Haematology

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Haematology

Aims of the session
• Brief overview of the haematological system• Leukaemias• Lymphomas• Myelomas and other paraproteinaemias• SBAs

http://library.med.utah.edu/WebPath/webpath.html
Webpath•SBAs•Tutorials•Images•Covers most major systems of the body

OSCE Scenario
• You are a GP and a 23-year old woman comes to visit your clinic complaining of decreased energy levels. Please take a history and attempt to formulate an appropriate management plan
(5 minutes)

Key Differentials - TATT
• Hypothyroidism• Infection• Menorrhagia• Lyphoma• Other Malignancies
NB: DON’T FORGET: 1) General Proforma 2) Systemic Symptoms 3) ICE

Terminally differentiated cells vs Partially differentiated
Hematopoiesis

Some definitions
• Blast cell
• Terminally differentiated
• Totipotent stem cell

Some definitions
• Blast cell – immature precursors of either lymphocytes (lymphoblasts) or myeloid cells (myeloblasts). They do not normally appear in peripheral blood. They can be recognized by their large size, and primitive nuclei (ie. the nuclei contain nucleoli).
• Terminally differentiated - cells which have specialized properties and functions. They are also unable to undergo cellular growth or multiplication.
• Totipotent stem cell – a cell that is capable of developing into any cell type including extraembyronic tissue.

Terminally differentiated cells vs Blast cells
Terminally differentiated Blast cellsUnlikely to transform to other cell types
Slow rate of cell turnover (tumours of terminally differentiated cells will take time to accumulate – chronic leukaemias
Low cell turnover means they are less responsive to chemotherapyHighly specialized cell
Ability to transform to many cell types
Rapidly replicating (tumours of blast cells can accumulate quickly causing aacute leukaemias)
High cell turnover means they are more responsive to chemotherapyNot very specialized

• Pluripotent stem cell
• Granulocyte
• Pancytopenia

• Pluripotent stem cell – a cell which has the ability to differentiate into more than one cell type. Pluripotent stem cells are derived from totipotent stem cells. Pluripotent stem cells can develop into any cell type except for the extraembryonic tissue.
• Granulocyte - a circulating white blood cell which has prominent granules in the cytoplasm and a nucleus of two or more lobes. They are derived from the myeloid lineage and including neutrophils, basophils and eosinophils
• Pancytopenia - a reduction in the number of red and white blood cells, as well as platelets. It occurs due to a problem with the bone marrow.


A B
Describe?

Classification of Leukaemias
Classified according to the cell lineage that is affected ie. myeloid or lymphoid
Also classified according to speed of onset ie acute due to accumulation of blast cells or chronic due to accumulation of a terminally differentiated cell.

Disorders of the myeloid lineage

Terminally differentiated cells vs Partially differentiated
Acute myeloid leukaemias

Terminally differentiated cells vs Partially differentiated
Acute myeloid leukaemias The myeloid stem cell can
differentiate into myeloid, monocytic, or erythroid cells, or into megakaryocytes

Terminally differentiated cells vs Partially differentiated
Acute myeloid leukaemias The myeloid stem cell can
differentiate into myeloid, monocytic, or erythroid cells, or into megakaryocytes
Therefore, AML can be derived from myeloblasts (MI-M2), promyelocytes (M3), a mixture of myeloblasts and monoblasts (M4), monoblasts (M5), erythroblasts (M6), or megakaryoblasts (M7).

Acute myeloid leukaemias
• Characterized by the rapid growth of abnormal white blood cells that accumulate in the bone marrow and interfere with the production of normal blood cells.
• The most common acute leukemia affecting adults.
• Two classification systems – WHO and the FAB
• FAB classification still widely used and clinically important

French American British (FAB) classification of AML
Classified based upon type of precursor / blast cell which is predominant
Type Name Cytogenetics Associated featuresM0 minimally differentiated acute myeloblastic leukemia M1 acute myeloblastic leukemia, without maturation Gum hypertrophy
M2 acute myeloblastic leukemia, with granulocytic maturation t(8;21)(q22;q12), t(6;9) Auer rods
M3 promyelocytic, or acute promyelocytic leukemia (APL) t(15;17) DIC and Auer rods
M4 acute myelomonocytic leukemia inv(16)(p13q22), del(16q)
M4eo myelomonocytic together with bone marrow eosinophilia inv(16), t(16;16) Eosinophilia
M5 acute monoblastic leukemia (M5a) or acute monocytic leukemia (M5b) del (11q), t(9;11), t(11;19) Hypokalemia
M6 acute erythroid leukemias, including erythroleukemia (M6a) and very rare pure erythroid leukemia (M6b)
M7 acute megakaryoblastic leukemia t(1;22) Downs syndrome

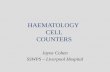
AML BLOOD FILM – WHAT CAN BE SEEN?

Bone marrow apsirate showing Auer rods
• Highly specific for AML subtypes M2 and M3

AML – Presentation• Patients present with pancytopaenia due to a hypercellular bone marrow
– Symptoms of anaemia– Infections– Bleeding
Other signs: Splenomegaly, Hepatomegaly, Lymphadenopathy
• Death in 6-12 weeks if left untreated.
• Best initial test is blood smear– Blast cells present (blasts have occupied all of the bone marrow and are now spilling
over into the blood)– WCC can be low, normal or high

Treatment of acute leukaemia
Supportive:
ProblemAnaemiaThrombocytopeniaDICInfection
Tumour lysis syndrome
Treatment

Treatment of acute leukaemia
Supportive:
ProblemAnaemiaThrombocytopeniaDICInfection
Tumour lysis syndrome
TreatmentPacked RBCsPlatelets (if <10)FFP, cyroprecipitateAntibiotics, reverse barrier nursingAllopurinol/rasburicase

Definitive treatment for AMLChemotherapy:• Induction 4-6w• Consolidation• Duanorubicin + Cytobarine
• Other • Add in all-trans-retinoic-acid (ATRA) in PML (M3) during induction• Monoclonal Ab• CNS radiotherapy• BM transplantation

The importance of the t(15;17) translocation
• The t(15;17) translocation is associated with PML (M3) and produces a PML-RARα fusion protein which binds to the retinoic acid receptor element in the promoters of several myeloid-specific genes and inhibits myeloid differentiation
• Treatment with Retinoic acid thus stimulates cellular differentiation and has a big impact on the prognosis of PML

Terminally differentiated cells vs Partially differentiated
Myeloproliferative disorders

Myeloproliferative disorders• A group of disorders which are due to over proliferation
of terminally differentiated cells of the myeloid lineage.• Are classified according to whether they are
Philadelphia chromosome positive or negative.
• Have the ability to transfrom into an acute myeloid leukaemia
Philadelphia positive Philadelphia negativeChronic myeloid leukaemia Polycythemia rubra vera
Essential thrombocytosis Myelofibrosis

PathophysiologyTwo classes of mutations may be required:

Terminally differentiated cells vs Partially differentiated
Chronic myeloid leukaemias

Stepped-up production of granulocytes and their precursors and failed apoptosis leads to insidious progression towards a blast crisis.
Epidemiology
•Incidence= 0.6-2/100,000•Can occur at any age but rare in children. Peak incidence at 40-60 •Less common than AML, CLL
Chronic myeloid leukaemia

Pathophysiology95% involve t(9;22)(q34;q11) translocation, resulting in the Philadelphia chromosome. This forms a fusion gene- BCR-ABL1 with constitutively active tyrosine kinase activity.

Usually asymptomatic!
•Examination-Splenomegaly- may be only feature at latent phase, massive later on
•Bloods-Anaemia- mild, worsens with progression-WBCs- extremely high-Smear- leukocytosis with granulocyte left-shift
Symptoms

Leukocytosis, increased numbers of banded neutrophils


•Imatinib-Tyrosine kinase inhibitor, targets BCR-ABL1. Greatly increases 5 year survival compared to older drug therapies
-Initial treatment, continued indefinitely if optimal response.
Other:•Monoclonals•Surgery
-Splenectomy for splenomegaly or pancytopenia•Radiotherapy
-Pallative for bulky LN or splenomegaly
Treatment of CML

Prognosis
• Median survival 5-6 years.• Chronic Accelerated Blast Transformation

Terminally differentiated cells vs Partially differentiated
Polycythemia rubra vera

• Clinical features– Night sweats– Hyperviscosity symptoms– Pruritus after a hot bath– Plethoric face– Splenomegaly– Haemorrhage– Hypertension– Gout
• Increased proliferation of erythrocytes, and sometimes thrombocytes. Rarely increased proliferation of granulocytes

• Important lab features– Increased Hb, HCT, Red cell mass– Low serum EPO– Increased platelet count– JAK2 mutation in 95%
• Treatment– Venesection– Cytotoxic myelosuppression
• Hydroxyurea• Busulphan
INCREASED RISK OF DEVELOPING ACUTE MYELOID LEUKAEMIA

Terminally differentiated cells vs Partially differentiated
Histiocytosis (too many dendritic cells and macrophages aka histiocytes)

Terminally differentiated cells vs Partially differentiated
Mastocytosis (too many mast cells)

Disorders of the lymphoid lineage

Terminally differentiated cells vs Partially differentiated
Lymphoproliferative disorders

Terminally differentiated cells vs Partially differentiated
Acute lymphoblastic leukaemias

Acute lymphoblastic leukaemia
Also known as ‘lymphocytic’.
Presents acutely with a pancytopenia and hypercellular bone marrow.
Epidemiology
•Incidence = 1/50,000. Slight male predominance.•Commonest type of childhood leukaemia (70%)•Peak age 2-5 years, but later increase >50.•Prognosis is poor if <1 year of age or >10 years of age.

PathophysiologyUNCONTROLLED PROLIFERATION
•Genetic Factors - dysregulation of proto-oncogene e.g. TEL-AML1 (25%).
• Environmental Factors – X Rays + DOWN’S
85% are derived from B-cell precursors.
-T-cell ALL
-B-cell ALL

Findings specific for ALL•Examination
-Lymphadenopathy-Splenomegaly (10-20% presentation)-CNS signs- more likely
•Bloods-Anaemia- usually severe, signs present-WBCs- variable, usually neutropenia-Smear- smallish basophilic blasts, few granules, hand-mirror cells-Clotting- 10% ALL presents with DIC
•Imaging-Mediastinal mass in some T cell ALL

Small basophilic blasts with few granules

Treatment of acute leukaemiaSupportive:
ProblemAnaemiaThrombocytopeniaDICInfection
Tumour lysis syndromeCNS prophylaxis
TreatmentPacked RBCsPlatelets (if <10)FFP, cyroprecipitateAntibiotics, reverse barrier nursingAllopurinol/uricase
Intrathecal chemo e.g. methotrexate, cytarabine

DefinitiveChemotherapy:•Induction 4-6w•Consolidation•Maintenance (ALL only) 1-2y
-Longer in boys
Other
•Monoclonal Ab•CNS radiotherapy•BM transplantation
•5 year survival -Children- 75%-Adults- 40%

Terminally differentiated cells vs Partially differentiated
Chronic lymphoid leukaemia/ lymphoma

98% develop from B cells.
Epidemiology
•Incidence = 4.2/100,000. Slight male predominance.•Most common form of leukaemia in the West•Usually >55, median age 72, rare <40.

Pathophysiology
Largely unknown with no specific genetic abnormalities.

Symptoms specific for CLL

Symptoms specific for CLLUsually asymptomatic!• Examination
-Lymphadenopathy/splenomegaly present in late disease.
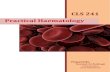
• Bloods-WBCs- extremely high-Smear- lymphocytosis with ‘smudge/basketball
cells’• Other
-Richter’s syndrome-Prolymphocytic transformation

Smudge cells- destruction of fragile lymphocytes during smear

Treatment of CLL
• Watchful waiting with regular monitoring• Chemotherapy. Indications:
– Severe systemic symptoms– Non-pred-responsive AI anaemia/thrombocytopenia– Progressive splenomegaly/lymphadenopathy– Increased WBC/reduced ‘doubling time’
• Surgery– -Splenectomy for splenomegaly or pancytopenia
• Radiotherapy– -Pallative for bulky LN or splenomegaly



What is the difference between lymphoma and CLL
• Are part of a continuum of disease• Leukemia usually refers to a condition in which the
abnormal cells populate the blood• But lymphoma usually initially populates LN,
spleen etc. to form a tumour mass.


Hodgkin’s lymphoma
Originates from B cells in the germinal centres of lymphoid tissue and is characterised by orderly spread from one LN group to another.
Epidemiology
•Incidence = 2.2/100,000, 30% of all lymphoma•Bimodal distribution with peaks at 15-30 and >50 years•Slight male predominance

Risk factors•Acquired
-HIV/AIDS- increases with CD4 count-Previous non-Hodgkin’s lymphoma-Autoimmune conditions
•Inherited-Immune defects-Family history of H/non-H lymphoma, CLL

PathogenesisSome proliferation of malignant Reed-Sternberg cells (probably of B cell lineage) and abnormal mononucleocytes.

Presentation•Painless non-tender rubbery enlarged LN
-Cervical involvement in 60-70%, axillary in 10-15%, inguinal in 6-12%-May increase/decrease in size spontaneously-May become ‘matted’ and non-mobile-Contiguous progression to nearby groups-Alcohol-induced pain
•Systemic symptoms-Especially fever (30%), may be cyclic-And severe pruritis (25%)
•Other-Early satiety due to splenomegaly

Investigations•FBC
-Exclude leukaemia, mononucleosis•ESR/CRP•LFTs•U&Es•CXR
-Lymphadenopathy, mediastinal expansion•CT
-Thorax, abdomen for staging•BM biopsy•Other
-HIV, Monospot, LDH, thoracentesis, PET, LP, MRI


Ann-Arbour staging
Automatic stage IV if extranodal involvement. Systemic symptoms = B, extranodal = E, >10cm = X, splenic involvement = S

TreatmentSupportive•Fertility•Cardiac function•Respiratory function•Tumour lysis syndrome•Others, as indicated (see leukaemias slide)

TreatmentDefinitive•IA/IIA
-Radiotherapy alone- affected nodes and prophylatically -Chemo with radiotherapy of affected nodes
•IB/IIB/III/IV-Chemo
•BM transplant-If still progressive despite chemo or after induction of remission after relapse

Non-Hodgkin’s lymphoma
A heterogeneous group of lymphoid tumours, mostly of B cell origin. Characterised by irregular pattern of spread and common extranodal disease, they vary in their aggressiveness.
Epidemiology•Incidence = 17/100,000•Median age is >50•Diffuse large B cell and follicular commonest

Risk factors•Acquired
-Infection e.g. EBV (Burkitt’s), HTLV-1 (T cell), HCV, HHV8 (Castleman’s), H. pylori (gastric MALT)-Previous chemotherapy/Hodgkin’s-Autoimmune disorders e.g. Sjogren’s, Hashimoto’s, coeliac-Immunodeficiency e.g. post-transplant, HIV/AIDS
•Inherited

Pathogenesis

Presentation•Painless non-tender rubbery enlarged LN
-Non-contiguous progression•Systemic symptoms
-Commoner in high-grade•Rash
-Cutaneous involvement e.g. mycosis fungoides, anaplastic large-cell etc.
•Abdominal pain, early satiety -Splenomegaly but unusual as rarely massive-Hepatomegaly
•Mass-Testicular-GI, symptoms of obstruction
•Shortness of breath, pleuritic chest pain, SVC syndrome-Mediastinal mass in high grade
•Neurological-Primary CNS lymphoma, commoner in immunosuppressed

Investigations•FBC
-Anaemia, thrombocytopenia, neutropenia-Thrombocytosis, lymphocytosis may occur
•ESR/CRP•LFTs•U&Es
-Obstructive nephropathy, hypercalcaemia•Serology
-HIV, HTLV-1, HCV•Imaging
-CXR-Intrathoracic lymphadenopathy, mediastinal expansion-CT-Thorax, abdomen for staging-Bone scan-PET-MRI- Brain, cord-USS- Scrotum
•BM biopsy-Should always be carried out

•Lymph node USS and excision biopsy

Treatment•Low grade
-Localised (rare)- radiotherapy, surgery-Disseminated- watch and wait or chemo when symptomatic/organ dysfunction-Gastric MALT- associated with H pylori, antibiotic therapy curative in 90%
•High grade-Aggressive chemo e.g. CHOP-Maintenance not needed-Allogenic stem cell transplantation-CNS prophylaxis in very high grade e.g. Burkitt’s

Prognosis of lymphoma
5 year survival rates•Hodgkin’s- highly curable
-I/II- 90%-IV- 65%-Long-term sequelae of treatment
•Non-Hodgkin’s- vary widely (see IPI)-Overall 63%-Indolent follicular lymphoma I/II- 91% but may not be curable-DLBLC- curable with aggressive chemo

Terminally differentiated cells vs Partially differentiated
Plasma cell neoplasm e.g. Multiple myeloma and Waldenstrom’s macroglobulinaemia

• Multiple Myeloma• MGUS• Waldenstrom’s macroglobulinaemia• (Non-Hodgkin lymphoma)• (CLL)

• Presdisposing factors– Radiation– Benzene– Pesticides
• Epidemiology– 4 per 100,000 per year– Median age 66 years
• Pathophysiology– Post germinal centre B cell proliferation
• Monoclonal antibody


• Hypercalcaemia• Renal impairment• Anaemia• Bone disease
• Hyperviscosity• Amyloidosis (AL)• Infection (recurrent)


• Amyloid L – Ig light chains– paraproteinaemias
• Amyloid A – Protein A– Chronic inflammation
• Amyloid TTR – Transthyretin– Transthyretin abnormality
• Polyneuropathy,• Restrictive cardiomyopathy
• Amyloid B2M – Beta 2 microglobulin– Occurs in dialysis
• Carpal tunnel
• Also associated with Alzheimer’s disease, Diabetes Mellitus

• FBC and film• ESR• Urine dipstick• 24 hour urine collection• U&Es• Urate• Albumin, calcium, phosphate, ALP• Serum and urinary electrophoresis• Serum Ig• X-ray• (BM Biopsy –diagnostic rather than screening)

1. Production of a single monoclonal antibody (paraprotein)– ‘M’ band in γglobulin region on serum/ urine
electrophoresis2.Increased clonal plasma cells in the bone
marrow– >20% monoclonal plasma cells on bone marrow
biopsy3. Evidence of organ damage (‘CRAB HAI’)

• Prognosis– MM remains an incurable disease– Mean survival 3-4 yrs from diagnosis
• Treatment– Specific– Supportive

• Intensive or non intensive– Intensive if <65– Non intensive if >65
• Intensive– 4-6 cycles chemotherapy
• Cyclophosphamide, dexamethasone, thalidomide– THEN autologous stem cell collection and
transplant• Non-intensive
– Chemo: Melphalan and cyclophosphamide

• Renal disease– rehydration – 3L/day
• Bone disease– Bisphosphonates– Radiotherapy to bony lesions– Corticosteroids
• Anaemia– Transfusion/ EPO
• Hyperviscosity– Plasmapheresis
• Infection– Broad spectrum Abx and antifungals

• Post germinal centre B cell proliferation• Monoclonal antibody/ paraprotein production
– M Band– BJP
• >20% monoclonal plasma cells in BM• ‘CRAB HAI’• Specific and supportive treatment• Outcome still poor

• Often discovered incidentally in elderly• Benign• Characterised by:
– Low levels of paraprotein, normal levels of Ig– <10% plasma cells in bone marrow– Absence of lytic bone lesions– Absent/minimal urinary BJP– Absence of end organ damage associated with MM
• 1% per year develop MM

• Lymphoplasmacytoid proliferation– Similarities with CLL
• IgM paraprotein– Plasma viscosity
• Organomegaly and lymphadenopathy more common than in MM– No end organ damage (cf MM)


A 67 year old lady is found to have an Hb of 18.9g/dL. Her erythropoeitin level is markedly raised. Which of the following is the least likely diagnosis?
A) COPDB) Eisenmenger’s syndromeC) Polycythaemia veraD) Renal cell carcinomaE) Nepalese woman living at high altitude

A 67 year old lady is found to have an Hb of 18.9g/dL. Her erythropoeitin level is markedly raised. Which of the following is the least likely diagnosis?
A) COPDB) Eisenmenger’s syndromeC) Polycythaemia veraD) Renal cell carcinomaE) Nepalese woman living at high altitude

Which one of the following is not consistent with a diagnosis of MGUS?
A) normal urinalysisB) normal renal functionC) 20% plasma cells in bone marrowD) Normochromic, normocytic anaemia with Rouleaux formationsE) Absence of lytic bone lesions

Which one of the following is not consistent with a diagnosis of MGUS?
A) normal urinalysisB) normal renal functionC) 20% plasma cells in bone marrowD) Normochromic, normocytic anaemia with Rouleaux formationsE) Absence of lytic bone lesions

A patient has a sharp M band on serum electrophoresis. Which of the following is least consistent with this result?
A) IgG MMB) Waldenstrom’ macroglobulinaemiaC) AA amyloidosisD) MGUSE) CLL

A patient has a sharp M band on serum electrophoresis. Which of the following is least consistent with this result?
A) IgG MMB) Waldenstrom’ macroglobulinaemiaC) AA amyloidosisD) MGUSE) CLL

Which ONE of these is the most likely clinical presentation of a child with acute lymphoblastic leukaemia?
a) A 6 month history of fatigue and repeated upper respiratory tract infectionb) Poor appetite and abdominal pain resulting from swollen spleenc) Swollen gums in the mouthd) Recent history of bruising and tirednesse) None- incidental finding

Which ONE of these is the most likely clinical presentation of a child with acute lymphoblastic leukaemia?
a) A 6 month history of fatigue and repeated upper respiratory tract infectionb) Poor appetite and abdominal pain resulting from swollen spleenc) Swollen gums in the mouthd) Recent history of bruising and tirednesse) None- incidental finding

A blood smear of a patients shows increased numbers of neutrophils, eosinophils and basophils. In addition, there are increased numbers of promyelocytes (but infrequent blast cells). What is the optimum treatment for this patient?
a)Allogenic stem cell transplantationb)Combination chemoc) Imatinibd)Blood transfusion to relieve symptomse)Rifampicin and isoniazid

A blood smear of a patients shows increased numbers of neutrophils, eosinophils and basophils. In addition, there are increased numbers of promyelocytes (but infrequent blast cells). What is the optimum treatment for this patient?
a)Allogenic stem cell transplantationb)Combination chemoc) Imatinibd)Blood transfusion to relieve symptomse)Rifampicin and isoniazid

A 59 year old man receiving chemotherapy for NonHodgkin’s Lymphoma develops painful haematuria. Which of the following is the most likely cause of his symptoms?
A) RituximabB) CyclophosphamideC) Adriamycin (doxorubicin/ hydroxydaunarubicin)D) Vincristine (oncovin)E) Prednisolone

A 59 year old man receiving chemotherapy for NonHodgkin’s Lymphoma develops painful haematuria. Which of the following is the most likely cause of his symptoms?
A) RituximabB) CyclophosphamideC) Adriamycin (doxorubicin/ hydroxydaunarubicin)D) Vincristine (oncovin)E) Prednisolone

A 50 year old woman is about to commence chemotherapy for treatment of AML. Which of the following medications should she be started on prior to chemotherapy?
A) ColchicineB) DexamethasoneC) DiclofenacD) AllopurinolE) Hydroxychloroquine

A 50 year old woman is about to commence chemotherapy for treatment of AML. Which of the following medications should she be started on prior to chemotherapy?
A) ColchicineB) DexamethasoneC) DiclofenacD) AllopurinolE) Hydroxychloroquine

A 6 year old boy from Kenya develops swelling of the jaw. The mass responds rapidly to chemotherapy. What is the most likely diagnosis?
a) Burkitt's lymphomab) Follicular lymphomac) Mycosis fungoidesd) Lymphoblastic lymphomae) Enteropathy-associated T cell lymphoma

A 6 year old boy from Kenya develops swelling of the jaw. The mass responds rapidly to chemotherapy. What is the most likely diagnosis?
a) Burkitt's lymphomab) Follicular lymphomac) Mycosis fungoidesd) Lymphoblastic lymphomae) Enteropathy-associated T cell lymphoma

A 22-year-old man presents with fever, sweating, particularly at night, pruritus and weight loss.
O/E: palpable, painless cervical lymph nodes and no skin manifestations. The most appropriate investigation would be:-
a) FBCb) Lymph Node Biopsyc) Chest Radiographd) CT scan of the neck and mediastinume) Mantoux Test

A 22-year-old man presents with fever, sweating, particularly at night, pruritus and weight loss.
O/E: palpable, painless cervical lymph nodes and no skin manifestations. The most appropriate investigation would be:-
a) FBCb) Lymph Node Biopsyc) Chest Radiographd) CT scan of the neck and mediastinume) Mantoux Test

25-year-old woman presents with a single, non-tender, enlarged cervical lymph node. She also complains of fever and night sweats. Lymph node biopsy reveals infiltration with histiocytes and lymphocytes and presence of cells with bilobed mirror-image nuclei. The most likely diagnosis is:-
a) Non-Hodgkin’s lymphomab) Hodkin’s lymphomac) Sarcoidosisd) Acute Lymphoblastic Leukemia (ALL)e) TB

25-year-old woman presents with a single, non-tender, enlarged cervical lymph node. She also complains of fever and night sweats. Lymph node biopsy reveals infiltration with histiocytes and lymphocytes and presence of cells with bilobed mirror-image nuclei. The most likely diagnosis is:-
a) Non-Hodgkin’s lymphomab) Hodkin’s lymphomac) Sarcoidosisd) Acute Lymphoblastic Leukemia (ALL)e) TB

30-year-old man has had a progressively worsening productive cough for one month. On physical examination, a few small non-tender lymph nodes are palpable in the axillae, and the tip of the spleen is palpable.
Hb 10.2 g/dl, Hct 31.1% MCV 90 fL, WBC count 67 x 10 9 / L Platelet count 36 x 10 9 / L.
Microscopic examination of his peripheral blood smear shows many blasts with Auer rods. Which of the following is the most likely diagnosis?
A) Leukemoid reaction B) Acute myelogenous leukemia C) Chronic lymphocytic leukemia D) Acute lymphoblastic leukemia E) Leukoerythroblastosis

30-year-old man has had a progressively worsening productive cough for one month. On physical examination, a few small non-tender lymph nodes are palpable in the axillae, and the tip of the spleen is palpable.
Hb 10.2 g/dl, Hct 31.1% MCV 90 fL, WBC count 67 x 10 9 / L Platelet count 36 x 10 9 / L.
Microscopic examination of his peripheral blood smear shows many blasts with Auer rods. Which of the following is the most likely diagnosis?
A) Leukemoid reaction B) Acute myelogenous leukemia C) Chronic lymphocytic leukemia D) Acute lymphoblastic leukemia E) Leukoerythroblastosis
Related Documents