1/11 Health and Human Rights with regard to Sanitation April 2013 Jorge Queiroz Introduction The scope of this paper is to provide a general dimension of what I consider to be one of the most vital and fundamental areas to human physical and mental health, and needless to say standard of living, which is conventionally known as sanitation 1 , with particular attention to how it is dealt with in Brazil, from a human rights, health and legal perspectives. Health, human rights and law have an extensive, long, intertwining and complex relationship internationally, and water and sanitation occupy a vital space in this field. When we speak of poor water quality and sanitation (which are directly interrelated), we speak of illnesses, poverty and risks to society. Lack of sanitation infrastructure also leads to devastating environmental problems, such as destruction/pollution of water sources (rivers, lakes, phreatic surface, and water basins), sea/shores, soil (agriculture) and air. This particular area represents a major problem for developing and underdeveloped countries 2 – 2.6 billion 3 low-income people are still without access 1 WHO definition: Sanitation generally refers to the provision of facilities and services for the safe disposal of human urine and feces. Inadequate sanitation is a major cause of disease world-wide and improving sanitation is known to have a significant beneficial impact on health both in households and across communities. The word 'sanitation' also refers to the maintenance of hygienic conditions, through services such as garbage collection and wastewater disposal. 2 World Bank/Global Practice Team Sanitation – The Political Economy of Sanitation: How can we increase investment and improve service for the poor/2011 – There is ongoing concern that governments, at many levels, are not devoting enough attention and resources to sanitation services. Existing sanitation investments and service provision rarely place sufficient stress upon the distinct and urgent needs of the poor. Enhance the design, implementation, and effectiveness of operations that provide pro-poor sanitation investments and services. The ultimate goal is to improve health and hygiene outcomes. The Action Framework stresses the importance of strengthened relationships of accountability among citizens, civil society organizations, and government and other service providers. While studies came across evidence of corrupt practices and rent-seeking behavior, it was overall not identified as the predominant feature distorting sanitation investment decisions. There is evidence that civil society and the private sector not only can contribute to strengthening accountability but also can be reliable and trusted partners for delivering sanitation services and creating community demand for sanitation provision. 3 Human Development Report 2006 (UNDP 2006) – about half of the world’s population lack access to basic sanitation.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1/11
Health and Human Rights with regard to Sanitation
April 2013
Jorge Queiroz
Introduction
The scope of this paper is to provide a general dimension of what I
consider to be one of the most vital and fundamental areas to human physical and
mental health, and needless to say standard of living, which is conventionally
known as sanitation1, with particular attention to how it is dealt with in Brazil, from
a human rights, health and legal perspectives.
Health, human rights and law have an extensive, long, intertwining and
complex relationship internationally, and water and sanitation occupy a vital space
in this field. When we speak of poor water quality and sanitation (which are
directly interrelated), we speak of illnesses, poverty and risks to society. Lack of
sanitation infrastructure also leads to devastating environmental problems, such
as destruction/pollution of water sources (rivers, lakes, phreatic surface, and water
basins), sea/shores, soil (agriculture) and air.
This particular area represents a major problem for developing and
underdeveloped countries2 – 2.6 billion3 low-income people are still without access
1 WHO definition: Sanitation generally refers to the provision of facilities and services for the safe disposal
of human urine and feces. Inadequate sanitation is a major cause of disease world-wide and improving sanitation is known to have a significant beneficial impact on health both in households and across communities. The word 'sanitation' also refers to the maintenance of hygienic conditions, through services such as garbage collection and wastewater disposal. 2 World Bank/Global Practice Team Sanitation – The Political Economy of Sanitation: How can we increase
investment and improve service for the poor/2011 – There is ongoing concern that governments, at many levels, are not devoting enough attention and resources to sanitation services. Existing sanitation investments and service provision rarely place sufficient stress upon the distinct and urgent needs of the poor. Enhance the design, implementation, and effectiveness of operations that provide pro-poor sanitation investments and services. The ultimate goal is to improve health and hygiene outcomes. The Action Framework stresses the importance of strengthened relationships of accountability among citizens, civil society organizations, and government and other service providers. While studies came across evidence of corrupt practices and rent-seeking behavior, it was overall not identified as the predominant feature distorting sanitation investment decisions. There is evidence that civil society and the private sector not only can contribute to strengthening accountability but also can be reliable and trusted partners for delivering sanitation services and creating community demand for sanitation provision. 3 Human Development Report 2006 (UNDP 2006) – about half of the world’s population lack access to basic
sanitation.
2/11
to improved sanitation worldwide4. Among the diseases caused by poor water
quality and sanitation are: diarrhoea, dengue fever5, hepatitis A, arsenicosis,
cholera, fluorosis, intestinal diseases, leptospirosis, malaria, schistosomiasis,
trachoma, typhoid.6 These illnesses will generate a host of other health problems,
many times causing permanent damage upon those infected, including death.
Over one-third of the world's population has no access to sanitation
facilities.
In developing countries, about 80% of illnesses are linked to poor water and
sanitation conditions.
At any one time, half of the world's hospital beds are occupied by patients
suffering from water-borne diseases.
1 out of every 4 deaths under the age of 5 worldwide is due to a water-
related disease.7
Case Analysis - Brazil
Improvement in water and sanitation infrastructure is at the top of the
agenda in Brazil8. Sewage is the main cause of water and soil contamination in
Brazil’s metropolitan areas and has a significant impact on the society as a whole,
more so on the poor living in its slums9 (favelas10), generating major health
4 WHO/UNEP – Going back in history, before the industrial revolution, it was possible to withdraw and
consume water to everyone’s satisfaction However, times have changed as demographic pressure in the last three centuries (for example, 1 billion inhabitants in 1800, 2 billion in 1900 and 6.6 billion at the end of 2007) no longer allows for the management of water without cooperation among communities. 5 Centers for Disease Control and Prevention – CDC reports that with more than one-third of the world’s
population living in areas at risk for transmission, dengue infection is a leading cause of illness and death in the tropics and subtropics. Dengue Fever (DF) and Dengue Hemorrhagic Fever (DHF) 6 WHO/UNICEF 2012
7 The Water Project – NGO 2012
8 Diverse legislation has been introduced in Brazil since late 1990’s.
9 UN 2012 defines slum as a run-down area of a city characterized by substandard housing, squalor, and
lacking in tenure security, combining to various extents the following particularities: inadequate access to safe water; little or no access to sanitation and other infrastructure; poor structural quality of housing; overcrowding; and insecure residential status (lack of personal/community land ownership). Slums are usually inhabited by the very poor or socially disadvantaged. Slum buildings vary from simple, one to multi-layered, shacks to permanent and well-maintained structures. About one billion people worldwide live in slums and this number is expected to double by 2030 10
Brazilian Institute of Geography and Statistics (IBGE) Demographic Census 2010 – 11.425.644 people in Brazil (6% of the population) live in subnormal poverty clusters - slums (favelas), property invasions, gullies, swamp houses, and the like. These types of poverty concentrations are also formed by narrow alleys of difficult personal access – and access by any public service. The lack of services such as routine garbage collection allows rubbish to accumulate in huge quantities. The lack of infrastructure such as sanitation is
3/11
problems – over 11 million people live in poverty clusters in Brazil (6% of the
population)
The vast majority of the population in Brazil live in metropolitan centers
and less than 20% of the sewage produced in urban areas is treated11, one of the
reasons being that slum dwellers do not have legal title of the land. Sewage that is
not treated ends up every day ‘in natura’ in rivers, lakes, hydrographic basins and
sea, with severe damage to the environment and health12.
In order for Brazil to reach universal access to sanitation, it would need
to invest substantially more than today – that is, 0.63% of GNP ($15.6 billion/year)
when a mere 1/3 of that ($5.4 billion/year) is currently invested.13 Only half of the
population has access to sewage collection system14 – in other words, roughly 100
million men, women and children in Brazil do not have access to this basic human
right to health, essential to their dignity. About 25% of the population does not
have access to treated water.15
Advances made in the last decades were largely offset by the rather
high rate of population growth, among other reasons – such as political resolve, for
instance.
“In socially and economically dynamic Brazil, persistence of sanitation
problems, although decreasing over time, remains a source of
embarrassment, as sanitation (especially sanitary sewerage) is
associated with modern society.”16
To put it into perspective, Brazil’s population went from 50 million to
almost 200 million people from 1970 to 2012 respectively. It is still characterized
by its dramatic inequality and concentration of income – in 2010 half of its families
also caused by the informal nature of settlement. Informal settlements also face the brunt of natural (tropical storms) and man-made disasters, such as floods and landslides. 11
Agencia Nacional de Aguas/ANA – Brazil’s National Department of Waters 12
ANA Brasil 13
IBGE 2010 – Istituto Brasileiro de Geografia e Estatistica / Brazilian Institute of Geography and Statistics – Síntese dos Indicadores de 2009 14
IBGE 2008 – Instituto Brasileiro de Geografia e Estatistica / Brazilian Institute of Geography and Statistics – Pesquisa Nacional de Saneamento Basico – National Data about Sanitation – In 2008 56% of domiciles did not have access to sewage collection. 15
Ministry of Cities, Department of Sanitation - SNIS 2010 – Sistema Nacional de Informacoes em Saneamento 2010 16
The World Bank – WSP/Water and Sanitation Program, The Political Economy of Sanitation – February 2011
4/11
lived on less than US$ 200 per month; the 10% richer accounted for 45% of total
income while the 10% poorer accounted for only 1%.17
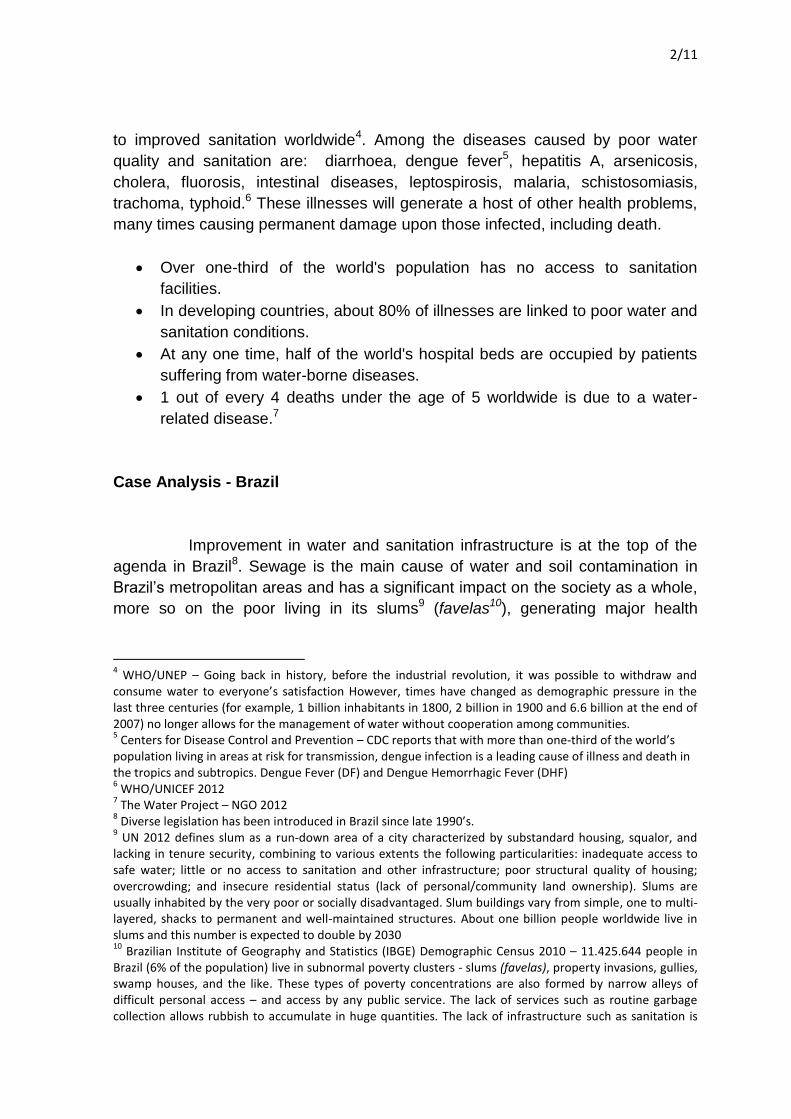
Dengue Fever and Dengue Hemorrhagic Fever18
Dengue fever19 (transmitted by the Aedes Aegypti mosquito which
belongs to the same family of that of yellow fever20) is directly linked sanitation
problems.
Dengue has emerged as a worldwide problem only since the 1950s and
it is endemic in Latin America and Southeast Asia.21
17
IBGE – Instituto Brasileiro de Geografia e Estatistica / Brazilian Institute of Geography and Statistics 18
See supra, page 1, introduction 19
Dengue fever is one of the main public health problems on earth (Brazil’s Ministry of Heath). 20
Instituto Oswaldo Cruz. Existence of the dengue virus in Brazil was proven by laboratorial analysis only in 1982. From 1982 to 2011 four types of dengue virus were identified. There is no vaccine to prevent dengue in the world. 21
WHO 2012
5/11
The incidence of dengue has grown dramatically around the world in
recent decades. Over 2.5 billion people – over 40% of the world's population – are
now at risk from dengue and as many as 100 million people are infected yearly. An
estimated 500 000 people with severe dengue require hospitalization each year, a
large proportion of whom are children. About 2.5% of those affected die.22
The threat of a possible outbreak of dengue fever now exists in Europe
and local transmission of dengue was reported for the first time in France,
Portugal, Croatia and other countries.
Aedes Aegypti Mosquito (Dengue Mosquito)
Dengue Fever in Brazil
Dengue fever reappeared in Brazil in 197623 and became critical in the
end of 1990s due to the fact that traditional methods employed were not effective
and that the dengue mosquito adapted quite well to the new environment created
by the accelerated disorganized increase of urban areas and corresponding
number of informal settlements (favelas and the like) together with the lack of
sanitation.
22
WHO 2012 23
According to CDC 2010 – Center for Disease Control and Prevention – dengue has emerged as a worldwide problem only since the 1950s. As many as 100 million people are infected yearly worldwide. The Pan-American Health Organization (PAHO/WHO) relates greater incidence of dengue and its expansion to regions not affected before to the global warming effect.
6/11
With this scenario the Ministry of Health created the Program for
Eradication of Dengue24 in 1996.25
The appearance of a new serotype (dengue 3) in Brazil in late 1990s,
which in the period of only three months spread to eight states made it clear that
there was a high risk of a new epidemic of dengue fever (DF) and dengue
hemorrhagic fever (DHF).
It has been a major health/sanitation related problem since then.26 This
alarming fact led to the intensification of governmental actions to combat the
dengue in 2002 through formal/specific nationwide federal programs, a task force
among federal, state and municipal authorities which proved to be quite effective,
reducing the incidence of dengue by 73% during the first six months of 2004.27
Nevertheless, it reached new epidemic levels in first quarter of 2013 (635
thousand cases/108 deaths in only 3 months) with an increase of 279% in
comparison to same period in 201228.
24
Programa de Erradicacao do Aedes Aegypti – PEAa 25
Among its findings were the fact that dengue could be solved only on a mid/long term basis. Only in 1995 the reporting of dengue infections became mandatory in Brazil. 26
Brazil’s Ministry of Health 2002 – Epidemic Surveillance 27
In 2002 the Ministry of Health created the PNCD – Programa Nacional de Controle da Dengue (National Program for the Control of Dengue). Further on (2003) and within the PNCD, it created and coordinated the National Mobilization Program against the Dengue with the participation of 40 representative departments, agencies and organizations in the country. Incidence was reduced by 73% from the first six months of 2003 to the same period in 2004 – down from 300 thousand to 84 thousand people infected nationally. Brazil’s Ministry of Health issued an epidemic alert due to the dramatic increase of reported cases of dengue fever in the first quarter of 2013 where it registered an increase of 279% in comparison to same period in 2012. In a period of only three months from Jan-Mar 2013, 635.161 cases were registered, among which 1.243 were considered serious with 108 deaths caused by dengue haemorrhagic fever.
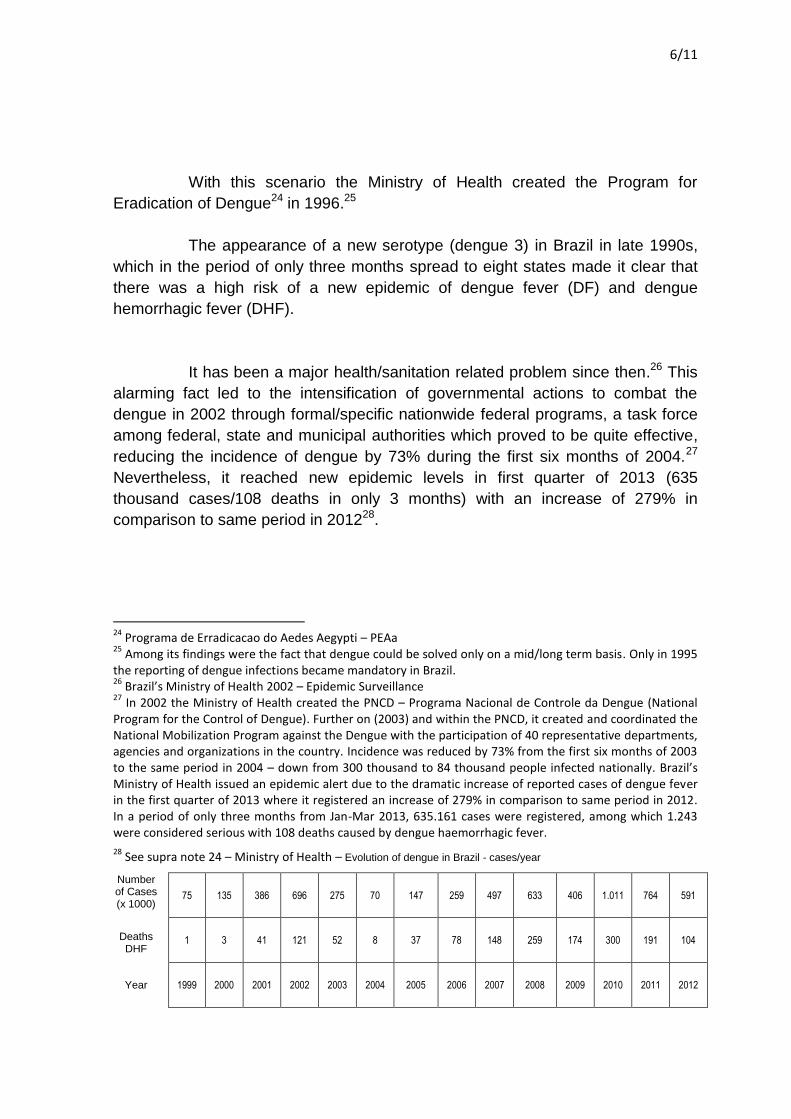
28 See supra note 24 – Ministry of Health – Evolution of dengue in Brazil - cases/year
Number of Cases (x 1000)
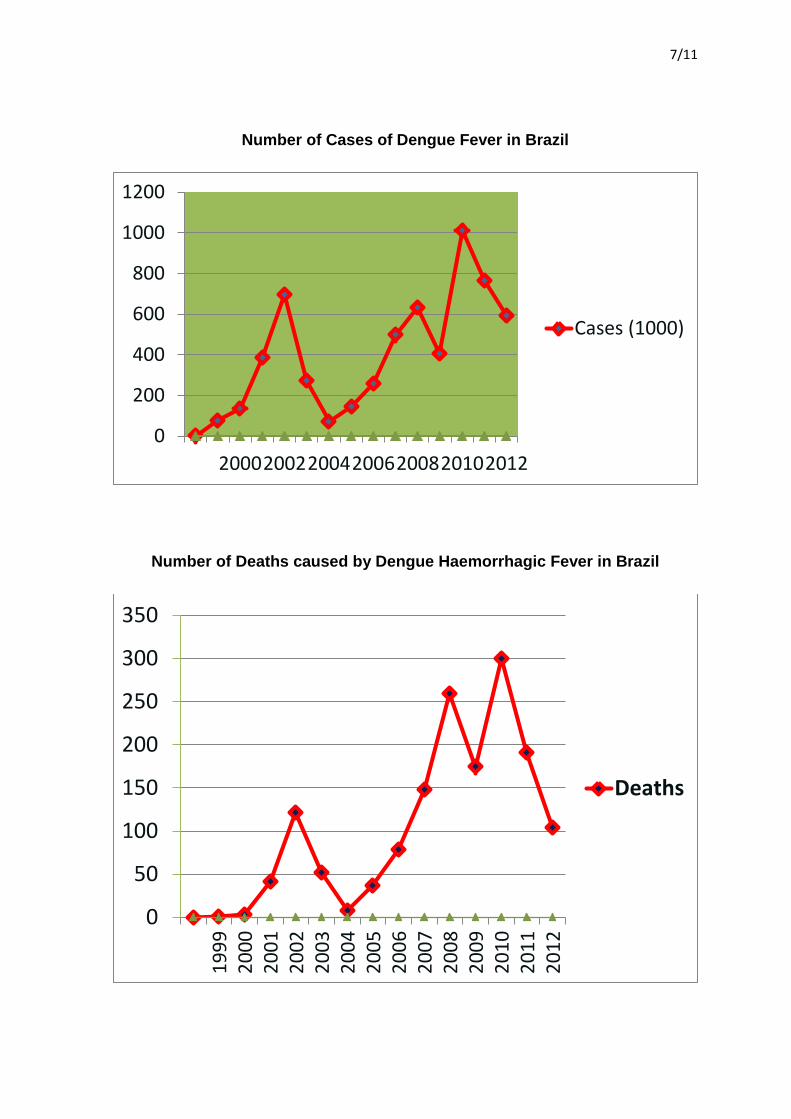
75 135 386 696 275 70 147 259 497 633 406 1.011 764 591
Deaths DHF
1 3 41 121 52 8 37 78 148 259 174 300 191 104
Year 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
7/11
Number of Cases of Dengue Fever in Brazil
Number of Deaths caused by Dengue Haemorrhagic Fever in Brazil
0
200
400
600
800
1000
1200
2000200220042006200820102012
Cases (1000)
0
50
100
150
200
250
300
350
19
99
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
20
09
20
10
20
11
20
12
Deaths
8/11
Legal Framework – Brazil
Sanitation is a theme addressed in Brazil’s Constitutional Reform of
1988. The constitution establishes how water and sanitation must be handled by
the three spheres of power – federal, state and municipal. It also determines that
all water resources including rivers, lakes and water basins are property of the
Brazilian State.
The principle of autonomy of the 26 different States and the capital
Brasilia, and that of distribution of powers are part of the essence of Brazil’s
constitutional pillars. The nature of these powers is political-administrative
(president/ governors/ mayors) and legislative (federal, state, municipality).
The constitution determines that all three spheres of power have the
political and administrative obligation to manage and control public health, to
protect the environment and control any and all forms of pollution (art. 23). Art. 241
establishes that the three levels of power must apply the entirety principle to the
administration of public services:
Art. 241 The three spheres of power shall discipline via legislation
the public partnerships and the partnerships of cooperation among
the three levels, authorizing joint-administration of public services
as well as total or partial transfer of responsibilities, services,
personnel and assets which are essential to the continuity of
services transferred.
Nonetheless, the specific matter of legislation regarding water systems,
sanitation, environmental protection and pollution control is under exclusive federal
jurisdiction. It must be noted that sanitation is inserted under the broader context
of Water Systems, art. 22 IV of the constitution, and that legislation related to the
use of waters, criteria to be adopted and priorities for its use are of sole federal
responsibility.
9/11
As determined by its art 21 XIX, federal law (Nr. 9433 of 1997) created
the Brazilian System for the Management of Water Systems29 and the National
Department of Waters – (L9984/2000)30.
Art. 21 XX prescribes that definition of directives for urban development,
including housing, sanitation and urban transportation, is also under federal
jurisdiction.
It is the responsibility of Congress and the President to provide
legislation establishing the rules that govern the area of Sanitation in Brazil.
Federal law 11445 (2007) stipulates the national sanitation directives as well as
federal sanitation policies. Public services related to sanitation need to comply with
the following fundamental principles:
Universality of access
Health and environmental safety
Efficiency and sustainability
Social participation
Safety, quality and regularity
Integration of sanitation infrastructure and services with the
efficient management of water sources
Brazil’s constitution determines that water resources are not part of the
public sanitation services. The use of water resources in public sanitary services,
including sewage collection, transportation and treatment, is subject to the federal
concession of right of use, regulations and state legislations in accordance to
federal law (L9433/97).
As a result of Brazil’s continental size (world’s 5th largest, closely
following Canada, China, US with Russia being an isolated 1st) with near 200
million people (also 5th)31 to be serviced, as well as the number of states and
municipalities involved in the sanitation and water supply systems, there is a
multiplicity of principals and agents involved in the complete process.
In observance to federal statute, Brazil employs a mixed system for the
operation of the sanitation services and stimulates cooperation among federal,
state and municipal levels. The result is a complex and gigantic network which
includes the 26 states, the capital and over 5570 municipalities.
29
Sistema Nacional de Gerenciamento de Recursos Hidricos 30
Agencia Nacional de Aguas – ANA (Ministry of Environment) 31
The World Bank 2012
10/11
As prescribed by law, in principle it is the responsibility of the
municipality to operate the sanitation system as a whole, with the exception of
water supply, which includes waste disposal, transportation and treatment, and all
interrelated services (control, public health, environment, and others) as well as
planning, construction and management of all necessary infrastructures.
In many cases such as the State of Sao Paulo, the system is operated
by a mixed capital corporation (SABESP) dully licensed to perform the sanitation
and water supply services in the greater metropolitan area of its capital (the city of
Sao Paulo) and other municipalities which together consist of a total of 365
municipalities in the state. It is the larger and most efficient sanitation and water
company in Brazil, providing32:
100% of treated water to 27.7 million people
Sewage collection to 90% of the area under its responsibility
Sewage treatment to 88% of the area covered
In number of customers (27.7 million), it is among the largest
sanitation companies in the world – it provides services to 67.2%
of the population of the whole Sao Paulo State (41.2 million
people), corresponding to almost twice the population of
Belgium. The Sao Paulo metropolitan area alone has a
population of 20 million people (Shanghai has approximately 23
million people; Beijing – 20 million; Mumbai – 18.4 million)
Number of employees – 14,896
Municipalities serviced – 365, which include the large
metropolitan area of the city of Sao Paulo (Sao Paulo state total
– 645)
Since 2002 its shares are listed in the Sao Paulo and New York
stock exchanges
New horizons – in addition to the State of Sao Paulo, it is now
ready to expand its activities to other states and countries
It is important to observe that SABESP does not operate in slums
(favelas) because of legal, technical, operating and environmental constraints33.
The number of people that live in what is officially classified as overcrowded
32
SABESP – Companhia de Saneamento Básico do Estado de São Paulo 33
Legal – no legal title of land (informal settlements), pathways do not exist for legal purposes / Technical-operating-logistics – narrow and winding (many times steep) alleys of difficult or no viable access; drug dealing and crime poses an additional problem / Environmental – many dwellings located in environmental sensitive areas (pollution, landslides, floods)

11/11
subnormal poverty concentrations in the Sao Paulo metropolitan area totals 2.2
million34.
Conclusions of Case Analysis
Brazil is a nation of contrasts, that carries the stigma of inequality which
places the country still far from fulfilling the right to dignity of millions of its citizens:
rich/poor, rich country/poor people, world’s 6th largest economy/85th ranking in
United Nation’s Human Development Index (HDI). It has a long-standing,
structurally poor social legacy of inequality and poverty with its origin in political-
administrative inefficiencies and corruption, with enormous health, environmental,
educational, socioeconomic and welfare hurdles to overcome.
In the area of sanitation Brazil has made significant progress in the last
decades and still has a long way to go as it ranks 9th in number of people without
toilets at home.35 It has a good legal framework to support the initiatives needed in
its route to universalization of the access to sanitation by its 200 million people.
Nevertheless, Brazil will not solve this problem of gigantic, ever growing, atypical
and unimaginable proportions with typical initiatives – solution necessarily goes
through political resolve and unconventional methods and efforts of the equal
dimension of the problem.
Most important is the fact that there is greater awareness and
involvement in the part of the society in a clear demonstration that it wants
concrete advances in these interconnected social, civil and human rights’ areas.
34
IBGE - 2010 Demographic Census (Brazilian Institute of Geography and Statistics) 35
WHO 2012
Related Documents











