Health Systems: Goals, Functions, Actors Health workforce Daniel Opoku Department of Health Care Management, Technische Universität Berlin (WHO Collaborating Centre for Health Systems Research and Management) European Observatory on Health Systems and Policies

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Health Systems: Goals, Functions, ActorsHealth workforce
Daniel OpokuDepartment of Health Care Management, Technische Universität Berlin
(WHO Collaborating Centre for Health Systems Research and Management)European Observatory on Health Systems and Policies

WHO 2007
25 Sept
25 Sept
26 Sept
26 Sept
27 Sept
01 Oct
02 Oct
02 Oct
03 Oct
03 Oct
2
Guiding framework for the module
24 September 2019 Frameworks 1
01 Oct
Summary: 27 Sept Performance assessment: 03 Oct
& other frameworks: 24/25 Sept
25 Sept
325 September 2019 Health workforce
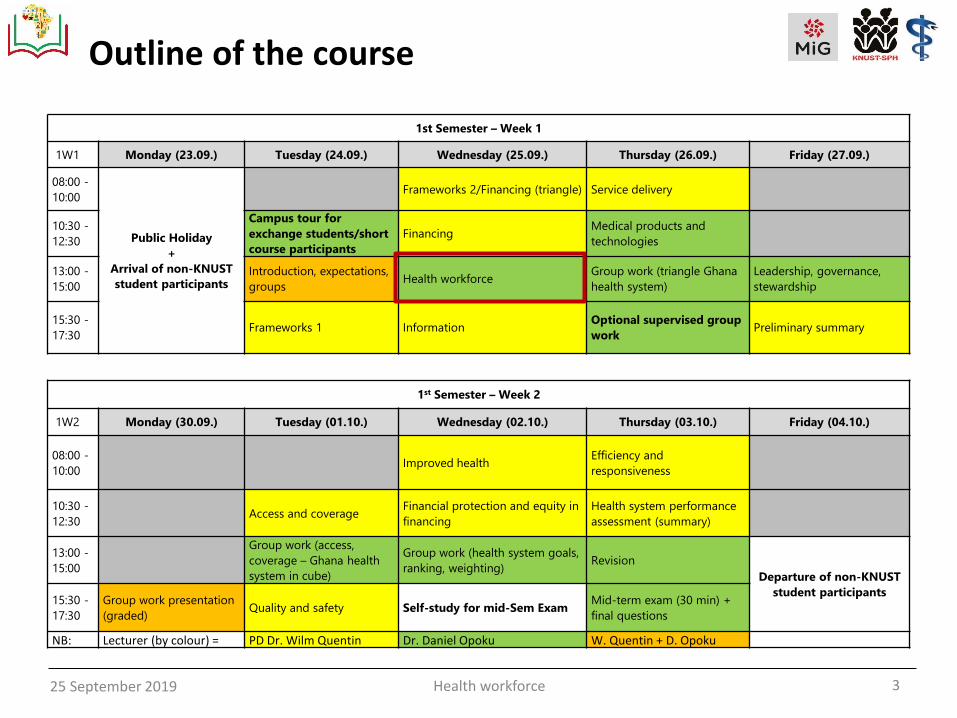
Outline of the course
1st Semester – Week 1
1W1 Monday (23.09.) Tuesday (24.09.) Wednesday (25.09.) Thursday (26.09.) Friday (27.09.)
08:00 -
10:00
Public Holiday
+
Arrival of non-KNUST
student participants
Frameworks 2/Financing (triangle) Service delivery
10:30 -
12:30
Campus tour for
exchange students/short
course participants
FinancingMedical products and
technologies
13:00 -
15:00
Introduction, expectations,
groupsHealth workforce
Group work (triangle Ghana
health system)
Leadership, governance,
stewardship
15:30 -
17:30Frameworks 1 Information
Optional supervised group
workPreliminary summary
1st Semester – Week 2
1W2 Monday (30.09.) Tuesday (01.10.) Wednesday (02.10.) Thursday (03.10.) Friday (04.10.)
08:00 -
10:00Improved health
Efficiency and
responsiveness
10:30 -
12:30Access and coverage
Financial protection and equity in
financing
Health system performance
assessment (summary)
13:00 -
15:00
Group work (access,
coverage – Ghana health
system in cube)
Group work (health system goals,
ranking, weighting)Revision
Departure of non-KNUST
student participants15:30 -
17:30
Group work presentation
(graded)Quality and safety Self-study for mid-Sem Exam
Mid-term exam (30 min) +
final questions
NB: Lecturer (by colour) = PD Dr. Wilm Quentin Dr. Daniel Opoku W. Quentin + D. Opoku

4
Agenda
25 September 2019 Health workforce
• Importance, definition and indicators of health workforce
• Distribution of health workforce & health staff shortage
• Shifting demands and rising pressures on health workers
• International mobility of health workforce

525 September 2019 Health workforce
High-income countries: Growth in health & social sector outpaces general employment growth, 1990-2014

625 September 2019 Health workforce
WHO 2016 OECD 2016
High on the international agenda (2016)

725 September 2019 Health workforce
High on the international agenda (2017)

825 September 2019 Health workforce
“Health workers are all people primarily engaged in actions with the primary intent of enhancing health.” (World Health Report 2006)
“A well-performing health workforce is one that works in ways that are responsive, fair and efficient, to achieve the best health outcomes possible, given available resources and circumstances.” (WHO, 2007)
Health workforce includes different occupations: • Physicians, nurses and midwifery personnel• Dentistry & pharmaceutical personnel• Laboratory health workers• Environmental and public health workers• Community and traditional health workers• Other health service providers• Health management and support workers
… working in curative, preventive and rehabilitative care services as well as health education, promotion and research.
Health workforce: definitions

925 September 2019 Health workforce
Source: A Universal Truth: No Health Without a Workforce
Third Global Forum on Human Resources for Health Report
Four critical dimensions of Human Resources for Health I

1025 September 2019 Health workforce
Availability Sufficient supply of health workers, with competencies and skill mix that correspond to population needs
Accessibility Equitable distribution of health workers in terms of travel time and transport (spatial), opening hours (temporal), referral mechanisms (organizational); direct and indirect cost of services (formal & informal)
Acceptability Characteristics and ability of the workforce to treat all patients with dignity, create trust and enable/promote demand for services (age/religion/social & cultural values etc.)
QualityCompetencies, skills, knowledge and behaviour of health worker as assessed according to professional norms and as perceived by users
Can these dimensions
be influenced and how?
- Governance! Based on data/evidence
- E.g. health workforce policies- Legislation & regulation,
e.g. incentives/ disincentives, education;
- non-legislative governance mechanisms
Four critical dimensions of Human Resources for Health II

1125 September 2019 Health workforce
Key indicators
Health worker density• measured by physician/nurse/
midwife/dentist or pharmacistrate per 1000 population
Distribution of health workers• health workers by occupation,
geographical region, facility type, country-of-birth, age and sex/the total number of health workers
Annual number of graduates • N° of graduates from health
profession educational institutions /total population
Skill mix/composition of workforce• nurse/physician ratio,
GP/physician ratio
Employment characteristics • Total annual number of working
hours/number of active health workers, defined in headcounts

1225 September 2019 Health workforce

1325 September 2019 Health workforce
Nursing and physician density in EU countries
3 : 1
2 : 1

1425 September 2019 Health workforce
Why health workforce is important
Source: World Health Report 2006

1525 September 2019 Health workforce
Ebola outbreak in West Africa in 2014
Source: https://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/distribution-map.html

1625 September 2019 Health workforce
Healthcare systems were too weak to control the outbreak
• Inadequate services and workforce to control the outbreak – cases other than Ebola were often not treated (malaria etc.)
• Problems with adequate and timely payment of health workers for their services as well as appropriate training and education
Source: http://allafrica.com/view/group/main/main/id/00032734.html
WHO defines minimum threshold of 2.3 doctors, nurses and midwives per 1 000 population that are necessary to deliver essential maternal and child health services (MDG 4).
Shortage of health workforce was a major challenge in controlling Ebola during the West African outbreak but workforce itself was also severely affected by the outbreak.

1725 September 2019 Health workforce
• Mortality: Ebola deaths among health workers? • Are health workers (more) at risk?
Ebola: Health workers essential, but too few andat risk
0.02 0.11 0.06
1.45
8.07
6.85
0
1
2
3
4
5
6
7
8
9
10
Ginea Liberia Sierra Leone
% mortality (caused by Ebola) among total population compared to health workforce
% mortality due to Ebola among total population
% mortality among doctor, nurse/midwive workforce
Source: Evans et al., Lancet 2015
x 70
x 80
x 100

1825 September 2019 Health workforce
Density of physicians (per 1000 population, 2014)
Liberia: 0.014Sierra Leone: 0.024Guinea: 0.097
Source: http://apps.who.int/gho/data/node.main.A1444?lang=en&showonly=HWF
Russia: 3.3
Australia: 3.4
Germany: 4.1
Norway: 4.4
USA: 2.6
Brazil: 1.8
Argentina 3.8
South Africa: 0.8
Libya: 2.1
India:0.7
China: 1.5
Canada: 2.5

1925 September 2019 Health workforce
Density of nurses & midwives (per 1000, 2014)
Liberia: 0.266Sierra Leone: 0.319Guinea: 0.466
Source: http://apps.who.int/gho/data/node.main.A1444?lang=en&showonly=HWF
USA: 9.9
Canada: 9.5
Brazil: 7.4Peru: 1.5
South Africa: 5.1
Libya 6.9
Turkey:2.5
Russia: 4.6
China: 1.7
Australia: 12.3
Norway: 17.4
Germany:13.5
India: 2.1
2025 September 2019 Health workforce
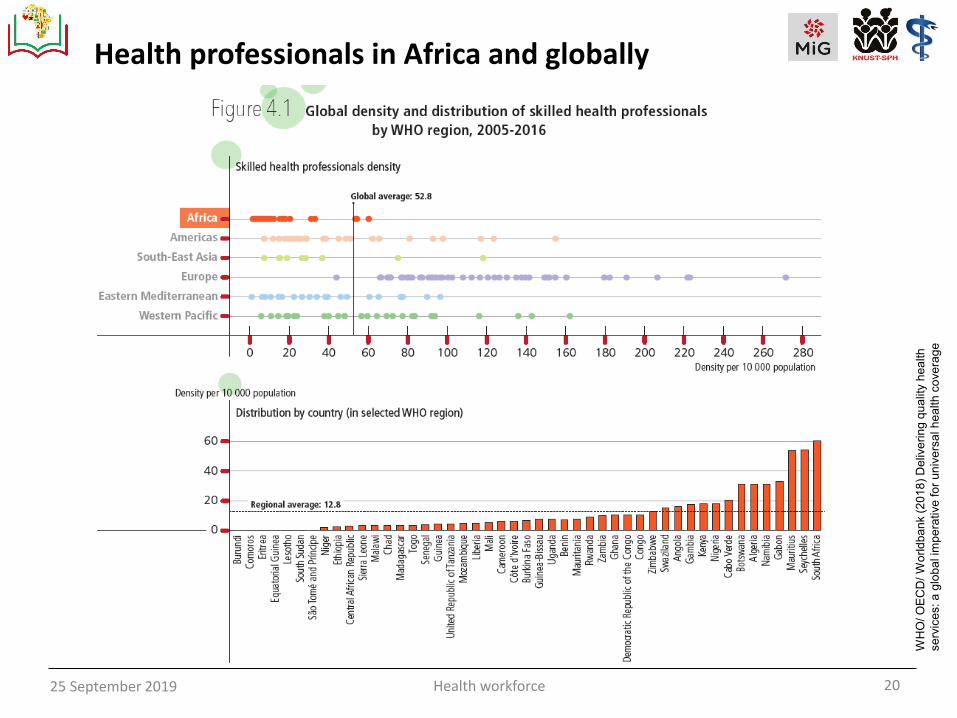
Health professionals in Africa and globally
WH
O/ O
EC
D/
Wo
rld
ban
k(2
01
8)
Deliv
eri
ng
qu
alit
y h
ea
lth
se
rvic
es: a
glo
ba
l im
pe
rative
fo
r u
niv
ers
al h
ea
lth
co
ve
rag
e

2125 September 2019 Health workforce
In Ghana?
WHO (2017). Africa Health Workforce Observatory. HRH Observatory.
Ghana http://www.hrh-observatory.afro.who.int/countries/ghana-2/
0.11
0.98
0.010.07
0.190.22
1.17
0.04 0.06
0.45
0
0.2
0.4
0.6
0.8
1
1.2
1.4
Physicians Nurses andMidwives
Dentists andtechnicians
Pharmacists andtechnicians
Community health
Den
sity
per
1,0
00
po
pu
lati
on
Density of health workforce in Ghana and WHO African region in 2008
Ghana
Africa

2225 September 2019 Health workforce
Source: WHO (2016) Health workforce requirements for universal health coverage and the
sustainable development goals.
Uneven distribution of health workers
10x
10x 6x
9x12x
6x

2325 September 2019 Health workforce
The uneven distribution of health workers …
… multiplies if burden of diseaseis taken into account
Source: WHO. 2006. The World Health Report 2006 -Working
Together for Health, page 9
3% vs.
25%
37% vs. 9%

2425 September 2019 Health workforce
Density levels also differ significantly within countries
Geographical variation in physician density per 100,000 population by countries’ national, highest and lowest physician density region (NUTS 2 level), 2014

2525 September 2019 Health workforce
316276
529
302
487
321
414 404
519
439
695
441
551
473
419464
604
501
588
529
689
867
95
160148
227 224
300
240275
129
286240
215
273300 313 328
351
298254
376 378
299
00
100
200
300
400
500
600
700
800
900
1,000
Highest density region lowest region 2014 national
25
Density levels also differ significantly within countries
Geographical variation in physician density per 100,000 population by countries’ national, highest and lowest physician density region (NUTS 2 level), 2014
Source: Maier 2017, based
on Eurostat database 2016
→ Maldistribution leads to both under- and over-served areas2.9x
2.9x
3.6x
3.3x
4.0x
1.1x
1.4x
1.4x
1.7x
1.3x
1.4x

2625 September 2019 Health workforce
x 2.6
x 2.3
x 1.0
x 1.2x 1.2
Urban-rural discrepancies:a different way to look at intra-country variation
x 2.5

2725 September 2019 Health workforce
Ghana? What data on urban/rural divide?
Source: http://apps.who.int/gho/data/node.main.A1444?lang=en&showonly=HWF
902
2346
990
551
2338
1564
5 18
236
0
500
1000
1500
2000
2500
Physicians Midwives Dentists Radiographers Medical assistants
Tota
l nu
mb
ers
of
hea
lth
wo
rkfo
rce
Total numbers of health workforce by geographic distribution in Ghana in 2004
Rural
Urban
-> Only absolute numbers and from 2004

2825 September 2019 Health workforce
Rising numbers of doctors in OECD countries
Source: OECD (2016) Health Workforce Policies in OECD Countries - Right Jobs, Right Skills, Right Places

2925 September 2019 Health workforce
Source: WHO (2016) Health workforce requirements for universal health coverage and the
sustainable development goals.
… but numbers should rise in low-income countries,especially in Africa, not in Europe

3025 September 2019 Health workforce
Ghana over time? Density of pysicians andnurses/midwives in Ghana 2004, 2007-10
Source: http://apps.who.int/gho/data/node.main.A1444?lang=en&showonly=HWF
0.160.07
0.11 0.09 0.10
0.950.99
1.05
0.93
0.00
0.20
0.40
0.60
0.80
1.00
1.20
2004 2007 2008 2009 2010
Den
sity
per
1,0
00
po
pu
lati
on
if no bars shown, no data available
Physicians Nurses and midwives

3125 September 2019 Health workforce
Source: World Health Report 2006
Global health workforce deficit
Driving forces are:
▪ population growth
▪ demographic and
epidemiological transitions
▪ ageing of the existing
health workforce
▪ international migration and
recruitment of health
personnel from low- and
middle-income countries
Global demand for health workers still far outstrips supply, and the gap
is growing every year.
3225 September 2019 Health workforce
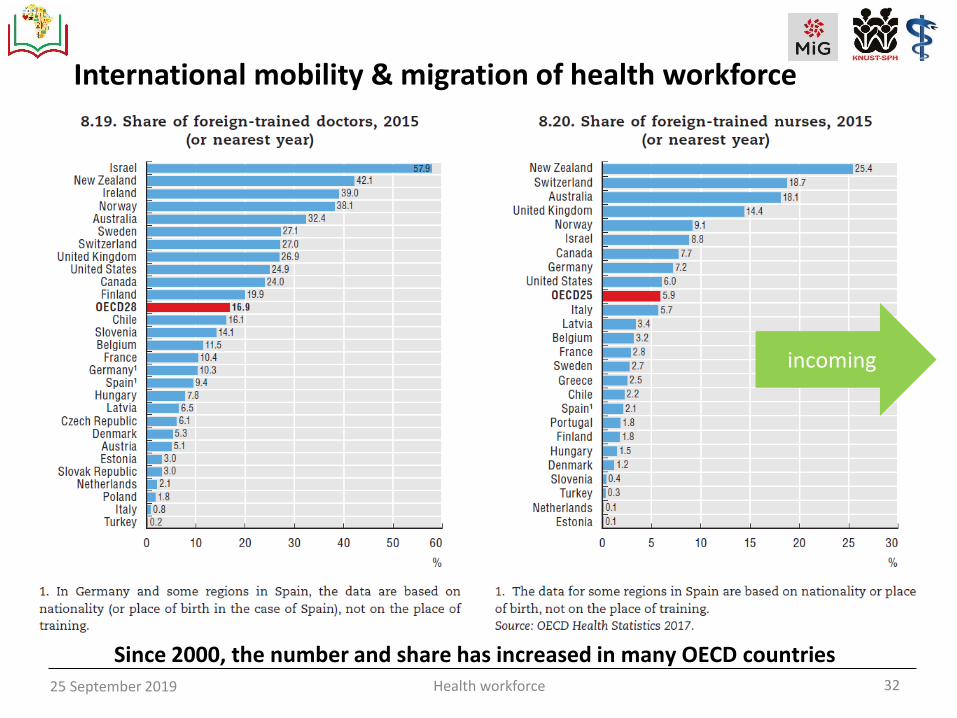
International mobility & migration of health workforce
Since 2000, the number and share has increased in many OECD countries
incoming

3325 September 2019 Health workforce
WHO Global Code of Practice on the International Recruitment of Health Personnel (2010)
➢ adopted by all 193 WHO member states➢ Aim: to stem the brain drain from poor to rich countries➢ establishes and promotes voluntary principles and practices
for the ethical international recruitment of health personnel
Global care chains’ impacts on health systems
incoming

3424 September 2019 Health workforce
outgoing

35
A closer look at Ghana
24 September 2019 Frameworks 1

3625 September 2019 Health workforce
• Physicians: annual registrations in the UK of from selected African countries: 1.1 % (Ghana), 2.0 % (South Africa), and 0.7 % (Zimbabwe) of the total number of doctors registering in the UK.
• Nurses: the number of nurses: 1% from Ghana, 0.6% (SA) and 2.6% (Zimbabwe) registering annually in the UK as a proportion of the total number of nurses registering in the UK; yearly increasing trend (Ghana)
(Source: Stilwell, Human Resources for Health 2003, Buchan & Dovlo for DFID 2004)
Source: Anarfi et al. 2010 Key Determinants of Migration among Health Professionals in Ghana https://www.researchgate.net/profile/John_Anarfi/publication/242579161_Key_Determinants_of_Migration_among_Health_Professionals_in_Ghana/links/5425841c0cf238c6ea7411cf.pdf
Ghana: migration of physicians and nurses
outgoing
incoming

3725 September 2019 Health workforce
Shifting demands on health professionals
Source: World Health Report 2006
Population growth
& ageing, epidemiological
transition
Retirement, supply ofgraduates

3825 September 2019 Health workforce12 September 2018 Health workforce 38
Public policy levers to shape health labour markets
Source: WHO (2016) Working for health and growth: investingin the health workforce. Report of the High-Level Commission on Health Employment and Economic Growth.

3925 September 2019 Health workforce
Take-home messages
• Health workers are the backbone of strong, resilient health systems.
• Demand for health workforce expected to increase (e.g. demographic and epidemiological transitions, technology, changing patients expectations) -> access to safe & quality health services
• Health workforce shortages widen inequities in access to & quality of health services -> economic consequences and development (HIV/AIDS / Ebola in West Africa)
• Equity? International health worker mobility affects low resource countries that already have shortages –> but mobility of health workers may also bring benefits to source nations (brain drain to brain gain/circular migration?)
Related Documents











