MILITARY MEDICINE, 168, 1:57,2003 Health Assessment of U.S. Army Rangers Guarantor: Patricia A. Deuster, PhD MPH Contributors: CAPT Anjali Sridhar, MC USA*; Patricia A. Deuster, PhD MPH*; William J. Becker, PhD*; Regina Call, RN*; MAJ Karen K. O'Brien, MC USAt; LTC Gaston Bathalon, AMSC USA; Purpose: Assess the health behaviors of U.S. Army Rangers, including their diet and physical activity patterns, and their use of alcohol, tobacco, and nutritional supplements. Meth- ods: Army Rangers (N= 38) completed selected self-report and food frequency questionnaires, and anthropometric measures (height, weight, circumferences) were taken. Results: Dietary patterns were collected from questionnaires that asked re- spondents to report the frequency of usual consumption from a list of foods over a period of 1 year. The data collected indicated a diet high in fat (38.0% of energy) and low in carbo- hydrates (41.9%). Protein intake (17.9% of energy) was consis- tent with recommendations for endurance and strength train- ing athletes. Hours engaged in physical activity averaged 12 per week. Overall, 76% of the volunteers reported using alco- hol on a regular basis, and 52.6%used some form of tobacco: 50%reported using either snuffor chewing tobacco. The use of supplements was high with 13%taking creatine and ephedrine products on a regular basis. Conclusion: Although physical activity patterns indicated a high level of activity, dietary and other health behaviors, such as smoking, alcohol use, and patterns of supplement use, suggest that health education programs may be important in this select Army population. Introduction H ealth assessments ofvariousgroups havebeen conducted over the yearsto document particular lifestyle patterns that may affect overall health. Numerous studies have shown the importance ofnutrition and other health behaviors forreducing the morbidity and mortality of the general population. For ex- ample, a diet that meets energy requirements and is low in fat has been associated with a reducedrisk of developing various chronic diseases.F In addition, combining a good diet with physical exercise and other positive health behaviors (nonsmok- ing' limiting alcohol intake) can substantiallyreduce the risk of chronic disease and morbidity. 1-3 U.S. citizens also believe that takingdietarysupplements may reducethe risk ofchronic diseaseand improve overall health."? Although the role of nutritional supplements in reducing chronic diseases is unknown, the use of nutritional supple- ments is prevalent. 4,6-8 This is particularly true among athletes with various reports indicating that 39% to 100% use supple- ments on a regular basis. 4 ,8- 12 Over the past several years, the use of supplementswithin both the military and civilian popu- lations has become a concern, because adverse events associ- *Department of Military andEmergency Medicine, Uniformed Services University of the Health Sciences, Bethesda, MD. tMartin Army Community Hospital, FortBenning, GA. *U.S. Army Institute ofEnvironmental Medicine, Natick, MA. The opinions and assertions expressed herein are those ofthe authors and should notbe construed as reflecting those ofthe U.S. Army, the Uniformed Services Uni- versity ofthe Health Sciences (USUHS), or the Department ofDefense. This manuscript was received for review in November 2001 and accepted for publication in June 2002. ated with selected supplements, in particular ephedrine-con- taining products, have been reported." Thus, the health behavior of supplement users must also be considered as a component ofa health assessment. The U.S. military is interested in the overall health and well- ness ofthe war fighter. In particular,the military leadership has become increasingly concerned withthe roleofhealthbehaviors in various aspects of military training. Dietary and physical activity patterns, supplement use, and alcohol and tobacco use are behaviors ofinterest.Onegroupof military personnel whose health behaviors are ofinterest is the U.S. Army Rangers. This elitegroupofmen undergoes rigorous physical and psycholog- icaltrainingjust tojointhis prestigious fighting organization. To date, no information regarding the health habits ofRangershas been reported, although health and nutritional surveys of other military populations, such as high ranking military officers, 14 the Navy SEALS, 15 newrecruits.' and Navy divers, 16 have been conducted. Because Rangers routinely undergo rigorous physical training and experience high levels of stress, their nutrition and health behaviors would be impor- tant for formulating recommendations regarding short-and long-termhealth objectives. The goal ofthis study was to conduct a health assessment of the U.S. Army Rangers. The overall information derived can be used by health care professionals for making recommen- dations about future desirablehealth behaviors. Tothat end, U.S. Army Rangers were provided a questionnaire to assess the weekly amount of aerobic and anaerobic exercise per- formed, nicotine and daily caffeine intake, alcohol habits, use of supplements, and dietary patterns, including the intake offat, carbohydrates, and protein. Specific questions to be answered by the study include the following: (1) Do intakes of carbohy- drates, fat, and protein meet the Dietary Guidelines for Ameri- cans, 2000 (DGA)l7 and the Military Dietary References In- takes?" (2) Do dietary patterns of the trainees conform to recommendations for endurance athletes? (3) What are their health behaviors in terms of nutritional supplement patterns, use of caffeine, alcohol and tobacco, and levels of daily physical activity? Methods The 38 subjects who volunteered forthis study were all qual- ified Ranger graduates assigned to Fort Benning, Georgia. The study was part of another study to examine the effects of crea- tine on military performance. Many subjects were briefed on the study, and then those interested in participating reported the next morning to the gymnasium for the Rangers. At that time, informed consent was obtained from each individual. All the participants came from similarmilitary training. Thestudywas approved by the Institutional Review Boards at the Uniformed 57 Military Medicine, Vol. 168, January 2003 Downloaded from https://academic.oup.com/milmed/article/168/1/57/4915738 by guest on 22 July 2022

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

MILITARY MEDICINE, 168, 1:57,2003
Health Assessment of U.S. Army Rangers
Guarantor: Patricia A. Deuster, PhD MPHContributors: CAPT Anjali Sridhar, MC USA*; Patricia A. Deuster, PhD MPH*; William J. Becker, PhD*;Regina Call, RN*; MAJ Karen K. O'Brien, MC USAt; LTC Gaston Bathalon, AMSC USA;
Purpose: Assess the health behaviors of U.S. Army Rangers,including their diet and physical activity patterns, and theiruse of alcohol, tobacco, and nutritional supplements. Methods: Army Rangers (N= 38) completed selected self-report andfood frequency questionnaires, and anthropometric measures(height, weight, circumferences) were taken. Results: Dietarypatterns were collected from questionnaires that asked respondents to report the frequency of usual consumption froma list of foods over a period of 1 year. The data collectedindicated a diet high in fat (38.0% of energy) and low in carbohydrates (41.9%). Protein intake (17.9% of energy) was consistent with recommendations for endurance and strength training athletes. Hours engaged in physical activity averaged 12per week. Overall, 76% of the volunteers reported using alcohol on a regular basis, and 52.6% used some form of tobacco:50%reported using either snuff or chewing tobacco. The use ofsupplements was high with 13%taking creatine and ephedrineproducts on a regular basis. Conclusion: Although physicalactivity patterns indicated a high level of activity, dietary andother health behaviors, such as smoking, alcohol use, andpatterns of supplement use, suggest that health educationprograms may be important in this select Army population.
Introduction
H ealth assessments ofvariousgroupshavebeen conductedover theyears todocument particularlifestyle patterns that
may affect overall health. Numerous studies have shown theimportance ofnutritionand otherhealth behaviors forreducingthe morbidity and mortality of the general population. For example, a diet that meets energy requirements and is low in fathas been associated with a reduced risk of developing variouschronic diseases.F In addition, combining a good diet withphysical exercise and otherpositive healthbehaviors (nonsmoking' limiting alcohol intake) can substantiallyreducethe risk ofchronic diseaseand morbidity. 1-3
U.S. citizens alsobelieve that takingdietarysupplements mayreducethe risk ofchronic diseaseand improve overall health."?Although the role of nutritional supplements in reducingchronic diseases is unknown, the use of nutritional supplements is prevalent.4,6-8 This is particularly true among athleteswith various reports indicating that 39% to 100% use supplements on a regularbasis.4,8- 12 Over the past several years, theuse ofsupplementswithinboth the military and civilian populations has become a concern, because adverse events associ-
*Department ofMilitary andEmergency Medicine, Uniformed Services University oftheHealth Sciences, Bethesda, MD.
tMartin Army Community Hospital, FortBenning, GA.*U.S. Army Institute ofEnvironmental Medicine, Natick, MA.The opinions andassertions expressed herein arethose oftheauthors andshould
notbe construed as reflecting those ofthe U.S. Army, the Uniformed Services University ofthe Health Sciences (USUHS), or the Department ofDefense.
This manuscript was received for review in November 2001 and accepted forpublication inJune 2002.
ated with selected supplements, in particular ephedrine-containing products, have been reported." Thus, the healthbehavior of supplement users must also be considered as acomponent ofa health assessment.
The U.S. military is interestedin the overall health and wellness ofthe warfighter. Inparticular,the military leadership hasbecome increasingly concerned withthe roleofhealthbehaviorsin various aspects of military training. Dietary and physicalactivity patterns, supplement use, and alcohol and tobacco useare behaviors ofinterest.Onegroupofmilitary personnel whosehealth behaviors are ofinterest is the U.S. Army Rangers. Thiselitegroupofmen undergoes rigorous physical and psychologicaltrainingjust tojointhis prestigious fighting organization. Todate, no information regarding the healthhabits ofRangershasbeen reported, although health and nutritional surveys ofother military populations, such as high ranking militaryofficers, 14 the Navy SEALS, 15 newrecruits.' and Navy divers, 16
have been conducted. Because Rangers routinely undergorigorous physical training and experience high levels ofstress, their nutrition and health behaviors wouldbe important for formulating recommendations regarding short-andlong-termhealth objectives.
Thegoal ofthis study was to conduct a health assessment ofthe U.S. Army Rangers. The overall information derived canbe used by health care professionals for making recommendations about future desirable health behaviors. Tothat end,U.S. Army Rangers were provided a questionnaire to assessthe weekly amount of aerobic and anaerobic exercise performed, nicotine and daily caffeine intake,alcohol habits, use ofsupplements, and dietary patterns, including the intake offat,carbohydrates, and protein. Specific questions to be answeredby the study include the following: (1) Do intakes of carbohydrates, fat, and proteinmeet the Dietary Guidelines forAmericans, 2000 (DGA)l7 and the Military Dietary References Intakes?" (2) Do dietary patterns of the trainees conform torecommendations for endurance athletes? (3) What are theirhealth behaviors in terms of nutritional supplement patterns,use ofcaffeine, alcohol and tobacco, and levels ofdaily physicalactivity?
Methods
The38 subjectswho volunteered forthis study were all qualified Ranger graduates assigned to Fort Benning, Georgia. Thestudy was part ofanother study to examine the effects ofcreatineon military performance. Many subjectswere briefed on thestudy, and then those interested in participating reported thenext morning to the gymnasium for the Rangers. At that time,informed consent was obtained from each individual. All theparticipantscamefrom similarmilitary training. Thestudywasapproved by the Institutional Review Boardsat the Uniformed
57 Military Medicine, Vol. 168, January 2003
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/168/1/57/4915738 by guest on 22 July 2022
58 HealthAssessmentof U.S. Army Rangers
oJ.J:=~~~~_mmIIIL.
TABLE I
DIETARY PATIERNS OF U.S. ARMY RANGERS
Ethnicity
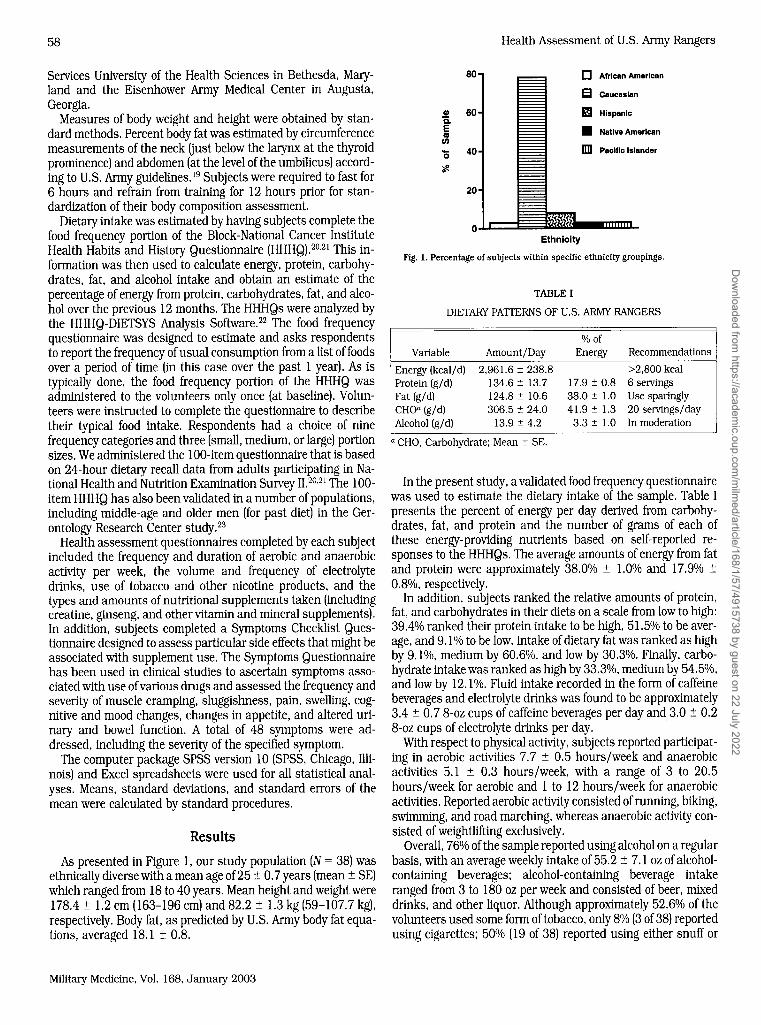
Fig. 1. Percentage of subjects within specific ethnicity groupings.
0 African American
EJ Caucasian
m Hispanic
• Native American
lID Pacific Islander
% ofEnergy Recommendations
>2,800 kcal17.9 ± 0.8 6 servings38.0 ± 1.0 Use sparingly41.9 ± 1.3 20 servings/day
3.3 ± 1.0 In moderation
Amount/Day
2,961.6 ± 238.8134.6 ± 13.7124.8 ± 10.6306.5 ± 24.0
13.9 ± 4.2
Variable
Energy (kcal/d)Protein (g/ d)Fat (g/d)cno-(g/d)Alcohol (g/ d)
a CHO, Carbohydrate; Mean ± SE.
G) 60Q.Easen'0 40
80
20
~o
In the present study,a validated food frequency questionnairewas used to estimate the dietary intake of the sample. Table Ipresents the percent of energy per day derived from carbohydrates, fat, and protein and the number of grams of each ofthese energy-providing nutrients based on self-reported responses to the HHHQs. Theaverage amounts ofenergy from fatand protein were approximately 38.00/0 ± 1.0% and 17.9% ±0.8%, respectively.
In addition, subjects ranked the relative amounts ofprotein,fat, and carbohydrates in their diets on a scalefrom low to high:39.4% ranked their proteinintake to be high, 51.50/0 to be average,and 9.1% to be low. Intakeofdietaryfatwasranked as highby 9.10/0, mediumby 60.60/0, and low by 30.30/0. Finally, carbohydrateintakewas rankedas highby33.3°Al, mediumby54.5%,and low by 12.1°Al. Fluidintake recorded in the form ofcaffeinebeverages and electrolyte drinks was foundto be approximately3.4 ± 0.7 8-ozcups ofcaffeine beverages per day and 3.0 ± 0.28-ozcups ofelectrolyte drinks per day.
Withrespectto physical activity, subjects reported participating in aerobic activities 7.7 ± 0.5 hours/week and anaerobicactivities 5.1 ± 0.3 hours/week, with a range of 3 to 20.5hours/week for aerobic and 1 to 12 hours/week for anaerobicactivities. Reported aerobic activity consistedofrunning,biking,swimming, and road marching, whereasanaerobic activity consisted ofweightlifting exclusively.
Overall, 76% ofthe samplereportedusingalcohol ona regularbasis, withan average weekly intake of55.2 ± 7.1 ozofalcoholcontaining beverages; alcohol-containing beverage intakeranged from 3 to 180 ozper weekand consistedofbeer, mixeddrinks, and other liquor. Although approximately 52.6% of thevolunteers used someform oftobacco, only8% (3of38) reportedusing cigarettes; 500/0 (19 of 38) reported using either snuff or
Results
As presented in Figure 1, our study population (N = 38)wasethnically diverse witha meanageof25 ± 0.7years (mean ± SE)whichrangedfrom 18to 40years. Mean heightand weight were178.4 ± 1.2em (163-196 cm) and 82.2 ± 1.3kg (59-107.7 kg),respectively. Body fat, as predicted by U.S. Army bodyfat equations, averaged 18.1 ± 0.8.
Services University of the Health Sciences in Bethesda, Maryland and the Eisenhower Army Medical Center in Augusta,Georgia.
Measures of bodyweight and height were obtained by standard methods. Percentbodyfatwas estimatedbycircumferencemeasurements ofthe neck (just below the larynxat the thyroidprominence) and abdomen(atthe level ofthe umbilicus) according to U.S. Army guidelines. 19 Subjectswererequiredto fast for6 hours and refrain from training for 12 hours prior for standardization of their bodycomposition assessment.
Dietary intakewas estimatedbyhavingsubjects complete thefood frequency portion of the Block-National Cancer InstituteHealth Habits and History Questionnaire (HHHQ}.20,21 This information was then used to calculateenergy, protein, carbohydrates, fat, and alcohol intake and obtain an estimate of thepercentage ofenergy from protein, carbohydrates, fat, and alcohol over the previous 12months. The HHHQs wereanalyzed bythe HHHQ-DIETSYS Analysis Software.F The food frequencyquestionnaire was designed to estimate and asks respondentsto report the frequency ofusual consumption from a list offoodsover a period of time (in this case over the past 1 year). As istypically done, the food frequency portion of the HHHQ wasadministered to the volunteers only once (at baseline). Volunteers wereinstructed to complete the questionnaire to describetheir typical food intake. Respondents had a choice of ninefrequency categories and three (small, medium, or large) portionsizes.We administered the 100-item questionnaire that is basedon 24-hour dietary recall data from adults participating in NationalHealthand Nutrition Examination Survey II.20,21 The 100itemHHHQ has alsobeenvalidated in a number ofpopulations,includingmiddle-age and older men (for past diet) in the Gerontology ResearchCenter study."
Healthassessment questionnairescompleted byeach subjectincluded the frequency and duration of aerobic and anaerobicactivity per week, the volume and frequency of electrolytedrinks, use of tobacco and other nicotine products, and thetypesand amounts ofnutritional supplements taken (includingcreatine,ginseng, and othervitaminand mineralsupplements).In addition, subjects completed a Symptoms Checklist Questionnairedesigned to assess particular sideeffects that mightbeassociatedwith supplementuse. The Symptoms Questionnairehas been used in clinical studies to ascertain symptoms associatedwithuse ofvariousdrugs and assessed the frequency andseverity ofmuscle cramping, sluggishness, pain, swelling, cognitive and mood changes, changes in appetite, and altered urinary and bowel function. A total of 48 symptoms were addressed, including the severity of the specified symptom.
The computer package SPSS version 10 (SPSS, Chicago, Illinois) and Excel spreadsheets wereused for all statistical analyses. Means, standard deviations, and standard errors of themean werecalculatedby standard procedures.
Military Medicine, Vol. 168, January 2003
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/168/1/57/4915738 by guest on 22 July 2022

Health Assessment of U.S. Anny Rangers
chewing tobacco. The average number of cans of smokelesstobacco used per day by subjects was 0.8 ::t 0.1.
Dailyuse of nutritional supplements was reported by 81.5% ofthe subjects for various reasons. including enhanced energy.weight loss. and increasing muscle mass . The most commonlyused nutritional supplements were carbohydrate/electrolyte fluidreplacement beverages. followed by protein powders. creatine.and ephedrine. Subjects also reported using other nutraceuticalproducts. such as ginseng. glutamine. and vitamins/minerals.The percentage of subjects taking various supplements is presented in Figure 2. Specifically. subjects reported taking 1.2 ::t0.16 doses/day of creatine. 1.3 ::t 0.3 doses/day of ephedrine.3.6::t 1.54doses/day ofprotein. and 3.3 ::t 1.3doses/day ofothervitamins and supplements. such as ginseng. glutamate. vitamins.and minerals.
All subjects completed a Symptoms Checklist Questionnaireto evaluate specific symptoms they had experienced dunngthepreceding week that might be associated with various supplements. Analysis of the questionnaire indicated that 34% and47% reported symptoms of dry mouth and thirst, respectively.and another 39%. 32%. 34%. and 26% reported symptoms ofmuscle stiffness . tiredness/lack of energy. sweating. and muscle weakness. respectively. No attempt was made to determinewhether there was a causal relationship between the supplements taken and symptoms reported.
Discussion
Obtaining accurate health and nutritional information by using questionnaires is a difficult task as the information obtainedoften has many inherent errors .15.23.24 Inherent errors includeinaccuracies and recall bias in reporting and estimation ofphysical activity and dietary and supplement intakes.24.25 Despitethese inherent errors. the obtained information is essential forany health assessment and can be useful for making recommendations about current and future health programs. Thepresent study is one of the first reports on the health habits ofU.S.Army Rangers. Although the Rangers are highly physicallyactive. their use of tobacco and alcohol and overall dietary intake suggest that educational programs promoting more healthful habits may be warranted.
Macronutrients and Fluid Intake
In the present study. a validated foodfrequency questionnairewas used to estimate the dietary intake of the sample. Overall,the U.S. Army Rangers reported dietary intakes that met the
0 CHOlE leclrol yle Beverages
100 0 Creatine81.6
IICl Ephedr ine Produ cts<::i: Protein PowdersI1l 75l- •CIl Other Nutraceutlcals
C.E 50'"en'0 23.7
'if. 25
Fig. 2. Percentage of sample reporting use of specific nutritional supplements.
59
Military Dietary References Intakes" but not the DGA.17 Theaverage amount of energy from fat exceeded the USDG recommendation of approximately 30% or less . and the recommendations from the Position of the Canadian and American DieteticAssociation and the American College of Sports Medicine saidthat 20% to 25% of the total energy should come from fat.26Although considerable data indicate that a high fat intake increases the risk of coronary artery disease and other chronicdiseases. whether the risk is also increased in populationswhose energy expenditures are high is unclear. Thus. the implications of a diet that exceed the DGA recommendations fordietary fat in this active population remain to be determined .Similar to fat intake in the present study and consistent withother studies ofmilitary and civilian populations. protein intakewas comparable with recommendations of 14% to 18% for endurance and strength training athletes." These values suggestthat protein and fat were the macronutrients of choice. andalthough fatty acids are clearly an important source of fuelduring exercise. protein is not. Protein contributes only 2% to10% of the total energy expended during exercise. and to date.no studies have demonstrated a dietary protein-induced benefitin exercise performance" even though commercial productssuggest otherwise.
The two main limiting factors of most physical activities arecarbohydrate stores and fluid intake .8.29 In contrast to fat andprotein. reported carbohydrate intake was 41.9% ::t 1.3% of thetotal energy consumed. a value low in comparison with therecommended guideltnes of 55% to 60% of total energy. Thissuggests that protein. alcohol, and fat were being consumed atthe expense ofcarbohydrates. and this lowlevelofcarbohydrateintake could potentially compromise exercise performance. inparticular for endurance activities common to Ranger training.8.29Studies have shown that endurance performance is usually superior after high. as compared with low. carbohydratediets. with recommended carbohydrate intakes of8 to 109/kg ofbodyweight.29-31There is no doubt that Ranger training is strenuous and sustained in nature. For example. one weekly routineconsists of a 10- to 20-mile road march while carrying approximately 45 pounds; such an event would require adequatestores of glycogen. However. on average. the subjects were consuming less than 4 g of carbohydrates per kilogram of bodyweight, much less than recommended for their activity level.Assuch. these data indicate that the energy intake patterns of theRangers may not have been consistent with optimal performance.
Fluid intake in the form of electrolyte drinks and caffeinebeverages was reported by all subjects in the health question naire to be lowrelative to the amount ofenergy expended dunngphysical activity by this group of individuals. However. theamount of water consumed was not listed in the health andnutrition questionnaire. and as such. the number reported doesnot reflect total fluid intake. During all field exercises and longmarches. subjects regularly ingested large amounts of waterbecause it was required. Although the amount of fluid in theform of electrolyte and water intake should be sufficient tomatch the water losses . if adequate fluid was not replaced. thenearly fatigue durtng exercise could ensue and hinder performance . The consequences of dehydration are potentially lifethreatening.s-" Adequate hydration allows the body to maintain
Military Medicine. Vol. 168.January 2003
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/168/1/57/4915738 by guest on 22 July 2022

60
critical thermoregulatory responses, whereas even a modestdehydration can result in measurabledeclines in cardiovascularand thermoregulatory function.v" Voluntary dehydration, astate commonly seen in athletes and subjects in our study, canseverely compromise physiological function such that the risk ofheat illness increases and exercise performance decltnes.v"Based on the obtained information, it appears that U.S. ArmyRangers attempt to maintain hydrationstatus in proportion tosweatlosses so that a high level ofphysical activity and endurance can be maintained.
SupplementUseThedata obtained from this study indicated that supplement
use amongRangers was high. According to publishedsources,we speculate that the reasons for using supplements are numerous, with the primary ones being weight loss, improvedphysical performance, and increasedmusclemass.' Othercommon reasons offered by publishedresources includemaintaining and/or improving health and self-treatment of a medicalcondition.' Although these are not the actual comments recorded from our subjects, webelieve that this information canbe correlated with the subjects in our study because populations in many other studies were predominately athletes. Thisintake of supplements is of concern in that it has been suggested that athletes do not need vitamins and supplements ifadequate energy to maintain body weight is obtained from avariety offoods. 20
The U.S. Army Rangers are comparable with competitive endurance and strength trainingathletes because ofthe rigorousexercise and trainingthat theyundergo on a daily basis. Proteinsupplements, whichwere taken by 24% of the subjects in thepresent study and 29% of U.S. Army specialoperations candidates." are used primarily to promote muscle strength, function, and possibly size." Studies have shown that the exactamount and composition ofan aminoacid supplementin additionto the timing ofingestion in relationto exercise is importantin determining the efficacy of protein supplementation in improving performance." Considering the high protein intake ofthe Rangers from food alone (approximately 1.6 g/kg), it isunlikely that supplemental protein by these individuals wouldbe necessary. Although this may also be true for vitamin andmineral supplements, the data from the present study are insufficient to make such a statement.
Creatine is anotherpopularsupplementused byRangers andmany other military personnel.4,33,34 Arsenaultet al.33reportedthat 180/0 of the U.S. Army Special Forces candidates tookcreatine, and a 2001 study by Stephens et al.' noted that creatineuse was reported by 230/0 of individuals enteringbasic militarytraining for enlisted service in the AirForce. Many people takecreatinefor the purported performance-enhancing claims, andin fact, many studies have reported improved performance inhigh-intensity, repetitive bouts ofexercise whensupplementingwith creatine,35,36 but this is not always the case.37-39 We recentlydemonstrated that creatineuse was not associated withimproved performance ofmilitary specific tasks but did cause asignificant increase in body weight, specifically fluid and/orfat-free mass." This evidence indicates that use of creatine isunnecessary in military personnel, unless weight gain is theobjective.
Lastly, over 13% ofthe Rangers weretakingephedrine/ ephe-
Military Medicine, Vol. 168, January 2003
Health Assessment of U.S. Army Rangers
dra in someform. Similarly, in a recent surveyofpeople 18andover in a metropolitan area, 12% ofthe samplereported takingephedra in the past 12 months." To date, ephedrine alkaloidshave not been shownto improve exercise performance, unlesstaken in combination with caffeine,'? but they do appear effective forweight loss. It is ofinterest that the military unit and theinstallationwhere this studywas conducted haveissued a command directed to discourage ephedrine use.
Despite no clear performance advantage, such supplementsare commonly used, particularly by athletes in training.4,5,9,37This is of increasing concern particularly because the use ofephedrine has beenlinkedto multiple adverse events, includingdeath.13 Adverse effects from supplementuse maybe magnifiedoramplified whenused while exercising under extreme environmental conditions, particularly warm or hot environments.However, interactions between over-the-counter supplements,physical exertion, and environmental extremes have not beenexamined. Coupled withthe potentialadverse effects, Stephenset al..' whichhad a study population ofN = 550, reported thatAirForce basic traineeswhohad taken supplements to improveperformance were morelikely to engage in high-risk behaviors,including heavy drinking and driving after drinking as compared with nonsupplement users. Whereas this finding is ofconcern, other studies have indicated that among U.S. ArmySpecial Forces and Ranger trainingschools, individuals whousesupplements, at least occasionally, were significantly less likelyto smoke (p< 0.05) and morelikely toexercise ona daily basis."We did not attempt to associatesupplementuse withany otherhealth habit due to the sample size. However, we did examinespecific self-reported physical symptoms that could be associated with or a stimulus for taking supplements. Many of thesubjectsreported drymouth and increasedthirst, whereasothers reported tirednessand lackofenergy. Clearly moreinformation regarding the association between supplementuse, symptom profiles, and other health habits and the role ofsupplements in military performance is needed because it isunlikely that the use ofsupplementswill decline in the comingyears.This is based on studies that suggestsupplementuse ison the rise, especially in endurance and strength-training athletes.? In addition, the perceived potential physical and performancebenefits, whether true or not, havealso played a role inpromoting supplementuse in this groupofindividuals.
Tobacco and Alcohol UseThe use of tobacco and alcohol was high among those sam
pled and is ofconcernas both substances are associated withhealth risks and compromised performance.v-"Themilitary, ingeneral, has a long-standing historyofhightobacco and alcoholuse42,43 that may be related to environmental influences andoccupational pressures likely encountered in the lifestyles ofthese individuals. Studies ofmilitary populations indicate that320/0 of U.S. Air Force" and 50.90/0 of Norwegian Army" basictrainees smoke. In contrast, smokeless tobacco appears to beused morefrequently by specialoperations soldiers. Arsenaultet al.33 found that 31% of special operations trainees usedsmokeless tobacco as compared with 12.9% whosmoked cigarettes.Thesevaluesare somewhat consistentwithour valuesof50% for smokeless and 7.90/0 for cigarettes. It appears thatspecial operations personnel havea muchhigherrate oftobaccouse than overall Army personnel whohavesmoking prevalence
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/168/1/57/4915738 by guest on 22 July 2022

Health Assessment of u.s. Army Rangers
rates of 260/0.25 Efforts to reduce the frequency of these behaviors in the militarywouldlower future morbidity and mortalityand possibly improve performance. A study of u.s. Air Forcebasic trainees showed that smokingwas related to risk factorsbelieved to decrease militaryreadiness, such as alcohol use anddecreased physical activity." Fromthe U.S. Surgeon General'spoint ofview, quitting smokingfor 1 year could reduce the riskofheart disease attributed to smokingbyone-half." Ofinterest isthe decision to ban tobacco use during Ranger school to helpprevent future tobacco use by Rangers and other special operations personnel.
Alcohol consumption,whichwas high in this population,hasbeen associated with a number ofhealth risks, but the benefitsoflowrisk drinkingcan be achieved byrefrainingfromsmoking,eating less dietary fat, and regular exercise.43
Daily Physical ActivityThe level of physical activity in this study population was
quite high, as would be expected, and was greater than therecommendations ofthe DGA that all persons should engagein30 minutes or more ofmoderatephysicalactivity on most (preferably all) days of the week. I? The recommendation has beenmade because exercise may protect against selected chronicdiseases.I? A study on the performance on an indoor militaryobstacle course revealed that top-performing individuals wereleaner, had a lower percent of body fat, and displayed manydiverse physicalcapabilities." How these physicalactivity habits and anthropomorphic indexes, in combination with the observed dietary, alcohol, and tobacco habits will affect futurehealth is as yet unknown.
In summary, our heath assessment revealed that the physicalactivity level ofour population ofu.S. Army Rangers should beconsistent with excellent physical conditionand exceeded recommended physical activity guidelines. In contrast, the dietaryhabits ofthe population,highfat and lowcarbohydrateintakes,werenot consistent with the DGA or Military DietaryReferencesIntakes. Dietaryrecommendations for these elite athletes needto be made to optimize their physical performance and, hopefully, decrease the risk oflong-term medicalcomplications. Nutritional supplement use was high, particularly the use of protein powders, creatine, ephedrine, and others (ginseng,glutamate). Theuse ofthese supplements is not indicatedbasedon the dietary intakes of the Rangers and on the lack of information regarding a beneficial effect. Importantly, the use ofthese supplements by this study population is of concern andneeds to be further addressed with specific recommendationsand regulationoftheir use to preventadverseoutcomes. Lastly,the smokingand alcoholuse in this study populationwas high.Thiswas consistent with previousstudies performed in U.S. AirForce basic trainees" and is of immediate concern for futuremilitary readiness and long-term health. Future programs andrecommendations to reduce the use of tobaccoand alcohol areneeded, along with recommendations regarding the use of dietary supplements, to sustain and support an elite fightingforce, such as the U.S. Army Rangers.
References1. Boden-Albala B, Sacco RL: Lifestyle factors and stroke risk: exercise, alcohol,
diet, obesity, smoking, drug use, and stress. Curr Atheroscler Rep 2000; 2:160-6.
61
2. Talcott GW, Poston WS 2nd, Haddock CK: Co-occurance use of cigarettes, alcohol, and caffeine in a retired military population. Milit Med 1998; 163: 133-8.
3. Manley AF: Cardiovascular implications of smoking: the Surgeon General's pointof view. J Health Care Poor Underserved 1997; 8: 303-10.
4. Stephens MB,Olsen C: Ergogenic supplements and health risk behaviors. J FamPract 2001; 50: 696-9.
5. Marriott BM:The role of dietary supplements in health: an overviewin the UnitedStates. Adv Exp Med BioI2001; 492: 203-17.
6. Harnack LJ, RydellSA,Stang J: Prevalenceofuse ofherbal products by adults in theMinneapolis/St. Paul, MNmetropolitan area. MayoClln Proc 2001; 76: 688-94.
7. Messerer M, Johansson SE, Wolk A: Use of dietary supplements and naturalremedies increased dramatically during the 1990s. J Intern Med 2001; 250:160-6.
8. Burke LM: Nutritional practices of male and female endurance cyclists. SportsMed 2001; 31: 521-32.
9. Krumbach CJ, Ellis DR, Driskell JA: A report ofvitamin and mineral supplementuse among university athletes in a division I institution. Int J Sport Nutr 1999; 9:416-25.
10. Deuster PA, KyleSB, Moser PB, Vigersky RA,Singh A, Schoomaker EB: Nutritional survey ofhighly trained women runners. AmJ Clin Nutr 1986; 45: 954-62.
11. DeBoltJE, Doubt TJ, Singh A, Moses FM,Ryan CJ, Deuster PA:Dietary patterns,gastrointestinal complaints and nutritional knowledge of recreational triathletes.Am J Clin Nutr 1990; 51: 690-7.
12. Singh A, Evans 0, Gallagher KL, Deuster PA: Dietary intakes and biochemicalprofiles ofnutritional status ofultramarathoners. MedSci Sports Exerc 1993; 25:328-34.
13. Haller CA, Benowitz NL: Adverse cardiovascular and central nervous systemevents associated with dietary supplements containing ephedra alkaloids. NEnglJ Med 2000; 343: 1833-8.
14. Deuster PA, Montgomery LC, Gilstad DR, Holland JC, Cowan ML,Newman RC:Health and fitness profiles of male military officers. Milit Med 1987; 152: 290-3.
15. DeBolt JE, Singh A, Day BA, Deuster PA: Nutritional survey of the U.S. NavySEALtrainees. Am J Clin Nutr 1988; 48: 1316-23.
16. Singh A, Deuster PA,Day BA,Smith DJ, DeBoltJE, Doubt TJ: Nutritional statusof land-based U.S. Navydivers. Undersea Biomed Res 1988; 15: 135-45.
17. U.S. Department of Agriculture, Agricultural Research Service, Dietary Guidelines Advisory Committee: Report of the Dietary Guidelines Advisory committeeon the Dietary Guidelines for Americans, 2000.
18. Army Regulation 40-25: Nutrition Standards and Education. BUMEDINST10110.6. AFI 44-141, June 15,2001.
19. U.S. Department of the Army:The Army Weight Control Program. Army Regulation 600-9. Washington, DC, October 1, 1986.
20. Block G, Dresser CM,Hartman AM,Carroll MD:Nutrient sources in the Americandiet: quantitative data from the NHANES II survey: I. Vitamins and minerals.Am J Epidemiol1985; 122: 13-26.
21. BlockG, DresserCM, Hartman AM,CarrollMD: Nutrient sources in the Americandiet: quantitative data from the NHANES II survey: II. Macronutrients and fats.Am J Epidemiol1985; 122: 27-40.
22. HHHQ-DIETSYS Analysis Software, Version 3:0. Rockville,MD, National CancerInstitute, 1993.
23. Sobell J, Block G, Koslowe P, Tobin J, Andres R: Validation of a retrospectivequestionnaire assessing diet 10-15 years ago. AmJ Epidemiol 1989; 130: 173-87.
24. Giovino GA: Epidemiology of tobacco use among U.S. adolescents. Nicotine TobRes 1999; l(Suppl): S31-40.
25. Yore MM, Bell NS, Senier L, Amoroso PJ: Progress toward attainment of theHealthy People 2000 objectives in the U.S. Army: measured by health risk appraisal results. Am J Prev Med 2000; 19: 87-93.
26. Position of the American Dietetic Association, Dietitians of Canada, and theAmerican Collegeof Sports Medicine: Nutrition and athletic performance. Can JDiet Pract Res 2000; 61: 176-92.
27. Fielding RA, Parkington J: What are the dietary protein requirements of physically active individuals? New evidence on the effects of exercise on protein utilization during post-exercise recovery. Nutr Clin Care 2002; 5: 191-6.
28. Wolfe RR: Protein supplements and exercise. Am J Clin Nutr 2000; 72(Suppl):5518-7S.
29. Jacobs KA, Sherman WM: The efficacy of carbohydrate supplementation andchronic high-carbohydrate diets for improving endurance performance. IntJ Sport Nutr 1999; 9: 92-115.
30. Burke LM: Nutritional needs for exercise in the heat. Comp Biochem Physiol AMol Integr Physiol2001; 128: 735-48.
31. Burke LM,Cox GR,Cummings NK, Desbrow B: Guidelines for daily carbohydrateintake: do athletes achieve them? Sports Med 2001; 31: 267-99.
Military Medicine, Vol. 168, January 2003
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/168/1/57/4915738 by guest on 22 July 2022
62
32. Mau ghan RJ: Fluid balance and exercise. Int J Sports Med 1992; 13(Suppl):SI 32-5 .
33. Arsenaul t J . KennedyJ: Dietary supplement use in U.S. Army Special Operation scand ida tes . Milit Med 1999; 164: 495-501.
34. Sheppard HL. Raichada SM, Kouri KM.Stenson -Bar -Maor L. Branch JD : Use ofcreatine an d other supplements by members ofcivilian and military health clubs:a cross-sectional survey, Int J Sports Nutr Exerc Metab 2000 : 10: 245-59.
35. Greenh alf PL. Casey A Short AH.Harris R, Soderlund K.Hultman E: Influence oforal creatine supplementation of muscle torque during repeated bout s of maximal exercise in man . Clin SCi 1993; 84: 565-71.
36. Kreider RB. Ferreira M. Wilson M. et aI: Effects of creatine suppl ementation onbody composition. strength , an d sprint performan ce. MedSCiSports Exerc 1998;30: 73- 82.
37. Bennett T. Bathalon G. Armstrong D. et aI: Effect of creatine on performanc e ofmilitarily relevant tasks and soldier health . Mllit Med 200 1; 166: 996 - 1002.
38. Balsom PD. Harndge SDR, Soderlund K, Sjodin B. Ekblom B: Creatine supple-
Military Medicine. Vol. 168. January 2003
Health Assess ment of U,S. Army Rangers
mentation per se does not enhance endu ran ce exercise performance. Acta PhysiolSCand 1993; 149: 52 1-3.
39. Cooke WH. GrandJean PW.Barnes WS: Effect of oral creatine supplementation onpower output and fatigue during bicycle ergometry. J Appl Physio! 1995; 78: 670 -3.
40. Bucci LR: Selected herbals an d human exercise performance . Am J Clin Nutr2000 : 72(Suppl): 6245-36S.
41. SChel E. Sogaard J : The impact of military service on young men's smokingbehavior. Prev Med 1994; 23: 242-8.
42. Haddock CK. Klesges RC. Talcott GW. Lando H. Stein RJ: Smoking prevalenceand risk factors for smoking in a population of United States Air Force basictrainees. Tob Control 1998; 7: 232-5.
43. Thakk er KD: An overview of health risks and benefits of alcohol cons umption.Alcohol Clin Exp Res 1998; 22(Suppl): 2855-985 .
44. Bishop PA. Fielitz LR, Crowder TA. Anderson CL. Smith JH . Derrick KR: Physiological determinants of performance on an indoor military obstacle course test.Millt Med 1999; 164: 891-6.
V1SH KID MOUY. AGE 6
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/168/1/57/4915738 by guest on 22 July 2022
Related Documents











