HEAD INJURY DR RAJESH T EAPEN ATLAS HOSPITAL RUWI MUSCAT

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

HEAD INJURY
DR RAJESH T EAPEN
ATLAS HOSPITAL
RUWI
MUSCAT
Any degree of traumatic brain injury ranging from
scalp laceration to LOC to focal neurological
deficits
Head Injury

Head injuries are among the most common types of trauma
encountered in emergency departments (EDs).
Many patients with severe brain injuries die before reaching a
hospital, with almost 90% of prehospital trauma-related deaths
involving brain injury.

About 75% of patients with brain injuries who receive medical
attention can be categorized as having minor injuries, 15% as
moderate, and 10% as severe.
Most recent United States data estimate 1,700,000 traumatic
brain injuries (TBIs) annually, including 275,000
hospitalizations and 52,000 deaths.


Head Injury
Causes
• Motor vehicle accidents
• Falls
• Assaults
• Sports-related injuries
• Firearm-related injuries

Head Injury
High potential for poor
outcome
Deaths occur at three points
in time after injury:
•Immediately after the injury
•Within 2 hours after injury
•3 weeks after injury

Head Injury
TYPES:
• Scalp laceration
• Skull Fractures
• Minor Head Trauma
Concussion and post-
concussion syndrome
• Major Head Trauma:
Cerebral contusion
Laceration

Intracranial Perfusion
Cranial volume fixed80% = Cerebrum, cerebellum & brainstem
12% = Blood vessels & blood
8% = CSF
Increase in size of one component
diminishes size of another
Inability to adjust = increased ICP

Head Injury
Scalp lacerations
• The most minor type of head trauma
• Scalp is highly vascular - profuse
bleeding
• Major complication is infection

Head Injury
Skull fractures :
• Linear Skull Fracture
• Depressed Skull Fracture
• Diastatic Skull Fracture
• Basal Skull Fracture
• Compound Skull Fracture
• Compound elevated Skull
Fracture
• Growing Skull Fracture
• Coup & Countercoup

Head Injury
• Skull fractures
Location of fracture alters the presentation of
the manifestations
• Facial paralysis
• Conjugate deviation of gaze
• Battle’s sign, Raccoon eyes

Basilar Skull Fracture
Battle’s sign Raccoon eyes

Basal Skull fractures
• CSF leak (extravasation) into
ear (Otorrhea) or nose
(Rhinorrhea)
• High risk infection or
meningitis
• ―HALO Sign ‖ on clothes or
linen
• Possible injury to Internal
carotid artery
• Permanent CSF leaks
possible
“HALO Sign ”
Head Injury

Investigations
• X-ray
• CT scan: standard modality
• MRI
• Bleeding from the ear or nose in cases of
suspected CSF leak -"halo" or "ring" sign ,
when dabbed on a tissue paper
• CSF leak - analyzing the glucose level and
by measuring tau-transferrin.

Management
Pre-hospital care:
• Patients with severe head injuries should be
assumed to have a cervical spine (C-spine) injury
and immobilized with cervical collar until clinical and
radiographic studies can prove otherwise
• Minimize CSF leak
• Bed flat
• Never suction orally; never insert NG tube; caution
patient not to blow nose
• Place sterile gauze/cotton ball around area
Definitive Rx:
• Measures to reduce ICP
• Supportive management
• Surgery

Head Injury
Minor head trauma
Concussion : head injury with a temporary
loss of brain function concussion can
cause a variety of physical, cognitive , and
emotional symptoms.
Cause: Sudden acceleration and
deceleration injury e.g.: Car accident,
sports injury, bicycle accident etc.

Head Injury
Types of Head Injuries
Concussion
Presentation:
Physical-headache, LOC, Amnesia,
s/s of ↑ ICP(Cushing’s triad) , convulsions
Cognitive : confusion, irritability, behavioral
changes

Head Injury
Minor head trauma
• Post-concussion syndrome
• 2 weeks to 2 months
• Persistent headache
• Lethargy
• Personality and behavior changes

Head Injury
Major head trauma
• Includes cerebral contusions and lacerations
• Both injuries represent severe trauma to the
brain

Head Injury
Major head trauma
Contusion
The bruising of brain tissue within a focal area
that maintains the integrity of the pia mater and
arachnoid layers associated with multiple micro-
hemorrhages, small vessel bleed into brain
tissue
Lacerations
Involve actual tearing of the brain tissue
Intracerebral hemorrhage is generally
associated with cerebral laceration

Cerebral Contusion Cerebral Laceration
Head Injury

Head Injury
Pathophysiology
Diffuse axonal injury (DAI)• Widespread axonal damage occurring after a mild, moderate,
or severe TBI
• Seen in half the cases of head injury
• Process takes approximately 12-24 hours

Head Injury
Pathophysiology
Diffuse axonal injury (DAI)Clinical signs:
• Level of Consciousness
• ICP
Decerebration or decortication
Global cerebral edema
90% regain consciousness from severe DAI

Intracranial Hemorrhage
• Extra- axial hemorrhage
Epidural hematoma
Subdural hematoma-
Acute
Chronic
Subarachnoid hemorrhage
• Intra-axial hemorrhage
• Intra-parenchymal
hemorrhage
• Intra-ventricular hemorrhage

Epidural and Subdural Hematomas
Epidural Hematoma
Subdural Hematoma
Epidural and Subdural Hematomas
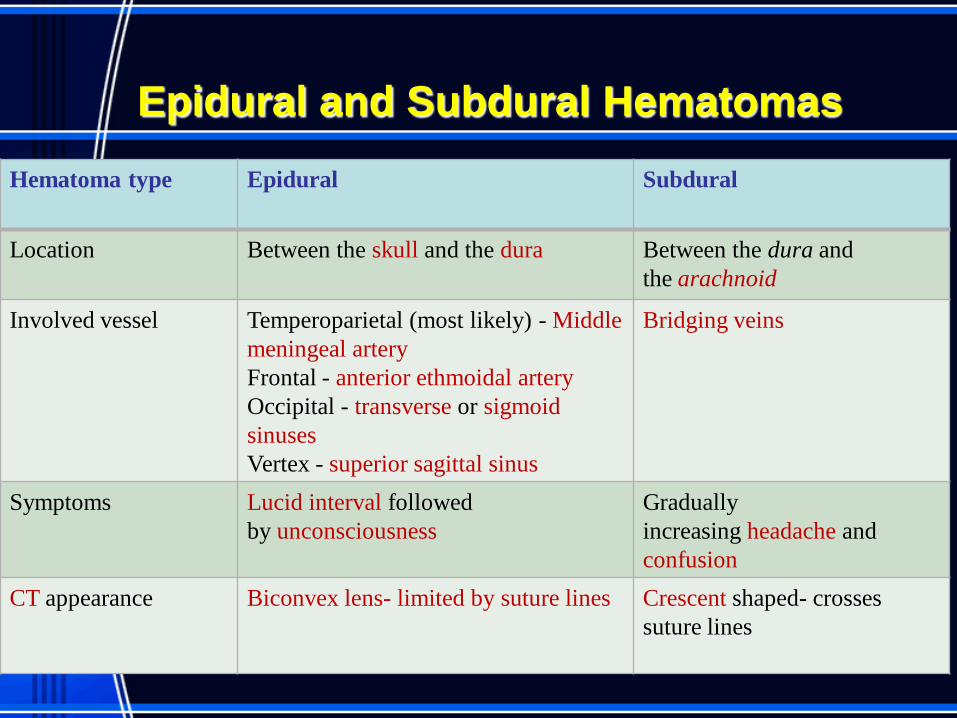
Hematoma type Epidural Subdural
Location Between the skull and the dura Between the dura and
the arachnoid
Involved vessel Temperoparietal (most likely) - Middle
meningeal artery
Frontal - anterior ethmoidal artery
Occipital - transverse or sigmoid
sinuses
Vertex - superior sagittal sinus
Bridging veins
Symptoms Lucid interval followed
by unconsciousness
Gradually
increasing headache and
confusion
CT appearance Biconvex lens- limited by suture lines Crescent shaped- crosses
suture lines

Subarachnoid Hemorrhage
Causes:
• Rupture of Berry aneurism(MCC)
• Trauma (fracture at the base of the skull
leading to internal carotid aneurysm)
• Amyloid angiopathy
• Blood dyscrasias
• Vasculitis
Clinical Features:
• Explosive or thunderclap headache, ―worst
headache of my life‖,
• Nausea and vomiting, decreased LOC or
coma.
• Signs of meningeal irritation

Intracerebral Hemorrhage (ICH)
Intracranial hemorrhage is hemorrhage that occurs
within the brain tissue itself; an intra-axial
hemorrhage.
Two main types:
• Intraparencymal hemorrahge- ICH extending into
brain parenchyma; MCC- HTNsive vasculopathy
• Intra-ventricular hemorrhage- ICH extending into
ventricles; MCC –trauma
Causes:
Hypertensive vasculopathy(70-80%)
Ruptured AVM
Trauma
Blood dyscrasias

Intracerebral Hemorrhage (ICH)
Clinical presentation: Rapidly progressive severe
headache, building over several minutes, often
accompanied by focal neurological deficits, nausea and
vomiting, decreased level of consciousness.
S/S depend site of hemorrhage:
Basal ganglia/internal capsule - hemiparesis,
dysphasia
Cerebellum - ataxia, vertigo
Pons - cranial nerve deficits, coma
Cerebral cortex- hemiparesis, hemi-sensory loss,
hemi-anopsia, dysphasia

Complications
• Neurological deficits or death
• Seizures
• Obstructive Hydrocephalus
• Spasticity
• Urinary complications
• Aspiration pneumonia
• Cushing’s ulcer
• Neuropathic pain
• Deep venous thrombosis
• Pulmonary emboli
• Cerebral herniation

Glasgow Coma Scale
Suspect severe brain injury GCS <9
32
*Decorticate posturing to pain
**Decerebrate posturing to pain



Diagnostic Studies
CT scan –
A GCS score less than 15 after blunt head
trauma warrants a patient with no intoxicating
consideration of an urgent CT scan.

CT findings
Epidural Hematoma Subdural Hematoma

CT findings
Subarachnoid hemorrhage Intracerebral hematoma

Diagnostic Studies
• MRI – superior for demonstrating the size of an acute
subdural hematoma.
• Cerebral angiogram if hemorrhage is confirmed (not
necessary in case of classic hypertensive hemorrhage)
• Cervical spine X-ray
• EEG
• Lumbar Puncture

Management
1) Supportive Measures:
• Endotracheal intubation for patients with
decreased level of consciousness and poor airway
protection.
• Cautiously lower blood pressure to a MAP less
than 130 mm Hg, but avoid excessive
hypotension.[10]
• Rapidly stabilize vital signs, and simultaneously
acquire emergent CT scan.
• Maintain euvolemia, using normotonic rather than
hypotonic fluids, to maintain brain perfusion
without exacerbating brain edema
• Avoid hyperthermia.
• Facilitate transfer to the operating room or ICU.

Management
2) Decrease cerebral edema:
• Modest passive hyperventilation to reduce
PaCO2
• Mannitol, 0.5-1.0 gm/kg slow iv push
• Furosemide 5-20 mg iv
• Elevate head 20-30 degrees, avoid any neck
vein compression
• Sedate and paralyze if necessary with
morphine and vecuronium (struggling, coughing
etc will elevate intracranial pressure)

Management
3) Surgical Evacuation of hematoma:No surgical intervention if collection <10ml
Indication of surgical decompression:
• The GCS score decreases by 2 or more points between the
time of injury and hospital evaluation
• The patient presents with fixed and dilated pupils
• The intracranial pressure (ICP) exceeds 20 mm Hg
Exception :
In Subdural hematoma with GCS=15- hematoma >10mm ,or
>5mm midline shift ---- requires Surgical decompression
SAH: when a cerebral aneurysm is identified on angiography,
clipping and coiling is done to prevent re-bleed

Management
Surgical Decompression contd..
Types:
• Burr-hole
• Craniotomy- bone flap is temporarily removed
from the skull to access the brain
• Craniectomy – in which the skull flap is not
immediately replaced, allowing the brain to
swell, thus reducing intracranial pressure
• Cranioplasty - surgical repair of a defect or
deformity of a skull.



Initial management of the patient with traumatic
brain injury (treatment option).

Initial management of the patient with traumatic brain
injury (treatment option). Contd….

Assessment parameters for the patient with a head
injury include (A) eye opening and responsiveness,
(B) vital signs

Assessment parameters for the patient with a head injury:
(C, D) motor response reflected in hand strength or
response to painful stimulus.

NURSING MANAGEMENT:
• Ineffective Cerebral tissue perfusion related
to increased ICP and decreased CPP
• Fluid volume deficit related to decrease LOC
and hormonal dysfunction.
• Risk for injury related to decreased level of
consciousness.
• Knowledge deficit regarding the treatment
modalities and current situation.

• Ineffective thermoregulation related to
damage to hypothalamic centres.
• Risk for Impaired skin integrity related to
compromised circulation shifting of fluid
from intra vascular to interstitial space.
• Anxiety related to outcome of diseases as
evidenced by poor concentration on work,
isolation from others, rude behaviour

Nursing Process: The Care of the Patient
with Brain Injury—Assessment
• Health history with focus upon the immediate
injury, time, cause, and the direction and force of
the blow
• Baseline assessment
• LOC—Glasgow Coma Scale
• Frequent and ongoing neurologic assessment
• Multisystem assessment
51

Nursing Process: The Care of the Patient
with Brain Injury—Diagnoses
Ineffective airway clearance and impaired gas exchange
Ineffective cerebral perfusion
Deficient fluid volume
Imbalanced nutrition
Risk for injury
Risk for imbalanced body temperature
Risk for impaired skin integrity
Disturbed thought patterns
Disturbed sleep pattern
Interrupted family process
Deficient knowledge52

Collaborative Problems/Potential
Complications
• Decreased cerebral perfusion
• Cerebral edema and herniation
• Impaired oxygenation and ventilation
• Impaired fluid, electrolyte, and nutritional
balance
• Risk of posttraumatic seizures
53

Nursing Process: The Care of the Patient with
Brain Injury—Planning
Major goals may include
Maintenance of patent airway,
Adequate cerebral perfusion pressure (CPP),
Fluid and electrolyte balance,
Adequate nutritional status,
Prevention of secondary injury,
Maintenance of normal temperature,
Maintenance of skin integrity,
Improvement of cognitive function,
Prevention of sleep deprivation,
Effective family coping,
Increased knowledge about rehabilitation process, and
Absence of complications. 54

Interventions
• Ongoing assessment and monitoring is vital
• Maintenance of airway
–Positioning to facilitate drainage of oral secretions with
HOB usually elevated 30° to decrease venous
pressure
–Suctioning with caution
–Prevention of aspiration and respiratory insufficiency
–Monitor ABGs, ventilation, and mechanical ventilation
–Monitor for pulmonary complications, potential ARDS
55

Interventions
• I&O and daily weights
• Monitor blood and urine electrolytes
osmolality and blood glucose
• Measures to promote adequate nutrition
• Strategies to prevent injury–Assessment of oxygenation
–Assessment of bladder and urinary output
–Assessment for constriction due to dressings and casts
–Pad side-rails
–Mittens to prevent self-injury; avoid restraints
56

Interventions
• Strategies to prevent injury–Reduce environmental stimuli
–Adequate lighting to reduce visual hallucinations
–Measures to minimize disruption of sleep-wake cycles
–Skin care
–Measures to prevent infection
• Maintaining body temperature–Maintain appropriate environmental temperature
–Use of coverings—sheets, blankets to patient needs
–Administration of acetaminophen for fever
–Cooling blankets or cool baths; avoid shivering
57

Interventions
• Support of cognitive function
• Support of family–Provide and reinforce information
–Measures to promote effective coping
–Setting of realistic, well-defined, short-term goals
–Referral for counseling
–Support groups
• Patient and family teaching
58

Promotion of Effective Breathing and Airway
Clearance
• Monitor carefully to detect potential respiratory
failure
–Pulse oximetry and ABGs
–Lung sounds
• Early and vigorous pulmonary care to prevent
and remove secretions
• Suctioning with caution
• Breathing exercises
• Assisted coughing
• Humidification and hydration59

Improving Mobility
• Maintain proper body alignment
• Turn only if spine is stable and as indicated by
physician
• Monitor blood pressure with position changes
• PROM at least four times a day
• Use neck brace or collar, as prescribed, when
patient is mobilized
• Move gradually to erect position
60

DIET PLAN
Amino Acids
• Protein is used for the growth, repair and
maintenance of nearly every tissue in the
body and is composed of amino acids.
• Those with traumatic brain injuries
require 0.55 to 0.73 grams of protein per
pound of body weight

• Other Foods
A person living with a brain injury should
consume a rounded diet that is rich in fruits,
vegetables and whole grains.
Avoid saturated fat, hydrogenated fats and sodium
because they may increase your risk of suffering
a stroke.

CALORIE REQUIREMENTS
• The Glasgow Coma Scale is a tool used by
medical professionals to measure someone's
level of consciousness.
• Someone with a GCS of 4 to 5 needs 22.7 to
27.3 calories per pound of body weight per day.
• Someone with a GCS of 6 to 7 needs 18.2 to
22.7 calories.
• Those with less-severe injuries who have a GCS
of 8 to 12 require 13.6 to 16 calories.


Preventive Measures
Health Promotion
• Prevent car and motorcycle accidents
• To wear safety helmets
Cognitive Rehabilitation Therapy
Physical Therapy
Speech Therapy
Mental Rehabilitation
Physical Exercise
Occupational Therapy
Rehabilitation

Rehabilitation
Ambulatory and Home Care
• Nutrition
• Bowel and bladder management
• Spasticity
• Dysphagia
• Seizure disorders
• Family participation and education

Related Documents




