Clinical Evaluation of Safoof Ziabetus In Management of Ziabetus Shakri By HAMID ALI Dissertation Submitted to the Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore. In Partial fulfilment of the requirements for the degree of MAHIRE TIB ( M. D. Unani) In MOALEJAT (Medicine) Department of Moalejat National Institute of Unani Medicine Bangalore 2007

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Clinical Evaluation of Safoof Ziabetus
In
Management of Ziabetus Shakri
By
HAMID ALI
Dissertation Submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore.
In Partial fulfilment of the requirements for the degree of
MAHIRE TIB ( M. D. Unani)
In
MOALEJAT
(Medicine)
Department of Moalejat
National Institute of Unani Medicine
Bangalore
2007
Clinical Evaluation of Safoof Ziabetus In
Management of Ziabetus Shakri
By
HAMID ALI
Dissertation Submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore. In Partial fulfilment of the requirements for the degree of
MAHIRE TIB ( M. D. Unani) In
MOALEJAT (Medicine)
Under the Guidance of
DR. MOHD ANWAR
Department of Moalejat National Institute of Unani Medicine
Bangalore
2007
Rajiv Gandhi University of Health Sciences, Karnataka
DECLARATION BY THE CANDIDATE
I hereby declare that the Dissertation entitled “Clinical Evaluation Of Safoof
Ziabetus In Management Of Ziabetus Shakri” is a bonafide and genuine
research work carried out by me under the guidance of Dr. Mohd Anwar,
Reader, Dept. of Moalejat, National Institute of Unani Medicine, Bangalore.
Date: HAMID ALI
Place: Bangalore
National Institute of Unani Medicine (Dept. of AYUSH, Ministry of Health & Family Welfare, Govt. of India)
Kottigepalya, Magadi Main Road, Bangalore‐91: 0‐580725
CERTIFICATE BY THE GUIDE
This is to certify that the Dissertation entitled “Clinical Evaluation Of Safoof
Ziabetus In Management Of Ziabetus Shakri” is a bonafide research work
done by HAMID ALI in partial fulfilment of the requirement for the degree of
“Mahire Tib (M.D. Unani) in Moalejat (Medicine)”.
Date : Dr. Mohd Anwar Place : Bangalore Reader
Department Of Moalejat
National Institute of Unani Medicine
Bangalore
National Institute of Unani Medicine (Dept. of AYUSH, Ministry of Health & Family Welfare, Govt. of India)
Kottigepalya, Magadi Main Road, Bangalore‐91: 083580725
ENDORSEMENT BY THE HOD, HEAD OF THE INSTITUTION
This is to certify that the Dissertation entitled “Clinical Evaluation of Safoof
Ziabetus in Management of Ziabetus Shakri” is a bonafide research work
done by HAMID ALI under the guidance of Dr. Mohd Anwar, Reader, Dept. of
Moalejat, National Institute of Unani Medicine, Bangalore.
Prof. Mansoor Ahmad Siddiqui Prof. M. A. Jafri
HOD, Department of Moalejat Director
National Institute of Unani Medicine National Institute of Unani Medicine
Date: Date:
Place: Bangalore Place: Bangalore
COPYRIGHT
Declaration by the Candidate
Thereby declare that the Rajiv Gandhi University of Health Sciences, Karnataka
shall have the rights to preserve, use and disseminate this Dissertation in print or
electronic format for academic / research purpose.
Date : HAMID ALI
Place: Bangalore
© Rajiv Gandhi University Of Health Sciences, Karnataka.
ACKNOWLEDGEMENT
“All praises to Almighty ALLAH the most beneficent the most merciful, the
omnipresent and creator of all living and non-living being, by thanking him
for best owing upon me to courage, mindset, patience strength and zeal that
enabled me to complete this work successfully."
‘After the praise of almighty ALLAH, Salam and Darood on our Prophet
Huzoor Mohammad Mustafa (SAW).’
I exceed my bliss height in expressing my deep sense of gratitude to
Prof. M. A. Jafri, Director, National Institute of Unani Medicine, Bangalore, for
his moral encouragement and providing me the necessary facilities that I needed
for my research work.
My sincere thanks are to Prof. M. A. Siddiqui, HOD, Department of
Moalejat, National Institute of Unani Medicine, Bangalore, for his valuable advice
and moral encouragement.
It is with a deep and abiding sense of gratitude that I acknowledge my debt
to my guide Dr. Mohd. Anwar, the fountainhead of the work enclosed in the
following pages. His sense of responsibility towards this work, constructive
criticism and wise counsel smoothed the rough patches and his able guidance
throughout, are the pillars upon which this dissertation stands. It was a pleasure to
have been under his supervision and his dynamism inspired me to efforts that I
would have otherwise been incapable of, my respect and admiration for him is
unbounded.
I deem it a sacred privilege to express my deep sense of gratitude and
obligation to my co- guide Dr. Tanzeel Ahmad, whose constructive guidance,
constant inspiration, valuable advice and moral encouragement has accelerated me
to reach my destination. His critical suggestions have added more dimension to the
study.
i
I pray that the soul of our beloved ‘Late Hakeem Ajmal Khan Sahab’
may rest in peace, who established A & U Tibbia College and Hospital and
stressed the need for research and the use of modern sciences indigenous
medicine, instead of blindly followed old prescriptions.
I exceed my bliss height in expressing my deep sense of gratitude to my
teacher ‘Dr. Rais-ur-Rahman Sahab, H.O.D. and Reader of Department of
Moalejat, A&U Tibbia College Karol Bagh, for his perpetual guidance and
constant encouragement. He has been my source of inspiration throughout the
course of my study, not only at post-graduate level but also during graduation
level. His guidance is a gift that I would cherish for the rest of my life.
I am indebted to all my esteemed teachers of the Deptt. Of Moalejat,
namely Prof. Syed Abrar, Dr. A. N. Ansari, Dr. M. A. Quamri, who have enlighten
me with their knowledge and experiences and provided academic support during
the course of my research work.
I wish great fully to acknowledge to my other teachers specially
Prof.Ghufran Ahmad, Dr.G. D. Sofi, Dr. Nasreen Jahan, and Dr. A. H. Ansari for
their constant sympathetic attitude and special blessing to me.
I am deeply thankful to Dr. Mohd. Nafees Khan, Dr. Mohd. Azam for their
help and co-operation.
I am also thankful to my colleagues Dr. Mohd. Zubair and Dr. Abdul
Hakeem for their kind co-operation and help during my research work.
I am deeply thankful to Mr.Ehtesham and Mr.Danish Ghani (NIUM library)
who never expressed signs of exhaustion in providing me literature.
I want to offer my gratitude with great honour and respect to my parents
whose love and prayers have always been a great source of strength to me and
have proved icon for the ship of my carrier. My heart goes out in reverence to
them for their tremendous patience, endurance and affections.
ii
I do not find adequate words to express my deep sense of respect and
sincere thanks to my elder brothers Er. Athar Mustafa and Er. Kausar Murtaza,
who left no stone unturned in enabling and whetting me to obtain and achieve the
aims and objectives in life, whose perennial patronization enabled me to beat the
impossible. Their inspirations and prayers have always been a driving force behind
my efforts.
My acknowledgement would remain incomplete without making a special
mention for the sustained help, encouragement moral boost up and kind co-
operation which I received from my Sisters Zehra Anjum, Dr.Wajida Tabassum,
Dr.Nigar Tabassum.
I am highly obliged and deeply touched by the pains taken by ‘Dr.Naghma
Chand (M.D.)’ who never expressed sign of exhaustion in providing me literature
and to the thesis to correct shape, her moral support and wishes are invaluable and
valuable advice to my life.
At this moment how can I forget to express my deep affection and thanks
for my beloved son Mohd. Hamd, who missed me during my academic period.
Lastly, and by no means least, I would specially like to mention the name
of my beloved wife Samreen Fatma, there is no way I could have completed this
work without her moral support, constant encouragement, persistent co-operation,
endless forbearance and inexhaustible store of affections that sustains me at each
and every step and helped me to bring this work to end.
Date : HAMID ALI
Place : Bangalore
iii
ABBREVIATIONS
Acetyl CoA : Acetyl Coenzyme A
Acyl CoA : Acyl-coenzyme A
AD : Anno Domain (after the death of Christ)
ALT : Alanine amino transferase
aq. : Aqua ( Water)
AST : Aspartate amino transferase
AT : After Treatment
ATP : Adenosine triphosphate
BC : Before Christ
BMI : Body mass index
BP : Blood Pressure
BT : Before Treatment
Cap : Capsule
cm : Centimetre
CRF : Case report form
cu.mm : Cubic millimetre
dl : Decilitre
DLC : Differential Leucocytes Count
DNA : Deoxyribonucleic acid
Dr : Doctor
E.coli : Escherichia coli
ECG : Electrocardiogram
ed. : Edition
iv
e.g. : example gratv (for example)
ESR : Erythrocyte sedimentation rate
et.al. : et alii or et alia (and other)
etc. : etcetera (and the rest)
FDA : Food and Drug Administration
FFA : Free fatty acid
GDM : Gestational Diabetes Mellitus
GLUTS : Glucose transporters
gm : Gram
GOD/ POD : Glucose Oxidase / Peroxidase
G.Sylvestre : Gymnema Sylvestre
Hb : Haemoglobin
HDL : High density lipoprotein
Hg : Mercury
HGP : Hepatic glucose production
HNF : Hepatocyte Nuclear Factor
hr : Hour
IBW : Ideal Body Weight
ICMR : Indian council of Medical research
IDDM : Insulin Dependent Diabetes Mellitus
IDF : International Diabetes federation
i.e. : “idest” (that is)
IFCC : International Federation of Clinical Chemistry
IPF : Insulin promoter factor
v
IU/L : International Units per Liter
JVP : Jugular Venous Pressure
Kcal : Kilo Calorie
KFT : Kidney Function Test
Kg : Kilogram
Lb : Pound
LFT : Liver Function Test
m2 : Square metre
m3 : Cubic millimetre
mg : Milligram
mg/dl : Milligram per decilitre
min : Minutes
mm : Millimetre
mmol/L : Millimol per litre
MODY : Maturity onset diabetes of the young
MUFA : Monounsaturated fatty acids
n : Total number
NAD : Nicotinamide adenine dinucleotide
NIDDM : Non Insulin Dependent Diabetes Mellitus
NIUM : National Institute of Unani Medicine
No. : Number
p : Probability of error
PNPP : p-Nitrophenyl Phosphate
PP cells : Polypeptide cells
vi
pts. : Points
PUFA : Polyunsaturated fatty acids
R. Br. : Roxburgh
RIA : Radio immunological assay
R.R. : Respiratory Rate
S.Cholesterol : Serum Cholesterol
SGOT : Serum glutamic oxaloacetic transaminase
SGPT : Serum glutamic pyruvic transaminase
Sol. : Solution
T.Cordifolia : Tinospora Cordifolia
Temp : Temperature
TLC : Total Leucocytes Count
UV : Ultra Violet
Vol. : Volume
WHO : World Health Organisation
Β : Beta
2nd : Second
% : Percentage
> : Greater than
> : Greater than or equal to
+ : Positive
_ : Negative
vii
Clinical evaluation of Safoof Ziabetus
In
Management of Ziabetus Shakri
ABSTRACT
_____________________________________________________________
Nowadays, Ziabetus Shakri (Diabetes Mellitus) has become a global problem in spite of
advances in modern science, and prevails all over the world. Globally it affects about 246
million peoples. It causes Disability through its complications like blindness, kidney
failure, coronary artery disease, gangrene of lower extremities. Owing to these
complications, the researchers of different system of medicine are concentrating
themselves for the development of the new antidiabetic drugs. The different antidiabetic
drugs have been already evaluated by main stream of medicine and have very much
potent and effective hypoglycaemic action, but the long term use of these drugs resulted
in development of various side effects. Hence, there is a dire need to develop safe and
effective drug for the management of Ziabetus Shakri. Unani physicians have been
treating Ziabetus Shakri since ancient times; they have described a number of Unani
drugs both single and compound for the management of Ziabetus Shakri. Recently
several single herbal drugs has been experimentally and clinically evaluated and reported
as hypoglycaemic agents. However, the scientific study of compound formulation is
largely ignored by the scientists and physicians despite the fact that a good number of
compound drugs have been described in Unani literature to be effective in Ziabetus
viii
condition as large number of physicians of Unani medicine are using them successfully
since long. Keeping this fact in mind a randomized single blind placebo diet control trial
was conducted on the “Clinical evaluation of Safoof Ziabetus in management of
Ziabetus Shakri”.
The trial was conducted on 50 newly diagnosed patients of Ziabetus Shakri, at National
Institute of Unani Medicine Hospital, Bangalore. They were divided into two Groups;
Group A (Test Group-30 Patients) was given test drug and Group B (Placebo-20
Patients) placebo in a dose of 6 gm thrice a day in capsule form orally with water,15
minutes before meal along with planned diet and exercise for the period of 45 days. This
study shows good response on blood sugar level of the cases treated with Unani
formulation i.e. Average reduction of 56.83 mg/dl (32.80 %) in fasting and 67.23 mg/dl
(26.94 %) in post prandial blood sugar was recorded. On comparing before treatment
observations of Blood sugar fasting and post prandial with their corresponding after
treatment observations, with the help of Student’s ‘t’ test, it was found significant
statistically (p < 0.05) [ Calculated value of ‘t’= 9.31 (Fasting) and 7.42 (Post prandial) ] .
Study also reveals that the Ziabetus Shakri is relatively more common in person having
age 40 years and above with har mizaj. The advantage of this treatment is that, it is very
much cost effective and offer maximum success without any adverse effect.
Keywords: Ziabetus Shakri; Antidiabetic drugs; Safoof Ziabetus; Clinical evaluation.
ix
TABLE OF CONTENTS
S.No. Contents Page No.
1. Introduction Page No. 1-6
2. Objectives Page No. 7-8
3. Review of Literature Page No. 9-71
4. Methodology Page No. 72-86
5. Results Page No. 87-118
6. Discussion Page No. 119-135
7. Conclusion Page No. 136-138
8. Summary Page No. 139-143
9. Bibliography Page No. 144-170
10. Annexures Page No. 171-192
x
LIST OF TABLES
S.No. Table No. Page No.
1. Table No.1 85
2. Table No.2 85
3. Table No.3 87
4. Table No.4A 89
5. Table No.4B 89
6. Table No.5A 91
7. Table No.5B 92
8. Table No.6A 94
9. Table No.6B 94
10. Table No.7A 96
11. Table No.7B 97
12. Table No.8A 99
13. Table No.8B 99
14. Table No.9A 102
15. Table No.9B 103
16. Table No.10A 107
17. Table No.10B 107
18. Table No.11A 110
19. Table No.11B 110
20. Table No.12A 112
21. Table No.12B 113
22. Table No.13A 114
23. Table No.13B 114
xi
LIST OF FIGURES
Figures Page No.
Photograph of Gurmar Booti 55
Photograph of Gilo Khushk 62
Photograph of Safoof Ziabetus and Placebo 82
Graph No.1 89
Graph No.2 89
Graph No.3 91
Graph No.4A 93
Graph No.4B 93
Graph No.5A 96
Graph No.5B 96
Graph No.6A 98
Graph No.6B 98
Graph No.7A 101
Graph No.7B 101
Graph No.8A 103
Graph No.8B 103
Graph No.9A 107
Graph No.9B 107
Graph No.10A 111
Graph No.10B 111
Graph No.11A 114
Graph No.11B 114
Graph No.12A 118
Graph No.12B 118
xii
DEDICATED TO
MY PARENTS
xiii
Introduction
INTRODUCTION
1
Introduction
INTRODUCTION
The term Ziabetus is a Greek word which means “to run through” or “Siphon”, is
characterized by hyperglycaemia, glycosuria, increased appetite, excessive thirst and
gradual loss of body weight. The concept of Ziabetus also exists in ancient world; it is
proved by the discovery of Ebers papyrus, written about 1550 BC. Ebers papyrus
contains descriptions of various diseases including a polyuric state resembling Ziabetus
Shakri. Although Buqrat “ The father of medicine” did not specifically mention
Ziabetus in his writings, but there are accounts in the Buqrat’s writings that are consistent
with the sign and symptoms of Ziabetus, like excessive urinary flow with wasting of the
body. After Buqrat, Arsyatoos (Aretaeus) was the first to use the term “Ziabetus” in
connection with this ailment, which means “to run through” or “Siphon” and provided the
accurate description of the symptoms of Ziabetus for the first time. After Arsyatoos,
Jalinoos described Ziabetus as a rare disease, and referred to the ailment as “Diarrhoea
Urinosa (Diarrhoea of Urine)”, and “Dipsakos (the thirsty disease)”. However, the
association of polyuria with a sweet tasting substance in the urine was first reported in
Sanskrit literature by Susruta, Charaka and Vaghbata (5th Century AD). They also
classified Ziabetus like condition into two: congenital and late onset, and described its
relationship with heredity, obesity, sedentary life and diet. During the same era, Chinese
and Japanese physicians also described the sweetness of urine and observed that people
with Ziabetus were prone to develop boils and an affliction which clinically resembles
tuberculosis. After that, during the Arabic era Ibne Sina described accurately the clinical
features of the disease and mentioned two specific complications of the disease, namely
2
Introduction
gangrene and the collapse of sexual function. No further progress was made in the
understanding of Ziabetus until the 16th century AD when Von Hohenheim (Paracelsus)
reported that urine of Diabetic patients contained an abnormal substance and concluded
that this substance was salt and that Diabetes was due to the deposition of salt in the
kidneys causing thirst of the kidney and polyuria. In 1674 AD Thomas Willis claimed
that Diabetes was primarily a disease of the blood and not the kidneys, he proposed that
the sweetness first appeared in the blood and was later found in the urine. Cullen was the
first person who distinguished Diabetes into two types. In this classification, we find first
time a distinction between Diabetes, with the urine of “the smell; colour and flavor of
honey,” and Diabetes, with limpid but not sweet urine. In 1798 AD John Rollo was the
first who use the adjective “ Mellitus” to distinguish the condition from other polyuric
diseases. In 1889 AD, Oskar Minkowski and Josef Von Mering established the role of
the pancreatic disorders in causing Diabetes. In June 1921 AD, the endocrine role of the
pancreas in metabolism and development of Diabetes was clarified by Banting and Best,
when they repeated the work of Von Mering and Minkowski, and went a step further and
isolated the hormone insulin from bovine Pancreas.
Now in present era due to resemblance in clinical features of the disease Ziabetus Shakri
has been correlated with Diabetes Mellitus, which is a chronic disorder of carbohydrate
metabolism and glucose intolerance. It is characterized by high blood glucose level and
glycosuria resulting from dysfunction of pancreatic β cells and insulin resistance. The
defective β cells result in lack of total or partial synthesis of insulin. Heredity, age,
obesity, diet, sex, sedentary life style, socio-economic status, hypertension and various
stresses are the common factors supposed to be involved in the aetiology of Diabetes
3
Introduction
Mellitus. Although Diabetes Mellitus is a disorder of carbohydrate metabolism, but in
long term it also affects metabolism of protein, lipids and electrolytes and results in the
development of Diabetic complications like blindness, renal failure, coronary artery
disease, gangrene of lower extremities, stupor, coma etc. Due to these dreadful
complications, Diabetes has become a global problem in spite of advances in modern
sciences. It is considered as one of the most common non-communicable disease,
globally. According to IDF, about 246 million people are affected with this disease all
over the world in 2007 and this number may increase to 380 million by 2025. Although
the prevalence rate of the disease varies from country to country. However, WHO has
been projected India as the country with the fastest growing population of Diabetes
patients. Depending upon its aetiology and treatment Diabetes Mellitus can be divided
into four types among them two are main i.e. Type 1 or Insulin Dependent Diabetes
Mellitus (IDDM) and Type 2 or Non-Insulin Dependent Diabetes Mellitus (NIDDM).
Type 2 Diabetes Mellitus accounts for over 85-95% of all Diabetic population and is
characterised by insulin resistance and / or abnormal insulin secretion. Depending upon
the nature of the disease, insulin and certain synthetic drugs like Glibenclamide,
Metformin, Gliclazide, Glimepiride, and Glipizide etc are widely used in its management.
Although the initial response of these drugs are usually good but long term use of oral
hypoglycaemic agents frequently loosing efficacy and results in development of "insulin
resistance" and side effects like Hypoglycaemic reactions, Agranulocytosis, Aplastic
anaemia and Haemolytic anaemia.
Owing to dreadful complications of Diabetes Mellitus and lack of safe and effective drug
for its management, it becomes a thrust area for research, in every field of medical
4
Introduction
science. The researchers of different systems of medicine are continuously concentrating
themselves for the development of safe and effective antidiabetic drugs. As far as the
Unani system of medicine is concerned, Ziabetus Shakri is being treated since Greco-
Arab period. Unani physicians claim to possess many safe and effective antidiabetic
agents for the management of Ziabetus Shakri. Therefore, it is one of the areas which
have to be given priority in scientific research in Tibbe Unani. Tibbe Unani possesses
large number of mufrad and murakkab drugs for the management of Ziabetus Shakri.
Many important and therapeutically effective murakkab drugs have been described to be
useful in Ziabetus Shakri in standard qarabadeen; they have not been evaluated
scientifically so far, for their described effect. Recently several herbal single drugs have
been experimentally and clinically evaluated and reported as good hypoglycaemic agents.
However, the scientific study of compound formulation is largely ignored by the
scientists and physicians despite the fact that a good number of compound drugs have
been described in Unani literature to be effective in Ziabetus condition as large number of
physicians of Unani medicine are using them successfully since long.
Safoof Ziabetus is one such drug described in various qarabadeen to be effective in
Ziabetus Shakri further inquiry with Unani physicians revealed that the drug is highly
effective and possess least chances of toxicity and side effects.
In view of the above a single blind placebo study was designed to investigate the
hypoglycaemic effect of Safoof Ziabetus in the patients of Ziabetus Shakri.
Safoof Ziabetus contains Gurmar booti (Gymnema Sylvestre) and Gilo khushk
(Tinospora Cordifolia) in 1:1 ratio, in the form of fine powder. The Powder was filled in
5
Introduction
capsules of 1gm capacity and 6 capsules was given 3 times a day orally with water,
15 minutes before breakfast, lunch, and dinner for 45 days. Total daily dose of Safoof
Ziabetus given to each patient was 18 gm in three divided doses. The study was
conducted at National Institute of Unani Medicine Hospital, Bangalore. After completion
of the trial, the data were analysed for the efficacy of drugs.
The study work includes the detailed Introduction, Description of Ziabetus Shakri
(Introduction of the Disease), History, Anatomy & Physiology of Pancreas, Definition,
Prevalence, Classification, Pathogenesis, Clinical features, Complications, Diagnostic
criteria and Management of Ziabetus Shakri in the light of literature available in Unani as
well as Modern system of Medicine. The study work also includes the literature review of
Unani drugs used for the treatment, the description of Material and Methods, Results,
Discussion, Summary, Conclusion of the clinical trial and Bibliography which has been
numbered consecutively in the order in which they are first mentioned in the text.
Proforma and Master Charts of study work are attached at the end of the dissertation.
Abbreviations details used in the dissertation are given under the heading of abbreviation.
6
Objectives
OBJECTIVES
7
Objectives
OBJECTIVES OF THE STUDY
To evaluate the effect of “SAFOOF ZIABETUS” in the management of
Ziabetus Shakri.
To validate the Unani claim for “SAFOOF ZIABETUS”.
To help in development of a safe and efficacious drug for Ziabetus Shakri.
8
Review of Literature (Classification)
CLASSIFICATION
According to Unani System of Medicine Ziabetus can be divided into two types:
(A) Ziabetus har or Shakri
(B) Ziabetus barid
This classification is based upon the nature of the disease (4, 7, 9, 12, 15, 20).
While on the other hand, in modern system of medicine, although all forms of Diabetes
Mellitus are characterized by hyperglycemia, the pathogenic mechanisms by which
hyperglycemia arises differ widely. Some forms of Diabetes Mellitus are characterized by
an absolute insulin deficiency or a genetic defect leading to defective insulin secretion,
whereas other forms share insulin resistance as their underlying etiology. Recent changes
in classification reflect an effort to classify Diabetes Mellitus on the basis of etiology.
Etiologic Classification Of Diabetes Mellitus
I. Type 1 Diabetes: Cell destruction, usually leading to absolute insulin deficiency
A. Immune mediated
B. Idiopathic
II. Type 2 Diabetes: May range from predominantly insulin resistance with relative
insulin deficiency to a predominantly secretory defect with insulin resistance.
35
Review of Literature (Classification)
III. Other Specific Types
A. Genetic Defects Of Cell Function
1. Chromosome 12, HNF-1 (MODY3) 2. Chromosome 7, glucokinase (MODY2)
3. Chromosome 20, HNF-4 (MODY1) 4. Chromosome 13, insulin promoter factor-1
(IPF-1; MODY4) 5. Chromosome 17, HNF-1 (MODY5) 6. Chromosome 2, NeuroD1
(MODY6) 7. Mitochondria DNA 8. Others
B. Genetic Defects In Insulin Action
1. Type A insulin resistance 2. Leprechaunism 3. Rabson-Mendenhall syndrome
4. Lipoatrophic Diabetes 5. Others
C. Diseases Of The Exocrine Pancreas
1. Pancreatitis 2. Trauma / pancreatectomy 3. Neoplasia 4. Cystic fibrosis
5. Hemochromatosis 6. Fibrocalculous pancreatopathy 7. Others
D. Endocrinopathies
1. Acromegaly 2. Cushing’s syndrome 3. Glucagonoma 4. Pheochromocytoma
5. Hyperthyroidism 6. Somatostatinoma 7. Aldosteronoma 8. Others.
E. Drug Or Chemical-Induced
1. Vacor 2. Pentamidine 3. Nicotinic acid 4. Glucocorticoids 5.Thyroid hormone
6. Diazoxide 7. Adrenergic agonists 8.Thiazides 9. Dilantin 10. Interferon 11. Others
F. Infections
1. Congenital rubella 2. Cytomegalovirus 3. Others
36
Review of Literature (Classification)
G. Uncommon Forms Of Immune-Mediated Diabetes
1. “Stiff-man” syndrome 2. Anti–insulin receptor antibodies 3. Others
H. Other Genetic Syndromes Sometimes Associated With Diabetes
1. Down’s syndrome 2. Klinefelter’s syndrome 3. Turner’s syndrome 4.Wolfram’s
syndrome 5. Friedreich’s ataxia 6. Huntington’s chorea 7. Laurence-Moon-Biedl
syndrome 8. Myotonic dystrophy 9. Porphyria 10. Prader-Willi syndrome 11. Others
IV. Gestational Diabetes Mellitus (GDM) (120)
37
Review of Literature (Clinical Features)
CLINICAL FEATURES OF ZIABETUS SHAKRI
In classical Unani literature it is described that, the disease Ziabetus always clinically
presents itself by:
1. Increased frequency of Micturition with excessive thirst and dryness of mouth.
2. Ants and flies are attracted on urine. (Due to presence sugar).
3. Patients feel heat in the back around the waist (In case of abnormal hot
temperament of kidney).
4. Dryness all over the body (Due to shortage of fluid in body)
(1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 20, 104)
While according to modern system of medicine, Type 2 Diabetes Mellitus develops
slowly. Many people have Type 2 Diabetes for several years before the condition is
diagnosed, often through routine screening tests. Typically, the earliest symptoms are
increased thirst and frequent urination. That's because excess glucose circulating in
body draws water from tissues, making patients dehydrated. To quench thirst, patients
drink more water and other beverages which lead to more frequent urination.
Other Signs And Symptoms Of Type-2 Diabetes Mellitus Include:
Flu-like symptoms: Sugar is an important fuel. When it doesn't reach to body cells,
patients feel tired and weak.
Weight fluctuations: Because body is trying to compensate for lost fluids and sugar,
patients eat more than usual and gain weight which causes body cells to become more
43
Review of Literature (Clinical Features)
resistant to the action of insulin. But the opposite also can occur. Patients may eat more
than normal but still lose weight because muscle tissues don't get enough glucose to
generate growth and energy.
Blurred vision: High levels of blood sugar pull fluid from body tissues, including the
lenses of eyes. This affects your ability to focus. In some cases, Diabetes can lead to
blindness.
Slow-healing of sores or Frequent infections: Diabetes affects body's ability to heal
and fight infection. Bladder and vaginal infections can be a particular problem for
women.
Nerve damage (Neuropathy): Excess sugar in blood can damage the small blood
vessels to nerves. Patients may feel tingling and loss of sensation in hands and feet, as
well as burning pain in arms, hands, legs and feet.
Red, swollen, tender gums: Diabetes increases the risk of infection in gums and in the
bones that hold teeth in place. (21,109,171)
44
Review of Literature (Complications)
COMPLICATIONS OF ZIABETUS SHAKRI
In Ziabetus as the vicious cycle of large intake of fluid and frequent urination
developed, it affects almost all body parts. First, it weakened the liver due to which there
is deficiency of fluid and nutrition to all body parts which initially results in generalized
weakness, but with the passage of time it results in development of generalized wasting
and dryness all over the body (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,21,104).
According To Modern Literature Complications Of Diabetes Mellitus Can Be
Divided Into Two Types:
Acute complications
Chronic complications
(1) Acute Complications
(A) Diabetic ketoacidosis.
(B) Nonketotic hyperosmolar coma.
(C) Hypoglycemia.
(D) Amputation
(2) Chronic Complications.
(A) Microvascular diseases
(a) Diabetic retinopathy
Severe vision loss .
Blindness.
45
Review of Literature (Complications)
(b) Diabetic neuropathy
Abnormal sensation
Decreased sensation.
Diabetic foot .
(c) Diabetic nephropathy
Chronic renal failure.
(B) Macrovascular disease
(a) Atherosclerosis
(b) Coronary artery disease, leading to myocardial infarction or angina .
(c) Stroke (mainly ischemic type)
(d) Peripheral vascular disease, which contributes to intermittent claudication
(exertion-related foot pain) as well as diabetic foot.
(e) Diabetic myonecrosis
(f) Diabetic foot often due to a combination of neuropathy and arterial disease.
(21, 109, 172)
46
Review of Literature (Definition)
ZIABETUS SHAKRI (DIABETES MELLITUS)
In classical literature of Unani Medicine, Diabetes is described under the heading
of Ziabetus.It is defined by various Unani philosophers as following:
1. Ziabetus is a disease in which patient excretes water as such through urinary passage
soon after its intake, as that of food without digestion from the stomach and intestine
like in “Zalaqul -ama”. (1, 2, 5, 10, 13)
2. Ziabetus is a disease in which patient excretes water in the form of urine soon after its
intake, but there is no incontinence of urine as found in Salesul-baul. (3, 6, 14, 15, 16)
3. Ziabetus is a disease in which patient always feel thirst and when he drinks water,
excrete it out through urine soon after its intake.(4, 7, 8, 9, 11, 12, 17, 18, 19, 20, 104)
Now, after discovery of Insulin the concept of disease is totally changed. In modern
literature it is defined as:
4. Diabetes Mellitus is a chronic, hereditary disease characterized by an abnormally high
level of glucose in the blood and the excretion of sugar in urine. The basic defect is an
absolute or relative lack of insulin which leads to abnormalities of metabolism, not
only of carbohydrate but also of protein and fat. (105)
5. Diabetes Mellitus is a disorder in which the level of blood glucose is persistently raised
above the normal range. (106)
6. Diabetes Mellitus is a syndrome with metabolic, vascular and neuropathic components
that are interrelated. The metabolic syndrome is characterized by alterations in
28
Review of Literature (Definition)
carbohydrate, fat and protein metabolism secondary to absent or markedly diminished
insulin secretion and / or ineffective insulin action. The vascular syndrome consists of
abnormalities in both large vessels (Macroangiopathy) and small vessels
(Microangiopathy).The Macroangiopathic changes cause cerebrovascular accidents,
myocardial infarction and peripheral vascular disease. Although these large vessel
sequelae occur in people without Diabetes, but in Diabetic patients they appear earlier
and are more severe. The clinical expressions of the microangiopathic changes are
Diabetic retinopathy and nephropathy. (107)
7. Diabetes Mellitus is a disease of excess glucose in the plasma, Qualitative
abnormalities of carbohydrate and lipid metabolism, characteristic pathologic changes
in the nerves and small blood vessels and intensification of atherosclerosis. (108)
8. Diabetes Mellitus is a clinical syndrome characterized by hyperglycaemia due to
absolute or relative deficiency of insulin. Lack of insulin whether absolute or relative
affects the metabolism of carbohydrate, protein, fat, water and electrolytes. Chronic
hyperglycaemia leads to complications of Diabetes and affects most characteristically
the eye, the kidney, the nervous system, the cardiovascular system and others such as
intercurrent infections, Diabetic foot ulcers. (109)
9. Diabetes Mellitus is characterized by hyperglycaemia and other metabolic
derangements that are caused by inadequate action of insulin on body tissues, either
because of reduced circulating levels of insulin or resistance of target tissues to its
actions. (110)
29
Review of Literature (Definition)
10. The term Diabetes Mellitus describes a metabolic disorder of multiple aetiology
characterized by chronic hyperglycaemia with disturbances of carbohydrate, fat and
protein metabolism resulting from defects in insulin secretion, insulin action, or both.
The effects of Diabetes Mellitus include long term damage, dysfunction and failure
of various organs. Diabetes Mellitus may present with characteristic symptoms such
as thirst, polyuria, blurring of vision, and weight loss. In its most severe forms,
Ketoacidosis or a non- ketotic hyperosmolar state may develop and lead to stupor,
coma and, in absence of effective treatment, death. Often symptoms are not severe,
or may be absent, and consequently hyperglycaemia sufficient to cause pathological
and functional changes may be present for a long time before the diagnosis is made.
The long term effects of Diabetes Mellitus include progressive development of the
specific complications of retinopathy with potential blindness, nephropathy that may
lead to renal failure, and / or neuropathy with risk of foot ulcers, amputation, Charcot
joints, and features of autonomic dysfunction, including sexual dysfunction. People
with Diabetes are at increased risk of cardiovascular, peripheral vascular and
cerebrovascular disease. Several pathogenetic processes are involved in the
development of Diabetes. These include processes which destroy the beta cells of the
pancreas with consequent insulin deficiency, and others that result in resistance to
insulin action. The abnormalities of carbohydrate, fat and protein metabolism are due
to deficient action of insulin on target tissues resulting from insensitivity or lack of
insulin. (111)
30
Review of Literature (Definition)
11. Diabetes mellitus is a metabolic cum-vascular syndrome of multiple aetiologies
characterized by chronic hyperglycaemia with disturbances of carbohydrate, fat, and
protein metabolism resulting from defects in insulin secretion, insulin action or both. This
disorder is frequently associated with long term damage, which can lead to failure of
organs like eyes, kidneys, nerves, heart, and blood vessels. (112, 113, 22)
31
Review of Literature (Introduction of the Disease)
REVIEW OF LITERATURE
9
Review of Literature (Introduction of the Disease)
INTRODUCTION OF THE DISEASE
The term Ziabetus is a Greek word which means “to run through” or “Siphon”, is
characterized by hyperglycaemia, glycosuria, increased appetite, excessive thirst and
gradual loss of body weight. Dayasqoomas (1,2,3,4), Qaramees (1,3,4), Dawwarah
(1,2,4,5,6,7,8,9),Dolab (1,2, 3,4,5, 6, 7,8,9,10, 11, ,12), Zalaq-ul-kuliya (1,2, 3,4, 6, 7, 8,
9,11,12),Salesul-baul (5,6,9,12), Istisqae anmas (5,6,12),Barkarya (3,4,5,6,7), Moattasa
(5,7) and Attasa (12) are the synonyms commonly used for Ziabetus in Unani System of
Medicine. In Ziabetus, the patient excretes water as such through urinary passage soon
after its intake. The ratio of fluid taken and the urinary output remains the same (Zalqul
majari) as that of solid without digestion from the stomach and intestine, a condition
known in Unani medicine as 'Zalqul-ama'. There is excessive thirst more intake of water
and its rapid discharge as urine. The patient also experiences a feeling of heat in the back
around the waist and in the right side of the body. When the disease takes the body
completely in its grip dryness will develop all over the body rendering it weak.
There are four major causes described in most of the classical Unani literature,
responsible for the development of Ziabetus:
1. Sue mizaj har kuliya (Abnormal hot temperament of kidney).
(1,2,3,4,5,6,7,8,10,11,13,14,15,16,17,18,19)
2. Zoufe-kuliya (Weakness of kidney). (1,2,5,7,8,11)
3. Majari ka kushada ho jana (Dilatation of renal vessels). (1,2,5,7,8,11)
4. Sue mizaj barid of tamam badan / kuliya / jigar (Abnormal cold temperament of
body / kidney / liver). (1,2,3,4,5,6,7,8,10,11,14,15,17,18)
10
Review of Literature (Introduction of the Disease)
Among all above mentioned causes, most emphasis was given to abnormal hot
temperament of kidney by most of the eminent Unani physicians during the
description of Ziabetus. They also described that weakness of kidney and dilatation of
renal vessels occurs due to abnormal hot temperament of kidney. (1, 2, 5, 6, 7, 8, 10,
11, 13, 18)
Ziabetus Can Be Divided Into Two Types:
(A) Ziabetus har and (B) Ziabetus barid
(A) Ziabetus har: In this disease the patient feels very much thirst and passes white
coloured urine frequently and the urine contains sugar. In fact it is the Diabetes in
true sense. The excretion of sugar renders the body weak, the muscles degenerated
and become lean and thin and the general health is run down. (4, 7, 9, 12, 15, 20)
(B) Ziabetus barid: In this condition the patient feels acute thirst and passes white
coloured urine in large quantity but does not contain sugar. This type of Ziabetus can
be matched with Diabetes Insipidus. (4, 7, 9, 12, 15, 20)
Nowadays the accepted concept of Diabetes mellitus is that, it is a chronic
disorder of carbohydrate metabolism and glucose intolerance, characterized by high
blood glucose level and glycosuria resulting from dysfunction of pancreatic β cells and
insulin resistance. The defective β cells result in lack of total or partial synthesis of
insulin. Chronic hyperglycaemia also affects metabolism of protein and lipids. (21)
11
Review of Literature (Introduction of the Disease)
There are four types of Diabetes Mellitus depending upon its aetiology and
treatment among them two are main: Type-1 or Insulin Dependent Diabetes Mellitus
(IDDM) and Type-2 or Non-Insulin Dependent Diabetes Mellitus (NIDDM).
Type-1 Diabetes Mellitus: Type-1 Diabetes (formerly known as Insulin-Dependent
Diabetes, childhood Diabetes, or juvenile-onset Diabetes) is most commonly diagnosed
in children and adolescents, but can occur in adults, as well. It is characterized by β-cell
destruction, which usually leads to an absolute deficiency of insulin. Most cases of Type-
1 Diabetes are immune-mediated characterized by autoimmune destruction of the β-cells
in the Islets of Langerhans of the pancreas, destroying them or damaging them
sufficiently to reduce insulin production. However, some forms of Type-1 Diabetes are
characterized by loss of the β-cells without evidence of autoimmunity. (22)
Type -2 Diabetes Mellitus: This form of Diabetes, previously referred to as Non-Insulin
Dependent Diabetes, Type-2 Diabetes, or adult-onset Diabetes, is a term used for
individuals who have insulin resistance and usually have relative (rather than absolute)
insulin deficiency (23, 24, 25, 26). At least initially, and often throughout their lifetime,
these individuals do not need insulin treatment to survive. The specific aetiologies of
this form of Diabetes are not known, but many factors like heredity, age, obesity, diet,
sex, sedentary life style, socio economic status, hypertension and various stresses are
supposed to be involved in the aetiology of Diabetes Mellitus. Most patients of Type-2
Diabetes Mellitus are obese, and obesity itself causes some degree of insulin resistance
(27, 28). Patients who are not obese by traditional weight criteria may have an increased
percentage of body fat distributed predominantly in the abdominal region (29).
Ketoacidosis seldom occurs spontaneously in this type of Diabetes; when seen, it usually
12
Review of Literature (Introduction of the Disease)
arises in association with the stress of another illness such as infection (30, 31, 32). This
form of Diabetes frequently goes undiagnosed for many years because the
hyperglycaemia develops gradually and at earlier stages is often not severe enough for
the patient to notice any of the classic symptoms of Diabetes (33, 34, 35). Nevertheless,
such patients are at increased risk of developing macro-vascular and micro-vascular
complications (35, 36, 37, 38, 39). Whereas patients with this form of Diabetes may have
insulin levels that appear normal or elevated, the higher blood glucose levels in these
Diabetic patients would be expected to result in even higher insulin values had their beta-
cell function been normal (40). Thus, insulin secretion is defective in these patients and
insufficient to compensate for the insulin resistance. The risk of developing this form of
Diabetes increases with age, obesity, and lack of physical activity (34, 41). It occurs
more frequently in women with prior GDM (Gestational Diabetes Mellitus) and in
individuals with hypertension or dyslipidemia, and its frequency varies in different
racial/ethnic subgroups (34, 35, 41). It is often associated with a strong genetic
predisposition, more so than is the autoimmune form of Type-1 Diabetes (42, 43).
However, the genetics of this form of Diabetes are complex and not clearly defined.
Classically, the age of onset of Type-2 Diabetes is above 40 years. However in
Indians it has been found to be a decade earlier than in the west. Occasional patients
might develop Type-2 Diabetes in the second decade of life. Obesity is not a common
feature in Type-2 Diabetes in India. Only about 50% of cases have a BMI > 25 kg / m2
while, 15-20 % of the patients are underweight. (21)
13
Review of Literature (Diagnostic Criteria)
DIAGNOSTIC CRITERIA
Revised criteria for diagnosing Diabetes Mellitus (Ziabetus Shakri) have been
issued by consensus panel of experts from the National Diabetes data group and the
world health organization. The revised criteria reflect new epidemiologic and metabolic
evidence and are based on the following premises:
1. The spectrum of fasting plasma glucose and the response to an oral glucose load varies
in normal individuals.
2. Diabetes Mellitus defined as the level of glycaemia at which Diabetes specific
complications are noted and not on the level of glucose tolerance from population based
viewpoint.
In the new diagnostic criteria the oral glucose tolerance test which was previously
recommended by the National Diabetes Data group has been replaced with the
recommendation that the diagnosis of Diabetes Mellitus be based on:
Two consecutive readings of fasting plasma glucose levels of 126 mg/dl
(7.0 mmol/L) or higher.
Other options for diagnosis include:
Two consecutive readings of casual plasma glucose concentration
(Random) 200 mg /dl (11.1 mmol / L) or higher with symptoms of
Diabetes i.e. polyuria, polydipsia or unexplained weight loss. Casual is
defined as any time of day without regard to time since last meal.
47
Review of Literature (Diagnostic Criteria)
Or
Finding of two consecutive readings of two hour post prandial plasma
glucose readings > 200 mg /dl during an oral glucose tolerance test.
Fasting plasma glucose is selected as the primary diagnostic test because it predicts
adverse outcomes (e.g. retinopathy) as well as the two hour post prandial blood glucose
test. But fasting plasma glucose is much more reproducible than oral glucose tolerance
test or the Random blood glucose test and easier to perform in a clinical setting.
Criteria For Testing For Diabetes Mellitus In Asymptomatic Undiagnosed Individuals:
1. Testing for Diabetes should be considered in all individuals at age 45 years and
above and, if normal, it should be repeated at 3 years intervals.
2. Testing should be considered at a young age or be carried out more frequently in
individuals who are
Obese ( > 120% desirable body weight or a BMI > 27 kg /m2 )
Habitually physically inactive.
Have a first degree relative with Diabetes.
Members of a high risk ethnic population.
Have delivered a baby weighing >9 lb (i.e.> 4.032 kg) or Have been diagnosed
with Gestational Diabetes Mellitus.
Hypertensive (BP > 140/90 mm Hg).
Have a HDL cholesterol level < 35 mg /dl (0.90 mmol /L) and / or a triglyceride
level > 250 mg /dl (2.82 mmol/L).
On previous testing, had Impaired Glucose Tolerance or Impaired Fasting
Glucose. ( 21, 22, 173)
48
Review of Literature (Gurmar Booti)
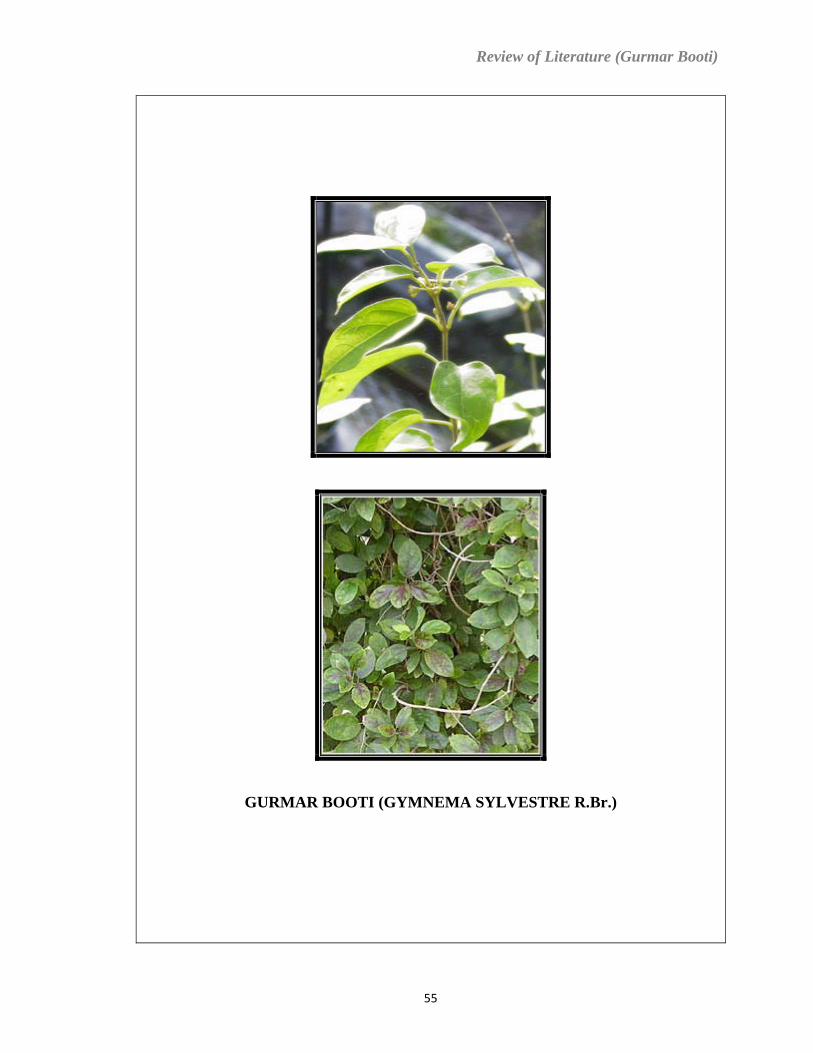
GURMAR BOOTI (GYMNEMA SYLVESTRE R.Br.)
55
Review of Literature (Gurmar Booti)
GURMAR BOOTI (GYMNEMA SYLVESTRE R.Br.)
1. Unani Name Gurmar booti (174, 175, 176, 177, 178)
2. Botanical Name Gymnema sylvestre R.Br. (176, 177, 178, 179, 180, 181, 182)
3. Family Asclepiadaceae (176, 177, 178, 179, 180, 181, 182)
4. Vernaculars
Bengali ..........Mera-singi, Chhota-dudhilata.
English.......... Gymnema sylvestre, Periploca of the woods.
Gujrati...........Dhuleti, Mardashingi.
Hindi.............Gur-mar, Merasingi.
Kannada ........Sannagerasehambu.
Marathi..........Kavali, Kalikardori, Vakundi.
Sanskrit..........Meshashringi ( Ram’s horn ), Madhu nashini,
Sarpadarushtrika.
Tamil .............Adigam, Cherukurinja.
Telagu............Padapatri.
Unani.............Gurmar booti. (174, 175, 177, 179, 180, 181, 182)
56
Review of Literature (Gurmar Booti)
5. Introduction
The description of Gurmar booti is not found in the classical text
books of Unani Medicine written by eminent scholars of Arab. However, Najmul Ghani
described this drug in his book “Khazainul Advia” with Indian reference. Gymnema
sylvestre is a shrubby climbing plant called Meshasringi, “ram’s horn” in Sanskrit, and
Gurmar booti in Hindi and Unani. It has been used for more than thousands of years in
India to treat Diabetes. Sushruta describes Gymnema sylvestre as a destroyer of
Madhumeha (Glycosuria) and other urinary disorders. On account of its property of
abolishing the taste of sugar it has been given the name of “Gurmar” meaning “sugar
destroying” and it is believed therefore, that it might neutralize the excess of sugar
present in the body of Diabetic patient. Its root also has been reported as a remedy for
snake bite for this purpose the powdered root being applied to the part bitten, and a
decoction given internally. In modern literature Gymnema sylvestre or Gurmar is first
described by Roxburgh under the name of “Asclepias geminate”, but he did not describe
anything about its medicinal properties. After Roxburgh, Mr.Edgeworth, noticed that on
chewing its leaves, it destroys the power of the tongue to appreciate the taste of sugar and
all saccharine substances. This property is later proved in 1887 AD by Dr. Hooper, who
says “After chewing one or two leaves it was proved undoubtedly that sugar had no taste
immediately afterwards”. But now it is a well established fact that this effect does not last
for 24 hours as stated, but for only one or two hours, after that time the tongue resumes
its appreciation of sweet taste. (177, 181, 182)
57
Review of Literature (Gurmar Booti)
6. Habitat: Woody climber found in central and southern India, on the Western Ghats,
in the Goa territory, and in the tropical Africa (177, 178, 180, 181, 182).
7. Morphology:
A large woody much branched climber running over the tops of high
trees; young stems and branches pubescent, often densely so, terete. Leaves are 3.2-5.0
cm by 1.3-3.2 cm ,ovate, elliptic, or ovate-lanceolate, acute or shortly acuminate; upper
surface dark green, shining, under surface pale green, more or less pubescent on both
sides; venation transverse and reticulate with a marginal vein; petioles 6-13 mm long ,
pubescent. Flowers in pedunculate or nearly sessile cymes; peduncles densely pubescent,
shorter than the petioles and arising from between them, sometimes producing successive
umbels or whorls of flowers; pedicels 3-13 mm long, pubescent; bracts minute, ovate-
oblong, hairy ciliate. Calyx pubescent, divided to the base or nearly so; segments 2mm
long, oblong, obtuse, ciliolate. Corolla yellow,4-5 mm across; tube campanulate,1.5 mm
long, about equalling the lobes; lobes thick, ovate-deltoid, speading, recurved, glabrous;
corona of 5 processes inserted on the corolla-tube, alternate with its lobes, free at the
short deltoid subacute tip which protrudes above the sinus, the lower adnate portion
decurrent, channelled and with strongly ciliate margins. Style apex thick,
subhemispherical, much exserted beyond the anthers, pearly white. Follicles 6.3-7.5 by
0.8 cm, terete, rigid. Lanceolate, attenuated into a beak, glabrous, one follicle often
suppressed. Seeds 1.3 cm long, narrowly ovoid-oblong, flat, with a thin broad marginal
wing, brown, glabrous. The taste of plant is bitter, acrid. According to Unani literature
58
Review of Literature (Gurmar Booti)
Gurmar booti is a shrubby climbing plant having dense branches. Its leaves are 4-5 inches
long and resembles with the leaves of Eagle Marmelos. On chewing leaves are bitter.
(174, 175, 177, 178, 179, 180, 182)
8. Parts Used: Leaves, Stem, Root. (174, 175, 176, 177, 178, 179, 180, 182)
9. Temperament:
Hot and Dry in second degree. (174, 175, 178)
10. Actions:
In Unani Literature : Muqawwie Meda (Stomachic), Qate Munashshiyat
( Anti-narcotic), Antidiabetic, Tiryaq (Antidote), Mulayyan
(Demulcent), Muharrike-Qalb wa Dorane-khoon (Stimulant to
Heart and Blood Circulation). (174, 175, 176, 177, 178)
In Modern Literature: Stomachic, Stimulant, Laxative, Diuretic, Astringent, Tonic,
Antiperiodic, Cooling, Alterative, Anthelmintic, Alexiteric,
Emetic, Expectorant .(179, 180, 181)
11. Uses:
It is commonly used as a remedy for Diabetes Mellitus and glycosuria. Its root
has long been used as a remedy for snake bite, its powder being dusted upon the wound,
or made into paste with water and applied and a decoction given internally. Leaves when
chewed paralyse the sense of taste for sweet and bitter substances for some time. A
59
Review of Literature (Gurmar Booti)
decoction of leaves is useful for fever and cough. Leaves triturated and mixed with castor
oil are applied to swollen glands and to enlargement of internal viscera as the liver and
spleen. A mixture of leaves and black pepper is given for cholera. Leaves are also useful
in eye complaints, cures opacities of the lens, cornea, and vitreous body. It is also useful
in heart diseases, piles, leucoderma, inflammations, burning sensation, biliousness,
bronchitis, asthma, ulcers and used to relieve irritation in plague. (174, 175, 176, 177,
178, 179, 180, 181)
12. Phytochemical Studies:
The leaves contain hentriacontane, pentatriacontane, a-and ß-chlorophylls, phytin, resins,
tartaric acid, formic acid, butyric acid, anthraqui-none derivatives, inositol, d -quercitol
and "gymnemic acid". The leaves give positive tests for alkaloids. Flavonol glycosides,
kaempferol and quercetin have been isolated from the aerial parts of the plant (183).
Three new oleanane-type triterpene glycosides were isolated from the leaves of the plant.
Six oleanane-type saponins (184, 185). Few new tritepenoid saponins, gymnemasins A,
B, C and D were also isolated from the leaves of Gymnema sylvestre. (186, 187)
13. Important Formulations: Qurs Ziabetus khas, Qurs Ziabetus. (178,188)
14. Muzir : Non-toxic (177)
15. Musleh : Not mentioned in books
16. Badal : Not mentioned in books
17. Dose : 4-6 gms (177, 178)
60
Review of Literature (Gurmar Booti)
18. Scientific Studies:
The hypoglycaemic action of Gymnema leaves was first documented in the late
1920s by Mhasker and caius (189). This action is attributed to members of a family of
substances called gymnemic acids (190, 191). According to research in healthy
volunteers, Gymnema leaves raise insulin levels (192, 193, 194). Based on animal
studies, this may be due to regeneration of the cells in the pancreas that secrete insulin
(195, 196, 197, 198) or by stimulation of β cell function and increasing the flow of
insulin from these cells (199, 200). Other animal researches shows that Gymnema can
also reduce glucose absorption from the intestine (201, 202), improve uptake of glucose
into cells, and prevent adrenal hormones from stimulating the liver to produce glucose,
thereby reducing blood sugar levels and increasing glucose tolerance (203, 204, 205, 206,
207, 208 ).Other animal studies have shown that extracts of Gymnema leaves can lower
serum cholesterol and triglycerides and prevent weight gain (209, 210, 211, 212, 213).
When placed directly on the tongue, gurmarin, another constituent of the leaves, and
gymnemic acid have been shown to block the ability in humans to taste sweets (214,215).
A preliminary trial in a group of type 1 and type 2 diabetics have shown promising results
with a dose of 800 mg per day of an extract standardized for 25 % gymnemic acid. (216)
61
Review of Literature (History)
HISTORY
Ziabetus is known since the age of antiquity, where symptoms of Ziabetus were
described. It is commonly believed that the history of medicine began with the Greeks,
and before the time of Buqrat (460 BC), Ancient Egypt (Misri) was the first civilization
known to have an extensive study of medicine and to have left behind written records of
its practices and procedures. It is proved by the discovery of the Ebers papyrus in the
graves of thabes by famous German Egyptologist Georg Ebers in 1862 AD. The Ebers
papyrus is one of the most famous document relating to the ancient practice of medicine,
written about 1550 BC. Ebers papyrus contains descriptions of various diseases including
a polyuric state resembling Ziabetus shakri (44,45,46). Although the Unani physician
Buqrat (460 BC) “The father of medicine” did not specifically mentioned Ziabetus in his
writings, there are accounts in the Buqrat’s writings that are consistent with the sign and
symptoms of Ziabetus, like excessive urinary flow with wasting of the body (46).
Arsyatoos ( Aretaeus ) and Jalinoos (Galen) were followers of Buqrat. Arsyatoos ( 81-
138 AD ) provided the first accurate description of the symptoms of Ziabetus. He was the
first who use the term “Ziabetus” in connection with this ailment,which means “to run
through” or “Siphon”. He described the disease as “Ziabetus is a dreadful affliction, not
very frequently among men, being a melting down of the flesh and limbs into urine”
(45,47,48,49,50). Jalinoos (131-201 AD), a contemporary of Arsyatoos, the most
influential medical writer of all time,discussed Ziabetus in a number of his books. He
described the condition as rare, as he had only seen two cases, he referred to the ailment
as “Diarrhoea Urinosa ( Diarrhoea of urine )” and “dipsakos ( the thirsty disease)”
14
Review of Literature (History)
(45,46,51). However, the association of polyuria with a sweet tasting substance in the
urine was first reported in Sanskrit literature dating from the 5th - 6th century AD at the
time of Susruta, Charaka and Vaghbata. They described the urine of polyuric patients
as having the taste like honey, being sticky to touch and strongly attracting the ants. The
Indian description of that time also contains Ziabetus like conditions of two types:
congenital and late onset. Also, the Indians noticed the relation of Ziabetus to heredity,
obesity, sedentary life and diet. During the same era, Chinese and Japanese physicians
also described Ziabetus and the sweetness of urine of Ziabetus patients, which apparently
attracted dogs. They also observed that people with Ziabetus were prone to develop boils
and an affliction which clinically resembles tuberculosis (45,46,52). During the 9th -11th
centuries AD, Arabic medicine was at its peak of achievements and Arabian physicians
translated the works of Buqrat and Jalinoos and enriched them with latest knowledge of
that era. Two prominent physicians of this era who contributed to the knowledge of
Ziabetus were Shaikh-Ul-Rais Bu Ali Ibne Sina (960-1037 AD) and Musa Bin
Maimoon ( 1135 AD). Ibne Sina described accurately the clinical features of the disease
and mentioned two specific complications of the disease,namely gangrene and the
collapse of sexual function. While on the other hand Musa Bin Maimoon claimed to have
seen more than 20 cases. He proposed that Ziabetus was caused by the sweet water of
river nile and the prevailing heat that spreads over the kidneys (45,46). No further
progress was made in the understanding of Ziabetus until the 16th century AD. When the
swiss physician Von Hohenheim ( Paracelsus ) reported that urine of Ziabetus (Diabetic)
patients contained an abnormal substance which remained as a white powder after
evaporation, he concluded that this substance was salt and that Diabetes was due to the
15
Review of Literature (History)
deposition of salt in the kidneys causing thirst of the kidney and polyuria (45). The
modern history of Diabetes began with the Thomas Willi’s ( 1621-1675 AD )
observations of Diabetes in 1674 AD and Matthew Dobson’s experiments in 1776 AD
that conclusively established the diagnosis of Diabetes in the presence of sugar in the
urine and blood. Diabetes was no longer considered a rare ailment. Thomas Willis
referred to Diabetes as the “Pissing evil” and noted that in patients with Diabetes, “The
urine was wonderfully sweet, as if it were imbued with honey or sugar”. He claimed that
Diabetes was primarily a disease of the blood and not the kidneys. Willis proposed that
the sweetness first appeared in the blood and was later found in the urine. During the
same era Thomas Sydenham ( 1624-1689 AD ) speculated that Diabetes was a systemic
disease arising in the blood where “Chyle” was incompletely digested and its non-
absorbed residue had to be excreted. After Thomas Sydenham, Johann Conrada
Brunner ( 1653-1727 AD ) came very close to discovering pancreatic Diabetes when he
observed in 1682 AD that, After the incomplete removal of the pancreas from a dog,
“…..the animal made water very frequently and that he was very thirsty, drinking largely
of water in proportion to the discharge of urine” (45,46,53,54,55,56,57). Cullen was the
first person who distinguished Diabetes into two types. In this classification, we find first
time a distinction between Diabetes, with the urine of “the smell; colour and flavor of
honey,” and Diabetes, with limpid but not sweet urine (46). The concept of Thomas
Sydenham was further elaborated by Matthew Dobson (1735-1784 AD), who provided
experimental evidence that people with Diabetes pass sugar in their urine. He gently
heated two quarts of urine to dryness. The remaining residue was a whitish cake,which
Dobson wrote “ was granulated and broke easily between the fingers; it smelled sweet
16
Review of Literature (History)
like brown sugar, neither could it be distinguished from sugar, except that the sweetness
left a slight sense of coolness on the palate”. Moreover he concluded that this substance
had previously existed in the serum rather than being formed in the kidneys. He wrote
“this idea of the disease explains its emaciating effects from so large a proportion of the
alimentary matter being drawn off by the kidneys, before it is perfectly assimilated and
applied to the purpose of nutrition (58). In 1788 AD Thomas Cawley described that
Diabetes may follow damage to the pancreas, such as through calculus formation (59).
Twenty years after the Matthew Dobson, in 1797 AD Matthew Baillie stated that “upon
examination of the kidneys……it seemed probable that Diabetes depends, in a
considerable degree, upon a deranged action of the secretory structure of the kidneys, by
which the blood there is disposed to new combinations” the effect of which is the
production of “a saccharine matter”. He also proposed that “the chyle may be so
imperfectly formed, as to make the blood be more readily changed into a saccharine
matter, by the action of the kidneys” (60). In 1798 AD, a year after the Matthew Baillie,
“John Rollo” a surgeon, expressed his opinion that “ the Diabetes Mellitus” is a disease
of the stomach and its immediate cause is a morbid condition of stomach evolving from
vegetable substances containing saccharine matter, which is quickly separated as a
foreign body by the kidney”(61). Further he was the first who use the adjective
“Mellitus” to distinguish the condition from other polyuric diseases in which glycosuria
was absent and urine was tasteless. Rollo made other contributions to the study of
Diabetes,including descriptions of “cataract due to Diabetes” and odour of acetone on the
breath of some Diabetes patients (62). In 1815 AD, Michel Eugene Chevreul (1786-1889
AD) published his experimental findings on urine and stated that sweet substance found
17
Review of Literature (History)
in urine of Diabetes patients was to be identical to grape sugar (63). In 1839 AD, John
Elliotson speaks about “grief”, “chills” and, “excess of venery” as possible etiological
factors for Diabetes in his “Principles and practice of medicine” (64). In the first half of
the 19th century Claude Bernard (1813-1878 AD) discovered that the liver releases a
substance that affects blood sugar levels. In 1875 AD, he isolated a starch like substance
that he called “Glycogen”, which was the precursor of glucose, “the internal secretion” of
the liver. This observation established the liver’s role as a vital organ in Diabetes. He also
demonstrated that the central nervous system was involved in controlling the blood
glucose concentration. He also performed many systematic experiments on the pancreas
(46, 65, 66, 67). During mid 19th century AD, William Prout (1785-1859 AD) described
“exposure to cold”, “attacks of rheumatism and gout”, “The drinking of cold fluids while
heated”, and “mental anxiety and distress” as the most frequent exciting causes of
Diabetes. He was the first, who recognized the coma as a complication of Diabetes (68).
Further in 1869 AD, H.D.Noyes, observed that a form of “retinitis” developed in
glycosuric patients (45), during the same year, Paul Langrhans ( 1847-1888 AD) had
noticed small clusters of ductless cells in teased preparations of pancreas, he simply
described these structures without speculating as to their possible function. It was only in
1893 AD that Edouard Laguesse (1861-1927 AD ) suggested that these clumps of cells
,which he named the “islets of langerhans” in honour of langerhans and suggested that
they might constitute the endocrine tissue of the pancreas (45,46,69,70). In 1874 AD,
Prof.A.Kussmaul (1822-1902 AD) described the “air hunger” of ketoacidosis (71). In
1875 AD, Dickinson published a paper “Diabetes, in his diseases of the kidneys”, in
which he defined Diabetes as “a disease of the nervous system characterized by the
18
Review of Literature (History)
secretion of saccharine containing urine” (72). In 1877 AD, Etienne Lancereaux (1829-
1910 AD) demonstrated a causal relationship between Diabetes and lesions of the
pancreas (73), and his friend, Apollinaire Bauchardat (1806-1886 AD), began the
modern therapy of Diabetes by limiting carbohydrates in the diet, advocating fast days,
and using exercise to help control glycosuria (74). In 1889 AD, Oskar Minkowski (1858-
1931 AD) and Josef Von Mering (1849-1908 AD) demonstrated conclusively that
removal of the pancreas from a dog results in the development of fatal Diabetes. This
observation firmly established the role of the pancreatic disorders in causing Diabetes
(75,76,77). Further in 1901 AD, Eugene Undsay Opie’s ( 1873-1962 AD ) pathologic
study on Diabetes Mellitus established that Diabetes is caused by a lesion of the pancreas,
and the lesion is of such kind in which the islands of langerhans are destroyed or injured
(78). In 1908 AD, Georg L.Zuelzer (1870-1949 AD) and Nicolas Paulesco ( 1869-1931
AD ) had prepared potent pancreatic extract before 1921 AD. In 1909 AD, Jean De
Meyer gave the name “ insulin” derived from the latin word insula ( insula=island ), to
the glucose lowering hormone, whose existence at that time was still hypothetical , which
he postulated was produced by the islet tissue (79). Further Moses Barron ( 1883 AD)
give conclusion regarding the relationship of islets of langerhans to Diabetes “…..that the
islets secrete a hormone directly into the lymph or blood streams (Internal
secretion),which has a controlling power over carbohydrate metabolism” (80). The
finding of Moses Barron triggered the investigations of Frederick Grant Banting (1891-
1941 AD) and Charles Herbert Best (1899 AD). In December 1921 AD, they got success
in isolation of insulin and published the results of their research on “The internal
secretion of the pancreas” in which they were able to demonstrate the reversal of the
19
Review of Literature (History)
metabolic changes of Diabetes by injection of a potent extract of the pancreatic islands
(81,82,83). On 11th Jan 1922 AD, the first patient of Diabetes a 14 year old boy named
Leonard Thombson was treated with insulin (54, 84). In 1923 AD Eli Lilly begins
commercial production of insulin, and called it "Isletin Insulin." In 1925 AD Home
testing for sugar in the urine through Benedict’s solution was introduced. In 1927 AD an
oral medication called "horment" or "glukohorment" was developed as a replacement for
insulin, but side effects are unacceptable and very soon dropped out. In 1930s AD Insulin
was further refined to Protamine zinc insulin, a long-acting insulin that provide more
flexibility. In 1936 AD Himsworth divided Diabetics into two types based on "insulin
sensitivity." In 1940's AD neutral protamine Hagedorn insulin was introduced and the
connection was established between Diabetes and long-term complications of kidney and
eye diseases. In late 1940's AD Helen Free developed the "dip-and-read" urine test
(Clinistix) allowing instant monitoring of blood glucose levels. In 1951 AD Lawrence
and Bornstein measured the amount of insulin in the blood and noted that older and
obese patients with Diabetes have insulin, but those who were young have none. In 1955
AD Oral drugs that help lower blood glucose levels was introduced. In 1959 AD, Two
major types of diabetes are recognized: Type 1 (Insulin-Dependent) Diabetes and Type 2
(Non-Insulin-Dependent) Diabetes. During the1959-1960 AD Yallow and Berson
developed the radioimmunological assay (RIA) procedure, to measure insulin with much
greater precision than earlier techniques, for that Yallow received the Nobel Prize in 1977
AD. In 1964 AD, The first strips for testing blood glucose were used. In1970 AD, First
blood glucose meter (Ames) and Insulin pumps were introduced. During the same year
Laser therapy was used to slow down or prevent blindness due to Diabetes. In1973 AD,
20
Review of Literature (History)
U-100 insulin is introduced. In 1976 AD, the glycosylated haemoglobin (A1C) test was
introduced as a monitor of glycaemic control. The manufacturing of insulin changed
dramatically with the advent of DNA technology that allows synthesis of a genetically
engineered "human" type of insulin, and in 1978 AD, production of the first recombinant
DNA insulin was announced. In 1979 AD, Type 1 and Type 2 Diabetes are formally
recognized by the American Diabetes Association. Type 1 is also called Insulin
Dependent Diabetes Mellitus (IDDM), and Type 2 is called Non Insulin Dependent
Diabetes Mellitus (NIDDM). In 1983 AD, the first biosynthetic human insulin, and
"Reflolux", later known as "Accu-Chek"(allows blood glucose self-monitoring) was
introduced .In 1996 AD, the FDA approved the first recombinant DNA human insulin
analogue, lispro (Humalog). In 2001 AD, FDA approved Cygnus' first-generation model
of the GlucoWatch Biographer for use by adults - the first frequent, automatic and non-
invasive glucose monitor. In 2003 AD, the names Insulin Dependent Diabetes Mellitus
(IDDM) for Type 1 and Non Insulin Dependent Diabetes Mellitus (NIDDM) for Type 2
diabetes are formally dropped. Today Researchers are working on an insulin patch and
inhaled insulin, Genetic engineering is being used to manipulate cells so they secrete
insulin. A sensor-computer-pump system that mimics the insulin response of the normal
pancreas is being developed to function as an "artificial pancreas". Apart from these,
various researches are still going on, to explore new aspects of Diabetes and its
management. (85, 86, 87, 88, 89, 90, 91, 92)
21
Review of Literature (Management)
MANAGEMENT OF ZIABETUS SHAKRI (DIABETES MELLITUS)
The goals of management in people with Ziabetus Shakri (Diabetes Mellitus) are:
To normalise the elevated blood sugar level.
Relief from Diabetic symptoms and improvement in quality of life.
Prevention of acute complications.
Prevention of microvascular complications like retinopathy, neuropathy and
nephropathy.
Prevention of macrovascular complications like cardiovascular, cerebrovascular
and peripheral vascular disease.
Prevention of infections.
Therefore the complete treatment of people with Diabetes Mellitus requires
advocating a healthy life style, Diabetes education with focus on proper balanced diet and
increased physical activity to attain and maintain desired body weight. Also meticulous
attention is to be given to achieve normoglycaemia, control of hypertension and
management of dyslipidemia with the help of Diet, Exercise, Oral hypoglycaemic agents
and insulin.
49
Review of Literature (Management)
1. Diabetes Education:
Diabetes education means empowering Diabetic patients with knowledge of Diabetes
and providing tools crucial for making them active partners in the Diabetes management,
these includes :
In depth information about Diabetes, its complications and treatment. Appropriate
self care skills.
Appropriate resources for self care.
A positive attitude.
Self monitoring skills.
2. Diet:
The aims of dietary management are to achieve and maintain ideal body weight,
euglycaemia and desirable lipid profile, prevent and postpone complications related to
Diabetes The dietary recommendations should be individualized according to person’s
ethnicity, cultural and family background, and personal preferences and associated co-
morbid conditions. It should be flexible in variety and preparation of food choices and
timing of meals according to person’s daily routine.
Dietary Recommendations:
A. Total Calorie Intake. The calorie requirements of Diabetic person depend on
physical activity and nutritional status as in a normal individual, unless there is
50
Review of Literature (Management)
glycosuria. Individual with > 120% of ideal weight is considered overweight and <
90% of ideal weight is underweight.
The ideal body weight (IBW) is calculated by formula:
IBW= (height in cm – 100) x 0.9
The caloric intake of person with Diabetes should be altered gradually, preferably not
more than 500 Kcal per day.
B. Total Calorie Distribution:
(i) Carbohydrate (55-60% of total calorie requirement):
Avoid sugar, honey, jaggery and sweets.
Restrict processed refined foods like maida-based products.
Main source should be cereals, mixed coarse grains, whole pulses, salads and
soybeans.
Roots and tubers should be used sparingly.
(ii) Protein (10-15% of total calorie requirement):
Protein from vegetable sources, low fat milk and milk products, fish and lean meat is
preferable.
(iii) Fat (20-25% of total calorie requirement):
Saturated fat - <7% of total caloric intake (including ghee and butter).
51
Review of Literature (Management)
Rest should be in from of MUFA and PUFA.
Trans-fatty acid (hydrogenated vegetable oils) should be avoided.
Dietary cholesterol should be minimal and in any case should not exceed 300mg
per day.
Use more than one edible oil.
Oils containing linoleic acid only such as ground nut, sesame, cotton seed, rice
bran and safflower should be used along with oils containing a-linoleic acid such
as soyabean, mustard, canola etc.
(iv) Fibers: Traditional Indian diet is rich in fibers. Fiber rich foods include whole
grains (ragi, jowhar, barley, oats etc.), whole pulses, soybean, green leafy vegetables and
fenugreek seeds.
(v) Fruits: Whole fruits are recommended in moderation (1-2 servings), however, very
sweet fruits and fruit juices should be avoided.
(vi) Common salt: Up to 6gm/day is permitted. Restrict pickles, papad, chatni and salty
processed foods
(vii) Alcohol: Alcohol intake is best avoided and if used, must be in moderation. It may
exacerbate, neuropathy, dyslipidemia, obesity and may worsen the control of Diabetes.
(viii) Artificial sweeteners: Use of artificial sweeteners in limited quantity is acceptable
but they are to be avoided during pregnancy and lactation.
(ix) Tobacco: Smoking and the use of tobacco in any form should be prohibited.
52
Review of Literature (Management)
C. Dietary Modifications In Special Situations
(i) Nephropathy: Dietary protein should be restricted to 0.6 gm/kg, and salt to 4 gm/day.
(ii) Hypertension: Dietary salt should be restricted to minimum.
(iii) Dyslipidemia: Total fat intake should be curtailed and diet to be modified by
increasing MUFA and dietary fibers by reducing saturated fatty acids.
(iv) Infections and acute illness: In such conditions, fasting should be avoided and
adequate caloric intake must be ensured.
3. Physical Activity
Regular physical activity is an essential component of management in persons
with Type 2 Diabetes. A careful assessment of an individual should be made by physician
while incorporating an exercise program in the management. Exercise programme should
be individualized according to individual capacity and disabilities. Exercise must be done
regularly such as brisk walk for 30 - 60 minutes or its equivalent physical activity. The
best form of exercise recommended to a Diabetic is a stepwise increase of aerobic
exercises. There are several benefits from a regular exercise schedule. These include
improvement in insulin sensitivity, reduction of hypertension, reduction in weight,
improvement in lipid profile (reduces serum triglycerides and increases HDL particularly
HDL2 cholesterol), improvement in cardiovascular function, increase in bone density,
improvement in the sense of physical and mental well being and improvement in quality
of life.
53
Review of Literature (Management)
Precautions During Exercise
Person with Diabetes and coronary artery disease should be prescribed
appropriate exercises after cardiac evaluation.
In proliferative Diabetic retinopathy, strenuous activity like diving, weight lifting
or bending may precipitate vitreous haemorrhage or retinal detachment. Walking
may be continued.
Person with Diabetes and overt nephropathy often have reduced capacity to
exercise.
Peripheral neuropathy results in loss of protective sensation in the feet. It is
advised to wear proper footwear. The person with Diabetes should be taught to
monitor for blisters and other damages to the feet before and after exercise.
Autonomic neuropathy may limit an individual's exercise capacity and increase
the risk of adverse cardiovascular events during exercise.
4. Oral Hypoglycemic Agents:
Oral hypoglycemic agents should be used in Type-2 Diabetes Mellitus in the
event of failure of diet and exercise. In Unani system of medicine certain drugs like Qurs
Dolabi, Safoof Tabasheer, Qurs Ziabetus, Qurs Nashkoor, Qurs Ziabetus khas, Safoof
Ziabetus are used, while in modern system of medicine various types of Oral
hypoglycemic agents are used like Tolbutamide, Glibenclamide, Glipizide, Metformin,
Phenformin etc. (112)
54
Review of Literature (Pancreas)
PANCREAS
The pancreas is a retroperitoneal gland, it is about 12 to 15 cm long and 2.5 cm
thick lies posterior to the greater curvature of the stomach. The pancreas consists of a
head, a body, and a tail and is connected to the duodenum by two ducts. Pancreatic
secretions pass from the secretory cells (Exocrine cells) in the pancreas into small ducts
that ultimately unite to form two large ducts that drain the secretions into the small
intestine. The larger of the two ducts is called the pancreatic duct (Duct of Wirsung). In
most people, the pancreatic duct joins the common bile duct from the liver and gall
bladder and enters the duodenum as a common duct called the Hepatopancreatic ampulla
(Ampulla of Vater). The smaller of the two ducts, the accessory duct (Duct of Santorini),
leads from the pancreas and empties into the duodenum about 2.5 cm superior to the
Hepatopancreatic ampulla. The pancreas is supplied by the pancreatic branches of the
splenic artery and pancreaticoduodenal arteries, and the venous drainage of pancreas is
via the pancreaticoduodenal veins which end up in the portal vein.
Histologically, the pancreas is composed of small clusters of glandular epithelial cells,
about 99 % of which are arranged in clusters called acini and constitute the exocrine
portion of the organ. The cells within acini secrete a mixture of fluid and digestive
enzymes called pancreatic juice. Remaining 1 % of the cells scattered amongst the acini
are the endocrine cells of the pancreas, in groups called the islets of Langerhans ,
arranged in clusters and cords and are crisscrossed by a dense network of capillaries. The
capillaries of the islets are lined by layers of endocrine cells, which are in direct contact
22
Review of Literature (Pancreas)
with blood vessels, by either cytoplasmic processes or by direct apposition. Islets of
Langerhans are composed of different kinds of cells:
Insulin-producing beta cells (50-80% of the islet cells).
Glucagon-releasing alpha cells (15-20%).
Somatostatin-producing delta cells (3-10%).
Pancreatic polypeptide-containing PP cells .
These cells are related with the regulation of blood glucose level. The levels of glucose in
the blood are monitored or regulated by different hormones liberated from these cells
with the help of negative feedback mechanism, to maintain the homeostasis. The most
important among them is insulin. Insulin is the “hormone of plenty”—it is released when
glucose is abundant and performs some important functions in the body.
Functions Of Insulin
In body it stimulates:
a) Muscle and fat cells to remove glucose from the blood
b) Body cells to breakdown glucose, releasing its energy in the form of ATP (via
glycolysis and the citric acid cycle)
c) The liver and muscles to store glucose as glycogen (short-term energy reserve)
d) Adipose tissues to store glucose as fat (long-term energy reserve) and inhibit fat
breakdown.
e) Cells to use glucose in protein synthesis.
23
Review of Literature (Pancreas)
Glucagon is the main hormone opposing the action of insulin and is released when food
is scarce. Glucagon triggers glycogen breakdown, which releases energy (a catabolic
effect), and also helps the body to switch to using resources other than glucose, such as
fat and protein, whereas insulin triggers the formation of glycogen (an energy-requiring
process, or an anabolic effect). Blood glucose level varies according to the body needs
and is regulated by hormones within a narrow range i.e. from 70 to 140 mg/dl. The blood
glucose level can rise because of diet, breakdown of glycogen, or through hepatic
synthesis of glucose. Eating produces a rise in blood glucose, the extent of which depends
on a number of factors such as the amount and the type of carbohydrate eaten (i.e. the
glycemic index), the rate of digestion, and the rate of absorption. Because glucose is a
polar molecule, its absorption across the hydrophobic gut wall requires specialized
glucose transporters (GLUTS of which there are five types GLUTS 1, GLUTS 2, GLUTS
3, GLUTS 4, GLUTS 5). In the gut, GLUT2 and GLUT5 are the most common.
The liver is a major producer of glucose—it releases glucose from the breakdown of
glycogen and also synthesizes glucose from intermediates of carbohydrate, protein, and
fat metabolism. The liver is also a major consumer of glucose and can buffer glucose
levels. It receives glucose-rich blood directly from the digestive tract via the portal vein,
and quickly removes large amounts of glucose from the circulation so that even after a
meal, the blood glucose levels rarely rise above 140 mg/dl in a non-diabetic. On the other
hand the rise in blood glucose following a meal is detected by the pancreatic beta cells,
which respond by releasing insulin. Insulin increases the uptake and use of glucose by
tissues such as skeletal muscles and fat cells. This rise in glucose also inhibits the release
of Glucagon, inhibiting the production of glucose from other sources, e.g., glycogen
24
Review of Literature (Pancreas)
break down. Once when the glucose enters inside the cells, some of the glucose is used
immediately via glycolysis. This is a central pathway of carbohydrate metabolism
because it occurs in all cells in the body and because sugar can be converted into glucose
and enters this pathway. During the well-fed state, the high levels of insulin and low
levels of Glucagon stimulate glycolysis, which releases energy and produces
carbohydrate intermediates that can be used in other metabolic pathways. The liver and
muscles take up any glucose that is not used immediately where it can be converted into
glycogen (glycogenesis). Insulin stimulates glycogenesis in the liver by:
a) Stimulating hepatic glycogen synthetase (the enzyme that catalyzes glycogen
synthesis in the liver).
b) Inhibiting hepatic glycogen phosphorylase (the enzyme that catalyzes glycogen
breakdown in the liver).
c) Inhibiting glucose synthesis from other sources (inhibits gluconeogenesis).
On the other hand Insulin also encourages glycogen formation in muscles, through a
different method. In muscles, it increases the number of glucose transporters (GLUT4) on
the cell surface. This leads to a rapid uptake of glucose that is converted into muscle
glycogen. When glycogen stores are fully replenished, excess glucose is converted into
fat by a process called lipogenesis. Glucose is converted into fatty acids that are stored as
triglycerides (three fatty acid molecules attached to one glycerol molecule) for storage.
Insulin promotes lipogenesis by:
a) Increasing the number of glucose transporters (GLUT4) expressed on the surface
of the fat cells, causing a rapid uptake of glucose.
25
Review of Literature (Pancreas)
b) Increasing lipoprotein lipase activity, this frees up more fatty acids for triglyceride
synthesis.
In addition to promoting fat synthesis, insulin also inhibits fat breakdown by inhibiting
hormone sensitive lipase (an enzyme that breaks down fat stores). As a result, there are
lower levels of fatty acids in the blood stream. Insulin also has an anabolic effect on
protein metabolism. It stimulates the entry of amino acids into cells and stimulates
protein production from amino acids. While during fasting blood sugar level fall and
inhibits insulin secretion and stimulates Glucagon release. Glucagon opposes many
actions of insulin. Most importantly, Glucagon raises blood sugar levels by stimulating
the mobilization of glycogen stores in the liver, providing a rapid burst of glucose. In 10–
18 hours, the glycogen stores are depleted, and if fasting continues, Glucagon continues
to stimulate glucose production by favoring the hepatic uptake of amino acids and
glycerol. In addition to low blood glucose levels, many other stimuli stimulate Glucagon
release including eating a protein-rich meal (the presence of amino acids in the stomach
stimulates the release of both insulin and Glucagon, Glucagon prevents hypoglycemia
that could result from unopposed insulin) and stress (the body anticipates an increased
glucose demand in times of stress).The metabolism of fatty acids (from adipose tissue) is
a major source of energy for organs such as the liver. Fatty acids are broken down to
acetyl-CoA, which is channeled into the citric acid cycle and generates ATP. As
starvation continues, the levels of acetyl-CoA increase until the oxidative capacity of the
citric acid cycle is exceeded. The liver processes these excess fatty acids into ketone
bodies (3-hydroxybutyrate) to be used by many tissues as an energy source. The most
important organ that relies on ketone production is the brain because it is unable to
26
Review of Literature (Pancreas)
metabolize fatty acids. During the first few days of starvation, the brain uses glucose as a
fuel. If starvation continues for more than two weeks, the level of circulating ketone
bodies is high enough to be used by the brain. This slows down the need for glucose
production from amino acid skeletons, thus slowing down the loss of essential proteins.
(93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103)
27
Review of Literature (Pathogenesis)
PATHOGENESIS OF ZIABETUS SHAKRI
Pathogenesis Of Ziabetus Shakri (Diabetes Mellitus) In Unani System Of Medicine
In Unani system of medicine, ancient Philosophers explained the pathogenesis of
Ziabetus Shakri (Diabetes Mellitus) logically and rationally. The mainstay of Ziabetus is
the development of abnormal hot temperament in the kidney. This altered hot
temperament renders the renal vessels paralyzed and hence dilated. The morbid hot
temperament disturbs the normal functioning of kidney and reduces the Quwwate Masika
(Retentive power) of kidney. In contrast to the reduced retentive power, the morbid hot
temperament, on the other hand increases the Quwwate Jazba (Absorptive power) of
kidney. The excessive thrust of Quwwate Jazba pulls and absorbs the excessively large
amount of water from the liver but as unable to digest and retain the fluid due to weak
Quwwate Masika and strengthen Quwwate Dafia, the fluid ultimately passes out towards
the urinary bladder and finally in the form of urine large amount of fluid excreted. The
deficit of fluid thus created in the liver is compensated by excessive absorption of fluid
from the Urooqe Masariqa (Mesenteric vessels). The Urooqe Masariqa absorbs the fluid
from stomach, and stomach demands plentiful fluid from outside in form of excessive
thirst. The concatenation of this demand and supply thus established between the organs,
produces a vicious cycle resulting in large intake of fluid as due to thirst and thereof
excessive and frequent urination.(1, 2, 5, 6, 7, 8, 10, 11, 13, 18)
38
Review of Literature (Pathogenesis)
Pathogenesis Of Diabetes Mellitus Type 2 In Modern System Of Medicine
Type-2 Diabetes Mellitus known as maturity onset type of Diabetes till 1979 AD
and non insulin dependent Diabetes thereafter, it accounts for 85 to 95 % of all patients
with Diabetes mellitus. Pathogenesis of this primary form of Diabetes Mellitus is
complex and varied. The disorder evolves slowly in course of several years with a
prolonged subclinical phase. Two distinct factors that work in tandem for the evolution
and progress of the disorder are:
A. Insulin secretory dysfunction i.e. failure of pancreatic β cells to release as much
insulin as required for metabolic control under the prevailing situation “relative
insulin deficiency”.
B. Impaired insulin action manifest as decreased insulin sensitivity of the target cells
i.e. “insulin resistance”.
Both insulin secretory function and sensitivity to insulin action are modulated by
hereditary and environmental factors. (21)
1. Insulin Secretory Dysfunction: Impaired insulin secretion is a uniform finding
in Type-2 Diabetic patients and the development of beta cell dysfunction has been well
characterized in diverse ethnic populations (121, 122, 123, 124, 125, 126, 127, 128, 129,
130, 131, 132). Early in the natural history of type-2 Diabetes Mellitus, insulin resistance
with loss or reduction of Ist phase and prolongation of 2nd phase of insulin secretion is
well established (121, 122, 127, 129, 130, 131, 133, 134, 135, 136, 137), but glucose
tolerance remains normal because of a compensatory increase in insulin secretion (121,
122, 125, 126, 127, 129, 130, 131, 134, 135, 136, 138, 139, 140). Within the normal
39
Review of Literature (Pathogenesis)
glucose tolerant population, approximately 20-25 % of individuals are severely resistant
to the action of insulin (141). However, insulin secretion in these insulin resistant Non-
Diabetic individuals is increased in proportion to the severity of insulin resistance and
glucose tolerance remains normal (141). As the fasting plasma glucose concentration
rises from 80 to 140 mg /dl, the fasting plasma insulin concentration increases
progressively, up to two to three fold above that in normal glucose tolerant subjects. The
progressive rise in fasting plasma insulin level is an adaptive response of the pancreas to
maintain normal glucose homeostasis. However, when the fasting plasma glucose
concentration rises above 140 mg/dl, it causes glucotoxicity to β cells and affects insulin
gene transcription, leading to decreased insulin synthesis and secretion (122, 123, 126,
127, 136, 142, 143). Hyperglycaemia and hypoinsulinaemia causes lipotoxicity to β cells
by increasing plasma free fatty acid (FFA) levels which make situation worse, because
prolonged exposure of β cells to elevated plasma FFA levels leads to further inhibition of
insulin secretion. Increased fatty acyl CoA levels within the β cells also impair beta cell
function and causes apoptosis of beta cells (144, 145, 146). Apart from gluco-
lipotoxicity, some other factors contribute to beta cell dysfunction and leads to impaired
insulin secretion like Incretin deficiency and / or incretin resistance (147,148,149,150)
and hyper secretion of amylin (151). Apart from these acquired causes some genetic
factors are also implicated in inducing defect in β cell function. Monogenic mutations
leading to defects in insulin secretion have been documented in five types of maturity
onset type of Diabetes in the young (MODY) and two clusters with mitochondrial DNA
mutation thus for such patients may account for 1 % of Non-insulin dependent Diabetes
40
Review of Literature (Pathogenesis)
among the Caucasians. Specification of genetic loci in the rest still continues to remain as
nightmare for geneticists. (21)
2. Impaired Insulin Action Or Insulin Resistance: Insulin resistance implies decreased
peripheral uptake of glucose as well as inadequate suppression of hepatic glucose
production and lipolysis in response to insulin. Relatively high levels of insulin at fasting
and in response to secretogogues are indicative of insulin resistance. Insulin resistance is
well known in obesity (21), because obesity is an extremely important diabetogenic
influence and not surprisingly, approximately 80 % of Type-2 Diabetes Mellitus patients
are obese. (152)
Seats Of Insulin Resistance
A. Muscle: Skeletal muscles and adipose tissues required insulin for optimal glucose
uptake and utilization. In Type-2 Diabetes Mellitus, entry of glucose into myocytes
occurs only through mass action as available insulin fails to recruit more GLUT 4 for
facilitated transport of glucose across the cell membrane, and result in reduction of
glucose uptake. Further insulin mediated augmentation of glucose utilization is impaired
in muscles of patients with Type-2 Diabetes Mellitus. Late increase in the contents of
triglycerides in skeletal muscles has been implicated to induce insulin resistance in the
muscles. (21)
B. Liver: In Type-2 Diabetes Mellitus restraining effects of insulin in hepatic glucose
production (HGP) is impaired and leads to increase HGP during post absorptive and
fasting states.(21)
41
Review of Literature (Pathogenesis)
C. Adipose Tissue: Free fatty acids are stored as triglycerides in adipocytes and serve as
an important energy source during conditions of fasting. Insulin is a potent inhibitor of
lipolysis and restrains the release of FFA from the adipocytes by inhibiting the enzyme
hormone sensitive lipase. In Type-2 Diabetics the ability of insulin to inhibit lipolysis and
reduce the plasma FFA concentration is markedly reduced. Prolonged elevation of
plasma FFA concentration leads to insulin resistance in muscles and liver thus impair
insulin secretion. (121, 122, 153, 154, 155, 156, 157, 158, 159, 160, 161)
Cellular Mechanism Of Insulin Resistance: The stimulation of glucose metabolism by
insulin requires that the hormone must first bind to specific receptors that are present on
the cell surface of all insulin target tissues. After insulin has bound to and activated its
receptor “second messengers” are generated which initiate a series of events that
eventually result in the stimulation of intracellular glucose metabolism under the control
of insulin (121, 162, 163, 164, 165, 166, 167, 168). In Type-2 Diabetes Mellitus insulin
binding to target tissue is reduced due to decreased number of receptors without change
in insulin receptor affinity. In addition to the decreased number of cell surface receptors,
a variety of defects in insulin receptor internalization and processing also occurred.
(169,170)
42
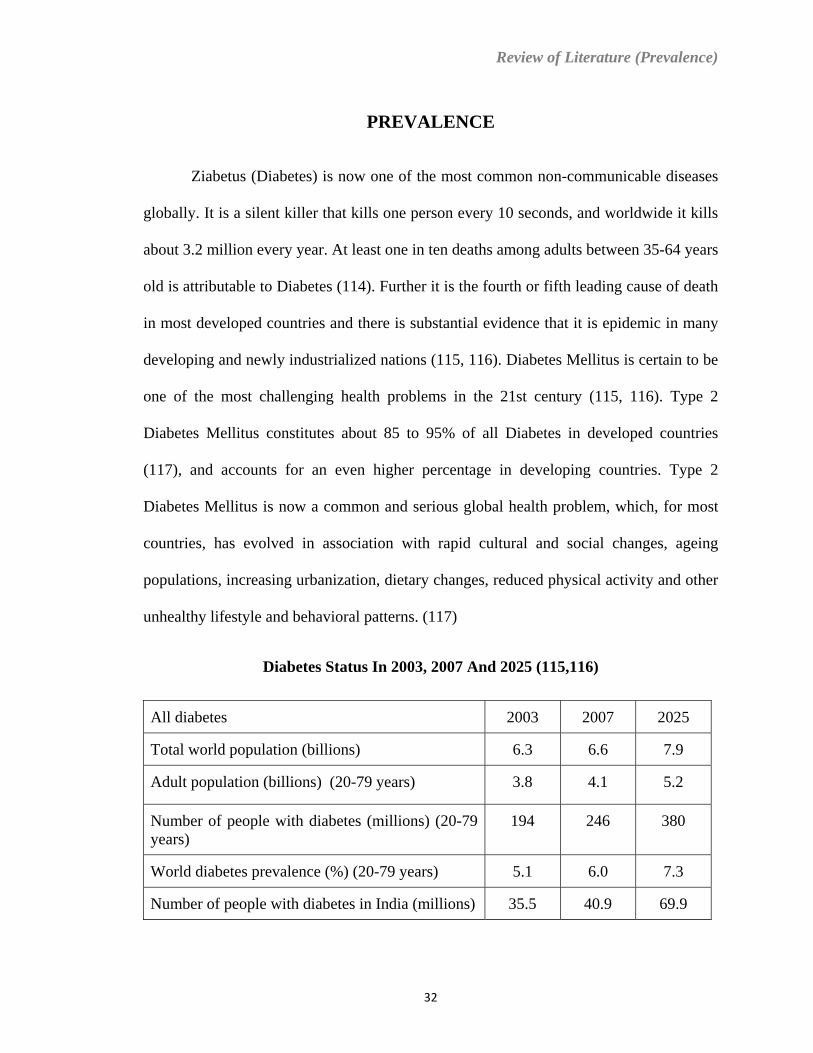
Review of Literature (Prevalence)
PREVALENCE
Ziabetus (Diabetes) is now one of the most common non-communicable diseases
globally. It is a silent killer that kills one person every 10 seconds, and worldwide it kills
about 3.2 million every year. At least one in ten deaths among adults between 35-64 years
old is attributable to Diabetes (114). Further it is the fourth or fifth leading cause of death
in most developed countries and there is substantial evidence that it is epidemic in many
developing and newly industrialized nations (115, 116). Diabetes Mellitus is certain to be
one of the most challenging health problems in the 21st century (115, 116). Type 2
Diabetes Mellitus constitutes about 85 to 95% of all Diabetes in developed countries
(117), and accounts for an even higher percentage in developing countries. Type 2
Diabetes Mellitus is now a common and serious global health problem, which, for most
countries, has evolved in association with rapid cultural and social changes, ageing
populations, increasing urbanization, dietary changes, reduced physical activity and other
unhealthy lifestyle and behavioral patterns. (117)
Diabetes Status In 2003, 2007 And 2025 (115,116)
All diabetes 2003 2007 2025
Total world population (billions) 6.3 6.6 7.9
Adult population (billions) (20-79 years) 3.8 4.1 5.2
Number of people with diabetes (millions) (20-79 years)
194 246 380
World diabetes prevalence (%) (20-79 years) 5.1 6.0 7.3
Number of people with diabetes in India (millions) 35.5 40.9 69.9
32
Review of Literature (Prevalence)
Current Prevalence:
It is estimated that currently (2007) some 246 million people worldwide, or 6.0% in the
adult population, have diabetes and that this will increase to 380 million, or 7.3%, by
2025. The Western pacific region with 67 million and the European region with 53
million will have the highest number of people with Diabetes in 2007. However, in terms
of prevalence, it is the Eastern Mediterranean and Middle East region which has the
highest rate (9.2%) followed by the North American region (8.4%). (115, 116, 117)
By 2025 the Diabetic prevalence of the South and Central American region is expected to
be nearly as high (9.3%) as that of North America region (9.7%). The Western Pacific
region will continue to have the highest number of people with Diabetes, with some 100
million, representing an almost 50 % increase from 2007. (115, 116)
Age Distribution
The 40-59 year age group currently has the highest number of persons of Diabetes with
some 113 million (46 % of total world Diabetic population), of which more than 70 %
live in developing countries. (115, 116, 118)
Gender distribution
The estimates for both 2003 and 2025 showed a female predominance in the number of
persons with diabetes. The female numbers were about 10% higher than for males. (115)
33
Review of Literature (Prevalence)
Urban/Rural distribution
In 2003, the number of people with diabetes in urban areas was 78 million, compared to
44 million persons with diabetes in rural areas. By 2025, it is expected that this
discrepancy will increase to 182 million urban and 61 million rural persons with diabetes.
In India prevalence of diabetes in urban population is 5.9 % and in rural population it is
2.7 %. ( 115, 119)
34
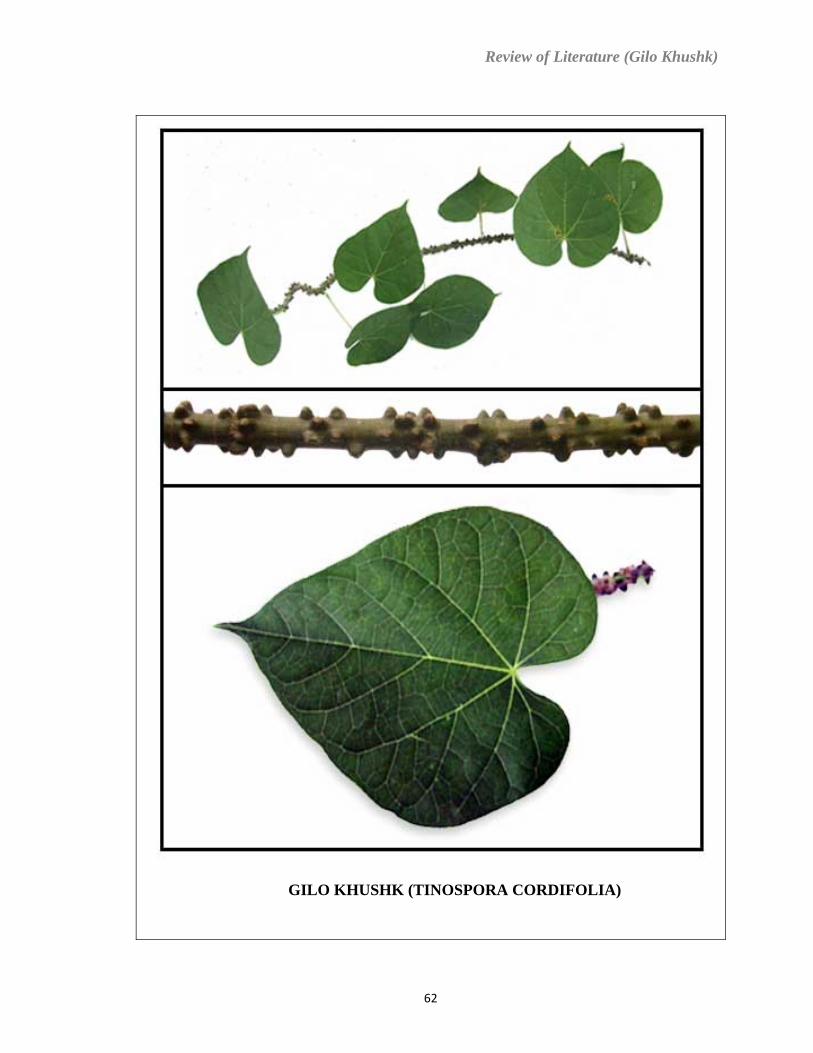
Review of Literature (Gilo Khushk)
GILO KHUSHK (TINOSPORA CORDIFOLIA)
62
Review of Literature (Gilo Khushk)
GILO KHUSHK (TINOSPORA CORDIFOLIA)
1. Unani Name : Gilo Khushk (174, 175, 217, 218, 219, 220, 221)
2. Botanical Name : Tinospora cordifolia (181, 182, 219, 220, 222, 223, 224)
3. Family : Menispermaceae (181, 182, 219, 222, 223, 224)
4. Vernaculars:
Arabic ……….......Jilo
Bengali………......Gadancha, Giloe, Gulancha, Guluncha, Nimgilo.
Ceylon……….......Chintil
China……….........K'uan Chu Hsing
French……….. .....Culancha
Goa………….........Amritvel, Amrityel
Gujarati……… ....Gado, Galo, Gulo, Gulwel
Hindi……….........Giloe, Gulancha, Gulbel, Gurach, Gurcha
Kannada…….......Amrytaballi, Madhuparne, Uganiballi
Malayalam…….....Amrytu, Peyamrytam, Sjttamrytu
Marathi……….....Ambarvel, Gharol, Giroli, Gulavela, Gulaveli, Guloe, Gulvel.
Nepal………….....Garjo
63
Review of Literature (Gilo Khushk)
Persian……… .....Gulbel.
Punjab…………...Batindu, Garham, Garum, Gilo, Gilogularich, Zakhmihaiyat
Sanskrit………..... Amrita, Amritalata, Amritavallari, Amritavalli, Bhishaka-priya,
Chakralakshana,Chakrangi,Chandrahasa,Chandrapasa, Chchinna,
Chehinnaruha.
Sikkim……….......Gurjo
Tamil……….........Amridavalli, Amudam, Asasi, Kaippuchindil, Kunali.
Telugu……….......Duyutige, Guduchi, Iruluchi, Jivantika, Madhuka, Manapala,
Somida.
Uriya………….....Gulancha, Gulochi.
Unani ……............Gilo (174, 175, 181, 182, 217, 220, 221, 222, 223, 224)
5. Introduction:
A large, glabrous, deciduous climbing shrub found throughout tropical
India known as “Gilo” in Unani, and Guduchi in Sanskrit. In ancient era it is commonly
used as a Dafe Nobat (Antiperiodic) in fevers, and as a Muqawwi (Tonic) and Moaddil
(Alterative); it is also credited with Muqawwie Bah (Aphrodisiac) properties. The fresh
plant is said to be more efficient than the dry; it is taken with milk in Wajaul Mafasil
(Rheumatism), Hurqate Baul (Acidity of urine) and Sue Hazm (Dyspepsia). Its juice with
64
Review of Literature (Gilo Khushk)
honey and pakhanbed is useful in Suzak (Gonorrhoea). In Gujarat, a necklace called
Kamala-ni-mala (Jaundice necklace) is made of small pieces of the stem, and is
supposed to cure that disease. The stem, if placed upon a bush in the open air, will retain
its vitality through the hot season, and when the rains commences, put forth leaves and
long whipcord-like roots, which soon reach the ground. A starch like substance is
prepared from its dry stem known as Sat Gilo. Tinospora cordifolia first time attracted the
Europeans during the early part of 19th century, by those who have tried it as a tonic,
antiperiodic and diuretic. Now at present it is an official part of Pharmacopoeia of India.
(174, 175, 181, 182, 220, 221, 222, 223, 224)
6. Habitat: Throughout tropical India, Ceylon and Burma. (181, 182, 220, 222, 223, 224)
7. Morphology
A woody climber, with perennial stems reaching 2 inches in diameter, with
a thick, soft, warted bark, the younger branches succulent with the bark smooth, giving
out adventitious roots sometimes many yards in length and excessively slender, which
lengthen downwards and at last reach the soil. Leaves alternate, on long flexuous
petioles, spreading, and 2—4 inches long, roundish-ovate, entire, cordate at the base,
acute at the apex, quite smooth, thin, somewhat glaucous beneath and resembles with the
betel leaves. Flowers dicecious, pedicellate, inconspicuous, yellow, in short, axillary,
long-stalked racemes, the male in small fascicles, the female solitary, bracts minute.
Male flowers :—Sepals 6 in two rows of 3- each, the outer short, roundish, the inner
twice as long, broadly obovate, concave, smooth; petals 6, opposite the sepals, and about
65
Review of Literature (Gilo Khushk)
half the length of the inner ones, clawed below, somewhat 3-lobed above, with the lateral
lobes involute, stamens 6, longer than the petals, immediately in front of which they stand
and by which they are partially enwrapped, filaments much thickened at the end, anther-
cells oblong, widely separated below; no rudiment of carpels.
Female flowers :—Sepals as in the male ; petals oblong-spathulate ;stamens reduced to
small oblong scales in front of the petals; carpeis 3, distinct, opposite the outer sepals,
elevated on a thick gynophobe, ovary oblong-ovoid, smooth, style short, thick, stigma
dilated, tongue-shaped, laciniate.
Fruit of 3 (or more usually less by abortion) shortly stalked, subglobose drupes, with
an apiculus on one side marking the position of the style, about as large as a pea, red,
pulp scanty, putamen thin, bony, convex outside, with a deep, large, hollow process
extending to the middle of the fruit on the ventral surface, making the cavity horse-shoe-
shaped. Seed similar in form to the cavity which it fills, embryo enclosed in the copious
endosperm which is ruminated on the hollow, ventral surface, radicle rounded, superior,
cotyledons leafy, ovate, veined, very divaricated.(174,175,182,217,219,220,222,223,224)
8. Parts Used: Stem, Root and Leaves. (174,175,181,182,217,220,221,222,223,224)
9. Temperament: Hot and dry in first degree (Dry)
Hot and wet in first degree (fresh)
According to Sharif khan Murakkabul- quwa. (174,175,218,219,221)
66
Review of Literature (Gilo Khushk)
10. Actions :
In Unani: Muqawwi (Tonic), Dafe Humma (Antipyretic), Dafe Nobat
(Antiperiodic), Muqawwie Meda (Stomachic), Katile Kirme
Shikam (Anthelmintic), Musaffie Khoon (Blood purifier),Mudire
Baul (Diuretic), Munaffise Balgham (Expectorant), Muqawwie
Bah (Aphrodisiac), Mushtahi (Appetiser), Dafe qae (Anti-emetic)
(174, 175, 217, 219, 220, 221).
In Modern: Anti-inflammatory, Adaptogenic, Antineoplastic, Antioxidant,
Hepatoprotective, Immunomodulator, Analgesic, Antispasmodic,
Hypoglycaemic. (181, 182, 222, 223, 224)
11. Uses:
• The stem is bitter stomachic, stimulates bile secretion, causes constipation, tonic,
and diuretic, enriches the blood, and cures jaundice, useful in skin diseases.
• The juice is useful in diabetes, vaginal and urethral discharges, Mild fevers and
enlarged spleen.
• Starch obtained from the roots and stems of plant known as Sate Gilo used in
chronic diarrhea and some form of chronic dysentery. But it is also a valuable
nutrient when there is intestinal irritability and inability to digest any kind of food.
In case of acid diarrhea due to acidity of the intestinal canal or acid dyspepsia. It
is also useful in relieving the symptoms of rheumatism.
67
Review of Literature (Gilo Khushk)
• Freshly prepared juice from the green plant is a powerful diuretic so given to cure
urinary tract infections and gonorrhea. For Gonorrhea it is also given with
pakhanbed and honey.
• The root and stem of T. Cordifolia are prescribed in combination with other drugs
as an antidote to snake bite and scorpion sting. The juice and decoction of the root
are applied to the part bitten, poured frequently into the eyes and administered
internally by mouth at intervals of half an hour.
• The root is a powerful emetic and used for visceral obstructions and its watery
extract is used in leprosy.
• A decoction of Gilo leaves is used for the treatment of gout, and young leaves,
bruised in milk, are used as a liniment in erysipelas. The leaves are beaten with
honey and used for ulcers.
• Dried and powdered fruit with ghee or honey is prescribed as a tonic and also in
the treatment of jaundice and rheumatism. T. Cordifolia is also widely used in
India for treating diabetes mellitus. (174, 175, 181, 182, 217, 218, 219, 221, 222,
223, 224, 225, 226)
12. Phytochemical Studies
A large number of compounds have been isolated from the aerial parts and roots of
T. cordifolia. In the early 1900s, giloin, gilenin, and gilosterol were found in the plant
together with the bitter principles columbin, chasmanthin, and palmarin (227). More
recently, a wide variety of sesquiterpenes and diterpenes have been isolated from the
68
Review of Literature (Gilo Khushk)
stems of the plant. The major isolated compounds include the following: Cordiofolisides
A, B, and C (new norditerpene furan glycosides) (228); tinocordifolin and
tinocordifolioside (daucane-type sesquiterpenes) (229,230); palmatosides C and F
(furanoid diterpene glucosides) (231); cordioside, tinosponone, and tinocordioside
(clerodane diterpenoids) (232, 233); tinosporaside (a novel 18-norclerodane diterpene
glucoside) (234), and tinocordiside (a new cadinane sesquiterpene glycoside) (235). In
addition, syringin, cordiol, cordioside, cordifoliosides A and B (new phenylpropene
disaccharides) were identified as the active principles with anticomplement and
immunomodulatory activities (236, 237). It has been shown that the stems of the plant
contain the alkaloid berberine, and cultures of stem callus from this plant have been
shown to have the capability of synthesizing this compound (238). Ecdysterone,
makisterone A, and 20β-hydroxyecdysone are the phytoecdysones isolated from the
aerial parts of the plant (239, 240, 241). Other constituents reported from T. cordifolia
include a new phenolic lignan and the following compounds: Octacosanol, nonacosan-15-
one, heptacosanol, β-sitosterol, tinosporidine, cordifol, cordifolone (242, 243),
magnoflorine, tembetarine (244), syringine, and syringine apiosylglycoside (245).The
roots of T. cordifolia contain isocolumbin, palmatine, tetrahydropalmatine, magnoflorine,
and jatrorrhizine. (246, 247)
12. Important Formulations: Safoof Sat-e-gilo (248), Safoof Gilo, Roghan Gilo (220).
13. Muzir: Little or no side effects. Toxicological studies on rabbit do not show any
Adverse effects. (249, 250)
14. Musleh: Tabasheer and Dana heel. (175)
69
Review of Literature (Gilo Khushk)
15. Badal: Sat-e-gilo (175)
16. Doses:
Powder: 4-6 Masha [Masha = Gram] (174)
1-2 Tola [Tola = 10 Gram] (175)
Decoction: 2-3 Tola (175)
17. Scientific Studies:
Experimental trials on T.cordifolia shows that it exhibits insulin
like activity, decreases the blood glucose level, and inhibit adrenaline-induced
hyperglycaemia in rats and rabbits. It also reduces serum and tissue cholesterol,
phospholipids, and free fatty acids levels and also reduces levels of brain lipids in rats
(251, 252, 253). Its aq.extract is found to exhibit antispasmodic activity in rabbit and also
found to decrease Blood pressure and producing bradycardia temporarily in anaesthetised
dogs (223). T.cordifolia is reported to benefit the immune system in a variety of ways
(254). The alcoholic and aqueous extracts of T.cordifolia have been tested successfully
for immunomodulatory activity (255). It helps by increasing the effectiveness of WBC
and builds up the body’s immune system. It also has significantly reduced the mortality
from E.coli induced peritonitis in mice. In clinical study, it has afforded protection in
cholestatic patients against E.coli infection (256).
In animals, it exhibits anti-oxidant and anti-inflammatory properties (257, 258, 259), and
also found to kill the HeLa cells very effectively in vitro hence shows Antineoplastic
activity (249). The anti-stress and tonic property of the plant was clinically tested and it
70
Review of Literature (Gilo Khushk)
was found that it brought about good response in children with moderate degree of
behaviour disorders and mental deficit (251). In other experimental trials it is found that
Tinospora cordifolia also exhibit Hepatoprotective property in goat, and in vitro
inactivating property against Hepatitis B and E surface antigen (260, 261). Other reported
properties of T.cordifolia includes Antimalarial, Antipyretic properties (246, 249, 258).
71
Methodology
METHODOLOGY
72

Methodology
MATERIAL AND METHODS
For the assessment of efficacy of Safoof Ziabetus the patients of Ziabetus Shakri
were selected from the National Institute of Unani Medicine Hospital, Bangalore. Before
conducting the trial, the proposed research project was submitted for the approval to the
Institutional Ethical Committee of National Institute of Unani Medicine, Bangalore, and
the same was approved by the Committee.
After obtaining ethical clearance, the patients were selected on the basis of detailed
history and pathological investigations. The findings were recorded on the prescribed
proforma designed for the study. The patients fulfilling the inclusion criteria were
included in the study after obtaining the informed consent in writing, while those patients
who did not qualify the inclusion criteria or came under exclusion criteria were excluded
from the study.
Criteria For The Selection Of Patients
1. Inclusion Criteria
A. All patients of Ziabetus Shakri confirmed by investigations.
B. Patients belonging to 30-60 years of age of either sex.
C. Patients able to participate in the study and ready to follow the instructions.
2. Exclusion Criteria
A. Patients below the age of 30 years and above the age of 60 years.
B. Female patients with pregnancy and lactation.
C. Patients with Cardiovascular diseases.
D. Patients with Renal diseases.
73
Methodology
E. Patients with Hepatic disorders.
F. Patients with Type-1 Diabetes Mellitus.
G. Patients having complications like Gangrene and Diabetic Ketoacidosis.
To exclude the patients from the study, detailed history, physical examination and the
following biochemical investigations were carried out:
• Kidney function test (Blood Urea, Serum Creatinine) was done to exclude renal
diseases.
• Liver function test (Serum Bilirubin, SGOT, SGPT, and Alkaline Phosphatase)
was done to exclude liver diseases.
• ECG was done to exclude Cardiac disorders (Angina, Myocardial Infarction etc.).
Following Investigations Were Carried Out In Patients Before The Treatment:
A. Haematological Investigations:
• Hb%
• TLC
• DLC
• ESR
B. Biochemical Investigations:
(i) Blood Sugar
• Fasting
• Post prandial
74
Methodology
(ii) Kidney Function Test
• Blood Urea
• Serum Creatinine
(ii) Liver Function Test
• Total Bilirubin
• SGPT (ALT)
• SGOT (AST)
• Alkaline Phosphatase
(iii) Serum Cholesterol
C. Urine Analysis
• Routine Examination
• Microscopic Examination
D. ECG
Assessment Of Mizaj (Temperament)
The temperament (Mizaj) of the patients was assessed evolving different parameters,
suggested by Unani authors for the purpose. Details of these parameters have been given
in the CRF proforma.
Clinical Evaluation Of The Disease
Patients suffering from Ziabetus Shakri were interrogated and subjected to complete
physical and clinical examination as per details given in the CRF proforma.
75
Methodology
Chief Complaints
The complaints which brought patient to the doctor were written in chronological order
with duration.
History Of Present Illness
A detailed history of development of present clinical symptoms Like Polyuria, Nocturia,
Polydipsia, Tiredness, General Weakness, Increased appetite, Wasting of muscles, Loss
of body Weight, Non-healing or Delayed healing of cuts and Wounds, Paraesthesia, Pain
in the limbs were recorded.
History Of Past Illness
All patients were thoroughly interrogated for history of past Illnesses like Obesity /
Overweight, Gestational Diabetes Mellitus, Pancreatitis, Hypertension, Ischemic heart
diseases etc. and the findings were noted.
Family History
History of specific diseases like Diabetes Mellitus, Hypertension, Ischemic heart
diseases, Stroke in family members like parents, brothers and sisters, were recorded.
General Physical Examination
General physical examination of all patients was done. Special emphasis was given to
examination of Pulse, Blood Pressure, Temperature, Respiratory rate, Weight, Pallor,
Oedema, Built, JVP, Cyanosis, and the eyes were observed for cataract.
76
Methodology
Systemic Examination
A. Cardiovascular System
The examination of Cardiovascular system was carried out and the findings
were recorded as follows:
(i) Inspection : To observe deformities, dilated vessels and impulses.
(ii) Palpation : To determine the site and character of apex beat, thrills and
other impulses.
(iii) Percussion : To determine area of cardiac dullness and other dullness’s.
(iv) Auscultation: At different areas to record heart sounds and other sounds like
murmurs, friction rub etc.
B. Respiratory System
The Respiratory System was thoroughly examined and the findings were
recorded as follows:
(i) Inspection : To observe shape and movements of chest and swelling or
lesion if any.
(ii) Palpation : To observe position of trachea, apex beat, movements of chest,
tenderness, vocal fremitus, swelling.
(iii) Percussion: To determine the percussion note of lungs, area of cardiac
dullness, upper border of liver dullness and other dullness’s.
(iv) Auscultation: To record breath sounds, vocal resonance and added
sounds.
77
Methodology
C. Digestive System :
The Digestive System was thoroughly examined and the findings were recorded as
follows:
(i) Inspection of :
(a) Mouth : To know the condition of teeth, tongue, and gums.
(b) Abdomen: For scar, distension, dilated veins, hernia, discolouration, masses
and movements.
(ii) Palpation and Percussion: To observe the condition of liver, spleen, kidney,
stomach, bladder etc.
(iii) Auscultation over the abdomen for bowel sounds and other added sounds.
D.Nervous System
The Nervous System was thoroughly examined for mental state, speech, neck
stiffness, cranial nerves, motor and sensory functions, reflexes and the findings
were recorded on the CRF Proforma.
E.Urogenital System
The Urogenital system was thoroughly examined by inspection, palpation,
percussion, and auscultation for any abnormality and the findings were recorded
on the CRF Proforma.
78
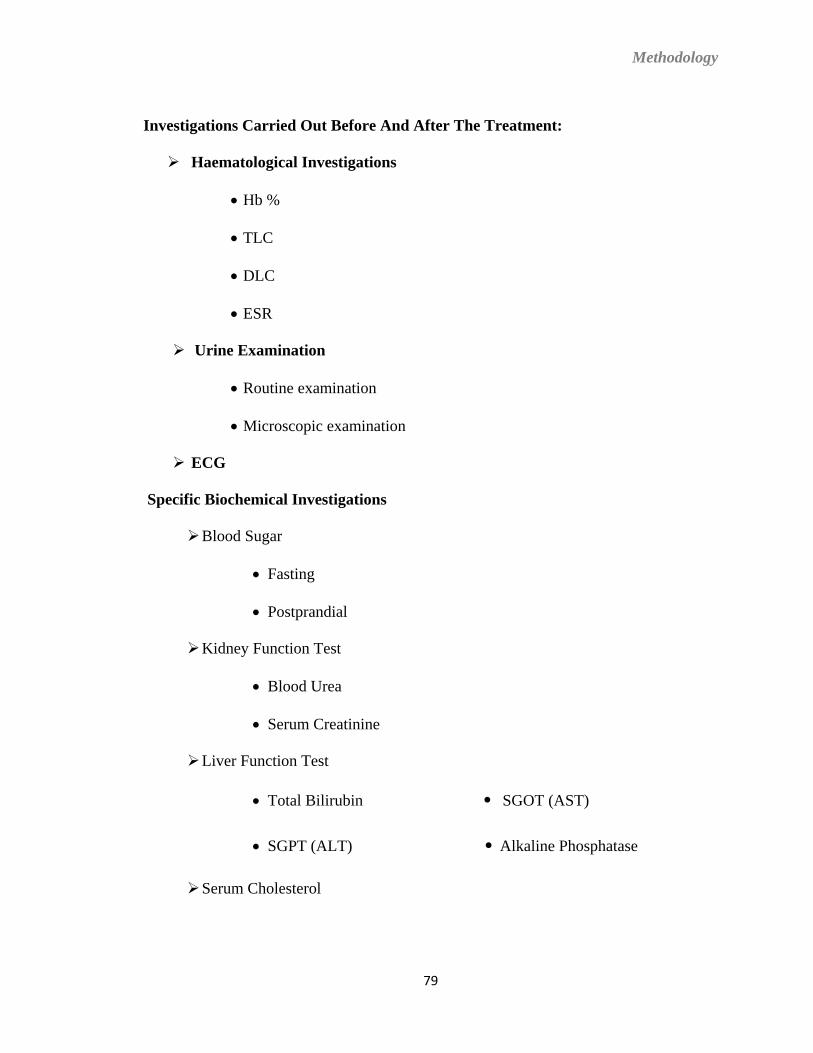
Methodology
Investigations Carried Out Before And After The Treatment:
Haematological Investigations
• Hb %
• TLC
• DLC
• ESR
Urine Examination
• Routine examination
• Microscopic examination
ECG
Specific Biochemical Investigations
Blood Sugar
• Fasting
• Postprandial
Kidney Function Test
• Blood Urea
• Serum Creatinine
Liver Function Test
• Total Bilirubin • SGOT (AST)
• SGPT (ALT) • Alkaline Phosphatase
Serum Cholesterol
79
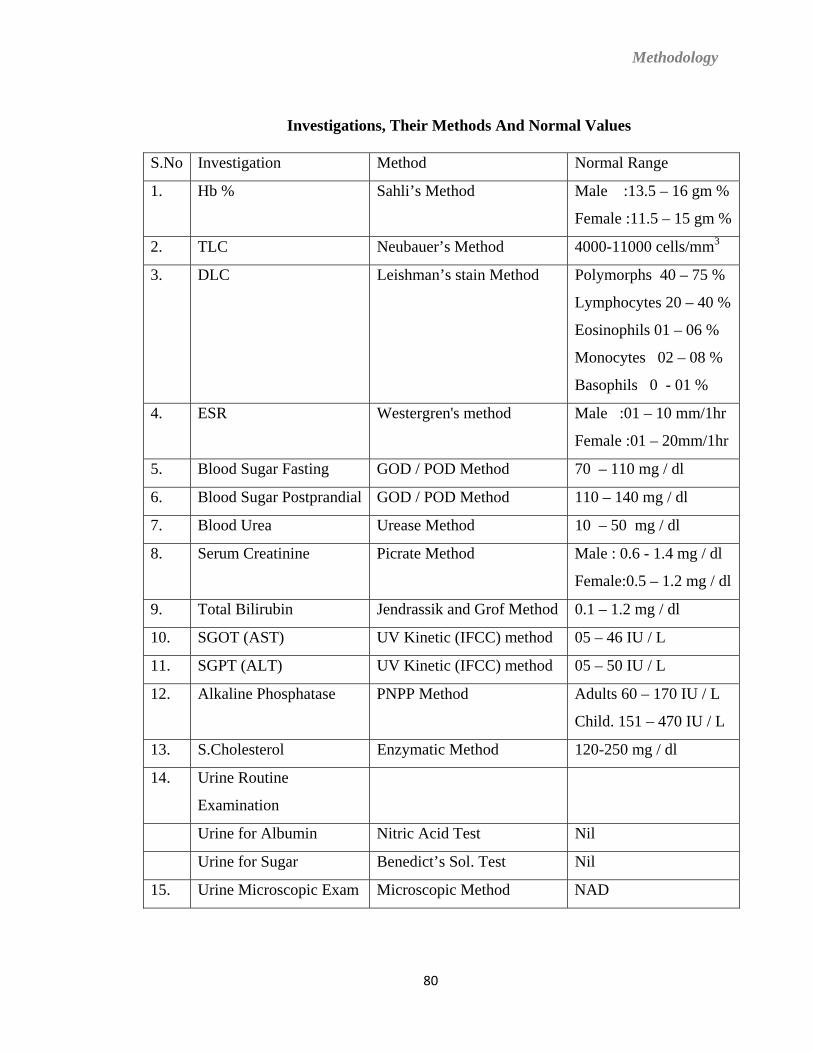
Methodology
Investigations, Their Methods And Normal Values
S.No Investigation Method Normal Range
1. Hb % Sahli’s Method Male :13.5 – 16 gm %
Female :11.5 – 15 gm %
2. TLC Neubauer’s Method 4000-11000 cells/mm3
3. DLC Leishman’s stain Method Polymorphs 40 – 75 %
Lymphocytes 20 – 40 %
Eosinophils 01 – 06 %
Monocytes 02 – 08 %
Basophils 0 - 01 %
4. ESR Westergren's method Male :01 – 10 mm/1hr
Female :01 – 20mm/1hr
5. Blood Sugar Fasting GOD / POD Method 70 – 110 mg / dl
6. Blood Sugar Postprandial GOD / POD Method 110 – 140 mg / dl
7. Blood Urea Urease Method 10 – 50 mg / dl
8. Serum Creatinine Picrate Method Male : 0.6 - 1.4 mg / dl
Female:0.5 – 1.2 mg / dl
9. Total Bilirubin Jendrassik and Grof Method 0.1 – 1.2 mg / dl
10. SGOT (AST) UV Kinetic (IFCC) method 05 – 46 IU / L
11. SGPT (ALT) UV Kinetic (IFCC) method 05 – 50 IU / L
12. Alkaline Phosphatase PNPP Method Adults 60 – 170 IU / L
Child. 151 – 470 IU / L
13. S.Cholesterol Enzymatic Method 120-250 mg / dl
14. Urine Routine
Examination
Urine for Albumin Nitric Acid Test Nil
Urine for Sugar Benedict’s Sol. Test Nil
15. Urine Microscopic Exam Microscopic Method NAD
80
Methodology
After thorough clinical examination and laboratory investigations, 79 diagnosed
patients of Ziabetus Shakri were included in the study. Out of 79 patients, 29 patients did
not complete full course of treatment. Only 50 patients completed the treatment during
the study.
For the assessment of efficacy of Unani formulation (Safoof Ziabetus), patients of
Ziabetus Shakri were divided into two groups i.e. “Group A and Group B". Group A
contained 30 patients while Group B contained 20 patients. Group A was given the test
drug (Safoof Ziabetus) whereas Group B placebo.
Preparation Of The Drug
The ingredients of Safoof Ziabetus [Gurmar Booti (Gymnema Sylvestre), Gilo Khushk
(Tinospora Cordifolia)] (262) were supplied by National Institute of Unani Medicine
Pharmacy, Bangalore.
Proper identification of ingredients was done by Chief Pharmacist of NIUM Pharmacy, to
ensure the originality and authenticity of the drugs. After proper identification, the
ingredient of Safoof Ziabetus was cleared from all impurities and ground to fine powder,
under the guidance of Dr. Mohd. Nafis Khan, Chief Pharmacist, NIUM Pharmacy,
Bangalore and filled in capsules of 1 gm capacity.
Similarly placebo was supplied by NIUM Pharmacy, and identified by Chief Pharmacist.
After proper identification the placebo was filled in capsules in same way as the test drug.
Study Design
The research design used for the study was randomized single blind placebo diet control.
81
Methodology
SAFOOF ZIABETUS
PLACEBO
82
Methodology
Sample Size
Total 50 patients [30 pts in Group A (Test drug) and 20 pts in Group B (Placebo drug)]
were included in the study.
Duration Of Protocol
The total duration of protocol was 45 days.
Drug Dose And Dosage Schedule
The Safoof Ziabetus filled in capsules was given to Group A in a dose of 6 gm thrice a
day (i.e. Six Capsules of 1 gm each) orally with water,15 minutes before breakfast, lunch
and dinner for 45 days. Total daily dose of Safoof Ziabetus given to each patient was 18
gm in three divided doses. Group B was treated in same way as the test group but with
placebo.
The capsules given to both Groups i.e. Group A and Group B were identical in size,
shape and colour.
Diet
All the patients of Ziabetus Shakri included in the study were advised to take their
tailored made diet as per ICMR Guidelines, to achieve and maintain ideal body weight,
euglycaemia and desirable lipid profile to prevent or at least postpone the complications
related with Ziabetus.
83
Methodology
Exercise
All the patients of Ziabetus Shakri included in the study were advised to follow exercise
programme as per ICMR Guidelines to do regular physical activity. The exercise
programme was individualized according to individual capacity and disabilities.
Follow-Up
All the patients of Ziabetus Shakri included in the study, were kept under strict
observation and asked to come every fortnightly for proper follow-up and assessment of
subjective and objective parameters. Findings were recorded on the prescribed CRF
proforma.
Criteria For Assessment Of Results
To assess the response of treatment on patients of Ziabetus Shakri in Group A and Group
B, following subjective and objective parameters were used in the study:
Subjective Parameters
1. Polyuria
2. Nocturia
3. Polydipsia
4. Tiredness
5. General Weakness
6. Increased appetite
7. Wasting of muscles
8. Weight gain without any apparent reason
9. Non-healing or Delayed healing of cuts and wounds.
10. Paraesthesia
84
Methodology
11. Pain in limbs
12. Defective vision
13. Impotence
14. Pruritus vulvae
15. Balanitis
16. Nausea
17. Vomiting
18. Depression
19. Irritability
Objective Parameters
1. Blood Sugar Fasting
2. Blood Sugar Post Prandial
3. Urine for Sugar
Procedure Of Study
After thorough clinical examination of the patients and laboratory investigations,
seventy nine diagnosed patients of Ziabetus Shakri who fulfilled the inclusion criteria
were selected for the study. Out of these 29 patients did not complete full course of
treatment. Only 50 patients completed the treatment during the study.
For the assessment of efficacy of Unani formulation (Safoof Ziabetus), patients of
Ziabetus Shakri were divided into two groups i.e. “Group A and Group B". Group A
contained 30 patients and Group B contained 20 patients. Group A was given test drug
(Safoof Ziabetus) and Group B placebo in a dose of 6 gm thrice a day in capsule form
orally with water,15 minutes before breakfast, lunch and dinner, for the period of 45
85
Methodology
days. During the study each patient was advised to take their tailored made diet and to
follow exercise programme as per ICMR Guidelines.
All the patients included in the trial were asked to come to the hospital every fortnightly
for proper follow-up. During the complete course of study each patient visited the
hospital four times i.e. at 0 day, 15th day, 30th day, and 45th day. Complete laboratory
investigations (As mentioned in the CRF proforma) were carried out before and after the
treatment. Besides, Blood Sugar Fasting and Postprandial, Urine for Sugar, and thorough
clinical examination carried out on every visit. The findings were recorded on the
prescribed CRF proforma.
Statistical Analysis
After completion of study, obtained data was analysed with the help of Student’s‘t’ test.
86
Results
RESULTS
87
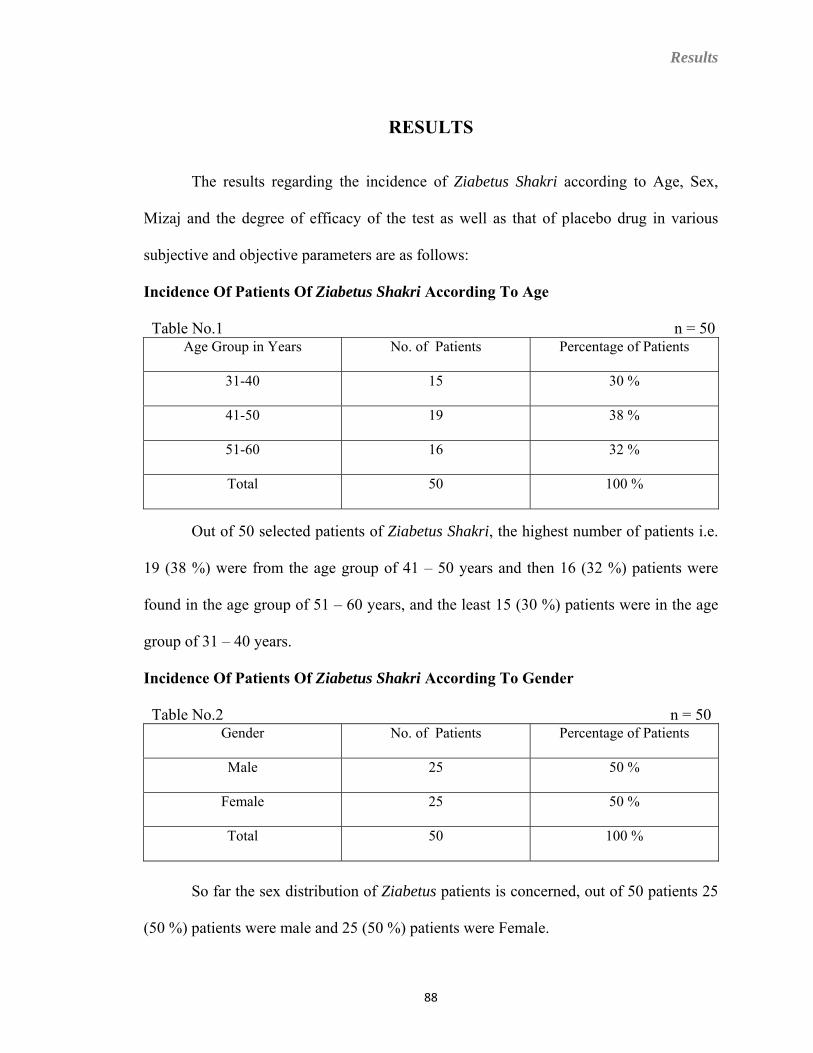
Results
RESULTS
The results regarding the incidence of Ziabetus Shakri according to Age, Sex,
Mizaj and the degree of efficacy of the test as well as that of placebo drug in various
subjective and objective parameters are as follows:
Incidence Of Patients Of Ziabetus Shakri According To Age
Table No.1 n = 50 Age Group in Years No. of Patients Percentage of Patients
31-40 15 30 %
41-50 19 38 %
51-60 16 32 %
Total 50 100 %
Out of 50 selected patients of Ziabetus Shakri, the highest number of patients i.e.
19 (38 %) were from the age group of 41 – 50 years and then 16 (32 %) patients were
found in the age group of 51 – 60 years, and the least 15 (30 %) patients were in the age
group of 31 – 40 years.
Incidence Of Patients Of Ziabetus Shakri According To Gender
Table No.2 n = 50 Gender No. of Patients Percentage of Patients
Male 25 50 %
Female 25 50 %
Total 50 100 %
So far the sex distribution of Ziabetus patients is concerned, out of 50 patients 25
(50 %) patients were male and 25 (50 %) patients were Female.
88
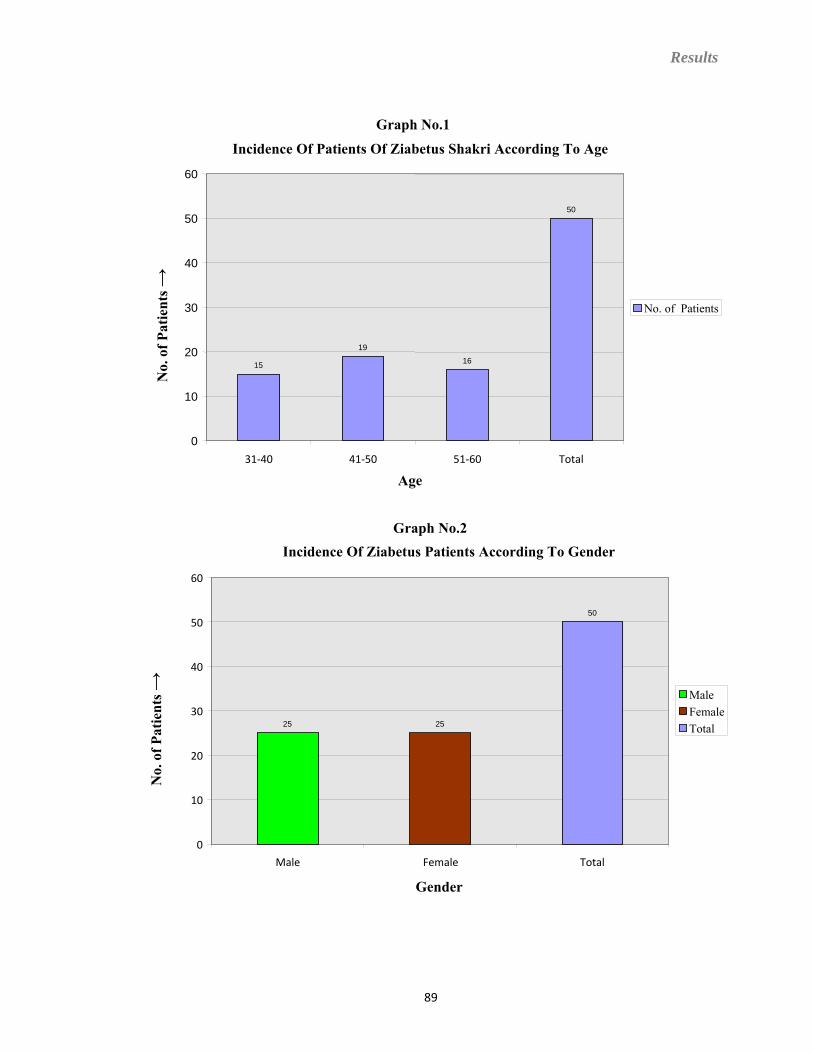
Results
Graph No.1
Incidence Of Patients Of Ziabetus Shakri According To Age
15
19
16
50
0
10
20
30
40
50
60
31‐40 41‐50 51‐60 Total
Age
No.
of P
atie
nts →
No. of Patients
Graph No.2 Incidence Of Ziabetus Patients According To Gender
25 25
50
0
10
20
30
40
50
60
Male Female Total
Gender
No.
of P
atie
nts →
MaleFemaleTotal
89
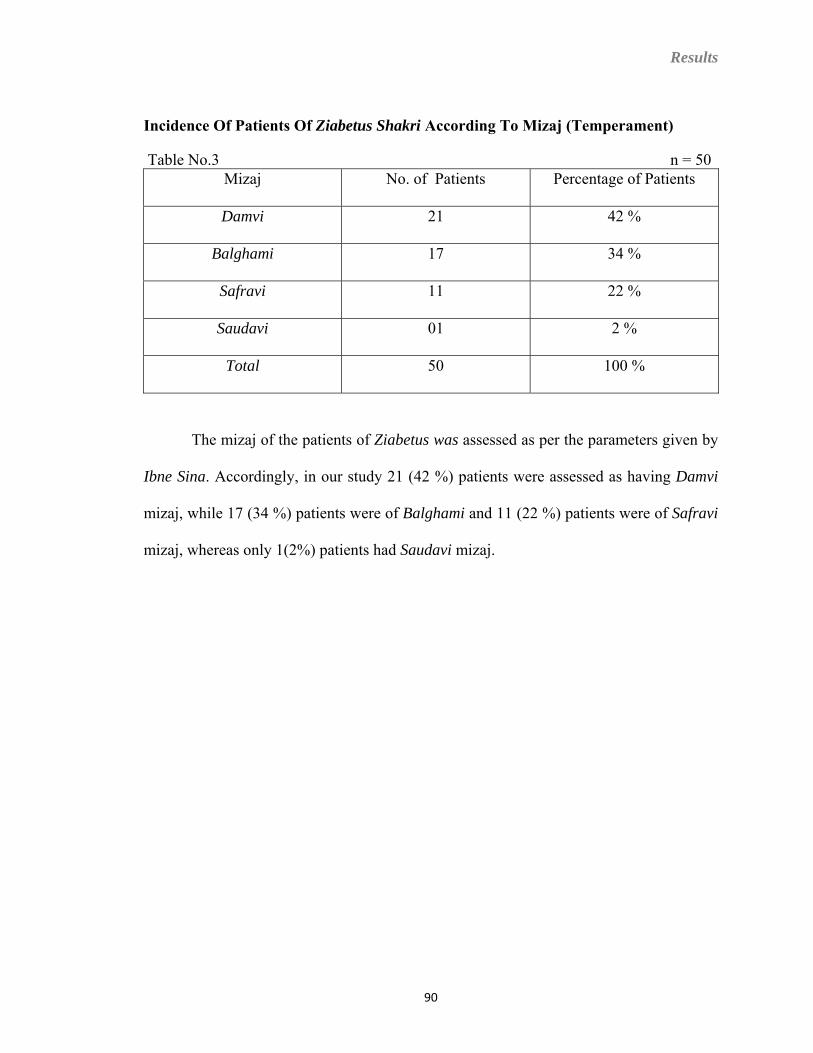
Results
Incidence Of Patients Of Ziabetus Shakri According To Mizaj (Temperament)
Table No.3 n = 50 Mizaj No. of Patients Percentage of Patients
Damvi 21 42 %
Balghami 17 34 %
Safravi 11 22 %
Saudavi 01 2 %
Total 50 100 %
The mizaj of the patients of Ziabetus was assessed as per the parameters given by
Ibne Sina. Accordingly, in our study 21 (42 %) patients were assessed as having Damvi
mizaj, while 17 (34 %) patients were of Balghami and 11 (22 %) patients were of Safravi
mizaj, whereas only 1(2%) patients had Saudavi mizaj.
90
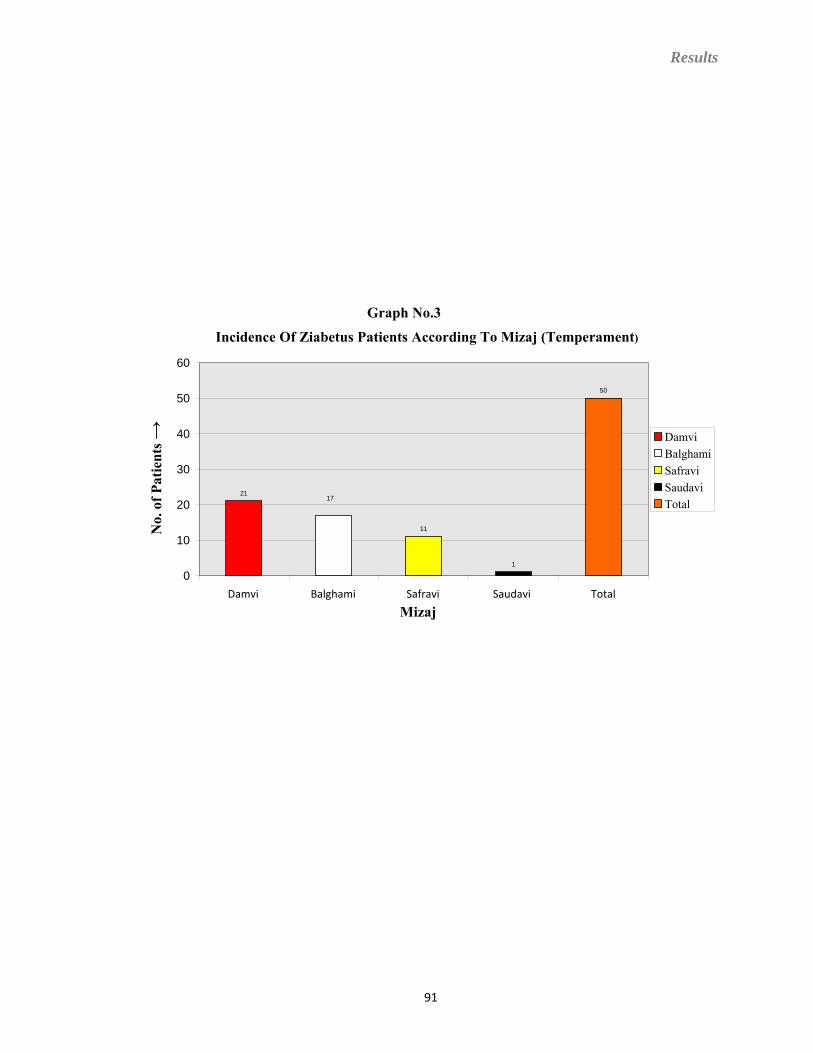
Results
Graph No.3
Incidence Of Ziabetus Patients According To Mizaj (Temperament)
21 17
11
1
50
0
10
20
30
40
50
60
Damvi Balghami Safravi Saudavi Total Mizaj
No.
of P
atie
nts →
DamviBalghamiSafraviSaudavi Total
91
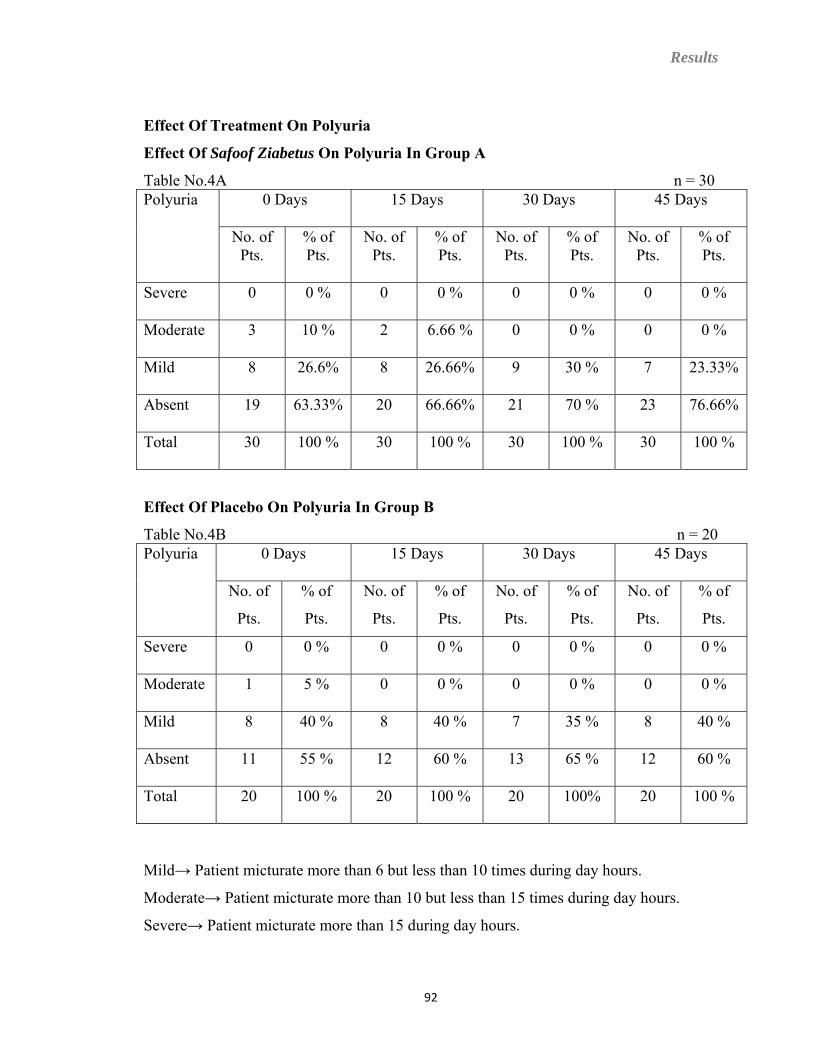
Results
Effect Of Treatment On Polyuria
Effect Of Safoof Ziabetus On Polyuria In Group A
Table No.4A n = 30 0 Days 15 Days 30 Days 45 Days Polyuria
No. of Pts.
% of Pts.
No. of Pts.
% of Pts.
No. of Pts.
% of Pts.
No. of Pts.
% of Pts.
Severe 0 0 % 0 0 % 0 0 % 0 0 %
Moderate 3 10 % 2 6.66 % 0 0 % 0 0 %
Mild 8 26.6% 8 26.66% 9 30 % 7 23.33%
Absent 19 63.33% 20 66.66% 21 70 % 23 76.66%
Total 30 100 % 30 100 % 30 100 % 30 100 %
Effect Of Placebo On Polyuria In Group B
Table No.4B n = 20
0 Days 15 Days 30 Days 45 Days Polyuria
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
Severe 0 0 % 0 0 % 0 0 % 0 0 %
Moderate 1 5 % 0 0 % 0 0 % 0 0 %
Mild 8 40 % 8 40 % 7 35 % 8 40 %
Absent 11 55 % 12 60 % 13 65 % 12 60 %
Total 20 100 % 20 100 % 20 100% 20 100 %
Mild→ Patient micturate more than 6 but less than 10 times during day hours.
Moderate→ Patient micturate more than 10 but less than 15 times during day hours.
Severe→ Patient micturate more than 15 during day hours.
92
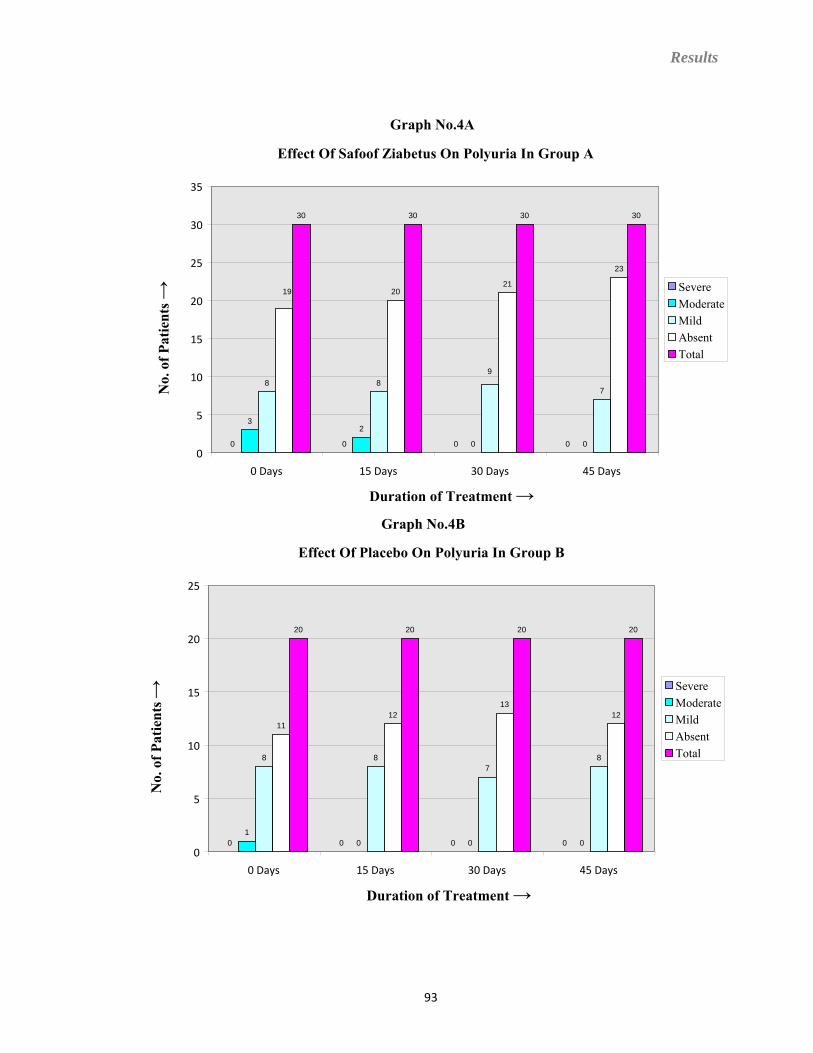
Results
Graph No.4A
Effect Of Safoof Ziabetus On Polyuria In Group A
0 0 0 0
32
0 0
8 89
7
19 2021
23
30 30 30 30
0
5
10
15
20
25
30
35
0 Days 15 Days 30 Days 45 Days
Duration of Treatment →
No.
of P
atie
nts →
SevereModerateMildAbsentTotal
Graph No.4B
Effect Of Placebo On Polyuria In Group B
0 0 0 01
0 0 0
8 87
8
1112
1312
20 20 20 20
0
5
10
15
20
25
0 Days 15 Days 30 Days 45 Days
Duration of Treatment →
No.
of P
atie
nts →
SevereModerateMildAbsentTotal
93
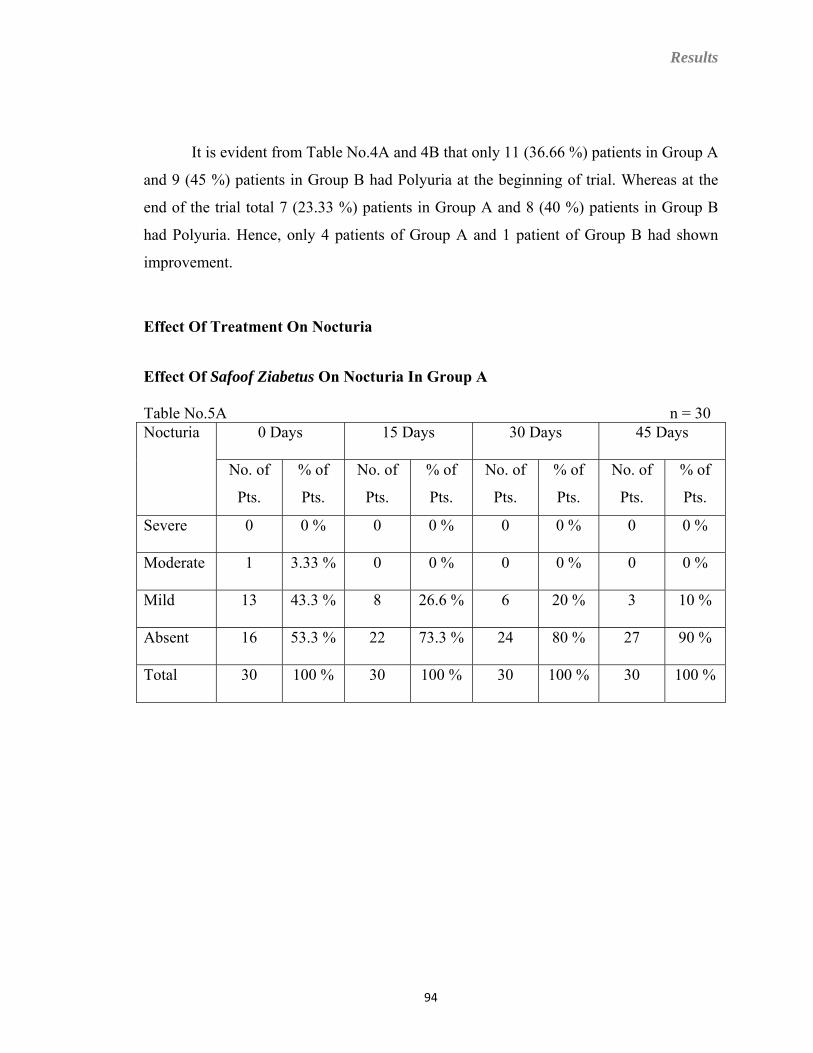
Results
It is evident from Table No.4A and 4B that only 11 (36.66 %) patients in Group A
and 9 (45 %) patients in Group B had Polyuria at the beginning of trial. Whereas at the
end of the trial total 7 (23.33 %) patients in Group A and 8 (40 %) patients in Group B
had Polyuria. Hence, only 4 patients of Group A and 1 patient of Group B had shown
improvement.
Effect Of Treatment On Nocturia
Effect Of Safoof Ziabetus On Nocturia In Group A
Table No.5A n = 30 0 Days 15 Days 30 Days 45 Days Nocturia
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
Severe 0 0 % 0 0 % 0 0 % 0 0 %
Moderate 1 3.33 % 0 0 % 0 0 % 0 0 %
Mild 13 43.3 % 8 26.6 % 6 20 % 3 10 %
Absent 16 53.3 % 22 73.3 % 24 80 % 27 90 %
Total 30 100 % 30 100 % 30 100 % 30 100 %
94
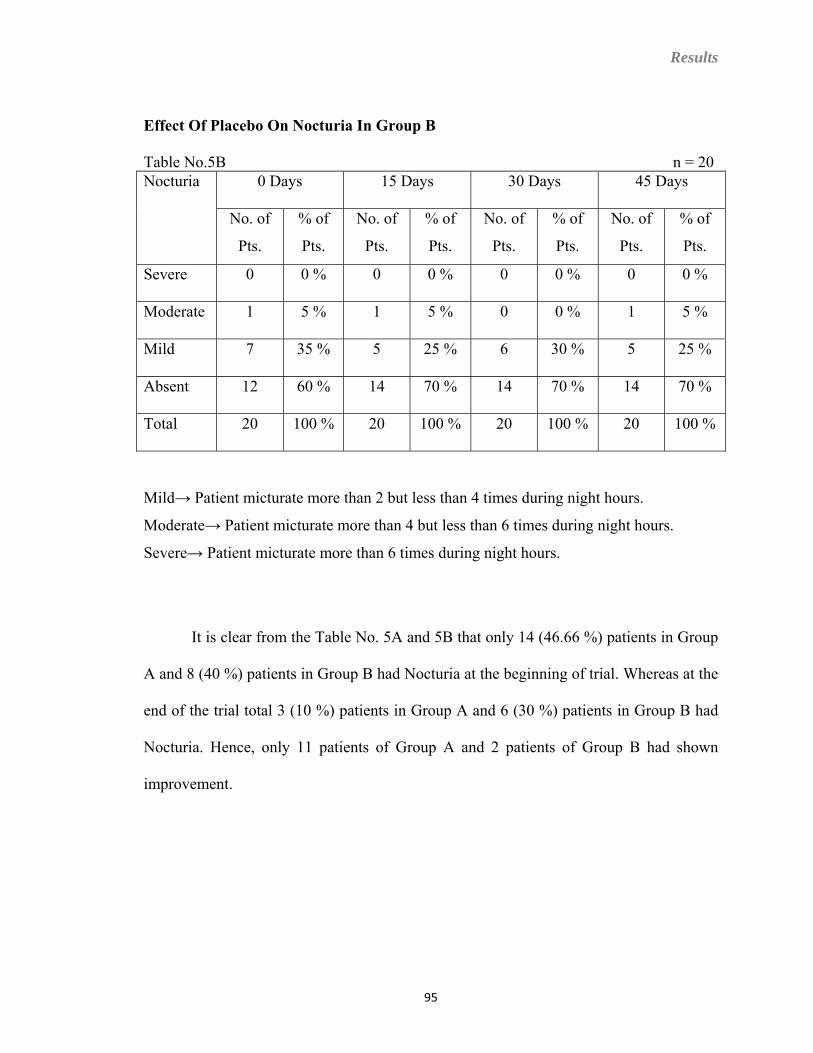
Results
Effect Of Placebo On Nocturia In Group B
Table No.5B n = 20 0 Days 15 Days 30 Days 45 Days Nocturia
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
Severe 0 0 % 0 0 % 0 0 % 0 0 %
Moderate 1 5 % 1 5 % 0 0 % 1 5 %
Mild 7 35 % 5 25 % 6 30 % 5 25 %
Absent 12 60 % 14 70 % 14 70 % 14 70 %
Total 20 100 % 20 100 % 20 100 % 20 100 %
Mild→ Patient micturate more than 2 but less than 4 times during night hours.
Moderate→ Patient micturate more than 4 but less than 6 times during night hours.
Severe→ Patient micturate more than 6 times during night hours.
It is clear from the Table No. 5A and 5B that only 14 (46.66 %) patients in Group
A and 8 (40 %) patients in Group B had Nocturia at the beginning of trial. Whereas at the
end of the trial total 3 (10 %) patients in Group A and 6 (30 %) patients in Group B had
Nocturia. Hence, only 11 patients of Group A and 2 patients of Group B had shown
improvement.
95
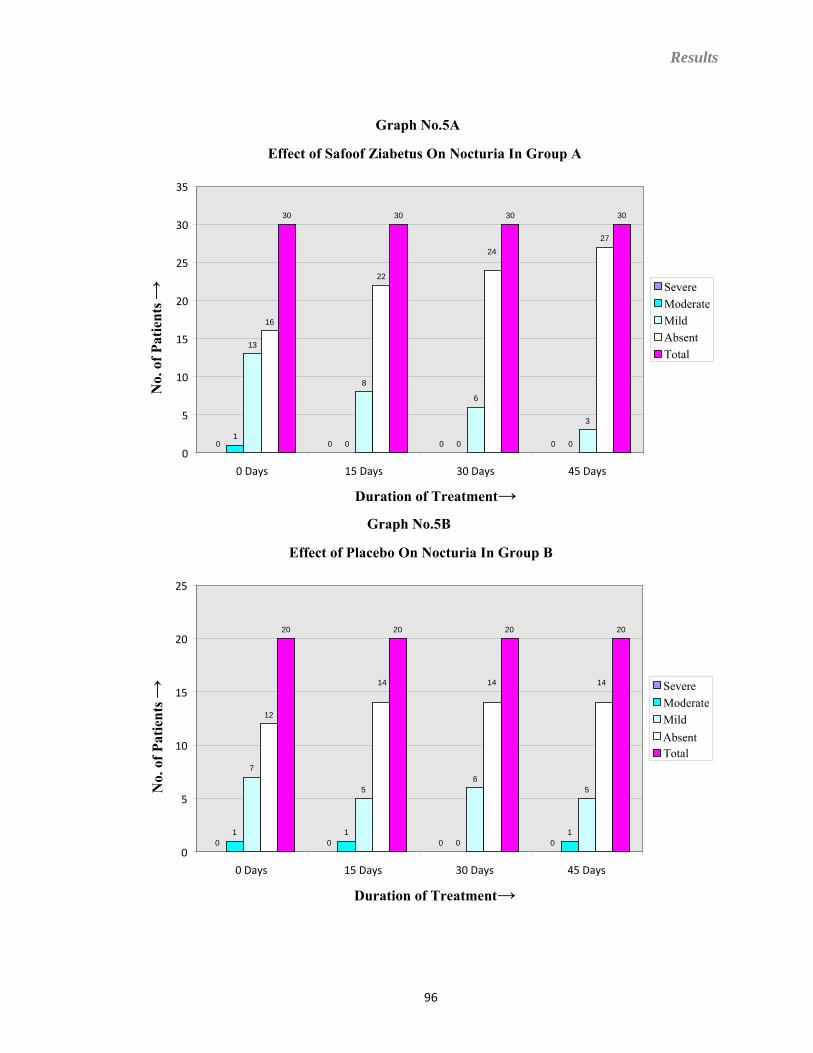
Results
96
Graph No.5A
Effect of Safoof Ziabetus On Nocturia In Group A
0 0 0 01
0 0 0
13
8
6
3
16
22
24
27
30 30 30 30
0
5
10
15
20
25
30
35
0 Days 15 Days 30 Days 45 Days
Duration of Treatment→
No.
of P
atie
nts →
SevereModerateMildAbsentTotal
Graph No.5B
Effect of Placebo On Nocturia In Group B
0 0 0 01 1
01
7
56
5
12
14 14 14
20 20 20 20
0
5
10
15
20
25
0 Days 15 Days 30 Days 45 Days
Duration of Treatment→
No.
of P
atie
nts →
SevereModerateMildAbsentTotal
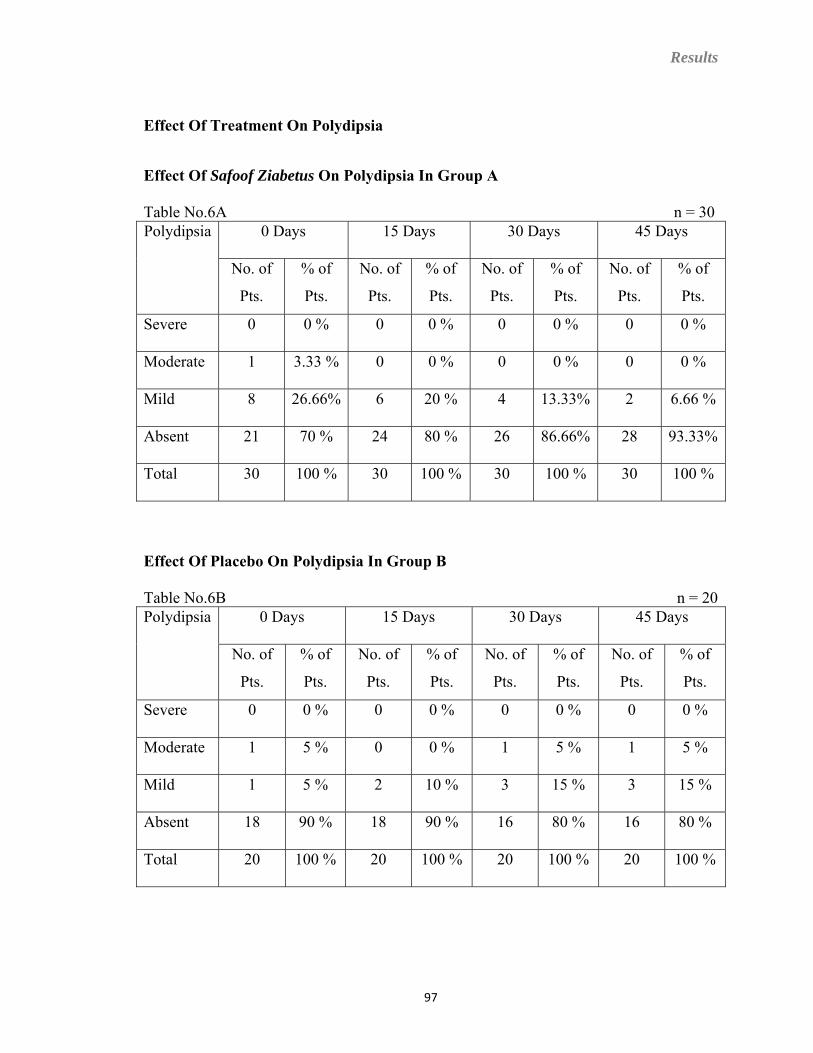
Results
Effect Of Treatment On Polydipsia
Effect Of Safoof Ziabetus On Polydipsia In Group A
Table No.6A n = 30 0 Days 15 Days 30 Days 45 Days Polydipsia
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
Severe 0 0 % 0 0 % 0 0 % 0 0 %
Moderate 1 3.33 % 0 0 % 0 0 % 0 0 %
Mild 8 26.66% 6 20 % 4 13.33% 2 6.66 %
Absent 21 70 % 24 80 % 26 86.66% 28 93.33%
Total 30 100 % 30 100 % 30 100 % 30 100 %
Effect Of Placebo On Polydipsia In Group B
Table No.6B n = 20 0 Days 15 Days 30 Days 45 Days Polydipsia
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
Severe 0 0 % 0 0 % 0 0 % 0 0 %
Moderate 1 5 % 0 0 % 1 5 % 1 5 %
Mild 1 5 % 2 10 % 3 15 % 3 15 %
Absent 18 90 % 18 90 % 16 80 % 16 80 %
Total 20 100 % 20 100 % 20 100 % 20 100 %
97
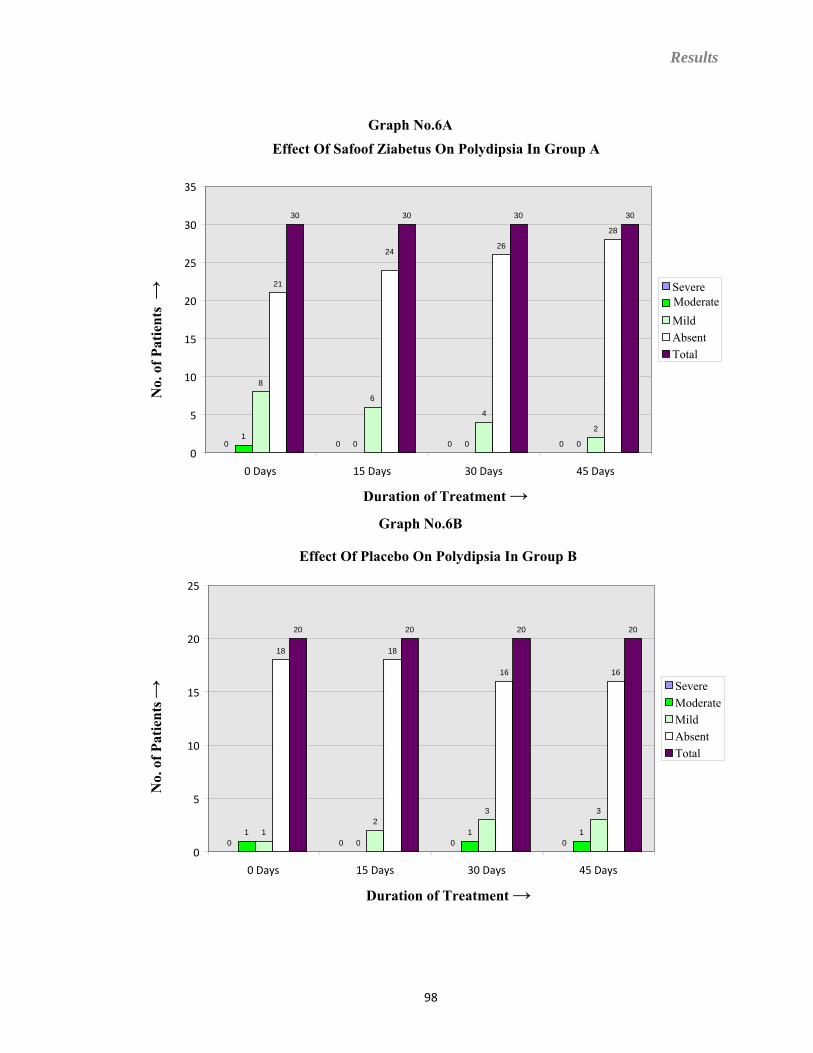
Results
Graph No.6B
Effect Of Placebo On Polydipsia In Group B
0 0 0 01
01 11
23 3
18 18
16 16
20 20 20 20
0
5
10
15
20
25
0 Days 15 Days 30 Days 45 Days
Duration of Treatment →
No.
of P
atie
nts →
SevereModerateMildAbsentTotal
Graph No.6AEffect Of Safoof Ziabetus On Polydipsia In Group A
0 0 0 01
0 0 0
8
6
4
2
21
2426
28
30 30 30 30
0
5
10
15
20
25
30
35
0 Days 15 Days 30 Days 45 Days
Duration of Treatment →
No.
of P
atie
nts →
Severe ModerateMildAbsentTotal
98
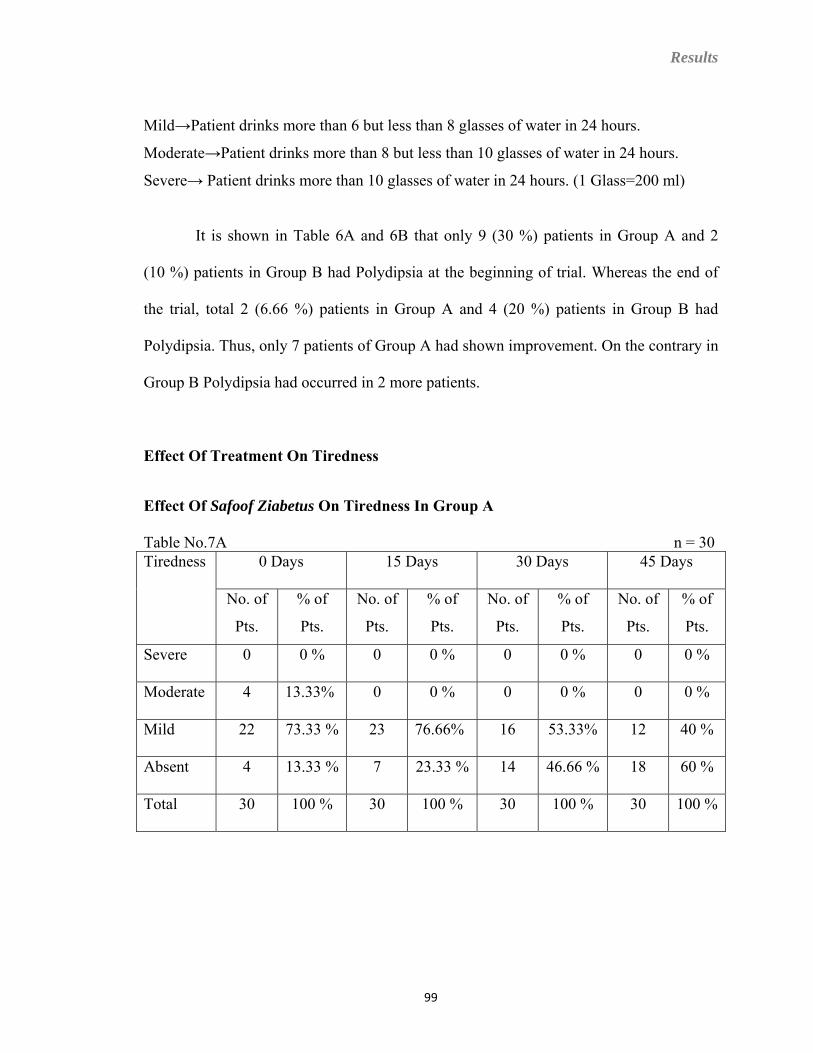
Results
Mild→Patient drinks more than 6 but less than 8 glasses of water in 24 hours.
Moderate→Patient drinks more than 8 but less than 10 glasses of water in 24 hours.
Severe→ Patient drinks more than 10 glasses of water in 24 hours. (1 Glass=200 ml)
It is shown in Table 6A and 6B that only 9 (30 %) patients in Group A and 2
(10 %) patients in Group B had Polydipsia at the beginning of trial. Whereas the end of
the trial, total 2 (6.66 %) patients in Group A and 4 (20 %) patients in Group B had
Polydipsia. Thus, only 7 patients of Group A had shown improvement. On the contrary in
Group B Polydipsia had occurred in 2 more patients.
Effect Of Treatment On Tiredness
Effect Of Safoof Ziabetus On Tiredness In Group A
Table No.7A n = 30 0 Days 15 Days 30 Days 45 Days Tiredness
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
Severe 0 0 % 0 0 % 0 0 % 0 0 %
Moderate 4 13.33% 0 0 % 0 0 % 0 0 %
Mild 22 73.33 % 23 76.66% 16 53.33% 12 40 %
Absent 4 13.33 % 7 23.33 % 14 46.66 % 18 60 %
Total 30 100 % 30 100 % 30 100 % 30 100 %
99
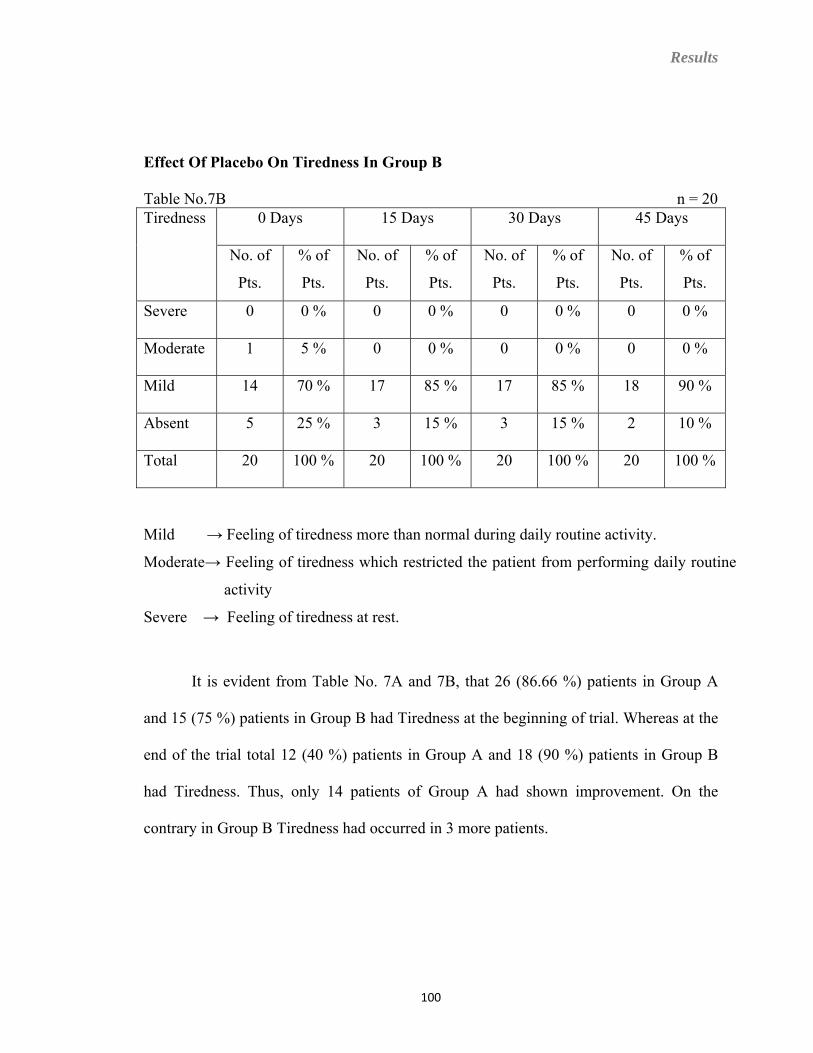
Results
Effect Of Placebo On Tiredness In Group B
Table No.7B n = 20 0 Days 15 Days 30 Days 45 Days Tiredness
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
Severe 0 0 % 0 0 % 0 0 % 0 0 %
Moderate 1 5 % 0 0 % 0 0 % 0 0 %
Mild 14 70 % 17 85 % 17 85 % 18 90 %
Absent 5 25 % 3 15 % 3 15 % 2 10 %
Total 20 100 % 20 100 % 20 100 % 20 100 %
Mild → Feeling of tiredness more than normal during daily routine activity.
Moderate→ Feeling of tiredness which restricted the patient from performing daily routine
activity
Severe → Feeling of tiredness at rest.
It is evident from Table No. 7A and 7B, that 26 (86.66 %) patients in Group A
and 15 (75 %) patients in Group B had Tiredness at the beginning of trial. Whereas at the
end of the trial total 12 (40 %) patients in Group A and 18 (90 %) patients in Group B
had Tiredness. Thus, only 14 patients of Group A had shown improvement. On the
contrary in Group B Tiredness had occurred in 3 more patients.
100
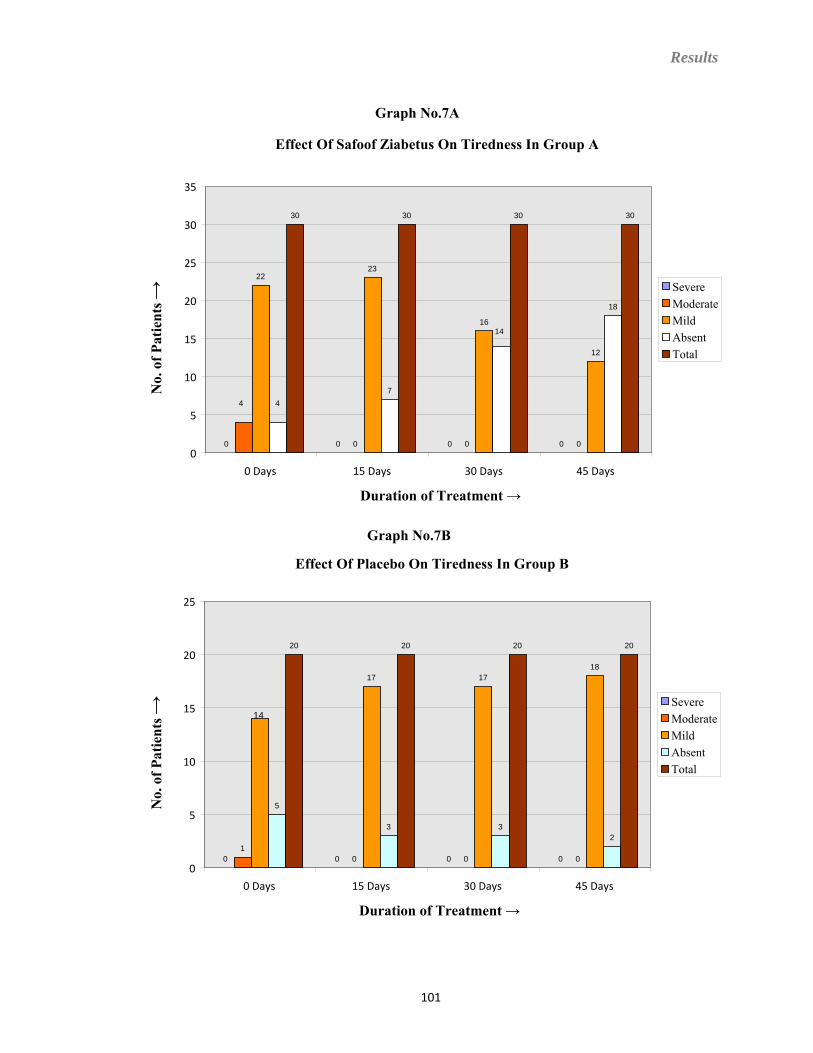
Results
101
Graph No.7A
Effect Of Safoof Ziabetus On Tiredness In Group A
0 0 0 0
4
0 0 0
2223
16
12
47
14
18
30 30 30 30
0
5
10
15
20
25
30
35
0 Days 15 Days 30 Days 45 Days
Duration of Treatment →
No.
of P
atie
nts →
SevereModerateMildAbsentTotal
Graph No.7B
Effect Of Placebo On Tiredness In Group B
0 0 0 01
0 0 0
14
17 1718
5
3 32
20 20 20 20
0
5
10
15
20
25
0 Days 15 Days 30 Days 45 Days
Duration of Treatment →
No.
of P
atie
nts →
SevereModerateMildAbsentTotal
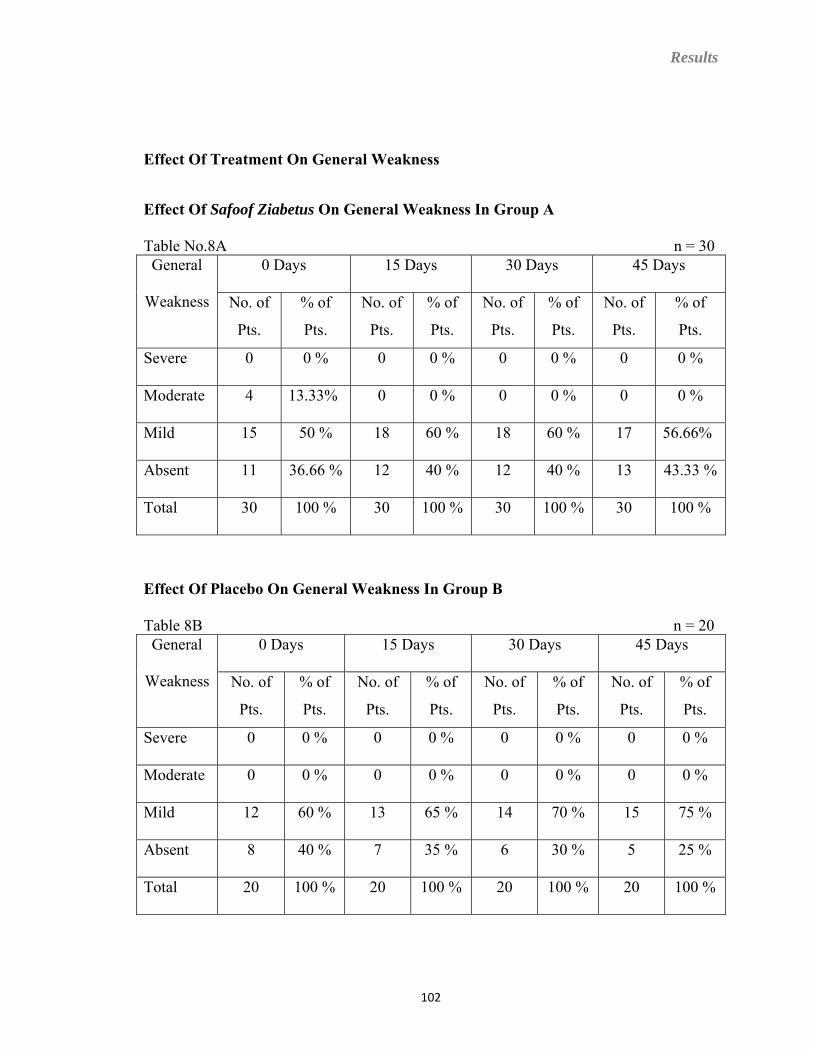
Results
Effect Of Treatment On General Weakness
Effect Of Safoof Ziabetus On General Weakness In Group A
Table No.8A n = 30 0 Days 15 Days 30 Days 45 Days General
Weakness No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
Severe 0 0 % 0 0 % 0 0 % 0 0 %
Moderate 4 13.33% 0 0 % 0 0 % 0 0 %
Mild 15 50 % 18 60 % 18 60 % 17 56.66%
Absent 11 36.66 % 12 40 % 12 40 % 13 43.33 %
Total 30 100 % 30 100 % 30 100 % 30 100 %
Effect Of Placebo On General Weakness In Group B
Table 8B n = 20 0 Days 15 Days 30 Days 45 Days General
Weakness No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
Severe 0 0 % 0 0 % 0 0 % 0 0 %
Moderate 0 0 % 0 0 % 0 0 % 0 0 %
Mild 12 60 % 13 65 % 14 70 % 15 75 %
Absent 8 40 % 7 35 % 6 30 % 5 25 %
Total 20 100 % 20 100 % 20 100 % 20 100 %
102
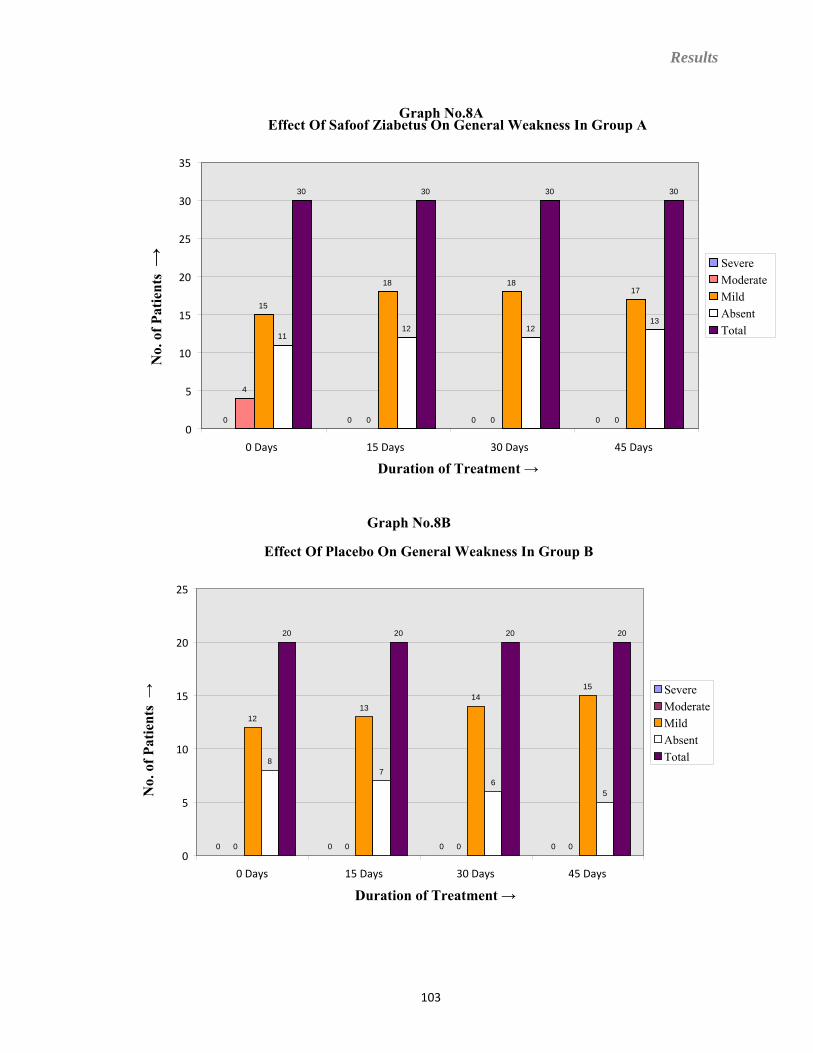
Results
Effect Of Safoof Ziabetus On General Weakness In Group A
0 0 0 0
4
0 0 0
15
18 1817
1112 12
13
30 30 30 30
0
5
10
15
20
25
30
35
0 Days 15 Days 30 Days 45 Days
Duration of Treatment →
No.
of P
atie
nts →
Graph No.8A
SevereModerateMildAbsentTotal
Graph No.8B
Effect Of Placebo On General Weakness In Group B
0 0 0 00 0 0 0
1213
1415
8 7
65
20 20 20 20
0
5
10
15
20
25
0 Days 15 Days 30 Days 45 Days
Duration of Treatment →
No.
of P
atie
nts →
SevereModerateMildAbsentTotal
103
Results
Mild→ Patient feels difficulty in performing only strenuous activity.
Moderate→ Patient feels difficulty in performing daily routine activity
Severe→ Patient feels exhausted and unable to do any work.
It is shown in Table 8A and 8B, that only 19 (63.33 %) patients in Group A and
12 (60 %) patients in Group B had General Weakness at the beginning of the study.
Whereas at the end of the study total 17 (56.66 %) patients in Group A and 15 (75 %)
patients in Group B had General Weakness. Hence, only 2 patients of Group A had
shown improvement. On the contrary in Group B General Weakness had occurred in 3
more patients.
104
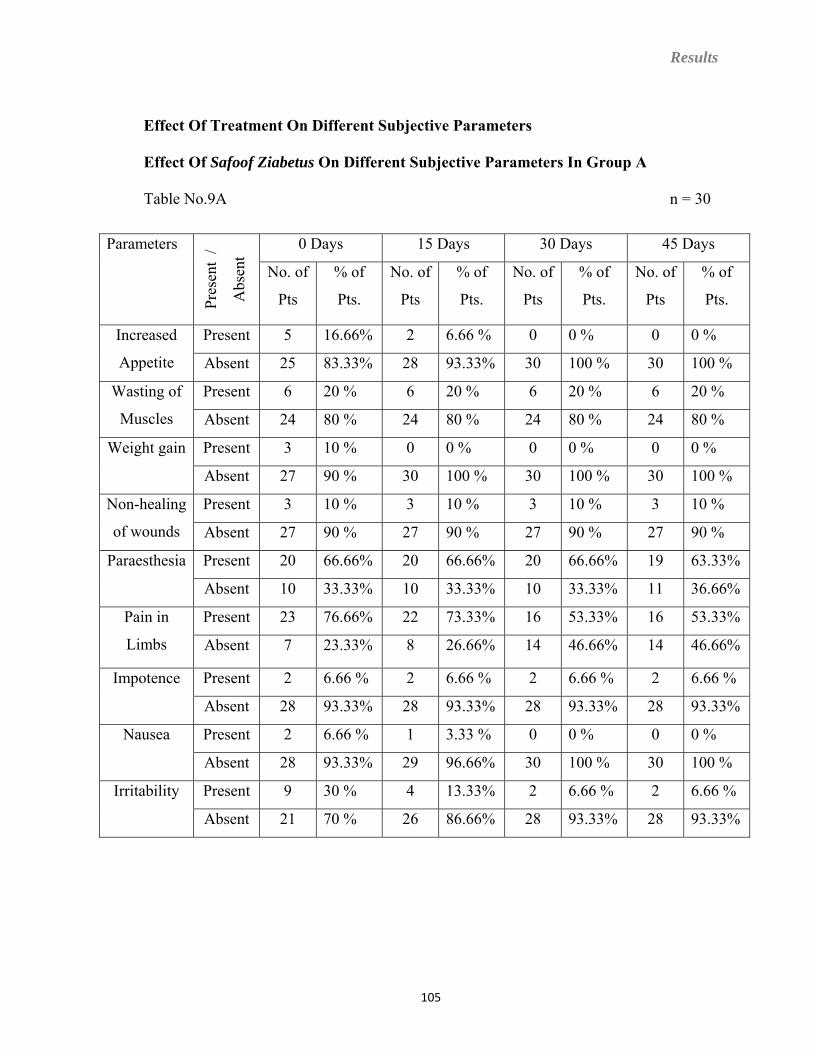
Results
Effect Of Treatment On Different Subjective Parameters
Effect Of Safoof Ziabetus On Different Subjective Parameters In Group A
Table No.9A n = 30
0 Days 15 Days 30 Days 45 Days Parameters
Pres
ent
/
Abs
ent
No. of
Pts
% of
Pts.
No. of
Pts
% of
Pts.
No. of
Pts
% of
Pts.
No. of
Pts
% of
Pts.
Present 5 16.66% 2 6.66 % 0 0 % 0 0 % Increased
Appetite Absent 25 83.33% 28 93.33% 30 100 % 30 100 %
Present 6 20 % 6 20 % 6 20 % 6 20 % Wasting of
Muscles Absent 24 80 % 24 80 % 24 80 % 24 80 %
Present 3 10 % 0 0 % 0 0 % 0 0 % Weight gain
Absent 27 90 % 30 100 % 30 100 % 30 100 %
Present 3 10 % 3 10 % 3 10 % 3 10 % Non-healing
of wounds Absent 27 90 % 27 90 % 27 90 % 27 90 %
Present 20 66.66% 20 66.66% 20 66.66% 19 63.33% Paraesthesia
Absent 10 33.33% 10 33.33% 10 33.33% 11 36.66%
Present 23 76.66% 22 73.33% 16 53.33% 16 53.33% Pain in
Limbs Absent 7 23.33% 8 26.66% 14 46.66% 14 46.66%
Present 2 6.66 % 2 6.66 % 2 6.66 % 2 6.66 % Impotence
Absent 28 93.33% 28 93.33% 28 93.33% 28 93.33%
Present 2 6.66 % 1 3.33 % 0 0 % 0 0 % Nausea
Absent 28 93.33% 29 96.66% 30 100 % 30 100 %
Present 9 30 % 4 13.33% 2 6.66 % 2 6.66 % Irritability
Absent 21 70 % 26 86.66% 28 93.33% 28 93.33%
105
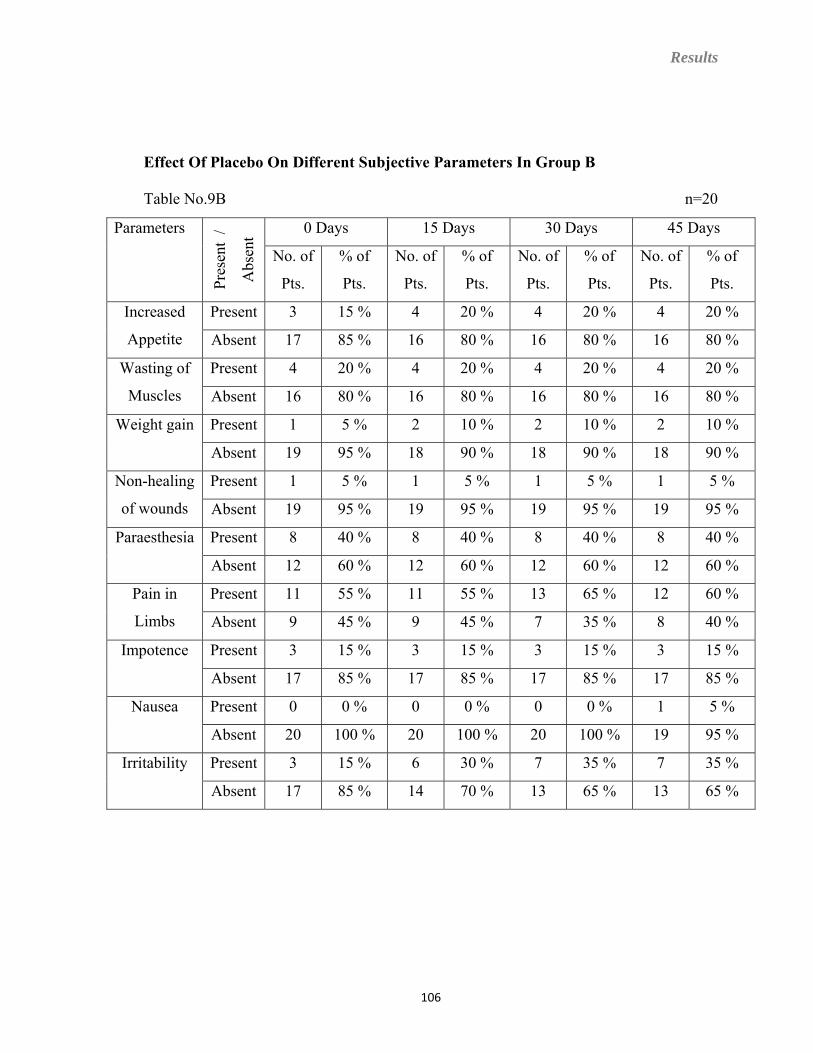
Results
Effect Of Placebo On Different Subjective Parameters In Group B
Table No.9B n=20
0 Days 15 Days 30 Days 45 Days Parameters Pr
esen
t /
Abs
ent
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
No. of
Pts.
% of
Pts.
Present 3 15 % 4 20 % 4 20 % 4 20 % Increased
Appetite Absent 17 85 % 16 80 % 16 80 % 16 80 %
Present 4 20 % 4 20 % 4 20 % 4 20 % Wasting of
Muscles Absent 16 80 % 16 80 % 16 80 % 16 80 %
Present 1 5 % 2 10 % 2 10 % 2 10 % Weight gain
Absent 19 95 % 18 90 % 18 90 % 18 90 %
Present 1 5 % 1 5 % 1 5 % 1 5 % Non-healing
of wounds Absent 19 95 % 19 95 % 19 95 % 19 95 %
Present 8 40 % 8 40 % 8 40 % 8 40 % Paraesthesia
Absent 12 60 % 12 60 % 12 60 % 12 60 %
Present 11 55 % 11 55 % 13 65 % 12 60 % Pain in
Limbs Absent 9 45 % 9 45 % 7 35 % 8 40 %
Present 3 15 % 3 15 % 3 15 % 3 15 % Impotence
Absent 17 85 % 17 85 % 17 85 % 17 85 %
Present 0 0 % 0 0 % 0 0 % 1 5 % Nausea
Absent 20 100 % 20 100 % 20 100 % 19 95 %
Present 3 15 % 6 30 % 7 35 % 7 35 % Irritability
Absent 17 85 % 14 70 % 13 65 % 13 65 %
106
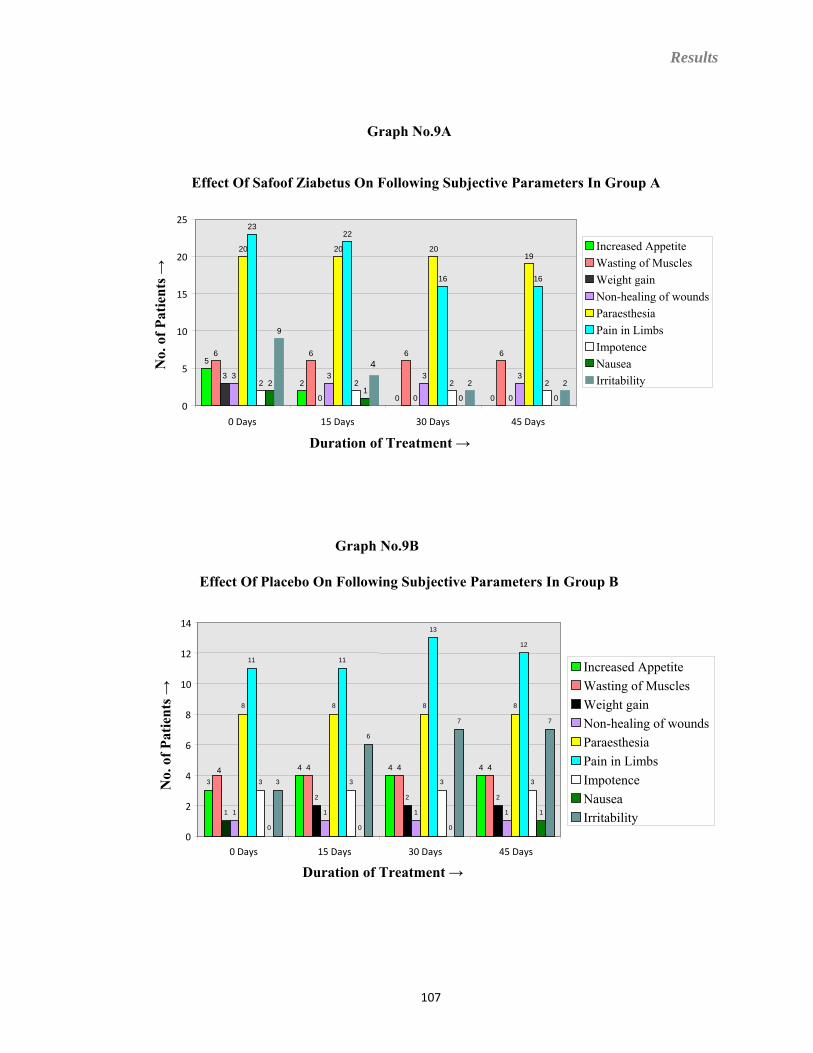
Results
Graph No.9A
Effect Of Safoof Ziabetus On Following Subjective Parameters In Group A
5
2
0 0
6 6 6 6
3
0 0 0
3 3 3 3
20 20 2019
2322
16 16
2 2 2 22 1
0 0
9
4
2 2
0
5
10
15
20
25
0 Days 15 Days 30 Days 45 Days
Duration of Treatment →
No.
of P
atie
nts →
Increased AppetiteWasting of MusclesWeight gainNon-healing of woundsParaesthesiaPain in LimbsImpotenceNauseaIrritability
Graph No.9B
Effect Of Placebo On Following Subjective Parameters In Group B
3 4 4 44 4 4 4
1 2 2 2
1 1 1 1
8 8 8 8
11 11
13
12
3 3 3 3
0 0 0
1
3
6
7 7
0
2
4
6
8
10
12
14
0 Days 15 Days 30 Days 45 Days
Duration of Treatment →
No.
of P
atie
nts →
Increased AppetiteWasting of MusclesWeight gainNon-healing of woundsParaesthesiaPain in LimbsImpotenceNauseaIrritability
107
Results
Effect Of Treatment On Increased Appetite
It is evident from Table No. 9A and 9B that only 5 (16.66 %) patients in Group A
and 3 (15 %) patients in Group B had Increased Appetite at the beginning of trial.
Whereas at the end of the trial 0 (0%) patient in Group A and 4 (20 %) patients in Group
B had Increased Appetite. Hence, all patients i.e. 5 patients of Group A had shown
improvement. On the contrary in Group B Increased Appetite had occurred in 1 more
patient.
Effect Of Treatment On Weight Gain
It is evident from Table No. 9A and 9B that only 3 (10 %) patients in Group A
and 1 (5 %) patient in Group B had Weight gain at the beginning of trial. Whereas at the
end of the trial 0 (0%) patient in Group A and 2 (20 %) patients in Group B had Weight
gain. Thus, all the patients i.e. 3 patients of Group A had shown improvement by the
treatment. On the contrary in Group B Weight gain had occurred in 1 more patient.
Effect Of Treatment On Paraesthesia
It is evident from Table No. 9A and 9B that only 20 (66.66 %) patients in Group
A and 8 (40 %) patients in Group B had Paraesthesia at the beginning of trial. Whereas at
the end of the trial 19 (63.33 %) patients in Group A and 8 (40 %) patients in Group B
had Paraesthesia. Hence, only 1 patient of Group A had shown improvement. On the
contrary there was no improvement observed in the Paraesthesia in Group B.
108
Results
Effect Of Treatment On Pain In Limbs
It is evident from Table No. 9A and 9B that only 23 (76.66 %) patients in Group
A and 11 (55 %) patients in Group B had Pain in Limbs at the beginning of trial. Whereas
at the end of the trial 16 (53.33 %) patient in Group A and 12 (60 %) patients in Group B
had Pain in Limbs. Thus, only 7 patients of Group A had shown improvement. On the
contrary in Group B Pain in Limbs had occurred in one more patient.
Effect Of Treatment On Nausea
It is evident from Table No. 9A and 9B that only 2 (6.66 %) patients in Group A
and no patient in Group B had Nausea at the beginning of trial. Whereas at the end of the
trial no patient in Group A and 1 (5 %) patient in the Group B had Nausea. Hence, all
patients i.e. 2 patients of Group A had shown improvement by the treatment. On the
contrary in Group B Nausea had occurred in one more patients.
Effect Of Treatment On Irritability
It is evident from Table No. 9A and 9B that only 9 (30 %) patients in Group A
and 3 (15 %) patients in Group B had Irritability at the beginning of trial. Whereas at the
end of the trial 2 (6.66 %) patients in Group A and 7 (35 %) patients in Group B had
irritability. Thus, only 7 patients of Group A had shown improvement. On the contrary in
Group B Irritability had occurred in 4 more patients.
109
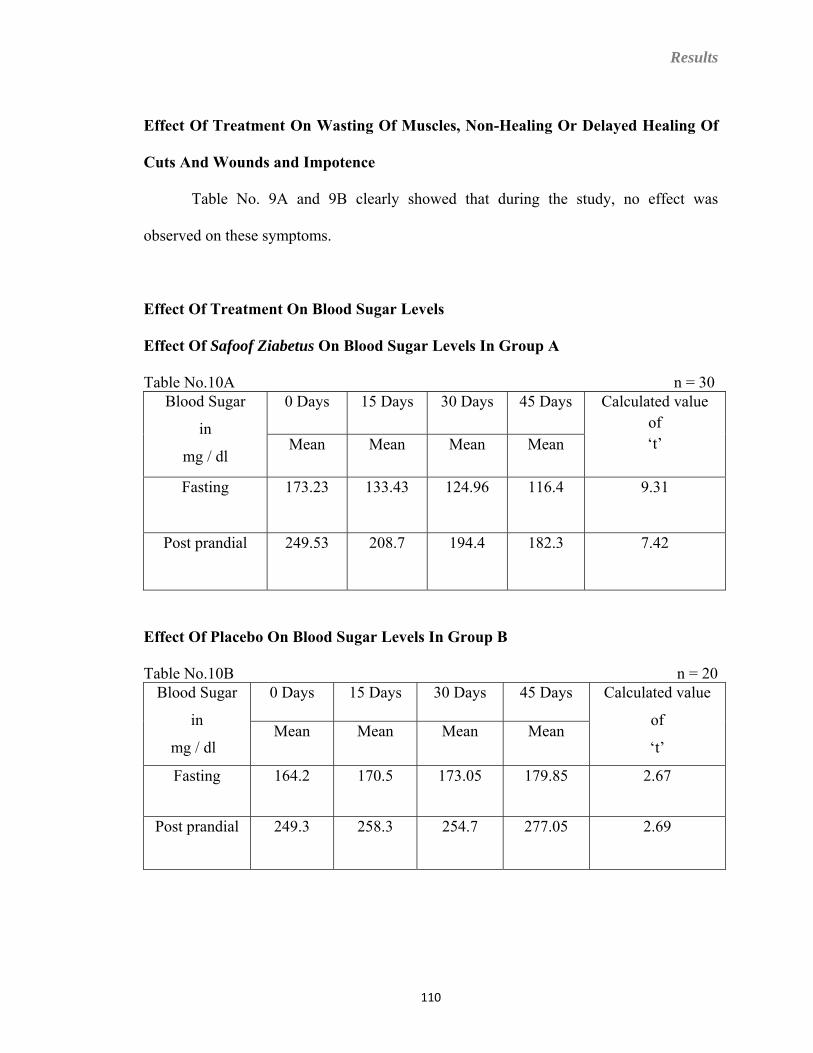
Results
Effect Of Treatment On Wasting Of Muscles, Non-Healing Or Delayed Healing Of
Cuts And Wounds and Impotence
Table No. 9A and 9B clearly showed that during the study, no effect was
observed on these symptoms.
Effect Of Treatment On Blood Sugar Levels
Effect Of Safoof Ziabetus On Blood Sugar Levels In Group A
Table No.10A n = 30 0 Days
15 Days 30 Days 45 Days Blood Sugar Calculated value
of in ‘t’ Mean Mean Mean Mean
mg / dl Fasting 173.23 133.43 124.96 116.4 9.31
Post prandial 249.53 208.7 194.4 182.3 7.42
Effect Of Placebo On Blood Sugar Levels In Group B
Table No.10B n = 20 0 Days 15 Days 30 Days 45 Days Blood Sugar Calculated value
of in Mean Mean Mean Mean
mg / dl ‘t’
164.2 Fasting 170.5 173.05 179.85 2.67
Post prandial 249.3 258.3 254.7 277.05 2.69
110
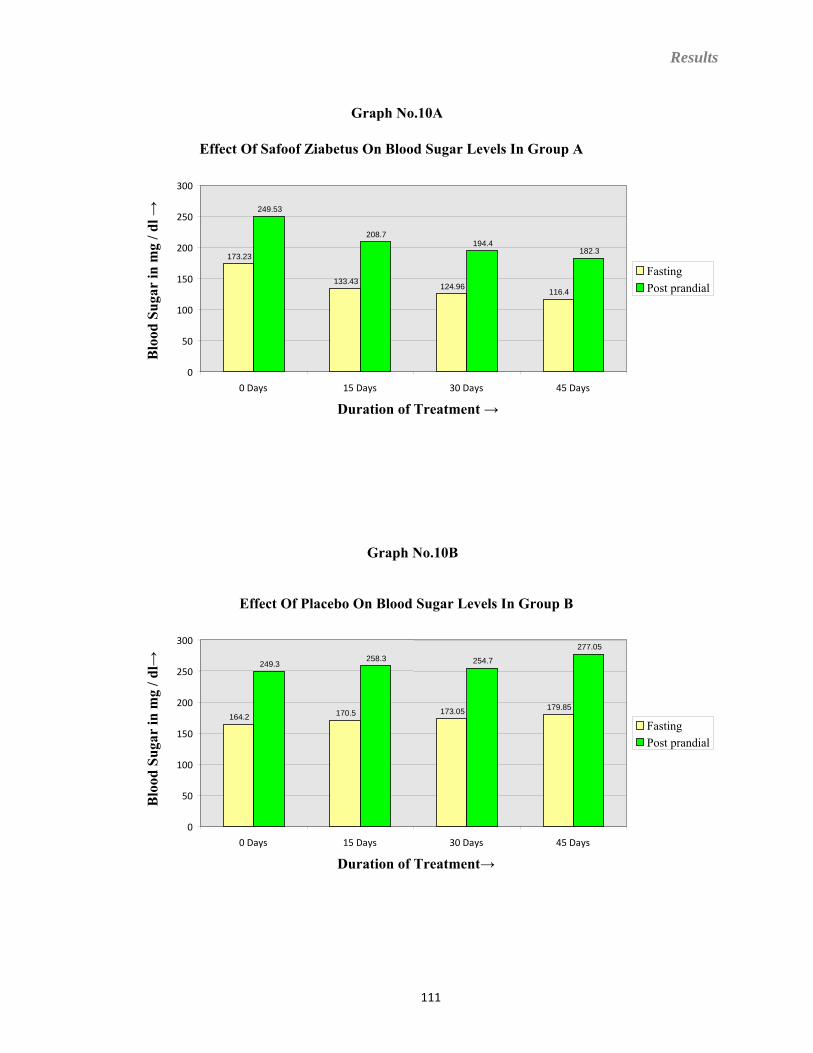
Results
Graph No.10A
Effect Of Safoof Ziabetus On Blood Sugar Levels In Group A
173.23
133.43 124.96116.4
249.53
208.7194.4
182.3
0
50
100
150
200
250
300
0 Days 15 Days 30 Days 45 Days
Duration of Treatment →
Blo
od S
ugar
in m
g / d
l →
FastingPost prandial
Graph No.10B
Effect Of Placebo On Blood Sugar Levels In Group B
164.2 170.5 173.05 179.85
249.3258.3 254.7
277.05
0
50
100
150
200
250
300
0 Days 15 Days 30 Days 45 Days
Duration of Treatment→
Blo
od S
ugar
in m
g / d
l→
FastingPost prandial
111
Results
Effect Of Treatment On Blood Sugar Fasting
It is evident from Table No.10A and 10B that before the treatment mean Blood
Sugar in the Fasting state was 173.23 mg/dl in Group A and 164.2 mg/dl in Group B.
Whereas at the end of the treatment it was reduced to 116.4 mg/dl (average reduction of
32.80 %) in Group A. On the contrary in Group B it was increased to 179.85 mg/dl
(average elevation of 9.53 %). On comparing Blood Sugar Fasting observations of
‘Group A’ with ‘Group B’ with the help of Student’s ‘t’ test, it was found significant
statistically (p<0.05). It means test drug reduces the Blood Sugar Fasting level
significantly as compared to placebo.
Effect Of Treatment On Blood Sugar Post Prandial
It is clearly shown in Table No.10A and 10B that before the treatment mean
Blood Sugar in the Post Prandial state was 249.53 mg/dl in Group A and 249.3 mg/dl in
Group B. Whereas at the end of the treatment it was reduced to 182.3 mg/dl (average
reduction of 26.94 %) in Group A. On the contrary in Group B it was increased to 277.05
mg/dl (average elevation of 11.13%). On comparing Blood Sugar Post Prandial
observations of ‘Group A’ with ‘Group B’ with the help of Student’s ‘t’ test, it was found
significant statistically (p<0.05). It means test drug reduces the Blood Sugar Post
Prandial level significantly as compared to placebo.
112
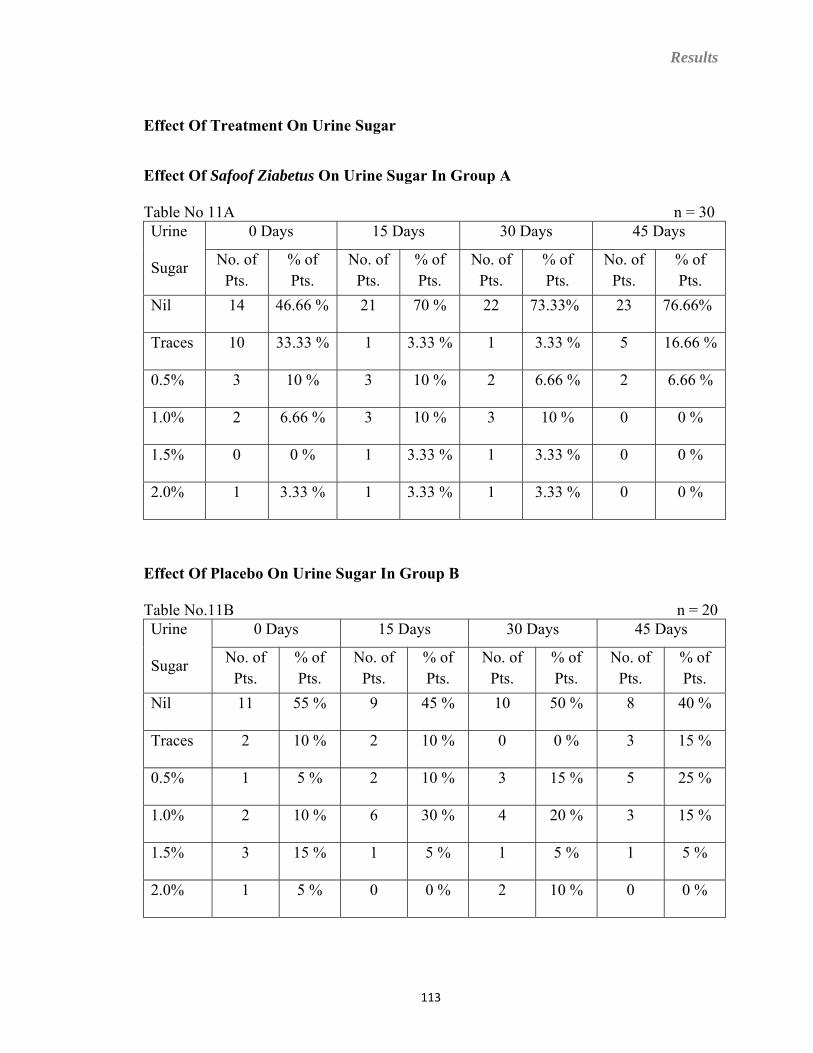
Results
Effect Of Treatment On Urine Sugar
Effect Of Safoof Ziabetus On Urine Sugar In Group A
Table No 11A n = 30 0 Days 15 Days 30 Days 45 Days Urine
Sugar No. of Pts.
% of Pts.
No. of Pts.
% of Pts.
No. of Pts.
% of Pts.
No. of Pts.
% of Pts.
Nil 14 46.66 % 21 70 % 22 73.33% 23 76.66%
Traces 10 33.33 % 1 3.33 % 1 3.33 % 5 16.66 %
0.5% 3 10 % 3 10 % 2 6.66 % 2 6.66 %
1.0% 2 6.66 % 3 10 % 3 10 % 0 0 %
1.5% 0 0 % 1 3.33 % 1 3.33 % 0 0 %
2.0% 1 3.33 % 1 3.33 % 1 3.33 % 0 0 %
Effect Of Placebo On Urine Sugar In Group B
Table No.11B n = 20 0 Days 15 Days 30 Days 45 Days Urine
Sugar No. of Pts.
% of Pts.
No. of Pts.
% of Pts.
No. of Pts.
% of Pts.
No. of Pts.
% of Pts.
Nil 11 55 % 9 45 % 10 50 % 8 40 %
Traces 2 10 % 2 10 % 0 0 % 3 15 %
0.5% 1 5 % 2 10 % 3 15 % 5 25 %
1.0% 2 10 % 6 30 % 4 20 % 3 15 %
1.5% 3 15 % 1 5 % 1 5 % 1 5 %
2.0% 1 5 % 0 0 % 2 10 % 0 0 %
113
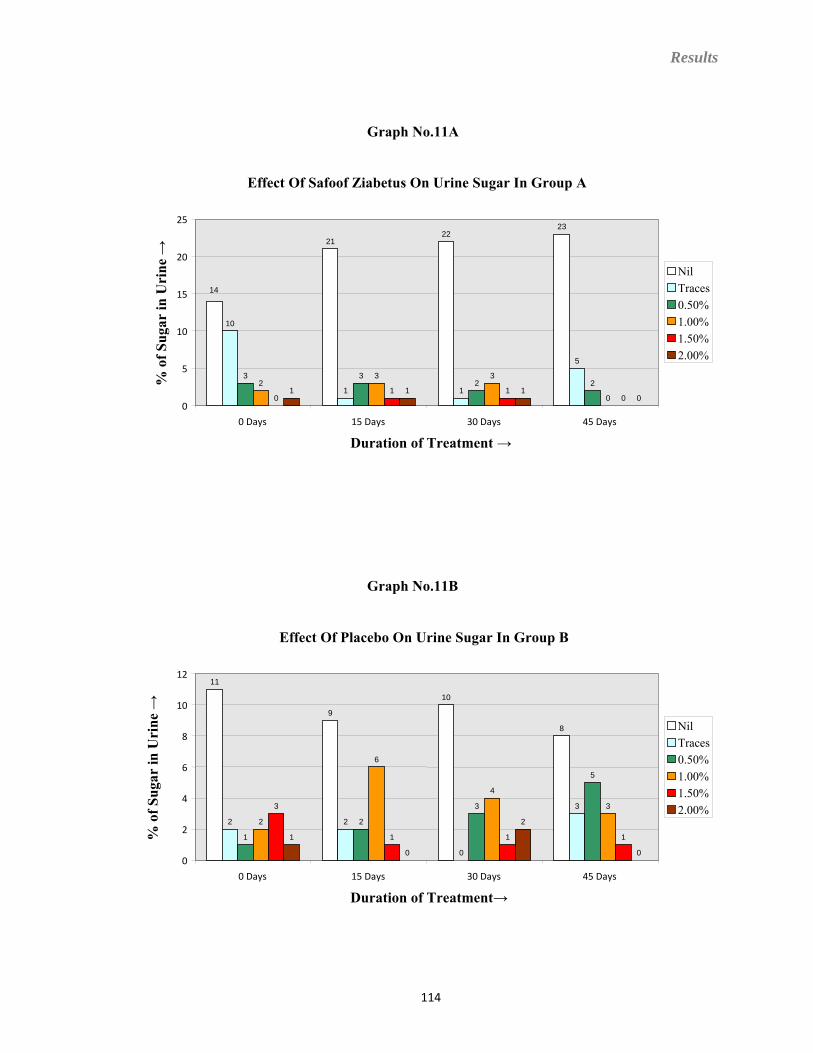
Results
Graph No.11A
Effect Of Safoof Ziabetus On Urine Sugar In Group A
14
2122
23
10
1 1
5
3 32 22
3 3
001 1
01 1 1
00
5
10
15
20
25
0 Days 15 Days 30 Days 45 Days
Duration of Treatment →
% o
f Sug
ar in
Uri
ne →
NilTraces0.50%1.00%1.50%2.00%
Graph No.11B
Effect Of Placebo On Urine Sugar In Group B
11
9
10
8
2 2
0
3
1
2
3
5
2
6
4
33
1 1 11 0
2
00
2
4
6
8
10
12
0 Days 15 Days 30 Days 45 Days
Duration of Treatment→
% o
f Sug
ar in
Uri
ne →
NilTraces0.50%1.00%1.50%2.00%
114
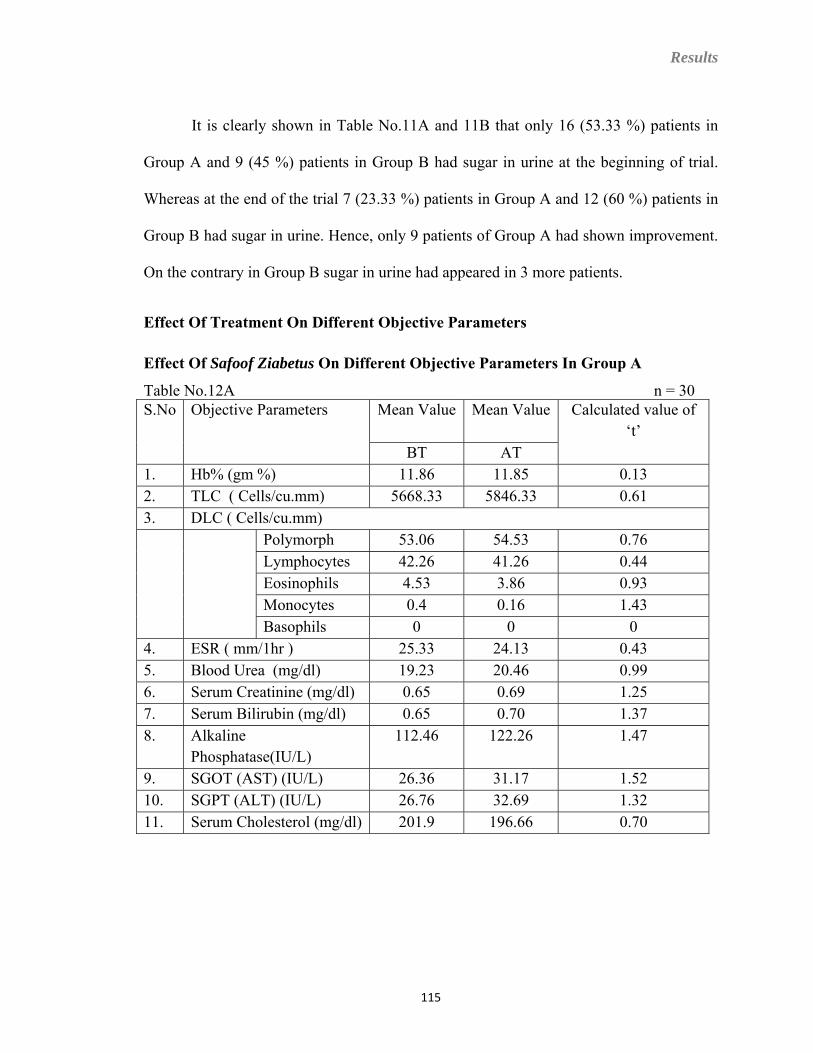
Results
It is clearly shown in Table No.11A and 11B that only 16 (53.33 %) patients in
Group A and 9 (45 %) patients in Group B had sugar in urine at the beginning of trial.
Whereas at the end of the trial 7 (23.33 %) patients in Group A and 12 (60 %) patients in
Group B had sugar in urine. Hence, only 9 patients of Group A had shown improvement.
On the contrary in Group B sugar in urine had appeared in 3 more patients.
Effect Of Treatment On Different Objective Parameters
Effect Of Safoof Ziabetus On Different Objective Parameters In Group A
Table No.12A n = 30 Mean Value
Mean ValueS.No Objective Parameters Calculated value of ‘t’
BT AT 1. Hb% (gm %) 11.86 11.85 0.13 2. TLC ( Cells/cu.mm) 5668.33 5846.33 0.61 3. DLC ( Cells/cu.mm)
Polymorph 53.06 54.53 0.76 Lymphocytes 42.26 41.26 0.44
Eosinophils 4.53 3.86 0.93 Monocytes 0.4 0.16 1.43 Basophils 0 0 0
4. ESR ( mm/1hr ) 25.33 24.13 0.43 5. Blood Urea (mg/dl) 19.23 20.46 0.99 6. Serum Creatinine (mg/dl) 0.65 0.69 1.25 7. Serum Bilirubin (mg/dl) 0.65 0.70 1.37 8. Alkaline
Phosphatase(IU/L) 112.46 122.26 1.47
9. SGOT (AST) (IU/L) 26.36 31.17 1.52 10. SGPT (ALT) (IU/L) 26.76 32.69 1.32 11. Serum Cholesterol (mg/dl) 201.9 196.66 0.70
115
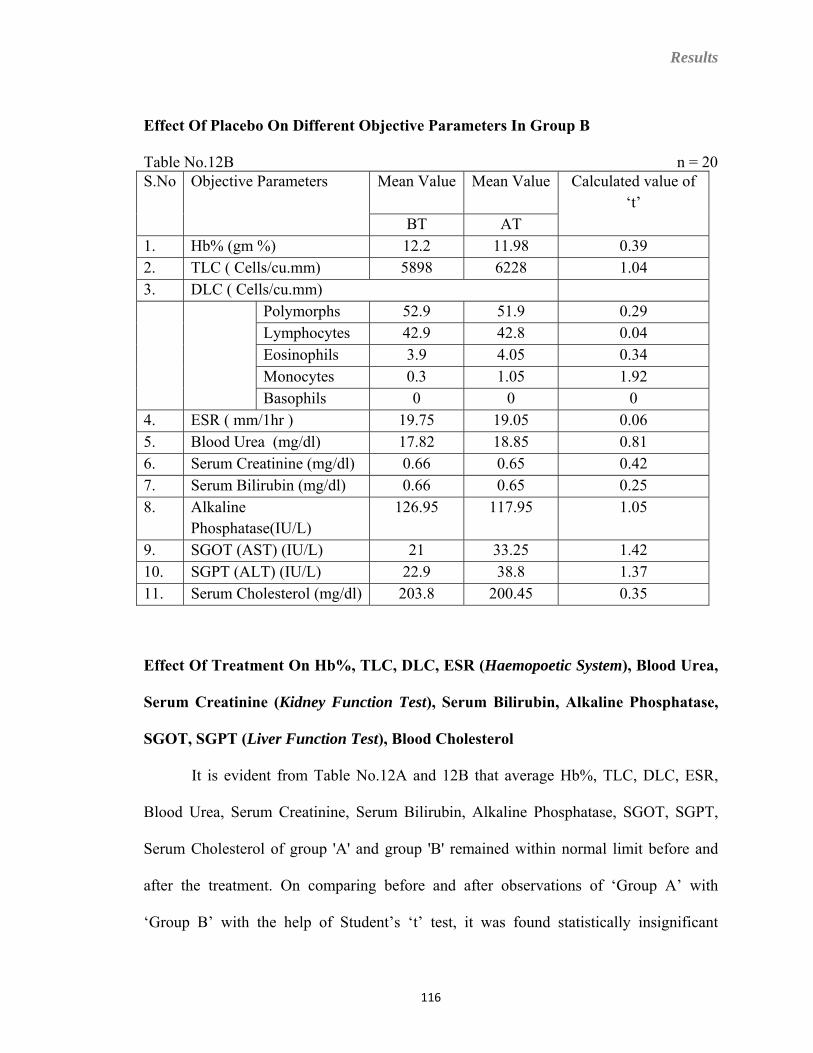
Results
Effect Of Placebo On Different Objective Parameters In Group B
Table No.12B n = 20 Mean Value Mean Value
S.No Objective Parameters Calculated value of
‘t’ BT AT
1. Hb% (gm %) 12.2 11.98 0.39 2. TLC ( Cells/cu.mm) 5898 6228 1.04 3. DLC ( Cells/cu.mm)
Polymorphs 52.9 51.9 0.29 Lymphocytes 42.9 42.8 0.04 Eosinophils 3.9 4.05 0.34 Monocytes 0.3 1.05 1.92 Basophils 0 0 0
4. ESR ( mm/1hr ) 19.75 19.05 0.06 5. Blood Urea (mg/dl) 17.82 18.85 0.81 6. Serum Creatinine (mg/dl) 0.66 0.65 0.42 7. Serum Bilirubin (mg/dl) 0.66 0.65 0.25 8. Alkaline
Phosphatase(IU/L) 126.95 117.95 1.05
9. SGOT (AST) (IU/L) 21 33.25 1.42 10. SGPT (ALT) (IU/L) 22.9 38.8 1.37 11. Serum Cholesterol (mg/dl) 203.8 200.45 0.35
Effect Of Treatment On Hb%, TLC, DLC, ESR (Haemopoetic System), Blood Urea,
Serum Creatinine (Kidney Function Test), Serum Bilirubin, Alkaline Phosphatase,
SGOT, SGPT (Liver Function Test), Blood Cholesterol
It is evident from Table No.12A and 12B that average Hb%, TLC, DLC, ESR,
Blood Urea, Serum Creatinine, Serum Bilirubin, Alkaline Phosphatase, SGOT, SGPT,
Serum Cholesterol of group 'A' and group 'B' remained within normal limit before and
after the treatment. On comparing before and after observations of ‘Group A’ with
‘Group B’ with the help of Student’s ‘t’ test, it was found statistically insignificant
116
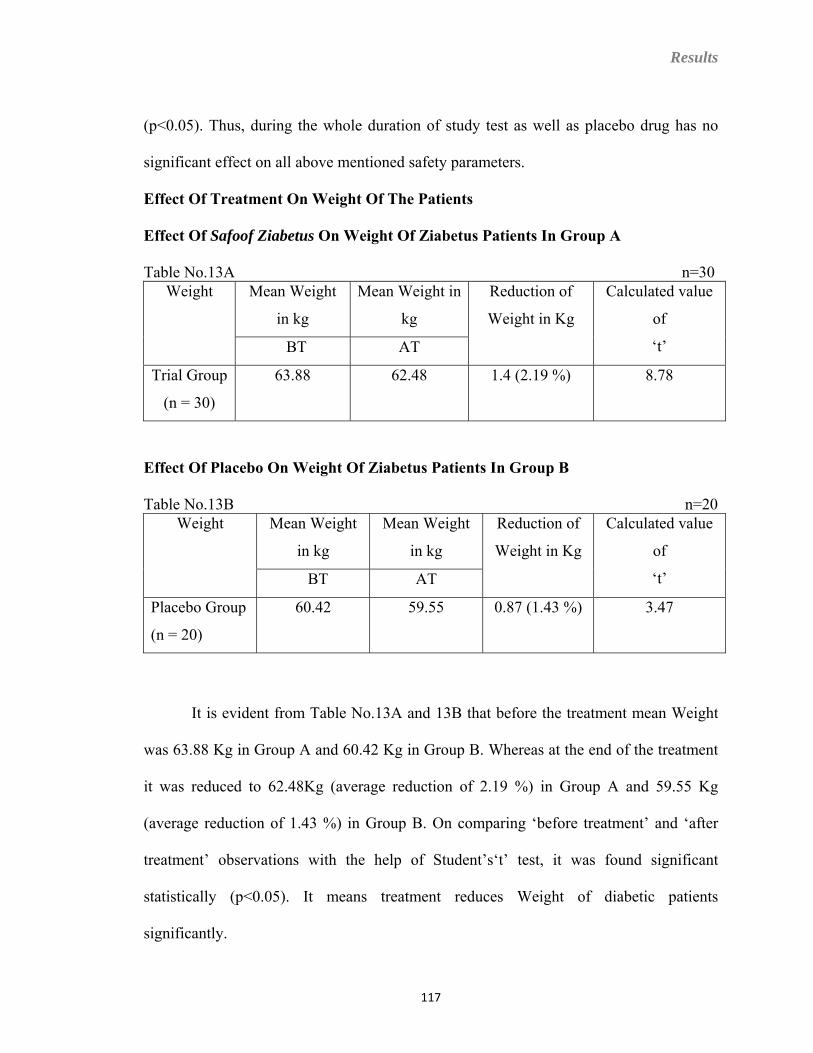
Results
(p<0.05). Thus, during the whole duration of study test as well as placebo drug has no
significant effect on all above mentioned safety parameters.
Effect Of Treatment On Weight Of The Patients
Effect Of Safoof Ziabetus On Weight Of Ziabetus Patients In Group A
Table No.13A n=30 Mean Weight
in kg
Mean Weight in
kg
Weight Reduction of
Weight in Kg
Calculated value
of
‘t’ BT AT
Trial Group
(n = 30)
63.88 62.48 1.4 (2.19 %) 8.78
Effect Of Placebo On Weight Of Ziabetus Patients In Group B
Table No.13B n=20 Mean Weight
in kg
Mean Weight
in kg
Weight Reduction of
Weight in Kg
Calculated value
of
‘t’ BT AT
Placebo Group
(n = 20)
60.42 59.55 0.87 (1.43 %) 3.47
It is evident from Table No.13A and 13B that before the treatment mean Weight
was 63.88 Kg in Group A and 60.42 Kg in Group B. Whereas at the end of the treatment
it was reduced to 62.48Kg (average reduction of 2.19 %) in Group A and 59.55 Kg
(average reduction of 1.43 %) in Group B. On comparing ‘before treatment’ and ‘after
treatment’ observations with the help of Student’s‘t’ test, it was found significant
statistically (p<0.05). It means treatment reduces Weight of diabetic patients
significantly.
117
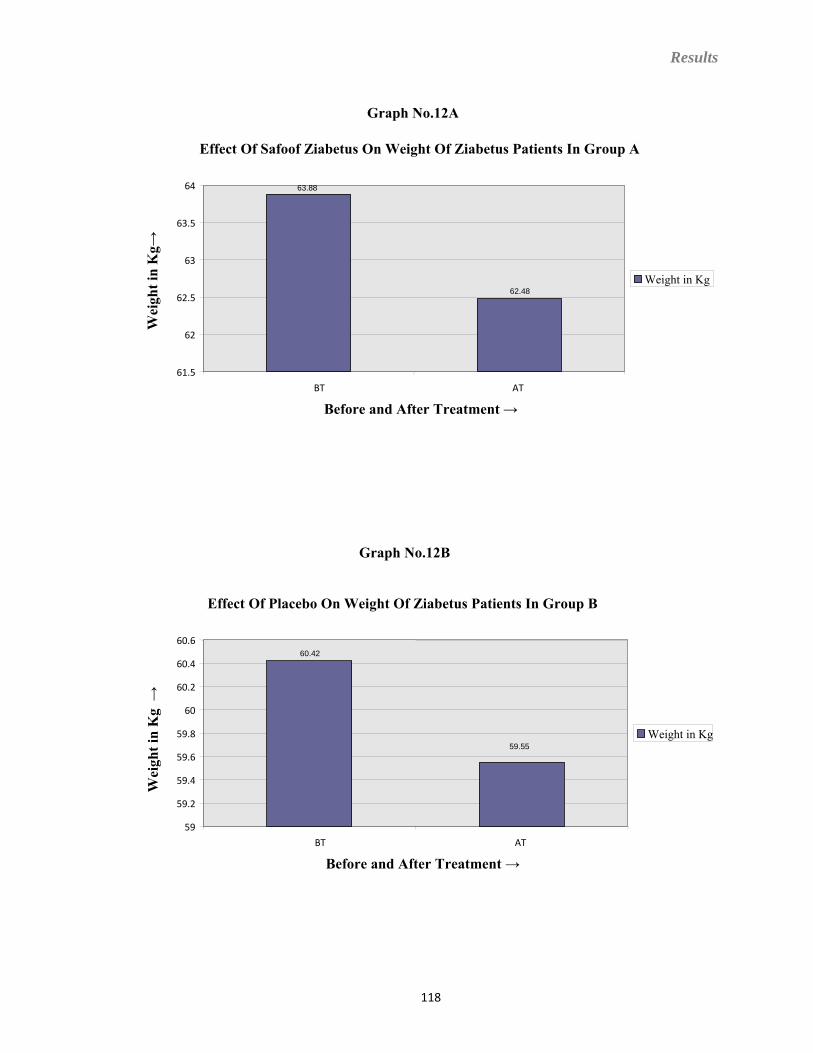
Results
Graph No.12A
Effect Of Safoof Ziabetus On Weight Of Ziabetus Patients In Group A
63.88
62.48
61.5
62
62.5
63
63.5
64
BT AT
Before and After Treatment →
Wei
ght i
n K
g→
Weight in Kg
Graph No.12B
Effect Of Placebo On Weight Of Ziabetus Patients In Group B
60.42
59.55
59
59.2
59.4
59.6
59.8
60
60.2
60.4
60.6
BT AT
Before and After Treatment →
Wei
ght i
n K
g →
Weight in Kg
118
Discussion
DISCUSSION
119
Discussion
DISCUSSION
The Ziabetus Shakri (Diabetes Mellitus) is a major public health problem and
considered as one of the most common non-communicable disease, globally. About 246
million people are affected with this disease all over the world in 2007 and this number
may increase to 380 million by 2025. Although the prevalence rate of the disease varies
from country to country. However, WHO has been projected India as the country with the
fastest growing population of Diabetes patients. Due to its severe consequences Diabetes
become a silent killer that kills one person every 10 seconds, and world wide it kills 3.2
millions every year. Owing to its dreadful complications such as Diabetic Ketoacidosis,
Diabetic Retinopathy, Diabetic Neuropathy, Atherosclerosis, Coronary artery disease and
Stroke the researchers of different system of medicine are concentrating themselves for
the development of new antidiabetic drugs. A number of antidiabetic drugs have been
evaluated by the researchers of main stream medicine such as Glibenclamide, Metformin,
Gliclazide, Glimepiride, Glipizide etc. These drugs have been found to possess potent and
effective hypoglycaemic activity, but the long term use of these drugs frequently leads to
the development of various side effects such as Hypoglycaemic reactions,
Agranulocytosis, Aplastic anaemia, and Haemolytic anaemia .
As far as the Unani system of medicine is concerned, Unani physicians have been treating
Ziabetus Shakri since Greco-Arab period. They have claimed to possess many safe and
effective antidiabetic agents for the management of Ziabetus Shakri. Therefore, it is one
of the areas which have to be given priority in scientific research in Tibbe Unani. Many
important and therapeutically effective murakkab drugs have been described to be useful
120
Discussion
in Ziabetus Shakri in standard qarabadeen; they have not been evaluated scientifically so
far for their described effect. Recently several herbal single drugs have been
experimentally and clinically evaluated and reported as good hypoglycaemic agents.
However, the scientific study of compound formulation is largely ignored by the
scientists and physicians despite the fact that a good number of compound drugs have
been described in Unani literature to be effective in Ziabetus condition. Safoof Ziabetus
is one such drug described in various qarabadeen to be effective in Ziabetus Shakri.
In view of the above a single blind placebo study was designed to investigate the
hypoglycaemic effect of Safoof Ziabetus in the patients of Ziabetus Shakri.
The results and observations obtained from the trial were depicted in Tables and Graphs.
The discussions regarding the incidence of Ziabetus Shakri according to Age, Sex, Mizaj,
and the efficacy of drug in various subjective and objective parameters are as follows:
Incidence Of Patients Of Ziabetus Shakri According To Age
As it is evident from Table No. 1 that out of 50 selected patients of Ziabetus
Shakri, the highest number of patients i.e. 19 (38 %) were from the age group of 41 – 50
years and then 16 (32 %) patients were found in the age group of 51 – 60 years. While the
least 15 (30 %) patients were in the age group of 31 – 40 years. This finding coincides
with the findings described by Anonymous. (115,116)
121
Discussion
Incidence Of Patients Of Ziabetus Shakri According To Gender
As it is clear from the Table No.2 that out of 50 patients of Ziabetus Shakri, 25
(50 %) patients were male and 25 (50 %) patients were Female. This finding does not
coincide with the findings described by Anonymous (115). One of the reasons for such
difference might be the small number of patients in the study. The size of our study is too
small containing only 50 patients. Hence, the exact distribution pattern of the disease
according to gender probably could not be determined accurately through this study.
Incidence Of Patients Of Ziabetus Shakri According To Mizaj (Temperament)
The mizaj of the patients of Ziabetus was assessed as per the parameters given by
Ibne Sina. In our study 21 (42 %) patients were assessed as having Damvi mizaj, while 17
(34 %) patients were of Balghami and 11 (22 %) patients were of Safravi mizaj, whereas
only 1 (2%) patients had Saudavi mizaj. It clearly indicated that most of the patients had
har mizaj. These findings are inconformity with the findings suggested by Razi, Ibne
Sina, Jurjani, Al-Baghdadi, Majusi, M.A.Arzani, N.Samarqandi, and Ajmal Khan. (1, 3,
5, 11, 14, 16, 18, 19, 20).
Effect Of Safoof Ziabetus On Polyuria In Group A
It is evident from the table No.4A that only 11 (36.66 %) patients had Polyuria at
the beginning of trial. Out of these 3 (10%) patients had moderate and 8 (26.6 %) patients
had mild degree of Polyuria. After 15 days of treatment only 2 (6.66 %) patients had
moderate and 8 (26.6 %) patients had mild degree of Polyuria and after 30 days of
122
Discussion
treatment only 9 (30 %) patients had mild degree of Polyuria. Whereas after 45 days of
treatment only 7 (23.33 %) patients had mild degree of Polyuria.
The improvement in this symptom appears to be due to the effect of test drug which
reduced the blood glucose level and that in turn decreased the frequency of micturition
(Polyuria). The exact mechanism of hypoglycaemic activity of test can not be described
at the moment but as per the description of Unani literature it may be attributed mainly to
the blood purifying activity of both Gilo Khushk and Gurmar Booti. These findings are
inconformity with the findings suggested by Najmul Ghani, Kabeeruddin, Nadkarni,
Kritikar and Basu, Stanely P et al, Mhasker and caius, Shanmugasundaram et al.
(174,175,179,181,189,192,193,222,252)
Effect Of Placebo On Polyuria In Group B
It is shown in table No.4B that only 9 (45 %) patients had Polyuria at the
beginning of trial. Out of these, 1 (5 %) patient had moderate and 8 (40 %) patients had
mild degree of Polyuria. After 15 days of treatment 8 (40 %) patients had mild degree of
Polyuria while after 30 days of treatment only 7 (35 %) patients had mild degree of
Polyuria. Whereas at the end of the trial total 8 (40 %) patients had mild degree of
Polyuria.
The mild improvement in this symptom might be attributed to diet and exercise
prescribed as per ICMR guidelines.
123
Discussion
Effect Of Safoof Ziabetus On Nocturia In Group A
It is clear from the table No.5A that only 14 (46.66 %) patients of Ziabetus Shakri
had Nocturia at the beginning of the treatment. Out of these, 1 (3.33%) patient had
moderate degree and 13 (43.33 %) patients had mild degree of Nocturia. After 15 days of
treatment 8 (26.6 %) patients had mild degree of Nocturia. While after 30 days of
treatment only 6 (20 %) patients had mild degree of Nocturia. Whereas at the end of the
study only 3 (10 %) patients had Nocturia of mild degree. The improvement in this
symptom appears to be due to the effect of test drug which reduced the blood glucose
level and that in turn decreased the Nocturia. The exact mechanism of hypoglycaemic
activity of test drug can not be described at the moment but as per the description of
Unani literature it may be attributed mainly to the blood purifying activity of both Gilo
Khushk and Gurmar Booti. These findings are inconformity with the findings suggested
by Najmul Ghani, Kabeeruddin, Nadkarni, Kritikar and Basu, Stanely P et al, Mhasker
and caius, Shanmugasundaram et al.( 174,175,179, 181,189, 192,193, 222,252)
Effect Of Placebo On Nocturia In Group B
It is evident from the table No 5B that only 8 (40 %) patients of Ziabetus Shakri
had Nocturia at the beginning of the treatment. Out of these, 1 (5 %) patient had moderate
degree of Nocturia and 7 (35 %) patients had mild degree of Nocturia. After 15 days of
treatment 1 (5 %) patient had moderate degree and 5 (25 %) patients had mild degree of
Nocturia. While after 30 days of treatment only 6 (30 %) patients had mild degree of
Nocturia. Whereas at the end of the trial 1 (5 %) patient had moderate degree and 5
124
Discussion
(25 %) patients had mild degree of Nocturia. The mild improvement in this symptom
might be attributed to diet and exercise prescribed as per ICMR guidelines.
Effect Of Safoof Ziabetus On Polydipsia In Group A
As it is evident from table No.6A only 9 (30 %) patients had Polydipsia at the
beginning of trial. Out of these, 1 (3.33 %) patient had moderate and 8 (26.6 %) patients
had mild degree of Polydipsia. After 15 days of treatment 6 (20 %) patients had mild
degree of Polydipsia, while after 30 days of treatment only 4 (13.33 %) patients had mild
degree of Polydipsia.Whereas at the end of the trial only 2 (6.66 %) patients had mild
degree of Polydipsia.
The improvement in this symptom might be due to reduction in blood glucose
level and decreased frequency of micturition. This effect may be attributed to the
ingredients of the test drug; as Gilo khushk reduces the thirst and Gurmar booti reduces
the Polyuria as described by Anonymous. (177,222)
Effect Of Placebo On Polydipsia In Group B
As it is clear from table No.6B only 2 (10 %) patients had Polydipsia at the
beginning of trial. Out of these, 1 (5 %) patient had moderate and 1 (5 %) patient had
mild degree of Polydipsia. After 15 days of treatment 2 (10 %) patients had mild degree
of Polydipsia, while after 30 days of treatment 1 (5 %) patient had moderate degree of
Polydipsia and 3 (15 %) patients had mild degree of Polydipsia. Whereas at the end of the
trial 1(5 %) patient had moderate and 3 (15 %) patients had mild degree of Polydipsia. It
clearly indicates that the placebo did not have any effect on this symptom. On the
125
Discussion
contrary in this group Polydipsia had occurred in two more patients during the study, it
might be due to fluctuation in the blood glucose level.
Effect Of Safoof Ziabetus On Tiredness In Group A
As it is shown in table No.7A total 26 (86.66 %) patients had Tiredness at the
beginning of trial. Out of these, 4 (13.33 %) patients had moderate and 22 (26.6 %)
patients had mild degree of Tiredness. After 15 days of treatment 23 (76.66 %) patients
had mild degree of Tiredness. While after 30 days of treatment only 16 (53.33 %) patients
had mild degree of Tiredness. Whereas at the end of the trial only 12 (6.66 %) patients
had mild degree of Tiredness.
Association of Tiredness with hyperglycaemia is now a well established and documented
fact. It can be inferred therefore that the improvement in the Tiredness of the patients is
mainly because of the improvement in diabetic condition of the patient. Further, since
Gilo and Gurmar has been reported to possess tonic, antioxidant, adaptogenic and
analgesic activities. The partial role of these effects in improving the Tiredness can not be
denied. These findings are inconformity with the findings suggested by Najmul Ghani,
Kabeeruddin, K.M.Nadkarni, Kirtikar and Basu, Dymock,W. et.al, Prince P, et al. ,
Mathew S, et al.(174, 175, 179, 181, 182, 222, 258, 259, 223)
Effect Of Placebo On Tiredness In Group B
As it is shown in table No.7B, 15 (75%) patients had Tiredness at the beginning
of trial. Out of these, 1 (5%) patient had moderate and 14 (70%) patients had mild degree
of Tiredness. After 15 and 30 days of treatment 17 (85%) patients had mild degree of
126
Discussion
Tiredness. Whereas at the end of the trial 18 (90%) patients had mild degree of Tiredness.
It clearly indicates that the placebo did not have any effect on this symptom. On the
contrary in this group Tiredness had occurred in three more patients during the study, it
might be due to fluctuation in the blood glucose level.
Effect Of Safoof Ziabetus On General Weakness In Group A
As evident from the table No.8A, total 19 (63.33 %) patients had General
Weakness at the beginning of trial. Out of these, 4 (13.33 %) patients had moderate and
15 (50 %) patients had mild degree of General Weakness. While after 15 and 30 days of
treatment 18 (60 %) patients had mild degree of General Weakness. Whereas at the end
of the study only 17 (56.66 %) patients had mild degree of General Weakness.
It is a well known and documented fact that in Ziabetus Shakri General Weakness
is mainly occurs due to reduction in utilisation of glucose. It is also documented that Gilo
khushk and Gurmar booti increases the utilisation of glucose, thereby improving the
General Weakness. Further, since Gilo has been reported to possess antioxidant, anti-
stress and tonic activity. The role of these effects in improving the General Weakness can
not be denied. (192,193,194,201, 202,203, 204,205, 251, 258,259)
Effect Of Placebo On General Weakness In Group B
As shown in table No.8B, total 12 (60%) patients had mild degree of General
Weakness at the beginning of trial. After 15 days of treatment 13 (65%) patients had mild
degree of General Weakness, while after 30 days 14 (70%) patients had mild degree of
General Weakness. Whereas after 45 days of treatment 15 (75%) patients had mild
127
Discussion
degree of General Weakness. It clearly indicates that the placebo did not have any effect
on this symptom. On the contrary in this group General Weakness had occurred in three
more patients during the study, it might be due to fluctuation in the blood glucose level.
Effect Of Safoof Ziabetus On Different Subjective Parameters In Group A
Out of 30 patients, 5 (16.66 %) patients were having Increased Appetite, 3 (10%)
patients were of Weight Gain before the treatment. During the study it was observed that
these two symptoms disappeared. Similarly, there were only 6 (20%) patients of Wasting
of Muscles, 3 (10%) patients of Non-healing of Wounds and 2 (6.66%) patients of
Impotence before the treatment. However, no improvement was observed in these
symptoms.
There were 20 (66.66%) patients of Paraesthesia, 23 (76.66%) patients of Pain in
Limbs and 9 (30%) patients of Irritability before the treatment. After 30 days of treatment
improvement was noted in only 7 (23.33%) patients of Pain in Limbs and 7 (23.33%)
patients of Irritability. At the end of the study Paraesthesia was absent in only one
patient. There were only 2 (6.66%) patients who complained of Nausea before the
treatment. One of them got relief after 15 days of treatment while other after 30 days .The
improvement in the symptom of Increased Appetite might be attributed to reduction in
blood sugar level, while improvement in Gaining of Weight might be attributed to diet
restriction and exercise programme advised to patients. The improvement in Paraesthesia
and Pain in the Limbs might be attributed to the analgesic property of Gilo khushk as
described in Wealth of India. As far as the improvement in Irritability was concerned it
might be occurred because of the overall improvement in health and feeling of wellness
128
Discussion
in patients. Improvement in the symptom of Nausea might be attributed to the anti-emetic
property of Gilo khushk as described in Najmul Ghani and Anonymous. (174, 222, 223)
Effect Of Placebo On Different Subjective Parameters In Group B
As evident from Table No. 9B out of 20 patients there were 3 (15 %) patients of
Increased Appetite, 1 (5%) patient of Weight Gain before the treatment. After 15, 30 and
45 days of treatment, there were 4 (20%) patients of Increased Appetite, 2 (10%) of
Weight Gain. Similarly, there were only 4 (20%) patients of Wasting of Muscles, 1 (5%)
patient of Non-healing of Wounds, 3 (15%) patients of Impotence and 8 (40%) patients of
Paraesthesia before the treatment. During the study no improvement was observed in
these symptoms.
There were 11 (55%) patients of Pain in Limbs, 3 (15%) patients of Irritability,
and no (0%) patient of Nausea before the treatment. After 15 days of treatment there
were 11 (55%) patients of Pain in Limbs, 6 (30%) patients of Irritability, and 0 patient of
Nausea, while after 30 days of treatment there were 13 (65%) patients of Pain in Limbs, 7
(35%) patients of Irritability and 0 patient of Nausea. Whereas at the end of the study
there were 12 (60%) patients of Pain in Limbs, 7 (35%) patients of Irritability and 1 (5%)
patient of Nausea. It indicates that the placebo did not have any effect on these
symptoms. On the contrary in this group all the above mentioned symptoms increases to
some extent, it might be due to fluctuation in the blood glucose level.
129
Discussion
Effect Of Safoof Ziabetus On Blood Sugar Levels In Group A
It is evident from table No.10A, the mean Blood Sugar in the Fasting state was
173.23 mg/dl at the beginning of the treatment, while after 15 days and 30 days of
treatment it was reduced to 133.43 mg/dl and 124.96 mg/dl, respectively. Whereas at the
end of the study mean Fasting Blood Glucose level reduced to 116.4 mg/dl.
Similarly, the mean Blood Sugar in the Post Prandial state was 249.53 mg/dl at
the beginning of the treatment, while after 15 days and 30 days of treatment it was
reduced to 208.7 mg/dl and 194.4 mg/dl, respectively. Whereas at the end of the study
mean Post Prandial Blood Glucose level reduced to 182.3 mg/dl. The improvement in
Blood Sugar level during the state of Fasting and Post Prandial is attributed to the
hypoglycaemic activity of test drug contained Gilo Khushk and Gurmar booti.
Experimental and clinical studies shows that Gurmar booti and Gilo khushk
increases the insulin level, reduces the glucose absorption from the intestine, improves
uptake of glucose into the cells and prevents adrenal hormone from stimulating the liver
to produce glucose, thereby reducing Blood Glucose level and increasing the glucose
tolerance. Hence, the finding of Blood Glucose reduction during Fasting and Post
Prandial state is inconformity with the description of Najmul Ghani, Kabeeruddin,
Nadkarni, Kritikar and Basu, Stanely P et al, Mhasker and caius, Shanmugasundaram et
al., Hirata and co-workers,Yoshikawa et al, Chattopadhyay. (174, 175,179,181,189, 192,
193,194,202,206,207,222,252).
On comparing ‘before treatment’ observations of Blood Sugar Fasting and Post Prandial
with their corresponding ‘after treatment’ observations, with the help of Student’s ‘t’ test,
130
Discussion
it was found significant statistically (p<0.05). Hence trial drug has significant effect on
Blood Sugar Fasting and Post Prandial.
Effect Of Placebo On Blood Sugar Levels In Group B
As it is evident from table No.10B, the mean Blood Sugar in the Fasting state was
164.2 mg/dl at the beginning of the treatment, while after 15 days and 30 days of
treatment it was increased to 170.5 mg/dl and 173.05 mg/dl, respectively. At the end of
the study mean Fasting Blood Glucose level increased to 179.85 mg/dl. Similarly, the
mean Blood Sugar in the Post Prandial state was 249.3 mg/dl at the beginning of the
treatment, while after 15 days and 30 days of treatment it was increased to 258.3 mg/dl
and 254.7 mg/dl, respectively. Whereas, at the end of the study mean Post Prandial Blood
Glucose level increased to 277.05 mg/dl. It clearly indicates that the placebo did not have
any effect on Blood Sugar levels. On the contrary in this group Blood Sugar levels i.e.
Fasting and Post Prandial increases during the study.
On comparing ‘before treatment’ observations of Blood Sugar Fasting and Post Prandial
with their corresponding ‘after treatment’ observations with the help of Student’s ‘t’ test,
it was found significant statistically (p<0.05). Hence, Placebo did not have any blood
glucose lowering effect.
Effect Of Safoof Ziabetus On Urine Sugar In Group A
As shown in table 11A out of 30 patients, 10 (33.33%) patients had sugar in urine
in traces at the start of the treatment. After 15 and 30 days there was only 1 (3.33%)
patient with sugar in urine. Whereas, at the end of the treatment there were only 5
131
Discussion
(16.66%) patients who had urinary sugar. Similarly, there were only 3 (10%) patients of
0.5%, 2 (6.66%) patients of 1% and 1 (3.33%) patient of 2% sugar in urine at the start of
the treatment. After 15 days of treatment there were 3 (10%) patients each of 0.5% and
1% sugar in the urine and 1 (3.33%) patient each of 1.5% and 2% sugar in urine. While
after 30 days of treatment there were 2 (6.66%) patients of 0.5%, 3 (10%) patients of 1%
and 1 (3.33%) patient each of 1.5% and 2% sugar in urine. Whereas at the end of the
study, there were 2 (6.66%) patients who had 0.5% sugar in the urine and no patient was
found to have 1%, 1.5%, and 2% sugar in urine. The improvement in urinary sugar level
is due to low level of sugar in the blood. As sugar in urine appears only when blood sugar
level exceeds the threshold value i.e.180 mg/dl and its quantity in the urine increases
proportionally as the sugar in blood increases..
Effect Of Placebo On Urine Sugar In Group B
As shown in table 11B out of 20, 2 (10%) patients had sugar in urine in traces at 0
and 15 days of treatment. While after 30 days no patient was found with sugar in urine.
Whereas at the end of the study, 3 (15%) patients had urinary sugar in traces. Similarly,
there were only 1 (5%) patient of 0.5%, 2 (10%) patients of 1% and 3 (15%) patients of
1.5% and 1 (5%) patient of 2% sugar in urine at the start of the treatment. After 15 days
of treatment there were 2 (10%) patients of 0.5%, 6 (30%) patients of 1%, 1 (5%) patient
of 1.5% and no patient of 2% sugar in urine. While after 30 days there were 3 (15%)
patients of 0.5%, 4 (20%) patients of 1%, 1 (5%) patient of 1.5% and 2 (10%) patients of
2% sugar in urine. Whereas at the end of the study, only 3 (15%) patients of traces, 5
132
Discussion
(25%) patients of 0.5%, 3 (15%) patients of 1%, and 1 (5%) patient of 1.5% were found.
Hence, the placebo has no effect on urinary sugar.
Effect Of Safoof Ziabetus On Different Objective Parameters In Group A
Effect On Haemopoetic System (Hb%, TLC, DLC, ESR)
Only slight variation was noted in parameters of Haemopoetic system, as shown
in Table No.12A. However, all the observations were still found within the normal limit.
On comparing ‘before treatment’ observations of each parameter with their
corresponding ‘after treatment’ observations with the help of Student’s‘t’ test, it was
found insignificant statistically (p<0.05). It may be concluded therefore that the test drug
does not posses any adverse effect on Haemopoetic system.
Effect On Kidney Function Test (Blood Urea, Serum Creatinine)
Only slight variation was observed in parameters of Kidney Function Test. As
evident from Table No.12A, all the observations were still found within normal limit. On
comparing ‘before treatment’ observations with their corresponding ‘after treatment’
observations with the help of Student’s‘t’ test, it was found insignificant statistically
(p<0.05). Hence trial drug has no adverse effect on Kidney Function Test.
133
Discussion
Effect On Liver Function Test (Serum Bilirubin, Alkaline Phosphatase, SGOT,
SGPT)
As shown in Table No.12A all the observations of Liver Function Test were
found within normal limit before and after the treatment. On comparing ‘before
treatment’ observations of all parameters with their corresponding ‘after treatment’
observations with the help of Student’s‘t’ test, it was found insignificant statistically
(p<0.05). Hence, it may be concluded that test drug has no adverse effect on Liver
Function Test.
Effect On Serum Cholesterol
Only slight variation was observed in S.Cholesterol level as shown in Table
No.12A. However, before and after observations were still found within normal limit. On
comparing ‘before treatment’ observation with ‘after treatment’ observation with the help
of Student’s‘t’ test, it was found insignificant statistically (p<0.05). Hence, it may be
concluded that test drug has no effect on Serum Cholesterol level.
Effect Of Placebo On Different Objective Parameters In Group B
As evident from Table No.12B, only slight variations were noted in all objective
parameters, but all the observations still found within normal limit. On comparing ‘before
treatment’ observations of each parameter with their corresponding ‘after treatment’
observations with the help of Student’s‘t’ test, it was found insignificant statistically
(p<0.05). Hence trial drug has no effect on these objective parameters.
134
Discussion
Effect Of Safoof Ziabetus On Weight Of Ziabetus Patients In Group A
It is evident from the table No.13A, mean Weight of Group A patients before the
treatment was 63.88 kg and after treatment it reduced to 62.48 kg. This improvement might be
attributed to diet and exercise programme advised to the patients. On comparing ‘before treatment
observations of Weight with their corresponding after treatment observations with the help of
Student’s‘t’ test, it was found significant statistically (p<0.05).
Effect Of Placebo On Weight Of Ziabetus Patients In Group B
As shown in table No.13B, mean Weight of Group B patients before the treatment
was 60.42 kg and after treatment it reduced to 59.55 kg. This improvement might be
attributed to diet and exercise programme advised to patients. On comparing before
treatment observations of Weight with their corresponding after treatment observations
with the help of Student’s‘t’ test, it was found significant statistically (p<0.05).
Although, the results of the present study are very encouraging and statistically
significant. But the duration of the study was only 45 days, which could not elaborate the
long term safety and efficacy of the Safoof Ziabetus. Hence, the long term study (Phase
III and IV Clinical Trial) is required to further explore the safety and efficacy of this
formulation and to make it a standard formulation for the long term management of
Ziabetus Shakri.
135
Conclusion
CONCLUSION
136
Conclusion
CONCLUSION
The clinical study on Ziabetus Shakri and review of literature presented in this
dissertation provide certain important and fruitful information regarding the usefulness of
Unani formulation in the management of Ziabetus Shakri. Ziabetus (Diabetes) has
become a global problem in spite of advances in modern sciences and considered as one
of the most common non-communicable disease globally. It is a major cause of disability
through its complications like blindness, renal failure, coronary artery disease, gangrene
of lower extremities. Owing to these complications, the researchers of different system of
medicine are concentrating themselves for the development of the new antidiabetic drugs.
The different antidiabetic drugs has been already evaluated by main stream of medicine
such as Glibenclamide, Metformin, Glipizide etc., these drugs have very much potent and
effective hypoglycaemic action, but the long term use of these drugs resulted in
development of various side effects like Hypoglycaemic reactions, Aplastic anaemia, and
Haemolytic anaemia. Hence, there is an increasing interest among diabetic patients and
health professionals in using alternative medicinal systems such as Unani system of
Medicine for the management of Ziabetus Shakri. Unani drugs are available in abundance
in surrounding and can provide safe, stable, standardise and efficacious treatment. The
therapeutic application of Unani drugs is based upon evidence handed down from
generation to generation and achieves their importance through experience and not by
experiments. Nevertheless their clinical efficacy is beyond doubt. Hence, Tibbe Unani
possesses large number of mufrad and murakkab drugs for the management of Ziabetus
Shakri; but they have not been evaluated scientifically so far for their described effect.
Hence, scientific evaluation of compound Unani drugs on the modern scientific approach
137
Conclusion
of research and treatment is quite necessary. Keeping this fact in mind a clinical trial was
conducted on the "Clinical evaluation of Safoof Ziabetus in management of Ziabetus
Shakri.” Safoof Ziabetus was selected from a long list of compound Unani formulations
used by the Unani physicians for the management of Ziabetus Shakri. It contains Gurmar
booti (Gymnema Sylvestre) and Gilo khushk (Tinospora Cordifolia) in equal quantity.
The trial was conducted on 50 newly diagnosed patients of Ziabetus Shakri [divided into
two groups "Group A (30 Patients) and Group B (20 Patients)"] at National Institute of
Unani Medicine Hospital, Bangalore. Group A was given the test drug (Safoof Ziabetus)
whereas Group B placebo in a dose of 6 gm thrice a day in capsule form orally with
water,15 minutes before breakfast, lunch, and dinner along with planned diet and exercise
for the period of 45 days. Study reveals that the Ziabetus Shakri is relatively more
common in person having age 40 years and above with har mizaj.
As evident from results and discussion, the cases treated with Safoof Ziabetus
showed good response; the results were encouraging and statistically significant.
Moreover, the drug was found relatively safe, as the safety parameters (Haemogram,
LFT, KFT and S.Cholesterol) remained within normal limits during the study. Since the
duration of the study was only 45 days, therefore the long term safety and efficacy of
Safoof Ziabetus can not be elaborate at the moment but for short term use, it was found
safe. Hence, long term study (Phase III and IV Clinical Trial) will be required to assess
the long term perspectives of test drug for its safety and toxicity and to make it a standard
formulation for the long term management of Ziabetus Shakri.
138
Summary
SUMMARY
139
Summary
SUMMARY
The term Ziabetus is a Greek word which means “to run through” or “Siphon”,
was first used by Arsyatoos,characterized by hyperglycaemia, glycosuria, increased
appetite, excessive thirst and gradual loss of body weight . It is a disease in which, patient
excretes water as such through urinary passage soon after its intake. The ratio of fluid
taken and the urinary output remains the same (Zalaqul majari) as that of solid without
digestion from the stomach and intestine, a condition known in Unani medicine as
'Zalaqul-ama'. There is excessive thirst more intake of water and its rapid discharge as
urine. When the disease takes the body completely in its grip there occurs dryness all
over the body rendering it weak. Sue mizaj har kuliya, Zoufe-kuliya, Majari ki
kushadgi,and Sue mizaj barid of tamam badan / kuliya / jigar ,are the four major causes
described in most of the classical Unani literature, responsible for the development of
Ziabetus. Now in present era due to resemblance in clinical features of the disease
Ziabetus Shakri has been correlated with Diabetes Mellitus, which is a chronic disorder
of carbohydrate metabolism and glucose intolerance. It is characterized by high blood
glucose level and glycosuria resulting from dysfunction of pancreatic β cells and insulin
resistance. Owing to its dreadful complications such as Diabetic Ketoacidosis, Diabetic
Retinopathy, Diabetic Neuropathy, Atherosclerosis, Coronary artery disease, Stroke etc.,
now Diabetes has become a global problem in spite of advances in modern sciences, and
prevails all over the world, and considered as one of the most common non-
communicable disease globally. In present study, the Introduction of Ziabetus Shakri,
History, Anatomy & Physiology of Pancreas, Definition, Prevalence, Classification,
140
Summary
Pathogenesis, Clinical features, Complications, Diagnostic criteria and Management has
been discussed in detail.
Age: The highest number of patients i.e. 19 (38 %) were found in the age group of 41–50
years showing higher incidence after 40 years.
Gender: 25 (50 %) patients were male and 25 (50 %) patients were Female, showing
equal incidence of disease in both sexes.
Mizaj (Temperament): The highest number of patients i.e. 21(42%) were of Damvi
Mizaj, showing higher incidence in har mizaj.
Effect Of Treatment On Different Subjective Parameters Of Ziabetus Shakri
[Group A contain 30 Patients and Group B contain 20 Patients]
Effect Of Treatment On Polyuria: Only 4 (36.36 %) patients of Group A and 1
(11.11 %) patients of Group B had shown improvement by the treatment.
Effect Of Treatment On Nocturia: Only 11 (78.57 %) patients of Group A and 2 (25 %)
patients of Group B had shown improvement by the treatment.
Effect Of Treatment On Polydipsia: Only 7 (77.77 %) patients of Group A had shown
improvement by the treatment. On the contrary in Group B Polydipsia had occurred in 2
more patients.
Effect Of Treatment On Tiredness: Only 14 (53.84 %) patients of Group A had shown
improvement by the treatment. On the contrary in Group B Tiredness had occurred in 3
(20 %) more patients.
Effect Of Treatment On General Weakness: Only 2 (10.52 %) patients of Group A had
shown improvement by the treatment. On the contrary in Group B General Weakness had
occurred in 3 (25 %) more patients.
141
Summary
Effect Of Treatment On Increased Appetite: All patients i.e. 5 (100 %) patients of
Group A had shown improvement by the treatment. On the contrary in Group B Increased
Appetite had occurred in 1 (33.33 %) more patients.
Effect Of Treatment On Weight Gain: All the patients i.e. 3 (100 %) patients of Group
A had shown improvement by the treatment. On the contrary in Group B Weight Gain
had occurred in 1 more patients.
Effect Of Treatment On Paraesthesia: Only 1 (5 %) patient of Group A had shown
improvement by the treatment. On the contrary no improvement was observed in the
Paraesthesia in Group B.
Effect Of Treatment On Pain In Limbs: Only 7 (30.43 %) patients of Group A had
shown improvement by the treatment. On the contrary in Group B Pain in Limbs had
occurred in one (9.09 %) more patients.
Effect Of Treatment On Nausea: All patients i.e.2 (100 %) patients of Group A had
shown improvement by the treatment. On the contrary in Group B Nausea had occurred
in one more patients.
Effect Of Treatment On Irritability: Only 7 (77.77 %) patients of Group A had shown
improvement by the treatment. On the contrary in Group B Irritability had occurred in 4
more patients.
Effect Of Treatment On Wasting Of Muscles, Non-Healing Or Delayed Healing Of
Cuts And Wounds, Impotence: During the study, no effect was observed on these
symptoms.
142
Summary
Effect Of Treatment On Different Objective Parameters Of Ziabetus Shakri
Effect Of Treatment On Blood Sugar Fasting: During the study average reduction of
56.83 mg/dl (32.80 %) in Group A, and average elevation of 15.65 mg/dl (9.53 %) in
Group B was recorded in Blood Sugar Fasting and statistically it was found significant.
Effect Of Treatment On Blood Sugar Post Prandial: During the study average
reduction of 67.23 mg/dl (26.94 %) in Group A, and average elevation of 27.75 mg/dl
(11.13%) in Group B was recorded in Blood Sugar Post Prandial and statistically it was
found significant.
Effect Of Treatment On Urine Sugar: Only 9 (56.25 %) patients of Group A had
shown improvement by the treatment. On the contrary in Group B, sugar in urine had
appeared in 3 (33.33 %) more patients
Effect Of Treatment On Hb%, TLC, DLC, ESR, Blood Urea, Serum Creatinine,
Serum Bilirubin, Alkaline Phosphatase, SGOT, SGPT, Serum Cholesterol
It was observed that average Hb%, TLC, DLC, ESR, Blood Urea, Serum
Creatinine, Serum Bilirubin, Alkaline Phosphatase, SGOT, SGPT, Serum Cholesterol of
group 'A' and group 'B' remained within normal limit before and after the treatment. On
comparing before and after observations of ‘Group A’ with ‘Group B’ with the help of
Student’s ‘t’ test, it was found statistically insignificant (p<0.05). Thus, during the whole
duration of study test as well as placebo drug has no significant effect on all above
mentioned safety parameters.
Effect Of Treatment On Weight Of The Patients: During the study, average reduction
of 1.4 Kg (2.19 %) in Group A and 0.87 Kg (1.43 %) in Group B was recorded and found
significant statistically (p<0.05).
143
Summary
SUMMARY
139
Summary
SUMMARY
The term Ziabetus is a Greek word which means “to run through” or “Siphon”,
was first used by Arsyatoos,characterized by hyperglycaemia, glycosuria, increased
appetite, excessive thirst and gradual loss of body weight . It is a disease in which, patient
excretes water as such through urinary passage soon after its intake. The ratio of fluid
taken and the urinary output remains the same (Zalaqul majari) as that of solid without
digestion from the stomach and intestine, a condition known in Unani medicine as
'Zalaqul-ama'. There is excessive thirst more intake of water and its rapid discharge as
urine. When the disease takes the body completely in its grip there occurs dryness all
over the body rendering it weak. Sue mizaj har kuliya, Zoufe-kuliya, Majari ki
kushadgi,and Sue mizaj barid of tamam badan / kuliya / jigar ,are the four major causes
described in most of the classical Unani literature, responsible for the development of
Ziabetus. Now in present era due to resemblance in clinical features of the disease
Ziabetus Shakri has been correlated with Diabetes Mellitus, which is a chronic disorder
of carbohydrate metabolism and glucose intolerance. It is characterized by high blood
glucose level and glycosuria resulting from dysfunction of pancreatic β cells and insulin
resistance. Owing to its dreadful complications such as Diabetic Ketoacidosis, Diabetic
Retinopathy, Diabetic Neuropathy, Atherosclerosis, Coronary artery disease, Stroke etc.,
now Diabetes has become a global problem in spite of advances in modern sciences, and
prevails all over the world, and considered as one of the most common non-
communicable disease globally. In present study, the Introduction of Ziabetus Shakri,
History, Anatomy & Physiology of Pancreas, Definition, Prevalence, Classification,
140
Summary
Pathogenesis, Clinical features, Complications, Diagnostic criteria and Management has
been discussed in detail.
Age: The highest number of patients i.e. 19 (38 %) were found in the age group of 41–50
years showing higher incidence after 40 years.
Gender: 25 (50 %) patients were male and 25 (50 %) patients were Female, showing
equal incidence of disease in both sexes.
Mizaj (Temperament): The highest number of patients i.e. 21(42%) were of Damvi
Mizaj, showing higher incidence in har mizaj.
Effect Of Treatment On Different Subjective Parameters Of Ziabetus Shakri
[Group A contain 30 Patients and Group B contain 20 Patients]
Effect Of Treatment On Polyuria: Only 4 (36.36 %) patients of Group A and 1
(11.11 %) patients of Group B had shown improvement by the treatment.
Effect Of Treatment On Nocturia: Only 11 (78.57 %) patients of Group A and 2 (25 %)
patients of Group B had shown improvement by the treatment.
Effect Of Treatment On Polydipsia: Only 7 (77.77 %) patients of Group A had shown
improvement by the treatment. On the contrary in Group B Polydipsia had occurred in 2
more patients.
Effect Of Treatment On Tiredness: Only 14 (53.84 %) patients of Group A had shown
improvement by the treatment. On the contrary in Group B Tiredness had occurred in 3
(20 %) more patients.
Effect Of Treatment On General Weakness: Only 2 (10.52 %) patients of Group A had
shown improvement by the treatment. On the contrary in Group B General Weakness had
occurred in 3 (25 %) more patients.
141
Summary
Effect Of Treatment On Increased Appetite: All patients i.e. 5 (100 %) patients of
Group A had shown improvement by the treatment. On the contrary in Group B Increased
Appetite had occurred in 1 (33.33 %) more patients.
Effect Of Treatment On Weight Gain: All the patients i.e. 3 (100 %) patients of Group
A had shown improvement by the treatment. On the contrary in Group B Weight Gain
had occurred in 1 more patients.
Effect Of Treatment On Paraesthesia: Only 1 (5 %) patient of Group A had shown
improvement by the treatment. On the contrary no improvement was observed in the
Paraesthesia in Group B.
Effect Of Treatment On Pain In Limbs: Only 7 (30.43 %) patients of Group A had
shown improvement by the treatment. On the contrary in Group B Pain in Limbs had
occurred in one (9.09 %) more patients.
Effect Of Treatment On Nausea: All patients i.e.2 (100 %) patients of Group A had
shown improvement by the treatment. On the contrary in Group B Nausea had occurred
in one more patients.
Effect Of Treatment On Irritability: Only 7 (77.77 %) patients of Group A had shown
improvement by the treatment. On the contrary in Group B Irritability had occurred in 4
more patients.
Effect Of Treatment On Wasting Of Muscles, Non-Healing Or Delayed Healing Of
Cuts And Wounds, Impotence: During the study, no effect was observed on these
symptoms.
142
Summary
Effect Of Treatment On Different Objective Parameters Of Ziabetus Shakri
Effect Of Treatment On Blood Sugar Fasting: During the study average reduction of
56.83 mg/dl (32.80 %) in Group A, and average elevation of 15.65 mg/dl (9.53 %) in
Group B was recorded in Blood Sugar Fasting and statistically it was found significant.
Effect Of Treatment On Blood Sugar Post Prandial: During the study average
reduction of 67.23 mg/dl (26.94 %) in Group A, and average elevation of 27.75 mg/dl
(11.13%) in Group B was recorded in Blood Sugar Post Prandial and statistically it was
found significant.
Effect Of Treatment On Urine Sugar: Only 9 (56.25 %) patients of Group A had
shown improvement by the treatment. On the contrary in Group B, sugar in urine had
appeared in 3 (33.33 %) more patients
Effect Of Treatment On Hb%, TLC, DLC, ESR, Blood Urea, Serum Creatinine,
Serum Bilirubin, Alkaline Phosphatase, SGOT, SGPT, Serum Cholesterol
It was observed that average Hb%, TLC, DLC, ESR, Blood Urea, Serum
Creatinine, Serum Bilirubin, Alkaline Phosphatase, SGOT, SGPT, Serum Cholesterol of
group 'A' and group 'B' remained within normal limit before and after the treatment. On
comparing before and after observations of ‘Group A’ with ‘Group B’ with the help of
Student’s ‘t’ test, it was found statistically insignificant (p<0.05). Thus, during the whole
duration of study test as well as placebo drug has no significant effect on all above
mentioned safety parameters.
Effect Of Treatment On Weight Of The Patients: During the study, average reduction
of 1.4 Kg (2.19 %) in Group A and 0.87 Kg (1.43 %) in Group B was recorded and found
significant statistically (p<0.05).
143
Bibliography
BIBLIOGRAPHY
144
Bibliography
BIBLIOGRAPHY
1. Ibne sina. Al-Qanoon Fit-Tib (Urdu translation by Kantoori GH). Vol-3, Part 2. Urdu
Bazar, Lahore (Pakistan) : Shaikh Mohd.Bashir and Sons; 1927: 201-202.
2. Sadidi G. Moalijate-sadidi (Urdu translation by Hussain A). Lucknow (India) : Matba
Munshi Nawal Kishore; 1845: 328.
3. Al-Baghdadi ABH. Kitab-ul-Mukhtarat Fit-Tib (Arabic). Hyderabad,Daccan (India) :
Dairahtul-Marrif Al-Usmaniyah; 1363 H: 425-427.
4. Sharif M. Miftahul-Hikmat.Vol-1. Lahore (Pakistan) : Daftarul-Hakeem-wa-Rafeequl-
Atibba-wa-Chashmae-Sehat; 1931: 1005-1023.
5. Samarqandi N. Sharah Asbab (Urdu translated by Ayyub M).Vol-2. Lucknow (India) :
Matba Munshi Nawal Kishore; 1918: 118-120.
6. Arzani MA. Tibbe-Akbar (Urdu).Vol-2. Lucknow (India) : Matba Munshi Nawal
Kishore; 1890: 69.
7. Kabiruddin M. Al-Ikseer. Vol-2. New Delhi (India): Aijaz Publishing House; 2003:
1195-1199.
8. Aqsarai J. Aqsarai Sharah Mojaz. (Urdu translation by Ayyub M). Lucknow (India):
Matba Munshi Nawal Kishore; 1908: 351-352.
9. Jeelani G.Makhzane-Hikmat. Lahore (Pakistan): Matba Nawal Kishore Steem Press;
1910:781.
10. Mohammad M. Kifayat Mansoori (Persian).NA:Dar Matba Mustafae-Mohd.Hussain
Khan; 1271 H: 119.
145
Bibliography
11. Jurjani AH. Zakheera Khwarzam Shahi (Urdu translation by Khan HH). Vol-2, Part-6.
Lucknow (India) :Matba Munshi Nawal Kishore; 1878: 1336-1337.
12. Hussain F. Tibe-Usmani Al-Maruf Kulliyate-Asrare-Nihani. Lahore (Pakistan) :
Union Salim Press; NA: 778-780.
13. Karim N. Shifaul-Amraz. Lucknow (India) : Matba Munshi Nawal Kishore; NA:
222-223.
14. Arzani MA. Meezane-tib (Urdu translation by Ali MH). Lucknow (India) : Matba
Tej Kumar Ltd.; 1976: 152.
15. Khan AD. Tarkeebul-Ilaj. Lucknow (India): Matba Munshi Nawal Kishore; 1905:
246-248.
16. Matees H. Mujarrabate-Farangi (Persian). Agra (India): Dar Matba Mufeede-Aam;
1896: 435-436.
17. Hameed A. Marjul-Behreen.Vol-2.Agra (India) ; Agra Akhbar Press; 1934: 305-311.
18. Razi MZ. Kitabul-Hawi( Urdu). Vol-10.New Delhi: CCRUM; 2002: 181-183.
19. Majusi AA. Kamilus-Sanah. (Urdu translation by Kantoori GH).Vol-1. Lucknow
(India) : Matba Munshi Nawal Kishore; 1889: 469-470.
20. Khan A. Bayaze-Ajmal. New Delhi (India): Aijaz publishing house; 1995: 146-147.
21. Shah SN, Anand MP (Ed). API Textbook of Medicine. 7th ed. Mumbai (India): The
Association of Physicians of India; 2003: 1102-1117.
22. American Diabetes Association: Report of the expert committee on the diagnosis and
classification of diabetes mellitus. Diabetes care 1998; 21(suppl.1): S5-S19.
23. Reaven GM, Bernstein R, Davis B, Olesfky JM. Nonketotic diabetes mellitus: insulin
deficiency or insulin resistance? Am J Med 1976; 60: 80-88.
146
Bibliography
24. Olefsky JM, Kolterman OG, Scarlett, JA. Insulin action and resistance in obesity and
noninsulin-dependent type II diabetes mellitus. Am J Physiol 1982; 243:E15-E30.
25. DeFronzo R, Deibert D, Hendler R, Felig P. Insulin sensitivity and insulin binding to
monocytes in maturity-onset diabetes. J Clin Invest 1979; 63: 939-946.
26. Turner RC, Holman, RR, Matthews D, Hockaday TDR, Peto J. Insulin deficiency
and insulin resistance interaction in diabetes: estimation of their relative contribution
by feedback analysis from basal plasma insulin and glucose concentrations.
Metabolism 1979; 28: 1086-1096.
27. Kolterman OG, Gray RS, Griffin J, Burstein P, Insel J, Scarlett JA, Olefsky JM.
Receptor and postreceptor defects contribute to the insulin resistance in noninsulin-
dependent diabetes mellitus. J Clin Invest 1981; 68: 957-969.
28. Bogardus C, Lillioja S, Mott DM, Hollenbeck C, Reaven G. Relationship between
degree of obesity and in vivo insulin action in man. Am J Physiol 1985; 248:E286-
E291.
29. Kissebah AH, Vydelingum N, Murray R, Evans DF, Hartz AJ, Kalkhoff RK, Adams
PW. Relationship of body fat distribution to metabolic complications of obesity.
J Clin Endocrinol Metab 1982; 54: 254-260.
30. Butkiewicz EK, Leibson C, O'Brien PC, Palumbo PJ, Rizza RA. Insulin therapy for
diabetic ketoacidosis. Diabetes Care 1995; 18: 1187-1190.
31. Banerji MA, Chaiken RL, Huey H, Tuomi T, Norin AJ, Mackay IR, et al.GAD
antibody negative NIDDM in adult black subjects with diabetic ketoacidosis and
increased frequency of human leukocyte antigen DR3 and DR4. Diabetes 1994; 43:
741-745.
147
Bibliography
32. Umpierrez GE, Casals MMC, Gebhart SSP, Mizon PS, Clark WS, Phillips LS.
Diabetic ketoacidosis in obese African-Americans. Diabetes 1995; 44: 79-85.
33. Harris MI. Impaired glucose tolerance in the U.S. population. Diabetes Care 1989;
12: 464-474.
34. Zimmet PZ: Kelly West Lecture 1991. Challenges in diabetes epidemiology: from
west to the rest. Diabetes Care 1992; 15: 232-252.
35. Fujimoto WY, Leonetti DL, Kinyoun JL, Shuman WP, Stolov WC, Wahl PW.
Prevalence of complications among second-generation Japanese-American men with
diabetes, impaired glucose tolerance or normal glucose tolerance. Diabetes 1987; 36:
739.
36. Moss SE, Klein R, Klein BEK, Meuer MS. The association of glycemia and cause-
specific mortality in a diabetic population. Arch Int Med 1984; 154: 2473-2479.
37. Kuusisto J, Mykknen L, Pyorala K, Laakso M. NIDDM and its metabolic control
predict coronary heart disease in elderly subjects. Diabetes 1994; 43: 960-967.
38. Andersson DKG, Svaardsudd K. Long-term glycemic control relates to mortality in
type II diabetes. Diabetes Care 1995; 18: 1534-1543.
39. Uusitupaa MIJ, Niskanen LK, Siitonen O, Voutilainen E, Pyorala K. Ten year
cardiovascular mortality in relation to risk factors and abnormalities in lipoprotein
composition in type 2 (non-insulin-dependent) diabetic and non-diabetic subjects.
Diabetologia 1993; 18: 1534-1543.
40. Polonsky KS, Sturis J, Bell GI. Non-insulin-dependent diabetes mellitus: a genetically
programmed failure of the beta cell to compensate for insulin resistance. N Engl J Med
1996; 334: 777-784.
148
Bibliography
41. Harris MI, Couric CC, Reiber G, Boyko E, Stern M, Bennett P (Eds.). Diabetes in
America. 2nd ed. Washington, DC, U.S. Govt. Printing Office, 1995 (NIH publ. no.
95-1468)
42. Newman B, Selby JV, Slemenda C, Fabsitz R, Friedman GD. Concordance for type 2
(non-insulin-dependent) diabetes mellitus in male twins. Diabetologia 1987;
30:763-738.
43. Barnett AH, Eff C, Leslie RDG, Pyke DA. Diabetes in identical twins. Diabetologia
1981; 20: 87-93.
44. Ebbel,B. The Papyrus Ebers: Capenhagen and Oxford. Oxford University Press;
1937:115.
45. Pickup,J. and William,G. Textbook of Diabetes. 2nd ed.,Vol-1. London: Blackwell
science; 1997: 3-10.
46. Sanders,L.J. From Thebes to Toronto and the 21st century:An incredible journey.
Diabeters Spectrum 2002; 15: 56-60.
47. Leopald,E.J. Aretaeus the cappadocian. Ann.med.Hist. 1930; 2: 424-455.
48. Henschen,F. On the term Diabetes in the work of Aretaeus and galen. Med.Hist.
1969; 13: 190-192.
49. Atretaeus: On Diabetes,The extant works,Edited and translated by F.Adams,London
Sydenham society;1856: 338-339.
50. Atretaeus C: On causes and symptoms of chronic diseases,Translated by Adams
CF;London(UK),London Sydenham society;1856:138.
51. Galen,Om sjukdomarnas lokalisation,translated by A.Renander,Stockholm; 1960:N.A.
149
Bibliography
52. Algaonkerss.Diabetes Mellitus as seen in ancient Ayurvedic medicine. In: Bajaj,
A.S.editor.Insulin and metabolism. Bombay (India):Indian press; 1972: 1-19.
53. Farmer L. Notes on the history of Diabetes Mellitus. Bulletin of New York Academy
of Medicine. 1952; 28: 408-416.
54. Mann RJ. Historical vignette: Honey urine to pancreatic Diabetes 600BC-1922AD.
Mayo clinic proceedings.1971; 46: 56-58.
55. Willis T. Pharmaceutice rationalis:or,an excercitation of the operations of medicines
in humane bodies,in his practice of physick,london,During,1684; sect 3: chapt.3.
56. Paton A. The English Diabetes (1674-1877). St.thomas hosp.Gaz. 1954; 52: 189-191.
57. Macleod JJR and Banting FG. The antidiabetic functions of the pancreas and the
successful isolation of the antidiabetic hormone-insulin;St.louis: CV Mosby
Company; 1923:7.
58. Dobson M. Experiments and observations on the urine in Diabetes. Med.obs.inq.1776;
5: 298-316.
59. Cawley TA. Singular case of Diabetes,consisting entirely in the quality of urine;with
an inquiry into the different theories of that diaease. Lon.Med.J. 1788; 9: 286-308.
60. Baillie M. Morbid Anatomy. 2nd edi.London : J.Johnson;1797.
61. Rollo J. Causes of the Diabetes Mellitus. 2nd edi. London : C.Dilly; 1798.
62. Rollo J. An account of two cases of the Diabetes Mellitus,with remarks as they arose
during the progress of the cure. London: C.Dilly;1797.
63. Chevreul ME. Note sur le sucre de diabetes. Ann.Chim. 1815; 95: 319-320.
64. Elliotson J. The principles and practice of medicine. London: J.Butler; 1839:NA
150

Bibliography
65. Mc Cradie AR. The discoveries in the field of Diabetes Mellitus and their
investigators. Med. Life. 1924; 31: 215-250.
66. Bernard C. Lecons de physialogie. Paris: Bailliere;1855: 289,296-313.
67. Bernard C. Memoire sur le pancreas. Paris: Bailliere; 1856. (Published as a
monograph of the physiological society. Academy press: London; 1985.)
68. Prout W. On the nature and treatment of stomach and renal diseases. 5th
edi.London:Churchill;1848.
69. Langerhans P. Beirage zur mikroskopischen Anatomie der Bauchspeicheldruse:
Inaugural dissertation. Berlin: Gustave lange; 1869.
70. Laguesse GE. Sur la formation des ilots de Langerhans dans le pancreas.
C.R.Soc.Biol.;Paris.1893;45: 819-820.
71. Kussmaul A. Zur Lehre vom Bailliere.Uber eine eigenthumliche to desart bei
Diabetischen,Uber Acetonamie.Glycerin-behandlung des Diabetes und
Einspritzungen von Diastase ins blit bei dieser Kranicheit.Deutsche Arch. Klin. Med.
1874;14: 1-46.
72. Dickinson WH. Diabetes,in his diseases of the kidney. London: Longmans,Green and
Co.;1875:pt.1.
73. Lancereaux E. Notes et reflixions a propos de deux cas de diabete sucre avec
alteration du pancreas. Bull. Acad. Med.Paris. 1877; 6: 1215-1240.
74. Padfield CI. A review of the history of the treatment of Diabetes Mellitus and the
search for oral hypoglycaewmic agents. Guy. Hosp. Rep.1964; 113: 45-54.
75. Von Mering J. and O.Minkowski. Diabetes Mellitus nach pankreasexstirpation.
Arch.Path.Pharmak. 1889-1890; 26: 371-387.
151
Bibliography
76. Minkowski O. Die Lehre vom pancreas- Diabetes in ihrer geschichtlichen
Entwicklung. Munch. Med.Wschr.1929; 76: 311-315.
77. Editorial: Oskar Minkowski (1858-1931):designer of experimental diabetes.
JAMA.1967; 199: 754-755.
78. Opie EL. The relation of Diabetes Mellitus to lesions of the pancreas: hyaline
degeneration of the islands of Langerhans. 1901; 5: 527-540.
79. Meyer JD. Sur la signification physiologique de la secretion interne du pancreas. zbl
physiol. 1904; 18: 826.
80. Barron M. The relation of the islets of langerhans to Diabetes with special reference
to cases of pancreatic lithiasis. Surg. Gynec.Obstet.1920; 31: 437-448.
81. Banting FG. and Best CH. The internal secretion of the pancreas. J. Lab. Clin. Med.
1922; 7: 251-266.
82. Banting FG. The history of insulin. Edinburg Med. J. 1929; 36: 1-18.
83. Murray I. The search for insulin. Scot.Med.J.1969; 14: 286-293
84. Wrenshall GA et.al. The story of insulin. London (UK): The Bodley Heod ltd;1962:
39-52.
85. http://www.britannica.com/eb/article/19-09-2007
86. http://www.cygn.com/overview/history.html / 19-09-2007
87. http://diabetes.about.com/library/blNIHdiabetesoverview8.htm/19-09-2007
88. http://www.diabetes.ca/Section_About/timeline.asp/19-09-2007
89.http://inventors.about.com/gi/dynamic/offsite.htm?site=http://web.mit.edu/invent/iow/
free.html/19-09-2007
90. http://www.postgradmed.com/issues/1997/04_97/diabetes.htm /19-09-2007
152
Bibliography
91. http://www.roche-diagnostics.com/press_lounge/history.html /19-09-2007
92. http://www.ddri.org/ResearchTimeline.asp/19-09-2007
93. Standring S, Ellis H, Healy JC, Johnson D, Williams A, Collins P, Wigley C. Gray’s
Anatomy: The Anatomical Basis of Clinical Practice. 38th edi. London (UK):
Elsevier (Churchill livingstone); 2005: 1231-1237.
94. Sinnatamby CS. Last’s Anatomy regional and applied. 10th edi.(reprint). London:
Churchill Livingstone; 2001: 261-264.
95. Chaurasia BD. Human anatomy. Vol-2. 3rd edi. New Delhi: CBS Publishers and
distributors; 1995: 246-250.
96. Keele CA, Neil E, Joels N. Samson Wright’s applied Physiology.13th edi. Delhi
(India): Oxford University Press; 1986: 508-511.
97. Tortora GJ and Grabowski SR. Principles of Anatomy and Physiology. 9th edi. New
York: Johnwiley and Sons,inc; 2000: 592-595,840.
98. Guyton AC and Hall EJ. Textbook of Medical Physiology. 10th edi. (reprint).
New Delhi : Saunders; 2003:74 6,884-894.
99. Bijlani RL. Understanding Medical Physiology. 3rd edi. New Delhi: Jaypee Brothers
Medical Publishers(p)ltd.; 2004: 382,552-555.
100.Chandramouli R. Textbook of physiology. 2nd edi. New Delhi: Jaypee Brothers
Medical Publishers(p)ltd.; 2003: 281,337-341.
101.Davies A, Blakeley AGH, Kidd C, McGeown JG. Human Physiology. London (UK):
Churchill Livingstone; 2001: 447-459
102.Chatterjee CC. Human physiology. Vol-2. 11th edi. (reprint). Kolkatta; Medical
Allied agency; 2002: 4(106-130).
153
Bibliography
103. Marya RK. Medical physiology. 2nd edi. New Delhi; CBS Publishers and
distributors; 2003: 365-368, 459-464.
104. Khan MS. Makhazine Taleem (Persian).Delhi: Dar Matba Farouq; 1323H: 210-211.
105. Marble A.et.al. Joslin’s Diabetes Mellitus. 11th edi. London: Henry kimpton
publishers; 1971: 2.
106. Oakley WG et.al. Diabetes and its management. 3rd edi. London: Blackwell
scientific publications ; 1978: 1.
107. Davidson MB. Diabetes Mellitus diagnosis and treatment. 4th edi. Pennsylvania;
W.B.Saunders company; 1998: 19106.
108. West KM. Epidemiology of Diabetes and its vascular lesions. New York : Elsevier;
1978: 19-39.
109. Haslett C, Chilvers ER, Hunter JAA, Boon NA (Ed.). Davidson’s Principles and
Practice of Medicine.18th ed.UK: Churchill Livingstone; 1999: 472-509.
110. Myers AR. Medicine (The National Medical Series for Independent Study). London:
Williams and Wilkins medical publications; 1986: 351.
111. Anonymous. Report of a WHO consultation;Diagnosis and classification of diabetes
mellitus. Geneva :WHO; 1999: 2.
112. Anonymous. ICMR Guidelines for the Management of Type-2 Diabetes mellitus-
2005. New Delhi: ICMR; 2005: 1-16.
113. Warrell DA et.al. Oxford Textbook of Medicine. Vol-2. 4th edi. Oxford: Oxford
university press; 2003: 12 (11.1).
114. Anonymous. Millions of diabetic can now walk at home. Deccan Herald : DH
Health (A world diabetes day special). Bangalore.2006 ;14 Nov: 1.
154
Bibliography
115. Anonymous. Diabetes Atlas. 2nd edi. Belgium: International Diabetes federation;
2003: 7-12.
116. Anonymous. Diabetes Atlas. 3rd edi. Belgium: International Diabetes federation;
2006: 1-20.
117. World Health Organization. Prevention of diabetes mellitus. Technical Report Series
No. 844.Geneva: WHO:1994.
118. King H, Rewers M. Global estimates for prevalence of diabetes mellitus and
impaired glucose tolerance in adults. WHO Ad Hoc Diabetes Reporting Group.
Diabetes Care 1993; 16:157-177.
119. Sadikot SM et.al. The burden of Diabetes and impaired glucose tolerance in India
using the WHO 1999 criteria; Prevalence of Diabetes in India study (PODIS).
Diabetes Research and clinical practice. 2004; 66: 301-307.
120. Anonymous. The expert committee on the diagnosis and classification of diabetes
mellitus; Report of the expert committee on the diagnosis and classification of
diabetes mellitus. Diabetes care.1997; 20; 1183-1197.
121. DeFronzo RA. Pathogenesis of type 2 diabetes mellitus: metabolic and molecular
implications for identifying diabetes genes. Diabetes.1997; 5: 117-269.
122. DeFronzo RA. Lilly Lecture. The triumvirate: beta cell, muscle, liver. A collusion
responsible for NIDDM. Diabetes. 1988; 37: 667-687.
123. Polonsky KS, Sturis J, Bell GI. Non-insulin-dependent diabetes mellitus - a
genetically programmed failure of the beta cell to compensate for insulin resistance.
N Engl J Med. 1996; 334:777-783.
155
Bibliography
124. Cerasi E. Insulin deficiency and insulin resistance in the pathogenesis of NIDDM: is
a divorce possible?. Diabetologia. 1995; 38: 992-997.
125. Sicree RA, Zimmet P, King HO, Coventry JO. Plasma insulin response among
Nauruans: Prediction of deterioration in glucose tolerance over 6 years.
Diabetes.1987; 36: 179-186.
126. Saad MF, Knowler WC, Pettitt DJ, Nelson RG, Mott DM, Bennett PH. Sequential
changes in serum insulin concentration during development of non-insulin-
dependent diabetes. Lancet.1989; i: 1356-1359.
127. Saad MF, Knowler WC, Pettitt DJ, Nelson RG, Mott DM, Bennett PH. The natural
history of impaired glucose tolerance in the Pima Indians. New Engl J Med. 1988;
319: 1500-1505.
128. Haffner SM, Miettinen H, Gaskill SP, Stern MP. Decreased insulin secretion and
increased insulin resistance are independently related to the 7-year risk of NIDDM
in Mexican-Americans. Diabetes.1995; 44: 1386-1391.
129. Weyer C, Hanson RL, Tataranni PA, Bogardus C, Pratley RE. A high fasting plasma
insulin concentration predicts type 2 diabetes independent of insulin resistance.
Evidence for a pathogenic role of relative hyperinsulinemia. Diabetes. 2000; 49:
2094-2101.
130. Weyer C, Bogardus C, Pratley RE. Metabolic characteristics of individuals with
impaired fasting glucose and/or impaired glucose tolerance. Diabetes.1999;
48:2197-2203.
156
Bibliography
131. Weyer C, Tataranni PA, Bogardus C, Pratley RE. Insulin resistance and insulin
secretory dysfunction are independent predictors of worsening of glucose tolerance
during each stage of type 2 diabetes development. Diabetes Care.2000; 24: 89-94.
132. Pimenta W, Korytkowski M, Mitrakou A, Jenssen T, Yki-Jarvinen H, Evron W,
Dailey G, Gerich J. Pancreatic beta-cell dysfunction as the primary genetic lesion in
NIDDM. Evidence from studies in normal glucose-tolerant individuals with a first
degree NIDDM relative. JAMA.1995; 273: 1855-1861.
133. Eriksson J, Franssila-Kallunki A, Ekstrand A, Saloranta C, Widen E, Schalin C,
Groop L. Early metabolic defects in persons at increased risk for non-insulin-
dependent diabetes mellitus. New Engl J Med. 1989; 321: 337-343.
134. Reaven GM, Hollenbeck CB, Chen YDI. Relationship between glucose tolerance,
insulin secretion, and insulin action in non-obese individuals with varying degrees
of glucose tolerance. Diabetologia. 1989; 32: 52-55.
135. Gulli G, Ferrannini E, Stern M, Haffner S, DeFronzo RA. The metabolic profile of
NIDDM is fully established in glucose-tolerant offspring of two Mexican-American
NIDDM parents. Diabetes. 1992; 41: 1575-1586.
136. Martin BC, Warram JH, Krolewski AS, Bergman RN, Soeldner JS, Kahn RC. Role
of glucose and insulin resistance in development of type 2 diabetes mellitus: results
of a 25-year follow-up study. Lancet. 1992; 340: 925-929.
137. Lillioja S, Mott DM, Zawadzki JK, Young AA, Abbott WG, Knowler WC, Bennett
PH, Moll P, Bogardus C. In vivo insulin action is familial characteristic in
nondiabetic Pima Indians. Diabetes.1987; 36: 1329-1335.
157
Bibliography
138. Kahn SE. Clinical Review 135. The importance of ß-cell failure in the development
and progression of type 2 diabetes. J Clin Endocrinol Metab. 2001; 86: 4047-4058.
139. Bergman RN, Finegood DT, Kahn SE. The evolution of ß-cell dysfunction and
insulin resistance in type 2 diabetes. European J Clin Invest. 2002; 32: 35-45.
140. Hansen BC, Bodkin NH. Heterogeneity of insulin responses: phases leading to type 2
(noninsulin-dependent) diabetes mellitus in the rhesus monkey. Diabetologia.1986;
29: 713-719.
141. Diamond MP, Thornton K, Connolly-Diamond M, Sherwin RS, DeFronzo RA.
Reciprocal variations in insulin-stimulated glucose uptake and pancreatic insulin
secretion in women with normal glucose tolerance. J Soc Gynecol Invest. 1995; 2:
708-715.
142. Jallut D, Golay A, Munger R, Frascarolo P, Schutz Y, Jequier E, Felber JP. Impaired
glucose tolerance and diabetes in obesity: a 6 year follow-up study of glucose
metabolism. Metabolism.1990; 39: 1068-1075.
143. Robertson RP, Olson IK, Zhang H-J. Differentiating glucose toxicity from glucose
desensitization: a new message from the insulin gene. Diabetes. 1994; 43: 1085-
1089.
144. Shimabukuro M, Zhou Y-T, Levi M, Unger RH. Fatty acid induced ß cell apoptosis:
a link between obesity and diabetes. Proc Natl Acad Sci.1998; 95: 2498-2502.
145. Zhou YP, Grill VE. Long-term exposure of rat pancreatic islets to fatty acids inhibits
glucose-induced insulin secretion and biosynthesis through a glucose fatty acid
cycle. J Clin Invest. 1994; 93: 870-876.
158
Bibliography
146. Shimabukuro M. Higa M. Zhou YT. Wang MY. Newgard CB. Unger RH.
Lipoapoptosis in beta-cells of obese prediabetic fa/fa rats. Role of serine
palmitoyltransferase overexpression. J Biol Chem.1998; 273: 32487-90.
147. Drucker DJ. Glucagon-like peptides. Diabetes. 1998; 47: 159-169.
148. Holst JJ, Gromada J, Nauck MA. The pathogenesis of NIDDM involves a defective
expression of the GIP receptor. Diabetologia. 1997; 40: 984-986.
149. Fehmann HC. Goke R. Goke B. Cell and molecular biology of the incretin hormones
glucagon-like peptide-I and glucose-dependent insulin releasing polypeptide.
Endocrine Reviews.1995; 16: 390-410.
150. Drucker DJ. Minireview: the glucagon-like peptides. Endocrinology.2001; 142:
521-527.
151. Kahn SE, Andrikopoulos S, Verchere CB. Islet amyloid. A long-recognized but
underappreciated pathological feature of type 2 diabetes. Diabetes 1999; 48: 241-253.
152. Cotran RS, Kumar V, Robbins SL. Pathologic Basis of Disease. 5th ed. USA: WB
Saunders Company; 1994: 915.
153. Jansson PA, Larsson A, Smith U, Lonroth P. Lactate release from the subcutaneous
tissue in lean and obese men. J Clin Invest 1994; 93: 240-246.
154. Boden G. Role of fatty acids in the pathogenesis of insulin resistance and NIDDM.
Diabetes 1997; 46: 3-10.
155. McGarry JD. Banting lecture 2001: dysregulation of fatty acid metabolism in the
etiology of type 2 diabetes. Diabetes 2002; 51: 7-18.
156. Reaven GM. Banting Lecture. Role of insulin resistance in human disease. Diabetes
1988; 37: 595-607.
159
Bibliography
157. Golay A, Felber JP, Jequier E, DeFronzo RA, Ferrannini E. Metabolic basis of
obesity and noninsulin-dependent diabetes mellitus. Diabetes Metab Rev 1988; 4:
727-747.
158. Thiebaud D, DeFronzo RA, Jacot E, Golay A, Acheson K, Maeder E, Jequier E,
Felber JP. Effect of long-chain triglyceride infusion on glucose metabolism in man.
Metabolism 1982; 31: 1128-1136.
159. Kelley De, Mandarino LJ. Fuel selection in human skeletal muscle in insulin
resistance. A reexamination. Diabetes 2000; 49: 677-683.
160. Kashyap S, Belfort R, Pratipanawatr T, Berria R, Pratipanawatr W, Bajaj M,
Mandarino L, DeFronzo R, Cusi K: Chronic elevation in plasma free fatty acids
impairs insulin secretion in non-diabetic offspring with a strong family history of
T2DM. Diabetes 2002; 51(Suppl 2): A12.
161. Carpentier A. Mittelman SD. Bergman RN. Giacca A. Lewis GF. Prolonged
elevation of plasma free fatty acids impairs pancreatic beta-cell function in obese
nondiabetic humans but not in individuals with type 2 diabetes. Diabetes 2000; 49:
399-408.
162. Saltiel AR, Kahn CR. Insulin signaling and the regulation of glucose and lipid
metabolism. Nature 2001; 414: 799-806.
163. Virkamaki A, Ueki K, Kahn CR. Protein-protein interaction in insulin signaling and
the molecular mechanisms of insulin resistance. J Clin Invest 1999; 103: 931-943.
164. Pessin JE, Saltiel AR. Signaling pathways in insulin action: molecular targets of
insulin resistance. J Clin Invest 2000; 106: 165-169.
160
Bibliography
165. Whitehead JP, Clark SF, Urso B, James DE. Signalling through the insulin receptor.
Current Opinion in Cell Biology 2000; 12: 222-228.
166. Wilden PA, Kahn CR. The level of insulin receptor tyrosine kinase activity
modulates the activities of phosphatidylinositol 3-kinase, microtubule-associated
protein, and S6 kinases. Mol Endo 1994; 8: 558-567.
167. Haring HU, Mehnert H. Pathogenesis of type 2 (non-insulin-dependent) diabetes
mellitus: candidates for a signal transmitter defect causing insulin resistance of the
skeletal muscle. Diabetologia 1993; 36: 176-182.
168. Wajtaszewski JFP, Hansen BF, Kiens B, Richter EA. Insulin signaling in human
skeletal muscle. Time course and effect of exercise. Diabetes 1997; 46: 1775-1781.
169. Molina JM, Ciaraldi TP, Brady D, Olefsky JM. Decreased activation rate of insulin-
mediated glucose transport in adipocytes from obese and NIDDM subjects.
Diabetes 1989; 38: 991-995.
170. Trichitta V, Brunetti A, Chiavetta A, Benzi L, Papa V, Vigneri R. Defects in insulin-
receptor internalization and processing in monocytes of obese subjects and obese
NIDDM patients. Diabetes 1989; 38: 1579-1584.
171. htpp://www.mayoclinic.com/24-01-2007.
172. Weiss J, Sumpio B. Review of prevalence and outcome of vascular disease in
patients with diabetes mellitus. Eur J Vasc Endovasc Surg 2006; 31 (2): 143-50.
173. American Diabetes Association; Diagnosis and classification of diabetes mellitus;
Diabetes care 2007 Jan; 30 (suppl.1): S42-S47.
174. Ghani NM. Khazainul Advia.Vol-2.Urdu Bazaar, Lahore (Pakistan): Shaikh Md.
Bashir and sons; N.A.: 54,569.
161
Bibliography
175. Kabeeruddin. Khawasul-Advia. New Delhi : Aijaz publishing house; NA :475-476.
176. Siddiqui B. Tiryaqul-Hayat. Chatta Bazaar, Hyderabad (India): Shamsul-Islam
Press; N.A.: 69-74.
177. Anonymous. Standardisation of Single Drugs of Unani Medicine. Part-III, New
Delhi: CCRUM; 1997: 115-121.
178. Hussain SM. Herbal Unani Medicine. Mumbai (India): Avicenna Research
Publication; 2004: 42.
179. Kirtikar KR and Basu BD. Indian Medicinal Plants. Vol-7. 2nd edi. Dehradun
(India): Oriental press; 2003: 2240-2244.
180. Anonymous. The wealth of India (Raw materials). Vol-4. New Delhi : NISCAIR;
2003: 276-277.
181. Nadkarni KM (Ed). Dr. K.M.Nadkarni’s Indian Materia Medica. Vol-1.2nd edi.
(3rd revised); 1982: 596-599, 1220-1221.
182. Dymock,W.et.al.; “ Pharmacographia indica ( A history of the principal drugs of
vegetable origin); Vol-1; 2005: 54-56 and Vol-2;2005: 405-455.
183. Liu X, Ye W, Yu B, Zhao S, Wu H, Che C. Two new flavonol glycosides from
Gymnema sylvestre and Euphorbia ebracteolata. Carbohydr Res. 2004; 339 (4):
891-895.
184. Ye W, Liu X, Zhang Q, Che CT, Zhao S. Anti-sweet saponins from Gymnema
sylvestre. J Nat Prod. 2001; 64(2): 232-235.
185. Ye WC, Zhang QW, Liu X, Che CT, Zhao SX. Oleanane saponins from Gymnema
sylvestre. Phytochemistry 2000; 53(8): 893-899.
162
Bibliography
186. Sahu NP, Mahato SB, Sarkar SK, Poddar G. Triterpenoid saponins from Gymnema
sylvestre. Phytochemistry1996; 41(4): 1181-1185.
187. Suttisri R, Lee IS, Kinghorn AD. Plant-derived triterpenoid sweetness inhibitors. J
Ethnopharmacol. 1995; 47(1): 9-26.
188. Anonymous; National Formulary of Unani Medicine; part-I; Urdu edi.; New Delhi :
Ministry of health and family welfare;1993: 99.
189. Mhasker KS, Caius JF. A study of Indian medicinal plants. II. Gymnema sylvestre
R.Br. Indian J Med Res Memoirs 1930; 16: 2–75.
190. Sugihara Y, Nojima H, Matsuda H, et al. Antihyperglycemic effects of gymnemic
acid IV, a compound derived from Gymnema sylvestre leaves in streptozotocin
diabetic mice. J Asian Nat Prod Res 2000; 2: 321–7.
191. Murakami N, Murakami T, Kadoya M, et al. New hypoglycemic constituents in
"gymnemic acid" from Gymnema sylvestre. Chem Pharm Bull (Tokyo) 1996 ;
44:469–71.
192. Shanmugasundaram KR, Panneerselvam C, Sumudram P, Shanmugasundaram ERB.
Insulinotropic activity of G. sylvestre, R.Br. and Indian medicinal herb used in
controlling diabetes mellitus. Pharmacol Res Commun 1981; 13: 475–86.
193.Shanmugasundaram ERB, Rajeswari G, Baskaran K, Kumar RBR,
Shanmugasundaram KR and Ahmath BK. Use of Gymnema sylvestre leaf
extract in the control of blood glucose in insulin-dependent diabetes mellitus. J.
Ethnopharmacol. 1990; 30: 281-94.
194. Hirata S, Abe T, and Imoto T. Effect of crude gymnemic acid on oral glucose
tolerance test in human being. J. Yonago Med Assoc. 1992; 43: 392-6.
163
Bibliography
195. Shanmugasundaram ER, Gopinath KL, Radha Shanmugasundaram K, Rajendran
VM. Possible regeneration of the islets of Langerhans in streptozotocin diabetic rats
given Gymnema sylvestre leaf extracts. J Ethnopharmacol 1990; 30: 265–79.
196. Prakash AO, Mather S, Mather R. Effect of feeding Gymnema sylvestre leaves on
blood glucose in beryllium nitrate treated rats. J Ethnopharmacol 1986; 18: 143–4.
197. Okabayashi Y, Tani S, Fujisawa T, Koide M, Hasegawa H, Nakamura T. et. al.
Effect of Gymnema sylvestre. R. Br. on glucose homeostasis in rats. Diabetes Res.
Clin. Pract. 1990; 9: 143-8.
198. Baskaran K, Ahmath BK, Shanmugasundaram KR and Shanmugasundaram ERB .
Antidiabetic effect of the leaf extract from Gymnema sylvestre in insulin-dependent
diabetes mellitus patients. J. Ethnopharmacol. 1990; 30: 295-300.
199. Persaud SJ, Al-Majed H, Raman A, Jones PM. Gymnema sylvestre stimulates
insulin release in vitro by increased membrane permeability. J Endocrinol 1999;
163: 207–12.
200. Shane-McWhorter L. Biological complementary therapies: a focus on botanical
products in diabetes. Diabetes Spectrum 2001; 14: 199–208.
201. Shimizu K, Iino A, Nakajima J, et al. Suppression of glucose absorption by some
fractions extracted from Gymnema sylvestre leaves. J Vet Med Sci 1997; 59: 245–51.
202. Yoshikawa M, Murakami T, Kadoya M, Li Y, Murakami N, Yamahara J, and
Matsuda H. Medicinal foodstuffs. IX. The inhibitors of glucose absorption from the
leaves of Gymnema sylvestre R. BR. (Asclepiadaceae): structures of gymnemosides
a and b. Chem. Pharm. Bull. (Tokyo). 1997a ; 45: 1671-6.
164
Bibliography
203. Anonymous; Gymnema sylvestre. Alt Med Rev 1999; 4: 46–7 [review].
204. Gholap S, Kar A. Effects of Inula racemosa root and Gymnema sylvestre leaf
extracts in the regulation of corticosteroid induced diabetes mellitus: involvement
of thyroid hormones. Pharmazie 2003; 58: 413–5.
205. Kar A, Choudhary BK and Bandyopadhyay NG. Preliminary studies of the
inorganic constituents of some indigenous hypoglycaemic herbs on oral glucose
tolerance test. J. Ethnopharmacol. 1999; 64: 179-84.
206. Chattopadhyay RR. Possible mechanism of antihyperglycemic effect of Gymnema
sylvestre Leaf extract: part 1. Gen Pharmac. 1998; 31: 495-6.
207. Chattopadhyay RR. A comparative evaluation of some blood sugar lowering agents
of plant origin. J. Ethnopharmacol. 1999; 67: 367-72.
208. Kar A, Choudhary BK, and Bandyopadhyay NG. Comparative evaluation of
hypoglycaemic activity of some Indian medicinal plants in alloxan diabetic rats.
J. Ethnopharmacol. 2003; 84: 105-8.
209. Bishayee A, Chatterjee M. Hypolipidemic and antiatherosclerotic effects of oral
Gymnema sylvestre R.Br. leaf extract in albino rats fed on a high fat diet. Phytother
Res 1994; 8: 118–20.
210. Shigematsu N, Asano R, Shimosaka M, Okazaki M. Effect of administration with
the extract of Gymnema sylvestre R. Br leaves on lipid metabolism in rats.Biol
Pharm Bull 2001; 24: 713–7.
211. Shigematsu N, Asano R, Shimosaka M, Okazaki M. Effect of long term-
administration with Gymnema sylvestre R. BR on plasma and liver lipid in rats.
Biol Pharm Bull 2001; 24: 643–9.
165
Bibliography
212. Nakamura Y, Tsumura Y, Tonogai Y, Shibata T. Fecal steroid excretion is increased
in rats by oral administration of gymnemic acids contained in Gymnema sylvestre
leaves. J Nutr 1999; 129: 1214–22.
213. Wang LF, Luo H, Miyoshi M, Imoto T, Hiji Y, and Sasaki T. Inhibitory effect of
gymnemic acid on intestinal absorption of oleic acid in rats. Can. J. Physiol.
Pharmacol. 1998; 76: 1017-23.
214. Min BC, Sakamoto K. Influence of sweet suppressing agent on gustatory brain
evoked potentials generated by taste stimuli. Appl Human Sci 1998; 17: 9–17.
215. Gent JF, Hettinger TP, Frank ME, Marks LE. Taste confusions following gymnemic
acid rinse. Chem Senses 1999; 24: 393–403.
216. Joffe DJ, Freed SH. Effect of extended release gymnema sylvestre leaf extract (Beta
Fast GXR) alone or in combination with oral hypoglycemics or insulin regimens
for type 1 and type 2 diabetes. Diabetes In Control Newsletter 2001; 76: NA.
217. Khan MA. Muheete-Aazam.Vol-IV. Part-1st.Kanpur (India): Matba Nizami; 3 1 3 H :
112.
218. Khan MS.Taleefe-Sharify. Delhi: Matba Darul-Islam;N.A.:146-147.
219. Lubhaya R. Goswami Bayanul-Advia. Vol-II. Delhi: Goswami Pharmaci;1984:
194-195.
220. Chughtai GM and Chughtai F. Rahnumae-Aqaqeer. Part-II. New Delhi: Aijaz
Publishing House; 2004: 250-260.
221. Hakeem MA. Bustanul Mufradat.New Delhi: Idara Kitabul shifa; 2002: 489
222. Kirtikar KR and Basu BD. Indian Medicinal Plants. Vol-1.2nd edi.Dehradun:
Oriental press; 2003:108-112.
166
Bibliography
223. Anonymous. The wealth of India (Raw materials). Vol-10. New Delhi: NISCAIR;
2003: 251-252.
224. Bentley R and Trimen H. Medicinal plants.Vol-1. New Delhi : R.Kumar Omsons
publications; 2002: 59-62
225. Materia Medica of India and their therapeutics by Rustorjee Naserwanjee Khory and
Nanabhai Navrosji Katrak; Komal Prakash: 31.
226. Zhaotf, Wang X, Rimando AM, Chec. Folk tonic medicinal plants : T.sgittata var.
Cravaniana and Mahonia beabi. PLANTA MED 1991; 57 : 505.
227. Chopra R, et al. Chopra's Indigenous Drugs of India . Kolkatta(India): B.K. Dhur of
Academic Publishers; 1982:426-28.
228. Gangan V, et al. Cordifolisides A, B, C: norditerpene furan glycosides from
Tinospora cordifolia . Phytochemistry 1994; 37(3): 781-86.
229. Maurya R, et al. Tinocordifolin, a sesquiterpene from Tinospora cordifolia .
Phytochemistry 1998; 49(5): 1343-45.
230. Maurya R, et al. A sesquiterpene glucoside from Tinospora cordifolia .
Phytochemistry 1997; 44(4): 749-50.
231. Gangan V, et al. Palmatosides C, F: diterpene furan glucosides from Tinospora
cordifolia -structural elucidation by 2D NMR spectroscopy. Indian J Chem, Sect B:
Org Chem Incl Med Chem 1996; 35B (6): 630-34.
232. Maurya R, et al. Clerodane diterpenoids from Tinospora cordifolia . Phytochemistry
1995; 38(3): 559-61.
233. Wazir V, et al. Cordioside, a clerodane furano diterpene glucoside from Tinospora
cordifolia . Phytochemistry 1995; 38(2): 447-49.
167
Bibliography
234. Khan M, et al. Tinosporaside, an 18-norclerodane glucoside from Tinospora
cordifolia . Phytochemistry 1988; 28(1): 273-75.
235. Ghosal S, et al. Tinocordiside, a new rearranged cadinane sesquiterpene glycoside
from Tinospora cordifolia . J Nat Prod 1997; 60(8): 839-41.
236. Kapil A, et al. Immunopotentiating compounds from Tinospora cordifolia . J
Ethnopharmacol 1997; 58(2): 89-95.
237. Maurya R, et al. Cordifolisides A and B, two new phenylpropene disaccharides from
Tinospora cordifolia possessing immunostimulant activity. Nat Prod Lett
1996;8(1):7-10.
238. Padhya M, et al. Biosynthesis of isoquinoline alkaloid berberine in tissue cultures of
Tinospora cordifolia . Indian Drugs 1986; 24(1): 47-48.
239. Pradhan P, et al. Two phytoecdysones from Tinospora cordifolia : structural
assignments by 2D NMR spectroscopy. Indian J Chem, Sect B: Org Chem Incl
Med Chem 1997; 36B (10): 958-62.
240. Gangan V, et al. Phytoecdysones from Tinospora cordifolia : structural elucidation
of ecdysterone and makisterone A by 2D NMR spectroscopy. Indian J Chem, Sect
B: Org Chem Incl Med Chem 1997; 36B (9): 787-92.
241. Pathak A, et al. NMR spectra investigations. 35. Studies on medicinal plants. 39.
NMR studies of 20β-hydroxyecdysone, a steroid isolated from Tinospora cordifolia.
Indian J Chem, Sect B: Org Chem Incl Med Chem 1995; 34B (7): 674-76.
242. Hanuman J, et al. A natural phenolic lignan from Tinospora cordifolia Miers.
J Chem Soc, Perkin Trans 1. 1986; 7: 1181-85.
168
Bibliography
243. Khaleque A, et al. Tinospora cordifolia . IV. Isolation of heptacosanol, β-sitosterol,
and three other compounds tinosporidine, cordifol, and cordifolone. Pak J Sci Ind
Res 1971; 14(6): 481-83.
244. Pachaly P, et al. Alkaloids from Tinospora cordifolia Miers. Arch Pharm 1981 ;
314 (3): 251-56.
245. Sipahimalani A, et al. Phenylpropanoid glycosides and tetrahydrofurofuranlignan
glycosides from the adaptogenic plant drugs Tinospora cordifolia and Drypetes
roxburghii.Planta Med 1994; 60(6): 596-97.
246. Sarma D, et al. Constituents of Tinospora cordifolia root. Fitoterapia 1998; 69(6):
541-42.
247. Sarma D, et al. Isolation of jatrorrhizine from Tinospora cordifolia roots. Planta Med
1995; 61(1): 98-99.
248. Kabiruddin. Bayaze-kabir (Delhi ke murakkabat).Vol.2. Hikmat book depot;
1978:96.
249. Jagetia G, et al. Evaluation of the antineoplastic activity of guduchi ( Tinospora
cordifolia ) in cultured HeLa cells. Cancer Letters 1998; 127(1-2): 71-82.
250. Ikram M, et al. Antipyretic studies on some indigenous Pakistani medicinal plants:
II. J Ethnopharmacol 1987; 19(2): 185-92.
251. Singh SS,Pandey SC,Srivastava S,Gupta VS,Patro B. chemistry and medicinal
properties of Tinospora cordifolia.Indian Journal of Pharmacology 2003; 35: 83-91
252. Stanely P, et al. Hypoglycaemic and other related actions of Tinospora cordifolia
roots in alloxan-induced diabetic rats. J Ethnopharmacol 2000; 70(1): 9-15.
169
Bibliography
253. Stanely P, et al. Hypolipidaemic action of Tinospora cordifolia roots in alloxan
diabetic rats. J Ethnopharmacol 1999; 64(1): 53-57.
254. Kapil A, Sharma S. Immuno potentiating compounds from T.cordifolia.
J Ethnopharmacol 1997; 58: 89-95.
255. Rege NN, Thatte UM, Dahanukar SA. Adaptogenic properties of six rasayana herbs
used in ayruvedic medicine.PHYTOTHER RES 1999; 13 : 275-91.
256. Dhuby J.N. Effect of some Indian herbs on macrophage functions in Ochraloxin
treated mice. J Ethnopharmacol 1997; 58 : 15-20.
257. Jana V, Chattopadhyay RN, Shw BP. Preliminary studies on anti-inflammatory
activity of Zingiber officinale Rosc, Vitex negundo Linn and T.cordifolia (Willid)
Miers in albino rats. INDIAN J.PHARM 1999; 31 : 232-3.
258. Prince P, et al. Antioxidant activity of Tinospora cordifolia roots in experimental
diabetes. J Ethnopharmacol 1999; 65(3): 277-81.
259. Mathew S, et al. Antioxidant activity of Tinospora cordifolia and its usefulness in
the amelioration of cyclophosphamide induced toxicity. J Exp Clin Cancer Res
1997; 16(4):407-11.
260. Mehrotra R, Katiyar CK, Gupta AP. Hepato protective compositions and
composition for treatment of conditions related to hepatitis B and E infection.US
PATENT 749296-2000.
261. Nagarkatti D, et al. Modulation of Kupffer cell activity by Tinospora cordifolia in
liver damage. J Postgrad Med 1994; 40(2): 65-67.
262. Kabiruddin. Moalijate Sharah Asbab.Part III. New Delhi: Aijaz Publishing House;
N.A.: 45.
170
Annexures (Proforma)
CLINICAL EVALUATION OF SAFOOF ZIABETES IN
MANAGEMENT OF ZIABETES SHAKRI
PROFORMA _______________________________________________________________________
Case No…… OPD/IPD No. Regd.No.
Name: …………………………….....Father/Husband’s Name…….......................
Age/Sex : …………………….................Religion:………………………….............
Marital status:…………………..............................................................................
Occupation:………………………... Monthly income:…………………................
Address:…………………………………………………………………….....................................................................................................................................................
Date of starting Treatment :………..... Date of stopping Treatment:………......
Chief complaints:
1. 2. 3. 4. 5.
History Of Present Illness: …………………………………………………............................................................
………………………………………………………………………...............................
History Of Past Illness:……………………………………………….........................
……………………………………………………………………………….....................
Past History Of Gestational Diabetes:………………………………........................
Family History Of Diabetes Mellitus:………………………………..........................
Treatment History :…………………………………………………............................
………………………………………………………………………………....................
171
Annexures (Proforma)
Personal History:
Appetite o Good o Fair o Poor
Diet
o Veg o Non –veg
Habit o Smoking o Alcohol intake
o Tobacco Chewing o Pan Chewing
Menstrual / Obstetrical History:……………………………………............... ………………………………………………………………………………..........
GENERAL PHYSICAL EXAMINATION
Look ………………........Cyanosis ………. ……….Clubbing …………..........
Built………………….....Paller……………………....Oedema…………...........
Expression………….....Icterus………………….......Dehydration………........
Lymphadenopathy………....JVP…………………...Weight …………............
Vitals :
Pulse B.P. Temp R.R.
SYSTEMIC EXAMINATION
CARDIOVASCULAR SYSTEM Inspection……………………………………………………………………….
Palpation…………………………………………………………………………..
Percussion…………………………………………………………………………
Auscultation………………………………………………………………………..
172
Annexures (Proforma)
RESPIRATORY SYSTEM
Inspection………………………………………………………………………….
Palpation…………………………………………………………………………..
Percussion…………………………………………………………………………
Auscultation……………………………………………………………………….
DIGESTIVE SYSTEM
Inspection………………………………………………………………………….
Palpation…………………………………………………………………………
Percussion…………………………………………………………………………
Auscultation………………………………………………………………………. NERVOUS SYSTEM
Mental state.................................................................................................
Speech..........................................................................................................
Neck stiffness..............................................................................................
Cranial nerves.............................................................................................
Motor and Sensory functions.......................................................................
Reflexes........................................................................................................
UROGENITAL SYSTEM
Inspection……………………………………………………………………….
Palpation………………………………………………………………………...
Percussion………………………………………………………………………
Auscultation……………………………………………………………………..
173
Annexures (Proforma)
INVESTIGATIONS
S.NO INVESTIGATION BEFORE TREATMENT AFTER TREATMENT
1. Hb%
2. TLC
3. DLC
4. ESR
5. Blood sugar fasting
6. Blood sugar post prandial
7. Blood Urea
8. Serum Creatinine
9. Serum bilirubin
10. Alkaline Phosphatase
11. SGOT (AST)
12. SGPT (ALT)
13. Serum Cholesterol
14 URINE Colour Appearance Reaction Sp.gravity Protein Glucose RBC Pus cells Cast Bacteria Epithelial Cells Crystals
15. ECG
16. Weight
174
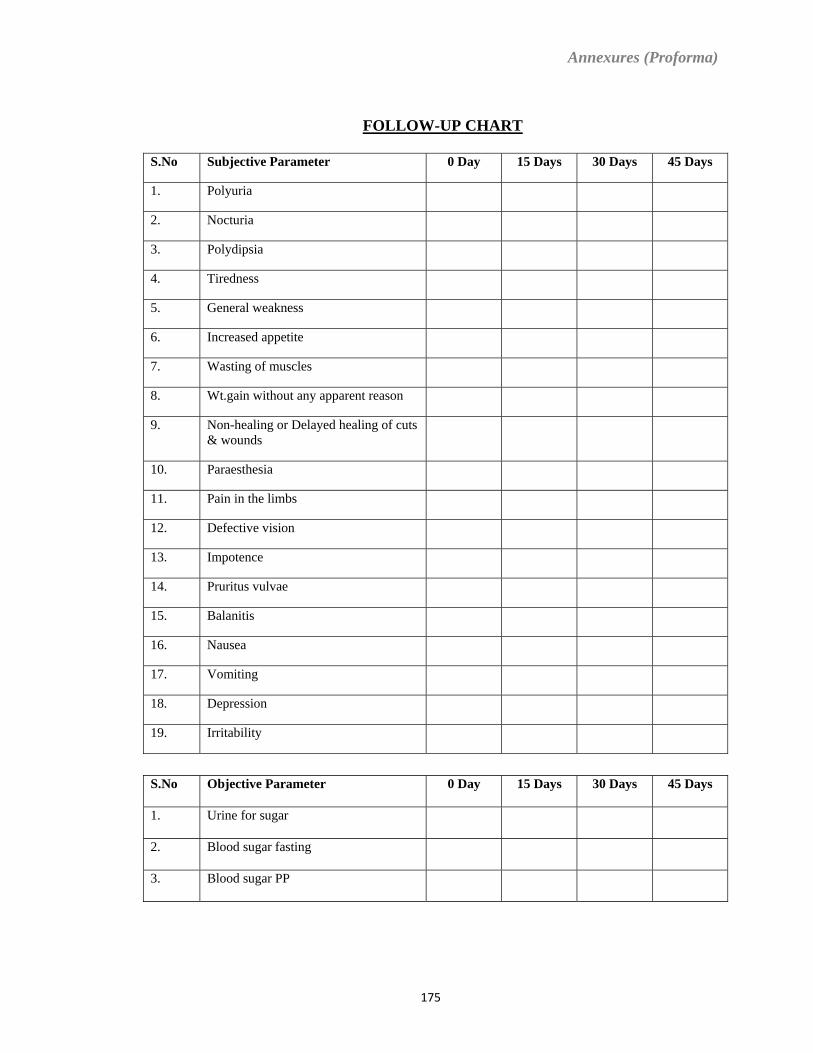
Annexures (Proforma)
FOLLOW-UP CHART
S.No Subjective Parameter 0 Day 15 Days 30 Days 45 Days
1. Polyuria
2. Nocturia
3. Polydipsia
4. Tiredness
5. General weakness
6. Increased appetite
7. Wasting of muscles
8. Wt.gain without any apparent reason
9. Non-healing or Delayed healing of cuts & wounds
10. Paraesthesia
11. Pain in the limbs
12. Defective vision
13. Impotence
14. Pruritus vulvae
15. Balanitis
16. Nausea
17. Vomiting
18. Depression
19. Irritability
S.No Objective Parameter 0 Day 15 Days 30 Days 45 Days
1. Urine for sugar
2. Blood sugar fasting
3. Blood sugar PP
175
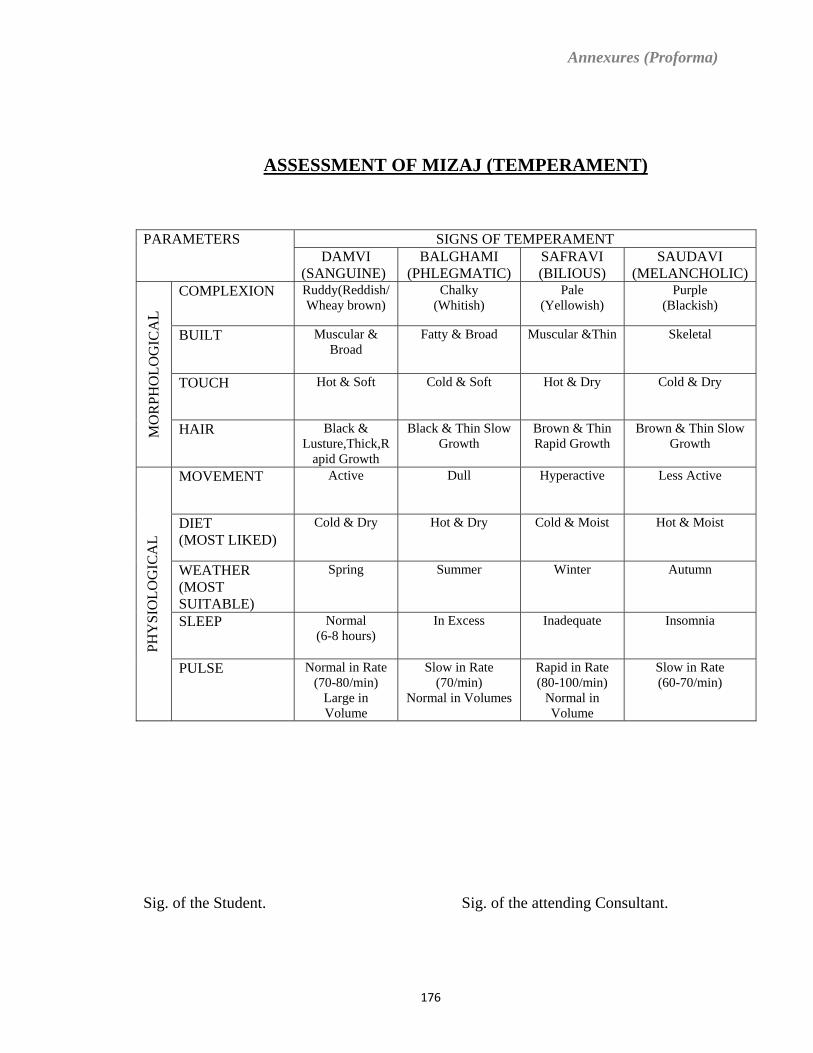
Annexures (Proforma)
ASSESSMENT OF MIZAJ (TEMPERAMENT)
SIGNS OF TEMPERAMENT PARAMETERS DAMVI
(SANGUINE) BALGHAMI
(PHLEGMATIC) SAFRAVI (BILIOUS)
SAUDAVI (MELANCHOLIC)
COMPLEXION Ruddy(Reddish/Wheay brown)
Chalky (Whitish)
Pale (Yellowish)
Purple (Blackish)
BUILT Muscular & Broad
Fatty & Broad Muscular &Thin Skeletal
TOUCH Hot & Soft Cold & Soft Hot & Dry Cold & Dry
MO
RPH
OLO
GIC
AL
HAIR Black & Lusture,Thick,R
apid Growth
Black & Thin Slow Growth
Brown & Thin Rapid Growth
Brown & Thin Slow Growth
MOVEMENT Active Dull Hyperactive Less Active
DIET (MOST LIKED)
Cold & Dry Hot & Dry Cold & Moist Hot & Moist
WEATHER (MOST SUITABLE)
Spring Summer Winter Autumn
SLEEP Normal (6-8 hours)
In Excess Inadequate Insomnia
PHY
SIO
LOG
ICA
L
PULSE Normal in Rate (70-80/min)
Large in Volume
Slow in Rate (70/min)
Normal in Volumes
Rapid in Rate (80-100/min)
Normal in Volume
Slow in Rate (60-70/min)
Sig. of the Student. Sig. of the attending Consultant.
176
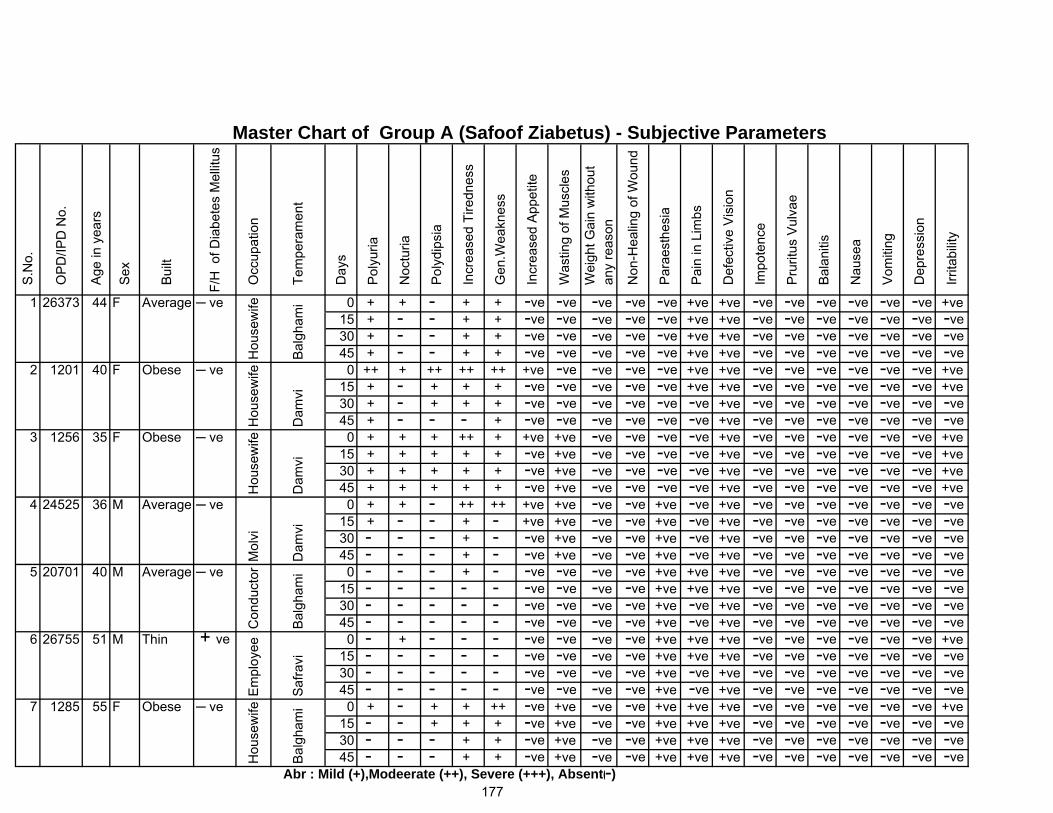
1 26373 44 F Average ─ ve 0 + + - + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve15 + - - + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 + - - + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve45 + - - + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve
2 1201 40 F Obese ─ ve 0 ++ + ++ ++ ++ +ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve15 + - + + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve30 + - + + + -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve45 + - - - + -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve
3 1256 35 F Obese ─ ve 0 + + + ++ + +ve +ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve +ve15 + + + + + -ve +ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve +ve30 + + + + + -ve +ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve +ve45 + + + + + -ve +ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve +ve
4 24525 36 M Average ─ ve 0 + + - ++ ++ +ve +ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve15 + - - + - +ve +ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - + - -ve +ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - + - -ve +ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve
5 20701 40 M Average ─ ve 0 - - - + - -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve15 - - - - - -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - - - -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - - - -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve
6 26755 51 M Thin + ve 0 - + - - - -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve +ve15 - - - - - -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - - - -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - - - -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve
7 1285 55 F Obese ─ ve 0 + - + + ++ -ve +ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve +ve15 - - + + + -ve +ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - + + -ve +ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - + + -ve +ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve
S.N
o.
Tem
pera
men
t
Abr : Mild (+),Modeerate (++), Severe (+++), Absent(-)
Noc
turia
-ve-ve
OP
D/IP
D N
o.
Age
in y
ears
F/H
of D
iabe
tes
Mel
litus
Sex
Bui
lt
-ve-ve
Day
s
Pol
yuria
Pol
ydip
sia
Inc
reas
ed T
iredn
ess
Occ
upat
ion
Gen
.Wea
knes
s
Was
ting
of M
uscl
es
-ve
-ve
-ve-ve
-ve
-ve
-ve
-ve-ve-ve
-ve
-ve
Irri
tabi
lity
-ve
Vom
iting
Dep
ress
ion
Bal
aniti
s
Nau
sea
Pai
n in
Lim
bs
Def
ectiv
e V
isio
n-ve-ve
-ve
-ve
-ve-ve-ve
-ve
-ve-ve
Master Chart of Group A (Safoof Ziabetus) - Subjective Parameters
Hou
sew
ife
Bal
gham
i
Im
pote
nce
Pru
ritus
Vul
vae
Wei
ght G
ain
with
out
any
reas
on
Par
aest
hesi
a
Non
-Hea
ling
of W
ound
Inc
reas
ed A
ppet
ite
Mol
viH
ouse
wife
Hou
sew
ifeE
mpl
oyee
Dam
viD
amvi
Dam
viB
algh
ami
Con
duct
orH
ouse
wife -ve
Bal
gham
iSa
fravi
177
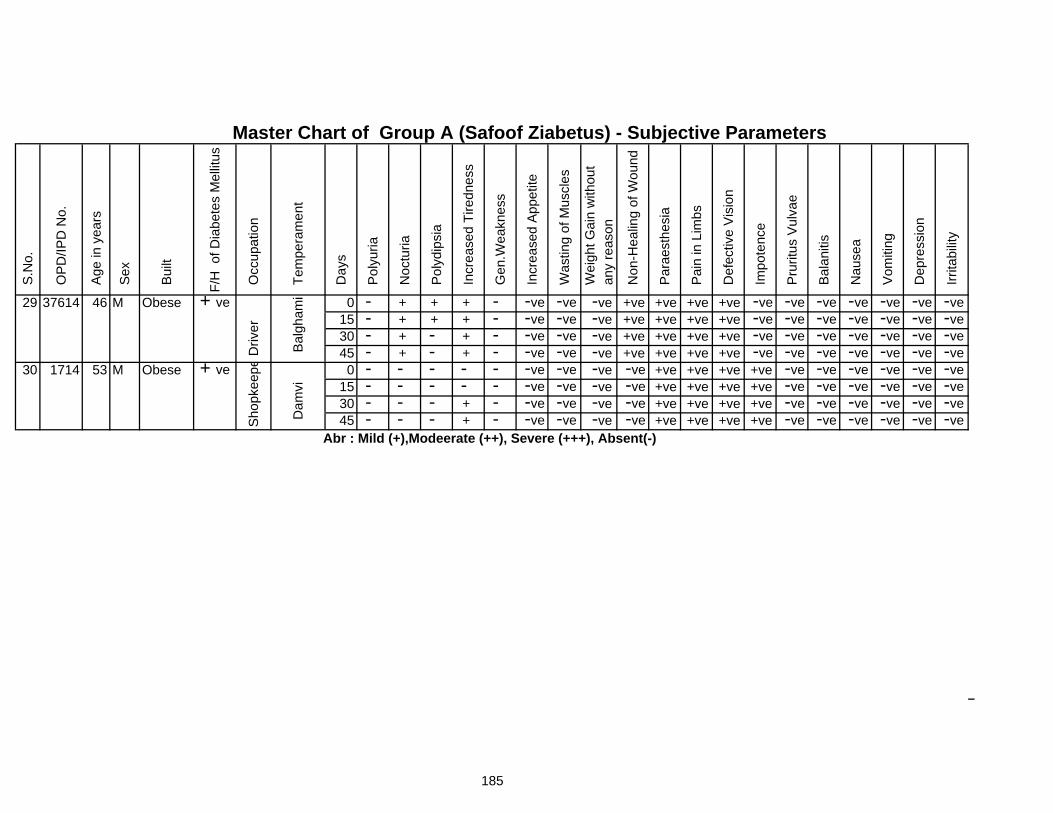
29 37614 46 M Obese + ve 0 - + + + - -ve -ve +ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve15 - + + + - -ve -ve +ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 - + - + - -ve -ve +ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve45 - + - + - -ve -ve +ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve
30 1714 53 M Obese + ve 0 - - - - - -ve -ve -ve +ve +ve +ve +ve -ve -ve -ve -ve -ve -ve15 - - - - - -ve -ve -ve +ve +ve +ve +ve -ve -ve -ve -ve -ve -ve30 - - - + - -ve -ve -ve +ve +ve +ve +ve -ve -ve -ve -ve -ve -ve45 - - - + - -ve -ve -ve +ve +ve +ve +ve -ve -ve -ve -ve -ve -ve
Master Chart of Group A (Safoof Ziabetus) - Subjective Parameters
Im
pote
nce
Pru
ritus
Vul
vae
Wei
ght G
ain
with
out
any
reas
on
Non
-Hea
ling
of W
ound
Par
aest
hesi
a
Gen
.Wea
knes
s
Pai
n in
Lim
bs
Def
ectiv
e V
isio
n
S.N
o.
OP
D/IP
D N
o.
Irri
tabi
lity
Bal
aniti
s
Nau
sea
Vom
iting
Dep
ress
ion
Sho
pkee
p e
Dam
vi
Pol
ydip
sia
Occ
upat
ion
Tem
pera
men
t
Day
s
Pol
yuria
Noc
turia
Driv
er
Bal
gham
i Inc
reas
ed T
iredn
ess
Inc
reas
ed A
ppet
ite
Was
ting
of M
uscl
es
-ve
-ve
-ve
Age
in y
ears
-ve
Sex
Bui
lt
F/H
of D
iabe
tes
Mel
litus
-ve
-ve
185
-ve
Abr : Mild (+),Modeerate (++), Severe (+++), Absent(-)
-ve
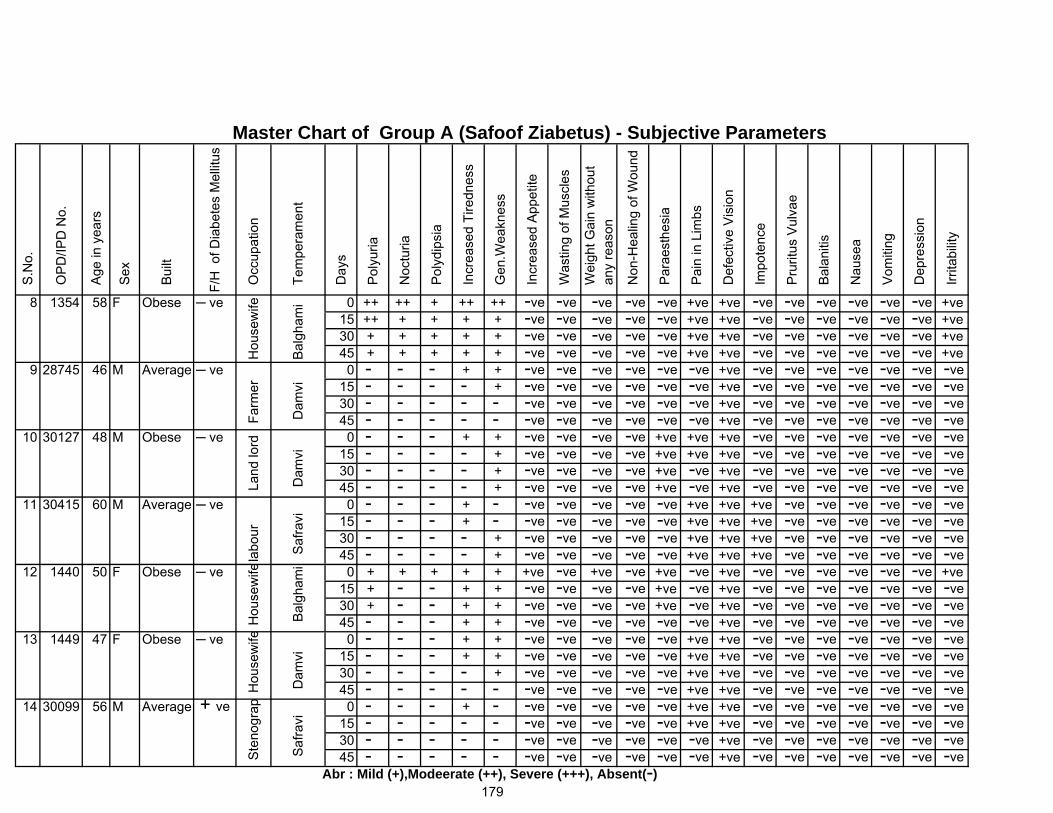
8 1354 58 F Obese ─ ve 0 ++ ++ + ++ ++ -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve15 ++ + + + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve30 + + + + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve45 + + + + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve
9 28745 46 M Average ─ ve 0 - - - + + -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve15 - - - - + -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - - - -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - - - -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve
10 30127 48 M Obese ─ ve 0 - - - + + -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve15 - - - - + -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - - + -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - - + -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve
11 30415 60 M Average ─ ve 0 - - - + - -ve -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve15 - - - + - -ve -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve30 - - - - + -ve -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve45 - - - - + -ve -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve
12 1440 50 F Obese ─ ve 0 + + + + + +ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve +ve15 + - - + + -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve30 + - - + + -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - + + -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve
13 1449 47 F Obese ─ ve 0 - - - + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve15 - - - + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - - + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - - - -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve
14 30099 56 M Average + ve 0 - - - + - -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve15 - - - - - -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - - - -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - - - -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve
179
Saf
ravi
Dam
vi D
amvi
Saf
ravi
Bal
gham
i D
amvi
Hou
sew
ife F
arm
er L
and
lord
labo
ur H
ouse
wife
Abr : Mild (+),Modeerate (++), Severe (+++), Absent(-)
-ve
-ve-ve-ve-ve-ve-ve
Ste
nogr
ap -ve-ve-ve-ve
Master Chart of Group A (Safoof Ziabetus) - Subjective Parameters
Hou
sew
ife
Bal
gham
i
Im
pote
nce
Pru
ritus
Vul
vae
Wei
ght G
ain
with
out
any
reas
on
Non
-Hea
ling
of W
ound
Par
aest
hesi
a
Gen
.Wea
knes
s
Irri
tabi
lity
-ve-ve-ve
Bal
aniti
s
Nau
sea
Vom
iting
Dep
ress
ion
Pai
n in
Lim
bs
Def
ectiv
e V
isio
n
-ve-ve
+ve-ve
-ve-ve-ve-ve
-ve-ve-ve-ve
S.N
o.
Pol
ydip
sia
Inc
reas
ed T
iredn
ess
Occ
upat
ion
Tem
pera
men
t
Day
s
Pol
yuria
F/H
of D
iabe
tes
Mel
litus
OP
D/IP
D N
o.
Age
in y
ears
Sex
Bui
lt
Noc
turia
-ve-ve
Inc
reas
ed A
ppet
ite
Was
ting
of M
uscl
es
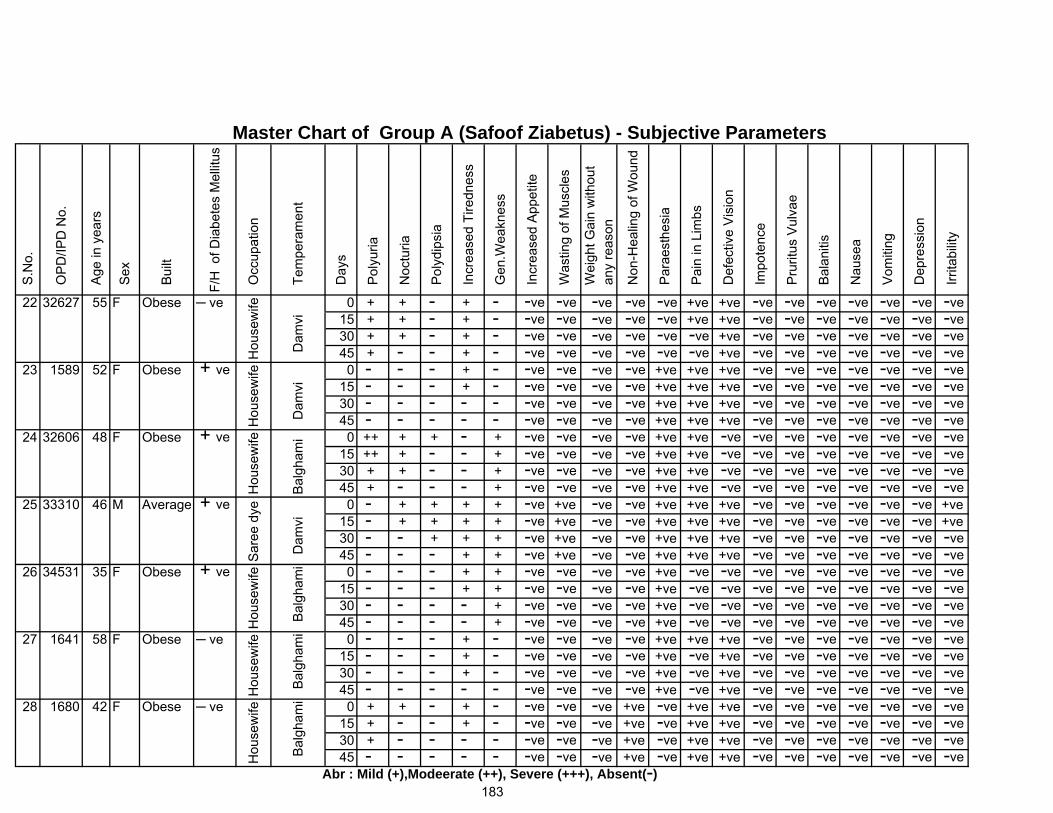
22 32627 55 F Obese ─ ve 0 + + - + - -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve15 + + - + - -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 + + - + - -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve45 + - - + - -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve
23 1589 52 F Obese + ve 0 - - - + - -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve15 - - - + - -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - - - -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - - - -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve
24 32606 48 F Obese + ve 0 ++ + + - + -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve -ve15 ++ + - - + -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve -ve30 + + - - + -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve -ve45 + - - - + -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve -ve
25 33310 46 M Average + ve 0 - + + + + -ve +ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve +ve15 - + + + + -ve +ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve +ve30 - - + + + -ve +ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - + + -ve +ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve
26 34531 35 F Obese + ve 0 - - - + + -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve -ve15 - - - + + -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve -ve30 - - - - + -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve -ve45 - - - - + -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve -ve
27 1641 58 F Obese ─ ve 0 - - - + - -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve15 - - - + - -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - + - -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - - - -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve
28 1680 42 F Obese ─ ve 0 + + - + - -ve -ve +ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve15 + - - + - -ve -ve +ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 + - - - - -ve -ve +ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - - - -ve -ve +ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve
S.N
o.
Tem
pera
men
t
Day
s
183
-ve-ve
Inc
reas
ed A
ppet
ite
Was
ting
of M
uscl
es
Sex
Bui
lt
F/H
of D
iabe
tes
Mel
litus
OP
D/IP
D N
o.
Age
in y
ears
-ve
Hou
sew
ife
Dam
vi
Gen
.Wea
knes
s
Pol
ydip
sia
Inc
reas
ed T
iredn
ess
Occ
upat
ion
Noc
turia
Pol
yuria
-ve-ve-ve-ve-ve-ve-ve-ve-ve-ve-ve
Irri
tabi
lity
-ve-ve-ve
Bal
aniti
s
Nau
sea
Vom
iting
Dep
ress
ion
Pai
n in
Lim
bs
Def
ectiv
e V
isio
n
Master Chart of Group A (Safoof Ziabetus) - Subjective Parameters
Im
pote
nce
Pru
ritus
Vul
vae
Wei
ght G
ain
with
out
any
reas
on
Non
-Hea
ling
of W
ound
Par
aest
hesi
a
-ve-ve-ve-ve
Abr : Mild (+),Modeerate (++), Severe (+++), Absent(-)
-ve
-ve-ve-ve-ve-ve-ve
Hou
sew
ifeH
ouse
wife
Sar
ee d
yeH
ouse
wife
Hou
sew
ifeH
ouse
wife
Bal
gham
i D
amvi
Bal
gham
i D
amvi
Bal
gham
i B
algh
ami
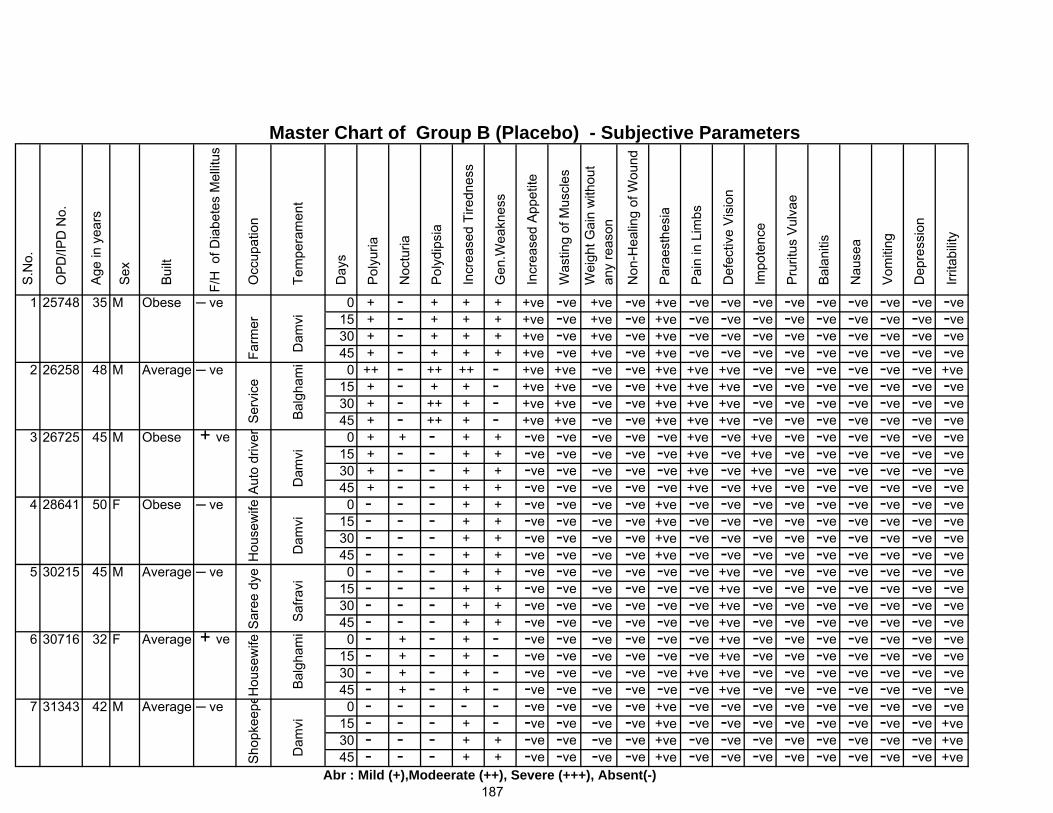
1 25748 35 M Obese ─ ve 0 + - + + + +ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve -ve15 + - + + + +ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve -ve30 + - + + + +ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve -ve45 + - + + + +ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve -ve
2 26258 48 M Average ─ ve 0 ++ - ++ ++ - +ve +ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve +ve15 + - + + - +ve +ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 + - ++ + - +ve +ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve45 + - ++ + - +ve +ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve
3 26725 45 M Obese + ve 0 + + - + + -ve -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve15 + - - + + -ve -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve30 + - - + + -ve -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve45 + - - + + -ve -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve
4 28641 50 F Obese ─ ve 0 - - - + + -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve -ve15 - - - + + -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve -ve30 - - - + + -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve -ve45 - - - + + -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve -ve
5 30215 45 M Average ─ ve 0 - - - + + -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve15 - - - + + -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - + + -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - + + -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve
6 30716 32 F Average + ve 0 - + - + - -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve15 - + - + - -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve30 - + - + - -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve45 - + - + - -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve
7 31343 42 M Average ─ ve 0 - - - - - -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve -ve15 - - - + - -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve +ve30 - - - + + -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve +ve45 - - - + + -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve +ve
187Abr : Mild (+),Modeerate (++), Severe (+++), Absent(-)
-ve-ve
Dam
vi D
amvi
Saf
ravi
Hou
sew
ifeS
hopk
eepe
Bal
gham
i D
amvi
Def
ectiv
e V
isio
n
Ser
vice
Aut
o dr
iver
Hou
sew
ifeS
aree
dye
-ve-ve
Master Chart of Group B (Placebo) - Subjective Parameters
Farm
er
Dam
vi
Wei
ght G
ain
with
out
any
reas
on
Non
-Hea
ling
of W
ound
Par
aest
hesi
a
Gen
.Wea
knes
s
Inc
reas
ed A
ppet
ite
Im
pote
nce
Irri
tabi
lity
+ve +ve +ve
Bal
aniti
s
Nau
sea
Vom
iting
Dep
ress
ion
Pru
ritus
Vul
vae
Pai
n in
Lim
bs-ve-ve
-ve-ve-ve-ve
-ve-ve-ve-ve
-ve-ve-ve-ve
-ve-ve-ve-ve
S.N
o.
Pol
ydip
sia
Inc
reas
ed T
iredn
ess
Occ
upat
ion
Tem
pera
men
t
Day
s
Pol
yuria
OP
D/IP
D N
o.
Noc
turia
-ve-ve
Age
in y
ears
Sex
Bui
lt
F/H
of D
iabe
tes
Mel
litus
Was
ting
of M
uscl
es
+ve
Bal
gham
i
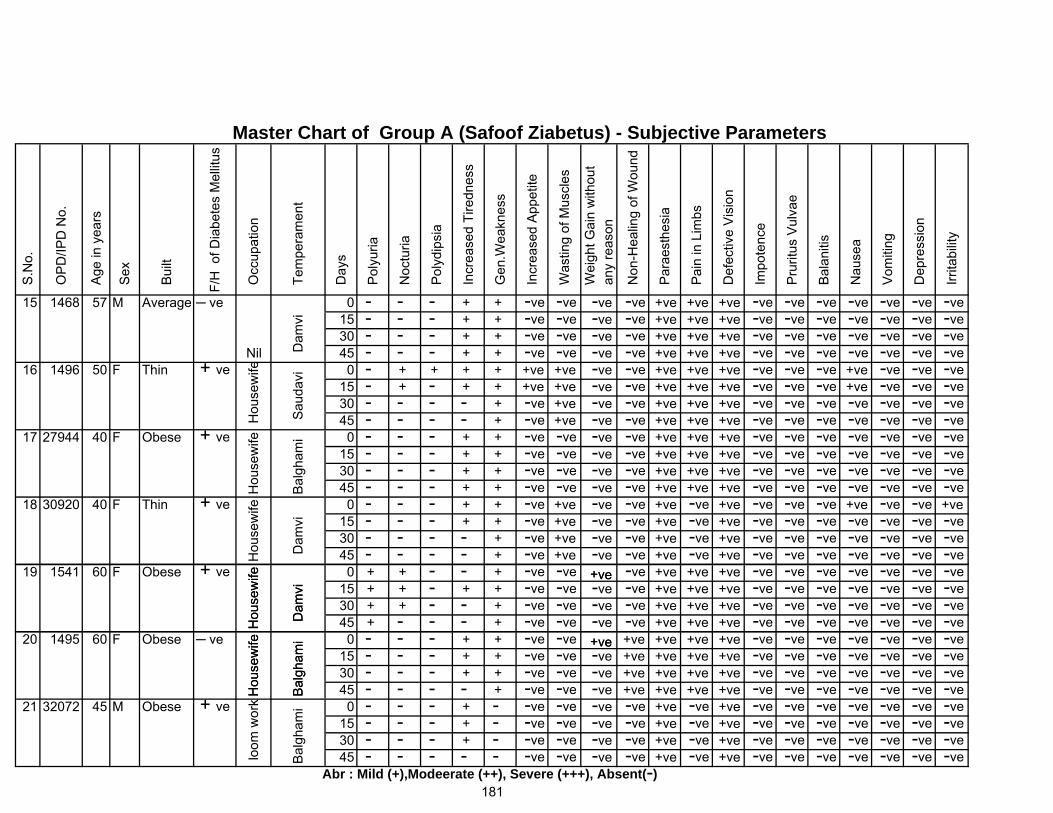
15 1468 57 M Average ─ ve 0 - - - + + -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve15 - - - + + -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - + + -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - + + -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve
16 1496 50 F Thin + ve 0 - + + + + +ve +ve -ve +ve +ve +ve -ve -ve -ve +ve -ve -ve -ve15 - + - + + +ve +ve -ve +ve +ve +ve -ve -ve -ve +ve -ve -ve -ve30 - - - - + -ve +ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - - + -ve +ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve
17 27944 40 F Obese + ve 0 - - - + + -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve15 - - - + + -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - + + -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - + + -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve
18 30920 40 F Thin + ve 0 - - - + + -ve +ve -ve +ve -ve +ve -ve -ve -ve +ve -ve -ve +ve15 - - - + + -ve +ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - - + -ve +ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - - + -ve +ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve
S.N
o.
Tem
pera
men
t
Day
s
-ve-ve
Inc
reas
ed A
ppet
ite
Was
ting
of M
uscl
es
Sex
Bui
lt
F/H
of D
iabe
tes
Mel
litus
OP
D/IP
D N
o.
Age
in y
ears
-ve
Nil Dam
vi
Gen
.Wea
knes
s
Pol
ydip
sia
Inc
reas
ed T
iredn
ess
Occ
upat
ion
Noc
turia
Pol
yuria
-ve-ve-ve-ve-ve-ve-ve-ve-ve
+ve
Irri
tabi
lity
-ve-ve-ve
Bal
aniti
s
Nau
sea
Vom
iting
Dep
ress
ion
Pai
n in
Lim
bs
Def
ectiv
e V
isio
n
Master Chart of Group A (Safoof Ziabetus) - Subjective Parameters
Im
pote
nce
Pru
ritus
Vul
vae
Wei
ght G
ain
with
out
any
reas
on
Non
-Hea
ling
of W
ound
Par
aest
hesi
a
-ve
Hou
sew
ifeH
ouse
wife
Hou
sew
ife H
ouse
wife
Sau
davi
Bal
gham
i D
amvi
Dam
vi
19 1541 60 F Obese + ve 0 + + - - + -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve15 + + - + + -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 + + - - + -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve45 + - - - + -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve
+ve-ve-ve-ve
+ve
Hou
sew
ifeH
ouse
wife
Dam
viB
algh
ami20 1495 60 F Obese ─ ve 0 - - - + + -ve -ve +ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve
15 - - - + + -ve -ve +ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - + + -ve -ve +ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - - + -ve -ve +ve +ve +ve +ve -ve -ve -ve -ve -ve -ve -ve
21 32072 45 M Obese + ve 0 - - - + - -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve15 - - - + - -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - + - -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - - - -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve
181
-ve-ve-ve-ve
Abr : Mild (+),Modeerate (++), Severe (+++), Absent(-)
+ve-ve-ve-ve
loom
wor
kH
ouse
wife
Bal
gham
iBa
lgha
mi
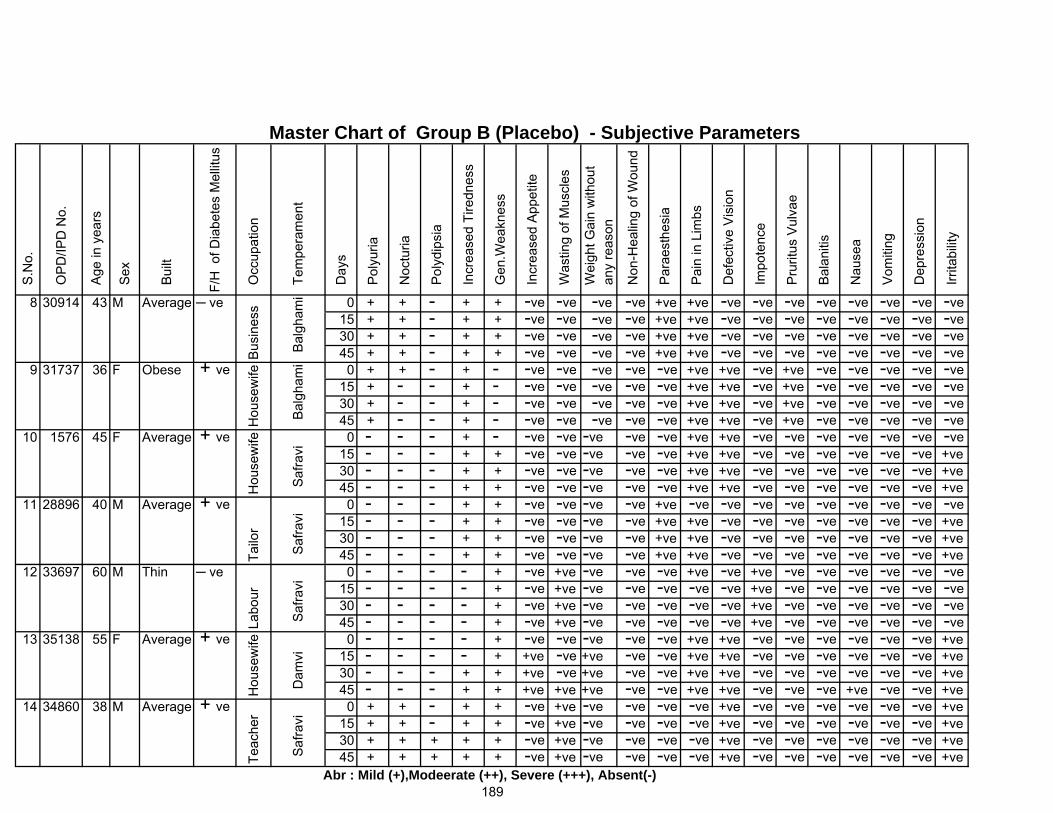
8 30914 43 M Average ─ ve 0 + + - + + -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve -ve15 + + - + + -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve -ve30 + + - + + -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve -ve45 + + - + + -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve -ve
9 31737 36 F Obese + ve 0 + + - + - -ve -ve -ve -ve +ve +ve -ve +ve -ve -ve -ve -ve -ve15 + - - + - -ve -ve -ve -ve +ve +ve -ve +ve -ve -ve -ve -ve -ve30 + - - + - -ve -ve -ve -ve +ve +ve -ve +ve -ve -ve -ve -ve -ve45 + - - + - -ve -ve -ve -ve +ve +ve -ve +ve -ve -ve -ve -ve -ve
10 1576 45 F Average + ve 0 - - - + - -ve -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve15 - - - + + -ve -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve30 - - - + + -ve -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve45 - - - + + -ve -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve
11 28896 40 M Average + ve 0 - - - + + -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve -ve15 - - - + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve +ve30 - - - + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve +ve45 - - - + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve +ve
12 33697 60 M Thin ─ ve 0 - - - - + -ve +ve -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve15 - - - - + -ve +ve -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve30 - - - - + -ve +ve -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve45 - - - - + -ve +ve -ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve
13 35138 55 F Average + ve 0 - - - - + -ve -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve15 - - - - + +ve -ve +ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve30 - - - + + +ve -ve +ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve45 - - - + + +ve +ve +ve -ve -ve +ve +ve -ve -ve -ve +ve -ve -ve +ve
14 34860 38 M Average + ve 0 + + - + + -ve +ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve +ve15 + + - + + -ve +ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve +ve30 + + + + + -ve +ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve +ve45 + + + + + -ve +ve -ve -ve -ve -ve +ve -ve -ve -ve -ve -ve -ve +ve
189
Saf
ravi
Saf
ravi
Dam
vi S
afra
vi S
afra
vi
Tailo
rLa
bour
Hou
sew
ifeTe
ache
r
-ve
Master Chart of Group B (Placebo) - Subjective Parameters
Bus
ines
s
Bal
gham
i Im
pote
nce
Pru
ritus
Vul
vae
Wei
ght G
ain
with
out
any
reas
on
Irri
tabi
lity
-ve
Vom
iting
Dep
ress
ion
-ve-ve
Bal
aniti
s
Nau
sea
Pai
n in
Lim
bs
Def
ectiv
e V
isio
n
Non
-Hea
ling
of W
ound
Par
aest
hesi
a
-ve-ve-ve-ve
Gen
.Wea
knes
s
Inc
reas
ed A
ppet
ite
Was
ting
of M
uscl
es
Pol
ydip
sia
Inc
reas
ed T
iredn
ess
Occ
upat
ion
Bui
lt
F/H
of D
iabe
tes
Mel
litus
S.N
o.
OP
D/IP
D N
o.
Age
in y
ears
Sex
Noc
turia
Tem
pera
men
t
Day
s
Pol
yuria
Abr : Mild (+),Modeerate (++), Severe (+++), Absent(-)
Hou
sew
ife
Bal
gham
i
Hou
sew
ife
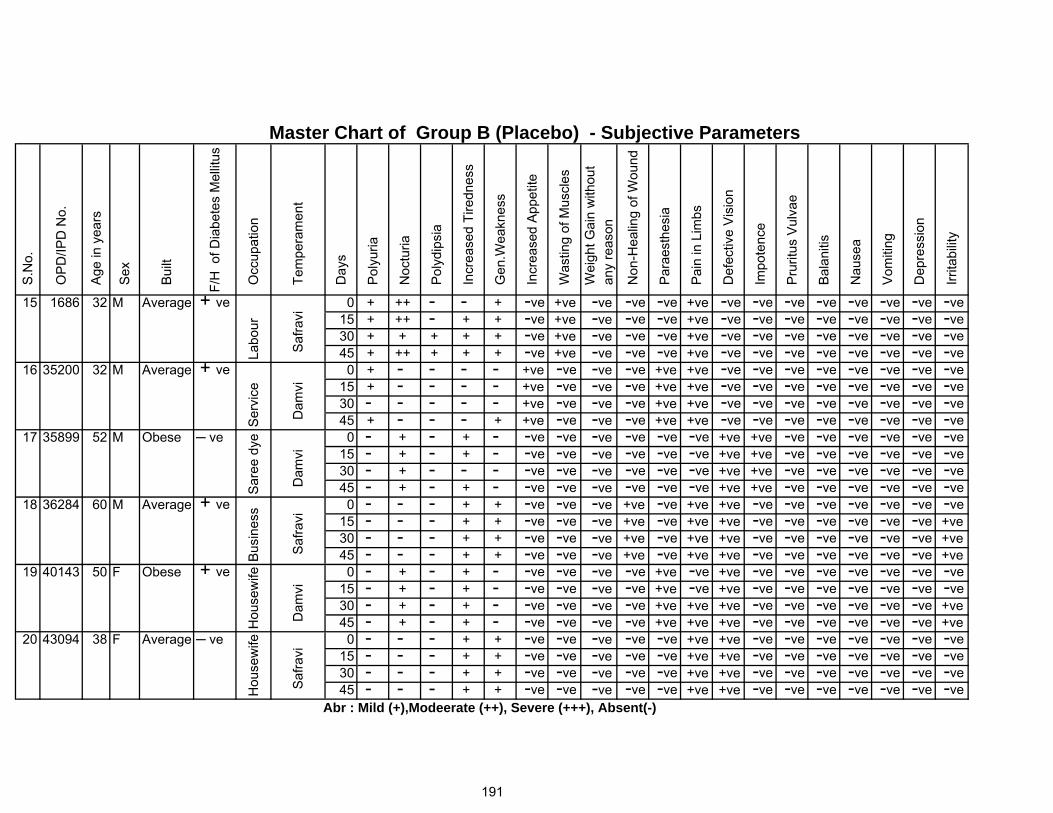
15 1686 32 M Average + ve 0 + ++ - - + -ve +ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve15 + ++ - + + -ve +ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve30 + + + + + -ve +ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve45 + ++ + + + -ve +ve -ve -ve +ve -ve -ve -ve -ve -ve -ve -ve -ve
16 35200 32 M Average + ve 0 + - - - - +ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve -ve15 + - - - - +ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve -ve30 - - - - - +ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve -ve45 + - - - + +ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve -ve
17 35899 52 M Obese ─ ve 0 - + - + - -ve -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve15 - + - + - -ve -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve30 - + - - - -ve -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve45 - + - + - -ve -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve
18 36284 60 M Average + ve 0 - - - + + -ve -ve +ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve15 - - - + + -ve -ve +ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve30 - - - + + -ve -ve +ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve45 - - - + + -ve -ve +ve -ve +ve +ve -ve -ve -ve -ve -ve -ve +ve
19 40143 50 F Obese + ve 0 - + - + - -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve15 - + - + - -ve -ve -ve +ve -ve +ve -ve -ve -ve -ve -ve -ve -ve30 - + - + - -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve +ve45 - + - + - -ve -ve -ve +ve +ve +ve -ve -ve -ve -ve -ve -ve +ve
20 43094 38 F Average ─ ve 0 - - - + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve15 - - - + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve30 - - - + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve45 - - - + + -ve -ve -ve -ve +ve +ve -ve -ve -ve -ve -ve -ve -ve
Bui
lt
F/H
of D
iabe
tes
Mel
litus
Noc
turia
S.N
o.
OP
D/IP
D N
o.
Age
in y
ears
Sex
Occ
upat
ion
Tem
pera
men
t
Day
s
Pol
yuria
Gen
.Wea
knes
s
Inc
reas
ed A
ppet
ite
Was
ting
of M
uscl
es
Pol
ydip
sia
Inc
reas
ed T
iredn
ess
-ve-ve-ve
-ve-ve-ve-ve
Irri
tabi
lity
-ve-ve-ve
Bal
aniti
s
Nau
sea
Vom
iting
Dep
ress
ion
Pai
n in
Lim
bs
Def
ectiv
e V
isio
n
-ve
Master Chart of Group B (Placebo) - Subjective Parameters
Labo
ur
Saf
ravi
Im
pote
nce
Pru
ritus
Vul
vae
Wei
ght G
ain
with
out
any
reas
on
Non
-Hea
ling
of W
ound
Par
aest
hesi
a
Dam
vi D
amvi
-ve
Ser
vice
Sar
ee d
yeB
usin
ess
Hou
sew
ife -ve-ve
Saf
ravi
Dam
vi
-ve
-ve-ve
-ve-ve
-ve
191
Saf
ravi
Hou
sew
ife
Abr : Mild (+),Modeerate (++), Severe (+++), Absent(-)
-ve-ve-ve-ve
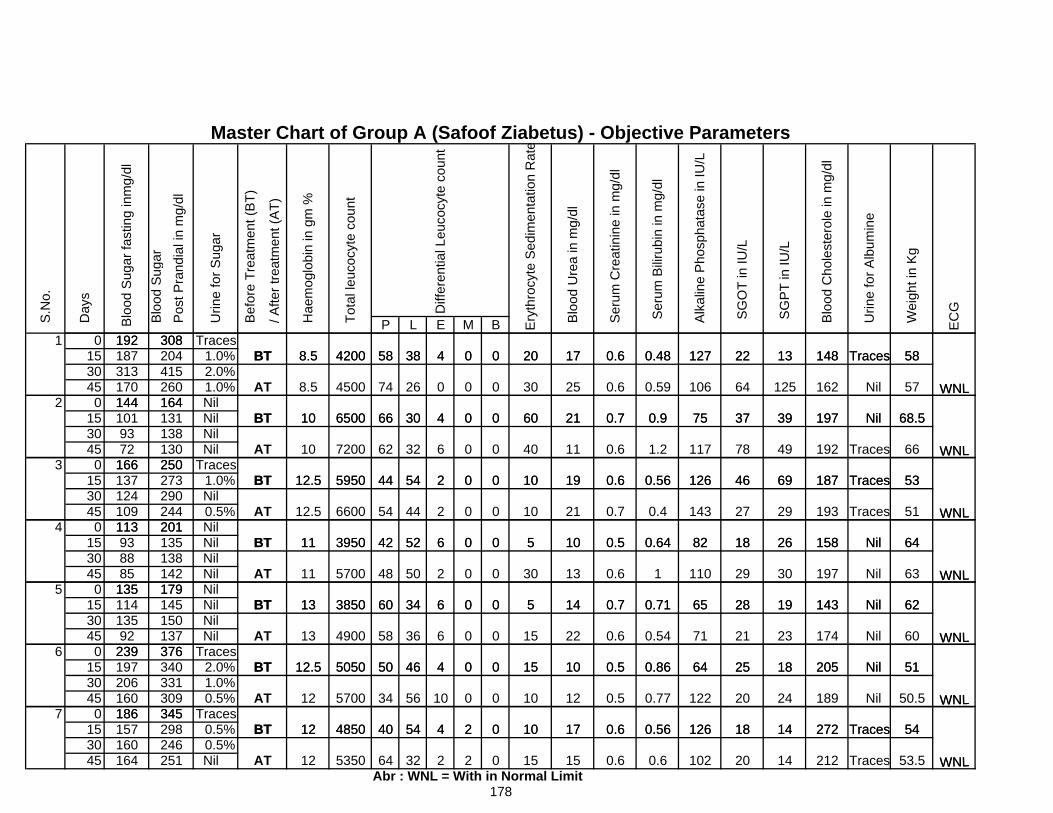
P L E M B
Master Chart of Group A (Safoof Ziabetus) - Objective Parameters
192
Pos
t Pra
ndia
l in
mg/
dl
WNL
308 T
otal
leuc
ocyt
e co
unt
Hae
mog
lobi
n in
gm
%
/ A
fter t
reat
men
t (A
T)
Bef
ore
Trea
tmen
t (B
T)
Urin
e fo
r Sug
ar
Ery
thro
cyte
Sed
imen
tatio
n R
ate
Diff
eren
tial L
euco
cyte
cou
nt
BT 588.5 4200
S
erum
Bilir
ubin
in m
g/dl
Alk
alin
e P
hosp
hata
se in
IU/L
Blo
od U
rea
in m
g/dl
Wei
ght i
n K
g
EC
G
S
GO
T in
IU/L
S
GP
T in
IU/L
Blo
od C
hole
ster
ole
in m
g/dl
Urin
e fo
r Alb
umin
e
Day
s
Ser
um C
reat
inin
e in
mg/
dl
S.N
o.
Blo
od S
u gar
Blo
od S
ugar
fast
ing
inm
g/dl
38 4 0 0 20 17 0.6 0.48 127 22 13 148 Traces 581 0 Traces
15 1.0%30 2.0%45 1.0%
192187313170144 164
WNL
WNL
260
BT 10
308204415
BT
AT
588.5
8.5
4200
4500
6500
38
26
3066
74
4
0
4
0
0
0
0
0
0
20
30
60
17
25
21
0.6
0.6
0.7
0.48
0.59
0.9
127
106
75
22
64
37
13
125
39
148
162
197
Traces
Nil
Nil
58
57
68.52 0 Nil
15 Nil30 Nil45 Nil
144101
164
WNL
WNL
BT
AT
10
10
131138130250166
93
BT
72
12.5 5950
7200 62
44
6500 3066
32
54
4
6
2
0
0
0
0
0
0
60
40
10
21
11
19
0.7
0.6
0.6
0.9
1.2
0.56
75
117
126
37
78
46
39
49
69
197
192
187
Nil
Traces
Traces
68.5
66
533 0 Traces
15 1.0%30 Nil45 0.5% WNL244
WNL
201
250166137 273
290124
113109
BT
AT
BT 11
12.5
12.5
3950
6600
5950
42
54
44 54
44
52
2
2
6
0
0
0
0
0
0
10
10
5
19
21
10
0.6
0.7
0.5
0.56
0.4
0.64
126
143
82
46
27
18
69
29
26
187
193
158
Traces
Traces
Nil
53
51
644 0 Nil
15 Nil30 Nil45 Nil
WNL
WNL
201
138142179
938885
135
113
BT
BT
AT
135 11
13
11
3850
5700
3950
60
48
42 52
50
34
6
2
6
0
0
0
0
0
0
5
30
5
10
13
14
0.5
0.6
0.7
0.64
1
0.71
82
110
65
18
29
28
26
30
19
158
197
143
Nil 64
Nil
Nil
63
625 0 Nil
15 Nil30 Nil45 Nil WNL
WNL
135137376
92239
150
179135BT114 145
AT
BT 12.5
13
13
5050
4900
3850
50
58
60 34
36
46
6
6
4
0
0
0
0
0
0
5
15
15
14
22
10
0.7
0.6
0.5
0.71
0.54
0.86
65
71
64
28
21
25
19
23
18
143
174
205
Nil
51
Nil
Nil
62
606 0 Traces
15 2.0%30 1.0%45 0.5% WNL309
345160186
376197206
239340331
BT 12.5
12
12AT
BT 4850
5700
5050
40
34
50 46
56
54
4
10
4
0
0
2
0
0
0
15
10
10
10
12
17
0.5
0.5
0.6
0.86
0.77
0.56
64
122
126
25
20
18
18
24
14
205
189
272
51
Nil
Traces
Nil
WNL
50.5
547 0 Traces
15 0.5%30 0.5%45 Nil
160164
345186157
Abr : WNL = With in Normal Limit 178
298246251 12AT
12BT
5350
4850
64
40 54
32
4
2
2
2
0
0
10
15
17
15
0.6
0.6
0.56
0.6
126
102
18
20
14
14
272
212 Traces
Traces
WNL
54
53.5

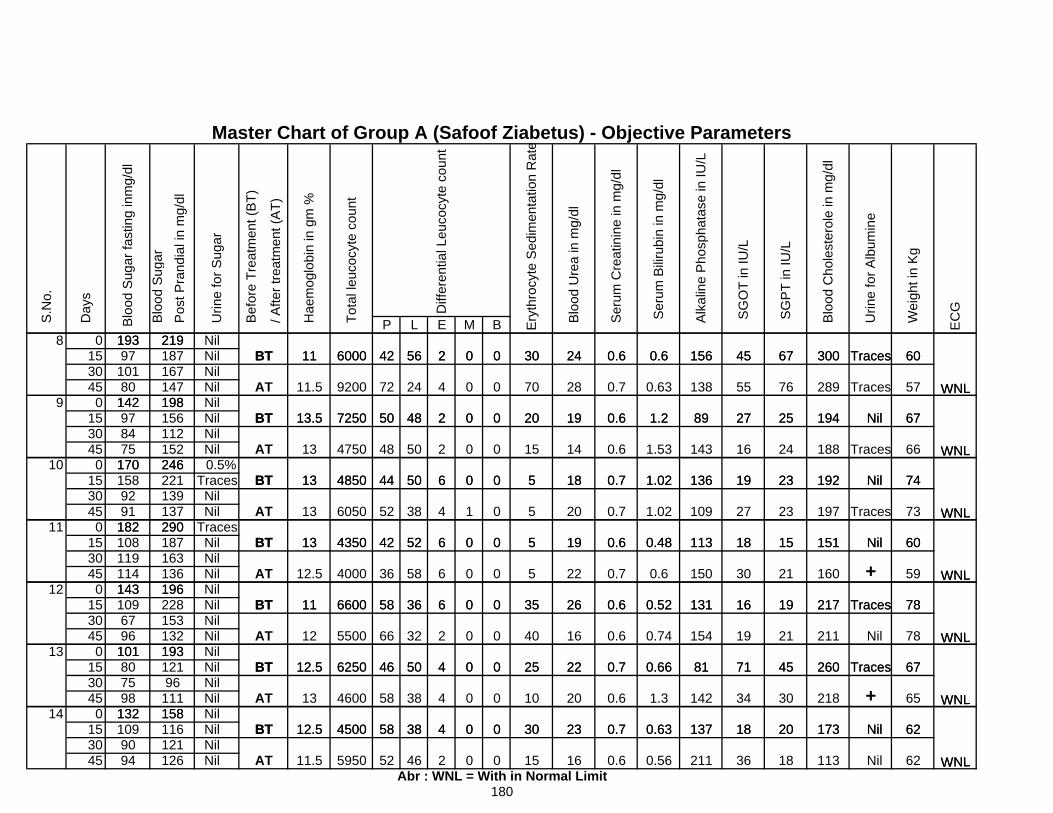
P L E M B
Master Chart of Group A (Safoof Ziabetus) - Objective Parameters
60Traces30067451560.60.6243000256
S.N
o.
Blo
od S
ugar
Blo
od S
ugar
fast
ing
inm
g/dl
Day
s
Blo
od U
rea
in m
g/dl
Ser
um C
reat
inin
e in
mg/
dl
Ery
thro
cyte
Sed
imen
tatio
n R
ate
Tot
al le
ucoc
yte
coun
t
Hae
mog
lobi
n in
gm
%
Wei
ght i
n K
g
EC
G
S
GO
T in
IU/L
S
GP
T in
IU/L
Blo
od C
hole
ster
ole
in m
g/dl
Urin
e fo
r Alb
umin
e
S
erum
Bilir
ubin
in m
g/dl
Alk
alin
e P
hosp
hata
se in
IU/L
6000193
BT219
/ A
fter t
reat
men
t (A
T)
Bef
ore
Trea
tmen
t (B
T)
Urin
e fo
r Sug
ar
WNL
Diff
eren
tial L
euco
cyte
cou
nt
4211
Pos
t Pra
ndia
l in
mg/
dl
8 0 Nil15 Nil30 Nil45 Nil
60
57
67
Traces
Traces
Nil
300
289
194
67
76
25
45
55
27
156
138
89
0.6
0.63
1.2
0.6
0.7
0.6
24
28
19
30
70
20
0
0
0
0
0
0
2
4
2
9200
7250
56
24
48BT
187
13.5 50
7211.5
600019397
101BT
AT
219
WNL
4211
WNL
16714780
142 1989 0 Nil15 Nil30 Nil45 Nil
74
67
66
Nil
Nil
Traces
192
194
188
23
25
24
19
27
16
136
89
143
1.02
1.2
1.53
0.7
0.6
0.6
18
19
14
5
20
15
0
0
0
0
0
0
6
2
250
50
7250 48
444850
4750
BT
AT
13
8475
170
13.5
13 48
50
BT246
WNL
97 156112
WNL
142 198
15210 0 0.5%
15 Traces30 Nil45 Nil
74
73
60
Nil
Traces
Nil
192
197
151
23
23
15
19
27
18
136
109
113
1.02
1.02
0.48
0.7
0.7
0.6
18
20
19
5
5
5
0
0
0
0
1
0
6
4
6
50
38
5242
52
444850
4350
6050
13
13
13
BT290
170BT
AT
1589291
182
246221139137 WNL
WNL
11 0 Traces15 Nil30 Nil45 Nil
78
60
59
Traces
Nil
+ 217
151
160
19
15
21
16
18
30
131
113
150
0.52
0.48
0.6
0.6
0.6
0.7
26
19
22
35
5
5
0
0
0
0
0
0
6
6
658
36
52
36
42
586600
4000
11
12.5
435013BT
AT
187290
108119 163
136196
BT
114143
182
WNL
WNL12 0 Nil
15 Nil30 Nil45 Nil
78
78
67
Traces
Nil
Traces
217
211
260
19
21
45
16
19
71
131
154
81
0.52
0.74
0.66
0.6
0.6
0.7
26
16
22
35
40
25
0
0
0
0
0
0
6
2
4
36
32
5046
66
58660011
6250
5500
12.5
12AT
BT
109196228 BT153132193
6796
101
143
WNL
WNL
13 0 Nil15 Nil30 Nil45 Nil
62
67
65
Nil
Traces
+ 173
260
218
20
45
30
18
71
34
137
81
142
0.63
0.66
1.3
0.7
0.7
0.6
23
22
20
30
25
10
0
0
0
0
0
0
4
4
438
38
50
58
58
46
4500
4600
625012.5
AT
BT
BT12196
111158
12.5
13
193807598
132
101
WNL
WNL
14 0 Nil15 Nil30 Nil45 Nil
62
62
Nil
Nil
173
113
20
18
18
36
137
211
0.63
0.56
0.7
0.6
23
16
30
15
0
0
0
0
4
2
38
4652
58
5950
4500BT116121126
158
180
11.5AT
12.5
Abr : WNL = With in Normal Limit
1099094
132
WNL

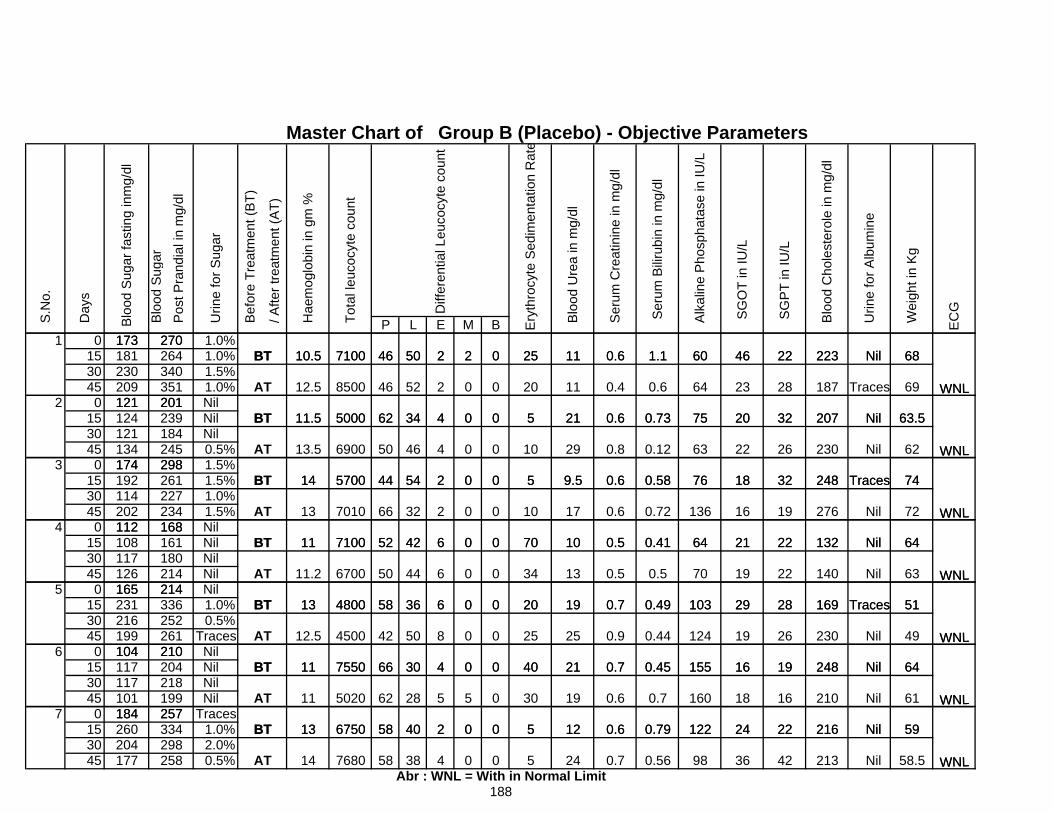
P L E M B Pos
t Pra
ndia
l in
mg/
dl
WNL
Ery
thro
cyte
Sed
imen
tatio
n R
ate
Tot
al le
ucoc
yte
coun
t
Hae
mog
lobi
n in
gm
%
/ A
fter t
reat
men
t (A
T)
Bef
ore
Trea
tmen
t (B
T)
Urin
e fo
r Sug
ar
Diff
eren
tial L
euco
cyte
cou
nt
173BT 4610.5 7100
S
erum
Bilir
ubin
in m
g/dl
Alk
alin
e P
hosp
hata
se in
IU/L
Blo
od U
rea
in m
g/dl
Ser
um C
reat
inin
e in
mg/
dl
Wei
ght i
n K
g
EC
G
S
GO
T in
IU/L
S
GP
T in
IU/L
Blo
od C
hole
ster
ole
in m
g/dl
Urin
e fo
r Alb
umin
e
Day
s
270
S.N
o.
Blo
od S
ugar
Blo
od S
ugar
fast
ing
inm
g/dl
50 2 2 0 25 11 0.6 1.1 60 46 22322 Nil
Master Chart of Group B (Placebo) - Objective Parameters
681 0 1.0%
15 1.0%30 1.5%45 1.0% WNL
WNL
340351209
121 201
264
11.5
8500
5000
173181230
BT
AT
4610.5
12.5
7100270
BT 62
46
50
52
34
2
2
4
2
0
0
0
0
0
25
20
5
11
11
21
0.6
0.4
0.6
1.1
0.6
0.73
60
64
75
46
23
20 32
223
187
207
22
28
Nil
Traces
Nil
68
69
63.52 0 Nil
15 Nil30 Nil45 0.5% WNL
WNL
121 201
245184
124 239 11.5 5000
BT298
121134174
BT
AT 13.5
14 5700
6900 50
62
44
34
46
54
4
4
2
0
0
0
0
0
0
5
10
5
21
29
9.5
0.6
0.8
0.6
0.73
0.12
0.58
75
63
76
20
22
18
32
26
32
207
230
Nil
Nil
Traces248
63.5
62
743 0 1.5%
15 1.5%30 1.0%45 1.5%
WNL
WNL202
BT
AT112
298261227234168
174192114
BT 11
13
14
7100
7010
5700
52
66
44 54
32
42
2
2
6
0
0
0
0
0
0
5
10
70
9.5
17
10
0.6
0.6
0.5
0.58
0.72
0.41
76
136
64
18
16
21 22
32
19
Traces
Nil
Nil
248
276
132 64
74
724 0 Nil
15 Nil30 Nil45 Nil WNL
WNL
108117126165
BT
180214214
112161168
BT
AT
13
11.2
11
4800
6700
7100
58
50
52 42
44
36
6
6
6
0
0
0
0
0
0
70
34
20
10
13
19
0.5
0.5
0.7
0.41
0.5
0.49
64
70
103
21
19
29
22
22
28 169
Nil
140
132 64
Nil
Traces
63
515 0 Nil
15 1.0%30 0.5%45 Traces WNL
WNL
216199104
165231 336
252261210
BT
AT
214
BT 11
12.5
13
7550
4500
4800
66
42
58 36
50
30
6
8
4
0
0
0
0
0
0
20
25
40
19
25
21
0.7
0.9
0.7
0.49
0.44
0.45
103
124
155
29
16
26
19
28
19 230
248
169 Traces
Nil
64 Nil
51
496 0 Nil
15 Nil30 Nil45 Nil WNL
104117117101184
58
WNL
40 2257
210
AT
BT
204218199
BT
13
11
11
6750
5020
7550
62
66 30
28
4
5
0
5
0
0
0
0
40
30
5
21
19
12
0.7
0.6
0.6
0.45
0.7
0.79
155
160
122
16
18
19
16
22
248 64
Nil
Nil
Nil
61
59
210
216247 0 Traces
15 1.0%30 2.0%45 0.5%
184260204177
Abr : WNL = With in Normal Limit58
58
WNL
40
38
2257
BT334298258 14AT
13
7680
6750
4
0
0
0
0
5
5
12
24
0.6
0.7
0.79
0.56
122
98
22 Nil
Nil
188
59
58.5
216
42 21336
24

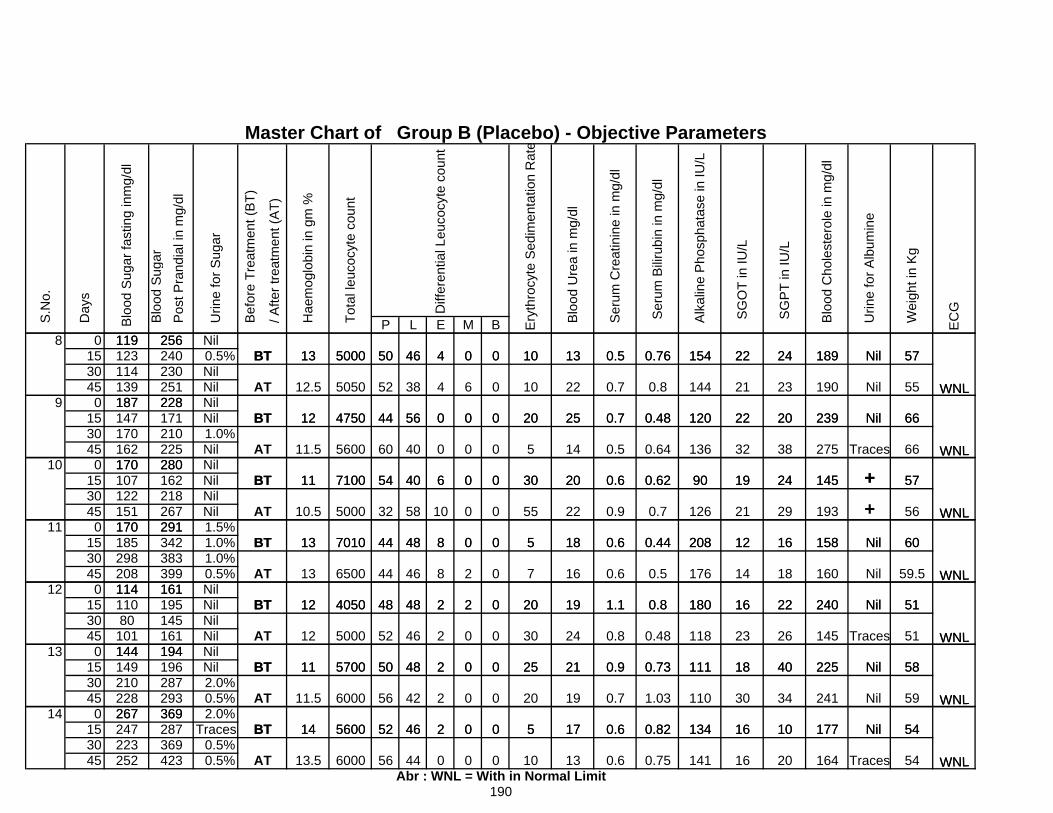
P L E M B
Master Chart of Group B (Placebo) - Objective Parameters
Pos
t Pra
ndia
l in
mg/
dl
/ A
fter t
reat
men
t (A
T)
Bef
ore
Trea
tmen
t (B
T)
Urin
e fo
r Sug
ar
WNL
S
erum
Bilir
ubin
in m
g/dl
Alk
alin
e P
hosp
hata
se in
IU/L
EC
GDiff
eren
tial L
euco
cyte
cou
nt
119BT 5013
2565000
Wei
ght i
n K
g
S
GO
T in
IU/L
S
GP
T in
IU/L
Blo
od C
hole
ster
ole
in m
g/dl
Urin
e fo
r Alb
umin
e
Blo
od U
rea
in m
g/dl
Day
s
Ser
um C
reat
inin
e in
mg/
dl
Ery
thro
cyte
Sed
imen
tatio
n R
ate
Tot
al le
ucoc
yte
coun
t
Hae
mog
lobi
n in
gm
%
S.N
o.
Blo
od S
ugar
Blo
od S
ugar
fast
ing
inm
g/dl
46 4 0 0 10 13 0.5 0.76 154 22 24 189 Nil 578 0 Nil
15 0.5%30 Nil45 Nil
230251139
187 228
WNL
WNL
119123114
BT
AT
5013256
12.5
5000
BT
240
12 44
525050
4750
46
38
56
4
4
0
0
6
0
0
0
0
10
10
20
13
22
25
0.5
0.7
0.7
0.76
0.8
0.48
154
144
120
22
21
22
24
23
20
189
190
239
Nil
Nil
Nil
57
55
669 0 Nil
15 Nil30 1.0%45 Nil
187 228
225
147 171210
WNL
WNL
280
BT
AT
BT
12
11.5 60
44170162170
11 7100
5600
54
4750 56
40
40
0
0
6
0
0
0
0
0
0
20
5
30
25
14
20
0.7
0.5
0.6
0.48
0.64
0.62
120
136
90
22
32
19
20
38
24
239
275
145
Nil
Traces
+
66
66
5710 0 Nil
15 Nil30 Nil45 Nil WNL
WNL
151170
280162218267
BT
AT
107122
BT291
17011
7010
5000
13
10.5
7100
44
32
54 40
58
48
6
10
8
0
0
0
0
0
0
30
55
5
20
22
18
0.6
0.9
0.6
0.62
0.7
0.44
90
126
208
19
21
12
24
29
16
145
193
158
+ + Nil
57
56
6011 0 1.5%
15 1.0%30 1.0%45 0.5%
WNL
WNL
170
BT
383399161
208114
185298
BT
AT
342291
12
13
701013
484050
6500 44
44 48
46
48
8
8
2
0
2
2
0
0
0
5
7
20
18
16
19
0.6
0.6
1.1
0.44
0.5
0.8
208
176
180
12
14
16
16
18
22
158
160
240
Nil
Nil
60
59.5
Nil 5112 0 Nil
15 Nil30 Nil45 Nil
WNL
WNL80
101144
145161194
195 BT161114
110
AT
BT 5700
5000
11
12
12
50
52
484050 48
46
48
2
2
2
2
0
0
0
0
0
20
30
25
19
24
21
1.1
0.8
0.9
0.8
0.48
0.73
180
118
111
16
23
18
22
26
40
240
145
225 Nil
Nil 51
51
58
Traces13 0 Nil
15 Nil30 2.0%45 0.5% WNL
WNL
267
144 194149210228 293
369
196287
BT
14
11.5AT
BT 5600
6000
570011
52
56
50
42
46
48
2
2
2
0
0
0
0
0
0
5
25
20
17
21
19
0.6
0.9
0.7
0.82
0.73
1.03
134
111
110
16
18
30
10
40
34
177
225
241
Nil
Nil
Nil 54
58
5914 0 2.0%
15 Traces30 0.5%45 0.5% WNL
267
Abr : WNL = With in Normal Limit
247223252
369287369423
190
13.5AT
14BT
6000
5600
56
52 46
44
2
0
0
0
0
0
5
10
17
13
0.6
0.6
0.82
0.75
134
141
16
16
10
20
177
164
Nil
Traces
54
54

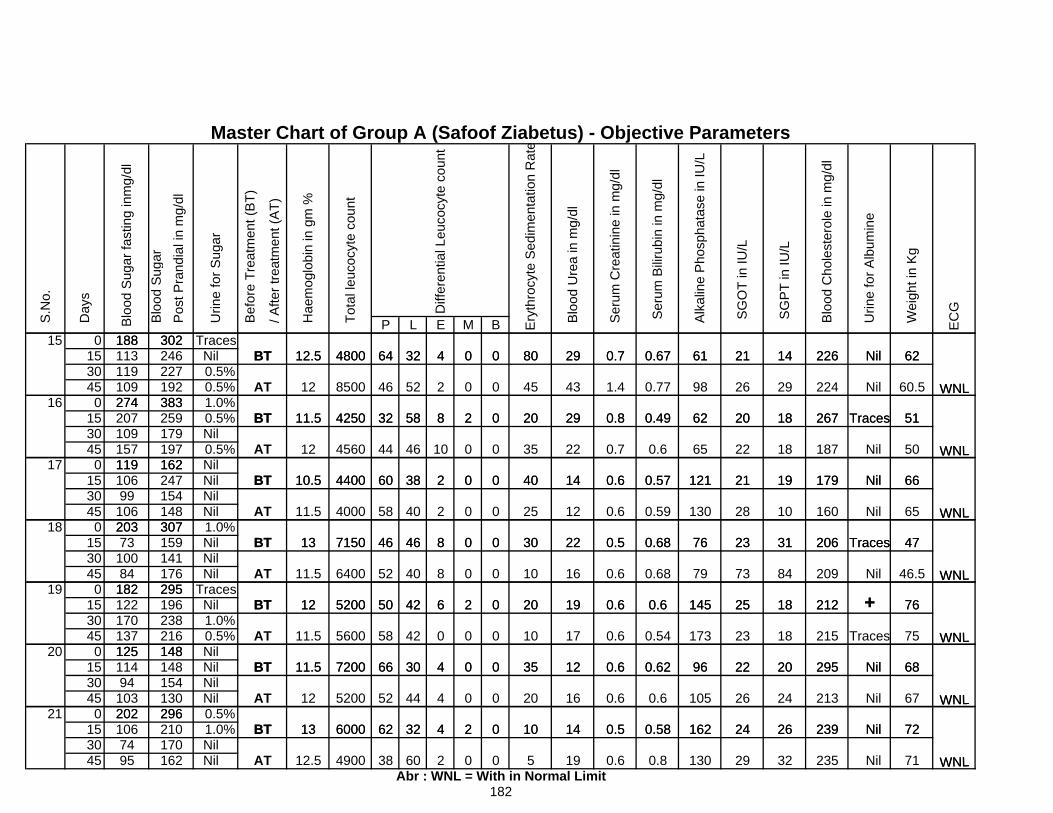
P L E M B
Master Chart of Group A (Safoof Ziabetus) - Objective Parameters
62 Nil2261421610.670.7298000432
S.N
o.
Blo
od S
ugar
Blo
od S
ugar
fast
ing
inm
g/dl
Day
s
Pos
t Pra
ndia
l in
mg/
dl
302
Wei
ght i
n K
g
EC
G
S
GO
T in
IU/L
S
GP
T in
IU/L
Blo
od C
hole
ster
ole
in m
g/dl
Urin
e fo
r Alb
umin
e
Alk
alin
e P
hosp
hata
se in
IU/L
Blo
od U
rea
in m
g/dl
Ser
um C
reat
inin
e in
mg/
dl
S
erum
Bilir
ubin
in m
g/dl
WNL
Bef
ore
Trea
tmen
t (B
T)
Ery
thro
cyte
Sed
imen
tatio
n R
ate
Diff
eren
tial L
euco
cyte
cou
nt
188BT
Tot
al le
ucoc
yte
coun
t
Hae
mog
lobi
n in
gm
%
/ A
fter t
reat
men
t (A
T)
6412.5 4800
Urin
e fo
r Sug
ar
15 0 Traces15 Nil30 0.5%45 0.5%
62
60.5
51
Nil
Nil
Traces
226
224
267
14
29
18
21
26
20
61
98
62
0.67
0.77
0.49
0.7
1.4
0.8
29
43
29
80
45
20
0
0
0
0
0
2
4
2
8
32
52
5832
46
BT
246302
WNL
WNL
188113119
BT
AT
6412.5
12
4800
11.5
8500
4250
227192109
274 38316 0 1.0%15 0.5%30 Nil45 0.5%
66 Nil
51
50
Traces
Nil
267
187
179
18
18
19
20
22
21
62
65
121
0.49
0.6
0.57
0.8
0.7
0.6
29
22
14
20
35
40
0
0
0
2
0
0
8
10
2
46
38
5832
44
604400
BT
AT109157119
207 259179
BT 10.5
WNL
WNL
11.5
12 4560
4250
162
274 383
19717 0 Nil
15 Nil30 Nil45 Nil
66
65
47
Nil
Nil
Traces
179
160
206
19
10
31
21
28
23
121
130
76
0.57
0.59
0.68
0.6
0.6
0.5
14
12
22
40
25
30
0
0
0
0
0
0
2
2
8
38
40
467150 46
58
60
4000
4400
BT307
11910699
BT
AT106203
13
11.5
10.5
WNL
WNL
162247154148
18 0 1.0%15 Nil30 Nil45 Nil 46.5
76
47
Nil
Traces
212 + 209
206
84
18
31
73
25
23
79
145
76
0.68
0.6
0.68
0.6
0.6
0.5
16
19
22
10
20
30
0
0
0
0
2
0
8
6
8
40
42
46
50
6400
7150
52
46
520012
BT
AT
159307
141176295
BT
20373
10084
18211.5
13
WNL
WNL
19 0 Traces15 Nil30 1.0%45 0.5%
76
75
68
215
295
212
Traces
Nil
+ 18
18
20
25
23
22
145
173
96
0.6
0.54
0.62
0.6
0.6
0.6
19
17
12
20
10
35
0
0
0
2
0
0
6
0
4
42
42
30
58
50
667200
5600
5200
11.5
11.5
12295
BT
BT
AT
196238216148125
182122
WNL
WNL
170137
20 0 Nil15 Nil30 Nil45 Nil 67
72
68
Nil
Nil239
295 Nil
21324
26
20
26
24
22
105
162
96
0.6
0.58
0.62
0.6
0.5
0.6
16
14
12
20
10
35
0
0
0
0
2
0
4
4
4
44
32
30
62
52
66
5200
7200
12
11.5148154
BT
AT
BT
130296
148
13 6000
11494
103202
125
WNL
WNL21 0 0.5%
15 1.0%30 Nil45 Nil
72
71
Nil239
Nil
26
32
24
29
162
130
0.58
0.8
0.5
0.6
14
19
10
5
0
0
2
0
4
2
32
6038
62210170162
BT296
1067495
Abr : WNL = With in Normal Limit12.5AT
13
4900
6000
235
202
WNL
182

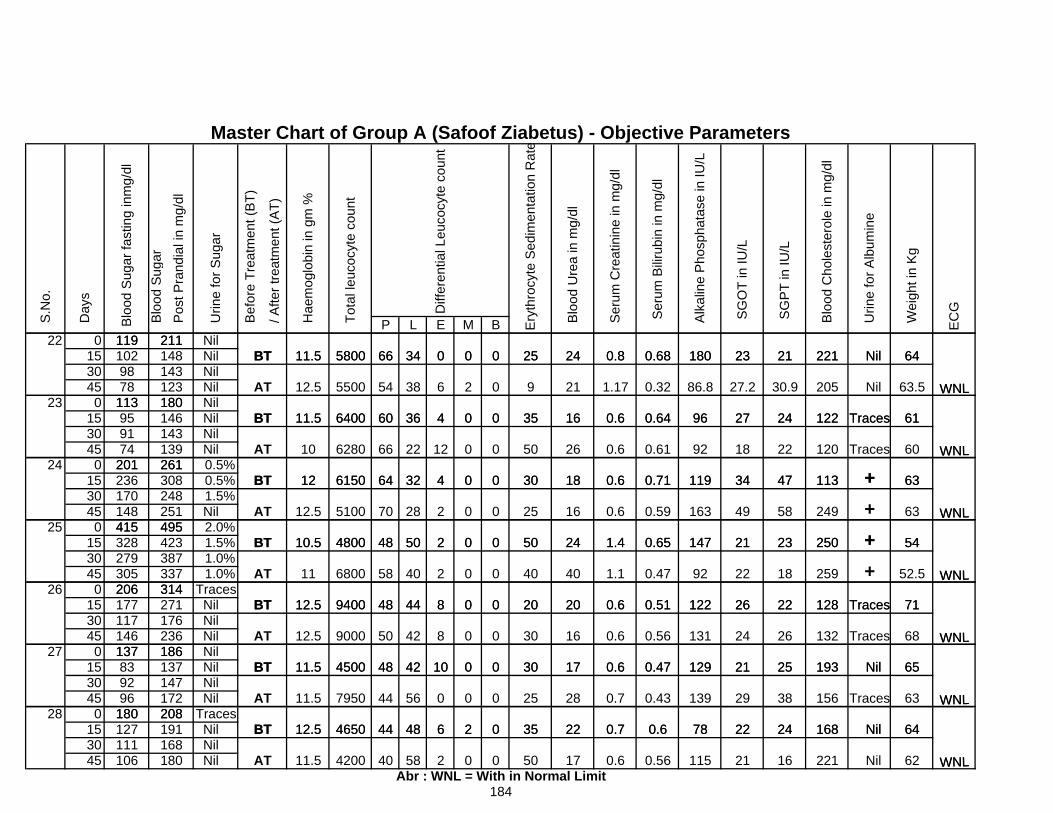
P L E M B
Master Chart of Group A (Safoof Ziabetus) - Objective Parameters
Pos
t Pra
ndia
l in
mg/
dl
WNL
Ery
thro
cyte
Sed
imen
tatio
n R
ate
Tot
al le
ucoc
yte
coun
t
Hae
mog
lobi
n in
gm
%
/ A
fter t
reat
men
t (A
T)
Bef
ore
Trea
tmen
t (B
T)
Urin
e fo
r Sug
ar
Diff
eren
tial L
euco
cyte
cou
nt
119BT 6611.5 5800
Alk
alin
e P
hosp
hata
se in
IU/L
Blo
od U
rea
in m
g/dl
Ser
um C
reat
inin
e in
mg/
dl
S
erum
Bilir
ubin
in m
g/dl
S
GO
T in
IU/L
S
GP
T in
IU/L
Blo
od C
hole
ster
ole
in m
g/dl
Urin
e fo
r Alb
umin
e
Day
s
211
S.N
o.
Blo
od S
ugar
Blo
od S
ugar
fast
ing
inm
g/dl
34 0 0 0 25 24 0.8 0.68 180 23 21 221 Nil 64
Wei
ght i
n K
g
EC
G
22 0 Nil15 Nil30 Nil45 Nil WNL
WNL
14814312378
113 180
11910298
BT
AT
6611.5
12.5
5800
11.5BT
211
5500
6400
34
38
3660
54
0
6
4
0
2
0
0
0
0
25
9
35
24
21
16
0.8
1.17
0.6
0.68
0.32
0.64
180
86.8
96
23
27.2
27
21
30.9
24
221
205
122
Nil
Nil
Traces
64
63.5
6123 0 Nil
15 Nil30 Nil45 Nil WNL
WNL
95113 180
139143146
BT 12
11.5
10 66
BT
AT 6280261
9174
20164
6400
6150
3660
22
32
4
12
4
0
0
0
0
0
0
35
50
30
16
26
18
0.6
0.6
0.6
0.64
0.61
0.71
96
92
119
27
18
34
24
22
47
122
120
113
Traces
Traces
+
61
60
6324 0 0.5%
15 0.5%30 1.5%45 Nil
WNL
WNL148
BT
AT
10.5
12.5
12
4800BT415
261308248251495
201236170
48
70
64
5100
6150 32
28
50
4
2
2
0
0
0
0
0
0
30
25
50
18
16
24
0.6
0.6
1.4
0.71
0.59
0.65
119
163
147
34
49
21
47
58
23
113
249
250
+ + +
63
63
5425 0 2.0%
15 1.5%30 1.0%45 1.0% WNL
328279305206
11
10.5
12.5BT 489400
6800
4800
314
BT
AT387337
415423495
58
48 50
40
44
2
2
8
0
0
0
0
0
0
50
40
20
24
40
20
1.4
1.1
0.6
0.65
0.47
0.51
147
92
122
21
22
26
23
18
22
250 + 259
128
+ Traces
54
WNL
52.5
7126 0 Traces
15 Nil30 Nil45 Nil
117146
271176236
137
206177
186AT 12.5
12.5BT
50
48
9000
9400314
BT 4811.5 4500
44
42
42
8
8
10
0
0
0
0
0
0
20
30
30
20
16
17
0.6
0.6
0.6
0.51
0.56
0.47
122
131
129
26
24
21
22
26
25
128
132
193
Traces
Traces
Nil
WNL
WNL
71
68
6527 0 Nil
15 Nil30 Nil45 Nil
137839296
180
186137147
44
WNL
208172 44
BT 48
12.5
11.5
11.5
AT
BT 4650
7950
4500 42
56
48
10
0
6
0
0
2
0
0
0
30
25
35
17
28
22
0.6
0.7
0.7
0.47
0.43
0.6
129
139
78
21
29
22
25
38
24 168
156
193 Nil
Traces
Nil
63
64
WNL
65
28 0 Traces15 Nil30 Nil45 Nil
180191168180
184
127111106
Abr : WNL = With in Normal Limit40
44
WNL62
208
AT
12.5BT
11.5 4200
4650 48
58
6
2
2
0
0
0
35
50
22
17
0.7
0.6
0.6
0.56
78
115
22
21
24
16
168
221
Nil
Nil
64

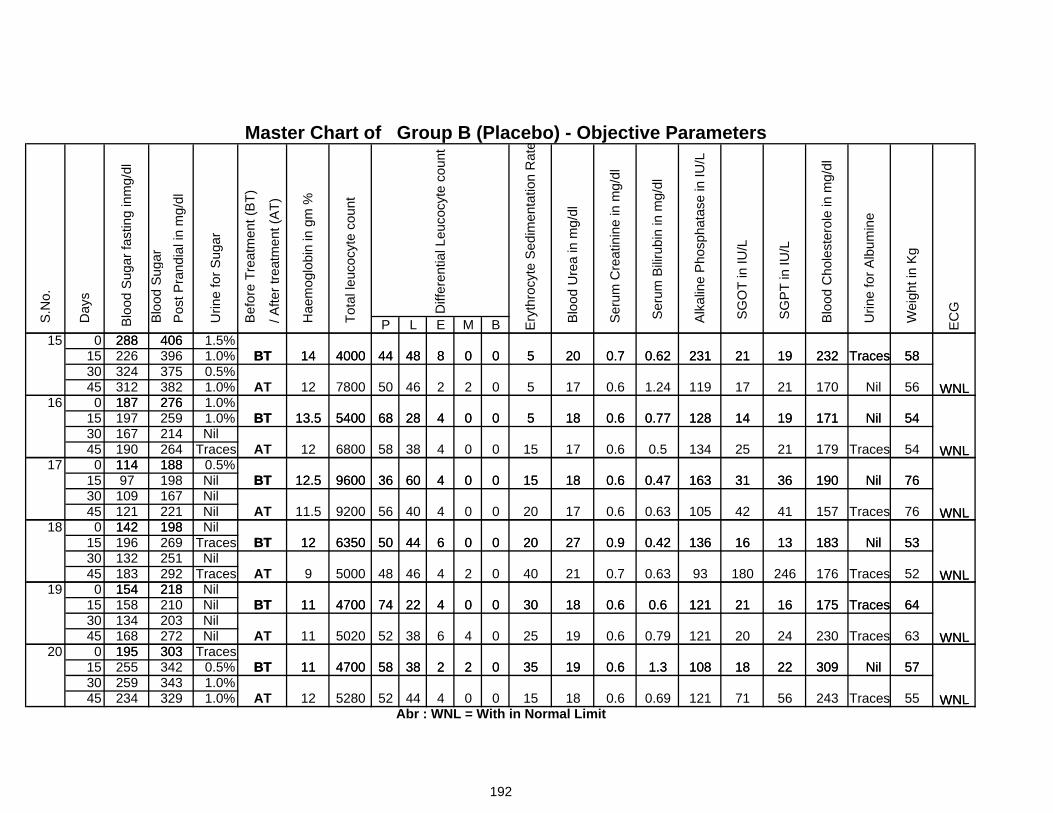
P L E M B
58Traces23219212310.620.72050084000 44
Blo
od U
rea
in m
g/dl
48 T
otal
leuc
ocyt
e co
unt
Diff
eren
tial L
euco
cyte
cou
nt
BT
Day
s
Wei
ght i
n K
g
EC
G
S
GO
T in
IU/L
S
GP
T in
IU/L
Blo
od C
hole
ster
ole
in m
g/dl
Urin
e fo
r Alb
umin
e
Alk
alin
e P
hosp
hata
se in
IU/L
Urin
e fo
r Sug
ar
Ser
um C
reat
inin
e in
mg/
dl
S.N
o.
Blo
od S
u gar
Blo
od S
ugar
fast
ing
inm
g/dl
288
/ A
fter t
reat
men
t (A
T)
Bef
ore
Trea
tmen
t (B
T)
Ery
thro
cyte
Sed
imen
tatio
n R
ate
S
erum
Bilir
ubin
in m
g/dl
Master Chart of Group B (Placebo) - Objective Parameters
Pos
t Pra
ndia
l in
mg/
dl
WNL
14406
Hae
mog
lobi
n in
gm
%
15 0 1.5%15 1.0%30 0.5%45 1.0%
58
56
54
Traces
Nil
Nil
232
170
171
19
21
19
21
17
14
231
119
128
0.62
1.24
0.77
0.7
0.6
0.6
20
17
18
5
5
5
0
0
0
0
2
0
8
2
4
4000 44
46
2868
50780012
5400
48BT
187 276
288226324
AT
13.5BT
WNL
375382312 WNL
14406396
16 0 1.0%15 1.0%30 Nil45 Traces
76
54
54
Nil
Nil
Traces
190
171
179
36
19
21
31
14
25
163
128
134
0.47
0.77
0.5
0.6
0.6
0.6
18
18
17
15
5
15
0
0
0
0
0
0
4
4
4
38
60
2868
58
3612.5 9600
214264
197 259 5400187 276
167190114
BT188
WNL
13.5
12
BT
AT 6800 WNL17 0 0.5%
15 Nil30 Nil45 Nil
76
76
53
Nil
Traces
Nil
190
157
183
36
41
13
31
42
16
163
105
136
0.47
0.63
0.42
0.6
0.6
0.9
18
17
27
15
20
20
0
0
0
0
0
0
4
4
6
40
44
60
6350
9200
50
56
3612.5 9600
12
11.5
BT
121 AT167109221198142
114BT
18897 198
WNL
WNL
18 0 Nil15 Traces30 Nil45 Traces
64Traces175
53
52
Nil
Traces
183
176
16
13
246
21
16
180
121
136
93
0.6
0.42
0.63
0.6
0.9
0.7
18
27
21
30
20
40
0
0
0
0
0
2
4
6
4
44
46
22
6350
48
50
74470011
9 5000
12BT
AT
196
154BT
251292218
183
198
132269
142
WNL
WNL
19 0 Nil15 Nil30 Nil45 Nil
64
63
57
Traces
Traces
Nil
175
230
309
16
24
22
21
20
18
121
121
108
0.6
0.79
1.3
0.6
0.6
0.6
18
19
19
30
25
35
0
0
0
0
4
2
4
6
2
38
38
22
58
52
744700
4700
5020
11
11
11
AT
BT
154BT
218210203272303
134168195
158
WNL
WNL
20 0 Traces15 0.5%30 1.0%45 1.0%
192
57
55
Nil
Traces
309
243
22
56
18
71
108
121
1.3
0.69
0.6
0.6
19
18
35
15
0
0
2
0
2
4
3858
5280
470011BT255 342343
303
329Abr : WNL = With in Normal Limit
12AT 4452234
195
259WNL
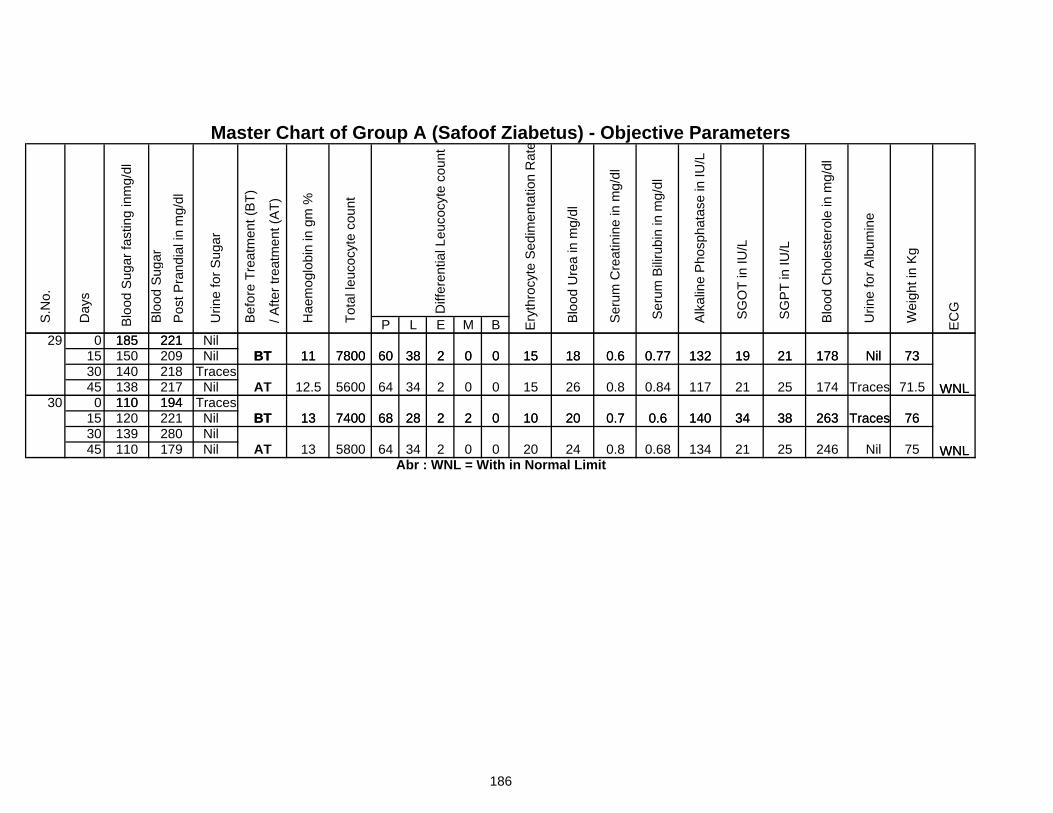
P L E M B
7321
EC
G
Urin
e fo
r Alb
umin
e
Wei
ght i
n K
g
WNL
Master Chart of Group A (Safoof Ziabetus) - Objective Parameters
Nil0.6181500238
Day
s
S.N
o.
Blo
od S
ugar
Blo
od S
ugar
fast
ing
inm
g/dl
Tot
al le
ucoc
yte
coun
t
Hae
mog
lobi
n in
gm
%
/ A
fter t
reat
men
t (A
T)
Bef
ore
Trea
tmen
t (B
T)
Ery
thro
cyte
Sed
imen
tatio
n R
ate
Diff
eren
tial L
euco
cyte
cou
nt
S
erum
Bilir
ubin
in m
g/dl
Blo
od U
rea
in m
g/dl
Ser
um C
reat
inin
e in
mg/
dl
S
GO
T in
IU/L
S
GP
T in
IU/L
Blo
od C
hole
ster
ole
in m
g/dl
Alk
alin
e P
hosp
hata
se in
IU/L
0.77 19 178132221
11
Pos
t Pra
ndia
l in
mg/
dl
BT185
Urin
e fo
r Sug
ar
7800 6029 0 Nil
15 Nil30 Traces45 Nil
73
76
21
25
38
WNLTraces 71.5
WNL
117
140 Traces
174
263
Nil
21
34
0.84
0.6
26
20
0
0
0.6
0.8
0.7
1815
15
10
00
0
2
34
28
2
2
2
38218217138
1400.77 19 178132
221150 209
AT
11
BT
BT185
194110740013
7800
68
64
60
560012.530 0 Traces
15 Nil30 Nil45 Nil
186
76
21
38
250.68 WNL
140
134 75246 Nil
Traces263340.6200
24
0.7
0.80
10
20
2
0
28 2
Abr : WNL = With in Normal Limit5800 2
139110 179 AT 13
280221 BT194
120110
740013
3464
68
Related Documents







![ETABS [Qaemi Hamid]](https://static.cupdf.com/doc/110x72/55cf8673550346484b97c22c/etabs-qaemi-hamid.jpg)



