Hatem Eleishi, MD Rheumatologist STILL’S DISEASE

Hatem Eleishi, MD Rheumatologist STILL’S DISEASE.
Dec 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Hatem Eleishi, MD
Rheumatologist
STILL’S DISEASE
Systemic onset juvenile rheumatoid arthritis (formerly called Still's disease)
is a subset of juvenile rheumatoid arthritis (JRA) that describes patients with:
Intermittent fever +/- rashArthritis
Children with this illness comprise between 10 and 15 percent of all cases of JRA.

By definition, systemic onset JRA does not occur after the age of 16 years.
Adult-onset Still's disease
Is the same disorder occurring in patients over the age of 16.
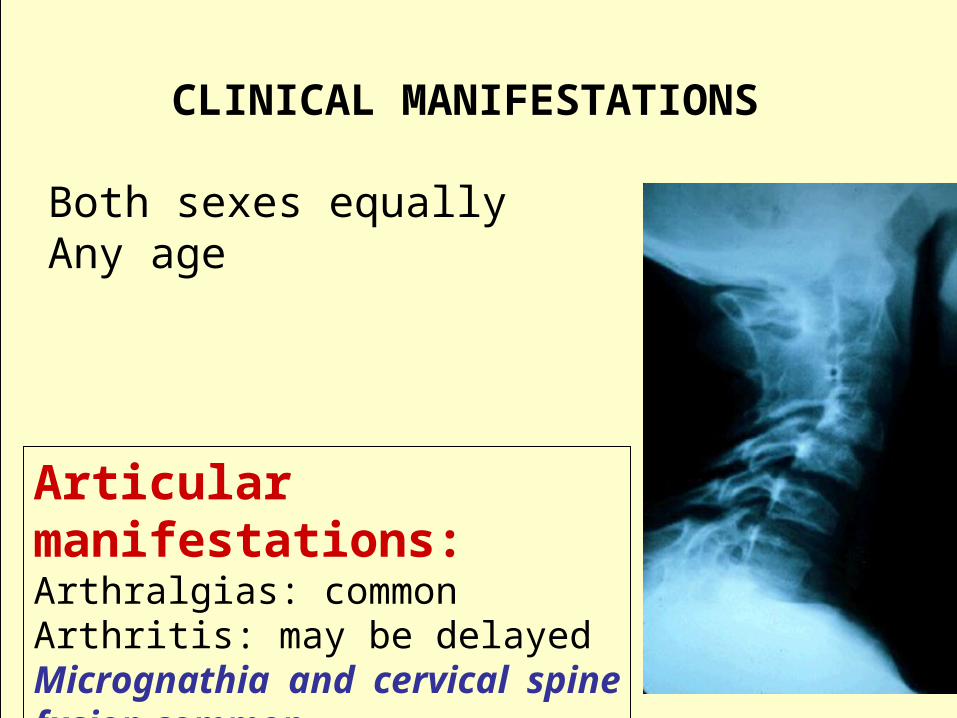
CLINICAL MANIFESTATIONS
Both sexes equallyAny age
Articular manifestations: Arthralgias: commonArthritis: may be delayedMicrognathia and cervical spine fusion common

Extra-articular manifestations: FeverMacular, salmon pink rash HepatomegalySplenomegalyLymphadenopathy Pericardial effusions

Disseminated intravascular coagulation (DIC) or Macrophage activation syndrome (MAS)
May occur within the first few days or weeks following: 1. Initiation of therapy with NSAIDs or gold salts 2. Viral and bacterial infections
Or may occurwithout any evident initiating event.
DIAGNOSIS:
A diagnosis of exclusion
Combination of intermittent daily fevers greater than 38.5°C and arthritis
For at least six weeks May be delayed
Hallmark

Laboratory findings:
Acute phase response
Neutrophilic leucocytosis: count in the 20,000 to 30,000/mm3 range
Marked reactive thrombocytosis
Anemia: commonly present and often profound
Elevated serum ferritin levels
Minor transaminitis

SOJRA may be the most difficult form of JRA to diagnose for the following reasons:
First:
Arthritis may not be evident early in the course of the disease.
Arthritis is important to make a
definite diagnosis

Second: Children often appear quite ill with:
High spiking feversRashes
Markedly elevated WBC countsAnemia
Hence, initially thought to have an infection
But, with no response to antibioticsAnd with >6weeks duration
**
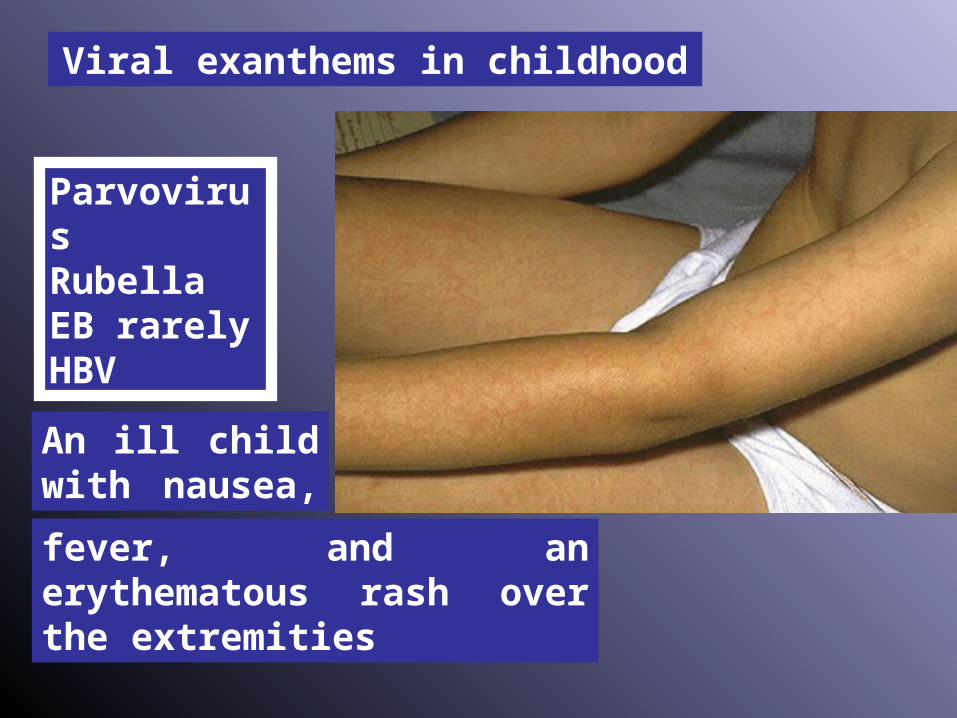
An ill child with nausea,
fever, and an erythematous rash over the extremities
Viral exanthems in childhood
ParvovirusRubellaEB rarelyHBV
Third: Children may have:
FeversMarkedly elevated WBC counts
AnemiaLymphadenopathy
Hence, leukemia considered
Clues to differentiation include

Systemic onset JRA is not associated with:
ThrombocytopeniaLymphocytosisExtreme pain*
LN biopsy shows reactive hyperplasia
c
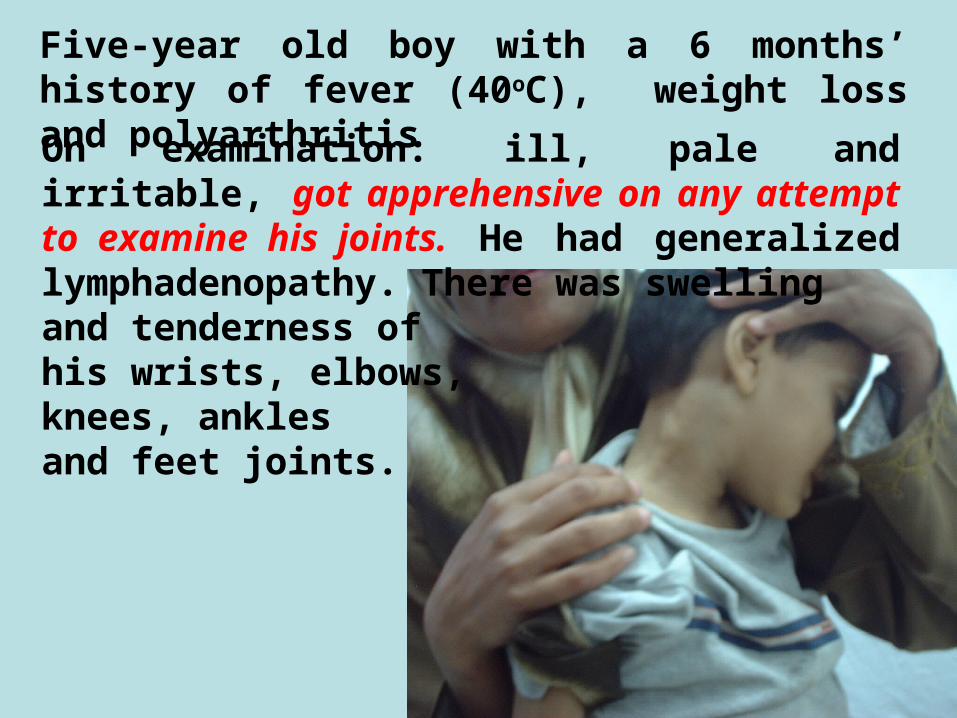
Five-year old boy with a 6 months’ history of fever (40oC), weight loss and polyarthritisOn examination: ill, pale and irritable, got apprehensive on any attempt to examine his joints. He had generalized lymphadenopathy. There was swellingand tenderness ofhis wrists, elbows, knees, anklesand feet joints.

His labs showed ESR 140Hb 2.3; MCV 56WBC 2.9Platelets 50Serum albumin 2.1ALT, AST: normalUrine: freeANA negative

Treatment: NSAIDs: Indomethacin
Corticosteroids: used judiciously to minimize toxicity (below 0.5 mg/kg per day of prednisone or its equivalent) and the duration of therapy should be less than six months
Methotrexate with a usual maximum oral dose of 15 mg per week.

Course and prognosis:
Highly variable, but in general:
The child who appears well after six months has a substantial probability of remaining well.
Poorer functional outcomes may occur in those with more than six months of fever, thrombocytosis, or corticosteroid therapy

In conclusion
In conclusion
SOJRA is:
Intermittent fever of at least 6 weeks’ duration
And arthritis
SOJRA is a diagnosis of exclusion

Treatment consists of corticosteroids that should be used judiciously and immunosuppressives as methotrexate
Prognosis can be predicted over the first 6 months of the course of the disease

Thank you
Related Documents