LEGIONELLA PLUS: FACILITIES MANAGEMENT • ASBESTOS • PATIENT SAFETY • SIGNAGE • SECURITY ENERGY HEALTHCARE IT VOLUME 14.6 www.healthbusinessuk.net A look at healthcare commissioning since the introduction of the Health and Social Care Act PROCURING HEALTH SERVICES FINANCE Mandatory food standards in the NHS contract for the first time CATERING RAISING FOOD QUALITY Advice for identifying and managing possible Ebola-infected patients EBOLA VIRUS DISEASE INFECTION CONTROL

Health Business 14.6
Apr 06, 2016
Business Information for Healthcare Professionals
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

LEGIONELLA
PLUS: FACILITIES MANAGEMENT • ASBESTOS • PATIENT SAFETY • SIGNAGE • SECURITY
ENERGYHEALTHCARE IT
VOLUME 14.6www.healthbusinessuk.net
A look at healthcare commissioning since the introduction of the Health and
Social Care Act
PROCURING HEALTH SERVICES
FINANCE
Mandatory food standards in the NHS contract for the first time
CATERING
RAISING FOOD QUALITY
Advice for identifying and managing possible Ebola-infected patients
EBOLA VIRUS DISEASE
INFECTION CONTROL
Tailored Solutions for your Waste Management and Disposal!Whether your clinical waste is infectious or non-infectious, using a specialist disposal company will make your waste management simple, help you meet your Duty of Care obligations, and save on costs!
With increasing legislation and financial demands, the pressure is on many organisations to balance the right disposal route, whilst getting the best value for money.
Talk to us today quoting S1801, about a tailor-made waste management solution to suit your business needs and your pocket.
Infectious & non-infectious clinical waste Pharmaceutical waste Dental waste Tailored solutions Nationwide service Licensed waste carrier
Tel: 029 2080 9090 email: [email protected] web: www.phswastemanagement.co.uk

Comm
entHEALTH BUSINESS MAGAZINE ISSUE 14.6
LEGIONELLA
PLUS: FACILITIES MANAGEMENT • ASBESTOS • PATIENT SAFETY • SIGNAGE • SECURITY
ENERGYHEALTHCARE IT
VOLUME 14.6www.healthbusinessuk.net
A look at healthcare commissioning since the introduction of the Health and
Social Care Act
PROCURING HEALTH SERVICES
FINANCE
Mandatory food standards in the NHS contract for the first time
CATERING
RAISING FOOD QUALITY
Advice for identifying and managing possible Ebola-infected patients
EBOLA VIRUS DISEASE
INFECTION CONTROL
© 2014 Public Sector Information Limited. No part of this publication can be reproduced, stored in a retrieval system or transmitted in any form or by any other means (electronic, mechanical, photocopying, recording or otherwise) without the prior written permission of the publisher. Whilst every care has been taken to ensure the accuracy of the editorial content the publisher cannot be held responsible for errors or omissions. The views expressed are not necessarily those of the publisher. ISSN 1362 - 2541
If you would like to receive all issues of Health Business magazine for £120 a year, please contact Public Sector Information Limited, 226 High Road, Loughton, Essex IG10 1ET. Tel: 020 8532 0055, Fax: 020 8532 0066, or visit the Health Business website at:
P ONLINE P IN PRINT P MOBILE P FACE TO FACE
www.healthbusinessuk.net
PUBLISHED BY PUBLIC SECTOR INFORMATION LIMITED226 High Rd, Loughton, Essex IG10 1ET. Tel: 020 8532 0055 Fax: 020 8532 0066 Web: www.psi-media.co.ukEDITOR Angela Pisanu EDITORIAL ASSISTANT Arthur Walsh EDITORIAL DIRECTOR Danny Wright PRODUCTION EDITOR Richard Gooding PRODUCTION CONTROL Jacqueline Lawford, Jo Golding WEBSITE PRODUCTION Reiss Malone ADVERTISEMENT SALES Jeremy Cox, Ben Plummer, Amber Oxley, Alexander Baker ADMINISTRATION Victoria Leftwich, Vickie Hopkins PUBLISHER Karen Hopps REPRODUCTION & PRINT Argent Media
Surgeons’ survival rates for public viewingAs part of the NHS’s quest for more transparency, patients will now be able to compare the survival rates of 5,000 surgeons from across the UK on an easy-to-use website called MyNHS.
Performance data will let patients know whether clinical outcomes for individual surgeons are within expected limits, and provide them with other information, such as data on local NHS food quality, staffing and patient safety. Eventually, it will also contain figures on one year and five year cancer survival rates for NHS trusts.
NHS England medical director Pr. Sir Bruce Keogh said: “This represents another major step forward on the transparency journey. It will help drive up standards, and we are committed to expanding publication into other areas.” Previously Sir Bruce had said that surgeons who fail to publish their mortality rates could face penalties.
But some critics say the data may be misleading and could lead to some consultants refusing difficult cases. Prof John MacFie, president of the Federation of Surgical Specialty Associations, said: “The publication of individual surgeons’ performance data is crude and can be misleading, and does not include essential information such as duration of hospital stay and returns to theatre.
“There is now good anecdotal evidence that shows publishing this data has encouraged risk averse behaviour, which is not in the interest of patients. I believe that the data should only be published after any concerns in a surgeon’s performance have been investigated. In reality very few deaths can be attributed to surgical error alone, and this data only attracts attention away from institutional failings. Put simply, hospitals should not be allowing surgeons to practice unless they can demonstrate their practice is safe.” Read the full story on page nine. Angela Pisanu, editor
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
3 Volume 14.6 | HEALTH BUSINESS MAGAZINE

Delivering paperless health care
“The right file for the right patient at the right time –
100% guaranteed”
“Patient care and clinical effectiveness
enchanced”
“Annual savings of £1.4m with the CCube
scan‑on‑demand solution”
“The system architecture enables easy integration with patient information systems”
Do you want compliance?
Do you want process efficiencies?
Visit www.ccubesolutions.com
Enterprise Software
2013 Winner
Advisory Trade Member
Call us now on 01908 677752 or email [email protected]

Contents
WAYFINDING
PLUS: FINANCE • LEADERSHIP • RECRUITMENT • SECURITY • FLEET MANAGEMENT
INFECTION CONTROLOCCUPATIONAL HYGIENE
VOLUME 14.5www.healthbusinessuk.net
A look at the NHS post-Francis Report
PATIENT SAFETY
MEASURING THE FRANCIS EFFECT
The DH’s recently updated guidance on NHS parking principles sparks up the debate
TO PAY OR NOT TO PAY
PARKING
How supermarket-style check out systems can be used in healthcare to improve safety
TRACKING TECHNOLOGY
HEALTHCARE IT
AMBULANCES
PLUS: DESIGN & BUILD • ENERGY • FLEET MANAGEMENT • HEALTHCARE EVENTS • TRANSLATION
HEALTHCARE IT
LITIGATION
VOLUME 14.4
www.healthbusinessuk.net
Making sure healthcare waste does not
pose a risk to public health or the environment
WASTE MANAGEMENT
BINNING CLINICAL WASTE
Using technology to deliver
savings and increase transparency
E-PROCUREMENT
STRATEGY
PURCHASING
The first line of defence for
infection control
HAND HYGIENE
INFECTION CONTROL
PROCUREMENT
PLUS: MARKET RESEARCH • LONE WORKER PROTECTION • FLEET MANAGEMENT & MORE
REFURBISHMENT
ENERGY
VOLUME 14.3www.healthbusinessuk.net
Cost-cutting can put vulnerable patients at risk, says the Building and EngineeringServices Association
LEGIONELLA
MAKINGWATER SAFE
Harnessing technical innovations to help keep hospitals bug-free
INFECTIONCONTROL
CLEANING
Bringing together clinicians, commissioners, providers and social care teams
HEALTH + CAREEVENT PREVIEW
ENERGY
PLUS: MEDICINES & MEDICAL DEVICES • FACILITIES MANAGEMENT • LEADERSHIP
FLEET MANAGEMENT
Using information to make care
better, safer and more affordable
THE POWER OF BIG DATA
HEALTHCARE IT
How a design-led solution can reduce
aggression and improve safety
TAMING EMOTIONS IN A&E
DESIGN & BUILD
INFECTION CONTROL
VOLUME 14.1
www.healthbusinessuk.net
Implementing the government’s recommendations
following the Francis Report
PATIENT SAFETY
A FINAL RESPONSE TO FRANCIS
LANDSCAPING
PLUS: HEALTH & SAFETY • ENERGY • FACILITIES MANAGEMENT • FLEET MANAGEMENT
DESIGN & BUILD
ERGONOMICS
VOLUME 14.2
www.healthbusinessuk.net
Effective wayfinding is important for
patients, staff and visitors alike
SIGNAGE
FINDING
YOUR WAY TO
BETTER HEALTH
What issues might a hospital face when
going ‘paperless’ and sharing patient records across
Primary and Secondary Care boundaries?
OVERCOMING
PAPERLESS HURDLES
HEALTHCARE IT
Health Business www.healthbusinessuk.net
CONTENTS
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
5 Volume 14.6 | HEALTH BUSINESS MAGAZINE
07 NEWS Care Quality Commission ranks GP surgeries by risk; Surgeons told to publish mortality rates or face sanctions; Welsh government invests in liver disease prevention 13 FINANCE Collaboration and competition between Trusts is the best way to improve healthcare commissioning, writes Stephen Childs of NHS North of England 17 HOSPITAL MANAGEMENT Outside expertise can make a real difference in how hospitals are governed
21 INFECTION CONTROL What are the risk factors for the spread of the Ebola virus and how can they be identified? Public Health England shares its most up to date guidelines 25 PATIENT SAFETY The MHRA’s Tony Sant comments on how the introduction of integrated error reporting and improved governance for medical equipment will assist patient care 29 HEALTHCARE IT What role do GS1 standards, which are mandated for use in NHS hospitals, play in healthcare delivery? 37 EVENT PREVIEW: HEALTHCARE IT EXCHANGE A look forward to the December event that focuses on how emerging technologies are revolutionising healthcare 41 INFORMATION DISPOSAL High profile instances of hospital data breaches highlight the importance of information destruction, the BSIA writes
44 SIGNAGE A Sign Design Society member talks about how a wayfinding trial in A&E departments has increased staff safety
47 ENERGY The BIFM’s Chris Moriarty on the steps building managers can take to implement a successful energy policy 53 FACILITIES MANAGEMENT How taking a proper look at heating, ventilation and air conditioning systems can lead to reduced costs 57 ASBESTOS IOSH documents a successful large-scale asbestos clean in a UK hospital 61 HEALTHCARE ESTATES A review of the event where ideas on the efficient running of hospitals were shared, with record visitors for 2014 65 LEGIONELLA The Water Management Society’s Susan Pearson talks about the organisation’s efforts to combat Legionella infection 71 BEST PRACTICE A review of October’s Best Practice 2014, the event where Jeremy Hunt addressed medical professionals 74 PARKING Health Business takes a look at new parking guidelines for hospitals that will see them offer reduced charges for certain groups 77 CATERING The government is set to enforce new rules to make hospital meals more nutritious and sustainable. Health Business sums up the changes
83 HEALTH BUSINESS AWARDS PREVIEW A look at the shortlists for this year’s award ceremony, held in London on 4 December
85 SECURITY The BSIA on the use of technology to combat aggression against hospital staff
21
29
47
77
W W W . C A N T A R U S . C O M
thedecorativepanelsgroup
YOUR PERFECT PARTNER
dp-BioCote® Quartz protected
*Tested in accordance with ISO22196:2011
Century House, Premier Way,Lowfields Business Park,Elland, West Yorkshire,HX5 9HF
T: +44 (0) 1484 658341 F: +44 (0) 1484 658812E: [email protected]
Download our app Scan for AndroidScan for AppleContact us for more information.
*A 99.9% germ free laminated board material suitable for furniture and fit out manufacture.
Significant reductions of harmful microbes within 15 minutes.
Available from stock in unicolour and woodgrain finishes.
Works continuously for the expected lifetime of the product.
dp-BioCote Quartz technology:
• Makes a product more hygienic, if it is likely to host harmful microbes.
• Keep a product fresher for longer, if it is likely to host odour-causing or staining microbes.
• Extend the usable lifetime of a product, if it is likely to host microbes which might degrade the surface.
• The surface is highly resistant to abrasion, far exceeding the abrasion resistance of high pressure worktops.
Produced in 2014

thedecorativepanelsgroup
YOUR PERFECT PARTNER
dp-BioCote® Quartz protected
*Tested in accordance with ISO22196:2011
Century House, Premier Way,Lowfields Business Park,Elland, West Yorkshire,HX5 9HF
T: +44 (0) 1484 658341 F: +44 (0) 1484 658812E: [email protected]
Download our app Scan for AndroidScan for AppleContact us for more information.
*A 99.9% germ free laminated board material suitable for furniture and fit out manufacture.
Significant reductions of harmful microbes within 15 minutes.
Available from stock in unicolour and woodgrain finishes.
Works continuously for the expected lifetime of the product.
dp-BioCote Quartz technology:
• Makes a product more hygienic, if it is likely to host harmful microbes.
• Keep a product fresher for longer, if it is likely to host odour-causing or staining microbes.
• Extend the usable lifetime of a product, if it is likely to host microbes which might degrade the surface.
• The surface is highly resistant to abrasion, far exceeding the abrasion resistance of high pressure worktops.
Produced in 2014
Public to compare surgeons’ survival rates for the first time on MyNHS website
HEALTHCARE DATA
Patients will be able to compare the survival rates of 5,000 surgeons from across the UK for the first time, as part of a major transparency drive by the NHS. Performance data for 13 different specialities – including heart, bariatric and orthopaedic surgery, will let patients know whether clinical outcomes for individual surgeons are within expected limits. The website will also include searchable information on local NHS food quality, staffing and patient safety, as well as local hospital performance, mental health care, social care and public health. Eventually, it will also contain figures on one year and five year cancer survival rates for NHS trusts. But some surgeons say the data may be “crude and misleading.” In a speech at the Foundation Trust Network Conference, Health Secretary Jeremy Hunt said: “Transparency is about patient outcomes not process targets. It uses the power of a learning culture and of peer review, not blame. “Healthcare globally has been slow to develop the kind of safety culture based on openness and transparency that has become normal in the airline, oil and nuclear industries. The NHS is now blazing a trail across the world as the first major health
economy to adopt this kind of culture.”NHS England medical director Prof Sir Bruce Keogh said: “This represents another major step forward on the transparency journey. It will help drive up standards, and we are committed to expanding publication into other areas. “The results demonstrate that surgery in this country is as good as anywhere in the western world and, in some specialities, it is better. The surgical community in this country deserves a great deal of credit for being a world leader in this area.”Prof Sir Bruce has previously said that surgeons who fail to publish their mortality rates could
face sanctions, with around 2,500 believed to not be taking part in the initiative. But some surgeons have warned the move could lead to some consultants refusing difficult cases. Prof John MacFie, president of the Federation of Surgical Specialty Associations, said: “The publication of individual surgeons’ performance data is crude and can be misleading, and does not include essential information such as duration of hospital stay and returns to theatre. “There is now good anecdotal evidence that shows publishing this data has encouraged risk averse behaviour, which is not in the interest of patients. “I believe that the data should only be published after any concerns in a surgeon’s performance have been investigated. “In reality very few deaths can be attributed to surgical error alone, and this data only attracts attention away from institutional failings. Put simply, hospitals should not be allowing surgeons to practice unless they can demonstrate their practice is safe.”
Research carried out by the Royal Voluntary Service has shown that elderly people who leave hospital without sufficient home support have more than double the risk of re-admission within three months compared to those with adequate care provision. The organisation’s campaign, ‘Let’s End Going Home Alone’, aims to minimise the unnecessary distress and costs that this can cause. The King’s Fund, who collaborated on the study, claim that making greater use of volunteers could help save the NHS as much as £40.4 million annually. The report’s authors estimate that roughly 200,00 people aged over 75 have been discharged without adequate home support over the last five years. David McCullough, chief executive of the Royal Voluntary Service, said: “The population is living longer, an achievement which should be celebrated – yet
it is presenting a challenge for the very organisation that has helped people live longer lives. “With local authority and hospital trusts facing budget cuts, we believe greater volunteer support through Home from Hospital schemes can improve the quality of older people’s lives long after a hospital stay and save the NHS millions of pounds. “Placing a caring volunteer at the centre of an older person’s recovery plan dramatically improves their experience, their confidence and their wellbeing, and helps them continue to live independent fulfilling lives. It also drives important efficiencies in hospitals enabling swift, well-managed discharge from wards. A strong warning sign identified in the report is the link between early discharge and readmission.”
Home support needed to prevent re-admission
TELECARE
The University of Westminster has been awarded a research grant of £620,000 to develop a portable device capable of testing bodily fluids to diagnose the virus. The EbolaCheck research initiative aims to create a portable, battery-operated device that can detect Ebola in a single process and give results within 40 minutes, which would make it more than eight times as quick as some existing laboratory techniques. Researchers working on the project, which is funded by the Department for International Development (DFID) and the Wellcome Trust, expect the device to be available for use as early as May 2015. Dr Sterghios A. Moschos, director of the Westminster Genomic Services Unit at the University of Westminster and leader of the EbolaCheck
research project, said: “We will use robust technologies to develop a simple but effective tool to diagnose this deadly virus similar to a blood glucose meter, and as reliable as hospital tests. Our portable device will be designed to run on batteries and only needs a small drop of blood to provide a result in less than 40 minutes. We then aim to make the whole process even safer by being able to use the device on saliva and urine. Early prototypes of this tool will be available for demonstration in a few months and we expect to begin testing it with patient samples by May.”
Westminster university to develop Ebola screening device
INFECTION CONTROL
New
s
READ MORE: tinyurl.com/og9zauf
READ MORE: tinyurl.com/k4zq75a
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
7 Volume 14.6 | HEALTH BUSINESS MAGAZINE

Tailored Solutions for your Waste Management and Disposal!Whether your clinical waste is infectious or non-infectious, using a specialist disposal company will make your waste management simple, help you meet your Duty of Care obligations, and save on costs!
With increasing legislation and financial demands, the pressure is on many organisations to balance the right disposal route, whilst getting the best value for money.
Talk to us today quoting S1801, about a tailor-made waste management solution to suit your business needs and your pocket.
Infectious & non-infectious clinical waste Pharmaceutical waste Dental waste Tailored solutions Nationwide service Licensed waste carrier
Tel: 029 2080 9090 email: [email protected] web: www.phswastemanagement.co.uk

New
s
INSPECTIONSNEWS IN BRIEF
‘Kitemark’ for NHS health appsNHS England chiefs have said that a ‘kitemark’ for approved healthcare apps is to be one of a number of technological initiatives to receive backing. This forms part of a bid to go ‘paperless’ in UK hospitals, and aims to reassure doctors that any apps that patients use to manage their condition is validated as being safe for use. This is expected to include a digital version of the red book used to record babies’ vaccinations.
Living wage for Derbyshire Health TrustDerbyshire Community Health Services NHS Foundation Trust in the East Midlands has agreed to pay each member of its staff living wage rates, raising the salaries of 65 employees in line with living wage guidelines. This constitutes an hourly rate of £7.65 for organisations based outside London, up from the national minimum wage of £6.50. Amanda Rawlings, Head of People and Organisational Effectiveness for the trust, said: “We are proud to be a living wage employer. “We believe that every member of staff deserves a living wage. “Adopting this initiative helps to improve morale, enhance quality of work and reduce sickness levels. “For the relatively few people within our organisation who were affected it has made a big difference and one we are proud to support.”
Shortlist announced for the Health Business Awards The shortlists for the 2014 Health Business Awards, which takes place in London on Thursday December 4, have been announced. The Awards, last held in 2011, recognise the efforts of organisations to improve and innovate the delivery of NHS services. Sixteen categories, which include awards for Clinical Commissioning and Patient Safety, will feature many examples of excellence and best practice. The Awards will be presented by BBC The One Show reporter and GP Dr Sarah Jarvis.
900 GP practices face CQC inspectionThe Care Quality Commission (CQC) has said that over a tenth of all GP practices are to face urgent inspection following the conclusion of regulators that they could be failing to provide adequate levels of care to their patients. Almost 900 practices were found to be at risk of breaching care standards, nearly a quarter of these being in London. Commonly cited issues within practices included insufficient access to doctors and difficulties in arranging breast cancer checks. Inspectors are to visit potentially failing practices over the winter period, while lower-risk surgeries are to be address over the next two years. The CQC has based practices’ risk ratings on 38 indicators taken from sources such as patient feedback forms and government statistics. Indicators include: the number of respondents to the GP patient survey who rated their care as fairly good or very good; flu vaccination percentage rates; dementia diagnosis rates; and the number of emergency admissions that could be addressed outside hospitals. Pulse magazine reports that GPs have been critical of the CQC’s risk assessments, with some accusing them of drawing on “simplistic” indicators and using data as “sticks to beat GPs with.” The CQC comments that these measures should not be seen as a judgement of care quality: “We will use our analysis of these indicators to raise questions, not make judgements, about the quality of care. Our judgements will always follow inspections, which take into account the results of our intelligent monitoring
and reports from other organisations.”Dr Richard Vautry, deputy chair of the General Practitioners Committee, said: “The art of general practice isn’t reflected within these very simplistic and bald statements, but also to provide this level of detail and information without any context on the practice from which it came from. There’s no link about what type of patients a particular practice provides services too. What funding levels they receive compared to other practices, the challenges practices face from premises, or support from community team. “They’re becoming more and more sticks to beat general practices with, and more and more targets – when we’ve seen the dangers of a target culture in mid-Staffs, and the consequences of organisations simply focusing on performance management targets, and there’s a risk of this happening to practices as well.”
NEW TRUST
New Trust for North MidlandsThe University Hospitals of North Midlands NHS Trust (UHNM) has been established with the help of more than a quarter of a billion pounds in investment. The Trust integrates the controversial Mid Staffordshire NHS Foundation Trust with the University Hospital of North Staffordshire. Dr Anne-Marie Houlder, chairman of Stafford and Surrounds Clinicial Commissioning Group, said that both Stafford and Surrounds and Cannock Chase CCG had been involved in the special administration process which saw the Mid Staffs Trust dissolved and in the transition of services. She said: “We now have a situation where we have a brand new hospital trust, University Hospitals of North Midlands (UHNM), with two hospitals – County Hospital in Stafford and Royal Stoke University Hospital. “It is vital that throughout this transition the quality of that care doesn’t suffer, so we have put in place a number of things to support the transition work and ensure that care stays at the high level which the people of Staffordshire both need and deserve.”
READ MORE: tinyurl.com/lppxfnd
ANTIBIOTICS
Misconceptions about antibiotics revealed in new surveyFour in ten people take antibiotics for a cough or runny nose despite both conditions normally clearing up without treatment, according to new research out today by Public Health England (PHE) for European Antibiotic Awareness Day (EAAD). The research also found 90 per cent of people are not aware bacteria that are resistant to antibiotics spreads easily from person to person, and more than one in seven don’t realise that healthy people can harbour these bacteria. People surveyed also mistakenly believed antibiotics can be used for fungal infections and allergic reactions, work as anti-inflammatory medication and can weaken the immune system. This confusion is contributing to inappropriate use of antibiotics, a factor in the growing threat of treatment-resistant bacteria.
READ MORE: tinyurl.com/kxwbwut
READ MORE: tinyurl.com/mglrhor
E TO READ MORE GO TO PAGE 83
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
9 Volume 14.6 | HEALTH BUSINESS MAGAZINE

37p+VAT
Print and Post
DOCMAIL PRESCRIBES:
IDEAL FLU RECALL PRINT & POST SOLUTION...
Find out why these practices simply LOVE Docmail!
Get in touch TODAY and find out how to start saving time, money and stress at Flu recall time!
● Huge time and cost savings● No contract! No minimum quantity! Free sign up!● Now even easier to use with Docmail PrintDriver● ONLY UK PRINT & MAIL COMPANY WITH 100% IG TOOLKIT
Martin’s Oak Surgery, Battle“We started using Docmail a couple of years ago to help reduce the burden of doing large mailings, and almost instantly we could see its appeal.
“Docmail has saved money, staff hours and elbow grease and once we learned how to format the documents and spreadsheets, it really was plain sailing. Furthermore, the helpdesk are invaluable - they are very responsive, understanding, and have some great hints and tips.
“For example, our flu campaign alone saves over £800 and by using EMIS Web searches cleverly; we can combine runs to offset costs even further.”
Carey Sinclair, Practice Manager
Portesham Surgery, West Dorset“We have used Docmail in our practice for the last five years - prior to which I used to spend a whole morning printing letters, and getting on my knees to stuff envelopes with our flu invitation letter! We use Docmail for mass mailings, including all our flu clinic invitations but also towards year-end to mail lists of patients who are missing something like a recent blood pressure reading.
“I have just estimated the mailings would cost almost twice as much if we did them in-house the traditional way. Based on sending out 1,000 letters, Docmail would cost just over £350, but including postage at 53p, envelopes, paper, and ink costs, plus staff time, it would cost us around £670 to do the same mailing, a saving of around over £300. The savings are amazing!”
Alison Dunbar, Practice Manager
Sunnyside Medical Centre, Portsmouth“Within a matter of weeks of signing up to Docmail, we were able to train all the administration team and secretaries to use the system.
“The step-by-step guide was a big help when training other staff members, and everyone has picked it up quickly. You only need to set everything up once - the headed paper, various templates, and mailing lists - which makes it more convenient for other staff members to log-on and use.
“We have undoubtedly cut our postage and stationery costs in half, and we have saved countless hours on mass-mailings. I would not hesitate to recommend Docmail to other medical practices.”
Stacey Windebank , Practice Administration and IT Assistant
01761 409701 / [email protected] - WWW.DOCMAIL.CO.UK
Part of
DM_Flu Advert v3.pdf 1 17/07/2014 10:07

37p+VAT
Print and Post
DOCMAIL PRESCRIBES:
IDEAL FLU RECALL PRINT & POST SOLUTION...
Find out why these practices simply LOVE Docmail!
Get in touch TODAY and find out how to start saving time, money and stress at Flu recall time!
● Huge time and cost savings● No contract! No minimum quantity! Free sign up!● Now even easier to use with Docmail PrintDriver● ONLY UK PRINT & MAIL COMPANY WITH 100% IG TOOLKIT
Martin’s Oak Surgery, Battle“We started using Docmail a couple of years ago to help reduce the burden of doing large mailings, and almost instantly we could see its appeal.
“Docmail has saved money, staff hours and elbow grease and once we learned how to format the documents and spreadsheets, it really was plain sailing. Furthermore, the helpdesk are invaluable - they are very responsive, understanding, and have some great hints and tips.
“For example, our flu campaign alone saves over £800 and by using EMIS Web searches cleverly; we can combine runs to offset costs even further.”
Carey Sinclair, Practice Manager
Portesham Surgery, West Dorset“We have used Docmail in our practice for the last five years - prior to which I used to spend a whole morning printing letters, and getting on my knees to stuff envelopes with our flu invitation letter! We use Docmail for mass mailings, including all our flu clinic invitations but also towards year-end to mail lists of patients who are missing something like a recent blood pressure reading.
“I have just estimated the mailings would cost almost twice as much if we did them in-house the traditional way. Based on sending out 1,000 letters, Docmail would cost just over £350, but including postage at 53p, envelopes, paper, and ink costs, plus staff time, it would cost us around £670 to do the same mailing, a saving of around over £300. The savings are amazing!”
Alison Dunbar, Practice Manager
Sunnyside Medical Centre, Portsmouth“Within a matter of weeks of signing up to Docmail, we were able to train all the administration team and secretaries to use the system.
“The step-by-step guide was a big help when training other staff members, and everyone has picked it up quickly. You only need to set everything up once - the headed paper, various templates, and mailing lists - which makes it more convenient for other staff members to log-on and use.
“We have undoubtedly cut our postage and stationery costs in half, and we have saved countless hours on mass-mailings. I would not hesitate to recommend Docmail to other medical practices.”
Stacey Windebank , Practice Administration and IT Assistant
01761 409701 / [email protected] - WWW.DOCMAIL.CO.UK
Part of
DM_Flu Advert v3.pdf 1 17/07/2014 10:07
New
s
Thinktank warns against healthcare ‘postcode lottery’
LOCALISM
The International Longevity Centre UK (ILC-UK) has warned that the decision in recent years to entrust local authorities with additional healthcare responsibilities could create a ‘postcode lottery’ and heighten the risk of political interference. While a report issued by ILC-UK says that localism could be beneficial, it should be rolled out with long term strategies in mind rather than short term targets, as politicians may not devote their energies to schemes that have no immediate impact on the ballot box. Jonathan Scrutton, senior policy and research officer at ILC-UK, said: “There is a huge invest-to-save argument. Early investment in preventing ill health in old age can reduce long-term care costs. “Localism has the potential to transform public health and deliver better and more targeted services. But if local authorities are to maximise the long-term benefit of investing in preventative health, they must not get drawn into simply achieving short-term targets.” Local authorities have been charged with
administering public health services since changes to the Health and Social Care Act were enacted in April 2013. The ILC-UK report comments on the positive side of this change, saying it “has the benefits that local health priorities can be addressed by targeted initiatives, and innovative strategies can be developed that encourage more integrated working between departments.” However, “it also has the potential to worsen the effects of the ‘postcode lottery’, where the quality and availability of NHS services older people can expect are defined by where they live.” A Department of Health spokesman said: “People’s health varies widely across the country, which is why we have scrapped a one-size-fits-all approach and are empowering communities to tackle their own specific problems, backed by billions of pounds in ring-fenced funding.But councils are held to account and must still prove their strategies are working.”
The Deputy Prime Minister, Nick Clegg, has announced that treatment for mental health conditions will be brought into line with other NHS services with the introduction of the first ever waiting time standards. There will also be £120 million to improve mental health services. For the first time, from April 2015, most patients needing talking therapies – for conditions like depression – will be guaranteed the treatment they need in as little as 6 weeks, with a maximum wait of 18 weeks. For many patients experiencing their first episode of psychosis, the NHS will start to provide treatment within 2 weeks of referral – bringing it into line with consultations for cancer. Evidence shows that treating psychosis rapidly can dramatically improve patients’ chances of recovery and potentially save £44 million each year in hospital admissions.
First ever NHS waiting time standards for mental health announced
MENTAL HEALTH
READ MORE: tinyurl.com/3pu8v9g
HEALTHCARE IT
The Welsh government has launched a new initiative to tackle the rate of deaths that occur as a result of liver disease. Together for Health – Liver Disease Delivery Plan, lays out a strategy for NHS Wales and its partners to improve services for people with liver disease, as well as working to minimise the effect of social inequalities. Plans are currently under consultation and are due to be finalised in April next year. Deputy health minister Vaughan Gething, said: “The Welsh Government will continue to take action to help positively influence people’s lifestyles. As outlined in the recent Public Health White Paper, we are exploring legislating to curb excessive
alcohol consumption by introducing a 50p minimum unit price for alcohol. “At the same time we want to help people be aware of these risks in their own lives and encourage people to take responsibility for their actions and shaping their own health. “The prudent healthcare approach means that we all have to be jointly involved in minimising avoidable harm. By paying better and more careful attention to our own health, we can often avoid causing damage.”
GPs could receive cash to buy IT systems
LIVER DISEASE
Welsh government to tackle liver disease
A report developed by NHS England along with the Department of Health, Monitor and other organisations says that the current system of central funding for IT systems in general practice could be terminated when the GP Systems of Choice scheme expires in April 2018. Practices would instead receive funding through per patient capitation payment. This would give surgeries leverage to purchase their own systems rather than choosing from a Government-approved list of suppliers. The report, titled ‘Personalised Health and Care 2020’, says: “The GPSoC contract for the central purchasing of GP systems and associated technology ends in April 2018, and NHS England and DH will consider carefully whether it is appropriate that it continues as a national contract or whether funding for GP systems should be incorporated into the capitation payments made to primary care providers, who will then be free to purchase systems from any supplier, subject to meeting national data and technology standards.” The report also mentions plans to provide patients with access to their medical records, allowing them to add comments to their GP medical records and an expansion of the care.data initiative by 2018.
READ MORE: tinyurl.com/o7sffan
READ MORE: tinyurl.com/pydfp74
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
11 Volume 14.6 | HEALTH BUSINESS MAGAZINE
Are you gearingup for a surge inpatient numbers?
With admissions on the rise and bed numbers fallingacross the UK, surge periods are adding to thepressure on hospital bed capacity. In addition, theCare Quality Commission has recently adopted theHospital Intelligent Monitoring System whichhighlights the NHS Trusts most at risk offalling standards. Elliott has developed anew standard rental fleet of wardblocks, designed to meet theneeds of NHS Trusts withcapacity issues.
For more information please contact us on
FREEPHONE 0800 085 8202 or email [email protected]
Available to rent now &installed on site in 8 weeks
**RDS and HTM/HBN Derogation sheets available on request.
BENEFITSRapidly increase capacity
Available for hire terms from 3 months upwards
Block design gives flexibilityon size and bed numbers
Designed with Patient care and dignity in mind
Cost effective solution
Off balance sheet solution
HTM/HBN Compliant where necessary**
Infection Controlapproved finishes
Medical Gasses
Up to 50 year design life
TECHNICALSOLUTION
8604 Elliott A4 Educ-Ad_Layout 1 16/04/2014 14:13 Page 1

Are you gearingup for a surge inpatient numbers?
With admissions on the rise and bed numbers fallingacross the UK, surge periods are adding to thepressure on hospital bed capacity. In addition, theCare Quality Commission has recently adopted theHospital Intelligent Monitoring System whichhighlights the NHS Trusts most at risk offalling standards. Elliott has developed anew standard rental fleet of wardblocks, designed to meet theneeds of NHS Trusts withcapacity issues.
For more information please contact us on
FREEPHONE 0800 085 8202 or email [email protected]
Available to rent now &installed on site in 8 weeks
**RDS and HTM/HBN Derogation sheets available on request.
BENEFITSRapidly increase capacity
Available for hire terms from 3 months upwards
Block design gives flexibilityon size and bed numbers
Designed with Patient care and dignity in mind
Cost effective solution
Off balance sheet solution
HTM/HBN Compliant where necessary**
Infection Controlapproved finishes
Medical Gasses
Up to 50 year design life
TECHNICALSOLUTION
8604 Elliott A4 Educ-Ad_Layout 1 16/04/2014 14:13 Page 1
Written by Stephen Childs, m
anaging director, NHS N
orth of England Comm
issioning Support Unit
We live in interesting times in the NHS. From the Lansley reforms to the NHS’s £30 billion deficit to Simon Stevens’ Five Year Forward View, it is a fascinating period to be working in this sector. A particularly interesting area that has seen dramatic change in recent years is commissioning. The Health and Social Care Act introduced by the current government completely changed the way commissioning takes place in the NHS, with Commissioning Support Units coming into operation to support GPs, providing services, solutions and support that would free up their time so they could focus on improving outcomes for patients and healthcare for local communities. Despite the dramatic change and challenges, huge progress has been made in the 18 months since the reforms came into effect and Commissioning Support Units are beginning to prove they can be a successful model. There have been some teething problems – for example, the number of CSUs has declined from 27 at inception to the nine that exist in England today. It’s also possible that this number will fall further,
although it will be important that enough are retained to give customers sufficient choice. But the successes far outweigh the challenges. The marketplace is viable and functioning well, and collaboration, innovation and efficiency are being put at the heart of the CSU model. An example of this came earlier in 2014 when a group of likeminded CSUs, including the North of England CSU which I lead, came together to form the Elis Group with the aim of working collaboratively to share best practice, benchmark, share expertise, and reduce development costs across a range of programme areas. The group now works
with more than 90 Clinical Commissioning Groups (CCGs) and other NHS organisations, covering almost half the UK population. While collaboration is championed, the Elis Group’s CSUs also compete against each other. This creates a dual dynamic of collaboration and competition that gives service providers – and even more importantly patients – the best deal possible.
THE FINANCIAL CHALLENGEAs the landscape has evolved over the past 18 months, the management resources available have continued to reduce and commissioners need to be even smarter with how they utilise resources for the benefit of their communities. It has been estimated that the spend on management resources is some 40 per cent lower than when Primary Care Trusts (PCTs) were at their ‘peak’ around five years ago – a saving of around £1 billion. But these financial pressures are far from disappearing. NHS England needs to find further 15 per cent management cost savings and CCGs 10-15 per cent by 2015/6. Logic tells you that working in an increasingly constrained financial environment should enable smarter E
Despite the dramatic change and challenges, huge progress has been made in the 18 months since reforms came into effect and Commissioning Support Units are beginning to prove they can be a successful model
CHAMPIONING COMMISSIONINGStephen Childs of NHS North of England comments on the progress that has been made to improve healthcare commissioning since the introduction of the Health and Social Care Act
Finance
COMISSISSIONING
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
13 Volume 14.6 | HEALTH BUSINESS MAGAZINE
SIMPLE SOLUTIONS DRAMATIC BENEFITS!
Leading
reward
creative
creative
inspireddesign
big
key
big
solution
inspiringbusiness
business
efficiencybest
create evolveinvent
invent
new
keyimagination
imagination
imagination
new
think big
concept
concept
brains
analysys
conceptthought
idea
ChangeIn the
Healthcaresector
MARSHALLbästLtd
+ 44 (0) 845 130 9074 • [email protected] • www.marbast.eu
✔ PERFECT – For conventional fabric cubicle curtains.Unique Marlux® “clip on – clip off ” glider can be attached to the curtain first thensimply snapped onto the cubicle curtain track with the curtain.
✔ PERFECT – For Marlux® Fast-Fit Disposable Curtains.Patented push button access & removal point allows curtains to be changedin seconds.
✔ PERFECT – For reducing the possibility of patient self-harm.When used with Marbäst® Magnetic Anti Ligature brackets each individualcubicle will collapse when an abnormal load is applied.
Unheard of until their launch in 2002 and brainchild of our CEO Laurence Marshall, disposableprivacy curtains are now a familiar sight in quality healthcare establishments throughout the UK &worldwide.
At Marshall bäst Ltd we believe that simple solutions can have a dramatic impact on the wellbeingof patients and that’s why our policy of developing simple solutions has served the trade so well forover 40 years!
Marlux® Hospital Cubicle Curtain Track is...

SIMPLE SOLUTIONS DRAMATIC BENEFITS!
Leading
reward
creative
creative
inspireddesign
big
key
big
solution
inspiringbusiness
business
efficiencybest
create evolveinvent
invent
new
keyimagination
imagination
imagination
new
think big
concept
concept
brains
analysys
conceptthought
idea
ChangeIn the
Healthcaresector
MARSHALLbästLtd
+ 44 (0) 845 130 9074 • [email protected] • www.marbast.eu
✔ PERFECT – For conventional fabric cubicle curtains.Unique Marlux® “clip on – clip off ” glider can be attached to the curtain first thensimply snapped onto the cubicle curtain track with the curtain.
✔ PERFECT – For Marlux® Fast-Fit Disposable Curtains.Patented push button access & removal point allows curtains to be changedin seconds.
✔ PERFECT – For reducing the possibility of patient self-harm.When used with Marbäst® Magnetic Anti Ligature brackets each individualcubicle will collapse when an abnormal load is applied.
Unheard of until their launch in 2002 and brainchild of our CEO Laurence Marshall, disposableprivacy curtains are now a familiar sight in quality healthcare establishments throughout the UK &worldwide.
At Marshall bäst Ltd we believe that simple solutions can have a dramatic impact on the wellbeingof patients and that’s why our policy of developing simple solutions has served the trade so well forover 40 years!
Marlux® Hospital Cubicle Curtain Track is...
thinking and commissioning, and we are seeing evidence 18 months on from the inception of CCGs that this is the case.
ENABLING EFFICIENCYCSUs were established to enable efficiency in two areas – management of the commissioning process, and management of the direct commissioning of health services themselves. Everything we do is focussed on being more efficient and effective – in particular through collaboration, spreading best practice and encouraging commissioners to work with outcomes front of mind when making key decisions. At their best CSUs can bring scale, resilience, standardised processes and levels of efficiency to enable the new system to work effectively. Not just for CCGs but for NHS England too. One recent example is the work we’ve done at North of England CSU (NECSU) around business intelligence. Prior to 2013 we had five PCT clusters in our region all either having established or in the process of establishing separate business intelligence tools. This meant the system of processing and collecting data across the primary and secondary care sectors was being replicated many times over at unnecessary cost. We quickly realised this did not make sense and by consolidating the best of the systems in development into a single business intelligence tool (RAIDR) we could share and exchange information more easily and at a significantly lower cost. So successful has this process been that not only is the system being used throughout the North East and Cumbria it has now been taken up by 43 CCGs from Suffolk to Yorkshire covering 20 per cent of the country. We are very proud that a product developed by the NHS for the NHS is leading the market. The competition is intense and our aim is to keep RAIDR ahead of the pack and for that reason we continue to invest heavily in its development – £0.5 million this year alone in new dashboards for our customers.
SHARING BEST PRACTICESharing best practice is at the heart of what we do. However, what might sound like a fairly simple concept is not without its challenges. The past few years has seen a number of initiatives from the Department of Health and NHS to foster a culture and climate of innovation and learning from others in the NHS. These include things like David Nicholson’s Innovation, Health and Wealth initiative and the NHS Innovation Challenge Prizes. But more work still needs to be done to highlight the benefits of sharing of
experiences and how learning from others can both prevent mistakes being repeated as well provide ideas for improvements that have already shown they work. Organisations should not be afraid to be open and transparent, to share and learn. A key initiative of the Elis Group has been to establish a Knowledge Hub. This is a web-based repository for best practice that can be accessed by all CSU customers. People are incentivised to use it in a number of ways, for example through their staff appraisal process. We work with CCGs to upload their case studies and experiences that can be built on by others in the field. There’s also a chat forum where people can post their good ideas and comments. It’s very much an iterative process and one that we hope will be opened up to a larger community in due course.
COLLABORATION, COLLABORATIONCompetition is clearly vital to ensure a strong and vibrant marketplace – but so is collaboration. We are seeing more and more evidence of how collaborating with our peers makes the best sense for patients and customers alike. We have experienced this ourselves partnering successfully for projects such as waiting list validation and
patient engagement contracts. We are also actively encouraging
collaboration to drive efficiency with a specific workstream
in place to drive business development across CSUs. For example, the CSUs that comprise the Elis Group have collaborated to establish the Elis Framework. This is a framework
that gives CSUs and their customers faster,
procurement compliant access to a range of small to medium
sized enterprises, as well as some larger suppliers, when they need to access additional expertise or capacity – saving the NHS money and speeding up service delivery.
DRIVING THOUGHT LEADERSHIPWe are also committed through the Elis Group to providing leadership in debating and solving some of the biggest issues around commissioning. We are planning to run a series of nationwide workshops that bring together leaders in primary care to address these issues, and ensure we maximise the collective intellectual experience and firepower that we have at our disposal. We are also establishing the Elis Group Academy, an educational initiative that brings together the brightest and the best minds to drive forward excellence in commissioning support. This virtual learning programme will enable staff to achieve an accredited academic qualification targeted at commissioning support services. This will also allow staff
to share best practice, ensuring high-quality commissioning is not delivered in silos.
TRANSFORMING HEALTHAs CSUs have evolved, we are steadily increasing the type of work we do to focus more on ‘transformational’ rather than ‘transactional’ work. As CCGs mature and grow in confidence we are seeing opportunities to work with them in more of a consultancy capacity. While ultimately commissioning decisions are in the hands of CCGs, we can play a valuable role in helping them identify where they can make the most significant improvements and where their investment will see the best return in improving the health of their communities. Third sector partnerships are also a key feature of our approach. While CCGs have their own local relationships with third sector partners, through the Elis Group we are seeking to engage with more organisations with a national footprint. This includes liaising closely with the Association of Chief Executives of Voluntary Organisations (ACEVO). We are particularly interested in drawing on their ideas on service redesign, patient experience and information, as well as their expertise in engagement and consultation with local communities.
THE FUTURESome have cast doubt on the future of Commissioning Support Units. However, I hope this shows you the opposite is the case. Innovations like the Elis Framework are boosting efficiency. A fascinating mix of collaboration and competition is creating a thriving marketplace that is driving innovation, investment and improvement. Knowledge sharing is creating a system where best practice is championed, not forgotten. In short, the future is bright for CSUs with innovation, efficiency and collaboration at the heart of what we are doing and achieving.
FURTHER INFORMATIONwww.necsu.nhs.uk
Finance
COMMISSIONING
About NECSU
NECSU is one of nine Commissioning Support Units across England. Based in the north of the country, it has over 700 staff working across Teesside, Durham, Tyne and Wear and Cumbria. Its customers include 13 Clinical Commissioning Groups (CCGs) across the north east and Cumbria, covering a population of over 3.5 million, as well as Yorkshire and Humber CSU, CCGs in Lancashire, Wigan, Suffolk and Anglia, NHS England, a number of Local Authorities and Foundation Trusts.
Competition
is clearly
vital to
ensure a
strong and
vibrant marketplace
– but so is
collaboration
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
15 Volume 14.6 | HEALTH BUSINESS MAGAZINE
Convergence: is Healthcare getting closer to FMCG, and vice-versa?
Demographic changes, an increasing demand for preventive products moving towards a mass consumer healthcare market, and more intense levels of competition are forcing the healthcare industry to renovate. A major trend to respond to these challenges lies in merging with
FMCG companies to complement organisational capabilities in terms of sales and marketing, production and distribution. FMCG companies are used to launching daily products for the mass market, and it seems a golden opportunity to combine this with the R&D expertise of pharmaceutical companies in order to respond to the market’s demand and launch consumer products with preventive care features. Naturally, to make this transition, some new challenges arise. For
example: to understand the new and best consumer channels; to adjust the supply chain to serve these channels in the most efficient way; to review the commercial structure and processes; and how to handle M&A activity in the best way possible. Are you ready to deal with these challenges?
Integration Management Consulting, a member of the MCA since 2013, is an international consultancy in strategy, management and operations that specialises in the design and the implementation of solutions. Founded in 1995, we now have over 200 professionals spread across our offices in Europe and Latin America. We have deep functional expertise in Marketing and Sales as well as Supply Chain, and we have used this expertise across a variety of industries. This cross-industry experience allows us to transfer ideas and best practices from one industry to another, and together with our proven track record of delivering more than 150 projects for global leaders in the healthcare industry and over 200 projects within FMCG, we have the capability to add real value to our customers.
We have helped our clients to grow and expand their reach, through new go-to-market strategies as well as roadmap
development covering all the areas of the company. Transformation is only possible when you are truly hands-on and fully engage the client team; Integration works like this with the client’s team to start building the new reality and changing things from day one.
Our broad experience in Marketing and Sales projects includes portfolio reviews, channel strategy and all the internal
processes to make sure your consumer is being reached. We also have extensive work developed in Supply Chain, from transfer order and logistic network reviews to make-or-buy decisions.
All our projects connect the strategy with the reality of both the market and of our clients, ensuring a smooth and successful
implementation. We are committed to guarantee that our recommendations are implementable and we work extremely closely with our clients to challenge, tailor and fine-tune our recommendations to ensure they are relevant, robust and realistic.
Some of our clients in the healthcare industry include:
www.integrationconsulting.com
In association with
Integration_HB14.6 - FP.indd 1 19/11/2014 11:48

Written by Alan Leam
an, ceo of MCA and M
ichael Allen, EY
The financial health of the NHS is rarely out of the news at the moment, and Simon Steven’s recent report confirms that this level of interest will only grow as we get nearer to the general election in May 2015. All our politicians will seek to reassure the public that our hospitals and GP services will be secure in their hands. However, a quick view of the facts reveals that the situation is far more complex than the competing parties often allow. Demographic pressures, a growing population and the availability of new treatments and drugs are all adding to costs. At the same time, public expectations and demands are rising as well. The UK’s management consulting firms are very alive to these challenges. Many
are working to relieve the pressure of rising costs, or to help trusts and others to manage demand effectively. They are able, often, to help introduce changes that both improve patient care and the use of valuable resources. One area where Management Consultancies Association (MCA) members have made a real impact in recent times is in helping hospital trusts and others on the front line to improve their financial and people management. Sometimes, it takes an extra pair of eyes to see where the problems are, or to bring people together in support of the best solutions. And it often requires consultants with deep financial and other skills to get to the bottom of how to put institutions on
a sustainable footing for the future. Engaging outside support when it is needed is a sign of real strength. The institutions of the NHS are entitled to draw on the best skills, insights and knowledge that is available. With the challenges facing trusts as great as ever, some of the problems can seem very difficult to disentangle due to the complexity of the task in hand. However, we can be optimistic and, critically, many of the changes that are required can be made without the need for recurrent investment.
PROVIDING BETTER CARE FOR LESSAny trust CEO will tell you their job is to manage the inherent tension between access, quality and cost – the three card trick. However, for many trusts delivering that trick is a challenge mainly due to increasing non-elective demand and the requirement to make recurrent savings of 4.5 per cent each year. The forecast increase in trust deficits from £400 million in 2013/14 to £800 million in 2014/15, alongside growing waiting lists and deterioration in A&E performance, confirms this challenge. However, this isn’t inevitable. Experience shows that quality care costs less – for example it is much better for an elderly patient with a fractured hip to have their operation within 12 hours of their fall than it is to keep them in hospital for several days before operating; it is also much cheaper. Experience also tells us that there is a E
SERVING MORE THAN JUST THE BOTTOM LINEAlan Leaman and Michael Allen share insights on how healthcare trusts can benefit from bringing in outside experts to resolve financial issues and improve hospital governance
Hospital Managem
ent
CONSULTANCIES
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
17 Volume 14.6 | HEALTH BUSINESS MAGAZINE
Convergence: is Healthcare getting closer to FMCG, and vice-versa?
Demographic changes, an increasing demand for preventive products moving towards a mass consumer healthcare market, and more intense levels of competition are forcing the healthcare industry to renovate. A major trend to respond to these challenges lies in merging with
FMCG companies to complement organisational capabilities in terms of sales and marketing, production and distribution. FMCG companies are used to launching daily products for the mass market, and it seems a golden opportunity to combine this with the R&D expertise of pharmaceutical companies in order to respond to the market’s demand and launch consumer products with preventive care features. Naturally, to make this transition, some new challenges arise. For
example: to understand the new and best consumer channels; to adjust the supply chain to serve these channels in the most efficient way; to review the commercial structure and processes; and how to handle M&A activity in the best way possible. Are you ready to deal with these challenges?
Integration Management Consulting, a member of the MCA since 2013, is an international consultancy in strategy, management and operations that specialises in the design and the implementation of solutions. Founded in 1995, we now have over 200 professionals spread across our offices in Europe and Latin America. We have deep functional expertise in Marketing and Sales as well as Supply Chain, and we have used this expertise across a variety of industries. This cross-industry experience allows us to transfer ideas and best practices from one industry to another, and together with our proven track record of delivering more than 150 projects for global leaders in the healthcare industry and over 200 projects within FMCG, we have the capability to add real value to our customers.
We have helped our clients to grow and expand their reach, through new go-to-market strategies as well as roadmap
development covering all the areas of the company. Transformation is only possible when you are truly hands-on and fully engage the client team; Integration works like this with the client’s team to start building the new reality and changing things from day one.
Our broad experience in Marketing and Sales projects includes portfolio reviews, channel strategy and all the internal
processes to make sure your consumer is being reached. We also have extensive work developed in Supply Chain, from transfer order and logistic network reviews to make-or-buy decisions.
All our projects connect the strategy with the reality of both the market and of our clients, ensuring a smooth and successful
implementation. We are committed to guarantee that our recommendations are implementable and we work extremely closely with our clients to challenge, tailor and fine-tune our recommendations to ensure they are relevant, robust and realistic.
Some of our clients in the healthcare industry include:
www.integrationconsulting.com
In association with
Integration_HB14.6 - FP.indd 1 19/11/2014 11:48

significant variation in the utilisation of resources such as operating theatres or clinic rooms. This variation exists not only between trusts but also within them. For example, it is quite common to see threefold variation in the number of patients seen by doctors in the same team during their clinics or operating lists. By identifying this variation, understanding the causes and taking steps to address it, trusts can make significant savings whilst concurrently improving access for patients. This principle also applies to differences in length of stay, day-case rates and the proportion of emergency patients managed through ambulatory care. Furthermore, there is a vast body of evidence which shows too many patients are admitted to hospital and that they stay in hospital too long once they have been seen. The management of patients with chronic diseases such as diabetes or chronic obstructive pulmonary disease is a good example of this. These patients account for a disproportionate number of hospital admissions, most of which can be avoided through improvements in community care, primary care, social care and improved use of technology.
TALENT MANAGEMENTGlobal competition for talent is a key challenge for all sectors of the economy. Thirty years after the introduction of general management in the NHS, this is especially true in the health service. Recent data shows that over 10 per cent of trusts do not have a director of finance or a director of operations. And the average tenure of a ceo is just 15 months. Making these positions more attractive to those already working in the service and professionals in the private sector is essential if we are to avoid decline in the calibre of leadership. This challenge is even more acute
when it comes to clinical managers and leaders. Good clinical leadership is essential to any well-run trust; however most clinicians view these roles as unattractive. Changing this perception is crucial.
GOVERNANCE AND CULTURAL CHANGEAchieving cultural change is just as critical to the future of the NHS as good governance. There is a growing interest in mutual ownership as a way to improve ownership and engagement. This is an interesting concept, which will undoubtedly appeal to some organisations and teams, although to succeed it must be underpinned by accurate and timely service line reports and performance data. Regulators, such as Monitor and the Care Quality Commission (CQC), recognise the importance of good governance and that it needs to be improved within the NHS. In the case of Monitor, the CQC and the Trust Development Authority, there is now consensus as to what governance should look like, and the features that they will be expecting when performing inspections. These new frameworks come in response to the Francis enquiry and will form a critical step in the transformation of NHS Trusts. The challenges facing NHS Trusts remain significant. However, with the right information, an engaged workforce, strong clinical leadership, the right incentives, a culture of innovation, appropriate governance and the right support, the trust sector can thrive.
Written by Alan Leaman, ceo of the Management Consultancies Association (MCA), and Michael Allen, director in the Health Practice at EY.
FURTHER INFORMATIONwww.mca.org.uk
Hosp
ital M
anag
emen
t
Case study 1Mid Yorkshire Hospitals NHS Trust wins MCA Award with EY for its work to restore financial health.
In April 2013, Mid Yorkshire Hospitals NHS Trust and consultancy EY won an MCA (Management Consultancies Association) award for their achievements in reducing one of the largest NHS budget deficits in history whilst improving outcomes and access for patients. The turnaround at the Trust has been quite remarkable – with recurrent savings of over £50 million made since April 2012 (equivalent to almost six per cent per annum) alongside a 21 point reduction in the mortality rate. The Trust is now on course to eliminate its deficit in 2016/17 – six years earlier than previously expected and has recently had its plans to reconfigure services in conjunction with partners in the Local Health Economy approved by the Secretary of State for Health. Just over two years after the Trust and EY started working together, the Trust also treats more patients than ever before, long-term care has improved, and plans are in place to provide better care for women in and after pregnancy.
Case study 2KPMG with University Hospitals Bristol NHS Foundation Trust (UHB).
KPMG with University Hospitals Bristol NHS Foundation Trust (UHB) was highly commended by the MCA in the Performance Improvement in the Public Sector category. KPMG’s analysis revealed that rather than the A&E itself, actually the problems were as a result of bottlenecks in the flow of patients through the hospital primarily due to wards being unable to release their beds when they were needed, interrupting flow through the hospital and resulting in long waits in A&E and a queuing of ambulances. Prior to KPMG’s involvement, the hospital had a very large number of projects, all intended to improve performance, but the large number resulted in a lack of focus and a lack of rapid progress. The consultancy therefore drastically reduced the number of projects to focus on a few, key clinical goals. Teams became clinician and nurse-led, to ensure that solutions were not imposed but created jointly, which had a critical impact on raising motivation and engagement levels. UHB is now exceeding the regulator’s target for time spent in A&E, with over 97 per cent of patients now treated in less than four hours (an improvement on 90 per cent achieved in March 2013).
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.618

In a recent Health Business article, Nick Gerrard discussed the Project Spotlight initiative undertaken at Mid Essex Hospital Services Trust. The use of innovative sourcing and procurement strategies not only achieved impressive savings but also led to a transformation in the role of procurement – now a business-focussed function contributing to improved patient care and enhanced level of service. These creative new approaches are essential in meeting the challenge of achieving more for less in today’s NHS. Some initiatives are major changes and are required at an organisational level. However, there are also quick wins to be had for those charged with finding savings – by helping individuals and teams to use their own skills to maximum effect. THE IMPORTANCE OF NEGOTIATIONPicture the scene: after weeks of preparation, it is now time to negotiate an important contract – one that will make a big difference not only to the performance of the organisation or department, but to the
morale and confidence of all those involved. Somehow though, things don’t quite go to plan. There’s too much dancing around before the key issues are discussed, while you and your colleagues find yourselves saying things you hadn’t intended to say. But through the awkward silences and power play, a deal of sorts is agreed. Leaving the room you wonder just how realistic the agreement is and know that a better outcome with greater savings could probably have been achieved. Days later, further contact with the other party reveals several misunderstandings, creating more work and uncertainty. This scenario is not untypical. In its work with NHS teams and in other organisations and industries, Huthwaite is frequently
told that people involved in bidding for and negotiating major agreements have received scant opportunity to develop their skills – yet they are expected to win business or shape agreements that will have a lasting impact on their organisation. Received wisdom about how to behave before and during negotiations can also have a detrimental effect on the outcome. When Huthwaite looked at the behaviours of skilled negotiators its research revealed some surprising results. VERBAL BEHAVIOURAL SKILLSHuthwaite’s research shows that the behavioural profile of skilled negotiators is a far cry from the traditional narrow-eyed, poker-faced silent character, or the table-thumping individual issuing ultimatums. Successful negotiators create a co-operative, collaborative climate wherever possible, using questioning skills and open language. The skilled negotiator has a wide portfolio of verbal skill, not only using certain behaviours to great effect but,
importantly, avoiding others. An example is giving feelings – perhaps somewhat surprisingly, successful negotiators express their feelings more often than unsuccessful ones. E.g. “I’m delighted we’ve made progress on this issue” or “I’m disappointed that you view this as unimportant”. Irritators – telling the other party “this is a good deal for you” or “I’m being very generous here” have the potential to irritate and annoy, and can damage the climate of the meeting. Skilled negotiators are not immune, and use these approximately twice per hour. Unsuccessful negotiators however averaged 10.8 times per hour. Counterproposals – responding to the other party’s proposal with an immediate
counterproposal can be damaging to the negotiation. It sends the message that the initial proposal has been ignored. Skilled negotiators spend much more time listening, seeking information and understanding the other side’s position, and in doing so make less than half the number of counterproposals made by their unskilled counterparts. Testing understanding and summarising – a key measure of successful negotiations is how implementable the agreement is and that often depends on the amount of clarity achieved during the discussions. Verbal behaviours that check understanding throughout, and clarify agreements through effective summarising, are essential in creating a workable agreement.
FLEXIBILITYAll these behaviours are just a part of the excellent negotiator’s skill set. They need to have the full range of behaviours in their repertoire together with the flexibility to use each as appropriate to the situation. Equally important is the way they prepare and plan. Average negotiators spend time preparing data and gathering information but fail to plan how best to use it. Skilled negotiators prepare well but then spend more time planning. They explore a wider range of possible issues and trades, identify their levers and how to use them, and know the real cost of any concessions they might make. Achieving more for less in the NHS is here to stay and ambitious new initiatives undoubtedly have a key role to play in shaping the future of the service. In addition, building the confidence and skill of those who have responsibility to negotiate can provide a relatively quick way of securing major savings whilst achieving the best outcomes for the organisation and most importantly, the patients and service users.
FURTHER INFORMATIONTel: 01709 710081 www.huthwaite.co.uk
“Combined with robust preparation and planning, effective negotiators need to have the full range of behaviours in their repertoire together with the flexibility to use each as appropriate to the situation”– Ali Morris, business director for healthcare, Huthwaite International
ADVERTISEMENT FEATURE
ACHIEVING MORE FOR LESS IN CHALLENGING TIMESIn this article, Ali Morris, business director for Healthcare at Huthwaite International considers how the often overlooked subject of personal skill in negotiation can help both non-clinical and clinical stakeholders to manage the pressure on costs and other resources
Advertisement Feature
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
19 Volume 14.6 | HEALTH BUSINESS MAGAZINE

Medi-Shower TM Benefits:
• Anti-bacterial
• Medi-Flush replaceable insert
• Low maintenance costs
• Reduced risk of infection
• Saves water and energy
•• Easy to clean/retrofit
• Medi-Shower has up to a five year warranty and a 5 year guarantee against limescale clogging when inserts are replaced on a quarterly basis.
Multishower GB Ltd, Medi-ShowerTM
PO Box 307, Londonderry, BT48 4EA
Tel +44 (0) 208 263 6095
Fax +44 (0) 208 263 6100
For distribution inquires please
contact: [email protected]
‘Best Product for Enhancing Infection
Prevention’Building Better Healthcare
Awards 2014
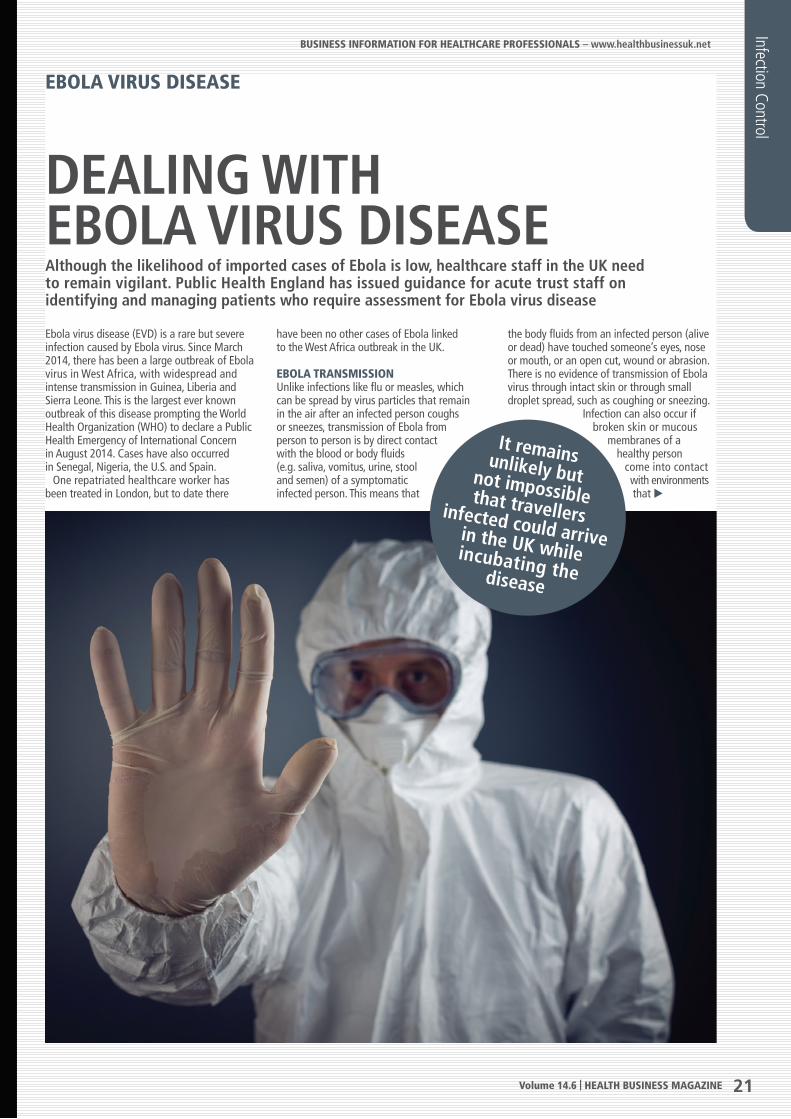
Ebola virus disease (EVD) is a rare but severe infection caused by Ebola virus. Since March 2014, there has been a large outbreak of Ebola virus in West Africa, with widespread and intense transmission in Guinea, Liberia and Sierra Leone. This is the largest ever known outbreak of this disease prompting the World Health Organization (WHO) to declare a Public Health Emergency of International Concern in August 2014. Cases have also occurred in Senegal, Nigeria, the U.S. and Spain. One repatriated healthcare worker has been treated in London, but to date there
have been no other cases of Ebola linked to the West Africa outbreak in the UK.
EBOLA TRANSMISSIONUnlike infections like flu or measles, which can be spread by virus particles that remain in the air after an infected person coughs or sneezes, transmission of Ebola from person to person is by direct contact with the blood or body fluids (e.g. saliva, vomitus, urine, stool and semen) of a symptomatic infected person. This means that
the body fluids from an infected person (alive or dead) have touched someone’s eyes, nose or mouth, or an open cut, wound or abrasion. There is no evidence of transmission of Ebola virus through intact skin or through small droplet spread, such as coughing or sneezing.
Infection can also occur if broken skin or mucous
membranes of a healthy person
come into contact with environments that E
EBOLA VIRUS DISEASE
DEALING WITH EBOLA VIRUS DISEASEAlthough the likelihood of imported cases of Ebola is low, healthcare staff in the UK need to remain vigilant. Public Health England has issued guidance for acute trust staff on identifying and managing patients who require assessment for Ebola virus disease
Infection Control
It remains unlikely but not impossible that travellers infected could arrive in the UK while incubating the disease
Medi-Shower TM Benefits:
• Anti-bacterial
• Medi-Flush replaceable insert
• Low maintenance costs
• Reduced risk of infection
• Saves water and energy
•• Easy to clean/retrofit
• Medi-Shower has up to a five year warranty and a 5 year guarantee against limescale clogging when inserts are replaced on a quarterly basis.
Multishower GB Ltd, Medi-ShowerTM
PO Box 307, Londonderry, BT48 4EA
Tel +44 (0) 208 263 6095
Fax +44 (0) 208 263 6100
For distribution inquires please
contact: [email protected]
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
21 Volume 14.6 | HEALTH BUSINESS MAGAZINE
REDUCINGINFECTION RISKNYMAS is dedicated to making healthcarewashing facilities safe, accessible andhygienic. Our Nyma®CARE range of productshas been carefully developed to minimise therisk of cross contamination in healthcareestablishments.
• Rimless sanitary ware
• Unique Nyma®GUARDanti-microbial protection
• Innovative flangeless grab rail
www.nymas.co.uk
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.622
High Effi ciency - Low Radiation - Modulating
Ranges from 8kg/hr - 2000kg/hr
CERTUSS (UK) LimitedUnit 45 Gravelly Industrial ParkTyburn RoadBirminghamB24 8TG
Tel: 0121 327 5362Fax: 0121 328 [email protected]

have become contaminated with an Ebola patient’s infectious fluids such as soiled clothing, bed linen, or used needles. The likelihood of contracting Ebola is considered low unless there has been this type of specific exposure. Ebola virus is not spread through routine, social contact (such as shaking hands or sitting next to someone) with asymptomatic individuals. People who have had social contact with symptomatic individuals with confirmed Ebola infection should be followed up as a contact through the local Health Protection Team. The Ebola virus is not a robust virus, and is readily inactivated, for example, by soap and water or by alcohol.
IDENTIFYING PATIENTS AT RISK Ebola is spread through direct contact with blood and body fluids from infected people. The incubation period ranges from two to 21 days. It remains unlikely but not impossible that travellers infected in one of the affected countries could arrive in the UK while incubating the disease and develop symptoms after their return. Although the likelihood of imported cases is low, healthcare staff in the UK need to remain vigilant. Individuals may present in several different
ways to hospitals: referral by NHS 111, referral by primary care, self-presentation directly to A&E, or transfer by ambulance. Triage mechanisms need to be able to quickly identify patients at risk so that they can be isolated and a risk assessment completed. Patients with a history of travel to an affected area within the last 21 days who have a fever (>380C), or a history of fever in the past 24 hours, should be isolated and any further assessment carried out by staff wearing appropriate personal protective equipment (PPE). Apart from fever, other symptoms of Ebola may include headache, sore throat, general malaise, diarrhoea, vomiting, bleeding and bruising. Additional information that may assist with the subsequent risk assessment includes whether the individual has come into contact with a person known/suspected to have Ebola, cared for anyone with a severe illness or who has died of an unknown cause, attended any funerals, had any contact with dead bodies, visited any traditional or spiritual healers, or been admitted to hospital in the affected areas. Guidance on the risk assessment and
management of viral haemorrhagic fevers (including Ebola) by the Advisory Committee on Dangerous Pathogens (ACDP) is the principal source of guidance for clinicians risk assessing and managing suspected cases.
CLEANING REQUIREMENTSThe following cleaning requirements have been written based on the ACDP guidance for the management of individuals with suspected or confirmed viral haemorrhagic fever, such as Ebola virus. This guidance applies for individuals who have been categorised as high possibility or confirmed Ebola. Specialist advice should be sought from the Health Protection Team, where required. All cleaning must be conducted wearing appropriate personal protective equipment (PPE) according to the standards described in the ACDP guidance. Where there has been no obvious contamination with blood or bodily fluids, affected areas should be disinfected with hypochlorite containing 10,000ppm available chlorine. Affected clothing or linen should be contained within an impermeable bag and treated and disposed of as category A waste. For areas where there has been contamination with blood or bodily fluids, the
above guidance should be followed as well as addition measures. Bodily fluids should be mopped up with absorbent material, such as disposable paper towels. The area should then be disinfected with freshly prepared hypochlorite solution containing 10,000ppm available chlorine ensuring a contact time of two minutes before wiping up with disposable paper towels, but do not mix hypochlorites with any other cleaning agents as this may create dangerous fumes. The surface should then be washed with warm water and detergent. For larger spills, where possible, allow any potential aerosols to settle out. Adequate ventilation must be ensured when disinfecting areas with chlorine based products Specialist contractors may consider fumigation necessary following assessment. All waste, including linen and potentially contaminated cleaning equipment, should be treated and disposed of as category A waste.
Source: Public Health England
FURTHER INFORMATION:Guidance from Public Health England can be downloaded from tinyurl.com/lce8ovc
The incubation period ranges from two to 21 days. It remains unlikely but not impossible that travellers infected in one of the affected countries could arrive in the UK while incubating the disease and develop symptoms after their return
Infection Control
EBOLA VIRUS DISEASE
Ebola should be suspected in patients presenting to primary care services who have a fever of >38°C OR have a history of fever in the past 24 hours AND have recently visited any of the affected areas (as outlined previously) within the previous 21 days OR Have a fever of >38°C OR have a history of fever in the past 24 hours AND have cared for / come into contact with body fluids of / handled clinical specimens (blood, urine, faeces, tissues, laboratory cultures) from an individual or laboratory animal known or strongly suspected to have VHF.
Ebola should be suspected in individuals with a fever [>38°C], or history of fever in the previous 24 hours, who have visited an affected area within the past 21 days (or who have cared for or come into contact with body fluids or clinical specimens from a live or dead individual or animal known or strongly suspected to have Ebola virus disease).Individuals should be isolated in a side room straightaway. They should not sit in the general waiting room before being assessed. The ACDP risk algorithm should be reviewed and a full history should be taken by a clinician trained in the use of and wearing appropriate PPE. The history includes details of travel history, return date to the UK, presenting symptoms and any contact with persons known or suspected to have Ebola infection. If the clinician is concerned about possible Ebola virus disease, then the case should be discussed with an Infection specialist at the local trust (ie consultant in microbiology, virology or infectious diseases physician). If the initial risk assessment indicates that there is a higher risk based on the patient’s symptoms, then the additional control measures will need to be put in place. Relevant diagnostic tests should not be delayed while awaiting the results of Ebola tests. These may include a malaria test, FBC, U&Es, LFTs, clotting screen, CRP, glucose and blood cultures. If appropriate, the infection specialist will then contact the Imported Fever Service to discuss testing and further management issues. The local health protection team should be contacted if a patient is being tested for Ebola or if there are additional public health issues.
Ebola management in acute trusts
Identifying patients at risk of Ebola virus
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
23 Volume 14.6 | HEALTH BUSINESS MAGAZINE
You wouldn’t risk infection here... ...so why risk it here?
For further information or to order please call: 0870 122 8822 or visit www.idealspec.co.uk
Scan with a QR code reader to view the Markwik21 video
Markwkwik21Total Disinfection ControlTotal Disinfection Control
Written by Tony Sant, m
anager, adverse incident reporting for medical devices, M
RHA
Healthcare professionals such as doctors, nurses and pharmacists are, almost without exception, dedicated to helping patients and ensuring patient safety. Unfortunately, on rare occasions the medicines and medical devices that healthcare staff use may not work as well as expected, or may not be used as intended by the manufacturer. That’s why the Medicines and Healthcare products Regulatory Agency (MHRA) and NHS England are working together to develop an integrated reporting route for healthcare professionals. The aim of this will be to improve the quantity and quality of incident reporting for medication errors and the full range of medical devices used in hospitals including defibrillators, infusion pumps, hip and knee implants, pacemakers, hospital beds, and operating tables. This joint work is in response to a number of strategic drivers including the implementation of the recommendations made by Sir Robert Francis QC and Professor Don Berwick on patient safety, and a review by Earl Howe into the MHRA’s handling of
the PIP breast implant fraud. It also takes into account the revised definition of adverse drug reaction to include medication errors in the EU Directive on Pharmacovigilance. These reports recommended taking steps to maximise the quality and quantity of adverse incident reports from healthcare organisations and the need to enhance the ability to learn from these adverse events.
REPORTING SYSTEMSCurrently, there are two national reporting systems for incidents involving medication errors and medical devices – one is operated by the MHRA and the other, the National Reporting and Learning System (NRLS), is operated by NHS England. The NRLS collects reports from healthcare professionals about patient safety incidents, which could have or did lead to harm for one or more patients receiving NHS care. NRLS patient safety reports include many types of incidents such as falls, diagnosis and surgery. These tend to be reports about system and use errors from
a human factors perspective rather than problems with individual products. The MHRA currently collects reports from healthcare professionals, manufacturers and the public about safety and performance issues specifically related to medicines, vaccines and medical devices. Reports for medicines and vaccines include all side-effects through the MHRA’s Yellow Card Scheme, but reports about serious and unexpected side-effects are particularly valuable as they can have a major influence upon the Agency’s assessment of the performance of the medicines and whether regulatory action is appropriate to protect patients. In the same way for medical devices, adverse incident reports help MHRA to monitor the safety and performance of medical devices in use in all healthcare settings.
BETTER PATIENT CAREWhile adverse incident reporting is not the only method of assessing the safety and performance of medicines and medical devices, it is a good indicator of how specific E
LEARNING FROM ERRORS IN HEALTHCARETony Sant of the Medicines and Healthcare Products Regulatory Agency examines how the development of an integrated reporting tool and improved governance for problems with medicines and medical equipment will play a vital role in raising standards for patient care
Patient Safety
INCIDENT REPORTING
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
25 Volume 14.6 | HEALTH BUSINESS MAGAZINE

medicines and medical devices are performing in real patient situations. After considerable engagement with healthcare commissioners and providers MHRA and NHS England jointly issued two patient safety alerts to healthcare providers. These officially started a process to improve the quality of reporting for both medication errors and medical device incidents within the National Reporting and Learning system. Through these alerts healthcare commissioners and large healthcare provider organisations (in the NHS and independent sector) are being asked to improve clinical governance arrangements for reporting and learning from medication errors and medical device incidents. They have been asked to identify board directors, multidisciplinary committees and safety officers who will have the responsibility to oversee and support incident reporting and learning in these important areas. The appointed medical device safety officers and medication safety officers will be specifically supported by new national networks. A key aim is to eliminate duplicate
adverse reporting data entry by healthcare professionals, as is currently the case in the present NRLS and MHRA reporting systems. The networks will also improve communication and feedback on reported safety issues, and enable safer practice to be discussed and shared through webinars, online
forums, conferences and workshops. Smaller healthcare provider
organisations should continue to report medication and
device incidents, take action to improve medication and device safety locally and work with the safety officers.
MAKING DATA AVAILABLE
The new integrated reporting route will
improve the quality of reporting medication and medical
device incidents and ensure specific details such as model numbers and the manufacturers of specific medical devices are available. Currently, these details can at times be missing in some adverse incident reports but the new safety officers will be asked to ensure that the MHRA and NRLS receive the information they need. The overall implementation of this work is being closely monitored by NHS
England and MHRA, who, based on earlier engagement with stakeholders believe that this is a good step forward for both organisations as it shows commitment to developing new ways to help improve patient safety through reporting, learning and the sharing of best practice. New technology is also being developed by the MHRA to help our surveillance of medical devices. We are working with a number of NHS trusts to pilot a new tracking system for high-risk medical devices such as hip implants and heart valves. The system will incorporate unique device identifier bar codes into patient electronic records. This information (suitably anonymised) will then be analysed by the Clinical Practice Research Datalink (CPRD) – a secure e-health research service – and will enable the MHRA to better assess the performance of high-risk medical devices and to trace patients in the event of a device recall or safety alert. This project is one of a number that MHRA has established to strengthen the implementation of existing controls; to meet the requirements of future EU medical device regulations and to help MHRA ensure that medical devices used to treat, diagnose and monitor health conditions are as safe as they can be.
FURTHER INFORMATIONwww.mhra.gov.uk
Patie
nt S
afet
y
INCIDENT REPORTING
The new
integrated
reporting route
will improve the
quality of reporting
medication and
medical device
incidents
The Marlux cubicle curtain track system is used extensively throughout the UK as it is the only product that satisfies three fundamental facilities requirements. Firstly, it is perfect for use with conventional fabric curtains because the unique ‘clip on - clip off’ glider can be detached from the track, attached to the curtain and then simply be snapped back onto the track along with the curtain. With other systems the bulky and often heavy curtain has to be lifted up and offered to the glider itself which is usually captured within the track channel. The Marlux system removes the need for step ladders making curtain changing safer for staff. The same track system also allows the option to use Marlux Fast-Fit Disposable Curtains and, by taking advantage of the push button access and removal plunger, disposable curtains can be removed and re-fitted in seconds, freeing up staff to use their valuable time more efficiently. Finally, when used with suitably configured Marbast magnetic anti-ligature fittings the system can be used in high-risk areas to reduce the opportunity for patient self-harm.
The precision designed magnetic device enables the system to stay in place during normal everyday use and only the individual bay or unit will collapse when an abnormal load is applied avoiding the unintended consequential damage to other patients and staff when adjacent cubicles collapse. The same magnetic system can also be used with vertical and roller blinds and,
providing magnetic rather than mechanical restraint, there’s nothing to wear out, break or jam and the system can simply be re-connected and used over and over again.
FURTHER INFORMATIONTel: 0845 130 [email protected] www.marbast.eu
Easy to use cubicle and window tracks designed specifically for healthcare environments
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.626

NEW
POLYFLOR LTD. PO BOX 3 RADCLIFFE NEW RD WHITEFIELD MANCHESTER M45 7NR
TEL: 0161 767 1122 E-MAIL: [email protected] WWW.POLYFLOR.COM/VERONA
New carborundum-free safety flooring with high decorative appeal
Fresh designs to create an uplifting environment to encourage patient wellbeing
Suited for all areas within a care facility where contamination occurs
18 subtle pastel shades complemented by bold statement colours
Fully HSE Compliant with sustainable wet slip resistance
Reinforced with Polysafe PUR for superior cleaning
Play with colour…encourage wellbeing
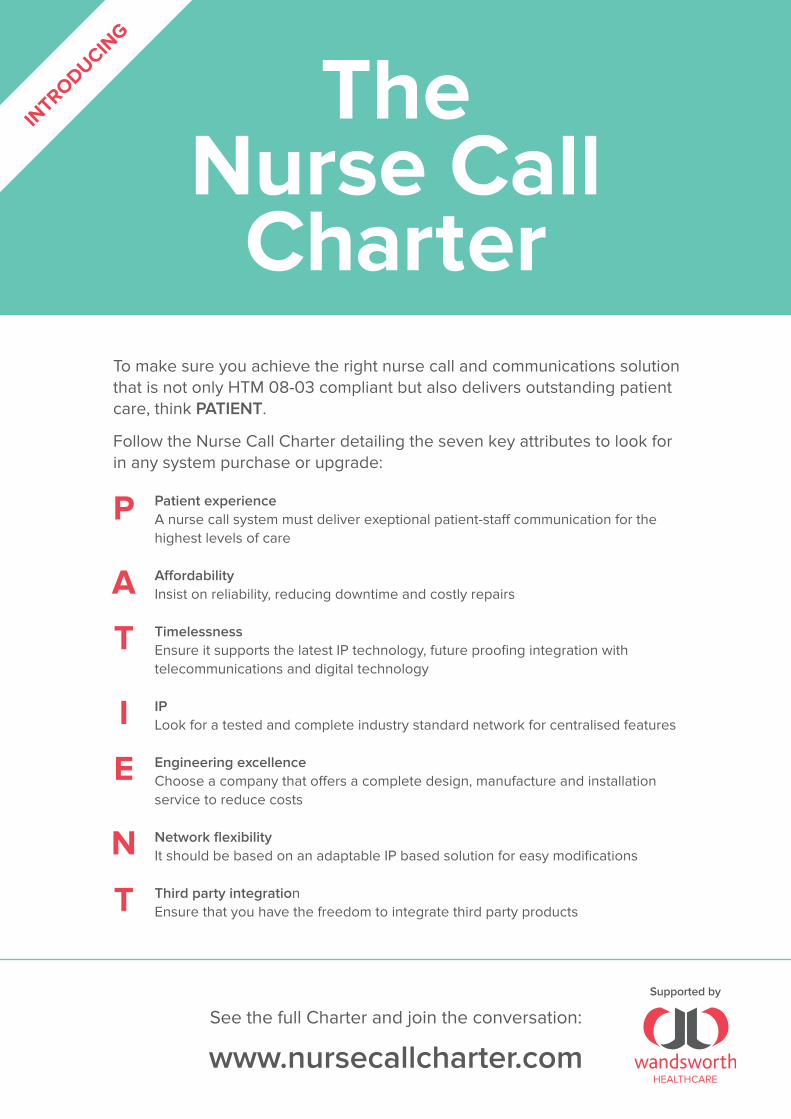
See the full Charter and join the conversation:
www.nursecallcharter.com
To make sure you achieve the right nurse call and communications solution that is not only HTM 08-03 compliant but also delivers outstanding patient care, think PATIENT.
Follow the Nurse Call Charter detailing the seven key attributes to look for in any system purchase or upgrade:
Patient experienceA nurse call system must deliver exeptional patient-staff communication for the highest levels of care
AffordabilityInsist on reliability, reducing downtime and costly repairs
TimelessnessEnsure it supports the latest IP technology, future proofing integration with telecommunications and digital technology
IPLook for a tested and complete industry standard network for centralised features
Engineering excellenceChoose a company that offers a complete design, manufacture and installation service to reduce costs
Network flexibilityIt should be based on an adaptable IP based solution for easy modifications
Third party integrationEnsure that you have the freedom to integrate third party products
The Nurse Call
Charter
VIP SponsorSupported by
P
A
T
I
E
N
T
INTRODUCIN
G
Nurse call charter ad FPv7.indd 1 15/08/2014 16:19

Written by Alaster Purchase, chief operating officer, G
S1 UK
It is well documented that the NHS possesses the greatest purchasing power of any business in the UK. Yet the procurement function has traditionally not been able to turn this status to true advantage – supply chain inefficiencies are widespread due to the sheer size and scale of the procurement operation, and trusts buying independently of each other has
led to inconsistencies between the amount they sometimes
spend on purchasing the same products. At a healthcare conference we held in June this year Rob Knott, national director for NHS procurement development at the Department of Health
(DH), spoke about the lack of focus on this area
on board agendas. He said: “Assurity of supply; risk; are our
patients being given the right products at the right time; are some products not arriving so we’ve had to cancel operations, and so on – [the lack of focus] is not discussed at board level, and yet it’s one of the most critical things to look at in the organisation.” Even so, the recognition that the hospital-wide procurement process needs to be reformed is long-standing, but leveraging capability – even that already widely used in other sectors – at the centre of possible solutions has not often been the approach taken. The challenging situation in which the NHS now finds itself has accelerated this need E
IDENTIFY, CAPTURE AND SHARE INFORMATIONGS1 standards were mandated for use in NHS hospitals by the eProcurement Strategy. So what is the actual purpose of them, and what is their wider role in improving healthcare delivery? Alaster Purchase, chief operating officer for GS1 UK explains
Healthcare IT
BARCODE TECHNOLOGY
The
patient care
pathway can be
tracked ensuring the
right patient, receives
the right treatment
at the right time
with the right
product See the full Charter and join the conversation:
www.nursecallcharter.com
To make sure you achieve the right nurse call and communications solution that is not only HTM 08-03 compliant but also delivers outstanding patient care, think PATIENT.
Follow the Nurse Call Charter detailing the seven key attributes to look for in any system purchase or upgrade:
Patient experienceA nurse call system must deliver exeptional patient-staff communication for the highest levels of care
AffordabilityInsist on reliability, reducing downtime and costly repairs
TimelessnessEnsure it supports the latest IP technology, future proofing integration with telecommunications and digital technology
IPLook for a tested and complete industry standard network for centralised features
Engineering excellenceChoose a company that offers a complete design, manufacture and installation service to reduce costs
Network flexibilityIt should be based on an adaptable IP based solution for easy modifications
Third party integrationEnsure that you have the freedom to integrate third party products
The Nurse Call
Charter
VIP SponsorSupported by
P
A
T
I
E
N
T
INTRODUCIN
G
Nurse call charter ad FPv7.indd 1 15/08/2014 16:19
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
29 Volume 14.6 | HEALTH BUSINESS MAGAZINE

Increase you contact centres productivity and effectiveness in partnership with Ultra’s dedicated team and real-time campaign management software.
Get in touch with one of our experts to see how we can support your organisation.
Enteprise-level solutions for contact centres in the healthcare market
Keep a eye on your inbound and outbound environments.
Explore your options with Ultra and we will improve your ROI.
0207 965 0207 [email protected] www.UltraComms.com
Leverage our expertise and experience in the healthcare sector and migrate to our platform. We can:
• Run in parallel with your existing contact centre.• Connect to your current phone system. • Fully integrate with your CRM software.• Enable PCI DSS compliance.
Helping to create healthy & safe environments in the healthcare sectorAt Qube Construction Management PLC our specialist team of surveyors are qualified to work with asbestos and together have over 30 years’ experience in the field. We will help you to determine and develop the right strategy, plans and processes for the management and development of your premises to meet your healthcare needs.
We offer the following asbestos services:• Asbestos Survey – Management Survey,
Refurbishment & Demolition Survey• Asbestos Removal • Asbestos Encapsulation• Asbestos Waste Carrier• Asbestos Awareness Training
Call us for an informal discussion around solutions to minimise risk of exposure on:
0800 468 1700
Canterbury House, Waterside Court, Neptune Way, Medway City Estate, Rochester, Kent ME2 4NZ www.qubecmplc.co.uk
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.630

however. DH published the eProcurement Strategy in May 2014, which estimated that trusts can save £1.5bn by the end of 2015-16 through taking a cohesive approach to procurement based on global GS1 standards, national framework and local delivery. In addition, after the initial investment has been made to support this shift, the cost savings will build and build over subsequent years.
STANDARDS & TECHNOLOGY GS1 standards were mandated for use in NHS hospitals by the eProcurement Strategy. So what is the actual purpose of them – what do they do? The simplest answer is that they uniquely identify ‘things’. The term has to be loose, as these things range from people (patients, care givers) and places (shelves, draws, wards, even bed locations) through to products (such as medicines, devices, surgical instruments) and items (such as medical records). These ‘things’ are coded with identifying numbers that are globally unique. This ensures that when suppliers, buyers or clinicians share information on that item, they can be certain that there will be no conflicts with other items and that supporting supply chain processes can operate efficiently. Once identified, the patient care pathway can also be fully tracked ensuring the right patient, receives the right treatment at the right time with the right
product without ambiguity. This is of particular importance in a hospital context, as it prevents avoidable mistakes such as when patients receive the wrong medicine and enables effective recalls should they become necessary. Identification standards are only part of the solution – having them in place massively increases operational efficiencies, but the eProcurement Strategy also ensures that supporting systems are deployed to help trusts get maximum benefit from standardisation. There are a number of new services being introduced to support the identification of people, places, products and assets as well as the integration of systems across the entire NHS.
SHARED PRODUCT INFORMATION The first of these is the use Product Information Management (PIM) catalogue being fed from a GS1-compliant ‘datapool’, which forms part of the Global Data Synchronisation Network (GDSN) – using this platform, trusts are able to access a shared repository of supplier managed accurate data on the items procured for use in the NHS. It also includes all the information about a product necessary to perform business transactions, which is synchronised
in a standardised way between suppliers and buyers to
make the trading process transparent and efficient
for all parties involved. The GDSN network already E
Healthcare IT
BARCODE TECHNOLOGYGS1 Standards and the eProcurement Strategy
Government’s eProcurement Strategy, underlined the fundamental requirement for GS1 standards in smarter NHS procurement. GS1 standards enable purchasing and logistics efficiencies and improve inventory management. They have been used in retail for nearly 40 years and are estimated to save the industry approaching £11billion per year. By providing a common language for identifying, locating, moving and trading medical supplies and assets quickly, adoption of these standards in the NHS is estimated to deliver savings in procurement costs, making a significant contribution towards the overall procurement savings target of £1.5bn by 2015-16. The eProcurement strategy sets a timeline for the adoption of GS1 standards in NHS procurement highlights plans for a GS1 NHS Datapool to provide visibility of purchasing across the NHS to ensure the purchasing efficiency of the service as a whole is maximised. In the short-term Trusts will need to develop a GS1 adoption plan in the next financial year.
Items
are coded
with globally
unique identifying
numbers, ensuring
that there will
be no conflicts
with other
items
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
31 Volume 14.6 | HEALTH BUSINESS MAGAZINE

All efficiencies made in the supply chain result in increased potential for improvements in patient care. Being able to know unequivocally what something is – and where – is such a fundamental point that it is easy to overlook just how important it is in ensuring everything else functions effectively contains almost one million products registered for the healthcare sector, mainly medical devices following the US Food and Drug Administration’s rule on unique device identification. The benefits to ensuring relevant parties are using shared, high quality data include improved availability of healthcare items in hospitals, reduced procurement costs, lowering risk of errors and never events and increased supply chain efficiency.
LOCATING STOCK EFFICIENTLYAs mentioned above, GS1 standards do not just provide unique identification for items – they can actually be applied to a wide range of different ‘things’. This includes locations such as shelves, wards or beds, which can be identified using a GS1 identifier called a Global Location Number (GLN). GLNs are specifically used to uniquely identify, deliver and store locations as well as electronic invoice and order points. The eProcurement Strategy sets out the requirement for the deployment of a central GLN registry. This registry will enable unambiguous identification for both the physical locations of where to deliver goods and the destination of all business messages necessary between trading partners (such as purchase orders, advance delivery notifications, proof of
delivery, invoices and remittance advice).If a PIM and datapool enables unequivocal identification of the products and services a hospital purchases (or what we might think of as the ‘what’ of procurement), then this registry covers the ‘where’.The combination of these solutions enables trusts to operate far more efficiently through access to accurate procurement data, good catalogue management and a consistent identification system to allow stock and equipment to be located quickly. Overall these support the roll-out of a fully integrated purchase-to-pay and product management process that substantially reduce the processing/management overhead.
GS1 AND PATIENT CAREAll efficiencies made in the supply chain ultimately result in increased potential for improvements in patient care.Being able to know unequivocally what something is – and where – seems like such a fundamental and obvious point that it is easy to overlook just how important it is in ensuring everything else functions effectively. For example – a joint survey with Nursing Times in 2010 found that nurses spend on average one hour in every eight-hour shift searching for missing stock or patient records. It is clear to see how consistent identification and tracking of items would free up time that
could be refocused on caring for patients.Electronic health records also have an important role to play in enhancing current processes, enabling automated completion at all stages of patient engagement in theatre, clinic and pharmacy, and providing verification for medicines and devices at the point of use. They can even form part of a system for automating stock replenishments where necessary in line with forecast requirements.The quality of the data within these records is a key factor in how effective they – and indeed all internal processes – are able to be.
NEXT STEPSThere are always challenges associated with widespread change, particularly where new technologies are introduced, and how this change is managed will be an important factor in determining its success. All trusts are now required to appoint a GS1 lead to help develop and oversee a GS1 standards adoption plan by 2015. The National Information Board also published the Personalised Health and Care Strategy 2020 in November – this paper sets out a framework for enabling England to become a global leader in the provision of digital health and care services that improve patient safety and transparency. We fully support the proposal set out in this paper to embrace GS1 standards and, building upon the approach set out in the eProcurement Strategy, we believe the foundations will be in place to develop an exemplar world-class healthcare service.Change may present challenges, but the potential benefits of implementing these solutions successfully – and consequences of not implementing this essential evolution – are far more significant.
FURTHER INFORMATIONwww.gs1ukinhealthcare.org
BARCODE TECHNOLOGY
Heal
thca
re IT BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.632

Practice managers, receptionists and now a growing number of GPs across the country, wake to the knowledge that the first few hours of the morning will be a battle against the torrent of calls that will ring their practice. This pressure of demand will have steadily built up over the previous twelve hours as patients for various reasons decide they need to contact their local practice. Busy practices respond to this demand by increasing staff count in the mornings and denying access to prescription and other services until the afternoons. These tactics, although effective in the short term, create a ripple of problems across the practice. The problem of staffing a practice over extended hours is made worse by the need to ‘front load’ your day, this makes you short of staff later in the afternoon and evening or increases your overall costs due to the increase in worked hours. PATIENT ACCESSPatient access is also compromised in this ‘morning model.’ Many patients decide they need to see a GP or access practice services in the evening or night before, but cannot act until the phone lines open in the morning. The dilemma and therefore frustration is that they don’t know if they will get a morning appointment ‘in the lottery’: should they stay at home and possibly be late for work if an appointment isn’t
available, or go to work to find they could have been seen first thing in the morning? The same model also has a potential effect on A&E attendances. Patients or parents of patients that have a health concern are more likely to go to A&E when they are unsure of how soon they will have access to medical expertise; having to wait until the morning causes increased anxiety and therefore drives greater numbers of patients to utilise other and more expensive NHS services. The lack of access also has an effect on DNA rates. Having received a text message to remind them of their upcoming appointment, the patient is unable to cancel or rearrange the appointment until the phones open in the morning, which compounds the access problem by reducing the amount of available appointments until the patient gets through to the already busy reception. A common result of this is that the patient tries, can’t get through and therefore DNAs.
WHAT IS THE ALTERNATIVE?Other sectors suffer similar telephone demands and have made changes to alleviate the problem. The move to web services has helped, although the health services have a particular issue in that its most needy users are often the elderly and/or the poorest in our society and therefore have the least access to the web. So the answer is to utilise the technology
to which virtually all patients have access. It may seem perverse, but the cause of many practices’ problems can actually be the solution. The key is to offer appointments and practice services 24/7, in the same way as other organisations have made their services available. Council, banking and other government departments can now all be accessed over the phone via automated systems. A growing number of practices are now also offering the same level of service to their patients. Offering 24/7 booking of appointments by the phone spreads the calls across the whole day, and importantly reduces the build-up of calls in the evening, which would then have to be dealt with in the morning. Anxious patients gain a level of control by knowing if they will be seen in the morning and are therefore less likely to utilise OOH or A&E services. The ability to cancel, check and rearrange appointments means that DNAs are reduced and appointment availability is increased, improving access for all. The frustrated patients now know if they should go to work, as they are now in control of their appointment times. BENEFITSOther services can also be made available, repeat prescriptions can be requested automatically over the phone 24/7, removing the need to only offer these services at certain times of the day. Triaging can be improved, by allowing patients to ring and request a triage call and at the same time leave a reason for the call back. This enables medical staff to prioritise calls to the patients they feel most need a call. The costs of these services are easily regained by the saving in staff time, the reduction in DNAs and the improvement of services. (As we know, banks wouldn’t offer these services if they didn’t think they were efficient.) A growing number of CCGs as well as individual practices, have invested in these services, with both Barnsley and Camden CCG purchasing Voice Connects’ Patient Partner solution. So quell that torrent of calls by embracing the very technology that causes you the problem, use the phone.
FURTHER INFORMATIONTel: 0116 232 [email protected]
ADVERTISEMENT FEATURE
USING TECHNOLOGY TO IMPROVE PATIENT ACCESSVoice Connect, the integrated communication specialist, has developed a range of computer telephony solutions to help practices save time and money
Advertisement Feature
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
33 Volume 14.6 | HEALTH BUSINESS MAGAZINE
My Stroke Guide
At the Stroke Association we understand stroke. Working closely with stroke survivors and carers we’ve developed My Stroke Guide, a unique online platform to support stroke survivors to make the best possible recovery.
The guide, built by award-winning web consultancy Cantarus, provides accessible information, a video library, goal setting and peer support enabling users to self-manage their condition day to day. Available through a smartphone, tablet, laptop or desktop PC, the guide improves stroke survivor’s knowledge of their condition and offers them tools to manage their condition.
We worked alongside Cantarus to develop My Stroke Guide by embracing a user-centred design approach. Everything from its look, language, features and content has been determined by working with stroke survivors and carers.
Features include:
Information tailored to the individual’s needs and local area
Peer-to-peer support, including an extensive video library and an online forum
Goal-setting tools and graphs which reflect the individual’s progress
Advice and signposting on the various issues people can face after stroke.
Continuous Improvement…
Our technical partnership with Cantarus – now in its sixth year – covers development, hosting and support. It enables My Stroke Guide to be an ever-evolving solution that leverages our expertise, and the feedback of its users, to continuously increase the value it offers to stroke survivors.
We’d love to work with you to tailor My Stroke Guide to your population. For more please email [email protected]
Designed for stroke survivors by stroke survivors
Stroke Association is a Company Limited by Guarantee, registered in England and Wales (No 61274). Registered office: Stroke AssociationHouse, 240 City Road, London EC1V 2PR. Registered as a Charity in England and Wales (No 211015) and in Scotland (SC037789). Also registered in Northern Ireland (XT33805) Isle of Man (No 945) and Jersey (NPO 369).
A staggering 74% of stroke survivors left hospital feeling more isolated1 while 73% lacked confidence after their stroke2. Without support this can lead to further problems and in some cases re-admission to hospital.
W W W . C A N T A R U S . C O M
stroke.org.uk
A unique online platform to support stroke survivors to make the best possible recovery.My Stroke Guide is an interactive online platform accessed through computers, tablets and smartphones. It is a highly accessible website, offering goal-setting tools and peer-to-peer support as well as information in a number of formats. The Guide empowers stroke survivors to make their best possible recovery.
1 - Stroke Association, Struggling to recover - Life After Stroke campaign briefing 2012 2- Stroke Association, Feeling overwhelmes - Life After Stroke campaign briefing 2013
“I would have loved to have had this when I came
out of hospital. Until you see the information like
that in the videos, you don’t take it in properly”
Mindy, stroke survivor
“There is a lack of information readily available
after stroke, you have to really hunt for it.
My Stroke Guide helps you to help yourself”
Colin, stroke survivor

My Stroke Guide
At the Stroke Association we understand stroke. Working closely with stroke survivors and carers we’ve developed My Stroke Guide, a unique online platform to support stroke survivors to make the best possible recovery.
The guide, built by award-winning web consultancy Cantarus, provides accessible information, a video library, goal setting and peer support enabling users to self-manage their condition day to day. Available through a smartphone, tablet, laptop or desktop PC, the guide improves stroke survivor’s knowledge of their condition and offers them tools to manage their condition.
We worked alongside Cantarus to develop My Stroke Guide by embracing a user-centred design approach. Everything from its look, language, features and content has been determined by working with stroke survivors and carers.
Features include:
Information tailored to the individual’s needs and local area
Peer-to-peer support, including an extensive video library and an online forum
Goal-setting tools and graphs which reflect the individual’s progress
Advice and signposting on the various issues people can face after stroke.
Continuous Improvement…
Our technical partnership with Cantarus – now in its sixth year – covers development, hosting and support. It enables My Stroke Guide to be an ever-evolving solution that leverages our expertise, and the feedback of its users, to continuously increase the value it offers to stroke survivors.
We’d love to work with you to tailor My Stroke Guide to your population. For more please email [email protected]
Designed for stroke survivors by stroke survivors
Stroke Association is a Company Limited by Guarantee, registered in England and Wales (No 61274). Registered office: Stroke AssociationHouse, 240 City Road, London EC1V 2PR. Registered as a Charity in England and Wales (No 211015) and in Scotland (SC037789). Also registered in Northern Ireland (XT33805) Isle of Man (No 945) and Jersey (NPO 369).
A staggering 74% of stroke survivors left hospital feeling more isolated1 while 73% lacked confidence after their stroke2. Without support this can lead to further problems and in some cases re-admission to hospital.
W W W . C A N T A R U S . C O M
stroke.org.uk
A unique online platform to support stroke survivors to make the best possible recovery.My Stroke Guide is an interactive online platform accessed through computers, tablets and smartphones. It is a highly accessible website, offering goal-setting tools and peer-to-peer support as well as information in a number of formats. The Guide empowers stroke survivors to make their best possible recovery.
1 - Stroke Association, Struggling to recover - Life After Stroke campaign briefing 2012 2- Stroke Association, Feeling overwhelmes - Life After Stroke campaign briefing 2013
“I would have loved to have had this when I came
out of hospital. Until you see the information like
that in the videos, you don’t take it in properly”
Mindy, stroke survivor
“There is a lack of information readily available
after stroke, you have to really hunt for it.
My Stroke Guide helps you to help yourself”
Colin, stroke survivor
14001
0844 811 0070 | [email protected] | www.pageone.co.uk
‘Apps for Smarter Working’Secure messaging & lone worker function for your smartphone
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.636

The conversation is no longer about the targets that the government has set – NHS Informatics leaders across the country are instead focusing on how they are going to address the problems that arise as they try to achieve these tasks within the set deadlines. Public and private organisations constantly need to drive greater efficiencies and improve the quality of patient care. An increasing drive to move care closer to home, the aging population and a rapidly emerging technology savvy generation are just some of the challenges faced by information management and technology (IM&T) directors and their organisations. These developments call for greater alignment between hospitals,
GPs and community services, implementation of new technologies, effective system integration and information sharing. IT is one of the key tools helping organisations achieve these goals. However, in times of budget constraints, doing more with a reduced budget, while improving the quality of patient care delivered is a massive challenge IM&T directors. Nonetheless, it is one which they need to get on top of to position IT as a strategic and innovative partner in the organisation. As such, for organisations that recognise the need to drive greater efficiencies and improve the quality of patient care through IT, the Healthcare IT Exchange provides a
platform to benchmark with an exclusive group of senior peers and solution providers capable of helping them define and successfully navigate this new territory. Moreover, the unique format lets you evaluate new technologies as well as provide a fresh perspective on what the latest changes and initiatives in healthcare IT mean for you.
WHO WILL BE THERE?Chief information officers (CIOs), IM&T directors, chief clinical information officers (CCIOs), government representatives and leading solution providers will be gathering at the fifth Healthcare IT Exchange in December. They will dissect and discuss how public and private organisations can drive greater efficiencies and improve quality of care in times of restrained budgets and change for the healthcare sector. Boasting a unique structure, seniority and exclusivity it is unlike other events in the industry, focusing on peer-to-peer learning and networking to help healthcare
“An excellent opportunity for networking with peers and information gathering for future developments” Head of Information and Performance, West Middlesex University Hospital
EVENT PREVIEW
NAVIGATING THE TARGETS SET FOR HOSPITAL ICTThe Healthcare IT Exchange on 1-3 December in Birmingham will examine the role of IT to drive greater efficiencies and improve the quality of patient care
Healthcare ITBUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
37 Volume 14.6 | HEALTH BUSINESS MAGAZINE
Heal
thca
re IT
Integrate your systems and automate your processes for better patient care
Talk to us about• Yoursystemsintegrationneeds• Improvingyouroperationalprocedures• Masterdatamanagement–alwaysknowingtherightpatient,
whateverthesetting• Automatingandactingonyourmedicaldeviceinformation
MeetusattheHealthcareITExchangeattheHiltonBirminghamMetropoleHotelon1stto3rdDecember2014orcontactus at: [email protected]+44 (0) 1372 700790
ENOVATION UKTheLodge,ThorncroftManor,DorkingRoad,Leatherhead,Surrey.KT228JBUKwww.enovation.co.uk
As a specialist provider of healthcare integration solutions with a 30 year heritage, ENOVATION has seen significant changes in the requirements for systems integration and interoperability. Today, its clients in the NHS and private healthcare sector face complex challenges in delivering continuous improvements in patient care across different settings and organisations. Clients also have to meet stringent operational targets and efficiency drives. The NHS directive to be paperless by 2018 is seen as essential in transforming services and improving the effectiveness of daily workloads. The ability to integrate different systems and technologies, to ensure information is available at the right time and place to support clinical pathways and workflows is fundamental to achieving service improvement. ENOVATION’s portfolio of solutions and services has grown to meet these challenges and comprises an integration engine, master data management system and robotic process automation, with an ‘integrate anything’ capability. The company also provides a medical device information system enabling
staff to connect, monitor, analyse and act on vital clinical information. Key to any successful implementation is ENOVATION’s staff and their ability to understand client specific needs, utilising and tailoring its solutions to deliver benefits in the most efficient and cost effective manner. One of ENOVATION’s recent large scale implementations took place at Croydon Health Services NHS Trust. Here, the company’s Cloverleaf integration engine supports systems interoperability with its new Electronic Patient Record solution. A first for the NHS in England, the Trust has recently been recognised as a leader in IT practice in healthcare by the international health information body – HIMSS Europe. The Trust has been awarded one of the highest grades of award for its use of IT systems to improve its patient care.
At Derby Hospital’s NHS Foundation Trust, Blue Prism software helps deliver integration and workflow requirements that supports the implementation of their new EPR. Mark Norwood, associate director of IM&T said: “Blue Prism has played a vital role in automating business processes around departmental patient flows and system registrations, which otherwise would have required extra staff and reduced timeliness of patient information to our clinical systems.” ENOVATION is a rapidly expanding company and is part of the VANAD Group which is based in The Netherlands – this leading international information and communications solutions provider is one of the few family owned businesses in the IT sector.
FURTHER INFORMATIONwww.enovation.co.uk
Integration and automation solutions from ENOVATION helps NHS trusts provide better care for patients
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.638

professionals find strategies that they can implement to drive efficiencies, utilise evolving technologies and help their organisation move towards an integrated approach to care.
WHO CAN YOU LEARN FROM?The agenda is focussed on interactive sessions, case studies and discussions rather than lecture-led sessions to ensure that attendees get the most out of their time and really find solutions to their challenges. Dr. Colin Brown, clinical director for Elective Medicine, and Informatics clinical lead, University Hospitals of Morecambe Bay NHS Foundation Trust is delivering a case study on the challenges of implementing an EPR across a major multi-hospital trust. Malcolm Senior, director of informatics, Taunton and Somerset NHS Foundation Trust will take part in a panel discussion on Open Source, as the first Trust to implement an open source EPR. Mr. Rowan Pritchard-Jones, consultant plastic surgeon and CCIO St Helens and Knowsley Health Informatics Service is sitting on the CCIO panel discussion: Art of the possible – how is IT being used innovatively to deliver patient care? Paul Duffy, co-director of IT and Telecommunications, Belfast Health and Social Care Trust will deliver a warts and all case study: Real life experiences of introducing mobile working and delivering digital data to clinicians at point of care – warts and all. Dr. Paul Upton, director of Transformation, The Royal Cornwall Hospitals NHS Trust will deliver a keynote presentation on how to shift an organisation’s thinking to prioritise IT.
WHAT WILL YOU LEARN?Visitors will be provided with key insights that can be implemented in healthcare
environments, including: how to build a secure mobile strategy to deliver new digital data to clinicians at the point of care; how to integrate multiple systems into one platform or front end; how to share data across primary, secondary, social and mental care; and ways to manage the higher level of data. There will also be guidance on how to maintain and upgrade infrastructure to support the adoption of new systems, as well as strategies to tackle the interim clinical risk of having a mixed economy of paper and electronic records.
TAILOR-MADE LEARNINGThe Healthcare IT Exchange offers a variety of unique learning styles and sessions, which you can select from to build a customised itinerary that reflects your current initiatives, priorities and future strategic objectives. The Exchange sessions reflect strategic issues that were identified during our research with IM&T leaders. The session formats include: Case Studies, Panel Discussions, Roundtables, BrainWeaves, Workshops and Masterclasses. An integral part of your agenda are the one-on-one business meetings with leading solution providers. Prior to attending the Healthcare IT Exchange, you will be able to assess the solution providers who will be attending and select six to eight who offer products and services that match your initiatives and priorities. You will be
matched with providers, based on your selections, and the pre-arranged meetings will be incorporated into your customised agenda. These private 30 minute one-on-one meetings give you the opportunity to hear from leading specialists, whose industry knowledge and experience enable them to make a valuable contribution to the requirements of your organisation.
BRAINWEAVE DISCUSSIONSThe signature BrainWeave sessions encourage discussion, debate and learning in an unscripted and informal setting, on topics which are front of mind issues. You will be able to select from a range of BrainWeave topics. These discussions will be moderated by an industry leader to ensure that the discussions stay on course and deliver maximum benefit to you. Ask questions, share experiences,ideas and find the right answers to your immediate concerns.
WHEN WILL IT TAKE PLACE?The Healthcare IT Exchange will take place on 1-3 December, Hilton, Birmingham Metropole, United Kingdom and will be supported by leading solution providers including Dell, Kainos, Scandox, Vocera, Orion Health, Cloud2, Enovation, Fortrus and many more.
FURTHER INFORMATIONwww.healthcareitexchange.co.uk
“Valuable and interesting blend of supplier meetings and conference sessions” Head of ICT, Leeds and York partnership NHS Foundation Trust
Healthcare IT
EVENT PREVIEW
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
39 Volume 14.6 | HEALTH BUSINESS MAGAZINE

wipe it clean with TGServices
Secure & Approved Data Elimination Services CESG StandardSales T: +44 (0)1285 642222 E: [email protected]
wipe it clean with TGServices
Secure & Approved Data Elimination Services CESG StandardSales T: +44 (0)1285 642222 E: [email protected]
Written by Jam
es Kelly, chief executive, BSIA
Transnationally, criminals and hackers are increasingly focusing on personal information from the health sector as a rich source of individuals’ personal details – a valuable commodity when it comes to activities like fraud and identity theft. The high value placed on medical records is due to the wealth of information they contain; i.e. names,
addresses, National Insurance numbers, employment information and sometimes even financial information. Indeed, a reported 12 million medical records have been hacked or stolen so far in the United States this year – a chilling trend which emphasises the importance of effective healthcare information maintenance worldwide. Professional information destruction (ID) is one of the most straightforward security measures a hospital or health centre can implement to help combat the risk of crime. While it may not be as immediately obvious as the need to protect valuable onsite equipment or the personal security of staff and patients, careless disposal of patient and staff records can lead to irrevocable reputational and financial damage. Therefore it is vital that, with the help of a trusted information destruction company,
hospitals and health centres alike can effectively protect private and confidential information from falling into fraudsters’ or criminals’ hands.
NHS SURREY BREACHAs recently as 2012, there was an information security breach at NHS Surrey wherein
computers containing confidential files were sold on eBay without the hard drives being wiped or destroyed securely. It was one of the biggest security breaches ever witnessed by the now dissolved NHS Surrey, and was primarily caused by the handing over of old computers to a new service provider who was not compliant with essential standards. Commenting at the time of the
NHS Surrey breach, Adam Chandler, chairman of the BSIA’s Information Destruction Section asserted: “Organisations tend to ‘turn a blind eye’ when it comes to selecting an information destruction service provider. The dangers associated with doing this were highlighted perfectly recently, when the Information Commissioner’s Office (ICO) issued a £200,000 fine to Surrey NHS for engaging with an unapproved supplier who was promising a cut price job for the value of the material they were supposed to be destroying. In this case, it was computer equipment – some of which ended up on eBay.”
WHO SHOULD BE RESPONSIBLE?There can sometimes be a question mark over who is responsible for ensuring the discarding of confidential documents. When asked about his experiences with information destruction in the health sector, Anthony Pearlgood, a member of the BSIA’s Information Destruction Section stated that: “Only a small fraction of organisational waste paper and data processing products such as hard drives, CDs, memory sticks and DVDs are destroyed annually by professional firms.” “It is important that key decision makers do
As recently as 2012, there was a breach at NHS Surrey wherein computers containing confidential files were sold on eBay without the hard drives being wiped or destroyed securely
A HEALTHY APPROACH TO INFORMATION SECURITYThe recent government push towards the centralisation of NHS data into a network of regional centres through the ‘accredited safe havens’ scheme has thrown information maintenance within the health sector into the forefront of public discussion, writes the BSIA’s James Kelly
Information Security
DATA DISPOSAL
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
41 Volume 14.6 | HEALTH BUSINESS MAGAZINE
Reisswolf London LtdTel: 01525 379405 Email: [email protected] Website: www.rw-london.co.uk
REISSWOLF NHSSHREDDING SERVICEWhether you’re after an ad-hoc or scheduled collection, Reisswolf are the company to TRUST for all of your DATA DESTRUCTION requirements.
Experienced in dealing with a number of NHS sites from HOSPITALS to MEDICAL CENTRES and SURGERIES throughout the UK. Reisswolf are fully compliant and accredited to the DATA PROTECTION ACT 1998 and BSIA standards, BS EN 15713, ISO 90001, 14001, 18001, 27001
SO IF YOUR OFFICE IS BOGGED DOWN WITH:
· Confidential Waste· Employee or Staff Records· CCTV tapes and discs· Reports· Financial Information
CALL US ON 01525 379405
PROTECTYOURSELF...
A risk assessment carried out by NHS
England revealed that 2 million NHS data
breaches have been logged since the
start of 2011.
Full recycling service also available – ask for details
C
M
Y
CM
MY
CY
CMY
K
Reisswolf 21.10.14.pdf 1 21/10/2014 15:00
FUTURE-PROOF YOUR CAFM• INTEGRATED ESTATES MANAGEMENT -greaterefficiency andcontrol
• FOR THE NHS BY THE NHS -directinputfrom NHSusers
• INTUITIVE WORK FLOWS -fastersystem performance
• REMOTE MOBILE CAPABILITY -improvedproductivity
calluson:0845 270 7747orvisit: www.fmfirst.co.uk
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.642

not make these choices lightly, and are sure to source a reputable supplier that meets the relevant standards,” he added.So what are the key considerations for decision makers when it comes to the destruction of healthcare information?
DON’T IGNORE DATA PROTECTIONNon-secure disposal of data can lead to the long-term damage of a hospital or health centres reputation. Such behaviour appears careless and incredibly disorganised to the public. Indeed, Since the Data Protection Act of 1998 (which aims to balance the rights of the individuals and organisations who are legitimately holding and using their information) proficient ID procedures have become much more strictly regulated. In 2010 the Information Commissioner’s Office (ICO) was given additional enforcement powers, enabling them to issue penalty fines of up to £500,000 in the case of a data breach. The Act regulates the processing of personal data, held both manually and on computer. It’s wise to be shrewd as to what constitutes ‘information’, as the term covers an array of things; i.e. paper, credit cards, SIM cards, media equipment, CDs, DVDS, hard disks, and hard drives. It is important to consider the processing of branded products such as uniforms also – should they fall into the wrong hands, unwanted intruders with malicious intentions could gain access to
restricted areas by impersonating healthcare personnel.
There are particular standards that need
to be adhered to by companies that are responsible
for information destruction. Such standards guarantee that the service being provided is secure and professional, an essential requirement of the Data Protection Act. Once they have served their purpose, all confidential materials should be destroyed (either on-site or off-site) to the extent that they may never be reconstructed. ID Companies should provide the customer (health institution) with a full audit trail, including a certification of destruction. A key European standard for ID (EN15713) details the range of requirements that an ID company must meet: they must have an administration office on-site where records and documentation are kept; premises should also be isolated from any other business or activities operating on the same site; intruder alarms that are closely monitored by an Alarm Receiving Centre (ARC) should be installed on the property; and finally, CCTV should be placed at the points where the unloading, storage and processing of information is conducted. The vehicles that transport the information due to be destroyed should also be fully secure. There is also a British standard (BS 8470) that ID companies should comply with. According to BS 8470 ID companies must identify product specific shredding sizes,
guaranteeing that the information is destroyed to the point of irreparability. The BSIA’s dedicated ID section comprises companies that are inspected to both of these standards, amongst many other important principles, making them reliable service providers.
SOURCE A REPUTABLE SUPPLIER When it comes to data security in the health sector, there is no room for complacency, particularly when it comes to sourcing a reliable ID provider. It is absolutely essential that decision makers are choosing a company that meets with the essential standards highlighted above. Members of the BSIA’s Information Destruction Section all adhere to these standards and meet with rigorous membership criteria. Further, the ID section of the BSIA follows a specific code of ethics that solidifies the section’s dedication to providing the best service for their customers. Adam Chandler, Chairman of the BSIA’s Information Destruction Section, comments: “The commitment of BSIA members to best practice enables us to help our customers at a time when their businesses are most at risk from fraud.” When it comes to ID there is no room for risk to healthcare providers, be it financial (in terms of fines) or reputational. To find out more about the ID section of the BSIA and their code of ethics, or to locate a trusted and professional ID service near you, visit the association’s website.
FURTHER INFORMATIONwww.bsia.co.uk/information-destruction
Information Security
DATA DISPOSAL
The ID
section of
the BSIA follows
a specific code of
ethics that solidifies
its dedication to
providing the
best service
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
43 Volume 14.6 | HEALTH BUSINESS MAGAZINE

Sign
age
The cost benefit analysis showed that for every £1 spent on the design solutions, £3 was generated in benefits
Hospital wayfinding has been the subject of much debate. In such a complex and highly stressful environment, the need for patients and visitors to find their way quickly and easily has a huge impact on the quality of their experience. As recent evidence has shown, good wayfinding is also critical in reducing potential violence and aggression, particularly in hospital A&E departments. Two years ago, my company Whybrow Wayfinding was asked to work with design agency PearsonLloyd on a project to redesign accident and emergency departments to help reduce violence and aggression. The project was commissioned by the Design Council and the Department of Health and funded through the Design Council’s Design Challenges programme, which poses open innovation competitions to develop practical solutions to social problems. The project, [A Better A&E], helped reduce patient aggression and violence by 50 per cent.
A COST TO THE SYSTEMAccording to the National Audit Office, violence and aggression towards hospital staff costs the NHS at least £69 million a year in staff absence, loss of productivity and additional security. The problem is particularly difficult to manage in the high-pressure environment of A&E, where pain and worry can alter the behaviour of patients and visitors, reducing their tolerance levels and making them more likely to behave aggressively. A Better A&E developed a set of three solutions aimed at improving the patient experience by reducing tension and hostility, and preventing more serious incidents caused by accumulated aggression. The solutions were piloted in two hospitals: Southampton General Hospital and St George’s Hospital, London, and focused on creating a calmer and more relaxing care environment through a combination of clear signage, A&E process maps and live information about waiting times. The first of our projects, the Guidance Solution, was targeted at patients to ensure they had all the basic information about the department and how it works. Designed to be implemented in any A&E department, this solution provided a
platform to communicate basic information to patients, such as where they are, what happens next, and why they’re waiting. We coordinated the production and installation of the information touch points across the two pilot hospitals, as well as two Trusts who have since implemented the Guidance Solution. Easily identifiable vertical information panels were applied throughout the A&E departments to explain the activities that took place in each space and how long these activities might take. They worked as standalone items, as well as a series, and were customised to each Trust. The panels were complemented by a full wall height process map illustrating the patient journey as a series of stages, from check-in to assessment, treatment and next steps so visitors can very quickly learn the process for receiving treatment. Easy and low cost implementation was critical, and after completing a value engineering exercise we settled on direct to substrate aluminium laminate prints, which are non-porous and hygienic. The prints were mounted to walls using the ‘3M Dual Lock’ system, enabling them to be removed easily for redecoration. Overstretched healthcare budgets require a scheme that can be retrofitted cheaply and quickly at almost any department in the country. 75 per cent of patients said the improved signage reduced their frustration during waiting times. A supplementary leaflet in the waiting room guided patients arriving at A&E through the process, including further information about the department and contact details for other urgent care centres in the local vicinity. A tear off questionnaire provided patients and visitors with an opportunity to give feedback. 88 per cent of patients felt the Guidance Solution clarified the A&E process A digital stream communicating live, up-to-date information about the department complemented the print material. Existing data stored in the computer systems automatically updated the electronic displays,
providing accurate and relevant
information at regular intervals.
PEOPLE SOLUTIONThe People Solution provided a forum for staff working in the department, supporting their interactions with frustrated or aggressive patients. For current staff, a reflective programme provided a space for staff to consider the factors that undermine their capacity to care for patients. The goal was to identify factors that impacted the collective mood and to work to remove the root causes and to prevent them from occurring in the future. PearsonLloyd worked with organisational psychologists Julian Lousada and Vyla Rollins to develop an eight-week programme that was conducted with eight to 10 members of staff across the department, using an external facilitator. A new tool, the Incident Tally Chart, was developed to help focus on different variables within the system that might hinder the ability of staff to deliver high quality care. Programme findings were
CLEAR SIGNAGE, SAFER WARDSThe Sign Design Society represents professionals and clients involved in the resolution of navigation problems in complex environments and the planning, design, manufacture and installation of signing solutions. Ian Whybrow of Whybrow Wayfinding describes a project in one of the most challenging environments
WAYFINDING
Writ
ten
by Ia
n W
hybr
ow fo
r the
Sig
n De
sign
Soci
ety
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.644

reported back to management, helping the department as a whole to understand, learn and improve ways of delivering care. The programme was supplemented by an induction pack for staff new to A&E, to inform them of issues they may encounter whilst working in the department. This ensured that staff, such as trainee nurses and junior medics, had the required knowledge to work in this highly pressured environment.
TOOLKIT SOLUTIONThe third solution took the form of an online guidance document, offering free high-level design recommendations, focused on the built environment or service changes. The toolkit was aimed at NHS managers, clinicians and healthcare planners, who want to develop and deliver a better service in effective and inspiring environments. The toolkit breaks the patient journey down into its different stages of the A&E process and presents case studies of best practice that are in place at other NHS Trusts. It was intended for use by all NHS staff, while also providing a reference source for architects or interior designers working on new-build projects.
IMPROVED EXPERIENCEResults from trials in the A&E departments of Southampton General Hospital and St George’s Hospital where the full set of solutions were piloted have been shown to improve patient behaviour. Frontier Economics and ESRO developed a methodology that involved collection of primary patient and staff data through immersive methods, secondary A&E data collection, and cost-benefit analysis to reveal the impact of the design solutions. Improved levels of patient experience, reduced hostility and non-violent aggression, and good value for money were all noted in the evaluation. Further installations have taken place at Newham Hospital, London and Addenbrooke’s Hospital, Cambridge, with work ongoing at Norfolk and Norwich University Hospital. The cost benefit analysis showed that for every £1 spent on the design solutions, £3 was generated in benefits. But the value of generated benefits is expected to rise as the scheme is more widely adopted and evaluated. Improving the visitor experience in difficult circumstances is really at the heart of this issue. We all accept that visiting
A&E is usually an unplanned and anxious event for anyone, especially when our children are involved. But this anxiety can be lessened by good, clear communication at every step along the journey – a silent arm around our shoulder.
FURTHER INFORMATIONwww.signdesignsociety.co.ukwww.whybrow.co.ukpearsonlloyd.com
Signage
About the author
Ian Whybrow is director of Whybrow Wayfinding, an award-winning agency based in London. Ian has designed and implemented wayfinding schemes for over twenty five years. He founded Whybrow Wayfinding in 1997, and since then has built a successful agency with a broad client base and a strong reputation for delivering high quality and cost-effective wayfinding.
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
45 Volume 14.6 | HEALTH BUSINESS MAGAZINE
www.spectrumenergysystems.co.uk
Speak to one of our renewable energy specialists today:
0845 47 47 604
PURCHASEENERGY FROM 5.5p / kWhUtilise your unused roofspace and save...Solar PV is one of the most reliable renewable energies available today.
A proven technology making it a great investment to generate savings.
High performance systems engineeredto save you money
Guaranteed income for 20 years
Experienced electrical engineers
Outright purchase or power purchaseagreement
We offer both roof and ground SolarPV systems
If you are a high energy user this enables you to
purchase green energy at non-premium prices
and protect you against future energy price rises.
No capital outlay is required
We supply, install and maintain the solar PVsystem on your roof or land
We then sell the energy generated back toyou at a discounted rate
For high energy users we can offer from 5.5pper kWh which is index linked for 20 years
PowerPurchaseAgreement (PPA)
info.spectrumenergysystems.co.uk
SPECTRUM AD_Health Business_Layout 1 20/10/2014 09:20 Page 1

Written by Chris M
oriarty, hed of insight and corporate affairs, BIFM
The use of energy is a hot topic. With organisations having to comply with increasing levels of legislation, and society demanding more sustainable and transparent practices, it is vital that organisations are fully aware their energy usage and whether they are adopting best practice wherever possible. A full energy audit is a methodical examination of energy use, and thus energy cost, and the procedures that impact on its use. Coupled with an energy policy, which can act as a driver for implementing and improving an organisation’s energy management system, you can demonstrate commitment to minimising energy use. This can be broken down in the six elements described below.
TOP LEVEL COMMITMENTIt starts at the top. The energy policy should be endorsed by senior management, ideally at board level, in order to demonstrate their commitment and ensure that the organisation allocates the staff time to maintain and enhance its efforts to improve energy efficiency and adapt energy use to its needs. Without that support you are likely to see any initiatives lose momentum and fail to get the widespread behaviour change that these types of projects require.
DEFINING THE STRATEGYIn the quest to reduce energy use it can be tempting to rush into quick fix solutions. Bolt-on renewable and low to zero carbon technologies, such as photovoltaic arrays, wind turbines and solar thermal, are often seen as the answer, although the capital cost can often be seen as a barrier. Whilst these all have a part to play, there should be a consistent strategy running from the energy policy. The standard published ISO 50001, Energy Management Systems, provides a framework for integrating energy performance into management practices. This enables organisations to: develop a policy for more efficient use of energy and fix targets and objectives to meet that policy; use data to better understand and make
decisions concerning energy use and consumption; measure
the results; review the effectiveness of the
policy; and continually improve energy management.The first step is always to understand current energy use by carrying out
energy use
ENERGY AUDITS
SWITCH ON TO THE ENERGY AGENDAA full energy audit, coupled with a robust energy policy, can demonstrate an organisation’s commitment to the sustainability agenda. Chris Moriarty from the British Institute of Facilities Management explains how to develop a successful energy policy
Energy
A full
energy audit
is a methodical
examination of
energy use, and thus
energy cost, and the
procedures that
impact on it
use
www.spectrumenergysystems.co.uk
Speak to one of our renewable energy specialists today:
0845 47 47 604
PURCHASEENERGY FROM 5.5p / kWhUtilise your unused roofspace and save...Solar PV is one of the most reliable renewable energies available today.
A proven technology making it a great investment to generate savings.
High performance systems engineeredto save you money
Guaranteed income for 20 years
Experienced electrical engineers
Outright purchase or power purchaseagreement
We offer both roof and ground SolarPV systems
If you are a high energy user this enables you to
purchase green energy at non-premium prices
and protect you against future energy price rises.
No capital outlay is required
We supply, install and maintain the solar PVsystem on your roof or land
We then sell the energy generated back toyou at a discounted rate
For high energy users we can offer from 5.5pper kWh which is index linked for 20 years
PowerPurchaseAgreement (PPA)
info.spectrumenergysystems.co.uk
SPECTRUM AD_Health Business_Layout 1 20/10/2014 09:20 Page 1
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
47 Volume 14.6 | HEALTH BUSINESS MAGAZINE
Seeking substantial cuts in energy costs and to meet your carbon reduction targets?
Hanergy Holding Group Ltd is a multinational clean-energy power generation company, as well as the world’s largest thin‑film solar company. Our global leading CIGS technology has the highest efficiency potential among thin‑film solar cell materials.
Hanergy provides customers with one-stop green energy service – from project development, finance, installation, to operational management.
To find out how Hanergy can turn your roof into a solar power station, please contact us today, our dedicated UK team will answer all of your questions.
T: +44 (0) 20 7337 6060 E: [email protected]: www.hanergy.eu / www.hanergy.com
Hanergy Solar Power UKPart of the Hanergy Holding Group
Across 86 buildings, powerPerfector is saving its healthcare clients over £805,000 every year. That’s the equivalent of...
One technology to save you money and protect your estate
38 Nurses
...or
...or
7.6 Ambulances
16 Doctors020 7262 6004
www.powerperfector.com [email protected]
Annual electricity reduction of £805,000. Equivalents based on a newly trained nurse salary of £21,176 (www.rcn.org.uk), ambulance cost of £106,000 (www.emas.nhs.uk), doctor’s salary of £50,322 (www.payscale.com).
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.648

audits from an analysis of regular meter readings. This will show, for example, if electricity or gas use is dominant and where improvement efforts should be focused.
DEFINING THE MAIN OBJECTIVESA long-term target should be developed with a series of stepping stones to maintain progress. For example, if you have multiple
buildings, consider initially restricting the policy objectives to a small number or even a single building. This will ensure that the project is manageable. It can be rolled out to cover all buildings later. This will also help you to understand the benefits of the policy at a smaller scale, helping inform the roll out across further buildings and informing target settings. It is important to define the area over which
To formulate the energy policy itself, once the scope is defined and a general picture of high level energy use understood, it is important to set targets and goals
Energy
ENERGY AUDITS
Developing an energy policyTop level commitment The energy policy should be endorsed by senior management to demonstrate their commitment and ensure enough time and resource is put towards it. Defining the strategy There should be a consistent strategy running from the energy policy. ISO 50001, Energy Management Systems, provides a framework for integrating energy performance into management practices. Define the main objectives A long-term target should be developed with a series of stepping stones. The objectives themselves should be simple and clear so that they can be understood by all. Cost and time resources Ensure that the energy audit does not focus solely on the financial costs and also consider the human effort and behaviour change required. Target and review periods It is important to set targets and goals; determine action plans; state time frames; and identify key personnel, including the sponsoring senior staff member. Continual improvement The energy policy should be an official, publicly available statement. It should illustrate a commitment to achieve energy management objectives and to do this by continual improvement.
the policy applies at any particular time.The objectives themselves should be simple and clear so that they can be understood by internal and external parties, such as employees, customers, public authorities and investors. They will form the basis for setting energy targets. COST AND TIME RESOURCESThere are certainly long term benefits to be had through better managed energy but these will be no overnight fix. We must also ensure that we do not focus solely on the financial costs and also consider the human effort required. Changes to the way in which we manage our energy requires behaviour change and for that you need to
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
49 Volume 14.6 | HEALTH BUSINESS MAGAZINE

When formulating an energy policy, there is no simple solution to tackling this complex challenge. Each building is different, each organisation is different. The journey towards better energy management will be unique
Ener
gy
ENERGY AUDITS
look at different techniques to build that movement from within the workforce. One approach would be to form an energy working party to feed ideas into the policy. By acting as advocates they can help establish commitment throughout multiple areas of the organisation. Consulting with people from a variety of skill sets and department will broaden input. It is also a good idea to identify ‘energy champions’, people who can support initiatives on a daily basis in their usual working lives.
TARGET AND REVIEW PERIODSTo formulate the energy policy itself, once the scope is defined and a general picture of high level energy use understood, it is important to: set targets and goals; determine action plans; state time frames; and identify key personnel, including the sponsoring senior staff member. This will allow roles and responsibilities to be transparent and identify building lifecycle factors. These steps will ensure that efforts are concentrated to optimum effect and that realistic targets and timeframes are set. It will also help you understand whether the project is working and where you may need to adapt approaches.
CONTINUAL IMPROVEMENTThe energy policy should be an official,
publicly available statement. It should illustrate a commitment to achieve energy management objectives such as to reduce greenhouse gas emissions and to do this by continual improvement. When formulating an energy policy, there is no simple solution to tackling this complex challenge. Each building is different, each organisation is different, and therefore the journey towards better energy management will be unique. That said, the above provides a framework to take the first steps. What is important is that full commitment is given to it from the start. Our work shows us that organisations are tackling the whole sustainability agenda either to comply with legislation or to enhance their public image. It is encouraging that organisations are reviewing their activity but doing it for these reasons threatens to undermine the benefits that can be realised. A full and sustained approach to becoming
a more sustainable business must be part of the DNA of an organisation; it cannot be a side project, it cannot be a short term goal. Increasingly organisations are becoming switched on to the topic, which is good news. I look forward to seeing how this important debate develops. The BIFM has developed an Energy Audits Good Practice Guide, which presents good practice for some of the important energy management procedures ranging from developing an energy policy to deciding which improvements to make. It enables facilities managers to compare the results of an energy audit with good practice in both energy use and energy related procedures in order to manage their organisation’s energy costs. Members can download the guide at www.bifm.org.uk.
FURTHER INFORMATION www.bifm.org.uk/gpgs
With years of experience in everything from small island off-grid to multi-mega watt funded solar PV systems, Sun Renewables offer the best value for money and return on investment available today.
Contact: Phone: 0845 3011061 Email: [email protected] Web: www.sunrenewables.com
Photovoltaic and Heat Pump Energy Systems
SUN RENEWABLES Ltd
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.650
What are the energy challenges that you see facing the healthcare sector?The NHS’s vast buying power and procurement organisations such as the Crown Commercial Service (CCS) framework have meant a lot has been done to reduce the unit price of energy charged to the sector. Despite this, the increase in demand for healthcare and advancements in technology have resulted in NHS energy bills almost tripling over the last 10 years. We know that healthcare organisations can make cost savings of 10 to 30 per cent through improved energy efficiency measures, depending on the condition of the building. However, there are several challenges, for example finances. Many NHS Trust budgets are being more tightly squeezed than ever before and capital funding for energy projects can be difficult to secure. There is concern among healthcare managers that energy costs can only go one way, which could put further strain on budgets for patient care. Plus challenging government carbon targets are requiring senior NHS managers to put carbon reduction plans in place. NHS buildings are also under increasing strain and staff are using more electrical equipment to improve the quality of diagnosis and treatment. Many buildings, along with their heating and cooling systems, are ageing and even newer buildings are experiencing
challenges improving their energy efficiency. We know that some NHS trusts we work with find it difficult to navigate the various technologies and frameworks to identify what will work for their needs. And it’s almost impossible to take the blueprint from one Trust and replicate that across the country. But there are strategies which can work for all NHS Trusts.
What options are available to overcome these issues? One of the best options available at the moment is an Energy Performance Contract (EPC). These are self-funding agreements designed to reduce energy consumption and costs by identifying the right measures based on an individual Trust’s needs and circumstances. British Gas was one of the first companies to offer EPCs when they were introduced to the UK from North America about three years ago, having been successful there for 20 years. A range of energy efficiency measures, from lighting, new boilers and cooling systems to solar panels and ground source heat pumps, are installed and maintained, often giving the ability to generate renewable energy on site. The measures then pay for themselves through reduced energy use over an agreed period of time.
One of our challenges is to make the process of such an offering simple to understand. As the savings are guaranteed by British Gas, we can also assure customers that these savings can contribute towards Cost Improvement Plan targets and are guaranteed to be bigger than the project costs.
Why are healthcare organisations taking up EPCs in the UK?From our experience, EPCs can help save a significant amount of money which can then be put back into patient care. In terms of Trusts we support, large hospitals like St George’s hospital in London can save around £1million per year, equivalent to 25 per cent off their annual energy bill. Even smaller NHS trust sites can achieve substantial savings each year – Northern Lincolnshire and Goole NHS trust are looking to save over £500,000 a year over three hospital sites. In fact, through our EPC contracts alone British Gas will save the NHS over £70 million in energy costs over the lifetime of our contracts. The NHS’s carbon footprint is 25 million tonnes of CO2 per year in England alone – reducing this is a key objective of the EPC. St George’s will save 6,000 tonnes annually, the equivalent of taking 3,000 cars off the road and Northern Lincolnshire and Goole will save 3,360 tonnes each year. Installing more effective heating, cooling and lighting systems can make buildings more comfortable and flexible for patients. In addition, many Trusts design and implement staff awareness programmes, which British Gas helps to deliver, which teach staff to think differently about the amount of energy they use in their day-to-day work.
Is British Gas unique in the market?Our vision is to make it easy for businesses to manage their energy, and that includes making energy more affordable. We know that one size doesn’t fit all, and we are unique in being able to offer a comprehensive range of energy efficiency measures which allows organisations to benefit from the best solution to match their situation. We are also confident in giving real guarantees and that we will be around for the next 10-15 years to ensure that the NHS can rely on us to deliver them energy savings year after year.
FURTHER INFORMATIONwww.britishgas.co.uk/business-services
ENERGY
SIMPLIFYING THE TRANSITION TO ENERGY EFFICIENT BUILDINGSMike Chessum, head of Energy Construction Services at British Gas Business, reflects on his experience of helping healthcare organisations to improve the energy efficiency of their estate
Advertisement Feature
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
51 Volume 14.6 | HEALTH BUSINESS MAGAZINE
thedecorativepanelsgroup
YOUR PERFECT PARTNER
dp-BioCote® Quartz protected
*Tested in accordance with ISO22196:2011
Century House, Premier Way,Lowfields Business Park,Elland, West Yorkshire,HX5 9HF
T: +44 (0) 1484 658341 F: +44 (0) 1484 658812E: [email protected]
Download our app Scan for AndroidScan for AppleContact us for more information.
*A 99.9% germ free laminated board material suitable for furniture and fit out manufacture.
Significant reductions of harmful microbes within 15 minutes.
Available from stock in unicolour and woodgrain finishes.
Works continuously for the expected lifetime of the product.
dp-BioCote Quartz technology:
• Makes a product more hygienic, if it is likely to host harmful microbes.
• Keep a product fresher for longer, if it is likely to host odour-causing or staining microbes.
• Extend the usable lifetime of a product, if it is likely to host microbes which might degrade the surface.
• The surface is highly resistant to abrasion, far exceeding the abrasion resistance of high pressure worktops.
Produced in 2014

thedecorativepanelsgroup
YOUR PERFECT PARTNER
dp-BioCote® Quartz protected
*Tested in accordance with ISO22196:2011
Century House, Premier Way,Lowfields Business Park,Elland, West Yorkshire,HX5 9HF
T: +44 (0) 1484 658341 F: +44 (0) 1484 658812E: [email protected]
Download our app Scan for AndroidScan for AppleContact us for more information.
*A 99.9% germ free laminated board material suitable for furniture and fit out manufacture.
Significant reductions of harmful microbes within 15 minutes.
Available from stock in unicolour and woodgrain finishes.
Works continuously for the expected lifetime of the product.
dp-BioCote Quartz technology:
• Makes a product more hygienic, if it is likely to host harmful microbes.
• Keep a product fresher for longer, if it is likely to host odour-causing or staining microbes.
• Extend the usable lifetime of a product, if it is likely to host microbes which might degrade the surface.
• The surface is highly resistant to abrasion, far exceeding the abrasion resistance of high pressure worktops.
Produced in 2014
A study by cost consultants EC Harris, identifying £1.5bn worth of savings the NHS could make by improving efficiency across its estate, was unveiled at the recent Healthcare Estates conference in Manchester. The current annual bill for NHS estates management stands at £7.2bn and is rising at almost eight per cent every year despite the austerity measures introduced by the coalition government. Conference delegates responded by urging the Department of Health to renew the publicly funded £50m pilot programme run by several trusts last year to trial energy saving strategies and to bolster the department’s own Encode sustainability design guidance. Trusts that ran the pilot schemes were able to reinvest their savings from reduced energy bills in frontline patient care. However, DoH spokesman Peter Sellars told the conference there was no more “capital spend available” for another round of energy efficiency schemes, although he said “the ministerial team are always asking us to do more about the energy efficiency agenda.” He urged trusts to look for alternative sources of funding such as the Green Investment Bank.“The evidence shows that the way we currently manage our estates is not sustainable,” Mr Sellars added.
LOW-HANGING FRUITExperts who spoke at a session organised by the Building and Engineering Services Association (B&ES) identified lots of ‘low hanging fruit’ that almost every healthcare facility can find to quickly and cheaply improve its energy efficiency. Estates managers were urged to carry out extensive measuring and monitoring to investigate how well their heating and cooling systems were operating. In many cases, they will find they are working against each other because occupants have been changing the temperature settings, the B&ES speakers said. This situation is often made worse by building users opening the windows because they feel hot, rather than turning the heating down. Even relatively new hospitals could benefit from extensive re-commissioning to eradicate this type of problem, delegates heard.Facilities managers (FMs) should make
sure there was a temperature ‘dead band’ programmed into the controls by optimising the set points to ensure the heating and cooling systems did not end up running at the same time and wasting huge amounts of energy. Darren Jones of specialist consultancy Low Carbon Europe also told the session that ventilation systems were always overlooked as a source of potential savings. He said that optimising the way air was supplied to just one operating theatre could save a hospital £5,000 in annual running costs. That could add up to £10m a year if replicated right across the whole of the NHS and would also avoid 80 tonnes of carbon emissions. He said that any ventilation fan that is over five years old is almost certainly inefficient and a replacement would pay for itself in less than three years. Healthcare FMs could cut running costs by 29 per cent by replacing the fans in their air handling units and the addition
of heat recovery to ventilation systems can reduce costs in non-clinical areas by up to 30 per cent. Even more basic measures like having grilles and filters cleaned regularly can save thousands of pounds a year. Mr Jones urged hospital FMs to measure air flow rates to get an idea of how well their systems were working and look for ‘free cooling’ opportunities – where the system will cool the building without the need for the refrigeration circuit to operate. “When we survey NHS buildings, we often find that the chillers have free cooling circuits that are not being used because the building managers are not familiar with the controls,” said Mr Jones.
He pointed out that partial free cooling was possible even when the outside temperature was as high as 18degC. “We need to train people to take advantage of this so that refrigerant plant only runs when it is really needed.” Variable speed drives are often installed in plant rooms, but have just been left at a constant speed setting, which defeats the object, Mr Jones added.
RECOVERINGDavid Fitzpatrick, sales and marketing director of Ruskin Air Management, told the conference that, because the primary focus tends to be on operating theatres and critical areas, the well-being of recovering patients and hospital staff can be forgotten. He said that his company’s research among bed management teams revealed their top priority was to help patients recover more quickly. This means that a high standard of indoor air quality (IAQ) is required in general
areas, according to Mr Fitzpatrick. “Things are already pretty fraught in A&E as it is, so having poor air quality is just going to make everyone feel even worse,” he said. “The ventilation, therefore, needs to be able to contend with airborne contaminants and VOCs; as well as cooking and body odours, but it was often not designed with any of those things in mind.” Ruskin is actively involved in the design and refurbishment of healthcare ventilation systems and Mr Fitzpatrick said that a big problem his team encountered was the fact that an area was often designed for one purpose, but was reconfigured and used for something else at a later date.
Facilities managers should make sure there was a temperature ‘dead band’ programmed into the controls by optimising the set points to ensure the heating and cooling systems did not end up running at the same time and wasting huge amounts of energy
HEATING & VENTILATION
STRATEGIES FOR ENERGY EFFICIENCYMillions of pounds could be shaved from NHS running costs if estates managers take a closer look at how their heating, ventilation and air conditioning systems are performing, according to the Building & Engineering Services Association
Facilities Managem
entBUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
53 Volume 14.6 | HEALTH BUSINESS MAGAZINE
David Fitzpatrick, sales and marketing director,
Ruskin Air Management

All Yeoman Shield materials/products
are sourced and manufactured in the
United Kingdom. ISO 9001 Certifi cate No 5887
YEOMAN SHIELD... WHEN YOUR DOORS NEED EMERGENCY TREATMENT
Yeoman Shield Wall and Door Protection - cuts out the need for repetitive and costly re-decoration.
Visit our website www.yeomanshield.com
Yeoman Shield Wall and Door Protection - cuts out the need for repetitive and costly re-decoration.
Visit our website www.yeomanshield.com
Yeoman Shield Wall and Door Protection - cuts out the need for repetitive and costly re-decoration.
Visit our website www.yeomanshield.comYeoman House, Whitehall Industrial Estate,
Whitehall Road, Leeds, LS12 5JBT: 0113 279 5854 F: 0113 231 0406 E: [email protected]
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.654

“We are seeing increased demand for a mixed approach to ventilation that combines natural, low energy solutions wherever possible with powered ventilation only where it is essential,” said Mr Fitzpatrick. “This provides the necessary amount of flexibility so the system can adapt to changing uses and conditions, but also keeps the initial capital cost down. “Natural ventilation measures are generally fairly easy to install, but the controls are critical to ensure the system works properly.” In fact, 80 per cent of ‘quick wins’ in hospitals are linked to making better use of Building Management Systems (BMS) that are already in place, but are not controlling as many of the building functions as they are capable of, the B&ES experts explained. Maintaining high levels of air purity in clinical and general healthcare facilities remains a major priority, but B&ES indoor air quality expert Peter Dyment said many FMs were missing the growing threat from increased outside air pollution. The increase in the concentration of diesel particulates, particularly in urban areas, since the government encouraged the adoption of diesel vehicles has led to a worrying rise in respiratory diseases, he said. However, the Health Technical Memoranda (HTM) used to guide NHS managers on a wide range of design issues do not cover contaminants that might enter the building from outside. “HTM guidance concentrates on the transmission of diseases inside hospitals and a lot more needs to be done about the potential health impacts of outdoor pollution,” he told the conference. “360,000 premature deaths in the EU are already down to worsening air pollution.” Mr Dyment, who is a consultant for Camfil Farr, cited newly revised guidance from B&ES: ‘Guide to Good Practice – Internal Cleanliness of Ventilation Systems’ (TR/19) as a good source of advice for healthcare premises managers on tackling the threat posed by poorly maintained ventilation systems.
BENEFITS“Many of the measures needed are very low cost, such as cleaning intake grilles, and will payback in hours because of the immediate running cost and health benefits,” he added. Increased use of air filtration will also help trusts maintain good indoor air quality, the conference heard.Mr Dyment explained that energy saving filters were now a much more significant section of the market ‘growing by 20-30 per cent per year. “They will also last two or three times as long as commodity products,” he said. Persuading NHS trust boards to spend money on remedial measures is not easy because they are fully focused on frontline patient care, but Mr Fitzpatrick said it was important to avoid talking about the technical issues and express the possible investment in terms of its direct impact on improving
conditions for patients and how energy savings can be reinvested in patient care. One very easy way to cut costs, while also improving ventilation rates, is to replace standard windows with louvred openings. These meet health, safety and security requirements, but can improve ventilation rates by 15 per cent due to their larger ‘free area’, he added. Many conventional windows have to be secured shut for safety reasons. B&ES Eastern Counties regional manager Mike Malina warned delegates against the use of renewables for ‘token’ reasons and said they should only be considered once an ‘energy hierarchy’ had been put in place first, i.e. measures to reduce energy demand along with energy efficiency improvements to existing systems.
He also said heat pumps could not be deployed as direct replacements for boilers unless other improvements to the building were first carried out such as better insulation and a proper controls strategy. “NHS managers usually say there is no money for energy efficiency measures, but relatively small investments can realise huge savings in such energy intensive buildings,” said Mr Malina. “There would be no need to raise taxes to pay for more investment in the NHS because energy efficiency improvements pay for themselves and free up more tax payers’ money for frontline patient care,” he added.
FURTHER INFORMATION www.b-es.org
“Many of the measures needed are very low cost, such as cleaning intake grilles, and will payback in hours because of the immediate running cost and health benefits” Peter Dyment, Consultant for Camfil Farr
Facilities Managem
ent
HEATING & VENTILATION
BUSINESS INFORMATION
55 Volume 14.6 | HEALTH BUSINESS MAGAZINE
Sperion’s management have over 20 years of experience providing solutions to public sector bodies including the NHS.
Sperion’s experience often enables clients to save and reduce spend of asbestos management and removal whilst still complying fully with regulation & legislation.
Sperion offer the full range of asbestos services to both the public and private sectors, predominantly within London, the South East and Home Counties. Sperion have experience of working within most environments including live retail outlets, educational establishments, hospitals, hotels, financial institutions, residential premises, public buildings and construction sites.
Sperion’s aim is to provide a fast, efficient service with quality and integrity.Sperion is a client-focused business that draws upon in excess of 40 years’ experience gained at the highest level within the asbestos removal and consultancy industry. The Directors and Senior Management have managed and worked within every project scenario and can provide an unrivalled service for any project.
See how Sperion can ensure compliance within your budget.• HSE Licenced Asbestos removal• Asbestos Refurbishment & Demolition surveys• Asbestos Management Surveys• Asbestos Consultancy
Asbestos management
Telephone: 0800 9996 900Email: [email protected]
Helping to create healthy & safe environments in the healthcare sectorAtQubeConstructionManagementPLCourspecialistteamof surveyorsarequalifiedtoworkwithasbestosandtogetherhaveover30years’experienceinthefield.Wewillhelpyoutodetermineanddeveloptherightstrategy,plansandprocessesforthemanagementanddevelopmentofyourpremisestomeetyourhealthcareneeds.
Weofferthefollowingasbestosservices:• AsbestosSurvey–ManagementSurvey,
Refurbishment&DemolitionSurvey• AsbestosRemoval• AsbestosEncapsulation• AsbestosWasteCarrier• AsbestosAwarenessTraining
Callusforaninformaldiscussionaroundsolutionstominimiseriskofexposureon:
0800 468 1700
CanterburyHouse,WatersideCourt,NeptuneWay,MedwayCityEstate,Rochester,KentME24NZwww.qubecmplc.co.uk
Expert, affordable asbestossolutions for your peace of mind
• Asbestos advice
• Management surveys
• Sample analysis
• Asbestos removal
• Refurbishment/Demolition surveys
• Asbestos encapsulation
Tel: 01722 321419www.sarumasbestos.co.uk
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.656
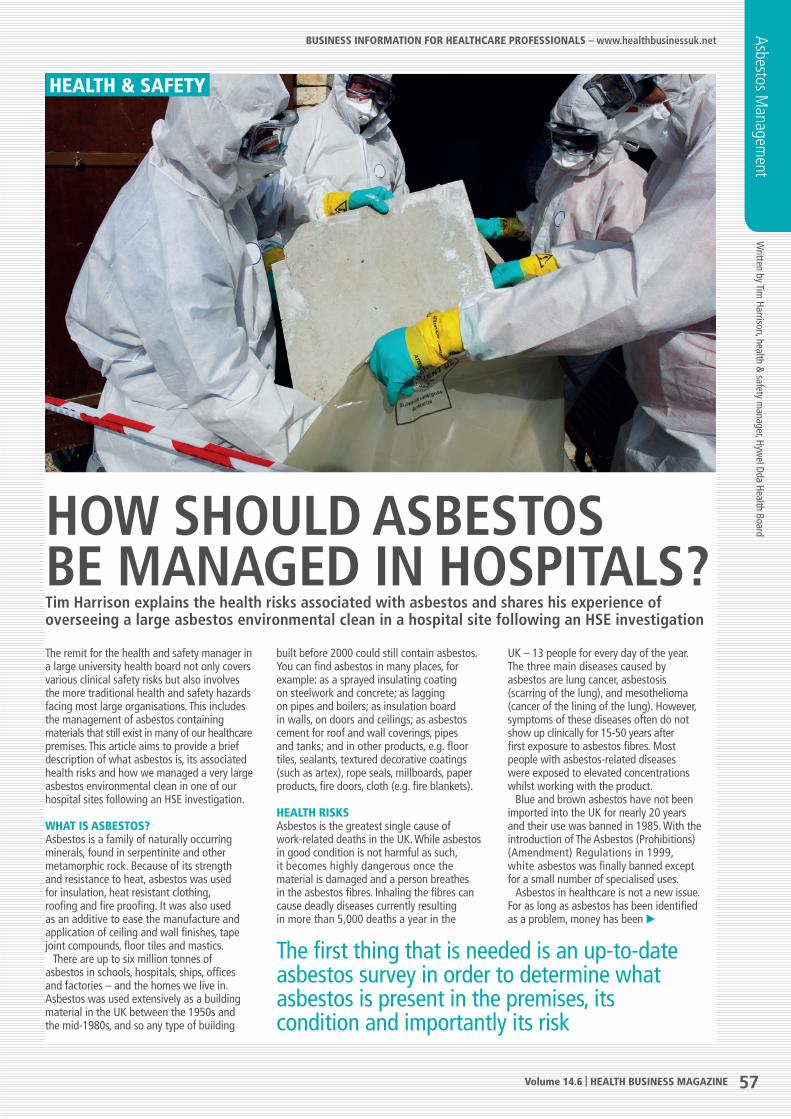
Written by Tim
Harrison, health & safety m
anager, Hywel Dda Health Board
The remit for the health and safety manager in a large university health board not only covers various clinical safety risks but also involves the more traditional health and safety hazards facing most large organisations. This includes the management of asbestos containing materials that still exist in many of our healthcare premises. This article aims to provide a brief description of what asbestos is, its associated health risks and how we managed a very large asbestos environmental clean in one of our hospital sites following an HSE investigation.
WHAT IS ASBESTOS?Asbestos is a family of naturally occurring minerals, found in serpentinite and other metamorphic rock. Because of its strength and resistance to heat, asbestos was used for insulation, heat resistant clothing, roofing and fire proofing. It was also used as an additive to ease the manufacture and application of ceiling and wall finishes, tape joint compounds, floor tiles and mastics. There are up to six million tonnes of asbestos in schools, hospitals, ships, offices and factories – and the homes we live in. Asbestos was used extensively as a building material in the UK between the 1950s and the mid-1980s, and so any type of building
built before 2000 could still contain asbestos. You can find asbestos in many places, for example: as a sprayed insulating coating on steelwork and concrete; as lagging on pipes and boilers; as insulation board in walls, on doors and ceilings; as asbestos cement for roof and wall coverings, pipes and tanks; and in other products, e.g. floor tiles, sealants, textured decorative coatings (such as artex), rope seals, millboards, paper products, fire doors, cloth (e.g. fire blankets).
HEALTH RISKSAsbestos is the greatest single cause of work-related deaths in the UK. While asbestos in good condition is not harmful as such, it becomes highly dangerous once the material is damaged and a person breathes in the asbestos fibres. Inhaling the fibres can cause deadly diseases currently resulting in more than 5,000 deaths a year in the
UK – 13 people for every day of the year.The three main diseases caused by asbestos are lung cancer, asbestosis (scarring of the lung), and mesothelioma (cancer of the lining of the lung). However, symptoms of these diseases often do not show up clinically for 15-50 years after first exposure to asbestos fibres. Most people with asbestos-related diseases were exposed to elevated concentrations whilst working with the product. Blue and brown asbestos have not been imported into the UK for nearly 20 years and their use was banned in 1985. With the introduction of The Asbestos (Prohibitions) (Amendment) Regulations in 1999, white asbestos was finally banned except for a small number of specialised uses. Asbestos in healthcare is not a new issue. For as long as asbestos has been identified as a problem, money has been
The first thing that is needed is an up-to-date asbestos survey in order to determine what asbestos is present in the premises, its condition and importantly its risk
HOW SHOULD ASBESTOS BE MANAGED IN HOSPITALS?Tim Harrison explains the health risks associated with asbestos and shares his experience of overseeing a large asbestos environmental clean in a hospital site following an HSE investigation
Asbestos Managem
ent
HEALTH & SAFETY
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
57 Volume 14.6 | HEALTH BUSINESS MAGAZINE

Now available on your tablet device......
app.greenfleet.net
GreenFleet magazine is now available on iOS and Android platforms, offering an interactive experience for fleet managers and those responsible for keeping transport emissions to a minimum.
Download your free copy from

Now available on your tablet device......
app.greenfleet.net
GreenFleet magazine is now available on iOS and Android platforms, offering an interactive experience for fleet managers and those responsible for keeping transport emissions to a minimum.
Download your free copy from
spent on removing it or managing its risk in hospitals and other healthcare premises.
HOSPITAL BUILDINGSA lot of healthcare premises are quite old and although new hospitals are being built, there are a large number of hospitals and healthcare buildings built using asbestos containing materials. These were often found in large boiler houses, lagging on steam pipes located in under floor voids/subways, asbestos insulating board protecting pipework in clinical environments all of which are realities of its use from not too long ago. From the patient’s viewpoint, however, these asbestos installations were not really likely to affect their health as the asbestos containing material tended to be in locations where only a limited number of staff or contractors worked and therefore did not impinge upon the patients or the majority of healthcare staff. This sadly was not the case for some hospital maintenance workers who worked in often cramped and difficult conditions within service ducts and service risers. Many have undeniably been exposed to asbestos fibres and some even died as a result. It is also possible that more will suffer as a result of their past exposure in the future.
DUTY TO MANAGESince 2004 the law has required that asbestos in healthcare premises, together with all non-domestic properties, should be managed. This management is intended to ensure those that occupy the buildings are not exposed to asbestos and those that work upon the fabric of the building are informed about the asbestos that is present, so that they can avoid it. The law requires that there be a duty holder. In many acute general hospitals this is normally the delegated responsibility of the estates department.
THE DUTY HOLDERThe first thing that is needed is an up to date asbestos survey in order to determine what asbestos is present in the premises, its condition and importantly its risk. This survey will then be used to produce an Asbestos Register, which provides information to not only hospital staff but also visiting contractors who may require access to areas of the hospital premises. The ‘duty holder’ should also prepare a management plan that shows how the organisation will manage asbestos within its premises. There is no need for a huge document – a straightforward statement of what is to be done and who will do it, highlighting problem areas if any exist.
During 2009 three individual NHS Trusts merged to form Hywel Dda Health Board, and as part of this process an internal review was undertaken to determine the level of compliance with the Asbestos at Work Regulations. This review discovered a number of concerns and the organisation informed the Health and Safety Executive of our findings. This resulted in a formal investigation relating to the historical management of asbestos at Bronglais General Hospital, Aberystwyth by the HSE during 2010/11. The HSE’s investigation report made several
recommendations including: the appointment of an estates
compliance manager with specific responsibility
for the management of asbestos; an electronic asbestos risk register, updated on a constant basis, that shows where asbestos containing
materials (ACM) are present, its condition
and control measures required; asbestos awareness
training to be provided to all estates staff including the estates
management teams; and respiratory face fit testing for all Estates staff requiring it. Finally, there was a recommendation for the health board to undertake a cleaning regime to ensure so far as is reasonably practicable that Asbestos Containing Materials (ACMs) are removed from under floor service voids and vertical service risers at Bronglais General Hospital. The specification for the project related to asbestos removal and decontamination works of the between floor voids and vertical service risers. It was planned that the works would be undertaken over an 18 month period.
CHALLENGESOne of the main problems facing both the Contractors and the Health Board was the project having to be carried out with the minimum disruption to clinical services. The only access into the floor voids were via floor hatches located in the main corridors located in ward areas. Therefore, the access required to undertake asbestos removal/cleaning works would have considerable impact on the day to day running of the hospital. In order to avoid this, the selected contractor had to create suitable access/egress points into the voids by breaching the exterior walls at a number of specified locations along the rear elevation of the hospital. These cut-out access points were often only 500mm in height therefore creating difficult conditions for the asbestos removal contractors working in confined spaces and working at considerable height. As the site was to remain a live working environment, the amounts of services that could be isolated were minimal. Services that
remained live were hot water for heating systems, live steam and electrical installations. Therefore hot work and heat stress were identified as being likely issues for the contractor’s staff. Hywel Dda Health Board had to co-operate with the principle contractor in reducing the risk that these hazards presented, by isolating hot services as far as practicable. The contractor had to have procedures in place for the regular assessment of the risk of heat stress and monitoring of employees and contingencies were put in place to supply suitable engineering and procedural controls e.g. additional cooling and ventilation, ‘cool’ rest areas, limiting working time in high risk areas etc.
A SUCCESSFUL PROJECTUndertaking the majority of the removal work externally avoided the temporary closure of clinical services for the duration of the contract. Vertical riser access did however impact slightly on the clinical environment with the only practical entry into these areas was via access doors on each landing, airlocks had to be assembled on each landing, and sufficient space was left on the stairwells and landings to allow these stairs to be used for emergency evacuation of the building. Also, suitable access was made through the windows on these stairs to allow removal operatives’ equipment and waste to transit in and out of the building via the scaffolding without entering the live areas of the hospital. Scaffolding was erected on the rear elevation of the hospital and had suitable protection to maintain enclosure integrity during poor weather. Prior to any breaches into the fabric of the building a thorough examination of the floor void was undertaken. The walls were breached under controlled conditions in specified locations. Enclosures were built for the breaching work to be undertaken in, with the aim of preventing air from flowing into the void to reduce the risk of disturbing any asbestos containing material in the void. Once the breaching works were finished and the enclosures complete, air locks and bag locks were located on the scaffolding, with negative pressure units in place. In order to test the integrity of the areas each void was smoke tested, which in itself was a risk in a fully occupied hospital. The project was extremely successful with very few incidents reported throughout the scheme, and these generally involved reassuring hospital staff of the actual work undertaken. The work has resulted in clean voids and risers that now provide a far safer environment for both our hospital maintenance staff and contractors who are required to access these areas.
Tim Harrison is the Health and Safety Manager for Hywel Dda Health Board and a member of the iosh Healthcare Group
FURTHER INFORMATIONwww.iosh.co.uk
Asbestos Managem
ent
HEALTH & SAFETY
The project
was extremely
successful
with very
few incidents
reported
throughout the
scheme
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
59 Volume 14.6 | HEALTH BUSINESS MAGAZINE
Safe, proven, affordable.
Aid Call wireless nurse call is safe, reliable and proven with over 3,000 systems installed nationwide, and at a fraction of the cost of a wired system.
0800 052 3616www.aidcall.co.uk
Why aren’t you wireless?
E N
300220 (2007)
Quote Ref: Hbus

Safe, proven, affordable.
Aid Call wireless nurse call is safe, reliable and proven with over 3,000 systems installed nationwide, and at a fraction of the cost of a wired system.
0800 052 3616www.aidcall.co.uk
Why aren’t you wireless?
E N
300220 (2007)
Quote Ref: Hbus
This year’s Healthcare Estates in Manchester on 7-8 October saw key senior directors, managers and their teams from healthcare facilities enjoy two days of debate and discussion on key issues affecting the sector, and network with exhibitors who showed many of the latest products and services and innovations on offer. Visitor attendance was up by 14 per cent this year, with an attendance of 1,515 compared to 1,350 the previous year. Steve Webb, show director, said: “Since the 2010 event, we have worked hard to deliver a key audience to the sectors leading healthcare event. This year saw even more key decision makers attend with a good growth in attendance.” The combined attendance with speakers, delegates, exhibitor guests,
VIPs and stand personnel saw over 3,000 attendees fill the exhibition floor, who along with delegates networked with 180 exhibitors to discuss and see the new ideas and developments available to them.
ENERGYEnergy featured heavily at Healthcare Estates with a dedicated stream on both days in the main conference and a theatre providing complimentary content on the exhibition floor. Against a world backdrop of increased concerns about energy security, price
fluctuations and, of course, the need to address climate change,
the organisers worked closely with the Carbon
Energy Fund (CEF) and BRE and key speakers to address the issue. Peter Sellars from the Department of Health
delivered an opening address on how estates and facilities can contribute towards a sustainable NHS, whilst assuring compliance and managing emerging priorities. On the back of the announcement of six new projects aimed at gaining a fuller understanding of how energy is managed in the country’s non-domestic buildings, Healthcare Estates delivered nine hours of content in this important area. Funded with £3 million from the Engineering and Physical Sciences Research Council (EPSRC), and carried out on behalf of the Research Councils UK Energy Programme (RCUKEP), the research addressed ways to use technology, data and information, mathematics, law and sociology to create better energy strategies and behaviours in public buildings, including hospitals and health centres. Non-domestic buildings currently account for approximately 18 per cent of UK carbon emissions and 13 per cent of final energy consumption, with the NHS being the biggest contributor overall. Professor Philip Nelson, EPSRC’s chief executive, said: “Improving energy efficiency is an important piece of the energy puzzle. Worldwide energy demand is rising, as are global temperatures and sea levels. We need to find smart solutions to how we use energy while improving the environment in which people have to work, rest or play. “These projects will go a long way to help improve our understanding of what goes on in non-domestic buildings and add to the armoury at the disposal of those managing these facilities.”
EVENT REVIEW
FOCUS ON HEALTH BUILDING MANAGEMENTHealthcare Estates 2014 took place on 7-8 October at Manchester Central and saw a record numbers of visitors sharing insights on running hospital estates efficiently and effectively
Healthcare Estates
Visitors
enjoyed two
days of debate
and discussion on
key issues affecting
the sector. Exhibitors
also showed many
of the latest
products
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
61 Volume 14.6 | HEALTH BUSINESS MAGAZINE
AustcoMaking it
Easier to Care
Nurse Call is a Lot Smarter Than it Used to be
What Would Happen if You....
Ramped up control of care for both staff and patients
Made mundane routines simpler and quicker
Massively improved communication
High Effi ciency - Low Radiation - Modulating
Ranges from 8kg/hr - 2000kg/hr
CERTUSS (UK) LimitedUnit 45 Gravelly Industrial ParkTyburn RoadBirminghamB24 8TG
Tel: 0121 327 5362Fax: 0121 328 [email protected]
Credit Card Keys specialises in the development, manufacture and supply of quality key storage systems for a wide range of industries. The company has been established for over 31 years and is one of the UK’s leading key storage manufacturers. Credit Card Keys employs the latest developments in key storage and key management technology to produce high quality, reliable and easy to operate systems. All key systems are built to the very highest standards and although they are extremely popular with obvious market areas such as the automotive trade, Credit Card Key’s key management systems are also used and are effective in other work environments.
For example, a Premier League Football Club not only uses the management systems to track keys but also walkie talkies. The Smart Box series can be used to secure a variety of valuable assets such as keys, tools, pharmaceuticals, mobile phones and PPE equipment. Credit Card Keys distributes its products throughout the UK and to global customers too. The company also supplies Sentinel Key Safes for the control access keys to homes, boats, lockers, caravans and planting equipment. For more information or to get a competitive quotation please visit the website.
FURTHER INFORMATIONwww.cckeys.com
Secure key storage and key management solutions
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.662

The new projects will be run at Imperial College London, University of Cambridge, University of Edinburgh, University of Oxford, University of Southampton and the University of Strathclyde.
PLANNING, DESIGN & CONSTRUCTIONPlanning, Design & Construction proved to be one of the most popular streams in the conference with a host of areas covered including an update on the new procurement regulations, new collaborative opportunities and how design teams and NHS clients can work together, which included real examples of smarter ways to procure services. David Whiteley, chief engineer and programme lead for the Department of Health presented on the new version of the NHS Premises Assurance Model (PAM), a management tool that provides NHS organisations with a way of assessing how safely and efficiently they run their estate and facilities services. It provides a nationally consistent approach to evaluating NHS estates and facilities performance against a common set of questions and metrics. It is a basis for providing assurance on the safety and suitability of healthcare premises. New for this year at the Healthcare Estates event was a Construction Industry Council & BIM Area. This area had workshops, software demonstrations, networking events, case studies, and BIM specific sessions. Companies involved included ADP Architects and Architects for Health. Supporting the area were leading architectural firms, including Stantec and ADP plus contractors who showcased recent and current projects.
AWARDSDay one concluded with the Healthcare Estates IHEEM annual dinner and awards, with guest presenter Fabrice Muamba, who famously suffered a heart attack playing for Bolton
at White Hart Lane against Spurs. His heart stopped beating for 78 mins, but remarkably he recovered to tell his tale. Fabrice was a refugee from Congo who despite coming to the country with no English at 7, went on to gain 10 GCSEs and 3 A Levels before embarking on his football career. The Product Innovation in Healthcare Award was presented to IDEXX Water for its Pseudalert rapid detection method which halves the time taken for the identification of Pseudomonas aeruginosa in hospital water systems. The Sustainable Achievement Award Winner
was awarded to Sussex Community NHS Trust working in partnership with Capita. The Trust has already achieved a 15 per cent reduction in absolute CO2 emissions against their 2010 baseline, despite an increase in clinical activity, meaning they have already met the interim 2015 reduction target. Leeds Teaching Hospitals NHS Trust scooped the 2014 Estates and Facilities Team Award.The team developed and embedded a range of key initiatives which have been key factors in improving the quality of patient safety and delivering financial improvements through increased productivity.
The Project Team of the Year Award, which goes to the team that has successfully delivered a new build or a refurbishment, was presented to AFL Architects, Interserve Construction and the Mid Chesire NHS Foundation Trust. The accomodation delivered includes eight state of the art operating theatres (4 with Ultra Clean Ventilation), 14 recovery bed spaces and 14 critical care bed spaces. The new facilities feature the most up to date equipment available for patients to receive truly first class treatment in a modern environment. The William E Schall Award recognises the
graduate who has made the best contribution while studying the Medical Technologies Foundation Degree Course. This year the award went to Daniel Couzens, a clinical engineer at Basildon University Hospital who performed excellently in his foundation degree course. He has spent the last two years completing a medical technologies foundation degree course at Kingston University in London.
ATTENDANCEOverall attendance to Healthcare Estates increased again and exceeded 3,000 with visitor attendance up by 14 per cent with an attendance of 1,515 compared to 1,350 the previous year. The total attendance of 3,186 includes visitors, delegates, speakers and exhibitor guests to this year’s Exhibition, Conference and Dinner held in Manchester in October. The attendance continues the increases seen since the move to Manchester, with attendees able to network with the 182 exhibitors representing more than 200 suppliers to the Healthcare sector. The attendance included 461 delegates and speakers to the conference – up 15 per cent on the previous year – and a record attendance at the IHEEM dinner of 450 who enjoyed a fantastic evening at the Mercure Piccadilly in Manchester. Healthcare Estates also saw over 350 NHS VIP’s representing many of the UK’s leading hospital trusts in the UK attended the event.
FURTHER INFORMATIONwww.healthcare-estates.com
Healthcare Estates
EVENT REVIEW
Overall attendance to Healthcare Estates increased again and exceeded 3,000 with visitor attendance up by 14 per cent with an attendance of 1,515 compared to 1,350 the previous year
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
63 Volume 14.6 | HEALTH BUSINESS MAGAZINE
!Legionella, are you at risk? !
!Hydrosense is a breakthrough technology for the rapid detection
of legionella. Get accurate on-site results in 25 minutes!!
!
!
!Rapid -The worlds fastest test!On-site - No transportation of samples!Self test - No training required!Accurate - More accurate than lab tests!Control - Record and report with our Smartphone app !
!
Hydrosense - Know your risk0131 560 [email protected] !www.hydrosense.biz

Written by Susan Pearson, W
MSoc
Legionella
“There has been great public interest in the increasing incidence of Legionnaire’s Disease. Outbreaks have been reported in Europe, Australasia, the USA, as well as the UK. The reported causes of this disease range from bacteria in showerheads to spray from cooling towers, air conditioning systems and even contaminated drinking water. There is uninformed theory and discussion which has not, at present, led to firm diagnosis of the cause or remedy.” So said the December 1980 issue of ‘Waterline’, the newsletter of the Industrial Water Society (IWS), in a preamble on the major conference on Legionnaires’ disease that the then IWS was due to host in May 1981 in order “to put the facts as currently known before the public, industries associated with the problem and before the world press.” First set up in 1976 as the Cooling Water Association, the IWS paved the way in encouraging companies to think about water consumption, to look at water use within buildings and ensure used water was cleaned up before being discharged to the drains. The society set up some of the first training courses and meetings on water management
issues and ran definitive conferences, such as the one described above, on the emerging problem of Legionnaires’ disease.
WHAT IS LEGIONELLA?The Health & Safety Executive defines Legionellosis as a collective term for diseases caused by legionella bacteria including the most serious Legionnaires’ disease, as well as the similar but less serious conditions of Pontiac fever and Lochgoilhead fever. Legionnaires’ disease is a potentially fatal form of pneumonia and everyone is susceptible to infection. The bacterium Legionella pneumophila and related bacteria are common in natural water sources such as rivers, lakes and reservoirs, but usually in low numbers. They may also be found in purpose-built water systems such as cooling towers, evaporative condensers, hot and cold water systems and spa pools.
If conditions are favourable, the bacteria may grow increasing the risks of Legionnaires’ disease and it is therefore important to control the risks by introducing appropriate measures outlined in Legionnaires’ disease – The Control of Legionella bacteria in water systems (L8).
THE CURRENT PICTUREIn present day, the ‘Water Management Society’ (WMSoc), as the IWS has been known since 1998, still aims to raise the bar as a leading source of expertise on Legionella awareness and training. It has a strong role in producing new guidance and was a collaborator alongside the Health and Safety Executive and other organisations in the recent review of the L8 Approved Code of Practice (ACOP) on [Legionella] (fourth edition) and this year’s accompanying technical guidance HSG274. Today, WMSoc provides up-to-date
instruction on how to prevent Legionnaires’ disease within
various water systems, including cooling towers,
and provides a forum for connecting members to other professionals and statutory bodies within the water management industry. The society also has a strong
focus on prevention of other waterborne
infections such as Pseudomonas aeruginosa and
Stenotrophomonas maltophilia.
CONFERENCEWMSoc’s most recent conference ‘Fifty Shades of Water Management’ covered a wide range of practical aspects of water engineering. On the health side it provided
LEARNING ABOUT LEGIONELLAHealth professionals need to be aware of the risks that waterborne legionella bacteria can pose patients and hospital staff. Susan Pearson talks about the work the Water Management Society is doing to bring healthcare professionals up to speed
HEALTH & SAFETY
Legionnaires’ disease is a potentially fatal form of pneumonia and everyone is susceptible to infection
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
65 Volume 14.6 | HEALTH BUSINESS MAGAZINE

Water Safety Plans What do they mean to me?
Thursday 11th December 2014Royal College of Surgeons35-43 Lincoln’s Inn Fields, London WC2A 3PE
Water Safety Plans and the formation of Water Safety Groups and
Teams are integral to the latest UK legislation and guidances, not
only for hospitals, but throughout the entire worldwide water
delivery programme.
The speakers will deliver their global viewpoints and how lessons
learned from their own experience can benefit others in very
different industries.
Presentations include Water Safety Plans
from the WHO, cruise ship industry,
FM sector and hospital perspectives.
Chaired by Prof Christopher L R Bartlett
SPEAKERS:
Dr Susanne Lee, Leegionella Ltd
Dr Barbara Mouchtouri, University of Thessaly
Paul Nolan, Water Hygiene Ltd
Dr Mike Weinbren, Chesterfield Royal Hospital
George McCracken, Belfast Health and Social Care Trust
For the full programme and to book delegate and trade spaces visit www.wmsoc.org.uk/conferences.php
E: [email protected] T: 01827 289558
THE WATER MANAGEMENT SOCIETY
TRADE STANDS
AVAILABLE
£650 +vat
THE WATER MANAGEMENT SOCIETY
5 CPD points awarded
a focus for delegates to learn more about a variety of potential waterborne pathogens from Professor Kevin Kerr of the Harrogate and District NHS Foundation Trust and Hull York Medical School, while Dr Sam Collins from Public Health England looked at the advantages and limitations of rapid testing for Legionella bacteria in water samples. This referenced DNA-based polymerase chain reaction (PCR) methods and immunomagnetic, MALDI ToF (matrix assisted laser desorption ionisation time of flight), looking at the relationship between results obtained using rapid techniques and classic culture methods. A fruitful discussion noted that PCR can be used to detect dormant but live (viable but not culturable [VBNC]) bacteria that cannot be detected by culture, and noted that results can be produced in hours rather than the days required by culture. How cutting edge procedures can be compromised by poor hand washing, and how first risk assessments need to be carried out at the design stage rather than failing to consult infection control professionals at this stage, were just some of the topics covered during the conference’s workshops. Another Water Management Society conference late last year focused on the new Pseudomonas aeruginosa guidance in the HTM 04-01 Addendum, ‘Pseudomonas aeruginosa – advice for augmented care units.’ Speakers discussed the contribution to the guidance
of the most recent thinking, research and experience, including from leading plumbing product manufacturers, on minimising the risk of growth and spread of the organism in healthcare plumbing systems. The guidance’s publication in March 2013 followed the death, just over a year earlier, of three young infants in the neonatal intensive care unit (NICU) at Belfast’s Royal Jubilee Maternity Hospital (RJMH) from Pseudomonas aeruginosa-related infection. The source was subsequently identified as six hand washbasins.
MEMBERSHIPWMSoc draws its membership from water treatment suppliers, scientists, engineers, manufacturers, consultants and facilities managers from both the UK and overseas. As a not-for-profit organisation, the society offers its members a wide range of benefits including: City and Guilds accredited training courses, such as practical risk assessment including an extensive practical element and
a detailed study of the HSE’s Approved Code of Practice; further practical and technical training on responsible management of water in both the public and private sectors; specialist on-site training; conferences and national and regional events and seminars; and publications at reduced rates. The society produces a wide range of publications on managing Legionnaires’ disease in different systems and provides the latest industry news and guidelines in the quarterly ‘Waterline’ journal. This features technical papers and articles, current thinking in water management, products and systems, case histories and plant descriptions. As WMSoc member, independent water consultant Paul Nolan, Water Hygiene Ltd, says: “WMSoc membership brings a broad approach to developing skills in the water hygiene world. For me, membership is continual learning and knowing I can obtain answers to challenges from the vast experience of other members and the Society ‘Waterline’ journal.”
Legionella
WMSoc has a strong role in producing new guidance and was a collaborator alongside the Health and Safety Executive and other organisations in the recent review of the L8 Approved Code of Practice
HEALTH & SAFETY
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
67 Volume 14.6 | HEALTH BUSINESS MAGAZINE
Member
Water Testing
ALcontrol Laboratories - Confidence to Actwww.alcontrol.co.uk
Total Viable Count & Endotoxin Testing
In compliance with CFPP 01-06
Legionella TestingIn compliance with ACOP L8
Pseudomonas aeruginosa Testing
In compliance with HTM 04-01
Water testing performed atRotherham | Dunstable
Newton Abbot | Bellshill
For more information call us on
08450 738808 email us at
[email protected] visit our website at
www.alcontrol.co.uk
Providers of bespoke Water Treatment and Hygiene Solutions within Healthcare Premises:
Legionella Risk AssessmentsPseudomonas Assessments for Augmented
Care UnitsLegionella and Pseudomonas Awareness Training
CoursesDisinfections of domestic water systemsWater Treatment of Cooling Towers and Closed
Water SystemsAuditing of Legionella and Pseudomonas
control records All works carried out in accordance with HSC ACOP L8, HSG274 and HTM04-01.
Telephone 01732 838331Email [email protected]
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.668

NEXT EVENTThe Water Management Society’s next event will be ‘Water Safety Plans: what do they mean to me?’, which will be held on 11 December in London. Water Safety Plans and Water Safety Groups and Teams are integral to the latest UK legislation and guidance on Legionella and Pseudomonas. Speakers will include Dr Susanne Lee, former Director of the Health Protection Agency’s London Regional, Food Water and Environmental Microbiology Services Laboratory (LFWE) and co-director of the Legionella consultancy, Dr Mike Weinbren, Consultant Microbiologist at the Chesterfield Royal Hospital and George McCracken of the Belfast Health and Social Care Trust (BHSCT). Mr McCracken is the head of estates at the Belfast Trust and was responsible for delivering engineering solutions to address the immediate aftermath of the Pseudomonas aeruginosa incidents described above.
FURTHER INFORMATIONwww.wmsoc.org.uk
LegionellaHEALTH & SAFETY
Where does legionella come from and how do people get it?
Legionella bacteria are widespread in natural water systems, e.g. rivers and ponds. However, the conditions are rarely right for people to catch the disease from these sources. Outbreaks of the illness occur from exposure to legionella growing in purpose-built systems where water is maintained at a temperature high enough to encourage growth, e.g. cooling towers, evaporative condensers, hot and cold water systems and spa pools used in all sorts of premises (work and domestic). People contract Legionnaires’ disease by inhaling small droplets of water (aerosols), suspended in the air, containing the bacteria. Certain conditions increase the risk from legionella, for example, if the water temperature in all or some parts of the system is between 20-45 °C, which is suitable for growth, if the water is stored and/or re-circulated, or if there are deposits that can support bacterial growth providing a source of nutrients for the organism e.g. rust, sludge, scale, organic matter and biofilms. It is also possible for breathable water droplets to be created and dispersed e.g. aerosol created by a cooling tower, or water outlets.
The Water Management Society’s next event will be ‘Water Safety Plans:
what do they mean to me?’ Speakers will include Dr
Mike Weinbren, Consultant Microbiologist at the
Chesterfield Royal Hospital and George McCracken
of the Belfast Health and Social Care Trust (BHSCT)
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
69 Volume 14.6 | HEALTH BUSINESS MAGAZINE
Want to end the wait to see a GP?
Many debate, some despair, few decide.Find out today how our award-winning intervention turns your decision into action, in weeks.
Email Jonathan Ratcliff [email protected] or call 01509 816293.
gpaccess.uk
GP Access_HB14.6 - FP NEW.indd 1 19/11/2014 10:08

Best Practice 2014 saw 2,354 GPs, practice managers, primary care professionals and suppliers gather at the NEC in Birmingham on 22-23 October to get information on running their practices successfully, with increased effectiveness and improve patient outcomes through clinical training. Best Practice 2014 gave delegates hard-hitting practical advice on how to maximise practice income, reduce expenditure and referrals, as well as a ground-breaking look at the future of general practice, exploring the new shape of general practice within the NHS, and how to survive and prosper whilst maintaining the highest levels of patient care.
MESSAGE FROM THE TOPHealth Secretary Jeremy Hunt set out his ambitions for transforming primary care at the Best Practice Show. He explained how the Conservative party wants to transform GP care in the next Parliament in the way that hospital care has been transformed in previous decades. But his commitment to funding primary care and resolving the workforce crisis was challenged by delegates. Hunt said developing a new model of primary care which embraced integrated out of hospital care was a priority. In addition he said he wanted to see more innovation, greater use of technology and sharing of GP records which could reduce GP visits by 20 per cent and more care provided during evenings and weekends. CCGs needed to become accountable care organisations and there needed to be a new open and transparent culture with data about performance and peer reviews driving up standards. National Association of Primary Care (NAPC) co-chair Dr Charles Alessi challenged Hunt to reverse the decline in resources for primary care that he said had been slashed year on year. “Thank you for acknowledging that primary care is the solution to the difficulties we have at the moment… but we need your commitment actively here, in public, to
allow us to find the solutions together for the problems that we have –
we are all in this together.”“You absolutely have that commitment,” responded Mr Hunt, “why wouldn’t I want to support you, who have been at the forefront of so much innovation, in primary care for so many years? “ He admitted that high
profile targets for hospital care – the 18-week wait and
A&E targets – had sucked resources out of primary care.
“But you can’t go on expanding capacity in A&E because in the end you have to tackle the issues at source which is why we need to invest properly in primary care,” he said.
EVENT REVIEW
PRIMARY CARE BEST PRACTICEHealth Secretary Jeremy Hunt set out his ambitions for transforming primary care at October’s Best Practice Show
Best Practice 2014
Health
Secretary
Jeremy Hunt set
out his ambitions for
transforming
primary care at the
Best Practice
Show
Want to end the wait to see a GP?
Many debate, some despair, few decide.Find out today how our award-winning intervention turns your decision into action, in weeks.
Email Jonathan Ratcliff [email protected] or call 01509 816293.
gpaccess.uk
GP Access_HB14.6 - FP NEW.indd 1 19/11/2014 10:08
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
71 Volume 14.6 | HEALTH BUSINESS MAGAZINE
BESPOKE • BATCH • IMPORTS • SPECIAL OBTAINS
97.6% of orders delivered by 12pm the Next Day (99.6% by 2pm)
26.5% of customers enjoy MyIPS online ordering
Over 20,000 lines available, inc. over 1500 Imports & Special Obtains
earning your trust since 2001
Tel: 0800 644 0747 Fax: 0800 783 0305 Email: [email protected] Online: www.ipsspecials.com
CONTACT US TO DISCUSS HOW WE CAN IMPROVE YOUR SPECIALS SUPPLY

BESPOKE • BATCH • IMPORTS • SPECIAL OBTAINS
97.6% of orders delivered by 12pm the Next Day (99.6% by 2pm)
26.5% of customers enjoy MyIPS online ordering
Over 20,000 lines available, inc. over 1500 Imports & Special Obtains
earning your trust since 2001
Tel: 0800 644 0747 Fax: 0800 783 0305 Email: [email protected] Online: www.ipsspecials.com
CONTACT US TO DISCUSS HOW WE CAN IMPROVE YOUR SPECIALS SUPPLY
Best Practice 2014 saw 2,354 primary care professionals and suppliers gather at the NEC
EVENT REVIEW
Best Practice 2014 WORKFORCE CRISISDr Rosemary Leonard, GP and media medic, said: “We have a terrible crisis in the GP workforce. I am one of the many, many practices where we have had a GP leave because of burn-out at the age of only 49 and we have been unable to replace her. We have places left unfilled on the GP training programme and the answer to this has been to say to those of us who are left – you are going to have to work seven days a week from 8-8 and oh, everyone’s got to be a named GP, you are going to be made even more responsible for patients. That seems to me to be knocking us when we are really down and under stress.” Another GP who works in a “super practice” in Surrey which provides telephone consultations, told Mr Hunt: “Some days I feel like a glorified call centre operative and I am worried I am becoming de-skilled.” Hunt said the pressure on GPs could be reduced by introducing networked GP practices to provide more appointments during evenings and weekends and by reducing QOF targets and bureaucracy. He said he had recently visited some not-for-profit GP organisations in America which provided holistic care and this reduced emergency admissions and GP burn-out. “I am ambitious for change,” he declared. He said the NAPC was key to driving innovation in primary care: “I have always seen the NAPC as the innovators in the NHS, people at the forefront, people who want to
do things differently, but things that are true to the NHS values that we all believe in. You have been blazing a trail for a lot of ideas that are now becoming absolutely mainstream.”
PROGRAMME OVERVIEWThe Dispensing Doctors’ Association (DDA) held its annual conference at the Best Practice event. The session saw industry professionals debate the challenges to primary care delivery, such as dispensing practices in the wider primary care landscape, CQC updates and challenges for dispensing practices, and essential facts on controlled drug regulations. The event held high-impact CPD-accredited clinical updates for GPs with the very latest evidence and guidelines on a wide-range of core conditions seen in day-to-day practice. Topics covered included assessing for cognitive impairment in dementia, respiratory disease, diabetes, ophthalmology, CVD, dermatology, gastroenterology, mental health, sexual health and paediatrics. Practice Business and Plenary Sessions involved advice, case-studies and expert panels on finance, regulation, contract, workforce, practice management and policy matters of direct relevance to your practice.
Topics included the 2014/15 contract, NHS England’s Primary Care Strategy, online access and care data, and preparing your practice for a seven-day NHS. New-style CQC inspections, threats to practice profits, and the A&E crisis were also discussed in this stream. In the Transforming Primary Care programme, delegates were able to hear inspirational case studies from the pioneers of transformation and discover new solutions to the biggest barriers in providing excellence within patient care. Topics included personalisation and how and why it will radically change the doctor/patient relationship, and what can be learned from the Prime Minister’s Challenge Programme. The Best Practice Workshops allowed delegates to develop skills in an array of areas of general practice through real-life workshops, providing practical solutions that can be implemented instantly in your practice. Topics included survival tips for locums in the new primary care landscape, using social media in practice, and early diagnosis and patient management.
FURTHER INFORMATIONwww.bestpracticeshow.co.uk
Bray Group manufactures and supplies medicines, medical devices and pharmacy sundries in the UK and also has extensive experience of exporting to other countries. Bray Groups manufacturing facility is located in Faringdon, Oxfordshire. The company is licenced as a manufacturer by the Medicines & Healthcare products Regulatory Agency (MHRA) in the UK and registered with the FDA in the USA as a manufacturer. The company specialises in the production of Silver Nitrate products, such as the Caustic Pencils for removal of Warts & Verrucas. Typical customers include National Health Service, hospitals, clinics, wholesalers, distributors, retail pharmacies, medical practitioners and complementary therapists. Products manufactured include, Avoca silver nitrate Caustic Applicators and silver nitrate
caustic pencils, Portia vaginal ring pessaries, NIX styptic pencils, and Portia pessary sizing guide. Bray group also holds and supports pessary trainings days all over the country on the sizing and fitting of ring pessaries. All training is carried out by Urogynae nurse professionals. Training booklets and attendance certificates are supplied. Please visit our websites below for further product information.
FURTHER INFORMATIONwww.bray.co.ukwww.avocamedical.com www.portiapessaries.com
Manufacturing healthcare solutions in the UK
University Hospitals Coventry and Warwickshire NHS Trust have utilised Docman’s electronic document transfer solution Docman Hub to send over 1 million patient letters electronically to GPs. The Trust reports a saving of around 50 pence for each patient letter sent, with further additional time savings for the Trust and Primary Care by removing the processes of handling paper. Mark Walker, Clinical Results Reporting manager said: “UHCW sends patient letters in real time to GP practices. Our previous process was to send paper letters to our GP colleagues; this was a costly and time consuming method”. Colin Sweeney, director of IT at King’s College hospital said: “When a patient is first referred to us, Docman RMS allows us to ensure patients are booked
into the right clinics without paper letters or faxes. It also gives us a full audit trail of the referral process, so that when patients ring the hospital we know where the referral is in the pathway. Previously, that would have meant hunting through piles of letters on desks.” Docman is a leading supplier of electronic document management, transfer and collaboration solutions for primary, secondary and social healthcare organisations. Docman GP is now centrally funded and available through GPSoC.
FURTHER INFORMATIONwww.docman.com
Electronic document management solutions for healthcare organisations
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
73 Volume 14.6 | HEALTH BUSINESS MAGAZINE

Park
ing
Following guidelines from the Department of Health in August, hospitals have been told to provide free, reduced, or capped parking charges to ‘priority groups.’ These include visitors with relatives who are seriously ill or are in hospital for a long time and frequent outpatient visitors. People with disabilities, including those that have temporary disabilities, should also qualify for reduced rates. Hospital parking policies are set by individual NHS trusts, and the guidance says that charges should be reasonable for the area. Some hospital staff, for example, those working shifts and unable to get public transport, should have slashed rates and other concessions should be considered locally for staff, such as for volunteers or staff who car-share. Priority for staff parking should be based on need, such as staff whose daily duties require them to travel by car. Such staff might also include nurses or therapists who visit patients at home. The guidance also suggests that routine travel between hospital sites might more sensibly be managed by providing internal transport.
PAY FOR THE TIME USEDThe Department for Health’s guidelines recommend hospitals should use pay-on-exit or similar schemes so car park users pay only for the time they use in a hospital car park. Additional charges should only be imposed where reasonable and should be waived when overstaying is beyond the driver’s control, such as when treatment takes longer than planned, or when staff are required to work beyond their scheduled shift. Jeremy Hunt, the health secretary, said: “Patients and families shouldn’t have to deal with the added stress of unfair parking charges. These clear ground rules set out our expectations and will help the public hold the NHS to account for unfair charges or practices.”
KEEP EVERYONE INFORMEDThe guidelines say that NHS trusts should make their parking policies and principles clear. Details of charges, concessions and additional charges should be well publicised including at car park entrances, wherever payment is made and inside the hospital. They should also be included on the hospital website and on patient letters and forms, where appropriate.
Information that NHS trusts should publish includes their parking policy; their implementation of the NHS car parking principles; financial information relating to their car parking; and summarised complaint information on car parking and actions taken in response. The Department of Health guidance has also made it clear trusts were responsible for the actions of private car parking contractors running facilities on their behalf. It said that NHS organisations should act against rogue contractors in line with the relevant codes of practice where applicable, and that contracts should not be let on any basis that incentivises additional charges, such as ‘income from parking charge notices only’. There are two trade associations – the British Parking Association and the Independent Parking Committee, which makes sure their members follow a code of conduct and provides an appeals service for motorists. The guidelines say that NHS organisations should consider imposing a requirement for contractors to be members of such an association.
FAIRER PARKINGMacmillan Cancer Support conducted research into the full cost of hospital parking in England, concluding that “cancer patients face a lottery in the price of hospital parking and the availability of discounts,” with some hospitals offering completely free parking, while others charge anything from £2 to £24 a day. It found that the average daily cost of using a hospital car park is £7.66. The research found that despite existing government guidance, 59 per cent of hospitals in England are still charging at least some cancer patients to use the car park, and almost 10 per cent of hospitals in England have ignored government guidance completely and continue to charge cancer patients the full price for parking. Duleep Allirajah, head of policy at the Macmillan, explained the problem: “The core principle of the NHS is to provide free healthcare for all at the point of access. But sadly some cancer patients in England are paying extortionate hospital car parking
charges in order to access
treatment for a life-threatening illness.
“Cancer patients receiving vital treatments
such as chemotherapy and radiotherapy will often need to make frequent trips to hospital and unaffordable charges are leaving many out of pocket.” Welcoming the Department for Health’s guidance, Allirajah went on to say: “Macmillan Cancer Support is pleased the Government has recognised this as a problem and has issued new guidelines advising hospitals to offer concessions, including free or reduced charges or caps for people with disabilities such as cancer. “Hospitals must not ignore Government guidance and commit to implementing the guidelines as a matter of urgency so that cancer patients do not continue to pay unfair hospital parking charges.” A spokesperson from the watchdog Healthwatch England, said that said: “The key will be making sure the public are aware of the changes so that they can challenge the system when they feel they are facing unfair charges. “The new rules will hopefully offer much-needed support for those who have to visit hospitals regularly, either for treatment or in support of a loved one receiving care.”
FURTHER INFORMATIONtinyurl.com/ny36o4d
GOVERNMENT GUIDELINES
A FAIRER HOSPITAL PARKING SYSTEMHospitals in England have been told to offer free, reduced or capped parking charges for certain groups under new government guidelines. Health Business summarises the new guidance
The guidelines
recommend
hospitals should use
pay-on-exit or similar
schemes so users
pay only for the
time the use
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.674

Parking
Call: 01604 696 800Visit: www.workflowdynamic.com Email: [email protected]
Helping you manage your parking efficiently
• Permitprocessing• Onlineapplicationprocessing•Mobileenforcement• Enforcementprocessing• Appealsandmailhandling• Internetpayment• Youretainallticketrevenue• Payperuse• Nocapitalexpenditure
DynamicParkingManagement
1st Stop Recruitment, founded by Lesley Whiting in 2002, has 27 years’ experience in the industry. After receiving formal training with a national agency, the company has become a leading recruiter in the Haverhill area. 1st Stop Recruitment is proud to offer a unique concept in recruitment and the company’s unrivalled experience and recruitment knowledge, teamed with its membership to the UK’s largest recruitment network makes 1st Stop Recruitment the obvious choice for local and national recruitment. The company works extremely closely with clients in all aspects of the recruitment process often reducing the time and cost. The company’s aim is to make recruitment as seamless as possible, leaving you to get
on with what you do best. 1st Stop Recruitment’s mobile-friendly website gives clients the opportunity to keep in touch any time and offers a scanner for mobile link to the web page. In November 2013, 1st Stop Recruitment was approved a GLA Licence enabling the company to further develop its business in a new sector. Licence no: STST00002.
FURTHER INFORMATIONTel: 01440-763021info@1ststoprecruitment.co.ukwww.1ststoprecruitment.co.uk
1st Stop Recruitment – a leading local and national recruitment provider
75 Volume 14.6 | HEALTH BUSINESS MAGAZINE

patients, releasing time to be spent on care activities rather than processes.
TRACKINGHydration is a key part of patient health, and goes hand in hand with the standards put forward. The Patient Feedback solution from Hospedia has been designed to provide hospitals with valuable real-time data regarding patient hydration. A Fluid Intake Tracker asks patients to identify how much liquid they have consumed on a given day, giving frontline staff a clear indication of where hydration issues may be present. This solution is mirrored by the associated Plate Waste Tracker. Reducing food wastage is a real priority, and asking patients to provide details of the estimated proportion of their meal that was consumed provides hospital staff with valuable data about waste and consumption. Combined with a Catering Satisfaction Survey, which allows patients to provide wider feedback about their meal experiences, staff can easily monitor adherence to the new nutritional standards.
A UNIFIED APPROACHTying together the available technologies supports hospitals in managing and monitoring compliance with the new standards, providing valuable data and reducing the time spent on processes. The aim of the standards is to improve patient care without creating an impossible burden for hospital staff; bedside technology ensures that hospitals can meet those standards quickly and cost-effectively, saving both time and money.
FURTHER INFORMATIONwww.hospedia.co.uk
The responsibility of hospitals to provide the highest level of care for their patients is a fundamental principle of the NHS, and new legally binding standards for nutrition and hospital food are to be introduced following the recommendations of the Hospital Food Panel. NHS hospitals must develop and maintain a food and hydration strategy that includes the nutrition and hydration needs of patients, healthier eating for the whole hospital community and sustainable procurement of food and catering services. The impact of these newly legislated standards will vary across the NHS, although existing technology capabilities can reduce the potential burden of managing and monitoring the required improvements.
BACKGROUNDThe Hospital Food Panel, set up by Dr Dan Poulter, Parliamentary Under Secretary for Health, was tasked with examining existing food standards and advising on how they should be applied, monitored and improved. The aim of the Panel was not to create a host of new standards, but to identify relevant existing standards that could be brought together, making it easier to commission,
provide and monitor food service. However any changes to how standards are viewed and measured will result in some level of process disruption, and utilising available technology will be a valuable way of meeting the new requirements while focusing on providing a better patient experience. Electronic Meal Ordering and Menu Display solutions, from point-of-care specialist Hospedia, are already supporting a number of hospitals in streamlining their catering processes, providing improved choice to patients and reducing cost and wastage. The solutions have a variety of features that align closely with the new standards. Other electronic solutions from Hospedia, including Patient Feedback and Patient Flow Management, provide hospitals with further tools to manage patient nutrition and hydration more generally.
STARTING FROM THE POINT OF ADMISSIONManaging patient nutrition begins at the point of admission. Identifying patients at risk of malnourishment is a key part of the new standards; such patients represent longer hospital stays and increased likelihood of complications during recovery. Once a patient has been flagged as malnourished following their admission assessment, it is vital that this information is accessible and up to date across care teams and catering services. Such information can be loaded into a hospital’s Patient Flow Management solution, to be immediately transmitted into the hospital’s PAS, patient notes and other computer systems, ensuring that all members of the care team associated with that patient have accurate, up to date information about the patient’s nutritional needs and can continue to monitor and update the patient status as necessary.
MEETING INDIVIDUAL NEEDSPatients at risk of malnutrition require additional calories within a small portion size. The new standards support both those patients and those who are managing obesity or related disorders
through reducing calorie intake. Catering staff and dieticians are starting to move away from the terminology ‘healthy eating’, with its implications of restricted-calorie diets, instead using the term ‘eating for health’ to describe the need for a therapeutic diet that is tailored to the individual. With the focus on tailoring meal choices to each patient’s needs, traditional ordering processes using paper menus will become more laborious and time consuming, requiring staff to individually inform patients of the restricted selections they are able to make from the master menu. Within the Hospedia Electronic Meal Ordering solution, the available selections can be tailored; patients are only presented with the choices suitable for them. Staff are not tasked with managing complex requirements for a ward of
CATERING
ACHIEVING NEW CATERING STANDARDS With new standards for nutrition and hospital food due to be introduced, NHS hospitals will be required to develop and maintain a food and hydration strategy tailored to individual patient needs
NHS hospitals must develop and maintain a food and hydration strategy that includes the nutrition and hydration needs of patients
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.676

New information is constantly coming to light that demonstrates the importance of good nutrition in helping people stay healthy for longer. In an ideal world this attention to balanced diets and well prepared meals would be nowhere more evident than in healthcare environments, where people depend on medical intervention to recover from illness and fight for their lives, but unfortunately this has not always been the case. Unappetising ward dinners are the stuff of grim folklore, and the data has borne out an unimpressive level of satisfaction with what is on offer in many hospitals – while a 2011 poll of NHS staff found that 98 per cent rated their hospital’s food offering as “good” or “excellent”, a survey of 64,000 patients carried out last year by the Care Quality Commission found that only 55 per cent felt the same. Around the time the second survey was published, Alex Jackson of the Campaign for Better Hospital Food issued a statement echoing the concerns of many, saying: “It is time for the government to come clean about
the sorry state of hospital food in England and set mandatory standards for patient meals. “This would only involve extending an existing policy which has seen it set mandatory standards for prison food and food served in government departments, to go alongside those that already exist for school food. Surely patients recovering in hospital have the same right to good food as government ministers, school kids and prisoners?” Calls for better service in this area go back some time, and the studies have mounted up over the years showing that the UK has traditionally underperformed, one finding that 60 per cent of all hospital meals contain more salt than a Big Mac. Although millions in public spending has been thrown
at the problem, complaints persist. Secretary of State for Health Jeremy Hunt recently approved a raft of measures designed to
tackle the issue – what are they and do they go far enough?
NEW MEASURESBack in August, the Department of Health reported on two new policies it was implementing as part of a wide-ranging drive to guarantee that
hospitals throughout the UK offer high quality,
nutritious meals to patients, visitors and staff. As a result of
these measures, hospital catering will be subject to legally binding food
standards that address dietary requirements and sustainable food procurement, and all hospitals will be ranked according to the quality of their food provision.
NEW STANDARDS
SERVING BETTER HEALTH ON A PLATEA raft of new measures introduced by the Department for Health will see hospitals held to strict catering standards, with poorly performing institutions named publicly. Health Business reports
Catering
Studies
show that the
UK has a history
of underperforming.
One found 60 per
cent of hospital meals
contain more salt
than a Big
Mac
77 Volume 14.6 | HEALTH BUSINESS MAGAZINE

Quality ingredients & service... Naturally!InterspiceBosse
www.bosse-interspice.co.uk
Formulated without wheat flour, our sponge mixtures produce such light and tasty results that no one will ever guess are completely GLUTEN FREE.

Quality ingredients & service... Naturally!InterspiceBosse
www.bosse-interspice.co.uk
Formulated without wheat flour, our sponge mixtures produce such light and tasty results that no one will ever guess are completely GLUTEN FREE.
This Government crackdown on poor quality hospital food came about after a report carried out by the Hospital Food Standards Panel made a number of recommendations, saying that the government needs to enforce five existing standards out of a potential fifty. The panel collaborated with professional organisations including royal colleges and nutritional experts to produce the report, which aims to help hospitals approach the issue in a more targeted way and penalise those that fail to. The authors write in their introduction that the way hospitals feed patients must take into account the UK’s worrying health statistics, pointing to that fact that 62 per cent of adults are overweight or obese and that many patients are “dealing with illness brought on by overconsumption.” VISIONSetting out their vision for hospital catering, the authors of the report say that it “should complement the patient’s care and enhance their stay. It should help staff and visitors choose a healthier lifestyle and it should support our economy and protect our environment. Hospital food can – and should – be a vehicle for improvement and a role model for food in the local community. Crucially, it should also be a source of pleasure and enjoyment. “Many hospitals provide food and drink
that demonstrates these ideals in action. But some struggle to deliver on one or more aspects, and variation across the country is too great. The NHS has a full array of catering services from on-site cooking to bought-in/delivered meals and from NHS employed staff to contract caterers. All are capable of delivering excellent food. Equally, all can
fail if they are not implemented properly.”Jeremy Hunt welcomed the report and its recommendations, saying: “We are making the NHS more transparent, giving patients the power to compare food on wards and incentivising hospitals to raise their game. Many hospitals are already offering excellent food to their patients and staff. But we want to know that all patients have nourishing and appetising food to help them get well faster and stay healthy, which is why we’re introducing tough new mandatory standards for the first time ever.”
ADOPTED STANDARDSThe first required standard for patient catering that is to be included in the NHS Standard Contract (making its adoption compulsory in all hospitals) is Nutrition Alliance’s 10 key characteristics of good nutritional care. The Alliance says that all healthcare service users should be screened
to identify whether they are malnourished or at risk of becoming malnourished, and that any nutritional care needs must be incorporated into their care support plan. Another listed characteristic of positive care is that hospital personnel are competent to meet patients’ needs and that they receive ongoing training to improve their skills. The report cites Royal Liverpool University Hospital as an example of this standard being used successfully. Recognising that routine meal times don’t work for all patients, staff reflected
“We are making the NHS more transparent, giving patients the power to compare food on wards and incentivising hospitals to raise their game”Jeremy Hunt
CateringNEW STANDARDS
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
79 Volume 14.6 | HEALTH BUSINESS MAGAZINE

SV 0951 Health Businesss November Hospital Testimonial V4.indd 1 06/11/2014 17:13

Public Health England’s Healthier and More Sustainable Catering – Nutrition Principles is the standard adopted by the panel for staff and visitor catering, and is to be applied as appropriate for patient catering
CateringNEW STANDARDS
on the 10 Key Characteristics and came up with a call order service that led to improved levels of patient satisfaction. The second standard is the British Dietetic Association’s Nutrition and Hydration Digest, which provides dietitians, clinicians and caterers with a toolkit to help them manage the needs of patients. This takes into account issues like patient safety and guidelines on how food should be delivered so that patients receive an “adequate overall intake” for key nutrients over the course of their stay. The implementation of this standard has been effective in Leeds Teaching Hospital NHS Trust. A review of the menu for older patients led to smaller, nutrient-meals being served at lunchtime, which is supplemented with an afternoon tea service. BAPEN’s Malnutrition Universal Screening Tool (MUST) allows healthcare professionals to assess in five steps whether malnutrition or obesity could play a role in illness as presented by patients. The tool includes quality frameworks for nutritional care and assessment criteria to monitor performance, and gives management guidelines to help coordinate patients’ diet plans according to their level of medical risk. The report gives the example of Poole Hospital NHS Foundation Trust. The Trust tasked nutrition nurse specialist Debbie Thompson with improving MUST nutrition screening. While a low rate of compliance (24 per cent) with the malnutrition screening measure was identified in 2011, the Trust’s efforts have in this area have led to a 96 per cent screening rate in 2014 – the vast majority taking place within 24 hours of admission. Public Health England’s Healthier and More Sustainable Catering – Nutrition Principles is the standard adopted by the panel for staff and visitor catering, and is to be applied as appropriate for patient catering. This publication gives a breakdown of average nutritional requirements by age as well as by population group – for example, individuals of African, African-Caribbean and South Asian descent may be at risk of Vitamin D deficiency, which should be recognised in their food plan. Bolton Hospital NHS Foundation Trust followed these suggestions to limit the impact of unhealthy foods on offer, for example by restricting high-sugar drinks to small portion sizes of no more than 330ml. Finally, Defra’s Government Buying Standard for Food and Catering Services “goes beyond production standards, resource efficiencies and nutrition helping provide a comprehensive tool for setting technical specifications and evaluating bids.” Hull and East Yorkshire Hospitals NHS Trust met this standard through effective engineering of their menus, for example by developing a range of energy-dense and dysphagia meals for nutritionally vulnerable patients.
RANKINGMeanwhile, a new inspection regime will see hospitals ranked by the quality of their
food, with results made available on the NHS Choices website for patients to see. The first set of assessments published by the DoH found that the Alastair Farquehar Centre in North East London and Witney Community Hospital in Oxford were among the worst performing in the country. Professor Edward Baker, deputy chief inspector of hospitals at the Care Quality Commission, said: “It’s really important for patients to have access to good quality food based on their own needs. “During our inspections, we speak to
patients and check records to ensure patients are receiving the right food for their individual needs. Our findings determine which hospitals need closer inspection of their food practices.”
RESPONSEWhile many are hopeful that the enforcement of these recommendation in the NHS Standard Contract will lead to an improved service, some feel that these measures do not go far enough. Alex Jackson of the Campaign for Better Hospital Food said that the government is “pulling the wool over our eyes,” saying: “We want to see hospital food standards set down in legislation, similarly to school food standards, and therefore universally applied to all
hospitals and protected by publicly elected representatives for generations to come. “But the government still refuses to do this and has only committed to including the standards in NHS commissioning contracts, which are long documents full of clauses that without proper enforcement and monitoring can be ignored by hospitals. “The government may have inserted a new clause in a legal document, but that won’t be what most people consider to be legally-binding. It’s woefully inadequate.” Meanwhile, shadow public health
minister Luciana Berger claims that Hunt has made a serious miscalculation in failing to ask patients how they would like the situation to change, adding: “Everyone wants to see the quality of hospital food improved, but without proper enforcement there is a risk that these new standards will simply be ignored.” In response to these criticisms, Hunt told the BBC that hospital compliance would be “treated very seriously” and said: “All of this is about looking after patients in the same way you would want your own friends or you own family to be looked after.”
FURTHER INFORMATIONtinyurl.com/oenbh3u
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
81 Volume 14.6 | HEALTH BUSINESS MAGAZINE

Prod
uct P
rofil
es
The Recruitment & Employment Confederation (REC) is the professional body for the recruitment industry. The REC represents 3,349 corporate members who have branches across all regions of the UK. In addition, the REC represents 5,759 individual members within the Institute of Recruitment Professionals (IRP). All members must abide by a code of professional practice. Above all, the REC is committed to raising standards and highlighting excellence throughout the recruitment industry. The REC breaks down its membership into specialist niche sectors, and the REC Health and Social Care Sector Group provides specialist support and advice to agencies who work across the health and social care space. Members include agencies that recruit nurses, locum doctors, allied health professionals, carers, social workers and clerical staff for the National Health Service and local authorities.
The health and social care sector faces some serious challenges, not least an ageing workforce, ever-tighter public sector budgets and a drive for efficiency in all public procurement frameworks. Through the REC Health and Social Care sector group, it is critical that we demonstrate the central role that the recruitment industry plays in providing a flexible, skilled workforce where and when it is needed. The REC represents the recruitment industry on the NHS Employers National Agency and Temporary Staffing Strategic Forum, the Department of Health’s National Procurement Council and the Local Government Association’s Employer Standards Advisory Group.
FURTHER INFORMATIONwww.rec.uk.com
REC – representing the recruitment industry
Swallow EMP are specialists in mobility aids that assist with moving wheelchair users and people with limited mobility up and down flights of stairs in a variety of environments including healthcare and education. The company is owned by Greg and Julia Pons who pride themselves on supplying the correct solution. When approached by a client they check the stairs and landings at the building and if it is for a wheelchair user, they check that the wheelchair and the stair climber are compatible and that the wheelchair user is happy with the proposed solution. SwallowEMP have stair climbers for people who are in wheelchairs or people with limited mobility, there are powered and non-powered designs for use on straight, spiral and flared stairs. The powered units go both up and down stairs
so can be used to cover access, egress and evacuation, and also lift break downs or outages. Simplicity and safety and reducing manual handling are the keys with the product range. SwallowEMP also supply stair climbers that take goods up and down stairs. Contact Swallowemp to find out about the options available to improve access, egress and evacuation.
FURTHER INFORMATIONTel: 0121 366 [email protected]
Swallow Evacuation & Mobility Products – offering people a choice
YPO is the UK’s largest publicly owned buying organisation, wholly owned by 13 local government member authorities and an expanding list of associate member authorities across the wider public sector. Established in 1974 as a Joint Committee of local authorities, YPO aggregates the procurement spend of its customers to drive efficiency savings for the public sector through its bulk buying power for supplies and contract services. YPO has a vision that every single public organisation achieves the best possible value for money when procuring its goods and services. Over the past four decades, YPO has worked tirelessly to help its customers make the best use of their ever squeezed budgets. From schools and charities to the NHS and emergency services, the organisation works across the entire public sector. The organisation has consistently returned its profits
to the public purse, giving back £105 million to date. YPO collaborates with competitor buying organisations, central government departments and industry bodies to help drive further efficiency savings for the benefit of the public sector. In 2014, YPO achieved ‘Best Public Procurement Project’ at the CIPS Supply Management Awards for its work with partner procurement organisations in establishing the RM958 Insurance Services framework agreement.
FURTHER INFORMATIONTel: 01924 834 [email protected]
Achieve the best possible value for money with YPO
PCMG is the leading provider of energy cost recovery services for NHS Trusts. The company can help you to meet your savings targets, or generate revenue to re-invest into energy efficiency initiatives. PCMG works with you to identify and secure cost recoveries and savings within your historical electricity, gas and water expenditure. The company operates on a contingency fee basis, which means that working with PCMG is without any risk or initial financial outlay. In addition to being cost recovery experts, the company has some of the UK’s leading expertise in non-commodity electricity and gas costs, such as network charges and environmental taxes. PCMG is the only cost consultant actively involved in energy network policy, and in recent years its unique regulatory policy work has resulted in millions of pounds being returned to its clients. In the past three years, PCMG has recovered £9.7
million for 129 NHS Trusts with success stories including: East and North Hertfordshire NHS Trust: £400,000; Royal United Bath NHS Trust: £202,000; Central Manchester University Hospitals NHS Foundation Trust: £262,000; Dartford & Gravesham NHS Trust: £54,000. Services can be accessed via public sector frameworks including NHS Shared Business Services [ref SBS/12/SG/ZMF/8296/08] and NHS Commercial Alliance [ref 2012004NC].
FURTHER INFORMATIONTel: 01253 361 600www.pcmg.co.uk
Energy cost recovery services for the NHS
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.682

We’re used to being faced with bad news about the NHS in the national media, with stories on medical errors and budgetary issues clocking up column inches on a regular basis. As a result, the good news coming from the people working tirelessly to care for the nation can sometimes receive less attention. To help set right this balance, the Health Business Awards come to Grange St. Paul’s Hotel in London this December to recognise those who strive to raise standards in the NHS.
This year’s ceremony is to be hosted by Dr Sarah Jarvis, an Oxford-trained GP who is familiar on our screens as the health and medical reporter for BBC’s The One Show. In addition to her media activities and her work for the West London practice where she has been based for
EVENT PREVIEW
REWARDING EXCELLENCEThe Health Business Awards take place on 4 December 2014 and will showcase the success stories in the health sector
Health Business Awards
over 20 years, Sarah has been the Women’s Health spokesperson for the Royal College of General Practitioners and chair of the Health Care Committee of the cholesterol charity HEART UK.
This year marks the inclusion of a new category, the Clinical Commissioning Award, sponsored by Medibooks. This award recognises the efforts of clinical commissioning groups (CCGs) to make the right decisions for patients in their local area. Nominees include: NHS West Cheshire CCG, whose Hospital@Home visit scheme has boosted patient satisfaction and saved £2.9 million through reducing hospital stays; NHS Bedfordshire CCG, who worked with local pharmacies to offer an enhanced service for diabetics; and NHS Crawley CCG, who helped to establish ‘Dementia Friendly Crawley’.
Health Business Awards 2014: the other shortlistsAIR AMBULANCE SERVICE OF THE YEARDorset and Somerset Air AmbulanceMidlands Air AmbulanceWales Air Ambulance East Anglian Air AmbulanceKent, Surrey & Sussex Air Ambulance
AMBULANCE TRUST OF THE YEARWest Midlands Ambulance ServiceNorth West Ambulance Service NHS TrustYorkshire Ambulance ServiceClinical Commissioning Award (sponsored by Medibooks)Chorley and South Ribble CCG / Greater Preston CCGNHS West Cheshire CCGNHS Bedfordshire CCGNHS Crawley CCGWarrington CCG
ENVIRONMENTAL PRACTICE AWARDEstates and Facilities Innovation Award (sponsored by Swallow Evacuation & Mobility Products)North Bristol NHS Trust: Hospital Move projectColchester Hospital University NHS Foundation Trust: Heat Recovery System Birmingham Childrens’ Hospital NHS Foundation Trust: Transport Booking / Patient meals systems
HEALTHCARE IT AWARDNHS Central Southern Commissioning Support UnitSt George’s Healthcare NHS TrustWrightington, Wigan and Leigh NHS Foundation TrustLiverpool Community Health NHS TrustUniversity Hospitals Birmingham NHS Foundation Trust
HEALTHCARE RECRUITMENT AWARD (SPONSORED BY THE RECRUITMENT & EMPLOYMENT CONFEDERATION)NHS Leadership AcademySandwell and West Birmingham Hospitals (SWBH) NHS TrustPlymouth Hospitals NHS TrustHospital Building Award (sponsored by Decorative Panels)Morgan Stanley Clinical Building: Great Ormond Street Hospital
Finchley Memorial Hospital (Central London Community Healthcare NHS Trust)Brunel Building: Southmead Hospital (North Bristol NHS Trust)Richard Desmond Childrens Eye Centre: Moorfields Eye Hospital NHS Foundation Trust
HOSPITAL CATERING AWARD (SPONSORED BY BOSSE INTERSPICE)Pennine Acute Hospitals NHS TrustSalisbury NHS Foundation Trust Sheffield Teaching Hospitals’ NHS TrustNottingham University Hospitals NHS TrustPrincess Alexandra Hospital NHS Trust
INNOVATION IN MENTAL HEALTH AWARD (SPONSORED BY ERS MEDICAL)Pennine Care NHS Foundation Trust: Flo telehealth text / Healthy MindsNorth East London NHS Foundation Trust: Coping Through Football Barnet, Enfield and Haringey Mental Health NHS Trust/Metropolitan Police Service: Fixated Threat Assessment Centre (FTAC) teamBirmingham and Solihull Mental Health NHS Foundation trust: ADHD/Smartphone app development projectsNottinghamshire Healthcare NHS trust: anti-stigma film
NHS COLLABORATION AWARD (SPONSORED BY YPO)Chorley and South Ribble CCG / Greater Preston CCG: Improvements to A&EOxleas NHS Foundation Trust / Greenwich CCG: Integrated Health & Social CareEast Lancashire Hospitals NHS Trust / Lancashire Constabulary: A&E Liaison Leicestershire Partnership NHS Trust: Health & Hate CrimesCardiff and Vale University Health Board: Alcohol Treatment Centre
NHS PUBLICITY CAMPAIGN AWARDNorth West Ambulance Service NHS Trust:#Team999Public Health England: Toxic Cycle anti-smoking campaign
NHS West Suffolk CCG: Emergency Department Cinema Campaign
OUTSTANDING ACHIEVEMENT IN HEALTHCARE (SPONSORED BY AUSTCO)Frimley Health NHS TrustRoyal Brompton & Harefield NHS Foundation TrustRoyal National Orthopaedic Hospital NHS TrustWest Midlands Ambulance ServiceWest Suffolk NHS Foundation Trust
PATIENT DATA AWARD (SPONSORED BY CCUBE SOLUTIONS)Milton Keynes Hospital NHS Foundation Trust: EDRM systemNottinghamshire Healthcare NHS Trust: Electronic Integrated Care Pathway (e-ICP)North West Ambulance Service NHS Trust: Electronic Referral Information Sharing System Liverpool Heart and Chest Hospital NHS Trust: EPR/backup system
PATIENT SAFETY AWARD (SPONSORED BY PENTLAND MEDICAL)Salford Royal NHS Foundation TrustNorthumberland, Tyne and Wear NHS Foundation TrustGreat Ormond Street Hospital Foundation NHS TrustYeovil District Hospital NHS Foundation trust
TELEHEALTH AWARD (SPONSORED BY CCUBE SOLUTIONS)East London NHS Foundation Trust: Telehealth EU accreditationStoke on Trent Clinical Commissioning Group/ PartnersBridgewater Community Healthcare NHS Trust/ Bristol City Council: Reablement Service
TRANSPORT & LOGISTICS AWARD (SPONSORED BY SAFER PARKING SCHEME)St Helens and Knowsley Teaching Hospitals NHS Trust and New HospitalsUniversity Hospitals Birmingham NHS Foundation Trust Royal Bournemouth and Christchurch NHS Trust
On the shortlist for the Outstanding Achievement in Healthcare Award, sponsored by Austco, are organisations such as: Frimley Health NHS Trust in Surrey, the first Trust to be rated ‘Outstanding’ in the new Care Quality Commission standards; West Midlands Ambulance Service, whose radical new approach to trauma care has saved resulted in an additional 81 survivors than was first projected; and the Royal National Orthopaedic Hospital NHS Trust, where a new osteoarthritis screening technique and integrated patient care model have helped to transform patient experience.
FURTHER INFORMATIONhbawards.co.uk
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
83 Volume 14.6 | HEALTH BUSINESS MAGAZINE

You know Pinpoint as the leading supplier of Sta� Personal Alarm Systems, but we
can do much, much more for you.
For further information telephone Simon Hemming on01333 421706 or email [email protected]
We would very much welcome the opportunity TODAY to discuss what more Pinpoint can do for you.
Pinpoint can provide, integrate and support...
....throughout Great Britain and Ireland
Disabled Refuge AlarmsCCTVDoor Entry SystemsIntruder Alarm SystemsPatient Movement Detection SystemsFire Alarm SystemsEnvironmental Monitoring SystemsANPR
Pinpoint Sta� Personal Alarm SystemsPinpoint Patient CallNurse Call SystemsVoice CommunicationDrugs Cupboard AlarmsPaging SystemsAccessible Toilet AlarmsAccess Control SystemsPerimeter Detection
www.pinpointlimited.com
YOUR NEEDSOUR PRIORITY
®

You know Pinpoint as the leading supplier of Sta� Personal Alarm Systems, but we
can do much, much more for you.
For further information telephone Simon Hemming on01333 421706 or email [email protected]
We would very much welcome the opportunity TODAY to discuss what more Pinpoint can do for you.
Pinpoint can provide, integrate and support...
....throughout Great Britain and Ireland
Disabled Refuge AlarmsCCTVDoor Entry SystemsIntruder Alarm SystemsPatient Movement Detection SystemsFire Alarm SystemsEnvironmental Monitoring SystemsANPR
Pinpoint Sta� Personal Alarm SystemsPinpoint Patient CallNurse Call SystemsVoice CommunicationDrugs Cupboard AlarmsPaging SystemsAccessible Toilet AlarmsAccess Control SystemsPerimeter Detection
www.pinpointlimited.com
YOUR NEEDSOUR PRIORITY
® Written by Jam
es Kelly, British Security Industry Association (BSIA)
Physical assaults against health service staff is a significant problem. For the year 2012-13, physical assaults against NHS staff in England were shown to have risen from 59,744 in 2011-12 to 63,199 in 2012-13, according to figures collated from NHS Trusts across the UK. Some healthcare staff are, of course, more at risk than others. Those who work in isolation, or out in the community, are at particular risk, and employers across the healthcare sector
should be committed to the development and implementation of a comprehensive lone worker policy to protect these employees, and the organisation at large. Such ‘lone working’ is commonplace in the health sector, with a 2012 study by the Royal College of Nursing revealing that more than 60 per cent of community nurses spend more than half their time as lone workers without immediate access to a colleague for
support. Over 70 per cent of respondents to this survey also reported that they had been subject to either physical assault or verbal abuse during the course of their jobs in the two years prior to the study.
LONE WORKER DEVICESThankfully, the use of lone worker devices by many NHS Trusts and private healthcare firms is helping to alleviate this situation. Working alongside their clients in the healthcare sector, several members of the British Security Industry Association have developed highly-effective lone worker devices, which are equipped with mobile phone type GSM technology to connect employees quickly and discreetly with an emergency response system that has direct links to the police. In fact, a number of products are now commercially available from BSIA member companies, including the Reliance Protect solution used largely across
Video Content Analysis can be used to automatically detect an intruder, or to count the number of people entering or leaving an area – beneficial, for instance, for keeping track of how many people have entered or left an emergency room during a given period of time
COMBATING THREATS TO HEALTHCARE STAFFFrom an increased risk of physical assault to high-profile data breaches, the security threats faced by the NHS are constantly evolving. James Kelly of the British Security Industry Association reports on the technology that can prevent violence against staff
Security
STAFF PROTECTION
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
85 Volume 14.6 | HEALTH BUSINESS MAGAZINE

the NHS, which is styled like an ID card holder.Working alongside private security providers is a key element of the NHS’s lone worker protection strategy, and NHS Protect – the central security management body for the National Health Service – is actively involved with the BSIA’s Lone Worker section committee, particularly its work in the development of the British Standard for lone worker protection, BS8484. The adoption of BS8484 lone worker solutions in the NHS is implemented largely through a national Framework Agreement. CHOOSING A SUPPLIERChris Allcard, Head of Lone Worker Services at Reliance High-Tech, comments: “Choosing a supplier whose lone worker protection
solutions fully adhere to BS8484 is an essential step in mitigating and eliminating the risks faced by lone workers in the healthcare sector. One of the key benefits of BS8484 solutions, aside from a top priority response from the police, is that they enable audio evidence to be captured, which can be used as part of taking action against aggressors and offenders, giving healthcare organisations an added layer of protection. “Integrating these solutions into an organisation’s lone working policies and procedures, coupled with ongoing compliance monitoring, can help provide
a comprehensive solution such as is currently evident within the NHS.” Other security technology used within the hospital, clinic or surgery setting can also help to reduce the risk of assault, while also protecting the vulnerable patients being cared for within. CCTV, for example, provides the healthcare sector with a mechanism to deter or detect criminals and trespassers, while monitoring the activity of authorised personnel such as staff, patients and visitors. In a hospital environment, such monitoring can offer peace of mind to both patients and visitors, knowing that no unwanted trespassers will infringe upon their privacy despite the hustle and bustle of a busy healthcare setting. Such security can stem beyond the four walls of the premises. Cameras can also be strategically installed around the perimeter, particularly around car parks. Hospitals, in particular, are vulnerable to thefts from their long-stay parking, with many visitors staying for a long period of time, particularly if their loved ones are undergoing extensive treatments or lengthy operations. Therefore, thieves may see these unattended vehicles as easy targets. CCTV can closely monitor these areas, deterring thieves from damaging or stealing this property and maintaining a safe environment for those passing through. VIDEO CONTENT ANALYSISOne particular element of CCTV that is being increasingly employed in a number of sectors, including healthcare, is that of Video Content Analysis (VCA). VCA is the name given to the automatic analysis of CCTV images, which is then used to create meaningful information regarding the content. For example, VCA can be used to automatically detect an intruder,
or to count the number of people entering or leaving an area – beneficial, for
instance, for keeping track of how many people have entered or
left an emergency room during a given period of time. If the area that needs protecting is particularly extensive – such as the multiple floors and rooms of a hospital building – then
multiple screens are often required to be monitored at
once. VCA can offer solutions to make this monitoring process as
efficient as possible, particularly during the night when fewer staff may be on duty. Advances in technology means that this process can be streamlined through the deployment of either motion sensors for the CCTV – where the cameras only start rolling when movement is detected – or by using fence-mounted vibration detectors that trigger an alert in the security control room.
FURTHER INFORMATIONwww.bsia.co.uk
Secu
rity
If the area that needs protecting is particularly extensive then multiple screens are often required
STAFF PROTECTION
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.686

Products & Services
Liquid Culture is passionate about all things refreshment; experts in coffee first and foremost, and specialists in providing the complete drink and snack service. Liquid Culture supplies a comprehensive range, from vending machines to professional coffee machines, and the best ingredients and products to serve with them. The company also shares its expertise and knowledge, offering business-to-business consultancy and a ‘Your Brew Buddy’ barista training service. Liquid Culture’s colleagues are knowledgeable and friendly and always willing to go the extra mile, whether they are chatting to you about new coffee blends, delivering your ingredients, or filling and maintaining your vending machine. Ideal for both retail and commercial venues, the Liquid Culture Espresso Tower offers exceptional quality at the touch of a button. It is exactly
the same concept as Costa Express and Starbucks to-go but supporting the independent coffee provider. Liquid Culture can also fully brand the towers to your requirements. So if your organisation serves refreshments to customers or staff, the company can design and deliver the optimum refreshment service. Liquid Culture strongly believes that every refreshment break deserves to be enjoyed – how totally refreshing.
FURTHER INFORMATIONwww.liquid-culture.co.uk
Liquid Culture – the experts in coffee
VENDING
GCSC (SW) is a South West based company providing specialist cleaning and maintenance services to the commercial kitchen industry including Cornwall and Devon. The cleaning of kitchen canopy systems is becoming increasingly necessary in order to comply with insurance companies’ requirements. At the same time, this process will also prevent a fire from spreading as a result of an out break of a fire within the kitchen, through regular cleaning of the kitchen extract ductwork, fan unit together with the plenum area behind the grease filters. Established in 2004, the company provides professional kitchen canopy and duct work cleaning, including extraction/intake fan units. All work is carried out in accordance with HVCA TR19 standards, and on completion GCSC provides its clients with certification and supporting photographic
evidence in order to comply with your insurance policy. GCSC also provides full commercial kitchen and appliance deep cleans, sale and hire of commercial chemical decarbonising dip tanks for the cleaning of canopy filters and kitchen utensils, and air filtration media. Cleaning is achieved on site to allow next day use. The company also supplies specifically designed chemicals for use within commercial kitchens. For a free no obligation quotation or for more information contact GCSC.
FURTHER INFORMATIONTel: 01840 211179www.gcscsw.co.uk
Commercial cleaning services for hospitals
CATERING
In Kenya, Computer Aid in partnership with AMREF has started training 26,000 Kenyan nurses online from certificate to diploma-level. This program – which will be completed in five years – would have taken 100 years under traditional methods without network access and IT equipment. Computer Aid International is a UK-registered charity which refurbishes and data-wipes donated IT equipment and sends them to those that need them around the world. Computer Aid works with overseas NGOs and governmental agencies in Africa and South America to ensure that every PC sent is used effectively and that the necessary training and technical support is available. Computer Aid has been distributing over 100 telemedicine kits to rural hospitals across East Africa for doctors to access life-saving
information online, improving HIV testing rates, facilitating research into malaria and cleft palate operations. The work Computer Aid does is reliant on donations of equipment from hospitals, doctor practices and health centres here in the UK. Its projects can only continue with more of the same support. Please help the company to bridge the digital gap by donating your unwanted IT equipment. Contact Computer Aid to arrange PC collection and make a difference.
FURTHER [email protected]
Transforming people’slives through ICT
ICT
The health sector handles sensitive personal data on a regular basis. The Data Protection Act places a legal obligation for organisations to ensure that this personal data is handled appropriately throughout the chain of custody. Did you know that your responsibilities under the Data Protection Act are not passed on as you discard personal data? Personal information that is collected by your organisation is your responsibility until it has been destroyed. Be sure you know that the files and records you dispose of are destroyed in a secure manner, by a reputable secure shredding service provider and in line with EN15713, the European standard for information destruction. A reputable company such as The Shred Centre will provide you with a complete audit trail from collection to
destruction. It’s fully auditable, secure shredding service for healthcare providers, gives you complete peace of mind. The company provides secure shredding services that ensure complete destruction of data recorded on paper, hard disk, X-rays or any other media format. The Shred Centre is a family run secure shredding company, offering first class service alongside complete security. Visit the website or call Patrick Stephens, MD today to find out how The Shred Centre can help you.
FURTHER INFORMATIONTel: 01388 448160www.theshredcentre.com
First class secure shredding services
DOCUMENT DESTRUCTION
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
87 Volume 14.6 | HEALTH BUSINESS MAGAZINE

Prod
ucts
& S
ervic
es
Access Cards is a one-stop-shop for all security consumables. Access Cards supplies at discounted rates cards from manufacturers such as HID, TDSI and Paxton as well as all ribbon cartridges from leading printer manufacturers, NHS logoed lanyards and Yo-yo reels. Healthcare environments present particular challenges for security and facilities teams managing access for temporary staff, particularly when those staff are playing a critical patient care role. Access Cards responds to your last minute requirements efficiently with same day and next day deliveries either to your office or directly to new members of staff. Templates for
different departments are created and Access Cards holds agreed amounts of pre-printed cards. This approach not only improves efficiencies but reduces costs for clients by more than 20 per cent. Access Cards guarantees to identify and supply any card. If you are not sure what card technology is used on your estate then call Access Cards or send a sample card to Access Cards, 25 Southampton Buildings, London, WC2A 1Al for identification and estimate quoting your name, organisation and email address.
FURTHER INFORMATIONTel: 0203 151 0200www.accesscards.co.uk
Your one-stop-shop for security consumables
SECURITY
Skyguard – Europe’s premier personal safety service, has been chosen as an approved supplier on the NHS Supply Chain’s Framework Agreement for electronic assistive technology products. The Framework encompasses a wide range of telehealthcare products which enable the severely disabled or elderly to live independently in their own homes, by making their day to day tasks easier and safer. Following the conclusion of an OJEU tender process, NHS Supply Chain (acting as agent for NHS Business Services Authority), selected Skyguard’s MySOS device for the personal safety alarms product category. Skyguard’s marketing director, Will Murray said: “Skyguard are delighted to be awarded onto this Framework which demonstrates our commitment to offering the highest quality products and
customer service, whilst delivering excellent value for money. We already work with over 100 NHS Trusts to protect lone workers and Telecare users, however,
this framework now makes it even easier for the NHS and other healthcare organisations to procure our products.” Under the Framework Agreement there are two different methods of supply: ‘Non-Direct’, whereby NHS Supply Chain can purchase products and make them available to NHS Trusts, private healthcare providers, and government departments and agencies. Alternatively, these organisations can purchase ‘Direct’ products, entering into a contract directly with the supplier through the framework.
FURTHER INFORMATIONwww.skyguardgroup.com
Telehealthcare products from Skyguard
SECURITY
Ductbusters is a specialist ventilation system cleaning and maintenance company offering full UK coverage with a directly employed, fully trained labour force working to B&ESA TR19, CIBSE TM26 and NHS HTM03-1 standards. The services offered include:Ductwork cleaning – ductwork is often located above ceilings and requires certain skills and techniques to obtain safe access and thoroughly clean. Air handling unit maintenance – the equipment that drives the air through the ductwork also needs attention to ensure the quality of the air inside the building is not contaminated. Kitchen extract cleaning – most catering operations have an extract system above their cooking range. This takes away steam and grease emissions and if not regularly cleaned will present a fire risk. Fire damper drop testing – any
ductwork that passes through a fire rated wall should have a fire damper fitted to help prevent the spread of flames. Regular testing to BS9999 and B&ESA SFG20 is essential to ensure correct operation. Ventilation risk assessment – all ventilation systems should be regularly inspected to ascertain what the level of internal contamination is. A team of experienced surveyors is available to conduct free site surveys of any potential application. To arrange a survey please call or visit the website.
FURTHER INFORMATIONTel: 0800 085 0403www.ductbusters.co.uk
Ventilation system maintenance services
FACILITIES MANAGEMENT
Shark Attack is a North London design studio that prides itself on delivering effective, engaging, top-tier design for both pixels and print. Available services include branding and identity design, promotional or informational literature, and web design. Whether your project requires just one of these disciplines, more than one, or something else entirely, Shark Attack will provide you with a stylish, integrated solution that looks great and does its job in a smart, elegant, intelligent way – exactly as it should. Furthermore, you won’t be stuck talking to an ‘account handler’; at Shark Attack the client gets to deal directly with the designer, ensuring
that you get exactly the design that you are looking for. No middlemen. With over two decades of industry experience, Shark Attack has satisfied clients around the world. Here in the UK the company has created compelling design solutions for the Metropolitan Police Service and the BBC, not to mention charities, pharmaceutical companies, and the music and publishing industries. Even if all you need is a business card, Shark Attack is here to help. Just call the studio and ask for Rick.
FURTHER INFORMATIONTel: 020 333 [email protected]
Supercharge your business message with design from Shark Attack
SMALL BUSINESS
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
HEALTH BUSINESS MAGAZINE | Volume 14.688

Products & Services
Chlorine Dioxide (ClO2) has been called the ‘ideal’ biocide because of its unique combination of properties. ClO2 is very effective at low dosage rates and is able to permeate and penetrate biofilms which are relatively resistant to other drinking water disinfectants such as chlorine. Its effectiveness against biofilms and legionella bacteria make it ideal to control the risk of Legionnaires’ Disease associated with hot and cold domestic water systems, cooling water systems, spas, hot tubs and leisure pools. For this reason, chlorine dioxide is increasingly being used to control legionella in healthcare water systems. However, traditional chlorine dioxide generators can be complex, unreliable and use hazardous chemicals. The Activ-Ox® systems from Feedwater are simpler and safer than other chlorine dioxide systems giving a high yield of chlorine dioxide instantly from low hazard precursors.
A range of systems are available suitable for either treating all the incoming water within a hospital or just the targeted dosing of a high risk area. Feedwater has been producing chlorine dioxide products for 20 years and as well as its own patented Activ-Ox® systems the company can also supply chemicals for other chlorine dioxide generators at competitive prices.To find out more about Chlorine Dioxide and see a video demonstration of Activ-Ox visit the website.
FURTHER INFORMATIONwww.feedwater.co.uk
CIO2 legionella control in the health care sector
LEGIONELLA
SSQC is an independent quality assurance company situated in Shetland that has been supporting clients since 1985 with specialist and time critical Microbiology services. SSQC’s Microbiology Laboratory is UKAS accredited No 2651. It is now also a member of the Legionella Control Association and undertakes sampling and analysis of potable water for the detection and enumeration of legionella species. The company has a dedicated team of experienced sampling officers on hand. The laboratory is UKAS accredited which includes the isolation and enumeration of legionella species and confirmation of legionella
pneumophila Sg 1-14. The laboratory works closely with the Scottish Legionella Reference Laboratory based at Glasgow Royal Infirmary. The laboratory participates in potable water external quality schemes, PHE legionella and QWAS. The laboratory also offers other accredited testing methods on Potable water. For further information on any of these services please refer to the SSQC website or contact Margaret Nugent, laboratory manager.
FURTHER INFORMATIONSSQC Ltd, Port Arthur, Scalloway, Shetland ZE1 0UNTel: 01595 772441www.ssqc.co.uk
New accreditation for legionella services
LEGIONELLA
Providing a total compliance solution throughout the UK, Expert Water Services specialises in the whole range of legionella control and water management, from risk assessment, monitoring, chlorination, RPZ valve/TMV installation and microbiological sampling, to remedial work, whole system commissioning and consultancy. With over 10 years experience, Expert Water Services offers unrivalled service in the water hygiene industry and place its clients’ needs first. Sensitive to the specific needs of the care sector, the company currently service local authorities as well as
privately run healthcare establishments, and understands the diversity of your properties and the need for compliance with current legislation and total peace of mind. Expert Water Services also provides specific legionella training and awareness courses for all manner of delegates, and the company is well versed in the delivery of such training, which can be tailored to suit all manner of clients and their specific requirements.
FURTHER INFORMATIONTel: 01226 214932Mobile: 07855174688www.expertwaterservices.co.uk
Water safety compliance for the care industry
LEGIONELLA
Established in April 2011, Deveron Water Solutions provides tailored water treatment services covering most aspects of water quality and hygiene. Services include: water storage tank and associated services; cleaning and disinfection (carried out in accordance with the BS 8558 and HTM 04-01 requirements); external mains water service; pressure testing/data logging and disinfection; RPZ valve testing and maintenance; pre commission chemical cleaning of LPHW and CHW systems; chemical supply and dosing; water sampling; legionella risk assessments (in accordance with BS 8580, ACoP L8 (4th edition 2013) and HSG 274 parts 1-3 requirements). Deveron Water Solutions’ experienced operatives have attained city and guilds
qualifications in building disinfections, RPZ valve testing (WRAS approved testers) and legionella risk assessment. All operatives hold CSCS and National Water Hygiene cards and are registered on the Energy and Utility Skills Register. Whatever your water treatment requirements, Deveron Water Solutions can design a bespoke programme to suit your needs. For further information or if you wish to discuss your requirements contact Deveron on the details below. FURTHER [email protected] www.deveronwater.com
Tailored water treatment services from Deveron
LEGIONELLA
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
89 Volume 14.6 | HEALTH BUSINESS MAGAZINE

Adve
rtise
rs In
dex
HEALTH BUSINESS MAGAZINE | Volume 14.690
BUSINESS INFORMATION FOR HEALTHCARE PROFESSIONALS – www.healthbusinessuk.net
With the ever present threat of austerity measures and pressure for improvements being a major focus for NHS trusts today, the benefits of professional and efficiently managed car parking facilities are often overlooked, whereas the truth is often that these valuable commodities represent areas of patient and customer service that can also deliver financial benefit to a trust. The need for stress free parking at hospitals has made car parking a key issue for NHS trusts. Hospitals have evolved with insufficient parking spaces to accommodate today’s demand. Lack of available space and poor car park and traffic management consistently leaves hospital visitors and patients with a poor first impression. These problems frequently add to distress and lead to missed appointments as well as financial loss through wasted staff hours. Excel Parking Services delivers tailor made solutions to fit the
specialist sector of hospital parking and security services and to ensure that the trust’s car parks are managed with the professionalism and attention to detail they deserve. The company’s aim is to provide the most effective and appropriate system of operation, utilising its portfolio of products and services to meet the client’s requirements. Whether you need to discourage long-stay parking or effectively manage available space or need advice on travel policies and parking equipment, please contact Excel Parking Services on the details below.
FURTHER INFORMATIONTel: 0114 267 8008 www.excelparking.co.uk
Professional parking management for the NHS
CAR PARKING
The health sector handles sensitive personal data on a regular basis. The Data Protection Act places a legal obligation for organisations to ensure that this personal data is handled appropriately throughout the chain of custody. Did you know that your responsibilities under the Data Protection Act are not passed on as you discard personal data? Personal information that is collected by your organisation is your responsibility until it has been destroyed. Be sure you know that the files and records you dispose of are destroyed in a secure manner, by a reputable secure shredding service provider and in line with EN15713, the European standard for information destruction. A reputable company such as The Shred Centre will provide you with a complete audit trail from collection to
destruction. It’s fully auditable, secure shredding service for healthcare providers, gives you complete peace of mind. The company provides secure shredding services that ensure complete destruction of data recorded on paper, hard disk, X-rays or any other media format. The Shred Centre is a family run secure shredding company, offering first class service alongside complete security. Visit the website or call Patrick Stephens, MD today to find out how The Shred Centre can help you.
FURTHER INFORMATIONTel: 01388 448160www.theshredcentre.com
First class secure shredding services
DOCUMENT DESTRUCTION
ADVERTISERS INDEXThe publishers accept no responsibility for errors or omissions in this free service
1st Stop Recruitment 75Access Cards 88Aidcall 60Alcontrol Laboratories 68Asckey Data Services 42Austco 62Bosse Interspice 78Bray Group 73British Gas 51Cantarus 34, 35CCube Solutions 4Certuss 62CFH Docmail 10Computer Aid International 87Cranegates 8Credit Card Keys 62Decorative Panels 6, 52Deveron Water Solutions 89Docman 73Ductbusters 88Elliott UK 12Enovation 38Excel Parking Services 90Expert Water Services 89
Feedwater 89GCSC 87GP Access 70Hanergy Solar Power UK 48Hospedia 76Howorth Air Technology 22Huthwaite International 19Hydrosense 64Integration Consulting 16IPS Specials 72Leviathan Water 68Liquid Culture 87Marshall Bast 14, 26McCain 80Neopost 68Newton Rigg College 36Nymas 22Page One Communications 36PHS Group IFCPin Point 84Polyflor 27Power Perfector 48Qube Construction 56Recruitment & Employment Confederation 82
Reisswolf Loondon 42Sarum Asbestos 56Shark Attack 88Skyguard 88Spectrum Energy Systems 46Sperion 56SSQC 89Sun Renewable 50Sundeala 54Swallow Evacuation & Mobility Products 82Sync Interactive 30Teknomek BCTG Services 40The Parking Shop 75The Shred Centre 87TM Electronics 68UK Parking Control IBCUltra Communications 30Visual UK 54Voice Connect 33Water Management Society 66Yeoman Shield 54YPO 82

We get right to the heart of your parking issues.Healthcare parking management is a sensitiveissue but also an essentialservice. UKPC offer sensible solutions that willprotect your car parks whilst serving your visitorsand staff with diligence,commitment and thehighest standards ofcustomer care.
ukparkingcontrol.com
© 2014 UK Parking Control Ltd
0844 800 8710 [email protected]
The Parking Professionals
UKPC Health Business magazine A4 Ad.indd 2 27/08/2014 09:57

ADJUSTABLE NON-MARKINGSTAINLESS STEEL FEET
NO PORES OR GAPS
SLOPING TOP FOR BETTER HYGIENE
SECRET FIXINGSREDUCE DIRT TRAPS
100% 304 GRADE STAINLESS STEEL CONSTRUCTION
view the full range 24/7
HYGIENIC FURNITUREAND EQUIPMENT
QUALITY OF SERVICE
QUALITY THROUGH MANUFACTURE
QUALITY BY DESIGN
CALL: 01603 788833ONLINE: teknomek.co.uk EMAIL: [email protected]
We design. We manufacture. We excel.
High quality stainless steel furniture and
equipment. See our full range and endless
options online at teknomek.co.uk
Made inthe UK
Related Documents











