Democratic Services ◦ Chief Executive’s Department ◦ Leicestershire County Council ◦ County Hall Glenfield ◦ Leicestershire ◦ LE3 8RA ◦ Tel: 0116 232 3232 ◦ Email: [email protected] www.twitter.com/leicsdemocracy www.facebook.com/leicsdemocracy www.leics.gov.uk/local_democracy Meeting: Health Overview and Scrutiny Committee Date/Time: Wednesday, 10 September 2014 at 2.00 pm Location: Sparkenhoe Committee Room, County Hall, Glenfield Contact: Mrs. R. Palmer (0116 305 6098) Email: rosemary.[email protected] Membership Dr. S. Hill CC (Chairman) Mrs. J. A. Dickinson CC Dr. T. Eynon CC Dr. R. K. A. Feltham CC Mr. W. Liquorish JP CC Mr. J. Miah CC Mr. M. T. Mullaney CC Mr. J. P. O'Shea CC Mr. A. E. Pearson CC Please note: this meeting will be filmed for live or subsequent broadcast via the Council’s web site at http://www.leics.gov.uk/webcast – Notices will be on display at the meeting explaining the arrangements. AGENDA Item Report by 1. Minutes of the meeting held on 11 June 2014 (Pages 5 - 12) 2. Question Time. 3. Questions asked by members under Standing Order 7(3) and 7(5). 4. To advise of any other items which the Chairman has decided to take as urgent elsewhere on the agenda. 5. Declarations of interest in respect of items on the agenda.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Democratic Services ◦ Chief Executive’s Department ◦ Leicestershire County Council ◦ County Hall
Glenfield ◦ Leicestershire ◦ LE3 8RA ◦ Tel: 0116 232 3232 ◦ Email: [email protected]
www.twitter.com/leicsdemocracy
www.facebook.com/leicsdemocracy
www.leics.gov.uk/local_democracy
Meeting: Health Overview and Scrutiny Committee
Date/Time: Wednesday, 10 September 2014 at 2.00 pm
Location: Sparkenhoe Committee Room, County Hall, Glenfield
Contact: Mrs. R. Palmer (0116 305 6098)
Email: [email protected]
Membership
Dr. S. Hill CC (Chairman)
Mrs. J. A. Dickinson CC
Dr. T. Eynon CC Dr. R. K. A. Feltham CC Mr. W. Liquorish JP CC
Mr. J. Miah CC Mr. M. T. Mullaney CC Mr. J. P. O'Shea CC Mr. A. E. Pearson CC
Please note: this meeting will be filmed for live or subsequent broadcast via the
Council’s web site at http://www.leics.gov.uk/webcast – Notices will be on display at the meeting explaining the arrangements.
AGENDA
Item Report by
1.
Minutes of the meeting held on 11 June 2014
(Pages 5 - 12)
2.
Question Time.
3.
Questions asked by members under Standing Order 7(3) and 7(5).
4.
To advise of any other items which the Chairman has decided to take as urgent elsewhere on the agenda.
5.
Declarations of interest in respect of items on the agenda.
6.
Declarations of the Party Whip in accordance with Overview and Scrutiny Procedure Rule 16.
7.
Presentation of Petitions under Standing Order 36.
8.
Quarterly Performance Report.
Chief Executive and GEM Commissioning Support Performance Service
(Pages 13 - 24)
9.
Leicester, Leicestershire and Rutland - Learning Lessons to Improve Care.
University Hospitals of Leicester NHS Trust and East Leicestershire Clinical Commissioning Group
(Pages 25 - 70)
10.
Better Care Fund Update.
Director of Health and Care Integration
(Pages 71 - 86)
11.
UHL Update on Current Issues.
University Hospitals of Leicester NHS Trust
(Pages 87 - 128)
12.
Arriva Transport Solutions.
East Leicestershire and Rutland Clinical Commissioning Group
(Pages 129 - 136)
13.
Date of next meeting
The next meeting of the Committee is scheduled to take place at 2.00pm on 21 November 2014. Meetings will be held at 2.00pm on the following dates during 2015:- 12 January 25 February 10 June 9 September 11 November
14.
Any other items which the Chairman has decided to take as urgent.
QUESTIONING BY MEMBERS OF OVERVIEW AND SCRUTINY
Members serving on Overview and Scrutiny have a key role in providing constructive yet robust
challenge to proposals put forward by the Cabinet and Officers. One of the most important skills is the
ability to extract information by means of questions so that it can help inform comments and
recommendations from Overview and Scrutiny bodies.
Members clearly cannot be expected to be experts in every topic under scrutiny and nor is there an
expectation that they so be. Asking questions of ‘experts’ can be difficult and intimidating but often
posing questions from a lay perspective would allow members to obtain a better perspective and
understanding of the issue at hand.
Set out below are some key questions members may consider asking when considering reports on
particular issues. The list of questions is not intended as a comprehensive list but as a general guide.
Depending on the issue under consideration there may be specific questions members may wish to
ask.
Key Questions:
• Why are we doing this?
• Why do we have to offer this service?
• How does this fit in with the Council’s priorities?
• Which of our key partners are involved? Do they share the objectives and is the service to be
joined up?
• Who is providing this service and why have we chosen this approach? What other options were
considered and why were these discarded?
• Who has been consulted and what has the response been? How, if at all, have their views been
taken into account in this proposal?
If it is a new service:
• Who are the main beneficiaries of the service? (could be a particular group or an area)
• What difference will providing this service make to them – What will be different and how will we
know if we have succeeded?
• How much will it cost and how is it to be funded?
• What are the risks to the successful delivery of the service?
If it is a reduction in an existing service:
• Which groups are affected? Is the impact greater on any particular group and, if so, which group
and what plans do you have to help mitigate the impact?
• When are the proposals to be implemented and do you have any transitional arrangements for
those who will no longer receive the service?
• What savings do you expect to generate and what was expected in the budget? Are there any
redundancies?
• What are the risks of not delivering as intended? If this happens, what contingency measures have
you in place?
This page is intentionally left blank
Minutes of a meeting of the Health Overview and Scrutiny Committee held at County Hall, Glenfield on Wednesday, 11 June 2014.
PRESENT
Dr. S. Hill CC (in the Chair)
Mrs. J. A. Dickinson CC Dr. T. Eynon CC Dr. R. K. A. Feltham CC Mr. W. Liquorish JP CC
Mrs. H. E. Loydall CC Mr. J. Miah CC Mr. A. E. Pearson CC Mr. P.G. Lewis CC
In attendance Paul St Clair, Assistant Director of Operations Leicester, Leicestershire and Rutland, East Midlands Ambulance Service (minute 10 refers) Tim Loveridge Director of Business Development and Strategy (minute 10 refers) Mrs. R. Camamile CC, Chairman of the Scrutiny Review Panel (minute 11 refers) Patricia Ford, Head of Nursing West Leicestershire Clinical Commissioning Group (minute 12 refers) Caroline Trevithick, Chief Nurse and Quality Lead, West Leicestershire CCG (minute 12 refers) Tracy Ward, Head of Service Compliance and Quality, Leicestershire County Council (minute 12 refers) Christine Richardson, NHS England (minutes 13 and 14 refer) Helen Thompson, Divisional Director, Leicester Partnership Trust (minute 14 refers) Neil Hemstock, Clinical Director for CAMHS (minute 14 refers)
Mike Sandys, Director of Public Health, Leicestershire County Council (minute 15 refers) Lisa Carter, Performance Manager, Leicestershire County Council (minute 15 refers)
1. Appointment of Chairman. That Dr S Hill CC be appointed Chairman of the Health Overview and Scrutiny Committee for the period ending with the date of the Annual Meeting of the County Council in 2015.
Dr S Hill CC in the Chair
2. Election of Deputy Chairman. That Mrs J A Dickinson CC be elected Deputy Chairman of the Health Overview and Scrutiny Committee for the period ending with the date of the Annual Meeting of the County Council in 2015.
3. Minutes of the meeting held on 12 March 2014. The minutes of the meeting held on 12 March 2014 were taken as read, confirmed and signed.
Agenda Item 15
4. Question Time. The Chief Executive reported that no questions had been received under Standing Order 35.
5. Questions asked by members under Standing Order 7(3) and 7(5). The Chief Executive reported that no questions had been received under Standing Order 7(3) and 7(5).
6. To advise of any other items which the Chairman has decided to take as urgent elsewhere on the agenda. There were no urgent items for consideration.
7. Declarations of interest in respect of items on the agenda. The Chairman invited members who wished to do so to declare any interest in respect of items on the agenda for the meeting. Dr. T. Eynon CC declared a personal interest in all items on the agenda as a salaried GP. Mrs. J. A. Dickinson declared a personal interest in all items relating to the University Hospital of Leicester NHS Trust on the agenda as her grandson was employed by the University Hospital of Leicester NHS Trust.
8. Declarations of the Party Whip in accordance with Overview and Scrutiny Procedure Rule 16. There were no declarations of the party whip.
9. Presentation of Petitions under Standing Order 36. The Chief Executive reported that no petitions had been received under Standing Order 36.
10. Progress Following Risk Summits and Outcome of CQC Inspection.
The Committee considered a report from East Midlands Ambulance Service (EMAS) that provided an update on progress made to service delivery since the two risk summits on October 2013 and February 2014. A copy of the report marked ‘Agenda item 10’ is filed with these minutes.
The Chairman welcomed Paul St Clair, Assistant Director of Operations for Leicester, Leicestershire and Rutland (LLR) and Tim Loveridge, Director of Business Development and Strategy to the meeting for this item. In the ensuing discussion the following points were raised:
i. Implementation of EMAS Estates Strategy was on hold to enable the organisation to focus on performance of quality of care; it was not known when implementation would recommence, however it was recognised that any changes made to the estate in the future would have to be self-funding. The closure of the ambulance station in Melton had not affected response times in the area, although EMAS was still looking for new premises in Melton Mowbray.
6
ii. The Committee welcomed the focus on recruitment of front line staff and was
reassured to note that the LLR division would have the correct level of staff by Sept 2014; it was also noted that staff turnover and sickness levels had reduced significantly within the service. The additional staff, in conjunction with additional fleet assets had led to an increase in patient carrying capacity and a reduction in time between first responder arrival and ambulance arrival.
iii. The Committee was pleased to note the increasing number of patients who were
treated on scene by EMAS and not taken to hospital (non-conveyance). The Committee was assured that data relating to the treatment of these people was clinically reviewed to ensure that the appropriate course of action had been taken. Further work would be undertaken to improve non-conveyance rates further.
iv. The Committee was assured that the improvements being made through the Better Care Plan were sustainable because they were being implemented incrementally over an 18 month programme. Delivery of the action plan was supported by good communication with staff at all levels and better engagement with partners. The Committee welcomed the improvements in cleanliness and infection control.
v. The Committee raised the issue of ambulances being delayed at Accident and
Emergency (A&E) due to delays in transferring the patient from paramedics to A&E staff. It was noted that this was beyond EMAS control; however EMAS was working with UHL to improve handover times including by deploying hospital liaison officers to A&E to manage groups of patients and assist with handovers. If handover time could be reduced to established targets then an additional 9000 working hours would be created for the service per annum.
RESOLVED: (a) That the update on the current issues, progress and challenges that face the East
Midlands Ambulance Service NHS Trust (EMAS) be noted; (b) That EMAS be requested to provide a further update on the performance of the
Better Patient Care Plan and performance issues to the Health Overview and Scrutiny Committee on 12 November 2014.
11. Report of the Scrutiny Review Panel on the Referral Pathway for Older People with
Anxiety and Depression. The Committee considered a report from the Scrutiny Review Panel outlining the conclusions and recommendations from the panel’s investigation into the referral pathway for older people with anxiety and depression. A copy of the report marked ‘Agenda item 11’ is filed with these minutes. The Chairman welcomed Mrs. R. Camamile CC, Chairman of the Scrutiny Review Panel to the meeting for this item. The Committee welcomed the report and noted that a small number of typographical changes would be made before the report would be presented to the Cabinet and Clinical Commission Group. It was noted that the Panel was proposing the screening of both new and existing care home residents for mental health problems. Changes in circumstances could lead to
7
anxiety or depression; however it was important not to generalise and to treat each person as an individual. RESOLVED:
a) That the report of the Scrutiny Review Panel on the Referral Pathway for Older People with Anxiety or Depression be supported and that the recommendations therein be referred to the Cabinet and County Clinical Commissioning Groups for consideration;
b) That recommendation (b) of the report be amended to include reference to Day
Centres;
c) That the Chairman of the Panel be requested to liaise with the appropriate Cabinet Lead Member, Chief Officer and partners with a view to monitoring progress made against the recommendations.
12. Emergency Hospital Admission Avoidance from Care Homes.
The Committee considered a report from West Leicestershire and East Leicestershire and Rutland Clinical Commissioning Groups on the work undertaken to avoid unnecessary hospital admissions from care homes in Leicestershire. A copy of the report marked ‘Agenda item 12’ is filed with these minutes. The Chairman welcomed Patricia Ford, Head of Nursing West Leicestershire Clinical Commissioning Group, Caroline Trevithick, Chief Nurse and Quality Lead, West Leicestershire CCG and Tracy Ward, Head of Service Compliance and Quality, Leicestershire County Council to the meeting for this item. Arising from discussion the following points were raised:
i. It was noted that the provision of bespoke data for emergency admissions was being piloted by West Leicestershire CCG and would be rolled out if successful across the county. The Committee felt that whilst emergency admissions from care homes had fallen, it would be useful to capture data on emergency admissions for a longer period than December 2013 - February 2014. However, the fact that the information could be used to give GPs more information on patients and highlight areas that generated disproportionate emergency admissions was seen as beneficial.
ii. The Committee discussed the need for care homes to have better trained staff
with better remuneration to increase skill base and reduce high staff turnover. As well as supporting qualified nurses in care homes who might have become isolated from other non-emergency facilities in the County, it was felt that these measures would reduce care home staff contacting emergency services. Other factors were identified which contributed to emergency admissions included the changeover of staff; use of agency staff and the need to change established practices in care homes of referring staff to emergency care.
iii. Concern was expressed regarding the quality of care plans. The Committee was advised that there was no national template for care plans, although the County Council had a range of documents that could be shared with providers and would support them to improve the quality of care plans. Both the County Council and NHS could require improvements as part of the contract monitoring process. In addition the care quality commission would look at care plans when assessing
8
residential care homes. Healthwatch also had the ability to act as an independent assessor in ensuring that care plans are followed. Access to a free advocacy service was available for social care patients who were dissatisfied with the quality of their care plans.
RESOLVED:
a) That the work undertaken to avoid unnecessary hospital admissions from care homes be noted;
b) That the key commissioning activities and quality improvement initiatives introduced in 2013/14 and for 2014/15 to improve outcomes for frail older people be noted;
c) That West Leicestershire Clinical Commissioning Group and East Leicestershire
and Rutland Clinical Commissioning Group be requested to submit a report on progress with the initiatives and activities designed to reduce unnecessary hospital admissions to the meeting of the Health Overview and Scrutiny Committee on 12 November 2014.
13. Perinatal Inpatient Mental Health Services in Leicestershire. The Committee considered a report from NHS England and West Leicestershire Clinical Commissioning Group which provided an update on the provision on inpatient perinatal mental health services in Leicestershire. A copy of the report marked ‘Agenda item 13’ is filed with these minutes. The Chairman welcomed Christine Richardson, NHS England, Head of Specialised Commissioning for the East Midlands to the meeting for this item. Concern was expressed that there was an apparent lack of demand for inpatient perinatal mental health services in Leicestershire which was not supported by demographic evidence. However, the Committee was pleased to note that the new pathways were working and that there had been no issues since the service provided by Leicestershire Partnership Trust (LPT) ceased. It was acknowledged that the facilities and staffing of the unit at LPT had not been fit for purpose whereas the new services model included well regarded units in both Nottingham and Derby. The new pathway also aimed to ensure consistency in the provision of community services across the East Midlands. RESOLVED: That the update on the provision of inpatient perinatal mental health services in Leicestershire be noted.
14. Proposed Relocation of Child and Adolescent Mental Health Inpatient Services. The Committee received a report from Leicester Partnership Trust (LPT) on the proposal to temporarily relocate the specialist inpatient child and adolescent mental health service (CAMHS) to Coalville Hospital. A copy of the report marked ‘Agenda item 14’ is filed with these minutes.
9
The Chairman welcomed Helen Thompson, Divisional Director, Leicester Partnership Trust, Christine Richardson, NHS England, Head of Specialised Commissioning for the East Midlands and Neil Hemstock, Clinical Director for CAMHS Trust to the meeting. Arising from discussion the following points were noted:
i. The Committee was concerned with the proposal to move CAMHS inpatient services to Coalville hospital as it would have poor transport links to the rest of the County making visitation by relatives difficult. The Committee was assured that, where appropriate, transport for families would be subsidised. Alternative sites had been considered; however no other suitable sites had been identified as they were either be occupied or were found to have an unsuitable environment for CAMHS patients.
ii. It was noted that, following a national review of the ‘tier 4 CAMHS’, the service
would be re-procured. There was therefore a risk to the long term provision of the service in Leicestershire. Should LPT be successful in tendering for the new service, the Leicester, Leicestershire and Rutland Estates strategy would be used to identify a long term solution. The Clinical ambition was for the service to from part of the Bradgate Unit; options included the refurbishment of a ward or developing a unit in partnership with a school.
iii. Concern was expressed that work to relocate the CAMHS inpatient service had not commenced early enough. However, the Committee was advised that the priorities in the Capital Programme following the sale of the Towers Site had been the Centre of Excellence and refurbishment of Adult Mental Health wards. The work on relocating CAMHS inpatient service had therefore not started until 2012 and had been further complicated by the lack of continuity in leadership at the Trust and the outsourcing of facilities management.
iv. The ward at Coalville was not fit for purpose and would have required refurbishing regardless of the relocation of CAMHS inpatient services. The worst case scenario for the cost of refurbishment was £2m. It was noted that the service would still not meet the national requirements as it had dormitories rather than individual rooms. This issue would be addressed through the location of the permanent site.
v. It was noted that the relocation of the CAMHS services to Coalville would enable LPT to deliver a good quality service within its existing footprint.
vi. The Committee expressed the view that CAMHS facilities provided may not be
sufficient to meet demand, which if lost would have a detrimental effect on other mental health services in Leicestershire. LPT were concerned that if the proposed plan contained in the report did not receive support then the service could be lost and CAMHS patients would be treated outside the East Midlands region.
RESOLVED: That the proposed relocation of Child and Adolescent Mental Health Services be supported, subject to Leicestershire Partnership NHS Trust being asked to give further consideration to the following areas of concern:- (a) The long term viability of the service; (b) Accessibility and transport.
10
15. Performance Report. The Committee considered a joint report from the Chief Executive and Director of Public Health which provided an overview of the performance framework across the health and wellbeing sector in Leicestershire and an overview of current performance A copy of the report marked ‘Agenda item 15’ is filed with these minutes. The Committee welcomed the report in particular the layout and content of the health and wellbeing corporate dashboards marked Appendices A and B as this would assist the Committee in identifying areas for scrutiny and showed the progress of the Better Care Fund project. It was noted that the ‘breast feeding at 6-8 weeks prevalence target’ was still not being met. Data has shown that uptake was lower in West Leicestershire so that area was being targeted through information provision, peer support and peer education. The position had improved recently, however it was acknowledged that there was an element of choice involved. RESOLVED:
a) That the progress made to date in developing the performance framework alongside reporting arrangements to support the Committee’s role be noted;
b) That the performance summary and issues identified this quarter be noted.
16. Date of next meeting.
It was noted that the next meeting of the Committee would be held on 10 September 2014 at 2.00pm.
17. Any other items which the Chairman has decided to take as urgent. There were no urgent items for consideration.
2.00 - 4.45 pm CHAIRMAN 11 June 2014
11
12
This page is intentionally left blank
HEALTH AND WELLBEING SCRUTINY COMMITTEE 10 SEPTEMBER 2014
REPORT OF COUNTY COUNCIL CHIEF EXECUTIVE AND GEM
COMMISSIONING SUPPORT PERFORMANCE SERVICE
PERFORMANCE REPORT AT END OF QUARTER 1 2014/15 Purpose of Report
1. To provide the Committee with an update on performance against current performance priorities set out in the Health and Wellbeing Board and Commissioner Performance Frameworks, based on data available at the end of quarter 1 2014/15.
Background
2. The Committee currently receives a joint report on performance from the County Council’s Chief Executive’s Department and the Greater East Midlands (GEM) Commissioning Support Service. This report encompasses:
a. Performance against key metrics and priorities set out in the Better Care
Fund plan and with progressing health and social care integration. b. An update on key provider performance issues and performance priorities
identified in Clinical Commissioning Group Plans. c. An update on the impact of delivery of actions and priorities identified in
the Joint Health and Wellbeing Strategy using a variety of related performance measures and targets. Also the impact on performance of service delivery with regard to key areas of adult social care, public health and children’s health services.
Performance Update
3. Since the last meeting the main change to the Health and Wellbeing Performance
Framework relates to the agreement by the County Council of a new Strategic Plan with supporting priorities, indicators and targets to 2018. These impact on certain elements of the health and wellbeing performance framework. There have also been some changes to the health performance system including a new ‘Everyone Counts’ dashboard updating parts of the NHS Constitution.
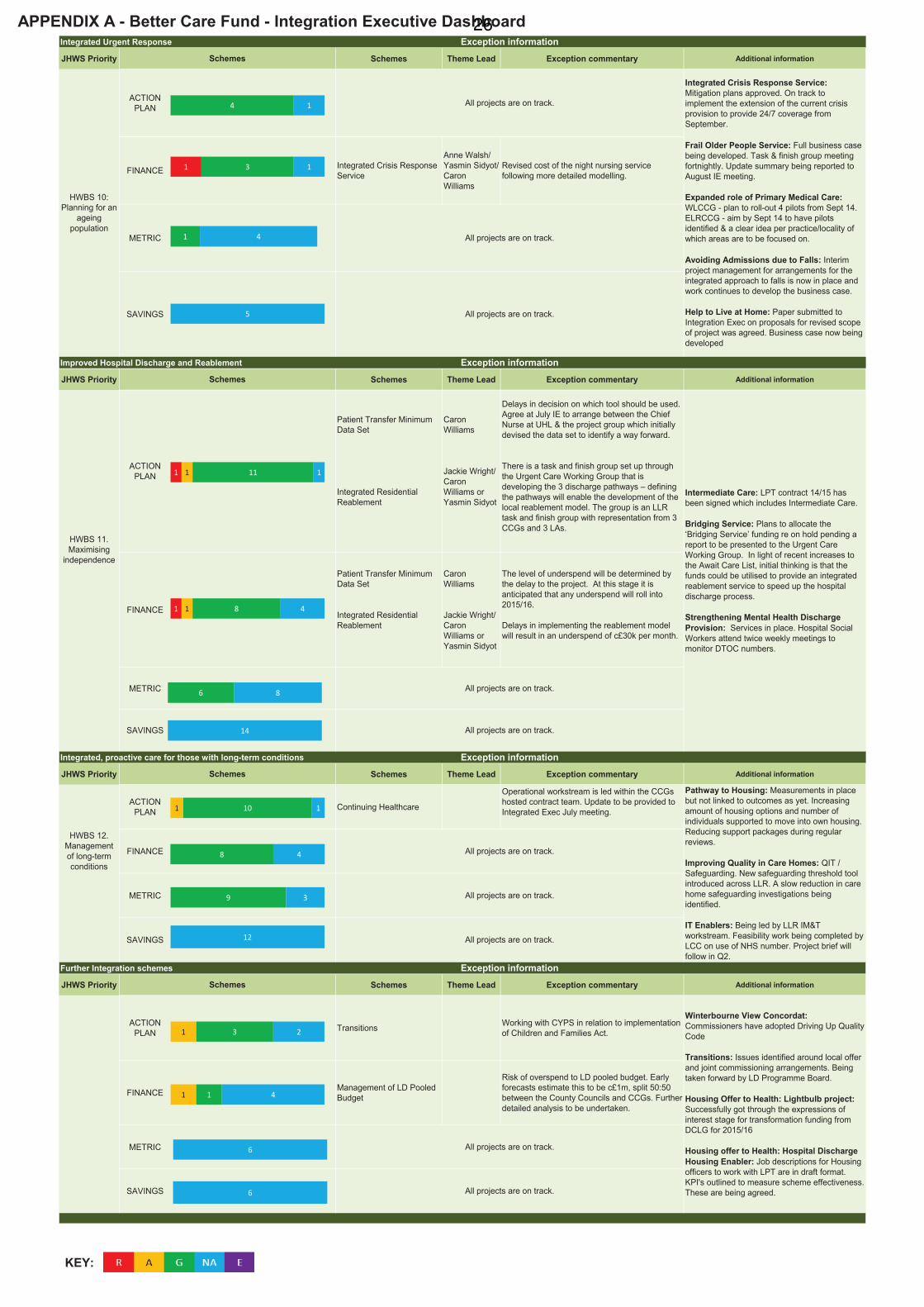
Better Care Fund and Integration Projects - Integration Executive Dashboard – Appendix A
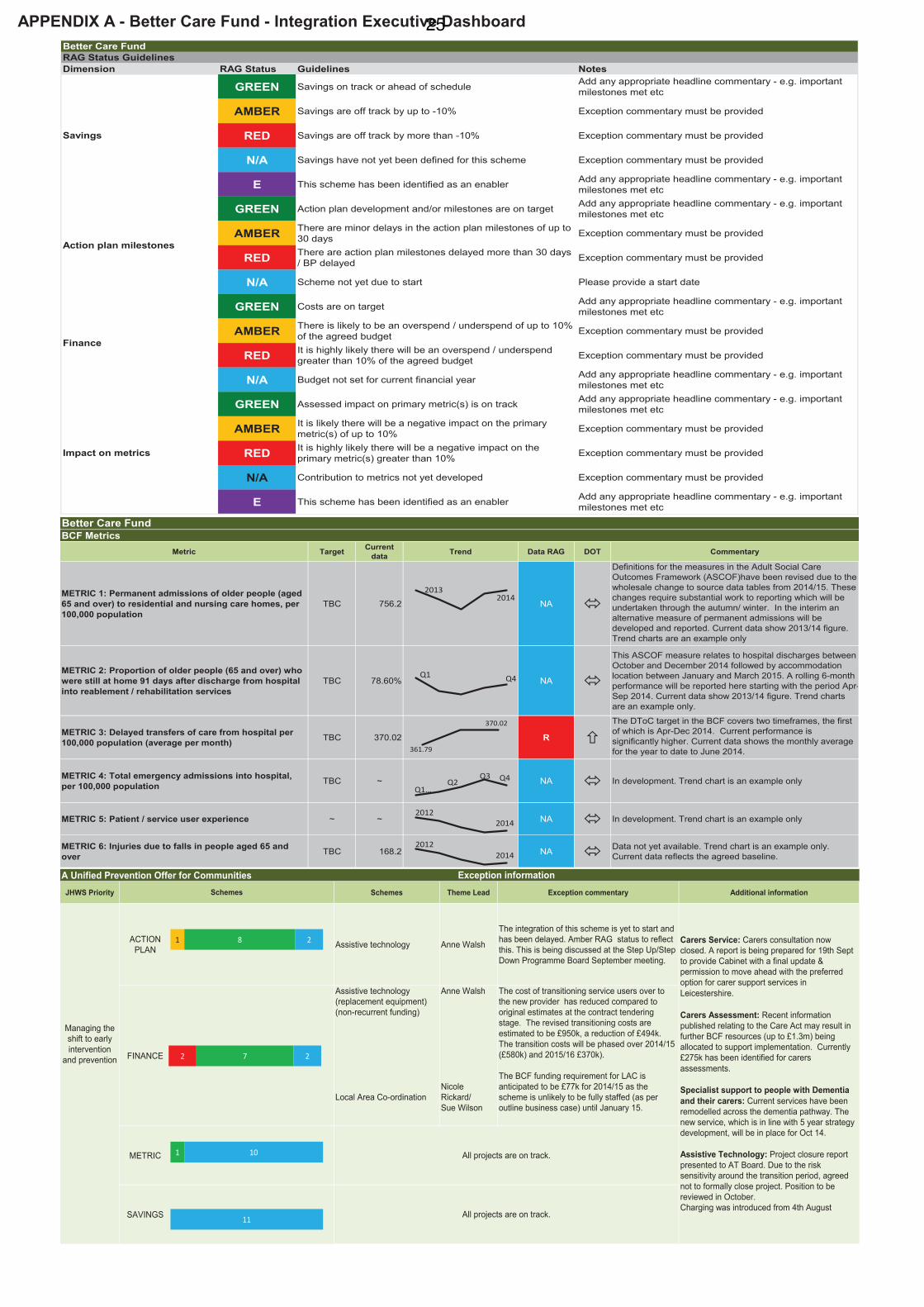
4. The dashboard attached as Appendix A summarises performance against the current schemes within the Better Care Fund (BCF). As a number of the schemes are still at an early stage of development or delivery the report highlights Amber and Red issues on an exception basis.
5. There is also a summary of the BCF Plan key metrics/targets and available
current baseline data against them. Where data is not yet available for the
Agenda Item 813
metrics and proposed targets the published baselines are shown. The trend charts are examples only and as data is published these will be used to show a view of whether the data is fluctuating or following a consistent upward or downward trend over a period of time.
6. However, nationally all Better Care Fund plans need to be resubmitted in the light
of national changes to the BCF process. The templates and technical guidance for this were released on July 25th and the Plan will need to be submitted by 19th September.
7. There is a new pay for performance scheme linked to a revised BCF metric which equates to a reduction of 3.5% in ‘total emergency admissions’ in 2015/16, rather than the current ‘avoidable emergency admissions’. The baselines for all the metrics in the BCF guidance have been changed so that these are all now calculated in 2013/14. This means all the metrics and trajectories in each BCF plan have to be recalculated/ revalidated. Further work has therefore been completed during July/August to assess the data quality and data capture for all BCF schemes.
8. The Integration Executive on 1st September will be considering the proposed
survey questions to be used for the patient experience metric and whether the injuries due to falls should remain as a local metric.
9. In Leicestershire our current performance in emergency admissions puts us in the
lowest performing quartile nationally and performance during the first quarter shows more people being admitted than accounted for in NHS commissioning plans. The Leicester, Leicestershire and Rutland (LLR) wide 5 year plan sets a trajectory to reduce emergency admissions by 5% per year. 3.5% of the 5% is now subject to pay for performance. However essentially we will have to make a reduction of 8% in emergency admissions in 2015/16 to achieve the 3.5% reduction per the 2013/14 baseline. A meeting is planned for 3 September to discuss the 3.5% metric and consider if any local flexibility is required.
10. National Better Care Fund resubmission templates require a much greater level
of detail about the benefits of each scheme linked to the metrics, and in particular the breakdown for total emergency admissions metrics. Work is underway to understand the impact of these changes. Analysis has been completed and for Leicestershire this would entail around 1,911 admissions to be avoided through BCF related interventions. It is anticipated that a number of the allocations may change in line with the BCF resubmission.
14
Performance Against Current BCF Metrics
11. Within the current outcome metrics, there have been a number of issues highlighted:
Metric Commentary
Metric 3: No of days of delayed transfers of care from hospital per 100,000 population (average per month)
The Delayed Transfer of Care (DToC) data shows deterioration in performance. This is a composite measure across settings of care (e.g. acute, community and mental health). University Hospitals Leicestershire (UHL) and partners through the Urgent Care Working Group are focusing on the changes needed to local discharge pathways, with a focus on tackling length of stay. There are a number of initiatives in place to improve the position. The Integration Executive have received assurance that the Leadership Group for Delayed Transfers of Care are working towards a single discharge process and a significant increase in reablement. See also paragraph 38.
Metric 5: Patient Experience
In terms of the metric to measure patient experience this will not now be prescribed nationally, so consideration is being given to using a relevant local metric. The approach to this for the BCF resubmission is being considered at the Integration Executive’s September meeting. NHS England have confirmed that more than one question can be used.
Local Metrics
Injuries due to falls in people aged 65 and over
It is being recommended that the local metric remains as falls due to injuries for the BCF Plan.
Length of Stay Additional work is being undertaken on the length of stay (LOS) metric and this will be reported locally. It is anticipated that by October 2014 a trajectory for improving LOS performance will be agreed as part of the urgent care and frail older people workstreams of the five year plan. The discharge pathways from the acute trust will be simplified to five clear routes with system performance including (delayed discharges) measured against these routes, by setting of care.
n.b. See also page 9 re emergency admissions performance.
12. Within the current Better Care Fund scheme delivery progress updates, a number of issues have been noted.
Scheme Commentary
Carers Assessment
Included in Leicestershire’s BCF allocation is £1.3m that has been identified by Government to implement aspects of the Care Act. Main areas include additional responsibilities for carers, new eligibility criteria, safeguarding and independent mental health advocacy. At the time of the BCF Plan submission in April only £0.3m was included for carers assessments, however new guidance received for the September resubmission states that the
15
BCF Plan needs to demonstrate how the full £1.3m has been allocated. This will increase BCF commitments by £1m.
Assistive Technology: replacement equipment
The contract for Leicestershire’s housing related support services has recently been awarded to a new provider. As part of the transition process it was anticipated that there would be a need to replace old/incompatible equipment. At the post tender stage the cost of this has been reduced by £494k. The transition period commences in 2014/15 and will continue into the first half of 2015/16. The new phasing of expenditure and reduced level of funding required will be reflected in the BCF resubmission.
Local Area Coordination
Anticipated underspend as the scheme is unlikely to be fully staffed until January 2015, although various options to mitigate this are being addressed.
Integrated Crisis Response Service
A £232k overspend for the Integrated Crisis Response Service relates to the night nursing element provided by Leicestershire Partnership NHS Trust (LPT). Original financial modelling in 2013 has since been updated resulting in the additional cost as the service delivery model was developed.
Patient Transfer Minimum Data Set
There have been some delays affecting the decision on which tool should be implemented for the minimum data set. This was due to be addressed at meeting arranged between the Chief Nurse at University Hospitals of Leicester and the project group which devised the minimum safe transfer data set to identify a way forward.
13. Recommendations on the patient experience metrics and baselines and
targets will be considered as part of the revised Better Care Fund Plan resubmission process.
Better Care - Adult Social Care Outcomes Framework Performance
14. The Better Care Fund process recognises that tackling pressure on the acute hospital sector needs supporting and integrated adult social and community care services. The Adult Social Care Outcomes Framework (ASCOF) is designed to highlight aspects of performance in adult social care services, some elements of which Better Care Fund Plan projects can potentially support.
15. New ASCOF comparative figures have recently been updated for 2013 -14 by the
Health and Social Care Information Centre and will be considered in detail by the Adults and Communities Scrutiny Committee in September. In summary they show a mixed comparative picture with good performance around safeguarding but room for improvement in relation to indicators in the domains of enhancing quality of life for people with care and support needs, delaying and reducing the need for care and support and ensuring people have a positive experience of care. Comments on Domain 2 are set out below.
ASFOF Domain 2: Delaying and Reducing the Need for Care and Support
16
The number of permanent admissions to residential or nursing care is the over-arching metric for this domain and for people aged 18-64 during 2013/14 was slightly lower than the national average and in the second quartile i.e. it is better to have a lower number of admissions. For those aged 65 or over however performance on the comparable indicator was slightly above average and in the third quartile.
Two key measures in the ASCOF relate to reducing delayed transfers of care from hospital. The first of these focuses on all delays regardless of which agency the delay is attributable to. In Leicestershire these are higher than the national average and in the third quartile. The number of delays attributable to either Adult Social Care specifically or jointly with the NHS are significantly lower than ‘all delays’ i.e. they don’t include those attributable to the NHS only. Nevertheless a rise in numbers through the year has meant an increase above the national average into the third quartile. The BCF performance reporting will in future cover the impact of care/health services in terms of reducing emergency hospital admissions.
16. In total 8 of the 19 ASCOF indicators are improving and 9 deteriorating. The County Council has identified ‘Better Care’ as one of the priorities in its Strategic Plan. This is supported by a programme of activity and variety of projects within the Council’s transformation programme as well as the projects in the Better Care Fund.
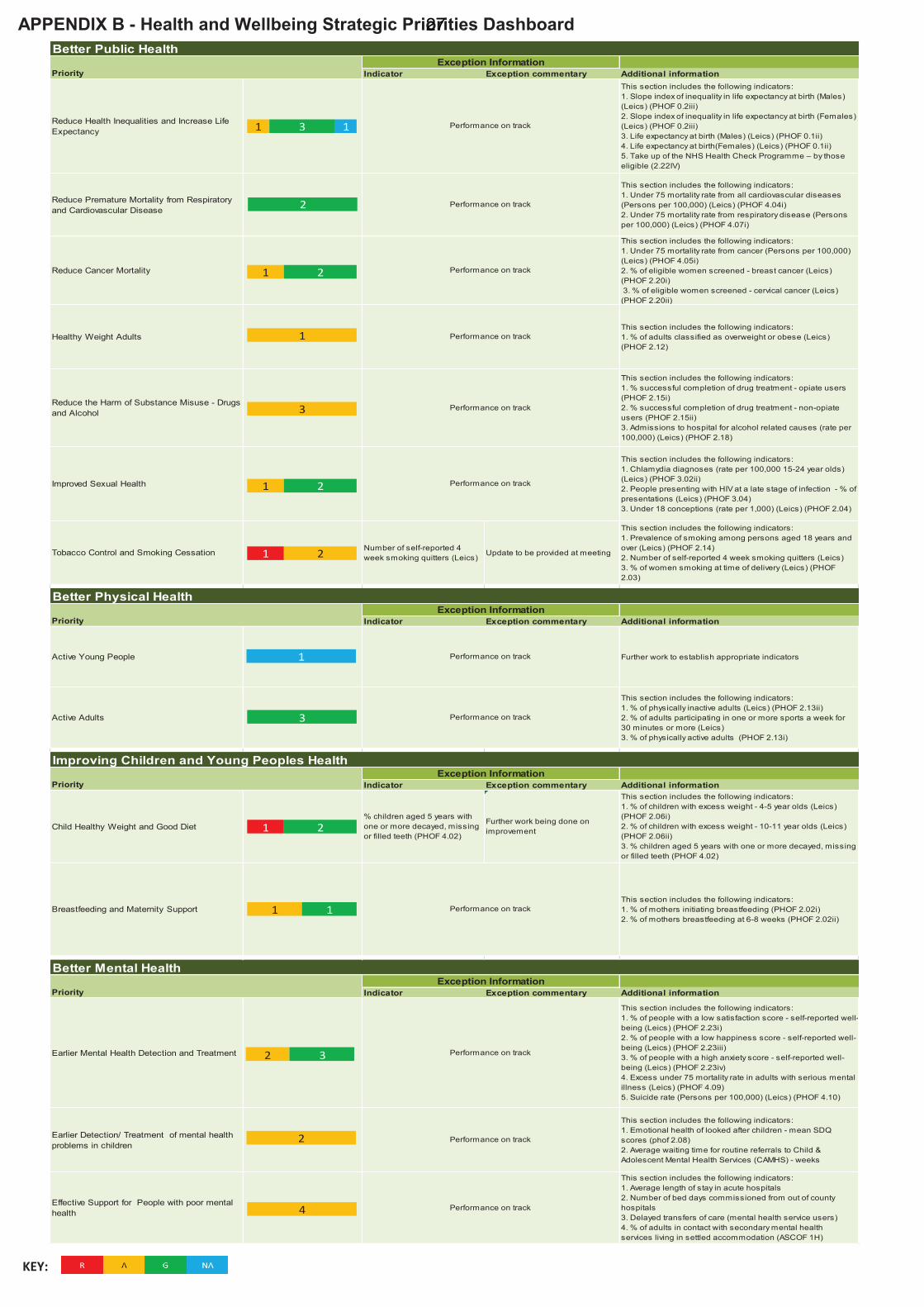
Health and Wellbeing Strategic Priorities Dashboard - Appendix B
17. Appendix B to this report is a dashboard summarising the performance against key strategic health and wellbeing priorities. The priorities include Better Public Health, Better Mental Health, Better Physical Health and improving Children and Young People’s Health.
18. The indicators included in each section are listed in the additional information box
and any RED exceptions are highlighted with performance commentary against them. A number of issues are highlighted below.
Public Health Performance
19. Public health performance nationally is looked at in terms of the Public Health Outcomes Framework (PHOF). In August Public Health England produced an update to PHOF figures. Overall the picture for Leicestershire shows good
comparative performance with just two areas flagged as below average – fuel poverty and chlamydia diagnosis (covered at the last meeting). Public Health England also pulls together a range of data into a health summary – an updated version of the summary was released in July. The summary shows a largely positive picture of health in Leicestershire with just three health/care issues flagged – incidence of malignant melanoma, diabetes and excess winter deaths.
20. The County Council has identified a number of targeted areas for performance
improvement including health inequalities and life expectancy, premature
17
mortality, cancer mortality, healthy weight adults, substance misuse, sexual health and tobacco control/smoking. These are a focus for a variety of public health contracts and interventions. There are no significant performance issues flagged for these areas at present.
Children’s Health
21. Child health indicator data provided by Public Health England is generally positive. Of the 32 indicators with national comparisons, only 3 child health ones are below average – level of development at the end of reception year, children with decayed, missing or filled teeth, and breastfeeding prevalence at 6-8 weeks. Provisional Leicestershire figures for the % of children with a good level of development have seen a good increase this year by around 11.7% to 58%. Breastfeeding prevalence and actions to improve this were reported at the last meeting.
22. The Harborough cluster of Children’s Centres was recently inspected and
judged to be ‘Good’. Five of the six clusters in Leicestershire have now been inspected with all receiving a ‘good’ rating from Ofsted. The 2014 Children’s Centres Satisfaction Survey took place between April and May 2014. A county headline summary report has been produced showing analyses of the 1,769 parents who responded. Initial results have found that 91% would recommend their centre.
23. The percentage of Looked After Children having health checks increased by 0.9% 2013 to 2014 and is now 74.2%. The percentage of Looked After Children having dental checks increased by 0.2% from 2013 to 2014 and is now 73.5%. The percentage of Looked After Children up to date with immunisations increased by 5.9% from 2013 to 2014 and is now 86.4%.
Mental Health
24. The Health and Wellbeing Board has identified mental health as an important priority in the Health and Wellbeing Strategy. The County Council has also updated its priorities and targets including reducing unhappiness and anxiety scores, reducing excess under 75 mortality in adults with a mental illness, reducing wait times for assessment/treatment and good emotional health of
children in care. Performance reporting on these areas is still being developed and will be reported to future meetings.
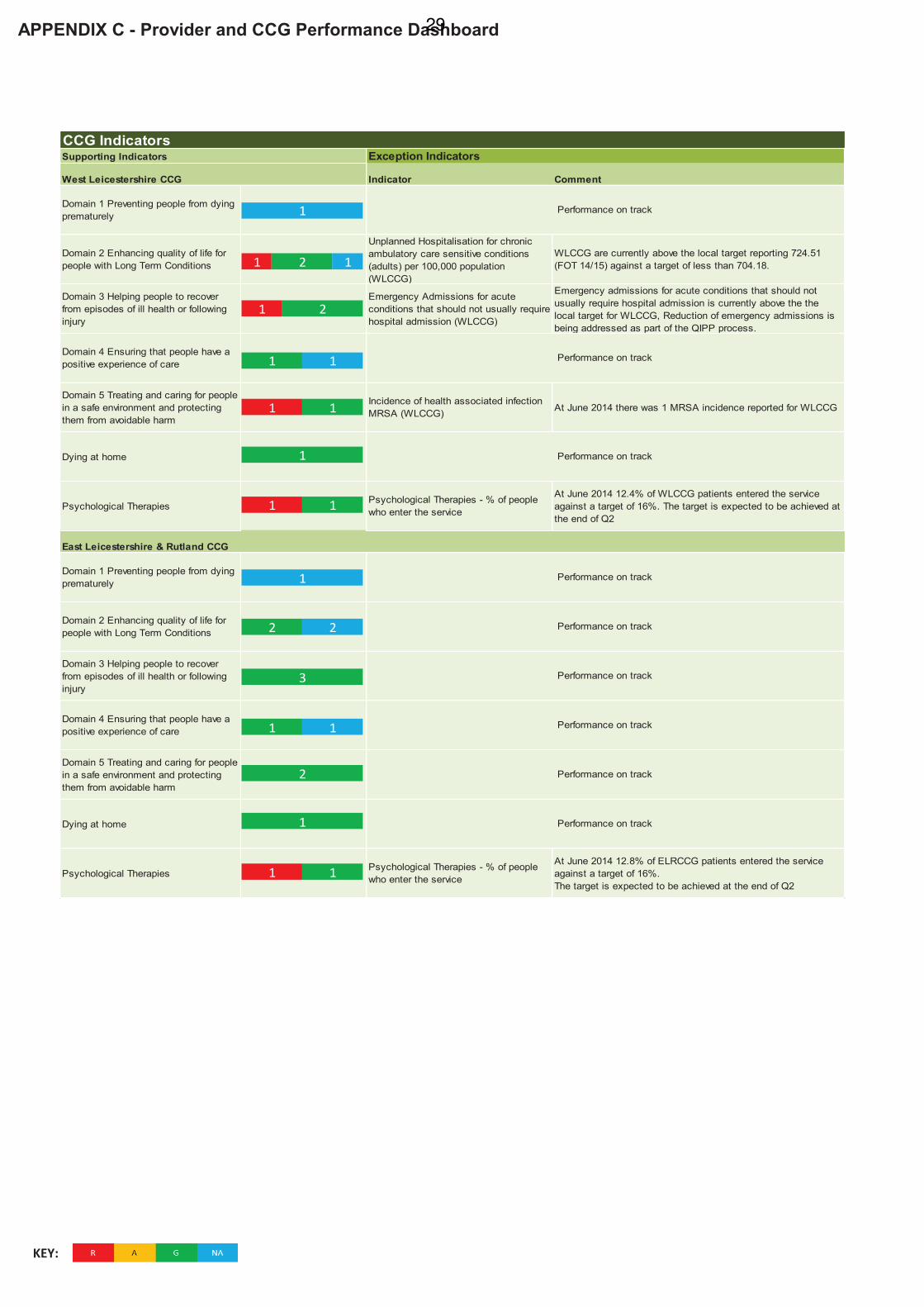
25. Performance in relation to access to psychological therapies (IAPT) is covered in the provider dashboard. At June 2014, patients accessing IAPT for both West Leicestershire Clinic Commissioning Group (WLCCG) and East Leicestershire and Rutland Clinical Commissioning Group (ELRCCG) have not achieved Q1 trajectory. WLCCG is at 12.4% and ELRCCG is at 12.8% against a 16% target. The provider of the service, Nottingham Healthcare NHS Trust, expects to achieve the national target at the end of Q2. This is due to early disruption in the service due to the transition from the previous provider. A number of other initiatives will begin to take affect which will improve the position. These include did not attend text reminders and pilots of self- referrals.
18
26. The following mental health related performance indicators have been updated from LPT Board reports.
Occupancy Rate – Mental Health
Performance against this indicator has decreased with mental health bed occupancy for the month of June at 91.3% against the trust target of 85% or below. Performance for the divisions stands at adult mental health and learning disability (91.3%) community health services (91.7%) and families, children and young people (89.5%)
% Delayed Patients (MH) Performance against this indicator has increased for the month of June to 4.6% from 6.2% and stays within the Monitor 7.5% target.
Total number of Home Treatment episodes carried out by Crisis Resolution team (year to date)
Performance against this indicator has improved significantly since June, with the current position being 97%
Suicides With regard to LPT 7 suicides have been reported in the year to date. Below the amount projected at 12. There have also been 2 attempted suicides by inpatients and 7 by outpatients in the year to date.
Child and Adolescent Mental Health Services
The average wait time for routine referrals was 9.1 weeks in 2013/14. In Q1 2014/15 this has reduced to 8.7 weeks. Urgent referrals have minimal wait times.
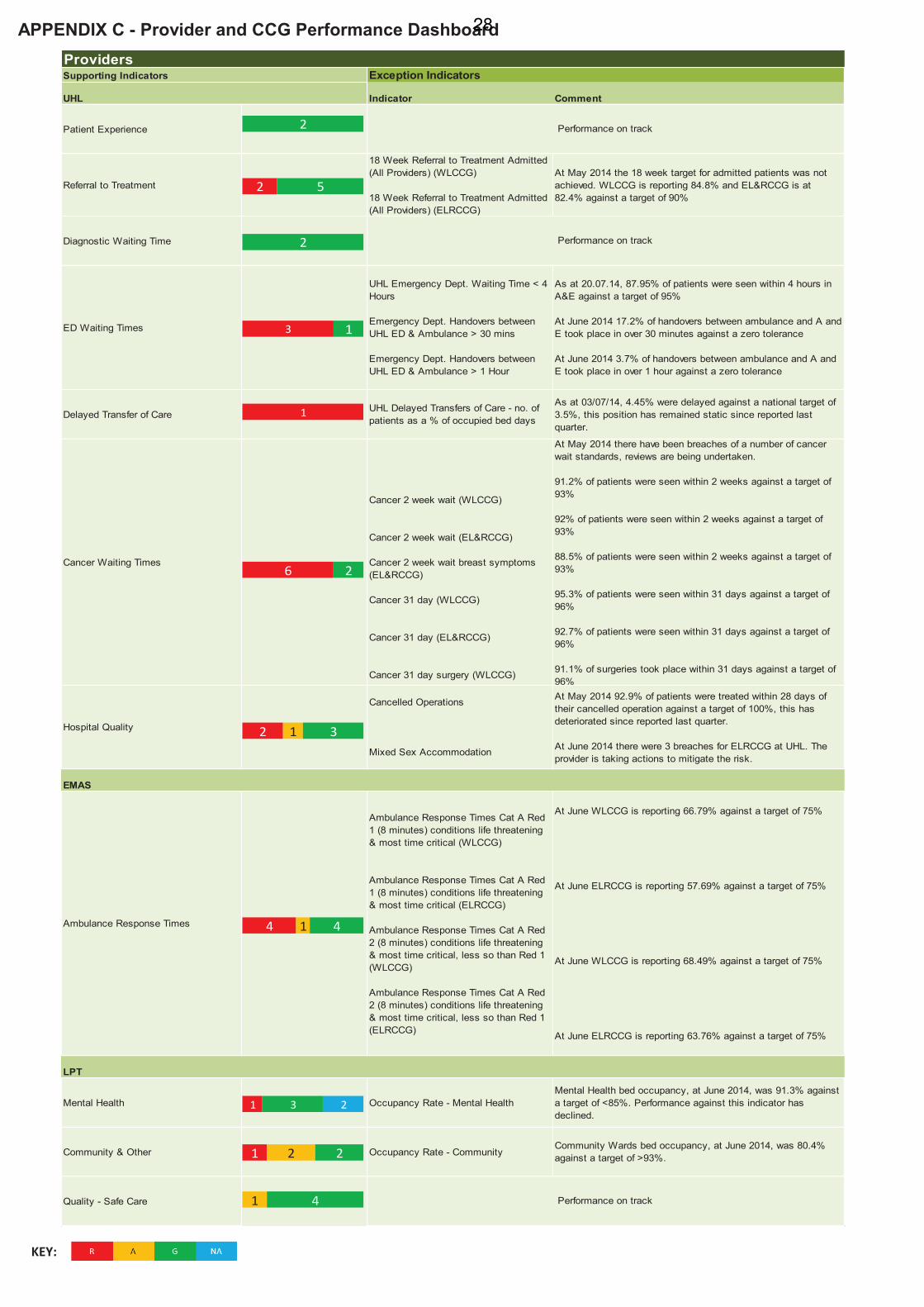
Provider and CCG Dashboard - Appendix C
27. Attached as Appendix C is a dashboard that summarises information on provider and CCG performance updated to reflect changes through ‘Everyone Counts’. The Everyone Counts Dashboard replaces the NHS Constitution, and sets the rights and pledges that patients are entitled to through the NHS.
28. The indicators within the dashboard are reported at CCG level. Data reported at
provider level does differ, and delivery actions indicate where this is a risk. EMAS - Ambulance Response Times
29. At June 2014, all ambulance response times in the east midlands regionally
achieved the national standards, which is an improvement on the 2013/14 position. Data at CCG level for June 2014 is reported as follows:
• Cat A (8 mins) Red 1 WL 66.79% and ELR 57.69% (Target 75%)
• Cat A (8 mins) Red 2 WL 68.49% and ELR 63.76% (Target 75%)
• Cat A (19 mins) WL 94.15% and ELR 91.45% (Target 95%)
30. There has been a significant increase in activity from NHS 111 of approximately 20-25%. ELRCCG are working collaboratively with EMAS and NHS 111 provider
19
to ensure delivery actions are in place. LLR Quality Commissioners are developing a process for local reporting, providing local quality assurance and information to improve Key Performance Indicator performance. Although recruitment is continuing, and productivity will improve by the beginning of Q3, the current requirements to achieve LLR targets by July 2014 are not expected to be achieved.
18 Weeks Referral to Treatment (Data is at CCG level)
31. The referral to treatment (RTT) operational standards are 90% of admitted (to
hospital) and 95% of non-admitted patients (out-patients) should start consultant-led treatment within 18 weeks of referral. In order to sustain delivery of these standards 92% of patients who have not yet started treatment should have been waiting no longer than 18 weeks.
32. At May 2014, the 18 week target for admitted patients was not achieved. WLCCG is reporting 84.8% and EL&R CCG is at 82.4% against a target of 90%. Overall the performance against the Remedial Action Plan (RAP) is monitored by the RTT Working Group with the Joint RTT Board establishing an oversight role involving NHS England and the Trust Development Authority (TDA). LLR CCG strategic plans are in place which complement contract management and include; level of commissioned activity; data integrity; identification and management of risk; commissioner delivery plans and sustainability. Operationally UHL Patient Tracking List (PTL) meetings are in place providing assurance of the internal management processes and alignment with the RTT Board, with focus on all specialties ensuring sustainability.
Accident and Emergency - 4 Hour Waiting Time
33. As at 20 July 2014, 87.95% of patients were seen within 4 hours in A and E against a target of 95%. The UHL Contract for 2014/15 was signed on 30 June 2014. This includes a newly agreed Remedial Action Plan (RAP) and trajectories that were agreed at the Escalation Meeting with NHS England and the Trust Development Authority (TDA) on 01 July 2014. Performance showed improvement during June 2014, with the month end position at 91.02%, and a year to date position of 87.04%. The work that an external consultant is undertaking with UHL and the wider system through clinical engagement appears to be having an impact. Work on inflow and discharge continues to support system change, with breaches being predominantly due to bed availability or Emergency Department process. A reduction in the number of patients waiting for a bed in the morning has impacted positively on flow.
Cancer Waits – 2 Week Waits, 2 Week Waits for Breast Symptoms, 31 Day Wait and 31 Day Waits for Surgery
34. At May 2014, there have been breaches of a number of cancer wait standards for WLCCG and ELRCCG. There has been an increase in cancer referrals between February and April 2014, with a high proportion being confirmed as breast cancer. An additional consultant and an extra theatre have been resourced at Glenfield. A cancer action group has been formed to assess patient trigger points, and potential breaches. Reviews of breaches are also being undertaken.
20
Mixed Sex Accommodation
35. At June 2014, there were 3 breaches for ELRCCG at UHL. The provider is taking actions to mitigate the risk, and the actions have been reviewed via the UHL Executive Quality Board and the CCG Clinical Quality Review Group. As a result of a Root Cause Analysis, staff education has been put in place.
Cancelled Operations – Non Readmitted within 28 Days
36. At May 2014, 92.9% of patients were seen against a target of 100%. This is deterioration since reported last quarter. A new standard to contact the patient within 48 hours of cancellation and rebook a “To Come In” date within 21 days has been initiated with associated escalation processes. A daily cancelled operations patient level report will be emailed via an automated route to service and operational mangers, highlighting the 21 day re-book date. At the Contract Performance Meeting with UHL on 3rd April 2014, UHL requested to revisit trajectories. UHL are identifying non-bed capacity related reasons for cancellations which equate to approximately 40% of cancellations and are analysing reasons for breaches to be reported to Commissioners in May 2014.
Ambulance Handovers
37. At June 2014, 17.2% of handovers between ambulance and Accident and Emergency took place in over 30 minutes against a zero tolerance. This position has deteriorated from 12.9% reported last quarter. EMAS is currently assessing issues with performance, and is undertaking further recruitment.
Delayed Transfers of Care (DTOC)
38. Delays are being reported as the number of patients discharged as a percentage of occupied bed days. As at 3 July, 4.45% were delayed against a national target of 3.5%. This position has remained static since reported last quarter. Actions in place include daily calls with all partners chaired by the CCGs; the Discharge Steering Group is in place to oversee the redesign of the discharge process, and a project plan is in place with LLR partner engagement. An analysis of discharges is undertaken weekly and report to the Urgent Care Working Group. Delayed discharge performance continues to fluctuate due to staff capacity.
Safety Thermometer
39. The NHS Safety Thermometer is a local improvement tool for measuring, monitoring and analysing patient harms and “harm free” care. At May 2014, UHL is reporting 94.66% against a target of 95% which remains in line with the national position.
40. CCGs, LPT and UHL have published a quality review into previous patient cases
in order to understand lessons which could be learnt and what improvements can be made. The quality review focused on healthcare to patients between March
21
2012 and June 2013 and looked at care before admission, during the stay in hospital, after discharge and care from the local GP and social care services. The reviewers found significant lessons to learn for all healthcare partners.
Clinical Commissioning Group Performance
Emergency Admissions
41. There are a number of indicators in the NHS Outcomes Framework that relate to emergency admissions. At May 2014, at WLCCG, unplanned hospitalisation for chronic ambulatory care sensitive conditions (adults) and emergency admissions for acute conditions that should not usually require hospital admission activity is above the local target. Reduction of emergency admissions is being picked up as part of the QIPP (Quality, Innovation, Productivity and Prevention) process with providers through contractual arrangements. For WLCCG this is also reported at locality level. Local schemes are in place within the CCGs, and will be reported for the next quarter when more activity data is available.
MRSA
42. At June 2014, there was 1 MRSA incidence reported for WLCCG. Following arbitration, an incidence reported in May 2014 was removed from WL and assigned to a third party. The case in June has also been sent to arbitration, the result of this should be made available during August 2014.
Leicestershire Partnership Trust (LPT)
43. Performance issues against ‘Efficient Services’ indicators are detailed below. Data and commentary are taken directly from the LPT Board Papers for May 2014.
% Occupancy Rate - Community
Performance for the month of June stands at 80.4% against the 93% or above target. Community wards with significantly lower bed occupancy during the month were Ashby General Ward, Melton Dalgleish Ward and Rutland Ward.
% Delayed Patients (Community )
Performance has increased compared to May at 2.20% for June against the target of 2.12%
Waiting times The clinical divisions have provided assurance that there are no patients waiting longer than 52 weeks. Additional waiting times funding has had the expected effect on waiting times performance.
44. Performance issues against ‘Quality – Safe Care’ indicators are detailed below.
Data and commentary are taken directly from the LPT Board papers for January 2014.
Compliance with hygiene code Podiatry services negotiating suitable timescale for appropriate works to be undertaken. Building works on Welford and
22
Kirby wards re facilities under review to ensure suitable equipment identified.
Infection control – C Diff (MH and Community)
Monitor targets reflect the annual de minimis limit set at 12 cases p.a. There have been no cases of CDiff for June which keeps the year to date position at 1 case.
Strategic Executive Information System (STEIS) – Serious Incident (SI) action plans implemented within timescales STEIS is the system used to report serious untoward incidents
Performance against this indicator for the month of June is 100% form 87.5% in May.
Background papers Leicestershire Partnership Trust Board Papers can be found at the following link: http://www.leicspart.nhs.uk/_Aboutus-Trustboardmeetings2014-July2014.aspx University Hospitals Leicester Trust Board meetings can be found at the following link: http://www.leicestershospitals.nhs.uk/aboutus/our-structure-and-people/board-of-directors/board-meeting-dates/ Further information on the health system can be found in a previous report to the Shadow Health and Wellbeing Board March 2013: http://politics.leics.gov.uk/ieListDocuments.aspx?CId=961&MId=3727&Ver=4 Recommendations 45. The Committee is asked to:
a) note the performance summary, issues identified this quarter and actions planned in response to improve performance; and
b) comment on any recommendations or other issues with regard to the report.
List of Appendices Appendix A - Better Care Fund - Integration Executive Summary Dashboard Appendix B - Health and Wellbeing Strategic Priorities Summary Dashboard Appendix C - Provider and CCG Performance Summary Dashboard Officers to Contact Kate Allardyce and Sarah Cooke - Performance Team (Leicester & Lincoln) Greater East Midlands Commissioning Support Unit
Tel: 0116 295 7272, Mobile: 07795126428 Email: [email protected]
23

Andy Brown, Performance & Business Intelligence Team Leader, Leicestershire County Council. Tel: 0116 305 6096 Email: [email protected]
24
APPENDIX A - Better Care Fund - Integration Executive Dashboard
A Unified Prevention Offer for Communities
JHWS Priority Schemes Theme Lead Exception commentary Additional information
ACTION
PLANAssistive technology Anne Walsh
The integration of this scheme is yet to start and
has been delayed. Amber RAG status to reflect
this. This is being discussed at the Step Up/Step
Down Programme Board September meeting.
FINANCE
Assistive technology
(replacement equipment)
(non-recurrent funding)
Local Area Co-ordination
Anne Walsh
Nicole
Rickard/
Sue Wilson
The cost of transitioning service users over to
the new provider has reduced compared to
original estimates at the contract tendering
stage. The revised transitioning costs are
estimated to be £950k, a reduction of £494k.
The transition costs will be phased over 2014/15
(£580k) and 2015/16 £370k).
The BCF funding requirement for LAC is
anticipated to be £77k for 2014/15 as the
scheme is unlikely to be fully staffed (as per
outline business case) until January 15.
METRIC
SAVINGS All projects are on track.
Exception information
Schemes
Managing the
shift to early
intervention
and prevention
All projects are on track.
Carers Service: Carers consultation now
closed. A report is being prepared for 19th Sept
to provide Cabinet with a final update &
permission to move ahead with the preferred
option for carer support services in
Leicestershire.
Carers Assessment: Recent information
published relating to the Care Act may result in
further BCF resources (up to £1.3m) being
allocated to support implementation. Currently
£275k has been identified for carers
assessments.
Specialist support to people with Dementia
and their carers: Current services have been
remodelled across the dementia pathway. The
new service, which is in line with 5 year strategy
development, will be in place for Oct 14.
Assistive Technology: Project closure report
presented to AT Board. Due to the risk
sensitivity around the transition period, agreed
not to formally close project. Position to be
reviewed in October.
Charging was introduced from 4th August
1 8 2
2 7 2
1 10
Dimension RAG Status Guidelines Notes
GREEN Savings on track or ahead of scheduleAdd any appropriate headline commentary - e.g. important
milestones met etc
AMBER Savings are off track by up to -10% Exception commentary must be provided
RED Savings are off track by more than -10% Exception commentary must be provided
N/A Savings have not yet been defined for this scheme Exception commentary must be provided
E This scheme has been identified as an enablerAdd any appropriate headline commentary - e.g. important
milestones met etc
GREEN Action plan development and/or milestones are on targetAdd any appropriate headline commentary - e.g. important
milestones met etc
AMBERThere are minor delays in the action plan milestones of up to
30 daysException commentary must be provided
REDThere are action plan milestones delayed more than 30 days
/ BP delayedException commentary must be provided
N/A Scheme not yet due to start Please provide a start date
GREEN Costs are on targetAdd any appropriate headline commentary - e.g. important
milestones met etc
AMBERThere is likely to be an overspend / underspend of up to 10%
of the agreed budget Exception commentary must be provided
REDIt is highly likely there will be an overspend / underspend
greater than 10% of the agreed budget Exception commentary must be provided
N/A Budget not set for current financial yearAdd any appropriate headline commentary - e.g. important
milestones met etc
GREEN Assessed impact on primary metric(s) is on trackAdd any appropriate headline commentary - e.g. important
milestones met etc
AMBERIt is likely there will be a negative impact on the primary
metric(s) of up to 10%Exception commentary must be provided
REDIt is highly likely there will be a negative impact on the
primary metric(s) greater than 10%Exception commentary must be provided
N/A Contribution to metrics not yet developed Exception commentary must be provided
E This scheme has been identified as an enablerAdd any appropriate headline commentary - e.g. important
milestones met etc
Impact on metrics
Better Care Fund
RAG Status Guidelines
Savings
Action plan milestones
Finance
11
Better Care Fund
BCF Metrics
Metric TargetCurrent
dataTrend Data RAG DOT Commentary
METRIC 1: Permanent admissions of older people (aged
65 and over) to residential and nursing care homes, per
100,000 population
TBC 756.2 NA ó
Definitions for the measures in the Adult Social Care
Outcomes Framework (ASCOF)have been revised due to the
wholesale change to source data tables from 2014/15. These
changes require substantial work to reporting which will be
undertaken through the autumn/ winter. In the interim an
alternative measure of permanent admissions will be
developed and reported. Current data show 2013/14 figure.
Trend charts are an example only
METRIC 2: Proportion of older people (65 and over) who
were still at home 91 days after discharge from hospital
into reablement / rehabilitation services
TBC 78.60% NA ó
This ASCOF measure relates to hospital discharges between
October and December 2014 followed by accommodation
location between January and March 2015. A rolling 6-month
performance will be reported here starting with the period Apr-
Sep 2014. Current data show 2013/14 figure. Trend charts
are an example only.
METRIC 3: Delayed transfers of care from hospital per
100,000 population (average per month)TBC 370.02 R ñ
The DToC target in the BCF covers two timeframes, the first
of which is Apr-Dec 2014. Current performance is
significantly higher. Current data shows the monthly average
for the year to date to June 2014.
METRIC 4: Total emergency admissions into hospital,
per 100,000 populationTBC ~ NA ó In development. Trend chart is an example only
METRIC 5: Patient / service user experience ~ ~ NA ó In development. Trend chart is an example only
METRIC 6: Injuries due to falls in people aged 65 and
overTBC 168.2 NA ó
Data not yet available. Trend chart is an example only.
Current data reflects the agreed baseline.
20132014
Q1Q4
Q1 …Q2
Q3 Q4
2012
2014
2012
2014
370.02
361.79
25
APPENDIX A - Better Care Fund - Integration Executive Dashboard
KEY:
Integrated Urgent Response
JHWS Priority Schemes Theme Lead Exception commentary Additional information
ACTION
PLAN
FINANCEIntegrated Crisis Response
Service
Anne Walsh/
Yasmin Sidyot/
Caron
Williams
Revised cost of the night nursing service
following more detailed modelling.
METRIC
SAVINGS
Improved Hospital Discharge and Reablement
JHWS Priority Schemes Theme Lead Exception commentary Additional information
ACTION
PLAN
Patient Transfer Minimum
Data Set
Integrated Residential
Reablement
Caron
Williams
Jackie Wright/
Caron
Williams or
Yasmin Sidyot
Delays in decision on which tool should be used.
Agree at July IE to arrange between the Chief
Nurse at UHL & the project group which initially
devised the data set to identify a way forward.
There is a task and finish group set up through
the Urgent Care Working Group that is
developing the 3 discharge pathways – defining
the pathways will enable the development of the
local reablement model. The group is an LLR
task and finish group with representation from 3
CCGs and 3 LAs.
FINANCE
Patient Transfer Minimum
Data Set
Integrated Residential
Reablement
Caron
Williams
Jackie Wright/
Caron
Williams or
Yasmin Sidyot
The level of underspend will be determined by
the delay to the project. At this stage it is
anticipated that any underspend will roll into
2015/16.
Delays in implementing the reablement model
will result in an underspend of c£30k per month.
METRIC
SAVINGS
Integrated, proactive care for those with long-term conditions
JHWS Priority Schemes Theme Lead Exception commentary Additional information
ACTION
PLANContinuing Healthcare
Operational workstream is led within the CCGs
hosted contract team. Update to be provided to
Integrated Exec July meeting.
FINANCE
METRIC
SAVINGS
Further Integration schemes
JHWS Priority Schemes Theme Lead Exception commentary Additional information
ACTION
PLANTransitions
Working with CYPS in relation to implementation
of Children and Families Act.
FINANCEManagement of LD Pooled
Budget
Risk of overspend to LD pooled budget. Early
forecasts estimate this to be c£1m, split 50:50
between the County Councils and CCGs. Further
detailed analysis to be undertaken.
METRIC
SAVINGS
Winterbourne View Concordat:
Commissioners have adopted Driving Up Quality
Code
Transitions: Issues identified around local offer
and joint commissioning arrangements. Being
taken forward by LD Programme Board.
Housing Offer to Health: Lightbulb project:
Successfully got through the expressions of
interest stage for transformation funding from
DCLG for 2015/16
Housing offer to Health: Hospital Discharge
Housing Enabler: Job descriptions for Housing
officers to work with LPT are in draft format.
KPI's outlined to measure scheme effectiveness.
These are being agreed.
All projects are on track.
All projects are on track.
All projects are on track.
All projects are on track.
Exception information
Pathway to Housing: Measurements in place
but not linked to outcomes as yet. Increasing
amount of housing options and number of
individuals supported to move into own housing.
Reducing support packages during regular
reviews.
Improving Quality in Care Homes: QIT /
Safeguarding. New safeguarding threshold tool
introduced across LLR. A slow reduction in care
home safeguarding investigations being
identified.
IT Enablers: Being led by LLR IM&T
workstream. Feasibility work being completed by
LCC on use of NHS number. Project brief will
follow in Q2.
All projects are on track.
All projects are on track.
HWBS 12.
Management
of long-term
conditions
All projects are on track.
All projects are on track.
Exception information
Schemes
Schemes
HWBS 11.
Maximising
independence
All projects are on track.
Exception information
Schemes
All projects are on track.
Schemes
HWBS 10:
Planning for an
ageing
population
Integrated Crisis Response Service:
Mitigation plans approved. On track to
implement the extension of the current crisis
provision to provide 24/7 coverage from
September.
Frail Older People Service: Full business case
being developed. Task & finish group meeting
fortnightly. Update summary being reported to
August IE meeting.
Expanded role of Primary Medical Care:
WLCCG - plan to roll-out 4 pilots from Sept 14.
ELRCCG - aim by Sept 14 to have pilots
identified & a clear idea per practice/locality of
which areas are to be focused on.
Avoiding Admissions due to Falls: Interim
project management for arrangements for the
integrated approach to falls is now in place and
work continues to develop the business case.
Help to Live at Home: Paper submitted to
Integration Exec on proposals for revised scope
of project was agreed. Business case now being
developed
Exception information
Intermediate Care: LPT contract 14/15 has
been signed which includes Intermediate Care.
Bridging Service: Plans to allocate the
‘Bridging Service’ funding re on hold pending a
report to be presented to the Urgent Care
Working Group. In light of recent increases to
the Await Care List, initial thinking is that the
funds could be utilised to provide an integrated
reablement service to speed up the hospital
discharge process.
Strengthening Mental Health Discharge
Provision: Services in place. Hospital Social
Workers attend twice weekly meetings to
monitor DTOC numbers.
4 1
1 3 1
1 1 11 1
1 1 8 4
6 8
1 10 1
8 4
9 3
1 3 2
1 1 4
6
1 4
5
14
12
6
26
APPENDIX B - Health and Wellbeing Strategic Priorities Dashboard
KEY:
Indicator Exception commentary Additional information
Reduce Health Inequalities and Increase Life
Expectancy
This section includes the following indicators:
1. Slope index of inequality in life expectancy at birth (Males)
(Leics) (PHOF 0.2iii)
2. Slope index of inequality in life expectancy at birth (Females)
(Leics) (PHOF 0.2iii)
3. Life expectancy at birth (Males) (Leics) (PHOF 0.1ii)
4. Life expectancy at birth(Females) (Leics) (PHOF 0.1ii)
5. Take up of the NHS Health Check Programme – by those
eligible (2.22IV)
Reduce Premature Mortality from Respiratory
and Cardiovascular Disease
This section includes the following indicators:
1. Under 75 mortality rate from all cardiovascular diseases
(Persons per 100,000) (Leics) (PHOF 4.04i)
2. Under 75 mortality rate from respiratory disease (Persons
per 100,000) (Leics) (PHOF 4.07i)
Reduce Cancer Mortality
This section includes the following indicators:
1. Under 75 mortality rate from cancer (Persons per 100,000)
(Leics) (PHOF 4.05i)
2. % of eligible women screened - breast cancer (Leics)
(PHOF 2.20i)
3. % of eligible women screened - cervical cancer (Leics)
(PHOF 2.20ii)
Healthy Weight Adults
This section includes the following indicators:
1. % of adults classified as overweight or obese (Leics)
(PHOF 2.12)
Reduce the Harm of Substance Misuse - Drugs
and Alcohol
This section includes the following indicators:
1. % successful completion of drug treatment - opiate users
(PHOF 2.15i)
2. % successful completion of drug treatment - non-opiate
users (PHOF 2.15ii)
3. Admissions to hospital for alcohol related causes (rate per
100,000) (Leics) (PHOF 2.18)
Improved Sexual Health
This section includes the following indicators:
1. Chlamydia diagnoses (rate per 100,000 15-24 year olds)
(Leics) (PHOF 3.02ii)
2. People presenting with HIV at a late stage of infection - % of
presentations (Leics) (PHOF 3.04)
3. Under 18 conceptions (rate per 1,000) (Leics) (PHOF 2.04)
Tobacco Control and Smoking CessationNumber of self-reported 4
week smoking quitters (Leics)Update to be provided at meeting
This section includes the following indicators:
1. Prevalence of smoking among persons aged 18 years and
over (Leics) (PHOF 2.14)
2. Number of self-reported 4 week smoking quitters (Leics)
3. % of women smoking at time of delivery (Leics) (PHOF
2.03)
Indicator Exception commentary Additional information
Active Young People Further work to establish appropriate indicators
Active Adults
This section includes the following indicators:
1. % of physically inactive adults (Leics) (PHOF 2.13ii)
2. % of adults participating in one or more sports a week for
30 minutes or more (Leics)
3. % of physically active adults (PHOF 2.13i)
Indicator Exception commentary Additional information
Child Healthy Weight and Good Diet
% children aged 5 years with
one or more decayed, missing
or filled teeth (PHOF 4.02)
Further work being done on
improvement
This section includes the following indicators:
1. % of children with excess weight - 4-5 year olds (Leics)
(PHOF 2.06i)
2. % of children with excess weight - 10-11 year olds (Leics)
(PHOF 2.06ii)
3. % children aged 5 years with one or more decayed, missing
or filled teeth (PHOF 4.02)
Breastfeeding and Maternity Support
This section includes the following indicators:
1. % of mothers initiating breastfeeding (PHOF 2.02i)
2. % of mothers breastfeeding at 6-8 weeks (PHOF 2.02ii)
Indicator Exception commentary Additional information
Earlier Mental Health Detection and Treatment
This section includes the following indicators:
1. % of people with a low satisfaction score - self-reported well-
being (Leics) (PHOF 2.23i)
2. % of people with a low happiness score - self-reported well-
being (Leics) (PHOF 2.23iii)
3. % of people with a high anxiety score - self-reported well-
being (Leics) (PHOF 2.23iv)
4. Excess under 75 mortality rate in adults with serious mental
illness (Leics) (PHOF 4.09)
5. Suicide rate (Persons per 100,000) (Leics) (PHOF 4.10)
Earlier Detection/ Treatment of mental health
problems in children
This section includes the following indicators:
1. Emotional health of looked after children - mean SDQ
scores (phof 2.08)
2. Average waiting time for routine referrals to Child &
Adolescent Mental Health Services (CAMHS) - weeks
Effective Support for People with poor mental
health
This section includes the following indicators:
1. Average length of stay in acute hospitals
2. Number of bed days commissioned from out of county
hospitals
3. Delayed transfers of care (mental health service users)
4. % of adults in contact with secondary mental health
services living in settled accommodation (ASCOF 1H)
Performance on track
Performance on track
Performance on track
Better Public Health
Priority
Exception Information
Exception Information
Performance on track
Performance on track
Better Physical Health
Priority
Performance on track
Performance on track
Improving Children and Young Peoples Health
Priority
Exception Information
Performance on track
Performance on track
Performance on track
Performance on track
Better Mental Health
Priority
Performance on track
Exception Information
1 2
1 1
1 3 1
2
1 2
1
3
1 2
1 2
1
3
2 3
2
4
27
APPENDIX C - Provider and CCG Performance Dashboard
KEY:
Supporting Indicators
UHL Indicator Comment
Patient Experience
Referral to Treatment
18 Week Referral to Treatment Admitted
(All Providers) (WLCCG)
18 Week Referral to Treatment Admitted
(All Providers) (ELRCCG)
At May 2014 the 18 week target for admitted patients was not
achieved. WLCCG is reporting 84.8% and EL&RCCG is at
82.4% against a target of 90%
Diagnostic Waiting Time
ED Waiting Times
UHL Emergency Dept. Waiting Time < 4
Hours
Emergency Dept. Handovers between
UHL ED & Ambulance > 30 mins
Emergency Dept. Handovers between
UHL ED & Ambulance > 1 Hour
As at 20.07.14, 87.95% of patients were seen within 4 hours in
A&E against a target of 95%
At June 2014 17.2% of handovers between ambulance and A and
E took place in over 30 minutes against a zero tolerance
At June 2014 3.7% of handovers between ambulance and A and
E took place in over 1 hour against a zero tolerance
Delayed Transfer of CareUHL Delayed Transfers of Care - no. of
patients as a % of occupied bed days
As at 03/07/14, 4.45% were delayed against a national target of
3.5%, this position has remained static since reported last
quarter.
Cancer Waiting Times
Cancer 2 week wait (WLCCG)
Cancer 2 week wait (EL&RCCG)
Cancer 2 week wait breast symptoms
(EL&RCCG)
Cancer 31 day (WLCCG)
Cancer 31 day (EL&RCCG)
Cancer 31 day surgery (WLCCG)
At May 2014 there have been breaches of a number of cancer
wait standards, reviews are being undertaken.
91.2% of patients were seen within 2 weeks against a target of
93%
92% of patients were seen within 2 weeks against a target of
93%
88.5% of patients were seen within 2 weeks against a target of
93%
95.3% of patients were seen within 31 days against a target of
96%
92.7% of patients were seen within 31 days against a target of
96%
91.1% of surgeries took place within 31 days against a target of
96%
Hospital Quality
Cancelled Operations
Mixed Sex Accommodation
At May 2014 92.9% of patients were treated within 28 days of
their cancelled operation against a target of 100%, this has
deteriorated since reported last quarter.
At June 2014 there were 3 breaches for ELRCCG at UHL. The
provider is taking actions to mitigate the risk.
EMAS
Ambulance Response Times
Ambulance Response Times Cat A Red
1 (8 minutes) conditions life threatening
& most time critical (WLCCG)
Ambulance Response Times Cat A Red
1 (8 minutes) conditions life threatening
& most time critical (ELRCCG)
Ambulance Response Times Cat A Red
2 (8 minutes) conditions life threatening
& most time critical, less so than Red 1
(WLCCG)
Ambulance Response Times Cat A Red
2 (8 minutes) conditions life threatening
& most time critical, less so than Red 1
(ELRCCG)
At June WLCCG is reporting 66.79% against a target of 75%
At June ELRCCG is reporting 57.69% against a target of 75%
At June WLCCG is reporting 68.49% against a target of 75%
At June ELRCCG is reporting 63.76% against a target of 75%
LPT
Mental Health Occupancy Rate - Mental Health
Mental Health bed occupancy, at June 2014, was 91.3% against
a target of <85%. Performance against this indicator has
declined.
Community & Other Occupancy Rate - CommunityCommunity Wards bed occupancy, at June 2014, was 80.4%
against a target of >93%.
Quality - Safe Care
ProvidersException Indicators
Performance on track
Performance on track
Performance on track
2 5
2
6 2
2 1 3
4 1 4
3 1
1
2
1 4
1 2 2
1 3 2
28
APPENDIX C - Provider and CCG Performance Dashboard
KEY:
Supporting Indicators
West Leicestershire CCG Indicator Comment
Domain 1 Preventing people from dying
prematurely
Domain 2 Enhancing quality of life for
people with Long Term Conditions
Unplanned Hospitalisation for chronic
ambulatory care sensitive conditions
(adults) per 100,000 population
(WLCCG)
WLCCG are currently above the local target reporting 724.51
(FOT 14/15) against a target of less than 704.18.
Domain 3 Helping people to recover
from episodes of ill health or following
injury
Emergency Admissions for acute
conditions that should not usually require
hospital admission (WLCCG)
Emergency admissions for acute conditions that should not
usually require hospital admission is currently above the the
local target for WLCCG, Reduction of emergency admissions is
being addressed as part of the QIPP process.
Domain 4 Ensuring that people have a
positive experience of care
Domain 5 Treating and caring for people
in a safe environment and protecting
them from avoidable harm
Incidence of health associated infection
MRSA (WLCCG)At June 2014 there was 1 MRSA incidence reported for WLCCG
Dying at home
Psychological TherapiesPsychological Therapies - % of people
who enter the service
At June 2014 12.4% of WLCCG patients entered the service
against a target of 16%. The target is expected to be achieved at
the end of Q2
East Leicestershire & Rutland CCG
Domain 1 Preventing people from dying
prematurely
Domain 2 Enhancing quality of life for
people with Long Term Conditions
Domain 3 Helping people to recover
from episodes of ill health or following
injury
Domain 4 Ensuring that people have a
positive experience of care
Domain 5 Treating and caring for people
in a safe environment and protecting
them from avoidable harm
Dying at home
Psychological TherapiesPsychological Therapies - % of people
who enter the service
At June 2014 12.8% of ELRCCG patients entered the service
against a target of 16%.
The target is expected to be achieved at the end of Q2
CCG IndicatorsException Indicators
Performance on track
Performance on track
Performance on track
Performance on track
Performance on track
Performance on track
Performance on track
Performance on track
Performance on track
1 2 1
1 2
1 1
1 1
1
2 2
3
1 1
2
1
1 1
1 1
1
1
29

30
This page is intentionally left blank
HEALTH OVERVIEW AND SCRUTINY COMMITTEE: 10 SEPTEMBER 2014
REPORT OF UNIVERSITY HOSPITALS OF LEICESER AND EAST LEICESTERSHIRE AND RUTLAND CLINICAL COMMISSIONING GROUP
LEARNING LESSONS TO IMPROVE CARE
Introduction
1. The following paper reports the findings of a clinical audit commissioned by
health organisations in Leicester, Leicestershire and Rutland to examine the quality care of patients and the action plan to address the areas of improvement identified.
2. This audit was prompted by the Summary Hospital Level Mortality Indicator (SHMI)* of University Hospitals of Leicester (UHL) being at or slightly above 1.05 since 2010/11. It must, however, be noted that this is within expected limits and the aim of the audit was to enable healthcare organisations to understand this issue better.
3. The findings of the audit, and the action plan developed as a result of the process, are being shared within the boards of all five partner local NHS organisations (East Leicestershire and Rutland Clinical Commissioning Group (ELRCCG), Leicester City Clinical Commissioning Group (LCCCG), West Leicestershire Clinical Commissioning Group (WLCCG), UHL and Leicestershire Partnership Trust (LPT)). Each individual organisation has reviewed the findings internally and identified their own actions, and in addition the audit demonstrated the need for cross organisational actions to be implemented to improve the quality of care for patients across the system.
Rationale for the Audit
4. This clinical audit was undertaken as a proactive step by the local health organisations to better understand the quality of care across the whole patient pathway.
Audit Methodology
5. Case notes from patients who had died in 2012-13 were reviewed by teams of doctors and nurses. 381 patients were identified from the cohort of patients who had been admitted to UHL in an emergency and died in hospital following an attempt at resuscitation, or had died on the Intensive Therapy Unit or had died within 30 days of discharge from hospital after changing their post code or GP.
6. The cases were deliberately chosen as those most likely to identify any clinical issues across the healthcare system. The audit was designed to shine a light on the quality and appropriateness of care rather than clinical outcomes.
Agenda Item 931
Findings
7. Of the 381 case notes audited, 208 (55%) were identified as having significant lessons to learn. Of these 89 (23%) were found to be below an acceptable standard. A thematic analysis of the findings identified 47 themes, the ‘Top 12’ being:
• DNAR orders
• Clinical reasoning
• Palliative care
• Clinical management
• Discharge summary
• Fluid management
• Unexpected deterioration
• Discharge
• Severity of illness
• Early Warning Score
• Antibiotics
• Medication
Duty of Candour
8. In order to demonstrate openness and transparency contact has been made with the next of kin of the 381 patients whose case notes were audited.
9. A call centre has been set up to allow them to talk through the care of their relative and escalate further concerns if necessary.
Five Point Action Plan
10. In response to the findings a Five Point Action Plan has been developed, the full
action plan is attached with the papers. This includes the following actions:
• Clinical Leadership and Task Force to address improvements
• Public and Patient Involvement
• Integrated care pathways
• Acute care pathway review and redesign
• End of life care transformation
Conclusion
11. This is a significant review for all Boards to consider of quality of patient care across LLR. It represent a positive step taken by the CCGs, UHL and LPT to allow the health community to make focussed improvements across the system. However, Boards should be aware that the findings could raise anxieties across many areas including patients, clinicians and the media.
32
12. System Leadership will play a key role in ensuring that the Five Point Action Plan will deliver the outcomes expected of it and boards should consider strategies for clinical leadership to support the delivery of safe high quality care across LLR. We need, also, to engender a culture that challenges healthcare practice and encourages patients to co-produce health care with clinicians.
13. An implementation group has been established to ensure that the actions included in the plan are implemented in line with agreed timescales. This Clinical Task Force will be co-chaired by Professor Mayur Lakhani and Dr Kevin Harris.
List of Appendices
• Appendix A - Learning Lessons to Improve Care: A joint review of the quality
of care delivered to patients who died in Leicester, Leicestershire and Rutland in 2012-13. Summary Document.
• Appendix B - Leicester, Leicestershire and Rutland (LLR) Joint Mortality
Review: Case Records Review (22 July 2014).
• Appendix C - Joint LLR Learning Lessons to Improve Care Action Plan.
33
34
This page is intentionally left blank
East Leicestershire and Rutland Clinical Commissioning Group Leicester City Clinical Commissioning Group
Leicestershire Partnership NHS Trust NHS England (Leicestershire & Lincolnshire Area)
University Hospitals of Leicester NHS Trust West Leicestershire Clinical Commissioning Group
Learning Lessons to Improve Care
A joint review of the quality of care delivered to patients who died in Leicester, Leicestershire and Rutland (LLR) in 2012-13
Summary Document
July 2014
35

36
28 July 2014 Page 1
1. Executive Summary
The Summary Hospital-Level Mortality Indicator (SHMI) of University Hospitals of Leicester (UHL) NHS Trust has been at or slightly above 1.05 since 2010/11. Although a SHMI of 1.05 (compared to a national average of 1.0) is within the expected range of NHS hospitals, local NHS organisations chose to request a joint primary and secondary care case records review of patients who died during the year of 2012/13, to ensure the care provided locally was of an acceptable standard.
In order to identify areas where the care delivered in Leicester, Leicestershire and Rutland (LLR) could be improved, local doctors and nurses reviewed the case records of a focused sample of patients who died in hospital or within 30 days of discharge following an emergency admission to UHL NHS Trust.
Reviewers found significant lessons to learn for all healthcare partners in 208 (55%) of the 381 cases reviewed, which included 89 cases (23%) where care was considered to be below an acceptable standard.
Comments made by reviewers as to how and where issues occurred in the 208 cases identified as having significant lessons to learn were grouped into themes. 47 themes were identified overall, which were ranked according to how many cases were affected.
The issues identified were wide-ranging and 99 of the 208 cases (48%) with significant lessons to learn involved more than one theme.
Furthermore, 23 of the 89 cases (26%) where care was considered to be below an acceptable standard involved services delivered in two or more local health and social care organisations. These data reflected how dependent the different organisations which make up the health and social care system in LLR are on each other and led reviewers to the conclusion that care quality must be improved not by addressing the issues individually, but by looking at the healthcare system as a whole.
‘Issues, Challenges and Next Steps’, which the LLR healthcare community would need to address in order to improve patient care, were identified following the review. These next steps included:
· Convincing People that the Problem is Theirs
· Convincing People that by Working Together a Solution can be Found
· Getting Data Collection and Monitoring Systems Right
· Making Changes that are Achievable and Sustainable
· Shifting Organisational Context and Culture
· Leadership, Oversight and Co-ordination
· Maintaining Momentum · Considering the Side Effects of Change
A vision document entitled ‘Reflection from the Future’ was completed which recommended the development of a LLR-wide healthcare ‘co-operation association’ through which all health and social care would be planned and delivered jointly by local organisations, with a focus on patient need and care quality and with input from patients and practitioners.
37
Summary of Documents LLR Joint Quality Review (2012-13)
Page 2 28 July 2014
2. Background for the Review
The quality of healthcare services is assessed using a number of different quality measures. One measurement of the standard of care provided in hospitals used nationally is the Summary Hospital-Level Mortality Indicator (SHMI)
1.
Since the publication of the SHMI for NHS Trusts in England in March 2011, University Hospitals of Leicester (UHL) NHS Trust’s SHMI has been at or slightly above 1.05. Although a SHMI above 1.00 does not mean that UHL NHS Trust is providing poor care, it is recommended that further investigation into the hospital’s performance is undertaken to ensure that the care provided is at an acceptable standard
2.
NHS England, on behalf of the Clinical Commissioning Groups for Leicester, Leicestershire and Rutland (LLR), Leicestershire Partnership NHS Trust (LPT) and UHL NHS Trust, requested the University of Leicester undertake a retrospective (historic) case record review to better understand whether there were common clinical issues and/or errors in the care received by patients who had died within the LLR healthcare system. It was understood that, should no common clinical issues and/or errors be identified, that further investigation into the data submitted by UHL to calculate the SHMI may be required.
The retrospective case record review was undertaken not to challenge the reported excess in the number of deaths in patients who receive care from UHL NHS Trust, or any other organisation providing health or social care services in LLR; rather it was completed as best practice to identify any areas where care and patient experience may be improved.
3. Context for the Review
From the outset, it was agreed that the review would look at the care provided by all NHS organisations in Leicester, Leicestershire and Rutland (LLR) and that the findings would have implications for all of the organisations involved.
It was therefore decided that a joint primary and secondary care case records review would be undertaken in which doctors and nurses from primary care, community health services and hospitals review primary care, community health and hospital case records together.
This type of joint review of NHS healthcare records has not been attempted before and so it was difficult to anticipate the findings or compare the findings with other reviews. Where previous reviews have included random patient samples, been completed by doctors only and focussed on the care delivered/deaths in hospitals, this review looked at a specific patient group, the care delivered in both the community and hospital setting, included patients who died up to 30 days after discharge from hospital and used nurses and doctors to retrospectively assess the standard of care provided.
1 SHMI average value for all NHS Trusts for England is 1.00. Values more than 1.00 suggest a higher than
expected number of deaths (after consideration of relevant differences in the patients). Values less than 1.00 indicate fewer deaths than expected. 2 Health and Social Care Information Centre. (2014) Summary Hospital-level Mortality Indicator (SHMI) –
Frequently Asked Questions (FAQs) (available at http://www.hscic.gov.uk/media/9926/SHMI-FAQs/pdf/SHMI_FAQ.pdf).
38
28 July 2014 Page 3
4. Summary of the Review Process
49 doctors and nurses from local primary, community and secondary healthcare services reviewed 381 selected case records. The records were of patients admitted to UHL NHS Trust as an emergency and subsequently died in hospital, following an attempt at resuscitation or in the Intensive Therapy Unit, or within 30 days of discharge from hospital after changing their postcode or registered GP. The change of postcode was assumed to demonstrate a move by the patient from independent living to supported living (e.g. move into a care home). This approach was used to select the cases most likely to help reviewers identify issues and/or errors that may exist across local healthcare services.
Each case record was reviewed by a pair of local doctors, one from primary care and the other from secondary care, and then discussed with the medical co-ordinator of the review. Only those case records that the doctors agreed had no ‘significant lessons to learn’ were reviewed by a pair of local nurses, one from community healthcare and the other from secondary care, who then discussed their findings with the nursing co-ordinator of the review.
The data collected during the review was managed in two ways. Any numerical data was collated and analysed to help identify trends in the care provided. The comments made by reviewers about how and where the issues occurred in the delivery of care were examined to identify common areas or ‘themes’.
5. Questions to be answered by the Review
The primary question was the proportion (percentage) of cases reviewed that had clinical care of at least an acceptable standard.
The secondary question was whether there were significant lessons that could be learnt from the clinical care provided.
5.1. Primary Question: Was the Clinical Care of at Least an Acceptable Standard?
‘Clinical care’ was defined as the processes of healthcare or social care services that affect a patient’s experience and/or the probability of an outcome for a patient. When deciding whether care was of an acceptable standard or not, the reviewers considered the implications for the patient’s experience or the probability of outcomes for the patient rather than whether the care would be considered as customary or usual practice.
The acceptable standard of care was considered as the absence of error. So, for care to be considered as not acceptable, an error had to be identified. The reviewers used the definition of error described by the Institute of Medicine’s Committee on Quality of Health Care in America in its report To err is human – building a safer health system (page 54)
3:
3 Kohn LT, Corrigan JM, Donaldson MS (eds) on behalf of the Committee on Quality of Health Care in America,
Institute of Medicine. To err is human – building a safer health system. Washington DC: National Academy Press; 2000.
39
Summary of Documents LLR Joint Quality Review (2012-13)
Page 4 28 July 2014
“Error is defined as the failure of a [correctly] planned action to be completed as intended (i.e. error of execution) or the use of a wrong plan to achieve an aim (i.e. error of planning).”
Note that an action or inaction does not have to be linked with an adverse event for it to be considered an error. So, the reviewers were not looking for adverse events or serious untoward incidents, nor were they looking to attribute blame to any practitioner or organisation. However, they were looking for errors of action or inaction. The theory is that a pattern of repeated errors reflects shortcomings in the systems of care, even if a patient was not harmed in a particular case.
5.2. Secondary Question: What Significant Lessons can be Learnt from the Care?
Any significant lessons that could be learnt from a case were described by the reviewers under one or more of the following headings:
● “Failure to Interpret” refers to the initial assessment of the patient and the failure to realise that an adverse event had happened or could happen based on what would reasonably be expected to be ascertained in the situation. ● “Failure to Investigate” refers to the follow-up of the patient after the initial assessment. This includes observations to monitor the patient, as well as laboratory tests, imaging or referral. ● “Failure in Instruction” refers to the conveying of information for others to take action once it is realised that such actions are necessary. The features of good communication are accuracy, completeness, relevance, clarity and timeliness. ● “Failure in Information” refers to the conveying of information for others to take note rather than for action. The features of good communication are accuracy, completeness, relevance, clarity and timeliness. ● “Failure to Implement” refers to the actions that should take place based on appropriate instructions conveyed correctly.
From the comments made by reviewers, issue ‘themes’ were identified.
Further details of the methods used to complete the LLR Joint Mortality Review and examples of the reviewer comments which were used to identify system themes can be found in the ‘Case Records Review’ document.
6. Summary of the Results of the Review
6.1. Answers to Review Questions
Reviewers found significant lessons to learn in 208 (55%) of the 381 cases reviewed, which included 89 cases (23%) where care was considered to be below an acceptable standard.
40
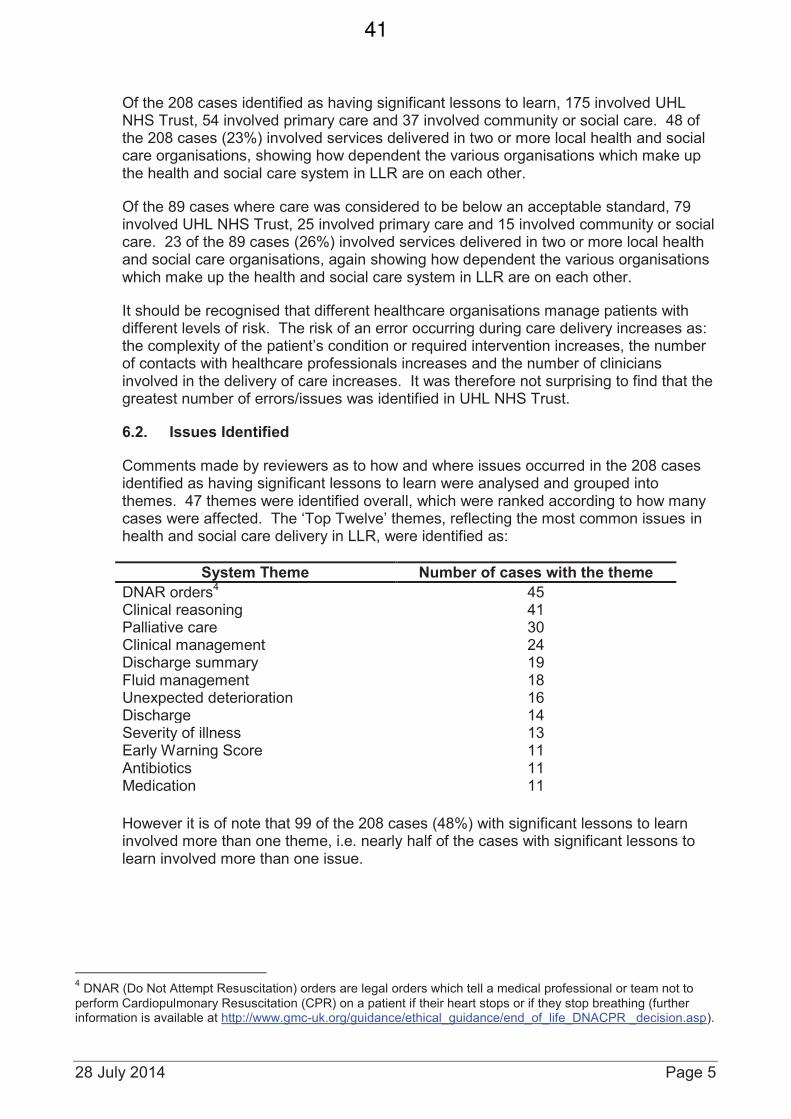
28 July 2014 Page 5
Of the 208 cases identified as having significant lessons to learn, 175 involved UHL NHS Trust, 54 involved primary care and 37 involved community or social care. 48 of the 208 cases (23%) involved services delivered in two or more local health and social care organisations, showing how dependent the various organisations which make up the health and social care system in LLR are on each other.
Of the 89 cases where care was considered to be below an acceptable standard, 79 involved UHL NHS Trust, 25 involved primary care and 15 involved community or social care. 23 of the 89 cases (26%) involved services delivered in two or more local health and social care organisations, again showing how dependent the various organisations which make up the health and social care system in LLR are on each other.
It should be recognised that different healthcare organisations manage patients with different levels of risk. The risk of an error occurring during care delivery increases as: the complexity of the patient’s condition or required intervention increases, the number of contacts with healthcare professionals increases and the number of clinicians involved in the delivery of care increases. It was therefore not surprising to find that the greatest number of errors/issues was identified in UHL NHS Trust.
6.2. Issues Identified
Comments made by reviewers as to how and where issues occurred in the 208 cases identified as having significant lessons to learn were analysed and grouped into themes. 47 themes were identified overall, which were ranked according to how many cases were affected. The ‘Top Twelve’ themes, reflecting the most common issues in health and social care delivery in LLR, were identified as:
However it is of note that 99 of the 208 cases (48%) with significant lessons to learn involved more than one theme, i.e. nearly half of the cases with significant lessons to learn involved more than one issue.
4 DNAR (Do Not Attempt Resuscitation) orders are legal orders which tell a medical professional or team not to
perform Cardiopulmonary Resuscitation (CPR) on a patient if their heart stops or if they stop breathing (further information is available at http://www.gmc-uk.org/guidance/ethical_guidance/end_of_life_DNACPR _decision.asp).
System Theme Number of cases with the theme
DNAR orders4 45
Clinical reasoning 41 Palliative care 30 Clinical management 24 Discharge summary 19 Fluid management 18 Unexpected deterioration 16 Discharge 14 Severity of illness 13 Early Warning Score 11 Antibiotics 11 Medication 11
41
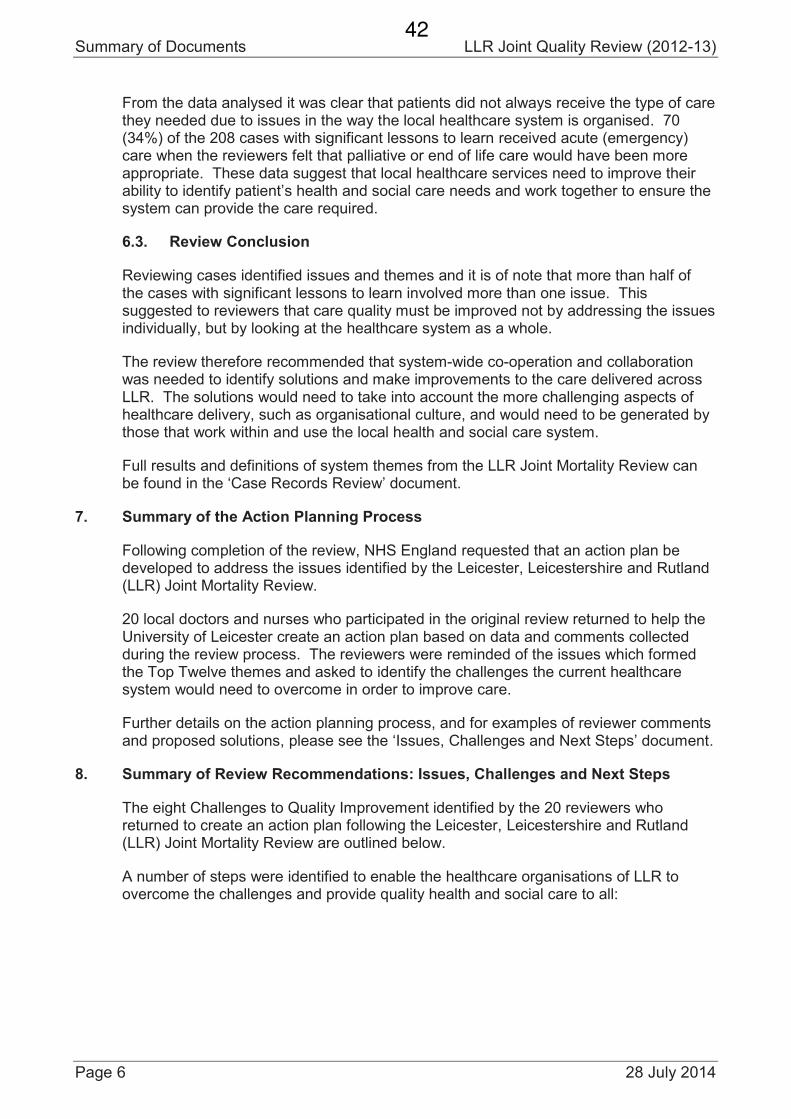
Summary of Documents LLR Joint Quality Review (2012-13)
Page 6 28 July 2014
From the data analysed it was clear that patients did not always receive the type of care they needed due to issues in the way the local healthcare system is organised. 70 (34%) of the 208 cases with significant lessons to learn received acute (emergency) care when the reviewers felt that palliative or end of life care would have been more appropriate. These data suggest that local healthcare services need to improve their ability to identify patient’s health and social care needs and work together to ensure the system can provide the care required.
6.3. Review Conclusion
Reviewing cases identified issues and themes and it is of note that more than half of the cases with significant lessons to learn involved more than one issue. This suggested to reviewers that care quality must be improved not by addressing the issues individually, but by looking at the healthcare system as a whole.
The review therefore recommended that system-wide co-operation and collaboration was needed to identify solutions and make improvements to the care delivered across LLR. The solutions would need to take into account the more challenging aspects of healthcare delivery, such as organisational culture, and would need to be generated by those that work within and use the local health and social care system.
Full results and definitions of system themes from the LLR Joint Mortality Review can be found in the ‘Case Records Review’ document.
7. Summary of the Action Planning Process
Following completion of the review, NHS England requested that an action plan be developed to address the issues identified by the Leicester, Leicestershire and Rutland (LLR) Joint Mortality Review.
20 local doctors and nurses who participated in the original review returned to help the University of Leicester create an action plan based on data and comments collected during the review process. The reviewers were reminded of the issues which formed the Top Twelve themes and asked to identify the challenges the current healthcare system would need to overcome in order to improve care.
Further details on the action planning process, and for examples of reviewer comments and proposed solutions, please see the ‘Issues, Challenges and Next Steps’ document.
8. Summary of Review Recommendations: Issues, Challenges and Next Steps
The eight Challenges to Quality Improvement identified by the 20 reviewers who returned to create an action plan following the Leicester, Leicestershire and Rutland (LLR) Joint Mortality Review are outlined below.
A number of steps were identified to enable the healthcare organisations of LLR to overcome the challenges and provide quality health and social care to all:
42
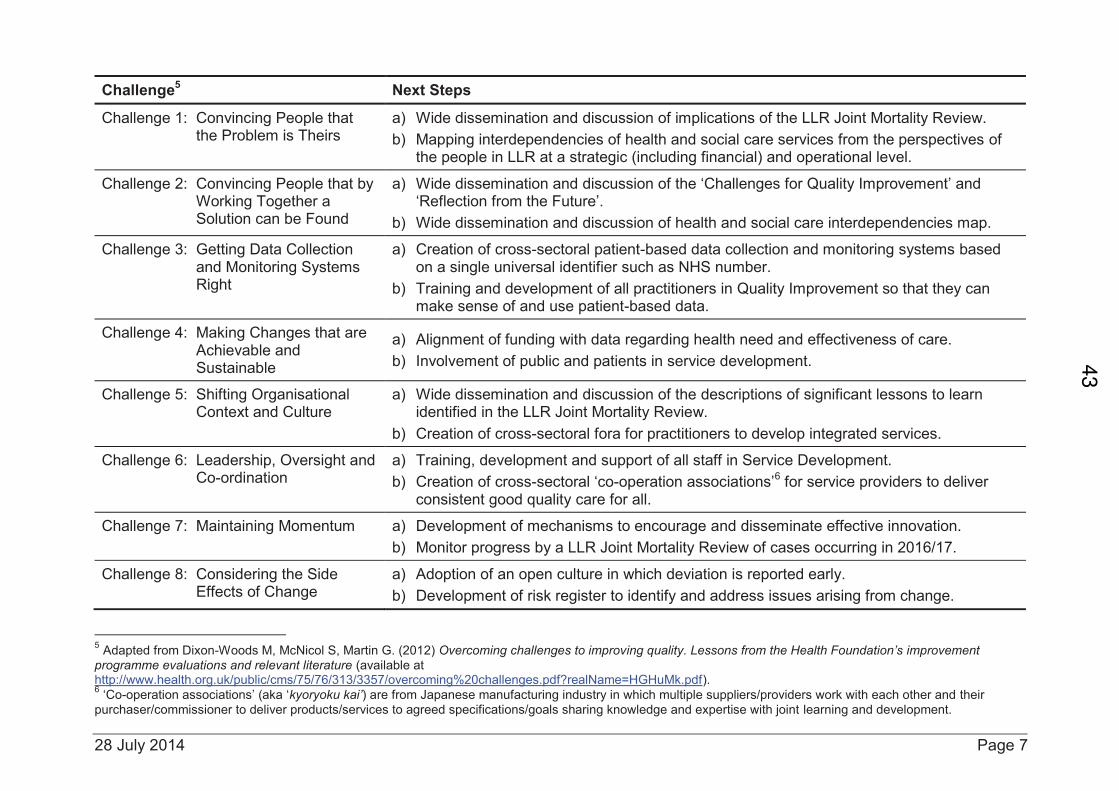
28 July 2014 Page 7
Challenge5 Next Steps
Challenge 1: Convincing People that the Problem is Theirs
a) Wide dissemination and discussion of implications of the LLR Joint Mortality Review.
b) Mapping interdependencies of health and social care services from the perspectives of the people in LLR at a strategic (including financial) and operational level.
Challenge 2: Convincing People that by Working Together a Solution can be Found
a) Wide dissemination and discussion of the ‘Challenges for Quality Improvement’ and ‘Reflection from the Future’.
b) Wide dissemination and discussion of health and social care interdependencies map.
Challenge 3: Getting Data Collection and Monitoring Systems Right
a) Creation of cross-sectoral patient-based data collection and monitoring systems based on a single universal identifier such as NHS number.
b) Training and development of all practitioners in Quality Improvement so that they can make sense of and use patient-based data.
Challenge 4: Making Changes that are Achievable and Sustainable
a) Alignment of funding with data regarding health need and effectiveness of care.
b) Involvement of public and patients in service development.
Challenge 5: Shifting Organisational Context and Culture
a) Wide dissemination and discussion of the descriptions of significant lessons to learn identified in the LLR Joint Mortality Review.
b) Creation of cross-sectoral fora for practitioners to develop integrated services.
Challenge 6: Leadership, Oversight and Co-ordination
a) Training, development and support of all staff in Service Development.
b) Creation of cross-sectoral ‘co-operation associations’6 for service providers to deliver
consistent good quality care for all.
Challenge 7: Maintaining Momentum a) Development of mechanisms to encourage and disseminate effective innovation.
b) Monitor progress by a LLR Joint Mortality Review of cases occurring in 2016/17.
Challenge 8: Considering the Side Effects of Change
a) Adoption of an open culture in which deviation is reported early.
b) Development of risk register to identify and address issues arising from change.
5 Adapted from Dixon-Woods M, McNicol S, Martin G. (2012) Overcoming challenges to improving quality. Lessons from the Health Foundation’s improvement
programme evaluations and relevant literature (available at http://www.health.org.uk/public/cms/75/76/313/3357/overcoming%20challenges.pdf?realName=HGHuMk.pdf). 6 ‘Co-operation associations’ (aka ‘kyoryoku kai’) are from Japanese manufacturing industry in which multiple suppliers/providers work with each other and their
purchaser/commissioner to deliver products/services to agreed specifications/goals sharing knowledge and expertise with joint learning and development.
43
Summary of Documents LLR Joint Quality Review (2012-13)
Page 8 28 July 2014
9. Summary of Vision: Reflection from the Future
‘Reflection from the Future’ is a vision document written to illustrate how health and social care in Leicester, Leicestershire and Rutland (LLR) could be delivered if the recommendations outlined in the ‘Issues, Challenges and Next Steps’ document were accepted and actioned.
The document describes a LLR-wide health and social care ‘co-operation association’, through which health and social care is planned and delivered jointly, with a focus on patient need and quality of care. The vision outlines how discussions and decisions about health and social care in LLR should involve every level of staff and every organisation affected, directly or indirectly, by the care process – including patients.
In the document the ‘co-operative association’ employs a funding system which rewards innovation and an education system which shares best practice to allow all of the organisations which form the ‘co-operation association’ to benefit equally and for patient care to be improved.
The vision relies on working relationship based on trust, quality and dependence which allows the ‘co-operative association’ to develop health and social care services which are organised, innovative, effective and high quality.
10. Summary of LLR Healthcare Provider Response
In response to the review findings, and subsequent recommendations and vision documents, the Clinical Commissioning Groups for Leicester, Leicestershire and Rutland (LLR), Leicestershire Partnership NHS Trust (LPT) and UHL NHS Trust completed two exercises:
10.1. Joint LLR Quality Review Action Plan
The first exercise outlined six priority areas for healthcare improvement in LLR. The Joint LLR Quality Review Action Plan also identified current quality improvement initiatives anticipated to address the priority areas and gaps where further work would be required. Opportunities for collaborative working were highlighted and deadlines for action jointly agreed. The six priority areas jointly agreed were:
· Advance Care Planning co-ordination (including DNAR orders, palliative care and end of life care)
· Use of, and compliance with, best practice policies and guidelines
· Patient-centred care for the frail older person
· Ensuring ongoing learning and feedback
· Completion of Individual Organisation Action Plans (see 10.2)
· Development of joint long term action plan to reflect recommendations outlined in Issues, Challenges and Next Steps document
44
28 July 2014 Page 9
10.2. Individual Organisation Quality Review Action Plans
The second exercise was the completion of individual action plans by the LLR Clinical Commissioning Groups, LPT and UHL NHS Trust detailing their role in the review response and the specific actions required by them to realise the Joint LLR Quality Review Action Plan.
A commitment was also made by all of the healthcare organisations involved in the review to use the review findings for educational purposes and share the learning across all organisations to improve healthcare planning and delivery in LLR.
11. Acknowledgements
The 49 doctors and nurses who participated in the Leicester, Leicestershire and Rutland (LLR) Joint Mortality Review would like to express their gratitude to the patients whose case records were reviewed and analysed. Each of the reviewers was personally touched by the experiences, both good and bad, of the patients described in the case records and are committed to ensuring lessons are learned from the review and that health and social care across LLR is improved.
Lucy Douglas-Pannett Specialty Registrar in Public Health On behalf of East Leicestershire Clinical Commissioning Group Leicester City Clinical Commissioning Group Leicestershire Partnership NHS Trust University Hospitals of Leicester NHS Trust West Leicestershire Clinical Commissioning Group
12. Bibliography
This document is a summary of original review documents and action plans, namely:
1. Leicester, Leicestershire and Rutland (LLR) Joint Mortality Review: Case Records Review (24 July 2014)
2. Joint LLR Quality Review Action Plan (July 2014)
The above documents are available on the following websites:
www.eastleicestershireandrutlandccg.nhs.uk
www.leicestercityccg.nhs.uk
www.leicestershospitals.nhs.uk
www.leicspart.nhs.uk
www.westleicestershireccg.nhs.uk
3. LLR Joint Mortality Review: Critique and Comparison (18 March 2014)
4. LLR Joint Mortality Review: Issues, Challenges and Next Steps (24 July 2014)
45
Summary of Documents LLR Joint Quality Review (2012-13)
Page 10 28 July 2014
5. LLR Joint Mortality Review: Reflection from the Future (18 March 2014)
6. Individual LLR Organisation Action Plans
The above documents are available from:
West Leicestershire Clinical Commissioning Group on 01509 567755 or
46
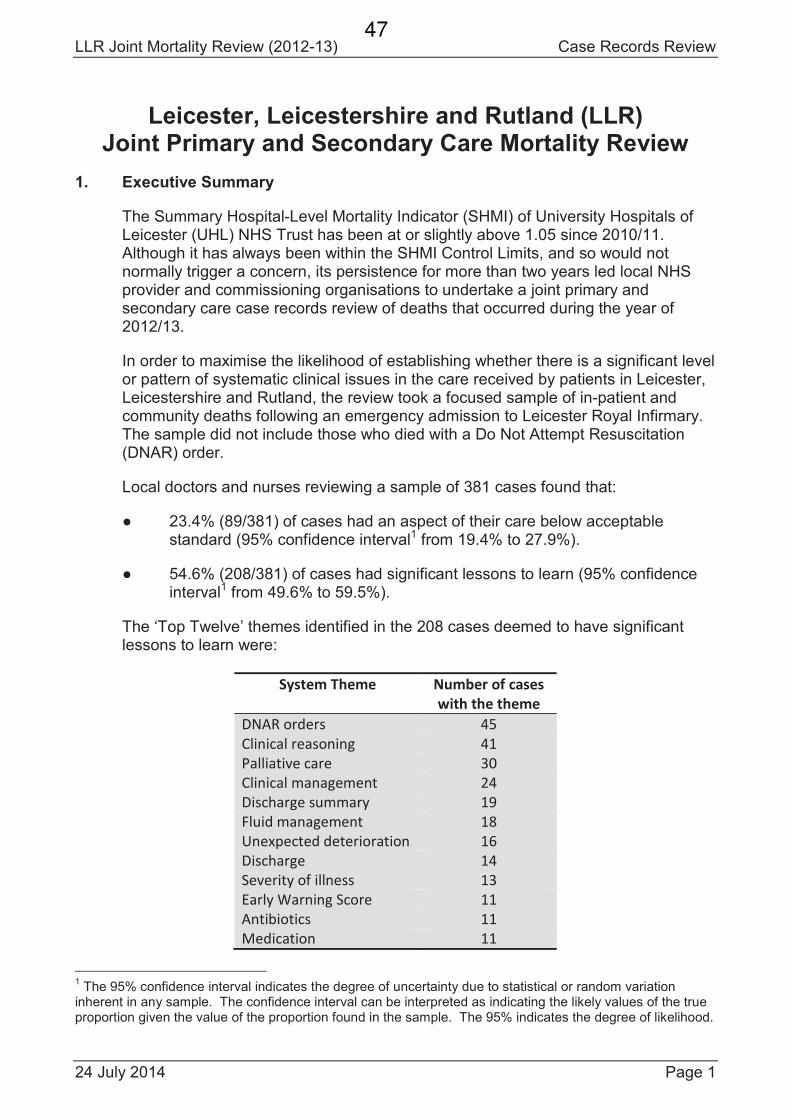
LLR Joint Mortality Review (2012-13) Case Records Review
24 July 2014 Page 1
Leicester, Leicestershire and Rutland (LLR)Joint Primary and Secondary Care Mortality Review
1. Executive Summary
The Summary Hospital-Level Mortality Indicator (SHMI) of University Hospitals of Leicester (UHL) NHS Trust has been at or slightly above 1.05 since 2010/11. Although it has always been within the SHMI Control Limits, and so would not normally trigger a concern, its persistence for more than two years led local NHS provider and commissioning organisations to undertake a joint primary and secondary care case records review of deaths that occurred during the year of 2012/13.
In order to maximise the likelihood of establishing whether there is a significant level or pattern of systematic clinical issues in the care received by patients in Leicester, Leicestershire and Rutland, the review took a focused sample of in-patient and community deaths following an emergency admission to Leicester Royal Infirmary.The sample did not include those who died with a Do Not Attempt Resuscitation (DNAR) order.
Local doctors and nurses reviewing a sample of 381 cases found that:
23.4% (89/381) of cases had an aspect of their care below acceptable standard (95% confidence interval1 from 19.4% to 27.9%).
54.6% (208/381) of cases had significant lessons to learn (95% confidence interval1 from 49.6% to 59.5%).
The ‘Top Twelve’ themes identified in the 208 cases deemed to have significant lessons to learn were:
System Theme Number of cases
with the theme
DNAR orders 45
Clinical reasoning 41
Palliative care 30
Clinical management 24
Discharge summary 19
Fluid management 18
Unexpected deterioration 16
Discharge 14
Severity of illness 13
Early Warning Score 11
Antibiotics 11
Medication 11
1The 95% confidence interval indicates the degree of uncertainty due to statistical or random variation
inherent in any sample. The confidence interval can be interpreted as indicating the likely values of the true proportion given the value of the proportion found in the sample. The 95% indicates the degree of likelihood.
47
Case Records Review LLR Joint Mortality Review (2012-13)
Page 2 24 July 2014
2. Case Records Review Panel Members
The review was undertaken by experienced doctors and nurses who are working or have worked in the health service in Leicester, Leicestershire or Rutland for many years. The analyses in this report are based on their review of case records.
2.1. Doctors’ Sub-Panel
Title Name Job Title Location Practice No. of cases
reviewed
Dr Dan O'Keeffe General Practitioner Retired - 57
Dr Pam Bowyer General Practitioner Coalville Dr NR Pulman & Partners 36
Dr Orest Mulka General Practitioner Retired - 35
Dr Sue Cullis General Practitioner Portfolio - 34
Dr Kath Packham Specialty Registrar Public Health - 28
Dr Simeon Rayner General Practitioner Billesdon Dr MWE Austin & Partners 28
Dr Ian Robinson General Practitioner Portfolio - 28
Dr Carol Furlong General Practitioner Coalville Dr NR Pulman & Partners 26
Dr Elizabeth Alun-Jones General Practitioner Hinckley Dr ID Cracknell & Partners 26
Dr Chris Williams – also on
Thematic Analysis Panel
General Practitioner Coalville Dr NR Pulman & Partners 26
Dr Chris Prideaux General Practitioner Portfolio - 21
Dr Hilary Fox General Practitioner Uppingham Dr JP Jones & Partners 18
Dr Geth Jenkins General Practitioner Earl Shilton Dr G Jenkins & Partners 13
Dr Karl Shergill General Practitioner Birstall Dr KS Shergill & Partners 5
Dr Ronald Hsu –
Doctors’ Co-ordinator
Teaching Fellow Public Health University of Leicester 0
Title Name Job Title Specialty Hospital No. of cases
reviewed
Mr Martin Dennis Hospital Consultant Vascular Surgery Leicester Royal Infirmary 64
Dr James Reid Hospital Consultant Geriatric Medicine Leicester Royal Infirmary 43
Dr Doug Skehan Hospital Consultant Cardiology Glenfield Hospital 33
Dr Fiona Miall Hospital Consultant Haematology Leicester Royal Infirmary 31
Dr Azri Nache – also on
Thematic Analysis Panel
Specialty Registrar General Medicine Leicester Royal Infirmary 31
Dr Mark Ardron Hospital Consultant Stroke Medicine Leicester Royal Infirmary 30
Dr Penny Eames Hospital Consultant Neurology Leicester General Hospital 21
Dr Alison Gallagher Hospital Consultant Endocrinology Leicester Royal Infirmary 21
Dr Lisa Turner Specialty Registrar General Medicine Leicester Royal Infirmary 21
Dr Ruth Denton-Beaumont Hospital Consultant Acute Medicine Leicester Royal Infirmary 18
Dr John Parker Hospital Consultant Anaesthetics Leicester Royal Infirmary 18
Dr Lee Walker Hospital Consultant Acute Medicine Leicester Royal Infirmary 15
Dr Barrie Rathbone Hospital Consultant Gastroenterology Leicester Royal Infirmary 13
Dr Patricia Hooper Specialty Registrar General Medicine Leicester Royal Infirmary 12
Dr Dilesh Lakhani Hospital Consultant Geriatric Medicine Leicester Royal Infirmary 10
Dr Miles Levy – also on
Thematic Analysis Panel
Hospital Consultant Endocrinology Leicester Royal Infirmary 0
48
LLR Joint Mortality Review (2012-13) Case Records Review
24 July 2014 Page 3
2.2. Nurses’ Sub-Panel
Title Name Job Title NHS
Organisation
Division No. of cases
reviewed
Mrs Debra Clarke Deputy Sister for District
Nursing Service
LPT NHS Trust Merlyn Vaz Health and Social
Care Centre
85
Ms Sara Lowe Releasing Time to Care
Nurse Facilitator
LPT NHS Trust Charnwood Mill 49
Mr Jonathan Dexter Advanced Nurse
Practitioner
LPT NHS Trust Charnwood Mill 27
Ms Zoe Harris Specialist Nurse Team
Manager for Long Term
Conditions
LPT NHS Trust Riverside House 25
Mrs Debbie Leafe Clinical Education Lead
for Adult Services
LPT NHS Trust Charnwood Mill 13
Mrs Louise Clayton Specialist Nurse for
Heart Failure
LPT NHS Trust Westcotes Health Centre 13
Ms Shelley Jacques Registered Nurse in
Nursing Bank
LPT NHS Trust St Matthews Health and
Community Centre
12
Ms Lesley Tooley Clinical Training and
Development Manager
LPT NHS Trust Charnwood Mill 12
Title Name Job Title NHS
Organisation
Hospital No. of cases
reviewed
Ms Julia Ball Divisional Head of
Nursing for Planned Care
UHL NHS Trust Leicester Royal Infirmary 29
Miss Amy Brown Registered Nurse in
Emergency Department
UHL NHS Trust Leicester Royal Infirmary 29
Ms Yvonne Kenmuir-Hogg Matron for Elective
Orthopaedic Surgery
UHL NHS Trust Leicester General Hospital 27
Mrs Helen Smalley Ward Sister for Specialist
and Vascular Surgery
UHL NHS Trust Leicester Royal Infirmary 26
Mrs Christine Bufton Lead Specialist Nurse for
Vascular Studies Unit
UHL NHS Trust Leicester Royal Infirmary 22
Ms Alison Hessey Matron for Planned Care UHL NHS Trust Glenfield Hospital 19
Mrs Natalie Nelson Ward Sister for
Orthopaedic Surgery
UHL NHS Trust Leicester Royal Infirmary 19
Ms Elizabeth Aryeetey Lead Specialist Nurse for
Congenital Heart Disease
UHL NHS Trust Glenfield Hospital 16
Mr Dominick Tompkins Releasing Time to Care
Nurse Facilitator
UHL NHS Trust Leicester Royal Infirmary 16
Ms Linda Zeleny Ward Sister for Brain
Injury Unit
UHL NHS Trust Leicester General Hospital 12
Mrs Lucy Douglas-Pannett –
Nurses’ Co-ordinator
Specialty Registrar in
Public Health
- - 10
Ms Margaret Kelly Deputy Sister for Acute
Medical Unit
UHL NHS Trust Leicester Royal Infirmary 9
3. Thematic Analysis Panel Members
The reviewers’ analyses were analysed for themes by the five clinicians in bold.
4. Report Authors
Dr R Hsu and Mrs L Douglas-Pannett compiled this report based on the analyses.
49
Case Records Review LLR Joint Mortality Review (2012-13)
Page 4 24 July 2014
5. Acknowledgements
All members of the LLR Mortality Case Records Review Panel and Thematic Analysis Panel would like to express our indebtedness to the patients whose case records we reviewed and analysed. Regardless of our years of clinical experience, each of us was personally touched by the experiences, both good and bad, of the patients as described in the case records. It is incumbent upon all of us to use the legacy that these patients left us to identify where and how care can be improved.
The doctors and nurses would not have been able to undertake the review without the support of the directors and managers of local NHS Trusts and Clinical Commissioning Groups:
University Hospitals of Leicester (UHL) NHS Trust – Dr Kevin Harris– Ms Carole Ribbins– Ms Rebecca Broughton
Leicestershire Partnership (LPT) NHS Trust – Ms Rachel Bilsborough– Ms Jude Smith
East Leicestershire and Rutland (ELR) CCG – Dr Dave Briggs– Ms Carmel O’Brien
Leicester City (LC) CCG – Dr Simon Freeman– Ms Dawn Leese
West Leicestershire (WL) CCG – Dr Nick Pulman– Ms Caroline Trevithick
Equally importantly was the work of the managerial, administrative and clerical staff who brought together primary care, community (SystmOne) and hospital records for the reviewers to review:
University Hospitals of Leicester (UHL) NHS Trust – Ms Linda Hutchinson– Ms Jo Lowry– Ms Enady Mussa– Ms Claire Willday
Greater East Midlands Commissioning Support Unit – Mr Phil Demmer
Finally, we would like to thank the following data analyst and clerks for collating the information necessary to identify those patients who were admitted to LRI and either seen by the LRI Resuscitation Team or treated in LRI Intensive Therapy Unit for adults:
UHL Business Intelligence – Mr Gareth Greaves
LRI Resuscitation Team – Ms Nicola McKay
LRI Intensive Therapy Unit for Adults – Ms Kim Clarkson– Ms Alexandra Smith
50
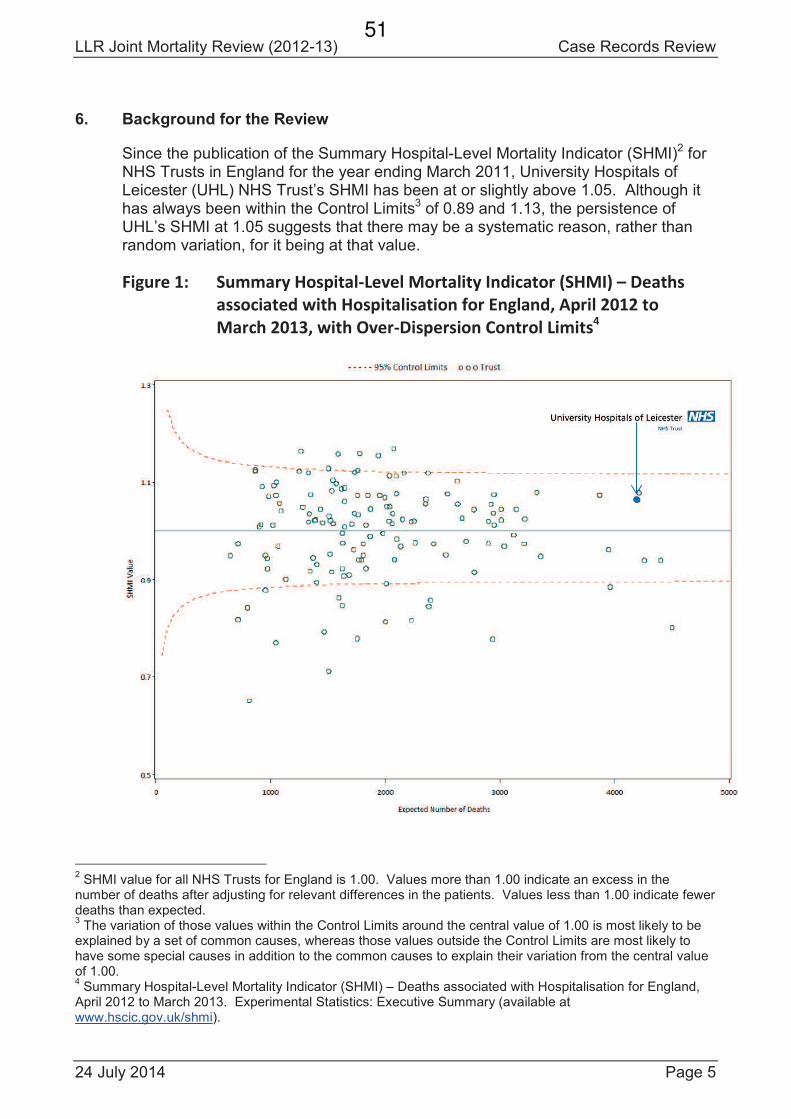
LLR Joint Mortality Review (2012-13) Case Records Review
24 July 2014 Page 5
6. Background for the Review
Since the publication of the Summary Hospital-Level Mortality Indicator (SHMI)2 for NHS Trusts in England for the year ending March 2011, University Hospitals of Leicester (UHL) NHS Trust’s SHMI has been at or slightly above 1.05. Although it has always been within the Control Limits3 of 0.89 and 1.13, the persistence of UHL’s SHMI at 1.05 suggests that there may be a systematic reason, rather than random variation, for it being at that value.
Figure 1: Summary Hospital-Level Mortality Indicator (SHMI) – Deaths
associated with Hospitalisation for England, April 2012 to
March 2013, with Over-Dispersion Control Limits4
2SHMI value for all NHS Trusts for England is 1.00. Values more than 1.00 indicate an excess in the
number of deaths after adjusting for relevant differences in the patients. Values less than 1.00 indicate fewer deaths than expected.3
The variation of those values within the Control Limits around the central value of 1.00 is most likely to be explained by a set of common causes, whereas those values outside the Control Limits are most likely to have some special causes in addition to the common causes to explain their variation from the central value of 1.00.4
Summary Hospital-Level Mortality Indicator (SHMI) – Deaths associated with Hospitalisation for England, April 2012 to March 2013. Experimental Statistics: Executive Summary (available at www.hscic.gov.uk/shmi).
51
Case Records Review LLR Joint Mortality Review (2012-13)
Page 6 24 July 2014
Local NHS organisations commissioned a retrospective case record review to ascertain whether there are systematic clinical issues in the care received by patients in Leicester, Leicestershire and Rutland. If such a retrospective case record review fails to find a significant level or pattern of systematic clinical issues, it would be reasonable to assume that systematic non-clinical issues, such as differences in clinical coding or unadjusted confounding, could explain the persistence of UHL’s SHMI at 1.05.
The commissioning of the retrospective case record review does not imply, and is not intended to imply, that there really is an excess in the adjusted number of deaths attributable to the care provided by University Hospitals of Leicester (UHL) NHS Trust or any other organisation providing health or social care services in Leicester, Leicestershire and Rutland.
7. Context for the Review
From the outset, it was agreed that the persistently high SHMI is an issue for all those providing NHS healthcare in Leicester, Leicestershire and Rutland, and notjust for University Hospitals of Leicester (UHL) NHS Trust.
So, it was agreed that a joint primary and secondary care case records review would be undertaken in which doctors and nurses from primary care, community health services and hospitals review primary care, community health (SystmOne) and hospital records together.
Such a comprehensive joint review of NHS healthcare records has never been attempted before, and so it is not possible to make direct comparisons with other reviews. However, there are two published reviews that give an indication of the results that could reasonably be expected in this review:
1. In a NCEPOD review of the care of patients who died in hospital between 1 October 2006 and 31 March 2007 within four days of admission5 on page 17: “However, in 34.2% (750/2195) of patients there was room for improvement and in 4.9% (108/2195) of cases care was judged to have been less than satisfactory by the advisors. In 107 cases there was insufficient data to assess the case.” Although not calculated by NCEPOD, the 95% confidence intervals for 34.2% would be 32.2% to 36.2% and for 4.9% they would be 4.09% to 5.91%.
2. In a retrospective case record review by Hogan H et al of 1,000 adults who died in 2009 in 10 acute hospitals in England6 on page 739: “131 (13.1%; 95% CI: 10.9% to 15.1%) patients were identified as having a problem in care that contributed to their death.” This is analogous to significant lessons to learn. Although not calculated by Hogan H et al, Table 3 in their article has 60 cases considered to have received poor quality of care and 10 very
5National Confidential Enquiry into Patient Outcome and Death. Caring to the End? A review of the care of
patients who died in hospital within four days of admission. London: NCEPOD; 2009 Nov.6
Hogan H, Healey F, Neale G, Thomson R, Vincent C, Black N. Preventable deaths due to problems in care in English acute hospitals: a retrospective case record review study. BMJ Quality and Safety 2012 Sep;21(9): 737-45.
52
LLR Joint Mortality Review (2012-13) Case Records Review
24 July 2014 Page 7
poor care, giving a total of 70 cases of the 1,000 records reviewed (7%; 95% CI: 5.57% to 8.76%). This is analogous to unacceptable care.
8. Sample Size Required for the Review
If the headline category is considered to be unacceptable care, and one considers the expected percentage in 1,000 eligible cases in a year to be 5%, the following sample sizes would give the following degrees of uncertainty as exemplified by the 95% confidence interval7:
Expected percentage Sample size 95% confidence interval
5% 440 from 3.48% to 6.52%5% 240 from 2.60% to 7.40%5% 144 from 1.70% to 8.30%
It was decided to sample 440 cases in order to minimise the degree of uncertainty to an expected percentage of 5% ± 1.5%. If the measured proportion turns out to be less than 5%, there will be a smaller degree of uncertainty, and if more than 5%(up to 50%), there will be a larger degree of uncertainty.
9. Sampling Strategy for the Review
The sampling strategy was to focus on admissions most likely to demonstrate any systematic clinical issues that may exist. That way, if no systematic clinical issues are found, then there is no need for any further comprehensive reviews as other samples are also unlikely to find systematic clinical issues.
A focused sample was undertaken of those patients from Leicester, Leicestershire or Rutland who either died in or were discharged from Leicester Royal Infirmary on or between 1 April 2012 and 31 March 2013 following an emergency admission to ahospital.
For those who died in Leicester Royal Infirmary, only those who died after involvement of the Resuscitation Team or in the Intensive Therapy Unit for adults were selected on the basis that they were not expected to die. If a patient was expected to die, one would expect a Do Not Attempt Resuscitation (DNAR) order to be in place and so the Resuscitation Team would not be called and the patient would not be treated in the Intensive Therapy Unit for adults.
For those who were discharged from Leicester Royal Infirmary, only those who died within 30 days of discharge and changed either their postcode or registered GP, indicating a change in residence, were selected on the basis that such changes increase the likelihood of systematic clinical issues arising.
Since the sample is not a random sample of either admissions or deaths, it is not possible to extrapolate the findings of this review to all admissions or all deaths in University Hospitals of Leicester (NHS) Trust or Leicester, Leicestershire and Rutland.
7The 95% confidence interval indicates the degree of uncertainty due to statistical or random variation
inherent in any sample. The confidence interval can be interpreted as indicating the likely values of the true proportion given the value of the proportion found in the sample. The 95% indicates the degree of likelihood.
53
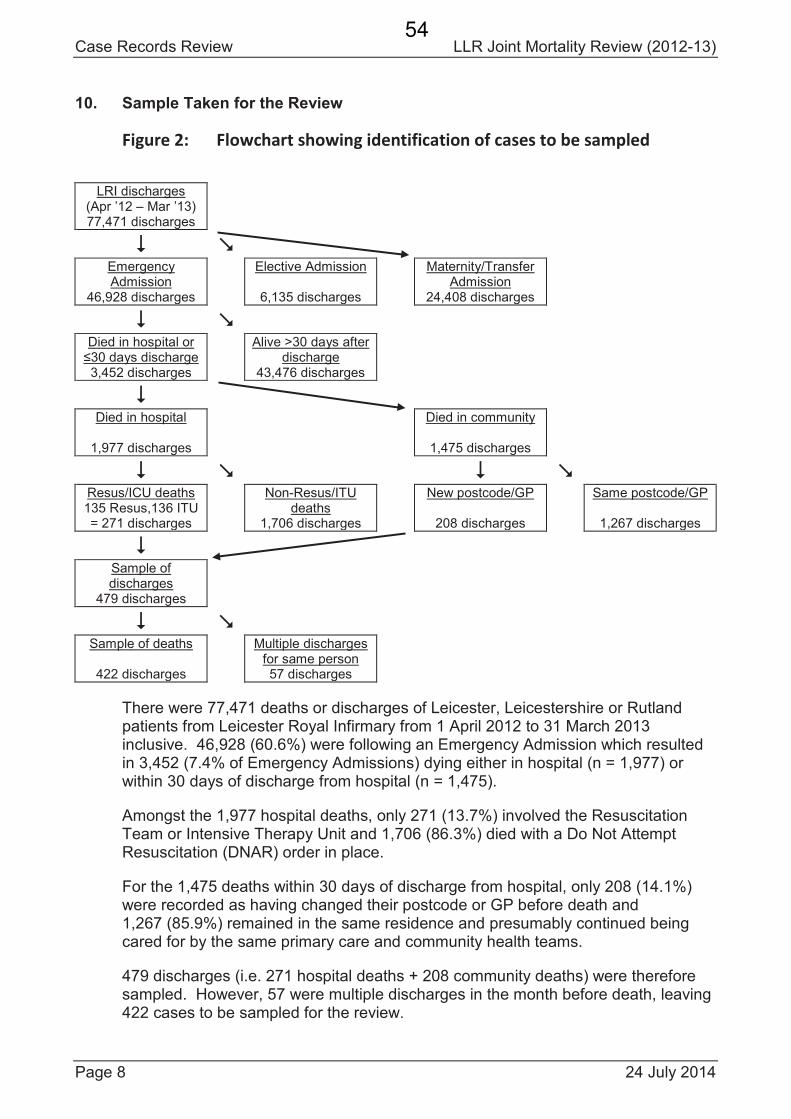
Case Records Review LLR Joint Mortality Review (2012-13)
Page 8 24 July 2014
10. Sample Taken for the Review
Figure 2: Flowchart showing identification of cases to be sampled
LRI discharges(Apr ’12 – Mar ’13)77,471 discharges
Emergency Admission
46,928 discharges
Elective Admission
6,135 discharges
Maternity/Transfer Admission
24,408 discharges
Died in hospital or
3,452 discharges
Alive >30 days after discharge
43,476 discharges
Died in hospital
1,977 discharges
Died in community
1,475 discharges
Resus/ICU deaths135 Resus,136 ITU= 271 discharges
Non-Resus/ITU deaths
1,706 discharges
New postcode/GP
208 discharges
Same postcode/GP
1,267 discharges
Sample of discharges
479 discharges
Sample of deaths
422 discharges
Multiple dischargesfor same person57 discharges
There were 77,471 deaths or discharges of Leicester, Leicestershire or Rutland patients from Leicester Royal Infirmary from 1 April 2012 to 31 March 2013 inclusive. 46,928 (60.6%) were following an Emergency Admission which resulted in 3,452 (7.4% of Emergency Admissions) dying either in hospital (n = 1,977) or within 30 days of discharge from hospital (n = 1,475).
Amongst the 1,977 hospital deaths, only 271 (13.7%) involved the Resuscitation Team or Intensive Therapy Unit and 1,706 (86.3%) died with a Do Not Attempt Resuscitation (DNAR) order in place.
For the 1,475 deaths within 30 days of discharge from hospital, only 208 (14.1%) were recorded as having changed their postcode or GP before death and 1,267 (85.9%) remained in the same residence and presumably continued being cared for by the same primary care and community health teams.
479 discharges (i.e. 271 hospital deaths + 208 community deaths) were therefore sampled. However, 57 were multiple discharges in the month before death, leaving 422 cases to be sampled for the review.
54
LLR Joint Mortality Review (2012-13) Case Records Review
24 July 2014 Page 9
11. Questions to be Answered by the Review
The primary question was the proportion of cases in the sample that had clinical care of at least an acceptable standard.
The secondary question was whether there were significant lessons that could be learnt from the clinical care reviewed.
11.1. Primary Question: Was the Clinical Care of at Least an Acceptable Standard?
Clinical care was considered to be the processes of healthcare or social care services that impact on a patient’s experience and/or the probability of outcomes for a patient. When deciding whether care was of an acceptable standard or not, the reviewers considered the implications for the patient’s experience or the probability of outcomes for the patient rather than whether the care would be considered as customary or usual practice of care.
The acceptable standard of care was considered as the absence of error. So, for care to be considered as not acceptable, an error had to be identified. The reviewers used the definition of error described by the Institute of Medicine’s Committee on Quality of Health Care in America in its report To err is human – building a safer health system8 (page 54):
“Error is defined as the failure of a [correctly] planned action to be completed as intended (i.e. error of execution) or the use of
a wrong plan to achieve an aim (i.e. error of planning).”
Note that an action or inaction does not have to be linked with an adverse event for it to be considered an error. So, the reviewers were not looking for adverse events or serious untoward incidents, nor were they looking to attribute adverse events or serious untoward incidents to an error. However,they were looking for errors of commission or omission. The assumption is that a pattern of repeated errors reflects deficiencies in the systems of care even if a patient was not harmed in a particular case.
Since no plan is perfect or implemented as intended, it is unrealistic to consider the presence of any error as defining care as not acceptable. Carewas considered as not of an acceptable standard only if an error was serious.In order to achieve a reasonable degree of validity and reliability in the assessment of seriousness of errors, an error was considered sufficiently serious if it demonstrably impacted on the patient’s experience (such as adelay in diagnosing pneumonia prolonging the presence of symptoms), or there was widely accepted evidence that the error was likely to have significantly increased the probability of an adverse event (such as lack of thromboembolism prophylaxis) or significantly decreased the probability of a beneficial event (such as failure to administer aspirin after a myocardial infarction).
8Kohn LT, Corrigan JM, Donaldson MS (eds) on behalf of the Committee on Quality of Health Care in
America, Institute of Medicine. To err is human – building a safer health system. Washington DC: National Academy Press; 2000.
55
Case Records Review LLR Joint Mortality Review (2012-13)
Page 10 24 July 2014
11.2. Secondary Question: What Significant Lessons can be Learnt from the Care?
Any significant lessons that could be learnt from a case were described by the reviewers under one or more of the following headings:
“Failure to Interpret” refers to the initial assessment of the patient and the failure to realise that an adverse event had happened or could happen based on what would reasonably be expected to be ascertained in the situation.
“Failure to Investigate” refers to the follow-up of the patient after the initial assessment. This includes observations to monitor the patient, as well as laboratory tests, imaging or referral.
“Failure in Instruction” refers to the conveying of information for others to take action once it is realised that such actions are necessary. The features of good communication are accuracy, completeness, relevance, clarity and timeliness.
“Failure in Information” refers to the conveying of information for others to take note rather than for action. The features of good communication are accuracy, completeness, relevance, clarity and timeliness.
“Failure to Implement” refers to the actions that should take place based on appropriate instructions conveyed correctly.
11.3. Index Admission and Period of Care Reviewed
The Index Admission was defined as the emergency admission involving an in-patient stay in Leicester Royal Infirmary (LRI) whose date of admission was the last one prior to the date of death.
The Period of Care reviewed was from the date of the last in-patient admission to University Hospitals of Leicester NHS Trust (UHL) prior to the Index Admission up to and including the date of death:
| PERIOD OF CARE TO BE REVIEWED || | |
Date of Date of Date ofPrior Admission Index Admission Death
11.4. Clinical Uncertainty
Whenever there was clinical uncertainty, the reviewers erred towards giving the benefit of doubt to the clinicians involved in the care of the patient. So, the default stance was always that the care received by a patient was of an acceptable standard and that there were no significant lessons to learn.There had to be evidence to the contrary for care to be considered otherwise.
56
LLR Joint Mortality Review (2012-13) Case Records Review
24 July 2014 Page 11
12. Case Records Review Panel
The Doctors’ Sub-Panel consisted of:13 General Practitioners (2 of whom retired recently) and 1 SpecialtyRegistrar in Public Health who was formerly a General Practitioner12 Hospital Consultants and 3 Specialty Registrars in their final year.
The Nurses’ Sub-Panel consisted of:8 nurses from City and County bases in the Community Health ServicesDivision of Leicestershire Partnership NHS Trust11 nurses from the three hospital sites of University Hospitals of Leicester(UHL) NHS Trust and 1 Specialty Registrar in Public Health who was formerly a nurse.
The Doctors’ and Nurses’ Sub-Panels worked independently in adjacent rooms.Each Sub-Panel had reviewers from primary care or community health services paired with reviewers from the acute hospital. All reviewers received a written protocol and attended a 30 minute training session on the protocol and data entry requirements before they started reviewing cases. After the first day, new reviewers were paired with experienced reviewers. Reviewers were rotated between pairs so that no reviewer reviewed with someone they worked with on a previous day.9
Each case was first reviewed by a pair in the Doctors’ Sub-Panel. If they decided that there were no significant lessons to learn, the case was reviewed by a pair in the Nurses’ Sub-Panel. This arrangement was necessary because there were fewer nurses than doctors reviewing cases. Since it is unlikely that a pair in the Nurses’ Sub-Panel would overrule a Doctors’ Sub-Panel’s finding of significantlessons to learn, this sub-group review by the Nurses’ Sub-Panel is unlikely to affect the number of cases with significant lessons to learn but is likely to lead to anunderestimate of the number of significant lessons to learn.
All pairs reviewed the primary care and hospital records, and had access to the community health services records on SystmOne as well as hospital computerised laboratory results and imaging. Both reviewers in a pair had to agree whether care was of an acceptable standard and whether there were any significant lessons to learn. Then the pair had to justify their decision about the standard of care and significant lessons to a Sub-Panel Co-ordinator who was a public health specialist with either a medical or nursing background. The pair’s review of a case was accepted only if the Sub-Panel Co-ordinator agreed with their decision about the standard of care and description of significant lessons to learn. Whenever there was uncertainty within a pair or between a pair and the Sub-Panel Co-ordinator, the case was discussed with all the pairs from the same Sub-Panel until a consensuswas reached.10 The pairs in each Sub-Panel were encouraged to discuss their cases with other pairs in the same Sub-Panel or other Sub-Panel, depending on the expertise required, as well as contact colleagues with specific areas of expertise. It took each pair an average of 45 minutes to review a case with the doctors’ pairsspending 43 minutes per case and the nurses’ pairs spending 47 minutes per case.
9On two occasions it was necessary to allow two nurses to work together twice.
10There were only 4 cases in which other pairs in the Sub-Panel changed the original pair’s decision:
2 cases from acceptable care to unacceptable care, 1 case from unacceptable care to acceptable care,1 case with acceptable care from significant lessons to learn to no significant lessons to learn.
57
Case Records Review LLR Joint Mortality Review (2012-13)
Page 12 24 July 2014
13. Thematic Analysis of Significant Lessons
The reviewers’ descriptions of significant lessons to learn were analysed to ascertain the following:
1. Care: whether the type of care11 the patient should have received was received
2. Decision Making: whether the correct plan was made at the correct time
3. Communication: whether the right message reached the right people
4. Delivery: whether the required care was delivered and was timely
5. Monitoring: whether the patient’s clinical condition was monitored appropriately
6. Responsiveness: whether there was an appropriate response to any unexpected deterioration in the patient’s clinical condition
7. System Themes: the themes raised by the reviewers’ in their descriptions.
14. Thematic Analysis Panel
The LLR Mortality Case Records Thematic Analysis Panel consisted of:one doctor with general practice expertise who had reviewed cases (Dr Chris Williams)one doctor with hospital medicine expertise who had reviewed cases (Dr Azri Nache)one doctor with hospital medicine expertise who had not reviewed cases (Dr Miles Levy)one doctor with public health expertise who had heard the reviewed cases as the Doctors’ Sub-Panel Co-ordinator (Dr Ronald Hsu)one nurse with public health expertise who had heard the reviewed cases as the Nurses’ Sub-Panel Co-ordinator (Mrs Lucy Douglas-Pannett).
The doctors on the Thematic Analysis Panel independently analysed the reviewers’descriptions of significant lessons to learn. Then they discussed their individual analyses and themes with each other. The collective analysis and themes for a case was agreed only when there was unanimity between the doctors on the Panel.
The Nurses’ Sub-Panel Co-ordinator, Mrs Lucy Douglas-Pannett, reviewed the analysis and themes agreed by the doctors and revised the analysis and themes in 38 cases after discussion with the Doctors’ Sub-Panel Co-ordinator, Dr Ronald Hsu.
Each doctor on the Thematic Analysis Panel took an average of 20 hours to analyse 208 cases and another 20 hours to agree the collective analysis and themes.
11Care was categorised into:
“Acute Care” where the intention of care was to improve the patient’s health state“Continuing Care” where the intention of care was to maintain or prevent decline in patient’s health state“Palliative Care” where the intention of care was to reduce the rate of decline in the patient’s health state“End of Life Care” where the intention of care was to support the patient during the declining health state
58
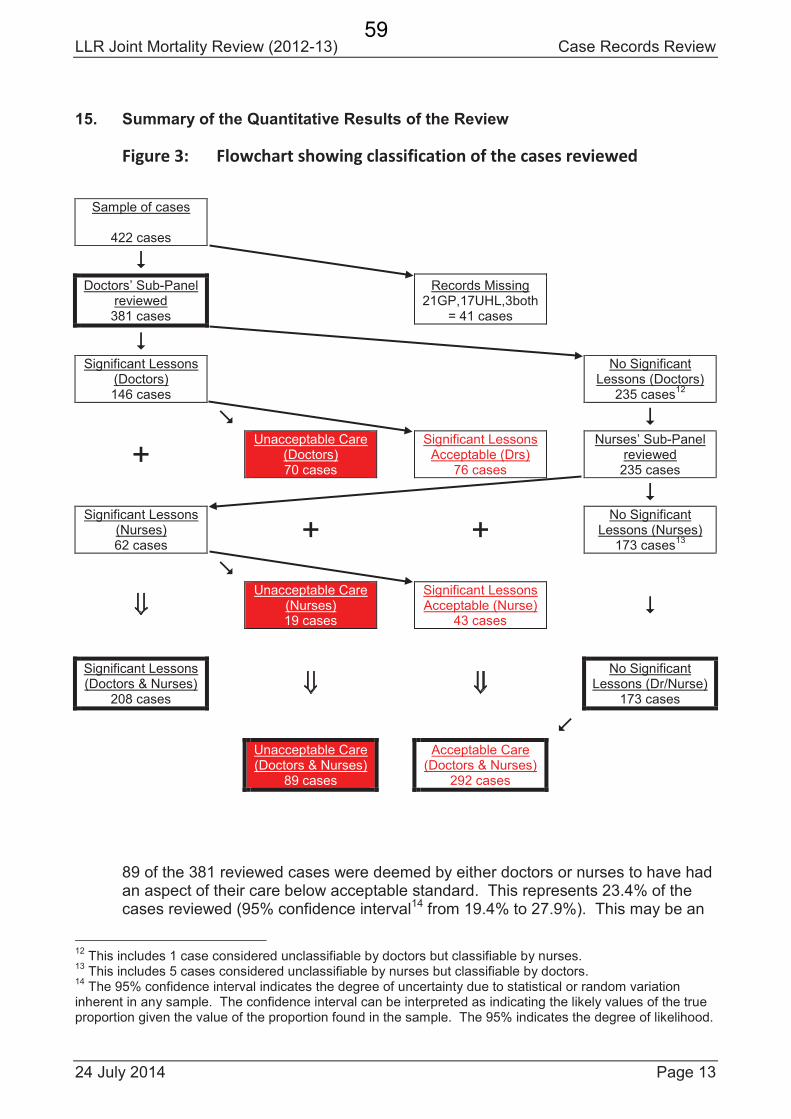
LLR Joint Mortality Review (2012-13) Case Records Review
24 July 2014 Page 13
15. Summary of the Quantitative Results of the Review
Figure 3: Flowchart showing classification of the cases reviewed
Sample of cases
422 cases
Doctors’ Sub-Panel reviewed381 cases
Records Missing21GP,17UHL,3both
= 41 cases
Significant Lessons (Doctors)146 cases
No Significant Lessons (Doctors)
235 cases12
+Unacceptable Care
(Doctors)70 cases
Significant Lessons Acceptable (Drs)
76 cases
Nurses’ Sub-Panel reviewed235 cases
Significant Lessons (Nurses)62 cases
+ +No Significant
Lessons (Nurses)173 cases
13
Unacceptable Care (Nurses)19 cases
Significant Lessons Acceptable (Nurse)
43 cases
Significant Lessons (Doctors & Nurses)
208 cases
No Significant Lessons (Dr/Nurse)
173 cases
Unacceptable Care (Doctors & Nurses)
89 cases
Acceptable Care (Doctors & Nurses)
292 cases
89 of the 381 reviewed cases were deemed by either doctors or nurses to have had an aspect of their care below acceptable standard. This represents 23.4% of the cases reviewed (95% confidence interval14 from 19.4% to 27.9%). This may be an
12This includes 1 case considered unclassifiable by doctors but classifiable by nurses.
13This includes 5 cases considered unclassifiable by nurses but classifiable by doctors.
14The 95% confidence interval indicates the degree of uncertainty due to statistical or random variation
inherent in any sample. The confidence interval can be interpreted as indicating the likely values of the true proportion given the value of the proportion found in the sample. The 95% indicates the degree of likelihood.
59
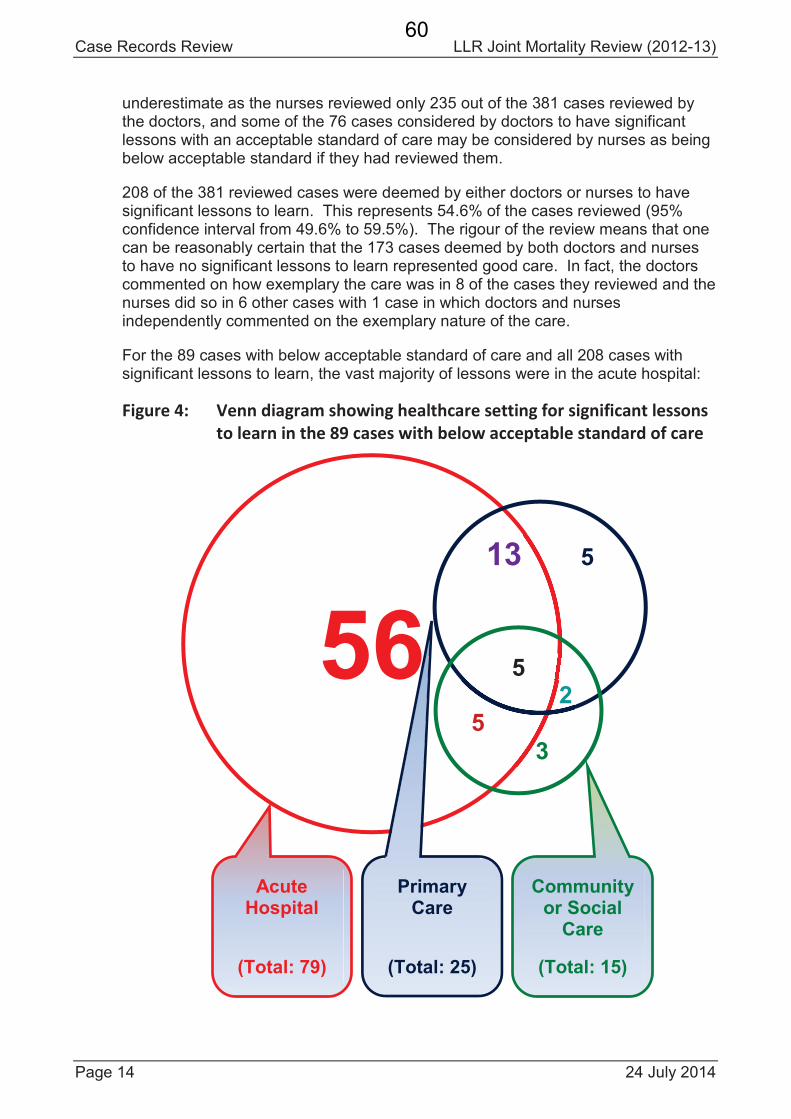
Case Records Review LLR Joint Mortality Review (2012-13)
Page 14 24 July 2014
underestimate as the nurses reviewed only 235 out of the 381 cases reviewed by the doctors, and some of the 76 cases considered by doctors to have significant lessons with an acceptable standard of care may be considered by nurses as being below acceptable standard if they had reviewed them.
208 of the 381 reviewed cases were deemed by either doctors or nurses to have significant lessons to learn. This represents 54.6% of the cases reviewed (95% confidence interval from 49.6% to 59.5%). The rigour of the review means that one can be reasonably certain that the 173 cases deemed by both doctors and nurses to have no significant lessons to learn represented good care. In fact, the doctors commented on how exemplary the care was in 8 of the cases they reviewed and the nurses did so in 6 other cases with 1 case in which doctors and nurses independently commented on the exemplary nature of the care.
For the 89 cases with below acceptable standard of care and all 208 cases with significant lessons to learn, the vast majority of lessons were in the acute hospital:
Figure 4: Venn diagram showing healthcare setting for significant lessons
to learn in the 89 cases with below acceptable standard of care
56
13 5
52
5
3
AcuteHospital
(Total: 79)
PrimaryCare
(Total: 25)
Community or Social
Care
(Total: 15)
60
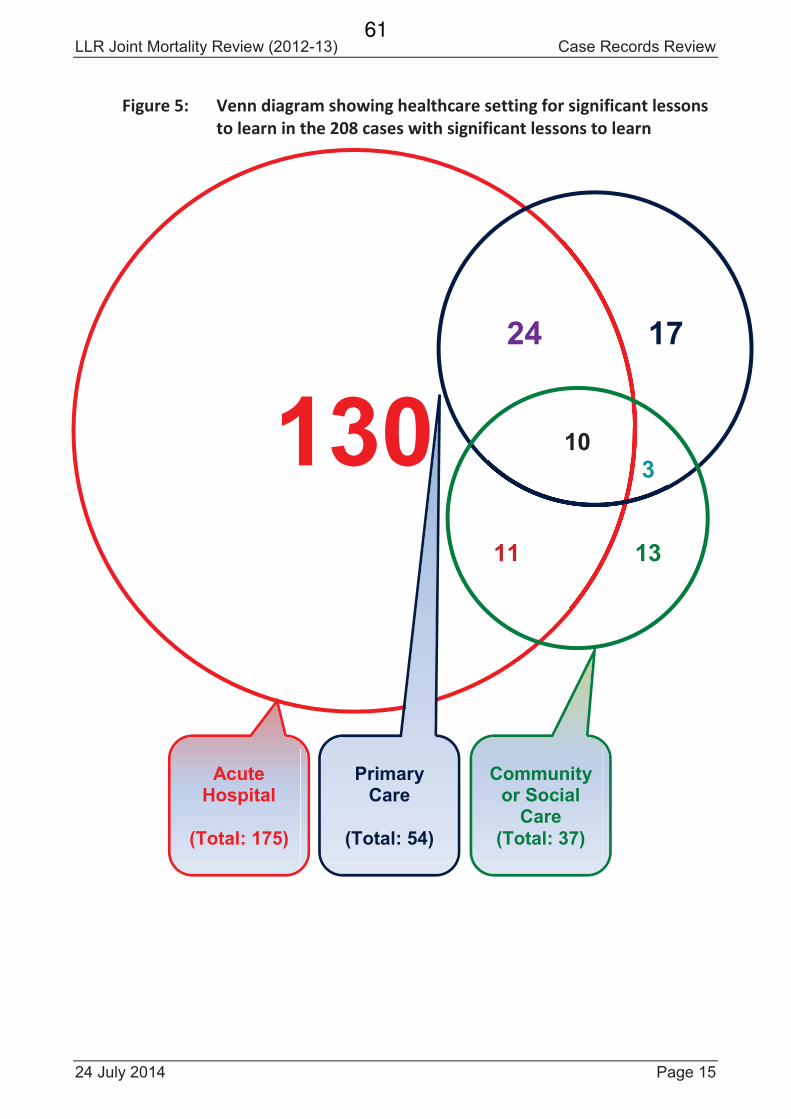
LLR Joint Mortality Review (2012-13) Case Records Review
24 July 2014 Page 15
Figure 5: Venn diagram showing healthcare setting for significant lessons
to learn in the 208 cases with significant lessons to learn
130
24 17
103
11 13
AcuteHospital
(Total: 175)
PrimaryCare
(Total: 54)
Community or Social
Care(Total: 37)
61
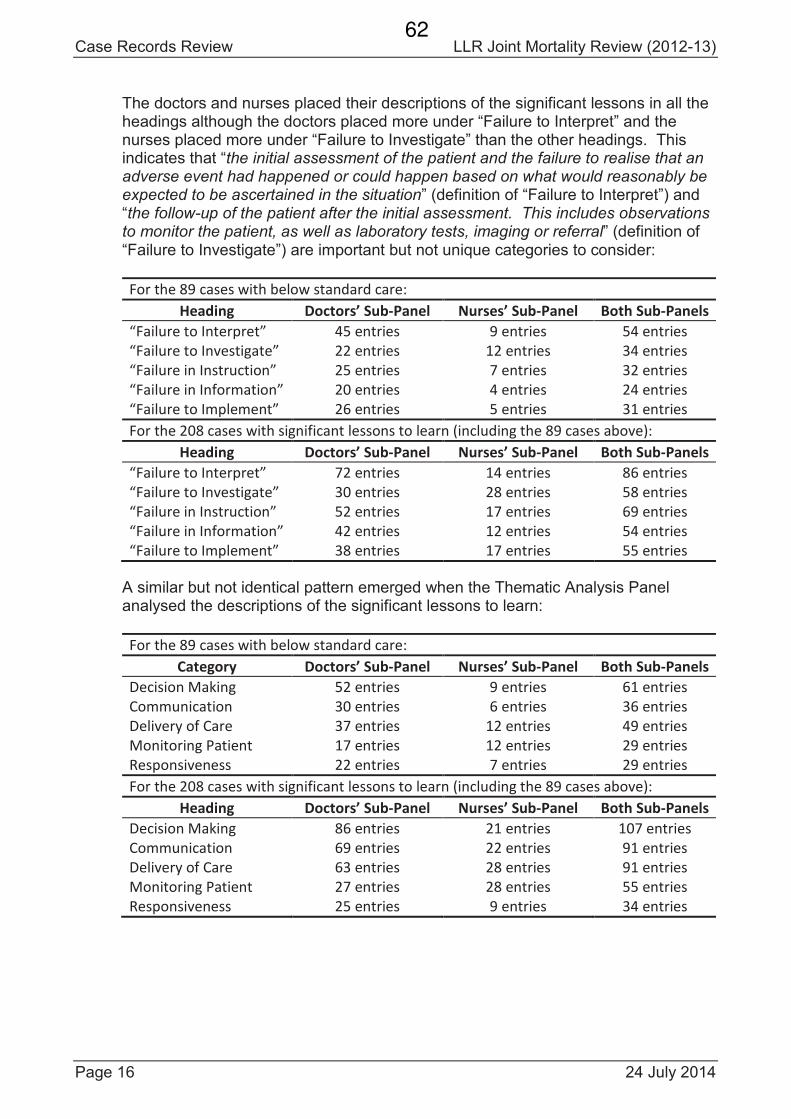
Case Records Review LLR Joint Mortality Review (2012-13)
Page 16 24 July 2014
The doctors and nurses placed their descriptions of the significant lessons in all the headings although the doctors placed more under “Failure to Interpret” and the nurses placed more under “Failure to Investigate” than the other headings. This indicates that “the initial assessment of the patient and the failure to realise that an adverse event had happened or could happen based on what would reasonably be expected to be ascertained in the situation” (definition of “Failure to Interpret”) and “the follow-up of the patient after the initial assessment. This includes observations to monitor the patient, as well as laboratory tests, imaging or referral” (definition of “Failure to Investigate”) are important but not unique categories to consider:
For the 89 cases with below standard care:
Heading Doctors’ Sub-Panel Nurses’ Sub-Panel Both Sub-Panels
“Failure to Interpret” 45 entries 9 entries 54 entries
“Failure to Investigate” 22 entries 12 entries 34 entries
“Failure in Instruction” 25 entries 7 entries 32 entries
“Failure in Information” 20 entries 4 entries 24 entries
“Failure to Implement” 26 entries 5 entries 31 entries
For the 208 cases with significant lessons to learn (including the 89 cases above):
Heading Doctors’ Sub-Panel Nurses’ Sub-Panel Both Sub-Panels
“Failure to Interpret” 72 entries 14 entries 86 entries
“Failure to Investigate” 30 entries 28 entries 58 entries
“Failure in Instruction” 52 entries 17 entries 69 entries
“Failure in Information” 42 entries 12 entries 54 entries
“Failure to Implement” 38 entries 17 entries 55 entries
A similar but not identical pattern emerged when the Thematic Analysis Panel analysed the descriptions of the significant lessons to learn:
For the 89 cases with below standard care:
Category Doctors’ Sub-Panel Nurses’ Sub-Panel Both Sub-Panels
Decision Making 52 entries 9 entries 61 entries
Communication 30 entries 6 entries 36 entries
Delivery of Care 37 entries 12 entries 49 entries
Monitoring Patient 17 entries 12 entries 29 entries
Responsiveness 22 entries 7 entries 29 entries
For the 208 cases with significant lessons to learn (including the 89 cases above):
Heading Doctors’ Sub-Panel Nurses’ Sub-Panel Both Sub-Panels
Decision Making 86 entries 21 entries 107 entries
Communication 69 entries 22 entries 91 entries
Delivery of Care 63 entries 28 entries 91 entries
Monitoring Patient 27 entries 28 entries 55 entries
Responsiveness 25 entries 9 entries 34 entries
62
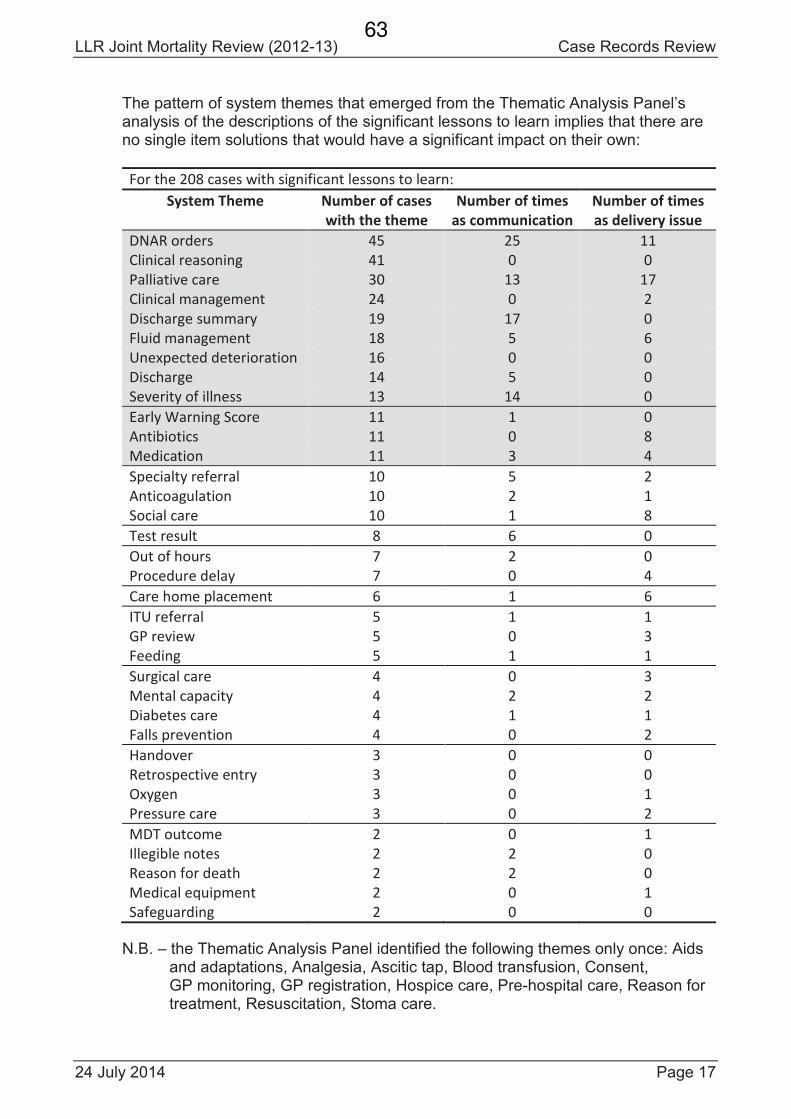
LLR Joint Mortality Review (2012-13) Case Records Review
24 July 2014 Page 17
The pattern of system themes that emerged from the Thematic Analysis Panel’s analysis of the descriptions of the significant lessons to learn implies that there are no single item solutions that would have a significant impact on their own:
For the 208 cases with significant lessons to learn:
System Theme Number of cases
with the theme
Number of times
as communication
Number of times
as delivery issue
DNAR orders 45 25 11
Clinical reasoning 41 0 0
Palliative care 30 13 17
Clinical management 24 0 2
Discharge summary 19 17 0
Fluid management 18 5 6
Unexpected deterioration 16 0 0
Discharge 14 5 0
Severity of illness 13 14 0
Early Warning Score 11 1 0
Antibiotics 11 0 8
Medication 11 3 4
Specialty referral 10 5 2
Anticoagulation 10 2 1
Social care 10 1 8
Test result 8 6 0
Out of hours 7 2 0
Procedure delay 7 0 4
Care home placement 6 1 6
ITU referral 5 1 1
GP review 5 0 3
Feeding 5 1 1
Surgical care 4 0 3
Mental capacity 4 2 2
Diabetes care 4 1 1
Falls prevention 4 0 2
Handover 3 0 0
Retrospective entry 3 0 0
Oxygen 3 0 1
Pressure care 3 0 2
MDT outcome 2 0 1
Illegible notes 2 2 0
Reason for death 2 2 0
Medical equipment 2 0 1
Safeguarding 2 0 0
N.B. – the Thematic Analysis Panel identified the following themes only once: Aids and adaptations, Analgesia, Ascitic tap, Blood transfusion, Consent, GP monitoring, GP registration, Hospice care, Pre-hospital care, Reason for treatment, Resuscitation, Stoma care.
63
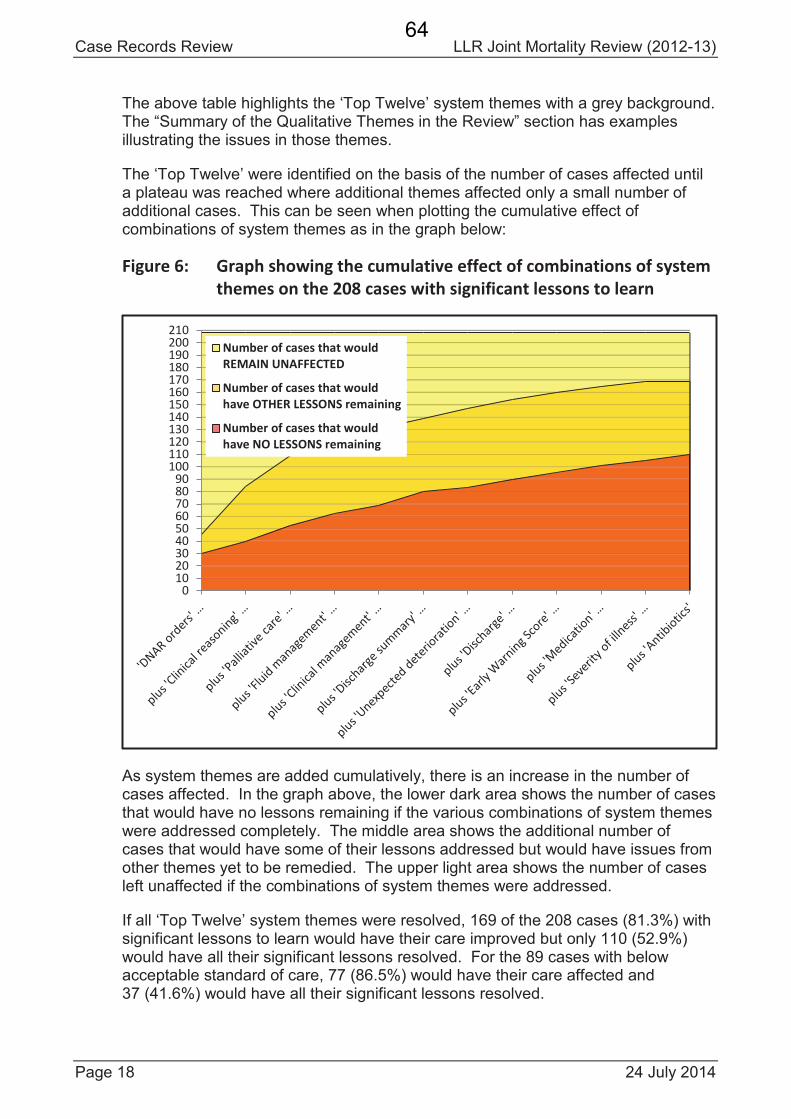
Case Records Review LLR Joint Mortality Review (2012-13)
Page 18 24 July 2014
The above table highlights the ‘Top Twelve’ system themes with a grey background. The “Summary of the Qualitative Themes in the Review” section has examples illustrating the issues in those themes.
The ‘Top Twelve’ were identified on the basis of the number of cases affected until a plateau was reached where additional themes affected only a small number of additional cases. This can be seen when plotting the cumulative effect of combinations of system themes as in the graph below:
Figure 6: Graph showing the cumulative effect of combinations of system
themes on the 208 cases with significant lessons to learn
As system themes are added cumulatively, there is an increase in the number of cases affected. In the graph above, the lower dark area shows the number of cases that would have no lessons remaining if the various combinations of system themes were addressed completely. The middle area shows the additional number of cases that would have some of their lessons addressed but would have issues from other themes yet to be remedied. The upper light area shows the number of cases left unaffected if the combinations of system themes were addressed.
If all ‘Top Twelve’ system themes were resolved, 169 of the 208 cases (81.3%) with significant lessons to learn would have their care improved but only 110 (52.9%) would have all their significant lessons resolved. For the 89 cases with below acceptable standard of care, 77 (86.5%) would have their care affected and 37 (41.6%) would have all their significant lessons resolved.
0102030405060708090
100110120130140150160170180190200210
Number of cases that would
REMAIN UNAFFECTED
Number of cases that would
have OTHER LESSONS remaining
Number of cases that would
have NO LESSONS remaining
64
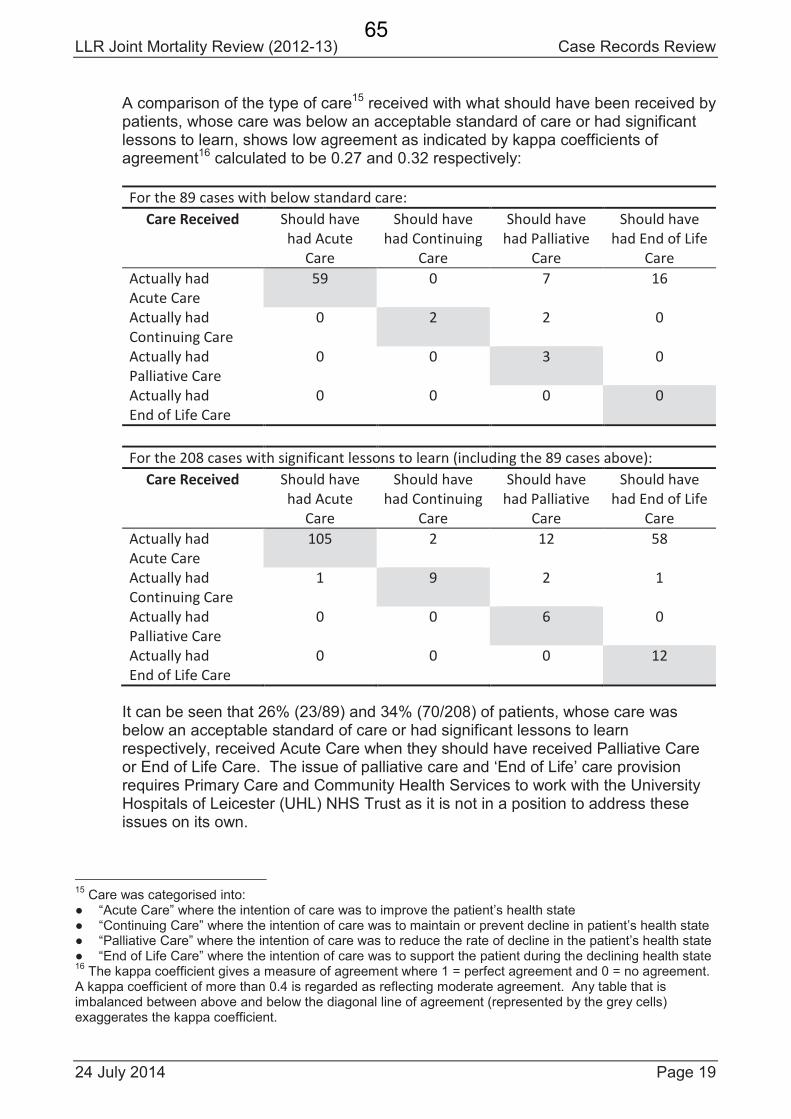
LLR Joint Mortality Review (2012-13) Case Records Review
24 July 2014 Page 19
A comparison of the type of care15 received with what should have been received by patients, whose care was below an acceptable standard of care or had significant lessons to learn, shows low agreement as indicated by kappa coefficients of agreement16 calculated to be 0.27 and 0.32 respectively:
For the 89 cases with below standard care:
Care Received Should have
had Acute
Care
Should have
had Continuing
Care
Should have
had Palliative
Care
Should have
had End of Life
Care
Actually had
Acute Care
59 0 7 16
Actually had
Continuing Care
0 2 2 0
Actually had
Palliative Care
0 0 3 0
Actually had
End of Life Care
0 0 0 0
For the 208 cases with significant lessons to learn (including the 89 cases above):
Care Received Should have
had Acute
Care
Should have
had Continuing
Care
Should have
had Palliative
Care
Should have
had End of Life
Care
Actually had
Acute Care
105 2 12 58
Actually had
Continuing Care
1 9 2 1
Actually had
Palliative Care
0 0 6 0
Actually had
End of Life Care
0 0 0 12
It can be seen that 26% (23/89) and 34% (70/208) of patients, whose care was below an acceptable standard of care or had significant lessons to learn respectively, received Acute Care when they should have received Palliative Care or End of Life Care. The issue of palliative care and ‘End of Life’ care provision requires Primary Care and Community Health Services to work with the University Hospitals of Leicester (UHL) NHS Trust as it is not in a position to address these issues on its own.
15Care was categorised into:
“Acute Care” where the intention of care was to improve the patient’s health state“Continuing Care” where the intention of care was to maintain or prevent decline in patient’s health state“Palliative Care” where the intention of care was to reduce the rate of decline in the patient’s health state“End of Life Care” where the intention of care was to support the patient during the declining health state
16The kappa coefficient gives a measure of agreement where 1 = perfect agreement and 0 = no agreement.
A kappa coefficient of more than 0.4 is regarded as reflecting moderate agreement. Any table that is imbalanced between above and below the diagonal line of agreement (represented by the grey cells) exaggerates the kappa coefficient.
65
Case Records Review LLR Joint Mortality Review (2012-13)
Page 20 24 July 2014
16. Summary of the Qualitative Themes in the Review
Excerpts from the reviewers’ descriptions of 10 cases are used to illustrate the issues raised by the 12 most common themes described by the Case Records Review Panel and identified by the Thematic Analysis Panel.
16.1. Do Not Attempt Resuscitation (DNAR) Orders
45 of the cases were found to have issues relating to Do Not Attempt Resuscitation (DNAR) orders. Frequently there was a lack of recognition for the need to broach the subject of DNAR with the patient and/or their next-of-kin resulting, at times, in inappropriate hospital admissions and treatment.
“No evidence of an 'End of Life' care plan, although the patient obviously fitted the criteria.”
“… the patient would have been better managed with palliative care.”
“… since no DNAR form had been completed, the patient received resuscitation which was unsuccessful.”
There are many reasons why DNAR orders may not be raised at the appropriate time but they need to be overcome to prevent inappropriate responses to clinical deterioration.
“If this was broached by doctors on the ward with the patient and family, it is very likely the patient would have had a hospital DNAR form and a good death.”
The role of Primary Care in initiating discussion of advance care directives, encompassing DNAR orders, needs to be reconsidered if inappropriate admission and treatment in hospital are to be prevented. The responsibility of hospital staff to check whether a community DNAR orders exists, and to carry a patient’s last wishes as set out in the order, needs to be re-emphasised.
A recurring issue identified by the reviewers was the communication of DNAR orders so that they could be acted upon.
“Preceding extensive discussion between GP and family about future care and a community DNAR form was agreed. Nurses and doctors on ward were unaware of this and, when patient had a cardiac arrest, resuscitation was unsuccessfully initiated.”
16.2. Clinical Reasoning
There were 41 cases where the reviewers felt that there were significant lessons to learn from poor clinical reasoning. Certain cases highlighted problems with the clinical assessment of patients by doctors and/or slow recognition of the need for clinical reassessment.
“… the issue of [investigative procedure] dominated discussions betweendoctors rather than the treatment of severe pneumonia in ITU.”
66
LLR Joint Mortality Review (2012-13) Case Records Review
24 July 2014 Page 21
“The patient was known to have metastatic [type of] cancer. The patient was bed bound in own home for [a number of] weeks due to pain. GP assessments did not diagnose pathological fracture neck of femur as the reason for being bed bound and in pain. …”
In some cases the significance of clinical findings were not considered and translated into an appropriate management plan.
“Blood results (sodium 155 mmol/L, potassium 3.3 mmol/L) indicating significant dehydration do not appear to have been acted upon.”
“As the patient was asymptomatic with no evidence that it would become symptomatic, we feel this could have been managed in the community hospital.”
In other cases the validity and timeliness of certain clinical decisions was questionable.
“GP did not arrange appropriately timed INR check after starting [antibiotics] for [condition] (checked 4 days after starting [antibiotics] but then not scheduled for 8 weeks) and patient subsequently admitted with INR > 10 and upper GI bleed.”
Several of the reviewed cases demonstrated a need in the hospital for routine procedures to be carefully monitored and for timely recognition and action when the clinical condition of a patient deviates from the norm or standard care pathway.
16.3. Palliative Care
Palliative care was cited as an issue in 30 reviewed cases. A number of cases alluded to patients being investigated and treated when it was no longer appropriate given the patient’s diagnosis/prognosis.
“… The patient was transferred from LRI to GGH but unfit to have [investigative procedure] and admitted to GGH ITU shortly afterwards. [Investigative procedure] then done, with little benefit to patient.”
Lack of familiarity with the patient in ‘Out of Hours’ care was found to interrupt palliative care plans. Coupled with poor documentation, this resulted in unnecessary hospital admissions.
“We feel that the decision to readmit the patient for the Index Admission may not have been in the patient's best interests. It is possible that this was due to either a failure of the information in the Discharge Summary for the Prior Admission to be conveyed or a failure of the relevance of the information to be recognised when a problem arose regarding the patient's medication. This decision was probably taken by an 'Out of Hours' GP and the hospital notes suggest that admission was advised without a face-to-face assessment.”
“The information from the Prior Admission, which would have informed a decision not to readmit, appears to have not been available to key decision makers.”
67
Case Records Review LLR Joint Mortality Review (2012-13)
Page 22 24 July 2014
“Therefore, an 'Out of Hours' GP was called, who recommended readmission as the Index Admission. This may not have been in the patient's best interests and may have resulted from inadequate information sharing.”
“Failure to implement an 'End of Life' care plan in the community.”
A number of these cases ultimately resulted in death away from the home environment. This could be avoided if palliative care was considered to be an active, rather than a passive, package of care and communicated as such to all involved in a clear and timely manner.
16.4. Clinical Management
There was a lack of clinical oversight in 24 cases which affected the ability to plan and implement appropriate clinical management of patients, especially those with multiple complex diseases. These cases highlighted the necessity of holistic care and the problems caused by managing clinical issues and physiological anomalies in isolation. Some aspects related specifically to a lack of co-ordination within and between specialties.
“Eventual diagnosis unclear but failure of physicians, surgeons and ITU to escalate treatment. We wonder if this was in part due to him having known mental health issues. Patient does not appear to have had a carer with him after his initial assessment.”
“The doctors in GGH concentrated on diagnosing the cause of the asymptomatic [arrhythmia] and ignored the delirium and functional decline of the patient for about 10 days.”
16.5. Discharge Summary
19 of the reviewed cases illustrated how an inadequate, or inadequately communicated, discharge summary contributed to inappropriate decisions by staff.
“The Discharge Summary for the Prior Admission did not fully convey the plan for a non-interventional, palliative approach although strongly implied.”
“The Discharge Summary did not convey the renal failure or the possible transient ischaemic attack (for which aspirin had been started) and stated that the ramipril had been stopped because the patient's blood pressure was controlled, rather than the patient's renal failure.”
Without comprehensive discharge summaries, GPs and other community care services were often having to reassess patients, frequently resulting in errors/omissions and the fragmentation of care; all of which could have been avoided with clear and timely discharge documentation.
This was exacerbated when the patient changed their address and/or GP. The discharge summary would still be sent to the patient’s previous GP as the patient had not registered with a new GP. Thus the information required by the new GP would not be available to them. So discussions and decisions in the hospital regarding circumstances requiring readmission and ‘End of Life’ planning would not be known to the new GP or the community health team, let alone the ‘Out of Hours’ GP service.
68
LLR Joint Mortality Review (2012-13) Case Records Review
24 July 2014 Page 23
16.6. Fluid Management
Fluid management was identified as an issue in 18 cases. Fluids were prescribed in a haphazard manner and records showed an inadequate level of monitoring which resulted in patients becoming dehydrated or overloaded.
“… Intravenous fluids appear to have been inadequately prescribed. There were no recorded instructions to nurses to record fluid balance.”
“After ITU discharge to ward, it seemed as though the patient's renal function was not measured. There were no fluid balance charts in the notes. The patient was readmitted as the Index Admission with a creatinine of 530 umol/L indicating renal failure which was the cause of death.”
The reviewed cases suggested an overall lack of understanding of the importance of fluid management, especially the recording and monitoring of patient fluid intake and output on the ward.
16.7. Unexpected Deterioration
In 16 cases, there was a failure to recognise an unexpected significant deterioration in a patient. At times, this occurred in the presence of a precipitous drop in oxygen saturation or an increased Early Warning Score (EWS). Thus clinicians missed the last window of opportunity to treat a patient proactively.
“Failure to act on ITU plan to immediately inform ITU if patient deteriorates. Patient suddenly had oxygen saturation of 74% on air but ITU was not informed. Patient had a cardiac arrest 2 hours later and died despite resuscitation attempt.”
Poor communication was deemed to be a significant issue in relation to the escalation of patient care when deterioration was identified.
“Observations taken during the 24 hours before death showed hypoxia with oxygen saturation of 80% on 2 separate occasions associated with systolic BP dropping from 130 mmHg to 96 mmHg, and rose only to 90%. No record in hospital notes of doctor being informed for subsequent assessment.”
“High EWS score should have been communicated and acted upon.”
“Nurses' requests for medical advice were not adequately responded to by on-call [specialty] doctors.”
These cases illustrate the importance of having a culture, structure and procedures in place that facilitate recognition and responsiveness to deviations from the norm or standard care pathways.
16.8. Discharge
Reviewers found a lack of clinical overview and co-ordination within the hospital in relation to discharge preparation, and between secondary and primary care post-discharge. Issues such as a lack of information regarding follow up requirements were often compounded by GPs not reviewing
69
Case Records Review LLR Joint Mortality Review (2012-13)
Page 24 24 July 2014
patients post-discharge and/or correctly identifying their post-discharge needs.
“The Discharge Summary included the stopping of [drug] but the information was not highlighted or obvious. There was no request for the GP to monitor renal function after discharge and there was no hospital follow-up plan.”
“This could have been due to either a failure of the information in the Discharge Summary for the Prior Admission to be conveyed or a failure of the relevance of the information to be recognised when a problem arose regarding the patient's medication.”
Discharges were delayed due to a lack of appropriate placements and/or funding.
“Fast Track forms may not have been completed.”
In some cases poor discharge planning and implementation prevented the patient from being discharged to and die in the place of their choice. This was considered to be below an acceptable standard of care by the reviewers.
16.9. Severity of Illness
Reviewers felt that there were 13 cases in which the severity of the patient’s illness was not recognised in a timely manner. By the time referral to an appropriate specialist was made, the delay in transfer of care compounded the situation for the patient.
“Failure to seek further specialist opinion despite multiple clinical signs of seriousness of illness.”
“Failure by both consultant and junior doctors to appreciate the seriousness of illness on several occasions despite multiple clinical signs.”
On some occasions it was found that protocols, pathways and procedures were followed but without assessment of the appropriateness and/or benefit of such for the patient when considering their long term prognosis.
“In the hospital, there was no record of any discussion with patient or family about suitability of operation and risk/benefit of operation given underlying disease [of known metastatic [type of] cancer].”
It was clear to the reviewers that a lack of appreciation of the severity of a patient’s illness often contributed to the delivery of inappropriate or excessive care and/or a missed opportunity to discuss patient’s wishes in relation to their long term treatment or palliative care.
16.10. Early Warning Score (EWS)
11 cases were found to have issues relating to the Early Warning Score (EWS) used to record and score patient observations made in hospitals. Inconsistent use of the EWS tool and errors in the calculation of the scores were noted. A lack of communication of increased scores was also an area of concern for the reviewers.
70
LLR Joint Mortality Review (2012-13) Case Records Review
24 July 2014 Page 25
“Nursing observations prior to actual discharge from ITU showed EWS of 5 (incorrectly calculated as 4). No evidence of communication by nurse to doctors about deterioration.”
Cases were identified where clinicians recorded the EWS but did not fully assess or appropriately respond to the patient’s presenting condition or symptoms. Thus resulting, again, in clinicians missing the last window of opportunity to treat a patient proactively.
“In hospital, a window of opportunity was lost for early identification ofdeterioration prior to death as oxygen saturation dropped to 80% but this does not seem to have been noticed as EWS only scored 1 on the basis of BP.”
There was evidence of nurses responding appropriately to a patient’s condition or Early Warning Score (EWS), but being reassured inappropriately by junior doctors.
“… junior doctor did not act on high post-operative EWS on return from ward. No entries in medical notes until Resuscitation Team called, although EWS entry in nursing notes suggests patient was seen by a junior doctor and no action was deemed necessary a few hours prior to death.”
16.11. Antibiotics
Antibiotics featured in 11 of the cases reviewed. The issues relating to antibiotics included delayed administration and ineffectual prescribing.
“Delay in antibiotic administration of 9 hours despite blood white cell count being 0.3 x 10^9/L.”
“Failure to recognise infection can be from other non-bacterial sources …[and] Microbiologist not involved until Day 5.”
16.12. Medication
Reviewers identified 11 cases in which medication was an area of concern. Although the reviewers appreciated that clinicians can differ in their assessment and treatment of a patient, poor prescribing practice was evident in a number of cases and decisions for changes to medication were often poorly documented.
“Seen by another consultant 3 days later on [date] who stated to restart warfarin. This did not affect the outcome in this patient as he never received the warfarin but odd contradiction in management plan that is not explained. ?plan by previous consultant not noticed.”
The reviewers felt that clear clinical leadership was key to avoiding these issues in the future.
71
Case Records Review LLR Joint Mortality Review (2012-13)
Page 26 24 July 2014
17. Conclusions of the Review
This joint primary and secondary care case records review was undertaken to establish whether there is a significant level or pattern of systematic clinical issues in the care received by patients in Leicester, Leicestershire and Rutland.
In this review, 23.4% of reviewed cases (95% CI: 19.4% to 27.9%) were found to bebelow acceptable standard. These were amongst the 54.6% of reviewed cases(95% CI: 49.6% to 59.5%) identified as having significant lessons to learn.
Although one should be wary of making direct comparisons between reviews with different methodologies and sampling strategies, it is likely that this joint case records review has established that there is a significant level or pattern of systematic clinical issues in the care received by patients in Leicester, Leicestershire and Rutland. In the ‘Critique of the Protocol and Comparison with Published Reviews’ document, the “Summary of Comparing with Comparable Studies” on page 29 is “In summary, the proportion of cases with unsatisfactory care ranged from 3% to 7% in studies of deaths in hospital. A sub-group analysis of the LLR Joint Mortality Review, based on the findings of doctors only and counting only cases with significant lessons for the hospital with/without other services, gave a range from 17% to 19% for ‘below an acceptable standard’ of care.”
Thematic analysis of the reviewers’ descriptions of cases with significant lessons to learn identified 47 system themes. The 12 most common system themes were found in 86.5% of cases with below acceptable standard of care and 81.3% of cases with significant lessons to learn. However, even if all 12 of the most common system themes were resolved, only 41.6% of cases with below acceptable standard of care and 52.9% of cases with significant lessons to learn, would have all their issues resolved. This illustrates why addressing single issues, even when done cumulatively, has limited impact on resolving all the issues for cases with concern.
Reviewing cases can only identify issues and themes. A system-wide approach through co-operation and collaboration is required to identify solutions and make improvements. Solutions need to take into account the intangible and intrinsic aspects of healthcare delivery such as organisational culture. Learning from this review, and any subsequent work, requires partnership with input from a cross-section of clinical and managerial staff and, most importantly, patients.
Dr Ronald HsuSenior Teaching Fellow in Epidemiology and Public HealthDepartment of Medical and Social Care EducationUniversity of Leicester
Mrs Lucy Douglas-PannettSpecialty Registrar in Public Health
72
1
Quality review action plans
Learning from the Leicester,
Leicestershire and Rutland (LLR) quality
review has identified a number of areas
that require improvements.
Page 1 provides numerous examples of
actions we had already started to
implement and some new actions we
have taken as a result of this review.
Should you wish to read the full version
of any of the healthcare organisations
action plans these are available on
request
In addition, we are also working together
across the health community on 5 key
areas of action (see pages 2 & 3)
East Leicestershire and Rutland Clinical Commissioning Group
Leicester City Clinical Commissioning Group
Leicestershire Partnership NHS Trust
NHS England (Leicestershire & Lincolnshire Area)
University Hospitals of Leicester NHS Trust
West Leicestershire Clinical Commissioning Group
LLR
Joint Action Plan
(See page 2)
Leicestershire Partnership NHS Trust Action Plan
We have developed advanced nurse practitioners (nurses who have undergone
further training and expanded their expertise) to lead care management in
community hospitals with support from University Hospitals of Leicester (UHL)
We have trained advance nurse practitioners to complete Do Not Attempt
Resuscitation (DNAR) forms for use across the LLR healthcare system.
We have developed a competency framework for nurses signing Do Not
Attempt Cardiopulmonary Resuscitation (DNA-CPR), which will be implemented
by the end of 2014.
We have created a 7 day face to face service between the hours of 9 to 5
supported by a 24 hour telephone advice service to support patients and family
at the end of life (Action for LOROS & LPT).
We have committed to “Care in the last days of life” and training of 1000 staff
by September 2014.
We have a co-ordinated community health service redesign work programme,
which is ongoing and in collaboration with social care and GP practises.
We have a ‘single point of access’ for scheduled (planned) and unscheduled
(unplanned) care.
University Hospitals of Leicester NHS Trust Action Plan
We have invested to recruit an additional 200 ward based nurses since 2013/14 which will improve
quality outcomes at ward level. The Trust has also committed to implementing ‘Supervisory Status’
of the Ward Sisters for 2 days a week on all wards to ensure quality standards are delivered.
We have standardised the approach to care for patients facing an uncertain recovery and who are at
risk of dying in the next one to two months and invested in staff training to deliver this.
We have implemented an electronic system to improve safety of prescribing, supply and
administration of medicines for inpatients and patients discharged from the medical wards at the
LRI.
We have strengthened our ward communication and staff handover systems to ensure all patients
have care and discharge plans in place, which are regularly reviewed with greater patient
involvement.
To ensure patients at nights, weekends and bank holidays receive continuity of care we have put in
place a multi-disciplinary team to oversee out of hours care.
We have redesigned our cardiac and respiratory care pathways to ensure appropriate patients are
directly admitted to the Cardiac and Respiratory Units at the Glenfield Hospital.
We have established an Older Persons Board which is executively led to ensure the needs of frail and
older patients are consistently met through various work streams and have already achieved the
Quality Mark for ‘Elder-Friendly Wards’ for 7 of our wards.
Our 14/15 Quality Commitment work-streams and quality improvement schemes, agreed with our
commissioners, include earlier recognition and response to the deteriorating patient, better care for
patients with diabetes and reducing medication errors
Clinical Commissioning Groups Action Plan
We have provided training in ‘Gold Standards Framework’ in end of life (EoL)
care for GPs/nurses/care homes.
All CCGs have end of life care schemes with national standards.
Computer templates for advance care planning in place.
All GPs have dementia screening in place through NHS Health Checks system.
We have implemented Advanced Care planning/Emergency Response Service to
enable people to remain at home if appropriate to avoid hospital admission.
We continue to deliver high quality, well-attended ‘Safeguarding’ training and
evaluation at appraisal.
All CCGs have been working alongside NHS England to identify practitioners in
need of development or where concerns relating to practice exist.
We have developed and implemented a GP feedback and reporting concerns
process across LLR to identify and take action on issues related to quality &
safety.
We undertake regular unannounced visits to assess the quality of
commissioned services- such as hospitals, care homes and health units.
We have GPs and nurse specialist measures in place to support EoL care across
all three CCGs areas.
Contact details
· East Leicestershire and Rutland CCG
www.eastleicestershireandrutlandccg.nhs.uk
· Leicester City CCG
www.leicestercityccg.nhs.uk
· Leicestershire Partnership NHS Trust www.leicspart.nhs.uk
· University Hospitals of Leicester NHS Trust www.leicestershospitals.nhs.uk
· West Leicestershire CCG
www.westleicestershireccg.nhs.uk
· NHS England
www.england.nhs.uk/mids-east
73
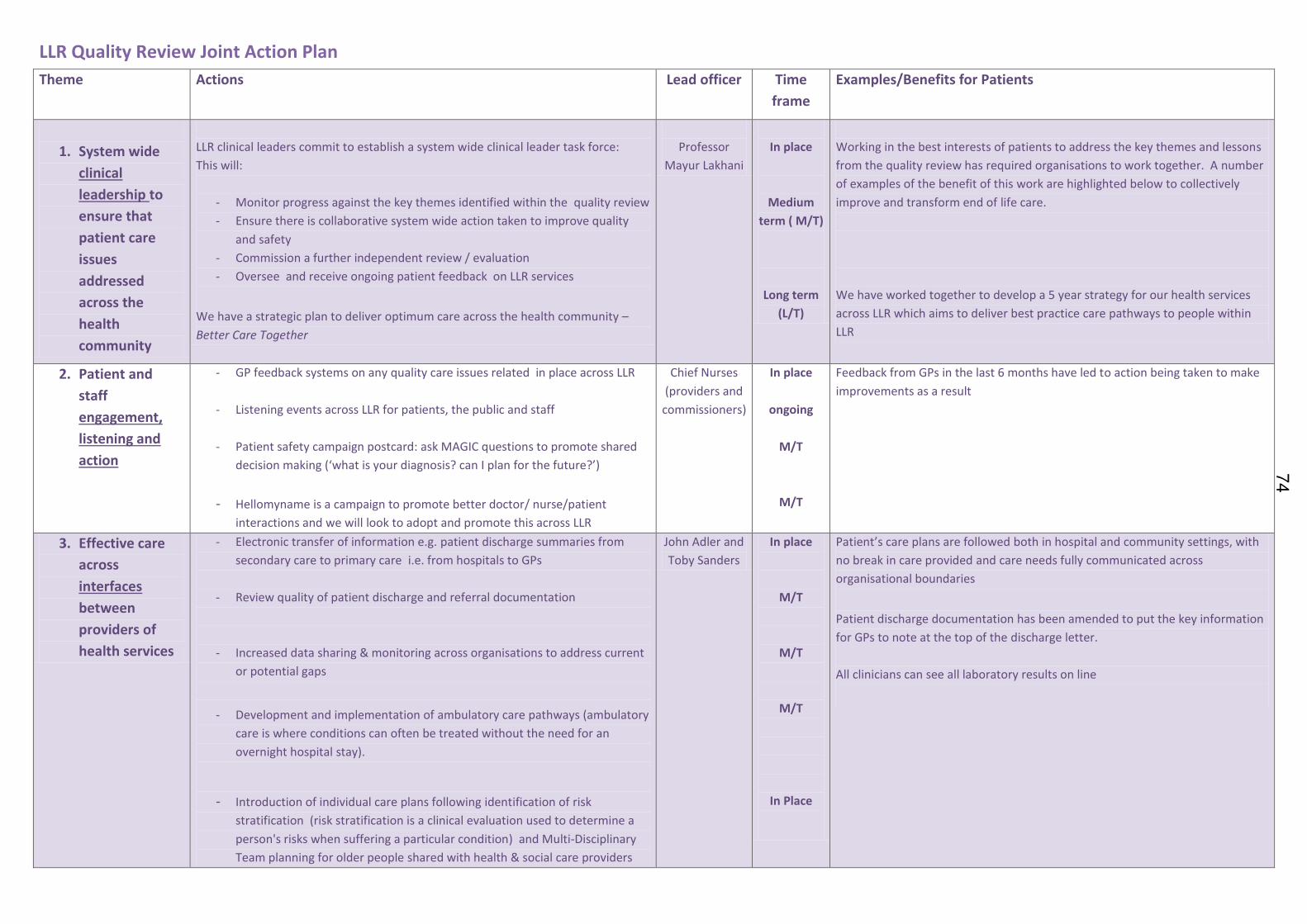
LLR Quality Review Joint Action Plan
Theme Actions Lead officer Time
frame
Examples/Benefits for Patients
1. System wide
clinical
leadership to
ensure that
patient care
issues
addressed
across the
health
community
LLR clinical leaders commit to establish a system wide clinical leader task force:
This will:
- Monitor progress against the key themes identified within the quality review
- Ensure there is collaborative system wide action taken to improve quality
and safety
- Commission a further independent review / evaluation
- Oversee and receive ongoing patient feedback on LLR services
We have a strategic plan to deliver optimum care across the health community –
Better Care Together
Professor
Mayur Lakhani
In place
Medium
term ( M/T)
Long term
(L/T)
Working in the best interests of patients to address the key themes and lessons
from the quality review has required organisations to work together. A number
of examples of the benefit of this work are highlighted below to collectively
improve and transform end of life care.
We have worked together to develop a 5 year strategy for our health services
across LLR which aims to deliver best practice care pathways to people within
LLR
2. Patient and
staff
engagement,
listening and
action
- GP feedback systems on any quality care issues related in place across LLR
- Listening events across LLR for patients, the public and staff
- Patient safety campaign postcard: ask MAGIC questions to promote shared
decision making (‘what is your diagnosis? can I plan for the future?’)
- Hellomyname is a campaign to promote better doctor/ nurse/patient
interactions and we will look to adopt and promote this across LLR
Chief Nurses
(providers and
commissioners)
In place
ongoing
M/T
M/T
Feedback from GPs in the last 6 months have led to action being taken to make
improvements as a result
3. Effective care
across
interfaces
between
providers of
health services
- Electronic transfer of information e.g. patient discharge summaries from
secondary care to primary care i.e. from hospitals to GPs
- Review quality of patient discharge and referral documentation
- Increased data sharing & monitoring across organisations to address current
or potential gaps
- Development and implementation of ambulatory care pathways (ambulatory
care is where conditions can often be treated without the need for an
overnight hospital stay).
- Introduction of individual care plans following identification of risk
stratification (risk stratification is a clinical evaluation used to determine a
person's risks when suffering a particular condition) and Multi-Disciplinary
Team planning for older people shared with health & social care providers
John Adler and
Toby Sanders
In place
M/T
M/T
M/T
In Place
Patient’s care plans are followed both in hospital and community settings, with
no break in care provided and care needs fully communicated across
organisational boundaries
Patient discharge documentation has been amended to put the key information
for GPs to note at the top of the discharge letter.
All clinicians can see all laboratory results on line
74
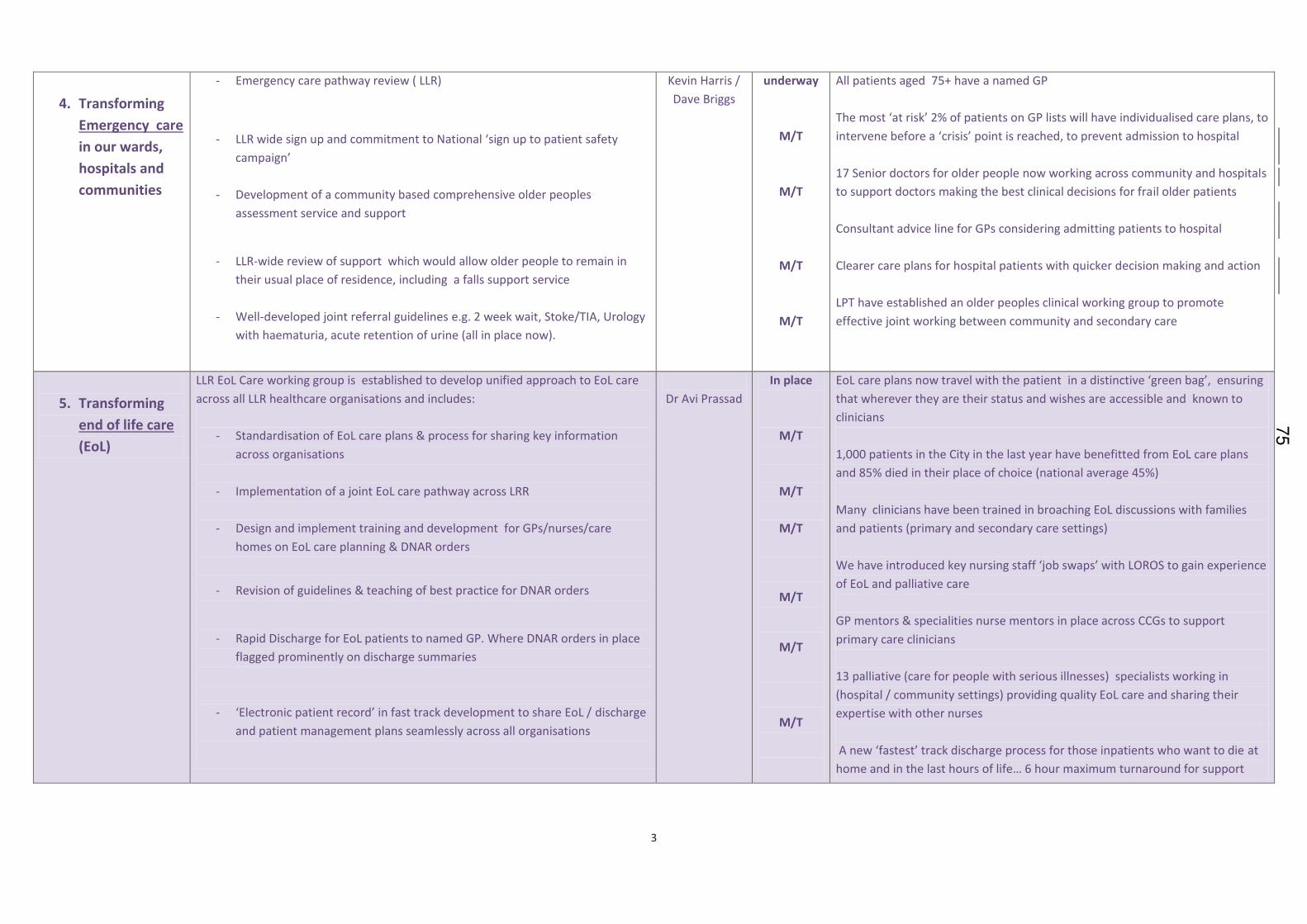
3
4. Transforming
Emergency care
in our wards,
hospitals and
communities
- Emergency care pathway review ( LLR)
- LLR wide sign up and commitment to National ‘sign up to patient safety
campaign’
- Development of a community based comprehensive older peoples
assessment service and support
- LLR-wide review of support which would allow older people to remain in
their usual place of residence, including a falls support service
- Well-developed joint referral guidelines e.g. 2 week wait, Stoke/TIA, Urology
with haematuria, acute retention of urine (all in place now).
Kevin Harris /
Dave Briggs
underway
M/T
M/T
M/T
M/T
All patients aged 75+ have a named GP
The most ‘at risk’ 2% of patients on GP lists will have individualised care plans, to
intervene before a ‘crisis’ point is reached, to prevent admission to hospital
17 Senior doctors for older people now working across community and hospitals
to support doctors making the best clinical decisions for frail older patients
Consultant advice line for GPs considering admitting patients to hospital
Clearer care plans for hospital patients with quicker decision making and action
LPT have established an older peoples clinical working group to promote
effective joint working between community and secondary care
5. Transforming
end of life care
(EoL)
LLR EoL Care working group is established to develop unified approach to EoL care
across all LLR healthcare organisations and includes:
- Standardisation of EoL care plans & process for sharing key information
across organisations
- Implementation of a joint EoL care pathway across LRR
- Design and implement training and development for GPs/nurses/care
homes on EoL care planning & DNAR orders
- Revision of guidelines & teaching of best practice for DNAR orders
- Rapid Discharge for EoL patients to named GP. Where DNAR orders in place
flagged prominently on discharge summaries
- ‘Electronic patient record’ in fast track development to share EoL / discharge
and patient management plans seamlessly across all organisations
Dr Avi Prassad
In place
M/T
M/T
M/T
M/T
M/T
M/T
EoL care plans now travel with the patient in a distinctive ‘green bag’, ensuring
that wherever they are their status and wishes are accessible and known to
clinicians
1,000 patients in the City in the last year have benefitted from EoL care plans
and 85% died in their place of choice (national average 45%)
Many clinicians have been trained in broaching EoL discussions with families
and patients (primary and secondary care settings)
We have introduced key nursing staff ‘job swaps’ with LOROS to gain experience
of EoL and palliative care
GP mentors & specialities nurse mentors in place across CCGs to support
primary care clinicians
13 palliative (care for people with serious illnesses) specialists working in
(hospital / community settings) providing quality EoL care and sharing their
expertise with other nurses
A new ‘fastest’ track discharge process for those inpatients who want to die at
home and in the last hours of life… 6 hour maximum turnaround for support
75

76
Th
is p
ag
e is
inte
ntio
nally
left b
lank
HEALTH OVERVIEW AND SCRUTINY COMMITTEE:
10 SEPTEMBER 2014
REPORT OF THE DIRECTOR OF HEALTH AND CARE INTEGRATION
BETTER CARE FUND UPDATE Purpose of report
1. The purpose of this report is to provide an update on the requirements for all Health and Wellbeing Boards to resubmit their Better Care Fund (BCF) plans by 19th September, in line with new policy and guidance issued nationally on 25th July
Policy Framework and Previous Decisions
2. Leicestershire’s Health and Wellbeing Board submitted a Better Care Fund Plan
in April 2014, in line with the previous national policy and guidance.
3. The operational development and delivery of the Better Care Fund plan is undertaken by the Integration Executive on a day to day basis, reporting to the Health and Wellbeing Board which has delegated responsibility to agree the Better Care Fund and plans arising from its use.
4. The Integration Executive oversees four areas of work prioritised through the
BCF plan plus four other ‘business as usual’ integration priorities between NHS partners and local government (including improvements to continuing health care services).
5. At a previous meeting of the Health Overview and Scrutiny Committee a request
was made for further information on the improvements being made to continuing health care arrangements locally, and the Housing Offer to Health.
Overview of National Developments during July and August 2014
6. The amount, type and depth of analysis needed for each BCF resubmission has changed substantially due to the new guidance, promoted by the need for more rigour in BCF plans nationally, in particular with reference to NHS acute sector impact. Specific changes include:-
• a new pay for performance scheme linked to a revised BCF metric which equates to a reduction of 3.5% in total emergency admissions in 2015/16.
Agenda Item 1077
• Changes to the baselines for all the metrics in the BCF guidance; these are all now calculated from within 2013/14. This means all the metrics and trajectories in each BCF plan have to be recalculated / revalidated.
7. BCF plans must also demonstrate assurance regarding:
• Protecting adult social care services;
• How the NHS number will be adopted;
• The arrangements for accountable leads professionals for care planning;
• How care act requirements have been met (with reference to the total allocation by Local Authority);
• How information governance has been addressed for records sharing;
• How a proportion of the funds will be commissioned from NHS providers outside of hospital;
• Alignment to local primary care strategies including co-commissioning plans with NHS England.
8. The publication of the new guidance raised a large number of questions and requests for clarification across the country. These have been handled through a number of routes, including national webinars, the development of an FAQs section of the website, a regular ebulletin and the issue of further guidance on a number of issues, including the 3.5% reduction in hospital admissions metric.
9. There has also been a requirement for templates to be submitted nationally
which test the readiness for resubmission at three specific dates between 25th July and 19th September.
10. In recognition of the more onerous and complex process for BCF resubmissions,
some additional (nationally procured) support was made available from 26th August in each region. This includes regional workshops, and additional “hands on” support to individual areas. In Leicestershire, this support will entail two days of consultancy time to provide an external review of the submission against the assurance process and external validation of the outcome of the review.
11. While the additional support is welcomed, feedback has been given that this
comes at a very late stage in the process raising some practical / logistical difficulties for local areas to make best use of this in sufficient time for the resubmission.
Update on BCF Assurance Process
12. The assurance process is an intensive process involving a technical desk top
review, triangulation of other evidence about the wider context of the financial and delivery challenges facing local health and care economies and a telephone interview with representatives from each BCF plan/Health and Wellbeing Board area.
13. The outcome of the review will be that all BCF plans fall into one of four
categories below, which have specific definitions:
78
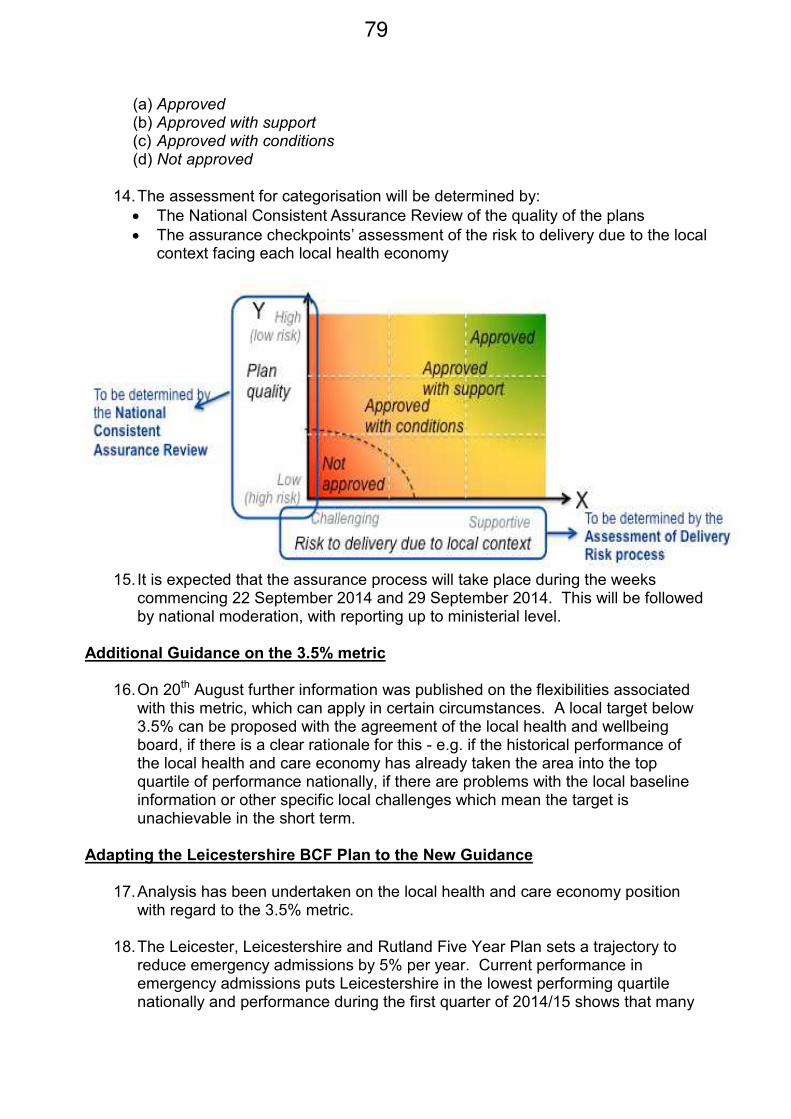
(a) Approved (b) Approved with support (c) Approved with conditions (d) Not approved
14. The assessment for categorisation will be determined by:
• The National Consistent Assurance Review of the quality of the plans
• The assurance checkpoints’ assessment of the risk to delivery due to the local context facing each local health economy
15. It is expected that the assurance process will take place during the weeks
commencing 22 September 2014 and 29 September 2014. This will be followed by national moderation, with reporting up to ministerial level.
Additional Guidance on the 3.5% metric
16. On 20th August further information was published on the flexibilities associated with this metric, which can apply in certain circumstances. A local target below 3.5% can be proposed with the agreement of the local health and wellbeing board, if there is a clear rationale for this - e.g. if the historical performance of the local health and care economy has already taken the area into the top quartile of performance nationally, if there are problems with the local baseline information or other specific local challenges which mean the target is unachievable in the short term.
Adapting the Leicestershire BCF Plan to the New Guidance
17. Analysis has been undertaken on the local health and care economy position with regard to the 3.5% metric.
18. The Leicester, Leicestershire and Rutland Five Year Plan sets a trajectory to
reduce emergency admissions by 5% per year. Current performance in emergency admissions puts Leicestershire in the lowest performing quartile nationally and performance during the first quarter of 2014/15 shows that many
79
more people are being admitted to hospital than NHS commissioning plans have accounted for this year. Some of this activity is the subject of contract queries between the local CCGs and UHL.
19. The baseline for the target was set at the end of the 2013/14 financial year. In
order to achieve a 3.5% reduction of the baseline, a real terms reduction of up to 8% during 2015/16 will need to be made. The financial risk associated with this metric is £2.84m for Leicestershire’s BCF plan. Local flexibility around the delivery of this metric is being sought.
20. The following actions have been taken to review the Leicestershire BCF plan in
the context of the new guidance:-
• Further impact assessment work has taken place on the BCF interventions that will contribute to the emergency admissions metric within the Leicestershire BCF plan;
• The proportion which the four main schemes contributing to this metric are estimated to contribute to a reduction in hospital admissions has been assessed, with individual trajectories developed based on the phasing and impact of these developments;
• All other BCF schemes and their contribution to metrics within the BCF plan have been reviewed, particularly to test the assumptions about scale of delivery and phasing of the impact.
• The impact analysis is being supported by a review of the evidence base for the interventions in the BCF plan, which is being undertaken by Public Health;
• The data quality and data capture for all BCF schemes has been assessed and recommendations have been made from this to show where the data that is being relied upon for achieving the metrics can be strengthened
• The BCF financial plan is being re-profiled to accommodate the contingency needed for the 3.5% target, additional Care Act requirements, and the re-phasing of BCF schemes per the impact assessment.
Conclusion
21. The following conclusions can be drawn:-
• The requirements for BCF resubmissions are substantial and the timescales are problematic.
• There has been a significant amount of new information to assimilate between July 25th and August 22nd during peak holiday season.
• The assurance process indicates that BCF plans in challenged health and care economies are likely to receive low ratings (e.g. approved with conditions).
80
• The 3.5% metric presents a specific challenge to the Leicestershire plan however 4 schemes have been identified that could contribute to achieving this metric.
• A timeline for the remaining four weeks has been prepared, including the governance steps needed ahead of the resubmission
Resource Implications
22. The Better Care Fund Plan is to be delivered via a pooled budget which will comprise £38m in 2015/16.
Timetable for Decisions
23. Appendix 1 of the paper outlines the governance milestones for the resubmission leading up to the 19th September.
24. Appendices 2 and 3 provide further information about the timescales affecting
improvements to the continuing care service and the integrated housing offer. Officer to Contact Cheryl Davenport Director of Health and Care Integration Tel: 0116 305 4212 Email: [email protected] Equalities and Human Rights Impact Assessment Implications
25. The BCF aims to improve outcomes and wellbeing for the people of Leicestershire, with effective protection of social care and integrated activity to reduce emergency and urgent health demand. As part of the implementation of the Plan, an Equalities and Human Rights Impact Assessment and other relevant impact assessments will be undertaken to ensure that there is a clear understanding of how various groups are affected.
81
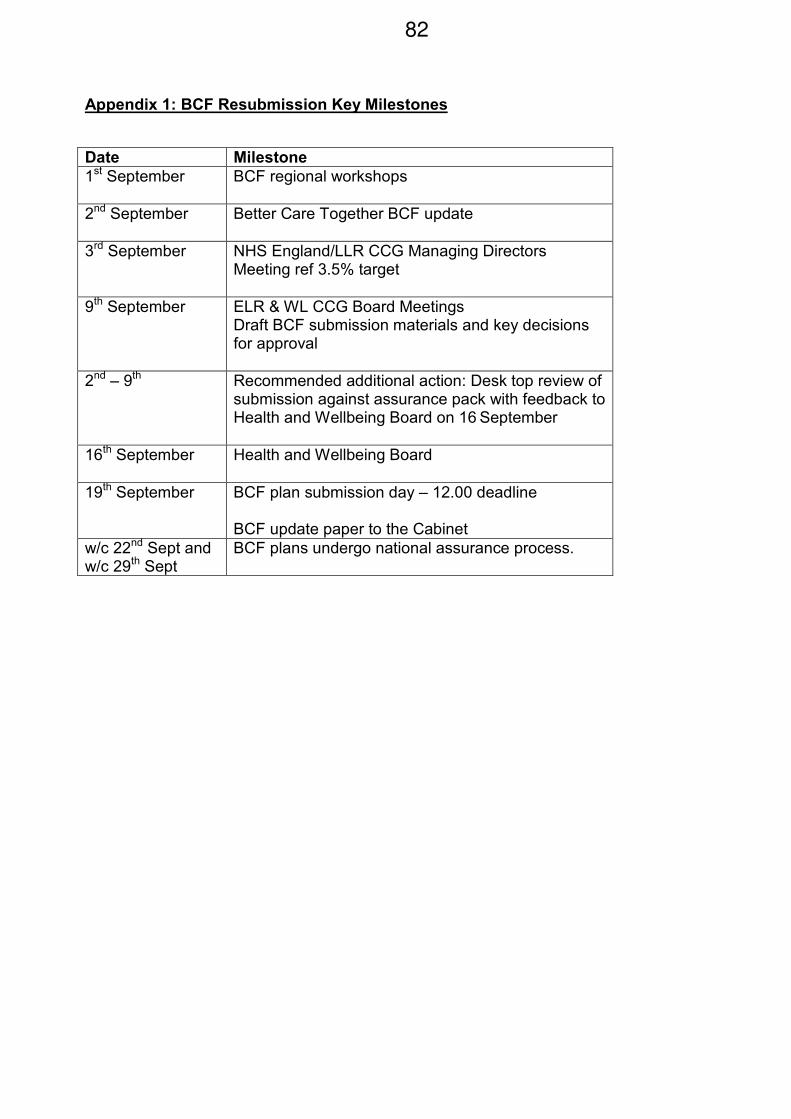
Appendix 1: BCF Resubmission Key Milestones
Date Milestone
1st September
BCF regional workshops
2nd September
Better Care Together BCF update
3rd September
NHS England/LLR CCG Managing Directors Meeting ref 3.5% target
9th September
ELR & WL CCG Board Meetings Draft BCF submission materials and key decisions for approval
2nd – 9th Recommended additional action: Desk top review of submission against assurance pack with feedback to Health and Wellbeing Board on 16 September
16th September
Health and Wellbeing Board
19th September
BCF plan submission day – 12.00 deadline BCF update paper to the Cabinet
w/c 22nd Sept and w/c 29th Sept
BCF plans undergo national assurance process.
82
Appendix 2 - Continuing Healthcare (CHC) Update
Background
1. ‘NHS continuing healthcare’ (CHC) means a package of ongoing care that is arranged and funded solely by the NHS where the individual has been found to have a ‘primary health need’ as set out in the National Framework for NHS Continuing Healthcare and NHS-funded Nursing Care guidance. Such care is provided to an individual aged 18 or over, to meet needs that have arisen as a result of disability, accident or illness. The actual services provided as part of the package should be seen in the wider context of best practice and service development for each client group. Eligibility for NHS CHC places no limits on the setting in which the package of support can be offered or on the type of service delivery.
2. ‘NHS-funded nursing care’ is the funding provided by the NHS to homes
providing nursing to support the provision of nursing care by a registered nurse. Since 2007 NHS-funded nursing care has been based on a single band rate. In all cases individuals should be considered for eligibility for NHS CHC before a decision is reached about the need for NHS-funded nursing care.
3. Individuals who need ongoing care / support may require services arranged by
CCGs and / or LAs. CCGs and LAs therefore have a responsibility to ensure that the assessment of eligibility for care / support and its provision take place in a timely and consistent manner. If a person does not qualify for NHS CHC, the NHS may still have a responsibility to contribute to that person’s health needs – either by directly commissioning services or by part-funding the package of support. Where a package of support is commissioned or funded by both an LA and a CCG, this is known as a ‘joint package’ of care. A joint package of care could include NHS-funded nursing care and other NHS services that are beyond the powers of a LA to meet. The joint package could also involve the CCG and the LA both contributing to the cost of the care package, or the CCG commissioning part of the package. Joint packages of care may be provided in a nursing or residential care home, or in a person’s own home.
4. In July 2013 a review of the current CHC process was carried out to examine
organisational responsibilities and barriers to a more streamlined process which has a high patient and carer satisfaction.
5. The review was undertaken involving key stakeholders and Healthwatch
Leicestershire, who undertook a call for evidence from the voluntary and community sector on patient experience of the NHS CHC process, completed in January 2014.
6. The review identified a number of key areas of improvement for consideration:
• Clarity of organisational responsibilities, transfer of information, and accountability.
• Pressure for early discharge from the acute sector and demands of ‘fast track referrals’.
83
• Patient satisfaction, lack of good co-ordination and communication about key stages of the process, and patient participation in the decision-making process.
• Timescales for assessment, support and funding agreements.
• Improved multi-disciplinary approach.
• Reduction of cost pressures and effective use of resources.
7. The review conclusion recommended an integrated approach that would seek to elevate a number of inefficiencies highlighted as a result of the review and to put the patient into the centre of the process.
Progress to date
8. Leicestershire County Council and East Leicestershire and Rutland CCG have had initial discussions to identify resources to enhance the current CHC team (hosted by Greater East Midlands Commissioning Support Unit), by providing dedicated social care workers to be part of the current clinical multi-disciplinary team (MDT) and to pilot an integrated pathway for CHC assessment.
9. The team will receive referrals and allocate a named CHC co-ordinator who will
be responsible for collating the specialist assessments needed to populate the CHC assessment for consideration by the multi-agency CHC Panel.
10. The co-ordinator will also be responsible for the engagement and involvement of
the patient and carers providing a person centred approach to the process.
11. Fast track referrals will not be the responsibility of this team, but ongoing review and case management post-fast track could be incorporated potentially.
12. Joint commissioning of support services would seem to be the best way forward
in securing good quality, cost effective service provision and initial discussions have been instigated to take forward this proposal.
13. Personal Health Budgets will also need to be available to CHC eligible patients
from October 2014. Personal budgets for social care support are already well established and an integrated approach for joint funded patients would ensure consistency in support provision with contracted and non-contracted providers and reduce hand offs when packages are reviewed and funding arrangements changed as a result.
Timescales for implementation September 2014 - December 2014 Planning and joint pathway agreements. December 2014 – March 2015 Pilot testing of integrated approach. March 2015 – March 2018 Implementation and evaluation of process, benefits and further development opportunities.
84
Appendix 3: Integrated Housing Offer Update: Light Bulb Project Background / Update
1. On 5 December 2013, the Health and Wellbeing Board (HWB) considered the
findings of the Housing Services Partnership’s (HSP) “Housing offer to Health” (HOTH) which had been developed in conjunction with the Chartered Institute for Housing.
2. The HWB agreed to support the delivery of the 5 initial key project areas as set
out below:
• Hospital housing action team - Involvement in the current work at UHL to understand delayed discharge issues and work with LPT around the Bradgate Unit discharge issues.
• Handy person support services – Link into the “Help to Live at Home” project which has housing services involved in the project.
• First Contact scheme in Primary Care – Discussions with CCGs and information from First Contact pilot GP practices to sell the idea to other practices.
• Keeping warm and well at home – Link into the “Help to Live at Home” project
• Older persons holistic support – Link into the “Help to Live at Home” project. The Light Bulb Project (Lead: Danny Myers, [email protected])
3. The HOTH has developed since the HWB’s initial consideration in December 2013. The biggest change has been the development of the Light Bulb Project which in effect absorbs and expands upon the “Keeping Warm and Well at Home” and “Handy Person Support Services” elements of the HOTH.
4. The Light Bulb Project is part of the Better Care Together approach to reduce
delayed transfers of care and reduce demand on expensive care settings for frail older people by integrating currently fragmented housing support services and developing a new integrated, easier to access and income generating housing support prevention offer.
5. The Project aims to enable and empower people, especially older people, to
remain independent at home for longer. The current housing support offer is too
complex - funded by two tiers of local authorities and delivered by a multitude of
public, private and landlord based providers. The project seeks to provide a
single point of access for Leicestershire residents to housing advice and support
and assessment services which can support residents through securing a wide
range of support which could include handyperson services, cost effective
recycled furniture, affordable warmth advice and practical support, and minor
and major adaptations (including DFGs).
6. The ambition is to improve access, broaden the advice and assessment process
and ensure that there are no hand offs between organizations. Light Bulb has
85
the potential to make all housing support services easier to access and more
efficient, which would be worth pursuing independently of the potential benefit
that this improved offer could have on the wider health and social care economy.
7. Hospital admissions for over 75s and residential placements cost Leicestershire’s
health and social care budgets approximately £93m in 2013-14. If a third of
hospital admissions were avoided, there is a potential saving of approaching
£17m which Light Bulb, as part of the wider Better Care Together approach, will
help generate.
8. The cost of Leicestershire’s funded social care placements is £48m and
assuming an annual cost of between £25,000 and £36,000 per annum per
resident, every care placement avoided or delayed represents a significant
opportunity for saving.
9. Partners in Leicestershire will be making this case in a final bid to be submitted to
the DCLG’s Transformation Challenge Award (TCA) on October 1st. The TCA has made available £105 million of grant funding in 2015 to 2016 to support local authorities re-engineer their business practices and redesign service delivery.
10. On June 24th the Integration Executive of the HWB agreed to support the
submission of an initial Expression of Interest to the DCLG. Consequently, the DCLG invited the county’s 8 local authorities to submit a final business case, which is currently in development.
86
HEALTH OVERVIEW AND SCRUTINY COMMITTEE - 10TH SEPTEMBER
2014
REPORT OF UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST
UPDATE ON CURRENT ISSUES
PURPOSE OF REPORT 1. The purpose of this report is to update the Health Overview and Scrutiny Committee on the following issues:-
(a) meeting the new cardiac review standards : paediatric congenital cardiac surgery;
(b) the proposed move of inpatient vascular services from the
Leicester Royal Infirmary to the Glenfield Hospital site; (c) emergency care; (d) nursing workforce; (e) Care Quality Commission inspection: action plan update; (f) financial position 2014/15.
2. The following officer will be in attendance at the Committee meeting to
present this report:-
• Ms. K. Shields, Director of Strategy. MEETING THE NEW CARDIAC REVIEW STANDARDS: PAEDIATRIC CONGENITAL CARDIAC SURGERY 3. The national review being carried out by NHS England has produced
draft standards highlighting key requirements expected of Specialist Surgical Centres within the Congenital Heart Network. The Trust and other stakeholders expect to hear soon what the final requirements will be for public consultation.
4. The latest iteration has highlighted two key points that impact on the services which the Trust provides:-
• surgical teams require a minimum of four surgeons each delivering a minimum of 125 cases and a total of 500 cases per annum. This is based on clinical evidence that indicates such activity provides the
Agenda Item 1187
necessary level of clinical quality needed to provide the service. It is clear that there will be some flexibility in the timescales allowed to meet these numbers, with an initial milestone at 375 cases, probably within three years; and
• all paediatric services need to be co-located on one site and not as previously indicated within 30 minutes contact time.
5. The Trust remains committed to the retention of paediatric congenital
cardiac surgery at the University Hospitals of Leicester NHS Trust (UHL).
6. Accordingly, the Trust Board has agreed to commission an urgent assessment of the potential to alter the Trust’s current reconfiguration plan to achieve co-location (i.e. moving children’s heart surgery from Glenfield Hospital to the Leicester Royal Infirmary); to pursuing the existing dialogue with Birmingham Children’s Hospital with a view to agreeing a network approach as soon as possible; with a business case to retain children’s heart surgery at UHL to be developed and presented to the Trust Board. 7. A further update on the direction of travel is to be presented to the public Trust Board at its next meeting on 25th September 2014. THE PROPOSED MOVE OF INPATIENT VASCULAR SERVICES FROM THE LEICESTER ROYAL INFIRMARY TO THE GLENFIELD HOSPITAL SITE Purpose 8. The purpose of this section is to advise the Committee on the proposed
move of inpatient vascular services from the Leicester Royal Infirmary (LRI) to the Glenfield Hospital (GH) site.
9. Specifically, the paper outlines: a. priorities for vascular services future delivery; b. alignment to the blueprint for Health and Social Care in Leicester,
Leicestershire and Rutland (LLR) 2014 – 2019; c. the priority for the service within the Trust’s Five Year Integrated
Business Plan (IBP); d. the impact on overall patient service delivery specific to vascular
services; e. engagement and consultation as part of developing the future
Business Case.
Service Planning Strategic Context
10. The Trust’s 2014 Clinical Strategy identifies that:
‘more specialised planned care specialities will be provided on the Glenfield site. Our tertiary cardiology services will expand to include complex aortic and mitral valve work. We will move our vascular
88
services to the Glenfield Hospital in order to optimise clinical interdependencies with cardiology and interventional radiology through the development of a hybrid theatre.’
11. Developing a comprehensive programme to clinically manage and surgically treat patients with aortic pathology is one of the major aims of the cardiac, thoracic and vascular surgeons.
12. Cardio-vascular disease affects 50% of the ‘older’ population and has a significant effect on quality of life and longevity. Addressing the main factors contributing to mortality including cardio-vascular disease is key to the blueprint for Health and Social Care in LLR 2014 – 2019. 13. For UHL, any future plans for service improvement and reconfiguration
must respond to the identified challenges in health need across LLR and make a significant contribution towards better outcomes. The co-location of cardio-vascular services on the GH site will provide the appropriate environment to drive up clinical and patient reported outcomes.
14. The relocation of vascular services has been identified as a priority for delivery within the next two years Trust Operational Plan and is integral to delivery of the Trust’s Clinical Strategy and Five Year Integrated Business Plan (IBP) as an enabler for the release of space on the LRI site.
15. The transfer of vascular services from the LRI to GH is fully aligned with
the corporate objectives and strategic principles of the Trust. The co-location with other specialised services at the GH will ensure that safe, high quality patient-centred healthcare is delivered to the population of LLR.
16. Nationally, the provision of vascular surgery now comes within the remit of specialised commissioning groups and there is a move towards locating tertiary (specialist) services into fewer larger units (Level One Regional Centres). Future Vascular Priorities for Delivery 17. The proposed move of vascular services to the GH site is in support of
realising the service ambition to become a Level One Regional Centre for complex endovascular services. The move will incorporate the transfer of vascular and supporting services from the LRI to the GH site, including:
i. an inpatient ward ii. surgical admissions area iii. vascular studies unit iv. angiography v. and the provision of a new hybrid theatre.
18. In the short term vascular outpatients will be retained on the LRI site pending a longer term approach to the provision of a dedicated Outpatient/Daycase (OP/DC) hub which will incorporate these services. This will be subject to public consultation as part of the future
89
configuration of services with the development of the proposed OP/DC hub at GH. 19. The move of vascular services supports the re-designation of UHL as a lead, level one centre and thereby ensures the long term sustainability of vascular, cardiac and cardiology services. The move is supported by both vascular and cardiology clinical teams. The co-location of vascular services with cardiology/cardiothoracic surgery at GH is a key foundation in the re-designation process for vascular services; and likewise any future designation as a thoracic aortic disease centre. 20. Loss of designation would not only incur a loss of income but more importantly impact on the availability of specialist vascular services to our local as well as regional population across the East Midlands. 21. Re-designation not only secures service sustainability but offers patients a high quality streamlined service supported by 21st century imaging solutions. Proposal 22. It is proposed to develop a Full Business Case (FBC) by March 2015 in support of the move. An Outline Business Case (OBC) proposal has been developed in support of the move and is under consideration by the National Trust Development Agency (NTDA).
23 The future delivery structure is currently under review and as part of this engagement and consultation is an integral part.
24. In respect of patient impact, based on 2013/14 activity, the proposed move will:
• Transfer 745 elective and 867 emergency inpatients from the LRI to GH per annum, plus 114 vascular day cases (this excludes radiology patients);
• Maintain 8,797 outpatients (this excludes non face to face contacts of 76 patients) on the LRI site as currently provided, pending the future consultation in respect of the proposed provision of an OP/DC hub on the GH site.
Timescales for Delivery
25. The high level milestones for delivery of the proposed move are outlined below:
Milestone Date
Detailed Design & Full Business Case (FBC) Development
August 2014 – January 2015
Capital Planning & Investment Committee February/March 2015
90
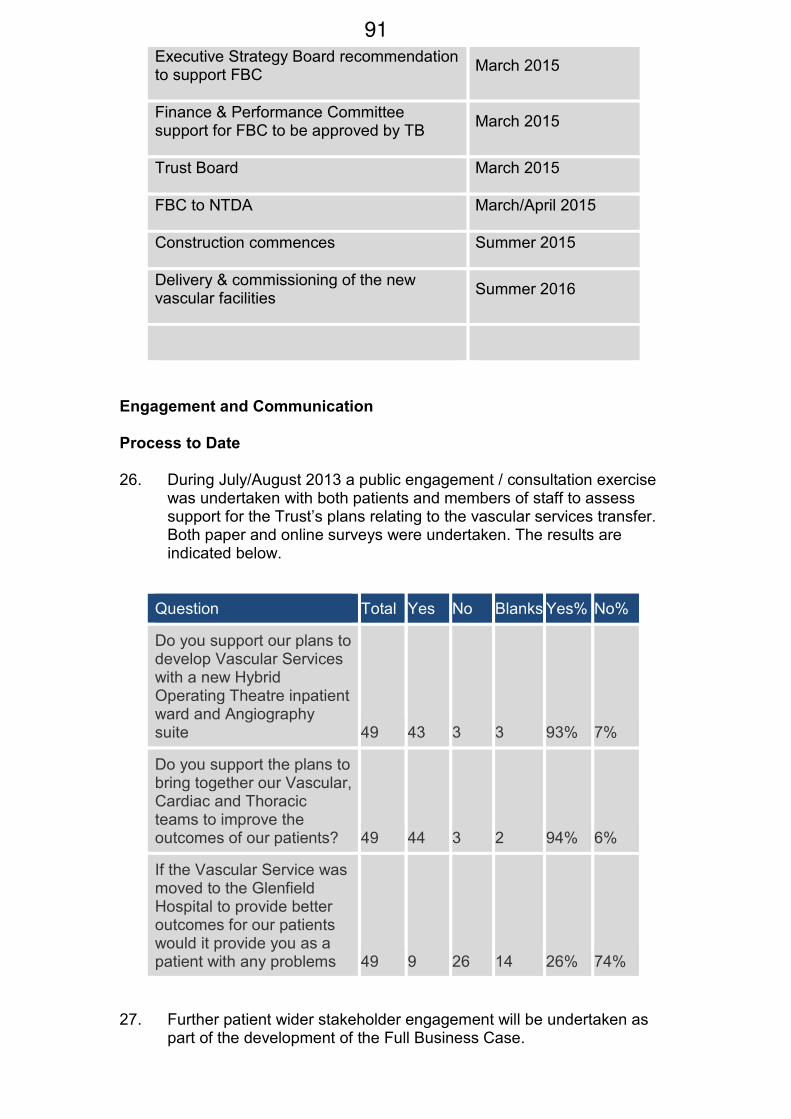
Executive Strategy Board recommendation to support FBC
March 2015
Finance & Performance Committee support for FBC to be approved by TB
March 2015
Trust Board March 2015
FBC to NTDA March/April 2015
Construction commences Summer 2015
Delivery & commissioning of the new vascular facilities
Summer 2016
Engagement and Communication
Process to Date
26. During July/August 2013 a public engagement / consultation exercise was undertaken with both patients and members of staff to assess support for the Trust’s plans relating to the vascular services transfer. Both paper and online surveys were undertaken. The results are indicated below.
Question Total Yes No Blanks Yes% No%
Do you support our plans to develop Vascular Services with a new Hybrid Operating Theatre inpatient ward and Angiography suite 49 43 3 3 93% 7%
Do you support the plans to bring together our Vascular, Cardiac and Thoracic teams to improve the outcomes of our patients? 49 44 3 2 94% 6%
If the Vascular Service was moved to the Glenfield Hospital to provide better outcomes for our patients would it provide you as a patient with any problems 49 9 26 14 26% 74%
27. Further patient wider stakeholder engagement will be undertaken as part of the development of the Full Business Case.
91
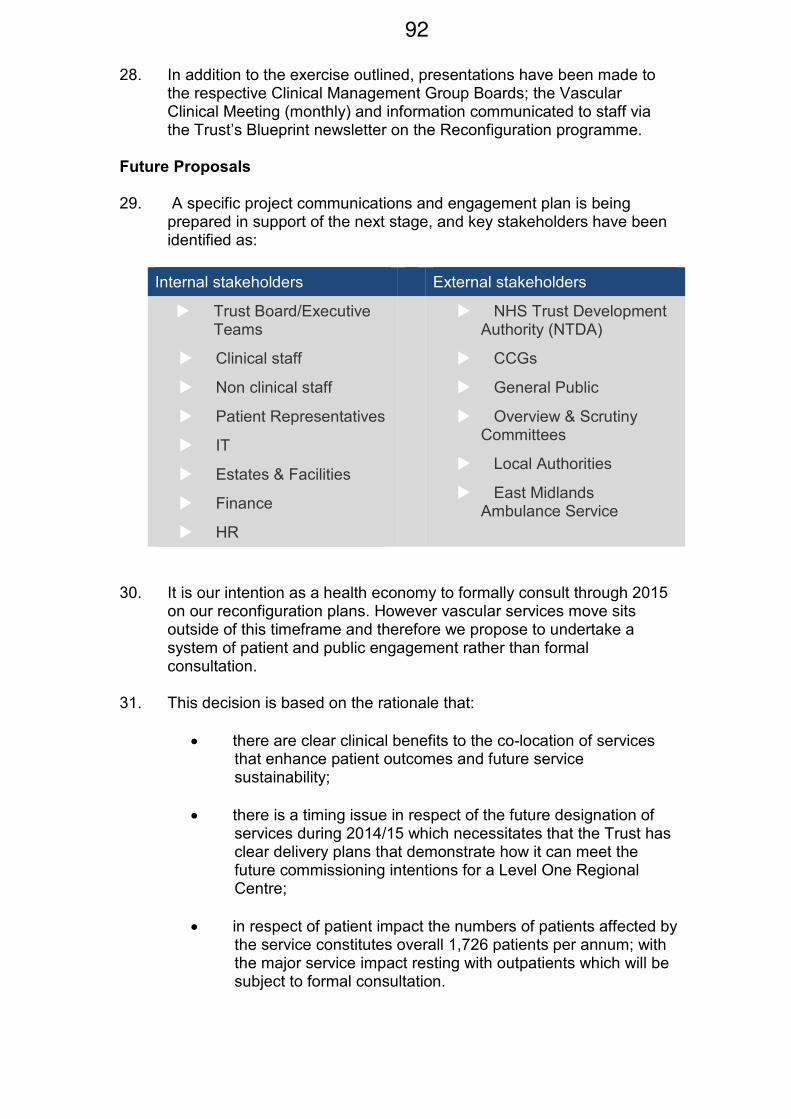
28. In addition to the exercise outlined, presentations have been made to the respective Clinical Management Group Boards; the Vascular Clinical Meeting (monthly) and information communicated to staff via the Trust’s Blueprint newsletter on the Reconfiguration programme. Future Proposals
29. A specific project communications and engagement plan is being prepared in support of the next stage, and key stakeholders have been identified as:
Internal stakeholders External stakeholders
� Trust Board/Executive Teams
� Clinical staff
� Non clinical staff
� Patient Representatives
� IT
� Estates & Facilities
� Finance
� HR
� NHS Trust Development Authority (NTDA)
� CCGs
� General Public
� Overview & Scrutiny Committees
� Local Authorities
� East Midlands Ambulance Service
30. It is our intention as a health economy to formally consult through 2015 on our reconfiguration plans. However vascular services move sits outside of this timeframe and therefore we propose to undertake a system of patient and public engagement rather than formal consultation.
31. This decision is based on the rationale that:
• there are clear clinical benefits to the co-location of services that enhance patient outcomes and future service sustainability;
• there is a timing issue in respect of the future designation of services during 2014/15 which necessitates that the Trust has clear delivery plans that demonstrate how it can meet the future commissioning intentions for a Level One Regional Centre;
• in respect of patient impact the numbers of patients affected by the service constitutes overall 1,726 patients per annum; with the major service impact resting with outpatients which will be subject to formal consultation.
92
Recommendations: 32. The Committee is asked to:
(a) note the future service priorities for vascular services as aligned to the blueprint for Health and Social Care in LLR 2014 – 2019;
(b) support the proposed location of services in accordance with
UHL’s Clinical Strategy 2014 and Five Year IBP; and (c) support the proposed approach to patient and public
engagement outlined in paragraphs 26-30 above.
EMERGENCY CARE 33. The key facts relating to UHL’s recent emergency care performance are summarised below:-
• performance against the 95% 4 hour target was 91.2% in June 2014; 92.52% in July 2014; and 91.26% in August 2014.
• emergency admissions are much higher than in the comparative period during 2013 (e.g. 9% increase for July 2014 compared to July 2013).
• delayed transfers of care remain continually above the agreed performance level (3.5%) at 4.7%; 27% of delays are attributable to UHL internal reasons; 49% are attributable to external matters; and 24% are attributable to nursing homes.
34. It is disappointing that the improvement in performance seen in
June and July was not sustained in August 2014. Waiting to be seen times and decision to treat/admit/discharge times in the Emergency Department remain high, especially out of hours. A series of further actions have therefore been agreed to improve performance, primarily through improving the level of specialty ‘in-reach’ into the Emergency Department between 5pm and midnight : two ‘super weeks’ of performance are to be trialled weeks commencing 15th September and 29th September, respectively.
35. Success is the sum of small efforts, repeated day in and day out. At present, UHL is failing in its aim to deliver high quality emergency care for all, day in, day out. Over the last couple of years, UHL has worked with the Emergency Care Improvement Support Team, the NHS Trust Development Authority (TDA), two management consultancies and now Dr Ian Sturgess, a national lead in emergency care to deliver improvement. The Trust has developed many improvement plans, some with partners in Leicester, Leicestershire and Rutland and have refined the actions when new challenges have presented themselves. Many improvements have been delivered and the provision of emergency care in UHL has significantly improved over the last 12 months, but the Trust is still not consistently delivering high quality care. The
93
Trust remains committed to working hard to resolve this deep- rooted problem. 36. In parallel, enabling works commenced at Leicester Royal Infirmary in May 2014 to pave the way for the eventual construction of the new Emergency Department. The Trust continues to discuss the Outline Business Case with the TDA and, at its meeting held on 28th August 2014, the Trust Board approved an updated Outline Business Case which will now be the subject of further review with the TDA. NURSING WORKFORCE 37. The headline nurse staffing figures for July 2014 are set out below:-
• the sum of budgeted whole time equivalent (WTE) posts for July 2014: 5,106
• the sum of nurses in post for July 2014: 4,565 WTE
• the sum of nurses waiting to start in July 2014: 320 WTE
• the sum of nurses waiting to leave in July 2014: 120 WTE
• the sum of total reported vacancies for July 2014: 341 WTE
International Recruitment 38. To date, 161 international nurses have joined the Trust and they have undertaken a very detailed and comprehensive induction programme. Further recruitment is planned with an additional 50 international recruits planned to join the Trust on 11th September 2014. Current plans are for a further 50 international nurses to join the Trust in November 2014. The plan for 2015 is for 5 cohorts of up to 30 international nurses to be recruited. Local Recruitment 39. Local recruitment activity continues, with monthly advertisements for Registered Nurses and bi-monthly advertisements for Healthcare Assistants. The Trust also proactively attends all Royal College of Nursing recruitment fairs across the country. The Trust continuously recruits from its local university (De Montfort University) twice a year and from this source has recruited 82 newly qualified Adult nurses, 25 Children’s nurses and 25 Midwives to join the Trust in November 2014. 40. Since 1st April 2013 the Trust has recruited 161 international nurses;
405 ‘clearing house’ nurses and local Registered Nurses; and 375 nursing assistants; giving a total of 941 Registered Nurses and Healthcare Assistants recruited since April 2013.
94
CARE QUALITY COMMISSION INSPECTION: ACTION PLAN UPDATE 41. The Trust has developed an action plan to respond to the findings of the Care Quality Commission following the Commission’s inspection in January 2014. 42. The action plan is reviewed monthly at the Trust’s Quality Assurance Committee, reporting to the Trust Board. 43. The latest version of the action plan, reviewed by the Quality Assurance Committee on 27th August 2014, is attached for information. 44. The final date for completion of all actions is March 2015 (assuming no slippage). FINANCIAL POSITION 2014/15 45. The Trust incurred a deficit of approximately £40m in 2013/14 and is forecasting a similar figure for 2014/15. This is one of the largest deficits in the country and is obviously a very serious situation. In the past, the Trust had appeared to be stronger financially but the underlying position was being masked by additional year-end funding from commissioners which is no longer available. 46. At month 4 2014/15, the Trust is approximately £1m adverse to plan but actions have been taken to ensure that the Trust does not exceed its planned deficit. 47. The Trust’s Cost Improvement Programme is performing strongly, with forecast savings of £48m in 2014/15, against a target of £45m. 48. The Trust’s Long Term Financial Model does not anticipate break even until the start of year 6 (i.e. 2019/20). 49. It is of note that recent research conducted by the Health Service Journal identified that nearly half of the hospital Trust sector is currently planning or forecasting a deficit for 2014/15. The gross deficit projected by those organisations is £940m. In contrast, the gross surplus projected by the 68 Trusts planning to finish the year in the black was £167m. CONCLUSION 50. The Committee is invited to receive and comment upon this report. A representative of the Trust will be in attendance at the Committee meeting (as identified in paragraph 2 above) to respond to the comments and questions of Members. OFFICER TO CONTACT Stephen Ward, Director of Corporate and Legal Affairs, UHL.
95
96
This page is intentionally left blank
CQC Action Plan
April 2014
Approved Quality Assurance Committee and Trust
Board April 2014
Appendix A
97
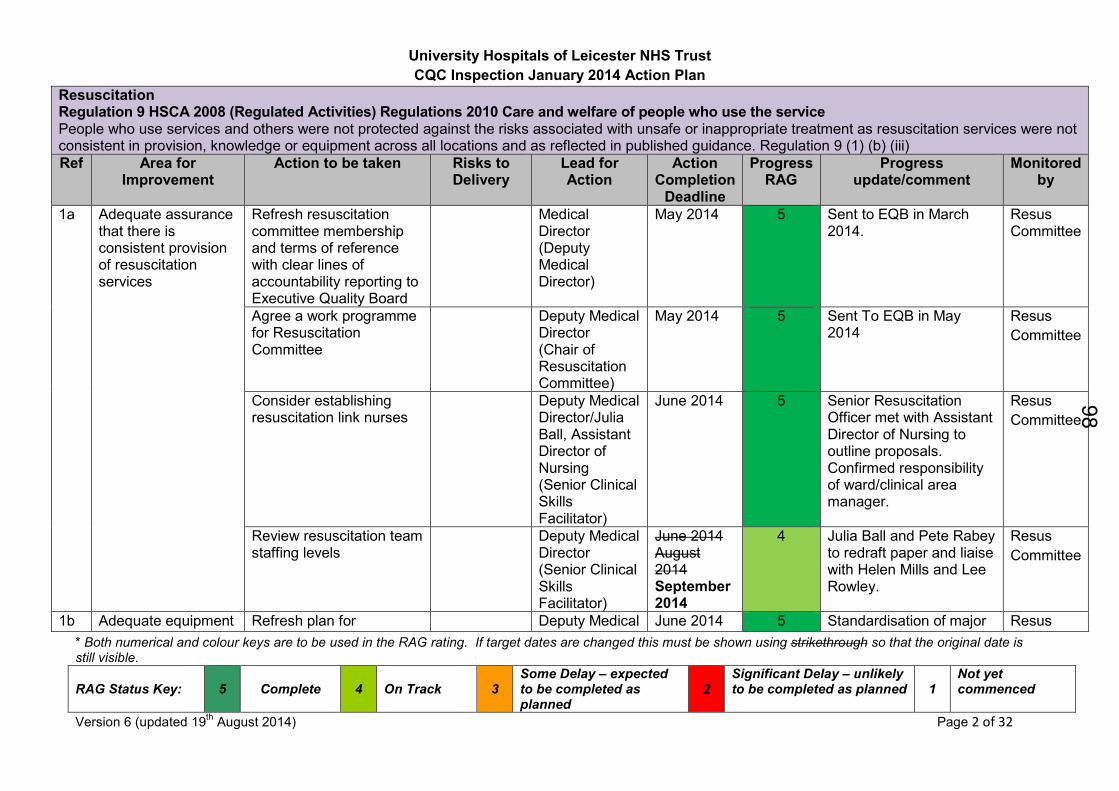
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 2 of 32
Resuscitation Regulation 9 HSCA 2008 (Regulated Activities) Regulations 2010 Care and welfare of people who use the service People who use services and others were not protected against the risks associated with unsafe or inappropriate treatment as resuscitation services were not consistent in provision, knowledge or equipment across all locations and as reflected in published guidance. Regulation 9 (1) (b) (iii)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
1a Adequate assurance that there is consistent provision of resuscitation services
Refresh resuscitation committee membership and terms of reference with clear lines of accountability reporting to Executive Quality Board
Medical Director (Deputy Medical Director)
May 2014 5 Sent to EQB in March 2014.
Resus Committee
Agree a work programme for Resuscitation Committee
Deputy Medical Director (Chair of Resuscitation Committee)
May 2014 5 Sent To EQB in May 2014
Resus
Committee
Consider establishing resuscitation link nurses
Deputy Medical Director/Julia Ball, Assistant Director of Nursing (Senior Clinical Skills Facilitator)
June 2014 5 Senior Resuscitation Officer met with Assistant Director of Nursing to outline proposals. Confirmed responsibility of ward/clinical area manager.
Resus
Committee
Review resuscitation team staffing levels
Deputy Medical Director (Senior Clinical Skills Facilitator)
June 2014 August 2014 September 2014
4 Julia Ball and Pete Rabey to redraft paper and liaise with Helen Mills and Lee Rowley.
Resus
Committee
1b Adequate equipment Refresh plan for Deputy Medical June 2014 5 Standardisation of major Resus
98
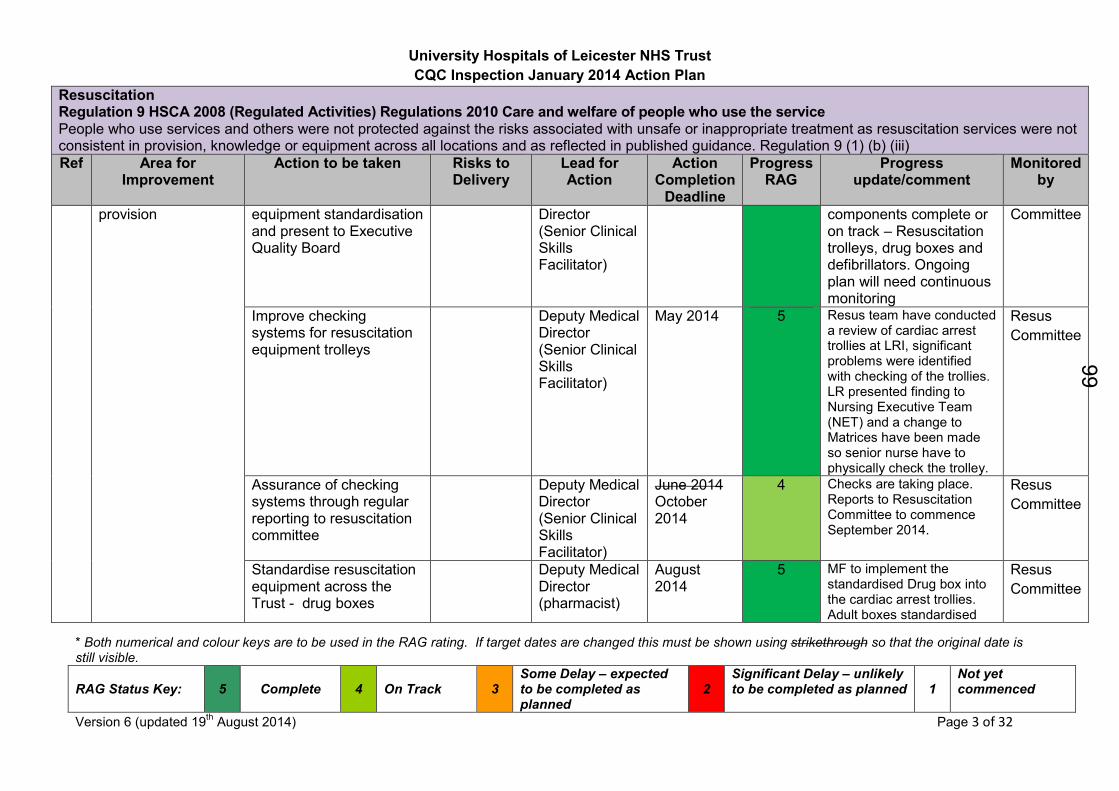
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 3 of 32
Resuscitation Regulation 9 HSCA 2008 (Regulated Activities) Regulations 2010 Care and welfare of people who use the service People who use services and others were not protected against the risks associated with unsafe or inappropriate treatment as resuscitation services were not consistent in provision, knowledge or equipment across all locations and as reflected in published guidance. Regulation 9 (1) (b) (iii)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
provision equipment standardisation and present to Executive Quality Board
Director (Senior Clinical Skills Facilitator)
components complete or on track – Resuscitation trolleys, drug boxes and defibrillators. Ongoing plan will need continuous monitoring
Committee
Improve checking systems for resuscitation equipment trolleys
Deputy Medical Director (Senior Clinical Skills Facilitator)
May 2014 5 Resus team have conducted a review of cardiac arrest trollies at LRI, significant problems were identified with checking of the trollies. LR presented finding to Nursing Executive Team (NET) and a change to Matrices have been made so senior nurse have to physically check the trolley.
Resus
Committee
Assurance of checking systems through regular reporting to resuscitation committee
Deputy Medical Director (Senior Clinical Skills Facilitator)
June 2014 October 2014
4 Checks are taking place. Reports to Resuscitation Committee to commence September 2014.
Resus
Committee
Standardise resuscitation equipment across the Trust - drug boxes
Deputy Medical Director (pharmacist)
August 2014
5 MF to implement the standardised Drug box into the cardiac arrest trollies. Adult boxes standardised
Resus
Committee
99
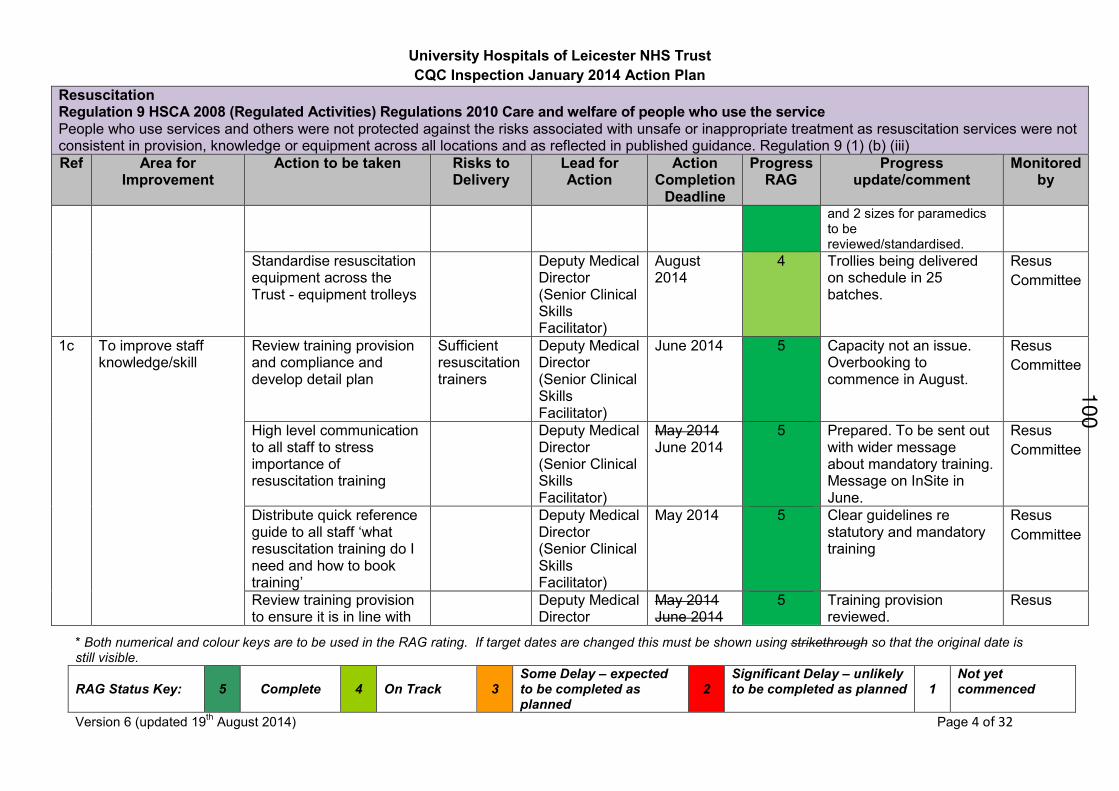
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 4 of 32
Resuscitation Regulation 9 HSCA 2008 (Regulated Activities) Regulations 2010 Care and welfare of people who use the service People who use services and others were not protected against the risks associated with unsafe or inappropriate treatment as resuscitation services were not consistent in provision, knowledge or equipment across all locations and as reflected in published guidance. Regulation 9 (1) (b) (iii)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
and 2 sizes for paramedics to be reviewed/standardised.
Standardise resuscitation equipment across the Trust - equipment trolleys
Deputy Medical Director (Senior Clinical Skills Facilitator)
August 2014
4 Trollies being delivered on schedule in 25 batches.
Resus
Committee
1c To improve staff knowledge/skill
Review training provision and compliance and develop detail plan
Sufficient resuscitation trainers
Deputy Medical Director (Senior Clinical Skills Facilitator)
June 2014 5 Capacity not an issue. Overbooking to commence in August.
Resus
Committee
High level communication to all staff to stress importance of resuscitation training
Deputy Medical Director (Senior Clinical Skills Facilitator)
May 2014 June 2014
5 Prepared. To be sent out with wider message about mandatory training. Message on InSite in June.
Resus
Committee
Distribute quick reference guide to all staff ‘what resuscitation training do I need and how to book training’
Deputy Medical Director (Senior Clinical Skills Facilitator)
May 2014 5 Clear guidelines re statutory and mandatory training
Resus
Committee
Review training provision to ensure it is in line with
Deputy Medical Director
May 2014 June 2014
5 Training provision reviewed.
Resus
100
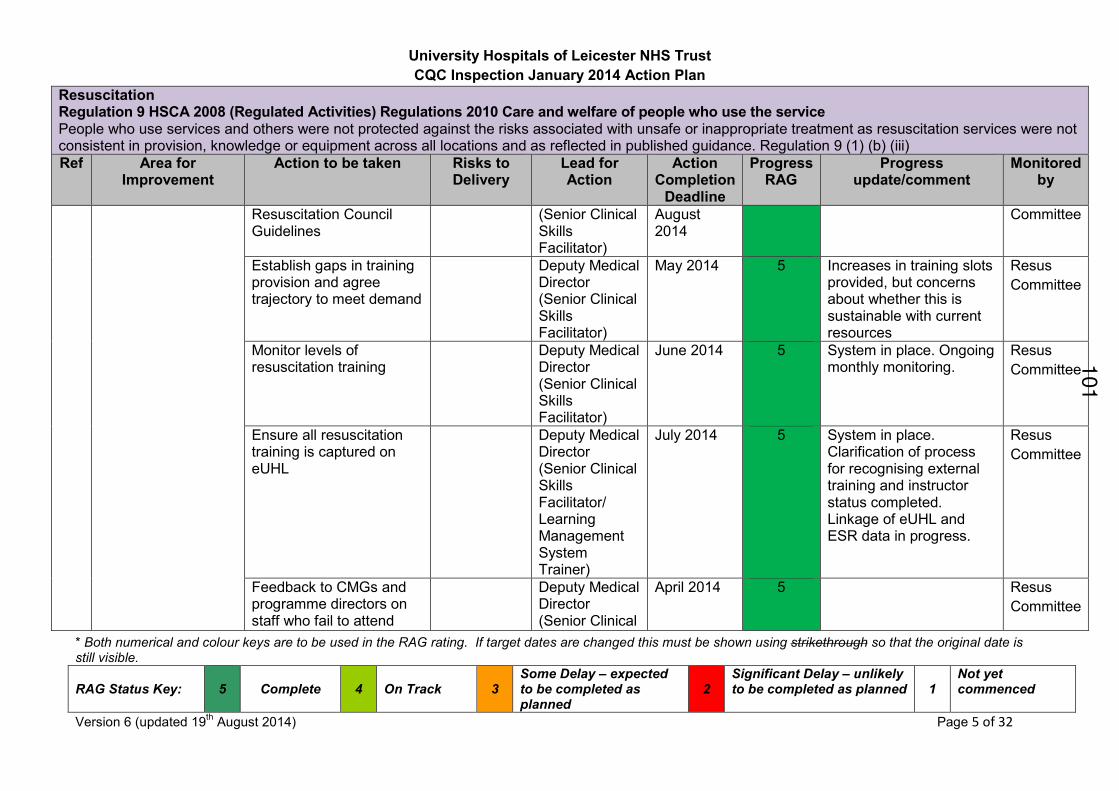
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 5 of 32
Resuscitation Regulation 9 HSCA 2008 (Regulated Activities) Regulations 2010 Care and welfare of people who use the service People who use services and others were not protected against the risks associated with unsafe or inappropriate treatment as resuscitation services were not consistent in provision, knowledge or equipment across all locations and as reflected in published guidance. Regulation 9 (1) (b) (iii)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
Resuscitation Council Guidelines
(Senior Clinical Skills Facilitator)
August 2014
Committee
Establish gaps in training provision and agree trajectory to meet demand
Deputy Medical Director (Senior Clinical Skills Facilitator)
May 2014 5 Increases in training slots provided, but concerns about whether this is sustainable with current resources
Resus
Committee
Monitor levels of resuscitation training
Deputy Medical Director (Senior Clinical Skills Facilitator)
June 2014 5 System in place. Ongoing monthly monitoring.
Resus
Committee
Ensure all resuscitation training is captured on eUHL
Deputy Medical Director (Senior Clinical Skills Facilitator/ Learning Management System Trainer)
July 2014 5 System in place. Clarification of process for recognising external training and instructor status completed. Linkage of eUHL and ESR data in progress.
Resus
Committee
Feedback to CMGs and programme directors on staff who fail to attend
Deputy Medical Director (Senior Clinical
April 2014 5 Resus
Committee
101
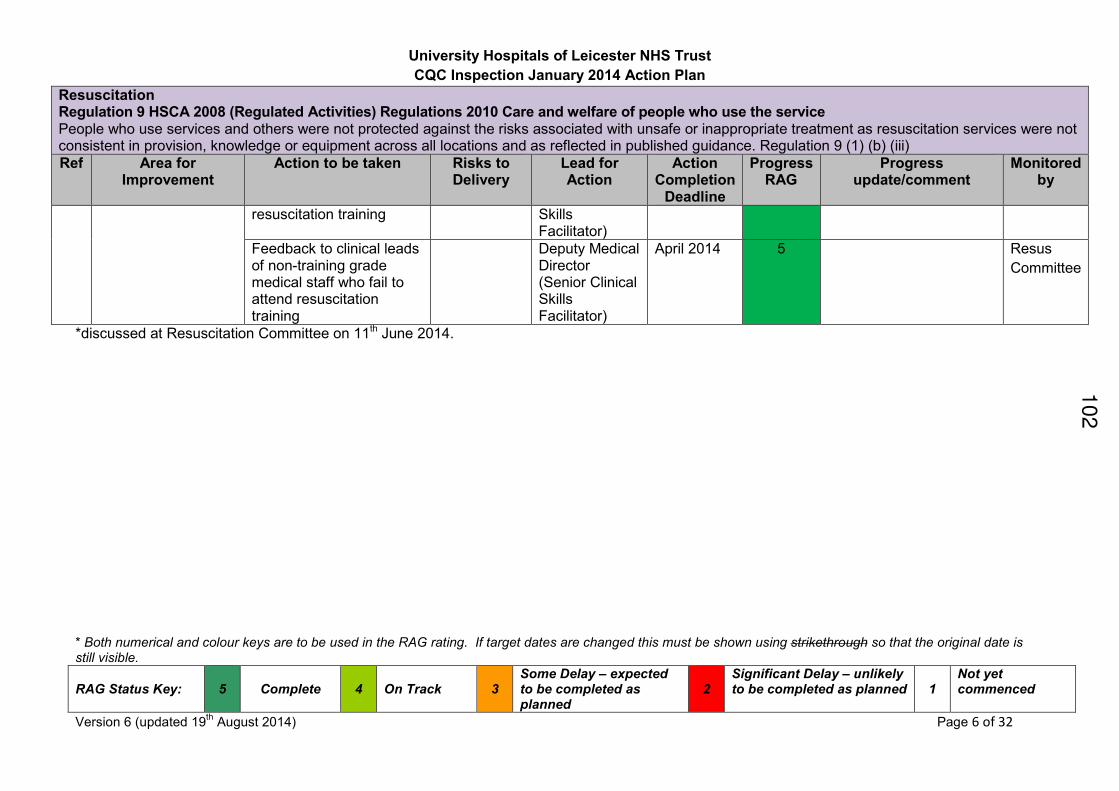
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 6 of 32
Resuscitation Regulation 9 HSCA 2008 (Regulated Activities) Regulations 2010 Care and welfare of people who use the service People who use services and others were not protected against the risks associated with unsafe or inappropriate treatment as resuscitation services were not consistent in provision, knowledge or equipment across all locations and as reflected in published guidance. Regulation 9 (1) (b) (iii)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
resuscitation training Skills Facilitator)
Feedback to clinical leads of non-training grade medical staff who fail to attend resuscitation training
Deputy Medical Director (Senior Clinical Skills Facilitator)
April 2014 5 Resus
Committee
*discussed at Resuscitation Committee on 11th June 2014.
102
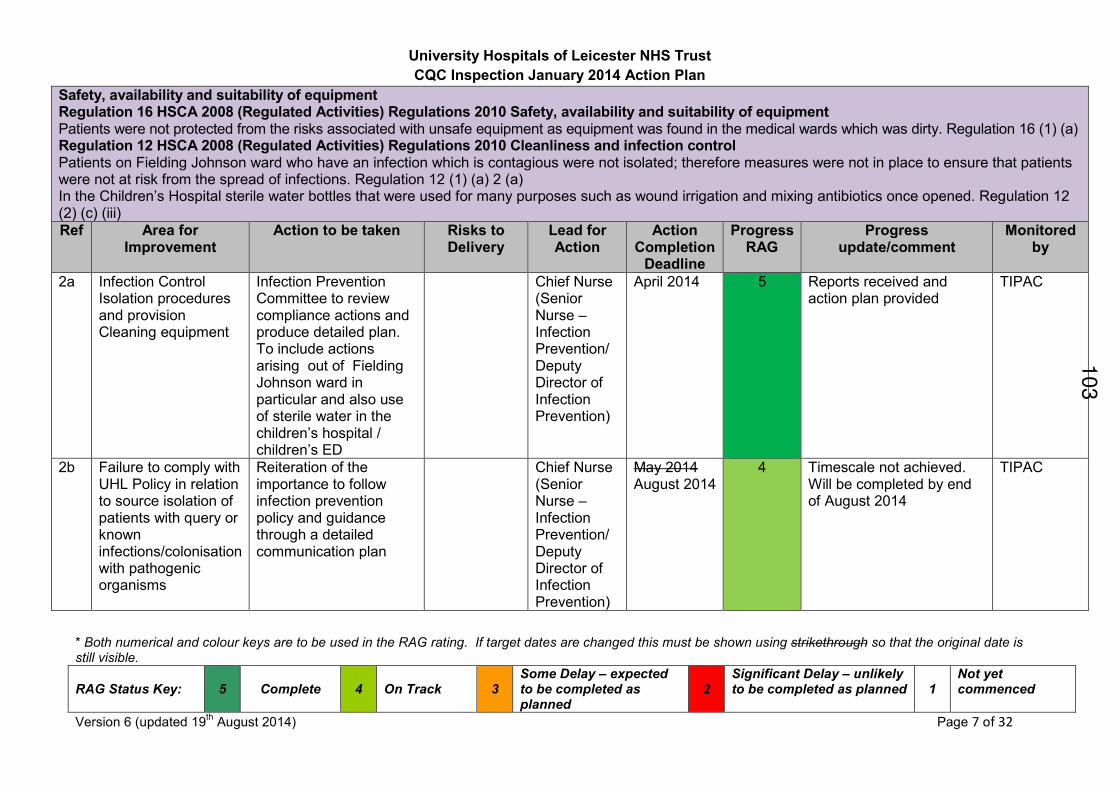
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 7 of 32
Safety, availability and suitability of equipment Regulation 16 HSCA 2008 (Regulated Activities) Regulations 2010 Safety, availability and suitability of equipment Patients were not protected from the risks associated with unsafe equipment as equipment was found in the medical wards which was dirty. Regulation 16 (1) (a) Regulation 12 HSCA 2008 (Regulated Activities) Regulations 2010 Cleanliness and infection control Patients on Fielding Johnson ward who have an infection which is contagious were not isolated; therefore measures were not in place to ensure that patients were not at risk from the spread of infections. Regulation 12 (1) (a) 2 (a) In the Children’s Hospital sterile water bottles that were used for many purposes such as wound irrigation and mixing antibiotics once opened. Regulation 12 (2) (c) (iii)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
2a Infection Control Isolation procedures and provision Cleaning equipment
Infection Prevention Committee to review compliance actions and produce detailed plan. To include actions arising out of Fielding Johnson ward in particular and also use of sterile water in the children’s hospital / children’s ED
Chief Nurse (Senior Nurse – Infection Prevention/ Deputy Director of Infection Prevention)
April 2014 5 Reports received and action plan provided
TIPAC
2b Failure to comply with UHL Policy in relation to source isolation of patients with query or known infections/colonisation with pathogenic organisms
Reiteration of the importance to follow infection prevention policy and guidance through a detailed communication plan
Chief Nurse (Senior Nurse – Infection Prevention/ Deputy Director of Infection Prevention)
May 2014 August 2014
4 Timescale not achieved. Will be completed by end of August 2014
TIPAC
103
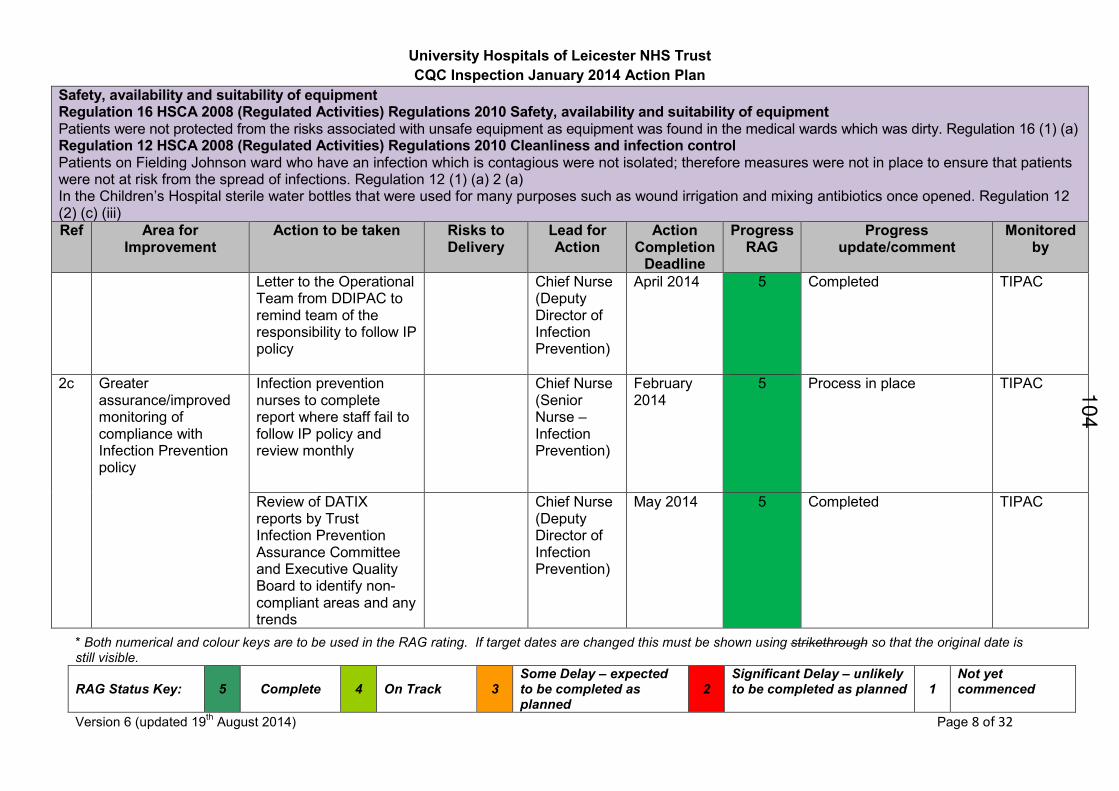
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 8 of 32
Safety, availability and suitability of equipment Regulation 16 HSCA 2008 (Regulated Activities) Regulations 2010 Safety, availability and suitability of equipment Patients were not protected from the risks associated with unsafe equipment as equipment was found in the medical wards which was dirty. Regulation 16 (1) (a) Regulation 12 HSCA 2008 (Regulated Activities) Regulations 2010 Cleanliness and infection control Patients on Fielding Johnson ward who have an infection which is contagious were not isolated; therefore measures were not in place to ensure that patients were not at risk from the spread of infections. Regulation 12 (1) (a) 2 (a) In the Children’s Hospital sterile water bottles that were used for many purposes such as wound irrigation and mixing antibiotics once opened. Regulation 12 (2) (c) (iii)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
Letter to the Operational Team from DDIPAC to remind team of the responsibility to follow IP policy
Chief Nurse (Deputy Director of Infection Prevention)
April 2014 5 Completed TIPAC
2c Greater assurance/improved monitoring of compliance with Infection Prevention policy
Infection prevention nurses to complete report where staff fail to follow IP policy and review monthly
Chief Nurse (Senior Nurse – Infection Prevention)
February 2014
5 Process in place TIPAC
Review of DATIX reports by Trust Infection Prevention Assurance Committee and Executive Quality Board to identify non-compliant areas and any trends
Chief Nurse (Deputy Director of Infection Prevention)
May 2014 5 Completed TIPAC
104
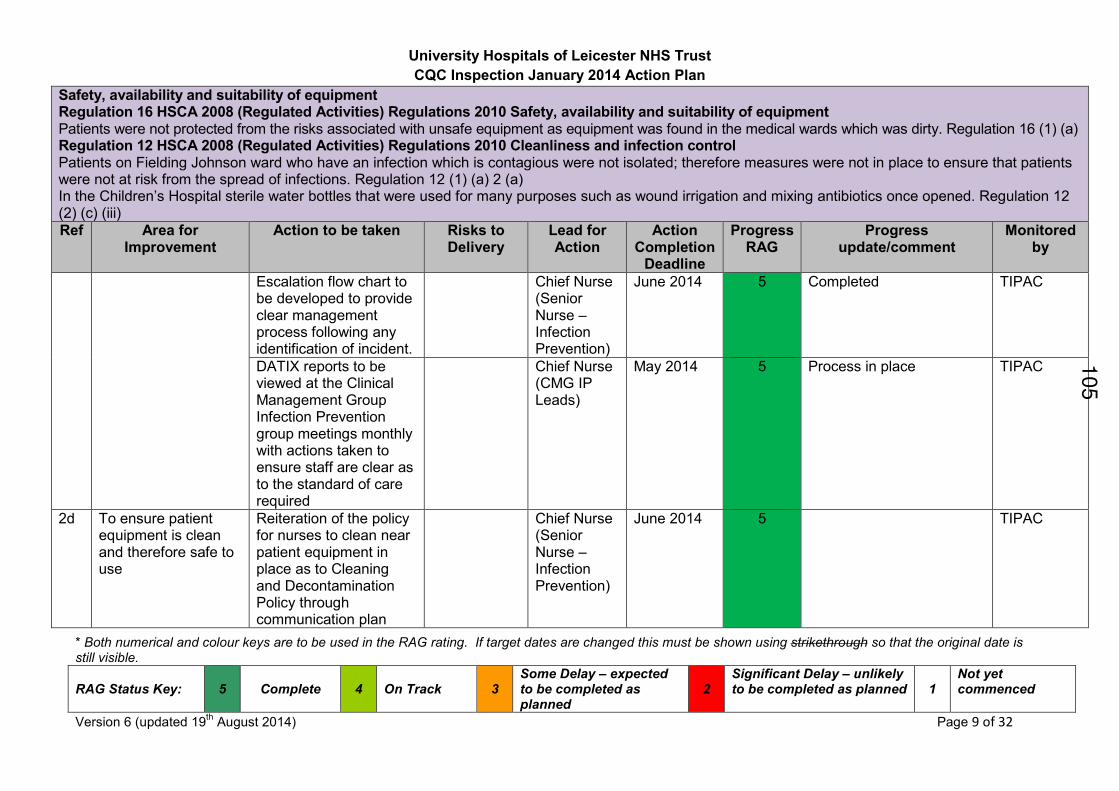
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 9 of 32
Safety, availability and suitability of equipment Regulation 16 HSCA 2008 (Regulated Activities) Regulations 2010 Safety, availability and suitability of equipment Patients were not protected from the risks associated with unsafe equipment as equipment was found in the medical wards which was dirty. Regulation 16 (1) (a) Regulation 12 HSCA 2008 (Regulated Activities) Regulations 2010 Cleanliness and infection control Patients on Fielding Johnson ward who have an infection which is contagious were not isolated; therefore measures were not in place to ensure that patients were not at risk from the spread of infections. Regulation 12 (1) (a) 2 (a) In the Children’s Hospital sterile water bottles that were used for many purposes such as wound irrigation and mixing antibiotics once opened. Regulation 12 (2) (c) (iii)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
Escalation flow chart to be developed to provide clear management process following any identification of incident.
Chief Nurse (Senior Nurse – Infection Prevention)
June 2014 5 Completed
TIPAC
DATIX reports to be viewed at the Clinical Management Group Infection Prevention group meetings monthly with actions taken to ensure staff are clear as to the standard of care required
Chief Nurse (CMG IP Leads)
May 2014 5 Process in place TIPAC
2d To ensure patient equipment is clean and therefore safe to use
Reiteration of the policy for nurses to clean near patient equipment in place as to Cleaning and Decontamination Policy through communication plan
Chief Nurse (Senior Nurse – Infection Prevention)
June 2014 5 TIPAC
105
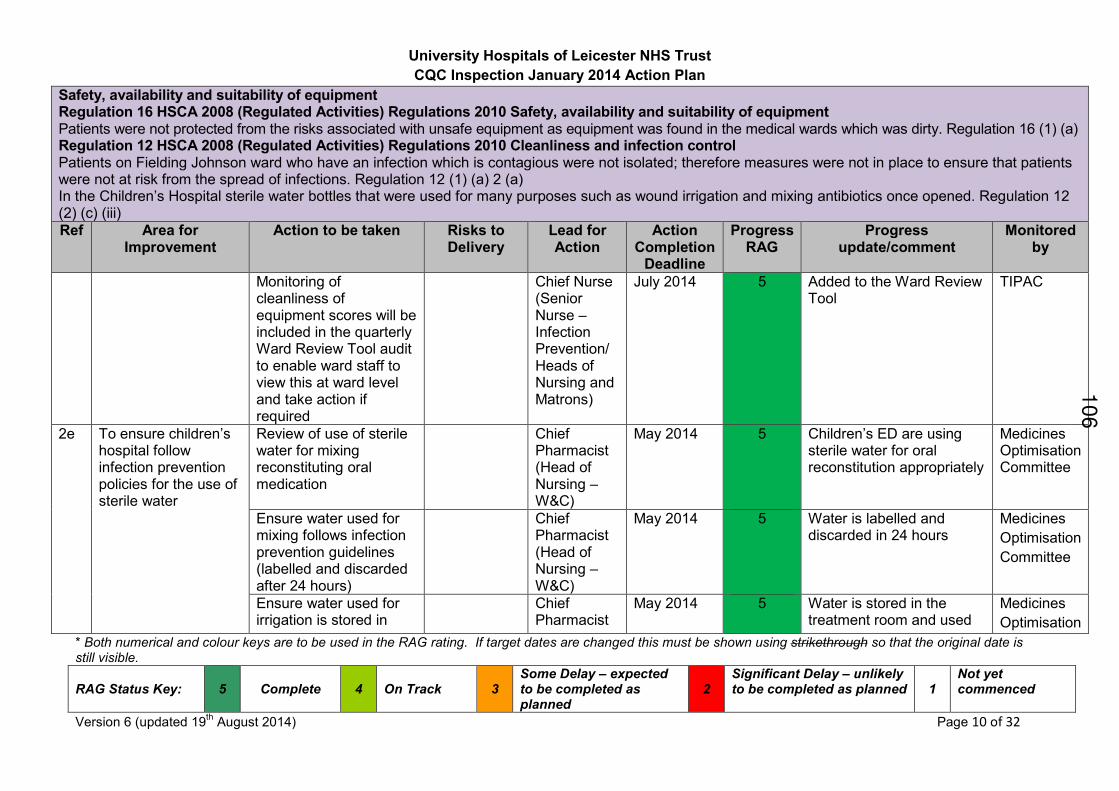
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 10 of 32
Safety, availability and suitability of equipment Regulation 16 HSCA 2008 (Regulated Activities) Regulations 2010 Safety, availability and suitability of equipment Patients were not protected from the risks associated with unsafe equipment as equipment was found in the medical wards which was dirty. Regulation 16 (1) (a) Regulation 12 HSCA 2008 (Regulated Activities) Regulations 2010 Cleanliness and infection control Patients on Fielding Johnson ward who have an infection which is contagious were not isolated; therefore measures were not in place to ensure that patients were not at risk from the spread of infections. Regulation 12 (1) (a) 2 (a) In the Children’s Hospital sterile water bottles that were used for many purposes such as wound irrigation and mixing antibiotics once opened. Regulation 12 (2) (c) (iii)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
Monitoring of cleanliness of equipment scores will be included in the quarterly Ward Review Tool audit to enable ward staff to view this at ward level and take action if required
Chief Nurse (Senior Nurse – Infection Prevention/ Heads of Nursing and Matrons)
July 2014 5 Added to the Ward Review Tool
TIPAC
2e To ensure children’s hospital follow infection prevention policies for the use of sterile water
Review of use of sterile water for mixing reconstituting oral medication
Chief Pharmacist (Head of Nursing – W&C)
May 2014 5 Children’s ED are using sterile water for oral reconstitution appropriately
Medicines Optimisation Committee
Ensure water used for mixing follows infection prevention guidelines (labelled and discarded after 24 hours)
Chief Pharmacist (Head of Nursing – W&C)
May 2014 5 Water is labelled and discarded in 24 hours
Medicines
Optimisation
Committee
Ensure water used for irrigation is stored in
Chief Pharmacist
May 2014 5 Water is stored in the treatment room and used
Medicines
Optimisation
106
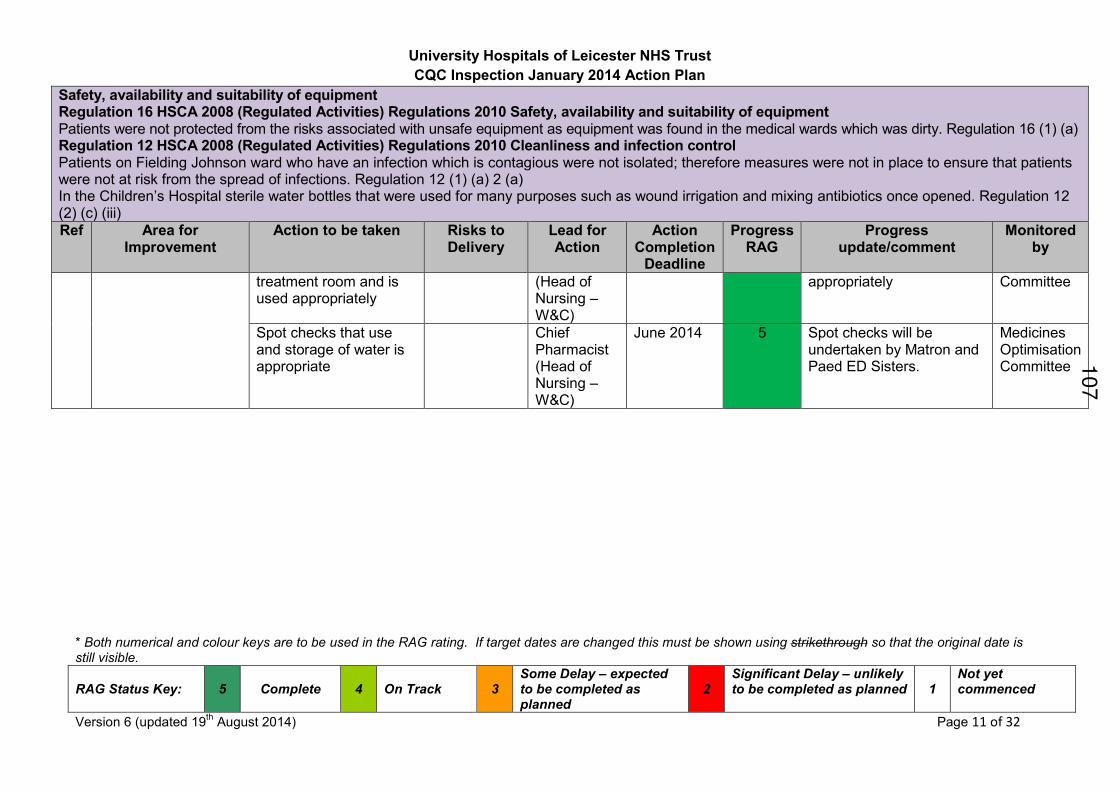
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 11 of 32
Safety, availability and suitability of equipment Regulation 16 HSCA 2008 (Regulated Activities) Regulations 2010 Safety, availability and suitability of equipment Patients were not protected from the risks associated with unsafe equipment as equipment was found in the medical wards which was dirty. Regulation 16 (1) (a) Regulation 12 HSCA 2008 (Regulated Activities) Regulations 2010 Cleanliness and infection control Patients on Fielding Johnson ward who have an infection which is contagious were not isolated; therefore measures were not in place to ensure that patients were not at risk from the spread of infections. Regulation 12 (1) (a) 2 (a) In the Children’s Hospital sterile water bottles that were used for many purposes such as wound irrigation and mixing antibiotics once opened. Regulation 12 (2) (c) (iii)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
treatment room and is used appropriately
(Head of Nursing – W&C)
appropriately Committee
Spot checks that use and storage of water is appropriate
Chief Pharmacist (Head of Nursing – W&C)
June 2014 5 Spot checks will be undertaken by Matron and Paed ED Sisters.
Medicines Optimisation Committee
107
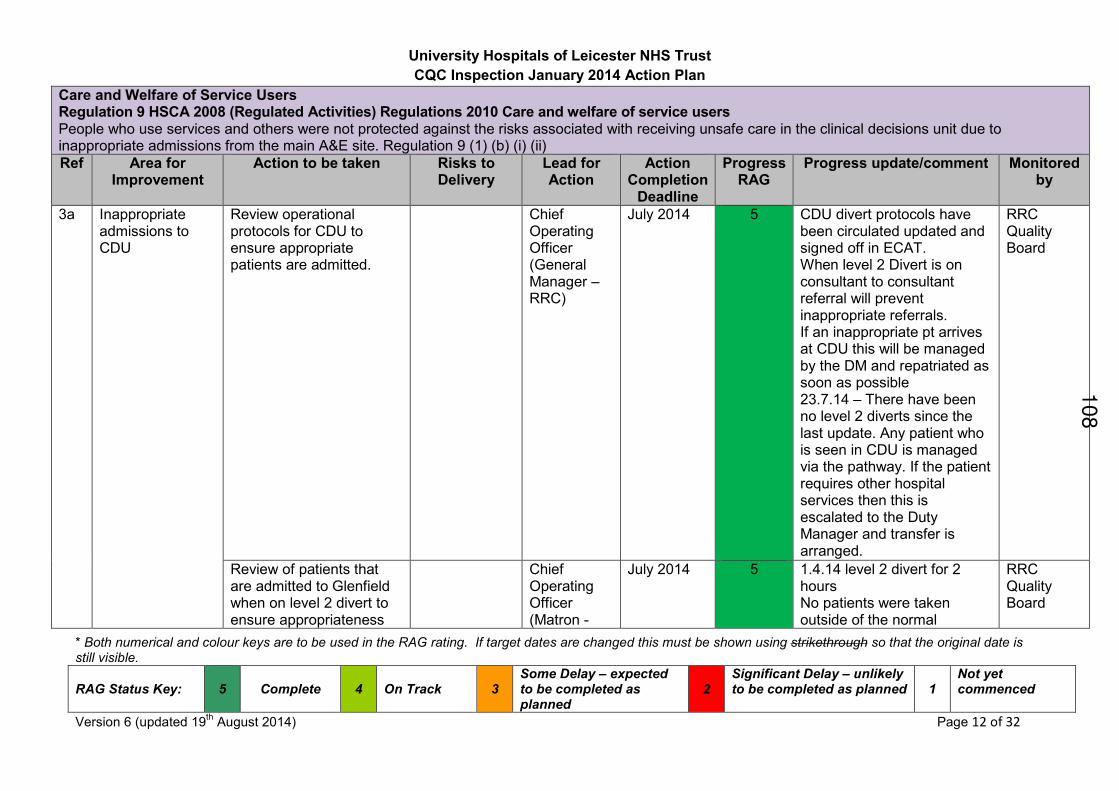
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 12 of 32
Care and Welfare of Service Users Regulation 9 HSCA 2008 (Regulated Activities) Regulations 2010 Care and welfare of service users People who use services and others were not protected against the risks associated with receiving unsafe care in the clinical decisions unit due to inappropriate admissions from the main A&E site. Regulation 9 (1) (b) (i) (ii)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment Monitored by
3a Inappropriate admissions to CDU
Review operational protocols for CDU to ensure appropriate patients are admitted.
Chief Operating Officer (General Manager – RRC)
July 2014 5 CDU divert protocols have been circulated updated and signed off in ECAT. When level 2 Divert is on consultant to consultant referral will prevent inappropriate referrals. If an inappropriate pt arrives at CDU this will be managed by the DM and repatriated as soon as possible 23.7.14 – There have been no level 2 diverts since the last update. Any patient who is seen in CDU is managed via the pathway. If the patient requires other hospital services then this is escalated to the Duty Manager and transfer is arranged.
RRC Quality Board
Review of patients that are admitted to Glenfield when on level 2 divert to ensure appropriateness
Chief Operating Officer (Matron -
July 2014 5 1.4.14 level 2 divert for 2 hours No patients were taken outside of the normal
RRC Quality Board
108

University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 13 of 32
Care and Welfare of Service Users Regulation 9 HSCA 2008 (Regulated Activities) Regulations 2010 Care and welfare of service users People who use services and others were not protected against the risks associated with receiving unsafe care in the clinical decisions unit due to inappropriate admissions from the main A&E site. Regulation 9 (1) (b) (i) (ii)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment Monitored by
CDU) respiratory / cardiology criteria. Monitoring by nurse in charge. 19.8.14 - No patients have been escalated as inappropriate
3b CDU design and flow
A working party will review the flow within CDU and implement any further improvement actions
Chief Operating Officer (General Manager – RRC)
October 2014
4 A working group has been established to discuss and implement improvements to flow and staffing. This is being feedback to ECAT. • Draft 1 staffing has been submitted to ECAT, Draft 2 is being worked on • DR Ian Sturgess is working with the team in assessing flow and suggested improvements • Matron has been appointed to provide senior nursing leadership and manage change (due to start in 2-3mths) • Targets have been set for diagnostics and imaging
RRC Quality Board 1
09
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 14 of 32
110
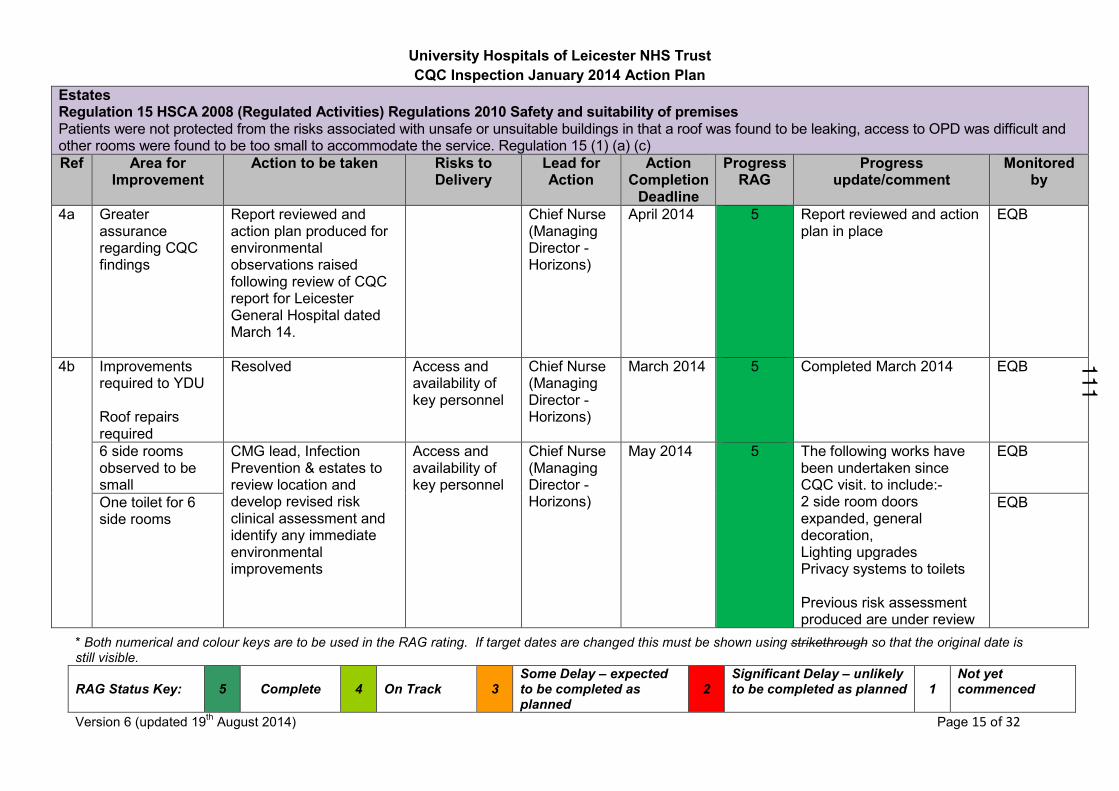
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 15 of 32
Estates Regulation 15 HSCA 2008 (Regulated Activities) Regulations 2010 Safety and suitability of premises Patients were not protected from the risks associated with unsafe or unsuitable buildings in that a roof was found to be leaking, access to OPD was difficult and other rooms were found to be too small to accommodate the service. Regulation 15 (1) (a) (c)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
4a Greater assurance regarding CQC findings
Report reviewed and action plan produced for environmental observations raised following review of CQC report for Leicester General Hospital dated March 14.
Chief Nurse (Managing Director - Horizons)
April 2014 5 Report reviewed and action plan in place
EQB
4b Improvements required to YDU Roof repairs required
Resolved Access and availability of key personnel
Chief Nurse (Managing Director - Horizons)
March 2014 5 Completed March 2014 EQB
6 side rooms observed to be small
CMG lead, Infection Prevention & estates to review location and develop revised risk clinical assessment and identify any immediate environmental improvements
Access and availability of key personnel
Chief Nurse (Managing Director - Horizons)
May 2014 5 The following works have been undertaken since CQC visit. to include:- 2 side room doors expanded, general decoration, Lighting upgrades Privacy systems to toilets Previous risk assessment produced are under review
EQB
One toilet for 6 side rooms
EQB
111
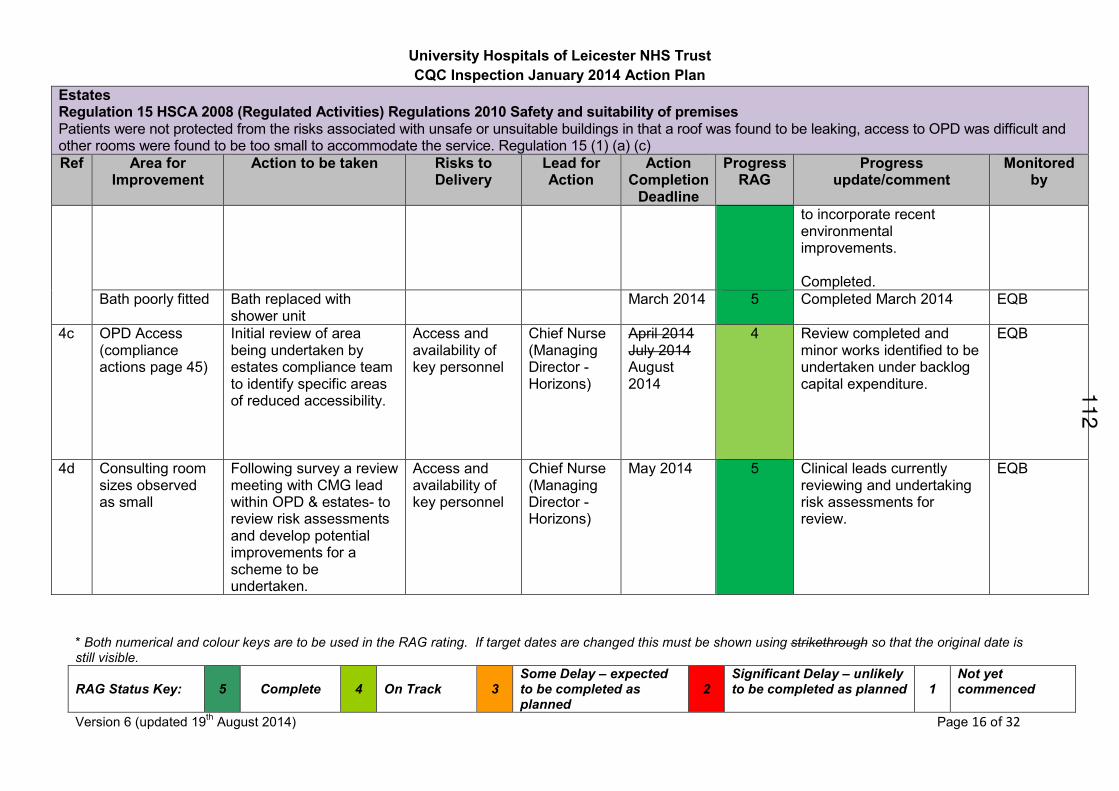
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 16 of 32
Estates Regulation 15 HSCA 2008 (Regulated Activities) Regulations 2010 Safety and suitability of premises Patients were not protected from the risks associated with unsafe or unsuitable buildings in that a roof was found to be leaking, access to OPD was difficult and other rooms were found to be too small to accommodate the service. Regulation 15 (1) (a) (c)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
to incorporate recent environmental improvements. Completed.
Bath poorly fitted
Bath replaced with shower unit
March 2014 5 Completed March 2014 EQB
4c OPD Access (compliance actions page 45)
Initial review of area being undertaken by estates compliance team to identify specific areas of reduced accessibility.
Access and availability of key personnel
Chief Nurse (Managing Director - Horizons)
April 2014 July 2014 August 2014
4 Review completed and minor works identified to be undertaken under backlog capital expenditure.
EQB
4d Consulting room sizes observed as small
Following survey a review meeting with CMG lead within OPD & estates- to review risk assessments and develop potential improvements for a scheme to be undertaken.
Access and availability of key personnel
Chief Nurse (Managing Director - Horizons)
May 2014 5 Clinical leads currently reviewing and undertaking risk assessments for review.
EQB
112
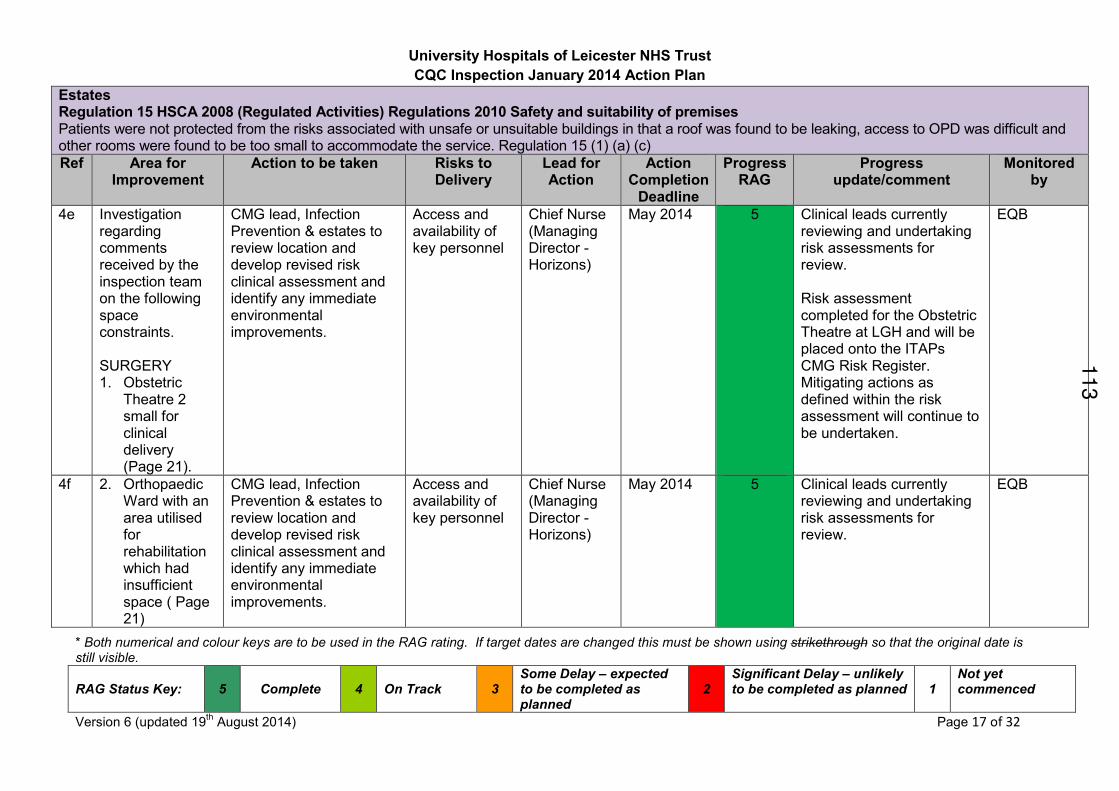
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 17 of 32
Estates Regulation 15 HSCA 2008 (Regulated Activities) Regulations 2010 Safety and suitability of premises Patients were not protected from the risks associated with unsafe or unsuitable buildings in that a roof was found to be leaking, access to OPD was difficult and other rooms were found to be too small to accommodate the service. Regulation 15 (1) (a) (c)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
4e Investigation regarding comments received by the inspection team on the following space constraints. SURGERY 1. Obstetric
Theatre 2 small for clinical delivery (Page 21).
CMG lead, Infection Prevention & estates to review location and develop revised risk clinical assessment and identify any immediate environmental improvements.
Access and availability of key personnel
Chief Nurse (Managing Director - Horizons)
May 2014 5 Clinical leads currently reviewing and undertaking risk assessments for review. Risk assessment completed for the Obstetric Theatre at LGH and will be placed onto the ITAPs CMG Risk Register. Mitigating actions as defined within the risk assessment will continue to be undertaken.
EQB
4f 2. Orthopaedic Ward with an area utilised for rehabilitation which had insufficient space ( Page 21)
CMG lead, Infection Prevention & estates to review location and develop revised risk clinical assessment and identify any immediate environmental improvements.
Access and availability of key personnel
Chief Nurse (Managing Director - Horizons)
May 2014 5 Clinical leads currently reviewing and undertaking risk assessments for review.
EQB
113
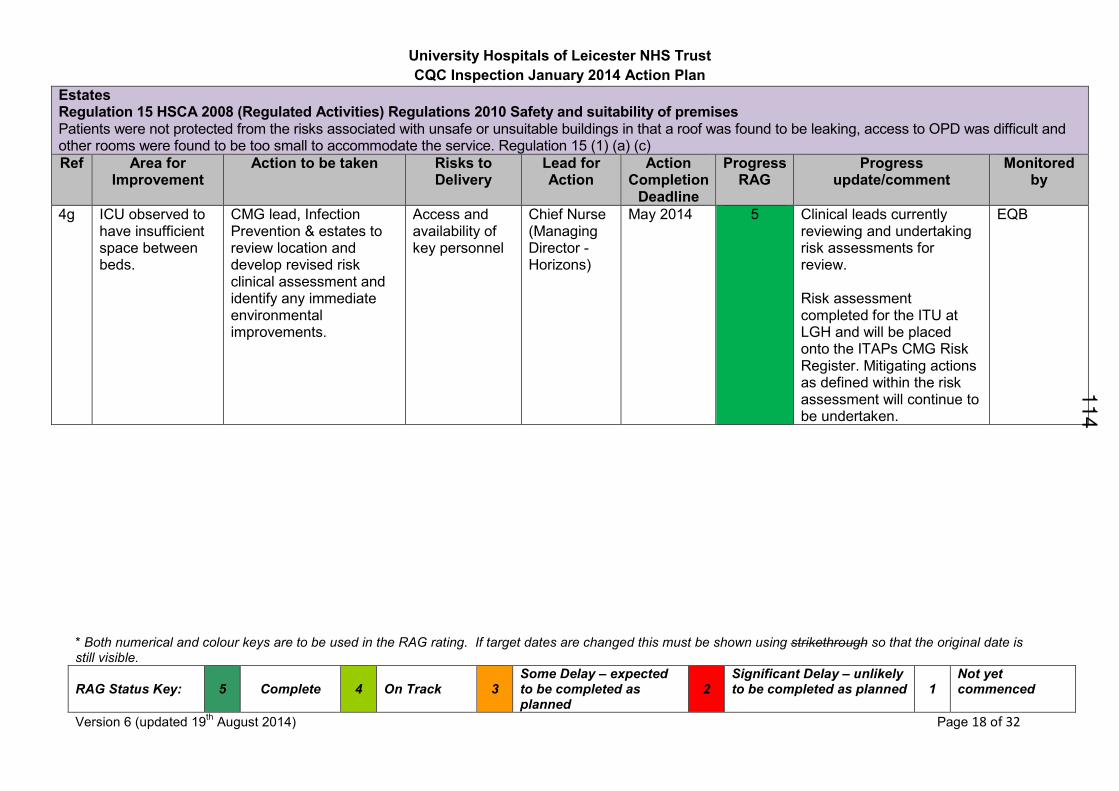
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 18 of 32
Estates Regulation 15 HSCA 2008 (Regulated Activities) Regulations 2010 Safety and suitability of premises Patients were not protected from the risks associated with unsafe or unsuitable buildings in that a roof was found to be leaking, access to OPD was difficult and other rooms were found to be too small to accommodate the service. Regulation 15 (1) (a) (c)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
4g ICU observed to have insufficient space between beds.
CMG lead, Infection Prevention & estates to review location and develop revised risk clinical assessment and identify any immediate environmental improvements.
Access and availability of key personnel
Chief Nurse (Managing Director - Horizons)
May 2014 5 Clinical leads currently reviewing and undertaking risk assessments for review. Risk assessment completed for the ITU at LGH and will be placed onto the ITAPs CMG Risk Register. Mitigating actions as defined within the risk assessment will continue to be undertaken.
EQB
114
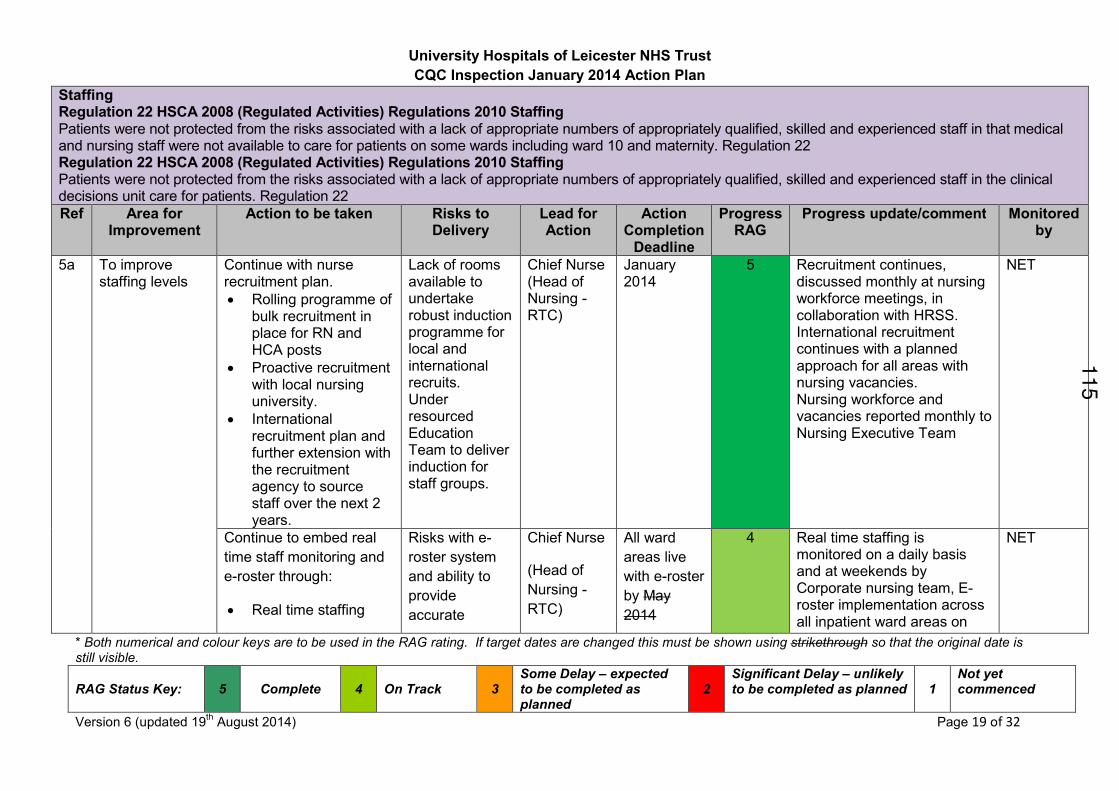
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 19 of 32
Staffing Regulation 22 HSCA 2008 (Regulated Activities) Regulations 2010 Staffing Patients were not protected from the risks associated with a lack of appropriate numbers of appropriately qualified, skilled and experienced staff in that medical and nursing staff were not available to care for patients on some wards including ward 10 and maternity. Regulation 22 Regulation 22 HSCA 2008 (Regulated Activities) Regulations 2010 Staffing Patients were not protected from the risks associated with a lack of appropriate numbers of appropriately qualified, skilled and experienced staff in the clinical decisions unit care for patients. Regulation 22
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment Monitored by
5a
To improve staffing levels
Continue with nurse recruitment plan.
• Rolling programme of bulk recruitment in place for RN and HCA posts
• Proactive recruitment with local nursing university.
• International recruitment plan and further extension with the recruitment agency to source staff over the next 2 years.
Lack of rooms available to undertake robust induction programme for local and international recruits. Under resourced Education Team to deliver induction for staff groups.
Chief Nurse (Head of Nursing - RTC)
January 2014
5 Recruitment continues, discussed monthly at nursing workforce meetings, in collaboration with HRSS. International recruitment continues with a planned approach for all areas with nursing vacancies. Nursing workforce and vacancies reported monthly to Nursing Executive Team
NET
Continue to embed real
time staff monitoring and
e-roster through:
• Real time staffing
Risks with e-
roster system
and ability to
provide
accurate
Chief Nurse
(Head of
Nursing -
RTC)
All ward
areas live
with e-roster
by May
2014
4 Real time staffing is monitored on a daily basis and at weekends by Corporate nursing team, E-roster implementation across all inpatient ward areas on
NET
115
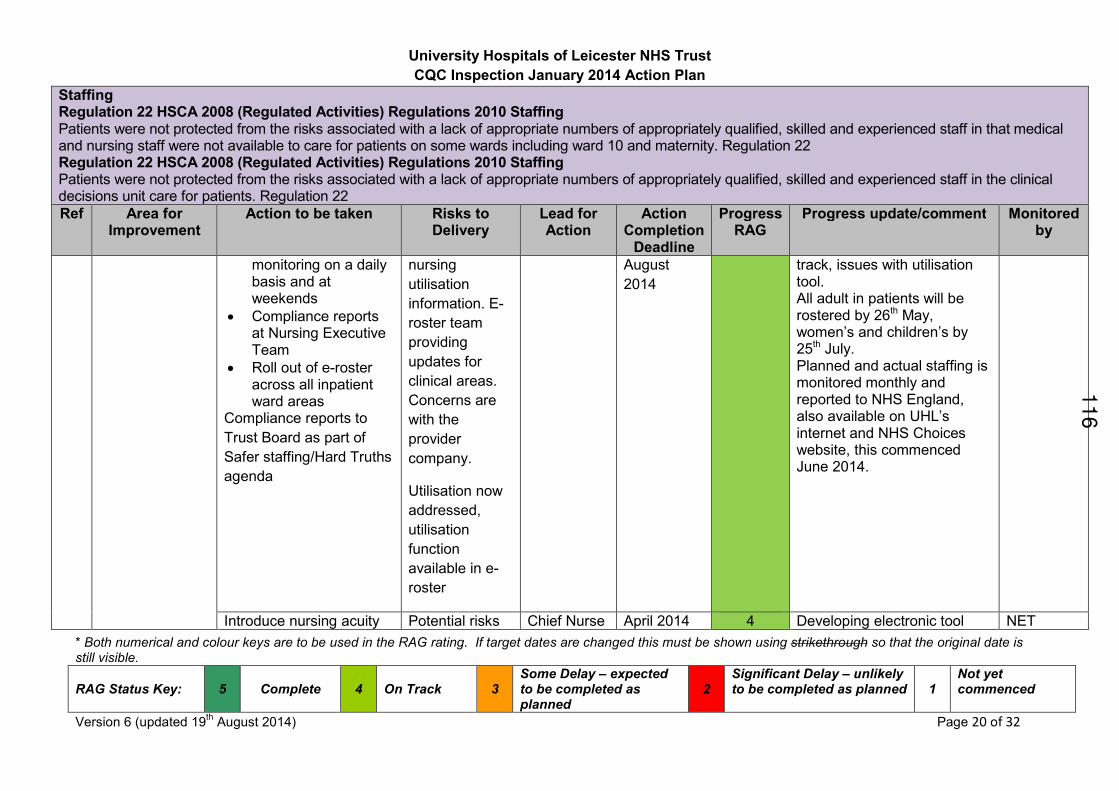
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 20 of 32
Staffing Regulation 22 HSCA 2008 (Regulated Activities) Regulations 2010 Staffing Patients were not protected from the risks associated with a lack of appropriate numbers of appropriately qualified, skilled and experienced staff in that medical and nursing staff were not available to care for patients on some wards including ward 10 and maternity. Regulation 22 Regulation 22 HSCA 2008 (Regulated Activities) Regulations 2010 Staffing Patients were not protected from the risks associated with a lack of appropriate numbers of appropriately qualified, skilled and experienced staff in the clinical decisions unit care for patients. Regulation 22
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment Monitored by
monitoring on a daily basis and at weekends
• Compliance reports at Nursing Executive Team
• Roll out of e-roster across all inpatient ward areas
Compliance reports to
Trust Board as part of
Safer staffing/Hard Truths
agenda
nursing
utilisation
information. E-
roster team
providing
updates for
clinical areas.
Concerns are
with the
provider
company.
Utilisation now
addressed,
utilisation
function
available in e-
roster
August
2014
track, issues with utilisation tool. All adult in patients will be rostered by 26th May, women’s and children’s by 25th July. Planned and actual staffing is monitored monthly and reported to NHS England, also available on UHL’s internet and NHS Choices website, this commenced June 2014.
Introduce nursing acuity Potential risks Chief Nurse April 2014 4 Developing electronic tool NET
116
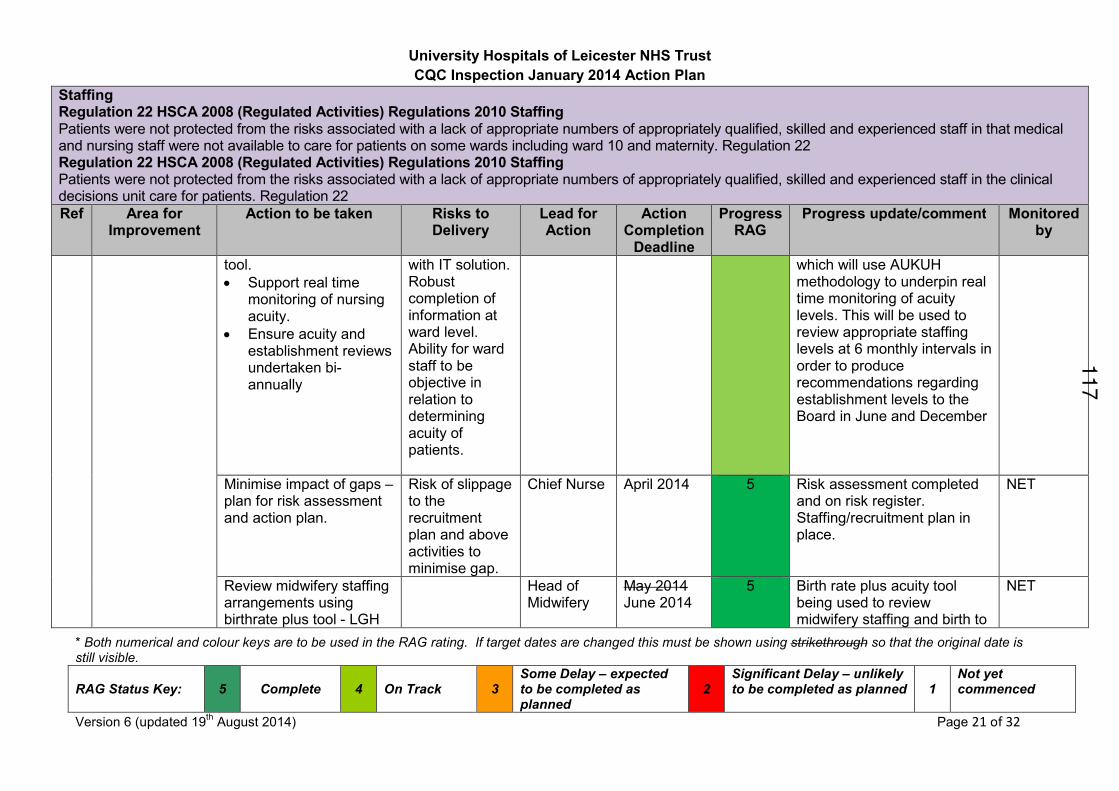
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 21 of 32
Staffing Regulation 22 HSCA 2008 (Regulated Activities) Regulations 2010 Staffing Patients were not protected from the risks associated with a lack of appropriate numbers of appropriately qualified, skilled and experienced staff in that medical and nursing staff were not available to care for patients on some wards including ward 10 and maternity. Regulation 22 Regulation 22 HSCA 2008 (Regulated Activities) Regulations 2010 Staffing Patients were not protected from the risks associated with a lack of appropriate numbers of appropriately qualified, skilled and experienced staff in the clinical decisions unit care for patients. Regulation 22
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment Monitored by
tool.
• Support real time monitoring of nursing acuity.
• Ensure acuity and establishment reviews undertaken bi-annually
with IT solution. Robust completion of information at ward level. Ability for ward staff to be objective in relation to determining acuity of patients.
which will use AUKUH methodology to underpin real time monitoring of acuity levels. This will be used to review appropriate staffing levels at 6 monthly intervals in order to produce recommendations regarding establishment levels to the Board in June and December
Minimise impact of gaps – plan for risk assessment and action plan.
Risk of slippage to the recruitment plan and above activities to minimise gap.
Chief Nurse April 2014 5 Risk assessment completed and on risk register. Staffing/recruitment plan in place.
NET
Review midwifery staffing arrangements using birthrate plus tool - LGH
Head of Midwifery
May 2014 June 2014
5 Birth rate plus acuity tool being used to review midwifery staffing and birth to
NET
117
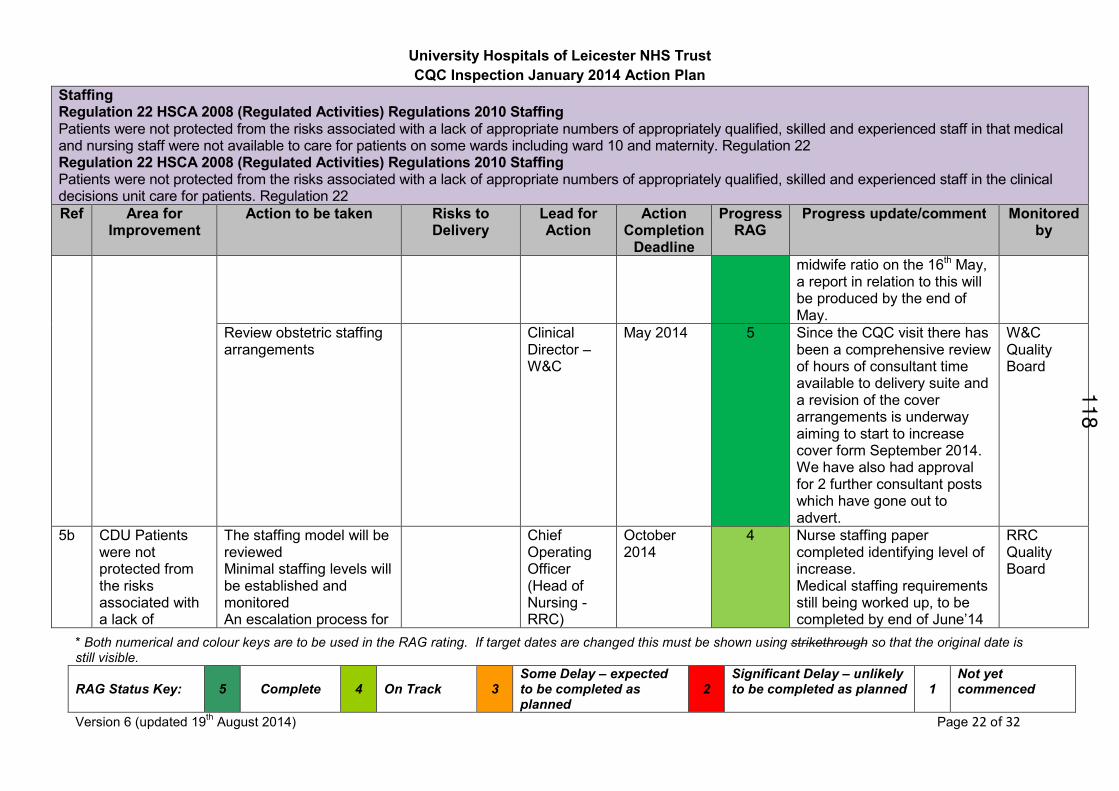
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 22 of 32
Staffing Regulation 22 HSCA 2008 (Regulated Activities) Regulations 2010 Staffing Patients were not protected from the risks associated with a lack of appropriate numbers of appropriately qualified, skilled and experienced staff in that medical and nursing staff were not available to care for patients on some wards including ward 10 and maternity. Regulation 22 Regulation 22 HSCA 2008 (Regulated Activities) Regulations 2010 Staffing Patients were not protected from the risks associated with a lack of appropriate numbers of appropriately qualified, skilled and experienced staff in the clinical decisions unit care for patients. Regulation 22
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment Monitored by
midwife ratio on the 16th May, a report in relation to this will be produced by the end of May.
Review obstetric staffing arrangements
Clinical Director – W&C
May 2014 5 Since the CQC visit there has been a comprehensive review of hours of consultant time available to delivery suite and a revision of the cover arrangements is underway aiming to start to increase cover form September 2014. We have also had approval for 2 further consultant posts which have gone out to advert.
W&C Quality Board
5b CDU Patients were not protected from the risks associated with a lack of
The staffing model will be reviewed Minimal staffing levels will be established and monitored An escalation process for
Chief Operating Officer (Head of Nursing - RRC)
October 2014
4 Nurse staffing paper completed identifying level of increase. Medical staffing requirements still being worked up, to be completed by end of June’14
RRC Quality Board
118
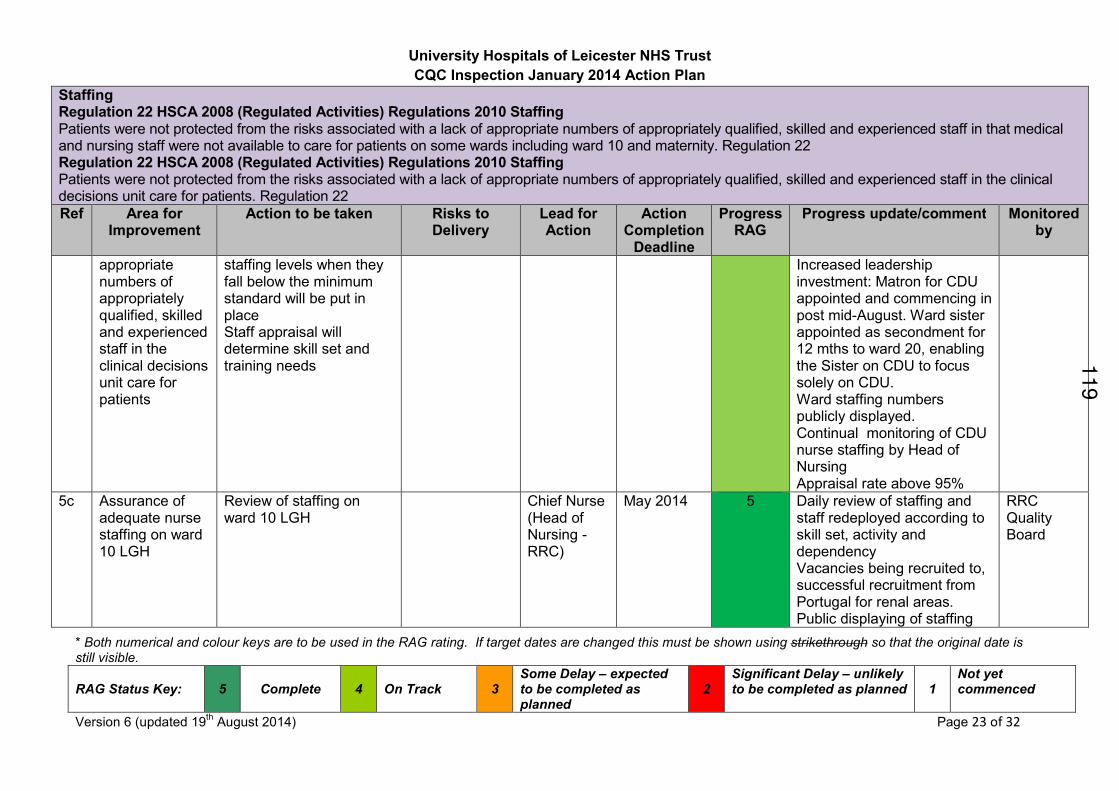
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 23 of 32
Staffing Regulation 22 HSCA 2008 (Regulated Activities) Regulations 2010 Staffing Patients were not protected from the risks associated with a lack of appropriate numbers of appropriately qualified, skilled and experienced staff in that medical and nursing staff were not available to care for patients on some wards including ward 10 and maternity. Regulation 22 Regulation 22 HSCA 2008 (Regulated Activities) Regulations 2010 Staffing Patients were not protected from the risks associated with a lack of appropriate numbers of appropriately qualified, skilled and experienced staff in the clinical decisions unit care for patients. Regulation 22
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment Monitored by
appropriate numbers of appropriately qualified, skilled and experienced staff in the clinical decisions unit care for patients
staffing levels when they fall below the minimum standard will be put in place Staff appraisal will determine skill set and training needs
Increased leadership investment: Matron for CDU appointed and commencing in post mid-August. Ward sister appointed as secondment for 12 mths to ward 20, enabling the Sister on CDU to focus solely on CDU. Ward staffing numbers publicly displayed. Continual monitoring of CDU nurse staffing by Head of Nursing Appraisal rate above 95%
5c Assurance of adequate nurse staffing on ward 10 LGH
Review of staffing on ward 10 LGH
Chief Nurse (Head of Nursing - RRC)
May 2014 5 Daily review of staffing and staff redeployed according to skill set, activity and dependency Vacancies being recruited to, successful recruitment from Portugal for renal areas. Public displaying of staffing
RRC Quality Board
119
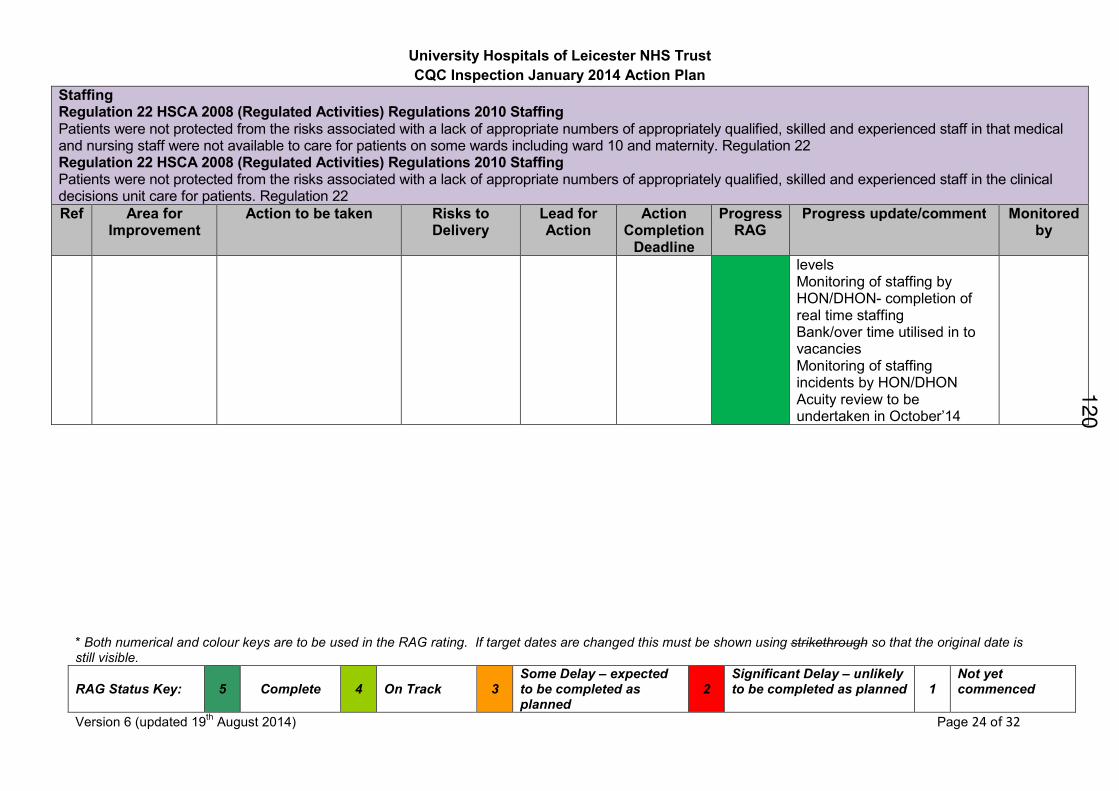
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 24 of 32
Staffing Regulation 22 HSCA 2008 (Regulated Activities) Regulations 2010 Staffing Patients were not protected from the risks associated with a lack of appropriate numbers of appropriately qualified, skilled and experienced staff in that medical and nursing staff were not available to care for patients on some wards including ward 10 and maternity. Regulation 22 Regulation 22 HSCA 2008 (Regulated Activities) Regulations 2010 Staffing Patients were not protected from the risks associated with a lack of appropriate numbers of appropriately qualified, skilled and experienced staff in the clinical decisions unit care for patients. Regulation 22
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment Monitored by
levels Monitoring of staffing by HON/DHON- completion of real time staffing Bank/over time utilised in to vacancies Monitoring of staffing incidents by HON/DHON Acuity review to be undertaken in October’14
120
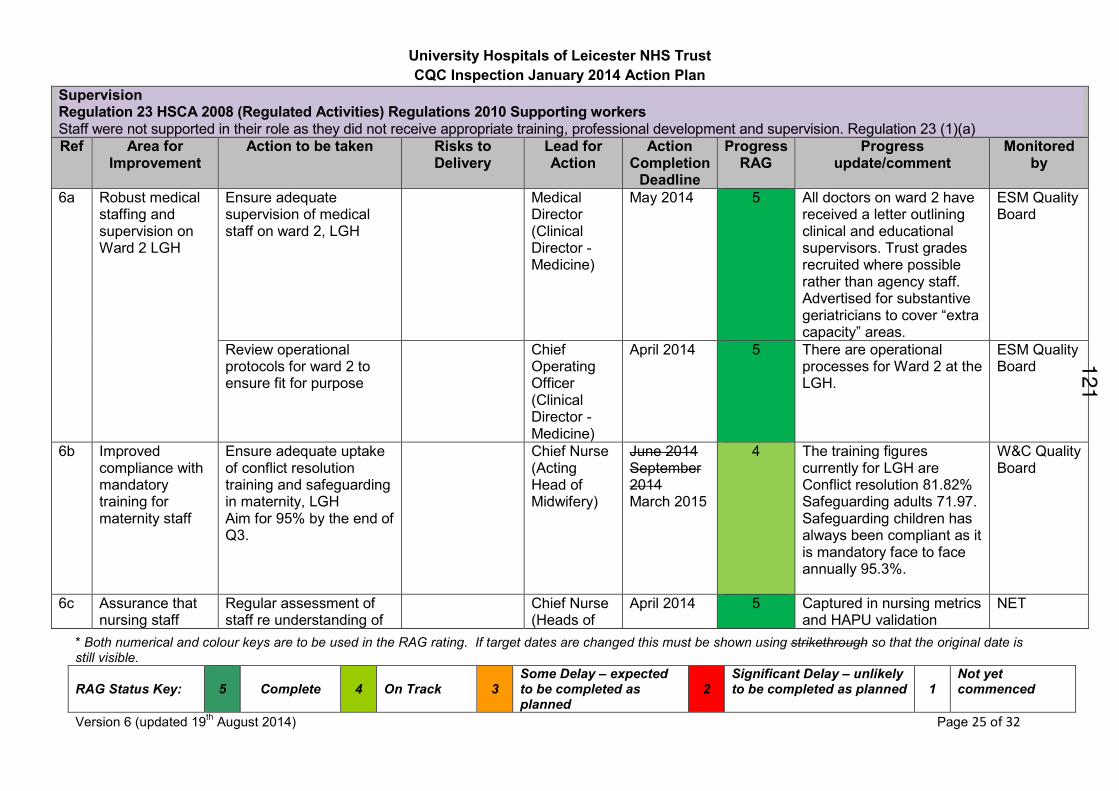
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 25 of 32
Supervision Regulation 23 HSCA 2008 (Regulated Activities) Regulations 2010 Supporting workers Staff were not supported in their role as they did not receive appropriate training, professional development and supervision. Regulation 23 (1)(a)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
6a Robust medical staffing and supervision on Ward 2 LGH
Ensure adequate supervision of medical staff on ward 2, LGH
Medical Director (Clinical Director - Medicine)
May 2014 5 All doctors on ward 2 have received a letter outlining clinical and educational supervisors. Trust grades recruited where possible rather than agency staff. Advertised for substantive geriatricians to cover “extra capacity” areas.
ESM Quality Board
Review operational protocols for ward 2 to ensure fit for purpose
Chief Operating Officer (Clinical Director - Medicine)
April 2014 5 There are operational processes for Ward 2 at the LGH.
ESM Quality Board
6b Improved compliance with mandatory training for maternity staff
Ensure adequate uptake of conflict resolution training and safeguarding in maternity, LGH Aim for 95% by the end of Q3.
Chief Nurse (Acting Head of Midwifery)
June 2014 September 2014 March 2015
4 The training figures currently for LGH are Conflict resolution 81.82% Safeguarding adults 71.97. Safeguarding children has always been compliant as it is mandatory face to face annually 95.3%.
W&C Quality Board
6c Assurance that nursing staff
Regular assessment of staff re understanding of
Chief Nurse (Heads of
April 2014 5 Captured in nursing metrics and HAPU validation
NET
121
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 26 of 32
Supervision Regulation 23 HSCA 2008 (Regulated Activities) Regulations 2010 Supporting workers Staff were not supported in their role as they did not receive appropriate training, professional development and supervision. Regulation 23 (1)(a)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
have had training in assessment of hospital acquired pressure ulcers
waterlow risk assessment through matron ward rounds, nursing metrics and HAPU validation monthly.
Nursing)
6d Assurance that staff are clear regarding training and induction for agency nurses
Ensure staff are clear about training and induction for agency nurses (LGH). Communication via heads of nursing and spot checks.
All agency staff sourced via the staff bank office will have required training; however local induction and orientation to the clinical area must be undertaken locally by the ward area and documented.
Head of Nursing - RTC and Heads of Nursing
May 2014 5 All agency staff sourced via the Staff Bank office, are compliant with all training requirements as legislated by UHL and NHSLA. Update information shared with all Heads of Nursing at Nursing Executive Team. Any concerns with agency staff performance must be escalated to the staff bank office for action. Agency checklist attached for information, which includes UHL specific in relation to safeguarding, and HAPU.
NET
6e Assurance that sufficient staff have had
Training needs analysis of nursing staff on ward 10 (dialysis training)
Chief Nurse (Head of Nursing -
May 2014 5 Complete. RRC Quality Board
122
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 27 of 32
Supervision Regulation 23 HSCA 2008 (Regulated Activities) Regulations 2010 Supporting workers Staff were not supported in their role as they did not receive appropriate training, professional development and supervision. Regulation 23 (1)(a)
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
dialysis training on ward 10 LGH
RRC)
123
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 28 of 32
Care and welfare of people who use services Regulation 9 HSCA 2008 (Regulated Activities) Regulations 2010 Care and welfare of people who use services Patients were not protected from the risk of receiving care that is inappropriate or unsafe because assessments of needs were not always completed.
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
7a To ensure there are robust systems for patients that protect them from the risk of receiving care that is inappropriate or unsafe because assessment of needs not always completed (regulation 9)
Increased audit of discharge lounge at LRI to ensure appropriate admission and assessment of patients including assessment for Hospital Acquired Pressure Ulcers
Chief Operating Officer (Senior Site Manager)
May 2014 5 A robust audit tool in place to ensure all patients are assessed and given on going care. A referral checklist for transfer to discharge lounge is being developed. Recruited new sister and have had input from an established sister at Glenfield.
NET
7b Prompt/appropriate assessment of children admitted
Reiterate appropriate use of CAU and admission of children overnight to beds
Heads of Nursing – W&C
May 2014 5
All staff have been reminded of the importance of not delaying admission to wards Monthly audit of delays through EDIS.
W&C Quality Board
Development of escalation policy for children’s hospital
Heads of Nursing – W&C
June 2014 August 2014
4
Lead Consultant for CAU in process of developing escalation policy. First draft has been proceed.
W&C Quality Board
Review paediatric bed capacity to ensure effective emergency and elective flow supports timely assessment
General Manager – W&C
July 2014 September 2014
3
Bed modelling being undertaken with support from EY team
W&C Quality Board
124
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 29 of 32
Care and welfare of people who use services Regulation 9 HSCA 2008 (Regulated Activities) Regulations 2010 Care and welfare of people who use services Patients were not protected from the risk of receiving care that is inappropriate or unsafe because assessments of needs were not always completed.
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
within the Children’s Hospital.
Regular audit of pain relief of children in all admission areas through monthly nursing metric
Head of Nursing – W&C
May 2014 5
Monthly metrics being undertaken.
W&C Quality Board
7c
Recovery of patients post dental extraction
To undertake an options appraisal to identify most suitable accommodation for recovery after paediatric dental extraction that meets privacy and dignity requirements (and maintains safety)
Presentation of option appraisal to CMG management team and escalation thereafter
Chief Operating Officer (Acting General Manager - ITAPS/ Matron - Theatres)
May 2014 July 2014
5 Option appraisal completed. UHL will need to make the service as nest a fit as it can in the current accommodation whilst new accommodation is sought. Meeting being pulled together.
EQB
Option appraisal presented to Executive Team.
Chief Operating Officer (Acting General Manager - ITAPS/
August 2014 September 2014
3 Discussion at ET on 19th August. Advised to discuss with commissioners and attend ET again in September.
EQB
125
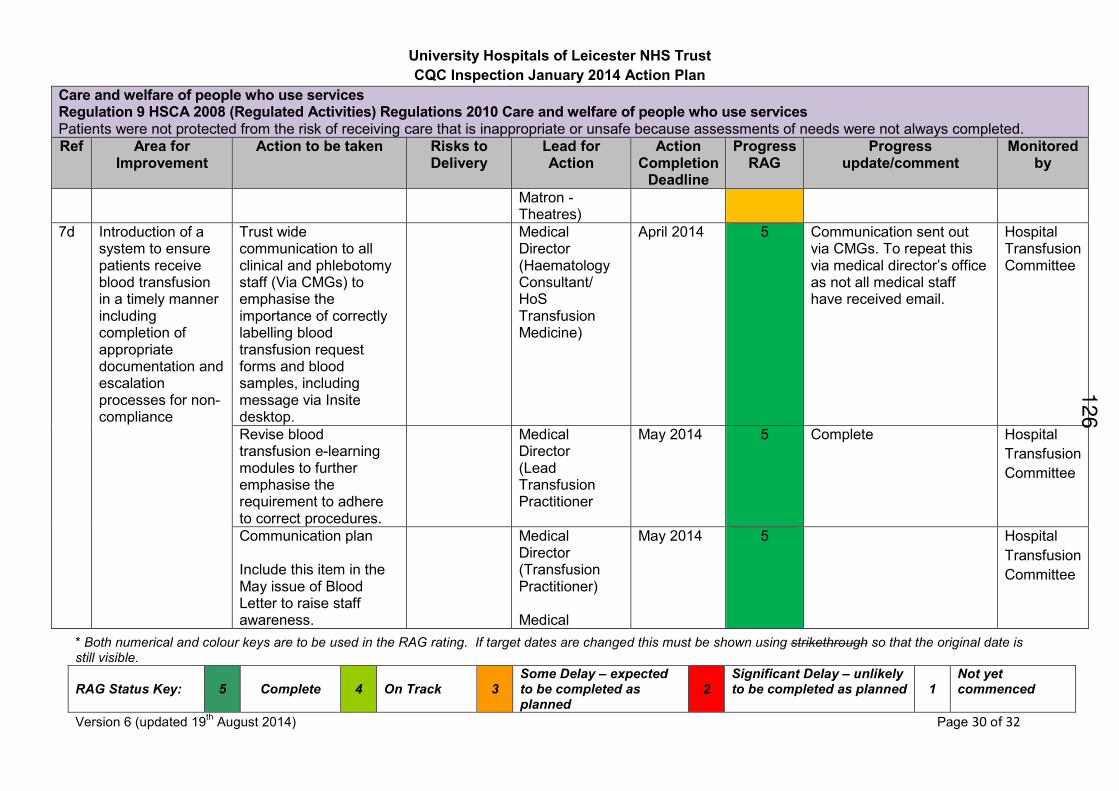
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 30 of 32
Care and welfare of people who use services Regulation 9 HSCA 2008 (Regulated Activities) Regulations 2010 Care and welfare of people who use services Patients were not protected from the risk of receiving care that is inappropriate or unsafe because assessments of needs were not always completed.
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
Matron - Theatres)
7d Introduction of a system to ensure patients receive blood transfusion in a timely manner including completion of appropriate documentation and escalation processes for non-compliance
Trust wide communication to all clinical and phlebotomy staff (Via CMGs) to emphasise the importance of correctly labelling blood transfusion request forms and blood samples, including message via Insite desktop.
Medical Director (Haematology Consultant/ HoS Transfusion Medicine)
April 2014 5 Communication sent out via CMGs. To repeat this via medical director’s office as not all medical staff have received email.
Hospital Transfusion Committee
Revise blood transfusion e-learning modules to further emphasise the requirement to adhere to correct procedures.
Medical Director (Lead Transfusion Practitioner
May 2014
5 Complete Hospital
Transfusion
Committee
Communication plan Include this item in the May issue of Blood Letter to raise staff awareness.
Medical Director (Transfusion Practitioner) Medical
May 2014 5 Hospital
Transfusion
Committee
126
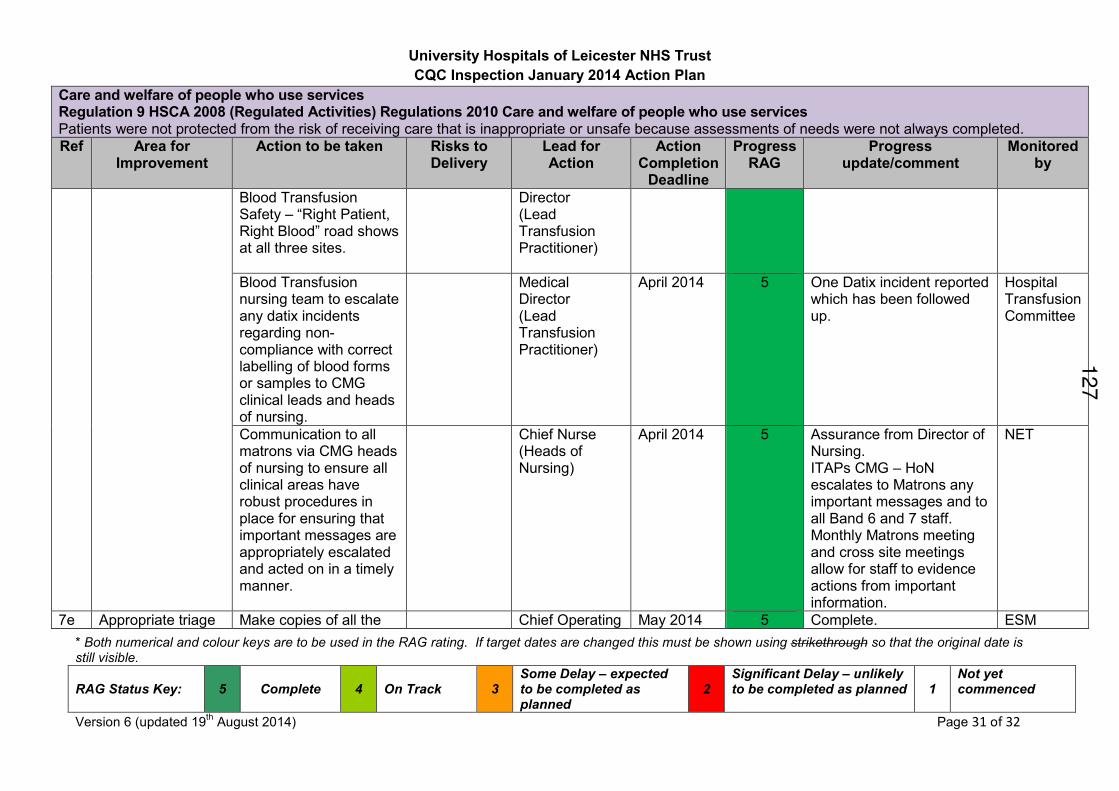
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 31 of 32
Care and welfare of people who use services Regulation 9 HSCA 2008 (Regulated Activities) Regulations 2010 Care and welfare of people who use services Patients were not protected from the risk of receiving care that is inappropriate or unsafe because assessments of needs were not always completed.
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
Blood Transfusion Safety – “Right Patient, Right Blood” road shows at all three sites.
Director (Lead Transfusion Practitioner)
Blood Transfusion nursing team to escalate any datix incidents regarding non-compliance with correct labelling of blood forms or samples to CMG clinical leads and heads of nursing.
Medical Director (Lead Transfusion Practitioner)
April 2014 5 One Datix incident reported which has been followed up.
Hospital Transfusion Committee
Communication to all matrons via CMG heads of nursing to ensure all clinical areas have robust procedures in place for ensuring that important messages are appropriately escalated and acted on in a timely manner.
Chief Nurse (Heads of Nursing)
April 2014 5 Assurance from Director of Nursing. ITAPs CMG – HoN escalates to Matrons any important messages and to all Band 6 and 7 staff. Monthly Matrons meeting and cross site meetings allow for staff to evidence actions from important information.
NET
7e Appropriate triage Make copies of all the Chief Operating May 2014 5 Complete. ESM
127
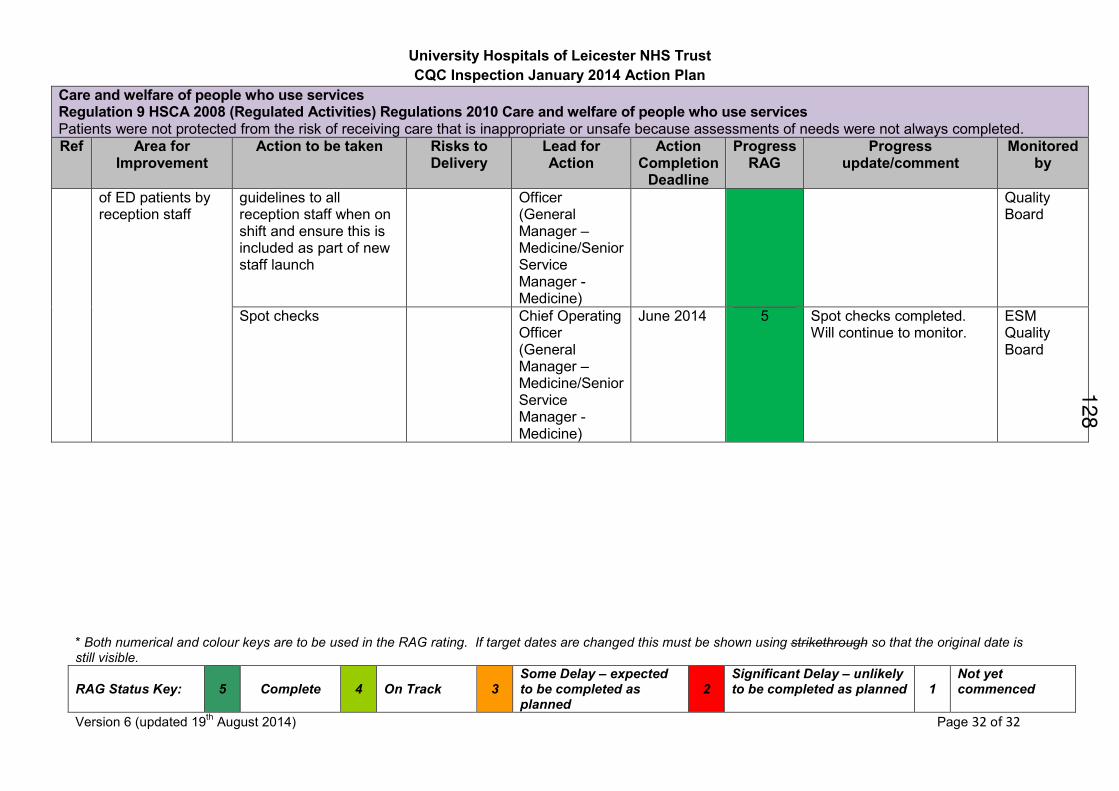
University Hospitals of Leicester NHS Trust
CQC Inspection January 2014 Action Plan
* Both numerical and colour keys are to be used in the RAG rating. If target dates are changed this must be shown using strikethrough so that the original date is still visible.
RAG Status Key:
5
Complete
4
On Track
3
Some Delay – expected to be completed as planned
2
Significant Delay – unlikely to be completed as planned
1
Not yet commenced
Version 6 (updated 19th August 2014) Page 32 of 32
Care and welfare of people who use services Regulation 9 HSCA 2008 (Regulated Activities) Regulations 2010 Care and welfare of people who use services Patients were not protected from the risk of receiving care that is inappropriate or unsafe because assessments of needs were not always completed.
Ref Area for Improvement
Action to be taken Risks to Delivery
Lead for Action
Action Completion
Deadline
Progress RAG
Progress update/comment
Monitored by
of ED patients by reception staff
guidelines to all reception staff when on shift and ensure this is included as part of new staff launch
Officer (General Manager – Medicine/Senior Service Manager - Medicine)
Quality Board
Spot checks Chief Operating Officer (General Manager – Medicine/Senior Service Manager - Medicine)
June 2014 5 Spot checks completed. Will continue to monitor.
ESM Quality Board
128
HEALTH OVERVIEW AND SCRUTINY COMMITTEE: 10 SEPTEMBER 2014
REPORT OF EAST LEICESTERSHIRE AND RUTLAND CCG
ARRIVA TRANSPORT SOLUTIONS LTD (ARRIVA) NON EMERGENCY
PATIENT TRANSPORT SERVICE – PERFORMANCE UPDATE Purpose of report 1. The purpose of this report is to inform the Committee as to Arriva’s progress in
meeting its contractual obligations in providing its Non-Emergency Patient Transport Service (NEPTS) to Leicester, Leicestershire and Rutland (LLR) patients.
Background 2. As a result of considerable recent media exposure concerning a number of negative
patient experiences in relation to the services provided by Arriva the performance of the provider against its contracted targets has been highlighted as a major concern to the health and wellbeing of the patients which rely upon the service.
3. Considerable efforts over the last 12 months have been made by the East Leicestershire and Rutland Clinical Commissioning Group (CCG), who performance manage the contract on behalf of the 3 LLR CCGs and consequently the health care requirements of patient users of the service, to understand the main drivers within the healthcare system which impact on patient transport and promote effective changes where required and to also address those elements of performance which are in the control of Arriva by utilising appropriate provisions and levers in the contract.
4. Arriva is on track to achieve compliance against the main contract targets by the end of October 2014 for those elements of the service where it has control. The CCGs are working with other providers in the health care system which utilise the services which Arriva operate and have a direct impact on its performance so as to make the patient transport service more efficient and provide a more positive patient experience.
5. Further details are provided in the Appendix to this report which is a report setting out performance issues and resolution plans.
Conclusions 6. The initial performance of Arriva against its key performance indicators as detailed in
the contract of July 2012 was unsatisfactory which caused considerable patient disquiet and complaint as well as contractual and financial consequences having to be imposed by the CCG commissioners where Arriva were in control of that performance.
Agenda Item 12129
7. Performance has improved since the beginning of 2014 following a number of measures put in place by Arriva, both managerial and operational, and the Company is on track to meet its main key performance indicators by the end of October 2014.
8. As a result of various ‘deep dive’ consultation/workshop initiatives with other provider/ stakeholders and meetings all instigated by the CCG Contract team it has become patently apparent that a large measure of the issues which involve Arriva with the greatest delays has been caused by ineffective discharge processes by the acute hospitals operated by University Hospitals Leicester. This ties up a large proportion of the fleet and support staff which should be more available during each working day.
Recommendations
9. The Committee is requested to: (a) Note the contents of the report;
(b) Note the steps taken to address performance at Arriva and the further actions being
undertaken by the CCG Contract and Quality team. Officer to Contact Dr David Briggs, Managing Director East Leicestershire and Rutland CCG Telephone: 0116 295 5105 Email: [email protected] List of Appendices Appendix – Report Providing Information as to Performance Issues and Resolution Plans
130
ARRIVA – Non-Emergency Patient Transport Service for Leicester, Leicestershire and Rutland
Report providing information as to Performance Issues and Resolution Plans
Background: 1. In 2012 Leicester City Primary Care Trust (PCT), as lead commissioner on behalf of
Leicester City and Leicestershire County and Rutland PCT’s, re-procured the Non- Emergency Patient Transport Service; this service was previously provided by the East Midlands Ambulance Service (EMAS). The contract was awarded to Arriva Transport Solutions Limited.
2. The contract period is for five years (July – June) with an option to extend by two
years and the financial value for the five years is £26m. 3. The contract has a baseline level of activity based on previous known historic
demand and usage to reflect expected journeys linked to a Points of Care (POC) list as well as an element that allows for journeys not part of the baseline to be undertaken and charged at a different rate over and above the baseline classed as Extra Contractual Journeys (ECJs).
4. Upon the contract being awarded to Arriva via the procurement process
(commencing 1st July 2012) the contract was being managed by Leicester City CCG for the benefit of all 3 LLR CCG’s.
5. With effect from 1st April 2013 the responsibility for the contract and performance
management of this contract transferred to East Leicestershire and Rutland CCG (ELRCCG). The contract was handed over to ELRCCG by LCCCG with a number of known and unresolved on-going issues
Hospital Discharge Issues: 6. During 2014 the CCGs in considering the impact of external factors on the
performance of Arriva established a number of factors which not only impacted on Arriva’s ability to achieve their targets but which have also impacted on the wider Urgent Care Service as follows: - Increase in activity at the Front Door of A&E. - The low level of discharges from the UHL discharge lounge and an increase
in discharges from wards requiring extra time to collect patients from wards, approximately two thirds of patients are being discharged from the wards and not the discharge lounge.
- The low level of discharges that are planned - currently only 20% which equates to approximately 250 journeys out of an average monthly discharge total of 1,250.
- The increase in discharges booked on the day - currently 80% which equates to approximately 1,000 journeys out of an average monthly discharge total of 1,250. Table 2 demonstrates by hour when discharges are being undertaken and clearly shows that very little activity takes place early in the day with a peak between the hours of 11am and 6pm.
APPENDIX 131
- The increase in levels of mobility, specifically a marked increase in requests for stretchers. The planned level of stretchers and actual requests are detailed at table 1.
- Inappropriate booking of stretchers and two man support wheelchairs when a lower level of mobility support (both vehicular and staffing) would have been sufficient.
- The cut off times for entry into Nursing/Care Homes, between 5pm and 7pm which is dictated by the nursing staff working hours and if not met (especially on a Friday evening means a re-bed over the whole weekend).
- The cut off times for entry into Community Hospitals approximately 9pm with the same effect as for the nursing homes.
- The level of cancelled and aborted journeys which range from between 10% – 20% aborted journeys and 15% - 30% cancelled journeys on an average month.
- Patients that are booked ready but are still awaiting the medication. (TTO’s) which means they are waiting many hours after notified release times before being able to be transported with vehicles and staff waiting outside. Arriva have advised that approximately 25% of discharges are delayed by over 10 minutes and that of those 80 – 85% are due to patients waiting for their medication.
Discharge Effects on Social and Adult Care Partners: 7. The hospital discharge issues detailed above has an obvious negative impact on
the services which are provided by the Local Authorities in having to provide extra unplanned support and services when patient transfers do not happen when planned and expected and rebidding of patients is required. This is a waste of time and resources, which also causes unwelcome amounts of anxiety to patients, their families and other care providers.
8. The contract with Arriva has a range of Key Performance Indicators built in to
enable effective monitoring of expected standards for this service. In addition there are penalty clauses for non-achievement of KPI’s at 1.5% of the annual contract value and an incentive payment linked to a year on year reduction of the aborted journeys. The KPI’s that were not achieved in years one and two have had penalties applied. In addition, two Contract Queries have been issued which reflect the Quality Concerns below:
• Patients within a 10 mile radius of the point of care will spend no longer than 60 minutes on the vehicle.
• Patients within a 10 – 35 mile radius of the point of care will spend no longer than 90 minutes on the vehicle.
• Patients within a 35 – 80 mile radius of the point of care will spend no longer than 120 minutes on the vehicle.
• Patients shall arrive within 60 minutes prior to their appointment/zone time at the appropriate point of care.
• Outpatient Return patients shall be collected within 60 minutes of request or agreed transport/or zone time.
132
• Discharge patients shall be collected within 120 minutes of request or agreed transport/or zone time.
• Arrival 30 minutes before appointment.
• Arrival before appointment.
• 30 minute travel time inwards/outbound.
• Departure after treatment (booked ready 30 minutes). 9. As a result a comprehensive Remedial Action Plan was put in place by Arriva and
approved by the CCGs which was monitored and managed until all required actions had been satisfactorily undertaken.
Contract Performance Management Key issues: 10. Two Contract Queries for Performance and Quality targets not being met were
issued. 11. Reporting issues were also identified, both contractual performance data reporting
and the indicators for quality compliance. Arriva have undertaken a number of data cleansing exercises and the commissioners now have improved confidence in their data and validation processes. In addition there were concerns with regards to the level of expertise of the Arriva performance management team, highlighted by the level of support that was required by them from the CCG Contract and Quality teams on a monthly basis including ensuring that an appropriate Remedial Action Plan was provided; in order to address this Arriva have restructured and appointed a new team of managers.
12. Following scrutiny and by working with both the Provider, partner CCG’s and
other stakeholders it has been established that the original procurement documents did not fully quantify the requirements of this service. This had a major negative effect on Arriva establishing the correct vehicle fleet and support staff required to meet patient needs.
2014 Situation: 13. An unannounced Quality Visit was undertaken on the 24 March 2014 at which
further evidence of on-going concerns in relation to complaints and incident reporting were found resulting in the CCG Quality leads agreeing a half day workshop with the provider which focused on supporting Arriva to deliver the Remedial Action Plan, to improve their reporting and to ensure they are able to provide appropriate evidence.
14. Concerns were raised with CCG Performance and Collaborative Commissioning Boards with regards to Arriva’s ability to meet the requirements of the contract as well as the Remedial Action Plan, however further detailed work with Arriva has been undertaken and a better understanding of the complexities of the actual demands on this service is now known, which has resulted in an adjustment to the defined complexity requirements that accurately reflect the mix of patient needs and
133
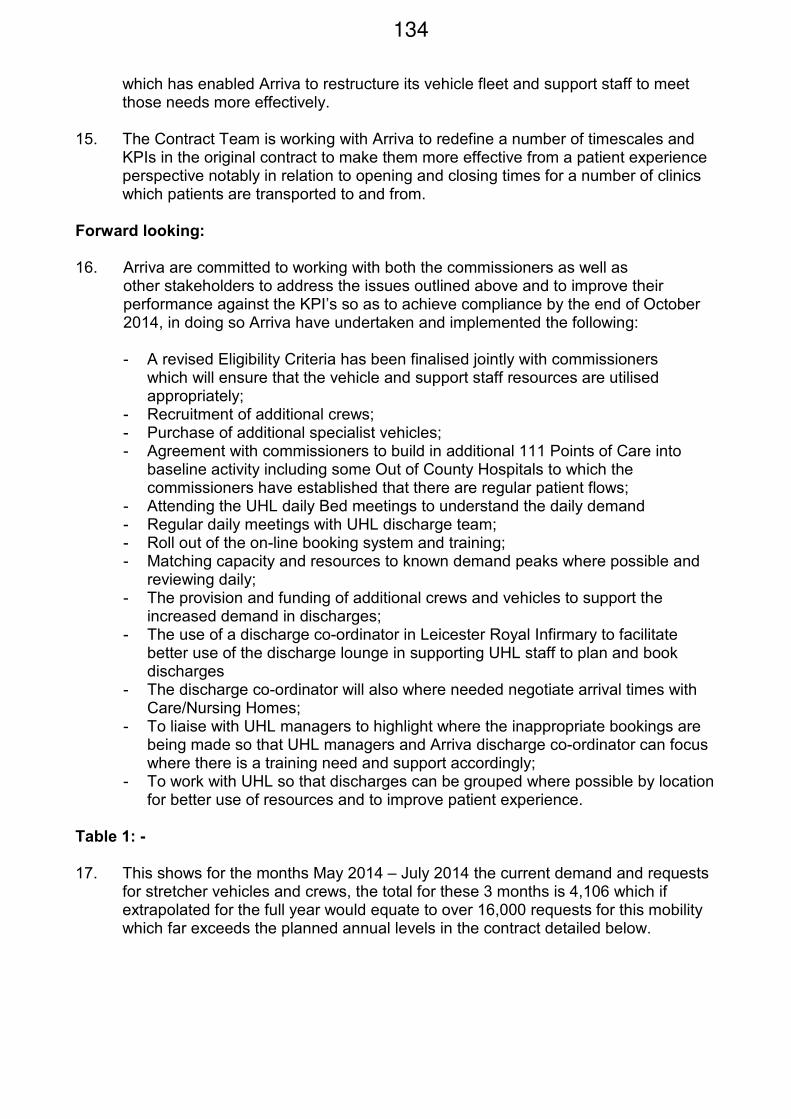
which has enabled Arriva to restructure its vehicle fleet and support staff to meet those needs more effectively.
15. The Contract Team is working with Arriva to redefine a number of timescales and
KPIs in the original contract to make them more effective from a patient experience perspective notably in relation to opening and closing times for a number of clinics which patients are transported to and from.
Forward looking: 16. Arriva are committed to working with both the commissioners as well as
other stakeholders to address the issues outlined above and to improve their performance against the KPI’s so as to achieve compliance by the end of October 2014, in doing so Arriva have undertaken and implemented the following:
- A revised Eligibility Criteria has been finalised jointly with commissioners
which will ensure that the vehicle and support staff resources are utilised appropriately;
- Recruitment of additional crews; - Purchase of additional specialist vehicles; - Agreement with commissioners to build in additional 111 Points of Care into
baseline activity including some Out of County Hospitals to which the commissioners have established that there are regular patient flows;
- Attending the UHL daily Bed meetings to understand the daily demand - Regular daily meetings with UHL discharge team; - Roll out of the on-line booking system and training; - Matching capacity and resources to known demand peaks where possible and
reviewing daily; - The provision and funding of additional crews and vehicles to support the
increased demand in discharges; - The use of a discharge co-ordinator in Leicester Royal Infirmary to facilitate
better use of the discharge lounge in supporting UHL staff to plan and book discharges
- The discharge co-ordinator will also where needed negotiate arrival times with Care/Nursing Homes;
- To liaise with UHL managers to highlight where the inappropriate bookings are being made so that UHL managers and Arriva discharge co-ordinator can focus where there is a training need and support accordingly;
- To work with UHL so that discharges can be grouped where possible by location for better use of resources and to improve patient experience.
Table 1: - 17. This shows for the months May 2014 – July 2014 the current demand and requests
for stretcher vehicles and crews, the total for these 3 months is 4,106 which if extrapolated for the full year would equate to over 16,000 requests for this mobility which far exceeds the planned annual levels in the contract detailed below.
134
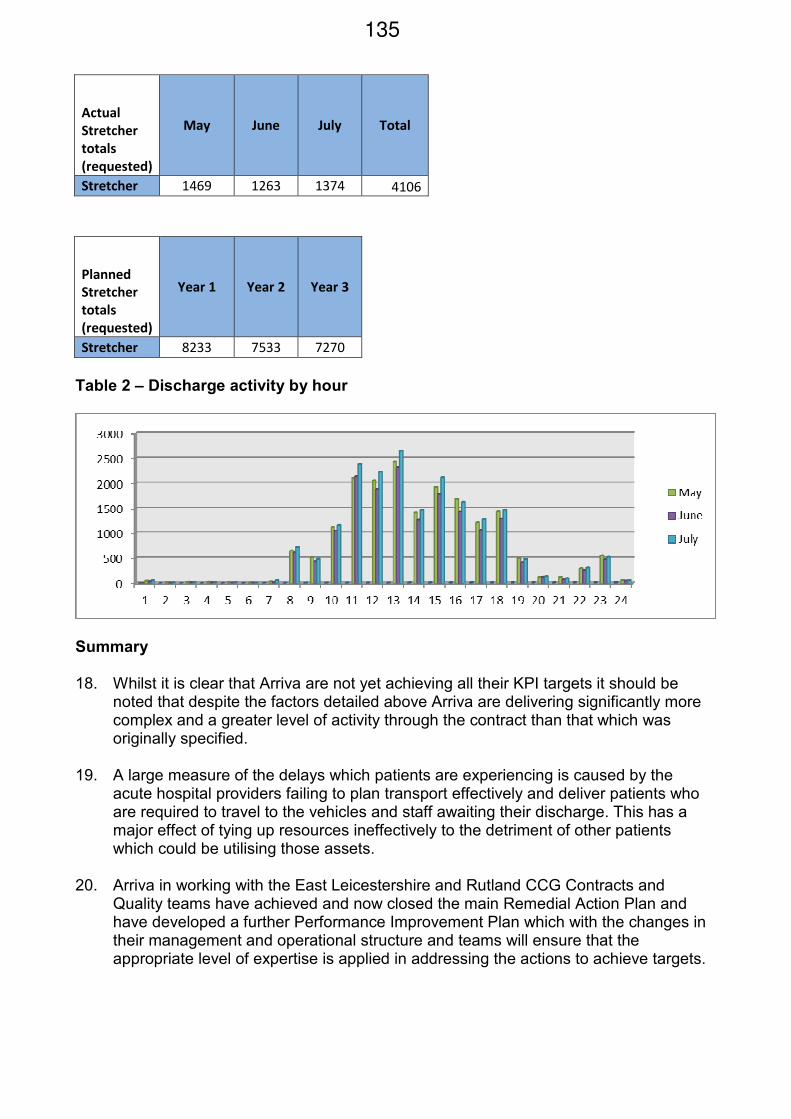
Actual
Stretcher
totals
(requested)
May June July Total
Stretcher 1469 1263 1374 4106
Planned
Stretcher
totals
(requested)
Year 1 Year 2 Year 3
Stretcher 8233 7533 7270
Table 2 – Discharge activity by hour
Summary
18. Whilst it is clear that Arriva are not yet achieving all their KPI targets it should be
noted that despite the factors detailed above Arriva are delivering significantly more complex and a greater level of activity through the contract than that which was originally specified.
19. A large measure of the delays which patients are experiencing is caused by the
acute hospital providers failing to plan transport effectively and deliver patients who are required to travel to the vehicles and staff awaiting their discharge. This has a major effect of tying up resources ineffectively to the detriment of other patients which could be utilising those assets.
20. Arriva in working with the East Leicestershire and Rutland CCG Contracts and
Quality teams have achieved and now closed the main Remedial Action Plan and have developed a further Performance Improvement Plan which with the changes in their management and operational structure and teams will ensure that the appropriate level of expertise is applied in addressing the actions to achieve targets.
135
21. The Committee is requested to note:
• The continued failures across the contract defined KPI’s, Performance and Quality;
• The provision and subsequent sign off of the Remedial Action Plan dealing formally with required actions to address performance issues;
• The provision of the Performance Improvement Plan;
• The other factors affecting this service that are outside of Arriva’s control and their impact on delivery;
• The provision of additional resources by Arriva;
• The restructure of the Arriva Management and Operational team;
• The recent improvements in delivery;
• The issues across Urgent Care that are impacting on this service including the increase in demand and the inefficiencies of other providers processes;
• The issues with discharges that are outside the control of Arriva;
• The provision of a discharge co-ordinator into Leicester Royal Infirmary and the restructuring and increases in the vehicle fleet and support staff to deal with changes in complexity of patient need;
• The further actions being undertaken by the CCG Contract and Quality team.
136
Related Documents











