Headache Dr. M. Aufa N

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

HeadacheDr. M. Aufa N

Nyeri kepala
primer
migrain
Tension type
headache
Cluster headache
sekunder
Headache
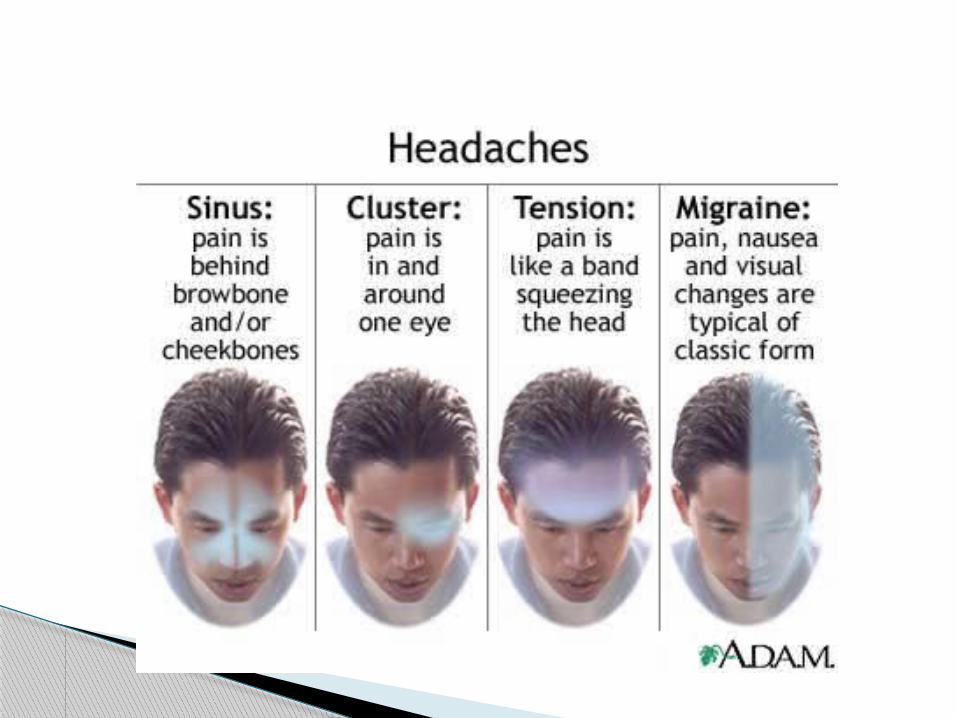

PRIMARY HEADACHE

Pulsatile Unilateral 4 – 72 hours Can’t do ADL (not relieving by rest) Can followed by : Photophobia &
Phonophobia (classical / aura)
Migrain

Stress Foods : MSG, tyramine, nitrite Coffein withdrawal Too little or too much sleep
Precipitating migrain

Non pharmacology :◦ Relaxation technique◦ Biofeedback◦ Dark, quite room◦ Avoid trigger◦ Adequate sleep, Avoid excessive sleep◦ Regular exercise
Migraine management

Pharmacologic :◦ Abortive
Ergotamine Sumatriptan
◦ Preventive Beta blocker Tricyclic antidepressant Asam valproate Calcium channel blocker
Migraine management

All round Tight like headache Pericranial muscle tenderness Relieving by rest Stress factor
Tension type headache

Strictly unilateral Ipsilateral autonomic symptoms –at least one of:
conjunctival injection, nasal blockage, facial sweating, miosis,ptosis
Bouts-typically 1/year lasting 6-12 weeks with discrete headaches 1-8times /day each lasting 30-60 mins
Age 20-40 M>F=7:1 Headache severe/excrutiating- restless
“banging head against wall”
Cluster headache

Subcutaneous sumatriptan 6mg
High dose/high flowrate oxygen
Intranasal triptans- not so effective
Cluster headaches-abortive treatment

Verapamil 240-960mg/day ( ECG)-bradycardia,hypotension,arrythmias,constipation,fatigue,oedema
Lithium 400-2000mg/day hypothyroidism,Diabetes insipidus, tremor,nausea, wt gain ataxia drowsiness, confusion seizure
Methylsergide 3-12mg/day vascular constrictive phenomena, fibrotic reactions ,muscle cramps, abdominal discomfort weight gain, mood change
Transitional treatments:High dose corticosteroids- 1mg/kg ( up to 60mg
daily for 5 days tapering over 2-3 weeks
rapid onset of action. Attack recurs once dose reduced. Initial add-on until other preventatives are effective
Cluster headache- preventive treatments

vertigo
Periferberputar
Neuritis vestibularis &
LabirinitisRiw infeksi +
lama
BPPV Perub posisi
+ detik
Menieretinitus
Sentraldizzines
- Cerebellum- Brain stem
13
vertigo

14

15
Dix Hallpike manouver (1)

16
Dix Hallpike manouver (1)

17
Pengobatan – Brand daroft

Terima kasih
Related Documents











