Health Overview and Scrutiny in Essex, Southend and Thurrock Good Practice Guidelines on Consultation relating to Service Variations and Developments Protocol on Health Scrutiny Studies February 2004

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Health Overview and Scrutiny in Essex, Southend and Thurrock
Good Practice Guidelines on Consultation relating to
Service Variations and Developments
Protocol on Health Scrutiny Studies
February 2004
2
Distribution list:
NHS Organisations:
David Brackenbury Chief Executive Southend Hospital NHS TrustRichard Coleman Chief Executive North Essex Mental Health Partnership
NHS TrustPam Court Chief Executive Harlow PCTJulie Garbutt Chief Executive Thurrock PCTPatrick Geoghegan Chief Executive South Essex Partnership NHS TrustJohn Gilham Chief Executive Princess Alexandra Hospital NHS TrustMark Halladay Chief Executive Chelmsford PCTTerry Hanafin Chief Executive Essex Strategic Health Authority Mike Harrison Chief Executive Maldon & South Chelmsford PCTManfred Hennessey Chief Executive Southend-on-Sea PCTAnthony Marsh Chief Executive Essex Ambulance Service NHS TrustMalcolm McCann Chief Executive Castle Point & Rochford PCTMary-Ann Munford Chief Executive Basildon PCTBrendan Osborne Chief Executive Colchester PCTHoward Perry Chief Executive Billericay, Brentwood & Wickford PCTAndrew Pike Chief Executive Mid Essex Hospital Services NHS TrustMike Pollard Chief Executive Essex Rivers Healthcare NHS TrustAidan Thomas Chief Executive Epping Forest PCTPaul Unsworth Chief Executive Tendring PCTStephen Welfare Chief Executive Essex Workforce Development
ConfederationAlan Whittle Chief Executive Basildon & Thurrock University Hospitals
NHS TrustPeta Wilkinson Chief Executive Uttlesford PCTDr Paul Zollinger-Read
Chief Executive Witham, Braintree & Halstead Care Trust
Local Authorities
Councillor Professor Roger Dyson
Chair Essex County Council Overview and Scrutiny Committee
Councillor Lesley Salter
Chair Southend-on Sea Borough Council Overview and Scrutiny Committee
Councillor George Watts
Chair Thurrock Council Overview and Scrutiny Committee
Local Authority Overview and Scrutiny Officers
Patient and Public Involvement Forums in Essex
Forum Support Organisations in Essex
Head of Patient and Public Involvement Unit, Department of Health
3
CONTENTS
Foreword
SECTION A Good Practice Guidelines on Consultation relating to Service Variations and Developments
SECTION B Protocol on Health Scrutiny Studies
4
FOREWORD
The Overview and Scrutiny of Health is a new power given to the Overview and Scrutiny Committees (OSCs) of some local authorities with effect from 1 January 2003. It is recognised as an important part of the Government's commitment to place patients and members of the public at the centre of health services and seen as a means by which democratically elected community leaders may voice the views of their constituents and require local NHS bodies to listen and respond.
Whilst the powers of overview and scrutiny of the NHS enable OSCs to review any matter relating to planning, provision and operation of health services in the area of the local authority, the subject matter of health scrutiny can be divided for practical purposes into the following principal categories:-
Consultation by NHS bodies on any proposal for a substantial development or variation in the provision of health services
In-depth scrutiny studies of particular health issues or services
Accordingly, in order to facilitate the development of health scrutiny in Essex, Southend and Thurrock, and to ensure that it operates efficiently and effectively in line with Ministerial Guidance to improve not only health services but also the health of local people, best practice guidelines and a protocol for the main subject areas, have been devised and agreed by Essex County Council, Southend-on-Sea Borough Council and Thurrock Borough Council, together with NHS organisations in Essex.
Part A of the document is designed to provide a best practice framework for consultations relating to any proposed service variations and developments by the NHS.
Part B is designed to apply primarily to in-depth scrutinies undertaken by the OSCs themselves, albeit following prior consultation with stakeholders, including relevant NHS bodies. However, there is no reason why the procedures in Protocol B should not apply to any major scrutiny arising from a substantial service variation or development, subject to the guidelines on service variation taking precedence of application in any such case.
Whilst the protocols lay the foundations for effective scrutiny, success will depend on all parties following the practices agreed in these documents and maintaining good communications with one another.
If there are any disagreements about the interpretation of these guidelines and protocol, reference should be made to the Health Overview and Scrutiny Regulations, Ministerial Guidance and Ministerial Directions.
…………………………………….. ……………………………………………..
Terry Hanafin Councillor Professor Roger DysonChief Executive ChairEssex Strategic Health Authority Essex Health Overview and Scrutiny
Partnership Forum

5
LIST OF SIGNATORY ORGANISATIONS
Essex Strategic Health Authority
NHS Trusts in Essex
Primary Care Trusts in Essex
The Essex, Southend and Thurrock Local Authorities
Community Health Councils in Essex

6
SECTION A
Good Practice Guidelines on Consultation relating to Service Variations and Developments
7
CONTENTS
Page
1. Why do we need to consult and on what? 8
2. Planning your consultation 10
3. Receiving and analysing feedback 15
4. The role of local authorities in relation to health service consultations 17
5. The role of Patient and Public Involvement Forum s 20
References 22
Appendix 1 Model continuum of involvement / consultation
Appendix 2 Flow chart illustrating stages of consultation
Appendix 3 Example of good practice in public and stakeholder involvement prior to the announcement of the formal consultation process
Appendix 4 Questions asked by the local authority health overview and scrutiny committee service variation panels
Appendix 5 Health service variations – local authority procedure
Appendix 6 Membership of the working group
Appendix 7 A template for your consultation project
8
1. WHY DO WE NEED TO CONSULT AND ON WHAT?
1.1 The Legal Framework
Consultation on changes to health services is not a new requirement. The Community Health Council Regulations, 1996, require Strategic Health Authorities (previously Health Authorities) to consult on proposals for any substantial development or variation to health services.
Under Section 7 of the Health and Social Care Act 2001, the regulations governing the powers of local authorities for overview and scrutiny of health now also place a duty on local NHS organisations to consult the overview and scrutiny committee or committees on any proposal for a substantial development of the health service or on any proposal to make a substantial variation in the provision of such service(s). With the abolition of Community Health Councils on 1 December 2003, these regulations will take the place of the Community Health Council Regulations.
1.2 The Context Of Consultation
Proposals for the development or variations to services are likely to span the whole spectrum of change, from very minor changes such as an extension of the opening hours of a particular clinic through to the reconfiguration of county-wide specialist services (e.g. specialist cancer services) or major capital (new build) projects.
It is good practice for health organisations to notify the relevant overview and scrutiny committee/s (and local Community Health Council/s until 1 December 2003) of any proposals for service development or change as early as possible. Early discussions should take place between representatives from the NHS and Overview and Scrutiny officers on the type of involvement / consultation planned and whether the proposed changes to services are considered to be substantial and therefore require a period of formal consultation. Government guidance on consultations states that full consultation should last for a minimum of twelve weeks, and that consultations should ensure that groups the NHS has traditionally found hard to reach and the wider community should be consulted (DOH, 2003 Overview and Scrutiny of Health Guidance).
It is important to remember that the section 11 duty to involve and consult patients and the public still applies whether or not a proposal constitutes a substantial variation or development (Department of Health: Strengthening Accountability Policy and Practice Guidance 2003).
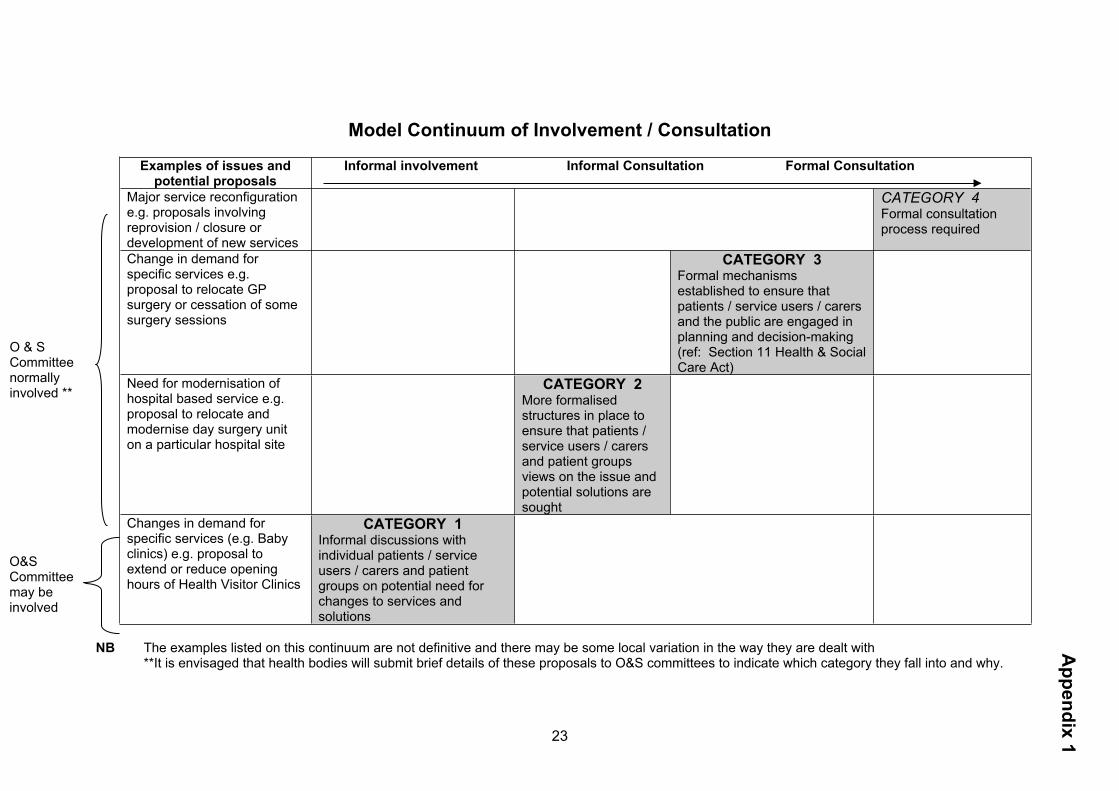
Appendix 1 provides examples of the types of service changes which may fall within this continuum of involvement / consultation.
1.3 Who Is Responsible For Consultation?
The Primary Care Trust (PCT) leading the commissioning process will normally be responsible for consultation. Where a proposal service spans more than one PCT, they will need to agree a process of joint consultation. The Board of each PCT should formally delegate the responsibility to a joint PCT committee, which should act as a single entity and be responsible for making the final decision following consultation.
9
The Strategic Health Authority has a responsibility for making sure that Trusts and PCTs involve patients and the public and that consultation is done well, in line with national guidance.
1.4 What Is A Substantial Variation In Service?
What constitutes a ‘substantial development’ or ‘variation’ is not defined in the legislation, in the guidance on overview and scrutiny of health (Department of Health, May 2003), or in the policy and practice guidance for Section 11 (Department of Health, February 2003). The guidance on overview and scrutiny of health recommends that local NHS organisations should aim to reach a local understanding or definition with their overview and scrutiny committee(s) on this issue and that this should be informed by discussions with other key stakeholders including Patients’ Forums.
The following guidelines, taken from the guidance on overview and scrutiny of health may help to inform these discussions and provide a provisional framework within which NHS organisations, overview and scrutiny committees and stakeholders in Essex should consider whether a proposal is substantial. Generally, the degree of impact of the change upon patients, carers and the public who use, or have the potential to use, a service should be considered. Issues for specific consideration include:
Changes in accessibility of services: e.g. both reductions and increases of services on a particular site or changes in opening times for a particular clinic.Communities attach considerable importance to the local provision of services, and local accessibility can be a key factor in improving population health, especially for disadvantaged and minority groups. At the same time, development in medical practice and in the effective organisation of health care services may call for reorganisation including the relocation of services. But changes to service locations can often be controversial. Thus there should be discussion of any proposal, which involves the alteration to, or withdrawal of, primary care, in-patient, day patient or diagnostic facilities.
The impact of the proposal on the wider community and other services, including economic impact, transport, regeneration.
The degree to which patients are affected: changes may affect the whole population (such as changes to accident and emergency services) or a small group of patients accessing a specialist service. If changes affect a small group of patients, the change may still be considered substantial, particularly if patients need to continue accessing that service for many years (e.g. patient access to a GP branch surgery in a particular locality or access for patients to renal services).
Changes to service models and methods of service delivery. Altering the way a service is delivered may be a substantial change – for example, moving a particular service into community settings rather than being hospital based. The views of patients, Patient and Public Involvement Forums and the general public will be essential in such cases.
1.5 When Are NHS Bodies Not Required To Consult?
Some exemptions exist in relation to the requirement for consultation. The requirement does not apply with respect to:
10
Any proposal to establish or dissolve a NHS Trust or Primary Care Trust unless that establishment or dissolution represents a substantial variation or development.
Pilot schemes within the meaning of Section 4 of the National Health Service (Primary Care) Act 1997(1).
Where a decision has to be taken immediately because of a risk to the safety or welfare of patients or staff. In such circumstances, the NHS body must notify the Overview and Scrutiny committee immediately, in writing, of the decision taken and the reason why no consultation has taken place. If an OSC is not satisfied that the reasons given are adequate, any difference of opinion may be settled by applying agreed protocols. If this is insufficient, the matter should be referred to the SHA and full HOSC(s).
2. PLANNING YOUR CONSULTATION
2.1 The Importance Of Planning
The Health Overview and Scrutiny Committee will ask how you have gone about your consultation and reacted to responses. In particular, it will test the extent to which you have involved patients and the public in determining the options for consultation. It may also ask you to provide evidence. Planning thoroughly means your consultation is much more likely to go well. Your key stakeholders will have an opportunity to participate and their views will have been carefully considered. It also means that you will have set objectives to identify how successful the process has been and identify what improvements you would make next time round. Remember people supported by health and social care services and the wider public should be involved in the continuous planning and development of services and not just asked to comment on a proposed major change. To do this properly, robust planning is essential. This section outlines key issues that you may want to consider when planning a consultation process.
2.2 Guidance On Consultation
Strengthening Accountability, the Department of Health's practice guidance on involving patients and the public gives an excellent outline of consultation tools. It covers recommended good practice on procedures such as informal consultation, listening exercises, discussion periods and formal consultation. Some methods will be more suitable in certain circumstances than others. The guidance fully explains these.
The practice guidance can be ordered free of charge directly from the Department of Health or is available on the department’s website at: www.doh.gov.uk/involvingpatients/index.htm
2.3 Preparatory Work
2.3.1 Be clear about why you consulting
11
By being focussed before you start means that you will have a clear understanding of why you are consulting, what needs to be done and how you will evaluate your progress. This will make it easier for your key audiences to understand what is expected of them and for Health Overview and Scrutiny to see your objectives. To have a greater chance of success, it may useful to consider the questions in the box below.
Questions to ask yourself before you start
What do you want to know?Try to be clear about the area or subject you want to investigate. For example, the views of patients with cancer are very wide. The information needs of women with breast cancer are narrower and more manageable. Do you want to give and/or receive information? What are you going to do with this information?What is the point of doing the public involvement initiative? For example, do you want to feed into service agreements? Are you undertaking a service review? What are you going to do with the information once you have obtained it?Think about how you are going to use the information. Many initiatives fail because there is nowhere for the findings to 'go', so changes never happen. Decide who you want to influence from the start.
Who is committed to the work? Who is not?Have you gained the support of key people in order that the results of the initiative can be used effectively? Be aware of who may not wish to support the initiative - have you explained your project clearly enough? Gain the commitment of those who are able to make change. What scope is there to make changes or influence decisions?Be very clear about what is feasible. If there are constraints say so at the beginning. For example, 'There is no additional funding to invest in the service but it is possible to rearrange clinic times to suit service users better'. Most public involvement work is long term. Don't raise people's expectations if you can't deliver in a short time. Be honest and realistic. How will you know if you have been successful?Define the outcomes you want to achieve at the beginning by thinking through the above questions. Has any other agency already undertaken this type of work?If someone else has undertaken a similar initiative, do you need to repeat one locally. Public involvement initiatives are often resource intensive and some groups in the community have consultation 'fatigue'. There may be very good reasons for doing a similar piece of work locally - local knowledge will dictate what is best.
Extract from The Reference Manual for Public Involvement, Barker, Bullen and de Ville 1999
12
2.3.2 Timing
Timing is vital to effective consultations. You need to make sure that your key stakeholders have enough time to be involved in the process. A minimum of three months is good practice and complies with the requirements of Section 7 and Section 11 guidance. It is important that you decide the timetable for the consultation process before you start so your stakeholders know what is happening and when they can expect a decision to be announced.
Producing consultation documents, organising events and analysing and summarising feedback can take a considerable amount of time. Remember to build this into your timetable. When planning the process, consider your key audiences and their schedules. For example, a consultation during school holidays may have a lower response rate.
2.3.3 Key audiences
Being aware of who the key audiences are for the consultation will ensure that you are able to invite them to participate and keep them up-to-date with developments. Preparing a list of individuals and organisations that need to be involved together with their contact details during the preparatory phase means that you will be able to keep in touch with each other. Your key audiences may include:
Advocacy services Community Health Councils Commission for Patient and Public Involvement in Health Colleagues in your organisation Councils for Voluntary Services District and borough councils Housing associations Essex County Council - including Health Overview and Scrutiny Committee Essex Strategic Health Authority Key non-statutory and voluntary organisations Local democratic forums Local individuals and community groups Media Minority groups who otherwise may be excluded by mainstream consultation MPs Service users and carers directly affected by proposals Patient and Public Involvement Forum(s) Primary Care Trusts and other NHS Trusts in north Essex The general public Unions Universities User and carers groups who support individuals who may directly affected by
the outcome of your consultation Keep Health Overview and Scrutiny informed at each stage of your consultation process and ask what involvement is required by the Committee and when this is will happen.
Overview and Scrutiny Committees should be informed of forthcoming NHS consultations as soon as possible and in good time for them to be included in OSCs’
13
annual overview and scrutiny plans; this is particularly important, as the consultation workload will affect the capacity of OSCs to undertake in-depth scrutiny studies. To this end, preparation of a rolling schedule of forthcoming consultations would be helpful (see also footnote to Appendix 1).
2.4 Consultation Stages
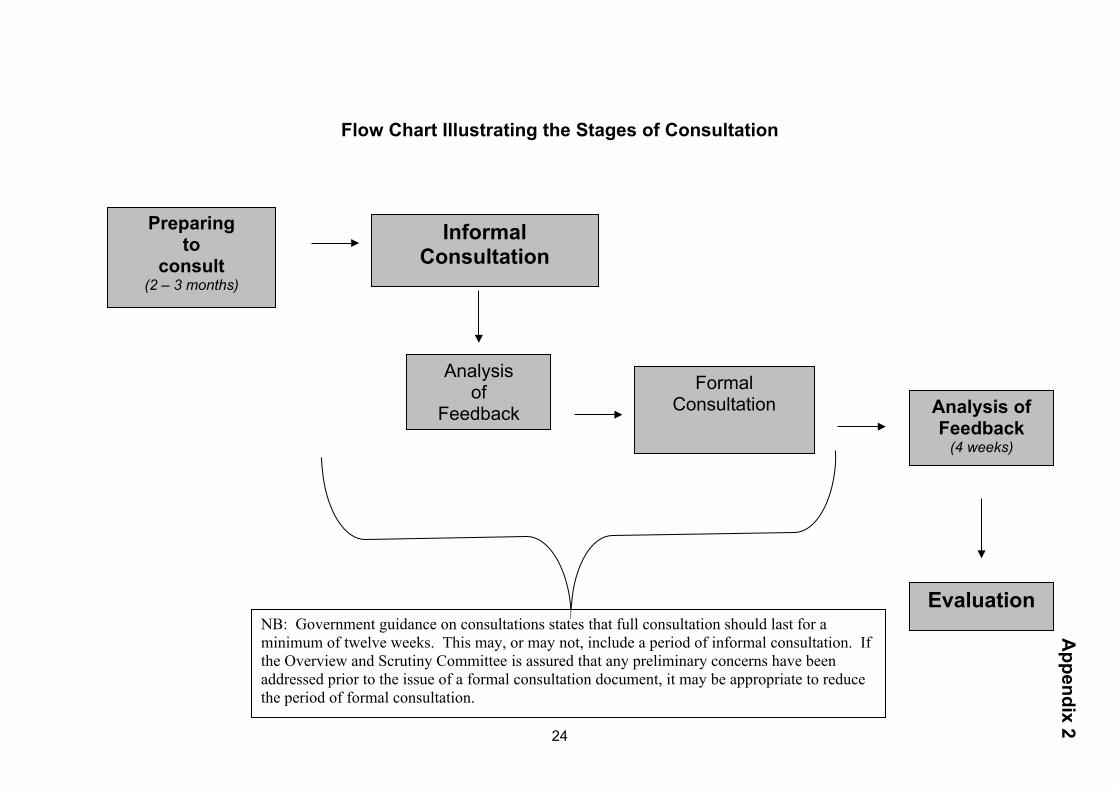
A flow chart illustrating the key stages in the consultation process is provided at Appendix 2.
2.4.1 Preparing to consult
Allow two to three months for preparation before embarking on the informal and formal stages of a consultation. This period will include preparatory dialogues with some key stakeholders such as Health Overview and Scrutiny Committees, Patient and Public Involvement Forum(s), the Commission for Patient and Public Involvement in Health and other local NHS organisations about your intentions to consult.
2.4.2 Informal consultation period
The informal discussion stage is an opportunity to involve stakeholders who may be directly affected by your proposals. Typically, you may be asking them:
How the proposals will impact on them Issues that need to be considered by the formal consultation How you are going to carry out formal consultation – eg what type of events
your stakeholders would like How you will evaluate and disseminate the responses
It is considered good practice to produce a discussion document that clearly explains the plans and a variety of opportunities for your stakeholders to talk about them with you and give their feedback. The discussion document should be available in different formats, not just written. For example, in Harlow, there are a high number of people who cannot read. Comments from your earlier preparatory discussion should inform your discussion document. Remember to allow time for writing and disseminating the discussion document, arranging events/meetings and producing supporting marketing materials.
Allow at least a month for this stage.
2.4.3 Analysis of feedback from informal discussions and preparation for formal consultation
During this period, you should: Analyse feedback from the informal stage - Section 3 provides more advice
about this Prepare your formal consultation document Arrange events/meetings to give stakeholders the opportunity to discuss the
proposals face-to-face with representatives of your organisation Prepare marketing material in a variety of formats to promote the formal
consultation
Allow at least three to four weeks for this stage.
14
2.4.4 Formal Consultation
By this stage your consultation and involvement activities should include all stakeholders who may have an interest in the proposed changes to services. Remember to make the information available to all stakeholders and be prepared to give individuals and groups the opportunity to talk about their feelings and views.
Allow at least a month for this stage.
2.4.5 Analysis of feedback from formal consultation
During this period, you should: Analyse feedback from the informal stage - Section 3 provides more advice
about this Prepare your report on the consultation process Prepare your communications activities to disseminate information about the
outcome of the involvement and consultation process.
2.5 Evaluation
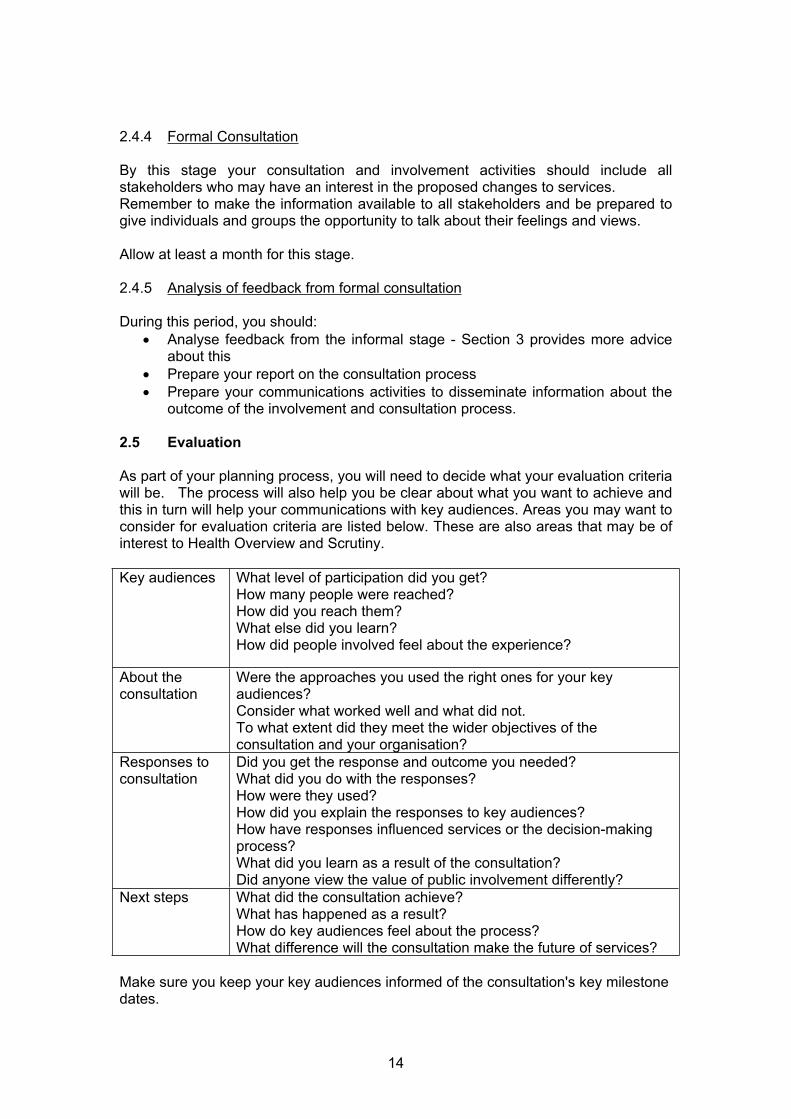
As part of your planning process, you will need to decide what your evaluation criteria will be. The process will also help you be clear about what you want to achieve and this in turn will help your communications with key audiences. Areas you may want to consider for evaluation criteria are listed below. These are also areas that may be of interest to Health Overview and Scrutiny.
Key audiences What level of participation did you get?How many people were reached?How did you reach them?What else did you learn?How did people involved feel about the experience?
About the consultation
Were the approaches you used the right ones for your key audiences?Consider what worked well and what did not.To what extent did they meet the wider objectives of the consultation and your organisation?
Responses to consultation
Did you get the response and outcome you needed?What did you do with the responses?How were they used?How did you explain the responses to key audiences?How have responses influenced services or the decision-making process?What did you learn as a result of the consultation?Did anyone view the value of public involvement differently?
Next steps What did the consultation achieve?What has happened as a result?How do key audiences feel about the process?What difference will the consultation make the future of services?
Make sure you keep your key audiences informed of the consultation's key milestone dates.
15
3. RECEIVING AND ANALYSING FEEDBACK
3.1 Guiding Principles For Receiving And Analysing Feedback
The process for receiving and analysing feedback needs to be carefully planned from the outset, as part of the consultation plan, because:
People will give their views in different ways e.g. orally, in writing, at meetings, via questionnaire, via organisations or via advocates or spokespeople
The nature of the consultation will vary e.g. it may be potentially contentious, such as closing a GP branch surgery, or it may relate to a very specialist area that will only affect a small number of people e.g. gynaecological cancer surgery
Thinking about how the feedback can be analysed should be linked to the design of questionnaires, interactive events etc.
People will need information about the proposals in a way that meets their needs and enables them to contribute informed views. The entire consultation plan should focus on how this can be achieved as the views of local people should be part of the decision making process.
Some situations, such as large public meetings, may not be appropriate if the consultation is likely to generate a lot of interest as in practice only a few people will be able to ask questions and contribute to the debate. Organising more structured events over a longer timescale may be better way of ensuring everyone is able to contribute.
Consultation is not a ballot and this needs to be taken into account when planning the consultation and analysing feedback. It is about enabling local people to shape and contribute to proposals. Other points to consider are:
Are efficient and methodical methods of recording feedback and activity in place
Who is going to do the analysis? Whom does the Outcome of Consultation Report need to be formally
presented to? How can local people be kept informed of the outcome of consultation?
3.2 Analysing Feedback
The analysis must be:
Open and easy to understand Fair Thorough Open to examination An accurate reflection of the views expressed during the consultation
3.2.1 Stages
(i) Informal consultation
16
Local people are to be involved at a very early stage of developing proposals. Records of views during this process should be used to help shape the proposals for formal consultation.
This will enable many concerns and issues to be addressed prior to formal consultation and will allow for the ideas and suggestions of local people and key stakeholders to be incorporated.
(ii) Formal consultation
3.3 Recording Activity And Views
Keep comprehensive records of the initial distribution of consultation materials i.e. how many consultation documents, summaries, posters were sent out, whom they went to. Also keep records of any additional copies requested
Record how the consultation was publicised, i.e. press releases, in newsletters, on websites etc
Keep a record of all consultation meetings, the numbers attending, the views expressed, for example:
o All consultation meetings o Any other meetings where the consultation is discussedo All written responses – letters, emails or feedback formso Any interactive exercises o Telephone conversationso One to one discussions
Establish a process for acknowledging feedback and responding to important issues that are raised during the consultation.
3.4 Producing The Outcome Of Consultation Report
Allow time to do this properly in order to ensure that all the views expressed as part of the consultation are represented fully and accurately
Ensure the right people are involved, for example those developing the proposals need to have access to all the feedback
Be careful about quantifying views, in particular with percentages. This can be very misleading especially if small numbers are involved. It is also difficult to do accurately, for example, an organisation will be responding on behalf of a large number of people.
Report on major themes and concerns or support but also on important points that may have been raised by a minority or an individual. Report ideas and suggestions.
Include original responses from key individuals/ organisations (such as the Community Health Councils) as an appendix to the report.
17
4. THE ROLE OF LOCAL AUTHORITIES IN RELATION TO HEALTH SERVICE CONSULTATION
4.1 Responsibilities
The Overview & Scrutiny Committee of each local authority with social services responsibilities has the power to consider substantial variations or developments in the local health service.
In May 2003 guidance was issued by the Secretary of Sate for Health (Department of Health) which clarified the legislation that provides local authority overview and scrutiny committees with this power.
Section 4 of The Local Authority (Overview and Scrutiny Committees Health Scrutiny Functions) Regulations 2002 stipulates that where a local NHS body has under consideration any proposal for a substantial development of the health service in the area of a local authority, or for a substantial variation in the provision of such service, it shall consult the overview and scrutiny committee of that authority.
The Overview and Scrutiny Committee has no desire to create additional layers and delay implementation of the Trust’s proposals and equally does not wish to overburden the committee’s proceedings with a plethora of consultation exercises. However, this is an important power and is the central element to the government’s proposals to make the NHS more accountable locally. It is therefore vital that there is a local understanding of what constitutes a substantial variation/development and the processes that have been put in place. The Overview and Scrutiny Committee must have an awareness of what proposals are planned and have the opportunity to ensure that local views have been sought and taken into consideration.
4.2 Role
The Role of the Overview and Scrutiny Committee is to consider:
(i) Whether, as a statutory body, the Overview and Scrutiny Committee has been properly consulted within the consultation process.
(ii) Whether, in developing the proposals for service changes, the health body concerned has taken into account the public interest through appropriate public and patient involvement and consultation.
(iii) Whether a proposal for change is in the interests of the local health service.
Full Consultation should last for a minimum of 12 weeks and should involve the wider community including hard to reach groups.
The OSC will consider 3 core principles for the development of proposals for the re-configuration of services:
Developing Options for change with people, not for them Focus on redesign of services rather than relocation Taking a whole systems view
18
4.3 Procedure Please note: Although the following provides a guide to the procedure, the order in which things happen may vary according to the complexity of the issue and other constraints.
The NHS body informally advises the Health Scrutiny Officer for the Health Overview and Scrutiny Committee and the appropriate Community Health Council(s) until their abolition on 1 December 2003, of the proposed service variation, in advance of the consultation process. Section 10.1.2 of the Ministerial Guidance states that NHS bodies should consult the OSC at an early stage to agree whether the proposal is substantial. Further guidance has also been issued on consulting with CHCs in the period until 1 December 2003 and the importance of these two bodies working together. These early discussions should include agreement about the length of time the consultation will last, identification of the population which may be affected and methods to be used taking into account local needs. It is important that NHS bodies inform the OSC (and CHCs) very early of any proposal for change, so that their consideration can be properly timetabled.
The Chairman of the Committee and local Members are advised of the proposals and provided with any supporting papers supplied by the NHS body.
At the beginning of the second phase of consultation, the Health Scrutiny Officer will write to the Project Manager dealing with the consultation for the NHS body to request a response to a set of questions within a given timeframe (an example of the type of questions that could be asked are set out in Appendix 4).
The Committee will consider the formal consultation document and may raise additional queries by way of a further letter with the health body. Answers will be requested within a specified timescale. The Committee will respond to NHS consultation within the stipulated timescale, and if it does not support the proposals, it will provide reasons and evidence for its view.
The Committee may also utilise its statutory powers to require a suitable representative(s) from the Health body to attend a meeting of the Committee to provide information. Adequate notice will be given to the Health body concerned.
If the Committee is satisfied with the information it has received from the Health body and no additional information is required it may then sign-off the service variation.
If the Committee is not satisfied with the information supplied by the health body it may request additional information/request the length of the consultation period to be extended or ultimately refer the matter to the Secretary of State for determination.
The Committee will provide the details of its final decision to the NHS body concerned within the time specified in the NHS consultation. Should the Committee be minded to refer the matter to the Secretary of State, the relevant NHS body will be given the opportunity to respond to the Committee’s comments and an effort at local resolution will be made.
An overview of the Local Authority procedure in relation to health overview and scrutiny is provided in Appendix 5.
19
4.4 Power Of Referral To The Secretary Of State
If the Overview and Scrutiny Committee is not satisfied:
a) With the content of the consultation with the committee by the NHS (not consultation with other stakeholders), or
b) That sufficient time has been allowed; or
c) That the reasons given for not carrying out consultation are adequate
it may report the matter to the Secretary of State in writing, setting out the reasons for referral. The SoS can require the NHS body concerned to carry out such consultation or further consultation with the Committee, as he considers appropriate.
If the Committee considers that the proposal is not in the interest of the health service in its area it may also refer the issue to the SoS in writing, who may make a final decision on the proposal. The SoS can require the NHS body to take such action or desist from taking such action as he (or she) may direct.
Decisions of this nature made by the Committee are formally recorded and are available to the public.
The Secretary of State may ask an Independent Reconfiguration Panel to take a judgement on the matter. This is a body that has been specifically set up to deal with referrals of this type.
4.5 Discharge Of Functions
Some local authorities may opt to discharge this function through the establishment of a Service Variation Panel, to help the Health Overview and Scrutiny Committee (OSC) deal with this workload. The Panel has delegated powers from the OSC to consider proposals for change. The prime reason for this process is to allow consultations by NHS bodies to be dealt with expeditiously. A Panel’s powers allow it to deal with all service variations and developments, subject to the proviso that any proposal to refer a matter to the Secretary of State must be referred back to the OSC for a decision. Since the Panel will take some decisions itself, its proceedings must be in public.
4.6 Joint Committees
Where a service change impacts on more than one OSC area, this will require the establishment of joint committees of OSCs to consider the change. Such joint committees exercise all the powers of an OSC and may not refer back to their ‘parent’ committees. However, ‘parent’ OSCs can exercise the power of referral to the Secretary of State following the receipt of comments back from the relevant health body(ies).
Many local authorities are currently in the process of clarifying arrangements for joint committees and there are some complexities surrounding the constitutional arrangements. These are likely to be resolved over the coming months and additional guidance will be incorporated in this section when the protocol is re-visited. Overall, the same procedure for dealing with variations will apply although there is likely to be
20
some additional information regarding the process, which will need to be co-ordinated between the authorities involved.
The NHS might need to set up a joint PCT committee for proposals involving several areas and the Strategic Health Authority might have a role in ensuring the full and relevant involvement of all stakeholders in such case.
5. THE ROLE OF PATIENT AND PUBLIC INVOLVEMENT FORUMS
5.1 Background
The primary legislation for Patients’ Forums is contained in sections 15 – 19 of the NHS Reform and Health Care Professions Act 2002.
Patients’ Forums are to be known as Patient and Public Involvement Forums – but they will not be referred to as such in regulations because this is not how they are referred to in the Act.
The draft regulations were laid before Parliament in early August and came into effect on 1 September 2003 at which point, the Patient and Public Involvement Forums were legally established (Statutory Instrument 2003 Nos. 2123 & 2124).
It is the responsibility of the Commission for Patient and Public Involvement in Health to appoint members to the Forums. The Commission will arrange to provide staff to Patients’ Forums, set quality standards, monitor how successfully those standards are met and make recommendations for improvement and assist and facilitate Forums in co-ordinating their activities. It will take time for Forums to have a full complement of members, however the Commission plan to have a minimum of seven members in place in each forum by 1 December 2003.
These members will be drawn from the local population who will represent the views of communities about the quality and configuration of health services provided and commissioned by PCTs and Trusts. They will be attached to, but independent from, every Trust and Primary Care Organisation.
A Patient and Public Involvement Forum member’s term of office shall be for a period of one to four years as agreed between the prospective member and the Commission at the time of the appointment.
5.2 The Role Of Patient And Public Involvement Forums
Patient and Public Involvement Forums will actively monitor and review NHS services in the following ways:
5.2.1 General
Obtaining the views of patients and carers about health services Provide advice, and make reports and recommendations to NHS
organisations about matters relating to the range and operation of services Inspect premises used by NHS patients including inspecting premises where
primary care and NHS care are provided by the independent sector Collect information on the range and operation of services, identify trends and
make reports to decision makers
21
Promote the involvement of the public in decisions and consultations on matters affecting their health
Put forward the views of the public to key local decision makers Provide a ‘one stop shop’ service by providing advice and information to the
public about public involvement, and complaints processes Monitor how well the local NHS is meeting its duty to involve and consult the
public Advise the relevant health bodies and other decision makers about how to
encourage the public to be involved in the decision making processes and in particular to meet their duty under Section 11 of the Health and Social Care Act
5.2.2 Patients Advice and Liaison Services - PALS and Independent Complaints Advocacy Service - ICAS
Forums will monitor the quality of Patient Advice and Liaison Services (PALS) in the area, and bring any shortcomings in the service to the attention of the relevant trust and if necessary to the Commission.
Primary Care Trust Forums will make arrangements to provide independent complaints advocacy to people wanting to complain about the NHS.
5.2.3 Overview and Scrutiny
Forums have powers to make referrals to Overview and Scrutiny Committees. This includes health services provided from a body outside the area of the local authority to inhabitants within it. Where a Forum considers that the NHS Trust or Primary Care Trust for which it was established is not carrying out its duty under Section 11 of the 2001 Act, or is not doing so in a satisfactory manner, it may refer the matter to a relevant overview and scrutiny committee who may decide to investigate further.
Forums should be involved in discussion with Overview and Scrutiny committees and with NHS bodies on what constitutes the understanding of ‘substantial variation and substantial development’
Forum members can participate in working groups or act as advisors to the committee
5.2.4 Commission for Patient and Public Involvement in Health
Forums can refer matters to the Commission and any other body they think appropriate
Forums can bring any shortcomings in the service to the attention of the relevant trust and if necessary to the Commission.
Forums are required to produce any information which appears to the Commission to be necessary for the effective carrying out of the CPPIH functions under specified regulations of the Act (with the exception of confidential information).
5.2.5 Additional points
Forum members may in the future (subject to changes in regulations) be nominated for consideration when Non Executive vacancies arise on Trust and PCT Boards.
Produce an annual report of their work and make their findings and reports available
22
References
Health Developments in Partnership: A good practice framework for public involvement in service changes in North Essex. North Essex Health Authority April 1999
Health and Social Care Act 2001Directions to Local Authorities (Overview and Scrutiny Committees, Health Scrutiny Functions)http://www.doh.gov.uk/involvingpatients/guidance.htm
How Community Health Council will Respond to Consultation documents. North East Essex Community Health Council Protocol. 1999.
Overview and Scrutiny of Health – Guidance. Department of Health. May 2003.
Patients’ Forums – Consultation on the Draft Regulations. Draft Statutory Instruments;
The Patients’ Forums (Membership and Procedure) Regulations 2003The Patients’ Forums (Functions) Regulations 2003
Department of Health, May 2003
Sections 7 – 10 Health and Social Care Act 2001http://www.legislation.hmso.gov.uk/acts/acts2001/20010015.htm
Section 38 Local Government Act 2000 http://www.legislation.hmso.gov.uk/acts/acts2000/20000022.htm
Statement of our Principles for Best Practice in Public Engagement. Essex County Council (date?)
Statutory Instrument 2002 No 3007 The Commission for Patient and Public Involvement in Health (Functions) Regulations 2002
Statutory Instrument 2002 No. 3048The Local Authority (overview and scrutiny Committees Health Scrutiny Regulations 2002 http://www.legislation.hmso.gov.uk/si/si2002/20023048.htm
Statutory Instrument 2003 No. 2123. The Patients’ Forum (Membership and Procedure) Regulations 2003 and Statutory Instrument 2003 No 2124 The Patients’ Forums (Functions) Regulations 2003 – 13 August 2003.
The Commission for Patient and Public Involvement in Health (Functions) Regulations 2002. Statutory Instrument 2002 No 3007. Department of Health 2002.
Strengthening Accountability: Involving Patients and the Public. Policy and Practice Guidance. Section 11 of the Health and Social Care Act 2001. Department of Health February 2003.
23
Model Continuum of Involvement / Consultation
Examples of issues and potential proposals
Informal involvement Informal Consultation Formal Consultation
Major service reconfiguration e.g. proposals involving reprovision / closure or development of new services
CATEGORY 4Formal consultation process required
Change in demand for specific services e.g. proposal to relocate GP surgery or cessation of some surgery sessions
CATEGORY 3Formal mechanisms established to ensure that patients / service users / carers and the public are engaged in planning and decision-making (ref: Section 11 Health & Social Care Act)
Need for modernisation of hospital based service e.g. proposal to relocate and modernise day surgery unit on a particular hospital site
CATEGORY 2More formalised structures in place to ensure that patients / service users / carers and patient groups views on the issue and potential solutions are sought
Changes in demand for specific services (e.g. Baby clinics) e.g. proposal to extend or reduce opening hours of Health Visitor Clinics
CATEGORY 1Informal discussions with individual patients / service users / carers and patient groups on potential need for changes to services and solutions
NB The examples listed on this continuum are not definitive and there may be some local variation in the way they are dealt with**It is envisaged that health bodies will submit brief details of these proposals to O&S committees to indicate which category they fall into and why.
Appendix 1
O & S Committeenormally involved **
O&S Committee may beinvolved
24
Flow Chart Illustrating the Stages of Consultation
Preparingto
consult(2 – 3 months)
Informal Consultation
Analysisof
FeedbackFormal
Consultation Analysis of Feedback
(4 weeks)
Evaluation
Appendix 2
NB: Government guidance on consultations states that full consultation should last for a minimum of twelve weeks. This may, or may not, include a period of informal consultation. If the Overview and Scrutiny Committee is assured that any preliminary concerns have been addressed prior to the issue of a formal consultation document, it may be appropriate to reduce the period of formal consultation.
25
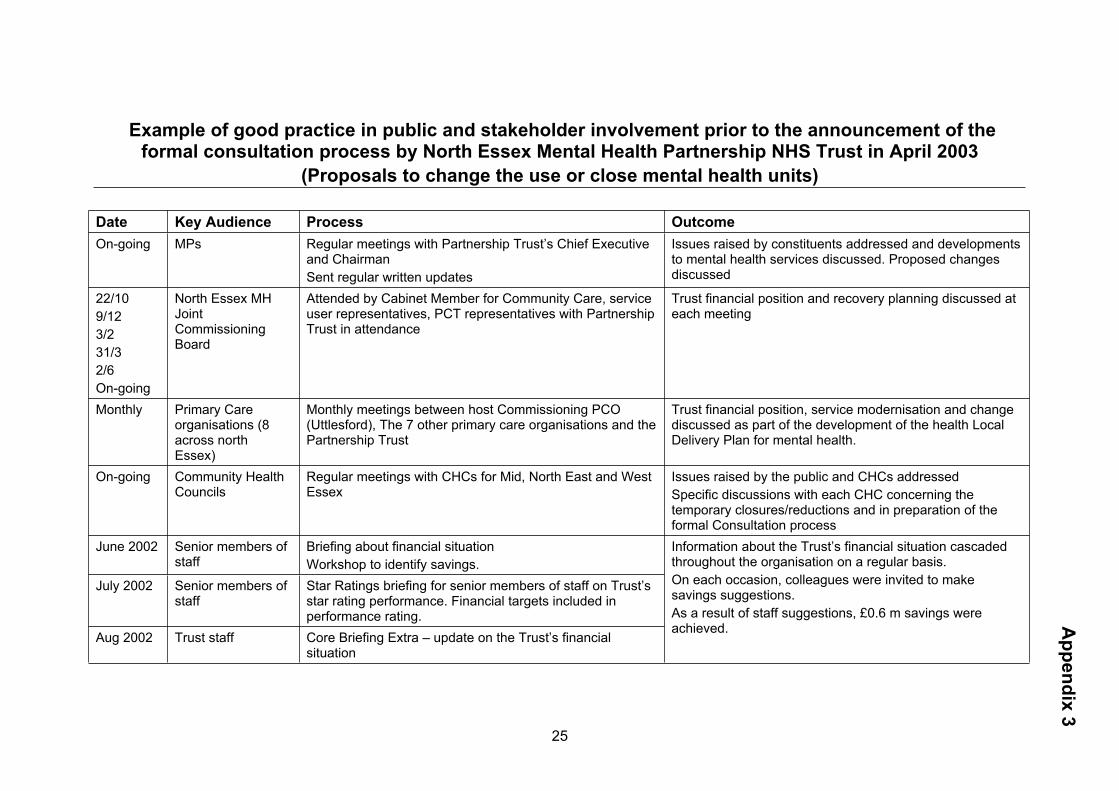
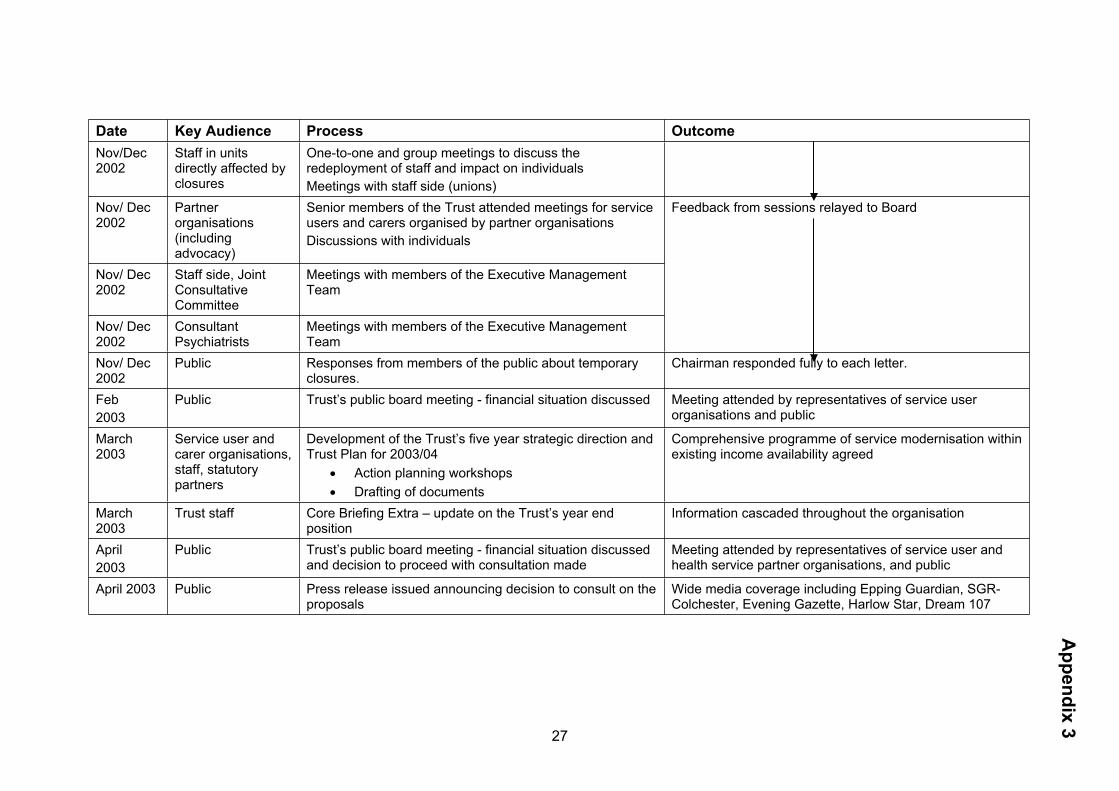
Example of good practice in public and stakeholder involvement prior to the announcement of the formal consultation process by North Essex Mental Health Partnership NHS Trust in April 2003
(Proposals to change the use or close mental health units)
Date Key Audience Process OutcomeOn-going MPs Regular meetings with Partnership Trust’s Chief Executive
and ChairmanSent regular written updates
Issues raised by constituents addressed and developments to mental health services discussed. Proposed changes discussed
22/109/123/231/32/6On-going
North Essex MH Joint Commissioning Board
Attended by Cabinet Member for Community Care, service user representatives, PCT representatives with Partnership Trust in attendance
Trust financial position and recovery planning discussed at each meeting
Monthly Primary Care organisations (8 across north Essex)
Monthly meetings between host Commissioning PCO (Uttlesford), The 7 other primary care organisations and the Partnership Trust
Trust financial position, service modernisation and change discussed as part of the development of the health Local Delivery Plan for mental health.
On-going Community Health Councils
Regular meetings with CHCs for Mid, North East and West Essex
Issues raised by the public and CHCs addressedSpecific discussions with each CHC concerning the temporary closures/reductions and in preparation of the formal Consultation process
June 2002 Senior members of staff
Briefing about financial situation Workshop to identify savings.
July 2002 Senior members of staff
Star Ratings briefing for senior members of staff on Trust’s star rating performance. Financial targets included in performance rating.
Aug 2002 Trust staff Core Briefing Extra – update on the Trust’s financial situation
Information about the Trust’s financial situation cascaded throughout the organisation on a regular basis. On each occasion, colleagues were invited to make savings suggestions. As a result of staff suggestions, £0.6 m savings were achieved. A
ppendix 3
26
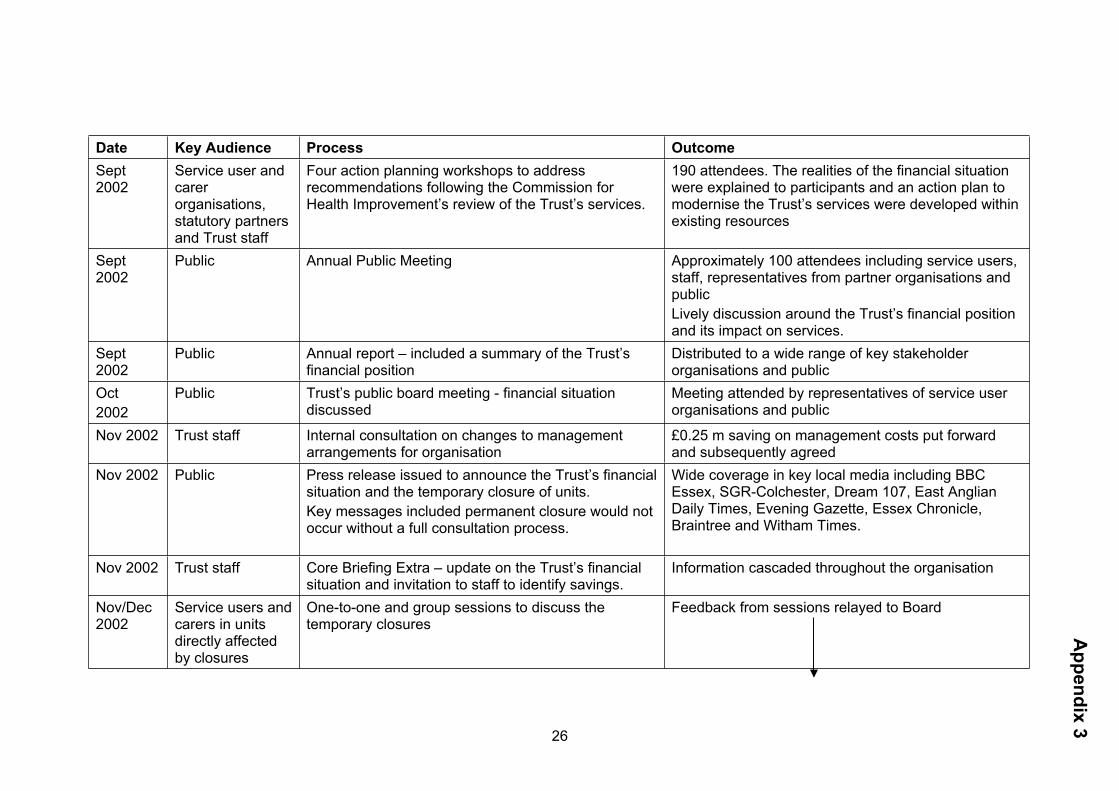
Date Key Audience Process OutcomeSept 2002
Service user and carer organisations, statutory partners and Trust staff
Four action planning workshops to address recommendations following the Commission for Health Improvement’s review of the Trust’s services.
190 attendees. The realities of the financial situation were explained to participants and an action plan to modernise the Trust’s services were developed within existing resources
Sept 2002
Public Annual Public Meeting Approximately 100 attendees including service users, staff, representatives from partner organisations and publicLively discussion around the Trust’s financial position and its impact on services.
Sept 2002
Public Annual report – included a summary of the Trust’s financial position
Distributed to a wide range of key stakeholder organisations and public
Oct2002
Public Trust’s public board meeting - financial situation discussed
Meeting attended by representatives of service user organisations and public
Nov 2002 Trust staff Internal consultation on changes to management arrangements for organisation
£0.25 m saving on management costs put forward and subsequently agreed
Nov 2002 Public Press release issued to announce the Trust’s financial situation and the temporary closure of units. Key messages included permanent closure would not occur without a full consultation process.
Wide coverage in key local media including BBC Essex, SGR-Colchester, Dream 107, East Anglian Daily Times, Evening Gazette, Essex Chronicle, Braintree and Witham Times.
Nov 2002 Trust staff Core Briefing Extra – update on the Trust’s financial situation and invitation to staff to identify savings.
Information cascaded throughout the organisation
Nov/Dec 2002
Service users and carers in units directly affected by closures
One-to-one and group sessions to discuss the temporary closures
Feedback from sessions relayed to Board
Appendix 3
27
Date Key Audience Process OutcomeNov/Dec 2002
Staff in units directly affected by closures
One-to-one and group meetings to discuss the redeployment of staff and impact on individuals Meetings with staff side (unions)
Nov/ Dec 2002
Partner organisations (including advocacy)
Senior members of the Trust attended meetings for service users and carers organised by partner organisationsDiscussions with individuals
Nov/ Dec 2002
Staff side, Joint Consultative Committee
Meetings with members of the Executive Management Team
Nov/ Dec 2002
Consultant Psychiatrists
Meetings with members of the Executive Management Team
Feedback from sessions relayed to Board
Nov/ Dec 2002
Public Responses from members of the public about temporary closures.
Chairman responded fully to each letter.
Feb2003
Public Trust’s public board meeting - financial situation discussed Meeting attended by representatives of service user organisations and public
March 2003
Service user and carer organisations, staff, statutory partners
Development of the Trust’s five year strategic direction and Trust Plan for 2003/04
Action planning workshops Drafting of documents
Comprehensive programme of service modernisation within existing income availability agreed
March 2003
Trust staff Core Briefing Extra – update on the Trust’s year end position
Information cascaded throughout the organisation
April2003
Public Trust’s public board meeting - financial situation discussed and decision to proceed with consultation made
Meeting attended by representatives of service user and health service partner organisations, and public
April 2003 Public Press release issued announcing decision to consult on the proposals
Wide media coverage including Epping Guardian, SGR-Colchester, Evening Gazette, Harlow Star, Dream 107
Appendix 3
28
Examples of questions that may be asked by Local Authority Health Overview & Scrutiny Committees
At the beginning of any second phase public consultation the Panel would request a response in writing from NHS bodies proposing service variations and developments to four basic questions as follows:
1) How the views of the public were obtained in the earlier stages of the change programme, including consultation procedures used, numbers involved, timescales for consultation and the questions asked.
2) What views were expressed by the public. We will be interested in how well informed, clear and representative these views are, and how they bear on the options available to the PCTs.
3) How these views were interpreted by the PCTs and factored into the development of your proposals, whether for or against the proposals.
4) What the public response is now to any proposals that differ from those submitted to the public in the initial round of consultation.
Upon receipt the Panel would determine if witnesses would be required to attend a future meeting and give oral evidence.
Appendix 4
29
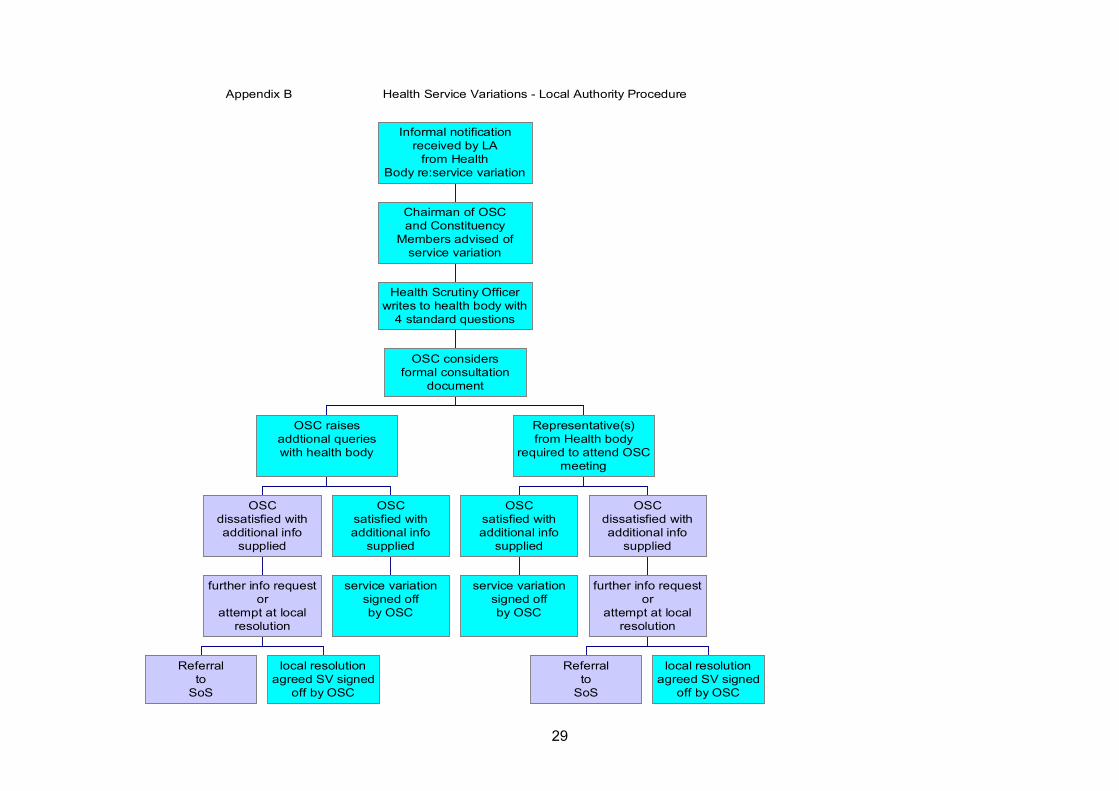
Appendix B Health Service Variations - Local Authority Procedure
Referralto
SoS
local resolutionagreed SV signed
off by OSC
further info requestor
attempt at localresolution
OSCdissatisfied withadditional info
supplied
service variationsigned offby OSC
OSCsatisfied withadditional info
supplied
OSC raisesaddtional querieswith health body
service variationsigned offby OSC
OSCsatisfied withadditional info
supplied
Referralto
SoS
local resolutionagreed SV signed
off by OSC
further info requestor
attempt at localresolution
OSCdissatisfied withadditional info
supplied
Representative(s)from Health body
required to attend OSCmeeting
OSC considersformal consultation
document
Health Scrutiny Officerwrites to health body with
4 standard questions
Chairman of OSCand Constituency
Members advised ofservice variation
Informal notificationreceived by LA
from HealthBody re:service variation
Appendix 5
30
Membership of the Working Group
Linda Barnard Communications Manager, Colchester Primary Care Trust
Lesley Edwards Principal Democratic Services Officer, Thurrock Council
Jennie Fisher Patient and Public Involvement Manager, Essex Strategic Health Authority
Karen Fulcher Head of Communications, North Essex Mental Health Partnership NHS Trust
Lee Harris Assistant Chief Executive, Southend-on-Sea Borough Council
Catherine Hodson Health Scrutiny Manager, Essex County Council
Joan Smith Chief Officer, North East Essex Community Health Council
Geoff Smalley Principal Committee Officer, Southend-on-Sea Borough Council
Appendix 6
31
Appendix 7
A TEMPLATE FOR YOUR CONSULTATION PROJECTThis is just a suggestion to help you get started. An initial plan is the best way to bring people together to gain agreement about the project and it will most likely give you a good precursor to your consultation document.Wendy SmithDirector of Communications, Essex Strategic Health Authority
Title of ProjectPatient, Public and Staff Involvement Plan
Insert author and date
Purpose
This paper advises on the latest guidance for patient and public involvement and proposes a plan to ensure that patients, public and staff are involved in insert project details.
Issue
Brief details explaining the proposals for service change or development. Try to sum it up simply in the first couple of lines then add another couple of short paragraphs of why this proposal is needed.
Main Impact of Service Change for Patients
What is the positive impact on patients?
Explain any drawbacks or compromises for patients or any possible negative public perception.
What is the scale of the effect? If it’s small scale, how many patients might be involved and who are they?
Anything else?
How Patients, Public and Staff Should be Involved
Patients, public and staff should:
have the opportunity to understand the aims of the recommendation and how it addresses the best interests of patients.
32
be involved in how the recommendation is implemented, thus bringing in the special expertise of patients, public and staff to the implementation plan, to ensure changes are designed to meet patients’ needs.
Add details of any specific decision-making input you want e.g. feedback will inform the outline business case, feedback will inform the option appraisal process.
Background
Insert details to explain how the proposals have come about e.g. difficulties with the current position, result of modernisation initiatives, any previous work that has been undertaken like a clinical review, any previous consultation that has happened and what the outcomes were.
New Procedures and National Guidance on Patient and Public Involvement
In previous years it was the responsibility of the health authority to consult the Community Health Council on any proposed service change. The Health and Social Care Act 2000 now places a duty to consult on NHS Trusts and Primary Care Trusts.
The latest national guidance on patient and public involvement emphasises closer ongoing involvement of patients and local people. This is happening through the new three-year planning framework to produce Local Delivery Plans. Through this mechanism Primary Care Trusts are engaging local communities in future service changes. Last year’s emerging Local Delivery Plans of both the Primary Care Trusts and the Strategic Health Authorities included planning intentions in insert your project if relevant.
As part of the new duty to consult, each local NHS body has a duty to consult the local overview and scrutiny committee(s) on any proposals it may have under consideration for any substantial development, or on any proposal to make any substantial variation. This is in addition to the discussions that NHS bodies will have with the local authority. The duty to consult the overview and scrutiny committee is also additional to the duty placed on NHS bodies to consult and involve patients and the public as an ongoing process under section 11 of the Health and Social Care Act.
Guidance recommends that the NHS body should discuss proposals with the overview and scrutiny committee at an early stage in order to agree whether or not the proposal is considered substantial and to discuss how consultation will be undertaken e.g. length of time and methods.
The PCT leading the commissioning process will normally be responsible for consultation. Where a proposed service spans more than one PCT, they will need to agree a process of joint consultation. The Board of each PCT should formally delegate the responsibility to a joint PCT committee, which should act as a single entity and be responsible for making the final decision following consultation. It may be that your project already has a Board or a Steering Group that would act as the consulting body on behalf of commissioners.
33
The Strategic Health Authority(ies) have a responsibility for making sure that Trusts and PCTs involve patients and the public and that consultation is done well, in line with national guidance.
The Plan for Involving Patients, Public, Staff and Professionals
Subject of Consultation
The following are given:
E.g. national policy concerning this project – NHS Plan targets, NICE guidance and other national guidance
E.g. the outcome of an independent expert clinical review or CHI inspection E.g. local policy agreed with full consultation E.g. financial position E.g. workforce issues – contractual issues, accreditation
The following are examples of decisions that need wider consultation:
E.g. how the new service can best meet the individual needs of patients and their families
E.g. how the proposed service change should be implemented E.g. how the new arrangements should be organised to ensure the greatest
efficiency and support to clinicians E.g. what is the preferred option
Basic Framework for Consultation
Period of informal discussion to introduce the issues and gather views that will inform the consultation process.
Minimum 12-week consultation period as recommended by guidelines. Could coincide with an options appraisal process. If the service is a major development, such as new hospital or a radically different way of running a major service like mental health care, there may be a need for more than one period of consultation to narrow down the options.
Details on how service users and carers could be engaged e.g. through existing groups, forums and networks. Details of one or more workshops for service users and carers. If networks are not well established you may decide to set up a user/carer panel of people who want to be consulted with one or more user groups of people who want to be involved. This infrastructure could go on throughout the development to become part of the future new service.
Distribution of consultation documents and feedback forms to all stakeholders, community representatives, staff and professionals (see proposed initial distribution list below). PCTs and Trusts will be responsible for ensuring that the information is cascaded and available to all relevant staff and professionals and will arrange any staff/team/professional discussions as necessary.
Specific consultation with representative bodies and Overview and Scrutiny Committees e.g. could include staff forums, Local Representative Committees,
34
trades union representatives, Local Strategic Partnerships. Meetings with groups also to be arranged by request.
Depending on the nature of your project you may have some special exercises e.g. professional survey or research, options appraisal exercise involving stakeholders and users.
Action Plan
1. State who is to be the consulting body. If this is to be on behalf of more than one PCT or Trusts and others in the network you will need to get formal agreement from the constituent bodies.
2. Essex Strategic Health Authority (SHA) Communications Directorate to provide advice and support, linking with colleagues in other SHAs and Department of Health if relevant.
3. xxxxx to identify key contacts, including overview and scrutiny committees, and send them proposals and plans for informal discussion and discussions about consultation process. This could include key staff groups.
4. Xxxxxx to prepare discussion and consultation materials: discussion document, feedback form, posters and fliers, presentations for discussion meetings, supporting press releases.
5. Xxxxxxxxxxxx to be involved in drafting and approving materials (see schedule of deadlines below).
6. Xxxxxxxxx to manage distribution including photocopying or printing as necessary, address labels and postage, email and website use.
7. PCTs and Trusts to prepare for cascade distribution to service users and representatives, hospital staff, relevant community staff, GPs, medical committees, executive committees, boards and any others as appropriate.
8. Xxxxxxxxxxxxxx to arrange dates, venues and process for workshop style sessions.
9. xxxxxxxxx to prepare to respond to OSCs as required.
10. xxxxxxxxxxx to prepare for discussion sessions to any group or organisation by request.
11. xxxxxxxxxxxxx to prepare for collation of feedback and to produce outcome reports for Board (or Steering Group) consideration that will inform implementation plans or business case or whatever is the next decision-making step.
Schedule for Discussion or Consultation Periods
After preliminary discussions with Overview and Scrutiny Committees and others, the following offers a typical timescale for work involved whether it is for an informal discussion period or a formal consultation period. In your actual plan you should insert dates.
35
2 weeks Produce first draft discussion/consultation document and distribute for comments
2 weeks Second draft for approval1 week Final amendments and approval1 week Distribution of documents, posters, fliers and press release12 weeks Formal consultation period2 weeks Collate and analyse feedback and prepare outcome report1 week Outcome report goes to Board or other decision-making body
Proposed Initial Distribution List
User GroupsSupport Groups and voluntary organisationsPosters and fliers to services and GP surgeriesOverview & Scrutiny CommitteesLocal Representative CommitteesIndependent sector providersPCTs, Trusts, SHAs, Workforce Development Confederation – cascade to GPs, staff, clinicians, medical committees and executive committees, service user groups and patient representatives, boardsRelevant staff and union representativesCVSs, CABs and general voluntary organisationsLocal authorities / democratic forums / strategic partnershipsMPs Press and mediaNeighbouring service networksDepartment of HealthSocial ServicesPatient and Public Involvement ForumsForum Support Organisations
Related Documents











