Haileyesus Getahun Stop TB Department WHO Re-conceptualizing ICF and IPT: global progress to date 14 th Core Group Meeting of the TB/HIV Working Group, Addis Ababa, Ethiopia.

Haileyesus Getahun Stop TB Department WHO
Jan 04, 2016
14 th Core Group Meeting of the TB/HIV Working Group, Addis Ababa, Ethiopia. Re-conceptualizing ICF and IPT: global progress to date. Haileyesus Getahun Stop TB Department WHO. Collaborative TB/HIV activities. A. Establish the mechanism for collaboration A.1. TB/HIV coordinating bodies - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Haileyesus GetahunStop TB Department
WHO
Re-conceptualizing ICF and IPT: global progress to date
14th Core Group Meeting of the TB/HIV Working Group, Addis Ababa, Ethiopia.

Collaborative TB/HIV activities
B. To decrease the burden of TB in PLWHA- Three IsB.1. Intensified TB case findingB.2. Isoniazid preventive therapyB.3. TB infection control in health care and other settings
A. Establish the mechanism for collaborationA.1. TB/HIV coordinating bodiesA.2. HIV surveillance among TB patientA.3. TB/HIV planningA.4. TB/HIV monitoring and evaluation
C. To decrease the burden of HIV in TB patientsC.1. HIV testing and counsellingC.2. HIV preventive methodsC.3. Cotrimoxazole preventive therapyC.4. HIV/AIDS care and supportC.5. Antiretroviral therapy to TB patients.
Joint HIV and TB
HIV programme
TB programme

Why re-conceptualisation?
99 5 1 4 4 4
92
5627 47 3 3 5
84
7226 25
7
3 3
118
104
4047
14
17 10
128
111
56
68
44
58
25
113
97
52
62
58
61
33
0.0
100.0
200.0
300.0
400.0
500.0
600.0
700.0
800.0
900.0
Tested for HIV HIV-positive CPT ART Screened forTB
Diagnosedwith TB
IPT
Th
ou
sa
nd
s o
f p
atie
nts
2002
2003
2004
2005
2006
2007
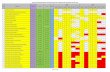
Diagnosis and treatment of HIV in TB patientsDiagnosis, treatment and prevention of TB
Collaborative TB/HIV activities, 2002–2007, GLOBAL PROGRESS

Countries with policy on ICF, 2006 (N=109)
Countries reporting ICF, 2006 (N=44)
Why re-conceptualisation?

Countries with policy on IPT, 2006 (N=82)
Countries reporting IPT, 2006 (N=24)
Why re-conceptualisation?

Re-conceptualisation of IPT and ICF
• Essential package of HIV care and treatment
• ICF as a gatekeeper for IPT and Infection control
• Simplified screening algorithm (WHO)
• Implementation on the grounds of human rights
WHO's Three Is Meeting, April 2008

Progress: Meta-analysis of primary data
Primary question What is the most sensitive clinical
algorithm to screen for culture-confirmed pulmonary TB in people
living with HIV? Objective
Develop a standardized evidence-based approach and guidelines to TB
screening and prevention (IPT) among PLHIV.

Progress: Meta-analysis of primary data
Inclusion criteria for studies
• Involved diagnosis of TB in PLHIV
• Culture of at least one sputum specimen was used to confirm the diagnosis of TB
• Sputum specimens were collected from PLHIV regardless of signs or symptoms
• Data was collected about symptoms and signs in PLHIV at the time that sputum specimens for culture were collected

Published and unpublished studies included in the meta-analysis
Principle investigator
Study site Sample size HIV-infected patients
Varma Thailand, Viet Nam, Cambodia
1782* 1782*
Maartens South Africa 129 129
Grants South Africa 1093 1093
Kimerling Cambodia 504 130
Corbett Zimbabwe 4668 874
Shah Ethiopia 453 453
Ayles Zambia 7963 2297
Corbett Zimbabwe 9068 1916
Churchyard South Africa 1955 567
Kimerling Cambodia 441 441
Bekker South Africa 174 174
Lawn South Africa 236 236
Total 28,466 10,092

Progress: Scaling up IPT as part of ICF
• IPT statement of WG finalised and widely disseminated.
• FAQ on IPT developed and will soon be posted on WHO website
• Paper submitted to the Lancet Summarise findings of global consultation Simplified strategy of scale-up suggested Critical steps for nationwide scale up
identified
• NTP to lessen its "control" over INH as a drug

Progress: demand generation
Living with HIV. Dying of TB
First ever protest at HIV ConferenceMexico city, August 2008

Conclusion
• Evidence based TB screening and prevention approach in progress by WHO
• Leadership and ownership from HIV stakeholders for IPT and ICF is needed
• Countries need to scale up ICF, as a gateway for IPT and infection control
• Dire need for increased community mobilisation and demand generation
• More research, research, research for the best tool
Related Documents