Health-related quality of life in HIV-1-infected patients on HAART: a five-years longitudinal analysis accounting for dropout in the APROCO-COPILOTE cohort (ANRS CO-8) Camelia Protopopescu Fabienne Marcellin Bruno Spire Marie Pre ´au Renaud Verdon Dominique Peyramond Franc ¸ois Raffi Genevie `ve Che ˆne Catherine Leport Maria-Patrizia Carrieri Received: 18 April 2006 / Accepted: 21 November 2006 / Published online: 1 February 2007 ȑ Springer Science+Business Media B.V. 2007 Abstract Background The long-term efficacy of Highly Active Antiretroviral Therapies (HAART) has enlightened the crucial role of health-related quality of life (HRQL) among HIV-infected patients. However, any analysis of such extensive longitudinal data necessi- tates a suitable handling of dropout which may corre- late with patients’ health status. Methods We analysed the HRQL evolution over 5 years for 1,000 patients initiating a protease inhibitor (PI)-containing therapy, using MOS SF-36 physical (PCS) and mental (MCS) scores. In parallel with a classical separate random effects model, we used a joint parameter-dependent selection model to account for non-ignorable dropout. Results HRQL evolved according to a two-phase pattern, characterized by an initial improvement during the year following HAART initiation and a relative stabilization thereafter. Immunodepression and self-reported side effects were found to be nega- tive predictors of both PCS and MCS scores. Hepatitis C virus coinfection and AIDS clinical stage were found to affect physical HRQL. Results were not significantly altered when accounting for dropout. Conclusion Such results, obtained on a large sample of HIV-infected patients with extensive follow-up, underline the need for a regular monitoring of patients’ immunological status and for a better management of their experience with hepatitis C and HAART. Keywords HIV HAART Quality of life Hepatitis C Dropout Introduction The introduction of Highly Active Antiretroviral Therapies (HAART) has led to a progressive decline in HIV-related mortality [1]. With HIV infection considered as a chronic illness, health-related quality of life (HRQL) has become an important marker in the follow-up of HIV-infected patients. In this context, our study aimed at analysing HRQL long-term evo- lution after initiation of a protease inhibitor (PI)-con- taining therapy and the clinical and sociobehavioral factors associated to HRQL changes. To that end, we C. Protopopescu F. Marcellin B. Spire M. Pre ´au M.-P. Carrieri Health and Medical Research National Institute (INSERM), Research Unit 379, Social Sciences Applied to Medical Innovation, 23, rue Stanislas Torrents, 13006 Marseilles, France C. Protopopescu (&) F. Marcellin B. Spire M. Pre ´au M.-P. Carrieri Southeastern Health Regional Observatory (ORS-PACA), 23, rue Stanislas Torrents, 13006 Marseilles, France e-mail: [email protected] R. Verdon CHU de la Co ˆ te de Nacre, Caen, France D. Peyramond Croix-Rousse Hospital, Lyon, France F. Raffi Ho ˆ tel-Dieu, Nantes, France G. Che ˆne INSERM Research Unit 330, Bordeaux, France C. Leport Faculte ´ Xavier Bichat, Paris, France 123 Qual Life Res (2007) 16:577–591 DOI 10.1007/s11136-006-9151-7

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Health-related quality of life in HIV-1-infected patients onHAART: a five-years longitudinal analysis accounting fordropout in the APROCO-COPILOTE cohort (ANRS CO-8)
Camelia Protopopescu Æ Fabienne Marcellin Æ Bruno Spire Æ Marie Preau ÆRenaud Verdon Æ Dominique Peyramond Æ Francois Raffi Æ Genevieve Chene ÆCatherine Leport Æ Maria-Patrizia Carrieri
Received: 18 April 2006 / Accepted: 21 November 2006 / Published online: 1 February 2007� Springer Science+Business Media B.V. 2007
Abstract
Background The long-term efficacy of Highly Active
Antiretroviral Therapies (HAART) has enlightened
the crucial role of health-related quality of life
(HRQL) among HIV-infected patients. However, any
analysis of such extensive longitudinal data necessi-
tates a suitable handling of dropout which may corre-
late with patients’ health status.
Methods We analysed the HRQL evolution over
5 years for 1,000 patients initiating a protease inhibitor
(PI)-containing therapy, using MOS SF-36 physical
(PCS) and mental (MCS) scores. In parallel with a
classical separate random effects model, we used a
joint parameter-dependent selection model to account
for non-ignorable dropout.
Results HRQL evolved according to a two-phase
pattern, characterized by an initial improvement
during the year following HAART initiation and a
relative stabilization thereafter. Immunodepression
and self-reported side effects were found to be nega-
tive predictors of both PCS and MCS scores. Hepatitis
C virus coinfection and AIDS clinical stage were found
to affect physical HRQL. Results were not significantly
altered when accounting for dropout.
Conclusion Such results, obtained on a large sample
of HIV-infected patients with extensive follow-up,
underline the need for a regular monitoring of patients’
immunological status and for a better management of
their experience with hepatitis C and HAART.
Keywords HIV � HAART � Quality of life �Hepatitis C � Dropout
Introduction
The introduction of Highly Active Antiretroviral
Therapies (HAART) has led to a progressive decline
in HIV-related mortality [1]. With HIV infection
considered as a chronic illness, health-related quality
of life (HRQL) has become an important marker in
the follow-up of HIV-infected patients. In this context,
our study aimed at analysing HRQL long-term evo-
lution after initiation of a protease inhibitor (PI)-con-
taining therapy and the clinical and sociobehavioral
factors associated to HRQL changes. To that end, we
C. Protopopescu � F. Marcellin � B. Spire �M. Preau � M.-P. CarrieriHealth and Medical Research National Institute(INSERM), Research Unit 379, Social Sciences Applied toMedical Innovation, 23, rue Stanislas Torrents, 13006Marseilles, France
C. Protopopescu (&) � F. Marcellin � B. Spire �M. Preau � M.-P. CarrieriSoutheastern Health Regional Observatory (ORS-PACA),23, rue Stanislas Torrents, 13006 Marseilles, Francee-mail: [email protected]
R. VerdonCHU de la Cote de Nacre, Caen, France
D. PeyramondCroix-Rousse Hospital, Lyon, France
F. RaffiHotel-Dieu, Nantes, France
G. CheneINSERM Research Unit 330, Bordeaux, France
C. LeportFaculte Xavier Bichat, Paris, France
123
Qual Life Res (2007) 16:577–591
DOI 10.1007/s11136-006-9151-7

used data collected among HIV-infected patients from
a French cohort study (APROCO-COPILOTE -
ANRS CO8) during 5 years after enrolment. However,
such longitudinal data always present missing assess-
ments due to patients’ temporary (missed clinical visit
or non-response to a questionnaire) or permanent
withdrawal from the study. The probability of with-
drawal may depend on HRQL itself, as for instance,
patients with low HRQL may be more likely to leave
the study than the others. In this case, the underlying
dropout process is informative or non ignorable, fol-
lowing the terminology of Little et al. [2], and valid
results for longitudinal inference can be obtained only
if this process is explicitly modelled [3]. Different
methods have been developed to address this issue
[4–7]. Guo and Carlin proposed a joint modelling of
longitudinal and event time data using Bayesian
methods [8]. We adapted this modelling approach to
the analysis of our study data, then we compared the
obtained results with those of the standard approach,
which does not take into account the possibly
non-ignorable dropout.
Methods
Study population
The French APROCO-COPILOTE (ANRS CO-8)
multicenter cohort study, setup in 1997, aimed at
describing clinical, immunological, virological and
socio-behavioral characteristics of HIV-1-infected
patients who were beginning combination antiretrovi-
ral therapy (HAART) that included a PI [9]. Entry in
the cohort (Month 0, M0) corresponded to the begin-
ning of combination therapy. Along with clinical and
socio-demographic data collection, which have been
extensively described elsewhere [9, 10], follow-up of
patients included longitudinal assessment of HRQL
using the Medical Outcome Study 36-item Short Form
Health Survey (MOS SF-36) [11–13] validated in
French [14, 15]. This self-administered questionnaire is
designed to analyse eight health concepts, each related
to a physical or mental dimension of HRQL. The
corresponding scores, converted into a scale ranging
from 0 to 100, can be combined to obtain two aggre-
gate scores: the physical component summary (PCS)
and the mental component summary (MCS), with high
scores corresponding to better HRQL. Patients were
asked to complete the MOS SF-36 questionnaire at
baseline (M0), and a total of six other measures were
collected during the follow-up: at 12 months (M12), at
28 months (M28), then every 8 months thereafter until
Month 60 (M60).
Statistical methods
The longitudinal evolution between M0 and M60 of the
PCS and MCS scores was analysed using linear models.
Scores were log-transformed (–ln(100 – PCS) and
–ln(100 – MCS)) in order to satisfy normality and het-
eroskedasticity assumptions. Factors associated with
physical and mental HRQL evolution were explored
among patients’ sociodemographic, behavioral and
HIV-related characteristics: age, gender, geographic
origin, stability and comfort of housing conditions,
presence of a stable partner, daily alcohol consumption,
HIV transmission group (homosexuals, intravenous
drug users IDU, others), antiretroviral naivety, CD4
count (<200 cells/mm3), number of self-reported
symptoms of lipodystrophy, number of self-reported
treatments’ side-effects excluding lipodystrophy.
In a first approach (separate modelling), HRQL
scores evolution was analysed using a random effects
or mixed model, where all missing data are considered
missing at random (MAR), cf. Little et al. [2]. As
descriptive analyses clearly showed a two-phase evo-
lution in HRQL scores with a change in the slope
1 year after initiation of combination therapy (Fig. 1a
and 1b), a piecewise linear model with a change point
at M12 was chosen for this analysis. Each factor con-
tribution to the model was made of three covariates: a
first one representing the principal effect of the factor,
and two interaction-with-time variables (slopes) rep-
resenting respectively the changes in the short-time
effect of the factor (M0–M12), and the changes in the
effect of the factor during the maintenance phase of
the treatment (M12–M60). For example, a positive
principal effect followed by a negative first slope,
smaller in absolute value, and a non-significant second
slope means that the corresponding factor has a global
positive effect on the response variable during the
study period, but this effect decreases during the first
year, then does not change significatively after M12.
The effect of each factor on patients’ HRQL was first
tested in univariate analyses, and the factors which
achieved a significance of P < .2 were considered eli-
gible for the multivariate model. The two interactions
with time were included in the multivariate model if at
least one of them was significant in the univariate
analysis (P < .2). The final multivariate model was
determined using likelihood ratio tests to validate the
number of random effects used and backward analyses
with P < .2 threshold for the selection of factors.
578 Qual Life Res (2007) 16:577–591
123
Patients drop out at a given visit if no HRQL
assessment is available from this visit onward (until
M60). This way, patients are defined as ‘‘drop out’’ for
HRQL if the last available measure occurs before M60
(censoring time). A discrete analogue of the continu-
ous proportional hazards (Cox) model [16] was used to
analyse separately the interval-censored time-to-drop-
out data. In this model, the effect of each factor can be
interpreted as in the classical Cox model.
In a second approach (joint modelling), HRQL
scores and time-to-dropout were simultaneously mod-
elled using the shared-parameter selection type-model
proposed by Henderson et al. [17] and Guo and Carlin
[8]. In this joint approach, the possible correlation
between the longitudinal and the time-to-dropout
models is modelled through two latent random vari-
ables and the common explanatory variables. Missing
data due to dropout are considered as non-ignorable,
while intermittent missing data are considered MAR.
All the analyses were performed using log-transformed
scores. In addition, each factor contribution to HRQL
between M0 and M12 was given for the untransformed
scores after translation back onto their original scale
(see Appendix). All the analyses were performed using
SAS software, version 9.1 for Windows [18]. A detailed
description of the statistical models and the SAS codes
are supplied in the Appendix.
Results
Description of dataset
Of the 1,281 patients who were enrolled in the AP-
ROCO-COPILOTE cohort (ANRS CO-8), 1,000 pa-
tients had completed the MOS SF-36 questionnaire at
M0, and were thus included in the analysis. There were
no significant differences in gender and viral load at
baseline between these patients and the 281 non-
respondents to the questionnaire. Respondents in-
cluded significantly higher proportions of young pa-
tients, patients infected through homosexual contacts,
patients not at AIDS-stage, and patients with low
baseline CD4 count (<200 cells/mm3) (data not shown).
Socio-demographic and clinical characteristics at
enrolment of the 1,000 study patients are presented in
Table 1.
n=1000 626 452 412 395 338 238
4949
.550
50.5
5151
.5
PC
S
0 12 28 36 44 52 60
Time (months)
Mean PCS Untransformed score SEs
Mean PCS Untransformed score SEs
n=1000 626 452 412 395 338 2384042
4446
48
MC
S
0 12 28 36 44 52 60
Time (months)
(a)
(b)
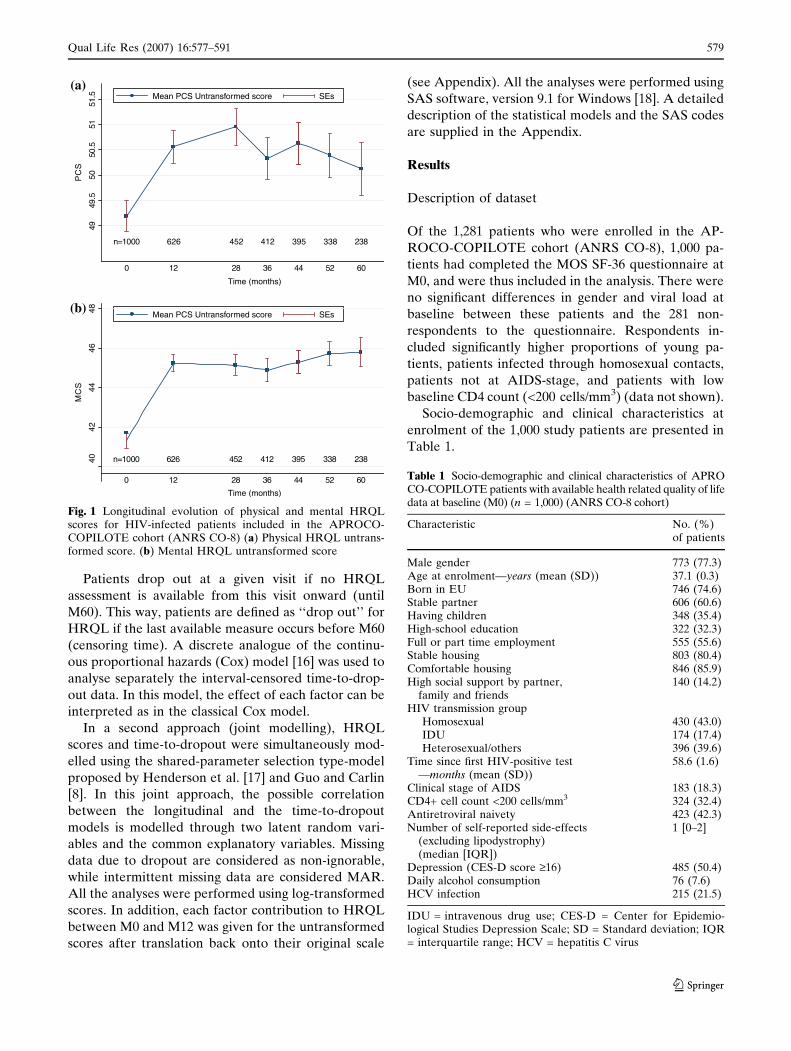
Fig. 1 Longitudinal evolution of physical and mental HRQLscores for HIV-infected patients included in the APROCO-COPILOTE cohort (ANRS CO-8) (a) Physical HRQL untrans-formed score. (b) Mental HRQL untransformed score
Table 1 Socio-demographic and clinical characteristics of APROCO-COPILOTE patients with available health related quality of lifedata at baseline (M0) (n = 1,000) (ANRS CO-8 cohort)
Characteristic No. (%)of patients
Male gender 773 (77.3)Age at enrolment—years (mean (SD)) 37.1 (0.3)Born in EU 746 (74.6)Stable partner 606 (60.6)Having children 348 (35.4)High-school education 322 (32.3)Full or part time employment 555 (55.6)Stable housing 803 (80.4)Comfortable housing 846 (85.9)High social support by partner,
family and friends140 (14.2)
HIV transmission groupHomosexual 430 (43.0)IDU 174 (17.4)Heterosexual/others 396 (39.6)
Time since first HIV-positive test—months (mean (SD))
58.6 (1.6)
Clinical stage of AIDS 183 (18.3)CD4+ cell count <200 cells/mm3 324 (32.4)Antiretroviral naivety 423 (42.3)Number of self-reported side-effects
(excluding lipodystrophy)(median [IQR])
1 [0–2]
Depression (CES-D score ‡16) 485 (50.4)Daily alcohol consumption 76 (7.6)HCV infection 215 (21.5)
IDU = intravenous drug use; CES-D = Center for Epidemio-logical Studies Depression Scale; SD = Standard deviation; IQR= interquartile range; HCV = hepatitis C virus
Qual Life Res (2007) 16:577–591 579
123
Most patients were male, natives of European
countries, mean age (SD) was 37.1 (0.3) years. There
were 174 patients (17.4%) infected through IDU, and
430 (43%) infected through homosexual contact. Mean
time (SD) since first HIV-positive test was 58.6 (1.6)
months. CD4 count was below 200 cells/mm3 in 32.4%
of patients, with a median [IQR] of 293 [154–440] cells/
mm3. As stated in the inclusion criteria, all patients
initiated an antiretroviral combination including a PI at
M0. Forty-two percent of patients had never received
antiretroviral therapy before (antiretroviral naive
patients). These patients had a significantly more
advanced HIV disease at baseline, characterized by a
CD4 count below 200 cells/mm3. They were also more
likely than the other patients to have unstable housing
conditions and to be infected through IDU. About one
fifth of all patients were coinfected with hepatitis C virus
(HCV). Between M0 and M60, a total of 78 patients died
and 46 patients signed a withdrawal request form.
We censored these 124 patients in the time to dropout
analysis, as we cannot consider that their quality of life
was observed at the time of dropout. The missing
HRQL data (intermittent and drop-out from the study)
for non-censored patients are due either to a missed
clinical visit, to a non-response to a self-administered
questionnaire or to a lost to follow-up. The proportion
of dropouts is quite high in this study: 37.4% of the 1,000
patients have dropped out after 1 year and 76.2% after
5 years. The distributions of the original aggregate PCS
and MCS scores and the number of individuals still in
the study at each of the seven dataset time points are
presented respectively in Fig. 1a, b.
Results using separate modelling
Multivariate random effects models estimated signifi-
cant positive slopes for both PCS and MCS scores from
M0 to M12 (‘‘Slope 1’’ in Tables 2a, 3a), thereby
underlining the increase in these two scores observed in
the first year after PI introduction (Fig. 1a, b). Slopes
estimated thereafter (‘‘Slope 2’’) were non-significantly
different from zero, underlining a relative stabilization
of the scores after M12, after accounting for the effect
of covariates.
Age, parenthood, experience of AIDS-defining
events and HCV coinfection were found to be inde-
pendent negative predictors of PCS score, while high
education level and homosexual HIV transmission
were associated with higher levels of physical HRQL.
CD4 count below 200 cells/mm3 and number of self-
reported treatment’ side effects excluding lipodystro-
phy were found to be negatively associated with both
physical and mental HRQL scores. However, the
impact of side effects on HRQL decreased over time,
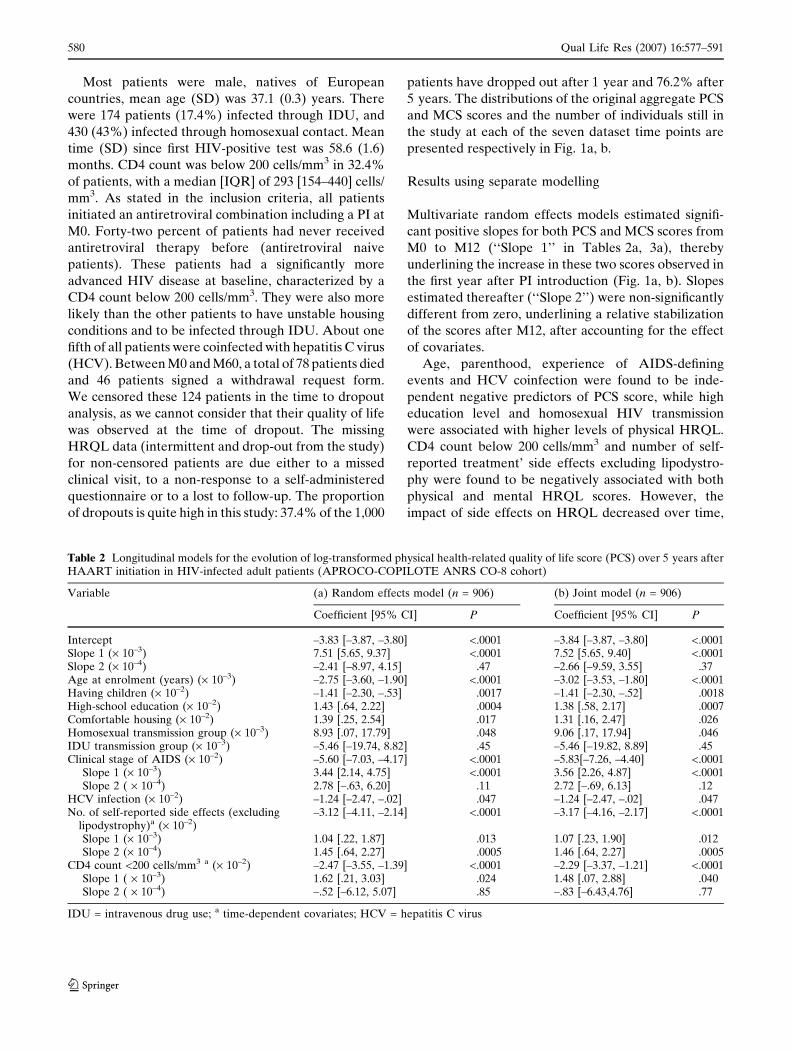
Table 2 Longitudinal models for the evolution of log-transformed physical health-related quality of life score (PCS) over 5 years afterHAART initiation in HIV-infected adult patients (APROCO-COPILOTE ANRS CO-8 cohort)
Variable (a) Random effects model (n = 906) (b) Joint model (n = 906)
Coefficient [95% CI] P Coefficient [95% CI] P
Intercept –3.83 [–3.87, –3.80] <.0001 –3.84 [–3.87, –3.80] <.0001Slope 1 (· 10–3) 7.51 [5.65, 9.37] <.0001 7.52 [5.65, 9.40] <.0001Slope 2 (· 10–4) –2.41 [–8.97, 4.15] .47 –2.66 [–9.59, 3.55] .37Age at enrolment (years) (· 10–3) –2.75 [–3.60, –1.90] <.0001 –3.02 [–3.53, –1.80] <.0001Having children (· 10–2) –1.41 [–2.30, –.53] .0017 –1.41 [–2.30, –.52] .0018High-school education (· 10–2) 1.43 [.64, 2.22] .0004 1.38 [.58, 2.17] .0007Comfortable housing (· 10–2) 1.39 [.25, 2.54] .017 1.31 [.16, 2.47] .026Homosexual transmission group (· 10–3) 8.93 [.07, 17.79] .048 9.06 [.17, 17.94] .046IDU transmission group (· 10–3) –5.46 [–19.74, 8.82] .45 –5.46 [–19.82, 8.89] .45Clinical stage of AIDS (· 10–2) –5.60 [–7.03, –4.17] <.0001 –5.83[–7.26, –4.40] <.0001
Slope 1 (· 10–3) 3.44 [2.14, 4.75] <.0001 3.56 [2.26, 4.87] <.0001Slope 2 ( · 10–4) 2.78 [–.63, 6.20] .11 2.72 [–.69, 6.13] .12
HCV infection (· 10–2) –1.24 [–2.47, –.02] .047 –1.24 [–2.47, –.02] .047No. of self-reported side effects (excluding
lipodystrophy)a (· 10–2)–3.12 [–4.11, –2.14] <.0001 –3.17 [–4.16, –2.17] <.0001
Slope 1 (· 10–3) 1.04 [.22, 1.87] .013 1.07 [.23, 1.90] .012Slope 2 (· 10–4) 1.45 [.64, 2.27] .0005 1.46 [.64, 2.27] .0005
CD4 count <200 cells/mm3 a (· 10–2) –2.47 [–3.55, –1.39] <.0001 –2.29 [–3.37, –1.21] <.0001Slope 1 ( · 10–3) 1.62 [.21, 3.03] .024 1.48 [.07, 2.88] .040Slope 2 ( · 10–4) –.52 [–6.12, 5.07] .85 –.83 [–6.43,4.76] .77
IDU = intravenous drug use; a time-dependent covariates; HCV = hepatitis C virus
580 Qual Life Res (2007) 16:577–591
123
as shown by the significant positive associated slopes.
In the same way, the impact of low CD4 count on
physical HRQL progressively decreased during the
first year of the follow-up, remaining constant there-
after. Having comfortable housing conditions was the
only positive predictor of both physical and mental
HRQL, but its impact on mental HRQL also de-
creased between M0 and M12. Additional predictors
of better mental HRQL were male gender and pres-
ence of a stable partner. HIV transmission through
IDU and number of self-reported symptoms of lip-
odystrophy1 were negatively associated with mental
HRQL score. The impact of antiretroviral naivety on
mental HRQL had a varying pattern over time: neg-
ative at baseline, positive at M12 and re-becoming
negative during the maintenance phase (M12–M60).
Depressive symptomatology, defined as a score ‡16 in
the French version of the Center for Epidemiological
Studies Depression Scale CES-D [19], was collinear
with poor mental HRQL, as 64% of patients with
CES-D score over 16 had mental HRQL below the
first quartile. Thus, depression could be considered to
be more a proxy than an explanatory variable of the
patients’ mental health status.
Results from the separate analysis for the dropout
process are presented in Table 4a.
Socio-demographic and behavioral characteristics
that were found independently associated with a higher
risk of dropout were: female gender, younger age,
difficult housing conditions (unstable or uncomfortable
housing), non-European origin and daily consumption
of alcohol (average number of alcohol units per day ‡1
[20]). Concerning HIV-related characteristics, risk
factors for a dropout included: homosexual and IDU
transmission, antiretroviral naivety and CD4 count
below 200 cells/mm3.
Results using joint modelling
Results using joint modelling of HRQL scores and
dropout process are presented in Tables 2b, 3b and 4b.
The coefficients associated with significant predictors
of HRQL estimated with the joint model were similar
to those obtained with separate models. Changes did
not exceed 10% in magnitude, except for the coeffi-
cient associated with the number of self-reported
symptoms of lipodystrophy, whose absolute value
changed by a rate of 11% between separate and joint
modelling. However, the 95% confidence intervals
obtained with the two methods for this coefficient
overlapped greatly. Some of the dropout model coef-
ficients exhibited marked changes, but remained in the
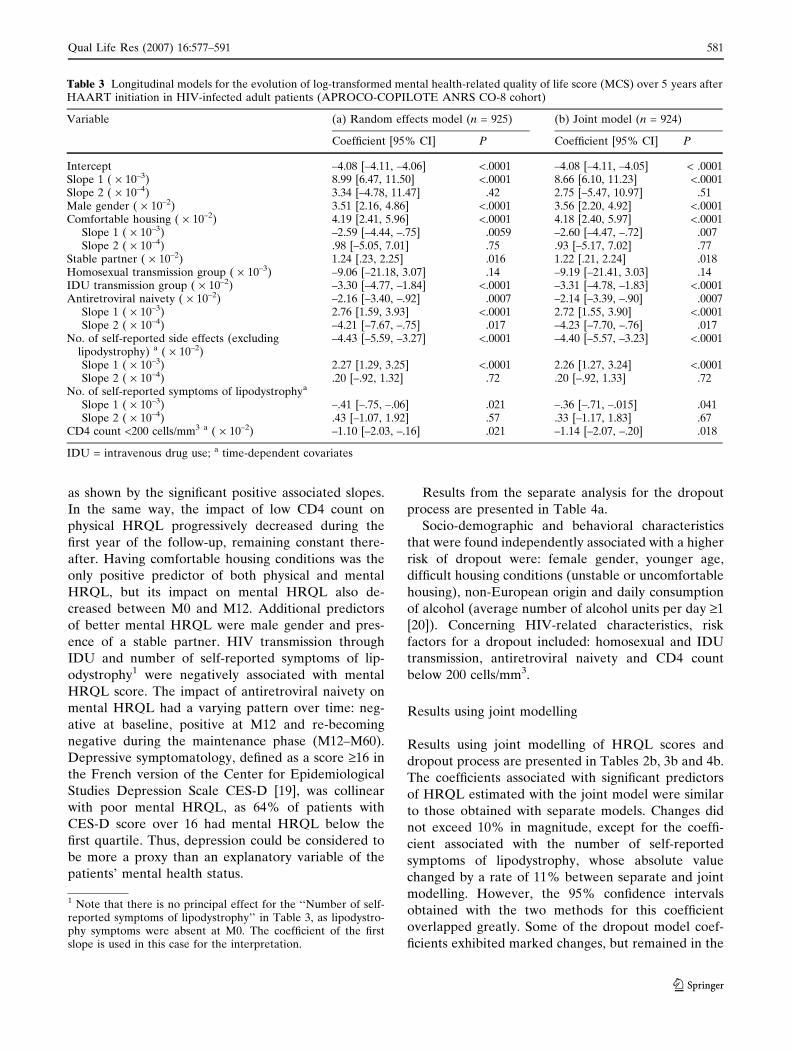
Table 3 Longitudinal models for the evolution of log-transformed mental health-related quality of life score (MCS) over 5 years afterHAART initiation in HIV-infected adult patients (APROCO-COPILOTE ANRS CO-8 cohort)
Variable (a) Random effects model (n = 925) (b) Joint model (n = 924)
Coefficient [95% CI] P Coefficient [95% CI] P
Intercept –4.08 [–4.11, –4.06] <.0001 –4.08 [–4.11, –4.05] < .0001Slope 1 ( · 10–3) 8.99 [6.47, 11.50] <.0001 8.66 [6.10, 11.23] <.0001Slope 2 ( · 10–4) 3.34 [–4.78, 11.47] .42 2.75 [–5.47, 10.97] .51Male gender ( · 10–2) 3.51 [2.16, 4.86] <.0001 3.56 [2.20, 4.92] <.0001Comfortable housing ( · 10–2) 4.19 [2.41, 5.96] <.0001 4.18 [2.40, 5.97] <.0001
Slope 1 ( · 10–3) –2.59 [–4.44, –.75] .0059 –2.60 [–4.47, –.72] .007Slope 2 ( · 10–4) .98 [–5.05, 7.01] .75 .93 [–5.17, 7.02] .77
Stable partner ( · 10–2) 1.24 [.23, 2.25] .016 1.22 [.21, 2.24] .018Homosexual transmission group ( · 10–3) –9.06 [–21.18, 3.07] .14 –9.19 [–21.41, 3.03] .14IDU transmission group ( · 10–2) –3.30 [–4.77, –1.84] <.0001 –3.31 [–4.78, –1.83] <.0001Antiretroviral naivety ( · 10–2) –2.16 [–3.40, –.92] .0007 –2.14 [–3.39, –.90] .0007
Slope 1 ( · 10–3) 2.76 [1.59, 3.93] <.0001 2.72 [1.55, 3.90] <.0001Slope 2 ( · 10–4) –4.21 [–7.67, –.75] .017 –4.23 [–7.70, –.76] .017
No. of self-reported side effects (excludinglipodystrophy) a ( · 10–2)
–4.43 [–5.59, –3.27] <.0001 –4.40 [–5.57, –3.23] <.0001
Slope 1 ( · 10–3) 2.27 [1.29, 3.25] <.0001 2.26 [1.27, 3.24] <.0001Slope 2 ( · 10–4) .20 [–.92, 1.32] .72 .20 [–.92, 1.33] .72
No. of self-reported symptoms of lipodystrophya
Slope 1 ( · 10–3) –.41 [–.75, –.06] .021 –.36 [–.71, –.015] .041Slope 2 ( · 10–4) .43 [–1.07, 1.92] .57 .33 [–1.17, 1.83] .67
CD4 count <200 cells/mm3 a ( · 10–2) –1.10 [–2.03, –.16] .021 –1.14 [–2.07, –.20] .018
IDU = intravenous drug use; a time-dependent covariates
1 Note that there is no principal effect for the ‘‘Number of self-reported symptoms of lipodystrophy’’ in Table 3, as lipodystro-phy symptoms were absent at M0. The coefficient of the firstslope is used in this case for the interpretation.
Qual Life Res (2007) 16:577–591 581
123
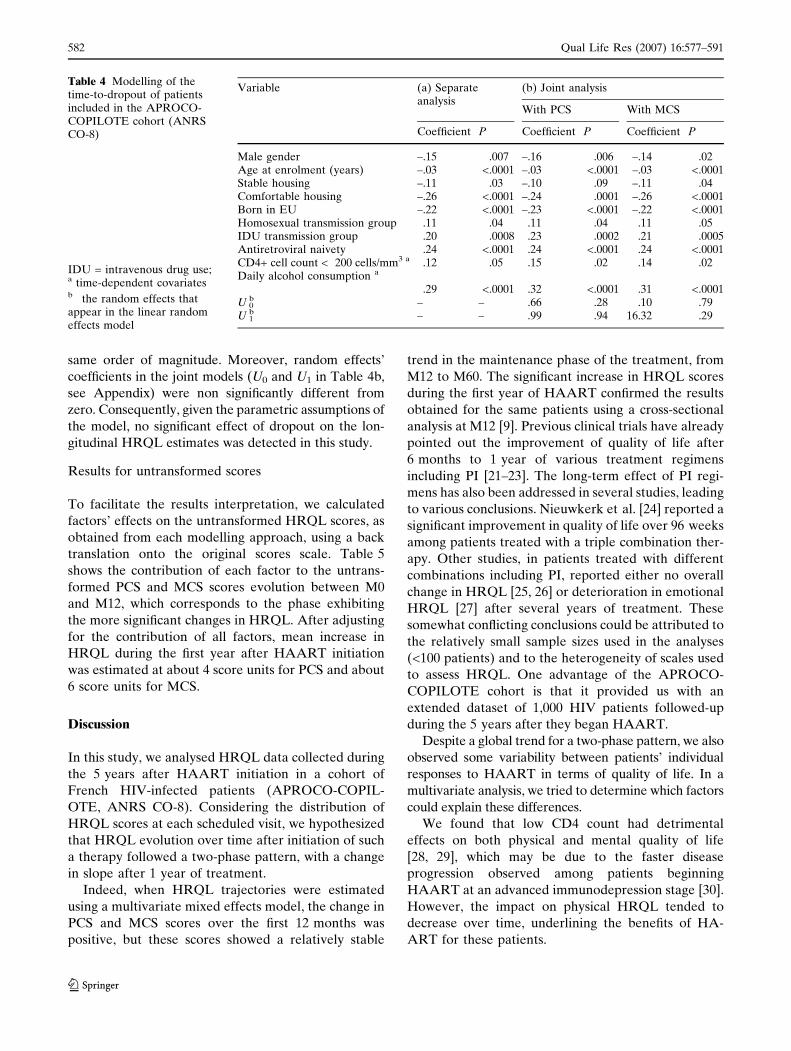
same order of magnitude. Moreover, random effects’
coefficients in the joint models (U0 and U1 in Table 4b,
see Appendix) were non significantly different from
zero. Consequently, given the parametric assumptions of
the model, no significant effect of dropout on the lon-
gitudinal HRQL estimates was detected in this study.
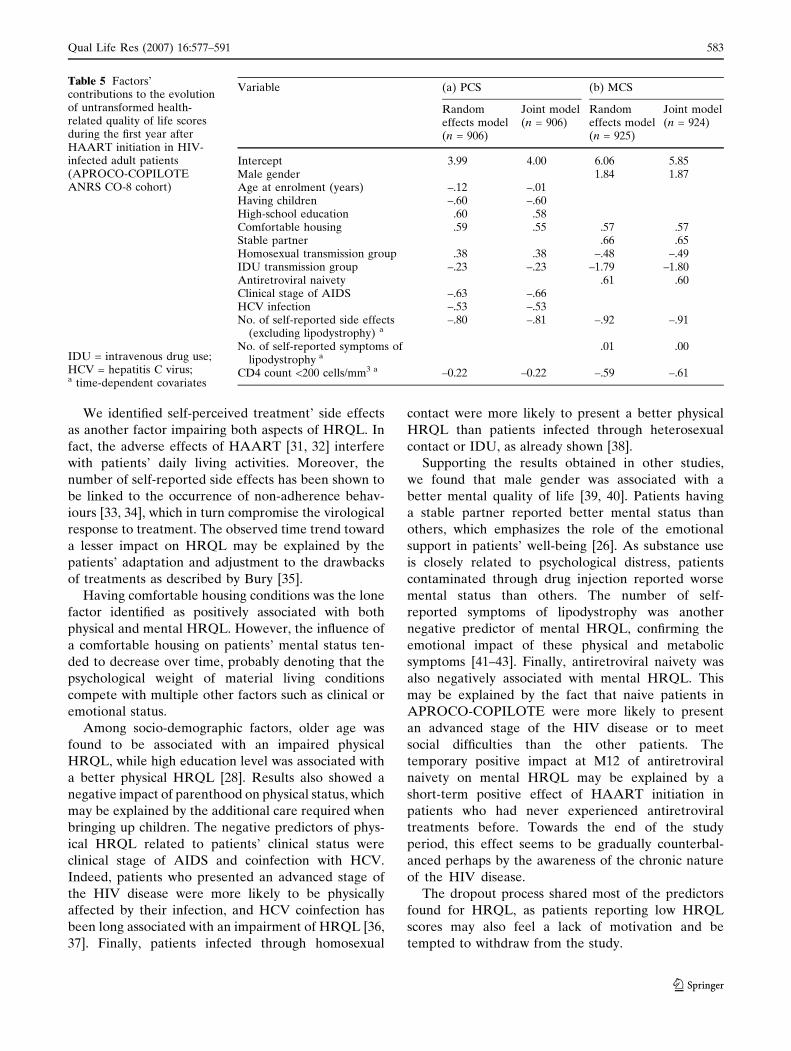
Results for untransformed scores
To facilitate the results interpretation, we calculated
factors’ effects on the untransformed HRQL scores, as
obtained from each modelling approach, using a back
translation onto the original scores scale. Table 5
shows the contribution of each factor to the untrans-
formed PCS and MCS scores evolution between M0
and M12, which corresponds to the phase exhibiting
the more significant changes in HRQL. After adjusting
for the contribution of all factors, mean increase in
HRQL during the first year after HAART initiation
was estimated at about 4 score units for PCS and about
6 score units for MCS.
Discussion
In this study, we analysed HRQL data collected during
the 5 years after HAART initiation in a cohort of
French HIV-infected patients (APROCO-COPIL-
OTE, ANRS CO-8). Considering the distribution of
HRQL scores at each scheduled visit, we hypothesized
that HRQL evolution over time after initiation of such
a therapy followed a two-phase pattern, with a change
in slope after 1 year of treatment.
Indeed, when HRQL trajectories were estimated
using a multivariate mixed effects model, the change in
PCS and MCS scores over the first 12 months was
positive, but these scores showed a relatively stable
trend in the maintenance phase of the treatment, from
M12 to M60. The significant increase in HRQL scores
during the first year of HAART confirmed the results
obtained for the same patients using a cross-sectional
analysis at M12 [9]. Previous clinical trials have already
pointed out the improvement of quality of life after
6 months to 1 year of various treatment regimens
including PI [21–23]. The long-term effect of PI regi-
mens has also been addressed in several studies, leading
to various conclusions. Nieuwkerk et al. [24] reported a
significant improvement in quality of life over 96 weeks
among patients treated with a triple combination ther-
apy. Other studies, in patients treated with different
combinations including PI, reported either no overall
change in HRQL [25, 26] or deterioration in emotional
HRQL [27] after several years of treatment. These
somewhat conflicting conclusions could be attributed to
the relatively small sample sizes used in the analyses
(<100 patients) and to the heterogeneity of scales used
to assess HRQL. One advantage of the APROCO-
COPILOTE cohort is that it provided us with an
extended dataset of 1,000 HIV patients followed-up
during the 5 years after they began HAART.
Despite a global trend for a two-phase pattern, we also
observed some variability between patients’ individual
responses to HAART in terms of quality of life. In a
multivariate analysis, we tried to determine which factors
could explain these differences.
We found that low CD4 count had detrimental
effects on both physical and mental quality of life
[28, 29], which may be due to the faster disease
progression observed among patients beginning
HAART at an advanced immunodepression stage [30].
However, the impact on physical HRQL tended to
decrease over time, underlining the benefits of HA-
ART for these patients.
Table 4 Modelling of thetime-to-dropout of patientsincluded in the APROCO-COPILOTE cohort (ANRSCO-8)
IDU = intravenous drug use;a time-dependent covariatesb the random effects thatappear in the linear randomeffects model
Variable (a) Separateanalysis
(b) Joint analysis
With PCS With MCS
Coefficient P Coefficient P Coefficient P
Male gender –.15 .007 –.16 .006 –.14 .02Age at enrolment (years) –.03 <.0001 –.03 <.0001 –.03 <.0001Stable housing –.11 .03 –.10 .09 –.11 .04Comfortable housing –.26 <.0001 –.24 .0001 –.26 <.0001Born in EU –.22 <.0001 –.23 <.0001 –.22 <.0001Homosexual transmission group .11 .04 .11 .04 .11 .05IDU transmission group .20 .0008 .23 .0002 .21 .0005Antiretroviral naivety .24 <.0001 .24 <.0001 .24 <.0001CD4+ cell count < 200 cells/mm3 a .12 .05 .15 .02 .14 .02Daily alcohol consumption a
.29 <.0001 .32 <.0001 .31 <.0001U 0
b – – .66 .28 .10 .79U 1
b – – .99 .94 16.32 .29
582 Qual Life Res (2007) 16:577–591
123
We identified self-perceived treatment’ side effects
as another factor impairing both aspects of HRQL. In
fact, the adverse effects of HAART [31, 32] interfere
with patients’ daily living activities. Moreover, the
number of self-reported side effects has been shown to
be linked to the occurrence of non-adherence behav-
iours [33, 34], which in turn compromise the virological
response to treatment. The observed time trend toward
a lesser impact on HRQL may be explained by the
patients’ adaptation and adjustment to the drawbacks
of treatments as described by Bury [35].
Having comfortable housing conditions was the lone
factor identified as positively associated with both
physical and mental HRQL. However, the influence of
a comfortable housing on patients’ mental status ten-
ded to decrease over time, probably denoting that the
psychological weight of material living conditions
compete with multiple other factors such as clinical or
emotional status.
Among socio-demographic factors, older age was
found to be associated with an impaired physical
HRQL, while high education level was associated with
a better physical HRQL [28]. Results also showed a
negative impact of parenthood on physical status, which
may be explained by the additional care required when
bringing up children. The negative predictors of phys-
ical HRQL related to patients’ clinical status were
clinical stage of AIDS and coinfection with HCV.
Indeed, patients who presented an advanced stage of
the HIV disease were more likely to be physically
affected by their infection, and HCV coinfection has
been long associated with an impairment of HRQL [36,
37]. Finally, patients infected through homosexual
contact were more likely to present a better physical
HRQL than patients infected through heterosexual
contact or IDU, as already shown [38].
Supporting the results obtained in other studies,
we found that male gender was associated with a
better mental quality of life [39, 40]. Patients having
a stable partner reported better mental status than
others, which emphasizes the role of the emotional
support in patients’ well-being [26]. As substance use
is closely related to psychological distress, patients
contaminated through drug injection reported worse
mental status than others. The number of self-
reported symptoms of lipodystrophy was another
negative predictor of mental HRQL, confirming the
emotional impact of these physical and metabolic
symptoms [41–43]. Finally, antiretroviral naivety was
also negatively associated with mental HRQL. This
may be explained by the fact that naive patients in
APROCO-COPILOTE were more likely to present
an advanced stage of the HIV disease or to meet
social difficulties than the other patients. The
temporary positive impact at M12 of antiretroviral
naivety on mental HRQL may be explained by a
short-term positive effect of HAART initiation in
patients who had never experienced antiretroviral
treatments before. Towards the end of the study
period, this effect seems to be gradually counterbal-
anced perhaps by the awareness of the chronic nature
of the HIV disease.
The dropout process shared most of the predictors
found for HRQL, as patients reporting low HRQL
scores may also feel a lack of motivation and be
tempted to withdraw from the study.
Table 5 Factors’contributions to the evolutionof untransformed health-related quality of life scoresduring the first year afterHAART initiation in HIV-infected adult patients(APROCO-COPILOTEANRS CO-8 cohort)
IDU = intravenous drug use;HCV = hepatitis C virus;a time-dependent covariates
Variable (a) PCS (b) MCS
Randomeffects model(n = 906)
Joint model(n = 906)
Randomeffects model(n = 925)
Joint model(n = 924)
Intercept 3.99 4.00 6.06 5.85Male gender 1.84 1.87Age at enrolment (years) –.12 –.01Having children –.60 –.60High-school education .60 .58Comfortable housing .59 .55 .57 .57Stable partner .66 .65Homosexual transmission group .38 .38 –.48 –.49IDU transmission group –.23 –.23 –1.79 –1.80Antiretroviral naivety .61 .60Clinical stage of AIDS –.63 –.66HCV infection –.53 –.53No. of self-reported side effects
(excluding lipodystrophy) a–.80 –.81 –.92 –.91
No. of self-reported symptoms oflipodystrophy a
.01 .00
CD4 count <200 cells/mm3 a –0.22 –0.22 –.59 –.61
Qual Life Res (2007) 16:577–591 583
123

The method that we chose for the analyses taking
into account the dropout process (use of a shared
parameter selection model) enabled us to estimate
in a single model the effects of each patients’ char-
acteristics on the evolution of their HRQL and the
impact of the time that they spent on study. This is
of particular interest in the context of a longitudinal
cohort study, in which study dropouts are relatively
frequent. Indeed, patients who withdrew before the
end of the study may have a particular clinical
profile, covering a large number of cases from the
patient presenting a satisfying global health status
who do not feel the need of maintaining regular
clinical visits, to the one who is lost of follow-up
because of a worsening health status. The proposed
joint model, derived from the one presented by Guo
and Carlin [8], can be easily fitted using standard
packages such as the NLMIXED procedure of SAS
(see Appendix).
Two limitations of our study must be underlined.
First, the use of the MOS SF-36 generic psychometric
instrument may not allow to take into account all the
specificities of HIV infection. Although this instru-
ment showed satisfying validity and reliability prop-
erties in a recent study invoving HIV-infected patients
[44], it neglects some important dimensions of quality
of life, especially sexual affective and cognitive func-
tioning or sleep problems. Second, the analysis ex-
cluded patients who did not complete the MOS SF-36
questionnaire at enrolment. A descriptive analysis
showed that these patients had a worse HIV status at
baseline than respondents.
To conclude, our study brought to light the early
effects of HAART on HIV patients’ quality of life,
characterized by a significant increase in both physical
and mental HRQL scores occurring during the first
year of treatment. Data collected over 5 years of
HAART showed no overall change in HRQL scores
after this initial increase. In addition, our study iso-
lated both immunodepression and coinfection with
HCV as being two negative predictors of patients’
quality of life, along with the number of self-reported
side-effects, and underlined the role of lipodystrophy
symptoms on patients’ mental status. These results,
obtained on a large sample of HIV-infected patients
followed up during an extended period of time, con-
firm those of previous studies conducted on fewer
subjects with a cross-sectional design. They underline
the necessity to investigate and manage the patients’
perception of treatments’ adverse effects throughout
their clinical follow-up. Besides, they confirm the need
for a careful monitoring of viral comorbidities and for
a prompt management of therapeutic failure to ensure
patients’ well-being.
Acknowledgements The authors would like to thank all pa-tients, nurses and physicians in clinical sites. The APROCO-COPILOTE Study Group is composed of the follow-ing:Steering Committee: Principal Investigators: C. Leport, F.Raffi; Methodology: G. Chene, R. Salamon; Social Sciences:J-P. Moatti, J. Pierret , B. Spire; Virology: F. Brun-Vezinet,H. Fleury, B. Masquelier; Pharmacology: G. Peytavin, R.Garraffo.Scientific Committee: Members of Steering Commit-tee and other members: D. Costagliola, P. Dellamonica, C.Katlama, L. Meyer, M. Morin, D. Salmon, A. Sobel; Projectcoordination: F. Collin; Events Validation Committee: L.Cuzin, M. Dupon, X. Duval, V. Le Moing, B. Marchou, T.May, P. Morlat, C. Rabaud, A. Waldner-Combernoux; Clini-cal Research Group : V. Le Moing, C. Lewden.Clinical cen-ters: Amiens (Pr Schmit), Angers (Dr Chennebault), Belfort(Dr Faller), Besancon (Dr Estavoyer, Pr Laurent, Pr Vuit-ton), Bordeaux (Pr Beylot, Pr Lacut, Pr Le Bras, Pr Rag-naud), Bourg-en-Bresse (Dr Granier), Brest (Pr Garre), Caen(Pr Bazin), Compiegne (Dr Veyssier), Corbeil-Essonne (DrDevidas), Creteil (Pr Sobel), Dijon (Pr Portier), Garches (PrPerronne), Lagny (Dr Lagarde), Libourne (Dr Ceccaldi),Lyon (Pr Peyramond), Meaux (Dr Allard), Montpellier (PrReynes), Nancy (Pr Canton), Nantes (Pr Raffi), Nice (PrCassuto, Pr Dellamonica), Orleans (Dr Arsac), Paris (PrBricaire, Pr Caulin, Pr Frottier, Pr Herson, Pr Imbert, DrMalkin, Pr Rozenbaum, Pr Sicard, Pr Vachon, Pr Vilde),Poitiers (Pr Becq-Giraudon), Reims (Pr Remy), Rennes (PrCartier), Saint-Etienne (Pr Lucht), Saint-Mande (Pr Roue),Strasbourg (Pr Lang), Toulon (Dr Jaureguiberry), Toulouse(Pr Massip), Tours (Pr Choutet).Data monitoring and statis-tical analysis: C. Alfaro, F. Alkaied, C. Barennes, S. Bouc-herit, AD. Bouhnik, C. Brunet-Francois, MP. Carrieri, JL.Ecobichon, V. El Fouikar, V. Journot, R. Lassalle, JP. Le-grand, M. Francois, E. Pereira, M. Preau, V. Villes, C. Pro-topopescu, H. Zouari, F. Marcellin.Promotion: AgenceNationale de Recherches sur le Sida (ANRS, CoordinatingAction n�7.) Other support: College des Universitaires deMaladies Infectieuses et Tropicales (CMIT ex APPIT), Si-daction Ensemble contre le Sida and associated pharmaceu-tical companies: Abbott, Boehringer-Ingelheim, Bristol-MyersSquibb, Glaxo- SmithKline, Merck Sharp et Dohme, Roche.
Appendix
The linear random effects model
Let yij be the transformed score (MCS or PCS) mea-
sured for patient i at time sj, i ¼ 1; . . . ;N; j ¼ 1; . . . ; 7.
We used a piecewise linear random effects model with
a change in the slope at M12, written as:
yij¼a0þx01i tj
� �b0þU0iþ a1þx02i tj
� �b1þU1i
� �min tj;12
� �
þ a2þx02i tj
� �b2þU2i
� �tj�12� �þþeij
Here x1iðtÞ and x2iðtÞ are vectors including fixed and
time-varying explanatory variables, and tj � 12� �þ
584 Qual Life Res (2007) 16:577–591
123
¼ tj � 12 if tj � 12 , and 0 otherwise. U0i is the subject-
specific intercept, U1i and U2i are the random slopes,
modelling the true individual level trajectories after
they have been adjusted for the overall mean trajectory
and the other fixed effects, such that U0i;U1i;U2ið Þ0�N 0;Gð Þ, and eij � N 0; r2
� �are mutually independent
measurement errors. The first term a0 þ x01i tj
� �b0 þU0i
includes principal effects of the factors, the second
term a1 þ x02i tj� �
b1 þU1i
� �represents the changes in
the short term evolution (M0–M12), and the third term
a2 þ x02i tj
� �b2 þU2i
� �represents the changes in the
long-term evolution (M12–M60).
We used the random effects covariance matrix G to
perform a likelihood ratio test for choosing the number
of random effects in the model. We tested whether we
needed a model with q = 3 random effects (i.e. two
random slopes: U1i;U2i) or whether a simpler model,
with only two random effects, would be more ade-
quate. We fitted both models with the same set of fixed
effects and recorded the deviance (–2 Log Likelihood)
for each of them. The distribution of the difference in
deviances is a mixture of a v2 with q degrees of free-
dom and a v2 with q–1 degrees of freedom [45].
For the MCS (resp. PCS) transformed score we
found an increase in the deviance of 16.2 (resp. 23.6) for
q = 3 degrees of freedom, so the test rejected the
specification with two random effects in both cases.
Nevertheless, the estimated G matrix for the model
with three random effects was almost singular, which
suggested that the variability in the last slope was very
small after considering heterogeneity which was
accounted for by the fixed factors. Moreover, the esti-
mated parameters and their P-values were very similar
for the two models, so we finally decided to include only
two random effects in the longitudinal model, which
allowed a faster estimation of the joint model.
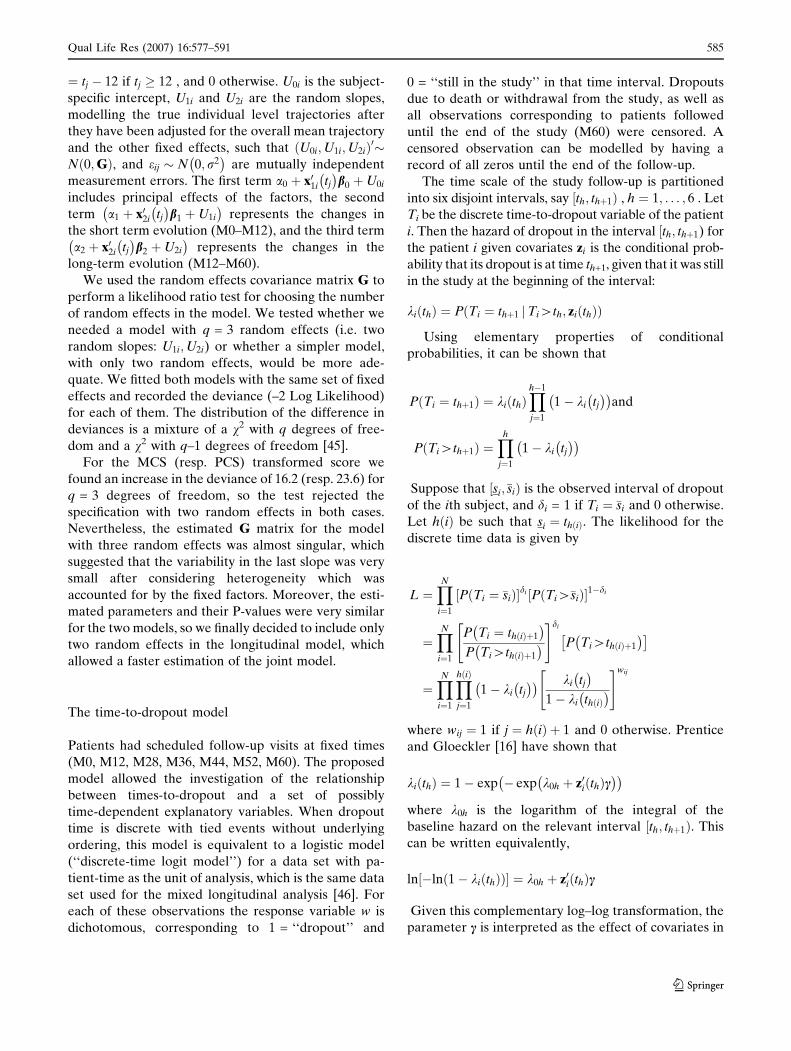
The time-to-dropout model
Patients had scheduled follow-up visits at fixed times
(M0, M12, M28, M36, M44, M52, M60). The proposed
model allowed the investigation of the relationship
between times-to-dropout and a set of possibly
time-dependent explanatory variables. When dropout
time is discrete with tied events without underlying
ordering, this model is equivalent to a logistic model
(‘‘discrete-time logit model’’) for a data set with pa-
tient-time as the unit of analysis, which is the same data
set used for the mixed longitudinal analysis [46]. For
each of these observations the response variable w is
dichotomous, corresponding to 1 = ‘‘dropout’’ and
0 = ‘‘still in the study’’ in that time interval. Dropouts
due to death or withdrawal from the study, as well as
all observations corresponding to patients followed
until the end of the study (M60) were censored. A
censored observation can be modelled by having a
record of all zeros until the end of the follow-up.
The time scale of the study follow-up is partitioned
into six disjoint intervals, say ½th; thþ1Þ , h ¼ 1; . . . ; 6 . Let
Ti be the discrete time-to-dropout variable of the patient
i. Then the hazard of dropout in the interval ½th; thþ1) for
the patient i given covariates zi is the conditional prob-
ability that its dropout is at time th+1, given that it was still
in the study at the beginning of the interval:
kiðthÞ ¼ P Ti ¼ thþ1 Ti[th; zi thð Þjð Þ
Using elementary properties of conditional
probabilities, it can be shown that
P Ti ¼ thþ1ð Þ ¼ ki thð ÞYh�1
j¼1
1� ki tj� �� �
and
P Ti[thþ1ð Þ ¼Yh
j¼1
1� ki tj
� �� �
Suppose that ½si;�siÞ is the observed interval of dropout
of the ith subject, and di = 1 if Ti ¼ �si and 0 otherwise.
Let h ið Þ be such that si ¼ th ið Þ. The likelihood for the
discrete time data is given by
L ¼YN
i¼1
P Ti ¼ �sið Þ½ �di P Ti[�sið Þ½ �1�di
¼YN
i¼1
P Ti ¼ th ið Þþ1
� �
P Ti[th ið Þþ1
� �
" #di
P Ti[th ið Þþ1
� �� �
¼YN
i¼1
Yh ið Þ
j¼1
1� ki tj
� �� � ki tj� �
1� ki th ið Þ� �
" #wij
where wij ¼ 1 if j ¼ hðiÞ þ 1 and 0 otherwise. Prentice
and Gloeckler [16] have shown that
kiðthÞ ¼ 1� exp � exp k0h þ z0i thð Þc� �� �
where k0h is the logarithm of the integral of the
baseline hazard on the relevant interval ½th; thþ1Þ. This
can be written equivalently,
ln �ln 1� kiðthÞð Þ½ � ¼ k0h þ z0i thð Þc
Given this complementary log–log transformation, the
parameter c is interpreted as the effect of covariates in
Qual Life Res (2007) 16:577–591 585
123

zi on the hazard rate of dropout, assuming the hazard
rate to be constant on each interval of the study.
As noted by Vonesh et al. [4], one advantage when
using such a model is that it allows the inclusion of
time-dependent covariates, defined at the start
of each interval ½th; thþ1Þ. In this way, the inclusion of
time-dependent covariates is not affected by the fact
that an actual measurement may not be available
for them at the time-of-dropout. Moreover, the
specification of the time-to-dropout model gives a
closed-form expression for the marginal and joint
likelihood, allowing us to use existing standard soft-
ware like the SAS procedure NLMIXED to estimate
both the separate and joint model (see also Guo and
Carlin [8]).
The log-likelihood function for the sample of indi-
viduals used in this study can then be given by
ln L ¼XN
i¼1
Xh ið Þ
j¼1
wij ln 1� exp � exp k0j þ z0i tj
� �c
� �� �� ��
þ 1� wij
� �� exp k0j þ z0i tj
� �c
� �� �g
This takes the form of a ‘‘sequential binary response’’
model with data in the ‘‘vertical’’ form with the ith
subject contributing h(i) observations. Allison [47
] and Jenkins [48–50] have shown that, for such
suitably organized data, the log-likelihood function is
the same as the log-likelihood for a generalized linear
model of the binomial family with complementary log–
log link function.
The joint model
In the joint approach, the linear random effects model
and the time-to-dropout model are estimated simulta-
neously (see Guo and Carlin [8]). The discrete-time
proportional hazard model is now written as follows:
ln � ln 1� kiðthÞð Þ½ � ¼ c0U0i þ c1U1i þ k0h þ z0iðthÞc;
where U0 and U1 are the random effects that appear in
the linear random effects model. In this way, the HRQL
model and the time-to-dropout model are connected
through the stochastic dependence on unobserved fac-
tors represented by these random variables. The
parameters c0 and c1 in the time-to-dropout model
measure the association between the two submodels
induced through these two common latent variables. In
the absence of association between the two models, the
parameters c0 and c1 are not statistically significant and
there is no gain from the joint analysis.
As in Guo and Carlin [8], the binary explanatory
variables were coded with 1 for the active modality and
–1 for the reference modality.
The SAS codes used to estimate the separate and
joint models for the MCS transformed score are given
below.
Determination of factors’ contribution to the
untransformed HRQL scores changes between
M0 and M12
In order to have an idea of the contribution of each
factor on the HRQL scores changes between M0 and
M12 on their original scale (varying between 0 and
100), we adopted the following approach. For each
factor, the corresponding univariate two–phase ran-
dom effects model on transformed HRQL scores was
translated back onto the original scale using the inverse
transformation of -ln (100-score). Then, the factor’s
contribution to the HRQL scores evolution during the
first year of HAART was calculated as the difference
between the score values estimated by the back
translated model at M12 and M0. The same approach
was used to determine the intercepts’ contribution,
from the two-phase random effects model without
covariates.
Random slopes and variance components
parametrization for the mixed model:
Here obstime1 and obstime2 are the two time
variables defined in the ‘‘Statistical methods’’ section
(i.e. minðtj; 12Þ and tj � 12� �þ
respectively). The legend
for the rest of the covariates is given at the end of this
Appendix. Multivariate influence analysis was per-
formed using the INFLUENCE option of the MODEL
proc mixed data = mydata covtest method=ml;
class patient;
model lnmcs = obstime1 obstime2 sexe_r naif_tr
naif_tr_1 naif_tr_2
part_pr confort confort_1 confort_2 homo
toxico cd4t_200 nbs30 nbs30_1
nbs30_2 nbtm_1 nbtm_2 / influence
(iter = 5 effect = patient est) s cl;
random obstime1 intercept /
subject = patient type = fa0(2);
ods output covparms = cp;
ods output solutionf = solf;
ods output Influence = inf;
run;
586 Qual Life Res (2007) 16:577–591
123
statement, in order to test the stability of the linear
mixed model to perturbations of the data. According to
the likelihood distance and Cook’s D measure [51], two
patients identified as influential observations were
dropped from the basis for each HRQL score.
As in Guo and Carlin [8], we used the FA0(q)
structure (No Diagonal Factor Analytic) for the G
matrix in the RANDOM statement of SAS PROC
MIXED, where q is the number of random effects.
This parametrization is equivalent to specifying a
Cholesky root for the G matrix, to constrain it to be
non-negative definite. The lower triangular Choleski
root of G is a lower triangular matrix C, with non-
negative diagonal elements that is a ‘square root’ of G
in the sense that CC¢=G.
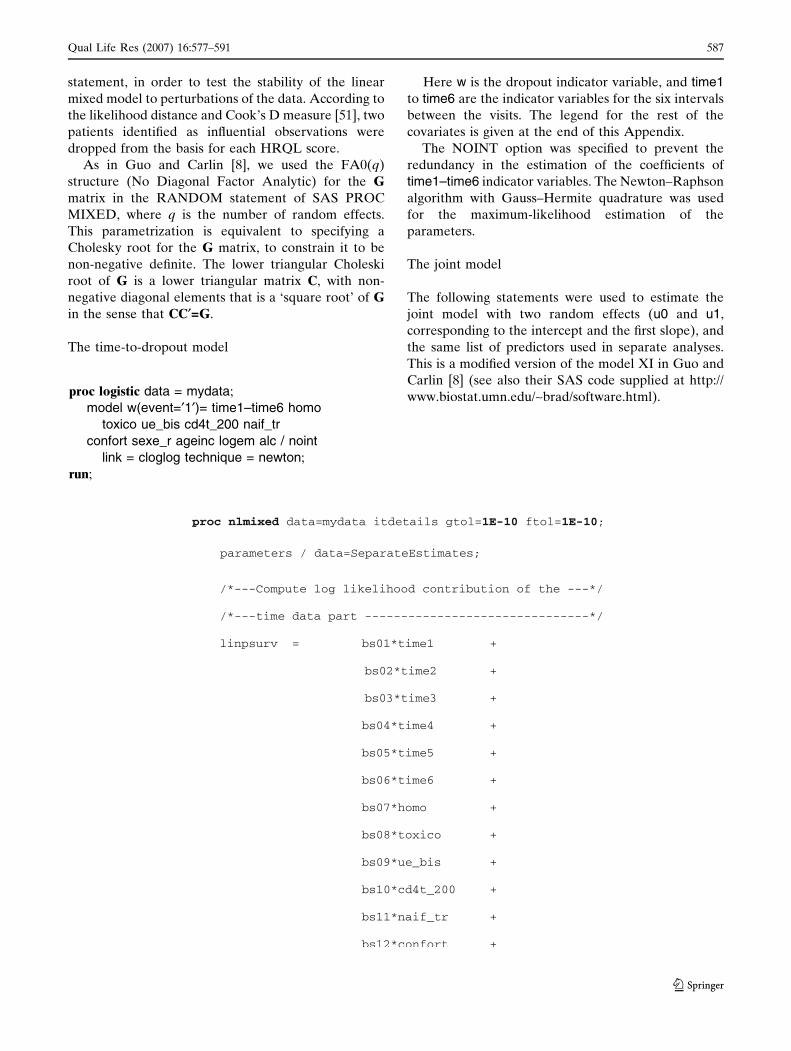
The time-to-dropout model
Here w is the dropout indicator variable, and time1
to time6 are the indicator variables for the six intervals
between the visits. The legend for the rest of the
covariates is given at the end of this Appendix.
The NOINT option was specified to prevent the
redundancy in the estimation of the coefficients of
time1–time6 indicator variables. The Newton–Raphson
algorithm with Gauss–Hermite quadrature was used
for the maximum-likelihood estimation of the
parameters.
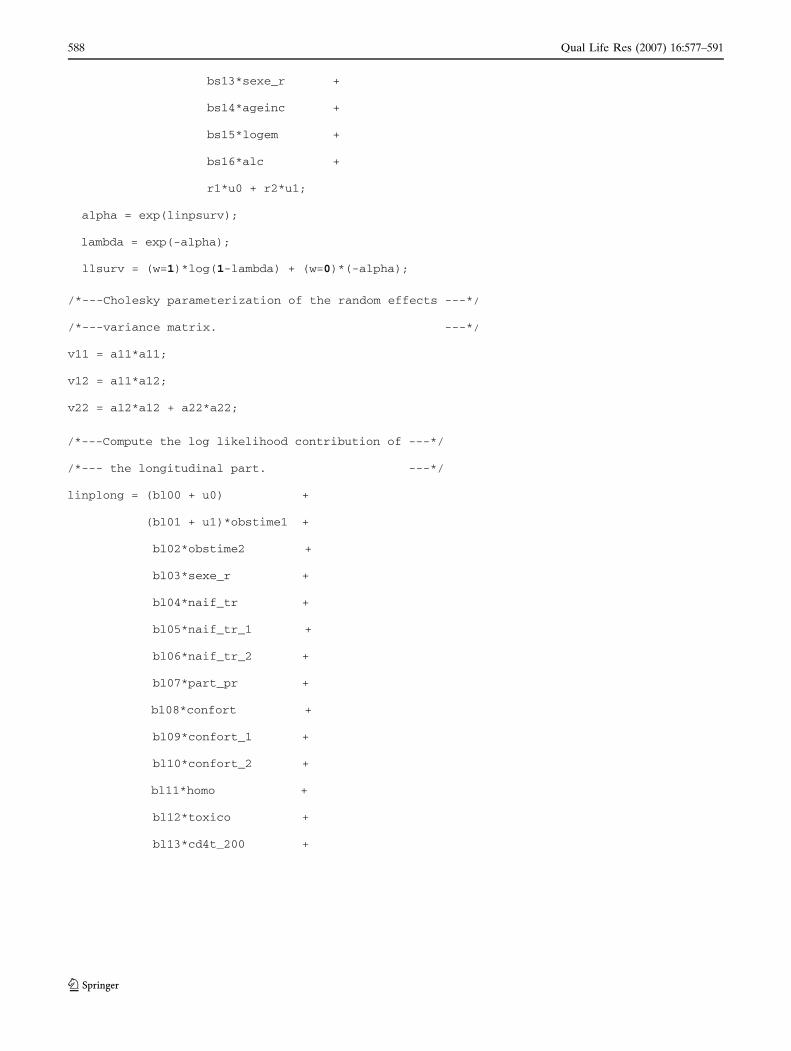
The joint model
The following statements were used to estimate the
joint model with two random effects (u0 and u1,
corresponding to the intercept and the first slope), and
the same list of predictors used in separate analyses.
This is a modified version of the model XI in Guo and
Carlin [8] (see also their SAS code supplied at http://
www.biostat.umn.edu/~brad/software.html).proc logistic data = mydata;
model w(event=¢1¢)= time1–time6 homo
toxico ue_bis cd4t_200 naif_tr
confort sexe_r ageinc logem alc / noint
link = cloglog technique = newton;
run;
Qual Life Res (2007) 16:577–591 587
123
588 Qual Life Res (2007) 16:577–591
123
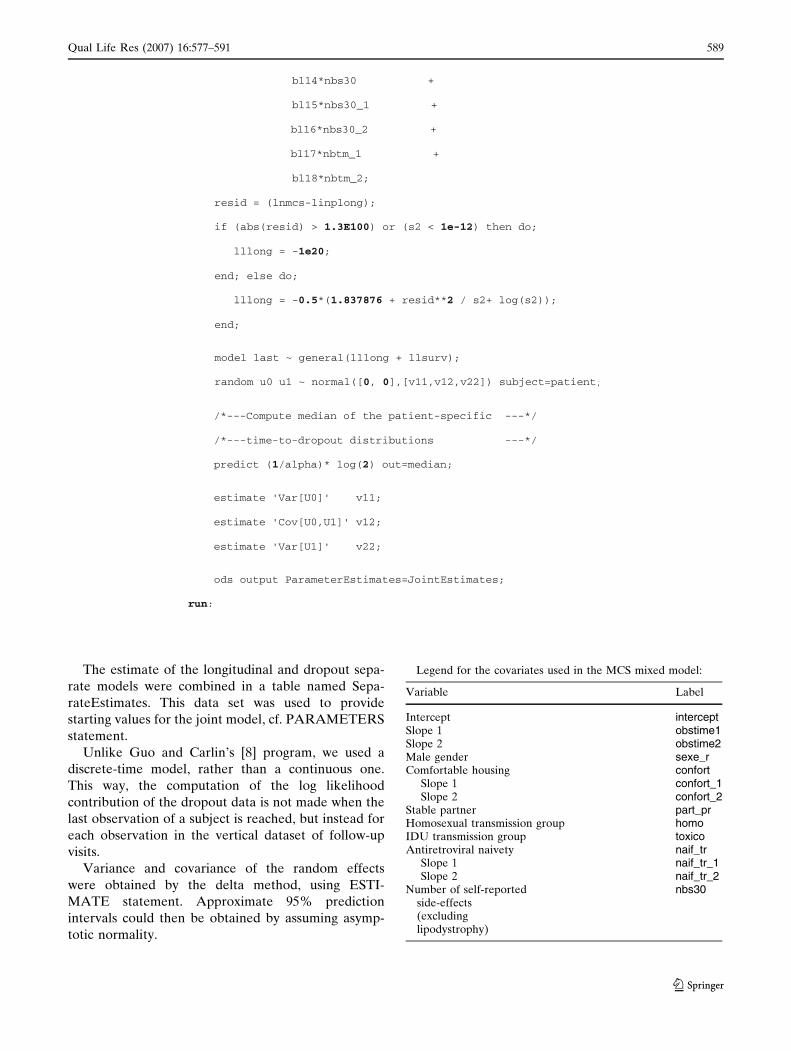
The estimate of the longitudinal and dropout sepa-
rate models were combined in a table named Sepa-
rateEstimates. This data set was used to provide
starting values for the joint model, cf. PARAMETERS
statement.
Unlike Guo and Carlin’s [8] program, we used a
discrete-time model, rather than a continuous one.
This way, the computation of the log likelihood
contribution of the dropout data is not made when the
last observation of a subject is reached, but instead for
each observation in the vertical dataset of follow-up
visits.
Variance and covariance of the random effects
were obtained by the delta method, using ESTI-
MATE statement. Approximate 95% prediction
intervals could then be obtained by assuming asymp-
totic normality.
Legend for the covariates used in the MCS mixed model:
Variable Label
Intercept interceptSlope 1 obstime1Slope 2 obstime2Male gender sexe_rComfortable housing confort
Slope 1 confort_1Slope 2 confort_2
Stable partner part_prHomosexual transmission group homoIDU transmission group toxicoAntiretroviral naivety naif_tr
Slope 1 naif_tr_1Slope 2 naif_tr_2
Number of self-reportedside-effects(excludinglipodystrophy)
nbs30
Qual Life Res (2007) 16:577–591 589
123

References
1. Palella, F. J., Jr., Delaney, K. M., Moorman, A. C., Loveless,M. O., Fuhrer, J., Satten, G. A., et al. (1998). Decliningmorbidity and mortality among patients with advanced hu-man immunodeficiency virus infection. HIV OutpatientStudy Investigators. New England Journal of Medicine, 338,853–860.
2. Little, R., & Rubin, D. (2002). Statistical analysis withmissing data.
3. Laird, N. M. (1988). Missing data in longitudinal studies.Statistics in Medicine, 7, 305–315.
4. Vonesh, E. F., Greene, T., & Schluchter, M. D. (2006). Sharedparameter models for the joint analysis of longitudinal dataand event times. Statistics in Medicine, 15, 143–163.
5. Hogan, J. W., Lin, X., & Herman, B. (2004). Mixtures ofvarying coefficient models for longitudinal data with discreteor continuous nonignorable dropout. Biometrics, 60, 854–864.
6. Lin, D. Y., & Ying, Z. (2003). Semiparametric regressionanalysis of longitudinal data with informative drop-outs.Biostatistics, 4, 385–398.
7. Hu, C., & Sale, M. E. (2003). A joint model for nonlinearlongitudinal data with informative dropout. Journal ofPharmacokinetics and Pharmacodynamics, 30, 83–103.
8. Guo, X., & Carlin, B. P. (2004). Separate and joint modelingof longitudinal and event time data using standard computerpackages. The American Statistician, 58, 1–9.
9. Carrieri, P., Spire, B., Duran, S., Katlama, C., Peyramond,D., Francois, C., et al. (2003). Health-related quality of lifeafter 1 year of highly active antiretroviral therapy. Journal ofAcquired Immune Deficiency Syndromes, 32, 38–47.
10. Carrieri, M. P., Leport, C., Protopopescu, C., Cassuto, J. P.,Bouvet, E., Peyramond, D., et al. (2006), Factors associatedwith nonadherence to highly active antiretroviral therapy: A5-year follow-up analysis with correction for the bias inducedby missing data in the treatment maintenance phase. Journalof Acquired Immune Deficiency Syndromes, 41, 477–485.
11. Ware, J. E., Jr., & Sherbourne, C. D. (1992). The MOS 36-item short-form health survey (SF-36). I. Conceptualframework and item selection. Medical Care, 30, 473–483.
12. McHorney, C. A., Ware, J. E., Jr., & Raczek, A. E. (1993).The MOS 36-Item Short-Form Health Survey (SF-36): II.Psychometric and clinical tests of validity in measuringphysical and mental health constructs. Medical Care, 31,247–263.
13. McHorney, C. A., Ware, J. E., Jr., Lu, J. F., & Sherbourne, C. D.(1994). The MOS 36-item Short-Form Health Survey (SF-36):
III Tests of data quality, scaling assumptions, and reliabilityacross diverse patient groups. Medical Care, 32, 40–66.
14. Ware, J. E., Jr., Keller, S. D., Gandek, B., Brazier, J. E., &Sullivan, M. (1995). Evaluating translations of health statusquestionnaires. Methods from the IQOLA project. Interna-tional Quality of Life Assessment. International Journal ofTechnology Assessment in Health Care, 11, 525–551.
15. Leplege, A., Mesbah, M., & Marquis, P. (1995). [Preliminaryanalysis of the psychometric properties of the French versionof an international questionnaire measuring the quality oflife: The MOS SF-36 (version 1.1)]. Revue d Epidemiologie etde Sante Publique, 43, 371–379.
16. Prentice, R. L., & Gloeckler, L. A. (1978). Regressionanalysis of grouped survival data with application to breastcancer data. Biometrics, 34, 57–67.
17. Henderson, R., Diggle, P., & Dobson, A. (2000). Jointmodelling of longitudinal measurements and event timedata. Biostatistics, 1, 465–480.
18. SAS/STAT 9.1 (2004). User’s Guide. Cary, NC, SAS Insti-tute Inc: SAS Publishing.
19. Furher, R., & Rouillon, F. (1989). La version francaise del’echelle CES-D. Description and translation of theauto-evaluation (in French). Psychiatrie et Psychobiologie, 4,163–166.
20. Bissell, D., Paton, A., & Ritson, B. (1982). ABC of alcohol.Help: Referral. British Medical Journal (Clinical ResearchEd), 284, 495–497.
21. Nieuwkerk, P. T., Gisolf, E. H., Colebunders, R., Wu, A. W.,Danner, S. A., & Sprangers, M. A. (2000). Quality of life inasymptomatic- and symptomatic HIV infected patients in atrial of ritonavir/saquinavir therapy. The Prometheus StudyGroup. Acquired Immune Deficiency Syndromes, 14, 181–187.
22. Cohen, C., Revicki, D. A., Nabulsi, A., Sarocco, P. W., &Jiang, P. (1998). A randomized trial of the effect of ritonavirin maintaining quality of life in advanced HIV disease. Ad-vanced HIV Disease Ritonavir Study Group. Acquired Im-mune Deficiency Syndromes, 12, 1495–1502.
23. Carr, A., Chuah, J., Hudson, J., French, M., Hoy, J., Law, M.,et al. (2000). A randomised, open-label comparison of threehighly active antiretroviral therapy regimens including twonucleoside analogues and indinavir for previously untreatedHIV-1 infection: The OzCombo1 study. Acquired ImmuneDeficiency Syndromes, 14, 1171–1180.
24. Nieuwkerk, P. T., Gisolf, E. H., Reijers, M. H., Lange, J. M.,Danner, S. A., & Sprangers, M. A. (2001). Long-term qualityof life outcomes in three antiretroviral treatment strategiesfor HIV-1 infection. Acquired Immune Deficiency Syn-dromes, 15, 1985–1991.
25. Burgoyne, R. W., Rourke, S. B., Behrens, D. M., & Salit, I.E. (2004). Long-term quality-of-life outcomes among adultsliving with HIV in the HAART era: The interplay of changesin clinical factors and symptom profile. Acquired ImmuneDeficiency Syndromes Behavior, 8, 151–163.
26. Burgoyne, R., & Renwick, R. (2004). Social support andquality of life over time among adults living with HIV in theHAART era. Social Science and Medicine, 58, 1353–1366.
27. Eriksson, L. E., Bratt, G. A., Sandstrom, E., & Nordstrom,G. (2005). The two-year impact of first generation proteaseinhibitor based antiretroviral therapy (PI-ART) on health-related quality of life. Health Quality of Life Outcomes, 3, 32.
28. Campsmith, M. L., Nakashima, A. K., & Davidson, A. J.(2003). Self-reported health-related quality of life in personswith HIV infection: Results from a multi-site interviewproject. Health Quality of Life Outcomes, 1, 12.
29. Jia, H., Uphold, C. R., Wu, S., Chen, G. J., & Duncan, P. W.(2005). Predictors of changes in health-related quality of life
continued
Variable Label
Slope 1 nbs30_1Slope 2 nbs30_2
Number of self-reportedsymptoms oflipodystrophySlope 1 nbtm_1Slope 2 nbtm_2
CD4+ cell count <200 cells/mm3 cd4t_200Born in EU ue_bisAge at enrolment ageincStable housing logemDaily alcohol consumption alc
590 Qual Life Res (2007) 16:577–591
123
among men with HIV infection in the HAART era. Ac-quired Immune Deficiency Syndromes Patient Care STDSPatient Care STDS, 19, 395–405.
30. Hogg, R. S., Yip, B., Chan, K. J., Wood, E., Craib, K. J.,O’Shaughnessy, M. V., & Montaner, J. S. (2001). Rates ofdisease progression by baseline CD4 cell count and viral loadafter initiating triple-drug therapy. JAMA, 286, 2568–2577.
31. Bonfanti, P., Valsecchi, L., Parazzini, F., Carradori, S., Pus-terla, L., Fortuna, P., et al. (2000). Incidence of adversereactions in HIV patients treated with protease inhibitors: acohort study Coordinamento Italiano Studio Allergia e In-fezione da HIV (CISAI) Group. Journal of Acquired Im-mune Deficiency Syndromes, 23, 236–245.
32. Fellay, J., Boubaker, K., Ledergerber, B., Bernasconi, E.,Furrer, H., Battegay, M., et al. (2001). Prevalence of adverseevents associated with potent antiretroviral treatment: SwissHIV Cohort Study. Lancet, 358, 1322–1327.
33. Ammassari, A., Murri, R., Pezzotti, P., Trotta, M. P.,Ravasio, L., De Longis, P., et al. (2001). Self-reportedsymptoms and medication side effects influence adherence tohighly active antiretroviral therapy in persons with HIVinfection. Journal of Acquired Immune Deficiency Syn-dromes, 28, 445–449.
34. Duran, S., Spire, B., Raffi, F., Walter, V., Bouhour, D.,Journot, V., et al. (2001). Self-reported symptoms after ini-tiation of a protease inhibitor in HIV-infected patients andtheir impact on adherence to HAART. HIV Clinical Trials,2, 38–45.
35. Bury, M. (1991). The sociology of chronic illness: A review ofresearch and prospects. Sociology of Health and Illness, 13,451–468.
36. Foster, G. R., Goldin, R. D., & Thomas, H. C. (1998).Chronic hepatitis C virus infection causes a significantreduction in quality of life in the absence of cirrhosis. Hep-atology, 27, 209–212.
37. Rodger, A. J., Jolley, D., Thompson, S. C., Lanigan, A., &Crofts, N. (1999). The impact of diagnosis of hepatitis C viruson quality of life. Hepatology, 30, 1299–1301.
38. Preau, M., Leport, C., Salmon-Ceron, D., Carrieri, P., Por-tier, H., Chene, G., et al. (2004). Health-related quality oflife and patient–provider relationships in HIV-infected pa-tients during the first three years after starting PI-containing
antiretroviral treatment. Acquired Immune Deficiency Syn-dromes Care, 16, 649–661.
39. Cederfjall, C., Langius-Eklof, A., Lidman, K., & Wredling, R.(2001). Gender differences in perceived health-related qual-ity of life among patients with HIV infection. Acquired Im-mune Deficiency Syndromes Patient Care STDS, 15, 31–39.
40. Mrus, J. M., Williams, P. L., Tsevat, J., Cohn, S. E., & Wu, A.W. (2005). Gender differences in health-related quality oflife in patients with HIV/AIDS. Quality of Life Research, 14,479–491.
41. Nicholas, P. K., Kirksey, K. M., Corless, I. B., & Kemppainen,J. (2005). Lipodystrophy and quality of life in HIV: Symptommanagement issues. Applied Nursing Research, 18, 55–58.
42. Collins, E., Wagner, C., & Walmsley, S. (2000). Psychosocialimpact of the lipodystrophy syndrome in HIV infection.Acquired Immune Deficiency Syndromes Read, 10, 546–550.
43. Preau, M., Bouhnik, A., Spire, B., Leport, C., Saves, M.,Pıcard, O., et al. (2006). Health related quality of life andlipodystrophy syndrome among HIV-infected patients.Encephale, 32, 713–719.
44. Hsiung, P. C., Fang, C. T., Chang, Y. Y., Chen, M. Y., Wang,J. D. (2005). Comparison of WHOQOLbREF and SF-36 inpatients with HIV infection. Quality of Life Research, 14,141–150.
45. Monnete, G., Shao, Q., & Kwan, E. (2002). A first look atmultilevel models. In S.C.S. Institute for Social Research.York University: Institute for Social Research. StatisticalConsulting Service, York University.
46. Allison, P. D. (1995). Survival analysis using the SAS system:A practical guide. The SAS Institute, Cary, NC.
47. Allison, P. D. (1982). Discrete-time methods for the analysisof event histories. Sociological Methodology, 15, 61–98.
48. Jenkins, S. P. (1995). Easy estimation methods for discrete-time duration models. Oxford Bulletin of Economics andStatistics, 57, 129–138.
49. Jenkins, S. P. (1997). Estimation of discrete time (groupedduration data) proportional hazards models: pgmhaz. StataTechnical Bulletin Reprints, STB 17, 1–12.
50. Jenkins, S. P. (2005). Survival analysis. In Institute for Socialand Economic Research, University of Essex.
51. Zewotir, T., & Galpin, J. S. (2005). Influence diagnostics forlinear mixed models. Journal of Data Science, 3, 153–177.
Qual Life Res (2007) 16:577–591 591
123
Related Documents











