Health Savings Accounts and Trends in Employee Health Benefits National Academy of Social Insurance Charles H. Klippel Senior Vice President and Deputy General Counsel Aetna Inc. January 27, 2005

Health Savings Accounts and Trends in Employee Health Benefits National Academy of Social Insurance Charles H. Klippel Senior Vice President and Deputy.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Health Savings Accountsand
Trends in Employee Health Benefits
National Academy of
Social Insurance
Charles H. Klippel
Senior Vice President
and Deputy General Counsel
Aetna Inc.
January 27, 2005

The Emergence and Future of Consumerism
• Drivers of change in plan design– Changes in preferences/ market forces– The role of a deductible – Tax policy
• Impact of change– Findings from Aetna’s experience
• Future directions– Further evolution in plan design– Employer disengagement– Other considerations
Policy follows the market
• HSAs are a consequence, not a cause, of change– Consumerism did not start in Washington– Not a “red” or “blue” idea– Not driven by health industry– Started with employers
• Not radical thinking– Role of deductible in health coverage– Response to employee concerns– Cost pressures– Preserving tax preference of benefit dollars
Deductibles in health plans
• Deductibles have always been a part of health insurance – Standard in almost all other forms of
insurance– Historically plans without a deductible are
the anomaly
• Health Maintenance OrganizationsSelected provider networkCare managed to protocols = Different benefit structure

The Role of a Deductible
Classic role of a deductible in insurance• Reduce “moral hazard”• Avoid high processing costs of smaller claims
Additional consideration in health• Increasing choice in treatment• Differing perceptions of value• Significant cost differences• Efficacy may not correlate with cost
Example: Pharmaceuticals

Supporting choice/ subsidizing risk
Options for the plan sponsor• Manage selection directly or in benefit design• Pay everything regardless of choice• Deductible (with financial assistance)
Focus defined benefit dollars on shared, unanticipated risks• Benefits typically a trade-off for wages• “Regressive” (in tax terms)• An inherent cross-subsidy related to use, not need

Health Reimbursement Accounts
• A portion of benefits structured as “fund”– Unused dollars roll over for future years
• Sanctioned by Treasury in June 2002– Must be employer dollars– No employee contributions– Employer defines rules– Money is not portable
• HRAs in practice– Typically self-funded plans– Accounts generally “first dollar”– May continue for retirees, otherwise lost
when employment ends
HRA

Health Savings Accounts
• Part of MMA in December 2003• Greater flexibility
– Permits employee funding• Consumer protections
– All money belongs to employee– Employer can’t restrict use– Fully portable– HDPH specifies minimum deductible and
maximum out-of-pocket (i.e., plans can be too rich or too limited to qualify)
HSA
Alternatives to fund structure
• Additional wages– Less tax efficient– Does not encourage savings
• Lower deductible, eliminate “fund”– “Doughnut-hole” argument– Less consumer risk (?)
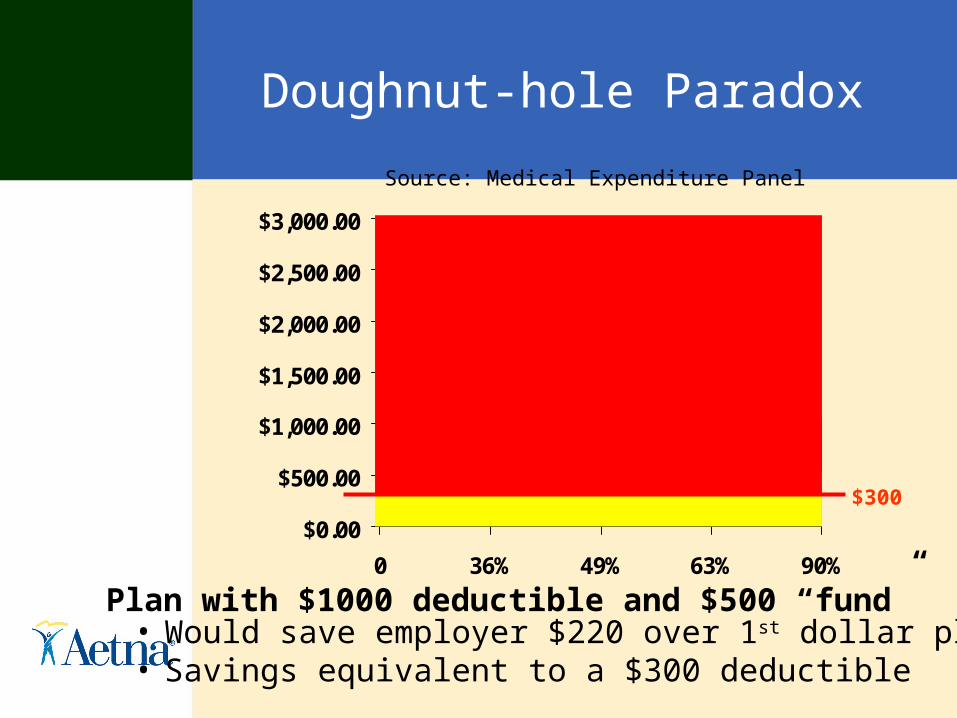
Doughnut-hole Paradox
$0.00
$500.00
$1,000.00
$1,500.00
$2,000.00
$2,500.00
$3,000.00
0 36% 49% 63% 90%
Source: Medical Expenditure Panel Survey (2002)
Plan with $1000 deductible and $500 “fund”• Would save employer $220 over 1st dollar plan• Savings equivalent to a $300 deductible
$300

Doughnut-hole Paradox
$0.00
$500.00
$1,000.00
$1,500.00
$2,000.00
$2,500.00
$3,000.00
0 36% 49% 63% 90%
$300 Deductible $1000 w/ $500 Fund
More expenses covered 43% 57%
Average % of expenses covered
45% 86%
% covered of $10,000 99.7% 99.5%
$0.00
$500.00
$1,000.00
$1,500.00
$2,000.00
$2,500.00
$3,000.00
0 36% 49% 63% 90%
Impact of plan design
• Aetna Health Fund®– HRA plan enrollees in 2003– 13,500 members enrolled in other Aetna
plans in the 2002– One full-replacement plan– Full-year 2002 to 2003 comparison – Also compared to 300,000 cohort-matched
individuals enrolled in other Aetna plans in 2003
Aetna Health Fund Study2002-2003
• Overall year-over-year trend: 3.7%• Full replacement customer trend: -11%• Specific utilization
– Primary visits (non-preventive): -11%– Specialist visits: +3%– Emergency room visits: -3%– Inpatient admissions: -5%
• Preventive services:– Preventive visits: +23% (+8%)*– Gynecological visits: +4% (+4%)– Child preventive exams
• 4-6 year olds: +4% (+5%)• 6-8 year olds: +8% (+6%)
*Comparison with cohort-matched population of 338,000 Aetna members
AHF
Aetna Health Fund StudyImpact on Pharmacy Costs
Full-year study results:• Overall pharmacy cost trend: -5.5%• Number of prescriptions: -13%• Generic Utilization: + 7%
Full replacement customer (2600 lives)*• Overall Rx trend: - 6.5%• Number of scripts: -11.1%• Generic utilization: + 29%*Nine months 1/03-9-03
AHF
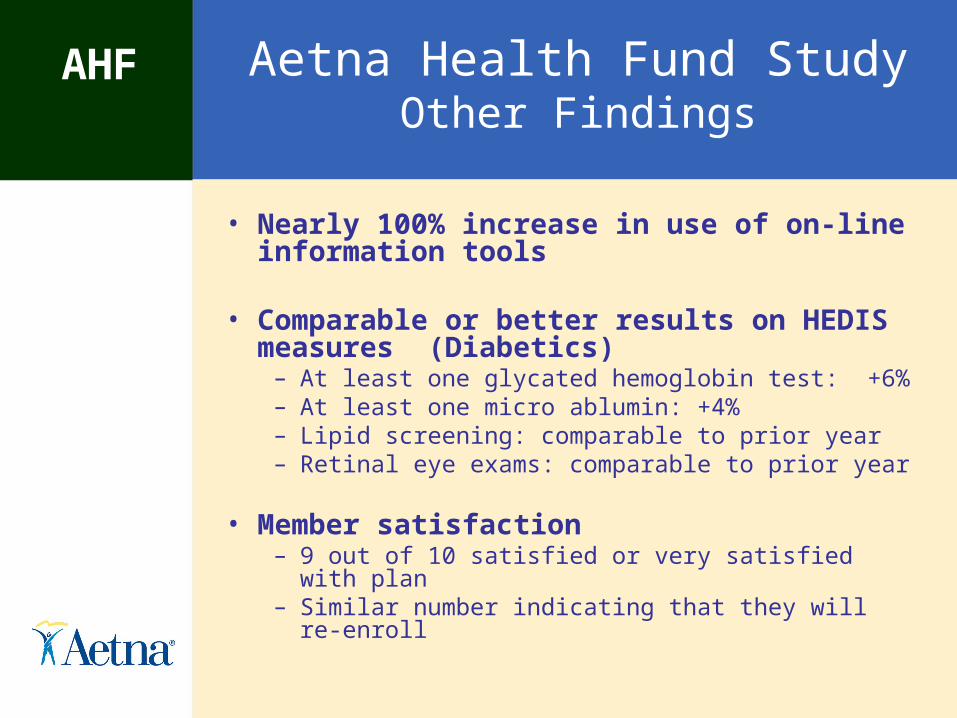
Aetna Health Fund StudyOther Findings
• Nearly 100% increase in use of on-line information tools
• Comparable or better results on HEDIS measures (Diabetics)
– At least one glycated hemoglobin test: +6%– At least one micro ablumin: +4%– Lipid screening: comparable to prior year– Retinal eye exams: comparable to prior year
• Member satisfaction– 9 out of 10 satisfied or very satisfied with plan– Similar number indicating that they will re-enroll
AHF
Looking forward
Where is plan design going from here?
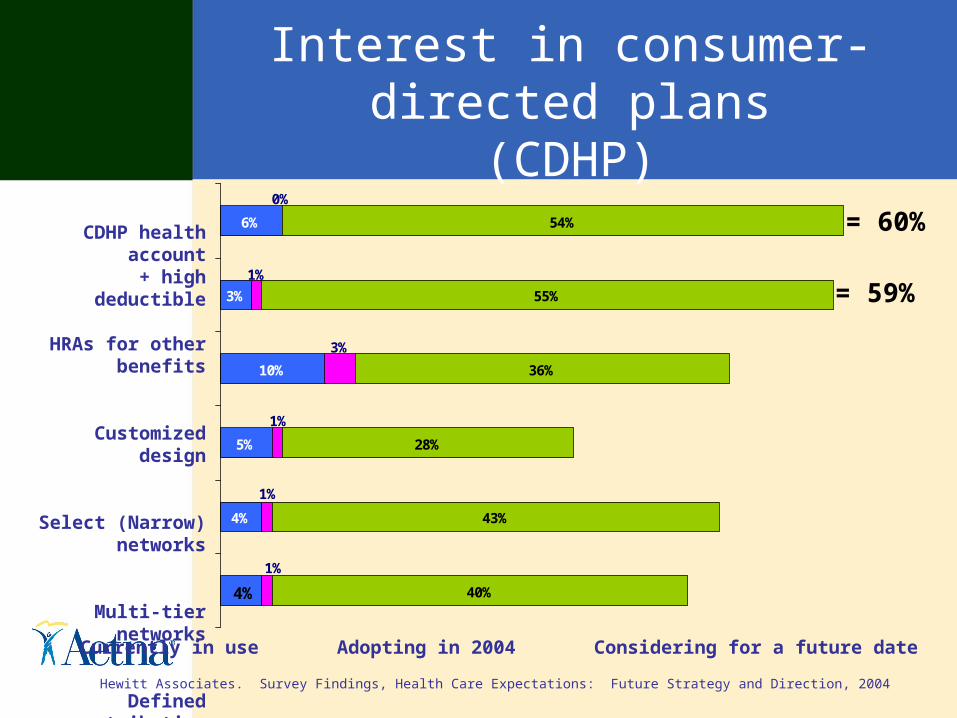
Interest in consumer-directed plans(CDHP)
4%
5%
10%
3%
6%
40%
43%
28%
36%
55%
54%
4%
1%
3%
1%
0%
1%
1%
CDHP health account + high deductible
HRAs for other benefits
Customized design
Select (Narrow) networks
Multi-tier networks
Defined contribution
Currently in use Adopting in 2004 Considering for a future date
Hewitt Associates. Survey Findings, Health Care Expectations: Future Strategy and Direction, 2004
= 59%
= 60%

Estimated CDHP adoption
1% 2% 3% 7% 12% 19% 24%4% 4% 4%
4%4%
4%4%
26% 26% 26%26%
25%
25%24%
52% 51% 49% 47% 43%38%
35%
18% 18% 18% 17% 16% 15% 13%
2004 2005 2006 2007 2008 2009 2010
POSPPOHMOConventionalConsumer-directed health plans
(percentages may not total 100 because of rounding)
Forrester Research, Inc., 2003
Other considerations
• Protecting vulnerable populations– Preventive benefits– Chronic disease coverage
• Contribution strategies– Higher contributions for lower-paid– Anticipating retirement
• Employee choice– Retaining traditional plan options– Member-selectable benefits – Buy-up options
• Trade-offs– Salary, bonus, severance, other benefits
Further change is needed
• Fully engaging consumers– Better cost and quality information– Reliable, trusted information on optimal
treatments– Consumer-relevant pricing models;
simplicity and disclosure– Targeted clinical support and financial risk
protection– New value options in care (e.g., Minute
Clinics, lower-cost pharmaceuticals)– Greater long-term savings… and still some challenging social choices
Related Documents




![[Friederike Klippel] Keep Talking Communicative F(BookFi.org)](https://static.cupdf.com/doc/110x72/56d6bfe01a28ab3016980726/friederike-klippel-keep-talking-communicative-fbookfiorg.jpg)






