This article was downloaded by: [University of Stellenbosch], [Harold M Lesch] On: 11 January 2012, At: 23:45 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Perspectives Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/rmps20 Health workers: idealistic expectations versus interpreters' competence Ilse Feinauer a & Harold M. Lesch a a Afrikaans and Dutch, Stellenbosch University, Cape Town, South Africa Available online: 29 Nov 2011 To cite this article: Ilse Feinauer & Harold M. Lesch (2011): Health workers: idealistic expectations versus interpreters' competence, Perspectives, DOI:10.1080/0907676X.2011.634013 To link to this article: http://dx.doi.org/10.1080/0907676X.2011.634013 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.tandfonline.com/page/terms-and- conditions This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
This article was downloaded by [University of Stellenbosch] [Harold M Lesch]On 11 January 2012 At 2345Publisher RoutledgeInforma Ltd Registered in England and Wales Registered Number 1072954 Registeredoffice Mortimer House 37-41 Mortimer Street London W1T 3JH UK
PerspectivesPublication details including instructions for authors andsubscription informationhttpwwwtandfonlinecomloirmps20
Health workers idealistic expectationsversus interpreters competenceIlse Feinauer a amp Harold M Lesch aa Afrikaans and Dutch Stellenbosch University Cape Town SouthAfrica
Available online 29 Nov 2011
To cite this article Ilse Feinauer amp Harold M Lesch (2011) Health workers idealistic expectationsversus interpreters competence Perspectives DOI1010800907676X2011634013
To link to this article httpdxdoiorg1010800907676X2011634013
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use httpwwwtandfonlinecompageterms-and-conditions
This article may be used for research teaching and private study purposes Anysubstantial or systematic reproduction redistribution reselling loan sub-licensingsystematic supply or distribution in any form to anyone is expressly forbidden
The publisher does not give any warranty express or implied or make any representationthat the contents will be complete or accurate or up to date The accuracy of anyinstructions formulae and drug doses should be independently verified with primarysources The publisher shall not be liable for any loss actions claims proceedingsdemand or costs or damages whatsoever or howsoever caused arising directly orindirectly in connection with or arising out of the use of this material
Health workers idealistic expectations versus interpretersrsquo competence
Ilse Feinauer and Harold M Lesch
Afrikaans and Dutch Stellenbosch University Cape Town South Africa
(Received 2 February 2010 final version received 17 October 2011)
Health care professionals sometimes have expectations that interpreters cannotmeet In this case interpreters are expected to declare in writing that they assistedthe medical investigator to explain the information in consent forms for parentsof paediatric burns patients and volunteers on antiretroviral therapy Theseconsent forms were translated from English into Afrikaans and isiXhosa Theyalso have to declare that the patients fully understand the content of the relevantdocument and all their questions were satisfactorily answered This investigationshows that the interpreters did not fully understand the information that theyhave to explain None of the interpreters interviewed would like to sign theagreement certifying that they explained the information of the trial in thepatientrsquos mother tongue and that the patient understood it
Interpreters have to take primary responsibility in bringing the message acrossTaking the level of education of the interpreters into account it seems impossiblefor them to explain the medical procedures so that the patients can make aninformed decision They are set up for failure when they are confronted withthis task and these documents The conflict between what is expected of theseinterpreters and the reality of their position is spelled out
Keywords interpreting applied translation interpreting studies
Introduction
This article concerns intercultural communication within the health sector where
health workers are required to communicate across cultural boundaries on a regular
basis South Africa which has 11 official languages is a truly multilingual and
consequently multicultural country This leads to a situation where fellow South
Africans themselves are not able understand one another effectively not simply a
matter of foreign citizens not being understood (Pienaar 2006 p 36) The official
languages in the Western Cape are Afrikaans English and isiXhosa The majority of
residents in the Western Cape are Afrikaans speakers 25 million people use
Afrikaans as their home and first language This amounts to 553 of all Western
Cape residents more than half the population of the province IsiXhosa is the
language spoken by the second largest proportion of the Western Cape population
11 million people which is 237 of the Western Cape population English is
spoken as a first language by only 875000 residents or 193 of the Western Cape
population (Census 2001)
This article discusses the communicative (in)adequacy of the Afrikaans and
isiXhosa target texts translated from English that are used as consent forms for
Corresponding author Email hleschsunacza
Perspectives Studies in Translatology
2011 116 iFirst article
ISSN 0907-676X printISSN 1747-6623 online
2011 Taylor amp Francis
httpdxdoiorg1010800907676X2011634013
httpwwwtandfonlinecom
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
parents of paediatric burn patients and volunteers on antiretroviral therapy In these
texts the interpreters have to declare by their signatures that they assisted the
relevant investigator by explaining the information in the document to the parent or
volunteer using the language medium of Afrikaans or isiXhosa They also have todeclare that the parent or volunteer fully understands the content of the document
and has had all their questions answered satisfactorily What will be investigated here
is not whether these texts communicate adequately with the parent or volunteer
but whether the interpreters fully understand the information that they have to
explain to parents or volunteers
The two issues discussed here are
Will the interpreters fully understand the information on the informed consentforms that they have to explain to parents or volunteers
Is it ethical to leave the explaining to the interpreters and then expect that they
should sign the informed consent forms declaring that the content has been
fully understood by the parents or volunteers
The aim of this article is to highlight the conflict between what is expected of the
interpreters and the reality of their position This will be done by reflecting on the
situation in the Western Cape South Africa The structure of the article will be asfollows sketching the situation by diagnosing the problem contextualising the
research within interpreting studies presenting the two sets of data ie the profile of
the interpreters and the comprehension test and finally the discussion of the results
The situation
The research on the informed consent forms concerned for the two projects was
conducted at the Tygerberg and Red Cross state hospitals respectively TygerbergHospital is linked to Stellenbosch University as a tertiary-level medical institution
The hospital was opened in 1976 and employs 1715 nurses and 536 doctors It treats
approximately 56000 in- and 590000 out-patients per year (Capegateway public
info 2009) The staff mainly has Afrikaans as their mother tongue with a small
proportion using English as first language The patients are also mainly Afrikaans
speakers with a small proportion with English as mother tongue IsiXhosa is the
predominant language among black patients (Williams 2005 in Saulse 2009 p 24)
Informed consent forms and information leaflets were distributed here among HIV-positive volunteer mothers who were using antiretroviral therapy with the title (see
Appendix1 Text 1) lsquoA DOUBLE-BLIND PLACEBO CONTROLLED RANDO-
MISED STUDY TO INVESTIGATE THE EFFICACY AND SAFETY OF LOW-
DOSE L-CARNITINEMAGNESIUM SUPPLEMENTATION IN PREVENT-
ING HYPERLACTINEMIA AND LACTIC ACIDOSIS IN HIV-INFECTED
SOUTH AFRICAN WOMEN ON STAVUDINE CONTAINING COMBINED
ANTIRETROVIRAL THERAPY (cART)rsquo
The Red Cross War Memorial Childrenrsquos Hospital is the only child healthinstitution in South Africa and is located near Cape Town It treats approximately
19700 in- and 216000 out-patients per year (Capegateway public info 2009) This
hospital is linked academically to the University of Stellenbosch the University
of Cape Town and the Faculty of Dentistry of the University of the Western Cape
The staff use both English and Afrikaans in equal proportions while the language
2 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
among patients is very diverse with English Afrikaans and isiXhosa being used on
an almost equal basis (Williams 2005 in Saulse 2009 p 24) Informed consent
forms were distributed here among the parents or legal guardians of burns patients
entitled (see Appendix 1 Text 2) lsquoVIRTUAL REALITY FOR PAIN RELIEF IN
PAEDIATRIC BURNS PATIENTSrsquo
Feinauer (2003) discussed the profile of typical state hospital patients in the
Western Cape they were mostly lay people from a low socio-economic level who are
language impoverished have low or no level of schooling lack communication skills
sometimes do not use the standard varieties of Afrikaans English or isiXhosa they
are economically deprived they have low concentration levels they are ill are
intimidated by the unfamiliar environment and are without any medical knowledge
(Feinauer 2003 pp 216217) Feinauer and Luttig (2005) find that sometimes the
gap between the source-text recipients and the target-text recipients is too big
to be bridged by merely changing the translation approach from linguistic to
functional An empirical study was undertaken on how to present information on
primary ailments (HIVAids and TB) in an accessible form to lay people Actual
target texts in both Afrikaans and isiXhosa were assessed in terms of their
communicative success by using questionnaires amongst state hospital patients
who were on a much lower level of literacy or knowledge than that of the source text
recipients
The main communicative problems were ascribed to the fact that these target
texts were almost exact replicas of the source texts in other words the translators
still used the linguistic approach The source texts were retranslated using the
functionalist approach by translators who played a much more important role in
designing the target texts keeping the target readers in mind the whole time The
target texts were reassessed using the same questionnaires but with different
respondents The respondents however were on the same level of literacy or
knowledge as that of the first group of respondents Then the big disappointment
came comprehension did improve slightly but after all the effort and time that went
into the retranslation the improvement was not statistically significant What did
become apparent in this research is that a target text as such irrespective of the
translation approach is not the means to convey the necessary knowledge to these
target recipients
This should be kept in mind to contextualise the enormity and the responsibility
of the task assigned to the interpreters Before we look at the profile of the
interpreters at these two hospitals and their understanding of the relevant
documents let us look at what is generally expected from health care interpreters
(HCIs) as well as the role that the interpreters are supposed to play during the
communication process
Interpreting theory
Obligations of health care interpreters
According to Angelelli (2006 p 186) health care organisations sometimes have
expectations (which are sometimes even included in job descriptions) beyond the
interpreterrsquos control One of her respondents reacted by noting that lsquoproviders can
easily put us in the position of doing other things which we are not entitled to
do we donrsquot have the training we donrsquot have the capacity to do those thingsrsquo
Perspectives Studies in Translatology 3
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
(Angelelli 2006 p 189) One of the reasons why HCIs are so often misused is because
it is so difficult to define their role in the system Angelelli (2006 p 175) says lsquoOne
of the most problematic issues is the role of interpreters Presumably this role should
be simple to describe the interpreter faithfully conveys a message from one
language to another while maintaining neutralityrsquo Angelelli (2006 p 182) identifies
the following roles that interpreters can play as they perform their task message
converter message clarifier cultural clarifier patient advocate
System agent
All four of these roles could be operative here but in this case the roles of message
converter and clarifier or as Jalbert (1998 in Leanza 2007 pp 1314) calls it the
role of bilingual professional will be the primary role Whatever role the interpreter
takes on here will be within the overarching role of the interpreter as the healthcare
provider or acting on behalf of the institutional or medical system Leanza (2007 p
17) refers to the interpreter playing the role of lsquosystem agentrsquo Here the interpreter is
in essentially the same (symbolic) position as the health care provider
The researchers want the interpreters to be translating machines in other words
to act as linguistic agents but to simultaneously act as health system agents since
they want the interpreter to get the parents or the volunteers to sign the informed
consent forms in order to be able to conduct their research The researcher explains
the relevant information on the informed consent forms to the interpreter(s) and
then the interpreter is left with the patient in a situation of dialogue and not in a
situation of trialogue which is usually the default situation for HCIs As Leanza
(2007 pp 1314) puts it the interpreter becomes the healthcare professional The
fact that the interpreter has to sign that the information was conveyed clearly to the
patient and that the patient understands the information implies that there is an
agreement between the health care provider and the interpreter before the discussion
starts between the interpreter and the patient The interpreterrsquos signature will indicate
that she has kept to the agreement
This is in direct opposition to the view that the interpreter is usually part of
the lsquotreating teamrsquo but is not regarded as the person with the primary responsibility
for the care and treatment of patients The interpreter is usually regarded as acting in
a secondary or supporting role The United States National Council on Interpreting
in Health Care (NCHIC 2004 16) states
Interpreters in health care understand that they are not there as primary participants inthe interaction and therefore are not in a position to make decisions to advise orcounsel Their function is that of a communication facilitator and as such theirresponsibility is to the process of communication and the facilitation of a mutualunderstanding of meaning It is not within the interpreterrsquos set of duties to give advice orto counsel either party with respect to the goals of the health care encounter
Here however the interpreter is pushed into the primary role and has to take
primary responsibility This according to Angelelli (2004 pp 78) would mean that
the interpreter aligns with the system and the interpreter alone has to construct the
conversation This means that the task for bringing the message across is the sole
responsibility of the interpreter This is not a new role for interpreters as seen from
various publications on the role of the interpreter such as the book by Pochhacker
4 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
and Shlesinger (2007 p 2) where one of the roles of the interpreter is described as
someone who could take over the interview and the article by Anthonissen (2008
p 171) which describes the mediating role of the interpreter as providing lsquoguided
constructive interventionrsquoThis more visible interpreter could only successfully step into the shoes of the
health care provider whilst also acting as message converter message clarifier and
cultural clarifier if she were able to fully understand the documents The interpreter
should provide the most faithful rendering possible of what these document say This
does not only entail an accurate translation of the words spokenwritten but also a
translation that formulates the information in such a way that it becomes coherent
within the world view of the patient In order to do this the interpreter needs to have
a deep and thorough knowledge of the subject matter as well as the language usedwithin that field It is obvious that the more explication needs to go into the
clarification of the message the better the interpreter ought to know the subject field
and its discourse The ability to interpret accurately and completely is to a large
extent dependent on how much background knowledge the interpreter has of the
content and context of the communication Romero (2008 p 19) states with respect
to court and legal interpreters that interpreters cannot interpret what they do not
know or understand Communication in the legal setting is guided by an under-
standing of the use of legal arguments protocol procedures laws and traditions Ifinterpreters are not prepared to handle this task they will get in the way or perform
poorly The same applies to HCIs especially if they don the white coat of the health
care provider
According to NCHIC (2004 p 18)
The ethical obligation of interpreters is to possess enough understanding of culture andcultural practices and beliefs to be able to facilitate communication across culturaldifferences seeking to minimize and if possible avoid potential misunderstanding andmiscommunication based on cultural assumptions andor stereotyping Under certainconditions such as clashing cultural beliefs or practices a lack of linguistic equivalencyor the inability of parties to articulate the differences in their own words the interpretershould assist by sharing cultural information or helping develop an explanation thatcan be understood by all (our emphasis)
NCICH (2004 pp 1314) also states that the language used by the provider is asource of data for the patient The patient therefore should be able to access both
the technical information and the information about the kind of relationship the
provider is attempting to establish in order to make decisions that will impact on
his or her health and wellbeing Here this is relevant since the parents or volunteers
have to sign informed consent forms In order for the parents or volunteers to
internalise the necessary information to make the correct and informed decision the
interpreter would have to have succeeded in making all the information clearly
understood
Community agent
The interpreters in this situation could also act as community agents who play an
advocacy role This is the counterpart of the role of system agent where the
interpreters are agents of the institution and spokespersons for the healthcare system
and its discourse As community agents the interpreters may act in accordance with
Perspectives Studies in Translatology 5
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
the cultural norms and values of their own community If the role of advocate is
adopted it presupposes once again that the interpreter is well informed about the
laws rules and procedures that need to be relayed (Leanza 2007 p 14) The task
of the interpreter is twofold here disclose all relevant information necessary for
making an informed choice about proposed procedures and ensure that the patient
understands the information received and the implications of giving consent (adapted
from Johnstone 1999 p 235 who applied this to the role of the nurse regarding
informed consent) Since this research deals with informed consent the interpreterrsquos
role here should rather be that of an advocate for parents and volunteers improving
their level of understanding and in that way helping them to make an informed
decision about taking part in the research or not
What is informed consent According to Robertson (1981 p 102 in Johnstone
1999 pp 210211)
The doctrine of informed consent although having a profound ethical dimension isessentially a legal doctrine developed partially out of recognition of the patientrsquos right toself-determination and partially out of the doctorrsquos duty to give the patient lsquolsquoinformationabout proposed treatment so as to provide him or her with the opportunity of makingan informed or rational choice as to whether to undergo the treatmentrsquorsquo
Johnstone (1999 pp 224225) also feels that the term lsquoinformed consentrsquo should be
abandoned in favour of lsquoinformed decision-makingrsquo Unlike the notion of lsquoinformed
consentrsquo this formulation seems to invite continuous re-evaluation of any decisions
made about care and treatment options Patients must also be informed of their
right to refuse a recommended medical or nursing procedure and should be kept
up to date on the relevant details pertaining to their cases This should be done
by interpreters who adopt the role of patientrsquos advocate Details which are not
readily understood should be explained (in understandable language) and reinforced
through planned patient health education programmes something that nurses
interpreters are educationally prepared to undertake Many factors can deter patients
from exercising informed and voluntary choices amongst which is poor commu-
nication The patientrsquos ability to understand entails whether the patient is able to
comprehend the risks benefits and alternatives to a proposed medical procedure as
well as the implications of giving consent The question could be asked concerning
just how sophisticated a patientrsquos understanding needs to be and in this case
how sophisticated the interpreterrsquos understanding needs to be in order to really
explain these procedures and to really support these parents and volunteers in
making their decisions
Data
Two phases of data collection were involved Both were done during one
consultation with the interpreters The first phase aimed at compiling a profile of
the relevant interpreters whereas the second phase entailed completing a compre-
hension test ie an exercise to ascertain whether the interpreters understand the test
that they were supposed to explain to the patient
6 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Profile of interpreters
The interpreters of the Tygerberg and Red Cross state hospitals were visited by the
researchers and asked to complete questionnaires on their training background
comprehension of the target text etc At Tygerberg only one interpreter was found
and at Red Cross only two Therefore we also visited the Groote Schuur state
hospital where another three interpreters were interviewed although the informed
consent forms were not meant for this hospital The Groote Schuur hospital has a
similar profile to that of the Tygerberg hospital The results of the survey are listed in
Table 1
Regarding the languages offered for TBH and RXH no interpreters were found
for Afrikaans whilst in both hospitals Afrikaans was either the most spoken
language or used on an equal basis with English and isiXhosa All six interpreters are
mother-tongue speakers of isiXhosa with English as their second language At
RXH Sesotho and isiZulu are offered as third languages and at GSH two of the
interpreters offer Afrikaans as their third language Regarding the interpretersrsquo
qualifications none has a tertiary education and not all have even completed their
secondary education Regarding their training as interpreters and the period that
they were interpreting the interpreter at TBH had no training but she was a nursing
ancillary who later just moved into an interpreting lsquopositionrsquo She has been doing
this for the past eight months on a freelance basis at the Tygerberg hospital
The two interpreters at RXH have been performing interpreting duties for the
past seven years They are full-time interpreters and had training in interpreting for
two years on an ad hoc basis from an NGO (non-governmental organisation)
namely the National Language Project (NLP) Apart from language and interpreting
skills they also had some training in counselling They presented themselves as very
professional The three interpreters at GSH had been doing lsquoformalrsquo interpreting
in this hospital for the past two years but were doing interpreting on an ad hoc
basis at the hospital for at least 10 years before that even though their job
description was that of lsquocleanerrsquo When they were appointed as interpreters they
underwent training for six weeks
Table 1 Interpreters consulted
HospitalNumber ofinterpreters Gender Age Qualifications Languages
Interpretertraining
Tygerberg(TBH)
1 Female 33 Matric Wasnursing ancillary
EnglishisiXhosa
None
Red Cross(RXH)
2 Female 35 53 Matric Post-matric studies(Adult basiceducationAncillary socialwork)
EnglishisiXhosaisiZuluEnglishisiXhosaSesotho
Two-yeartrainingSometraining incounselling
GrooteSchuur(GSH)
3 MaleFemale(2)
43 46 48 Busy with matricWere cleaners
EnglishisiXhosaEnglishisiXhosaAfrikaansEnglishisiXhosaAfrikaans
6-weektraining
Perspectives Studies in Translatology 7
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Comprehension test
They were also tested on their comprehension of the English source texts since
all of them offered English and since the source-text documents would have
been explained to them in English The translations into Afrikaans and isiXhosa
are very close linguistic translations of the original so if they did not understand
the source text they would not understand the target text either Questions were
also put on textual issues such as sentence and paragraph length paragraph
coherence and stylistic and lexical suitability (Table 2)
According to Gile (1995 p 34) the following criteria for quality can be applied
universally to all interpreting acts ideational clarity (the message of the sender
should be clear and comprehensible to the receiver) linguistic acceptability (the
interpreter should use grammar which is acceptable for the situation and the other
participants) and terminological accuracy (the interpreter should use the correct
target language equivalent for medical terms in the source language) From the
responses it can be deduced that none of these criteria could be met here
Question 1 addresses the ideational clarity and no interpreter completely agreed
that they clearly understood the message of the senders Linguistic acceptability
and terminological accuracy are addressed by questions 5 and 6 and here no one
agreed that the vocabulary and style of these texts was appropriate for this
situation Other remarks on the texts as such are that they found the texts too
long to explain but they did not think they themselves would be able to paraphrase
them in order to shorten the time with the patients Only one the male interpreter
from GSH felt that if he were given enough time to work with the texts he would
be able to explain the contents to the parents or volunteers The other interpreters
did not feel comfortable explaining the information of the texts so that the patients
or their parents could come to an informed decision as to whether they should sign
the document or not Needless to say none of the interpreters would like to sign
the agreement certifying that they explained the information of the trial in the
patientrsquos mother tongue and that the patient understood what was explained See
Appendix 2 for the section of the Informed Consent forms where the interpreters
are required to sign
If these interpreters were to be confronted with this task the ethical response
would be to withdraw from the assignment unless they are supplied with a much
Table 2 Responses on English source texts
No Question1Donrsquot agree
at all 2Donrsquot agree 3Agree4Completely
agree
1 I clearly understand thetexts
GSH 1 TBH 1 RXH 1 GSH 2 RXH 1
2 The length of thesentences is good
GSH 1 TBH 1 RXH 2 GSH 2
3 The paragraphs arecoherent
RXH 1 RXH 1 GSH3 TBH 1
4 The length of theparagraphs is good
RXH 1 GSH3 TBH 1
RXH 1
5 The vocabulary isappropriate
GSH 2 RXH 2 GSH 1TBH 1
6 The style of the text isappropriate
GSH 3 RXH 2 TBH 1
8 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
simpler document or preferably have a health care provider with them doing the
actual explanation Then they could revert to their more passive role of interpreting
as part of a trialogue The NCICH (2004 p 16) also makes the point that lsquoTo work
within the professional boundaries of the interpreter role also means that interpretersare aware of the limitations of their duties as well as the limitations of their abilities as a
health care interpreterrsquo (our emphasis)
Discussion
Regardless of the role of the interpreter either as system or community agent the
basic goal of medical discourse is mutual understanding Clear verbal commu-
nication is a necessary component of an effective clinical encounter Even when
patients and providers are educated in the same language faulty communication
can lead to distortions and miscommunications between the parties let aloneeducated health care providers and uneducated patients and semi-educated
interpreters (Kaufert amp Putsch 1997 in Angelelli 2004 p 18) Communicative
failure will inevitably be the result here since neither interpreters nor parents or
volunteers have the same level of literacy or knowledge as the compilers of the
source texts in both these instances the compilers were medical researchers The
parents or volunteers would therefore not be able to make informed decisions
about agreeing to take part in the research projects or not
What is equally disturbing is that the interpreters are set up for failure whenthey are confronted with a task of this scope and these types of documents These
target texts will not be comprehensible enough to be viewed as providing an effective
service to the customer According to Gile (1995 pp 7980) one is not able to fully
comprehend something simply on the grounds of knowledge of the language or
extra-linguistic knowledge The content of the speech may be too difficult it may
deviate from generally accepted linguistic standards or the level of knowledge of the
language and extra linguistic knowledge of the receiver may not be high enough
Then it is necessary to analyse the discourse itself to a much greater extent than onewould analyse discourse with regard to comprehension in everyday situations
Therefore to fully comprehend one does not only need knowledge of the language
and extra-linguistic knowledge but the discourse also need purposeful analysis This
type of analysis could not be performed by most of the HCIs in South Africa and
should rather be left to the health care providers or to trained translators working
with the health care providers in rendering a much simpler target text
It is high time to shift the focus in research on health care interpreting to the
way in which the health care provider deals with the HCIs so as not to expectfar more than what their duties entail and their training predicts The education
and career profile of the six interpreters described above is fairly typical of HCIs in
South Africa and health care providers should keep this in mind This is evident
from the following job advertisement for an interpreter with a medical background
but no mention is made of interpreting or translation training The typical
requirements are matric the speaking andor writing skills in the languages needed
and nursing or other medical experience
Mouldmed Locum International Exchange Ltd is looking for a translatorinterpreterwho is able to speak and write three languages fluently (preferably English Afrikaansand Xhosa) The candidate must be able to start immediately and must have a Matric
Perspectives Studies in Translatology 9
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
qualification and a medical background This is a three-month contract with the optionto extend Working hours are 0730 1600 (30-minute lunch) Monday to Friday Thejob entails office work and patient communication A senior assistant nurse with theselanguage requirements would also qualify for the position
Responsibility and ethical behaviour standards towards interpreters should also be
laid down for the health care provider and not only for the interpreter NCICH
(2004 p 19) notes the responsibility of the health care provider lsquoProviders have the
duty to present their knowledge clearly and objectively so that the patient is able
to make informed choicesrsquo If even interpreters are not monitored to meet their
obligations who is going to monitor the health care providers
Further research that could flow from this could be competency testing of the
interpreters to see how well they actually understand the information which had
been communicated by the health care provider and after the interpreters have
explained the information to the patients the same competency testing could be
done on the patientsrsquo understanding This can be established by asking patients
probing questions and inviting them to repeat the information they have received
(Roth et al 1983 p 175 in Johnstone 1999 pp 225227)
A retranslation of the source texts could also be done into Afrikaans and
isiXhosa using the functionalist approach and the interpreters could then be
retested to see whether they now understand the target texts better and whether
they would be able to paraphrase and explain the content better to the patient
Keeping in mind the socio-economic and educational level of the prototypical
patient for whom these informed consent forms are intended we would still
dissuade the interpreters from attempting to convey the message without a health
care provider present and from signing the document
Notes
1 Each of the nine provinces has its own set of official languages eg English Afrikaansand one or more of the indigenous languages On a national level all 11 of these languagesare recognised as official In the case of the Western Cape Province there are thus threeofficial languages as stated
2 Groote Schuur Hospital is linked to the University of Cape Town and situated in theObservatory area in Cape Town a mainly English-speaking area It employs 524 doctorsand 1370 nurses The hospital treats approximately 44000 in-and 575000 out-patientsper year (Capegateway public info 2009) The staff use both Afrikaans and English on anequal basis and a small proportion use African languages The patients are alsopredominantly Afrikaans and English and a large proportion use African or otherlanguages (Williams 2005 in Saulse 2009 p 24)
3 This is the highest level of secondary schooling that can be obtained within the SouthAfrican context This gives access to tertiary education
Notes on contributors
Ilse Feinauer is associate professor in the Department of Afrikaans and Dutch and isresponsible for teaching Translation Studies and Practice to undergraduate and postgraduatestudents She also teaches Afrikaans linguistics She is coordinator for the MPhil inTranslation Studies She has extensive experience both as a translator and scholar intranslation theory
Harold Lesch is a senior lecturer also in the Department of Afrikaans and Dutch and holds aqualification in Translation Studies He is currently coordinator of the Post Graduate Diploma
10 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
in Translation and Interpreting and is responsible for teaching Interpreting Studies andPractice
References
Angelelli C (2004) Medical interpreting and cross-cultural communication CambridgeCambridge University Press
Angelelli C (2006) Validating professional standards and codes Challenges and opportu-nities Interpreting 8 175193
Anthonissen C (2008) On interpreting the interpreter experiences of language practitionersin mediating for the TRC Journal of Multicultural Discourses 3 165188
Capegateway public info (2009) httpwwwwesterncapegovzaengyour_gov5987Census (2001) Primary tables 1996 and 2001 compared Accessed at httpwwwstatssagovza
census01htmlC2001PrimTablesaspFeinauer I (2003) TB or not TB The communicative success of translated medical texts in
South Africa In W Botha (Ed) n Man wat beur rsquon Huldigingsbundel vir Dirk vanSchalkwyk (pp 213223) Stellenbosch Buro of the WAT
Feinauer I amp Luttig L (2005) Functionalism is not always the remedy Perspectives Studiesin Translatology 13 123131
Gile D (1995) Basic concepts and models for interpreter and translator training AmsterdamJohn Benjamins
Johnstone M-J (1999) Bioethics A nursing perspective Sydney HarcourtLeanza Y (2007) Role of community interpreters in pediatrics as seen by interpreters
physicians and researchers In F Pochhacker amp M Shlesinger (Eds) Healthcareinterpreting Discourse and interaction (pp 1134) Amsterdam Benjamins
Pienaar M (2006) Kommunikasie tussen staat en burgers die stand van tolkdienste SabinetOnline 40 3546
Pochhacker F amp Shlesinger M (Eds) (2007) Healthcare interpreting Discourse andinteraction Amsterdam Benjamins
Romero B (2008) Here are your right hands exploring interpreter qualifications Universityof Dayton Law Review 34 1533
Saulse B (2009) Interpreting within the Western Cape Health Care Sector A DescriptiveOverview (Unpublished masterrsquos thesis) University of Stellenbosch South Africa
United States National Council on Interpreting in Health Care (2004) A national code ofethics for interpreters in health care The National Council on Interpreting in Health CareWorking Papers Series httpwwwncihcorg
Appendix A
Text 1
A DOUBLE-BLIND PLACEBO CONTROLLED RANDOMISED STUDY TO INVESTI-GATE THE EFFICACY AND SAFETY OF LOW-DOSE L-CARNITINEMAGNESIUMSUPPLEMENTATION IN PREVENTING HYPERLACTINEMIA AND LACTIC ACIDO-SIS IN HIV-INFECTED SOUTH AFRICAN WOMEN ON STAVUDINE CONTAININGCOMBINED ANTIRETROVIRAL THERAPY (cART)
Introduction
We are doing a study to see if a l-carnitine magnesium combination product that could help toprevent high blood lactate levels which are known to be one of the side effects of some of themedications used in the treatment of HIV-infection (anti retroviral drugs)
The ability to decrease the way the virus multiplies is achieved by combined anti retroviraltherapy HIV positive (HIV ) patients receiving a combination of these drugs survive by
Perspectives Studies in Translatology 11
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
keeping the infection under control but not by killing the virus altogether This treatment hasindeed increased the quality of life in HIV individuals
One of the drugs the nucleotidic reverse transcriptase inhibitors (NRTIrsquos) can alter the energyproducing part of cells in the body and this that can lead to effects such as the high bloodlactate Twenty five percent of patients with high lactate levels donrsquot have any symptoms whileonly a smaller percentage less than 10 percent develops symptoms including loss of weightand abdominal pain
What is the purpose of this trial
A previous study showed that the low dose l-carnitine and magnesium was absorbed in healthymale volunteers and that the supplement was safe to administer
We want to determine if a dose of two capsules per day of the study drug over a period of ayear prevents the build up of lactic acid in the blood We also want to show if the l-carnitineand magnesium is absorbed in HIV positive subjects on combined anti-retroviral therapy anddetermine what the concentration levels of the anti-retroviral drugs are after a period of 6months and 12 months
To achieve this the study drug must be compared with a placebo (these are capsules that looksthe same as the study drug which are filled with a harmless compound in this case lactose)An extra 20 ml of blood and 50ml of urine apart from the normal routine bloods will be takenbefore starting anti-retroviral therapy and 30ml of blood and 50ml of urine will be taken 6monthly thereafter up to 12 months
The levels of lactic acid cholesterol triglycerides LDL - HDL- and Lp(a) lipoproteins andanti-retroviral drugs will be determined in the blood and those of the l-carnitine with itssupporting metabolites (the organic acid - amino acid-and major and trace element profileswhich includes magnesium) will be determined in the blood and urine These results of thosesubjects that are on the study drug will be compared with those of the placebo group to show ifthere are statistical relevant differences
Text 2
PARTICIPANT INFORMATION SHEET AND CONSENT FORM FOR USE BYPARENTSLEGAL GUARDIANS
Virtual Reality for pain relief in paediatric burns patients
What is this research study all aboutYour child has been admitted to this unit because of their burn injury Every child in this burnsunit has dressing changes on a daily basis Your child will be given the normal medication thatshehe receives during any dressing change These dosages of medication have been prescribedby the doctor when your child was admitted to the burns unit With all burn injuries one ofthe biggest problems that our patients experience is pain At the moment the professionals inthe burns unit do not know if there is something other than pain medication that can help todecrease your childrsquos pain Certain studies have proven that using a technique called VirtualRealty (VR) can distract a child and thereby decrease their pain during a specific procedureVirtual Reality is a program that we will use to allow your child to watch a video game throughgoggles that will be placed on their face Half of the treatment will be done using only the painmedication The other half of the dressing change will be done using the pain medication andthe VR We will then interview yourself and your child to find out how you your child feltabout this process and if you feel that Virtual reality can help to decrease your childrsquos painDuring the interviews with youyour child and nursing staff information may be recorded on a
12 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
tape recorder so that we can check all our information We will also be videotaping alldressing changes and using information from those tapes to help us with this study
Why has your child been invited to participateIn order to see if this process of VR is going to worknot work we have to assess it on at least250 children All children who are over the age of 5 and who do not have a face burn can takepart in this study You and your child have the option to participate in this study andparticipation is completely VOLUNTARY
What will your responsibilities beBy agreeing to let your child participate in this study you will allow us to ask your child tocomplete a questionnaire You will also be interviewed
Will your child benefit from taking part in this researchAt this stage we cannot say if your child will benefit from the study that we are doing If whatwe are doing does work then your child will experience less pain during the dressing changesIf the results are positive then it means that in the future more patients with similar injuries toyour child can be helped when they are experiencing pain during dressing changes
Are there any risks involved in your child taking part in this researchThere are no reported risks The only reported side effect of the VR is sickness If your childdoes experience any sickness due to the VR it will be stopped immediately
If you do not agree to allow your child to take part what alternatives does your child haveYou and your child have the option not to participate in this study participation is completelyVOLUNTARY Your child will only be entered into the study with your permission If youchoose not to enter the study we will still treat your child to the best of our ability and it willnot change the way you are treated You can leave the study at any time after you join
Who will have access to your childrsquos medical recordsAny information gained from this study and testing will be kept strictly private and no oneoutside of the people in the study will know youryour childrsquos results without your permissionIf the information is published to educate other health care professionals we will not use anynames Thus you and your child will never be able to be identified by anyone except studypersonnel Similarly no person outside of the study will have access to audio and videorecordings that may have been made during the dressing changes
Will you or your child be paid to take part in this study and are there any costs involvedYou or your child will not be paid to take part in the study and there will be no costs involvedfor you if your child does take part
Perspectives Studies in Translatology 13
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
14 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Health workers idealistic expectations versus interpretersrsquo competence
Ilse Feinauer and Harold M Lesch
Afrikaans and Dutch Stellenbosch University Cape Town South Africa
(Received 2 February 2010 final version received 17 October 2011)
Health care professionals sometimes have expectations that interpreters cannotmeet In this case interpreters are expected to declare in writing that they assistedthe medical investigator to explain the information in consent forms for parentsof paediatric burns patients and volunteers on antiretroviral therapy Theseconsent forms were translated from English into Afrikaans and isiXhosa Theyalso have to declare that the patients fully understand the content of the relevantdocument and all their questions were satisfactorily answered This investigationshows that the interpreters did not fully understand the information that theyhave to explain None of the interpreters interviewed would like to sign theagreement certifying that they explained the information of the trial in thepatientrsquos mother tongue and that the patient understood it
Interpreters have to take primary responsibility in bringing the message acrossTaking the level of education of the interpreters into account it seems impossiblefor them to explain the medical procedures so that the patients can make aninformed decision They are set up for failure when they are confronted withthis task and these documents The conflict between what is expected of theseinterpreters and the reality of their position is spelled out
Keywords interpreting applied translation interpreting studies
Introduction
This article concerns intercultural communication within the health sector where
health workers are required to communicate across cultural boundaries on a regular
basis South Africa which has 11 official languages is a truly multilingual and
consequently multicultural country This leads to a situation where fellow South
Africans themselves are not able understand one another effectively not simply a
matter of foreign citizens not being understood (Pienaar 2006 p 36) The official
languages in the Western Cape are Afrikaans English and isiXhosa The majority of
residents in the Western Cape are Afrikaans speakers 25 million people use
Afrikaans as their home and first language This amounts to 553 of all Western
Cape residents more than half the population of the province IsiXhosa is the
language spoken by the second largest proportion of the Western Cape population
11 million people which is 237 of the Western Cape population English is
spoken as a first language by only 875000 residents or 193 of the Western Cape
population (Census 2001)
This article discusses the communicative (in)adequacy of the Afrikaans and
isiXhosa target texts translated from English that are used as consent forms for
Corresponding author Email hleschsunacza
Perspectives Studies in Translatology
2011 116 iFirst article
ISSN 0907-676X printISSN 1747-6623 online
2011 Taylor amp Francis
httpdxdoiorg1010800907676X2011634013
httpwwwtandfonlinecom
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
parents of paediatric burn patients and volunteers on antiretroviral therapy In these
texts the interpreters have to declare by their signatures that they assisted the
relevant investigator by explaining the information in the document to the parent or
volunteer using the language medium of Afrikaans or isiXhosa They also have todeclare that the parent or volunteer fully understands the content of the document
and has had all their questions answered satisfactorily What will be investigated here
is not whether these texts communicate adequately with the parent or volunteer
but whether the interpreters fully understand the information that they have to
explain to parents or volunteers
The two issues discussed here are
Will the interpreters fully understand the information on the informed consentforms that they have to explain to parents or volunteers
Is it ethical to leave the explaining to the interpreters and then expect that they
should sign the informed consent forms declaring that the content has been
fully understood by the parents or volunteers
The aim of this article is to highlight the conflict between what is expected of the
interpreters and the reality of their position This will be done by reflecting on the
situation in the Western Cape South Africa The structure of the article will be asfollows sketching the situation by diagnosing the problem contextualising the
research within interpreting studies presenting the two sets of data ie the profile of
the interpreters and the comprehension test and finally the discussion of the results
The situation
The research on the informed consent forms concerned for the two projects was
conducted at the Tygerberg and Red Cross state hospitals respectively TygerbergHospital is linked to Stellenbosch University as a tertiary-level medical institution
The hospital was opened in 1976 and employs 1715 nurses and 536 doctors It treats
approximately 56000 in- and 590000 out-patients per year (Capegateway public
info 2009) The staff mainly has Afrikaans as their mother tongue with a small
proportion using English as first language The patients are also mainly Afrikaans
speakers with a small proportion with English as mother tongue IsiXhosa is the
predominant language among black patients (Williams 2005 in Saulse 2009 p 24)
Informed consent forms and information leaflets were distributed here among HIV-positive volunteer mothers who were using antiretroviral therapy with the title (see
Appendix1 Text 1) lsquoA DOUBLE-BLIND PLACEBO CONTROLLED RANDO-
MISED STUDY TO INVESTIGATE THE EFFICACY AND SAFETY OF LOW-
DOSE L-CARNITINEMAGNESIUM SUPPLEMENTATION IN PREVENT-
ING HYPERLACTINEMIA AND LACTIC ACIDOSIS IN HIV-INFECTED
SOUTH AFRICAN WOMEN ON STAVUDINE CONTAINING COMBINED
ANTIRETROVIRAL THERAPY (cART)rsquo
The Red Cross War Memorial Childrenrsquos Hospital is the only child healthinstitution in South Africa and is located near Cape Town It treats approximately
19700 in- and 216000 out-patients per year (Capegateway public info 2009) This
hospital is linked academically to the University of Stellenbosch the University
of Cape Town and the Faculty of Dentistry of the University of the Western Cape
The staff use both English and Afrikaans in equal proportions while the language
2 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
among patients is very diverse with English Afrikaans and isiXhosa being used on
an almost equal basis (Williams 2005 in Saulse 2009 p 24) Informed consent
forms were distributed here among the parents or legal guardians of burns patients
entitled (see Appendix 1 Text 2) lsquoVIRTUAL REALITY FOR PAIN RELIEF IN
PAEDIATRIC BURNS PATIENTSrsquo
Feinauer (2003) discussed the profile of typical state hospital patients in the
Western Cape they were mostly lay people from a low socio-economic level who are
language impoverished have low or no level of schooling lack communication skills
sometimes do not use the standard varieties of Afrikaans English or isiXhosa they
are economically deprived they have low concentration levels they are ill are
intimidated by the unfamiliar environment and are without any medical knowledge
(Feinauer 2003 pp 216217) Feinauer and Luttig (2005) find that sometimes the
gap between the source-text recipients and the target-text recipients is too big
to be bridged by merely changing the translation approach from linguistic to
functional An empirical study was undertaken on how to present information on
primary ailments (HIVAids and TB) in an accessible form to lay people Actual
target texts in both Afrikaans and isiXhosa were assessed in terms of their
communicative success by using questionnaires amongst state hospital patients
who were on a much lower level of literacy or knowledge than that of the source text
recipients
The main communicative problems were ascribed to the fact that these target
texts were almost exact replicas of the source texts in other words the translators
still used the linguistic approach The source texts were retranslated using the
functionalist approach by translators who played a much more important role in
designing the target texts keeping the target readers in mind the whole time The
target texts were reassessed using the same questionnaires but with different
respondents The respondents however were on the same level of literacy or
knowledge as that of the first group of respondents Then the big disappointment
came comprehension did improve slightly but after all the effort and time that went
into the retranslation the improvement was not statistically significant What did
become apparent in this research is that a target text as such irrespective of the
translation approach is not the means to convey the necessary knowledge to these
target recipients
This should be kept in mind to contextualise the enormity and the responsibility
of the task assigned to the interpreters Before we look at the profile of the
interpreters at these two hospitals and their understanding of the relevant
documents let us look at what is generally expected from health care interpreters
(HCIs) as well as the role that the interpreters are supposed to play during the
communication process
Interpreting theory
Obligations of health care interpreters
According to Angelelli (2006 p 186) health care organisations sometimes have
expectations (which are sometimes even included in job descriptions) beyond the
interpreterrsquos control One of her respondents reacted by noting that lsquoproviders can
easily put us in the position of doing other things which we are not entitled to
do we donrsquot have the training we donrsquot have the capacity to do those thingsrsquo
Perspectives Studies in Translatology 3
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
(Angelelli 2006 p 189) One of the reasons why HCIs are so often misused is because
it is so difficult to define their role in the system Angelelli (2006 p 175) says lsquoOne
of the most problematic issues is the role of interpreters Presumably this role should
be simple to describe the interpreter faithfully conveys a message from one
language to another while maintaining neutralityrsquo Angelelli (2006 p 182) identifies
the following roles that interpreters can play as they perform their task message
converter message clarifier cultural clarifier patient advocate
System agent
All four of these roles could be operative here but in this case the roles of message
converter and clarifier or as Jalbert (1998 in Leanza 2007 pp 1314) calls it the
role of bilingual professional will be the primary role Whatever role the interpreter
takes on here will be within the overarching role of the interpreter as the healthcare
provider or acting on behalf of the institutional or medical system Leanza (2007 p
17) refers to the interpreter playing the role of lsquosystem agentrsquo Here the interpreter is
in essentially the same (symbolic) position as the health care provider
The researchers want the interpreters to be translating machines in other words
to act as linguistic agents but to simultaneously act as health system agents since
they want the interpreter to get the parents or the volunteers to sign the informed
consent forms in order to be able to conduct their research The researcher explains
the relevant information on the informed consent forms to the interpreter(s) and
then the interpreter is left with the patient in a situation of dialogue and not in a
situation of trialogue which is usually the default situation for HCIs As Leanza
(2007 pp 1314) puts it the interpreter becomes the healthcare professional The
fact that the interpreter has to sign that the information was conveyed clearly to the
patient and that the patient understands the information implies that there is an
agreement between the health care provider and the interpreter before the discussion
starts between the interpreter and the patient The interpreterrsquos signature will indicate
that she has kept to the agreement
This is in direct opposition to the view that the interpreter is usually part of
the lsquotreating teamrsquo but is not regarded as the person with the primary responsibility
for the care and treatment of patients The interpreter is usually regarded as acting in
a secondary or supporting role The United States National Council on Interpreting
in Health Care (NCHIC 2004 16) states
Interpreters in health care understand that they are not there as primary participants inthe interaction and therefore are not in a position to make decisions to advise orcounsel Their function is that of a communication facilitator and as such theirresponsibility is to the process of communication and the facilitation of a mutualunderstanding of meaning It is not within the interpreterrsquos set of duties to give advice orto counsel either party with respect to the goals of the health care encounter
Here however the interpreter is pushed into the primary role and has to take
primary responsibility This according to Angelelli (2004 pp 78) would mean that
the interpreter aligns with the system and the interpreter alone has to construct the
conversation This means that the task for bringing the message across is the sole
responsibility of the interpreter This is not a new role for interpreters as seen from
various publications on the role of the interpreter such as the book by Pochhacker
4 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
and Shlesinger (2007 p 2) where one of the roles of the interpreter is described as
someone who could take over the interview and the article by Anthonissen (2008
p 171) which describes the mediating role of the interpreter as providing lsquoguided
constructive interventionrsquoThis more visible interpreter could only successfully step into the shoes of the
health care provider whilst also acting as message converter message clarifier and
cultural clarifier if she were able to fully understand the documents The interpreter
should provide the most faithful rendering possible of what these document say This
does not only entail an accurate translation of the words spokenwritten but also a
translation that formulates the information in such a way that it becomes coherent
within the world view of the patient In order to do this the interpreter needs to have
a deep and thorough knowledge of the subject matter as well as the language usedwithin that field It is obvious that the more explication needs to go into the
clarification of the message the better the interpreter ought to know the subject field
and its discourse The ability to interpret accurately and completely is to a large
extent dependent on how much background knowledge the interpreter has of the
content and context of the communication Romero (2008 p 19) states with respect
to court and legal interpreters that interpreters cannot interpret what they do not
know or understand Communication in the legal setting is guided by an under-
standing of the use of legal arguments protocol procedures laws and traditions Ifinterpreters are not prepared to handle this task they will get in the way or perform
poorly The same applies to HCIs especially if they don the white coat of the health
care provider
According to NCHIC (2004 p 18)
The ethical obligation of interpreters is to possess enough understanding of culture andcultural practices and beliefs to be able to facilitate communication across culturaldifferences seeking to minimize and if possible avoid potential misunderstanding andmiscommunication based on cultural assumptions andor stereotyping Under certainconditions such as clashing cultural beliefs or practices a lack of linguistic equivalencyor the inability of parties to articulate the differences in their own words the interpretershould assist by sharing cultural information or helping develop an explanation thatcan be understood by all (our emphasis)
NCICH (2004 pp 1314) also states that the language used by the provider is asource of data for the patient The patient therefore should be able to access both
the technical information and the information about the kind of relationship the
provider is attempting to establish in order to make decisions that will impact on
his or her health and wellbeing Here this is relevant since the parents or volunteers
have to sign informed consent forms In order for the parents or volunteers to
internalise the necessary information to make the correct and informed decision the
interpreter would have to have succeeded in making all the information clearly
understood
Community agent
The interpreters in this situation could also act as community agents who play an
advocacy role This is the counterpart of the role of system agent where the
interpreters are agents of the institution and spokespersons for the healthcare system
and its discourse As community agents the interpreters may act in accordance with
Perspectives Studies in Translatology 5
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
the cultural norms and values of their own community If the role of advocate is
adopted it presupposes once again that the interpreter is well informed about the
laws rules and procedures that need to be relayed (Leanza 2007 p 14) The task
of the interpreter is twofold here disclose all relevant information necessary for
making an informed choice about proposed procedures and ensure that the patient
understands the information received and the implications of giving consent (adapted
from Johnstone 1999 p 235 who applied this to the role of the nurse regarding
informed consent) Since this research deals with informed consent the interpreterrsquos
role here should rather be that of an advocate for parents and volunteers improving
their level of understanding and in that way helping them to make an informed
decision about taking part in the research or not
What is informed consent According to Robertson (1981 p 102 in Johnstone
1999 pp 210211)
The doctrine of informed consent although having a profound ethical dimension isessentially a legal doctrine developed partially out of recognition of the patientrsquos right toself-determination and partially out of the doctorrsquos duty to give the patient lsquolsquoinformationabout proposed treatment so as to provide him or her with the opportunity of makingan informed or rational choice as to whether to undergo the treatmentrsquorsquo
Johnstone (1999 pp 224225) also feels that the term lsquoinformed consentrsquo should be
abandoned in favour of lsquoinformed decision-makingrsquo Unlike the notion of lsquoinformed
consentrsquo this formulation seems to invite continuous re-evaluation of any decisions
made about care and treatment options Patients must also be informed of their
right to refuse a recommended medical or nursing procedure and should be kept
up to date on the relevant details pertaining to their cases This should be done
by interpreters who adopt the role of patientrsquos advocate Details which are not
readily understood should be explained (in understandable language) and reinforced
through planned patient health education programmes something that nurses
interpreters are educationally prepared to undertake Many factors can deter patients
from exercising informed and voluntary choices amongst which is poor commu-
nication The patientrsquos ability to understand entails whether the patient is able to
comprehend the risks benefits and alternatives to a proposed medical procedure as
well as the implications of giving consent The question could be asked concerning
just how sophisticated a patientrsquos understanding needs to be and in this case
how sophisticated the interpreterrsquos understanding needs to be in order to really
explain these procedures and to really support these parents and volunteers in
making their decisions
Data
Two phases of data collection were involved Both were done during one
consultation with the interpreters The first phase aimed at compiling a profile of
the relevant interpreters whereas the second phase entailed completing a compre-
hension test ie an exercise to ascertain whether the interpreters understand the test
that they were supposed to explain to the patient
6 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Profile of interpreters
The interpreters of the Tygerberg and Red Cross state hospitals were visited by the
researchers and asked to complete questionnaires on their training background
comprehension of the target text etc At Tygerberg only one interpreter was found
and at Red Cross only two Therefore we also visited the Groote Schuur state
hospital where another three interpreters were interviewed although the informed
consent forms were not meant for this hospital The Groote Schuur hospital has a
similar profile to that of the Tygerberg hospital The results of the survey are listed in
Table 1
Regarding the languages offered for TBH and RXH no interpreters were found
for Afrikaans whilst in both hospitals Afrikaans was either the most spoken
language or used on an equal basis with English and isiXhosa All six interpreters are
mother-tongue speakers of isiXhosa with English as their second language At
RXH Sesotho and isiZulu are offered as third languages and at GSH two of the
interpreters offer Afrikaans as their third language Regarding the interpretersrsquo
qualifications none has a tertiary education and not all have even completed their
secondary education Regarding their training as interpreters and the period that
they were interpreting the interpreter at TBH had no training but she was a nursing
ancillary who later just moved into an interpreting lsquopositionrsquo She has been doing
this for the past eight months on a freelance basis at the Tygerberg hospital
The two interpreters at RXH have been performing interpreting duties for the
past seven years They are full-time interpreters and had training in interpreting for
two years on an ad hoc basis from an NGO (non-governmental organisation)
namely the National Language Project (NLP) Apart from language and interpreting
skills they also had some training in counselling They presented themselves as very
professional The three interpreters at GSH had been doing lsquoformalrsquo interpreting
in this hospital for the past two years but were doing interpreting on an ad hoc
basis at the hospital for at least 10 years before that even though their job
description was that of lsquocleanerrsquo When they were appointed as interpreters they
underwent training for six weeks
Table 1 Interpreters consulted
HospitalNumber ofinterpreters Gender Age Qualifications Languages
Interpretertraining
Tygerberg(TBH)
1 Female 33 Matric Wasnursing ancillary
EnglishisiXhosa
None
Red Cross(RXH)
2 Female 35 53 Matric Post-matric studies(Adult basiceducationAncillary socialwork)
EnglishisiXhosaisiZuluEnglishisiXhosaSesotho
Two-yeartrainingSometraining incounselling
GrooteSchuur(GSH)
3 MaleFemale(2)
43 46 48 Busy with matricWere cleaners
EnglishisiXhosaEnglishisiXhosaAfrikaansEnglishisiXhosaAfrikaans
6-weektraining
Perspectives Studies in Translatology 7
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Comprehension test
They were also tested on their comprehension of the English source texts since
all of them offered English and since the source-text documents would have
been explained to them in English The translations into Afrikaans and isiXhosa
are very close linguistic translations of the original so if they did not understand
the source text they would not understand the target text either Questions were
also put on textual issues such as sentence and paragraph length paragraph
coherence and stylistic and lexical suitability (Table 2)
According to Gile (1995 p 34) the following criteria for quality can be applied
universally to all interpreting acts ideational clarity (the message of the sender
should be clear and comprehensible to the receiver) linguistic acceptability (the
interpreter should use grammar which is acceptable for the situation and the other
participants) and terminological accuracy (the interpreter should use the correct
target language equivalent for medical terms in the source language) From the
responses it can be deduced that none of these criteria could be met here
Question 1 addresses the ideational clarity and no interpreter completely agreed
that they clearly understood the message of the senders Linguistic acceptability
and terminological accuracy are addressed by questions 5 and 6 and here no one
agreed that the vocabulary and style of these texts was appropriate for this
situation Other remarks on the texts as such are that they found the texts too
long to explain but they did not think they themselves would be able to paraphrase
them in order to shorten the time with the patients Only one the male interpreter
from GSH felt that if he were given enough time to work with the texts he would
be able to explain the contents to the parents or volunteers The other interpreters
did not feel comfortable explaining the information of the texts so that the patients
or their parents could come to an informed decision as to whether they should sign
the document or not Needless to say none of the interpreters would like to sign
the agreement certifying that they explained the information of the trial in the
patientrsquos mother tongue and that the patient understood what was explained See
Appendix 2 for the section of the Informed Consent forms where the interpreters
are required to sign
If these interpreters were to be confronted with this task the ethical response
would be to withdraw from the assignment unless they are supplied with a much
Table 2 Responses on English source texts
No Question1Donrsquot agree
at all 2Donrsquot agree 3Agree4Completely
agree
1 I clearly understand thetexts
GSH 1 TBH 1 RXH 1 GSH 2 RXH 1
2 The length of thesentences is good
GSH 1 TBH 1 RXH 2 GSH 2
3 The paragraphs arecoherent
RXH 1 RXH 1 GSH3 TBH 1
4 The length of theparagraphs is good
RXH 1 GSH3 TBH 1
RXH 1
5 The vocabulary isappropriate
GSH 2 RXH 2 GSH 1TBH 1
6 The style of the text isappropriate
GSH 3 RXH 2 TBH 1
8 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
simpler document or preferably have a health care provider with them doing the
actual explanation Then they could revert to their more passive role of interpreting
as part of a trialogue The NCICH (2004 p 16) also makes the point that lsquoTo work
within the professional boundaries of the interpreter role also means that interpretersare aware of the limitations of their duties as well as the limitations of their abilities as a
health care interpreterrsquo (our emphasis)
Discussion
Regardless of the role of the interpreter either as system or community agent the
basic goal of medical discourse is mutual understanding Clear verbal commu-
nication is a necessary component of an effective clinical encounter Even when
patients and providers are educated in the same language faulty communication
can lead to distortions and miscommunications between the parties let aloneeducated health care providers and uneducated patients and semi-educated
interpreters (Kaufert amp Putsch 1997 in Angelelli 2004 p 18) Communicative
failure will inevitably be the result here since neither interpreters nor parents or
volunteers have the same level of literacy or knowledge as the compilers of the
source texts in both these instances the compilers were medical researchers The
parents or volunteers would therefore not be able to make informed decisions
about agreeing to take part in the research projects or not
What is equally disturbing is that the interpreters are set up for failure whenthey are confronted with a task of this scope and these types of documents These
target texts will not be comprehensible enough to be viewed as providing an effective
service to the customer According to Gile (1995 pp 7980) one is not able to fully
comprehend something simply on the grounds of knowledge of the language or
extra-linguistic knowledge The content of the speech may be too difficult it may
deviate from generally accepted linguistic standards or the level of knowledge of the
language and extra linguistic knowledge of the receiver may not be high enough
Then it is necessary to analyse the discourse itself to a much greater extent than onewould analyse discourse with regard to comprehension in everyday situations
Therefore to fully comprehend one does not only need knowledge of the language
and extra-linguistic knowledge but the discourse also need purposeful analysis This
type of analysis could not be performed by most of the HCIs in South Africa and
should rather be left to the health care providers or to trained translators working
with the health care providers in rendering a much simpler target text
It is high time to shift the focus in research on health care interpreting to the
way in which the health care provider deals with the HCIs so as not to expectfar more than what their duties entail and their training predicts The education
and career profile of the six interpreters described above is fairly typical of HCIs in
South Africa and health care providers should keep this in mind This is evident
from the following job advertisement for an interpreter with a medical background
but no mention is made of interpreting or translation training The typical
requirements are matric the speaking andor writing skills in the languages needed
and nursing or other medical experience
Mouldmed Locum International Exchange Ltd is looking for a translatorinterpreterwho is able to speak and write three languages fluently (preferably English Afrikaansand Xhosa) The candidate must be able to start immediately and must have a Matric
Perspectives Studies in Translatology 9
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
qualification and a medical background This is a three-month contract with the optionto extend Working hours are 0730 1600 (30-minute lunch) Monday to Friday Thejob entails office work and patient communication A senior assistant nurse with theselanguage requirements would also qualify for the position
Responsibility and ethical behaviour standards towards interpreters should also be
laid down for the health care provider and not only for the interpreter NCICH
(2004 p 19) notes the responsibility of the health care provider lsquoProviders have the
duty to present their knowledge clearly and objectively so that the patient is able
to make informed choicesrsquo If even interpreters are not monitored to meet their
obligations who is going to monitor the health care providers
Further research that could flow from this could be competency testing of the
interpreters to see how well they actually understand the information which had
been communicated by the health care provider and after the interpreters have
explained the information to the patients the same competency testing could be
done on the patientsrsquo understanding This can be established by asking patients
probing questions and inviting them to repeat the information they have received
(Roth et al 1983 p 175 in Johnstone 1999 pp 225227)
A retranslation of the source texts could also be done into Afrikaans and
isiXhosa using the functionalist approach and the interpreters could then be
retested to see whether they now understand the target texts better and whether
they would be able to paraphrase and explain the content better to the patient
Keeping in mind the socio-economic and educational level of the prototypical
patient for whom these informed consent forms are intended we would still
dissuade the interpreters from attempting to convey the message without a health
care provider present and from signing the document
Notes
1 Each of the nine provinces has its own set of official languages eg English Afrikaansand one or more of the indigenous languages On a national level all 11 of these languagesare recognised as official In the case of the Western Cape Province there are thus threeofficial languages as stated
2 Groote Schuur Hospital is linked to the University of Cape Town and situated in theObservatory area in Cape Town a mainly English-speaking area It employs 524 doctorsand 1370 nurses The hospital treats approximately 44000 in-and 575000 out-patientsper year (Capegateway public info 2009) The staff use both Afrikaans and English on anequal basis and a small proportion use African languages The patients are alsopredominantly Afrikaans and English and a large proportion use African or otherlanguages (Williams 2005 in Saulse 2009 p 24)
3 This is the highest level of secondary schooling that can be obtained within the SouthAfrican context This gives access to tertiary education
Notes on contributors
Ilse Feinauer is associate professor in the Department of Afrikaans and Dutch and isresponsible for teaching Translation Studies and Practice to undergraduate and postgraduatestudents She also teaches Afrikaans linguistics She is coordinator for the MPhil inTranslation Studies She has extensive experience both as a translator and scholar intranslation theory
Harold Lesch is a senior lecturer also in the Department of Afrikaans and Dutch and holds aqualification in Translation Studies He is currently coordinator of the Post Graduate Diploma
10 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
in Translation and Interpreting and is responsible for teaching Interpreting Studies andPractice
References
Angelelli C (2004) Medical interpreting and cross-cultural communication CambridgeCambridge University Press
Angelelli C (2006) Validating professional standards and codes Challenges and opportu-nities Interpreting 8 175193
Anthonissen C (2008) On interpreting the interpreter experiences of language practitionersin mediating for the TRC Journal of Multicultural Discourses 3 165188
Capegateway public info (2009) httpwwwwesterncapegovzaengyour_gov5987Census (2001) Primary tables 1996 and 2001 compared Accessed at httpwwwstatssagovza
census01htmlC2001PrimTablesaspFeinauer I (2003) TB or not TB The communicative success of translated medical texts in
South Africa In W Botha (Ed) n Man wat beur rsquon Huldigingsbundel vir Dirk vanSchalkwyk (pp 213223) Stellenbosch Buro of the WAT
Feinauer I amp Luttig L (2005) Functionalism is not always the remedy Perspectives Studiesin Translatology 13 123131
Gile D (1995) Basic concepts and models for interpreter and translator training AmsterdamJohn Benjamins
Johnstone M-J (1999) Bioethics A nursing perspective Sydney HarcourtLeanza Y (2007) Role of community interpreters in pediatrics as seen by interpreters
physicians and researchers In F Pochhacker amp M Shlesinger (Eds) Healthcareinterpreting Discourse and interaction (pp 1134) Amsterdam Benjamins
Pienaar M (2006) Kommunikasie tussen staat en burgers die stand van tolkdienste SabinetOnline 40 3546
Pochhacker F amp Shlesinger M (Eds) (2007) Healthcare interpreting Discourse andinteraction Amsterdam Benjamins
Romero B (2008) Here are your right hands exploring interpreter qualifications Universityof Dayton Law Review 34 1533
Saulse B (2009) Interpreting within the Western Cape Health Care Sector A DescriptiveOverview (Unpublished masterrsquos thesis) University of Stellenbosch South Africa
United States National Council on Interpreting in Health Care (2004) A national code ofethics for interpreters in health care The National Council on Interpreting in Health CareWorking Papers Series httpwwwncihcorg
Appendix A
Text 1
A DOUBLE-BLIND PLACEBO CONTROLLED RANDOMISED STUDY TO INVESTI-GATE THE EFFICACY AND SAFETY OF LOW-DOSE L-CARNITINEMAGNESIUMSUPPLEMENTATION IN PREVENTING HYPERLACTINEMIA AND LACTIC ACIDO-SIS IN HIV-INFECTED SOUTH AFRICAN WOMEN ON STAVUDINE CONTAININGCOMBINED ANTIRETROVIRAL THERAPY (cART)
Introduction
We are doing a study to see if a l-carnitine magnesium combination product that could help toprevent high blood lactate levels which are known to be one of the side effects of some of themedications used in the treatment of HIV-infection (anti retroviral drugs)
The ability to decrease the way the virus multiplies is achieved by combined anti retroviraltherapy HIV positive (HIV ) patients receiving a combination of these drugs survive by
Perspectives Studies in Translatology 11
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
keeping the infection under control but not by killing the virus altogether This treatment hasindeed increased the quality of life in HIV individuals
One of the drugs the nucleotidic reverse transcriptase inhibitors (NRTIrsquos) can alter the energyproducing part of cells in the body and this that can lead to effects such as the high bloodlactate Twenty five percent of patients with high lactate levels donrsquot have any symptoms whileonly a smaller percentage less than 10 percent develops symptoms including loss of weightand abdominal pain
What is the purpose of this trial
A previous study showed that the low dose l-carnitine and magnesium was absorbed in healthymale volunteers and that the supplement was safe to administer
We want to determine if a dose of two capsules per day of the study drug over a period of ayear prevents the build up of lactic acid in the blood We also want to show if the l-carnitineand magnesium is absorbed in HIV positive subjects on combined anti-retroviral therapy anddetermine what the concentration levels of the anti-retroviral drugs are after a period of 6months and 12 months
To achieve this the study drug must be compared with a placebo (these are capsules that looksthe same as the study drug which are filled with a harmless compound in this case lactose)An extra 20 ml of blood and 50ml of urine apart from the normal routine bloods will be takenbefore starting anti-retroviral therapy and 30ml of blood and 50ml of urine will be taken 6monthly thereafter up to 12 months
The levels of lactic acid cholesterol triglycerides LDL - HDL- and Lp(a) lipoproteins andanti-retroviral drugs will be determined in the blood and those of the l-carnitine with itssupporting metabolites (the organic acid - amino acid-and major and trace element profileswhich includes magnesium) will be determined in the blood and urine These results of thosesubjects that are on the study drug will be compared with those of the placebo group to show ifthere are statistical relevant differences
Text 2
PARTICIPANT INFORMATION SHEET AND CONSENT FORM FOR USE BYPARENTSLEGAL GUARDIANS
Virtual Reality for pain relief in paediatric burns patients
What is this research study all aboutYour child has been admitted to this unit because of their burn injury Every child in this burnsunit has dressing changes on a daily basis Your child will be given the normal medication thatshehe receives during any dressing change These dosages of medication have been prescribedby the doctor when your child was admitted to the burns unit With all burn injuries one ofthe biggest problems that our patients experience is pain At the moment the professionals inthe burns unit do not know if there is something other than pain medication that can help todecrease your childrsquos pain Certain studies have proven that using a technique called VirtualRealty (VR) can distract a child and thereby decrease their pain during a specific procedureVirtual Reality is a program that we will use to allow your child to watch a video game throughgoggles that will be placed on their face Half of the treatment will be done using only the painmedication The other half of the dressing change will be done using the pain medication andthe VR We will then interview yourself and your child to find out how you your child feltabout this process and if you feel that Virtual reality can help to decrease your childrsquos painDuring the interviews with youyour child and nursing staff information may be recorded on a
12 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
tape recorder so that we can check all our information We will also be videotaping alldressing changes and using information from those tapes to help us with this study
Why has your child been invited to participateIn order to see if this process of VR is going to worknot work we have to assess it on at least250 children All children who are over the age of 5 and who do not have a face burn can takepart in this study You and your child have the option to participate in this study andparticipation is completely VOLUNTARY
What will your responsibilities beBy agreeing to let your child participate in this study you will allow us to ask your child tocomplete a questionnaire You will also be interviewed
Will your child benefit from taking part in this researchAt this stage we cannot say if your child will benefit from the study that we are doing If whatwe are doing does work then your child will experience less pain during the dressing changesIf the results are positive then it means that in the future more patients with similar injuries toyour child can be helped when they are experiencing pain during dressing changes
Are there any risks involved in your child taking part in this researchThere are no reported risks The only reported side effect of the VR is sickness If your childdoes experience any sickness due to the VR it will be stopped immediately
If you do not agree to allow your child to take part what alternatives does your child haveYou and your child have the option not to participate in this study participation is completelyVOLUNTARY Your child will only be entered into the study with your permission If youchoose not to enter the study we will still treat your child to the best of our ability and it willnot change the way you are treated You can leave the study at any time after you join
Who will have access to your childrsquos medical recordsAny information gained from this study and testing will be kept strictly private and no oneoutside of the people in the study will know youryour childrsquos results without your permissionIf the information is published to educate other health care professionals we will not use anynames Thus you and your child will never be able to be identified by anyone except studypersonnel Similarly no person outside of the study will have access to audio and videorecordings that may have been made during the dressing changes
Will you or your child be paid to take part in this study and are there any costs involvedYou or your child will not be paid to take part in the study and there will be no costs involvedfor you if your child does take part
Perspectives Studies in Translatology 13
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
14 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
parents of paediatric burn patients and volunteers on antiretroviral therapy In these
texts the interpreters have to declare by their signatures that they assisted the
relevant investigator by explaining the information in the document to the parent or
volunteer using the language medium of Afrikaans or isiXhosa They also have todeclare that the parent or volunteer fully understands the content of the document
and has had all their questions answered satisfactorily What will be investigated here
is not whether these texts communicate adequately with the parent or volunteer
but whether the interpreters fully understand the information that they have to
explain to parents or volunteers
The two issues discussed here are
Will the interpreters fully understand the information on the informed consentforms that they have to explain to parents or volunteers
Is it ethical to leave the explaining to the interpreters and then expect that they
should sign the informed consent forms declaring that the content has been
fully understood by the parents or volunteers
The aim of this article is to highlight the conflict between what is expected of the
interpreters and the reality of their position This will be done by reflecting on the
situation in the Western Cape South Africa The structure of the article will be asfollows sketching the situation by diagnosing the problem contextualising the
research within interpreting studies presenting the two sets of data ie the profile of
the interpreters and the comprehension test and finally the discussion of the results
The situation
The research on the informed consent forms concerned for the two projects was
conducted at the Tygerberg and Red Cross state hospitals respectively TygerbergHospital is linked to Stellenbosch University as a tertiary-level medical institution
The hospital was opened in 1976 and employs 1715 nurses and 536 doctors It treats
approximately 56000 in- and 590000 out-patients per year (Capegateway public
info 2009) The staff mainly has Afrikaans as their mother tongue with a small
proportion using English as first language The patients are also mainly Afrikaans
speakers with a small proportion with English as mother tongue IsiXhosa is the
predominant language among black patients (Williams 2005 in Saulse 2009 p 24)
Informed consent forms and information leaflets were distributed here among HIV-positive volunteer mothers who were using antiretroviral therapy with the title (see
Appendix1 Text 1) lsquoA DOUBLE-BLIND PLACEBO CONTROLLED RANDO-
MISED STUDY TO INVESTIGATE THE EFFICACY AND SAFETY OF LOW-
DOSE L-CARNITINEMAGNESIUM SUPPLEMENTATION IN PREVENT-
ING HYPERLACTINEMIA AND LACTIC ACIDOSIS IN HIV-INFECTED
SOUTH AFRICAN WOMEN ON STAVUDINE CONTAINING COMBINED
ANTIRETROVIRAL THERAPY (cART)rsquo
The Red Cross War Memorial Childrenrsquos Hospital is the only child healthinstitution in South Africa and is located near Cape Town It treats approximately
19700 in- and 216000 out-patients per year (Capegateway public info 2009) This
hospital is linked academically to the University of Stellenbosch the University
of Cape Town and the Faculty of Dentistry of the University of the Western Cape
The staff use both English and Afrikaans in equal proportions while the language
2 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
among patients is very diverse with English Afrikaans and isiXhosa being used on
an almost equal basis (Williams 2005 in Saulse 2009 p 24) Informed consent
forms were distributed here among the parents or legal guardians of burns patients
entitled (see Appendix 1 Text 2) lsquoVIRTUAL REALITY FOR PAIN RELIEF IN
PAEDIATRIC BURNS PATIENTSrsquo
Feinauer (2003) discussed the profile of typical state hospital patients in the
Western Cape they were mostly lay people from a low socio-economic level who are
language impoverished have low or no level of schooling lack communication skills
sometimes do not use the standard varieties of Afrikaans English or isiXhosa they
are economically deprived they have low concentration levels they are ill are
intimidated by the unfamiliar environment and are without any medical knowledge
(Feinauer 2003 pp 216217) Feinauer and Luttig (2005) find that sometimes the
gap between the source-text recipients and the target-text recipients is too big
to be bridged by merely changing the translation approach from linguistic to
functional An empirical study was undertaken on how to present information on
primary ailments (HIVAids and TB) in an accessible form to lay people Actual
target texts in both Afrikaans and isiXhosa were assessed in terms of their
communicative success by using questionnaires amongst state hospital patients
who were on a much lower level of literacy or knowledge than that of the source text
recipients
The main communicative problems were ascribed to the fact that these target
texts were almost exact replicas of the source texts in other words the translators
still used the linguistic approach The source texts were retranslated using the
functionalist approach by translators who played a much more important role in
designing the target texts keeping the target readers in mind the whole time The
target texts were reassessed using the same questionnaires but with different
respondents The respondents however were on the same level of literacy or
knowledge as that of the first group of respondents Then the big disappointment
came comprehension did improve slightly but after all the effort and time that went
into the retranslation the improvement was not statistically significant What did
become apparent in this research is that a target text as such irrespective of the
translation approach is not the means to convey the necessary knowledge to these
target recipients
This should be kept in mind to contextualise the enormity and the responsibility
of the task assigned to the interpreters Before we look at the profile of the
interpreters at these two hospitals and their understanding of the relevant
documents let us look at what is generally expected from health care interpreters
(HCIs) as well as the role that the interpreters are supposed to play during the
communication process
Interpreting theory
Obligations of health care interpreters
According to Angelelli (2006 p 186) health care organisations sometimes have
expectations (which are sometimes even included in job descriptions) beyond the
interpreterrsquos control One of her respondents reacted by noting that lsquoproviders can
easily put us in the position of doing other things which we are not entitled to
do we donrsquot have the training we donrsquot have the capacity to do those thingsrsquo
Perspectives Studies in Translatology 3
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
(Angelelli 2006 p 189) One of the reasons why HCIs are so often misused is because
it is so difficult to define their role in the system Angelelli (2006 p 175) says lsquoOne
of the most problematic issues is the role of interpreters Presumably this role should
be simple to describe the interpreter faithfully conveys a message from one
language to another while maintaining neutralityrsquo Angelelli (2006 p 182) identifies
the following roles that interpreters can play as they perform their task message
converter message clarifier cultural clarifier patient advocate
System agent
All four of these roles could be operative here but in this case the roles of message
converter and clarifier or as Jalbert (1998 in Leanza 2007 pp 1314) calls it the
role of bilingual professional will be the primary role Whatever role the interpreter
takes on here will be within the overarching role of the interpreter as the healthcare
provider or acting on behalf of the institutional or medical system Leanza (2007 p
17) refers to the interpreter playing the role of lsquosystem agentrsquo Here the interpreter is
in essentially the same (symbolic) position as the health care provider
The researchers want the interpreters to be translating machines in other words
to act as linguistic agents but to simultaneously act as health system agents since
they want the interpreter to get the parents or the volunteers to sign the informed
consent forms in order to be able to conduct their research The researcher explains
the relevant information on the informed consent forms to the interpreter(s) and
then the interpreter is left with the patient in a situation of dialogue and not in a
situation of trialogue which is usually the default situation for HCIs As Leanza
(2007 pp 1314) puts it the interpreter becomes the healthcare professional The
fact that the interpreter has to sign that the information was conveyed clearly to the
patient and that the patient understands the information implies that there is an
agreement between the health care provider and the interpreter before the discussion
starts between the interpreter and the patient The interpreterrsquos signature will indicate
that she has kept to the agreement
This is in direct opposition to the view that the interpreter is usually part of
the lsquotreating teamrsquo but is not regarded as the person with the primary responsibility
for the care and treatment of patients The interpreter is usually regarded as acting in
a secondary or supporting role The United States National Council on Interpreting
in Health Care (NCHIC 2004 16) states
Interpreters in health care understand that they are not there as primary participants inthe interaction and therefore are not in a position to make decisions to advise orcounsel Their function is that of a communication facilitator and as such theirresponsibility is to the process of communication and the facilitation of a mutualunderstanding of meaning It is not within the interpreterrsquos set of duties to give advice orto counsel either party with respect to the goals of the health care encounter
Here however the interpreter is pushed into the primary role and has to take
primary responsibility This according to Angelelli (2004 pp 78) would mean that
the interpreter aligns with the system and the interpreter alone has to construct the
conversation This means that the task for bringing the message across is the sole
responsibility of the interpreter This is not a new role for interpreters as seen from
various publications on the role of the interpreter such as the book by Pochhacker
4 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
and Shlesinger (2007 p 2) where one of the roles of the interpreter is described as
someone who could take over the interview and the article by Anthonissen (2008
p 171) which describes the mediating role of the interpreter as providing lsquoguided
constructive interventionrsquoThis more visible interpreter could only successfully step into the shoes of the
health care provider whilst also acting as message converter message clarifier and
cultural clarifier if she were able to fully understand the documents The interpreter
should provide the most faithful rendering possible of what these document say This
does not only entail an accurate translation of the words spokenwritten but also a
translation that formulates the information in such a way that it becomes coherent
within the world view of the patient In order to do this the interpreter needs to have
a deep and thorough knowledge of the subject matter as well as the language usedwithin that field It is obvious that the more explication needs to go into the
clarification of the message the better the interpreter ought to know the subject field
and its discourse The ability to interpret accurately and completely is to a large
extent dependent on how much background knowledge the interpreter has of the
content and context of the communication Romero (2008 p 19) states with respect
to court and legal interpreters that interpreters cannot interpret what they do not
know or understand Communication in the legal setting is guided by an under-
standing of the use of legal arguments protocol procedures laws and traditions Ifinterpreters are not prepared to handle this task they will get in the way or perform
poorly The same applies to HCIs especially if they don the white coat of the health
care provider
According to NCHIC (2004 p 18)
The ethical obligation of interpreters is to possess enough understanding of culture andcultural practices and beliefs to be able to facilitate communication across culturaldifferences seeking to minimize and if possible avoid potential misunderstanding andmiscommunication based on cultural assumptions andor stereotyping Under certainconditions such as clashing cultural beliefs or practices a lack of linguistic equivalencyor the inability of parties to articulate the differences in their own words the interpretershould assist by sharing cultural information or helping develop an explanation thatcan be understood by all (our emphasis)
NCICH (2004 pp 1314) also states that the language used by the provider is asource of data for the patient The patient therefore should be able to access both
the technical information and the information about the kind of relationship the
provider is attempting to establish in order to make decisions that will impact on
his or her health and wellbeing Here this is relevant since the parents or volunteers
have to sign informed consent forms In order for the parents or volunteers to
internalise the necessary information to make the correct and informed decision the
interpreter would have to have succeeded in making all the information clearly
understood
Community agent
The interpreters in this situation could also act as community agents who play an
advocacy role This is the counterpart of the role of system agent where the
interpreters are agents of the institution and spokespersons for the healthcare system
and its discourse As community agents the interpreters may act in accordance with
Perspectives Studies in Translatology 5
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
the cultural norms and values of their own community If the role of advocate is
adopted it presupposes once again that the interpreter is well informed about the
laws rules and procedures that need to be relayed (Leanza 2007 p 14) The task
of the interpreter is twofold here disclose all relevant information necessary for
making an informed choice about proposed procedures and ensure that the patient
understands the information received and the implications of giving consent (adapted
from Johnstone 1999 p 235 who applied this to the role of the nurse regarding
informed consent) Since this research deals with informed consent the interpreterrsquos
role here should rather be that of an advocate for parents and volunteers improving
their level of understanding and in that way helping them to make an informed
decision about taking part in the research or not
What is informed consent According to Robertson (1981 p 102 in Johnstone
1999 pp 210211)
The doctrine of informed consent although having a profound ethical dimension isessentially a legal doctrine developed partially out of recognition of the patientrsquos right toself-determination and partially out of the doctorrsquos duty to give the patient lsquolsquoinformationabout proposed treatment so as to provide him or her with the opportunity of makingan informed or rational choice as to whether to undergo the treatmentrsquorsquo
Johnstone (1999 pp 224225) also feels that the term lsquoinformed consentrsquo should be
abandoned in favour of lsquoinformed decision-makingrsquo Unlike the notion of lsquoinformed
consentrsquo this formulation seems to invite continuous re-evaluation of any decisions
made about care and treatment options Patients must also be informed of their
right to refuse a recommended medical or nursing procedure and should be kept
up to date on the relevant details pertaining to their cases This should be done
by interpreters who adopt the role of patientrsquos advocate Details which are not
readily understood should be explained (in understandable language) and reinforced
through planned patient health education programmes something that nurses
interpreters are educationally prepared to undertake Many factors can deter patients
from exercising informed and voluntary choices amongst which is poor commu-
nication The patientrsquos ability to understand entails whether the patient is able to
comprehend the risks benefits and alternatives to a proposed medical procedure as
well as the implications of giving consent The question could be asked concerning
just how sophisticated a patientrsquos understanding needs to be and in this case
how sophisticated the interpreterrsquos understanding needs to be in order to really
explain these procedures and to really support these parents and volunteers in
making their decisions
Data
Two phases of data collection were involved Both were done during one
consultation with the interpreters The first phase aimed at compiling a profile of
the relevant interpreters whereas the second phase entailed completing a compre-
hension test ie an exercise to ascertain whether the interpreters understand the test
that they were supposed to explain to the patient
6 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Profile of interpreters
The interpreters of the Tygerberg and Red Cross state hospitals were visited by the
researchers and asked to complete questionnaires on their training background
comprehension of the target text etc At Tygerberg only one interpreter was found
and at Red Cross only two Therefore we also visited the Groote Schuur state
hospital where another three interpreters were interviewed although the informed
consent forms were not meant for this hospital The Groote Schuur hospital has a
similar profile to that of the Tygerberg hospital The results of the survey are listed in
Table 1
Regarding the languages offered for TBH and RXH no interpreters were found
for Afrikaans whilst in both hospitals Afrikaans was either the most spoken
language or used on an equal basis with English and isiXhosa All six interpreters are
mother-tongue speakers of isiXhosa with English as their second language At
RXH Sesotho and isiZulu are offered as third languages and at GSH two of the
interpreters offer Afrikaans as their third language Regarding the interpretersrsquo
qualifications none has a tertiary education and not all have even completed their
secondary education Regarding their training as interpreters and the period that
they were interpreting the interpreter at TBH had no training but she was a nursing
ancillary who later just moved into an interpreting lsquopositionrsquo She has been doing
this for the past eight months on a freelance basis at the Tygerberg hospital
The two interpreters at RXH have been performing interpreting duties for the
past seven years They are full-time interpreters and had training in interpreting for
two years on an ad hoc basis from an NGO (non-governmental organisation)
namely the National Language Project (NLP) Apart from language and interpreting
skills they also had some training in counselling They presented themselves as very
professional The three interpreters at GSH had been doing lsquoformalrsquo interpreting
in this hospital for the past two years but were doing interpreting on an ad hoc
basis at the hospital for at least 10 years before that even though their job
description was that of lsquocleanerrsquo When they were appointed as interpreters they
underwent training for six weeks
Table 1 Interpreters consulted
HospitalNumber ofinterpreters Gender Age Qualifications Languages
Interpretertraining
Tygerberg(TBH)
1 Female 33 Matric Wasnursing ancillary
EnglishisiXhosa
None
Red Cross(RXH)
2 Female 35 53 Matric Post-matric studies(Adult basiceducationAncillary socialwork)
EnglishisiXhosaisiZuluEnglishisiXhosaSesotho
Two-yeartrainingSometraining incounselling
GrooteSchuur(GSH)
3 MaleFemale(2)
43 46 48 Busy with matricWere cleaners
EnglishisiXhosaEnglishisiXhosaAfrikaansEnglishisiXhosaAfrikaans
6-weektraining
Perspectives Studies in Translatology 7
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Comprehension test
They were also tested on their comprehension of the English source texts since
all of them offered English and since the source-text documents would have
been explained to them in English The translations into Afrikaans and isiXhosa
are very close linguistic translations of the original so if they did not understand
the source text they would not understand the target text either Questions were
also put on textual issues such as sentence and paragraph length paragraph
coherence and stylistic and lexical suitability (Table 2)
According to Gile (1995 p 34) the following criteria for quality can be applied
universally to all interpreting acts ideational clarity (the message of the sender
should be clear and comprehensible to the receiver) linguistic acceptability (the
interpreter should use grammar which is acceptable for the situation and the other
participants) and terminological accuracy (the interpreter should use the correct
target language equivalent for medical terms in the source language) From the
responses it can be deduced that none of these criteria could be met here
Question 1 addresses the ideational clarity and no interpreter completely agreed
that they clearly understood the message of the senders Linguistic acceptability
and terminological accuracy are addressed by questions 5 and 6 and here no one
agreed that the vocabulary and style of these texts was appropriate for this
situation Other remarks on the texts as such are that they found the texts too
long to explain but they did not think they themselves would be able to paraphrase
them in order to shorten the time with the patients Only one the male interpreter
from GSH felt that if he were given enough time to work with the texts he would
be able to explain the contents to the parents or volunteers The other interpreters
did not feel comfortable explaining the information of the texts so that the patients
or their parents could come to an informed decision as to whether they should sign
the document or not Needless to say none of the interpreters would like to sign
the agreement certifying that they explained the information of the trial in the
patientrsquos mother tongue and that the patient understood what was explained See
Appendix 2 for the section of the Informed Consent forms where the interpreters
are required to sign
If these interpreters were to be confronted with this task the ethical response
would be to withdraw from the assignment unless they are supplied with a much
Table 2 Responses on English source texts
No Question1Donrsquot agree
at all 2Donrsquot agree 3Agree4Completely
agree
1 I clearly understand thetexts
GSH 1 TBH 1 RXH 1 GSH 2 RXH 1
2 The length of thesentences is good
GSH 1 TBH 1 RXH 2 GSH 2
3 The paragraphs arecoherent
RXH 1 RXH 1 GSH3 TBH 1
4 The length of theparagraphs is good
RXH 1 GSH3 TBH 1
RXH 1
5 The vocabulary isappropriate
GSH 2 RXH 2 GSH 1TBH 1
6 The style of the text isappropriate
GSH 3 RXH 2 TBH 1
8 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
simpler document or preferably have a health care provider with them doing the
actual explanation Then they could revert to their more passive role of interpreting
as part of a trialogue The NCICH (2004 p 16) also makes the point that lsquoTo work
within the professional boundaries of the interpreter role also means that interpretersare aware of the limitations of their duties as well as the limitations of their abilities as a
health care interpreterrsquo (our emphasis)
Discussion
Regardless of the role of the interpreter either as system or community agent the
basic goal of medical discourse is mutual understanding Clear verbal commu-
nication is a necessary component of an effective clinical encounter Even when
patients and providers are educated in the same language faulty communication
can lead to distortions and miscommunications between the parties let aloneeducated health care providers and uneducated patients and semi-educated
interpreters (Kaufert amp Putsch 1997 in Angelelli 2004 p 18) Communicative
failure will inevitably be the result here since neither interpreters nor parents or
volunteers have the same level of literacy or knowledge as the compilers of the
source texts in both these instances the compilers were medical researchers The
parents or volunteers would therefore not be able to make informed decisions
about agreeing to take part in the research projects or not
What is equally disturbing is that the interpreters are set up for failure whenthey are confronted with a task of this scope and these types of documents These
target texts will not be comprehensible enough to be viewed as providing an effective
service to the customer According to Gile (1995 pp 7980) one is not able to fully
comprehend something simply on the grounds of knowledge of the language or
extra-linguistic knowledge The content of the speech may be too difficult it may
deviate from generally accepted linguistic standards or the level of knowledge of the
language and extra linguistic knowledge of the receiver may not be high enough
Then it is necessary to analyse the discourse itself to a much greater extent than onewould analyse discourse with regard to comprehension in everyday situations
Therefore to fully comprehend one does not only need knowledge of the language
and extra-linguistic knowledge but the discourse also need purposeful analysis This
type of analysis could not be performed by most of the HCIs in South Africa and
should rather be left to the health care providers or to trained translators working
with the health care providers in rendering a much simpler target text
It is high time to shift the focus in research on health care interpreting to the
way in which the health care provider deals with the HCIs so as not to expectfar more than what their duties entail and their training predicts The education
and career profile of the six interpreters described above is fairly typical of HCIs in
South Africa and health care providers should keep this in mind This is evident
from the following job advertisement for an interpreter with a medical background
but no mention is made of interpreting or translation training The typical
requirements are matric the speaking andor writing skills in the languages needed
and nursing or other medical experience
Mouldmed Locum International Exchange Ltd is looking for a translatorinterpreterwho is able to speak and write three languages fluently (preferably English Afrikaansand Xhosa) The candidate must be able to start immediately and must have a Matric
Perspectives Studies in Translatology 9
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
qualification and a medical background This is a three-month contract with the optionto extend Working hours are 0730 1600 (30-minute lunch) Monday to Friday Thejob entails office work and patient communication A senior assistant nurse with theselanguage requirements would also qualify for the position
Responsibility and ethical behaviour standards towards interpreters should also be
laid down for the health care provider and not only for the interpreter NCICH
(2004 p 19) notes the responsibility of the health care provider lsquoProviders have the
duty to present their knowledge clearly and objectively so that the patient is able
to make informed choicesrsquo If even interpreters are not monitored to meet their
obligations who is going to monitor the health care providers
Further research that could flow from this could be competency testing of the
interpreters to see how well they actually understand the information which had
been communicated by the health care provider and after the interpreters have
explained the information to the patients the same competency testing could be
done on the patientsrsquo understanding This can be established by asking patients
probing questions and inviting them to repeat the information they have received
(Roth et al 1983 p 175 in Johnstone 1999 pp 225227)
A retranslation of the source texts could also be done into Afrikaans and
isiXhosa using the functionalist approach and the interpreters could then be
retested to see whether they now understand the target texts better and whether
they would be able to paraphrase and explain the content better to the patient
Keeping in mind the socio-economic and educational level of the prototypical
patient for whom these informed consent forms are intended we would still
dissuade the interpreters from attempting to convey the message without a health
care provider present and from signing the document
Notes
1 Each of the nine provinces has its own set of official languages eg English Afrikaansand one or more of the indigenous languages On a national level all 11 of these languagesare recognised as official In the case of the Western Cape Province there are thus threeofficial languages as stated
2 Groote Schuur Hospital is linked to the University of Cape Town and situated in theObservatory area in Cape Town a mainly English-speaking area It employs 524 doctorsand 1370 nurses The hospital treats approximately 44000 in-and 575000 out-patientsper year (Capegateway public info 2009) The staff use both Afrikaans and English on anequal basis and a small proportion use African languages The patients are alsopredominantly Afrikaans and English and a large proportion use African or otherlanguages (Williams 2005 in Saulse 2009 p 24)
3 This is the highest level of secondary schooling that can be obtained within the SouthAfrican context This gives access to tertiary education
Notes on contributors
Ilse Feinauer is associate professor in the Department of Afrikaans and Dutch and isresponsible for teaching Translation Studies and Practice to undergraduate and postgraduatestudents She also teaches Afrikaans linguistics She is coordinator for the MPhil inTranslation Studies She has extensive experience both as a translator and scholar intranslation theory
Harold Lesch is a senior lecturer also in the Department of Afrikaans and Dutch and holds aqualification in Translation Studies He is currently coordinator of the Post Graduate Diploma
10 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
in Translation and Interpreting and is responsible for teaching Interpreting Studies andPractice
References
Angelelli C (2004) Medical interpreting and cross-cultural communication CambridgeCambridge University Press
Angelelli C (2006) Validating professional standards and codes Challenges and opportu-nities Interpreting 8 175193
Anthonissen C (2008) On interpreting the interpreter experiences of language practitionersin mediating for the TRC Journal of Multicultural Discourses 3 165188
Capegateway public info (2009) httpwwwwesterncapegovzaengyour_gov5987Census (2001) Primary tables 1996 and 2001 compared Accessed at httpwwwstatssagovza
census01htmlC2001PrimTablesaspFeinauer I (2003) TB or not TB The communicative success of translated medical texts in
South Africa In W Botha (Ed) n Man wat beur rsquon Huldigingsbundel vir Dirk vanSchalkwyk (pp 213223) Stellenbosch Buro of the WAT
Feinauer I amp Luttig L (2005) Functionalism is not always the remedy Perspectives Studiesin Translatology 13 123131
Gile D (1995) Basic concepts and models for interpreter and translator training AmsterdamJohn Benjamins
Johnstone M-J (1999) Bioethics A nursing perspective Sydney HarcourtLeanza Y (2007) Role of community interpreters in pediatrics as seen by interpreters
physicians and researchers In F Pochhacker amp M Shlesinger (Eds) Healthcareinterpreting Discourse and interaction (pp 1134) Amsterdam Benjamins
Pienaar M (2006) Kommunikasie tussen staat en burgers die stand van tolkdienste SabinetOnline 40 3546
Pochhacker F amp Shlesinger M (Eds) (2007) Healthcare interpreting Discourse andinteraction Amsterdam Benjamins
Romero B (2008) Here are your right hands exploring interpreter qualifications Universityof Dayton Law Review 34 1533
Saulse B (2009) Interpreting within the Western Cape Health Care Sector A DescriptiveOverview (Unpublished masterrsquos thesis) University of Stellenbosch South Africa
United States National Council on Interpreting in Health Care (2004) A national code ofethics for interpreters in health care The National Council on Interpreting in Health CareWorking Papers Series httpwwwncihcorg
Appendix A
Text 1
A DOUBLE-BLIND PLACEBO CONTROLLED RANDOMISED STUDY TO INVESTI-GATE THE EFFICACY AND SAFETY OF LOW-DOSE L-CARNITINEMAGNESIUMSUPPLEMENTATION IN PREVENTING HYPERLACTINEMIA AND LACTIC ACIDO-SIS IN HIV-INFECTED SOUTH AFRICAN WOMEN ON STAVUDINE CONTAININGCOMBINED ANTIRETROVIRAL THERAPY (cART)
Introduction
We are doing a study to see if a l-carnitine magnesium combination product that could help toprevent high blood lactate levels which are known to be one of the side effects of some of themedications used in the treatment of HIV-infection (anti retroviral drugs)
The ability to decrease the way the virus multiplies is achieved by combined anti retroviraltherapy HIV positive (HIV ) patients receiving a combination of these drugs survive by
Perspectives Studies in Translatology 11
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
keeping the infection under control but not by killing the virus altogether This treatment hasindeed increased the quality of life in HIV individuals
One of the drugs the nucleotidic reverse transcriptase inhibitors (NRTIrsquos) can alter the energyproducing part of cells in the body and this that can lead to effects such as the high bloodlactate Twenty five percent of patients with high lactate levels donrsquot have any symptoms whileonly a smaller percentage less than 10 percent develops symptoms including loss of weightand abdominal pain
What is the purpose of this trial
A previous study showed that the low dose l-carnitine and magnesium was absorbed in healthymale volunteers and that the supplement was safe to administer
We want to determine if a dose of two capsules per day of the study drug over a period of ayear prevents the build up of lactic acid in the blood We also want to show if the l-carnitineand magnesium is absorbed in HIV positive subjects on combined anti-retroviral therapy anddetermine what the concentration levels of the anti-retroviral drugs are after a period of 6months and 12 months
To achieve this the study drug must be compared with a placebo (these are capsules that looksthe same as the study drug which are filled with a harmless compound in this case lactose)An extra 20 ml of blood and 50ml of urine apart from the normal routine bloods will be takenbefore starting anti-retroviral therapy and 30ml of blood and 50ml of urine will be taken 6monthly thereafter up to 12 months
The levels of lactic acid cholesterol triglycerides LDL - HDL- and Lp(a) lipoproteins andanti-retroviral drugs will be determined in the blood and those of the l-carnitine with itssupporting metabolites (the organic acid - amino acid-and major and trace element profileswhich includes magnesium) will be determined in the blood and urine These results of thosesubjects that are on the study drug will be compared with those of the placebo group to show ifthere are statistical relevant differences
Text 2
PARTICIPANT INFORMATION SHEET AND CONSENT FORM FOR USE BYPARENTSLEGAL GUARDIANS
Virtual Reality for pain relief in paediatric burns patients
What is this research study all aboutYour child has been admitted to this unit because of their burn injury Every child in this burnsunit has dressing changes on a daily basis Your child will be given the normal medication thatshehe receives during any dressing change These dosages of medication have been prescribedby the doctor when your child was admitted to the burns unit With all burn injuries one ofthe biggest problems that our patients experience is pain At the moment the professionals inthe burns unit do not know if there is something other than pain medication that can help todecrease your childrsquos pain Certain studies have proven that using a technique called VirtualRealty (VR) can distract a child and thereby decrease their pain during a specific procedureVirtual Reality is a program that we will use to allow your child to watch a video game throughgoggles that will be placed on their face Half of the treatment will be done using only the painmedication The other half of the dressing change will be done using the pain medication andthe VR We will then interview yourself and your child to find out how you your child feltabout this process and if you feel that Virtual reality can help to decrease your childrsquos painDuring the interviews with youyour child and nursing staff information may be recorded on a
12 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
tape recorder so that we can check all our information We will also be videotaping alldressing changes and using information from those tapes to help us with this study
Why has your child been invited to participateIn order to see if this process of VR is going to worknot work we have to assess it on at least250 children All children who are over the age of 5 and who do not have a face burn can takepart in this study You and your child have the option to participate in this study andparticipation is completely VOLUNTARY
What will your responsibilities beBy agreeing to let your child participate in this study you will allow us to ask your child tocomplete a questionnaire You will also be interviewed
Will your child benefit from taking part in this researchAt this stage we cannot say if your child will benefit from the study that we are doing If whatwe are doing does work then your child will experience less pain during the dressing changesIf the results are positive then it means that in the future more patients with similar injuries toyour child can be helped when they are experiencing pain during dressing changes
Are there any risks involved in your child taking part in this researchThere are no reported risks The only reported side effect of the VR is sickness If your childdoes experience any sickness due to the VR it will be stopped immediately
If you do not agree to allow your child to take part what alternatives does your child haveYou and your child have the option not to participate in this study participation is completelyVOLUNTARY Your child will only be entered into the study with your permission If youchoose not to enter the study we will still treat your child to the best of our ability and it willnot change the way you are treated You can leave the study at any time after you join
Who will have access to your childrsquos medical recordsAny information gained from this study and testing will be kept strictly private and no oneoutside of the people in the study will know youryour childrsquos results without your permissionIf the information is published to educate other health care professionals we will not use anynames Thus you and your child will never be able to be identified by anyone except studypersonnel Similarly no person outside of the study will have access to audio and videorecordings that may have been made during the dressing changes
Will you or your child be paid to take part in this study and are there any costs involvedYou or your child will not be paid to take part in the study and there will be no costs involvedfor you if your child does take part
Perspectives Studies in Translatology 13
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
14 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012

among patients is very diverse with English Afrikaans and isiXhosa being used on
an almost equal basis (Williams 2005 in Saulse 2009 p 24) Informed consent
forms were distributed here among the parents or legal guardians of burns patients
entitled (see Appendix 1 Text 2) lsquoVIRTUAL REALITY FOR PAIN RELIEF IN
PAEDIATRIC BURNS PATIENTSrsquo
Feinauer (2003) discussed the profile of typical state hospital patients in the
Western Cape they were mostly lay people from a low socio-economic level who are
language impoverished have low or no level of schooling lack communication skills
sometimes do not use the standard varieties of Afrikaans English or isiXhosa they
are economically deprived they have low concentration levels they are ill are
intimidated by the unfamiliar environment and are without any medical knowledge
(Feinauer 2003 pp 216217) Feinauer and Luttig (2005) find that sometimes the
gap between the source-text recipients and the target-text recipients is too big
to be bridged by merely changing the translation approach from linguistic to
functional An empirical study was undertaken on how to present information on
primary ailments (HIVAids and TB) in an accessible form to lay people Actual
target texts in both Afrikaans and isiXhosa were assessed in terms of their
communicative success by using questionnaires amongst state hospital patients
who were on a much lower level of literacy or knowledge than that of the source text
recipients
The main communicative problems were ascribed to the fact that these target
texts were almost exact replicas of the source texts in other words the translators
still used the linguistic approach The source texts were retranslated using the
functionalist approach by translators who played a much more important role in
designing the target texts keeping the target readers in mind the whole time The
target texts were reassessed using the same questionnaires but with different
respondents The respondents however were on the same level of literacy or
knowledge as that of the first group of respondents Then the big disappointment
came comprehension did improve slightly but after all the effort and time that went
into the retranslation the improvement was not statistically significant What did
become apparent in this research is that a target text as such irrespective of the
translation approach is not the means to convey the necessary knowledge to these
target recipients
This should be kept in mind to contextualise the enormity and the responsibility
of the task assigned to the interpreters Before we look at the profile of the
interpreters at these two hospitals and their understanding of the relevant
documents let us look at what is generally expected from health care interpreters
(HCIs) as well as the role that the interpreters are supposed to play during the
communication process
Interpreting theory
Obligations of health care interpreters
According to Angelelli (2006 p 186) health care organisations sometimes have
expectations (which are sometimes even included in job descriptions) beyond the
interpreterrsquos control One of her respondents reacted by noting that lsquoproviders can
easily put us in the position of doing other things which we are not entitled to
do we donrsquot have the training we donrsquot have the capacity to do those thingsrsquo
Perspectives Studies in Translatology 3
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
(Angelelli 2006 p 189) One of the reasons why HCIs are so often misused is because
it is so difficult to define their role in the system Angelelli (2006 p 175) says lsquoOne
of the most problematic issues is the role of interpreters Presumably this role should
be simple to describe the interpreter faithfully conveys a message from one
language to another while maintaining neutralityrsquo Angelelli (2006 p 182) identifies
the following roles that interpreters can play as they perform their task message
converter message clarifier cultural clarifier patient advocate
System agent
All four of these roles could be operative here but in this case the roles of message
converter and clarifier or as Jalbert (1998 in Leanza 2007 pp 1314) calls it the
role of bilingual professional will be the primary role Whatever role the interpreter
takes on here will be within the overarching role of the interpreter as the healthcare
provider or acting on behalf of the institutional or medical system Leanza (2007 p
17) refers to the interpreter playing the role of lsquosystem agentrsquo Here the interpreter is
in essentially the same (symbolic) position as the health care provider
The researchers want the interpreters to be translating machines in other words
to act as linguistic agents but to simultaneously act as health system agents since
they want the interpreter to get the parents or the volunteers to sign the informed
consent forms in order to be able to conduct their research The researcher explains
the relevant information on the informed consent forms to the interpreter(s) and
then the interpreter is left with the patient in a situation of dialogue and not in a
situation of trialogue which is usually the default situation for HCIs As Leanza
(2007 pp 1314) puts it the interpreter becomes the healthcare professional The
fact that the interpreter has to sign that the information was conveyed clearly to the
patient and that the patient understands the information implies that there is an
agreement between the health care provider and the interpreter before the discussion
starts between the interpreter and the patient The interpreterrsquos signature will indicate
that she has kept to the agreement
This is in direct opposition to the view that the interpreter is usually part of
the lsquotreating teamrsquo but is not regarded as the person with the primary responsibility
for the care and treatment of patients The interpreter is usually regarded as acting in
a secondary or supporting role The United States National Council on Interpreting
in Health Care (NCHIC 2004 16) states
Interpreters in health care understand that they are not there as primary participants inthe interaction and therefore are not in a position to make decisions to advise orcounsel Their function is that of a communication facilitator and as such theirresponsibility is to the process of communication and the facilitation of a mutualunderstanding of meaning It is not within the interpreterrsquos set of duties to give advice orto counsel either party with respect to the goals of the health care encounter
Here however the interpreter is pushed into the primary role and has to take
primary responsibility This according to Angelelli (2004 pp 78) would mean that
the interpreter aligns with the system and the interpreter alone has to construct the
conversation This means that the task for bringing the message across is the sole
responsibility of the interpreter This is not a new role for interpreters as seen from
various publications on the role of the interpreter such as the book by Pochhacker
4 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
and Shlesinger (2007 p 2) where one of the roles of the interpreter is described as
someone who could take over the interview and the article by Anthonissen (2008
p 171) which describes the mediating role of the interpreter as providing lsquoguided
constructive interventionrsquoThis more visible interpreter could only successfully step into the shoes of the
health care provider whilst also acting as message converter message clarifier and
cultural clarifier if she were able to fully understand the documents The interpreter
should provide the most faithful rendering possible of what these document say This
does not only entail an accurate translation of the words spokenwritten but also a
translation that formulates the information in such a way that it becomes coherent
within the world view of the patient In order to do this the interpreter needs to have
a deep and thorough knowledge of the subject matter as well as the language usedwithin that field It is obvious that the more explication needs to go into the
clarification of the message the better the interpreter ought to know the subject field
and its discourse The ability to interpret accurately and completely is to a large
extent dependent on how much background knowledge the interpreter has of the
content and context of the communication Romero (2008 p 19) states with respect
to court and legal interpreters that interpreters cannot interpret what they do not
know or understand Communication in the legal setting is guided by an under-
standing of the use of legal arguments protocol procedures laws and traditions Ifinterpreters are not prepared to handle this task they will get in the way or perform
poorly The same applies to HCIs especially if they don the white coat of the health
care provider
According to NCHIC (2004 p 18)
The ethical obligation of interpreters is to possess enough understanding of culture andcultural practices and beliefs to be able to facilitate communication across culturaldifferences seeking to minimize and if possible avoid potential misunderstanding andmiscommunication based on cultural assumptions andor stereotyping Under certainconditions such as clashing cultural beliefs or practices a lack of linguistic equivalencyor the inability of parties to articulate the differences in their own words the interpretershould assist by sharing cultural information or helping develop an explanation thatcan be understood by all (our emphasis)
NCICH (2004 pp 1314) also states that the language used by the provider is asource of data for the patient The patient therefore should be able to access both
the technical information and the information about the kind of relationship the
provider is attempting to establish in order to make decisions that will impact on
his or her health and wellbeing Here this is relevant since the parents or volunteers
have to sign informed consent forms In order for the parents or volunteers to
internalise the necessary information to make the correct and informed decision the
interpreter would have to have succeeded in making all the information clearly
understood
Community agent
The interpreters in this situation could also act as community agents who play an
advocacy role This is the counterpart of the role of system agent where the
interpreters are agents of the institution and spokespersons for the healthcare system
and its discourse As community agents the interpreters may act in accordance with
Perspectives Studies in Translatology 5
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
the cultural norms and values of their own community If the role of advocate is
adopted it presupposes once again that the interpreter is well informed about the
laws rules and procedures that need to be relayed (Leanza 2007 p 14) The task
of the interpreter is twofold here disclose all relevant information necessary for
making an informed choice about proposed procedures and ensure that the patient
understands the information received and the implications of giving consent (adapted
from Johnstone 1999 p 235 who applied this to the role of the nurse regarding
informed consent) Since this research deals with informed consent the interpreterrsquos
role here should rather be that of an advocate for parents and volunteers improving
their level of understanding and in that way helping them to make an informed
decision about taking part in the research or not
What is informed consent According to Robertson (1981 p 102 in Johnstone
1999 pp 210211)
The doctrine of informed consent although having a profound ethical dimension isessentially a legal doctrine developed partially out of recognition of the patientrsquos right toself-determination and partially out of the doctorrsquos duty to give the patient lsquolsquoinformationabout proposed treatment so as to provide him or her with the opportunity of makingan informed or rational choice as to whether to undergo the treatmentrsquorsquo
Johnstone (1999 pp 224225) also feels that the term lsquoinformed consentrsquo should be
abandoned in favour of lsquoinformed decision-makingrsquo Unlike the notion of lsquoinformed
consentrsquo this formulation seems to invite continuous re-evaluation of any decisions
made about care and treatment options Patients must also be informed of their
right to refuse a recommended medical or nursing procedure and should be kept
up to date on the relevant details pertaining to their cases This should be done
by interpreters who adopt the role of patientrsquos advocate Details which are not
readily understood should be explained (in understandable language) and reinforced
through planned patient health education programmes something that nurses
interpreters are educationally prepared to undertake Many factors can deter patients
from exercising informed and voluntary choices amongst which is poor commu-
nication The patientrsquos ability to understand entails whether the patient is able to
comprehend the risks benefits and alternatives to a proposed medical procedure as
well as the implications of giving consent The question could be asked concerning
just how sophisticated a patientrsquos understanding needs to be and in this case
how sophisticated the interpreterrsquos understanding needs to be in order to really
explain these procedures and to really support these parents and volunteers in
making their decisions
Data
Two phases of data collection were involved Both were done during one
consultation with the interpreters The first phase aimed at compiling a profile of
the relevant interpreters whereas the second phase entailed completing a compre-
hension test ie an exercise to ascertain whether the interpreters understand the test
that they were supposed to explain to the patient
6 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Profile of interpreters
The interpreters of the Tygerberg and Red Cross state hospitals were visited by the
researchers and asked to complete questionnaires on their training background
comprehension of the target text etc At Tygerberg only one interpreter was found
and at Red Cross only two Therefore we also visited the Groote Schuur state
hospital where another three interpreters were interviewed although the informed
consent forms were not meant for this hospital The Groote Schuur hospital has a
similar profile to that of the Tygerberg hospital The results of the survey are listed in
Table 1
Regarding the languages offered for TBH and RXH no interpreters were found
for Afrikaans whilst in both hospitals Afrikaans was either the most spoken
language or used on an equal basis with English and isiXhosa All six interpreters are
mother-tongue speakers of isiXhosa with English as their second language At
RXH Sesotho and isiZulu are offered as third languages and at GSH two of the
interpreters offer Afrikaans as their third language Regarding the interpretersrsquo
qualifications none has a tertiary education and not all have even completed their
secondary education Regarding their training as interpreters and the period that
they were interpreting the interpreter at TBH had no training but she was a nursing
ancillary who later just moved into an interpreting lsquopositionrsquo She has been doing
this for the past eight months on a freelance basis at the Tygerberg hospital
The two interpreters at RXH have been performing interpreting duties for the
past seven years They are full-time interpreters and had training in interpreting for
two years on an ad hoc basis from an NGO (non-governmental organisation)
namely the National Language Project (NLP) Apart from language and interpreting
skills they also had some training in counselling They presented themselves as very
professional The three interpreters at GSH had been doing lsquoformalrsquo interpreting
in this hospital for the past two years but were doing interpreting on an ad hoc
basis at the hospital for at least 10 years before that even though their job
description was that of lsquocleanerrsquo When they were appointed as interpreters they
underwent training for six weeks
Table 1 Interpreters consulted
HospitalNumber ofinterpreters Gender Age Qualifications Languages
Interpretertraining
Tygerberg(TBH)
1 Female 33 Matric Wasnursing ancillary
EnglishisiXhosa
None
Red Cross(RXH)
2 Female 35 53 Matric Post-matric studies(Adult basiceducationAncillary socialwork)
EnglishisiXhosaisiZuluEnglishisiXhosaSesotho
Two-yeartrainingSometraining incounselling
GrooteSchuur(GSH)
3 MaleFemale(2)
43 46 48 Busy with matricWere cleaners
EnglishisiXhosaEnglishisiXhosaAfrikaansEnglishisiXhosaAfrikaans
6-weektraining
Perspectives Studies in Translatology 7
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Comprehension test
They were also tested on their comprehension of the English source texts since
all of them offered English and since the source-text documents would have
been explained to them in English The translations into Afrikaans and isiXhosa
are very close linguistic translations of the original so if they did not understand
the source text they would not understand the target text either Questions were
also put on textual issues such as sentence and paragraph length paragraph
coherence and stylistic and lexical suitability (Table 2)
According to Gile (1995 p 34) the following criteria for quality can be applied
universally to all interpreting acts ideational clarity (the message of the sender
should be clear and comprehensible to the receiver) linguistic acceptability (the
interpreter should use grammar which is acceptable for the situation and the other
participants) and terminological accuracy (the interpreter should use the correct
target language equivalent for medical terms in the source language) From the
responses it can be deduced that none of these criteria could be met here
Question 1 addresses the ideational clarity and no interpreter completely agreed
that they clearly understood the message of the senders Linguistic acceptability
and terminological accuracy are addressed by questions 5 and 6 and here no one
agreed that the vocabulary and style of these texts was appropriate for this
situation Other remarks on the texts as such are that they found the texts too
long to explain but they did not think they themselves would be able to paraphrase
them in order to shorten the time with the patients Only one the male interpreter
from GSH felt that if he were given enough time to work with the texts he would
be able to explain the contents to the parents or volunteers The other interpreters
did not feel comfortable explaining the information of the texts so that the patients
or their parents could come to an informed decision as to whether they should sign
the document or not Needless to say none of the interpreters would like to sign
the agreement certifying that they explained the information of the trial in the
patientrsquos mother tongue and that the patient understood what was explained See
Appendix 2 for the section of the Informed Consent forms where the interpreters
are required to sign
If these interpreters were to be confronted with this task the ethical response
would be to withdraw from the assignment unless they are supplied with a much
Table 2 Responses on English source texts
No Question1Donrsquot agree
at all 2Donrsquot agree 3Agree4Completely
agree
1 I clearly understand thetexts
GSH 1 TBH 1 RXH 1 GSH 2 RXH 1
2 The length of thesentences is good
GSH 1 TBH 1 RXH 2 GSH 2
3 The paragraphs arecoherent
RXH 1 RXH 1 GSH3 TBH 1
4 The length of theparagraphs is good
RXH 1 GSH3 TBH 1
RXH 1
5 The vocabulary isappropriate
GSH 2 RXH 2 GSH 1TBH 1
6 The style of the text isappropriate
GSH 3 RXH 2 TBH 1
8 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
simpler document or preferably have a health care provider with them doing the
actual explanation Then they could revert to their more passive role of interpreting
as part of a trialogue The NCICH (2004 p 16) also makes the point that lsquoTo work
within the professional boundaries of the interpreter role also means that interpretersare aware of the limitations of their duties as well as the limitations of their abilities as a
health care interpreterrsquo (our emphasis)
Discussion
Regardless of the role of the interpreter either as system or community agent the
basic goal of medical discourse is mutual understanding Clear verbal commu-
nication is a necessary component of an effective clinical encounter Even when
patients and providers are educated in the same language faulty communication
can lead to distortions and miscommunications between the parties let aloneeducated health care providers and uneducated patients and semi-educated
interpreters (Kaufert amp Putsch 1997 in Angelelli 2004 p 18) Communicative
failure will inevitably be the result here since neither interpreters nor parents or
volunteers have the same level of literacy or knowledge as the compilers of the
source texts in both these instances the compilers were medical researchers The
parents or volunteers would therefore not be able to make informed decisions
about agreeing to take part in the research projects or not
What is equally disturbing is that the interpreters are set up for failure whenthey are confronted with a task of this scope and these types of documents These
target texts will not be comprehensible enough to be viewed as providing an effective
service to the customer According to Gile (1995 pp 7980) one is not able to fully
comprehend something simply on the grounds of knowledge of the language or
extra-linguistic knowledge The content of the speech may be too difficult it may
deviate from generally accepted linguistic standards or the level of knowledge of the
language and extra linguistic knowledge of the receiver may not be high enough
Then it is necessary to analyse the discourse itself to a much greater extent than onewould analyse discourse with regard to comprehension in everyday situations
Therefore to fully comprehend one does not only need knowledge of the language
and extra-linguistic knowledge but the discourse also need purposeful analysis This
type of analysis could not be performed by most of the HCIs in South Africa and
should rather be left to the health care providers or to trained translators working
with the health care providers in rendering a much simpler target text
It is high time to shift the focus in research on health care interpreting to the
way in which the health care provider deals with the HCIs so as not to expectfar more than what their duties entail and their training predicts The education
and career profile of the six interpreters described above is fairly typical of HCIs in
South Africa and health care providers should keep this in mind This is evident
from the following job advertisement for an interpreter with a medical background
but no mention is made of interpreting or translation training The typical
requirements are matric the speaking andor writing skills in the languages needed
and nursing or other medical experience
Mouldmed Locum International Exchange Ltd is looking for a translatorinterpreterwho is able to speak and write three languages fluently (preferably English Afrikaansand Xhosa) The candidate must be able to start immediately and must have a Matric
Perspectives Studies in Translatology 9
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
qualification and a medical background This is a three-month contract with the optionto extend Working hours are 0730 1600 (30-minute lunch) Monday to Friday Thejob entails office work and patient communication A senior assistant nurse with theselanguage requirements would also qualify for the position
Responsibility and ethical behaviour standards towards interpreters should also be
laid down for the health care provider and not only for the interpreter NCICH
(2004 p 19) notes the responsibility of the health care provider lsquoProviders have the
duty to present their knowledge clearly and objectively so that the patient is able
to make informed choicesrsquo If even interpreters are not monitored to meet their
obligations who is going to monitor the health care providers
Further research that could flow from this could be competency testing of the
interpreters to see how well they actually understand the information which had
been communicated by the health care provider and after the interpreters have
explained the information to the patients the same competency testing could be
done on the patientsrsquo understanding This can be established by asking patients
probing questions and inviting them to repeat the information they have received
(Roth et al 1983 p 175 in Johnstone 1999 pp 225227)
A retranslation of the source texts could also be done into Afrikaans and
isiXhosa using the functionalist approach and the interpreters could then be
retested to see whether they now understand the target texts better and whether
they would be able to paraphrase and explain the content better to the patient
Keeping in mind the socio-economic and educational level of the prototypical
patient for whom these informed consent forms are intended we would still
dissuade the interpreters from attempting to convey the message without a health
care provider present and from signing the document
Notes
1 Each of the nine provinces has its own set of official languages eg English Afrikaansand one or more of the indigenous languages On a national level all 11 of these languagesare recognised as official In the case of the Western Cape Province there are thus threeofficial languages as stated
2 Groote Schuur Hospital is linked to the University of Cape Town and situated in theObservatory area in Cape Town a mainly English-speaking area It employs 524 doctorsand 1370 nurses The hospital treats approximately 44000 in-and 575000 out-patientsper year (Capegateway public info 2009) The staff use both Afrikaans and English on anequal basis and a small proportion use African languages The patients are alsopredominantly Afrikaans and English and a large proportion use African or otherlanguages (Williams 2005 in Saulse 2009 p 24)
3 This is the highest level of secondary schooling that can be obtained within the SouthAfrican context This gives access to tertiary education
Notes on contributors
Ilse Feinauer is associate professor in the Department of Afrikaans and Dutch and isresponsible for teaching Translation Studies and Practice to undergraduate and postgraduatestudents She also teaches Afrikaans linguistics She is coordinator for the MPhil inTranslation Studies She has extensive experience both as a translator and scholar intranslation theory
Harold Lesch is a senior lecturer also in the Department of Afrikaans and Dutch and holds aqualification in Translation Studies He is currently coordinator of the Post Graduate Diploma
10 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
in Translation and Interpreting and is responsible for teaching Interpreting Studies andPractice
References
Angelelli C (2004) Medical interpreting and cross-cultural communication CambridgeCambridge University Press
Angelelli C (2006) Validating professional standards and codes Challenges and opportu-nities Interpreting 8 175193
Anthonissen C (2008) On interpreting the interpreter experiences of language practitionersin mediating for the TRC Journal of Multicultural Discourses 3 165188
Capegateway public info (2009) httpwwwwesterncapegovzaengyour_gov5987Census (2001) Primary tables 1996 and 2001 compared Accessed at httpwwwstatssagovza
census01htmlC2001PrimTablesaspFeinauer I (2003) TB or not TB The communicative success of translated medical texts in
South Africa In W Botha (Ed) n Man wat beur rsquon Huldigingsbundel vir Dirk vanSchalkwyk (pp 213223) Stellenbosch Buro of the WAT
Feinauer I amp Luttig L (2005) Functionalism is not always the remedy Perspectives Studiesin Translatology 13 123131
Gile D (1995) Basic concepts and models for interpreter and translator training AmsterdamJohn Benjamins
Johnstone M-J (1999) Bioethics A nursing perspective Sydney HarcourtLeanza Y (2007) Role of community interpreters in pediatrics as seen by interpreters
physicians and researchers In F Pochhacker amp M Shlesinger (Eds) Healthcareinterpreting Discourse and interaction (pp 1134) Amsterdam Benjamins
Pienaar M (2006) Kommunikasie tussen staat en burgers die stand van tolkdienste SabinetOnline 40 3546
Pochhacker F amp Shlesinger M (Eds) (2007) Healthcare interpreting Discourse andinteraction Amsterdam Benjamins
Romero B (2008) Here are your right hands exploring interpreter qualifications Universityof Dayton Law Review 34 1533
Saulse B (2009) Interpreting within the Western Cape Health Care Sector A DescriptiveOverview (Unpublished masterrsquos thesis) University of Stellenbosch South Africa
United States National Council on Interpreting in Health Care (2004) A national code ofethics for interpreters in health care The National Council on Interpreting in Health CareWorking Papers Series httpwwwncihcorg
Appendix A
Text 1
A DOUBLE-BLIND PLACEBO CONTROLLED RANDOMISED STUDY TO INVESTI-GATE THE EFFICACY AND SAFETY OF LOW-DOSE L-CARNITINEMAGNESIUMSUPPLEMENTATION IN PREVENTING HYPERLACTINEMIA AND LACTIC ACIDO-SIS IN HIV-INFECTED SOUTH AFRICAN WOMEN ON STAVUDINE CONTAININGCOMBINED ANTIRETROVIRAL THERAPY (cART)
Introduction
We are doing a study to see if a l-carnitine magnesium combination product that could help toprevent high blood lactate levels which are known to be one of the side effects of some of themedications used in the treatment of HIV-infection (anti retroviral drugs)
The ability to decrease the way the virus multiplies is achieved by combined anti retroviraltherapy HIV positive (HIV ) patients receiving a combination of these drugs survive by
Perspectives Studies in Translatology 11
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
keeping the infection under control but not by killing the virus altogether This treatment hasindeed increased the quality of life in HIV individuals
One of the drugs the nucleotidic reverse transcriptase inhibitors (NRTIrsquos) can alter the energyproducing part of cells in the body and this that can lead to effects such as the high bloodlactate Twenty five percent of patients with high lactate levels donrsquot have any symptoms whileonly a smaller percentage less than 10 percent develops symptoms including loss of weightand abdominal pain
What is the purpose of this trial
A previous study showed that the low dose l-carnitine and magnesium was absorbed in healthymale volunteers and that the supplement was safe to administer
We want to determine if a dose of two capsules per day of the study drug over a period of ayear prevents the build up of lactic acid in the blood We also want to show if the l-carnitineand magnesium is absorbed in HIV positive subjects on combined anti-retroviral therapy anddetermine what the concentration levels of the anti-retroviral drugs are after a period of 6months and 12 months
To achieve this the study drug must be compared with a placebo (these are capsules that looksthe same as the study drug which are filled with a harmless compound in this case lactose)An extra 20 ml of blood and 50ml of urine apart from the normal routine bloods will be takenbefore starting anti-retroviral therapy and 30ml of blood and 50ml of urine will be taken 6monthly thereafter up to 12 months
The levels of lactic acid cholesterol triglycerides LDL - HDL- and Lp(a) lipoproteins andanti-retroviral drugs will be determined in the blood and those of the l-carnitine with itssupporting metabolites (the organic acid - amino acid-and major and trace element profileswhich includes magnesium) will be determined in the blood and urine These results of thosesubjects that are on the study drug will be compared with those of the placebo group to show ifthere are statistical relevant differences
Text 2
PARTICIPANT INFORMATION SHEET AND CONSENT FORM FOR USE BYPARENTSLEGAL GUARDIANS
Virtual Reality for pain relief in paediatric burns patients
What is this research study all aboutYour child has been admitted to this unit because of their burn injury Every child in this burnsunit has dressing changes on a daily basis Your child will be given the normal medication thatshehe receives during any dressing change These dosages of medication have been prescribedby the doctor when your child was admitted to the burns unit With all burn injuries one ofthe biggest problems that our patients experience is pain At the moment the professionals inthe burns unit do not know if there is something other than pain medication that can help todecrease your childrsquos pain Certain studies have proven that using a technique called VirtualRealty (VR) can distract a child and thereby decrease their pain during a specific procedureVirtual Reality is a program that we will use to allow your child to watch a video game throughgoggles that will be placed on their face Half of the treatment will be done using only the painmedication The other half of the dressing change will be done using the pain medication andthe VR We will then interview yourself and your child to find out how you your child feltabout this process and if you feel that Virtual reality can help to decrease your childrsquos painDuring the interviews with youyour child and nursing staff information may be recorded on a
12 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
tape recorder so that we can check all our information We will also be videotaping alldressing changes and using information from those tapes to help us with this study
Why has your child been invited to participateIn order to see if this process of VR is going to worknot work we have to assess it on at least250 children All children who are over the age of 5 and who do not have a face burn can takepart in this study You and your child have the option to participate in this study andparticipation is completely VOLUNTARY
What will your responsibilities beBy agreeing to let your child participate in this study you will allow us to ask your child tocomplete a questionnaire You will also be interviewed
Will your child benefit from taking part in this researchAt this stage we cannot say if your child will benefit from the study that we are doing If whatwe are doing does work then your child will experience less pain during the dressing changesIf the results are positive then it means that in the future more patients with similar injuries toyour child can be helped when they are experiencing pain during dressing changes
Are there any risks involved in your child taking part in this researchThere are no reported risks The only reported side effect of the VR is sickness If your childdoes experience any sickness due to the VR it will be stopped immediately
If you do not agree to allow your child to take part what alternatives does your child haveYou and your child have the option not to participate in this study participation is completelyVOLUNTARY Your child will only be entered into the study with your permission If youchoose not to enter the study we will still treat your child to the best of our ability and it willnot change the way you are treated You can leave the study at any time after you join
Who will have access to your childrsquos medical recordsAny information gained from this study and testing will be kept strictly private and no oneoutside of the people in the study will know youryour childrsquos results without your permissionIf the information is published to educate other health care professionals we will not use anynames Thus you and your child will never be able to be identified by anyone except studypersonnel Similarly no person outside of the study will have access to audio and videorecordings that may have been made during the dressing changes
Will you or your child be paid to take part in this study and are there any costs involvedYou or your child will not be paid to take part in the study and there will be no costs involvedfor you if your child does take part
Perspectives Studies in Translatology 13
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
14 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012

(Angelelli 2006 p 189) One of the reasons why HCIs are so often misused is because
it is so difficult to define their role in the system Angelelli (2006 p 175) says lsquoOne
of the most problematic issues is the role of interpreters Presumably this role should
be simple to describe the interpreter faithfully conveys a message from one
language to another while maintaining neutralityrsquo Angelelli (2006 p 182) identifies
the following roles that interpreters can play as they perform their task message
converter message clarifier cultural clarifier patient advocate
System agent
All four of these roles could be operative here but in this case the roles of message
converter and clarifier or as Jalbert (1998 in Leanza 2007 pp 1314) calls it the
role of bilingual professional will be the primary role Whatever role the interpreter
takes on here will be within the overarching role of the interpreter as the healthcare
provider or acting on behalf of the institutional or medical system Leanza (2007 p
17) refers to the interpreter playing the role of lsquosystem agentrsquo Here the interpreter is
in essentially the same (symbolic) position as the health care provider
The researchers want the interpreters to be translating machines in other words
to act as linguistic agents but to simultaneously act as health system agents since
they want the interpreter to get the parents or the volunteers to sign the informed
consent forms in order to be able to conduct their research The researcher explains
the relevant information on the informed consent forms to the interpreter(s) and
then the interpreter is left with the patient in a situation of dialogue and not in a
situation of trialogue which is usually the default situation for HCIs As Leanza
(2007 pp 1314) puts it the interpreter becomes the healthcare professional The
fact that the interpreter has to sign that the information was conveyed clearly to the
patient and that the patient understands the information implies that there is an
agreement between the health care provider and the interpreter before the discussion
starts between the interpreter and the patient The interpreterrsquos signature will indicate
that she has kept to the agreement
This is in direct opposition to the view that the interpreter is usually part of
the lsquotreating teamrsquo but is not regarded as the person with the primary responsibility
for the care and treatment of patients The interpreter is usually regarded as acting in
a secondary or supporting role The United States National Council on Interpreting
in Health Care (NCHIC 2004 16) states
Interpreters in health care understand that they are not there as primary participants inthe interaction and therefore are not in a position to make decisions to advise orcounsel Their function is that of a communication facilitator and as such theirresponsibility is to the process of communication and the facilitation of a mutualunderstanding of meaning It is not within the interpreterrsquos set of duties to give advice orto counsel either party with respect to the goals of the health care encounter
Here however the interpreter is pushed into the primary role and has to take
primary responsibility This according to Angelelli (2004 pp 78) would mean that
the interpreter aligns with the system and the interpreter alone has to construct the
conversation This means that the task for bringing the message across is the sole
responsibility of the interpreter This is not a new role for interpreters as seen from
various publications on the role of the interpreter such as the book by Pochhacker
4 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
and Shlesinger (2007 p 2) where one of the roles of the interpreter is described as
someone who could take over the interview and the article by Anthonissen (2008
p 171) which describes the mediating role of the interpreter as providing lsquoguided
constructive interventionrsquoThis more visible interpreter could only successfully step into the shoes of the
health care provider whilst also acting as message converter message clarifier and
cultural clarifier if she were able to fully understand the documents The interpreter
should provide the most faithful rendering possible of what these document say This
does not only entail an accurate translation of the words spokenwritten but also a
translation that formulates the information in such a way that it becomes coherent
within the world view of the patient In order to do this the interpreter needs to have
a deep and thorough knowledge of the subject matter as well as the language usedwithin that field It is obvious that the more explication needs to go into the
clarification of the message the better the interpreter ought to know the subject field
and its discourse The ability to interpret accurately and completely is to a large
extent dependent on how much background knowledge the interpreter has of the
content and context of the communication Romero (2008 p 19) states with respect
to court and legal interpreters that interpreters cannot interpret what they do not
know or understand Communication in the legal setting is guided by an under-
standing of the use of legal arguments protocol procedures laws and traditions Ifinterpreters are not prepared to handle this task they will get in the way or perform
poorly The same applies to HCIs especially if they don the white coat of the health
care provider
According to NCHIC (2004 p 18)
The ethical obligation of interpreters is to possess enough understanding of culture andcultural practices and beliefs to be able to facilitate communication across culturaldifferences seeking to minimize and if possible avoid potential misunderstanding andmiscommunication based on cultural assumptions andor stereotyping Under certainconditions such as clashing cultural beliefs or practices a lack of linguistic equivalencyor the inability of parties to articulate the differences in their own words the interpretershould assist by sharing cultural information or helping develop an explanation thatcan be understood by all (our emphasis)
NCICH (2004 pp 1314) also states that the language used by the provider is asource of data for the patient The patient therefore should be able to access both
the technical information and the information about the kind of relationship the
provider is attempting to establish in order to make decisions that will impact on
his or her health and wellbeing Here this is relevant since the parents or volunteers
have to sign informed consent forms In order for the parents or volunteers to
internalise the necessary information to make the correct and informed decision the
interpreter would have to have succeeded in making all the information clearly
understood
Community agent
The interpreters in this situation could also act as community agents who play an
advocacy role This is the counterpart of the role of system agent where the
interpreters are agents of the institution and spokespersons for the healthcare system
and its discourse As community agents the interpreters may act in accordance with
Perspectives Studies in Translatology 5
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
the cultural norms and values of their own community If the role of advocate is
adopted it presupposes once again that the interpreter is well informed about the
laws rules and procedures that need to be relayed (Leanza 2007 p 14) The task
of the interpreter is twofold here disclose all relevant information necessary for
making an informed choice about proposed procedures and ensure that the patient
understands the information received and the implications of giving consent (adapted
from Johnstone 1999 p 235 who applied this to the role of the nurse regarding
informed consent) Since this research deals with informed consent the interpreterrsquos
role here should rather be that of an advocate for parents and volunteers improving
their level of understanding and in that way helping them to make an informed
decision about taking part in the research or not
What is informed consent According to Robertson (1981 p 102 in Johnstone
1999 pp 210211)
The doctrine of informed consent although having a profound ethical dimension isessentially a legal doctrine developed partially out of recognition of the patientrsquos right toself-determination and partially out of the doctorrsquos duty to give the patient lsquolsquoinformationabout proposed treatment so as to provide him or her with the opportunity of makingan informed or rational choice as to whether to undergo the treatmentrsquorsquo
Johnstone (1999 pp 224225) also feels that the term lsquoinformed consentrsquo should be
abandoned in favour of lsquoinformed decision-makingrsquo Unlike the notion of lsquoinformed
consentrsquo this formulation seems to invite continuous re-evaluation of any decisions
made about care and treatment options Patients must also be informed of their
right to refuse a recommended medical or nursing procedure and should be kept
up to date on the relevant details pertaining to their cases This should be done
by interpreters who adopt the role of patientrsquos advocate Details which are not
readily understood should be explained (in understandable language) and reinforced
through planned patient health education programmes something that nurses
interpreters are educationally prepared to undertake Many factors can deter patients
from exercising informed and voluntary choices amongst which is poor commu-
nication The patientrsquos ability to understand entails whether the patient is able to
comprehend the risks benefits and alternatives to a proposed medical procedure as
well as the implications of giving consent The question could be asked concerning
just how sophisticated a patientrsquos understanding needs to be and in this case
how sophisticated the interpreterrsquos understanding needs to be in order to really
explain these procedures and to really support these parents and volunteers in
making their decisions
Data
Two phases of data collection were involved Both were done during one
consultation with the interpreters The first phase aimed at compiling a profile of
the relevant interpreters whereas the second phase entailed completing a compre-
hension test ie an exercise to ascertain whether the interpreters understand the test
that they were supposed to explain to the patient
6 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Profile of interpreters
The interpreters of the Tygerberg and Red Cross state hospitals were visited by the
researchers and asked to complete questionnaires on their training background
comprehension of the target text etc At Tygerberg only one interpreter was found
and at Red Cross only two Therefore we also visited the Groote Schuur state
hospital where another three interpreters were interviewed although the informed
consent forms were not meant for this hospital The Groote Schuur hospital has a
similar profile to that of the Tygerberg hospital The results of the survey are listed in
Table 1
Regarding the languages offered for TBH and RXH no interpreters were found
for Afrikaans whilst in both hospitals Afrikaans was either the most spoken
language or used on an equal basis with English and isiXhosa All six interpreters are
mother-tongue speakers of isiXhosa with English as their second language At
RXH Sesotho and isiZulu are offered as third languages and at GSH two of the
interpreters offer Afrikaans as their third language Regarding the interpretersrsquo
qualifications none has a tertiary education and not all have even completed their
secondary education Regarding their training as interpreters and the period that
they were interpreting the interpreter at TBH had no training but she was a nursing
ancillary who later just moved into an interpreting lsquopositionrsquo She has been doing
this for the past eight months on a freelance basis at the Tygerberg hospital
The two interpreters at RXH have been performing interpreting duties for the
past seven years They are full-time interpreters and had training in interpreting for
two years on an ad hoc basis from an NGO (non-governmental organisation)
namely the National Language Project (NLP) Apart from language and interpreting
skills they also had some training in counselling They presented themselves as very
professional The three interpreters at GSH had been doing lsquoformalrsquo interpreting
in this hospital for the past two years but were doing interpreting on an ad hoc
basis at the hospital for at least 10 years before that even though their job
description was that of lsquocleanerrsquo When they were appointed as interpreters they
underwent training for six weeks
Table 1 Interpreters consulted
HospitalNumber ofinterpreters Gender Age Qualifications Languages
Interpretertraining
Tygerberg(TBH)
1 Female 33 Matric Wasnursing ancillary
EnglishisiXhosa
None
Red Cross(RXH)
2 Female 35 53 Matric Post-matric studies(Adult basiceducationAncillary socialwork)
EnglishisiXhosaisiZuluEnglishisiXhosaSesotho
Two-yeartrainingSometraining incounselling
GrooteSchuur(GSH)
3 MaleFemale(2)
43 46 48 Busy with matricWere cleaners
EnglishisiXhosaEnglishisiXhosaAfrikaansEnglishisiXhosaAfrikaans
6-weektraining
Perspectives Studies in Translatology 7
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Comprehension test
They were also tested on their comprehension of the English source texts since
all of them offered English and since the source-text documents would have
been explained to them in English The translations into Afrikaans and isiXhosa
are very close linguistic translations of the original so if they did not understand
the source text they would not understand the target text either Questions were
also put on textual issues such as sentence and paragraph length paragraph
coherence and stylistic and lexical suitability (Table 2)
According to Gile (1995 p 34) the following criteria for quality can be applied
universally to all interpreting acts ideational clarity (the message of the sender
should be clear and comprehensible to the receiver) linguistic acceptability (the
interpreter should use grammar which is acceptable for the situation and the other
participants) and terminological accuracy (the interpreter should use the correct
target language equivalent for medical terms in the source language) From the
responses it can be deduced that none of these criteria could be met here
Question 1 addresses the ideational clarity and no interpreter completely agreed
that they clearly understood the message of the senders Linguistic acceptability
and terminological accuracy are addressed by questions 5 and 6 and here no one
agreed that the vocabulary and style of these texts was appropriate for this
situation Other remarks on the texts as such are that they found the texts too
long to explain but they did not think they themselves would be able to paraphrase
them in order to shorten the time with the patients Only one the male interpreter
from GSH felt that if he were given enough time to work with the texts he would
be able to explain the contents to the parents or volunteers The other interpreters
did not feel comfortable explaining the information of the texts so that the patients
or their parents could come to an informed decision as to whether they should sign
the document or not Needless to say none of the interpreters would like to sign
the agreement certifying that they explained the information of the trial in the
patientrsquos mother tongue and that the patient understood what was explained See
Appendix 2 for the section of the Informed Consent forms where the interpreters
are required to sign
If these interpreters were to be confronted with this task the ethical response
would be to withdraw from the assignment unless they are supplied with a much
Table 2 Responses on English source texts
No Question1Donrsquot agree
at all 2Donrsquot agree 3Agree4Completely
agree
1 I clearly understand thetexts
GSH 1 TBH 1 RXH 1 GSH 2 RXH 1
2 The length of thesentences is good
GSH 1 TBH 1 RXH 2 GSH 2
3 The paragraphs arecoherent
RXH 1 RXH 1 GSH3 TBH 1
4 The length of theparagraphs is good
RXH 1 GSH3 TBH 1
RXH 1
5 The vocabulary isappropriate
GSH 2 RXH 2 GSH 1TBH 1
6 The style of the text isappropriate
GSH 3 RXH 2 TBH 1
8 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
simpler document or preferably have a health care provider with them doing the
actual explanation Then they could revert to their more passive role of interpreting
as part of a trialogue The NCICH (2004 p 16) also makes the point that lsquoTo work
within the professional boundaries of the interpreter role also means that interpretersare aware of the limitations of their duties as well as the limitations of their abilities as a
health care interpreterrsquo (our emphasis)
Discussion
Regardless of the role of the interpreter either as system or community agent the
basic goal of medical discourse is mutual understanding Clear verbal commu-
nication is a necessary component of an effective clinical encounter Even when
patients and providers are educated in the same language faulty communication
can lead to distortions and miscommunications between the parties let aloneeducated health care providers and uneducated patients and semi-educated
interpreters (Kaufert amp Putsch 1997 in Angelelli 2004 p 18) Communicative
failure will inevitably be the result here since neither interpreters nor parents or
volunteers have the same level of literacy or knowledge as the compilers of the
source texts in both these instances the compilers were medical researchers The
parents or volunteers would therefore not be able to make informed decisions
about agreeing to take part in the research projects or not
What is equally disturbing is that the interpreters are set up for failure whenthey are confronted with a task of this scope and these types of documents These
target texts will not be comprehensible enough to be viewed as providing an effective
service to the customer According to Gile (1995 pp 7980) one is not able to fully
comprehend something simply on the grounds of knowledge of the language or
extra-linguistic knowledge The content of the speech may be too difficult it may
deviate from generally accepted linguistic standards or the level of knowledge of the
language and extra linguistic knowledge of the receiver may not be high enough
Then it is necessary to analyse the discourse itself to a much greater extent than onewould analyse discourse with regard to comprehension in everyday situations
Therefore to fully comprehend one does not only need knowledge of the language
and extra-linguistic knowledge but the discourse also need purposeful analysis This
type of analysis could not be performed by most of the HCIs in South Africa and
should rather be left to the health care providers or to trained translators working
with the health care providers in rendering a much simpler target text
It is high time to shift the focus in research on health care interpreting to the
way in which the health care provider deals with the HCIs so as not to expectfar more than what their duties entail and their training predicts The education
and career profile of the six interpreters described above is fairly typical of HCIs in
South Africa and health care providers should keep this in mind This is evident
from the following job advertisement for an interpreter with a medical background
but no mention is made of interpreting or translation training The typical
requirements are matric the speaking andor writing skills in the languages needed
and nursing or other medical experience
Mouldmed Locum International Exchange Ltd is looking for a translatorinterpreterwho is able to speak and write three languages fluently (preferably English Afrikaansand Xhosa) The candidate must be able to start immediately and must have a Matric
Perspectives Studies in Translatology 9
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
qualification and a medical background This is a three-month contract with the optionto extend Working hours are 0730 1600 (30-minute lunch) Monday to Friday Thejob entails office work and patient communication A senior assistant nurse with theselanguage requirements would also qualify for the position
Responsibility and ethical behaviour standards towards interpreters should also be
laid down for the health care provider and not only for the interpreter NCICH
(2004 p 19) notes the responsibility of the health care provider lsquoProviders have the
duty to present their knowledge clearly and objectively so that the patient is able
to make informed choicesrsquo If even interpreters are not monitored to meet their
obligations who is going to monitor the health care providers
Further research that could flow from this could be competency testing of the
interpreters to see how well they actually understand the information which had
been communicated by the health care provider and after the interpreters have
explained the information to the patients the same competency testing could be
done on the patientsrsquo understanding This can be established by asking patients
probing questions and inviting them to repeat the information they have received
(Roth et al 1983 p 175 in Johnstone 1999 pp 225227)
A retranslation of the source texts could also be done into Afrikaans and
isiXhosa using the functionalist approach and the interpreters could then be
retested to see whether they now understand the target texts better and whether
they would be able to paraphrase and explain the content better to the patient
Keeping in mind the socio-economic and educational level of the prototypical
patient for whom these informed consent forms are intended we would still
dissuade the interpreters from attempting to convey the message without a health
care provider present and from signing the document
Notes
1 Each of the nine provinces has its own set of official languages eg English Afrikaansand one or more of the indigenous languages On a national level all 11 of these languagesare recognised as official In the case of the Western Cape Province there are thus threeofficial languages as stated
2 Groote Schuur Hospital is linked to the University of Cape Town and situated in theObservatory area in Cape Town a mainly English-speaking area It employs 524 doctorsand 1370 nurses The hospital treats approximately 44000 in-and 575000 out-patientsper year (Capegateway public info 2009) The staff use both Afrikaans and English on anequal basis and a small proportion use African languages The patients are alsopredominantly Afrikaans and English and a large proportion use African or otherlanguages (Williams 2005 in Saulse 2009 p 24)
3 This is the highest level of secondary schooling that can be obtained within the SouthAfrican context This gives access to tertiary education
Notes on contributors
Ilse Feinauer is associate professor in the Department of Afrikaans and Dutch and isresponsible for teaching Translation Studies and Practice to undergraduate and postgraduatestudents She also teaches Afrikaans linguistics She is coordinator for the MPhil inTranslation Studies She has extensive experience both as a translator and scholar intranslation theory
Harold Lesch is a senior lecturer also in the Department of Afrikaans and Dutch and holds aqualification in Translation Studies He is currently coordinator of the Post Graduate Diploma
10 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
in Translation and Interpreting and is responsible for teaching Interpreting Studies andPractice
References
Angelelli C (2004) Medical interpreting and cross-cultural communication CambridgeCambridge University Press
Angelelli C (2006) Validating professional standards and codes Challenges and opportu-nities Interpreting 8 175193
Anthonissen C (2008) On interpreting the interpreter experiences of language practitionersin mediating for the TRC Journal of Multicultural Discourses 3 165188
Capegateway public info (2009) httpwwwwesterncapegovzaengyour_gov5987Census (2001) Primary tables 1996 and 2001 compared Accessed at httpwwwstatssagovza
census01htmlC2001PrimTablesaspFeinauer I (2003) TB or not TB The communicative success of translated medical texts in
South Africa In W Botha (Ed) n Man wat beur rsquon Huldigingsbundel vir Dirk vanSchalkwyk (pp 213223) Stellenbosch Buro of the WAT
Feinauer I amp Luttig L (2005) Functionalism is not always the remedy Perspectives Studiesin Translatology 13 123131
Gile D (1995) Basic concepts and models for interpreter and translator training AmsterdamJohn Benjamins
Johnstone M-J (1999) Bioethics A nursing perspective Sydney HarcourtLeanza Y (2007) Role of community interpreters in pediatrics as seen by interpreters
physicians and researchers In F Pochhacker amp M Shlesinger (Eds) Healthcareinterpreting Discourse and interaction (pp 1134) Amsterdam Benjamins
Pienaar M (2006) Kommunikasie tussen staat en burgers die stand van tolkdienste SabinetOnline 40 3546
Pochhacker F amp Shlesinger M (Eds) (2007) Healthcare interpreting Discourse andinteraction Amsterdam Benjamins
Romero B (2008) Here are your right hands exploring interpreter qualifications Universityof Dayton Law Review 34 1533
Saulse B (2009) Interpreting within the Western Cape Health Care Sector A DescriptiveOverview (Unpublished masterrsquos thesis) University of Stellenbosch South Africa
United States National Council on Interpreting in Health Care (2004) A national code ofethics for interpreters in health care The National Council on Interpreting in Health CareWorking Papers Series httpwwwncihcorg
Appendix A
Text 1
A DOUBLE-BLIND PLACEBO CONTROLLED RANDOMISED STUDY TO INVESTI-GATE THE EFFICACY AND SAFETY OF LOW-DOSE L-CARNITINEMAGNESIUMSUPPLEMENTATION IN PREVENTING HYPERLACTINEMIA AND LACTIC ACIDO-SIS IN HIV-INFECTED SOUTH AFRICAN WOMEN ON STAVUDINE CONTAININGCOMBINED ANTIRETROVIRAL THERAPY (cART)
Introduction
We are doing a study to see if a l-carnitine magnesium combination product that could help toprevent high blood lactate levels which are known to be one of the side effects of some of themedications used in the treatment of HIV-infection (anti retroviral drugs)
The ability to decrease the way the virus multiplies is achieved by combined anti retroviraltherapy HIV positive (HIV ) patients receiving a combination of these drugs survive by
Perspectives Studies in Translatology 11
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
keeping the infection under control but not by killing the virus altogether This treatment hasindeed increased the quality of life in HIV individuals
One of the drugs the nucleotidic reverse transcriptase inhibitors (NRTIrsquos) can alter the energyproducing part of cells in the body and this that can lead to effects such as the high bloodlactate Twenty five percent of patients with high lactate levels donrsquot have any symptoms whileonly a smaller percentage less than 10 percent develops symptoms including loss of weightand abdominal pain
What is the purpose of this trial
A previous study showed that the low dose l-carnitine and magnesium was absorbed in healthymale volunteers and that the supplement was safe to administer
We want to determine if a dose of two capsules per day of the study drug over a period of ayear prevents the build up of lactic acid in the blood We also want to show if the l-carnitineand magnesium is absorbed in HIV positive subjects on combined anti-retroviral therapy anddetermine what the concentration levels of the anti-retroviral drugs are after a period of 6months and 12 months
To achieve this the study drug must be compared with a placebo (these are capsules that looksthe same as the study drug which are filled with a harmless compound in this case lactose)An extra 20 ml of blood and 50ml of urine apart from the normal routine bloods will be takenbefore starting anti-retroviral therapy and 30ml of blood and 50ml of urine will be taken 6monthly thereafter up to 12 months
The levels of lactic acid cholesterol triglycerides LDL - HDL- and Lp(a) lipoproteins andanti-retroviral drugs will be determined in the blood and those of the l-carnitine with itssupporting metabolites (the organic acid - amino acid-and major and trace element profileswhich includes magnesium) will be determined in the blood and urine These results of thosesubjects that are on the study drug will be compared with those of the placebo group to show ifthere are statistical relevant differences
Text 2
PARTICIPANT INFORMATION SHEET AND CONSENT FORM FOR USE BYPARENTSLEGAL GUARDIANS
Virtual Reality for pain relief in paediatric burns patients
What is this research study all aboutYour child has been admitted to this unit because of their burn injury Every child in this burnsunit has dressing changes on a daily basis Your child will be given the normal medication thatshehe receives during any dressing change These dosages of medication have been prescribedby the doctor when your child was admitted to the burns unit With all burn injuries one ofthe biggest problems that our patients experience is pain At the moment the professionals inthe burns unit do not know if there is something other than pain medication that can help todecrease your childrsquos pain Certain studies have proven that using a technique called VirtualRealty (VR) can distract a child and thereby decrease their pain during a specific procedureVirtual Reality is a program that we will use to allow your child to watch a video game throughgoggles that will be placed on their face Half of the treatment will be done using only the painmedication The other half of the dressing change will be done using the pain medication andthe VR We will then interview yourself and your child to find out how you your child feltabout this process and if you feel that Virtual reality can help to decrease your childrsquos painDuring the interviews with youyour child and nursing staff information may be recorded on a
12 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
tape recorder so that we can check all our information We will also be videotaping alldressing changes and using information from those tapes to help us with this study
Why has your child been invited to participateIn order to see if this process of VR is going to worknot work we have to assess it on at least250 children All children who are over the age of 5 and who do not have a face burn can takepart in this study You and your child have the option to participate in this study andparticipation is completely VOLUNTARY
What will your responsibilities beBy agreeing to let your child participate in this study you will allow us to ask your child tocomplete a questionnaire You will also be interviewed
Will your child benefit from taking part in this researchAt this stage we cannot say if your child will benefit from the study that we are doing If whatwe are doing does work then your child will experience less pain during the dressing changesIf the results are positive then it means that in the future more patients with similar injuries toyour child can be helped when they are experiencing pain during dressing changes
Are there any risks involved in your child taking part in this researchThere are no reported risks The only reported side effect of the VR is sickness If your childdoes experience any sickness due to the VR it will be stopped immediately
If you do not agree to allow your child to take part what alternatives does your child haveYou and your child have the option not to participate in this study participation is completelyVOLUNTARY Your child will only be entered into the study with your permission If youchoose not to enter the study we will still treat your child to the best of our ability and it willnot change the way you are treated You can leave the study at any time after you join
Who will have access to your childrsquos medical recordsAny information gained from this study and testing will be kept strictly private and no oneoutside of the people in the study will know youryour childrsquos results without your permissionIf the information is published to educate other health care professionals we will not use anynames Thus you and your child will never be able to be identified by anyone except studypersonnel Similarly no person outside of the study will have access to audio and videorecordings that may have been made during the dressing changes
Will you or your child be paid to take part in this study and are there any costs involvedYou or your child will not be paid to take part in the study and there will be no costs involvedfor you if your child does take part
Perspectives Studies in Translatology 13
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
14 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012

and Shlesinger (2007 p 2) where one of the roles of the interpreter is described as
someone who could take over the interview and the article by Anthonissen (2008
p 171) which describes the mediating role of the interpreter as providing lsquoguided
constructive interventionrsquoThis more visible interpreter could only successfully step into the shoes of the
health care provider whilst also acting as message converter message clarifier and
cultural clarifier if she were able to fully understand the documents The interpreter
should provide the most faithful rendering possible of what these document say This
does not only entail an accurate translation of the words spokenwritten but also a
translation that formulates the information in such a way that it becomes coherent
within the world view of the patient In order to do this the interpreter needs to have
a deep and thorough knowledge of the subject matter as well as the language usedwithin that field It is obvious that the more explication needs to go into the
clarification of the message the better the interpreter ought to know the subject field
and its discourse The ability to interpret accurately and completely is to a large
extent dependent on how much background knowledge the interpreter has of the
content and context of the communication Romero (2008 p 19) states with respect
to court and legal interpreters that interpreters cannot interpret what they do not
know or understand Communication in the legal setting is guided by an under-
standing of the use of legal arguments protocol procedures laws and traditions Ifinterpreters are not prepared to handle this task they will get in the way or perform
poorly The same applies to HCIs especially if they don the white coat of the health
care provider
According to NCHIC (2004 p 18)
The ethical obligation of interpreters is to possess enough understanding of culture andcultural practices and beliefs to be able to facilitate communication across culturaldifferences seeking to minimize and if possible avoid potential misunderstanding andmiscommunication based on cultural assumptions andor stereotyping Under certainconditions such as clashing cultural beliefs or practices a lack of linguistic equivalencyor the inability of parties to articulate the differences in their own words the interpretershould assist by sharing cultural information or helping develop an explanation thatcan be understood by all (our emphasis)
NCICH (2004 pp 1314) also states that the language used by the provider is asource of data for the patient The patient therefore should be able to access both
the technical information and the information about the kind of relationship the
provider is attempting to establish in order to make decisions that will impact on
his or her health and wellbeing Here this is relevant since the parents or volunteers
have to sign informed consent forms In order for the parents or volunteers to
internalise the necessary information to make the correct and informed decision the
interpreter would have to have succeeded in making all the information clearly
understood
Community agent
The interpreters in this situation could also act as community agents who play an
advocacy role This is the counterpart of the role of system agent where the
interpreters are agents of the institution and spokespersons for the healthcare system
and its discourse As community agents the interpreters may act in accordance with
Perspectives Studies in Translatology 5
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
the cultural norms and values of their own community If the role of advocate is
adopted it presupposes once again that the interpreter is well informed about the
laws rules and procedures that need to be relayed (Leanza 2007 p 14) The task
of the interpreter is twofold here disclose all relevant information necessary for
making an informed choice about proposed procedures and ensure that the patient
understands the information received and the implications of giving consent (adapted
from Johnstone 1999 p 235 who applied this to the role of the nurse regarding
informed consent) Since this research deals with informed consent the interpreterrsquos
role here should rather be that of an advocate for parents and volunteers improving
their level of understanding and in that way helping them to make an informed
decision about taking part in the research or not
What is informed consent According to Robertson (1981 p 102 in Johnstone
1999 pp 210211)
The doctrine of informed consent although having a profound ethical dimension isessentially a legal doctrine developed partially out of recognition of the patientrsquos right toself-determination and partially out of the doctorrsquos duty to give the patient lsquolsquoinformationabout proposed treatment so as to provide him or her with the opportunity of makingan informed or rational choice as to whether to undergo the treatmentrsquorsquo
Johnstone (1999 pp 224225) also feels that the term lsquoinformed consentrsquo should be
abandoned in favour of lsquoinformed decision-makingrsquo Unlike the notion of lsquoinformed
consentrsquo this formulation seems to invite continuous re-evaluation of any decisions
made about care and treatment options Patients must also be informed of their
right to refuse a recommended medical or nursing procedure and should be kept
up to date on the relevant details pertaining to their cases This should be done
by interpreters who adopt the role of patientrsquos advocate Details which are not
readily understood should be explained (in understandable language) and reinforced
through planned patient health education programmes something that nurses
interpreters are educationally prepared to undertake Many factors can deter patients
from exercising informed and voluntary choices amongst which is poor commu-
nication The patientrsquos ability to understand entails whether the patient is able to
comprehend the risks benefits and alternatives to a proposed medical procedure as
well as the implications of giving consent The question could be asked concerning
just how sophisticated a patientrsquos understanding needs to be and in this case
how sophisticated the interpreterrsquos understanding needs to be in order to really
explain these procedures and to really support these parents and volunteers in
making their decisions
Data
Two phases of data collection were involved Both were done during one
consultation with the interpreters The first phase aimed at compiling a profile of
the relevant interpreters whereas the second phase entailed completing a compre-
hension test ie an exercise to ascertain whether the interpreters understand the test
that they were supposed to explain to the patient
6 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Profile of interpreters
The interpreters of the Tygerberg and Red Cross state hospitals were visited by the
researchers and asked to complete questionnaires on their training background
comprehension of the target text etc At Tygerberg only one interpreter was found
and at Red Cross only two Therefore we also visited the Groote Schuur state
hospital where another three interpreters were interviewed although the informed
consent forms were not meant for this hospital The Groote Schuur hospital has a
similar profile to that of the Tygerberg hospital The results of the survey are listed in
Table 1
Regarding the languages offered for TBH and RXH no interpreters were found
for Afrikaans whilst in both hospitals Afrikaans was either the most spoken
language or used on an equal basis with English and isiXhosa All six interpreters are
mother-tongue speakers of isiXhosa with English as their second language At
RXH Sesotho and isiZulu are offered as third languages and at GSH two of the
interpreters offer Afrikaans as their third language Regarding the interpretersrsquo
qualifications none has a tertiary education and not all have even completed their
secondary education Regarding their training as interpreters and the period that
they were interpreting the interpreter at TBH had no training but she was a nursing
ancillary who later just moved into an interpreting lsquopositionrsquo She has been doing
this for the past eight months on a freelance basis at the Tygerberg hospital
The two interpreters at RXH have been performing interpreting duties for the
past seven years They are full-time interpreters and had training in interpreting for
two years on an ad hoc basis from an NGO (non-governmental organisation)
namely the National Language Project (NLP) Apart from language and interpreting
skills they also had some training in counselling They presented themselves as very
professional The three interpreters at GSH had been doing lsquoformalrsquo interpreting
in this hospital for the past two years but were doing interpreting on an ad hoc
basis at the hospital for at least 10 years before that even though their job
description was that of lsquocleanerrsquo When they were appointed as interpreters they
underwent training for six weeks
Table 1 Interpreters consulted
HospitalNumber ofinterpreters Gender Age Qualifications Languages
Interpretertraining
Tygerberg(TBH)
1 Female 33 Matric Wasnursing ancillary
EnglishisiXhosa
None
Red Cross(RXH)
2 Female 35 53 Matric Post-matric studies(Adult basiceducationAncillary socialwork)
EnglishisiXhosaisiZuluEnglishisiXhosaSesotho
Two-yeartrainingSometraining incounselling
GrooteSchuur(GSH)
3 MaleFemale(2)
43 46 48 Busy with matricWere cleaners
EnglishisiXhosaEnglishisiXhosaAfrikaansEnglishisiXhosaAfrikaans
6-weektraining
Perspectives Studies in Translatology 7
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Comprehension test
They were also tested on their comprehension of the English source texts since
all of them offered English and since the source-text documents would have
been explained to them in English The translations into Afrikaans and isiXhosa
are very close linguistic translations of the original so if they did not understand
the source text they would not understand the target text either Questions were
also put on textual issues such as sentence and paragraph length paragraph
coherence and stylistic and lexical suitability (Table 2)
According to Gile (1995 p 34) the following criteria for quality can be applied
universally to all interpreting acts ideational clarity (the message of the sender
should be clear and comprehensible to the receiver) linguistic acceptability (the
interpreter should use grammar which is acceptable for the situation and the other
participants) and terminological accuracy (the interpreter should use the correct
target language equivalent for medical terms in the source language) From the
responses it can be deduced that none of these criteria could be met here
Question 1 addresses the ideational clarity and no interpreter completely agreed
that they clearly understood the message of the senders Linguistic acceptability
and terminological accuracy are addressed by questions 5 and 6 and here no one
agreed that the vocabulary and style of these texts was appropriate for this
situation Other remarks on the texts as such are that they found the texts too
long to explain but they did not think they themselves would be able to paraphrase
them in order to shorten the time with the patients Only one the male interpreter
from GSH felt that if he were given enough time to work with the texts he would
be able to explain the contents to the parents or volunteers The other interpreters
did not feel comfortable explaining the information of the texts so that the patients
or their parents could come to an informed decision as to whether they should sign
the document or not Needless to say none of the interpreters would like to sign
the agreement certifying that they explained the information of the trial in the
patientrsquos mother tongue and that the patient understood what was explained See
Appendix 2 for the section of the Informed Consent forms where the interpreters
are required to sign
If these interpreters were to be confronted with this task the ethical response
would be to withdraw from the assignment unless they are supplied with a much
Table 2 Responses on English source texts
No Question1Donrsquot agree
at all 2Donrsquot agree 3Agree4Completely
agree
1 I clearly understand thetexts
GSH 1 TBH 1 RXH 1 GSH 2 RXH 1
2 The length of thesentences is good
GSH 1 TBH 1 RXH 2 GSH 2
3 The paragraphs arecoherent
RXH 1 RXH 1 GSH3 TBH 1
4 The length of theparagraphs is good
RXH 1 GSH3 TBH 1
RXH 1
5 The vocabulary isappropriate
GSH 2 RXH 2 GSH 1TBH 1
6 The style of the text isappropriate
GSH 3 RXH 2 TBH 1
8 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
simpler document or preferably have a health care provider with them doing the
actual explanation Then they could revert to their more passive role of interpreting
as part of a trialogue The NCICH (2004 p 16) also makes the point that lsquoTo work
within the professional boundaries of the interpreter role also means that interpretersare aware of the limitations of their duties as well as the limitations of their abilities as a
health care interpreterrsquo (our emphasis)
Discussion
Regardless of the role of the interpreter either as system or community agent the
basic goal of medical discourse is mutual understanding Clear verbal commu-
nication is a necessary component of an effective clinical encounter Even when
patients and providers are educated in the same language faulty communication
can lead to distortions and miscommunications between the parties let aloneeducated health care providers and uneducated patients and semi-educated
interpreters (Kaufert amp Putsch 1997 in Angelelli 2004 p 18) Communicative
failure will inevitably be the result here since neither interpreters nor parents or
volunteers have the same level of literacy or knowledge as the compilers of the
source texts in both these instances the compilers were medical researchers The
parents or volunteers would therefore not be able to make informed decisions
about agreeing to take part in the research projects or not
What is equally disturbing is that the interpreters are set up for failure whenthey are confronted with a task of this scope and these types of documents These
target texts will not be comprehensible enough to be viewed as providing an effective
service to the customer According to Gile (1995 pp 7980) one is not able to fully
comprehend something simply on the grounds of knowledge of the language or
extra-linguistic knowledge The content of the speech may be too difficult it may
deviate from generally accepted linguistic standards or the level of knowledge of the
language and extra linguistic knowledge of the receiver may not be high enough
Then it is necessary to analyse the discourse itself to a much greater extent than onewould analyse discourse with regard to comprehension in everyday situations
Therefore to fully comprehend one does not only need knowledge of the language
and extra-linguistic knowledge but the discourse also need purposeful analysis This
type of analysis could not be performed by most of the HCIs in South Africa and
should rather be left to the health care providers or to trained translators working
with the health care providers in rendering a much simpler target text
It is high time to shift the focus in research on health care interpreting to the
way in which the health care provider deals with the HCIs so as not to expectfar more than what their duties entail and their training predicts The education
and career profile of the six interpreters described above is fairly typical of HCIs in
South Africa and health care providers should keep this in mind This is evident
from the following job advertisement for an interpreter with a medical background
but no mention is made of interpreting or translation training The typical
requirements are matric the speaking andor writing skills in the languages needed
and nursing or other medical experience
Mouldmed Locum International Exchange Ltd is looking for a translatorinterpreterwho is able to speak and write three languages fluently (preferably English Afrikaansand Xhosa) The candidate must be able to start immediately and must have a Matric
Perspectives Studies in Translatology 9
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
qualification and a medical background This is a three-month contract with the optionto extend Working hours are 0730 1600 (30-minute lunch) Monday to Friday Thejob entails office work and patient communication A senior assistant nurse with theselanguage requirements would also qualify for the position
Responsibility and ethical behaviour standards towards interpreters should also be
laid down for the health care provider and not only for the interpreter NCICH
(2004 p 19) notes the responsibility of the health care provider lsquoProviders have the
duty to present their knowledge clearly and objectively so that the patient is able
to make informed choicesrsquo If even interpreters are not monitored to meet their
obligations who is going to monitor the health care providers
Further research that could flow from this could be competency testing of the
interpreters to see how well they actually understand the information which had
been communicated by the health care provider and after the interpreters have
explained the information to the patients the same competency testing could be
done on the patientsrsquo understanding This can be established by asking patients
probing questions and inviting them to repeat the information they have received
(Roth et al 1983 p 175 in Johnstone 1999 pp 225227)
A retranslation of the source texts could also be done into Afrikaans and
isiXhosa using the functionalist approach and the interpreters could then be
retested to see whether they now understand the target texts better and whether
they would be able to paraphrase and explain the content better to the patient
Keeping in mind the socio-economic and educational level of the prototypical
patient for whom these informed consent forms are intended we would still
dissuade the interpreters from attempting to convey the message without a health
care provider present and from signing the document
Notes
1 Each of the nine provinces has its own set of official languages eg English Afrikaansand one or more of the indigenous languages On a national level all 11 of these languagesare recognised as official In the case of the Western Cape Province there are thus threeofficial languages as stated
2 Groote Schuur Hospital is linked to the University of Cape Town and situated in theObservatory area in Cape Town a mainly English-speaking area It employs 524 doctorsand 1370 nurses The hospital treats approximately 44000 in-and 575000 out-patientsper year (Capegateway public info 2009) The staff use both Afrikaans and English on anequal basis and a small proportion use African languages The patients are alsopredominantly Afrikaans and English and a large proportion use African or otherlanguages (Williams 2005 in Saulse 2009 p 24)
3 This is the highest level of secondary schooling that can be obtained within the SouthAfrican context This gives access to tertiary education
Notes on contributors
Ilse Feinauer is associate professor in the Department of Afrikaans and Dutch and isresponsible for teaching Translation Studies and Practice to undergraduate and postgraduatestudents She also teaches Afrikaans linguistics She is coordinator for the MPhil inTranslation Studies She has extensive experience both as a translator and scholar intranslation theory
Harold Lesch is a senior lecturer also in the Department of Afrikaans and Dutch and holds aqualification in Translation Studies He is currently coordinator of the Post Graduate Diploma
10 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
in Translation and Interpreting and is responsible for teaching Interpreting Studies andPractice
References
Angelelli C (2004) Medical interpreting and cross-cultural communication CambridgeCambridge University Press
Angelelli C (2006) Validating professional standards and codes Challenges and opportu-nities Interpreting 8 175193
Anthonissen C (2008) On interpreting the interpreter experiences of language practitionersin mediating for the TRC Journal of Multicultural Discourses 3 165188
Capegateway public info (2009) httpwwwwesterncapegovzaengyour_gov5987Census (2001) Primary tables 1996 and 2001 compared Accessed at httpwwwstatssagovza
census01htmlC2001PrimTablesaspFeinauer I (2003) TB or not TB The communicative success of translated medical texts in
South Africa In W Botha (Ed) n Man wat beur rsquon Huldigingsbundel vir Dirk vanSchalkwyk (pp 213223) Stellenbosch Buro of the WAT
Feinauer I amp Luttig L (2005) Functionalism is not always the remedy Perspectives Studiesin Translatology 13 123131
Gile D (1995) Basic concepts and models for interpreter and translator training AmsterdamJohn Benjamins
Johnstone M-J (1999) Bioethics A nursing perspective Sydney HarcourtLeanza Y (2007) Role of community interpreters in pediatrics as seen by interpreters
physicians and researchers In F Pochhacker amp M Shlesinger (Eds) Healthcareinterpreting Discourse and interaction (pp 1134) Amsterdam Benjamins
Pienaar M (2006) Kommunikasie tussen staat en burgers die stand van tolkdienste SabinetOnline 40 3546
Pochhacker F amp Shlesinger M (Eds) (2007) Healthcare interpreting Discourse andinteraction Amsterdam Benjamins
Romero B (2008) Here are your right hands exploring interpreter qualifications Universityof Dayton Law Review 34 1533
Saulse B (2009) Interpreting within the Western Cape Health Care Sector A DescriptiveOverview (Unpublished masterrsquos thesis) University of Stellenbosch South Africa
United States National Council on Interpreting in Health Care (2004) A national code ofethics for interpreters in health care The National Council on Interpreting in Health CareWorking Papers Series httpwwwncihcorg
Appendix A
Text 1
A DOUBLE-BLIND PLACEBO CONTROLLED RANDOMISED STUDY TO INVESTI-GATE THE EFFICACY AND SAFETY OF LOW-DOSE L-CARNITINEMAGNESIUMSUPPLEMENTATION IN PREVENTING HYPERLACTINEMIA AND LACTIC ACIDO-SIS IN HIV-INFECTED SOUTH AFRICAN WOMEN ON STAVUDINE CONTAININGCOMBINED ANTIRETROVIRAL THERAPY (cART)
Introduction
We are doing a study to see if a l-carnitine magnesium combination product that could help toprevent high blood lactate levels which are known to be one of the side effects of some of themedications used in the treatment of HIV-infection (anti retroviral drugs)
The ability to decrease the way the virus multiplies is achieved by combined anti retroviraltherapy HIV positive (HIV ) patients receiving a combination of these drugs survive by
Perspectives Studies in Translatology 11
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
keeping the infection under control but not by killing the virus altogether This treatment hasindeed increased the quality of life in HIV individuals
One of the drugs the nucleotidic reverse transcriptase inhibitors (NRTIrsquos) can alter the energyproducing part of cells in the body and this that can lead to effects such as the high bloodlactate Twenty five percent of patients with high lactate levels donrsquot have any symptoms whileonly a smaller percentage less than 10 percent develops symptoms including loss of weightand abdominal pain
What is the purpose of this trial
A previous study showed that the low dose l-carnitine and magnesium was absorbed in healthymale volunteers and that the supplement was safe to administer
We want to determine if a dose of two capsules per day of the study drug over a period of ayear prevents the build up of lactic acid in the blood We also want to show if the l-carnitineand magnesium is absorbed in HIV positive subjects on combined anti-retroviral therapy anddetermine what the concentration levels of the anti-retroviral drugs are after a period of 6months and 12 months
To achieve this the study drug must be compared with a placebo (these are capsules that looksthe same as the study drug which are filled with a harmless compound in this case lactose)An extra 20 ml of blood and 50ml of urine apart from the normal routine bloods will be takenbefore starting anti-retroviral therapy and 30ml of blood and 50ml of urine will be taken 6monthly thereafter up to 12 months
The levels of lactic acid cholesterol triglycerides LDL - HDL- and Lp(a) lipoproteins andanti-retroviral drugs will be determined in the blood and those of the l-carnitine with itssupporting metabolites (the organic acid - amino acid-and major and trace element profileswhich includes magnesium) will be determined in the blood and urine These results of thosesubjects that are on the study drug will be compared with those of the placebo group to show ifthere are statistical relevant differences
Text 2
PARTICIPANT INFORMATION SHEET AND CONSENT FORM FOR USE BYPARENTSLEGAL GUARDIANS
Virtual Reality for pain relief in paediatric burns patients
What is this research study all aboutYour child has been admitted to this unit because of their burn injury Every child in this burnsunit has dressing changes on a daily basis Your child will be given the normal medication thatshehe receives during any dressing change These dosages of medication have been prescribedby the doctor when your child was admitted to the burns unit With all burn injuries one ofthe biggest problems that our patients experience is pain At the moment the professionals inthe burns unit do not know if there is something other than pain medication that can help todecrease your childrsquos pain Certain studies have proven that using a technique called VirtualRealty (VR) can distract a child and thereby decrease their pain during a specific procedureVirtual Reality is a program that we will use to allow your child to watch a video game throughgoggles that will be placed on their face Half of the treatment will be done using only the painmedication The other half of the dressing change will be done using the pain medication andthe VR We will then interview yourself and your child to find out how you your child feltabout this process and if you feel that Virtual reality can help to decrease your childrsquos painDuring the interviews with youyour child and nursing staff information may be recorded on a
12 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
tape recorder so that we can check all our information We will also be videotaping alldressing changes and using information from those tapes to help us with this study
Why has your child been invited to participateIn order to see if this process of VR is going to worknot work we have to assess it on at least250 children All children who are over the age of 5 and who do not have a face burn can takepart in this study You and your child have the option to participate in this study andparticipation is completely VOLUNTARY
What will your responsibilities beBy agreeing to let your child participate in this study you will allow us to ask your child tocomplete a questionnaire You will also be interviewed
Will your child benefit from taking part in this researchAt this stage we cannot say if your child will benefit from the study that we are doing If whatwe are doing does work then your child will experience less pain during the dressing changesIf the results are positive then it means that in the future more patients with similar injuries toyour child can be helped when they are experiencing pain during dressing changes
Are there any risks involved in your child taking part in this researchThere are no reported risks The only reported side effect of the VR is sickness If your childdoes experience any sickness due to the VR it will be stopped immediately
If you do not agree to allow your child to take part what alternatives does your child haveYou and your child have the option not to participate in this study participation is completelyVOLUNTARY Your child will only be entered into the study with your permission If youchoose not to enter the study we will still treat your child to the best of our ability and it willnot change the way you are treated You can leave the study at any time after you join
Who will have access to your childrsquos medical recordsAny information gained from this study and testing will be kept strictly private and no oneoutside of the people in the study will know youryour childrsquos results without your permissionIf the information is published to educate other health care professionals we will not use anynames Thus you and your child will never be able to be identified by anyone except studypersonnel Similarly no person outside of the study will have access to audio and videorecordings that may have been made during the dressing changes
Will you or your child be paid to take part in this study and are there any costs involvedYou or your child will not be paid to take part in the study and there will be no costs involvedfor you if your child does take part
Perspectives Studies in Translatology 13
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
14 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012

the cultural norms and values of their own community If the role of advocate is
adopted it presupposes once again that the interpreter is well informed about the
laws rules and procedures that need to be relayed (Leanza 2007 p 14) The task
of the interpreter is twofold here disclose all relevant information necessary for
making an informed choice about proposed procedures and ensure that the patient
understands the information received and the implications of giving consent (adapted
from Johnstone 1999 p 235 who applied this to the role of the nurse regarding
informed consent) Since this research deals with informed consent the interpreterrsquos
role here should rather be that of an advocate for parents and volunteers improving
their level of understanding and in that way helping them to make an informed
decision about taking part in the research or not
What is informed consent According to Robertson (1981 p 102 in Johnstone
1999 pp 210211)
The doctrine of informed consent although having a profound ethical dimension isessentially a legal doctrine developed partially out of recognition of the patientrsquos right toself-determination and partially out of the doctorrsquos duty to give the patient lsquolsquoinformationabout proposed treatment so as to provide him or her with the opportunity of makingan informed or rational choice as to whether to undergo the treatmentrsquorsquo
Johnstone (1999 pp 224225) also feels that the term lsquoinformed consentrsquo should be
abandoned in favour of lsquoinformed decision-makingrsquo Unlike the notion of lsquoinformed
consentrsquo this formulation seems to invite continuous re-evaluation of any decisions
made about care and treatment options Patients must also be informed of their
right to refuse a recommended medical or nursing procedure and should be kept
up to date on the relevant details pertaining to their cases This should be done
by interpreters who adopt the role of patientrsquos advocate Details which are not
readily understood should be explained (in understandable language) and reinforced
through planned patient health education programmes something that nurses
interpreters are educationally prepared to undertake Many factors can deter patients
from exercising informed and voluntary choices amongst which is poor commu-
nication The patientrsquos ability to understand entails whether the patient is able to
comprehend the risks benefits and alternatives to a proposed medical procedure as
well as the implications of giving consent The question could be asked concerning
just how sophisticated a patientrsquos understanding needs to be and in this case
how sophisticated the interpreterrsquos understanding needs to be in order to really
explain these procedures and to really support these parents and volunteers in
making their decisions
Data
Two phases of data collection were involved Both were done during one
consultation with the interpreters The first phase aimed at compiling a profile of
the relevant interpreters whereas the second phase entailed completing a compre-
hension test ie an exercise to ascertain whether the interpreters understand the test
that they were supposed to explain to the patient
6 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Profile of interpreters
The interpreters of the Tygerberg and Red Cross state hospitals were visited by the
researchers and asked to complete questionnaires on their training background
comprehension of the target text etc At Tygerberg only one interpreter was found
and at Red Cross only two Therefore we also visited the Groote Schuur state
hospital where another three interpreters were interviewed although the informed
consent forms were not meant for this hospital The Groote Schuur hospital has a
similar profile to that of the Tygerberg hospital The results of the survey are listed in
Table 1
Regarding the languages offered for TBH and RXH no interpreters were found
for Afrikaans whilst in both hospitals Afrikaans was either the most spoken
language or used on an equal basis with English and isiXhosa All six interpreters are
mother-tongue speakers of isiXhosa with English as their second language At
RXH Sesotho and isiZulu are offered as third languages and at GSH two of the
interpreters offer Afrikaans as their third language Regarding the interpretersrsquo
qualifications none has a tertiary education and not all have even completed their
secondary education Regarding their training as interpreters and the period that
they were interpreting the interpreter at TBH had no training but she was a nursing
ancillary who later just moved into an interpreting lsquopositionrsquo She has been doing
this for the past eight months on a freelance basis at the Tygerberg hospital
The two interpreters at RXH have been performing interpreting duties for the
past seven years They are full-time interpreters and had training in interpreting for
two years on an ad hoc basis from an NGO (non-governmental organisation)
namely the National Language Project (NLP) Apart from language and interpreting
skills they also had some training in counselling They presented themselves as very
professional The three interpreters at GSH had been doing lsquoformalrsquo interpreting
in this hospital for the past two years but were doing interpreting on an ad hoc
basis at the hospital for at least 10 years before that even though their job
description was that of lsquocleanerrsquo When they were appointed as interpreters they
underwent training for six weeks
Table 1 Interpreters consulted
HospitalNumber ofinterpreters Gender Age Qualifications Languages
Interpretertraining
Tygerberg(TBH)
1 Female 33 Matric Wasnursing ancillary
EnglishisiXhosa
None
Red Cross(RXH)
2 Female 35 53 Matric Post-matric studies(Adult basiceducationAncillary socialwork)
EnglishisiXhosaisiZuluEnglishisiXhosaSesotho
Two-yeartrainingSometraining incounselling
GrooteSchuur(GSH)
3 MaleFemale(2)
43 46 48 Busy with matricWere cleaners
EnglishisiXhosaEnglishisiXhosaAfrikaansEnglishisiXhosaAfrikaans
6-weektraining
Perspectives Studies in Translatology 7
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Comprehension test
They were also tested on their comprehension of the English source texts since
all of them offered English and since the source-text documents would have
been explained to them in English The translations into Afrikaans and isiXhosa
are very close linguistic translations of the original so if they did not understand
the source text they would not understand the target text either Questions were
also put on textual issues such as sentence and paragraph length paragraph
coherence and stylistic and lexical suitability (Table 2)
According to Gile (1995 p 34) the following criteria for quality can be applied
universally to all interpreting acts ideational clarity (the message of the sender
should be clear and comprehensible to the receiver) linguistic acceptability (the
interpreter should use grammar which is acceptable for the situation and the other
participants) and terminological accuracy (the interpreter should use the correct
target language equivalent for medical terms in the source language) From the
responses it can be deduced that none of these criteria could be met here
Question 1 addresses the ideational clarity and no interpreter completely agreed
that they clearly understood the message of the senders Linguistic acceptability
and terminological accuracy are addressed by questions 5 and 6 and here no one
agreed that the vocabulary and style of these texts was appropriate for this
situation Other remarks on the texts as such are that they found the texts too
long to explain but they did not think they themselves would be able to paraphrase
them in order to shorten the time with the patients Only one the male interpreter
from GSH felt that if he were given enough time to work with the texts he would
be able to explain the contents to the parents or volunteers The other interpreters
did not feel comfortable explaining the information of the texts so that the patients
or their parents could come to an informed decision as to whether they should sign
the document or not Needless to say none of the interpreters would like to sign
the agreement certifying that they explained the information of the trial in the
patientrsquos mother tongue and that the patient understood what was explained See
Appendix 2 for the section of the Informed Consent forms where the interpreters
are required to sign
If these interpreters were to be confronted with this task the ethical response
would be to withdraw from the assignment unless they are supplied with a much
Table 2 Responses on English source texts
No Question1Donrsquot agree
at all 2Donrsquot agree 3Agree4Completely
agree
1 I clearly understand thetexts
GSH 1 TBH 1 RXH 1 GSH 2 RXH 1
2 The length of thesentences is good
GSH 1 TBH 1 RXH 2 GSH 2
3 The paragraphs arecoherent
RXH 1 RXH 1 GSH3 TBH 1
4 The length of theparagraphs is good
RXH 1 GSH3 TBH 1
RXH 1
5 The vocabulary isappropriate
GSH 2 RXH 2 GSH 1TBH 1
6 The style of the text isappropriate
GSH 3 RXH 2 TBH 1
8 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
simpler document or preferably have a health care provider with them doing the
actual explanation Then they could revert to their more passive role of interpreting
as part of a trialogue The NCICH (2004 p 16) also makes the point that lsquoTo work
within the professional boundaries of the interpreter role also means that interpretersare aware of the limitations of their duties as well as the limitations of their abilities as a
health care interpreterrsquo (our emphasis)
Discussion
Regardless of the role of the interpreter either as system or community agent the
basic goal of medical discourse is mutual understanding Clear verbal commu-
nication is a necessary component of an effective clinical encounter Even when
patients and providers are educated in the same language faulty communication
can lead to distortions and miscommunications between the parties let aloneeducated health care providers and uneducated patients and semi-educated
interpreters (Kaufert amp Putsch 1997 in Angelelli 2004 p 18) Communicative
failure will inevitably be the result here since neither interpreters nor parents or
volunteers have the same level of literacy or knowledge as the compilers of the
source texts in both these instances the compilers were medical researchers The
parents or volunteers would therefore not be able to make informed decisions
about agreeing to take part in the research projects or not
What is equally disturbing is that the interpreters are set up for failure whenthey are confronted with a task of this scope and these types of documents These
target texts will not be comprehensible enough to be viewed as providing an effective
service to the customer According to Gile (1995 pp 7980) one is not able to fully
comprehend something simply on the grounds of knowledge of the language or
extra-linguistic knowledge The content of the speech may be too difficult it may
deviate from generally accepted linguistic standards or the level of knowledge of the
language and extra linguistic knowledge of the receiver may not be high enough
Then it is necessary to analyse the discourse itself to a much greater extent than onewould analyse discourse with regard to comprehension in everyday situations
Therefore to fully comprehend one does not only need knowledge of the language
and extra-linguistic knowledge but the discourse also need purposeful analysis This
type of analysis could not be performed by most of the HCIs in South Africa and
should rather be left to the health care providers or to trained translators working
with the health care providers in rendering a much simpler target text
It is high time to shift the focus in research on health care interpreting to the
way in which the health care provider deals with the HCIs so as not to expectfar more than what their duties entail and their training predicts The education
and career profile of the six interpreters described above is fairly typical of HCIs in
South Africa and health care providers should keep this in mind This is evident
from the following job advertisement for an interpreter with a medical background
but no mention is made of interpreting or translation training The typical
requirements are matric the speaking andor writing skills in the languages needed
and nursing or other medical experience
Mouldmed Locum International Exchange Ltd is looking for a translatorinterpreterwho is able to speak and write three languages fluently (preferably English Afrikaansand Xhosa) The candidate must be able to start immediately and must have a Matric
Perspectives Studies in Translatology 9
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
qualification and a medical background This is a three-month contract with the optionto extend Working hours are 0730 1600 (30-minute lunch) Monday to Friday Thejob entails office work and patient communication A senior assistant nurse with theselanguage requirements would also qualify for the position
Responsibility and ethical behaviour standards towards interpreters should also be
laid down for the health care provider and not only for the interpreter NCICH
(2004 p 19) notes the responsibility of the health care provider lsquoProviders have the
duty to present their knowledge clearly and objectively so that the patient is able
to make informed choicesrsquo If even interpreters are not monitored to meet their
obligations who is going to monitor the health care providers
Further research that could flow from this could be competency testing of the
interpreters to see how well they actually understand the information which had
been communicated by the health care provider and after the interpreters have
explained the information to the patients the same competency testing could be
done on the patientsrsquo understanding This can be established by asking patients
probing questions and inviting them to repeat the information they have received
(Roth et al 1983 p 175 in Johnstone 1999 pp 225227)
A retranslation of the source texts could also be done into Afrikaans and
isiXhosa using the functionalist approach and the interpreters could then be
retested to see whether they now understand the target texts better and whether
they would be able to paraphrase and explain the content better to the patient
Keeping in mind the socio-economic and educational level of the prototypical
patient for whom these informed consent forms are intended we would still
dissuade the interpreters from attempting to convey the message without a health
care provider present and from signing the document
Notes
1 Each of the nine provinces has its own set of official languages eg English Afrikaansand one or more of the indigenous languages On a national level all 11 of these languagesare recognised as official In the case of the Western Cape Province there are thus threeofficial languages as stated
2 Groote Schuur Hospital is linked to the University of Cape Town and situated in theObservatory area in Cape Town a mainly English-speaking area It employs 524 doctorsand 1370 nurses The hospital treats approximately 44000 in-and 575000 out-patientsper year (Capegateway public info 2009) The staff use both Afrikaans and English on anequal basis and a small proportion use African languages The patients are alsopredominantly Afrikaans and English and a large proportion use African or otherlanguages (Williams 2005 in Saulse 2009 p 24)
3 This is the highest level of secondary schooling that can be obtained within the SouthAfrican context This gives access to tertiary education
Notes on contributors
Ilse Feinauer is associate professor in the Department of Afrikaans and Dutch and isresponsible for teaching Translation Studies and Practice to undergraduate and postgraduatestudents She also teaches Afrikaans linguistics She is coordinator for the MPhil inTranslation Studies She has extensive experience both as a translator and scholar intranslation theory
Harold Lesch is a senior lecturer also in the Department of Afrikaans and Dutch and holds aqualification in Translation Studies He is currently coordinator of the Post Graduate Diploma
10 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
in Translation and Interpreting and is responsible for teaching Interpreting Studies andPractice
References
Angelelli C (2004) Medical interpreting and cross-cultural communication CambridgeCambridge University Press
Angelelli C (2006) Validating professional standards and codes Challenges and opportu-nities Interpreting 8 175193
Anthonissen C (2008) On interpreting the interpreter experiences of language practitionersin mediating for the TRC Journal of Multicultural Discourses 3 165188
Capegateway public info (2009) httpwwwwesterncapegovzaengyour_gov5987Census (2001) Primary tables 1996 and 2001 compared Accessed at httpwwwstatssagovza
census01htmlC2001PrimTablesaspFeinauer I (2003) TB or not TB The communicative success of translated medical texts in
South Africa In W Botha (Ed) n Man wat beur rsquon Huldigingsbundel vir Dirk vanSchalkwyk (pp 213223) Stellenbosch Buro of the WAT
Feinauer I amp Luttig L (2005) Functionalism is not always the remedy Perspectives Studiesin Translatology 13 123131
Gile D (1995) Basic concepts and models for interpreter and translator training AmsterdamJohn Benjamins
Johnstone M-J (1999) Bioethics A nursing perspective Sydney HarcourtLeanza Y (2007) Role of community interpreters in pediatrics as seen by interpreters
physicians and researchers In F Pochhacker amp M Shlesinger (Eds) Healthcareinterpreting Discourse and interaction (pp 1134) Amsterdam Benjamins
Pienaar M (2006) Kommunikasie tussen staat en burgers die stand van tolkdienste SabinetOnline 40 3546
Pochhacker F amp Shlesinger M (Eds) (2007) Healthcare interpreting Discourse andinteraction Amsterdam Benjamins
Romero B (2008) Here are your right hands exploring interpreter qualifications Universityof Dayton Law Review 34 1533
Saulse B (2009) Interpreting within the Western Cape Health Care Sector A DescriptiveOverview (Unpublished masterrsquos thesis) University of Stellenbosch South Africa
United States National Council on Interpreting in Health Care (2004) A national code ofethics for interpreters in health care The National Council on Interpreting in Health CareWorking Papers Series httpwwwncihcorg
Appendix A
Text 1
A DOUBLE-BLIND PLACEBO CONTROLLED RANDOMISED STUDY TO INVESTI-GATE THE EFFICACY AND SAFETY OF LOW-DOSE L-CARNITINEMAGNESIUMSUPPLEMENTATION IN PREVENTING HYPERLACTINEMIA AND LACTIC ACIDO-SIS IN HIV-INFECTED SOUTH AFRICAN WOMEN ON STAVUDINE CONTAININGCOMBINED ANTIRETROVIRAL THERAPY (cART)
Introduction
We are doing a study to see if a l-carnitine magnesium combination product that could help toprevent high blood lactate levels which are known to be one of the side effects of some of themedications used in the treatment of HIV-infection (anti retroviral drugs)
The ability to decrease the way the virus multiplies is achieved by combined anti retroviraltherapy HIV positive (HIV ) patients receiving a combination of these drugs survive by
Perspectives Studies in Translatology 11
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
keeping the infection under control but not by killing the virus altogether This treatment hasindeed increased the quality of life in HIV individuals
One of the drugs the nucleotidic reverse transcriptase inhibitors (NRTIrsquos) can alter the energyproducing part of cells in the body and this that can lead to effects such as the high bloodlactate Twenty five percent of patients with high lactate levels donrsquot have any symptoms whileonly a smaller percentage less than 10 percent develops symptoms including loss of weightand abdominal pain
What is the purpose of this trial
A previous study showed that the low dose l-carnitine and magnesium was absorbed in healthymale volunteers and that the supplement was safe to administer
We want to determine if a dose of two capsules per day of the study drug over a period of ayear prevents the build up of lactic acid in the blood We also want to show if the l-carnitineand magnesium is absorbed in HIV positive subjects on combined anti-retroviral therapy anddetermine what the concentration levels of the anti-retroviral drugs are after a period of 6months and 12 months
To achieve this the study drug must be compared with a placebo (these are capsules that looksthe same as the study drug which are filled with a harmless compound in this case lactose)An extra 20 ml of blood and 50ml of urine apart from the normal routine bloods will be takenbefore starting anti-retroviral therapy and 30ml of blood and 50ml of urine will be taken 6monthly thereafter up to 12 months
The levels of lactic acid cholesterol triglycerides LDL - HDL- and Lp(a) lipoproteins andanti-retroviral drugs will be determined in the blood and those of the l-carnitine with itssupporting metabolites (the organic acid - amino acid-and major and trace element profileswhich includes magnesium) will be determined in the blood and urine These results of thosesubjects that are on the study drug will be compared with those of the placebo group to show ifthere are statistical relevant differences
Text 2
PARTICIPANT INFORMATION SHEET AND CONSENT FORM FOR USE BYPARENTSLEGAL GUARDIANS
Virtual Reality for pain relief in paediatric burns patients
What is this research study all aboutYour child has been admitted to this unit because of their burn injury Every child in this burnsunit has dressing changes on a daily basis Your child will be given the normal medication thatshehe receives during any dressing change These dosages of medication have been prescribedby the doctor when your child was admitted to the burns unit With all burn injuries one ofthe biggest problems that our patients experience is pain At the moment the professionals inthe burns unit do not know if there is something other than pain medication that can help todecrease your childrsquos pain Certain studies have proven that using a technique called VirtualRealty (VR) can distract a child and thereby decrease their pain during a specific procedureVirtual Reality is a program that we will use to allow your child to watch a video game throughgoggles that will be placed on their face Half of the treatment will be done using only the painmedication The other half of the dressing change will be done using the pain medication andthe VR We will then interview yourself and your child to find out how you your child feltabout this process and if you feel that Virtual reality can help to decrease your childrsquos painDuring the interviews with youyour child and nursing staff information may be recorded on a
12 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
tape recorder so that we can check all our information We will also be videotaping alldressing changes and using information from those tapes to help us with this study
Why has your child been invited to participateIn order to see if this process of VR is going to worknot work we have to assess it on at least250 children All children who are over the age of 5 and who do not have a face burn can takepart in this study You and your child have the option to participate in this study andparticipation is completely VOLUNTARY
What will your responsibilities beBy agreeing to let your child participate in this study you will allow us to ask your child tocomplete a questionnaire You will also be interviewed
Will your child benefit from taking part in this researchAt this stage we cannot say if your child will benefit from the study that we are doing If whatwe are doing does work then your child will experience less pain during the dressing changesIf the results are positive then it means that in the future more patients with similar injuries toyour child can be helped when they are experiencing pain during dressing changes
Are there any risks involved in your child taking part in this researchThere are no reported risks The only reported side effect of the VR is sickness If your childdoes experience any sickness due to the VR it will be stopped immediately
If you do not agree to allow your child to take part what alternatives does your child haveYou and your child have the option not to participate in this study participation is completelyVOLUNTARY Your child will only be entered into the study with your permission If youchoose not to enter the study we will still treat your child to the best of our ability and it willnot change the way you are treated You can leave the study at any time after you join
Who will have access to your childrsquos medical recordsAny information gained from this study and testing will be kept strictly private and no oneoutside of the people in the study will know youryour childrsquos results without your permissionIf the information is published to educate other health care professionals we will not use anynames Thus you and your child will never be able to be identified by anyone except studypersonnel Similarly no person outside of the study will have access to audio and videorecordings that may have been made during the dressing changes
Will you or your child be paid to take part in this study and are there any costs involvedYou or your child will not be paid to take part in the study and there will be no costs involvedfor you if your child does take part
Perspectives Studies in Translatology 13
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
14 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012

Profile of interpreters
The interpreters of the Tygerberg and Red Cross state hospitals were visited by the
researchers and asked to complete questionnaires on their training background
comprehension of the target text etc At Tygerberg only one interpreter was found
and at Red Cross only two Therefore we also visited the Groote Schuur state
hospital where another three interpreters were interviewed although the informed
consent forms were not meant for this hospital The Groote Schuur hospital has a
similar profile to that of the Tygerberg hospital The results of the survey are listed in
Table 1
Regarding the languages offered for TBH and RXH no interpreters were found
for Afrikaans whilst in both hospitals Afrikaans was either the most spoken
language or used on an equal basis with English and isiXhosa All six interpreters are
mother-tongue speakers of isiXhosa with English as their second language At
RXH Sesotho and isiZulu are offered as third languages and at GSH two of the
interpreters offer Afrikaans as their third language Regarding the interpretersrsquo
qualifications none has a tertiary education and not all have even completed their
secondary education Regarding their training as interpreters and the period that
they were interpreting the interpreter at TBH had no training but she was a nursing
ancillary who later just moved into an interpreting lsquopositionrsquo She has been doing
this for the past eight months on a freelance basis at the Tygerberg hospital
The two interpreters at RXH have been performing interpreting duties for the
past seven years They are full-time interpreters and had training in interpreting for
two years on an ad hoc basis from an NGO (non-governmental organisation)
namely the National Language Project (NLP) Apart from language and interpreting
skills they also had some training in counselling They presented themselves as very
professional The three interpreters at GSH had been doing lsquoformalrsquo interpreting
in this hospital for the past two years but were doing interpreting on an ad hoc
basis at the hospital for at least 10 years before that even though their job
description was that of lsquocleanerrsquo When they were appointed as interpreters they
underwent training for six weeks
Table 1 Interpreters consulted
HospitalNumber ofinterpreters Gender Age Qualifications Languages
Interpretertraining
Tygerberg(TBH)
1 Female 33 Matric Wasnursing ancillary
EnglishisiXhosa
None
Red Cross(RXH)
2 Female 35 53 Matric Post-matric studies(Adult basiceducationAncillary socialwork)
EnglishisiXhosaisiZuluEnglishisiXhosaSesotho
Two-yeartrainingSometraining incounselling
GrooteSchuur(GSH)
3 MaleFemale(2)
43 46 48 Busy with matricWere cleaners
EnglishisiXhosaEnglishisiXhosaAfrikaansEnglishisiXhosaAfrikaans
6-weektraining
Perspectives Studies in Translatology 7
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Comprehension test
They were also tested on their comprehension of the English source texts since
all of them offered English and since the source-text documents would have
been explained to them in English The translations into Afrikaans and isiXhosa
are very close linguistic translations of the original so if they did not understand
the source text they would not understand the target text either Questions were
also put on textual issues such as sentence and paragraph length paragraph
coherence and stylistic and lexical suitability (Table 2)
According to Gile (1995 p 34) the following criteria for quality can be applied
universally to all interpreting acts ideational clarity (the message of the sender
should be clear and comprehensible to the receiver) linguistic acceptability (the
interpreter should use grammar which is acceptable for the situation and the other
participants) and terminological accuracy (the interpreter should use the correct
target language equivalent for medical terms in the source language) From the
responses it can be deduced that none of these criteria could be met here
Question 1 addresses the ideational clarity and no interpreter completely agreed
that they clearly understood the message of the senders Linguistic acceptability
and terminological accuracy are addressed by questions 5 and 6 and here no one
agreed that the vocabulary and style of these texts was appropriate for this
situation Other remarks on the texts as such are that they found the texts too
long to explain but they did not think they themselves would be able to paraphrase
them in order to shorten the time with the patients Only one the male interpreter
from GSH felt that if he were given enough time to work with the texts he would
be able to explain the contents to the parents or volunteers The other interpreters
did not feel comfortable explaining the information of the texts so that the patients
or their parents could come to an informed decision as to whether they should sign
the document or not Needless to say none of the interpreters would like to sign
the agreement certifying that they explained the information of the trial in the
patientrsquos mother tongue and that the patient understood what was explained See
Appendix 2 for the section of the Informed Consent forms where the interpreters
are required to sign
If these interpreters were to be confronted with this task the ethical response
would be to withdraw from the assignment unless they are supplied with a much
Table 2 Responses on English source texts
No Question1Donrsquot agree
at all 2Donrsquot agree 3Agree4Completely
agree
1 I clearly understand thetexts
GSH 1 TBH 1 RXH 1 GSH 2 RXH 1
2 The length of thesentences is good
GSH 1 TBH 1 RXH 2 GSH 2
3 The paragraphs arecoherent
RXH 1 RXH 1 GSH3 TBH 1
4 The length of theparagraphs is good
RXH 1 GSH3 TBH 1
RXH 1
5 The vocabulary isappropriate
GSH 2 RXH 2 GSH 1TBH 1
6 The style of the text isappropriate
GSH 3 RXH 2 TBH 1
8 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
simpler document or preferably have a health care provider with them doing the
actual explanation Then they could revert to their more passive role of interpreting
as part of a trialogue The NCICH (2004 p 16) also makes the point that lsquoTo work
within the professional boundaries of the interpreter role also means that interpretersare aware of the limitations of their duties as well as the limitations of their abilities as a
health care interpreterrsquo (our emphasis)
Discussion
Regardless of the role of the interpreter either as system or community agent the
basic goal of medical discourse is mutual understanding Clear verbal commu-
nication is a necessary component of an effective clinical encounter Even when
patients and providers are educated in the same language faulty communication
can lead to distortions and miscommunications between the parties let aloneeducated health care providers and uneducated patients and semi-educated
interpreters (Kaufert amp Putsch 1997 in Angelelli 2004 p 18) Communicative
failure will inevitably be the result here since neither interpreters nor parents or
volunteers have the same level of literacy or knowledge as the compilers of the
source texts in both these instances the compilers were medical researchers The
parents or volunteers would therefore not be able to make informed decisions
about agreeing to take part in the research projects or not
What is equally disturbing is that the interpreters are set up for failure whenthey are confronted with a task of this scope and these types of documents These
target texts will not be comprehensible enough to be viewed as providing an effective
service to the customer According to Gile (1995 pp 7980) one is not able to fully
comprehend something simply on the grounds of knowledge of the language or
extra-linguistic knowledge The content of the speech may be too difficult it may
deviate from generally accepted linguistic standards or the level of knowledge of the
language and extra linguistic knowledge of the receiver may not be high enough
Then it is necessary to analyse the discourse itself to a much greater extent than onewould analyse discourse with regard to comprehension in everyday situations
Therefore to fully comprehend one does not only need knowledge of the language
and extra-linguistic knowledge but the discourse also need purposeful analysis This
type of analysis could not be performed by most of the HCIs in South Africa and
should rather be left to the health care providers or to trained translators working
with the health care providers in rendering a much simpler target text
It is high time to shift the focus in research on health care interpreting to the
way in which the health care provider deals with the HCIs so as not to expectfar more than what their duties entail and their training predicts The education
and career profile of the six interpreters described above is fairly typical of HCIs in
South Africa and health care providers should keep this in mind This is evident
from the following job advertisement for an interpreter with a medical background
but no mention is made of interpreting or translation training The typical
requirements are matric the speaking andor writing skills in the languages needed
and nursing or other medical experience
Mouldmed Locum International Exchange Ltd is looking for a translatorinterpreterwho is able to speak and write three languages fluently (preferably English Afrikaansand Xhosa) The candidate must be able to start immediately and must have a Matric
Perspectives Studies in Translatology 9
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
qualification and a medical background This is a three-month contract with the optionto extend Working hours are 0730 1600 (30-minute lunch) Monday to Friday Thejob entails office work and patient communication A senior assistant nurse with theselanguage requirements would also qualify for the position
Responsibility and ethical behaviour standards towards interpreters should also be
laid down for the health care provider and not only for the interpreter NCICH
(2004 p 19) notes the responsibility of the health care provider lsquoProviders have the
duty to present their knowledge clearly and objectively so that the patient is able
to make informed choicesrsquo If even interpreters are not monitored to meet their
obligations who is going to monitor the health care providers
Further research that could flow from this could be competency testing of the
interpreters to see how well they actually understand the information which had
been communicated by the health care provider and after the interpreters have
explained the information to the patients the same competency testing could be
done on the patientsrsquo understanding This can be established by asking patients
probing questions and inviting them to repeat the information they have received
(Roth et al 1983 p 175 in Johnstone 1999 pp 225227)
A retranslation of the source texts could also be done into Afrikaans and
isiXhosa using the functionalist approach and the interpreters could then be
retested to see whether they now understand the target texts better and whether
they would be able to paraphrase and explain the content better to the patient
Keeping in mind the socio-economic and educational level of the prototypical
patient for whom these informed consent forms are intended we would still
dissuade the interpreters from attempting to convey the message without a health
care provider present and from signing the document
Notes
1 Each of the nine provinces has its own set of official languages eg English Afrikaansand one or more of the indigenous languages On a national level all 11 of these languagesare recognised as official In the case of the Western Cape Province there are thus threeofficial languages as stated
2 Groote Schuur Hospital is linked to the University of Cape Town and situated in theObservatory area in Cape Town a mainly English-speaking area It employs 524 doctorsand 1370 nurses The hospital treats approximately 44000 in-and 575000 out-patientsper year (Capegateway public info 2009) The staff use both Afrikaans and English on anequal basis and a small proportion use African languages The patients are alsopredominantly Afrikaans and English and a large proportion use African or otherlanguages (Williams 2005 in Saulse 2009 p 24)
3 This is the highest level of secondary schooling that can be obtained within the SouthAfrican context This gives access to tertiary education
Notes on contributors
Ilse Feinauer is associate professor in the Department of Afrikaans and Dutch and isresponsible for teaching Translation Studies and Practice to undergraduate and postgraduatestudents She also teaches Afrikaans linguistics She is coordinator for the MPhil inTranslation Studies She has extensive experience both as a translator and scholar intranslation theory
Harold Lesch is a senior lecturer also in the Department of Afrikaans and Dutch and holds aqualification in Translation Studies He is currently coordinator of the Post Graduate Diploma
10 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
in Translation and Interpreting and is responsible for teaching Interpreting Studies andPractice
References
Angelelli C (2004) Medical interpreting and cross-cultural communication CambridgeCambridge University Press
Angelelli C (2006) Validating professional standards and codes Challenges and opportu-nities Interpreting 8 175193
Anthonissen C (2008) On interpreting the interpreter experiences of language practitionersin mediating for the TRC Journal of Multicultural Discourses 3 165188
Capegateway public info (2009) httpwwwwesterncapegovzaengyour_gov5987Census (2001) Primary tables 1996 and 2001 compared Accessed at httpwwwstatssagovza
census01htmlC2001PrimTablesaspFeinauer I (2003) TB or not TB The communicative success of translated medical texts in
South Africa In W Botha (Ed) n Man wat beur rsquon Huldigingsbundel vir Dirk vanSchalkwyk (pp 213223) Stellenbosch Buro of the WAT
Feinauer I amp Luttig L (2005) Functionalism is not always the remedy Perspectives Studiesin Translatology 13 123131
Gile D (1995) Basic concepts and models for interpreter and translator training AmsterdamJohn Benjamins
Johnstone M-J (1999) Bioethics A nursing perspective Sydney HarcourtLeanza Y (2007) Role of community interpreters in pediatrics as seen by interpreters
physicians and researchers In F Pochhacker amp M Shlesinger (Eds) Healthcareinterpreting Discourse and interaction (pp 1134) Amsterdam Benjamins
Pienaar M (2006) Kommunikasie tussen staat en burgers die stand van tolkdienste SabinetOnline 40 3546
Pochhacker F amp Shlesinger M (Eds) (2007) Healthcare interpreting Discourse andinteraction Amsterdam Benjamins
Romero B (2008) Here are your right hands exploring interpreter qualifications Universityof Dayton Law Review 34 1533
Saulse B (2009) Interpreting within the Western Cape Health Care Sector A DescriptiveOverview (Unpublished masterrsquos thesis) University of Stellenbosch South Africa
United States National Council on Interpreting in Health Care (2004) A national code ofethics for interpreters in health care The National Council on Interpreting in Health CareWorking Papers Series httpwwwncihcorg
Appendix A
Text 1
A DOUBLE-BLIND PLACEBO CONTROLLED RANDOMISED STUDY TO INVESTI-GATE THE EFFICACY AND SAFETY OF LOW-DOSE L-CARNITINEMAGNESIUMSUPPLEMENTATION IN PREVENTING HYPERLACTINEMIA AND LACTIC ACIDO-SIS IN HIV-INFECTED SOUTH AFRICAN WOMEN ON STAVUDINE CONTAININGCOMBINED ANTIRETROVIRAL THERAPY (cART)
Introduction
We are doing a study to see if a l-carnitine magnesium combination product that could help toprevent high blood lactate levels which are known to be one of the side effects of some of themedications used in the treatment of HIV-infection (anti retroviral drugs)
The ability to decrease the way the virus multiplies is achieved by combined anti retroviraltherapy HIV positive (HIV ) patients receiving a combination of these drugs survive by
Perspectives Studies in Translatology 11
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
keeping the infection under control but not by killing the virus altogether This treatment hasindeed increased the quality of life in HIV individuals
One of the drugs the nucleotidic reverse transcriptase inhibitors (NRTIrsquos) can alter the energyproducing part of cells in the body and this that can lead to effects such as the high bloodlactate Twenty five percent of patients with high lactate levels donrsquot have any symptoms whileonly a smaller percentage less than 10 percent develops symptoms including loss of weightand abdominal pain
What is the purpose of this trial
A previous study showed that the low dose l-carnitine and magnesium was absorbed in healthymale volunteers and that the supplement was safe to administer
We want to determine if a dose of two capsules per day of the study drug over a period of ayear prevents the build up of lactic acid in the blood We also want to show if the l-carnitineand magnesium is absorbed in HIV positive subjects on combined anti-retroviral therapy anddetermine what the concentration levels of the anti-retroviral drugs are after a period of 6months and 12 months
To achieve this the study drug must be compared with a placebo (these are capsules that looksthe same as the study drug which are filled with a harmless compound in this case lactose)An extra 20 ml of blood and 50ml of urine apart from the normal routine bloods will be takenbefore starting anti-retroviral therapy and 30ml of blood and 50ml of urine will be taken 6monthly thereafter up to 12 months
The levels of lactic acid cholesterol triglycerides LDL - HDL- and Lp(a) lipoproteins andanti-retroviral drugs will be determined in the blood and those of the l-carnitine with itssupporting metabolites (the organic acid - amino acid-and major and trace element profileswhich includes magnesium) will be determined in the blood and urine These results of thosesubjects that are on the study drug will be compared with those of the placebo group to show ifthere are statistical relevant differences
Text 2
PARTICIPANT INFORMATION SHEET AND CONSENT FORM FOR USE BYPARENTSLEGAL GUARDIANS
Virtual Reality for pain relief in paediatric burns patients
What is this research study all aboutYour child has been admitted to this unit because of their burn injury Every child in this burnsunit has dressing changes on a daily basis Your child will be given the normal medication thatshehe receives during any dressing change These dosages of medication have been prescribedby the doctor when your child was admitted to the burns unit With all burn injuries one ofthe biggest problems that our patients experience is pain At the moment the professionals inthe burns unit do not know if there is something other than pain medication that can help todecrease your childrsquos pain Certain studies have proven that using a technique called VirtualRealty (VR) can distract a child and thereby decrease their pain during a specific procedureVirtual Reality is a program that we will use to allow your child to watch a video game throughgoggles that will be placed on their face Half of the treatment will be done using only the painmedication The other half of the dressing change will be done using the pain medication andthe VR We will then interview yourself and your child to find out how you your child feltabout this process and if you feel that Virtual reality can help to decrease your childrsquos painDuring the interviews with youyour child and nursing staff information may be recorded on a
12 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
tape recorder so that we can check all our information We will also be videotaping alldressing changes and using information from those tapes to help us with this study
Why has your child been invited to participateIn order to see if this process of VR is going to worknot work we have to assess it on at least250 children All children who are over the age of 5 and who do not have a face burn can takepart in this study You and your child have the option to participate in this study andparticipation is completely VOLUNTARY
What will your responsibilities beBy agreeing to let your child participate in this study you will allow us to ask your child tocomplete a questionnaire You will also be interviewed
Will your child benefit from taking part in this researchAt this stage we cannot say if your child will benefit from the study that we are doing If whatwe are doing does work then your child will experience less pain during the dressing changesIf the results are positive then it means that in the future more patients with similar injuries toyour child can be helped when they are experiencing pain during dressing changes
Are there any risks involved in your child taking part in this researchThere are no reported risks The only reported side effect of the VR is sickness If your childdoes experience any sickness due to the VR it will be stopped immediately
If you do not agree to allow your child to take part what alternatives does your child haveYou and your child have the option not to participate in this study participation is completelyVOLUNTARY Your child will only be entered into the study with your permission If youchoose not to enter the study we will still treat your child to the best of our ability and it willnot change the way you are treated You can leave the study at any time after you join
Who will have access to your childrsquos medical recordsAny information gained from this study and testing will be kept strictly private and no oneoutside of the people in the study will know youryour childrsquos results without your permissionIf the information is published to educate other health care professionals we will not use anynames Thus you and your child will never be able to be identified by anyone except studypersonnel Similarly no person outside of the study will have access to audio and videorecordings that may have been made during the dressing changes
Will you or your child be paid to take part in this study and are there any costs involvedYou or your child will not be paid to take part in the study and there will be no costs involvedfor you if your child does take part
Perspectives Studies in Translatology 13
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
14 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
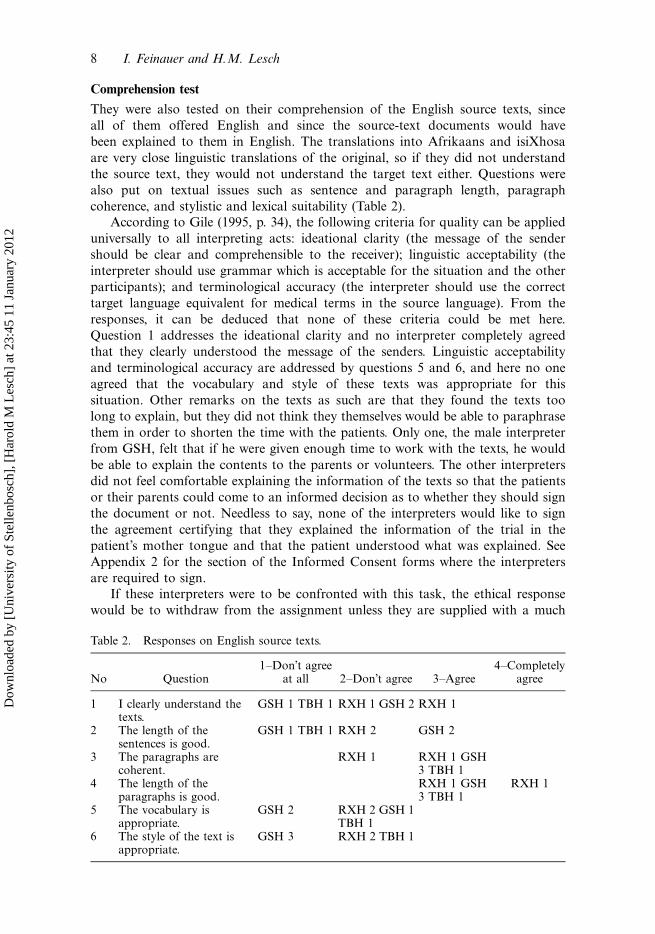
Comprehension test
They were also tested on their comprehension of the English source texts since
all of them offered English and since the source-text documents would have
been explained to them in English The translations into Afrikaans and isiXhosa
are very close linguistic translations of the original so if they did not understand
the source text they would not understand the target text either Questions were
also put on textual issues such as sentence and paragraph length paragraph
coherence and stylistic and lexical suitability (Table 2)
According to Gile (1995 p 34) the following criteria for quality can be applied
universally to all interpreting acts ideational clarity (the message of the sender
should be clear and comprehensible to the receiver) linguistic acceptability (the
interpreter should use grammar which is acceptable for the situation and the other
participants) and terminological accuracy (the interpreter should use the correct
target language equivalent for medical terms in the source language) From the
responses it can be deduced that none of these criteria could be met here
Question 1 addresses the ideational clarity and no interpreter completely agreed
that they clearly understood the message of the senders Linguistic acceptability
and terminological accuracy are addressed by questions 5 and 6 and here no one
agreed that the vocabulary and style of these texts was appropriate for this
situation Other remarks on the texts as such are that they found the texts too
long to explain but they did not think they themselves would be able to paraphrase
them in order to shorten the time with the patients Only one the male interpreter
from GSH felt that if he were given enough time to work with the texts he would
be able to explain the contents to the parents or volunteers The other interpreters
did not feel comfortable explaining the information of the texts so that the patients
or their parents could come to an informed decision as to whether they should sign
the document or not Needless to say none of the interpreters would like to sign
the agreement certifying that they explained the information of the trial in the
patientrsquos mother tongue and that the patient understood what was explained See
Appendix 2 for the section of the Informed Consent forms where the interpreters
are required to sign
If these interpreters were to be confronted with this task the ethical response
would be to withdraw from the assignment unless they are supplied with a much
Table 2 Responses on English source texts
No Question1Donrsquot agree
at all 2Donrsquot agree 3Agree4Completely
agree
1 I clearly understand thetexts
GSH 1 TBH 1 RXH 1 GSH 2 RXH 1
2 The length of thesentences is good
GSH 1 TBH 1 RXH 2 GSH 2
3 The paragraphs arecoherent
RXH 1 RXH 1 GSH3 TBH 1
4 The length of theparagraphs is good
RXH 1 GSH3 TBH 1
RXH 1
5 The vocabulary isappropriate
GSH 2 RXH 2 GSH 1TBH 1
6 The style of the text isappropriate
GSH 3 RXH 2 TBH 1
8 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
simpler document or preferably have a health care provider with them doing the
actual explanation Then they could revert to their more passive role of interpreting
as part of a trialogue The NCICH (2004 p 16) also makes the point that lsquoTo work
within the professional boundaries of the interpreter role also means that interpretersare aware of the limitations of their duties as well as the limitations of their abilities as a
health care interpreterrsquo (our emphasis)
Discussion
Regardless of the role of the interpreter either as system or community agent the
basic goal of medical discourse is mutual understanding Clear verbal commu-
nication is a necessary component of an effective clinical encounter Even when
patients and providers are educated in the same language faulty communication
can lead to distortions and miscommunications between the parties let aloneeducated health care providers and uneducated patients and semi-educated
interpreters (Kaufert amp Putsch 1997 in Angelelli 2004 p 18) Communicative
failure will inevitably be the result here since neither interpreters nor parents or
volunteers have the same level of literacy or knowledge as the compilers of the
source texts in both these instances the compilers were medical researchers The
parents or volunteers would therefore not be able to make informed decisions
about agreeing to take part in the research projects or not
What is equally disturbing is that the interpreters are set up for failure whenthey are confronted with a task of this scope and these types of documents These
target texts will not be comprehensible enough to be viewed as providing an effective
service to the customer According to Gile (1995 pp 7980) one is not able to fully
comprehend something simply on the grounds of knowledge of the language or
extra-linguistic knowledge The content of the speech may be too difficult it may
deviate from generally accepted linguistic standards or the level of knowledge of the
language and extra linguistic knowledge of the receiver may not be high enough
Then it is necessary to analyse the discourse itself to a much greater extent than onewould analyse discourse with regard to comprehension in everyday situations
Therefore to fully comprehend one does not only need knowledge of the language
and extra-linguistic knowledge but the discourse also need purposeful analysis This
type of analysis could not be performed by most of the HCIs in South Africa and
should rather be left to the health care providers or to trained translators working
with the health care providers in rendering a much simpler target text
It is high time to shift the focus in research on health care interpreting to the
way in which the health care provider deals with the HCIs so as not to expectfar more than what their duties entail and their training predicts The education
and career profile of the six interpreters described above is fairly typical of HCIs in
South Africa and health care providers should keep this in mind This is evident
from the following job advertisement for an interpreter with a medical background
but no mention is made of interpreting or translation training The typical
requirements are matric the speaking andor writing skills in the languages needed
and nursing or other medical experience
Mouldmed Locum International Exchange Ltd is looking for a translatorinterpreterwho is able to speak and write three languages fluently (preferably English Afrikaansand Xhosa) The candidate must be able to start immediately and must have a Matric
Perspectives Studies in Translatology 9
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
qualification and a medical background This is a three-month contract with the optionto extend Working hours are 0730 1600 (30-minute lunch) Monday to Friday Thejob entails office work and patient communication A senior assistant nurse with theselanguage requirements would also qualify for the position
Responsibility and ethical behaviour standards towards interpreters should also be
laid down for the health care provider and not only for the interpreter NCICH
(2004 p 19) notes the responsibility of the health care provider lsquoProviders have the
duty to present their knowledge clearly and objectively so that the patient is able
to make informed choicesrsquo If even interpreters are not monitored to meet their
obligations who is going to monitor the health care providers
Further research that could flow from this could be competency testing of the
interpreters to see how well they actually understand the information which had
been communicated by the health care provider and after the interpreters have
explained the information to the patients the same competency testing could be
done on the patientsrsquo understanding This can be established by asking patients
probing questions and inviting them to repeat the information they have received
(Roth et al 1983 p 175 in Johnstone 1999 pp 225227)
A retranslation of the source texts could also be done into Afrikaans and
isiXhosa using the functionalist approach and the interpreters could then be
retested to see whether they now understand the target texts better and whether
they would be able to paraphrase and explain the content better to the patient
Keeping in mind the socio-economic and educational level of the prototypical
patient for whom these informed consent forms are intended we would still
dissuade the interpreters from attempting to convey the message without a health
care provider present and from signing the document
Notes
1 Each of the nine provinces has its own set of official languages eg English Afrikaansand one or more of the indigenous languages On a national level all 11 of these languagesare recognised as official In the case of the Western Cape Province there are thus threeofficial languages as stated
2 Groote Schuur Hospital is linked to the University of Cape Town and situated in theObservatory area in Cape Town a mainly English-speaking area It employs 524 doctorsand 1370 nurses The hospital treats approximately 44000 in-and 575000 out-patientsper year (Capegateway public info 2009) The staff use both Afrikaans and English on anequal basis and a small proportion use African languages The patients are alsopredominantly Afrikaans and English and a large proportion use African or otherlanguages (Williams 2005 in Saulse 2009 p 24)
3 This is the highest level of secondary schooling that can be obtained within the SouthAfrican context This gives access to tertiary education
Notes on contributors
Ilse Feinauer is associate professor in the Department of Afrikaans and Dutch and isresponsible for teaching Translation Studies and Practice to undergraduate and postgraduatestudents She also teaches Afrikaans linguistics She is coordinator for the MPhil inTranslation Studies She has extensive experience both as a translator and scholar intranslation theory
Harold Lesch is a senior lecturer also in the Department of Afrikaans and Dutch and holds aqualification in Translation Studies He is currently coordinator of the Post Graduate Diploma
10 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
in Translation and Interpreting and is responsible for teaching Interpreting Studies andPractice
References
Angelelli C (2004) Medical interpreting and cross-cultural communication CambridgeCambridge University Press
Angelelli C (2006) Validating professional standards and codes Challenges and opportu-nities Interpreting 8 175193
Anthonissen C (2008) On interpreting the interpreter experiences of language practitionersin mediating for the TRC Journal of Multicultural Discourses 3 165188
Capegateway public info (2009) httpwwwwesterncapegovzaengyour_gov5987Census (2001) Primary tables 1996 and 2001 compared Accessed at httpwwwstatssagovza
census01htmlC2001PrimTablesaspFeinauer I (2003) TB or not TB The communicative success of translated medical texts in
South Africa In W Botha (Ed) n Man wat beur rsquon Huldigingsbundel vir Dirk vanSchalkwyk (pp 213223) Stellenbosch Buro of the WAT
Feinauer I amp Luttig L (2005) Functionalism is not always the remedy Perspectives Studiesin Translatology 13 123131
Gile D (1995) Basic concepts and models for interpreter and translator training AmsterdamJohn Benjamins
Johnstone M-J (1999) Bioethics A nursing perspective Sydney HarcourtLeanza Y (2007) Role of community interpreters in pediatrics as seen by interpreters
physicians and researchers In F Pochhacker amp M Shlesinger (Eds) Healthcareinterpreting Discourse and interaction (pp 1134) Amsterdam Benjamins
Pienaar M (2006) Kommunikasie tussen staat en burgers die stand van tolkdienste SabinetOnline 40 3546
Pochhacker F amp Shlesinger M (Eds) (2007) Healthcare interpreting Discourse andinteraction Amsterdam Benjamins
Romero B (2008) Here are your right hands exploring interpreter qualifications Universityof Dayton Law Review 34 1533
Saulse B (2009) Interpreting within the Western Cape Health Care Sector A DescriptiveOverview (Unpublished masterrsquos thesis) University of Stellenbosch South Africa
United States National Council on Interpreting in Health Care (2004) A national code ofethics for interpreters in health care The National Council on Interpreting in Health CareWorking Papers Series httpwwwncihcorg
Appendix A
Text 1
A DOUBLE-BLIND PLACEBO CONTROLLED RANDOMISED STUDY TO INVESTI-GATE THE EFFICACY AND SAFETY OF LOW-DOSE L-CARNITINEMAGNESIUMSUPPLEMENTATION IN PREVENTING HYPERLACTINEMIA AND LACTIC ACIDO-SIS IN HIV-INFECTED SOUTH AFRICAN WOMEN ON STAVUDINE CONTAININGCOMBINED ANTIRETROVIRAL THERAPY (cART)
Introduction
We are doing a study to see if a l-carnitine magnesium combination product that could help toprevent high blood lactate levels which are known to be one of the side effects of some of themedications used in the treatment of HIV-infection (anti retroviral drugs)
The ability to decrease the way the virus multiplies is achieved by combined anti retroviraltherapy HIV positive (HIV ) patients receiving a combination of these drugs survive by
Perspectives Studies in Translatology 11
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
keeping the infection under control but not by killing the virus altogether This treatment hasindeed increased the quality of life in HIV individuals
One of the drugs the nucleotidic reverse transcriptase inhibitors (NRTIrsquos) can alter the energyproducing part of cells in the body and this that can lead to effects such as the high bloodlactate Twenty five percent of patients with high lactate levels donrsquot have any symptoms whileonly a smaller percentage less than 10 percent develops symptoms including loss of weightand abdominal pain
What is the purpose of this trial
A previous study showed that the low dose l-carnitine and magnesium was absorbed in healthymale volunteers and that the supplement was safe to administer
We want to determine if a dose of two capsules per day of the study drug over a period of ayear prevents the build up of lactic acid in the blood We also want to show if the l-carnitineand magnesium is absorbed in HIV positive subjects on combined anti-retroviral therapy anddetermine what the concentration levels of the anti-retroviral drugs are after a period of 6months and 12 months
To achieve this the study drug must be compared with a placebo (these are capsules that looksthe same as the study drug which are filled with a harmless compound in this case lactose)An extra 20 ml of blood and 50ml of urine apart from the normal routine bloods will be takenbefore starting anti-retroviral therapy and 30ml of blood and 50ml of urine will be taken 6monthly thereafter up to 12 months
The levels of lactic acid cholesterol triglycerides LDL - HDL- and Lp(a) lipoproteins andanti-retroviral drugs will be determined in the blood and those of the l-carnitine with itssupporting metabolites (the organic acid - amino acid-and major and trace element profileswhich includes magnesium) will be determined in the blood and urine These results of thosesubjects that are on the study drug will be compared with those of the placebo group to show ifthere are statistical relevant differences
Text 2
PARTICIPANT INFORMATION SHEET AND CONSENT FORM FOR USE BYPARENTSLEGAL GUARDIANS
Virtual Reality for pain relief in paediatric burns patients
What is this research study all aboutYour child has been admitted to this unit because of their burn injury Every child in this burnsunit has dressing changes on a daily basis Your child will be given the normal medication thatshehe receives during any dressing change These dosages of medication have been prescribedby the doctor when your child was admitted to the burns unit With all burn injuries one ofthe biggest problems that our patients experience is pain At the moment the professionals inthe burns unit do not know if there is something other than pain medication that can help todecrease your childrsquos pain Certain studies have proven that using a technique called VirtualRealty (VR) can distract a child and thereby decrease their pain during a specific procedureVirtual Reality is a program that we will use to allow your child to watch a video game throughgoggles that will be placed on their face Half of the treatment will be done using only the painmedication The other half of the dressing change will be done using the pain medication andthe VR We will then interview yourself and your child to find out how you your child feltabout this process and if you feel that Virtual reality can help to decrease your childrsquos painDuring the interviews with youyour child and nursing staff information may be recorded on a
12 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
tape recorder so that we can check all our information We will also be videotaping alldressing changes and using information from those tapes to help us with this study
Why has your child been invited to participateIn order to see if this process of VR is going to worknot work we have to assess it on at least250 children All children who are over the age of 5 and who do not have a face burn can takepart in this study You and your child have the option to participate in this study andparticipation is completely VOLUNTARY
What will your responsibilities beBy agreeing to let your child participate in this study you will allow us to ask your child tocomplete a questionnaire You will also be interviewed
Will your child benefit from taking part in this researchAt this stage we cannot say if your child will benefit from the study that we are doing If whatwe are doing does work then your child will experience less pain during the dressing changesIf the results are positive then it means that in the future more patients with similar injuries toyour child can be helped when they are experiencing pain during dressing changes
Are there any risks involved in your child taking part in this researchThere are no reported risks The only reported side effect of the VR is sickness If your childdoes experience any sickness due to the VR it will be stopped immediately
If you do not agree to allow your child to take part what alternatives does your child haveYou and your child have the option not to participate in this study participation is completelyVOLUNTARY Your child will only be entered into the study with your permission If youchoose not to enter the study we will still treat your child to the best of our ability and it willnot change the way you are treated You can leave the study at any time after you join
Who will have access to your childrsquos medical recordsAny information gained from this study and testing will be kept strictly private and no oneoutside of the people in the study will know youryour childrsquos results without your permissionIf the information is published to educate other health care professionals we will not use anynames Thus you and your child will never be able to be identified by anyone except studypersonnel Similarly no person outside of the study will have access to audio and videorecordings that may have been made during the dressing changes
Will you or your child be paid to take part in this study and are there any costs involvedYou or your child will not be paid to take part in the study and there will be no costs involvedfor you if your child does take part
Perspectives Studies in Translatology 13
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
14 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012

simpler document or preferably have a health care provider with them doing the
actual explanation Then they could revert to their more passive role of interpreting
as part of a trialogue The NCICH (2004 p 16) also makes the point that lsquoTo work
within the professional boundaries of the interpreter role also means that interpretersare aware of the limitations of their duties as well as the limitations of their abilities as a
health care interpreterrsquo (our emphasis)
Discussion
Regardless of the role of the interpreter either as system or community agent the
basic goal of medical discourse is mutual understanding Clear verbal commu-
nication is a necessary component of an effective clinical encounter Even when
patients and providers are educated in the same language faulty communication
can lead to distortions and miscommunications between the parties let aloneeducated health care providers and uneducated patients and semi-educated
interpreters (Kaufert amp Putsch 1997 in Angelelli 2004 p 18) Communicative
failure will inevitably be the result here since neither interpreters nor parents or
volunteers have the same level of literacy or knowledge as the compilers of the
source texts in both these instances the compilers were medical researchers The
parents or volunteers would therefore not be able to make informed decisions
about agreeing to take part in the research projects or not
What is equally disturbing is that the interpreters are set up for failure whenthey are confronted with a task of this scope and these types of documents These
target texts will not be comprehensible enough to be viewed as providing an effective
service to the customer According to Gile (1995 pp 7980) one is not able to fully
comprehend something simply on the grounds of knowledge of the language or
extra-linguistic knowledge The content of the speech may be too difficult it may
deviate from generally accepted linguistic standards or the level of knowledge of the
language and extra linguistic knowledge of the receiver may not be high enough
Then it is necessary to analyse the discourse itself to a much greater extent than onewould analyse discourse with regard to comprehension in everyday situations
Therefore to fully comprehend one does not only need knowledge of the language
and extra-linguistic knowledge but the discourse also need purposeful analysis This
type of analysis could not be performed by most of the HCIs in South Africa and
should rather be left to the health care providers or to trained translators working
with the health care providers in rendering a much simpler target text
It is high time to shift the focus in research on health care interpreting to the
way in which the health care provider deals with the HCIs so as not to expectfar more than what their duties entail and their training predicts The education
and career profile of the six interpreters described above is fairly typical of HCIs in
South Africa and health care providers should keep this in mind This is evident
from the following job advertisement for an interpreter with a medical background
but no mention is made of interpreting or translation training The typical
requirements are matric the speaking andor writing skills in the languages needed
and nursing or other medical experience
Mouldmed Locum International Exchange Ltd is looking for a translatorinterpreterwho is able to speak and write three languages fluently (preferably English Afrikaansand Xhosa) The candidate must be able to start immediately and must have a Matric
Perspectives Studies in Translatology 9
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
qualification and a medical background This is a three-month contract with the optionto extend Working hours are 0730 1600 (30-minute lunch) Monday to Friday Thejob entails office work and patient communication A senior assistant nurse with theselanguage requirements would also qualify for the position
Responsibility and ethical behaviour standards towards interpreters should also be
laid down for the health care provider and not only for the interpreter NCICH
(2004 p 19) notes the responsibility of the health care provider lsquoProviders have the
duty to present their knowledge clearly and objectively so that the patient is able
to make informed choicesrsquo If even interpreters are not monitored to meet their
obligations who is going to monitor the health care providers
Further research that could flow from this could be competency testing of the
interpreters to see how well they actually understand the information which had
been communicated by the health care provider and after the interpreters have
explained the information to the patients the same competency testing could be
done on the patientsrsquo understanding This can be established by asking patients
probing questions and inviting them to repeat the information they have received
(Roth et al 1983 p 175 in Johnstone 1999 pp 225227)
A retranslation of the source texts could also be done into Afrikaans and
isiXhosa using the functionalist approach and the interpreters could then be
retested to see whether they now understand the target texts better and whether
they would be able to paraphrase and explain the content better to the patient
Keeping in mind the socio-economic and educational level of the prototypical
patient for whom these informed consent forms are intended we would still
dissuade the interpreters from attempting to convey the message without a health
care provider present and from signing the document
Notes
1 Each of the nine provinces has its own set of official languages eg English Afrikaansand one or more of the indigenous languages On a national level all 11 of these languagesare recognised as official In the case of the Western Cape Province there are thus threeofficial languages as stated
2 Groote Schuur Hospital is linked to the University of Cape Town and situated in theObservatory area in Cape Town a mainly English-speaking area It employs 524 doctorsand 1370 nurses The hospital treats approximately 44000 in-and 575000 out-patientsper year (Capegateway public info 2009) The staff use both Afrikaans and English on anequal basis and a small proportion use African languages The patients are alsopredominantly Afrikaans and English and a large proportion use African or otherlanguages (Williams 2005 in Saulse 2009 p 24)
3 This is the highest level of secondary schooling that can be obtained within the SouthAfrican context This gives access to tertiary education
Notes on contributors
Ilse Feinauer is associate professor in the Department of Afrikaans and Dutch and isresponsible for teaching Translation Studies and Practice to undergraduate and postgraduatestudents She also teaches Afrikaans linguistics She is coordinator for the MPhil inTranslation Studies She has extensive experience both as a translator and scholar intranslation theory
Harold Lesch is a senior lecturer also in the Department of Afrikaans and Dutch and holds aqualification in Translation Studies He is currently coordinator of the Post Graduate Diploma
10 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
in Translation and Interpreting and is responsible for teaching Interpreting Studies andPractice
References
Angelelli C (2004) Medical interpreting and cross-cultural communication CambridgeCambridge University Press
Angelelli C (2006) Validating professional standards and codes Challenges and opportu-nities Interpreting 8 175193
Anthonissen C (2008) On interpreting the interpreter experiences of language practitionersin mediating for the TRC Journal of Multicultural Discourses 3 165188
Capegateway public info (2009) httpwwwwesterncapegovzaengyour_gov5987Census (2001) Primary tables 1996 and 2001 compared Accessed at httpwwwstatssagovza
census01htmlC2001PrimTablesaspFeinauer I (2003) TB or not TB The communicative success of translated medical texts in
South Africa In W Botha (Ed) n Man wat beur rsquon Huldigingsbundel vir Dirk vanSchalkwyk (pp 213223) Stellenbosch Buro of the WAT
Feinauer I amp Luttig L (2005) Functionalism is not always the remedy Perspectives Studiesin Translatology 13 123131
Gile D (1995) Basic concepts and models for interpreter and translator training AmsterdamJohn Benjamins
Johnstone M-J (1999) Bioethics A nursing perspective Sydney HarcourtLeanza Y (2007) Role of community interpreters in pediatrics as seen by interpreters
physicians and researchers In F Pochhacker amp M Shlesinger (Eds) Healthcareinterpreting Discourse and interaction (pp 1134) Amsterdam Benjamins
Pienaar M (2006) Kommunikasie tussen staat en burgers die stand van tolkdienste SabinetOnline 40 3546
Pochhacker F amp Shlesinger M (Eds) (2007) Healthcare interpreting Discourse andinteraction Amsterdam Benjamins
Romero B (2008) Here are your right hands exploring interpreter qualifications Universityof Dayton Law Review 34 1533
Saulse B (2009) Interpreting within the Western Cape Health Care Sector A DescriptiveOverview (Unpublished masterrsquos thesis) University of Stellenbosch South Africa
United States National Council on Interpreting in Health Care (2004) A national code ofethics for interpreters in health care The National Council on Interpreting in Health CareWorking Papers Series httpwwwncihcorg
Appendix A
Text 1
A DOUBLE-BLIND PLACEBO CONTROLLED RANDOMISED STUDY TO INVESTI-GATE THE EFFICACY AND SAFETY OF LOW-DOSE L-CARNITINEMAGNESIUMSUPPLEMENTATION IN PREVENTING HYPERLACTINEMIA AND LACTIC ACIDO-SIS IN HIV-INFECTED SOUTH AFRICAN WOMEN ON STAVUDINE CONTAININGCOMBINED ANTIRETROVIRAL THERAPY (cART)
Introduction
We are doing a study to see if a l-carnitine magnesium combination product that could help toprevent high blood lactate levels which are known to be one of the side effects of some of themedications used in the treatment of HIV-infection (anti retroviral drugs)
The ability to decrease the way the virus multiplies is achieved by combined anti retroviraltherapy HIV positive (HIV ) patients receiving a combination of these drugs survive by
Perspectives Studies in Translatology 11
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
keeping the infection under control but not by killing the virus altogether This treatment hasindeed increased the quality of life in HIV individuals
One of the drugs the nucleotidic reverse transcriptase inhibitors (NRTIrsquos) can alter the energyproducing part of cells in the body and this that can lead to effects such as the high bloodlactate Twenty five percent of patients with high lactate levels donrsquot have any symptoms whileonly a smaller percentage less than 10 percent develops symptoms including loss of weightand abdominal pain
What is the purpose of this trial
A previous study showed that the low dose l-carnitine and magnesium was absorbed in healthymale volunteers and that the supplement was safe to administer
We want to determine if a dose of two capsules per day of the study drug over a period of ayear prevents the build up of lactic acid in the blood We also want to show if the l-carnitineand magnesium is absorbed in HIV positive subjects on combined anti-retroviral therapy anddetermine what the concentration levels of the anti-retroviral drugs are after a period of 6months and 12 months
To achieve this the study drug must be compared with a placebo (these are capsules that looksthe same as the study drug which are filled with a harmless compound in this case lactose)An extra 20 ml of blood and 50ml of urine apart from the normal routine bloods will be takenbefore starting anti-retroviral therapy and 30ml of blood and 50ml of urine will be taken 6monthly thereafter up to 12 months
The levels of lactic acid cholesterol triglycerides LDL - HDL- and Lp(a) lipoproteins andanti-retroviral drugs will be determined in the blood and those of the l-carnitine with itssupporting metabolites (the organic acid - amino acid-and major and trace element profileswhich includes magnesium) will be determined in the blood and urine These results of thosesubjects that are on the study drug will be compared with those of the placebo group to show ifthere are statistical relevant differences
Text 2
PARTICIPANT INFORMATION SHEET AND CONSENT FORM FOR USE BYPARENTSLEGAL GUARDIANS
Virtual Reality for pain relief in paediatric burns patients
What is this research study all aboutYour child has been admitted to this unit because of their burn injury Every child in this burnsunit has dressing changes on a daily basis Your child will be given the normal medication thatshehe receives during any dressing change These dosages of medication have been prescribedby the doctor when your child was admitted to the burns unit With all burn injuries one ofthe biggest problems that our patients experience is pain At the moment the professionals inthe burns unit do not know if there is something other than pain medication that can help todecrease your childrsquos pain Certain studies have proven that using a technique called VirtualRealty (VR) can distract a child and thereby decrease their pain during a specific procedureVirtual Reality is a program that we will use to allow your child to watch a video game throughgoggles that will be placed on their face Half of the treatment will be done using only the painmedication The other half of the dressing change will be done using the pain medication andthe VR We will then interview yourself and your child to find out how you your child feltabout this process and if you feel that Virtual reality can help to decrease your childrsquos painDuring the interviews with youyour child and nursing staff information may be recorded on a
12 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
tape recorder so that we can check all our information We will also be videotaping alldressing changes and using information from those tapes to help us with this study
Why has your child been invited to participateIn order to see if this process of VR is going to worknot work we have to assess it on at least250 children All children who are over the age of 5 and who do not have a face burn can takepart in this study You and your child have the option to participate in this study andparticipation is completely VOLUNTARY
What will your responsibilities beBy agreeing to let your child participate in this study you will allow us to ask your child tocomplete a questionnaire You will also be interviewed
Will your child benefit from taking part in this researchAt this stage we cannot say if your child will benefit from the study that we are doing If whatwe are doing does work then your child will experience less pain during the dressing changesIf the results are positive then it means that in the future more patients with similar injuries toyour child can be helped when they are experiencing pain during dressing changes
Are there any risks involved in your child taking part in this researchThere are no reported risks The only reported side effect of the VR is sickness If your childdoes experience any sickness due to the VR it will be stopped immediately
If you do not agree to allow your child to take part what alternatives does your child haveYou and your child have the option not to participate in this study participation is completelyVOLUNTARY Your child will only be entered into the study with your permission If youchoose not to enter the study we will still treat your child to the best of our ability and it willnot change the way you are treated You can leave the study at any time after you join
Who will have access to your childrsquos medical recordsAny information gained from this study and testing will be kept strictly private and no oneoutside of the people in the study will know youryour childrsquos results without your permissionIf the information is published to educate other health care professionals we will not use anynames Thus you and your child will never be able to be identified by anyone except studypersonnel Similarly no person outside of the study will have access to audio and videorecordings that may have been made during the dressing changes
Will you or your child be paid to take part in this study and are there any costs involvedYou or your child will not be paid to take part in the study and there will be no costs involvedfor you if your child does take part
Perspectives Studies in Translatology 13
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
14 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012

qualification and a medical background This is a three-month contract with the optionto extend Working hours are 0730 1600 (30-minute lunch) Monday to Friday Thejob entails office work and patient communication A senior assistant nurse with theselanguage requirements would also qualify for the position
Responsibility and ethical behaviour standards towards interpreters should also be
laid down for the health care provider and not only for the interpreter NCICH
(2004 p 19) notes the responsibility of the health care provider lsquoProviders have the
duty to present their knowledge clearly and objectively so that the patient is able
to make informed choicesrsquo If even interpreters are not monitored to meet their
obligations who is going to monitor the health care providers
Further research that could flow from this could be competency testing of the
interpreters to see how well they actually understand the information which had
been communicated by the health care provider and after the interpreters have
explained the information to the patients the same competency testing could be
done on the patientsrsquo understanding This can be established by asking patients
probing questions and inviting them to repeat the information they have received
(Roth et al 1983 p 175 in Johnstone 1999 pp 225227)
A retranslation of the source texts could also be done into Afrikaans and
isiXhosa using the functionalist approach and the interpreters could then be
retested to see whether they now understand the target texts better and whether
they would be able to paraphrase and explain the content better to the patient
Keeping in mind the socio-economic and educational level of the prototypical
patient for whom these informed consent forms are intended we would still
dissuade the interpreters from attempting to convey the message without a health
care provider present and from signing the document
Notes
1 Each of the nine provinces has its own set of official languages eg English Afrikaansand one or more of the indigenous languages On a national level all 11 of these languagesare recognised as official In the case of the Western Cape Province there are thus threeofficial languages as stated
2 Groote Schuur Hospital is linked to the University of Cape Town and situated in theObservatory area in Cape Town a mainly English-speaking area It employs 524 doctorsand 1370 nurses The hospital treats approximately 44000 in-and 575000 out-patientsper year (Capegateway public info 2009) The staff use both Afrikaans and English on anequal basis and a small proportion use African languages The patients are alsopredominantly Afrikaans and English and a large proportion use African or otherlanguages (Williams 2005 in Saulse 2009 p 24)
3 This is the highest level of secondary schooling that can be obtained within the SouthAfrican context This gives access to tertiary education
Notes on contributors
Ilse Feinauer is associate professor in the Department of Afrikaans and Dutch and isresponsible for teaching Translation Studies and Practice to undergraduate and postgraduatestudents She also teaches Afrikaans linguistics She is coordinator for the MPhil inTranslation Studies She has extensive experience both as a translator and scholar intranslation theory
Harold Lesch is a senior lecturer also in the Department of Afrikaans and Dutch and holds aqualification in Translation Studies He is currently coordinator of the Post Graduate Diploma
10 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
in Translation and Interpreting and is responsible for teaching Interpreting Studies andPractice
References
Angelelli C (2004) Medical interpreting and cross-cultural communication CambridgeCambridge University Press
Angelelli C (2006) Validating professional standards and codes Challenges and opportu-nities Interpreting 8 175193
Anthonissen C (2008) On interpreting the interpreter experiences of language practitionersin mediating for the TRC Journal of Multicultural Discourses 3 165188
Capegateway public info (2009) httpwwwwesterncapegovzaengyour_gov5987Census (2001) Primary tables 1996 and 2001 compared Accessed at httpwwwstatssagovza
census01htmlC2001PrimTablesaspFeinauer I (2003) TB or not TB The communicative success of translated medical texts in
South Africa In W Botha (Ed) n Man wat beur rsquon Huldigingsbundel vir Dirk vanSchalkwyk (pp 213223) Stellenbosch Buro of the WAT
Feinauer I amp Luttig L (2005) Functionalism is not always the remedy Perspectives Studiesin Translatology 13 123131
Gile D (1995) Basic concepts and models for interpreter and translator training AmsterdamJohn Benjamins
Johnstone M-J (1999) Bioethics A nursing perspective Sydney HarcourtLeanza Y (2007) Role of community interpreters in pediatrics as seen by interpreters
physicians and researchers In F Pochhacker amp M Shlesinger (Eds) Healthcareinterpreting Discourse and interaction (pp 1134) Amsterdam Benjamins
Pienaar M (2006) Kommunikasie tussen staat en burgers die stand van tolkdienste SabinetOnline 40 3546
Pochhacker F amp Shlesinger M (Eds) (2007) Healthcare interpreting Discourse andinteraction Amsterdam Benjamins
Romero B (2008) Here are your right hands exploring interpreter qualifications Universityof Dayton Law Review 34 1533
Saulse B (2009) Interpreting within the Western Cape Health Care Sector A DescriptiveOverview (Unpublished masterrsquos thesis) University of Stellenbosch South Africa
United States National Council on Interpreting in Health Care (2004) A national code ofethics for interpreters in health care The National Council on Interpreting in Health CareWorking Papers Series httpwwwncihcorg
Appendix A
Text 1
A DOUBLE-BLIND PLACEBO CONTROLLED RANDOMISED STUDY TO INVESTI-GATE THE EFFICACY AND SAFETY OF LOW-DOSE L-CARNITINEMAGNESIUMSUPPLEMENTATION IN PREVENTING HYPERLACTINEMIA AND LACTIC ACIDO-SIS IN HIV-INFECTED SOUTH AFRICAN WOMEN ON STAVUDINE CONTAININGCOMBINED ANTIRETROVIRAL THERAPY (cART)
Introduction
We are doing a study to see if a l-carnitine magnesium combination product that could help toprevent high blood lactate levels which are known to be one of the side effects of some of themedications used in the treatment of HIV-infection (anti retroviral drugs)
The ability to decrease the way the virus multiplies is achieved by combined anti retroviraltherapy HIV positive (HIV ) patients receiving a combination of these drugs survive by
Perspectives Studies in Translatology 11
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
keeping the infection under control but not by killing the virus altogether This treatment hasindeed increased the quality of life in HIV individuals
One of the drugs the nucleotidic reverse transcriptase inhibitors (NRTIrsquos) can alter the energyproducing part of cells in the body and this that can lead to effects such as the high bloodlactate Twenty five percent of patients with high lactate levels donrsquot have any symptoms whileonly a smaller percentage less than 10 percent develops symptoms including loss of weightand abdominal pain
What is the purpose of this trial
A previous study showed that the low dose l-carnitine and magnesium was absorbed in healthymale volunteers and that the supplement was safe to administer
We want to determine if a dose of two capsules per day of the study drug over a period of ayear prevents the build up of lactic acid in the blood We also want to show if the l-carnitineand magnesium is absorbed in HIV positive subjects on combined anti-retroviral therapy anddetermine what the concentration levels of the anti-retroviral drugs are after a period of 6months and 12 months
To achieve this the study drug must be compared with a placebo (these are capsules that looksthe same as the study drug which are filled with a harmless compound in this case lactose)An extra 20 ml of blood and 50ml of urine apart from the normal routine bloods will be takenbefore starting anti-retroviral therapy and 30ml of blood and 50ml of urine will be taken 6monthly thereafter up to 12 months
The levels of lactic acid cholesterol triglycerides LDL - HDL- and Lp(a) lipoproteins andanti-retroviral drugs will be determined in the blood and those of the l-carnitine with itssupporting metabolites (the organic acid - amino acid-and major and trace element profileswhich includes magnesium) will be determined in the blood and urine These results of thosesubjects that are on the study drug will be compared with those of the placebo group to show ifthere are statistical relevant differences
Text 2
PARTICIPANT INFORMATION SHEET AND CONSENT FORM FOR USE BYPARENTSLEGAL GUARDIANS
Virtual Reality for pain relief in paediatric burns patients
What is this research study all aboutYour child has been admitted to this unit because of their burn injury Every child in this burnsunit has dressing changes on a daily basis Your child will be given the normal medication thatshehe receives during any dressing change These dosages of medication have been prescribedby the doctor when your child was admitted to the burns unit With all burn injuries one ofthe biggest problems that our patients experience is pain At the moment the professionals inthe burns unit do not know if there is something other than pain medication that can help todecrease your childrsquos pain Certain studies have proven that using a technique called VirtualRealty (VR) can distract a child and thereby decrease their pain during a specific procedureVirtual Reality is a program that we will use to allow your child to watch a video game throughgoggles that will be placed on their face Half of the treatment will be done using only the painmedication The other half of the dressing change will be done using the pain medication andthe VR We will then interview yourself and your child to find out how you your child feltabout this process and if you feel that Virtual reality can help to decrease your childrsquos painDuring the interviews with youyour child and nursing staff information may be recorded on a
12 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
tape recorder so that we can check all our information We will also be videotaping alldressing changes and using information from those tapes to help us with this study
Why has your child been invited to participateIn order to see if this process of VR is going to worknot work we have to assess it on at least250 children All children who are over the age of 5 and who do not have a face burn can takepart in this study You and your child have the option to participate in this study andparticipation is completely VOLUNTARY
What will your responsibilities beBy agreeing to let your child participate in this study you will allow us to ask your child tocomplete a questionnaire You will also be interviewed
Will your child benefit from taking part in this researchAt this stage we cannot say if your child will benefit from the study that we are doing If whatwe are doing does work then your child will experience less pain during the dressing changesIf the results are positive then it means that in the future more patients with similar injuries toyour child can be helped when they are experiencing pain during dressing changes
Are there any risks involved in your child taking part in this researchThere are no reported risks The only reported side effect of the VR is sickness If your childdoes experience any sickness due to the VR it will be stopped immediately
If you do not agree to allow your child to take part what alternatives does your child haveYou and your child have the option not to participate in this study participation is completelyVOLUNTARY Your child will only be entered into the study with your permission If youchoose not to enter the study we will still treat your child to the best of our ability and it willnot change the way you are treated You can leave the study at any time after you join
Who will have access to your childrsquos medical recordsAny information gained from this study and testing will be kept strictly private and no oneoutside of the people in the study will know youryour childrsquos results without your permissionIf the information is published to educate other health care professionals we will not use anynames Thus you and your child will never be able to be identified by anyone except studypersonnel Similarly no person outside of the study will have access to audio and videorecordings that may have been made during the dressing changes
Will you or your child be paid to take part in this study and are there any costs involvedYou or your child will not be paid to take part in the study and there will be no costs involvedfor you if your child does take part
Perspectives Studies in Translatology 13
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
14 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012

in Translation and Interpreting and is responsible for teaching Interpreting Studies andPractice
References
Angelelli C (2004) Medical interpreting and cross-cultural communication CambridgeCambridge University Press
Angelelli C (2006) Validating professional standards and codes Challenges and opportu-nities Interpreting 8 175193
Anthonissen C (2008) On interpreting the interpreter experiences of language practitionersin mediating for the TRC Journal of Multicultural Discourses 3 165188
Capegateway public info (2009) httpwwwwesterncapegovzaengyour_gov5987Census (2001) Primary tables 1996 and 2001 compared Accessed at httpwwwstatssagovza
census01htmlC2001PrimTablesaspFeinauer I (2003) TB or not TB The communicative success of translated medical texts in
South Africa In W Botha (Ed) n Man wat beur rsquon Huldigingsbundel vir Dirk vanSchalkwyk (pp 213223) Stellenbosch Buro of the WAT
Feinauer I amp Luttig L (2005) Functionalism is not always the remedy Perspectives Studiesin Translatology 13 123131
Gile D (1995) Basic concepts and models for interpreter and translator training AmsterdamJohn Benjamins
Johnstone M-J (1999) Bioethics A nursing perspective Sydney HarcourtLeanza Y (2007) Role of community interpreters in pediatrics as seen by interpreters
physicians and researchers In F Pochhacker amp M Shlesinger (Eds) Healthcareinterpreting Discourse and interaction (pp 1134) Amsterdam Benjamins
Pienaar M (2006) Kommunikasie tussen staat en burgers die stand van tolkdienste SabinetOnline 40 3546
Pochhacker F amp Shlesinger M (Eds) (2007) Healthcare interpreting Discourse andinteraction Amsterdam Benjamins
Romero B (2008) Here are your right hands exploring interpreter qualifications Universityof Dayton Law Review 34 1533
Saulse B (2009) Interpreting within the Western Cape Health Care Sector A DescriptiveOverview (Unpublished masterrsquos thesis) University of Stellenbosch South Africa
United States National Council on Interpreting in Health Care (2004) A national code ofethics for interpreters in health care The National Council on Interpreting in Health CareWorking Papers Series httpwwwncihcorg
Appendix A
Text 1
A DOUBLE-BLIND PLACEBO CONTROLLED RANDOMISED STUDY TO INVESTI-GATE THE EFFICACY AND SAFETY OF LOW-DOSE L-CARNITINEMAGNESIUMSUPPLEMENTATION IN PREVENTING HYPERLACTINEMIA AND LACTIC ACIDO-SIS IN HIV-INFECTED SOUTH AFRICAN WOMEN ON STAVUDINE CONTAININGCOMBINED ANTIRETROVIRAL THERAPY (cART)
Introduction
We are doing a study to see if a l-carnitine magnesium combination product that could help toprevent high blood lactate levels which are known to be one of the side effects of some of themedications used in the treatment of HIV-infection (anti retroviral drugs)
The ability to decrease the way the virus multiplies is achieved by combined anti retroviraltherapy HIV positive (HIV ) patients receiving a combination of these drugs survive by
Perspectives Studies in Translatology 11
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
keeping the infection under control but not by killing the virus altogether This treatment hasindeed increased the quality of life in HIV individuals
One of the drugs the nucleotidic reverse transcriptase inhibitors (NRTIrsquos) can alter the energyproducing part of cells in the body and this that can lead to effects such as the high bloodlactate Twenty five percent of patients with high lactate levels donrsquot have any symptoms whileonly a smaller percentage less than 10 percent develops symptoms including loss of weightand abdominal pain
What is the purpose of this trial
A previous study showed that the low dose l-carnitine and magnesium was absorbed in healthymale volunteers and that the supplement was safe to administer
We want to determine if a dose of two capsules per day of the study drug over a period of ayear prevents the build up of lactic acid in the blood We also want to show if the l-carnitineand magnesium is absorbed in HIV positive subjects on combined anti-retroviral therapy anddetermine what the concentration levels of the anti-retroviral drugs are after a period of 6months and 12 months
To achieve this the study drug must be compared with a placebo (these are capsules that looksthe same as the study drug which are filled with a harmless compound in this case lactose)An extra 20 ml of blood and 50ml of urine apart from the normal routine bloods will be takenbefore starting anti-retroviral therapy and 30ml of blood and 50ml of urine will be taken 6monthly thereafter up to 12 months
The levels of lactic acid cholesterol triglycerides LDL - HDL- and Lp(a) lipoproteins andanti-retroviral drugs will be determined in the blood and those of the l-carnitine with itssupporting metabolites (the organic acid - amino acid-and major and trace element profileswhich includes magnesium) will be determined in the blood and urine These results of thosesubjects that are on the study drug will be compared with those of the placebo group to show ifthere are statistical relevant differences
Text 2
PARTICIPANT INFORMATION SHEET AND CONSENT FORM FOR USE BYPARENTSLEGAL GUARDIANS
Virtual Reality for pain relief in paediatric burns patients
What is this research study all aboutYour child has been admitted to this unit because of their burn injury Every child in this burnsunit has dressing changes on a daily basis Your child will be given the normal medication thatshehe receives during any dressing change These dosages of medication have been prescribedby the doctor when your child was admitted to the burns unit With all burn injuries one ofthe biggest problems that our patients experience is pain At the moment the professionals inthe burns unit do not know if there is something other than pain medication that can help todecrease your childrsquos pain Certain studies have proven that using a technique called VirtualRealty (VR) can distract a child and thereby decrease their pain during a specific procedureVirtual Reality is a program that we will use to allow your child to watch a video game throughgoggles that will be placed on their face Half of the treatment will be done using only the painmedication The other half of the dressing change will be done using the pain medication andthe VR We will then interview yourself and your child to find out how you your child feltabout this process and if you feel that Virtual reality can help to decrease your childrsquos painDuring the interviews with youyour child and nursing staff information may be recorded on a
12 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
tape recorder so that we can check all our information We will also be videotaping alldressing changes and using information from those tapes to help us with this study
Why has your child been invited to participateIn order to see if this process of VR is going to worknot work we have to assess it on at least250 children All children who are over the age of 5 and who do not have a face burn can takepart in this study You and your child have the option to participate in this study andparticipation is completely VOLUNTARY
What will your responsibilities beBy agreeing to let your child participate in this study you will allow us to ask your child tocomplete a questionnaire You will also be interviewed
Will your child benefit from taking part in this researchAt this stage we cannot say if your child will benefit from the study that we are doing If whatwe are doing does work then your child will experience less pain during the dressing changesIf the results are positive then it means that in the future more patients with similar injuries toyour child can be helped when they are experiencing pain during dressing changes
Are there any risks involved in your child taking part in this researchThere are no reported risks The only reported side effect of the VR is sickness If your childdoes experience any sickness due to the VR it will be stopped immediately
If you do not agree to allow your child to take part what alternatives does your child haveYou and your child have the option not to participate in this study participation is completelyVOLUNTARY Your child will only be entered into the study with your permission If youchoose not to enter the study we will still treat your child to the best of our ability and it willnot change the way you are treated You can leave the study at any time after you join
Who will have access to your childrsquos medical recordsAny information gained from this study and testing will be kept strictly private and no oneoutside of the people in the study will know youryour childrsquos results without your permissionIf the information is published to educate other health care professionals we will not use anynames Thus you and your child will never be able to be identified by anyone except studypersonnel Similarly no person outside of the study will have access to audio and videorecordings that may have been made during the dressing changes
Will you or your child be paid to take part in this study and are there any costs involvedYou or your child will not be paid to take part in the study and there will be no costs involvedfor you if your child does take part
Perspectives Studies in Translatology 13
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
14 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
keeping the infection under control but not by killing the virus altogether This treatment hasindeed increased the quality of life in HIV individuals
One of the drugs the nucleotidic reverse transcriptase inhibitors (NRTIrsquos) can alter the energyproducing part of cells in the body and this that can lead to effects such as the high bloodlactate Twenty five percent of patients with high lactate levels donrsquot have any symptoms whileonly a smaller percentage less than 10 percent develops symptoms including loss of weightand abdominal pain
What is the purpose of this trial
A previous study showed that the low dose l-carnitine and magnesium was absorbed in healthymale volunteers and that the supplement was safe to administer
We want to determine if a dose of two capsules per day of the study drug over a period of ayear prevents the build up of lactic acid in the blood We also want to show if the l-carnitineand magnesium is absorbed in HIV positive subjects on combined anti-retroviral therapy anddetermine what the concentration levels of the anti-retroviral drugs are after a period of 6months and 12 months
To achieve this the study drug must be compared with a placebo (these are capsules that looksthe same as the study drug which are filled with a harmless compound in this case lactose)An extra 20 ml of blood and 50ml of urine apart from the normal routine bloods will be takenbefore starting anti-retroviral therapy and 30ml of blood and 50ml of urine will be taken 6monthly thereafter up to 12 months
The levels of lactic acid cholesterol triglycerides LDL - HDL- and Lp(a) lipoproteins andanti-retroviral drugs will be determined in the blood and those of the l-carnitine with itssupporting metabolites (the organic acid - amino acid-and major and trace element profileswhich includes magnesium) will be determined in the blood and urine These results of thosesubjects that are on the study drug will be compared with those of the placebo group to show ifthere are statistical relevant differences
Text 2
PARTICIPANT INFORMATION SHEET AND CONSENT FORM FOR USE BYPARENTSLEGAL GUARDIANS
Virtual Reality for pain relief in paediatric burns patients
What is this research study all aboutYour child has been admitted to this unit because of their burn injury Every child in this burnsunit has dressing changes on a daily basis Your child will be given the normal medication thatshehe receives during any dressing change These dosages of medication have been prescribedby the doctor when your child was admitted to the burns unit With all burn injuries one ofthe biggest problems that our patients experience is pain At the moment the professionals inthe burns unit do not know if there is something other than pain medication that can help todecrease your childrsquos pain Certain studies have proven that using a technique called VirtualRealty (VR) can distract a child and thereby decrease their pain during a specific procedureVirtual Reality is a program that we will use to allow your child to watch a video game throughgoggles that will be placed on their face Half of the treatment will be done using only the painmedication The other half of the dressing change will be done using the pain medication andthe VR We will then interview yourself and your child to find out how you your child feltabout this process and if you feel that Virtual reality can help to decrease your childrsquos painDuring the interviews with youyour child and nursing staff information may be recorded on a
12 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
tape recorder so that we can check all our information We will also be videotaping alldressing changes and using information from those tapes to help us with this study
Why has your child been invited to participateIn order to see if this process of VR is going to worknot work we have to assess it on at least250 children All children who are over the age of 5 and who do not have a face burn can takepart in this study You and your child have the option to participate in this study andparticipation is completely VOLUNTARY
What will your responsibilities beBy agreeing to let your child participate in this study you will allow us to ask your child tocomplete a questionnaire You will also be interviewed
Will your child benefit from taking part in this researchAt this stage we cannot say if your child will benefit from the study that we are doing If whatwe are doing does work then your child will experience less pain during the dressing changesIf the results are positive then it means that in the future more patients with similar injuries toyour child can be helped when they are experiencing pain during dressing changes
Are there any risks involved in your child taking part in this researchThere are no reported risks The only reported side effect of the VR is sickness If your childdoes experience any sickness due to the VR it will be stopped immediately
If you do not agree to allow your child to take part what alternatives does your child haveYou and your child have the option not to participate in this study participation is completelyVOLUNTARY Your child will only be entered into the study with your permission If youchoose not to enter the study we will still treat your child to the best of our ability and it willnot change the way you are treated You can leave the study at any time after you join
Who will have access to your childrsquos medical recordsAny information gained from this study and testing will be kept strictly private and no oneoutside of the people in the study will know youryour childrsquos results without your permissionIf the information is published to educate other health care professionals we will not use anynames Thus you and your child will never be able to be identified by anyone except studypersonnel Similarly no person outside of the study will have access to audio and videorecordings that may have been made during the dressing changes
Will you or your child be paid to take part in this study and are there any costs involvedYou or your child will not be paid to take part in the study and there will be no costs involvedfor you if your child does take part
Perspectives Studies in Translatology 13
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
14 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012

tape recorder so that we can check all our information We will also be videotaping alldressing changes and using information from those tapes to help us with this study
Why has your child been invited to participateIn order to see if this process of VR is going to worknot work we have to assess it on at least250 children All children who are over the age of 5 and who do not have a face burn can takepart in this study You and your child have the option to participate in this study andparticipation is completely VOLUNTARY
What will your responsibilities beBy agreeing to let your child participate in this study you will allow us to ask your child tocomplete a questionnaire You will also be interviewed
Will your child benefit from taking part in this researchAt this stage we cannot say if your child will benefit from the study that we are doing If whatwe are doing does work then your child will experience less pain during the dressing changesIf the results are positive then it means that in the future more patients with similar injuries toyour child can be helped when they are experiencing pain during dressing changes
Are there any risks involved in your child taking part in this researchThere are no reported risks The only reported side effect of the VR is sickness If your childdoes experience any sickness due to the VR it will be stopped immediately
If you do not agree to allow your child to take part what alternatives does your child haveYou and your child have the option not to participate in this study participation is completelyVOLUNTARY Your child will only be entered into the study with your permission If youchoose not to enter the study we will still treat your child to the best of our ability and it willnot change the way you are treated You can leave the study at any time after you join
Who will have access to your childrsquos medical recordsAny information gained from this study and testing will be kept strictly private and no oneoutside of the people in the study will know youryour childrsquos results without your permissionIf the information is published to educate other health care professionals we will not use anynames Thus you and your child will never be able to be identified by anyone except studypersonnel Similarly no person outside of the study will have access to audio and videorecordings that may have been made during the dressing changes
Will you or your child be paid to take part in this study and are there any costs involvedYou or your child will not be paid to take part in the study and there will be no costs involvedfor you if your child does take part
Perspectives Studies in Translatology 13
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
14 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
14 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Perspectives Studies in Translatology 15
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
16 I Feinauer and HM Lesch
Dow
nloa
ded
by [
Uni
vers
ity o
f St
elle
nbos
ch]
[H
arol
d M
Les
ch]
at 2
345
11
Janu
ary
2012
Related Documents











