can analyze a person’s complete DNA sequence quickly and identify which anomalies may be causing their medical condition. The problem is the huge amount of genetic information that needs to be processed. Each person's DNA chain, made up of the four different chemical bases of DNA, called A, C, G and T, contains 6 billion components, which can differ from "normal" at more than 3 million points. Doctors are still learning the full medical significance of most of those variations.
That information could revolutionize the treatment of genetically-related diseases. Har-old Varmus, director of the National Cancer In-stitute, said that genetic sequencing analysis is, “the biggest change I've ever seen in oncology. Doctors are taking genetic information they see in patients' tumors and changing therapy in dra-matic ways."
Biotechnology companies are now develop-ing small, user-friendly DNA sequencers with software that doctors can use to diagnose and treat specific diseases. One of the new machines is the size of an I-pod and can be used to test patients for infections and drug responses.
Martin Reese, the CEO of one of these com-panies, Omicia, described his goal. "We're taking a process, hand annotation of the genome, that can take up to six months to do, and automating it so that it takes just a half hour or an hour."
At his office, Jay Flatley, the CEO of Illumina, demonstrated an Apple iPad loaded with an ap-plication that displayed his own genome. He quickly skipped from screen to screen filled with, text and color icons, stopping at one describing a gene that determines his body’s response to the blood-thinner warfarin. "I'm in the high-sen-sitivity category, so I should get a lower dose."
The potential of the new technology was dramatically demonstrated by Joe Beery, an in-formation technology expert working for Life Technologies Corp. With the help of his compa-ny’s DNA sequencers, researchers at Baylor were able to correctly diagnose his 12-year-old twins, Alexis and Noah, after standard diagnostic tech-niques had failed.
The twins suffered from recurring vomit-ing, muscle weakness, seizures, and occasional breathing difficulties. They had been misdiag-nosed at age 2 with cerebral palsy, but the stan-
dard treatments did not work. When they were 5 1/2 years old, their mother, Retta Beery, learned of a rare disorder of the nervous system called a "dystonia" caused by a deficiency in the chemi-cal dopamine that seemed to fit.
At first, the standard drug treatment for dys-tonia seemed to help, but the eventually some of the symptoms returned, especially for the daughter, Alexis. In 2009, after more diagnostic tests failed to reveal any more clues, the Beery’s turned to Joe’s company for help. It put the Beer-ys’ in touch with a team of doctors and scientists at Baylor College of Medicine's Human Genome Sequencing Center in Houston. They decoded the twins’ DNA sequence by hand, a process that took two months, with Joe’s company and Baylor research funds covering the cost.
The analysis revealed that the children also had a second genetic condition that interfered with another chemical in the nervous system called serotonin. When the standard pharmaco-logical substitute for serotonin was administered to the Beery twins, their symptoms disappeared completely.
Recently, Life Technologies introduced a new $150,000 machine capable of sequencing an en-tire human genome in a day for about $1,000, less than the typical cost of a colonoscopy, and is marketing it to hospitals, clinics and testing laboratories as well as researchers.
The Beerys said that while they had always prayed for guidance, they never dreamed that the answer to their children's health mystery would arise from his job. "Genome sequencing literally saved her life," Retta Beery said."The fact that I ended up where I ended up, you have to believe those prayers were answered," her hus-band added.
But other obstacles still loom before this DNA diagnostic technology becomes generally avail-able to patients who are not the subject of clini-cal research studies, or capable of paying for the sequencing and analysis out of pocket.
Health insurers are already expressing re-luctance to cover the cost of full genome se-quencing and analysis, even if it is just $1,000. According to a spokesman for America's Health Insurance Plans, an industry umbrella group, in-surers will first demand much more proof of its accuracy and utility in improving the outcome of medical treatment.
Thus, once again, after medical science has given us a new and more effective tool to fight disease, patients will either need to wait, pay for it out of their own pockets, if they can, or wage another battle with the health insurance system to reap the same benefits that the Beery twin have gained from it.
Yaakov Kornreich is a veteran Anglo-Jewish journalist. He is
the Senior Editor of Building Blocks, published by the Jewish
Press, and this Health & Living supplement. He can be con-
tacted at [email protected].

FEBRUARY 2012
10
RA
ISIN
G O
UR
CH
ILD
REN
10
Kid Snack Attack!By Ita Yankovich
Snack is under attack in America. Mayor Bloom-berg and even First Lady Michelle Obama are on a mission to eliminate unhealthy snacks from
our schools’ lunches, vending machines and even grocery lists. American kids snack three times a day on chips, candy and other junk foods which now ac-count for more than 27 percent of children’s daily caloric intake, according to a recent study. Kids’ fast paced- lifestyle often make them prefer grazing on small snacks rather than consuming 3 solid meals.
Many Americans don’t appreciate politicians getting involved in their family’s eating patterns, but the fact remains that in the U.S alone at least 1 in 5 kids is overweight and the numbers continue to grow. Because most children do not purchase their own food, we have to look toward parents and caregivers as to why this epidemic exists. These days, many households do not have sit-down fam-ily dinners. That is because the parents are too busy working overtime trying to make ends meet, tak-ing care of elderly parents, running errands after work, and shuffling children to afterschool activi-ties to prepare proper meals for their families. To
satisfy their parental guilt, they often decide that the easiest way to remedy the problem is by allow-ing their children to eat convenient, high-calorie snacks to satisfy their cravings and eliminate com-plaints.
Government surveys from the mid-2000’s show that the average American ate 2,375 calories a day, one third more than in the late 70’s. The biggest contributor to this increase has been the rise in the number of snacks people eat a day. Americans have gone from eating 3.8 snacks and meals a day to 4.9 on average.
Many parents have also been confused by sur-prising reports which found that adolescents who ate more snacks were less overweight and had a higher energy level than those youth who ate few-er snacks. In a recent government survey of 5,800 teenagers, it was reported in the American Journal of Clinical Nutrition that the rates of obesity went down as the number of snacks the kids ate each day went up.
Clearly the debate will continue, but in the mean time we have to be smart about how and what we allow our kids to snack upon.
Kids are not going to eat healthy foods on their own; why should they choose trail mix and broccoli when they can eat an assortment of neon-colored, bubblegum-flavored snacks? So it is our job to help them make wiser decisions.
When introducing a new healthy snack, studies recommend that just by telling your kids that the new food tastes good rather than “it is good for them” will improve the chances of success. Many children will reject a food without even tasting it if they see the word ‘healthy’ on the food packaging, because they assume it will taste bad.
It is better to let kids be kids, and allow them to enjoy their favorite treats once in a while. Many par-ents are more relaxed about healthy food choices on Shabbos and Chagim for example, and let their kids eat their favorite nosh from the store or drink a little soda as a Shabbos treat, knowing that the more you make unhealthy food off-limits, the more kids will be tempted to eat them.
Children are also more likely to eat foods they had a hand in preparing it. Experts suggest set-ting aside time on the weekend or evenings when parents and kids together can prepare snacks for the week ahead. This not only establishes quality time, but also creates a stock of healthy after-school snacks that will be readily accessible when they feel the urge to snack. By giving children a sense of own-ership over the healthy snacks they have created, we also make them more likely to eat them.
The Center for Science in the Public Interest has published a list of some of the nutrition-ally worst popular snacks on the market today. They are: Chips Ahoy!, Oreo cookies, Pepsi and Coca-Cola, artificial fruit juices, Hostess snack cakes, and Keebler Club & Cheddar Sandwich Crackers. The group also listed the nutritional-ly worst candy bars, citing Kit Kat Big Kat and Snickers, along with Starburst Fruit Chews. Below are some of the worst and best snacks.

FEBRUARY 2012
1111
RA
ISIN
G O
UR
CH
ILD
REN
Worst Snacks• Potato chips- The problem with most chips is that
they are addictive. The old TV commercial was right -- usually you can’t just eat one. Most 1oz bags of chips have 225 calories and very little real nutri-tion. When eating chips, your child is just consum-ing fat, carbs and hydrogenated oils and salt. Po-tatoes in general are healthy and are loaded with potassium, but a much better way to get those benefits would be by eating a baked potato.
• Cookies-Cookies and milk used to be a staple snack for kids coming home from school, but to-day we know that it is a bad choice since most cookies are loaded with sugar and little nutri-tional value, and the amount of butterfat in whole milk is unhealthy for all children over the age of 2.
• Chicken nuggets- There is too little chicken in these treats and too much deep-fried bread, fat and so-dium.
• Cereal- Don’t be fooled by misleading claims of “whole grain” or “High in Fiber” or “Rich in Vi-tamin D” on your kids’ sweetened cereal boxes. ABC News reported that a shocking 44 children’s cereals contain more than 11 grams of sugar per serving. In fact, only a quarter of today’s cereals meet voluntary proposed guidelines of the feder-al Interagency Working Group on Food Marketed to Children which, recommends no more than 26 percent added sugar by weight. Good cereal choices are Cheerios, Cornflakes and Kix.
Best Snacks• Cut up Fruit/veggies-Kids often will reject this so
make it interesting by cutting it in fun shapes and sizes and offering a side dip like hummus, guaca-mole or homemade salsa
• Crackers- Whole wheat crackers are best especially when spread with peanut butter, ‘real’ cheese or hummus.
• Yogurt-Yogurt supplies lots of calcium--275 to 450 milligrams per 8-ounce container. Look for brands that do not contain NutraSweet or aspartame, choose those with “live and active cultures,” which are beneficial bacteria for your child’s intes-tines.
• Nuts and Raisin Mix-Kids love small crunchy foods (think BBQ twists) so replace that with an assortment of seeds and nuts. Seeds are high in fat but they are ‘healthy unsaturated fats.’ Sunflower seeds are a good choice. The US Journal of Agricultural and Food Chemistry reports, sunflower seeds proved to be the best source of phytosterols — as well as being a good source of magnesium, iron, copper, manganese, and vitamin E. Add some raisins into the mix for some sweet flavor and you’ve just increased their potas-sium and iron intake for the day.
• Popcorn - Popcorn is a good source of fiber, car-bohydrates, and rich in antioxidants, plus your kids will love watching and hearing it pop! You can make it in the microwave or do it ‘old school’ in a non-stick sauce pan. When making or buying pop-corn, keep it healthy by avoiding the addition of butter, oil or salt. One cup of air popped popcorn has only 30 calories.
Ita Yankovich teaches English Literature and Writing at
Kingsborugh and Touro College. She is also a freelance
writer who has authored several articles in various publi-
cations. She can be reached at [email protected]
Best and Worst Snacks
Educating the next generation of health care professionalsExplore our programs in:NURSING Associate in Applied Science —Brooklyn*
OCCUPATIONAL THERAPY BS/MS—Bay Shore, Manhattan
OCCUPATIONAL THERAPY ASSISTANT Associate in Applied Science—Manhattan
PHYSICAL THERAPY BS/DPT—Bay Shore, Manhattan
PHYSICIAN ASSISTANT BS/MS—Bay Shore, Manhattan, Mineola
SPEECH-LANGUAGE PATHOLOGY Master of Science—Brooklyn
* A portion of this program must be taken in Manhattan.
Plus we off er baccalaureate degree programs in BIOLOGY and PSYCHOLOGY
through the Undergraduate Studies Department in Bay Shore
Touro College is an Equal Opportunity Institution
BAY SHORE CAMPUSPrograms represented include: Occupational Therapy, Physical Therapy,
Physician Assistant-Long Island, Undergraduate Studies-Psychology, Biology
1700 Union Blvd., Bay Shore, NY 11706
MANHATTAN CAMPUS Programs represented include: Nursing, Occupational Therapy, Occupational Therapy
Assistant, Physical Therapy, Physician Assistant-Manhattan, Speech-Language Pathology
27 West 23rd St., 6th Floor, New York, NY 10010
INFORMATION SESSIONS FOR 2012-13 ACADEMIC YEAR
INFORMATION SESSIONS WILL BE HELD FROM 6PM-7:30PM. SIGN-IN BEGINS AT 5:45PM, AND PRESENTATIONS BEGIN PROMPTLY AT 6:15 EACH NIGHT.
FOR MORE INFORMATION:
CALL 1-866-TOURO4U
OR VISIT TOURO.EDU/SHS
FOR MORE INFORMATION:
CALL 1-866-TOURO4U
OR VISIT TOURO.EDU/SHS

FEBRUARY 2012
1212
RA
ISIN
G O
UR
CH
ILD
REN
Twins Are MultiplyingBy Amy A. Dubitsky
Having twins used to be a novelty. Now, if you think that you are seeing double everywhere you go, it is not your imagination. The National
Center for Health Statistics (NCHS), under the aus-pices of the Centers for Disease Control and Preven-tion (CDC), published a study last month noting the sharp increase in twin births over the past three decades. According to the study, the twin birth rate rose 76% from 1980 through 2009. In 1980, one in every fifty-three babies was a twin. In 2009, one in
every thirty babies was a twin. This study did not ad-dress births of higher multiple pregnancies.
Dr. Michael Feinman, a fertility specialist at HRC Fertility in the Los Angeles area, says that the increase in twin births “is not a natural occurrence, but due to assisted reproductive technology and women giving birth at an older age.” Dr. Feinman explained that one reason for this is that after age 35, women naturally produce higher FSH levels, which is the hormone that is used in fertility treat-ments. The higher levels of this hormone increase the incidence of twin births. According to the CDC study, this only accounts for about one third of the rise in twinning over 30 years.
Another reason for the increase in twinning is as-sisted reproductive treatments. Many eggs are no longer viable for pregnancy in women over age 35, and they are unsuccessful in getting pregnant on their
own. The fertility treatments used often result in twin or higher multiple births. While ovulation stimulation medications, which are hormones taken by women to increase the chance that they will get pregnant, have no control over the number of embryos produced, Dr. Feinman is pleased that the medical field has been able to cut down on the number of triplet births caused by in vitro fertilization (IVF). When women use IVF, the doctor selects the number of embryos implanted. The method has been advanced to a level that, according to Feinman, “in a generally healthy women under the age of thirty-five, two embryos would be implanted on day three of their cycle or one embryo on day five
of their cycle. There is a growing body of evidence to prove that implanting more than one embryo in some scenarios does not increase the pregnancy rate.”
Dr. Feinman doesn’t recommend planning a twin birth and his view is reinforced by the findings of the CDC. “Thinking that you are saving money on additional procedures by having twins is a fallacy. Other medical expenses usually accompany mul-tiple births as well as other long-lasting problems. Fifty percent of the time, twins are born premature, and the incidence of cerebral palsy is eight times higher in twins than [in] single births, and forty times higher in triplets.”
He also points out an increase in divorce rate in parents of multiples.
When selecting a doctor for reproductive as-sistance, many patients ask for the doctor’s success rate. Dr. Feinman explains that doctors use the “clini-
cal pregnancy rate,” which is when a heart beat is de-tected on an ultra-sound monitor. It doesn’t account for those patients that have miscarriages at 18 or 20 weeks gestation, which are more frequent with twins.
The study by the CDC was done to evaluate the elevated health risks and accompanying greater health care costs due to twin births. Of the 865,000 twins born during the 1980-2009 study period, over 50% were low birth weight, and one in ten were very low birth weight.
Dr. Feinman works closely with the Puah Insti-tute, a non-profit organization that assists couples facing infertility, and guides them on how to pro-
ceed with treatments in accordance with Jewish law. He understands the emotions involved when couples are having difficulty getting pregnant, but makes the following recommendation: “Women un-der age thirty-eight who have not been successful in getting pregnant for six months should see a doctor, just for testing. If there is an obvious problem that can be corrected, there is no reason to wait longer. If there is no obvious problem, I recommend waiting a year before resorting to treatment. In women over 38 it would be [on] a case by case basis.”
Couples facing infertility should consult with their personal physicians and Rabbis for guidance. And if twins are on the way- you should all be blessed with good health and an easy delivery.
Amy Dubitsky is a freelance writer and marketing professional
in Phoenix, AZ.

FEBRUARY 2012
1313
RA
ISIN
G O
UR
CH
ILD
REN
The Sunshine Vitamin
By Dana Ledereich
Vitamin D is critical for healthy bone development and for a healthy immune system. Vitamin
D enables the body to absorb calcium and thereby fosters bone growth and strength. Insufficient vitamin D can cause anemia and increased suscepti-bility to a variety of illnesses.
Vitamin D is naturally available in certain foods including beef liver, egg yolks and fatty fish such as salmon and sardines. It is also available in vitamin D-fortified foods including certain milks and cereals.
Vitamin D is produced by the body when the skin absorbs ultraviolet rays from the sun, which is why Vitamin D is known as the “sunshine vitamin.” Sunshine is the body’s main source of vitamin D. It can produce all of the Vitamin D it needs with just ten min-utes outdoors, with exposed skin on the face and arms, three times a week, between 11-2 PM. Vitamin D defi-ciency is a byproduct of the industrial age, when people went from spend-ing most of their day outdoors work-ing in the fields or on farms to largely working indoors in stores, offices and factories.
The use of sunscreen has made it more difficult to get vitamin D from spending time outdoors. An SPF of 8 has been found to reduce vitamin D production by up to 95 percent! While the critical importance of sunscreen as a protection against skin cancer can-not be overstated, it does have a nega-tive impact on vitamin D production.
The body’s vitamin D production typically falls during wintertime as well. That is because much less time is spent outdoors, and when we do go outside, more of our skin is covered to protect against the cold, and not exposed to the sun’s ultraviolet rays that it needs to produce vitamin D. It is important for parents to provide their children with alternate forms of vita-min D during this time. Meals should include foods that are natural sources of vitamin D or that are fortified with vitamin D. Also, the time spent out-doors in the spring, summer and fall months does enable the body to de-velop a reserve of vitamin D to support the body through the winter.
People who cover their skin for modesty or cultural purposes are also at a greater risk for vitamin D deficien-
cy. They should make sure they ingest enough vitamin D through natural and fortified food sources to make up the difference.
Even babies in-utero need vitamin D. The growing fetus draws the vita-min D from its mother. If a pregnant woman does not have enough vita-min D, it places the fetus at risk for vi-tamin D deficiency. Pregnant woman should be vigilant in their vitamin D consumption to ensure better health of their growing baby.
Breastfed babies are also at risk for vitamin D deficiency. As baby skin is sensitive and delicate, it is not safe for a baby to spend time outdoors with exposed skin. If breast milk is the sole source of a baby’s nutrition, consult a pediatrician about vitamin D supple-mentation. Most infant formula is for-tified with enough vitamin D to meet a baby’s needs.
Vitamin D deficiency causes rick-ets, which is a softening and weak-ening of the bones in children. Doc-tors have known for years about the importance of vitamin D for bone growth and bone density and its importance in preventing fractures. More recently, they have discovered the importance of vitamin D to im-mune system health.
Vitamin D is crucial for people of all ages – from fetuses in-utero to older adults. Deficiencies in adults have been linked to osteoporosis, certain cancers, heart disease and diabetes. In children, in addition to rickets, vita-min D deficiencies have been linked to stunted growth, muscle weakness, anemia and increased susceptibility to infections such as pneumonia.
While the cold winter weather lasts, make sure to consume foods with higher amounts of vitamin D. Be-fore you know it spring will be here. Then you can go outside, get some fresh air and make your own Vitamin D!
Dana Ledereich, MA, OT/L is a pediatric oc-
cupational therapist who works in Yeshiva
of Flatbush and also maintains a private
practice. She evaluates and treats children
age birth-13 years with sensory processing
issues, poor handwriting, developmental
concerns and neurological issues. She has
lectured to both parents and professionals
on various topics in sensory processing and
handwriting development. She is available
for lectures as well as to mentor new thera-
pists. She can be reached at 718-252-2939.
718.629.1000
5350 KINGS HIGHWAY
BROOKLYN, NY 11203
WWW.REVIVALHHC.ORG

FEBRUARY 2012
1414
RA
ISIN
G O
UR
CH
ILD
REN
Helping Children with Health Challenges Develop Healthy Self-Esteem
By Melanie Kwestel
There’s no doubt that a diagnosis of serious medical illness compli-cates both a child’s emotional de-
velopment and the family’s dynamics. But even the most serious illness or disability is not a barrier to developing the healthy sense of self that children require to reach their potential.
Clinical psychologist Rabbi Dr. Jer-ry Lob addressed the challenges faced by families of chronically ill children at Chai Lifeline’s LH Financial Services Annual Winter Family Retreat. The event, held in January, brought more than 350 parents, patients, profession-als, and volunteers together to share outlooks and strategies.
Dr. Lob outlined what he called the “three ‘S’s of parenting and family growth,” which is an appropriate strat-egy for all families.
SafetyIn addition to physical safety
(knowing and feeling that their par-ents are providing for their needs), children feel safer when they are confident that they can express their feeling and concerns to their par-ents.
“Children need to feel that their opinions matter,” Dr. Lob stated. “They don’t need a vote (in how the household is run), but they do need a voice. They need to feel that they will be heard.”
Taking the time to listen and ac-cept the feelings of all the children in a family is important as well. Dr. Lob related the story of a sibling of a child with special needs who was never allowed to express negative feelings.
“At first I thought he was exag-gerating when he told me that he was not allowed to be negative. But when I spoke to the mother, she con-firmed his statements. She felt that her healthy son’s life could never be as ‘bad’ as that of her special needs child. Therefore he could never express sad-ness or anger about his situation.”
The child’s anger eventually led him off the derech and into dangerous behavior. For all intents and purposes, the young man was lost to his family.
StrengthChildren need strong parents who
set appropriate boundaries with both
rewards and consequences. Parents should be unified and confident in the decisions they make for their families. Children feel safer when they under-stand the limits in which they and their families function.
Strong and close relationships with each child are critically impor-tant. While it is natural for parents to spend more time caring for their sick child whose condition requires it, mothers and fathers need to be aware and responsive to the needs of their other children as well.
“The amount of time you spend
with each child won’t be the same,” Dr. Lob cautioned, “but both mothers and fathers should make time for each child and engage him or her in the most ap-propriate way for that child. For some, it may be learning together; for others, it could be having a catch outside.”
Strong parents make demands of their children based on realistic as-sessments of their children’s abilities. Children do not have to be perfect, but they do need to feel that they can and will live up to their parents’ expec-tations for them.
“Treating a child who is ill or who has any kind of special need as being less than capable in the areas where they can succeed is a disservice. Reaching for a goal will help a child develop self-esteem.”
Dr. Lob emphasized that self-es-teem is directly related to strong par-enting. “Strong parents,” he said, “help build self esteem.” He outlined three strategies parents can use to promote
healthy self images in their children:Give real compliments. Compli-
ments that reward children for real accomplishments encourage children to reach for the next level. Look for be-haviors and achievements to compli-ment, and be generous with praise.
When it comes to criticism, choose your battles. Dr. Lob recalled a conver-sation he had with Rabbi Yechiel Michal Twerski. He asked how Rabbi Twerski’s parents had managed to raise children who had achieved so much in their lives. “Our parents were half-blind,” Rabbi Twerski replied. “They didn’t no-
tice every silly thing we did. When they critiqued, it was constructive.”
“Have less of an ayin ra and more of an ayin tov,” said Dr. Lob. “Catch your children doing good.”
Set realistic, achievable goals, but don’t sell your children short. Children develop self-esteem when they go be-yond what they thought they could do. Feeling good about themselves comes from liking what they see when they look in the mirror. While parents should not have unrealistic expectations of any of their children, they need to be particularly in tune to children who have physical, emotional, or academic challenges and help them meet their goals. Don’t let children off the hook. It can create resentment among siblings, and in the final analysis, will lower the child’s self esteem.
SimchaCreate an environment of Simcha
within your home. Look for ways to
spend time together as a family, for example, by reserving some Shabbos meals that will be “family only” time.
Understand and respond to your children’s unique abilities and per-sonalities. Dr. Lob recalled a rabbi who has two autistic children. Every day he comes home, turns on music, and dances with these two children, bringing simcha to their lives, and to his own.
Parents also need to find time for themselves and to strengthen their marriage. Children feel more simchak-dik when parents really care about each other. Each parent must do something that she or he enjoys, and couples need to find ways to have fun with each other. There’s no question that it is more challenging to find time for oneself and one’s spouse when parenting a child who is ill or disabled. But children are happier when they can see that their parents get along and are happy together.
One of the ways that we as Jews create simcha in our lives and our homes is through our belief in Hash-em. Remind your children and your-self that Hashem loves us and remains with us throughout our travails.
Dr. Lob illustrated the concept with a d’var Torah from Harav Chaim Shmulevitz. When our forefather Yosef was sold into slavery by his brothers, he was transported in the caravan of a spice dealer. Rashi stated that the caravan usually carried foul-smelling goods, and that the presence of besa-mim comforted Yosef. Though his life had taken a disastrous turn, and he was worried about his father and the future of klal Yisrael, the sweet, famil-iar odor was a comfort to him. Harav Matisyahu Solomon added that Yo-sef took their presence as a sign that Hashem was still with him.
The message to us is not to be oblivious to the positive signs that Hashem sends us. Though it is often a struggle for parents to raise children with the self-esteem necessary to succeed in life, our mission is to see the signs that Hashem has not for-saken us and to smell the besamim in our lives.
Melanie Shimoff Kwestel is the director of
communications for Chai Lifeline. Chai Life-
line provides emotional, social, and financial
support that enables families of seriously ill
children to cope with crises and daily chal-
lenges of pediatric illness.

FEBRUARY 2012
1515
RA
ISIN
G O
UR
CH
ILD
REN
See how much more we all can do this year.
365 days a year
24 hours a day,
through good days
and sad times,
Chai Lifeline
makes living
with pediatric
illness easier.
Last year,
Chai Lifelinebrought
joy and hope to
4,297lives impacted by
pediatric illness.
Become a partner.
45,621 Meals to hospitals and homes
20,938 Visits to sick children by trained volunteers
22,981 Rides to hospitals and medical centers
36,229 Opportunities for fun and support
1,961 Hours of professional tutoring
1,267 Hours of counseling
3,873 Trained, compassionate volunteers
263 Family days, holiday parties, recreation events and retreats
204 Crisis intervention workshops in schools, camps, and communities following tragedies
8 Weeks in Camp Simcha and Camp Simcha Special, “the happiest place on earth” for children with cancer or chronic illnesses.
Regional Offices California | Florida | Illinois | New Jersey | Canada | England | Antwerp | IsraelChai Family Centers Brooklyn | Long Island | New York City | Monsey | Chicago | N. Miami BeachChai House Philadelphia Goldman River Retreat Mahwah
151 West 30th Street, New York, NY 10001
(877) CHAI-LIFE (212) 465-1300www.chailifeline.org
Helping the child, the family, and the community
Exercise and Academic Performance
By Dana Ledereich
Recent studies have confirmed what occupational therapists have been saying for years:
Physical exercise has a positive ef-fect on academic performance.
The amount of time allotted to physical education during the school day has declined over the years. Decreasing school budgets and increased pressure from stan-dardized tests have forced many schools to cut down or even elimi-nate physical education class from the curriculum in favor of more class time. However, studies show that this policy does not result in better academic performance. In some cases, more time in physical education class has led to improved grades overall and improved test scores on standardized exams. In controlled studies, children who increased their physical activity through physical education class or other school-based physical activ-ity either maintained or improved their scores on standardized tests even though they received less classroom instruction than children in the control group.
More and more American chil-dren are classified as obese. Some would even argue that childhood obesity has reached epidemic pro-portions. While some of the blame can be placed on processed food and on larger food portions, de-creased physical activity plays a strong role as well. Children spend more time in front of a computer screen or texting on a cell phone than they do playing organized sports or just playing on the play-ground. There have been initiatives designed to encourage schools to serve healthy food in more appro-priate portion sizes, but many of these same schools have cut back on physical education classes and thus deprive their students of regu-lar physical exercise.
The exact relationship between physical activity and academic per-formance is not fully understood, but physically fit and active children tend to demonstrate better academ-ic achievement. It has been suggest-ed that exercise increases the flow of blood and oxygen to the brain. Exer-cise has also been found to lead to
increased levels of norepinephrine and endorphins, substances that are important for reducing stress.
Regular, intermittent breaks for physical exercise can also have a positive effect on overall behavior and concentration. This exercise can be in the form of jumping jacks near the students’ desks, wall push-ups, or simply walking around the desk a few times. Rather than creating a chaotic environment, the physical exercise stimulates better attention. For children more challenged by a decreased attention span, occupa-tional therapists often recommend an air-filled seat cushion or a ball chair -- Both these options provide opportunity for movement to en-hance the student’s ability to attend to the lesson.
Incorporating physical exercise into the school day is especially challenging during the winter. Dur-ing recess, the cold weather forces students to remain indoors in their classrooms. Although they may be allowed to stand or eat a snack dur-ing this 10-15 minute break, there is no opportunity for physical exercise. Teachers would be best advised to keep some jump ropes and Chinese jump ropes in the classroom for these times. Balloons also come in handy as a safe alternative to balls and are a fun way to provide physi-cal exercise within the confines of the classroom.
In this era of increased empha-sis on standardized test scores, schools would find it advantageous to increase the emphasis on physi-cal education and exercise during the school day. Moreover, if teach-ers provide opportunities for physi-cal exercise within the confines of their classroom, they can expect improved classroom behavior and performance.
Dana Ledereich, MA, OT/L is a pediatric oc-
cupational therapist who works in Yeshiva
of Flatbush and also maintains a private
practice. She evaluates and treats children
age birth-13 years with sensory processing
issues, poor handwriting, developmental
concerns and neurological issues. She has
lectured to both parents and profession-
als on various topics in sensory process-
ing and handwriting development. She is
available for lectures as well as to mentor
new therapists. She can be reached at
718-252-2939.

FEBRUARY 2012
1616
RA
ISIN
G O
UR
CH
ILD
REN
Advocates Fear a Proposed Redefinition of Autism
By Yaakov Kornreich
The American Psychiatric Asso-ciation (APA) has come up with a controversial new definition
for autism, which is scheduled to be published by the end of this year in the fifth edition of its Diagnostic and Statistical Manual of Mental Disor-ders. Widely known as the DSM, it is the medical establishment’s "bible" for all psychiatric diagnoses. While the new definition has not yet been finalized, its outlines have already taken shape. Those familiar with work of the APA’s working committee of autism experts say that they have reached a broad consensus on doing away with the three distinct subtypes which were defined in the fourth edi-tion of the DSM, published in 1994, as autism, Asperger Syndrome, and Pervasive Developmental Disorder-Not Otherwise Specified, widely known as PDD-NOS.
In the fifth edition, already known as DSM-5, there will be only one rec-ognized diagnostic category -- au-tism spectrum disorder -- that would replace the three current subtypes that, taken together, are already widely referred to as the autism spec-trum. This will not just be a change in terminology. The committee is also changing the criteria that is currently being used by mental health prac-titioners to diagnose children with one of the three currently recognized subtypes, in an effort to give an au-tism diagnosis greater precision.
The estimated rate of autism for children in the United States has sky-rocketed since the definition was changed in the DSM-IV. Using the di-agnostic criteria established in 1994, the rate of autism has been measured to be as high as one in every 110 chil-dren, many times the rate observed before those criteria were set. Some experts say that the sharp increase in the number of autism cases now being
diagnosed is authentic, and a cause for serious concern. Others contend that it is the result of the subjective nature of the diagnostic guidelines in the DSM-IV, which encourages mental health professionals to label more borderline cases to be one of the three autism spectrum subtypes than they would have under the pre-1994 guidelines.
There are also the autism skeptics who suggest that mental health prac-titioners are diagnosing more cases today because autism is in the head-lines. As a result, more parents are bringing in their children for screen-ing at a much younger age, when the symptoms of autism are much more ambiguous and difficult to interpret.
According to Geraldine Dawson, the chief science officer for Autism Speaks, and a professor of psychiatry at the University of North Carolina, "This is not an academic exercise. These changes in the diagnostic cri-teria will have a real impact on peo-ple's ability to obtain services."
According to Dawson, at least two studies of the new definition be-ing proposed for DSM-5 show that it would sharply decrease the number of people who would be diagnosed with autism in the future, and who would therefore become eligible for health, educational and social servic-es from the government. According to a presentation at a recent meeting of the Icelandic Medical Association, less than half the children who were diagnosed with autism in a 1993 study would qualify under the new proposed new DSM-5 criteria.
For example, under the DSM-IV criteria, a mental health professional would have to identify impairment in only three of eight categories to con-firm an Asperger’s diagnosis, while under the proposed DSM-5 defini-tion, an impairment in five of seven categories would be necessary.
Dawson says that under the new definition, far fewer higher functioning individuals, including many now diag-nosed with Asperger syndrome, would meet the autism spectrum disorder criteria. She agrees that the DSM-IV cri-teria do need updating because there is no clear differences between the three currently recognized subtypes as to their likely causes or recommended treatments. But she adds, "We have to keep in mind the real-world implica-tions. In particular, we have to be very
careful that through this process that we're not excluding people from receiv-ing services that they need and deserve."
In addition to making it harder to diagnose new cases, parents of chil-dren already diagnosed with disorders on the autism spectrum and receiving treatment for it, worry that the DSM-5 definition might cause them to lose that designation, and the insurance and government benefits that go with it.
Members of the APA's autism working group say that they are con-fident that their new definition and diagnostic criteria will not disqualify those who are truly autistic, but the research they say they have to back up that claim is still unpublished, and is thus not yet subject to scrutiny and verification by others in the field.
Autism advocates say that the lives of too many people will be affected by a redefinition of autism to simply allow a committee of experts to do it by fiat. They are calling on the APA to put the proposed new definition to the test, and to release the results of that test well before the December 31st deadline for finalizing the DSM-5. That way, any fears and doubts about the new autism defi-nition can be put to rest in advance, and there will be enough time to revise it, if necessary, before it goes into effect.
The fourth edition of the Diagnostic
and Statistical Manual of Mental
Disorders (DSM-IV), published by the
American Psychiatric Association, is
the ultimate mental health reference
for professionals in the field, providing
the definitive diagnostic criteria for
all mental disorders. The DSM-IV was
published in 1994, and is now being
updated. The fifth edition, DSM-5, is
due to be published in early 2013.

FEBRUARY 2012
1717
RA
ISIN
G O
UR
CH
ILD
REN
19 Unvaccinated Arizona Children Quarantined
By Joel Mandel
A case of the mumps diagnosed in a fourth-grad-er attending a public school in Gilbert, Arizona, a suburb of Phoenix, has led to the removal of
19 other students who have not been vaccinated against the disease, and who may have been ex-posed to the infected child on or before February 2. They will not be allowed to return to the Higley Elementary and Middle School until the end of the quarantine period, which in this case is February 28, as long as no additional mumps cases are reported before then. While the 19 children are kept at home, their school, with the help of county officials, will provide them with their daily homework.
The move was a public health precaution against the unvaccinated children spreading the mumps to others. Bob England, the director of the Maricopa County Department of Health, said that, “we don’t do this unless we think we really need to. In order to cut it off before it has a chance to turn into a bigger outbreak, we have to make sure we’ve got herd immunity around that first case, meaning everybody around that first case im-munized. … Hopefully, with this one, we can nip
it right in the bud and there won’t be any more cases.”
"We hate to kick kids out of school," England added. "But every time a parent signs an exemp-tion and chooses not to vaccinate their child, they've got to know this is possible."
Arizona is one of the states which permits par-ents to opt out of the usual requirement for all children to receive their scheduled vaccinations in order to be admitted into class at the start of each school year. In Arizona, parents can request an ex-emption on personal or religious grounds, including fears that some vaccines could be harmful to their child’s health. The requirements in other states vary.
Mumps is caused by a highly contagious virus. It used to be a common childhood disease, but out-breaks in the US have become relatively rare since vaccination became widespread in the late 1960's.
Mumps is not serious, and leaves no lasting ill ef-fects in children. Its symptoms include fever, head-ache, and a painful swelling of the salivary glands. Most children in the US are routinely vaccinated against the disease between the ages of 12 months and 15 months as part of the MMR shot (measles, mumps and rubella) and receive a second dose between 4 and 6 years old. The vaccine is about 80% effective.
Older adults are likely immune to the mumps because it was so prevalent when they were young, but children and younger adults who have not been fully vaccinated may be at risk.
The safety of the MMR vaccine has been ques-tioned. In 1998, Dr. Andrew Wakefield. published a paper in the British medical journal Lancet which claimed there may be an association between the MMR vaccine and onset of autism. This contention led many parents in the UK and around the world to resist the mandatory vaccination of their chil-dren. In 2004, evidence was uncovered that Wake-field had falsified his research. In 2010 Lancet re-tracted his paper, and Wakefield was reprimanded by his peers.
Nevertheless, some parents still question the safety of vaccines, even though the consensus of the medical community is that the risks that they pose are small, and that universal vaccination is es-sential to public health.
For example, in the summer of 2009, there was an outbreak of measles in several New York religious communities. It was started by an unvac-cinated child who contracted the measles virus in Great Britain, and then spread it while attending a summer camp in the Catskills.

FEBRUARY 2012
1818
WO
MEN
'S H
EALT
H
Are Working Mothers Happier and Healthier Than Stay-at-Home Mothers?
By Ita Yankovich
Mrs. Green is rushing off to work. She brushes away a strand of hair from her baby’s eyes, kisses her pudgy cheeks goodbye, while giv-
ing the babysitter last minute instructions for the day, all while adjusting her sheital, fumbling for her keys, and answering a ringing cell phone. In an-other household, Mrs. Abrams is keeping her eye on lunch sizzling on the fryer while folding laun-dry and singing ‘Twinkle Twinkle’ to her giggling infant in the bouncer. Her toddler is whining that he’s bored and demands that she play Lego with him, so she lowers the heat on the stovetop, puts the laundry aside and uses her left leg to move the bouncer all the while.
The old debate over who has it ‘harder,’ stay-at-home mothers or working mothers, has never been clearly resolved. Some studies claim that stay-at-home mothers are more satisfied while working mothers are plagued with guilt, while other studies suggest the opposite. To date, much of the research on maternal employment has been inconsistent and focused on how it affects the chil-dren’s upbringing, rather than how it affects the woman. Some studies have shown that the more a
mother works, the better off her children are, while other studies suggest the contrary. Finally, there are studies that haven’t even discerned a clear cor-relation. A recent report published in The Ameri-can Psychological Association’s Journal of Family Psychology, claims that working mothers tend to be happier and even healthier than stay-at-home moms.
That study found that mothers who are em-ployed part-time reported better overall health and fewer symptoms of depression than stay-at-home moms, and that there were no reported differences in general health or depressive symp-toms between moms who were employed part time and those who worked full time. Mothers employed part time were just as involved in their child’s school as stay-at-home moms, and more involved than moms who worked full time. In ad-dition, mothers working part time appeared more sensitive with their pre-school children and pro-vided more learning opportunities for toddlers than stay-at-home moms and moms working full time. Mothers who participated in the study were from 10 locations across the U.S. The number of mothers employed part time remained at about 25 percent of the total during the study, although some of the mothers moved into and out of part-time work.
Researchers then examined the data collected by a 10-year study by the National Institute for Child Health and Human Development, which tracked 1,364 mothers beginning in 1991 when their ba-bies were 6 months old, and interviewing them seven times, and culminating when their children were fifth-graders. They compared stay-at-home moms to those who worked part-time or full-time (more than 32 hours a week) and concluded that in many areas, there was no difference in emotional well-being between the full- and part-timers. In general, part-time working moms reported less work-family conflict than full-time working moms, but the rates of depression and overall health lev-els were about the same for the two groups.
The most significant differences arose when comparing stay-at-home moms to those who worked part-time. The part-timers were less de-pressed, had better health, were more sensitive to their children and were better able to provide them with learning opportunities. That may be a function of employment, which improves people’s social skills and increases awareness of what’s go-ing on in the community. For example, part-time moms said they were as active in their kids’ schools as moms who didn’t work and, not surprisingly, were able to devote more time than moms who worked full-time.
Tzivy Reiter, LCSW, and author of the soon to be released book, Briefcase & Baby Bottles: The Work-ing Mother’s Guide to Nurturing Jewish Home, inter-viewed over 20 working mothers to gain insight into their daily lives. She believes that there is no one size fits all approach to the issue; whether or not a woman works is a very individual choice that
is based on a myriad of personal variables. “A wom-an’s happiness with her choice will depend in large part on the support she is given by her family and community, as well as the strength of the connec-tion she has with her family,” Reiter explains.
The financial-management website, Mint, published an estimate of how much a homemaker would earn if she were paid market prices for her work. The result was nearly $100,000 a year. Data like this vindicates stay-at-home moms who feel their work is undervalued. The salary was calculat-ed by adding the daily cost of a chef, cleaning lady, babysitter, a personal driver, and a professional laundry service.
Shira Offer, a Professor of sociology at Bar Ilan University in Israel, authored a study where she reported that working women today feel overbur-dened by their multitasking and lack of spousal do-mestic support compared to stay-at-home moth-ers. While today’s generation of fathers is expected to be involved in housework and child care, Offer still finds that most women feel that it is their pri-mary role. “We expect mothers to be good workers who are highly committed to their work, but they are also the ones held accountable for how their children do and how their households are run,” says Offer.
Socially, we are conflicted on how we feel about working moms vs. stay–at-home moms. In an online blog survey, when asked who has it harder, 39% polled believed that the answer is working mothers while 26% reported that all par-enting is difficult, and 18% said it depends on the circumstance. “We live in a society that sends us mixed messages-extolling the virtues of the stay at home mom, yet denigrating her lack of career achievement,” says Reiter. This leads mothers to doubt their choices-whether that choice is to stay at home or work. This is why Reiter believes that being part-time working mothers allows them to have the best of both worlds-investment in a ca-reer, yet still affording them the flexibility to spend meaningful time with their children. Whether a woman chooses to stay at home or work it is im-perative, as Reiter claims, that, “she feel supported in those decisions and comfortable that it can still yield a happy and positive outcome for their fami-lies”.
Personally, as someone who has delved into both options, I can honestly say that I didn’t find one to be easier or more rewarding than the other. I think we all are just trying to be good “Yiddishe Mamas” in a modern, fast-paced world. Those who work feel the financial pressure to contribute and often feel conflicted when at home and at the of-fice, while those who are at home all day can feel overwhelmed and isolated. The main take away point from this study is that we mothers have to take care of ourselves if we want to take care of our families. If it takes a village to raise a child, then shouldn’t it take at least for us, as women, to be plugged into our own mental health in order to take care of ourselves?
Serving Tucson, Arizona since 1963
HANDMAKER
Assisted LivingPost Hospital RehabSkilled NursingAdult Day ProgramsLong Term Memory Care
520.322.7035www.handmaker.org
FEBRUARY 2012
1919
WO
MEN
'S H
EALT
H
New Clues Found To Explain the Course of Lupus
By Joel Mandel
Lupus is an autoimmune disease which affects an estimated 1.5 million Americans, striking mostly
women of child-bearing age (15-44) 9 times more often than men.
It can be difficult to diagnose be-cause its symptoms tend to mimic those of other ailments. The most distinctive sign of lupus, which oc-curs in many but not all cases, is a facial rash that resembles the wings of a butterfly unfolding across both cheeks.
Nobody knows why lupus causes the body’s immune system to attack healthy tissue in the kidney, blood vessels in the lungs, coronary arteries and the brain. However, a paper by Italian researchers, published in the Annals of Rheumatic Diseases identi-fied a DNA sequence in people with a particularly intense form of lupus which appears to accelerate the pro-gression of the disease.
These DNA "enhancers" in a se-quence called HS1.2 accelerate the ac-tivation of neighboring genes respon-sible for the most severe form of the disease, which results in joint pain, fe-ver, skin rashes, hair loss and anemia.
Scientists already knew that some people are born with a tendency to-ward developing lupus, which may be then triggered by infections, certain drugs or even exposure to sunlight. In addition, no two cases of lupus are ex-actly alike. Its symptoms may come on suddenly or gradually. The disease can flare up, becoming severe, and then, inexplicably start to improve or dis-appear completely over time. This is
why scientists have been eager to find more clues to accurately predict the course of the disease in each patient.
The Italian researchers may have found part of the answer. They believe that the HS1.2 accelerator, which is
found in over 30% of lupus patients, activates "transcription factor NF-KB," a molecule that turns on the genes which boost the production of the im-mune system antibodies that attack the healthy tissues of the body, which is the fundamental way in which lupus works.
The HS1.2 genetic sequence also plays a role in other autoimmune dis-eases such as rheumatoid arthritis, and its presence in an individual may
indicate a greater susceptibility to all kinds of autoimmune diseases.
Current treatments for lupus in-clude cortisone, a powerful and dan-gerous steroid, as well as a variety of anti-malarial drugs and immune sys-tem suppressants. The discovery of the accelerator sequence could lead to new treatments for lupus based upon medicines specifically designed to "turn off" the accelerator effect.
According to the head researcher for the study, Gianfranco Ferraccioli of the Catholic University of Sacred Heart in Rome, “new drugs that turn off the enhancer HS1.2, or inhibit its effect on NF-KB, may stop the disease with-out the need for immunosuppressive drugs or other therapies which have many dangerous side effects."
The discovery could lead to a new diagnostic test for lupus sufferers, in which the presence or absence of the enhancer DNA sequence helps doc-tors to come up with a more precise prognosis for each patient, and more personalized care."
No two cases of lupus are exactly alike. Its symptoms may come on suddenly or gradually. The disease can flare up,
becoming severe, and then, inexplicably start to improve or disappear completely.
We Are Here to Help.
That is why we have a team of experts especially for you.
Our Heritage Program has patient navigators that serve asliasons with physicians and medical staff to guide patients and
families during their hospital stay. Call us anytime.
Richard Friedman, MD, FACSDirector and Physician Liason
(917) 710-4896
Joseph DeutschPatient Navigator(917) 509-4441
Dov JacobPatient Navigator(917) 886-3865

FEBRUARY 2012
2020
WO
MEN
'S H
EALT
H
Cholesterol Drug May Fight Breast CancerBy Rachel Wizenfeld
A new study published found possible benefits of using statins, a drug commonly used to lower cholestrol, to treat certain types of breast
cancer patients, researchers and doctors say. The new research was published in the Jan. 20
issue of the journal Cell, and a Health Day News ar-ticle said the study author, Dr. Carol Prives who is chair of the department of biological sciences at Co-lumbia University in New York City, is cautious in her enthusiasm about the results and their implications.
The study looked at a specific cell mutation called p53, which is found in roughly 20-40% of breast cancer tumors, according to Dr. Homayoon Sanati, oncologist and director of the MemorialCare Breast Center at Orange Coast Memorial Medical Center in Fountain Valley, CA. Cells with this p53 mutation have elevated levels of genes in a certain pathway called the mevalonate pathway, which is also involved in cholestrol synthesis. Stains are used to block this pathway to lower cholesterol, and
concurrently, when p53 breast cancer cells were exposed to statins in a laboratory, their growth rate went down.
“Basically, that’s a signal in lab findings that statins can be useful in breast cancer patients that have this gene,” said Dr. Hanati. “It might be a mech-anism to block their growth.”
He cautioned that these findings are very pre-liminary, and additional research may be difficult since most of the statins drugs are becoming ge-neric, the drug companies are not going to invest money in research. Thus government-sponsored cooperatives and other groups are needed to fund a study that will identify patients with this p53 muta-tion, give them statins, and see if it makes an impact on their breast cancer. Oftentimes it may take five to ten years to get a concept from a lab to actual clini-cal practice, Dr. Hanati said.
Another study reported in 2005 also noted a link between breast cancer and statins. The ob-servational study, reported at an American So-ciety in Clinical Oncology meeting in Orlando looked at 40,000 patients in the VA system and
identified 500 who had breast cancer. Of those 500, patients who were taking statins versus those who were not had a reduced breast cancer risk of 50%.
The problem with observational studies is that researchers don’t have complete information about the patients, including family history and what addi-tional hormones they may be taking, Dr. Sanati said, but studies like these are possible in the VA system because of their excellent health records.
Statins are also commonly used to treat heart disease, which is currently the most prevalent cause of death among women. Although another recent study has found increased risks of diabetes for statins-users, doctors agree that the benefits of statins far outweigh the risks.
“Statins changed the landscape of coronary artery disease and for that reason many women should be on it,” said Dr. Sanati.
Rachel Wizenfeld is a frequent contributor to publications like
The Jewish Press, The Jewish Journal and the New York Blue-
print. She lives in Los Angeles.
Breast Cancer Screening Caught in Controversy Over Planned Parenthood
Once again, the bitter running controversy between right-to-life and pro-choice factions in this country has spilled over to impact the cause of promoting women’s health by damag-ing the credibility of the largest orga-nization in this country fighting breast cancer, the Susan G. Komen for the Cure foundation. Komen was plunged into partisan political controversy on January 31 when it announced a cut off in its ongoing funding for breast cancer screening conducted by the Planned Parenthood organization.
The foundation had been giving Planned Parenthood about $700,000 a year to provide the screening to all women seeking its family planning services. According to Planned Par-enthood, over the past five years, the Komen grants paid for 170,000 breast cancer screenings at Planned Par-enthood’s health centers across the country. The total amount of money involved, about $700,000 a year, rep-resents a tiny fraction of the nearly $2 billion that Komen has spent fighting breast cancer since its inception in 1982.
The Komen foundation has al-ways been relatively conservative in its outlook. Its founder, Nancy Brinker, is a major Republican donor; who was appointed the US ambassador to Hungary by President George W. Bush. However, until now, her personal po-
litical orientation never intruded on the Komen foundation’s activities.
However, the group’s previous grants to Planned Parenthood had drawn criticism from some pro-life advocates. They argued that giving Planned Parenthood money, even for a worthwhile purpose freed up other funds in its budget to pay for more of its abortion and other family planning services which pro-life advocates be-lieve are immoral.
Komen foundation officials were careful not to tie the funding cutoff to the right to life issue. Instead they cited a rule Komen instituted last year which requires it to withdraw its fund-ing to any group under any federal, state of local investigation. They then noted that Planned Parenthood is un-der investigation by Republicans in the House into whether it was violat-ing the Hyde Amendment, which pro-hibits any federal health funding to be used to provide abortion services.
The ruse fooled nobody. The lead-ership of Komen was severely criti-
cized by Democrats in Congress and women’s health advocates for bowing to the pressure from the pro-life fac-tion, and allowing the fight against breast cancer to be politicized. It quickly became a public relations di-saster for Komen foundation, which is the largest, most widely known, and best-funded breast cancer organiza-tion in the United States.
Planned Parenthood actually wound up reaping a fund-raising bo-
nanza from the cutoff. Within three days of the announcement, a total of $3 million from over 10,000 do-nors around the country, including a $250,000 matching grant from New York City’s billionaire mayor, Michael Bloomberg.
The intense criticism in the media forced the leadership of Komen to go into damage control mode, and search for a face-saving way out. Instead of simply admitting that they had blun-dered, they decided to change the rule which they had used as an excuse for the cutoff in the first place.
On February 3rd, the Komen board issued a statement to "apolo-gize to the American public for recent decisions that cast doubt upon our commitment to our mission of sav-ing women's lives." It also said that Komen "will continue to fund exist-ing grants, including those of Planned Parenthood, and preserve their eligi-bility to apply for future grants." It also announced that the rule would be changed to "make clear that disquali-fying investigations must be criminal and conclusive in nature and not po-litical. That is what is right and fair." The announcement stopped short of committing the foundation to provide new funding for Planned Parenthood, and merely stated its eligibility to ask for it.
Planned Parenthood then issued a statement saying, "We are enormous-ly grateful that the Komen Foundation has clarified its grant-making criteria, and we look forward to continuing our partnership with Komen partners, leaders and volunteers."
Then it was the turn of pro-life groups to express their disappoint-ment that Komen had backed away from the cutoff, but by then it had be-come clear to everyone that the big-gest loser from the episode was the effort by Komen to mobilize unified and bi-partisan public support for the war against breast cancer.
"Over the past five years, the Komen grants paid for 170,000 breast cancer screenings at Planned Parenthood’s health centers across the country."
21
FEBRUARY 2012
2222
GO
LDEN
YEA
RS
Diabetes - The Silent KillerBy Yaakov Kornreich
The world-wide diabetes epidemic and its re-lated precursor, obesity, are the fastest grow-ing public health menaces of the 21st century.
FEBRUARY 2012
2323
GO
LDEN
YEA
RS
AT A GLANCE - DIABETES
(Also known as: Diabetes Mellitus)
Definition: A metabolic condition in which the body suffers from exces-sively high blood sugar (glucose) levels.
Estimated number of cases world-
wide: Over 300 million
Diagnostic Criterion
(Type 1 and Type 2)
Hemoglobin A1c test: Pre-diabetes: 5.7% - 6.4%Diabetes: 6.5% or higher
Fasting blood glucose level:Pre-diabetes: 100-125 mg/dLDiabetes: 126 mg/dL or higher
Symptoms (all types):
• Increased thirst• Increased urination• Blurry eyesight• Fatigue• Weight loss despite increased ap-
petite• Numbness or tingling in the extremi-
ties (Type 1 & Type 2)• Nausea and vomiting (Type 1 & Ges-
tational)
Major Complications (Type 1 & Type 2):
• Damage to eyesight, leading to blindness
• Cardiovascular disease leading to heart attack or stroke
• Kidney damage leading to end stage renal failure
• Nerve damage leading to loss of feeling
• Circulatory problems in the legs and feet leading to infections and amputation
Diabetes mellitus is a chronic condition re-sulting from the body’s inability to properly control blood sugar (glucose). Normally, the
body controls the glucose level with a hormone produced in the pancreas called insulin. Those who have diabetes have either lost the ability to produce enough insulin, or the cells in their body no longer respond properly to the insulin that is being produced.
More than 90% of diabetes cases in the US to-day are Type 2, and less than 10% are Type1.
Diabetes was well known to the ancients, but the current epidemic of Type 2 diabetes is a phenomenon of modern living. It is largely the re-sult of eating an unhealthy diet combined with a sedentary lifestyle. As a result, diabetes is nearly four times as common today as all types of cancer combined, and it causes more deaths each year than breast and prostate cancer combined.
More than 25 million Americans already have diabetes, and more than double that number have blood sugar numbers high enough to clas-sify them as suffering from pre-diabetes. That means that they are likely to develop the full blown Type 2 diabetes in the near future if they do not make the necessary changes in their diet and lifestyles to prevent it.
Type 1 and Type 2 diabetes have many of the same symptoms and potentially deadly conse-quences, but different causes. Type 1 diabetes is also known as “juvenile diabetes” because in most cases it appears in childhood, in contrast with Type 2, which used to occur only in adults, which is why it was formerly known as adult-onset dia-betes.
Type 1 is an autoimmune disease, like Rheu-matoid Arthritis and Lupus, in which something triggers the body’s own immune system to attack the insulin-producing beta cells in the part of the pancreas known as the islets of Langerhans.
Type 1 cannot be cured, but it can be effec-tively managed. Proper insulin therapy, combined with regular monitoring of blood sugar levels, can allow people with Type 1 diabetes to lead a nor-mal and healthy life.
One of the most insidious aspects of Type 2 diabetes is that by the time people are diagnosed
with it, they may have already developed a seri-ous long term complication of the condition. Type 2 doubles the risk of cardiovascular disease, which ultimately kills 52% of people with diabe-tes. People diagnosed with Type 2 also have dou-ble the risk of suffering a stroke within 5 years. Al-most one in three will eventually develop kidney disease, and diabetes is one of the leading causes of adult blindness.
Diabetes is also associated with circulation problems in the lower extremities. This can result in the slow healing or infection of wounds on the feet and legs. This is further complicated by the fact that high blood sugar due to diabetes can cause damage to the nerves that sense pain. This means that diabetes patients may not realize that they have a wound on their leg or foot until after it has become dangerously infected. This can ulti-mately lead to the need for amputation.
Type 2 diabetes is also a condition related to aging. Approximately 20% of the population over 60 have the condition, and an equal number have its precursor. It is no longer called “juvenile” diabetes because of the shocking relatively recent result of the obesity epidemic, the discovery of Type 2 diabetes, for the first time, in grossly over-weight teenagers and young adults.
Type 2 is typically treated with oral medica-tions such as metformin, and it, too, requires the monitoring of blood sugar levels. The good news is that pre-diabetes or mild cases of Type 2 can also be controlled through appropriate changes in diet and lifestyle and weight loss. These are more effective, but require a lot more work and discipline, than taking pills. In fact, there is evi-dence that Type 2 diabetes can actually be re-versed, in at least some cases, with sufficiently aggressive and strictly observed diet and lifestyle changes and weight loss.
There are other types of diabetes, the most common being gestational diabetes, a temporary condition which affects 2-5% of pregnant women and generally subsides after the baby is born. The symptoms are similar to those of Type 2 diabetes, and women who have had gestational diabetes are at higher risk of developing Type 2 diabetes later in life.
Women with gestational diabetes must be treated and closely monitored, because of the potential danger from the diabetes to the health of both the mother and the fetus. Gestational dia-betes in the mother puts the baby at greater risk for high birth weight, cardiac and central nervous system problems, respiratory distress and skel-etal muscle malformations. The damage done to blood vessels could impair the function of the placenta, causing fetal distress requiring early de-livery through the induction of labor or cesarean section.
Metabolic syndrome is the name for an in-creasingly common cluster of symptoms exhib-ited together in the same patient which are likely due to common factors. People with metabolic syndrome are at increased risk for coronary artery disease, stroke, and type 2 diabetes. The great-est risk factor for metabolic syndrome is obesity in which most of the extra weight, in the form of fat, is found in the chest and abdomen, giving the body an “apple” shape. It is also commonly associ-ated with the phenomenon of insulin resistance,
Continued on page 24
"Medical expenses for people with diabetes are more than two times higher
than for people without diabetes."Source: National Diabetes Fact Sheet, 2011 - published by the Centers for Disease Control and Prevention
RESOURCES
Friends With Diabeteswww.friendswithdiabetes.orgA Rockland County-based support group for
religious Jews with diabetes. Distributes diabetes-safe recipes, sponsors meetings (separated by gender and age), and presentations by renowned rabbonim. Publications, edited by Rabbi Hirsch Meisels, in English, Hebrew and Yiddish, address halachic, social and health challenges facing frum Jews living with diabetes.
Jewish Diabetes Associationhttp://jewishdiabetes.comAn organization devoted to diabetes education
and advocacy offering its website, magazine and contact persons in both Hebrew and English.
Living With Diabeteswww.mendosa.comInformational website
American Diabetes Organizationhttp://www.diabetes.orgAn organization dedicated to preventing and
curing diabetes and improving the lives of all peo-ple affected by the disease.

FEBRUARY 2012
2424
GO
LDEN
YEA
RS
in which the body is unable to use insulin prop-erly to control blood sugar and fat levels, leading to pre-diabetes. Other risk factors for metabolic syndrome include age, lack of exercise, and ge-netic factors.
While not yet proven, scientists have a theory about how excess fat, especially in the abdomen, leads to Type 2 diabetes. Dr. Naveed Sattar, pro-fessor of metabolic medicine at the University of Glasgow, in Scotland, believes that if too much fat is stored in the abdomen, it can interfere with the way the pancreas produces insulin, and the way that the liver uses it to control blood sugar and fat levels in the body.
Glucose is one of the main fuels for the cells of the body. It is released into the bloodstream by the digestion of the carbohydrates in our food. Insulin is used by the body to help main-tain a constant level of glucose in the blood-stream by stimulating the liver and muscle cells to store excess glucose in the form of glycogen. When there is too much glycogen to be conve-niently stored, the body turns it into fat which is stored in fat cells.
According to Dr. Sattar, Type 2 diabetes may be the result of the body being unable “to make and store fat safely. Some people can store fat subcutaneously (under the skin). With others, it goes straight to the liver and pancreas. That's the classic big waist, pot belly shape; the fat isn't dis-tributed around the body." According to the the-ory, at some point that excess fat interferes with the proper functioning of the liver and pancreas.
The classic symptoms of uncontrolled dia-betes include increased frequency of urination accompanied by increased thirst, and increased hunger. The symptoms develop more rapidly (over a few weeks or months) in type 1 diabetes while in type 2 diabetes they usually develop much more gradually and may therefore be more difficult to notice.
Another symptom of uncontrolled diabetes is blurred vision, because of changes caused by high blood glucose levels in the shape of the lens of the eye.
Many of the long term complications from di-abetes are the result of its accumulated damage to blood vessels throughout the body, including the coronary arteries, the veins in the legs, and the tiny blood vessels found in the retina of the eye and in the kidneys.
How does one get diabetes? Scientists are not sure, but for Type 1, heredity plays only a minor role. Less than 10% of people with Type 1 have a family history of the condition. Scientists believe that even those with a genetic predisposition still must be exposed to an unknown triggering mechanism for the autoimmune reaction which destroys the body’s ability to produce insulin.
Type 2 has a much stronger hereditary com-ponent, particularly when both parents have the condition. But even those who have those ge-netic factors can lower their risk by maintaining a proper weight and exercising regularly.
While there is no cure for Type 1 diabetes, there
has been encouraging progress in its treatment. A new generation of miniaturized insulin infusion pumps is being developed which includes a con-tinuous blood glucose monitoring system. Once perfected, the system would be implanted under the skin to function like an artificial pancreas.
There are also ongoing experiments with transplants of pancreatic cells or stem cells to start producing insulin in the body again. But for now, most people with the condition still must rely on daily insulin injections.
However, for people with Type 2 diabetes, there are viable alternatives to lifelong depen-dence on medications. In a recent study, more than 70% of subjects with Type 2 who underwent bariatric (gastric bypass or lap band) surgery, and who lost more than 30 pounds of body weight, appeared to be free of the condition. Similar ben-efits can be obtained by following a very low-car-bohydrate diet, combined with regular exercise, which is intended not only to eliminate body weight, but also to slash the amount of fat around the liver and pancreas.
According to Dr. Joel Goodman, the head of the Department of Endocrinology and Metabo-lism at Brookdale University Hospital and Medical Center, in Brooklyn, NY, a low-carb diet is most ap-propriate for people treating their Type 2 diabe-tes.
Jews appreciate good food, and perversely, diabetes actually increases the body’s cravings for food, making it more difficult to curb one’s appetite. Yet today, religious Jews with diabetes can, within certain limitations, eat the traditional foods they love on Shabbos, Yom Tov and even Passover without endangering their health. Read-ily available resources provide diabetes-safe reci-pes for Jewish delicacies, halachic guidance, sup-port and counseling.
The obesity epidemic and the climbing dia-betes statistics amount to a nationwide public health emergency. Yet, thanks to modern medical science, we have a much better understanding of this silent killer. Jews with diabetes, in particular, are no longer faced with the dilemma of being forced to choose between following our tradi-tions and beliefs or protecting our health.
Continued from page 23
AT A GLANCE - DIABETES - THREE COMMON VARIATIONS:
Type 1 (formerly known as Juvenile Diabetes)
Prevalence: Less than 10% of all casesCause: An autoimmune reaction destroying the body’s ability to make insulinTriggering Mechanism: UnknownDuration: ChronicOnset: SuddenDiagnosed population: Children or young adultsFamily History Risk Factor: Minor, less than 10% of cases have a family historyOther Risk Factors: UnknownTreatment: Daily insulin injections with close moni-toring of blood sugar levels
Type 2 (formerly known as Adult Onset Diabetes)
Prevalence: More than 90% of all cases, growing quicklyCause: Improper body reaction to insulin (insulin re-sistance)Triggering Mechanism: Suspected interference of fat with pancreas and liver functionDuration: ChronicOnset: Gradual, often marked by rising blood sugar levels (pre-diabetes)Diagnosed population: Older adults and others who are morbidly obese and sedentaryFamily History Risk Factor: Significant, especially in certain ethnic populationsOther Risk Factors: Obesity and a sedentary life style (Metabolic Syndrome)Treatment: Oral medication, combined with change of diet and regular exercise
Gestational Diabetes
Prevalence: 2-5% of all pregnant womenCause: Similar to Type 2Triggering Mechanism: Interactions with pregnan-cy hormonesSeverity: Generally mildOnset: Midway through pregnancyDuration: Temporary - symptoms disappear after deliveryFamily History Risk Factor: YesOther Risk Factors: Overweight, high blood pres-sure, ageTreatment: Adjust diet to maintain safe blood sugar levelsComplications: Babies tend to be larger than normalMother at increased risk of Type 2 diabetes later in life
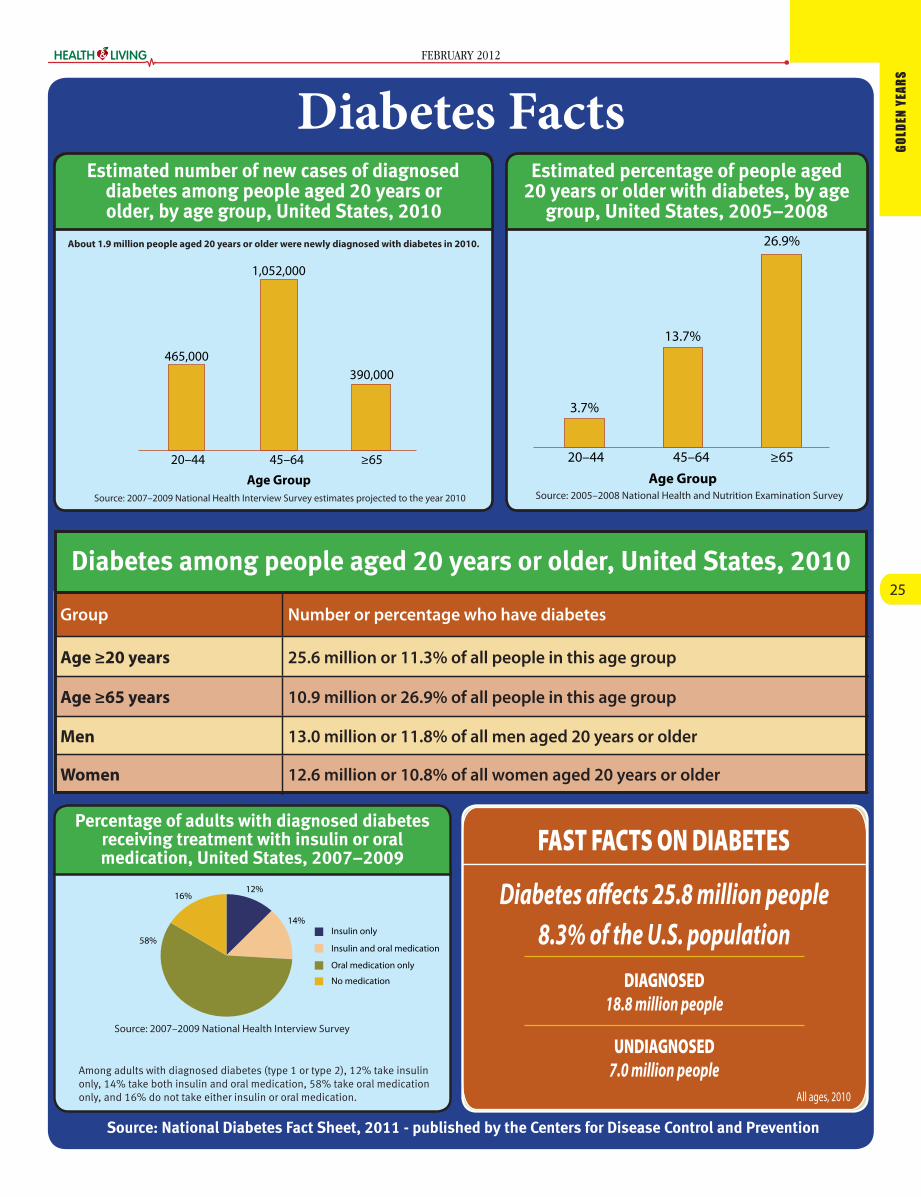
FEBRUARY 2012
2525
GO
LDEN
YEA
RS
FAST FACTS ON DIABETES
Diabetes affects 25.8 million people 8.3% of the U.S. population
DIAGNOSED 18.8 million people
UNDIAGNOSED 7.0 million people
All ages, 2010
Group Number or percentage who have diabetes
Age ≥20 years 25.6 million or 11.3% of all people in this age group
Age ≥65 years 10.9 million or 26.9% of all people in this age group
Men 13.0 million or 11.8% of all men aged 20 years or older
Women 12.6 million or 10.8% of all women aged 20 years or older
Diabetes among people aged 20 years or older, United States, 2010
Source: 2005–2008 National Health and Nutrition Examination Survey
tage of people aged 20 years or older with diagnosed and undiagby age group, United States, 2005–2008
3.7%
13.7%
26.9%
20–44 45–64
Age Group
d and undiagnosed diabetesEstimated percentage of people aged 20 years or older with diabetes, by age
group, United States, 2005–2008
Source: 2007–2009 National Health Interview Survey estimates projected to the year 2010
Estimated number of new cases of diagnosed diabetes among people aged 20 years or older, by age group, United States, 2010
465,000
1,052,000
390,000
20–44 45–64
Age Group
About 1.9 million people aged 20 years or older were newly diagnosed with diabetes in 2010.
w cases of diagnosed diabetesEstimated number of new cases of diagnosed diabetes among people aged 20 years or older, by age group, United States, 2010
Insulin only
Insulin and oral medication
Oral medication only
No medication
16%12%
14%
58%
Source: 2007–2009 National Health Interview Survey
Percentage of adults with diagnosed diabetes receiving treatment with insulin or oral medication, United States, 2007–2009
Among adults with diagnosed diabetes (type 1 or type 2), 12% take insulin only, 14% take both insulin and oral medication, 58% take oral medication only, and 16% do not take either insulin or oral medication.
Diabetes Facts
Source: National Diabetes Fact Sheet, 2011 - published by the Centers for Disease Control and Prevention

FEBRUARY 2012
2626
GO
LDEN
YEA
RS
Understanding CataractsBy Dr. Morris Shamah
Your doctor just told you that you have a cataract. He ex-plained to you in a few words
what a cataract is, and asked when you want to schedule surgery. You are stunned.
What? A cataract? A film in my eye? Am I going blind? The doctor briefly reassures you, but, a little confused, you say you want to go home and discuss it with your fam-ily. He gives you a look, and with a shrug of his shoulders, he agrees, but you really do not understand what’s going on.
What is a cataract. What has to be done? What is the overall picture of your future vision?
We are all born with a lens in our eye. The lens is just behind the pupil, or behind the iris. It is, in an adult, about the size of two large lentils, side by side. The purpose of this lens is to focus an image of what we see on our retina, the op-tical sensor at the back of our eye. When we are born the lens is crystal
clear. As we age, it gets cloudy, dark, filled with little vacuoles, much like a dirty window. After a long while, the lens becomes really opaque and the image that is transmitted to the retina becomes just a blur of light.
Why does this happen?In a minority of cases, it is due to
certain diseases, to exposure to cer-tain toxins or to radiation. But in most cases, it is a normal consequence of aging. Perhaps sunlight, chemicals in our diets, poor living and other fac-tors add to the insult to the lens to make it cloudy. We know that diabet-ics get cataracts at a somewhat ear-lier age than non-diabetics. And we do know that some diabetics do get a particular type of cataract.
But, in most people, a cataract is just a result of normal aging.
Why?Think of an egg white. As you
crack a fresh egg, the white is nearly clear, transparent. But as you heat it, beat it, or shake it, it becomes cloudier and cloudier, until it is fi-nally opaque and white. That why
we call it an “egg white” and not an “egg clear.” What is happening when we heat the egg white is that we are changing the nature of a clear pro-
tein and altering it so that it is no longer transparent. The same thing happens over time with the lens in our eyes. It is first a clear crystalline protein, but, with exposure over time, that protein becomes cloudy.
This cloudiness usually does not happen suddenly, but rather gradu-ally. The cloudiness can develop in different sections of the lens – in the front, middle, back, or throughout. The amount of opacity and its loca-tion is what determines if and how it affects your vision.
For example, early on you could just have a bit of yellowing in the middle of the lens. This would cause almost no noticeable symptoms. Your doctor would tell you that you have an early cataract. At this stage, the cataract really needs no care. After a bit more time, this type cata-ract might cause slight darkening of your vision and a small change in your eyeglass prescription. A year or two later, you may find that things just do not appear as clear as they once were, that colors are changing (warm colors, like yellow, are more intense, cool colors, like blue, are less intense).
Now your doctor would then check your glasses prescription, to see how much your vision can be improved, and discuss other symp-toms from your cataract. If he and you together decide that vision will not improve enough with a change in the prescription of your glasses, he would then present you with the option of undergoing cataract surgery, to remove the cloudy lens inside your eye and replace it with a clear one.
We will discuss the nature of this operation in the second part of this ar-
ticle, but first, we will discuss the vari-ous kinds of cataract development.
Cataracts that develop on the very back of the lens – known as “posterior sub capsular” -- often cause a great deal of glare, even in the early stages. The glare from such cataracts can make night driv-ing and walking in the sun terribly uncomfortable. And yet, in medium lighting, one might still see very well with such a cataract.
These types of cataracts tend to develop in younger people and of-ten progress rapidly. The decision as to whether or not to operate on this type of cataract would depend on the level of disability that it causes. For example, someone who drives at night would be a more likely can-didate for surgery.
There are various types of cata-racts, including cataracts which af-fect newborns, that must be taken care of early. But in most cases, the decision on when surgery is neces-sary is a judgment call that the doc-tor and patient must make together after a glasses exam (refraction) is done. The decision is usually based on the level of patient disability and discomfort. If it is not necessary to remove the cataract immediately, an appointment is made for an-other visit to check on it in several months.
It should here be said that there are some physicians who, for rea-sons that will go unmentioned, will surgically remove just about any opacity.
It also should be noted that op-tometrists cannot, not by training and not by law, perform any eye surgery. So, in some cases an op-tometrist might try to nurse a pa-tient with a cataract along by selling them new glasses when what they really require is a referral to an eye MD, an ophthalmologist, for surgi-cal removal of the cataract. We will explain what that entails in part two of this article.
Dr. Morris Shamah is an ophthalmologist,
with a sub-specialty of glaucoma. He has
headed the division of glaucoma for over
20 years at Brookdale Hospital. He is cur-
rently involved in full time clinical practice.
Dr. Shamah is a founding member of the
Ophthalmic Laser Surgical Society and is
founder and chairman of the Brooklyn
Glaucoma Society. He prides himself in re-
sisting the trend of factory type medicine
and runs a ‘super modern‘ but old fash-
ioned type personal medical practice.

FEBRUARY 2012
2727
GO
LDEN
YEA
RS
New Insights into Parkinson's
By Sandy Eller
While more than 50,000 new cases of Parkinson’s Disease are diagnosed annually in the
United States, sources as early as an ancient Egyptian papyrus describe symptoms that resemble those of this degenerative neurological disease. The first formal study of the disease was an 1817 write-up by British apothecary James Parkinson entitled “An Essay on the Shaking Palsy.” Today scientists are attempting to discover both the cause of and a still elusive cure for Parkinsons, and new treatments for the disease con-tinue to evolve.
Parkinson’s is a brain disease that creates problems with movement. Its four main symptoms -- tremors, stiff-ness of the limbs and trunk, slowness of movement and impaired balance -- de-velop gradually and worsen over time. It is more prevalent in men and tends to develop at around age 60. High profile Americans who suffer from Parkinson’s include former boxer Muhammad Ali, former attorney general Janet Reno and actor Michael J. Fox, whose Michael J. Fox Foundation for Parkinson’s Research aims at finding a cure for the disease by funding Parkinson’s research.
While medications and surgical op-tions exist to treat Parkinson’s, none actually reverse the effects of the dis-ease but merely alleviate its symptoms. Medications to treat Parkinson’s include levadopa, developed in the 1960s and still the most effective treatment avail-able; dopamine agonists, which trick the brain into thinking it is receiving dopamine; anitcholinergics, which help control tremors; and MAO-B and COMT inhibitors, which help prolong the ef-fects of levadopa.
For many years Parkinson’s was thought to involve a lack of the neu-rotransmitter dopamine, caused by the death of dopamine-releasing cells in a particular area of the brain. But scien-tists now have reason to believe that the onset of Parkinson’s actually begins in other parts of the brain. According to Dr. Edward Fon, chair of the Scientific Advisory Board of Parkinson’s Society Canada, many Parkinson’s patients have a medical history of loss of smell, abnormal REM (rapid eye movement) sleep, excessive sleepiness and chronic constipation, among other conditions. Dr. Fon hopes that by being aware of these non-motor manifestations of the
disease, Parkinson’s patients can be identified long before crucial dopamine producing brain cells begin to die out.
The discovery in 1997 of an abnor-mal gene that appeared to be respon-sible for early onset Parkinson’s, which accounts for a small percentage of Parkinson’s patients, was a significant breakthrough, as Parkinson’s had long been thought not to have a genetic component. Since that time, research-ers have identified mutations in seven genes that are directly linked to devel-oping Parkinson’s. While this accounts only for a minority of Parkinson’s cases, it has opened up new doors in the re-search of this disease.
Deep Brain Stimulation (DBS) is an existing surgical option that was approved by the Food and Drug Ad-ministration for Parkinson’s treatment in 2002. In a small group of patients it has dramatically relieved their symp-toms for as long as five years. A recent study on DBS effectiveness indicates that it may hold the key to significant improvements for Parkinson’s patients.
“This study validates the use of mild electrical currents delivered to specific brain structures in order to improve Par-kinson’s disease in select patients with advanced symptoms and additionally it explored a new stimulation paradigm,” said Dr. Michael S. Okun, administrative director of the University of Florida Col-lege of Medicine’s Center for Movement Disorders and Neurorestoration. “Fu-ture improvements in devices and the delivery systems for DBS will hopefully provide exciting new opportunities for Parkinson’s sufferers.”
Recent research also suggests that an abnormal protein in the brain called alpha-synuclein may be one of the causes of the cellular damage that plagues Parkinson’s patients. If this is true, then developing drugs that could either stop or slow the spread of this protein could have significant bearing on the disease.
“It is an exciting time to work on Parkinson’s Disease,” Dr. Fon told Di-mensions, a publication of the National Research Institute Canada, Canada’s premier organization for research and development.
Sandy Eller is a freelance writer who has writ-
ten for various websites, newspapers, maga-
zines and private clients in addition to hav-
ing written song lyrics and scripts for several
full scale productions. She can be contacted
Services are available 24 hours a day, 7 days a week.For more information about our home care services, please call us:
1-877-55-GEFEN( 1 - 8 7 7 - 5 5 4 - 3 3 3 6 )
www.gefenseniorcare.com
(718) 575-9090
A company of the GEFEN Senior Care Group
(includes accomodating chronically ill, diabetic, and KOSHER needs)
Our Services Include:
Our aids are specially trained for your KOSHER needs.
Our Homecare Locations Include:MAIN OFFICES
113-15 76th Road,
Forest Hills, NY 11375
Tel: (718) 575-9090
Fax: (718) 575-9099
111 Beaver Dam Road,
Brookhaven, NY 11719
Tel: (631) 286-4786
Fax: (631) 286-5229
RECRUITING OFFICES
3099 Coney Island Avenue,
Brooklyn, NY 11235
Tel: (347) 462-2900
Fax: (347) 462-2899
372 E. 204th Street, Suite A,
Bronx, NY 10467
Tel: (347) 945-2040
Fax: (347) 945-2041

FEBRUARY 2012
2828
GO
LDEN
YEA
RS
Effect of Antioxidants on Longevity
Irina Lenkovskiy, MS, RD, CDN
The most common medical con-dition currently affecting the elderly in the United States is
coronary heart disease, followed by stroke. Most seniors are plagued with some sort of ailments usually related to heart conditions, demen-tia, and osteoporosis, diabetes, and Parkinson’s disease, cancer and/or eye problems. We are so focused on drugs to manage these illnesses, that we neglect to consider how nutrition and a person’s diet play a very large role in keeping a person healthy and controlling some of these conditions, often preventing many of these dis-eases from even surfacing.
Antioxidants in the blood are vi-tal to overall health. Antioxidants is the collective name for the vitamins, minerals, carotenoids, and poly-phenols that protect the body from harmful free radicals, which are the molecules produced when the body breaks down food, or by environmen-tal exposures like tobacco smoke and radiation. Free radicals can damage cells, and may play a role in heart dis-ease, cancer and other diseases. Low levels of antioxidants, or inhibition of the antioxidant enzymes, cause a chemical imbalance and may dam-age or kill cells.
Antioxidants come from a va-riety of food sources, including fruits, vegetables, whole grain cere-als, nuts and some other surprising sources such as coffee, chocolate, and red wine. Antioxidant sub-stances are found in beta-carotene (found in large concentration in car-rots), lutein (found in green, leafy vegetables), lycopene (absorbed from cooked tomatoes products), selenium (found in rice and wheat), vitamin A, vitamin C, and vitamin E.
Vitamin E destroys free radicals in cell membranes and protects unsaturated fatty acids from lipid peroxidation. Vitamin E can block hydrogen peroxide production and the resulting cytotoxicity. Thus vita-min E may slow the progression of Alzheimer’s disease. According to recent studies, vitamin E concentra-tion in the blood was lower among demented patients as compared with non-demented ones. Thus, a lower level of vitamin E may relate to developing Alzheimer’s disease.
The recent studies indicate that people who consume the highest amounts of vitamin C experience a reduced risk of ischemic stroke. An-tioxidants can also protect against inflammation, atherosclerosis, en-hance immune defense, protects eyes against cataracts and macular degeneration. They can slow and
possibly prevent the development of cancer.
Antioxidants can have nega-tive effects as well. High doses can be dangerous by working as pro-oxidants which promote rather than neutralize oxidation. In addition, not all free radicals are harmful. Some of them can attack harmful bacteria or cancer cells in the body and are therefore necessary. Thus, very high intake of antioxidants may destroy or slow the effect of the protective free radicals. Maintaining the proper level is very important; this is where professionals can step in.
There is no simple approach to taking antioxidants. Many seniors are overly cautious and are not getting enough while others are taking too much for their medical conditions. Medical professionals warn that seniors can cause harm to themselves from overmedicat-ing with antioxidants via supple-ments. For instance, when it was
recommended that patients should increase their Vitamin D to 600-800 milligrams a day, studies have shown that high, daily doses of over 2,000 can put patients at risk for up-per gastro-intestinal cancers such as pancreatic cancer. Another study suggested that smokers who took beta-carotene were at an increased
risk for getting lung cancer, and the debate still rages over the benefits vs. the risks of cancer patients taking antioxidants.
A dietician especially trained to work with the elderly popula-tion can discuss and emphasize the benefits of antioxidants, which can slow their aging process and prolong lives. A dietician can rec-ommend healthy food options that contain antioxidants in a daily diet and explain the drawback of an-tioxidants when they are taken in the wrong amounts. Seniors can-not decide independently the level and quantities of their antioxidants; these specifications are determined by multiple factors such as: autoim-mune disease, menopause, and car-diovascular issues.
Seniors and their relatives may be surprised to know that the better home care agencies, such as Ameri-care, an agency providing skilled and paraprofessional services to
patients in their own home, employ dieticians which will be very benefi-cial to patients.
An elderly person’s diet has a very strong effect on their aging process and medical condition. It is therefore beneficial for the elderly and their caregivers to seek the ad-vice of a Registered Dietician.
Irina Lenkovskiy is a Registered Dietitian
and Certified Dietitian Nutritionist. She
has a masters of Science degree in nutri-
tion and has been working with the elder-
ly for the last seven years. She is currently
employed by Americare CSS as a nutri-
tionist providing direct counseling to the
patients and continuing education/con-
sultation to Americare’s nurses. Ameri-
care CSS is a Certified Home Health Agen-
cy. The Americare Companies, founded
in 1982, provide high quality home care
services in the N.Y. metro area, including
the 5 boros, Long Island, and Westches-
ter, Rockland, Orange, Dutchess, Putnam,
Sullivan, and Ulster counties, in the Hud-
son Valley. Americare integrates compas-
sionate patient care with family needs
and is ready to serve 24/7 with registered
nurses, home health aides, PT’s, OT’s,
speech therapists, registered dieticians,
and social workers. For further informa-
tion call Penina Mezei at 917-992-5529,
or e-mail [email protected] for
any questions regarding Americare or
home care services.

FEBRUARY 2012
2929
GO
LDEN
YEA
RS
Seniors and Technology Do Go Together
By Shimon Lewin
With so many new devices filling today’s technology market, picking one that fits
your needs can be daunting and frustrating for someone who hasn’t used such devices before. Seniors, especially, may question if they actu-ally need any of these gadgets. Many people think the new devices coming out are geared mostly for young peo-ple, but to their surprise, I have shown them how several of the devices can be of great use to them. The good news is that even though technology is getting more and more ad-vanced, it is also getting easier to use.
Besides for laptops, there are other types of de-vices that one can carry around with them and en-joy the many benefits that these machines have to offer. In this article, we will mention two: the smart-phone and the tablet.
The Smartphone: A smartphone is a phone that does more than
just make telephone calls. For instance, it can give
you the ability to see pictures and video of family members thousands of miles away. It can also help you keep track and schedule your daily tasks.
The smartphone has four main operating sys-tems in the U.S. This is the software that provides functionality to the phone. The companies that pro-vide the operating systems are Apple (the iPhone), Blackberry, Google (Android devices) and Windows.
The smartphone market was at first dominated by the Blackberry, but in recent years, Apple has pret-ty much taken over, while Google’s Android has been catching up. In last place are Windows-based phones.
The Tablet:A tablet is a device that can do most things that
a computer can do but is lighter and more portable thereby providing greater ease of use. Picking out a tablet can be relatively easy if you are getting an Apple, as there is one basic line to choose from- the iPad series. If you decide to purchase a Google-based tablet, there is a little more research involved when choosing among the different options. I would rec-ommend a screen that is 10.1 inches as opposed to the cheaper seven-inch screens. The bigger screens will allow you to see more and make the view clearer thereby enhancing your day to day usage. Other tablets are produced by companies like Barnes and Noble and Amazon, but that’s a topic for another dis-cussion.
These devices can greatly improve your way of living. Some of the apps (programs that can be pur-chased for the device) are briefly mentioned below, and will hopefully be discussed more in depth in fu-ture articles.
Keeping track of medications. Remembering which medications to take and when can become a challenge when there are many pills to keep track of. There are apps designed to help you keep track of your meds, with the appropriate schedules.
Planning a road trip? Visiting a friend who just moved out to a new neighborhood? Paying a visit to a new doctor? Google Maps will be able to assist you in getting to your destination in unfamiliar territory. You can actually see pictures of the streets (depend-ing on the area) of where you need to go. You will
Continued on page 31

FEBRUARY 2012
3030
GO
LDEN
YEA
RS
Preventing Alzheimer’s Disease With Brain-Healthy Habits
By Tzivia Emmer
As the first wave of baby-boomers hits their mid-60’s, the scientific community is paying close atten-
tion to the escalation of Alzheimer’s dis-ease and other forms of dementia that affect an aging population. Alzheimer’s disease is becoming a global health cri-sis that is expected to exceed 100 mil-lion by 2050.
So far, with clinical trials underway in a number of research centers, the only current medical treatment consists of drugs that can ease or delay symp-toms in some patients.
At the same time, a growing body of research indicates that lifestyle fac-tors can effectively push back the tick-ing Alzheimer’s clock, allowing people to be free of symptoms well into old age, even past age 100.
Senility was once thought to be a normal part of aging, but we now know that Alzheimer’s is a specific disease that causes structural and functional
changes in the brain. In 1906, the German neurologist
and psychiatrist Alois Alzheimer ap-plied chemical stains to slides of brain tissue obtained after the death of a patient with early-onset dementia. He saw deposits of abnormal waxy protein fragments and twisted fibers -- the “am-yloid plaques” and “tau tangles” that currently define Alzheimer’s disease.
Advances in imaging technology eventually showed that these protein deposits were present in nearly all older people if they lived long enough, and that they accumulated over a long pe-riod of time.
“We now know that the pathol-ogy underlying AD is present years, if not decades, prior to development of symptoms,” said Jeffrey R. Petrella M.D., a leader of Alzheimer’s researcher at the Duke University School of Medicine in Durham N.C.
In addressing a session of the yearly meeting of the Radiological Society of North America, Petrella gave an over-view of how research using MRI, posi-
tron emission tomography (PET scans) and biomarkers such as cerebrospinal fluid have allowed scientists to observe what happens inside the brain of a liv-ing person. As a result of such research, the National Institutes on Aging and the Alzheimer’s Association have changed the definition of Alzheimer’s disease to recognize several stages, beginning with mild cognitive impairment (MCI). Previously, the only stage diagnosed was that of dementia, when significant cognitive decline has already occurred.
Gary Small, M.D., who also spoke at the RSNA conference, emphasized the importance of lifestyle factors in fore-stalling the symptoms of Alzheimer’s disease.
Small, the director of UCLA’s Lon-gevity Center and author of the book, The Alzheimer’s Prevention Program, recommends a defensive arsenal of good habits to preserve brain health but he warns that “doing it for a few days isn’t going to help very much.” The point is to establish genuine habits, and to do so as early as possible.
Small’s defensive strategy includes: • Diet, especially the Mediterranean
diet, which emphasizes fruits and vegetables, healthy fats (such as olive oil), and fish (especially those with a high concentration of Ome-ga-3 fatty acids). Those who dislike fish might want to explore and try different types of fish especially in light of MRI studies at the Universi-ty of Pittsburgh Medical Center that suggest eating baked or broiled fish every week can reduce the risk of developing mild cognitive im-pairment and Alzheimer’s disease. Other dietary recommendations in-clude antioxidant-containing foods, moderate caffeine intake, whole grain and high fiber foods, alcohol in moderation including red wine, and a number of spices, including turmeric. (Interestingly, the inci-dence of Alzheimer’s is relatively low in India, where curry is the na-tional dish.)
• Exercise. Couch potatoes take note: Sedentary people who begin a fit-ness program increase the size of their brains in the hippocampus
and frontal lobes, areas related to memory. Researchers at Harvard found that 90 minutes of brisk walking per week, or about 15 min-utes a day, could delay cognitive decline. Any type of aerobic activity will serve the purpose: The goal is to get the heart pumping faster so that it delivers more oxygen and nu-trients to the brain.
• Brain training. Memory games and puzzles are becoming popular for improving brain function. But do they work? We now know that the brain can change and remodel it-self in response to the right kind of stimulation. It can literally grow new neurons to improve informa-tion processing, memory, creative thinking and problem solving.
Alzheimer’s disease spreads
throughout the brain, ultimately
affecting the areas of the cerebral
cortex that control language,
reasoning, sensory processing, and
conscious thought
Courtesy NIH/NIA
Continued on page 31
TELL US YOUR FAMILIES STORIES ABOUT LIVING
WITH ALZHEIMER'S, TO APPEAR IN OUR MAY 2012 ISSUE.
EMAIL US AT [email protected] Madison Ave. Lakewood, NJ 08701 Ph: 732.905.2055 Fax: 732.905.4030
www.lakewoodcourtyard.com
Chanah Daina, CALADirector of Marketing
732.865.8130
R. G
RO
SS
MA
N 7
18.6
77.6
757
A GLATT KOSHER
Assisted & Independent
living community
living at a NEW level
Schedule a tour of our newly decorated Assisted Living Community
Combining the warmth of home with resort ambiance
PHOTO CREDITS: EMES STUDIOS

FEBRUARY 2012
3131
GO
LDEN
YEA
RS
never have to fumble with an outdat-ed map, or rely on unclear or incorrect instructions from friends. It really is amazing to be able to see places you have never been to in such great de-tail and depth!
Apps that connect you to devices to monitor your home while you are away. There are some great devices and apps out there that can help you see your home when you are thou-sands of miles away -- No more won-
dering or worrying about your prop-erty while you are on vacation.
The list of things these tablets can do with the right apps installed on them is endless. It is important to keep in mind that technology can be of great use to people of all ages. Once you learn a little bit about the dif-ferent devices out there, it’s really not as intimidating as it may seem at first.
Shimon Lewin is IT director for The Jewish
Press and the author of numerous articles on
technology and software. He can be reached
via email: [email protected]
Seniors and Technology Do Go Together Continued from page 29
In other words, mental exercise “builds brain muscle.”In addition, a recently released PET scan study at Washington Universi-ty in St. Louis showed that people who are mentally active throughout their lives had lower levels of beta amyloid in their brains than those who were less mentally active. Since amyloid begins accumulat-ing in the brain long before cogni-tive decline occurs, the best ap-proach is to keep learning, reading, writing or engaging in intellectually stimulating activities throughout life.
• De-stress. Among other studies, researchers in Sweden who fol-lowed a group of 1100 women for 35 years found that frequent stress in midlife led corresponded with a 65 percent higher risk of Alzheim-
er’s disease. Defensive strategies against stress include getting enough sleep, not multi-tasking, meditation, physical activity, and meditative exercise such as yoga and tai chi.
Although the National Institutes of Health (NIH) has yet to declare positive-ly that lifestyle habits prevent mental decline, 80 million baby boomers en-tering the age of risk don’t have to wait around but can incorporate the strate-gies in the anti-Alzheimer’s arsenal into a healthy lifestyle.
And meanwhile, as Dr. Petrella told the RSNA attendees, “the cure could be in someone’s test tube right now.”
Tzivia Emmer is a freelance writer and part-
ner with medical physicist Bruce Emmer,
DABR, DABMP, in Emmer Communications,
a copywriting and content team serving the
radiology industry. They can be reached at
Ronald Reagan, the 40th president of the U.S., was one of many prominent
people afflicted with Alzheimer’s disease, including Aaron Copland, Norman
Rockwell and Sugar Ray Robinson.
164-11 Chapin Parkway, Jamaica Hills, NY 11432718-298-7800 • www.margarettietz.org
Centrally located near the Queens communities of Kew Gardens Hills, Hillcrest & Jamaica Estates. Only 20 minutes from Brooklyn, Manhattan & the Five Towns.
adlib
unlim
ited
.com
Expansive Rehab Gym,well-stocked with the latest cutting edge equipment.
IS ON THE MAP*
Plans forExpanded
Kosher Kitchen,with two dedicated
& fabulous chefs.
New Director of Guest Relations –Rebbetzin Lonni Oppenheimer,
beloved Rebbetzin of Young Israel of Forest Hills, to make sure our
Residents feel at home.
Brand new luxurious setting
featuring newly renovated rooms & upscale ambiance.
and our numbers have increased to match!
Margaret TietzNursing & Rehabilitation Center
*We created our very own
Neighborhood Eruv Map & Guide, a highly popular piece that’s now in its second printing!
*
Providing SPIRITual
Sustenanceas your body recovers!™
Continued from page 30

FEBRUARY 2012
3232
HEA
LTH
Y L
IVIN
G
The Okinawan Lifestyle: A Secret to Longevity?
By Leah Lebel
For most people, celebrating at a friend’s or loved one’s one-hundredth birthday is considered a rar-ity. With an average world lifespan of just over 70,
it’s quite likely that most of us will not have the privi-lege of celebrating our own centennial. In one seg-regated part of Japan, however, it’s rather common to meet someone who has celebrated this milestone. Okinawa, one of the Ryukyu Island group, boasts a community of people enjoying the longest life spans on earth. They seem to have access to some secret fountain of youth. In fact, not only are these people older than those in most other cultures, but they are also relatively more active, have fewer chronic health problems, lower rates of dementia, healthier bone densities and appear more youthful than those who are two decades younger. They have the lowest mor-tality rates from some of the most prevalent chronic diseases in the United States, including cancer, heart disease, and strokes.
For years, people have been trying to uncover what became known as “The Okinawan Secret to Reaching Old Age.” While many had hoped to dis-cover some mysterious herbal remedy, or perhaps a recipe for a youth potion, the reality is that there is no easy or quick way to achieve the staggeringly long lives that the Okinawans are fortunate to reach. Indeed, their longevity has a lot more to do with their lifestyle than with luck or a mysterious ritual. The Oki-nawans are living examples of just what far-reaching effects a healthful diet, coupled with a healthful lifestyle, can have. There’s nothing unfamiliar about what their diets contain. In fact, it’s mostly what’s been preached to us by public health officials for years. The problem is that behavior change is easier read about than accomplished. Moreover, many of the central characteristics of the Okinawan lifestyle are not readily adaptable to the fast-paced world we live in today. However, there are several noteworthy lifestyle adaptations that we can, to a limited extent, imitate and implement, with a little motivation and perhaps a powerful will to live longer. Here are some aspects of their healthy lifestyle that you can begin practicing right now: • The Okinawans do not overeat: When it comes to
moderation, there are few who understand limits better than the Okinawans. This culture regularly practices calorie control by a simple cultural prin-ciple that they refer to as “hara hachi bu.” Odd pronunciation aside, this is essentially a method of eating whereby they stop when they are only eighty-percent full. Through Hara Hachi Bu, the Okinawans manage to maintain low BMIs (body-mass indexes), which is likely one of the secrets to their living long.
• Their lower body weights: The average BMI of an Okinawan is twenty, significantly higher than the average in (surprise!) the United States. The new agenda for US public health is now addressing an overweight, rather than a healthy-weight, popula-tion. More than half of the American population
now has a BMI of over 25, making the majority of us overweight. A BMI above 25 puts one at in-creased risk for atherosclerosis and many chronic diseases. There are many benefits from achieving a healthier BMI that many of us can enjoy. Perhaps striving for a BMI that’ll decrease the risk of having a heart attack will increase the odds of extending our life spans.
• Physical Activity: Even at extremely old ages, the Okinawans are anything but sedentary. They maintain high rates of physical activity every day, a recommendation that’s been made by the Acad-emy of Nutrition and Dietetics (formerly known as American Dietetic Association) for many years. The Okinawans garden, dance, and practice martial arts (some members of the Okinawan community still participate in competitive sports past the age of one-hundred).
• What they eat: The Okinawans eat a diet that’s natu-rally high in whole grains and contains a plethora of foods rich in antioxidants and phytochemicals. They consume extraordinarily high amounts of omega-3 fatty acids and monounsaturated fats from sources such as fatty fish. They also consume relatively low amounts of saturated and trans-fats. They eat diets quite rich in fruits and vegetables, which, like main-taining lower BMIs and achieving high physical ac-tivity rates, have been correlated with lower rates of mortality from many chronic diseases.
• Other potential contributors: In addition to eating an ideal diet composition, the Okinawans main-tain social networks and keep strong interpersonal bonds, which is yet another factor that has been associated with good health. Moreover, they have
a non-pressurized and easygoing lifestyle, a strong sense of earthly purpose, and are optimistic. While many of us strive to slow down or squeeze in an-other hour of relaxation in our continuously busy schedules, the Okinawans take it easy and as a re-sult, seem to have more time on their hands in the long run too.
Although there is much evidence that the Oki-nawan practices correlate with longer life spans, there are still many people that are flummoxed and do not understand the staggering impact that mere-ly leading healthful and non-stressful lifestyle can lead to. Truthfully, diet and lifestyle alone does not necessarily guarantee a longer lifespan, but it can of-fer a greater quality of life, if a longer life in itself is not attained.
Another potential factor in the longevity of the Okinawan people, in addition to their healthy life-
style is their genetics. Science does not yet have a conclusive answer to the question of whether ge-netics or lifestyle has a larger impact on determining lifespan. Nonetheless, many are striving to emulate the ways of the Okinawans in the hope of extending their lives. Some consider this a futile quest, but oth-ers will not be surprised if the Okinawan emulators increase their chance to become fortunate enough to attend a very special hundredth birthday party—their own.
Leah Lebel is the former editor-in-chief of the Touro College
newspaper. She graduated with honors and an award along-
side her bachelor’s in biology and psychology and is now pur-
suing a Master’s degree in Nutrition at Brooklyn College.

FEBRUARY 2012
3333
HEA
LTH
Y L
IVIN
G
Juice, the Whole Juice and Nothing but the Juice
By Ita Yankovich
Most people turn to fruit juices as a healthy alter-native to soda and coffee. Whether it’s apple, orange or grape, most of us enjoy at least one
refreshing glass a day. Many are unaware; however, that drinking juice can be just as unhealthy as soda, harmful and damaging to one’s health and even deadly.
Medicine and JuiceWhen taking medicine it is best to take it with plain
water since many fruit juices do not interact well with drugs. Grapefruit juice specifically has been proven to counteract with many medications. The American Chemical Society recently conducted a study where they gave patients taking the allergy drug fexofena-dine, either a glass of water or juice. When the drug was taken with grapefruit juice, for instance, only half of the dose was absorbed into the bloodstream, compared to taking it with water. Grapefruit also doesn’t mix with the popular drug Lipitor causing possible liver dam-age. Scientist have also found that grapefruit, orange and apple juices reduce absorption of the anticancer drug etoposide; certain beta blockers used to treat high blood pressure; cyclosporine, used to prevent rejection of transplanted organs; and certain antibiotics.
European scientists have found high levels of an-timony, a chemical linked to cancer, in a number of popular juice brands. In some cases, the levels were 10 times higher than that what is considered ‘safe' under EU guidelines. It is believed the substance is leached into fruit juices from the plastic bottles.
Children and JuiceMany parents think they are doing the right thing
by filling their kids’ bottles, Sippy cups and glasses with juice, but beware since many juices are not that much better than soda, due to their high sugar content.
The American Academy of Pediatrics issued guide-lines saying fruit juice should not be given to children younger than 6 months, and that there is no nutritional reason to give it to them before their first birthday. Chil-dren 1-6 years old should only have 4-6 ounces of juice a day and older children 8-12 ounces day.
The problem with juices is that their high sugar and calorie count promote obesity in children and makes them lose their appetite for healthier options such as low-fat milk. In addition, by opting for the juice rather than the actual fruit, kids miss out on important fruit fibers.
Fruit juices also promote tooth decay in children especially, when they are allowed to take a bottle or Sippy cup with juice to sleep with them. The prolonged contact allows the sugar in the juice to penetrate the enamel in the child’s teeth more deeply.
Parents should make also sure that they are giving their kids only 100% pasteurized fruit juice, in which any harmful organisms that may be present have been killed by the pasteurization process.
Arsenic found in apple juice has been getting a lot of attention since Dr. Oz, a prominent television talk show host, announced that apple juice contains potentially
dangerous levels of inorganic arsenic, a known carcin-ogen. The FDA at first discredited the report, but then Consumer Reports conducted its own apple juice tests, and found that 10 percent of juices tested contained high arsenic levels. That led the FDA to announce that it was considering tighter apple juice restrictions while it conducts its own research.
Diabetics and JuiceWhen consuming juice, diabetics need to keep a
close watch on their blood sugar levels since some juic-es (cranberry) are absorbed at a quicker rate and lead to a more rapid rise in blood sugar levels compared to unfiltered apple juice or vegetable juice with are ab-sorbed at a slower pace. A limited amount of juice is allowed for diabetics, but they must consider how it fits in as part of a well-rounded diet in keeping within the recommendations of their physician. For diabetics who must take insulin, having a small container of juice readily available is highly recommended. Drinking the juice can serve as a quick antidote in cases of an insu-lin overdose, leading to the risk of passing out due to blood sugar levels falling too low.
Interestingly, an Israeli study has found that pome-granate juice, although it contains sugars, does not worsen sugar levels in the blood, and in fact cut the risk of atherosclerosis.
Decoding the Juice BoxThis article is not intended to discourage juice
drinking, but rather to be smarter about how and what kind of juice we drink. Fruit juices can be a vital part of a well-balanced diet, but consumers need to be edu-cated and understand how to interpret the labels, so they are actually drinking juice and not a concoction of water, dye and sugar.
Tropicana and Nestlé’s Juicy Juice were criticized by the FDA for printing misleading labels, which had con-sumers thinking they were purchasing a 100% blend of orange and tangerine juice, when in fact the product was mostly made up of flavored apple juice. The term used to describe the juice is important. In the USA, fruit juice can only legally be used to describe a product which is 100% fruit juice. A blend of fruit juice(s) with other ingredients is labeled “juice cocktail” or “juice drink.”
Read the ingredient list. Make sure that you’re getting 100% juice. Often times, you think you are drinking cranberry juice, for example, buy you’re re-ally drinking a mixture of apple, grape and cranberry juice, with added cranberry flavor, so don’t be fooled by the picture on the bottle. Check out how many grams of sugar are in the drink and if there are any artificial sweeteners and flavors. Just because the label claims to be sugar –free that doesn’t mean that the liquid is void of all sugars since the fruit contains natural sugars. Misleadingly labeled juice drinks can be dangerous for diabetics and bad for those trying to lose weight.
Ita Yankovich teaches English Literature and Writing at Kings-
borugh and Touro College. She is also a freelance writer who
has authored several articles in various publications. She can
be reached at [email protected]
is a not-for-profit organization services are free of charge to all families.
For more information call TAFKID at (718) 252-2236 or
e-mail: [email protected]
TAFKID assists families whose children
have been diagnosed with a variety of disabilities and special needs.
Services provided by TAFKID include: Family Support Services & Information Educational Advocacy Individual Case Consultation Referrals to Doctors, Therapists,
Schools and Government Programs Parent Matching Family Recreation Programs Parent Training and Meetings Guest Lecturers Community Sensitivity and Training Informational Publications Pediatric Equipment Lending Program Tape/Video Lending

FEBRUARY 2012
3434
HEA
LTH
Y L
IVIN
G
Fitting Fitness into a Busy Man’s Lifestyle
By Isaac Hyman
When it comes to staying healthy, many men elect to focus on healthy eating to maintain a healthy life-
style. Without proper fitness and condition-ing, however, you may miss out on a vital part of healthy living. Think of health and fit-ness as two business partners - steady, sup-portive, growth oriented, and unforgiving when you have one misstep. The problem lies in defining what proper fitness means to the busy working man who considers walking up a flight of stairs to be a strenu-ous exercise. We live in a world of speed and convenience, which means we’re more effi-cient workers but less healthy people. Still, we can do small things to modify our daily commute to and from work to improve fitness. Try getting off one stop earlier on your subway, or walk up the five flights of stairs instead of using the elevator. In-
stead of rid-i n g
the escalator, make double time by walk-ing them also. These small steps will get you thinking fit in all aspects of your day.
Posture issues from non-ergonomic seating, carpal tunnel syndrome, and cramping are all work-related health is-sues that affect body and mind. We’re not giving up computers, chairs, or cramped work spaces anytime soon, but a solid car-dio and aerobic routine in the morning will leave you feeling refreshed and awake to start the day. And for those who just want to shake off the stresses and strains of sit-ting all day, hit the area gym before head-ing home.
In business, time is money. If you value achieving something, then you’ll spend more than five minutes on it. And that goes for your fitness routine. A customized fit-ness routine is a better investment of your time than a 5 minute abs workout.
A great fitness routine goes hand in hand with healthy eating habits. It’s im-portant to remember to hydrate through-out the day with liquids other than coffee. Avoid snacking on chips and opt for a ba-nana instead, a significantly filling and nu-tritious food. Stock your work fridge with yogurts or granola bars that you can grab and go.
By eating healthy and keeping a steady fitness routine, you’ll have more fuel and
energy to do more, achieve more, and keep your ca-
reer moving as fast as you want.
Fit and Trim
TREADMILL TIPS & TRICKS
Vary your workout.In other words, DO NOT do the same action ev-
ery time you get on the treadmill. If you’ve been walking, run a little. If you always run, try power walking for a change. You can play around with the intensity, duration, and incline levels, all to change the type of workout. When you do the same thing, your body just gets used to it and stops reacting. So always change it up.
Add some weights.Try putting on a pair of wrist weights, or ankle
weights. This may slow you down, as it will be hard-
er to move, but it will work your muscles, and give you more of a challenging workout.
Go climbing.On the treadmill that is. Raise the incline level on
your treadmill. You can start with a 2.0 incline and work your way up to whatever feels comfortable (yet challenging). Again, this will slow you down but give you more of a challenge and vary your workout.
Interval training is STILL the best.Interval training, mixing a warm up, jogs, runs
and hill climbing, is considered the best way to burn
fat. That is because after interval training, your body continues to burn fat throughout the day.
Don’t forget to warm up, cool down, and stretch.
Your body is like a car; it is “cold” when not in opera-tion, so give yourself a full five minutes of warm up before you start running or jogging. Walk at a moderate pace, and move your arms as well. When you are done, do NOT just jump off the treadmill with your heart rate so elevat-ed. Slow it down gradually by decreasing the speed until you feel that your heart rate slowly went down (Around 5 minutes). Don’t forget to stretch when you are done.
A Working Woman’s Health Routine
By Tanya Rosen
Media conglomerate CEO Martha Stewart has a packed day, starting at 5
AM and ending at 12 AM. But no matter what her schedule de-mands, Martha makes time to do two workout routines - one complete fitness routine in the morning and a yoga session in the afternoon.
The lesson is obvious - if Martha Stewart, at 69 years old, can make time for two fitness routines, all working women should consider adding a disci-plined fitness routine into their daily or weekly schedules.
For working women like me, juggling a family and a career, the key to a healthy - and mod-erately stress free life - is a sched-ule. Just like you have a weekly planner for all your tasks, buy a weekly fitness planner to track your fitness routine. And stick to it! By schedul-ing your fitness, you won’t miss a beat in your routine.
Lunch time workouts are ris-ing in popularity so
use that extra hour to your ad-vantage. Research any gyms that are within a five minute of your workplace. Not interested in changing and feeling sweaty all day? Opt instead for an in-of-fice workout utilizing chairs for tricep dips and stairs for a great cardio routine. No matter which option you select, make sure to focus on intensity. But most im-portantly - be sure to eat lunch at some point. You’ll need to re-fuel for the rest of the day.
Take it from me - staying fit and eating healthy are impor-tant ingredients for a maintain-ing a healthy lifestyle in the workplace and in your home.
Tanya Rosen is the co-owner of Shape Fitness, an all women’s fitness studio in Flatbush. Tanya is a certified nutritionist, per-
sonal trainer, and Aerobics Instructor, specializing in pre and post natal fitness. The first ever kosher workout DVD by Shape is
now available in Judaica stores or online at www.shapefitnessgym.com, where personal training packages and class schedules
can be viewed as well. To contact Tanya or Shape, please call (718) 338-8700
Isaac Hyman is a Certified Personal Trainer, pushing Jewish
men and youth to stay fit, think fit, and act fit every day. He
can be reached at 908.906.1857 or at MaccabiFitness@
gmail.com

FEBRUARY 2012
3535
HEA
LTH
Y L
IVIN
G
Make Tonight’s Dinner Tomorrow’s Lunch!
By Nina Safar
Want your resolution to eat healthy this year to last? Skip boring meals made out of bland ingredients and go for zesty dishes that are
bursting with flavor. The more flavorful the meal, the more filling it will be! Cilantro, lime, honey, soy sauce, ginger and garlic should all be staples in your kitchen. Carefully blended, these can be used to make even the simplest recipes taste delicious.
When shopping for ingredients, plan ahead to make enough dinner that there will be leftovers for tomorrow’s lunch! This way, you won’t be tempted to order in greasy takeout or munch on muffins, donuts and chips when in the office.
* All of the recipes below can be served over brown rice, quinoa or steamed veggies for dinner; they also taste great in a whole wheat wrap with crisp lettuce and some avocado, or over a salad, for lunch.
Honey Lime Grilled ChickenSome nights I crave carbs like pizza and pasta.
Then there are the nights when all I want is a fresh garden salad topped with juicy slices of perfectly grilled chicken. This marinade blends together some of my favorite ingredients to create a sweet-ly glazed chicken that has just the right kick of lime.
Ingredients:
• 4 boneless, skinless chicken breasts• 1/4 cup olive oil• 1/4 cup soy sauce• Juice of 1 lime• 3 tablespoons honey• 3 cloves of garlic, diced• 1 tablespoon of ginger, diced• 1 teaspoon Grill Mates® Montreal Steak Sea-
soning.
Directions:
Combine the olive oil, soy sauce, lime, honey, garlic, ginger and steak seasoning in a large zip lock bag. Place the chicken inside and marinate for several hours. Heat grill pan to medium high and grill chicken for approximately 6 minutes each side, or until juices run clear. Squeeze some fresh lime on top before serving.
Baked Salmon with Lemon & Cilantro:My husband has never been a fan of salmon
until we had it for dinner one night at our friends, Mira & Levi. I have to admit, at first I was jealous that she was able to get him to eat two servings of something that he would never finish at home. But then I gave myself a mental slap and realized it would be ridiculous for me to not ask her for the recipe. I’m glad I did, since I now make this for din-ner at least once a week!
Ingredients:
• 2 tablespoons olive oil• 2 tablespoons lemon juice• 1/2 teaspoon Montreal Steak Seasoning• Chopped cilantro• 3 pieces of salmon
Directions:
Combine the olive oil, lemon juice and steak seasoning and drizzle some over the fish, leaving half of the mixture on the side. Bake the salmon in a 500 degree oven for 20 minutes, uncovered. After you remove the salmon from the oven, place the chopped cilantro in the remaining olive oil and lemon juice mixture and pour over the freshly baked salmon.
Teriyaki Grilled Tofu:I love a good burger or a zesty chicken dish,
however sometimes it’s nice to switch things up and keep the menu lighter with a vegetarian din-ner. Going meatless doesn’t mean skimping on flavor! The glaze in this recipe is good enough to eat solo, but tastes even better drizzled over veg-gies and grilled tofu.
Ingredients:
• 4 tablespoons soy sauce• 2 tablespoon rice vinegar• 1/4 cup honey• 2 garlic cloves, minced• 1 teaspoon peeled fresh ginger, minced• 1 package of extra firm tofu
Directions:
Remove tofu from package and pat dry with paper towels to remove moisture. Then, cut into triangles and grill the tofu on a grill pan over medium heat (do not heat with oil!). Meanwhile, combine the remaining ingredients on stovetop and stir until thickens. Once the tofu has been cooked, serve over steamed string beans and drizzle the sauce on top.
When Nina Safar is not updating recipes on Kosher in the
Kitch, she enjoys playing hostess. Never having too much
time in the kitchen, she likes recipes that taste great and
are easy to make. Kosher in the Kitch features recipes from
experienced foodies as well as experimenting cooks. You
don’t have to be a chef to cook a good meal! For more great
menu ideas and tasty recipes, check out www.kosher-
inthekitch.com for your next favorite dish.
Crunchy Cravings: Low Cal Snacks!When you are craving something salty and
crunchy, stay away from snacks loaded with emp-ty calories such as potato chips, and reach for a healthier more filling (and still crispy!) snack in-stead.
- Apple slices with peanut butter- Carrot sticks with hummus- Almonds - Frozen Grapes- Roasted chickpeas
FEBRUARY 2012
3636
HEA
LTH
Y L
IVIN
G
New Approach in Natural
HealingBy Jenny Azar CMT
In an age of technical and at times, imper-sonal medicine, massage offers a drug-free, non-invasive and humanistic ap-
proach based on the body’s natural ability to heal itself.
So what exactly are the benefits to re-ceiving regular massage and/or bodywork treatments? • Increases circulation, allowing the body
to pump more oxygen and nutrients into tissues and vital organs.
• Stimulates the flow of lymph, the body’s natural defense system, against toxic invaders. For example, in breast cancer patients, massage has been shown to in-crease the cells that fight cancer.
• Increased circulation of blood and lymph systems improves the condition of the body’s largest organ the skin.
• Relaxes and softens injured and overused muscles.
• Reduces muscle spasms and cramping.• Increases joint flexibility. • Reduces recovery time, helps prepare for
strenuous workouts and eliminates sub-sequent pains of the athlete at any level.
• Releases endorphins the body’s natural painkiller. Massage is now being widely used in chronic illness, injury and recov-ery from surgery to control and relieve pain.
• Reduces post-surgery adhesions and edema, and can be used to reduce and realign scar tissue after healing has oc-curred.
• Improves range-of-motion and decreases discomfort for patients with low back pain.
• Relieves pain for migraine headache suf-ferers and decreases the need for medica-tion.
• Provides exercise and stretching for atro-phied muscles and reduces shortening of the muscles for those with restricted range of motion.
• Promotes shorter labors for women giv-ing birth, as well as reducing the need for medication, relieving depression and anxiety, and shortening hospital stays.
Jenny Azar is a Certified Massage Therapist special-
izing in pre/post natal massage at Bavia Health in
Monmouth Medical Center. She is also a teachers as-
sistant at The Institute for Therapeutic Massage. For
more info call 732-936-911 or log onto http://www.
massageprogram.com.
Sit Stronger to Control Back Pain
By Dr. Steven Weiniger
If you have back pain, you probably already know your posture isn’t good. And if you sit for much of your waking day, you know you’re training your
body to be slumped over into folded, or “weak” pos-ture. However, even though you may never be per-
fectly straight, there are ways to relieve your pain by strengthening your posture.
Low back pain from sitting results from mechani-cal stress on the body. This is called poor bio-me-chanics, and when the body is not mechanically well aligned posture, and balance, is weak. The simple act of balancing when you stand up with weak posture will overwork some muscles and stress joints. The key to reducing this strain is to improve balance, and the ability to control HOW you balance, to retrain muscles and nerves for less pain and better function.
Step one towards stronger posture is improv-ing the symmetry of how your body moves on each side. In fact, just changing the position from which you move can help free up locked and stiff joints and become the first step to stronger posture and less pain.
The SITTING LEG CROSS StrongPosture Stretch
is an easy back and hip stretch you can do at your desk. You can use your office chair, or if you want to challenge yourself with an exercise taught by pos-ture professionals, do the Sitting Leg Cross while sit-ting on a ball.
A: Sit tall and strong on the front edge of chair or ball as you cross your left leg over the right knee. Pull your belly in to brace your core. As you
exhale, keep your head and shoulders aligned as you pull your body forward. Take 2 or 3 breaths, and come up with your posture still strong. Re-peat on other side.
B: Repeat above, but this time cross your legs at the knee.
Do this to help you become aware of and im-prove your lower body symmetry, and to start your own daily posture exercise program.
Steven Weiniger literally wrote the book on posture exercise:
Stand Taller~Live Longer-An Anti-Aging Strategy. He created
the StrongPosture™ exercise programs taught by Certified
Posture Exercise Professionals (CPEPs), chiropractors, PTs,
massage therapists and other body professionals who pro-
mote the importance of posture with annual posture pictures
and daily posture awareness. For more info see www.Body-
Zone.com.

FEBRUARY 2012
3737
HEA
LTH
Y L
IVIN
G
Raw Food DietBy Sheryl Mayer MS RD CDN
It seems like we will do anything to lose twenty pounds before Pesach (or any holiday), whether it entails
getting rid of bad carbs, fats, sweets, caffeine or well, almost everything. Many of my patients are asking me about the raw food diet being popu-larized by celebrities in the media. This diet requires us to eliminate al-most everything we are used to out of our diets, and replace it or just keep foods that are raw. Proponents of the diet believe that a diet made up of mainly uncooked and unpro-cessed plant foods leads to a thin-ner body, more radiant skin and hair, and more physical and mental en-ergy. It also claims to prevent many chronic diseases that are rampant in our times.
Because the diet consists of over 75% raw fruits and vegetables (pref-erably organic), the diet takes a lot of commitment and a lot of time. There is a lot of investment in the kitchen, chopping, blending, juic-ing and dehydrating. The staples
of the diet are fresh fruits and veg-etables, nuts, seeds, beans, grains, legumes, dried fruits, seaweeds, sun-dried fruits, fresh fruit and veg-etable juices, and purified water. People who are true “raw foodists” put a lot of effort into making yeast “cheeses”, cashew milk (from soaked cashews), and sprouted beans. Dairy and animal products are not allowed. Foods cannot be heated higher than 115 to 118 degrees. A dehydrator is a machine that uses heat of the aforementioned low temperature to dry out fruits and vegetables and can help devoted dieters prepare homemade cookies or fruit leathers. The principle be-hind this temperature restriction is that high heat deactivates enzymes naturally found in food and makes the body’s organs work harder to produce the enzymes needed for digestion. Also, heating foods at high temperature tends to produce carcinogens.
I don’t believe that implement-ing this overly restrictive diet is ben-eficial long term. While it is definitely beneficial to eat an abundance of
raw produce, many are unaware that cooking some vegetables (such as tomatoes or carrots) actually boosts the bioavailability of the phytonu-trients. So eating everything raw means that some nutrients won’t be as efficiently absorbed in the di-gestive tract. In the absence of dairy and meat, it can also be challenging to meet your needs for key vitamins and minerals including calcium, iron, zinc, B12, omega 3 fatty acids and protein.
But that doesn’t mean the core concept of the raw food diet is for naught. Meal preparation, using minimal prep and the least pro-cessed ingredients, is usually the healthiest way to go. The best way to transform your diet into a healthy and energizing one is to aim to have two-thirds of your plate made up of healthy plant foods, like vegetables, fruits, whole grains and beans. Then have the remaining one-third made up of protein, preferably fish, lean poultry, and very limited amounts of red meat. To add flavor, use moder-ate amounts of healthy oils, herbs, spices, citrus and vinegars.
Mango avocado salad• 2 Ripe Mangoes, peeled and
chopped• 1 Ripe Avocado, peeled and
chopped• 1 tbsp Lime Juice• 2 tsp Extra Virgin Olive Oil• 1 tbsp chopped basil• 1 tsp Black Sesame Seeds (option-
al)Mix all ingredients together, chill
for a few hours and serve.
Sheryl Mayer MS RD CDN is a registered
dietitian with an M.S. in Health and Nutri-
tion. She is the owner of Nutritionista, a
nutrition consulting service. Due to mul-
tiple requests, a weight loss group is
forming for overweight teens. (Separate
groups for boys and girls). Nutritional
counseling and therapy in a group setting
(in addition to regular private consulta-
tion) will be used to help teens learn how
to lose weight and keep it off permanently.
To inquire about this group, please call
347-850-3438 or email at SherylMayer@
Nutritionistainc.com. Please visit the web-
site www.nutritionistainc.com

FEBRUARY 2012
3838
H&
L TE
CH The Truth about Hair Replacement
By Barry Katz
Unless you are among the lucky 15 percent of males, you will experience some hair loss by the time you reach 50, according to
statistics from the American Hair Loss Associa-tion. Men losing their hair are not the minority; in fact, by age 21, one in four men will have lost some of their hair.
Years ago, men had few viable options for disguising hair loss. Aside from buying a larger yarmulke, one could wear a toupee, perhaps not the most natural look. Furthermore, there are halachic considerations with regard to don-ning tefillin atop a toupee. Some poskim hold that it is assur to do so, which would necessitate removing the fake hair -- thereby defeating its purpose. Rabbi Moshe Feinstein allows for one to place tefillin atop a toupee while in shul, as long as the wearer donned his phylacteries on his bare head at home beforehand. This hardly seems worth the trouble.
A major change took place during the 1980s, when doctors prescribed a medication called minoxidil for patients suffering from high blood pressure. People soon discovered that one of its side effects was the thickening of hair. Thus, in 1988, Rogaine launched a product containing
minoxidil that promised to regrow hair. Thanks to a heavy dose of marketing, Rogaine was soon a household name. While their website boasts that 85 percent of men regrew their hair after four months, the company fails to mention a number of downsides. First, the product is cost-ly. A three-month supply of their topical solu-tion – which may or may not work, as the num-bers indicate – sells for $49.95. This adds up to several hundred dollars a year, and thousands of dollars over one’s lifetime.
Second, the product needs to be applied twice a day. This is quite time consuming. Addi-tionally, when one stops using the product the hair that had regrown, falls out, leaving the user back to the original situation.
Finally, users have mentioned that although Rogaine is FDA approved, it may cause side ef-fects such as dry scalp and itching.
Longer-lasting solutions include hair resto-ration surgery. The idea is to implant hair into the scalp that will re-establish blood flow and allow the hair to grow normally. Various tech-niques are used to transplant hair. As with most technologies, hair grafting has come a long way since it was introduced about a half century ago.
The first hair transplant surgery took place in 1959. Over the next 20 years, the method
was to implant about 12 hairs in a 3-4 millime-ter round. In one session the surgeon would implant about 50 of these grafts. Patients with large bald spots often required multiple visits. This was both time consuming and expensive. Another issue was that the density of the grafts next to the spots without hairs led to a tooth-brush-like effect. These surgeries were there-fore unpopular.
During the 1980s the grafts became small-er. These days, five hairs per graft and smaller rounds give the hair a more natural appearance. Technology also allows for inserting more grafts per visit. Nevertheless, upon close inspection a discerning eye can see the differences between one with a transplant and one with naturally full hair. Another disadvantage is it can take a long time for the hair to be fully restored; the transplanted hair might first fall out before new hair grows in, so anyone expecting quick results will be disappointed. Finally, as with all hair replacement methods, insurance will not reimburse these treatments, which range from $4,000 to $20,000.
Another method is called a scalp flap. Hair from another part of the head is grown long and inserted into the scalp. While this method
Continued on page 41

FEBRUARY 2012
3939
H&
L TE
CHDemystifying Defibrillators
By Jason Esses
If you’ve seen a defibrillator used in movies or television, you come away with an image that evokes heroism, speed, and technological
success. A doctor or paramedic sees an individ-ual in cardiac arrest and quickly grabs a defibril-lator to shock the person back to life. You might think that all that’s needed is the opportunity to defibrillate and everything will be all right.
If only it were that easy. Actually, it all depends on time. Even in a
hospital setting, and I’ve seen many cardiac ar-rests in many hospitals, it could sometimes take more than ten minutes, an eternity, to defibril-late someone in cardiac arrest.
Several types of defibrillators are available. The two general categories are external and in-ternal. External defibrillators come in two variet-ies: the simple-to-use, automated external defi-brillators or AEDs, and the ones typically seen in hospitals, which are the more sophisticated, manual or semi-automatic kind.
The internal defibrillator is automatic and implantable, hence the name Automatic Im-plantable Cardio-defibrillator or AICD, and a lit-tle larger than a typical permanent pacemaker. Let’s first focus on the external kind.
Just what do defibrillators do?
The heart has multiple, interconnected sys-tems: the pumping system, i.e. the heart cham-bers; the plumbing system, i.e. the coronary ar-teries; and the electrical system, i.e. the special-ized conduction tissue of the heart. Defibrilla-tors target problems with the electrical system,
although not all problems. The electrical system may stop working partially or completely, or it could “short-circuit” -- both being potentially life-threatening situations.
Two examples of “short-circuiting,” or ar-rhythmias, are ventricular fibrillation (VF), or ventricular tachycardia (VT). During Ventricu-lar Fibrillation or Ventricular Tachycardia, the heart functionally stops pumping, immediately endangering organs such as the brain. Within minutes, approximately three to five, neurons in the brain start to have irreversible damage. Although Cardio-Pulmonary Resuscitation (CPR) is thought to help, the only real treatment is ef-fectively targeting the Ventricular Fibrillation or Ventricular Tachycardia by applying high electri-cal energy on the heart. This is what a defibrilla-tor does. It does not correct a cessation of elec-trical activity, which only a pacemaker can treat.
According to the American Heart Associa-tion, approximately 300,000 out-of-hospital cardiac arrests occur annually, many of them to people who appear healthy and have no known heart problems or risk factors. Eighty percent of these arrests happen at home, and a meager eight percent survive.
Although not all causes of cardiac arrest are due to ventricular fibrillation or ventricu-lar tachycardia, a significant percentage is. These occurrences are potentially treatable by defibrillation. Upon application, AEDs are de-signed to recognize one of these arrhythmias,
Continued on page 41

FEBRUARY 2012
4040
H&
L TE
CH Protect Your Hearing
in the Digital AgeBy Rachel Wizenfeld
Lovers of the iPod and iPhone may rave about their music collections, but their ears often tell a different story. Due to the increased prevalence of ear buds and
personal listening devices (PDAs) throughout the world, at least one leading doctor estimates that hearing loss is going to hit people at younger and younger ages.
“It’s going to shift the curve,” said Ronald Hoff-man, MD, director of The Ear Institute at the NY Eye & Ear Infirmary. “If we would normally see hearing loss at say, 62, I think it’s going to go to 56. It’s going
to shift the curve down – people are going to get in trouble earlier.”
Any loud noise can damage hearing, he explains, but the real risks come with long-term exposure – whether it’s a noisy work environment, constant listening to earphones or frequent rock concerts or other loud music venues (shall we mention Jewish weddings?).
He quoted a recent study out of Israel, which
found that a large percentage of young people who use PDAs are experiencing hearing loss.
Indicators of hearing loss are very subtle, he said, but signs include difficulty hearing through background noise and being unable to hear phone beeps or the ticking of your wristwatch. High-pitched, high-frequency sounds are usually the first sounds to go, he warns.
“When using a PDA, try to set the sound at the lowest level that you can comfortably hear what you need to hear,” said Dr. Hoffman. “If after using a PDA or noise exposure your ears feel clogged or stuffy and you hear ringing, that sound was too loud. If we tested your hearing at that moment, we would measure a hearing loss…that loss is re-
versible, but if you repeatedly suffer these types of hearing loss, they eventually become perma-nent.”
The Occupational Safety and Health Adminis-tration (OSHA) has recommended an upper limit of 80 decibels for PDAs, according to John Weigand, AUD, director of audiology at SUNY Downstate Medical Center. Dr. Weigand noted that many mp3 players and other music devices have limiting con-
trols, so parents can keep the sound output at de-sired levels for their children.
“But if my own son said he’s going to listen to music at 79 decibels for 8 hours a day, which is lower than the OSHA limit, it’s still too loud,” he said. “It’s common sense: if you’re using ear-phones and someone else can hear the music, it’s too loud.”
Dr. Weigand mentioned the three-foot rule: “If you and I are talking in an environment with back-ground noise, music or traffic, and we’re three feet away from each other and we have to raise our voices, we’re in a place that could be hazardous to hearing over time.”
And while there are steps that everyone can – and should – take to prevent hearing loss, it is still very individual, he said. He’s had patients who expe-rienced hearing damage from just one loud event, and then seen people like a cabinet maker, who used power tools for 25 years, eight hours a day, whose hearing was barely affected. “People are pre-disposed to it,” he said.
Certain health problems are associated with hearing loss, including diabetes, high blood pres-sure and smoking, “anything that affects blood flow can affect the way the inner ear is getting enough oxygen,” Dr. Weigand said. He advises people with these conditions to take extra pre-cautions.
He said that there’s no evidence that a child’s ear is more sensitive than an adult’s, but “it’s natural to take extra precautions – children have a longer way to go in life so they will need their hearing much longer.”
Wearing disposable earplugs from the pharma-cy is an easy way to protect hearing in noisy work environments, whether in a band or near a con-struction site.
“Weddings of all faiths get loud,” Dr. Weigand re-ports, “and usually the band will not turn the music down. Most people attend an average of five wed-dings a year, and if that’s the loudest environment they’re in, it’s not such a problem. If you’re playing in the band five times a month or more, there may be problems.”
Tips to Protect Hearing
• Keep volume levels on PDAs, phones and music devices at the lowest level that you can comfort-ably hear.
• Keep music levels below 80 decibels; if you have kids, implement controls on your children’s mu-sic devices so they can’t surpass this level.
• Be conscious of feelings of ringing or stuffiness after listening to music – if you have these sen-sations, lower the volume or limit your listening time.
• Wear properly-inserted earplugs, available at the drugstore, if frequently exposed to loud environ-ments.
Rachel Wizenfeld is a frequent contributor to publications like
The Jewish Press, The Jewish Journal and the New York Blue-
print. She lives in Los Angeles.

FEBRUARY 2012
4141
H&
L TE
CH
and announce to bystanders if a shock is to be delivered. All the bystander has to do is press the shock button. The more sophisti-cated, semi-automatic or manual defibrillators found in hospitals require rhythm interpretation by a healthcare professional prior to defibrillation.
Case in point: In November 2010, while announcing for a high school football game at Midwood High School in Brooklyn, Erasmus Hall athletic director Marshall Tames suffered a cardiac arrest. One of the coaches started CPR, and a local physician grabbed an AED and saved the man’s life. The entire event was broadcast over the public announcement system. The man recovered nicely after open-heart surgery, and equally important, he didn’t suffer any significant brain damage, because the AED was nearby. If the first re-sponders had had to wait for the paramedics to supply the AED, he could have suffered permanent-ly brain damage even if doctors could have subsequently treated his heart problem.
The implantable defibrillator, or AICD, is offered to two categories of patients. Some patients who have had a prior cardiac arrest
need an AICD for prevention of a repeat event, i.e. secondary pre-vention. And some patients are at risk for cardiac arrest even if they have never had such an episode i.e. primary prevention.
Risk factors for cardiac arrest include congestive heart failure, or a “weak and damaged” heart from prior heart attacks. In the last year, several studies have revealed that the AICD is under-utilized by the medical community, even though it is more effective at saving lives than most of the common medica-tions that patients take to prevent heart attacks.
We all should be asking the fol-lowing questions: Does my local synagogue or community center have an AED? How about the cater-ing hall or summer camp? If so, do we know where it is and how to use it? Would we even know to look for it? If not, then we need to do some-thing about it. AEDs are relatively inexpensive. AEDs can save not just the body but also the quality of productive “life” as it was meant to be lived.
For more information about de-fibrillators, see the American Heart Association online, www.heart.org.
Jason Esses is an attending cardiologist
practicing in Brooklyn, affiliated with
Maimonides Medical Center.
Demystifying Defibrillators
The Truth about Hair Replacement
Continued from page 39
Continued from page 38
In Our Next Issue of
Using Technology to Enhance the
Shabbos ExperienceIn our May 2012 issue, Health &
Living will look at various ways in which new technologycan enhance our enjoyment of Shabbos and Yom Tov within the bounds of Jewish law.
If you have any novel implementations of technology to suggest for inclusion in this story, please email us at [email protected]
produces instant results, the surgery is more complicated. Besides the health risks that accompany all medi-cal procedures, this method will most likely produce uneven results unless it is performed by an expert surgeon.
A third variation of hair replace-ment surgery is scalp reduction. It is exactly as it sounds: Excessive bald skin is removed, and the parts of the scalp with hair are stretched and sewn together. Often this is combined with one of the previous methods. Cutting open the scalp carries the risk of infection, scar-ring and swelling of surrounding areas, including the face.
When electing to undergo one of these surgeries, one must evalu-ate whether the potentially im-proved appearance is worth the possible side effects, the risk that the results will look unnatural, and the cost. If opting for surgery, how-ever, experts advise using only rec-ommended and known surgeons, even though the cost will be much higher.
For those unwilling to pay the big bucks, there is always the big-ger yarmulke.
Barry Katz is a college administrator and
adjunct professor who lives in Brooklyn, NY
with his wife and three children. You can
contact him at [email protected].
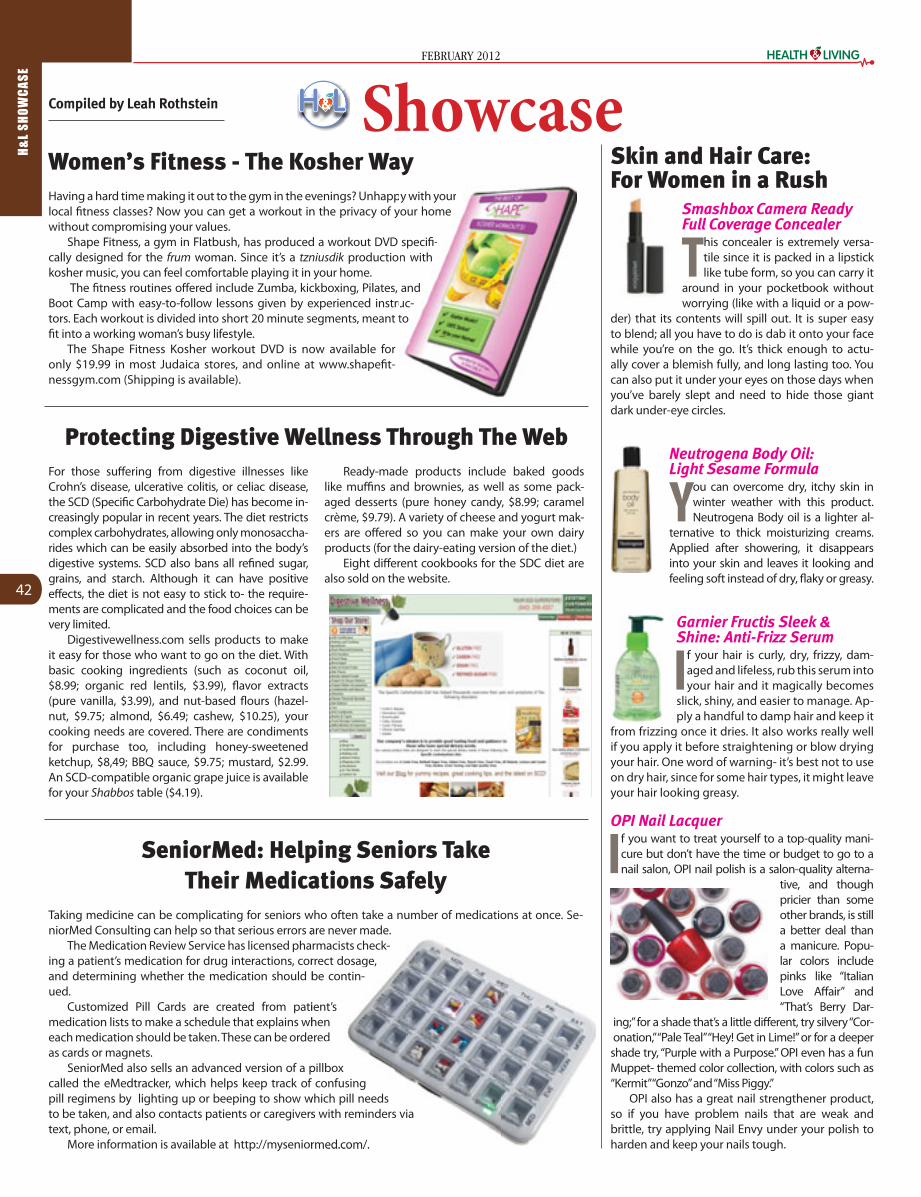
FEBRUARY 2012
4242
H&
L S
HO
WC
AS
E
Garnier Fructis Sleek & Shine: Anti-Frizz Serum
If your hair is curly, dry, frizzy, dam-aged and lifeless, rub this serum into your hair and it magically becomes
slick, shiny, and easier to manage. Ap-ply a handful to damp hair and keep it
from frizzing once it dries. It also works really well if you apply it before straightening or blow drying your hair. One word of warning- it’s best not to use on dry hair, since for some hair types, it might leave your hair looking greasy.
Having a hard time making it out to the gym in the evenings? Unhappy with your local fitness classes? Now you can get a workout in the privacy of your home without compromising your values.
Shape Fitness, a gym in Flatbush, has produced a workout DVD specifi-cally designed for the frum woman. Since it’s a tzniusdik production with kosher music, you can feel comfortable playing it in your home.
The fitness routines offered include Zumba, kickboxing, Pilates, and Boot Camp with easy-to-follow lessons given by experienced instruc-tors. Each workout is divided into short 20 minute segments, meant to fit into a working woman’s busy lifestyle.
The Shape Fitness Kosher workout DVD is now available for only $19.99 in most Judaica stores, and online at www.shapefit-nessgym.com (Shipping is available).
Smashbox Camera Ready Full Coverage Concealer
This concealer is extremely versa-tile since it is packed in a lipstick like tube form, so you can carry it
around in your pocketbook without worrying (like with a liquid or a pow-
der) that its contents will spill out. It is super easy to blend; all you have to do is dab it onto your face while you’re on the go. It’s thick enough to actu-ally cover a blemish fully, and long lasting too. You can also put it under your eyes on those days when you’ve barely slept and need to hide those giant dark under-eye circles.
OPI Nail Lacquer
If you want to treat yourself to a top-quality mani-cure but don’t have the time or budget to go to a nail salon, OPI nail polish is a salon-quality alterna-
tive, and though pricier than some other brands, is still a better deal than a manicure. Popu-lar colors include pinks like “Italian Love Affair” and “That’s Berry Dar-
ing;” for a shade that’s a little different, try silvery “Cor-onation,” “Pale Teal” “Hey! Get in Lime!” or for a deeper shade try, “Purple with a Purpose.” OPI even has a fun Muppet- themed color collection, with colors such as “Kermit” “Gonzo” and “Miss Piggy.”
OPI also has a great nail strengthener product, so if you have problem nails that are weak and brittle, try applying Nail Envy under your polish to harden and keep your nails tough.
py with your your home
specifi-n with
and uc-to
Skin and Hair Care: For Women in a Rush
Women’s Fitness - The Kosher Way
Neutrogena Body Oil: Light Sesame Formula
You can overcome dry, itchy skin in winter weather with this product. Neutrogena Body oil is a lighter al-
ternative to thick moisturizing creams. Applied after showering, it disappears into your skin and leaves it looking and feeling soft instead of dry, flaky or greasy.
Protecting Digestive Wellness Through The WebFor those suffering from digestive illnesses like Crohn’s disease, ulcerative colitis, or celiac disease, the SCD (Specific Carbohydrate Die) has become in-creasingly popular in recent years. The diet restricts complex carbohydrates, allowing only monosaccha-rides which can be easily absorbed into the body’s digestive systems. SCD also bans all refined sugar, grains, and starch. Although it can have positive effects, the diet is not easy to stick to- the require-ments are complicated and the food choices can be very limited.
Digestivewellness.com sells products to make it easy for those who want to go on the diet. With basic cooking ingredients (such as coconut oil, $8.99; organic red lentils, $3.99), flavor extracts (pure vanilla, $3.99), and nut-based flours (hazel-nut, $9.75; almond, $6.49; cashew, $10.25), your cooking needs are covered. There are condiments for purchase too, including honey-sweetened ketchup, $8,49; BBQ sauce, $9.75; mustard, $2.99. An SCD-compatible organic grape juice is available for your Shabbos table ($4.19).
Ready-made products include baked goods like muffins and brownies, as well as some pack-aged desserts (pure honey candy, $8.99; caramel crème, $9.79). A variety of cheese and yogurt mak-ers are offered so you can make your own dairy products (for the dairy-eating version of the diet.)
Eight different cookbooks for the SDC diet are also sold on the website.
SeniorMed: Helping Seniors Take Their Medications Safely
Taking medicine can be complicating for seniors who often take a number of medications at once. Se-niorMed Consulting can help so that serious errors are never made.
The Medication Review Service has licensed pharmacists check-ing a patient’s medication for drug interactions, correct dosage, and determining whether the medication should be contin-ued.
Customized Pill Cards are created from patient’s medication lists to make a schedule that explains when each medication should be taken. These can be ordered as cards or magnets.
SeniorMed also sells an advanced version of a pillbox called the eMedtracker, which helps keep track of confusing pill regimens by lighting up or beeping to show which pill needs to be taken, and also contacts patients or caregivers with reminders via text, phone, or email.
More information is available at http://myseniormed.com/.
are never made.rmacists check-rrect dosage,be contin-
ient’s hen
ered
pillbox f confusing
which pill needs s with reminders via
rmed.com/.
ShowcaseCompiled by Leah Rothstein

FEBRUARY 2012
4343
H&
L S
HO
WC
AS
E
Living Tree Community FoodsLiving Tree sells olive oils, dried fruits, nuts, and
other products that are both organic and in sync with the raw foods movement. They cater to the kosher consumer, with a list available on their website http://livingtreecommunity.com/store2/prod-uct-list.asp clearly labeling which of their products are kosher (certified by the Vaad Hakashrus of Northern California).
The main categories of products sold on the website are: dried fruits/veg-etables, edible seeds, wild rice/grains, co-conut products, nut butters, tahini, pes-tos, olive oils, and honey. They also offer international produce, including some exotic products that can be hard to find (a good
opportunity to make the blessing of shehechiyanu), such as goji berries, agave nectar, and raw cacao beans.
The products come directly from family farmers- the almonds and olives are grown in California’s Central Valley region. For the allergy-concerned, all of the nut butters sold are entirely peanut-free. As a special offer, nursing mothers and seniors get a free package of or-ganic sundried raisins with their order. Don’t forget the chocolates, which are made entirely without sugar- honey is used as a sweetener instead. Tasty and organic gift packs are available for you
to send as shalach manot.
Tokyo Hibachi: Kosher Asian RestaurantWhen you think of exotic restaurant destina-
tions, the first place you think of is probably not Springfield, NJ. Yet Tokyo Hibachi is right there, serving Japanese-style glatt kosher hibachi grilled meat. They also have sushi meat, due to customer demand- but don’t worry, the meat isn’t raw.
New Jersey Jewish News reports that the restau-rant is owned by Amy and Tony Pan, from Indonesia and China respectively. The couple hopes to eventu-ally add more items to the menu from their native cuisines, but it’s hard to find all the ingredients they need here in America, particularly since they need to find kosher versions.
The restaurant is under the supervision of Vaad Harabbonim of MetroWest.
Is Your IPhone Pesachdik?Tired of shlepping around printed directories of
Kosher for Passover products and fumbling through pages of listings when doing your Pesach shop-ping? Now there is a better way.
The OU has released a free app for the iPhone, iPod Touch or IPad which allows you to search for the kind of OU certified product you are looking for on your smartphone while you are in the aisle of the supermarket. Products are listed by category and brand and specify what kind of kosher symbol should be printed on the package.
Users have their choice of searching only for products that are Kosher for Passover or all OU certi-fied kosher products for year round use. The app will also display current OU kosher alerts, listings of new certified products, and provide access to the OU ko-sher question hotline.
The new app, which was released in January, is in addition to an app which was released last
year which searches only for OU Kosher for Pass-over foods either by name or by category. Both are available free for download from the Apple iTunes store.
Showcase
DO YOU HAVE A PRODUCT OR SERVICE THAT YOU WOULD LIKE US TO FEATURE?
EMAIL US AT - [email protected]

FEBRUARY 2012
4444
CO
MM
UN
ITY
PR
OFI
LE
By: Sandy Eller
Founded just over four years ago, Kids of Courage is rapidly mak-ing a name for itself as the only
year round program to provide free medically supervised trips for children with a wide range of illnesses and dis-abilities. In that short period of time, co-founders Ari Adlerstein, Dr. Stuart Ditchek and Howard Kafka have cre-ated an organization whose slogan “Conquering Illness Through Adven-ture” has given a new lease on life to both children who are coping with serious medical situations and their families.
Kids of Courage serves over four hundred families and their list of pa-tient diagnoses is staggering: familial dysautonomia, muscular dystrophy, nemaline myopathy, cancer, seizure disorder, neurofibtomatosis, cere-bral palsy, quadriplegia, paraplegia, spina bifida, liver, kidney and heart transplant, Fanconi’s anemia, total brain injury, stroke, glycogen storage disease, Gaucher disease, multiple genetic disorders, and cystic fibrosis. While some children suffer from long term disabilities, others are dealing with life threatening illnesses. Kids of Courage selects campers based on medical need, targeting the most seriously ill children who are cogni-tively appropriate for their age group. It arranges events and trips with full medical supervision that allow these children and young adults to escape and have some good old fashioned fun despite their fragile medical con-ditions.
The Kids of Courage annual ski weekend is the world’s largest adap-tive ski event. This past year’s three day trip, which took place in early January at Vermont’s Mount Snow in conjunction with Ability PLUS, gave close to sixty children, including some on ventilators, the opportunity
to enjoy a day on the slopes using both regular and adaptive ski equip-ment.
The most impressive Kids of Cour-age program is the annual summer
camp trip. One hundred and fifty chil-dren from twelve different states, Israel, England and Canada participated in the 2011 trip which featured an eight day visit to San Francisco. The itiner-ary included visits to Six Flags Discov-ery Kingdom, an Oakland A’s baseball game, the Golden Gate Bridge, Raging Waters, and tours of Alcatraz, the NASA center and the Jelly Belly factory. Put-ting together a trip of this magnitude is a Herculean effort.
“The average cost per camper with accompanying staff is $5000, which includes air travel, medical equipment rentals, hotel, food, event admis-sion and medications,” explained Dr. Ditchek. “All trips require a minimum of a one to one counselor/camper ra-tio for the least complicated campers and up to a three to one ratio for the most demanding patients, in addition to medical and logistics staff.”
New for 2011 was the TD Bank Five Boro Bike Tour, a forty mile fundraising race that attracted one hundred and
sixty riders, including fifteen campers on adaptive cycles. The event raised over $180,000. Kids of Courage is hoping to attract two hundred riders to this year’s bike tour, which will take place on May 6th.
Kids of Courage runs approximate-ly six Shabbatons, two major trips and several smaller events sprinkled throughout the year. As a precaution, the trips are limited to locations that are near sophisticated medical facili-ties. In most cases, however, the full complement of volunteer medical staff that is an integral part of each
event is able to handle the emergen-cies that inevitably arise.
“To date we have had one case that we weren’t able to handle on our own and required hospitalization,” said Dr. Ditchek. “We deal with medi-cal situations on every flight and have never had to divert a plane due to medical emergency.”
Kids of Courage relies exclusively on private donors and foundations and receives no government funding. The organization has one part time paid administrative employee and
a staff of 1400 volunteers from New York, New Jersey, Florida, Los Angeles, Toronto, Chicago, Detroit, Maryland, Denver, Washington DC, Israel and other locations..
For the dedicated volunteers who donate countless hours, it is an oppor-tunity to give back to those who are less fortunate, and to gain valuable life lessons.
“While I have spent the past four years donating much of my free time towards Kids of Courage, the time I have spent with these children has hardly been unidirectional,” offered volunteer Moishe Gamss. “These kids and their families maintain so-cial normalcy in spite of their daily complications. Seeing this provides me with an obligation to view my comparably uneventful life in a new light. I realize how trivial some of my past discomforts have been and cherish everything I have so much more.”
One of the main priorities for Kids of Courage is to provide a social struc-ture and a network of friends to chil-dren whose medical conditions typi-cally take them outside the normal realm of socialization. Many campers communicate through the Kids of Courage Facebook page, which fea-tures videos, pictures and an opportu-nity for social networking.
“These kids are often home-bound,” said Dr. Ditchek. “Facebook and Skype have presented many great opportunities to our kids. Our goal is to create new opportuni-ties for our campers, providing year round friendship and medical sup-port and to demonstrate to the world that having an illness doesn’t mean that you stop living or experiencing exciting things.”
They can be visited at www.kidsoc.org and Facebook: www.facebook.com/kidsofcourage
BY THE NUMBERSFounded: 2008
Number of Families in Program: 400+
Number of Volunteers: 1400
Number of Paid Full Time Employees: 0Number of Paid Part Time Employees: 1
Community Profile

FEBRUARY 2012
454545
CO
MM
UN
ITY
PR
OFI
LE
Medical Profile

FEBRUARY 2012
4646
CO
MM
UN
ITY
PR
OFI
LE
NYM Adds Bariatric Gastric Bypass to Robotic-Assisted Surgery Program
Adding to its advanced robotic-as-sisted surgery program, New York Meth-odist Hospital now offers minimally in-vasive, robotic gastric bypass surgery to help obese patients achieve weight loss of up to 70 percent of body fat. Obesity is defined as having a body mass index, or ratio of height to weight, of greater than 35. NYM is one of only three hospitals in the Northeast to offer robotic gastric by-pass surgery.
“Weight loss surgery can greatly im-prove the quality of life of many patients,” said Steven J. Carryl, M.D., attending sur-geon, Department of Surgery at NYM. “With better results, less post-operative symptoms and a shorter recovery time, minimally invasive bariatric surgery can be a good option for many obese
patients who need to lose a significant amount of weight.”
Robotic gastric bypass surgery helps patients lose weight by permanently reducing the stomach size and rerout-ing the digestive track. Because of its decreased size, the patient’s stomach will only be able to hold small amounts of food.
The robot, which is controlled by a surgeon, allows for increased precision and enhanced magnification for the surgeon, which results in less pain and a shorter recovery time for the patient, as the minimally invasive procedure means smaller incisions. The patient also experi-ences less blood loss and less scarring than a patient who undergoes traditional gastric bypass surgery.
Because it is irreversible, gastric by-pass surgery should only performed when all other weight loss methods have failed.
For patients who may only need to lose up to 45 percent of their body fat, NYM offers laparoscopic band surgery, a minimally invasive, reversible bariatric procedure that restricts the amount of food a patient can eat by placing an ad-justable band around the stomach.
New York Methodist Hospital also provides customized weight loss plans through its Comprehensive Weight Management Program for overweight or obese patients who do not need or want to undergo sur-gery. Program participants receive a medical evaluation and may meet
with a nutritionist, fitness expert and behavior modification specialist. Monthly follow-up visits with their weight loss “team” allow participants to monitor their progress.
For more information about the Comprehensive Weight Management Program at NYM, call 718.246.8580. To speak with a Hospital staff member about gastric bypass or laparoscopic band surgeries, call 718.780.5293.
Brooklyn Hospital Offers Minimally Invasive Kidney Stone Treatment
New York Methodist Hospital is now using an improved technology, known as the Sonolith i-move, for the dissolution of kidney stones. Ex-tracorporeal shock-wave lithotripsy (ESWL) is a minimally invasive surgical procedure used to treat patients with kidney stones. Physicians in NYM’s Division of Urology, headed by Ivan Grunberger, M.D., make up the first
team in the United States to use the new lithotripsy device, which offers improved results.
Kidney stones are solid masses of tiny crystals that can form in the kid-neys and cause bleeding, kidney dam-age, or ongoing urinary tract infections. It is estimated that more than one mil-lion patients with ESWL are treated an-nually in the United States.
The new lithotripter can also monitor patient movements in real time with revolutionary infrared tracking: if the patient moves slightly during the procedure, the machine locates the kidney stone and com-pletes treatment. The extended pen-etration depth of the shockwaves also allows for treatment of patients who are obese.
Newly Transformed Tietz Center a Must-SeeFollowing the culmination of a
$16 million renovation project, the community is invited to see the brand new Margaret Tietz Nursing and Rehabilitation Center. Central-ly located in the heart of Queens, this 200 bed skilled nursing facility boasts state-of-the-art sub-acute and long-term care in an upscale and luxurious ambiance.
The Tietz Center’s newest AME-Nities™ for the body and soul in-clude a thoroughly remodeled rehab gym that doubled in size, as well as a new décor that pervades the entire facility.
The Center caters to the spe-cific needs of the Jewish com-
munity offering daily minyan prayers, which take place in its very own synagogue with their own on-site Rabbi who also leads Torah study groups. A beauti-fully furnished Shabbos apart-ment is conveniently available for the comfort of visiting fam-ily members, and residents enjoy delicious and healthy glatt kosher cuisine certified by the Vaad Har-abonim of Queens.
The 140 private and 30 semi-private rooms, are well appointed and provide patients and residents with a haven of wall-to-wall com-fort. The Tietz Center offers the ideal environment for recovery following
surgery or a debilitative illness and specializes in quick recovery for or-thopedic conditions. Physical, Occu-pational and Speech Therapies are provided utilizing the most innova-tive techniques and technologically advanced equipment. In addition to Short Term Rehabilitation, the Tietz Center provides Long Term Care, In Patient Hospice/Palliative Care and Adult Day Care.
Medicare, Medicaid, and most HMOs are accepted; a Medicaid Co-ordinator is available to assist with Medicaid applications.
For more information call Steph-anie Zim, Director of Admissions at (718) 298-7800 ext. 2264.
L-R: Angelish Kumar, M.D., Edward
Zoltan, M.D., Ivan Colon, M.D., and
Ivan Grunberger, M.D., chief of
urology at NYM, with the Sonolith
i-move machine.
Steven J. Carryl, M.D., attending
surgeon at NYM, poses with the da
Vinci robot.
Rehabilitating in the state-of-the-
art Rehab room at Margaret Tietz
Nursing and Rehabilitation Center is
enhanced by the presence of Rabbi
Zavel Pearlman and visiting students
from nearby Chofetz Chaim Yeshiva.
Community Provider Bulletin

FEBRUARY 2012
474747
CO
MM
UN
ITY
PR
OFI
LE
Community Provider Bulletin
Community CalendarMARCH
Weight Loss Surgery Support Group Where: Hekemian Auditorium 30 Pros-
pect Ave. Hackensack, NJ. Hours: 6:30-7:30 PM Free support group run by registered nurses and nurse practioners providing on-going peer support and edu-cation to the post-operative bariatric surgery patient. For more information call (201) 966-2193.
North Shore Hospital- Women's Pavilion TourWhere: 125 Community Drive Great
Neck, NY. For more information call 516-465-2552.
JASA Presents: The Annual Volunteer Ventures Expo for New Yorkers 50+
Where: UJA Federation of New York - 130 E. 59 St. New York, NY. Hours: 10AM-2PM. A conference and volunteer opportunities fair for adults 50+ Register in advance at jasa.org
Maimonides Birthing TourWhere: 4802 10th Ave. Brooklyn, NY. For more information call (718) 283-6000.
MARCH CONTINUED
Medical Ethics ConferenceWhere: 3700 Henry Hudson Pkwy, 2nd Fl. Riverdale, NY
Yeshivat Chovevei Torah Rabbinical School of Medical ethics conference will be a three day con-ference with a community event on the night of March 20. For more information call (212) 666-0036.
Save Your Vision - Crescent Tower Community Where: 23-22 39th Astoria, NY: 11:3 AM.
Speaker: Dr. Chad Haller
APRIL
Elaine Kramer Child Development Workshops. Where: UJA Federation 130 East
59St. between Lexington and Park Avenues NY, NY Using Music to Promote Emotional Expression and Build Social SkillsContact Roni Katz at [email protected] or (212) 690-7234. $30 per workshop
Young Child's Expo-9th Annual Conference Where: Hotel Pennsylvania
MAY
Flatbush Satmar Bikur Cholim Annual Spring TeaWhere: Ateres Chynka
Hatzolah of Flatbush Annual Gala AuctionWhere: Cong. Shaarei Zion
Hatzolah of Boro Park Annual Melaveh Malkah (for men)Where: Ateres Golda
Hatzolah of Boro Park Annual Gala Auction Event (for women)
Where: Ateres Golda
Partners for Life Gala-Organization: Gift of Life Bone Marrow Foundation
Where: Grand Hyatt- 109 E 42nd St New York, NY. 6pm-10pmGift of Life will honor its marrow donors, trans-plant recipients, volunteers and financial sup-porters. This year actress Mayim Bialik will serve as the event's emcee. Cocktail hour 6PM Dinner 7PM.Contact: Barby A. Sloven Phone: 561-982-2914 or E-mail: [email protected]
1
4
7
12
21
18
1
6
19
20
17
18-20
20-23
Specialty Care Group & Health Services Centers now in Boro Park
Boro Park Center, located at 4915-10th Av-enue is one of Centers for Specialty Care Group’s newest NYC nursing home and rehabilitation centers. The home specializes in long and short term rehab, bariatric recovery, and hip and knee rehabilitation, among other specialty treat-ments.
"Centers for Specialty Care Group prides itself on servicing the community. At the Boro Park Center, we understand what that involves, and therefore make it our goal to be there for the com-munity," said Kenneth Rozenberg, CEO of CFSCG. Since Boro Park Center has joined the group, the management has made many positive changes to reflect that mission.
Recently, the facility celebrated the opening of
a magnificent shul. The shul was the brainchild of Jeremy B. Strauss, Executive Director and Kenneth Rozenberg, CEO. The Shul at Boro Park Center is for the convenience of residents and their families,” said Strauss. It is brand new, beautifully decorated and fully stocked with seforim. It is especially comforting for residents to have the shul conveniently located on premises.
BPC has full time Resident Ambassadors on site to make certain that all residents’ needs are being met. These ambassadors facilitate the comfort of each individual, ensuring that every resident feels at home at Boro Park Center.
Boro Park Center now has a free courtesy shuttle for the convenience of all members of the com-munity. Schedule for the shuttle can be obtained
through a Resident Ambassador.A brand new, lavish Bikur Cholim Room is avail-
able to all guests. The room is stocked with food, drink and other amenities.
Centers for Specialty Care Group is a compre-hensive and well-respected health services group based in New York City. The group operates an ex-tensive network of health care centers throughout the boroughs in New York City and upstate New York as well as facilities throughout South Jersey. CFSCG facilities have full time on-site physicians, nurses, and many other health care professionals dedicated to providing caring treatment. With many locations throughout New York State, a Centers for Specialty Care facility is never far from you. Now,with Boro Park Center as a member, it is closer than ever.
TO SUBMIT AN EVENT FOE THIS LISTING OR FOR THE WEEKLY JEWISH PRESS: EMAIL [email protected]

FEBRUARY 2012
4848
CO
MM
UN
ITY
PR
OFI
LE
How to Pick the Right Pharmacy
Location/ConvenienceWhen you or your loved ones are
sick, the last thing you need to be concerned about is getting in your car and driving miles to pick up their medication. You want to make sure that the pharmacy is close to where you live or work. It would also be helpful if they had a parking lot or curb-side pickup.
You also want the pharmacy to be convenient with long hours and weekend hours. It would be nice to have a 24 hour operated pharmacy, but small (Shomer Shabbos) pharma-cies cannot do that, so focus instead on finding a pharmacy open at least from 8am to 9pm. On the weekends,
hours are not as important, unless your doctor’s office is also open on Sunday to give you new prescriptions.
InsuranceYou want a pharmacy that accepts a
variety of insurance plans because there is a chance you may have to switch in-surance companies due to work, age, medical or financial issues. If you are a Medicare recipient, you want to make sure that the pharmacy accepts ALL Medicare Part D plans. As a Medicare Part D patient, sometimes one plan be-comes cheaper than another. You want to make sure that if you change plans you won’t have to change pharmacies.
Friendly and Personal Service You want a pharmacy that takes
the time to answer all your questions, that will work with your doctor on dosing and refill issues and that will deal with the insurance company. 7
Look for special perks that some pharmacies offer such as: blood sugar
or blood pressure testing and weight scale. Seek out pharmacies that offer private counseling or stock asthma inhalers or even crutches for injuries. Some pharmacies will mix flavored syrup into liquid medicines for chil-dren to make the taste more palat-able.
HIPAA ComplianceThe Health Insurance Portabil-
ity and Accountability Act deals with patients’ rights. When choosing a pharmacy, make sure that they com-ply with the current HIPAA laws. Most pharmacies will have a sign posted about private consultations and a pa-tient’s right to privacy.
Online PharmacyMany consumers are turning to
the Internet to have their prescrip-tions filled. They do it for the conve-nience and for the potential of great discounts, but there are dangers in-volved if you choose the wrong on-
line pharmacy, so make sure that it follows these guidelines:• The pharmacy must require a pre-
scription.• The pharmacy must ask for a medi-
cal and prescription history. With-out this information, the online pharmacy has no way of checking for drug interactions or inappropri-ate prescribing.
• The pharmacy does not advertise or offer to sell any narcotics or con-trolled substances. It is illegal for any Internet pharmacy to sell or ship these products.
• The Pharmacy should be a fully li-censed Internet pharmacy located in Canada, the U.S., Western Eu-rope, Asia, Australia or New Zea-land. You should be able to spot their licensing number on their website, and if you can’t then ask them for it, and verify it with the li-censing organization.
Local PharmaciesAD Pharmacy1310 48th StreetBrooklyn NY(718) 972-5750
Apple Drugs376 Kingston AvenueBrooklyn, NY (718) 467-6700
Boardwalk RX3100 Ocean Pkwy.Brooklyn, NY(718) 996-7600
Boro Park Pharmacy4723 13th Ave.Brooklyn, NY(718) 437-0505
Cropsey Pharmacy2527 Cropsey Ave.Brooklyn, NY(718) 449-0434
D-Best Pharmacy490 Ave. PBrooklyn, NY(718) 336-7168
Dear Drugs490 Avenue pBrooklyn, NY(718) 375-1282
Eisenberg Pharmacy203 Brighton Beach Ave. Brooklyn NY(718) 743-1200
Eliyahu’s Pharmacy573 Kings HighwayBrooklyn, NY (718) 627-0485
Ezra604 Central AvenueCedarhurst, NY(516) 569-7821
Family Pharmacy3692 Nostrand Ave. Brooklyn, NY (718) 769-9600
Get Well Pharmacy5218 8th Ave.Brooklyn, NY(718) 686-0812
Good Neighbor Pharmacy1614 Ave. MBrooklyn, NY 11230(718) 375-8900
Grand Central Pharmacy420 Central AvenueCedarhurst, NY (516) 295-8880
Hamilton Drugs Corp.4514 Fort Hamilton Pkwy. Brooklyn, NY (718) 435-8800
Haven Pharmacy1211 Ave. UBrooklyn, NY(718) 382-9616
Island Pharmacy1841 Coney Island Ave. Brooklyn, NY (718) 336-2800
J Drugs Pharmacy1205 Ave. JBrooklyn, NY(718) 258-6686
J Drugs II Pharmacy3402 Avenue NBrooklyn, NY(718) 258-5858
Just in Time Pharmacy2126 Knapp St.Brooklyn, NY(718) 332-5474
Kings Bay Chemists3610 Nostrand AvenueBrooklyn, NY(718) 891-3447
Klein’s Pharmacy4818 13th Ave. Brooklyn, NY (718) 633-1548
Lane Pharmacy4623 13th Ave.Brooklyn, NY
Lieb Pharmacy4924 16th Ave. Brooklyn, NY (718) 633-5770
Modern Chemists1630 Coney Island Ave. Brooklyn, NY (718) 258-4200
Metro Drugs5027 New Utrecht AveBrooklyn, NY (718) 431-8000
New Utrecht Pharmacy4624 New Utrecht AveBrooklyn, NY (718) 436-9300
New Age Pharmacy2918 Ave. J Brooklyn, NY(718) 253-1700
Navar Pharmacy3002 Ave. M Brooklyn, NY (718) 677-5811
Noor Pharmacy2036 Bedford Ave. Brooklyn, NY(718) 282-8982
Community Service Directory
Focus on
Pharmacies

FEBRUARY 2012
494949
CO
MM
UN
ITY
PR
OFI
LE
Oceanna Pharmacy6716 18th Ave. Brooklyn, NY(718) 232-2288
Park Pharmacy3205 Quentin Rd. Brooklyn, NY (718) 645-3200
Quick Aid Pharmacy3814 13th Ave. Brooklyn, NY (718) 854-7722
Shalom’s Pharmacy1106 Ave. K. Brooklyn, NY(718) 253-4900
Shimon’s Pharmacy115 Lee Ave. Brooklyn, NY(718) 384-0234
Sunshine Pharmacy411 Kingston AveBrooklyn, NY (718) 773-2020
Supreme RX Pharmacy3011 Ave. N Brooklyn, NY (718) 677-6600
National ChainsCVS PharmacyVisit website for locations www.cvs.com
Duane Reade PharmacyVisit website for locations www.duanereade.com
Rite AidVisit website for locations www.RiteAid.com
Walgreens PharmacyVisit website for locations www.walgreens.com
Community Service
Directory

FEBRUARY 2012
5050
CO
MM
UN
ITY
PR
OFI
LE
by Dr. Robert Van Amerongen
Preventing Medical ErrorsIn 2001, the National Institutes of Health (NIH)
published a groundbreaking report documenting for the first time one of the most serious new medi-cal problems of our day, avoidable medical errors. According to the NIH, medical errors are responsible for between 40,00-100,000 deaths annually among patients in US hospitals, and up to 30% of them could be avoided.
Sometimes the problem is simple human error. But in an increasing number of cases, the true culprit behind the medical error is the dizzying complexity of the modern health care system itself. After careful investigation, we often find that a medical error is the end result of a combination of failures in which the hu-man mistake is just the last link in a long chain.
As the head of the Pediatric Emergency Services department at New York Methodist Hospital in Brook-lyn, I learned of one such chain of events which took place at another hospital. One day, two teenage girls came in at almost the same time complaining of simi-lar symptoms, severe pain in the abdomen, leading the doctors on duty to suspect appendicitis. The two girls also, by chance, had very similar names, and were assigned to adjacent beds.
Diagnostic blood tests were ordered on them both, and one quickly came back with a high white blood cell count, indicating an infection. Doctors placed an order into the hospital’s computer for the pharmacy to send up a dose of antibiotics for the girl with the high white cell count, and sent her to another department to get a CAT scan. Meanwhile, there was a shift change for the nurses on duty. The antibiotics arrived at the ward while the first girl was still away getting the CAT scan. One of the new nurses went to the computer to verify who should receive the medi-cation, but the hospital’s computer system was tem-porarily down. The name on the antibiotic was close to that of the second girl, and she was the only one there at the time with the right set of symptoms, so the nurse gave her the antibiotic, unaware that it was intended for another patient she had never seen.
This could easily have been a tragic mistake, espe-cially if the second girl had suffered an allergic reac-tion to the medication. Fortunately, that did not hap-pen, and when the first girl returned to the ward, the mistake was quickly discovered and rectified.
No serious harm was done, but it could have eas-ily turned out differently. A subsequent investigation would have blamed the nurse, but the error was ac-tually caused by a “perfect storm” of unpredictable events which defeated the safeguards in place to pre-vent such mistakes. It was, in fact, a system error, an example of a modernized version of Murphy’s Law by former NASA official Charles P. Boyle who said, “Suc-cess can be insured only by devising a defense against failure of the contingency plan.”
To explain how these errors happen, experts in the field compare a hospital’s medical safety systems to an onion with overlapping layers. In this case, one
layer of protection was the computerized system which the nurse should have been able to use to verify which patient should receive the antibiotics. But that layer failed because the computer was down. Another layer of the safety onion was the medical training of the nurse, but in this case, the medication was consis-tent with what she knew of the patient’s symptoms, so the error slipped through that layer as well.
Imagine that the errors are small peas being dropped on a constantly shifting stack of Swiss cheese slices, with each slice representing a medical safety system. In most cases, the pea will be stopped by the topmost slice, or it may fall through a hole in the top slice to be stopped by the slice below that. However, if you keep dropping peas long enough, eventually a hole in each of the shifting slices will line up exactly with the others, just for an instant, allowing the error to get all the way through the stack.
Small medical errors of all kinds happen every day, but the built-in safeguards in the system catch the vast majority of them before they can do harm. For ex-ample, if a nurse or a patient reaches for one of several bottles of pills in a medicine cabinet, and accidently picks up the wrong one, they will usually be able to tell immediately by the unique size, shape and color of the pill that they made a mistake.
The problem is that the great complexity in the practice of medicine today has created new ways that medical errors can evade detection. For example, doctors routinely check their patient’s medications to spot dangerous drug interactions, and the patient’s pharmacist is supposed to double check. However, if a patient is seeing several different specialists, one of them can easily be unaware of an incompatible medi-cation that another doctor has prescribed. If that pa-tient also shops around at different pharmacies to get the cheapest price on each drug, that layer of protec-tion against drug interactions will fail as well.
Chai Lifeline’s Camp Simcha Special is a program for children with very serious medical problems who
are usually taking multiple prescription medications and need various types of special treatment. To guard their health, the camp’s medical staff, under my direc-tion, carefully checks and double checks every drug called for on each child’s medical record against the drugs which the child brings with them to camp. Then we have our supervising pharmacist check the drugs again for possible bad interactions, just to make sure.
Today, American hospitals are being held more accountable to stop medical errors. Hospitals now have quality assurance officers on staff working to improve their safety systems, and their efforts have begun to bring down the number of medical errors being made.
A major government-supported effort is now underway to computerize all US medical records to improve accuracy and facilitate sharing, in order to help doctors and nurses make the right treatment decisions.
But if today’s war against medical errors is to be won, parents and the patients themselves must join in the fight. Parents must make sure that they are fully knowledgeable about every aspect of their child’s medical condition. They must serve as their child’s advocates, informing any doctor treating their child about every allergy, every medication their child is taking, and other relevant information, including their child’s accurate weight, which is crucial in determining proper dosages.
The same holds true when looking after the medi-cal needs of an elderly family member. If they are see-ing several doctors, make sure that they are all aware of the total picture. Whenever a new prescription is issued, make sure that the drug name and dosage is clear, and get all the prescriptions filled through the same source, so that the pharmacist can catch any po-tential interactions that were overlooked.
The rule of thumb for stopping medical errors is the same as for stopping terrorists: “If you see some-thing, say something!” If you have a question, don’t be reluctant to ask it. If you suspect that a doctor or nurse is about to make a treatment mistake, speak up!
Today, we truly live in an age of medical miracles. However, as parents and caring family members, we still need to be vigilant to make sure that those treat-ing our loved ones have the complete and accurate information they need to deliver the proper medical care.
Reference: For more information on the various causes of
medical errors, read “How Doctors Think” by Dr. Jerome Groop-
man.
Dr. Robert Van Amerongen is a graduate of Yeshiva University
and the Albert Einstein School of Medicine. He completed a resi-
dency in pediatrics at North Shore University Hospital, and a fel-
lowship in Pediatric Emergency Medicine at Bellevue Hospital/
NYU Medical Center. He is the director of the Pediatric Emergen-
cy Services at New York Methodist Hospital in Brooklyn. He has
served as the Medical Director of Camp Simcha Special since
2008. Dr. Van Amerongen is a resident of the Five Towns and
a Hatzalah volunteer. He is also the Medical Director of Priority
Pediatrics, an urgent pediatric care facility located at 444 Mer-
rick Road in Lynbrook, Long Island - (516) 599-5437.
From the Doctor's Desk
"Dr. Van" taking care of the kids at Camp Simcha
Special

51

52
FEBRUARY 2012
53
2 columns

FEBRUARY 2012
54 AD - FULL PAGESize 8,625"x11,1875"
FEBRUARY 2012
55
AD - 1/2 PAGESize 8,625"x5,5"
AD - 1/4 PAGESize 6,5"x5,5"
AD - 1/8 PAGESize 6,5"x2,67"
AD - 1/8 PAGESize 6,5"x

FEBRUARY 2012
56
AD - 1/2 PAGESize 4,2"x11,1875"
FEBRUARY 2012
57
3 columns

FEBRUARY 2012
58
AD - 1/3 PAGESize 2,75"x11,1875"
AD - 1/6 PAGESize 2,75"x5,5"
These sizes - only for 3 columns
AD - 1/6 PAGESize 5,7"x2,67"