HEALTH ANXIETY AMONG OLDER ADULTS: ASSESSING THE EFFICACY OF COGNITIVE BEHAVIOURAL TREATMENT A Thesis Submitted to the Faculty of Graduate Studies and Research In Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy in Clinical Psychology University of Regina by Michelle D. Bourgault-Fagnou Regina, Saskatchewan December 2010 Copyright 2010: M. D. Bourgault-Fagnou HEALTH ANXIETY AMONG OLDER ADULTS: ASSESSING THE EFFICACY OF COGNITIVE BEHAVIOURAL TREATMENT A Thesis Submitted to the Faculty of Graduate Studies and Research In Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy in Clinical Psychology University of Regina by Michelle D. Bourgault-Fagnou Regina, Saskatchewan December 2010 Copyright 2010: M. D. Bourgault-Fagnou

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
HEALTH ANXIETY AMONG OLDER ADULTS: ASSESSING THE EFFICACY OF
COGNITIVE BEHAVIOURAL TREATMENT
A Thesis
Submitted to the Faculty of Graduate Studies and Research
In Partial Fulfillment of the Requirements
for the Degree of
Doctor of Philosophy
in Clinical Psychology
University of Regina
by
Michelle D. Bourgault-Fagnou
Regina, Saskatchewan
December 2010
Copyright 2010: M. D. Bourgault-Fagnou
HEALTH ANXIETY AMONG OLDER ADULTS: ASSESSING THE EFFICACY OF
COGNITIVE BEHAVIOURAL TREATMENT
A Thesis
Submitted to the Faculty of Graduate Studies and Research
In Partial Fulfillment of the Requirements
for the Degree of
Doctor of Philosophy
in Clinical Psychology
University of Regina
by
Michelle D. Bourgault-Fagnou
Regina, Saskatchewan
December 2010
Copyright 2010: M. D. Bourgault-Fagnou

1+1
NOTICE:
Library and Archives Canada
Published Heritage Branch
395 Wellington Street Ottawa ON K1 A ON4 Canada
The author has granted a non-exclusive license allowing Library and Archives Canada to reproduce, publish, archive, preserve, conserve, communicate to the public by telecommunication or on the Internet, loan, distribute and sell theses worldwide, for commercial or non-commercial purposes, in microform, paper, electronic and/or any other formats.
The author retains copyright ownership and moral rights in this thesis. Neither the thesis nor substantial extracts from it may be printed or otherwise reproduced without the author's permission.
Bibliotheque et Archives Canada
Direction du Patrimoine de redition
395, rue Wellington Ottawa ON KlA ON4 Canada
Your file Votre reference ISBN: 978-0-494-79975-8 Our file Notre reference ISBN: 978-0-494-79975-8
AVIS:
L'auteur a accord& une licence non exclusive permettant a Ia Bibliotheque et Archives Canada de reproduire, publier, archiver, sauvegarder, conserver, transmettre au public par telecommunication ou par ('Internet, preter, distribuer et vendre des theses partout dans le monde, a des fins commerciales ou autres, sur support microforme, papier, electronique et/ou autres formats.
L'auteur conserve Ia propriete du droit d'auteur et des droits moraux qui protege cette these. Ni Ia these ni des extraits substantiels de celle-ci ne doivent etre imprimes ou autrement reproduits sans son autorisation.
In compliance with the Canadian Privacy Act some supporting forms may have been removed from this thesis.
While these forms may be included in the document page count, their removal does not represent any loss of content from the thesis.
141
Canada
Conformement a Ia loi canadienne sur la protection de la vie privee, quelques formulaires secondaires ont ete enleves de cette these.
Bien que ces formulaires aient inclus dans la pagination, it n'y aura aucun contenu manquant.
1*1 Library and Archives Canada
Published Heritage Branch
395 Wellington Street OttawaONK1A0N4 Canada
Bibliotheque et Archives Canada
Direction du Patrimoine de I'edition
395, rue Wellington Ottawa ON K1A 0N4 Canada
Your file Votre reference ISBN: 978-0-494-79975-8 Our We Notre reference ISBN: 978-0-494-79975-8
NOTICE: AVIS:
The author has granted a nonexclusive license allowing Library and Archives Canada to reproduce, publish, archive, preserve, conserve, communicate to the public by telecommunication or on the Internet, loan, distribute and sell theses worldwide, for commercial or noncommercial purposes, in microform, paper, electronic and/or any other formats.
L'auteur a accorde une licence non exclusive permettant a la Bibliotheque et Archives Canada de reproduire, publier, archiver, sauvegarder, conserver, transmettre au public par telecommunication ou par I'lnternet, preter, distribuer et vendre des theses partout dans le monde, a des fins commerciales ou autres, sur support microforme, papier, electronique et/ou autres formats.
The author retains copyright ownership and moral rights in this thesis. Neither the thesis nor substantial extracts from it may be printed or otherwise reproduced without the author's permission.
L'auteur conserve la propriete du droit d'auteur et des droits moraux qui protege cette these. Ni la these ni des extra its substantiels de celle-ci ne doivent etre imprimes ou autrement reproduits sans son autorisation.
In compliance with the Canadian Privacy Act some supporting forms may have been removed from this thesis.
Conformement a la loi canadienne sur la protection de la vie privee, quelques formulaires secondaires ont ete enleves de cette these.
While these forms may be included in the document page count, their removal does not represent any loss of content from the thesis.
Bien que ces formulaires aient inclus dans la pagination, il n'y aura aucun contenu manquant.
1+1
Canada

UNIVERSITY OF REGINA
FACULTY OF GRADUATE STUDIES AND RESEARCH
SUPERVISORY AND EXAMINING COMMITTEE
Ms. Michelle Denise Bourgault-Fagnou, candidate for the degree of Doctor of Philosophy in Psychology, has presented a thesis titled, Health Anxiety Among Older Adults: Assessing The Efficacy Of Cognitive Behavioural Treatment, in an oral examination held on December 15, 2010. The following committee members have found the thesis acceptable in form and content, and that the candidate demonstrated satisfactory knowledge of the subject material.
External Examiner: **Dr. Patricia Furer, Faculty of Medicine, University of Manitoba
Supervisor: Dr. Heather Hadjistavropoulos, Department of Psychology
Committee Member: Dr. Gordon Asmundson, Department of Psychology
Committee Member: *Dr. Thomas Hadjistavropoulos, Department of Psychology
Committee Member: Dr. Ron Martin, Faculty of Education
Chair of Defense: Dr. Ian Germani, Department of History
*Not present at defense **Via Video Conference
UNIVERSITY OF REGINA
FACULTY OF GRADUATE STUDIES AND RESEARCH
SUPERVISORY AND EXAMINING COMMITTEE
Ms. Michelle Denise Bourgault-Fagnou, candidate for the degree of Doctor of Philosophy in Psychology, has presented a thesis titled, Health Anxiety Among Older Adults: Assessing The Efficacy Of Cognitive Behavioural Treatment, in an oral examination held on December 15, 2010. The following committee members have found the thesis acceptable in form and content, and that the candidate demonstrated satisfactory knowledge of the subject material.
External Examiner: *Dr. Patricia Furer, Faculty of Medicine, University of Manitoba
Supervisor: Dr. Heather Hadjistavropoulos, Department of Psychology
Committee Member: Dr. Gordon Asmundson, Department of Psychology
Committee Member: "Dr. Thomas Hadjistavropoulos, Department of Psychology
Committee Member: Dr. Ron Martin, Faculty of Education
Chair of Defense: Dr. Ian Germani, Department of History
*Not present at defense **Via Video Conference

ABTRACT
The purpose of this research was to assess the effectiveness of a six-session enhanced
cognitive behavioural therapy (ECBT) program for health anxiety in older adults (i.e.,
learning and memory aids), and to examine whether the program fostered the therapeutic
alliance and motivation for psychotherapy as compared to a standard cognitive
behavioural therapy (SCBT) program and wait-list control (WLC) condition. In Study 1,
57 community dwelling seniors 60 years of age and over with elevated levels of health
anxiety were randomly assigned to six weeks of SCBT, ECBT, or WLC. At pre-
treatment, post-treatment, and three-month follow-up, participants completed
questionnaires on health anxiety and its dimensions, and measures of anxiety sensitivity,
state and trait anxiety, depression, pain, and health-related quality of life. Participants
also completed measures of therapeutic alliance and motivation for psychotherapy.
Participants were asked to complete open-ended questions at pre-treatment on the nature
of health anxiety and at post-treatment on the experience of therapy. In Study 2, a control
group of 57 community participants matched with the older adult group on sex and
Whiteley Index (WI) score was used as a comparison on measures of health anxiety and
its dimensions. In Study 1, the results of the mixed factorial ANCOVAs indicated
participants in the SCBT and ECBT groups showed significantly lower levels of health
anxiety on the WI, with significant reductions in both group on subscales measuring
disease fear and bodily preoccupation. There was also a significant improvement in the
SCBT group on the physical component of health-related quality of life when compared
to the WLC group. Using paired samples t-tests to examine pre- to post-treatment scores,
ii
ABTRACT
The purpose of this research was to assess the effectiveness of a six-session enhanced
cognitive behavioural therapy (ECBT) program for health anxiety in older adults (i.e.,
learning and memory aids), and to examine whether the program fostered the therapeutic
alliance and motivation for psychotherapy as compared to a standard cognitive
behavioural therapy (SCBT) program and wait-list control (WLC) condition. In Study 1,
57 community dwelling seniors 60 years of age and over with elevated levels of health
anxiety were randomly assigned to six weeks of SCBT, ECBT, or WLC. At pre-
treatment, post-treatment, and three-month follow-up, participants completed
questionnaires on health anxiety and its dimensions, and measures of anxiety sensitivity,
state and trait anxiety, depression, pain, and health-related quality of life. Participants
also completed measures of therapeutic alliance and motivation for psychotherapy.
Participants were asked to complete open-ended questions at pre-treatment on the nature
of health anxiety and at post-treatment on the experience of therapy. In Study 2, a control
group of 57 community participants matched with the older adult group on sex and
Whiteley Index (WI) score was used as a comparison on measures of health anxiety and
its dimensions. In Study 1, the results of the mixed factorial ANCOVAs indicated
participants in the SCBT and ECBT groups showed significantly lower levels of health
anxiety on the WI, with significant reductions in both group on subscales measuring
disease fear and bodily preoccupation. There was also a significant improvement in the
SCBT group on the physical component of health-related quality of life when compared
to the WLC group. Using paired samples t-tests to examine pre- to post-treatment scores,
ii
participants in the SCBT group demonstrated significant improvements on all three
measures of health anxiety, state and trait anxiety, depression, and both physical and
mental components of health-related quality of life; participants in the ECBT group
demonstrated significant improvements on two measures of health anxiety (WI, Short
Health Anxiety Inventory), hypochondriacal somatic symptoms, anxiety sensitivity, and
depression. Only one measure showed improvement in the WLC group. On both the
ANCOVAs and paired samples t-tests, from post-treatment to follow-up, treatment gains
were maintained and improvements were seen on select measures. These findings, along
with findings from examination of clinically significant change, maintenance of gains at
follow-up, and post-treatment responses to open-ended questions, suggested both SCBT
and ECBT were effective in improving scores on measures. Qualitative analysis of open-
ended responses at pre-treatment identified five themes describing the development of
health anxiety in older adults including Anxiety as Genetic, Anxiety as a Learned
Response, Vulnerability to Illness and Disease, Awfulness of Illness, Inability to Cope,
and Inadequacy of Physicians/Medical Care. In Study 2, the younger adult group was
significantly higher than the older adult group on all measures with the exception of a
subscale measuring disease fear/phobia. Although the results from Study 1 were mixed,
overall, the findings indicated that cognitive behavioural therapy is effective for reducing
aspects of health anxiety in older adults. The results contributed to the understanding of
therapeutic factors and the cognitive behavioural model of health anxiety in older adults.
Additional study implications, contributions, limitations, and future directions are
discussed.
iii
participants in the SCBT group demonstrated significant improvements on all three
measures of health anxiety, state and trait anxiety, depression, and both physical and
mental components of health-related quality of life; participants in the ECBT group
demonstrated significant improvements on two measures of health anxiety (WI, Short
Health Anxiety Inventory), hypochondriacal somatic symptoms, anxiety sensitivity, and
depression. Only one measure showed improvement in the WLC group. On both the
ANCOVAs and paired samples t-tests, from post-treatment to follow-up, treatment gains
were maintained and improvements were seen on select measures. These findings, along
with findings from examination of clinically significant change, maintenance of gains at
follow-up, and post-treatment responses to open-ended questions, suggested both SCBT
and ECBT were effective in improving scores on measures. Qualitative analysis of open-
ended responses at pre-treatment identified five themes describing the development of
health anxiety in older adults including Anxiety as Genetic, Anxiety as a Learned
Response, Vulnerability to Illness and Disease, Awfulness of Illness, Inability to Cope,
and Inadequacy of Physicians/Medical Care. In Study 2, the younger adult group was
significantly higher than the older adult group on all measures with the exception of a
subscale measuring disease fear/phobia. Although the results from Study 1 were mixed,
overall, the findings indicated that cognitive behavioural therapy is effective for reducing
aspects of health anxiety in older adults. The results contributed to the understanding of
therapeutic factors and the cognitive behavioural model of health anxiety in older adults.
Additional study implications, contributions, limitations, and future directions are
discussed.
iii

ACKNOWLEDGEMENTS
Many people contributed their time and knowledge to this dissertation and provided
valuable advice and assistance throughout the process. First and foremost, I would like to
extend my deepest gratitude to my supervisor, Dr. Heather Hadjistavropoulos. She has
been an ongoing source of support and guidance through all the phases of this project.
Her expertise, assistance, and feedback were essential to the completion of this study. I
am very grateful to have such an inspiring and supportive advisor who always took the
time to provide encouragement and guidance. I would also like to thank the members of
my committee, Drs. Gordon Asmundson, Thomas Hadjistavropoulos, and Ron Martin,
for their time, expertise, support, and efficiency. All three have contributed substantially
and my dissertation benefited as a result. I would especially like to thank my participants
who contributed their time and information to this study. Without their help, this
dissertation would not have been possible. Also, a special thank you to Amy Janzen,
Amanda Lints-Martindale, and Jocelyne Leclerc for their assistance in data collection. I
would like to thank the Centre on Aging and Health at the University of Regina for
providing me with SGI Graduate Fellowships in Aging and Health to assist in the funding
of my program. I would also like to acknowledge the Faculty of Graduate Studies and
Research for providing teaching assistantships and scholarships to help fund my studies
and research.
iv
ACKNOWLEDGEMENTS
Many people contributed their time and knowledge to this dissertation and provided
valuable advice and assistance throughout the process. First and foremost, I would like to
extend my deepest gratitude to my supervisor, Dr. Heather Hadjistavropoulos. She has
been an ongoing source of support and guidance through all the phases of this project.
Her expertise, assistance, and feedback were essential to the completion of this study. I
am very grateful to have such an inspiring and supportive advisor who always took the
time to provide encouragement and guidance. I would also like to thank the members of
my committee, Drs. Gordon Asmundson, Thomas Hadjistavropoulos, and Ron Martin,
for their time, expertise, support, and efficiency. All three have contributed substantially
and my dissertation benefited as a result. I would especially like to thank my participants
who contributed their time and information to this study. Without their help, this
dissertation would not have been possible. Also, a special thank you to Amy Janzen,
Amanda Lints-Martindale, and Jocelyne Leclerc for their assistance in data collection. I
would like to thank the Centre on Aging and Health at the University of Regina for
providing me with SGI Graduate Fellowships in Aging and Health to assist in the funding
of my program. I would also like to acknowledge the Faculty of Graduate Studies and
Research for providing teaching assistantships and scholarships to help fund my studies
and research.
iv

DEDICATION
I would like to thank my parents, Gerry and Louise, for their unwavering support during
the course of this work. Without their help, I could not have completed this dissertation.
A well-deserved thank you also goes to my siblings and my friends for their help,
empathy, and support. Most importantly, I would like to acknowledge my husband,
Andre, for the many sacrifices he made in order to support me in completing this work.
Thank you for your endless patience, understanding, and support.
v
DEDICATION
I would like to thank my parents, Gerry and Louise, for their unwavering support during
the course of this work. Without their help, I could not have completed this dissertation.
A well-deserved thank you also goes to my siblings and my friends for their help,
empathy, and support. Most importantly, I would like to acknowledge my husband,
Andre, for the many sacrifices he made in order to support me in completing this work.
Thank you for your endless patience, understanding, and support.
v
TABLE OF CONTENTS
ABSTRACT ii
ACKNOWLEDGEMENTS iv
DEDICATION v
TABLE OF CONTENTS vi
LIST OF TABLES x
LIST OF FIGURES xiii
LIST OF APPENDICES xvi
1. INTRODUCTION 1
1.1 Overview 1
1.2 Health Anxiety Versus Hypochondriasis 4
1.3 Features Associated with Health Anxiety 9
1.3.1 Cognitive and Somatic Features 9
1.3.2 Behaviours Associated with Health Anxiety 10
1.3.3 Patient-Physician Relationships 12
1.4 Theoretical Approach to Health Anxiety 14
1.4.1 Misinterpretations and Maintenance of Health Anxiety 16
1.5 Health Anxiety Among Seniors 26
1.5.1 How Does the Cognitive Behavioural Model of Health 29
Anxiety Apply to Older Adults?
1.6 Other Forms of Anxiety Among Seniors 30
1.6.1 Symptoms of Anxiety: Trait and State Anxiety 30
vi
TABLE OF CONTENTS
ABSTRACT ii
ACKNOWLEDGEMENTS iv
DEDICATION v
TABLE OF CONTENTS vi
LIST OF TABLES x
LIST OF FIGURES xiii
LIST OF APPENDICES xvi
1. INTRODUCTION 1
1.1 Overview 1
1.2 Health Anxiety Versus Hypochondriasis 4
1.3 Features Associated with Health Anxiety 9
1.3.1 Cognitive and Somatic Features 9
1.3.2 Behaviours Associated with Health Anxiety 10
1.3.3 Patient-Physician Relationships 12
1.4 Theoretical Approach to Health Anxiety 14
1.4.1 Misinterpretations and Maintenance of Health Anxiety 16
1.5 Health Anxiety Among Seniors 26
1.5.1 How Does the Cognitive Behavioural Model of Health 29
Anxiety Apply to Older Adults?
1.6 Other Forms of Anxiety Among Seniors 30
1.6.1 Symptoms of Anxiety: Trait and State Anxiety 30
vi

1.6.2 Anxiety Sensitivity 32
1.7 Depression and Its Relationship to Health Anxiety in Seniors 33
1.8 Treatment Issues 34
1.8.1 Treatment of Health Anxiety 34
1.8.2 Enhancing CBT for Use with Older Adults 44
1.8.3 Reason Why CBT May Be Effective with Older Adults 46
1.8.4 Fostering the Therapeutic Alliance 47
1.8.5 Motivation in Psychotherapy 50
1.9 Research Problem and Purpose 52
1.10 Hypotheses 55
1.10.1 Hypotheses: Study 1 55
1.10.2 Hypotheses: Study 2 56
2. METHOD 57
2.1 Study 1 57
2.1.1 Participants 57
2.1.2 Measures 60
2.1.2.1 Primary Outcome Measures 64
2.1.2.2 Secondary Outcome Measures 75
2.1.2.3 Therapy Programs: Measures of the
Therapeutic Relationship and
Motivation for Psychotherapy 79
2.1.3 Standard Cognitive Behavioural Therapy (SCBT) and
vii
1.6.2 Anxiety Sensitivity 32
1.7 Depression and Its Relationship to Health Anxiety in Seniors 33
1.8 Treatment Issues 34
1.8.1 Treatment of Health Anxiety 34
1.8.2 Enhancing CBT for Use with Older Adults 44
1.8.3 Reason Why CBT May Be Effective with Older Adults 46
1.8.4 Fostering the Therapeutic Alliance 47
1.8.5 Motivation in Psychotherapy 50
1.9 Research Problem and Purpose 52
1.10 Hypotheses 55
1.10.1 Hypotheses: Study 1 55
1.10.2 Hypotheses: Study 2 56
2. METHOD 57
2.1 Study 1 57
2.1.1 Participants 57
2.1.2 Measures 60
2.1.2.1 Primary Outcome Measures 64
2.1.2.2 Secondary Outcome Measures 75
2.1.2.3 Therapy Programs: Measures of the
Therapeutic Relationship and
Motivation for Psychotherapy 79
2.1.3 Standard Cognitive Behavioural Therapy (SCBT) and
vii

Enhanced Cognitive Behavioural Therapy (ECBT) 81
2.1.4 Procedure 83
2.1.5 Design and Analyses 85
2.1.5.1 Analyses 85
2.1.5.2 Preparation of the Data for Analysis 87
2.1.5.3 Qualitative Data Analysis 88
2.2 Study 2 90
2.2.1 Participants and Procedure 90
2.2.2 Preparation of the Data for Analysis 91
3. RESULTS 95
3 1 Study 1 95
3.1.1 Preliminary Analyses 95
3.1.2 Testing Hypothesis 1 105
3.1.2.1 Subscale Comparisons 110
3.1.2.2 Secondary Outcome Measures 114
3.1.3 Testing Hypotheses 2 and 3: Stability of Improvements 120
3.1.4 Hypothesis 4 and 5 — Therapeutic Alliance and Motivation
for Psychotherapy 124
3.1.5 Process and Significance of Change 127
3.1.5.1 Treatment Specific Change 127
3.1.5.2 Clinically Significant Change 137
3.1.6 Supplementary Analyses 141
viii
Enhanced Cognitive Behavioural Therapy (ECBT) 81
2.1.4 Procedure 83
2.1.5 Design and Analyses 85
2.1.5.1 Analyses 85
2.1.5.2 Preparation of the Data for Analysis 87
2.1.5.3 Qualitative Data Analysis 88
2.2 Study 2 90
2.2.1 Participants and Procedure 90
2.2.2 Preparation of the Data for Analysis 91
3. RESULTS 95
3.1 Study 1 95
3.1.1 Preliminary Analyses 95
3.1.2 Testing Hypothesis 1 105
3.1.2.1 Subscale Comparisons 110
3.1.2.2 Secondary Outcome Measures 114
3.1.3 Testing Hypotheses 2 and 3: Stability of Improvements 120
3.1.4 Hypothesis 4 and 5 - Therapeutic Alliance and Motivation
for Psychotherapy 124
3.1.5 Process and Significance of Change 127
3.1.5.1 Treatment Specific Change 127
3.1.5.2 Clinically Significant Change 137
3.1.6 Supplementary Analyses 141
viii

3.1.6.1 Relationship Between Health Anxiety and the Therapeutic
Relationship and Motivation for Psychotherapy at Post-
Treatment 141
3.1.6.2 Analysis of Change in the WLC Group 146
3.1.7 Results of the Qualitative Analysis 155
3.1.7.1 Pre-Treatment Responses 155
3.1.7.2 Post-Treatment Responses 163
3.2 Study 2 173
3.2.1 Comparison on Anxiety Measures 173
4. DISCUSSION 176
4.1 Assessment of Hypotheses 177
4.2 Qualitative Analysis Examining Experience of Health Anxiety 190
Among Seniors
4.3 Comparison of Older and Younger Adults on Health Anxiety 192
4.4 Contributions 195
4.5 Limitations 196
4.6 Future Directions 199
4.7 Conclusion 201
5. REFERENCES 202
ix
3.1.6.1 Relationship Between Health Anxiety and the Therapeutic
Relationship and Motivation for Psychotherapy at Post-
Treatment 141
3.1.6.2 Analysis of Change in the WLC Group 146
3.1.7 Results of the Qualitative Analysis 155
3.1.7.1 Pre-Treatment Responses 155
3.1.7.2 Post-Treatment Responses 163
3.2 Study 2 173
3.2.1 Comparison on Anxiety Measures 173
4. DISCUSSION 176
4.1 Assessment of Hypotheses 177
4.2 Qualitative Analysis Examining Experience of Health Anxiety 190
Among Seniors
4.3 Comparison of Older and Younger Adults on Health Anxiety 192
4.4 Contributions 195
4.5 Limitations 196
4.6 Future Directions 199
4.7 Conclusion 201
5. REFERENCES 202
ix

LIST OF TABLES
Table
1. Background Characteristics by Group 59
2. Comparisons of Background Characteristics between Groups 61
3. Summary of Participants' Health Conditions by Group 62
4. Demographic Information and Scale Scores for Matched Participants 92
5. Summary of Participants' Health Conditions by Group 93
6. Means and Standard Deviations for Primary and Secondary Outcome
Measures 96
7. Means and Standard Deviations for WI, SHAI, and IAS Subscales 99
8. Means and Standard Deviations for WAI and NML-2 Subscales 101
9. Correlations Between Measures at Pre-Treatment 103
10. Mixed-Factor 3 (Treatment) x 2 (Time) ANCOVAs for Primary
Outcome Measures 106
11. Comparisons from Pre- to Post-Treatment for Primary Dependent
Variables 109
12. Mixed-Factor 3 (Treatment) x 2 (Time) ANCOVAs for WI, SHAI, and
IAS Subscales 111
13. Comparisons from Pre- to Post-Treatment for WI Subscale 113
14. Mixed-Factor 3 (Treatment) x 2 (Time) ANCOVAs for Secondary
Outcome Measures 117
LIST OF TABLES
Table
1. Background Characteristics by Group 59
2. Comparisons of Background Characteristics between Groups 61
3. Summary of Participants'Health Conditions by Group 62
4. Demographic Information and Scale Scores for Matched Participants 92
5. Summary of Participants'Health Conditions by Group 93
6. Means and Standard Deviations for Primary and Secondary Outcome
Measures 96
7. Means and Standard Deviations for WI, SHAI, and IAS Subscales 99
8. Means and Standard Deviations for WAI and NML-2 Subscales 101
9. Correlations Between Measures at Pre-Treatment 103
10. Mixed-Factor 3 (Treatment) x 2 (Time) ANCOVAs for Primary
Outcome Measures 106
11. Comparisons from Pre- to Post-Treatment for Primary Dependent
Variables 109
12. Mixed-Factor 3 (Treatment) x 2 (Time) ANCOVAs for WI, SHAI, and
IAS Subscales 111
13. Comparisons from Pre- to Post-Treatment for WI Subscale 113
14. Mixed-Factor 3 (Treatment) x 2 (Time) ANCOVAs for Secondary
Outcome Measures 117

15. Comparisons from Pre- to Post-Treatment for Secondary Outcome
Measures 119
16. Comparisons from Post-Treatment to Follow-Up for the Primary
Outcome Measures 121
17. Comparisons from Post-Treatment to Follow-Up for the WI, SHAI,
and IAS Subscales 122
18. Comparisons from Post-Treatment to Follow-Up for the Secondary
Outcome Measures. 123
19. Mixed-Factor 3 (Time) x 2 (Treatment) ANCOVAs for WAI and
NML-2 Subscales 125
20. Comparisons from Session 1, Session 3, and Session 6 on the WAI-
Goals Subscale 126
21. Paired T-Tests for Each Primary Outcome Measure 129
22. Paired T-Tests for Each Subscale on WAI, SHAI, and IAS 131
23. Paired T-Tests for Each Secondary Outcome Measure 134
24. Correlations Between the WAI and NML-2 and the Health Anxiety
Measures Change Scores in the SCBT Group 142
25. Correlations Between the WAI and NML-2 and the Health Anxiety
Measures Change Scores in the ECBT Group 144
26. WLC Group Analyses at Time 1, 2, and 3 for the Primary Outcome
Measures 147
27. WLC Group Analyses at Time 1, 2, and 3 for the Secondary Outcome
xi
15. Comparisons from Pre- to Post-Treatment for Secondary Outcome
Measures 119
16. Comparisons from Post-Treatment to Follow-Up for the Primary
Outcome Measures 121
17. Comparisons from Post-Treatment to Follow-Up for the WI, SHAI,
and IAS Subscales 122
18. Comparisons from Post-Treatment to Follow-Up for the Secondary
Outcome Measures. 123
19. Mixed-Factor 3 (Time) x 2 (Treatment) ANCOVAs for WAI and
NML-2 Subscales 125
20. Comparisons from Session 1, Session 3, and Session 6 on the WAI-
Goals Subscale 126
21. Paired T-Tests for Each Primary Outcome Measure 129
22. Paired T-Tests for Each Subscale on WAI, SHAI, and IAS 131
23. Paired T-Tests for Each Secondary Outcome Measure 134
24. Correlations Between the WAI and NML-2 and the Health Anxiety
Measures Change Scores in the SCBT Group 142
25. Correlations Between the WAI and NML-2 and the Health Anxiety
Measures Change Scores in the ECBT Group 144
26. WLC Group Analyses at Time 1, 2, and 3 for the Primary Outcome
Measures 147
27. WLC Group Analyses at Time 1, 2, and 3 for the Secondary Outcome
xi

Measures 149
28. WLC Group Analyses at Time 1, 2, and 3 for the WI and SHAI
Subscales 151
29. Themes and Sub-Themes of the Development of Health Anxiety in
Seniors 156
30. Themes and Sub-Themes of Older Adults' Experiences and
Perceptions of Psychological Treatment for Health Anxiety 165
31. Scale Scores for Matched Participants 174
xii
Measures 149
28. WLC Group Analyses at Time 1, 2, and 3 for the WI and SHAI
Subscales 151
29. Themes and Sub-Themes of the Development of Health Anxiety in
Seniors 156
30. Themes and Sub-Themes of Older Adults' Experiences and
Perceptions of Psychological Treatment for Health Anxiety 165
31. Scale Scores for Matched Participants 174
xii
LIST OF FIGURES
Figure
1. Cognitive behavioural model of the development of health anxiety 15
2. Relationship between enhancements, factors affecting seniors in
therapy, and outcome in psychotherapy 54
3. Flow of participants through the treatments 86
4. Mean WI scores by treatment condition at pre-treatment and post-
treatment 108
5. Mean WI — Disease Fear/Phobia scores by treatment condition at pre-
treatment and post-treatment 115
6. Mean SF-12-PCS scores by treatment condition at pre-treatment and
post-treatment 118
7. Mean WAI - Goal scores by treatment condition at Session 1, Session
2, and Session 3 128
8. Proportion of participants in each treatment condition who
demonstrated clinically significant change, according to Jacobson and
Truax's (1992) definition, on the WI 139
9. Proportion of participants in each treatment condition who had WI
scores below 8 at post-treatment 141
10. Model of the development of health anxiety in older adults 157
11. Model of older adults' experiences and perceptions of psychological
treatment for health anxiety 164
LIST OF FIGURES
Figure
1. Cognitive behavioural model of the development of health anxiety 15
2. Relationship between enhancements, factors affecting seniors in
therapy, and outcome in psychotherapy 54
3. Flow of participants through the treatments 86
4. Mean WI scores by treatment condition at pre-treatment and post-
treatment 108
5. Mean WI - Disease Fear/Phobia scores by treatment condition at pre-
treatment and post-treatment 115
6. Mean SF-12-PCS scores by treatment condition at pre-treatment and
post-treatment 118
7. Mean WAI - Goal scores by treatment condition at Session 1, Session
2, and Session 3 128
8. Proportion of participants in each treatment condition who
demonstrated clinically significant change, according to Jacobson and
Truax's (1992) definition, on the WI 139
9. Proportion of participants in each treatment condition who had WI
scores below 8 at post-treatment 141
10. Model of the development of health anxiety in older adults 157
11. Model of older adults' experiences and perceptions of psychological
treatment for health anxiety 164
xiii
LIST OF APPENDICES
Appendix
A Recruitment Poster 233
B Information Sheet and Consent Form 234
C Outline of Videos 238
D University of Regina Research Ethics Board Approval 245
E Questionnaires 246
F Online Classified Notice 269
G Information Sheet and Consent Form for Online Study 270
xiv
LIST OF APPENDICES
Appendix
A Recruitment Poster 233
B Information Sheet and Consent Form 234
C Outline of Videos 238
D University of Regina Research Ethics Board Approval 245
E Questionnaires 246
F Online Classified Notice 269
G Information Sheet and Consent Form for Online Study 270
xiv

1. INTRODUCTION
1.1 Overview
Factors associated with aging, such as higher rates of medical illness, physical
frailty, and a heightened sense of mortality, may contribute to excessive preoccupation
with health-related issues among older adults (Snyder & Stanley, 2001). In fact, 10% to
15% of seniors exhibit a marked concern about their health (Ables, 1997). This is
problematic as heightened levels of anxiety among older adults have been found to be
associated with increased depression (Jeste, Hays, & Steffens, 2006), increased morbidity
(Ostir & Goodwin, 2006), chronic health conditions (Diala & Muntaner, 2003), and
markedly higher health care costs (Simon, Ormel, VonKoff, & Barlow, 1995). The
negative implications of anxiety demonstrate the importance of performing additional
research on the nature of anxiety as well as methods for reducing anxiety in the older
adult population.
The nature of anxiety can be best understood by examining both what it is and
what it is not. The construct of anxiety can be differentiated from the construct of fear,
for example. There is a great deal of evidence to suggest that anxiety and fear reactions
differ psychologically and physically (Barlow, Brown, & Craske, 1994). Fear can be
described as an immediate emotional reaction to an imminent threat or danger and it is
characterized by strong escapist action tendencies and activation of the autonomic
nervous system (e.g., increased heart rate and blood pressure; Barlow et al., 1994). The
term anxiety, on the other hand, is used to describe a future-oriented mood-state
characterized by marked negative affect, bodily symptoms of tension, and apprehension
1
1. INTRODUCTION
1.1 Overview
Factors associated with aging, such as higher rates of medical illness, physical
frailty, and a heightened sense of mortality, may contribute to excessive preoccupation
with health-related issues among older adults (Snyder & Stanley, 2001). In fact, 10% to
15% of seniors exhibit a marked concern about their health (Abies, 1997). This is
problematic as heightened levels of anxiety among older adults have been found to be
associated with increased depression (Jeste, Hays, & Steffens, 2006), increased morbidity
(Ostir & Goodwin, 2006), chronic health conditions (Diala & Muntaner, 2003), and
markedly higher health care costs (Simon, Ormel, VonKoff, & Barlow, 1995). The
negative implications of anxiety demonstrate the importance of performing additional
research on the nature of anxiety as well as methods for reducing anxiety in the older
adult population.
The nature of anxiety can be best understood by examining both what it is and
what it is not. The construct of anxiety can be differentiated from the construct of fear,
for example. There is a great deal of evidence to suggest that anxiety and fear reactions
differ psychologically and physically (Barlow, Brown, & Craske, 1994). Fear can be
described as an immediate emotional reaction to an imminent threat or danger and it is
characterized by strong escapist action tendencies and activation of the autonomic
nervous system (e.g., increased heart rate and blood pressure; Barlow et al., 1994). The
term anxiety, on the other hand, is used to describe a future-oriented mood-state
characterized by marked negative affect, bodily symptoms of tension, and apprehension
1

about the future because one cannot predict or control upcoming events (Barlow, 1988).
The focus of this research will be on anxiety regarding health among the older adult
population.
Several specific types of anxiety have been identified in the literature, such as
anxiety disorders, and trait, state, and health anxiety. Research focused on the prevalence
of specific anxiety disorders suggests they are a significant issue for older adults. Most
recently, Byers, Yaffe, Covinsky, Friedman, and Bruce (2010) examined nationally
representative estimates of age-specific 12-month prevalence rates of the Diagnostic and
Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV-TR; American
Psychiatric Association [APA], 2000) anxiety disorders among 2575 community-
dwelling adults 55 years of age and older in the National Comorbidity Survey Replication
(NCS-R) in the United States. Using the Composite International Diagnostic Interview
(CIDI; Kessler & Ustun, 2004), Byers et al. (2010) found that the most prevalent 12-
month anxiety disorder was specific phobia (6.5%), followed by social phobia (3.5%),
posttraumatic stress disorder (2.1%), generalized anxiety disorder (GAD) (2.0%), panic
disorder (1.3%), and agoraphobia without panic disorder (0.8%). The total prevalence of
anxiety disorders measured was 11.6%. The authors also found that the prevalence of
pooled anxiety disorder declined with age, with rates among women significantly more
prominent than men.
Rates of anxiety are even higher when significant but subsyndromal levels of
anxiety are assessed among older adults. For example, significant levels of anxiety have
ranged from 17% to as high as 47% using the State-Trait Anxiety Inventory (STAI,
2
about the future because one cannot predict or control upcoming events (Barlow, 1988).
The focus of this research will be on anxiety regarding health among the older adult
population.
Several specific types of anxiety have been identified in the literature, such as
anxiety disorders, and trait, state, and health anxiety. Research focused on the prevalence
of specific anxiety disorders suggests they are a significant issue for older adults. Most
recently, Byers, Yaffe, Covinsky, Friedman, and Bruce (2010) examined nationally
representative estimates of age-specific 12-month prevalence rates of the Diagnostic and
Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV-TR; American
Psychiatric Association [APA], 2000) anxiety disorders among 2575 community-
dwelling adults 55 years of age and older in the National Comorbidity Survey Replication
(NCS-R) in the United States. Using the Composite International Diagnostic Interview
(CIDI; Kessler & Ustun, 2004), Byers et al. (2010) found that the most prevalent 12-
month anxiety disorder was specific phobia (6.5%), followed by social phobia (3.5%),
posttraumatic stress disorder (2.1%), generalized anxiety disorder (GAD) (2.0%), panic
disorder (1.3%), and agoraphobia without panic disorder (0.8%). The total prevalence of
anxiety disorders measured was 11.6%. The authors also found that the prevalence of
pooled anxiety disorder declined with age, with rates among women significantly more
prominent than men.
Rates of anxiety are even higher when significant but subsyndromal levels of
anxiety are assessed among older adults. For example, significant levels of anxiety have
ranged from 17% to as high as 47% using the State-Trait Anxiety Inventory (STAI,
2

Spielberger, 1983) in community dwelling seniors (Himmelfarb & Murrell, 1984; Kvaal,
Macijauskiene, Engedal, & Laake, 2001). Using the Goldberg Anxiety Scale (GS-A;
Goldberg, Bridges, Duncan-Jones, & Grayson, 1988), Richardson, Simning, He, and
Conwell (2010) found that among 377 community dwelling older adults, 27.3% had
clinically significant symptoms of anxiety (GS-A > 6).
Researchers have also investigated worry (apprehensive expectation) themes of
older adults. Montorio, Nuevo, Marquez, Izal, and Losada (2003) found that the most
frequent contents of worry among a sample of 85 older adults were related mainly to
family and personal health. Similarly, Skarborn and Nicki (1996) found health-related
worries to be the most prevalent concern among a sample of 100 community-dwelling
Canadian seniors (aged 65 and older). Wisocki (1988) found that the primary health-
related worries of 94 community seniors included worry about sensory and motor losses,
failing memory, illness or accident involving family members, loss of independence, and
depression. Rodin and Timko (1992) suggest that older adults are especially susceptible
to anxiety about failing health since it is a situation that threatens to reduce the control
they have or perceive to have over their lives.
In samples of community dwelling and primary care seniors, the prevalence and
nature of anxiety disorders indicate that health anxiety is a significant concern (Snyder &
Stanley, 2001). Health-related anxiety is also an important factor in GAD, phobias, panic
disorder, and obsessive-compulsive disorder among older adults (Snyder & Stanley,
2001). The research that has been completed to date provides evidence to suggest that a
considerable number of older adults may experience significant levels of health anxiety.
3
Spielberger, 1983) in community dwelling seniors (Himmelfarb & Murrell, 1984; Kvaal,
Macijauskiene, Engedal, & Laake, 2001). Using the Goldberg Anxiety Scale (GS-A;
Goldberg, Bridges, Duncan-Jones, & Grayson, 1988), Richardson, Simning, He, and
Conwell (2010) found that among 377 community dwelling older adults, 27.3% had
clinically significant symptoms of anxiety (GS-A > 6).
Researchers have also investigated worry (apprehensive expectation) themes of
older adults. Montorio, Nuevo, Marquez, Izal, and Losada (2003) found that the most
frequent contents of worry among a sample of 85 older adults were related mainly to
family and personal health. Similarly, Skarborn and Nicki (1996) found health-related
worries to be the most prevalent concern among a sample of 100 community-dwelling
Canadian seniors (aged 65 and older). Wisocki (1988) found that the primary health-
related worries of 94 community seniors included worry about sensory and motor losses,
failing memory, illness or accident involving family members, loss of independence, and
depression. Rodin and Timko (1992) suggest that older adults are especially susceptible
to anxiety about failing health since it is a situation that threatens to reduce the control
they have or perceive to have over their lives.
In samples of community dwelling and primary care seniors, the prevalence and
nature of anxiety disorders indicate that health anxiety is a significant concern (Snyder &
Stanley, 2001). Health-related anxiety is also an important factor in GAD, phobias, panic
disorder, and obsessive-compulsive disorder among older adults (Snyder & Stanley,
2001). The research that has been completed to date provides evidence to suggest that a
considerable number of older adults may experience significant levels of health anxiety.
3

There is only a limited amount of research that has examined health anxiety
among older adults, and no research that has examined outcomes of treatment for health
anxiety with this population. The focus of the present research was to gain a better
understanding of health anxiety among older adults and to assess the efficacy of cognitive
behavioural therapy (CBT) for health anxiety in both a standard format and a format
enhanced for older adults. In the following literature review, a description of health
anxiety followed by a summary of the cognitive behavioural (CB) theory of health
anxiety will be provided. Next, a review of research that has been conducted on health
anxiety among the older adult population and a review of some of the major research
findings associated with health anxiety in other populations that could contribute to our
knowledge of seniors will be provided. In addition, the research on anxiety among
seniors will be summarized. Attention will then be given to the CB approach to health
anxiety and treatment studies in this area to date. Finally, a summary of the issues around
enhancing the therapeutic alliance and motivation for psychotherapy among older adults
will be provided.
1.2 Health Anxiety versus Hypochondriasis
Although health anxiety and hypochondriasis share common features, they are
considered distinct constructs. Health anxiety has been conceptualized as a dimensional
construct that varies considerably from person to person, ranging in severity from mild to
severe (e.g., Barsky, Wyshak, & Klerman, 1986a; Ferguson, 2009; Salkovskis &
Warwick, 1986). Supporting this conceptualization in a recent taxometric analysis with
711 adults using the nine-item version of the Whiteley Index (WI; Pilowsky, 1967)
4
There is only a limited amount of research that has examined health anxiety
among older adults, and no research that has examined outcomes of treatment for health
anxiety with this population. The focus of the present research was to gain a better
understanding of health anxiety among older adults and to assess the efficacy of cognitive
behavioural therapy (CBT) for health anxiety in both a standard format and a format
enhanced for older adults. In the following literature review, a description of health
anxiety followed by a summary of the cognitive behavioural (CB) theory of health
anxiety will be provided. Next, a review of research that has been conducted on health
anxiety among the older adult population and a review of some of the major research
findings associated with health anxiety in other populations that could contribute to our
knowledge of seniors will be provided. In addition, the research on anxiety among
seniors will be summarized. Attention will then be given to the CB approach to health
anxiety and treatment studies in this area to date. Finally, a summary of the issues around
enhancing the therapeutic alliance and motivation for psychotherapy among older adults
will be provided.
1.2 Health Anxiety versus Hypochondriasis
Although health anxiety and hypochondriasis share common features, they are
considered distinct constructs. Health anxiety has been conceptualized as a dimensional
construct that varies considerably from person to person, ranging in severity from mild to
severe (e.g., Barsky, Wyshak, & Klerman, 1986a; Ferguson, 2009; Salkovskis &
Warwick, 1986). Supporting this conceptualization in a recent taxometric analysis with
711 adults using the nine-item version of the Whiteley Index (WI; Pilowsky, 1967)
4

scored on a five-point Likert-type scale (Barsky, Wyshak, & Klerman, 1990a), Ferguson
(2009) concluded that the pattern of results indicated that health anxiety is better
represented as a dimensional rather than a categorical construct. In another recent study
with 1,083 undergraduate students, Longley, Broman-Fulks, Calamari, Noyes, Wade, and
Orlando (in press) conducted a taxometric analysis of self report measures of
hypochondriasis to more comprehensively assess the full range of the construct.
Longley et al. (in press) evaluated the nature of these self report measures of
hypochondriasis using taxometric analysis of the following four empirically derived
symptom indicators: (a) cognitive—conviction that one is ill despite contrary evidence;
(b) perceptual—somatic sensitivity to body sensations; (c) behavioural—reassurance
seeking used to allay illness fears; and (d) affective—worry about health and illness. The
composite indicators included items from the Multidimensional Inventory of
Hypochondriacal Traits (Longley, Watson, & Noyes, 2005), Illness Attitudes Scale (IAS;
Kellner, 1987), and the WI. Longley et al. (in press) concluded that the results of
analyses provided convergent support that these self report measures of hypochondriasis
had a dimensional latent structure.
In contrast to health anxiety, hypochondriasis as specifically defined by the DSM-
IV-TR is a categorical construct and it can be distinguished from nonclinical health
anxiety by the degree of worry and conviction about having a serious disease, distress,
and interference in functioning (Barsky, Fama, Bailey, & Ahern, 1998). The presence of
health anxiety is necessary, but not sufficient, to assign a diagnosis of hypochondriasis.
To meet the diagnostic criteria for hypochondriasis, a person is required to have a six-
5
scored on a five-point Likert-type scale (Barsky, Wyshak, & Klerman, 1990a), Ferguson
(2009) concluded that the pattern of results indicated that health anxiety is better
represented as a dimensional rather than a categorical construct. In another recent study
with 1,083 undergraduate students, Longley, Broman-Fulks, Calamari, Noyes, Wade, and
Orlando (in press) conducted a taxometric analysis of self report measures of
hypochondriasis to more comprehensively assess the full range of the construct.
Longley et al. (in press) evaluated the nature of these self report measures of
hypochondriasis using taxometric analysis of the following four empirically derived
symptom indicators: (a) cognitive—conviction that one is ill despite contrary evidence;
(b) perceptual—somatic sensitivity to body sensations; (c) behavioural—reassurance
seeking used to allay illness fears; and (d) affective—worry about health and illness. The
composite indicators included items from the Multidimensional Inventory of
Hypochondriacal Traits (Longley, Watson, & Noyes, 2005), Illness Attitudes Scale (IAS;
Kellner, 1987), and the WI. Longley et al. (in press) concluded that the results of
analyses provided convergent support that these self report measures of hypochondriasis
had a dimensional latent structure.
In contrast to health anxiety, hypochondriasis as specifically defined by the DSM-
IV-TR is a categorical construct and it can be distinguished from nonclinical health
anxiety by the degree of worry and conviction about having a serious disease, distress,
and interference in functioning (Barsky, Fama, Bailey, & Ahern, 1998). The presence of
health anxiety is necessary, but not sufficient, to assign a diagnosis of hypochondriasis.
To meet the diagnostic criteria for hypochondriasis, a person is required to have a six-
5

month duration of symptoms, persistence despite medical reassurance following
appropriate medical evaluation, non-delusional intensity of beliefs regarding health, and
clinically significant interference in social, occupational, or other important areas of
functioning (APA, 2000).
Hypochondriasis is not the only disorder characterized by severe health anxiety
(Asmundson, Taylor, Sevgur, & Cox, 2001). Frequently, health anxiety co-occurs with
other clinical disorders, such as mood and anxiety disorders (e.g., illness phobia, panic
disorder; Noyes et al., 1994), and somatization disorder (Barsky, Barnett, & Cleary,
1994). Health anxiety is also commonly associated with various health conditions (e.g.,
cardiac conditions, chronic pain; Eifert, Zvolensky, & Lejuez, 2001; Hadjistavropoulos,
Owens, Hadjistavropoulos, & Asmundson, 2001). Due to the limited research on health
anxiety as a separate construct to hypochondriasis, a great deal of the research reviewed
in this paper was conducted with samples of individuals diagnosed with hypochondriasis.
This limitation should be kept in mind in reviewing the research that follows.
In the upcoming fifth edition of the Diagnostic and Statistical Manual of Mental
Disorders (APA, 2010) to be published in May 2013, the Work Group for Somatic
Symptom Disorders, which includes hypochondriasis, is recommending that this disorder
be subsumed into a new disorder called Complex Somatic Symptom Disorder (CSSD).
CSSD includes the previous diagnoses of Somatization Disorder, Undifferentiated
Somatoform Disorder, Hypochondriasis, Pain Disorder Associated With Both
Psychological Factors and a General Medical Condition, and Pain Disorder Associated
6
month duration of symptoms, persistence despite medical reassurance following
appropriate medical evaluation, non-delusional intensity of beliefs regarding health, and
clinically significant interference in social, occupational, or other important areas of
functioning (APA, 2000).
Hypochondriasis is not the only disorder characterized by severe health anxiety
(Asmundson, Taylor, Sevgur, & Cox, 2001). Frequently, health anxiety co-occurs with
other clinical disorders, such as mood and anxiety disorders (e.g., illness phobia, panic
disorder; Noyes et al., 1994), and somatization disorder (Barsky, Barnett, & Cleary,
1994). Health anxiety is also commonly associated with various health conditions (e.g.,
cardiac conditions, chronic pain; Eifert, Zvolensky, & Lejuez, 2001; Hadjistavropoulos,
Owens, Hadjistavropoulos, & Asmundson, 2001). Due to the limited research on health
anxiety as a separate construct to hypochondriasis, a great deal of the research reviewed
in this paper was conducted with samples of individuals diagnosed with hypochondriasis.
This limitation should be kept in mind in reviewing the research that follows.
In the upcoming fifth edition of the Diagnostic and Statistical Manual of Mental
Disorders (APA, 2010) to be published in May 2013, the Work Group for Somatic
Symptom Disorders, which includes hypochondriasis, is recommending that this disorder
be subsumed into a new disorder called Complex Somatic Symptom Disorder (CSSD).
CSSD includes the previous diagnoses of Somatization Disorder, Undifferentiated
Somatoform Disorder, Hypochondriasis, Pain Disorder Associated With Both
Psychological Factors and a General Medical Condition, and Pain Disorder Associated
6

With Psychological Factors. As outlined by the APA (2010), to meet criteria for CSSD,
criteria A, B, and C are necessary:
A. Somatic symptoms: One or more somatic symptoms that are distressing and/or result
in significant disruption in daily life.
B. Overwhelming concern or preoccupation with symptoms and illness: At least three
of the following are required to meet this criterion:
(1) High level of health-related anxiety.
(2) A tendency to fear the worst about one's health or bodily symptoms
(catastrophizing).
(3) Belief in the medical seriousness of one's symptoms despite evidence to the
contrary.
(4) Health concerns and/or symptoms assume a central role in one's life
(ruminative preoccupation).
C. Chronicity: Although any one symptom may not be continuously present, the state of
being symptomatic is chronic (at least 6 months).
The following optional specifiers may be applied to a diagnosis of CSSD where
one of the following dominates the clinical presentation (APA, 2010):
1. Multiplicity of somatic complaints (previously, somatization disorder).
2. High health anxiety (previously, hypochondriasis). If patients present solely with
health-related anxiety in the absence of somatic symptoms, they may be more
appropriately diagnosed as having an anxiety disorder.
7
With Psychological Factors. As outlined by the APA (2010), to meet criteria for CSSD,
criteria A, B, and C are necessary:
A. Somatic symptoms: One or more somatic symptoms that are distressing and/or result
in significant disruption in daily life.
B. Overwhelming concern or preoccupation with symptoms and illness: At least three
of the following are required to meet this criterion:
(1) High level of health-related anxiety.
(2) A tendency to fear the worst about one's health or bodily symptoms
(catastrophizing).
(3) Belief in the medical seriousness of one's symptoms despite evidence to the
contrary.
(4) Health concerns and/or symptoms assume a central role in one's life
(ruminative preoccupation).
C. Chronicity: Although any one symptom may not be continuously present, the state of
being symptomatic is chronic (at least 6 months).
The following optional specifiers may be applied to a diagnosis of CSSD where
one of the following dominates the clinical presentation (APA, 2010):
1. Multiplicity of somatic complaints (previously, somatization disorder).
2. High health anxiety (previously, hypochondriasis). If patients present solely with
health-related anxiety in the absence of somatic symptoms, they may be more
appropriately diagnosed as having an anxiety disorder.
7
3. Pain disorder. This classification is reserved for individuals presenting
predominantly with pain complaints who also have many of the features described
under criterion B. Patients with other presentations of pain may better fit other
psychiatric diagnoses, such as adjustment disorder or psychological factors
affecting a medical condition.
The Somatic Symptom Disorders Work Group and the Anxiety, Obsessive-
Compulsive Spectrum, Posttraumatic, and Dissociative Disorders Work Group are
considering the possibility that what was described as Hypochondriasis in the DSM-IV-
TR may represent a heterogeneous disorder in which some individuals may be better
considered to have CSSD and some may be better considered to have an anxiety disorder.
The website indicates that there will be ongoing discussion of this issue (APA, 2010).
Numerous researchers are in favour of viewing hypochondriasis as an anxiety
disorder given significant similarities between hypochondriasis and anxiety disorders
(e.g., Olatunji, Deacon, & Abramowitz, 2009). Like obsessive-compulsive disorder,
hypochondriasis involves intrusive, distressing thoughts and repetitive behaviours
(Olatunji, et al., 2009). In both hypochondriasis and obsessive-compulsive disorder,
dysfunctional beliefs (e.g., overestimation of the likelihood and severity of having an
illness, intolerance of uncertainty about the meaning of feared stimuli) are associated with
increased anxiety and distress, and subsequent attempts to check or seek reassurance
about the symptoms are associated with an immediate decrease in anxiety (Olatunji et al.,
2009).
8
3. Pain disorder. This classification is reserved for individuals presenting
predominantly with pain complaints who also have many of the features described
under criterion B. Patients with other presentations of pain may better fit other
psychiatric diagnoses, such as adjustment disorder or psychological factors
affecting a medical condition.
The Somatic Symptom Disorders Work Group and the Anxiety, Obsessive-
Compulsive Spectrum, Posttraumatic, and Dissociative Disorders Work Group are
considering the possibility that what was described as Hypochondriasis in the DSM-IV-
TR may represent a heterogeneous disorder in which some individuals may be better
considered to have CSSD and some may be better considered to have an anxiety disorder.
The website indicates that there will be ongoing discussion of this issue (APA, 2010).
Numerous researchers are in favour of viewing hypochondriasis as an anxiety
disorder given significant similarities between hypochondriasis and anxiety disorders
(e.g., Olatunji, Deacon, & Abramowitz, 2009). Like obsessive-compulsive disorder,
hypochondriasis involves intrusive, distressing thoughts and repetitive behaviours
(Olatunji, et al., 2009). In both hypochondriasis and obsessive-compulsive disorder,
dysfunctional beliefs (e.g., overestimation of the likelihood and severity of having an
illness, intolerance of uncertainty about the meaning of feared stimuli) are associated with
increased anxiety and distress, and subsequent attempts to check or seek reassurance
about the symptoms are associated with an immediate decrease in anxiety (Olatunji et al.,
2009).
8

The prominent preoccupation with bodily symptoms in both hypochondriasis and
panic disorder has also been identified (Barky, Barnett, & Clearly, 1994). The cognitive
and behavioural mechanisms that maintain hypochondriasis also appear similar to those
that maintain panic disorder, with the exception that the feared catastrophe is foreseen as
occurring immediately in panic disorder, resulting in the urge to escape right away
(Olatunji et al., 2009). In addition, both panic disorder and hypochondriasis involve
hypervigilance to bodily sensations and acute sensitivity to harmless or normal bodily
sensations (Olatunji, Deacon, Abramowitz, & Valentiner, 2007). This tendency to
misinterpret innocuous bodily symptoms as physically harmful (i.e., anxiety sensitivity)
is associated with both panic disorder and hypochondriasis (Deacon & Abramowitz,
2008). The combination of excessive body vigilance and high anxiety sensitivity leads to
the catastrophic misinterpretations of somatic cues (`this symptom means I have cancer'),
which evokes hypochondriacal fear and panic attacks. The coping strategies, such as
body checking and seeking medical reassurance (Deacon, Lickel, & Abramowitz, 2008),
that individuals with hypochondriasis and panic disorder use to manage their anxiety
paradoxically appear to maintain or even exacerbate the cognitive mechanisms that
underlie these disorders (Olatunji et al., 2009). In this study, the focus will be on those
individuals identified as having elevated health anxiety as compared to hypochondriasis.
1.3 Features Associated with Health Anxiety
1.3.1 Cognitive and Somatic Features of Health Anxiety
The cognitive features associated with excessive health anxiety include disease
conviction, disease preoccupation, hypervigilance for bodily changes, and difficulty with
9
The prominent preoccupation with bodily symptoms in both hypochondriasis and
panic disorder has also been identified (Barky, Barnett, & Clearly, 1994). The cognitive
and behavioural mechanisms that maintain hypochondriasis also appear similar to those
that maintain panic disorder, with the exception that the feared catastrophe is foreseen as
occurring immediately in panic disorder, resulting in the urge to escape right away
(Olatunji et al., 2009). In addition, both panic disorder and hypochondriasis involve
hypervigilance to bodily sensations and acute sensitivity to harmless or normal bodily
sensations (Olatunji, Deacon, Abramowitz, & Valentiner, 2007). This tendency to
misinterpret innocuous bodily symptoms as physically harmful (i.e., anxiety sensitivity)
is associated with both panic disorder and hypochondriasis (Deacon & Abramowitz,
2008). The combination of excessive body vigilance and high anxiety sensitivity leads to
the catastrophic misinterpretations of somatic cues ('this symptom means I have cancer'),
which evokes hypochondriacal fear and panic attacks. The coping strategies, such as
body checking and seeking medical reassurance (Deacon, Lickel, & Abramowitz, 2008),
that individuals with hypochondriasis and panic disorder use to manage their anxiety
paradoxically appear to maintain or even exacerbate the cognitive mechanisms that
underlie these disorders (Olatunji et al., 2009). In this study, the focus will be on those
individuals identified as having elevated health anxiety as compared to hypochondriasis.
1.3 Features Associated with Health Anxiety
1.3.1 Cognitive and Somatic Features of Health Anxiety
The cognitive features associated with excessive health anxiety include disease
conviction, disease preoccupation, hypervigilance for bodily changes, and difficulty with
9

acceptance of medical reassurance (APA, 2000). Individuals with health anxiety believe
strongly that they are physically ill; that is, they have strong disease conviction,
adamantly believing that they have a serious disease that has been undetected by medical
examinations. Disease conviction is associated with preoccupation with one's bodily
appearance and functioning and hypervigilance for bodily sensations. People with
elevated health anxiety also typically resist the idea that they are suffering from a mental
disorder. However, they are often able to recognize, at least in their calmer moments,
that their health concerns are overstated (Taylor & Asmundson, 2004).
People with high levels of health anxiety also have a tendency to misinterpret the
seriousness of harmless, natural bodily sensations, and appear to overestimate the
seriousness of symptoms of general medical conditions (Cote et al., 1996). Complaints
may be in the form of highly specific symptoms, or vague, variable, and generalized (e.g.,
aching "all over") symptoms. Frequent specific symptoms include localized pain, bowel
complaints (e.g., changes in bowel habits), and cardio-respiratory sensations (e.g., chest
tightness).
1.3.2 Behaviours Associated with Health Anxiety
Abramowitz, Schwartz, and Whiteside (2002) indicate that engaging in certain
behaviours to bring about safety is a logical and adaptive response for someone who
believes himself or herself to be in danger. These safety-seeking behaviours act to reduce
anxiety regarding the danger or potential for threat. However, if the perception of danger
is based on an incorrect belief, Abramowitz et al. (2002) indicate that safety-seeking
behaviours also have the effect of preventing someone from noticing that their fear is
10
acceptance of medical reassurance (APA, 2000). Individuals with health anxiety believe
strongly that they are physically ill; that is, they have strong disease conviction,
adamantly believing that they have a serious disease that has been undetected by medical
examinations. Disease conviction is associated with preoccupation with one's bodily
appearance and functioning and hypervigilance for bodily sensations. People with
elevated health anxiety also typically resist the idea that they are suffering from a mental
disorder. However, they are often able to recognize, at least in their calmer moments,
that their health concerns are overstated (Taylor & Asmundson, 2004).
People with high levels of health anxiety also have a tendency to misinterpret the
seriousness of harmless, natural bodily sensations, and appear to overestimate the
seriousness of symptoms of general medical conditions (Cote et al., 1996). Complaints
may be in the form of highly specific symptoms, or vague, variable, and generalized (e.g.,
aching "all over") symptoms. Frequent specific symptoms include localized pain, bowel
complaints (e.g., changes in bowel habits), and cardio-respiratory sensations (e.g., chest
tightness).
1.3.2 Behaviours Associated with Health Anxiety
Abramowitz, Schwartz, and Whiteside (2002) indicate that engaging in certain
behaviours to bring about safety is a logical and adaptive response for someone who
believes himself or herself to be in danger. These safety-seeking behaviours act to reduce
anxiety regarding the danger or potential for threat. However, if the perception of danger
is based on an incorrect belief, Abramowitz et al. (2002) indicate that safety-seeking
behaviours also have the effect of preventing someone from noticing that their fear is
10

inaccurate. One safety-seeking behaviour identified in individuals with elevated health
anxiety is reassurance seeking (e.g., from family physicians). When individuals with
elevated health anxiety turn to physicians, medical reference books, or family and friends
for reassurance, he or she will often experience a temporary reduction in anxiety and
distress. Abramowitz et al. (2002) indicate that this kind of reassurance seeking becomes
a habit, and the individual will come to rely on such reassurance to relieve health anxiety
which, in turn, strengthens inaccurate beliefs about health. Frequent checking of one's
body (e.g., recurrent prodding of the abdomen) is another safety-seeking behaviour, and it
not only prevents disconfirmation of inaccurate beliefs, but also increases the symptoms
that were the initial source of the misinterpretation (Abramowitz et al., 2002). For
instance, individuals who are focused on particular bodily sensations often perform
repeated examinations on the affected areas (e.g., excessively checking blood pressure).
These repeated examinations can have the effect of increasing discomfort in the area,
which is then misinterpreted as a sign of illness (Abramowitz et al., 2002). Searching for
other sources of information on the disease (e.g., checking the Internet), and trying
various kinds of remedies (e.g., herbal medications) are also types of common safety-
seeking behaviours (Taylor & Asmundson, 2004).
Avoidance and escape from stimuli that the individual believes to be associated
with disease are other common safety-seeking behaviours (Taylor & Asmundson, 2004).
For example, a highly health anxious individual may avoid medical buildings such as
clinics and hospitals, avoid sickly looking people, and limit contact with people who
come in contact with illness such as physicians and nurses (Taylor & Asmundson, 2004).
11
inaccurate. One safety-seeking behaviour identified in individuals with elevated health
anxiety is reassurance seeking (e.g., from family physicians). When individuals with
elevated health anxiety turn to physicians, medical reference books, or family and friends
for reassurance, he or she will often experience a temporary reduction in anxiety and
distress. Abramowitz et al. (2002) indicate that this kind of reassurance seeking becomes
a habit, and the individual will come to rely on such reassurance to relieve health anxiety
which, in turn, strengthens inaccurate beliefs about health. Frequent checking of one's
body (e.g., recurrent prodding of the abdomen) is another safety-seeking behaviour, and it
not only prevents disconfirmation of inaccurate beliefs, but also increases the symptoms
that were the initial source of the misinterpretation (Abramowitz et al., 2002). For
instance, individuals who are focused on particular bodily sensations often perform
repeated examinations on the affected areas (e.g., excessively checking blood pressure).
These repeated examinations can have the effect of increasing discomfort in the area,
which is then misinterpreted as a sign of illness (Abramowitz et al., 2002). Searching for
other sources of information on the disease (e.g., checking the Internet), and trying
various kinds of remedies (e.g., herbal medications) are also types of common safety-
seeking behaviours (Taylor & Asmundson, 2004).
Avoidance and escape from stimuli that the individual believes to be associated
with disease are other common safety-seeking behaviours (Taylor & Asmundson, 2004).
For example, a highly health anxious individual may avoid medical buildings such as
clinics and hospitals, avoid sickly looking people, and limit contact with people who
come in contact with illness such as physicians and nurses (Taylor & Asmundson, 2004).
11

Inaccurate beliefs that could be self-corrected if the person had faced the feared stimuli
and the feared negative outcomes did not materialize (Abramowitz et al., 2002) are
maintained through avoidance.
Studies have demonstrated the significance of safety behaviours in health anxious
individuals. Abramowitz and Moore (2007) demonstrated that performing personally
relevant safety behaviours produced a quick reduction in anxiety in individuals who met
DSM-IV-TR criteria for hypochondriasis, when compared with individuals who engaged
in non-safety behaviour activities. In addition, Abramowitz et al. (2007) found that in
medically healthy university students, health anxiety was a significant predictor of safety
behaviours, which is consistent with the CB model of health anxiety.
1.3.3 Patient-Physician Relationships
Patients with health anxiety and physicians have often been found to have
problematic relationships. Frustration and resentment on the part of both the physician
and patient are fairly common (APA, 2000). For example, Persing, Stuart, Noyes, and
Happel (2000) interviewed 20 patients with DSM-III-R (APA, 1987) hypochondriasis and
26 patients without hypochondriasis from a general medicine clinic to obtain information
on the patients' recent health problems and medical care. Patients with hypochondriasis
and patients without hypochondriasis made an equal number of positive comments, but
patients with hypochondriasis made significantly more negative comments about
physicians' professional characteristics (e.g., ineffective, hurried or careless, not
accepting), patients' own characteristics (e.g., helpless, hopeless, reluctant to seek
medical care), and total negative comments. Many patients viewed physicians they had
12
Inaccurate beliefs that could be self-corrected if the person had faced the feared stimuli
and the feared negative outcomes did not materialize (Abramowitz et al., 2002) are
maintained through avoidance.
Studies have demonstrated the significance of safety behaviours in health anxious
individuals. Abramowitz and Moore (2007) demonstrated that performing personally
relevant safety behaviours produced a quick reduction in anxiety in individuals who met
DSM-IV-TR criteria for hypochondriasis, when compared with individuals who engaged
in non-safety behaviour activities. In addition, Abramowitz et al. (2007) found that in
medically healthy university students, health anxiety was a significant predictor of safely
behaviours, which is consistent with the CB model of health anxiety.
1.3.3 Patient-Physician Relationships
Patients with health anxiety and physicians have often been found to have
problematic relationships. Frustration and resentment on the part of both the physician
and patient are fairly common (APA, 2000). For example, Persing, Stuart, Noyes, and
Happel (2000) interviewed 20 patients with DSM-III-R (APA, 1987) hypochondriasis and
26 patients without hypochondriasis from a general medicine clinic to obtain information
on the patients' recent health problems and medical care. Patients with hypochondriasis
and patients without hypochondriasis made an equal number of positive comments, but
patients with hypochondriasis made significantly more negative comments about
physicians' professional characteristics (e.g., ineffective, hurried or careless, not
accepting), patients' own characteristics (e.g., helpless, hopeless, reluctant to seek
medical care), and total negative comments. Many patients viewed physicians they had
12

seen as unskilled and uncaring. They indicated that, in many instances, their
relationships with physicians had suffered from poor communication and cooperation.
Notably, although these patients were diagnosed with hypochondriasis by Persing et al.
(2000), none were assigned a diagnosis of hypochondriasis by their own physician.
Similarly, Warwick and Salkovskis (1989) indicated that individuals with health anxiety
believe that their physicians see them as excessively concerned about their health, which
may actually be a realistic assessment of their physicians' appraisal. When Barsky,
Wyshak, Latham, and Klerman (1991) examined physicians' assessments of the patients
with hypochondriasis, they found that the physicians' use of the term hypochondriasis
was closely associated with their frustration with the patient. They also found that
physicians complained that patients with hypochondriasis bring forth baseless
complaints, and are demanding, difficult, and ungrateful (Barsky, Wyshak, Latham, et al.,
1991).
More recent research conducted by Noyes et al. (2003) examined the relationship
between health anxiety and the patient-physician relationship among 162 patients
attending a general medicine clinic. They found that increased health anxiety was
negatively correlated with perceived physician characteristics and satisfaction with care.
A further study conducted by many of the same researchers, Noyes, Longley, Langbehn,
Stuart, and Kukoyi (2010), examined the association between health anxiety using the
IAS and the physician-patient relationship using the Physician-Patient Relationship Scale
(Noyes et al., 2010) with a sample of 310 family medicine patients. Noyes et al. (2010)
13
seen as unskilled and uncaring. They indicated that, in many instances, their
relationships with physicians had suffered from poor communication and cooperation.
Notably, although these patients were diagnosed with hypochondriasis by Persing et al.
(2000), none were assigned a diagnosis of hypochondriasis by their own physician.
Similarly, Warwick and Salkovskis (1989) indicated that individuals with health anxiety
believe that their physicians see them as excessively concerned about their health, which
may actually be a realistic assessment of their physicians' appraisal. When Barsky,
Wyshak, Latham, and Klerman (1991) examined physicians' assessments of the patients
with hypochondriasis, they found that the physicians' use of the term hypochondriasis
was closely associated with their frustration with the patient. They also found that
physicians complained that patients with hypochondriasis bring forth baseless
complaints, and are demanding, difficult, and ungrateful (Barsky, Wyshak, Latham, et al.,
1991).
More recent research conducted by Noyes et al. (2003) examined the relationship
between health anxiety and the patient-physician relationship among 162 patients
attending a general medicine clinic. They found that increased health anxiety was
negatively correlated with perceived physician characteristics and satisfaction with care.
A further study conducted by many of the same researchers, Noyes, Longley, Langbehn,
Stuart, and Kukoyi (2010), examined the association between health anxiety using the
IAS and the physician-patient relationship using the Physician-Patient Relationship Scale
(Noyes et al., 2010) with a sample of 310 family medicine patients. Noyes et al. (2010)
13

also found that among family medical patients, health anxiety was associated with a
poorer therapeutic patient-physician relationship.
1.4 Theoretical Approach to Health Anxiety
There are several theories or models of health anxiety, such as psychodynamic,
biological, behavioural, interpersonal, and CB. Based on their review of the empirical
literature, Taylor and Asmundson (2004) suggest that the CB theory of health anxiety is
particularly informative in terms of usefulness of the theory to explain predisposing
factors or vulnerabilities, precipitating factors, maintaining factors, and protective factors
(prevention of development, persistence, or increase of the problem). The CB theory is
also empirically supported, whereas there is limited evidence to support the alternative
theories (see Taylor & Asmundson, 2004; Taylor, Asmundson, & Coons, 2005). As
such, this approach will be the focus in the current research.
According to the CB model of health anxiety (see Figure 1), individuals suffering
from persistent health anxiety are expected to misinterpret benign physical sensations,
bodily variations, and other health information as signs of serious physical illness
(Salkovskis, 1989, 1996; Salkovskis & Clark, 1993; Salkovskis & Warwick, 1986;
Warwick & Salkovskis, 1990). The greater the level of threat perceived by the sufferer,
the greater are the consequences of this misinterpretation. The level of threat is predicted
to be a function of the interactions among the perceived probability of the disease,
perceived dreadfulness or cost of the disease (e.g., pain and suffering caused by the
disease, emotional impact on family and friends), perceived ability to prevent the disease
from worsening, and perceived likelihood of being able to affect the course of the disease
14
also found that among family medical patients, health anxiety was associated with a
poorer therapeutic patient-physician relationship.
1.4 Theoretical Approach to Health Anxiety
There are several theories or models of health anxiety, such as psychodynamic,
biological, behavioural, interpersonal, and CB. Based on their review of the empirical
literature, Taylor and Asmundson (2004) suggest that the CB theory of health anxiety is
particularly informative in terms of usefulness of the theory to explain predisposing
factors or vulnerabilities, precipitating factors, maintaining factors, and protective factors
(prevention of development, persistence, or increase of the problem). The CB theory is
also empirically supported, whereas there is limited evidence to support the alternative
theories (see Taylor & Asmundson, 2004; Taylor, Asmundson, & Coons, 2005). As
such, this approach will be the focus in the current research.
According to the CB model of health anxiety (see Figure 1), individuals suffering
from persistent health anxiety are expected to misinterpret benign physical sensations,
bodily variations, and other health information as signs of serious physical illness
(Salkovskis, 1989, 1996; Salkovskis & Clark, 1993; Salkovskis & Warwick, 1986;
Warwick & Salkovskis, 1990). The greater the level of threat perceived by the sufferer,
the greater are the consequences of this misinterpretation. The level of threat is predicted
to be a function of the interactions among the perceived probability of the disease,
perceived dreadfulness or cost of the disease (e.g., pain and suffering caused by the
disease, emotional impact on family and friends), perceived ability to prevent the disease
from worsening, and perceived likelihood of being able to affect the course of the disease
14

Previous illness experience and other medical factors
pretatton and resulting anxiety
Perceived likelihood of
A nviety illness
Perceived X cost awfulness
burden of the illness
Perceived ability Perception of extent that to cope with the X external rescue factors illness will help
Adapted from Salkovskis & Warwick 2001
Figure 1. Cognitive behavioural model of the development of health anxiety
Note. From Salkovskis, P. M., & Warwick, H. M. C. (2001). Making sense of
hypochondriasis: A cognitive model of health anxiety. In G.J.G. Asmundson, S. Taylor,
and B.J. Cox (Eds.), Health Anxiety. Copyright 2001 by John Wiley & Sons, Ltd.
15
Previous illness experience and other medical factors
Misinterpretafctoti and rssultfliE anxiety
Anxietr =
Perceived likelihood of illness
Perceived cost awfiikiess, burden of the ittness
Perceived ability Perception of extent that to cope with the X external rescue factors iBness will help
Adapted iram Salkovskis & Warwick, 2901
Figure I. Cognitive behavioural model of the development of health anxiety
Note. From Salkovskis, P. M., & Warwick, H. M. C. (2001). Making sense of
hypochondriasis: A cognitive model of health anxiety. In G.J.G. Asmundson, S. Taylor,
and B.J. Cox (Eds.), Health Anxiety. Copyright 2001 by John Wiley & Sons, Ltd.
15

(i.e., being able to cope with the disease and the likelihood of outside factors coming to
the aid of the individual).
1.4.1 Misinterpretations and Maintenance of Health Anxiety
According to the CB model, it is hypothesized that the tendency to misinterpret
health-related information is a function of the individual's specific knowledge and past
experiences of illness, which have lead to the formation of inflexible or negative
assumptions about symptoms, disease, medical care, etc. These inflexible or negative
assumptions about health, coupled with a critical incident, are expected to generate
specific misinterpretations about health (Salkovskis & Warwick, 2001). General health-
related assumptions can arise from a wide variety of sources, including early health- and
illness-related experiences, later events such as unexpected or unpleasant illness in the
person's social group, and information in the media (Salkovskis & Warwick, 2001).
However, when these assumptions are relatively inflexible and extreme, it is expected
that this will lead to more severe and persistent health anxiety (Salkovskis & Warwick,
2001). For example, it is common for people to believe that persistent and intense
physical pain of an unusual and unexplained type could be a sign of ill health (Salkovskis
& Warwick, 2001). In an individual prone to health anxiety, however, he or she would
have a tendency to believe that any unexplained change in their body is always going to
be a sign of serious illness (Salkovskis & Warwick, 2001).
Marcus, Gurley, Marchi, and Bauer (2007) conducted a review of the literature
examining tenants of the CB model including: (a) whether health-anxious individuals
hold distinct assumptions about health and illness and cognitive processes involved in
16
(i.e., being able to cope with the disease and the likelihood of outside factors coming to
the aid of the individual).
1.4.1 Misinterpretations and Maintenance of Health Anxiety
According to the CB model, it is hypothesized that the tendency to misinterpret
health-related information is a function of the individual's specific knowledge and past
experiences of illness, which have lead to the formation of inflexible or negative
assumptions about symptoms, disease, medical care, etc. These inflexible or negative
assumptions about health, coupled with a critical incident, are expected to generate
specific misinterpretations about health (Salkovskis & Warwick, 2001). General health-
related assumptions can arise from a wide variety of sources, including early health- and
illness-related experiences, later events such as unexpected or unpleasant illness in the
person's social group, and information in the media (Salkovskis & Warwick, 2001).
However, when these assumptions are relatively inflexible and extreme, it is expected
that this will lead to more severe and persistent health anxiety (Salkovskis & Warwick,
2001). For example, it is common for people to believe that persistent and intense
physical pain of an unusual and unexplained type could be a sign of ill health (Salkovskis
& Warwick, 2001). In an individual prone to health anxiety, however, he or she would
have a tendency to believe that any unexplained change in their body is always going to
be a sign of serious illness (Salkovskis & Warwick, 2001).
Marcus, Gurley, Marchi, and Bauer (2007) conducted a review of the literature
examining tenants of the CB model including: (a) whether health-anxious individuals
hold distinct assumptions about health and illness and cognitive processes involved in
16

health anxiety, (b) if triggering these assumptions leads to increased health anxious
concerns, and (c) whether these individuals perceive their bodily sensations differently
from others (i.e., experience greater somatosensory amplification). In their review,
Marcus et al. (2007) examined which aspects of the CB model have been subjected to
empirical testing and they meta-analyzed the results of these studies to determine the
magnitude of the support for the model.
Dysfunctional Assumptions about Health and Illness and Cognitive Processes in
Health Anxiety. As reviewed by Marcus et al. (2007), researchers have been able to
examine the extent to which individuals with elevated health anxiety hold dysfunctional
assumptions about health by asking participants to either indicate which illness they
would assume they had if they experienced an ambiguous symptom or to estimate the
likelihood that such certain ambiguous symptoms are a sign of a catastrophic illness.
Overall, Marcus et al.'s (2007) review suggested that individuals with elevated health
anxiety do indeed hold dysfunctional assumptions about health. Several studies outlined
by Marcus et al. (2007) serve to highlight these findings. For example, Hitchcock and
Mathews (1992) found that college students higher in health anxiety, as measured by the
IAS, were more likely to interpret bodily sensations (e.g., chest tightness) as indicative of
catastrophic illness (e.g., having a heart attack) than were students who scored lower on
the IAS. Marcus (1999) found that among college students, IAS scores positively
correlated with estimates of the likelihood that ambiguous symptoms (e.g., headache)
were indicative of serious illnesses (e.g., brain tumour). Barsky, Coeytaux, Remy,
Sarnie, and Cleary (1993) found that patients diagnosed with hypochondriasis identify
17
health anxiety, (b) if triggering these assumptions leads to increased health anxious
concerns, and (c) whether these individuals perceive their bodily sensations differently
from others (i.e., experience greater somatosensory amplification). In their review,
Marcus et al. (2007) examined which aspects of the CB model have been subjected to
empirical testing and they meta-analyzed the results of these studies to determine the
magnitude of the support for the model.
Dysfunctional Assumptions about Health and Illness and Cognitive Processes in
Health Anxiety. As reviewed by Marcus et al. (2007), researchers have been able to
examine the extent to which individuals with elevated health anxiety hold dysfunctional
assumptions about health by asking participants to either indicate which illness they
would assume they had if they experienced an ambiguous symptom or to estimate the
likelihood that such certain ambiguous symptoms are a sign of a catastrophic illness.
Overall, Marcus et al.'s (2007) review suggested that individuals with elevated health
anxiety do indeed hold dysfunctional assumptions about health. Several studies outlined
by Marcus et al. (2007) serve to highlight these findings. For example, Hitchcock and
Mathews (1992) found that college students higher in health anxiety, as measured by the
IAS, were more likely to interpret bodily sensations (e.g., chest tightness) as indicative of
catastrophic illness (e.g., having a heart attack) than were students who scored lower on
the IAS. Marcus (1999) found that among college students, IAS scores positively
correlated with estimates of the likelihood that ambiguous symptoms (e.g., headache)
were indicative of serious illnesses (e.g., brain tumour). Barsky, Coeytaux, Remy,
Sarnie, and Cleary (1993) found that patients diagnosed with hypochondriasis identify
17

more physical symptoms as indicating that a person is "not healthy" than do medical
patients who do not have hypochondriasis.
Also reviewed by Marcus et al. (2007) was the extent to which information
processing biases may exist in individuals with health anxiety. This was of interest as
information processing biases are predicted to occur in individuals with elevated health
anxiety when they inadvertently gather evidence to support inaccurate beliefs (Salkovskis
& Warwick, 2001). For example, a self-maintaining confirmatory bias can occur once a
critical incident (e.g., noticing unfamiliar bodily sensations, hearing details of illness in a
close family member, or reading information about illness) has activated health-related
assumptions and resulted in misinterpretations of bodily symptoms. This would result in
the individual selectively attending to information that is consistent with illness beliefs
and ignoring information that is inconsistent with these beliefs. That is, once these illness
concerns are activated, the person will focus their attention on previously unnoticed
bodily variations. These bodily changes are viewed as new phenomena and are
consistent with the belief that illness or disease is present. Adding to this process, people
with excessive health anxiety may spend a great deal of time attending to their bodies,
thereby increasing the chances of noticing bodily sensations (Kellner, Abbott, Winslow,
& Pathak, 1987).
As reviewed by Marcus et al. (2007), an attentional bias towards certain types of
information among individuals with heightened levels of health anxiety has been reported
by researchers using various research protocols. In one such study, investigators
identified that university students with high scores on the IAS performed more poorly
18
more physical symptoms as indicating that a person is "not healthy" than do medical
patients who do not have hypochondriasis.
Also reviewed by Marcus et al. (2007) was the extent to which information
processing biases may exist in individuals with health anxiety. This was of interest as
information processing biases are predicted to occur in individuals with elevated health
anxiety when they inadvertently gather evidence to support inaccurate beliefs (Salkovskis
& Warwick, 2001). For example, a self-maintaining confirmatory bias can occur once a
critical incident (e.g., noticing unfamiliar bodily sensations, hearing details of illness in a
close family member, or reading information about illness) has activated health-related
assumptions and resulted in misinterpretations of bodily symptoms. This would result in
the individual selectively attending to information that is consistent with illness beliefs
and ignoring information that is inconsistent with these beliefs. That is, once these illness
concerns are activated, the person will focus their attention on previously unnoticed
bodily variations. These bodily changes are viewed as new phenomena and are
consistent with the belief that illness or disease is present. Adding to this process, people
with excessive health anxiety may spend a great deal of time attending to their bodies,
thereby increasing the chances of noticing bodily sensations (Kellner, Abbott, Winslow,
&Pathak, 1987).
As reviewed by Marcus et al. (2007), an attentional bias towards certain types of
information among individuals with heightened levels of health anxiety has been reported
by researchers using various research protocols. In one such study, investigators
identified that university students with high scores on the IAS performed more poorly
18
during an attention-concentration task than students with low scores on the IAS (Pauli,
Schwenzer, Brody, Rau, & Birbaumer, 1993). Participants were informed that they
would receive a painful stimulus during the second part of a test, while the first part
would be pain-free. The expectancy of a forthcoming pain stimulus reduced the
performance of students with high IAS scores in both parts of the test. Students with low
scores on the IAS, on the other hand, displayed significantly better performance in the
first, pain-free part of the test compared to the second, pain-related part of the test.
Individuals with elevated levels of health anxiety appeared to have difficulty distracting
their attention from the pain stimulus and concentrating on the task at hand, even though
they were aware that the pain stimulus would not be applied until after they had reached a
certain point in the task (Pauli et al., 1993). However, two studies by Brown, Kosslyn,
Delamater, Fama, and Barsky (1999) that examined recall of health-related words yielded
inconsistent results. They found that individuals with elevated health anxiety did not
perceive more health-related words than words not related to health. In fact, these
individuals showed an unexpected bias against reporting health-related words. That is,
individuals with elevated health anxiety committed more errors of omission for health
than for nonhealth words, whereas the group without health anxious beliefs correctly
reported similar numbers of each. These findings, however, were not replicated in the
clinical sample (Brown et al., 1999).
Owens, Asmundson, Hadjistavropoulos, and Owens (2004) identified that
individuals with heightened levels of health anxiety spent significantly more time
attending to illness-related words than individuals with lower levels of health anxiety.
19
during an attention-concentration task than students with low scores on the IAS (Pauli,
Schwenzer, Brody, Rau, & Birbaumer, 1993). Participants were informed that they
would receive a painful stimulus during the second part of a test, while the first part
would be pain-free. The expectancy of a forthcoming pain stimulus reduced the
performance of students with high IAS scores in both parts of the test. Students with low
scores on the IAS, on the other hand, displayed significantly better performance in the
first, pain-free part of the test compared to the second, pain-related part of the test.
Individuals with elevated levels of health anxiety appeared to have difficulty distracting
their attention from the pain stimulus and concentrating on the task at hand, even though
they were aware that the pain stimulus would not be applied until after they had reached a
certain point in the task (Pauli et al., 1993). However, two studies by Brown, Kosslyn,
Delamater, Fama, and Barsky (1999) that examined recall of health-related words yielded
inconsistent results. They found that individuals with elevated health anxiety did not
perceive more health-related words than words not related to health. In fact, these
individuals showed an unexpected bias against reporting health-related words. That is,
individuals with elevated health anxiety committed more errors of omission for health
than for nonhealth words, whereas the group without health anxious beliefs correctly
reported similar numbers of each. These findings, however, were not replicated in the
clinical sample (Brown et al., 1999).
Owens, Asmundson, Hadjistavropoulos, and Owens (2004) identified that
individuals with heightened levels of health anxiety spent significantly more time
attending to illness-related words than individuals with lower levels of health anxiety.
19

Specifically, on a modified Stroop task, individuals with high health anxiety had
significantly slower colour-naming response times to illness-related words when
compared to individuals with low to moderate health anxiety. The specificity of the bias
was supported by a failure to find slower response times for either negative or positive
groups of words. Thus, these results indicate that individuals with elevated levels of
health anxiety appear to display an attentional bias for illness-related information. Also
in support of this finding, medical patients with hypochondriasis have been found to
recall more pain-related words (e.g., stinging, burning) than medical patients without
hypochondriasis (Pauli & Alpers, 2002). Lecci and Cohen (2002), on the other hand,
only found this Stroop interference of illness-related words when they first induced
illness-concern in their participants by telling them that their blood pressure was too high.
In the control condition, which was similar to Owens et al.'s (2004) procedure, there was
no Stroop interference for illness-related words.
Marcus et al. (2007) indicated that some of the positive findings in this area
suggest that future research examining cognitive processes in health anxiety may prove to
be confirming of the predictions, but there is not yet sufficient evidence to conclude that
individuals with health anxiety process illness-related materials differently from
nonhypochondriacal individuals, even if the contents of their health-related beliefs do
differ.
Triggers for Health Anxiety. Again, as summarized in Marcus et al. (2007),
researchers have also examined Salkovskis and Warwick's (1986) supposition that
exposure to illness-related materials triggers increased hypochondriacal concerns or
20
Specifically, on a modified Stroop task, individuals with high health anxiety had
significantly slower colour-naming response times to illness-related words when
compared to individuals with low to moderate health anxiety. The specificity of the bias
was supported by a failure to find slower response times for either negative or positive
groups of words. Thus, these results indicate that individuals with elevated levels of
health anxiety appear to display an attentional bias for illness-related information. Also
in support of this finding, medical patients with hypochondriasis have been found to
recall more pain-related words (e.g., stinging, burning) than medical patients without
hypochondriasis (Pauli & Alpers, 2002). Lecci and Cohen (2002), on the other hand,
only found this Stroop interference of illness-related words when they first induced
illness-concern in their participants by telling them that their blood pressure was too high.
In the control condition, which was similar to Owens et al.'s (2004) procedure, there was
no Stroop interference for illness-related words.
Marcus et al. (2007) indicated that some of the positive findings in this area
suggest that future research examining cognitive processes in health anxiety may prove to
be confirming of the predictions, but there is not yet sufficient evidence to conclude that
individuals with health anxiety process illness-related materials differently from
nonhypochondriacal individuals, even if the contents of their health-related beliefs do
differ.
Triggers for Health Anxiety. Again, as summarized in Marcus et al. (2007),
researchers have also examined Salkovskis and Warwick's (1986) supposition that
exposure to illness-related materials triggers increased hypochondriacal concerns or
20

anxiety in health-anxious individuals. Lecci and Cohen (2002) reported on two studies in
which they primed college student participants by giving them a medical exam and
informing them that their blood pressures were dangerously high. In both studies,
students in the experimental condition who reported high levels of somatosensory
amplification (i.e., a tendency to perceive normal somatic and visceral sensations as being
relatively intense, disturbing and noxious; Barsky, Wyshak, & Klerman, 1990) displayed
greater interference on a modified Stroop task for illness-related words, suggesting that
the bogus medical feedback activated illness-related concerns. Furthermore, in both
studies, students in the experimental condition who reported high levels of illness
preoccupation on the WI displayed greater Stroop interference for all words, perhaps
resulting from increased arousal and anxiety.
In another study, Marcus (1999) attempted to trigger anxiety in college students
using a scrambled sentences task that included illness-related words (e.g., cancer).
Although IAS scores were positively related to state anxiety scores for students in the
control condition, contrary to the CB model, there was no relationship between IAS
scores and anxiety in the priming condition. In other words, priming with illness-related
words did not lead those students who were more health anxious to become more
anxious. Instead, it appeared that the students lower in health anxiety became as anxious
as the students with elevated health anxiety. Marcus et al. (2007) indicated that Marcus's
(1999) priming task was more indirect and subtle than the one used by Lecci and Cohen
(2002), but they felt the inconsistent results could also be due to the very different
dependent variables that were used in each study (i.e., Stroop interference versus self-
21
anxiety in health-anxious individuals. Lecci and Cohen (2002) reported on two studies in
which they primed college student participants by giving them a medical exam and
informing them that their blood pressures were dangerously high. In both studies,
students in the experimental condition who reported high levels of somatosensory
amplification (i.e., a tendency to perceive normal somatic and visceral sensations as being
relatively intense, disturbing and noxious; Barsky, Wyshak, & Klerman, 1990) displayed
greater interference on a modified Stroop task for illness-related words, suggesting that
the bogus medical feedback activated illness-related concerns. Furthermore, in both
studies, students in the experimental condition who reported high levels of illness
preoccupation on the WI displayed greater Stroop interference for all words, perhaps
resulting from increased arousal and anxiety.
In another study, Marcus (1999) attempted to trigger anxiety in college students
using a scrambled sentences task that included illness-related words (e.g., cancer).
Although IAS scores were positively related to state anxiety scores for students in the
control condition, contrary to the CB model, there was no relationship between IAS
scores and anxiety in the priming condition. In other words, priming with illness-related
words did not lead those students who were more health anxious to become more
anxious. Instead, it appeared that the students lower in health anxiety became as anxious
as the students with elevated health anxiety. Marcus et al. (2007) indicated that Marcus's
(1999) priming task was more indirect and subtle than the one used by Lecci and Cohen
(2002), but they felt the inconsistent results could also be due to the very different
dependent variables that were used in each study (i.e., Stroop interference versus self-
21
reported state anxiety). Marcus et al. (2007) stated that because there were only three
published studies and the findings from these studies were not consistent, they felt it was
not appropriate to perform a meta-analysis on the triggers component. Given that the
findings were not consistent, Marcus et al. (2007) also state that if health anxious
concerns are better conceptualized as chronic concerns instead of dormant cognitive
contents triggered by certain events as hypothesised in the CB model, then health anxiety
may be better conceptualized as an ongoing state of mind rather than a discreet series of
events.
Studies of Perception and Amplification of Bodily Sensations. A final area that
was examined by Marcus et al. (2007) was the extent to which physiological reactions,
including heightened experience of bodily sensations, maintain health anxiety. This part
of the CB model predicts that heightened levels of anxiety about health will generally
lead to physiological arousal as part of the normal reaction to stress (Salkovskis &
Warwick, 2001). The combination of increased physiological arousal and the health
anxious person's tendency to monitor and misinterpret bodily sensations is predicted to
lead to more anxiety and thus more symptoms, resulting in a vicious cycle of symptoms,
catastrophic misinterpretations, and anxiety (Salkovskis & Warwick, 2001). In support
of this aspect of the model, studies have examined the relationship between health
anxiety and scores on the Somatosensory Amplification Scale (SSAS; Barsky et al.,
1990c), a self-report scale that assesses sensitivity to bodily sensations. Generally, SSAS
scores have been moderately positively correlated with self-reported health anxiety scores
22
reported state anxiety). Marcus et al. (2007) stated that because there were only three
published studies and the findings from these studies were not consistent, they felt it was
not appropriate to perform a meta-analysis on the triggers component. Given that the
findings were not consistent, Marcus et al. (2007) also state that if health anxious
concerns are better conceptualized as chronic concerns instead of dormant cognitive
contents triggered by certain events as hypothesised in the CB model, then health anxiety
may be better conceptualized as an ongoing state of mind rather than a discreet series of
events.
Studies of Perception and Amplification of Bodily Sensations. A final area that
was examined by Marcus et al. (2007) was the extent to which physiological reactions,
including heightened experience of bodily sensations, maintain health anxiety. This part
of the CB model predicts that heightened levels of anxiety about health will generally
lead to physiological arousal as part of the normal reaction to stress (Salkovskis &
Warwick, 2001). The combination of increased physiological arousal and the health
anxious person's tendency to monitor and misinterpret bodily sensations is predicted to
lead to more anxiety and thus more symptoms, resulting in a vicious cycle of symptoms,
catastrophic misinterpretations, and anxiety (Salkovskis & Warwick, 2001). In support
of this aspect of the model, studies have examined the relationship between health
anxiety and scores on the Somatosensory Amplification Scale (SSAS; Barsky et al.,
1990c), a self-report scale that assesses sensitivity to bodily sensations. Generally, SSAS
scores have been moderately positively correlated with self-reported health anxiety scores
22

(Barsky & Wyshak, 1990) and medical patients diagnosed with hypochondriasis score
higher on the SSAS than do other medical patients (Barsky et al., 1990c).
Other studies have used in vivo procedures to examine whether individuals with
elevated health anxiety are in fact more sensitive to physical sensations or more accurate
in their perceptions of bodily processes. In this case, women with high levels of health
anxiety have been found to evidence greater pain sensitivity on a cold pressor task (i.e.,
they rated the task as more unpleasant, withdrew their hands more quickly, and had a
greater elevation in heart rate) than women with lower levels of health anxiety (Gramling,
Clawson, & McDonald, 1996). However, despite higher SSAS scores, patients with
elevated health anxiety have not been found to be more accurate on a heartbeat detection
task than patients without elevated health anxiety. In fact, in this research, there was a
trend toward greater accuracy among the patients without elevated health anxiety (Barsky
et al., 1995). Similarly, Haenen, Schmidt, Schoenmakers, and van der Hout (1996) found
that although patients with a diagnosis of hypochondriasis had higher SSAS scores, they
were no more sensitive to tactile stimuli (assessed with a two two-point discrimination
task) than a control group of healthy adults. Marcus et al. (2007) have interpreted the
findings to indicate health anxiety is probably not related to increased physical sensations
per se, but rather to increased misinterpretations of sensations. Overall, Marcus et al.
(2007) concluded that the results of their meta-analysis suggest that the CB model holds
significant promise.
Other Maintaining Factors. As described above, within the CB model, safety-
seeking behaviours, such as avoidance, checking, and reassurance seeking are similarly
23
(Barsky & Wyshak, 1990) and medical patients diagnosed with hypochondriasis score
higher on the SSAS than do other medical patients (Barsky et al., 1990c).
Other studies have used in vivo procedures to examine whether individuals with
elevated health anxiety are in fact more sensitive to physical sensations or more accurate
in their perceptions of bodily processes. In this case, women with high levels of health
anxiety have been found to evidence greater pain sensitivity on a cold pressor task (i.e.,
they rated the task as more unpleasant, withdrew their hands more quickly, and had a
greater elevation in heart rate) than women with lower levels of health anxiety (Gramling,
Clawson, & McDonald, 1996). However, despite higher SSAS scores, patients with
elevated health anxiety have not been found to be more accurate on a heartbeat detection
task than patients without elevated health anxiety. In fact, in this research, there was a
trend toward greater accuracy among the patients without elevated health anxiety (Barsky
et al., 1995). Similarly, Haenen, Schmidt, Schoenmakers, and van der Hout (1996) found
that although patients with a diagnosis of hypochondriasis had higher SSAS scores, they
were no more sensitive to tactile stimuli (assessed with a two two-point discrimination
task) than a control group of healthy adults. Marcus et al. (2007) have interpreted the
findings to indicate health anxiety is probably not related to increased physical sensations
per se, but rather to increased misinterpretations of sensations. Overall, Marcus et al.
(2007) concluded that the results of their meta-analysis suggest that the CB model holds
significant promise.
Other Maintaining Factors. As described above, within the CB model, safety-
seeking behaviours, such as avoidance, checking, and reassurance seeking are similarly
23

hypothesized to maintain health anxiety (Salkovskis & Warwick, 2001). When a person
tries to avoid or check for physical disease (e.g., avoiding strenuous exercise or contact
with disease; reading medical information from the Internet; frequently consulting with
physicians; bodily checking, manipulation, and inspection) this is expected to sustain
anxiety by increasing symptoms that form the focus of the misinterpretation.
Seeking reassurance from medical professionals, family, or friends is
hypothesized to increase health anxiety and worry through an increase in the likelihood
that the individual with elevated health anxiety will receive ambiguous or false positive
results of medical tests, and through inconsistencies in the information given by different
people on different occasions. Safety-seeking behaviour is thought to have a significant
effect on the maintenance of health anxiety when the individual believes that his or her
safety-seeking behaviour has the immediate and direct effect of preventing the health-
related problem. When this occurs, the person experiences short-term relief because he
or she feels safe. However, the individual also gains no evidence to disconfirm erroneous
assumptions.
In support of this aspect of the model, researchers have found that individuals
with elevated levels of health anxiety respond less positively to information typically
interpreted as reassuring. Lucock, Morley, White, and Peake (1997) found that
reassurance, even when initially effective, does not remain effective in the long-term.
After 49 out of 50 patients, who underwent a gastroscopy, had their physician
consultation, negative diagnostic findings led to an immediate feeling of reassurance
(Lucock et al., 1997). However, when these patients were separated into three groups
24
hypothesized to maintain health anxiety (Salkovskis & Warwick, 2001). When a person
tries to avoid or check for physical disease (e.g., avoiding strenuous exercise or contact
with disease; reading medical information from the Internet; frequently consulting with
physicians; bodily checking, manipulation, and inspection) this is expected to sustain
anxiety by increasing symptoms that form the focus of the misinterpretation.
Seeking reassurance from medical professionals, family, or friends is
hypothesized to increase health anxiety and worry through an increase in the likelihood
that the individual with elevated health anxiety will receive ambiguous or false positive
results of medical tests, and through inconsistencies in the information given by different
people on different occasions. Safety-seeking behaviour is thought to have a significant
effect on the maintenance of health anxiety when the individual believes that his or her
safety-seeking behaviour has the immediate and direct effect of preventing the health-
related problem. When this occurs, the person experiences short-term relief because he
or she feels safe. However, the individual also gains no evidence to disconfirm erroneous
assumptions.
In support of this aspect of the model, researchers have found that individuals
with elevated levels of health anxiety respond less positively to information typically
interpreted as reassuring. Lucock, Morley, White, and Peake (1997) found that
reassurance, even when initially effective, does not remain effective in the long-term.
After 49 out of 50 patients, who underwent a gastroscopy, had their physician
consultation, negative diagnostic findings led to an immediate feeling of reassurance
(Lucock et al., 1997). However, when these patients were separated into three groups
24

based on their levels of health anxiety (as assessed by the IAS), individuals with the
highest levels of health anxiety no longer felt reassured 24 hours following the
consultation. In fact, their level of worry about their health and illness conviction
returned to levels equal to those found prior to receiving their test results. At one-year
follow-up, the group with the highest levels of health anxiety continued to be concerned
about their symptoms.
Individuals with elevated levels of health anxiety have also been found to be
significantly more likely to immediately interpret health information provided by their
physician as less reassuring than the physicians had perceived their feedback to be
(Lucock, White, Peake, & Morley, 1998). When measured again at one-month follow-
up, patient reassurance ratings were found to have decreased further. Similarly,
individuals with moderate levels of health anxiety rated the level of reassurance provided
by their physician lower after one month had elapsed.
Another maintaining factor in health anxiety is affect, particularly anxiety and
depression (Salkovskis & Warwick, 2001). For instance, mood disturbances have been
linked to negative or maladaptive patterns of thinking, which then leads to further
increases in mood disturbance (Salkovskis & Warwick, 2001). These cognitive processes
in anxiety and depression generally are thought to prime ruminative worries about health
problems and the implications of the feared consequences (Salkovskis & Warwick,
2001).
25
based on their levels of health anxiety (as assessed by the IAS), individuals with the
highest levels of health anxiety no longer felt reassured 24 hours following the
consultation. In fact, their level of worry about their health and illness conviction
returned to levels equal to those found prior to receiving their test results. At one-year
follow-up, the group with the highest levels of health anxiety continued to be concerned
about their symptoms.
Individuals with elevated levels of health anxiety have also been found to be
significantly more likely to immediately interpret health information provided by their
physician as less reassuring than the physicians had perceived their feedback to be
(Lucock, White, Peake, & Morley, 1998). When measured again at one-month follow-
up, patient reassurance ratings were found to have decreased further. Similarly,
individuals with moderate levels of health anxiety rated the level of reassurance provided
by their physician lower after one month had elapsed.
Another maintaining factor in health anxiety is affect, particularly anxiety and
depression (Salkovskis & Warwick, 2001). For instance, mood disturbances have been
linked to negative or maladaptive patterns of thinking, which then leads to further
increases in mood disturbance (Salkovskis & Warwick, 2001). These cognitive processes
in anxiety and depression generally are thought to prime ruminative worries about health
problems and the implications of the feared consequences (Salkovskis & Warwick,
2001).
25

1.5 Health Anxiety Among Seniors
There is a commonly held belief that older adults display greater health-related
concerns compared with younger adults (Snyder & Stanley, 2001). Factors associated
with aging, such as higher rates of medical illness, physical frailty, and a heightened
sense of mortality, may contribute to excessive preoccupation with health-related issues
(Snyder & Stanley, 2001). Available prevalence estimates of hypochondriasis from older
community samples range from 3.9% to 33.0% (Palmore, 1970; Stenback, Kumpulainen,
& Vauhkenen, 1978) as compared with similar estimates of 4.2% to 13.8% for
hypochondriasis in general medical patients (Barsky, Wyshak, & Klerman, 1990a; Noyes
et al., 1993). Barsky, Frank, Cleary, Wyshak, and Klerman (1991) examined the
relationship between hypochondriasis and age in 60 patients who met the DSM-III-R
diagnostic criteria for hypochondriasis and 100 comparison patients from a general
medical clinic. Barsky, Frank, Cleary, et al. (1991) concluded that hypochondriasis is
found to some degree in all patients and appeared to be unrelated to age. They also found
that patients with hypochondriasis aged 65 years and over did not differ significantly
from younger patients with hypochondriasis in hypochondriacal attitudes, somatization,
tendency to amplify bodily sensation, or global assessment of their overall health, even
though they had higher level of physical difficulties. A non-significant trend was noted
in that the older adult group endorsed less disease anxiety and disease conviction when
compared with the younger patients. When examining the social and functional activity
levels of participants, older patients reported greater difficulty participating in social
events and activities of daily living than younger patients. This decline in functioning
26
1.5 Health Anxiety Among Seniors
There is a commonly held belief that older adults display greater health-related
concerns compared with younger adults (Snyder & Stanley, 2001). Factors associated
with aging, such as higher rates of medical illness, physical frailty, and a heightened
sense of mortality, may contribute to excessive preoccupation with health-related issues
(Snyder & Stanley, 2001). Available prevalence estimates of hypochondriasis from older
community samples range from 3.9% to 33.0%> (Palmore, 1970; Stenback, Kumpulainen,
& Vauhkenen, 1978) as compared with similar estimates of 4.2% to 13.8% for
hypochondriasis in general medical patients (Barsky, Wyshak, & Klerman, 1990a; Noyes
et al., 1993). Barsky, Frank, Cleary, Wyshak, and Klerman (1991) examined the
relationship between hypochondriasis and age in 60 patients who met the DSM-III-R
diagnostic criteria for hypochondriasis and 100 comparison patients from a general
medical clinic. Barsky, Frank, Cleary, et al. (1991) concluded that hypochondriasis is
found to some degree in all patients and appeared to be unrelated to age. They also found
that patients with hypochondriasis aged 65 years and over did not differ significantly
from younger patients with hypochondriasis in hypochondriacal attitudes, somatization,
tendency to amplify bodily sensation, or global assessment of their overall health, even
though they had higher level of physical difficulties. A non-significant trend was noted
in that the older adult group endorsed less disease anxiety and disease conviction when
compared with the younger patients. When examining the social and functional activity
levels of participants, older patients reported greater difficulty participating in social
events and activities of daily living than younger patients. This decline in functioning
26

with age was not observed in the comparison group, despite similar medical morbidity.
Snyder and Stanley (2001) suggest that older patients with hypochondriasis are less
functional than younger patients despite similarities in hypochondriacal symptoms, and
that severe health anxiety may be more incapacitating in older adults even when symptom
severity is similar to that of younger patients.
Bourgault-Fagnou and Hadjistavropoulos (2009) examined predictors of health
anxiety in a sample of older adults with varying levels of frailty receiving home health
care services using a medically adjusted version of the IAS. Frailty is conceptualized as a
multidimensional, heterogeneous, and unstable state of vulnerability for mortality and
morbidity (distinguishing it from disability or aging alone) (Hogan, MacKnight, &
Bergman, 2003). The score on the medically adjusted version of the IAS was calculated
by summing items that reflected worry about illness, anxiety about health, and bodily
preoccupation, as well as items that were not confounded by whether the individual was
suffering from an illness. Using mediation analysis, Bourgault-Fagnou and
Hadjistavropoulos (2009) found that emotional preoccupation coping mediated the
relationship between frailty and health anxiety, which they felt suggested that frailty
alone may not necessarily lead to health anxiety. Instead, frailty seemed to be associated
with emotional preoccupation coping which then fully accounted for its relationship with
health anxiety among older adults.
Similarly, Boston and Merrick (2010) examined health anxiety among 145 older
adults recruited from community-based organizations and retirement village communities
in Australia. Using the Short Health Anxiety Inventory (SHAI; Salkovskis, Rimes,
27
with age was not observed in the comparison group, despite similar medical morbidity.
Snyder and Stanley (2001) suggest that older patients with hypochondriasis are less
functional than younger patients despite similarities in hypochondriacal symptoms, and
that severe health anxiety may be more incapacitating in older adults even when symptom
severity is similar to that of younger patients.
Bourgault-Fagnou and Hadjistavropoulos (2009) examined predictors of health
anxiety in a sample of older adults with varying levels of frailty receiving home health
care services using a medically adjusted version of the IAS. Frailty is conceptualized as a
multidimensional, heterogeneous, and unstable state of vulnerability for mortality and
morbidity (distinguishing it from disability or aging alone) (Hogan, MacKnight, &
Bergman, 2003). The score on the medically adjusted version of the IAS was calculated
by summing items that reflected worry about illness, anxiety about health, and bodily
preoccupation, as well as items that were not confounded by whether the individual was
suffering from an illness. Using mediation analysis, Bourgault-Fagnou and
Hadjistavropoulos (2009) found that emotional preoccupation coping mediated the
relationship between frailty and health anxiety, which they felt suggested that frailty
alone may not necessarily lead to health anxiety. Instead, frailty seemed to be associated
with emotional preoccupation coping which then fully accounted for its relationship with
health anxiety among older adults.
Similarly, Boston and Merrick (2010) examined health anxiety among 145 older
adults recruited from community-based organizations and retirement village communities
in Australia. Using the Short Health Anxiety Inventory (SHAI; Salkovskis, Rimes,
27

Warwick, & Clark, 2002), approximately 7.6% of participants reported scores of 15 or
higher, indicating acute health anxiety (Rode, Salkovskis, Dowd, & Hanna, 2006). The
majority of the group also reported some physical illness. The authors indicated that the
SHAI scores for this group were similar to those reported in other studies for younger
people with chronic illness (Abramowitz, Deacon, & Valentiner, 2007; Rode et al., 2006;
Salkovskis et al., 2002).
Given the findings by Boston and Merrick (2010) described above, research
examining the prevalence of health anxiety among younger individuals with chronic
health conditions was examined. Research in this area is limited as only three studies
have addressed this topic area. Rode et al. (2006) assessed health anxiety in individuals
referred to a specialist chronic pain clinic using the SHAI. Severe and persistent health
anxiety was identified in 37% of these participants. Similar to this, Grassi, Sabato, Rossi,
Biancosino, and Marmai (2005) used the Diagnostic Criteria for Psychosomatic Research
System (Fava et al., 1995) to assess 146 patients with cancer for psychiatric morbidity
and psychosocial syndromes. They found that approximately 38% of mixed cancer
patients experienced persistent health anxiety. In contrast, using the SHAI, lower rates of
health anxiety were found among 246 individuals with multiple sclerosis, with
approximately 25% reporting severe and persistent health anxiety (Kehler &
Hadjistavropoulos, 2008). The findings suggest that health anxiety is substantial among
individuals with chronic health conditions, but also that variability may exist in the
prevalence of health anxiety depending on the chronic health condition examined.
28
Warwick, & Clark, 2002), approximately 7.6% of participants reported scores of 15 or
higher, indicating acute health anxiety (Rode, Salkovskis, Dowd, & Hanna, 2006). The
majority of the group also reported some physical illness. The authors indicated that the
SHAI scores for this group were similar to those reported in other studies for younger
people with chronic illness (Abramowitz, Deacon, & Valentiner, 2007; Rode et al., 2006;
Salkovskis et al , 2002).
Given the findings by Boston and Merrick (2010) described above, research
examining the prevalence of health anxiety among younger individuals with chronic
health conditions was examined. Research in this area is limited as only three studies
have addressed this topic area. Rode et al. (2006) assessed health anxiety in individuals
referred to a specialist chronic pain clinic using the SHAI. Severe and persistent health
anxiety was identified in 37% of these participants. Similar to this, Grassi, Sabato, Rossi,
Biancosino, and Marmai (2005) used the Diagnostic Criteria for Psychosomatic Research
System (Fava et al., 1995) to assess 146 patients with cancer for psychiatric morbidity
and psychosocial syndromes. They found that approximately 38% of mixed cancer
patients experienced persistent health anxiety. In contrast, using the SHAI, lower rates of
health anxiety were found among 246 individuals with multiple sclerosis, with
approximately 25% reporting severe and persistent health anxiety (Kehler &
Hadjistavropoulos, 2008). The findings suggest that health anxiety is substantial among
individuals with chronic health conditions, but also that variability may exist in the
prevalence of health anxiety depending on the chronic health condition examined.
28

These findings suggest that elevated health anxiety may not be part of the normal
experience for seniors, even when a health condition is present. However, although
health anxiety appears to occur less in older adults when compared to younger adults, it is
still a concern for a number of individuals. Given the limited research on health anxiety
among older adults, the following sections outline the CB model as it applies to older
persons and research on other specific forms of anxiety that affect seniors.
1.5.1 How Does the Cognitive Behavioural Model of Health Anxiety Apply to Older
Adults?
Boston and Merrick (2010) and Snyder and Stanley (2001) indicate that the CB
model of health anxiety may be applicable to older adults. First, the CB model posits that
innocuous bodily sensations are misinterpreted as a serious threat to health or a sign of
illness (Salkovskis & Warwick, 2001). There are a number of factors associated with
aging, such as increased somatic changes, decreased physical agility, greater medical
morbidity, and greater physical frailty that may cause an older adult to focus his or her
attention to health and bodily sensations (Barsky, 1993; Snyder & Stanley), and possibly
increase the chance of misinterpretation.
Second, certain common experiences seniors encounter during later life may serve
as critical incidents in the emergence of health-related anxiety (Snyder & Stanley, 2001).
For instance, older adults are likely to experience a higher number of health-related
distressing events, including the illness or death of a spouse, family member, or friend,
disease themselves, and falls or bodily injuries. The physiological changes associated
with aging may intensify difficulties seniors have coping with health anxiety (Snyder &
29
These findings suggest that elevated health anxiety may not be part of the normal
experience for seniors, even when a health condition is present. However, although
health anxiety appears to occur less in older adults when compared to younger adults, it is
still a concern for a number of individuals. Given the limited research on health anxiety
among older adults, the following sections outline the CB model as it applies to older
persons and research on other specific forms of anxiety that affect seniors.
1.5.1 How Does the Cognitive Behavioural Model of Health Anxiety Apply to Older
Adults?
Boston and Merrick (2010) and Snyder and Stanley (2001) indicate that the CB
model of health anxiety may be applicable to older adults. First, the CB model posits that
innocuous bodily sensations are misinterpreted as a serious threat to health or a sign of
illness (Salkovskis & Warwick, 2001). There are a number of factors associated with
aging, such as increased somatic changes, decreased physical agility, greater medical
morbidity, and greater physical frailty that may cause an older adult to focus his or her
attention to health and bodily sensations (Barsky, 1993; Snyder & Stanley), and possibly
increase the chance of misinterpretation.
Second, certain common experiences seniors encounter during later life may serve
as critical incidents in the emergence of health-related anxiety (Snyder & Stanley, 2001).
For instance, older adults are likely to experience a higher number of health-related
distressing events, including the illness or death of a spouse, family member, or friend,
disease themselves, and falls or bodily injuries. The physiological changes associated
with aging may intensify difficulties seniors have coping with health anxiety (Snyder &
29
Stanley, 2001). That is, given that older adults experience greater frailty and disease, this
may intensify pre-existing health anxiety or decrease perceived ability to function in
people with pre-existing health anxiety.
Third, Boston and Merrick (2010) suggest that older people have developed
coping behaviours throughout their lives. Although for most people these coping
behaviours are adaptive, in some more vulnerable people they may develop into
problematic safety-seeking behaviours which serve to reinforce and maintain health
anxiety (Snyder and Stanley, 2001). In addition, it is possible that decreasing physical
function and cognitive decline may render coping mechanisms less effective (Boston &
Merrick, 2010).
Only one study has empirically tested the applicability of aspects of the CB model
of health anxiety to older adults. Boston and Merrick (2010) found that, consistent with
the CB model of health anxiety, health anxiety as measured by the SHAI predicted safety
behaviours and medical utilization in a community sample of 145 older adults in
Australia. Boston and Merrick (2010) concluded that the findings of this study were a
step towards empirical support for the applicability of the CB model of health anxiety to
older adults.
1.6 Other Forms of Anxiety Among Seniors
1.6.1 Symptoms of Anxiety: Trait and State Anxiety
As outlined above, anxiety disorders affect a significant number of older adults.
Rates of anxiety are also significant when sub-clinical levels of anxiety are assessed in
older adults. For example, in a survey of community dwelling elders, Himmelfarb and
30
Stanley, 2001). That is, given that older adults experience greater frailty and disease, this
may intensify pre-existing health anxiety or decrease perceived ability to function in
people with pre-existing health anxiety.
Third, Boston and Merrick (2010) suggest that older people have developed
coping behaviours throughout their lives. Although for most people these coping
behaviours are adaptive, in some more vulnerable people they may develop into
problematic safety-seeking behaviours which serve to reinforce and maintain health
anxiety (Snyder and Stanley, 2001). In addition, it is possible that decreasing physical
function and cognitive decline may render coping mechanisms less effective (Boston &
Merrick, 2010).
Only one study has empirically tested the applicability of aspects of the CB model
of health anxiety to older adults. Boston and Merrick (2010) found that, consistent with
the CB model of health anxiety, health anxiety as measured by the SHAI predicted safety
behaviours and medical utilization in a community sample of 145 older adults in
Australia. Boston and Merrick (2010) concluded that the findings of this study were a
step towards empirical support for the applicability of the CB model of health anxiety to
older adults.
1.6 Other Forms of Anxiety Among Seniors
1.6.1 Symptoms of Anxiety: Trait and State Anxiety
As outlined above, anxiety disorders affect a significant number of older adults.
Rates of anxiety are also significant when sub-clinical levels of anxiety are assessed in
older adults. For example, in a survey of community dwelling elders, Himmelfarb and
30

Murrell (1984) found that 17% of males and 21% of females experienced anxiety
symptoms of sufficient severity to warrant intervention. When using the STAI
(Spielberger, 1983) in a sample of 73 geriatric inpatients, Kvaal, Macijauskiene, Engedal,
and Laake (2001) found that 41% of the female patients and 47% of the male patients had
a STAI state scale score above the cut-off of 39-40 points for significant anxiety
symptoms (Kvaal et al., 2001). In a follow-up study with the same patients, it was found
that the score on the STAI state scale had increased one to three months after discharge
(Kvaal & Laake, 2003). Bourgault-Fagnou and Hadjistavropoulos (2009) examined
levels of trait anxiety in a sample of 112 seniors receiving home care services. The
sample was classified into a low-frailty group and a high-frailty group. The authors
found that the low-frailty group was experiencing average levels of trait anxiety
(compared with a normative sample; Spielberger et al., 1983). However, they also found
that the group classified as being high-frailty was experiencing above-average levels of
trait anxiety (compared with a normative sample; Spielberger et al., 1983), suggesting
higher levels of trait anxiety among those individuals with poorer health.
Trait and state anxiety and health anxiety are similar, yet distinct concepts. Trait
anxiety is described as a relatively enduring predisposition to respond to stress with
anxiety, along with a tendency to view a broad range of situations as potentially
threatening (Nixon & Steffeck, 1977). State anxiety, however, can be described as one's
current subjective experience of apprehension and arousal of the autonomic system in
response to stress (Nixon & Steffeck, 1977). In hypothesized hierarchical fear structures,
trait anxiety is situated at one of the higher levels, whereas more specific fears are lower
31
Murrell (1984) found that 17% of males and 21% of females experienced anxiety
symptoms of sufficient severity to warrant intervention. When using the STAI
(Spielberger, 1983) in a sample of 73 geriatric inpatients, Kvaal, Macijauskiene, Engedal,
and Laake (2001) found that 41% of the female patients and 47% of the male patients had
a STAI state scale score above the cut-off of 39-40 points for significant anxiety
symptoms (Kvaal et al., 2001). In a follow-up study with the same patients, it was found
that the score on the STAI state scale had increased one to three months after discharge
(Kvaal & Laake, 2003). Bourgault-Fagnou and Hadjistavropoulos (2009) examined
levels of trait anxiety in a sample of 112 seniors receiving home care services. The
sample was classified into a low-frailty group and a high-frailty group. The authors
found that the low-frailty group was experiencing average levels of trait anxiety
(compared with a normative sample; Spielberger et al., 1983). However, they also found
that the group classified as being high-frailty was experiencing above-average levels of
trait anxiety (compared with a normative sample; Spielberger et al., 1983), suggesting
higher levels of trait anxiety among those individuals with poorer health.
Trait and state anxiety and health anxiety are similar, yet distinct concepts. Trait
anxiety is described as a relatively enduring predisposition to respond to stress with
anxiety, along with a tendency to view a broad range of situations as potentially
threatening (Nixon & Steffeck, 1977). State anxiety, however, can be described as one's
current subjective experience of apprehension and arousal of the autonomic system in
response to stress (Nixon & Steffeck, 1977). In hypothesized hierarchical fear structures,
trait anxiety is situated at one of the higher levels, whereas more specific fears are lower
31
order factors (Taylor, 1995; Zinbarg, Barlow, & Brown, 1997). Researchers have found
a moderate correlation between trait anxiety and health anxiety, but suggest that they
remain distinct constructs (Bourgault-Fagnou & Hadjistavropoulos, 2009; Hitchcock &
Mathews, 1992; Stewart & Watt, 2000).
1.6.2 Anxiety Sensitivity
Due to the increased attention paid to bodily sensations among those with
elevated health anxiety, anxiety sensitivity may be another important construct associated
with health anxiety in older adults. Anxiety sensitivity is an individual's tendency to fear
his or her own anxiety and anxiety-related symptoms because such symptoms are
believed to have harmful consequences (Reiss & McNally, 1985). Anxiety sensitivity is
believed to be a stable, trait-like characteristic and has been described as a risk factor for
anxiety-related disorders such as panic disorder (Schmidt & Joiner, 2002). It is
considered to be a dimensional construct consisting of three distinct, but related,
dimensions including physical concerns (i.e., fear of negative physical consequences of
anxiety-related somatic sensations), mental incapacitation (i.e., fear of negative
psychological consequences of anxiety-related cognitive sensations), and social concerns
(i.e., fear of negative social consequences of publicly observable anxiety sensations)
(Zinbarg, Mohlman, & Hong, 1999).
Anxiety sensitivity has been shown to be a significant predictor, albeit a separate
and distinct construct, of health anxiety in clinical (Otto, Demopulos, McLean, Pollack,
& Fava, 1998; Otto, Pollack, Sachs, & Rosenbaum, 1992) and non-clinical samples
(Stewart & Watt, 2000). Recently, Olatunji, Wolitzky-Taylor, Elwood, Connolly,
32
order factors (Taylor, 1995; Zinbarg, Barlow, & Brown, 1997). Researchers have found
a moderate correlation between trait anxiety and health anxiety, but suggest that they
remain distinct constructs (Bourgault-Fagnou & Hadjistavropoulos, 2009; Hitchcock &
Mathews, 1992; Stewart & Watt, 2000).
1.6.2 Anxiety Sensitivity
Due to the increased attention paid to bodily sensations among those with
elevated health anxiety, anxiety sensitivity may be another important construct associated
with health anxiety in older adults. Anxiety sensitivity is an individual's tendency to fear
his or her own anxiety and anxiety-related symptoms because such symptoms are
believed to have harmful consequences (Reiss & McNally, 1985). Anxiety sensitivity is
believed to be a stable, trait-like characteristic and has been described as a risk factor for
anxiety-related disorders such as panic disorder (Schmidt & Joiner, 2002). It is
considered to be a dimensional construct consisting of three distinct, but related,
dimensions including physical concerns (i.e., fear of negative physical consequences of
anxiety-related somatic sensations), mental incapacitation (i.e., fear of negative
psychological consequences of anxiety-related cognitive sensations), and social concerns
(i.e., fear of negative social consequences of publicly observable anxiety sensations)
(Zinbarg, Mohlman, & Hong, 1999).
Anxiety sensitivity has been shown to be a significant predictor, albeit a separate
and distinct construct, of health anxiety in clinical (Otto, Demopulos, McLean, Pollack,
& Fava, 1998; Otto, Pollack, Sachs, & Rosenbaum, 1992) and non-clinical samples
(Stewart & Watt, 2000). Recently, Olatunji, Wolitzky-Taylor, Elwood, Connolly,
32

Gonzales, and Armstrong (2009) confirmed a relationship between anxiety sensitivity and
symptoms of health anxiety. More specifically, Olatunji et al. (2009) found that the
anxiety sensitivity dimension of physical concerns had the largest relationship with health
anxiety, particularly illness likelihood and body vigilance aspects of health anxiety (as
measured by the SHAI).
With respect to the older adult population, Bravo and Silverman (2001) examined
the role of anxiety sensitivity, anxiety, and depression in 53 clinic referred (i.e.,
outpatient mental health programs) and 53 non-clinic referred older adults and their
relation to hypochondriacal concerns and medical illnesses. The results indicated that
anxiety sensitivity was significantly elevated in the clinic-referred group relative to the
non-clinic referred group, was negatively associated with a history of medical illnesses,
was strongly associated with health anxious concerns, and was a better predictor of health
anxious concerns than depression and trait anxiety.
1.7 Depression and Its Relationship to Health Anxiety in Seniors
Depression is one of the most common psychiatric disorders diagnosed in seniors
(Blazer, 1998; Hawranik, 1991). In the general population, approximately 10% to 15%
of seniors request help or require intervention for depressive complaints (Brodarty, 1993;
Beekman, Deeg, Braam, Smit, & van Tilburg, 1997). Because of this high rate of
depression among older adults, it is important to consider its relationship with health
anxiety. Symptoms of health anxiety have been found to be prevalent among seniors
with depression (Blazer, 1998). Koenig, Cohen, Blazer, Krishnan, and Sibert (1993)
examined the profile of depressive symptoms in younger and older male medical
33
Gonzales, and Armstrong (2009) confirmed a relationship between anxiety sensitivity and
symptoms of health anxiety. More specifically, Olatunji et al. (2009) found that the
anxiety sensitivity dimension of physical concerns had the largest relationship with health
anxiety, particularly illness likelihood and body vigilance aspects of health anxiety (as
measured by the SHAI).
With respect to the older adult population, Bravo and Silverman (2001) examined
the role of anxiety sensitivity, anxiety, and depression in 53 clinic referred (i.e.,
outpatient mental health programs) and 53 non-clinic referred older adults and their
relation to hypochondriacal concerns and medical illnesses. The results indicated that
anxiety sensitivity was significantly elevated in the clinic-referred group relative to the
non-clinic referred group, was negatively associated with a history of medical illnesses,
was strongly associated with health anxious concerns, and was a better predictor of health
anxious concerns than depression and trait anxiety.
1.7 Depression and Its Relationship to Health Anxiety in Seniors
Depression is one of the most common psychiatric disorders diagnosed in seniors
(Blazer, 1998; Hawranik, 1991). In the general population, approximately 10% to 15%
of seniors request help or require intervention for depressive complaints (Brodarty, 1993;
Beekman, Deeg, Braam, Smit, & van Tilburg, 1997). Because of this high rate of
depression among older adults, it is important to consider its relationship with health
anxiety. Symptoms of health anxiety have been found to be prevalent among seniors
with depression (Blazer, 1998). Koenig, Cohen, Blazer, Krishnan, and Sibert (1993)
examined the profile of depressive symptoms in younger and older male medical
33

inpatients aged 20-39 years (n = 116) and aged 70-102 years (n = 332), consecutively
admitted to the medical and neurological services of a medical centre. They found that,
among older men, loss of interest, insomnia, suicidal thoughts, and somatic concerns
most strongly differentiated depressed from non-depressed patients. Lyness, King,
Conwell, Cox, and Caine (1993) found that increasing age and depressive
symptomatology were predictors of greater somatic concern in 109 psychiatric inpatients
with DSM-III-R major depression. More recently, Bourgault-Fagnou and
Hadjistavropoulos (2009) examined predictors of health anxiety in sample of 112 seniors
receiving home care services. The authors found that higher levels of depression, along
with higher levels of pain, frailty, trait anxiety, and emotional preoccupation coping,
predicted higher health anxiety as measured by the IAS.
1.8 Treatment Issues
1.8.1 Treatment of Health Anxiety
Treatment provided under the CB orientation involves helping the individual with
health anxiety see that what they believe to be health-threatening symptoms can
alternatively be the result of normal bodily functioning (Warwick, 1989). CBT can also
assist the person in developing an understanding of bodily sensations and effective ways
of coping with preoccupation with bodily symptoms. As psychologically-oriented
treatment may be seen as potentially threatening in and of itself, and, as health problems
may be ignored and, in the meantime, worsen, it is important to point out the benefits of
this approach (Warwick, 1989).
34
inpatients aged 20-39 years (n = 116) and aged 70-102 years (n = 332), consecutively
admitted to the medical and neurological services of a medical centre. They found that,
among older men, loss of interest, insomnia, suicidal thoughts, and somatic concerns
most strongly differentiated depressed from non-depressed patients. Lyness, King,
Conwell, Cox, and Caine (1993) found that increasing age and depressive
symptomatology were predictors of greater somatic concern in 109 psychiatric inpatients
with DSM-III-R major depression. More recently, Bourgault-Fagnou and
Hadjistavropoulos (2009) examined predictors of health anxiety in sample of 112 seniors
receiving home care services. The authors found that higher levels of depression, along
with higher levels of pain, frailty, trait anxiety, and emotional preoccupation coping,
predicted higher health anxiety as measured by the IAS.
1.8 Treatment Issues
1.8.1 Treatment of Health Anxiety
Treatment provided under the CB orientation involves helping the individual with
health anxiety see that what they believe to be health-threatening symptoms can
alternatively be the result of normal bodily functioning (Warwick, 1989). CBT can also
assist the person in developing an understanding of bodily sensations and effective ways
of coping with preoccupation with bodily symptoms. As psychologically-oriented
treatment may be seen as potentially threatening in and of itself, and, as health problems
may be ignored and, in the meantime, worsen, it is important to point out the benefits of
this approach (Warwick, 1989).
34

Taylor and Asmundson (2004) outline several interventions used in CBT for
health anxiety to help the person abandon dysfunctional beliefs and accept more adaptive
ways of thinking about health and disease. CBT for health anxiety generally includes the
following strategies: treatment engagement strategies, psychoeducation, goal setting,
cognitive restructuring, behavioural exercises, stress management techniques, and relapse
prevention methods (Taylor & Asmundson, 2004).
Treatment engagement strategies are used to enhance treatment motivation and
encourage more adaptive ways of thinking about health and disease. For example, the
therapist may use motivational interviewing techniques (MI; Miller & Rollnick, 2002)
such as open-ended questions, reflective listening, summary statements, and differential
reinforcement of the patient's utterances in order to elicit self-motivating statements from
the patient and to decrease the patient's reluctance to engage fully in therapy.
Psychoeducation involves providing alternative, noncatastrophic explanations of
the patient's bodily changes or sensations. Explanations should include both
physiological and psychological explanations in order to help the patient understand that
their symptoms are real, and a result of normal bodily processes (Sharpe, Bass, & Mayou,
1995). The explanation should also discuss how beliefs, emotions, and bodily changes
and sensations are interrelated (Smith, 1985).
The patient and therapist may also work together to develop a set of goals to work
on in the course of therapy. Common treatment goals for health anxiety can include
decreased disease conviction, decreased health-related worry, decreased medical
35
Taylor and Asmundson (2004) outline several interventions used in CBT for
health anxiety to help the person abandon dysfunctional beliefs and accept more adaptive
ways of thinking about health and disease. CBT for health anxiety generally includes the
following strategies: treatment engagement strategies, psychoeducation, goal setting,
cognitive restructuring, behavioural exercises, stress management techniques, and relapse
prevention methods (Taylor & Asmundson, 2004).
Treatment engagement strategies are used to enhance treatment motivation and
encourage more adaptive ways of thinking about health and disease. For example, the
therapist may use motivational interviewing techniques (MI; Miller & Rollnick, 2002)
such as open-ended questions, reflective listening, summary statements, and differential
reinforcement of the patient's utterances in order to elicit self-motivating statements from
the patient and to decrease the patient's reluctance to engage fully in therapy.
Psychoeducation involves providing alternative, noncatastrophic explanations of
the patient's bodily changes or sensations. Explanations should include both
physiological and psychological explanations in order to help the patient understand that
their symptoms are real, and a result of normal bodily processes (Sharpe, Bass, & Mayou,
1995). The explanation should also discuss how beliefs, emotions, and bodily changes
and sensations are interrelated (Smith, 1985).
The patient and therapist may also work together to develop a set of goals to work
on in the course of therapy. Common treatment goals for health anxiety can include
decreased disease conviction, decreased health-related worry, decreased medical
35
utilization, decreased bodily checking, improved health habits, improved overall quality
of life, and so forth (Taylor & Asmundson, 2004).
Cognitive interventions are used to challenge and alter disease-related beliefs.
The aim of cognitive interventions is to promote the development of alternative,
nonthreatening explanations of bodily events (Warwick, 1995). Cognitive interventions
are used to help patients identify and objectively examine their health-related beliefs,
which are usually catastrophic in nature, and to create reasonable, noncatastrophic
alternatives (Taylor & Asmundson, 2004).
Behavioural methods play a large role in treating fear, avoidance, and maladaptive
safety behaviours such as excessive checking and reassurance seeking. Behavioural
exercises generally require the person with health anxiety to be exposed to the feared
stimuli in a systematic, controlled fashion (Taylor & Asmundson, 2004). Behavioural
exercises can include behavioural experiments that test the effects of beliefs and
behaviours (e.g., testing the effects of performing vs. not performing safety behaviours),
situational exposure (i.e., exposure to harmless but fear-evoking stimuli), interoceptive
exposure (i.e., sensation-inducing exercises), and imaginal exposure (e.g., try to imagine
all the components of the feared situation as vividly as possible; Taylor & Asmundson,
2004).
Stress management techniques can be used to reduce a person's anxious arousal.
Typical stress management procedures that are often used to reduce health anxiety
include psychoeducation for stress management, applied relaxation training (e.g.,
36
utilization, decreased bodily checking, improved health habits, improved overall quality
of life, and so forth (Taylor & Asmundson, 2004).
Cognitive interventions are used to challenge and alter disease-related beliefs.
The aim of cognitive interventions is to promote the development of alternative,
nonthreatening explanations of bodily events (Warwick, 1995). Cognitive interventions
are used to help patients identify and objectively examine their health-related beliefs,
which are usually catastrophic in nature, and to create reasonable, noncatastrophic
alternatives (Taylor & Asmundson, 2004).
Behavioural methods play a large role in treating fear, avoidance, and maladaptive
safety behaviours such as excessive checking and reassurance seeking. Behavioural
exercises generally require the person with health anxiety to be exposed to the feared
stimuli in a systematic, controlled fashion (Taylor & Asmundson, 2004). Behavioural
exercises can include behavioural experiments that test the effects of beliefs and
behaviours (e.g., testing the effects of performing vs. not performing safety behaviours),
situational exposure (i.e., exposure to harmless but fear-evoking stimuli), interoceptive
exposure (i.e., sensation-inducing exercises), and imaginal exposure (e.g., try to imagine
all the components of the feared situation as vividly as possible; Taylor & Asmundson,
2004).
Stress management techniques can be used to reduce a person's anxious arousal.
Typical stress management procedures that are often used to reduce health anxiety
include psychoeducation for stress management, applied relaxation training (e.g.,
36
progressive muscle relaxation), breathing retraining, a general approach to problem
solving, and time management techniques (Taylor & Asmundson, 2004).
Relapse prevention methods are used to maintain and extend treatment gains,
including methods for dealing with future episodes of elevated anxiety. A CBT program
for health anxiety should provide the patient with a review of treatment progress, attempt
to establish expectations for post-treatment functioning, provide a written maintenance
plan, outline how to deal with relapse preventions, and, if possible, arrange for periodic
check-ins with the therapist (Taylor & Asmundson, 2004).
Adding to the above description, Furer, Walker, and Freeston (2001) highlight,
several important considerations for the treatment of health anxiety among individuals at
risk for or with chronic medical conditions. First, they highlight the use of problem-
focused coping, such as increasing activities and fully immersing oneself in these
activities in an effort to help to reduce distress. Second, Furer and colleagues suggest that
with slight modifications, many of the core CB techniques may prove beneficial. They
caution that the aim should be to decrease excessive preoccupation with disease and its
negative consequences as opposed to attempting to convince the individual that the
disease and its associated consequences can be avoided. Realistic concern about one's
health is seen as normal, and individuals should be encouraged to be involved in their
health care and to obtain appropriate medical management and tests.
Case studies and several non-randomized controlled studies have been published
on the treatment of elevated health anxiety and hypochondriasis and they suggest that
CBT (6-16 weekly sessions) can effectively reduce health anxiety and hypochondriasis.
37
progressive muscle relaxation), breathing retraining, a general approach to problem
solving, and time management techniques (Taylor & Asmundson, 2004).
Relapse prevention methods are used to maintain and extend treatment gains,
including methods for dealing with future episodes of elevated anxiety. A CBT program
for health anxiety should provide the patient with a review of treatment progress, attempt
to establish expectations for post-treatment functioning, provide a written maintenance
plan, outline how to deal with relapse preventions, and, if possible, arrange for periodic
check-ins with the therapist (Taylor & Asmundson, 2004).
Adding to the above description, Furer, Walker, and Freeston (2001) highlight,
several important considerations for the treatment of health anxiety among individuals at
risk for or with chronic medical conditions. First, they highlight the use of problem-
focused coping, such as increasing activities and fully immersing oneself in these
activities in an effort to help to reduce distress. Second, Furer and colleagues suggest that
with slight modifications, many of the core CB techniques may prove beneficial. They
caution that the aim should be to decrease excessive preoccupation with disease and its
negative consequences as opposed to attempting to convince the individual that the
disease and its associated consequences can be avoided. Realistic concern about one's
health is seen as normal, and individuals should be encouraged to be involved in their
health care and to obtain appropriate medical management and tests.
Case studies and several non-randomized controlled studies have been published
on the treatment of elevated health anxiety and hypochondriasis and they suggest that
CBT (6-16 weekly sessions) can effectively reduce health anxiety and hypochondriasis.
37
For example, Warwick and Marks (1988) evaluated the effectiveness of a CBT for illness
phobia or hypochondriasis with 17 patients with an International Statistical
Classification of Diseases and Related Health Problems 9th Revision (World Health
Organization, 1977) diagnosis. Treatment consisted of seven sessions, on average, during
which exposure and response prevention (i.e., the patient confronts their fears and then
discontinues the usual escape response) was implemented to address avoidance
behaviours (exercise avoidance) and reassurance seeking. Significant improvements
were observed on severity of the patient's main worries (e.g., heart disease), designated
target behaviour(s), vocational and recreational functioning, and on the Fear
Questionnaire (Marks & Mathews, 1979). Treatment gains were maintained for 6 of 13
patients who were followed a median of 5 years.
Bouman and Visser (1998) compared cognitive therapy to behaviour therapy (i.e.,
in vivo exposure plus response prevention) among 17 patients meeting DSM-IV (APA,
1994) criteria for hypochondriasis. Because of the small sample size, patients were used
as their own controls by observing pre- and post-baseline periods of four weeks without
treatment. After the initial interviews, patients were randomly assigned to either of the
two treatment conditions. Patients in both treatment conditions improved on specific
measures of hypochondriasis and depression. The two treatments were found to be
equally effective.
The efficacy of individual CBT for hypochondriasis has also been demonstrated
in five randomized controlled trials (e.g., Barsky & Ahem, 2004; Visser & Bouman,
2001). Warwick, Clark, Cobb, and Salkovskis (1996) were one of the first groups to
38
For example, Warwick and Marks (1988) evaluated the effectiveness of a CBT for illness
phobia or hypochondriasis with 17 patients with an International Statistical
Classification of Diseases and Related Health Problems 9th Revision (World Health
Organization, 1977) diagnosis. Treatment consisted of seven sessions, on average, during
which exposure and response prevention (i.e., the patient confronts their fears and then
discontinues the usual escape response) was implemented to address avoidance
behaviours (exercise avoidance) and reassurance seeking. Significant improvements
were observed on severity of the patient's main worries (e.g., heart disease), designated
target behaviour(s), vocational and recreational functioning, and on the Fear
Questionnaire (Marks & Mathews, 1979). Treatment gains were maintained for 6 of 13
patients who were followed a median of 5 years.
Bouman and Visser (1998) compared cognitive therapy to behaviour therapy (i.e.,
in vivo exposure plus response prevention) among 17 patients meeting DSM-IV (APA,
1994) criteria for hypochondriasis. Because of the small sample size, patients were used
as their own controls by observing pre- and post-baseline periods of four weeks without
treatment. After the initial interviews, patients were randomly assigned to either of the
two treatment conditions. Patients in both treatment conditions improved on specific
measures of hypochondriasis and depression. The two treatments were found to be
equally effective.
The efficacy of individual CBT for hypochondriasis has also been demonstrated
in five randomized controlled trials (e.g., Barsky & Ahern, 2004; Visser & Bouman,
2001). Warwick, Clark, Cobb, and Salkovskis (1996) were one of the first groups to
38

evaluate the effectiveness of a controlled trial of CBT for hypochondriasis. Thirty-two
patients meeting the DSM-III-R criteria for hypochondriasis were randomly assigned to a
CBT or a wait-list control (WLC) condition. The patients in the active treatment
condition received 16 individual treatment sessions, spread over 4 months. The active
treatment group showed significantly greater improvements than the WLC group on
patient ratings including global problem severity, disease conviction when anxious and
when calm, need for reassurance, time spent worrying about health, health anxiety,
frequency of checking behaviour, depression, and general anxiety. Only frequency of
avoidance behaviours showed no significant differences. The active treatment group also
showed significant improvements compared to the WLC group on therapist ratings of
global problem severity, need for reassurance, health anxiety, and disease conviction.
Finally, the active treatment group showed significant improvements compared to the
WLC group on assessor (blind to treatment allocation) ratings including global problem
severity, disease conviction when anxious and when calm, time spent wanting
reassurance, and strength of need for reassurance. The improvements were maintained at
three months follow-up. The authors concluded that CBT is an acceptable and effective
treatment for hypochondriasis, but they also mentioned a number of limitations of their
study. All treatments were carried out by only one therapist (the first author), so it is
unclear whether other therapists would obtain similar results. One other limitation
included the fact that the follow-up period of three months was relatively short.
In another randomized controlled trial, Clark et al. (1998) compared three
conditions: (1) CBT, (2) behavioural stress management (BSM), and (3) WLC. BSM
39
evaluate the effectiveness of a controlled trial of CBT for hypochondriasis. Thirty-two
patients meeting the DSM-III-R criteria for hypochondriasis were randomly assigned to a
CBT or a wait-list control (WLC) condition. The patients in the active treatment
condition received 16 individual treatment sessions, spread over 4 months. The active
treatment group showed significantly greater improvements than the WLC group on
patient ratings including global problem severity, disease conviction when anxious and
when calm, need for reassurance, time spent worrying about health, health anxiety,
frequency of checking behaviour, depression, and general anxiety. Only frequency of
avoidance behaviours showed no significant differences. The active treatment group also
showed significant improvements compared to the WLC group on therapist ratings of
global problem severity, need for reassurance, health anxiety, and disease conviction.
Finally, the active treatment group showed significant improvements compared to the
WLC group on assessor (blind to treatment allocation) ratings including global problem
severity, disease conviction when anxious and when calm, time spent wanting
reassurance, and strength of need for reassurance. The improvements were maintained at
three months follow-up. The authors concluded that CBT is an acceptable and effective
treatment for hypochondriasis, but they also mentioned a number of limitations of their
study. All treatments were carried out by only one therapist (the first author), so it is
unclear whether other therapists would obtain similar results. One other limitation
included the fact that the follow-up period of three months was relatively short.
In another randomized controlled trial, Clark et al. (1998) compared three
conditions: (1) CBT, (2) behavioural stress management (BSM), and (3) WLC. BSM
39

therapy was a non-specific treatment based on the rationale that some people react to
stress by becoming worried about their health. Thus, such worries are best dealt with by
acquiring a comprehensive set of stress management techniques including relaxation
training, exposure and desensitization, problem solving, assertiveness, time-management
skills, and a stimulus control procedure for postponing worry until a specified "worry
time." Forty-eight patients with hypochondriasis were randomly assigned to one of these
conditions. Each treatment consisted of up to 16 weekly one-hour sessions in the first
four months and up to three booster sessions in the next three months. Both treatment
groups led to significantly improved outcomes as compared to the WLC group. Further,
the CBT group showed improved outcomes as compared to stress-management therapy
on measures of health anxiety at posttreatment, but at 12-month follow-up the advantages
of CBT were no longer evident.
Employing a similar design, Visser and Bouman (2001) conducted a controlled
study to compare the efficacy of in vivo exposure plus response prevention, cognitive
therapy, and WLC. Seventy-eight patients with a DSM-IV-TR diagnosis of
hypochondriasis were randomly assigned to one of these conditions. Each active
treatment consisted of 12 weekly sessions, followed by a four-week interval without
treatment. At both post-treatment and seven-month follow-up, the two forms of
treatment were deemed equally effective and produced significantly improved outcomes
(i.e., reduced health anxiety, illness behaviour, somatosensory amplification, symptoms
of somatization, ratings of idiosyncratic hypochondriacal situations and cognitions,
symptoms of depression, obsessive-compulsive complaints, and general mental
40
therapy was a non-specific treatment based on the rationale that some people react to
stress by becoming worried about their health. Thus, such worries are best dealt with by
acquiring a comprehensive set of stress management techniques including relaxation
training, exposure and desensitization, problem solving, assertiveness, time-management
skills, and a stimulus control procedure for postponing worry until a specified "worry
time." Forty-eight patients with hypochondriasis were randomly assigned to one of these
conditions. Each treatment consisted of up to 16 weekly one-hour sessions in the first
four months and up to three booster sessions in the next three months. Both treatment
groups led to significantly improved outcomes as compared to the WLC group. Further,
the CBT group showed improved outcomes as compared to stress-management therapy
on measures of health anxiety at posttreatment, but at 12-month follow-up the advantages
of CBT were no longer evident.
Employing a similar design, Visser and Bouman (2001) conducted a controlled
study to compare the efficacy of in vivo exposure plus response prevention, cognitive
therapy, and WLC. Seventy-eight patients with a DSM-IV-TR diagnosis of
hypochondriasis were randomly assigned to one of these conditions. Each active
treatment consisted of 12 weekly sessions, followed by a four-week interval without
treatment. At both post-treatment and seven-month follow-up, the two forms of
treatment were deemed equally effective and produced significantly improved outcomes
(i.e., reduced health anxiety, illness behaviour, somatosensory amplification, symptoms
of somatization, ratings of idiosyncratic hypochondriacal situations and cognitions,
symptoms of depression, obsessive-compulsive complaints, and general mental
40

functioning) compared to the WLC group. However, the high drop-out rate in this study
(28.2%) limits the generalizability of the findings.
More recently, using a randomized, usual care control group design, Barsky and
Ahern (2004) found support for the efficacy of a six session CB intervention. One
hundred and two individuals who exceeded the cut-off score on a self-report
hypochondriasis questionnaire were assigned to CBT and 85 were assigned to medical
care as usual. CBT was administered individually in six sessions at weekly intervals.
Factors that are thought to be related to patient amplification of somatic symptoms and
misattribution of these factors to serious disease were covered, including attention and
bodily hypervigilance, beliefs about symptom etiology, circumstances and context, illness
and sick role behaviours, and mood. Each session consisted of educational information
about the symptom amplifiers, an illustrative exercise, and a discussion to personalize the
material presented. The CBT group showed significantly improved outcomes (i.e.,
reduced hypochondriacal symptoms, attitudes and beliefs, health-related anxiety,
somatosensory amplification, and intermediate activities of daily living) as compared to
the WLC group at both 6- and 12-month follow-up. At 12-month follow-up, CBT
patients had significantly lower levels of hypochondriacal symptoms, beliefs and
attitudes, and health-related anxiety. Significant improvements in social functioning
were not identified until the 12-month follow-up. They also had significantly less
impairment of intermediate activities of daily living. Hypochondriacal somatic
symptoms were not improved significantly by treatment, but this was not one of the aims
of treatment, since the focus was on helping the patients cope with these symptoms.
41
functioning) compared to the WLC group. However, the high drop-out rate in this study
(28.2%o) limits the generalizability of the findings.
More recently, using a randomized, usual care control group design, Barsky and
Ahem (2004) found support for the efficacy of a six session CB intervention. One
hundred and two individuals who exceeded the cut-off score on a self-report
hypochondriasis questionnaire were assigned to CBT and 85 were assigned to medical
care as usual. CBT was administered individually in six sessions at weekly intervals.
Factors that are thought to be related to patient amplification of somatic symptoms and
misattribution of these factors to serious disease were covered, including attention and
bodily hypervigilance, beliefs about symptom etiology, circumstances and context, illness
and sick role behaviours, and mood. Each session consisted of educational information
about the symptom amplifiers, an illustrative exercise, and a discussion to personalize the
material presented. The CBT group showed significantly improved outcomes (i.e.,
reduced hypochondriacal symptoms, attitudes and beliefs, health-related anxiety,
somatosensory amplification, and intermediate activities of daily living) as compared to
the WLC group at both 6- and 12-month follow-up. At 12-month follow-up, CBT
patients had significantly lower levels of hypochondriacal symptoms, beliefs and
attitudes, and health-related anxiety. Significant improvements in social functioning
were not identified until the 12-month follow-up. They also had significantly less
impairment of intermediate activities of daily living. Hypochondriacal somatic
symptoms were not improved significantly by treatment, but this was not one of the aims
of treatment, since the focus was on helping the patients cope with these symptoms.
41

Taylor, Asmundson, and Coons (2005) conducted a meta-analysis of 25 trials
examining various treatments for health anxiety, in order to gain a greater understanding
of the relative efficacy of these interventions. Psychosocial treatments that were
reviewed included psychoeducation, explanatory therapy (an approach based primarily on
providing a large amount of reassurance, anxiolytic medication when the patient becomes
anxious, and psychoeduction; Kellner, 1979; Taylor & Asmundson, 2004), cognitive
therapy, exposure and response prevention, CBT, and behavioural stress management.
Four different types of drug treatments were reviewed and included paroxetine,
fluoxetine, fluvoxamine, and nefazodone. Participants in the studies that were included
either had full or abridged hypochondriasis (i.e., differs from full-blown hypochondriasis
in that one or more of the diagnostic features of hypochondriasis are not present; Taylor
& Asmundson, 2004). They were typically aged in their 30s or 40s, and approximately
two-thirds were female. The duration of health anxiety, when reported, was typically
several years. Patients in drug trials were on their medications at the time of the post-
treatment assessment. For studies of full-blown hypochondriasis, the post-treatment
effect sizes for measures of hypochondriasis suggested that CBT and fluoxetine yielded
the largest effects for treatment completers. The mean estimated effect size for CBT was
2.05 and the mean estimated effect size for fluoxetine was 1.92.
Taylor et al. (2005) suggested the following from the meta-analysis results. First,
for measures of hypochondriasis, all of the psychosocial and drug treatments had larger
effect sizes than WLCs. This indicates that the clinician's skills are useful in the
treatment of health anxiety. When treatment acceptability, and strength, breadth, and
42
Taylor, Asmundson, and Coons (2005) conducted a meta-analysis of 25 trials
examining various treatments for health anxiety, in order to gain a greater understanding
of the relative efficacy of these interventions. Psychosocial treatments that were
reviewed included psychoeducation, explanatory therapy (an approach based primarily on
providing a large amount of reassurance, anxiolytic medication when the patient becomes
anxious, and psychoeduction; Kellner, 1979; Taylor & Asmundson, 2004), cognitive
therapy, exposure and response prevention, CBT, and behavioural stress management.
Four different types of drug treatments were reviewed and included paroxetine,
fluoxetine, fluvoxamine, and nefazodone. Participants in the studies that were included
either had full or abridged hypochondriasis (i.e., differs from full-blown hypochondriasis
in that one or more of the diagnostic features of hypochondriasis are not present; Taylor
& Asmundson, 2004). They were typically aged in their 30s or 40s, and approximately
two-thirds were female. The duration of health anxiety, when reported, was typically
several years. Patients in drug trials were on their medications at the time of the post-
treatment assessment. For studies of full-blown hypochondriasis, the post-treatment
effect sizes for measures of hypochondriasis suggested that CBT and fluoxetine yielded
the largest effects for treatment completers. The mean estimated effect size for CBT was
2.05 and the mean estimated effect size for fluoxetine was 1.92.
Taylor et al. (2005) suggested the following from the meta-analysis results. First,
for measures of hypochondriasis, all of the psychosocial and drug treatments had larger
effect sizes than WLCs. This indicates that the clinician's skills are useful in the
treatment of health anxiety. When treatment acceptability, and strength, breadth, and
42

durability of effects were taken into consideration, Taylor et al. (2005) suggested that
CBT is the treatment of choice for full hypochondriasis. However, for mixed full and
abridged hypochondriasis, they suggest that psychoeducation might be adequate for many
patients with mild health anxiety, especially if the person is not depressed. If depression
plays a factor in cases of abridged hypochondriasis, CBT for health anxiety may be more
beneficial because it appeared to be superior to psychoeducation in reducing depression.
The results, however, need to be interpreted with caution as the sample sizes tended to be
small in most of the studies included.
Since the time of this review, Seivewright et al. (2008) conducted a randomised
controlled trial to compare the efficacy of CBT versus WLC in the treatment of health
anxiety. Twenty-three patients were randomised to the CBT group and 26 patients were
randomised to the WLC control group. The active treatment consisted of an average of
4.3 sessions (range 0-13) of 45-60 minutes over a six-month period. Participants in the
active treatment received CBT supplemented by a booklet (bibliotherapy). At both post-
treatment and six-month follow-up, CBT produced significantly improved outcomes on
health anxiety, generalized anxiety, and depression compared to the WLC control group.
In another recent randomized controlled trial, Sorensen, Birket-Smith, Wattar, and
Salkovskis (in press) compared three conditions: (1) CBT, (2) short-term psychodynamic
psychotherapy (STPP), and (3) WLC in the treatment of hypochondriasis. Eighty
patients with hypochondriasis were randomly assigned to one of these conditions. The
CBT program consisted of eight individual sessions and eight group sessions. The STPP
program consisted of 16 weekly sessions. Patients in the WLC group were asked to keep
43
durability of effects were taken into consideration, Taylor et al. (2005) suggested that
CBT is the treatment of choice for full hypochondriasis. However, for mixed full and
abridged hypochondriasis, they suggest that psychoeducation might be adequate for many
patients with mild health anxiety, especially if the person is not depressed. If depression
plays a factor in cases of abridged hypochondriasis, CBT for health anxiety may be more
beneficial because it appeared to be superior to psychoeducation in reducing depression.
The results, however, need to be interpreted with caution as the sample sizes tended to be
small in most of the studies included.
Since the time of this review, Seivewright et al. (2008) conducted a randomised
controlled trial to compare the efficacy of CBT versus WLC in the treatment of health
anxiety. Twenty-three patients were randomised to the CBT group and 26 patients were
randomised to the WLC control group. The active treatment consisted of an average of
4.3 sessions (range 0-13) of 45-60 minutes over a six-month period. Participants in the
active treatment received CBT supplemented by a booklet (bibliotherapy). At both post-
treatment and six-month follow-up, CBT produced significantly improved outcomes on
health anxiety, generalized anxiety, and depression compared to the WLC control group.
In another recent randomized controlled trial, Sorensen, Birket-Smith, Wattar, and
Salkovskis (in press) compared three conditions: (1) CBT, (2) short-term psychodynamic
psychotherapy (STPP), and (3) WLC in the treatment of hypochondriasis. Eighty
patients with hypochondriasis were randomly assigned to one of these conditions. The
CBT program consisted of eight individual sessions and eight group sessions. The STPP
program consisted of 16 weekly sessions. Patients in the WLC group were asked to keep
43
in touch with their family physician, and they were instructed not to begin any other
treatment during the study period. The patients receiving CBT had significant
improvements compared to the WLC group on measures of health anxiety, generalized
anxiety, and depression and compared to the STPP group on measures of health anxiety
and depression. The STPP group did not show significant improvements relative to the
WLC group on any measures. At follow-up, CBT did significantly better than STPP on
all measures with the exception of one generalized anxiety measure. The above
described results suggest that CBT is effective in the treatment of health anxiety.
1.8.2 Enhancing CBT for Use with Older Adults
Empirical evidence for the effectiveness of CB interventions with seniors has
grown over the past 30 years (Satre, Knight, & David, 2006). These studies have used
treatment manuals specifically adapted for older adults, taking into account the changes
that occur through the aging process (Mohlman et al., 2003; Stanley, Diefenbach, &
Hopko, 2004). A number of adaptations for treatment of older adults have been
suggested in the gerontological literature. For example, some older adults may
experience cognitive decline, which can be problematic during psychotherapy (Snyder &
Stanley, 2001). In order to facilitate patient understanding, abbreviated sessions focused
on concrete tasks have been suggested as a way to improve outcome. Treatment may
also take a greater number of sessions compared with younger adults (Snyder & Stanley,
2001). To facilitate comprehension, terms should be simplified, removing possible
communication barriers between therapist and the older patient (Snyder & Stanley, 2001).
Clinicians should consider any modifications of terms necessary to fit the patient's
44
in touch with their family physician, and they were instructed not to begin any other
treatment during the study period. The patients receiving CBT had significant
improvements compared to the WLC group on measures of health anxiety, generalized
anxiety, and depression and compared to the STPP group on measures of health anxiety
and depression. The STPP group did not show significant improvements relative to the
WLC group on any measures. At follow-up, CBT did significantly better than STPP on
all measures with the exception of one generalized anxiety measure. The above
described results suggest that CBT is effective in the treatment of health anxiety.
1.8.2 Enhancing CBT for Use with Older Adults
Empirical evidence for the effectiveness of CB interventions with seniors has
grown over the past 30 years (Satre, Knight, & David, 2006). These studies have used
treatment manuals specifically adapted for older adults, taking into account the changes
that occur through the aging process (Mohlman et al., 2003; Stanley, Diefenbach, &
Hopko, 2004). A number of adaptations for treatment of older adults have been
suggested in the gerontological literature. For example, some older adults may
experience cognitive decline, which can be problematic during psychotherapy (Snyder &
Stanley, 2001). In order to facilitate patient understanding, abbreviated sessions focused
on concrete tasks have been suggested as a way to improve outcome. Treatment may
also take a greater number of sessions compared with younger adults (Snyder & Stanley,
2001). To facilitate comprehension, terms should be simplified, removing possible
communication barriers between therapist and the older patient (Snyder & Stanley, 2001).
Clinicians should consider any modifications of terms necessary to fit the patient's
44

educational background, cognitive skills, and preferences (e.g., nervous or concerned
instead of worried; classes rather than treatment sessions; Stanley et al., 2004). Written
materials summarizing the information covered during treatment sessions might also be
useful as a reference for between-session reviews (Snyder & Stanley, 2001). Further, the
addition of learning and memory aids designed to increase homework compliance,
strengthen memory for techniques, and facilitate the use of these techniques have been
found to be useful in psychotherapy with older adults (Mohlman et al., 2003). For
instance, modifications of homework assignments may be necessary for some patients
(e.g., use of audiotapes, enlarged homework forms, simplified checklists). In other cases,
treatment may need to occur at a generally slower pace than is recommended, and with
less intensive homework assignments overall (e.g., practicing only one skill each day). In
addition, some patients may find the cognitive restructuring component difficult to
comprehend. In these cases, the overall amount of time spent on cognitive restructuring
can be decreased (Stanley et al., 2004).
A number of studies have adapted CBT specifically for seniors and have used
modifications, such as making examples more relevant to older people (e.g., Wetherall,
Gatz, & Craske, 2003). Mohlman and colleagues (2003) compared the efficacy of an
enhanced individual-format CBT administered in a mental health clinic for treatment of
late-life GAD to a standard CBT format. Study 1 compared the standard version of CBT
with a WLC group. Study 2 compared an enhanced version (ECBT) that included
learning and memory aids designed to make the therapy more effective with older adults
to a WLC. These enhancements were derived from articles and workshop materials
45
educational background, cognitive skills, and preferences (e.g., nervous or concerned
instead of worried; classes rather than treatment sessions; Stanley et al., 2004). Written
materials summarizing the information covered during treatment sessions might also be
useful as a reference for between-session reviews (Snyder & Stanley, 2001). Further, the
addition of learning and memory aids designed to increase homework compliance,
strengthen memory for techniques, and facilitate the use of these techniques have been
found to be useful in psychotherapy with older adults (Mohlman et al., 2003). For
instance, modifications of homework assignments may be necessary for some patients
(e.g., use of audiotapes, enlarged homework forms, simplified checklists). In other cases,
treatment may need to occur at a generally slower pace than is recommended, and with
less intensive homework assignments overall (e.g., practicing only one skill each day). In
addition, some patients may find the cognitive restructuring component difficult to
comprehend. In these cases, the overall amount of time spent on cognitive restructuring
can be decreased (Stanley et al, 2004).
A number of studies have adapted CBT specifically for seniors and have used
modifications, such as making examples more relevant to older people (e.g., Wetherall,
Gatz, & Craske, 2003). Mohlman and colleagues (2003) compared the efficacy of an
enhanced individual-format CBT administered in a mental health clinic for treatment of
late-life GAD to a standard CBT format. Study 1 compared the standard version of CBT
with a WLC group. Study 2 compared an enhanced version (ECBT) that included
learning and memory aids designed to make the therapy more effective with older adults
to a WLC. These enhancements were derived from articles and workshop materials
45
focused on tailoring CBT to older adults (Knight & Satre, 1999) or were devised by
Mohlman himself. Immediately following completion of the intervention, Study 1 CBT
participants showed significant improvement on GAD severity ratings. Study 2 EBCT
participants showed significant improvement on two self-report measures, rates of post-
treatment GAD, and GAD severity ratings. ECBT resulted in improvement on more
measures and yielded larger effect sizes than standard CBT, when each was compared
against a WLC group (Mohlman et al., 2003). This data remain preliminary as no further
follow-up data have been published.
1.8.3 Reasons Why CBT May Be Effective with Older Adults
Morris and Morris (1991) state that there are a number of reasons why CB
interventions can be particularly effective with older people. First, CBT is focused on the
`here and now.' The individual's current needs are identified and interventions are
developed to target specific stressors. Second, CBT is skills enhancing and practical.
The organized nature of therapy can help to keep the person oriented to tasks within and
across sessions. Homework is used to keep the individual focused on managing
problems. Third, CBT encourages self-monitoring. The individual is taught to recognize
mood fluctuations and emotional vulnerabilities and to develop strategies that enhance
coping ability. Fourth, it is educative. The connection between thoughts, mood, and
behaviour is explained, and the model explains the impact of negative cycles of
problematic emotion states (e.g., depression, anxiety) upon the person's activity level and
vice versa. Fifth, CBT is goal oriented. Interventions are developed to challenge
stereotyped beliefs (i.e., 'You can't teach an old dog new tricks').
46
focused on tailoring CBT to older adults (Knight & Satre, 1999) or were devised by
Mohlman himself. Immediately following completion of the intervention, Study 1 CBT
participants showed significant improvement on GAD severity ratings. Study 2 EBCT
participants showed significant improvement on two self-report measures, rates of post-
treatment GAD, and GAD severity ratings. ECBT resulted in improvement on more
measures and yielded larger effect sizes than standard CBT, when each was compared
against a WLC group (Mohlman et al., 2003). This data remain preliminary as no further
follow-up data have been published.
1.8.3 Reasons Why CBT May Be Effective with Older Adults
Morris and Morris (1991) state that there are a number of reasons why CB
interventions can be particularly effective with older people. First, CBT is focused on the
'here and now.' The individual's current needs are identified and interventions are
developed to target specific stressors. Second, CBT is skills enhancing and practical.
The organized nature of therapy can help to keep the person oriented to tasks within and
across sessions. Homework is used to keep the individual focused on managing
problems. Third, CBT encourages self-monitoring. The individual is taught to recognize
mood fluctuations and emotional vulnerabilities and to develop strategies that enhance
coping ability. Fourth, it is educative. The connection between thoughts, mood, and
behaviour is explained, and the model explains the impact of negative cycles of
problematic emotion states (e.g., depression, anxiety) upon the person's activity level and
vice versa. Fifth, CBT is goal oriented. Interventions are developed to challenge
stereotyped beliefs (i.e., 'You can't teach an old dog new tricks').
46

As described above, individual CBT for health anxiety has proven to be effective
in a variety of samples. However, this treatment awaits testing in samples of older adults.
Nonetheless, it would appear that with some modifications CBT could be applied to
samples of seniors. Given the limited resources of the health care system it is also
important to investigate less costly methods of providing CBT for health anxiety. In this
regard, examining the effectiveness of providing patients with a brief intervention for
health anxiety is a worthy endeavour.
1.8.4 Fostering the Therapeutic Alliance
Although some patients receiving treatment for health anxiety will be
apprehensive about psychological interventions, this may be especially true for older
adults who are often unsure about seeking treatment for psychological difficulties
(Lasocki, 1986). Small (1997) attributed this reluctance to the fact that some older adults
associate psychological problems with 'being crazy' or as a sign that they are weak. This
is often reinforced by physicians who tell the older adult that their problems are 'all in
their head' because they cannot find a biomedical cause for reported symptoms (Snyder
& Stanley, 2001). As a result, the relationship between the client and therapist is
especially important when treating older adults with health anxiety. Their potential lack
of trust for mental health professionals and possible disappointment at being referred by
their physicians can be improved through the development of a strong relationship
(Snyder & Stanley, 2001). Thus, treatment programs specifically tailored to the older
adult population may help to foster the relationship between the client and therapist,
47
As described above, individual CBT for health anxiety has proven to be effective
in a variety of samples. However, this treatment awaits testing in samples of older adults.
Nonetheless, it would appear that with some modifications CBT could be applied to
samples of seniors. Given the limited resources of the health care system it is also
important to investigate less costly methods of providing CBT for health anxiety. In this
regard, examining the effectiveness of providing patients with a brief intervention for
health anxiety is a worthy endeavour.
1.8.4 Fostering the Therapeutic Alliance
Although some patients receiving treatment for health anxiety will be
apprehensive about psychological interventions, this may be especially true for older
adults who are often unsure about seeking treatment for psychological difficulties
(Lasocki, 1986). Small (1997) attributed this reluctance to the fact that some older adults
associate psychological problems with 'being crazy' or as a sign that they are weak. This
is often reinforced by physicians who tell the older adult that their problems are 'all in
their head' because they cannot find a biomedical cause for reported symptoms (Snyder
& Stanley, 2001). As a result, the relationship between the client and therapist is
especially important when treating older adults with health anxiety. Their potential lack
of trust for mental health professionals and possible disappointment at being referred by
their physicians can be improved through the development of a strong relationship
(Snyder & Stanley, 2001). Thus, treatment programs specifically tailored to the older
adult population may help to foster the relationship between the client and therapist,
47

commonly known as the therapeutic alliance, resulting in greater improvement in mental
health.
The therapeutic alliance pertains to the collaborative nature of the relationship, the
affective bond between therapist and patient, the patient's trust in the therapist, and
agreement on goals by both the therapist and patient (Bordin, 1979; Horvath & Symonds,
1991). Several studies have shown that the therapeutic alliance is related to outcome
(e.g., Barber, Connolly, Crits-Christoph, Gladis, & Siqueland, 2000; Krupnick et al.,
1996; Martin, Garske, & Davis, 2000). Moreover, Horvath and Symonds (1991) showed
that, in general, the better the therapeutic alliance, the better the outcome. Marmar,
Gaston, Gallagher, and Thompson (1989) reported that for older patients with depression
treated in behavioural, cognitive, or brief dynamic psychotherapy, the alliance assessed
early in treatment was moderately associated with outcome, with the strongest results in
cognitive therapy. In the same sample of participants, Gaston, Marmar, Gallagher, and
Thompson (1991) examined the relationship between the therapeutic alliance and
outcome over and above initial symptomatology and in-treatment symptomatic change.
To measure therapy progress, participants completed the California Psychotherapy
Alliance Scales (CALPAS; Marmar, Weiss, & Gaston, 1989), after the 5th, 10th, and 15th
sessions. For the whole sample, no substantial association was found between alliance
and outcome. However, within treatment conditions, the alliance uniquely contributed to
outcome with increasing variance accounted for as therapy progressed, and especially in
behavioural and cognitive therapy; from 19% and 32% at the 5th session, to 36% and
57% at the 15th session.
48
commonly known as the therapeutic alliance, resulting in greater improvement in mental
health.
The therapeutic alliance pertains to the collaborative nature of the relationship, the
affective bond between therapist and patient, the patient's trust in the therapist, and
agreement on goals by both the therapist and patient (Bordin, 1979; Horvath & Symonds,
1991). Several studies have shown that the therapeutic alliance is related to outcome
(e.g., Barber, Connolly, Crits-Christoph, Gladis, & Siqueland, 2000; Krupnick et al.,
1996; Martin, Garske, & Davis, 2000). Moreover, Horvath and Symonds (1991) showed
that, in general, the better the therapeutic alliance, the better the outcome. Marmar,
Gaston, Gallagher, and Thompson (1989) reported that for older patients with depression
treated in behavioural, cognitive, or brief dynamic psychotherapy, the alliance assessed
early in treatment was moderately associated with outcome, with the strongest results in
cognitive therapy. In the same sample of participants, Gaston, Marmar, Gallagher, and
Thompson (1991) examined the relationship between the therapeutic alliance and
outcome over and above initial symptomatology and in-treatment symptomatic change.
To measure therapy progress, participants completed the California Psychotherapy
Alliance Scales (CALPAS; Marmar, Weiss, & Gaston, 1989), after the 5th, 10th, and 15th
sessions. For the whole sample, no substantial association was found between alliance
and outcome. However, within treatment conditions, the alliance uniquely contributed to
outcome with increasing variance accounted for as therapy progressed, and especially in
behavioural and cognitive therapy; from 19% and 32% at the 5th session, to 36% and
57% at the 15th session.
48

Recently, Zuroff and Blatt (2006) examined the impact of the patient's perception
of the quality of the therapeutic relationship and involvement of the therapeutic alliance
to treatment outcome during brief treatments of depression among 191 outpatients with
nonbipolar, nonpsychotic major depressive disorder. Patients were randomly assigned to
four treatment conditions including CBT, interpersonal therapy (IPT), and two separate
conditions for clinical management with medication. The authors demonstrated that a
positive therapeutic relationship perceived by the client early in treatment predicted more
rapid reduction in emotional difficulties following the initial relationship assessment.
This effect occurred equally across all four treatment conditions. A positive early
therapeutic relationship also predicted better emotional adjustment throughout the 18-
month follow-up as well as development of greater enhanced coping. Controlling a wide
range of patient characteristics did not eliminate the effects of the therapeutic relationship
on rate of improvement during treatment and on enhanced coping. Thus, Zuroff and Blatt
(2006) suggest that, independent of type of treatment and early clinical improvement, the
therapeutic relationship contributes directly to positive therapeutic outcome.
Unfortunately, the therapeutic alliance has not been widely assessed or discussed with
respect to older adults.
Hyer and Kramer (2004) have some suggestions for how CBT with older adults
can be altered to foster the therapeutic alliance. First, enhancing common therapy factors
and building a strong alliance are proactive initiatives that require a planned, focused
effort to conduct psychotherapy within the client's frame of reference. Second, with older
people, considerable effort should be directed toward increasing the client's involvement
49
Recently, Zuroff and Blatt (2006) examined the impact of the patient's perception
of the quality of the therapeutic relationship and involvement of the therapeutic alliance
to treatment outcome during brief treatments of depression among 191 outpatients with
nonbipolar, nonpsychotic major depressive disorder. Patients were randomly assigned to
four treatment conditions including CBT, interpersonal therapy (IPT), and two separate
conditions for clinical management with medication. The authors demonstrated that a
positive therapeutic relationship perceived by the client early in treatment predicted more
rapid reduction in emotional difficulties following the initial relationship assessment.
This effect occurred equally across all four treatment conditions. A positive early
therapeutic relationship also predicted better emotional adjustment throughout the 18-
month follow-up as well as development of greater enhanced coping. Controlling a wide
range of patient characteristics did not eliminate the effects of the therapeutic relationship
on rate of improvement during treatment and on enhanced coping. Thus, Zuroff and Blatt
(2006) suggest that, independent of type of treatment and early clinical improvement, the
therapeutic relationship contributes directly to positive therapeutic outcome.
Unfortunately, the therapeutic alliance has not been widely assessed or discussed with
respect to older adults.
Hyer and Kramer (2004) have some suggestions for how CBT with older adults
can be altered to foster the therapeutic alliance. First, enhancing common therapy factors
and building a strong alliance are proactive initiatives that require a planned, focused
effort to conduct psychotherapy within the client's frame of reference. Second, with older
people, considerable effort should be directed toward increasing the client's involvement
49

in therapy. This, combined with presentation of the principles underlying the symptoms
and therapeutic process, is the main goal of socialization. Blazer (1998) noted that the
best path to communication with the older client is to conduct an effective interview
during which the therapist validates and gives both respect and dignity to the client. This
allows the client time to express concerns and feel as though they are being listened to.
The principles of therapy are repeated across all sessions to foster retention (Gallagher-
Thompson & Thompson, 1995). Normalizing symptoms and providing perspective on
the role of the client are parts of this process. Third, the emphasis within therapy is on
coping and a positive view of problems, as aging can be a time in which change and
decline in functioning often occurs, resulting in problems, disease, and loss. The focus of
therapy is doing the best with what one has.
1.8.5 Motivation in Psychotherapy
Patient motivation for treatment has been considered to be vital to psychotherapy
progress and outcome (Keijsers, Schaap, Hoogduin, Hoogsteyns, & de Kemp, 1999). In
psychotherapy, the client not only receives treatment but must actively participate in it.
Thus, motivation to participate is a vital factor in the outcome of treatment (Krause,
1966). Treatment motivation is often seen as important because there is an assumed
relationship with treatment-related behaviour such as adherence, compliance, or treatment
engagement (Drieschner, Lammers, & van der Staak, 2004). For example, Ryan, Plant,
and O'Malley (1995) noted that lack of motivation is one of the most frequently
mentioned reasons for client dropout, failure to comply, relapse, and other negative
treatment outcomes.
50
in therapy. This, combined with presentation of the principles underlying the symptoms
and therapeutic process, is the main goal of socialization. Blazer (1998) noted that the
best path to communication with the older client is to conduct an effective interview
during which the therapist validates and gives both respect and dignity to the client. This
allows the client time to express concerns and feel as though they are being listened to.
The principles of therapy are repeated across all sessions to foster retention (Gallagher-
Thompson & Thompson, 1995). Normalizing symptoms and providing perspective on
the role of the client are parts of this process. Third, the emphasis within therapy is on
coping and a positive view of problems, as aging can be a time in which change and
decline in functioning often occurs, resulting in problems, disease, and loss. The focus of
therapy is doing the best with what one has.
1.8.5 Motivation in Psychotherapy
Patient motivation for treatment has been considered to be vital to psychotherapy
progress and outcome (Keijsers, Schaap, Hoogduin, Hoogsteyns, & de Kemp, 1999). In
psychotherapy, the client not only receives treatment but must actively participate in it.
Thus, motivation to participate is a vital factor in the outcome of treatment (Krause,
1966). Treatment motivation is often seen as important because there is an assumed
relationship with treatment-related behaviour such as adherence, compliance, or treatment
engagement (Drieschner, Lammers, & van der Staak, 2004). For example, Ryan, Plant,
and O'Malley (1995) noted that lack of motivation is one of the most frequently
mentioned reasons for client dropout, failure to comply, relapse, and other negative
treatment outcomes.
50

Motivation for psychotherapy among individuals with health anxiety is an
important factor. Individuals with health anxiety seek therapy for a number of different
reasons (Taylor & Asmundson, 2004). Some individuals recognize that they have a
problem with anxiety and it needs to be treated. Others are persuaded or even coerced
into seeking therapy by their family or physicians. These individuals may be reluctant to
engage in therapy and may, in fact, have the goal of proving that their problems are not
"all in their head" and that they are not mentally disordered (Warwick, 1995). These
individuals may not fully participate in therapy because they believe that medical
intervention would be of greater help than psychological intervention. Thus, strategies
that enhance motivation are often a vital prerequisite (Taylor & Asmundson, 2004).
In CBT, considerable attention has been paid to ways of motivating patients to
comply with treatment techniques and homework assignments (e.g., Curtis, 1984;
Horvath, 1993). Several researchers have conceptualized patient motivation as a state of
readiness for change prior to the beginning of treatment interventions (Keijsers et al.,
1999). Conceptualized in this way, patient motivation includes the acknowledgement of
problems, level of distress, commitment for change, or credibility or acceptance of
psychological treatment (e.g., Miller & Rollnick, 1992; Nelson & Borkovec, 1989).
Other researchers have focused on criteria for patients' actual participation, cooperation,
or compliance during the course of treatment (Keijsers et al., 1999). Because complaint
reduction has been attributed in large part to the patients' accomplishment and
implementation of new and more effective coping behaviour, this suggests that treatment
51
Motivation for psychotherapy among individuals with health anxiety is an
important factor. Individuals with health anxiety seek therapy for a number of different
reasons (Taylor & Asmundson, 2004). Some individuals recognize that they have a
problem with anxiety and it needs to be treated. Others are persuaded or even coerced
into seeking therapy by their family or physicians. These individuals may be reluctant to
engage in therapy and may, in fact, have the goal of proving that their problems are not
"all in their head" and that they are not mentally disordered (Warwick, 1995). These
individuals may not fully participate in therapy because they believe that medical
intervention would be of greater help than psychological intervention. Thus, strategies
that enhance motivation are often a vital prerequisite (Taylor & Asmundson, 2004).
In CBT, considerable attention has been paid to ways of motivating patients to
comply with treatment techniques and homework assignments (e.g., Curtis, 1984;
Horvath, 1993). Several researchers have conceptualized patient motivation as a state of
readiness for change prior to the beginning of treatment interventions (Keijsers et al.,
1999). Conceptualized in this way, patient motivation includes the acknowledgement of
problems, level of distress, commitment for change, or credibility or acceptance of
psychological treatment (e.g., Miller & Rollnick, 1992; Nelson & Borkovec, 1989).
Other researchers have focused on criteria for patients' actual participation, cooperation,
or compliance during the course of treatment (Keijsers et al., 1999). Because complaint
reduction has been attributed in large part to the patients' accomplishment and
implementation of new and more effective coping behaviour, this suggests that treatment
51

compliance is a more direct predictor of CBT outcome than initial patient motivation
(Keijsers et al., 1999).
In the majority of studies investigating patient initial motivation in CBT,
motivation was found to be significantly related to outcome (Haan et al., 1997; Hoogduin
& Duivenvoorden, 1988; Nelson & Borkovec, 1989; Schefft & Kanfer, 1987; Simpson &
Joe, 1993). High initial motivation appears to be associated with better treatment
outcome and lower dropout rate. However, motivation in CBT among older adults has
not been examined. Thus, one purpose of this study is to assess whether motivation for
therapy improved over six sessions of therapy.
To help enhance the therapeutic alliance and foster motivation for psychotherapy
in this sample of older adults, an enhanced cognitive behavioural therapy (ECBT) for
health anxiety will be tested. Memory and learning aids as well as a short video (one for
each of the six sessions) with an older adult actor demonstrating and giving a testimonial
of how the program improved their symptoms will be shown to participants. The goal of
using these videos will also be to enhance the therapeutic alliance and patient motivation,
and ultimately improve health anxiety and its related symptoms.
1.9 Research Problem and Purpose
Two separate studies were conducted. The purpose of Study 1 was to examine the
efficacy of a standard and an enhanced six-session CB intervention for health anxiety for
older adults in comparison to a WLC group. To date, no research has examined the
effectiveness of CBT for health anxiety among older adults. Results from previous
research assessing the efficacy of ECBT in comparison with standard cognitive
52
compliance is a more direct predictor of CBT outcome than initial patient motivation
(Keijsers etal., 1999).
In the majority of studies investigating patient initial motivation in CBT,
motivation was found to be significantly related to outcome (Haan et al., 1997; Hoogduin
& Duivenvoorden, 1988; Nelson & Borkovec, 1989; Schefft & Kanfer, 1987; Simpson &
Joe, 1993). High initial motivation appears to be associated with better treatment
outcome and lower dropout rate. However, motivation in CBT among older adults has
not been examined. Thus, one purpose of this study is to assess whether motivation for
therapy improved over six sessions of therapy.
To help enhance the therapeutic alliance and foster motivation for psychotherapy
in this sample of older adults, an enhanced cognitive behavioural therapy (ECBT) for
health anxiety will be tested. Memory and learning aids as well as a short video (one for
each of the six sessions) with an older adult actor demonstrating and giving a testimonial
of how the program improved their symptoms will be shown to participants. The goal of
using these videos will also be to enhance the therapeutic alliance and patient motivation,
and ultimately improve health anxiety and its related symptoms.
1.9 Research Problem and Purpose
Two separate studies were conducted. The purpose of Study 1 was to examine the
efficacy of a standard and an enhanced six-session CB intervention for health anxiety for
older adults in comparison to a WLC group. To date, no research has examined the
effectiveness of CBT for health anxiety among older adults. Results from previous
research assessing the efficacy of ECBT in comparison with standard cognitive
52
behavioural therapy (SCBT) for GAD among older adults suggested that it may be
important to enhance CBT for it to be effective with older adults (Mohlman et al., 2003).
Therefore, comparison of ECBT to a SCBT and a WLC condition was expected to
demonstrate that learning and memory aids and educational videos would lead to greater
reduction in symptoms of health anxiety among older adults (see Figure 2, pg. 37). A
further purpose of Study 1 was to examine whether the ECBT program promoted a higher
level of therapeutic alliance and motivation for psychotherapy as compared to the SCBT
program. This research was thought to be valuable because establishing and fostering a
strong therapeutic alliance and motivation for psychotherapy has been related to outcome
in psychotherapy (Snyder & Stanley, 2001), but could be challenging to establish with
older adults. A further objective of Study 1 was to gain a greater understanding of the
nature of health anxiety among older adults. This was examined through qualitative
analysis of the participants' responses to semi-structured interview questions regarding
development and maintenance of health anxiety. Study 1 was also used to collect
qualitative information from older participants on their experiences with CBT. A
secondary study was conducted to clarify the relationship between age and health anxiety.
The purpose of Study 2 was to examine differences between an older adult group and a
younger adult group control group with similar levels of health anxiety as measured by a
common measure of health anxiety. The goal was to examine whether the nature of the
two groups' concerns on various dimensions of health anxiety was comparable or
whether the pattern of responses differed. Specifically, the older adult and younger adult
53
behavioural therapy (SCBT) for GAD among older adults suggested that it may be
important to enhance CBT for it to be effective with older adults (Mohlman et al., 2003).
Therefore, comparison of ECBT to a SCBT and a WLC condition was expected to
demonstrate that learning and memory aids and educational videos would lead to greater
reduction in symptoms of health anxiety among older adults (see Figure 2, pg. 37). A
further purpose of Study 1 was to examine whether the ECBT program promoted a higher
level of therapeutic alliance and motivation for psychotherapy as compared to the SCBT
program. This research was thought to be valuable because establishing and fostering a
strong therapeutic alliance and motivation for psychotherapy has been related to outcome
in psychotherapy (Snyder & Stanley, 2001), but could be challenging to establish with
older adults. A further objective of Study 1 was to gain a greater understanding of the
nature of health anxiety among older adults. This was examined through qualitative
analysis of the participants' responses to semi-structured interview questions regarding
development and maintenance of health anxiety. Study 1 was also used to collect
qualitative information from older participants on their experiences with CBT. A
secondary study was conducted to clarify the relationship between age and health anxiety.
The purpose of Study 2 was to examine differences between an older adult group and a
younger adult group control group with similar levels of health anxiety as measured by a
common measure of health anxiety. The goal was to examine whether the nature of the
two groups' concerns on various dimensions of health anxiety was comparable or
whether the pattern of responses differed. Specifically, the older adult and younger adult
53

Perspective-taking strategies
Demonstration videos
Mid-week troubleshooting
phone calls Weekly readings
Factors Affecting Seniors in Therapy
Possible Cognitive Decline Excessive Preoccupations
Medical and physical problems Social Isolation
Simplified terms
v
Weekly graphing of mood
Significant Improvement in Outcomes
Symptom Reduction Increased Therapeutic Alliance
Increased Motivation for Psychotherapy
Figure 2. Relationship between enhancements, factors affecting seniors in therapy, and
outcome in psychotherapy.
54
Perspective-taking strategies
Demonstration videos
Mid-week troubleshooting
phone calls
1 Factors Affecting Seniors in
Therapy
Possible Cognitive Decline Excessive Preoccupations
Medical and physical problems Social Isolation
Simplified terms
Weekly graphing of mood
Significant Improvement in Outcomes
Symptom Reduction Increased Therapeutic Alliance
Increased Motivation for Psychotherapy
Figure 2. Relationship between enhancements, factors affecting seniors in therapy, and
outcome in psychotherapy.
54

groups were matched on their overall level of health anxiety as assessed by the WI. This
allowed for examination of how the younger and older adults would differ on
subdimensions of health anxiety, such as bodily preoccupation, fear of disease, and
disease conviction. This study was felt to be important to address questions that exist in
the literature with regard to the impact of age on health anxiety.
1.10 Hypotheses
1.10.1 Hypotheses: Study 1
Based on the results of earlier investigations (e.g., Barsky & Ahern, 2004;
Mohlman et al., 2003), it was hypothesized that:
1. Participants receiving SCBT and ECBT, but not those in WLC, would evidence
improvements in health anxiety, frequency of hypochondriacal thoughts,
hypochondriacal somatic symptoms, tendency to experience bodily sensations as
distressing, state and trait anxiety, depression, pain, and health-related quality of
life from pre-treatment to post-treatment.
2. In keeping with the findings of Mohlman et al. (2003), participants treated with
ECBT would demonstrate the greatest overall improvement at post-treatment and
follow-up on each of the measures indicated in the first hypothesis in comparison
to SCBT and WLC.
3. For participants treated with each of SCBT and ECBT, all expected improvements
would be maintained three months following the conclusion of treatment.
4. Participants treated with ECBT would demonstrate a higher level of therapeutic
alliance at three and six weeks than those receiving SCBT.
55
groups were matched on their overall level of health anxiety as assessed by the WI. This
allowed for examination of how the younger and older adults would differ on
subdimensions of health anxiety, such as bodily preoccupation, fear of disease, and
disease conviction. This study was felt to be important to address questions that exist in
the literature with regard to the impact of age on health anxiety.
1.10 Hypotheses
1.10.1 Hypotheses: Study 1
Based on the results of earlier investigations (e.g., Barsky & Ahern, 2004;
Mohlman et al., 2003), it was hypothesized that:
1. Participants receiving SCBT and ECBT, but not those in WLC, would evidence
improvements in health anxiety, frequency of hypochondriacal thoughts,
hypochondriacal somatic symptoms, tendency to experience bodily sensations as
distressing, state and trait anxiety, depression, pain, and health-related quality of
life from pre-treatment to post-treatment.
2. In keeping with the findings of Mohlman et al. (2003), participants treated with
ECBT would demonstrate the greatest overall improvement at post-treatment and
follow-up on each of the measures indicated in the first hypothesis in comparison
to SCBT and WLC.
3. For participants treated with each of SCBT and ECBT, all expected improvements
would be maintained three months following the conclusion of treatment.
4. Participants treated with ECBT would demonstrate a higher level of therapeutic
alliance at three and six weeks than those receiving SCBT.
55

5. Participants treated with ECBT would demonstrate a higher level of motivation
for psychotherapy at three and six weeks than those receiving SCBT.
6. We did not make any hypotheses regarding the qualitative responses.
1.10.2 Hypotheses: Study 2
1. It was hypothesized that participants in the older group would have significantly
higher scores than the control group on the Somatic Symptoms/Bodily
Preoccupation subscale of the WI, the Negative Consequences of Illness subscale
of the SHAI, and the Symptoms Effects subscale of the IAS. There were no other
hypothesized differences on other subscales.
56
5. Participants treated with ECBT would demonstrate a higher level of motivation
for psychotherapy at three and six weeks than those receiving SCBT.
6. We did not make any hypotheses regarding the qualitative responses.
1.10.2 Hypotheses: Study 2
1. It was hypothesized that participants in the older group would have significantly
higher scores than the control group on the Somatic Symptoms/Bodily
Preoccupation subscale of the WI, the Negative Consequences of Illness subscale
of the SHAI, and the Symptoms Effects subscale of the IAS. There were no other
hypothesized differences on other subscales.
56
2. METHOD
2.1 Study 1
2.1.1 Participants
Recruitment of participants was accomplished through newspaper advertisements,
appearances by the author on radio and cable television programs, short information
presentations by the author to seniors' groups, and posted announcements in seniors'
centres (e.g., seniors' community residences, other community organizations) and
physicians' offices in Regina, Saskatchewan (see Appendix A). Participants were asked
to inquire about their eligibility to participate if they were experiencing anxiety or worry
about their health. Interested participants were screened first by telephone with a short
questionnaire (i.e., WI) assessing their level of health anxiety. Those participants with a
significant amount of health anxiety were then invited to participate in the study.
Inclusion criteria consisted of the following: (a) a score of 8 or higher on the WI, (b)
willingness to keep medication status stable while participating in the study (i.e., no
change in psychotropic medication type or increase in dose), (c) no evidence of suicidal
ideation, (d) no evidence of current substance abuse, (e) no evidence of current psychotic
condition, and (f) aged 60 years of age and older (Barsky & Ahern, 2004). A consent
form was presented to participants before they began any questionnaires or therapy (see
Appendix B). All participants were randomly assigned to one of three conditions (WLC,
SCBT, or ECBT).
Participants were recruited from September 2007 until April 2009. The
recruitment goal for this study was to obtain 93 participants (31 per treatment group) with
57
2. METHOD
2.1 Study 1
2.1.1 Participants
Recruitment of participants was accomplished through newspaper advertisements,
appearances by the author on radio and cable television programs, short information
presentations by the author to seniors' groups, and posted announcements in seniors'
centres (e.g., seniors' community residences, other community organizations) and
physicians' offices in Regina, Saskatchewan (see Appendix A). Participants were asked
to inquire about their eligibility to participate if they were experiencing anxiety or worry
about their health. Interested participants were screened first by telephone with a short
questionnaire (i.e., WI) assessing their level of health anxiety. Those participants with a
significant amount of health anxiety were then invited to participate in the study.
Inclusion criteria consisted of the following: (a) a score of 8 or higher on the WI, (b)
willingness to keep medication status stable while participating in the study (i.e., no
change in psychotropic medication type or increase in dose), (c) no evidence of suicidal
ideation, (d) no evidence of current substance abuse, (e) no evidence of current psychotic
condition, and (f) aged 60 years of age and older (Barsky & Ahern, 2004). A consent
form was presented to participants before they began any questionnaires or therapy (see
Appendix B). All participants were randomly assigned to one of three conditions (WLC,
SCBT, or ECBT).
Participants were recruited from September 2007 until April 2009. The
recruitment goal for this study was to obtain 93 participants (31 per treatment group) with
57
significantly elevated health anxiety (i.e., a score of 8 or higher on the WI). The sample
size was estimated using power analysis (Faul & Erfelder, 1992). Setting the significance
criterion at 0.01 and assuming a moderate effect size (0.30) based on previous studies
(e.g., Barksy & Ahern, 2004; Mohlman et al., 2003), estimations of sample size using
power analysis lead to the conclusion that approximately 93 participants were required to
achieve a generally acceptable power of 0.80 (Cohen, 1988).
A total of 110 potential participants responded to recruitment advertisements. Of
these individuals, 73 met eligibility criteria and initially agreed to participate in the study.
However, 19 participants later declined to participate prior to completing questionnaires
due to lack of interest, difficulty with the time commitment, and not wanting to engage in
therapy. Another three participants (two participants from the SCBT group and one from
the ECBT group) dropped-out before completing all the sessions. Thus, a total of 54
participants completed the study. Although the goal to recruit 93 participants was not
met, the number of individuals who completed the study is similar to a number of prior
research samples assessing the effectiveness of CBT for health anxiety (e.g., Bouman &
Visser, 1998; Clark et al., 1998; Seivewright et al., 2008; Visser & Bouman, 2001;
Warwick et al., 1996; Warwick & Marks, 1988).
In total, 19 participants in the SCBT group completed the treatment and two
dropped out; 17 participants in the ECBT group completed the treatment and one dropped
out; and all 18 WLC participants completed the study. Table 1 outlines the participants'
demographic information for each group. Independent samples t-tests (for age, number
of health conditions) and chi-square analyses (for sex, marital status, education level)
58
significantly elevated health anxiety (i.e., a score of 8 or higher on the WI). The sample
size was estimated using power analysis (Faul & Erfelder, 1992). Setting the significance
criterion at 0.01 and assuming a moderate effect size (0.30) based on previous studies
(e.g., Barksy & Ahern, 2004; Mohlman et al., 2003), estimations of sample size using
power analysis lead to the conclusion that approximately 93 participants were required to
achieve a generally acceptable power of 0.80 (Cohen, 1988).
A total of 110 potential participants responded to recruitment advertisements. Of
these individuals, 73 met eligibility criteria and initially agreed to participate in the study.
However, 19 participants later declined to participate prior to completing questionnaires
due to lack of interest, difficulty with the time commitment, and not wanting to engage in
therapy. Another three participants (two participants from the SCBT group and one from
the ECBT group) dropped-out before completing all the sessions. Thus, a total of 54
participants completed the study. Although the goal to recruit 93 participants was not
met, the number of individuals who completed the study is similar to a number of prior
research samples assessing the effectiveness of CBT for health anxiety (e.g., Bouman &
Visser, 1998; Clark et a l , 1998; Seivewright et al, 2008; Visser & Bouman, 2001;
Warwick et a l , 1996; Warwick & Marks, 1988).
In total, 19 participants in the SCBT group completed the treatment and two
dropped out; 17 participants in the ECBT group completed the treatment and one dropped
out; and all 18 WLC participants completed the study. Table 1 outlines the participants'
demographic information for each group. Independent samples t-tests (for age, number
of health conditions) and chi-square analyses (for sex, marital status, education level)
58

Table 1
Background Characteristics by Group
Characteristics SCBT
(n = 21)
ECBT
(n= 18)
WLC
(n = 18)
Total
(n = 57)
Age
Total Health Conditions
Mean (SD) Mean (SD) Mean (SD) Mean (SD)
69.00 (6.81)
2.43 (1.50)
68.17 (6.84)
2.11 (1.18)
68.88 (7.47)
2.12 (1.54)
68.72 (6.92)
2.30 (1.46)
Number % Number % Number % Number %
Sex
Female 16 (76.2) 12 (66.7) 16 (88.9) 44 (77.2)
Male 5 (23.8) 6 (33.3) 2 (11.1) 13 (22.8)
Marital Status
Married/ 6 (28.6) 10 (55.6) 9 (50.0) 25 (43.9)
Common-Law
Not Married 15 (71.4) 8 (44.4) 9 (50.0) 32 (56.1)
Education
< High School 9 (42.9) 6 (33.3) 8 (44.4) 23 (40.3)
> = High School 12 (57.1) 12 (66.7) 10 (55.6) 34 (59.7)
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control
59
Table 1
Background Characteristics by Group
Characteristics SCBT
(w = 21)
ECBT
(n=18)
WLC
(w=18)
Total
(n = 57)
Mean (SD) Mean (SD) Mean (SD) Mean (SD)
Age 69.00(6.81) 68.17(6.84) 68.88(7.47) 68.72 (6.92)
Total Health Conditions 2.43(1.50) 2.11(1.18) 2.12(1.54) 2.30(1.46)
Sex
Female
Male
Marital Status
Married/
Common-Law
Not Married
Education
< High School
> = High School
Number %
16(76.2)
5 (23.8)
6 (28.6)
15(71.4)
9 (42.9)
12(57.1)
Number %
12 (66.7)
6(33.3)
10 (55.6)
8 (44.4)
6 (33.3)
12 (66.7)
Number %
16 (88.9)
2(11.1)
9 (50.0)
9 (50.0)
8 (44.4)
10(55.6)
Number %
44 (77.2)
13 (22.8)
25 (43.9)
32(56.1)
23 (40.3)
34 (59.7)
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control
59

were used to compare demographic information between groups. This showed no
differences in age, number of health conditions, sex, marital status, and education
between groups (see Table 2). A summary of participants' health conditions is presented
in Table 3. The most common conditions cited were arthritis (55.6%), high blood
pressure (44.4%), and osteoporosis (31.5%). Other common health conditions reported
included hearing problems, heart disease, vision problems, and respiratory disease.
2.1.2 Measures
Questionnaires were chosen to assess health anxiety, frequency of
hypochondriacal thoughts, hypochondriacal somatic symptoms, tendency to experience
bodily sensations as distressing, state and trait anxiety, anxiety sensitivity, depression,
pain, health-related quality of life, therapeutic alliance, and motivation for psychotherapy.
The questionnaires described below fall into three separate areas — primary outcome
measures, secondary outcome measures, and measures of therapeutic alliance and
motivation. Primary outcome measures are identified as those relating to health anxiety,
frequency of hypochondriacal thoughts, and hypochondriacal somatic symptoms (i.e.,
measures that are most directly related to health anxiety). Secondary outcome measures
are identified as those questionnaires relating to anxiety sensitivity, state and trait anxiety,
depression, pain, and health-related quality of life. The measures of therapeutic alliance
and motivation for psychotherapy relate to aspects of the therapist or therapy and
participant motivation for herapy. In addition, demographic information was collected
and all participants were invited to share their perceptions and experiences through open-
ended questions at pre-treatment and at post-treatment. As part of the pre-treatment
60
were used to compare demographic information between groups. This showed no
differences in age, number of health conditions, sex, marital status, and education
between groups (see Table 2). A summary of participants' health conditions is presented
in Table 3. The most common conditions cited were arthritis (55.6%), high blood
pressure (44.4%), and osteoporosis (31.5%). Other common health conditions reported
included hearing problems, heart disease, vision problems, and respiratory disease.
2.1.2 Measures
Questionnaires were chosen to assess health anxiety, frequency of
hypochondriacal thoughts, hypochondriacal somatic symptoms, tendency to experience
bodily sensations as distressing, state and trait anxiety, anxiety sensitivity, depression,
pain, health-related quality of life, therapeutic alliance, and motivation for psychotherapy.
The questionnaires described below fall into three separate areas - primary outcome
measures, secondary outcome measures, and measures of therapeutic alliance and
motivation. Primary outcome measures are identified as those relating to health anxiety,
frequency of hypochondriacal thoughts, and hypochondriacal somatic symptoms (i.e.,
measures that are most directly related to health anxiety). Secondary outcome measures
are identified as those questionnaires relating to anxiety sensitivity, state and trait anxiety,
depression, pain, and health-related quality of life. The measures of therapeutic alliance
and motivation for psychotherapy relate to aspects of the therapist or therapy and
participant motivation for herapy. In addition, demographic information was collected
and all participants were invited to share their perceptions and experiences through open-
ended questions at pre-treatment and at post-treatment. As part of the pre-treatment
60
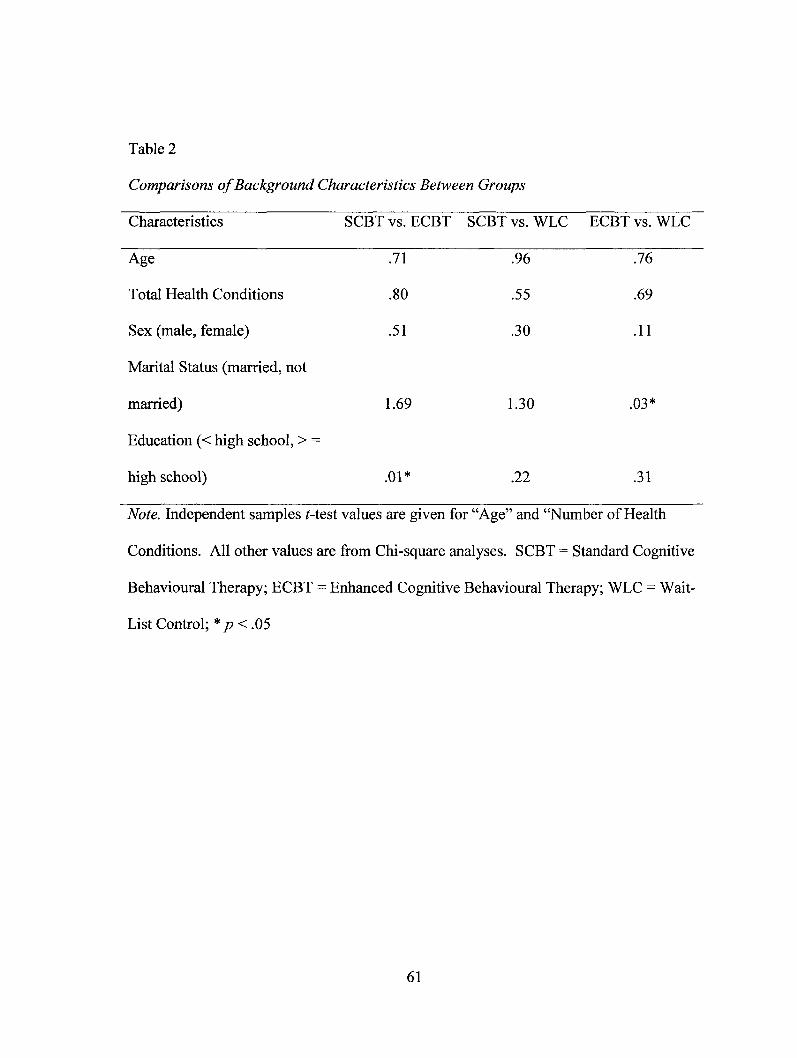
Table 2
Comparisons of Background Characteristics Between Groups
Characteristics SCBT vs. ECBT SCBT vs. WLC ECBT vs. WLC
Age .71 .96 .76
Total Health Conditions
Sex (male, female)
Marital Status (married, not
married)
Education (< high school, > —
high school)
.80 .55 .69
.51 .30 .11
1.69 1.30 .03*
.01* .22 .31
Note. Independent samples t-test values are given for "Age" and "Number of Health
Conditions. All other values are from Chi-square analyses. SCBT = Standard Cognitive
Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; * p < .05
61
Table 2
Comparisons of Background Characteristics Between Groups
Characteristics
Age
Total Health Conditions
Sex (male, female)
Marital Status (married, not
married)
Education (< high school, > =
high school)
SCBT vs. ECBT
.71
.80
.51
1.69
.01*
SCBT vs. WLC
.96
.55
.30
1.30
.22
ECBT ' vs. WLC
.76
.69
.11
.03*
.31
Note. Independent samples Mest values are given for "Age" and "Number of Health
Conditions. All other values are from Chi-square analyses. SCBT = Standard Cognitive
Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; * p<.05
61

Table 3
Summary of Participants' Health Conditions by Group
Health Condition SCBT
(n = 21)
ECBT
(n = 18)
WLC
(n = 18)
Total
(n = 57)
Arthritis
Number % Number % Number % Number %
10 (47.6) 8 (44.4) 12 (66.7) 32 (56.1)
Cancer 0 2 (11.1) 1 (5.6) 4 (7.0)
Diabetes 1 (4.8) 0 2 (11.1) 3 (5.3)
Hearing Problems 7 (33.3) 4 (22.2) 2 (11.1) 15 (26.3)
Heart Disease 4 (19.0) 2 (11.1) 4 (22.2) 10 (17.5)
High Blood Pressure 12 (21.1) 4 (22.2) 9 (50.0) 25 (43.9)
Kidney Disease 1 (4.8) 0 0 1 (1.8)
Osteoporosis 6 (28.6) 7 (38.9) 5 (27.8) 18 (31.66)
Parkinson's Disease 0 1 (5.6) 0 1 (1.8)
Respiratory Disease 3 (14.3) 1 (5.6) 4 (22.2) 8 (14.0)
Stroke 2 (9.5) 2 (11.1) 0 4 (7.0)
Vision Problems 4 (19.0) 4 (22.2) 3 (16.7) 11 (19.3)
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control
62
Table 3
Summary of Participants' Health Conditions by Group
Health Condition SCBT ECBT WLC Total
(« = 21) (n =18) (w=18) (AI = 57)
Number % Number % Number % Number %
Arthritis
Cancer
Diabetes
Hearing Problems
Heart Disease
High Blood Pressure
Kidney Disease
Osteoporosis
Parkinson's Disease
Respiratory Disease
Stroke
Vision Problems
10 (47.6)
0
1 (4.8)
7(33.3)
4(19.0)
12(21.1)
1 (4.8)
6 (28.6)
0
3 (14.3)
2 (9.5)
4 (19.0)
8 (44.4)
2(11.1)
0
4 (22.2)
2(11.1)
4 (22.2)
0
7 (38.9)
1 (5.6)
1 (5.6)
2(11.1)
4 (22.2)
12 (66.7)
1 (5.6)
2(11.1)
2(11.1)
4 (22.2)
9 (50.0)
0
5 (27.8)
0
4 (22.2)
0
3 (16.7)
32(56.1)
4 (7.0)
3 (5.3)
15 (26.3)
10(17.5)
25 (43.9)
1(1.8)
18(31.66)
1(1.8)
8 (14.0)
4 (7.0)
11(19.3)
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control
62

questionnaire package, all participants were asked to respond in writing to the following
questions: (1) What are your previous illness experiences? During childhood? Family
members and friends affected?; (2) Why do you believe you worry about your health?;
(3) What do you do to cope with your worry?; and (4) With respect to your health, what
do you worry about? Participants who completed the SCBT and ECBT treatments were
also asked the following questions: (1) Do you feel the program helped improve your
worries about health? If so, how?; (2) What did you find most helpful about the
program?; (3) What did you find least helpful about the program?; (4) How did you feel
about your relationship with the therapist?; (5) In your opinion, was there anything about
the program that helped strengthen your relationship? If so, please explain.; (6) In your
opinion, was there anything about the therapist that helped strengthen your relationship?
If so, please explain.; (7) Did your motivation for doing the program change throughout
the sessions? If so, how and why do you think that is?; (8) In your opinion, was there
anything about the program that helped motivate you to try and practice some of the
techniques in the program? If so, please explain.; and (9) In your opinion, was there
anything about the therapist or what she did that helped motivate you to try and practice
some of the techniques in the program? If so, please explain. Open-ended questions
were included so participants could provide additional information, comments, feedback,
and experiences in a qualitative form. The Structured Clinical Interview for the DSM-IV
Axis I Disorders (SCID-I), Clinician Version (First, Spitzer, Gibbon, & Williams, 1996)
was administered to all participants during the initial assessment in order to accurately
63
questionnaire package, all participants were asked to respond in writing to the following
questions: (1) What are your previous illness experiences? During childhood? Family
members and friends affected?; (2) Why do you believe you worry about your health?;
(3) What do you do to cope with your worry?; and (4) With respect to your health, what
do you worry about? Participants who completed the SCBT and ECBT treatments were
also asked the following questions: (1) Do you feel the program helped improve your
worries about health? If so, how?; (2) What did you find most helpful about the
program?; (3) What did you find least helpful about the program?; (4) How did you feel
about your relationship with the therapist?; (5) In your opinion, was there anything about
the program that helped strengthen your relationship? If so, please explain.; (6) In your
opinion, was there anything about the therapist that helped strengthen your relationship?
If so, please explain.; (7) Did your motivation for doing the program change throughout
the sessions? If so, how and why do you think that is?; (8) In your opinion, was there
anything about the program that helped motivate you to try and practice some of the
techniques in the program? If so, please explain.; and (9) In your opinion, was there
anything about the therapist or what she did that helped motivate you to try and practice
some of the techniques in the program? If so, please explain. Open-ended questions
were included so participants could provide additional information, comments, feedback,
and experiences in a qualitative form. The Structured Clinical Interview for the DSM-IV
Axis I Disorders (SCID-I), Clinician Version (First, Spitzer, Gibbon, & Williams, 1996)
was administered to all participants during the initial assessment in order to accurately
63

assess the participants' backgrounds, history, and current difficulties. This was not used
in the analyses.
2.1.2.1 Primary Outcome Measures
Whiteley Index (WI; Pilowsky, 1967). The WI was developed to assess the core
features of hypochondriasis. Respondents answer 'yes' or 'no' to each of 14 questions,
including items such as "Do you often worry about the possibility that you have a serious
illness?" and "Is it hard for you to believe the doctor when he tells you there is nothing to
worry about?" In the original paper on the measure, Pilowsky (1967) reported that
principal components analysis of the WI items yielded three factors: (1) disease fear,
which refers to the fear of having or developing a serious illness; (2) disease conviction,
which describes the subjective impression of the patient as suffering from multiple bodily
symptoms and pains; and (3) bodily preoccupation, which is said to represent the strength
of the patients' belief that they suffer from a serious illness. To score the measure, the
three subscales can be scored separately or summed to yield a total score. Its test-retest
reliability and discriminant and convergent validity have been established (Beaber &
Rodney, 1984; Hanback & Revelle, 1978; Pilowsky, 1967, 1978). The intrascale
consistency of the WI among a sample of general medical outpatients was 0.85
(Cronbach alpha), and the test-retest reliability was 0.84 (Pearson's product-moment
correlation) over a mean interval of 25.6 days (Barsky, Wyshak, & Klerman, 1990c).
The WI predicts both treatment outcome and health care utilization (Barsky, Cleary,
Wyshak, Spitzer, Williams, & Klerman, 1992).
64
assess the participants' backgrounds, history, and current difficulties. This was not used
in the analyses.
2.1.2.1 Primary Outcome Measures
Whiteley Index (WI; Pilowsky, 1967). The WI was developed to assess the core
features of hypochondriasis. Respondents answer 'yes' or 'no' to each of 14 questions,
including items such as "Do you often worry about the possibility that you have a serious
illness?" and "Is it hard for you to believe the doctor when he tells you there is nothing to
worry about?" In the original paper on the measure, Pilowsky (1967) reported that
principal components analysis of the WI items yielded three factors: (1) disease fear,
which refers to the fear of having or developing a serious illness; (2) disease conviction,
which describes the subjective impression of the patient as suffering from multiple bodily
symptoms and pains; and (3) bodily preoccupation, which is said to represent the strength
of the patients' belief that they suffer from a serious illness. To score the measure, the
three subscales can be scored separately or summed to yield a total score. Its test-retest
reliability and discriminant and convergent validity have been established (Beaber &
Rodney, 1984; Hanback & Revelle, 1978; Pilowsky, 1967, 1978). The intrascale
consistency of the WI among a sample of general medical outpatients was 0.85
(Cronbach alpha), and the test-retest reliability was 0.84 (Pearson's product-moment
correlation) over a mean interval of 25.6 days (Barsky, Wyshak, & Klerman, 1990c).
The WI predicts both treatment outcome and health care utilization (Barsky, Cleary,
Wyshak, Spitzer, Williams, & Klerman, 1992).
64

Hiller, Rief, and Fichter (2002) determined that a cut-off score of 8 provided
optimal sensitivity (71% of hypochondriacal patients correctly identified) and specificity
(80% of controls correctly identified) for determining cases of hypochondriasis versus
non-hypochondriacal cases. The WI has demonstrated good psychometric properties
when used to assess hypochondriasis in a broad-aged sample that included older adult
patients (Barsky, Frank, Cleary, et al., 1991). Specific psychometric data for this
measure exclusively with older adults was not reported.
Despite favorable psychometric properties, the factor structure of the WI has not
been found to be robust across studies (Asmundson, Carleton, Bovell, & Taylor, 2008).
In a study examining the factor analysis of the WI, Asmundson et al. (2008) reviewed a
number of published studies examining the factor structure of the WI in clinical samples
using exploratory factor-analytic (EFA) procedures (Asmundson et al., 2008; Hiller, Rief,
& Fichter, 2002; Pilowsky, 1967; Speckens, Spinhoven, Sloekers, Bolk, & van Hemert,
1996), confirmatory factor analytic (CFA) procedures (Conradt, Cavanaugh, Franklin, &
Rief, 2006), and a combination of both EFA and CFA procedures (Fink et al., 1999).
Varying results were found. Asmundson et al. (2008) suggested that the inconsistent
findings are likely the result of these studies using different practices with regard to factor
identification and item retention. Moreover, differences in factor solutions may have
resulted from using samples that differed significantly with respect to range and severity
of health anxiety. Asmundson et al. (2008) then tested a total of nine different models
that have been found in past research on a sample of 300 undergraduate students. They
concluded that the greatest support was found for a two-factor solution with three items
65
Hiller, Rief, and Fichter (2002) determined that a cut-off score of 8 provided
optimal sensitivity (71% of hypochondriacal patients correctly identified) and specificity
(80% of controls correctly identified) for determining cases of hypochondriasis versus
non-hypochondriacal cases. The WI has demonstrated good psychometric properties
when used to assess hypochondriasis in a broad-aged sample that included older adult
patients (Barsky, Frank, Cleary, et al., 1991). Specific psychometric data for this
measure exclusively with older adults was not reported.
Despite favorable psychometric properties, the factor structure of the WI has not
been found to be robust across studies (Asmundson, Carleton, Bovell, & Taylor, 2008).
In a study examining the factor analysis of the WI, Asmundson et al. (2008) reviewed a
number of published studies examining the factor structure of the WI in clinical samples
using exploratory factor-analytic (EFA) procedures (Asmundson et al., 2008; Hiller, Rief,
& Fichter, 2002; Pilowsky, 1967; Speckens, Spinhoven, Sloekers, Bolk, & van Hemert,
1996), confirmatory factor analytic (CFA) procedures (Conradt, Cavanaugh, Franklin, &
Rief, 2006), and a combination of both EFA and CFA procedures (Fink et al., 1999).
Varying results were found. Asmundson et al. (2008) suggested that the inconsistent
findings are likely the result of these studies using different practices with regard to factor
identification and item retention. Moreover, differences in factor solutions may have
resulted from using samples that differed significantly with respect to range and severity
of health anxiety. Asmundson et al. (2008) then tested a total of nine different models
that have been found in past research on a sample of 300 undergraduate students. They
concluded that the greatest support was found for a two-factor solution with three items
65

on each factor. These factors were labelled Somatic Symptoms/Bodily Preocupation and
Disease Worry/Phobia.
In this study, following past researchers, we calculated the total score of the WI
and used a cut off score of eight to identify individuals with significant health anxiety
(Hiller et al., 2002). In analyses of patient outcomes we examined both the total score
and the two subscale scores identified by Asmundson et al. (2008).
Short Form Health Anxiety Inventory (SHAI; Salkovskis et al., 2002). The SHAI
was designed to be a comprehensive measure for anxiety about health across the
continuum of symptom severity (Salkovskis et al., 2002). The inventory can be given to
patients with medical problems and used to distinguish these individuals from those with
other anxiety-based disorders. The 18 items comprising the short form of this scale are
closely aligned with the model of health anxiety proposed by Warwick and Salkovskis
(1990). To complete this inventory, individuals are asked for each item to choose one of
four statements that most closely resembles their thoughts and feelings (there is the
option to choose more than one statement). Response choices are then scored from 0 to 3
(if multiple responses were selected on an item, the highest score is used for total score
computation) and summed to form a total score. Subscales include a negative
consequences scale that assesses differences between individual perceptions of the
negative consequences of illness and a general scale reflecting key aspects of health
anxiety (i.e., disease conviction, perceived vulnerability to illness, fear and worry about
illness, preoccupation, interference and bodily awareness, psychological reactions to
66
on each factor. These factors were labelled Somatic Symptoms/Bodily Preocupation and
Disease Worry/Phobia.
In this study, following past researchers, we calculated the total score of the WI
and used a cut off score of eight to identify individuals with significant health anxiety
(Hiller et al., 2002). In analyses of patient outcomes we examined both the total score
and the two subscale scores identified by Asmundson et al. (2008).
Short Form Health Anxiety Inventory (SHAI; Salkovskis et al., 2002). The SHAI
was designed to be a comprehensive measure for anxiety about health across the
continuum of symptom severity (Salkovskis et al., 2002). The inventory can be given to
patients with medical problems and used to distinguish these individuals from those with
other anxiety-based disorders. The 18 items comprising the short form of this scale are
closely aligned with the model of health anxiety proposed by Warwick and Salkovskis
(1990). To complete this inventory, individuals are asked for each item to choose one of
four statements that most closely resembles their thoughts and feelings (there is the
option to choose more than one statement). Response choices are then scored from 0 to 3
(if multiple responses were selected on an item, the highest score is used for total score
computation) and summed to form a total score. Subscales include a negative
consequences scale that assesses differences between individual perceptions of the
negative consequences of illness and a general scale reflecting key aspects of health
anxiety (i.e., disease conviction, perceived vulnerability to illness, fear and worry about
illness, preoccupation, interference and bodily awareness, psychological reactions to
66

bodily sensations, deliberate action after a bodily sensation, concerns about death,
attitudes of self and others towards health anxiety, avoidance and reassurance).
A cut-off score of 18 or higher has been used to identify individuals who have a
high likelihood of having a DSM-IV diagnosis of hypochondriasis. Cut-off scores
between 15 and 17 identify individuals who have been found to be highly health anxious
but who are not likely to meet clinical criteria for a diagnosis of hypochondriasis. Scores
lying between 15 and 17 have been found to be three standard deviations above norms of
non-clinical controls (Rode et al., 2006).
The scale has good internal consistency, alpha equal to .89, when administered to
a sample of individuals diagnosed with hypochondriasis, anxious controls (i.e., panic
disorder and social phobia), non-clinical controls, general practice clinic clients, and
medical outpatients (Salkovskis et al., 2002). Assessment of the test-retest reliability of
the full version of the scale produced a correlation of .76 with on average a 22-day
interval between questionnaire completion dates. Discrimination between scores from
individuals with hypochondriasis or anxious controls and non-clinical or medical patients
was significant (Salkovskis et al., 2002). Responsiveness to treatment progress was
demonstrated by a significantly greater change in full scale (Salkovskis et al., 2002) and
short form (Barsky & Ahern, 2004) scores among a group of patients actively engaged in
treatment versus a group awaiting treatment using the full scale (Salkovskis et al., 2002)
and the short form (Barsky & Ahern, 2004). Specific psychometric data for this measure
exclusively with older adults is not yet available. Boston and Merrick (2010) used the
SHAI to assess health anxiety in an older adult sample, but did not report any
67
bodily sensations, deliberate action after a bodily sensation, concerns about death,
attitudes of self and others towards health anxiety, avoidance and reassurance).
A cut-off score of 18 or higher has been used to identify individuals who have a
high likelihood of having a DSM-IV diagnosis of hypochondriasis. Cut-off scores
between 15 and 17 identify individuals who have been found to be highly health anxious
but who are not likely to meet clinical criteria for a diagnosis of hypochondriasis. Scores
lying between 15 and 17 have been found to be three standard deviations above norms of
non-clinical controls (Rode et al., 2006).
The scale has good internal consistency, alpha equal to .89, when administered to
a sample of individuals diagnosed with hypochondriasis, anxious controls (i.e., panic
disorder and social phobia), non-clinical controls, general practice clinic clients, and
medical outpatients (Salkovskis et al., 2002). Assessment of the test-retest reliability of
the full version of the scale produced a correlation of .76 with on average a 22-day
interval between questionnaire completion dates. Discrimination between scores from
individuals with hypochondriasis or anxious controls and non-clinical or medical patients
was significant (Salkovskis et al., 2002). Responsiveness to treatment progress was
demonstrated by a significantly greater change in full scale (Salkovskis et al., 2002) and
short form (Barsky & Ahern, 2004) scores among a group of patients actively engaged in
treatment versus a group awaiting treatment using the full scale (Salkovskis et al., 2002)
and the short form (Barsky & Ahern, 2004). Specific psychometric data for this measure
exclusively with older adults is not yet available. Boston and Merrick (2010) used the
SHAI to assess health anxiety in an older adult sample, but did not report any
67

psychometric properties. Moreover, because the inventory can be given to patients with
medical problems and used to distinguish these individuals from those with other anxiety-
based disorders, it was chosen for this study.
Factor analysis of the scale by Salkovskis et al. (2002) confirmed the two
previously identified subscales. However, subsequent factor analyses have produced
different results; this may reflect differences in subsamples. Abramowitz et al. (2007),
for instance, conducted an EFA with the 18-item SHAI using a sample of 442 students.
A three-factor solution was determined, with the factors labeled as Illness Likelihood,
Illness Severity, and Body Vigilance. Olatunji (2009) conducted a second EFA using
principal components analysis with a sample of 498 students. Again, an interpretable
three factor solution was indicated and Olatunji (2009) retained the same factor labels as
those identified by Abramowitz et al. (2007), with only slight variations in the items
contained within each factor. Illness Likelihood assesses the intrusive cognitions about
health beliefs about the probability of acquiring a serious illness, Illness Severity
measures the perceived burden of having serious illness, and Body Vigilance assesses
attention towards bodily sensations.
A CFA was conducted to test the goodness-of-fit of three competing models of
the latent structure of the SHAI (Abramowitz et al., 2007). The single-factor model
provided a poor fit to the data, whereas the two- and three-factor models were identified
as having adequate and similar model fit. As a result, the authors recommended the two-
factor model reported by Salkovskis et al. (2002) on the basis of parsimony, labeling their
factors Illness Likelihood and Negative Consequences. Illness Likelihood comprised 14
68
psychometric properties. Moreover, because the inventory can be given to patients with
medical problems and used to distinguish these individuals from those with other anxiety-
based disorders, it was chosen for this study.
Factor analysis of the scale by Salkovskis et al. (2002) confirmed the two
previously identified subscales. However, subsequent factor analyses have produced
different results; this may reflect differences in subsamples. Abramowitz et al. (2007),
for instance, conducted an EFA with the 18-item SHAI using a sample of 442 students.
A three-factor solution was determined, with the factors labeled as Illness Likelihood,
Illness Severity, and Body Vigilance. Olatunji (2009) conducted a second EFA using
principal components analysis with a sample of 498 students. Again, an interpretable
three factor solution was indicated and Olatunji (2009) retained the same factor labels as
those identified by Abramowitz et al. (2007), with only slight variations in the items
contained within each factor. Illness Likelihood assesses the intrusive cognitions about
health beliefs about the probability of acquiring a serious illness, Illness Severity
measures the perceived burden of having serious illness, and Body Vigilance assesses
attention towards bodily sensations.
A CFA was conducted to test the goodness-of-fit of three competing models of
the latent structure of the SHAI (Abramowitz et al., 2007). The single-factor model
provided a poor fit to the data, whereas the two- and three-factor models were identified
as having adequate and similar model fit. As a result, the authors recommended the two-
factor model reported by Salkovskis et al. (2002) on the basis of parsimony, labeling their
factors Illness Likelihood and Negative Consequences. Illness Likelihood comprised 14
68
items concerning beliefs about the likelihood of developing a serious illness and focus on
bodily sensations and the four items of the Negative Consequences factor measured
catastrophic cognitions about the burden and outcome of having a serious medical
condition. Based on this research, we also chose to calculate the SHAI subscales as
outlined by Salkvoskis et al. (2002).
Illness Attitudes Scale (IAS; Kellner, 1986; Kellner et al., 1987). The IAS is a 29-
item self-report questionnaire assessing fears, beliefs, and attitudes associated with health
anxiety. It is comprised of nine subscales, each assessing aspects of abnormal illness
behaviour and beliefs including 1) worry about illness, 2) concerns about pain, 3) health
habits, 4) hypochondriacal beliefs, 5) thanatophobia, 6) disease phobia, 7) bodily
preoccupations, 8) treatment experiences, and 9) effects of symptoms. Each scale is
comprised of three items ranked on a 5-point scale with endpoints labelled 'no' (0) and
`most of the time' (4). A score, ranging from 0 to a maximum of 108, is calculated for
the IAS by summing all responses. Higher scores reflect greater health anxiety. Two
additional questions ask the respondent for further information about illness and
treatment, but they are not calculated in the scoring of the scale.
Factor analyses of the IAS using various populations have revealed that the
original factor solution outlined by Kellner et al. (1987) may not be the most suitable fit
for the IAS items. Varying models have emerged including two-factor, four-factor, and
five-factor solutions. Hiller et al. (2002), Speckens et al. (1996), and Wise and Sheridan
(2001) all found similar two-factor solutions. Speckens et al. (1996) conducted an EFA
using principal components analysis with 130 general medical outpatients, 113 general
69
items concerning beliefs about the likelihood of developing a serious illness and focus on
bodily sensations and the four items of the Negative Consequences factor measured
catastrophic cognitions about the burden and outcome of having a serious medical
condition. Based on this research, we also chose to calculate the SHAI subscales as
outlined by Salkvoskis et al. (2002).
Illness Attitudes Scale (IAS; Kellner, 1986; Kellner et al., 1987). The IAS is a 29-
item self-report questionnaire assessing fears, beliefs, and attitudes associated with health
anxiety. It is comprised of nine subscales, each assessing aspects of abnormal illness
behaviour and beliefs including 1) worry about illness, 2) concerns about pain, 3) health
habits, 4) hypochondriacal beliefs, 5) thanatophobia, 6) disease phobia, 7) bodily
preoccupations, 8) treatment experiences, and 9) effects of symptoms. Each scale is
comprised of three items ranked on a 5-point scale with endpoints labelled 'no' (0) and
'most of the time' (4). A score, ranging from 0 to a maximum of 108, is calculated for
the IAS by summing all responses. Higher scores reflect greater health anxiety. Two
additional questions ask the respondent for further information about illness and
treatment, but they are not calculated in the scoring of the scale.
Factor analyses of the IAS using various populations have revealed that the
original factor solution outlined by Kellner et al. (1987) may not be the most suitable fit
for the IAS items. Varying models have emerged including two-factor, four-factor, and
five-factor solutions. Hiller et al. (2002), Speckens et al. (1996), and Wise and Sheridan
(2001) all found similar two-factor solutions. Speckens et al. (1996) conducted an EFA
using principal components analysis with 130 general medical outpatients, 113 general
69

practice patients, and 204 participants from the general population. The two factors
identified were labelled Health Anxiety and Illness Behaviour (Speckens et al., 1996).
Dammen et al. (1999) conducted an EFA using principal components analysis with 199
patients referred to cardiological outpatient investigation because of chest pain. Dammen
et al.'s (1999) two factors identified were also labelled Health Anxiety and Illness
Behaviour. Hiller et al. (2002) conducted an EFA using principal components analysis
with 570 patients with mental and psychophysiological disorders. Again, similar to
Speckens et al. (1996), the two factors found by Hiller et al. (2002) were labelled Health
Anxiety and Illness Behaviour.
Studies concluding that a four-factor solution provided the best fit for the items
include Ferguson and Daniel (1995), Hadjistavropoulos et al. (1999), and Stewart and
Watt (2000). Ferguson and Daniel (1995) conducted an EFA using principal components
analysis in a sample of 101 undergraduate students. Ferguson and Daniel's (1995) four
factors were named (1) General Hypochondriacal Fears and Beliefs, (2) Symptom
Experience and Frequency of Treatment, (3) Thanatophobia, and (4) Fear of Coronary
Heart Disease and Associated Health Habits. Hadjistavropoulos et al. (1999) conducted,
in two parts, a factor analysis of the IAS. In Study 1, they used principal components
analysis with a sample of 390 undergraduate students. In Study 2, Hadjistavropoulos et
al. (1999) employed CFA to compare seven different factor models of the IAS with the
sample of undergraduate students. Based on the results of the CFA, as well as previous
research and theoretical considerations, Hadjistavropoulos et al. (1999) concluded that a
four factor solution received the greatest support and could be conceptualized as
70
practice patients, and 204 participants from the general population. The two factors
identified were labelled Health Anxiety and Illness Behaviour (Speckens et al., 1996).
Dammen et al. (1999) conducted an EFA using principal components analysis with 199
patients referred to cardiological outpatient investigation because of chest pain. Dammen
et al.'s (1999) two factors identified were also labelled Health Anxiety and Illness
Behaviour. Hiller et al. (2002) conducted an EFA using principal components analysis
with 570 patients with mental and psychophysiological disorders. Again, similar to
Speckens et al. (1996), the two factors found by Hiller et al. (2002) were labelled Health
Anxiety and Illness Behaviour.
Studies concluding that a four-factor solution provided the best fit for the items
include Ferguson and Daniel (1995), Hadjistavropoulos et al. (1999), and Stewart and
Watt (2000). Ferguson and Daniel (1995) conducted an EFA using principal components
analysis in a sample of 101 undergraduate students. Ferguson and Daniel's (1995) four
factors were named (1) General Hypochondriacal Fears and Beliefs, (2) Symptom
Experience and Frequency of Treatment, (3) Thanatophobia, and (4) Fear of Coronary
Heart Disease and Associated Health Habits. Hadjistavropoulos et al. (1999) conducted,
in two parts, a factor analysis of the IAS. In Study 1, they used principal components
analysis with a sample of 390 undergraduate students. In Study 2, Hadjistavropoulos et
al. (1999) employed CFA to compare seven different factor models of the IAS with the
sample of undergraduate students. Based on the results of the CFA, as well as previous
research and theoretical considerations, Hadjistavropoulos et al. (1999) concluded that a
four factor solution received the greatest support and could be conceptualized as
70

hierarchical in nature, with four lower-order factors loading on a single higher-order
factor. The factors were labelled (1) Fear of Illness and Pain, (2) Symptom Effects, (3)
Treatment Experiences, and (4) Disease Conviction (Hadjistavropoulos et al., 1999).
Stewart and Watt (2000) presented an EFA using principal components analysis with a
sample of 197 undergraduate students. Similar to Hadjistavropoulos et al. (1999),
examination of the results revealed that a four-factor solution at the lower-order level
(with lower-order dimensions tapping illness-related Fears, Behaviour, Beliefs and
Effects), and a unifactorial measure at the higher-order level (i.e., higher-order dimension
tapping General Hypochondriacal Concerns) provided the best fit for the data.
Two studies found that a five-factor solution best fit the IAS items.
Hadjistavropoulos and Asmundson (1998) conducted an EFA using principal components
analysis with a sample of 198 chronic pain patients. The factors were named (1) Fear of
Illness and Pain, (2) Effects of Symptoms, (3) Health Habits, and (4) Disease Phobia and
Conviction, and (5) Fear of Death. Cox et al. (2000) conducted an EFA using principal
components analysis with a sample of 309 undergraduate students. Cox et al. (2000) also
produced a five-factor solution. The five factors identified were named (1) Fear of Illness
and Death, (2) Treatment Experience, (3) Symptom Effects, (4) Disease Phobia and
Conviction, and (5) Health Habits.
Of the above-reviewed studies, the highest quality study appears to have been
conducted by Hadjistavropoulos et al. (1999), who conducted the factor analysis with a
sample of 390 undergraduate students, and employed EFA and CFA procedures, with
comparison of various models. Thus, in the analyses of patient outcomes, we examined
71
hierarchical in nature, with four lower-order factors loading on a single higher-order
factor. The factors were labelled (1) Fear of Illness and Pain, (2) Symptom Effects, (3)
Treatment Experiences, and (4) Disease Conviction (Hadjistavropoulos et al., 1999).
Stewart and Watt (2000) presented an EFA using principal components analysis with a
sample of 197 undergraduate students. Similar to Hadjistavropoulos et al. (1999),
examination of the results revealed that a four-factor solution at the lower-order level
(with lower-order dimensions tapping illness-related Fears, Behaviour, Beliefs and
Effects), and a unifactorial measure at the higher-order level (i.e., higher-order dimension
tapping General Hypochondriacal Concerns) provided the best fit for the data.
Two studies found that a five-factor solution best fit the IAS items.
Hadjistavropoulos and Asmundson (1998) conducted an EFA using principal components
analysis with a sample of 198 chronic pain patients. The factors were named (1) Fear of
Illness and Pain, (2) Effects of Symptoms, (3) Health Habits, and (4) Disease Phobia and
Conviction, and (5) Fear of Death. Cox et al. (2000) conducted an EFA using principal
components analysis with a sample of 309 undergraduate students. Cox et al. (2000) also
produced a five-factor solution. The five factors identified were named (1) Fear of Illness
and Death, (2) Treatment Experience, (3) Symptom Effects, (4) Disease Phobia and
Conviction, and (5) Health Habits.
Of the above-reviewed studies, the highest quality study appears to have been
conducted by Hadjistavropoulos et al. (1999), who conducted the factor analysis with a
sample of 390 undergraduate students, and employed EFA and CFA procedures, with
comparison of various models. Thus, in the analyses of patient outcomes, we examined
71

both the total score and the four subscales on the IAS identified by Hadjistavropoulos et
al. (1999).
Researchers have also examined the sensitivity and specificity of the scale and
determined that a cut-off point of 45 maximized the precision of the scale (Cox et al.,
2000). Sensitivity equalled 72% and specificity equalled 73% when distinguishing
hypochondriacal patients from patients with other somatoform disorders, and specificity
climbing to 79% when the controls had psychiatric conditions other than somatoform
disorders. In an alternate sample of 246 medical outpatients, sensitivity and specificity
remained high at 79% and 84%, respectively (Speckens, van Hemert, Spinhoven, & Bolk,
1996). These findings are interpreted to mean that the IAS has acceptable levels of
sensitivity and specificity and thereby is susceptible to only low frequencies of Type I
and Type II errors. The scale has also been found to discern advances in treatment (Cox
et al., 2000). Among seniors aged 65 years and over, the internal consistency coefficient
(a) of the total scale has ranged from 0.84 to 0.85 (Bourgault-Fagnou &
Hadjistavropoulos, 2009; Bravo & Silverman, 2001).
Somatic Symptom Inventory (SSI; Barsky, Wyshak, & Klerman, 1986a and b).
The SSI is a 26-item questionnaire assessing somatic symptoms or bodily complaints
often associated with hypochondriasis. In this inventory, the patients' degree of
discomfort for each symptom is rated on 5-point linear scales (`not at all,' a little bit,'
`moderately,' quite a bit,' and 'a great deal'). The items were derived from the MMPI
hypochondriasis scale and the Symptom Checklist-90 somatization subscale. Among
medical outpatients, scores on this instrument have been found to correlate moderately (r
72
both the total score and the four subscales on the IAS identified by Hadjistavropoulos et
al. (1999).
Researchers have also examined the sensitivity and specificity of the scale and
determined that a cut-off point of 45 maximized the precision of the scale (Cox et al.,
2000). Sensitivity equalled 72% and specificity equalled 73%) when distinguishing
hypochondriacal patients from patients with other somatoform disorders, and specificity
climbing to 79% when the controls had psychiatric conditions other than somatoform
disorders. In an alternate sample of 246 medical outpatients, sensitivity and specificity
remained high at 79% and 84%, respectively (Speckens, van Hemert, Spinhoven, & Bolk,
1996). These findings are interpreted to mean that the IAS has acceptable levels of
sensitivity and specificity and thereby is susceptible to only low frequencies of Type I
and Type II errors. The scale has also been found to discern advances in treatment (Cox
et al., 2000). Among seniors aged 65 years and over, the internal consistency coefficient
(a) of the total scale has ranged from 0.84 to 0.85 (Bourgault-Fagnou &
Hadjistavropoulos, 2009; Bravo & Silverman, 2001).
Somatic Symptom Inventory (SSI; Barsky, Wyshak, & Klerman, 1986a and b).
The SSI is a 26-item questionnaire assessing somatic symptoms or bodily complaints
often associated with hypochondriasis. In this inventory, the patients' degree of
discomfort for each symptom is rated on 5-point linear scales ('not at all,' 'a little bit,'
'moderately,' 'quite a bit,' and 'a great deal'). The items were derived from the MMPI
hypochondriasis scale and the Symptom Checklist-90 somatization subscale. Among
medical outpatients, scores on this instrument have been found to correlate moderately (r
72
= 0.52 — 0.65) with those of the WI (Barsky et al., 1995; Noyes et al., 2003). The scale
also has been found to be significantly correlated with depressive symptoms and
utilization of medical services in a general medical outpatient setting (Barsky et al.,
1986a; Barsky et al., 1986b). Among a sample of 75 general medical clinic patients, the
SSI had a test-retest reliability of 0.86, and an internal consistency of 0.95. The SSI has
demonstrated good psychometric properties when used to assess hypochondriasis in a
broad-aged sample that included older adult patients (Barsky et al., 1991). Specific
psychometric data for this measure exclusively with older adults was not reported.
However, the SSI has demonstrated strong intercorrelations with the WI and together the
two measures accurately identify hyponchondriacal patients in medical settings (Barsky
et al., 1986).
Somatosensory Amplification Scale (SSAS; Barksy, Wyshak, & Klerman, 1990b).
The SSAS is a 10-item self-report questionnaire designed to measure the tendency to
experience bodily sensations as being unusually intense, aversive, or distressing. The
scale assesses the individual's sensitivity to a range of mild bodily experiences (e.g.,
hunger contractions), which are uncomfortable and unpleasant, but are not typical
symptoms of disease. The SSAS asks the respondent to indicate the degree to which each
statement is characteristic of them in general, on an ordinal scale from 1 (`not at all') to 5
(`extremely'). Internal consistency values for this scale have ranged from alpha = .71 to
.82, and test-retest reliability coefficients have ranged from r = 0.87 (4 weeks) to 0.79 (10
weeks) (Barsky et al., 1990b; Speckens, van Hemert, Spinhoven, & Bolk, 1996). SSAS
scores have been shown to be highly correlated with IAS and WI scores, indicating
73
= 0.52 - 0.65) with those of the WI (Barsky et al., 1995; Noyes et al., 2003). The scale
also has been found to be significantly correlated with depressive symptoms and
utilization of medical services in a general medical outpatient setting (Barsky et al.,
1986a; Barsky et al., 1986b). Among a sample of 75 general medical clinic patients, the
SSI had a test-retest reliability of 0.86, and an internal consistency of 0.95. The SSI has
demonstrated good psychometric properties when used to assess hypochondriasis in a
broad-aged sample that included older adult patients (Barsky et al., 1991). Specific
psychometric data for this measure exclusively with older adults was not reported.
However, the SSI has demonstrated strong intercorrelations with the WI and together the
two measures accurately identify hyponchondriacal patients in medical settings (Barsky
eta l , 1986).
Somatosensory Amplification Scale (SSAS; Barksy, Wyshak, & Klerman, 1990b).
The SSAS is a 10-item self-report questionnaire designed to measure the tendency to
experience bodily sensations as being unusually intense, aversive, or distressing. The
scale assesses the individual's sensitivity to a range of mild bodily experiences (e.g.,
hunger contractions), which are uncomfortable and unpleasant, but are not typical
symptoms of disease. The SSAS asks the respondent to indicate the degree to which each
statement is characteristic of them in general, on an ordinal scale from 1 ('not at all') to 5
('extremely'). Internal consistency values for this scale have ranged from alpha = .71 to
.82, and test-retest reliability coefficients have ranged from r = 0.87 (4 weeks) to 0.79 (10
weeks) (Barsky et al., 1990b; Speckens, van Hemert, Spinhoven, & Bolk, 1996). SSAS
scores have been shown to be highly correlated with IAS and WI scores, indicating
73

convergent validity (Speckens, van Hemert, Spinhoven, & Bolk, 1996). Responsiveness
to treatment progress was demonstrated by a significant reduction of SSAS scores among
a group of patients actively engaged in treatment versus a group awaiting treatment
(Barsky & Ahern, 2004). Specific psychometric data for this measure exclusively with
older adults has not been reported.
Hypochondriacal Cognitions Questionnaire (Barsky & Ahern, 2004). This two-
part, 36-item measure was designed to assess frequency of hypochondriacal thoughts. In
Part I, the patient is required to rate how often each of the 18 disease-related thoughts
occurs on a 5-point scale (`thought never occurs,' thought rarely occurs,' thought occurs
during half of the times when I am nervous or concerned,' thought usually occurs,' and
`thought always occurs'). In Part II, the patient is required to rate how often each of the
same 18 disease-related thoughts occurs on a scale from 0-100 CI do not believe this
thought at all' to 'I am completely convinced this thought is true'). The individual items
in each part can be summed to get the overall score. Only Part I was used in this study.
Responsiveness to treatment progress was demonstrated by a significant reduction of
hypochondriacal thought frequency among a group of patients actively engaged in
treatment versus a group awaiting treatment (Barsky & Ahern, 2004). Specific
psychometric data for this measure exclusively with older adults has not been reported.
As this appeared to be the only measure available at the time that assessed
hypochondriacal cognitions, it was chosen for this study.
74
convergent validity (Speckens, van Hemert, Spinhoven, & Bolk, 1996). Responsiveness
to treatment progress was demonstrated by a significant reduction of SSAS scores among
a group of patients actively engaged in treatment versus a group awaiting treatment
(Barsky & Ahern, 2004). Specific psychometric data for this measure exclusively with
older adults has not been reported.
Hypochondriacal Cognitions Questionnaire (Barsky & Ahern, 2004). This two-
part, 36-item measure was designed to assess frequency of hypochondriacal thoughts. In
Part I, the patient is required to rate how often each of the 18 disease-related thoughts
occurs on a 5-point scale ('thought never occurs,' 'thought rarely occurs,' 'thought occurs
during half of the times when I am nervous or concerned,' 'thought usually occurs,' and
'thought always occurs'). In Part II, the patient is required to rate how often each of the
same 18 disease-related thoughts occurs on a scale from 0-100 (T do not believe this
thought at all' to T am completely convinced this thought is true'). The individual items
in each part can be summed to get the overall score. Only Part I was used in this study.
Responsiveness to treatment progress was demonstrated by a significant reduction of
hypochondriacal thought frequency among a group of patients actively engaged in
treatment versus a group awaiting treatment (Barsky & Ahern, 2004). Specific
psychometric data for this measure exclusively with older adults has not been reported.
As this appeared to be the only measure available at the time that assessed
hypochondriacal cognitions, it was chosen for this study.
74

2.1.2.2 Secondary Outcome Measures
Anxiety Sensitivity Index (ASI; Reiss, Peterson, Gursky, & McNally, 1986). The
ASI is a 16-item measure assessing concern regarding anxiety-related bodily sensations
(Reiss et al., 1986). Each item of the scale is responded to on a 5-point Likert scale that
ranges from 'very little' to 'very much'. The scale has good test-retest reliability. A
reliability of 0.75 was found when assessed over a 2-week interval (Reiss et al., 1986),
0.65 over a 5-week interval (Schmidt, Lerew, & Jackson, 1997), and 0.71 over a 3-year
interval (Maller & Reiss, 1992). The internal consistency of the scale is good and has
ranged from 0.82 to 0.91 (Peterson & Heilbronner, 1987; Schmidt & Joiner, 2002;
Taylor, Koch, & Crockett, 1991; Telch, Shermis, & Lucas, 1989). Within a sample of
community dwelling older adults, the internal consistency of the ASI was found to be
0.92 (Bravo & Silverman, 2001). Research has confirmed the criterion, convergent, and
discriminant validities of the scale (Reiss et al., 1986). Factor analytic research of the
ASI has led to a diversity of findings concerning its factor structure (e.g., Peterson &
Heilbronner, 1987; Schmidt & Joiner, 2002; Telch et al., 1989). However, at this time,
the consensus appears to be that the structure of the ASI is hierarchical with one higher-
order general factor and three lower-order factors assessing physical, mental, and social
concerns (Zinbarg et al., 1997; Zinbarg, Brown, Barlow, & Rapee, 2001). There is some
evidence to suggest that the physical subscale is most strongly associated with heightened
fear during physiological challenges (e.g., hyperventilation; Zinbarg et al., 2001) and
hypervigilance for bodily sensations (Zvolensky & Forsyth, 2002), whereas the mental
75
2.1.2.2 Secondary Outcome Measures
Anxiety Sensitivity Index (ASI; Reiss, Peterson, Gursky, & McNally, 1986). The
ASI is a 16-item measure assessing concern regarding anxiety-related bodily sensations
(Reiss et al., 1986). Each item of the scale is responded to on a 5-point Likert scale that
ranges from 'very little' to 'very much'. The scale has good test-retest reliability. A
reliability of 0.75 was found when assessed over a 2-week interval (Reiss et al., 1986),
0.65 over a 5-week interval (Schmidt, Lerew, & Jackson, 1997), and 0.71 over a 3-year
interval (Mailer & Reiss, 1992). The internal consistency of the scale is good and has
ranged from 0.82 to 0.91 (Peterson & Heilbronner, 1987; Schmidt & Joiner, 2002;
Taylor, Koch, & Crockett, 1991; Telch, Shermis, & Lucas, 1989). Within a sample of
community dwelling older adults, the internal consistency of the ASI was found to be
0.92 (Bravo & Silverman, 2001). Research has confirmed the criterion, convergent, and
discriminant validities of the scale (Reiss et al., 1986). Factor analytic research of the
ASI has led to a diversity of findings concerning its factor structure (e.g., Peterson &
Heilbronner, 1987; Schmidt & Joiner, 2002; Telch et al., 1989). However, at this time,
the consensus appears to be that the structure of the ASI is hierarchical with one higher-
order general factor and three lower-order factors assessing physical, mental, and social
concerns (Zinbarg et al., 1997; Zinbarg, Brown, Barlow, & Rapee, 2001). There is some
evidence to suggest that the physical subscale is most strongly associated with heightened
fear during physiological challenges (e.g., hyperventilation; Zinbarg et al., 2001) and
hypervigilance for bodily sensations (Zvolensky & Forsyth, 2002), whereas the mental
75

subscale is most strongly associated with depression (Zinbarg et al., 2001) and emotional
avoidance (Zvolensky & Forsyth, 2002).
A CFA was used to test the adequacy of the model proposed by Zinbarg et al.
(1997) to a sample of 322 community dwelling older adults aged 65 to 97 (Mohlman &
Zinbarg, 2000). The results of the CFA indicated that a bifactor model with a higher
order factor (i.e., anxiety sensitivity) and three first-order factors (Physical Concerns,
Mental Incapacitation Concerns, and Social Concerns) corresponding to Zinbarg et al.'s
(1997) model provided the best fit.
State-Trait Anxiety Inventory (STAI-Form Y; Spielberger, Gorsuch, Lushene,
Montouri, & Platsek, 1983). The STAI was designed to assess both a stable propensity to
experience anxiety in stressful situations and tendencies to perceive stressful situations as
anxiety-provoking (Spielberger, 1983). The portions of the STAI that measure trait and
state anxiety consist of 20 items each (Spielberger, 1983). In the section assessing state
anxiety, respondents indicate on a 4-point rating scale how they feel at this moment.
Response choices include 'not at all,' somewhat,"moderately so,' very much so.' For
each trait anxiety item, respondents indicate on a 4-point rating scale how they generally
feel. Response choices include: 'almost never,' sometimes,"often,' and 'almost
always.' The individual items on each scale can be summed to get the anxiety score.
Scores range from 20-80 on the STAI and higher scores indicate greater anxiety. The
STAI has been found to have good internal consistency (alpha found to range from 0.86
to 0.95), and discriminant and concurrent validity (Spielberger, 1983). The trait scale
76
subscale is most strongly associated with depression (Zinbarg et al., 2001) and emotional
avoidance (Zvolensky & Forsyth, 2002).
A CFA was used to test the adequacy of the model proposed by Zinbarg et al.
(1997) to a sample of 322 community dwelling older adults aged 65 to 97 (Mohlman &
Zinbarg, 2000). The results of the CFA indicated that a bifactor model with a higher
order factor (i.e., anxiety sensitivity) and three first-order factors (Physical Concerns,
Mental Incapacitation Concerns, and Social Concerns) corresponding to Zinbarg et al.'s
(1997) model provided the best fit.
State-Trait Anxiety Inventory (STAI-Form Y; Spielberger, Gorsuch, Lushene,
Montouri, & Platsek, 1983). The STAI was designed to assess both a stable propensity to
experience anxiety in stressful situations and tendencies to perceive stressful situations as
anxiety-provoking (Spielberger, 1983). The portions of the STAI that measure trait and
state anxiety consist of 20 items each (Spielberger, 1983). In the section assessing state
anxiety, respondents indicate on a 4-point rating scale how they feel at this moment.
Response choices include 'not at all,' 'somewhat,' 'moderately so,' 'very much so.' For
each trait anxiety item, respondents indicate on a 4-point rating scale how they generally
feel. Response choices include: 'almost never,' 'sometimes,' 'often,' and 'almost
always.' The individual items on each scale can be summed to get the anxiety score.
Scores range from 20-80 on the STAI and higher scores indicate greater anxiety. The
STAI has been found to have good internal consistency (alpha found to range from 0.86
to 0.95), and discriminant and concurrent validity (Spielberger, 1983). The trait scale
76

further has been shown to have good test-retest reliability (range of 0.73 to 0.86;
Spielberger, 1983).
Among two older adult community subsamples, one with GAD and the other with
no anxiety disorder, internal consistency reliability for the STAI ranged from 0.79-0.94
(Stanley, Beck & Zebb, 1996). The STAI State and Trait scales have demonstrated good
discriminant validity (Dennis, Boddington, & Funnell, 2007). The STAI has been found
to differentiate between older adults with a current anxiety disorder and controls with no
diagnosable psychiatric disorders (Kabacoff, Segal, Hersen, & Van Hesselt, 1997; Kvaal,
Ulstein, Nordhus, & Engedal, 2005). Kvaal et al. (2005) found that a cut-off point of
54/55 on the total STAI state mean sum score discriminated best between those with a
mental disorder and those without. Comprehensive normative data for older adults has
yet to be established, although means and standard deviations are available from the
original authors in an age band spanning 50-69.
Geriatric Depression Scale (GDS; Brink, Yesavage, Lum, Heirsema, Adey, &
Rose, 1982; Yesavage et al., 1983). The GDS is a brief self-report depression scale that
has been specifically designed to assess depression in older people. It consists of 30
items, has a yes-no format, and assesses affective and behavioural symptoms of
depression. Scores on the GDS range from 0-30 and can be categorized into three
groups: (1) 0-9 is normal, (2) 10-19 is mild depression, and (3) 20-30 is severe
depression. One advantage of the GDS over other screening instruments is that it focuses
on psychological aspects of depression by not emphasising somatic items (Tuokko &
Hadjistavropoulos, 1998). The scale can also be read to the participant as the yes-no
77
further has been shown to have good test-retest reliability (range of 0.73 to 0.86;
Spielberger, 1983).
Among two older adult community subsamples, one with GAD and the other with
no anxiety disorder, internal consistency reliability for the STAI ranged from 0.79-0.94
(Stanley, Beck & Zebb, 1996). The STAI State and Trait scales have demonstrated good
discriminant validity (Dennis, Boddington, & Funnell, 2007). The STAI has been found
to differentiate between older adults with a current anxiety disorder and controls with no
diagnosable psychiatric disorders (Kabacoff, Segal, Hersen, & Van Hesselt, 1997; Kvaal,
Ulstein, Nordhus, & Engedal, 2005). Kvaal et al. (2005) found that a cut-off point of
54/55 on the total STAI state mean sum score discriminated best between those with a
mental disorder and those without. Comprehensive normative data for older adults has
yet to be established, although means and standard deviations are available from the
original authors in an age band spanning 50-69.
Geriatric Depression Scale (GDS; Brink, Yesavage, Lum, Heirsema, Adey, &
Rose, 1982; Yesavage et al., 1983). The GDS is a brief self-report depression scale that
has been specifically designed to assess depression in older people. It consists of 30
items, has a yes-no format, and assesses affective and behavioural symptoms of
depression. Scores on the GDS range from 0-30 and can be categorized into three
groups: (1) 0-9 is normal, (2) 10-19 is mild depression, and (3) 20-30 is severe
depression. One advantage of the GDS over other screening instruments is that it focuses
on psychological aspects of depression by not emphasising somatic items (Tuokko &
Hadjistavropoulos, 1998). The scale can also be read to the participant as the yes-no
77
format makes it agreeable to such administration when the participant has problems that
could interfere with reading. The GDS has well-established internal consistency, with
high Cronbach's alpha reliabilities reported ranging from .87 to .94 (Adams, 2001;
Yesavage et al., 1983), and established reliability among independent community
residents, those receiving medical or psychiatric treatments in outpatient and inpatient
settings, as well as institutionalized older adults (Yesavage et al., 1983).
Geriatric Pain Measure (GPM; Ferrell, Stein, & Beck, 2000). The GPM is a
multidimensional pain measure developed for older persons undergoing comprehensive
geriatric assessment. It examines the impact that pain has on function, mood,
engagement in activities, and quality of life. The GPM consists of 24 items that can be
either interview-administered or self-administered and takes approximately five minutes
to complete. Twenty-two items are scored dichotomously and two items scored
categorically on a 0-10 scale. The total score is obtained by summing the "yes"
responses to the dichotomous items with the numerical responses to the categorical items
to give the total score (range = 0 to 42). Factor analysis revealed five clusters of
components: pain intensity, disengagement, pain with ambulation, pain with strenuous
activities, and pain with other activities. Satisfactory internal consistency (alpha = .94;
Brink et al., 1982) and good test-retest reliability (r = .85; Koenig Meador, Cohen, &
Blazer, 1988) have been demonstrated.
Short Form-12 Health Survey (SF-12; Ware, Kosinski, & Keller, 1996). The SF-
12 is a self-administered questionnaire consisting of 12 items derived from the SF-36
Health Survey. The SF-12 measures eight domains of health, including physical
78
format makes it agreeable to such administration when the participant has problems that
could interfere with reading. The GDS has well-established internal consistency, with
high Cronbach's alpha reliabilities reported ranging from .87 to .94 (Adams, 2001;
Yesavage et al., 1983), and established reliability among independent community
residents, those receiving medical or psychiatric treatments in outpatient and inpatient
settings, as well as institutionalized older adults (Yesavage et al., 1983).
Geriatric Pain Measure (GPM; Ferrell, Stein, & Beck, 2000). The GPM is a
multidimensional pain measure developed for older persons undergoing comprehensive
geriatric assessment. It examines the impact that pain has on function, mood,
engagement in activities, and quality of life. The GPM consists of 24 items that can be
either interview-administered or self-administered and takes approximately five minutes
to complete. Twenty-two items are scored dichotomously and two items scored
categorically on a 0-10 scale. The total score is obtained by summing the "yes"
responses to the dichotomous items with the numerical responses to the categorical items
to give the total score (range = 0 to 42). Factor analysis revealed five clusters of
components: pain intensity, disengagement, pain with ambulation, pain with strenuous
activities, and pain with other activities. Satisfactory internal consistency (alpha = .94;
Brink et al., 1982) and good test-retest reliability (r = .85; Koenig Meador, Cohen, &
Blazer, 1988) have been demonstrated.
Short Form-12 Health Survey (SF-12; Ware, Kosinski, & Keller, 1996). The SF-
12 is a self-administered questionnaire consisting of 12 items derived from the SF-36
Health Survey. The SF-12 measures eight domains of health, including physical
78

functioning (ability to perform daily activities as well as strenuous activities), role-
physical (limitations of one's physical health on work or other activities), bodily pain
(amount of pain felt and its interference on normal activities), general health (perceived
general health), vitality (tiredness and energy), social functioning (whether physical and
emotional health affects one's social activities), role-emotional (extent to which work or
other activities are limited due to emotional problems), and mental health (emotional
well-being) (Ware, Kosinski, Turner-Bowker, & Gandek, 2002). For ease of use, the
eight domain scales have been combined into two larger component scales including (1)
physical component summary (PCS) (physical functioning, role-physical, bodily pain,
general health), and (2) mental component summary (MCS) (vitality, social functioning,
role-emotional, mental health) (Ware et al., 2002). The SF-36 and SF-12 component
scales are highly correlated, r = .95 for PCS and r = .97 for MCS (Ware et al., 1996).
Test-retest reliability (two weeks) of the PCS-12 ranges from 0.86 to 0.89, and 0.76 to
0.77 for the MCS-12 (Ware et al., 1996). For the eight domain scale scores, test-retest
reliability was 0.63 to 0.91 (Ware et al., 1996). Relative validity coefficients for the PCS-
12 ranged from 0.43 to 0.78, and from 0.93 to 0.98 for the MCS-12 (Ware et al., 2002).
2.1.2.3 Measures of the Therapeutic Relationship and Motivation for Psychotherapy
The Working Alliance Inventory — Client Form (WAI; Horvath & Greenberg,
1989). The WAI is a 36 item self-report scale designed to assess the therapeutic
relationship. The WAI comprises three scales, including the Bond scale, which measures
the therapeutic bond (e.g., attachment, mutual liking, trust), the Tasks scale, which
measures agreement on joint tasks (e.g., techniques and strategies of treatment), and the
79
functioning (ability to perform daily activities as well as strenuous activities), role-
physical (limitations of one's physical health on work or other activities), bodily pain
(amount of pain felt and its interference on normal activities), general health (perceived
general health), vitality (tiredness and energy), social functioning (whether physical and
emotional health affects one's social activities), role-emotional (extent to which work or
other activities are limited due to emotional problems), and mental health (emotional
well-being) (Ware, Kosinski, Turner-Bowker, & Gandek, 2002). For ease of use, the
eight domain scales have been combined into two larger component scales including (1)
physical component summary (PCS) (physical functioning, role-physical, bodily pain,
general health), and (2) mental component summary (MCS) (vitality, social functioning,
role-emotional, mental health) (Ware et al., 2002). The SF-36 and SF-12 component
scales are highly correlated, r = .95 for PCS and r = .97 for MCS (Ware et al., 1996).
Test-retest reliability (two weeks) of the PCS-12 ranges from 0.86 to 0.89, and 0.76 to
0.77 for the MCS-12 (Ware et al., 1996). For the eight domain scale scores, test-retest
reliability was 0.63 to 0.91 (Ware et al., 1996). Relative validity coefficients for the PCS-
12 ranged from 0.43 to 0.78, and from 0.93 to 0.98 for the MCS-12 (Ware et al., 2002).
2.1.2.3 Measures of the Therapeutic Relationship and Motivation for Psychotherapy
The Working Alliance Inventory - Client Form (WAI; Horvath & Greenberg,
1989). The WAI is a 36 item self-report scale designed to assess the therapeutic
relationship. The WAI comprises three scales, including the Bond scale, which measures
the therapeutic bond (e.g., attachment, mutual liking, trust), the Tasks scale, which
measures agreement on joint tasks (e.g., techniques and strategies of treatment), and the
79

Goals scale, which measures agreement about treatment goals (e.g., areas targeted for
change). Participants respond to each item on a 7-point Likert scale that ranges from
`does not correspond at all' to 'corresponds exactly." The reliability estimate for the
client form of the WAI has been reported at Cronbach's a = 0.98, and test-retest reliability
was r = 0.83 across a 2-week period (Tracey & Kokotovic, 1989). For the purpose of this
study, the WAI was administered on the first, third, and last sessions. The WAI was
chosen because it is based on Bordin's transtheoretical model (Bordin, 1979) of the
therapeutic alliance. Specific psychometric data for this measure exclusively with older
adults has not been reported.
Nijmegen Motivation List-2 (NML-2; Keijsers et al., 1999) is a 24 item instrument
designed to measure patient motivation for CBT. The participant rates the extent to
which each statement applied to him or her on a 6-point scale, ranging from 'not at all
applicable' to 'very applicable.' A factor analysis by Keijsers et al. (1999) of the NML-2
resulted in three factors: (1) Preparedness, which measures the patient's preparedness to
actively invest in treatment and to make sacrifices; (2) Distress, which measures pressure
by others and level of distress; and (3) Doubt, which measures doubt about the
investment in treatment, the treatment itself, and the possibility of gaining from it.
Internal consistencies for the factors were reasonable and the Cronbach's alphas ranged
from .71 to .84 (Keijsers et al., 1999). Test-retest reliabilities for the three subscales
ranged from .69 to .78. The NML-2 predicted decreases in GAD symptoms at 6- and 24-
month follow-ups in a sample of 52 adults with a principal diagnosis of GAD received
CBT (Dugas et al., 2003). This measure was chosen because it was specifically designed
80
Goals scale, which measures agreement about treatment goals (e.g., areas targeted for
change). Participants respond to each item on a 7-point Likert scale that ranges from
'does not correspond at all' to 'corresponds exactly." The reliability estimate for the
client form of the WAI has been reported at Cronbach's a = 0.98, and test-retest reliability
was r = 0.83 across a 2-week period (Tracey & Kokotovic, 1989). For the purpose of this
study, the WAI was administered on the first, third, and last sessions. The WAI was
chosen because it is based on Bordin's transtheoretical model (Bordin, 1979) of the
therapeutic alliance. Specific psychometric data for this measure exclusively with older
adults has not been reported.
Nijmegen Motivation List-2 (NML-2; Keijsers et al., 1999) is a 24 item instrument
designed to measure patient motivation for CBT. The participant rates the extent to
which each statement applied to him or her on a 6-point scale, ranging from 'not at all
applicable' to 'very applicable.' A factor analysis by Keijsers et al. (1999) of the NML-2
resulted in three factors: (1) Preparedness, which measures the patient's preparedness to
actively invest in treatment and to make sacrifices; (2) Distress, which measures pressure
by others and level of distress; and (3) Doubt, which measures doubt about the
investment in treatment, the treatment itself, and the possibility of gaining from it.
Internal consistencies for the factors were reasonable and the Cronbach's alphas ranged
from .71 to .84 (Keijsers et al., 1999). Test-retest reliabilities for the three subscales
ranged from .69 to .78. The NML-2 predicted decreases in GAD symptoms at 6- and 24-
month follow-ups in a sample of 52 adults with a principal diagnosis of GAD received
CBT (Dugas et al., 2003). This measure was chosen because it was specifically designed
80
to measure patient motivation for CBT. Specific psychometric data for this measure
exclusively with older adults has not been reported.
2.1.3 Therapy Programs: Standard Cognitive Behavioural Therapy (SCBT) and
Enhanced Cognitive Behavioural Therapy (ECBT)
The SCBT program was designed by Barsky and Ahern (2004) and is consistent
with principles of the CB model of health anxiety. This program was chosen because it
was brief (six sessions) and written in English. Further, permission was granted by Dr.
Barsky for us to use and adapt his program. This program has been found to be effective
for the treatment of hypochondriasis with younger adults (Barsky & Ahern, 2004). The
topics that were covered in both the SCBT and ECBT programs include the following:
(1) education about the nature of health anxiety, (2) improving understanding and ability
to control health anxiety using psychological means (e.g., coping strategies, attention and
distraction techniques), (3) self-monitoring (i.e., keeping track of anxiety and methods
one can use to deal with it), (4) improving the understanding and management of stress,
(5) examining thoughts and beliefs about health anxiety, (6) improving behaviours and
activities that have an impact on health anxiety, (7) improving other emotional states
(e.g., depression) that have an impact on health anxiety, and (8) maintaining
improvements in emotional functioning.
The ECBT program covered the same topics but also included learning and
memory aids and videos designed to make the therapy more effective with older adults
(see Appendix C for outline of videos) following recommendations by Mohlman and
81
to measure patient motivation for CBT. Specific psychometric data for this measure
exclusively with older adults has not been reported.
2.1.3 Therapy Programs: Standard Cognitive Behavioural Therapy (SCBT) and
Enhanced Cognitive Behavioural Therapy (ECBT)
The SCBT program was designed by Barsky and Ahern (2004) and is consistent
with principles of the CB model of health anxiety. This program was chosen because it
was brief (six sessions) and written in English. Further, permission was granted by Dr.
Barsky for us to use and adapt his program. This program has been found to be effective
for the treatment of hypochondriasis with younger adults (Barsky & Ahern, 2004). The
topics that were covered in both the SCBT and ECBT programs include the following:
(1) education about the nature of health anxiety, (2) improving understanding and ability
to control health anxiety using psychological means (e.g., coping strategies, attention and
distraction techniques), (3) self-monitoring (i.e., keeping track of anxiety and methods
one can use to deal with it), (4) improving the understanding and management of stress,
(5) examining thoughts and beliefs about health anxiety, (6) improving behaviours and
activities that have an impact on health anxiety, (7) improving other emotional states
(e.g., depression) that have an impact on health anxiety, and (8) maintaining
improvements in emotional functioning.
The ECBT program covered the same topics but also included learning and
memory aids and videos designed to make the therapy more effective with older adults
(see Appendix C for outline of videos) following recommendations by Mohlman and
81

colleagues (2003). The following learning and memory aids were added to the SCBT
program:
■ Weekly reading assignments meant to reinforce session material (this written
information can be used as a reference throughout the weeks).
■ Graphing exercises in which participants chart numerical mood ratings averaged
over each week (meant to highlight gradual progress, reveal patterns in moods, and
facilitate discussion).
■ Mid-week homework reminder/troubleshooting calls from the therapist for the first
four assignments (meant to alleviate participants' ambivalence about asking for
help and review the procedures and goals of the assignment, decrease social
isolation often common among seniors).
■ A perspective-taking strategy to facilitate evidence generation in cognitive-
restructuring exercises (i.e., each participant was asked to generate a list of three to
five individuals who they believe are good problem solvers and generate evidence
that refutes automatic thoughts from the perspective of each person on the list)
which was meant to reduce automatic thoughts through the enhancement of
generative thinking abilities and broadened perspectives.
■ Short videos with older adults giving personal testimonials about the program
which were used to help socialize the client to treatment and ultimately to enhance
motivation.
82
colleagues (2003). The following learning and memory aids were added to the SCBT
program:
• Weekly reading assignments meant to reinforce session material (this written
information can be used as a reference throughout the weeks).
• Graphing exercises in which participants chart numerical mood ratings averaged
over each week (meant to highlight gradual progress, reveal patterns in moods, and
facilitate discussion).
• Mid-week homework reminder/troubleshooting calls from the therapist for the first
four assignments (meant to alleviate participants' ambivalence about asking for
help and review the procedures and goals of the assignment, decrease social
isolation often common among seniors).
• A perspective-taking strategy to facilitate evidence generation in cognitive-
restructuring exercises (i.e., each participant was asked to generate a list of three to
five individuals who they believe are good problem solvers and generate evidence
that refutes automatic thoughts from the perspective of each person on the list)
which was meant to reduce automatic thoughts through the enhancement of
generative thinking abilities and broadened perspectives.
• Short videos with older adults giving personal testimonials about the program
which were used to help socialize the client to treatment and ultimately to enhance
motivation.
82

2.1.4 Procedure
Ethics approval for this study was obtained from the University of Regina Research
Ethics Board (see Appendix D). All participants were screened first by telephone with
the WI to assess levels of health anxiety. The WI was used to eliminate individuals who
clearly did not have health anxiety and would not benefit from the treatment being
offered. Potential participants were also asked to report their age. It was decided, due to
difficulties with recruitment, that two participants both aged 57 years (one from the
SCBT group and one from the ECBT group) and above would be allowed to participate.
Other researchers who conduct research with older adults often include those above the
age of 55 (e.g., Byers et al., 2010). Those participants with a score of eight or higher on
the WI were then invited to our clinic for completion of the questionnaire package and
semi-structured interview. A member of the research team met with the participants to
fill out the questionnaires at the Psychology Training Clinic at the University of Regina
or at an otherwise convenient location (e.g., participant's home). A consent form was
presented to participants before they began any questionnaires or therapy. Following
this, participants were randomly assigned to SCBT, ECBT, or to the WLC group. The
randomized allocation sequence was computer generated in blocks of 10. Allocation of
participants to the specific group was concealed from the initial assessor until after the
assessment was complete and the participant was deemed to meet eligibility criteria. The
questionnaire package was completed on three different occasions: once when the study
began, once immediately after the study was over, and one final time three months after
the treatment program ended. The questionnaire package consisted of a section assessing
83
2.1.4 Procedure
Ethics approval for this study was obtained from the University of Regina Research
Ethics Board (see Appendix D). All participants were screened first by telephone with
the WI to assess levels of health anxiety. The WI was used to eliminate individuals who
clearly did not have health anxiety and would not benefit from the treatment being
offered. Potential participants were also asked to report their age. It was decided, due to
difficulties with recruitment, that two participants both aged 57 years (one from the
SCBT group and one from the ECBT group) and above would be allowed to participate.
Other researchers who conduct research with older adults often include those above the
age of 55 (e.g., Byers et al., 2010). Those participants with a score of eight or higher on
the WI were then invited to our clinic for completion of the questionnaire package and
semi-structured interview. A member of the research team met with the participants to
fill out the questionnaires at the Psychology Training Clinic at the University of Regina
or at an otherwise convenient location (e.g., participant's home). A consent form was
presented to participants before they began any questionnaires or therapy. Following
this, participants were randomly assigned to SCBT, ECBT, or to the WLC group. The
randomized allocation sequence was computer generated in blocks of 10. Allocation of
participants to the specific group was concealed from the initial assessor until after the
assessment was complete and the participant was deemed to meet eligibility criteria. The
questionnaire package was completed on three different occasions: once when the study
began, once immediately after the study was over, and one final time three months after
the treatment program ended. The questionnaire package consisted of a section assessing
83

demographic and background information (Appendix D), the SHAI, IAS, SSAS, SSI,
HCQ, STAI, ASI, GDS, GPM, and SF-12. The questionnaires assessing health anxiety
were placed first in order in the package given the results of a previous study that
demonstrated that focusing on one's own health can influence ratings of health anxiety
(Lister, Rode, Farmer, & Salkovskis, 2002). At three-month follow-up, the demographic
and background information sections, semi-structured interview, WAI, and NML-2 were
omitted from the questionnaire package. Participants were asked to complete the WAI in
order to provide information on the relationship with their therapist after the first, third
session, and again after the final session. The NML-2 was also completed after the first,
third, and final sessions. Open-ended questions, which have been described above, were
also included at pre-treatment and at post-treatment.
Participants randomly assigned to the two experimental conditions received either
the SCBT or ECBT program immediately after the initial questionnaires were completed.
The participants in these conditions attended the intervention once a week for one hour,
over a six week period. Participants who were randomly assigned to the WLC group
were offered the ECBT health anxiety treatment program no later than six weeks
following their enrolment in the study. Therapy was conducted by the researcher and
three other graduate students in the Clinical Psychology programme at the University of
Regina who were trained in provision of the treatment program. Training of the student
therapists consisted of a review of the treatment manual, review of the treatment videos,
and direction provided by the researcher. Supervision was provided by Heather
Hadjistavropoulos, Ph.D., a registered doctoral psychologist, while doctoral students
84
demographic and background information (Appendix D), the SHAI, IAS, SSAS, SSI,
HCQ, STAI, ASI, GDS, GPM, and SF-12. The questionnaires assessing health anxiety
were placed first in order in the package given the results of a previous study that
demonstrated that focusing on one's own health can influence ratings of health anxiety
(Lister, Rode, Farmer, & Salkovskis, 2002). At three-month follow-up, the demographic
and background information sections, semi-structured interview, WAI, and NML-2 were
omitted from the questionnaire package. Participants were asked to complete the WAI in
order to provide information on the relationship with their therapist after the first, third
session, and again after the final session. The NML-2 was also completed after the first,
third, and final sessions. Open-ended questions, which have been described above, were
also included at pre-treatment and at post-treatment.
Participants randomly assigned to the two experimental conditions received either
the SCBT or ECBT program immediately after the initial questionnaires were completed.
The participants in these conditions attended the intervention once a week for one hour,
over a six week period. Participants who were randomly assigned to the WLC group
were offered the ECBT health anxiety treatment program no later than six weeks
following their enrolment in the study. Therapy was conducted by the researcher and
three other graduate students in the Clinical Psychology programme at the University of
Regina who were trained in provision of the treatment program. Training of the student
therapists consisted of a review of the treatment manual, review of the treatment videos,
and direction provided by the researcher. Supervision was provided by Heather
Hadjistavropoulos, Ph.D., a registered doctoral psychologist, while doctoral students
84

conducted the six week intervention. Sessions were offered at Psychology Training
Clinic at the University of Regina. See Figure 3 for a profile of the randomized control
trial. The procedure described above follows the Consolidated Standards of Reporting
Trials (CONSORT) as outlined by Schulz, Altman, and Moher (2010).
2.1.5 Design and Analyses
2.1.5.1 Analyses
In order to test the hypothesis that participants receiving SCBT and ECBT, but
not those in the WLC, would evidence improvements in health anxiety, frequency of
hypochondriacal thoughts, hypochondriacal somatic symptoms, tendency to experience
bodily sensations as being distressing, state anxiety, depression, pain, and health-related
quality of life from pre-treatment to post-treatment, a series of mixed factor analyses of
covariance (ANCOVAs) were used to compare the treatment group and control group
scores on the dependent variables (i.e., WI, SHAI, IAS, SSI, SSAS, HCQ, ASI, STAI-S,
STAI-T, GDS, GPM, SF-12-PCS, SF-12-MCS) at baseline and post-treatment, with the
pre-treatment value of the measure of interest in the analysis set as the covariate. This
analytic method has more power than analysis of variance when treatment assignment is
randomized (van Breukelen, 2006; Vickers, 2004), as was the case for this study.
To test the hypotheses (1) that participants treated with ECBT would demonstrate
the greatest overall improvement (as assessed by the dependent measures) at follow-up in
each of the areas indicated in the first hypothesis, and (2) that participants treated with
both SCBT and ECBT would maintain improvements at three months following the
85
conducted the six week intervention. Sessions were offered at Psychology Training
Clinic at the University of Regina. See Figure 3 for a profile of the randomized control
trial. The procedure described above follows the Consolidated Standards of Reporting
Trials (CONSORT) as outlined by Schulz, Altman, and Moher (2010).
2.1.5 Design and Analyses
2.1.5.1 Analyses
In order to test the hypothesis that participants receiving SCBT and ECBT, but
not those in the WLC, would evidence improvements in health anxiety, frequency of
hypochondriacal thoughts, hypochondriacal somatic symptoms, tendency to experience
bodily sensations as being distressing, state anxiety, depression, pain, and health-related
quality of life from pre-treatment to post-treatment, a series of mixed factor analyses of
covariance (ANCOVAs) were used to compare the treatment group and control group
scores on the dependent variables (i.e., WI, SHAI, IAS, SSI, SSAS, HCQ, ASI, STAI-S,
STAI-T, GDS, GPM, SF-12-PCS, SF-12-MCS) at baseline and post-treatment, with the
pre-treatment value of the measure of interest in the analysis set as the covariate. This
analytic method has more power than analysis of variance when treatment assignment is
randomized (van Breukelen, 2006; Vickers, 2004), as was the case for this study.
To test the hypotheses (1) that participants treated with ECBT would demonstrate
the greatest overall improvement (as assessed by the dependent measures) at follow-up in
each of the areas indicated in the first hypothesis, and (2) that participants treated with
both SCBT and ECBT would maintain improvements at three months following the
85

110 individuals assessed for eligibility
v57 individuals randomly
assigned
53 individuals were excluded • 37 did not meet inclusion
criteria • 19 declined to participate
SCBT - 21 individuals completed questionnaires and allocated
19 individuals in analyses at post-treatment • 2 individuals
dropped out
19 individuals in analyses at follow-up
ECBT - 18 individuals completed questionnaires and allocated
17 individuals in analyses post-treatment • 1 individual
dropped out
17 individuals in analyses at follow-up
• WLC - 18 individuals completed questionnaires and allocated
•18 individuals completed at post-treatment
Figure 3. Flow of participants through the treatments.
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control
86
SCBT-21 individuals completed questionnaires and allocated
19 individuals in analyses at post-treatment • 2 individuals
dropped out
110 individuals assessed for eligibility
57 individuals randomly assigned
ECBT-18 individuals completed questionnaires and allocated
17 individuals in analyses post-treatment • 1 individual
dropped out
1 '
19 individuals in analyses at follow-up
i '
17 individuals in analyses at follow-up
53 individuals were excluded • 37 did not meet inclusion
criteria • 19 declined to participate
WLC-18 individuals completed questionnaires and allocated
18 individuals completed at post-treatment
Figure 3. Flow of participants through the treatments.
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control
86

conclusion of treatment, a series of mixed model ANCOVAs were used to compare the
SCBT and ECBT on each of the dependent variables. In order to test the hypotheses that
participants treated with ECBT would demonstrate a higher level of therapeutic alliance
and motivation for treatment at three and six weeks than those receiving SCBT, a series
of mixed model ANCOVAs were used to compare the SCBT and ECBT on each of the
dependent variables.
An intent-to-treat (ITT) analysis was conducted in order to evaluate pre- to post-
treatment effects for all participants who intended to participate, regardless of whether he
or she dropped out or not. Thus, in addition to the participants who completed treatment,
all participants who were randomized to either the SCBT or ECBT conditions and
completed all pre-treatment questionnaires and at least one treatment session (two from
the SCBT group and one from the ECBT group) were included in the ITT analysis.
2.1.5.2 Preparation of the Data for Analysis
The alpha level for the mixed factor ANCOVAs tests was set at .05. Results of
evaluation of assumptions of normality and homogeneity of variance-covariance matrixes
were satisfactory. The assumption of sphericity for all repeated measures analyses was
met or was corrected for using the Greenhouse-Geisser correction provided by SPSS.
Assessment for outliers was conducted by examining the z-scores for each dependent and
independent variable. Based on the recommended criteria that z-scores greater than 3.29
should be considered outliers (Tabachnick & Fidell, 2001), there were no outlying data
points identified. Next, the pattern of missing data was examined and mean substitution
was used to replace the missing value in those instances where there was only very
87
conclusion of treatment, a series of mixed model ANCOVAs were used to compare the
SCBT and ECBT on each of the dependent variables. In order to test the hypotheses that
participants treated with ECBT would demonstrate a higher level of therapeutic alliance
and motivation for treatment at three and six weeks than those receiving SCBT, a series
of mixed model ANCOVAs were used to compare the SCBT and ECBT on each of the
dependent variables.
An intent-to-treat (ITT) analysis was conducted in order to evaluate pre- to post-
treatment effects for all participants who intended to participate, regardless of whether he
or she dropped out or not. Thus, in addition to the participants who completed treatment,
all participants who were randomized to either the SCBT or ECBT conditions and
completed all pre-treatment questionnaires and at least one treatment session (two from
the SCBT group and one from the ECBT group) were included in the ITT analysis.
2.1.5.2 Preparation of the Data for Analysis
The alpha level for the mixed factor ANCOVAs tests was set at .05. Results of
evaluation of assumptions of normality and homogeneity of variance-covariance matrixes
were satisfactory. The assumption of sphericity for all repeated measures analyses was
met or was corrected for using the Greenhouse-Geisser correction provided by SPSS.
Assessment for outliers was conducted by examining the z-scores for each dependent and
independent variable. Based on the recommended criteria that z-scores greater than 3.29
should be considered outliers (Tabachnick & Fidell, 2001), there were no outlying data
points identified. Next, the pattern of missing data was examined and mean substitution
was used to replace the missing value in those instances where there was only very
87

minimal missing data (e.g., if a participant did not complete one whole questionnaire or
left blank more than two questions in a row data was not replaced). In total, less than one
percent of the data were replaced. All analyses were conducted on an ITT basis. The
analyses included all subjects with a pre-treatment measurement, regardless of the
duration of their treatment. For the three drop-outs, pre-treatment data were carried
forward to serve as post-treatment scores (last-observation carried-forward (LOCF)
technique) (Greeven, van Balkom, van der Leeden, Merkelbach, van den Heuvel, &
Spinhoven, 2007; Sorensen et al., in press).
2.1.5.3 Qualitative Data Analysis
The current data was comprised of participants' responses to the open-ended
questions completed at pre-treatment and post-treatment by participants in both the SCBT
and ECBT groups. The questions described in the Method section were attached at the
end of the questionnaire packages and participants were asked to respond to questions in
writing. All the responses were read and then entered into a Microsoft Word document.
After inputting all the responses, the following coding process took place.
Coding. Analysis from a grounded theory perspective is a systematic process that
occurs in various stages (Strauss & Corbin, 1998). Data were analyzed using a three-
stage coding process which included open, axial, and selective coding procedures
(Strauss & Corbin, 1998).
Open coding. For the open coding stage, raw data were named and categorized
after being broken down into discrete parts, examined closely, compared for similarities
and differences, interpreted, and reconstructed to establish conceptual labels or
88
minimal missing data (e.g., if a participant did not complete one whole questionnaire or
left blank more than two questions in a row data was not replaced). In total, less than one
percent of the data were replaced. All analyses were conducted on an ITT basis. The
analyses included all subjects with a pre-treatment measurement, regardless of the
duration of their treatment. For the three drop-outs, pre-treatment data were carried
forward to serve as post-treatment scores (last-observation carried-forward (LOCF)
technique) (Greeven, van Balkom, van der Leeden, Merkelbach, van den Heuvel, &
Spinhoven, 2007; Sorensen et al., in press).
2.1.5.3 Qualitative Data Analysis
The current data was comprised of participants' responses to the open-ended
questions completed at pre-treatment and post-treatment by participants in both the SCBT
and ECBT groups. The questions described in the Method section were attached at the
end of the questionnaire packages and participants were asked to respond to questions in
writing. All the responses were read and then entered into a Microsoft Word document.
After inputting all the responses, the following coding process took place.
Coding. Analysis from a grounded theory perspective is a systematic process that
occurs in various stages (Strauss & Corbin, 1998). Data were analyzed using a three-
stage coding process which included open, axial, and selective coding procedures
(Strauss & Corbin, 1998).
Open coding. For the open coding stage, raw data were named and categorized
after being broken down into discrete parts, examined closely, compared for similarities
and differences, interpreted, and reconstructed to establish conceptual labels or
88
interpretative schemes (Strauss & Corbin, 1998). An initial list of open codes was
developed for the pre-treatment responses and for the post-treatment responses through
examination of participants' responses to the open-ended questions.
Axial coding. In the axial coding stage, categories pertaining to the research
questions were derived from the emerging concepts (Strauss & Corbin, 1998).
Specifically, ideas that were conceptually related were grouped together. At this stage of
the coding process, open codes were collapsed to develop categories. Then, direct quotes
from the responses that were conceptually related were cut from original document and
pasted together to emphasize a particular category. Higher order concepts within each
category began to emerge and they were compared to establish abstract concepts (Strauss
& Corbin, 1998).
Selective coding. To facilitate the development of models that describe older
adults' experiences of health anxiety and older adults' experiences of the psychological
treatment of health anxiety, selective coding procedures were subsequently employed. In
the selective coding stage, comparisons and links were made across categories (Strauss &
Corbin, 1998). The core tasks in this stage were to identify the core themes and sub-
themes to form a model of older adults' development of health anxiety and older adults'
experiences in the psychological treatment of health anxiety. The diagrammatic
representations of the emergent models based on the themes derived from the original
data provide a visual description (Strauss & Corbin, 1998). These both appear in the
Results section. To represent the emergent themes of the final analysis and the
integrated perceptions and experiences of the older adults, verbatim quotes were selected
89
interpretative schemes (Strauss & Corbin, 1998). An initial list of open codes was
developed for the pre-treatment responses and for the post-treatment responses through
examination of participants' responses to the open-ended questions.
Axial coding. In the axial coding stage, categories pertaining to the research
questions were derived from the emerging concepts (Strauss & Corbin, 1998).
Specifically, ideas that were conceptually related were grouped together. At this stage of
the coding process, open codes were collapsed to develop categories. Then, direct quotes
from the responses that were conceptually related were cut from original document and
pasted together to emphasize a particular category. Higher order concepts within each
category began to emerge and they were compared to establish abstract concepts (Strauss
& Corbin, 1998).
Selective coding. To facilitate the development of models that describe older
adults' experiences of health anxiety and older adults' experiences of the psychological
treatment of health anxiety, selective coding procedures were subsequently employed. In
the selective coding stage, comparisons and links were made across categories (Strauss &
Corbin, 1998). The core tasks in this stage were to identify the core themes and sub-
themes to form a model of older adults' development of health anxiety and older adults'
experiences in the psychological treatment of health anxiety. The diagrammatic
representations of the emergent models based on the themes derived from the original
data provide a visual description (Strauss & Corbin, 1998). These both appear in the
Results section. To represent the emergent themes of the final analysis and the
integrated perceptions and experiences of the older adults, verbatim quotes were selected
89
from the responses to the open-ended questions. Those quotes are also presented in the
Results section.
To ensure reliability of the coding of the themes and sub-themes, a second
researcher examined the raw data, coding, themes, and sub-themes, engaging in the same
process described above. Any differences in opinion were resolved via discussion.
2.2 Study 2
2.2.1 Participants and Procedure
In order to recruit control participants for comparison with the older adult sample
recruited in Study 1, the research was advertised on online classified websites across
Canada (e.g., www.craigslist.com, www.usedregina.com). Participants were informed of
the nature of the study and invited to take part in the 30 minute study by connecting to the
survey via a link posted on the advertisement (Appendix F). The main page of the survey
described the nature and purpose of the study (Appendix G), and required the participants
to indicate whether they consented to participate before moving forward with the survey.
Participants completed a battery of self-report questionnaires including the WI, SHAI,
IAS, SSI, SSAS, HCQ, ASI, and STAI (all measures are described above). Once all
questionnaires were completed and submitted, participants had the option of entering
their name in a draw to win one of three $20 Chapters gift certificates.
A total of 296 potential control participants responded to recruitment
advertisements. Of these individuals, 220 fully completed all the questionnaires.
Participants from the control group were then matched to the older adult participants by
sex and WI score (a score of greater than or equal to 8). Sex and WI score matches were
90
from the responses to the open-ended questions. Those quotes are also presented in the
Results section.
To ensure reliability of the coding of the themes and sub-themes, a second
researcher examined the raw data, coding, themes, and sub-themes, engaging in the same
process described above. Any differences in opinion were resolved via discussion.
2.2 Study 2
2.2.1 Participants and Procedure
In order to recruit control participants for comparison with the older adult sample
recruited in Study 1, the research was advertised on online classified websites across
Canada (e.g., www.craigslist.com, www.usedregina.com). Participants were informed of
the nature of the study and invited to take part in the 30 minute study by connecting to the
survey via a link posted on the advertisement (Appendix F). The main page of the survey
described the nature and purpose of the study (Appendix G), and required the participants
to indicate whether they consented to participate before moving forward with the survey.
Participants completed a battery of self-report questionnaires including the WI, SHAI,
IAS, SSI, SSAS, HCQ, ASI, and STAI (all measures are described above). Once all
questionnaires were completed and submitted, participants had the option of entering
their name in a draw to win one of three $20 Chapters gift certificates.
A total of 296 potential control participants responded to recruitment
advertisements. Of these individuals, 220 fully completed all the questionnaires.
Participants from the control group were then matched to the older adult participants by
sex and WI score (a score of greater than or equal to 8). Sex and WI score matches were
90

made for 57 pairs of the older adult sample (n = 57) and control sample (n = 57)
participants. The mean age of participants in the control group was 33.05 (SD = 9.50)
years of age, compared to 68.70 (SD = 6.92) years of age in the older adult group. Both
groups were comprised of 44 (77.2%) females (there was no significant difference, X2 (1,
114) = .000, p = 1.00. There was no significant difference found between groups with
regard to relationship status, X2 (1, 114) = .04,p = .85. In both groups, the majority of
participants were not married (older adult group — N = 32, 56.1%; control group = N = 31,
54.4%). There was a statistically significant difference in participants' highest level of
education, X2 (1, 114) = 13.37, p = .0001, with 89.5% of control participants (n = 51)
having more than a high school education, compared to 59.6% (n = 34) of the older adult
participants having more than a high school education. Control participants also had a
significantly lower average number of health conditions than the older adult group, t(112)
= 7.79,p = .0001 (older adult group: M= 2.30, SD = 1.46; control group: M .54, SD =
.87) (see Table 4 for demographic information). The most common conditions cited for
the older adults were arthritis (56.1%), high blood pressure (43.9%), and osteoporosis
(31.7%). For the younger adults, the most common conditions cited were arthritis
(14.0%), vision problems (12.3%), and hearing problems (8.8%) (see Tables 4 and 5).
2.2.2 Preparation of the Data for Analysis
Prior to conducting the analyses, the data set was cleaned and screened for
accuracy. Assessment for outliers was conducted by examining the z-scores for each
dependent and independent variable. Based on the recommended criteria that z-scores
greater than 3.29 should be considered outliers (Tabachnick & Fidell, 2001), there were
91
made for 57 pairs of the older adult sample (n = 57) and control sample (n = 57)
participants. The mean age of participants in the control group was 33.05 (SD = 9.50)
years of age, compared to 68.70 (SD = 6.92) years of age in the older adult group. Both
groups were comprised of 44 (77.2%) females (there was no significant difference, x2 (1,
114) = .000, p = 1.00. There was no significant difference found between groups with
regard to relationship status, x2 (1, 114) = .04,p = .85. In both groups, the majority of
participants were not married (older adult group - iV = 32, 56.1 %; control group = TV = 31,
54.4%»). There was a statistically significant difference in participants' highest level of
education, x2 (1, 114) = 13.37, p = .0001, with 89.5% of control participants (n = 51)
having more than a high school education, compared to 59.6% (n = 34) of the older adult
participants having more than a high school education. Control participants also had a
significantly lower average number of health conditions than the older adult group, ^(112)
= 7.79,p = .0001 (older adult group: M= 2.30, SD = 1.46; control group: M= .54, SD =
.87) (see Table 4 for demographic information). The most common conditions cited for
the older adults were arthritis (56.1%), high blood pressure (43.9%), and osteoporosis
(31.7%). For the younger adults, the most common conditions cited were arthritis
(14.0%)), vision problems (12.3%), and hearing problems (8.8%) (see Tables 4 and 5).
2.2.2 Preparation of the Data for Analysis
Prior to conducting the analyses, the data set was cleaned and screened for
accuracy. Assessment for outliers was conducted by examining the z-scores for each
dependent and independent variable. Based on the recommended criteria that z-scores
greater than 3.29 should be considered outliers (Tabachnick & Fidell, 2001), there were
91

Table 4
Demographic Information and Scale Scores for Matched Participants
Demographic Characteristic Older Adult
Group
Matched
Control Group
M (SD) M (SD) T
Age 68.70 6.92 33.05 (9.50) 22.90***
Number of Health Conditions 2.30 1.46 .54 (0.87) 7.79***
N % N % x2 Sex
Female 44 77.2 44 77.2 .000
Male 13 22.8 13 22.8
Marital Status
Married/Common-Law 25 43.9 26 45.6 .04
Not Married 32 56.1 31 54.4
Education
< High School 23 40.4 6 10.5 13.37***
> = High School 34 59.6 51 89.5
Notes: *p < .05, **p < .01, ***p < .001
92
Table 4
Demographic Information and Scale Scores for Matched Participants
Demographic Characteristic
Age
Number of Health Conditions
Sex
Female
Male
Older Adult
Group
M
68.70
2.30
N
44
13
(SD)
6.92
1.46
%
77.2
22.8
Matched
Control Group
M
33.05
.54
N
44
13
(SD)
(9.50)
(0.87)
%
77.2
22.8
T
22.90***
7 79***
7?
.000
Marital Status
Married/Common-Law 25 43.9 26 45.6 .04
Not Married
Education
< High School
> = High School
32
23
34
56.1
40.4
59.6
31
6
51
54.4
10.5
89.5
13 37***
Notes: *p < .05, **p < .01, ***p < .001
92
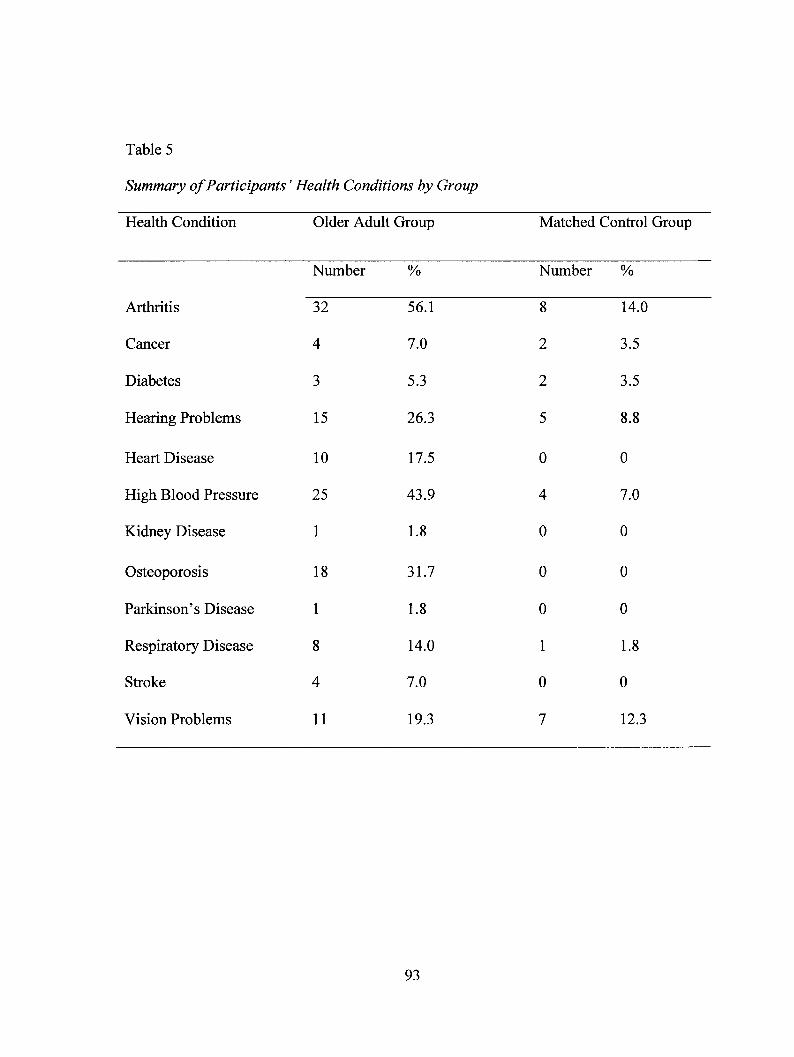
Table 5
Summary of Participants' Health Conditions by Group
Health Condition Older Adult Group Matched Control Group
Number % Number %
Arthritis 32 56.1 8 14.0
Cancer 4 7.0 2 3.5
Diabetes 3 5.3 2 3.5
Hearing Problems 15 26.3 5 8.8
Heart Disease 10 17.5 0 0
High Blood Pressure 25 43.9 4 7.0
Kidney Disease 1 1.8 0 0
Osteoporosis 18 31.7 0 0
Parkinson's Disease 1 1.8 0 0
Respiratory Disease 8 14.0 1 1.8
Stroke 4 7.0 0 0
Vision Problems 11 19.3 7 12.3
93
Table 5
Summary of Participants' Health Conditions by Group
Health Condition
Arthritis
Cancer
Diabetes
Hearing Problems
Heart Disease
High Blood Pressure
Kidney Disease
Osteoporosis
Parkinson's Disease
Respiratory Disease
Stroke
Vision Problems
Older Adult
Number
32
4
3
15
10
25
1
18
1
8
4
11
Group
%
56.1
7.0
5.3
26.3
17.5
43.9
1.8
31.7
1.8
14.0
7.0
19.3
Matched Control Group
Number
8
2
2
5
0
4
0
0
0
1
0
7
%
14.0
3.5
3.5
8.8
0
7.0
0
0
0
1.8
0
12.3
93

no outlying data points identified. Next, the pattern of missing data was examined and
mean substitution was used to replace the missing value in those instances where the
missing data appeared to be the result of random occurrence. In cases where the
participants did not complete one whole questionnaire or left blank more than two
questions in a row, then the missing information was not altered. Normality, linearity and
homoscedasticity were examined via histograms and scatterplots, and no substantial
deviations were noted.
94
no outlying data points identified. Next, the pattern of missing data was examined and
mean substitution was used to replace the missing value in those instances where the
missing data appeared to be the result of random occurrence. In cases where the
participants did not complete one whole questionnaire or left blank more than two
questions in a row, then the missing information was not altered. Normality, linearity and
homoscedasticity were examined via histograms and scatterplots, and no substantial
deviations were noted.
94
3. RESULTS
3.1 Study 1
3.1.1 Preliminary Analyses
Means and standard deviations for each dependent variable (DV) and each
subscale, at each time of measurement for each group are reported in Tables 6, 7, and 8.
Reliability analyses on the following pre-treatment measures showed good internal
consistency: WI a = .81; SHAI a = .80; IAS a = .82, IAS-Fear of Illness and Pain a = .71,
IAS-Symptom Effects a = .70, HCQ a = .82; ASI a = .87; STAI-S a = .93; STAI-T a =
.91; GDS a = .88; GPM a = .82; SF-12 a = .83; WAI-Tasks a — .86, WAI-Bond a = .85,
WAI-Goal a = .87; and NML-2: Preparedness a = .72. Reliability analyses on the
following pre-treatment measures showed acceptable internal consistency: WI-Somatic
Symptoms/Bodily Preoccupation a = .68; WI-Disease Fear/Phobia a = .68; WI- SSI a =
.61; SSAS a = .69; NML-2: Distress a = .68 NML-2: Doubt a = .68; SHAI-Negative
Consequences Subscale a = .63; IAS-Treatment Experience a = .60; and IAS-Disease
Conviction a = .64; (Zinbarg, Revelle, Yovel, & Li, 2005).
Correlations among measures were assessed at pre-treatment and are provided in
Table 9. Examination of the correlation matrix indicates that many of the questionnaires
were significantly related to one another. Further, a number of the health anxiety
measures were found to be correlated. Specifically, the WI was found to moderately
correlate with the other two measures of health anxiety — the SHAI and the IAS —
suggesting that those participants with elevated health anxiety on the WI were more
95
3. RESULTS
3.1 Study 1
3.1.1 Preliminary Analyses
Means and standard deviations for each dependent variable (DV) and each
subscale, at each time of measurement for each group are reported in Tables 6, 7, and 8.
Reliability analyses on the following pre-treatment measures showed good internal
consistency: WI a = .81; SHAI a = .80; IAS a = .82, IAS-Fear of Illness and Pain a = .71,
IAS-Symptom Effects a = .70, HCQ a = .82; ASI a = .87; STAI-S a = .93; STAI-T a =
.91; GDS a = .88; GPM a = .82; SF-12 a = .83; WAI-Tasks a = .86, WAI-Bond a = .85,
WAI-Goal a = .87; and NML-2: Preparedness a = .72. Reliability analyses on the
following pre-treatment measures showed acceptable internal consistency: Wl-Somatic
Symptoms/Bodily Preoccupation a = .68; WI-Disease Fear/Phobia a = .68; WI- SSI a =
.61; SSAS a = .69; NML-2: Distress a = .68 NML-2: Doubt a = .68; SHAI-Negative
Consequences Subscale a = .63; IAS-Treatment Experience a = .60; and IAS-Disease
Conviction a = .64; (Zinbarg, Revelle, Yovel, & Li, 2005).
Correlations among measures were assessed at pre-treatment and are provided in
Table 9. Examination of the correlation matrix indicates that many of the questionnaires
were significantly related to one another. Further, a number of the health anxiety
measures were found to be correlated. Specifically, the WI was found to moderately
correlate with the other two measures of health anxiety - the SHAI and the IAS -
suggesting that those participants with elevated health anxiety on the WI were more
95

Table 6
Means and Standard Deviations for Primary and Secondary Outcome Measures
Measure SCBT (N = 21) ECBT (N = 18) WLC (N = 18)
Mean SD Mean SD Mean SD
Whiteley Index
Pre-treatment 8.86 1.28 9.39 1.20 9.11 1.18
Post-treatment 4.95 3.23 6.28 3.63 8.50 1.38
Follow-up 4.62 2.46 5.17 2.73
Short Health Anxiety Inventory
Pre-treatment 14.07 4.52 17.37 4.93 16.82 5.30
Post-treatment 11.63 4.01 15.11 6.29 16.00 4.41
Follow-up 11.45 2.90 13.78 5.24
Illness Attitudes Scale
Pre-treatment 45.43 12.61 54.04 9.29 49.75 10.19
Post-treatment 40.71 11.91 50.48 11.40 49.81 11.59
Follow-up 39.30 10.42 46.08 10.74
Somatic Symptom Inventory
Pre-treatment 31.68 7.52 31.88 6.74 31.27 7.37
Post-treatment 31.10 8.55 28.95 5.32 31.56 9.93
Follow-up 30.48 8.05 28.71 5.45
96
Table 6
Means and Standard Deviations for Primary and Secondary Outcome Measures
Measure SCBT(#=21) ECBT(JV=18) WLC (TV =18)
Mean SD Mean SD Mean SD
Whiteley Index
Pre-treatment 8.86 1.28 9.39 1.20 9.11 1.18
Post-treatment 4.95 3.23 6.28 3.63 8.50 1.38
Follow-up 4.62 2.46 5.17 2.73
Short Health Anxiety Inventory
Pre-treatment 14.07 4.52 17.37 4.93 16.82 5.30
Post-treatment 11.63 4.01 15.11 6.29 16.00 4.41
Follow-up 11.45 2.90 13.78 5.24
Illness Attitudes Scale
Pre-treatment 45.43 12.61 54.04 9.29 49.75 10.19
Post-treatment 40.71 11.91 50.48 11.40 49.81 11.59
Follow-up 39.30 10.42 46.08 10.74
Somatic Symptom Inventory
Pre-treatment 31.68 7.52 31.88 6.74 31.27 7.37
Post-treatment 31.10 8.55 28.95 5.32 31.56 9.93
Follow-up 30.48 8.05 28.71 5.45
96

Measure SCBT (N = 21) ECBT (N = 18) WLC (N = 18)
Mean SD
Somatosensory Amplification Scale
Mean SD Mean SD
Pre-treatment 28.91 5.85 28.47 4.91 27.33 6.08
Post-treatment 27.86 5.68 27.29 7.02 27.03 4.66
Follow-up 27.86 5.91 25.48 4.42
Health Cognitions Questionnaire
Pre-treatment 29.29 10.01 29.78 7.59 29.11 8.16
Post-treatment 26.62 8.18 28.47 6.68 25.91 7.42
Follow-up 26.34 6.43 26.87 7.94
Anxiety Sensitivity Index
Pre-treatment 26.60 12.41 28.59 9.37 28.94 10.09
Post-treatment 23.10 9.83 24.59 11.27 29.86 10.84
Follow-up 22.16 9.24 20.89 9.29
State Trait Anxiety Inventory - State Scale
Pre-treatment 41.65 11.04 38.63 10.01 42.75 10.25
Post-treatment 36.24 9.90 36.87 8.29 39.80 10.61
Follow-up 40.30 10.09 34.71 8.89
State Trait Anxiety Inventory - Trait Scale
Pre-treatment 45.31 10.67 44.32 10.44 44.26 9.10
Post-treatment 41.53 10.47 42.98 8.00 42.50 10.44
Follow-up 40.30 10.09 40.82 9.32
97
Measure SCBT (TV =21) ECBT(N=18) WLC(JV=18)
Mean SD Mean SD Mean SD
Somatosensory Amplification Scale
Pre-treatment 28.91 5.85 28.47 4.91 27.33 6.08
Post-treatment 27.86 5.68 27.29 7.02 27.03 4.66
Follow-up 27.86 5.91 25.48 4.42
Health Cognitions Questionnaire
Pre-treatment 29.29 10.01 29.78 7.59 29.11 8.16
Post-treatment 26.62 8.18 28.47 6.68 25.91 7.42
Follow-up 26.34 6.43 26.87 7.94
Anxiety Sensitivity Index
Pre-treatment 26.60 12.41 28.59 9.37 28.94 10.09
Post-treatment 23.10 9.83 24.59 11.27 29.86 10.84
Follow-up 22.16 9.24 20.89 9.29
State Trait Anxiety Inventory - State Scale
Pre-treatment 41.65 11.04 38.63 10.01 42.75 10.25
Post-treatment 36.24 9.90 36.87 8.29 39.80 10.61
Follow-up 40.30 10.09 34.71 8.89
State Trait Anxiety Inventory - Trait Scale
Pre-treatment 45.31 10.67 44.32 10.44 44.26 9.10
Post-treatment 41.53 10.47 42.98 8.00 42.50 10.44
Follow-up 40.30 10.09 40.82 9.32
97

Measure SCBT (N = 21) ECBT (N = 18) WLC (N = 18)
Mean SD Mean SD Mean SD
Geriatric Depression Scale
Pre-treatment 13.28 7.53 14.37 6.16 11.45 5.41
Post-treatment 10.23 8.61 10.92 6.34 10.46 6.00
Follow-up 10.22 8.26 10.61 4.97
Geriatric Pain Measure
Pre-treatment 18.04 11.25 18.78 11.84 18.90 11.04
Post-treatment 17.26 11.17 16.42 10.96 20.36 9.39
Follow-up 17.90 11.65 14.80 9.43
Short-Form 12 - Physical Summary Score
Pre-treatment 39.47 11.60 37.36 13.58 43.48 10.72
Post-treatment 42.00 11.55 38.68 13.07 40.41 11.04
Follow-up 39.49 12.71 40.11 15.20
Short-Form 12 - Mental Summary Score
Pre-treatment 42.02 11.69 43.96 10.61 43.53 11.04
Post-treatment 46.05 9.85 47.21 6.91 44.54 11.62
Follow-up 44.70 11.11 48.67 10.32
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control
98
Measure SCBT(N=21) ECBT(iV=18) WLC(N=18)
Mean SD Mean SD Mean SD
Geriatric Depression Scale
Pre-treatment 13.28 7.53 14.37 6.16 11.45 5.41
Post-treatment 10.23 8.61 10.92 6.34 10.46 6.00
Follow-up 10.22 8.26 10.61 4.97
Geriatric Pain Measure
Pre-treatment 18.04 11.25 18.78 11.84 18.90 11.04
Post-treatment 17.26 11.17 16.42 10.96 20.36 9.39
Follow-up 17.90 11.65 14.80 9.43
Short-Form 12 - Physical Summary Score
Pre-treatment 39.47 11.60 37.36 13.58 43.48 10.72
Post-treatment 42.00 11.55 38.68 13.07 40.41 11.04
Follow-up 39.49 12.71 40.11 15.20
Short-Form 12 - Mental Summary Score
Pre-treatment 42.02 11.69 43.96 10.61 43.53 11.04
Post-treatment 46.05 9.85 47.21 6.91 44.54 11.62
Follow-up 44.70 11.11 48.67 10.32
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control
98
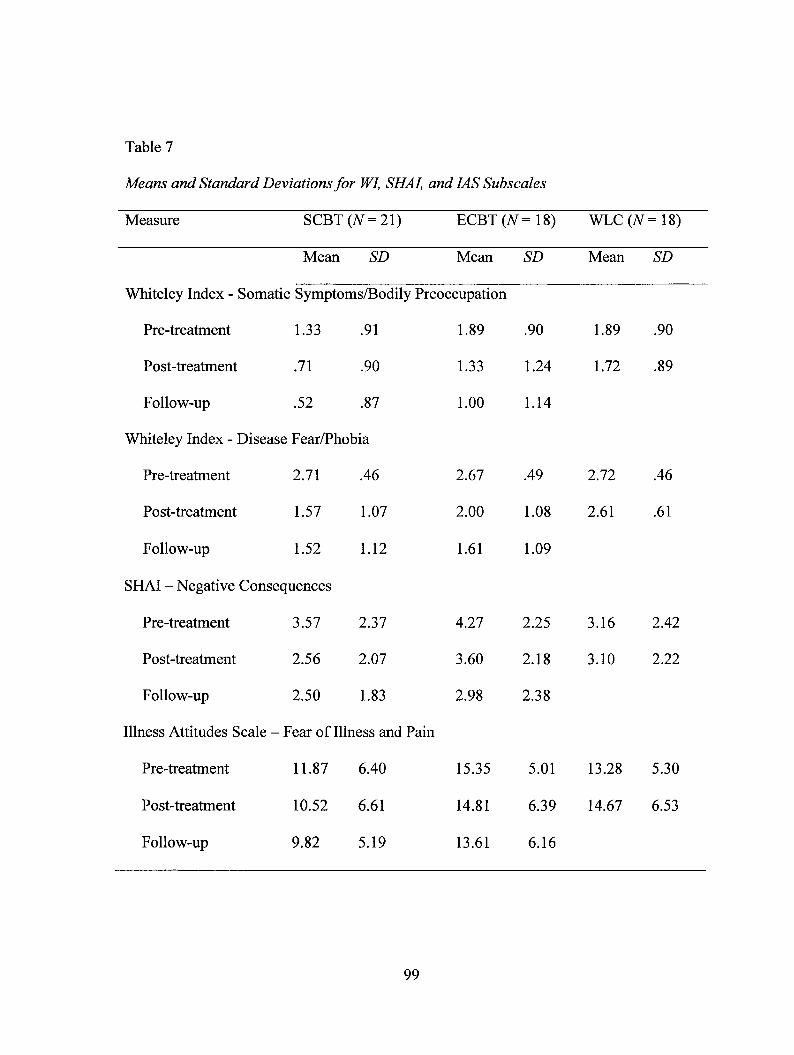
Table 7
Means and Standard Deviations for WI, SHAI, and IAS Subscales
Measure SCBT (N = 21) ECBT (N = 18) WLC (N = 18)
Mean SD Mean SD Mean SD
Whiteley Index - Somatic Symptoms/Bodily Preoccupation
Pre-treatment 1.33 .91 1.89 .90 1.89 .90
Post-treatment .71 .90 1.33 1.24 1.72 .89
Follow-up .52 .87 1.00 1.14
Whiteley Index - Disease Fear/Phobia
Pre-treatment 2.71 .46 2.67 .49 2.72 .46
Post-treatment 1.57 1.07 2.00 1.08 2.61 .61
Follow-up 1.52 1.12 1.61 1.09
SHAI - Negative Consequences
Pre-treatment 3.57 2.37 4.27 2.25 3.16 2.42
Post-treatment 2.56 2.07 3.60 2.18 3.10 2.22
Follow-up 2.50 1.83 2.98 2.38
Illness Attitudes Scale - Fear of Illness and Pain
Pre-treatment 11.87 6.40 15.35 5.01 13.28 5.30
Post-treatment 10.52 6.61 14.81 6.39 14.67 6.53
Follow-up 9.82 5.19 13.61 6.16
99
Table 7
Means and Standard Deviations for WI, SHAI, and IAS Subscales
Measure SCBT(7V=21) ECBT (N = 18) WLC (N = 18)
Mean SD Mean SD
Whiteley Index - Somatic Symptoms/Bodily Preoccupation
Pre-treatment 1.33 .91 1.89 .90
Post-treatment .71 .90
Follow-up .52 .87
Whiteley Index - Disease Fear/Phobia
Pre-treatment 2.71 .46
Post-treatment 1.57 1.07
Follow-up 1.52 1.12
SHAI - Negative Consequences
Pre-treatment 3.57 2.37
Post-treatment 2.56 2.07
Pre-treatment
Post-treatment
11.87 6.40
10.52 6.61
1.33
1.00
2.67
2.00
1.61
4.27
3.60
Follow-up 2.50 1.83 2.98
Illness Attitudes Scale - Fear of Illness and Pain
15.35
14.81
1.24
1.14
.49
1.08
1.09
2.25
2.18
2.38
Mean SD
1.89
1.72
2.72
2.61
3.16
3.10
.90
.89
.46
.61
2.42
2.22
5.01 13.28 5.30
6.39 14.67 6.53
Follow-up 9.82 5.19 13.61 6.16
99

Measure SCBT (N = 21) ECBT (N = 18) WLC (N = 18)
Illness Attitudes Scale
Mean SD Mean SD Mean SD
- Symptom Effects
Pre-treatment 6.24 3.16 6.89 3.25 6.97 1.93
Post-treatment 4.90 3.19 6.83 3.24 6.53 2.92
Follow-up 4.72 2.82 6.00 3.12
Illness Attitudes Scale - Disease Conviction
Pre-treatment 4.12 3.08 5.95 3.20 5.00 2.43
Post-treatment 3.02 3.12 4.77 3.06 4.61 2.45
Follow-up 3.04 2.57 3.91 2.84
Illness Attitudes Scale - Treatment Experience
Pre-treatment 8.77 2.97 9.85 2.03 9.06 2.75
Post-treatment 8.76 2.64 9.28 3.02 8.17 2.06
Follow-up 8.52 2.87 8.66 2.44
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control
100
Measure SCBT(iV=21) ECBT (TV =18) WLC (TV =18)
Mean SD Mean SD Mean SD
Illness Attitudes Scale - Symptom Effects
Pre-treatment 6.24 3.16 6.89 3.25 6.97 1.93
Post-treatment 4.90 3.19 6.83 3.24 6.53 2.92
Follow-up 4.72 2.82 6.00 3.12
Illness Attitudes Scale - Disease Conviction
Pre-treatment 4.12 3.08 5.95 3.20 5.00 2.43
Post-treatment 3.02 3.12 4.77 3.06 4.61 2.45
Follow-up 3.04 2.57 3.91 2.84
Illness Attitudes Scale - Treatment Experience
Pre-treatment 8.77 2.97 9.85 2.03 9.06 2.75
Post-treatment 8.76 2.64 9.28 3.02 8.17 2.06
Follow-up 8.52 2.87 8.66 2.44
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control
100

Table 8
Means and Standard Deviations for WAI and NML-2 Subscales
Measure SCBT (N = 20) ECBT (N = 18)
Mean SD Mean SD
Working Alliance Inventory - Tasks
Session 1 72.20 9.40 71.22 7.35
Session 3 72.20 8.08 71.56 10.09
Session 6 75.00 8.57 72.17 10.77
Working Alliance Inventory - Bond
Session 1 76.09 6.97 74.36 7.30
Session 3 75.45 6.64 75.07 7.17
Session 6 75.75 7.83 72.71 3.32
Working Alliance Inventory - Goal
Session 1 71.91 9.62 71.94 7.45
Session 3 72.83 9.14 71.81 9.71
Session 6 75.55 9.37 71.38 10.76
Nijmegen Motivation List-2 - Preparedness
Session 1 46.95 6.55 48.17 5.66
Session 3 48.42 6.09 45.48 8.92
Session 6 48.68 5.01 46.05 8.62
101
Table 8
Means and Standard Deviations for WAI and NML-2 Subscales
Measure SCBT(N=20) ECBT (#=18)
Mean
Working Alliance Inventory - Tasks
Session 1
Session 3
Session 6
Working Alliance Inventory - Bond
Session 1 76.09
Session 3
Session 6
75.45
75.75
Working Alliance Inventory - Goal
Session 1 71.91
Session 3
Session 6
72.83
75.55
SD
6.97
6.64
7.83
9.62
9.14
9.37
Nijmegen Motivation List-2 - Preparedness
Session 1 46.95 6.55
Session 3
Session 6
48.42
48.68
6.09
5.01
Mean
74.36
75.07
72.71
SD
- Tasks
72.20
72.20
75.00
9.40
8.08
8.57
71.22
71.56
72.17
7.35
10.09
10.77
7.30
7.17
3.32
71.94
71.81
71.38
7.45
9.71
10.76
48.17
45.48
46.05
5.66
8.92
8.62
101

Measure SCBT (N = 20) ECBT (N = 18)
Mean SD Mean SD
Nijmegen Motivation List-2 — Distress
Session 1 13.68 4.96 15.22 5.36
Session 3 13.16 4.96 14.61 4.34
Session 6 12.21 4.36 13.44 5.41
Nijmegen Motivation List-2 — Doubt
Session 1 14.08 5.35 14.39 4.96
Session 3 13.87 5.28 13.75 4.40
Session 6 12.35 4.89 13.86 5.78
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy
102
Measure SCBT (N = 20) ECBT (#=18)
Mean SD Mean SD
Nijmegen Motivation List-2 - Distress
Session 1 13.68 4.96 15.22 5.36
Session 3 13.16 4.96 14.61 4.34
Session 6 12.21 4.36 13.44 5.41
Nijmegen Motivation List-2 - Doubt
Session 1 14.08 5.35 14.39 4.96
Session 3 13.87 5.28 13.75 4.40
Session 6 12.35 4.89 13.86 5.78
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy
102

Table 9
Correlations Between Measures at Pre-Treatment
WI SHAI IAS SSI SSAS HCQ ASI STAI-S STAI-T GDS GPM MCS PCS
WI -- .39** .50*** .03 -.07 .17 .11 .09 .12 .13 -.03 .05 -.24
SHAI .78*** .32* .14 .61*** .53*** .26 .23 .18 .15 -.19 .04
IAS .31* .33* .56*** .65*** .38** .41** .39** .07 -.13 -.16
SSI ---- .55*** .46*** .33* .12 .20 .20 .63*** -.46*** -.09
SSAS .21 .35** .23 .29* .22 .33* -.21 -.17
HCQ .52*** .24 .13 .08 .17 -.25 .07
ASI .49*** .37** .34* .08 -.08 -.09
STAI-S .71*** .53*** .01 .08 -.44**
STAI-T .81*** .19 -.06 -.69***
GDS .28* -.17 -.69***
GPM -.74*** -.10
MCS -.21
103
Table 9
Correlations Between Measures at Pre-Treatment
WI SHAI IAS SSI SSAS HCQ ASI STAI-S STAI-T GDS GPM MCS PCS
WI -- .39** .50*** .03 -.07 .17 .11 .09 .12 .13 -.03 .05 -.24
SHAI — .78*** .32* .14 .61*** .53*** .26 .23 .18 .15 -.19 .04
IAS — .31* .33* .56*** .65*** .38** .41** .39** .07 -.13 -.16
SSI — .55*** .46*** .33* .12 .20 .20 .63*** -.46*** -.09
SSAS — .21 .35** .23 .29* .22 .33* -.21 -.17
HCQ — .52*** .24 .13 .08 .17 -.25 .07
ASI — .49*** .37** .34* .08 -.08 -.09
STAI-S — .71*** .53*** .01 .08 -.44**
STAI-T — .81*** .19 -.06 -.69***
GDS -— .28* -.17 ..69***
GPM -— -.74*** _ 1 0
MCS -— -.21
103

Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; WI = Whiteley Index; SHAI = Short Health Anxiety Inventory; IAS = Illness Attitudes Scale; SSI = Somatic
Symptoms Inventory; SSAS = Somatosensory Amplification Scale; HCQ = Health Cognitions Questionnaire; ASI = Anxiety
Sensitivity Index; STAI-S = State Trait Anxiety Inventory — State Scale; STAI-T = State Trait Anxiety Inventory — Trait Scale;
GDS = Geriatric Depression Scale; GPM = Geriatric Pain Measure; PCS = Short-Form — 12 — Physical Summary Score; and
MCS = Short-Form — 12 — Mental Summary Score; * p < .05, ** p < .01, *** p < .001
104
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; WI = Whiteley Index; SHAI = Short Health Anxiety Inventory; IAS = Illness Attitudes Scale; SSI = Somatic
Symptoms Inventory; SSAS = Somatosensory Amplification Scale; HCQ = Health Cognitions Questionnaire; ASI = Anxiety
Sensitivity Index; STAI-S = State Trait Anxiety Inventory - State Scale; STAI-T = State Trait Anxiety Inventory - Trait Scale;
GDS = Geriatric Depression Scale; GPM = Geriatric Pain Measure; PCS = Short-Form - 12 - Physical Summary Score; and
MCS = Short-Form - 12 - Mental Summary Score; * p < .05, ** p < .01, *** p < .001
104
likely to have increased health anxiety on the SHAI and IAS. The SHAI correlated
strongly with the IAS, HCQ, and ASI, and correlated moderately with the SSI, suggesting
those participants with elevated levels of health anxiety on the SHAI were more likely to
have increased health anxiety on the IAS, frequent hypochondriacal thoughts and
hypochondriacal somatic symptoms, and also experience bodily sensations as being
distressing. The IAS correlated strongly with the HCQ and ASI, and correlated
moderately with the SSI, SSAS, STAI-S, STAI-T, and GDS, suggesting that those
participants with elevated health anxiety on the IAS were more likely to have increased
hypochondriacal somatic symptoms, state and trait anxiety symptoms, and depressive
symptoms.
3.1.2 Testing Hypothesis 1
In order to test Hypothesis 1, 3 (treatment: SCBT, ECBT, WLC) x 2 (time: pre-
treatment and post-treatment) mixed factor ANCOVAs were conducted on each of these
DVs including the WI, SHAI, IAS, SSAS, SSI, and HCQ, with the pre-treatment value of
the measure of interest in the analysis set as the covariate. The independent variables
included one between groups variable, time, with two levels (pre-treatment and post-
treatment) and one within subject variable, group, with three levels (SCBT, ECBT, and
WLC).
The results from the mixed factor ANCOVAs assessing change in each primary
outcome measure, across all three groups from pre-treatment to post-treatment are shown
in Table 10. (Note: Treatment main effects are not reported in the table as the treatment
main effects are not of interest and do not provide relevant information; Huck &
105
likely to have increased health anxiety on the SHAI and IAS. The SHAI correlated
strongly with the IAS, HCQ, and ASI, and correlated moderately with the SSI, suggesting
those participants with elevated levels of health anxiety on the SHAI were more likely to
have increased health anxiety on the IAS, frequent hypochondriacal thoughts and
hypochondriacal somatic symptoms, and also experience bodily sensations as being
distressing. The IAS correlated strongly with the HCQ and ASI, and correlated
moderately with the SSI, SSAS, STAI-S, STAI-T, and GDS, suggesting that those
participants with elevated health anxiety on the IAS were more likely to have increased
hypochondriacal somatic symptoms, state and trait anxiety symptoms, and depressive
symptoms.
3.1.2 Testing Hypothesis 1
In order to test Hypothesis 1, 3 (treatment: SCBT, ECBT, WLC) x 2 (time: pre-
treatment and post-treatment) mixed factor ANCOVAs were conducted on each of these
DVs including the WI, SHAI, IAS, SSAS, SSI, and HCQ, with the pre-treatment value of
the measure of interest in the analysis set as the covariate. The independent variables
included one between groups variable, time, with two levels (pre-treatment and post-
treatment) and one within subject variable, group, with three levels (SCBT, ECBT, and
WLC).
The results from the mixed factor ANCOVAs assessing change in each primary
outcome measure, across all three groups from pre-treatment to post-treatment are shown
in Table 10. (Note: Treatment main effects are not reported in the table as the treatment
main effects are not of interest and do not provide relevant information; Huck &
105

Table 10
Mixed-Factor 3 (Treatment) x 2 (Time) ANCOVAs for Primary Outcome Measures
Measure Time Time x Covariate Time x Treatment
F p 112 F P ri2 F p i2
WI .305 .58 .006 .13 .73 .002 7.43 .001** .22
SHAI 1.97 .17 .04 7.36 .009** .12 2.97 .06 .10
IAS 4.26 .04* .07 6.82 .01* .11 2.31 .11 .08
SSI 1.50 .23 .03 3.27 .08 .06 1.26 .29 .05
SSAS 10.87 .002** .17 13.01 .001*** .20 .05 .95 .002
HCQ 6.52 .01* .11 10.62 .002** .17 1.06 .36 .04
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control; WI = Whiteley Index; SHAI = Short
Health Anxiety Inventory; IAS = Illness Attitudes Scale; SSI = Somatic Symptom
Inventory; SSAS = Somatosensory Amplification Scale; HCQ - Health Cognitions
Questionnaire; * p < .05, ** p < .01, *** p < .001
106
Table 10
Mixed-Factor 3 (Treatment) x 2 (Time) ANCOVAs for Primary Outcome Measures
Measure Time Time x Covariate Time x Treatment
WI
SHAI
IAS
SSI
SSAS
HCQ
F
.305
1.97
4.26
1.50
10.87
6.52
P
.58
.17
.04*
.23
.002**
.01*
r,2
.006
.04
.07
.03
.17
.11
F
.13
7.36
6.82
3.27
13.01
10.62
P
.73
.009**
.01*
.08
.001***
.002**
r,2
.002
.12
.11
.06
.20
.17
F
7.43
2.97
2.31
1.26
.05
1.06
P
.001**
.06
.11
.29
.95
.36
r,2
.22
.10
.08
.05
.002
.04
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control; WI = Whiteley Index; SHAI = Short
Health Anxiety Inventory; IAS = Illness Attitudes Scale; SSI = Somatic Symptom
Inventory; SSAS = Somatosensory Amplification Scale; HCQ = Health Cognitions
Questionnaire; * p < .05, **p<. 01, ***/?<. 001
106
MacLean, 1975). These analyses revealed main effects for time on the IAS (p = .04),
SSAS (p = .002), and HCQ (p = .01). In addition, the covariate (i.e., the pre-treatment
value of the measure of interest in the analysis) was significantly related to outcome at
post-treatment on the SHAI (p = .009), IAS (p = .01), SSAS (p = .001), and HCQ (p =
.002). Of particular interest were the interactions between group and time, after
controlling for the variability in pre-treatment scores. In this case, a statistically
significant time x treatment group interaction was found on the WI (p = .001). Figure 4
depicts the significant findings of the 3 x 2 analyses.
To examine the interaction further, 2 (treatment: SCBT and ECBT or WLC) x 2
(time: pre-treatment and post-treatment) repeated measures ANCOVAs were conducted
to determine specifically how treatment conditions influenced the DVs over time. More
specifically, the SCBT condition was compared to the WLC condition, the ECBT
condition was compared to the WLC condition, and the SCBT and ECBT conditions
were compared to each other. The pre-treatment value of the measure of interest in each
analysis was set as the covariate. Table 11 shows the results of the 2 x 2 analyses (Note:
Treatment main effects are not reported in the table as the treatment main effects are not
of interest and do not provide relevant information; Huck & MacLean, 1975). After
controlling for the effect of the pre-treatment score on the measure of interest, from pre-
treatment and post-treatment, individuals in the SCBT group evidenced greater
improvements than did individuals in the WLC group on the WI (p = .0001). From pre-
treatment to post-treatment, individuals in the ECBT group also evidenced greater
107
MacLean, 1975). These analyses revealed main effects for time on the IAS (p = .04),
SSAS (p = .002), and HCQ (p = .01). In addition, the covariate (i.e., the pre-treatment
value of the measure of interest in the analysis) was significantly related to outcome at
post-treatment on the SHAI (p = .009), IAS (p = .01), SSAS (p = .001), and HCQ (p =
.002). Of particular interest were the interactions between group and time, after
controlling for the variability in pre-treatment scores. In this case, a statistically
significant time x treatment group interaction was found on the WI (p = .001). Figure 4
depicts the significant findings of the 3 x 2 analyses.
To examine the interaction further, 2 (treatment: SCBT and ECBT or WLC) x 2
(time: pre-treatment and post-treatment) repeated measures ANCOVAs were conducted
to determine specifically how treatment conditions influenced the DVs over time. More
specifically, the SCBT condition was compared to the WLC condition, the ECBT
condition was compared to the WLC condition, and the SCBT and ECBT conditions
were compared to each other. The pre-treatment value of the measure of interest in each
analysis was set as the covariate. Table 11 shows the results of the 2 x 2 analyses (Note:
Treatment main effects are not reported in the table as the treatment main effects are not
of interest and do not provide relevant information; Huck & MacLean, 1975). After
controlling for the effect of the pre-treatment score on the measure of interest, from pre-
treatment and post-treatment, individuals in the SCBT group evidenced greater
improvements than did individuals in the WLC group on the WI (p = .0001). From pre-
treatment to post-treatment, individuals in the ECBT group also evidenced greater
107

10
9
8
7
6
5
4
3
2
1
0
Pre Post
- • —'SCBT
ECBT
—A—WLC
Figure 4. Mean WI scores by treatment condition at pre-treatment and post-treatment.
(Treatment Conditions: SCBT = Standard Cognitive Behavioural Therapy; ECBT =
Enhanced Cognitive Behavioural Therapy; WLC = Wait-List Control). Original in
Colour.
108
3 -2 -1 -0 -J
Pre Post
Figure 4. Mean WI scores by treatment condition at pre-treatment and post-treatment.
(Treatment Conditions: SCBT = Standard Cognitive Behavioural Therapy; ECBT =
Enhanced Cognitive Behavioural Therapy; WLC = Wait-List Control). Original in
Colour.
108

Table 11
Comparisons from Pre- to Post-Treatment for Primary Dependent Variables
Measure Treatment Time Time x Covariate Time x Treatment
F p 112 F p Ti2 F p 112
WI SCBT vs ECBT 2.48 .12 .07 .42 .52 .01 .42 .52 .01
SCBT vs WLC 1.58 .22 .04 4.01 .051 .10 17.59 .0001*** .33
ECBT vs WLC .85 .36 .03 .13 .72 .004 9.63 .004** .23
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; WI = Whiteley Index; * p < .01, ** p < .001
109
Table 11
Comparisons from Pre- to Post-Treatment for Primary Dependent Variables
Measure Treatment Time Time x Covariate Time x Treatment
F p r|2 F p r|2 F p rj2
WI SCBT vs ECBT 2.48 A2 !(J7 4̂2 5̂2 M A2 S2. M
SCBT vs WLC 1.58 .22 .04 4.01 .051 .10 17.59 .0001*** .33
ECBT vs WLC .85 .36 .03 .13 .72 .004 9.63 .004** .23
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; WI = Whiteley Index; * p < .01, ** p < .001
109

improvements than did individuals in the WLC group on the WI (p = .004). There was
no difference between the SCBT and ECBT groups.
3.1.2.1 Subscale comparisons
Because the WI, SHAT, and IAS have subscales, secondary analyses focusing on
the two WI subscales (i.e., Somatic Symptoms/Bodily Preoccupation; Disease
Fear/Phobia), one SHAI subscale (i.e., Negative Consequences), and four IAS subscales
(i.e., Fear of Illness and Pain, Symptom Effects, Treatment Experience, Disease
Conviction) were conducted in order to determine if the constructs measured by the
specific subscales were differentially affected by treatment condition over time. Seven 3
(treatment) x 2 (time) repeated measures ANCOVAs were conducted utilizing the above-
listed subscales as the DVs. The pre-treatment value of the measure of interest in each
analysis was set as the covariate. (Note: Treatment main effects are not reported in the
table as the treatment main effects are not of interest and do not provide relevant
information; Huck & MacLean, 1975).
The results indicated main effects for time on IAS-Disease Conviction (p = .01.
In addition, the covariate (i.e., the pre-treatment value of the measure of interest in the
analysis) was significantly related to outcome at post-treatment on the WI-Somatic
Symptoms/Bodily Preoccupation (p = .001), SHAI-Negative Consequences (p = .003),
and IAS-Fear of Illness and Pain (p = .04). Of relevance, there were time by treatment
interactions on WI-Disease Fear/Phobia (p = .002), after controlling for the effect of the
pre-treatment score on the measure of interest. See Table 12 for the results.
110
improvements than did individuals in the WLC group on the WI (p = .004). There was
no difference between the SCBT and ECBT groups.
3.1.2.1 Subscale comparisons
Because the WI, SHAI, and IAS have subscales, secondary analyses focusing on
the two WI subscales (i.e., Somatic Symptoms/Bodily Preoccupation; Disease
Fear/Phobia), one SHAI subscale (i.e., Negative Consequences), and four IAS subscales
(i.e., Fear of Illness and Pain, Symptom Effects, Treatment Experience, Disease
Conviction) were conducted in order to determine if the constructs measured by the
specific subscales were differentially affected by treatment condition over time. Seven 3
(treatment) x 2 (time) repeated measures ANCOVAs were conducted utilizing the above-
listed subscales as the DVs. The pre-treatment value of the measure of interest in each
analysis was set as the covariate. (Note: Treatment main effects are not reported in the
table as the treatment main effects are not of interest and do not provide relevant
information; Huck & MacLean, 1975).
The results indicated main effects for time on IAS-Disease Conviction (p = .01.
In addition, the covariate (i.e., the pre-treatment value of the measure of interest in the
analysis) was significantly related to outcome at post-treatment on the Wl-Somatic
Symptoms/Bodily Preoccupation (p = .001), SHAI-Negative Consequences (p = .003),
and LAS-Fear of Illness and Pain (p = .04). Of relevance, there were time by treatment
interactions on WI-Disease Fear/Phobia (p = .002), after controlling for the effect of the
pre-treatment score on the measure of interest. See Table 12 for the results.
110

Table 12
Mixed-Factor 3 (Treatment) x 2 (Time) ANCOVAs for WI, SHAI, and IAS Subscales
Measure Time Time x Covariate Time x Treatment
112
WI - SS 1.95 .17 .04 12.19 .001** .19 2.83 .07 .10
WI - DF .66 .42 .01 .02 .89 .0001 7.14 .002** .21
SHAI - NC 1.66 .20 .03 9.96 .003** .16 2.23 .12 .08
IAS - Fear 3.38 .07 .06 4.36 .04* .08 1.83 .17 .07
IAS - Eff .21 .65 .004 2.23 .14 .04 2.61 .08 .09
IAS - Exp 2.68 .11 .05 12.65 .001 .38 .99 .38 .04
IAS - Con 6.83 .01* .11 10.55 .002 .17 .85 .43 .03
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; WI - SS = Whiteley Index - Somatic Symptoms/Bodily Preoccupation; WI - DF = Whiteley Index - Disease
Fear/Phobia; SHAI - NC = Short Health Anxiety Inventory - Negative Consequences; IAS - Fear = Illness Attitudes Scale -
111
Table 12
Mixed-Factor 3 (Treatment) x 2 (Time) ANCOVAs for WI, SHAI, and IAS Subscales
Measure Time Time x Covariate Time x Treatment
WI-SS
WI-DF
SHAI - NC
IAS - Fear
IAS - Eff
IAS - Exp
IAS - Con
F
1.95
.66
1.66
3.38
.21
2.68
6.83
P
.17
.42
.20
.07
.65
.11
.01*
r,2
.04
.01
.03
.06
.004
.05
.11
F
12.19
.02
9.96
4.36
2.23
12.65
10.55
P
.001**
.89
.003**
.04*
.14
.001
.002
r,2
.19
.0001
.16
.08
.04
.38
.17
F
2.83
7.14
2.23
1.83
2.61
.99
.85
P
.07
.002**
.12
.17
.08
.38
.43
r,2
.10
.21
.08
.07
.09
.04
.03
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; WI - SS = Whiteley Index - Somatic Symptoms/Bodily Preoccupation; WI - DF = Whiteley Index - Disease
Fear/Phobia; SHAI - NC = Short Health Anxiety Inventory — Negative Consequences; IAS - Fear = Illness Attitudes Scale -
111

Fear of Illness and Pain; IAS — Eff = Illness Attitudes Scale — Symptom Effects; IAS — Exp = Illness Attitudes Scale —
Treatment Experience; IAS — Con = Illness Attitudes Scale — Disease Conviction; * p < .05, ** p < .01, *** p < .001
112
Fear of Illness and Pain; IAS - Eff = Illness Attitudes Scale - Symptom Effects; IAS - Exp = Illness Attitudes Scale -
Treatment Experience; IAS - Con = Illness Attitudes Scale - Disease Conviction; * p < .05, ** p < .01, *** p < .001
112
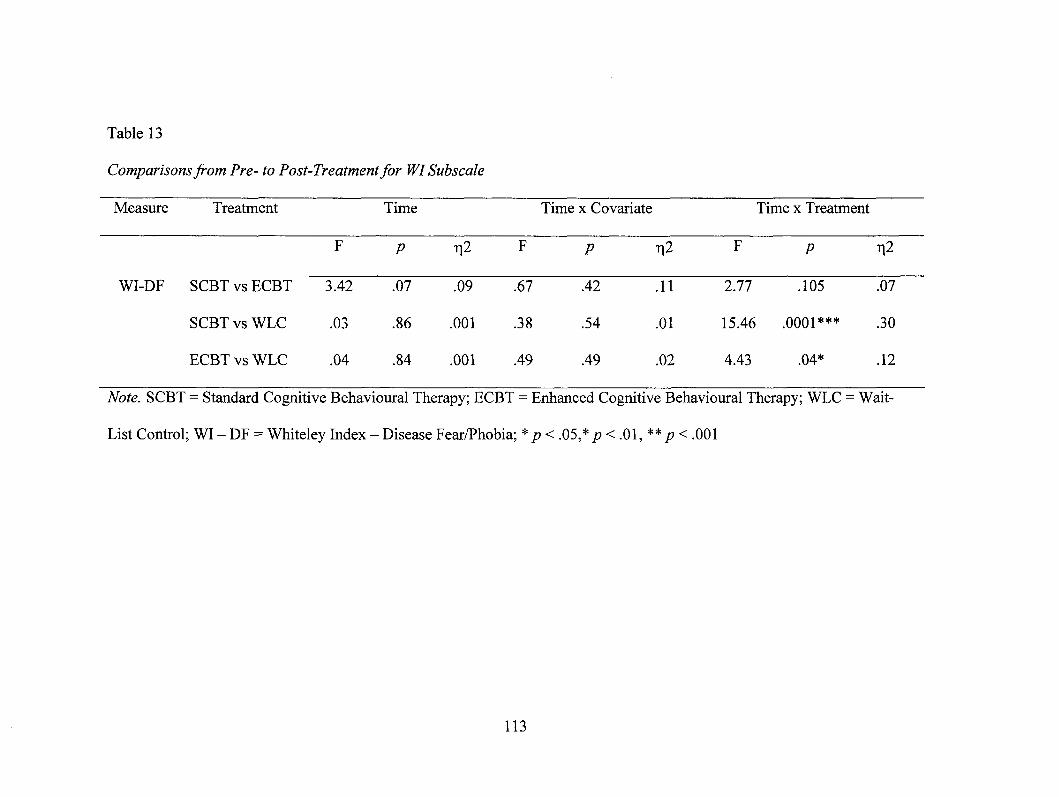
Table 13
Comparisons from Pre- to Post-Treatment for WI Subscale
Measure Treatment Time Time x Covariate Time x Treatment
F p n2 F p t12 F p 112
WI-DF SCBT vs ECBT 3.42 .07 .09 .67 .42 .11 2.77 .105 .07
SCBT vs WLC .03 .86 .001 .38 .54 .01 15.46 .0001*** .30
ECBT vs WLC .04 .84 .001 .49 .49 .02 4.43 .04* .12
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; WI — DF = Whiteley Index — Disease Fear/Phobia; * p < .05,* p < .01, ** p < .001
113
Table 13
Comparisons from Pre- to Post-Treatment for WI Subscale
Measure Treatment Time Time x Covariate Time x Treatment
F p r|2 F p r|2 F P ^2
WI-DF SCBT vs ECBT 3.42 0̂7 !(J9 67 4̂2 H 2/77 T05 !07
SCBT vs WLC .03 .86 .001 .38 .54 .01 15.46 .0001*** .30
ECBT vs WLC .04 .84 .001 .49 .49 .02 4.43 .04* .12
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; WI - DF = Whiteley Index - Disease Fear/Phobia; * p < .05,* p < .01, ** p < .001
113
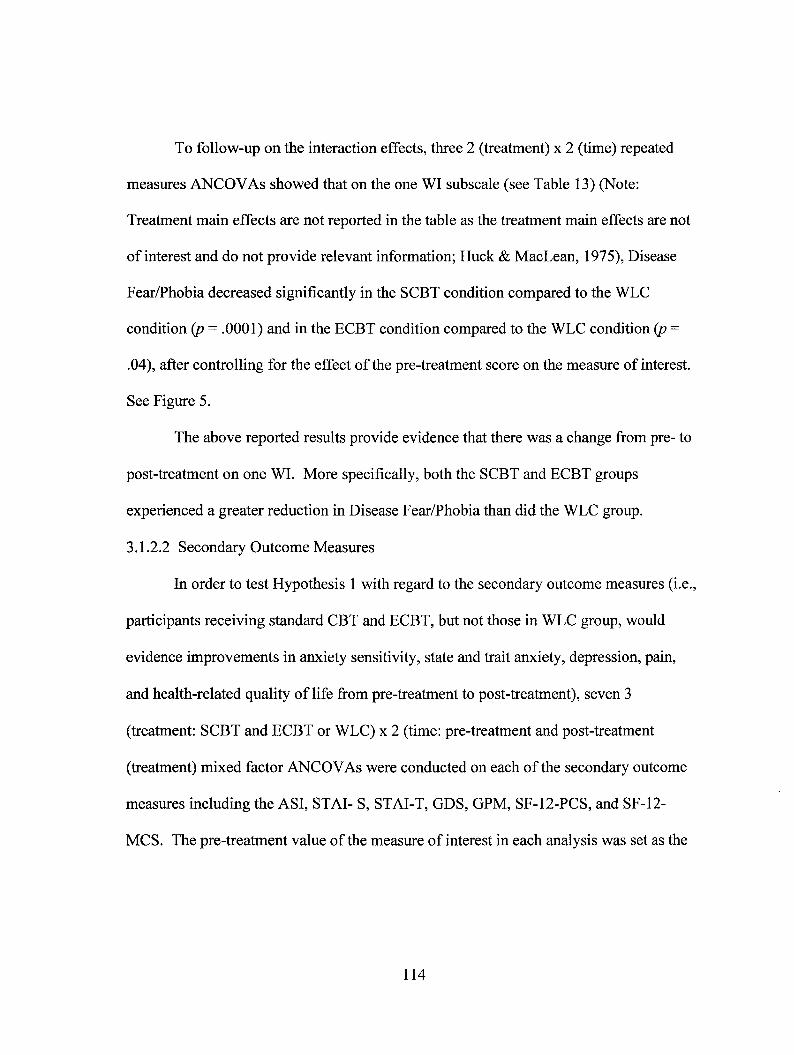
To follow-up on the interaction effects, three 2 (treatment) x 2 (time) repeated
measures ANCOVAs showed that on the one WI subscale (see Table 13) (Note:
Treatment main effects are not reported in the table as the treatment main effects are not
of interest and do not provide relevant information; Huck & MacLean, 1975), Disease
Fear/Phobia decreased significantly in the SCBT condition compared to the WLC
condition (p = .0001) and in the ECBT condition compared to the WLC condition (p =
.04), after controlling for the effect of the pre-treatment score on the measure of interest.
See Figure 5.
The above reported results provide evidence that there was a change from pre- to
post-treatment on one WI. More specifically, both the SCBT and ECBT groups
experienced a greater reduction in Disease Fear/Phobia than did the WLC group.
3.1.2.2 Secondary Outcome Measures
In order to test Hypothesis 1 with regard to the secondary outcome measures (i.e.,
participants receiving standard CBT and ECBT, but not those in WLC group, would
evidence improvements in anxiety sensitivity, state and trait anxiety, depression, pain,
and health-related quality of life from pre-treatment to post-treatment), seven 3
(treatment: SCBT and ECBT or WLC) x 2 (time: pre-treatment and post-treatment
(treatment) mixed factor ANCOVAs were conducted on each of the secondary outcome
measures including the ASI, STAI- S, STAI-T, GDS, GPM, SF-12-PCS, and SF-12-
MCS. The pre-treatment value of the measure of interest in each analysis was set as the
114
To follow-up on the interaction effects, three 2 (treatment) x 2 (time) repeated
measures ANCOVAs showed that on the one WI subscale (see Table 13) (Note:
Treatment main effects are not reported in the table as the treatment main effects are not
of interest and do not provide relevant information; Huck & MacLean, 1975), Disease
Fear/Phobia decreased significantly in the SCBT condition compared to the WLC
condition (p = .0001) and in the ECBT condition compared to the WLC condition (p =
.04), after controlling for the effect of the pre-treatment score on the measure of interest.
See Figure 5.
The above reported results provide evidence that there was a change from pre- to
post-treatment on one WI. More specifically, both the SCBT and ECBT groups
experienced a greater reduction in Disease Fear/Phobia than did the WLC group.
3.1.2.2 Secondary Outcome Measures
In order to test Hypothesis 1 with regard to the secondary outcome measures (i.e.,
participants receiving standard CBT and ECBT, but not those in WLC group, would
evidence improvements in anxiety sensitivity, state and trait anxiety, depression, pain,
and health-related quality of life from pre-treatment to post-treatment), seven 3
(treatment: SCBT and ECBT or WLC) x 2 (time: pre-treatment and post-treatment
(treatment) mixed factor ANCOVAs were conducted on each of the secondary outcome
measures including the ASI, STAI- S, STAI-T, GDS, GPM, SF-12-PCS, and SF-12-
MCS. The pre-treatment value of the measure of interest in each analysis was set as the
114
3
2.5
2
1.5
1
0.5
0
P re Post
—•— SCBT
—II— ECBT
—fr- W LC
Figure 5. Mean WI — Disease Fear/Phobia scores by treatment condition at pre-treatment
and post-treatment. (SCBT = Standard Cognitive Behavioural Therapy; ECBT =
Enhanced Cognitive Behavioural Therapy; WLC = Wait-List Control). Original in
Colour.
115
2.5
2
1.5
l H
0.5
0
Pre Post
Figure 5. Mean WI - Disease Fear/Phobia scores by treatment condition at pre-treatment
and post-treatment. (SCBT = Standard Cognitive Behavioural Therapy; ECBT =
Enhanced Cognitive Behavioural Therapy; WLC = Wait-List Control). Original in
Colour.
115
covariate. (Note: Treatment main effects are not reported in the table as the treatment
main effects are not of interest and do not provide relevant information; Huck &
MacLean, 1975).
The results from the mixed factor ANCOVAs assessing change in each secondary
outcome measure, across all three groups from pre-treatment to post-treatment are shown
in Table 14. There were main effects for time on the STAI-S (p = .001), STAI-T (p =
.02), GPM (p = .02), and SF-12-MCS (p = .0001). In addition, the covariate (i.e., the pre-
treatment value of the measure of interest in the analysis) was significantly related to
outcome at post-treatment on the STAI-S (p = .0001), STAI-T (p = .004), GPM (p —
.006), and SF-12-MCS (p = .0001). Of particular interest, a statistically significant time x
treatment group interaction was found on the SF-12-PCS (p = .04), after controlling for
the effect of the pre-treatment score on the measure of interest. Figure 8 depicts the
significant findings of the 3 x 2 analyses.
Two (treatment: SCBT and ECBT or WLC) x 2 (time: pre-treatment and post-
treatment) repeated measures comparisons were conducted to examine the relevant
interaction effect further. Table 15 shows the results of the 2 x 2 analyses (Note:
Treatment main effects are not reported in the table as the treatment main effects are not
of interest and do not provide relevant information; Huck & MacLean, 1975). From pre-
treatment to post-treatment, individuals in the SCBT group evidenced greater
improvements than did individuals in the WLC group on the SF-12-PCS (p = .002),
indicating an improvement in self-rated physical health.
116
covariate. (Note: Treatment main effects are not reported in the table as the treatment
main effects are not of interest and do not provide relevant information; Huck &
MacLean, 1975).
The results from the mixed factor ANCOVAs assessing change in each secondary
outcome measure, across all three groups from pre-treatment to post-treatment are shown
in Table 14. There were main effects for time on the STAI-S (p = .001), STAI-T (p =
.02), GPM (p = .02), and SF-12-MCS (p = .0001). In addition, the covariate (i.e., the pre-
treatment value of the measure of interest in the analysis) was significantly related to
outcome at post-treatment on the STAI-S (p = .0001), STAI-T (p = .004), GPM (p =
.006), and SF-12-MCS (p = .0001). Of particular interest, a statistically significant time x
treatment group interaction was found on the SF-12-PCS (p = .04), after controlling for
the effect of the pre-treatment score on the measure of interest. Figure 8 depicts the
significant findings of the 3 x 2 analyses.
Two (treatment: SCBT and ECBT or WLC) x 2 (time: pre-treatment and post-
treatment) repeated measures comparisons were conducted to examine the relevant
interaction effect further. Table 15 shows the results of the 2 x 2 analyses (Note:
Treatment main effects are not reported in the table as the treatment main effects are not
of interest and do not provide relevant information; Huck & MacLean, 1975). From pre-
treatment to post-treatment, individuals in the SCBT group evidenced greater
improvements than did individuals in the WLC group on the SF-12-PCS (p = .002),
indicating an improvement in self-rated physical health.
116

Table 14
Mixed-Factor 3 (Treatment) x 2 (Time) ANCOVAs for Secondary Outcome Measures
Measure Time Time x Covariate Time x Treatment
F P 112 F P 1-12 F p n2
ASI 3.29 .08 .06 9.54 .003 .15 1.53 .23 .05
STAI-S 13.39 .001** .20 20.80 .0001*** .28 .69 .51 .03
STAI-T 5.42 .02* .09 9.00 .004** .15 .65 .53 .02
GDS .02 .90 .0001 4.16 .05 .07 .68 .51 .03
GPM 5.65 .02* .10 8.34 .006** .14 1.07 .35 .04
SF-12-PCS 4.23 .05 .07 4.19 .05 .07 3.58 .04* .12
SF-12-MCS 24.12 .0001*** .31 17.60 .0001*** .25 1.07 .35 .04
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; ASI = Anxiety Sensitivity Index; STAI-S = State Trait Anxiety Inventory - State Scale; STAI-T = State Trait
Anxiety Inventory - Trait Scale; GDS = Geriatric Depression Scale; GPM = Geriatric Pain Measure; SF-12-PCS = Short-
Form-12 - Physical Summary Score; and MCS = Short-Form-12 - Mental Summary Score; * p < .05, ** p < .01, *** p < .001
117
Table 14
Mixed-Factor 3 (Treatment) x 2 (Time) ANCOVAs for Secondary Outcome Measures
Measure Time Time x Covariate Time x Treatment
F P ri2~ F P r^2 F p ^
ASI 3.29 ^08 M 9M M3 15 L53 23 0̂5
STAI-S 13.39 .001** .20 20.80 .0001*** .28 .69 .51 .03
STAI-T 5.42 .02* .09 9.00 .004** .15 .65 .53 .02
GDS .02 .90 .0001 4.16 .05 .07 .68 .51 .03
GPM 5.65 .02* .10 8.34 .006** .14 1.07 .35 .04
SF-12-PCS 4.23 .05 .07 4.19 .05 .07 3.58 .04* .12
SF-12-MCS 24.12 .0001*** .31 17.60 .0001*** .25 1.07 .35 .04
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; ASI = Anxiety Sensitivity Index; STAI-S = State Trait Anxiety Inventory - State Scale; STAI-T = State Trait
Anxiety Inventory - Trait Scale; GDS = Geriatric Depression Scale; GPM = Geriatric Pain Measure; SF-12-PCS = Short-
Form-12 - Physical Summary Score; and MCS = Short-Form-12 - Mental Summary Score; * p < .05, ** p < .01, *** p < .001
117

50
45 -
40
35 -
30 -
25
Pre Post
"SCBT
ECBT
—2z— WIC
Figure 6. Mean SF-12-PCS scores by treatment condition at pre-treatment and post-
treatment. (SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced
Cognitive Behavioural Therapy; WLC = Wait-List Control). Original in Colour.
118
Pre Post
Figure 6. Mean SF-12-PCS scores by treatment condition at pre-treatment and post-
treatment. (SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced
Cognitive Behavioural Therapy; WLC = Wait-List Control). Original in Colour.
118
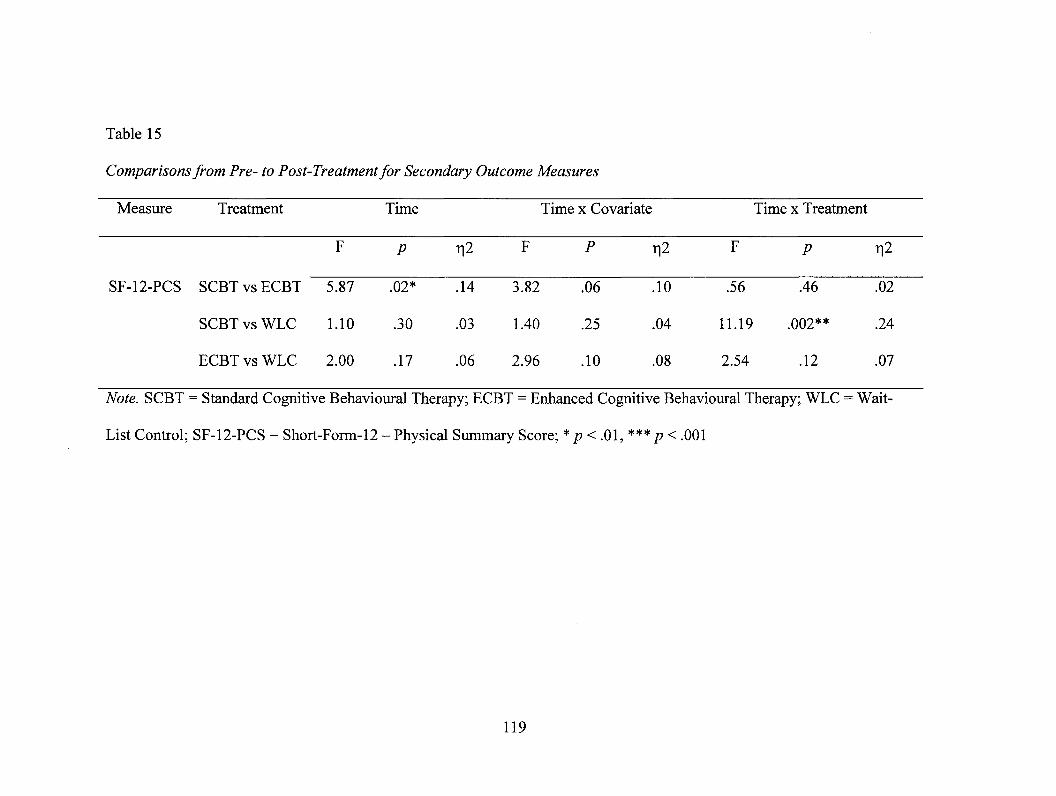
Table 15
Comparisons from Pre- to Post-Treatment for Secondary Outcome Measures
Measure Treatment Time Time x Covariate Time x Treatment
F p ri2 F P ri2 F p Ti2
SF-12-PCS SCBT vs ECBT 5.87 .02* .14 3.82 .06 .10 .56 .46 .02
SCBT vs WLC 1.10 .30 .03 1.40 .25 .04 11.19 .002** .24
ECBT vs WLC 2.00 .17 .06 2.96 .10 .08 2.54 .12 .07
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; SF-12-PCS = Short-Form-12 — Physical Summary Score; * p < .01, *** p < .001
119
Table 15
Comparisons from Pre- to Post-Treatment for Secondary Outcome Measures
Measure Treatment Time Time x Covariate Time x Treatment
F p TJ2 F P r̂ 2 F p n T
SF-12-PCS SCBT vs ECBT 5.87 1)2* T4 3l*2 M TO 16 A6 1)2
SCBT vs WLC 1.10 .30 .03 1.40 .25 .04 11.19 .002** .24
ECBT vs WLC 2.00 .17 .06 2.96 .10 .08 2.54 .12 .07
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; SF-12-PCS = Short-Form-12 - Physical Summary Score; * p < .01, *** p < .001
119

3.1.3 Testing Hypotheses 2 and 3: Stability of Improvements
In keeping with the findings of Mohlman et al. (2003), participants treated with
ECBT were predicted to demonstrate the greatest overall improvement at post-treatment
and at three-month follow-up on each of the primary outcome and secondary outcome
measures indicated in the Hypothesis 1. For participants treated with both SCBT and
ECBT, all expected improvements were hypothesized to be maintained three months
following the conclusion of treatment.
Twenty 2 (treatment) x 2 (time) repeated measures ANCOVAs were conducted to
assess change from post-treatment to follow-up in both the SCBT and ECBT conditions
(see Tables 16, 17, and 18 for results of the analyses) (Note: Treatment main effects are
not reported in the table as the treatment main effects are not of interest and do not
provide relevant information; Huck & MacLean, 1975). The post-treatment value of the
measure of interest in each analysis was set as the covariate. The analyses revealed
statistically significant main effects for time on the WI (p = .004), SHAI (p = .002), IAS
(p = .01), SSAS (p = .001), IAS-Fear Illness and Pain (p = .03), IAS-Disease Conviction
(p = .02), STAI-S (p = .005), and GDS (p = .04). Of relevance, there were statistically
significant time by treatment effects for the STAI-State (p = .02) and the SF-12-PCS (p =
.04), after controlling for the effect of the pre-treatment score on the measure of interest.
This indicated that from post-treatment to follow-up, individuals in the SCBT group
evidenced an increase in anxiety and the ECBT group evidenced a slight decline in
anxiety on the STAI-State. No other significant differences emerged.
120
3.1.3 Testing Hypotheses 2 and 3: Stability of Improvements
In keeping with the findings of Mohlman et al. (2003), participants treated with
ECBT were predicted to demonstrate the greatest overall improvement at post-treatment
and at three-month follow-up on each of the primary outcome and secondary outcome
measures indicated in the Hypothesis 1. For participants treated with both SCBT and
ECBT, all expected improvements were hypothesized to be maintained three months
following the conclusion of treatment.
Twenty 2 (treatment) x 2 (time) repeated measures ANCOVAs were conducted to
assess change from post-treatment to follow-up in both the SCBT and ECBT conditions
(see Tables 16, 17, and 18 for results of the analyses) (Note: Treatment main effects are
not reported in the table as the treatment main effects are not of interest and do not
provide relevant information; Huck & MacLean, 1975). The post-treatment value of the
measure of interest in each analysis was set as the covariate. The analyses revealed
statistically significant main effects for time on the WI (p = .004), SHAI (p = .002), IAS
(p = .01), SSAS (p = .001), IAS-Fear Illness and Pain (p = .03), LAS-Disease Conviction
(p = .02), STAI-S (p = .005), and GDS (p = .04). Of relevance, there were statistically
significant time by treatment effects for the STAI-State (p = .02) and the SF-12-PCS (p =
.04), after controlling for the effect of the pre-treatment score on the measure of interest.
This indicated that from post-treatment to follow-up, individuals in the SCBT group
evidenced an increase in anxiety and the ECBT group evidenced a slight decline in
anxiety on the STAI-State. No other significant differences emerged.
120
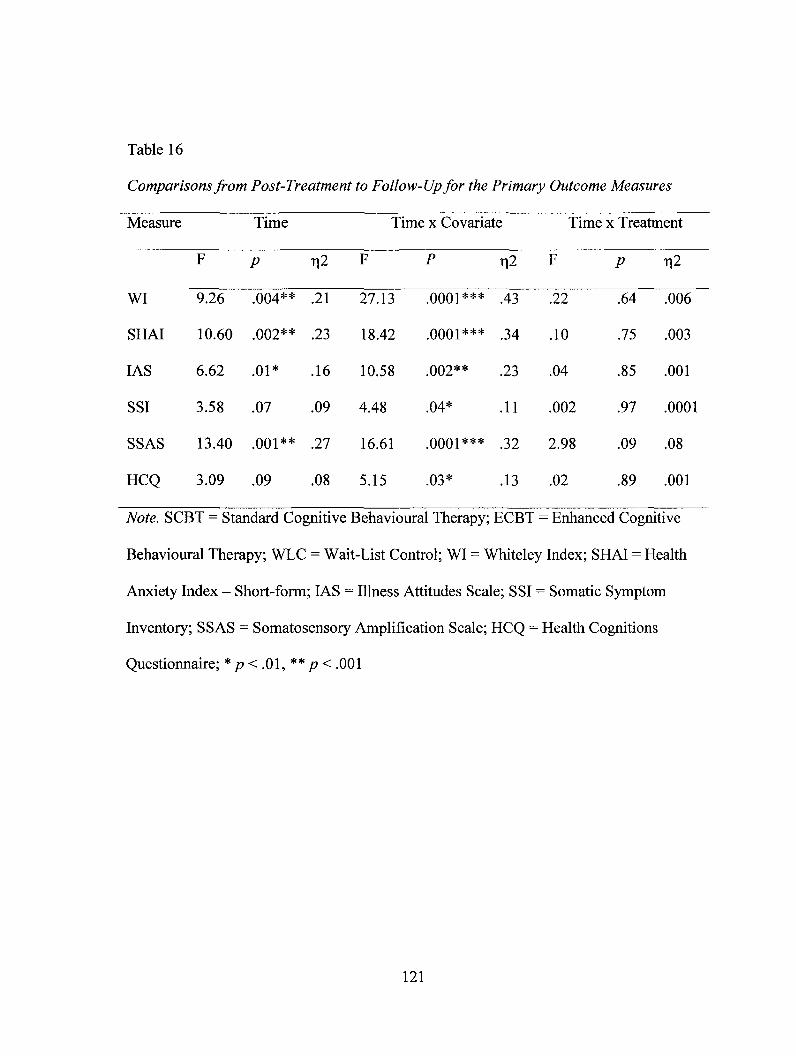
Table 16
Comparisons from Post-Treatment to Follow-Up for the Primary Outcome Measures
Measure Time Time x Covariate Time x Treatment
F p i2 F P i2 F p 112
WI 9.26 .004** .21 27.13 .0001*** .43 .22 .64 .006
SHAI 10.60 .002** .23 18.42 .0001*** .34 .10 .75 .003
IAS 6.62 .01* .16 10.58 .002** .23 .04 .85 .001
SSI 3.58 .07 .09 4.48 .04* .11 .002 .97 .0001
SSAS 13.40 .001** .27 16.61 .0001*** .32 2.98 .09 .08
HCQ 3.09 .09 .08 5.15 .03* .13 .02 .89 .001
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control; WI = Whiteley Index; SHAI = Health
Anxiety Index - Short-form; IAS = Illness Attitudes Scale; SSI = Somatic Symptom
Inventory; SSAS = Somatosensory Amplification Scale; HCQ = Health Cognitions
Questionnaire; * p < .01, ** p < .001
121
Table 16
Comparisons from Post-Treatment to Follow-Up for the Primary Outcome Measures
Measure Time Time x Covariate Time x Treatment
WI
SHAI
IAS
SSI
SSAS
HCQ
F
9.26
10.60
6.62
3.58
13.40
3.09
P
.004**
.002**
.01*
.07
.001**
.09
r,2
.21
.23
.16
.09
.27
.08
F
27.13
18.42
10.58
4.48
16.61
5.15
P
.0001***
.0001***
.002**
.04*
.0001***
.03*
r,2
.43
.34
.23
.11
.32
.13
F
.22
.10
.04
.002
2.98
.02
P
.64
.75
.85
.97
.09
.89
r,2
.006
.003
.001
.0001
.08
.001
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control; WI = Whiteley Index; SHAI = Health
Anxiety Index - Short-form; IAS = Illness Attitudes Scale; SSI = Somatic Symptom
Inventory; SSAS = Somatosensory Amplification Scale; HCQ = Health Cognitions
Questionnaire; * p < .01, ** p < .001
121
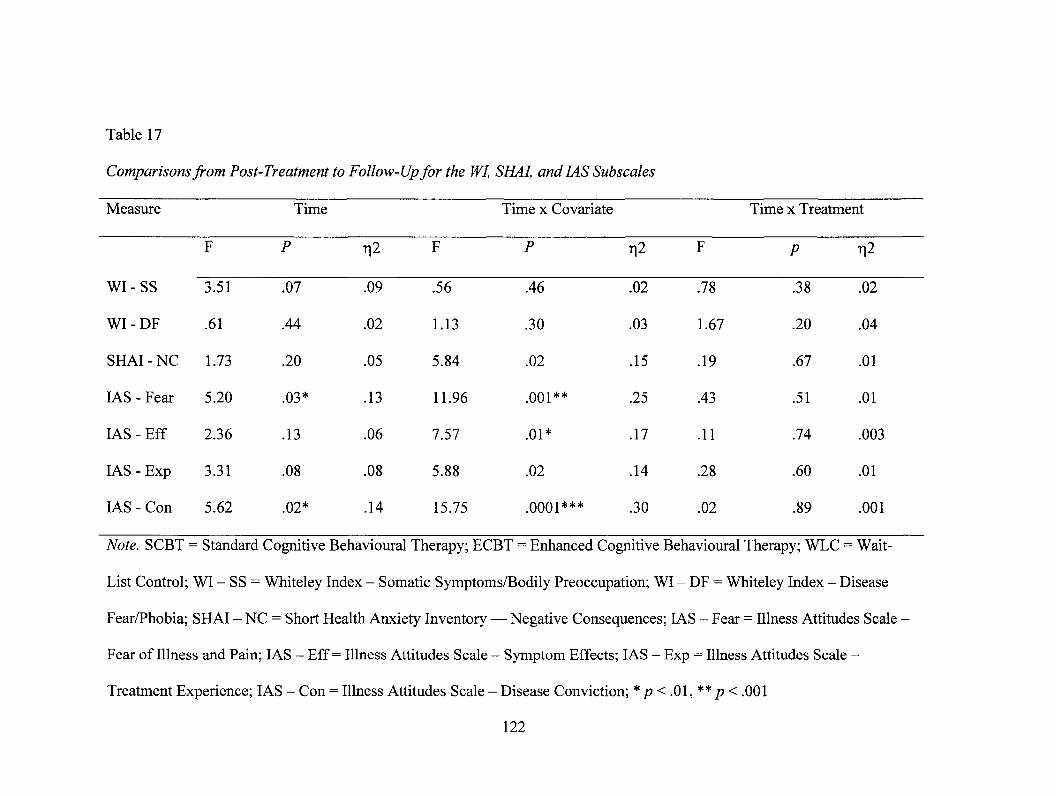
Table 17
Comparisons from Post-Treatment to Follow-Up for the WI, SHAI, and IAS Subscales
Measure Time Time x Covariate Time x Treatment
F P i2 F P T12 F p 112
WI - SS 3.51 .07 .09 .56 .46 .02 .78 .38 .02
WI - DF .61 .44 .02 1.13 .30 .03 1.67 .20 .04
SHAI - NC 1.73 .20 .05 5.84 .02 .15 .19 .67 .01
IAS - Fear 5.20 .03* .13 11.96 .001** .25 .43 .51 .01
IAS - Eff 2.36 .13 .06 7.57 .01* .17 .11 .74 .003
IAS -Exp 3.31 .08 .08 5.88 .02 .14 .28 .60 .01
IAS - Con 5.62 .02* .14 15.75 .0001*** .30 .02 .89 .001
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; WI - SS = Whiteley Index - Somatic Symptoms/Bodily Preoccupation; WI - DF = Whiteley Index - Disease
Fear/Phobia; SHAI - NC = Short Health Anxiety Inventory - Negative Consequences; IAS - Fear = Illness Attitudes Scale -
Fear of Illness and Pain; IAS - Eff = Illness Attitudes Scale - Symptom Effects; IAS - Exp = Illness Attitudes Scale -
Treatment Experience; IAS - Con = Illness Attitudes Scale - Disease Conviction; * p < .01, ** p < .001
122
Table 17
Comparisons from Post-Treatment to Follow-Up for the WI, SHAI, and IAS Subscales
Measure
WI-SS
WI-DF
SHAI - NC
IAS - Fear
IAS - Eff
IAS - Exp
IAS - Con
F
3.51
.61
1.73
5.20
2.36
3.31
5.62
Time
P
.07
.44
.20
.03*
.13
.08
.02*
r,2
.09
.02
.05
.13
.06
.08
.14
F
.56
1.13
5.84
11.96
7.57
5.88
15.75
Time x Covariate
P
.46
.30
.02
.001**
.01*
.02
.0001***
r,2
.02
.03
.15
.25
.17
.14
.30
F
.78
1.67
.19
.43
.11
.28
.02
Time x Treatment
P
.38
.20
.67
.51
.74
.60
.89
r,2
.02
.04
.01
.01
.003
.01
.001
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; WI - SS = Whiteley Index - Somatic Symptoms/Bodily Preoccupation; WI - DF = Whiteley Index - Disease
Fear/Phobia; SHAI - NC = Short Health Anxiety Inventory — Negative Consequences; IAS - Fear = Illness Attitudes Scale •
Fear of Illness and Pain; IAS - Eff = Illness Attitudes Scale - Symptom Effects; IAS - Exp = Illness Attitudes Scale -
Treatment Experience; IAS - Con = Illness Attitudes Scale - Disease Conviction; * p < .01, ** p < .001
122

Table 18
Comparisons from Post-Treatment to Follow-Up for the Secondary Outcome Measures
Measure Time Time x Covariate Time x Treatment
F p 112 F P rl2 F p 112
ASI 7.27 .01 .17 15.08 .0001*** .30 1.02 .32 .03
STAI-S 9.03 .005** .20 8.41 .006** .19 5.79 .02* .14
STAI-T 2.20 .15 .06 3.02 .09 .08 1.15 .29 .03
GDS 4.66 .04* .12 8.19 .007** .19 .04 .85 .001
GPM 1.05 .31 .03 2.61 .12 .07 2.46 .13 .06
SF-12-PCS .21 .65 .01 .10 .76 .01 4.26 .04* .11
SF-12-MCS 1.12 .30 .03 1.15 .29 .03 1.32 .26 .04
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control; ASI = Anxiety Sensitivity Index; STAI-
S = State Trait Anxiety Inventory - State Scale; STAI-T = State Trait Anxiety Inventory
- Trait Scale; GDS = Geriatric Depression Scale; GPM = Geriatric Pain Measure; SF-12-
PCS = Short-Form-12 - Physical Summary Score; and MCS = Short-Form-12 - Mental
Summary Score; * p < .01, ** p < .001
123
Table 18
Comparisons from Post-Treatment to Follow-Up for the Secondary Outcome Measures
Measure Time Time x Covariate Time x Treatment
ASI
STAI-S
STAI-T
GDS
GPM
SF-12-PCS
SF-12-MCS
F
7.27
9.03
2.20
4.66
1.05
.21
1.12
P
.01
.005**
.15
.04*
.31
.65
.30
r,2
.17
.20
.06
.12
.03
.01
.03
F
15.08
8.41
3.02
8.19
2.61
.10
1.15
P
.0001***
.006**
.09
.007**
.12
.76
.29
r,2
.30
.19
.08
.19
.07
.01
.03
F
1.02
5.79
1.15
.04
2.46
4.26
1.32
P
.32
.02*
.29
.85
.13
.04*
.26
r,2
.03
.14
.03
.001
.06
.11
.04
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control; ASI = Anxiety Sensitivity Index; STAI-
S = State Trait Anxiety Inventory - State Scale; STAI-T = State Trait Anxiety Inventory
- Trait Scale; GDS = Geriatric Depression Scale; GPM = Geriatric Pain Measure; SF-12-
PCS = Short-Form-12 - Physical Summary Score; and MCS = Short-Form-12 - Mental
Summary Score; * p < .01, ** p < .001
123
3.1.4 Hypothesis 4 and 5 — Therapeutic Alliance and Motivation for Psychotherapy
It was hypothesized that participants treated with ECBT would demonstrate
higher levels of therapeutic alliance and motivation for psychotherapy at three and six
weeks than those receiving SCBT. In order to test these hypotheses, 2 (treatment: SCBT,
ECBT) x 3 (time: Session 1, Session 3, Session 6) mixed factor ANCOVAs were
conducted on the WAI subscales (Tasks, Bond, Goals) and the NML-2 subscales
(Preparedness, Distress, Doubt). The Session 1 value of the measure of interest in each
analysis was set as the covariate. The results from the mixed factor ANCOVAs assessing
change in the WAI and NML-2 across both groups from Session 1 to Session 6 are shown
in Table 19. These analyses revealed a statistically significant main effect for time on the
WAI - Tasks (p = .02), NML-2-Preparedness (p = .047), NML-2-Distres (p = .02), and
NML-2-Doubt (p = .03). The covariate (i.e., the Session 1 value of the measure of
interest in the analysis) was significantly related to outcome at post-treatment on the
WAI-Bond (p = .02), NML-2-Preparedness (p = .044), NML-2-Distres (p = .004), and
NML-2-Doubt (p = .008), and a statistically significant time x treatment group interaction
on the WAI — Goals Subscale (p = .04).
To examine the interaction further, 2 (treatment: SCBT, ECBT) x 2 (time: Session
1, Session 3, or Session 6) repeated measures ANCOVAs were conducted to determine
specifically how treatment conditions influenced the DV over time. More specifically,
the SCBT condition was compared to the ECBT condition. The pre-treatment value of
the measure of interest in each analysis was set as the covariate. Table 20 shows the
124
3.1.4 Hypothesis 4 and 5 - Therapeutic Alliance and Motivation for Psychotherapy
It was hypothesized that participants treated with ECBT would demonstrate
higher levels of therapeutic alliance and motivation for psychotherapy at three and six
weeks than those receiving SCBT. In order to test these hypotheses, 2 (treatment: SCBT,
ECBT) x 3 (time: Session 1, Session 3, Session 6) mixed factor ANCOVAs were
conducted on the WAI subscales (Tasks, Bond, Goals) and the NML-2 subscales
(Preparedness, Distress, Doubt). The Session 1 value of the measure of interest in each
analysis was set as the covariate. The results from the mixed factor ANCOVAs assessing
change in the WAI and NML-2 across both groups from Session 1 to Session 6 are shown
in Table 19. These analyses revealed a statistically significant main effect for time on the
WAI - Tasks (p = .02), NML-2-Preparedness (p = .047), NML-2-Distres (p = .02), and
NML-2-Doubt (p = .03). The covariate (i.e., the Session 1 value of the measure of
interest in the analysis) was significantly related to outcome at post-treatment on the
WAI-Bond (p = .02), NML-2-Preparedness (p = .044), NML-2-Distres (p = .004), and
NML-2-Doubt (p = .008), and a statistically significant time x treatment group interaction
on the WAI - Goals Subscale (p = .04).
To examine the interaction further, 2 (treatment: SCBT, ECBT) x 2 (time: Session
1, Session 3, or Session 6) repeated measures ANCOVAs were conducted to determine
specifically how treatment conditions influenced the DV over time. More specifically,
the SCBT condition was compared to the ECBT condition. The pre-treatment value of
the measure of interest in each analysis was set as the covariate. Table 20 shows the
124

Table 19
Mixed-Factor 3 (Time) x 2 (Treatment) ANCOVAs for WAI and NML-2 Subscales
Measure Time Time x Covariate Time x Treatment
F P 112 F P i2 F p ri2
WAI - Tasks 2.68 .08 .14 3.09 .06 .15 1.52 .23 .08
WAI - Bond 4.67 .02* .22 4.58 .02* .21 1.12 .34 .06
WAI - Goals 1.03 .37 .06 1.09 .35 .06 3.62 .04* .18
NML-2 -
Preparedness 3.35 .047* .17 3.45 .044* .17 1.87 .17 .10
NML-2 - Distress 4.30 .02* .21 6.71 .004** .29 .10 .91 .006
NML-2 - Doubt 3.90 .03* .19 5.63 .008** .25 .85 .44 .05
Note. WAI-T = Working Alliance Inventory - Tasks Subscale; WAI-B = Working Alliance Inventory - Bond Subscale; WAI-
G = Working Alliance Inventory - Goals Subscale; NML-2 - P = Nijmegen Motivation List-2 - Preparedness Subscale; NML-
2 - Di = Nijmegen Motivation List-2 - Distress Subscale; NML-2 - P = Nijmegen Motivation List-2 - Doubt Subscale. * p <
.05, ** p <.01, ***p <.001
125
Table 19
Mixed-Factor 3 (Time) x 2 (Treatment) ANCOVAs for WAI and NML-2 Subscales
Measure
WAI-Tasks
WAI - Bond
WAI - Goals
NML-2 -
Preparedness
NML-2 - Distress
NML-2 - Doubt
F
2.68
4.67
1.03
3.35
4.30
3.90
Time
P
.08
.02*
.37
.047*
.02*
.03*
r,2
.14
.22
.06
.17
.21
.19
F
3.09
4.58
1.09
3.45
6.71
5.63
Time x Covariate
P
.06
.02*
.35
.044*
.004**
.008**
r,2
.15
.21
.06
.17
.29
.25
F
1.52
1.12
3.62
1.87
.10
.85
Time x Treatment
P
.23
.34
.04*
.17
.91
.44
r,2
.08
.06
.18
.10
.006
.05
Note. WAI-T = Working Alliance Inventory - Tasks Subscale; WAI-B = Working Alliance Inventory - Bond Subscale; WAI-
G = Working Alliance Inventory - Goals Subscale; NML-2 - P = Nijmegen Motivation List-2 - Preparedness Subscale; NML-
2 - Di = Nijmegen Motivation List-2 - Distress Subscale; NML-2 - P = Nijmegen Motivation List-2 - Doubt Subscale. * p <
.05, **/?<.01, ***/?<.001
125
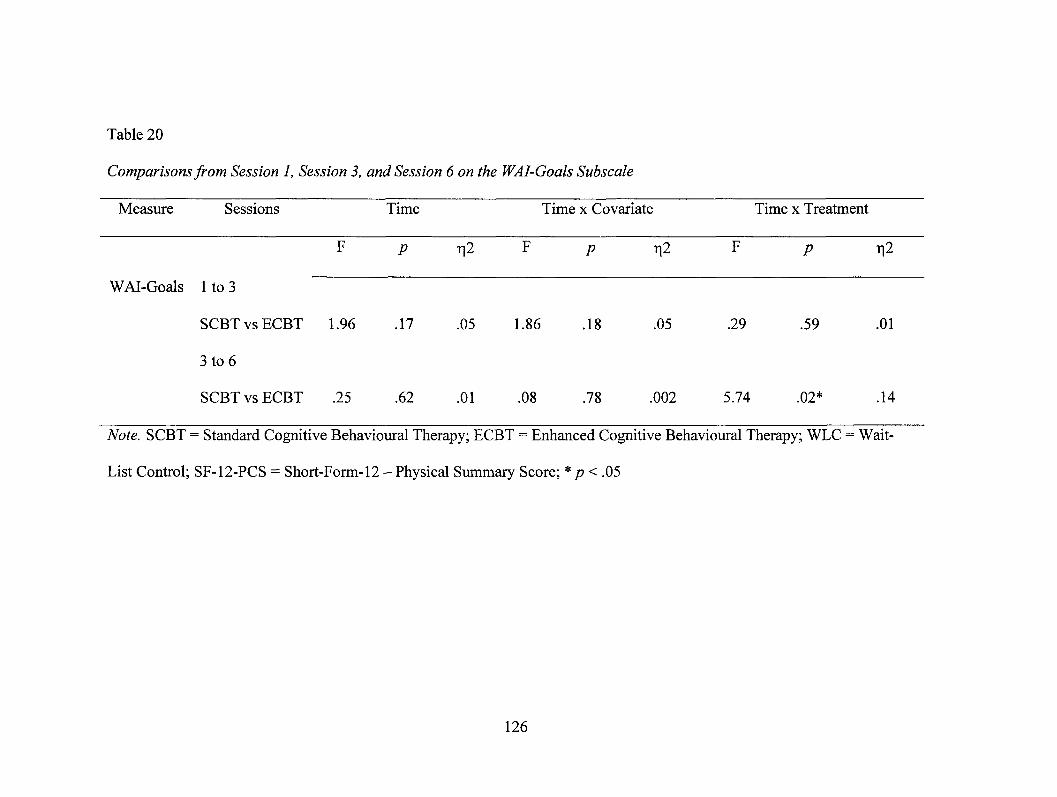
Table 20
Comparisons from Session 1, Session 3, and Session 6 on the WAI-Goals Subscale
Measure Sessions Time Time x Covariate Time x Treatment
F p 712 F p i2 F p rig
WAI-Goals 1 to 3
SCBT vs ECBT 1.96 .17 .05 1.86 .18 .05 .29 .59 .01
3 to 6
SCBT vs ECBT .25 .62 .01 .08 .78 .002 5.74 .02* .14
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; SF-12-PCS = Short-Form-12 — Physical Summary Score; * p < .05
126
Table 20
Comparisons from Session 1, Session 3, and Session 6 on the WAI-Goals Subscale
Measure Sessions Time Time x Covariate Time x Treatment
F p r|2 F p r(l F p r|2
WAI-Goals 1 to 3
SCBT vs ECBT 1.96 .17 .05 1.86 .18 .05 .29 .59 .01
3 to 6
SCBT vs ECBT .25 .62 .01 .08 .78 .002 5.74 .02* .14
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive Behavioural Therapy; WLC = Wait-
List Control; SF-12-PCS = Short-Form-12 - Physical Summary Score; * p < .05
126

results of the 2 x 3 analyses (Note: Treatment main effects are not reported in the table as
the treatment main effects are not of interest and do not provide relevant information;
Huck & MacLean, 1975). After controlling for the effect of the Session 3 score on the
measure of interest, from Session 3 to Session 6, individuals in the SCBT group
evidenced greater improvements than did individuals in the ECBT group on the WAI-
Goals (p = .02). These findings indicate that from Session 3 to Session 6, the WAI —
Goals Subscale score significantly increased in the SCBT group as compared to the
ECBT group. Figures 7 depict only the significant results of the 3 x 2 analyses.
3.1.5 Process and Significance of Change
3.1.5.1 Treatment Specific Change
The repeated measures factorial analyses consistently indicated a main effect for
time for many of the DVs amongst both the primary and secondary outcome measures.
Following other researchers (e.g., Greeven et al., 2007), paired-samples t-tests were
conducted on each DV for each treatment group to compare change from pre- to post-
treatment and post-treatment to follow-up in order to identify which treatment conditions
produced improvements on each DV. Tables 21, 22, and 23 illustrate the relevant data,
including Cohen's d effect sizes. Participants in the SCBT treatment group demonstrated
significant improvements from pre- to post-treatment on the WI (p = .0001), SHAI (p =
.001), IAS (p = .04), STAI-State (p = .01), STAI-Trait (p = .02), GDS (p = .02), SF-12-
PCS (p = .04), SF-12-MCS (p = .007), WI-Somatic Symptoms/Bodily Preoccupation (p
= .02), WI-Disease Fear/Phobia (p = .0001), SHAI-Negative Consequences (p = .02),
and IAS-Effects (p = .02). Participants in the ECBT treatment group demonstrated
127
results of the 2 x 3 analyses (Note: Treatment main effects are not reported in the table as
the treatment main effects are not of interest and do not provide relevant information;
Huck & MacLean, 1975). After controlling for the effect of the Session 3 score on the
measure of interest, from Session 3 to Session 6, individuals in the SCBT group
evidenced greater improvements than did individuals in the ECBT group on the WAI-
Goals (p = .02). These findings indicate that from Session 3 to Session 6, the WAI -
Goals Subscale score significantly increased in the SCBT group as compared to the
ECBT group. Figures 7 depict only the significant results of the 3 x 2 analyses.
3.1.5 Process and Significance of Change
3.1.5.1 Treatment Specific Change
The repeated measures factorial analyses consistently indicated a main effect for
time for many of the DVs amongst both the primary and secondary outcome measures.
Following other researchers (e.g., Greeven et al., 2007), paired-samples Mests were
conducted on each DV for each treatment group to compare change from pre- to post-
treatment and post-treatment to follow-up in order to identify which treatment conditions
produced improvements on each DV. Tables 21, 22, and 23 illustrate the relevant data,
including Cohen's d effect sizes. Participants in the SCBT treatment group demonstrated
significant improvements from pre- to post-treatment on the WI (p = .0001), SHAI (p —
.001), IAS (p = .04), STAI-State (p = .01), STAI-Trait (p = .02), GDS (p = .02), SF-12-
PCS (p = .04), SF-12-MCS (p = .007), Wl-Somatic Symptoms/Bodily Preoccupation (p
= .02), WI-Disease Fear/Phobia (p = .0001), SHAI-Negative Consequences (p = .02),
and IAS-Effects (p = .02). Participants in the ECBT treatment group demonstrated
127

76
75
74
73
72
71
70
69
Session 1 Session 2 Session 3
•••'"'SCBT
ECBT
Figure 7. Mean WAI - Goal scores by treatment condition at Session 1, Session 3, and
Session 6. (SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced
Cognitive Behavioural Therapy). Original in Colour.
128
'SCBT
•ECBT
Session 1 Session 2 Session 3
Figure 7. Mean WAI - Goal scores by treatment condition at Session 1, Session 3, and
Session 6. (SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced
Cognitive Behavioural Therapy). Original in Colour.
128

Table 21
Paired T-Tests for Each Primary Outcome Measure
Measure Comparisons t-test
Treatments Times T Df Sig (2 tailed) d
WI SCBT 1 vs 2 5.58 20 .000*** 1.63
2 vs 3 .79 20 .44 .12
ECBT 1 vs 2 4.60 17 .000*** 1.18
2 vs 3 2.08 17 .04* .36
WLC 1 vs 2 1.43 17 .17 .49
SHAI SCBT 1 vs 2 3.91 20 .001** .59
2 vs 3 .67 20 .51 .05
ECBT 1 vs 2 2.45 17 .03* .41
2 vs 3 1.69 17 .11 .24
WLC 1 vs 2 .82 17 .42 .17
IAS SCBT 1 vs 2 2.15 20 .04* .39
2 vs 3 .73 20 .47 .13
ECBT 1 vs 2 1.66 17 .11 .35
2 vs 3 2.60 17 .02* .41
WLC 1 vs 2 -.03 17 .98 .01
SSI SCBT 1 vs 2 .48 20 .64 .07
2 vs 3 .99 20 .34 .08
129
Table 21
Paired T-Tests for Each Primary Outcome Measure
Measure
WI
SHAI
IAS
SSI
Comparisons
Treatments
SCBT
ECBT
WLC
SCBT
ECBT
WLC
SCBT
ECBT
WLC
SCBT
Times
l v s 2
2vs3
1 vs2
2vs3
1 vs2
1 vs2
2vs3
1 vs2
2 v s 3
1 vs2
1 vs2
2vs3
l v s 2
2vs3
1 vs2
1 vs2
2vs3
T
5.58
.79
4.60
2.08
1.43
3.91
.67
2.45
1.69
.82
2.15
.73
1.66
2.60
-.03
.48
.99
/-test
Df
20
20
17
17
17
20
20
17
17
17
20
20
17
17
17
20
20
Sig (2 tailed)
.000***
.44
.000***
.04*
.17
.001**
.51
.03*
.11
.42
.04*
.47
.11
.02*
.98
.64
.34
d
1.63
.12
1.18
.36
.49
.59
.05
.41
.24
.17
.39
.13
.35
.41
.01
.07
.08
129
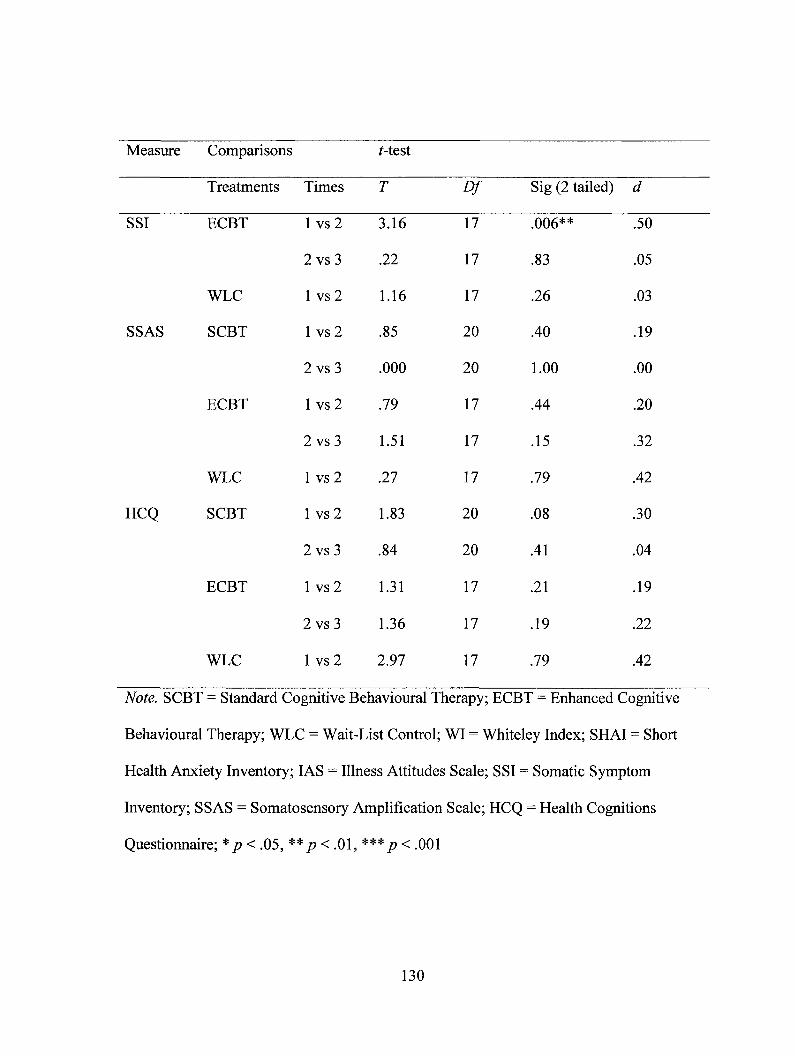
Measure Comparisons t-test
Treatments Times T Df Sig (2 tailed) d
SSI ECBT 1 vs 2 3.16 17 .006** .50
2 vs 3 .22 17 .83 .05
WLC 1 vs 2 1.16 17 .26 .03
SSAS SCBT 1 vs 2 .85 20 .40 .19
2 vs 3 .000 20 1.00 .00
ECBT 1 vs 2 .79 17 .44 .20
2 vs 3 1.51 17 .15 .32
WLC 1 vs 2 .27 17 .79 .42
HCQ SCBT 1 vs 2 1.83 20 .08 .30
2 vs 3 .84 20 .41 .04
ECBT 1 vs 2 1.31 17 .21 .19
2 vs 3 1.36 17 .19 .22
WLC 1 vs 2 2.97 17 .79 .42
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control; WI = Whiteley Index; SHAI = Short
Health Anxiety Inventory; IAS = Illness Attitudes Scale; SSI = Somatic Symptom
Inventory; SSAS = Somatosensory Amplification Scale; HCQ = Health Cognitions
Questionnaire; * p < .05, ** p < .01, *** p < .001
130
Measure Comparisons Mest
Treatments Times T Df
SSI ECBT l v s 2 3.16 17
2 v s 3 .22 17
WLC l v s 2 1.16 17
SSAS SCBT 1 vs 2 .85 20
2 vs 3 .000 20
ECBT l v s 2 .79 17
2vs3 1.51 17
WLC l v s 2 .27 17 .79 .42
Sig (2 tailed)
.006**
.83
.26
.40
1.00
.44
.15
d
.50
.05
.03
.19
.00
.20
.32
1 vs2
2vs3
1.83
.84
20
20
.08
.41
.30
.04
HCQ SCBT
ECBT l v s 2 1.31 17 .21 .19
2vs3 1.36 17 .19 .22
WLC l v s 2 2.97 17 .79 .42
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control; WI = Whiteley Index; SHAI = Short
Health Anxiety Inventory; IAS = Illness Attitudes Scale; SSI = Somatic Symptom
Inventory; SSAS = Somatosensory Amplification Scale; HCQ = Health Cognitions
Questionnaire; *p < .05, ** p < .01, ***p < .001
130

Table 22
Paired T-Tests for Each Subscale on the WI, SHAI, and MS
Measure Comparisons t-test
Treatments Times t df Sig (2 tailed) d
WI - SS SCBT 1 vs 2 2.65 20 .02* .70
2 vs 3 1.71 20 .10 .20
ECBT 1 vs 2 2.76 17 .01* .53
2 vs 3 1.84 17 .08 .29
WLC 1 vs 2 .68 17 .51 .20
WI - DF SCBT 1 vs 2 5.75 20 .0001*** 1.42
2 vs 3 .24 17 .82 .05
ECBT 1 vs 2 3.12 17 .006** .82
2 vs 3 2.12 17 .05* .37
WLC 1 vs 2 .70 17 .50 .21
SHAI - NC SCBT 1 vs 2 2.46 20 .02* .47
2 vs 3 .11 20 .92 .03
ECBT 1 vs 2 1.35 17 .20 .31
2 vs 3 1.55 17 .14 .28
WLC 1 vs 2 .18 17 .86 .03
IAS - Fear SCBT 1 vs 2 1.15 20 .26 .21
2 vs 3 .77 20 .45 .12
131
Table 22
Paired T-Tests for Each Subscale on the WI, SHAI, and IAS
Measure Comparisons Mest
Treatments Times t df Sig (2 tailed) d
W I - S S SCBT 1 vs2 2^65 20 !(J2* ?70~
2vs3 1.71 20 .10 .20
ECBT l v s 2 2.76 17 .01* .53
2vs3 1.84 17 .08 .29
WLC l v s 2 .68 17 .51 .20
W I - D F SCBT l v s 2 5.75 20 .0001*** 1.42
2vs3 .24 17 .82 .05
ECBT l v s 2 3.12 17 .006** .82
2vs3 2.12 17 .05* .37
WLC l v s 2 .70 17 .50 .21
SHAI-NC SCBT 1 vs 2 2.46 20 .02* .47
2vs3 .11 20 .92 .03
ECBT l v s 2 1.35 17 .20 .31
2vs3 1.55 17 .14 .28
WLC l v s 2 .18 17 .86 .03
IAS-Fear SCBT l v s 2 1.15 20 .26 .21
2vs3 .77 20 .45 .12
131

Measure Comparisons t-test
Treatments Times t df Sig (2 tailed) d
IAS - Fear ECBT 1 vs 2 1.65 17 .67 .10
2 vs 3 .44 17 .67 .20
WLC 1 vs 2 -1.22 17 .24 .24
IAS - Eff SCBT 1 vs 2 2.84 20 .01* .43
2 vs 3 .43 20 .67 .06
ECBT 1 vs 2 .12 17 .91 .02
2 vs 3 2.24 17 .04* .27
WLC 1 vs 2 1.07 17 .29 .18
IAS - Exp SCBT 1 vs 2 .03 20 .98 .00
2 vs 3 -.03 20 .98 .09
ECBT 1 vs 2 2.12 17 .22 .39
2 vs 3 1.55 17 .04* .30
WLC 1 vs 2 1.47 17 .16 .16
IAS - Con SCBT 1 vs 2 1.74 20 .10 .32
2 vs 3 .62 20 .54 .01
ECBT 1 vs 2 1.28 17 .22 .23
2 vs 3 1.72 17 .10 .23
WLC 1 vs 2 .77 17 .45 .38
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control; WI - SS = Whiteley Index - Somatic
132
Measure Comparisons Mest
Treatments Times t df Sig (2 tailed) d
IAS - Fear ECBT 1 vs 2 L65 17 67 I(F
2vs3 .44 17 .67 .20
WLC
IAS - Eff SCBT
ECBT
1 vs2
1 vs2
2vs3
1 vs2
2vs3
1 vs2
1 vs2
2vs3
-1.22
2.84
.43
.12
2.24
1.07
.03
-.03
17
20
20
17
17
17
20
20
.24
.01*
.67
.91
.04*
.29
.98
.98
.24
.43
.06
.02
.27
.18
.00
.09
WLC
IAS - Exp SCBT
ECBT l v s 2 2.12 17 .22 .39
2vs3 1.55 17 .04* .30
WLC l v s 2 1.47 17 .16 .16
IAS-Con SCBT l v s 2 1.74 20 .10 .32
2 v s 3 .62 20 .54 .01
ECBT l v s 2 1.28 17 .22 .23
2vs3 1.72 17 .10 .23
WLC l v s 2 .77 17 .45 .38
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control; WI - SS = Whiteley Index - Somatic
132

Symptoms/Bodily Preoccupation; WI — DF = Whiteley Index — Disease Fear/Phobia;
SHAI — NC = Short Health Anxiety Inventory Negative Consequences; IAS — Fear =
Illness Attitudes Scale — Fear of Illness and Pain; IAS — Eff = Illness Attitudes Scale —
Symptom Effects; IAS — Exp = Illness Attitudes Scale — Treatment Experience; IAS —
Con = Illness Attitudes Scale — Disease Conviction; * p < .05, ** p < .01, *** p < .001
133
Symptoms/Bodily Preoccupation; WI - DF = Whiteley Index - Disease Fear/Phobia;
SHAI - NC = Short Health Anxiety Inventory — Negative Consequences; IAS - Fear =
Illness Attitudes Scale - Fear of Illness and Pain; IAS - Eff = Illness Attitudes Scale -
Symptom Effects; IAS - Exp = Illness Attitudes Scale - Treatment Experience; IAS -
Con = Illness Attitudes Scale - Disease Conviction; * p < .05, ** p < .01, *** p < .001
133

Table 23
Paired T-Test for Each Secondary Outcome Measure
Measure Comparisons t-test
Treatments Times T Df Sig (2 tailed) d
ASI SCBT 1 vs 2 1.94 20 .07 .32
2 vs 3 .65 20 .52 .10
ECBT 1 vs 2 2.19 17 .04* .40
2 vs 3 1.87 17 .08 .37
WLC 1 vs 2 .38 17 .71 .09
STAI-S SCBT 1 vs 2 2.68 20 .01* .53
2 vs 3 -2.18 20 .04* .42
ECBT 1 vs 2 .80 17 .43 .21
2 vs 3 .97 17 .35 .26
WLC 1 vs 2 1.20 17 .25 .29
STAI-T SCBT 1 vs 2 2.62 20 .02* .37
2 vs 3 -.13 20 .90 .12
ECBT 1 vs 2 .70 17 .49 .13
2 vs 3 1.27 17 .22 .26
WLC 1 vs 2 1.38 17 .19 .18
GDS SCBT 1 vs 2 2.56 20 .02* .39
2 vs 3 .02 20 .99 .00
ECBT 1 vs 2 2.60 17 .02* .57
134
Table 23
Paired T-Testfor Each Secondary Outcome Measure
Measure Comparisons Mest
ASI
Treatments Times Df
SCBT l v s 2 1.94
2 vs 3 .65
20
20
Sig (2 tailed) d
.07
.52
.32
.10
STAI-S
STAI-T
GDS
ECBT
WLC
SCBT
ECBT
WLC
SCBT
ECBT
WLC
SCBT
ECBT
l v s 2
2vs3
1 vs2
1 vs2
2vs3
1 vs2
2vs3
1 vs2
1 vs2
2vs3
1 vs2
2vs3
1 vs2
1 vs2
2vs3
1 vs2
2.19
1.87
.38
2.68
-2.18
.80
.97
1.20
2.62
-.13
.70
1.27
1.38
2.56
.02
2.60
17
17
17
20
20
17
17
17
20
20
17
17
17
20
20
17
.04*
.08
.71
.01*
.04*
.43
.35
.25
.02*
.90
.49
.22
.19
.02*
.99
.02*
.40
.37
.09
.53
.42
.21
.26
.29
.37
.12
.13
.26
.18
.39
.00
.57
134

Measure Comparisons t-test
Treatments Times T Df Sig (2 tailed) d
GDS ECBT 2 vs 3 .37 17 .72 .06
WLC 1 vs 2 1.07 17 .30 .18
GPM SCBT 1 vs 2 .52 20 .61 .07
2 vs 3 -.81 20 .43 .06
ECBT 1 vs 2 .64 17 .53 .21
2 vs 3 1.25 17 .23 .16
WLC 1 vs 2 -1.42 17 .18 .15
SF-12-PCS SCBT 1 vs 2 -2.20 20 .04* .22
2 vs 3 2.24 20 .04* .21
ECBT 1 vs 2 -.69 17 .50 .11
2 vs 3 -.90 17 .38 .10
WLC 1 vs 2 3.04 17 .007** .29
SF-12-MCS SCBT 1 vs 2 -2.98 20 .007** .38
2 vs 3 .71 20 .49 .13
ECBT 1 vs 2 -1.65 17 .12 .37
2 vs 3 -.84 17 .41 .17
WLC 1 vs 2 -.77 17 .45 .09
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control; ASI = Anxiety Sensitivity Index; STAI-
S = State Trait Anxiety Inventory - State Scale; STAI-T = State Trait Anxiety Inventory
135
Measure Comparisons /-test
Treatments Times T Df Sig (2 tailed) d
GDS ECBT 2vs3 37 17 J 2 ~M
WLC l v s 2 1.07 17 .30 .18
GPM SCBT l v s 2 .52 20
2vs3 -.81 20
ECBT l v s 2 .64 17
2vs3 1.25 17
WLC l v s 2 -1.42 17
SF-12-PCS SCBT l v s 2 -2.20 20
2 vs 3 2.24 20
ECBT l v s 2 -.69 17
2vs3 -.90 17
WLC l v s 2 3.04 17
SF-12-MCS SCBT 1 vs 2 -2.98 20
2vs3 .71 20
ECBT l v s 2 -1.65 17
2 v s 3 -.84 17
WLC l v s 2 -.77 17
Note. SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control; ASI = Anxiety Sensitivity Index; STAI-
S = State Trait Anxiety Inventory - State Scale; STAI-T = State Trait Anxiety Inventory
.61
.43
.53
.23
.18
.04*
.04*
.50
.38
.007**
.007**
.49
.12
.41
.45
.07
.06
.21
.16
.15
.22
.21
.11
.10
.29
.38
.13
.37
.17
.09
135

— Trait Scale; GDS = Geriatric Depression Scale; GPM = Geriatric Pain Measure; SF-12-
PCS = Short-Form — 12 — Physical Summary Score; and MCS = Short-Form — 12 —
Mental Summary Score; * p < .05, ** p < .01, *** p < .001
136
- Trait Scale; GDS = Geriatric Depression Scale; GPM = Geriatric Pain Measure; SF-12-
PCS = Short-Form - 12 - Physical Summary Score; and MCS = Short-Form - 12 -
Mental Summary Score; * p < .05, ** p < .01, *** p < .001
136

significant improvements from pre- to post-treatment on the WI (p = .0001), SHAI (p =
.03), SSI (p = .006), ASI (p = .04), GDS (p = .02), WI-Somatic Symptoms/Bodily
Preoccupation (p = .01) and WI-Disease Fear/Phobia (p = .04); and from post-treatment
to follow-up on the IAS (p = .02), WI-Disease Fear/Phobia (p = .02), IAS-Symptom
Effects (p = .04), and IAS-Treatment Experience (p = .04). There were no significant
improvements evidenced on any of the DVs for the WLC group from pre-treatment to
post-treatment, which was on the SF-12-PCS (p = .007).
The change demonstrated by the SCBT and ECBT participants was not always
significantly greater than the change demonstrated by participants in WLC group as
illustrated in the previous mixed factorial repeated measures ANCOVAs. However, the
results suggest that improvements did occur in both the SCBT and ECBT groups after
treatment. Further, the changes appeared to have been maintained in both treatment
groups and improvement continued in the ECBT group on some measures.
3.1.5.2 Clinically Significant Change
Clinically significant change has been defined by Jacobson and Truax (1991) as
"the extent to which therapy moves someone outside the range of the dysfunctional
population or within the range of the functional population" (p. 12). Jacobson and Truax
(1991) indicated that one approach of identifying clinically significant change is to
determine whether the post-treatment score falls outside two standard deviations of the
mean of the population being examined. In the present study, Jacobson and Truax's
(1991) definition was used with WI scores from pre-treatment to post-treatment. The WI
was chosen to assess clinically significant change because it was a primary outcome
137
significant improvements from pre- to post-treatment on the WI (p = .0001), SHAI (p =
.03), SSI (p = .006), ASI (p = .04), GDS (p = .02), Wl-Somatic Symptoms/Bodily
Preoccupation (p = .01) and WI-Disease Fear/Phobia (p = .04); and from post-treatment
to follow-up on the IAS (p = .02), WI-Disease Fear/Phobia (p = .02), IAS-Symptom
Effects (p = .04), and IAS-Treatment Experience (p = .04). There were no significant
improvements evidenced on any of the DVs for the WLC group from pre-treatment to
post-treatment, which was on the SF-12-PCS (p = .007).
The change demonstrated by the SCBT and ECBT participants was not always
significantly greater than the change demonstrated by participants in WLC group as
illustrated in the previous mixed factorial repeated measures ANCOVAs. However, the
results suggest that improvements did occur in both the SCBT and ECBT groups after
treatment. Further, the changes appeared to have been maintained in both treatment
groups and improvement continued in the ECBT group on some measures.
3.1.5.2 Clinically Significant Change
Clinically significant change has been defined by Jacobson and Truax (1991) as
"the extent to which therapy moves someone outside the range of the dysfunctional
population or within the range of the functional population" (p. 12). Jacobson and Truax
(1991) indicated that one approach of identifying clinically significant change is to
determine whether the post-treatment score falls outside two standard deviations of the
mean of the population being examined. In the present study, Jacobson and Truax's
(1991) definition was used with WI scores from pre-treatment to post-treatment. The WI
was chosen to assess clinically significant change because it was a primary outcome
137

measure, and the WI scores were integral in determining eligibility for participation.
Figure 8 indicates the proportion of participants in each treatment condition who
demonstrated clinically significant change according to the definition provided by
Jacobson and Truax (1991). Chi-square analyses using Fisher's Exact Test showed a
greater proportion of participants demonstrated clinically significant change in the SCBT
condition compared to the WLC condition, x2 (1, 39) — 13.37, p < .0001, and the ECBT
condition compared to the WLC condition, x2 (1, 39) = '7.26,p = .02. No difference was
found between the SCBT and EBCT conditions, x2 (1, 39) = 1.19,p = .34.
The proportion of individuals who no longer met criteria for being categorized as
having high health anxiety was also of interest as an indicator of the clinical significance
of change produced by each treatment. This method of assessing clinically significant
change has been utilized in prior research (e.g., Openshaw, Waller, & Sperlinger, 2004).
Figure 9 shows the proportion of participants in each treatment group with a WI score
below eight (the cut-off for entry into the study) at post-treatment and follow-up,
respectively. Chi-square analyses using Fisher's Exact Test showed a greater proportion
of participants demonstrated clinically significant change in the SCBT condition
compared to the WLC condition, x2(1, 39) = 16.52,p < .0001, and the ECBT condition
compared to the WLC condition, x,2(1, 39) = 11.69, p = .002. No difference was found
between the SCBT and EBCT conditions, x2(1, 39) = .43,p = .72.
138
measure, and the WI scores were integral in determining eligibility for participation.
Figure 8 indicates the proportion of participants in each treatment condition who
demonstrated clinically significant change according to the definition provided by
Jacobson and Truax (1991). Chi-square analyses using Fisher's Exact Test showed a
greater proportion of participants demonstrated clinically significant change in the SCBT
condition compared to the WLC condition, x2 (1, 39) = 13.37,/* < .0001, and the ECBT
condition compared to the WLC condition, x2 (1, 39) = 7.26,p = .02. No difference was
found between the SCBT and EBCT conditions, %2(l,39)=lA9,p = .34.
The proportion of individuals who no longer met criteria for being categorized as
having high health anxiety was also of interest as an indicator of the clinical significance
of change produced by each treatment. This method of assessing clinically significant
change has been utilized in prior research (e.g., Openshaw, Waller, & Sperlinger, 2004).
Figure 9 shows the proportion of participants in each treatment group with a WI score
below eight (the cut-off for entry into the study) at post-treatment and follow-up,
respectively. Chi-square analyses using Fisher's Exact Test showed a greater proportion
of participants demonstrated clinically significant change in the SCBT condition
compared to the WLC condition, x2(l, 39) = 16.52,/? < .0001, and the ECBT condition
compared to the WLC condition, x2(l, 39) = 11.69, p = .002. No difference was found
between the SCBT and EBCT conditions, x2(l, 39) = .43,p = .72.
138
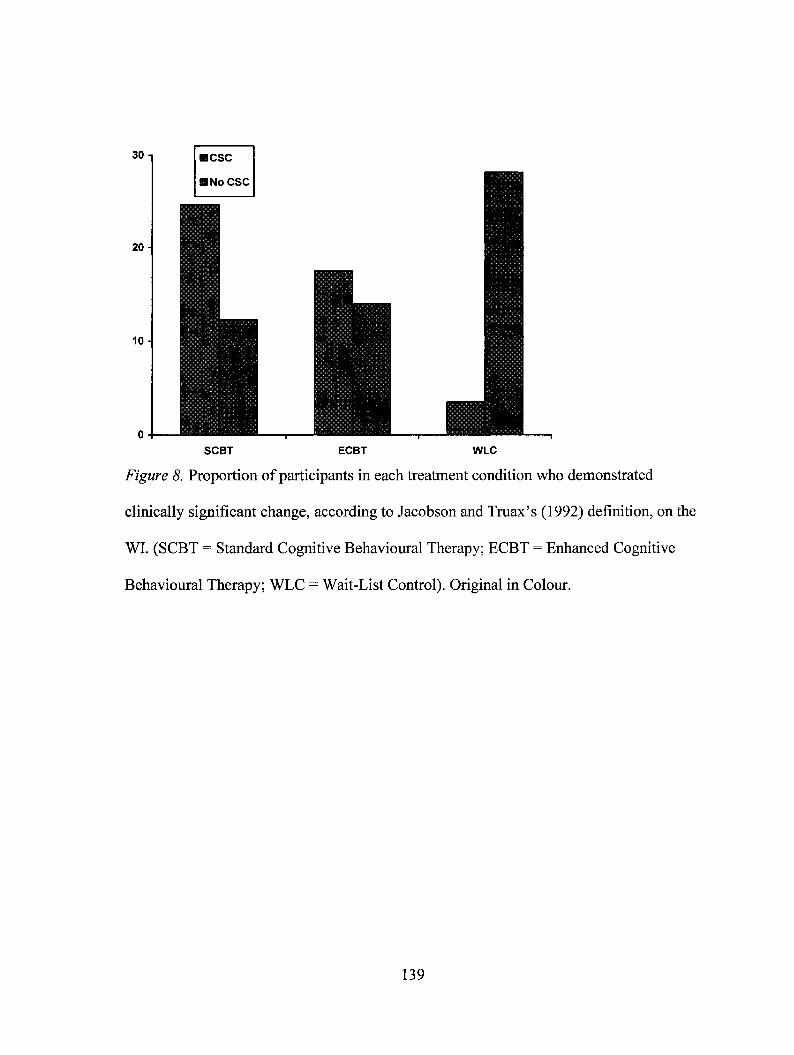
SCBT ECBT WLC
Figure 8. Proportion of participants in each treatment condition who demonstrated
clinically significant change, according to Jacobson and Truax's (1992) definition, on the
WI. (SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control). Original in Colour.
139
SCBT ECBT WLC
Figure 8. Proportion of participants in each treatment condition who demonstrated
clinically significant change, according to Jacobson and Truax's (1992) definition, on the
WI. (SCBT = Standard Cognitive Behavioural Therapy; ECBT = Enhanced Cognitive
Behavioural Therapy; WLC = Wait-List Control). Original in Colour.
139

E< 8
II1= > 8
SCBT ECBT WLC
Figure 9. Proportion of participants in each treatment condition who had WI scores
below 8 at post-treatment. (SCBT = Standard Cognitive Behavioural Therapy; ECBT =
Enhanced Cognitive Behavioural Therapy; WLC = Wait-List Control). Original in
Colour.
140
i < 8
l = > 8
SCBT ECBT WLC
Figure 9. Proportion of participants in each treatment condition who had WI scores
below 8 at post-treatment. (SCBT = Standard Cognitive Behavioural Therapy; ECBT
Enhanced Cognitive Behavioural Therapy; WLC = Wait-List Control). Original in
Colour.
140
3.1.6 Supplementary Analyses
3.1.6.1 Relationship Between Health Anxiety and the Therapeutic Relationship and
Motivation for Psychotherapy at Post-Treatment
Pearson correlation coefficients were calculated to evaluate the relationships
between the therapeutic alliance and motivation for psychotherapy and change in scores
from pre-treatment to post-treatment on the health anxiety measures in both of the SCBT
and ECBT groups. More specifically, the relationships between both the WAI and NML-
2 subscales scores at Session 6 and the WI, SHAI, and IAS change scores from pre-
treatment to post-treatment (change score was computed by calculating the difference in
score from pre-treatment to post-treatment) were examined. These results are presented
in Table 23 and 24. In the SCBT groups, Doubt as measured by the NML-2 was found to
be moderately negatively correlated with health anxiety as measured by the WI. In the
ECBT group, Distress as measured by the NML-2 was found to be moderately negatively
correlated with health anxiety as measured by the WI. The results suggest that among
participants treated with SCBT, lower levels of Doubt (i.e., doubt about the investment in
treatment, the treatment itself, and the possibility of gaining from it) at Session 6 were
related to greater improvements in health anxiety as measured by the WI at post-
treatment. In the ECBT group, lower levels of Distress (i.e., pressure by others and level
of distress) at Session 6 were related to greater improvements in health anxiety as
measured by the WI at post-treatment.
141
3.1.6 Supplementary Analyses
3.1.6.1 Relationship Between Health Anxiety and the Therapeutic Relationship and
Motivation for Psychotherapy at Post-Treatment
Pearson correlation coefficients were calculated to evaluate the relationships
between the therapeutic alliance and motivation for psychotherapy and change in scores
from pre-treatment to post-treatment on the health anxiety measures in both of the SCBT
and ECBT groups. More specifically, the relationships between both the WAI and NML-
2 subscales scores at Session 6 and the WI, SHAI, and IAS change scores from pre-
treatment to post-treatment (change score was computed by calculating the difference in
score from pre-treatment to post-treatment) were examined. These results are presented
in Table 23 and 24. In the SCBT groups, Doubt as measured by the NML-2 was found to
be moderately negatively correlated with health anxiety as measured by the WI. In the
ECBT group, Distress as measured by the NML-2 was found to be moderately negatively
correlated with health anxiety as measured by the WI. The results suggest that among
participants treated with SCBT, lower levels of Doubt (i.e., doubt about the investment in
treatment, the treatment itself, and the possibility of gaining from it) at Session 6 were
related to greater improvements in health anxiety as measured by the WI at post-
treatment. In the ECBT group, lower levels of Distress (i.e., pressure by others and level
of distress) at Session 6 were related to greater improvements in health anxiety as
measured by the WI at post-treatment.
141

Table 24
Correlations Between the WAI and NML-2 and the Health Anxiety Measures Change Scores in the SCBT Group
WI SHAI IAS WAI-T WAI-B WAI- G NML-2-P NML-2-Di NML-2-Do
WI .28 .16 .12 .13 .19 .23 -.20 -.61**
SHAI .79*** .12 .13 .19 -.01 -.23 -.30
IAS -.20 -.16 -.12 -.21 -.03 -.01
WAI-T .90*** .97*** .35 -.50* -.78***
WAI-B .85*** .23 -.33 -.65**
WAI-G .30 -.54* _.77***
NML-2-P .09 -.39
NML-2-Di .46*
NML-2-Do
Note. WI = Whiteley Index; SHAI = Short Health Anxiety Inventory; IAS = Illness Attitudes Scale; WAI-T = Working
Alliance Inventory - Tasks Subscale; WAI-B = Working Alliance Inventory - Bond Subscale; WAI-G = Working Alliance
Inventory - Goals Subscale; NML-2 - P = Nijmegen Motivation List-2 - Preparedness Subscale; NML-2 - Di = Nijmegen
142
Table 24
Correlations Between the WAI and NML-2 and the Health Anxiety Measures Change Scores in the SCBT Group
WI SHAI IAS WAI-T WAI-B WAI-G NML-2-P NML-2-Di NML-2-Do
WI — .28 .16 .12 .13 .19 .23 -.20 -.61**
SHAI - — .79*** .12 .13 .19 -.01 -.23 -.30
IAS - — -.20 -.16 -.12 -.21 -.03 -.01
WAI-T .90*** .97*** .35 .50* .73***
WAI-B - — .85*** .23 -.33 -.65**
WAI-G -— .30 -.54* ..77***
NML-2-P - — .09 -.39
NML-2-Di -— .46*
NML-2-Do
Note. WI = Whiteley Index; SHAI = Short Health Anxiety Inventory; IAS = Illness Attitudes Scale; WAI-T = Working
Alliance Inventory - Tasks Subscale; WAI-B = Working Alliance Inventory - Bond Subscale; WAI-G = Working Alliance
Inventory - Goals Subscale; NML-2 - P = Nijmegen Motivation List-2 - Preparedness Subscale; NML-2 - Di = Nijmegen
142

Motivation List-2 — Distress Subscale; NML-2 — Do = Nijmegen Motivation List-2 — Doubt Subscale; * p < .05, ** p < .01,
*** p < .001
143
Motivation List-2 - Distress Subscale; NML-2 - Do = Nijmegen Motivation List-2 - Doubt Subscale; * p < .05, ** p < .01,
***/?<.001

Table 25
Correlations Between the WAI and NML-2 and the Health Anxiety Measures Change Scores in the ECBT Group
WI SHAI IAS WAI-T WAI-B WAI- G NML-2-P NML-2-Di NML-2-Do
WI .51* .31 -.003 -.04 .01 -.17 -.51* -.37
SHAI .79*** -.29 -.33 -.25 -.32 -.05 -.003
IAS .22 .08 .17 -.28 -.29 -.15
WAI-T .91*** .93*** .10 -.13 -.38
WAI-B .95*** .16 .16 -.37
WAI-G .13 .13 -.36
NML-2-P -.16 .10
NML-2-Di .55*
NML-2-Do
Note. WI = Whiteley Index; SHAI = Short Health Anxiety Inventory; IAS = Illness Attitudes Scale; WAI-T = Working
Alliance Inventory - Tasks Subscale; WAI-B = Working Alliance Inventory - Bond Subscale; WAI-G = Working Alliance
Inventory - Goals Subscale; NML-2 - P = Nijmegen Motivation List-2 - Preparedness Subscale; NML-2 - Di = Nijmegen
144
Table 25
Correlations Between the WAI and NML-2 and the Health Anxiety Measures Change Scores in the ECBT Group
WI SHAI IAS WAI-T WAI-B WAI-G NML-2-P NML-2-Di NML-2-Do
WI — .51* .31 -.003 -.04 .01 -.17 -.51* -.37
SHAI .79*** -.29 -.33 -.25 -.32 -.05 -.003
IAS - — .22 .08 .17 -.28 -.29 -.15
WAI-T - — .91*** .93*** .10 -.13 -.38
WAI-B - — .95*** .16 .16 -.37
WAI-G — - .13 .13 -.36
NML-2-P - — -.16 .10
NML-2-Di -— .55*
NML-2-Do
Note. WI = Whiteley Index; SHAI = Short Health Anxiety Inventory; IAS = Illness Attitudes Scale; WAI-T = Working
Alliance Inventory - Tasks Subscale; WAI-B = Working Alliance Inventory - Bond Subscale; WAI-G = Working Alliance
Inventory - Goals Subscale; NML-2 - P = Nijmegen Motivation List-2 - Preparedness Subscale; NML-2 - Di = Nijmegen
144

Motivation List-2 — Distress Subscale; NML-2 — Do = Nijmegen Motivation List-2 — Doubt Subscale; * p < .05, ** p < .01,
*** p < .001
145
Motivation List-2 - Distress Subscale; NML-2 - Do = Nijmegen Motivation List-2 - Doubt Subscale; * p < .05, ** p < .01,
***/?<.001

3.1.6.2 Analysis of Change in the WLC Group
Data were collected from the WLC group on three occasions (Time 1 — baseline;
Time 2 — six weeks post-baseline; Time 3 — post-treatment with ECBT). A total of 11
participants completed questionnaires at all three time points. The majority of
participants were female (90.9%), and the mean age was 67.73 (SD = 7.35) years. The
majority of participants were also married or common-law (54.5%) and had completed
high school or above (54.5%). These participants had an average of 2.45 (SD = 1.86)
health conditions. The most common health conditions cited were arthritis (63.6%), high
blood pressure (54.5%), and heart disease (27.7%).
We decided to conduct one-way repeated measures ANOVAs on all primary and
secondary outcome measures with the 11 participants who underwent the treatment and
completed measures at all three time points as a way to examine further the effects of
CBT with older adults with health anxiety. All WLC participants were treated with
ECBT after the six week waiting period. Means and standard deviations on all measures
appear in Tables 25, 26, and 27.
The results from the one-way repeated measures ANOVAs assessing change in
each primary outcome measure, across all three time points are shown in Table 26.
These analyses revealed significant differences on scores on the WI (p < .0001) and the
SHAI (p = .003). On the WI, pairwise comparisons indicated that scores at Time 3 were
significantly lower than scores at Time 1 (p = .002) and at Time 2 (p = .03). On the
SHAI, pairwise comparisons indicated that scores at Time 3 were significantly lower than
scores at Time 1 (p = .01).
146
3.1.6.2 Analysis of Change in the WLC Group
Data were collected from the WLC group on three occasions (Time 1 - baseline;
Time 2 - six weeks post-baseline; Time 3 - post-treatment with ECBT). A total of 11
participants completed questionnaires at all three time points. The majority of
participants were female (90.9%), and the mean age was 67.73 (SD = 7.35) years. The
majority of participants were also married or common-law (54.5%) and had completed
high school or above (54.5%). These participants had an average of 2.45 (SD = 1.86)
health conditions. The most common health conditions cited were arthritis (63.6%), high
blood pressure (54.5%), and heart disease (27.7%).
We decided to conduct one-way repeated measures ANOVAs on all primary and
secondary outcome measures with the 11 participants who underwent the treatment and
completed measures at all three time points as a way to examine further the effects of
CBT with older adults with health anxiety. All WLC participants were treated with
ECBT after the six week waiting period. Means and standard deviations on all measures
appear in Tables 25, 26, and 27.
The results from the one-way repeated measures ANOVAs assessing change in
each primary outcome measure, across all three time points are shown in Table 26.
These analyses revealed significant differences on scores on the WI (p < .0001) and the
SHAI (p = .003). On the WI, pairwise comparisons indicated that scores at Time 3 were
significantly lower than scores at Time 1 (p = .002) and at Time 2 (p = .03). On the
SHAI, pairwise comparisons indicated that scores at Time 3 were significantly lower than
scores at Time 1 (p = .01).
146

Table 26
WLC Group Analyses at Time 1, 2, and 3 for the Primary Outcome Measures
Mean (SD) F(2,20) p T12 Time 1- Time 2 P Time 1 - Time 3 p Time 2 - Time 3 p
WI
Time 1 9.18 (1.67) 12.47 .0001 .56 .64 (9.18-8.55) 1.00 4.29 (9.18-4.90) .002 3.65 (8.55-4.90) .03
Time 2 8.55 (1.63)
Time 3 4.90 (2.52)
SHAI
Time 1 16.82 (4.62) 7.82 .003 .44 1.00 (16.82-15.82) 1.00 4.73 (16.82-12.09) .01 3.73 (15.82-12.09) .06
Time 2 15.82 (3.92)
Time 3 12.09 (4.69)
IAS
Time 1 50.64 (8.37) 1.97 .17 .16
Time 2 49.83 (10.11)
Time 3 45.64 (10.98)
SSI
Time 1 29.87 (6.56) 1.56 2.4 .14
147
Table 26
WLC Group Analyses at Time I, 2, and 3 for the Primary Outcome Measures
Mean (SO) F(2,20) p TT2 Time 1-Time 2 P Time 1-Time 3 p Time 2-Time 3 p
WI
Timel 9.18(1.67) 12.47 .0001 .56 .64(9.18-8.55) 1.00 4.29(9.18-4.90) .002 3.65(8.55-4.90) .03
Time 2 8.55(1.63)
Time 3 4.90 (2.52)
SHAI
Timel 16.82(4.62) 7.82 .003 .44 1.00(16.82-15.82) 1.00 4.73(16.82-12.09) .01 3.73(15.82-12.09) .06
Time 2 15.82(3.92)
Time 3 12.09 (4.69)
IAS
Timel 50.64(8.37) 1.97 .17 .16
Time 2 49.83(10.11)
Time 3 45.64(10.98)
SSI
Timel 29.87(6.56) 1.56 2.4 .14
147
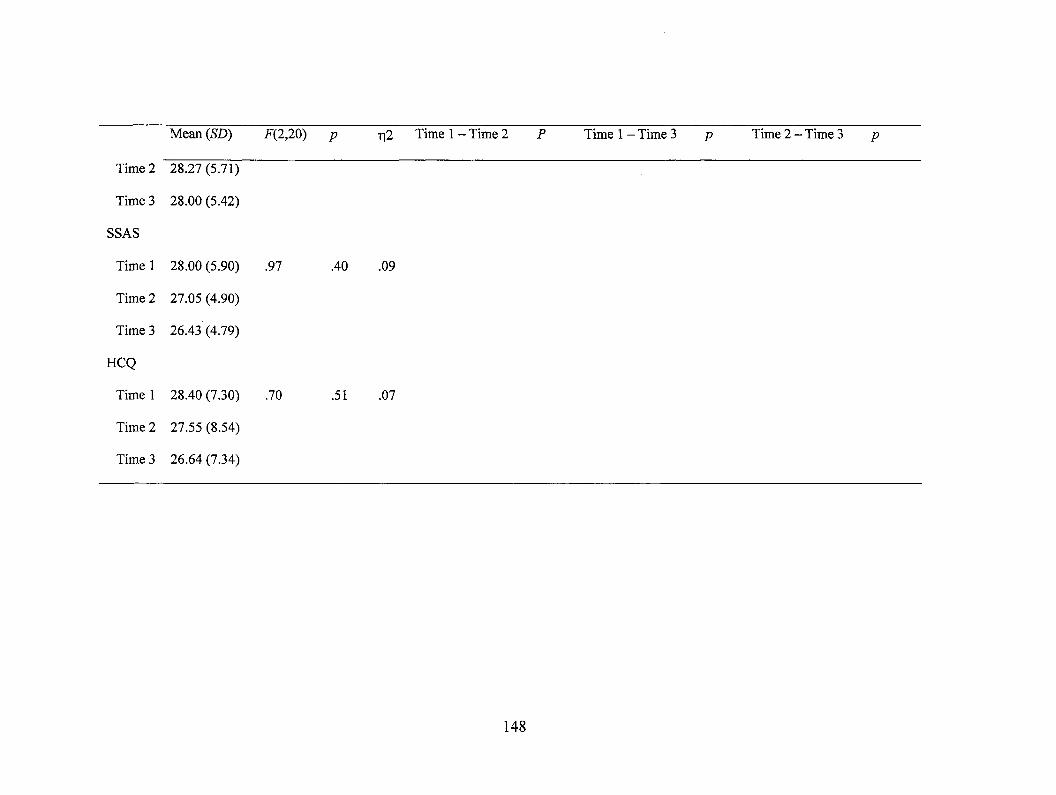
Time 2
Time 3
SSAS
Mean (SD) F(2,20) p n2 Time 1— Time 2 P Time 1— Time 3 p Time 2 — Time 3
28.27 (5.71)
28.00 (5.42)
Time 1 28.00 (5.90) .97 .40 .09
Time 2 27.05 (4.90)
Time 3 26.43 (4.79)
HCQ
Time 1 28.40 (7.30) .70 .51 .07
Time 2 27.55 (8.54)
Time 3 26.64 (7.34)
148
Mean (SD) F(2,20) p y\2 Time 1 - Time 2 P Time 1 - Time 3 p Time 2 - Time 3 p
Time 2 28.27 (5.71)
Time 3 28.00 (5.42)
SSAS
Timel 28.00(5.90) .97 .40 .09
Time 2 27.05 (4.90)
Time 3 26.43 (4.79)
HCQ
Timel 28.40(7.30) .70 .51 .07
Time 2 27.55 (8.54)
Time 3 26.64 (7.34)
148

Table 27
WLC Group Analyses at Time 1, 2, and 3 for the Secondary Outcome Measures
Mean (SD) F(2,20) p n2 Time 1— Time 2 P Time 1— Time 3 p Time 2 — Time 3 p
ASI
Time 1 27.33 (11.33) 2.92 .10 .23
Time 2 27.60 (11.42)
Time 3 23.82 (8.34)
STAI-S
Time 1 45.08 (10.55) 9.77 .001 .49 8.68 (45.08-36.40) .02 10.08(45.08-35.00) .01 1.40 (36.40-35.00) 1.00
Time 2 36.40 (9.78)
Time 3 35.00 (8.12)
STAI-T
Time 1 45.42 (8.28) 3.07 .07 .24
Time 2 42.11 (7.81)
Time 3 42.27 (8.72)
GDS
Time 1 12.43 (5.48) 1.35 .28 .12
149
Table 27
WLC Group Analyses at Time I, 2, and 3 for the Secondary Outcome Measures
Mean (SD) F(2,20) p rfi Time 1 - Time 2 P Time 1 - Time 3 p Time 2 - Time 3 p
ASI
Timel 27.33(11.33) 2.92 .10 .23
Time 2 27.60(11.42)
Time 3 23.82 (8.34)
STAI-S
Timel 45.08(10.55) 9.77 .001 .49 8.68(45.08-36.40) .02 10.08(45.08-35.00) .01 1.40(36.40-35.00) 1.00
Time 2 36.40 (9.78)
Time 3 35.00(8.12)
STAI-T
Timel 45.42(8.28) 3.07 .07 .24
Time 2 42.11(7.81)
Time 3 42.27 (8.72)
GDS
Timel 12.43(5.48) 1.35 .28 .12
149

Time 2
Time 3
GPM
Mean (SD) F(2,20) p ri2 Time 1— Time 2 P Time 1— Time 3 p Time 2 — Time 3 P
10.77 (5.48)
10.48 (4.90)
Time 1 19.71 (12.52) .52 .60 .05
Time 2 21.01 (10.10)
Time 3 20.91 (12.58)
PCS
Time 1 42.83 (11.96) .70 .51 .07
Time 2 40.59 (12.21)
Time 3 42.70 (12.25) 1.56 .23 .14
MCS
Time 1 42.24 (10.92) 1.54 .24 .13
Time 2 45.41 (11.09)
Time 3 45.16 (7.72)
Note. ASI = Anxiety Sensitivity Index; STAI-S = State Trait Anxiety Inventory — State Scale; STAI-T = State Trait Anxiety Inventory — Trait
Scale; GDS = Geriatric Depression Scale; GPM = Geriatric Pain Measure; PCS = Short-Form — 12 — Physical Summary Score; and MCS =
Short-Form — 12 — Mental Summary Score; * p < .05, ** p < .01, *** p < .001
150
Mean (SD) F(2,20) p r|2 Time 1 - Time 2 P Time 1 - Time 3 p Time 2 - Time 3 p
Time 2 10.77 (5.48)
Time 3 10.48 (4.90)
GPM
Timel 19.71(12.52) .52 .60 .05
Time 2 21.01(10.10)
Time 3 20.91(12.58)
PCS
Timel 42.83(11.96) .70 .51 .07
Time 2 40.59(12.21)
Time 3 42.70(12.25) 1.56 .23 .14
MCS
Timel 42.24(10.92) 1.54 .24 .13
Time 2 45.41(11.09)
Time 3 45.16(7.72)
State Scale; STAI-T = State Trait Anxiety Inventory - Trait
Short-Form - 12 - Physical Summary Score; and MCS =
Note. ASI = Anxiety Sensitivity Index; STAI-S = State Trait Anxiety Inventory
Scale; GDS = Geriatric Depression Scale; GPM = Geriatric Pain Measure; PCS
Short-Form - 12 - Mental Summary Score; *p< .05, ** p < .01, *** p< .001
150

Table 28
WLC Group Analyses at Time 1, 2, and 3 for the WI and SHAT Subscales
Mean (SD) F(2,20) p 1-12 Time 1— Time 2 P Time 1 — Time 3 p Time 2 — Time 3 p
WI-SS
Time 1 2.00 (1.00) 7.04 .01 .61 0.00 (2.00-2.00) 1.00 1.06 (2.00-.94) .02 1.06 (2.00-.94) .02
Time 2 2.00 (.77)
Time 3 .94 (.92)
WI-DF
Time 1 2.82 (.40) 8.18 .009 .65 .36 (2.82-1.48) .11 1.34 (2.82-1.48) .007 .97 (2.45-1.48) .05
Time 2 2.45 (.69)
Time 3 1.48 (1.21)
SHAI-
NC
Time 1 3.27 (2.41) 2.10 .18 .32
Time 2 3.37 (2.33)
Time 3 2.58 (1.54)
151
Table 28
WLC Group Analyses at Time I, 2, and 3 for the WI and SHAI Subscales
Mean (SD) F(2,20) p TJ2 Time 1 - Time 2 P Time 1 - Time 3 p Time 2 - Time 3
WI-SS
Timel 2.00(1.00) 7.04 .01 .61 0.00(2.00-2.00) 1.00 1.06 (2.00-.94) .02 1.06 (2.00-.94) .02
Time 2 2.00 (.77)
Time 3 .94 (.92)
WI-DF
Timel 2.82 (.40) 8.18 .009 .65 .36(2.82-1.48) .11 1.34(2.82-1.48) .007 .97(2.45-1.48) .05
Time 2 2.45 (.69)
Time 3 1.48(1.21)
SHAI-
NC
Timel 3.27(2.41) 2.10 .18 .32
Time 2 3.37(2.33)
Time 3 2.58(1.54)
151

Mean (SD) F(2,20) p 112 Time 1 — Time 2 P Time 1 — Time 3 p Time 2 — Time 3 p
IAS-
Fear
Time 1 13.30 (5.44) 2.81 .12 .41
Time 2 14.30 (6.25)
Time 3 12.00 (6.29)
IAS-Eff
Time 1 7.31 (1.90) .33 .72 .07
Time 2 7.04 (2.24)
Time 3 6.90 (2.59)
IAS-
Exp
Time 1 4.35 (2.06) .97 .42 .20
Time 2 4.75 (2.44)
Time 3 3.70 (3.50)
152
Mean (SD) F(2,20) p r\2 Time 1 - Time 2 P Time 1 - Time 3 p Time 2 - Time 3 p
Fear
Timel 13.30(5.44) 2.81 .12 .41
Time 2 14.30 (6.25)
Time 3 12.00 (6.29)
IAS-Eff
Timel 7.31(1.90) .33 .72 .07
Time 2 7.04 (2.24)
Time 3 6.90 (2.59)
IAS-
Exp
Timel 4.35(2.06) .97 .42 .20
Time 2 4.75 (2.44)
Time 3 3.70 (3.50)
152

Mean (SD) F(2,20) p Ti2 Time 1 — Time 2 P Time 1 — Time 3 p Time 2 — Time 3 p
IAS-
Con
Time 1 4.35 (2.06) .97 .42 .20
Time 2 4.75 (2.44)
Time 3 3.70 (3.50)
Note. WI — SS = Whiteley Index — Somatic Symptoms/Bodily Preoccupation; WI — DF = Whiteley Index — Disease Fear/Phobia; SHAI — NC =
Short Health Anxiety Inventory — Negative Consequences; IAS — Fear = Illness Attitudes Scale — Fear of Illness and Pain; IAS — Eff = Illness
Attitudes Scale — Symptom Effects; IAS — Exp = Illness Attitudes Scale — Treatment Experience; IAS — Con = Illness Attitudes Scale — Disease
Conviction; * p < .05, ** p < .01, *** p < .001
153
Mean (SD) F(2,20) p TI2 T i m e * ~Time 2 p T i m e * ~Time 3 P T i m e 2 _ T i m e 3 /> _ _
Con
Timel 4.35(2.06) .97 .42 .20
Time 2 4.75 (2.44)
Time 3 3.70 (3.50)
Note. WI - SS = Whiteley Index - Somatic Symptoms/Bodily Preoccupation; WI - DF = Whiteley Index - Disease Fear/Phobia; SHAI - NC =
Short Health Anxiety Inventory — Negative Consequences; IAS - Fear = Illness Attitudes Scale - Fear of Illness and Pain; IAS - Eff = Illness
Attitudes Scale - Symptom Effects; IAS - Exp = Illness Attitudes Scale - Treatment Experience; IAS - Con = Illness Attitudes Scale - Disease
Conviction; *p< .05, **p< .01, ***p< .001
153

The results from the one-way repeated measures ANOVAs assessing change in
each secondary outcome measure, across all three time points are shown in Table 26.
These analyses revealed significant differences on scores on the STAI-State (p = .001).
Pairwise comparisons indicated that scores at Time 2 were significantly lower than scores
at Time 1 (p = .02), and scores at Time 3 were significantly lower than scores at Time 1
(p = .01). There was no significant difference found between scores at Time 2 and Time
3.
One-way repeated measures ANOVAs assessing change in the WI, SHAI, and
IAS subscales across all three time points were conducted (results shown in Table 30).
These analyses revealed significant differences on scores on the WI-Somatic
Symptoms/Bodily Preoccupation (p = .01) and WI-Disease Fear/Phobia (p = .009). On
WI-Somatic Symptoms/Bodily Preoccupation, pairwise comparisons indicated that scores
at Time 3 were significantly lower than scores at Time 1 (p = .02), and scores at Time 3
were significantly lower than scores at Time 2 (p = .02). On WI-Disease Fear/Phobia,
pairwise comparisons indicated that scores at Time 3 were significantly lower than scores
at Time 1 (p = .007), and scores at Time 3 were significantly lower than scores at Time 2
(p = .05). There were no other significant differences noted.
These results suggest that in this WLC group that was administered ECBT after
the six week waiting period, ECBT was effective in significantly reducing health anxiety
as measured by the WI and the SHAI.
154
The results from the one-way repeated measures ANOVAs assessing change in
each secondary outcome measure, across all three time points are shown in Table 26.
These analyses revealed significant differences on scores on the STAI-State (p = .001).
Pairwise comparisons indicated that scores at Time 2 were significantly lower than scores
at Time 1 (p = .02), and scores at Time 3 were significantly lower than scores at Time 1
(p = .01). There was no significant difference found between scores at Time 2 and Time
3.
One-way repeated measures ANOVAs assessing change in the WI, SHAI, and
IAS subscales across all three time points were conducted (results shown in Table 30).
These analyses revealed significant differences on scores on the Wl-Somatic
Symptoms/Bodily Preoccupation (p = .01) and WI-Disease Fear/Phobia (p = .009). On
Wl-Somatic Symptoms/Bodily Preoccupation, pairwise comparisons indicated that scores
at Time 3 were significantly lower than scores at Time 1 (p = .02), and scores at Time 3
were significantly lower than scores at Time 2 (p = .02). On WI-Disease Fear/Phobia,
pairwise comparisons indicated that scores at Time 3 were significantly lower than scores
at Time 1 (p = .007), and scores at Time 3 were significantly lower than scores at Time 2
(p = .05). There were no other significant differences noted.
These results suggest that in this WLC group that was administered ECBT after
the six week waiting period, ECBT was effective in significantly reducing health anxiety
as measured by the WI and the SHAI.
154

3.1.7 Results of the Qualitative Analysis
3.1.7.1 Pre-Treatment Responses
A further purpose of the above study was to gather qualitative information about
health anxiety from the older adult participants and to examine this information in
relation to the CB model of health anxiety. From this analysis, six main themes
emerged as potential mechanisms for the development of health anxiety including
Anxiety is Genetic, Anxiety is a Learned Response, Vulnerability to Illness and Disease,
Awfulness of Illness, Inability to Cope, and Inability of Medical Care to Help. Several of
these themes also had subthemes (see Table 28 for outline of themes and sub-themes, and
Figure 10 for the model of the development of health anxiety in older adults).
Theme: Anxiety is Genetic. Some participants appeared to believe they were
naturally anxious or had been born that way. They reported that anxiety, worrying, and
nervousness was normal to them, because this had always been the case. For example,
one participant indicated that she worried about her health because "I am a natural
worrier."
Theme: Anxiety is a Learned Response. Some participants appeared to believe
that they had learned to respond with anxiety to health-related stressors. These
participants indicated they had learned to respond with anxiety through watching their
parents respond to health-related stressors. These participants appeared to learn that one
must be vigilant about one's health to avoid illness and disease and that health problems
were something to fear. For example, one participant indicated: "I worry about my health
because I observed my parents' approach to aches and pains, which was negative and to
155
3.1.7 Results of the Qualitative Analysis
3.1.7.1 Pre-Treatment Responses
A further purpose of the above study was to gather qualitative information about
health anxiety from the older adult participants and to examine this information in
relation to the CB model of health anxiety. From this analysis, six main themes
emerged as potential mechanisms for the development of health anxiety including
Anxiety is Genetic, Anxiety is a Learned Response, Vulnerability to Illness and Disease,
Awfulness of Illness, Inability to Cope, and Inability of Medical Care to Help. Several of
these themes also had subthemes (see Table 28 for outline of themes and sub-themes, and
Figure 10 for the model of the development of health anxiety in older adults).
Theme: Anxiety is Genetic. Some participants appeared to believe they were
naturally anxious or had been born that way. They reported that anxiety, worrying, and
nervousness was normal to them, because this had always been the case. For example,
one participant indicated that she worried about her health because "I am a natural
worrier."
Theme: Anxiety is a Learned Response. Some participants appeared to believe
that they had learned to respond with anxiety to health-related stressors. These
participants indicated they had learned to respond with anxiety through watching their
parents respond to health-related stressors. These participants appeared to learn that one
must be vigilant about one's health to avoid illness and disease and that health problems
were something to fear. For example, one participant indicated: "I worry about my health
because I observed my parents' approach to aches and pains, which was negative and to
155

Table 29
Themes and Sub-Themes of the Development of Health Anxiety in Seniors
Themes Sub-themes
Anxiety is Genetic
Anxiety is a Learned Response •
•
Experience with Illness
Experience with Death
Vulnerability to Illness
Awfulness of Illness •
•
•
•
Fear of Death
Fear of Pain
Fear of Disability & Dependence
Fear of Missing Out
Inability to Cope
Inability of Medical Care to Help
156
Table 29
Themes and Sub-Themes of the Development of Health Anxiety in Seniors
Themes
Anxiety is Genetic
Anxiety is a Learned Response
Vulnerability to Illness
Awfulness of Illness
Inability to Cope
Inability of Medical Care to Help
Sub-themes
• Experience with Illness
• Experience with Death
• Fear of Death
• Fear of Pain
• Fear of Disability & Dependence
• Fear of Missing Out
156

Genetics
HEALTH
ANXIETY
i Core Belief About Health &
Illness • Vulnerability to Disease • Inability to Cope • Awful Consequences • Inadequacy of
Physicians/Medical Care
Learning • Experience with
Illness • Experience with
Death
Figure 10. Model of the development of health anxiety in older adults
157
Genetics Learning
• Experience with Illness
• Experience with Death
Core Belief About Health & Illness
• Vulnerability to Disease • Inability to Cope • Awful Consequences • Inadequacy of
Physicians/Medical Care
Figure 10. Model of the development of health anxiety in older adults
157

be endured." In addition, participants appeared to believe their own experience with
illness and death contributed to their learning that health and illness should be feared.
Further analysis of the data revealed two sub-themes that illustrated the more specific
experiences that participants had with learning about illness including Experience with
Illness and Experience with Death.
Sub-theme: Experience with Illness. Many of the participants reported various
personal experiences with illness and health-related issues, such as experience with their
own personal health issues and with the health issues of family and friends, both mental
and physical. Some participants recalled noteworthy experiences with illness and health
issues beginning in childhood. For example, one participant indicated she had
experienced "unpleasant visits to doctors and hospitals. [I] became very frightened of
brick buildings and developed a fear of hospitals." Participants also reported significant
experiences with mental health issues: "I was hospitalized for anxiety and depression. I
have been treated for both over time." Finally, some participants also reported
experiencing current significant and life-changing health problems. For example, one
participant reported that "I had a stroke (trans ischemic attack) in 2000. I wasn't sure
what it was at first, but I had a great fear that something bad was going to happen to me."
Many of the older adults reported witnessing, throughout their lifetime, family
members, especially parents and friends', experiences of illness and health concerns. It
appeared that many of these participants were significantly negatively impacted by these
experiences. For example, one participant reported: "My mom and other family members
have both diabetes and heart disease. I worry about it." Other participants reported
158
be endured." In addition, participants appeared to believe their own experience with
illness and death contributed to their learning that health and illness should be feared.
Further analysis of the data revealed two sub-themes that illustrated the more specific
experiences that participants had with learning about illness including Experience with
Illness and Experience with Death.
Sub-theme: Experience with Illness. Many of the participants reported various
personal experiences with illness and health-related issues, such as experience with their
own personal health issues and with the health issues of family and friends, both mental
and physical. Some participants recalled noteworthy experiences with illness and health
issues beginning in childhood. For example, one participant indicated she had
experienced "unpleasant visits to doctors and hospitals. [I] became very frightened of
brick buildings and developed a fear of hospitals." Participants also reported significant
experiences with mental health issues: "I was hospitalized for anxiety and depression. I
have been treated for both over time." Finally, some participants also reported
experiencing current significant and life-changing health problems. For example, one
participant reported that "I had a stroke (trans ischemic attack) in 2000. I wasn't sure
what it was at first, but I had a great fear that something bad was going to happen to me."
Many of the older adults reported witnessing, throughout their lifetime, family
members, especially parents and friends', experiences of illness and health concerns. It
appeared that many of these participants were significantly negatively impacted by these
experiences. For example, one participant reported: "My mom and other family members
have both diabetes and heart disease. I worry about it." Other participants reported
158
witnessing family members with mental health issues. For example, "I have a bad family
history of suicide — father, sister, aunt, cousin."
Sub-theme: Experience with Death. Many of the participants reported personal
experiences with death that were significant and, for some, problematic. Some
participants reported their own personal close calls with death and many participants
reported having a difficult time coping with deaths of family members. These close calls
occurred in childhood for some and throughout adulthood for others. For example, one
participant reported: "At three weeks of age, I developed whooping cough and almost
died. I was a sickly child." Others reported medical emergencies that were dangerous
and life-threatening. For example, one participant indicated "I experienced a severe post-
partum haemorrhage and had to receive blood transfusions. I almost died..."
Some participants recalled witnessing the death of family members and friends
from health-related issues or complications. Many indicated these experiences had been
difficult and distressing. For example, one participant indicated that "My mother and
sister both died in their 60's from cancer. These were horrible, painful deaths." Another
participant indicated that "My father passed away at the age of 60 because of kidney
failure. There was no dialysis at the time. I've had a sister and brother die from cancer.
That was traumatic."
Theme: Vulnerability to Illness. Some participants reported they felt vulnerable to
illness and at greater risk for developing various diseases. Some participants reported
that due to poor health habits, such as smoking and not taking care of themselves, they
felt at higher risk for developing illness and disease. One participant reported that "I
159
witnessing family members with mental health issues. For example, "I have a bad family
history of suicide - father, sister, aunt, cousin."
Sub-theme: Experience with Death. Many of the participants reported personal
experiences with death that were significant and, for some, problematic. Some
participants reported their own personal close calls with death and many participants
reported having a difficult time coping with deaths of family members. These close calls
occurred in childhood for some and throughout adulthood for others. For example, one
participant reported: "At three weeks of age, I developed whooping cough and almost
died. I was a sickly child." Others reported medical emergencies that were dangerous
and life-threatening. For example, one participant indicated "I experienced a severe post
partum haemorrhage and had to receive blood transfusions. I almost died..."
Some participants recalled witnessing the death of family members and friends
from health-related issues or complications. Many indicated these experiences had been
difficult and distressing. For example, one participant indicated that "My mother and
sister both died in their 60's from cancer. These were horrible, painful deaths." Another
participant indicated that "My father passed away at the age of 60 because of kidney
failure. There was no dialysis at the time. I've had a sister and brother die from cancer.
That was traumatic."
Theme: Vulnerability to Illness. Some participants reported they felt vulnerable to
illness and at greater risk for developing various diseases. Some participants reported
that due to poor health habits, such as smoking and not taking care of themselves, they
felt at higher risk for developing illness and disease. One participant reported that "I
159

smoked a pack [of cigarettes] a day until I was 40. I keep expecting to get lung cancer."
Another participant reported "When my husband was sick...things went downhill from
there. It started with rheumatoid arthritis. When he died that was hard and that was
when I started worrying about [my own] health. I didn't take care of myself because I
was taking care of my husband."
Other participants appeared to feel that, because of their family history of health
issues, they were at increased risk for developing health-related issues. One other
participant wrote the following: "It crosses my mind that I would get cancer because my
parents both had cancer."
Theme: Awfulness of Illness. Another prominent concern among participants was
the perception that illness or disease would result in various serious negative
consequences. Many reported feeling fearful and anxious about what would accompany
the illness/disease. Further analysis of the data revealed five sub-themes that illustrated
the more specific experiences that participants had with awfulness of illness including
Fear of Death, Fear of Pain, Fear of Disability and Dependence, and Fear of Missing
Out on Life.
Sub-theme: Fear of Death. Some participants reported they were fearful that they
would die as a result of a health-related issue or disease. When asked what it was about
health that she worried about, one participant wrote: "When I get short of breath I
worry...worry that I will die. I don't think it's my time, and I got lots of things yet to do."
Another participant wrote: "[I worry] about having another stoke when my heart is
160
smoked a pack [of cigarettes] a day until I was 40. I keep expecting to get lung cancer."
Another participant reported "When my husband was sick...things went downhill from
there. It started with rheumatoid arthritis. When he died that was hard and that was
when I started worrying about [my own] health. I didn't take care of myself because I
was taking care of my husband."
Other participants appeared to feel that, because of their family history of health
issues, they were at increased risk for developing health-related issues. One other
participant wrote the following: "It crosses my mind that I would get cancer because my
parents both had cancer."
Theme: Awfulness of Illness. Another prominent concern among participants was
the perception that illness or disease would result in various serious negative
consequences. Many reported feeling fearful and anxious about what would accompany
the illness/disease. Further analysis of the data revealed five sub-themes that illustrated
the more specific experiences that participants had with awfulness of illness including
Fear of Death, Fear of Pain, Fear of Disability and Dependence, and Fear of Missing
Out on Life.
Sub-theme: Fear of Death. Some participants reported they were fearful that they
would die as a result of a health-related issue or disease. When asked what it was about
health that she worried about, one participant wrote: "When I get short of breath I
worry...worry that I will die. I don't think it's my time, and I got lots of things yet to do.v
Another participant wrote: "[I worry] about having another stoke when my heart is
160

beating fast, and the threat of another one bothers me. [I worry] that I will end up being
disabled and dead."
Sub-theme: Fear of Pain. Other participants appeared to be most fearful of the
pain that often accompanies illness and disease. One participant indicated that "As I get
older, I have more aches and pains. I am worried about how far that will go." As another
example, one participant indicated that "Arthritis and osteoporosis have the potential to
be painful so I need to manage these as well as possible."
Sub-theme: Fear of Disability and Dependence. Other participants reported a fear
of becoming disabled or dependent on others as a result of a health problem or disease.
One participant indicated: "[I am] worried about the loss of independence and how I'll
manage physically." Another participant reported that "I worry that I will end up being
disabled. I saw [my] aunt who was paralyzed from a stroke and [I have] the idea that this
could happen to me."
Sub-theme: Fear of Missing Out on Experiences. Some participants reported that
they felt that if they became ill or their health deteriorated, they would miss out on
various important life experiences or opportunities. They felt that they still had things to
accomplish, and they appeared fearful that an illness or disease would interfere with that.
Still others felt that they had only a limited amount of time left in life and they did not
want to spend those years being sick. For example, one participant indicated that "[I
worry] that the cancer is going to come back and that the Crohn's disease will come back
because this will affect things in my life. That I will end up running out of time to do all
the things that I want to do."
161
beating fast, and the threat of another one bothers me. [I worry] that I will end up being
disabled and dead."
Sub-theme: Fear of Pain. Other participants appeared to be most fearful of the
pain that often accompanies illness and disease. One participant indicated that "As I get
older, I have more aches and pains. I am worried about how far that will go." As another
example, one participant indicated that "Arthritis and osteoporosis have the potential to
be painful so I need to manage these as well as possible."
Sub-theme: Fear of Disability and Dependence. Other participants reported a fear
of becoming disabled or dependent on others as a result of a health problem or disease.
One participant indicated: "[I am] worried about the loss of independence and how I'll
manage physically." Another participant reported that "I worry that I will end up being
disabled. I saw [my] aunt who was paralyzed from a stroke and [I have] the idea that this
could happen to me."
Sub-theme: Fear of Missing Out on Experiences. Some participants reported that
they felt that if they became ill or their health deteriorated, they would miss out on
various important life experiences or opportunities. They felt that they still had things to
accomplish, and they appeared fearful that an illness or disease would interfere with that.
Still others felt that they had only a limited amount of time left in life and they did not
want to spend those years being sick. For example, one participant indicated that "[I
worry] that the cancer is going to come back and that the Crohn's disease will come back
because this will affect things in my life. That I will end up running out of time to do all
the things that I want to do."
161

Theme: Inability to Cope. Some participants reported they believed that they
would be unable to cope with illness and disease. These participants appeared to fear that
they would be unable to cope because they were alone and they did not have anyone to
help them. Others indicated they felt that after learning they had an illness or disease,
they would be emotionally unable to cope with the disease. One participant indicated
that "I am worried about getting old and my health steadily declining. I am also worried
about not being able to cope with the problems of old age and illness in myself and my
spouse." One participant indicated that "I worry about my heart, having a stroke, and
cancer. How would I cope if I was told I had a serious illness? I feel I would [have] a
serious case of depression."
Theme: Inadequacy of Medical Care. Another concern reported by participants
was the belief that the medical system and physicians would be unable to help them if
they became ill. They described having little confidence in their physician to diagnose or
treat their health-related issues. For example, one participant indicated that "Sometimes
when [I] go to the doctor, I feel like they are not listening to me or they might be missing
something. I know what's in my body, I know something's not right and they won't
check it out. Feel pretty helpless when seeing the doctor and they aren't checking
everything. Since I've had cancer, they are supposed to have a complete body check.
When the doctor says things are fine, what can you do even when you know there is
something wrong?"
162
Theme: Inability to Cope. Some participants reported they believed that they
would be unable to cope with illness and disease. These participants appeared to fear that
they would be unable to cope because they were alone and they did not have anyone to
help them. Others indicated they felt that after learning they had an illness or disease,
they would be emotionally unable to cope with the disease. One participant indicated
that "I am worried about getting old and my health steadily declining. I am also worried
about not being able to cope with the problems of old age and illness in myself and my
spouse." One participant indicated that "I worry about my heart, having a stroke, and
cancer. How would I cope if I was told I had a serious illness? I feel I would [have] a
serious case of depression."
Theme: Inadequacy of Medical Care. Another concern reported by participants
was the belief that the medical system and physicians would be unable to help them if
they became ill. They described having little confidence in their physician to diagnose or
treat their health-related issues. For example, one participant indicated that "Sometimes
when [I] go to the doctor, I feel like they are not listening to me or they might be missing
something. I know what's in my body, I know something's not right and they won't
check it out. Feel pretty helpless when seeing the doctor and they aren't checking
everything. Since I've had cancer, they are supposed to have a complete body check.
When the doctor says things are fine, what can you do even when you know there is
something wrong?"
162
3.1.7.2 Post-Treatment Responses
A model of older adult's therapy experiences was generated based on the
qualitative data analysis (see Figure 11). This model encompassed four themes that
emerged from the analysis: Essential Components of the Therapy Experience, Essential
Components of the Therapeutic Relationship, Benefits of the Therapy Experience, and
Issues with the Therapy Program (see Table 29 for outline of themes and sub-themes).
Theme: Essential Components of the Therapy Experience. Participants described
what they felt to be the most helpful and essential components of the therapy experience.
Further analysis of the data revealed five sub-themes that illustrated more specifically the
essential components of the therapy experience including Act of Talking to Someone
about Issues, Specific Self-Management Skills, Education and Information, and
Assignment of Homework
Sub-theme: Act of Talking to Someone about Issues. Many participants appeared
to feel that the act of discussing their issues with a professional was beneficial and
therapeutic. Participants indicated that having time to discuss problematic issues in their
lives with a therapist, and being given support and reassurance by the therapist was an
essential component of making the therapy a positive experience. For example, one
participant indicated that "talking to a professional was therapeutic [because I talked]
through the feelings I was having due to my health issues." Another participant, when
asked what she found most beneficial about the therapy program, wrote: "Just to be
speaking together. Simply, a way of speaking one-to-one with a professional
psychologist to release pent up concerns about mental, emotional, and physical
163
3.1.7.2 Post-Treatment Responses
A model of older adult's therapy experiences was generated based on the
qualitative data analysis (see Figure 11). This model encompassed four themes that
emerged from the analysis: Essential Components of the Therapy Experience, Essential
Components of the Therapeutic Relationship, Benefits of the Therapy Experience, and
Issues with the Therapy Program (see Table 29 for outline of themes and sub-themes).
Theme: Essential Components of the Therapy Experience. Participants described
what they felt to be the most helpful and essential components of the therapy experience.
Further analysis of the data revealed five sub-themes that illustrated more specifically the
essential components of the therapy experience including Act of Talking to Someone
about Issues, Specific Self-Management Skills, Education and Information, and
Assignment of Homework.
Sub-theme: Act of Talking to Someone about Issues. Many participants appeared
to feel that the act of discussing their issues with a professional was beneficial and
therapeutic. Participants indicated that having time to discuss problematic issues in their
lives with a therapist, and being given support and reassurance by the therapist was an
essential component of making the therapy a positive experience. For example, one
participant indicated that "talking to a professional was therapeutic [because I talked]
through the feelings I was having due to my health issues." Another participant, when
asked what she found most beneficial about the therapy program, wrote: "Just to be
speaking together. Simply, a way of speaking one-to-one with a professional
psychologist to release pent up concerns about mental, emotional, and physical
163

Essential Components of Essential Components of Therapy Program Therapeutic Relationship
Self-Management
Skills
Education & Information
Addresses Issues
Act of Talking to a
Professional
Positive Therapy Experience • Knowledge & Skill • Normalization • Time for Self-Care • Insight and Awareness • Confidence & Autonomy
Homework & Practice
Therapist Qualities
Empathic Professional Calm and relaxed Optimistic Friendly Non-judgemental Trustworthy Genuinely interested Invested in Outcome Honest and Sincere
Therapist Actions • Being present — face to face • Putting client at ease • Encouraging and reinforcing • Communicating belief in
therapy program • Instilling hope
Figure 11. Model of older adults ' experiences and perceptions of psychological treatment
for health anxiety
164
Essential Components of Therapy Program
Essential Components of Therapeutic Relationship
Act of Talking to a
Professional
Self-Management
Skills
Education & Information
Addresses Issues
Therapist Qualities
Empathic Professional Calm and relaxed Optimistic Friendly Non-judgemental Trustworthy Genuinely interested Invested in Outcome Honest and Sincere
Homework & Practice
Therapist Actions • Being present - face to face • Putting client at ease • Encouraging and reinforcing • Communicating belief in
therapy program • Instilling hope
Figure 11. Model of older adults' experiences and perceptions of psychological treatment
for health anxiety
164

Table 30
Themes and Sub-themes of Older Adults ' Experiences and Perceptions of Psychological
Treatment for Health Anxiety
Themes Sub-themes
Essential Component of Therapy
Program
• Act of Talking to a Professional
• Self-Management Skills
• Education & Information
• Homework & Practice
Essential Components of Therapeutic
Relationship
• Therapist Qualities
• Empathic
• Professional
• Calm and relaxed
• Optimistic
• Friendly
• Non-judgemental
• Trustworthy
• Genuinely interested
• Invested in Outcome
• Honest and Sincere
• Therapist Actions
• Being present — face to face
165
Table 30
Themes and Sub-themes of Older Adults' Experiences and Perceptions of Psychological
Treatment for Health Anxiety
Themes
Essential Component of Therapy
Program
Essential Components of Therapeutic
Relationship
Sub-themes
• Act of Talking to a Professional
• Self-Management Skills
• Education & Information
• Homework & Practice
• Therapist Qualities
• Empathic
• Professional
• Calm and relaxed
• Optimistic
• Friendly
• Non-judgemental
• Trustworthy
• Genuinely interested
• Invested in Outcome
• Honest and Sincere
• Therapist Actions
• Being present - face to face
165

• Putting client at ease
• Encouraging and reinforcing
• Communicating belief in therapy
program
• Instilling hope
Benefits of Therapy Experience • Knowledge & Skill
• Normalization
• Time for Self-Care
• Insight & Awareness
• Confidence & Autonomy
Issue with the Therapy Program • Did Not Adequately Address Problems
166
Benefits of Therapy Experience
Issue with the Therapy Program
• Putting client at ease
• Encouraging and reinforcing
• Communicating belief in therapy
program
• Instilling hope
• Knowledge & Skill
• Normalization
• Time for Self-Care
• Insight & Awareness
• Confidence & Autonomy
• Did Not Adequately Address Problems
166

behaviours" was helpful.
Sub-theme: Specific Self-Management Skills. Participants' experience of the
helpfulness of the various self-management techniques in decreasing anxiety and
improving well-being was a prominent theme among the responses. Most participants
reported at least one technique that they found useful but many participants listed a
number of the techniques for reducing their anxiety including relaxation techniques,
cognitive restructuring, goal setting, and distraction techniques. For example, one
participant wrote the following: "So now I can take on my health anxiety and use some of
the techniques I learned in the program — breathing exercises to calm you down and
distraction techniques"; and Coping techniques: 1) substituting new attitudes for negative
ones — new ways of looking at a situation; self-talk — rid myself of 'all or nothing'
attitude; diaphragmatic breathing for stress relief; distractions useful if unhealthy
thoughts bother me."
Sub-theme: Education and Information. Some participants reported they felt that
the provision of education and information to be an important and beneficial component
of the therapy programs. Participants indicated that education and information on
anxiety, coping, and self-management were helpful and that having written information
to review outside of therapy was a useful reminder or explanation for what had been
discussed during therapy. For example, one participant wrote "I was given information
which has helped me with my Parkinson's [disease] and the physical sensations
associated with the disease. I learned that I could deal with the anxiety and stress related
to my Parkinson's disease by doing the relaxation exercises to stay calm and found it
167
behaviours" was helpful.
Sub-theme: Specific Self-Management Skills. Participants' experience of the
helpfulness of the various self-management techniques in decreasing anxiety and
improving well-being was a prominent theme among the responses. Most participants
reported at least one technique that they found useful but many participants listed a
number of the techniques for reducing their anxiety including relaxation techniques,
cognitive restructuring, goal setting, and distraction techniques. For example, one
participant wrote the following: "So now I can take on my health anxiety and use some of
the techniques I learned in the program - breathing exercises to calm you down and
distraction techniques"; and Coping techniques: 1) substituting new attitudes for negative
ones - new ways of looking at a situation; self-talk - rid myself of 'all or nothing'
attitude; diaphragmatic breathing for stress relief; distractions useful if unhealthy
thoughts bother me."
Sub-theme: Education and Information. Some participants reported they felt that
the provision of education and information to be an important and beneficial component
of the therapy programs. Participants indicated that education and information on
anxiety, coping, and self-management were helpful and that having written information
to review outside of therapy was a useful reminder or explanation for what had been
discussed during therapy. For example, one participant wrote "I was given information
which has helped me with my Parkinson's [disease] and the physical sensations
associated with the disease. I learned that I could deal with the anxiety and stress related
to my Parkinson's disease by doing the relaxation exercises to stay calm and found it
167

helped me settle down." Another participant wrote the following: "The therapist brought
in new ideas that I had not considered before. When I have sensations of burning,
especially in the facial area, I remember to say to myself, 'This is no worse than it has
been previous, so it will ease up.' I never realized how powerful the mind is."
Sub-theme: Homework Some participants reported that they found that the
assignment of homework which resulted in having to practice the various self-
management skills to be helpful in learning how to manage their anxiety. For example,
one participant wrote that what helped motivate her to continue with the program was
"homework and going back to my list and to the handout book. Practice, practice how I
was thinking about sensations." Another participant wrote the following: "At every
session, we always discussed the methods I was using to counter stress — applied
relaxation or the diaphragmatic breathing exercise to reduce as much stress as possible.
We also discussed the rest of the techniques that I was using. As this was discussed at
every session, I understood that it was my responsibility to implement these exercises if I
wanted to change and feel better about myself and my health."
Theme: Essential Components of the Therapeutic Relationship. Most participants
indicated that they felt the therapeutic relationship had been a good one and described
positive experiences with their therapist. They also described what they felt to be the
most helpful and essential components of the therapeutic relationship. Further analysis of
the data revealed two sub-themes that illustrated more specifically the essential
components of the therapeutic relationship including Therapist Qualities and Therapist
Actions.
168
helped me settle down." Another participant wrote the following: "The therapist brought
in new ideas that I had not considered before. When I have sensations of burning,
especially in the facial area, I remember to say to myself, 'This is no worse than it has
been previous, so it will ease up.' I never realized how powerful the mind is."
Sub-theme: Homework. Some participants reported that they found that the
assignment of homework which resulted in having to practice the various self-
management skills to be helpful in learning how to manage their anxiety. For example,
one participant wrote that what helped motivate her to continue with the program was
"homework and going back to my list and to the handout book. Practice, practice how I
was thinking about sensations." Another participant wrote the following: "At every
session, we always discussed the methods I was using to counter stress - applied
relaxation or the diaphragmatic breathing exercise to reduce as much stress as possible.
We also discussed the rest of the techniques that I was using. As this was discussed at
every session, I understood that it was my responsibility to implement these exercises if I
wanted to change and feel better about myself and my health."
Theme: Essential Components of the Therapeutic Relationship. Most participants
indicated that they felt the therapeutic relationship had been a good one and described
positive experiences with their therapist. They also described what they felt to be the
most helpful and essential components of the therapeutic relationship. Further analysis of
the data revealed two sub-themes that illustrated more specifically the essential
components of the therapeutic relationship including Therapist Qualities and Therapist
Actions.
168

Sub-theme: Therapist Qualities. Most participants reported that they believed
specific therapist qualities positively impacted on the therapeutic relationship and their
level of motivation for therapy. Participants consistently indicated that the following
therapist qualities were important for fostering the therapeutic relationship and
motivation for psychotherapy: empathic; professional — knowledgeable, effective
communicator; calm and relaxed; optimistic; friendly; non-judgemental; trustworthy,
genuinely interested in the patient; invested in therapy outcome; and honest and sincere.
For example, one participant wrote "The therapist was excellent in her knowledge of
anxiety disorders and how it related to me. There was excellent communication between
us and she was very cooperative and helpful to me, and that strengthened the
relationship." When asked what she felt helped strengthen the therapeutic relationship,
another participant wrote "[The therapist] was a good listener, non-judgemental, guided
me in the right direction, she was friendly and she smiled, and she was easy to talk to."
Sub-theme: Therapist Actions. Most participants reported they believed specific
therapist actions positively impacted on the therapeutic relationship and their level of
motivation for psychotherapy. Participants consistently indicated that the following
therapist actions were important for fostering the therapeutic relationship and motivation
for therapy: being present or face-to-face, putting the client at ease, encouraging and
reinforcing, communicating belief in the therapy program, and instilling hope. For
example, one participant, when asked what helped motivate her during therapy, wrote
that "[The therapist] seemed to 'so believe' in the program and that it could help me that I
tried to participate fully." Another participant wrote "I think [my therapist] encouraged
169
Sub-theme: Therapist Qualities. Most participants reported that they believed
specific therapist qualities positively impacted on the therapeutic relationship and their
level of motivation for therapy. Participants consistently indicated that the following
therapist qualities were important for fostering the therapeutic relationship and
motivation for psychotherapy: empathic; professional - knowledgeable, effective
communicator; calm and relaxed; optimistic; friendly; non-judgemental; trustworthy,
genuinely interested in the patient; invested in therapy outcome; and honest and sincere.
For example, one participant wrote "The therapist was excellent in her knowledge of
anxiety disorders and how it related to me. There was excellent communication between
us and she was very cooperative and helpful to me, and that strengthened the
relationship." When asked what she felt helped strengthen the therapeutic relationship,
another participant wrote "[The therapist] was a good listener, non-judgemental, guided
me in the right direction, she was friendly and she smiled, and she was easy to talk to."
Sub-theme: Therapist Actions. Most participants reported they believed specific
therapist actions positively impacted on the therapeutic relationship and their level of
motivation for psychotherapy. Participants consistently indicated that the following
therapist actions were important for fostering the therapeutic relationship and motivation
for therapy: being present or face-to-face, putting the client at ease, encouraging and
reinforcing, communicating belief in the therapy program, and instilling hope. For
example, one participant, when asked what helped motivate her during therapy, wrote
that "[The therapist] seemed to 'so believe' in the program and that it could help me that I
tried to participate fully." Another participant wrote "I think [my therapist] encouraged
169

me quite a lot — I was sorry that the sessions had to end because I really felt that I
benefitted from our relationship."
Theme: Benefits of the Therapy Experience. All but two participants reported
they experienced a number of benefits from engaging in the therapy experience, and that
therapy had been worthwhile. Further analysis of the data revealed five sub-themes that
illustrated the more specific benefits that participants had with the therapy experience
including Knowledge and Skill, Normalization, Time for Self-care, Insight and
Awareness, and Confidence and Autonomy.
Sub-theme: Knowledge and Skill: Many participants reported that, during
therapy, they were able to gain knowledge and skills related to the management of health
anxiety. More specifically, many participants indicated they gained knowledge and skill
related to coping strategies, the construct of health anxiety and worry, and future
maintenance of mental health. For example, one participant wrote that "[The program
helped improve my worries about my health] by providing me with ideas on how to cope
and by educating [me] on how this (anxiety) has become an obstacle in my life and could
eventually become all consuming if not recognized and stopped." Another participant
indicated "Yes, the program did help. I realized more that health and other kinds of
worries affect what that I do and my behaviour shows it. My behaviour can influence the
amount of health anxiety I have and cope with my problems. So I now can take on my
health anxiety and use some of the techniques I learned in the program — i.e., 1) breath
exercise to calm you down, 2) distraction techniques. The techniques and strategies I
170
me quite a lot - 1 was sorry that the sessions had to end because I really felt that I
benefitted from our relationship."
Theme: Benefits of the Therapy Experience. All but two participants reported
they experienced a number of benefits from engaging in the therapy experience, and that
therapy had been worthwhile. Further analysis of the data revealed five sub-themes that
illustrated the more specific benefits that participants had with the therapy experience
including Knowledge and Skill, Normalization, Time for Self-care, Insight and
Awareness, and Confidence and Autonomy.
Sub-theme: Knowledge and Skill: Many participants reported that, during
therapy, they were able to gain knowledge and skills related to the management of health
anxiety. More specifically, many participants indicated they gained knowledge and skill
related to coping strategies, the construct of health anxiety and worry, and future
maintenance of mental health. For example, one participant wrote that "[The program
helped improve my worries about my health] by providing me with ideas on how to cope
and by educating [me] on how this (anxiety) has become an obstacle in my life and could
eventually become all consuming if not recognized and stopped." Another participant
indicated "Yes, the program did help. I realized more that health and other kinds of
worries affect what that I do and my behaviour shows it. My behaviour can influence the
amount of health anxiety I have and cope with my problems. So I now can take on my
health anxiety and use some of the techniques I learned in the program - i.e., 1) breath
exercise to calm you down, 2) distraction techniques. The techniques and strategies I
170

learn here will allow me to maintain my behaviour and replace them with ways that will
increase my well being."
Sub-theme: Normalization. Some participants indicated they felt their anxiety
issues were normalized during therapy. For example, one participant indicated that the
program helped her by "showing me that it's normal to have a few worries about my
health and how I think about them. I now recognize sensations as normal and redirect
them with good feelings." Another participant indicated that the program helped improve
his worries about his health by "becoming aware that others feel the same [as I do]."
Sub-theme: Time for Self-Care. A few participants reported they felt they were
able to give themselves some time for self-care without feeling guilty about doing so.
One participant indicated that what she found most helpful was "not feeling guilty about
doing this for myself." Another participant indicated that what she found most helpful
about the program was that she was able to "devote time to [herself] by going" to
therapy.
Sub-theme: Insight and Self-Awareness. Some participants reported they gained
insight and awareness about themselves and their anxiety issues. One participant
indicated that what she found most helpful about the program was "by educating me and
becoming more aware of my patterns, I could use the different suggestions to minimize
or eliminate my anxiety." Other participants indicated that "It made me realize how
anxiety can affect all areas of my life."
Sub-theme: Confidence and Autonomy. Many participants reported they gained
confidence that they could effectively manage their anxiety and worry and that they could
171
learn here will allow me to maintain my behaviour and replace them with ways that will
increase my well being."
Sub-theme: Normalization. Some participants indicated they felt their anxiety
issues were normalized during therapy. For example, one participant indicated that the
program helped her by "showing me that it's normal to have a few worries about my
health and how I think about them. I now recognize sensations as normal and redirect
them with good feelings." Another participant indicated that the program helped improve
his worries about his health by "becoming aware that others feel the same [as I do]."
Sub-theme: Time for Self-Care. A few participants reported they felt they were
able to give themselves some time for self-care without feeling guilty about doing so.
One participant indicated that what she found most helpful was "not feeling guilty about
doing this for myself." Another participant indicated that what she found most helpful
about the program was that she was able to "devote time to [herself] by going" to
therapy.
Sub-theme: Insight and Self-Awareness. Some participants reported they gained
insight and awareness about themselves and their anxiety issues. One participant
indicated that what she found most helpful about the program was "by educating me and
becoming more aware of my patterns, I could use the different suggestions to minimize
or eliminate my anxiety." Other participants indicated that "It made me realize how
anxiety can affect all areas of my life."
Sub-theme: Confidence and Autonomy. Many participants reported they gained
confidence that they could effectively manage their anxiety and worry and that they could
171

continue this successfully after the treatment sessions were completed. Participants also
indicated they gained hope that their anxiety and worry could decrease if they continued
to attend therapy and if they practiced the various anxiety management techniques that
were discussed during the sessions. For example, one participant indicated she felt the
program helped improve her worries about her health by "recognizing that I had the
knowledge and confidence to deal with problems." Other participants also indicated that
they felt they gained the knowledge and confidence to more effectively cope with
anxiety: "I feel more confident that I'm doing the right things to cope with anxiety." For
example, when asked if the program helped improve her worries about her health, one
participant wrote that "[It] gave me a better attitude, so I feel more positive about the
future of my health. I felt very negative and depressed about the future when I began the
sessions, mostly due to the fact that my sister had very recently died of cancer and I felt
extremely upset and discouraged about my own health chances in the future. [I] feel
much more positive about it now."
Theme: Issue with the Therapy Program. Although the large majority of
participants described a positive experience from participating in the programs, two
participants indicated they did not feel they experienced many benefits from the program.
The main concern reported by these two participants was that they did not feel the
program adequately addressed their concerns or problems, and, thus, they did not receive
the desired benefits. For example, one participant wrote: "I started to doubt as I felt that
it did not address my problems."
172
continue this successfully after the treatment sessions were completed. Participants also
indicated they gained hope that their anxiety and worry could decrease if they continued
to attend therapy and if they practiced the various anxiety management techniques that
were discussed during the sessions. For example, one participant indicated she felt the
program helped improve her worries about her health by "recognizing that I had the
knowledge and confidence to deal with problems." Other participants also indicated that
they felt they gained the knowledge and confidence to more effectively cope with
anxiety: "I feel more confident that I'm doing the right things to cope with anxiety." For
example, when asked if the program helped improve her worries about her health, one
participant wrote that "[It] gave me a better attitude, so I feel more positive about the
future of my health. I felt very negative and depressed about the future when I began the
sessions, mostly due to the fact that my sister had very recently died of cancer and I felt
extremely upset and discouraged about my own health chances in the future. [I] feel
much more positive about it now."
Theme: Issue with the Therapy Program. Although the large majority of
participants described a positive experience from participating in the programs, two
participants indicated they did not feel they experienced many benefits from the program.
The main concern reported by these two participants was that they did not feel the
program adequately addressed their concerns or problems, and, thus, they did not receive
the desired benefits. For example, one participant wrote: "I started to doubt as I felt that
it did not address my problems."
172

3.2 Study 2 — Results
3.2.1 Comparison on Anxiety Measures.
Independent samples t-tests were used to compare the matched control group to
the older adult participants. Hypothesis 1 proposed that the older adult participants
specifically would have significantly higher scores than the control group on the Somatic
Symptoms/Bodily Preoccupation subscale of the WI, the Negative Consequences of
Illness subscale of the SHAI, and the Symptoms Effects subscale of the IAS.
Although the hypothesis was not confirmed, there were a number of significant
differences found between the two groups (see Table 30). The matched control group
had significantly higher scores than the older adult group on the SHAI, t(112) = -4.16,p
— .0001; IAS, t(112) = -2.22,p = .03; SSI, t(112) = --3.22,p = .002; HCQ, t(112) = -2.98,
p = .003; ASI, t(112) = -8.33,p = .0001; STAI-S, t(112) = -3.39,p = .001; and STAI-T,
t(112) = -5.34, p = .0001. The matched control group also had significantly higher scores
than the older adult group on various WI, SHAI, and IAS subscales, including IAS — Fear
of Illness and Pain, t(112) = -2.70,p = .008; IAS — Symptom Effects, t(112) = -3.51,p —
.001. The older adult group had significantly higher scores than the matched control
group on WI — Disease Fear/Phobia, t(112) = -2.24,p = .03.
173
3.2 Study 2 - Results
3.2.1 Comparison on Anxiety Measures.
Independent samples /-tests were used to compare the matched control group to
the older adult participants. Hypothesis 1 proposed that the older adult participants
specifically would have significantly higher scores than the control group on the Somatic
Symptoms/Bodily Preoccupation subscale of the WI, the Negative Consequences of
Illness subscale of the SHAI, and the Symptoms Effects subscale of the IAS.
Although the hypothesis was not confirmed, there were a number of significant
differences found between the two groups (see Table 30). The matched control group
had significantly higher scores than the older adult group on the SHAI, t(l 12) = -4.16, p
= .0001; IAS, t(l 12) = -2.22, p = .03; SSI, t(\ 12) = --3.22,/? = .002; HCQ, t(\ 12) = -2.98,
p = .003; ASI, t(U2) = -8.33,/? = .0001; STAI-S, t(U2) = -3.39,/? = .001; and STAI-T,
t(l 12) = -5.34, p = .0001. The matched control group also had significantly higher scores
than the older adult group on various WI, SHAI, and IAS subscales, including IAS - Fear
of Illness and Pain, t(\ 12) = -2.70, p = .008; IAS - Symptom Effects, /(l 12) = -3.51, p =
.001. The older adult group had significantly higher scores than the matched control
group on WI - Disease Fear/Phobia, t(\ 12) = -2.24,p = .03.
173

Table 31
Scale Scores for Matched Participants
Measure Older Adult Matched
Group Control Group
M (SD) M (SD) t
Whiteley Index
Total Score 9.11 1.22 9.12 1.23 -.06
Somatic Symptoms 1.68 .93 1.75 .46 -.39
Disease Fear/Phobia 2.70 1.01 2.44 .76 2.24*
Short Health Anxiety Inventory
Total Score 15.99 5.00 19.94 5.13 -4.16***
Negative Consequences 2.30 .31 2.48 .33 -.98
Illness Attitudes Scale
Total 49.46 11.20 54.54 13.16 -2.22*
Fear of Illness and Pain 13.42 5.74 16.89 7.86 -2.70**
Symptom Effects 6.67 2.83 8.54 2.86 -3.51**
Treatment Experience 9.20 2.63 9.25 2.92 -.09
Disease Conviction 4.98 2.98 5.43 2.66 -.86
Somatic Symptom Inventory 31.62 7.05 36.75 9.77 -3.22**
Somatosensory Amplification Scale 28.17 5.59 27.97 6.77 .18
Health Cognitions Questionnaire 29.53 8.57 35.80 13.35 -2.98**
Anxiety Sensitivity Index 27.47 10.80 45.32 12.05 -8.33***
174
Table 31
Scale Scores for Matched Participants
Measure Older Adult
Group
Matched
Control Group
Whiteley Index
Total Score
Somatic Symptoms
Disease Fear/Phobia
Short Health Anxiety Inventory
Total Score
Negative Consequences
Illness Attitudes Scale
Total
Fear of Illness and Pain
Symptom Effects
Treatment Experience
Disease Conviction
M (SD)
9.11 1.22
1.68 .93
2.70 1.01
15.99 5.00
2.30 .31
49.46 11.20
13.42 5.74
6.67 2.83
9.20 2.63
4.98 2.98
Somatic Symptom Inventory 31.62 7.05
Somatosensory Amplification Scale 28.17 5.59
Health Cognitions Questionnaire 29.53 8.57
Anxiety Sensitivity Index 27.47 10.80
M (SD)
9.12 1.23
1.75 .46
2.44 .76
2.48 .33
16.89 7.86
9.25 2.92
5.43 2.66
36.75 9.77
.06
-.39
2.24'
19.94 5.13 -4.16 * * *
-.98
54.54 13.16 -2.22*
-2.70 * *
8.54 2.86 -3.51**
.09
.86
-3.22**
27.97 6.77 .18
35.80 13.35 -2.98**
45.32 12.05 -8.33***
174
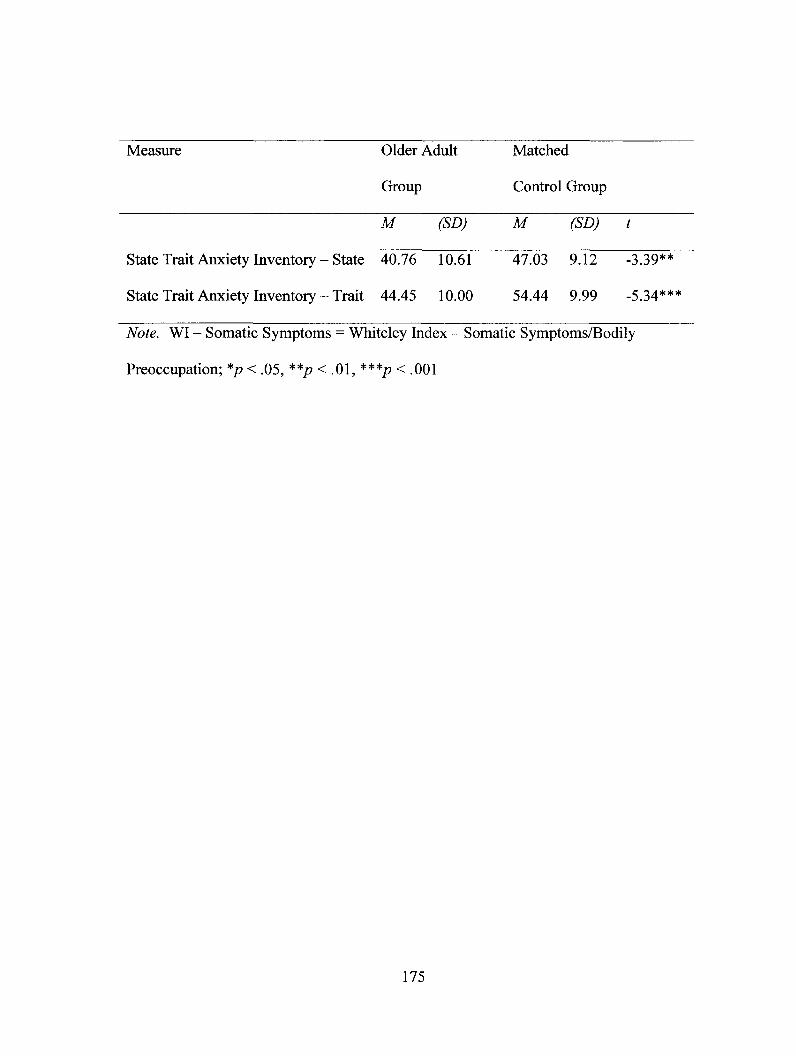
Measure Older Adult Matched
Group Control Group
M (SD) M (SD) t
State Trait Anxiety Inventory — State 40.76 10.61 47.03 9.12 -3.39**
State Trait Anxiety Inventory — Trait 44.45 10.00 54.44 9.99 -5.34***
Note. WI — Somatic Symptoms = Whiteley Index — Somatic Symptoms/Bodily
Preoccupation; *p < .05, **p < .01, ***p < .001
175
Measure Older Adult Matched
Group Control Group
M (SD) M (SD) t
State Trait Anxiety Inventory - State 40.76 10.61 47.03 9T2 -3.39**
State Trait Anxiety Inventory - Trait 44.45 10.00 54.44 9.99 -5.34***
Note. WI - Somatic Symptoms = Whiteley Index - Somatic Symptoms/Bodily
Preoccupation; *p < .05, **/? < .01, ***p < .001
175

4. DISCUSSION
Heightened levels of anxiety among older adults are associated with increased
depression (Jeste, Hays, & Steffens, 2006), increased morbidity (Ostir & Goodwin, 2006),
chronic health conditions (Diala & Muntaner, 2003), and markedly higher health care costs
(Simon, Ormel, VonKoff, & Barlow, 1995). Although aging does not inevitably result in
increases in health anxiety (Boston & Merrick, 2010; Bourgault-Fagnou &
Hadjistavropoulos, 2009), the negative effects of anxiety validate the importance of
having effective methods for reducing health anxiety among the older adult population.
Unfortunately, one of the significant limitations of the health anxiety treatment
literature is the almost exclusive focus on younger adults. Seniors have been consistently
underrepresented in research on health anxiety in spite of how common health concerns
are in the lives of older adults. Thus, most of the literature on health anxiety does not
focus attention on the unique concerns of older adults with health anxiety and specifically
on the outcome of treatment in this population. As a result, questions have been raised
about the appropriateness of generalising psychological interventions for health anxiety
developed and tested with younger adults to seniors (Snyder & Stanley, 2001). There is
empirical support, although very limited, that the CB model of health anxiety may be
applicable to older adults (Boston & Merrick, 2010). There is other evidence with other
psychological disorders that it is important to adapt treatment to meet the needs of older
adults, taking into account the changes that occur through the aging process (Mohlman et
al., 2003; Stanley, Diefenbach, Hopko, 2004). As such, psychological treatments based
176
4. DISCUSSION
Heightened levels of anxiety among older adults are associated with increased
depression (Jeste, Hays, & Steffens, 2006), increased morbidity (Ostir & Goodwin, 2006),
chronic health conditions (Diala & Muntaner, 2003), and markedly higher health care costs
(Simon, Ormel, VonKoff, & Barlow, 1995). Although aging does not inevitably result in
increases in health anxiety (Boston & Merrick, 2010; Bourgault-Fagnou &
Hadjistavropoulos, 2009), the negative effects of anxiety validate the importance of
having effective methods for reducing health anxiety among the older adult population.
Unfortunately, one of the significant limitations of the health anxiety treatment
literature is the almost exclusive focus on younger adults. Seniors have been consistently
underrepresented in research on health anxiety in spite of how common health concerns
are in the lives of older adults. Thus, most of the literature on health anxiety does not
focus attention on the unique concerns of older adults with health anxiety and specifically
on the outcome of treatment in this population. As a result, questions have been raised
about the appropriateness of generalising psychological interventions for health anxiety
developed and tested with younger adults to seniors (Snyder & Stanley, 2001). There is
empirical support, although very limited, that the CB model of health anxiety may be
applicable to older adults (Boston & Merrick, 2010). There is other evidence with other
psychological disorders that it is important to adapt treatment to meet the needs of older
adults, taking into account the changes that occur through the aging process (Mohlman et
al., 2003; Stanley, Diefenbach, Hopko, 2004). As such, psychological treatments based
176

on CB principles and with specific adaptations for older adults may be useful in treating
older adults with health anxiety.
The aim of the present study was to gain a better understanding of health anxiety
among older adults and to assess the efficacy of ECBT for health anxiety for older adults,
in comparison to a SCBT treatment and a WLC condition. Fifty-seven older adults with
health anxiety were randomly assigned to one of the three treatment conditions and were
assessed at pre- and post-treatment. Participants in both the experimental groups were
also assessed at three months following the end of treatment. The analyses addressed
several other relevant issues, including an examination of the therapeutic alliance,
motivation for psychotherapy, and clinical significance of the treatments for older adults
in the two treatment groups. Furthermore, we aimed to gain a greater understanding of
the nature of health anxiety and the experience of therapy among older adults through
qualitative analysis of open-ended questions. Finally, with this dataset we were able to
determine if older adults scored differently on health anxiety measures compared to a
younger adult sample by examining the differences between the older adult group and a
younger adult group control group. Findings from the study and how they inform the CB
model and current treatment protocols are discussed below.
4.1 Assessment of Hypotheses
According to Hypothesis 1, participants receiving SCBT and ECBT, but not those
in WLC group, would evidence improvements in health anxiety, frequency of
hypochondriacal thoughts, hypochondriacal somatic symptoms, tendency to experience
bodily symptoms as distressing, state and trait anxiety, depression, pain, and health-
177
on CB principles and with specific adaptations for older adults may be useful in treating
older adults with health anxiety.
The aim of the present study was to gain a better understanding of health anxiety
among older adults and to assess the efficacy of ECBT for health anxiety for older adults,
in comparison to a SCBT treatment and a WLC condition. Fifty-seven older adults with
health anxiety were randomly assigned to one of the three treatment conditions and were
assessed at pre- and post-treatment. Participants in both the experimental groups were
also assessed at three months following the end of treatment. The analyses addressed
several other relevant issues, including an examination of the therapeutic alliance,
motivation for psychotherapy, and clinical significance of the treatments for older adults
in the two treatment groups. Furthermore, we aimed to gain a greater understanding of
the nature of health anxiety and the experience of therapy among older adults through
qualitative analysis of open-ended questions. Finally, with this dataset we were able to
determine if older adults scored differently on health anxiety measures compared to a
younger adult sample by examining the differences between the older adult group and a
younger adult group control group. Findings from the study and how they inform the CB
model and current treatment protocols are discussed below.
4.1 Assessment of Hypotheses
According to Hypothesis 1, participants receiving SCBT and ECBT, but not those
in WLC group, would evidence improvements in health anxiety, frequency of
hypochondriacal thoughts, hypochondriacal somatic symptoms, tendency to experience
bodily symptoms as distressing, state and trait anxiety, depression, pain, and health-
177

related quality of life from pre-treatment to post-treatment. The results of the analyses
examining change from pre-treatment to post-treatment were mixed. Consistent with the
hypothesis, individuals receiving SCBT and ECBT showed significantly lower levels of
health anxiety (as measured by the WI), with reductions on the subscale measuring
disease fear/phobia, when compared to the WLC group. No other significant differences
were found at post-treatment on the primary outcome measures.
When viewing the results on the secondary outcome measures, individuals
receiving the SCBT showed significantly improved scores on the physical component of
health-related quality of life (SF-12-PCS; a high score equals higher physical health
related quality of life) when compared to the WLC group from pre-treatment to post-
treatment. No other significant differences were found on the secondary outcome
measures.
In order to evaluate the long-term effectiveness of the CBT programs,
questionnaires were completed by the experimental participants (but for ethical reasons
not the WLC participants) three months following the completion of the therapy program.
Hypothesis 2 indicated that participants treated with ECBT would demonstrate the
greatest overall improvement at post-treatment and follow-up on each of the measures
indicated in the first hypothesis. For participants treated with both SCBT and ECBT, all
expected improvements would be maintained three months following the conclusion of
treatment. Again, the findings were mixed. Improvements in scores on the WI and
Disease Fear/Phobia for participants in both treatment groups were maintained. There
were no significant declines on the measures, with the exception of one measure, in the
178
related quality of life from pre-treatment to post-treatment. The results of the analyses
examining change from pre-treatment to post-treatment were mixed. Consistent with the
hypothesis, individuals receiving SCBT and ECBT showed significantly lower levels of
health anxiety (as measured by the WI), with reductions on the subscale measuring
disease fear/phobia, when compared to the WLC group. No other significant differences
were found at post-treatment on the primary outcome measures.
When viewing the results on the secondary outcome measures, individuals
receiving the SCBT showed significantly improved scores on the physical component of
health-related quality of life (SF-12-PCS; a high score equals higher physical health
related quality of life) when compared to the WLC group from pre-treatment to post-
treatment. No other significant differences were found on the secondary outcome
measures.
In order to evaluate the long-term effectiveness of the CBT programs,
questionnaires were completed by the experimental participants (but for ethical reasons
not the WLC participants) three months following the completion of the therapy program.
Hypothesis 2 indicated that participants treated with ECBT would demonstrate the
greatest overall improvement at post-treatment and follow-up on each of the measures
indicated in the first hypothesis. For participants treated with both SCBT and ECBT, all
expected improvements would be maintained three months following the conclusion of
treatment. Again, the findings were mixed. Improvements in scores on the WI and
Disease Fear/Phobia for participants in both treatment groups were maintained. There
were no significant declines on the measures, with the exception of one measure, in the
178

three months following the end of treatment. Individuals in the SCBT group evidenced
an increase in state anxiety (STAI-S) and the ECBT group evidenced a slight decline in
state anxiety. However, there were no other significant differences found between SCBT
and ECBT, indicating that, overall, ECBT did not demonstrate that greatest overall
improvement when compared to SCBT.
While the results of the effectiveness of the two active treatment programs were
not entirely consistent with predictions, results provided a number of important insights
about the treatment of health anxiety among older adults. First, these findings provide
some support for both SCBT and ECBT as effective treatments for addressing certain
cognitive and behavioural aspects of health anxiety as well as the physical component of
health-related quality of life. Both programs appeared effective in reducing fear of
having or developing a serious illness. These findings are consistent with other studies
examining the efficacy of CBT for health anxiety (e.g., Barsky & Ahern, 2004;
Seivewright et al., 2008; Sorensen et al., in press; Visser & Bouman, 2001; Warwick et
al., 1996), which have consistently shown that CBT is effective in reducing health
anxiety.
Overall, it appears that the components of our CBT program successfully targeted
specific variables for change. For instance, there is evidence to suggest that the CBT
programs challenged some of the maladaptive thoughts and beliefs seniors were having
around the fear of having a disease. This is important because these beliefs (e.g., that one
should be fearful of disease) are hypothesized to have a negative impact on mood and
anxiety as well as on behaviours that maintain problematic beliefs (e.g., reassurance
179
three months following the end of treatment. Individuals in the SCBT group evidenced
an increase in state anxiety (STAI-S) and the ECBT group evidenced a slight decline in
state anxiety. However, there were no other significant differences found between SCBT
and ECBT, indicating that, overall, ECBT did not demonstrate that greatest overall
improvement when compared to SCBT.
While the results of the effectiveness of the two active treatment programs were
not entirely consistent with predictions, results provided a number of important insights
about the treatment of health anxiety among older adults. First, these findings provide
some support for both SCBT and ECBT as effective treatments for addressing certain
cognitive and behavioural aspects of health anxiety as well as the physical component of
health-related quality of life. Both programs appeared effective in reducing fear of
having or developing a serious illness. These findings are consistent with other studies
examining the efficacy of CBT for health anxiety (e.g., Barsky & Ahern, 2004;
Seivewright et al., 2008; Sorensen et al., in press; Visser & Bouman, 2001; Warwick et
al., 1996), which have consistently shown that CBT is effective in reducing health
anxiety.
Overall, it appears that the components of our CBT program successfully targeted
specific variables for change. For instance, there is evidence to suggest that the CBT
programs challenged some of the maladaptive thoughts and beliefs seniors were having
around the fear of having a disease. This is important because these beliefs (e.g., that one
should be fearful of disease) are hypothesized to have a negative impact on mood and
anxiety as well as on behaviours that maintain problematic beliefs (e.g., reassurance
179

seeking, focusing attention on bodily symptoms, bodily checking, avoidance) (Salkovskis
& Warwick, 2001).
Second, fears and beliefs related to illness decreased in comparison to somatic
symptoms. This finding, when examined, appears to make sense. Both treatment
protocols (SCBT and ECBT), which were based on Barsky and Ahern's (2004) CBT for
hypochondriasis, were intended to improve coping with symptoms rather than
eliminating them outright. In designing the treatment, Barsky and Ahern (2004)
indicated that individuals generally have better treatment outcomes when they learn to
cope with distressing bodily sensations rather than attempting to eliminate their somatic
sensations. Barsky and Ahern (2004) also explained that, conceptually, hypochondriacal
somatic symptoms cannot simply be stripped away with symptomatic treatment because
they exist for underlying psychological and interpersonal reasons. As such, it appears
that realistic goals in treating health anxiety include a reduction in fears and beliefs that
are distressing and an improvement in coping, rather than the elimination of somatic
symptoms.
However, improvement on the primary and secondary outcome measures in both
studies was relatively low when compared to what is typically seen in younger health
anxious samples. For example, Barsky and Ahern (2004) found that participants treated
with CBT significantly improved on measures of health anxiety (WI and SHAI),
hypochondriacal thought frequency, and somatosensory amplification. Seivewright et al.
(2008) and Sorenson et al. (2010) found that participants showed significantly greater
improvement on health anxiety as measured by the SHAI. Further, in clinical trials of
180
seeking, focusing attention on bodily symptoms, bodily checking, avoidance) (Salkovskis
& Warwick, 2001).
Second, fears and beliefs related to illness decreased in comparison to somatic
symptoms. This finding, when examined, appears to make sense. Both treatment
protocols (SCBT and ECBT), which were based on Barsky and Ahern's (2004) CBT for
hypochondriasis, were intended to improve coping with symptoms rather than
eliminating them outright. In designing the treatment, Barsky and Ahern (2004)
indicated that individuals generally have better treatment outcomes when they learn to
cope with distressing bodily sensations rather than attempting to eliminate their somatic
sensations. Barsky and Ahern (2004) also explained that, conceptually, hypochondriacal
somatic symptoms cannot simply be stripped away with symptomatic treatment because
they exist for underlying psychological and interpersonal reasons. As such, it appears
that realistic goals in treating health anxiety include a reduction in fears and beliefs that
are distressing and an improvement in coping, rather than the elimination of somatic
symptoms.
However, improvement on the primary and secondary outcome measures in both
studies was relatively low when compared to what is typically seen in younger health
anxious samples. For example, Barsky and Ahern (2004) found that participants treated
with CBT significantly improved on measures of health anxiety (WI and SHAI),
hypochondriacal thought frequency, and somatosensory amplification. Seivewright et al.
(2008) and Sorenson et al. (2010) found that participants showed significantly greater
improvement on health anxiety as measured by the SHAI. Further, in clinical trials of
180

CBT for health anxiety, reductions in associated symptoms (e.g., generalised anxiety,
depression) have also been found. For example, Seivewright et al. (2008) and Sorenson
et al. (2010) found that generalized anxiety and depression significantly improved in
individuals treated with CBT when compared with a control group. Given the differences
in findings, there are some possible explanations. First, our results may suggest that
health anxiety in late-life is more entrenched than health anxiety occurring in young
adulthood. Thus, older adults may require more than six sessions of treatment for
significant improvements to occur. In addition, it may be possible that CBT is not as
effective in older individuals with elevated health anxiety as it is in younger adults. Also,
because the improvements in levels of health anxiety were somewhat limited, there may
not have been the opportunity for accompanying reductions in anxiety sensitivity,
generalised anxiety, mood, and pain.
Another potential explanation for the lack of findings in our study is the small
sample size and statistical power needed to detect true differences between groups
(Tabachnick & Fidell, 2001). As described above, the outcome measures from pre- to
post-treatment and post-treatment to follow-up evidenced some, but only limited,
statistically significant change in those receiving the two treatments versus WLC. The
change demonstrated by the SCBT and ECBT participants was generally not significantly
greater than the change demonstrated by participants in WLC group, with the exception
of health anxiety (WI) and the physical component of health-related quality of life (SF-
12-PCS). However, the results of the paired sample t-tests and the examination of
clinically significant change suggest that improvements did occur in both the SCBT and
181
CBT for health anxiety, reductions in associated symptoms (e.g., generalised anxiety,
depression) have also been found. For example, Seivewright et al. (2008) and Sorenson
et al. (2010) found that generalized anxiety and depression significantly improved in
individuals treated with CBT when compared with a control group. Given the differences
in findings, there are some possible explanations. First, our results may suggest that
health anxiety in late-life is more entrenched than health anxiety occurring in young
adulthood. Thus, older adults may require more than six sessions of treatment for
significant improvements to occur. In addition, it may be possible that CBT is not as
effective in older individuals with elevated health anxiety as it is in younger adults. Also,
because the improvements in levels of health anxiety were somewhat limited, there may
not have been the opportunity for accompanying reductions in anxiety sensitivity,
generalised anxiety, mood, and pain.
Another potential explanation for the lack of findings in our study is the small
sample size and statistical power needed to detect true differences between groups
(Tabachnick & Fidell, 2001). As described above, the outcome measures from pre- to
post-treatment and post-treatment to follow-up evidenced some, but only limited,
statistically significant change in those receiving the two treatments versus WLC. The
change demonstrated by the SCBT and ECBT participants was generally not significantly
greater than the change demonstrated by participants in WLC group, with the exception
of health anxiety (WI) and the physical component of health-related quality of life (SF-
12-PCS). However, the results of the paired sample t-tests and the examination of
clinically significant change suggest that improvements did occur in both the SCBT and
181

ECBT groups after treatment; but given the small sample size and limited statistical
power, these improvements were not evidenced in the repeated measures analyses.
More specifically, the results of the paired samples t-tests indicated that
participants in the SCBT treatment group demonstrated significant improvements from
pre- to post-treatment on measures of health anxiety (WI, HAI, IAS) and their subscales
of Somatic Symptoms/Bodily Preoccupation, Disease Fear/Phobia (WI); Negative
Consequences (SHAI); Symptom Effects (IAS); state and trait anxiety; depression; and
health-related quality of life — mental and physical; and from post-treatment to follow-up
on state anxiety and the physical component of health-related quality of life (SF-12-PCS).
Participants in the ECBT treatment group demonstrated significant improvements from
pre- to post-treatment on measures of health anxiety (WI, SHAD and their subscales of
Somatic Symptoms/Bodily Preoccupation, Disease Fear/Phobia (WI); hypochondriacal
somatic symptoms (S SI); anxiety sensitivity; and depression; and from post-treatment to
follow-up on IAS health anxiety, and the subscales of Symptom Effects and Treatment
Experience; and Disease Fear/Phobia (WI). To the contrary, there was only one
improvement evidenced on any of the DVs for the WLC group from pre-treatment to
post-treatment, which was the physical component of health-related quality of life (SF-
12-PCS).
In addition, the changes that did occur from post-treatment to follow-up in our
study appeared to be maintained in both groups. This is consistent with a number of
studies examining the efficacy of CBT for health anxiety among younger adults (e.g.,
Seivewright et al., 2008; Sorensen et al., in press). Researchers have generally found that
182
ECBT groups after treatment; but given the small sample size and limited statistical
power, these improvements were not evidenced in the repeated measures analyses.
More specifically, the results of the paired samples Mests indicated that
participants in the SCBT treatment group demonstrated significant improvements from
pre- to post-treatment on measures of health anxiety (WI, HAI, IAS) and their subscales
of Somatic Symptoms/Bodily Preoccupation, Disease Fear/Phobia (WI); Negative
Consequences (SHAI); Symptom Effects (IAS); state and trait anxiety; depression; and
health-related quality of life - mental and physical; and from post-treatment to follow-up
on state anxiety and the physical component of health-related quality of life (SF-12-PCS).
Participants in the ECBT treatment group demonstrated significant improvements from
pre- to post-treatment on measures of health anxiety (WI, SHAI) and their subscales of
Somatic Symptoms/Bodily Preoccupation, Disease Fear/Phobia (WI); hypochondriacal
somatic symptoms (SSI); anxiety sensitivity; and depression; and from post-treatment to
follow-up on IAS health anxiety, and the subscales of Symptom Effects and Treatment
Experience; and Disease Fear/Phobia (WI). To the contrary, there was only one
improvement evidenced on any of the DVs for the WLC group from pre-treatment to
post-treatment, which was the physical component of health-related quality of life (SF-
12-PCS).
In addition, the changes that did occur from post-treatment to follow-up in our
study appeared to be maintained in both groups. This is consistent with a number of
studies examining the efficacy of CBT for health anxiety among younger adults (e.g.,
Seivewright et al., 2008; Sorensen et al., in press). Researchers have generally found that
182

treatment gains are often maintained with CBT. For example, Barsky and Ahern (2004)
found that gains on health anxiety, frequency of hypochondriacal thoughts, and
somatosensory amplification were maintained and 6- and 12-months follow-ups.
Further evidence for the effectiveness of our CBT programs for treating health
anxiety in older adults comes from an examination of clinically significant change
defined by Jacobson and Truax (1992). These authors indicated that clinically significant
change could be determined when post-treatment scores fall outside two standard
deviations of the mean of the population being examined. Of the 21 participants who
were assigned to and completed the SCBT treatment, of the 18 participants who were
assigned to and completed the ECBT treatment, and of the 18 participant who were
assigned to the WLC group, 14 of the SCBT group, 10 of the ECBT group, and 2 of the
WLC group finished with WI scores less than 8 — the score necessary for initial inclusion
in the trial. Thus, not only did 66.7% of the SCBT participants and 55.6% of ECBT
participants no longer meet criteria for elevated health anxiety as measured by the WI,
these improvements were significantly greater than those demonstrated by individuals in
the WLC group (only 11% made improvements), suggesting that both SCBT and ECBT
are effective treatments for reducing health anxiety as measured by the WI. These
findings appear consistent with those reported by Greeven et al. (2007), who found that
45% of the CBT participants had a decrease of more than one standard deviation on the
main outcome measure as opposed to a 14% decrease in the placebo group.
Qualitative analysis of post-treatment responses also provided evidence for the
effectiveness of our CBT programs for treating health anxiety in older adults. When
183
treatment gains are often maintained with CBT. For example, Barsky and Ahern (2004)
found that gains on health anxiety, frequency of hypochondriacal thoughts, and
somatosensory amplification were maintained and 6- and 12-months follow-ups.
Further evidence for the effectiveness of our CBT programs for treating health
anxiety in older adults comes from an examination of clinically significant change
defined by Jacobson and Truax (1992). These authors indicated that clinically significant
change could be determined when post-treatment scores fall outside two standard
deviations of the mean of the population being examined. Of the 21 participants who
were assigned to and completed the SCBT treatment, of the 18 participants who were
assigned to and completed the ECBT treatment, and of the 18 participant who were
assigned to the WLC group, 14 of the SCBT group, 10 of the ECBT group, and 2 of the
WLC group finished with WI scores less than 8 - the score necessary for initial inclusion
in the trial. Thus, not only did 66.7% of the SCBT participants and 55.6% of ECBT
participants no longer meet criteria for elevated health anxiety as measured by the WI,
these improvements were significantly greater than those demonstrated by individuals in
the WLC group (only 11 % made improvements), suggesting that both SCBT and ECBT
are effective treatments for reducing health anxiety as measured by the WI. These
findings appear consistent with those reported by Greeven et al. (2007), who found that
45%) of the CBT participants had a decrease of more than one standard deviation on the
main outcome measure as opposed to a 14% decrease in the placebo group.
Qualitative analysis of post-treatment responses also provided evidence for the
effectiveness of our CBT programs for treating health anxiety in older adults. When
183

asked whether they felt the program helped improve their worries about health, all but
two participants reported they experienced a number of benefits from engaging in the
therapy experience. Participants indicated they gained knowledge and skills to help
improve their ability to cope with their health anxiety and related issues. Others
indicated that their experiences with health anxiety were normalized during therapy and
they felt less different from other people. Participants reported an improvement in their
ability to engage in self-care by taking time for themselves without guilt. Others reported
an increase in insight and awareness about themselves and their issues with health
anxiety, and an increase in confidence that they could effectively manage their anxiety
and worry. Finally, participants indicated that they gained confidence and autonomy that
they could effectively manage their anxiety and worry even after treatment was
completed.
Additionally, participants were surveyed about what they believed to be helpful
during the therapy experience. They identified a number of components which they
found to be most helpful in improving their coping. Participants indicated that the act of
talking to someone about their issues was beneficial. Also reported was that the inclusion
of specific self-management skills such as relaxation techniques, cognitive restructuring,
and distraction techniques was helpful to participants during treatment. In addition,
education and information on health anxiety and the assignment of homework for weekly
practice were indicated as important aspects of therapy. Only two participants indicated
they did not feel they experienced many benefits from the program. The main concern
reported was that the program did not adequately address their concerns or problems.
184
asked whether they felt the program helped improve their worries about health, all but
two participants reported they experienced a number of benefits from engaging in the
therapy experience. Participants indicated they gained knowledge and skills to help
improve their ability to cope with their health anxiety and related issues. Others
indicated that their experiences with health anxiety were normalized during therapy and
they felt less different from other people. Participants reported an improvement in their
ability to engage in self-care by taking time for themselves without guilt. Others reported
an increase in insight and awareness about themselves and their issues with health
anxiety, and an increase in confidence that they could effectively manage their anxiety
and worry. Finally, participants indicated that they gained confidence and autonomy that
they could effectively manage their anxiety and worry even after treatment was
completed.
Additionally, participants were surveyed about what they believed to be helpful
during the therapy experience. They identified a number of components which they
found to be most helpful in improving their coping. Participants indicated that the act of
talking to someone about their issues was beneficial. Also reported was that the inclusion
of specific self-management skills such as relaxation techniques, cognitive restructuring,
and distraction techniques was helpful to participants during treatment. In addition,
education and information on health anxiety and the assignment of homework for weekly
practice were indicated as important aspects of therapy. Only two participants indicated
they did not feel they experienced many benefits from the program. The main concern
reported was that the program did not adequately address their concerns or problems.
184
These qualitative findings are consistent with the CB treatment literature, which
indicates that CBT that includes such components as education and information, the
teaching and provision of specific self-management skills (e.g., behavioural, emotional,
and cognitive), and assignment of homework are effective in the treatment of various
disorders including hypochondriasis (e.g., Barsky & Ahern, 2004; Seivewright et al.,
2008). These findings are also consistent with other qualitative investigations of
participants' experiences of psychotherapy. For example, Timulak (2007) applied meta-
analytic procedures to qualitative studies indentifying key client experiences repeatedly
described as helpful in psychotherapy. Timulak's (2007) findings indicated that through
psychotherapy, participants gained awareness/insight/self-understanding; new strategies
to attain goals; empowerment; relief; emotional exploration/experiencing; the feeling of
being understood; an opportunity for active participation; reassurance/support/safety; and
personal contact with a fellow human being.
Finally, the results from the supplementary analyses examining change in the
WLC group where participants were used as their own controls by observing changes in
baseline, post-baseline of six weeks without treatment, and post-treatment with ECBT
scores on all measures also provided evidence to the effectiveness of CBT for health
anxiety among older adults. These results indicated that participants demonstrated
significant improvements after receiving ECBT on measures of health anxiety (WI and
SHAI) that were not observed while they were waiting.
The results from the paired samples t-tests, examination of clinical change,
examination of the maintenance of gains, qualitative analysis of the post-treatment
185
These qualitative findings are consistent with the CB treatment literature, which
indicates that CBT that includes such components as education and information, the
teaching and provision of specific self-management skills (e.g., behavioural, emotional,
and cognitive), and assignment of homework are effective in the treatment of various
disorders including hypochondriasis (e.g., Barsky & Ahern, 2004; Seivewright et al.,
2008). These findings are also consistent with other qualitative investigations of
participants' experiences of psychotherapy. For example, Timulak (2007) applied meta-
analytic procedures to qualitative studies indentifying key client experiences repeatedly
described as helpful in psychotherapy. Timulak's (2007) findings indicated that through
psychotherapy, participants gained awareness/insight/self-understanding; new strategies
to attain goals; empowerment; relief; emotional exploration/experiencing; the feeling of
being understood; an opportunity for active participation; reassurance/support/safety; and
personal contact with a fellow human being.
Finally, the results from the supplementary analyses examining change in the
WLC group where participants were used as their own controls by observing changes in
baseline, post-baseline of six weeks without treatment, and post-treatment with ECBT
scores on all measures also provided evidence to the effectiveness of CBT for health
anxiety among older adults. These results indicated that participants demonstrated
significant improvements after receiving ECBT on measures of health anxiety (WI and
SHAI) that were not observed while they were waiting.
The results from the paired samples t-tests, examination of clinical change,
examination of the maintenance of gains, qualitative analysis of the post-treatment
185

responses, and findings from our supplementary analyses are consistent with previous
studies examining treatment of CBT. As such, they are important because they suggest
that SCBT and ECBT are more effective than was suggested by our other analyses.
However, additional evidence will be needed before any of these possible explanations
can be argued strongly. Thus, given these findings, further research with larger samples
of older adults appears to be warranted.
With respect to the lack of evidence that ECBT was superior to SCBT, examination
of the findings related to therapeutic alliance and motivation for psychotherapy could
potentially help to explain this finding. Hypotheses 4 and 5 stated, respectively, that
participants treated with ECBT would demonstrate a higher level of therapeutic alliance
and motivation for psychotherapy at three and six weeks than those receiving SCBT.
These hypotheses, for the most part, were not confirmed. When comparing the two
groups on the therapeutic alliance and motivation for psychotherapy, there was only one
significant difference found between the SCBT and ECBT groups, which was on the
WAI — Goals subscale, which measures agreement between client and therapist about
treatment goals or areas targeted for change. The SCBT group had significantly higher
scores on the WAI — Goals subscale at follow-up when compared to the ECBT group,
suggesting that participants in the SCBT had an increase in agreement with the therapist
about treatment goals.
In addition, in the supplementary analyses examining the relationship between
degree of change in health anxiety from pre-treatment to post-treatment and the
therapeutic relationship and motivation for psychotherapy at post-treatment, there were
186
responses, and findings from our supplementary analyses are consistent with previous
studies examining treatment of CBT. As such, they are important because they suggest
that SCBT and ECBT are more effective than was suggested by our other analyses.
However, additional evidence will be needed before any of these possible explanations
can be argued strongly. Thus, given these findings, further research with larger samples
of older adults appears to be warranted.
With respect to the lack of evidence that ECBT was superior to SCBT, examination
of the findings related to therapeutic alliance and motivation for psychotherapy could
potentially help to explain this finding. Hypotheses 4 and 5 stated, respectively, that
participants treated with ECBT would demonstrate a higher level of therapeutic alliance
and motivation for psychotherapy at three and six weeks than those receiving SCBT.
These hypotheses, for the most part, were not confirmed. When comparing the two
groups on the therapeutic alliance and motivation for psychotherapy, there was only one
significant difference found between the SCBT and ECBT groups, which was on the
WAI - Goals subscale, which measures agreement between client and therapist about
treatment goals or areas targeted for change. The SCBT group had significantly higher
scores on the WAI - Goals subscale at follow-up when compared to the ECBT group,
suggesting that participants in the SCBT had an increase in agreement with the therapist
about treatment goals.
In addition, in the supplementary analyses examining the relationship between
degree of change in health anxiety from pre-treatment to post-treatment and the
therapeutic relationship and motivation for psychotherapy at post-treatment, there were
186
no significant relationships found between outcome and the therapeutic alliance. When
examining outcome and motivation for psychotherapy, there were very few significant
relationships found. However, in participants treated with SCBT, lower levels of Doubt
(i.e., doubt about the investment in treatment, the treatment itself, and the possibility of
gaining from it) at Session 6 were found to be related to greater improvements in health
anxiety as measured by the WI change score from pre-treatment to post-treatment. In the
ECBT group, lower levels of Distress (i.e., pressure by others and level of distress) at
Session 6 were related to greater improvements in health anxiety as measured by the WI
change score from pre-treatment to post-treatment.
Although building the alliance and motivating patients for treatment was a focus
in the ECBT program, there is limited evidence to suggest that ECBT was superior to
SCBT. This was somewhat surprising initially. The ECBT program was specifically
designed for older adults and extra components were added which included weekly
reading assignments meant to reinforce session material, graphing exercises in which
participants chart numerical mood ratings averaged over each week, mid-week
homework reminder/troubleshooting calls from the therapist for the first four
assignments, a perspective-taking strategy (described above) to facilitate evidence
generation in cognitive restructuring exercises, and short videos with an older adult
giving personal testimonials about the program. Although we attempted to incorporate
components into our programs that would help to engage participants in therapy, given
the results from the supplementary analysis, it appears as though these enhancements
187
no significant relationships found between outcome and the therapeutic alliance. When
examining outcome and motivation for psychotherapy, there were very few significant
relationships found. However, in participants treated with SCBT, lower levels of Doubt
(i.e., doubt about the investment in treatment, the treatment itself, and the possibility of
gaining from it) at Session 6 were found to be related to greater improvements in health
anxiety as measured by the WI change score from pre-treatment to post-treatment. In the
ECBT group, lower levels of Distress (i.e., pressure by others and level of distress) at
Session 6 were related to greater improvements in health anxiety as measured by the WI
change score from pre-treatment to post-treatment.
Although building the alliance and motivating patients for treatment was a focus
in the ECBT program, there is limited evidence to suggest that ECBT was superior to
SCBT. This was somewhat surprising initially. The ECBT program was specifically
designed for older adults and extra components were added which included weekly
reading assignments meant to reinforce session material, graphing exercises in which
participants chart numerical mood ratings averaged over each week, mid-week
homework reminder/troubleshooting calls from the therapist for the first four
assignments, a perspective-taking strategy (described above) to facilitate evidence
generation in cognitive restructuring exercises, and short videos with an older adult
giving personal testimonials about the program. Although we attempted to incorporate
components into our programs that would help to engage participants in therapy, given
the results from the supplementary analysis, it appears as though these enhancements
187

may not have been necessary for improving the therapeutic alliance and motivation for
psychotherapy.
Although the findings indicate that ECBT was not superior to SCBT with respect
to enhancing the therapeutic alliance and motivation for psychotherapy, the results do
suggest that lower levels of Distress in the SCBT group and lower levels of Doubt in the
ECBT group were related to improved outcomes. These findings are consistent with
previous research which indicates that motivation is related to outcome in psychotherapy
(Keijsers et al., 1999). The findings also suggest that addressing Doubt and Distress
during therapy sessions could be critical for improving outcomes.
In addition, when examining the scores obtained by participants on the subscales
of the WAI and NML-2, overall, they were found to be higher than average (Horvath &
Greenberg, 1989; Nijmegen et al., 2004). This suggests there may not have been
sufficient room for improvement in scores. This may be due to the fact that our sample
of participants saw the advertisements for the study and then volunteered to take part. As
such, those who completed the therapy already were motivated and eager to help. As a
result, the extra components that were in the ECBT program may not have been
necessary for this sample of participants since they were already motivated and interested
in talking about their problems. Perhaps in different samples with lower motivation and
ability to connect, the ECBT program would be beneficial.
Further evidence that the therapeutic relationship was high was found when
examining participants' responses at post-treatment to open-ended questions. With
respect to the therapeutic relationship, all participants indicated that they felt the
188
may not have been necessary for improving the therapeutic alliance and motivation for
psychotherapy.
Although the findings indicate that ECBT was not superior to SCBT with respect
to enhancing the therapeutic alliance and motivation for psychotherapy, the results do
suggest that lower levels of Distress in the SCBT group and lower levels of Doubt in the
ECBT group were related to improved outcomes. These findings are consistent with
previous research which indicates that motivation is related to outcome in psychotherapy
(Keijsers et al., 1999). The findings also suggest that addressing Doubt and Distress
during therapy sessions could be critical for improving outcomes.
In addition, when examining the scores obtained by participants on the subscales
of the WAI and NML-2, overall, they were found to be higher than average (Horvath &
Greenberg, 1989; Nijmegen et al., 2004). This suggests there may not have been
sufficient room for improvement in scores. This may be due to the fact that our sample
of participants saw the advertisements for the study and then volunteered to take part. As
such, those who completed the therapy already were motivated and eager to help. As a
result, the extra components that were in the ECBT program may not have been
necessary for this sample of participants since they were already motivated and interested
in talking about their problems. Perhaps in different samples with lower motivation and
ability to connect, the ECBT program would be beneficial.
Further evidence that the therapeutic relationship was high was found when
examining participants' responses at post-treatment to open-ended questions. With
respect to the therapeutic relationship, all participants indicated that they felt the
188

therapeutic relationship had been transformative and described positive experiences with
their therapist. They also described the therapist qualities and actions that helped to
establish the therapeutic relationship and foster motivation for therapy. Therapist
qualities reported included being empathic, professional, relaxed, optimistic, friendly,
non-judgemental, trustworthy, genuinely interested in the patient, invested in therapy
outcome, honest, and sincere. Essential therapist actions included being present or face-
to-face, putting the patient at ease, encouraging and reinforcing, communicating belief in
the therapy program, and instilling hope.
Ackerman and Hilsenroth (2003) conducted a review of the literature on therapist
qualities and the therapeutic alliance and the findings revealed that specific therapist's
personal attributes were significantly related to the development and maintenance of a
positive relationship. They also suggest that a possible explanation for these findings is
that the therapist's personal qualities such as dependability, compassion, responsiveness,
and experience help patients gain the confidence and trust that their therapist has the
ability to both understand and help them cope with the issues that brought them to
therapy. Further, a caring and compassionate connection between the patient and
therapist helps create a warm, accepting, and supportive therapeutic climate that may
increase the opportunity for therapeutic patient change. If a patient believes the treatment
relationship is a collaborative effort between her/himself and the therapist, she or he may
be more likely to invest more in the treatment process and in turn experience greater
therapeutic gains. The responses provided by participants in our study appear consistent
with the findings by Ackerman and Hilsenroth (2003).
189
therapeutic relationship had been transformative and described positive experiences with
their therapist. They also described the therapist qualities and actions that helped to
establish the therapeutic relationship and foster motivation for therapy. Therapist
qualities reported included being empathic, professional, relaxed, optimistic, friendly,
non-judgemental, trustworthy, genuinely interested in the patient, invested in therapy
outcome, honest, and sincere. Essential therapist actions included being present or face-
to-face, putting the patient at ease, encouraging and reinforcing, communicating belief in
the therapy program, and instilling hope.
Ackerman and Hilsenroth (2003) conducted a review of the literature on therapist
qualities and the therapeutic alliance and the findings revealed that specific therapist's
personal attributes were significantly related to the development and maintenance of a
positive relationship. They also suggest that a possible explanation for these findings is
that the therapist's personal qualities such as dependability, compassion, responsiveness,
and experience help patients gain the confidence and trust that their therapist has the
ability to both understand and help them cope with the issues that brought them to
therapy. Further, a caring and compassionate connection between the patient and
therapist helps create a warm, accepting, and supportive therapeutic climate that may
increase the opportunity for therapeutic patient change. If a patient believes the treatment
relationship is a collaborative effort between her/himself and the therapist, she or he may
be more likely to invest more in the treatment process and in turn experience greater
therapeutic gains. The responses provided by participants in our study appear consistent
with the findings by Ackerman and Hilsenroth (2003).
189

4.2 Qualitative Analysis Examining Experience of Health Anxiety Among Seniors
In order to gain a greater understanding of the nature of health anxiety and the
experience of therapy among older adults, participant responses to open-ended questions
at pre-treatment were analysed qualitatively. Participants were asked about their
experiences regarding health and anxiety, and they reported a number of common
experiences that were analysed to form a model of the development of health anxiety in
older adults. When questioned about why they believed they experienced difficulties
with anxiety, some participants reported that they believed they had always been anxious
or that anxiety was genetic. Others reported they believed their anxiety to be a learned
response, typically from their parents and from other illness experiences. These results
are consistent with the literature on health anxiety which suggests that genetic and
environmental factors (e.g., learning) both play a role in the development of health
anxiety, although environmental factors appear to play a larger role (Taylor, Thordarson,
Jang, & Asmundson, 2006).
Participants also reported various past and current experiences with illness in
themselves and others as well as the experience of death. Participants' reports of past
experience with illness and death are consistent with the literature outlining the CB
model of health anxiety (Salkovskis & Warwick's, 1986). The CB model indicates that
past experience with illness, (e.g., early health- and illness-related experience, later
events such as unexpected or unpleasant illness in the person's social group, and
information in the media) and death lead to the formation of inflexible or negative
assumptions about symptoms, disease, medical care, and so forth. These negative
190
4.2 Qualitative Analysis Examining Experience of Health Anxiety Among Seniors
In order to gain a greater understanding of the nature of health anxiety and the
experience of therapy among older adults, participant responses to open-ended questions
at pre-treatment were analysed qualitatively. Participants were asked about their
experiences regarding health and anxiety, and they reported a number of common
experiences that were analysed to form a model of the development of health anxiety in
older adults. When questioned about why they believed they experienced difficulties
with anxiety, some participants reported that they believed they had always been anxious
or that anxiety was genetic. Others reported they believed their anxiety to be a learned
response, typically from their parents and from other illness experiences. These results
are consistent with the literature on health anxiety which suggests that genetic and
environmental factors (e.g., learning) both play a role in the development of health
anxiety, although environmental factors appear to play a larger role (Taylor, Thordarson,
Jang, & Asmundson, 2006).
Participants also reported various past and current experiences with illness in
themselves and others as well as the experience of death. Participants' reports of past
experience with illness and death are consistent with the literature outlining the CB
model of health anxiety (Salkovskis & Warwick's, 1986). The CB model indicates that
past experience with illness, (e.g., early health- and illness-related experience, later
events such as unexpected or unpleasant illness in the person's social group, and
information in the media) and death lead to the formation of inflexible or negative
assumptions about symptoms, disease, medical care, and so forth. These negative
190
assumptions then lead to a tendency to initially misinterpret information that is health-
related.
Finally, participants reported a number of dysfunctional core beliefs about the
nature of health and illness (e.g., increased vulnerability or risk for developing various
diseases either due to their poor health habits or to a family history of illness and disease;
fear of death, fear of pain, fear of disability and dependence, and fear of missing out on
life). These findings about dysfunctional beliefs in this older adult sample are consistent
with previous literature examining dysfunctional beliefs in individuals with elevated
health anxiety. Taylor and Asmundson (2004) indicate that health anxiety has a large
cognitive component with anxiety arising from misinterpretations of benign bodily
changes or sensations. In turn, the tendency to misinterpret sensations may be a result of
one's beliefs about sickness and health (Barsky & Klerman, 1983; Salkovskis &
Warwick, 2000). Cognitive studies have shown that individuals with elevated health
anxiety, compared with controls without anxiety, show a greater tendency to overestimate
the likelihood of contracting diseases, and to overestimate the dangerousness of diseases
(Ditto, Jemmott, & Darley, 1988; Easterling & Leventhal, 1989). Individuals with
elevated health anxiety also are more likely to regard themselves as being at greater risk
for developing various diseases, but do not view themselves as being at greater risk for
being the victim of an accident or criminal assault (Barsky et al., 2001; Haenen, de Jong,
Schmidt, Stevens, & Visser, 2000). Further, individuals with elevated health anxiety are
more likely to believe they are weak and unable to tolerate stress (Rief, Hiller, &
Margraf, 1998).
191
assumptions then lead to a tendency to initially misinterpret information that is health-
related.
Finally, participants reported a number of dysfunctional core beliefs about the
nature of health and illness (e.g., increased vulnerability or risk for developing various
diseases either due to their poor health habits or to a family history of illness and disease;
fear of death, fear of pain, fear of disability and dependence, and fear of missing out on
life). These findings about dysfunctional beliefs in this older adult sample are consistent
with previous literature examining dysfunctional beliefs in individuals with elevated
health anxiety. Taylor and Asmundson (2004) indicate that health anxiety has a large
cognitive component with anxiety arising from misinterpretations of benign bodily
changes or sensations. In turn, the tendency to misinterpret sensations may be a result of
one's beliefs about sickness and health (Barsky & Klerman, 1983; Salkovskis &
Warwick, 2000). Cognitive studies have shown that individuals with elevated health
anxiety, compared with controls without anxiety, show a greater tendency to overestimate
the likelihood of contracting diseases, and to overestimate the dangerousness of diseases
(Ditto, Jemmott, & Darley, 1988; Easterling & Leventhal, 1989). Individuals with
elevated health anxiety also are more likely to regard themselves as being at greater risk
for developing various diseases, but do not view themselves as being at greater risk for
being the victim of an accident or criminal assault (Barsky et al., 2001; Haenen, de Jong,
Schmidt, Stevens, & Visser, 2000). Further, individuals with elevated health anxiety are
more likely to believe they are weak and unable to tolerate stress (Rief, Hiller, &
Margraf, 1998).
191

The current qualitative study was intended to guide the application of the CB
theory of health anxiety to older adults. It aimed to provide a more in-depth exploration
of health anxiety experiences in older adults, and was intended to supplement the
experimental study undertaken and outlined above. Given the consistency of our
qualitative findings with previous findings from studies with younger adults and with
information provided by Snyder and Stanley (2001), it is promising that the CB model of
health anxiety can be applied to seniors. However, the following observation should be
taken into consideration in future research and clinical applications of the model to older
adults. In our sample, we had a number of participants experiencing current health-
related issues and significant concern about these problems. Their focus appeared to be
on coping with the current health issues and potential deterioration, rather than on the
possibility of becoming ill in the future. This would fit with Snyder and Stanley's (2001)
hypothesis that seniors with significant levels of health anxiety actually may be unduly
preoccupied with and worried about their existing health problems and symptoms rather
than actually misinterpreting their bodily sensations (Snyder & Stanley, 2001). Future
research with older adults should examine the role of actual illness in health anxiety.
4.3 Comparison of Older and Younger Adults on Health Anxiety
The purpose of Study 2 was to compare a health anxious older adult sample to a
sex and WI score matched health anxious younger adult sample in order to examine
whether the nature of the two groups' concerns on various anxiety measures were
comparable or whether the pattern of responses differed. We hypothesized that
participants in the older group would have significantly higher scores than the control
192
The current qualitative study was intended to guide the application of the CB
theory of health anxiety to older adults. It aimed to provide a more in-depth exploration
of health anxiety experiences in older adults, and was intended to supplement the
experimental study undertaken and outlined above. Given the consistency of our
qualitative findings with previous findings from studies with younger adults and with
information provided by Snyder and Stanley (2001), it is promising that the CB model of
health anxiety can be applied to seniors. However, the following observation should be
taken into consideration in future research and clinical applications of the model to older
adults. In our sample, we had a number of participants experiencing current health-
related issues and significant concern about these problems. Their focus appeared to be
on coping with the current health issues and potential deterioration, rather than on the
possibility of becoming ill in the future. This would fit with Snyder and Stanley's (2001)
hypothesis that seniors with significant levels of health anxiety actually may be unduly
preoccupied with and worried about their existing health problems and symptoms rather
than actually misinterpreting their bodily sensations (Snyder & Stanley, 2001). Future
research with older adults should examine the role of actual illness in health anxiety.
4.3 Comparison of Older and Younger Adults on Health Anxiety
The purpose of Study 2 was to compare a health anxious older adult sample to a
sex and WI score matched health anxious younger adult sample in order to examine
whether the nature of the two groups' concerns on various anxiety measures were
comparable or whether the pattern of responses differed. We hypothesized that
participants in the older group would have significantly higher scores than the control
192
group on the Bodily Preoccupation subscale of the WI, the Body Vigilance subscale of
the SHAI, and the Disruptive Effects of Symptoms subscale of the IAS. Although the
hypotheses were not confirmed, there were a number of significant differences found
between the two groups. Overall, the younger adult sample had consistently higher
scores on most of the measures even though they were matched with the older adult
sample on the WI. The older adult sample had only one significantly higher score than
the younger adult sample, which was on disease fear. The matched younger control
group had significantly higher scores than the older adult group on health anxiety (SHAI
and IAS), hypochondriacal somatic symptoms (SSI, SSAS), frequency of
hypochondriacal thoughts, tendency to experience bodily symptoms as distressing, and
state and trait anxiety, and on the subscales measuring disease conviction, illness
likelihood, body vigilance, fears of illness, hypochondriacal beliefs and disease
conviction, and disruptive effects of symptoms on functioning.
These findings are consistent with findings in the literature on health anxiety in
older adults. Although there is a commonly held belief that older adults display greater
health-related concerns compared with younger adults (Snyder & Stanley, 2001),
researchers have found that older adults do not differ significantly than younger adults
with respect to health anxiety (Barsky, Frank, Cleary, et al., 1991). Bourgault-Fagnou
and Hadjistavropoulos (2009) found that health anxiety among medically frail older
adults was similar to that of younger adults. Those individuals who were less frail had
lower levels of health anxiety than younger adults. Boston and Merrick (2010) similarly
found that the health anxiety scores for a community dwelling older adult group were
193
group on the Bodily Preoccupation subscale of the WI, the Body Vigilance subscale of
the SHAI, and the Disruptive Effects of Symptoms subscale of the IAS. Although the
hypotheses were not confirmed, there were a number of significant differences found
between the two groups. Overall, the younger adult sample had consistently higher
scores on most of the measures even though they were matched with the older adult
sample on the WI. The older adult sample had only one significantly higher score than
the younger adult sample, which was on disease fear. The matched younger control
group had significantly higher scores than the older adult group on health anxiety (SHAI
and IAS), hypochondriacal somatic symptoms (SSI, SSAS), frequency of
hypochondriacal thoughts, tendency to experience bodily symptoms as distressing, and
state and trait anxiety, and on the subscales measuring disease conviction, illness
likelihood, body vigilance, fears of illness, hypochondriacal beliefs and disease
conviction, and disruptive effects of symptoms on functioning.
These findings are consistent with findings in the literature on health anxiety in
older adults. Although there is a commonly held belief that older adults display greater
health-related concerns compared with younger adults (Snyder & Stanley, 2001),
researchers have found that older adults do not differ significantly than younger adults
with respect to health anxiety (Barsky, Frank, Cleary, et al., 1991). Bourgault-Fagnou
and Hadjistavropoulos (2009) found that health anxiety among medically frail older
adults was similar to that of younger adults. Those individuals who were less frail had
lower levels of health anxiety than younger adults. Boston and Merrick (2010) similarly
found that the health anxiety scores for a community dwelling older adult group were
193

similar to those reported in other studies for younger people with chronic illness
(Salkovskis et al., 2002; Rode et al., 2006; Abramowitz et al., 2007). However, although
older adults may report lower levels of anxiety, Snyder and Stanley (2001) suggest that
older patients with hypochondriasis are less functional than younger patients despite
similarities in hypochondriacal symptoms, and that severe health anxiety may be more
incapacitating in older adults even when symptom severity is similar to that of younger
patients. As a result, they may be worried less, but they may have higher levels of
distress and may in fact be engaging in more problematic behaviours to alleviate their
anxiety.
These results also may have been impacted by the dichotomous response options
on the WI. When screening for health anxiety, participants were asked to answer either
"yes" or "no" to the items on the WI. Dichotomous response options have been
respondent-rated as more difficult to use and less suitable for accurately representing
options than Likert scales (Preston & Colman, 2000). This may be particularly relevant
with regards to health anxiety and its contemporary conceptualization as a continuous
construct (Asmundson, Carleton, Bovell, & Taylor, 2008). Thus, the WI may not have
been able to discriminate between a respondent occasionally being fearful of life
threatening illness (e.g., fearful of cancer when a friend or loved one is diagnosed with
the disease) and a respondent who reported being excessively preoccupied with worries
of developing, or fears that they have already developed, a life threatening disease
(Welch, Carleton, & Asmundson, 2009). Although the WI with the "yes/no" format was
given to potential participants because it was rapid and straightforward to administer over
194
similar to those reported in other studies for younger people with chronic illness
(Salkovskis et al., 2002; Rode et al., 2006; Abramowitz et al., 2007). However, although
older adults may report lower levels of anxiety, Snyder and Stanley (2001) suggest that
older patients with hypochondriasis are less functional than younger patients despite
similarities in hypochondriacal symptoms, and that severe health anxiety may be more
incapacitating in older adults even when symptom severity is similar to that of younger
patients. As a result, they may be worried less, but they may have higher levels of
distress and may in fact be engaging in more problematic behaviours to alleviate their
anxiety.
These results also may have been impacted by the dichotomous response options
on the WI. When screening for health anxiety, participants were asked to answer either
"yes" or "no" to the items on the WI. Dichotomous response options have been
respondent-rated as more difficult to use and less suitable for accurately representing
options than Likert scales (Preston & Colman, 2000). This may be particularly relevant
with regards to health anxiety and its contemporary conceptualization as a continuous
construct (Asmundson, Carleton, Bovell, & Taylor, 2008). Thus, the WI may not have
been able to discriminate between a respondent occasionally being fearful of life
threatening illness (e.g., fearful of cancer when a friend or loved one is diagnosed with
the disease) and a respondent who reported being excessively preoccupied with worries
of developing, or fears that they have already developed, a life threatening disease
(Welch, Carleton, & Asmundson, 2009). Although the WI with the "yes/no" format was
given to potential participants because it was rapid and straightforward to administer over
194

the phone, future research in this area may consider using the 5-point Likert scale version
developed by Barsky et al., (1992).
4.4 Contributions
Considering the limited amount of literature with respect to health anxiety in
seniors, this study makes several important contributions. First, this is only study to date
that has evaluated the effectiveness of a CBT program designed specifically for older
adults with health anxiety. Most of the literature on health anxiety does not focus
attention on the concerns of older adults and on the outcome of psychological treatment
in this population. As a result, questions have been raised about the appropriateness of
generalizing psychological interventions for health anxiety developed and tested with
younger adults to seniors (Snyder & Stanley, 2001). Although the results provide mixed
evidence to support the effectiveness of a CBT program with respect to changing
thoughts and behaviours related to health anxiety, the findings from the paired samples t-
tests, analysis of clinically significant change, examination of the maintenance of gains,
supplementary analysis using the WLC group, and qualitative analysis of the post-
treatment responses should be viewed as providing promising evidence in support of
CBT for health anxiety for use with seniors. Participation in such a program is likely to
provide some benefit to seniors with elevated health anxiety.
Second, the treatment protocols used in this study were for six sessions of CBT.
Given the trend toward the use of shorter-term therapies and the limited access that
individuals have to psychological services due to limited resources, research on short-
term therapies provides direction for clinicians working with these patients.
195
the phone, future research in this area may consider using the 5-point Likert scale version
developed by Barsky et al., (1992).
4.4 Contributions
Considering the limited amount of literature with respect to health anxiety in
seniors, this study makes several important contributions. First, this is only study to date
that has evaluated the effectiveness of a CBT program designed specifically for older
adults with health anxiety. Most of the literature on health anxiety does not focus
attention on the concerns of older adults and on the outcome of psychological treatment
in this population. As a result, questions have been raised about the appropriateness of
generalizing psychological interventions for health anxiety developed and tested with
younger adults to seniors (Snyder & Stanley, 2001). Although the results provide mixed
evidence to support the effectiveness of a CBT program with respect to changing
thoughts and behaviours related to health anxiety, the findings from the paired samples t-
tests, analysis of clinically significant change, examination of the maintenance of gains,
supplementary analysis using the WLC group, and qualitative analysis of the post-
treatment responses should be viewed as providing promising evidence in support of
CBT for health anxiety for use with seniors. Participation in such a program is likely to
provide some benefit to seniors with elevated health anxiety.
Second, the treatment protocols used in this study were for six sessions of CBT.
Given the trend toward the use of shorter-term therapies and the limited access that
individuals have to psychological services due to limited resources, research on short-
term therapies provides direction for clinicians working with these patients.
195

Third, the qualitative responses provided further information in support that the
CB model of health anxiety appears to be appropriate for older adults. These findings
provide further support that the thoughts and beliefs of health anxious older adults are
similar among younger and older adults, although further research in this area is needed
to confirm this information empirically. The findings from the qualitative analysis also
suggest that actual illness or disease, rather than worry about the possibility of becoming
ill in the future, may be a greater concern for older adults with health anxiety. Thus,
further research examining the role of health conditions and illness in individuals with
excessive health anxiety appears warranted.
Finally, the comparison of the older adult group and younger adult group
provided further support that younger adults are scoring consistently higher on measures
of health anxiety even when matched by score on a measure of health anxiety (WI)
(Bourgault-Fagnou & Hadjistavropoulos, 2009). However, our older sample of
participants clearly indicated difficulties coping with the reported levels of anxiety.
Given these findings, it is important that clinicians working with these individuals assess
for and address sub-clinical symptoms of health anxiety.
4.5 Limitations
Although this study has advanced the literature on the experience and treatment of
health anxiety, there were several limitations to the present study. First, there were the
difficulties recruiting the intended 31 participants per treatment condition and the need to
settle for a relatively small sample size (n = 57). The difficulty in recruiting the expected
number of participants was the result of several factors. Although we had a number of
196
Third, the qualitative responses provided further information in support that the
CB model of health anxiety appears to be appropriate for older adults. These findings
provide further support that the thoughts and beliefs of health anxious older adults are
similar among younger and older adults, although further research in this area is needed
to confirm this information empirically. The findings from the qualitative analysis also
suggest that actual illness or disease, rather than worry about the possibility of becoming
ill in the future, may be a greater concern for older adults with health anxiety. Thus,
further research examining the role of health conditions and illness in individuals with
excessive health anxiety appears warranted.
Finally, the comparison of the older adult group and younger adult group
provided further support that younger adults are scoring consistently higher on measures
of health anxiety even when matched by score on a measure of health anxiety (WI)
(Bourgault-Fagnou & Hadjistavropoulos, 2009). However, our older sample of
participants clearly indicated difficulties coping with the reported levels of anxiety.
Given these findings, it is important that clinicians working with these individuals assess
for and address sub-clinical symptoms of health anxiety.
4.5 Limitations
Although this study has advanced the literature on the experience and treatment of
health anxiety, there were several limitations to the present study. First, there were the
difficulties recruiting the intended 31 participants per treatment condition and the need to
settle for a relatively small sample size (n = 57). The difficulty in recruiting the expected
number of participants was the result of several factors. Although we had a number of
196

participants indicate their interest in participating in the study and meet criteria for
inclusion in the study, there were a number of participants who declined to participate
prior to enrolment in the study. Many participants indicated they had changed their mind
or did not want to commit to the time involvement. Further, our study required
participants to attend sessions at the University clinic, which, in retrospect, may have
reduced the number of eligible participants due to increased mobility concerns that are
known to be present in older adults. Another difficulty in obtaining the desired sample
size was the limited population that was available. Recruitment for this study occurred
over a 24-month period in a small western Canadian city, and entailed multiple forms of
advertisement (e.g., posters, newspaper advertisements, radio and television appearances,
presentations to seniors' groups) conducted at multiple time points. With successive
recruitment attempts there was a notable decrease in the number of volunteers, suggesting
that the number of potential candidates was dwindling.
Second, is the lack of a long-term follow-up for the WLC group and longer-term
follow-up (e.g., 12 month) for the two treatment groups. We were not able to compare
the WLC condition to the two active treatments at follow-up, which would have been
more informative, given that psychological disorders have been found to improve over
time irrespective of specific treatment (Seivewright et al., 2008) and improvement in
treatment could reflect normal symptom fluctuation (Westen & Morrison, 2001). Though
having the WLC group complete the questionnaires would have allowed us to compare
this group to the two treatment groups, for ethical reasons, we were not comfortable
having participants who were in distress wait for treatment longer than six weeks. In
197
participants indicate their interest in participating in the study and meet criteria for
inclusion in the study, there were a number of participants who declined to participate
prior to enrolment in the study. Many participants indicated they had changed their mind
or did not want to commit to the time involvement. Further, our study required
participants to attend sessions at the University clinic, which, in retrospect, may have
reduced the number of eligible participants due to increased mobility concerns that are
known to be present in older adults. Another difficulty in obtaining the desired sample
size was the limited population that was available. Recruitment for this study occurred
over a 24-month period in a small western Canadian city, and entailed multiple forms of
advertisement (e.g., posters, newspaper advertisements, radio and television appearances,
presentations to seniors' groups) conducted at multiple time points. With successive
recruitment attempts there was a notable decrease in the number of volunteers, suggesting
that the number of potential candidates was dwindling.
Second, is the lack of a long-term follow-up for the WLC group and longer-term
follow-up (e.g., 12 month) for the two treatment groups. We were not able to compare
the WLC condition to the two active treatments at follow-up, which would have been
more informative, given that psychological disorders have been found to improve over
time irrespective of specific treatment (Seivewright et al., 2008) and improvement in
treatment could reflect normal symptom fluctuation (Westen & Morrison, 2001). Though
having the WLC group complete the questionnaires would have allowed us to compare
this group to the two treatment groups, for ethical reasons, we were not comfortable
having participants who were in distress wait for treatment longer than six weeks. In
197

addition, though a longer follow-up is clearly warranted, only a three-month post-
treatment follow-up for the two treatment groups was conducted due to the time
constraints of conducting doctoral research. However, a 12-month follow-up would have
enabled us to evaluate the long-term efficacy of the treatments.
Third, the sample had an unbalanced gender representation. As previously
indicated, 77% of the participants were female. Although this ratio is common in
research with older adults (e.g., Boston & Merrick, 2010; Mohlman & Zinbarg, 2000), it
is important to be aware that these findings may be more applicable to females. Future
research should replicate the current study either using a more gender balanced sample or
a sample exclusively consisting of men.
Fourth, the therapists in this study were relatively inexperienced (i.e., supervised
graduate students in clinical psychology). It is possible that experienced therapists would
have produced more beneficial results for the participants. This possibility remains open
for further study. In addition, there were three therapists providing the interventions, but
the majority of treatment was provided by one main therapist (the author). Specifically,
the main therapist provided treatment to 30 participants, while the other two therapists
provided treatment to eight participants and one participant, respectively. In addition, the
same therapist provided therapy in both the ECBT and SCBT condition. Although this is
beneficial in terms of controlling for therapist differences across conditions, this could
have inadvertently resulted in similarities between the two treatment conditions. Given
these numbers, an examination of the potential effect of therapist could not be conducted.
Future research should ensure each therapist provides treatment to an equal distribution
198
addition, though a longer follow-up is clearly warranted, only a three-month post-
treatment follow-up for the two treatment groups was conducted due to the time
constraints of conducting doctoral research. However, a 12-month follow-up would have
enabled us to evaluate the long-term efficacy of the treatments.
Third, the sample had an unbalanced gender representation. As previously
indicated, 77% of the participants were female. Although this ratio is common in
research with older adults (e.g., Boston & Merrick, 2010; Mohlman & Zinbarg, 2000), it
is important to be aware that these findings may be more applicable to females. Future
research should replicate the current study either using a more gender balanced sample or
a sample exclusively consisting of men.
Fourth, the therapists in this study were relatively inexperienced (i.e., supervised
graduate students in clinical psychology). It is possible that experienced therapists would
have produced more beneficial results for the participants. This possibility remains open
for further study. In addition, there were three therapists providing the interventions, but
the majority of treatment was provided by one main therapist (the author). Specifically,
the main therapist provided treatment to 30 participants, while the other two therapists
provided treatment to eight participants and one participant, respectively. In addition, the
same therapist provided therapy in both the ECBT and SCBT condition. Although this is
beneficial in terms of controlling for therapist differences across conditions, this could
have inadvertently resulted in similarities between the two treatment conditions. Given
these numbers, an examination of the potential effect of therapist could not be conducted.
Future research should ensure each therapist provides treatment to an equal distribution
198
of participants in order to prevent biased treatment results due to the effect of the
therapist rather than due to the program.
Fifth, only self-report measures were included in the design. Aiken (2002)
indicates that individuals may over-report symptoms in order to make their situation seem
worse, or they may under-report the severity or frequency of symptoms in order to
minimize their problems. Unfortunately, there are few practical and well-standardized
indirect and non-reactive measures of the psychological variables of interest in this study.
Future studies may find it informative to examine health care utilization as a more
objective measure of change.
4.6 Future Directions
Given the dearth of literature in the area investigating health anxiety among
seniors, future directions for research are abundant. First, further well-designed trials of
CBT for health anxiety among seniors are required. These studies should include larger
numbers of participants; longer follow-up times; multiple sites; and different treatment
protocols and formats such as treatments that include a greater number of sessions, group
treatments, and in-home sessions for those who are not mobile. It was observed by this
author that a number of participants were interested in and enquired about the possibility
of group therapy.
Although the enhanced components of our CBT program were based on the
literature, the current findings did not support the superiority of ECBT over SCBT.
Further trials should also be designed to assess not only whether the CBT program is
effective, but also which components of the therapy are active for older adults, including
199
of participants in order to prevent biased treatment results due to the effect of the
therapist rather than due to the program.
Fifth, only self-report measures were included in the design. Aiken (2002)
indicates that individuals may over-report symptoms in order to make their situation seem
worse, or they may under-report the severity or frequency of symptoms in order to
minimize their problems. Unfortunately, there are few practical and well-standardized
indirect and non-reactive measures of the psychological variables of interest in this study.
Future studies may find it informative to examine health care utilization as a more
objective measure of change.
4.6 Future Directions
Given the dearth of literature in the area investigating health anxiety among
seniors, future directions for research are abundant. First, further well-designed trials of
CBT for health anxiety among seniors are required. These studies should include larger
numbers of participants; longer follow-up times; multiple sites; and different treatment
protocols and formats such as treatments that include a greater number of sessions, group
treatments, and in-home sessions for those who are not mobile. It was observed by this
author that a number of participants were interested in and enquired about the possibility
of group therapy.
Although the enhanced components of our CBT program were based on the
literature, the current findings did not support the superiority of ECBT over SCBT.
Further trials should also be designed to assess not only whether the CBT program is
effective, but also which components of the therapy are active for older adults, including
199
components of the enhanced therapy. In addition, further research examining ECBT with
older adults from a community mental health setting or psychiatric setting is warranted.
With seniors with lower levels of motivation, more advanced age, or greater disability,
ECBT may prove to be more valuable. The comparison of CBT to other treatment
modalities (e.g., brief dynamic therapy, behaviour therapy) would also be of benefit given
that not all participants responded favourably to CBT.
Further research examining the theoretical model of health anxiety as it applies to
seniors appears warranted. Given our qualitative findings that the CB model of health
anxiety appears to be appropriate for older adults but that our sample had a number of
current health concerns, empirical validation of these findings would help to provide
further insight into the thoughts and beliefs of older adults with elevated health anxiety,
problematic behaviours, and other maintaining factors which could then be specifically
targeted in psychological treatments. The role that health conditions play in elevated
health anxiety among older adults is another area for future research.
Although only a small number (i.e., three) of participants dropped out of
treatment and only two participants indicated in the qualitative questions at post-
treatment that they did not find the treatment helpful, future therapy trials should include
an assessment of treatment acceptability. It would be helpful to know what participants
did not find helpful so that other alternative treatment options could be developed.
Finally, to facilitate healthcare planning and economic evaluation for older adults, future
trials should include an assessment of effect on healthcare resource use.
200
components of the enhanced therapy. In addition, further research examining ECBT with
older adults from a community mental health setting or psychiatric setting is warranted.
With seniors with lower levels of motivation, more advanced age, or greater disability,
ECBT may prove to be more valuable. The comparison of CBT to other treatment
modalities (e.g., brief dynamic therapy, behaviour therapy) would also be of benefit given
that not all participants responded favourably to CBT.
Further research examining the theoretical model of health anxiety as it applies to
seniors appears warranted. Given our qualitative findings that the CB model of health
anxiety appears to be appropriate for older adults but that our sample had a number of
current health concerns, empirical validation of these findings would help to provide
further insight into the thoughts and beliefs of older adults with elevated health anxiety,
problematic behaviours, and other maintaining factors which could then be specifically
targeted in psychological treatments. The role that health conditions play in elevated
health anxiety among older adults is another area for future research.
Although only a small number (i.e., three) of participants dropped out of
treatment and only two participants indicated in the qualitative questions at post-
treatment that they did not find the treatment helpful, future therapy trials should include
an assessment of treatment acceptability. It would be helpful to know what participants
did not find helpful so that other alternative treatment options could be developed.
Finally, to facilitate healthcare planning and economic evaluation for older adults, future
trials should include an assessment of effect on healthcare resource use.
200

4.7 Conclusion
In summary, this study was the first to examine the effectiveness of CBT for
health anxiety among older adults. Although results were mixed, overall, the findings
indicated that CBT is effective for reducing some of the health anxious thoughts and
beliefs in older adults. The results also contributed to the understanding of the
therapeutic relationship, motivation for psychotherapy, and the CB model of health
anxiety as it applies to older adults. Future research is needed to clarify the role of
specific therapy components and their usefulness in alleviating symptoms.
201
4.7 Conclusion
In summary, this study was the first to examine the effectiveness of CBT for
health anxiety among older adults. Although results were mixed, overall, the findings
indicated that CBT is effective for reducing some of the health anxious thoughts and
beliefs in older adults. The results also contributed to the understanding of the
therapeutic relationship, motivation for psychotherapy, and the CB model of health
anxiety as it applies to older adults. Future research is needed to clarify the role of
specific therapy components and their usefulness in alleviating symptoms.
201

5. REFERENCES
Ables, N. (1997). What practitioners should know about working with older adults.
Washington, DC: American Psychological Association.
Abramowitz, J. S., Deacon, B. J., & Valentiner, D. P. (2007). The short health
anxiety inventory in an undergraduate sample: Implications for a cognitive-
behavioral model of hypochondriasis. Cognitive Therapy and Research, 31,
871-883. doi:10.1007/s10608-006-9058-1
Abramowitz, J. S., & Moore, E. L. (2007). An experimental analysis of hypochondriasis.
Behaviour Research and Therapy, 45, 413-424. doi:10.1016/j.brat.2006.04.005
Abramowitz, J. S., Schwartz, S. A., & Whiteside, S. P. (2002). A contemporary
conceptual model of hypochondriasis. Mayo Clinic Proceedings, 77, 1323-1330.
doi:10.4065/77.12.1323
Ackerman, S. J., & Hilsenroth, M. J. (2003). A review of therapist characteristics and
techniques positively impacting the therapeutic alliance. Clinical Psychology
Review, 23, 1-33. doi:10.1016/S0272-735
Adams, K. B. (2001). Depressive symptoms, depletion, or developmental change?
Withdrawal, apathy, and lack of vigor in the Geriatric Depression Scale. The
Gerontologist, 41, 768-777. doi:10.1093/geront/41.6.768
Aiken, L. R. (2002). Psychological Testing and Assessment. New York, NY. Allyn &
Bacon.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental
disorders, fourth edition — Text revision. Washington, DC: same as author.
202
5. REFERENCES
Abies, N. (1997). What practitioners should know about working with older adults.
Washington, DC: American Psychological Association.
Abramowitz, J. S., Deacon, B. J., & Valentiner, D. P. (2007). The short health
anxiety inventory in an undergraduate sample: Implications for a cognitive-
behavioral model of hypochondriasis. Cognitive Therapy and Research, 31,
871-883. doi:10.1007/sl0608-006-9058-l
Abramowitz, J. S., & Moore, E. L. (2007). An experimental analysis of hypochondriasis,
Behaviour Research and Therapy, 45, 413^424. doi:10.1016/j.brat.2006.04.005
Abramowitz, J. S., Schwartz, S. A., & Whiteside, S. P. (2002). A contemporary
conceptual model of hypochondriasis. Mayo Clinic Proceedings, 77, 1323-1330.
doi:10.4065/77.12.1323
Ackerman, S. J., & Hilsenroth, M. J. (2003). A review of therapist characteristics and
techniques positively impacting the therapeutic alliance. Clinical Psychology
Review, 23, 1-33. doi:10.1016/S0272-735
Adams, K. B. (2001). Depressive symptoms, depletion, or developmental change?
Withdrawal, apathy, and lack of vigor in the Geriatric Depression Scale. The
Gerontologist, 41, 768-777. doi:10.1093/geront/41.6.768
Aiken, L. R. (2002). Psychological Testing and Assessment. New York, NY. Allyn &
Bacon.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental
disorders, fourth edition - Text revision. Washington, DC: same as author.
202

American Psychiatric Association. (2010). DSM-IV: The future of psychiatric diagnosis.
Retrieved July 3, 2010, from http://www.dsm5.org/Pages/Default.aspx
Asmundson, G. J. G., Carleton, R. N., Bovell, C. V., & Taylor, S. (2008). Comparison of
unitary and multidimensional models of the Whiteley Index in a nonclinical
sample: Implications for understanding and assessing health anxiety. Journal of
Cognitive Psychotherapy: An International Quarterly, 22, 87-96.
doi:10.1891/0889-8391.22.2.87
Asmundson, G. J. G., Taylor, S., Sevgur, S., & Cox, B. J. (2001). Health anxiety:
Classification and clinical features. In G.J.G. Asmundson, S. Taylor, & B.J. Cox
(Eds.), Health Anxiety: Clinical and Research Perspectives on Hypochondriasis
and Related Disorders (pp. 32-21). New York: John Wiley & Sons.
Barber, J. P., Connolly, M. B., Crits-Christoph, P., Gladis, L., & Siqueland, L. (2000).
Alliance predicts patients' outcome beyond in-treatment change in symptoms.
Journal of Consulting and Clinical Psychology, 68, 1027-1032.
doi:10.1080/10503300802609680
Barlow, D. H. (1988). Anxiety and its disorders: The nature and treatment of anxiety and
panic. New York: The Guilford Press.
Barlow, D. H., Brown, T. A., & Craske, M. G. (1994). Definitions of panic attacks and
panic disorder in DSM-IV: Implications for research. Journal of Abnormal
Psychology, 103, 553-554. doi: 10.1111/j.1468-2850.1996.tb00075.x
Barsky, A. J. (1993). The diagnosis and management of hypochondriacal concerns in the
elderly. Journal of Geriatric Psychiatry, 26, 129-141.
203
American Psychiatric Association. (2010). DSM-IV: The future of psychiatric diagnosis.
Retrieved July 3, 2010, from http://www.dsm5.org/Pages/Default.aspx
Asmundson, G. J. G., Carleton, R. N., Bovell, C. V., & Taylor, S. (2008). Comparison of
unitary and multidimensional models of the Whiteley Index in a nonclinical
sample: Implications for understanding and assessing health anxiety. Journal of
Cognitive Psychotherapy: An International Quarterly, 22, 87-96.
doi:10.1891/0889-8391.22.2.87
Asmundson, G. J. G., Taylor, S., Sevgur, S., & Cox, B. J. (2001). Health anxiety:
Classification and clinical features. In G.J.G. Asmundson, S. Taylor, & B.J. Cox
(Eds.), Health Anxiety: Clinical and Research Perspectives on Hypochondriasis
and Related Disorders (pp. 32-21). New York: John Wiley & Sons.
Barber, J. P., Connolly, M. B., Crits-Christoph, P., Gladis, L., & Siqueland, L. (2000).
Alliance predicts patients' outcome beyond in-treatment change in symptoms.
Journal of Consulting and Clinical Psychology, 68, 1027-1032.
doi:10.1080/10503300802609680
Barlow, D. H. (1988). Anxiety and its disorders: The nature and treatment of anxiety and
panic. New York: The Guilford Press.
Barlow, D. H., Brown, T. A., & Craske, M. G. (1994). Definitions of panic attacks and
panic disorder in DSM-IV: Implications for research. Journal of Abnormal
Psychology, 103, 553-554. doi: 10.111 l/j,1468-2850.1996.tb00075.x
Barsky, A. J. (1993). The diagnosis and management of hypochondriacal concerns in the
elderly. Journal of Geriatric Psychiatry, 26, 129-141.
203

Barsky, A. J., & Ahern, D. K. (2004). Cognitive behaviour therapy for hypochondriasis:
A randomized controlled trial. Journal of the American Medical Association, 291,
1464-1470. doi:10.1001/jama.291.12.1464
Barsky, A. J., Barnett, M. C., & Cleary, P. D. (1994). Hypochondriasis and panic
disorder: Boundary and overlap. Archives of General Psychiatry, 51, 918-925.
Retrieved from http://archpsyc.ama-assn.org/
Barsky, A. J., Cleary, P. D., Wyshak, G., Spitzer, R. L., Williams, J. B. W., & Klerman,
G. J. (1992). A structured diagnostic interview for hypochondriasis: A proposed
criteria standard. The Journal of Nervous and Mental Disease, 180, 20-27.
Retrieved from http://journals.1ww.com/jonmd/pages/default.aspx
Barsky, A. J., Fama, J. M., Bailey, E. D., & Ahern, D. K. (1998). A prospective 4- to 5-
year study of DSM-III hypochondriasis. Archives of General Psychiatry, 55, 737-
744. Retrieved from http://archpsyc.ama-assn.org/
Barsky, A. J., Frank, C. B., Cleary, P. D., Wyshak, G., & Klerman, G. L. (1991). The
relation between hypochondriasis and age. American Journal of Psychiatry, 148,
923-928. Retrieved from http://ajp.psychiatryonline.org/index.dtl
Barsky, A. J., & Klerman, G. L. (1983). Overview: Hypochondriasis, bodily complaints,
and somatic styles. American Journal of Psychiatry, 140, 273-283. Retrieved
from http://ajp.psychiatryonline.org/index.dt1
Barsky, A. J., & Cleary, P. D., Coeytaux, R. R., & Ruskin, J. N. (1995). The clinical
course of palpitations in medical outpatients. Archives of Internal Medicine, 155,
1782-1788. doi:10.1016/1062-1458(96)82286-0
204
Barsky, A. J., & Ahem, D. K. (2004). Cognitive behaviour therapy for hypochondriasis:
A randomized controlled trial. Journal of the American Medical Association, 291,
1464-1470. doi:10.1001/jama.291.12.1464
Barsky, A. J., Barnett, M. C , & Cleary, P. D. (1994). Hypochondriasis and panic
disorder: Boundary and overlap. Archives of General Psychiatry, 51, 918-925.
Retrieved from http ://archpsyc. ama-assn. org/
Barsky, A. J., Cleary, P. D., Wyshak, G., Spitzer, R. L., Williams, J. B. W., & Klerman,
G. J. (1992). A structured diagnostic interview for hypochondriasis: A proposed
criteria standard. The Journal of Nervous and Mental Disease, 180, 20-27.
Retrieved from http://ioumals.lww.com/jonmd/pages/default.aspx
Barsky, A. J., Fama, J. M., Bailey, E. D., & Ahem, D. K. (1998). A prospective 4- to 5-
year study of DSM-III hypochondriasis. Archives of General Psychiatry, 55, 737-
744. Retrieved from http://archpsyc.ama-assn.org/
Barsky, A. J., Frank, C. B., Cleary, P. D., Wyshak, G., & Klerman, G. L. (1991). The
relation between hypochondriasis and age. American Journal of Psychiatry, 148,
923-928. Retrieved from http://ajp.psvchiatryonline.org/index.dtl
Barsky, A. J., & Klerman, G. L. (1983). Overview: Hypochondriasis, bodily complaints,
and somatic styles. American Journal of Psychiatry, 140, 273-283. Retrieved
from http://ajp.psychiatryonline.org/index.dtl
Barsky, A. J., & Cleary, P. D., Coeytaux, R. R., & Ruskin, J. N. (1995). The clinical
course of palpitations in medical outpatients. Archives of Internal Medicine, 155,
1782-1788. doi:10.1016/1062-1458(96)82286-0
204

Barsky, A. J., & Wyshak, G. (1990). Hypochondriasis and somatosensory amplification.
British Journal of Psychiatry, 157, 404-409. Retrieved from http://bip.rcpsych.org/
Barsky, A. J., Wyshak, G., & Klerman, G. L. (1986a). Hypochondriasis: An evaluation of
the DSM-III-R criteria in medical outpatients. Archives of General Psychiatry, 43,
493-500. Retrieved from http://archpsyc.ama-assn.org/
Barsky, A. J., Wyshak, G., & Klerman, G. L. (1986b). Medical and psychiatric
determinants of outpatient medical utilization. Medical Care, 24, 548-560.
Retrieved from http://journals.1ww.com/lww-medicalcare/pages/defaultaspx
Barsky, A. J., Wyshak, G. and Klerman, G. L. (1990a). Transient hypochondriasis.
Archives of General Psychiatry, 47, 746-752. Retrieved from http://archpsyc.ama-
assn.org/
Barsky, A. J., Wyshak, G., & Klerman, G. L. (1990b). The prevalence of hypochondriasis
in medical outpatients. Social Psychiatry and Psychiatric Epidemiology, 25, 89-
94. doi:10.1007/BF00794988
Barsky, A. J., Wyshak, G., & Klerman, G. L. (1990c). The Somatosensory Amplification
Scale and its relationship to hypochondriasis. Journal of Psychiatric Research,
24, 323-334. doi:10.1016/0022-3956(90)9005-B
Barsky, A. J., Wyshak, G., Latham, K., & Klerman, G. (1991). Hypochondriacal patients,
their physicians and their medical care. Journal of Nervous and Mental Disease,
180, 20-27.
Beaber, R. J., & Rodney, W. M. (1984). Underdiagnosis of hypochondriasis in family
practice. Psychosomatics, 25, 39-46.
205
Barsky, A. J., & Wyshak, G. (1990). Hypochondriasis and somatosensory amplification.
British Journal of Psychiatry, 157, 404-409. Retrieved from http://bip.rcpsych.org/
Barsky, A. J., Wyshak, G., & Klerman, G. L. (1986a). Hypochondriasis: An evaluation of
the DSM-III-R criteria in medical outpatients. Archives of General Psychiatry, 43,
493-500. Retrieved from http://archpsyc.ama-assn.org/
Barsky, A. J., Wyshak, G., & Klerman, G. L. (1986b). Medical and psychiatric
determinants of outpatient medical utilization. Medical Care, 24, 548-560.
Retrieved from http://ioumals.lww.com/lww-medicalcare/pages/default.aspx
Barsky, A. J., Wyshak, G. and Klerman, G. L. (1990a). Transient hypochondriasis.
Archives of General Psychiatry, 47, 746-752. Retrieved from http ://archpsyc.ama-
assn.org/
Barsky, A. J., Wyshak, G., & Klerman, G. L. (1990b). The prevalence of hypochondriasis
in medical outpatients. Social Psychiatry and Psychiatric Epidemiology, 25, 89-
94. doi:10.1007/BF00794988
Barsky, A. J., Wyshak, G., & Klerman, G. L. (1990c). The Somatosensory Amplification
Scale and its relationship to hypochondriasis. Journal of Psychiatric Research,
24, 323-334. doi:10.1016/0022-3956(90)9005-B
Barsky, A. J., Wyshak, G., Latham, K., & Klerman, G. (1991). Hypochondriacal patients,
their physicians and their medical care. Journal of Nervous and Mental Disease,
180, 20-27.
Beaber, R. J., & Rodney, W. M. (1984). Underdiagnosis of hypochondriasis in family
practice. Psychosomatics, 25, 39-46.
205

Beekman, A. T. F., Deeg, D. J. H., Braam, A. W., Smit, J. H., & van Tilburg, W. (1997).
Consequences of major and minor depression in later life: A study of disability,
well-being and service utilization. Psychological Medicine, 27, 1397-1409.
doi:10.1017/S0033291797005734
Blazer, D. (1998). Emotional problems in later life: Investigative strategies for
professional caregivers. New York: Springer Publishing Company.
Bordin, E. S. (1979). The generalizability of the psychoanalytic concept of the working
alliance. Psychotherapy: Theory, Research and Practice, 16, 252-260.
Boston, A. F., & Merrick, P. L. (2010). Health anxiety among older people: An
exploratory study of health anxiety and safety behaviors in a cohort of older
adults in New Zealand. International Psychogeriatrics, 22, 549-548.
doi:10.1017/S1041610209991712
Bouman, T. K., & Visser, S. (1998). Cognitive and behavioural treatment of
hypochondriasis. Psychotherapy and Psychosomatics, 463, 214-221.
doi:10.1159/000012283
Bourgault-Fagnou, M. D., & Hadjistavropoulos, H. D. (2009). Understanding health
anxiety among community dwelling seniors with varying degrees of frailty. Aging
and Mental Health, 13, 226-237. doi:10.1080/13607860802380664
Brink, T. L., Yesavage, J. A., Lum, 0., Heirsama, P., Adey, M., & Rose, T. L. (1982).
Screening tests for geriatric depression. Clinical Gerontologist, 1, 37-73.
206
Beekman, A. T. F., Deeg, D. J. H., Braam, A. W., Smit, J. H., & van Tilburg, W. (1997).
Consequences of major and minor depression in later life: A study of disability,
well-being and service utilization. Psychological Medicine, 27, 1397-1409.
doi:10.1017/S0033291797005734
Blazer, D. (1998). Emotional problems in later life: Investigative strategies for
professional caregivers. New York: Springer Publishing Company.
Bordin, E. S. (1979). The generalizability of the psychoanalytic concept of the working
alliance. Psychotherapy: Theory, Research and Practice, 16, 252-260.
Boston, A. F., & Merrick, P. L. (2010). Health anxiety among older people: An
exploratory study of health anxiety and safety behaviors in a cohort of older
adults in New Zealand. International Psychogeriatrics, 22, 549-548.
doi:10.1017/S1041610209991712
Bouman, T. K., & Visser, S. (1998). Cognitive and behavioural treatment of
hypochondriasis. Psychotherapy and Psychosomatics, 463, 214-221.
doi:l 0.1159/000012283
Bourgault-Fagnou, M. D., & Hadjistavropoulos, H. D. (2009). Understanding health
anxiety among community dwelling seniors with varying degrees of frailty. Aging
and Mental Health, 13, 226-237. doi:l 0.1080/13607860802380664
Brink, T. L., Yesavage, J. A., Lum, O., Heirsama, P., Adey, M., & Rose, T. L. (1982).
Screening tests for geriatric depression. Clinical Gerontologist, 1, 37-73.
206

Bravo, I. M., & Silverman, W. K. (2001). Anxiety sensitivity, anxiety and depression in
older patients and their relation to hypochondriacal concerns and medical
illnesses. Aging and Mental Health, 5, 349-357. doi:10.1080/13607860120080305
Brodarty, H. (1993). Think of depression—atypical presentations in the elderly.
Australian Family Physician, 22, 1195-1203.
Busse, E. W. (1976). Hypochondriasis in the elderly: A reaction to social stress. Journal
of the American Geriatrics Society, 24, 145-149.
Byers, A. L., Yaffe, K., Covinsky, K. E., Friedman, M. B., & Bruce, M. L. (2010). High
occurrence of mood and anxiety disorders among older adults. Archives of
General Psychiatry, 67, 489-496. Retrieved from http://archpsyc.ama-assn.org/
Clark, D. M., Salkovskis, P. M., Hackmann, A., Wells, A., Fennell, M., Ludgate, J.,
Ahmad, S., Richards, H. C., & Gelder, M. (1998). Two psychological treatments for
hypochondriasis: A randomised controlled trial. British Journal of Psychiatry, 173,
218-225. Retrieved from http://bip4cpsych.ornZ
Cohen, G. D. (1990). Psychopathology and mental health in the mature and older adult.
In J. E. Birren & K. W. Schaie (Eds.), Handbook of the psychology of aging (pp.
359-368). San Diego, CA: Academic Press, Inc.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2" edition).
Hillsdale, New Jersey: Lawrence Erlbaum Associates, Publishers.
Cote, G., O'Leary, T., Barlow, D. H., Strain, J. J., Salkovskis, P. M., Warwick, H. M. C.,
Clark, D. M., Rapee, R., & Rasmussen, S. A. (1996). Hypochondriasis. In T. A.
Widgier, A. J., Francis, H. A. Pincus, R. Ross, M. B. First, & W. W. Davis (Eds.).
207
Bravo, I. M., & Silverman, W. K. (2001). Anxiety sensitivity, anxiety and depression in
older patients and their relation to hypochondriacal concerns and medical
illnesses. Aging and Mental Health, 5, 349-357. doi:10.1080/13607860120080305
Brodarty, H. (1993). Think of depression—atypical presentations in the elderly.
Australian Family Physician, 22, 1195-1203.
Busse, E. W. (1976). Hypochondriasis in the elderly: A reaction to social stress. Journal
of the American Geriatrics Society, 24, 145-149.
Byers, A. L., Yaffe, K., Covinsky, K. E., Friedman, M. B., & Bruce, M. L. (2010). High
occurrence of mood and anxiety disorders among older adults. Archives of
General Psychiatry, 67, 489-496. Retrieved from http://archpsyc.ama-assn.org/
Clark, D. M., Salkovskis, P. M., Hackmann, A., Wells, A., Fennell, M., Ludgate, J.,
Ahmad, S., Richards, H. C , & Gelder, M. (1998). Two psychological treatments for
hypochondriasis: A randomised controlled trial. British Journal of Psychiatry, 173,
218-225. Retrieved from http://bjp.rcpsych.org/
Cohen, G. D. (1990). Psychopathology and mental health in the mature and older adult.
In J. E. Birren & K. W. Schaie (Eds.), Handbook of the psychology of aging (pp.
359-368). San Diego, CA: Academic Press, Inc.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd edition).
Hillsdale, New Jersey: Lawrence Erlbaum Associates, Publishers.
Cote, G., O'Leary, T., Barlow, D. H., Strain, J. J., Salkovskis, P. M., Warwick, H. M. C ,
Clark, D. M., Rapee, R., & Rasmussen, S. A. (1996). Hypochondriasis. In T. A.
Widgier, A. J., Francis, H. A. Pincus, R. Ross, M. B. First, & W. W. Davis (Eds.).
207
DSM-IV sourcebook (Vol. 2, pp. 933-947). Washington, DC: American
Psychiatric Association.
Cox, B. J., Borger, S. C., Asmundson, G. J. G., & Taylor, S. (2000). Dimensions of
hypochondriasis and the five-factor model of personality. Personality and
Individual Differences, 29, 99-108. doi:10.1016/S0191-8869(99)00180-4
Curtis, J. M. (1984). Motivational techniques for individual and group psychotherapy.
Psychological Reports, 54, 271-277.
Deacon, B. J., & Abramowitz, J. S. (2008). Is hypochondriasis related to OCD, panic
disorder, or both? An empirical evaluation. Journal of Cognitive Psychotherapy, 22,
115-127. doi:10.1891/0889-8391.22.2.115
Deacon, B. J., Lickel, J., & Abramowitz, J. S. (2008). Medical utilization across the
anxiety disorders. Journal of Anxiety Disorders, 22, 344-350.
doi:10.1016/j janxdis.2007.03.004
Dennis, R. E., Boddington, S. J. A., & Funnell, N. J. (2007). Self-report measures of
anxiety: Are they suitable for older adults? Aging and Mental Health, 11, 668-677.
doi:10.1080/13607860701529916
Diala, C., & Muntaner, C. (2003). Mood and anxiety disorders among rural, urban, and
metropolitan residents in the United States. Community Mental Health Journal, 39,
239-252. doi:10.1023/A:1023342307323
Ditto, P. H., Jemmott, J. B. III, & Darley, J. M. (1988). Appraising the threat of illness: A
mental representational approach. Health Psychology, 7, 183-201.
doi:10.1037/0278-6133.7.2.183
208
DSM-IVsourcebook (Vol. 2, pp. 933-947). Washington, DC: American
Psychiatric Association.
Cox, B. J., Borger, S. C , Asmundson, G. J. G., & Taylor, S. (2000). Dimensions of
hypochondriasis and the five-factor model of personality. Personality and
Individual Differences, 29, 99-108. doi:10.1016/S0191-8869(99)00180-4
Curtis, J. M. (1984). Motivational techniques for individual and group psychotherapy.
Psychological Reports, 54, 271-277.
Deacon, B. J., & Abramowitz, J. S. (2008). Is hypochondriasis related to OCD, panic
disorder, or both? An empirical evaluation. Journal of Cognitive Psychotherapy, 22,
115-127. doi: 10.1891/0889-8391.22.2.115
Deacon, B. J., Lickel, J., & Abramowitz, J. S. (2008). Medical utilization across the
anxiety disorders. Journal of Anxiety Disorders, 22, 344-350.
doi: 10.1016/j .janxdis.2007.03.004
Dennis, R. E., Boddington, S. J. A., & Funnell, N. J. (2007). Self-report measures of
anxiety: Are they suitable for older adults? Aging and Mental Health, 11, 668-677.
doi:10.1080/13607860701529916
Diala, C , & Muntaner, C. (2003). Mood and anxiety disorders among rural, urban, and
metropolitan residents in the United States. Community Mental Health Journal, 39,
239-252. doi: 10.1023/A: 1023342307323
Ditto, P. H., Jemmott, J. B. Ill, & Darley, J. M. (1988). Appraising the threat of illness: A
mental representational approach. Health Psychology, 7, 183-201.
doi:10.1037/0278-6133.7.2.183
208

Drieschner, K. H., Lammers, S. M., & van der Staak, C. P. (2004). Treatment motivation:
An attempt for clarification of an ambiguous concept. Clinical Psychology
Review, 23, 1115-1137. doi:10.1016/j.cpr.2003.09.003
Dugas, M. J., Ladouceur, R., Leger, E., Freeston, M. H., Langlois, F., Provencher, M. D.,
& Boisvert, J.M. (2003). Group cognitive-behavioral therapy for generalized
anxiety disorder: Treatment outcome and long-term follow-up. Journal of
Consulting and Clinical Psychology, 71, 821-825. Doi:10.1037/0022-
006X.71.4.821g
Easterling, D. V., & Leventhal, H. (1989). Contribution of concrete cognition to emotion:
Neutral symptoms as elicitors of worry about cancer. Journal of Applied
Psychology, 74, 787-796. Retrieved from http://www.apa.org/pubs/journals/apl/
Eifert, G. H., Zvolensky, M. J., & Lejuez, C. W. (2001). Heart-focused anxiety in
medical and anxiety-related psychological conditions. In G. J. G. Asmundson, S.
Taylor, & B. J. Cox (Eds.), Health anxiety: Clinical and research perspectives on
hypochondriasis and related conditions (pp. 277-297). Baffins Lane, Chichester:
John Wiley & Sons.
Faul, F., & Erdfelder, E. (1992). GPOWER: A priori, post-hoc, and compromise power
analyses for MS-DOS [Computer program]. Bonn, FRG: Bonn University,
Department of Psychology.
Ferguson, E. (2009). A taxometric analysis of health anxiety. Psychological Medicine,
39, 277-285. doi:10.1017/S0033291708003322
209
Drieschner, K. H., Lammers, S. M., & van der Staak, C. P. (2004). Treatment motivation:
An attempt for clarification of an ambiguous concept. Clinical Psychology
Review, 23, 1115-1137. doi: 10.1016/j.cpr.2003.09.003
Dugas, M. J., Ladouceur, R., Leger, E., Freeston, M. H., Langlois, F., Provencher, M. D.,
& Boisvert, J.M. (2003). Group cognitive-behavioral therapy for generalized
anxiety disorder: Treatment outcome and long-term follow-up. Journal of
Consulting and Clinical Psychology, 71, 821-825. Doi:10.1037/0022-
006X.71.4.821g
Easterling, D. V., & Leventhal, H. (1989). Contribution of concrete cognition to emotion:
Neutral symptoms as elicitors of worry about cancer. Journal of Applied
Psychology, 74, 787-796. Retrieved from http://www.apa.org/pubs/joumals/apl/
Eifert, G. H., Zvolensky, M. J., & Lejuez, C. W. (2001). Heart-focused anxiety in
medical and anxiety-related psychological conditions. In G. J. G. Asmundson, S.
Taylor, & B. J. Cox (Eds.), Health anxiety: Clinical and research perspectives on
hypochondriasis and related conditions (pp. 277-297). Baffins Lane, Chichester:
John Wiley & Sons.
Faul, F., & Erdfelder, E. (1992). GPOWER: A priori, post-hoc, and compromise power
analyses for MS-DOS [Computer program]. Bonn, FRG: Bonn University,
Department of Psychology.
Ferguson, E. (2009). A taxometric analysis of health anxiety. Psychological Medicine,
39, 277-285. doi:10.1017/S0033291708003322
209

Ferrell, B. A., Stein, W. M., & Beck, J. C. (2000). The Geriatric Pain Measure: Validity,
reliability and factor analysis. Journal of the American Geriatrics Society, 48,
1669-1673. Retrieved from http://www.wiley.com/bw/journal.asp?ref=0002-
8614&site=1
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1996). Structured Clinical
Interview for DSM-IV Axis I Disorders (SCID). Washington, DC, American
Psychiatric Press.
Furer, P., Walker, J. R., & Freeston, M. H. (2001). Approaches to individual and group
cognitive-behavior therapy. In G. J. G. Asmundson, S. Taylor, & B. J. Cox (Eds.),
Health anxiety: Clinical and research perspectives on hypochondriasis and
related conditions (pp. 161-192). Baffins Lane, Chichester: John Wiley & Sons
Ltd.
Gallagher-Thompson, D., & Thompson, L. W. (1995). Psychotherapy with older adults in
theory and practice. In B. Boner & L. Beutler (Eds.), Comprehensive textbook of
psychotherapy (pp. 357-379). New York: Oxford University Press.
Gaston, L., Mannar, C. R., Gallagher, D., & Thompson, L. W. (1991). Alliance
prediction of outcome beyond in-treatment symptomatic change a psychotherapy
processes. Psychotherapy Research, 1, 104-113.
doi:10.1080/10503309112331335531
Goldberg, D., Bridges, K., Duncan-Jones, P., & Grayson, D. (1988). Detecting anxiety
and depression in general medical settings. British Medical Journal, 297, 897-
899. Retrieved from http://www.jstor.org/stable/29701082
210
Ferrell, B. A., Stein, W. M., & Beck, J. C. (2000). The Geriatric Pain Measure: Validity,
reliability and factor analysis. Journal of the American Geriatrics Society, 48,
1669-1673. Retrieved from http://www.wiley.com/bw/ioumal.asp?ref=0002-
8614&site=l
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1996). Structured Clinical
Interview for DSM-IV Axis I Disorders (SCID). Washington, DC, American
Psychiatric Press.
Furer, P., Walker, J. R., & Freeston, M. H. (2001). Approaches to individual and group
cognitive-behavior therapy. In G. J. G. Asmundson, S. Taylor, & B. J. Cox (Eds.),
Health anxiety: Clinical and research perspectives on hypochondriasis and
related conditions (pp. 161-192). Baffins Lane, Chichester: John Wiley & Sons
Ltd.
Gallagher-Thompson, D., & Thompson, L. W. (1995). Psychotherapy with older adults in
theory and practice. In B. Boner & L. Beutler (Eds.), Comprehensive textbook of
psychotherapy (pp. 357-379). New York: Oxford University Press.
Gaston, L., Marmar, C. R., Gallagher, D., & Thompson, L. W. (1991). Alliance
prediction of outcome beyond in-treatment symptomatic change a psychotherapy
processes. Psychotherapy Research, 1, 104-113.
doi:10.1080/10503309112331335531
Goldberg, D., Bridges, K., Duncan-Jones, P., & Grayson, D. (1988). Detecting anxiety
and depression in general medical settings. British Medical Journal, 297, 897-
899. Retrieved from http://www.jstor.org/stable/29701082
210

Gramling, S. E., Clawson, E. P., & McDonald, M. K. (1996). Perceptual and cognitive
abnormality model of hypochondriasis: Amplification and physiological
reactivity in women. Psychosomatic Medicine, 58, 423-431. Retrieved from
http://www.psychosomaticmedicine.org/
Grassi, L., Sabato, S., Rossi, R., Biancosino, B., & Marmai, L. (2005). Use of the
diagnostic criteria for psychosomatic research in oncology. Psychotherapy and
Psychosomatics, 74,100-107 . doi:10.1159/000083168
Greeven, A., van Balkom, A. J., van der Leeden, R., Merkelbach, J. W., van den Heuvel,
0.A., & Spinhoven, P. (2009). Cognitive behavioural therapy versus paroxetine
in the treatment of hypochondriasis: An 18-month naturalistic follow-up. Journal
of Behavior Therapy and Experimental Psychiatry, 40, 487-496.
doi:10.1016/j.btep.2009.06.005
Haan, E. de, Oppen, P. van, Balkom, A. J. L. M. van, Spinhoven, P., Hoogduin, K. A. L.,
& Van Dyck, R. (1997). Prediction of outcome and early vs. late improvement in
OCD patients treated with cognitive behaviour therapy and pharmacotherapy.
Acta Psychiatrica Scandinavica, 96, 354-361. doi: 10.1111/j.1600-
0447.1997.tb09929.x
Hadjistavropoulos, H. D., & Asmundson, G. J. G. (1998). Factor analytic investigation of
the Illness Attitudes Scales in a chronic pain sample. Behaviour Research and
Therapy, 36, 1185-1195. doi:10.1016/S0005-7967(98)00077-1
Hadjistavropoulos, H. D., Frombach, I. K., & Asmundson, G. J. G. (1999). Exploratory
and confirmatory factor analytic investigations of the Illness Attitudes Scale in a
211
Gramling, S. E., Clawson, E. P., & McDonald, M. K. (1996). Perceptual and cognitive
abnormality model of hypochondriasis: Amplification and physiological
reactivity in women. Psychosomatic Medicine, 58, 423-431. Retrieved from
http://www.psychosomaticmedicine.org/
Grassi, L., Sabato, S., Rossi, R., Biancosino, B., & Marmai, L. (2005). Use of the
diagnostic criteria for psychosomatic research in oncology. Psychotherapy and
Psychosomatics, 74, 100-107. doi: 10.1159/000083168
Greeven, A., van Balkom, A. J., van der Leeden, R., Merkelbach, J. W., van den Heuvel,
O.A., & Spinhoven, P. (2009). Cognitive behavioural therapy versus paroxetine
in the treatment of hypochondriasis: An 18-month naturalistic follow-up. Journal
of Behavior Therapy and Experimental Psychiatry, 40, 487-496.
doi:10.1016/j.btep.2009.06.005
Haan, E. de, Oppen, P. van, Balkom, A. J. L. M. van, Spinhoven, P., Hoogduin, K. A. L.,
& Van Dyck, R. (1997). Prediction of outcome and early vs. late improvement in
OCD patients treated with cognitive behaviour therapy and pharmacotherapy.
Acta Psychiatrica Scandinavica, 96, 354-361. doi: 10.1111/j.1600-
0447.1997.tb09929.x
Hadjistavropoulos, H. D., & Asmundson, G. J. G. (1998). Factor analytic investigation of
the Illness Attitudes Scales in a chronic pain sample. Behaviour Research and
Therapy, 36, 1185-1195. doi:10.1016/S0005-7967(98)00077-l
Hadjistavropoulos, H. D., Frombach, I. K., & Asmundson, G. J. G. (1999). Exploratory
and confirmatory factor analytic investigations of the Illness Attitudes Scale in a
211

nonclinical sample. Behaviour Research and Therapy, 37, 671-684.
doi:10.1016/S005-7967(98)00159-4
Hadjistavropoulos, H. D., Owens, K. M. B., Hadjistavropoulos, T., & Asmundson, G. J.
G. (2001). In G. J. G. Asmundson, S. Taylor, & B. J. Cox (Eds.), Health anxiety:
Clinical and research perspectives on hypochondriasis and related conditions
(pp. 298-323). Baffins Lane, Chichester: John Wiley & Sons Ltd.
Haenen, M. A., de Jong, P. J., Schmidt, A. J. M., Stevens, S., & Visser, L. (2000).
Hypochondriacs' estimation of negative outcomes: Domain-specificity and
responsiveness to reassuring and alarming information. Behaviour Research and
Therapy, 38, 819-833. doi:10.1016/50005-7967(99)00128-X
Haenen, M. A., Schmidt, A. J. M., Kroeze, S., & van den Hout, M. A. (1996).
Hypochondriasis and symptom reporting-The effect of attention versus
distraction. Psychotherapy and Psychosomatics, 65, 43-48.
Hanback, J. W., & Revelle, W. (1978). Arousal and perceptual sensitivity in
hypochondriacs. Journal of Abnormal Psychology, 87, 523-530. Retrieved from
http://psycnet.apa.org/journals/abn/87/5/523/
Hawranik, P. (1991). A clinical possibility: Preventing health problems after the age of
65. Journal of Gerontological Nursing, 17, 20-25.
Hiller, W., Rief, W., & Fichter, M. M. (2002). Dimensional and categorical approaches to
hypochondriasis. Psychological Medicine, 32, 707-718.
doi:10.1017/S0033291702005524
212
nonclinical sample. Behaviour Research and Therapy, 37, 671-684.
doi: 10.1016/S005-7967(98)00159-4
Hadjistavropoulos, H. D., Owens, K. M. B., Hadjistavropoulos, T., & Asmundson, G. J.
G. (2001). In G. J. G. Asmundson, S. Taylor, & B. J. Cox (Eds.), Health anxiety:
Clinical and research perspectives on hypochondriasis and related conditions
(pp. 298-323). Baffins Lane, Chichester: John Wiley & Sons Ltd.
Haenen, M. A., de Jong, P. J., Schmidt, A. J. M., Stevens, S., & Visser, L. (2000).
Hypochondriacs' estimation of negative outcomes: Domain-specificity and
responsiveness to reassuring and alarming information. Behaviour Research and
Therapy, 38, 819-833. doi:10.1016/S0005-7967(99)00128-X
Haenen, M. A., Schmidt, A. J. M., Kroeze, S., & van den Hout, M. A. (1996).
Hypochondriasis and symptom reporting-The effect of attention versus
distraction. Psychotherapy and Psychosomatics, 65, 43-48.
Hanback, J. W., & Revelle, W. (1978). Arousal and perceptual sensitivity in
hypochondriacs. Journal of Abnormal Psychology, 87, 523-530. Retrieved from
http://psycnet.apa.Org/ioumals/abn/87/5/523/
Hawranik, P. (1991). A clinical possibility: Preventing health problems after the age of
65. Journal of Gerontological Nursing, 17, 20-25.
Hiller, W., Rief, W., & Fichter, M. M. (2002). Dimensional and categorical approaches to
hypochondriasis. Psychological Medicine, 32, 707-718.
doi:10.1017/S0033291702005524
212

Himmelfarb, S., & Murrell, S. A. (1984). The prevalence and correlates of anxiety
symptoms in older adults. The Journal of Psychology, 116, 159-167.
Hitchcock, P. B., & Mathews, A. (1992). Interpretation of bodily symptoms in
hypochondriasis. Behaviour Research and Therapy, 30, 223-234.
doi:10.1016/0005-7967(92)90068-R
Hogan, D. B., MacKnight, C., & Bergman, H. (2003). Models, definitions, and criteria
for frailty. Aging Clinical and Experimental Research, 15 (3-Sup), 3-29.
Hoogduin, C. A. L., & Duivenvoorden, H. J. (1988). A decision model in the treatment of
obsessive-compulsive neuroses. British Journal of Psychiatry, 152, 516-521.
Horvath, A. T. (1993). Enhancing motivation for treatment of addictive behaviour:
Guidelines for the psychotherapist. Psychotherapy: Theory, Research, Practice,
Training, 30, 473-480. doi:10.1037/0033-3204.30.3.473
Horvath, A. 0., & Greenberg, L. S. (1989). The development and validation of the
Working Alliance Inventory. Journal of Counseling Psychology, 36, 223-233.
Horvath, A. 0., & Symonds, B. D. (1991). Relation between working alliance and
outcome in psychotherapy. Journal of Counseling Psychology, 38, 139-149.
doi:10.1037/0022-0167.36.2.223
Hyer, L., Kramer, D., & Sohnle, S. (2004). CBT with older people: Alterations and the
value of the therapeutic alliance. Psychotherapy: Theory, Research, Practice,
Training, 41, 276-291. doi:10.1037/0033-3204.41.3.276
213
Himmelfarb, S., & Murrell, S. A. (1984). The prevalence and correlates of anxiety
symptoms in older adults. The Journal of Psychology, 116, 159-167.
Hitchcock, P. B., & Mathews, A. (1992). Interpretation of bodily symptoms in
hypochondriasis. Behaviour Research and Therapy, 30, 223-234.
doi: 10.1016/0005-7967(92)90068-R
Hogan, D. B., MacKnight, C , & Bergman, H. (2003). Models, definitions, and criteria
for frailty. Aging Clinical and Experimental Research, 15 (3-Sup), 3-29.
Hoogduin, C. A. L., & Duivenvoorden, H. J. (1988). A decision model in the treatment of
obsessive-compulsive neuroses. British Journal of Psychiatry, 152, 516-521.
Horvath, A. T. (1993). Enhancing motivation for treatment of addictive behaviour:
Guidelines for the psychotherapist. Psychotherapy: Theory, Research, Practice,
Training, 30, 473^180. doi: 10.1037/0033-3204.30.3.473
Horvath, A. O., & Greenberg, L. S. (1989). The development and validation of the
Working Alliance Inventory. Journal of Counseling Psychology, 36, 223-233.
Horvath, A. O., & Symonds, B. D. (1991). Relation between working alliance and
outcome in psychotherapy. Journal of Counseling Psychology, 38, 139-149.
doi:10.1037/0022-0167.36.2.223
Hyer, L., Kramer, D., & Sohnle, S. (2004). CBT with older people: Alterations and the
value of the therapeutic alliance. Psychotherapy: Theory, Research, Practice,
Training, 41, 276-291. doi:10.1037/0033-3204.41.3.276
213

Jacobson, N.S., & Truax, P. (1991). Clinical significance: a statistical approach to
defining meaningful change in psychotherapy research. Journal of Consulting and
Clinical Psychology, 59, 12 -19. doi:10.1037/0022-006X.59.1.12
Jeste, N. D., Hays, J. C., & Steffens, D. C. (2006). Clinical correlates of anxious
depression among elderly patients with depression. Journal of Affective Disorders,
90, 37-41. doi:10.1016/j.jad.2005.10.007
Kabacoff, R. I., Segal, D. L., Hersen, M., & Van Hesselt, V. B. (1997). Psychometric
properties and diagnostic utility of the Beck Anxiety Inventory and the State-Trait
Anxiety Inventory with older adult psychiatric outpatients. Journal of Anxiety
Disorders, 11, 33-47. doi:10.1016/S0887-6185(96)00033-3.
Kehler, M. D., & Hadjistavropoulos, H. D. (2009). Is health anxiety a significant problem
for individuals with multiple sclerosis? Journal of Behavioral Medicine, 32, 150-
161. doi:10.1007/s10865-008-9186-z
Keijsers, G. P. J., Schaap, C. P. D. R., Hoogduin, C. A. L., Hoogsteyns, B., & de Kemp,
E. C. M. (1999). Preliminary results of a new instrument to assess patient
motivation for treatment in cognitive-behaviour therapy. Behavioural and Cognitive
Psychotherapy, 27, 165-179. Retrieved from
http://journals.cambridge.org/action/displayJournal?jid=BCP
Kellner, R. (1979). Psychotherapeutic strategies in the treatment of psychophysiologic
disorders. Psychotherapy and Psychosomatics, 32 (Suppl. 4), 91-100.
Kellner, R. (1986). Somatization and hypochondriasis. New York: Praeger.
214
Jacobson, N.S., & Truax, P. (1991). Clinical significance: a statistical approach to
defining meaningful change in psychotherapy research. Journal of Consulting and
Clinical Psychology, 59, 12 -19. doi:10.1037/0022-006X.59.1.12
Jeste, N. D., Hays, J. C , & Steffens, D. C. (2006). Clinical correlates of anxious
depression among elderly patients with depression. Journal of Affective Disorders,
90, 37-41. doi: 10.1016/j.jad.2005.10.007
Kabacoff, R. I., Segal, D. L., Hersen, M., & Van Hesselt, V. B. (1997). Psychometric
properties and diagnostic utility of the Beck Anxiety Inventory and the State-Trait
Anxiety Inventory with older adult psychiatric outpatients. Journal of Anxiety
Disorders, 11, 33-47. doi: 10.1016/S0887-6185(96)00033-3.
Kehler, M. D., & Hadjistavropoulos, H. D. (2009). Is health anxiety a significant problem
for individuals with multiple sclerosis? Journal of Behavioral Medicine, 32, 150-
161.doi:10.1007/sl0865-008-9186-z
Keijsers, G. P. J., Schaap, C. P. D. R., Hoogduin, C. A. L., Hoogsteyns, B., & de Kemp,
E. C. M. (1999). Preliminary results of a new instrument to assess patient
motivation for treatment in cognitive-behaviour therapy. Behavioural and Cognitive
Psychotherapy, 27, 165-179. Retrieved from
http://joumals.cambridge.org/action/displavJoumal?iid=BCP
Kellner, R. (1979). Psychotherapeutic strategies in the treatment of psychophysiologic
disorders. Psychotherapy and Psychosomatics, 32 (Suppl. 4), 91-100.
Kellner, R. (1986). Somatization and hypochondriasis. New York: Praeger.
214

Kellner, R., Abbott, P., Winslow, W. W., & Pathak, D. (1987). Fears, beliefs, and
attitudes in DSM-III hypochondriasis. Journal of Nervous and Mental Disease, 175,
20-25.
Kessler, R. C., & Ustun, T. B. (2004). The World Mental Health (WMH) Survey
Initiative version of the World Health Organization (WHO) Composite
International Diagnostic Interview (CIDI). International Journal of Methods in
Psychiatric Research, 13(2), 93-121. Retrieved from
http://www.ingentaconnect.com/content/whudijmpr/2004/00000013/00000002
Knight, B. G., & Satre, D. D. (1999). Cognitive behavioral psychotherapy with older
adults. Clinical Psychology: Science and Practice 6, 188-203.
doi:10.1093/clipsy.6.2.188
Koenig, H. G., Cohen, H. J., Blazer, D. G., Krishnan, K. R., & Sibert, T. E. (1993).
Profile of depressive symptoms in younger and older medical inpatients with
major depression. Journal of the American Geriatrics Society, 41, 1169-1176.
Koenig, H. G., Meador, K. G., Cohen, H. J., & Blazer, D. G. (1988). Depression in
elderly hospitalised patients with medical illness. Archives of Internal Medicine,
148, 1929-1936.
Kramer-Ginsberg, E., Greenwald, B., Aisen, P., & Brod-Miller, C. (1989).
Hypochondriaisis in the elderly depressed. Journal of American Geriatric
Psychiatry, 5, 211-215.
Krause, M. S. (1966). A cognitive theory of motivation for treatment. The Journal of
General Psychiatry, 75, 9-19.
215
Kellner, R., Abbott, P., Winslow, W. W., & Pathak, D. (1987). Fears, beliefs, and
attitudes in DSM-III hypochondriasis. Journal of Nervous and Mental Disease, 175,
20-25.
Kessler, R. C , & Ustun, T. B. (2004). The World Mental Health (WMH) Survey
Initiative version of the World Health Organization (WHO) Composite
International Diagnostic Interview (CIDI). International Journal of Methods in
Psychiatric Research, 13(2), 93-121. Retrieved from
http://www.ingentaconnect.com/content/whurr/iimpr/2004/00000013/00000002
Knight, B. G., & Satre, D. D. (1999). Cognitive behavioral psychotherapy with older
adults. Clinical Psychology: Science and Practice 6, 188-203.
doi:10.1093/clipsy.6.2.188
Koenig, H. G., Cohen, H. J., Blazer, D. G., Krishnan, K. R., & Sibert, T. E. (1993).
Profile of depressive symptoms in younger and older medical inpatients with
major depression. Journal of the American Geriatrics Society, 41, 1169-1176.
Koenig, H. G., Meador, K. G., Cohen, H. J., & Blazer, D. G. (1988). Depression in
elderly hospitalised patients with medical illness. Archives of Internal Medicine,
148, 1929-1936.
Kramer-Ginsberg, E., Greenwald, B., Aisen, P., 8c Brod-Miller, C. (1989).
Hypochondriaisis in the elderly depressed. Journal of American Geriatric
Psychiatry, 5, 211-215.
Krause, M. S. (1966). A cognitive theory of motivation for treatment. The Journal of
General Psychiatry, 75,9-19.
215

Krupnick, J. L., Sotsky, S. M., Simmens, S., Moyer, J., Elkin, I., Watkins, J., & Pilkonis,
P. A. (1996). The role of the therapeutic alliance in psychotherapy and
pharmacotherapy outcome: Findings in the National Institute of Mental Health
Treatment of Depression Collaborative Research Program. Journal of Consulting
and Clinical Psychology, 64, 532-539. doi:10.1037/0022-006X.64.3.532
Kvaal, K., & Laake, K. (2003). Anxiety and well-being in older patients after discharge
from hospital. Journal of Advanced Nursing, 44, 271-277. doi: 10.1046/j.1365-
2648.2003.02802.x
Kvaal, K., Laake, K., & Engedal, K. (2001). Psychometric properties of the state part of
the Spielberger State-Trait Anxiety Inventory (STAI) in geriatric patients.
International Journal of Geriatric Psychiatry, 16, 980-986. doi: 10.1002/gps.458
Kvaal, K., Macijauskiene, J., Engedal, K., & Laake, K. (2001). High prevalence of
anxiety symptoms in hospitalized geriatric patients. International Journal of
Geriatric Psychiatry, 16, 690-693. doi: 10.1002/gps.405
Kvaal, K., Ulstein, I., Nordhus, I. H., & Engedal, K. (2005). The Spielberger State-Trait
Inventory (STAI): the state scale in detecting mental disorders in geriatric
patients. International Journal of Geriatric Psychiatry, 20, 629-634. doi:
10.1002/gps.1330
Lasocki, M. (1986). Reasons for low utilization of mental health services by the elderly.
In T. L. Brink (Ed.), Clinical gerontology:• A guide to assessment and intervention
(pp.1-18). New York: The Haworth Press.
216
Krupnick, J. L., Sotsky, S. M., Simmens, S., Moyer, J., Elkin, I., Watkins, J., & Pilkonis,
P. A. (1996). The role of the therapeutic alliance in psychotherapy and
pharmacotherapy outcome: Findings in the National Institute of Mental Health
Treatment of Depression Collaborative Research Program. Journal of Consulting
and Clinical Psychology, 64, 532-539. doi:10.1037/0022-006X.64.3.532
Kvaal, K., & Laake, K. (2003). Anxiety and well-being in older patients after discharge
from hospital. Journal of Advanced Nursing, 44, 271-277. doi: 10.1046/J.1365-
2648.2003.02802.x
Kvaal, K., Laake, K., & Engedal, K. (2001). Psychometric properties of the state part of
the Spielberger State-Trait Anxiety Inventory (STAI) in geriatric patients.
International Journal of Geriatric Psychiatry, 16, 980-986. doi: 10.1002/gps.458
Kvaal, K., Macijauskiene, J., Engedal, K., & Laake, K. (2001). High prevalence of
anxiety symptoms in hospitalized geriatric patients. International Journal of
Geriatric Psychiatry, 16, 690-693. doi: 10.1002/gps.405
Kvaal, K., Ulstein, I., Nordhus, I. H., & Engedal, K. (2005). The Spielberger State-Trait
Inventory (STAI): the state scale in detecting mental disorders in geriatric
patients. International Journal of Geriatric Psychiatry, 20, 629-634. doi:
10.1002/gps.l330
Lasocki, M. (1986). Reasons for low utilization of mental health services by the elderly.
In T. L. Brink (Ed.), Clinical gerontology: A guide to assessment and intervention
(pp. 1-18). New York: The Haworth Press.
216

Lecci, L., & Cohen, D. J. (2007). Altered processing of health threat words as a function
of hypochondriacal tendencies and experimentally manipulated control beliefs.
Cognition and Emotion, 21, 211-224. doi:10.1080/02699930600625248
Lister, A., Rode, S., Farmer, A., & Salkovskis, P. M. (2002). Does thinking about
personal health risk increase anxiety? Journal of Health Psychology, 7, 409-414.
doi:10.1177/1359105302007004330
Longley, S. L., Broman-Fulks, J. J., Calamari, J. E., Noyes, R., Wade, M., & Orlando, C.
M. (in press). A taxometric study of hypochondriasis symptoms. Behavior
Therapy. doi:10.1016/j .beht.2010.02.002
Longley, S., Watson, D., & Noyes, R. (2005). Assessment of the hypochondriasis
domain: The Multidimensional Inventory of Hypochondriacal Traits (MIHT).
Psychological Assessment, 17, 3-14. doi:10.1037/1040-3590.17.1.3
Lucock, M. P., Morley, S., White, C., & Peake, M. D. (1997). Responses of consecutive
patients to reassurance after gastroscopy: results of self administered questionnaire
survey. British Medical Journal, 315, 1-4. Retrieved from http://www.bmj.com/
Lucock, M. P., White, C., Peake, M. D., & Morley, S. (1998). Biased perception and
recall of reassurance in medical patients. British Journal of Health Psychology, 3,
237-243.
Lyness, J., King, D., Conwell, Y., Cox, C., & Caine, E. (1993). Somatic worry and
medical illness in depressed patients. The American Journal of Geriatric
Psychiatry, 1, 288-295.
217
Lecci, L., & Cohen, D. J. (2007). Altered processing of health threat words as a function
of hypochondriacal tendencies and experimentally manipulated control beliefs.
Cognition and Emotion, 21, 211-224. doi: 10.1080/02699930600625248
Lister, A., Rode, S., Farmer, A., & Salkovskis, P. M. (2002). Does thinking about
personal health risk increase anxiety? Journal of Health Psychology, 7, 409-414.
doi: 10.1177/1359105302007004330
Longley, S. L., Broman-Fulks, J. J., Calamari, J. E., Noyes, R., Wade, M., & Orlando, C.
M. (in press). A taxometric study of hypochondriasis symptoms. Behavior
Therapy, doi: 10.1016/j.beht.2010.02.002
Longley, S., Watson, D., & Noyes, R. (2005). Assessment of the hypochondriasis
domain: The Multidimensional Inventory of Hypochondriacal Traits (MIHT).
Psychological Assessment, 17, 3-14. doi:10.1037/1040-3590.17.1.3
Lucock, M. P., Morley, S., White, C , & Peake, M. D. (1997). Responses of consecutive
patients to reassurance after gastroscopy: results of self administered questionnaire
survey. British Medical Journal, 315, 1-4. Retrieved from http://www.bmj .com/
Lucock, M. P., White, C , Peake, M. D., & Morley, S. (1998). Biased perception and
recall of reassurance in medical patients. British Journal of Health Psychology, 3,
237-243.
Lyness, J., King, D., Conwell, Y., Cox, C , & Caine, E. (1993). Somatic worry and
medical illness in depressed patients. The American Journal of Geriatric
Psychiatry, 1, 288-295.
217
Mailer, R. G., & Reiss, S. (1992). Anxiety sensitivity in 1984 and panic attacks in 1987.
Journal of Anxiety Disorders, 6, 241-247. doi:10.1016/0887-6185(92)90036-7
Marcus, D. K. (1999). The cognitive-behavioral model of hypochondriasis:
Misinformation and triggers. Journal of Psychosomatic Research, 47, 79-91.
Marcus, D. K., Gurley, J. R., Marchi, M. M., & Bauer, C. (2007). Cognitive and
perceptual variables in hypochondriasis and health anxiety: A systematic
review. Clinical Psychology Review, 27, 127-139. doi:10.1016/j.cpr.2006.09.003
Marks, I. M., & Mathews, A. M. (1979). Brief standard self-rating for phobic patients.
Behaviour Research and Therapy, 17, 263-267.
Marmar, C. R., Gaston, L., Gallagher, D., & Thompson, L. W. (1989). Therapeutic
alliance and outcome in behavioral, cognitive, and brief dynamic psychotherapy
in latelife depression. Journal of Nervous and Mental Disease, 177, 464-472.
Marmar, C., Weiss, D., & Gaston, L. (1989). Towards the validation of the California
Therapeutic Alliance Rating System. Psychological Assessment, 1, 46-52.
doi:10.1037/1040-3590.1.1.46
Martin, D. J., Garske, J. P., & Davis, M. K. (2000). Relation of the therapeutic alliance
with outcome and other variables: A meta analytic review. Journal of Consulting
and Clinical Psychology, 68, 438-450. doi:10.1037/0022-006X.68.3.438
Miller, W., & Rollnick, S. (2002). Motivational interviewing: Preparing people to
change (2nd edition). New York, NY: Guilford Press.
Mohl, P. C., Martinez, D., Ticknor, C., Huang, M., & Cordell, L. (1991). Early dropouts
from psychotherapy. Journal of Nervous and Mental Disorders, 179, 478-481.
218
Mailer, R. G., 8c Reiss, S. (1992). Anxiety sensitivity in 1984 and panic attacks in 1987.
Journal of Anxiety Disorders, 6, 241-247. doi:10.1016/0887-6185(92)90036-7
Marcus, D. K. (1999). The cognitive-behavioral model of hypochondriasis:
Misinformation and triggers. Journal of Psychosomatic Research, 47, 79-91.
Marcus, D. K., Gurley, J. R., Marchi, M. M., & Bauer, C. (2007). Cognitive and
perceptual variables in hypochondriasis and health anxiety: A systematic
review. Clinical Psychology Review, 27, 127-139. doi:10.1016/j.cpr.2006.09.003
Marks, I. M., & Mathews, A. M. (1979). Brief standard self-rating for phobic patients.
Behaviour Research and Therapy, 17, 263-267.
Marmar, C. R., Gaston, L., Gallagher, D., & Thompson, L. W. (1989). Therapeutic
alliance and outcome in behavioral, cognitive, and brief dynamic psychotherapy
in latelife depression. Journal of Nervous and Mental Disease, 177, 464-472.
Marmar, C , Weiss, D., & Gaston, L. (1989). Towards the validation of the California
Therapeutic Alliance Rating System. Psychological Assessment, 1, 46-52.
doi: 10.103 7/1040-3590.1.1.46
Martin, D. J., Garske, J. P., & Davis, M. K. (2000). Relation of the therapeutic alliance
with outcome and other variables: A meta analytic review. Journal of Consulting
and Clinical Psychology, 68, 438-450. doi:10.1037/0022-006X.68.3.438
Miller, W., & Rollnick, S. (2002). Motivational interviewing: Preparing people to
change (2nd edition). New York, NY: Guilford Press.
Mohl, P. C , Martinez, D., Ticknor, C , Huang, M., & Cordell, L. (1991). Early dropouts
from psychotherapy. Journal of Nervous and Mental Disorders, 179, 478-481.
218
Mohlman, J., Gorenstein, E. E., Kleber, M., de Jesus, M., Gorman, J., & Papp, L. A.
(2003). Standard and enhanced cognitive-behavior therapy for late-life
generalized anxiety disorder: Two pilot investigations. American Journal of
Geriatric Psychiatry, 11, 24-32. Retrieved from
http://journals.1ww.com/ajgponline/pages/default.aspx
Mohlman, J., & Zinbarg, R. E. (2000). The structure and correlates of anxiety sensitivity
in older adults. Psychological Assessment, 12, 440-446. doi:10.1037/1040-
3590.12.4.440
Montorio, I., Nuevo, R., Marquez, M., Izal, M., & Losada, A. (2001). Characterization of
worry according to severity of anxiety in elderly living in the community. Aging
and Mental Health, 7, 334-341. doi:10.1080/1360786031000150694
Nelson, R. A., & Borkovec, T. D. (1989). Relationship of client participation to
psychotherapy. Journal of Behavior Therapy and Experimental Psychiatry, 20,
155-162. doi:10.1016/0005-7916(89)90048-7
Nixon, G. F., & Steffeck, J. C. (1977). Reliability of the State-Trait Anxiety Inventory.
Psychological Reports, 40, 357-358.
Noyes, R. Jr., Kathol, R. G., Fisher, M. M., Phillips, B. M., Suelzer, M. T., & Holt, C. S.
(1993). The validity of DSM-III-R hypochondriasis. Archives of General
Psychiatry, 50, 961-970.
Noyes, R. Jr., Kathol, R. G., Fisher, M. M., Phillips, B. M., Suelzer, M., & Woodman, C.
L. (1994). Psychiatric comorbidity among patients with hypchondriasis. General
Hospital Psychiatry, 16, 78-87.
219
Mohlman, J., Gorenstein, E. E., Kleber, M., de Jesus, M., Gorman, J., & Papp, L. A.
(2003). Standard and enhanced cognitive-behavior therapy for late-life
generalized anxiety disorder: Two pilot investigations. American Journal of
Geriatric Psychiatry, 11, 24-32. Retrieved from
http://iournals.lww.com/aigponline/pages/default.aspx
Mohlman, J., & Zinbarg, R. E. (2000). The stmcture and correlates of anxiety sensitivity
in older adults. Psychological Assessment, 12, 440-446. doi:10.1037/1040-
3590.12.4.440
Montorio, I., Nuevo, R., Marquez, M., Izal, M., & Losada, A. (2001). Characterization of
worry according to severity of anxiety in elderly living in the community. Aging
and Mental Health, 7, 334-341. doi:10.1080/1360786031000150694
Nelson, R. A., & Borkovec, T. D. (1989). Relationship of client participation to
psychotherapy. Journal of Behavior Therapy and Experimental Psychiatry, 20,
155-162. doi: 10.1016/0005-7916(89)90048-7
Nixon, G. F., & Steffeck, J. C. (1977). Reliability of the State-Trait Anxiety Inventory.
Psychological Reports, 40, 357-358.
Noyes, R. Jr., Kathol, R. G., Fisher, M. M., Phillips, B. M., Suelzer, M. T., & Holt, C. S.
(1993). The validity of DSM-III-R hypochondriasis. Archives of General
Psychiatry, 50, 961-970.
Noyes, R. Jr., Kathol, R. G., Fisher, M. M., Phillips, B. M., Suelzer, M., & Woodman, C.
L. (1994). Psychiatric comorbidity among patients with hypchondriasis. General
Hospital Psychiatry, 16, 78-87.
219

Noyes, R. Jr., Longley, S. L., Langbehn, D. R., Stuart, S. P., & Kukovi, 0. A. (2010).
Hypochondriacal symptoms associated with a less therapeutic physician-patient
relationship. Psychiatry, 73, 57-69. doi:10.1521/psyc.2010.73.1.57
Noyes, R. Jr., Stuart, S. P., Langbehn, D. R., Happel, R. L., Longley, S. L., Muller, B.A.,
& Yagla, S. J. (2003). Test of an interpersonal model of hypochondriasis.
Psychosomatic Medicine, 65, 292-300.
doi:10.1097/01.PSY.0000058377.50240.64
Olatunji, B. 0. (2009). Incremental specificity of disgust propensity and sensitivity in the
prediction of health anxiety dimensions. Journal of Behavior Therapy and
Experimental Psychiatry, 40, 230-239. doi:10.1016/j.jbtep.2008.10.003
Olatunji, B. 0., Deacon, B. J., & Abramowitz, J. S. (2009). Is hypochondriasis an
anxiety disorder? British Medical Journal, 194, 481-482.
doi:10.1192/bjp.bp.108.061085
Olatunji, B., Deacon, B., Abramowitz, J. S., &Valentiner, D. P. (2007). Body vigilance in
nonclinical and anxiety disorder samples: Structure, correlates, and prediction of
health concerns. Behavior Therapy, 38, 392-401. doi:10.1016/jbeth.2006.09.002
Olatunji, B. 0., Wolitzky-Taylor, K. B., Elwood, L., Connolly, K., Gozales, B., &
Armstrong, T. (2009). Anxiety sensitivity and health anxiety in a nonclinical
sample: Specificity and prospective relations with clinical stress. Cognitive
Therapy and Research, 33, 416-424. doi:10.1037/a0017428
Openshaw, C., Waller, G., & Sperlinger, D. (2004). Group cognitive-behaviour therapy
for bulimia nervosa: Statistical versus clinically significant change in symptoms
220
Noyes, R. Jr., Longley, S. L., Langbehn, D. R., Stuart, S. P., & Kukovi, O. A. (2010).
Hypochondriacal symptoms associated with a less therapeutic physician-patient
relationship. Psychiatry, 73, 57-69. doi:10.1521/psyc.2010.73.1.57
Noyes, R. Jr., Stuart, S. P., Langbehn, D. R., Happel, R. L., Longley, S. L., Muller, B.A.,
& Yagla, S. J. (2003). Test of an interpersonal model of hypochondriasis.
Psychosomatic Medicine, 65, 292-300.
doi:10.1097/01.PSY.0000058377.50240.64
Olatunji, B. O. (2009). Incremental specificity of disgust propensity and sensitivity in the
prediction of health anxiety dimensions. Journal of Behavior Therapy and
Experimental Psychiatry, 40, 230-239. doi: 10.1016/j.jbtep.2008.10.003
Olatunji, B. O., Deacon, B. J., & Abramowitz, J. S. (2009). Is hypochondriasis an
anxiety disorder? British Medical Journal, 194, 481-482.
doi:10.1192/bjp.bp.l08.061085
Olatunji, B., Deacon, B., Abramowitz, J. S., &Valentiner, D. P. (2007). Body vigilance in
nonclinical and anxiety disorder samples: Stmcture, correlates, and prediction of
health concerns. Behavior Therapy, 38, 392-401. doi:10.1016/jbeth.2006.09.002
Olatunji, B. O., Wolitzky-Taylor, K. B., Elwood, L., Connolly, K., Gozales, B., &
Armstrong, T. (2009). Anxiety sensitivity and health anxiety in a nonclinical
sample: Specificity and prospective relations with clinical stress. Cognitive
Therapy and Research, 33, 416-424. doi:10.1037/a0017428
Openshaw, C , Waller, G., & Sperlinger, D. (2004). Group cognitive-behaviour therapy
for bulimia nervosa: Statistical versus clinically significant change in symptoms
220

across treatment. International Journal of Eating Disorders, 36, 363-375.
doi:10.1002/eat.20042
Ostir, G. V., & Goodwin, J. S. (2006). Anxiety in persons 75 and older: Findings from a
tri-ethnic population. Ethnicity and Disease, 16, 22-27. Retrieved from
http://www.ishib.org/ED index.asp
Otto, M., Demopulos, C., McLean, N., Pollack, M., & Fava, M. (1998). Additional
findings on the association between anxiety sensitivity and hypochondriacal
concerns: Examination of patients with major depression. Journal of Anxiety
Disorders, 12, 225-232. doi:10.1016/S0887-6185(98)00011-5
Otto, M., Pollack, M., Sachs, G., & Rosenbaum, J. (1992). Hypochondriacal concerns,
anxiety sensitivity, and panic disorder. Journal of Anxiety Disorders, 6, 93-104.
doi:10.1016/0887-6185(92)90008-U
Owens, K. M. B., Asmundson, G. J. G., Hadjistavropoulos, T., & Owens, T. J.
(2004). Attentional bias toward illness threat in individuals with elevated
health anxiety. Cognitive Therapy and Research, 28, 57-66.
doi:10.1023/B:COTR.0000016930.85884.29
Palmore, E. (1970). Normal aging. Durham, NC: Duke University Press.
Pauli, P., & Alpers, G. W. (2002). Memory bias in patients with hypochondriasis and
somatoform pain disorders. Journal of Psychosomatic Research, 52, 45-53.
doi:10.1016/S0022-3999(01)00295-1
221
across treatment. International Journal of Eating Disorders, 36, 363-375.
doi:10.1002/eat.20042
Ostir, G. V., & Goodwin, J. S. (2006). Anxiety in persons 75 and older: Findings from a
tri-ethnic population. Ethnicity and Disease, 16, 22-27. Retrieved from
http://www.ishib.org/ED index.asp
Otto, M., Demopulos, C , McLean, N., Pollack, M., & Fava, M. (1998). Additional
findings on the association between anxiety sensitivity and hypochondriacal
concerns: Examination of patients with major depression. Journal of Anxiety
Disorders, 12, 225-232. doi:10.1016/S0887-6185(98)00011-5
Otto, M., Pollack, M., Sachs, G., & Rosenbaum, J. (1992). Hypochondriacal concerns,
anxiety sensitivity, and panic disorder. Journal of Anxiety Disorders, 6, 93-104.
doi:10.1016/0887-6185(92)90008-U
Owens, K. M. B., Asmundson, G. J. G., Hadjistavropoulos, T., & Owens, T. J.
(2004). Attentional bias toward illness threat in individuals with elevated
health anxiety. Cognitive Therapy and Research, 28, 57-66.
doi:10.1023/B:COTR.0000016930.85884.29
Palmore, E. (1970). Normal aging. Durham, NC: Duke University Press.
Pauli, P., & Alpers, G. W. (2002). Memory bias in patients with hypochondriasis and
somatoform pain disorders. Journal of Psychosomatic Research, 52, 45-53.
doi:10.1016/S0022-3999(01)00295-l
221
Pauli, P., Schwenzer, M., Brody, S., Rau, H., & Birbaumer, N. (1993). Hypochondriacal
attitudes, pain sensitivity, and attentional bias. Journal of Psychosomatic
Research, 37, 745-752. doi:10.1016/0022-3999(93)90103-M
Persing, J. S., Stuart, S. P., Noyes, R. Jr., & Happel, R. L. (2000). Hypochondriasis: The
patient's perspective. International Journal of Psychiatry in Medicine, 30, 329-342.
Retrieved from http://baywood.metapress.com/
Peterson, R. A., & Heilbronner, R. L. (1987). The Anxiety Sensitivity Index: Construct
validity and factor analytic structure. Journal of Anxiety Disorders, 1, 117-121.
doi:10.1016/0887-6185(87)9002-8
Pilowsky, I. (1967). Dimensions of hypochondriasis. British Journal of Psychiatry, 113,
89-93.
Preston, C. C., & Colman, A. M. (2000). Optimal number of response categories in rating
scales: Reliability, validity, discriminating power, and respondent preferences.
Acta Psychologica, 104, 1-15. doi:10/1016/S0001-6918(99)00050-5
Rief, W., Hiller, W., & Margraf, J. (1998). Cognitive aspects of hypochondriasis and the
somatisation syndrome. Journal of Abnormal Psychology, 107, 587-595.
doi:10.1037/0021-843X.107.4.587
Reiss, S. & McNally, R. J. (1985). The expectancy model of fear. In S. Reiss & R. R.
Bootzin (Eds.), Theoretical issues in behavior therapy. New York: Academic
Press.
222
Pauli, P., Schwenzer, M., Brody, S., Rau, H., & Birbaumer, N. (1993). Hypochondriacal
attitudes, pain sensitivity, and attentional bias. Journal of Psychosomatic
Research, 37, 745-752. doi:10.1016/0022-3999(93)90103-M
Persing, J. S., Stuart, S. P., Noyes, R. Jr., & Happel, R. L. (2000). Hypochondriasis: The
patient's perspective. International Journal of Psychiatry in Medicine, 30, 329-342.
Retrieved from http://bavwood.metapress.com/
Peterson, R. A., & Heilbronner, R. L. (1987). The Anxiety Sensitivity Index: Construct
validity and factor analytic stmcture. Journal of Anxiety Disorders, 1, 117-121.
doi:10.1016/0887-6185(87)9002-8
Pilowsky, I. (1967). Dimensions of hypochondriasis. British Journal of Psychiatry, 113,
89-93.
Preston, C. C , & Colman, A. M. (2000). Optimal number of response categories in rating
scales: Reliability, validity, discriminating power, and respondent preferences.
Acta Psychologica, 104, 1-15. doi:10/1016/S0001-6918(99)00050-5
Rief, W., Hiller, W., & Margraf, J. (1998). Cognitive aspects of hypochondriasis and the
somatisation syndrome. Journal of Abnormal Psychology, 107, 587-595.
doi:10.1037/0021-843X.107.4.587
Reiss, S. & McNally, R. J. (1985). The expectancy model of fear. In S. Reiss & R. R.
Bootzin (Eds.), Theoretical issues in behavior therapy. New York: Academic
Press.
222
Reiss, S., Peterson, R. A., Gursky, D. M., & McNally, R. J. (1986). Anxiety sensitivity,
anxiety frequency, and the prediction of fearfulness. Behaviour Research and
Therapy, 24, 1-8. doi:10.1016/0005-7967(86)90143-9
Richardson, T. M., Simning, A., He, H., & Conwell, Y. (in press). Anxiety and its
correlates among older adults accessing aging services. International Journal of
Geriatric Psychiatry. doi:10.1002/gps.2474
Rode, S., Salkovskis, P., Dowd, H., & Hanna, M. (2006). Health anxiety levels in chronic
pain clinic attenders. Journal of Psychosomatic Research, 60, 155-161.
doi:10.1016/j jpsychores.2005.07.005
Rodin, J., & Timko, C. (1992). Sense of control, aging, and health. In M. G. Ory, & R. P.
Abeles (Eds.), Aging, health and behaviour (pp. 174-206). Thousand Oaks, Sage.
Ryan, R. M., Plant, R.W., & O'Malley, S. (1995). Initial motivations for alcohol
treatment: Relations with patient characteristics, treatment involvement, and
dropout. Addictive Behaviors, 20, 279-297. doi:10.1016/0306-4603(94)00072-7
Salkovskis, P. M. (1989). Somatic Problems. In K. Hawton, P. M. Salkovskis, J. Kirk, &
D. M. Clark (Eds.), Cognitive therapy for psychiatric problems: A practical guide
(pp. 23 5-276). Oxford: Oxford University Press.
Salkovskis, P. M. (1996). The cognitive approach to anxiety: Threat beliefs, safety
seeking behaviour, and the special case of health anxiety and obsessions. In P. M.
Salkovskis (Ed.), Frontiers of cognitive therapy (pp. 48-74). New York: Guilford.
223
Reiss, S., Peterson, R. A., Gursky, D. M., & McNally, R. J. (1986). Anxiety sensitivity,
anxiety frequency, and the prediction of fearfulness. Behaviour Research and
Therapy, 24, 1-8. doi: 10.1016/0005-7967(86)90143-9
Richardson, T. M., Simning, A., He, H., & Conwell, Y. (in press). Anxiety and its
correlates among older adults accessing aging services. International Journal of
Geriatric Psychiatry. doi:10.1002/gps.2474
Rode, S., Salkovskis, P., Dowd, H., & Hanna, M. (2006). Health anxiety levels in chronic
pain clinic attenders. Journal of Psychosomatic Research, 60, 155-161.
doi:10.1016/j.jpsychores.2005.07.005
Rodin, J., & Timko, C. (1992). Sense of control, aging, and health. In M. G. Ory, & R. P.
Abeles (Eds.), Aging, health and behaviour (pp. 174-206). Thousand Oaks, Sage.
Ryan, R. M., Plant, R.W., & O'Malley, S. (1995). Initial motivations for alcohol
treatment: Relations with patient characteristics, treatment involvement, and
dropout. Addictive Behaviors, 20, 279-297. doi: 10.1016/0306-4603(94)00072-7
Salkovskis, P. M. (1989). Somatic Problems. In K. Hawton, P. M. Salkovskis, J. Kirk, &
D. M. Clark (Eds.), Cognitive therapy for psychiatric problems: A practical guide
(pp. 235-276). Oxford: Oxford University Press.
Salkovskis, P. M. (1996). The cognitive approach to anxiety: Threat beliefs, safety
seeking behaviour, and the special case of health anxiety and obsessions. In P. M.
Salkovskis (Ed.), Frontiers of cognitive therapy (pp. 48-74). New York: Guilford.
223
Salkovskis, P. M., & Clark, D. M. (1993). Panic disorder and hypochondriasis. Advances
in Behaviour Research and Therapy, 15, 23-48. doi:10.1016/0146-
6402(93)900024
Salkovskis, P. M., Rimes, K. A., Warwick, H. M. C., & Clark, D. M. (2002). The Health
Anxiety Inventory: development and validation of scales for the measurement of
health anxiety and hypochondriasis. Psychological Medicine, 32, 843-853.
doi:10.1017/S0033291702005822
Salkovskis, P. M. & Warwick, H. M. C. (1986). Morbid preoccupation, health anxiety
and reassurance: a cognitive behavioural approach to hypochondriasis. Behaviour
Research and Therapy, 24, 597-602. doi:10.1016/0005-7967(86)90041-1
Salkovskis, P. M., & Warwick, H. M. C. (2001). Making sense of hypochondriasis: A
cognitive model of health anxiety. In G.J.G. Asmundson, S. Taylor, and B.J. Cox
(Eds.), Health Anxiety. John Wiley & Sons.
Satre, D. D., Knight, B. G., David, S. (2006). Cognitive-behavioral interventions with
older adults: Integrating clinical and gerontological research. Professional
Psychology.• Research and Practice, 37, 489-498. doi:10.1037/0735-
7028.37.5.489
Schefft, B. K., & Kanfer\, F. H. (1987). The utility of a process model in therapy: A
comparative study of treatment effects. Behavior Therapy, 18, 113-134.
doi:10.1016.S0005-7894(87)80036-9
224
Salkovskis, P. M., & Clark, D. M. (1993). Panic disorder and hypochondriasis. Advances
in Behaviour Research and Therapy, 15, 23-48. doi:10.1016/0146-
6402(93)90002-J
Salkovskis, P. M., Rimes, K. A., Warwick, H. M. C , & Clark, D. M. (2002). The Health
Anxiety Inventory: development and validation of scales for the measurement of
health anxiety and hypochondriasis. Psychological Medicine, 32, 843-853.
doi:10.1017/S0033291702005822
Salkovskis, P. M. & Warwick, H. M. C. (1986). Morbid preoccupation, health anxiety
and reassurance: a cognitive behavioural approach to hypochondriasis. Behaviour
Research and Therapy, 24, 597-602. doi:10.1016/0005-7967(86)90041-l
Salkovskis, P. M., & Warwick, H. M. C. (2001). Making sense of hypochondriasis: A
cognitive model of health anxiety. In G.J.G. Asmundson, S. Taylor, and B.J. Cox
(Eds.), Health Anxiety. John Wiley & Sons.
Satre, D. D., Knight, B. G., David, S. (2006). Cognitive-behavioral interventions with
older adults: Integrating clinical and gerontological research. Professional
Psychology: Research and Practice, 37, 489-498. doi:10.1037/0735-
7028.37.5.489
Schefft, B. K., & Kanfer\, F. H. (1987). The utility of a process model in therapy: A
comparative study of treatment effects. Behavior Therapy, 18, 113-134.
doi:10.1016.S0005-7894(87)80036-9
224
Schmidt, N. B., & Joiner, T. E. (2002). Structure of the Anxiety Sensitivity Index
psychometrics and factor structure in a community sample. Journal of Anxiety
Disorders, 16, 33-49. doi:10.1016/S0887-6185(01)00087-1
Schmidt, N. B., Lerew, D. R., & Trakowski, J. H. (1997). Body vigilance in panic
disorder: Evaluating attention to bodily perturbations. Journal of Consulting and
Clinical Psychology, 65, 214-220. doi:10.1037/0022-006X.65.2.214
Schmidt, N. B., Lerew, D. R., & Jackson, R. J. (1997). The role of anxiety sensitivity in
the pathogenesis of panic: Prospective evaluation of spontaneous panic attacks
during acute stress. Journal of Abnormal Psychology, 106, 355-364.
doi:10.1037/0021-843X.106.3.355
Seivewright, H., Green, J., Salkovskis, P., Barrett, B., Nur, U., & Tyrer, P. (2008).
Cognitive-behavioural therapy for health anxiety in a genitourinary medicine clinic:
Randomised controlled trial. British Journal of Psychiatry, 193, 332-337.
doi:10.1192/bjp.bp.108.052936
Sharpe, M., Bass, C., & Mayou, R. (1995). An overview of the treatment of functional
somatic symptoms. In R. Mayou, C. Bass, & M. Sharpe (Eds.), Treatment of
functional somatic symptoms (pp. 66-86). Oxford, UK: Oxford University Press.
Simon, G., Ormel, J., VonKorff, M., & Barlow, W. (1995). Health care costs associated
with depressive and anxiety disorders in primary care. American Journal of
Psychiatry, 152, 352-357. Retrieved from http://alp.psychiatryonline.org/index.dt1
225
Schmidt, N. B., & Joiner, T. E. (2002). Structure of the Anxiety Sensitivity Index
psychometrics and factor stmcture in a community sample. Journal of Anxiety
Disorders, 16, 33-49. doi: 10.1016/S0887-6185(01)00087-1
Schmidt, N. B., Lerew, D. R., & Trakowski, J. H. (1997). Body vigilance in panic
disorder: Evaluating attention to bodily perturbations. Journal of Consulting and
Clinical Psychology, 65, 214-220. doi:10.1037/0022-006X.65.2.214
Schmidt, N. B., Lerew, D. R., & Jackson, R. J. (1997). The role of anxiety sensitivity in
the pathogenesis of panic: Prospective evaluation of spontaneous panic attacks
during acute stress. Journal of Abnormal Psychology, 106, 355-364.
doi:10.1037/0021-843X.106.3.355
Seivewright, H., Green, J., Salkovskis, P., Barrett, B., Nur, U., & Tyrer, P. (2008).
Cognitive-behavioural therapy for health anxiety in a genitourinary medicine clinic:
Randomised controlled trial. British Journal of Psychiatry, 193, 332-337.
doi: 10.1192/bjp.bp. 108.052936
Sharpe, M., Bass, C , & Mayou, R. (1995). An overview of the treatment of functional
somatic symptoms. In R. Mayou, C. Bass, & M. Sharpe (Eds.), Treatment of
functional somatic symptoms (pp. 66-86). Oxford, UK: Oxford University Press.
Simon, G., Ormel, J., VonKorff, M., & Barlow, W. (1995). Health care costs associated
with depressive and anxiety disorders in primary care. American Journal of
Psychiatry, 152, 352-357. Retrieved from http://aip.psychiatryonline.org/index.dtl
225

Simpson, D. D., & Joe, G. W. (1993). Motivation as a predictor of early drop-out from
drug abuse treatment. Psychotherapy: Theory, Research, Practice, Training, 2,
357-368. doi:10.1037/0033-3204.30.2.357
Skarborn, M., & Nicki, R. (1996). Worry among Canadian seniors. International Journal
of Aging and Human Development, 43, 169-178. Retrieved from
http://www.baywood.com/journals/
Small, G. (1997). Recognizing and treating anxiety in the elderly. Journal of Clinical
Psychiatry, 58, (Suppl. 3) 41-57. Retrieved from
http://www.psychiatrist.com/default2.asp
Smith, R. C. (1985). A clinical approach to the somatizing patient. Journal of Family
Practice, 21, 294-301.
Snyder, A. G., & Stanley, M. A. (2001). Hypochondriasis and health anxiety in the
elderly. In G.J.G. Asmundson, S. Taylor, & B.J. Cox (Eds.). Health Anxiety:
Clinical and Research Perspectives on Hypochondriasis and Related Disorders
(pp. 246-274). New York: John Wiley & Sons.
Sorensen, P., Birket-Smith, M., Wattar, U., Buemann, I., & Salkovskis, P. (in press). A
randomized clinical trial of cognitive behavioural therapy versus short-term
psychodynamic psychotherapy versus no intervention for patients with
hypochondriasis. Psychological Medicine. doi:10.1017/50033291710000292
Speckens, A. E. M., van Hemert, A., M., Spinhoven, P., & Bolk, J. H. (1996). The
diagnostic and prognostic significance of the Whitely Index, the Illness Attitude
226
Simpson, D. D., & Joe, G. W. (1993). Motivation as a predictor of early drop-out from
drug abuse treatment. Psychotherapy: Theory, Research, Practice, Training, 2,
357-368. doi:10.1037/0033-3204.30.2.357
Skarbom, M., & Nicki, R. (1996). Worry among Canadian seniors. International Journal
of Aging and Human Development, 43, 169-178. Retrieved from
http://www.bavwood.com/ioumals/
Small, G. (1997). Recognizing and treating anxiety in the elderly. Journal of Clinical
Psychiatry, 58, (Suppl. 3) 41-57. Retrieved from
http://www.psvchiatrist.com/default2.asp
Smith, R. C. (1985). A clinical approach to the somatizing patient. Journal of Family
Practice, 21, 294-301.
Snyder, A. G., & Stanley, M. A. (2001). Hypochondriasis and health anxiety in the
elderly. In G.J.G. Asmundson, S. Taylor, & B.J. Cox (Eds.). Health Anxiety:
Clinical and Research Perspectives on Hypochondriasis and Related Disorders
(pp. 246-274). New York: John Wiley & Sons.
Sorensen, P., Birket-Smith, M., Wattar, U., Buemann, I., & Salkovskis, P. (in press). A
randomized clinical trial of cognitive behavioural therapy versus short-term
psychodynamic psychotherapy versus no intervention for patients with
hypochondriasis. Psychological Medicine. doi:10.1017/S0033291710000292
Speckens, A. E. M., van Hemert, A., M., Spinhoven, P., & Bolk, J. H. (1996). The
diagnostic and prognostic significance of the Whitely Index, the Illness Attitude
226

Scales and the Somatosensory Amplification Scale. Psychological Medicine, 26,
1085-1090. doi:10.1017/S0033291700035418
Speckens, A. E. M., Spinhoven, P., Sloekers, P. P. A., Bolk, J. H., & van Hemert, A. M.
(1996). A validation study of the Whitely Index, the Illness Attitude Scale, and the
Somatosensory Amplification Scale in general medical and general practice
patients. Journal of Psychosomatic Research, 40, 95-104. doi:10.1016/022-
3999(95)00561-7
Spielberger, C. D. (1983). Manual for the State-Trait Anxiety Inventory STAI (Form Y).
Palo Alto, CA: Consulting Psychologists Press.
Stanley, M. A., Beck, J. G., & Zebb, B. J. (1996). Psychometric properties of four anxiety
measures in older adults. Behaviour Research and Therapy, 34, 827-838.
doi:10.1016/005-7967(96)00064-2
Stanley, M. A., Diefenbach, G. J., & Hopko, D. R. (2004). Cognitive behavioural
treatment for older adults with generalized anxiety disorder: A therapist manual for
primary care settings. Behavior Modification, 28, 73-117. doi:
10.1177/0145445503259259
Stenback, A., Kumpulainen, M., & Vauhkenen, M. (1978). Illness and health in
septuagenarians. Journal of Gerontology, 33, 57-61.
Stewart, S. H., & Watt, M. C. (2000). Illness Attitudes Scale dimensions and their
associations with anxiety related constructs in a non-clinical sample. Behavior
Research and Therapy, 38, 83-99. Doi:10.1016/S005-7967(98)00207-1
227
Scales and the Somatosensory Amplification Scale. Psychological Medicine, 26,
1085-1090. doi:10.1017/S0033291700035418
Speckens, A. E. M., Spinhoven, P., Sloekers, P. P. A., Bolk, J. H., & van Hemert, A. M.
(1996). A validation study of the Whitely Index, the Illness Attitude Scale, and the
Somatosensory Amplification Scale in general medical and general practice
patients. Journal of Psychosomatic Research, 40, 95-104. doi: 10.1016/022-
3999(95)00561-7
Spielberger, C. D. (1983). Manual for the State-Trait Anxiety Inventory STAI (Form Y).
Palo Alto, CA: Consulting Psychologists Press.
Stanley, M. A., Beck, J. G., & Zebb, B. J. (1996). Psychometric properties of four anxiety
measures in older adults. Behaviour Research and Therapy, 34, 827-838.
doi: 10.1016/005-7967(96)00064-2
Stanley, M. A., Diefenbach, G. J., & Hopko, D. R. (2004). Cognitive behavioural
treatment for older adults with generalized anxiety disorder: A therapist manual for
primary care settings. Behavior Modification, 28, 73-117. doi:
10.1177/0145445503259259
Stenback, A., Kumpulainen, M., & Vauhkenen, M. (1978). Illness and health in
septuagenarians. Journal of Gerontology, 33, 57-61.
Stewart, S. H., & Watt, M. C. (2000). Illness Attitudes Scale dimensions and their
associations with anxiety related constructs in a non-clinical sample. Behavior
Research and Therapy, 38, 83-99. Doi:10.1016/S005-7967(98)00207-1
227
Strauss, A., & Corbin, J. (1998). Basics of qualitative research: Techniques and
procedures for developing grounded theory (2nd edition). Thousand Oaks, CA:
Sage Publications, Inc.
Stuart, S., & Noyes, R. (1999). Attachment and interpersonal communication in
somatisation. Psychosomatics, 40, 34-43. Retrieved from
http://psy.psychiatryonline.org/index.dt1
Tabachnick, B. G. & Fiddell, L. S. (2001). Using multivariate statistics (4th ed.).
Needham Heights, MA: Allyn & Bacon.
Taylor, S. (1995). Anxiety sensitivity: Theoretical perspectives and recent findings.
Behaviour Research and Therapy, 33, 243-258. doi:10.1016/005-7967(94)00063-
P
Taylor, S., & Asmundson, G. J. G. (2004). Treating health anxiety: A cognitive-
behavioral approach. New York, NY: The Guilford Press.
Taylor, S., Asmundson, G. J. G., & Coons, M. J. (2005). Current directions in the
treatment of hypochondriasis. Journal of Cognitive Psychotherapy: An
International Quarterly, 19, 285-304. Retrieved from
http://www.springerpub.com/product/08898391
Taylor, S., Koch, W. J., & Crockett, D. J. (1991). Anxiety sensitivity, trait anxiety, and
the anxiety disorders. Journal of Anxiety Disorders, 5, 293-311.
doi:10/1016/0887-6185(91)90030-W
228
Strauss, A., & Corbin, J. (1998). Basics of qualitative research: Techniques and
procedures for developing grounded theory (2" edition). Thousand Oaks, CA:
Sage Publications, Inc.
Stuart, S., 8c Noyes, R. (1999). Attachment and interpersonal communication in
somatisation. Psychosomatics, 40, 34-43. Retrieved from
http://psy.psychiatryonline.org/index.dtl
Tabachnick, B. G. & Fiddell, L. S. (2001). Using multivariate statistics (4th ed.).
Needham Heights, MA: Allyn & Bacon.
Taylor, S. (1995). Anxiety sensitivity: Theoretical perspectives and recent findings.
Behaviour Research and Therapy, 33, 243-258. doi:10.1016/005-7967(94)00063-
P
Taylor, S., & Asmundson, G. J. G. (2004). Treating health anxiety: A cognitive-
behavioral approach. New York, NY: The Guilford Press.
Taylor, S., Asmundson, G. J. G., & Coons, M. J. (2005). Current directions in the
treatment of hypochondriasis. Journal of Cognitive Psychotherapy: An
International Quarterly, 19,285-304. Retrieved from
http://www.springerpub.com/product/08898391
Taylor, S., Koch, W. J., & Crockett, D. J. (1991). Anxiety sensitivity, trait anxiety, and
the anxiety disorders. Journal of Anxiety Disorders, 5, 293-311.
doi: 10/1016/0887-6185(91)90030-W
228

Teich, M. J., Shermis, M. D., & Lucas, J. A. (1989). Anxiety sensitivity: Unitary
personality trait or domain-specific appraisals? Journal of Anxiety Disorders, 3,
25-32. doi:10.1016/0887-6185(89)90026-1
Taylor, S., Thordarson, D. S., Jang, K. L., & Asmundson, G. J. (2006). Genetic and
environmental origins of health anxiety: A twin study. World Psychiatry, 5, 47-
50. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/journals/297/
Timulak, L. (2007). Identifying core categories of client-identified impact of helpful
events in psychotherapy: A qualitative meta-analysis. Psychotherapy Research,
17, 305-314. doi:10.1080/10503300600608116
Tracey, T. J., & Kokotovic, A. M. (1989). Factor structure of the Working Alliance
Inventory. Psychological Assessment: A Journal of Consulting and Clinical
Psychology, 1, 207-210. doi:10.1037/1040-3590.1.3.207
Tuokko, H., & Hadjistavropoulos, T. (1998). An assessment guide to geriatric
neuropsychology. Mahwah, NJ: Lawrence Erlbaum Associates, Inc.
van Breukelen, G. J. P. (2006). ANCOVA versus change from baseline had more power
in randomized studies and more bias in nonrandomized studies. Journal of
Clinical Epidemiology, 59, 920-925. doi:10.1016/j .j clinepi.2006.02.007
Vickers, A. J. (2004). Statistical reanalysis of four recent randomized trials of
acupuncture for pain using analysis of covariance. Clinical Journal of Pain, 20,
319-323. Retrieved from http://journals.1ww.com/clinicalpain/pages/default.aspx
229
Telch, M. J., Shermis, M. D., & Lucas, J. A. (1989). Anxiety sensitivity: Unitary
personality trait or domain-specific appraisals? Journal of Anxiety Disorders, 3,
25-32. doi: 10.1016/0887-6185(89)90026-1
Taylor, S., Thordarson, D. S., Jang, K. L., & Asmundson, G. J. (2006). Genetic and
environmental origins of health anxiety: A twin study. World Psychiatry, 5, 47-
50. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/ioumals/297/
Timulak, L. (2007). Identifying core categories of client-identified impact of helpful
events in psychotherapy: A qualitative meta-analysis. Psychotherapy Research,
17, 305-314. doi:10.1080/10503300600608116
Tracey, T. J., & Kokotovic, A. M. (1989). Factor stmcture of the Working Alliance
Inventory. Psychological Assessment: A Journal of Consulting and Clinical
Psychology, 1, 207-210. doi:10.1037/1040-3590.1.3.207
Tuokko, H., & Hadjistavropoulos, T. (1998). An assessment guide to geriatric
neuropsychology. Mahwah, NJ: Lawrence Erlbaum Associates, Inc.
van Breukelen, G. J. P. (2006). ANCOVA versus change from baseline had more power
in randomized studies and more bias in nonrandomized studies. Journal of
Clinical Epidemiology, 59, 920-925. doi:10.1016/j.jclinepi.2006.02.007
Vickers, A. J. (2004). Statistical reanalysis of four recent randomized trials of
acupuncture for pain using analysis of covariance. Clinical Journal of Pain, 20,
319-323. Retrieved from http://ioumals.lww.com/clinicalpain/pages/default.aspx
229

Visser, S., & Bouman, T. K. (2001). The treatment of hypochondriasis: Exposure plus
response prevention vs cognitive therapy. Behaviour Research and Therapy, 39,
423-442. doi:10/1016/S0005-7967(00)00022-X
Ware, J., Kosinski, M., & Keller, S. (1996). A 12-item short-form health survey:
Construction of scales and preliminary tests of reliabililty and validity. Medical
Care, 34, 220-233. Retrieved from http://journals.1ww.com/lww-
medicalcare/pages/defaultaspx
Ware, J. E., Kosinski, M., Turner-Bowker, D. M. & Gandek, B. (2002). How to score
Version 2 of the SF-12 Health Survey. Lincoln, RI: Quality Metric Incorporated.
Warwick, H. M. (1989). A cognitive-behavioural approach to hypochondriasis and health
anxiety. Journal of Psychosomatic Research, 33, 705-711. doi:10.1016/0022-
3999(89)90086-X
Warwick, H. M. C. (1995). Treatment of hypochondriasis. In R. Mayou, C. Bass, & M.
Sharpe (Eds.), Treatment of functional somatic symptoms (pp. 163-174). Oxford,
UK: Oxford University Press.
Warwick, H. M. C., Clark, D. M., Cobb, A. M., & Salkovskis, P. M. (1996). A controlled
trial of cognitive-behavioural treatment of hypochondriasis. British Journal of
Psychiatry, 169, 189-195. Retrieved from http://bjp.rcpsych.org/
Warwick, H. M. C., & Marks, I. M. (1988). Behavioural treatment of illness phobia and
hypochondriasis: A pilot study of 17 cases. British Journal of Psychiatry, 152, 239-
241. Retrieved from http://bjp.rcpsych.org/
230
Visser, S., & Bouman, T. K. (2001). The treatment of hypochondriasis: Exposure plus
response prevention vs cognitive therapy. Behaviour Research and Therapy, 39,
423-442. doi: 10/1016/S0005-7967(00)00022-X
Ware, J., Kosinski, M., & Keller, S. (1996). A 12-item short-form health survey:
Construction of scales and preliminary tests of reliabililty and validity. Medical
Care, 34, 220-233. Retrieved from http://ioumals.lww.com/lww-
medicalcare/pages/defauitaspx
Ware, J. E., Kosinski, M., Turner-Bowker, D. M. & Gandek, B. (2002). How to score
Version 2 of the SF-12 Health Survey. Lincoln, RI: Quality Metric Incorporated.
Warwick, H. M. (1989). A cognitive-behavioural approach to hypochondriasis and health
anxiety. Journal of Psychosomatic Research, 33, 705-711. doi:10.1016/0022-
3999(89)90086-X
Warwick, H. M. C. (1995). Treatment of hypochondriasis. In R. Mayou, C. Bass, & M.
Sharpe (Eds.), Treatment of functional somatic symptoms (pp. 163-174). Oxford,
UK: Oxford University Press.
Warwick, H. M. C , Clark, D. M., Cobb, A. M., & Salkovskis, P. M. (1996). A controlled
trial of cognitive-behavioural treatment of hypochondriasis. British Journal of
Psychiatry, 169, 189-195. Retrieved from http://bip.rcpsych.org/
Warwick, H. M. C , & Marks, I. M. (1988). Behavioural treatment of illness phobia and
hypochondriasis: A pilot study of 17 cases. British Journal of Psychiatry, 152, 239-
241. Retrieved from http://bip.rcpsych.org/
230

Warwick, H. M. C., & Salkovskis, P. M. (1989). Cognitive and behavioural
characteristics of primary hypochondriasis. Scandinavian Journal of Behaviour
Therapy, 18, 85-92.
Warwick, H. M. C., & Salkovskis, P. M. (1990). Hypochondriasis. Behaviour Research
and Therapy, 28, 105-117. doi:10.1016/0005-7967(90)90023-C
Welch, P. G., Carleton, R. N., & Asmundson, G. J. (2009). Measuring health anxiety:
Moving past the dichotomous response option of the original Whiteley Index.
Journal of Anxiety Disorders, 23, 1002-1007. doi:10.1016/j.janxdis.2009.05.006
Westen, D., & Morrison, K. (2001). A multidimensional meta-analysis of treatments for
depression, panic, and generalized anxiety disorder: An empirical examination of
the status of empirically supported therapies. Journal of Consulting and Clinical
Psychology, 69, 875-899. doi:10.1037/0022-006X.69.6.875
Wetherall, J. L., Gatz, M., & Craske, M. G. (2003). Treatment of generalized anxiety
disorder in older adults. Journal of Consulting and Clinical Psychology, 71, 31-
40. doi:1oA037/0022-006X.71.1.31
Wisocki, P. A. (1988). Worry as a phenomenon relevant to the elderly. Behavior
Therapy, 19, 369-379. doi:10.1016/S0005-7894(88)80009-1
Yesavage, J. A., Brink, T.L., Rose, T. L., Lum, 0., Huang, V., Adey, M. B., & Leirer, V.
0. (1983). Development and validation of a geriatric depression screening scale:
A preliminary report. Journal of Psychiatric Research, 17, 37-49.
doi:10.1016/0022-3956(82)90033-4
231
Warwick, H. M. C , & Salkovskis, P. M. (1989). Cognitive and behavioural
characteristics of primary hypochondriasis. Scandinavian Journal of Behaviour
Therapy, 18, 85-92.
Warwick, H. M. C , & Salkovskis, P. M. (1990). Hypochondriasis. Behaviour Research
and Therapy, 28, 105-117. doi:10.1016/0005-7967(90)90023-C
Welch, P. G., Carleton, R. N., & Asmundson, G. J. (2009). Measuring health anxiety:
Moving past the dichotomous response option of the original Whiteley Index.
Journal of Anxiety Disorders, 23, 1002-1007. doi:10.1016/j.janxdis.2009.05.006
Westen, D., & Morrison, K. (2001). A multidimensional meta-analysis of treatments for
depression, panic, and generalized anxiety disorder: An empirical examination of
the status of empirically supported therapies. Journal of Consulting and Clinical
Psychology, 69, 875-899. doi:10.1037/0022-006X.69.6.875
Wetherall, J. L., Gatz, M., & Craske, M. G. (2003). Treatment of generalized anxiety
disorder in older adults. Journal of Consulting and Clinical Psychology, 71, 31 -
40. doi:10.1037/0022-006X.71.1.31
Wisocki, P. A. (1988). Worry as a phenomenon relevant to the elderly. Behavior
Therapy, 19, 369-379. doi:10.1016/S0005-7894(88)80009-l
Yesavage, J. A., Brink, T.L., Rose, T. L., Lum, O., Huang, V., Adey, M. B., & Leirer, V.
O. (1983). Development and validation of a geriatric depression screening scale:
A preliminary report. Journal of Psychiatric Research, 17, 37-49.
doi:10.1016/0022-3956(82)90033-4
231

Zinbarg, R., Barlow, D. H., & Brown, T. A. (1997). The hierarchical structure and
general factor saturation of the Anxiety Sensitivity Index: Evidence and
implications. Psychological Assessment, 9, 277-284. doi:10.1037/1040-
3590.9.3.277
Zinbarg, R. E., Brown, T. A., Barlow, D. H., & Rapee, R. M. (2001). Anxiety sensitivity,
panic, and depressed mood: a reanalysis teasing apart the contributions of the two
levels in the hierarchical structure of the Anxiety Sensitivity Index. Journal of
Abnormal Psychology, 110, 372-377. doi:10.1037/0021-843X.110.3.372
Zinbarg, R. E., Mohlman, J., & Hong, N. N. (1999). Dimensions of anxiety sensitivity. In
S. Taylor (Ed.), Anxiety sensitivity: Theory, research, and treatment of the fear of
anxiety (pp. 83-114). Mahwah, NJ: Erlbaum.
Zuroff, D. C., & Blatt, S. J. (2006). The therapeutic relationship in the brief treatment of
depression: Contributions to clinical improvement and enhanced adaptive
capacities. Journal of Consulting and Clinical Psychology, 74, 130-140.
doi:10.1037/0022-006X.74.1.130
Zvolensky, M. J., & Forsyth, J. P. (2002). Anxiety sensitivity dimensions in the
prediction of body vigilance and emotional avoidance. Cognitive Therapy and
Research, 26, 449-460. doi:10.1023/A:1016223716132
232
Zinbarg, R., Barlow, D. H., & Brown, T. A. (1997). The hierarchical stmcture and
general factor saturation of the Anxiety Sensitivity Index: Evidence and
implications. Psychological Assessment, 9, 277-284. doi:10.1037/1040-
3590.9.3.277
Zinbarg, R. E., Brown, T. A., Barlow, D. H., & Rapee, R. M. (2001). Anxiety sensitivity,
panic, and depressed mood: a reanalysis teasing apart the contributions of the two
levels in the hierarchical stmcture of the Anxiety Sensitivity Index. Journal of
Abnormal Psychology, 110, 372-377. doi: 10.1037/0021-843X.110.3.372
Zinbarg, R. E., Mohlman, J., & Hong, N. N. (1999). Dimensions of anxiety sensitivity. In
S. Taylor (Ed.), Anxiety sensitivity: Theory, research, and treatment of the fear of
anxiety (pp. 83-114). Mahwah, NJ: Erlbaum.
Zuroff, D. C , & Blatt, S. J. (2006). The therapeutic relationship in the brief treatment of
depression: Contributions to clinical improvement and enhanced adaptive
capacities. Journal of Consulting and Clinical Psychology, 74, 130-140.
doi:10.1037/0022-006X. 74.1.130
Zvolensky, M. J., & Forsyth, J. P. (2002). Anxiety sensitivity dimensions in the
prediction of body vigilance and emotional avoidance. Cognitive Therapy and
Research, 26, 449-460. doi:10.1023/A:1016223716132
232

Appendix A
Recruitment Poster
UNIVERSITY OF
4, REGINA
Do You Experience a Lot of Worry About Your Health?
Michelle Bourgault-Fagnou, M.A., & Heather Hadjistavropoulos, Ph.D. from the University of Regina are seeking individuals to participate in a study that is looking to improve the way that worry about health is treated among older adults.
If you are 65 years of age and older and find that you worry a lot about your health, you are eligible to participate. Your participation would involve six weekly individual meetings that last approximately 45 to 60 minutes each and completion of several questionnaires.
Potential benefits of participating in this study include a reduction in worry and negative emotions, improved overall health, and an increased quality of life.
If you would like to participate in this study or would like further information, please call 585-5369.
233
Appendix A
Recruitment Poster
|Sl¥] UNIVERSITY OF
l v REGINA Do You Experience a Lot of Worry
About Your Health?
Michelle Bourgault-Fagnou, M.A., & Heather Hadjistavropoulos, Ph.D. from the University of Regina are seeking individuals to participate in a study that is looking to improve the way that worry about health is treated among older adults.
If you are 65 years of age and older and find that you worry a lot about your health, you are eligible to participate. Your participation would involve six weekly individual meetings that last approximately 45 to 60 minutes each and completion of several questionnaires.
Potential benefits of participating in this study include a reduction in worry and negative emotions, improved overall health, and an increased quality of life.
If you would like to participate in this study or would like further information, please call 585-5369.
233

Appendix B
Information Sheet and Consent Form
UNIVERSITY OF
*REGINA [email protected]
Information for Participants
DEPARTMENT OF PSYCHOLOGY Regina, Saskatchewan Canada S4S 0A2 phone: (306) 585-4221 fax: (306) 585-5429 email:
If the page contains any information that is unclear, please ask the researcher for an explanation of the information that is not clear to you.
Title Testing the Efficacy of a Cognitive Behavioural Treatment of Health Anxiety Among Seniors
Background Factors associated with aging may contribute to excessive preoccupation with health-related issues and increased levels of health anxiety. This study is being done to improve the way health anxiety is treated among older adults. A health anxiety treatment program (described below) is being tested to determine if it is effective in helping older adults deal with their health anxiety more effectively.
Procedure This program will involve six weekly individual meetings that last approximately 45 to 60 minutes each. The meetings will take place at the Psychology Training Clinic at the University of Regina. The treatments are based on a programme developed by Barsky & Ahern (2004) which has previously been found to be effective for the treatment of hypochondriasis. Participants will be randomly assigned to one of three groups: (1) Therapy 1, (2) Therapy 2, or (3) waitlist.
Therapy 1 will cover the following: • Education about the nature of health anxiety • Improving your understanding and ability to control your health anxiety using
psychological means (e.g., coping strategies, attention and distraction techniques) • Self-monitoring (i.e., keeping track of your anxiety and methods you use to deal with
it) • Improving the understanding and management of stress • Examination of thoughts and beliefs about health anxiety • Improving behaviours and activities that have an impact on health anxiety
234
Appendix B
Information Sheet and Consent Form
iffl^l UNIVERSITY OF DEPARTMENT OF PSYCHOLOGY
JjfiL REGINA psychology [email protected]
Information for Participants
If the page contains any information that is unclear, please ask the researcher for an explanation of the information that is not clear to you.
Title Testing the Efficacy of a Cognitive Behavioural Treatment of Health Anxiety Among Seniors
Background Factors associated with aging may contribute to excessive preoccupation with health-related issues and increased levels of health anxiety. This study is being done to improve the way health anxiety is treated among older adults. A health anxiety treatment program (described below) is being tested to determine if it is effective in helping older adults deal with their health anxiety more effectively.
Procedure This program will involve six weekly individual meetings that last approximately 45 to 60 minutes each. The meetings will take place at the Psychology Training Clinic at the University of Regina. The treatments are based on a programme developed by Barsky & Ahem (2004) which has previously been found to be effective for the treatment of hypochondriasis. Participants will be randomly assigned to one of three groups: (1) Therapy 1, (2) Therapy 2, or (3) waitlist.
Therapy 1 will cover the following: • Education about the nature of health anxiety • Improving your understanding and ability to control your health anxiety using
psychological means (e.g., coping strategies, attention and distraction techniques) • Self-monitoring (i.e., keeping track of your anxiety and methods you use to deal with
it) • Improving the understanding and management of stress • Examination of thoughts and beliefs about health anxiety • Improving behaviours and activities that have an impact on health anxiety
234
Regina, Saskatchewan Canada S4S 0A2 phone: (306) 585-4221 fax: (306) 585-5429 email:

■ Improving other emotional states (e.g., depression) that have an impact on health anxiety
■ Maintaining improvements in emotional functioning
Therapy 2 will cover the following: ■ Will contain the same components as Therapy 1 but with added learning and memory
aids (e.g., weekly reading assignments, graphing exercises, expanded reviews of all session material) and instructional videos.
Waitlist Group ■ Participants assigned to the waitlist group will wait up to 12 weeks before beginning
Therapy 2. You will be asked to complete questionnaires about your levels of anxiety and mood (approximately 90 minutes in total), on three different occasions: once when the study begins, once immediately after the study is over, and one final time three months after the treatment program ends. A member of the research team will meet with you to fill out the questionnaires at the Psychology Training Clinic at the University of Regina or at an otherwise convenient location (e.g., your home). In addition, you will be asked to provide information on the relationship with your therapist and motivation for treatment during treatment sessions. Finally, you will be asked to take part in two short interviews, once at the beginning of treatment and once at the end, about your health anxiety, experience with the treatment program, the therapy and motivation for treatment.
Voluntary Participation Participation in this study is voluntary. Should you choose not to participate, or if you wish to withdraw from the study at any time after starting, you may do so without any consequences to your present or future health care.
Confidentiality Only the researchers will know that you are participating in this study. The information and test results obtained in the questionnaires will be stored in locked cabinets or storage rooms. Responses will be coded so that no one knows the identity of clients or caregivers. All responses and test results will be combined into summary data so that it is not possible to identify individual responses. In addition, there are certain limits to confidentiality. For example, if you pose immediate threat to your life or to other individuals, confidentiality may be broken in order to prevent harm. If you disclose information suggesting that any child is at risk of abuse, the Ministry of Social Services will have to be notified. Also, if you become involved in a legal case the judge has the right to subpoena any information relevant to the legal problem.
Possible Benefits & Risks
There are no anticipated risks from your participation. This research may help participants to deal with their health anxiety more effectively in a variety of ways. Further, if the treatment program is judged to be effective, it may help other older adults
235
• Improving other emotional states (e.g., depression) that have an impact on health anxiety
• Maintaining improvements in emotional functioning
Therapy 2 will cover the following: • Will contain the same components as Therapy 1 but with added learning and memory
aids (e.g., weekly reading assignments, graphing exercises, expanded reviews of all session material) and instructional videos.
Waitlist Group • Participants assigned to the waitlist group will wait up to 12 weeks before beginning
Therapy 2. You will be asked to complete questionnaires about your levels of anxiety and mood (approximately 90 minutes in total), on three different occasions: once when the study begins, once immediately after the study is over, and one final time three months after the treatment program ends. A member of the research team will meet with you to fill out the questionnaires at the Psychology Training Clinic at the University of Regina or at an otherwise convenient location (e.g., your home). In addition, you will be asked to provide information on the relationship with your therapist and motivation for treatment during treatment sessions. Finally, you will be asked to take part in two short interviews, once at the beginning of treatment and once at the end, about your health anxiety, experience with the treatment program, the therapy and motivation for treatment.
Voluntary Participation Participation in this study is voluntary. Should you choose not to participate, or if you wish to withdraw from the study at any time after starting, you may do so without any consequences to your present or future health care.
Confidentiality Only the researchers will know that you are participating in this study. The information and test results obtained in the questionnaires will be stored in locked cabinets or storage rooms. Responses will be coded so that no one knows the identity of clients or caregivers. All responses and test results will be combined into summary data so that it is not possible to identify individual responses. In addition, there are certain limits to confidentiality. For example, if you pose immediate threat to your life or to other individuals, confidentiality may be broken in order to prevent harm. If you disclose information suggesting that any child is at risk of abuse, the Ministry of Social Services will have to be notified. Also, if you become involved in a legal case the judge has the right to subpoena any information relevant to the legal problem.
Possible Benefits & Risks There are no anticipated risks from your participation. This research may help participants to deal with their health anxiety more effectively in a variety of ways. Further, if the treatment program is judged to be effective, it may help other older adults
235

who experience health anxiety. A summary of the results will be sent to all interested participants at the end of the study and may take up to one year.
Contact Information and Ethics Approval
If you have questions regarding this study, we encourage you to contact Michelle Bourgault-Fagnou, Department of Psychology, University of Regina, at 585-5369 or by mail at Department of Psychology, University of Regina, Regina, SK, S4S 0A2. You may also contact the Dr. Heather Hadjistavropoulos, Department of Psychology, University of Regina, Regina SK, S4S 0A2 at 585-5133.
This project was approved by the Research Ethics Board, University of Regina. If you have any questions or concerns about your rights or treatment, you can contact the Chair of the Research Ethics Board at 585-4775 or email: research.ethics(&,uregina.ca.
236
who experience health anxiety. A summary of the results will be sent to all interested participants at the end of the study and may take up to one year.
Contact Information and Ethics Approval If you have questions regarding this study, we encourage you to contact Michelle Bourgault-Fagnou, Department of Psychology, University of Regina, at 585-5369 or by mail at Department of Psychology, University of Regina, Regina, SK, S4S 0A2. You may also contact the Dr. Heather Hadjistavropoulos, Department of Psychology, University of Regina, Regina SK, S4S 0A2 at 585-5133.
This project was approved by the Research Ethics Board, University of Regina. If you have any questions or concerns about your rights or treatment, you can contact the Chair of the Research Ethics Board at 585-4775 or email: [email protected].
236
Consent Form
I, , have been informed of the nature of the study
(Print Name) entitled, "Testing the Efficacy of a Cognitive Behavioural Treatment of Health Anxiety Among Seniors," and freely consent to take part. A copy of the form entitled "Information for Potential Participants" and this consent form have been provided to me. I have read the information sheet and understand it.
I understand that my taking part is fully voluntary and that I may decline to take part or withdraw at any time without affecting my current or future health care. I understand that information gained from the study is confidential and may only be shared with members of the research team. I also understand that this information will be used for research purposes and that any details that may reveal my identity will be excluded from study reports and presentations.
• If I have questions I can call the researcher Michelle Bourgault-Fagnou at (306) 585-5369 or call Dr. Heather Hadjistavropoulos at (306) 585-5133.
• I may also contact the Chair of the Research Ethics Board at the University of Regina at (306) 585-4775 or by e-mail: research.ethics uregina.ca.
The content of this consent form has been explained to me and I agree to take part in this study. I have received a copy of this consent form for my records.
Printed Name of Participant:
Signature of Participant:
Signature of Investigator: Date
Your participation is greatly appreciated.
237
Consent Form
I, , have been informed of the nature of the study
(Print Name) entitled, "Testing the Efficacy of a Cognitive Behavioural Treatment of Health Anxiety Among Seniors," and freely consent to take part. A copy of the form entitled "Information for Potential Participants" and this consent form have been provided to me. I have read the information sheet and understand it.
I understand that my taking part is fully voluntary and that I may decline to take part or withdraw at any time without affecting my current or future health care. I understand that information gained from the study is confidential and may only be shared with members of the research team. I also understand that this information will be used for research purposes and that any details that may reveal my identity will be excluded from study reports and presentations.
• If I have questions I can call the researcher Michelle Bourgault-Fagnou at (306) 585-5369 or call Dr. Heather Hadjistavropoulos at (306) 585-5133.
• I may also contact the Chair of the Research Ethics Board at the University of Regina at (306) 585-4775 or by e-mail: research.ethics(5),uregina.ca.
The content of this consent form has been explained to me and I agree to take part in this study. I have received a copy of this consent form for my records.
Printed Name of Participant:
Signature of Participant:
Signature of Investigator: Date
Your participation is greatly appreciated.
237
Appendix C
Outline of Videos
Video 1:
■ Hello, my name is and I have worried a great deal about my health for a
number of years. I had found that since I had gotten older and experienced some
difficulties with my health, my worries about my health had gotten a lot worse. I
found that worrying and feeling anxious took up a lot of my time. Because of this, I
decided to give this approach a try. I've learned a number of ways to cope with my
worry. I've also had to learn how to think differently about my health and bodily
sensations. Overall, I worry a lot less and it has improved my mood and quality of
life. I found that attending all six sessions and trying all the different techniques and
assignments made a big difference in my life.
■ One of the most helpful things I learned in therapy was that I actually had many
beliefs about health that were not correct. These thoughts had a powerful influence
on me. As an example, I used to think "every sensation I had should be able to be
explained by my doctor." I learned in therapy that many bodily sensations actually
have no clear cause, or medical explanation. There are also many symptoms of
chronic conditions that never completely disappear. I was then able to learn several
ways to handle these sensations more effectively.
■ The second belief I had for a very long time was that "somewhere there is a doctor
who can cure my symptoms." I realized that it is much more helpful to change my
goal from finding a cure for many of my body sensations, to learning to live with
238
Appendix C
Outline of Videos
Video 1:
• Hello, my name is and I have worried a great deal about my health for a
number of years. I had found that since I had gotten older and experienced some
difficulties with my health, my worries about my health had gotten a lot worse. I
found that worrying and feeling anxious took up a lot of my time. Because of this, I
decided to give this approach a try. I've learned a number of ways to cope with my
worry. I've also had to learn how to think differently about my health and bodily
sensations. Overall, I worry a lot less and it has improved my mood and quality of
life. I found that attending all six sessions and trying all the different techniques and
assignments made a big difference in my life.
• One of the most helpful things I learned in therapy was that I actually had many
beliefs about health that were not correct. These thoughts had a powerful influence
on me. As an example, I used to think "every sensation I had should be able to be
explained by my doctor." I learned in therapy that many bodily sensations actually
have no clear cause, or medical explanation. There are also many symptoms of
chronic conditions that never completely disappear. I was then able to leam several
ways to handle these sensations more effectively.
• The second belief I had for a very long time was that "somewhere there is a doctor
who can cure my symptoms." I realized that it is much more helpful to change my
goal from finding a cure for many of my body sensations, to learning to live with
238

sensations that doctors have said are not caused by serious illness or they don't know
how to cure. Learning to cope with sensations made me feel like I had control over
my health.
■ Another thought I had that I think is funny now is that "being healthy meant that I
would have no bodily sensations. I used to think that if I did experience different
sensations, they must be symptoms of a disease." During therapy, I learned that
many bodily sensations come from normal bodily changes, such as indigestion, not
having enough sleep, or not having enough exercise. Other sensations come from
stress or strong emotion. The average healthy person has meaningless sensations
every four to six days.
■ By following this approach and learning about how my thoughts make me feel, I
realized the powerful effect that these thoughts have on me. I have learned that it is
okay to have bodily sensations because everybody has them and living with
sensations you don't understand or symptoms from a chronic illness is possible.
Video 2:
■ Hello, my name is , and I have worried a great deal about my health for a
number of years. I have a few health concerns, and because of this, I found myself
always worrying about my health and what my bodily sensations meant. I found that
I sometimes couldn't sleep or I was not able to get as much work done around the
house as I wanted to because I spent a lot of my time worrying and feeling anxious.
■ One of the most helpful things I learned in therapy was that the amount of attention I
pay to my body and different sensations, influences how strong the sensations
239
sensations that doctors have said are not caused by serious illness or they don't know
how to cure. Learning to cope with sensations made me feel like I had control over
my health.
• Another thought I had that I think is funny now is that "being healthy meant that I
would have no bodily sensations. I used to think that if I did experience different
sensations, they must be symptoms of a disease." During therapy, I learned that
many bodily sensations come from normal bodily changes, such as indigestion, not
having enough sleep, or not having enough exercise. Other sensations come from
stress or strong emotion. The average healthy person has meaningless sensations
every four to six days.
• By following this approach and learning about how my thoughts make me feel, I
realized the powerful effect that these thoughts have on me. I have learned that it is
okay to have bodily sensations because everybody has them and living with
sensations you don't understand or symptoms from a chronic illness is possible.
Video 2:
• Hello, my name is , and I have worried a great deal about my health for a
number of years. I have a few health concerns, and because of this, I found myself
always worrying about my health and what my bodily sensations meant. I found that
I sometimes couldn't sleep or I was not able to get as much work done around the
house as I wanted to because I spent a lot of my time worrying and feeling anxious.
• One of the most helpful things I learned in therapy was that the amount of attention I
pay to my body and different sensations, influences how strong the sensations
239

actually feel. I learned that the more attention I give to a sensation, the more it hurt or
bothered me.
■ For example, when I was at home alone, I would often notice and worry about my
back pain and if it actually meant that my condition was getting worse. The pain
would bother me all day long and I would have trouble getting anything done because
the pain was so bad. But then I learned about distraction and how taking part in
activities that are fun can really help me to take my mind off my bodily sensations.
When I play cards in the afternoon with friends or watch a good movie on television,
I hardly notice my pain. I started taking part in more activities that are enjoyable so
that I have less time to think about and notice my bodily sensations.
■ I also found that relaxation such as abdominal breathing was useful for when I was at
home alone and started to worry about my bodily sensations. When I focus on
relaxing, this takes my mind off my bodily sensations. It also helps reduce my
anxiety. Everyday, I try to find about 10 minutes to spend doing the relaxation I
learned in therapy.
Video 3:
■ One of the most important things I learned in therapy was that stress is one of the
main reasons I experience unpleasant bodily sensations.
■ What I learned is that when I am under stress, my body reacts like it needs to get
prepared for an emergency....to run away or fight someone off. For example, if I am
under a lot of stress, I notice that my heart beats faster, my breathing increases, my
240
actually feel. I learned that the more attention I give to a sensation, the more it hurt or
bothered me.
• For example, when I was at home alone, I would often notice and worry about my
back pain and if it actually meant that my condition was getting worse. The pain
would bother me all day long and I would have trouble getting anything done because
the pain was so bad. But then I learned about distraction and how taking part in
activities that are fun can really help me to take my mind off my bodily sensations.
When I play cards in the afternoon with friends or watch a good movie on television,
I hardly notice my pain. I started taking part in more activities that are enjoyable so
that I have less time to think about and notice my bodily sensations.
• I also found that relaxation such as abdominal breathing was useful for when I was at
home alone and started to worry about my bodily sensations. When I focus on
relaxing, this takes my mind off my bodily sensations. It also helps reduce my
anxiety. Everyday, I try to find about 10 minutes to spend doing the relaxation I
learned in therapy.
Video 3:
• One of the most important things I learned in therapy was that stress is one of the
main reasons I experience unpleasant bodily sensations.
• What I learned is that when I am under stress, my body reacts like it needs to get
prepared for an emergency... .to run away or fight someone off. For example, if I am
under a lot of stress, I notice that my heart beats faster, my breathing increases, my
240

muscles feel tight, and my thoughts go a mile a minute. I used to find these
sensations really scary and uncomfortable.
■ The thing I came to realize is that my brain gets ready for an emergency and my body
reacts like this whether there is a true emergency happening or I am just thinking
about something stressful or I am stressed out by little events that are bothering me.
■ For example, when I used to work, I got severe stomach pains and increased heart
rate the moment I stepped into the office every morning. This never happened on the
weekend, unless I started to think about things that had to be done at work.
■ I learned during therapy that stress can be relieved without medications, alcohol, or
quitting all my activities. Instead, I started using the relaxation exercises I used during
therapy to help me relax. I also found that just understanding that these sensations
were brought on when I was feeling under stress, helped me relax.
Video 4:
■ One of the most helpful things I learned in therapy was how to figure out the types of
things that bring on my bodily sensations. It took some thought to figure out which
situations brought on my physical sensations. But once I figured this out, this helped
me figure out how to control my sensations.
■ For example, I noticed that on days where I woke up with stomach pain and I was
under more stress or had an unpleasant meeting scheduled, I was more likely to say to
myself, "Oh no! Now I won't be able to have fun, I'll be feeling terrible all day, and
hopefully this stomach pain isn't something serious, like cancer. Forget even going!"
However, I also noticed that at times where I wasn't under stress, and I woke up with
241
muscles feel tight, and my thoughts go a mile a minute. I used to find these
sensations really scary and uncomfortable.
• The thing I came to realize is that my brain gets ready for an emergency and my body
reacts like this whether there is a tme emergency happening or I am just thinking
about something stressful or I am stressed out by little events that are bothering me.
• For example, when I used to work, I got severe stomach pains and increased heart
rate the moment I stepped into the office every morning. This never happened on the
weekend, unless I started to think about things that had to be done at work.
• I learned during therapy that stress can be relieved without medications, alcohol, or
quitting all my activities. Instead, I started using the relaxation exercises I used during
therapy to help me relax. I also found that just understanding that these sensations
were brought on when I was feeling under stress, helped me relax.
Video 4:
• One of the most helpful things I learned in therapy was how to figure out the types of
things that bring on my bodily sensations. It took some thought to figure out which
situations brought on my physical sensations. But once I figured this out, this helped
me figure out how to control my sensations.
• For example, I noticed that on days where I woke up with stomach pain and I was
under more stress or had an unpleasant meeting scheduled, I was more likely to say to
myself, "Oh no! Now I won't be able to have fun, I'll be feeling terrible all day, and
hopefully this stomach pain isn't something serious, like cancer. Forget even going!"
However, I also noticed that at times where I wasn't under stress, and I woke up with
241

the same kind of pain, I would instead usually say "This will go away as soon as I
have a good breakfast and a walk in the fresh air."
■ By paying attention, I began to notice what made me feel worse and what made me
feel better. So, if I was in a situation that was stressful, I would try relaxation or
distraction to reduce my stress. I would also try to spend more time doing activities
that made me feel good like exercising and spending time with my friends. I now
worry and feel anxious a lot less than I used to.
Video 5:
■ Some of the most helpful things I learned in therapy were different ways for coping
with my upsetting bodily sensations. I learned there are two main things that I can
use to deal with bothersome sensations. The first is making sure I do activities that
are good for my health like exercising and not avoiding these things because they
bring on normal body sensations. The second thing is stopping to do things that
unnecessarily made me anxious.
■ For example, I quit walking because I noticed that I would get completely out of
breath and tired, often worrying that something was really wrong with me. I decided
to begin walking again as a way to exercise and because it was something that I used
to enjoy and hadn't done for a long time. What I did initially was to walk about half
as far as I used to as a way to build up my strength. I really made an effort to take
note of how my sensations felt before and after the walk. I would have to remind
myself that avoiding exercise is more likely the cause of tiredness.
242
the same kind of pain, I would instead usually say "This will go away as soon as I
have a good breakfast and a walk in the fresh air."
• By paying attention, I began to notice what made me feel worse and what made me
feel better. So, if I was in a situation that was stressful, I would try relaxation or
distraction to reduce my stress. I would also try to spend more time doing activities
that made me feel good like exercising and spending time with my friends. I now
worry and feel anxious a lot less than I used to.
Video 5:
• Some of the most helpful things I learned in therapy were different ways for coping
with my upsetting bodily sensations. I learned there are two main things that I can
use to deal with bothersome sensations. The first is making sure I do activities that
are good for my health like exercising and not avoiding these things because they
bring on normal body sensations. The second thing is stopping to do things that
unnecessarily made me anxious.
• For example, I quit walking because I noticed that I would get completely out of
breath and tired, often worrying that something was really wrong with me. I decided
to begin walking again as a way to exercise and because it was something that I used
to enjoy and hadn't done for a long time. What I did initially was to walk about half
as far as I used to as a way to build up my strength. I really made an effort to take
note of how my sensations felt before and after the walk. I would have to remind
myself that avoiding exercise is more likely the cause of tiredness.
242

■ I also learned to stop doing things that made me unnecessarily anxious. For
example, I would often obsessively read medical articles or articles that were related
to health which often made me think I had the disease they were talking about or
would make me worry more about my own problems. I set the goal of not reading
medical articles for one week. What I noticed was that I was thinking less about
medical problems during the week. Now before I start reading a medical article, I
really think about whether it will be helpful to me or if I am just searching to see if I
am sick.
■ Changing these two things were difficult for me... but I think they made the biggest
difference. Instead of reading about being sick, it makes a lot of sense to me to focus
on doing things that are good for me and will help me stay strong and healthy.
Video 6:
• One of the most helpful things I learned in therapy was how my emotions affect my
physical symptoms. I learned that when I feel depressed or anxious, this causes
changes in body. For example, when I get anxious, I often feel it physically in terms
of an increased heart rate, muscle tension, sweating, flushing, dry mouth, stomach
churning, and increased pain. As an anxious person, I am more aware of bodily
sensations, and often have the tendency to believe new and worrisome conditions are
developing. I used to believe these sensations meant that I had a serious medical
problem.
243
• I also learned to stop doing things that made me unnecessarily anxious. For
example, I would often obsessively read medical articles or articles that were related
to health which often made me think I had the disease they were talking about or
would make me worry more about my own problems. I set the goal of not reading
medical articles for one week. What I noticed was that I was thinking less about
medical problems during the week. Now before I start reading a medical article, I
really think about whether it will be helpful to me or if I am just searching to see if I
am sick.
• Changing these two things were difficult for me... but I think they made the biggest
difference. Instead of reading about being sick, it makes a lot of sense to me to focus
on doing things that are good for me and will help me stay strong and healthy.
Video 6:
• One of the most helpful things I learned in therapy was how my emotions affect my
physical symptoms. I learned that when I feel depressed or anxious, this causes
changes in body. For example, when I get anxious, I often feel it physically in terms
of an increased heart rate, muscle tension, sweating, flushing, dry mouth, stomach
churning, and increased pain. As an anxious person, I am more aware of bodily
sensations, and often have the tendency to believe new and worrisome conditions are
developing. I used to believe these sensations meant that I had a serious medical
problem.
243

• I also learned that my mood changes how I think about health and illness. When in a
good mood, I feel like I can handle having an illness. When in a bad mood, however,
I feel like being sick is the worst thing in the world.
■ During therapy, I learned different strategies that I can use to feel better when I am
anxious or mildly depressed. To reduce anxiety, I practice relaxation; do things I
enjoy or postpone worrying until later in the day when I have to really think about
what is bothering me and problem solve. To lift my mild depression, I like going for
walks, being with friends, watching movies, and generally try to focus on positive
things in my life rather than the negative. I make an effort to feel good.
■ Overall, I've found that living with a chronic health problem required an attitude
adjustment on my part. First, I had to accept that my condition may be chronic, and
there are limits to effective treatment. Instead, I have turned my efforts towards
coping with symptoms rather than eliminating them. I have also made a conscious
decision to control the condition as much as possible, rather than letting it control my
life. I now try modifying the situations that make my bodily sensations worse. I have
reduced the stress in my life as much as possible. Another thing I try to do is to
distract my mind from constant worries with relaxation techniques, and pleasurable
activities. And finally, I try to participate in the activities that give me satisfaction as
often as possible, such as spending time with family and friends.
■ I have now realized that having a health problem is not the end of the world and I
now have a number of coping techniques that I can use to deal with problems if they
do arise.
244
• I also learned that my mood changes how I think about health and illness. When in a
good mood, I feel like I can handle having an illness. When in a bad mood, however,
I feel like being sick is the worst thing in the world.
• During therapy, I learned different strategies that I can use to feel better when I am
anxious or mildly depressed. To reduce anxiety, I practice relaxation; do things I
enjoy or postpone worrying until later in the day when I have to really think about
what is bothering me and problem solve. To lift my mild depression, I like going for
walks, being with friends, watching movies, and generally try to focus on positive
things in my life rather than the negative. I make an effort to feel good.
• Overall, I've found that living with a chronic health problem required an attitude
adjustment on my part. First, I had to accept that my condition may be chronic, and
there are limits to effective treatment. Instead, I have turned my efforts towards
coping with symptoms rather than eliminating them. I have also made a conscious
decision to control the condition as much as possible, rather than letting it control my
life. I now try modifying the situations that make my bodily sensations worse. I have
reduced the stress in my life as much as possible. Another thing I try to do is to
distract my mind from constant worries with relaxation techniques, and pleasurable
activities. And finally, I try to participate in the activities that give me satisfaction as
often as possible, such as spending time with family and friends.
• I have now realized that having a health problem is not the end of the world and I
now have a number of coping techniques that I can use to deal with problems if they
do arise.
244

Appendix D
University of Regina Research Ethics Board Approval
LNIVERSIT\ OF
t y REGINA
DATE July 10 2005
TO Michelle Bourgault-Fagnou Psychology
I- kt•t •€4 RA.
mE\IOR,•DL
FROM W Wessel Acting Chair Research Ethics Board
Re. Testing the Efficacy of a Cognitive Behavioural Treatment of Health Anxiety Among Seniors (78S0506)
Please be advised that the University of Regina Research Ethics Board has reviewed your proposal and found it to be
ACCEPTABLE AS SUBMITTED Only applicants with this designation have ethical approval to proceed with their research as descnbed in their applications The Tn-Council Policy Statement on Ethical Conduct for Research Involving Humans requires the researcher to send the Chair of the REB annual reports and notice of project conclusion for research lasting more than one year (Section IF! ETHICAL CLEARANCE MUST BE RENEWED BY SUBMITTING A BRIEF STATUS REPORT EVERY TWELVE MONTHS Clearance will be revoked unless a satisfactory status report is received
2 ACCEPTABLE SUBJECT TO CHANGES AND PRECAUTIONS (SEE ATTACHED) Changes must be submitted to 'he REB and subsequently approved prior to beginning research Pease address 'he concerns raised by the reviewer(s) by means of a supplementary memo to the Chair of the REB Do not submit a new application Please provide the supplementary memorandum** or contact the REB concerning the progress of the project before September 10, 2006 in order to keep your tie active Once changes are deemed acceptable approval will be granted
L.) "1 3 UNACCEPTABLE AS SUBMITTED Please contact the Chair of the REB for advice on how the project proposal might be revised
Dr Warren Wessel
c Dr H Hadistavropoulos supervisor (Psychologyi
KAaatt11.2 CO.
**supplementary memorandum should be 'chive-cad to the Crair of the Research Ethics Board at the Office of Research Services 1AH 505 or by e-ma to research eth cs@uregtha ca
245
Appendix D
University of Regina Research Ethics Board Approval
R E G I N A Mt \ ioR, \Dui
DATE July 10 2005
TO Michelle Bourgault-Fagnou Psychology
FROM W Wessel Acting Chair Research Ethics Board
Re' Testing the Efficacy of a Cognitive Behavioural Treatment of Health Anxiety Among Seniors (78S0506)
Please be advised that the University of Regina Research Ethics Board has reviewed your proposal and found it to be
\Z 1 ACCEPTABLE AS SUBMITTED Only applicants with this designation have ethical approval to proceed with their research as descnbed in their applications The Tn-Counal Policy Statement on Ethical Conduct for Research Involving Humans requires the researcher to send the Chair of the REB annual reports and notice of project conclusion for research lasting more than one year (Section 1 Fi ETHICAL CLEARANCE MUST BE RENEWED BY SUBMITTING A BRIEF STATUS REPORT EVERY TWELVE MONTHS Clearance will be revoked unless a satisfactory status report is 'eceived
Z 2 ACCEPTABLE SUBJECT TO CHANGES AND PRECAUTIONS (SEE ATTACHEDi Changes must be subr-itttec to 'he REB and subsequently approved prior to beginning research P'ease address 'he concerns raised by the reviewer(s) by means of a supplementary memo to the Chair of the REB Do not submit a new application Please provide the supplementary memorandum" or contact the REB concerning the progress of the project before September 10, 2006 in order to keep your fiie active Once changes are deemed acceptable approval will be granted
• 3 UNACCEPTABLE AS SUBMITTED Please contact the Chair of the REB for advice on how the project proposal might be revised
/ < Dr Warren Wessel
c Dr H Hadistavropoulos supervisor (Psychologyi
" supplementary memorandum should be 'orwa-aed to the Crair of the Research Ethics Board at the Office of Research Services |AH 505 or by e-Ta <o researcl et* cs@u'egira ca
245
Sex: ❑ Male ❑ Female / /
(Day/Month/Year) Marital Status: ❑ Single ❑ Common Law ❑ Widowed
Appendix E
Questionnaires
Background Information
Age:
Education: ❑ less than high school ❑ college certificate or some university ❑ Other
Health Conditions: ❑ Alzheimer's Disease ❑ Cancer ❑ Hearing Problems ❑ High Blood Pressure ❑ Liver Disease ❑ Parkinson's Disease ❑ Stroke ❑ Other, please specify
Date of Birth:
❑ Married ❑ Separated/divorced ❑ Other
❑ high school diploma ❑ university degree
❑ Arthritis ❑ Diabetes ❑ Heart Disease ❑ Kidney Disease ❑ Osteoporosis ❑ Respiratory Disease ❑ Vision Problems
List all current medications (and their dosages):
Medication Dosage Times taken per day
246
Appendix E
Questionnaires
Background Information
Sex: • Male • Female Age: Date of Birth: / /
(Day/Month/Year) Marital Status: • Single • Married • Common Law • Separated/divorced • Widowed • Other
Education: a less than high school a high school diploma p college certificate or some university a university degree • Other
Health Conditions: • Alzheimer's Disease p Cancer • Hearing Problems • High Blood Pressure p Liver Disease p Parkinson's Disease p Stroke p Other, please specify
List all current medications (and their dosages):
Medication Dosage Times taken per day
p Arthritis p Diabetes p Heart Disease p Kidney Disease p Osteoporosis p Respiratory Disease p Vision Problems
246

Whiteley Index
Here are some questions about your health. Circle either YES or NO to indicate our answer to each question.
1) Do you often worry about the possibility that you have got a serious illness?
Yes No
2) Are you bothered by many pains and aches? Yes No 3) Do you find that you are often aware of various things happening in your
body? Yes No
4) Do you worry a lot about your health? Yes No 5) Do you often have the symptoms of very serious illness? Yes No 6) If a disease is brought to your attention (through radio, television,
newspapers, or someone you know) do you worry about getting it yourself??
Yes No
7) If you feel ill and someone tells you that you are looking better, do you become annoyed?
Yes No
8) Do you find that you are bothered by many different symptoms? Yes No 9) Is it easy for you to forget about yourself, and think about all sorts of
other things? Yes No
10) Is it hard for you to believe the doctor when he or she tells you there is nothing for you to worry about?
Yes No
11) Do you get the feeling that people are not taking you illness seriously enough?
Yes No
12) Do you think that you worry about your health more than most people? Yes No 13) Do you think there is something seriously wrong with your body? Yes No 14) Are you afraid of illness? Yes No
247
Whiteley Index
Here are some questions about your health. Circle either YES or NO to indicate your answer to each question. ^ ^ _ 1) Do you often worry about the possibility that you have got a serious
illness? 2) Are you bothered by many pains and aches? 3) Do you find that you are often aware of various things happening in your
body? 4) Do you worry a lot about your health? 5) Do you often have the symptoms of very serious illness? 6) If a disease is brought to your attention (through radio, television,
newspapers, or someone you know) do you worry about getting it yourself??
7) If you feel ill and someone tells you that you are looking better, do you become annoyed?
8) Do you find that you are bothered by many different symptoms? 9) Is it easy for you to forget about yourself, and think about all sorts of
other things? 10) Is it hard for you to believe the doctor when he or she tells you there is
nothing for you to worry about? 11) Do you get the feeling that people are not taking you illness seriously
enough? 12) Do you think that you worry about your health more than most people? 13) Do you think there is something seriously wrong with your body? 14) Are you afraid of illness?
Yes
Yes Yes
Yes Yes Yes
Yes
Yes Yes
Yes
Yes
Yes Yes Yes
No
No No
No No No
No
No No
No
No
No No No
247

Health Anxiety Inventory
Instructions: Each question in this section consists of a group of four statements. Please read each group of statements carefully and then select the one which best describes your feelings, over the past week. Identify the statement by ringing the letter next to it, i.e., if you think that statement (a) is correct, ring statement (a); it may be that more than one statement applies, in which case, please ring any that are applicable.
1. (a) I do not worry about my health. (b) I occasionally worry about my health. (c) I spend much of my time worrying about my health. (d) I spend most of my time worrying about my health.
2. (a) I notice aches/pains less than most other people (of my age). (b) I notice aches/pains as much as most other people (of my age). (c) I notice aches/pains more than most other people (of my age). (d) I am aware of aches/pains in my body all the time.
3. (a) As a rule I am not aware of bodily sensations or changes. (b) Sometimes I am aware of bodily sensations or changes. (c) I am often aware of bodily sensations or changes. (d) I am constantly aware of bodily sensations or changes.
4. (a) Resisting thoughts of illness is never a problem. (b) Most of the time I can resist thoughts of illness. (c) I try to resist thoughts of illness but am often unable to do so. (d) Thoughts of illness are so strong that I no longer even try to resist them.
5. (a) As a rule I am not afraid that I have a serious illness. (b) I am sometimes afraid that I have a serious illness. (c) I am often afraid that I have a serious illness. (d) I am always afraid that I have a serious illness.
6. (a) I do not have images (mental pictures) of myself being ill. (b) I occasionally have images of myself being ill. (c) I frequently have images of myself being ill. (d) I constantly have images of myself being ill.
7. (a) I do not have any difficulty taking my mind off thoughts about my health. (b) I sometimes have difficulty taking my mind off thoughts about my health. (c) I often difficulty in taking my mind off thoughts about my health. (d) Nothing can take my mind off thoughts about my health.
248
Health Anxiety Inventory
Instructions: Each question in this section consists of a group of four statements. Please read each group of statements carefully and then select the one which best describes your feelings, over the past week. Identify the statement by ringing the letter next to it, i.e., if you think that statement (a) is correct, ring statement (a); it may be that more than one statement applies, in which case, please ring any that are applicable.
1. (a) I do not worry about my health. (b) I occasionally worry about my health. (c) I spend much of my time worrying about my health. (d) I spend most of my time worrying about my health.
2. (a) I notice aches/pains less than most other people (of my age). (b) I notice aches/pains as much as most other people (of my age). (c) I notice aches/pains more than most other people (of my age). (d) I am aware of aches/pains in my body all the time.
3. (a) As a mle I am not aware of bodily sensations or changes. (b) Sometimes I am aware of bodily sensations or changes. (c) I am often aware of bodily sensations or changes. (d) I am constantly aware of bodily sensations or changes.
4. (a) Resisting thoughts of illness is never a problem. (b) Most of the time I can resist thoughts of illness. (c) I try to resist thoughts of illness but am often unable to do so. (d) Thoughts of illness are so strong that I no longer even try to resist them.
5. (a) As a mle I am not afraid that I have a serious illness. (b) I am sometimes afraid that I have a serious illness. (c) I am often afraid that I have a serious illness. (d) I am always afraid that I have a serious illness.
6. (a) I do not have images (mental pictures) of myself being ill. (b) I occasionally have images of myself being ill. (c) I frequently have images of myself being ill. (d) I constantly have images of myself being ill.
7. (a) I do not have any difficulty taking my mind off thoughts about my health. (b) I sometimes have difficulty taking my mind off thoughts about my health. (c) I often difficulty in taking my mind off thoughts about my health. (d) Nothing can take my mind off thoughts about my health.
248
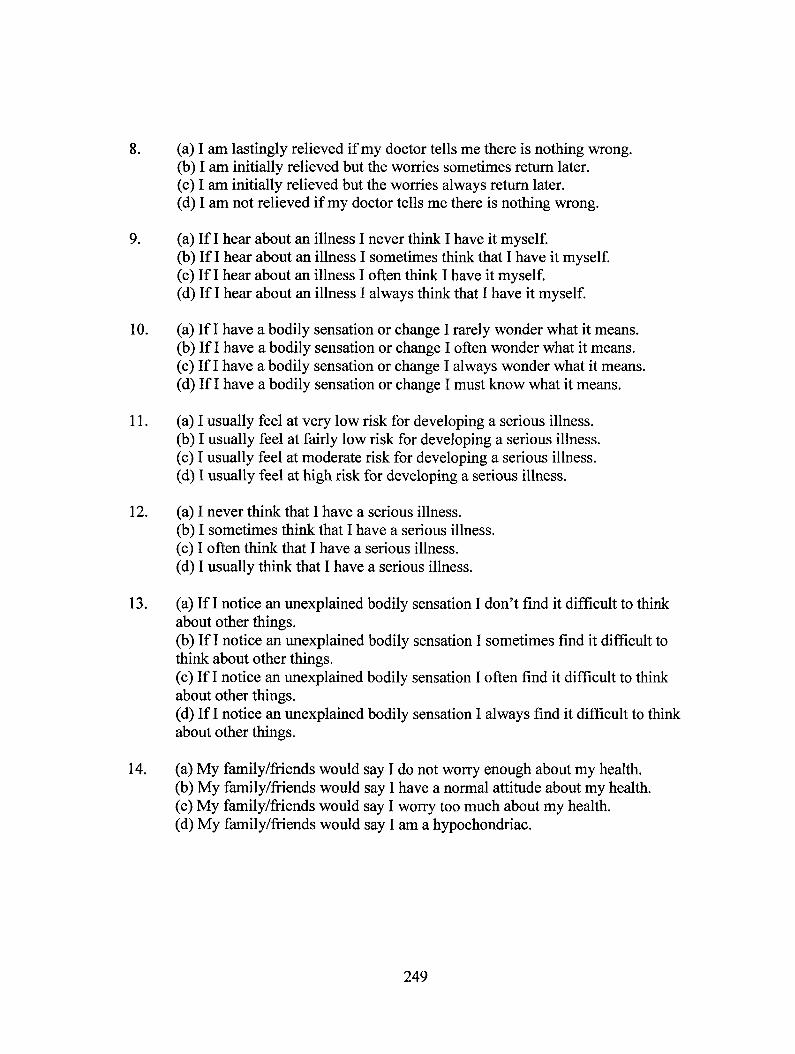
8. (a) I am lastingly relieved if my doctor tells me there is nothing wrong. (b) I am initially relieved but the worries sometimes return later. (c) I am initially relieved but the worries always return later. (d) I am not relieved if my doctor tells me there is nothing wrong.
9. (a) If I hear about an illness I never think I have it myself. (b) If I hear about an illness I sometimes think that I have it myself. (c) If I hear about an illness I often think I have it myself. (d) If I hear about an illness I always think that I have it myself.
10. (a) If I have a bodily sensation or change I rarely wonder what it means. (b) If I have a bodily sensation or change I often wonder what it means. (c) If I have a bodily sensation or change I always wonder what it means. (d) If I have a bodily sensation or change I must know what it means.
11. (a) I usually feel at very low risk for developing a serious illness. (b) I usually feel at fairly low risk for developing a serious illness. (c) I usually feel at moderate risk for developing a serious illness. (d) I usually feel at high risk for developing a serious illness.
12. (a) I never think that I have a serious illness. (b) I sometimes think that I have a serious illness. (c) I often think that I have a serious illness. (d) I usually think that I have a serious illness.
13. (a) If I notice an unexplained bodily sensation I don't find it difficult to think about other things. (b) If I notice an unexplained bodily sensation I sometimes find it difficult to think about other things. (c) If I notice an unexplained bodily sensation I often find it difficult to think about other things. (d) If I notice an unexplained bodily sensation I always find it difficult to think about other things.
14. (a) My family/friends would say I do not worry enough about my health. (b) My family/friends would say I have a normal attitude about my health. (c) My family/friends would say I worry too much about my health. (d) My family/friends would say I am a hypochondriac.
249
8. (a) I am lastingly relieved if my doctor tells me there is nothing wrong. (b) I am initially relieved but the worries sometimes return later. (c) I am initially relieved but the worries always return later. (d) I am not relieved if my doctor tells me there is nothing wrong.
9. (a) If I hear about an illness I never think I have it myself. (b) If I hear about an illness I sometimes think that I have it myself. (c) If I hear about an illness I often think I have it myself. (d) If I hear about an illness I always think that I have it myself.
10. (a) If I have a bodily sensation or change I rarely wonder what it means. (b) If I have a bodily sensation or change I often wonder what it means. (c) If I have a bodily sensation or change I always wonder what it means. (d) If I have a bodily sensation or change I must know what it means.
11. (a) I usually feel at very low risk for developing a serious illness. (b) I usually feel at fairly low risk for developing a serious illness. (c) I usually feel at moderate risk for developing a serious illness. (d) I usually feel at high risk for developing a serious illness.
12. (a) I never think that I have a serious illness. (b) I sometimes think that I have a serious illness. (c) I often think that I have a serious illness. (d) I usually think that I have a serious illness.
13. (a) If I notice an unexplained bodily sensation I don't find it difficult to think about other things. (b) If I notice an unexplained bodily sensation I sometimes find it difficult to think about other things. (c) If I notice an unexplained bodily sensation I often find it difficult to think about other things. (d) If I notice an unexplained bodily sensation I always find it difficult to think about other things.
14. (a) My family/friends would say I do not worry enough about my health. (b) My family/friends would say I have a normal attitude about my health. (c) My family/friends would say I worry too much about my health. (d) My family/friends would say I am a hypochondriac.
249

For the following questions, please think about what it might be like if you had a serious illness of a type which particularly concerns you (such as heart disease, cancer, multiple sclerosis and so on). Obviously you cannot know for definite what it would be like; please give your best estimate of what you think might happen, basing your estimate on what you know about yourself and serious illness in general.
15. (a) If I had a serious illness I would still be able to enjoy things in my life quite a lot. (b) If I had a serious illness I would still be able to enjoy things in my life a little. (c) If I had a serious illness I would still be almost completely unable to enjoy things in my life. (d) If I had a serious illness I would be completely unable to enjoy life at all.
16. (a) If I developed a serious illness there is a good chance that modern medicine would be able to cure me. (b) If I developed a serious illness there is a moderate chance that modern medicine would be able to cure me. (c) If I developed a serious illness there is a very small chance that modern medicine would be able to cure me. (d) If I developed a serious illness there is no chance that modern medicine would be able to cure me.
17. (a) A serious illness would ruin some aspects of my life. (b) A serious illness would ruin many aspects of my life. (c) A serious illness would ruin almost every aspect of my life. (d) A serious illness would ruin every aspect of my life.
18. (a) If I had a serious illness I would not feel that I had lost my dignity. (b) If I had a serious illness I would feel that I had lost a little of my dignity. (c) If I had a serious illness I would feel that I had lost quite a lot of my dignity. (d) If I had a serious illness I would feel that I had totally lost my dignity.
250
For the following questions, please think about what it might be like if you had a serious illness of a type which particularly concerns you (such as heart disease, cancer, multiple sclerosis and so on). Obviously you cannot know for definite what it would be like; please give your best estimate of what you think might happen, basing your estimate on what you know about yourself and serious illness in general.
15. (a) If I had a serious illness I would still be able to enjoy things in my life quite a lot. (b) If I had a serious illness I would still be able to enjoy things in my life a little. (c) If I had a serious illness I would still be almost completely unable to enjoy things in my life. (d) If I had a serious illness I would be completely unable to enjoy life at all.
16. (a) If I developed a serious illness there is a good chance that modem medicine would be able to cure me. (b) If I developed a serious illness there is a moderate chance that modem medicine would be able to cure me. (c) If I developed a serious illness there is a very small chance that modem medicine would be able to cure me. (d) If I developed a serious illness there is no chance that modem medicine would be able to cure me.
17. (a) A serious illness would ruin some aspects of my life. (b) A serious illness would min many aspects of my life. (c) A serious illness would min almost every aspect of my life. (d) A serious illness would min every aspect of my life.
18. (a) If I had a serious illness I would not feel that I had lost my dignity. (b) If I had a serious illness I would feel that I had lost a little of my dignity. (c) If I had a serious illness I would feel that I had lost quite a lot of my dignity. (d) If I had a serious illness I would feel that I had totally lost my dignity.
250
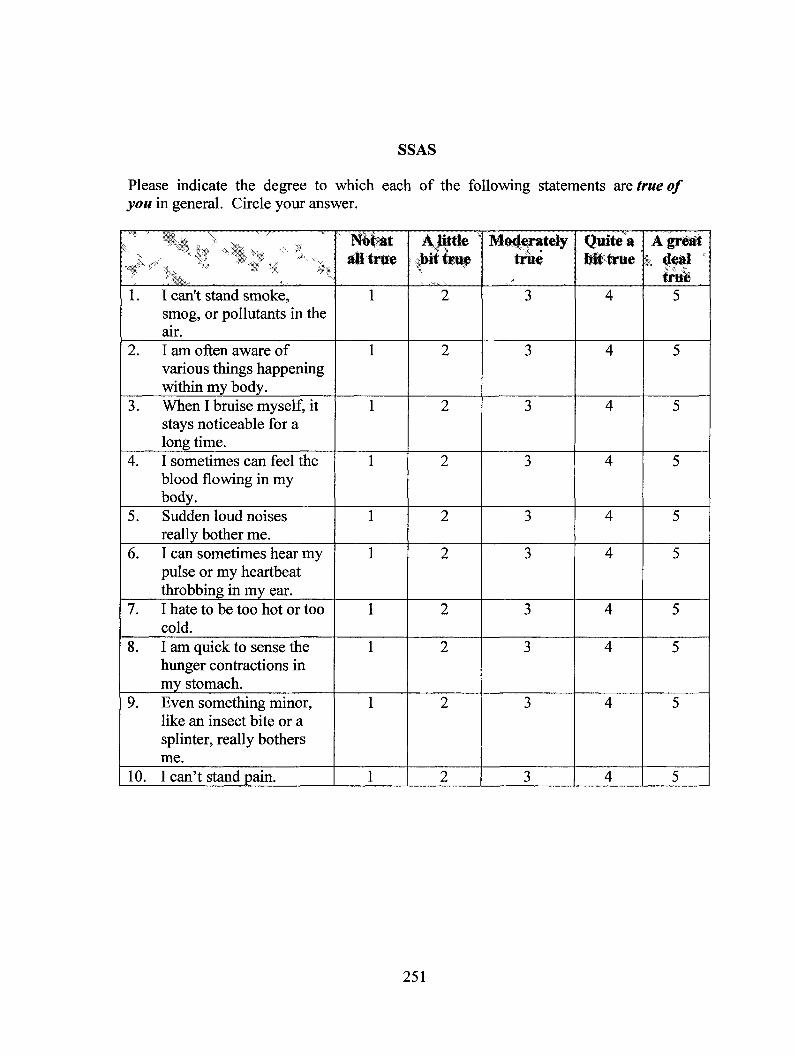
SSAS
Please indicate the degree to which each of the following statements are true of you in general. Circle your answer.
...;\ ,----
N,.
Not-at all true
A little , obit true
-.. \
Moderately true
Quite a bit true
A great i deal '
true 1. I can't stand smoke,
smog, or pollutants in the air.
1 2 3 4 5
2. I am often aware of various things happening within my body.
1 2 3 4 5
3. When I bruise myself, it stays noticeable for a long time.
1 2 3 4 5
4. I sometimes can feel the blood flowing in my body.
1 2 3 4 5
5. Sudden loud noises really bother me.
1 2 3 4 5
6. I can sometimes hear my pulse or my heartbeat throbbing in my ear.
1 2 3 4 5
7. I hate to be too hot or too cold.
1 2 3 4 5
8. I am quick to sense the hunger contractions in my stomach.
1 2 3 4 5
9. Even something minor, like an insect bite or a splinter, really bothers me.
1 2 3 4 5
10. I can't stand pain. 1 2 3 4 5
251
SSAS
Please indicate the degree to which each of the following statements are true of you in general. Circle your answer.
"W5? "•> 5^" ^..-7„, „™w™.
. ^Safex i.., ...
1. I can't stand smoke, smog, or pollutants in the air.
2. I am often aware of various things happening within my body.
3. When I bruise myself, it stays noticeable for a long time.
4. I sometimes can feel the blood flowing in my body.
5. Sudden loud noises really bother me.
6. I can sometimes hear my pulse or my heartbeat throbbing in my ear.
7. I hate to be too hot or too cold.
8. I am quick to sense the hunger contractions in my stomach.
9. Even something minor, like an insect bite or a splinter, really bothers me.
10. I can't stand pain.
aUtrwe
2
2
2
2
2
2
2
2
2
2
Moderately trite
3
3
3
3
3
3
3
3
3
3
Quite a WNrtie
4
4
4
4
4
4
4
4
4
4
A grist k 4#al s
true 5
5
5
5
5
5
5
5
5
5
251

S.S.I.
Below is a list of symptoms. For each one, please circle the number indicating how much it has bothered you over the past 6 months.
N\ - ,
1. Not it w
all ' A little
bit Moderately Quite *,
bit A great
deal 1. Nausea or vomiting 1 2 3 4 5 2. Soreness in your muscles 1 2 3 4 5 3. Pains or cramps in your
abdomen 1 2 3 4 5
4. Feeling faint or dizzy 1 2 3 4 5 5. Trouble with your vision 1 2 3 4 5 6. Your muscles twitching
or jumping 1 2 3 4 5
7. Feeling fatigued, weak, or tired all over
1 2 3 4 5
8. A fullness in your head or nose
1 2 3 4 5
9. Pains in your lower back 1 2 3 4 5 10. Constipation 1 2 3 4 5 11. Trouble catching your
breath 1 2 3 4 5
12. Hot or cold spells 1 2 3 4 5 13. A ringing or buzzing in
your ears 1 2 3 4 5
252
S.S.I.
Below is a list of symptoms. For each one, please circle the number indicating how much it has bothered you over the past 6 months.
mjmagjSj *N s \ *A
. . 9 **>: 1 \ , . 1. Nausea or vomiting 2. Soreness in your muscles 3. Pains or cramps in your
abdomen 4. Feeling faint or dizzy 5. Trouble with your vision 6. Your muscles twitching
or jumping 7. Feeling fatigued, weak,
or tired all over 8. A fullness in your head
or nose 9. Pains in your lower back 10. Constipation 11. Trouble catching your
breath 12. Hot or cold spells 13. A ringing or buzzing in
your ears
IVnt itt A ttftt , Wt
2 2 2
2 2 2
2
2
2 2 2
2 2
Moderately \ v.
3 3 3
3 3 3
3
3
3 3 3
3 3
Qu i t e*
4 4 4
4 4 4
4
4
4 4 4
4 4
Agre^tr
5 5 5
5 5 5
5
5
5 5 5
5 5
252
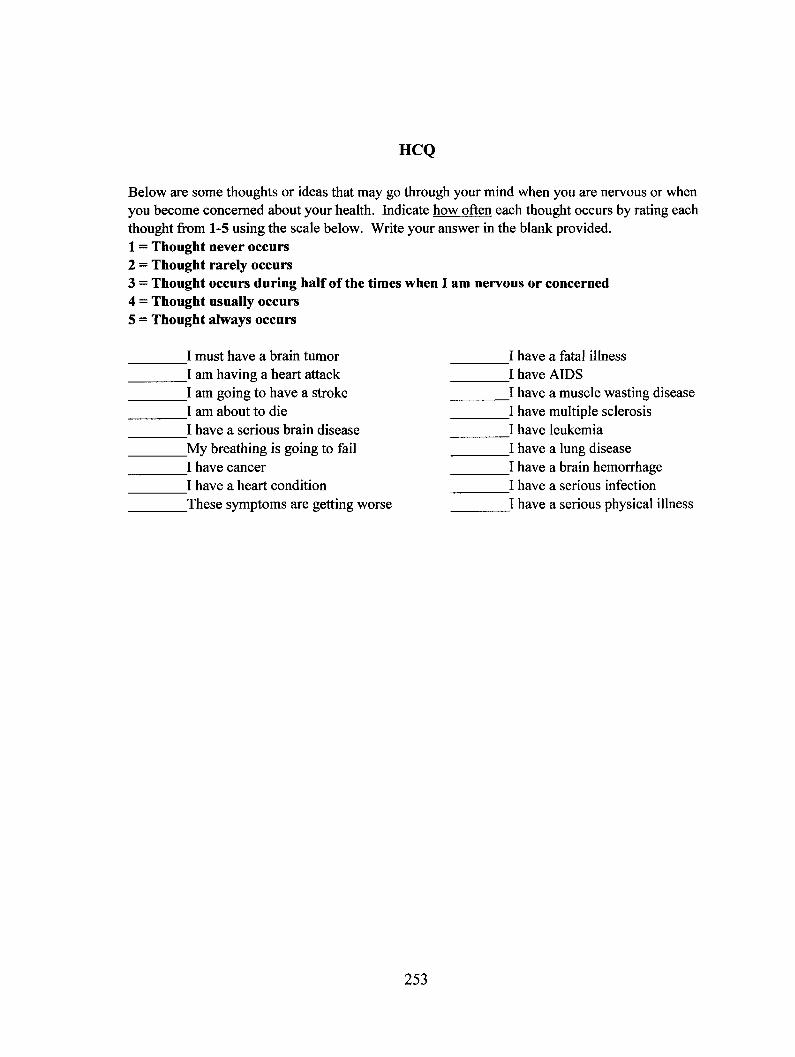
HCQ
Below are some thoughts or ideas that may go through your mind when you are nervous or when you become concerned about your health. Indicate how often each thought occurs by rating each thought from 1-5 using the scale below. Write your answer in the blank provided. 1= Thought never occurs 2 = Thought rarely occurs 3 = Thought occurs during half of the times when I am nervous or concerned 4 = Thought usually occurs 5 = Thought always occurs
I must have a brain tumor I am having a heart attack I am going to have a stroke I am about to die I have a serious brain disease My breathing is going to fail I have cancer I have a heart condition These symptoms are getting worse
253
I have a fatal illness I have AIDS I have a muscle wasting disease I have multiple sclerosis I have leukemia I have a lung disease I have a brain hemorrhage I have a serious infection I have a serious physical illness
HCQ
Below are some thoughts or ideas that may go through your mind when you are nervous or when you become concerned about your health. Indicate how often each thought occurs by rating each thought from 1-5 using the scale below. Write your answer in the blank provided. 1 = Thought never occurs 2 = Thought rarely occurs 3 = Thought occurs during half of the times when I am nervous or concerned 4 = Thought usually occurs 5 = Thought always occurs
I must have a brain tumor I am having a heart attack I am going to have a stroke I am about to die I have a serious brain disease My breathing is going to fail I have cancer I have a heart condition These symptoms are getting worse
I have a fatal illness _I have AIDS I have a muscle wasting disease I have multiple sclerosis I have leukemia I have a lung disease I have a brain hemorrhage I have a serious infection I have a serious physical illness
253

Anxiety Sensitivity Index
Instructions: Circle the one number that best represents the extent to which you agree with the item. If any of the items concern something that is not part of your experience (e.g., "it scares me when I feel shaky" for someone who has never trembled or had the "shakes"), answer on the basis of how you might feel if you had such an experience. Otherwise, answer all the items on the basis of your own experience.
--‘ . , Ver
Little eA Little Some Much
Very Much
1. It is important to me not to appear nervous. 1 2 3 4 5
2. When I cannot keep my mind on a task, I worry that I might be going crazy. 1 2 3 4 5
3. It scares me when I feel "shaky" (trembling). 1 2 3 4 5
4. It scares me when I feel faint. 1 2 3 4 5
5. It is important to me to stay in control of my emotions. 1 2 3 4 5
6. It scares me when my heart beats rapidly. 1 2 3 4 5
7. It embarrasses me when my stomach growls. 1 2 3 4 5
8. It scares me when I am nauseous. 1 2 3 4 5
9. When I notice that my heart is beating rapidly, I worry that I might have a heart attack.
1 2 3 4 5
10. It scares me when I become short of breath. 1 2 3 4 5
11. When my stomach is upset, I worry that I might be seriously ill. 1 2 3 4 5
12. It scares me when I am unable to keep my mind on a task. 1 2 3 4 5
13. Other people notice when I feel shaky. 1 2 3 4 5
254
Anxiety Sensitivity Index
Instructions: Circle the one number that best represents the extent to which you agree with the item. If any of the items concern something that is not part of your experience (e.g., "it scares me when I feel shaky" for someone who has never trembled or had the "shakes"), answer on the basis of how you might feel if you had such an experience. Otherwise, answer all the items on the basis of your own experience.
1. It is important to me not to appear nervous.
2. When I cannot keep my mind on a task, I worry that I might be going crazy.
3. It scares me when I feel "shaky" (trembling).
4. It scares me when I feel faint.
5. It is important to me to stay in control of my emotions.
6. It scares me when my heart beats rapidly.
7. It embarrasses me when my stomach growls.
8. It scares me when I am nauseous.
9. When I notice that my heart is beating rapidly, I worry that I might have a heart attack.
10. It scares me when I become short of breath.
11. When my stomach is upset, I worry that I might be seriously ill.
12. It scares me when I am unable to keep my mind on a task.
13. Other people notice when I feel shaky.
Little
1
1
1
1
1
1
1
1
1
1
1
1
1
A Little
2
2
2
2
2
2
2
2
2
2
2
2
2
Some
3
3
3
3
3
3
3
3
3
3
3
3
3
Much
4
4
4
4
4
4
4
4
4
4
4
4
4
Very •Much
5
5
5
5
5
5
5
5
5
5
5
5
5
254

14. Unusual body sensations scare me. 1 2 3 4 5
15. When I am nervous, I worry that I might be mentally ill. 1 2 3 4 5
16. It scares me when I am nervous. 1 2 3 4 5
255
14. Unusual body sensations scare me.
15. When I am nervous, I worry that I might be mentally ill.
16. It scares me when I am nervous.
1
1
1
2
2
2
3
3
3
4
4
4
5
5
5
255

State-Trait Anxiety Inventory — State (Form Y; STAI-S)
Directions: A number of statements which people have used to describe themselves are given below. Read each statement and then circle the appropriate number to the right of the statement to indicate how you feel right now, that is, at this moment. There are no right or wrong answers. Do not spend too much time on any one statement but give the answer which seems to describe your present feelings best.
• . , ,,, , - ,,,
" , •
Not at -All
Somewhpt Moderately so
Very Much
SO ' 1. I feel calm 1 2 3 4
2. I feel secure 1 2 3 4
3. I am tense 1 2 3 4
4. I feel strained 1 2 3 4 5. I feel at ease 1 2 3 4
6. I feel upset 1 2 3 4
7. I am presently worrying over possible misfortunes
1 2 3 4
8. I feel satisfied 1 2 3 4 9. I feel frightened 1 2 3 4 10. I am comfortable 1 2 3 4
11. I feel self-confident 1 2 3 4
12. I feel nervous 1 2 3 4
13. I am jittery 1 2 3 4
14. I feel indecisive 1 2 3 4
15. I am relaxed 1 2 3 4
16. I feel content 1 2 3 4
17. I am worried 1 2 3 4
18. I feel confused 1 2 3 4 19. I feel steady 1 2 3 4 20. I feel pleasant 1 2 3 4
256
State-Trait Anxiety Inventory - State (Form Y; STAI-S)
Directions: A number of statements which people have used to describe themselves are given below. Read each statement and then circle the appropriate number to the right of the statement to indicate how you feel right now, that is, at this moment. There are no right or wrong answers. Do not spend too much time on any one statement but give the answer which seems to describe your present feelings best.
1.
2.
3.
4. 5.
6.
7.
8. 9. 10. 11.
12.
13.
14.
15.
16.
17.
18. 19. 20.
I feel calm
I feel secure
I am tense
I feel strained I feel at ease
I feel upset
I am presently worrying over possible misfortunes I feel satisfied I feel frightened I am comfortable I feel self-confident
I feel nervous
I am jittery
I feel indecisive
I am relaxed
I feel content
I am worried
I feel confused I feel steady I feel pleasant
Not at All
Somewhat
2
2
2 2 2 2
2
2 2 2 2
2
2
2
2
2
2
2 2 2
' 'so • *-; 3
3
3 3 3 3
3
3 3 3 3
3
3
3
3
3
3
3 3 3
4
4
4 4 4 4
4
4 4 4 4
4
4
4
4
4
4
4 4 4
256

State-Trait Anxiety Inventory — Trait (Form Y; STAI-T)
Instructions: A number of statements which people have used to describe themselves are given below. Read each statement and then circle the appropriate number to the right of the statement to indicate how you generally feel. There are no right or wrong answers. Do not spend too much time on any one statement but give the answer that seems to describe how you generally feel.
Almost Never Sometimes Often
Almost ,-, Always
21. I feel pleasant 1 2 3 4
22. I feel nervous and restless 1 2 3 4
23. I feel satisfied with myself 1 2 3 4
24. I wish I could be as happy as others seem to be 1 2 3 4
25. I feel like a failure 1 2 3 4
26. I feel rested 1 2 3 4
27. I am "calm, cool, and collected" 1 2 3 4
28. I feel that difficulties are piling up so that I cannot overcome them 1 2 3 4
29. I worry too much over something that really doesn't matter
1 2 3 4
30. I am happy 1 2 3 4 31. I have disturbing thoughts 1 2 3 4
32. I lack self-confidence 1 2 3 4
33. I feel secure 1 2 3 4
34. I make decisions easily 1 2 3 4
35. I feel inadequate 1 2 3 4
36. I am content 1 2 3 4
37. Some unimportant thoughts run through my mind and bothers me 1 2 3 4
38. I take disappointments so keenly that I can't put them out of my mind 1 2 3 4
39. I am a steady person 1 2 3 4
40. I get in a state of tension or turmoil as I think over my recent concerns and interests
1 2 3 4
257
State-Trait Anxiety Inventory - Trait (Form Y; STAI-T)
Instructions: A number of statements which people have used to describe themselves are given below. Read each statement and then circle the appropriate number to the right of the statement to indicate how you generally feel. There are no right or wrong answers. Do not spend too much time on any one statement but give the answer that seems to describe how you generally feel.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30. 31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
I feel pleasant
I feel nervous and restless
I feel satisfied with myself
I wish I could be as happy as others seem to be I feel like a failure
I feel rested
I am "calm, cool, and collected"
I feel that difficulties are piling up so that I cannot overcome them I worry too much over something that really doesn't matter I am happy I have disturbing thoughts
I lack self-confidence
I feel secure
I make decisions easily
I feel inadequate
I am content
Some unimportant thoughts run through my mind and bothers me
I take disappointments so keenly that I can't put them out of my mind
I am a steady person
I get in a state of tension or turmoil as I think over my recent concerns and interests
Almost Newr,
1
Sometimes 2
2
2
2 2 2
2
2 2
2 2
2
2
2
2
2
2
2
2
2
Often 3
3
3
3 3 3
3
3 3
3 3
3
3
3
3
3
3
3
3
3
Almost Always *.
4
4
4
4 4 4
4
4 4
4 4
4
4
4
4
4
4
4
4
4
257

Mood Assessment Scale
Instructions: Choose the best answer for how you have felt over the past week:
1) Are you basically satisfied with your life? Yes No 2) Have you dropped many of your activities and interests? Yes No 3) Do you feel that your life is empty? Yes No 4) Do you often get bored? Yes No 5) Are you hopeful about the future? Yes No 6) Are you bothered by thoughts you can t get out of your head? Yes No 7) Are you in good spirits most of the time? Yes No 8) Are you afraid that something bad is going to happen to you? Yes No 9) Do you feel happy most of the time? Yes No 10) Do you often feel helpless? Yes No 11) Do you often get restless and fidgety? Yes No 12) Do you prefer to stay at home, rather than going out and doing new
things? Yes No
13) Do you frequently worry about the future? Yes No 14) Do you feel you have more problems with memory than most? Yes No 15) Do you think it is wonderful to be alive now? Yes No 16) Do you often feel downhearted and blue? Yes No 17) Do you feel pretty worthless the way you are now? Yes No 18) Do you worry a lot about the past? Yes No 19) Do you find life very exciting? Yes No 20) Is it hard for you to get started on new projects? Yes No 21) Do you feel full of energy? Yes No 22) Do you feel that your situation is hopeless? Yes No 23) Do you think that most people are better off than you are? Yes No 24) Do you frequently get upset over little things? Yes No 25) Do you frequently feel like crying? Yes No 26) Do you have trouble concentrating? Yes No 27) Do you enjoy getting up in the morning? Yes No 28) Do you prefer to avoid social gatherings? Yes No 29) Is it easy for you to make decisions? Yes No 30) Is your mind as clear as it used to be? Yes No
258
Mood Assessment Scale
Instructions: Choose the best answer for how you have felt over the past week:
1) Are you basically satisfied with your life? 2) Have you dropped many of your activities and interests? 3) Do you feel that your life is empty? 4) Do you often get bored? 5) Are you hopeful about the future? 6) Are you bothered by thoughts you can t get out of your head? 7) Are you in good spirits most of the time? 8) Are you afraid that something bad is going to happen to you? 9) Do you feel happy most of the time? 10) Do you often feel helpless? 11) Do you often get restless and fidgety? 12) Do you prefer to stay at home, rather than going out and doing new
things? 13) Do you frequently worry about the future? 14) Do you feel you have more problems with memory than most? 15) Do you think it is wonderful to be alive now? 16) Do you often feel downhearted and blue? 17) Do you feel pretty worthless the way you are now? 18) Do you worry a lot about the past? 19) Do you find life very exciting? 20) Is it hard for you to get started on new projects? 21) Do you feel full of energy? 22) Do you feel that your situation is hopeless? 23) Do you think that most people are better off than you are? 24) Do you frequently get upset over little things? 25) Do you frequently feel like crying? 26) Do you have trouble concentrating? 27) Do you enjoy getting up in the morning? 28) Do you prefer to avoid social gatherings? 29) Is it easy for you to make decisions? 30) Is your mind as clear as it used to be?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
No No No No No No No No No No No No
No No No No No No No No No No No No No No No No No No
258

Geriatric Pain Measure
Instructions: Please answer each question.
1) Do you or would you have pain with vigorous activities such as Yes No running, lifting heavy objects or participating in strenuous sports?
2) Do you or would you have pain with moderate activities such as Yes No moving a heavy table, pushing a vacuum cleaner, bowling or playing golf?
3) Do you or would you have pain with lifting or carrying groceries? Yes No 4) Do you or would you have pain climbing more than one flight of Yes No
stairs? 5) Do you or would you have pain climbing only a few steps? Yes No 6) Do you or would you have pain walking more than one block? Yes No 7) Do you or would you have pain walking one block or less? Yes No 8) Do you have pain with bathing or dressing? Yes No 9) Have you cut down the amount of time you spend on work or other
activities because of pain? Yes No
10) Have you been accomplishing less than you would like to because Yes No of pain?
11) Have you limited the kind of work or other activities you do because of pain?
Yes No
12) Does the work or activities you do require extra effort because of Yes No pain?
13) Do you have trouble sleeping because of pain? Yes No 14) Does pain prevent you from attending religious activities? Yes No 15) Does pain prevent you from enjoying any other social or Yes No
recreational activities (other than religious services)? 16) Does or would pain prevent you from traveling or using standard Yes No
transportation? 17) Does pain make you feel fatigued or tired? Yes No 18) Do you have to rely on family members or friends for help because Yes No
of pain? 19) On a scale of zero to ten, with zero meaning no pain, and ten
meaning the worst pain you can imagine, how severe is your pain today?
0 1 2 3 4 5 6 7 8 9 10 (0-10)
20) In the last seven days, on a scale of zero to ten, with zero meaning no pain, and ten meaning the worst pain you can imagine, how severe has your pain been on average?
0 1 2 3 4 5 6 7 8 9 10 (0-10)
259
Geriatric Pain Measure
Instructions: Please answer each question.
1) Do you or would you have pain with vigorous activities such as running, lifting heavy objects or participating in strenuous sports?
2) Do you or would you have pain with moderate activities such as moving a heavy table, pushing a vacuum cleaner, bowling or playing golf?
3) Do you or would you have pain with lifting or carrying groceries? 4) Do you or would you have pain climbing more than one flight of
stairs? 5) Do you or would you have pain climbing only a few steps? 6) Do you or would you have pain walking more than one block? 7) Do you or would you have pain walking one block or less? 8) Do you have pain with bathing or dressing? 9) Have you cut down the amount of time you spend on work or other
activities because of pain? 10) Have you been accomplishing less than you would like to because
of pain? 11) Have you limited the kind of work or other activities you do
because of pain? 12) Does the work or activities you do require extra effort because of
pain? 13) Do you have trouble sleeping because of pain? 14) Does pain prevent you from attending religious activities? 15) Does pain prevent you from enjoying any other social or
recreational activities (other than religious services)? 16) Does or would pain prevent you from traveling or using standard
transportation? 17) Does pain make you feel fatigued or tired? 18) Do you have to rely on family members or friends for help because
of pain? 19) On a scale of zero to ten, with zero meaning no pain, and ten
meaning the worst pain you can imagine, how severe is your pain today?
0 1 2 3 4 5 6 7 8 9 10
20) In the last seven days, on a scale of zero to ten, with zero meaning no pain, and ten meaning the worst pain you can imagine, how severe has vour pain been on average?
0 1 2 3 4 5 6 7 8 9 10
Yes
Yes
Yes Yes
Yes Yes Yes Yes Yes
Yes
Yes
Yes
Yes Yes Yes
Yes
Yes Yes
No
No
No No
No No No No No
No
No
No
No No No
No
No No
(0-10)
(0-10)
259

21) Do you have pain that never completely goes away? Yes No 22) Do you have pain every day? Yes No 23) Do you have pain several times a week? Yes No 24) Over the last seven days, has pain caused you to feel sad or Yes No
depressed?
260
21) Do you have pain that never completely goes away? 22) Do you have pain every day? 23) Do you have pain several times a week? 24) Over the last seven days, has pain caused you to feel sad or
depressed?
Yes Yes Yes Yes
No No No No
260

SF-12
The SF-12 is copy-righted so was not included here.
261
SF-12
The SF-12 is copy-righted so was not included here.
261

Working Alliance Inventory — Client Form
Below there are sentences that describe some of the different ways a person might think or feel about his or her therapist (counselor). If the statement describes the way you always feel (or think) circle the number 7; if it never applies to you circle the number 1. Use the number in between to describe the variations between these extremes.
Work fast, your first impressions are the ones we would like to see. (PLEASE DON'T FORGET TO RESPOND TO EVERY ITEM.)
1. I feel uncomfortable with my therapist. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
2. My therapist and I agree about the things I will need to do in therapy to help improve my situation. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
3. I am worried about the outcome of these sessions. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
4. What I am doing in therapy gives me new ways of looking at my problems. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
5. My therapist and I understand each other. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
6. My therapist perceives accurately what my goals are. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
262
Working Alliance Inventory - Client Form
Below there are sentences that describe some of the different ways a person might think or feel about his or her therapist (counselor). If the statement describes the way you always feel (or think) circle the number 7; if it never applies to you circle the number 1. Use the number in between to describe the variations between these extremes.
Work fast, your first impressions are the ones we would like to see. (PLEASE DON'T FORGET TO RESPOND TO EVERY ITEM.)
1. I feel uncomfortable with my therapist. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
2. My therapist and I agree about the things I will need to do in therapy to help improve my situation. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
3. I am worried about the outcome of these sessions. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
4. What I am doing in therapy gives me new ways of looking at my problems. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
5. My therapist and I understand each other. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
6. My therapist perceives accurately what my goals are. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
262

7. I find what I am doing in therapy confusing. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
8. I believe my therapist likes me. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
9. I wish my therapist and I could clarify the purpose of our sessions. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
10. I disagree with my therapist about what I ought to get out of therapy. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
11. I believe the time my therapist and I are spending together is not spent efficiently. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
12. My therapist does not understand what I am trying to accomplish in therapy. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
13. I am clear on what my responsibilities are in therapy. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
14. The goals of these sessions are important to me. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
15. I find what my therapist and I are doing in sessions is unrelated to my concerns. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
263
7. I find what I am doing in therapy confusing. 1 2 3 4
Never Rarely Occasionally Sometimes 5
Often 6
Very Often
7 Always
8. I believe my therapist likes me. 1 2 3 4
Never Rarely Occasionally Sometimes
9. I wish my therapist and I could clarify the purpose 1 2 3 4
Never Rarely Occasionally Sometimes
10.1 disagree with my therapist about what I ought to 1 2 3 4
Never Rarely Occasionally Sometimes
11.1 believe the time my therapist and I are spending 1 1 2 3 4
Never Rarely Occasionally Sometimes
12. My therapist does not understand what I am trying 1 2 3 4
Never Rarely Occasionally Sometimes
5 Often
6 Very Often
of our sessions. 5
Often 6
Very Often
get out of therapy. 5
Often
:ogether is 5
Often
6 Very Often
7 Always
7 Always
7 Always
not spent efficiently. 6
Very Often
to accomplish in therapy 5
Often 6
Very Often
7 Always
7 Always
13.1 am clear on what my responsibilities are in therapy. 1 2 3 4
Never Rarely Occasionally Sometimes 5
Often 6
Very Often
7 Always
14. The goals of these sessions are important to me. 1 2 3 4
Never Rarely Occasionally Sometimes 5
Often 6
Very Often
7 Always
15.1 find what my therapist and I are doing in sessions is unrelated to my concerns. 1 2 3 4
Never Rarely Occasionally Sometimes 5
Often 6
Very Often
7 Always
263
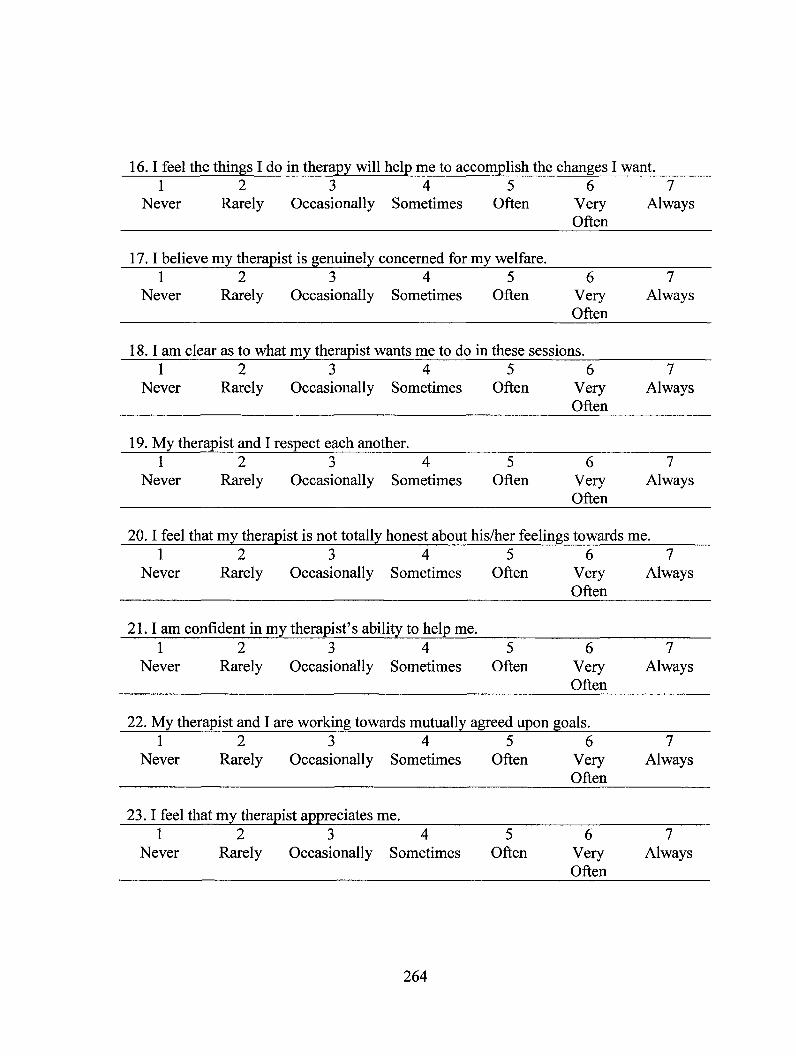
16. I feel the things I do in therapy will help me to accomplish the changes I want. 1 2 3 4
Never Rarely Occasionally Sometimes 5
Often 6
Very Often
7 Always
17. I believe my therapist is genuinely concerned for my welfare. 1 2 3 4
Never Rarely Occasionally Sometimes 5
Often 6
Very Often
7 Always
18. I am clear as to what my therapist wants me to do in these sessions. 1 2 3 4
Never Rarely Occasionally Sometimes 5
Often 6
Very Often
7 Always
19. My therapist and I respect each another. 1 2 3 4
Never Rarely Occasionally Sometimes 5
Often 6
Very Often
7 Always
20. I feel that my therapist is not totally honest about his/her feelings towards me. 1 2 3 4
Never Rarely Occasionally Sometimes 5
Often 6
Very Often
7 Always
21. I am confident in my therapist's ability to help me. 1 2 3 4
Never Rarely Occasionally Sometimes 5
Often 6
Very Often
7 Always
22. My therapist and I are working towards mutually agreed upon goals. 1 2 3 4
Never Rarely Occasionally Sometimes 5
Often 6
Very Often
7 Always
23. I feel that my therapist appreciates me. 1 2 3 4
Never Rarely Occasionally Sometimes 5
Often 6
Very Often
7 Always
264
16.1 feel the things I do in therapy will help me to accomplish the changes I want. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
17.1 believe my therapist is genuinely concerned for my welfare. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
18.1 am clear as to what my therapist wants me to do in these sessions. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
19. My therapist and I respect each another. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
20.1 feel that my therapist is not totally honest about his/her feelings towards me. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
21.1 am confident in my therapist's ability to help me. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
22. My therapist and I are working towards mutually agreed upon goals. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
23.1 feel that my therapist appreciates me. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
264

24. We agree on what is important for me to work on. 1 2 3
Never Rarely Occasionally 4
Sometimes 5
Often 6
Very Often
7 Always
25. As a result of these sessions, I am clearer as to how I might be able to change. 1 2 3
Never Rarely Occasionally 4
Sometimes 5
Often 6
Very Often
7 Always
26. My therapist and I trust one another. 1 2 3
Never Rarely Occasionally 4
Sometimes 5
Often 6
Very Often
7 Always
27. My therapist and I have different ideas on what my problems are. 1 2 3
Never Rarely Occasionally 4
Sometimes 5
Often 6
Very Often
7 Always
28. My relationship with my therapist is very important to me. 1 2 3
Never Rarely Occasionally 4
Sometimes 5
Often 6
Very Often
7 Always
29. I have the feeling that if I say or do the wrong things my therapist will stop working with me. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
30. My therapist and I collaborate on setting goals for my therapy. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
31. I am frustrated by the things I am doing in therapy. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
265
24. We agree on what is important for me to work on. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
25. As a result of these sessions, I am clearer as to how I might be able to change. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
26. My therapist and I trust one another. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
27. My therapist and I have different ideas on what my problems are. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
28. My relationship with my therapist is very important to me. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
29.1 have the feeling that if I say or do the wrong things my therapist will stop working with me. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
30. My therapist and I collaborate on setting goals for my therapy. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
31.1 am frustrated by the things I am doing in therapy. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
265

32. We have established a good understanding of the kinds of changes that would be good for me. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
33. The things that my therapist is asking me to do don't make sense. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
34. I don't know what to expect as a result of therapy. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
35. I believe the way we are working with my problem is correct. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
36. I feel my therapist cares about me even when I do things that he/she does no approve of. 1 2 3 4 5 6 7
Never Rarely Occasionally Sometimes Often Very Always Often
266
32. We have established a good xmderstanding of the kinds of chang good for me. 1 2 3 4 5
Never Rarely Occasionally Sometimes Often
;es that would be
6 Very Often
7 Always
33. The things that my therapist is asking me to do don't make sense. 1 2 3 4 5
Never Rarely Occasionally Sometimes Often 6
Very Often
7 Always
34.1 don't know what to expect as a result of therapy. 1 2 3 4 5
Never Rarely Occasionally Sometimes Often 6
Very Often
7 Always
35.1 believe the way we are working with my problem is correct. 1 2 3 4 5
Never Rarely Occasionally Sometimes Often 6
Very Often
36.1 feel my therapist cares about me even when I do things that he/she does of. 1 2 3 4 5
Never Rarely Occasionally Sometimes Often 6
Very Often
7 Always
no approve
7 Always
266

NML-2
Rate the extent to which each statement applies to you on a 6-point scale, ranging from 1, "not at all applicable" to 6, "very applicable".
to,,,,_,N. w , ,,
Not at all applicable -
Wry appiic le
6 1. My problems make me profoundly unhappy.
1 2 3 4 5
2. Because of my problems a number of people are extra nice to me.
1 2 3 4 5 6
3. I will do anything to get rid of my problems.
1 2 3 4 5 6
4. I do not believe that this is the right treatment for me.
1 2 3 4 5 6
5. I urgently need help in solving my problems.
1 2 3 4 5 6
6. I'm certain that I shall also practice at home the things I learn in treatment.
1 2 3 4 5 6
7. I expect to benefit more from therapy if I actively participate in it.
1 2 3 4 5 6
8. Actually, I embarked upon therapy on the insistence of other people.
1 2 3 4 5 6
9. I'm willing to put work or other activities aside in order to attend treatment sessions.
1 2 3 4 5 6
10. My problems make me feel ashamed.
1 2 3 4 5 6
11. I keep my appointment, no matter what.
1 2 3 4 5 6
12. I'm not very optimistic about the outcome of the treatment I'm about to begin.
1 2 3 4 5 6
13. I'm prepared to work on myself for awhile.
1 2 3 4 5 6
14. I think I'm difficult to treat. 1 2 3 4 5 6 15. I can really talk about my
problems with a number of people.
1 2 3 4 5 6
16. I'm willing to postpone other 1 2 3 4 5 6
267
NML-2 Rate the extent to which each statement applies to you on a 6-point scale, ranging from 1, "not at all applicable" to 6, "very applicable".
' ) * * - . . . » . . . , J* .. . . » . # *
1. My problems make me profoundly unhappy.
2. Because of my problems a number of people are extra nice to me.
3. I will do anything to get rid of my problems.
4. I do not believe that this is the right treatment for me.
5. I urgently need help in solving my problems.
6. I'm certain that I shall also practice at home the things I learn in treatment.
7. I expect to benefit more from therapy if I actively participate in it.
8. Actually, I embarked upon therapy on the insistence of other people.
9. I'm willing to put work or other activities aside in order to attend treatment sessions.
10. My problems make me feel ashamed.
11. I keep my appointment, no matter what.
12. I'm not very optimistic about the outcome of the treatment I'm about to begin.
13. I'm prepared to work on myself for awhile.
14. I think I'm difficult to treat. 15. I can really talk about my
problems with a number of people.
16. I'm willing to postpone other
Not at all Very applicable k , apflic#le
1
1
1
1
1
1
1
1
1
1
1
1
1
1 1
1
2
2
2
2
2
2
2
2
2
2
2
2
2
2 2
2
3
3
3
3
3
3
3
3
3
3
3
3
3
3 3
3
4
4
4
4
4
4
4
4
4
4
4
4
4
4 4
4
5
5
5
5
5
5
5
5
5
5
5
5
5
5 5
5
6
6
6
6
6
6
6
6
6
6
6
6
6
6 6
6
267
appointments to attend treatment.
17. The cause of my problems lies primarily in my circumstances.
1 2 3 4 5 6
18. I made the right decision in attending therapy.
1 2 3 4 5 6
19. I can only be helped by the very best therapist.
1 2 3 4 5 6
20. My problems make me a nuisance to others.
1 2 3 4 5 6
21. I do not know whether I'll find sufficient time to carry out homework assignments as well.
1 2 3 4 5 6
22. My problems will disappear of their own accord.
1 2 3 4 5 6
23. Previous treatment did not help me.
1 2 3 4 5 6
24. I've tried everything to get rid of my problems.
1 2 3 4 5 6
25. My problems do not bother me. 1 2 3 4 5 6 26. I can't help having problems. 1 2 3 4 5 6 27. I think it's a nuisance having to
carry out homework assignments as well.
1 2 3 4 5 6
28. I believe that this treatment will help me get rid of my problems.
1 2 3 4 5 6
29. Other people notice that I'm functioning less well.
1 2 3 4 5 6
30. I'm known as someone who perseveres.
1 2 3 4 5 6
31. I don't get much support from those around me.
1 2 3 4 5 6
32. Despite my problems I can function well in daily life.
1 2 3 4 5 6
33. There are more quarrels at home because of my problems.
1 2 3 4 5 6
34. If there was medicine that was effective for my problems as therapy, I would prefer to take that.
1 2 3 4 5 6
268
appointments to attend treatment.
17. The cause of my problems lies primarily in my circumstances.
18. I made the right decision in attending therapy.
19. I can only be helped by the very best therapist.
20. My problems make me a nuisance to others.
21. I do not know whether I' 11 find sufficient time to carry out homework assignments as well.
22. My problems will disappear of their own accord.
23. Previous treatment did not help me.
24. I've tried everything to get rid of my problems.
25. My problems do not bother me. 26. I can't help having problems. 27. I think it's a nuisance having to
carry out homework assignments as well.
28. I believe that this treatment will help me get rid of my problems.
29. Other people notice that I'm functioning less well.
30. I'm known as someone who perseveres.
31. I don't get much support from those around me.
32. Despite my problems I can function well in daily life.
33. There are more quarrels at home because of my problems.
34. If there was medicine that was effective for my problems as therapy, I would prefer to take that.
2
2
2
2
2
2
2
2
2 2 2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3 3 3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4 4 4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5 5 5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6 6 6
6
6
6
6
6
6
6
268
Appendix F
Online Classified Notice
Title: University of Regina seeking Volunteers!
We are looking for individuals aged 18-55 years to participate in an online questionnaire on health-related anxiety. Participation is voluntary and anonymous.
Time: 30 minute Internet based questionnaire
Compensation: All participants will be invited to enter their name in a draw for one of three $20 gift certificates.
This research has been approved by the University of Regina Ethics Board
Please visit the following website: http://www.surveymonkey.com/s/2X5YSMH In order to access the survey, you will need to type in the password: anxiety
Or you may contact Michelle Bourgault-Fagnou: bourmich uregina.ca or call 306-585-5369
269
Appendix F
Online Classified Notice
Title: University of Regina seeking Volunteers!
We are looking for individuals aged 18-55 years to participate in an online questionnaire on health-related anxiety. Participation is voluntary and anonymous.
Time: 30 minute Internet based questionnaire
Compensation: All participants will be invited to enter their name in a draw for one of three $20 gift certificates.
This research has been approved by the University of Regina Ethics Board
Please visit the following website: http://www.surveymonkev.eom/s/2X5YSMH In order to access the survey, you will need to type in the password: anxiety
Or you may contact Michelle Bourgault-Fagnou: [email protected] or call 306-585-5369
269

Appendix G
Information Sheet and Consent Form for Online Study
Information Page
Information for Potential Participants
Project Title: Testing the Efficacy of a Cognitive Behavioural Treatment of Health Anxiety Among Seniors
We are seeking volunteers aged 18 to 55 years to participate in a study examining health anxiety, which is worry you may experience due to bodily sensations or anxiety about health related information. This study is part of a larger study designed to examine the nature and extent of health anxiety among older adults and the efficacy of a cognitive behavioural treatment of health anxiety among seniors. By comparing older adults' scores to younger adults' scores on certain health anxiety measures, we hope to gain a greater understanding of the unique aspects of health anxiety among the older adult population. The principal investigator, Michelle Bourgault-Fagnou, is a Doctoral student in Clinical Psychology in the Department of Psychology, University of Regina. Her supervisor, Dr. Heather Hadjistavropoulos, is a Professor of Psychology, University of Regina.
Voluntary Participation Your participation in this research is completely voluntary. You have the right to withdraw at any time throughout the research project without any consequences or penalty.
Procedure If you agree to participate, you will complete a series of brief questionnaires online about your levels of health anxiety and related symptoms. As you complete the survey, your responses will be saved and you will be asked to click "Next" at the bottom of each page to move onto the next page of questions. At the conclusion of the survey, you will be asked to click "Done" to exit the survey. After you complete the survey, you may enter your e-mail address in a draw to win one of three $20 gift certificates.
Risks and Benefits There are no known risks associated with this online battery of questionnaires. The only cost to you will be the time required to complete the questionnaire. The
270
Appendix G
Information Sheet and Consent Form for Online Study
Information Page
Information for Potential Participants
Project Title: Testing the Efficacy of a Cognitive Behavioural Treatment of Health Anxiety Among Seniors
We are seeking volunteers aged 18 to 55 years to participate in a study examining health anxiety, which is worry you may experience due to bodily sensations or anxiety about health related information. This study is part of a larger study designed to examine the nature and extent of health anxiety among older adults and the efficacy of a cognitive behavioural treatment of health anxiety among seniors. By comparing older adults' scores to younger adults' scores on certain health anxiety measures, we hope to gain a greater understanding of the unique aspects of health anxiety among the older adult population. The principal investigator, Michelle Bourgault-Fagnou, is a Doctoral student in Clinical Psychology in the Department of Psychology, University of Regina. Her supervisor, Dr. Heather Hadjistavropoulos, is a Professor of Psychology, University of Regina.
Voluntary Participation Your participation in this research is completely voluntary. You have the right to withdraw at any time throughout the research project without any consequences or penalty.
Procedure If you agree to participate, you will complete a series of brief questionnaires online about your levels of health anxiety and related symptoms. As you complete the survey, your responses will be saved and you will be asked to click "Next" at the bottom of each page to move onto the next page of questions. At the conclusion of the survey, you will be asked to click "Done" to exit the survey. After you complete the survey, you may enter your e-mail address in a draw to win one of three $20 gift certificates.
Risks and Benefits There are no known risks associated with this online battery of questionnaires. The only cost to you will be the time required to complete the questionnaire. The
270
results of this study may help us gain more information on the nature and extent of health anxiety in the adult population.
Confidentiality You will not be asked to provide your name in order to complete this survey. Any information gathered from you for this study will be kept confidential by the researchers. All results will be summarized into group data, and no identifying information will be used in published works. If you provide your e-mail address for the gift certificate draw, it will not be linked to the information you provide.
Confidentiality and Internet Surveys There is a very small chance that your privacy may not be guaranteed by participating in this online study. Descriptions of the risks are listed below:
a. In order to protect the integrity of the study and to prevent multiple submissions from the same source this survey will record your computer's internet address. All Internet Service Providers assign an identification number to every computer. This number will be temporarily stored in a file until the research is completed. After completion of the research the principal investigator will delete the entire file. The principal investigator will not have access to this information, and it will not be used to identify individuals.
b. When submitting your survey answers via the Internet, there is small possibility your information will be intercepted by unauthorized third parties using sophisticated tools. It should be noted that this rarely occurs and is a risk that can occur at anytime, not just with online surveys, when using a computer connected to the internet.
c. Any computer connected to the Internet will store information about visited websites on the Internet browser's history list and its disk cache. The responses to this survey are only temporarily stored on your computer until you close down your browser window. In other words, after you complete and submit your survey, your computer will automatically delete this information. You may also delete this information by clearing your history list and disk cache.
d. After completion of your survey, the information will be sent directly to the survey software website. The information will then be sent to a private folder that is only accessible by the primary researcher. All responses will be downloaded daily and kept in a secure location by the researcher until completion of the study. The results will be stored on disks, and the information will not be linked to your Internet address.
271
results of this study may help us gain more information on the nature and extent of health anxiety in the adult population.
Confidentiality You will not be asked to provide your name in order to complete this survey. Any information gathered from you for this study will be kept confidential by the researchers. All results will be summarized into group data, and no identifying information will be used in published works. If you provide your e-mail address for the gift certificate draw, it will not be linked to the information you provide.
Confidentiality and Internet Surveys There is a very small chance that your privacy may not be guaranteed by participating in this online study. Descriptions of the risks are listed below:
a. In order to protect the integrity of the study and to prevent multiple submissions from the same source this survey will record your computer's internet address. All Internet Service Providers assign an identification number to every computer. This number will be temporarily stored in a file until the research is completed. After completion of the research the principal investigator will delete the entire file. The principal investigator will not have access to this information, and it will not be used to identify individuals.
b. When submitting your survey answers via the Internet, there is small possibility your information will be intercepted by unauthorized third parties using sophisticated tools. It should be noted that this rarely occurs and is a risk that can occur at anytime, not just with online surveys, when using a computer connected to the internet.
c. Any computer connected to the Internet will store information about visited websites on the Internet browser's history list and its disk cache. The responses to this survey are only temporarily stored on your computer until you close down your browser window. In other words, after you complete and submit your survey, your computer will automatically delete this information. You may also delete this information by clearing your history list and disk cache.
d. After completion of your survey, the information will be sent directly to the survey software website. The information will then be sent to a private folder that is only accessible by the primary researcher. All responses will be downloaded daily and kept in a secure location by the researcher until completion of the study. The results will be stored on disks, and the information will not be linked to your Internet address.
271

Questions and Contact Information Please feel free to contact any the researchers if you have additional questions about the procedures or purpose of this research. If you have questions about this study, feel free to e-mail the researcher, Michelle Bourgault-Fagnou, at [email protected] or call (306) 585-5369. You may also contact Dr. Heather Hadjistavropoulos, at [email protected] or call (306) 585-5133.
Ethics Approval This study has been approved by the Research Ethics Board at the University of Regina. If you have any questions about your rights as a participant in this study you can contact the Chair of the Research Ethics Board at the University of Regina at (306) 585-4775 or by e-mail: [email protected]. If you are calling long distance, please call collect.
Study Results_ A summary of study results will be posted on the website once all data have been collected-and analyzed. You may also contact the researchers, Michelle Bourgault-Fagnou or Dr. Hadjistavropoulos for the research findings. Please see contact information below.
If you prefer to correspond in writing, please use the addresses listed below:
Michelle Bourgault-Fagnou Department of Psychology University of Regina Regina, SK; S4S 0A2 E-mail: [email protected] Phone: (306) 585-5369
Dr. Heather Hadjistavropoulos Department of Psychology University of Regina Regina, SK, S4S 0A2 E-mail: [email protected] Phone: (306) 585-5133
272
Questions and Contact Information Please feel free to contact any the researchers if you have additional questions about the procedures or purpose of this research. If you have questions about this study, feel free to e-mail the researcher, Michelle Bourgault-Fagnou, at [email protected] or call (306) 585-5369. You may also contact Dr. Heather Hadjistavropoulos, at [email protected] or call (306) 585-5133.
Ethics Approval This study has been approved by the Research Ethics Board at the University of Regina. If you have any questions about your rights as a participant in this study you can contact the Chair of the Research Ethics Board at the University of Regina at (306) 585-4775 or by e-mail: [email protected]. If you are calling long distance, please call collect.
Study Results. A summary of study results will be posted on the website once all data have been collected and analyzed. You may also contact the researchers, Michelle Bourgault-Fagnou or Dr. Hadjistavropoulos for the research findings. Please see contact information below.
If you prefer to correspond in writing, please use the addresses listed below:
Michelle Bourgault-Fagnou Dr. Heather Hadjistavropoulos Department of Psychology Department of Psychology University of Regina University of Regina Regina, SK; S4S 0A2 Regina, SK, S4S 0A2 E-mail: [email protected] E-mail: [email protected] Phone: (306) 585-5369 Phone: (306) 585-5133
272
Consent Page
Project Title: Testing the Efficacy of a Cognitive Behavioural Treatment of Health Anxiety Among Seniors:
Are you 18 years of age or older? Yes No
Have you read and understood the information page? Yes No
Do you freely and voluntarily consent to take part in the research? Yes No
Completion of this online questionnaire implies consent to participate in this project.
If you have questions, you may e-mail the researcher, Michelle Bourgault-Fagnou, at [email protected] or 306-585-5369
Or, you may contact her supervisor, Dr. Heather Hadjistavropoulos, at heather.hadjistavropoulosguregina.ca or 306-585-5133
You may also contact the Chair of the Research Ethics Board at the University of Regina at (306) 585-4775 or by e-mail: [email protected]
273
Consent Page
Project Title: Testing the Efficacy of a Cognitive Behavioural Treatment of Health Anxiety Among Seniors:
Are you 18 years of age or older? Yes No
Have you read and understood the information page? Yes No
Do you freely and voluntarily consent to take part in the research? Yes No
Completion of this online questionnaire implies consent to participate in this project.
If you have questions, you may e-mail the researcher, Michelle Bourgault-Fagnou, at [email protected] or 306-585-5369
Or, you may contact her supervisor, Dr. Heather Hadjistavropoulos, at [email protected] or 306-585-5133
You may also contact the Chair of the Research Ethics Board at the University of Regina at (306) 585-4775 or by e-mail: [email protected]
273
Related Documents