TEE RELATSVITY OF SOCIAL CONSTRUCTION: TûWARDS A CONSULTATIVE APPROACH TO UNDERSTANDING HEALTH, ILLNESS AND DISEASE Todd Onam Smith A thesis submitted in conformity with the requirements for the degree of Ph. D. Graduate Department of Community Health University of Toronto @ Copyright by Todd Onan Smith (1997)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
TEE RELATSVITY OF SOCIAL CONSTRUCTION: TûWARDS A CONSULTATIVE APPROACH TO UNDERSTANDING
HEALTH, ILLNESS AND DISEASE
Todd Onam Smith
A thesis submitted in conformity with the requirements for the degree of Ph. D.
Graduate Department of Community Health University of Toronto
@ Copyright by Todd Onan Smith (1997)
National Library 191 of Canada Bibliothkque nationale du Canada
Acquisitions and Acquisitions et Bibliographic Services services bibliographiques
395 Wellington Street 395. rue Wellington Ottawa ON K1A ON4 OttawaON KIAON4 Canada Canada
The author has granted a non- exclusive licence aüowing the National Library of Canada to reproduce, loan, distribute or sell copies of this thesis in rnicrofom, paper or electronic formats.
The author retains ownership of the copyright in this thesis. Neither the thesis nor substantîal extracts *om it may be p ~ t e d or otherwise reproduced without the author's permission.
L'auteur a accordé une licence non exclusive permettant a la Bibliothèque nationale du Canada de reproduire, prêter, distribuer ou vendre des copies de cette thèse sous la forme de microfichelfi, de reproduction sur papier ou sur format électronique.
L'auteur conserve la propriété du droit d'auteur qui protège cette thèse. Ni la thèse ni des extraits substantiels de celle-ci ne doivent être imprimés ou autrement reproduits sans son autorisation.
ABSTRACT
CONSTRUCTION : THE SOCIAL
TOWARDS A CONSIJLTATIVE APPROACH TO UNDERSTANDING
HEALTH, ILLNESS AND DISEASE
Todd Smith, Ph-D. (1997)
Department of Community Health
University of Toronto
This dissertation constitutes a first step in the development
of what 1 am calling the consultative approach to understanding
health, illness and disease. It primary concern is to outline a
rationale for, and delineate the theoretical tools to help think
about, the relativity of the social construction of disease.
Particular emphasis is placed on the medical construction of
disease, and how medicine constructs some diseases more than it
does others. To this end, a preliminary typology is suggested p p p p p p - - - - - - - - -
for "mapping" the degree topwhich di£ f erent diseases are
constructed. This has implications for the social
constructionist position, and what is referred to more broadly
as horizontalism, because it suggests that medicine, while
certainly constructing diseases, may also be getting at certain
(many) diseases for more or less what they are. It also has
consequences for verticalism - an epistemological and
ontological orientation inforrning rnuch of current biomedicine -
because it challenges, along w i t h social constructionism, the
idea that medicine, or any paradigmatic orientation for that
matter, has special access to the "real" workings of the body.
Finally, various philosophical implications that follow £rom the
relativity of the social construction of disease are discussed.
As 1 see it, developing the consultative approach involves t w o
major projects. The first is to demonstrate the utility of
meaningful interparadigmatic collaboration for achieving better
understanding of disease (and reality, more generally). The
second is to establish the power of a particular communicative
process termed "consultation" for achieving such collaboration.
While, for the most part, 1 leave these two projects for
subsequent study, this dissertation lays the theoretical
foundation for the first. I Say this because, if different
paradigms can (at least potentially) see and penetrate into
(aspects of) reality (or disease, more specifically), then there
is utility, theoretically speaking, in fostering meaningful
interparadigmatic collaboration. And as discussed, different
paradigms (such as medicine and social constructionisrn, as
discussed herein), can indeed (at least potentially s o ) , see and
penetrate. This is confirmed by the relativity of the social
construction of reality (of disease) .
III

1 am privileged to have worked under the guidance of Robin
Badgley. Robin opened the door to the intellectual journey 1
have begun with this dissertation, a journey that both
celebrates and seeks to unify diversity. He was very receptive
to my work and yet extremely penetrating in his analysis of it.
As such, he gave coherent direction to my ideas. He was also
encouraging . Indeed, he was empowering, releasing the potential
within me to academically produce in ways 1 had never produced
before.
1 am similarly grateful to the two other full-time members of
my cortunittee, Ann Robertson and Joan Eakin who, while in many
ways responsive to my ideas, were also helpfully critical of
them. I am grateful to Ann for continuously challenging me to
delve more and more deeply into fundamental thernes, and to Joan
for highlighting issues 1 would have otherwise taken for
granted. 1 am also thankful to them for having prevented me
from t a k i n g on too much while concurrently allowing me
sufficient latitude to explore what 1 conslder to be certain
novelties.
1 would also like to mention Dorothy Pawluch, David Locker and
David Coburn who were al1 present at my defense and who each
raised issues that warrant rnuch attention. Future developments
of this study are bound to reflect their valuable input.
1 am particularly indebted to my family. My father David
Smith and mother Meim Smith, rny father-in-law Pat Lord and
mother-in-law Jean Lord, my two brothers Darron and Brett and
their wives Deb and Maureen, my grandmother Peggy Breckenridge,
and many other members of my family, were al1 so supportive both
emotionally and intellectually, and in some cases, financially.
I've found that writing a dissertation af te r years of

undergraduate and graduate work, is nothing less than an ordeal
for the writer. It is similarly an ordeal for those closest to
him (or ber, as the case rnay be) . There is an overwhelming
tendency amongst everyone to wonder when it will finally be
finished. Happily, my family did not allow that tendency to
overshadow the value they saw in me writing it.
To my dear wife Sandy, and my two boys Grayden and Connor, 1
give special thanks. Of everyone, Sandy was most acutely aware
of rny struggle to finish this dissertation. She was also most
supportive in times of stress. Her input, moreover, was no less
a source of support and inspiration. And as for my boys, who
had no clue about what 1 was doing, they enlivened me by simply
being around.
Finally, 1 want to thank my many friends who took the time to
read my dissertation or sections thereof, to provide me with
feedback, and/or to inspire me in some way. Among them is Ms.
Brenda Radford. One of my intentions for this thesis was to
break with traditional academic writing. Brenda helped me to do
just that. Others include Michael Dragornan, Peter Tamas,
Jonathan Menon, Andrea Robarts, Dan Jaciw and Duncan Hanks.

TABLE OF CONTENTS
m m D m m S ................................................. IV
TABLE OF CONTENTS .............................................. VI
LIST OF TABLES .................................................. X
LIST OF FIGURES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XI
CHAPmR 1: INTRODUCTION ......................................... 1 OBJECTIVE ....................................................... 1
S t a t e d Br ie f ly : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 M y Specific Concern . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . In Response to "So What?" 3
INTRODUCTION: CONTEXT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
VERTICAL VERSUS HORIZONTAL APPROACHES TO REALITY . . . . . . . . . . . . . . . 12 . . . . . . . . . . . . . . THE CONSULTATIVE APPROACH: SOME B A S I C ASSUMPTIONS 1 8
U n i t y in Diversity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Consultation and Seeing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 3
. . . . . . . . . . . . . . . . . . . . . . . . . In Short (see Table 1 f o r a summary) 28
SUMMARY OF PURPOSE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . CHAPTER OUTLINE 32
THE IRONY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33 SOME DEFINITIONS ................................................. 33
Illness and Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33 Medicine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Regarding Truth .............................................. 3 5
JOURNEY NOTES .................................................. 39
INTRODUCTION ................................................. 40
SCIENTISM AS VERTICALISM ....................................... 48 ....................................... MEDICINE AND VERTICALISM 53
Medicine and Naturalist Ontology and Cosmology . . . . . . . . . . . . . . . 53 Medicine and Naturalist Epistemology ......................... 55 In Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 6
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . VERTICALISM: ONE FINAL EXAMPLE 56
JOURNEY NOTES .................................................. 61 INTRODUCTION .............................................. 62
THE AMBIGUITY OF THINGS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
SO much . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71 THE SOCIAL CONSTRUCTION OF THINGS .............................. 71 Nietzsche .................................................... 71 Rorty ........................................................ 73
................................ Reality as a social construct 78
. . . . . . . . . . . . . . . . . . . . . . The Medical Mode1 as a Social Construct 8 1
Health, Illness and Disease as Metaphors . . . . . . . . . . . . . . . . . . . . . 8 3
SOCIAL CONSTRUCTION, POWER AND MEDICINE . . . . . . . . . . . . . . . . . . . . . . . . 86 Medicalization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89 Foucault . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
IN CONCLUSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100 CHAPTER 4 : THE RELATIVTTY OF SOCIAL CONSTRUCTION : THEORY PART 1
J O W E Y NOTES ................................................. 107
INTRODUCTION ................................................... 109
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . THE OMNIPOTENT SOCIAL? 114
THE RELATIVITY OF SOCIAL CONSTRUCTION . . . . . . . . . . . . . . . . . . . . . . . . . 122
REALITY AS CONSTRAINT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 125
The Body as Constraint ...................................... 129

The Impact of Phenomenal Tangibility ...................... ..,1 33 Revisiting the Paradi gm ..................................... 136 Meanings. Seeing and Constructing .......,.......... ......... 143
TANGIBILITY TYPES ............................................. 146 General Tangibility ......................................... 147 Anomalic Tangibility ........................................ 148 Fabricated Tangibility ................................... 149
Specified Tangibility ...................................... -150
Reality and the Relativity of Social Construction . . . . . . . . . . . 152 Finally . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155
SOME ADDITIONAL THOUGHTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155 The Relativity of Relativity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . -155 Unity Amidst the Diversity .................................. 158
CHAPTER 5 : PARADIGMATIC ARTICULATION. EXTENSION AND
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . INTENSIFICATION: TEEORY PART II 163
JOURNEY NOTES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163 INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 166 THE DRIVE TO PARADIGMATICALLY ARTICULATE ...................... 167 Introduction .................................................. 167
The Universal Drive to Construct . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167 Rationalization and Medicalization . . . . . . . . . . . . . . . . . . . . . . . . . . 174 TO Summarize . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 178
THE DUALITY OF PARADIGMATIC ARTICULATION . . . . . . . . . . . . . . . . . . . . . . 179 Paradigmatic Extension . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . - 1 8 1
Paradigrnatic Intensification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 187 Proactive Intensification and Education . . . . . . . . . . . . . . . . . . . . . 193 Extension, Intensification and Anomaly . . . . . . . . . . . . . . . . . . . . . . 194
PAFWDIGMATIC ARTICULATION AND THE CONSTRUCTION O F . . . . . . . . . . . . . 196 SOME FINAL THOUGHTS CONCERNING PARADIGMS AND THEIR PROCESSES .. 198 CEAPTER 6 : MAPPING THE RELATIVITY OF TEiE SOCIAL CONSTRUCTION OF
DIS-E ....................................................... 205
JOURNEY NOTES ................................................. 205
INTRODUCTION .................................................. 207
The Issue ................................................... 207 Tools for Thinking about the Relativity of Social Construc . . . 208
Things Remember
SOCIALLY-CONCEIVED-DISEASES ...... Introduction ................................................ 221 Hysteria ................................................... .222
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 254 AIDS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 255
SOCIALLY-AUGMENTED-DISEASES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 263 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 263
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Certain Infectious Diseases 264
HENCE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 276
CEAPTER 7 : KNOWING AND NOT KNawING ïN DZVERSITY . . . . . . . . . . . . . . . 284
J O W E Y NOTES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284 INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 285 UNIFYING THE CONCEPTUAL DIVERSITY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 285 ASSESSING THE TYPOLOGY ........................................ 290 IMPLICATIONS: TOWARDS THE UTILITY OF INTERPARADIGMATIC
COLLABOMTION ................................................. 306 INTERPARADIGMATIC COLLABORATION BETWEEN MEDICINE AND SOCIAL
... CONSTRUCTIONISM. ......................................... 312
In Summary .................................................. 314 SOME PHILOSOPHICAL IMPLICATIONS - IN BRIEF .................... 315 The Question of Eternal Questions ........................... 317 The Issue of Representation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 318
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Truth, Chess and Consultation 323
REFERENCES .................................................... 337
LIST OF TABLES
Table 1. Summary of assumptions as distinguished between the
verticalist, horizontalist and consu l t a t i ve approaches ............... 29
Table 2 . Matching the concepts with the categories of
disease ............................................................................................................................................................ 2 8 6

LIST OF FIGURES
Figure 1: The r e l a t i v i t y of the social construction of
......................................................................................................................................................... phenornena 13 7
Figure 2: The relativity of the r e l a t i v i t y of t he social
......................................................................................................... construction of phenornena 1 5 7
- -
INTRODUCTION
OBJECTIVE
S t a t e d Briefly :
The o b j e c t i v e of t h i s book is t o begin developing what I am
c a l l i n g t h e consultative approach t o understanding h e a l t h ,
i l l n e s s and d i sease . The c o n s u l t a t i v e approach i s con t r a s t ed to
what a r e r e f e r r e d t o as t h e verticalist approach and the
horizontalist approach. ' Broadly speaking, by verticalism i s meant an epis temologica l
and on to log i ca l o r i e n t a t i o n t h a t holds t h a t t r u t h of t h i n g s i s
acce s s ib l e , t h a t r e a l i t y i s pene t r ab l e , but t h a t i t i s so only
v i a c e r t a i n ways and by c e r t a i n i n v e s t i g a t i v e communities. That
is: some can see t h e way t h i n g s are while o t h e r s rnay see th ings
more d i s t o r t e d l y , whi le ye t o t h e r s may not r e a l l y see t h ings a t
a l l . Science and medicine a r e v e r t i c a l i s t i n t h i s s ense
(al though, as d i scussed l a t e r , t h e r e are q u a l i f i c a t i o n s t o
cons ider) . By horizontalism i s meant t h e ep i s t emolog ica l and on to log i ca l
o r i e n t a t i o n t h a t the truth of t h i n g s i s i nacce s s ib l e , and more
r a d i c a l l y , t h a t t h e r e r e a l l y i s n f t any t r u t h "out there" t o
access anyway. I n f a c t , t r u t h , i f anything, i s t r u t h
cons t ruc ted . And so i t r epud i a t e s t h e v e r t i c a l i s t tendency t o
champion c e r t a i n approaches t o r e a l i t y ( l i k e sc ience and
medicine) over o the r s . Soc i a l cons t ruc t ionis rn i s ve ry much
h o r i z o n t a l i s t i n t h i s sense (a l though , a s d i scussed l a t e r , t h e r e
a r e q u a l i f i c a t i o n s t o c o n s i d e r ) .
T h e consu l t a t i ve approach d i f f e r s from bo th t h e v e r t i c a l i s t
and h o r i z o n t a l i s t p o s i t i o n s whi le r e t a i n i n g elements from each.
I t r e j e c t s , along with t h e h o r i z o n t a l i s t , t h e v e r t i c a l i s t
p r e d i l e c t i o n t o exclude c e r t a i n approaches whi le championing

others. It, moreover, shares with the horizontalist a profound
recognition for the socially constructed nature of truth. There
is definitely made truth. We definitely construct truth, reify
it, internalize it and reconstruct it.
Yet, according to the consultative approach, not al1 truths
are constructed truths. With the verticalist position it holds
there is truth "out there" to be known. And like the
verticalist position, it holds we have the potential to approach
- if not to thoroughly penetrate - such truth. We have the
potential to approach - if not to thoroughly penetrate - for example, the way things are with health, illness and disease.
But, the consultationist goes on to Say - and this is the
crucial point - that this potential is not something unique to
any one paradigmatic approach. Instead, it pervades (perhaps in
varying degrees) our paradigmatic diversity. There is,
therefore, tremendous utility in looking to this diversity,
indeed, in facilitating an atmosphere of meaningful
interparadigmatic collaboration. There is tremendous utility in
meaningfully tapping this diversity in order to release the
wealth of possibility to know.
The consultationist, rnoreover, goes on to suggest a par t i cu la r
method for facilitating such interparadigmatic collaboration. To
this end, s/he champions a communicative process termed
consultation.
There are, therefore, two major pro jects involved in
delineating the consultative approach as 1 see it. The first is
to demonstrate the utility of meaningful interparadigmatic
collaboration for achieving better understandings of - for
penetrating more deeply into - reality. The second is to
demonstrate the power of the communicative process of
consul ta tion for facilitat ing meaningf ul interparadigmatic
collaboration so that more adequate understandings of reality
can be achieved.
My Specif ic Concern . . . . . . in this book is to begin the first project. More
precisely, it is to outline the theoretical rationale for taking
the utility of meaningful interparadigmatic collaboration
seriously. My premise is that the utility of interparadigmatic
collaboration stems from the possibility that we (relatively)
see, in al1 our diversity, (perhaps different) things about
reality, about truth. The possibility of seeing, of penetrating
reality as it is, therefore, needs to be established. This, 1
maintain, is accomplished through demonstrating the validity of
the daim: some t h i n g s are more s o c i a l l y c o n s t r u c t e d than
o t h e r s . Taking disease as my focus, my central objective, therefore,
to:
demonstrate the r e l a t i v i t y of t h e s o c i a l ,
medical cons t ruc t ion o f d i s e a s e .
is, moreover, to
and i n p a r t i c u l a r ,
explore the epis temologica l and o n t o l o g i c a l r a m i f i c a t i o n s tha t
follow £rom the r e l a t i v i t y of the social ( m e d i c a l )
c o n s t r u c t i o n of disease.
so doing, and as a particular case study, 1 aim to provide a
t h e o r e t i c a l ra t i o n a l e for the utility of f ostering
interparadigmatic collaboration between medicine and social
constructionism. To actually demonstrate such utility, thus
completing the first project, 1 leave for subsequent research.
In Response to "So What?"
The point behind developing the consultative approach, of
which this book is a first step, boils down to one thing: to
create a more adequate approach for preventing and allevia t i n g
suffering.
The premise is that much suffering is a consequence of, and is
sustained and/or exacerbated by, the imposition of certain
concepts of health, illness and disease, concepts that are
alienating to many, hence inappropriate to the sufferings of
many, hence, inadequate to the alleviation of the sufferings of
many. They are, moreover, inadequate to the seeing of certain
diseases. They do not "get at" those diseases as they really
are.
The problem of alienation is something of which social
constructionism is only too conscious. By defining our bodies
in certain ways, by propounding certain models of disease, by
systematically ignoring or qualifying certain complaints in ways
that conform to its own paradigmatic approach to health, illness
and disease, biomedicine is engaged in the process of
constructing a reality that is, in many ways, oppressive. And
yet, ironically, social constwuctionism is prone to the same
criticisrn. As will be discussed: in its analysis of the
deficiencies of medicine, in its depiction of medicine as a
social arrangement that dominates today; that gets at nothing
foundational - nothing essential about disease nor the workings of the natural in general - despite its claims; that imposes
such nonessentialities on the rest of us, either intentionally
or not; that is, by systernatically repudiating medicine in these
ways, social constructinnism is constructing its own version of
what health, illness and disease are, wittingly or not. It is
itself constructing a reality, a reality, moreover, that
excludes, that imposes, that subjugates, that alienates.
But what if both medicine and social constructionism, despite
their deficiencies, despite their constructions, are hitting
upon certain truths? What if both have something of value to
say about health, illness and disease? What if both see certain
things about the way reality is, about the way certain diseases
are?
(And the p o i n t o f t h i s s t u d y is t o d e m o n s t r a t e the very p o s s i b i l i t y that both d o ! )
Then it would seem advantageous for each to look to the other to
see what it can offer. Then it would seem their meaningful
interparadigmatic interaction would be most beneficial. For
such interaction can only lead to better understandings of
health, illness and disease, and hence better understandings on
how to reduce suffering.
In short (and not limiting things to the relationship between
medicine and social constructionism) :
T h e p o i n t of the c o n s u l t a t i v e approach is to d e m o n s t r a t e the
u t i l i t y o f m e a n i n g f u l i n t e r p a r a d i g m a tic c o l l a b o r a t i o n achieved
through a particular c o m m u n i c a t i v e p r o c e s s t e r m e d
c o n s u l t a t i o n . Through consul t a t i o n , paradigma t i c d i v e r s i t y i s
t apped , more adequate u n d e r s t a n d i n g s o f health, i l l n e s s and
d i s e a s e a r e achieved, a l i e n a t i o n is r e d u c e d , and c o n s e q u s n tly,
s u f f e r i n g is a l l e v i a t e d .
INTRODUCTION: CONTEXT
Now to flesh things out a bit.
In particular, what 1 want to do is outline some of the issues
and major convictions informing this study. Foremost among my
convictions is the principle of unity in diversity as outlined
by Baha'u'llah.
To begin, let me pose a few observational questions:
First, why is it that we have such a systematic need to
envelop ourselves in particular ways of thinking? Second, why
is it that we feel such a pressing need to hold on to and
perpetuate these ways of thinking? Third, why are we so
interested in disassociating ourselves from other ways of

thinking and attacking them by incessantly mining for and
exposing their deficiencies? These are not idle questions;
indeed, they address a reality that continues to permeate our
society at many levels. Think of the masses of students who
enter universities, are exposed to a variety of theoretical
views in a given area, and then find themselves latching ont0
one while devoting their lives to lambasting the others. Think
of party politics: can you recall a time when one party has
officially said of another party's position 'What a great idea!
Let's support it!" Now think of the myriad talk shows that
flood television these days: how often do you see a show in
which a frank yet meaningful discussion between estranged guests
occurs and culminates in a reconciliation of their- differences?
How often do these guests even seriously entertain the
possibility that their adversaries may have a point or two? And
the audience members: how often are they willing to entertain
the same possibility among those guests whom they are
predisposed to slander? If I were to venture perhaps an overly
hasty response to these questions, 1 would Say "never!" To be
fairer, 1 will simply respond "rarely" . Here are a few more questions:
Have you ever had the experience of being exposed to a nurnber
of viewpoints on an issue and, before finding yourself consumed
by one, in allied relationships to some and in hostile
relationships to the others, f ound yourself murmuring "Well,
they al1 make a pretty good case, donft they?" More concretely,
have you ever investigated a variety of available
philosophical/sociologica~ approaches to a given social issue
and, before making a choice among thern which then serves as your
paradigrnatic orientation to understanding and solving social
problems in general, said to yourself "1 can see validity in
each. Do I really need to choose?" Relatedly, have you ever
thought that, although so different and antagonistic in many
ways, Weberian, feminist, Parsonian, Marxist, phenomenological,
hermeneutic, structuralist, post-structuralist and other
approaches to understanding society al1 make at least some sense
- that they each speak to at least some truth about society?
Our general tendency is to devalue such thoughts and feelings of
eclectic sympathy. Instead, a pervasive drive to demarcate, to
hierarchize, to raise one position to lofty heights while
debasing al1 others that would have things otherwise, seems to
exist. There exists a powerful will to paradigmatic mastery.
This is not a new insight. Postmodernists and other critics
have been condemning modernisrn for the drive to dominate and
exclude for a while now. Let's take Lyotard as an example. For
~~otard', modernism is characterized by the quest for truth. It
is an era premised on the belief that we have the ability to
progress towards truth. But it is more than this. Modernism
also privileges some paradigmatic approaches (science, for
example) over others. Some are considered more apt to lead the
way to truth. And their dominance is legitimated by what
Lyotard terms the "metanarrative". Much like Plato's allegory
of the cave3, metanarratives - such as Hegel's dialectic of
Spirit, Marx' s ernancipation of the worker, the Enlightenment
view of humanity progressing and achieving greater and greater
liberty - guide us in our journey. They provide the overarching
criteria for distinguishing between what in fact constitutes
relevant knowledge, and more specifically, what speaks
truthfully about the world and what does not. Consequently,
certain knowledges prevail while others are lost in their wake.
But, as far as Lyotard is concerned, we are moving into a
postmodern age now, and happily so. Postmodernism is
characterized by an increasing incredulity towards, and a
collapse of, the metanarrative and its role as legitimator.

Correspondingly, the classical dividing lines between different
disciplines are evaporating. Knowledge hierarchies are
blurring, totalizing theories are crumbling, and in their place,
diversified, decentralized (and frequently competing) knowledges
are emerging.
Foucault is al1 for this. With Lyotard, he advocates the
"insurrection of s u b j u g a ted knowledgesu4. He is for l i t t l e
stories, localized knowledges, knowledges that, in our quest for
truth, have been suppressed, trarnpled on and disqualified as
naive and insufficient to the goals laid out by the more
totalizing theories (such as science, again), that have managed
to impose themselves and the specific aims they propound.
Foucault employs his genealogical approach5 as a means for
emancipating local knowledges from such tyranny. He explains
that
. . . in contrast to the various projects which aim to inscribe knowledges in the hierarchical order of power associated with science, a genealogy should be seen as a kind of atternpt to emancipate historical knowledges £rom that subjection, to render them, that is, capable of opposition and of struggle against the coercion of a theoretical, unitary, formal and scientific discourse. It is based on a reactivating of local knowledges . . . in opposition to the scientific hierarchization of knowledges and the effects intrinsic to their power: this, then is the project of these disordered and fragmentary
6 genealogies.
Foucault is for diversity, and is so at the expense of unity.
For him, unity is uniformity, constraint and subjugation.
Diversity, contrarily, is liberty - it is to be promoted, celebrated.
Now to be more specific.
Medicine, it is claimed, is one of these totalizing 7 f rameworks . Conrad and schneidere, for example, argue that
western society has seen three major and distinct cosmological
systems in place to help us understand and deal with the world
and its contingencies . Recently, the medical paradigm has
emerged as the third system, supplanting law and its forerunner
religion. Although some would argue that the power of medicine 9 is waning for various reasons , there are others who view
medicine as the chief definer of what constitutes deviance, and
by extension, normality. These others hold that more of life is
being defined and dealt with according to medical interpretation
and practice; that more of life is being understood in terms of
medical conceptions of health and illness. 10 This, among other
things, is what is meant by medicalization, which, for many, has
insidious implications. Medical conceptions are defining our
relationships with Our fellow humans, with the world, and with
ourselves, and doing so in ways that have alienating and
oppressive con~equences'~. Medicine is the latest incarnation of
paradigmatic mastery.
This view is shared by a number of approaches that participate
in the sociology of health and illness, including Parsonian,
feminist, Marxist and post-structuralist approaches, each of
which links the "evolution" of medicine to dominance with
Parsonian analysis shows how the medical profession acts to control rnotivated deviance. Marxist analysis links it with the development of capitalism; the feminists with patriarchy; and the Foucauldian position links it with the development of
12 modern society . Common to them all, however, is some version of the social
constructionist position which in turn "blends elements of these
perspectives. ,,13
Social constructionism, as its name suggests, views medicine
as sirnply that: a social construction. That medicine exists as
the dominant approach to understanding and dealing with those

"deviant" categories we cal1 illness is purely a socio-
historical contingency. Medicine did not have to emerge as it
has. Indeed, it need not have emerged at all. The fact that it
did simply indicates that certain
(patriarchal/capitalist/rationa~ist) interests won out over
others. Medicine is a child of social forces: there is nothing
inherently true nor essential about it: things could be
otherwise.
The popularity of such a view is relatively new within
sociology since it vas not long ago that medicine seemed immune
as an object of social inquiry. According to Wright and
~reacher'~, medical knowledge was, until recently, considered by
many to be self evident - it was, for the most part, taken for granted. Medicine was considered privileged, penetrating into
the realm of disease entities, entities understood to be both
natural and existing "out there". It was considered autonomous
to society given its roots in the modern sciences. As Lock
explains the situation:
For many years social scientists left unquestioned the dominant ideology of their tirne; scientific " f ac t s " were reified, assumed to be pristine and beyond the realrn of social analysis. Anthropologists were particularly blind in this respect, and while they blithely examined the exotic healing ceremonies and rituals of other cultures and situated them in local cosmologies, they stubbornly ignored modern medicine, assuming it to have evolved beyond the superstition, religion, and value laden beliefs so clear to them in traditional medicine. 15
Medicine was believed to hold a unique status by virtue of
having 'special access to the real workings of Nature."16 But for
the social constructionist now,
Medical categories ... are social through and through; they are the outcome of a web of social practices and bear their imprint. When we speak of tuberculosis we are not reading the

label on a discrete portion of nature, 'out therer; we are instead ... employing a social meaning that has been generated by the activities of many different social groups. 17
So, for the social constructionist, medicine is a (if not the)
paramount example of paradigmatic mastery. It has achieved a
towering influence over us all, and yet there is nothing
inherently profound about it. It does not speak to nor address
anything that is essentially true about the world especially
since, according to this view, there is no truth to the world of
which to speak in the first place. And the corollary: medicine
is 'only one of a number of alternative frameworks with no
higher claim to ultimate "truth" than any othcr. l8
The constructionist view can lead to different consequences.
On the one hand, it can lead to despair, since, if there is no
ultimate truth out there to be tapped, then wherein lies the
purpose of existence? This is characteristic of many forms of
existentialisrn. 19 On the other hand, it can lead to a great
sense of freedorn also characteristic of existentialism as well
as other views. No truth means no essential/eternal
requirements which in turn means we can create who and/or what
we want to be. It also means we can discard cosrnological
systems like the rnedical approach and fashion others in its
place, ones which (ostensibly) more aptly suit Our interests.
And we can do this as individuals as tJietzsche2' and ~artre" 22 would have it, or as comrnunities as Rorty would have it.
Notwithstanding the consequences, however, the constructionist
view means a rejection of our tendency to privilege certain ways
of knowing over others based on the modern belief that they
grant us "special access to the real workings of Nature", and
more generally, to ultimate truth.
Now whatrs interesting is that constructionism makes these
clairns about the non-existence of truth, and yet we can ask:
"are not these claims theniselves truth claims?" Social
construction falls into a paradox no matter how you shuffle the
cards. On the one hand it can adopt the superior position that
only it sees the truth - i.e. that reality and truth are socially constructed. But thatfs a contradiction. On the other
hand, it can adopt the humble position - one more in line with its own tenets - that it too is merely a social construction. But then what reason do we have for taking it so seriously? In
either case, social constructionism seems to undercut its own
significance as an approach to dealing with and understanding
other approaches to reality, let alone reality itself. But 1
have to admit that of the two, 1 prefer the latter position
since the former is tantamount to just one more attempt at
paradigmatic mastery, and hypocritically so.
1s there a way out of this conundrtm? 1 think there is . . . but 1 will get to this later. 2 3
VERTICAL VERSUS HORIZONTAL APPROACHES TO REALITY
Let me try and summarize where we are so far. To begin, there
exists this tendency to paradigmatic mastery. There exists this
pervasive drive to differentiate, exclude and subordinate
certain views so that others, in the name of truth, can flourish
and dominate. This is indicative of the modern condition (and
certain historical conditions as well, it should be said), and
is argued by constructionists to be manifestly clear in the case
of medicine. Constructionists of al1 sorts criticize and
repudiate the tendency to erect totalizing theories. For them,
and most clearly in the postmodern formulation, there is no
truth out there to be had. Truth is fabrication. So the
constuctionist seeks the following . S/he seeks to undemine
totalizing theories by highlighting their contingent origins,
and in so doing, to dissolve the traditional hierarchies of ways
to know. In short, s/he is after the liberation and celebration

of knowledge in al1 its diversity. (Whether constructionism is
to remain just one of those knowledges on par with al1 others,
is itself a question. )
Now, before 1 go any further, 1 need to point out that 1 have
been employing the term 'social constructionism" fairly loosely
to this point; 1 have included a number of relatively disparate
theoretical approaches under its umbrella, and perhaps unfairly
so. For instance, although both are very constructionist,
postmodernism24 takes issue with Marxism which it sees as
propounding just one more grand narrativezs to be repudiated.
Moreover, although common to many approaches, social
constructionism is also a unique approach having its own origins
and orientations that one cannot fully reconcile with Marxist,
feminist, postmodern or any other approaches. So, in order to
speak of certain cornonalties between most, if not al1 of these
approaches, 1 will employ the term horizontalist approach.
Moreover, throughout this work, the horizontalist approach is
contrasted with its polarity, the verticalist approach. These
terms are adapted £rom Rortyf s distinction between two estranged
philosophical traditions:
There, then, are two ways of thinking about var ious things. 1
have drawn them up as reminciers of the differences between a philosophical tradition which began, more or less, with Kant, and one which began, more or less with Hegel's Phenomenology. The first tradition thinks of truth as a vertical relationship between representation and what is represented. The second tradition thinks of truth horizontally ... This tradition does not ask how representations are related to nonrepresentations,
2 6 but how representations can be seen as hanging together.
Rorty, as does the social constructionist position outlined so
far, favors the horizontalist approach. For the horizontalist,
there is no absolute truth to be represented, no essential
reality to be accessed; ontologically, there is no essential

"what is". And even if there were, there is no way of
transcending what we create (our language, culture, ways of
knowing) to establish whether or not it is an adequate
representation of (or rnirrors) such a reality;
epistemologically, there is no fundamental way to know about
"what is". As Rorty puts it:
What we cannot do is rise above al1 human communities, actual and possible. We cannot find a skyhook which lifts us out of mere coherence - mere agreement - to something like "correspondence with reality as it is in itself". 2 7
In contrast, the verticalist approach daims we can.
Ontologically, verticalists assume there is something (there is
truth) out there to know. Epistemologically, verticalists also
hold that we can know it and moreover, that there are sorne ways
of knowing that are far superior to others. Hence, the drive
towards paradigrnatic mastery and domination.
What follows are three more ways to distinguish between the
verticalist and horizontalist orientations as 1 intend to use
t h e m . These examples are closely related, but hopefully they
will give a more comprehensive picture of how the two approaches
differ.
1. Regarding essentialism: Verticalists have it that there
are entities out there in the world that have essences - that
there are (as Aristotle sees it) real things made up of primary
characteristics that make them what they are. The point is to
uncover these entities as they are in themselves, thus revealing
how things fit together. The point of inquiry, moreover, is to
converge on an accurate understanding of what those essences
are. Horizontalists, contrarily, hold that no such essences
exist, and that even if they do, we can never know what they
are. Instead, any essence "uncovered" is really an essence
created - created either by a free individual from the
existentialist point of view, or by the
community/culture/language/the powerful from the post-
structuralist (or pragmatist or postmodern, to name a few) point
of view. Essences are simply constructions of convenience.
Illness, for example,
is not a fixed reality waiting to be discovered by the application of more and more precise and standardized methods; rather, illness is socially constructed, and any definition and diagnosis depends on the selection of particular signs and
28 symptoms as relevant.
Illness is nothing more than what we (or the powerful) make it.
Since verticalists are essentialists, they are also
foundationalists. They are foundationalist because they
attribute priority to the real. The body, for example, is given
priority as a real entity. The body impinges and conditions in
various ways. As Turner explains:
Foundationalist frameworks are concerned to understand the body as a lived experience, or to comprehend the phenomenology of embodiment, or to understand how the biological conditions of existence impinge upon the everyday life and rnacro
2 9 organization of human populations . . . Horizontalist approaches, on the other hand, are largely anti-
foundationalist. They have no concern for ontology. Instead,
they put discourse and metaphor in center stage and link them to
the processes of social construction and the exercises of power
in society.
By contrast, anti-foundationalist perspectives conceptualize the body as a discourse about the nature of social relations, or comprehend the body as a system of symbols, or seek to understand how bodily practices are metaphors for larger social structures, or they understand the body as a social construction of power and knowledge in society, or perceive the body as an effect of social discourse. 3 0
2 . Rega~ding human identity: Human identity is a particular
category of essence. Vertical approaches to understanding the
human condition place emphasis on human identity. Although
horizontalist in many ways, Marxism is no exception. The
younger Marx in particular assumes a creative human being that
is alienated frorn his or her creative potential (as well as in
other ways) under the capitalist mode of production.
Consequently, he wants to release the human condition Exom this 3 1 oppressive situation. Most political theory, in fact, stems
frorn certain understandings of human nature, saying basically
that since humans are essentially "X", we need to create a "Y" 32 society to deal with/foster 'X". Micro sociologists of health
and illness, although constructionist in many ways, focus on the
self as well. Their primary concern is with the way in which the
self is affected by the experience of being ill, by the stigrna
associated with illness, etc. 3 3 Horizontalists, and in
particular post-structuralists, on the other hand, repudiate any
notion of an essential self, let alone a universal human
identity. They de-center the self granting it no autonomy.
They approach the self as a product - fully so - of society. 3 4
To make the d a i m that an individual (or humanity) is 'X" is to
create or propound a fiction for the sake of dealing with the
world in a certain way.
3. Regarding progress: Verticalists hold that we are
progressing towards truth. We may have our setbacks; we may get
sidetracked. But in the large scheme of things, we are getting
a better and better handle on the way things are; we are
penetrating deeper and deeper into the way the world works. (We
are obtaining greater and greater knowledge into the realm of
health, illness and disease.) Once again, horizontalists
disagree. They see progress as a fiction. If there is no truth
out there, if there is no essential reality to the world and the
things in it, if there is no universal human identity underneath
a superficial diversity, then there is nothing towards which to
progress, nothing essential that is. The only progress that
exists is one of convenience, one defined according to our
created goals.
Now it should be clear that by "verticalist" and
"horizontalist" 1 am referring to ideal type orientations in the
Weberian sense. 1 am doing this for essentially heuristic
purposes. My analytical concern is the disparity between
horizontalist and verticalist tendencies which are shared in 3 5 varying ways and degrees by different theoretical approaches. 1
think it is accurate to Say that there are certain approaches
that can be categorized neatly as either verticalist in
orientation, or horizontalist. There are others, however, that
cannot be so neatly classified, having some affinities with both
camps. The Marxist and phenomenological approaches are clear
examples. As such, any exhaustive classification of theories as
either verticalist or horizontalist would be forcing the issue.
However, 1 do think the following summary is helpful:
1. Verticalist approaches include: realism, positivism and
other approaches that are more foundationalist, essentialist,
anti-constructionist and modernist in orientation.
2. Horizontalist approaches include: relativism, pragmatism
(as per Rorty) and post-structuralism, al1 of which are anti-
realist, anti-foundationalist, anti-essentialist,
constructionist and more postrnodernist in orientation. 3 6
3. Approaches that have both verticalist and horizontalist
traits include: Marxism, feminism, symbolic interactionism and
phenornenology, among others. As we have seen, Marxism is
verticalist in that it is concerned (at least in some of its
manifestations) with a creative human potential that is
alienated under capitalism. Many feminist formulations share a
similar view, but see patriarchy as the villain. Phenomenology
is also verticalist given its foundationalist concerns. But
each of these approaches is horizontalist in at least one
critical way. Each stresses, to some degree, the social
construction of reality.
THE CONSULTATIVE APPROACH: SOME BASIC ASSUMPTIONS
Tc recap: adopting a purely verticalist orientation means
wanting to penetrate the essence and identity of things; to be
concerned with foundations and how they impinge; to assume
universal and eternal truth; to daim that certain ways of
knowing (science, medicine) are making progress in discovering
the way things are, while other ways of knowing are insufficient
to this task. To adopt a purely horizontalist orientation is to
repudiate al1 these daims. There are no necessary essences,
foundations nor truths. Hence, there are no privileged ways of
knowing. Taken to its relativistic extreme, the horizontalist
approach regards any way as equal to any other. So letf s forget
the modernist p e s t for absolute truth, the horizontalist says.
Letr s celebrate instead the many ways we have of functioning in
the world; and let's ensure, this time, that we sanctify none of
them.
Now for a new approach to these issues.
What fo l lows is a brief overview of some the characteristics
of the consultative approach as 1 see it, which, as concerned
with health, illness and disease, is the subject of this study.
The consultative approach has affinities with both the
verticalist and horizontalist positions, but it is satisfied
with neither. Along with the horizontalist, it does not share
the verticalist drive to totalize and exclude. Instead, it
champions diversity. Along with the verticalist it does not
share the horizontalist daim that al1 truths, essences and
foundations are sirnply social constructions. Instead, it
accepts that truths exist and that we can have some knowledge of
what they are. Social construction does takes place, but it
does not account for everything on its own. So the
consultationist says "let's celebrate diversity", and s/he says
this for the sake of liberation. But s/he says this for another
reason as well. S/he says: "Let's celebrate diversity because
we may each have, in al1 Our myriad ways of knowing, the
potential to shed some light on reality."
This is a pivotal claim. Different ways of knowing are simply
that. They are different approaches each with the possibility
of revealing or penetrating or highlighting, at least to some
degree, certain realities - certain truths out there. There is
no room for unconditional paradigmatic mastery here. Instead,
what is called for is a constant willingness to entertain
diverse approaches to reality given the possibility they can see
certain truths - tmths other approaches rnay miss, ignore, distort. Like (sorne forrns of) horizontalism, the consultative
approach is profoundly interdisciplinary - and more generally,
interparadigmatic - in orientation. But it is so not for
postmodern reasons. It does not disregard the existence of
absolute, nor universals, nor empirical truth, nor our ability
to approach such truth. It accepts their existence and the
possibility, even the feasibility, of their discovery.
And it is for this very reason (to digress a little here),
that we can seriously entertain the social constructionist
position without falling into the trap it has, perhaps
unwittingly, set for itself. Social constructionism has
uncovered a certain truth about the world, namely that social
construction does indeed take place. However, social
constructionism runs into difficulties when it carries its claim
too far by attaching an illimitable status to the reality of 3 7 social construction.
Uni* in Diversity
So diversity is good. But is it sufficient on its own? For
the consultationist it is not. And herein lies the essential
assumption: celebrating diversity is essential, but it is
invariably found lacking unless informed by something else -
unless informed by a spirit of unity. Yet by unity is not meant
uniformity, normalization, or totalization - themes of
modernism. Rather, by unity is meant something more alive than
this, something that responds to and thrives on diversity. What
the consultationist is after is a unity in diversity.
The principle of unity in diversity is appropriated directly
£rom the writings of Baharu1 ll&h3' whose primary teaching is the
oneness of humanity. For him, "the history of humanity as one
people is now beginning."39 We are seeing a trend that has been
gaining greater and greater "momentum during the last hundred
years: the trend toward ever-increasing interdependence and
integration of h~manit~.''~~ This is evidenced by a number of
phenornena, f rom
the fusion of world financial markets, which in turn reflect humanityfs reliance on diverse and interdependent sources of energy, food, raw materials, technology and knowledge, to the construction of globe-girdling systems of communications and transportation. It is ref lected in the scientif ic understanding of the earthf s interconnected biosphere, which has in turn given a new urgency to the need for global
4 1 cooperation.
These processes are forcing us to recognize that we have many
universal commonalities. They are compelling governments to
think globally. The world is shrinking, and it is shrinking
fast. We can attempt to resist the trend, but to what avail?
Instead, perhaps it is time to intensify collective strategies
to address common issues, strategies premised on our fundamental
oneness .

Once again, this oneness is not a oneness of uniformity. Tt
is not about achieving homogeneity. Instead, it is one premised
on a profound regard for the diversity of races, cultures and
creeds that exist in the world. A helpful analogy is to compare
the world to the human body:
Human society is composed not of a mass of rnerely differentiated cells but of associations of individuals, each one of whom is endowed with intelligence and will; nevertheless, the modes of operation that characterize man's biological nature illustrate fundamental principles of existence. Chief among these is that of unity in diversity. Paradoxically, it is precisely the wholeness and complexity of the order constituting the human body - and the perfect integration into it of the body's cells - that permit the full realization of the distinctive capacities inherent in each of these cornponent elements. No ce11 lives apart £rom the body, whether in contributing to its functioning or in deriving its share £rom the well-being of the whole. 4 2
Others have probably used the body as an analogy to understand
the world as a whole. And it is certainly the case that the
analogy has been used to understand society at a national level.
Hegel takes an organicist view of s ~ c i e t ~ ' ~ as do others who 4 4 propound collectivist political theories. Such theories,
however, use the analogy in a way that helps to elevate the
state. Here the individual is considered irrelevant to, or
viewed as a pawn of, society. The "cell" fades in importance.
Contrarily, those who reject the analogy of the body tend
towards the opposite pole. Society, for thern, is nothing more
than a collection of individuals. The individual is paramount.
The c u l t of individualism dominates.
Baha'u'llah shares neither of these orientations. He shares
neither a system's theory approach, for example, nor its
opposite - libertarianism, for example. Instead, his view is
one of reciprocity between society and the individual. The
individual is a trust of society with certain rights and
freedoms that must be guaranteed. Society has a tremendous
responsibility to the individual. But society does not lose as
a consequence. Instead, by nourishing its "cells" it is in fact
nourishing itself. By imbuing the individual with certain
freedoms society is liberating the individual to contribute in
hidher own unique way to the well-being of the whole. In this
way, an otherwise homogenized and moribund body is given
vitality. Releasing creativity, in its diversity, gives life to
the whole, distinguishing "unity from homogeneity or
unifomity. " 4 5
So the diversity of humanity must be tapped. But it must be
tapped in a way that promotes the oneness of humanity.
Much like the role played by the gene pool in the biological life of humankind and its environrnent, the immense wealth of cultural diversity achieved over thousands of years is vital to the social and economic development of a human race experiencing its collective coming-of-age. It represents a heritage that must be permitted to bear its fruit in a global
4 6 civilization.
Unity without diversity is uniformity and lifelessness.
Diversity witnout unity is chaos and ineffectual (even perilous)
to our collective situation and ourselves. Hence the principle
of unity in diversity.
Now, horizontalists Say that diversity has been stifled; that
the individual creativity has been stifled; that humanity has
been stifled. According to Nietzsche, we have been stifled by
the Socratic principle to rationalize, to render everything
subject to reason. In The B i r t h of Tragedy, Nietzsche sees a
powerful struggle running through the ages, namely that between
two forces - the Dionysian and Socratic principles47. The
Dionysian principle of passion represents the "explosive,
ungoverned force of creati~n"~~. But it also represents a force
t h a t has f o r t h e most p a r t l o s t out i n i t s s t r u g g l e with t h e
Soc ra t i c p r i n c i p l e . Passion, f o r example, does not inform a r t
un le s s i t does s o i n conformity with reason. Beauty i s beauty
only in so fa r a s it appeals t o i n t e l l i g i b i l i t y , Nietzsche
rejects t h i s . Nietzsche r e j e c t s the crushing f o r c e of S o c r a t i c
reason. H e denounces it a s u n j u s t l y oppressive, e spec i a l ly
given i t s l a c k of grounding i n anything s u b s t a n t i a l l i k e e t e r n a l
t r u t h . So he c a l l s f o r t h e Superman, one who can shed t h e
f i c t i o n a l garments of reason and t r u t h and exe rc i se h i s /he r
c r e a t i v e capacity t o become.
T h e consu l t a t i ve approach a l s o promotes the need f o r
ind iv idua l becoming. But it does so always wi th the p r i n c i p l e
of un i ty i n m i n d . Without such an o r i e n t a t i o n w e invar iab ly end
up with a n t a g o n i s t i c becomings, then wi th c o n f l i c t , and then
wi th domination a l 1 over again . So, while d i v e r s i t y gives l i f e
t o uni ty , unity i s i n t u r n e s s e n t i a l t o d i v e r s i t y . I t fxees t h e
c r e a t i v e i n d i v i d u a l p o t e n t i a l so key t o i t s own v ivac i ty .
And why wouldn't we want t o be o r i en t ed towards unity, a u n i t y
i n which w e are each f r e e t o exerc i se Our c r e a t i v e p o t e n t i a l s ?
An o r i e n t a t i o n t o uni ty means we a re o r i en t ed t o each o the r . It
means we a r e o r i en t ed towards shar ing with, and learning from,
each o ther . W e a l 1 benefit.
Consultation and Seeing
W e benecit f o r many reasons one of which i s t h a t it i s
poss ib le t h a t each o f us may see, t o some ex ten t o r another, i n
our d iverse ways of knowing, d i f f e r e n t th ings about r e a l i t y .
This, once again , i s a c e n t r a l claim o f t he consu l t a t i ve
approach. From our var ious vantage p o i n t s , some of us rnay see
some things i n r e a l i t y w h i l e o thers may see o t h e r things about
r e a l i t y . Moreover, w e each may see d i f f e r e n t a spec t s of the
same th ing i n r e a l i t y . Some may see hyperkinesis as a d i sease
with b i o l o g i c a l foundations while o the r s may s e e i t as a s o c i a l

construction fabricated in order to individualize what rnay in 4 9 fact constitute a social problem. One may be right and the
other wrong in this case. On the other hand, both may be
penetrating into different aspects of the sarne phenomenon and
hence, different aspects that are true of it. Then again, one
aspect of the phenomenon may have more to it than any other, in
which case one approach may be more revealing (truth bound) than
any other. In any case, we lose if we do not collaborate - we lose the possibility of gaining a more comprehensive insight
into the phenomenon (and the opportunity to more effectively
reduce suffering associated with any "illness") . We lose by
simply promoting diversity.
Turnerr s "strategy of inclusion"50 is along the lines of what I
am talking about. "[His] approach is to think about problems
that interest [him] from diverse starting points. His reason
for this is that "no single paradigm or perspective can ever be
theoretically adequate. "52 In particular, he states that " [el ach
of the major traditions within medical sociology can be
criticized for its limitations and lacunae. "53 So whatr s the
point of adhering to one of them over al1 the others? Why not
draw from each, learn from each? Different paradigms can reveal
different things about phenornena. Turner's approach to anorexia
nervosa is particularly enlightening in this regard. He
demonstrates the utility of using three different, even
disparate, sociological paradigms for revealing different
aspects of this condition.
Anorexia should be approached conceptually and theoretically at three levels ... At the phenornenological level, we may understand loss of appetite as a pseudo-solution to communicative problems between the developing personality and the domestic environment of the overprotective home. At the social level, anorexia is a sick role which provides 'solutionsr to the demands of a cornpetitive middle-class
culture through the secondary gains of the sick role. At the societal level, it is an effect of fashions relating to food, consumption and life-style. Anorexia is peculiarly expressive of the persona1 and social dilemas of educated, middle-class women, because it articulates various aspects of their powerlessness within an environment that also demands their
5 4 cornpetitive success.
Similarly, different approaches are amenable to understanding
dif ferent phenomena. Turner reasons that
sociologists don' t have to choose. . .between levels. For example, it seems perfectly sensible for a medical sociologist to be interested in the question of human pain, and 1 felt that the best approach to that was the work of Merleau-Ponty on phenomenology. However, it was equally sensible for sociologists to be interested in the interaction between doctors and patients, and 1 felt that the legacy of Parson's 'sick role' ... was the most appropriate approach to that level. Finally, 1 felt that neither Merleau-Ponty nor Parsons was adequate for understanding the impact of the state or the environment of social class on the distribution of health and illness globally. 5 s
In brief,
Sociological theory is often written as if one had to choose between competing and incommensurable paradigms. My own view, which could be called methodological pragnatism, is that the epistemological standpoint, theoretical orientation and methodological technique which a social scientist adopts, should be at least in part determined by the nature of the
5 6 problern ai:d by the level of explanation which is required.
The consultative approach is pragmatic in this sense.
Different paradigms see different things (at least potentially),
so what's the point of devoting Our lives to refuting some for
the sake of others? Instead, wouldn't it be more fruitful to
see what each can offer, to take what each can offer, and to do
so with an ever expanding orientation to include as much diverse
knowledge as we can in Our overall approach to phenornena, their
various aspects, and to the world in general?
Assuming the answer is "yes", then other questions emerge,
such as: how is such an orientation to be put into practice?
Or: through what method are we to foster meaningful
interparadigmatic interaction? And: through what method are we
to feel confident that such interaction has the benefit of
getting at and integrating into our knowledge base the truths
the different paradigms are able to highlight, while at the same
time weeding out the deficiencies they invariably harbor? These
questions are reserved for the final chapter of this volume, and
discussed in depth in the next volume. But for the sake of
closure, it should be said briefly that for the consultationist,
there is only one method for this particular job. Not
surprisingly, the method is called consultation.
Here, consultation refers to something other than its ordinary
usage, i . e., a process "of deliberation, advice-seeking, and information-gathering from various sources... "57 Instead, it
denotes a process in which
a small or large number of individuals, representing themselves, institutions, nations, or any other group of people, communicate with one another in an atmosphere of complete unity and frankness. Their purpose is to seek out the truth about the object of their deliberation and to find ways and means in which individual and societal needs for justice, equality, freedom, and progress are met. They also deliberate on ways human conflicts can be resolved without the abuse of power or the manipulation or denial and violation of human rights of any people, whether or not they are directly
58 involved in these consultative processes.
It is, moreover, a process
in which the individual participants strive to transcend their respective points of view, in order to function as rnembers of a body with its own interests and goals. In such an
atmosphere, characterized by both candor and courtesy, ideas belong not to the individual to whom they occur during a discussion but to the group as a whole, to take up, discard, or revise as seems to best serve the goal pursued. Consultation succeeds to the extent that al1 participants support the decisions arrived at, regardless of the individual opinions with which they entered the discussion. Under such circumstances an earlier decision can be readily reconsidered
59 if experience exposes any shortcomings.
Put another way, consultation as described here, is a particular
mode of communication where:
1.the views of everyone, in al1 their diversity, are always
treated as potentially relevant to an issue (to understanding
a phenornenon), and are thus rigorously sought;
2. views are expressed freely but with prudence and with respect
and consideration for others and their views;
3.individuals (and groups) are detached from their own views
such that they see them not as finalities, but rather as
opinions that belong to the group for it to work with, mold or
discard in light of other views and evidence;
4.the ultimate objective is to achieve a unity of thought, but
if this is not attainable, a majority opinion prevails;
5. everyone supports the decision of the group in unity; and
6. the group is able to return to the consultative process upon
evidence of any deficiencies with the decision.
Obviously, consultation requires work on the part of the
individual. For many, it requires an attitudinal adjustment of
massive proportions. Most significantly, it requires an
orientation to otherness, an orientation to "releasing the
potentialities [in their wonderful diversity] latent within the
human consciou~ness"~~.
In Short (see Table 1 for a swnmary)
Verticalists like to think that they can penetrate into
reality and see the way things are. But they clah there are
only certain privileged ways of doing this. Other knowledges
are excluded, subjugated, relegated to minor positions on the
hierarchy, or rendered completely invalid. The approach tends
towards an oppressive uniformity. Horizontalists, on the other
hand, deny any access to truth or that there is even such thing
as truth; everything is a social construction. With this denial
of truth cornes the dissolution of every knowledge hierarchy, and
in their place, the liberation to create ourselves and our own
persona1 or community "truths" (assuming that the corresponding
realization of anomie, of ambiguity, is not too much for us
handle) . So the verticalists are seduced by the quest for truth
(leading to uniformity) while the horizontalists are seduced by
the opportunity for creativity (leading to diversity). The
consultative approach, however, says "why not be seduced by
both?" And if that sounds good, then it says "letf s accomplish
both through consultation, a communicative process founded on
the principle of unity in diversity."
SOMMARY OF PURPOSE
My grand purpose is to provide a rationale for, and delineate,
a consultative approach to understanding health, illness and
disease. This means undertaking two related projects. The
first, is to:
d e m o n s t r a t e the utility of meaningful i n t e r p a r a d i g m a t i c
collaboration f o r ach iev ing bet ter under s tand ings of - for
p e n e t r a t i n g more d e e p l y into - heal th, i l l n e s s and disease
(and r e a l i t y ) . The second is to:
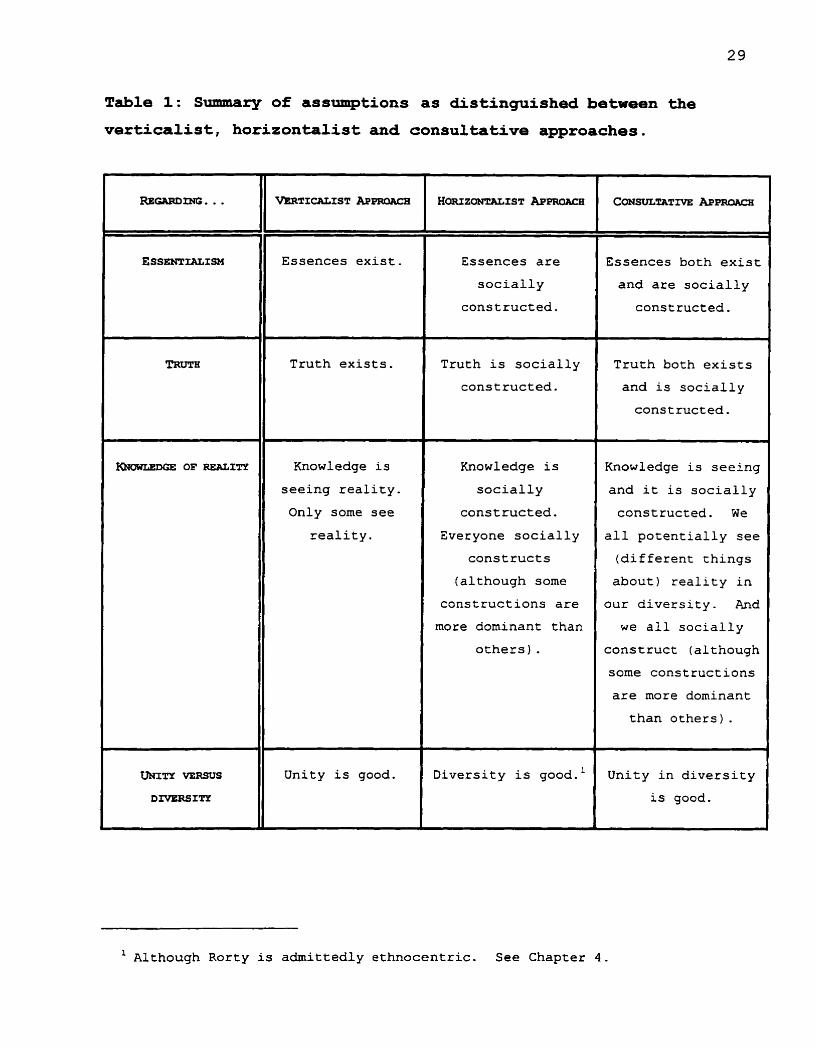
Table 1: S~lmmary of assumptions as distinguished between the
verticalist, horizontalist and consultative approaches.
Essences are
socially
constructed.
REGARD=. . .
ESSENTIALISM
TRUTII
OF REA~ITY
L
UNXTY VERSUS
DIVERSITY
Truth is socially
constructed.
V~TXCALIST A P ~ R O A ~ B
Essences exist.
Truth exists.
Knowledge is
seeing reality.
Only some see
reality.
Unity is good.
Knowledge is
socially
constructed.
Everyone socially
cons t ruc t s
(although some
constructions are
more dominant than
others) .
Diversity is good.'
Essences both exist
and are socially
cons tructed .
Truth both exists
and is socially
constructed.
Knowledge is seeing
and it is socially
constructed. We
a l 1 potentially see
(different things
about) reality in
our diversity. And
w e al1 socially
construct (although
some constructions
are more dominant
than others) .
Unity in diversity
is good.
l Although Rorty is admittedly ethnocentric. See Chapter 4.
demonstra t e the power o f the communicative p r o c e s s o f
consu l t a t i o n f o r f a c i l i t a ting m e a n i n g f u l i n t e rparad igma t i c
c o l l a b o r a t i o n s o that more adequate u n d e r s t a n d i n g s of heal t h ,
illness and disease (and reality) c a n be a c h i e v e d .
As mentioned, the latter 4-5 beyond the scope of this book, as is
the completion of the former. My concern, rather, is simply to
lay the theoretical foundation for the former.
Here is the thinking in brie£:
Different perspectives can be thought of as spotlights,
illuminating different phenornena (aspects) of reality. Sorne may
shine more intensely than others. Some may illuminate more
broadly t h a n others. But it is always possible that each
illuminates something about reality - some truth. So why not
look to each to see what it c m offer? The more light there is,
the more we see and the better off we are.
Underlying this thesis is the principle of unity in diversity.
Through an orientation to diversity, an otherwise singular and
oppressive approach to health, illness and disease
transforms/expands/bifurcates into one more responsive,
flexible, and imbued with greater meaning for all. Through an
orientation to unity, an otherwise scattered and (often)
conflictual diversity is thoroughly explored, and its advantages
integrated for the benefit of all.
This is obviously a case for interdisciplinarity, and more
broadly, for interparadigmatic collaboration. But this case is
being made for very specific reasons. 1 am suggesting, along
with the horizontalist, that the totalizing theories of
modernism are inadequate, and often oppressive. But unlike the
horizontalist, 1 am also suggesting that there is something
beyond social construction out there, something deep, to know,
that it can be known at least to some extent, and that it can be
known in different ways. This means that totalizing approaches

such a s medicine, and s c i ence more broadly, have, i n a l 1
l i k e l i h o o d , and d e s p i t e t h e i r de£ i c i e n c i e s , h i t upon and
exp la ined c e r t a i n t r u t h s . I n f a c t , they may have h i t upon many
truths, deep ly p e n e t r a t i n g i n t o them f o r what t h e y are. But i t
also means t h a t o the r approaches may have done so a s we l l ,
perhaps i n t o o t h e r areas o r a spec t s of r e a l i t y .
T h a t d i f f e r e n t approaches may see d i f f e r e n t r e a l i t i e s f o r more
o r less what t hey are is t h e proposed r a t i o n a l e f o r f o s t e r i n g
i n t e rpa r ad igma t i c co l l abo ra t i on . The p o s s i b i l i t y of
paradigmat ic seeing, t h e r e f o r e , needs t o be e s t a b l i s h e d .
I nva r i ab ly , t h a t i s what t h i s book i s about .
And it begins i t t h u s . It begins by demonstrat ing t h e
v i a b i l i t y o f , and exp lo r ing the r a m i f i c a t i o n s o f , a c r i t i c a l
c l a im made by Turner. 6 1 I t begins i t with an assessrnent of t h e
claim: some things are more socially constructed than others.
For i f t h i s claim is c o r r e c t , i f some d i s ea se s , f o r example, a r e
more (and hence, some less) s o c i a l l y cons t ruc ted than o t h e r s by
medicine, then, t h e o r e t i c a l l y , there i s u t i l i t y i n t ak ing
medicine s e r i o u s l y because i t means medicine may a c t u a l l y see
some d i s e a s e s (more o r l e s s ) f o r what t h e y a r e . Concurrent ly,
t h e r e i s , aga in t h e o r e t i c a l l y , u t i l i t y i n t a k i n g s o c i a l
cons t ruc t ion i sm s e r i o u s l y because i t means s o c i a l
cons t ruc t i on i sm may a c t u a l l y sec some d i s ea se s ( m o r e o r less)
f o r what t hey are. There is, t h e r e f o r e , and t h e o r e t i c a l l y yet
again , u t i l i t y i n each t a k i n g the o t h e r s e r i o u s l y - f o r each t o
cons ide r t he o t h e r a s ( a t l e a s t ) a ( p o t e n t i a l ) source of
va luab le informat ion about t h e t r u t h of hea l t h , i l l n e s s and
d i s e a s e .
Thus, my e s s e n t i a l concern is t o
demonstrate the relativity of the social, and i n particular,
medi cal construction of disease.
I t i s , moreover, t o
' explore the epistemological and antological implications that follow front the r e l a t i v i t y of the social ( m e d i c a l )
construction of d i s e a s e .
CHAPTER OUTLINE
In Chapters 2 and 3 my aim is to outline in more depth what is
rneant by the verticalist and horizontalist approaches
respectively, highlighting medicine and social constructionism
as prime examples, while Chapters 4 and 5 are concerned with
developing the theory informing the consultative approach. In
Chapter 4, I look in particular at the relativity of the social
construction of reality, its viability as a concept, what it
looks like, and its epistemological and ontological
ramifications. In this chapter 1 also introduce a number of the
conceptual tools that are utilized throughout the rest of the
book. In Chapter 5, I continue developing the theory by
addressing in depth the nature of paradigmatic articulation.
Most prorninently, the proposa1 that paradigmatic articulation,
while certainly involving social construction, concurrently
involves the possibility of penetrating into (getting to know in
more depth) reality, is examined. This possibility is pivotal
since it means, once again, that there is, within any paradigm,
(potential) relativity to how different things are both seen and
constructed; since it means that any paradigm can (potentially)
offer (deeper and deeper) insights into reality. In Chapter 6,
the theory is then applied very specifically to medicine in an
analysis of the varying degrees to which a range of diseases are
socially (medically) constructed. This is accomplished with the
introduction of a provisional typology to help think about the
relativity of the social construction of disease. Finally, in
Chapter 7, conclusions are drawn concerning the possibility of
seeing and their implications for the utility of
interparadigmatic collaboration between medicine and social
constructionism. The typology used to demonstrate the
relativity of the social construction of disease, thus
legitimating the utility of interparadigmatic collaboration, is
also assessed and potential weaknesses identified. Finally,
certain phifosophical ramifications are introduced.
1 also begin each chapter with what 1 am calling "Journey
Notes" the purpose of which is to provide brief overviews of
some of the most salient themes to that point, as well as to
introduce the next stage in the discussion.
Before going on, 1 should also point to...
THE IRONY
. . . involved in my focus on biomedicine and social constructionism. The irony stems from the fact that the former
f a l l s within the verticalist tradition as 1 am defining it,
while the latter falls within the horizontalist tradition as I
am defining it. And while the consultative approach as 1 am
defining it, is satisfied with neither, it is in many ways
informed by both - by many of their respective precepts. More
precisely, verticalisrn and horizontalism (specifically, social
constructionism) are drawn upon in order to make a theoretical- p p p p p p p p p p p - p - - - - - - - - - - - - - -
- - - - -
case for the utility of interparadigmatic interaction between
medicine and social constructionism. Even more ironic, and by
extension, they are drawn upon in order to make a theoretical
case for the utility of interparadigmatic interaction in
general, which would include their own interaction. This, no
doubt, is a notion that will vex proponents in both camps.
SOME DEFINITIONS
Illness and Disease
It is common within the sociology of health and illness to set
out a distinction between illness and disease. Whereas the
latter refers to physiological malfunctions, to objective signs
of illness, the former refers to the social psychological state

of the person af fli~ted~~, to his/her subjective awareness of the 6 3 disorder. The distinction is made in order to "avoid
unnecessary confusion between the two realms of culturally
defined and medically defined. problems. "64
However, this distinction doesn't necessarily hold within the
social constructionist literature. First of all, many social
constructionists would protest the stress placed on the
objectivity of disease. There are variations within
constructionism. Some constructionists are much more
constructionist than others.
Some, like Eisenberg, retain a view of disease as a biomedical reality while at the same t i m e recognizing the existence of alternative views of the problem; the latter are the non- medical or "folk" theories of illness. Other investigators are more drastically relativistic [as quoted above] and view the biomedical definitions as only one of a number of alternative frameworks with no higher claim to ultimate "truth" than any other. 6 5
Second of all, when social constructionists s p e a k of illness,
they often s p e a k of it in terms of social conceptions of 'what
is "really" or "basically" wrong with the person. ' 66 Thus spoken, illness refexs to a social designation rather than to an
individual experience (although many would argue the latter is
conditioned, if not determined, by the former) . A comrnon
concern is with the way in which illness designations are both
medically determined and believed to have an objective basis.
It is with this sense in mind, and not the more subjective sense
of the term in mind, that 1 employ the term illness.
And by disease 1 simply mean with Conrad and Kern
"biophysiological phenomena that manifest themselves as changes
in and rnalfunctions of the human body."67 And 1 do so emphasizing
that diseases are phenomena that are, like any other phenomena,
subject to interpretation, and hence, construction by any
paradigm.
Medicine
When 1 refer to "medicinet' 1 am referring to allopathie or
biomedicine as opposed to "alternativer' or "complementary"
medicine; the Western style of medicine that tends to dominate
today . Regarding T r u t h
1 think it is important at this point to emphasize that when 1
speak of truth, 1 place little ernphasis on distinguishing
between essential (foundational, eternal, universal) truth and
empirical or contingent truth. Since my primary aim is to
compare verticalism with horizontalism, the paramount question
is simply whether or not truth as "out there" of any kind exists
and whether or not it can be seen - truth, that is, besides constructed truth. In fact, the distinction between truth and
constructed truth is my primary concern £rom this point until
Chapter 7. In Chapter 7, 1 consider the various kinds of truth,
namely foundational, empirical, pragmatic and constructed truth.
1 "Verticalism" and "horisontalisrn" are terms adapted from a distinction
introduced by Rorty. See later in this Chapter.
2 See, for example, Lyotard (1993).
3 The allegory of the cave is a story meant to legitirnate the importance of
the philosophic/rational quest to transcend the knowledge we obtain through
other means (prejudice, belief, sense experience). The true philosophic goal
is to discover and become one with the realm of immutable truth (the realm of
the Forms ) . Most of us are like cave dwellers, Plato says, content with the
evanescent shadows we see on the walls of the cave. These shadows constitute
what we know. But then some of us are able to break away, to escape this
limited situation and see the light - to see the world of perfection as it is
in al1 its glory. Only true philosophers are able to take this step. See
the Republic pp. 240-243 for more details.
4 Foucault (1980), p. 81. Foucaultrs italics.
5 Foucault's genealogical method is discussed in more depth in Chapter 3.
6 Foucault (1980), p. 85.
7 This is a major theme within the sociology of health and illness. Some of
the more foundational contributions to this view include Conrad and Schneider
(1980); Freidson (1972); and Zola (1978).
8 Conrad and Schneider (1980) . 9 See for example Coburn (1988, 1988a, 1992 1 ; Coburn and Biggs (1986) ; Coburn
et al. (1981) ; McKinlay and Arches (1985) ; and Wahn (1987) . 10 Zola (1978).
11 Feminist sociologists of health, for example, see rnedicine in this way.
As White (1991, p. 51) explains, feminists "have examined medicalization at a
number of levels. Medical textsbooks and journals have been criticized for
their sexist attitudes ... Micro analyses of doctor-fernale patient interactions have revealed the daily workings of sexism...Barrett and Roberts ... analyzed the interactions between male doctors and middle aged fernale patients and
found that 'women were remorsely confirmed in traditional family and domestic
roles and more than one instance of a woman's refusal to do housework
resulted eventually in hospitalization and electro-convulsive therapyf."
12 White, (Iggl), p. 2.
13 Ibid.
14 Wright and Treacher (1982). See their Introduction.
15 Lock (1988). p. 3.
16 Wright and Treache- (1982),-p-. 6 % - - - - - - - - - - - - - - - - - - -
p p p p p p p - - - - -
17 Wright and Teacher, (19821, p. 10.
18 Mishler (l98l), p. 142.
19 A good overview on the subject is provided by Raymond (1991). Pascal's
Pensees gives a specific account of the despair we feel in the face of an
ambiguous existence.
20 Nietzsche, (1969).
21 Sartre (1956).
22 Rorty, (1989).
23 In Chapter 5, to be precise.
24 Which is i t se l f a mishmash of differing views. See Roseneau (1992)
Chapter 1 on this.
25 ... with its emphasis (in some of its formulations) on historical materialism and the inevitable emancipation of the worker and the emergence
of the classless society. These are themes to which Lyotard speaks. See

Sarup (1993) p. 145, for a brief word on Lyotardf s position with regard to
Marxism.
26 Rorty (19821, p. 92.
27 See Rorty in Brown (19941, p. 34.
28 Mishler (1981), p. 148.
29 Turner, (1992), p. 48.
30 Ibid.
31 This theme is particularly prominent in Marx's The German Ideology.
(1970).
32 The political theories of Hobbes (1968), Locke (1988) and Rousseau (1973)
a l1 begin with a theory of humankind in the natural state.
33 See Charmaz (1983; 1987), for example, regarding the impact that chronic
illness has on the sense of self. Goffman's Stigma (1963), is another good
example.
34 See, for example, Foucaultf s History of Sexuality (1978 . 35 That is, my concern is not with the different approaches themselves.
Rather, the different approaches are drawn upon in light of verticalist
and/or horizontalist themes.
36 1 should point out that this relativistic conclusion is not shared by al1
horizontalists. Certain pragmatists, for example, would take issue with such
extreme relativism. Rorty actually disavows relativism regarding some
beliefs as better than others. He States, for example, that '"Relativism" is
the view that every belief on a certain topic, or perhaps about any topic, is p p p p p p p p p p p - - - - - - - - - - - - - - - - - - - - -
as good aspevery other. No one holds this view. Except for the occasional
cooperative freshman, one cannot find anybody who says that two incompatible
opinions on an important topic are equally good.' (Quoted in Bernstein, 1991,
p - 201) . (See also Rorty (lggl), p. 212 for another example. ) Just because
there are no foundations does not mean we have to treat every view equally.
And Rorty certainly does not. As we shall see later, he is in fact quite
ethnocentric. Other horizontalists, however, are avowadly relativist.
Feyerabend, for example, says that ' . . . traditions. . . become good or bad (rational/irrational' pious/impious; advanced/"primitiveW;
humanitarian/vicious; etc.) only when looked at £rom the point of view of
some other tradition. "Objectively" there is not much to choose between
anti-semitism and humanitarianism. But racism will appear viciouz to a
humanitarian while humanitarianism will appear vapid to a racist. Relat ivsm
(in the old and simple sense of Protagoras) gives an adequate account of the
situation which thus emerges. ' (Quoted in Berstein, 1991, p. 200) . 37 Once again, see Chapter 5 for an elaboration on this theme.
38 Baha'u'llah is the founder of the Baha'i Faith.
39 Baha'i International Community (1995), p. 1.
40 Baha'i International Community (l99Sa}, p. 2.
41 Ibid.
42 Bahali International Comunity (19951, p. 4.
43 See Hegel' s Phenomenology of Mind (1969) , for his doctrine of organicism which he employs to understand philosophy, human personalities, societies,
etc.
44 See Marchak (1992) . p. 60. 45 Baha'i International Community, (19951, p. 4-
46 Baha'i International Community, (19951, p. 8.
47 This duality supplanted the Apollian-Dionysian duality that dominated
Greece before Socrates' influence took over. See Zeitlin (l994), p. 18.
48 Zeitlin (1994)' p. 6.
49 Conrad (1975).
50 Turner (1992), p. 235.
51 Ibid, p. 235-236.
52 Turner (1995), p. 211; my italics.
53 Ibid.
54 Turner (1992), p. 220.
55 Ibid, p. 236.
56 Ibid, p. 57.
57 Danesh (1986), p. 116.
58 Ibid.
59 Baha'i International Community (1995), p. 9.
60 Ibid.
61 Turner (1992) . 62 Conrad and Kern (1994), p. 7.
63 Turner (1992), p. 2.
64 Mishler (1981) , p. 142.
65 Ibid, p. 142.
66 Freidson (1970)' p. 209.
67 (1992), p. 7.

JOORNEY NOTES The o b j e c t i v e of t h i s chap te r i s t o e x p l o r e i n some d e p t h the
v e r t i c a l i s t approach t o r e a l i t y , and i n p a r t i c u l a r , t o h e a l t h , i l l n e s s and d i s e a s e .
T h e gist o f t h e c h a p t e r is t h i s : The d r i v e t o uncover - t o m i r r o r r e a l i t y - has captured the
imaginat ion over the c e n t u r i e s . T h e v e r t i c a l i s m s of Pla t o , Descartes and H u s s e r l a r e ment ioned a s examples . Each, i n h i s own way, makes the v e r t i c a l i s t a t t e m p t t o p e n e t r a t e i n t o the t r u t h of t h i n g s . The d r i v e t o p e n e t r a t e , moreover , c o n t i n u e s i n t o t h e present d a y , a drive r e p r e s e n t e d perhaps most p rominen t l y by science.
S c i e n t i s m i s a v e r s i o n o f v e r t i c a l i s m . Assuminq t h e r e is a r e a l i t y t o be uncovered, s c i e n t i s m h o l d s t h a t s c i e n c e i s t h e best way t o uncover i t , to uncover n a t u r e , t o uncover e s s e n c e - t o know what i s " o u t there". S c i e n c e i s t h e r e f o r e cons idered the best form of knowledge t oday .
Medicine is s i m i l a r l y v e r t i c a l i s t - a t l e a s t t h i s is what s o c i a l c o n s t r u c t i o n i s t s h o l d . Premised upon na t u r a l i s t on t o l o g y and epis temology , m e d i c i n e r egards i t s e l f a s h i t t i n g upon objective and u n i v e r s a l t r u t h s concern ing health, i l l n e s s and d i s e a s e , and a s h a v i n g a unique a b i l i t y t o do s o .
Werve heard a lot about the information age recently. We've
heaxd a lot from people like Lyotard that we are moving into a
postmodern era where the quest for "truth" is passé. We hear
that performativity - "the best possible input/output equationw'- is what really counts. The new attitude seems to be
this: whereas before we sought after loftiness, now itf s time
that we got down to earth. Forget eternality; let's deal with
practicality.
The question...now asked by the professionalist student, the State, or institutions of higher education is no longer "1s it true?" but "What use is it?" . . . What no longer makes the grade is competence as defined by other criteria true/false, justhnjust, etc. - and, of course, low performativity in
2 general.
This attitude has implications for power and its augmentation.
Power, Lyotard says, is performativity. Perfomativity
increases with the amount of information at one's disposal. 3
Power, then, is very much related to accessibility to
information and its efficient use.
The performativity of an utterance .. . increases proportionally to the amount of information about its referent one has at one's disposal. Thus the growth of power, and its self- legitimation, are now taking the route of data s torage and
4 accessibility, and the operativity of information.
Performativity is becoming increasingly important. I don't
want to deny that. But 1 don't think w e can conclude that the
search f o r truth is no longer captivating. Our fascination with
the prospect of being able to unearth the essence of things
continues to linger with us, if not to dominate us. The drive
to penetrate reality remains a powerful force in our society.
The conviction t h a t science can lead the way in this endeavor is
still profound. And 1 donlt think Lyotard would unequivocally
repudiate these observations. Indeed, 1 think it is correct to
maintain that he feels we are still in some ways captivated by
this mode of functioning. Otherwise he would not be urging us
to divest ourselves of the grand metanarratives that continue to
inform the quest for truth. 5
A recent cover story in T i m e titled "Glimpses of the ~ i n d " ~
provides a clear example of Our enduring captivation with truth.
Since Plato and before, we have wanted to understand the mind,
to locate it, to categorize it. Plato placed the mind within
the head, Aristotle within the neart, and Descartes somewhere
within the head again, portraying it as an inunaterial entity,
fundamentally distinguished from the materiality that houses it.
The mind has traditionally figured as one of the great subjects
of philosophical inquiry. Now science has made it one of its
many concerns.
Naturally, as a subject of probing scientific scrutiny, the
mind and its qualities (memory, emotion, consciousness) have
been tenaciously linked to materiality. In one scientific view,
the mind is simply a derivative of the brain. Consciousness,
for example, "rnay be nothing more than an evanescent by-product
of more mundane, wholly physical processes - much as a rainbow
is the result of the interplay of light and raindrops ."?
And why not? It makes sense. Take a chunk out of the brain
and funny things happen. Remove a portion of the hippocampus
and you may end up with someone like HM who is able to remember
things prior to surgery, but who is also unable to form any
post-surgery memories. Remove another part of the brain and you
may end up with an individual seemingly normal in many ways, but
who is also systematically indecisive, unreliable, prone to
making bad money investments, and what's more, indifferent to
these problerns. Different sections of the brain seern to be
directly correlated with different aspects of the mind. This is
the clairn that neuroscientists and other scientists are making
based on their use of special technologies such as magnetic
resonance imaging (MRI) and positron-emission tornography (PET) . These technologies ostensibly provide
a window on the human brain, letting scientists watch a thought taking place, see the red glow of fear erupting from the structure known as the amygdala, or note the telltale firing of neurons as a long-buried rnernory is reconstructed. 8
It may be taking things too far to clairn that science is
wholly materialist about the mind. Science rnay not take
materialism to the extent that Dernocritus did, who claimed
everything, even the soul, is made up of diverse eternal
building blocks - atoms - cornbined togethew in various formations. But it is most definitely leaning in that
direction. For many scientists, the mind is rooted in biologyg.
And the corollary they draw is this: no biological account, no
existence. For example: given there is no physical place for
the "self" to exist in the brain, there is no self. This is the
conclusion scientists have corne to after a century of
investigation. The "Time" article ends by saying: "It may be
that scientists will eventually have to acknowledge the
existence of something beyond their ken - something that rnight
be described as the soul. "'O To share a bias of mine, 1 agree.
But for now, scientists are after the physical foundations of
what Descartes originally distinguished as a mental (and
therefore, distinct from physical) substance.
The point of this is to begin to illustrate the verticalist
position as 1 am using it. The verticalist position vis-à-vis
science, for example, says that science can s e e ; science can see
a great deal. It can penetrate into phenomena we previously
held impervious to scientific investigation. And it can do so
with increasing precision and scope. The mind, before so

elusive and subject only to philosophical inquiry, is being
grounded by science. Science is going 'where no-one has gone
bef ore"".
This verticalist drive to penetrate the way things are, to get
at the absolute truth of things, is further revealed in a
special issue of T i m e called "The Frontief s of Medicine. ""
Consider, for example, the title of its introductory essay: "An
Epidemic of ~ i s c o v e r y " ' ~ ; or the position espoused in the same
essay regarding the discovery of the double-helix structure of
DNA :
The entire process of achievement took a major turn toward today's exuberant state in the 1950s. The demonstration of the double-helix structure of DNA by James Watson and Francis Crick in 1953 was the long-awaited key that opened the door to a rich trove of f u n d a m e n t a l biological knowledge. In time this discovery did nothing less than b r i n g to l i g h t the secrets hidden within the membrane of each of the 200 different varieties into which the hurnan body's 75 trillion cells are divided. 14
Or the title of the article devoted to genetics in the same
issue - "Keys to the Kingdom" - and its introductory statement: The discovery and manipulation of human genes - together with the use of special new drugs - are unlocking a future in which the human body promises to confound and defeat its ancient
15 enemies . It seems clear that verticalisrn and the quest for truth remains
a powerful force in our society.
It is, moreover, a force informed by a powerful tradition.
Humanity and its theorists, although not always scientific in
the modern sense, are certainly no strangers to the prospect of
penetrating reality. Take Plato, for instance. If anyone does,
he epitomizes the quest for truth. And his concerns are lofty,
to Say the least. For Plato,
The true lover of knowledge naturally strives for truth, and is not content with common opinion, but soars with undirnmed and unwearied passion till he grasps the essential nature of things . 16 Plato sees two worlds. The first is the material shadow
world, the world of transient things and common opinion. It
concerns him only insofar as it can entrap us and prevent us
from pursuing our main objective in life which is to uncover the
secrets of the real world, the world of the Forms. This is the
world of independent, universal, eternal realities. It is a
world unspoiled by particularity and ephemerality. It consists
of changeless ideas (the perfect good, justice, tree, horse,
color yellow, triangle) of which every corresponding particular
is simply a deficient emulation. It is the world of perfection.
For Plato, there is only one way to access this world, and
that is through reason. The senses misguide us. They leave us
captivated by the shadows of change. They distract us from what
is truly real. But we can know truth because we have all
experienced it. How? Plato believes in the immortality of the
soul and its transmigration. As such, he believes that we have
been reincarnated numerous times. We have therefore been able
to see the other world numerous times, and hence, those things 17 eternal. Thus, knowledge is not about acquisition, it is about
1 E! "rememberingf' or "reminiscing". And how do we rernember? How do
we recover knowledge? Through the practice of reason, and more
precisely, by exercising the Socratic method of questioning. The
Socratic method allows us to give birth to the knowledge latent
within us - to recollect. 19
Our fundamental aim, then , is to be in touch with our
reincarnated soul - the repository of absolute wisdom. It is to
disrobe ourselves of surface changeful knowledges so that we can
penetrate the light of reality.

If it is true, then, we must conclude that education is not what it is said to be by some, who profess to put into a soul knowledge that was not there before - rather as if they could put sight into blind eyes. On the contrary, Our argument indicates that this is a capacity which is innate in each man's soul, and that the faculty by which he learns is like an eye which cannot be turned £rom darkness to light unless the whole body is turned; in the same way the entire soul must be turned away from this world of change until its eye can bear to look straight at reality, and at the brightest of al1 realities which we have called the Good. 2 0
But, in the end, Plato does not universalize our capacity to see
the Good. Instead, he calls for a class of philosopher
guardians, a class both predisposed2' and fully trained to rule
humanity based on its privileged ability to approach Truth.
The history of western thought is filled with verticalists,
filled with personages concerned with the way things are in the
world. Aristotle, Augustine, Aquinus, and Bacon are just some.
So is Descartes. But Descartesf verticalism has a unique
foundation. It begins with the famous egocentric premise:
cogito ergo sum: I think, therefore 1 am. The fact that he
thinks - doubts, understands, imagines - means that he
indubitably exists.
Descartes' original concern is to refute radical skepticism,
the view that we cannot know, and more forcefully, that there is
nothing to know anyway. The world is an illusion. Descartes
sets out to invalidate skepticism by embracing it and pressing
it to its logical conclusions. He designs and applies a rnethod
of radical and systematic doubt through which he discards
anything the existence of which can be questioned in the
slightest. He even posits an evil demon with powers to deceive
him about the most obvious of things . 1 will suppose therefore that not God, who is supremely good and the source of truth, but rather some malicious demon of
the utmost power and cunning has employed al1 his energies in order to deceive me. 1 shall think that the sky, the air, the earth, colors, shapes, sounds and al1 external things are rnerely the delusions of dreams which he has devised to ensnare my judgment . 2 2
But in the end, one thing remains.
In that case 1 too undoubtedly exist, if he is deceiving me; and let him deceive me as much as he can, he will never bring it about that 1 am nothing so long as I think that 1 am something. So after considering everything very thoroughly, I rnust finally conclude that this proposition, 1 am, 1 exist, is necessarily true whenever it is put forward by me or conceived in rny mind. 2 3
So the cogito is his rock solid foundation. It is as
axiomatic to his knowledge of existence as 1+1=2 is to the rest
of mathematics. Upon it he seeks to build the edifice of
knowledge, one made up of clear and distinct ideas. His first
step is to confirm the existence of God (which he attempts
through a few deductive proofs). His second step is to
demonstrate the existence of the external world. Having proved
that God exists and that God is benevolent, he concludes that
God is no deceiver. Anything that we are convinced is t r u e -
that is clear and distinct to us - God validates. Hence, the
fact that we have a clear and distinct belief that the external
world exists means that it is no delusion. The idea of it as a
reality is true since it has been implanted within us by a non-
dece iving God . In short, for Descartes there is truth to be had. It is
"within human powers to arrive at a systematic and true
understanding of nature. . . "24 . And it is to be had through the
exercise of reason the fruits of which are confirmed by God.
Husserl is after certainty in much the same way that Descartes
is. His methods for achieving it are similar as well. Husserl
wants to create a "presuppositionless" philosophy25, a philosophy
oriented to getting at only what is perfectly evident. He seeks
to do so through the method of phenomenal reduction which
involves "bracketing out" or "parenthesizing" anything that can
be questioned as true. By doing this he feels he can reveal the
pith of a phenomenon, disclosing it in al1 its authenticity.
Thus to each psychic lived process there corresponds through the device of phenornenological reduction a pure phenomenon, which exhibits its intrinsic (immanent) essence...as an absolute datum. 2 6
Through phenomenal reduction, Husserl claims he can pierce
through the level of (mental, social) constructions, and get to
the level of "apodicticity" - the level of absolute reality. Like Plato and Descartes, he is after the true essence of
things . Plato wrote in the fourth century B.C., Descartes in the 17th
century and Husserl in the beginning of the 20th century.
That's a spread of well over two rnillennia and yet these
philosophers are the same in a very important sense. They
exemplify an entire philosophical tradition consumed with the
prospect of finding the best way to discover/represent reality.
As Rorty explains,
The picture which holds traditional philosophy captive is that of the mind as a great mirror, containing various representations - some accurate, some not - and capable of
2 7 being studied by pure, nonempirical methods.
Our task is to try and achieve "more accurate representations by
inspecting, repairing, and polishing the mirror, so to
speak.. . ,,28 . But, according to this tradition, certain ways of
polishing the mirror are more suitable than others. Thus,
Philosophy's central concern is to be a general theory of representation, a theory which will divide culture up into the areas which represent reality well, those which represent it
less well, and those which do not represent it at al1 (despite their pretense of doing so) . 2 9 This is verticalism as 1 am using it. There are things out
there to be known, and for some like Plato, Descartes and
~usserl~~, these things are absolute. We can know and accurately
represent them. But some ways of knowing, or representing, are
better than others. The verticalist task, therefore, is to
establish the hierarchy of representational strategies; to
elevate some (or one) as adequate to the task while lowering
(even denigrating) the others. This is what the philosophic
quest has entailed. And the result to date? Most prominently
it is the elevation of science to dominance.
SCIENTISM AS VERTICALISM
'In this century scientism in philosophy" writes Sorell, "has
already had one high point, and it may be enjoying a
resurgence."31 The 1920s were a great tirne for science with the
Vienna Circle working diligently to establish a program for its
unity. Today, science is ernerging to prominence once again,
perhaps dominating the way in which we address reality.
Traditionally, scientisrn has f a l l e n within the empirical - - - - - - - -
t-radrtron, h rradltlon that has repudiated the search for
metaphysical truth - a rationalist enterprise. More recently,
realists with interests in "deeper" issues have emerged within
the scientism camp. So there is controversy within the camp.
Yet both empiricists and realists share a profound concern for
the acquisition of truth, whether it be empirical or
foundational truth. Moreover, both hold that science is the
best way to access truth. Scientism is thus verticalism applied
to science. Consider Sorell's definition:
Scientism is the belief that science, especially natural science, is much the most valuable part of human learning - much the most valuable part because it is much the most
a u t h o r i t a t i v e , o r ser ious , o r b e n e f i c i a l . Other b e l i e f s r e l a t e d t o t h i s one may a l s o be regarded as s c i e n t i s t i c , e.g., the b e l i e f t h a t sc ience i s t h e o n l y valuable p a r t of human learning, o r the view t h a t it i s always good f o r sub jec t s t h a t do not belong t o sc ience t o be placed on a s c i e n t i f i c foot ing. When, a s has happened f requent ly s ince t h e seventeenth century, philosophers claim t o have made morals , or h i s t o r y , o r p o l i t i c s , o r a e s t h e t i c s , o r t h e study of t h e human rnind i n t o a sc ience , t h e y take it f o r granted t h a t f o r a sub jec t t o
become a sc ience i s fo r it t o go up i n the world. 3 2
Scientism makes sc ience the s tandard t o which a l 1 e l s e i s
But l e t ' s g e t more spec i f i c . What exac t ly are t h e claims
being made fo r sc ience? S o r e l l i s o l a t e s f i v e . One i s t h a t
science i s un i f i ed . By t h i s i s meant t h a t t h e laws and
t h e o r e t i c a l tems used by one s c i e n t i f i c theory are t r a n s l a t a b l e
i n t o any o t h e r s c i e n t i f i c theory. They axe in t e r -de f inab le
among t h e o r i e s . Theories a r e t h e r e f o r e conunensurable. A second
i s that sc ience is unr iva led i n i t s a b i l i t y t o p r e d i c t ,
explain and cont ro l . Science can tap i n t o t h e workings of
th ings and it can do s o b e t t e r than anything e l s e . S o r e l l
quotes Hempell on t h i s who says t h a t " the p r a c t i c a l app l ica t ion
of s c i e n t i f i c i n s i g h t s i s giving us an ever i nc reas ing rneasure
of con t ro l over the fo rces of na tu re and the m i n d s of
The a b i l i t y of sc ience t o e x e r c i s e g r e a t e r and g rea t e r con t ro l
i s p a r a l l e l e d by i t s a b i l i t y t o expand i n t o broader and broader
a r eas . I n f a c t , sc ien t i sm holds t h a t t h e reaches of sc ience a re
immeasurable. That i t s knowledge i s boundless. This i s t h e
t h i r d claim, and it i s a d a i m t h a t r i n g s loud and c l e a r with
Carnap who proclaims t h a t \\ [w] hen we Say t h a t s c i e n t i f i c
knowledge is unlimited, w e mean: there i s no question whose
answer is in p r i n c i p l e unattainable by science. ,,35
The fourth claim is that the methods of science guarantee
objectivity and that we are getting closer to the truth about
things. For logical positivists like Ayer, the best nethod is 3 6 one of verification. Any proposition that is meaningful is
either analytically or empirically verifiable. Al1 else is
senseless and not worth pursuing. When a proposition is
analytic it means that it is true by definition. ft is a
tautology. By empirically verifiable is meant that it can be
supported by experience. But - to digress a little - verificationism runs into problems, not least of which is its
own status as a principle. To daim that "[elvery genuine
proposition must be either analytic or empirically verifiable" 3 7 is itself neither analytic nor empirically verifiable. By its
own standards, verificationism is self-refuting.
For realists like Popper, the true method of science is that
of falsificationisrn. Falsificationism is asymmetrically related
to verificationism. The latter is purely inductive in that it
is bent on creating theories - and universal laws - out of the evidence. We must build from the evidence up. But the problem
with this approach3* is that we can never be sure that the
evidence we have is enough. How can we know that things will
not behave dif ferently in the future? How can we be sure that
As will always be As and not Bs? This was Hume's point. Past
events are no indication of what will happen in the future.
Al1 probable arguments are built on the supposition, that there is this conformity betwixt the future and the past, and therefore can never prove it. This conformity is a matter of fact, and if it must be proved, will admit of no proof but from experience. But our experience in the past can be a proof of nothing for the future, but upon a supposition, that there is a resemblance betwixt them. This therefore is a point, which can admit of no proof at all, and which we take
3 9 for granted without proof.
T h e sun ro se today, but what's t o Say t h a t i t w i l l r i s e
tornorrow. That w e assume it w i l l is nothing more t h a n t h a t - an
assumption.
So i f w e can't proceed induc t ive ly , we can proceed through
r e f u t a t i o n . W e can pos i t theories and test them. We can fo l low
modus t o l l e n s . Whereas w e can never decidedly prove a theory
t r u e s i n c e any sample of cor robora t ing evidence, no mat te r how
ex tens ive , i s always f i n i t e , we can unambiguously f a l s i f y a
theory . I t only t a k e s one "bad" i n s t ance t o do s o . So Popper
urges us t o proceed through r e f u t a t i o n . H e urges us t o c r e a t e
t h e o r i e s t h a t a r e f a l s i f i a b l e , and he says t h e more f a l s i f i a b l e ,
t h e better. The bolder , t h e b e t t e r . This , f o r him, i s the mark
how t r u e sc ience advances.
Moreover, i t is t he way i n which we can know w e are g e t t i n g
somewhere. The aim i s t o ge t c l o s e r t o t h e t r u t h . The ex ten t
t o which a theory mi r ro r s t h e t r u t h Popper calls its
v e r i s i m i l i t u d e . The e x t e n t t o which a t heo ry ' s v e r i s i m i l i t u d e
i nc r ea se s depends on i t s a b i l i t y t o withstand f a l s i f i c a t i o n .
The g r e a t e r t h e f i t n e s s of a theory - the g r e a t e r i t s a b i l i t y t o
defy r e f u t a t i o n - t h e more conf ident we can be that it
r ep re sen t s t r u t h .
W e can never make a b s o l u t e l y c e r t a i n t h a t Our theory is not l o s t . Al1 w e can do i s t o sea rch for t h e falsity con ten t o f our b e s t theory. W e do s o by t r y i n g t o refute our theory; t h a t is, by t ry ing t o t e s t it seve re ly i n t h e l i g h t of a l 1 our ob j ec t i ve knowledge and al1 Our ingenuity. I t i s , of course, always pos s ib l e t h a t t h e theory may be false even i f it passes a l 1 t h e s e tests; t h i s is allowed f o r by our search f o r v e r i s i m i l i t u d e . But i f it passes a l 1 these t e s t s then we m a y have good reason to conjecture t h a t our theory, which as we
know h a s a greater t r u t h content t han i t s predecessor, may have no g r e a t e r f a l s i t y content . And if w e f a i l t o r e f u t e t h e new theory , e s p e c i a l l y i n f i e l d s i n which i t s predecessor has been re fu ted , then w e can c l a i m t h i s as one of the ob j ec t i ve
reasons for the conjecture t h a t the new theory is a better approximation to truth t h a n the old theory. 4 O
And it is for these reasons that we can speak of scientific
progress. Why has science progressed? The explanation,
according to Newton-Smith is very simple: Our theories are 4 L getting closer to the truth. New theories are eclipsing older
ones - they are achieving greater and greater verisimilitude. Finally, the fifth claim is that science is beneficial.
Science, given its unlimited ability to approach truth, fosters
progress like no other knowledge form (especially compared to
religion, which is understood to stifle progress42). Its value
to humanity is unique, extensive and profound.
I should emphasize that there are different versions of
scientism. The distinction between logical positivism and its
rival, scientif ic realism, is particularly notable. The former
has nothing to do with metaphysical issues, deep causes,
theoretical entities, etc. Such things cannot be seen nor
experienced. They are, therefore, meaningless and represent
"nothing but sophistry and illusion"43. So positivism insists
that we focus our concerns on that which can be known
experientially. 'With a firm grip on observable reality the
positivist can do what he wants with the r e ~ t . " ~ ~
Realists, on the other hand, are intent upon getting
underneath the surface of things. For them, metaphysical
entities - like electrons and the mind - are real and can be known. We can penetrate and discover them in al1 their
primordial existence. R e a l i s r n is concerned with things both
observable and unobservable.
But logical positivism and realism are similar in fundamental
ways. They both Say that truth exists and that it can be known.
They are both prescriptive. They both Say that truth can only
be known through the methods of scientific inquiry which
guarantee objectivity, and allow us to find "...Truth naked,
relative to no des~ri~tion."'~ Both logical positivism and
realism hold that
[tlhere is a truth of matters, and the methods described by positivists and realists are adequate to the discovery of that truth. This assumes the capacity of the methods of empirical science, construed as guarantors of context independence, to fully reveal the actual character of things. 4 6
Both are verticalist in the purest sense.
MEDICINE AND VERTICAL~SM~'
Now for medicine (modern biomedicine). Medicine is modeled on
the natural sciences and is thus verticalist in orientation. It
revolves around two fundamental claims: 1. biomedical theory is
neutral; and 2. biomedical theory is universal in application.
By the former is meant that it has unique access to the workings
of nature, and more precisely, the body, The latter stems £rom
the former. By the latter is meant that since biomedical
findings are neutral, they speak to universal truths. They are
therefore universal in application.
But things are a little more involved than this. Gordon
provides a u s e f u l picture of the medical approach in her article
"Tenacious Assumptions in Western ~edicine"~'. What f ollows owes
much to her. In particular, Gordonf s depiction of the
naturalism of medicine and the way in which medicine understands
nature (the body) largely in terms of "the canons of the
enlic~htenment"~~ is informative. She divides her presentation
into two areas: 1. naturalist ontology/cosmology; and 2.
naturalist episternology.
Medicine and Natuzalist Ontology and Cosmology
Ontological concerns are concerns with what exists, with what
is real. They are concerns with the nature of being.
Cosmological concerns have to do with the ways in which the
world is put together and ordered.
Medical ontoiogy/cosmology is naturalist which means a few
things. In general, i t means that nature is approached as an
autonomous realm. Illnesses are viewed as entities, or made up
of entities, "out there". The naturalist tendency is to see
diseases independently of anything like culture, morality, the
supernatural, human consciousness, time and space.
To elaborate, consider illness in light of ... 1. Materialism: We have already touched on the dualism of
Descartes. For him, there are two fundamental substances in the
world - one is mental, the other material. The naturalism of
medicine not only perpetuates this division, but gives priority
to the latter. This is an emblematic outcome of the
Enlightenrnent, the tendency of which was to "disenchant" nature
and see it in mechanistic rather than in spiritual terms.
Medicine sees nothing 'divine" about illness. It strips illness
of its "evi l" foundations. Medicine understands illness in
terms of what it sees as the autonomous mechanisrns of nature,
and defines it in terms of materialist indicators (such as blood
pressure) . It understands illnesses by reducing them to
disordered bodily functions. This is physical reductionism.
2. Consciousness: Nature is a reality "out there" according to
naturalism. Thus, diseases are realities 'out there" according
to medicine. They are indif ferent to Our perceptions of them,
and as such, have definite realities. They are things-in-
themselves and to be understood accordingly. As such, medicine
defines illness and health in terms of objective criteria. The
concerns or feelings of patients are irrelevant. To make them
relevant is to conflate thing-in-themselves with emotional
responses to them, objectivity with subj ectivity, materiality

with mentality, "out there" with "in there". It is to rnuddle an
otherwise authentic entity.
3. Atornisrn: Medicine is atomistic which means that it
conceives of the body as little more than the sum of its various
parts. The parts, in their cause/effect relationships, form a
mechanical system which determines the whole. The whole is
therefore derivative of the parts while the opposite is not the
case. This means that the parts (much like the parts of a car)
can be looked at, assessed or dealt with as distinct phenomena.
They can be "decontextualized" and treated accordingly.
4. The Social: Nature is autonomous to social phenomena like
culture, values, morality, society and power. The social gives
rise to diversity, but this diversity is a superficial one. It
is transient and does not correspond to the essence of things.
There is a fundamental sameness to us all, one that underlies
and is indifferent to our diversity. The point is to permeate
the confusion of diversity in order to expose the light of
universality.
As far as disease is concerned this is what taxonomies have
done. Taxonomies are atternpts to mirror the diseases of nature
as they are in-themselves.
5. Time and Space: Medicine is getting better at mirroring
nature's diseases. It is capturing more and more of what nature
and its diseases, in al1 their universality, eternality and
omnipresence, are about. Medicine is on the cumulative path
greater truth, a truth that is neither tirne, nor location
specific.
Medicine and Naturalist Epistemology
Epistemological concerns are concerns about truth (whether
not there is truth) and what/how we can know of it. Naturalist
epistemology assumes there is truth and that there are very
s p e c i f i c ways w e can know of it. Medicine a d o p t s t h i s
epistemology.
Heref s how:
I t s ays t h a t s i n c e t h e r e i s an o b j e c t i v e n a t u r a l r e a l i t y ou t
t h e r e , w e need t o f i nd ways t o r e p r e s e n t it. W e need t o c r e a t e
models, a language, t h e o r i e s , t h a t correspond t o i l l n e s s as it
r e a l l y i s . W e can begin t o do t h i s by tapping i n t o our sensual
knowledge which i s a h i s t o r i c a l . But al though t h i s i s e s s e n t i a l ,
it i s no t enough. To g e t a t na tu r e we a l s o need t o manipulate
it, t o vex it, t o p lace it under a r t i f i c i a l s e t t i n g s and fo r ce
it t o unadu l t e r a t ed presence . This , obviously, i s what t h e
experiment i s al1 about.
But again , t h i s i s no t enough. W e a l s o have t o a l t e r
ou r se lve s when w e a l t e r n a t u r e . W e must disengage ourse lves
from ou r se lve s . W e must achieve adequate d i s t a n c e from Our
b i a s e s , va lues and preconceptions; achieve detachment so t h a t we
can perce ive t h e ob j ec t ( n a t u r e ) f o r what it r e a l l y i s .
When t h e s e c r i t e r i a a r e m e t , w e a r e on the way t o obta in ing ,
and hence adequate ly r e f l e c t i n g , t h e t r u t h about r e a l i t y
( n a t u r e ) . 5 0 In Conclusion . . .
. . . na tu r a l i sm inco rpo ra t e s a ve ry s p e c i f i c b l u e p r i n t f o r how
t o know what t r u l y e x i s t s . Biomedicine buys into, is based on,
and pe rpe tua t e s natural isrn. I t t he r eby lays s p e c i a l d a i m over
a s p e c i f i c domain of na tu r e , namely h e a l t h , i l l n e s s and d i s e a s e .
Hence the v e r t i c a l i s m of medicine.
mRTICALISM: ONE FINAL EXAMPLE
One month a f t e r T i m e publ i shed i t s a r t i c l e on t h e b ra in , it
came o u t with ano the r cover s t o r y t i t l e d "The Evolut ion of
~ e ~ r e s s i o n ~ ' ~ ~ . 1 mention t h i s because it provides one more
c u r r e n t example of our con t inu ing v e r t i c a l i s t (and i n t h i s case ,
naturalist), fascination with essences. Human nature is the
pivotal theme of the story.
Wright begins his article by saying that " [a] new field of
science examines the mismatch between our genetic makeup and the
modern world, looking for the source of our pervasive sense of
discontent." This new field of science is evolutionary
psychology, a field that seems to be evolving in the direction
of "mismatch theory". According to this theory, humans are
designed to live under conditions radically different than our
present situation seerns to allow. Because of the disparity
between our natural constitution and the social way of doing
things, the prevalence of many disorders - including depression, clinical anxiety disorder, and suicide - is up. Our present situation is one of social isolation. Our natural
situation is one of social cohesion. We yearn for the latter
but persist with the former. We look forward to watching shows
like Cheers where we can, if only for a fleeting moment, immerse
ourselves in a woxld "where everyone knows your name"; where
life bxings
regular, random encounters with friends, and not j u s t occasional, carefully scheduled lunches with them; where there [are] spats and rivalries, yes, but where grievances [are] usually heard in short order and tensions thus resolved. 5 2
But social transparency prevails. Subways are filled every
morning with emotionless faces staring off into space. Women
and men leave their suburban homes and drop their children off
at daycare £ive days a week only to return home to flick on the
TV. Acquaintances are dodged in the mean tirne. Think of what
the e l e c t r i c garage-door opener has done for uss3: now it is
possible to open the garage from our cars, scoot immediately
into the safety of our homes, and thus avoid the agony of a
courteous chat with our neighbors.

We do these things, but they are not natural. We champion the
free market and cornpetition but w e are really by nature much
more cooperative than that. We promote capitalism and produce
technologies (the TV, cars) thoroughly antithetical to our
natural ways of being. This is what mismatch theory s a y s . And
it says that, as a consequence, we feel guilt and a n x i e t y . If
we could just function in a way that corresponds more closely to
what Our genes require, things would be so much better. If we
could cultivate a n environment of warmth, affection and
camaraderie, we would be so much happier . There is a human nature rooted in our biology, the demands of
which we are systematically ignoring. Because we are ignoring
them, we are more depressed.
These are verticalist daims.
And they are d a i m s , like many others, that horizontalists
relentlessly dispute ...
1 Lyotard (1993), p. 46.
2 Ibid, p. 51.
3 Ibid, p. 47.
4 Ib id .
5 Ib id , p. 4 6 .
6 By Lernonick (1995).
7 Ib id , , p. 3 7 .
8 Ibid. Such technologies a l so l e t u s see the d i f f e r ences between how women
and men think, Women, apparently, use both sides of t h e bxain i n a more
i n t eg ra t ed way than men whose minds seem t o be more compartmentalized.
9 For others , the mind i s equated t o a computer. See i b id .
1 0 Ibid, p. 42.
11 S t a r Trek
1 2 Fa11 ( 1 9 9 6 ) .
13 By Nuland. My i t a l i c s .
1 4 Ibid., p. 7 . My i t a l i c s .
15 By J a ro f f . My italics.
1 6 A s quoted i n Ayer and OrGrady (1994) , p . 354.
17 Raymond (1991), p. 6 .
18 Z e i t l i n (1993), p. 109.
1 9 The theory of r e c o l l e c t i o n i s r a i s e d i n var ious p l ace s . Both t h e Meno and
t h e Phaedo provide good examples. In the former, f o r example, P l a to has
Socrates e l i c i t c o r r e c t answers regarding a geometr ical puzzle frorn a simple
s l a v e boy. Socrates is a b l e to do t h i s only because t h e s lave boy harbors a
p r i o r knowledge of geometry, knowledge he had h e r e t o f o r e forgot ten, knowledge
he ju s t needed t o recover, knowledge stermning from h i s s o u l t s p r i o r con tac t
with t he Forms.
20 A s quoted i n Ayer and OfGrady (1994) , p . p. 3 5 4 .
2 1 P la to a c t u a l l y recommends eugenic planning. For example, i n T h e Republic,
he wr i tes : "It follows £rom our conclusions so f a r t h a t sex should preferably
t ake p lace between men and women who a r e outs tandingly good, and should occur
as l i t t l e a s poss ible between men and women of a v a s t l y i n f e r i o r stamp." (p .
1 7 3 ) .
22 A s quoted i n Ayer and O'Grady (1994) , p. 111.
2 3 Ibid. Not my i t a l i c s .
2 4 S o r e l l ( l g g l ) , p. 29.
25 See Raymond ( l 9 9 l ) , p. 236.
26 Husserl quoted i n Raymond (1991), p. 238.
27 (1980), p. 12.
28 Ib id .
29 I b i d , , p. 3 .
30 I say f o r some s i n c e empirc is ts , who are v e r t i c a l i s t as well , a r e not
a f t e r absolute t r u th . Their concern l i e s w i th t r u t h t h a t can be experienced
through t he senses, through observation. That is, while they repudiate the
metaphysical, they s e e k observat ional t r u t h .
31 (1991), p . 3 .
32 Ib id , , p. 1 . Not my i t a l i c s .
33 1 am not proceeding i n t h e same oxder t h a t S o r e l l p resen ts them.
34 (1991), p . 7 .
35 Quoted Ibid ( l g g l ) , p . 6 . Not my i t a l i c s .
36 See Cottingham (1984), p. 105-111, fo r a b r i e f overview.
37 See Shand (1994), p. 271.
38 O r , r a t he r , "a" problem with t h i s approach. H o r i z o n t a l i s t s r a i s e numerous
i s sues with it. Chapter 3 explores many of them.
39 A s quoted i n Ayer and OfGrady (1994), p. 199. Not rny i t a l i c s .

40 In ibid., p . 357. Not my italics.
41 See Brown (1994), p. 10.
42 Sorel1 (lggl), p. 8.
43 Hume (1990) p. 165.
44 Hacking, (l994), p. 169.
45 Rorty i n Baynes et al. (1987), p. 61.
46 Longino ( l g g O ) , p. 179.
47 1 want to be clear at this point, that the following characterization of
medicine represents a horizontalist, and more precisely, a social
constructionist (within the sociology of health and illness) understanding.
It is difficult to Say how accurate a characterization it really is. For
example, although medicine may incorporate naturalist tendencies, it may be
too categorical to Say medicine is fully naturalist in the sense outlined.
Perhaps the characterization of medicine as naturalist is i tself a social
construction, one (more or less) fabricated for the purposes of social
constructionist analysis into the medical enterprise? This notwithstanding,
the discussion of naturalism which follows is informative, speaking at least
to a tendency within medicine if not to something it unequivocally endorses,
propounds . 48 (l988), pp. 19-56.
49 Ibid, p. 21.
50 Once again, from a constructionistfs point of view..
51 By Wright (August 2 8 , l99S), pp. 32-38.
52 Ibid, p. 35.
53 Ibid, p. 36.

JOflRPJEY NOl!ES Having discussed ve r t i ca l i sm , the o b j e c t i v e of this chapter is
t o explore i n depth i t s a n t i t h e s i s - the h o r i z o n t a l i s t approach t o r e a l i t y , and i n par t icu lar , t o hea l th , i l l n e s s and disease .
Here are some o f the main ideas: Horizontalism repudiates t he mind-as-mirror metaphor so dear
t o ve r t i ca l i sm . I t emphasizes, ins tead , two r e l a t e d po in t s . F i r s t : things a r e ambiguouç and cannot be known a s they are in- themselves; t hey can only be known i n l i g h t of social expec ta t ions , background assumptions; t h e y a r e meaningful on l y when paradigmatically d ic ta ted a s such; t hey mean nothing i n the absence o f perspec t ive . Second: things-in-themsel ves do no t r e a l l y e x i s t anyway (Nietzsche and Rorty, among o ther s , propound t h i s ant i -ontological view) ; th ings are constructed; t ru th is made. Hence, the world need not be a s it i s and can c e r t a i n l y be reconstructed i f we so wish i t t o be.
Having explored these two emphases, Berger's model o f t he social construct ion o f r e a l i t y i s introduced and then elaborated. Special emphasis i s then placed on the m e d i c a l model as a soc ia l construct , and on h e a l t h , i l l n e s s and d i sease a s metaphors of soc i e ta l t ens ions . The role o f power i n soc ia l construct ion i s a l s o emphasized. From various perspect ives - Parsonian, f emin is t and Marxist - medicine is depic ted a s t h e dominant producer of r e a l i t y today. I t is a l s o depicted a s the preeminen t agent of social control today, regula t i n g sociecy through medical i z a t i o n and through the 1 egitima t i o n o f dominant soc i e ta l expec ta t ions . The micro-interaction between doctor and pa t i en t is a l s o discussed a s a major forum for such l eg i t ima t ion .
T h e chapter ends w i t h the Foucauldian approach t o medicine. Foucault says that truth is power manipulated and t h a t medicine a s a "true" discourse - a s one representing the w a y things are with hea l th , i l l n e s s and disease - i s a c t u a l l y a contingent arrangement, one l i nked t o bio-power and i ts emergence t o prominence over t he l a s t couple cen tur ies .
INTRODUCTION
There are two p a r t s t o t h i s in t roduc t ion .
F i r s t , a shor t d ia logue:
It's 12rZ5pm. A verticalist and a h o r i z o n t a l i s t are h a v i n g
lunch together in a university cafeteria. It is a p l e a s a n t
meeting at first.
Verticalist: Hey, d i d you read the a r t i c l e i n t h i s weekf s T i m e ?
Hor izon ta l i s t : Which one?
Verticalist: T h e one about mismatch theory.
Hor i zon ta l i s t : Oh, you mean t h e cover s t o r y about human na tu re
and depression?
Verticalist: Yeah. What did you think?
Hor i zon ta l i s t : Waste of t ime!
V e r t i c a l i s t : What do you mean "waste of time"? How is it a
waste of tirne? I t could be r i g h t you know, and i f it i s , it
says a l o t about t h e problems with our s o c i e t y today and t h e
measures we need t o take t o solve them. 1 mean, i f we a r e by
na ture s o c i a l , t h e r e are a l o t o f changes t h a t we need t o . . . Hor izon ta l i s t : Yah r i g h t !
V e r t i c a l i s t : You c u t me o f f !
Horizontalist: 1 know 1 did, Youfre beginning t o i r r i t a t e m e
with t h a t d r ibb l e . You want t o know what 1 t h i n k ?
V e r t i c a l i s t : I f m n o t sure 1 do, anymore.
Hor i zon ta l i s t : W e l l , 1'11 t e l l you anyway. Mismatch theory says
t h a t human na ture i s i n h e r e n t l y s o c i a l , r i g h t ? T h a t i t s i n
Our genes t o be m o r e gregar ious and cooperat ive . But then 1
ask: Where i s t h i s view of human nature r e a l l y coming from?
What a r e i t s s o c i a l o r ig in s? Are these evo lu t ionary
psychologists a c t u a l l y g e t t i n g a t something profoundly t r u e
about us, o r a r e they j u s t seeing what they want t o see, what
their paradigmatic biases d i c t a t e ? Maybe they have j u s t
happened upon a f r u i t f u l s t r a t e g y t o l e g i t i m a t e another
fiction, even if unwittingly so. And here a r e some more
questions: what role does such a conception of human nature
play? Whose interests does it promote? Maybe it j u s t amounts
to one more attempt at makking some sense of this nebulous
world we live in.. . because, you know, there is nothing more to
this world than that: ambiguity. There is no deep t r u t h to
it . Truth, essence, human nature ... these are al1 fantasies of pragmatic convenience.
[Pause]
Wow! A horizontalist like myself can have a lot of fun with
mismatch theory!
The verticalist grimaces.
Horizontalist : What?
Verticalist: I think 1% going to go have lunch with someone
else now.
T h e verticalist leaves the tab le . The h o r i z o n t a l i s t s h r u g s .
Second, Chomsky versus ~oucault':
Noam Chomsky is another who posits a fixed and universal human
nature. He says that there is "a foundation for whatever it is
that- we 40 w i É h - o u z mental-mpacities; Por I f thërë wërë fiop
such foundation, we could not explain how it is that we are so
capable of learning and using language to the extent that we do,
We could not explain how it is that we can learn to use language
so creatively, producing sentences the likes of which are
totally unique. He says there must be something about our human
nature that allows us to be so linguistically innovative.
To elaborate, Chomsky finds it curious t h a t ,
... having mastered a language, one is able to understand an indefinite number of expressions that are new to one's experience . . . ; and one is able, with g r e a t e r or less facility, to produce such expressions on an appropriate occasion,
desp i t e t h e i r novel ty and independently of d e t e c t a b l e s t imulus conf igurat ions , and t o be understood by o thers who share t h i s s t i l l rnysterious a b i l i t y . The normal use of language is, i n t h i s sense, a c r e a t i v e a c t i v i t y . 3
Chomsky s t r e s s e s t h a t t h e language d a t a w e experience are
minuscule and cannot account f o r t h e prof ic iency w e manifest a s
language users. He exp la ins
The cornpetence of a n adu l t , o r even a young c h i l d , is such t h a t we must a t t r i b u t e t o him a knowledge o f language t h a t extends f a r beyond anything t h a t he has learned. Compared wi th the number of sentences t h a t a c h i l d can produce o r i n t e r p r e t wi th ease, t h e number of seconds i n a l i f e t i m e i s
r i d i c u l o u s l y small. Hence t h e data ava i lab le as input a r e on ly a minute sarnple of t h e l i n g u i s t i c mate r ia l that has been thoroughly mastered, a s indicated by ac tua l performance. 4
So what accounts fo r our language prof ic iency? According t o
Chomsky, there i s a "un iversa l grammar", a "gene t i ca l ly
determined language facu l ty" o r "language a c q u i s i t i o n devicew5
t h a t i s ingrained i n each of us . This device al lows us, when
confronted wi th the d a t a of any language, t o l e a r n , i n t e r p r e t
and use t h a t language c r e a t i v e l y .
T h i s un iversa l grammar i s immanent t o us a l l . But i t does not
c o n s t i t u t e everything t h a t is un ive r sa l ly t rue of us . chornsky6
contends t h a t we a r e fundamentally t h e same i n o t h e r ways a s
we11. For ins tance , he makes the Marxist claim t h a t there i s a
un ive r sa l human need f o r c r e a t i v e work. There i s a l s o a
un ive r sa l human need f o r f r e e inquiry . And l i k e mismatch
theory, he argues t h a t Our present s o c i o - p o l i t i c a l s i t u a t i o n i s
incompatible with such needs. I t is a n t i t h e t i c a l t o human
na tu re , and hence, it i s un jus t .
T h i s is a l 1 very v e r t i c a l i s t of Chomsky.
Enter Foucault.

Foucault will have nothing to do with any of this. He is not
concerned with whether or not there is a human nature. Instead,
he asks questions like: "How it is that we have such a
conception?" and, "What role does it play in our society?" To
posit a human
is suspicious
exist, but if
transcend our
nature is to posit a universal truth, and Foucault
of any claims to universal truth. Truth may
it does, we can never know of it7. We can never
historical/societal situation to achieve eternal
certainty. What we can do, however, is determine the social
origins of truth claims. We can see, for example, how it is
that certain concepts of human nature - as either evil or good,
selfish or altruistic, cornpetitive or cooperative, egocentric or
social, prosaic or creative - emerged and how they have functioned within society.
Foucault's basic technique is to historicize any truth clairn.
Truth is historically conditioned, historically made. It is
truth for that time, truth made by specific socio-historical
circumstances. This is very horizontalist of him. It is also
directly contrary to any verticalist conclusions.
. . . . . . . . . What follows is a relatively in-depth (though, in no way
comprehensive) look at the horizontalist position. Throughout 1
refer to a nwnber of theorists, some of whom are more
horizontalist than others. All, however, have horizontalist
contributions to make, and it is these which provide the focus
of this chapter.
In outlining the position, I find it useful to divide
horizontal emphases into two categories: 1. the ambiguity of
things; and 2. the social construction of things. By "things" 1
mean facts, data, states of affairs, evidence, signs, symptoms,
phenornena, entities, reality, etc. 1 find that the latter
category incorporates the former. 1, therefore, devote more
space to it later in this chapter where special emphasis is also
placed on the social construction of illness and the
relationship of medicine to power.
Now, with the former. . . TBE AMBIGUITY OF THINGS
Francis Bacon compares the mind to "a false mirror, which,
receiving rays irregularly distorts and discolors the nature of
things by mingling its own nature with it."' The mind, for Bacon,
is a cloudy thing; it is full of veils; it harbors different
"idols" al1 of which inhibit us from seeing the world as it
really is. As Bertrand Russell surmarizes, Bacon enmerates
four "idols of understanding":
'Idols of the tribe' are those that are inherent in hwnan nature; [Bacon] mentions in particular the habit of expecting more order in natural phenomena than is actually to be found. 'Idols of the cavef are persona1 prejudices, characteristic of the particular investigator. 'Idols of the market-place' are those that have to do with the tyranny of words. 'Idols of the theaterf are those that have to do with received wisdom of thought; of these, naturally Aristotle and the scholastics afforded him the most noteworthy instances. 9
The senses put us into contact with reality, but that is not
enough. Thatrs just scraping the surface of reality. The idea
iç to go deeper; to uncover how reality really works. But the
mind, on its own, is not up to the challenge.
Bacon goes on to talk about the importance of the experiment
in helping to get a better picture of reality, but that takes us
back to verticalism again. What's important from a
horizontalist point of view is the emphasis that Bacon places on
how the mind can limit/distort/transform what we see.
Horizontalism not only agrees with this, but takes it much
further. Data, for example, are not just data when we get hold
of them. They do not simply appear to us in some unadulterated
lucidity. Instead, they appear to us in ways molded to Our
theoretical, pre judicial, linguistic, mythical, social
expectations. They appear to us in ways paradigmatically
conformed. As we shall see, this is very much Kuhnf s position.
What this means is that the same data can mean different
things to different people/cultures, and in different historical
eras. Hence the problem with induction. Data do not speak for
themselves, nor do they stand unquestionably as some objective
state of a£ fairs. They actually donf t evince anything
meaningful unless they are paradigrnatically recognized as doing
so. To imagine that a single true theory can emerge out of a
given sample of "objective" data is simply nonsense. Instead,
the opposite seems to be the case. Scientists, for example,
. . .invariably describe and explain phenomena in terms of a specific theory which they have invented or constructed. But, formally speaking, an endless number of theories can be constructed to be consistent with a particular body of data, just as an endless number of curves can be constructed to pass through any finite number of points. Logically, the notion of a single correct, or best-supported theory is, to Say the least, an extremely dubious one; but historically it is a notion which scientists routinely and effectively employ, which is indeed essential in scientific research. 10
Likewise, it is possible for any body of data to be described in
terms of any theory: "The data can always be described in a way
which makes them compatible with the presuppositions of the
research tradition. "l'
Ponder the f ollowing:
1. The case of the hatL2:
Imagine you and your friend, upon entering Sandyfs home, find
a gray hat hanging on the banister. You both Say, "Great, Dan
is here." But when Sandy, who has just arrived home herself,
asks why you both have corne to that conclusion, you each give
different answers.
You Say: 'Well, 1 only know one person who wears a gray hat like
that, and its Dan."
But your friend says: "No, the reason I Say its Dan is because
Dan is the only one 1 know who leaves his hat hanging on the
banister like that."
As it turns out, Dan is in the house and he is helping himself
to some left oves Szechwan Chinese food. But the point is this:
The same state of affairs (the gray hat on the banister) is
used in different ways by you and your friend. You each
emphasize different aspects of the same state of affairs, and in
this case, come to the same conclusion. But what if your friend
believed instead that only another friend, Brett, hangs his hat
on the banister? Ln that case, you would each have come to
different conclusions.
A given state of affairs does not stand for anything in
itself. It stands for something only in light of certain
expectations, in light of what Longino refers to as "background
assumptions". Different background assumptions can highlight
the same state of affairs in different ways, and yet lead to the
same conclusions. A given state of affairs (the gray hat is on
the banister) may speak to one person in a way that is entirely
different to the way it speaks to another person, but then stand
for the same conclusion (Dan is in the house). On the other
hand, different beliefs may lead each to draw quite different
conclusions (Dan is in the house versus Brett is in the house)
from the same state of affairs (the gray hat is on the
banister) . Moreover, dif ferent beliefs rnay also take as
evidence completely different states of affairs, once again
leading to either the s m e or to different conclusions. In
Longinors words:
. . . how one determines evidential relevance, why one takes sorne state of affairs as evidence for one hypothesis rather than for another, depends on one's other beliefs, which we can cal1 background beliefs or assumptions. Thus, a given state of affairs can be taken as evidence for the same hypothesis in light of differing background beliefs, and it can be taken as evidence for quite different and even conflicting hypotheses given appropriately conflicting background beliefs. Similarly, different aspects of one state of affairs can be taken as evidence for the same hypothesis in light of differing background beliefs, and they can serve as evidence for different and even conflicting hypotheses given appropriately conflicting background beliefs. 13
To put this al1 another way, a given state of affairs is never
evidentially relevant, even apparent, unless paradigmatically
imbued a s such. (From Sandyf s point of view, the gray hat on
the banister may have no evidential import. For her, the
paucity of left over Chinese food may be the more relevant state
of affairs . )
2. The case of the two sexist pictures:
Although we live in a profoundly sexist society, although the
reaches of patriarchy are insidiously rampant, it remains
interesting to note that some can so easily read sexism into
practically everything they see. Here's an illustration of what
Imagine a picture of a man positioned behind a woman, both of
whorn are portrayed only £rom the waist up. The man is slightly
taller than the woman and a little to her right. They are both
looking straight ahead, each with little emotion on their faces.
There are many ways to interpret this picture. One way is to
see it as a sexist depiction/promulgation of stereotypical male
and female roles. With an inclination to (with background
assumptions that) see sexism in everything, one might rnake the
following interpretation: " H e r e is a typical depiction of a man
playing the protective role- The woman, on the other hand, is
portrayed as the weaker of the two, reliant upon the man for his
presence, strength and guidance. "
Now, imagine a second picture where the positions of the man
and woman are completely reversed. Based on what the first
picture evokes, one might conclude that this second one,
representing the opposite state of affairs, would evoke an
interpretation like: "Here the woman is finally portrayed
holding the more powerful of the two roles; she is watching over
the man who is in turn relying on her for her strength." But
that doesn' t necessarily happen. A new interpretation is made,
al1 right, but it is, like the first, consistent with the
assumption that sexism is omnipresent. This time: "The man is
depicted as setting the direction, leading the way. The woman,
on the other hand, is in her "proper" place, that is, behind the
more powerful man."
These two scenarios are intended to illustrate how background
assumptions can work to make basically the same thing - draw the same conclusions - out of radically different states of affairs. The paradigm is a powerful thing. It has a profound ability to
manipulate what it sees. And this it can do so even to the
point of fabricating sameness out of antithesis - sexism out of
antithesis.
3. The case of Pierre Rivière: 14 This third example comes from Foucault, Pierre Rivière was a
peasant who, in 1835, committed parricide, killing his mother,
sister and brother. While detained he wrote a mernoir recounting
particulars of his life and explaining the crime he comrnitted.
His memoir, however, led to disputes, being as it was
interpreted differently by different groups. On the one hand,
there were the doctors who concluded Rivière was mad, his memoir
providing unequivocal evidence to this end. The lawyers, on the
other hand, drawing upon the same memoir, reasoned he was sane.
The doctors emphasized the strangeness of his behavior while the
lawyers imputed full responsibility to Rivière for his actions.
In other words, the memoir (the evidence) was looked upon as
proof for two fundamentally opposed sets of conclusions. It
spoke entirely differently to the two paradigms.
So m u a . . . . . . for the independence of things l i k e facts, evidence, S t a t e s
of affairs, data (etc. ) , and hence, the phenornena they
ostensibly represent. So much for the autonomy of "objective"
criteria standing for things. So much for what Feyerabend
refers to as the "autonomy principle"'5. For the horizontalist,
facts (etc.) do not stand alone. They are not given. They make
no noise unless evoked by a paradigm. And when evoked, they
speak with a paradigmatic voice.
"There are no f acts, only interpretations . ,16 Facts (etc. ) are paradigmatically laden, and thoroughly sa.
TEE SOCIAL CONSTRUCTION OF TflïNGS
To begin, here is a taste of what two horizontalists - Nietzsche and Rorty - have to Say about reality and our p p p p p p p p p p p p p p p - p - - - - - - - - - - - -
- -
relationship to it. First:
Nietzsche
Nietzsche writes:
Have you not heard of that madman who lit a lantern in the bright morning hours, ran to the market place, and cried incessantly: '1 seek God! 1 seek God!'...'Wither is God?' he cried; '1 will tell you. Ne have k i l l e d him - you and 1. Al1 of us are his murderers. But how did we do this? . . . Who gave us the sponge to wipe away the e n t i r e horizon? . . . God is dead. God remains dead. And w e have killed him . . . There has never
17 been a greater deed ... But he also writes that we have not yet conquered Godf s shadow".
Our long-standing belief in God has had a powerful influence on

us, one w e have no t f u l l y escaped. W e s t i l l funct ion a s i f
the re were t ranscendent t h ings t o t h i s world we l i v e i n . W e
hold ont0 values t r e a t i n g them a s i f they were fundamental t o
the way th ings are and should be. W e seek and propound purpose
t o t h i s world, and search f o r an underlying order t o it. But
the re are no fundamental va lues , t h e r e is no purpose, the re is
no order. "The way" according t o za ra thus t ra lg , 'that does no t
e x i s t . W e t h ink t h a t as s c i e n t i s t s w e have escaped the i n £ luence of
God's shadow. But t h i s too i s f a l l a c i o u s . T o espouse the
o b j e c t i v i t y of sc i ence i s t o be t r ay a lingering metaphysical
f a i t h i n t r u t h e t e r n a l , a f a i t h which r e l i g i o n s share and which
l i nks t r u t h t o d i v i n i t y . But i f God does n o t exist, t r u t h
e t e r n a l does not e x i s t e i t h e r .
So w e must l e t it go. We must l e t t r u t h expire . W e must
expel God's shadow once and for a l l .
This rneans accepting t r u t h f o r what it r e a l l y i s , which i s
nothing more than
A mobile army of metaphors, metonyms, and anthropomorphisms - i n sho r t , a sum of human r e l a t i o n s , which have been enhanced, transposed, and embellished p o e t i c a l l y and r h e t o r i c a l l y , and which a f t e r long use seem firm, canonical , and ob l iga to ry t o a people: t r u t h s are i l l u s i o n s about which one has fo rgo t ten t h a t t h i s i s what they are ; metaphors which a r e worn out and without sensuous power; co ins which have l o s t t h e i r p i c tu re s
21 and now matter on ly as metal, no longer as coins.
I t means accept ing t h a t t r u t h i s nothing more than s o c i a l
const ruct ion, i t s o r i g i n s gene ra l l y f orgo t t en .
And since t h i s is a l 1 t r u t h is , we can c r e a t e the t r u t h s we
want. Why, f o r ins tance , should we be t i e d t o c e r t a i n
mora l i t i e s? Nietzsche f inds what he terms "s lave moral i ty" -
t he moral i ty of C h r i s t i a n i t y - p a r t i c u l a r l y d i s t a s t e f u l . I t has
debased humanity . Human passion, c r e a t i v i t y , magnificence -
these have all been stifled. The morality of Christianity has
ruled for two thousand years and it has achieved nothing,
nothing but mediocrity that is.
Nietzsche wants those of us who can to let it go and to
replace it with his own "master morality." But he knows that is
a burdensorne thing to do. Itrs burdensome to see the world f o r
what it really is - a human fabrication. To repudiate the
inertia of 2000 years of Christianity, to see it as unnecessary?
What a scary thought!** Only the strongest among us c m do this.
So he calls for the superman who can throw out the old, build
and build again the new, and do so making no appeal nor claims
to finality. While the weak pursue shelter within the confines
of commonality and (presumed) eternal morality and truth, while
they live in bad faithz3, the superman shakes free, pursues
his/her own ends and effects hidher own becoming. 2 4
Rorty
Rorty raises a number of related concerns. Put briefly, he
talks about:
1. The Liberal Ironist: Nietzsche calls for the superman;
Rorty calls for the "liberal ironist". Like the superman, the
liheral i rmis t I-s-happy-te embrace khê ambigukty -of exi-sten~~,
and to realize that there is nothing essential about the way
things are. Unlike the superman, the liberal ironist champions
l i be ra l democracy. Rorty thinks liberal democracy is the best
thing going (although there is no transcendental justification
for it). Nietzsche hates liberal democracy - he's of the
opinion that it perpetuates weakness and normality.
But let's dwell on the similarities between the two. By
'ironistr Rorty means
... the sort of person who faces up to the contingency of his or her own most central beliefs and desires - someone sufficiently historicist and nominalist to have abandoned the

i d e a t h a t t h o s e c e n t r a l beliefs and d e s i r e s r e f e r back t o something beyond the reach of t i m e and chance. 2 5
The i r o n i s t i s someone who recognizes t h a t
t h e r e i s no th ing deep down i n s i d e us except what w e have put t h e r e ourse lves , no c r i t e r i o n t h a t we have n o t c r ea t ed i n the course of c r e a t i n g a p r a c t i c e , no s tandard of r a t i o n a l i t y t ha t i s not an appea l t o such a c r i t e r i o n , no r i go rous argumentation t h a t i s n o t obedience t o our own convention. 2 6
There is no t r u t h except t h a t which w e have c r e a t e d .
So on what basis does t h e l i b e r a l i r o n i s t condemn repugnant
t h i n g s l i k e the Holocaust and t h e Naz i regime? On what b a s i s
does s/he r epud ia t e oppression, t o r t u r e , murder? C e r t a i n l y not
by appeal ing t o something divine, abso lu t e o r necessary. Such
t h i n g s do not e x i s t . The i r o n i s t recognizes t h a t h i s / h e r only
refuge a r e t h e values s /he , a s a rnenber of a community, has corne
t o p r e f e r . A l 1 we can do as i r o n i s t s i s compare our own c u l t u r e
and va lues \ \ i n s id ious ly w i th o the r s by r e f e r ence t o our own
s tandards" . 27
One might s a y Rorty is e t h n o c e n t r i c . Well he i s , and he
admits it. 2 8
And from a ph i l o soph ica l po in t of view, t h i s i s a l 1 ve ry
i r r i t a t i n g :
Rorty d iv ide s philosophy i n t o t r anscenden ta l philosophy and 2 9 e m p i r i c i s t phi losophy. The fo rmer i s represen ted by t h e
P l a t o n i s t s whi le t h e l a t t e r i s represen ted by t h e p o s i t i v i s t s .
They a r e d i s t i n c t i n t h a t P l a t o n i s t s a r e metaphysica l ly
o r i en t ed . P l a t o n i s t s a r e a f t e r t r u t h s t h a t t r anscend what
sc ience can r e v e a l . P o s i t i v i s t s , on t h e o t h e r hand, s ee sc ience
as t h e f i n a l r e cou r se . Science d e a l s with t h e ( a l b e i t
temporary) f a c t s of t h i s world, which, p o s i t i v i s t s i n s i s t , i s
a l 1 t h a t can be done. But both s ee themselves as seeking t r u t h ,
not producing i t . They bo th want t h i n g s (our c u l t u r e , f o r

i n s t a n c e ) " to be guided, cons t ra ined , not left t o its own
de vice^."^' Get t ing a t the t r u t h o f t h i n g s g i v e s us that
guidance.
But t h e l i b e r a l i r o n i s t s ays t he r e i s no necessa ry t r u t h t o be
found. There is no "the way t h e world i s . "31 Hence, there is
nothing beyond us t o he lp us g e t on with l i f e . W e on ly have
each o the r , Our community and the t r u t h s w e c r e a t e and dec ide t o
che r i s h . That which w e c r e a t e goes a l 1 the way d o m s o t o 3 2 speak. There is nothing deeper t o t h e worfd, The l i b e r a l
i r o n i s t i s cap t i va t ed by no i l l u s i o n s : t h e r e i s nothing b u t t h a t
which w e c r e a t e .
2 . Science a s a Tool: Drawing on the work of James and Dewey,
Rorty argues t h a t t r u t h is whatever we decide works f o r u s .
Drawing on t h e work of Heidegger, Rorty s t r e s s e s t h a t ne are not
detached observers , but a r e f i rs t and foremost beings-in- the-
world; we a r e coping beings. Truth i s not t r u t h because it
corresponds to some e t e r n a l r e a l i t y . I t i s t r u t h because 'lit
j u s t p l a i n enables us t o tope- ,/ 3 3
It i s w i t h t h i s i n mind t h a t we should understand s c i e n c e .
Science i s simply one more coping s t r a t e g y - al though i t may
seem t o be a good one - a t our d i sposa l . That i s all.
Philosophy has revered it making it t h e model t o which a l 1 forms
of i n q u i r y should conform. But there i s no j u s t i f i c a t i o n f o r
t h i s . I t i s one among innumerable cont ingent vocabu l a r i e s
a v a i l a b l e t o u s . Physics, f o r example, i s a con t ingen t
i n t e r p r e t i v e endeavor: "After each pedes t r i an pe r i od of
science, [physicists] dream up a new model, a new p i c t u r e , a new
vocabulary, and then they announce t h a t t he t r u e meaning o f the
Book [of Nature] has been discovered. ''34 They begu i l e thernselves
i n t o t h ink ing something l i k e " t h i s t ime werve f i n a l l y got Nature
r i g h t . " I n t h e p r a c t i c a l sense they may be r i g h t - now t h e y can
more effectively cope with Nature in ways they deem important;
in the sublime sense, however, they are delusional.
This means there is no reason to presume Galileo discovered a
way to go about things that corresponds more accurately with the
way the world i s than Aristotle's way. What Galileo did do was
"hit upon a tool [a vocabulary] which happened to work better
for certain purposes than any previous tool. " And \\ [O] nce we
found out what could be done with a Galilean vocabulary, nobody
was much interested in doing the things which used to be
done. . . with an Aristotelian vocabulary . "35 As such, we lost
interest in what Aristotle had to offer. Its role as a tool
became obsolete.
3. New Language, New Garne, New Reality: Wittgenstein compares 36 language to a game . His point is that when we are speaking a
language, we use words in much the sarne way that we use, for
example, the pieces in a chess game. Consider the game of
chess. The meaning of any piece (pawn, queen, king, knight)
ernerges entirely £rom the role it has in the game. The same
holds for the words of any language. The meaning of any word
(or concept) makes sense only in light of how it is used in a
particular language. Words derive their meaning not by virtue
of their correspondence to, nor because they stand for,
something. Their meanings are fully exhausted by their
application within the language game to which they belong.
Rorty is tired of the language garne of philosophy. It has
changed over time, but it has also remained consistent enough to
ceaselessly produce problems like "What is truth?", "What does
it mean to be a human being?", "What is the essence of human
nature?", "How can we best represent reality?", etc. It has
obsessed over the mind as the mirror of nature. And it has done
so to no avail. There has been no pay off. So he feels it's
time to let these problems go, tirne to be practical for once.

Rorty suggests t ha t w e t r y t h ink ing i n a new way, one t h a t
al lows us t o "ignore t h e apparen t ly f u t i l e t r a d i t i o n a l
quest ions . "37 He urges t h a t we " s t a r t a f r e s h ~ ' ~ ~ , t h a t we s e t about
c r e a t i n g new vocabularies i n which such problems do no t emerge - i n which they have no meaning. J u s t l i k e d i f f e r e n t background
b e l i e f s h igh l igh t d i f f e r e n t t h ings (da ta , s t a t e s of a f f a i r s ,
e tc . ) , di f f e r e n t vocabularies g ive r i se t o d i f f e ren t problems39.
Creating new vocabularies becomes poss ib l e when w e recognize
t h e r e i s nothing e s s e n t i a l about any vocabulary (language game);
t h a t there a r e no language games o u t t h e r e t h a t speak more
adequately of t r u t h than any o the r ( s i n c e t h e r e i s no t r u t h t o
speak of anyway); t h a t each language game i s productive of i t s
o m " t ruths" . But how a r e d i f f e r e n t language games produced?
Rorty turns t o t h e l i t e r a r y c u l t u r e for answers. 4 0
Poetry and o t h e r l i t e r a r y p u r s u i t s a r e powerful genera tors of
metaphor (novel ways o f using language) . Moreover, t h e metaphor
i s a fundamental source of language game innovation and hence,
of new "truth". 4 1 Imagine, f o r example, a game of chess with
three kings. The game would not be t h e same. The same holds
f o r metaphors and language games. Sometirnes a metaphor catches
on wi thin a c e r t a i n language game. When it does, it l o s e s i t s
metaphoric q u a l i t i e s , it becomes normalized and the language
game a l t e r s . The language game becomes a (moderately? o r
r a d i c a l l y ? ) new t o o l f o r coping.
Now, one might ask whether i t is p o s s i b l e t o ever f u l l y leave
c e r t a i n problems behind. 1s it p o s s i b l e , f o r example, t o ever
succes s fu l ly c r e a t e a language game i n which t h e problems of
t r u t h and essence do not , a t some p o i n t , and i n some way,
emerge? My f e e l i n g is t h a t it i s n o t . But t h a t r s g e t t i n g a
l i t t l e ahead of things . . . 42
Reality as a social constsuct
How about a few points to help summarize where we are so f a r ?
Horizontalists hold that :
1. there is no state of a£ fairs (body of data, evidence, etc. )
that means anything on its own. It acquires meaning only when
paradigmatically imbued; thus
2. the verticalist drive for objectivity is a misguided
pursuit.
Horizontalists also claim that:
3. Truth (essence, purpose to the world, etc. ) does (do) not
exist, although we certainly have our truths; but such
4. truths are nothing more than social constructions; thus
5. there is no reason for incessantly clinging to truths that
do not work for us - that have become tired. Let's be pragmatic
(and in Nietzsche's case, egocentric) and produce those truths
that suit us best. It may be difficult to repudiate the current
and build anew, but it can be done.
. . . . . . . . . . So reality is produced. But how so?
Berger and Luckman state that "[slociety is a human product.
Society is an objective reality. Man is a social pr~duct."~'
put another way by Berger alone: "Society is a dialectic
phenornenon in that it is a human product, and nothing but a
human product, that yet continuously acts back upon its
producer . " 4 4
There is an interactive relationship between human beings and
the society of which they are a part. While society is created
by humans, while it is nothing more than a product of human
consciousness and interaction, humans nevertheless ascribe to it
something far greater than that. They reify it, they treat it
as an exalted thing - a thing transcendent. Consequently,
society becomes coercive of its creators - a force with profound
effects. Humans become victims of their own creation.
Breaking things dom, Berger and Luckman outline three moments
of social construction. These are:
1. Externalization: Externalization is the outpouring of human
beings into the world (which is accomplished through human
interaction, mental activity, physical activity, etc. ) . It is
essential that we externalize. We must fashion Our world since
w e are un£ inished beings4'. We lack a pre-established
relationship with the world, so we create our society (its
institutions, practices, values, etc. ) in an attempt to rnake up
for this lack. To get comfortable.
But we do more than just create. We also imbue our creations
with stability. We clothe them in permanence, granting them an
existence both external to, and indifferent to, us. This we do
for survival reasons. We cannot live knowing that reality is
nothing more than what we have made it . Life, Our existence -
they would have no meaning. So we disguise the contingent
origins of reality. We objectify it, deify it (through
religion, etc. ) . As Turner explains Bergerr s position:
. . . al1 reality is socially constructed, as a consequence of Man's incompleteness, but human beings require stable meanings and cannot live in permanent awareness of the socially constructed and precarious nature of everyday reality, and they are forced to clothe these uncertainties in permanent significance. The precarious nature of the continuously- socially-constructed-world is disguised by the sacred canopy of shared realities. This reality-formation is proved by
4 6 religion.
NOW, 1 should be clear that this is Berger's view, and what
Berger says is not altogether horizontalist of him. Berger
holds (with Gehlen) that it is in our nature to create in order
to redress our inherent lacks. This is too essentialist for

horizontalists like Foucault and Rorty. The former, for
example, would probably want to know how such a conception of
human nature emerged. So, while Berger marries his
horizontalism with more than a hint of verticalism, Foucault
takes things a step further by completely displacing the
meaning-giving essential human subject. For him, there is only
the socially produced subject. 4 7
Anyway, Berger's emphasis on the human need to create and
disguise evokes the second moment of social construction which
is
2. Objectification: Through objectification, the socially
constructed reality (society, institutions, etc. ) takes on a
life of its own. It then confronts the individual as a
reification external to and other than him/herself. Reality is
rendered inexorable. It takes on an appearance of finality when
it is r e a l l y a nothing more than a contingency - a human
product . Finally, there is
3. Internalization: This refers to the process of re-
appropriating reality into our own consciousness. Through
internalization, we make that which we have created an essential
part of us, a determining component of Our subjective being.
Take language as an example. Language is nothing more than a
human product, but we encounter it as an objectivity - as an
entity with a life of its own. We then internalize it and find
ourselves interacting with the world through it.
The justice system prcvides another example. From a social
constructionist point of view, it's intriguing that so many have
such faith in it. A relatively comrnon position, for exa~n~le~~,
is that, while one may not agree with the verdict decided at a
certain trial, one would never question the integrity of the
legal system as a consequence. To do so would be
insurrectionary of him/her. A certain decision rnay be faulty,
but the system - thatfs another issue, one not to be touched.
The system is essential, eternal, true, good, and it must, at
al1 costs, be upheld. To suggest otherwise ... w e l l , only an
anarchist would do that!
But the systern is not essential. It does not tap into
anything necessary about the world. It is purely a human
construct we have corne to deify for our own comfort. It could
be otherwise.
The same holds for medicine. Medicine could be otherwise.
That is, one can see
The Medical Mode1 as a Social Constrvct
... and, building on the themes of Nietzsche, Berger, Foucault and others, this is exactly what social constructionists
propound.
To explain:
I n the previous chapter, 1 outlined the characteristics of
naturalist ontology/cosmology and epistemology. Naturalisrn
constitutes the very specific verticalism of biomedicine. To
review and summarize, this means that 'the medical
profession.. .sees medical knowledge as an assernbly of "proven,
timeless objective facts"'. To continue, it means that the
rnedical world view depends on belief in a reality in which a l 1 is orderly, predictable and stable. A world in which disequilibrium is materially generated (whether by viruses, bacteria, parasites or some other cause), can be empirically observed and externally corrected . . . Above all, it is a world which is knowable, but only by those who honor the rules of the scientific method. 4 9
Moreover, according to the verticalism of medicine,
if science [is] the accurate reading of Naturef s study with eyes undistorted by social interest or cultural prejudice,
[then] medicine [is] the benevolent application of some of what ris] found there. 5 0
Now :
What 1 want to do is outline t h e assumptions of the biomedical
model itselfS1. There is definitely some overlap here, but it is
worth delineating nonetheless.
Assumption :
1. Mind-Body Dualism: The assumption, based on Descartes
conception, is that the mind and body are dichotomous phenornena.
There is no causal interaction between them. s2 This means that
the body should be treated as a thing separate from the
individual.
2. Physical Reductionisrn: Disease is a function of disordered
bodily functions. As such, disease is sought, and addressed,
within the body. Social, psychological and behavioral
dimensions are ignored.
3. The Doctrine of S p e c i f i c Etiology: Each dysfunction has a
specific biomedical cause. This assumption leads t o the "magic
bullet" approach to healing - one dysfunction, one cause, one cure. Hence the abundance of pharmaceutical solutions.
4 The Bady as-a-Machine: T h e body -is viewed a s a o m p l e x - -
biomedical machine. It is made up of parts that need, every
once in a while, to be taken in to the "repair shop. "
5. The Body is the Proper Object of Medical Regimen and
Control: It is assumed t h a t the s i c k body should be given over
to, examined and treated by, the medical establishment. Only
the establishment has access to the relevant knowledge. The
treatment regimen it recommends, therefore, should be complied
~ i t h ~ ~ .
For the horizontalist, there is nothing necessary about this
model. Consider assumption 4. The machine metaphor is
contingent. Other cultures use different ~neta~hors~~ to
understand the body, metaphors which denote different
cosmological beliefs about the world in general. The Chinese
tradition, to cite an instance, understands the body in terms of
a necessary balance between two forces in the world - Yin and
Yang. Western civilization shared a similar view of the body at
one tirne. Aristotle saw the universe in terms of harmony; Galen
saw the body in the same way, positing an essential equilibrium
between four humors within the body (which correspond to the
four elements in the world - air, water, fire and earth) . 55 For Galen, illness emerged with an imbalance among the humors.
Herer s another example:
Fleck argues that the anatomical drawings of the middle ages convey the view of the world of that period - they are about the inevitability of death, Godf s organization of nature, and the human place in the cosmos. This contrasts with modern anatornical drawings which are different in significant ways. Most importantly, the presentation of the body is now that of a mechanical ob j ect . 5 6
Different times and places, di£ ferent world views, dif ferent
metaphors - thatrs the equation. Each body description is a
metaphor for broader cosmological beliefs. It helps us deal
with the body in light of those beliefs. It corresponds to, and
adequately reflects, nothing essential about the body itself.
The machine metaphor, therefore, is but a contingent tool for
coping. The same holds for the other four assumptions of the
medical model. Hence the contingency of the medical mode1
itself.
H e a l t h , Illness and Disease as Metaphots
According to Turner, Berger (and Luchann) does not take his
own conclusions far enough. Berger talks about the social
construction of reâ l i ty , but his primary concern is with social
reality. On the other hand,

a more radical constructionist view of knowledge would Say that knowledge of al1 reality (natural and social) is socially produced. This view would be supported by, for example, the work of Ludwik Fleck.. . who demonstrated that scientific facts are the products of what he called 'thought communitiesf . This point is merely to note that Berger's radical sociology should also be applied to scientific discourses. 5 7
It should, therefore, also be applied to the discourse on
health, illness and disease.
Health, illness, disease, the body ... these are al1 socially produced. They amount to little more than symbolic
manifestations of the values, tensions and anxieties that exist
in society. One can think of them as by-products of an
antecedent socially constructed reality. By the same token,
they can also be seen as metaphors for that realityS8. Such is
the case with the "body as machine" metaphor. Such is the case
with health, illness and disease in general.
Put another way: "Discourse about illness [health and disease]
conveys a message about the whole of so~iety."~~ crawford6' argues
that health and illnesses are not objective entities. Rather,
they axe "categories of Our experience that reveal tacit
assumptions about individual and social reality'? Tapping the
meaning of health, for example, reveals key features in the
structure of social reality, and more specifically, the values
championed by the social group whose reality it is.
Crawford identifies two discourses on health. The first, more
prevalent arnong middle class persons, he calls the discourse of
"health as self control". Within this discourse, being healthy
means being fit and trim. To be so is to celebrate and exhibit
a devotion to values like discipline and being on top of things.
To let your body go is to be out of control. In Crawford' s
words, " [ t] he body and 'personal responsibilityf for health is,
1 believe, the symbolic terrain upon which the desire for

con t ro l and t h e d i s p l a y of c o n t r o l is e n a ~ t e d . " ~ ~ T h e second
d i scourse , more p r eva l en t arnong lower class persons, he c a l l s
"hea l th as r e l ea se" . This conception i s informed by d i f f e r e n t
va lues such as the a b i l i t y t o adopt a c a sua l approach t o
problems along w i t h the a b i l i t y t o do what one wants when one
wants . There is, t h e r e f o r e , nothing f ixed nor e t e r n a l about what i t
means t o be hea l t hy . Heal th iness i s both d e r i v a t i v e o f , and
symbolic o f , wider s o c i a l c ~ n c e r n s ~ ~ .
The same goes f o r both i l l n e d 4 and d i sea se . Disease
c a t e g o r i e s o f t en manifes t s o c i a l cons te rna t ions . Hyster ia is a
c l e a r example. Hys te r i a symbolizes an h i s t o r i c a l example of
p a t r i a r c h a l a n x i e t y over women' s bodies and s e x u a l i t y , both of
which were "seen as t h r ea t en ing t o the moral and s o c i a l f a b r i c
of human s o c i e t i e s . " To go on,
Soc i a l anx ie ty about s e x u a l i t y was d i r e c t e d a g a i n s t women and t h i s anx ie ty has been expressed h i s t o r i c a l l y through a variety of medical c a t e g o r i e s which pinpoint and a r t i c u l a t e the subordinat ion of women t o p a t r i a r c h a l a u t h o r i t y . . . The h i s t o r y of h y s t e r i a is probably t h e most dramatic example of
p a t r i a r c h a l medicine; it most c l e a r l y expresses t h e subordinat ion of women, t h e not ion of s e x u a l i t y a s dangerous and the n e c e s s i t y t o regulate women i n t h e i n t e r e s t s o f s o c i a l
6 5 orde r .
Condit ions such as menopause, pre-rnenstrual syndrome and
i n f e r t i l i t y a r e s i r n i l a r examples. Chapter 7 de lves i n t o t h e
s o c i a l c o n s t r u c t i o n of these "diseasesff i n more dep th .
F ina l l y , like h e a l t h , i l l n e s s and disease, t h e body is a
cons t ruc ted phenornenon. This w e have seen, but a s another
example, e ourdi eu^^ shows how t h e body iç shaped and i n sc r ibed
d i f f e r e n t l y by d i f f e r e n t c l a s s e s . The body i s t h e symbolic
t e r r a i n upon which c l a s s d i f f e r e n c e s a r e expressed. Dif f e r en t
class values and activities r e s u l t i n d i f f e r e n t b o d i l y p u r s u i t s ,
and hence, with different understandings of what the body truly
is . As Turner summarizes Bourdieuf s position:
The body. . . is the consequence of (class ) practices . For example, weight lifting articulates working class bodies, while jogging and tennis produce a body which is at ease in the middle-class milieu or habitus. Class practices are i n sc r ibed on the body, which is also a social product of special class activities . 6 7
The body, therefore, is a constructed phenomenon, a figurative
exhibition of a particular class proclivity.
Reality, society, institutional structures, the judicial
system, the medical model, the body, health, illness and disease
are al1 social constructions. There is nothing true nor
essential about any of them. Some (illnesses, for example) are
symbolic articulations of others ( firrnly held beliefs, for
example) - metaphors of justification. Al1 are contingencies.
But, as hinted at in the case of hysteria, there is more to
the equation, and its name is power.
SOCIAL CONSTRUCTION, POWER AND MEDICINE
We are not al1 equal in Our ability to socially construct.
Some have more Say than others. In f ac t , some have much more
Say than others. This seems clear upon examination of the
origins of society, its institutions, its values, laws and
ethics. These have been constructed, for example, from a
predominantly patriarchal point of view. There is no disputing
that. There have been some changes of late such that women may
have become more powerful. But they do not dominate. Nor can
we deny that, historically, women have enjoyed very little Say
in the production of reality. The male reality as objective
reality - this is what women have had to face. This is what
women have internalized.
Now to be more specific.

Medicine is a powerful constructor. Health and illness, at
least in their current formulations are, for the most part,
medically constructed realities. As Freidson puts it: "The
medical profession has first d a i m to jurisdiction over the
label illness and anything to which it rnay be attached,
irrespective of its capacity to deal with it effecti~el~"~~.
Illness is a medically constructed objectivity to which we
generally concede. It is one to which persons thus afflicted 69 feel compelled to subrnit. Thus,
by virtue of being the authority on what illness "really" is, medicine creates the social possibilities for acting sick. In this sense, medicine's monopoly includes the right to create
7 O illness as an official social ro le .
This is clear in the case of mental illness. Goffman, in his
study ~ s ~ l u m s ' ~ , finds that mental illness is a learned social
role. Once labeled ill, patients learn to comply with that
label. There is nothing inherent to the illness. It is a
medical construct full of arbitrary expectations. It is, as
previously quoted, "social through and through. . . the outcome of a web of social practices that bear their ir~t~rint."'~ But it is
perceived otherwise. It is seen a s an objective reality. Once
admitted to the hospital, the patient is expected to act
accordingly, to manifest those behaviors that go along with
his/her label. Generally the patient does. S/he eventually
internalizes what is expected of him/her. The individual
him/herself thus becornes someone new: S/he is him/herself
(re) con~tructed'~.
The same can be s a i d of blind persons . According to ~cott?~,
The disability of blindness is a learned social role. The various attitudes and patterns of behavior that characterize people who are blind are not inherent in their condition but, rather, are acquired through ordinary processes of social learning .

Blind persons acqu i re behaviors t h a t correspond t o dominant
conceptions of what i t means t o be b l ind . This means they
become h e l p l e s s , dependent, d o c i l e , serious-rninded. While b l i n d
persons may begin the rapy wi th a l t e r n a t i v e views of what it
means t o be b l ind , such views a r e d i s c r e d i t e d i n va r ious ways by
t h e prof e s s i o n a l s working wi th them. " [BI y
manipulat ing. . . rewards and punishments, workers a r e a b l e t o
p ressure t h e c l i e n t i n t o r e j e c t i n g persona1 conceptions of
problems i n favor of t h e worker' s own def i n i t i o n s of them. "75
Blindness a s dependency, d o c i l i t y , e t c . , becomes b l indness as
objectivity. The b l i n d person l e a r n s t o see it as such, t o
i n t e r n a l i z e it, t o l i v e it. L i k e t h e menta l ly il1 person, s /he
i s thus , h im/herse l f , ( re ) cons t ruc t ed .
So i l l n e s s e s a r e cons t ruc ted , and with them, il1 persons .
This i ç what l a b e l i n g t h e o r i ~ t s ~ ~ say about deviance7' and deviant
persons. For them, t h e r e is no th ing i n t r i n s i c about any deviant
behavior. Deviant behavior i s simply t h a t which t he (more
powerful i n t h e ) cornmunity has corne t o d e f i n e as dev i an t . T h e
deviant i nd iv idua l i s simply an ind iv idua l who has managed t o
commit a s o c i a l l y determined d e v i a n t a c t , and t o be ef f e c t i v e l y
labeled f o r doing so . Deviance i s a s o c i a l cons t ruc t conferred
upon c e r t a i n i nd iv idua l s . Nothing more. But t he a t t r i b u t i o n
has imp l i ca t i ons . The i n d i v i d u a l suf fers s t i g m a t i z a t i o n , i s
excluded from normal i n t e r a c t i o n s , e t c . . So s /he adap ts , and
does so more o f t e n t h a n not by conforming t o t h e community
expec ta t ion (an apparent o b j e c t i v i t y ) of what t h e dev i an t ac t
means and consequently, what s / h e i s a s a dev i an t . I n l abe l i ng
ternis, s / h e f a l l s i n t o "secondary dev ia t ion" and takes on t h e
new r o l e of "deviant" person.
Back t o medicine.
Medicine dominates over d e f i n i t i o n s of health, i l l n e s s and
d i sease . But t h e r e i s more. The medical paradigm is spreading

its wings. It is becoming the dominant world view through which
reality i tself is being understood/constructed. Some even claim
the medical paradigm is the dominant framework through which we
now organize and make sense of the world7'; that it has become
the home of "truth"; that it has achieved cosmological
ascendance. In reference to Mary Douglas, Wright and Treacher
write :
[Mlodern science and medicine can themselves be understood as cosmologies: as systems of natural symbols which we today use to make sense of the world. Modern medicine, it seems, is not simply a body of knowledge but serves as a set of categories that we use both to filter and construct our experience. 79
Biology, for example, has become "the source of models and
metaphors for twentieth-century thought . "'O But why medicine? Well, one reason may be its (until perhaps
more recently) successful claim to unadulterated knowledge, a
knowledge unaffected by the workings of everyday life. Medicine
is part of a scientific tradition that can apparently penetrate
into objective nature, that can apparently get at things as they
are "deep dom". Thus (and to re-quote) , while The priest can always be countered by advocating atheism or another religion; the [medical] expert, on the contrary, is apparently irresistible; he claims - and it is usually a he - special access to the real workings of Nature; and if he can be challenged at all, then it is only £rom within his own technical discipline and in terms of the criteria there. 8 1
The belief in medicinefs objectivity lends credence to the
medical mode1 and its particular way of seeing (more and more)
of reality.
Medicalization
"Medicalization" is the name given to the process through
which more and more of life is defined and dealt with according
to medical interpretation and practicea2. It is "the process by
which human experiences are redefined as medical problems. "83
While other societies employ religion to explain the ambiguous,
western society relies on biomedicine to fulfill this role.
Impetus for medicalization may occur when a social status does not readily fit within [western] society's cultural systems. When a status is considered ambiguous, deviant, or in some way marginal to social noms and expectations, its legitimacy is questioned, and social rules for its management are arbitrary . . . Relegating such a condition to the health care system has been one way of managing difference £rom the
8 4 nom. . . In fact, social constructionists feel that much of life has been
medicalized - that which is considered deviance in particular. At one time deviance was closely associated with sin; at a later
time it was equated with crime. But now the medical paradigm
has taken over. Now deviance is thought of more in terms of
illness than anything else. 8 5
Indeed, medicalization is an infectious thing. It makes
medical problems out of phenomena that could easily be
understood in different ways. It makes medical problems, for
example, out of what could otherwise be interpreted as social
problems . Consider ~yperkinesis~~: hyperkinesis is a medical
category used to address hyperactive behavior. It is an
individualization of a particular "disorder". But must
hyperactivity be addressed in this way? Maybe the behavior is
better understood as an adaptation to, or symptomatic of, a
"disorder" within the social situation (at home or at school,
for example)? The medical construction is not amenable to such
an interpretation. Consequently, the social aspect goes
unnoticed and remains the status quo. 8 7
Medicalization also makes medical problems out of what could
otherwise be interpreted as a "normal" occurrence. Consider 88 menopause : every woman experiences menopause sometime during
her aging process. What could be more natural? Nonetheless,
medicine treats menopause as an aberration. It treats it as an
estrogen deficiency disease or as an ovarian dysfunction
accornpanied by a variety of physical and ernotional problems.
Menopause is rendered rnedically problematic. But perhaps this
is unwarranted. Look at how other cultures treat it. Chinese
and Indian cultures, for example, see menopause as a good thing, 89 one that frees women from certain burdensome roles. (1 w i l l
examine menopause-as-disease in Chapter 6.)
Moreover, through the drive to medicalize, individual cases of
"normality" are turned into specific cases requiring medical
intervention. Consider Turner' s summary of Bakwin' s study
describing the process by which 942 of 1000 school children were
invariably recommended for tonsillectomy:
Of these children, 610 had their tonsils removed after a preliminary investigation. The remaining children were then examined by another group of physicians and 174 were selected for tonsillectomy. Another group of doctors were then asked to examine the remaining group of children and of these 99 were judged to require tonsillectomy. Yet another group of doctors were employed to examine the remaining children and nearly one-half of these were recommended for the operation. This procedure left 58 children with their tonsils still
9 0 intact.
One wonders what would have happened if the process had
continued. Perhaps no children would have been left with
tonsils intact.
To recap:
1. Medicine dominates the construction of health and illness.
2. More and more of life (and individual scenarios) is (are)
being defined in terms of the medical paradigm.
That's where we are so far. This is the horizontalist
position.
But there is more from the horizontalist position, and it is
this: medicine is an agent of social control. It functions,
perhaps subtly, in the name of social order.
One finds this phenornenon first argued by the structural
functionalist ~arsons~l who clairns that professions like medicine
functions to control deviance. Although a little deviance is a
good thing, he says (as it helps to reaf f i r r n our values), too
much deviance is a bad thing (as it can bring the systern
crashing down). So we need agents of social control to make
sure that the level of deviance in society doesnft get out of
hand . We have two such agentsg2 - the legal agencies and the medical
agencies. Both perform two functions: 1. to isolate deviants so
that the rest of the "normal" population is not infected; and 2.
to rehabilitate the deviants so they can reenter society. The
two agencies differ in the rnanner in which they exercise social
control. The former is more inclined to use force than the
latter. The latter relies more on the enactment of certain
socialized expectations. That is, when sick, w e are expected to
play out an internalized script, to take on what Parsonfs refers
to 2 s the s i x k roh. - Iil-tkis way, the individual i s e f f e c t i v e l y
dealt with, rehabilitated and returned to normal functioning.
To elaborate, according to Parsons, the sick role has two
rights and two obligations. This is how it functions as a
mechanism of social control. These are: Right 1: the individual
is not responsible for his/her ailment. Right 2: the individual
is exempt from carrying out his/her normal activities.
Obligation 1: being sick is not a desirable thing, hence the
individual is obliged to get better. Obligation 2: in his/her
attempt to get better, the individual rnust seek out competent
help, namely medical assistance, and comply with it. These four
components constitute a societally instilled rnechanism that
operates to both manage deviance (sickness) and transform it
into normality. This is essential to a society that thrives on
productivity. Society canrt have too many sick people running
(or rather, lying) around. It needs active people carrying out
their daily obligations if it is to prosper. The sick role
ensures that any individual hiatus due to illness is short and
sweet.
Parson's formulation of the sick role is one way to approach
rnedicine as a systern of social control. And it has its 9 3 problems. Another way is to see medicine as a legitimator of
dominant values in society. From this perspective, medicine
performs the ideological function, for example, of reproducing
capitalisrn by diverting attention from its evils. One way it
does this is by individualizing social problems. This I have
mentioned. However, to put it from a Marxist point of view (in
the w a y White describes it) '': The rnedical profession is seen as central to the control of labor. . .and contemporary theories of disease perforrn an ideological function in stabilizing the status quo. The dominant class supports a conception of illness as an individual phenomenon and denies the salience- ofsocial
p p p p p p p - - - - - - - - - - - - - -
structures in the production of ill-health.
The tensions of capitalisrn are ideologically veiled by medical
practice. Labor is thus fooled and appeased,
And this is accomplished at both the conceptual, as well as at
the everyday micro l e v e l - within the doctor-patient
interaction, in particular. White goes on to explain the
Marxist position, and in particular Mishlerrs findings which
describe how:
. . . doctors strip the patient's information of its social context and redefine it in terms adequate to their technological framework. . . [Tl he dialogue between the doctor and the patient is one in which the doctor asserts the primacy

of the technical and the irmnutability of the social factors that the patient thinks might be a part of their problem. 9 5
Waitzkin cornes to similar conclusions arguing that doctors
"implicitly act as agents of social control ... by rendering public issues into prioate troubles. "96 In Waitzkinf s own words :
In medical encounters, technical statements help direct patient' s responses to ob jectified symptoms, signs and treatment. This reification shifts attention away from the totality of social relations and the social issues that are often root causes of persona1 trouble. 9 7
I corne back to Waitzkin a little later ... Feminists adopt a similar position, but ernphasize instead
medicine's role in perpetuating a patriarchal society. From a
feminist point of view, medicine acts to control women and
subordinate them to patriarchal authority in dif f erent waysge . It serves to legitimate, for example, women as domestic
laborers. It, for example, treats "suburban neurosis with
valium" thus reinforcing "the traditional role of women which
they are seeking to escape. rr 99
One way medicine controls women is by defining women's bodies
from a male perspective. For instance: p p p p p p p p p - - - - - - - -
- - -
Throughout the nineteenth century medical explanations were used to subordinate women . . . [Glynaecology was used to attack the f irst wave of feminism. Obstetricians and gynaecologists located the cause of women's psychological problems in the vagina and castrated women in their thousands. 100
In particular, medicine has created numerous medical categories
such as hysteria, anorexia nervosa and agoraphobia "which both
label [women] and control them ... and which express tensions and the social relations of so~iet~.'~'~' Which, in other words,
express and embody most fundamentally, patriarchal anxieties.
Medicine has been particularly concerned with women's
sexuality. Gynecology t e x t ç l o 2 have consistently def ined normal
sexuality for women in ways quite inconsistent with womenfs
actual experiences. In the 1950s, for example, they held that
vaginal orgasms were "the appropriate re~~onse"'~~ despite their
infrequency. From this it followed that the woman' s sex drive
was inferior to the man's, which in turn supported the view that
the woman should be the more passive of the two during sexual
intercourse. Medicine, and more precisely, gynecology, thus
authorized the view of "woman as passive". Gynecology, from the
feminist point of view, was (and is) "medicine practiced on
women for the benefit of men. "'O4
Another way medicine legitimates patriarchy is by controlling
interventions into women's bodies, Medicine has taken over
women' s 'problems" like ~nenstruation'~~, PMS and menopause. It
also controls intervention into their reproductive capacities.
Childbirth, for example, is a medical concern: to let the mid-
wife handle it, to opt to give birth at home - these would be silly things for a woman to do, even dangerous. 106
Finally, medicine works to legitimate patriarchy during the
micro-interactions between doctors and their patients. The
doctor-patient interaction takes place within the context of
certain societal values and assumpti~ns. They operate on the
basis of those assumptions, and in so doing, reproduce them in
turn. This is something that Waitzkin talks about as discussed
above, although he is not specifically concerned with
patriarchy. To elaborate, he states that
In their encounters with patients, doctors may interpret personal problems and encourage individual behaviors in directions that are consistent with societyfs dominant ideologic patterns. 107
He says that doctors will,
[b] y questioning, by interrupting, and by otherwise shifting the direction of conversation from nontechnical problems to technical ones...exclude certain topics from talk and include
others. Of particular interest here are the verbal techniques that divert attention £rom sources of persona1 distress in the
108 social context.
By diverting critical attention away from the lifeworld, doctors reinforce the ideas that pattern of the lifeworld and rnay help win acquiescence to those features of the lifeworld that patients find rnost disconcerting. 109
This doctors rnay do, although they rnay do so unwittingly.
This doctors rnay also do by modifying their treatment of
certain patients. Sometimes, for example, a male doctor rnay
have a female patient who deviates £rom his particular
understanding of what a woman (her demeanor, pursuits) should be
like. When she does, things can go awry, but more to the
detriment of the patient who is dependent upon her doctor's
valuation of her.
In our society, the man-woman and the doctor-patient relationships recapitulate and reinforce each other, locking male physician and female patient in an asymrnetrical relationship - a relationship in which female patients are dependent on their male physicians' judgments about them as
110 women . When a female patient defies expectation, she in turn threatens
the (ob jectively "out there") man-woman relationship. In
consequence, the physician may react. His negative appraisal of
her rnay lead to an alteration in "the remaining exchange of
information and the delivery of health care" he provides her"'.
In this way the woman is penalized while taken for granted
values and expectations are thus affirmed.
There !
Without claiming to have done so comprehensively, there are
the Parsonian, Marxist and Feminist approaches (stressing their
horizontalism) to medicine and its role as a social control
agent. Now for one more view £rom the pen of ... Foucault
While Chomsky propounds a human nature, Foucault (to put rny
words in his mouth) asks the question: "From whence the notion
of human nature?" His first move is to historicize such
conceptions. His concern is not whether or not there is a human
nature, but rather, how it is that questions concerning human
nature emerge. This we have seen. Chomsky also thinks that
"some firm and humane concept of the human essence or human
natureuu2 is politically indispensable. It iç essential if we
are to work Our way out of Our current plight. So he looks to a
superexcellent knowledge, one that rises above the vicissitudes
of social conflict, one whose light can guide humanity in its
quest for socio-political renewal. For Foucault, there is no
such knowledge.
Foucault says "[tlhe political question . . . is not error, illusion, alienated consciousness, or ideology; it is truth
itself. Hence the importance of Nietzsche. , /113 People like
Chomsky think society is missing the mark. Some Marxists have
it that the worker is alienated in capitalist society; that s/he
is ideologically duped into supporting a system that alienates
him/her. These sentiments assume there is a natural human path
we should be following, a path from which we have severely
deviated as a society. If we could just get back on it things
would be so much better. But there is no such path for
Foucault. Right versus wrong, truth versus falsehood, good
versus evil - in the eternal sense there is no distinction between them. Truth in any form is truth produced. More
specifically, its formulation at any one time is a manipulation
in the interests of power. According to Foucault:
... w e a r e forced t a produce t h e t r u t h of power t h a t Our s o c i e t y demands, of which it has need, i n order t o func t ion : we must speak t he t r u t h ; w e a r e cons t ra ined o r condemned t o confess o r t o discover the t r u t h . Power never cea se s its i n t e r r o g a t i o n , its i n q u i s i t i o n , i t s r e g i s t r a t i o n of t r u t h : it i n s t i t u t i o n a l i z e s , p ro fe s s iona l i ze s and rewards i t s p u r s u i t . I n t h e l a s t ana lys i s , we must produce t r u t h a s w e must produce wealth, indeed w e must produce t r u t h i n order t o produce wealth i n t h e f i r s t place. 114
Truth and power a r e f i rmly l inked . Power feeds on, and is
sus t a ined and fu r the red by, t h e product ion of t r u t h . Truth i s
power extended.
Foucault performs genealogy i n h i s a t t empt t o uncover t h e
o r i g i n s of t r u t h d a i m s , t o determine why they developed a s t h e y
d id , how they were used, t o r e v e a l t h e i r l i n k s t o domination.
Genealogy d i f f e r s r a d i c a l l y from the h i s t o r i a n ' s h i s t o r y . The
genea log i s t makes no t e l e o l o g i c a l assumptions. S/he sees no
d e s t i n y t o humanity nor any purposive rnovement towards any
ul t i rna te goa l . There i s no unfolding o f t r u t h , no progress , no
un ive r sa l s . Ins tead, s /he i s concerned wi th pa ins tak ing ly
i d e n t i f y i n g t h e
acc iden t s , t h e minute dev i a t i ons - o r conversely, t h e complete r e v e r s a l s - the e r r o r s , t h e f a l s e a p p r a i s a l s , and t h e f a u l t y c a l c u l a t i o n s t h a t gave b i r t h t o those t h ings t h a t continue t o e x i s t and have value f o r us; i t i s t o d iscover t h a t t r u t h o r being does not l i e a t t h e r o o t of what w e know and what w e a r e , bu t t h e e x t e r i o r i t y of a cc iden t s . 115
Genealogy r evea l s t he contingency of t h i n g s . When t h e claim:
"Now we've f i n a l l y h i t upon t h e t r u t h ! " i s made, t h e genea log i s t
says: "Don't be deceived i n t o th ink ing t h e r e t s anything deep
about it t h i s time. Last t ime, t h i s tirne, next t i m e . . . i t ' s
doesn ' t much mat ter . Notwithstanding how good it looks , t r u t h
i s only, and always w i l l be, a product ion of circumstances.
Here, le t ' s see how t h i s t r u t h emerged ..."

The same goes for the disciplines, any discipline. Foucault
pays particular attention to the human sciences, which, he says,
have their origins in the Enlightenment drive to find more
rational ways to govern"6. They are the manifestations of "an
aàministered society in which the centralization of information
about citizens is essential for some form of social planning. "Il7
Spawned significantly by radical transitions in demography and
the rise of urban-based industrial capitalism, the Enlightenment
brought with it new govermental concerns. Before, questions
regarding the nature of the state, how to remain in power - these were the primary concerns. However, beginning in the 16th
century, the f ocus changedlla. The individual, his /her relations
with others, the individual as productive and efficient, the
surveying and management of populations - these became the new concerns . And with these concerns emerged a new power in society, one
that revolved around two distinct poles - the human species
(regulating populations) and the human body (disciplining the
individual). The power was bio-power, and it was one that
operated at al1 levels (including micro-interactions like the
doctor-patient encounter), finding extension and legitimization
through the development and consolidation of certain knowledges
and practices (through disciplines like demography, statistics,
epidemiology, psychiatry) . The central issue was how to produce an orderly society of
normalized, disciplined, productive bodies that could be put to
use in the most economic of ways possible"g. This gave rise to
a number of disciplinary technologies, technologies epitomized
by Bentham's ~ano~ticon'~~. It also gave rise to the human
sciences which specialize in identifying deviation, in
determining how pervasive it is, in managing, rectifying and
normalizing it. And this they did (and do) through developing
prescriptions on how to live, prescriptions which, through the
mechanisms of power, we internalize thus determining how we act
and what we come to see as truth. 12 1
Hence, with bio-power the human sciences spawned and/or
developed. With the human sciences, bio-power secured its hold
and flourished, flourishing into the present day.
Foucault also talks in particular about medicinefs link to
power. Turner summarizes Foucault's position on this matter
well:
To understand the nature of modern conceptions of disease, we need to look at the historical emergence of medical categories as separate and distinctive forms of discourse ... Furthermore, it is argued that medicine has its historical roots in the institutional apparatus of social control, and that rnedicine is an important part of what Foucault had in mind by the notion of micro-politics, that is foms of political practice which are decentralized and operate locally through various institutional. settings such as the anatomical theater and the medical clinic. 122
IN CONCLUSION
To be verticalist is to advance the claim that one (or one's
discipline, or onef s epistemological community) knows the way to
penetrate reality and represent it. To be verticalist is to
d a i m authoritative knowledge of the way things are. '23 1t is to
propound the claim: "This is the truth, and this is how to
access it."
There have existed different versions of verticalism.
Theological, philosophical, mythical and scientific verticalism
are examples. The medical version is a sub-formulation of the
latter, and it dominates today. This is what horizontalists
claim. But horizontalists also see medicine as just one more
language gante, j u s t one more discourse formulation, just one
more paradigm caught up in itself.

Medicine is social through and through. Al1 horizontalists
believe this. And they believe, rnoreover, that any label, any
condition, whether it be hysteria, agoraphobia, menopause, AIDS,
diabetes, or l e s i o n , is the construct of socio-historical
conditions. Then there are some horizontalists who propound
something even more disquieting. For them, medicine is nothing
but a contingent arrangement produced (wittingly or not) in the
interests of domination. Its labels, its medical categories,
rnoreover, are contingent tools for the purpose of control, for
the purpose of manufacturing the disciplined (efficient, normal)
individual. Given no ties to power, they Say, there would be no
biomedical "truthff as we know it today.
1 In what follows, 1 am drawing upon Rabinow's (1984) juxtaposition of
Foucault and Choms ky . See Rabinow (1984), p . 3.
Chomsky (1968), p. 100.
Chomsky (1975), p. 123.
Quoted in Ayer and Of Brady (l994), p. 88.
As Rabinow (1984) explains in his Introduction.
Other horizontalists donft even allow for its existence. Nietzsche and
Rorty are good examples, both of whom are discussed in this chapter.
8 See Sorel1 (1991), p. 33.
9 Russel (l993), pp. 528-529.
10 Barnes in Skinner (1991), p. 86.
11 Ibid, p. 92.
12 An example adapted from Longino (1990), pp. 42-43.
13 (1990), p. 43.
14 (1975).
15 (1993), p.26.
16 Nietzsche, See Ayer and O'Grady (1994), p. 318.
17 See Ibid, p. 317.
18 See Zeitlin (19941, p. 5.
19 Nietzsche's protagonist in Thus Spake Z a r a t h u s t r a (1969) . 20 See Raymond (1991), p. 177.
21 See Ayer and O'Grady (1994), p. 317.
22 And it is not only Christianity that he is rejecting, but any system that
propounds a fundamental ontology. Platonism and the Forms would be another
example.
23 Sartre (1956).
24 But where does this leave us? To be strong means to self-create despite
the values, concerns, etc. of others. But doesn't that invariably lead to a
conflict of wills? To the doctrine "might is right"? And if sot doesn't
that lead us into trouble? These are just sorne of the issues that follow
£rom Nietzsche's conclusions. See Zeitlin (1994)' pp. 119 - 125, on this. 25 (1989), p. XV.
26 (1987), p. 60.
27 See Sorel1 (1991), p. 121.
28 See various selections from Rorty (1991) for pointed discussions on his
ethnocentrism.
29 (1987)' pp. 29-29 and 56-57.
30 Ibid, p. 57. Not my italics.
31 Quoted in Geras (1995).
32 Geras regarding Rorty (1995) . 33 (1987), p . 31.
34 Rorty (l982), p. 90.
35 Rorty (1989), p. 19.
36 Wittgenstein (1974) . 37 Rorty (1989), p. 9.
38 Rorty, (1991), p. 36.
39 This is one of Derrida's main themes as well. See Hoy (1991) for a
helpful introduction to Derrida. As well, see Derrida (1981).
40 (1989), p. 2 0 .
41 Ibid, p. 18.
42 See Chapter 7 on this.
43 (1967), p. 6 1 .
44 (1967), p. 1.
45 See Turner (1992), p. 113 on this.
46 Ibid, p. 117.
47 In fact, this is Foucault's major theme. His main purpose "has been to
create a history of the different modes by which, in Our culture, human
beings are made subjects." (Foucault in Dreyfus and Rabinow, 1983, p. 208).
And t h i s i s what he means by "the d e a t h of t h e sub jec t . " Foucault d i sp l ace s
t h e sub j ec t a s a determining e n t i t y .
4 8 One t h a t seemed t o predominate t h e a f t enna th of t h e O . J . Simpson c r imina l
t r i a l .
4 9 Kaufert i n Lock and Gordon (19881, p. 331.
50 Wright and Treacher ( l 982 ) , p . 4 .
5 1 A s summarized by Freund and McGuire (1995). Once again, t h i s i s from the
pe r spec t i ve of s o c i a l constructionism, and more precise ly , as Freund and
McGuire descr ibe it, c r i t i c a l sociology. One may wonder whether o r no t t h i s
d e p i c t i o n i s too extreme - a convenient f i c t i o n f o r the c r i t i c a l s o c i o l o g i s t .
52 Although, as d i scussed i n the previous chap te r , the mind is being thought
o f more and more as a bi-product of t h e brain.
5 3 Parsons speaks t o t h i s . See l a t e r i n t h i s Chapter.
54 Here t h e not ion of metaphor is t r e a t e d d i f f e r e n t l y than Rorty (1989)
treats i t . Rorty s e e s it as something novel, something which, once accepted,
once an habi tua1 p a r t of our speech and way of thinking, is no longer a
metaphor. See p. 18.
55 See White ( l g g l ) , p. 62 .
56 Ib id , p. 59 .
57 Turner (1992), p . 118.
58 One o f Mary Douglasr (1966; 1970) major themes.
59 Herz l i ch and Pierret ( l 985 ) , p . 150.
60 (1984) . p p p p p p p p p p p p p - - - - - - - - - - - - -
6r n id , -pT 627 -
62 I b i d . , p . 81.
63 Pierret cornes t o t h e same conclusion, although she i d e n t i f i e s four h e a l t h
cons t ruc t s : 1. hea l t h - i l l ne s s ; 2 . heal th- tool ; 3 . health-product; and 4 .
h e a l t h - i n s t i t u t i o n . Each construct f i t s i n to a "global system of
i n t e r p r e t a t i o n t h a t s i t u a t e [ s ] t h e ind iv idua l i n soc ie ty ( p . 1 2 ) .
64 Herz l i ch ( 1 9 7 3 ) o u t l i n e s three kinds of i l l n e s s conceptions: 1. illness as
d e s t r u c t i v e ; 2 . i l l n e s s as a l i b e r a t o r ; 3 . i l l n e s s as an occupation. The
conception adopted depends on the i nd iv idua l ' s r e l a t i onsh ip wi th soc i e ty .
E a c h no t i on of i l l n e s s "represents a s p e c i f i c view of i l h e s s , each o r i en t ed
b y d i f f e r e n t conceptions of the r e l a t i o n s of t h e individual t o soc ie ty . " (p .
128) The t h r ee conceptions of i l l n e s s , moreover, correspond t o t h r ee
coherent s t r a t e g i e s each wi th d i f f e r e n t ends: With t he f i r s t , t h e s t r a t e g y i s
not to be ill; with the second, the strategy is to be ill; with the third,
the strategy is to be a good patient.
65 Turner, (1995), p. 90.
66 (1984).
67 (1992), p. 88.
68 See Zola (1978), p. 86.
69 Although, 1 have to Say that this view ignores the potential impact of
human agency, of human defiance, etc.
70 Freidson (l97O), p. 206.
71 (1961).
72 Wright and Treacher (1982), p. 10.
73 Whatrs interesting is that the patient as mentally il1 is legitimated
through what Goffman (1961) refers to as retrospective construction on the
part of the medical s t a f f . Medical s t a f f need to justify the presence of the
patient, the label s/he has been assigned, as well as their role in dealing
with him/her: "The medical elements of the staff ... also need evidence that they are still in the trade they were trained for. These problems are eased,
no doubt unintentionally, by the case-history construction that Fs placed on
the patient's past life, that he finally became very sick, and that if he had
not been hospitalized much worse things would have happened to him ..." 74 (1969).
75 Ibid,
76 Lemert (1993), Becker (1993), and Erickson 1 9 9 3 ) - - - - - - -
- p p p p p p - - - - - - -
- -
77 And "residual deviance". This is Scheff's (1963) term for "unnamable"
instances of deviance. Mental illness i s one such instance.
78 Zola (1978); Conrad and Schneider (1980).
79 (1982), p. 6.
80 Longino (lggl), p. 163.
81 Wright and Treacher (1882), p. 6. My italics.
82 For a more complete characterization, see Zola (1978).
83 Becker and Nachtigall (l992), p. 456.
84 Ibid, p. 457.
85 Conrad and Schneider (1980) . Turner (1995) draws similar conclusions.
86 Conrad (1975).
87 The medicalization of wife abuse is another example. See Stark et al.
(1983), for example. . 88 Kaufert (1988).

See Chapter 6 for a fuller discussion.
Turner (19951, p. 42.
(1939).
see Parson (1959). Wolinsky (1980) Chapter 4, provides a good summary.
Parsons' sick sole concept does not, for example, adequately deal with
things like chronic illness, stigmas associated with certain illnesses,
impairment, etc. It is also based on the assumptions that patient help-
seeking is simple - that the patient actually willingly goes to the doctor
and does not seek help elsewhere; that patients willingly comply with
physician definitions and treatments; that physicians practice universalism
in their treatment of patients. See Galagher (1976), Ronig-Parnass (1981)'
Segall (1976) and Turner (1995: 42-45) for more detailed discussions on the
weaknesses of the sick role concept.
94 White (lggl), p . 27.
95 Ibid, p. 37.
96 Ibid, p. 38.
97 cited in Ibid, p. 38.
98 Ibid, p. 50.
99 Ibid, p. 53.
100 Ibid, p. 51.
101 Ibid, p. 57.
102 Scully and Bart (1978).
10p3pIbid,pp. 218- - - - - -
104 Ibid, p. 219.
105 Although Bransen (1992) would disagree. She argues that the
medicalization of menstruation is very much circumsribed, and the doctorrs
role limited. The degree to which it is circumscribed and the doctor's role
limited varies from genre (ways of talking) to genre. In one genre, for
example, the doctor is seen as critical. In another s/he is seen as
superf luous, etc.
106 An attitude prevalent especially in America. See discussion of childbirth
in Chapter 7.
107 Waitskin (l989), p. 224.
108 Ibid., p. 231. Not my italics..
109 Ibid., p. 232.
110 Fisher and Groce (1985), p. 346.
111 Ibid., p. 361.
112 Quoted in Rabinow (1984), p. 5.
113 Quoted in Ibid, p. 7 5 .
114 (1980), p. 93.
115 Quoted Rabinow (1984), p . 81.
116 See Foucault (1977 and 1 9 7 8 ) .
117 White (lggl), p. 66.
118 1 am drawing upon Rabinow (1984) here.
119 A necessary precursor ta capitalism, 1 should mention.
120 Foucault (1977) . Consider his description of the panopticon (p. 200) : "...at the periphery, an amular building; at the center, a tower; this tower
is pierced with wide windows that open ont0 the i ~ e r side of the ring; the
peripheric building is divided into cells , each of which extends the whole
width of the building; they have two windows, one on the inside,
corresponding to the windows of the tower; the other, on the outside, allows
the light to cross the ce11 from one end to the other. Ail that is needed,
then, is to place a supervisor in a central tower and to shut up in each ce11
a madman, a patient, a condemned man, a worker or a schoolboy. By the effect
of backlighting, one can observe from the tower, standing out precisely
against the light, the small captive shadows in the cells of the periphery.
They are like so many cages, so many small theaters, in which each actor is
alone, perfectly individualized and constantly visible. The panoptic
mechanism arranges spatial unities that make it possible to see constantly
and to recognize immediately." p p p p p p p p - - - - - - - - - - - - - - - -
12i Foücaurt Tiescribes the power process and its effects as follows: "When 1
think of the mechanics of power, 1 think of its capillary fonn of existence,
of the extent to which power seeps into the very grain of the individuals,
reaches right i n t o their bodies, permeates their gestures, their posture,
what they say, how they learn to live and work with other people" (cited in
White (19911, p. 56).
122 (1995), p. 19.
123 Derrida uses the term logocentrism in a similar way. See Fox (1994), p.
8.
CHAPTER 4
THE RELATMTY OF SOC= CONSTRUCTION: TffEORY PART I
JOURNEY NOTES Having o u t l i n e d the major t e n e t s o f t h e v e r t i c a l i s t and
h o r i z o n t a l i s t p o s i t i o n s , t h e o b j e c t i v e of t h i s chapter i s t o beg in t o devel op t he t h e o r y behind t h e consul t a t i v e approach . I t s t a r t s w i t h a demonstration of, and i n v e s t i g a t i o n i n t o t h e r a m i f i c a t i o n s o f , the fo l lowing claim:
Some things are more s o c i a l l y constructed than others. T h i s i s a c la im appropriated from ~ u r n e r ' by which I take t o mean t h a t while some th ings (such a s c e r ta in d i s ease s ) are soc ia l cons t ruc t i ons through and through ( i n t h e interests o f soc ia l o rder , for example), o t h e r s are more t r u e t o r e a l i t y - t h e y more c l o s e l y r e f l e c t t h e way r e a l i t y is, t h e way the natural i s . From t h i s I t h i n k i t is fair t o Say t h a t the degree t o which d i f f e r e n t phenomena are s o c i a l l y constructed i s r e l a t i v e . We can t he re fo re speak of the r e l a t i v i t y o f soc ia l cons t ruc t ion .
To speak of t h i s i s t o be n e i t h e r v e r t i c a l i s t i n o r i e n t a t i o n (i. e . , s t r e s s i n g t h e a b i l i t y o f some compared t o o the r s t o s ee ) , nor h o r i z o n t a l i s t i n o r i e n t a t i o n (i. e., s t r e s s i n g the omnipotence of soc ia l c o n s t r u c t i o n ) . Rather, t o speak o f such r e l a t i v i t y i s t o recognize a n i n t e r a c t i v e and dynamic r e l a t i o n s h i p between r e a l i t y and d i f f e r e n t paradigms, one t h a t v a r i e s wi th t h e s p e c i f i c phenomena under cons truct ion along w i t h the paradigm do ing the cons t ruc t i ng . Neither t h e phenomenon nor the paradigm is omnipotent, b u t then again, n e i t h e r i s impotent .
To p u t t h i s another way, the degree t o which a phenomenon is c o n s t r u c t e d d-egends on_ i_ts t rans lucen t -presencz - - iL s , wha G f - - - - -
term " t a n g i b i l i t y " - along wi th the power of t h e p a r t i c u l a r paradigm doing t h e cons t ruc t i ng t o a c t u a l l y cons t ruc t the way it would have t he phenomenon. Think of the fo l lowing metaphor: r e a l i t y and s o c i a l cons t ruc t ion are i n a t u g o f war with each o t h e r , Sometimes the former ho lds grea ter sway; a t o t he r t imes the l a t t e r predominates. O r t h i nk o f it i n t h i s way: soc ia l cons t ruc t i on t a k e s work. Some t h inqs , however, are e a s i e r t o work w i t h than o t h e r s .
The theme is the r e l a t i v i t y of soc ia l cons t ruc t ion . The p r e c i s e sub jec t mat ter f o r ana l y s i s is t h e d i s p a r i t y between medicine and t h e soc ia l c o n s t r u c t i o n i s t approach t o medicine. T h e former i s l a r g e l y v e r t i c a l i s t i n o r i e n t a t i o n claiming t h a t it h a s privileged access t o t h e way t h i n g s are wi th heal t h , illness and d i s e a s e . Heal t h , illness and d i sease are de f i ned by medic ine . The soc ia l cons t r u c t i o n i s t approach, horizon t a 1 i s t i n o r i e n t a t i o n and b lending i n various ways f e m i n i s t , Marxis t , p o s t - s t r u c t u r a l i s t , and o t h e r concerns, denies any p r i v i l ege t o

medicine. There i s no th ing unadul tera t e d / s a c r e d / p r i v i l e g e d about what med ic ine " f i n d s " and t h u s d e f i n e s a s hea l t h , i l l n e s s o r d i s e a s e . I n s t e a d , any and a l 1 d i s e a s e s are s i m p l y c o n s t r u c t i o n s of a c e r t a i n paradigma t i c p o s i t i o n tha t has m a n a g e d to achieve dominance i n our society. This does no t mean that there is no under ly inq r e a l i t y . I t j u s t means t h a t the a c t u a l wor ld we f u n c t i o n in i s s o c i a l l y c o n s t r u c t e d and c o n s t r u c t e d p r i m a r i l y from a medical p o i n t of v i e w . W e cannot escape our m e d i c a l l y constructed r e a l i t y i n such a way that allows us to see how adequate i t is t o t h e " r e a l " w o r l d . W e can only escape i n t o and c r i t i c i z e medic ine from a l t e r n a t i v e constructed r e a l i t i e s .
M y s p e c i f i c a i m is t o demonstrate t h e r e l a t i v i t y o f s o c i a l c o n s t r u c t i o n , and what such r e l a tivity l o o k s l i k e . Having done t h i s , one can n e i t h e r accept t h e medical nor the s o c i a l c o n s t r u c t i o n i s t approach i n whole. Rather , they should each be understood a s pos s ib l y having valuable c o n t r i b u t i o n s t o make, con t r i b u t i o n s which, when t a k e n toge t h e r , p o s s i b l y crea t e a more adequa t e approach t o understanding and address ing h e a l t h , i l l n e s s and d i s e a s e than e i t h e r one a lone . Taken a p a r t , b o t h g e t c a r r i e d a w a y w i t h t h e i r own p r o j e c t s , both fa11 i n t o the t rap o f p a r a d i p a t i c e x c l u s i v i t y , and no one b e n e f i t s .

INTRODUCTION
[Note: What follows is a short parable i n which three
disparate accounts of the sun are shared. While each account
may (or rnay not) resemble authentic views t h a t have existed o r
do exist, it is not my concern that they necessarily be
representat ional of such views.]
Parable: Three Views of the Sun
Three persons from d i f f e r e n t t i m e s and far o f f places suddenly
f i n d themselves on a beach together . The d a y i s warm and c l e a r ,
and t he sea is calm. They s i t w i t h each o ther i n an t i c ipa t ion
f o r they know - somehow - t h a t they have been summoned for a
purpose. Soon they find t ha t they can ta l k t o each other , th is
notwithstanding they speak d i f f e r e n t languages . S o they proceed
t o converse and do so i n an attempt t o make sense of their
mysterious encounter.
In time they n o t i c e a f i gure o f f i n the distance. They w a i t
i n s i l ence a s the f i g u r e approaches. When she arr i ve s she s i t s
with them. She then nods t o each in t u r n and introduces h e r s e l f
a s t h e I n q u i s i t o r .
Inquisitor: Welcome t o you all. Please, have some food.
She hands them each some bread and dr ink . They finish both
and f e e l rep len ished , t ranqui l and a t home.
Inquisitor: I have brought you here s o t h a t you may be
questioned. I will not keep you l o n g .
B u t the t h r e e visitors would l i k e to s tay l ong and they say
s o . T h e I n q u i s i t o r srniles.
Inquisitor: My ob j ective is simple.
The I n q u i s i t o r waits until the three repos i t i on themselves.
They are i n t r i g u e d , once again, focused. They wait for t h e
Inqu i s i t o r t o continue. She does.
Inquisitor: 1 would like for each of you to tell me what you
know about t h e Sun.

The visitors seem a little puzzled by the r e q u e s t , b u t they
see no reason not t o respond. The Inqu i s i t o r motions t o V i s i t o r
1 who begins.
Visitor 1: The Sun is that resplendent £ire up there that soars
across the sky everyday.
T h e v i s i t o r po in t s t o the sun and t h e n motions its d a i l y
rou t ine . The others follow his ges t i cu la t ions . V i s i t o r 1
cont inues .
Visitor 1: The Gods, in their magnificence, have willed it that
we should have light. So they have given us the Sun.
V i s i t o r 1 becomes s i l e n t and contemplative, and then speaks
again.
Visitor 1: For this wonderful g i f t we should be truly grateful.
Each morning the Sun God awakens to the same entrustment.
He fashions a great fire £rom an immortal flame. You can see
the fire maturing with the d a m as its rays emanate with
increasing intensity and splendor from the ends of the earth.
You can watch i t s flames gradually permeate and then break the
night . And when the fire has grown immense, its light
flooding the heavens, the Sun God lifts it into His mighty
hands and throws it westward. The distance is long and so the
Sun stays with us long, warming us, consoling us. Finally it
falls into the Abyss of the West where the Sun God catches it
and fondles it a s it slowly dirninishes once again to its
immutable essence. He then harbors the £lame through the
night while we sleep in peace, comforted in knowing that He
will, in H i s grace, awaken before long to His momentous task
once again.
The Sun God is truly benevolent.
T h e I n q u i s i t o r smiles and thanks the f i r s t v i s i t o r . She then
motions t o the second v i s i t o r . Visitor 2 is visibly i r r i t a t e d .

Visitor 2: I'm afraid 1 do not share my new friend's beliefs.
What is a l 1 this talk about "gods"? There are no "gods"!
There is only one God, and 1 cari assure you She has more
powers than any Sun god. The world is Her creation. The
stars, the Sun and moon were al1 put into motion by Her
benevolent hand. She fashioned the universe and did so
placing the Earth at the center of Her cosmos. And we - humanity - we are the object of Her omnipresent love. The
rest is in every respect tangential, supplementary to our
existence on Earth.
The sun takes its course from east to west in a perfect
circular motion while the Earth remains transfixed as its
center. We rely on the Sun to be sure. Like my friend has
said, it is a gift to us, one we cannot live without. Our
purpose is to be obedient to that which the Great One has
decreed, to progress within the bounds of spiritual ordinance.
The Sun, with its light and warmth, was created so that we
might do just that in this life.
But it is important to recognize that this is an ernbodied
life. When we die we shed our physicality and are reborn into
a new world. We are born into a world in which we need no
longer rely on the Sun, nor the rain, nor the air. This new
world, my friends, is the world of veridical life. It is the
world of life eternal for which we must al1 prepare. It is
the true home of God.
T h e Sun helps us to spiritually prepare for a glorious
rebir th by providing for essential physical needs. The sun is
a rneans to eternal rapture.
Inquisitor: Thank you. Your views are most welcome.
S h e t u r n s t o V i s i t o r 3 who is l o o k i n g a l i t t l e smug.
fnquisitor: And you, my friend, what can you tell us of the sun?
Visitor 3: Well, to begin, 1 have to admit t h a t what I have
heard here is a little too pietistic for me. In my world
t h e r e are no gods whatsoever - not even one. You want to
account for the Sun, existence, why we are here? Well, let me
give you rny account: you cannot. It is a waste of time to
think you can. The universe j u s t happened. There is no
explanation beyond that. And the Sun, the earth upon which we
live, our existence - the whole package is nothing but one grand serendipity . Now, this accident of a universe we live in holds many stars
one of which is the Sun. The earth revolves around the Sun
and not vice versa, and it does so in an elliptical fashion,
not a circular one. It may seem that the Sun is the one t h a t
is moving, but that is an illusion t h a t stems from our limited
perspective as observers here on earth.
1 can tell you more about the Sun, but before I do, I just
want to emphasize how really unnecessary it is to bekeve in
any god. 1 mean. . . The I n q u i s i t o r interrupts.
Inquisitor: 1 would ask that we stay in keeping with the subject
at hand. Can you tell us anything more about the sun?
Visitor 3: Yes. The Sun is a gaseous bal1 of fire millions of
miles from us. It is massive in that it is many tirnes g r e a t e r
than the earth in size, and yet it is t h e smallest star we
know of.
Visitor 3 is done. There is a pause w h i l e the three look to
t h e I n q u i s i t o r wi th curiosi ty. She l o o k s t h o u g h t f u l . Inquisitor: I want to thank each of you. 1 am g r a t e f u l t o you
for being so forthcoming. You have been borrowed from your
regular lives s o that 1 may be enlightened, and this has been
accomplished.
Heref s what 1 have learned f rom you. 1 see t h a t you a r e a t
variance with each o t h e r . You have each spoken of the Sun,
but i n so doing, you have rendered so much more. You have
a l s o shared accounts of your broader cosmological
understandings. There is much d i v e r s i t y between them. There
i s much d i v e r s i t y between you.
B u t t h i s i s t o be expected a s I'm su re you would agree.
There a re many generations and rnany leagues that separa te you.
You are of d i f f e r e n t worlds. T h i s i s a s p e c i a l place. Here
you can communicate w i t h each other, understand each other.
I n your worlds you cannot. You speak d i f f e r e n t languages, you
have d i f f e r e n t customs, you champion d i f f e r e n t values. I f you
were t o meet under a l t e r n a t i v e circumstances you would be
a l i e n s t o each other and perhaps even becorne enemies. Your
d i v e r s i t y would be a p o t e n t i a l source of mutual t h r e a t . 1 Say
t h i s because h i s to ry has t o l d t h e s t o r y many t i m e s ... Suddenly, the Inquisitor hesitates. She l ooks t h e m over , each
in turn. Then she continues.
Inquisitor: And yet , 1 wonder: a r e you r e a l l y so d i f f e r e n t £rom
each other? Your percept ions , your world views : are t h e y
- r e a l l y sa &ifparate?- qerkaps- tiley-are-. - Your-accoun€spof - thep
Sun would seem t o i n d i c a t e they a r e . But then ... Here. 1 have one more request of you. I would l i k e t o
probe i f 1 may. It seems t o m e t h a t you each va lue t h e Sun.
T h i s is something t o which the t h r e e of you have a l luded i f
not emphasized. Please, be succ inc t and t e l l m e why t h a t is
once again.
The Inquis i tor nods t o V i s i t o r 1.
Visitor 1: The sun provides l i g h t and warmth t o t h e ear th .
Without it we could not l i v e and grow.
Visitor 2: 1 must Say t h a t 1 agree with t h a t . The sun i s that
grea t n a t u r a l phenomenon towards which a l 1 corporeal ex i s tence
yearns. The sun g ives v i t a l i t y t o t h e physical .
Inquisitor: And you?
She l ooks t o Visitor 3.
Visitor 3: There is no denying what my two f r i ends have just
sa id . But what's as ton ish ing is t h a t t h e e a r t h happens t o be
a t exactly the r i g h t d i s tance £rom the Sun. I f t h e e a r t h were
any nearer o r further from it , w e would not exist. A s it
s tands , w e rece ive t h e p rec i se amount of heat w e need from t h e
Sun - that a l 1 th ings need, I should Say. (Although, with t h e
ozone l a y e r th inn ing the way it i s , the Sun f e e l s a l i t t l e
h o t t e r than it should a t times.)
Visitor 3 f i n i s h e s . The Inquisitor b r i n g s a n end t o her
inquiry .
Inquisitor: The sun renders warmth. The Sun renders l i g h t . T h e
Sun makes l i f e pos s ib l e . You al1 be l i eve these t h i n g s , don' t
you?
The t h r e e i n d i c a t e their agreement. They c e r t a i n l y do.
The Inquisitor then surveys her small assembly and nods one
l a s t t i m e i n thanks. And with that, the v i s i t o r s a r e gone.
She then r ises and continues on her way , her face content.
There is oneness, she thinks t o herse l f . Be i t disguised by
fundamental d i s c r e p a n c i e s , there is s t i l l oneness t o be found.
A t l e a s t with certain t h i n g s there is.. . THE OmIPOTENT SOCIAL?
1s everything pure ly s o c i a l cons t ruc t ion? Does medicine have
no foundations i n anything r e a l ? 1s i l l n e s s a fancy of the
times, a play with power? 1s it devoid of anything s u b s t a n t i a l ,
of anything deep, of anything t r u e bes ides made t r u t h ? The
emphatic h o r i z o n t a l i s t answers yes t o each of these questions.
The verticalist answers a definite no. And the consultationist?
S\he s e e s relevance to both sides.
There are degrees of horizontalism, to be sure. Many
constructionists, for example, acknowledge an underlying
biological reality. They concede there is something there,
something other than the social. Wright and Treacher write that
"[iJllnesses really do exist, but as sufferings which have no
necessary, transhistorical, universal shape ...'? Similarly,
Mishler writes that although cultural variation predominates,
"[tlhis does not mean that the same biological processes would
not be observed in different cultures, but that they will be
given different meanings. "3 Lock says the same. While she and
or don' want "to demonstrate the social and cultural character of al1 medical knowledge," Lock expla ins that they
are not denying the existence of real, painful stress and suffering. There is, of course, a biological reality, but the moment that efforts are made to explain, order, and manipulate that reality, then a process of contextualization takes place in which the dynamic relationship of biology with cultural values and the social order has to be considered. 5
Acknowledgments are made. That is not to be denied.
Moreover, there are definitely constructionists who are overtly
essentialist, granting significant weight to the biological, to
the natural. Bryan S. Turner, as shall become very evident
l a t e r in this chapter, is one such constructionist.
But 1 think is it is also fair to suggest that constructionism
can be sornewhat unilateral in its emphasis on the social as
compared to the natural. This is implied by the excerpts above,
but to elaborate, White, for example, in his "Trend Report: The
Sociology of Health and Illness" in 1991, expresses
dissatisfaction with critical sociology which he says "has not
freed itself from the clairns of medicine; it grants primacy to
the biological fact of disease and then adds the social ."6 And

White doesn't want to just add the social. He advocates,
instead, the social constructionist approach in which whether or
not something is a disease (like repetition strain injury), "or
will become a disease, is a political issue, and the outcome,
n o t o f b i o l o g i c a l factors, but social relationships."' He drawç
in particular on the work of Fleck who argues that '" [i]n
sciences, just as in art and in l i f e , o n l y that which is true t o 8 culture i s t r u e t o nature."' Not: that which is true to nature
is true to culture. In White's understanding of social
constructionism, nature is de-emphasized under the sway of the
social. Again: "[tlhe relationship of nature and society ... has moved into the center of the sociology of knowledge, with nature
l o s i n g its privileged epistemological status ."g
And it would seem that other constructionists would agree,
despite their acknowledgment of the biological. Wright and
Treacher, in their initial characterization of the social
constructionist approach, place tremendous stress on the social.
As quoted before, they Say: " [ m ] e d i c a l categories, we would
contend, a r e s o c i a l th rough and t h r o u g h ; they are the outcome of
a web of social practices and bear their irnprint."1° And they go
on to Say: " . . . e v e r y t h i n g i n medicine, however seemingly
technical or recondite, i s regarded as s o c i a l , though no t , of
course, the product of the same forxn of social practice in every
case. "'l Turner also says sornething very similar . Drawing upon
the work of Foucault, he writes:
This epistemology associated with the works of Foucault has radical implications for medical sociology. We can no longer regard 'diseases' as natural events in the world which occur outside the language with which they are described. A disease
e n t i t y i s the product o f m e d i c a l discourses which in turn reflect the dominant mode of thinking (the episteme in Foucault's teminology) within a society. 12
Now, it may be an exaggeration to Say with Fox the following:
Approaches which recognize that there is a nature, but that what is interesting about it is the way that culture uses it to create social relations, are well represented in the SHH? Here, nature is conceptualized as basically ineffectual and able to be bracketed out of the equation. Hence food taboos are seen as a consequence of cultural systems whereby nature is classified, rather than being explicatory of any 'real' danger associated with the foods themselves. 14
. . .by which, in my understanding, Fox is saying that constructionists pay lip service to nature, anà then set it
aside. That the dynamic relationship turns out to be not so
dynamic after a l l . That the relationship is more unidirectional
than any concessions would at first imply, with the social
exercising most, if not a l l , of the sway. That nature is
diminished, ignored. That, indeed, nature is forsaken in the
sweep of social constructionist analysis.
That is, it rnay be an exaggeration to conclude that social
constructionists, generally speaking, trivialize the impact of
nature to the extent that Fox suggests. There is diversity
within the paradigmatic approach, with some granting more weight
to nature than others. Nonetheless, it does seem reasonable to
conclude that £rom a social constructionist point of view
generally, whether or not something is considered a disease is
invariably a social issue. As Rosenberg summarizes it: "disease
is constructed not discovered. "15 Medical categories, moreover,
are contingent (dominant) social arrangements. They are not
adequate representations, of what is "out there".
And it seems reasonable to further characterize the
constructionist approach as calling into question any theory of
illness, and in particular, any scientif ically "correctf' theory
that claims attunernent with the natural. Such theories are
scrutinized for their social origins, which, when found, supply
constructionism with grounds to dismantle their verticalism and
any d a i m s they make to superiority. From a constructionist
point of view, any given scientific theory can be exposed for
its social origins, no matter how sound it may seem. This is
what Foucault's genealogy is a l 1 about. Sirnilarly, this is what
the "strong program" within sociology is about, a position that
holds scientific theorizing is "a social process, consequent
upon interests or non-scientif ic belief S . . . "16 . This means that
a scientific theory is just as contingent as the next (albeit a
lay) theory . "Correct" knowledges, "incorrect"
knowledges ... they al1 amount to the same thing: contingent social arrangements.
Moreover, because medicine has dominated, social
constructionism has paid particular attention to medicine and
its approach to health. And although Fox may be exaggerating
once again, there is definitely some truth to the notion that:
The sociology of health and illness has defined itself, at least in part, through its illustrations of the darker side to caring relationships. The healers are exposed as manipulative and/or oppressive characters, quick to make judgmental and moral evaluations of their patients, or as agents of a deterministic social or political system. . . [FI rom Eliot
- -
Freidscx-onwards there r a n have b e e n few passages emanatping from the pens of medical sociologists which have dwelt on the positive aspects of medical practice ...
. . .Medical sociological critiques of rnedicine articulated with a general disillusion with establishment values and centralized systems: to knock the powerful was trendy and
17 progressive.
Fox goes on to Say that, consequently, an opposition has
resulted
between medicine and health c a r e as the negative, controlling discipline, while the SHH [is] defined (and privileged) as the positive, empowering discipline - on the side of the oppressed and the vulnerable . . . [ an] opposition, which . . . variously
construct[s] a human subject which is essentialist and/or over-socialized or determined. 18
In short, it seems clear that while many constructionists
admit the presence and impact of nature (of biology, of
foundations) - while many are definitely essentialist in orientation, while many acknowledge the foundational - within
the social constructionist approach generally, the social
preponderates over the natural. The dynamic relationship is not
evidentially explored. Instead, the social is explored, and it
would seem, elevated. Moreover, claims to truth about the
natural (about the essential) are challenged and invariably
rendered social contingencies.
My concern, therefore, is to assess very specifically the
validity of this dynamic relationship between the natural and
the social that Lock, Wright and Teacher and others acknowledge,
and to explore, further, what it means both epistemologically
and ontologically to take this relationship seriously. Such an
exploration, I feel, will lead to conclusions that differ
notably £rom those which follow from the constructionist
approach (although not so much that social constructionism does
not figure), as well as radically £rom those which follow from
the anti-foundationalist position, a position that pays no heed
to nature whatsoever, that has no interest in making any avowals
to foundational impact.
Anti-foundationalism, I should make clear, is distinguished
from constructionism by virtue of its disavowal of ontology - of
any concrete prior-to-social reality. Turnerf s distinction is
helpful :
For the sake of clarification, we can say that constructionism is a position within the sociology of knowledge, which claims that our knowledge of reality is the consequence of social processes. There are no discursively autonomous and neutral 'knowledges' of the world: the most 'concrete' facts about
reality are social constructs. Ariti-foundationalism is a form of social ontology which says that there are no 'thingsf or conditions which are not the product of social processes. There are no essential foundations outside ongoing social
19 processes: the most concrete things are social products.
Constructionisrn, in the ideal sense of the term, is concerned
with "knowledge of" things - how "knowledge of" is socially
formulated. Anti-foundationalism places ernphasis on the things
themselves - how the things themselves are socially constructed
Some, like ~errida~', claim there is no independent realrn beyond
that of language and signification. The Saussurian practice of
dividing reality up into signifiers and what they signify
(signif ieds) is fallacious . Everything, for Derrida, signifies . Moreover, signifiers lead to other signif iers ad infini tum.
That is our world. If you logocentricallyZ1 (vertically) think
that youf ve uncovered some impregnable f oundat ion, that you' ve
got a legitimate clah to unqualified presence, guess again: the
foundation invariably slips away. No matter how solid it may
seem at first, it does not - cannot - stand alone. It
incorporates traces from other things. It thus refers on to
other things, which in turn refer on to yet other things, which
in turn refer back again as well as on to other things . . . The world is an endless play of referral. There can be no daims to
solid presence. Presence dissolves within an infinity of
signification.
Reality is a tapestry of signifiers. This is Derridean anti-
foundationalism in brie£. Put more generally, anti-
foundationalism has it that reality itself, not just our
knowledge of it, is (completely ! ) socially determined. With
anti-foundationalism, therefore, the biological is shown little
attention beyond triviality. Ontologically, the world is
(diseases are), constructed. In contrast, with social

constructionism proper, the biological is acknowledged, but
invariably the social is privileged. Epistemologically, the
world is (diseases are), constructed.
However, as Turner goes on to Say, although we can, in
principle, distinguish between constructionism and anti-
foundationalism, it is not uncommon for them to converge. 2 2
Indeed, he feels that ''in practice, these positions are likely
to be held simultaneously. "23 Thus, when 1 refer to the social
constructionist position, 1 refer to it in the ideal type sense
as horizontalist. And 1 do so not feeling too uncomfortable
given the inclination within social constructionism to grant
primacy to the social. thus overlooking the real-social dynamic.
However, 1 do so also noting that 1 am forcing the issue
somewhat, as there is most assuredly diversity within the social
constructionist paradigm - some constructionists (that is, some more than others), do indeed acknowledge (if not truly explore),
foundational impact.
So, once again, my objective here is to investigate the
epistemological and ontological ramifications that follow from
taking the dynamic relationship between the natural (the real)
and the social seriously. Both are considered since, as will be
demonstrated, the how of "knowledge-of" and the nature of "what
is" have consequences for each other. "What is" informs
"knowledge of"; "knowledge of" inf o m s "what is" . Turner asks :
"[aire diseases merely the products of different types of
classificatory procedure? Or are diseases the effects of our
biological and physiological constituti~n?"~~ From what f ollows,
1 Say diseases are both. They are both foundational and
constructed. But there is a qualification: the extent to which
they are both varies from disease to disease. This
qualification has pivotal epistemological, and therefore
ontological, ramifications.
THE RELATMTY OF SOCIAL CONSTRUCTION
The social holds sway. That is definitely granted. But let
me ask again: does it hold al1 of the sway as the anti-
foundationalist holds? In al1 situations? And if it does not,
then how should we understand this dynamic relationship between
the biological and the social that Lock talks about? What does
such a relationship actually look like? My feeling is that
Turner provides the key to these questions when he says "1 see
no reason to doubt the proposition that the body is socially
constructed. However, some things ( 'hysteria ') may be more
s o c i a l l y constructed than others ( 'gout') . " 2 5 The objective of
this chapter is to investigate the validity of such a daim as
well as to b u i l d on, modify and extend it.
To proceed, I employ two terms as heuristic tools: 1. the
paradigm; and 2. the phenornenon.
1. The Paradigm: Kuhn was the first to popularize this term in
his seminal work, The Structure of Sc ien t i f i c ~evolutions~~,
although there was much confusion over what he actually meant by
it. Some have even claimed that he used the term in over 22
different ways2'. Later, however, he came to refer to "paradigm"
in two very distinct ways, the first of which he preferred.
This one c m be referred to as paradigm-as-achievement28. A
(scientific) 29 paradigm in this sense is an "exempiary [way] of
conceptualizing and intervening in particular empirical
contexts . "'O It is a fundamental achievement - an exemplar - that
provides criteria for dealing with new empirical situations. As
Rouse explains, accepting a paradigm is like acquiring and
applying multiple skills. It involves
applying concepts, employing mathematical techniques (not just calculating, but choosing the right mathematics, applying it correctly to an empirical situation, knowing its limitations and approximations, etc.), using instrumentation and other

apparatus, and recognizing opportunities for varying or intervening in particular theoretical or experimental situations. 3 1
It involves "understanding how to treat new situations like old
ones, to do for them what has already been done in the exemplary
case. u3*
This is the narrow sense of the term, but one which, as Kuhn
explains, was also expanded to denote 'all shared group
commitments, all components of what [Kuhn] now wish[es] to call
the disciplinary matrix. "33 This second sense of the paradigm is
the paradigm-as-set-of -shared-~alues~~, which is more global in
scope and includes a group's ideological orientation, a group's
shared set of fundamental beliefs, values, vocabulary and
standards for what constitutes a relevant problem and what its
solution should look like. It is a theoretical world view
incommensurable with others, a view that conditions the way in
which we observe and deal with phenomena.
My use of the term paradigm has similarities with Kuhn's
second use. I use it because, although Kuhn may favor the
first, it is the second that has taken off within the philosophy
of science and, more generally, as part of the horizontalist's
view of things. This view of the paradigm emerges from a
relatively common reading of Kuhn, a reading which Kuhn in many
ways rejects in his 1969 postscript to Structure, much to the
discontent of some. Alan Musgravers reaction is indicative:
Kuhnfs Postscript left me feeling a little disappointed. I find the new, more real Kuhn who emerges in it but a pale reflection of the old, revolutionary Kuhn. Perhaps this revolutionary never really existed - but then it was necessary to invent him. 35
Horizontalists like Rorty prefer the revolutionary Kuhn, the
Kuhn that says science 'creates the world it attempts to
describe"36; the one that says science does so in line with the
paradigmatic assumptions that prevail at the time. The
paradigm, in this sense, has similarities with Wittgenstein's
language games, with Rorty's related emphasis on language and
how it cannot be transcended, with Foucault's discourses, etc.
Horizontalists variously emphasize language, discourse, the
epistemes, the paradigm etc., as the frameworks that guide, if
not determine, understanding and action.
Thus, by paradigm 1 mean to denote a particular framework
within which knowing, addressing and constructing reality
occurs. The paradigm is a lens through which individuals and/or
groups see reality. It is also a tool with which individuals
and/or groups both relate to and fashion reality (and/or more
narrowly, a specific class of phenornena, such as health, illness
and disease) . But my use of paradigm is not to discount the importance of
Kuhn's first use - paradigm-as-achievement. It is not to
discount Kuhn's insight into how new situations, new problerns,
are approached, interpreted and dealt with in light of past
successes. Rather, it is to draw a distinction: Kuhn refers to
past successes as paradigms; 1 refer to them simply as
exempl ars . Moreover, I do not restrict the meaning of exemplars to that
of successes. Rather, I see them as significant experiences in
general, experiences that can, on the one hand, spawn a
paradigmatic approach and then serve as fundamental sources of
paradigmatic justification. To experience oppression in one
situation, for example, rnay lead one to understand and treat
successive situations as oppressive as well. Likewise, a
negative experience with a "minority" may lead one to harbor
prejudicial attitudes towards "minorities" in general. On the
other hand, a paradigm rnay spawn an exemplar. It rnay take hold
of a particular experience (with a minority), paradigmatically
imbue it (see it as typical in a bad way), and then treat it as
lending critical support for the paradigmatic approach
(prejudicial attitudes towards minorities). It may elevate the
experience to the status of exemplar, to the status of pivotal
paradigmatic justification.
2. Phenomenon: By phenomenon I mean simply an event, process
or thing.
REALITY AS CONSTRAINT
To suggest that some things are more socially constructed than
others means to take the dynamic relationship between reality
and social construction seriously. This in t u r n means taking
reality and its impact on the relationship seriously. And there
seem to be good reasons for doing just that. Barnes, (a
constructionist, 1 might add), thinks there are:
[I]t is important not to lose sight of the connection which does exist between knowledge and the real world .. .Hence knowledge is found useful precisely because the world is as it is; and it is to t h a t extent a function of what is real, and not the pure product of thought and imagination. mowledge arises out of our encounters with reality and i s continually subject t o feedback-correction from these encounters, as failures of prediction, manipulation and control occur. 3 7
What follows are some more reasons for taking the impact of
reality seriously.
To begin, let me ask a question: is it possible to m a k e a
boulder of a feather?
Let me be more precise in what 1 am asking: is it possible to
socially construct a feather such that it is understood, related
to, and addressed in exactly the same way that a three ton
boulder is understood, related to, and addressed? 1s it
possible to thoroughly perceive a feather and boulder in exactly
the same way? For t h e m t o have precisely the same meanings
attached to them? Perhaps it is possible. But I would suggest
that it is unlikely. 1 would suggest that it is doubtful that
any paradigm would so construct a feather. Why? Well, most
fundamentally, reality exercises constraints over how it is
understood and what is made of it. It impinges, it dernands. In
a manner of speaking, it has a say. It thus moderates the
extent to which social construction can have its way with it.
Feyerabend says that "Scientists [and, for that matter, al1
members of relatively uniform cultures] are sculptors of
reality. "38 But sculptors need materials with which to work,
otherwise they cannot sculpt. And those materials must retain
properties, otherwise they would not be materials. And those
properties must involve conditions, otherwise they would not be
properties. And those conditions must impose demands, otherwise
they would not be conditions. And those demands must constrain,
otherwise they would not be demands. Hence, social
construction, like sculpting, has its limitations, limitations
which stem directly from the stuff it is constructing.
It follows that the social construction of "feather" has its
limitations. The feather imposes certain constraints,
constraints which allow it to be constructed only so far - within certain parameters, that 1 s . Social construction can
make many things of the phenornenon "feather". It cannot,
however, make it into j u s t anything. 1 doubt - to get back to the example - that it could make of it a boulder. And if it
could, 1 doubt the construction "feather-as-boulderf' would last
very long. Both the feather and the boulder would demand
otherwise (once again, in a manner of speaking) . Their feed-
back, upon encounter, would invariably diffuse any such
construction.
Think of an even more ridiculous example, such as the making
of a rock out of a rainbow. 1s such possible? Considering the
logic presented above, 1 suggest probably not, at least as

regards a sustained construction. Reality (the rainbow and
rock) upon feedback, would demand otherwise,
Social construction orders and manipulates reality . It imbues
phenomena with meanings. But reality and its phenomena (some
more so than others - 1 get to this later) can only be
manipulated so fa r . Reality sets parameters such that social
construction does not proceed unrestrained. It may be that
some, for example, see green as a distinct color while others
see it as simply a variation on the color blue. Green is thus
categorized differently, constructed differently by different
groups or individuals. But there are restraints to its
construction, and thus, to the variation in its constructions.
Green is less likely to be categorized as a variation of red,
for example (unless those perceiving are color blind). And even
less likely is the possibility of it being categorized as a
shape, like a triangle. The fact that it remains a color and
not a shape speaks to the reality of constraint.
The fact, moreover, that different musicians' interpretations
of Pachelbel's Canon and Gigue actually sound more or less
similar, and more or less like Pachelbel's Canon and Gigue as
demanded by the score, speaks to the reality of constraint. Not
too many musicians, 1 would venture, interpret the score -
construct it - to sound like "Mary Had a Little L A . "
Longino says that 'There is "something out there" that imposes
limits on what we can say about it. ' 39 1 agree and paraphrase: There are things out there that impose l i m i t s on our
constructions of t h e m .
Now, it should be emphasized that while reality limits, the
fact that it does necessarily means that it enables as w e l l .
One cannot sculpt unless there is something (with properties,
hence conditions, hence demands, hence constraints ) to sculpt . Real i ty-as-cons training and real ity-as-enabling are two sides of
the same coin. This means, moreover, that reality is
foundational. The foundations of reality (of phenomena) may be
manipulable, somewhat vacuous at times and therefore imbuable,
but they exist nonetheless. If they did not, social
construction could not proceed: it would have nothing to grab
hold of: it would have nothing with which to play. What I am
saying is in line with Gerasr response to Rorty. He writes:
Where one view. . . is that language' s sovereignty over al1 access to the world means there cannot be a way things are just in themselves, the argument put here is that there must be a segment of the world which is already - in itself, and however we rnay then further construct or conceptualize that world - structured, sornewhat stable and dif£erentiated. Otherwise language across the public space with shared symbols would be impossible. 4 O
This view contrasts with the central maxim of Sartrean
existentialism: "existence before essence". By this maxim is
meant that things (existences) have their different essences
only because they are endowed (by us) with t hose essences. This
in turn means that the essences of things are without necessity
and are purely transmutable. We are free to make of things what
we wish of them. The fact that we donf t exercise this freedom
is because the prospect of the inessentiality of things is a
scary one. We think: "If things are not the way they are out of
necessity, then what is the meaning of things? Indeed, what is
the meaning of life?" We feel little comfort with such
thoughts. So we avoid thém and thus avoid Our freedom to
create.
But the question is: can we actually create in the absence of
necessity? Can we create without conditions? Analogously: can
a house be built without materials? If not, then must not those
materials have certain qualities (conditions) that allow them to
be used in certain ways ...q ualities which, if absent, would make
it impossible to build unless other materials (with related, yet
perhaps different qualities/conditions, but with
qualities/conditions nonetheless) were used? If the answer is
"yes" to this last question and "no" to the othe r s , then 1 think
it is fair to draw a few related conclusions:
The freedom to construct is impossible in the absence of (at
least sone) vestige of necessity. 4 1
Social construction is impossible in the absence of (at least
some) phenornenal foundations.
And - dealing with the existentialist claim:
The social assignment/production of essence is impossible in
the absence of (at least some) prior-to-social essence.
Foundational essence conditions constructed essence.
Think of.. . The Body as Constraint
. . . and this al1 becomes more clear. Turner helps t o make it clear.
He writes that :
[I]t would be wrong to construe my sociology of the body as merely a social constructionist viewpoint ... 1 do not believe that rea-ty-is discourse, that is, 1 da not- beLieue t h a t - -
- - - - -
social reality is merely an issue of representation. 4 2
Horizontalism, speaking ontologically, says that is al1 reality
is. This we have seen. It also says that is al1 the body is.
Foucault, in particular, rejects the objectivity of the body and
maintains that the body is nothing but a product of knowledçe,
or rather, that it Y s an effect of practices which embody such
f orms of knowledge. " In particular, Foucault' s
... research fis] concerned with how 'bodies' are produced by discourses and his primary theme Lis] the normalization of the body and populations by the social sciences and the institutions which [articulate] scientific knowledge. 4 3
Turner is not about to reject the impact of knowledge,
discourse, social construction, practices, or what have you.
Their role is profound and he knows it. He insists that the
body is more than a social product. The body has organic
foundations. It has objectivity. It has actuality. The body
is a concrete potentiality that is socially/culturally
elaborated in different ways. In his words, " [tlhe body
provides the foundational potentialities upon which endless
cultural practices can be ere~ted."~~ So the body is both
foundational and anti-foundational; it is both natural and
cultural; it is both objective and constructed.
Take walking or any of the other basic "body techniques" such
as sitting, standing, gesticulating. From culture to culture
one can observe variations in the ways in which people
walk/sit/stand/gesticulate. Walking etc. 'are developed modes
of operation which are specific to given cultures"45. And as
such, they are social constructions. But that is not al1 they
are. Far from it. Remove their organic foundations and what do
you have left? Nothing. Walking, sitting, etc., are better
understood as elaborations on certain commonalties - on certain
foundational (biological) potentialities, that is.
Take sex differences. Turner writes that
. . . even if sexuality is produced by classificatory systems, it still seems to me that male and female bodies are organically, physi~logically~ biochernically different phenomena. 1 know there are problems in classifying biological sex differences. Biological difference is socially produced by the endless reproduction of human beings, but the classificatory systems can be seen as reflections upon differences in natural
46 phenomena.
Classifications produce. Different classifications produce
differently. Thatfs aàmitted. But it is also the case that
different classifications are variations on a foundational
distinction located at the organic level. Natural sex
differences constitute t he potentiality - the stuff - upon which
social construction erects its var ied elaborations of sex
differences. Without the natural, classification could not
ensue. Thus, while there is "a lot of theorizing [that]
entirely emphasizes classificatory processes", the question is:
"classification of ~hat?"~' There needs to be something there,
sornething real to construct, to classify.
Finally, take birth and death. Both are social processes.
Both are elaborated in myriad ways. And yet both are processes
common to us all. They are foundational to us all. The
diversity of social practices associated with them speaks to the
power of social construction. The fact that every culture deals
with them in some way, however, speaks to their foundational
impact.
It also speaks to something else - it speaks to a shared human ontology . Despite the prof ound di£ ferences that exist between
us, "there are fundamental human experiences which are
transcultural or universalistic.. They rnay be addressed in
different ways. They may have different meanings attached to
them. They rnay be variously constructed. But at core, they are
universal.
To sum up: social construction is powerful, but it has no
power unless it is in some way linked to foundations. To
proceed, social construction must have anchors in the stuff of
reality . Or: to work, social construction must have anchors in the
stuff of reality.
Or: to enable coping (coping with nature for example), social
construction must have anchors in t he stuff of reality (of
nature).

This means that coping is possible only because the social has
some attunement with the foundational. And it is for this
reason that I would suggest that a purely pragmatist, or purely
antirepresentationalist, or purely horizontalist approach is
lacking. Rorty says that the pragmatist "drops the notion of
truth as correspondence with reality altogether, and says that
modern science does not enable us to cope because it
corresponds, it just plain enables us to What I am
suggesting is that there is no coping unless there is (at least
some) correspondence with reality. Why? Because coping requires
that there be something with which to cope, which means that
there must be demands with which to work, and thus constraints
within which to innovate. There can be no coping unless coping
is tied in sorne way to, is prernised upon some understanding of,
corresponds to some degree to, the way things are.
Think of it this way. The only reason a sculptor can chisel a
piece of marble is because by doing sor s/he is addressing, upon
impact, sornething essential about the way marble is - the way marble breaks, for example. Indeed, the very act of using a
chisel to chip away rnarble implies some attunement on the part
of the sculptor with this very aspect of marble. Why? Because
if there were no such attunement on the part of the sculptor,
then the sculptor would perceive no distinction between
chiseling marble and chiseling water, for instance. Moreover,
we can be sure that upon taking the chisel to both marble and
water, the sculptor would become immediately attuned to an
essential difference between the two - to an essential
difference between how they each "break". Hence, coping entails
attunement - if only to some extent (if only to the extent of being able to distinguish between the breaking of marble and the
"breaking" of water) .

And to continue: why is it that a sculptor is able to make
"better" chisels (chisels more adequate to the task of chipping
marble)? 1s it not because, upon encounters with the marble - upon blows and chipping - the sculptor becomes more in tune with the way marble breaks? And even perhaps why it breaks the way
it breaks? Indeed, it would seem that the very act of designing
better chisels necessarily involves greater attunement with the
way marble breaks.
The sculptor copes (chisels), therefore, by virtue of (some)
attunement with the foundational (with the way rnarble breaks).
And the sculptor creates better chisels by virtue of greater
attunement with the foundational (with the way marble breaks).
No f oundations, no demands, no coping whatsoever . Coping
entails working within constraints and this in turn entails
attunement with the way things are (if only in some way and to
some degree) . It, rnoreover, entails the prospect of
correspondence, of representation. This becomes more clear with
the following. . . The Impact of Phenomenal Tangibility
Reality cons t ra ins soc ia l cons t ruc t ion . Reality enables
social cons t ruc t i on .
Organic foundations cons t ra in the soc ia l cons truct ion o f the
body. Organic foundations enable t h e soc ia l cons truct ion o f the
body*
That' s where we are so far . But thatr s just the beginning.
This picture needs to be modified somewhat for it is not
complete. In the first place, the power of t h e paradigm t o
construct needs t o be re-emphasized. In the second place, the
power of r e a l i t y t o cons train /enable needs t o be qualified. Let
me proceed with the latter modification first.
It begins as follows:

The power t o cons t ra in /enab le is n o t uni form across phenomena.
Hence t h e relativity of the social cons t ruc t ion of phenomena.
To explain, 1 would like to introduce a new analytical tool,
namely the term tangibility. The sway of social construction is
affected by what is real, and more specifically, by the
tangibility of what is real. The tangibility of a phenomenon
refers to the extent to which the independent-of-social-
"whatness" of a phenomenon is indisputably clear and obvious.
It therefore refers to the extent to which it constrains.
Complete tangibility (full constraint) is never achieved (as
discussed later). But the degree to which it is achieved is
critical in that the ambiguity of a given phenomenon has
consequences for its elaboration. Put another way, the clarity
and "liveliness" (to use Hume's terni in a modified way) of a
phenomenon acts very much like an anchor, reducing in proportion
to its weight as a tangible (constraining) phenomenon, the
degree to which social construction goes about constructing
it ... although . . . (to continue modifying)
. . . this implies a negative linear relationship between tangibility and social construction: the less tangible the
phenomenon (the less it constrains), the more it is socially
constructed. This is fallacious since it means that the
greatest degree of social construction occurs where there is no
tangibility (where there are no constraints) - where there is no
link to what is real. And that is impossible. Links to reality
are essential to social construction. This has been discussed.
So what 1 would like to suggest instead is the following: social
construction is greatest when it concerns semi-tangible (semi-
constraining) phenomena.
(If ve emphasized suf f iciently the relationship between
tangibility and constraint, 1 presume) .
1 suggest this because high degrees of tangibility mean less
latitude for social construction - tangible phenornena are more obvious about what they are; they are more demanding.
Similarly, with zero tangibility social construction is
paralyzed. In this case there is nothing to grab ont0 - there is no basis upon which to create; there a re no demands
forthcoming. With semi-tangibility, however, the condition is
set for extensive (and creative) social construction. The
demands are there but they are very indeterminate, highly
negotiable, extrernely supple.
A n analogy may help:
Imagine a c l a y a r t i s t who we w i l l c a l 1 Sandy, and who, on one
o c c a s i o n i s p r e s e n t e d w i t h a p i e c e o f c l a y . From a f a r , Sandy
l o o k s a t i t o b s e r v i n g i t s d i m e n s i o n s and p o t e n t i a l f o r
m a n i p u l a t i o n . She t h e n p r o c e e d s t o p i c k i t up, and much t o her
d i s s a t i s f a c t i o n , f i n d s t h a t i t i s a hardened p i e c e and t h a t i t
h a s a l r e a d y seen the k i l n . Sandy p u t s i t down and d e s p o n d e n t l y
a c c e p t s i t for what i t i s . I t s hardnes s - its t a n g i b i l i t y -
res t r ic t s Sandy from c r e a t i n g . She cou ld a t t e m p t t o f a s h i o n i t
i n her c a p a c i t y a s a c l a y a r t i s t , o r she c o u l d proceed t o smash
i t a g a i n s t the table i n f r o n t o f her, b u t would either approach
r e a l l y be t o h e r advantage? T h e e f f o r t wouldn't be worth it -
the r e s u l t s would n e v e r conform t o her p a r t i c u l a r e x p e c t a t i o n s
a s a c l a y a r t i s t .
On a n o t h e r o c c a s i o n , Sandy i s p r e s e n t e d w i t h a b u c k e t o f w a t e r
and a s p a r s e s c a t t e r i n g o f c l a y remnants . T h i s t i m e she i s
c o n f u s e d . Her r e a c t i o n : what i s t h e r e t o work w i t h h e r e ? A
very good q u e s t i o n . In t h i s case, Sandy e x p e r i e n c e s non-
t a n g i b i l i t y .
F i n a l l y , on a t h i r d o c c a s i o n , Sandy i s p r e s e n t e d w i t h what she
d e s i r e s m o s t a s a c l a y a r t i s t , a s a c r e a t o r - s o f t moldable
c lay. W i t h zea l and s k i l l , she f a s h i o n s i t t o her s a t i s f a c t i o n ,

shaping it i n conformity t o what she finds meaningful. With
semi-tangibility, Sandy finally gets her way.
In br i e f , semi-tangibility encourages social construction
because it is by definition pliant. A phenomenon with semi-
tangibility is a phenomenon profoundly amenable to social
moldability.
This means that some things are more socially constructed than
others as Turner contends. However, taking things a step
further, 1 would like to modify his contention by suggesting
that the social construction of things is curv i l i near l y r e l a t e d
t o the tangibility of those things (see Figure 1). The greater
the serni-tangibility of those things, the greater their 5 0 amenability to social construction. (Although, as will be
pointed out later in this chapter, even the most tangible things
have some construction to them - having meanings-attached. Hence why the curve is more definite with intangibility).
Revisiting the Paradigm
Now, to re-emphasize the power of the paradigm.
Tangibility is not something necessarily inherent to a
phenomenon. The extent to which any given phenomenon radiates
tangibility (exercises constraints) is in large measure - but in
no way totally - paradigmatically conditioned. The picture 1 have painted so far is one in which social
construction is seen to fil1 the voids that semi-tangibility
creates. With semi-tangibility, the paradigm latches ont0 and
molds, bends, constitutes the phenomenon to its will. But this
assumes the semi-tangibility of the phenomenon is independently
given - prior to social construction. It isdt - it isn't
necessarily, that is.
The paradigm is omnipresent. It is forever there in one form
or another like some perpetual fog, contextualizing our
observations of phenomena and constituting those same phenomena.
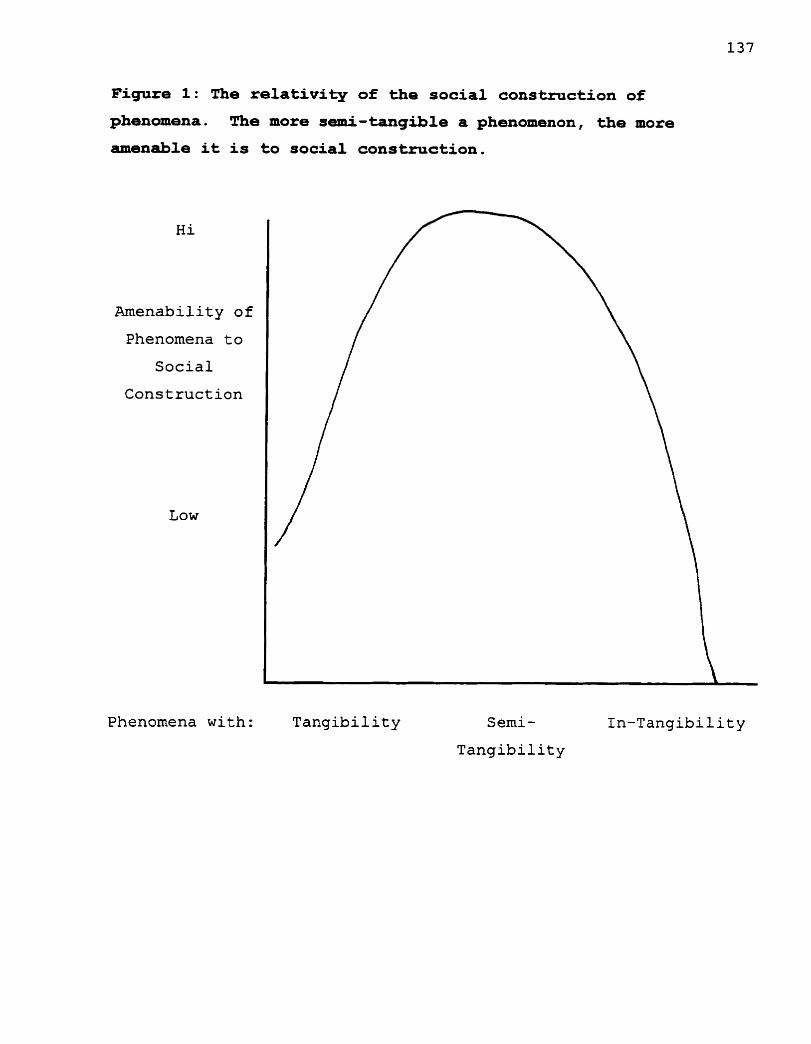
Figure 1: The relativity of the social construction of
phenomena. The more semi-tangible a phenomenon, the more
amenable it is to social construction.
Amenability of
Phenomena t O
Social
Construction
Low
Phenomena with: T a n g i b i l i t y Semi-
Tangibility
In-Tangibility
It forms a framework that shepherds (if not determines) both the
investigation of phenomena as well as their social construction.
This was discussed at length in Chapter 3 where it was seen that
illnesses emerge (and fully so from a horizontalist point of
view) in accordance with contextual values and anxieties.
To elaborate, it is useful to draw a distinction between
paradigmatic seeing and constructing, although they are integral
to each other.
Regarding seeing:
A helpful way to think of the paradigm is to compare it to a
lens. This is a common analogy and has been mentioned already.
The world is perceived by different people/groups through
di£ ferent lensesS1. The paradigm is the Lens through which a
group/individual sees.
As such, the paradigm conditions the tangibility of phenomena,
although it does so to some more than to others. As discussed
later in this chapter, certain phenomena (or rather, certain
aspects of phenomena) are rather universally tangible. They are
rather irresistible to any paradigm. For example, not many
would deny the hotness of a burner switched to high upon
accidentally placing a hand on it (except perhaps hot coal
walkers). Not many who would see/construct the hotness of the
burner as coldness, this notwithstanding our paradigmatic
differences. Here the hotness "burns" through the diversity of
paradigmatic fog. It constrains the paradigmatic fog.
But in general: through the paradigm, some phenomena radiate
tangibility, even translucence. Through it others are
distorted, rendered semi-tangible. Through it still others are
made intangible, hidden £rom view. Put another way: phenomena
speak out, but they speak with differing impact. Within the
paradigmatic ear some ring loud and clear, others with static,
and others not at all.

Put y e t ano the r way: a phenornenon r a d i a t e s t a n g i b i l i t y when
t h e paradigm I s i n sync with i t s phenomenal demands, i t s
c o n s t r a i n t s .
Put a f i n a l way: imagine you are enclosed i n a s p h e r i c a l
e d i f i c e of va r i ega ted g l a s s . I n some places t h e e d i f i c e is
t h i n n e r and more t r an spa ren t . I n o the r s i t is v a r i o u s l y
t h i c k e r , dense r , colored. T h i s e d i f i c e is your paradigm. What
you see through the t h i nne r , c l e a r e r s p o t s i s what's t ang ib l e t o
you. What you see through t h e rest i s v a r i o u s l y opaque -
v a r i o u s l y d i s c e r n i b l e , v a r i o u s l y muddled, va r i ous ly s e m i -
t a n g i b l e t o you. Indeed, through some s p o t s you s e e noth ing - you exper ience i n t a n g i b i l i t y .
Regarding cons t ruc t ing :
The power of t h e paradigm t o cons t ruc t is enormous.
~ u h n ' ~ , f o r example, çays that s c i e n t i s t ç a r e h a b i t u a l l y
involved i n what he c a l l s "normal science" - puzz le so lv ing
w i th in a s p e c i f i c paradigrnatic f ramework. B y t h i s he meanss3
t h a t t h e paradigm s e t s ou t t h e r u l e s , the s t anda rds and the
problems t o be solved, and t h e s c i e n t i s t , ab id ing by t h e s e r u l e s
and s t anda rds , embarks on a miss ion t o solve these problems.
What d r i v e s t h e s c i e n t i s t , what chal lenges him/her "is the
conv i c t i on t h a t , i f only he i s s k i l l f u l enough, he w i l l succeed
i n s o l v i n g a puzz le t h a t no one be fo r e has so lved o r solved so
~ e 1 1 " ~ ~ . Moreover, l i k e t he j igsaw puzzle where only one
s o l u t i o n i s acceptable , t h e s c i e n t i s t so lve s t he problem only
when h i s / h e r so lu t i on conforms t o t h e narrow expec t a t i ons of t h e
paradigm. The t r i c k i s f o r t h e s c i e n t i s t t o a r r i v e a t t h i s
s o l u t i o n , s i n c e i t is only t h e n t h a t s/he proves h i s / h e r
b r i l l i a n c e .
Normal science i s about " f i t t i n g " phenomena within the
pa rad igmat ic framework b e t t e r than anyone else has done. It is
consequently about constructing phenomena from the paradigmatic
point of view.
This we al1 do. Through Our paradigms we fashion Our world,
and we do so in different ways. Some phenomena we grab hold of
and then rnold. We understand the Sun, for example, in unique
ways. We attribute to it unique essences. Other phenornena, it
seems, we actually impute into existence. "Finding" biological
foundations for socially constructed deviance, is perhaps one
example. Then there are those phenomena we metaphorically
create. Certain phrases like " t h e is money" and "take it easy"
and "the world is an organism", are cases in point, And those
other phenomena we literally create such as technologies, 55 concrete manipulations of nature.
And once created, these phenomena become integral to each
other and to the world in which we live, thus articulatingke-
forming/shaping, indeed cons t ra in ing , the reality (paradigm)
through which further construction proceeds.
It is useful to distinguish between two types of creations to
make things a little clearer: 1. knowledge-of creations, and 2.
performance creations. The former include al1 those things that
emerge - to some extent or another - out of our attempts to
understand and address reality. Every attempt to penetrate
nature, to uncover its laws, to identify disease as they really
are, to make sense of deviance in light of illness, to confirm
that "such and suchf' is an eternal value, that it appeals to
some eternal truth - every such attempt invariably results in a phenomenal construction of one sort or another, in some degree
or another. A particular illness label like hyperkinesis is an
example of what 1 mean. The label incorporates the attempt to
deal with a particular phenomenon (hyper behavior among school
children) in a certain way (by individualizing the problem).
The latter - performance creations - include, for example, technologies. Technologies are created with the goal "to better
achievef' in mind. Some technologies are created for the sake of
achieving a more accurate understanding of what reality is al1
about. Through them, it is believed, we can penetrate the
workings of nature. Science, for instance, has manufactured an
extensive array of technologies with the aim of "getting at"
phenornena as they are in themselves. These technologies - the microscope, the ultrasound machine, etc. - are the devices through which phenornena are seen and thus understood. Other
technologies are created for the purpose of achieving greater
control and expediency. This is what Lyotard says technology is
created for. In his view, technology ernerges for the sake of
enhancing performativity - it has no necessary relationship to
truth.
Technical devices ... follow a principle, and it is the principle of optimal performance: maxirnizing output (the information of modifications obtained) and minimizing input (the energy expended in the process). Technology is therefore a game pertaining not to the true, the just, or the beautiful, etc., but to ef ficiency: a technical "move" is "good" when it does bette= md/er-expends 3 e s s energy-than another?"
Notwithstanding why they are created, however, technologies
are similar in at least two ways. In the first place, they have
roots in reality in that they are constructed out of knowledges
about reality. They have their roots in knowledge-of-reality
constructions. On the other hand, once created they have
consequences for the way in which we corne to see reality.
Whether created for the specific purpose of penetrating reality,
or for other reasons, they become part of our world. They
become part of the paradigm - itself articulated/modified/transformed by these creations - through
which reality is further understood.

Through technology, for example, the previously exceptional is
transformed into the mundane. Such is the case with artificial 5 7 heart implantation. This is Koenig's point. She begins by
quoting the New York Times which reported on February 18, 1985
that :
Though it was only the second time the Humana team performed an artificial heart implant, there was a sense of the routine. "Boy this is a du11 operation," one of the nurses who had participated in Mr. Schroederfs operations said, according to Dr. Jarvik. "That was great, " Dr. Jarvik said, "because nothing exciting is going on, there didnft seem to be any danger, any risk here."
And then says:
On reflection these remarks seem truly extraordinary. To describe the physical rernoval of a man's ailing heart and its replacement with a mechanical substitute as "routine," indeed, "just a dayf s work, " expresses something of the power of medical technology over the modern imagination.
Technology also has consequences for the way in which
inevitable processes and events are constructed. The impact of
technology on the wayç dying and death are conceptualized is a 5 8 good example. Technclogical along with pharmaceutical advances
have given physicians unprecedented "control over both the
process of dying and the timing of death. Physicians have
become the gatekeepers of dying. Death, now, "is seen as
something that can be controlled, postponed, and potentially
reversed, its timing elective, planned, and managed. This is
in stark contrast to a previous conception of death in which it
was 'looked upon as a familiar and timely "surrender of the self
to destiny". . . Dying, moreover, is something that Y s not
simply a biological "given" [anymore] but is shaped by
physiciansr interpretations of certain cues and inf~rmation"~~ - interpretations which are inf ormed by biomedicineC s cornmitment
to curative therapy and the prevalent assumption that
technological application "will r e s u l t in the alleviation of
suffering and the betterment of the world in general. "63
In short, performance creations, 6 4 along with knowledge-of
creations, condition or constrain the emergence of new
knowledge-of creations. They constitute part of the lens through
which we further see and construct that which we aim to see. In
Berger's tems, they become objectivities we internalize and
which provide the criteria upon which furthes paradigrnatic
discovery/creation of the knowledge-of type ensues.
Meanings, Seeing and Constructing
1 have stressed that things are always socially constructed:
nothing is completely immune from social construction - nothing (semi-) tangible that is. But why do I Say this? 1 Say this
because meanings are always involved with any phenomenon, no
matter how tangible the phenomencn, no matter how clearly the
phenomenon is seen for what it is. With semi-tangible
phenomena, the paradigm goes to work in full force producing
profoundly constructed realities. With tangible phenomena, on
the other hand, the paradigm is more restricted. Tangible
phenomena are bettes seen and are therefore less constructed.
They are less likely to be made into things they truly are not.
But they are socially constructed, nonetheless. Social meanings
are always attached to phenomena no matter how tangible they are
(hence why the curve is the way it is in Figure 1).
Take the Sun as an exarnple. The Sun provides light to the
earth. This aspect of the Sun is perhaps universally tangible.
Indeed, it seems impossible that this aspect could be
constructed otherwise - unless, for some reason, the sun stopped providing light and we were able to survive to witness it.
However, the light of the sun can have different meanings
attached to it. Some, for example, may view it in a positive
way. Someone lying on a beach during a well deserved vacation,
f o r example, rnay cons ide r it a b l e s s ing . Another, however,
a f f l i c t e d w i th sk in cancer due t o spending too rnuch time on t h e
beach, may harbor nega t i ve f e e l i n g s towards it . Here, d i f f e r e n t
meanings are a t t a ched t o t he same a s p e c t , an aspect t h a t i s
otherwise c l e a r l y s een from both pe r spec t i ve s .
Take ano the r example :
Both a daughter and her f a t h e r rnay be wel l aware t h a t h e r
d i r t y shoes a r e on t h e k i tchen t a b l e . They rnay bo th see t h i s
f a c t c l e a r l y . B u t t h e meanings they a t t a c h t o t h i s f a c t rnay
va ry . The former rnay s e e i t a s no b i g deal while t h e l a t t e r rnay
see it a s completely i napp rop r i a t e .
And ano the r example:
From wi th in a p a r t i c u l a r s c i e n t i f i c paradigm, it rnay seem
c l e a r how t o address a p a r t i c u l a r problem of n a t u r e . However,
for t h e neophyte and h i s mentor, the meanings t h e y a t t a c h t o the
s o l u t i o n rnay vary. The neophyte rnay a t t a c h much i n t e r e s t t o i t
while t h e mentor, having had a long and d i s t i n g u i s h e d ca r ee r ,
rnay cons ide r it t r i t e . She rnay have g r e a t e r i n t e r e s t i n new
problems, i n more cha l l eng ing problems.
I n each example, t h e phenomenon ( a s p e c t ) i s understood i n much
t h e sarne a c r o s s pe r spec t ives , o r between persons. The
phenornenon ( a spec t ) i s t a n g i b l e - seen f o r what it i s - across pe r spec t i ve s , o r between persons . Yet, t h e meanings a t t ached t o
t h i s same phenomenon ( a s p e c t ) , vary. And it i s i n t h i s way t h a t
s o c i a l cons t ruc t i on is n e c e s s a r i l y an i s s u e , no ma t t e r how
t a n g i b l e t h e phenornenon ( a spec t ) . So meanings and assumptions can i n h i b i t seeing, i n h i b i t
unders tanding a phenomenon f o r what it i s . Indeed, they can
becorne i n t i m a t e l y involved with a phenomenon, imbuing i t ,
manipulat ing it, and t h u s cons t ruc t i ng it. But meanings can
a l s o p lay a more superf luous r o l e , remaining noth ing more t h a n
meanings-attached t o t h a t which i s seen. This occurs i n the
case of tangible phenornena. And it a l w a y s occurs in the case of
tangible phenomena since meanings in one form or another are
ub iqu i tous . It is in this way that tangible phenomena are
constructed.
A final example helps summarize the main points:
Imagine a hi11 at an incline of 45 degrees. Some see this
t r u t h of the hi11 more clearly than others. Some are more
attuned to the steepness of the hi11 than others: the steepness
is more tangible to them. Consequently, they are less prone to
construct the hi11 otherwise. Those flying in an airplane
directly overhead, for example, rnay not be so attuned to the
steepness of the hill. Upon looking at it out their airplane
windows, they rnay see sornething quite contrary to the reality of
the hill. From their vantage point, it rnay not be so clear to
them what the hi11 is really like. It may be opaque to them,
semi-tangible to them. Indeed, it may not seem like a hi11 to
them at all. And so they rnay construct the hi11 accordingly - they may even flatten it.
Compare them with a group of runners making their way up the
hill. For these runners, the hi11 is indeed a hill. They are
more attuned to the steepness of the hill. Its steepness is
relatively tangible to them. And so their construction of it is
likely to be more in tune with the way things are with the hill.
From the running-paradigmatic-view, the steepness of the hi11 is
better seen and hence less constructed than it is frorn the
airplane-paradigmatic-view . Yet, within the running-paradigrn, constructions can Vary.
While being similarly attuned to the steepness of the hill, the
meanings the different runners attach to it can Vary
significantly. The stronger runners, for example, rnay attach
the meaning "welcome challenge" to the steepness of the hill.
The weaker runners, on the other hand, rnay attach to the same
aspect the meaning "unwelcome challenge." Here, they both see
its steepness, and yet attach opposite meanings to it.
Now it rnay also be that these meanings-attached become more
than that. It may be that these meanings have consequences for
how the hi11 is seen. The weaker runners may see it as steeper
than the stronger runners, and thus construct the hill. Yet,
this notwithstanding, there remains an affinity between the
weaker and stronger runners' conceptions of the hill. Although
their constructions of the hi11 may Vary frorn each other, they
share, nonetheless, an affinity they do not share with those
championing the airplane-paradigmatic construction. For al1
runners, the hi11 is a hill. It has perceivable steepness to
it.
Therefore, the hi11 is socially constructed no matter what.
It is constructed if only by virtue of having rneanings-attached.
But some constructions are more attuned to the hillness of the
hi11 than others. Some constructions, that is, are more attuned
with this particular foundational reality.
TANGIBILITY TYPES
My objective, so far, has been to build on Turner's daim that
some things are more socially constructed than others, and
further, that the extent to which things are constructed depends
upon their tangibility: the more semi-tangible they are, the
more amenable they are to social construction. This led
invariably into a discussion of the "how" of tangibility and to
the conclusion that the tangibility of a phenomenon is not
something necessarily given. It is in large measure conditioned
by the paradigm through which it is observed/constructed.
Tangibility, in other words, is a function of phenornenal-
p a r a d i g m a t i c fit, a fit that varies according to both the
phenomenon and the paradigm in question.
This done, what I want to do now is move from the relativity
of tangibility to discuss the various types of tangibility. In
my thinking, four such types are distinguishable (although, most
certainly, there may be more) : general tangibility, anomalic
tangibility, fabricated tangibility and specified tangibility.
General T a n g i b i l i t y
By "general" 1 mean "universal".
Phenornena with general tangibility are phenomena that are
(virtually) indiscriminate radiators of tangibility. They
permeate (ahost) any paradigrnatic fog. They appear focused
(basically) to any lens . They are (essentially) universally
unavoidable. 1 (qualify) for two reasons: 1. because there are
probably no phenomena perfectly tangible - social construction is always an issue; and 2. because there may be some paradigms
that are severely out of tune with them. But 1 would also
suggest that if there are, they are (invariably), only with
great - and perhaps acute - difficulty. Most, if not al1
paradigms are in tune with them ... or... ... with certain phenomenal aspects. Consider once again the
Sun. 1s there any question that the Sun provides the planet
light and warxnth? That if it were to perish, we would perish
along with it - at least in our current state of being? 1s
there any paradigm that would deny such a thing? We can make a
lot of different things of the Sun. We can socially construct
it in many ways. That is something the Inquisitor found in the
simile that began this chapter. But she also found that there
are concurrently aspects to it that seem invariable to us all,
around which our various constructions of the sun seem to
revolve. The two aspects - "provides heat" and "provides light" - seem (at least for the most part) interparadigmatically shared.
Consider the wheel. 1s there any doubt the roundness of a
wheel is what makes it useful as a wheel - that if it were
rectangular, its utility as a wheel would be diminished? And
the shadow. 1s there any doubt that a dense object placed in
front of a light castes a shadow on a nearby surface, and that
it does so every time?
The sun gives light. The roundness of a wheel is essential to
the wheel. Light on an object results in a shadow. These are
al1 tangible things, perhaps even universally so. They,
therefore, hold universal sway. They restrict what we do with
them. They ground any paradigmatic elaboration.
Thus, some (aspects of) phenomena e x e r t ( w e l l -nigh) universal
p u l l .
There are others, however, that exert more distinctive pulls -
that are more paradigmatically specific. 1 would like to
distinguish between two groups of these the first of which are
phenomena with :
Anomalic Tangibility
Let's cal1 these phenomena (or more precisely, once again,
their aspects) anomalies. Anomalies are novel ties, b u t
novelties that can cha l l enge paradigmatic e x p e c t a t i o n s . They
are instances of negative feedback, instances that can ring with
brazen clarity, that can demand with impudence, that can serve
testirnony to paradigmatic fallibility.
Every anomaly is a contravention of paradigmatic expectation.
And yet, it is for that very reason that it achieves
tangibility. As Kuhn explains, "[a]nornaly appears only against
the background provided by the paradigm. The more precise and
far-reaching that paradigm is, the more sensitive an indicator
it provides of anomaly. . . 1/65 . The more precise and far reaching
the paradigm, the more extensively the paradigm is compared with

the world; hence, the greater the likelihood that instances of
bad fit will emerge into view.
Anomalies are not necessarily threatening things. In fact,
they can be quite positive things. They can represent
opportunities for paradigmatic articulation. They can represent
puzzles one can expect to solve if one is ingenuous enough,
discrepancies one can expect to resolve in light of paradigmatic
expectations. Such anomalies are semi-tangible phenomena and
are dealt with as such. Here the paradigm dominates. It takes
these phenomena in, bandies them about, and then spits thern out
paradigmatically articulated. It makes of thern things
paradigmatically meaningful, paradigmatically tangible.
The paradigm, in other words, turns thern into phenomena with
Fabricated Tangibil i ty
On the other hand, and getting back to anomalie tangibility,
some anomalies, are not looked upon so favorably. Some are
truly irritants. And they are irritants because they challenge
the fundamental expectations of the paradigm. This is
dlsturbing and leads the defenders of the paradigm to do al1
they can to account for such anomalies without jeopardizing that
which is fundamental to the paradigm. As Kuhn explains,
defenders "will devise numerous articulations and ad hoc
modifications of their theory in order to eliminate apparent
conflict . " 6 6 To subrnit, to acknowledge the anomalies for what
they indicate, would require a reassessment of what the
defenders have corne to champion. It would jeopardize the very
foundations upon which their (normal scientific) work is based.
It would mean entertaining the severe limitations of their
paradigmatic understandings. These are tough notlons. So
attempts are made to neutralize anomalies, to assimilate thern
within (albeit modified, but not fundamentally so) paradigmatic
expectations, to fabxicate t h e m .

But not al1 anomalies can be successfully assimilated. And
the result? According to Kuhn, the result is paradigmatic
crisis leading to its invariable demise. As Barnes explains
Kuhn's position:
. . . a residue of recalcitrant anomalies may nonetheless persist and accumulate. Such a residue, growing ever larger over tirne, and growing ever more formidable as it resists attempt after attempt to re-assimilate it, may eventually prompt the suspicion that something is miss with the currently accepted paradigm, and set the stage for its demise. 6 7
These anomalies are tangible and glaringly so. They are not so
easily conformed nor ignored. Instead, this time it is the
paradigmatic view that does the conforming, or more precisely
(as Kuhn would have it) the metarnorphosing into something
altogether new.
The second group exerting distinctive pulls are phenomena with
Specif i ed Tangibility
These are phenomena that are relatively tangible to specific
parad igms . When a phenomenon has specified tangibility, it
means that there is a paradigm out there that is uniquely
attuned to its dernands, to its constraints. Certain paradigms
can be "in touch" with certain phenomena, or more accurately,
with certain phenomenal aspects.
Longino, for example, says that background assumptions \\ can . . . lead us to highlight certain aspects of a phenomenon over
others, thus determining the way it is described and the kind of
data it pro~ides."~' She contrasts her position with that of Kuhn
who argues that when an Aristotelian and a Galilean physicist
observe a swinging stone, they see d i f f e r e n t things: "the
Aristotelian sees a body falling with difficulty, a case of
constrained fall, while the Galilean sees oscillatory motion, a
pendulum. But as Longino explains, they are seeing dif ferent
aspects of the same thing:
The A r i s t o t e l i a n b e l i e v e s t h a t t h e n a t u r a l motion of a l 1 i tems (e lements) i n t h e sublunary sphere i s i n a s t r a i g h t l i n e t o t h e i r n a t u r a l p lace . This belief a b o u t mot ion determines what features o f t h e swinging stone are going t o be i m p ~ r t a n t , and c l e a r l y what is important i n t h e s i t u a t i o n is t h a t t h e s t one (whose n a t u r a l p l ace i s a t t h e c en t e r of t h e e a r t h ) even tua l l y cornes t o rest a t a p o s i t i o n which is a s c l o s e t o t h e c e n t e r as it can g e t (given t h a t it is cons t r a ined by t h e s t r i n g of chain) and hence t h a t t h e s tone , swinging, is i n a s t a t e of unna tu ra l motion u n t i l it cornes t o r e s t a t i t s f i n a l p o s i t i o n .
The Ga l i l e an , i n accounting for t h i s same phenomenon, i s
ope ra t i ng wi th t h e impetus t h e o r y of motion t h a t a l r e a d y had a theory of t h e o s c i l l a t o r y motion of v i b r a t o r y s t r i n g s . I n the c o n t e x t of t h i s t h e o r y , f e a t u r e s o t h e r t han those t h a t strike t h e A r i s t o t e l i a n become more i m p o r t a n t , i n p a r t i c u l a r t h e r e p e t i t i v e and o s c i l l a t o r y c h a r a c t e r of t h e s t o n e f s motion. I n t h i s r e spec t t h e motion of t h e s tone i s analogous t o t h a t of t h e v i b r a t i n g s t r i n g and i s g iven an analogous exp lana t ion .
Therefore,
It is no t ... necessary t o Say that t h e A r i s t o t e l i a n and t h e Ga l i l e an a r e see ing d i f f e r e n t t h i n g s . R a t h e r w e can say that they a r e s e e i n g t h e same t h i n g but a t t e n d i n g t o different
70 a s p e c t s o f i t .
Such may be t h e case wi th d i f f e r e n t approaches t o i l l n e s s .
Soc i a l c o n s t r u c t i o n i s t s may be i n touch w i t h how a c e r t a i n
i l l n e s s h a s been cons t ruc ted . Medical e x p e r t s , on t h e o t h e r
hand, rnay have s p e c i f i e d i n s i g h t s i n t o i t s b i o l o g i c a l
foundat ions . Both may be r i g h t . Both may be see ing d i f f e r e n t
a spec t s o f t h e same phenomenon.
S imi l a r l y , d i f f e r e n t paradigms rnay be i n touch with d i f f e r e n t
phenornena. Turner i s of t h e opin ion they are. He says t h a t an
i n t e r p r e t i v e socio logy is amenable t o understanding " s ickness 7 1 and i l l n e s s a t t h e l e v e l of the s o c i a l indiv idual" , whi le
Parson's s i c k r o l e t heo ry sheds l i g h t on t h e i n t e r a c t i o n between
doc to r s and p a t i e n t s . 7 2 Y e t Parson's s i c k r o l e theory f a l l s s h o r t
(a long with the i n t e r p r e t i v e approach) a s i t does not adequa te ly
address another phenomenon, namely the dominance of the medical
profession (which falls short in ways that the former two do
not). To address this, "the sociology of knowledge has proved
to be particularly important and prominent.. . "'3 Finally, to
understand macro-societal processes and the distribution of
health, neo-Marxist or political economy approaches have some
things to Say. 7 4
D i f f erent paradigms see different (aspects of) phenomena for
what they are. At least - to qual i fy - they do so potentially.
And when they do, the phenornena they see are phenomena with
specified tangibility. Thus, unlike with anomalic tangibility,
s p e c i f i e d t a n g i b i l i t y is an i n s t a n c e of p o s i t i v e f e e d b a c k . I t is
a case of mutual affinity between the paradigm and the
phenomenon (aspect). Rather than contravene paradigmatic
expectations, it conf irms them. Where there i s specified
t a n g i b i l i t y , the real-social t u g of war is replaced by a rea l -
s o c i a l embrace of unan imi ty .
Reality and the Relativity of Social Construction
There are times when my four year old son insists there are
monsters in the basement (this is 1997) . When we look together
we establish together that they are no monsters. But invariably
the rnonsters return - they return for him.
1 wonder whose conception, whose construction, whose
representation, is more in tune with the way things really are
on this matter. I would suggest mine is, and I presume most
would agree. But even if 1 am wrong and my son is right, the
same conclusion necessarily follows: one of us is less in tune
with the way reality really is on this matter; one of us is
making much more out of reality than the other.
Hence: the relativity of the social construction of reality.
Whereas Rorty writes . . .
Fossils are constituted as fossils by a web of relationships to other fossils and to the speech of the paleontologists who describe such relationships. If you canrt grasp some of these relationships, the fossil will remain, to you, a mere rock. Anything is, for purposes of being inquired into, "constituted" by a web of meanings. 7 5
... 1 would suggest not exactly. 1 would modify this by saying
instead that anything that exists is more or less constituted by
a web of meanings. In the case of fossils it may be more than
less, while in the case of other things it may be less than
more. But even where it is more than less, there always remains
some (perhaps ambiguous) hint of reality. Notice, for instance,
that in the absence of paleontologist speech, the fossil remains
a mere rock and not a rainbow.
Whereas Hacking says that ... The representations of physics are entirely different £rom simple, non-representational assertions about the location of my typewriter. There is a truth of the matter about the typewriter. In physics there is no final truth of the matter,
7 6 only a barrage of more or less instructive representations.
... 1 would modify this by saying the two situations are not entirely different - they are different in degree. Reality
constrains what we do with it. But it is not unifom in how it
constrains. There is a continuum of constraint here. Sometimes
reality speaks in a more tangible voice. Sometimes its speaks
truth about itself in ways that most, if not all, paradigms can
hardly ignore. The typewriter on the table is a relatively
tangible thing, and perhaps generally so. Can any paradigm
construct it otherwise? Perhaps. But it's unlikely, although 77
meanings will be attached to it. Other times, however, reality
speaks in a less tangible or more semi-tangible voice. When it
does, the paradigm goes to work. It imbues the ambiguous
phenornena, renders them paradigrnatically meaningful, constitutes

them, produces t h e m . Hence the barrage of representations
within physics . And yet other times - to modify even further - reality speaks
with a selective voice. It manifests specified tangibility
where a clarity equivalent to Yhere is a typewriter on the
table" is unique to a given paradigm. Thus, among the barrage
of representations within physics, there may be some that
actually conform quite nicely to reality.
Hence: the relativity of the social construction of reality.
Finally, Turner says chat "ontologies of the body tend to
bifurcate around foundationalism and anti-foundationalism". He
says that the question that divides them is as follows:
1s the fundamental nature of the body produced by social processes, in which case the body is not a unitary or universal phenomenon, or is the body an organic reality which exists independently of its social representation?
The answer, 1 think, is that reality (the body) is both
foundational and anti-foundational. It is both actual and
constructed. As Longino puts it, it is "a product of the
interaction between the external material reality that is "the
world" and our own pragmatic and intellectual [paradigmatic]
needsu7*. And the interaction is a dynamic one. Sornetimes
reality holds sway as it radiates unmistakable (anornalic,
general) tangibility. Then sometimes the paradigm holds sway as
it çoes to work on (imbues, manipulates, constructs) semi-
tangibility. Then there are those instances of close accord
between a singular paradigm and an aspect of reality by virtue
of specified tangibility.
To sum up:
There is this reality out there, but it is a mishmash of
constructions and foundations. From different paradigmatic
orientations, it consists of differently constituted things,
some of which:
Just b a s i c a l l y are the way they are (with s o c i a l meanings attached) . A r e profoundly constructed.
A r e somewha t const ructed.
Hence: the relativity of t h e social construction of reality.
Finally
From a logical point of view there doesnrt seem to be any
other viable conclusion to this matter. Consider the
alternative contention that al1 things are equally socially
constructed. There are distinct problerns with such a
contention. Most preeminently, it is impossible to take such a
contention seriously since the contention cancels itself out.
Since al1 things are equally constructed, the contention itself
is a construction on par with al1 other constructions. It,
therefore, has no serious claim to validity. In fact, the only
way to maintain its validity is to maintain that no things are
socially constructed. If the contention "al1 things are equally
socially constructed" is true - if it is itself not a construction - then it follows, by definition, that nothing is socially constructed; that al1 things just are . And this,
obviously, is false.
Hence: the relativity of social construction of reality.
SOME ADDITIONAL THOUGHTS
Before 1 go ont0 the next chapter, 1 would like to make two
additional points. The first is this:
R e l a t i v i t y i s itself a r e l a t i v e thing.
Let m e explain:
The Relativity of Relativity
The concept goes as follows.
There is an infinity of ways in which any one phenornenon can
be constructed. The relativity between the ways, however,
varies with the extent to which the phenornenon radiates general
tangibility.
Or, the affinity amongst the infinity of ways a phenornenon can
be constructed varies with the extent to which the phenomenon
radiates general tangibility.
To explain, consider the following ideal type (perhaps non-
existent) scenarios (see Figure 2) :
When a phenornenon has complete general tangibility, there is
well-nigh universal paradigmatic attunement with the phenornenon
as it-is-in-itself. Here, besides meanings-attached, the
relativity between the phenornenon's paradigmatic constructions
is nonexistent. Here the phenomenon exudes universal constraint
resulting in a basic similitude between the various
constructions (once again, excepting meanings-attached) - constructions which are really not constructions at all, but
conformities with the phenornenon as it truly is.
General semi-tangibility results in extreme relativity. Here
the diversity between paradigmatic constructions achieves its
greatest magnitude. By virtue of its universal semi-tangibility
each paradigm does with the phenomenon what it wills. Each goes
to work on the phenomenon in its own unique way. Each produces
a distinct construction, a construction very much in accordance
with its paradigrnatic expectations.
General intangibility results in hornogeneity once again. But
the reason for homogeneity, this time, is different. This time
there is nothing to construct. Whereas with general tangibility
there is constraint in the form of unquestionable presence, with
general intangibility there is constraint in the form of lack.

Figure 2 : The selativity of the relativity of the social
construction of phenomena.
Degree of
Relativity
Between
Phenomenal
Constructions
Low
General General General
Tangibility Semi- Intangibility
Tangibility
Here's another analogy t o h e l p c l a r i f y :
Upon e n t e r i n g the c l a s s r o o m , the s t u d e n t s a r e each g i v e n a
piece of c l a y . T h e pieces a r e s m a l l and r o u n d . They a r e h a r d .
L i k e Sandy's f i r s t piece they h a v e each b e e n f i r e d on the k i l n .
T h e s t u d e n t s ' r e a c t i o n s a r e c o n s i s t e n t , a l t h o u g h some a r e more
p l e a s e d t h a n o t h e r s . They r e s p o n d s i m i l a r l y . They a l 1 Say
s o m e t h i n g t o the effect of: "What can 1 t o d o w i t h this? M y
p i e c e of c l a y i s as it i s and t h a t ' s a l 1 there i s t o it. "
The n e x t d a y the same s t u d e n t s a r e g i v e n workab le clay. T h i s
t i m e the s t u d e n t s get t o w o r k , e a c h one i n t e n t on a c t u a l i z i n g t o
the best of h i s / h e r a b i l i t i e s h is /her own u n i q u e a n t i c i p a t i o n s
and s k i l l s . T h e r e s u l t i s a n a r r a y o f d i v e r s e c o n s t r u c t i o n s ,
e a c h o n e imbued w i t h u n i q u e m e a n i n g s .
T h e t h i r d d a y the c l a s s is g i v e n n o c l a y . The s t u d e n t s
c o n c l u d e t h e r e i s n o t h i n g for them t o d o . They l e a v e and go t o
an e a r l y l u n c h .
~ h u s ~ ' :
Genera l t a n g i b i l i t y g e n e r a t e s l i m i t e d r e l a t i v i t y . Genera l s e r n i - t a n g i b i l i t y g e n e r a t e s e x t e n s i v e r e l a tivity. General i n t a n g i b i l i t y g e n e r a t e s l i m i t e d ( z e r o ) r e l a t i v i t y o n c e a g a i n .
The second point i s t h a t t h e r e i s
U n i t y Amidst the Diversity
No mat te r how d i v e r s e our s e p a r a t e understandings, our
paradigrnatic views, Our cosmologies, there is , a t l e a s t with
c e r t a i n t h ings (phenornena, a s p e c t s ) , u n i t y t o be found i n what
we see , know and c o n s t r u c t . T h i s is what t h e I n t e r p r e t e r found
w i t h t h e t h r e e v i s i t o r s who agreed, d e s p i t e t h e i r d ive rgen t
cons t ruc t i ons of it, t h a t t h e sun g ives h e a t and l i g h t and i s
e s s e n t i a l t o l i f e .
What t h e I n t e r p r e t e r d i d n o t conclude, however, i s t h a t while
t h e peoples of t h e world rnay c o n s t r u c t and e l a b o r a t e i n

d i v e r s i t y - i n t h e i r diverse ways of knowing and dealing with
r e a l i t y - t h e y may also see different things for what they are,
precisely because of t he i r diversity. Anomalic and s p e c i f i e d
tangibility are possibilities for any paradigmatic view.
1 Turner (1992).
2 Wright and Teacher (1982) , p. 14. 3 Mishler (l98l), p. 142.
4 (1988).
5 (1988), p. 7.
6 p. 72.
7 p. 76. My italics.
8 p. 60. My italics.
9 p. Il. My italics.
10 (1982), p. 10; my italics.
Il Ibid; my italics.
12 (l995), p. 11; my italics.
13 SHH is the acronym for sociology of health and illness.
14 (l994), p. 14.
15 quoted in White (1991), p. 5.
16 Fox (l994), p. 15.
17 Ibid, p. 70.
18 Ibid, p. 71. It might be said that constructionism (within the sociology
of health and illness), achieves paradigmatic articulation through its
refutation of medicine. To invalidate medicine is to define and extend the
constructionist paradigm. But thatts getting a little ahead of things . . . See Chapter 5 on this.
19 (l992), p. 105.
20 (1976, 1981).
21 Derridar s word.
22 (l992), p. 105.
23 Ibid.
24 Turner (1995), p. 18.
25 (l992), p. 26.
26 (1970).
27 Hacking (1983), p. 10.
28 Ibid.

29 Science is Kthn's focus.
30 Rouse (l987), p. 30.
31 Ibid.
32 Ibid.
33 (1977), p. 319.
34 Hacking (1983), p. 10.
35 In Rouse (l987), p. 37.
36 Brown (1994), p. 33. Not my italics.
37 See Nicholson and McLaughlin.
38 (l993), p. 269.
39 Longino (IggZ!), p. 222.
40 (1995), p. 119.
41 Rorty, perhaps unwittingly, lends support to this view. If it were not
for constructions, he says, deconstruction would be impossible. He says:
"The non-Kantian knows that the edifice will itself one day be deconstructed,
and the great deeds reinterpreted, and reinterpreted again, and again. But
of course the non-Kantian is a parasite - flowers could not sprout from the
dialectical vine unless there were an edifice into whose chinks it could
insert its tendrils. No constructors, no deconstructors." (1982, p. 108)
For deconstruction to proceed, there nust be something w i t h which t o work, to
deconstruct . Well, the same holds true for construction! For construction
to proceed, there must be something w i t h which t o work, with which t o
construct .
4 2 Turner (1992), p. 41.
43 Ibid, p. 52.
44 Ibid, p. 118.
45 Ibid, p. 92.
46 Ibid, p. 256.
47 Ibid, p. 255.
48 Ibid, p. 252.
49 Rorty (1987), p. 30-31.
50 In other words: The more semi-tangible a thing, the more enabling it is.
The more tangible it is, the more restrictive is - restrictive by virtue of
its "concreteness". The more intangible beyond semi-tangible it is, the more
restrictive it is once again - restrictive by virtue of its "lackness". 51 Some of which, incidentally, are more dominant than others.
52 (1970).

53 1 am talking about the "revolutionary" K u h n now..
54 (1970), p. 3 8 .
55 Although, since every creation is understood through the paradigmatic
lens, "concrete" manipultations are concurrently metaphoric constructions.
56 (1993), p. 44.
57 (1988), p. 465.
58 Muller and Koenig (1988) .
59 Ibid, , p. 353. 60 Ibid, , p. 354.
61 Ibid,.
62 Ibid, p. 352.
63 Ibid, p. 367.
64 Daniel Bell (1974 and 1978) affords another example concerning the impact
of technology. In fact, he talks of technological determinism. Very
briefly, he sees the growth of technology as having radical consequences for
society, its n o m s and values. With the emergence of electronic technology
in particular, there takes place, for example, a societal shift from favoring
ascetic workism to championing secular hedonism. Hedonistic consumption
takes over as the nom. Moreover, the importance of obtaining knowledge - of going to university - is emphasized, thus diffusing mass production via
Fordism and similar rneans. Consequently, the middle class takes over as the
revolutionary class, displacing Marx's working class.
65 (l97O), p. 65.
66 (1970).
67 (19911, p. 91.
68 Longino (l99O), p. 216.
69 Ibid, p. 53.
70 Ibid, pp. 53 - 54; my italics. 71 Turner (1995), p. 205.
72 Turner (l992), p. 237.
73 Turner (1995), p. 208.
74 Ibid.
75 Rorty (l982), p. 199.
76 Hacking (1983), p. 145.
77 One may see it in a positive light: It's there poised for work. Another
may see it less positively: It represents work, something s/he is tired of
and wants to get away from.

7 8 Longino (19901, p. 221.
79 Although, it may be l eg i t i rna te ly asked: What about cases in-between? And
what about o u t l i e r s ? I leave such questions for fu tu re w o r k ,

PARADXGtMATIC ARTICULATION, EXTENSION AND m N S I F I C A T I O N : THEORY
PART II
JOClRBEY NOTES To Recap: The point o f Chapter 4 was t o beg in t o o u t l i n e t h e t heore t i ca l
r a t i o n a l e f o r interparadigma t i c c o l 1 aboration, e spec ia l l y between medicine and soc ia l construct ionism. Most s i g n i f i c a n t t o t h i s end was t o provide a t heore t i ca l r a t i o n a l e for t h e p o s s i b i l i t y that d i f f e r e n t paradigms can see. It was argued , moreover, tha t t h i s p o s s i b i l i t y emerges w i t h another p o s s i b i l i t y , namely, tha t some t h i n g s are more soc ia l ly constructed than o thers .
T h e chapter , however, was somewhat involved. Consider t h e fo l lowing summary for some o f the h i g h l i g h t s :
1 . Contra t h e h o r i z o n t a l i s t p o s i t i o n - and more s p e c i f i c a l l y the social c o n s t r u c t i o n i s t p o s i t i o n - there is good reason t o take t he impact o f reality s e r i o u s l y . Social cons t ruc t ion does not proceed unhindered. I t i s constrained by r e a l i t y , l i m i t e d by it, fraught with i t s demands. On t he o ther hand, i t i s by v i r t u e of such cons t ra in t t h a t s o c i a l cons t ruc t ion is a b l e t o proceed a t a l l . Social cons t ruc t ion i s not omnipotent. R e a l i t y cons t ra ins soc ia l cons t ruc t ion; r e a l i t y enables soc ia l cons t ruc t ion . The body, f o r example, both cons t ra ins and enables its social cons t ruc t ion .
2 . Some th ings a r e more s o c i a l l y constructed than o ther s . The degree t o which any phenomenon (o r phenomenal aspect) i s cons t ruc t ed v a r i e s accord ing Ca t h e e x t e n t t o which i t - - -
cons t ra ins . Put another way, phenomenal cons t ruc t ion v a r i e s according t o phenomenal t a n q i b i l i t y - t o the degree t o which the phenomenon man i f e s t s translucence.
3 . O r more accurate ly: t he more semi-tangible t h e phenomenon (or a s p e c t ) , t h e more amenable it is t o social cons t ruc t i on , The more t ang ib l e the phenomenon, the l e s s amenable it i s t o soc ia l construction and the more it i s perceived by the paradigm (doing the perceiv ing) for what i t is. The more i n tang ib l e the
phenomenon, the l e s s amenable i t is to social cons t ruc t ion given i t s absence from paradigmatic view - given i t s u t t e r lack o f cons t ra in t over t he paradigm. There is, therefore, a curv i l i near r e la t i onsh ip between t a n g i b i l i t y and social cons t ruc t ion .
4 . The degree t o which a phenomenon (aspect ) m a n i f e s t s t a n g i b i l i t y is not neces sar i l y given. I t is larqely, although no t determinably, paradigma t i c a l l y condi t ioned. Some phenomena (a spec t s ) seem t o permeate almost any paradigma t i c f o g .
5. Four t a n g i b i l i t y t y p e s a r e i d e n t i f i e d . T h e y a r e : a . phenornena (or phenomenal a s p e c t s ) wi t h g e n e r a l t a n g i b i l i t y - phenomena t h a t a r e u n i v e r s a l l y t a n g i b l e ; b. phenomena w i t h s p e c i f i e d t a n g i b i l i t y - phenomena posi t i v e l y t a n g i b l e t o s p e c i f i c p a r a d i g m s ; c . phenomena with a n o m e l i c t a n g i b i l i t y - phenomena n e g a t i v e l y t a n g i b l e t o s p e c i f i c p a r a d i g m s ; a n d d . phenomena w i t h f a b r i c a t e d t a n g i b i l i t y - phenomena r e n d e r e d p a r a d i g m a t i c a l l y t a n g i b l e .
6 . R e l a t i v i t y i s i t s e l f a re lat ive t h i n g . T h e d i s p a r i t y b e t w e e n the ways i n w h i c h a phenomenon i s v a r i o u s l y c o n s t r u c t e d v a r i e s w i t h the d e g r e e t o w h i c h the phenomenon m a n i f e s t s g e n e r a l ( u n i v e r s a l ) t a n g i b i l i t y * To Continue: T h e t h e o r e t i c a l j u s t i f i c a t i o n f o r i n t e r p a r a d i g r n a t i c
c o l l a b o r a t i o n i s f u r t h e r b a s e d upon a n e x p l o r a t i o n i n t o the paradigma tic d r i v e t o s e l f a r t i c u l a t e . Such a n e x p l o r a t i o n r e v e a l s how i t i s t h a t some t h i n g s corne t o be more s o c i a l l y c o n s t r u c t e d t h a n others.
N e e a c h f e e l a n e e d t o s o l i d i f y , i f n o t t o f u r t h e r , Our very spec i f ic ways o f k n o w i n g . W e a l 1 h a v e a n e e d t o make s e n s e of the w o r l d a t least i n some way and t o perpetuate/develop/sxpand these ways o f k n o w i n g . S o c i a l c o n s t r u c t i o n i s t s a g r e e w i t h t h i s , b u t 1 would a l s o l i k e t o i n c l u d e them under the same o b s e r v a t i o n .
T h i s d r i v e t o a r t i c u l a t e , h o w e v e r , h a s a d u a l i t y t o i t . On the o n e h a n d , i t c a n f o l l o w a n e g a t i v e p a t h , o n e t h a t l e a d s t o paradigma t i c excl u s i v i t y , e x p a n s i o n and m a s t e r y , a d r i v e I refer t o a s p a r a d i g m a t i c e x t e n s i o n . M e d i c a l i z a t i o n i s one very clear e x a m p l e o f p a r a d i g m a t i c e x t e n s i o n . S o is the s o c i a l c o n s t r u c t i o n i s t a t t e m p t t o d i s m a n t l e the m e d i c a l e m p i r e w h i l e l a y i n g o u t i t s own program ( p e r h a p s u n w i t t i n g l y s o ) a s a n a l t e r n a t i v e . On the other h a n d , the d r i v e t o a r t i c u l a t e can f o l l o w a m o r e p o s i t i v e p a t h . I t can r e s u l t i n a g r e a t e r a b i l i t y o f a n y p a r t i c u l a r p a r a d i g m t o see c e r t a i n phenomena ( o r c e r t a i n a s p e c t s t h e r e o f ) . I t can r e s u l t i n p a r a d i g m a t i c i n t e n s i f i c a t i o n . T h u s , w h i l e both m e d i c i n e and s o c i a l c o n s t r u c t i o n i s m p a r a d i g m a t i c a l l y e x t e n d , it i s p o s s i b l e t h a t they i n t e n s i f y a s w e l l . I t i s p o s s i b l e t h a t they d e l v e r e l a t i v e l y d e e p l y i n t o c e r t a i n r e a l i t i e s . 1
These, h o w e v e r , a r e i d e a l t y p e s c e n a r i o s o f a r t i c u l a t i o n t n a t p r o b a b l y d o n o t o c c u r i n i s o l a t i o n f rom each o t h e r . P e r h a p s a m o r e l i k e l y s c e n a r i o is o n e t h a t sees a m i n g l i n g o f these two p r o c e s s e s , w i t h o n e h o l d i n g more s w a y t h a n the o t h e r d e p e n d i n g on the n a t u r e o f the phenomenon i n v o l v e d . I f s o , t h e n t h e p a r a d i g m becomes a n e n t a n g l ed h o d g e p o d g e o f i n t e r c o n n e c t e d i d e a s t h a t r a n g e from r e l a t i v e l y p u r e r e f l e c t i o n s of r e a l i t y t o v e r i t a b l e c o n s t r u c t i o n s .

T h i s i s c r i t i c a l t o the o v e r a l l p r o j e c t o f e s t a b l i s h i n g the u t i l i t y o f i n t e r p a r a d i g m a t i c c o m m u n i c a t i o n , e s p e c i a l l y b e t w e e n m e d i c i n e and social c o n s t r u c t i o n i s m . F o r if t h i s h y p o t h e s i s is r i g h t : i f the d r i v e t o a r t i c u l a t e resul ts i n v a r i a t i o n s i n the d e g r e e t u which d i f f e r e n t phenomena are c o n s t r u c t e d by any one paradigrn (we a r e back t o the r e l a t i v i t y o f s o c i a l c o n s t r u c t i o n t h e m e ) ; if, w i t h i n a n y paradigm, there l i e s the p o t e n t i a l t h a t some " c o n s t r u c t i o n s " , t h r o u g h paradigma t i c i n t e n s i f i c a t i o n , are r e l a t i v e l y t r u e t o reali t y ; i f both s o c i a l c o n s t r u c t i o n i s m and m e d i c i n e , a s they a r t i c u l a t e , are c o n c u r r e n t l y ( a t l e a s t p o t e n t i a l l y ) g e t t i n g a t ( d i f f e r e n t ) t r u t h s about the way things a r e w i t h h e a l t h , i l l n e s s and disease, t h e n i t i s p l a u s i b l e t o s u g g e s t there i s u t i l i t y i n the i r i n t e r p a r a d i g m a t i c c o l l a b o r a t i o n .

INTRODUCTION
Construction is a relative thing.
Yet, the fact is, we do construct. The world we occupy is in
many ways a humanly produced thing. Horizontalism (social
constructionism) has a valid point, one not to be denigrated.
It has - perhaps unwittingly so - hit upon an empirical (or, contrarily, maybe even an eternal?) truth!
Moreover, the drive to construct is a powerful one. I ' m not
one to deny that. We as humans seek perpetuation, development,
legitimation and expansion of our particular ways of knowing and
dealing with the world as discussed in Chapter 3. We seek
paradigmatic articulation. Part of the aim of this chapter is
to outline some of the reasons scholars have given for why this
is. However, 1 would also like to introduce a modification to
horizontalist conceptions of paradigmatic articulation, namely,
the d r i v e t o a r t i c u l a t e has a d u a l i t y t o i t . While on the one
hand it leads to phenomenal construction through a process
termed paradigmatic ex tens ion , it is also possible for it to
lead to phenomenal revelation through a process termed
paradigmatic i n t e n s i f i c a t i o n . This is important because, i t
due t o t h e p o s s i b i l i t y o f i n t e n s i f i c a t i o n tha t there i s
r e l a t i v i t y t o the social cons t ruc t ion of r e a l i t y . Moreover,
is due to t h e p o s s i b i l i t y of i n t e n s i f i c a t i o n that w e might
sugges t t h e r e is utility i n meaningful interparadigma t i c
c o l l a b o r a t i o n . Intensification means getting closer and closer
to the truth. Meaningful interparadigmatic collaboration means
more and more about truth gets shared.
In what follows, 1 begin with a discussion concerning the
nature of paradigmatic articulation, what drives it and what
informs it, and do so highlighting the horizontalist position
(which, incidentally, invariably appeals to verticalist
notions), and its ernphasis on how paradigmatic articulation

results in a constructed world. Having set the stage thus, I
then go on to introduce the innovation of duality. In
particular, 1 suggest that paradigmatic articulation as
described and legitimated by horizontalism is really better
understood as paradigmatic extension, while paradigmatic
intensification is, concurrently, always a possibility.
THE DRJXE TO PARADIGMATICALfiY ARTICULATE
Intzoduction
Why is it that we construct? More precisely, why is it that
we go about articulating the paradigms we hold dear?
Interestingly, scholars, even those firmly propounding
horizontalist views, have made sense of the phenornenon through
appeals to verticalist assumptions. Most basically, they Say
there exists a universal human need to feel at ease with the
world. This concept was introduced in Chapter 3. But
paradigmatic articulation is conditioned by socio-historical
circumstances as w e l l . It is rendered idiosyncratic in terms of
the path it takes and the manner in which it proceeds by virtue
of having foundations in, and being caught up in, a particular
ethos, for example. Rationaiization and rnedicalization can be
understood as particular types of paradigrnatic articulation
specific to the modern drive to dominate in the most efficient,
systematic and regulatory way possible.
The Universal Drive to Constsuct
Theorists like Berger, Sartre and Nietzsche are horizontalist
in orientation - at least in the sense that 1 am using it. They
Say things like the world is a construction, essence is
attributed, truth is made, etc. But their horizontalisms
invariably betray verticalist assumptions.
This is clear with ~ e r ~ e r ~ , as we have seen. To review and
elaborate:
Berger, building on Gelhen among others, begins with the
notion that humans are by nature unfinished beings. We have no
species-specific reality so we go about "finishing" ourselves
through social construction, Social construction is the
inorganic manner by which we countervail our organic
indeterminancies, our natural lacks. It is compensation for an 3 inherently deficient human biology. It is, consequently, an
endless human pursuit.
A n endless human pursuit, moreover, we conceal from ourselves
- something we must inexorably do as far as Berger is concerned.
Otherwise we face something very disconcerting. Otherwise we
face the ambiguity of existence, the contingency of the ways
things are. To see the world as social construction is to
conf ront the ines sent iality of things , to conf ront chaos, to confront anomie. So we wrap that which we have created in
signif icance; we dress it in eternality, ob jectivity. In
Turner' s words :
. . . al1 reality is socially constructed, as a consequence of Man's incompleteness, but human beings require stable meanings and cannot live in permanent awareness of the socially constructed and precarious nature of everyday reality, and they are forced to clothe these uncertainties with permanent
4 signif icance . We mask its arbitrary origins, render solid its frailties. We
legitimate that which we construct.
Or more critically - throwing inequality into the equation - the powerful legitimate that which they construct and impose
5 upon everyone else. And how do they legitimate? One way they
do so is through the production of religion. At least this is
Bergerr s reasoning. Illustrating with a fanciful example, he
If one imagines oneself as a fully aware founder of a society, a kind of combination of Moses and Machiavelli, one could ask

oneself the following question: How can the futu~e continuation of the institutional order, now established e x
nihilo, be best ensured?
That is, while
... al1 the means of power have been effectively employed ... There still remains the problem of legitimation, al1 the more urgent because of the novelty and thus highly conscious precariousness of the new order.
And how is this problem solved? Berger says the answer is
simple. It is
solved by applying the following xecipe: Let the institutional order be so interpreted as to hide, as rnuch as possible, its constructed character.
That is,
Let that which has been stamped out of the ground ex nihilo appear as the manifestation of something that has been existent from the beginning of tirne, or at least from the beginning of this group. Let the people forget that this order was established by men and continues to be dependent upon the consent of men. Let them believe that, in acting out the institutional programs that have been imposed upon them, they are but realizing the deepest aspirations of their own being and putting themselves in haxmony with the fundamental order of the universe. In sum: Set up religious legitimations.
Religion, as far as Berger is concerned, is the supreme
legitimator. Through it, precarious social arrangements are
f i r rn ly established by virtue of their links to divine schemes.
Through it, ambiguities are solidified and discrepancies
elirninated.
Religion legitimates social institutions by bestowing upon them an ultimately valid ontological status, that is, by l oca t i n g them within a sacred and cosmic frame of reference. The historical constructions of human activity are viewed from a vantage point that, in its own self-definition, transcends both history and man. This can be done in different ways.
Probably the most ancient form of this legitimation is the conception of the institutional order as directly reflecting or manifesting the divine structure of the cosmos, that is, the conception of the relationship between society and cosmos as one between microcosm and macrocosm. Everything "here below" has its analogue "up above."
Berger's emphasis on religion is close to what other theorists
say about the role of ideology in general for justifying
contingent societal constructions that appeal to the powerful.
Marx, for example, emphasized how ideology is used by the
bourgeoisie to legitimate capitalism, keeping the proletariat
exploited by ensuring that s/he is ideologically deceived into
thinking that capitalism is the natural way things should be.
Sirnilarly, critical theoxists highlight medicine as the
legitimator today, actively legitimating on behalf of the
powerful both capitalism, and - as far as feminists are 7 concerned - patriarchy .
The early Sartre is another who builds his philosophy on
verticalist assumptions. He is criticized, for example, by
Heidegger and Derrida for privileging the autonomous,
constituting human consciousness, for making the huan b e i n g the 8 center of things. In Derrida's view there is no "Man". There
is no subject. The subject is a fictitious entity, a
construction, a relic of liberal humanism, a "position in 9 language", a mere "ef fect of discourse".
Sartre privileges the human being and hidher freedom.
Contrary to the Platonic view of an autonomous world of perfect
and eternal forms, one indifferent to humanity and its
activities, Sartre says that hurnans are the meaning makers of
the world. That 1 am my own meaning maker. There is nothing
out there that needs to be as it is. 1, for example, am the
architect of any value.
Value...can be revealed only to an active freedom which makes it exist as value by the sole fact of recognizing it as such. It follows that my freedom is the unique foundation of values and that nothing, absolutely nothing, justifies me in adopting this or that particular value, this or that particular scale
1 O of values.
1 am the architect of any essence, of any meaning.
. . . 1 discover myself suddenly as the one who gives its meaning to the alarm clock, the one who by a signboard forbids himself to walk on a flower bed or on the la m... the one finally who makes the values exist in order to determine his action by their demands. 11
1 am the architect of worthy activity.
..,al1 human activities are equivalent . . . Thus it amounts to the same thing whether one gets drunk alone or is a leader of nations. If one of these activities takes precedence over the other, this will not be because of its real goal but because of the degree of consciousness which it possesses of its ideal
12 goal. . . In the absence of anything like God, the inexorable laws of
science, Platofs eternal Forms, I am free to choose rny own
truths, to constitute my own world.
But this is a dreadful freedom 1 have. It is a freedom of
anxiety, of anguish. The infinity of possibilities available to
me, the utter responsibility of total choice that is mine,
choice completely devoid of support or constraint emergent from
any foundation or essentially, is tough to face. The only thing
1 have no choice over is my freedom. 1 am therefore condemned
to be free.
So what do 1 do? 1 seek escape. 1 seek a way out of my
freedom and the anxiety it provokes. And so 1 deceive rnyself
into believing that the world is the way it is because it
reflects the ways things must be. I attribute eternality to
contingency, meaning to human whirn, necessity to human
construction and to the way society is. Through appeal to
society and its "taken-for-granted structureff, I am able to
shield myself
from the naked terrors of [my] condition. The 'okay worldff provides routines and rituals through which these terrors are organized in such a way that [Il can face them with a measure of calm. 13
In other words, I render fundamental the accepted paradigmatic
approach to dealing with the world. 1 flee into what Sartre
calls bad faith, and live, according to Heidegger,
inauthentically.
It might be said, therefore, that construction anew emerges
through self-freedorn exercised; and that construction
a r t i c u l a t e d ernerges though self-freedom denied. The drive to
articulate is consequent upon the human weakness to be at ease
with the world.
Nietzsche despises this weakness, this herd mentality that the
generality of humanity has adopted. He despises commonality,
conforrnity, mediocrity. He despises entities like the state
"where everyone, good and bad, is a poison drinker: the state
where everyone, good and bad, loses hirnself: the state where
universal slow suicide is called - life.''14 Instead, Nietzsche
venerates the solitary individual, the one able to devise
his/her o m virtues, the one who the "good and justff would have
crucified". He venerates the one who can create for
him/herself, the unitary constructor, the anti-superfluous one,
the Superman.
As with Berger and Sartre, however, there is a verticalism
behind Nietzsche's creative horizontalism. In particular,
Nietzsche posits the metaphysical concept16 of a will-to-power
inherent to al1 organisms: "To al1 organic beings, to al1
organisms or bodies - from amoebae to humans - the will to power

i s basic."" T h e concept i s introduced by Nietzsche 's protagonis t
Zara thust ra , who speaks thus:
But t h a t you may understand my teach ing about good and e v i l , 1 s h a l l r e l a t e t o you my teaching about l i f e and about t h e na ture of a l 1 l i v i n g c r ea tu re s .
1 have followed the l i v i n g c r e a t u r e , 1 have followed t h e g r e a t e s t and the srnallest paths, t h a t 1 might understand i t s na ture .
L i s t en now t o my teaching, you w i s e s t men! Test i n e a r n e s t whether f have crept i n t o the h e a r t of l i f e i t s e l f and d o m t o t h e roo t s of i t s hear t !
Where 1 found a l i v i n g creature , t h e r e 1 found w i l l t o power; and even i n the w i l l of t h e se rvan t 1 found the w i l l t o be master. 18
This will-to-power i s a pos i t i ve c r e a t i v e d e s i r e , one tending
towards self-expression, self-becoming. I t i s "an ac t ive
p r i n c i p l e of becorning other , as opposed t o r e a c t i v i t y and
pass ivi ty ." lg B u t it i s a l s o one t h a t has been suppressed under
t h e domination of the Apollo (o r S o c r a t i c ) p r i n c i p l e , and i n
p a r t i c u l a r , under t h e sway of r e l i g i o u s values, standards of
good and e v i l , reason, e t c . The o b j e c t i v e is t o overcome one 's
immersion i n t hese fabr ica t ions of t h e herd ( t h e superfluous,
t h e weak), t he se f ab r i ca t ions t h a t can lead on ly t o mediocrity
and indolence. The ob jec t ive is t o occasion f r e e p lay t o one 's
d e s i r e , t o oner s will-to-power.
In summary: Berger, S a r t r e and Nietzsche a l 1 make foundational
c la ims. O n t h e one hand t h e dr ive t o a r t i c u l a t e emerges from
the need t o avoid uncer ta in ty . Soc i a l cons t ruc t ion emerges out
of t h e powerful human d e s i r e t o f e e l i n sync with t h e wowld, t o
r e s t assured t h a t i t s laws and demands have been mastered. So
w e impute t r u t h s - laws and demands - t o it and then forget t h a t
we have imputed them. W e fo rge t t h e i r o r ig in s and t h a t w e a r e
the constitutors of reality. But Sartre and Nietzsche go on to
Say "let's not forget such things"; and then invite us to "feel
free to create afresh". In fact, Nietzsche, divulging another
verticalist premise (another supposed truth), contends that to
live is to create afresh, to release the inherent will-to-power,
to fashion anew. Al1 else is mediocrity - slow suicide. Rationalization and Medicalization
Weber was another who ernphasized the universal human West for 2 0 mastery over the "contingencies of life". This quest is met
largely through what he termed rationalization, a process cornmon
to al1 of human history and associated very strongly with
religion. Through rationalization, the problematics of
religious beliefs are articulated, accounted for and rendered
intelligible. Or at least so it would seem. In fact, what
really happens is that rationalization creates deeper
contradictions - more pressing anomalies we might Say - engendering an Ympulse for religious innovation. "" (See the Appendix following this Chapter for an elaboration on this
theme) . The theme for now is that while rationalization is a universal
phenornenon stemming from the universal need to make sense of the
world, it has taken a singular path of late, one unique to
western society and informed very specifically by western
rationality - a f omal means-ends rationalityz2. As Turner explains, Weber had it that "the emergence of a modern form of
consciousness . . . is set within a rational tradition. "23 A tradition, moreover, that paradoxically has its origins in
something highly "irrational", i.e. the Protestant, and in
particular the Calvinistic quest for salvational security. A
quest that gave rise "by a process of unintended consequences to
a culture that emphasized reason, stability, coherence,
discipline and world-mastery. "24
It did so in different ways. In the Protestant Ethic and
S p i r i t of c a p i t a l i s m t S Weber explained that it, and in particular
capitalism - one of the rationalizing forces in our tirnest6- emerged out of the Calvinist doctrine which preached
predestination - the view that one had no Say in whether or not
one would be among the saved. But one could have an idea if one
were among the saved through a sign, and the sign was economic
success. So a new ethic developed, one based on the ascetic
standards of frugality, industriousness, and one that encouraged
the rational and methodical pursuit of econornic profit, a 27 pursuit that led to capitalism. Moreover, the Reformation,
through its devaluation of the priest, through its emphasis on
the autonorny of the individual with regard to the church,
through its denial of "the magical efficacy of the sacraments"
thus opening further the door to the world of science, was
a major catalyst in the transfomation of western urban culture that stimulated a new form of rationality characteristic of urban bourgeoisie, a rational culture spreading ultimately to al1 classes and groups within western
2 8 civilization.
According to Weber, rationalization based on this rationality,
has permeated and corne to regulate every aspect of Our lives.
It has, he larnentably concluded, resulted in an iron cage from
which there is no escape. It has resulted in the subordination
of substantive questions of value to that of formal (means-ends)
logic. It has produced a world without meaning, a world without
moral direction, a world dorninated by bureaucracy and the goals
of ef f iciency, order, calculabilityZg . . . . . . and control . Control of the body, for example.
Turner argues that while "Weber's discussion of
rationalization as an historical process can be seen as a
discussion of . . . the emergence of a particular form of
consciousness", it can also be seen 'as the analysis of the
ernergence of new forms of discipline that regulated and
organized the energies of the body. "'O In pre-capitalist
societies, the disciplines targeted human passion. Religion
penetrated into the realm of sexual emotions, imposing
restraints upon them. Then, with the Protestant Reformation,
significant transitions took place. In the first place, there
was an explosion of regulation expanding £rom the specificity of
the monastery to the generality of the household, an explosion
occasioned by the new ethic of world-mastery. In the second
place, regulation took on a new target, shifting from the inner
structures of human emotion to the surfaces of the body, a shift
occasioned by the Protestant disenchantment with the world and
the concomitant focus on the secular. Having their origins in
both religion and the amy, the modern scientific disciplines
developed increasingly rational ways to train, restrain and
discipline the human body by "diet, drill, exercise and
groorning . "31 This is one of Foucault's major preoccupations. As discussed
in Chapter 3, he says that around 17th and 18th centuries, a new
form of power came into being, a bio-power concerned with tne
management and regulation of both the human population and the
human body. There thus emerged a host of disciplines concerned
with the development of technologies that could be applied in a
number of settings - in prisons, in schools, in hospitals - for the purpose of observing, disciplining and producing the body3' - for the purpose of controlling and forging docile bodies
amenable to training, manipulation and improvement3. This was
(and continues to be to this day) accomplished in different
ways: 'through drills and training of the body, through
standardization of actions over t h e , and through the control of
~ ~ a c e . " ~ ~ It was (and continues to be to this day) facilitated
through the systematization of knowledge, through the
development of "examinations, tirnetables, taxonomies,
classifications and registers"35 - through the development of
rational methods of surveillance.
What emerges with bio-power is the rationalized, normalized,
efficient body. Difference is squashed. And this, as we have
seen, bothers Foucault. One can read Foucault as someone
sharing Weber's distress with the ethic of world mastery, an
ethic the basis upon which the historical process of
rationalization has ensued; and Nietzsche's disgust with the 3 6 subjugation of Dionysian passion.
And it is in this light that Foucault understands the
emergence and functioning of medicine. The body is a target and
site of rational disciplinary invasions, the target of myriad
disciplines concerned with its regulation. Medicine is one such
discipline, and a predorninant one at that, emerging with
rationalization and the drive to master and regulate. Its iocus
is the body and its function is that of effecting an efficient
goverment of embodiment . More specifically, its foci include
sexuality, human emotion, social deviance. Its objectives
include control over reproduction, the normalization of emotion
- the determination of normal emotion, that is - and the standardization of illness amenable to bureaucratic management.
Its objective is the management of embodiment through the
medical regimen.
Medicine, in this view, has become the guarantor of social
order. Tt is the latest societal response to the problems of
embodiment and the interaction between embodied persons,
supplanting religion and law and their roles in this regard3'.
The rise of medicine to prominence occurred with the emergence
of the anatomo-clinical gaze. In the Birth of the clinic3*,
Foucault refers to the gaze as the "great break" for medicine.

Through it, patients were objectified, rendered exposed.
Through it, patients were seen in a whole new way. Foucault
says of the autopsy, for example, that "the living night [was]
dissipated in the brightness of death.ff39 In later works, such as
Discipline and Punish, Foucault builds on the theme of the gaze,
describing it more generally as a technology of power through
which the object - the patient, the prisoner, the factory
worker, etc. - is laid bare. The panopticon is Foucaultr s
paradigmatic example of disciplinary technology and the most
efficient employment of the gaze. 4 0 Through the gaze, a
knowledge is achieved which is "codified and organizedff, and
which then "becomes a resource by which the observer develops
bath an expertise, and a control over those s/he observes.fr41
Foucault has it that medicine has developed this expertise and
is in a powerful position to exert control. We are thus seeing
the rnedicalization of society, one that involves the ever-
increasing management of life by medicine in the interests of
regulation and normality.
To Stimmarize
Ironically, theorists - some more up front about it than
others - harbor verticalist assumptions for why it is we construct, perpetuate, legitimate, rationalize, paradigmatically
articulate. We do so to avoid anomie, anxiety, despair. We
paradigmatically articulate to render meaning to the world.
Moreover, some see this as a weakness on Our part, insisting we
should face the ambiguity of our existence and create anew, each
one of us for ourselves. But in so doing they betray once again
a certain verticalism, propounding ideas like the inherent
freedom of the individual, and the individualrs inherent will-
to-powex.
But while paradigmatic articulation may have its vertical
roots, both Weber and Foucault have given reason to suggest that

it is also socio-historically conditioned. Since the 17th
century onwards, for example, a major form of paradigmatic
articulation has come to dorninate the West - rationalization based on formal rationality - one that has foundations in various features of the Protestant Ethic - in the ethic of
world-mastery, for example. Medicalization as paradigmatic
articulation can be understood in a similar way, emerging and
proceeding as a secular answer to the moral problems of
embodiment and its effective regulation.
THE DUALITY OF PARADIGMATIC ARTICULATION
So we construct. We paradigmatically articulate in the
interest of maintaining a meaningful reality, or in the interest
of creating a new (egocentric) meaningful reality. And there
are foundational reasons for why it is we do so. Moreover, how
we do so is socio-historically conditioned. These are sorne of
the themes raised so far, themes 1 have uncritically outlined.
Kuhn says that
scientific theories taken as a group are obviously more and more articulated. In the process they are matched to nature at an increasing number of points and with increasing precision. Or again, the number of subject m a t t e r s to which the puzzle-solving approach can be applied clearly grows with
4 2 t ime .
How? Kuhn explains t h a t
Al1 theories can be modified by a variety of ad hoc adjustments without ceasing to be, in their main lines, the same theories. It is important, furthemore, that this should be so, for it is often by challenging observations or adjusting theories that scientific knowledge grows. Challenges and adjustments are a standard part of normal
4 3 research in ernpirical science. . . Science proceeds for the most part through normal science -
through the articulation of a particular scientific paradigm.
But it is not only science that does this. We al1 do this to

some degree or another. We al1 articulate. We al1
"interpret . . . evidence so that it f its [our] fanciful ideas, eliminate difficulties by ad hoc procedures, push them aside, or
simply refuse to take them seriously. lJ4'
Think of it this way:
We latch ont0 the world in certain ways. We get comfortable
with those ways of latching, come to see them as inexorable, and
then seek to perpetuate them. And upon continued encounter with
the world, we also seek to ex tend Our ways of latching; we seek
to latch ont0 more and more things in line with the particular
ways we have come to latch. And when our particular ways of
latching are challenged, we adjust them. But when we adjust
them, we adjust them more often than not conservatively,
supportively. We make adjustments that will both sustain and
legitimate that which is fundamental to the ways in which we
have come to latch.
Thus, for Kuhn, normal science Y s to a great extent self-
validating: it produces a world in which it is true.. .' 4 5 . More
generally, paradigrnatic articulation is to a great extent self-
validating: we paradigmatically produce worlds in which our
paradigms are (more and more) true. (Unless, of course, we are
strong enough to construct otherwise).
The horizontalist daim is that the ways we do our latching,
the ways we construct, the ways we paradigmatically understand
and deal with the world, get at nothing profound. They are just
ways, ways getting at nothing necessary about the way things
are; ways penetrating into no f oundational truths, no essences,
no realities as-they-are-in-themselves. If anything, they are
the constructors of profundity, essence, reality. And it is on
this point that I would like to introduce a modification, which
is this :
P a r a d i g m a t i c a r t i c u l a t i o n h a s a d u a l i t y tu it. On the one
h a n d , p a r a d i g m a t i c a r t i c u l a t i o n does r e s u l t very much so i n the
( i n c r e a s e d ) c o n s t r u c t i o n of reality. O n t h e other hand, there
is s u f f i c i e n t reason t o a t l e a s t e n t e r t a i n the p o s s i b i l i t y that
paradigma tic a r t i c u l a t i o n can a l s o r e s u l t i n the p e n e t r a tion of
( c e r t a i n aspects of, p e r h a p s ) r e a l i t y . Thus, p a r a d i g m a t i c
a r t i c u l a t i o n i n v o l v e s what 1 shall c a l l paradigmatic extension.
B u t along with paradigmatic extension, it can a l s o involve w h a t
1: skia11 c a l l paradigmatic intensification. 4 6
Paradigmatic Extension
By paradigmatic extension 1 mean very much what has been
highlighted as paradigmatic articulation so far. To be clear,
paradigmatic extension refers to the process of incorporating
more and more phenomena into the purview of the paradigm - into its way of organizing reality. It does so by preying upon
phenomena - particularly those phenomena semi-tangible to it - by taking them in and churning thern about until they obtain
paradigmatic palatability. To paradigmatically extend is to
construct more and more of reality from the paradigmatic point
of view. And when other views are subjugated in consequence, it
is to territorialize reality, to colonize and imperialize. And
this may be consciously done. Paradigmatic extension may
accornpany the conscious belief that one's view is the more
valuable view, if not the only view that matters.
It might be said that the scientism of the scientific
empiricisrn of Carnap and others is a good example of
paradigmatic extension. At the turn of the century there was a
'unity of sciencef movement, one which held that the physical
sciences "enjoyed an implicit unity, one which formalization
would make explicit ... ""; but which also held that the unity
needed to spread. The goal was to extend the methods and
concepts of science to other spheres. This meant that a wider
unity, encompassing the social and human sciences, for example,
"had to be manufactured, by the introduction into previously
unscientific subjects - ethics, for example, or history - the concepts and methodology of established sciences."48 Scientism
is the extension (imposition) of scientific understandings into
areas previously untouched by science, based moreover, on the
belief that such is desirable, even necessary.
The thought behind the forging of this unity - that it is highly desirable for the concepts and methodology of established sciences to be spread, and unsatisfactory for, for example, ethics or history to be left in their prescientific state - captures the scientism in scientific empiricism. 49
Medicalization is a current example of paradigmatic extension.
It is the process by which more and more of life is described
and dealt with in light of the medical paradigm. It is the
process by which more and more phenomena are constructed from a
rnedical point of view and then imposed. We live very much in a
medical reality as a consequence of medicalization. Medicine
has achieved a substantial imperialism. These themes have been
dealt with at some length already, so 1 won't elaborate upon
them here.
Instead, let me turn to something a little more ironic. Those
who criticize medicine for its paradigmatic imperialism may
themselves, wittingly or not, be involved in affecting their own
paradigmatic imperialism. They may themselves be involved l n
affecting their own paradigmatic extension, and doing so through
the denigration of another paradigmatic approach - through the denigration of medicine. 1 am speaking here of my own
discipline - the sociology of health and illness - and in particular, horizontalist sociology by which 1 mean the (perhaps
radical) social constructionist position within sociology.
There are a few issues here:
Focusing on the body, Turner writes (referring to sociology
itself - Ifm not sure 1 would be so general), that
we can safely assume that within sociology there is a broad consensus around the ideas that (1) human nature is infinitely, or at least highly, malleable and plastic; (2) human nature is socially constructed, and as a consequence (3) there is little that one could Say in general about human nature... The body, and especially the female body, is seen to
5 O be a 'fabricationf.. . These are encompassing ideas. These are broad unyielding ideas.
And they are ideas, as has been discussed, that extend to
reality in general. From the social constructionist point of
view (to limit, somewhat, the generalization Turner adopts) , reality is basically a social construction. This is the
paradigmatic approach it has adopted.
Yet, why the general claims?
It is interesting to note that, in practice, social
constructionists tend to highlight social constructionism in
certain cases, for example where "there already exists a
political struggle around the existence of a disease; 'pre-
menstrual tensionf is a classic illustrati~n"~~ as are
AIDS, tran-sexualism, repetitive strain injury, eating disorder, minerf s lung, mental illness and psychosomatic illness generally [ a l1 of which] are areas of constructionist research rather than goitre, gout or gonorrhoeal arthritis. 5 2
It focuses on the politically charged. It invokes social
construction to explain the existence of these specific
conditions. And yet it also makes the general claim that
reality is socially constructed.
It seems that social constructionism (or rather, proponents of
it) is (are) doing exactly the same thing that it claims
medicine and science are doing. It is doing normal science. It
is making compelling arguments regarding certain cases, and then
constructing the rest of reality in light of those arguments.

One could Say that the politically charged cases constitute the
exemplars of the constructionist paradigm. They constitute the
preerninent scenarios of the paradigm. They are the points of
paradigmatic appeal, of paradigmatic justification. They are
the standards that inform further constructionist research into
reality, that fortify i t s extension.
And not just extension, but imperialism. As with rnedicine and
science, social constructionism can have its imperialist 5 3 tendencies. Like other professions, it is not beyond it to
insist upon its 'own claim to authority with something valid to
Say. And so it generates its own terms, develops its own
discourse around the notion that reality is socially
constructed, and then conforms/constructs reality accordingly. 5 5
And it does so in particular by feeding upon that which other
disciplines such as science and medicine, a£ firm. Fox says that
"the natural is simply denied to ensure the ascendancy of the
social/political position. "56 AS discussed before, this may be
too strong a generalization - constructionists generally
acknowledge the impact of the natural. But constructionism
generally does attribute greater weight to social/political
forces than to the natural. By doing so analytically,
constructionism f inds itself on the road to credence and thus,
credibility . But the irony continues, since, can it ever truly be on the
road to credence if by its own d a i m everything is socially
constructed? Wouldnft that mean that social constructionism
itself is a social construction? That it is in no position,
therefore, to make a truth claim? A c l a i m about the w a y things
a r e ? That it is in no position to make the daim "reality is
socially constructed"? And if so, wherefore its credence? Why
take it so seriously? Why not go with something else? With
another discourse? Here we have, it seems, a paradox. 5 7
And yet there is a way out.
The way out, however, does not include the contention that
only social constructionism has got things right. It does not
include the position that "sociology has developed the tools
which provide it with resources to protect it from generating
false pictures of realityu5' - not an uncommon position as Fox
goes on to explain:
Sornehow, sociologyfs analysis of the historical or social factors are the only ones to be free of their own social determination; we are supposed to believe that the sociological analysis is 'methodologically sound' ... In retaining its own d a i m to (social) scientific status, the strong program fails to subject its own discourse to the analysis which it demands of other sciences . . . 59
But that's contradictory. It means that, for some reason or
another, social constructionism is able to tap the truth of
things while maintaining the constructionist notion that there
is no truth to be tapped; that it is has uncovered the truth of
things when there is no such thing as truth. The paradox
remains . And it remains when the not-so-hypocritical-position is
adopted, a position perhaps more common among postmodernists.
Some, like Derrida for example, relativize everything. And in
accordance with that, they relativize their own views,
attributing to them nothing privileged. But in so doing, they
get into trouble in two ways. On the one hand, they undermine
their own position that al1 things are relative. Concurrently,
they irnplicitly affirm the possibility of a particular truth6' - the truth that there is no truth and that a l 1 things are
relative. They irnplicitly affirm a particular ontology. The
paradox thus persists, since, to deny truth is to promote a
particular truth; to deny ontology is to promote a particular
ontology; to deny the verticalist project is to promote a
particular verticalism; to promote horizontalism is to promote a
particular verticalism.
The way out is to let go of the unconditional claim that there
is no truth and that al1 is construction. It is not to deny
that social construction takes place, but to embrace the reality
that some things are more socially constructed than others.
Then the paradox dissolves. Then sociologists are in a
legitimate position to make truth claims (whether they intend to
or not) like:
Society is a dialectic phenomenon in that it is a human product . . . that yet continuously acts back upon its
6 1 producer . What makes power hold good, what makes it accepted, is simply the fact that it doesnf t only weigh on us as a force that says no, but that it traverses and produces things, it induces pleasure, f orms knowledge, produces discourse. 62
... medical ideas of the body and its diseases are ... socially constructed realities that are subject to social biases and limitations. Biomedical ideas are based upon a number of historical assumptions about the body and ways of knowing about the body ... 6 3
As the practice of modern medicine becomes increasingly a technical enterprise, 1t is more incumbent upon us than ever before to recognize that the human body is not a machine, that health and illness are not merely biological states, but rather that they are conditions which are intimately related to and constituted by the social nature of human life. 6 4
Gynecology is a specialty practiced (some Say perpetrated) on women by men and for men. 6 5
Or truth claims like:
The medical mode1 is . . . ( see Chapter 3).
Illness X is a metaphor of society and is therefore a social construction (see Chapter 3) .
* This is how illness X has been socially constructed (see Chapter 6) .
Then it is possible to Say that social constructionism is
en j oying
Paradigmatic Intensification
By paradigmatic intensification 1 mean the process whereby the
(any) paradigm becomes further attuned to (an aspect of) a
phenomenon. To paradigmatically intensify is to further reveal,
to further get at, to further uncover, to further penetrate a
particular reality.
Intensification is always a possibility.
It is always a possibility because tangibility is always a
possibility, and tangibility is always a possibility because
reality constrains. 66
Moreover, the possibility of intensification increases as
tangibility increases. As tangibility increases, the parameters
of possible investigation narrow - they become more directive. Tangibility is both the doorway and the funnel to phenomenal
(aspectual) penetration. The more tangible the phenomenon
(aspect) , the more ajar the door and the more directive the funnel. The more tangible the phenomenon, the more f e a s i b l e its
paradigmatic intensification and the more guided its
penetration.
So paradigmatic intensification is possible. And it's a good
thing it is because if it were not, there would be no reason to
take seriously any claim nor any confirmational analysis.
There would be no reason to take seriously the daim
"illnesses are socially constructed" unless it were possible
that the claim speaks to a certain reality, a reality, moreover,
that happens to be relatively tangible to a certain paradigmatic
point of view. There would be no reason to take seriously any
corroborative analysis to the claim unless there were some
possibility that the analysis penetrates into the "whatness" of
social construction; unless there were some possibility that it
reveals how certain illnesses are socially constructed, how
certain illnesses are metaphors for societal anxieties, how
power produces knowledge of illness not to mention illness
itself, how medicine medicalizes. To Say that illnesses are
socially constructed, that hysteria is a metaphor for
patriarchal anxieties over female sexuality, that medicine is a
dominant producer of illness, and that life is becoming more and
more medicalized is to make t r u t h c l a i m s - to speak to possible
realities. And if they are indeed realities, then to accurately
delve into and analyze them is to intensify.
And isnr t it possible that this is exactly what social
constructionism is doing, at least with regard to certain
conditions (such as pre-menstrual syndrome, menopause,
repetition strain injury, etc. ) ? Isnf t it possible that social
constructionisrn is hitting upon certain realities - tapping into certain tangibilities - and then accurately investigating those realities in more and more depth? In other words, isn't it
possible t h a t soc ia l constructionism is intensifying?
To maintain "no" is to maintain the invalidity of social
constructionism. The validity of social constructionism does
not stem £rom its own paradoxical daim that al1 is
construction. Rather, it stems from the possibility that it
sees a reality - that social construction is a reality; and from
the possibility that it can unveil the "how" of this reality -
how it is that things are socially constructed.
And it is for the same reasons that we can take Foucault
seriously :
Ironically, Foucault makes truth claims about what truth is.
In one spot he says: '"[tlruth" is linked in a circular relation
with systems of power which produce and sustain it, and to
effects of power which it induces and which extends it. f O7 In
another, he says that:
... in a society such as ours, but basically in any society, there are manifold relations of power which permeate, characterize and constitute the social body, and these relations of power cannot themselves be established, consolidated nor implemented without t h e production, accumulation, circulation and functioning of a discourse. There can be no possible exercise of power without a certain economy of discourses of truth which operates through and on the basis of this association. We are subjected to the production of truth through power and we cannot exercise power except through the production of truth. This is the case for every society, but I believe that in ours the relationship between power, right and truth is organized in a highly specific fashion. 68
1 italicize in places to make a point. In making his case
against deep universal truth, Foucault himself appeals to a deep
universal truth. His anti-essentialism/foundationalism is
informed by an essentialism/foundationalisrn - that truth is everywhere, and at al1 times, produced by power. He also
suggests an empirical truth - t h a t there is a "specific fashion"
in which truth, power and r i g h t are organized i n our society
today.
To adopt the Foucauldian position in full, therefore, is to
embrace paradox. It is to champion anti-ontology through an
(albeit implicit) appeal to a certain ontology. So 1 would
suggest that the Foucauldian position in full is erroneous. But
that doesn't mean that 1 think his position should be totally
thrown out. It may be that there is some truth to what he is
saying. It may be that his truth claims about truth are
speaking to a certain reality, be it foundational or empirical.
Moreover, it may be that he has penetrated into this reality,
that through his genealogical approach in particular, he has
penetrated deeply into the workings of power and the ways it
produces truth. It may be that his genealogy has permitted him
to intensify into this particular aspect of truth.
Hence the possible importance of Foucault.
And hence the possible importance of medicine.
That is, is it not possible that there are some things
tangible to medicine? And is it not possible that medicine has
intensified into some of those things? The avid horizontalist
says not a chance. Medicine is just a dominant discourse that
corresponds in no way to a reality "out there" because there is
no reality independent of discourse - the anti-foundationalist
position. Medicine creates its own reality, a reality which
happens to be imposed upon the rest of us. But when you think
of it, it is extremely verticalist of the horizontalist to be so
categorical. Indeed, it is very imperialist of him/her, not to
mention contradictory. To maintain this position is to practice
exclusion, and it is to do so, once again, by promoting a
certain truth: the truth that there is no truth to be accessed
by medicine or anyone else. A truth, moreover, of which only
the horizontalist seems to be aware; a truth only the
horizontalist seems to have penetrated. Indeed, to adopt this
position is to adopt an inconsistent position. It is to
paradigmatically extend, to paradigmatically territorialize, to
pronounce finality while contemporaneously denouncing the meta-
narrative, the dominant discourse, the final word on things.
Thus, to be consistent:
Just as it may be that sociology can see and penetrate, it may
also be that medicine can see and penetrate, albeit into
different phenomena (aspects). It may be, for example, that
medicine has come to grips with various health conditions - with certain acute illnesses, for example - with what they are about,
how they are to be addressed, etc. The success medicine has
enjoyed with certain illnesses suggests this possibility. Its
pragmatic success may have something to do with its
investigative responsiveness to certain phenomenal constraints.
My son, to give a persona1 example, has a congenital heart
condition called aortic stenosis which is defined by a narrowing
of the aortic valve making it more difficult for the heart to
pump blood to the body. The regular condition of the valve is
to have three cusps. With the condition stenosis, however, the
valve may have only one or two cusps, cusps which are thickened
and/or stiff resulting in a valve that is relatively narrow and
less flexible thus limiting the regular flow of blood. The
medical position has it that when the condition is severe, it
needs to be treated, otherwise the heart goes into failure and
the person dies. Now herefs the question: has medicine
constructed aortic stenosis, or has it intensified into a
particular biological reality? Well, I think it is undeniable
that rnedicine has constructed the phenomenon - at least to some
extent. Construction always occurs in some way, and to some
degree. But is it not also possible that medicine has
intensified into the phenomenon as well? 1s it not possible
that medicine has accomplished more than sirnply making this
condition up? It seems reasonable to assume that had my son not
been surgically treated for the condition, he would have died.
That had not his valve been widened through surgery, the blood
flow to the body would have remained obstructed adding undue
pressure on the heart causing it to go into failure. This is
what happens to individuals with severe cases of untreated
aortic stenosis. It may very well be, therefore, that aortic
stenosis is one of those conditions that is relatively tangible
to medicine. While it may be a construction (in some way), it
may also be a construction that reflects very closely a certain
reality, a reality into which medicine has intensified in much
the same way that "reality as socially constructed" rnay reflect
a reality into which sociology has intensified.
Similarly, it rnay be that medicine has penetrated into certain
everyday workings of the body. To give another example:
Within medicine, and science more generally, there is a
distinction made between two types of ce11 division: mitosis and
rneiosis. The former denotes cell division within the body
generally in which two daughter cells obtain identical copies of
chromosomes from the nucleus of the original cell. The latter
denotes ce11 division unique to the ovaries and testes in which
an original ce11 with 46 chromosomes in its nucleus, through two
successive ce11 divisions, generates four germ cells (sperms or
eggs) with 23 unique chromosomes each. Now, once again, herefs
the question: is the distinction not a legitimate one? Does it
not represent an intensification into cellular workings? Or
does the distinction represent simply a construction in the
service of some ideological agenda? 1 think it is fair to
entertain the possibility that medicine (or science more
generally) rnay have penetrated into something true of biological
reality. That it didn't just make this distinction up. That it
really sees something truly different about ce11 division within
the body generally, and within the ovaries and testes more
specifically. And that, while its understanding of these two
processes rnay change in the future, its identification of a
distinction is valid, speaking to a reality, if only
imperf ectly . To conclude "no distinction", in other words,
would be erroneous. In short, is it not fair to conclude that
science rnay have tapped into a specific biological phenomenon in
the same way that social constructionism rnay have penetrated
into a particular social phenomenon?
Rorty says that language (science, the paradigm) is nothing
more than a tool for coping. I would like to suggest that it is
concurrently, at least potentially so, a tool for
intensification.
Proactive Intensification and Education
Intensification is possible. Thatfs the point.
And it is due to its possibility that we can speak of
learning, of education, of acquiring a knowledge of how things
are, which is exactly what the various disciplines, and in
particular the sciences and social sciences, claim they are
about. They are about learning about reality in their various
ways. They are about fur ther intensifying into reality in their
various ways. They are about engaging in various proactive
intensifications. They are about actively penetrating into the
way things are so that things can be known, tapped, utilized,
etc. Hence the potential importance of these disciplines.
Hence the potential importance of medicine. Hence the potential
importance of sociology. 6 9 Hence one of the reasons education is so important, education
being the vehicle through which knowledge intensified is
imparted . . . . . . although - and here is the problem . . . ... education is also the vehicle through which knowledge
extended is imparted.
Within every discipline there lies both the possibility of
proactive intensification and its antithesis, proactive
extension. To medicalize, for example, is to proactively
extend. To medicalize is to actively promote the medical view
as applicable to a growing range of phenornena, and to do so
erroneously. Applying social construction exhaustively to every
illness and disease is another example of proactive extension.
And 1 Say "proactive" extension because 1 want to distinguish
it from reactive extension, extension that occurs despite no
deliberate intent to actively promote a paradigmatic point of

view, Here, extension occurs as a reaction to anomalic
challenge. The proponents of the paradigm react by extending
their paradigrnatic view to envelop the phenomenon and manipulate 7 0
it in line with expectation.
Extension, ~ ~ t r n s i f i c a t i o n and Anomaly
TO this point, 1 have been discussing extension and
intensification as ideal type processes occurring in isolation
from each other. Their mingling is perhaps the more likely
case, however, with one or the other holding more sway depending
on the phenornenon under paradigmatic investigation: the more
tangible the phenornenon, the more likely it is that
intensification will dominate, while the more semi-tangible the
phenornenon, the more likely it is that extension wiil dominate.
But we must also rernember that tangibility is in many ways
paradigmatically conditioned. More precisely, it is in many
ways conditioned by previous paradigmatic activity - by the mix
of antecedent intensifications and extensions into other
realities. ~ h e result is a paradigm made up of a mesh of
concepts, concepts that range in degree from relatively pure
truths (intensifications) to veritable fabrications
(extensions) ,
New it may çeem that extension stifles tangibility, but that
is not necessarily the case. In fact, extension can induce
tangibility and thus lead ultimateiy to its antithesis - intensification. To explain, the paradigm, being a mix of
intensifications anci extensions, can be thought of in terms of
the ratio extension/intensification (e/i). The greater the
ratio, the more the paradigm has extended relative to
intensifieci. The smaller the ratio, the more it has
intensified. ~ o w , consider the following: as e/i increases,
the likelihood of anomaly increases. Anornaly appears against
the paradigmatic background: "[tlhe more f a r reaching and
precise the paradigm, the more the paradigm is compared with the
world; hence the greater the likelihood that instances of bad
fit wil1 ernerge into view." This was said and discussed in
Chapter 4. Now to add: the more erroneously far reaching and
precise the paradigm, the greater the potential for that
reality, upon feedback, to protest. Hence, the greater the
likelihood of anomaly - of anomalic tangibility. The emerging
discontent with medical intervention as a whole can be
understood as a response to the anomalic effects of (discontent
with) medical extension into areas such as chronic illness,
aging, women' s "problems", etc., areas perhaps more adequately
dealt with and understood in other ways.
And with anomalic tangibility there is the possibility of
intensification, intensification of a radical kind, no less.
Intensification that can lead to novel experimentation and to
the articulation of new ways of thinking; that can lead to new
approaches; that can Lead to the reasserting of suppressed
approaches. It can lead to women reclaiming their bodies, to
renewed emphases on preventive health care, to renewed
validations of rnid-wifery, to the promotion of chiropractie -
al1 things that are happening today. It can also lead to legal
action that challenges the prevailing orientation of medical
practice. B r i e f l y , anomalic tangibility can lead to
intensification that foregoes heretofore held paradigmatic
expectations, and around which new paradigmatic expectations
form. It may even lead to paradigmatic shift, to paradigmatic
revolution.
With every paradigm there is the possibility of
intensification. This is so even with highly "extendedf'
paradigms. Extension can breed trouble, trouble that can in
turn prompt or rejuvenate intensification into new corners of
reality.
PARADIGMATIC ARTICULATION AND THE CONSTRUCTION OF A PHENOMENON
Finally, both paradigmatic extension and paradigmatic
intensification can lead to the construction of a phenomenon.
Why? Because both can lead to what 1 shall term
aspectualization, the situation where a phenomenon is understood
in light of one, or some, of its many (~nlimited?~~) aspects - in
light of very specific information about it. This is sornething
I have only alluded to so far.
I would actually suggest that aspectualization, in some degree
or another, is unavoidable. For if it were avoidable, then
total understanding would be possible. Then a perspectiveless
understanding of phenomena would be possible. Then absolute
freedom from paradigmatic constraints would be possible. And I
think we can safely assume that such freedom is rare if not
nonexistent.
Instead, through our paradigmatic ways of seeing the world, of
seeing phenomena, we select some information and exclude other
information. We select certain phenomenal aspects over others,
and then see/construct the world, see/construct phenomena, in
light of those aspects. And to select/exclude is inevitable.
We always do it, Some of us, for example, make heroes out of
good runners because we value good running. It doesn't much
matter that some good runners may also be good at other things,
like inventing cultural theory. Such information we exclude as
we select, indeed, highlight, their running ability - as we
select t h i s aspect of who they are. And yet others among us
make heroes out of cultural theorists because we value incisive
cultural criticism. For us others, it doesnf t much matter that
some of these cultural theorists may also be good runners. Such
information we exclude as we select, indeed, highlight,
theoretical ability - as we select t h i s aspect of who they are. 7 2
Dorothy smithY3 found sornething similar when she gave her

students the assignment of writing about someone they knew to be
mentally ill. She found that her students, in carrying out
their assignment, would actually look for mental illness, and
that they would do so by extracting some information while
excluding other information about their subjects, information
that supported their conceptions of mental illness. In this way
the students defined - constructed - their subjects. The issue, once again, is not whether or not things are
constructed, but rather the degree to which things are
constructed. This, it seems, is conditioned very much by the
extent to which aspects selected fa11 under the sway of
paradigmatic extension as opposed to paradigmatic
intensification. The degree to which phenomena are constructed
depends on the extent to which their aspects selected are
themselves semi-tangible and thus constructed, as opposed to
tangible and t h u s amenable to exploration. In the case of the
former, the aspects are open to profound construction which
means the phenomenon is understood in light of highly
constructed aspects. In the case of the latter, the aspects are
not so amenable to social construction which neans that the
phenomenon is understood in light of aspects both seen and
penetrated into. (And, incidentally, it is in this way that we
need to understand the intensification of phenomena - such really entails intensification into certain of their aspects.)
The former, therefore, is the more constructed of the two
phenomena, while the latter is the less constructed of the two
phenomena.
T a k i n g everything together, the social construction of a
phenomenon from any paradigmatic point of view can be understood
to involve at least three processes:
1. Aspectual Selection: Where some phenomenal aspects are selected (or weighted with more significance) while others

are excluded (or given less weight). This rneans that phenornena are seenkonstructed in light of certain aspects.
2.Aspectual Constntction: Those aspects selected may or may not be tangible to the paradigm. If they are, then intensification can ensue resulting in a phenomenon seen/constructed in l i g h t of aspec t s better and better seen. Here, the social construction of the phenomenon amounts to little more than an issue of aspectual selection (and meaning attachment - see below) . If they are not, however - if they are semi-tangible to the paradigm - then paradigmatic extension ensues resulting in a phenomenon seen/constructed in l i g h t of h i g h l y cons t ruc ted aspects. The result is a phenornenon constructed to a much greater extent. Indeed, in the extreme case, the aspects selected may be little more than social imputations, having little attunement with reality. If so, then the phenomenon itself turns out to be vexy much a construction.
3.Meaning Attachment: No matter how tangible the aspects aspectualized, meanings are always attached to them, and thus, to the phenomenon itself.
So, when we talk about the relativity of the social
construction of phenornena, 1 would suggest that such relativity
results primarily as a consequence of the second process - as a consequence of aspectual construction which is itself very much
a relative affair.
SOM3 FINAL THOUGRTS CONCERNING PARADIGMS AND TBEIR PROCESSES
Now, before 1 go to the next chapter, I just want to mention
one or two things - to offer a few speculations, nothing more - regarding certain allusions made throughout this chapter. The
theme of paradigmatic crisis and revolution is one such
allusion, and is one of Kuhnfs major themes. 7 4
Kuhn, for example, talks about how discovery is seldom an
instantaneous affair. Discovery is a process, he says, one t h a t
passes through three stages. It commences with an awareness of
recalcitrant anomalies, with an awareness that (normal) science
is being violated in some way. It then moves into the second
stage - the stage of extended exploration - if it is felt that the anomalies warrant further investigation and that they should
not be ignored nor relegated to ad hoc explanation. During this
stage, science becomes more speculative, possibly leading to the
third stage, the stage in which the anomalous is no longer t h e 75 anomalous, but the expected. At this point, discovery is
complete. That is, when this occurs there is a paradigmatic
shift, a s h i f t in which the previously anomalous is rendered the
stafidard, the basis upon which, the exemplar around which, a new
paradigm f lourishes . Now, while this is a particularly attractive model, 1 would
l i k e to propose two ways in which it might be modified. In the
first place, there may be certain factors that condition
paradigmatic shift in light of anomalic presence. Power, for
example, rnay play a big role in sustaining a certain
paradigmatic reality despite its ev iden t difflculties - its evident bad fit. In the second volume 1 tackle this and related
issues again.
In the second place, paradigmatic shift may not have to entai1
an a l 1 out shift. A s quoted earlier, Kuhn says that " [a] 11
theories can be rnodified by a variety of ad hoc adjustments
without ceasing to be, in their main lines, the same theories."
To put this another way, it is conceivable that paradigmatlc
shifts of a lesser kind can occur, shifts t h a t do not affect the
essence of the paradigm - that do not affect that which is integral to the paradigm. That do not, for instance, result in
the expulsion of any exemplars.
For heuristic purposes, think of the paradigm in terms of two
levels: a primary and a secondary level. The primary level
refers to the essence of the paradigrn. It consists of those
concepts that make the paradigm what it is. It is the rigid and
enduring quality of the paradigm. It is not so rigid that it
does not develop - articulate - through intensification and extension. This it certainly does. But it is not like t he
secondary level which is the more fluid level, the level of
flux. The secondary level is derivative of the prirnary level,
yet it is more flexible in the sense that it permits sorne
paradigmatic adaptation to phenomenal discrepancies. That is,
it permits what I shall t e m "accommodation."
Accommodation is a special case of extension. So far 1 have
presented extension as the process of incorporating more and
more phenomena into the paradigmatic view by distorting them,
conforrning them, etc.. Accommodation, however, is that aspect
of ext-ension that yields to anomalies, that takes them in
without any major attempts to socially (re)construct them in
line with paradigrnatic expectations. Accommodation thus results
in paradigmatic shifts, but shifts of the minor kind, since the 7 6 essence of the paradigm, its primary level, remains intact.
In this sense, we can think also in terms of primary and
secondary anomalies. Secondary anomalies are phenomena which
present little challenge to the essence of the paradigm.
Through extension they may be successfully reshaped so that they
conform to paradigmatic expectations, or they may be
accommodated since they are perceived as insignificant
challenges to paradigmatic coherence. In the latter case, the
orientation can be summed up as "why bother with them", with the 7 7
result once again being paradigmatic shifts of a minor kind.
But primary anomalies are dangerous. They are like negative
exemplars. They fundèmentally challenge that which is essential
to the paradigm. Consequently, much effort goes into their
conformity since their accommodation entails paradigmatic
demise.
The paradigm, therefore, is both rigid and dynamic. It is
dynamic in three ways: first, it articulates through
intensification; second, it articulates through extension;
third, it undergoes rninor shifts through a s p e c i f i c process of
extension termed accommodation, a process which gives the
paradigm its fluidity. The paradigm is rigid in that it is
incapable of accomodating primary anomalies without finding
itself fundamentally challenged. Moreover, it may be this rigid
quality which, i r o n i c a l l y , conditions its own demise - which facilitates its final act of dynamism - since it is against this rigidity that anomalies are most glaring.
But these, once again, 1 offer j u s t as speculations.
I And it is due to this possibility that w e can speak of "learning". That
is, while it is possible that any knowledge can see certain realities, it rnay
also be that only some, more than others, are actively striving to intensify
- to further penetrate - into what they see, and doing so with some success.
Perhaps the various sciences along with medicine are examples of knowledges
seeking to intensify, and doing so successfully to some extent. Perhaps
social constructionisrn is another example. This is dicussed in more depth in
this Chapter.
2 (1967); and with Luchann (1967).
3 For a good summary of Berger's position, see Turner (1992), p. 113-118.
4 Turner (1992), p. 117.
5 Which is Foucault's point about the knowledge/power nexus.
6 The ensuing quotes are from Berger (1967), p. 33-34.
7 Chapter 3 goes into this in some detail.
8 Boy in Skinner (1991), p. 48.
9 Rosenau (l992), pp. 42-43.
10 (1956), p. 34.
11 Ibid., p. 39.
12 Ibid., p. 629.
13 Berger (l963), p. 147
14 (1969), p. 77. Foucault shares this sentiment, warning us against a l 1
discourses that totalize, normalize and universalize.

15 Ibid, p. 90.
16 Zeitlin (l994), p. Il.
17 Lash (19911, p. 70.
18 Nietzsche (1969), p. 137.
19 Fox (l994), p. 131-
20 Swidler (1993), p. xiv.
21 Ibid, p. xv.
22 See Ritzer (1988), p. 123 for a good summary.
23 Turner (1992a), p. 116.
24 Ibid, p. 116.
25 (1958).
26 The other being bureaucracy.
27 1 should be clear that Weber does not deny the impact of material
conditions, the role of economic circumstances in the emergence of
capitalism. Indeed, one of his major objectives is to demonstxate the
likelihood of a plurality of causes, that one should prioritize neither
economic nor ideologic causes like the Protestant Ethic. As he States in The
Protestant E t h i c : "...it nevertheless cannot be the intention to substitute
for a one-sidedly 'materialist' interpretation of cultural and historical
causes an equally one-sidedly 'spiritualistf interpretation. Both are
equally possible, but both are of equally little service to the interests of
historical tr~th if they daim to be, not preliminaries to inquiry, but its
conclusions." (See Runciman (19871, p. 1 7 2 ) .
28 Turner (l992a), p. 116.
29 Ibid, p. 115.
30 Ibid, p. 117 .
31 Ibid, p. 119.
32 Turner (lggîa), p. 180.
33 This is Foucaultf s major theme in Discipline and Punish (1977) . 34 Rabinow (1984), p. 17.
35 Turner (1992a), p. 180.
36 Ibid, p. 21.
37 See Chapter 3 on this.
38 (1973).
39 Ibid, p. 146.
40 (l977),
41 Fox (1994), p. 24.
42 (l977), p. 289.
43 Ibid., p. 281.
44 Feyerabend (1993) , p. 148. 45 Barnes (1991), p. 92.
46 Longino says something similar to this. She says "both knowledge
extension and truth can guide scientific inquiry and serve as fundamental,
but not necessarily compatible, values determining its assessments," (1990,
p. 36).
47 Sorel1 (lggl), p. 9.
48 Ibid, p. 9.
49 Ibid, p. 9.
50 Turner (1992), p. 104.
51 Ibid, p. 106.
52 Ibid, p. 105.
53 Strong (1979). Strong talks about sociology more generally.
54 Fox (19941, p. 13.
55 It delineates a particular version of the medical model, for example,
squeezing medicine into a particular understanding of what medicine is al1
about - that it is purely naturalistic, for example (See Chapter 2). 56 (l994), p. 13.
57 This paradox is a common criticism of social constructionism.
58 Fox (l994), p. 6.
59 Ibid, p. 16.
&OpR~sgne~~(~992~,-p.90 - - - - - - - - - - -
61 Berger (l967), p. 3.
62 Foucault in Rabinow (198 4 ) , p . 61.
63 Freund and McGuire (1995), p. 5.
64 Lock (1988), p. 8.
65 Scully and Bart (1978), p. 213.
66 This is one of the major points of Chapter 4.
67 In Rabinow (1984), p. 74.
68 (1980), p. 93; my italics.
69 My emphasis is on "knowledge-of" as opposed to the acquisition of trades,
crafts, skills, performativity, etc., al1 of which are important parts of
education as w e l l .
70 Note: Paradigmatic extension, whether proactive or reactive, may not be
seen as such by those who champion the paradigm - by its proponents. Rather,
it may be seen as contributing to the refinement, integrity and coherence of
their particular view. They may see extension as intensification. In this
way they may deceive themselves thus making it possible for proactive and
reactive extension to occur.
71 Here's an interesting set of questions: hon many aspects does it take to
make a phenornenon? Do some phenomena have more aspects than others? Or do
al1 have an infinite number? And here's another question: what makes an
aspect an aspect? What are its parameters? What are the parameters of a
phenornenon? These are important questions each of which rnay imply a weakness
in my theoretical development. However, 1 leave such questions to others to
debate and proceed with the understanding of "aspect" as an ideal type
conceptual tool.
72 One more example would be when kids cal1 one of their classrnates "four-
eyes". Here they are defining him/her in iight of his/her having to wear
glasses.
73 (1978),
74 ( 1 9 7 0 ) .
75 Ibid, p . 53.
76 1 want to suggest, at this point, that paradigmatic fluidity also arises
as a consequence of the uniqueness of different individuals. While
individuals of a particular paradigmatic community share a commonality of
view, they do so most importantly at the prirnary level, at the level of
paradigmatic essence. This is the source-and the fogdatZonof their unity. - p p p p p p p p p p p - - - - - - - - - - -
But at the secondary level, their perspectives may Vary. Different
individuals may accommodate different phenomena into their paradigmatic view.
This results in paradigmatic fluidity across individuals. Moreover, given
the secondary nature of such fluidity, such diversity, the unity of the
paxaaigm, its essence, remains intact.
77 Although, the possibility of there being too m a n y accommodations at the
secondary level should be considered. Perhaps a given paradigm has a certain
tolerance level that is simply greater for secondary anomalies than for
primary anomalies, but one that, nevertheless, is not infinite.
MAPPING THE RELATIVITY OF THE SOCIAL CONSTRUCTION OF DISEASE
JOt3RPilEY NO!l?ES To Recsp: Not o n l y i s i t p o s s i b l e t h a t d i f f e r e n t paradigms s e e d i f f e r e n t
phenornena ( a s p e c t s ) , i t i s a l s o p o s s i b l e t h a t as t h e y a r t i c u l a t e , t h e y p e n e t r a t e more d e e p l y i n t o t h e t h i n g s t h e y see. Hence t h e r e l a t i v i t y o f t h e s o c i a l c o n s t r u c t i o n o f r e a l i t y .
Chapter 1 began by a s k i n g why i t i s we feel such a need t o envelope and perpe tua te Our p a r t i c u l a r ways o f t h i n k i n g ; why i t is, i n o t h e r words, we f e e l such a need t o parad igmat i ca l l y a r t i c u l a t e . Chapter 5 opened by o u t l i n i n g some o f the answers t o t h i s q u e s t i o n . In t e r e s t i n g l y , and i r o n i c a l l y , t h e answers a r e g e n e r a l l y v e r t i c a l i s t o n e s , speaking t o something e s s e n t i a l about human b e i n g s . But w h i l e e s s e n t i a l l y cornpelled, paradigma t i c a r t i c u l a t i o n i s c o n c u r r e n t l y s o c i a l l y cond i t i o n e d . Both r a t i o n a l i z a t i o n (based on formal r a t i o n a l i t y ) and m e d i c a l i z a t i o n , f o r example (the t w o dominant forms o f paradigmatic a r t i c u l a t i o n today, t h e l a t t e r perhaps a sub- ca tegory o f t h e former) have foundat ions i n , and are cond i t ioned by, p a r t i c u l a r s o c i o - h i s t o r i c a l c o n t i n g e n c i e s .
No m a t t e r what i t s o r i g i n s n o r its s o c i a l c o n d i t i o n s , however, t h e e s s e n t i a l p o i n t i s t h a t paradigmat ic a r t i c u l a t i o n has a d u a l i t y t o i t . On the one hand, i t i n v o l v e s paradigmatic e x t e n s i o n . On t h e o t h e r , i t ( p o t e n t i a l l y ) i n v o l v e s paradigma t i c i n t e n s i f i c a t i o n . The former r e f e r s t o the process o f conforming semi- tangib le phenomena i n l i n e w i th paradigma t i c e x p e c t a t i o n s . The l a t t e r refers t o t h e p r o c e s s of p e n e t r a t i n g more d e e p l y i n t o phenomena r e l a t i v e l y t a n g i b l e t o the paradigm. And t h i s may be e x a c t l y what medicine i s do ing - a t l e a s t with regard t o c e r t a i n phenomena. I t may a l s o be what s o c i a l cons t ruc t ion i sm i s do ing . To deny t h e p o s s i b i l i t y o f i n t e n s i f i c a t i o n i s t o undermine t h e s o c i a l c o n s t r u c t i o n i s t paradigma t i c v iew i t s e l f . We can t a k e s o c i a l cons t ruc t ion i sm s e r i o u s l y o n l y by v i r t u e o f the p o s s i b i l i t y that it is i t s e l f p e n e t r a t i n g i n t o a c e r t a i n r e a l i t y : t h e r e a l i t y t h a t r e a l i t y i s (more o r l e s s ) s o c i a l l y c o n s t r u c t e d .
Chapter 5 a l s o d e s c r i b e s what i s r e f e r r e d t o as a s p e c t u a l i z a t i o n - the process o f c o n s t r u c t i n g phenomena i n l i g h t of c e r t a i n a s p e c t s . A major d i f f e r e n c e i n t h e degree t o phenomena a r e c o n s t r u c t e d , t h e r e f o r e , i s t h e degree t o which their r e s p e c t i v e a s p e c t s - a s p e c t u a l i z e d a r e themselves c o n s t r u c t e d . To Continue:
In t h i s chapter, t h e a i m i s t o be more concrete . It is t o demonstra t e w i t h specific cases the relativi t y o f s o c i a l cons t ruc t ion u t i l i z i n g t h e concepts h igh l i gh t ed so far. To t h i s end, a typology of four ca t e g o r i e s represen t i n g different degrees of s o c i a l cons t ruc t ion is o f f e r e d a s an ana l y t i ca l t o o l . While the typology can be applied t o a n y paradigm, it is used a s a framework t o understand the r e l a t i v i t y o f the soc ia l (medical) cons t ruc t ion of var ious diseases.
INTRODUCTION
The Issue
A number of concepts have been introduced so far: phenornenal
tangibility, serni-tangibility, intangibility; generalized,
specified, anornalous and fabricated tangibility; paradigmatic
articulation, intensification, extension and aspectualization.
These have al1 been introduced in light of the clah that
different paradigms may both see and penetrate into various
phenomena - or perhaps more accurately, phenomenal aspects. Other phenomena (aspects), on the other hand, rnay be more
constructed, the results of paradigmatic extension and the
aspectualization of semi-tangible aspects. Hence the central
daim: some things are more socially constructed than others.
The discussion so far, however, has been largely a theoretical
one. In this chapter, my purpose is to apply the theory. In
Chapter 7, 1 provide conclusions and an assessment of rny
application.
To begin, it will be remembered that 1 see the tension between
medicine and social construction as largely an unnecessary
tension, a consequence of both paradigmatic approaches getting
carried away with their own projects, of both approaches getting
carried away with themselves. Medicine daims special and
evolving access to the "whatness" of the workings of the body
and its abnormalities. This is its verticalist claim. Social
constructionisrn counters with the horizontalist claim that the
putative diseases identified by medicine are social
constructions. In rny view, both have sornething - much - to offer, but within limits. And yet, both take their positions
much too far. Both lapse into paradigmatic extension. Both
(needlessly) construct health, illness, disease and the body.
Both (needlessly) construct reality.
Indeed, the medical and the social constructionist paradigms
are very much at variance, with medicine insisting upon its
being able to see diseases and the like, and social
constructionism insisting upon the unfounded imperialism of the
medical point of view (which, apparently, it s e e s - a verticalist claim, ironically) . The doorway to meaningful
interaction between them is consequently very much closed. But
if there is relativity to the social cons t ruc t ion of things - if
t h e r e i s r e l a t i v i t y t o the medical cons t ruc t ion of disease, for
example - t hen , the l o g i c goes, t he re are grounds t o f l i n g the
door wide open. There are grounds for each to look seriously to
t h e other for insight. Why? Because the relativity of the
medical construction of disease rneans two things. I t means: 1.
medicine may see and intensify into certain diseases, or aspects
thereof, relatively well - their physiological reality, for
example; and 2. social constructionism may see and intensify
into other diseases (and some of the same diseases), or aspects
thereof, relatively well - their socially constructed reality,
for example.
So, taking disease as the focus, the aim of this chapter is to
examine the social, and more particularly, the medical
construction of disease. Various conditions are assessed and
categorized according to the degree to which they a r e socially
(medically) constructed as diseases.
Tools for Thinking about the Relativity of Social Construction
As discussed, social construction is always a factor. There
exist no phenomena - of which there is at least sorne social awareness - fully disconnected from paradigmatic assumptions, that have no links to social meanings. The i s s u e , rather, is
t h e e x t e n t t o which paradigma tic assumptions/meanings infiltra t e
the phenomenon, imbue the phenomenon, cons t ruc t the phenomenon.
Relatedly, the issue is the extent to which paradigmatic

assumptions/rneanings debar seeing and intensification into the
phenomenon. Among the theoretical claims made so far is that
the more tangible the phenomenon to a paradigm, the more clearly
it is seen by the paradigm, the less amenable it is to
construction by the paradigm.
To demonstrate and better understand the relativity of social
construction, the following typology is offered as an analytical
tool in which four phenomena types are distinguished:
1. phenomena that are socially conceived, referred to here as
socially-conceived-phenornena ;
2. phenomena that are socially manipulated, referred to here
as socially-manipula ted-phenomena;
3. phenornena that are socially augmented, referred to here as
s o c i a l l y - a ugmented-phenornena;
4. phenomena that are socially transfixed, referred to here as
soc ia l l y - t rans f ixed-phenornena . These should be understood as ideal type categories, and the
entire scheme as a useful - and preliminary! - device for mapping the degree to which phenomena are constructed, with the
first category including the most constructed phenomena, and the
fourth the least constructed phenomena. (In fact, the fourth
category consists only of intangible phenomena or non-existent
phenomena. Any phenomenon perceived is a phenomenon constructed
somehow, and to some degree, as already said. There are no
perceivable phenomena impervious to social construction.)
It is according to this scheme that 1 demonstrate the
relativity of the social construction of disease. You will
remember that by disease 1 am utilizing Conrad and Kern's
definition which is that diseases are "biophysiological
phenomena that manifest thernselves as changes in and
malfunctions of the human body."' More broadly, 1 also refer to
"disorder" in order to incorporate malfunctions of the
psychological kind.
The problem, however, is that not everything we cal1 "disease"
conforms so well to disease in the sense defined. In fact, no
diseases are purely thus. Al1 diseases are constructed to sorne
extent or another. Al1 diseases are made sense of in terms of
social assumptions. Yet, the point once again, is that some
diseases are more socially constructed than others. This means
that some diseases correspond less well than others to
"malfunctions of the body" although, to those constructing them,
to those reifying them, they appear to correspond equally. In
fact, some diseases are o n l y what 1 s h a l l refer to a s " d i s e a s e s "
mean ing they have no v e r i f i a b l e and/or l e g i t i m a t e claim to
" m a l f u n c t i o n of the human body". This does not mean that, as
social constructions, the real biological does not figure.
Indeed it often does. But it figures more often than not as an
effect of the construction reified. Once constructed, such
"diseases" can produce serious physiological disorders. Here:
kill the social construct and the physical dies with it.
Then there are diseases that are diseases in the sense
defined, that have veritable roots in the biological. While
they are definitely constructed (to some extent), they are
constructed more or less in line with their realities as
diseases, as malfunctions. Here: kill the social construct and
the physical remains, only to stimulate the birth of another(?)
social construct . In any event, utilizing the typology above, I distinguish
between four types of disease constructions:
1. diseases that are socially conceived, or s o c i a l l y -
conceived-diseases;
2. diseases that are socially manipulated, or socially-
m a n i p u l a t e d - d i s e a s e s ;
3. diseases that are socially augmented, or socially-
augmented-diseases;
4. diseases that are socially transfixed, or socially-
transfixed-diseases . with the first category representing the most constructed
diseases (being only "diseases" with little or no correspondence
to the definition), and the fourth representing the hast
(encapsulating intangible on non-existent diseases).
And by these categories 1 mean the following:
1. Socially-conceived-àiseases. Socially-conceived-diseases
are social reifications manufactured out of the semi-tangible.
Where there is ambiguity, there is extensive amenability to
social construction. Hence, whexe there is physiological
ambiguity, where these is ambiguity about whether or not the
physiological constitutes a disease, there is extensive
amenability to social construction. Here, the physiological
(or, more broadly, the body) is constructed. Social (medical)
meanings imbue and pervade ambiguous physiological (corporeal)
realities making of them abnormalities, physical "diseases" or
psychological "disorders" with which to reckon.
Socially-conceived-diseases emerge as the ambiguous natural is
suf fused with the social (with medical assumptions/meanings) . This means that socially-conceived-diseases are stand-ins for
the social. They are social (medical) anxieties manifested and
imputed into the real, into "malfunctions of the bodyff. They
are "diseases" thoroughly social in constitution, social
epiphenomena reified through paradigmatic extension as the real
thing . This is not to Say that they are not associated with
physiological (or psychological) suffering. They often are.
But such suffering is, in many circumstances, better understood
as a consequence of the construction rather than visa versa.
Those "afflicted" buy into socially-conceived-dises as
d i s e a s e s , and "live out" their physiological (or psychological)
prescriptions. In this way, the constructed disease produces
real suffering. (1 Say this, however, with some reservation
since 1 do not want to totally discount the fact that such
"diseases" can also emerge through the attempt to explain
instances of real suffering; "diseases" which, when once
constwucted, induce more suffering.)
This raises an important distinction: socially-conceived-
diseases should not be confla ted with socially produced
diseases. Both emerge through the social, but while the former
refer to epistemological constructs with ontological
ramifications (and thus, invariably, physical ramifications in
the form of suffering), the latter refer to afflictions
generated through exposure to deleterious social arrangements
(in the way that silicosis or lung cancer emerges through
exposure to certain noxious work conditions in minesi; or in the
way that insufficient socioeconomic conditions lead to higher
rates of illness3) . When speaking of socially produced diseases,
the (more or less constructed) categories we use to designate
and understand them are generally taken for granted.
2. Socially-manipulated-diseases: There is a profound
qualitative disparity between socially-conceived-diseases and
socially-manipulated-dises. Socially-conceived-diseases have
no verifiable (or, to put it more forcefully, veritable) roots
in malfunctions in the physiological. Socially-manipulated-
diseases, on the other hand, are clearly diseases in that they
are rnalfunctions of the biological. Upon experience, there are
few, notwithstanding Our diversity, who would see or construct
them, otherwise. Socially-manipulated-diseases have generalized
tangibility as diseases (so defined). They permeate basically
any paradigm as diseases. The social, in other words, is

constrained by them. The social cannot so easily make of them
rainbows, or feathers, or rocks, for example. As diseases, they
are too dernanding, too evident, too tangible for that.
But while it is relatively tangible that they are diseases,
they nevertheless remain highly ambiguous phenornena. The actual
"whatness" of them - of what they are about, of how to deal with
them, of the why of them - is deeply semi-tangible. They are consequently shoe-ins for social construction. As evident
threats to health, to the well-being of society, there quickly
emerges an active social attempt to make sense of and address
them. Through paradigmatic extension once again, the social
goes to work on them, latching onto them (or rather, ont0 their
semi-tangible aspects), imbuing them, conditioning them. In so
doing, it invariably manipulates tkem in line with (dominant,
medical) social anxieties.
3. Socially-augmented-dises. A socially-augmented-disease
is a disease that is in certain ways socially "filled-out"
(exaggerated) , and/or "added-on-to" (supplernented) . In the
first sense, the disease is constructed through
aspectualization. More accurately, aspects belonging to it are
socially exaggerated to the point where they basically becorne
the disease. Aspectualization, to be sure, is not unique to
this category. Socially-conceived-diseases and socially-
manipulated-diseases are understood most significantly in light
of certain aspects - in light of certain aspects-aspectualized.
The difierence, however, is that socially-augrnented-diseases are
also understood in light of relatively tangible aspects, aspects
paradigmatically intensified into, aspects less infused with
paradigmatic assumptions/meanings than in the case of socially-
conceived and socially-manipulated-diseases. But they are
aspectualized nonetheless.
Socially-augmented-diseases in this sense are diseases with
certain (intensified into) aspects selected, highlighted, while
others are concurrently eclipsed (relegated to the background,
screened from paradigmatic perception).
Augmentation also involves "adding-to" or supplementation.
Again, the degree to which social assumptions/meanings
infiltrate the disease, distort it, etc., diminishes with its
tangibility. With socially-augmented-diseases, there is little
to no such social infiltration. Rather, the social either
exaggerates a tangible aspect, and/or attaches meanings to the
disease, meanings that remain ancillary to it. In this second
sense, meanings do not get in the way of paradigmatic seeing and
intensification. Rather, here, socially-augmented-diseases are
diseases with meanings-attached, nothing more.
Now, there is probably no such thing as an socially-augmented-
disease in this second sense alone. Any disease perceived is
likely, and at very minimum, a disease both socially
supplemented and aspectualized. Why? Because one can never see
everything there is to see about a disease, or any phenornenon
for that matter. Aspectualization is always a factor. The
issue, rather, is simply the extent to which aspectualization is
a factor (not to mention the degree to which the aspect
aspectualized is constructed as opposed to seen).
4 . Socially-transfixed-diseases. A disease devoid of any
construction whatsoever, a socially-transfixed-disease is either
intangible or nonexistent.
Some Things to Remember
Before I proceed to examples of the various disease types,
there are a few caveats that need to be stated up front. It is
only with these in mind that 1 can comfortably urge you, the
reader, to continue reading. They are the following:
1. The schema, the typology, is meant as a preliminary tool. 1
alluded to this already, but it is important to be clear.
1 am not about to daim that the schema constitutes the
definitive tool for representing the relativity of the social
construction of disease. Rather, the schema is offered as a
provisional tool to assist with seeing the relativity of the
social construction of disease which is the main point. 1 clairn
for it nothing more than j u s t one way of mapping the variable
degree to which social assumptions/meanings infiltrate and
construct different disease phenornena. Its strengths and
weaknesses as a tool, and the extent to which it accurately
encapsulates different diseases, will be taken up in Chapter 7.
2 . The four disease categories represent ideal types. Thus,
when 1 assign disease X to category N, 1 do so with the
understanding that the placement is, to some degree, forced.
There are probably no diseases that fit p e r f e c t l y within any one
of the categories, except the fourth, especially since the
schema itself is tentative. Any disease assigned, for example,
will jncorporate aspects perhaps better placed within other
categories, or somewhere in between two categories, or
otherwise. So, when I assign disease X to category N, 1 do so
only because, upon reflection, t h e category seems most relevant
to understanding its construction as a total phenornenon. When 1
categorize a disease, 1 am doing so in light of what seems most
prominent about the phenornenon in the degree to which it has
been socially constructed, especial ly when compared to other
diseases . Thus, a socially-manipulated-disease is relatively
more socially manipula ted than a socially-augmented-disease; a
socially-conceived-disease is relatively more socially conceived
than a socially-manipulated or socially-augmented-disease, etc..
As mentioned above, 1 plan to spend some time discussing the
merits and otherwise of these categories in Chapter 7.
3. The diseases do not represent a cross-section. In what
follows, I am not concerned with representing each disease type
with an abundance of diverse examples. I see tremendous value
in the attempt to categorize the many diseases (or "diseases")
that exist according to this, or to some other more adequate
typology, characterizing the relativity of the social
construction of disease. However, my primary purpose at this
time is to simply demonstrate the relativity of the social
construction of disease. And this, I think, can be accomplished
with one or two examples £rom each category which is al1 1
present in this chapter. Indeed, the goal would be achieved by
simply demonstrating disparity in the degree to which t w o
diseases are socially constructed. Once again, other diseases
(or "diseases") will be considered in Chapter 7.
1 should also point out that most of the examples 1 use centre
around womenfs conditions or conditions of sexuality as their
analyses as social constructions are plentiful within the social
constructionist literature. The problem, as indicated before, is
that such examples are prone to be treated as the exemplars of
the social constructionist paradigm, as justifications for the
clairn that al1 diseases are social through and through. But 1
draw upon them nonetheless to demonstrate very clearly that such
is not warranted. In the first place, as we shall see, other
diseases are less constructed than they are. In the second
place, there is variation in the extent to which they are
themselves constructed. For these reasons, 1 have chosen to
make them the focus of my analysis in this chapter.
4 . The disease placements are provisional. My placements are
necessarily provisional due to my own inclination to see,
organize and construct according to my own paradigmatic point of
view. To daim for my placements anything more solid than
provisional status would be tantamount to claiming that I can

see the way diseases are socially constructed, the degree to
which they are constructed, etc. It would be tantamount to my
claiming unadulterated access into this particular reality. Now
it may be that 1 am seeing this reality and am accurately
placing diseases into the appropriate categories of social
construction. The possibility of my seeing and representing the
reality of the social construction of disease does exist. But
it is only a possibility. My placements should, therefore, be
understood as constituting a submission subject to refinement,
modification . . . maybe even total rejection. What follows is an
initial attempt at something new, and so 1 make no claim to
expertise in the area.
I affirm this especially since, for the most part (and this is
important), rny analyses are informed by the sociological
literature concerned with health and illness. But 1 would also
suggest that while my analyses are guided by this literature,
they are not determined by it . If they were, then 1 would
probably not be atternpting to demonstrate the relativity of the
social construction of disease. Instead, 1 would Say my
analyses are guided by my own paradigmatic framework which is
definitely informed by the sociological, and in particular, the
constructionist literature, but within which the constructionist
approach is considered inadequate on its own, manifesting as 1
see it, many ironies.
Some of these ironies 1 have already highlighted in previous
chapters, especially in Chapter 5. In the present chapter,
however, examples abound as I draw so heavily on the
sociological/constructionist literature. For instance, you will
note that while the avid constructionist says everything is
construction, that truth does not exist, etc., truth claims of
the following nature are nevertheless made:
A. this is how disease X is constructed;
is" and "knowledge of" as discussed in Chapter 4. The "what" of
a disease has implications for what we come to know of it;
similarly, what we come to know of it has implications for the
"what" of it - for how it occupies a place in Our world, for its
essence. Yet, there is also the possibility - indeed, the
likelihood - that in what follows (and previously) , 1 needlessly conflate(ed) the ontological with the epistemological. This, 1
suggest, is a (potential) difficulty that is not resolved here,
but something that definitely requires attention.
1 also want to be clear concerning the contrast 1 draw between
disease and 'disease". As 1 see it, they are (ontologically?)
very different. By the former I mean a veritable malfunction of
the body (as defined above). In the case of the latter, 1 mean
a condition irnputed into existence with no veritable status as
"rnalfunction of the body", but one perceived/treated/lived as
such nonetheless. (Perhaps this means that epistemologically
they hold the same status? Although the episternological. informs
the ontological . . . ) . The distinction, 1 fee l , is somewhat
cumbersorne, but for the time being 1 leave it as such and
relegate it to further work, or to others, to refine.
6 . Medicine is the focus but not a w i l l i n g , nor a singular,
villain. Various analyses of the medical construction of
disease tend to depict medicine as intentionally seeking ways to
define more and more of reality from a medical perspective.
Sometimes it even cornes across as if medicine is involved in
some sort of a conspiracy to this end, in this way buttressing
its dominance and/or controlling us al1 on behalf of society.
Maybe this is the case at times. Generally speaking,
however, I t h i n k i t is more u s e f u l t o t h i n k of medic ine a s
engaged i n s o m e t h i n g we a r e a l 1 e n g a g e d i n : p a r a d i g m a t i c
a r t i c u l a t i o n . And this involves, either wittingly or not, both
paradigmatic extension as well the possibility of paradigmatic
intensification. The only real differences between the medical
approach and other paradigmatic approaches is that 1. medicine
happens to be more dominant at this time than other approaches,
especially vis-à-vis health, illness and disease; and 2.
medicine is the focus of this analysis. Social constructionism
could just as easily be the focus of a similar analysis. Any
paradigm could be the focus of a similar analysis. Any paradigm
could be exposed, in the way medicine is here, for its
deficiencies and strengths as an articulator.
This is important since, based on the analysis that follows,
one may easily form the impression that I harbour an implicit
hostility towards medicine. Let me be very clear that 1 harbour
no such hostility. If my analysis is trenchant, it is so
because 1 am dealing - at least for the most part until 1 get to socially-augmented-diseases - with what 1 see (in my own limited
way) as palpable examples of how medicine has extended. Medical
paradigmatic extension figures as the primary subject of rny
critique, not the medical paradigm as a totality. For there is
much more to the medical paradigm than its extensions, much more
to it (at least potentially s o ) that is worthwhile. This should
be clear given the discussion in Chapter 5 and elsewhere. In
short, extension is the problem as far as I am concerned, and my
specific focus (case study) throughout the bulk of this chapter
happens to be m e d i c a l extension. This is not to isolate
medicine as somehow uniquely deficient nor villainous since al1
paradigms e x t e n d , w i t t i n g l y or n o t , and could, as said, easily
be the focus of a similar analysis.
I should also be clear that, for the most part, 1 treat
medicine as an ideal type category. 1 do this for the sake of
simplicity, but because 1 do, 1 am also not being totally fair.
For there is diversity among those who champion the medical
paradigm at core, as there is among those who champion the

social constructionist paradigm, or any paradigm. There is
diversity manifested if only at the secondary paradigmatic level
(see Appendix 1 post Chapter 5) . Some physicians, for example,
would no doubt take issue with the general stance medicine has
adopted and propagated, as I understand it, concerning certain
diseases (or "diseases") . ..*......
With these caveats in mind, consider the first category
SOCIALLY -CONCEIVED-DISEASES
to which I assign the greatest level of social construction.
Introduction
As discussed in Chapter 4, social construction can proceed
only when it has something with which to work. To construct
something out of nothing, out of intangibility that is, is
impossible. Even at this level of social construction, this
deepest and most profound level, there is something with which
social construction is working. This is the level at which
phenomena are literally socially constructed; the level at which
phenomena are socially contrived out of other phenomena, semi-
tangible phenornena; the level at which paradigmatic extension
holds full sway.
Here, that which is contrived is a stand-in for that which
remains otherwise unarticulated. And it is the contrivance that
is reified. The facade, in other words, is ascribed its own
reality and thus becomes the real (to those who construct it).
The facade is objectified as something that exists "out there".
As such, it has real consequences, with those who buy into it
"playing outff the disease and thus manifesting the appropriate
(physical, psychological) symptoms. As such, the construction
of disease translates into the production of disease.
Certain "diseases" fit this description, being manifestations
of particular social anxieties or paradigmatic assumptions.
Clear examples abound. Menopause 1 suggest is one, being a
present day social elaboration of particular corporeal semi-
tangibilities, an elaboration that combines these together into
a disease. Hysteria - being more of an historical example while
in some ways still current - is anothex, and perhaps even more profoundly so than menopause (suggesting variation within this
category in the degree to which different diseases are socially
constructed), having no foundational roots in biological
dysfunction whatsoever. Its roots lay in the (supposedly)
"irrational" (woman) body from which the "diseasef' is
constructed, and the biological imputed. Both are products of
medical paradigmatic extension, extension inf ormed by broader
social values.
In what follows, I discuss hysteria first, and then menopause.
In Chapter 7, 1 allude to other conditions that may fa11 into
this category.
Eysteria
The history of hysteria is a debatable subject. Foucault bas
its o r i g i n s largely in the 19th century medical discourses on
sexuality. Others insist instead that the condition can be 6 traced back to early Egyptian and Greek times. And there are
still others who argue that hysteria has been given a history
that does not in fact exist, being erroneously attached in more
recent centuries to the tradition of suffocation of the womb as
expounded upon by Hippocrates. As in^^ puts it: Nineteenth-century hysteria, a parasite in search of a history, grafts itself by name and lineage ont0 the centuries- old tradition of suffocation of the womb, thus making Hippocrates its adopted father .
Classical hysteria, therefore, "is in reality but a mare's nest,
a spurious entity invented by later physicians in the Middle
Ages and Renaissance and legitimated a f t e r the event by medical
223
historians. "' In Kingf s view, \' [il t is tirne that father disowned
his hybrid child. "' No matter w h a t its historical origins, however, one fact
remains indisputable: the "disease" hysteria was (and still
by some) invariably tied to (presumable) corporeal
abnormalities, abnormalities, moreover, unique to women.
Landouzy in 18461°, for example, clairned that:
There is an organic cause f o r this affliction, the great majority of recorded cases with pathological evidence showing some type of lesion of the female reproductive apparatus, and particularly the uterus and ovaries.
It was not until Charcot and Freud that the biological basis for
hysteria f e l l into serious disrepute. But even then, the
condition was inexorably tied to the female constitution, and in
particular, to female sexuality.
Keeping Kingf s reservations in mind, what follows is a brief
history of the condition as generally told £rom the
constructionist position. Its status as a disease is then
assessed.
Most argue that the term "hysteria" derived from the Greek
w o r d "hystera" which means uterus or womb. 11 In its beginnings
as a disease, the condition - characterized by uncontrollable
crying, moodiness, tantrums, fainting, etc. - was believed to have ultimate foundations in certain aberrations of the womb.
It w a s therefore, treated a s a uniquely female disorder.
The earliest evidence of hysteria actually cornes from Egyptian
society, where it was identified in the oldest known medical
papyrus dating £rom around 1900 BC. The papyrus dealt
specifically with hysterical disorders and their requisite 12 treatrnents. Here, as it would be for centuries to come, the
condition was tied directly to the womb. Considered an
independent organism able to wander throughout the body, the

womb was held to cause various disturbances when estranged £rom
its normal position, and inducing hysterical disorders when
colliding with the brain. Any cure, therefore, worked to return
the womb back to its proper place.
Cure for this anomalous displacement could be attempted from two directions: the wornan's sexual parts could be fumigated with fragrant substances to attract the migratory uterus from below, or vile-tasting and foul-smelling potions could be ingested to drive the deviant womb back from above. 13
Also implied in the papyri was the connection to "abnormal"
sexual activity which lead to womb wandering. 14 Through sexual
abstinence and, thus, lack of pregnancy, the womb became dried
out inducing it to take flight from its home, The implied cure,
therefore, was pregnancy, a condition that ensured female well-
being. "(Plregnancy was normal, desirable and indeed a
necessary rnedical condition for women in order to preserve their
sanity. ,# 15
The notion that a women's sanity was linked to her sexuality,
to her role in society, and in particular, to her reproductive
system, is a consistent "theme that runs through the history of 16 the disease". Beyond implication, it was firmly implanted in
the Greek medical undeirstanding. Here, as with the Egyptians,
hysteria was once again viewed as a disease of the wandering
uterus applying pressure on the brain (which, incidentally, was
believed to be located within the heart and diaphragm). So
displaced, it provoked, arnong other symptoms, convulsions. This
time, however, the treatments prescribed were very specifically
sexually oriented. While scent therapy, irritant pessaries and 17 herbal concoctions were suggested, the treatments considered
most effective were intercourse, rnarriage and pregnancy. Where
normal sexuality oriented to pregnancy within the confines of
marriage was lacking, hysteria invariably presented.
This , o s t e n s i b l y , was Hippocrates view, a l though King' s
r e s e r a a t i o n s , once aga in , are important t o cons ider . According
t o King, while Hippocra tes c e r t a i n l y t a l ked of the wandering
womb, he d i d not a t t a c h ' hys te r i a" t o t he range of symptoms he
i d e n t i f i e d . I n f a c t , he placed g r e a t e r emphasis on t h e symptoms
themselves, and when he did group them, he grouped them
according t o t h e part of t he body t h e womb happened t o be
v i s i t i n g . Moreover, Hippocra tes did not recommend marr iage and
pregnancy f o r any th ing bu t hypochondria ( ano the r d i s e a s e of t h e
womb). The unders tanding t h a t he recommended it as a cure f o r
h y s t e r i a i s simply an e r r o r i n r e t r o s p e c t i v e i n t e r p r e t a t i o n . I n
King' s words :
It can be seen t h a t t h e Hippocra t i c t e x t s do indeed work by d e s c r i b i n g symptoms r a t h e r t h a n g iv ing a s i n g l e d i s e a s e name t o t h e s e chap t e r s , and that where they group symptoms and t h e r a p i e s t o g e t h e r t h e y do so according t o t h e p a r t of t h e
body t o which t he womb i s be l i eved t o have moved. O f these
t h e r a p i e s , t h e recommendation of marriage/pregnancy occurs only i n t h e d i s c u s s i o n of womb movement t o t h e hypochondria i n Diseases of Women.. .which ends by saying t h a t , a f t e r fumigation, the patient should s l e e p with her husband: "release £rom t h i s d i s ea se , when she is pregnant . "la
P la to a l s o p r e s c r i b e d marr iage and pregnancy as cures f o r t h e 19 wandering womb. H e wrote i n t he T i m a e u s t h a t :
The womb i s an animal which l ongs t o genera te c h i l d r e n . When it remains ba r r en t o o long a f t e r puberty, it is d i s t r e s s e d and s o r e l y d i s t u rbed , and s t r a y i n g about i n t h e body and c u t t i n g o f f the passages o f b rea th , it impedes r e s p i r a t i o n and b r i ngs t h e s u f f e r e r i n t o the extremist anguish and provokes a l 1
2 O manner of d i s e a s e s be s ide s .
Moreover, (as Turner exp l a in s P l a t o f s position), " [t] h e s e
d i s tu rbances cont inued u n t i l the womb was s a t i s f i e d by i t s
reproduct ive func t i on . "2'
Galen sha red much the same p o s i t i o n , although he introduced
some key innova t ions . 22 H e , l i k e t h e o the r s , l inked h y s t e r i a t o
women's reproductive activity, to deficiencies in sexual
intercourse and reproduction. But his reasons for doing so were
different. From b i s perspective, there was no such thing as a
wandering womb. Instead, sexual abstinence resulted in the
retainment of female "seminal secretions . . . within the womh bringing about putrefaction, contamination and finally
hysteria. "23 He also suggested that men could experience
hysteria, a notion that was later disavowed given the f i rm
conviction that hysteria was ultimately and causally tied to the
uterus . The link between hysteria and reproduction certainly had its
recesses. The Christian view leading up to the Renaissance, for
example, propounded the alternative notion that hysteria was
linked to the devil or to evil spirits. Of particular interest
here was the connection made between hysteria and witchcraft, a
position, "largely sustained by a virulent rnisogyny . "24 Consider,
for example, the not so uncommon attitude towards women as
expressed in Witches' Hammer, a work written in the fifteenth
century by Dominican monks :
What else is woman but a foe to friendship, an inescapable punishment, a necessary evil, a natural temptation, a desirable calamity, a domestic danger, a delectable detriment, an evil of nature, painted with fair c o l ~ u r s ! ~ ~
From such a perspective, one could only expect women to be in
league with the devil. Here, every woman was a potential
witch. 26 Every woman including Elizabeth Jackson who, in 1602,
was accused by another woman Mary Glover for the latter's
hysteria, and in particular, for her convulsions whenever
Jackson came near her. Jackson, who in an heated exchange with
Glover, wished upon Glover an evil death, was subsequently
convicted for her witchcraft, the apparent cause of Gloverfs
hysterical episodes. She was convicted, moreover, despite

Doctor Edward Jorden's efforts to disabuse those who were "apt
to make every thing a supernaturall work which they do not
unde r s t and". 27
The Christian view at this time, also held sexual behavior in 2 8 low regard, it being itself an evil act. Intercourse,
therefore, was no cure for hysteria.
Later, during the Renaissance and the Classical age, the link
between hysteria and the womb was further effaced, but for
different reasons. Leonardo Da Vinci with his drawings of
anatomy, Gabriele Fallopio's contributions concerning
reproduction, Harvey' s discovery of the circulation of blood,
al1 served to discount any links between the womb and hysteria.
Links, instead, were found elsewhere. Of particular note was
the connection made to female psychology and a womanfs
constitution as espoused by Willis and Sydenham in the
seventeenth century, both of whom "questioned the uterine
explanation of hysteria"Zg. In their view, women were more
likely to be afflicted with hysteria due to their more delicate
constitutions and inabilities to deal with difficulty. They
considered women more delicate because they saw thern as less
'dense and firmly organized" internally than men, thus allowing
any out of balance "animal spirits" within them to traverse and
produce disorder with ease. 30
" T h a t is why [hysteria] attacks women more than mentff writes Sydenham, "because they have a more delicate, less f i rm constitution, because they lead a softer life, and because they are accustomed to the luxuries and commodities of life and not to sufiering.
As before, patriarchal morality came into powerful play,
suffusing the female body and thus constructing the phenornenon
hysteria.
It is a similar moral stance that informed the work of
Philippe Pinel in Paris in the early nineteenth century, who
constructed his own version of hysteria. 32 In fact, Pinel
attributed a purely moral, and more specifically, sexual, origin
to hysteria. In his view, hysteria emerged as a physiological
and psychological response to deviant sexual activity. The
cure, once again, was normal sexual activity - marriage. (Pinel
also advised productive work as a cure. ) It was, moreover,
under his influence that an increase in the number of (supposed)
women hysterics occurred, with doctors becoming more and more
"provoked and outraged by what they perceived as female
treachery, malingering, and irmn~rality."~~ This lead to a
"medical reaction so violent that extreme rernedies such as
ovariectomies and clitoral cauterization were advocated by
certain specialists in cases of intractable hysteria. "34
Then ~ h a r c o t ~ ~ appeared on the scene in the late nineteenth
century, and did so suggesting the unique innovation that
hysteria was, at least in part, a learned disorder, a mimicked
disorder. He also suggested, like Galen, that men could
experience hysteria. But it was Freud's contribution that
changed the face of hysteria forever. It was also his
contribution that, despite his intentions, ultimately destroyed
hysteria as a disease. As Rousseau and Porter put it, "Freud
was not the beginning of anything new in the history and
conception of the condition but rather the end of a long wave. rr 3 6
Freud's chief contribution lay in the idea that "the symptoms
of hysteria were symbolic expressions of unresolved
psychodynamic conflicts and were typically sexual in nature. " j 7
Whereas, previously (and even in the nineteenth century as
observed at the beginning of this section), hysteria was held by
many to have an organic base, Freud (as did Charcot), found its
cause in the psychological. For psychological disorders devoid

of an organic base could nonetheless produce physical symptoms.
One could get parlor from anger, or heart palpitations from 38 fear, etc. . And one could get hysterical symptoms from the
repression of sexual conflict. Thus, with Freud the
pathological imagination of women, the pathological sexual
imagination of women, took over as the etiological agent of
hysteria . The problem, however, was that Freud's analyses of his
hysterical patients were overwhelmingly informed by particular
assumptions concerning female sexuality, assumptions which,
obviously, he took for granted. In his analyses, Freud
constructed away supposedly aberrant notions of sexuality,
notions that didn't sit well with the "patriarchal fantasies of
fernininity and female s e x ~ a l i t ~ " ~ ~ he championed. This is
evident in the case of Dora (who, incidentally, he recognized as
having been unsuccessful in curing) . As explained by Moi:
There are ... ideological tendencies to sexisrn at work in his text. Freud, for instance, systematically refuse [dl to consider female sexuality as an active, independent drive. Again and again, he exhort[ed] Dora to accept herself as an object for Herr K. Every time Dora reveal [ed] active sexual desires, Freud interpret [ed] them away, either by assuming that Dora [was] expressing masculine identification . . . or by supposing that she desirerd1 to be penetrated by the male. 4 0
According to Freud, Dora was actually aroused by Herr Krs (a
friend of her father's) pursuit of her. Her (hysterical)
problern lay, at core, in her inability to acknowledge it. 4 1
Thus, towards the end of the nineteenth century, hysteria
remained in large measure tied to the sexuality of wornen - to her deviances from the n o m s of sexual practice. While, with
Freud it was no longer tied to a wandering womb, it was firmly
tied to female corporeality and the supposed psychology that
goes with it. In this way, it was also tied to the roles she

was expected to play in society, to her specific roles as
reproducer and wife. This means that single, divorced or
widowed women, or women pursuing education or careers, were
highly susceptible to hysteria. They were the "superfluous"
among women in society because such pursuits/roles prevented
them £rom engaging in "normal sexual activity designed to bring 4 2 about reproduction". And as the superfluous, they were likely
to become the hysterical.
The implication of this medical mode1 was that women could only lead healthy lives in so far as they were sexually connected to a man in a lawful marriage which had the aim of reproduction. Sexual relations outside marriage were associated with another sexual disorder, namely nymphomania. The medical theory of the hysterical woman supported the status inequalities between men and women, supported the medical analysis of the social and psychological values of pregnancy inside marriage, and finally acted as an argument against further education for women on health grounds. A protracted period of education would delay the necessary functions of reproduction and satisfaction inside marriage and therefore professional women were particularly exposed to the
4 3 damaging implications of delayed pregnancy.
Hysteria in the 19th Century, with its varying etiology over
the years, is best understood as a descendant - one confirmed and re-confirrned (one constructed and re-constructed), in
different ways - of broader patriarchal values and concerns. It
was also a synibolization through which patriarchal concerns were
both rnanifested and worked-out. This understanding is further
evidenced by the dramatic decline in hysterical behavior since
the turn of the century, a decline most likely fostered by
social restrictions on various behaviors generally associated
with hysteria, such as thrashing about and fainting. Whereas,
in the 19th century it was fashionable to faint, the 20th
century began to see it as socially inappropriate. 4 4
This decline also lends credence to one current idea that
hysteria should be seen as a learned social role rather than a
disease entity 'out there". In one sense, for example, hysteria
can interpreted as a role that women adopted as an expression of
revolt against the impossible (patriarchal) situation they were
compelled to incessantly endure.
The hysteric's symptom-statements [were] ironic exaggerations of the Victorian ideal female stereotype. They [said], in effect: "You want me to be sickly, passive, and dependent? Watch me - 1'11 do it better than you believed possible - and youf 11 be sorry!" For carried to hyperbolic heights, stereotypical female modes of behaviour [were] inconvenient and irritating to those who [held] power . . . 4 5
And in Doraf s case:
[the] symptoms, seen as i ron ic communications, fulfill [ed] their purpose admirably. The aphonia: "1 cannot speak: 1 am woman, 1 have no Say. So 1 will Say nothing." The malaise . . . 1 am inactive, uninvolved, because 1 am unable to take initiative." The stomach pains: '1 am in pain, in the very region that defines me as a woman, and 1 need to be taken care of." And the suicide gesture: ' I ' m just a woman - maybe I shouldnrt be allowed to live. 46
On the other hand, the hysteria role can also be read as a being
a declaration of defeat, or
the realization that there is no other way out. Hysteria [was] . . .a cry for help when defeat [became] real, when the woman [saw] that she [was] efficiently gagged and chained to
4 7 her ferninine role.
In either case, hysteria was not a disease inexorably tied to a
womanfs natural constitution. Instead, it was a role played-out
in reaction to an oppressive social situation. Hysteria was not
a disease "out there" that afflicts the sexually deviant woman.
It was a social construct lived by wornen who found in it
(consciously or not) a method by which to manifest the
intolerability of their social situation. This does not mean

that t h e physical was not involved. It often was, but as
syrnptoms that emerged through immersion in the role.
Since Freud, less and less credence has been invested in the
idea of hysteria as a disease. In 1952, for example, with the
publication of the first version of the Diagnostic and
S t a t i s t i c a l Manual of Mental Disorders, the "disease" did not
appear, having been deleted in the precursor manual, the Mental 4 8 Disorders Diagnostic Manual . As Libbrecht indicates, this
institutionalized the trend beginning around the dawning of this
century, a trend spurred on by the likes of Dubois in 1904 who
clairneci that "within a few years the concept of hysteria will
belong to history ... t h e r e is no such disease, and there never
has been"; and Gaupp who in 1911 exclaimed tha.t: " [nlowadays the
cry is ever louder: away with the name and the concept of / 4 9 hysteria: there is no such thing. . . . This does not mean that
the diagnosis is no longer made. It still is. But when it is
made, it is made with some regret, and more often than not, as a
means by which to avoid confrontation with ignorance. Faced
with symptoms that cannot be made sense of, there are doctors
who "find an easy way out in relegating them to a category, to a
diagnosis, \hysteriar . . . " 5 0 As Ey puts it, making I would suggest
sornewhat of a bold over-generalization:
Every doctor knows in his clinical experience that he is bound to fa11 back on the magic word hysteria, and at the same time is loath to do so, because it has so little definite meaning. In fact, we are al1 obliged to make use of it when we are faced with paradoxical clinical manifestations which do not coincide wi th the pathology with which we are familiar, and which do not fit into the framework of illnesses which to us are 'real illnesses', which obey the general laws of anatomy and physiology. 5 1
Even though pathological changes cannot be demonstrated,
hysteria is still "ernployed as if it refers to a disease.. . "52
Here, hysteria is a spurious entity constructed, conceived, as
a stand-in for medical inadequacy. Here practitioners extend,
conforming the anomalous in order to safeguard (what they see
as) paradigmatic integrity, relegating it to the psychosomatic.
Such, to elaborate upon this medical phenornenon, is not only
the case with hysteria. For example, when physicians cannot
locate the cause of a complaint, when they are unable t o deal
with it in line with their medical training, some may very well
respond by psychologizing the complaint. The result is a unique
sort of construction, a construction of something that is
potentially real in nature, real in the body, into the
psychosornatic, even the morally depraved. In Kirmayerfs words:
" [t] he diagnosis of a psychosomatic condition transforms the
real into the imaginary, the innocent into the culpable . "53
Conditions are dismissed as imaginary, pseudoseisures,
pseudoangina, etc.; and patients are described as histrionic,
malingering, crocks, hypochondriacs, hysterics, psych cases, 5 4 etc.
Consider the following example: 5 5
A thirty-four year old professional woman with low back pain continues working despite her family doctorfs prescription of strict bed rest. Her doctor describes her as 'a workaholic, a driven perfectionist." She endures one year of pain with little changes in her life-style. Eventually, her pain worsens and she undergoes tests which dernonstrate a collapsed intervertegral disc. A neurosurgeon operates on her spinal column to decornpress t h e pinched nerve root. The patient feels better immediately after the operation but within a few days has recurrent pain. Without performing an examination, the surgeon tells the family doctor that he has corrected the back problem so there should be nothing wrong and suggests that the problem is "behavioral." He refuses to see the patient and advises she seek psychiatric help. (ft is subsequently found on myelogram X-ray that the patient has a new nerve r o o t compression from a re-extruded disc.)
The patient's expression of pain is discounted, psychologized.
Why? Because, for this doctor, it does not conform to the
biomedical mode1 within which he is immersed. In the first
place, the patient did not conform to expected standards of
behavior - she lived with the pain for a year without doing
anything about it. In the second place, she complained of pain
after the cause was ostensibly removed. As Kirmayer sumarizes
the case:
The disease revealed by the physical examination and technical instruments is at once more real and more important than the patient's subjective distress. The rational order of medicine eclipses the bodily-felt reality of the patient. If biology provides no rationale for suffering then medicine can wash its hands of the patient who must be responsible for her own recalcitrant problem. 5 6
This statement too, generalizes the response of medicine. And
it is not clear that such generalizations are fair. Not al1
doctors respond in such ways. However, the physician in the
above examples does. He articulates his biomedical paradigm,
extends it. And he feels compelled to do so. In the face of
anomaly - distress with no perceived biological cause - he feels compelled to make sense of it, to construct it in line with the
assumptions he has available to him, and in particular, with the
assumption of individual responsibility. He paradigmatically
extends the semi-tangibility with which he is faced. In this
way he leaves his biomedical world intact, and his failure to
address his patientf s pain, rationalized. His maneuver acts 'to
maintain the rationality and coherence of the biomedical world
view. . . ,,57 Moreover, his maneuver imposes an assumption that may
not apply - t h a t may be inappropriate - as evidenced by the
subsequent discovery of a new nerve root compression.
Now, 1 want to be clear. I am not suggesting that
psychosomatic illnesses do not exist. They probably do exist.

And 1 am not suggesting that physicians unequivocally or
purposefully misrepresent problems in line with their
assumptions when identifying patients as psychosomatic. What I
am suggesting, however, is that the attribution psychosomatic
illness may be inappropriate in certain cases, being nothing
more legitimate than a transformation of the anomalous into the
paradigmatically conformed. The attribution is much more common
among patients, for example, whose conditions challenge and
confuse the medical model, whose conditions, for example, are
"characterized by chronic, relapsing, and unpredictable course,
often with a poor prognosis"; whose conditions are "less
controllable by conventional medical treatments . In the face
of individual anomalies, clinicians may very well
respond ... by increasingly "psychologizing" the condition - Le., by shifting responsibility for etiology of £lare-ups [for example] to patientsf emotions, personality, or early psychological experiences. 5 9
And it is this "psychological" condition which is then
objectified, which is then made a part of reality.
Moreover, it is the emotions, the personality and the early
psychological experiences that are objectified as the causes of
the condition, that are "split off and reified as impersonal
causal agents responsible for the patientf s illne~s."~~ These
emotions, personalities and psychological experiences become the
reality, the reality, moreover, to which patients often succumb.
Patients often corne to explain '"their chronic ill-health by
def ining themselves as too "obsessive, " as "perfectionists, " as
"anal, " as "sensitive, " or as people who "hold to rnuch in"' . 6 1 Hysterics, similarly, fa11 into their prescribed role.
To sum up: Slavneyf s62 approach to hysteria is, 1 think,
particularly valuable. In his view, we need to see hysteria
from a variety of perspectives to see what each reveals. He
talks in particular about four perspectives within the field of
psychiatry - the disease perspective, the dimensional perspective, the behavioural perspective and the life-story
perspective. From the viewpoint of the disease-perspective,
however, which demands an etiology, he concludes there is
nothing much to see. It reveals little if anything about the
condition. Wandering wombs are a fabrication, and in their
absence, nothing else, no malfunction, no broken part, exists . Thus, we cannot conclude that hysteria is something someone has.
Still, it may be sornething sorneone is or does, by playing out a
prescribed role, for example. In any case, medicine, in having
claimed d i s e a s e (1 am speaking historically) for hysteria, 6 3 exceeded its \'compass". In "trying to Say everything, it . . . made
insupportable claims. " 6 4 In other words, it p a r a d i g m a t i c a l l y
extended and imputed into e x i s t e n c e a f a b r i c a t i o n . I t c o n c e i v e d
a c o u n t e r f e i t .
And this, I am suggesting, describes much of the history of
hysteria. While individuals have c e r t a i n l y behaved
"hysterically", the "disease" hysteria was little more than a
social construct created to rnake sense of certain aberrant
behaviors, a manifestation of particular social anxieties
exercised through medicine, a product of paradigma tic extension
inforrned by patriarchy, a product, moreover, emergent through
the social infiltration of women' s (threatening and semi-
t a n g i b l e - £rom this perspective) corporeal existence, and prescriptive of the role certain "deviant" women played out. As
such, hysteria was a socially-conceived-disease, the
manufactured fruit of a particular medical articulation that
went the way of extension.
These are strong claims, and they are premised rnost
significantly on the notion that there was (and is) nothing
biologically foundational to hysteria-as-disease. That is, the
construct hysteria-as-disease boasted no ties to veritable
malfunctions (besides the patriarchal notion that femaleness was
i t s e l f malfunction, which, of course, it was (and is) not) . Then again, perhaps 1 am too q u i c k to dismiss the biological
here. Maybe there was (and is) something foundational to
hysteria, something that underlayed it, some malfunction that
sought expression. But even if there was, let me suggest that
it was highly ambiguous, ambiguous in the sense that there was
nothing about the body that cried "malfunction" in the way that
it cries "malfunction" with TB, or heart attacks, or scurvy, or
strokes.
Relatedly, there is the issue of causality: did hysterical
malfunctions originate in the body, or were they produced
through living-out the hysterical role? (Or another option:
maybe they both originated in the body, and were produced
through living-out the hysterical role. . . . ) As noted, I take
the latter position. But let me note as well that my position
betrays a (potentially unwarranted) bias on my part, one that
may require further justification.
Menopause
Unlike hysteria, menopause is clearly associated with an
underlying biological reality. The reality that aging occurs,
that fertility loss occurs, that the cessation of menstruation
occurs, is undeniable. 65 1, therefore, consider rnenopause-as-
disease as less a construction than hysteria which, for me,
indicates variation within the category socially-conceived-
diseases. For this reason, 1 have decided to include it as an
example.
Menopause has ties in biological processes that really occur,
unlike a wandering womb. And yet, from a sociological point of
view, "menopause is a social construct and not a separate, 6 6 independent, biological entity". More specifically, the

disease menopause (referred to as an estrogen deficiency disease
or as an ovarian dysfunction6'), is a social construct. 6 8 ~t is a
"disease. " As Kauf ert and Gilbert put it : " . . .menopause can be interpreted as the imposition of a structure and a set of
boundaries on a reality that is essentially a m ~ r ~ h o u s " ~ ~ - on a
reality that is essentially semi-tangible. Questions like: how
should we address this reality? Does it constitute a disease or
just a normal part of life? are addressed, and essentially so,
in line with social assumptions. Such questions are not
answered so clear ly by the phenornenon itself, as in the case of
AIDS as we shall see, or stroke. In other words, menopause-as-
disease can be interpreted as the product of the social, of the
medical paradigmatic pervasion of real physiological processes.
It is, as with hysteria, a disease conceived through
medicalization, through paradigmatic extension by proponents
championing the medical model. This becomes clear when
contrasted to the alternative notion of menopause-as-normal as
discussed below.
When you think of it , the construction menopause-as-disease is not surprising. As a reality it demands attention, affecting
the "lives of women in a pronounced way. . . by ending menstruation and the ability to conceive . . . " Viewed in this way, "it seems
both predictable and logical that menopause should take on
special significance in the specific cultural traditions in
which the process takes place. "70 It is logical that, in our
society where medicine plays such a significant role, it should
take on the special significance of disease. And this it
certainly has.
Consider the following medical descriptions of the condition: 7 1
"The postmenopause should be regarded as a sex-linked endocrine deficiency disease which requires careful
evaluation, management and follow-up." (An Australian gynecologist )
The menopause Y s a hormonal deficiency state and, like al1 endocrinopathies, should be managed as vigorously as need be and without a necessary limitation of time." (Dr. Don Gambrell, Professor of Endocrinology and Obstetrics at the Medical College of Georgia)
And there are a plethora of other examples such as:
The menopause is an inevitable consequence of aging in the woman. Evidence demonstrating the adverse effects of the accompanying loss of ovarian hormone secretion has made the treatment of the menopause a major therapeutic and preventive health issue. 72
Kaufert et al. characterize this medical position well:
Within the language of medicine .. . menopause has been given many of the characteristics of a disease. Reading the medical literatuxe, a physician will find patients defined as menopausal in much the same fashion as they are labelled diabetic or arthritic. Symptoms are attributed to menopause just as they are attributed to gall bladder disease and stomach ulcer. In the literature, menopause is a condition to be diagnosed and treated. The phrases used to describe menopause, such as "ovarian f ailure" or "estrogen def iciency, " create an impression of pathology, which is heightened by menopause being blamed for an increase in the risk for coronary heart disease, osteoporosis, and urinary incontinence. Physicians are told that they must act preventively and protect their patients by replacing the lost estrogen. Al1 these words - diagnosis, prevention, treatment, symptoms - signify disease in the lexicon of medicine. 7 3
Having quoted this, we are faced with the question of how fair
such a statement is. Perhaps it makes too much of a
generalization where generalization is not wholly warranted.
Does the idea of menopause-as-disease really pervade the medical
establishment to the extent the above statement implies?
Such reservations notwithstanding, there remains little doubt
that the construct menopause-as-disease has received much
credence within the medical paradigm. And so rny focus is: why
treat it as a disease? The answer is quite simple as implied
already. The notion of menopause-as-disease fits well within
the rnedical view, a view that tends to dominate. Lt, moreover,
"irnplies a concrete medical course of action.ff74
On the other hand, medicine certainly did not always recognize
menopause as a disease. The mid-life women seeking medical
assistance for her troubles was commonly treated not so long ago
as a "stateless refugee" one denied "citizenship in the land of
the sick. ff75 She was a hypochondriac, a person devoid of any
legitimate claim to complaint. She was frowned upon, often
patronized.
But this al1 changed. The mid-life woman has become
medicalized, and her disease made the focus of a massive medical
undertaking. She has become the prime sub j ect for intervention
while the remainder of her life is characterized as problernatic
and dependent upon medicine for a return to normality. At least
much of medicine has corne to depict her life as such.
Statements such as the following, made as recently as 1994, are
indicative:
As the "baby boomers" are approaching mid-life and looking at menopause and andropause looming on the horizon, our society is suddenly demanding that the medical profession focus its attention on the golden age of life. Nearly one third of a womanf s life is now spent beyond the age of 50. In this context, we felt it was imperative to address specifically, and in a comprehensive rnanner, the rnedical issues which
76 pertain to the menopause.
The fact that the above is quoted in the preface to a book
titled Comprehensive Management of Menopause containing articles
by a range of medical experts that in large measure (but with
some notable exceptions), support and/or take for granted the

idea of the need for medical management, is even more
indicative.
How did we get to this point?
In Bellf sT7 oiew, menopause was defined as a "deficiency
disease" in the 1930s and 1940s, and has remained defined as
such ever since. The medicalization of menopause ernerged for a
number of reasons. In the first place, it reflected the
perspective of a small group of physicians who belonged to the 7 8 medical elite at that time. Bell goes on to Say that, given the
sway of these elite, their ability to publish their findings in
influential journals, etc., it was only too likely that their
definition would prevail." This does not mean they were being
entrepreneurial about defining menopause as such. It just means
they happen to have been influential in promoting what they
assumed was an appropriate way of understanding the phenomenon.
In the second place, and relatedly, medicalization was
wbstantiated by the discovery of a theory of etiology of
menopause. " [Ml ade possible by the paradigm of sex
endrocrin~lo~~"~~, the "disease" menopause was linked to hormonal
changes, and in particular, to the depletion of regularly
produced estrogen, the onset of which occurs with menopause.
This was further substantiated in the 1960s with the advent of 81 radioimmunoassay technique. In the third place, menopause-as-
disease - as an estrogen deficiency disease - was authenticated with the formulation of DES (diethylstilbestrol), an inexpensive
synthetic estrogen replacement which allowed for the management
and treatment of the deficiency state. 8 2
For coopere3, the introduction of hormone replacement therapy
(HRT) was the most significant step in solidifying the idea of
menopause as a hormone deficiency condition, a disease . Cooper,
moreover, considers it the greatest blessing, it being "a
practical working treatment already changing the lives of
coun t l e s s women. "84 She h a i l s it - from her very s p e c i f i c
f emin i s t pe r spec t i ve - a s a major f o r c e i n what she c a l l s
"Bio log ica l L ibe ra t i on , " providing mid- l i f e and o lder women with
t h e oppor tuni ty t h e y have been waiting fo r , the oppor tun i ty t o
rec la im t h e i r l i v e s , t o rec la im t h e i r womanhood. Like t h e
con t racep t ive p i l l , it bas f a c i l i t a t e d a second revo lu t ion , one
o r i e n t e d not t o change, b u t t o p reven t ing t h e dreaded "change of
l i f e . "85 Estrogen i s the key t o wornen' s h e a l t h and happiness,
Cooper says . Estrogen replacement therapy i s t h e g i f t t h a t
p l ace s t h e key i n t h e hands of women f o r l i f e . Comparing her
mo the r f s menopause with h e r own, Rowntree expresses t h e s e
sent iments wel l :
I t ' s b r ea th t ak ing how s w i f t l y t h e l i t t l e t r a n s p a r e n t patch 1 s t i c k on my burn d ispenses well-being throughout rny
system.. . I f m s o lucky, 1 t h i n k g u i l t i l y , next time 1 f a c e rny mother. She's looking a t m e cu r ious ly , h e r eyes f u l l of unmasked ques t i ons . You were born too e a r l y , 1 s i l e n t l y t e l l he r ; I f m going t o escape what happened t o you.
. . . Mother, 1 loa thed you once. You made my f l e s h creep. 1
wanted t o smash you, wipe you o u t . Never f e l t t h a t about anyone e l s e - nor about you s ince . It w a s your menopause.
And who i s t o thank f o r t h i s most prec ious of g i f t s ? One man
s t ands ou t : D r . Robert Wilson. And i f HRT i s t h e g i f t , then
Robert Wilson is t h e knight i n sh in ing amour . A t least t h i s is
how he i s dep i c t ed i n t he forward t o h i s book Ferninine Forever
by h i s f r i e n d D r . Greenbla t t :
Like a g a l l a n t knight he has come t o rescue his f a i r l a d y not a t t h e time of her bloom and f lower ing but i n h e r de spa i r i ng years ; a t a t i m e of h e r l i f e when t h e p r e se rva t i on and prolongat ion o f h e r femaleness are s o paramount. 8 6
These a r e de spa i r i ng years i n D r . Wilson's view. Every man
mar r ies a d e l i g h t f u l c r e a t u r e , an Aphrodite, a Helen of Troy, he
says , bu t when menopause k i cks i n , she fades. Her beauty, her
femaleness, fades. Her muscles weaken, h e r s k i n s ags , her bones 8 7 b r i t t l e and her vagina sh r inks . And more than that, she
achieves redundancy. Having l o s t her c a p a c i t y t o reproduce, she 8 8 o u t l i v e s he r b i o l o g i c a l use fu lness . Indeed, she o u t l i v e s her
use fu lness , per iod . Other mammals l i k e dogs, o r cows, can
reproduce a f t e r mid- l i f e . Women canf t . They a r e , t he r e fo re ,
"neuters" o r "eunuchs". While men remain m e n u n t i l dea th , women
degenera te t o t h e s t a t u s " ca s t r a t e " . 89
But e s t rogen t he r apy changes a l 1 t h a t , he goes on t o Say. It
may no t r e t a i n t h e woman's capac i t y t o reproduce, b u t it
s u s t a i n s he r p h y s i c a l i t y . H e r beauty i s sustained. Through it,
women a r e r e s to r ed , p u t t i n g them back on t h e road t o a l i f e 9 O worth l i v i n g . Through it t h e p a t h o l o g i c a l woman is rendered
normal. Without it, Wilson t e l l s us, wornen face "un to ld 9 1 misery".
Through t h i s s o r t of exaggerat ion of t he phys i ca l , and through
b u i l d i n g on and promoting severe sexual s t e r e o t y p e s , Wilson
propounded menopause as a de f i c i ency d i s e a s e r e q u i r i n g t reatment
by doc to r s . I n f a c t , Coney has i t t h a t Wilson "almost s ingle-
handedly cemented t h e idea of menopause a s a disease. "" H i s
i d e a s d i d n ' t ca tch on a t f i r s t wi th in t h e medical comrnunity;
none the less , h i s book sold w e l l while e s t r o g e n sales increased 9 3 by 400 pe rcen t between 1966 and 1 9 7 6 . In promoting t h e concep t ,
he a l s o compared menopause t o d i s ea se s l i k e diabetes.
"Diabet ics l a ck i n s u l i n ; t h e menopausal wornan lacks es t rogen.
Both. . .=an be rep laced . "" The cornparison was powerful, f o r
" [ w l r i t e r a f t e r w r i t e r [ s ince] has compared menopause t o
d i a b e t e ~ . " ~ ~ Writer a f t e r w r i t e r s i nce has t r e a t e d menopause a s a
disease.
And thus began what Coney r e f e r s t o a s the "menopause
i n d u s t r y . " By d e f i n i n g women a s d e f i c i e n t wi th t h e onse t of
l as t menses, as defect ive corne mid- l i f e due t o e s t r o g e n l a c k ,
t h e market, i n many ways, const ruc ted the range of p o s s i b l e
choice a v a i l a b l e t o women, Proponents w i th in medicine (and the
market) a s p e c t u a l i z e d and s o cons t ruc ted a r e a l i t y t o which
women were encouraged t o succumb f o r t h e i r own good. I n t h i s
way, they aspectualized the phenomenon menopause i n l i g h t of
es trogen d e f i c i e n c y , a phenomenon perhaps tangible t o m e d i c i n e
(perhaps even i n t e n s i f i e d into), and it was by v i r t u e o f t h i s
de f i c iency t h a t menopause w a s understood as a d i s e a s e . 96 For, as
t h e reasoning went, " the l o g i c a l response to a d e f i c i e n c y
cond i t ion is t o r ep l ace what is l o s t " ; hence, t h e app rop r i a t e
"response is t o r ep l ace t h e e ~ t r o ~ e n . " ~ '
This view has had a tremendous impact, be ing r e i f i e d and
propagated through t h e market . B y 1975, f o r example, "estrogens
had becorne t h e f i f t h most f requen t ly p r e sc r i bed drug i n t h e
United S t a t e ~ . " ~ ~ Through es t rogen therapy, women were able t o
r ep len i sh the lack. Through it , youth w a s no longer something
t o be l e f t behind. A s one woman desc r ibes i t s impact:
The drug companies have c l e a r l y done a sp l end id promotional job on hormone replacement therapy, because 1 never hear o r read a word a g a i n s t it. I t is a panacea. I t will make us a l 1 young and b e a u t i f u l f o r e v e r - and never mind the s i de - e f f ec t s . For every uncornfortable o r pa in fu l symptom ( inc lud ing s t a t e s of mind), t h e r e i s an appropr ia te drug. . . O h wow, have we got age by t h e t h r o a t ! Have w e got dea th a t bay! Al1 t h a t ' s needed is a chee r fu l , o p t i m i s t i c a t t i t u d e and loadsamoney. 9 9
Moreover, accord ing t o the market, women need it because
[slornething t e r r i b l e happens t o women a t around the age of f i f t y , something superadded t o t h e process of aging, which
t u r n s them i n t o monsters . I t i s t h i s : they a r e no l onge r women ( i n t h e sense of be ing de s i r ab l e p a r t n e r s f o r men), yet they persist i n behaving as i f t hey were. 100
This i s med i ca l i z a t i on , medical paradigmatic ex tens ion i n i t s
p u r e s t iorm. Here,

the definition of menopause as an estrogen deficiency condition turns it from being a stage in the normal processes of aging into a hazard to health and associates it with such long-term deficiency conditions as diabetes or amenia. Menopause becomes a disease and, therefore, the legitimate concern of the medical profession rather than a private experience of the individual woman. 101
Here, what we have is a normal process - menopause - socially imbued and thus constructed into a fiction. Through medical
paradigmatic extension we have a normal process constructed into
menopause-as-disease. Informed by patriarchy, those who
propound this view so c o n s t r u c t s menopause, and s o nourish
patriarchy in return. And it is this construct, this
reification, that women have faced, and continue to face. "Fear
[is] planted in the psyche of the mid-life woman. If she
ignores the siren cal1 of the medical industry, offering her
longer life and the prolongation of her youth" she will pay for 102 it somehow in the end. Furthemore, as she is estrogen
deficient for the rest of her life, she must, in this view, give
herself over to permanent medical management.lo3 Otherwise she
will invariably yield to the disease.
- And, t e go en7 t h 5 s j;S 710t a pretty disease, s h g is told ( & c e
again, by those who propound this view). Her beauty decline
aside, menopause is also responsible for '"a bizarre train of
symptoms which may completely upset the normal equilibrium of 104 even the well-balanced individual"' . Women have only to look
forward to hot flushes, night sweats, insornnia and lessening o r 105 loss of libido; depression, dizziness and incapacitation; 106
anxiety, increased tension, mood swings, emotionality and
irritability. 107 At least, this is what much of the literature
says, what the market has propounded. 108
The point, however, is that this picture of menopause is the
progeny of a specific paradigmatic extension. For if it
werenft, if it were the adequate reflection of a specific
paradigrnatic intensification, one would expect most, if not al1
women, to actually experience these symptoms. Women certainly
do experience thern, yet the fact is, it is only a small minority
of them who do. 10 9 The cross cultural data suggest that few, if
any of these symptoms, are reliably universally associated with 110 menopause. These symptorns seem, in many ways, culturally
specific, with the bulk of them native to western culture. : 11
These are suggestive claims, so let me justify them.
According to an alternative perspective on menopause: "most of
the symptoms of menopausal syndrome are a response to
psychosocial factors, 11112 Few, if any, have ties in the
biological. The clairn, more generally, is that the symptoms
experienced by women during menopause may have more do to with
the meanings and roles attributed to menopause in western
culture than anything biological. T h i s is indicated by the fact
that, in other cultures, where menopause is given different
meanings and roles, the same symptoms do not present. I have
already alluded to this in Chapter 3. However, to elaborate:
arnong Indian women, menopause prec ip i t a tes a role change, a
change for the better, one that allows women to "freely leave
their veiled seclusion, visit and joke with men...". i 13
Similarly, menopause can have positive meanings for Chinese
women. In Chinese culture where age is respected, "menopause
may be seen as a transition to a higher status. ,114 Women in
parts of Micronesia, Taiwan and rural Mexico also benefit from
menopause and the freedom it grants them. ils In such cultures,
where menopause is looked upon favorably, women do not
experience many (if any) of the symptoms outlined above. The
same goes for women from Yucatan and Evia, who "see menopause as
a life stage free of taboos and restrictions, offering increased
freedom to participate in many activities such as going to
church and visiting friends . ""' In both societies, old age is respected, and so menopause offers entry into a better life.
The same also goes for Indian South African women, especially
the younger women who see rnenopause as a positive life event
that hinders them in no way, that in fact liberates them to
pursue their professions or other interests. Upon rnenopause,
these women come into their own, no longer tied to certain
biological functions or roles. For many such women, life before
menopause is "being dominated and punished as a child,
physically abused as a bride, and frequently ignored as an adult
h~memaker.""~ It is a life of resentment. It is "only in the
post-reproductive stage her life that a wornan...soon to achieve
the enviable statuses mother-in-law and grandmother, cornes into
her own. "'la Finally, an implied consideration is that menopause
may have positive significance in many countries where
contraceptive use is limited. For such women, menopause can
mean f reedom from having children . Of al1 the symptoms attributed to menopause, the only one that
seems to achieve something close to universality is the hot
flash or hot flush. :19 But even this symptom varies cross-
culturally. The Japanese, for example, have "no one phrase
[that] unequivocally signifies the hot flush" since it occupies L2G little importance in their view. Nor do menopausal women
everywhere view hot flushes in a negative way. In Wales they
signify good health and are, therefore, sornething to b~ valued,
not disdained . 121 In North American society, however, where menopause has
received a more negative valuation, a higher ratio of women
experience these symptorns. And where menopause represents
decreased status, where it is devalued and contributes little or
nothing to greater freedom for women, the symptoms are more
prevalent.
At the same time, it is important to point out that even
within North American society, most menopausal women do not
experience such symptoms, despite the marketing. In the United
States it is estimated that 85 percent of wornen experience few
or no problems with the onset of last menses. 12 2 Moreover, women
who do experience adverse symptoms are more likely to be women
who fa11 into socially less privileged groups, or who have had
long-standing dif ficulties (emotional, financial, etc. ) . Still,
menopause is promoted as problematic for al1 women, a problem
encapsulating the various symptoms constituting menopausal
syndrome. This notwithstanding the fact that the majority of
women manifesting such symptoms are women who report poor health 123 - chronic illness, depression, etc. - prior to menopause. As
Hunter summarizes:
Overall, women are not more likely to be depressed during the menopause than at other times. The most relevant factors influencing a womanfs quality of life during the menopausal transition appear to be her previous emotional and physical health, her social situation, her experience of vasomotor symptoms, and her beliefs about the menopause. Psychosocial factors are the strongest predictors of rnood and well-being during the menopause transition. 124
Having said al1 this, it is also important to recognize that a
transformation may be taking place within the biomedical
paradigm in Western society. Menopause is being seen less and
less as a disease, and more and more as a disease-causing 12 5 agent, with the disease it is ostensibly causing being
osteopoxosis. For those advancing this medical point of view,
estrogen therapy is legitimated because it prevents
osteoporosis, a condition in which bone loss occurs, leading to
increased risk for fracture. But the social consequences of
this construction rernain the same for women. Women still need
to be educated in order to adopt estrogen therapy. They need to
submit themselves to this particular manifestation of medical
management. Silverman et (in 1990) claim that only 12% of
postmenopausal females at any one time take long-term estrogen
in the United States. They Say the goal of the Department of
Health and Human Services is to increase that number up to 30%
by the year 2000. For this to occur, women need to see
menopause as a medical condition, and their doctors "as the most
important person in a womanfs decision" regarding her estrogen
use. They go on to talk about various
in order to convince their patients to
treatment . But this is yet another construction,
paradigmatic extension within medicine
socially-conceived to be more precise.
methods doctors can adopt
comply with this
another consequence of
- another phenornenon And it is so in so many
ways. For, how serious a problem is osteoporosis? In asking
this, 1 don't intend to imply osteoporosis does not exist, nor
that it is not a serious condition. Osteoporosis, I think, is a
legitimate medical condition, one specifiably tangible to
medicine, one that medicine has intensified into. Its
characterization and link to menopause, however, is
questionable, exaggerated. In the var ious campaigns promoting
hormone replacement therapy, for example, women are bombarded
with pictures of a hunched over old woman suffering £rom 127 osteoporosis. Thus figuratively legitimated, estrogen therapy
is promoted as the panacea. Indeed, the "imagery is so powerful
that we donft stop to think how often in real life we actually
see a wornan with a dowager's hump. We donf t see one very
often. Coney reports that only "5% to 7% of 70-year olds will
show vertebral collapse". And she goes on: "1 have a very big
referral practice, and I have very few bent-over patients ... ,,129 Once again, the cross-cultural evidence serves to further
deflate the medical construction under scrutiny here. The
simple fact is that there are societies in which osteoporosis
does not present itself nearly to the extent it does here. In 130 some, it is basically unknown. For example, while Asian women
in North America are at risk for it, "their counterparts in
China or Japan rarely develop osteoporosis . "13' This may suggest
something about the medical paradigm in such countries. (It may
Say something about how physicians are not trained to see the
condition osteoporosis in the way physicians are trained to see
it in Western society). On the other hand, it may also Say
something about the tenuous relationship between estrogen
deficiency and osteoporosis. The incidence of osteoporosis may
have more to do with factors other than estrogen deficiency,
such as calcium deficiency, physical activity, fertility, 132 genetic make-up, etc. .
Even more ironic and suggestive is that osteoporosis occurs
amongst men. Men have about one half the number of hip
fractures as women. They are also more l i k e l y than women to die 133 from hip fractures. Yet the picture generally painted depicts
osteoporosis as a womanfs disease caused by loss of estrogen.
And since, according to this perspective, menopause, and thus
estrogen def iciency, is universal to women, estrogen replacement
therapy is touted as the cure-all. It is clearly not the cure-
al1 as the cross-cultural and inter-sex evidence suggests. That
we should aim to treat al1 women with estrogen therapy is
therefore, fallacious . 13 4 In short, according to these perspectives within medicine
under scrutiny here (perspectives that have also been
extensively promulgated through the menopause industry):
menopause is not a normal life stage but a disease (or disease-causing condition) that affects al1 wonen;
women at mid-life have the possibility of ill-health hanging over them;
medical surveillance of [womenfs] lives is necessary to ward this off. 135
This is medicalization in its purest form. This is m e d i c a l
paradigmatic a r t i c u l a t i o n a s extens ion in i ts pures t form.
Working £rom a profound paradigmatic orientation to disease, to
redress lack, medicine latches ont0 the phenomenon menopause,
imbues the aspect estrogen de£ iciency, aspectualizes it, and
renders the mid-life-until-she-doth-die woman diseased in light
of it. Menopause-as-disease is the colonization, construction,
of an otherwise natural phenomenon. The natural is transmuted
into menopause-as-disease. And, from the perspective 1 am
espousing, it is "natural" - "normal" - because disease is deviation from the normal, the standard, the typical, the
natural. 1 suggest, with Kaufert, that it is quite normal,
standard, typical, natural, for a woman's ovaries to fail 136 between 40 and 60. For her estrogen levels to decrease. 1 Say
this because they do so throughout the world, and they do so
consistently. As Coney puts it:
Natural bodily processes and physiological changes such as menopause should be defined by what ordinarily happens, not by experience which is d i f f e r e n t , A better word than symptom would be "signs" of menopause, meaning indicators or signals of a normal event. 13 7
The message, according to medicine, is that il1 health is the
fate of post-menopausal women (and their "signs" symptoms to
treat), their fate unless they subject themselves to its
understanding and its solutions. It says: for women's
(estrogen) lack, medicine possesses the (estrogen) cure. Women
need only succuxnb to it to avoid the perils of the menopause and
post-menopause years. This is the case, incidentally, and
ironically so, even though men experience similar troubles at a
similar stage in life. If men "are forgetful, and find
themselves putting the milk into the cupboard rather than the

fridge, [we] may laugh it off as old age or as too trivial t o
worry about." I f women do the same thing, we are only too
likely to "blame it on menopause. ,f 138
This is not to Say that the suffering of women at time of
menopause should be discounted. There are women who do suffer,
who may very well benefit from medical treatment, and
specifically, hormone replacement treatment. And the last thing
we should want by describing the process as "normal" is to deny
the legitimate experiences of suffering women. But they are, by
no means the majority. There are other women who see menopause
as a liberating thing, as a time of rebirth, as a process that 13 9 sets them free. And because many women see menopause this way,
it seems inadequate t o the experiences of women to construct i t
as a disease necessarily subject to rnedical management. 1 4 0
In wrapping up, 1 want to reemphasize that when 1 refer to
medicine, 1 am referring to a perspective within it. Medicine
is not some monolithic hornogeneous enterprise. There is
diversity within it. There is, consequently, a diversity of
ideas about menopause within it. Matthews et depart
somewhat £rom my depiction of the medical view so far. They
underscore the multifaceted nature of menopause, and the
variation in the way different women experience it, with many
seeing it in a positive way. This, they stress, has treatment
implications. Yet the construction of menopause-as-disease (and
more lately, menopause-as-disease-causing-agent), has played a
powerful role in both the rnedical and (through the market), the
public imagination. As such, it is a major exanple of medical
paradigmatic extension, being the product of the medical
imbuement and aspectualization of a semi-tangible biological
reality. While 1 would say estrogen deficiency itself is an
instance of something specifiably tangible to medicine, its
implications, what it means and entails, are very much
ambiguous. This means they are ripe for construction. And they
are constructed: our patriarchal society demands explanation for
bodily changes, especially bodily changes in women. Through the
process of medical paradigmatic articulation, and specifically,
of medical paradigmatic extension, the reality of menopause has
been (and still is) transfomed into a socially-conceived-
disease.
But while claiming it a socially-conceived-disease, 1 would
also l i k e to maintain that it is less socially-conceived than
hysteria (which, to reiterate, is why I chose menopause as an
example). As mentioned, there is variation in the degree to
which diseases are constructed within this category. There is
variation because menopause is indisputably tied to a biological
reality, to a biological reality that demands attention, that
demands social response. For this reason, its construction as a
disease may have more validity - it may make more sense, for
lack of better words - than the construction hysteria-as-
disease - a condition with no tangible ties in the biological. Undeniably, hysteria has been variously associated with
otherwise unexplainable physical or psychological symptoms.
Contrarily, it also produces physical or psychological
su£ fering. It has, however, no verif iable grounding in a
distinct biological reality Iike menopause dues. 1 4 2
Finally, despite the divergence between them, both can be
categorized as socially-conceived-dises since they do not
exist as diseases "out there". They are constructions i n the
most fundamental way, manifestations of paradigmatic extension
that symbolize (and function to deal with) particular social
anxieties. They are wholly imputed into existence. Whether or
not they take on the status of disease is more a matter of
values, politics, paradigmatic expectations, than anything else.
Rere the social infiltrates the (semi-tangible) real and
produces the sham; it then objectifies the sham - the socially-
conceived-disease.
SOCfALLY-MANIPtTLATED-DISUES
Introduction
And it is this that sets them apart from the remaining two
categories of disease - socially-manipulated-diseases and
socially-augmented-diseases (not to mention socially-transfixed-
diseases). The latter two share in common the following: they
both involve real diseases, diseases that exist "out there".
Both constitute malfunctions of the biological. What
differentiates them is the degree to which social construction
grabs a hold of them and bends them about. What dif ferentiates
them is the degree to which social construction has its way with
them as diseases .
Socially-manipulated-dises are very much under the sway of
social construction. Why? Because they are tangibly
threatening while, concurrently, shrouded in mystery. The fact
that they are diseases is relatively tangible, and often
generalizeably so. Upon experience with thern, few to none would
deny their detrimental impact. Contrarily, the why of them, how
they operate, their cures - these aspects are not so tangible.
These aspects are much more indeterminate. As such, the disease
phenomenon is a semi-tangible phenomenon, subject to intense
construction. Because they are so threatening to health,
because they so obviously cause suf£ering, there is a drive to
deal with them. Because it is not so clear how to deal with
them, because received knowledge and practice proves inadequate
to address them, because they are semi-tangible in these most
critical ways, this makes them are al1 the more threatening. So
they are dealt with otherwise. The social takes them over in an
attempt to make sense of them, to render them paradigmatically
meaningful. In this way, they become diseases manipulated in

line with social anxieties, diseases 'heavily burdened by 1 4 3 metaphorical thinking", diseases dripping with sociopolitical
rhetoric, diseases immersed in cultural meanings, assumptions ... . . . and rnorality. And as moral diseases, they become
stigmatized diseases, and their victirns - deviants. Epilepsy,
diabetes, cancer and leprosy are al1 classic examples. Today,
AIDS is the prime example. It is also the one that 1 give
special attention to in this section.
MDS
AIDS is a disease - and it is a disease in the sense defined -
caught up in a whirl of metaphors and meanings. It is a disease
deeply infiltrated by the social, a disease profoundly
rnanipulated in conformity with social meanings and assumptions.
There has been no avoiding the AIDS phenomenon.
The facts are sobering. Since its existence was first detected in 1981, acquired immune deficiency syndrome has become a global phenomenon and quite likely the rnost serious new menace to human h e a l t h around the world to appear in this
1 4 4 century ... Indeed, "AIDS has made us the unwilling spectators of a seldom
occurring event: the outbreak of a new illness, its sudden ,,i45 irruption into public l i f e and collective consciousness.
AIDS as a threat to health and well-being is, to Say the
l e a s t , evident. "The emergency is real. As a disease that
kills it boasts something very c lo se to generalized tangibility.
Y t doesn't matter from what angle you look: AIDS is a terrible
thing. ""' Its deleterious stipulations are too portentous for us to construct it otherwise. It seems unlikely, for example, that
anyone could reasonably transform it into a psychosomatic
illness, and then sustain the construction. The construction
AIDS-as-psychosomatic-illness would be short-lived, being a
construction fundamentally contrary to the actual demands of the
phenomenon. For dernands it makes. Powerful demands. So
powerful that AIDS is reshaping "many aspects of society, its
institutions, its noms and values, its interpersonal
relationships, and its cultural representations . "14' ït is
penetrating the social, "altering our awareness of the social
body from one of health to one of fatal di~ease.""~ Like it or
not, AIDS is forcing us to adapt.
Contrast this to hysteria. Hysteria has no status as a
disease 'out there" in the way AIDS does. "AIDS is real, and
utterly indifferent to what we Say about it."l5' It also
constrains what we Say about it. Conversely, hysteria as
disease is totally dependent upon what we Say about it
(although, as a reified construction, it certainly imposes
constraints on what we say about it; but it does so as a reified
construction). Cease the talk and the "disease" hysteria dies.
Cease the talk and the disease AIDS lives on.
But while tangible as a disease, AIDS is fraught with
ambiguity. The "what" of it as a disease is semi-tangible.
This has proved very distressing. 151 Here we have an infectious
condition that kills for which there are no known cures - a disease that has so far evaded the benefits of the medical
approach. As such, it has become a significant social concern.
We have had to deal with it in some way. Anddeal with it we
have - by constructing it in line with predominant assumptions; by manipulating and thus fashioning the phenomenon into
something distinct £rom what it could be ... by enveloping it in metaphor. For ' [ w l e repair to rnetaphor constantly . . . especially in discussions where meaning is inherently up for grabs ... ,, 15: Especially when faced with threatening diseases riddled with
semi-tangibility. Then the social goes to work, and rigorously
so. We feel compelled to "struggle to achieve some sort of
understanding of AIDS, a reality that is frightening, widely
publicized, and yet finally neither directly nor fully
knowable . ''153 Then, various moralities go to work:
Medicine, as we have seen, "imagines itself able to
describe ... natural categories without being implicated i n its
own descriptions, able to penetrate to their essence while still
only reflecting them in their natural intact tat te."'^^ It imagines itself able to intensify. But paradigmatic
intensification is something it (any paradigm) only more or less
accomplishes, depending on the essence in question. And with
AIDS, there is much to suggest that medicine has accomplished
little intensification, at least compared to the amount of
paradigmatic extension that has taken place - the ideological extension. Like cancer, AIDS carries with it "a heavy burden of
moral anxiety . . . 1,155 As a devastating disease imrnersed i n semi-
tangibility, it is subject to technical discourses imbued with
prejudicial meaning. In the face of bewildering threat, in the
Pest to contain it, resolve it, rnedicine (we) , invariably lapses into a blame mode. For to focus blame, to adopt the
moral stance, helps to resolve (however tentatively) some of the
~~erta~t_-- - - - - - - - - - - - - - - - - - - - - - -
This means, in turn, that AIDS as a semi-tangible phenomenon
also serves as an ideal vehicle for the propagation of certain
moralities. As an indeterminate, semi-tangible, reality, it
provides the ideal stuff out of which to construct that which
legitimates various ideological b i a s e s . Thus, "AIDS . . . [ cornes]
to symbolize whatever [is] threatening or sharneful . . . [ not to
mention] its victims [who become the] targets of accusations and
discrimination. "lS6 The examples in this regard, the i d e o l o g i c a l
manipulations, are numerous. AIDS has been characterized, for
example, as:
A gay plague, probably emanating from San Francisco
A condemnation to celibacy or death
A fascist plot to destroy hornosexuals
A CIA plot to destroy subversives
A disease that turns fruits into vegetables
The price to be paid for the sixties
A Soviet plot to destroy capitalists
etc. 1 5 7
In each case, AIDS is employed as a justification for social
prejudices. As one anonymous doctor employed it: "We used to
hate faggots on an emotional basis. Now we have good reason. ,, 158
Moreover, persons with AIDS are similarly manipulated,
manipulated into much more than persons afflicted with a certain
disease, much more, that is, than "person [ s ] experiencing the
progressive exposure of fragile vital organs to the ravages of
common infections. "15' TO say someone has AIDS means
that he or she is a certain t ype of person, socially and morally defined. Tragically, for those afflicted, it is also to Say that he or she is dangerous and untouchable. But it also means still more, for the metaphoric predication of AIDS opens a door to the dark musty cellar of cultural associations of the profane, the defiled, the denied, the unshown, the f orbidden, the f eared. 160
The victirn is stigmatized, and heavily so. The victim is 161 contaminated, and so s/he is feared. S/he is a penalized body,
the one to be blarned, the site of contagion, the one t o be 162 despised. S/he is a manipulated-body.
Now, while fueled by the serni-tangibility of AIDS, it is also
the case that these, and other metaphors, perpetuate the semi-
tangibility of AIDS. What emerges is a vicious circle: the
semi-tangibility of AIDS is resolved in (prejudicial) metaphor;
(pre judicial) rnetaphor in turn hinders (medical) paradigmatic
intensification into AIDS as a reality.
Metaphor perpetuates semi-tangibility because it highlights,
imbues and thus constructs according t o prevalent assumptions.
It constructs, for example, by prrld11cing certain images t h a t
socially fixate on certain phenomenal aspects while directing
attention away from others. It saturates and aspectualizes some
information - information that appears to substantiate certain asswnptions - and does so while masking, or diminishing, other
information. In other words:
.. .metaphor tends to designate, by exclusion, the "irrelevant" and close off our attention to it . . .Metaphor focuses our attention by crystallizing specific constellations of meaning and orienting our thought in particular directions, while simultaneously obscuring or blocking Our orientations to other possible avenues of seeing and knowing. Li?
Metaphor aspectualizes the constructed semi-tangible. "4 The
metaphoric affirmations of AIDS as a disease of the "dangerous ,,165 other, ,,166 or as a "gay plague, have done just that. They have
influenced profoundly the perception of AIDS and hence,
investigations into it as a disease. They have hampered
intensification into its foundational realities . One such reality includes the varicus ways by which the
disease is transmitted. The characterization of AIDS as a gay 167 and drug user's disease, for example, has had profound
implications for intensification into the realities of HIV
transmission. Initially fueled by early AIDS research conducted
mostly in the U.S. and Western Europe "where t h e high risk
populations were gay men and IV drug users who shared needles
for inje~tin~"'~~, the characterization has had the consequence
of directing attention to particular modes of transmission,
emphasizing t h o s e modes, excluding others, and thus creating the
illusion that the "virtuous" heterosexual population was safe.
This notwithstanding the fact that the majority "of AIDS cases
around the world resulted from heterosexual activity. ,,I69 In
fact,
[wlhen the World Health Organization announced that 80 percent of AIDS cases worldwide were found in Africa and had been heterosexually transrnitted, the Western public reacted in disbelief, did not attend to the facts because they concerned members of a remote, distinct population, or added Third World and African to the multiple stigma. 170
Similarly:
Between mid-1983 and mid-1986, the anomaly to [the] explanation [transmitted sexually by gay men] posed by the existence of heterosexual Haitian and African cases was avoided by assuming the Haitians were lying and the Africans
17 L were engaging in heterosexual anal intercourse.
In other words, the anomaly was in various wayç suppressed,
rationalized, modified. There was no roorn for it "as it was"
within the prevailing metaphoric construction of AIDS.
In this and other ways, metaphoric constructions of the AIDS
phenornenon have plagued research into its mode of transmission,
dramatically affecting, for example, the classification of AIDS
cases. As Murray and Payne explain:
The identification of AIDS as a "gay disease" has been continuously reinforced by the C D C f s classification system. Rather than report al1 cases with each characteristic, AIDS reports in MMWR suppressed interaction effects (e.g., a gay IV drug user was categorized as a gay case, a Haitian IV drug user as an IV drug user, etc.). Such tidy classification precludes independent judgment of the relative weight of risk factors and of their prevalence in the population at risk. 172
It was not until 1986 that the Centres for Disease Control
expanded its "4-H l i s t" of high risk categories, namely
homosexuals, hemophiliacs, heroin addicts, and Haitians. This
list, \'structured evidence collection . . . and contributed to a view that the major risk factor in acquiring AIDS is being a
particular kind of person rather than doing particular
things . f '173 The image of AIDS as a "gay disease" or one of the
three other "discreditable person diseases", "proved too
alluring to abandon. ,, i7 4
Such metaphors have also hindered investigation into the
actual "whatness" of the disease. For example, when the disease
was f i r s t identified as G R I D (Gay Related Immune Deficiency) , little attention was paid to it. When it was later recognized
as a threat to the heterosexual population and renamed AIDS,
"enormous increases in research funding enabled scientists to
identify several variants of the syndrome and to describe some
of the complex ways it can damage the body"17'. The
redefinition, the social reorientation to the disease, prompted
and facilitated (relatively) greater intensification into more
of its aspects.
But the history of AIDS is largely a history of clinging to
cornfortable metaphors. Despite the evidence
that AIDS constitutes a threat to the health of f a r more individuals (al1 of us?) than those lumped in received categories of the afflicted "other," American discourses on AIDS continue to reproduce metaphoric predications of the disease based on little other t h an images of the profane (i.e.
illicit sex, drug abuse, etc. ) . 176 And it has taken a lot to shake these metaphors. They have
become our reality, luring us into illusion. But they have not
remained immutable. Perhaps one of the most profound threats to
prevalent AIDSt constructions was Magic Johnson's announcement
that he was HIV positive and that he had contracted the 177 condition through promiscuous heterosexual activity. This
event was "deeply disconcerting because it notified everyone
that their assumptions about AIDS were erroneous and their
metaphors mechanisms to instill a false sense of security. ,178
His announcement spoke loud ly on behalf of an anomalous reality,
and did so with anomalic tangibility. It posed a powerful
challenge to the prevailing construction - social manipulation - of the AIDS disease.
In fact, these and other AIDS' metaphors have been challenged
more and more. The picture of AIDS has become much more
complicated of late as new types of AIDS "cases" have been 179 acknowledged. Consequently, new rneanings have been "built up
around AIDS and forced upon everyone, even if some [have] wanted
to deny it." New metaphors have emerged that highlight
something ominous, that highlight 'a concrete threat that
concern [s] everybody, not just homosexuals" a threat, moreover,
"against late twentieth-century values and culture. " Reference
has been made to the "AIDS effect" and the "AIDS social
phenomenon", for example. It might be said that AIDS has become
a new disease as the demands of reality - powerful, tangible
anomalies - have progressively exposed the inadequacies of its
previous social formulations.
At any rate, AIDS needs to be understood as a duaL phenomenon
- a biological malfunction, a disease in the purest sense of the
word, and as a social phenomenon, a social manipulation. Put
another way, it is a disease that has entered our world "on two
primary levels: as a biological event that infects Our bodies
and as a social event to which a variety of rneanings is 181 attached" according to Our social predilections. Put yet
another way, 'it is simuitaneously an epidemic of a
transmissible lethal disease and an epidemic of meanings or
signification. " lB2 The f ight against AIDS, theref ore, "has been
as much a fight against the misperceptions, misrepresentations
and misuse of the disease as against a pernicious biological 1 8 3 enemy .
Here we have a disease that is constructed as a disease, but
far less so than hysteria or menopause. It is relatively less
constructed than either of them because it is, undeniably -
tangibly, and acutely so - a disease. Like hysteria it is
heavily social. Unlike hysteria, it boasts undeniable roots in
the physical. 1 like the way Rosenberg puts it:
If diseases can be seen as occupying points along a spectrum, ranging from the most firmly based in a verifiable pathological mechanisrn, to those, like hysteria or alcoholism, with no well-understood mechanisms but with a highly charged social profile - AIDS occupies a place at both ends of the
184 spectrum.
It occupies a place as a socially constructed d i s e a s e , not a
fabrication or socially constructed "disease". It occupies a
place as a socially-rnanipulated-disease.
To sum up: AIDS is a socially-manipulated-disease, a disease
subject to intense social construction. As a threat, as a
disease, it is highly tangible. Otherwise, what to make of it
is highly semi-tangible in many ways. This makes it highly
amenable to social construction. Because it is so tangibly
threatening and yet so ambiguous in terms of what it is, there
is a powerful social drive to deal with it. It is, therefore,
constructed - infused with social meanings. It is latched upon
and paradigmatically manipulated into a meaningiul reality. It
is then understood/treated in light of that which is manipulated
about it. This means there is little paradigmatic
intensification (relatively speaking) that goes into a socially-
manipulated-disease. Instead, the disease (AIDS) is very much a
product of paradigmatic extension, its constructed semi-tangible
aspects aspectualized.
Introduction
With socially-augmented-diseases, however, the situation is
different. Once again there is aspectualization, but this time
there is aspectualization of aspects that are seen relatively
tangibly, of aspects that are (or have been) intensified into.

A socially-augmented-disease is constructed in so far as some of
its aspects are diminished while the aspect (s) seen is (are)
augmented, or socially exaggerated to the point where it (they)
becomes (become) the phenomenon. In other words, the disease
phenomenon is the aspect(s) seen (intensified into) . At least this is the first sense in which 1 mean augmentation.
The other has to do with meanings-attached, which 1 will get to
later.
Certain Infectious Diseases
... I would suggest, are good examples of socially-augmented- diseases in the first sense, especially as medicine knows them
today . Herefs how. Like al1 approaches, the medical approach is
lirniting in many ways. It adheres, for example, to a certain
doctrine - the doctrine of specific etiology (the notion that
each disease has a specifiable cause like a germ). This has
been discussed. But while limiting with so many diseases, while
blinding medicine to certain realities, it seems reasonable to
suggest that this doctrine also facilitates medicine's
intensification into other realities. The doctrine may be
particufarly suited to understanding certain diseases, and more
precisely, certain of their aspects: some disease aspects may be
specifiably tangible to the medical approach by virtue of its
adherence to the doctrine of specific etiology.
Medicine, for example, has identified tuberculosis (TB) (of
the lungs) as a condition caused by the bacterium mycobacterium
tuberculosis, or tubercle bacillus transmitted by "droplet
infection" (through sneezing, coughing, etc. ) . The bacterium,
according to medicine, is breathed into the lungs where it
multiplies and forms an infected area, leading to coughing,
chest pains, shortness of breath, loss of weight, fatigue, etc.
And if not thwarted by the body's immune system, medicine goes
ont0 explain that it can spread to the lymph nodes through the
vessels of the lymphatic system. Similarly, medicine has
identified typhoid fever as a condition caused by the
consumption of water, milk or food contaminated by the bacterium
s a l m o n e l l a typhi, or the typoid bacillus; and pneumonia as an
in£ lammation of the lungs that can be caused by, among others,
the bacterium streptococcus p n e u m o n i a ; and diphtheria as an
acute bacterial condition caused by the bacillus corynebacterium
diph therae.
Are these identifications constructions, or do they constitute
vexitable intensification' s into certain realities? Well,
everything is constructed to some extent or another. The very
naming of sornething - of a disease, of a bacterium - involves some degree of construction. It involves, at minimum,
aspectualization - choosing and highlighting some aspects of the phenornenon over others. But the point is this. It may be,
indeed it seems likely, that medicine has paradigmatically
intensified, at least somewhat, into these four diseases. It
seems likely that it has acquired some legitimate knowledge into
some aspects of their workings, into some aspects of their
causes, i n t o at l eas t p a r t of w h a t they are about. And why not?
Take away the causal bacterium identified by medicine in any one
of the four cases listed above, and the corresponding disease no
longer exists. Administer the appropriate vaccination, and the
disease is inhibited. In each case, medicine seems attuned to
this reality, to this aspectual demand. In each case,
medicinefs construction of the disease is constrained - purified - by virtue of having access to the workings of at least part of
(to an aspect ( s ) of) that disease. This separates such a
disease from other "diseases" like hysteria where causes are
purely socially irnputed. It separates it, as well, from a
disease like AIDS the etiology of which, the means of control of
which, and mode of transmission of which, have been (and very
much still are in the case of the former two), inadequately
understood as a consequence of metaphoric pre judices . Now, 1 donf t want to be too hasty on this point, especially
given the fact that 1 have included TB as an exarnple of a
socially-augmented-disease. In the first place, 1 would suggest
that TB, being one of the oldest of known human disea~es'~',
spent the bulk of its known existence as a socially-manipulated-
disease. In the second place, given its recent heightened
prevalence due its link with A I D S , 1 would also suggest that it
may be degenerating back to one of social-manipulation. In both
cases (historically, and most recently), it is a disease that is
clearly a disease, a tangible threat to corporeal existence, 18 6 recognized as the greatest killer, and yet, a disease shrouded
in rnystery - in semi-tangibility. It is only until quite
recently, and for only a brief time - maybe thirty years - that medicine manâged to elevate it to a place among the socially-
augmented.
Historically, TB underwent numerous social manipulations, was
associated with varied metaphors, was transformed in so many
socially convenient ways. In the eighteenth century, for
example, TB, understood primarily as consumption (a disease that
ravishes the body), was socially constructed into a disease of
passion, of romance, and persisted as such. It was reified
". . .as a sign of superior nature, as a becoming frailty." It
became the "the sensitive young ar t i s t ' s disease [as evidenced
by] O'Neill's Long Day's Journey i n t o N i g h t . ,, 187
The disease was also made very specifically into a spiritual
phenornenon, a condition that incited "pleasing melancholy, even
pious exhilaration. "las
[O] f al1 diseases tuberculosis had a reputation more calculated to draw admiration than repulsion ... For among
illnesses, tuberculosis was seen as the most spiritual, the most ennobling, a purger of base qualities and a distiller of
189 lofty ones.
So transfigured was it that its hideous physical symptorns became
secondary matters. Instead, consumption was held to progress
within the individual in such a way that "the encumbering
accretions of his personality melted away, revealing the
spiritual matrices out of which the transitory and illusory
accidents of his character had been formed. "lgO
It was also made into the disease of nobility where nobility
meant the ability to consume in an extravagant manner. The
reasoning: '[if] a wasteful consumption of food, drink, and
fancy goods is proof of nobility and refinement, how much
greater a leap in distinction must it not be if one can
similarly waste onef s own body? "lgl The disease was a harbinger
of death. It was, concurrently, an engineer of human
distinction,
These are just some of the ways in which TB was constructed in
the last couple of centuries.
To continue: such constructions rernain intact only until that
which causes the disease, how to clearly identify it, and how to
treat it, are established. Thus, when TB was discovered to be a
bacterial infection, the manipulations, the extensions (of
nobility), began to deteriorate. Koch is arguably the notable
personage here, being the one to irrefutably establish the link
between TB and the tubercle b a c i l l u s in 1882 - this aspect. In
so doing (and along with the subsequent identification of the
mode of transmission of the disease), he relegated TB "to the
group of infectious diseases", his finding dispelling the
mysteriousness of TB and serving as a compelling anomaly to
other predominant doctrines (such as TB as a hereditary 192 disease) . The social constructions of TB were further

delegitimated through the development of certain tools - now
more than ever at the disposa1 of the physician - tools of
intensification. Through radiology, microbiology and serology, 193 diagnosis of TB became a simplicity. They facilitated
intensification into TB, or aspects thereof . Finally, when
treatment was established in the form of isoniazid in 1952 (and
later, in the form of a combination between streptomycin and
paraminosalicytic acid (PAS)) the social manipulations received
another, lasting, powerful blow. 194
Although there is much more to TB than its link to the
bacillus (such as predisposing factors, maybe even heredity, 195
the role of socioeconomic conditionsLg6, etc. ) , the f a c t that it
is tied to the bacillus, that there are tools to see it thus,
and that there are treatments to address it thus, do much to
dispel the constructions, to constrain the social-manipulations,
to make of TB a socially-augmented-disease rather than a
socially-manipulated-dise. And 1 Say "socially-augmented"
because it is a disease that is seen very much in line with its
specifiably tangible link to the bacillus - in line with this
particular rnedical intensification.
1, moreover, Say medical intensification because if it were a
medical extension, the treatments for TB would not have worked
the way they have. TB would not have been eradicated to the
extent that it has (up until recently) . As discussed in Chapter
4, for an approach to work, it must have some foundations in, it
must be in some way informed by, what is real. And for an
approach to work w e l l , for an approach to successfully eradicate
a disease, for example, it must have (relatively) special
attunement with that which is true of the disease (or rather
true of aspects of it). In cases where there is minimal
attunement, where there is minimal intensification, where there
is ambiguity - semi-tangibili ty - the social (medicine)
compensates through paradigmatic extension. The social
(medicine) constructs in ways that do little to preclude the
disease from pursuing its deadly course. TB still killed as a
romantic, spiritual, noble disease . On the other hand, the social-augmentation of a paradigmatic
intensification can also lead to detrimental consequences. For,
once having aspectualized the intensification, once having so
dealt with the disease, there exists for us (medicine) the
danger of falling into complacency vis-à-vis the disease. There
exists the danger of seeing the disease in a limited way, thus
remaining unattuned to that which is also true of it, thus
setting ourselves up for another crisis.
Recently, TB has taken us by surprise and presented us with a
significant crisis. Having had much success with TB, having
tamed the universal killer, and having for the most part put it
aside, it has reernerged, challenging as ever. Indeed, it has
exploded with compelling force once again into Our lives in
various parts of the world. On October 17, 1990, the New York
Post headline read "Highly Contagious Tuberculosis Close to
Epidernic Level in ~it~"'~'. In the same year, an expert of the
World Health Organization made the claim "Africa is lost". 198
Tuberculosis has reached wide-spread prevalence, and to make
things worse, medicine is no longer sure how best to deal with
it. It has appeaxed in a new guise, one so far impervious to
standard approaches and treatments.
This new serni-tangibility (what do we do?) of TB is due,
f i r s t l y , to its link with AIDS. The HIV infection causes
immunocomprornization which dramatically increases susceptibility
to TB. 199 In fact, infection with HIV is held to be the greatest
risk factor in securing TB. 'O0 (TB, it is believed, also
triggers the onset of AIDS) . Its semi-tangibility is also due
to the particularly frightening reality that tubercular bacter ia
have developed the capacity for resistance, possessing
extraordinary mutation capabilities making standard treatrnent
for TB highly ineffectual. We, therefore, have a global time
bomb on our hands. According to one headline in the
International H e r a l d Tribune on January 25-26, 1992, "Drug-
Resistant Strains of Tuberculosis are 'Out of Controlr, U.S.
Says ." What this means is that TB has transfomed from something
understood - from something familiar - into something ambiguous - into something highly semi-tangible. Now it is ripe, once
again, for social-manipulation. Medicine, having intensified
into TB in one of its guises, is now faced with it once again,
but in another seemingly intractable guise, one resistant to
heretofore medical intensifications. In other words, having
augmented it and so satisfied ourselves that rnedicine actually
beat it, we (medicine) neglected it. And we (medicine) did so
to Our detriment. Through our neglect we undermined what we
saw. We aspectualized what we knew, what medicine saw, what
rnedicine intensified into, and so blanketed the unknown -
relegated it to some obscure corner. We social ly-augmen ted wha t
rnedicine had i n t e n s i f i e d i n t o , and so fooled ourselves i n t o
t h i n k i n g we had essentially vanquished t h e e n t i r e phenomenon.
N o w , with penetrating anomalic force, TB is here with us once
more, as enigmatic and orninous as ever. The unknown has
displaced the known, and not only that, has asserted itself with
a vengeance, proclaiming TB as one of the greatest health 20 1 challenges since the bubonic plague. This it has done through
an alliance with AIDS (another enigmatic and ominous disease, a
disease, moreover, we have yet to beat for the first time).
In short, once a vanquished phenomenon, TB has reemerged as a
tangible threat drenched in semi-tangibility. From my
analytical point of view, it has, therefore, regressed from the
status socially- (medically-) augmented-disease into (as it once
was) , the socially-manipulable. m . . . . o...
Speaking of infectious diseases more generally, 1 want to be
clear about something. My point is not that the
aspectualization of the tangible necessarily has the same
deleterious consequence for every disease: the invariable
undermining of what is seen through neglect of what is not seen.
There exists, with every disease, only the possibility of
undermining what is seen through neglect of what is not seen.
Moreover, within the category of socially-augmented-diseases,
the following general comment also applies: here, diseases are
socially constructed, medically constructed, by virtue of
medicine over-emphasizing that which it sees. In each case,
medicine makes of the phenomenon what it sees in the phenomenon.
The doctrine of specific etiology, while facilitating medicinefs
capacity to see and intensify into certain disease aspects,
concurrentfy blinds itself to other aspects. The tremendous
credence medicine has placed in medical measures such as
immunizations and inoculations to address infectious diseases,
for example, has concurrently limited medicine. As McKinlay and
McKinlay explain:
It is not uncommon today for biotechnological knowledge and specific medical interventions to be invoked as the major reason for most of the modern (twentieth century) decline in mortality. 202
But if you examine the evidence, it appears that such
interventions were of less importance in the decline than at
f i r s t imagined. In fact, according to McKinley and McKinlay,
medical measures such as the introduction of izoniazid for
tuberculosis, chloramphenicol for typhoid, sulphonomide for
pneumonia and toxoid for diptheria, among others

... appear to have contributed little to the overall decline in mortality in the United States since about 1900 - having in many instances been introduced several decades after a marked decline had already set in and having no detectable influence
203 in most instances.
On the other hand, other measures such as improvements in
nutrition, housing, population control, an emphasis on hygiene,
control over the water supply, etc., were far more important
factors in the decline of such diseases, and hence mortality. 294
McKoewn comes to similar conclusions, although he allows for a
greater role played by immunizations post 1935. In his words:
... the decline of mortality which was responsible for the modern improvement in health and growth of population . . . was due initially to a large increase in food supplies, which changed the relationship between micro-organisms and man, against the parasite and in favor of the host. From the second half of the nineteenth century this advance was supported powerfully by reduction of exposure to infection, which resulted indirectly £rom the falling prevalence of disease and directly improved hygiene, affecting, in the first instance, the quality of water and food. With the exception of vaccination against smallpox, the effect of immunization and treatment of disease was restricted to the twentieth century, mainly since 1935, and although now significant, over the whole period since the eighteenth century they have been less important than the other influences. 2 0 5
Let me underscore that immunizations play a role. Medicine,
in my view, has rnost definitely got that right. Medicine has
most definitely intensified into this reality. But medicine has
also hyperbolized the magnitude of the role immunizations play.
It has, in this way, socially-augmented these diseases. It has
intensified into certain aspects of these diseases, emphasized
those aspects in line with the doctrine of specific etiology,
those aspects specifiably tangible to it, and thus constructed
these diseases. It has come to understand them in light of the
assumption: unitary causality; in light of the assumption: germ-
begets-disease; in light of the magic bullet approach to
eradicating disease. To compare: although medicine doesn't
necessarily deny multi-causality, others place greater emphasis
on such a mode1 - one i n which the body, mind and environment
"interact to produce disease or to cure it.. . u 2 0 6 . Such i s the
case, for example, with Board of Health for the City of Toronto,
which places stress, in its Healthy Toronto 2000, on a mode1 of
health that incorporates four factors: human biology, persona1
behaviour, the psycho-social environment and the physical
environment, These factors, in turn, it is maintained, are
affected by wider cornmunity factors, including values,
standards, support systems and environmental influences. The
approach highlights the many determinants of health, as well as
the interplay between these determinants on the individual.
This is no longer an uncommon approach. Multi-causality is
very much in vogue, especially within the public health field.
And 1 would Say that medicine is opening up to it. But more
importantly, it is an approach that in no way denies that which
medicine has identified about disease, and in this case,
infectious disease. Those aspects rernain intact. And they
remain intact because, to put it plainly, medicine has a point;
because, as discussed, medicine is seeing and has penetrated
into some things legitimate, into some things t r u e , about these
diseases. At the same time, these aspects - having been rendered supreme by medicine - are relatively deflated under the
multi-causal approach.
. . . - . . . . . Then there are those diseases, or syndromes or conditions,
upon which medicine may have yet an even a greater, a more
pervasive, handle. Think of the myriad acute conditions that
medicine handles everyday. Think, for example, of the myriad

conditions that appear so frequently in the emergency room:
twisted ankles, bruised heads, gaping wounds. As conditions
they nay be constructed, but we can hardly conclude they are
constructed to the same extent that other diseases are
constructed, "diseases" like hysteria, or menopause. There are
bodily realities to them that demand, that constrain their
construction, that are both generalizably tangible as particular
threats to health, and specifiably tangible to medicine as
treatable entities (relatively speaking) . In other words: is there not something much more legitimate
about a toothache or a bone fracture, than the disease hysteria?
With Turner, 1 would have to Say that "my answer is rather like
Shakespeare's: 1 have yet to meet a philosopher who hadn't
suffered from toothache-" And has medicine not intensified into
such conditions, into their workings, and learned ways - even effective ways - to deal with them? The obvious success of
207 medicine in treating them would suggest a positive response.
1 am not suggesting that these conditions are immune from
construction. At very minimum, meanings always corne into play.
Rather, the issue is the extent to which those meanings get in
the way of seeing these conditions, of penetrating into their
workings, their foundations. It would seem that meanings, here,
do not infiltrate nearly to the same degree that they do with
the other diseases (or "diseases") discussed so far. It would
seem, for instance, that meanings do not get in the way and
construct (hinder seeing and socially manipulate) a twisted
ankle like they do AIDS, or a burned hand like they do
menopause. They rernain, instead, basically (and relatively
speaking!) ancillary, supplemental, and so constitute a second
way in which certain diseases are augmented.
~ c u l l ~ ~ ~ ~ , talks about how some conditions are more interesting
to physicians than others. Generally, they are acute, dramatic,
challenging conditions, conditions that present opportunities to
test out new techniques. Conditions that demand ingenuity.
Puzzles. Once mastered, however, they lose their novelty. The
rnedical interest in them fades while new challenges are sought.
The same conditions rnay have different meanings attached to thern
over time. This, however, does not necessarily mean that the
medical understandinq of these conditions changes as well, that
the medical intensification into appendicitis as an acute
inflammation of the appendix resulting in abdominal pain, for
example; or the medical understanding of hyperpyrexia as a life-
threatening condition characterized by overheating caused by an
overexposure to heat; or the medical understanding of myocardial
infarction as the death of a part of the heart muscle, changes.
Interest level notwithstanding, medicinefs knowledge of what
they are remains essentially uncompromised.
Similarly, a physician rnay attach contrary meanings to the
same condition under different circumstances, and yet understand
the what-it-is of each case in basically the same way - in
accordance with prevalent rnedical intensifications into the
phenomenon.
Imagine a physician who receives two patients each with gaping
wounds. The first patient is an assailant while the second is
the victim who managed to slash the assailant in self-defense.
Here, the two wounds rnay take on rather different meanings to
the physician, and immediately so. In the case of the former -
i.e. the "assailant wound" - the physician rnay come to see it as something well deserved, even as something to be fostered,
exacerbated . . . if only s/he hadnft taken that oath! Meanwhile, the "victim wound" rnay take on a rather different meaning to the
physician. S/he rnay come to see it as undeserved, and
therefore, as something to be treated immediately. In both
cases, the "whatness" of the wound, the physician' s perception

that it is a serious threat to the bodily health of the
individual, its workings and thus how to deal with it, remain
relatively and consistently tangible to the physician. The
medical understanding of that which constitutes a gaping wound -
a relatively intensified understanding it rnight be added -
remains (relatively) unadulterated by the meanings attached in
each case.
Thus, certain diseases or conditions are supplementally
constructed and in this way socially-augmented. They are
diseases seen relatively clearly for what they are, but diseases
that are variously associated with meanings that neither
infiltrate, nor obscure, nor manipulate, nor transform the
disease. Such meanings exist as addendums to the disease. 209
And this is in relative contrast to conceived and manipulated
diseases where meanings play a much more penetrating role, where
meanings largely take over resulting in veritable phenomenal
transfigurations. This is also in contrast to a myriad other
diseases and conditions not discussed in this chapter, but
alluded to in Chapter 7.
HENCE
It is to Chapter 7 that 1 now turn where 1 summarize and
analyze the foregoing, and set out the implications for
interparadigmatic collaboration, among others implications.
- -
1(1994), p. 7.
2 Leyton (1987).
3 Syme and Berkrnan (1994),
4 Tardive Dyskinesia is a case in point. While a pervasive iatrogenic side
effect of antipsychotic (neuroleptic) drugs, 'a seriously debilitating, often
irréversible disorder of the central nervous system, characterized by a
variety of involuntary movernents, most notably of the lips, jaw, and
tongueW4; a disorder that was not recognized as such by medicine because "it
hurt the economic and political interests of many clinicians" and their
desire to "control the deviant behavior of patients" with such drugs. (Freund
and McGuire (l995), p. 199) . 5 See Chapter 5 on this.
6 Turner (1995), p. 90-94.
7 King (1993), p. 64.
8 Rousseau and Porter (1993), p - xi.
9 (1993), p. 64.
10 In Merskey (lgïg), p. 12.
11 Veith (1965), is a case in point.
12 Bernheimer (1985), p. 2.
13 Ibid.
14 Ibid, p . 3 .
15 Turner (1995), p. 90.
16 Rodin (1992), p. 50.
17 King (19931, p. 14.
18 fbid, p. 22.
19 Turner (1995), p. 92.
20 Quoted in Veith (19651, p. 7-8.
21 (l99S), p. 92.
22 Ibid, p. 92.
23 Ibid, p. 93.
24 Bernheimer (1985), p. 3.
25 Quoted in I b i d . - - - - - - - -
26 Ibid .
27 Quoted in MacDonald (1991}, p. xxviii. It should be noted that although
Jorden is not successful in saving Elizabeth Jackson from her fate as a
witch, his l a te r work on the subject of hysteria would help to "secure the
decline of witchcraft" and its link to hysteria. In it he emphasizes the
natural causes of h y s t e r i a .
28 Rodin (1992), p. 50-
29 Bernheirner (19851, p. 4.
30 Ibid.
31 Quoted in Ibid.
32 Pinel is famous for t a k i n g the chains off inmates at the Bicetre Hospital
in Paris.
33 Bernheimer (1985), p. 5.
34 Ibid .
35 T u r n e r (1995 1, p . 94 .
36 ( l 9 9 3 ) , p . ix.
37 Rodin, p. 51.
38 Merskey ( l 9 7 9 ) , p. 10.
39 Ramas ( l 9 8 5 ) , p. 151 .
40 ( 1 9 8 5 ) , p . 191.
4 1 Ramas ( 1 9 8 5 ) , p. 51 .
4 2 Turner ( l 9 9 5 ) , p . 91.
4 3 I b i d , p . 91-92.
4 4 I b i d , p. 94.
45 Lackof f and Coyne ( 1 9 9 3 ) , p . 119.
46 Ibid.
47 M o i ( 1 9 9 5 ) , 192.
48 Libbrecht ( 1 9 9 5 ) , p . 167.
4 9 Both quoted i n Lewis ( 1 9 8 2 ) , p. 22 .
50 Slater ( l 9 8 2 ) , p . 39.
5 1 ( 1 9 8 2 ) , p . 3 .
52 Slavney ( l g g O ) , p . 2 .
53 ( 1 9 8 8 ) , p. 65.
54 Ibid, p. 65 - 66.
55 C i t e d i n i b i d , p . 61.
56 I b i d .
57 I b i d , p . 58.
58 Helman ( 1 9 8 8 ) , p . 1 1 7 .
59 I b i d .
60 Kirmayer ( 1 9 8 8 ) , p. 65.
61 Helman ( 1 9 8 8 ) , p . 1 1 7 .
62 ( 1 9 9 0 ) .
63 I b i d , p. 5.
64 I b i d .
65 K a u f e r t ( 1 9 8 8 ) , p . 331; Goodman ( l 9 9 O ) , p. 1 3 3 .
66 K a u f e r t ( l 9 8 8 ) , p . 331.
67 Freund and McGuire ( 1 9 9 5 ) , p . 197.
68 Menopause i s indexed in t h e International C l a s s i f i c a t i o n o f Diseases i n
the U.S. Department of H e a l t h and Human S e r v i c e s ( 1 9 8 9 ) , pp. 524-525.
69 ( 1 9 8 7 ) , p. 174.
70 Kearns a n d C h r i s t o p h e r s o n ( 1 9 9 2 ) , p . 191.
71 Here, 1 am drawing upon Coney (19941, p. 61-
72 Korenman (l99O), p. vii.
73 (l994), p. 59.
74 Freund and McGuire (l995), p. 198.
75 Coney (1994), p. 18.
76 Lorrain (l994), p. vii.
77 (1990).
78 Ibid., p. 46.
79 This notwithstanding the inherent limitations to many studies on
menopausal women, limitations due, for example, to nonrepresentative samples.
Clinical research generally drew upon women whose symptoms were already
"defined as severe enough to warrant treatment" for their samples. Y e t , the
conclusions made concerning these women were eventually "treated as
facts.. .presumably generalizeable to al1 women."
80 Bell (1990), p. 47.
81 Goodman (lggO), p. 139.
82 Bowles (l99O), p. 159.
83 (1975).
84 Ibid, p. 12.
85 Ibid, p. 20.
86 See Delaney et al (1976), p. 172.
87 Cooper (1975), p. 20.
88 Coney (l994), p. 72.
89 Ibid.
90 Cooper (1975), p. 35.
91 See Coney (l994), p. 73.
92 Ibid, p. 69.
93 da Lilva (l994), p. 213.
94 Coney (19941, p. 75.
95 Ibid.
96 Kaufert and Gilbert (1987), p. 175.
97 Ibid, p. 174.
98 Freund and McGuire (1995), p. 198. This despite the costs of estrogen
therapy. In the 1970s, for example, estrogen therapy was being associaced
with various iatrogenic diseases (p. 198), including uterine cancer (Goodman,
1990, p. 149). DES has also been implicated in the development of vaginal
cancer among daughters whose mothers were treated with the therapy during
p r e g n a n c y i n o r d e r t o p r e v e n t t h r e a t e n e d m i s c a r r i a g e . See Weiss (1983) o n
t h i s - 9 9 MacLeod ( 1 9 9 4 ) , p. 1 1 5 .
100 Ibid, p. 1 0 9 ,
1 0 1 K a u f e r t and G i l b e r t ( 1 9 8 7 ) p. 174 .
102 Coney ( l 9 9 4 ) , p. 20 .
1 0 3 Ibid, p. 61.
104 B e l l ( l 9 9 O ) , p . 58.
1 0 5 Goodman, p. 1 4 0 .
106 Towsend and Carbone ( d a t e ) , p . 231 .
107 I b i d , p . 235.
108 See Judd (1990) f o r a review of some of the m e d i c a l l i t e r a t u r e on
menopausa l r e l a t e d symptoms.
1 0 9 H u n t e r ( 1 9 9 4 ) ' p . 119 .
110 Townsend and Carbone ( 1 9 8 0 1 , p. 231; Goodman ( 1 9 9 0 ) , p. 140-141.
111 Beyene i n Dan and Lewis ( 1 9 9 2 ) , p . 1 6 9 .
112 Townsend and Carbone (1980j, p. 229.
1 1 3 I b i d , p . 231-
114 Bowles ( 1 9 9 0 ) , p . 1 6 1 .
1 1 5 Towsend and Carbone ( 1 9 8 0 1 , p . 231.
1 1 6 Beyene ( l g g î ) , p . 171 .
117 du T o i t ( 1 9 9 0 ) , p . 291 .
118 I b i d .
119 K e a r n s ( l 9 9 2 ) , p . 1 9 1 .
1 2 0 K a u f e r t e t a l ( 1 9 9 4 ) , p . 6 3 .
1 2 1 Coney ( 1 9 9 4 ) , p . 96.
122 Freund and McGuire ( 1 9 9 5 ) , p. 198.
1 2 3 Ibid, p. 198.
124 ( 1 9 9 4 ) , p. 123.
1 2 5 Beyene ( l 9 9 2 ) , p . 176 .
1 2 6 ( 1 9 9 0 ) , p . 129 .
127 See examples of the v a r i o u s a d v e r t i z e m e n t s for e s t r o g e n u s e as l i n k e d
w i t h a v o i d i n g o s t e o p o r o s i s , i n Chapter 8 o f Coney (1994) . 1 2 8 Coney ( 1 9 9 4 ) , p . 128 .
1 2 9 I b i d , p. 129.
130 O 'Lea ry Cobb (19941, p. 5 4 .
1 3 1 I b i d , p. 53
132 Ibid, p. 54.
133 Coney (1994), p. 131.
134 Notelovitz in Coney (19941, p. 329.
135 Coney (1994), p. 328.
136 Kaufert et al- (1994), p. 59.
137 Coney (l994), p. 84.
138 Kaufert et al, 1994, p. 59-
139 This is certainly how Heilbrun sees it in her Forward to A Certain Age:
Reflecting On Menopause (l994), and in contradistinction t o the Miller who
wrote an alternative Forward.
140 Delaney et al (l976), p. 176.
141 (1990),
142 And yet, 1 am making an assumption here - that estrogen deficieny is seen and intensified into, whereas the biological realities historically
associated with hysteria were mythological.
143 Bolton (l989), p. 99.
144 Ibid, p. 93.
145 Herzlich and Pierret (l993), p. 60.
146 Bolton (1989), p. 96.
147 Fortunato (l987), p. 1.
148 Nelkin et al. (1991), p. 2 .
149 Murphy (1995), p. 13.
150 Treichler (l988a), p. 195.
151 Murray and Payne (l989), p. 116.
152 Clatts and Mutchler (l989), p. 106.
153 Treichler (1988), p. 31.
154 Waldby (l996), p. 140.
155 Weeks (l989), p. 2.
156 Herz l ich and Pierret (l993), p. 64.
157 See Treichler in Crimp (1988) pp. 32-33, for these and more.
158 Quoted in Crimp (l988), p. 8.
159 Clatts and Mutchler (1989), p. 108.
160 Ibid.
161 Pryor and Reeder (1993).
162 Murphy (1995), p. 6. The emergence of urban myths is acother indicator
of the social need to make sense of threats immersed in semi-tangibility, and
to do so in line with current prejudices. According to Bloor (1995: 2): "A
widely popular HIV/AIDS myth which occurs in several related forms is the
morning-after message from the 'sevenger infector. Sometimes it is a message
written in lipstick or shaving foam in the bathroom ... Other times, it is a message opened on the return flight from the romantic holiday. But the
content of the message is always the same: 'Welcome to AIDS club.'" And as
Bloor goes on to explain: "The suitability of th2 H I V / A I D S epidemic as a
topic for urban myth-making hardly needs stating - the marginalized and vilified character of many persons with AIDS (drug injectors, gay men, black
Africans), the popular dichotomy ... which divides partners into guilty predators and innocent victims, and so on. "
163 Clatts and Mutchler (l989), p. 112.
164 Note: in cases of tangibility, it aspectualizes as well.
165 Clatts and Mutchler, p. 111.
166 Bolton (l989), p. 99.
167 Albrecht and Zimmerman (1993) , p. 4. 168 Ibid, p. 12.
169 Ibid.
170 Ibid, p. 3.
171 Murray and Payne (1989), p. 122.
172 (l989), p. 119.
173 Treichler (1988), p . 44.
174 Ibid.
175 Freund and McGuire (1995), p. 196.
176 Albrecht and Zimmerman (l993), p. 4.
177 Albrecht and Zimmennan (1993), p. 4.
178 Ibid.
179 Ibid, p. 3.
180 Herzlich and Pierret (1993), p. 66.
181 Murphy (1995), p. 13.
182 Treichler in Crimp (1988), p. 32.
183 Bolton (l989), p. 98.
184 In Fee and Fox (l988), p. 28.
185 Evans (1994), p. 1.
186 Ryan (1992), p. x i x . .
187 Sontag (1978), p. 34.
188 Caldwell (l988), p. 17.
189 Ibid.
190 Ibid .
191 Ib id . , p . 22.
192 Keers (l978), p. 60-61.
193 King (l982), p. 16.
194 Sontag (l978), p. 35.
195 King (1982), p. 68.
196 Evans (l994), p. S . [ i n Davies]
197 See Ryan (1992), p. 389.
198 Ibid.
199 Davies (1994), p. 401.
200 Ryan (1992) , p. 398.
201 Ibid, p. 391.
202 In Conrad and Kern (1994), p. 10.
203 Ibid, p. 20.
204 McKeown (1979).
205 McKeown (1979), p. 10-11.
206 Ehrenreich (l978), p . 13.
207 For there is no true success without i n t e n s i f i c a t i o n . See Chapter 4 on
this . 208 (1980) . 209 Now it may be t h a t meanings can take over a t some point, i n f i l t r a t i n g the
phenomenon. If so, then the phenomenon loses i t s s t a t u s a s an augmented-
disease. B y the same token, a manipulated-disease may "move up" i n s t a t u s as _ - - - - - - - - - -
i-ntensification i n c o It-s workïngs aspapd i sea se evolves .

JO-Y NOTES To sum up.. .

INTRODUCTION
The first five chapters of this book were devoted to outlining
the rationale for, as well as building a theory for, the
relativity of the social construction of disease. In Chapter 6,
1 took this objective a step further and outlined a typology to
help understand such relativity. In so doing, 1 drew upon the
concepts delineated in the previous chapters. In this chapter,
my primary concern is to attempt to bring the concepts and
typology together into an integrated format. This is followed
with an assessrnent of the typology through a brief consideration
of other diseases (or "diseases") and their fit within the
typology. Finally, 1 discuss the significance of my conclusions
for the first project of the consultative approach, namely, the
utility of interparadigmatic communication (between medicine and
social constructionism in particulax); and then finish with a
section on some of the implications of this study.
U N X N I N G THE CONCEPTUAL DIVERSITY
The following table (Table 2 - see over) consists of the major concepts discussed so fa r , and an illustration of their
relationships to the four categories of disease ranging £rom the
most constructed to the least constructed. Let me state up
front that 1 consider this presentation to be in some ways
forced. As with most integrative analyses, there are anomalies
with which to reckon. These 1 will highlight subsequent to rny
summary.
To begin: the major distinction between socially-conceived-
diseases and the rest, is that, whether or not the former are
granted status as diseases in the sense defined - that is, as
malfunctions of the body - is purely a social issue. What makes
a socially-conceived-disease a disease, is its social imputation
as such, its construction as such. This does not mean that it
is not associated with suffering; its construction may have ties

to legitimate physical experiences (women with menopause
experience hot flushes; women with hysteria faint) . But
suffering is very often a consequence of internalization, a
consequence of becoming immersed in the role - of living out the
Tangible as Disease I l X I X l I
1 1 I I
1 Constructed as Disease 1 x 1 1 1
Theoretics1 C o n r + ~ t s S-A-D
Tangible (aspect (s) )
S-T-D
x
Semi-Tangible (aspects (s) )
Intangible
Paradigmatic Intensification
I Aspectualization (Selection) I I l X I
x
x
Paradigmatic Extension
1 Aspectualization (Seiec./Construc.) ( x 1 x ( I
x
x
T a b l e 2 . Matching the Concepts w i t h the Categories of Disease
x
x
Meanings-Attached
prescription of the social reification. Here, deconstruct the
concept (in t h e literal sense) and we deconstruct the disease
S-C-D = SOCIALLY-CONCEIVED-DISEASES S-M-D = SOCIALLY-MANIPULATED-DISEASES S-A-D = SOCIALLY-AUGMENTED-DISEASES S-T-D = SOCIALLY-TRANSFIXED-DISEASES
x
("disease") . Eradicate menopause-as-disease and we are left
with menopause-as-normal. Eradicate hysteria-as-disease, and we
x
are left with some women (and men!) who rnay behave hysterically
x
on this or t h a t occasion. Where the social dictates otherwise,
as it has in the case of hysteria, and as it may be doing in the
case of menopause, the "disease" disintegrates from (perceived)
objective reality to myth of the past.

This is in direct contrast to both socially-manipulated-
diseases and socially-augmented-diseases where the social is
constrained. In both cases, there is no question about whether
or not we are dealing with diseases . There is an objective
reality to these diseases in the sense that they are "out
there". They demand attention as such. They may even have
generalizable tangibility as such, making trenchant claims,
piercing upon collision most, if not any, paradigmatic
impedance. Few, especially those afflicted, would (or could)
deny their detrimental (to body) reality, their objective
detrimental reality. Few with AIDS would deny the truth of AIDS
as a debilitating corporeal affliction. Few would deny the
killing capacity of TB - century after century, it has undeniably killed. Deny hysteria and it fades from
significance, but deny AIDS or TB, and they persist, and
tangibly so, as real forces with which to reckon - they persist
as diseases. As threats, both are tangible. As threatening
diseases, both are ( far) less constructed than socially-
conceived-diseases.
Moving on: while similar in this way, socially-manipulated-
diseases are, nevertheless, more socially constructed than
socially-augmented-diseases. They are so by virtue of the semi-
tangibility that engulfs thern. While highly tangible as
threats, socially-manipulated-diseaseses are, concurrently, highly
mysterious phenornena. What should we make of them? How do they
operate? How should we deal with them? There are no clear
answers to these questions, only uncertainties. This makes them
al1 the more threatening rendering them, in turn, al1 the more
ripe for social construction. And so they are taken in,
infiltrated with, and thus manipulated in line with, prevalent,
dominant, social anxieties - rnoralities. This is clearly what

has occurred, and still occurs, with AIDS. The very idea of
AIDS evokes condemation.
It is also what occurred with TB, the very idea of which,
however, (historically) evoked the opposite - nobility, spirituality. But TB only remained a moral disease until the
serni-tangibility of it, or rather, of certain aspects of it,
dissipated: until medicine found a way to penetrate the disease,
to paradigmatically intensify into it: until medicine understood
what caused it and how it could be addressed. Then TB (slowly)
died as a social-manipulation and became a social-augmentation.
While understood and s o c i a l l y lived for the bulk of its history
in light of certain semi-tangible aspects, in light of selected
constructed aspects - while having been aspectualized in th i s
way - T B underwent a social transformation. Through significant
medical discovery, it became understood in a new light: in light
of certain aspects (relatively) seen, in light of aspects
medically i n t e n s i f i e d into. In other words, TB (or rather,
aspects thereof) became specifiably tangible to medicine. (This,
until TBf s recent alliance with AIDS. )
Al1 things considered, we might Say that (recent) TB (as an
example of a socially-augmented-disease) 3s distinguished from
AIDS, menopause and hysteria, in three ways. It boasts 1. the
(specif ied to medicine) tangibility of certain of its aspects,
which have undergone 2. (medical) paradigmatic intensification,
and 3. aspectualization in the form of (medical) selection.
Contrarily, AIDS as a socially-manipulated-disease, and
menopause and hysteria as socially-conceived-diseases, share in
common: 1. aspectual semi-tangibility, leading to 2. (medical)
paradigmatic extension, achieved through 3. aspectualization in
the f o m of (medical) selecti~n and construction.
These factors make TB (again, until recently) less constructed
as a disease, than the others. And while AIDS is highly

constructed as a disease, while it is manipulated through
paradigmatic extension, it is far less a construction as a
disease than either hysteria or menopause, because AIDS, like TB
is a disease , and tangibly so. Contrarily, hysteria and
menopause as diseases, are social fabrications through and
through. They are "diseases".
But there is more. Under the category socially-augmented-
diseases 1 also mentioned acute conditions within which medicine
sees a lot. Whereas I would suggest aspectualization in the
form of selection is always an issue, it may be less so with
conditions such as gaping wounds, heart attacks, broken bones,
toothaches, etc. But even where aspectualization is reduced,
the social still cornes into play, and it does so in the form of
meanings-attached. Indeed, meanings-attached are probably
relevant to every category except the last, since, it will be
remembered, socially-transfixed-diseases are either intangible
or do not exist. In either case, the social has literally no
power over them since tangibility is a prerequisite for social
construction to ensue.
Finally, I've mentioned that there are inadequacies to rny
analytical summary. One has to do with how menopause fits with
it. While 1 maintain that the construction menopause-as-disease
is a construction in the most radical sense, it may be forcing
the issue to suggest that there is nothing (specifiably)
tangible (to medicine) about it . Menopause has grounding in
veritable and identifiable biological processes. Estrogen
deficiency, for example, is an aspect seen. In this sense, it
is distinguishable from hysteria. Yet, what to make of these
biological processes is very much semi-tangible. Whether they
imply disease, is a social matter. Here, aspectualization
involves both selection and construction which means
paradigmatic articulation proceeds as paradigmatic extension.
A second inadequacy has to do with the rnutual exclusivity
implied between paradigmatic intensification and extension for
each category. In Chapter 5 it was emphasized that paradigmatic
articulation always involves both, but in varying degrees, such
that we can think in terms of the ratio e/i: the greater the
ratio, the greater the paradigmatic extension compared to
intensification; hence, the more constructed the phenornenon.
More to the point is that extension is always an issue, even in
the case of socially-augmented-diseases. While such diseases
involve paradigmatic intensification, extension concurrently
ensues if only because of aspectual selection. For aspectual
selection means that other aspects are relegated to the
background, constructed from paradigmatic view, aspects that may
l a te r emerge with unbridled anornalic force challenging our
understanding of what the phenornenon truly is. TB and its link
to AIDS is a case in point.
A third inadequacy directly involves the four categories that
make up the typology. The typology is deficient to the task of
classifying al1 diseases. 1 have mentioned that my concern was
not to create the perfect typology, but to create a provisional p p p p p p p - - - - - - - - - - -
Cool-for understandingPthep relativity of the social construction
of disease, a tool subject to alteration. At the same time, it
is important to provide insights into its strengths and
weaknesses in order to assist with future endeavours concerned
with delineating a more adequate tool.
ASSESSING TEE TYPOLOGY
To this end, consider the following diseases (or "diseases"),
and their adequacy of fit within the typology. What follows are
simply snapshots - 1 make no attempt to deal with them in any
depth.
1. Three Historical ttDiseasesrf. To begin, the following three
conditions, in my estimation, fit well within the first category

- socially-conceived-diseases - as 1 see them as social constructions through and through. They are realities infused
by the social, thus constructed by the social, thus rendered
"txue" by the s o c i a l ; mbiguities, t h a t i s , made intelligible
and controllable by their transformation into discrete entities
sub ject to medical understanding.
In the 1850s two "diseases of the Negro race" included
"drapetomania" and "dysaethesia"'. The f orner disease was held
to explain the phenornenon of slaves running away from their
masters (as if it were normal for them to want to remain as
s l aves ) . It was believed that drapetomania caused this
peculiar, this abnomal act which led, subsequently, to a
"technological innovation", namely "the surgical removal of the
big toes, thereby making f light a physical impossibility. "' Similarly, the latter - dysaethesia aethiopis - was held to explain the "laggard work habits among slaved"' (as if it were
normal for slaves to want to work as slaves).
My suggestion is that there are no such diseases, nor have
there ever been, in the sense being malfunctions of the body.
These are "diseases", constructions pure and simple, innovations
[that] could only exist in circumstances of the subjugation of one group of people by another, with the dominant group defining the activities of the other groups as b e i n g so unacceptable that [they] must the product [s] of disease. 4
They are transformations, illegitimate surrogates reif ied. Like
the hysterla of old, they are social anxieties articulated in
the guise of biological abnormalities, abnormalities that do not
truly exist "out thereff.
The same can be said o f another historical disease:
"revolutiona". This disease was "discovered" during the
American Revolution. It was held to account for 'irrational
opposition to the "natural rule" of the English rnonarchr '. Once
again, this disease is an obvious construction, a "disease", one
symbolizing a very specific social desire of the times - a
desire to see the monarch rule unchallenged. A symbol,
moreover, that was socially elevated to the status of "real".
As such, these "diseases" fit well within the category
socially-conceived-diseases.
2. Childbirth. In my view, childbirth-as-disease (or medical
problem) does not fit well within any of the four categories,
although, if 1 had to choose, 1 would place it along with
menopause in the first.
In one sense, like menopause, childbirth is an obvious
reality. It occurs and there isn't a culture around the world
that doesnft acknowledge and respond to it in some way.
However, the ways in which it is described, defined, dealt with 6 and managed, are diverse. Childbirth has many incarnations.
This fact speaks to its rather generalized semi-tangibility as a
total phenornenon. What to make of it, how to deal with it,
whether or not it constitutes a problem requiring special
rnedical attention, etc. - these are al1 things semi-tangible about it, things very much subject to social whim.
- - -
- -Yet-sente -incarnati-oirs -arePmre -dominant than oth&rs. The
rnedical version is perhaps the most dominant today - at least in
western society - determining the physical location of
childbirth "for nearly three million women each year. " ' And yet
its definition may be nothing more than the pervasion of a
particular process with dominant meanings. Under the impact of
medicalization, of medical paradigmatic extension, childbirth
has become a medical event. It has become a "problem" (if not a
disease) subject to a particular method of treatrnent.
To illustrate, let me contrast the medical view with another
view, namely, the "alternative" view of childbirth as
represented by ~reichler', among others. The alternative view
offers insights into the socially constructed character of the
medical view while exposing i t s e l f as a social construction. 9
The alternative view perceives childbirth as a natural
process, a process that is disrupted under medical conceptions
and interventions. 10 It perceives childbirth as a process
requiring fittle or no medical intervention. 1 I Intervention is
necessary only under certain circumstances. Under most
circumstances, the woman and child are healthy. Labor and
delivery do not normally constitute a problem. This is
evidenced by the many cultures around the world that seem to
manage childbirths outside the hospital setting, and do so with
success. It is also supported by scientific evidence suggesting
obstetrical intervention is necessary "only under certain
circumstances . n12
The alternative approach also takes issue with some of the
implications of the concept "childbirth is a problem". This
concept, it says, has the consequence of thrusting women into a
certain role during labor and delivery, a role which condemns
them to relative passivity, to becoming the-acted-upon; a role
in which they are expected to adopt demeaning bodily positions -
analienatingrole m z e r a l L - So -the-aJter-native approach
advocates the reappropriation of the birth process by women.
Women are promoted as active, and indeed the foremost,
participants in a t r u l y natural process. 13 This attitude is
illustrated in ~ u r f a c i n ~ ' ~ , in which Margaret Atwood gives a
vivid picture of a motherrs act of reappropriation:
This tirne I will do it by rnyself, squatting on old newspapers in a corner alone; or on leaves, dry leaves, a heap of them, t h a t f s cleaner. The baby will slip out easily as an egg, a kitten, and 1'11 lick it off and bite the cord, the blood returning to the ground where it belongs; the moon will be full, pulling.
Seen £ r o m the alternative perspective, the medical conception
of childbirth is a natural process medically constructed.
Childbirth as a medical problem can be understood as an example
of a physicality socially infiltrated, a natural reality totally
pervaded with medical meanings and assumptions. These meanings
permeate the reality of childbirth producing a medical problem -
a problern that has both dorninated our understandings of
childbirth and alienated mothers £rom an otherwise normal and
persona1 experience. From this perspective, childbirth-as-
medical-problern belongs to the first category, as a socially-
conceived-problem (if not disease, per se.)
On the other hand, to categorize it as such may be forcing the
issue. 1 Say this because the alternative perspective may be
doing somewhat of an injustice to the medical approach. For is
it not the case, for example, that prior to the medicalization
of childbirth, there were much greater rates of fetal loss? And
did not mothers die during childbirth in more significant
numbers? Moreover, is it not the case that the medicalization
of this "natural" phenomenon has lead to success in reducing
such rnortality rates? If so, then there may be more legitimacy
to the medical construction of childbirth-as-a-problem than that
allowed by the alternative approach. And if so, then its
classification within in the first category is stretching things
a little. Nor does it belong in the second or third category as
childbirth is definitely not a disease.
Perhaps, childbirth requires a new category altogether.
3. Infertility: Infertility provides another anomalous
example.
Infertility can also be understood as a socially pervaded
phenomenon, an ambiguity imbued by the social (the medical) . While constituting a biological reality - a perceivable one at that - not so tangible is what exactly to make of it. What it
means as a phenornenon (is it a disease? or a problem? or is it
just another physiological state?) is essentially up for social
grabs. And so the social goes to work on it, making it into
something socially conformed, into something perhaps
unnecessary .. .making it into a disease. Becker and Nachtigall take the position that "infertility is
not a disease", but Say that
it is treated like one in the health care system. The way in which infertility is medically defined and treated is based on the biomedical assurnptions that lead to the categorization of infertility as a disease entity, a medical statement that it is abnormal to be unable to reproduce biologically. 15
This statement is informed by the cultural understanding that
involuntary childlessness is a social problem that needs to be
fixed. That it is a deviant reality that needs to be managed
and addressed. Thus, in this age of medicalization, it has been
relegated to medicine to handle. This medicine has done as
evidenced by
the replacement of the words, involuntary childlessness, in the social science literature by the word, infertility, reflecting a discourse increasingly dominated by biomedicine. 16
There are other options, however, to the notion that
involuntary childlessness is deviance, to the notion that
infertility is a disease. Rectifying the '\diseaset' infertility
is just one approach a society could take. Others could include
"remaining childless, adoption, and other modes of incorporating
children into daily life, such as fostering othersf
children. . . But such options are devalued in our society.
With medicine, the focus is the disease entity infertility; and
the solution is infertility treatment, a treatment, rnoreover,
that constitutes
a symbol of negative cultural attitudes about childlessness, as it inadvertently reinforces a sense of abnormality by

juxtaposing that which is considered normal against that which is not. Instead of diminishing feelings of abnormality when treatment is sought, values that are embedded in the health care system facilitate the growth of such feelings. 18
In sum, and from this perspective, here we have a biological
reality - the inability to have children - infused with a social value - the value that involuntary childlessness is abnormal, deviant. Under the sway of medicalization, the result is a
constructed reality - infertility as a disease entity; a
constructed reality, moreover, the treatment of which operates
to perpetuate the value infused.
But this, again, is just one way to understand infertility.
From this perspective, it is a "disease", a socially-conceived-
disease. However, if we grant the earlier notion that disease
represents deviation from the n o m (as we did in the case of
menopause), then infertility becomes a disease and the issue
becomes what to rnake of it as a d i s e a s e . As a threat to the
value of being able to produce children, it is ready for social
construction as a disease. Maybe it is better classified as a
socially-manipulated-disease. But then, as a socially-
manipulated-disease, it would have tangibility as a threat. And
f o r those who do not devalue childlessness, it has no
tangibility as such. For them, it may even represent a good
thing . How to place it within the typology is unclear. Perhaps, like
childbirth, requires another category . 19 4 . Leprosy. With leprosy, however, things seem, once again,
a little more clear, especially with regard to its historical
formulation.
Here we have, in my view, another socially-manipulated-
disease, for, as "the scourge of the Middle es"^', it w a s a
major threat to western society, to the health of the

population. Having first appeared in the seventh century, it
spread quickly over the region, remaining a significant health
issue up until the late fifteenth century. As such, there was
no doubt about one thing: here was a problem - a disease - that needed, somehow, to be addressed. Less tangible, however, was
what exactly to rnake of it, and thus, how to address it. But
something had to be made of it, and it needed to be addressed.
Its ominous and expanding presence demanded resolution.
Social assumptions came into play. One, in particular, played
a critical role - the belief in a powerful connection between spiritual health and physical health. This, linked with the
medieval scientific and religious belief that leprosy and
venereal disease had much in comrnon, led to the construction of
leprosy
as a disease brought about by moral failure, especially adultery and promiscuity. It was further assumed that leprosy actually expanded sexual desire so that lepers were thought to be particularly debauched. 2 1
Leprosy became a disease of exclusion. With its development as
a tangible threat, lepers were excluded in various ways. They
were institutionalized, for example, relegated to leprosaria or
l a za r houses. Moreover,
the Church developed a number 0 5 ritual activities £or the ritualized exclusion of lepers. For example, lepers were forbidden ordinary social relations with children and strangers, being forced to Wear special clothing including the
22 clapper and begging bowl.
The Church also "developed a special ritual called the office at
the seclusion of lepers where the leper was pronounced
symbolically dead and excluded from social contacts. ,,23
As such, leprosy was a socially-rnanipulated-disease. While
leprosy was tangibly threatening, while i-t: was clearly a disease
with which to reckon, what to make of it was very much up for
grabs, it being a muddle of semi-tangibility. It fell victim to
the social assumptions of the tirne, and was manipulated to fit
with those assumptions. It became the focus of ritual (and
otherwise) exclusionary practices, representing the boundary
between the human and the not human, representing hwnan
membership annulled.
5 . Mental Disease. There is a tendency within the
constructionist literature to treat mental disease in general as
a fiction, which, if true, would give it a place among socially-
conceived-diseases. 1% not convinced we can treated it so
generally.
Definitely, 1 would agree that many cases or types of mental
illness are heavily socially constructed. At the same time, 1
am disinclined to go as f a r a s scheff2' who is rnuch more
categorical. Briefly, Scheff says t h a t deviance, in the form of
mental i l l n e s s ( o r what he refers to a "residual deviance"), is
a function not of rule-breaking (of showing signs of mental
illness) per se, but of the way in which the community responds
to the individual breaking the rules. "Mental illness" is a
function primarily of the extent to which society reacts
unfavorably toward "deviantl' individuals. In making his point,
Scheff argues that while the frequency of residual rule-breaking
is high in the "normal1' population, only some take on the role
of "rnentally illtl. Such individuals are those who have been
successfully stigmatized by the community.
Scheff goes on to argue that the labeling process is
contingent upon a number of factors, including how visible the
abnomal behavior is; the power of the individual; the status of
the individual in relation to those in positions of social
control; and the leniency of the community towards rule-
breaking. Loring and ~ o w e l l ' ~ lend credence to this view,
axguing that incongruities between the status characteristics

(such as age and sex) of psychiatrists and their clients,
significantly affect diagnoses: the larger the incongruity, the
more likely it is that the psychiatrists label their clients
mentally il1 . Rosenfield agrees , and f inds that " [n] onwhite
male patients are seen more negatively because they are judged
by a higher status group of white male physicians"26.
Frorn this labeling perspective, then, mental illness is
largely a social phenornenon. Its fundamental determinant is the
quality of the response of the social environment. One is
mentally il1 insofar as s/he is labelled so, and insofar as s/he
is unable to combat the labelling process and the meanings
associated with being labelled.
Does this mean that mental illness does not exist "out therem?
According to ove^^ and his supporters, mos t persons identified as mentally il1 have in fact severe psychiatric disorders
2 8 notwithstanding the labelling process. They occupy the deviant
category "mentally ill" because they have legitimate mental 29 disorders "quite apart from any secondary deviance". Moreover,
stigma is not an issue. Although individuals may be
stigmatized, its effects on individuals are not nearly as severe
as Scheff and others have made them out to be. The stigma
process does not necessarily generate a self-fulfilling prophecy
such that the individual is hindered £rom escaping the master
status "deviantt'. 3 O
My inclination, without attempting to adequately substantiate
it here, is that, while disorders of the psychiatric kind
certainly exist, certain cases of mental illness may be more
socially constructed than others by virtue of the labelling
process and the social tendency to single out certain
individuals, lower status individuals, for example. Moreover, a
given "normal" case may be just as constructed as a given
"mentally ill" case. An individual may habour a legitimate
psychological disorder that the community, because of his/her
social standing or hidher relationship to others, refuses to
recognize. Yarrow et al3' provide evidence to this end. They
find that wives ni11 do their utmost to construct their
husbandrs behaviour as something other t han deviant. Here,
wives do al1 they can to rationalize their husbandf s erratic
behaviour because of their closeness to them. Only when the
situation becomes intolerable (penetratingly tangible) do they
identify their husbands as mentally ill. 3 2
In any case, 1 am suggesting there is diversity among mental
diseases. As with al1 diseases, some are more constructed than
others. It is, therefore, impossible to place them as a group
into the category socially-conceived-disease, let any of the
three remaining categories. There may be some, however, that
fit somewhere within the categories.
6. Repetition Strain Injury. Finally, repetition strain i n j u r y
presents an anomaly to my typology. If 1 were to adopt a purely
social constructionist point of view and criticize the disease
mode1 of it, 1 would have to categorize it as a socially-
conceived-disease* However, 1 am not convinced that there is
nothing physiological about it, nothing that is, beyond that
which i s psychosocially produced. T o make things even more
complicated, there exists no u n i f i e d understanding of what RSI
is, even within the medical community.
Repetition strain i n j u r y (RSI) constitutes a very recent
condition that has been psychologized, emotionalized, even
moralized by many. In the early 1980s in Australia, RSI - a
condition involving pain in the hands, arms and neck resulting
from repetitious work under modern office conditions,
particularly among women - broke out in epidemic proportions. 3 3 It formed the new industrial epidemic of Australia, becoming
the most common cause for taking time off work. 3 4 In so doing,
it sparked tremendous debate, debate particularly over whether
or not RSI constitutes a legitirnate disease, and more precisely
from the standard medical point of view, a work related organic 3 5 i n j u r y . There were, and are, many answers, representing, as
Bammer and Martin put it, 'an obvious tendency for analysts to
use frameworks compatible with their professional field and
persona1 commitments . "16 Some, "generally representatives of the unions involved"
attribute it to a deleterious working environment. They focus
on "the equipment and work processes suggesting that the
conditions of employment in modern offices, with the lack of
control experienced by the worker, and the drudgery of the work,
inevitably give rise to the cornplaint. "37 ~ i l l i a m s ~ ~ adopts this
position, arguing that new forms of work organization are needed
to prevent RSI. The socioeconomic conditions in Australia, he
says, have fostered the emergence of RSI. Others resist such
interpretations, insisting that RSI is neither organic nor that 3 9 it has work related origins. There are those, for example,
"generally the employers - [who take the position that RSI] is the outcome of a general lack of tone, poor posture and
a ~ f i t i i e s s ; ~ O - - T h e y also i n s l s t that aches and pains are a normal
part of certain work processes; that women with RSI are
rnalingerers intent upon securing workerfs compensation; that RSI
is "a compensation neurosis" taken on by those seeking
"secondary gain in the form of compensation payrnents, relief
from work, the sick role etc.""
Many psychiatrists c l a h that RSI is an hysterical conversion
disorder4*, or "a flight into physical symptoms from unresolved
psychological and emotional conflicts by those . . . p owerless to
change their situation^."^^ ~ u c i r e ~ ~ provides an argument to this
end, pointing out that the functional disorder was recognized as
a neurosis for over 100 years; that "conversion disorder" rnakes

sense since "the somatic presentation of unrecognized depression
or psychosis is common"; and that, to abandon such an
interpretation in favour of a medical explanation only feeds the
neurosis by legitimating the complaints. It similarly, detracts
from a more holistic approach to the problem.
Judge John Prosser QC sums up the contra-standard-medical-
model-view in a particularly derogatory manner, stating that
" R S I [is] meaningless and [has] no place in the medical books"
and that those who claim to suffer from RSI are "eggshell
personalities who [need] to get a grip on themselves". 4 5
But to get a grip on the "whatness" of RSI has, itself, proven
very problematic. RSI is an elusive phenomenon because it has
no succinct, no (specif iably) tangible (to medicine) biological
foundation. Rather, from what can be seen about it so far, it
is
a constellation of non-specific symptorns and experiences, rarely accornpanied by signs and without an identifiable pathological basis . It [does] not conform to conventional criteria for a disease or injury, nor [does] it respond to
4 6 treatrnent . Many treatments have been tried, including "analgesics, steroid
p p p p p p p p p p p - p - - - - - - - - - - -
InJectXons, occupational therapy, chiropractic, counselling,
acupuncture, immobilization by splints, plaster, physiotherapy,
hot washes and surgical ope ration^."^^ None have worked. No
"magic bullet" has been found.
As a consequence of this semi-tangibility, a serious debate
has ensued within the medical profession. The orthopedic and
rheurnatology communities in particular, "have engaged in
conflicting legitimatory discourses and constructed particular
models of RSI in efforts to persuade other experts of the
facticity, or otherwise, of the condition. ""
As well, a more general, debate has occurred over whether or
not RSI even exists. Some, like ~adler~', are insistent that it
does not. Relatedly, many doctors and other professionals
propound the psychosomatic view, drawing upon wider cultural
values and moralistic assumptions to explain the disorder. 5 0
Some daim women are lying. Some make comments on the
importance of women staying at home, of women doing housework,
of women being good rnothers, on the therapeutic value of
pregnancy, etc.. Their reasoning: women would not have RSI if
they conformed to such standards. Relatedly, there are those
who understand RSI to have foundations in psychological factors
unique to women, factors "having to do with their gender, family
circumstances, body shapes and esnotional di~tress."~~ Women are
in various ways implicated for their (supposed) distress. As
Reid et al. explain, " [w] omen [are] judged guilty (and [feel]
guilty) for experiencing pain which [can] not be located,
explained or banished. ,f 52 In this view, RSI is a manifestation
of psychological/moral weakness, while the person so afflicted
is a psychological, moral deviant. The result for women,
moreover, has been quite negative. According to Reid et al,
women are forced into a "pilgrimage of pain," into a seemingly
endless journey to find credibility for both their conditions
and themselves, to find some professional who will recognize and
alleviate their suffering.
But the confusion, the conflict, is to be expected. Where
there is semi-tangibility (where there is no identifiable,
systematic biological base; where there are no clinical signs or
identifiable underlying pathologies; where there is no clear fit
with the biomedical mode1 of disease or the doctrine of specific 5 3 etiology), linked with tangible threat (people taking off work,
and doing so more and more for (so they say) physiological
reasons), al1 manner of construction is only to be expected.

Having said this, there rnay be legitimacy to the psychological
profile of the condition. ~urner'~ points out that
there may be certain psychological factors which predispose some workers to suffer frorn this form of muscular problem, since it is clearly the case that not al1 workers exposed to the same set of conditions claim to experience pains in the upper part of the a m . These factors of vulnerability may be related to anger and stress.
As well, there is the issue of "why R S I appeared in Australia at
the particular time it did, why it achieved epidemic proportions
in the early 1980s, and why it was contained within certain
states and work areas."
On the other hand, RSI is receiving more credibility as a
legitimate biological disorder. In its spring issue of "At
Work", The Institute for Work and Health announced the launching
of the RSI Watch project in Ontario. The Watch is based on the
conviction that " [rlepeditive strain injuries are muscle, nerve,
and tendon disorders that affect hands, wrists, shoulders, arms,
or elbows and are associated with work and non-work factors."55
The purpose of the Watch is to help detennine the "nature of the
RSI problem, the reasons for it, how best to approach it, and
the action w e need to take to reduce it? There is currently
an interest in addressing a real "work-related musculoskeletal
disorder. "!j7
Now, 1 am not about to attempt to resolve the debate over that
'what" of RSI. Maybe it is a conversion disorder; maybe it has
real physiological foundations; maybe it iç a convenient excuse
for malingerers. Maybe there is some truth to a l1 these ways of
seeing RSI: maybe each is seeing something different yet
(relatively) true about RSI. I donr t know.
Whatever the case, 1 am unclear how to categorize RSI. If it
were to be concretely demonstrated to have no physiological
foundation in the way that hysteria and drapetornania have no
(verifiable) physiological f oundation, and yet be constructed as
a disease as hysteria and drapetomania were, then it would fa11
into the first category as hysteria and drapetomania do. On the
o the r hand, 1 am inclined to treat RSI-as-moral-failure as a
socially-conceived-phenornenon (if not disease) - as a reified symbolic stand-in for certain (patriarchal) moralities. But 1
do so hesitatingly, for there may be (at least) something t o the
malingering hypothesis: lousy work conditions can easily inspire
malingering. There may also be something to the conversion
disorder hypothesis: emotional stress, depression, etc., due to
lousy work conditions, can easily translate into physiological
pain..,
1 could go on. The main point is that 1 am unclear as to how
to classify RSI. 1 am unclear for two reasons. First, I am
ambivalent about how best to understand RSI. Second, my
typology is insufficient, from what 1 can tell, to help me
understand it.
. . . . . . . . . Nevertheless, whether my typology is sufficient or
insufficient is, for my purposes, a secondary issue. Again, my
intention has been simply to provide a provisional typology to
help think about the relativity of the social construction of
disease - to illustrate that the relativity of social construction of disease is a reality. To this end, 1 would like
to suggest that the typology is a useful one, for while it does
not adequately account for the many ways and degrees in which
diseases or "diseases" like childbirth, infertility, a variety
of mental illnesses, and R S I are (medically) constructed, it
does account for such variation in diseases or "diseases" like
hysteria, menopause, AIDS, TB and other infectious diseases,
various acute conditions, slave "diseases" and leprosy.
Now to the implications that follow from the relativity of the
social construction of disease. In what follows, the
theoretical utility of interparadigmatic collaboration is
highlighted.
IMPLICATIONS: TaWARDS THE UTILITY OF INTERPARADIGMATIC
COLUBORATION
'Abdu'l-Baha writes:
Whatsoever thou dost see about thee - wondrous products of human worhanship, inventions, discoveries and like evidences -each one of these was once a secret hidden away in the realrn of the unknown. The human spirit laid that secret bare, and drew it forth from the unseen into the realrn of the visible . . . [ Elach and every one of these was once a mystery, a closely guarded secret, yet the human spirit unravelled these secrets and brought them out of the invisible into the light of day. 5 8
He also writes:
... when you meet those whose opinions dif fer f rom your own, do not turn away your face from them. Al1 are seeking the truth, and there are many roads leading thereto. Truth has many
5 9 aspects. . . As expected, the avowed horizontalist would take issue with
the first statement. Both s/he and the avowed verticalist would
take issue with second statement. But they would do so for
radically different reasons. The latter would insist upon there
being only one road, or some best road, to truth. The former
would refute the existence of any truth besides made truth.
S/he would insist that no mysteries have been revealed since
there are no veritable mysteries nor secrets. There are only
made mysteries, made secrets. There are no roads to truth, only
roads to construction.
This book lays the theoretical foundation for adopting an
entirely di£ ferent approach to knowledge and truth, one that
differs from both the verticalist and the horizontalist
approaches while retaining elements £rom each. Relatedly, it
lays the theoretical rationale for taking the utility of
meaningful interparadigmatic collaboration seriously. It lends
credence to the orientation that says: "[l]etrs give this branch
of knowledge, and this one and this one, a meaningful chance.
Indeed, let's examine each closely to see what each can o f f e r .
Maybe they have some profound insights into reality. And maybe
we have sornething to o f f e r them in r e t u r n . "
1 Say this for two reasons. First: any particular way of
knowing, any paradigmatic view, may see something (relatively
clearly) about reality. This point first emerged in Chapter 4
in which tangibility - and hence, the relativity of social
construction - was introduced. For any given paradigm,
(relative) phenomenal (aspectual) tangibility (whether it be
general, specified o r anomalic tangibility) i s always a
possibility. It is always a possibility because, first and
forernost, reality imposes demands. More precisely, phenornena
(or aspects thereof) impose demands. They constrain (and
enable! ) what we say of them, what we construct of them. But
they do so in different ways and to different degrees.
Sometimes they impose constraints across (basically) a l 1
paradigms and so radiate general tangibility. "The Sun is hot"
is one such case. "The typewriter is on the table" is another.
These are obvious facts about the way things are, that in a
manner of speaking, clamour to be known as what they are. 6 O
Similarly:
If my cat is asleep on the bed, or if a certain group of men did not plant the bombs they are in jail for supposedly having planted, or if the Nazis brought about the deaths of millions of Jews, there is some core 'way things are' about this ... It constrains adequate belief. 6 1
I f it doesn ' t , then t o paraphrase Geras, t h e r e would be no such
t h i n g s a s a l i e i n our un iverse . 6 2 Other t imes, phenonena ( o r
a s p e c t s thereof) impose s e l e c t i v e c o n s t r a i n t s . They r a d i a t e
s p e c i f i e d o r anomalic t a n g i b i l i t y i n d i f f e r e n t ways/degrees t o
d i f f e r e n t paradigms. The manner and degree t o which t h e y do s o
depends i n l a r g e measure upon t h e paradigmatic l e n s through
which t h e y are seen ( o r not seen as t h e ca se may b e ) . The
r e s u l t i s t h e r e l a t i v i t y of t h e s o c i a l cons t ruc t i on of r e a l i t y .
Second, and once again l e a d i n g t o t h e r e l a t i v i t y of the s o c i a l
c o n s t r u c t i o n of r e a l i t y : it i s a l s o p o s s i b l e t h a t any p a r t i c u l a r
way of knowing can ( is) i n t e n s i f y (ing) i n t o what i t sees . That
it can ( i s ) unravel ( l i n g ) a c e r t a i n mystery of reality.
Paradigms extend a s they a r t i c u l a t e . They conform, d i s t o r t ,
c o n s t r u c t a s they articulate. B u t it i s a l s o p o s s i b l e t h a t a s
t hey a r t i c u l a t e , they i n t e n s i f y . This was the major point of
Chapter 5 .
Taken t oge the r , t h e c o r o l l a r y i s t h a t any p a r t i c u l a r way o f
knowing may be ab le t o shed some l i g h t on some a s p e c t ( s ) o f
r e a l i t y - on some phenomenon; while it d e f i n i t e l y cons t ruc t s ,
any p a r t i c u l a r way of knowing rnay be a l s o able t o h igh l i gh t
something of s i gn i f i c ance , t o h igh l i gh t sorne a spec t of t r u t h .
There is knowledge - a t l e a s t p o t e n t i a l l y - t o be gleaned from
Our d i v e r s i t y . So why not t a p our d i v e r s i t y t o s e e what it can
o f f e r ? W e remain unnecessa r i ly l im i t ed o therwise . W e remain
paradigmat ic extenders , even i m p e r i a l i s t s , o therwise . Hence,
t h e t h e o r e t i c a l r a t i o n a l e for t ak ing the u t i l i t y o f
in terparadigrnat ic c o l l a b o r a t i o n s e r i ous ly .
Consider t h e following analogy t o h e l p s o l i d i f y mat te r s :
Given copies of the same t e x t , the t w o readers go of f to read
them. They do so with h i g h l i g h t e r s i n hand. A s t h e y read, they
h i g h l i g h t the t e x t i n their own ways, focusing on certain
aspec t s . T h e t e x t exer t s a certain p u l l c r e a t i n g some overlap
between what is highl ighted by the two readers, b u t t h e pu l l i s
not so strong such that what they highlight achieves conformity.
The r e a d e r s ' d i s t i n c t paradigma tic expecta t i o n s exert t h e i r own
pulls.
Having finished reading, the t w o r e a d e r s then zero in on their
respective h igh l igh t s , perhaps underl ining them on one occasion,
h igh l igh t ing them with a second color on yet another occasion.
And this they do f o r the purpose o f accentuating the aspects
h i g h l i g h t e d - i n the attempt t o intensify their understandings
of them.
Yet, a s they h igh l igh t , underl ine, and h igh l igh t a g a i n , the
readers progressively lose s ight o f the rest of the t e x t . T n e y
a s p e c t u a l i z e and t h u s diminish the text -in -between . Through
h igh l igh t ing e t c . , the text-in-between fades from poten t ia l
prominence becoming the s u p e r f l u o u s , or the tangent ia l , or the
s i l e n t , or the understood-in-light-of - t h e - h i g h l i g h t e d ( i n light
o f t h a t which they see t o sorne extent) . The h igh l igh t s become
the t e x t t o each reader. The original text is thus limited,
a l t e red , distorted, constructed.
Then the two readers meet t o snare with each other their
respective i n s i g h t s on the t e x t . On that occasion they find,
upon listening t o each other, that they have missed some things
- tha t t hey have missed/ignored/forgotten certain a s p e c t s t o the
t e x t . As they collaborate, their knowledge of the text
develops. I t broadens and becomes more comprehensive.
In shor t , here' s the equation in brief :
1 . W i t h each paradigm there lies the possibility of seeing
(reiatively clear ly) , of intensif ying, and hence, of aspectual (phenomenal) illumination.
2. T h e more aspects revealed, the more comprehensive the textual
(phenomenal, r e a l i t y ) picture .
3. There is, therefore, (at least theoretically) tremendous
benefit to looking to each paradigm for insight. Otherwise w e
are certain to remain partly (if not predorninantly) blind to
reality (to any given phenomenon).
Galileo says that " . . . t h e r e is not a single effect in nature,
even the least that exists, such that the most ingenious
theorist c m arrive at a complete understanding of it."63 1 would
suggest t h a t perhaps a complete understanding of it is never
achievable no matter what. But a more comprehensive, more
penetrating one is definitely a possibility with
interparadigmatic collaboration.
Thus, I am inclined to agree with Nietzsche when he says:
There is only a perspective seeing, only a perspective 'knowingf; and the more emotions we allow to speak about one thing, the more eyes, different eyes, we can use to observe one thing, the more complete will Our 'conceptf of this thing, our 'ob j ectivityf , be . 6 4
(Although Nietzsche does not believe that a more complete
concept is a more true concept.) And with Feyerabend when he
says :
Still, there are many things we can learn from the sciences. But we can also learn £rom the humanities, from religion and £rom the remnants of ancient traditions that survived the onslaught of Western Civilization. No area is unified and perfect, few areas are repulsive and completely without
65 merit
And with Sorel1 when he says that:
A framework is needed that enables one to recognize the considerabfe value of science alongside the considerable value of rnany other parts of learning. 6 6
And with Turner when he advocates a 'strategy of inclusion' as
opposed to a 'strategy of exclusionf, the latter being an
unfortunate tendency in sociology
where people adopt a particular theoretical tradition, or a social theorist, or a particular paradigm, and then proceed to destroy al1 the other traditions, theorists or paradigms as competitive or incompatible with their preferred position. 67
A tendency, moreover, that is not lirnited to sociology. As
Feyerabend explains :
No idea is ever examined in al1 its ramifications and no view is ever given al1 the chances it deserves. Theories are abandoned and superseded by more fashionable accounts long before they have had an opportunity to show their virtues. 6 8
The only thing that should be excluded is the strategy of
exclusion itself. To adopt a strategy of exclusion is to retard
potential accesses, to suppxess potential penetrations into
reality. To exclude is to lose as any paradigm may surprise. 6 9
Yet, when I Say this, 1 want to be clear on something,
something essential. By discounting the strategy of exclusion 1
am not suggesting that every paradigm should remain as it is,
that paradigms should never alter, nor develop, nor dissolve.
T h e object ive is n o t to sa f eguard the paradigm a s it is. T h a t
would be a fxuitless objective. That would entai1 safeguarding
paradigmatic extensions along with possible paradigmatic
intensifications. That would even entail safeguarding highly
extended paradigms, paradigms that may concurrently have l i t t l e
to offer in the way of intensification. And the whole point is
to reduce extension. Paradigmatic extension is the problem.
Comprehensive intensification is the objective.
Instead, my point is that when paradigmatic change occurs, it
should occur as a consequence of interparadigmatic
collaboration. It should occur as a consequence of new insights
gained. With new insights cornes (moderate, radical,
evolutionary, dissolutionary) paradigmatic change - beneficial
change.
Now, having said al1 this, I have begged a number of
questions. First: is interparadigmatic interaction really
possible? Second: if it is, then how is it to be rneaningfully
fostered? Third: can interparadigmatic interaction really
affect more adequate, and more comprehensive, intensifications
into the truth of things? These are questions, however, that 1
address in future work. (Although, to give j u s t a hint of
things to corne: the daim is that interparadigmatic interaction
can occur; that it can be meaningfully fostered; that it can
ef fect more adequate, more comprehensive intensifications into
the truth of things; and that it can do so effectively only
through the communicative process consul ta tion. )
For now, the theme is simply that there is utility to
interparadigmatic collaboration - at least theoretically
speaking. The relativity of social construction implies
potential within any paradigm to see and intensify. The
potential within any paradigm to see and intensify is the
theoretical rationale for fostering meaningful interparadigmatic
comunication.
More specifically, the potential (indeed, reality) within p p p p p p p p p p p p p - - - - - - - - - - - - - -
- - - -
medicine and social constructionism to variously see and
intensify as indicated by the relativity of the social (medical)
construction of different diseases (like hysteria compared to
menopause, compared to AIDS, compared to (recent) TB), 1 would
like to suggest, theoretically justifies the utility in
fostering meaningful
INTERPARADICMATIC COLfrABORATION BETWEEN MEDI CINE AND SOC=
CONSTRUCTIONISM
Thus, 1 would like to suggest that for social constructionism
to devote itself solely to the refutation of medicine - or any
other approach for that matter - is for social constructionism to be engaged in an unfortunate enterprise. It is, in truth,
for social constructionism to practice exclusion. For rnedicine
to medicalize and to do so based on claims to privileged access
to the way things are with health, illness and disease, is
sirnilarly for medicine to be engaged in an unfortunate
enterprise. It is for medicine to practice exclusion. Both
enterprises involve paradigms getting caught up in themselves,
extending, "imperializing". Both are verticalist, logocentric
enterprises . . . p resumptuous enterprises.
That medicine is lirnited is more than clear. It is limited in
the sense that it does fabricate, in that it does construct
diseases. This is especially true in the case of socially-
conceived-diseases like hysteria, menopause and drapetomania,
"diseases" that have corne to exist because medicine ( o f t e n in
lins with dominant social assumptions, more generally) has
conceived them so. As socially-conceived-diseases, they are
reifications devoid of any grounding in that which is true of
disease. The sarne cannot be said of rnanipulated-diseases like
AIDS and leprosy, however, which are definitely real diseases,
thus indicating relativity in the medical construction of
disease. At the same time, medicine has had a hand in their
construction as w e l l , suffusing them and thus manipulating them
into realities they need not be. 7 O
Then again, there are certain diseases that are relatively
tangible to medicine as both threats and otherwise, indicating
even greater variation in the degree to which diseases are
(medically) constructed. Socially-augmented-diseases,
conditions like aortic stenosis, gout, gonorrheal arthritis,
gaping wounds, broken bones, toothaches, various inf ectious
diseases, TB (until recently) are, I would suggest, good
examples. While constructed through aspectualization and
supplernentation, there are aspects to these diseases that
medicine (relatively) sees and has intensified into. There is,
t h e r e fo r e , u t i l i t y i n looking t o medicine. I t sees t h e s e
d i seases , o r c e r t a i n of t he i r a s p e c t s . I t , t he r e fo r e , has much
t o o f f e r .
So does s o c i a l cons t ruc t ion i sm have much t o o f f e r , as t h e r e
are th ings r e l a t i v e l y t a n g i b l e t o it. The med ica l i z a t i on of
menopause i s , 1 would sugges t , a good example. The s o c i a l
cons t ruc t i on of hysteria a s disease, i s a n o t h e r . Both medicine
and s o c i a l cons t ruc t ion i sm c o n s t r u c t d i s ea se ; both also s e e
things about d i s e a s e . They see , moreover, d i f f e r e n t t h i n g s , and
so cons t ruc t some things less so t h a n o t h e r s . Medicine s e e s
more about t h e r e a l i t y of i n f e c t i o u s d i s e a s e and so c o n s t r u c t s
i t l e s s than it does o t h e r d i s e a s e s ; s o c i a l cons t ruc t ionis rn sees
more about t h e reality of h y s t e r i a , and s o c o n s t r u c t s i t less
t h a n when it goes on t o Say t h a t a l 1 d i s e a s e s are social
cons t ruc t s .
I n short, i t would seem t h e r e is u t i l i t y i n medicine and
s o c i a l cons t ruc t ionis rn looking t o each o t h e r f o r i n s i g h t . T h e i r
mutual i n t e r a c t i o n can he lp abate t h e medical c o n s t r u c t i o n of
d i s e a s e . I t can he lp aba t e t h e social c o n s t r u c t i o n i s t
construction of d i s e a s e . F ina l ly , it can y i e l d a more
comprehensive p i c t u r e i n t o any p a r t i c u l a r disease, not t o
mention h e a l t h , i l l n e s s and d i s e a s e i n gene ra l .
This i s a s i g n i f i c a n t conclus ion , having d i r e c t implications
for the a l l e v i a t i o n of su f f e r i ng , s i nce , t o r epea t , the more we
know about d i s e a s e , t h e b e t t e r w e equipped w e are t o add re s s it,
t o eliminate i t s d e l e t e r i o u s consequences.
In Sunimary
Let m e pu t t h i s a l 1 one f i n a l way:
While the s o c i a l c o n s t r u c t i o n i s t approach t o medicine and
medicalization i n p a r t i c u l a r has m e r i t , 1 am h e s i t a n t t o s t r i p
medicine completely o f i t s v a l i d i t y , rendering it simply a
manifestation of socia l /power p rocesses . I n f a c t , t o deny
medicine its relative validity - to deny that there are things which are relatively tangible to it, that there are diseases it
has not ( relatively) constructed, on the grounas that everything
is perspective - is to reject social constructionism itself as valid. But social constructionism has validity because there
are phenomena that are relatively tangible to it. There are
phenomena it has not (highly) constructed. It claims, and does
so justifiably as we have seen, that the social construction of
disease occurs. The social construction of these phenomena
(some more than others) , is a phenomenon with (relative) specified tangibility to the social constructionist approach.
Thus, unless we are going to grant privileged status to social
constructionisrn raising it to some super-paradigrnatic fevel such
that only it can know - a contradiction given its emphasis on perspectivisrn and zero truth besides made truth - we have to accept the possibility that rnedicine has some validity - that for medicine, some things (many things!) are relatively
tangible. That while medicine extends and so constructs a lot
of things, it also intensifies into a lot of things. The
relativity of the medical construction of hysteria cornpared to
AIDS compared to (recent) TB compared to toothache, as
demonstrated herein, speaks to this reality, and hence the
(relative) validity of the medical approach.
Hence the utility in their interparadigmatic collaboration ... ... at least theoretically speaking. It still remains to
demonstrate such utility with concrete examples. But this 1
leave for another book.
Now for ... SOME PHILOSOPHICAL IMPLICATIONS - ZN BRIEF
First, this study lends much credence to Turner's formulation
that some things are more socially constructed than othexs. But
it also goes beyond it, articulating, for example, how such

relativity occurs, its curvilinear relationship to tangibility
(see Chapter 4), its implications for interparadigmatic
collaboration, etc.
Second, it challenges both the verticalist and horizontalist
approaches to reality. As far as the former is concerned, it
repudiates the idea that there is one best way to get at the
truth of things. As far as the latter is concerned, it
repudiates the antifoundationalist notions of theorists like
Foucault, Rorty and Derrida, that truth and reality are purely
social (language, epistemic, paradigmatic) ai fairs . There is
truth beyond created truth, essence beyond imputed essence.
Third, it builds on and modifies t y p i c a l understandings, based
in large measure on the wowk of Kuhn, of the nature of
paradigmatic articulation. The most essential innovation
involves the recognition of the dual processes of paradigmatic
extension and intensification. This has implications for how we
go about investigating reality, as our concern (presumably)
would be to prevent, as much as possible, our lapsing into
paradigmatic extension.
Fourth, it has very specific implications for how social - p p p p p p p p p p p p p - - - - - - - - - - - - - - - - -
constructionists think about disease. As discussed, the
tendency among constructionists is to take exernplar cases like
hysteria, menopause and RSI, demonstrate their social
construction, and then see/claim al1 diseases as constructions.
The analysis in Chapter 6 provides justification to offset any
such predilection.
But these, by now, are obvious implications. Hence, the
brevity with which 1 treat them. There are others, however,
epistemological/ontological ones, that I have only alluded to so
far, but which deserve some introduction before corning to a
close. One is the question of eternality, and in particular

The Question of Bternal Questions
It may be recalled that horizontalists like Rorty are tired of
what they refer to as the language game of philosophy. (This
was mentioned in Chapter 3.) They are tired of the perpetual
verticalist attempt to tap into the way things are, to solve the
"deep" problems of philosophy. For Rorty, there are no deep
problems. There are only temporary problems, problems produced
by certain vocabularies. The real questions are
What sort of people would see these problems? What vocabulary, what image of man, would produce such problems? Why, insofar as we are gripped by these problems, do we see them as deep rather than as reductiones ad absurdum of a ~ o c a b u l a r ~ ? ~ ~
The "eternal" problems of philosophy are simply that: the
eternal problems of philosophy - or more accurately, traditional philosophy, verticalist philosophy. They are, therefore,
temporary constructions, unnecessary constructions: "[Tlhere are
no problems which bind the generations together into a natural
kind cal1 "humanity. "" Create a new vocabulary, eschew
verticalist philosophy, and you get new problems. And this is
exactly what Rorty is after. He is after a new kind of human
that can relinquish the questions that have plagued us for so
long, a liberal ironist capable of creating anew, and doing so
over and over again. In his words:
A sense of human history as the history of successive metaphors would let us see the poet, in the generic sense of the maker of new words, the shaper of new languages, as the
73 vanguard of the species.
New metaphors, new languages, new creations. New metaphors, new
languages, new problems - new constructed problems, that is - with which to grapple.
But herefs the question: Can w e ever totally avoid certain
problems? Can we ever construct a language such that certain

problems are forever forgotten? Forever buried? Are there not
problems that plague us all? Are there not questions that
transcend the diversity? That ground the diversity? That
demand of us universally? That have always demanded of us? I
think there are. As Jostein Gaarder's protagonist Alberto Knox
says: "We know of no culture which has not concerned itself with
what man is and where the world came from. rr 7 4
I certainly do not deny that there is some truth to what Rorty
and other horizontalists are saying. Definitely the equation
"new language, new problems" makes sense, at least to a point.
Different languages unquestionably give rise to different
problems. One only has to point to the cross cultural variation
to confirm this fact. But I would also suggest that amongst the
diversity there exists a perpetual unity - that there are
certain concerns we can never fully escape. Every language,
every paradigm, is invariably lured in by thern. Every language,
every paradigm invariably succumbs to them. Every language,
every paradigm is somehow founded upon answers given to them.
The equation, "new language, new problems (invariably) coupled
with eternal problems", seems to make more sense.
Cons ider
The Issue of Representation
and this becomes clearer.
Both Rorty and Derrida think the project of representation as
correspondence t o r e a l i t y has run its course. Rorty wants to
deny "that the notion of 'representation,' ... has any useful role in philosophy. ' r 7 5 AS ~ e r a s ~ ~ explains Rorty' s position:
we should let go of any idea ... of knowledge or truth as correspondence. This is 'an uncashable and outworn metaphor' of which several hundred years of effort have failed to make u s e f u l sense.
It is an outworn metaphor because

. . .there is not.. .a w a y t h i n g s . . . a r e d o m t h e r e , n o t 'a Way The World 1s' . . . The i d e a of 'something which i s what it i s a p a r t from language, a p a r t frorn any d e s c r i p t i o n ' [Ror ty says] i s one of ' t h e psuedo-problerns c r e a t e d by the e s s e n t i a l i s t t r a d i t i o n f . 'A p ragmat i s t must . . . i n s i s t ' , Rorty says , ' t h a t t h e r e i s no such t h ing as the way the t h i n g is i n i t s e l f , under no d e s c r i p t i o n , a p a r t from any use t o which human beings might want t o pu t i t . '
W e should, t h e r e f o r e ,
. . . j e t t i s o n a whole group of metaphors t h a t i s ent renched w i th in our t h i n k i n g about knowledge and t r u t h : metaphors of v i s i o n and mir ro r ing ; ' t h e p i c t u r e theory of languager and t r u t h a s accuracy o r r e p r e s e n t a t i o n ; what John Dewy c a l l e d the ' spec ta to r theory ' .
Moreover,
[ w l i t h those metaphors [would a l s o go] the i d e a o f sorne r e p r e s e n t a t i o n s vocabu la r i e s having more 'adequate' r e l a t i o n t o r e a l i t y . 'There i s no d e s c r i p t i o n which i s somehow "c loser" . . . ' t o what i s being expla ined, t h e r e i s only t h e exp lana t ion which best s u i t s a given
7 7 purpose.
Derr ida a g r e e s . Derr ida ' s work is " the l a t e s t a t tempt . . . t o
s h a t t e r the Kantians ' ingenious image of themselves a s
a c c u r a t e l y r ep r e sen t i ng how th ings r e a l l y are ."78 With Rorty,
Derr ida has it t h a t " [ b l y cons t ruc t i ng and u s i n g an a l t e r n a t i v e
t h e o r e t i c a l vocabulary i n which t h e metaphor of r e p r e s e n t a t i o n
d i d no t occur, t h e [ "e te rna l " ] problems would d i sappear . , 7 9
Con t r a r i l y , I would l i k e t o propose t h a t t o (more o r less)
r ep re sen t r e a l i t y i s unavoidable, f o r a t l e a s t two reasons .
F i r s t : t h e r e is a world out t h e r e , and it, more o r l e s s , and i n
d i f f e r e n t ways, cons t r a in s what we do wi th it, how we c o n s t r u c t
it. Accordingly, what w e c o n s t r u c t of it is , more o r l e s s , an
adequate r ep r e sen t a t i on o f i t . The degree t o which w e
adequate ly r e p r e s e n t it is a ma t t e r o f phenomenal-paradigmatic
f i t , which i s i n t u r n a f u n c t i o n of t a n g i b i l i t y . (See Chapter
4 . ) And t h e r e are definitely degrees to representational
adequacy. Some 'tools" (concepts, theories, pictures) represent
things about reality much better than others. Gerasr
illustration in this regard 3s telling:
1 Say, f o r example, knowing or believing it to be so, 'Richard Rorty is in the vicinity. Please find him; he looks like this. ' 1 hold up my copy of Contingency, Irony, and So l idar i t y , bearing a photograph of Rorty on its front cover. What tool or irnplement would serve as effecti~el~?'~
I ' m p r e t t y sure that were either of rny t w o sons to draw crayon
pictures of Rorty, as tools t h e y would not serve nearly as
effectively. My own drawing of him would probably do the job
little better.
Second: as Hacking says: "People represent. That is part of 8 2 what it is to be a person. "*' We are homo depictor. At the same
tirne, according to Searle, "representing lies at the heart of
language. Representation is of the essence of language. "83 We
cannot escape it. We must represent.
In one sense, horizontalists would agree with this last
statement. They would agree insofar as they maintain that the
world is a tapestry of representations (or signifiers as Derrida - - - - - - - - - - - - - - - - - - - - -
- - - - - 8 4 - - - - - - p u t s Tt ) . They would not agree, however, insofar as
representation means correspondence (to reality, or truth) . But
representation as correspondence, 1 want to maintain, is
inescapable, at least relatively so. Not even horizontalists
can f u l l y escape it. Think of what horizontalists are doing
when they go about criticizing the verticalist attempt to
represent reality. Think of what they are doing when they
propound antirepresentationalism? They are (more or l e s s )
represen t i n g an tirepresenta tional ism. They are saying " this is
what we mean by antirepresentationalisrn." Indeed, they write
volumes about how to be a good horizontalist, a good liberal
ironist, a good superman, a good antirepresentationalist. They
write volumes describing, representing, their novel approaches
to antirepresentationlism, to anti-essentialism, to the de-
centred (wo)rnan, to anti-philosophy, to how to deal with a
nebulous world. And when horizontalists set about answering
their verticalist (and other) critics, they are representing al1
over again.
On the one hand: in line with their antirepresentationalist
stance, they Say things like "full power to the reader". They
permit "the reader unlirnited f reedom in reading, complete
autonomy, the liberty or license to interpret the text without
constraint." They grant the reader "an unprecedented
significance by subjectively constructing meaning." Indeed,
" [il n the extreme" they give "each reader. . . absolute power, holding the right to any interpretation without restraint of
evidence, objective cues £rom the text, or the wishes of the
author.. ."85 The text is wide open to the whims of the reader.
It is at the mercy of the reader. It is, therefore,
nonrepresentational, at least authoritatively.
On the other hand: if this is the case, one might ask why it
is that horizontalists bother to reply to critical assessments
of their texts? For in the very act of replying, in the very
act of explicating their text, their position, and in the very
act of returning criticism, horizontalists assume that which
they ostensibly repudiate. By replying they implicitly assume,
for example, that :
their critics are misrepresenting their texts and what they are trying to say, or that the critical readings of their critics are somehow deficient. This implicitly means that the text (like reality) has a certain weight to it - a weight infused by the author. That the full autonomy of the reader is impossible. It also implicitly means that the horizontalistrs point of view is the more valid view.

they need to clarify what they actually mean by an earlier text . That they need to represent what they mean by an earlier text. Foucault, for example, gives many clarifications by what he means by the workings of power and the relationship between power and truth.
the full autonomy of the reader is not really desirable. Horizontalists writing about antirepresentationalism would like their texts to be understood. That is, they would like their particular representations of what they are saying about antirepresentationalisrn (and other things) to be understood as they represent them.
As with every other language game, as with every other
paradigmatic approach to how to do things, horizontalism,
antirepresentationalism, strives towards, and more or less
engages in representation as correspondence. Representation is
more or less inescapable, but inescapable nonetheless. It is
eternal.
Having said this, I want to be clear that 1 think the
horizontalist has a va l id point if not carried too far. 1 do
think that representation, for example, can be stifling. As has
been discussed, certain knowledges, certain representations of
the world, have dominated, imperialized, and subjugated others.
Diversity, consequently, has been squashed. This is what
totalizing theories have done and continue to do. They flourish
at the expense of other, perhaps just as valid, perhaps even
more valid, knowledges. But 1 would also suggest that the
solution does not lie in the attempt to create new languages
where representation does not figure. Such is a futile
endeavor. Instead, we are better to adopt an approach that
lo 'oks to the myriad representations in al1 their diversity, that
seeks to foster their meaningful cornparison and secure their
rnany fruits.

Now, to finish with one more simile concerned with the nature
of truth.
Truth , Chess and Consultation
In Chapter 3, we saw that Wittgenstein drew an analogy with
the game of chess. He compared it to a language game and how
each piece derives its meaning £rom the context of the game of
which it is a part.
What 1 want to do now is draw a different analogy using the
same game. 1 do this in the hopes that it will help to solidify
some of the major themes raised throughout this study. I do
this also as a way to help think about truth. Finally, 1 do
this as a way to highlight the power of interparadigmatic
collaboration for achieving truth, thus introducing the next
step in the development of the consultative approach.
Throughout this study 1 have been contrasting truth with
constructed truth. My distinction has been for the most part a
binary one, althcugh one that recognizes a profound
intermingling between truth and constructed truth, an
intemingling that varies in extent depending on the paradigm
and the phenornenon the paradigm is seeing/constructing. In the p p p p p - - - - - - - -
foklowrnng analogyPI expand thep d1sptinct ion to one that involves
an intemingling between four truth types. These truth types
are: foundational truth, empirical truth, constructed truth and
pragmatic truth. The analogy thus lends credence to the
possibility that the realist, the positivist, the social
constructionist and the pragmatist approaches each have
significant contributions to make with regard to episternology
and ontology. It consequently lends credence to the notion that
the realist, the positivist, the social constructionist and the
pragmatist should look to each other for insight . . . . . . although ...
. . . t h i s is just a simile. 1 am not about to d a i m that it
proves anything definitively. Instead, rny intention with this
simile is simply to stimulate an investigation into the
possibility/feasibility of such m a t t e r s .
W i t h t h e s e introductory remarks i n mind, here's t h e premise:
Darron is p l a y i n g a g a i n s t his computer i n a game of chess.
T h e game r e p r e s e n t s r e a l ity.
Now here' s the simile:
To Begin: Concerning Constructed T r u t h & Fouadational T r u t h
Darron i s very fond o f h i s two k n i g h t s . In f a c t , he is
obsessed w i t h h i s two k n i g h t s . When h e sits down to a game of
chess, h i s f i r s t and p r e v a i l i n g i n s t i n c t i s t o l o o k t o h i s
k n i g h t s , t o champion h i s k n i g h t s . Whenever h i s opponen t
c a p t u r e s h i s kniqhts, he gets very upset. He feels a sense of
l o s s u n l i k e when he l o s e s any of his o t h e r p i e c e s , u n l i k e when
h e loses R i s b i s h o p s , for example. Darron cares l i t t l e f o r h i s
b i s h o p s .
Darron i s e s p e c i c l l y adept a t f o rk ing h i s opponent with his
k n i g h t s , p a r t i c u l a r l y h i s opponent's k i n g and queen. His
k n i g h t s a r e h i s secret agen t s . When he looks t o the chessboard, - - - - - - - - - - -
Pris k n - i g l i t s - g l i t t e r w h i l e h i s otherppieces -fade t o al1 b u t
i n s i g n i f i c a n c e .
Darron t h u s sees the game o f c h e s s , i n d e e d , every s p e c i f i c
game, i n l i g h t of what h e can do w i t h h i s k n i g h t s . H e p lays
tbrough h i s k n i g h t s . His k n i g h t s are his panacea .
Darron has thus " k n i g h t i z e d " the game of c h e s s . Kn igh t i z ed
c h e s s i s Darron's cons t ruc ted c h e s s , his r e a l i t y , his t r u t h .
Now, cons ider t h e f o l l o w i n g q u e s t i o n s : to what e x t e n t i s
Darronfs c o n s t r u c t i o n a c o n s t r u c t i o n ? 1s i t n o t w i t h o u t i t s
foundat ions? 1s it n o t grounded, r i d d l e d w i t h e s s e n t i a l
demands? In o t h e r words: is it not limited, q u a l i f i e d , by the
real ?
With regard t o the f i na l ques t ion , t h e answer i n s h o r t is:
yes , i t i s .
Here's why:
Darron's cons t ruc t i on i s n e c e s s a r i l y t i e d t o t h e r e a l , t o the
foundational . It is t i e d , f o r example, t o c e r t a i n e s s e n t i a l s ;
t u , f o r example, t he f ac t t h a t : 1 . kn igh t s can o n l y make L-
shaped moves; 2 . kn igh t s are prone tc capture; 3 . k i n g s need t o
be protec ted from checkmate; 4 . no two pieces can occupy t he
same square; and 5 . knights cannot move, nor can any p i e c e , if
it means p u t t i n g the team's k ing i n t o check; etc. . When Darron
t ransgresses any of t he se fundamental c o n s t r a i n t s , when he
contravenes any of t he se foundational t r u t h s , he ge t s feedback
o f the neqa t i ve (con t rad ic tory ) s o r t . H e faces anomaly. And
sometimes it is glar ing anomaly. Sometimes the c o m p t e r f reezes
t h e game and emits messages l i k e : "Knights make L-shaped moves
on ly !" o r "You cannot put your k ing i n t o check!"
So Darron ' s cons t ruc t ion i s s i m u l taneously a y i e l d i n g of
s o r t s . I t is a cons t ruc t ion that conforms ( t o some d e g r e e ) t o
c e r t a i n demands; t h a t p e r s i s t s w i th in c e r t a i n c o n s t r a i n t s .
Darron does n o t , for example, cons t ruc t kn igh t s t h a t are
c a p t u r e 1 e s s f p much l e s s -knightsP tha t can share squares wi t h o ther
p i e c e s , nor kn igh t s that make Z-shaped moves. Darron is too
at tuned t o t h e L-shaped-movement r e a l i t y of h i s k n i g h t s , no t t o
mention certain o ther reali ties.
Sometimes, however, t he anomaly he faces is n o t so g la r ing .
I t i s no t so g la r ing , f o r example, when Darron l o s e s his bishop
t o h i s opponent. This is not t o Say t h a t he doesn' t feel a
twinge of recogni t ion when he l o s e s his bishop. This he does.
O n such occasions he is prodded and o f t e n t h l n k s t o h i m s e l f
something l i k e : "Bishops mcve diagonal ly ; I should have moved it
a few squares t o avoid the capture." B u t i t i s o n l y a m i ld
twinge he feels . I t i s o n l y a g e n t l e prodding he feels s ince he
cares l i t t l e for h i s b i shop . f i s main concern are h i s kn igh t s .
Darron is, t h e r e f o r e , much more detached from c e r t a i n
foundational t r u t h s than o thers . Why? Because he sees t h e game
through h i s kn igh t g la s se s . H e t hu s l o s e s touch with h i s o ther
p i e c e s , w i t h t h e i r foundational reali t ies. And so he cons t ruc t s
them accord ing ly . Through his kn igh t g l a s s e s he ex t ends . He
d e f i n e s t h e r e a l i t y o f the bishop, the r e a l i t y of t h e c a s t l e ,
the r e a l i t y o f the pawn, i n l i g h t o f the knight. H e knightizes
the b i s hop , t h e c a s t l e , the pawn.
And, yet again , h i s k n i g h t i z a t i o n of them he can t a k e o n l y so
f a r . R e a l i t y a l lows him t o cons t ruc t only s o f a r . A s he
k n i g h t i z e s , h e i n v a r i a b l y cornes up agains t c o n s t r a i n t s . N e
never , f o r example, g e t s t o the p o i n t o f rnaking a k n i g h t o u t of
h i s b i shop . For i f he t r i e s , he faces anomaly. H e i s reminded
t h a t b i shops o n l y move along diagonals . That t o move d iagona l ly
i s e s s e n t i a l t o b i shops . A s he cannot move them i n L-shapes, he
can never make o f them kn igh t s . So, by k n i g h t i z i n g his bishops
he dues something e l s e . H e cons t ruc t s them b y r e d u c i n g them, by
devaluing them: he d imin i shes them: he d im in i she s b u t does not - - - - - - - - - -
&fi t e r a t e fzheir e s s e n f i a l - capac typ to i o v e d i a g o n a l ly.
In s h o r t , Darronrs cons t ruc t i ons are cons tra ined by,
i n termingled w i th , the foundational . More p r e c i s e l y , they are
tied i n vary ing degrees t o v a r i o u s r e a l i t i e s . This m e a n s t ha t
he is a t tuned t o t h e foundat ional , but that he i s so t o v a r i o u s
e x t e n t s . Darron, f o r example, i s a t tuned to the fact t h a t
k n i g h t s make L-shaped moves only . H e i s l e s s attuned the
d i a g o n a l power o f t h e b i shop .
To Continue: Adding Eupirical T r u t h t o the Mix
These t r u t h s are in termingled w i t h the empir ica l as w e l l . I n
the f i r s t p lace , t h e empir ical incorporates t h e foundat ional .
An empixical s i t u a t i o n i n v o l v e s the "whatness" o f the p i e c e s

comprising t he s i t u a t i o n . But more t o t h e po in t , the "whatness"
o f t h e s e p ieces , along w i t h t h e i r pos i t i o n i n g e t c . , i s seen and
cons tructed through kn igh t l e n s e s . As Darron p l a y s , he sees
each s i t u a t i o n i n l i g h t of h i s kn igh t s , i n l i g h t o f what he can
do wi th his kn igh t s . In o t h e r words, Darron k n i g h t i z e s each
empirical s i t u a t i o n . He t h u s cons t ruc t s each empir ical
s i t u a t i o n .
But h i s cons t ruc t ions , once again, are not simply
cons t ruc t ions . They i n v o l v e attunement t o the emp i r i ca l , i f
o n l y t o some extent. They i n vo l ve pene t ra t ion i n t o ce r ta in
empir ical p o s s i b i l i t i e s , i f o n l y t o some e x t e n t . They invo lve
con formi ty t o cer ta in empir ica l c o n s t r a i n t s , if o n l y t o some
e x t e n t .
Consider t h e fo l lowing scenar io:
I t is Darron's move.
Upon i n ve s t i ga t i on o f the par t i cu la r s i t u a t i o n , Darron becomes
a t tuned t o t h e empirical truth tha t i f he moves one o f h i s
k n i g h t s , he puts h i s k i n g i n t o check. So he knows he can ' t move
t h i s kn igh t unless he wants t o l o se . However, he a l s o becomes
v e r y a t tuned t o another empir ica l t r u t h - t h a t h i s second knight
is i n p o s i t i o n t o capture h i s opponent's c a s t l e . Wi th one
simple L-shaped move, h i s opponent 's c a s t l e is h i s t o r y . And
what's even more e x c i t i n g , the move r e s u l t s i n a fork. By
moving h i s knight t o t ake h i s opponent's c a s t l e , Darron
concurren t l y places h i s opponent 's queen and bishop i n a f o r k .
This is great news for Darron.
Thus , through h i s k n i g h t s , c e r ta in empir ical real i t i e s shine.
They become apparent t o h i m . He becomes at tuned t o them. And
y e t , he becomes more than just attuned t o them. H e becomes
f i x a t e d on them. H e a s p e c t u a l i z e s them rendering the e n t i r e
empirical s i t u a t i o n seen/cons tructed i n l i g h t of these very
s p e c i f i c empir ical t r u t h s . H e t hus c o n s t r u c t s the e n t i r e
empir ical s i t u a t i o n into a golden oppor tun i t y t o fork.
Yet, as l u c k would have it, Darron constructs it so to his
inevitable l o s s .
Why? Well ( t o cont inue wi th t h i s p a r t i c u l a r scenar io ) , because
Darronf s f i x a t i o n i n h i b i t s h i m from see ing c e r t a i n o t h e r
r e a l i t i e s i n h e r e n t t o the empir ical s i t u a t i o n . S o fixated is
Darron on h i s k n i g h t s and what t h e y can do, so f ixa ted i s he
upon tak ing his opponent's c a s t l e and making the f o r k , t h a t he
i s simul taneous ly r a t h e r una t t u n e d , even blind, t o o t h e r
va luab le empir ical in format ion . In f a c t , a s i t t u r n s o u t , he
renders h i m s e l f b l i n d n o t o n l y t o va luable in format ion , b u t t o
c r i t i c a l in format ion a s w e l l . Darron f a i l s t o s e e that upon
ntoving h i s k n i g h t he c o n c u r r e n t l y opens h i s queen t o cap ture by
h i s opponent's queen. H e moreover, f a i l s t o s e e that upon
l o s i n g h i s queen i n t h i s way, his k i n g is concurren t l y p l a c e d
i n t o checkmate.
I n o t h e r words, Darron i s i n a d e q u a t e l y a t t u n e d to h i s
opponent 's queen. H e knows i t s l o c a t i o n . H e also knows that i t
c m move both d iagona l l y a s well a s v e r t i c a l l y and l a t e r a l l y a s
a l 1 queens can. B u t he a l s o sees i t i n a c e r t a i n way. H e sees
i t through k n i g h t l e n s e s . And s o t h e queen is k n i g h t i z e d . She
appears t o him o n l y in one way - a s a p iece open t o f o r k i n g .
That is a l l .
And so Darron makes h i s move and then l o s e s . H i s fork - h i s
focus - proves t o his d e t r i m e n t . Darron thus manufactures h i s
own demise.
Now it rnay be t h a t Darron's paradigmatic cons t ruc t ion is
shaken a s a consequence. I t may be t h a t he beg ins t o look t o
his other pieces w i t h more interest; t h a t he b e g i n s t o explore
what they can do . T h a t ' s one p o s s i b i l i t y .
Another p o s s i b i l i t y is t h a t Darron r e a c t s more i n f a v o r of the
s t a t u s quo. That he p e r s i s t s w i t h e v e n greater v i g o r t o
v i n d i c a t e h i s knights. T h a t i n so d o i n g , he manages t o d i s t o r t
and t h u s t o s q u e e z e h i s d e f e a t i n t o h i s "normal" parad igma t i c
box. That he r a t i o n a l i z e s : "If o n l y 1 cou ld focus more
i n t e n s e l y on what m y knights can d o , t h e n 1 wou ldn ' t end up
making the same m i s t a k e a g a i n . " T h a t , w h i l e s h a k e n , he d o e s no t
g i v e up on h i s k n i g h t s , b u t sets o u t i n s t e a d t o s a l v a g e t h e m ,
and t o do so w i t h purpose . Tha t h e commits w i t h r e n e w e d vigor
t o their r e s u s c i t a t i o n , t o their r e - l e g i t i m a t i o n , a s h i s key
a g e n t s .
I f s o , then Darron, d e s p i t e h i s c o n v i c t i o n s , remains l i m i t e d .
H e remains l i m i t e d because he c o n t i n u e s t o see and c o n s t r u c t
t h rough h i s k n i g h t s . T r u e : sometirnes t h i s h e d o e s t o his
b e n e f i t . Somet imes h i s k n i g h t i z e d a s s e s s m e n t of an e m p i r i c a l
s i t u a t i o n l e a d s t o b e n e f i c i a l consequences . Sometimes it even
l e a d s t o s u c c e s s i v e t r i u m p h s , and c o n s e q u e n t l y , t o games won.
Y e t , many times t h i s h e d o e s t o h i s d e t r i m e n t . Many times he
g e t s c a r r i e d away. Because he s e e s , c o n s t r u c t s and a d d r e s s e s
t h rough h i s k n i g h t s , h e t e n d s t o miss c e r t a i n e m p i r i c a l truths,
t o forego c e r t a i n oppor t uni ties no tw i t h s t a n d i n g his c o n v i c t i o n s
t o have t h i n g s o t h e r w i s e . He r e n d e r s himself u n a t t u n e d t o them.
H e a l s o r e n d e r s h i m s e l f una t tuned t o the f o u n d a t i o n a l
c a p a b i l i t i e s and e m p i r i c a l p o t e n t i a l i t i e s o f his o t h e r p i e c e s .
And so he misses some very c r i t i c a l o p p o r t u n i t i e s .
And s o Darron loses many games.
T o Finish: Appxoachiag Pragmat ic T z u t h
Then, one day, Darron is joined by his w i f e Debra and h i s
s i s t e r - i n - l a w Maureen. As l u c k would h a v e i t , Debra Zikes
b i s h o p s . She i s prone t o b i s h o p i z e the game. Maureen, on t h e
other hand, favors queens . S h e t e n d s to q u e e n i z e t h e game.
And together, one o f the f o l l o w i n g t w o s c e n a r i o s e n s u e :
Scenario 1 : Having seemingly incompatible v iews, Darron, Debra
and Maureen s t rugg le w i th every move. As t hey p lay , as each
empirical s i t u a t i o n emerges, t hey see i t , cons t ruc t i t ,
d i f f e r e n t l y . They make different worlds of it, they see
d i f f e r e n t o p p o r t u n i t i e s within i t , they e l e v a t e some and thus
diminish o ther p i eces , and they dev i s e incompatible s t ra t e g i e s
a t every t u r n . They s t r u g g l e a s much with themselves a s they d o
with t h e i r common enemy, and perhaps even more so .
S o t hey lose a l o t of games.. . . . .and so we sha l l pretend tha t it is t h e second scenario that
a c t u a l l y ensues .
Scenario 2: Darron, Debra and Maureen look t o each o t h e r f o r
i npu t . mile i n i t i a l l y at tached t o t h e i r own ways o f seeing and
addressing, t h e y commit t o working i n co l labora t ion . Th is leads
t o changes. O v e r t i m e , t h e y become more attuned t o more
foundational r e a l i t i e s . Darron, f o r example, becomes more
apprec ia t i ve of the diagonal capac i ty o f the bishop , o f i t s
po t en t ia l a s a diagonal mover. H e thus l ooks t o the bishop more
and devalues i t l e s s than he d i d before. H e devalues the cas t le
and pawn less and l e s s a s we l l . In other w o r d s , he de-
knight-izes ehc er-p - - - - - - - - - - - - - - - - - - -
And t h i s he does w i t h empirical s i t u a t i o n s a s we l l . While he
continues t o see them through his two k n i g h t s , he does so t h i s
time i n ways more cognizant of h i s l i m i t a t i o n s , i n ways more
cognizant of h i s paradigmatic cons t ra in t s . Su he l i s t e n s w i t h
i n t e r e s t t o Debra's bishopized and Maureen's queenized analyses
o f t he s i t u a t i o n . H e even p roac t i ve l y seeks t h e i r i n s i g h t . And
t h e y seek h i s and each o t h e r ' s a s we l l .
And t h i s they do for good reasons. To i l l u s t r a t e , c o n s i d e r
the scenario discussed above i n which Darron l o s t , but this time
wi th a l1 t h ree co l labora t ing on what t o do. T h e r e s u l t s a r e
f r u i t f u l .
To begin : Darron i s wi thheld from manufacturing demise.
N h i l e Darron i n i t i a l l y t ends towards the p o s s i b i l i t y of
f o rk ing , Maureen p o i n t s t o t h e danger Darron's proposed move
p u t s both t h e i r queen i n of c a p t u r e , and what's worse, their
k i n g i n danger o f being mated. Darron i s h e s i t a n t a t f i r s t . H e
s t r u g g l e s f o r a flaw i n Maureen's observat ion . But then he
yields upon i n v e s t i g a t i o n , upon i n t e n s i f i c a t i o n i n t o the way
things are . There are no buts about it - he sadly concludes -
h i s fork means their demise. H e i s unable t o c o n s t r u c t it
otherwise.
Then Debra s u g g e s t s another move. She i n d i c a t e s that one o f
t h e i r bishops i s p o i s e d t o take t h e i r opponent 's queen. A l 1
three examine t h e p o s s i b i l i t y from t h e i r var ious van t a g e p o i n t s .
A l 1 three conclude it looks v iab l e . And so they proceed thus .
Eventual ly , t h e y win t h e game.. .And then go on t o win many
games.
Though such c o l l a b o r a t i o n t h e i r r e s p e c t i v e hor i zons widen.
The i r cons truc ted truths a l t e r a s the range o f cont ingent truths
in each s i t u a t i o n widens, and a s more and more foundational
t r u t h s are tapped and i n t e n s i f i e d i n t o . And w h i l e Darron, Debra
and Maureen con t inue t o favor t h e k n i g h t , the b i shop and the
queen r e s p e c t i v e l y ; w h i l e they cont inue t o see and address
s i t u a t i o n s , a t l eas t i n i t i a l l y , through t h e i r f a v o r i t e p i e c e s ,
t h e y do so i n w a y s more open t o , i n ways more encouraging o f ,
each o ther ' s approaches.
In o ther words, t o g e t h e r t h e y d e v i s e more adequate s t r a t e g i e s
than they do s e p a r a t e l y . Hence, more games are won.
In o ther words, t o g e t h e r , t h e y t a p more adequa te ly t h e
founda t i o n a l and p e r c e i v e more comprehensively t h e empir ical .
And so informed, they devise b e t t e r ways t o proceed. Hence,
more games a r e won.
In other words, toge ther , and w i t h each move, they approach
pragmatic t r u t h . Hence, more games a r e won.
Now, it may be asked, similes aside: how is it they do this?
The answer, 1 subrnit, is this: they do it through a particular
communicative process termed c o n s u l t a t i o n ,
I t i s t h u s t o c o n s u l t a t i o n and the utility of
interparadigmatic co l l abo ra t i on that 1 t u r n . . . i n another book.
1 S e e F r e u n d and McGuire ( 1 9 9 5 ) , p. 193.
2 Whi te ( 1 9 9 1 ) ' p . 79.
3 Freund and McGuire ( 1 9 9 5 ) , p. 193.
4 Whi te ( l g g l ) , p . 78 .
5 F r e u n d and McGuire ( 1 9 9 5 ) p . 193 .
6 T r e i c h l e r ( l g g O ) , p. 117.
7 I b i d , p. 1 1 6 .
8 ( 1 9 9 0 ) .
9 I b i d , p. 1 3 1 .
1 0 The tirnetables m e d i c i n e imposes upon the b i r t h process, for example , a r e
d i s r u p t i v e , being e r r o n e o u s c o n s t r u c t i o n s o f t h e p r o c e s s c r e a t e d i n line w i t h
medical assumptions. See Rothman (1994) o n t h i s .
11 T r e i c h l e r (1990), p. 114.
1 2 I b i d .
1 3 I b i d , p . 122 .
1 4 S e e Ibid, p. 122 .
15 Becker and N a c h t i g a l l ( 1 9 9 2 ) ' p. 458.
1 6 I b i d , p. 457.
17 I b i d , p . 468.
1 8 I b i d , p. 468.
1 9 Here, 1 draw h e a v i l y o n T u r n e r (1987, p. 63) f r o m his c h a p t e r "Madness a n d
C i v i l i z a t i o n " written i n the first e d i t i o n o f Medical Power and Social
Knowledge, and r e p l a c e d in the s e c o n d by Col in Samson ' s "Madness and
P s y c h i a t r y " . 20 I b i d .
2 1 I b i d .
22 I b i d .
2 3 Ibid.
24 ( 1 9 6 3 ) .
25 ( 1 9 8 8 ) .
26 (19841, p . 1 9 .
27 ( 1 9 7 0 ) .
28 ( 1 9 7 9 ) .
29 ( 1 9 7 0 ) , p . 882.
30 Chauncey ( 1 9 7 5 1 ) ~ p. 249.
31 See Gove ( 1 9 7 0 ) .
32 Rosenberg ( 1 9 8 4 ) , p. 298.
33 Ferguson ( 1 9 8 4 ) .
34 W i l l i s ( l 9 9 4 ) , 1 3 3 .
35 See Bammer and Martin ( l 9 9 2 ) , 222 .
36 I b i d . , p. 220 .
37 White ( 1 9 9 1 ) , pp. 75-76.
38 ( 1 9 8 5 ) .
39 Reid e t . a l . ( l g g l ) , p . 601 .
40 White ( l 9 9 1 ) , p. 7 5 .
4 1 R e i d e t a l . ( 1 9 9 1 ) , p . 601.
4 2 Ibid, p. 602.
4 3 I b i d .
4 4 ( 1 9 8 6 ) .
4 5 See Arksey ( l 9 9 4 ) , p. 4 4 9 . p p p p p p p p - p - - - - - - - - - -
46 ae id -ee crf . ( 9 % j, p . 610-611.p
47 Willis ( l 9 9 4 ) , p. 1 4 5 .
4 8 Arksey (1994), p. 462.
49 ( 1 9 9 6 ) .
5 0 Reid e t a l . ( 1 9 9 1 ) .
5 1 Ibid, p. 610.
52 Ibid.
53 Bammer and Martin ( 1 9 9 2 ) , p. 222 .
5 4 (19921, p. 1 5 .
55 p. 1.
56 McIntosh quoted in Ibid, p . 6.
57 Ibid, p. 1.
58 (19781, p. 170.
59 'Abdu' l-Baha ( 1 9 9 5 ) , p. 53.
60 Geras (19951, p. 135.
61 Ibid, p. 140.
62 Ibid, p . 136.
63 Quoted in Brown (1994), p. 82.
64 See Ayer and O' Grady (1994) , p. 3 1 8 .
65 (1993), p. 249. Feyerabend's discussion of methodology lends credence to
the same conclusions. He ernphasizes how futile it is to cling to a
particular methodology to the expense of any other. In the first place, we
invariably let go anyway: "there is not a single rule, however plausible, and
however firmly grounded in epistemology, that is not violated at some time or
another." (p. 14) In the second place, there is utility in being flexible:
"Indeed ... events and developments, such as the invention of atomisrn in antiquity, the Copernican Revolution, the r i se of modern atomisrn ... the gxadual emergence of the wave theory of light, occurred only because some
thinkers either decided not to be bound by certain 'obviousr methodological
rules, or because they unwi t tingly broke them. " (p. 1 4 . ) Thus, while
accepted methodological prescriptions may have their benefits, they are not
sufficient. Hacking agrees. He asks: "Why should there be the method of
science? There is not just one way to build a house, or even to grow
tomatoes. We should not expect something as motley as the growth of
knowledge to be strapped to one methodology." (1983, p. 153)
66 (1991), p. 1.
67 (1992), p. 235.
68 Feyerabend (1993), p. 35.
69 1 should also Say that the strategy of exclusion spells loss for another
reason as well. It may be that the excluder itself has little to offer
besides a multitude of extensions, extensions perhaps intermingled with a few
sporadic intensifications.
70 Relatedly, medicine is limited by virtue of its tendency to grapple with
that which it cannot adequately address. The changing nature of rnorbidity,
for example, is exposing trenchant weaknesses in the biomedical approach.
Medicine, with its emphasis on acute illness, falls short in its capacity to
deal effectively with geriatric conditions, with chronic conditions, etc.
Medicine's extension into these areas, its medicalization of them, its
construction of them, is proving tangibly anornalic. In fact, the conspicuous
weaknesses of rnedicine in this regard are opening doors to alternative
approaches - among thern medical sociology - to the problems of morbidity:
. . . [ TJhe relevance of medical sociology appears to be enhanced by the
growing importance of chronicity in the character of disease in the
twentieth century. The aging of populations, the increasing importance of
chronic illness, the impact of environmental changes on the disease
structure, and growing public criticism of both the ineffective character
of much contemporary allopathie medicine in fundamentally changing the
current pattern of morbidity and mortality and its costs have created an
environment within which social science appears to be able to offer an
alternative perspective on long-term illnesses which are not amenable to
conventional scientific medical intervention. (Turner, 1992, p. 155)
Medicine, it seems, has extended beyond its valid scope of concern - beyond that which is relatively tangible to it. The same, however, goes for social
constructionism- Medicine medicalizes reality. Social constructionism
"constxuctionalizes" reality. Through demonstrating the medical construction
of certain conditions - which can be thought of as its exemplar cases - it then talks of the medical (and more broadly, social) construction of a vast
spectrum of life.
71 Rorty (l987), p . 50.
72 Rorty (19891, p - 20.
73 Ibid.
74 (19951, p. 13.
75 (1991), p. 2.
76 (19951, p. 112. - - - - - - - - - -
77 Ibid, p. 111.
78 Rorty (l982), p. 9 3 -
79 Hoy in Skinner (19911, p. 43.
80 (19951, p. 116.
81 (19831, p. 1 4 4 .
82 (Ibid), p. 132. This evokes another debate, that is, whether or not there
is a human nature. The anti-essentialist position, of course, is that there
is not. As per Rorty, language goes al1 the way d o m (Geras, 1995: l l S ) ,
socialization goes al1 the way down (p. 50). There is nothing to humans
except what culture (language) makes of us (p. 45) . This is a vast topic and
can in no way be dealt with adequately here. However, I think Geras provides
some valuable insight into the inadequacies of the no-human nature position.
He focuses in particular on Rortyts unwitting appeal to universal human
capacities such as the capacity for language and the capacity for "symbolic
inventiveness and individuality" (p. 53). Rorty also makes reference to
universal traits such as our susceptibility to pain (a trait we share with
anlmals), and our susceptibility to a par t icular sort of pain: humiliation (a
trait we do not share with animals). While he claims no foundation for his
position that everyone has the "'right to be understood'," this right "is
clearly related to [his] goal of sparing people that specially human pain of
being humiliated." (p. 58.)
83 In Magee (date), p. 344.
84 See Chapter 4 on this.
85 Rosenau (lggî), p . 3 8 .
'Abdu' 1-Baha (1978 1 . Selections from the Writings of 'Abdu 'l- Baha. Southharnpton: The Camelot Press Limited.
------- (1979) . Paris Talks. London: Bahaf i Publishing Trust. Albrecht, Gary L. and Rick S. Zimmerman (1993) . "What Does AIDS Teach Us About Social Sciences?" The Social and Behavioural Aspects of AIDS. Advances in Medical Sociology, 3: 1-18.
Arksey, Hilary (1994) . "Expert and Lay Participation in the Construction of Medical Knowledge . " Sociology of Heal th and Illness, 1 6 (4) : 448-468.
Ayer, A. J. and Jane O r Grady (eds. ) (1994) . A Dictionary of Philosophical Quota tions. Cambridge : Blackwell .
B a h a ' i International Community (1995a) . T u r n i n g Point for Al1 Nations. A Statement of the Baha'i International Community on the Occasion of the 50th Anniversary of the United Nations. New York.
Baha ' i International Community of Public Information (1995) . The Prosperity of Humankind. New York.
Bamrner, Gabriele and Brian Martin (1992) . "Repetition Strain Injury in Australia: Medical Knowledge, Social Movernent, and De Facto Partisanship. " Social Problems, 3 : 219-234.
Barnes, Barry (1991). Thomas Kuhn. In Skinner, Quentin (ed.), The R e t u r n o f Grand Theory in the Human Sciences. Cambridge: Cambridge University Press.
Becker, Gay and Robert D. Nachtigall (1992). "Eager for Medicalization: The Social Production of Infertility as a Disease. " Sociology of Heal th and i l l ne s s 1 4 ( 4 ) : 456-471 .
Becker, Howard S. (1993) . "Moral Entrepreneurs : The Creation and Enforcement of Deviant Categories." Reprinted in Kelly, Delos H. (ed.), Deviant Behaviour: A Text Reader in the Sociology of Deviance, f o u r t h edition. New York: St. Martin's Press.
Bell, Daniel (1974) . The Coming of the Post-Industrial Soc ie ty . New York: Basic Books.
----a-- (1978) . The Cultural Contradictions of Capitalism. New York: Basic Books.
Bell, Susan (1990). "Changing Ideas: The Medicalization of Menopause. " In Fromanek, R. (ed. ) , The Meanings of Menopause: Historieal, Medical and Clinical Perspectives. Hillsdale, NJ: The Analytic Press.
Berger, Peter (1963) . Invitation to Sociology. Toronto : Anchor Books.
------- (1967) . The Sacred Canopy: Elements of a Sociological Theory of Religion. Toronto: Anchor Books.

Berger, Peter and Thomas Luclanan (1969) . The Social Construction of Reality. Garden City, N.Y.: Anchor.
Bernheimer, Charles (1985) . "Introduction: Part 1. " In Bernheimer, Charles and Claire Kahane (eds. ) , In Dora's Case: Freud - Hysteria - F e m i n i s m . New York: Columbia University Press.
Bernstein, Richard (1991) . Beyond Objectivism and Relativism: Science as Hemeneutics, and Praxis. Philadelphia: University of Pennsylvania Press.
Beyene, Yewoubdar (1992). "Menopause: A Biological Event." In Dan, Alice J. and Linda L. Lewis ( e d s . ) , Menstrual Health in Women's Lives. Chicago : University of Illinois Press.
Bloor, Michael (1995) . The Sociology of HIV Transmission. London: SAGE Publications.
Bolton, Ralph (1989) . "Introduction: The AIDS Pandemic, a Global Emergency. " Medical Anthropology, 10 : 93-104.
Bourdieu, P. (1984) . Distinction, a Social Critique of the Judgement of T a s t e . London: Routledge & Kegan Paul.
Bowles, Cheryl L. (1990) . "The Menopause Experience: Sociocultural Influences and Theoretical Models." In Forrnanek, Ruth (ed. ) The Meaning of Menopause: Historical, Medical and Clinical Perspectives. Hillsdale, N. J. The Analytic Press.
Bransen, E. (1992). "Has Menstruation Been Medicalized? Or Will It Never Happen. . . . '' Sociology of Heal th and Illness, 14 (1) : 98-110.
Brown, James Robext (1994) . Smoke and Mirrors: How Science Reflects Reality. New York: Routledge.
Caldwell, Mark (1 988) . The Last Crusade: The War on Consumption, 1862 - 1954. New York: Antheneum.
Chamaz, Kathy (1983) . "Loss of Self: A Fundamental Form of Suffering in the Chronically Ill." Sociology of Health and Illness, 5 ( 2 ) : 168-197.
------- (1987) . "Struggling for a Self: Identity Levels of the Chronically 111." Research in the Sociology of Health Care, 6: 283-321.
Chauncey, Robert L . (1975) . 'Comment on the "Labelling Theory of Mental Illness. " American Sociological Review, 40 ( 2 ) 248-252.
Chomsky, N o m (1968) . Language and Mind. New York: Harcourt, Brace & World.
------- (1975). "Recent Contributions to the Theory of Innate Ideas. " Reprinted in Stitch, S. P. (ed. ) , Inna te Ideas. Berkeley: University of California Press.
Clatts, Michael C., and Kevin M. Mutchler (1989) . "AIDS and the Dangerous Other: Metaphors of Sex and Deviance in the Representation of Disease. " Medical Anthropology, 10: 105-114.
Coburn, David ( 198 8 ) . "Canadian Medicine : Dominance or Proletarianization?" The Milbank Quarterly, 66 ( 2 ) : 92-116.
------- (1988a) . "The Development o f Canadian Nursing: P ro f e s s iona l i z a t i on and P r o l e t a r i a n i z a t i o n . " The International Journal o f Heal t h Se rv ices , 18 ( 3 ) : 43 7-66.
------- ( 1 9 9 2 ) . "Freidson Then and Now: An " I n t e r n a l i s t " C r i t i q u e o f Freidonr s Pas t and Present V i e w s of the Medical Profession. " The I n t e r n a t i o n a l Journa l o f H e a l t h Se rv i ce s , 22(3 ) : 497-512.
Coburn, David and C . L . Biggs (1986) . " L i m i t s t o Medical Dominance: The Case o f Chiroprac t ic . ' ' S o c i a l Sc ience and Medicine, 22 (19 ) : 1035-1046.
Coburn, David, George M . Torrance and Joseph M . Kaufert (1981) . "Medical Dominance i n Canada i n H i s t o r i c a l Pe r spec t i ve : T h e Rise and F a l l of Medicine. " I n t e r n a t i o n a l J o u r n a l o f Health Services , 1 3 ( 3 ) : 407-432.
Coney, Sandra (1994) . The Menopause Indus t ry : How the Medical Establishment Exploi ts Women. Alameda CA: Hunter House.
Conrad, Peter (1975) . "The Discovery of Hyperkinesis : Notes on t h e Medical izat ion of Deviant Behaviour . " S o c i a l Probl ems, 2 3 (October) : 12-21 .
Conrad Peter and Rochelle Kern (1994) . "Part One: The S o c i a l Production o f Disease. " I n Conrad and Kern (eds . ) , The Sociology o f Heal th and I l l n e s s : C r i t i c a l Pe r spec t i ve s . New York: S t . Mar t in ' s P r e s s .
Conrad P . and J. Schneider (1980) . Deviance and Medical iza t ion: From Badness t o Sickness. S t . L o u i s : Mosby.
Cooper, Wendy (1975) . No Change: A Bio log ica l Revolut ion f o r Women. London : Hutchison .
Cottingham, John (198 4 ) . Rat ional i sm. London: Paladin books. Crawford, Robert (1984) . "A C u l t u r a l Account of "Health":
Control , Release and t h e Soc i a l B o d y . " I n McXinley, J. B. ( e d . ) , Issues i n the P o l i t i c a l Econorny o f Health C a r e . N . Y . : Tavis tok .
Crimp, Douglas (1988) . "AIDS, Homophobia, and Biomedical Discourse: An Epidemic o f S i g n i f i c a t i o n . " I n C r i m p , Douglas (ed. ) , AIDS: Cultural Analysis , Cu l t u r a l Activism. Cambridge: MIT Press.
da S i l va , M. Ol ive i r a (1994) . 'Choice of a Prepafa te i n HRT, C l i n i c a l Aspects w i t h E s t r a d i o l Valerate/Cyproterone Ace ta t e . '' I n Crosignani, P.G. e t a l . (eds . ) Women's Hea l th i n M e n o p a u s e : Behaviour, Cancer, Cardiovascular Disease, Hormone Replacement Therapy. Houston: Kluwer Academic Pub l i she r s .
Danesh, Hossain ( 1 9 8 6 ) . U n i t y : T h e Creative Foundation for Peace. Ottawa: Bahali Studies Pub l i ca t i ons .
Davies, P. D. O . (11994) . "Conclusions. " I n Davies, P. D. O. (ed. ) , C l i n l c a l Tuberculosis. New York: Chapman & H a l l Medical.
Delaney, Janice, Mary Jane Lupton and Emily To th ( 1 9 7 6 ) . T h e C u r s e : A Cultural History of Menst ra t ion . Toronto: A Mentor Book.
Derr ida , Jacques (1976) . O f Grammatology. T r a n s l a t e d by G . Spivak. Balt imore, M.D.: Johns Hopkins W i v e r s i t y P ress .
------- (1981) . P o s i t i o n s . T r a n s l a t e d by Alan Bass. Chicago: T h e U n i v e r s i t y of Chicago Press.
Douglas, Mary (1966) . P u r i t y and Danger: an A n a l y s i s of the Concepts o f P o l l u t i o n and Taboo. London: Rout ledge & Kegan Pau l .
------- (1970). Natura l Symbols, E x p l o r a t i o n s i n Cosrnology. Harmonsdworth: Penguin Books.
Dreyfus, Hubert L. and Paul Rabinow (1993) . Michel Foucaul t : Beyond S t r u c t u r a l i s m and Hermeneutics, second e d i t i o n . Chicago: The U n i v e r s i t y o f Chicago P r e s s .
Ehrenre ich , John (1978) . ' I n t r o d u c t i o n : The C u l t u r a l Crisis of Modern Medicine. " I n E h r e n r i c h , B. (ed. ) The C u l t u r a l C r i s i s o f Modern Medic ine , New York: Monthly R e v i e w Press.
Erickson, Kai T . (1993) . "On the Sociology of Deviance ." R e p r i n t e d i n Kelly, Delos H . (ed.) , Deviant Behaviour: A Text R e a d e r i n t h e Sociology o f Deviance, f o u r t h e d i t i o n . New York: St. Mar t in r s Press.
Evans, C . C . (1994) . " H i s t o r i c a l Background.'' I n Davies, P. D. O. (ed. ) , C l i n i c a l Tubercu los i s . N e w York: Chapman & Hal l Medical .
E y , Henr i ( 1 9 8 2 ) . "His tory and Analys is of t h e Concept . " I n Roy, A. (ed. ) , H y s t e r i a . Toronto: John Wily & Sons.
Ferguson, D . (1984) . 'The 'new" I n d u s t r i a l Epidemic. ' M e d i c a l J o u r n a l o f A u s t r a l i a , 140: 318-319.
Feyerabend, Paul (1993) . Against Method, t h i r d e d i t i o n . m & G n + v e r s o 7 p p - - - - - - - - - - - - - - - - - - - - - - - -
F i s h e r , Sue and Stephen B. Groce (1985) . "Doctor-Pat ient N e g o t i a t i o n of C u l t u r a l Assumptions." Soc io logy of Health and I I I n e s s , 7 ( 3 ) : 343-374.
Fortunato, John E. (1987) . AIDS: The S p i r i t u a l Dilemma. San Franc i sco : Harper & Row.
Foucau l t , Michel (1973) . T h e Birth of t h e Clinic. London: T a v i s t o c k .
------a (1975) . I r P i e r r e R i v i e r e , having s l a u g h t e r e d m y mother ,
m y sister and m y b r o t h e r . . . A Case o f Pa r r i c ide i n t h e 1 9 t h Century. T r a n s l a t e d by F. J e l l i n e k . New York.
------- (1977) . D i s c i p l i n e a n d Punish: The B i r t h of the P r i s o n . London: Tav i s tock .
------- (1978) . H i s t o r y o f S e x u a l i t y , Volume 1: An I n t r o d u c t i o n . T r a n s l a t e d by Robert Hur ley . Toronto: Random House.
------- (1979) . The H i s t o r y o f S e x u a l i t y , vol . 1 : An
Introduction. London: A l l e n Lane/Penguin Books.
------- (1980) . Power/Knowledge: Selected Interviews and Other
Writings 1972-1977. Edited by Colin Gordon. New York : Pantheon Books.
Fox, Nicholas J. (1994 . Postmodernism, Sociology and Heal th. Toronto: Universi ty of Toronto Press.
Freidson, E l i o t (1970) . Profession o f M e d i c i n e : A Study of the Socio l ogy o f Applied Knowledge . Chicago : Univers i ty of Chicago Press.
Freund, Peter E . S . and Meredith B.McGuire (1995) . Health, I l l n e s s and the S o c i a l Body, second e d i t i o n . N e w Jersey: Prentice-Hall , Inc .
Gaarder, Jostein (1994) . Sophie's World. New York: Berkley Books.
Galagher, Eugene B. ( 1 9 7 6 ) . "Lines of Reconstruct ion and Extension i n t h e Parsonian Sociology of I l l n e s s . " Socia l Science and Medicine, 10: 207-218.
Gera;, Norman (1995) . S o l i d a r i t y i n the Conversation o f Humankind: The Ungroundabl e L i b e r a l ism o f Richard Rorty. London: Verso.
Goffman, Erving (1961). Asylums: Essays on the Social Si tua t ion o f Mental Pa t i en t s and Other Inma tes . Toronto : Anchor Books.
------- (1963) . Stigma: Notes on the Management o f Spoiled
I d e n t i t y . Toronto: Simon and Schuster , I nc . . Goodman, Madeleine 3. (1990) . " T h e Biomedical Study of
Menopause. " I n Formanek, Ruth (ed. ) The Meaning o f Menopause: H i s t o r i c a l , Medical and C l i n i c a l Perspectives. Hi l l sda l e , N . J . The Analyt ic P re s s .
Gordon, Deborah R . (1988) . "Tenacious Assumptions i n Western Medicine", I n Lock, Margaret and Deborah R . Gordon (eds . ) , Biomedicine Examined. Dordrecht : Kluwer Academic Publ ishers .
Gove, Walter R . ( 1970) . "Socie ta l Reaction a s an Explanation o f Mental I l l n e s s : An Evaluat ion. " American Soc io log ica l Review, 35: 873-884.
------- (1979) . "The Labell ing Versus the Psych ia t r i c Explanation of Mental I l l n e s s : A Debate t h a t has Become Subs tan t ive ly Irreievant." Journa l of Health and Soc ia l Behaviour, 20 : 301-304.
Hacking, I an (1983) . Representing and Intervening. Cambridge: Cambridge Universi ty Press.
Hadler, Norman M . ( 1 9 9 6 ) . 'Ed i to r i a l : A Keyboard fo r "Daubert ."' JOEM, 38 (5) : 469-476.
Hegel, Georg Wilhelm F r i e d r i c (1969) . Phenomenology o f M i n d . Tran la ted by J. B. B a i l l i e . New York: Harper Torchbook.
Heilbrun, Carolyn G. (1994) . "Forward. " I n Coldsworty, Joanna (ed. ) , A Certa in Age: Ref l ec t ing on Menopause. N e w York: Columbia Universi ty Press.
Helman, Cecil G. (1988) . "Psyche, Soma, and Society: The Social Construction of Psychosornatic Disorders", In Lock, Margaret and Deborah R. Gordon (eds . ) , Biomedicine Examined. Dordrecht: Kluwer Academic Publishers.
Herzlich, Claudine (1973). "Health and Illness: A Social- psychological Analysis . " European Monographs i n Soc ia l Psycho1 ogy, vol. 5 . London : Academic Press.
Herzlich, Claudine and Janine Pierret (1985). "The Social Construction of the Patient: Patients and Illnesses in Other Ages . " Social Sc ience and Medicine, 2 0 ( 2 ) : 145-151.
------- (1993) . "From Epidemic to Modern Illness: The Social Construction of AIDS in France." The Soc ia l and Behavioural Aspects of AIDS. Advances i n Medical Sociology, volume 3 . J A I Press Inc.
Hobbes, Thomas (1968) . Leviathan. MacPherson, C. B . (ed. ) . Harmondsworth: Penguin.
Honig-Parnass, Tikvah (1981) . "Lay Concepts of the Sick-Role: An Examination of the Professionalist Bias in Parsonsf Model." Scc ia l Science and Medicine, 15A: 615-623.
Hoy, David (1991) . "Derrida. " In Skinner, Quentin (ed. ) , The Return of Grand Theory i n the Human Sc iences . Cambridge: Cambridge University Press.
Hume, David ( 1990) . Enquir ies Ccncerning Human Understanding and Concerning the Pr inc ip l e s of Morals, t h i r d e d i t i o n . Text Revised by P. H. Nidditch. Oxford: Clarendon Press.
Hunter, M.S. (1994). 'Psychosocial Factors Influencing Experience of the Menopause and Help-Seeking Behaviour." In Crosignani, P.G. et al. (eds.), Women's Health i n Menopause: Behaviour, Cancer, Cardiovascular Disease, Hormone Replacemen t Thexapy. London: Kluwer Academic Publishers.
(1989) In terna t iona l C l a s s i f i c a t i o n of Diseases, 9'" revision, clinical modification, 3ed edition. Washington: U. S. Department of Health and Human Services, Public Services.
Institute for Work and Health (1996) . 'At Work." Jaroff, Leon (1996) . "Keys to the Kingdom." In T i m e . Fall, pp.
18-23. Judd, Howard L. (1990) . "Physiological Consequences of Ovarian Failure. " In Korenman, Stanley G. (ed. ) , The Menopause: Bio logical and C l i n i c a l Consequences of Ovarian Fa i lure : Evolut ion and Management. Serono Syrnposia, USA,
Kaufert, Patricia (1988) . "Menopause as Process of Event: The Creation of Definitions in Biomedicine." In Lock, Margaret and Deborah R. Gordon (eds . ) , Biomedicine Examined. Dordrecht: Kluwer Academic Publishers.
Kaufert, Patricia and Penny Gilbert (1987) . "Medicalization and the Menopause. " In Coburn et al. (eds. ) , Heal t h and Canadian
Society: Sociological Perspectives, second edition. Richmond Hill: Fitzhenry and Whiteside.
Kaufert Patria A., Margaret Lock, Sonj a McKinlay and Nancy Avis (1994) . "Menopause as a Normal Physiological Event or as a Disease. '' In Lorrain, Jacques, et a1 (eds . ) , Comprehensive Management of Menopause. New York: Springer-Verlag.
Kearns, Jean Ruley and Victor A. Christopherson (1992) . "Mexican-American Womenf s Perceptions of Menopause. " In Dan, Alice J. and Linda L. Lewis (eds . ) , Menstrual Heal th in Women's Lives. Chicago: University of Illinois Press.
Keers, R. Y. (1978 1 . Pulmonary Tuberculosis: A Journey Down the Centuries. London: Bailliere Tindall.
King, Helen (1993) . "Once Upon a Text: Hysteria from Hippocrates." In Gilrnan et al. (eds.), Hysteria Beyond Freud. Berkeley: University of California Press.
Kimayer, Laurence J. (1988) . "Mind and Body as Metaphors : Hidden Values in Biomedicine", In Lock, Margaret and Deborah R. Gordon (eds. ) , Biomedicine Examined. Dordrecht : Kluwer Academic Publishers.
Koenig, Barbara A. (1988) . "The Technological Imperative in Medical Practice: The Social Creation of a "Routine" Treatment", In Lock, Margaret and Deborah Gordon (eds. ) Biomedicine Examined. Dordrecht: Kluwer Academic Publishers.
Korenman, Stanley G. (1990). "Preface." In Korenman, Stanley G. (ed. ) , The Menopause. Serono Symposia, USA.
Kuhn, Thomas S. (1970) . The Structure of Scientific Revolutions. Chicago: The University of Chicago Press.
------- (1977) . The Essential Tension: Selected Studies in Scientific Tradition and Change. Chicago: The University of Chicago Press.
Lakoff, Robin Tolmach and James C. Coyne (1993) . Father Knows Best: The Use and Abuse of Power in Freud's Case of Dora. New York: Teachers College Press.
Lash, Scott (1991) . Sociology of Postmodernism. New York: Routledge.
Lemert, Edwin M. (1993) . "Primary and Secondary Deviation. " Reprinted in Kelly, Delos H. (ed. ) , Deviant Behaviour: A Text Reader in the Sociology of Deviance, fourth edition. New York: St. Martin's Press.
Lemonick, Michael D. (1995). "Glimpses of the Mind." In Time. July 31, pp. 34-42.
Lewis, Aubrey (1982) . "The Survival of Hysteria. " In Roy, A. (ed. ) , Hysteria. Toronto: John Wily & Sons.
Leyton, Elliott (1987) . "Dying Hard: Industrial Carnage and Social Responsibility. " In Coburn et al. (eds. ) , Health and Canadian Society, second edition. Richmond Hill: Fitzhenry and Whiteside.
Libbrecht, Katrien (19951, Hysterical PsychosisL A H i s t o r i c a l Survey. London: Transaction Publishers .
Lock, Margaret (1988) . "Introduction." In Lock, Margaret and Deborah R. Gordon ( E d s . ) B i o m e d i c i n e Examined. Dordrecht : Klewer Academic Publishers .
Lock, Margaret and Deborah R . Gordon (1988) . "Relationships Between Society, Culture, and Biomedicine: Introduction to the Essays", in Lock and Gordon (eds.) Biomedicine Examined. Dordrecht: K l u w e r Academic Publishers .
Locke, John (1988) . Two Trea lises of G o v e r n m e n t . Laslett, Peter (ed. ) . Cambridge : Cambridge University Press.
Longino, Helen E. (1990) . S c i e n c e a s Social K n o w l e d g e : Values and Objectivity in Scientific Inquiry. Princeton: Princeton University Press.
Loring, Marti and Brian Powell (1988). "Gender, Race and DSM- III: A Study of the Objectivity of Psychiatric Diagnostic Behaviour . " Journal of Heal th and Human Development . 29 : 1- 22.
Lucire, Yolande (1986) . "Neurosis in the Workplace." Tne M e d i c a l Journal of Australia, 145: 323-326.
Lyotard, Jean-François ( 1993) . The Postmodern Condition : A Report on Knowl edge. Minneapolis : University of Minnesota Press.
MacDonald, Michael (1991). "Introduction." In MacDonald, Michael (ed. ) , Wi tchcraft and Hysteria i n E l i z a b e t h a n L o n d o n . New york: Tavistock/Routledge.
MacLeod, Sheila (1994). "Drunken Drowning." In Goldsworthy, Joanna (ed.), A C e r t a i n Age: Reflecting on Menopause. New York: Columbia University Press.
Marchak, Patricia (1992) . "Ideology and Social - - - - - - - Organi~ation,"~ - In - Teppermam; Lorne aKd d-J3mespCurtisp ( e d u , Everyday L i f e : A Reader. Toronto: McGraw-Hill Ryerson Limited.
Marx, Karl (1970). The German Ideology. Arthur, C.J. (ed.). New York: International Publishers.
Matthews, Karen A., Joyce Bromberger and Grace Egeland (1990) . "Behavioural Antecedents and Consequences of the Menopause." In Korenman, Stanley G. (ed. ) , The M e n o p a u s e : B i o l o g i c a l and C l inical Consequences of Ovarian F a i l ure: Evol u t i o n and M a n a g e m e n t . Serono Symposia, U S A .
McKeown, Thomas (1979). "The Deterrninants of Hurnan Health: Behaviour, Environment and Therapy. "
McKinlay, John B. and Joan Arches (1985) . "Towards the Proletarianization of Physicians. " International Journal of Health Services, 15 (2) : 161-19s.
McKinlay, John B. and Sonja M. McKinlay (1994) . "Medical Measures and the Decline of Mortality." In Conrad and Kern

( e d s . ) , The Sociology of Heal th and Illness: Cri t i c a l Perspectives. New York: St . Martin' s Press.
Merskey, Harold (1979) . The h a l y s i s of Hysteria. London: Baillière Tindall.
Miller, Nancy K. (1994) . "Forward. " In Coldsworty, Joanna (ed. ) , A C e r t a i n Age: Reflecting on Menopause. New York: Columbia University Press.
Mishler, Elliot G. (1981). "The Social Construction of Illness." In Mishler, Elliot et al. (Eds. ) S o c i a l C o n t e x t s of Wealth, Illness and Patient Care . Cambridge: Cambridge University Press.
Moi, Toril (1985) . "Representation of Patriarchy : Sexuality and Epistemology in Freud's Dora." In Bernheimer, Charles and Claire Kahane (eds . ) , In Dora's Case: Freud - Hysteria - F e m i n i s m . New York: Columbia University Press.
Muller, Jessica H. and Barbara A. and Koenig (1988). "On the Boundary of Live and Death: The Definition of Dying by Medical Residents", Lock, Magaret and Deborah Gordon (eds . ) Biomedicine Examined. Dordrecht: Kluwer Acadernic Publishers.
Murphy, Julien S. (1995) . The Constructed Body: AIDS, Reproductive Technology, and Etbics. Albany: State University of New York Press.
Murray and Payne (1989) . "The Social Classification of AIDS in American Epidemiology . " Medical h thropoloqy, 10 : 115-128.
Nelkin, Dorothy, David P. Willis and Scott V. Parris (1991). A Disease of Society: Cultural and Institutional Responses tu AIDS. Cambridge: Cambridge University Press.
Nicholson and McLaughlin (1987). "A Reply to M.R. Bury." Nietzsche, Friedrich (19691 . T h u s Spoke Zara t h u s t r a . Translated by R. 3 . Hollingdale, London: Penguin Books.
Notelovitz i n Coney, p. 329. Nuland, Sherwin B. (1996) . "An Epidemic of Discovery. " In
T i r n e . Fall, pp. 4-9.. OfLeary Cobb, Janine (1994). "Where the Woman Are." In Lorrain,
Jacques, e t a l (eds . ) , Comprehensive Management of Menopause. New York: Springer-Verlag.
Parson, Talcott (1939). 'The Professions and the Social Structure. " Social F o r c e s , 17 : 457-67.
------- (1952). The S o c i a l System. London: Routledge & Kegan Paul.
Pascal, Blaise (1941). Pensees. Translated by W. F. Trotter. New York: Modern Library.
Pier re t , Janine . "Constructing Discourses about Health and Their Social Determinants." In Radely, Alan (ed. ) , N o r l d s of Illness: Biographical and Cul tural Perspectives on Heal th and Disease. New York: Routledge.
Plato. The Republic. Translated by Robin Waterfield. Oxford: Oxford University Press
------- O Meno.
------- . Phaedo in The Last Days of Socrates. Tranlated by Hugh
Tredennick and Harold Tarrant. London: Penguin Books. Powell (1988) . Pryor, John B. and Glenn D. Reeder (1993) . "Collective and Individual Representations of HIV/AIDs Stigma." In Pryor, John E . and Glenn D. Reeder (eds . ) , The Social Psychology of HIV Infection. New Jersey: Lawrence Erlbaum Associates, Publishers.
Rabinow, Paul (1984) . In Rabinow, Paul (ed. ) , The F o u c a u l t Reader. New York: Pantheon Books.
Ramas, Maria (1985) . "Freudf s Dora, Doraf s Hysteria. " In Bernheimer, Charles and Claire Kahane ( e d s . ) , In Dora's Case: Freud - Hysteria - Feminism. New York: Columbia University Press.
Raymond, Diane Barsoum (1991) . Existentialism and the P h i l o s o p h i c a l Tradition. New Jersey: Prentice-Hall .
Reid, Janice, Christine Ewan and Eva Lowy (1991) . "Pilgrirnage of Pain: The Illness Experiences of Women with Repetition Strain Injury and the Search for Credibility." Social Science and Medicine, 32 ( 5 ) : 601-612.
Ritzer, George (1988) . Sociological Theory, second edi tion. N e w york: Knopf.
Rodin, Mari (1992) . "The Social Construction of Premenstrual Syndrome. " Social Science and Medicine, 35 (1) : 49-56.
Rorty, Richard (1980) . Philosophy and the Mirror of Nature. Princeton: Princeton University Press.
------- - - - - - ( 1 9 8 2 ) . Jonsequences _of P r a g m a t i s m . - Mnneapolis : University of Minnesota Press.
------- (1987) ."Pragmatisrn and Philosophy." In Baynes, Kenneth, James Bohman and Thomas McCarthy (eds.), After Philosophy: End or Transformation. The MIT Press.
------- (1989) . Con tingency, Irony and Sol idarity. Cambridge:
Cambridge University Press. ------- (1991) . Objectivity, R e l a t i v i s m and Truth: Philosophical Papers Vol une 1. Cambridge : Cambridge University Press.
Rosenberg, Charles E. (1988). "Disease and Social Order in America: Perceptions and Expectations." In Fee, Elizabeth and Daniel M. Fox (eds. ) , AIDS, The Burdens of History. Los Angeles: University of California Press.
Rosenberg, Morris (1984). "A Symbolic Interactionist View of Psychosis. " Journal of Health and Social B e h a v i o u r , 25: 289- 302.

Roseneau, Pauline Marie (1992) . Post-Modernism and the Social Sciences : Insights, Inxoads, and Intrusions. Princeton: Princeton University Press.
Rosenf ield, Sarah (1984) . "Race Dif ferences in Involuntary Hospitalization: Psychiatrie versus Labelling Perspectives." Journal of Health and Social Behaviour, 25: 14-23.
Rothman, Barbara Katz (1994). "Midwives in Transition: T h e Structure of a Clinical Revolution." In Conrad, Peter and Rochelle Kern (eds . ) , The Sociology of Heal th and Illness: Critical Perspectives, fourth edition. New York: St . Martin's Press.
Rouse, Joseph (1987). Knowledge and Power: Toward a Political Philosophy of Science. Ithaca: Corne11 University Press.
Rousseau, G. S. and Roy Porter (1993) . "Introduction: The Destinies of Hysteria. " In Gilman et al. (eds. ) , Hysteria Beyond Freud. Berkeley: University of California Press.
Rousseau, Jean-Jacques (1973) . The Social Con tract and Discourses. Cole, G. D. H. et al (eds. ) . London: Everyman.
Runciman, W. G. (1987) . Weber: Selections in Translation. Translated by Eric Matthews. Cambridge: Cambridge University Press.
Russell, Bertrand (1993) . History of Western Philosophy. London: Routledge.
Ryan, Frank (1992). Tuberculosis: The Greatest Story Never T o l d . Worcestershire, England: Swift Publishers.
Sartre, Jean-Paul (1956) . Being and Nothingness. Translated by Hazel Barnes. New York: Washington Press.
Saxup, Madan (1993) . Post-Structuralism and Postmodernism, second edition. Athens: T h e University of Georgia Press.
Scheff, Thomas (1963). " T h e Role of the Mentally III and the Dynarnics of the Mental Disorder: A Research Framework." Sociometry, 26: 436-453.
Scott, R. (1969) . The Making of Blind Men. New York: Russel. Sage.
Scully, Diana (1980) . Men Who Control Women's Health: The Miseducation of Obstetrician-Gynecologists. Boston: Houghton Mifflin.
Scully, Diana and Pauline Bart (1978). "A Funny Thing Happened on the Way to the Orifice: Women in Gynecology Textbooks." In Ehrenrich, B. (ed. ) The Cultural Crisis of Modern Medicine, New York: Monthly Review Press.
Searle, John (1987) . Wittgenstein. In Magee, Bryan (ed. ) , The Great Philosophers. Oxford: Oxford University Press.
Segall, Alexander (1976). "The Sick Role Concept: Understanding Illness Behaviour." Journal of Health and Social Behaviour, 17 (June) : 163-170.
Shand, John (1994) . Philosophy and Phi losophera . London: Penguin Books.
Silverman S t u a r t L . , Maria Greenwald and Arthur Huberman (1990) . "Decisions on Menopausal Therapy : The P r a c t i t i o n e r ' s Viewpoint . " I n Korenman, Stanley G. (ed . ) , T h e Menopause: B i 0 1 o g i c a l and Cl i n i c a l Consequences o f Ovarian F a i l ure: Evol u t i o n and Management. Serono Symposia, USA.
S l a t e r , E l i o t ( 1 9 8 2 ) . "What i s Hyster ia?" I n Roy, A. (ed. ) , Hysteria. Toronto: John Wily & Sons.
Slavney, P h i l l i p R . (1990) . Perspectives on Hys t e r i a . Bal t imore : The Johns Hopkins Univers i ty P r e s s .
Smith, Dorothy ( 1 9 7 8 ) . "K is Mentally Ill: The Anatomy of a Fac tua l Account . " Sociology, 12 (1) : 23-53.
Sontag, Susan (1978) . I l l n e s s a s Metaphor. New York: Fa r ra r , S t raus and Giroux.
Sorel , Tom (1991) . Scientism: Philosophy and the I n f a t u a t i o n with Science. London: Routledge.
Stark , Evan, Anne F l i t c r a f t and W i l l i a m F r az i e r ( 1 9 8 3 ) . "Medicine and P a t r i a r c h a l Violence: The S o c i a l Const ruc t ion o f a "Pr iva te" Event . " In Fee, E . (ed. ) , Wornen and Health: The Pol i t i c s o f Sex i n Medicine. Farmingdale, N . Y . : Baywood.
Strong (1979) . Swidler, Ann (1993) . Forward t o Weber' s T h e Socio logy of
Rel ig ion . Boston: Beacon Press. Syme, Leonard S. and Lisa F. Berkman (1994) . "Soc ia l Class,
S u s c e p t i b i l i t y , and Sickness ." I n Conrad, Peter and Rochelle Kern (eds. ) , The Sociology o f Heal th and I l l n e s s : C r i t i c a l Pe r spec t ives , f o u r t h e d i t i o n . New York: S t . Mar t in ' s Press.
Towsend, John M. and Cyntia L . Carbone (1980) . "Menopausal Syndrome: I l l n e s s of S o c i a l Role - A T r a n s c u l t u r a l Analysis." C u l t u r e , Medicine, and Psychia t ry , 4 : 229-248.
Treichler , Paula A. (1988) . "AIDS, Homophobia, and Biomedical Discourse: An Epidemic of S i g n i f i c a t i o n . " In Crimp, Douglas (ed. ) AIDS: C u l t u r a l Analysis , C u l t u r a l Activism. Cambridge:
MIT Press. ------- (1988a) . "AIDS, Gender, and Biomedical Discourse:
Current Contes ts f o r Meaning." In Fee, El i zabe th and Daniel M . Fox ( e d s . ) , A I D S , The Burdens o f H i s to ry . Los Angeles: Univers i ty of C a l i f o r n i a P r e s s .
_C_-___ (1990) . "Feminism, Medicine, and the Meaning of C h i l d b i r t h . " i n Jacobus M . e t a l . ( ed s . ) , Body/Poli t i c s : Women and the Discourses of Science. New York: Routledge.
Turner, Bryan S . (1987) . Medical Power and S o c i a l Knowledga, first edi t ion . London: Sage Pub l i ca t i ons .
--a---- (1992) . Regula t ing Bodies: Essays i n Medical Sociology. London: Routledge.
------- (1992a) . Max Weber: From History to Modernity. N e w York : Routledge .
Turner, Bryan S. with Colin Samson (1995) . Medical Power and Social Knowledge, second edition. London: Sage Publications.
Veith, Ilza (1965) . Hysteria: The History of a Disease. Chicago: The University of Chicago Press.
Waitskin, Howard (1989) . 'A Critical Theory of Medical Discourse: Ideology, Social Control, and the Processing of Social Context in Medical Encounters. " Journal of Heal th and Social Behaviour, 30 (June) : 220-239.
Waldby, Catherine (1996) . AIDS and the Body Politic: Biomedicine and Sexual Difference. New York : Routledge .
Weber, Max (1958) . The Protestant Ethic and the Spirit of Capitalism. . New York: Scribner' S.
Weeks, Jeffrey (1989) . "AIDS: The Intellectual Agenda. '' In Aggleton, Peter et al. (eds) , AIDS: Social Representa t i o n s , Social Practices. New York: The Falmer Press.
Weiss, Kay (1983) . "Vaginal Cancer: An Iatrogenic Disease?" in Fee, E. (ed. ) , Women and Health: The Politics of Sex in Medicine. Farmingdale, NY: Baywood.
Wahn, Michael (1987). "The Decline of Medical Dominance in Hospitals ." In Coburn et al (Eds. ) , Health and Canadian Society: Sociol ogical Perspectives. Richmond Hill : Fit zhenry and Whiteside.
White, Kevin (1991) . "Trend Report: The Sociology of Health and Illness." Current Sociology, 39 ( 2 ) : 1 -134 .
Williams, Trevor A. (1985) . "Visual Display Technology, Worker Disablement, and Work Organization. " Human Relations, 38 (11) : 1065-1084.
Willis, Evan (1994) . Illness and Social Relations: Issues in the Sociology of Heal th Care. NSW Australia: Allen 6 Unwin.
Wittgenstein, Ludwick (1974) . Philosophical Investigations. G. E. M. Anscombe and R. Rhees (eds. ) . Oxford: Basil Blackwell.
Wolinsky, F. (1980) . The Sociology of Health. Toronto: Little Brown.
Wright, Peter and Andrew Treacher (1982). The P r o b l e m af Medical Knowledge: Examining the Social Construction of Knowledge. Edinburgh: Edinburgh University Press.
Wright, Robert (1995). In Time. August 28, pp. 32-38. Zeitlin, Irving (1993) . P l a t o f s Vision: The Classical Origins of Social & Political Thought. N e w Jersey: Prentice Hall.
------- (1994) . Nietzsche: A Re-Examination. Cambridge: Polity Press. .
Zola, Irving (1978) . "Medicine as an Institution of Social Control. " In Ehrenrich, B. (ed. 1 The Cultural Crisis of Modern Medicine, New York: Monthly Review Press.
IMAGE EVALUATION TEST TARGET (QA-3)
APPLIED IMAGE. lnc - = 1653 East Main Street
O 1993. Applied Image. Inc.. All RighD Reserved
Related Documents











