OFFICE OF THE ASSISTANT SECRETARY OF DEFENSE 1200 DEFENSE PENTAGON WASHINGTON, DC 20301-1200 SEP 2 5 2018 HEALTH AFFAIRS MEMORANDUM FOR ASSISTANT SECRETARY OF THE ARMY (MANPOWER AND RESERVE AFFAIRS) ASSISTANT SECRETARY OF THE NAVY (MANPOWER AND RESERVE AFFAIRS) ASSISTANT SECRETARY OF THE AIR FORCE (MANPOWER AND RESERVE AFFAIRS) DIRECTOR, JOINT STAFF DIRECTOR, DEFENSE HEALTH AGENCY SUBJECT: Personal Protective Equipment Policy Guidance for Healthcare Personnel with Potentia l for Exposure to Infectious Agents This memorandum provides policy guidance to Department of Defense (DoD) healthcare personnel (HCP) concerning how to more efficiently organize and stockpile personal protective equipment (PPE), and select protective clothing and equipment in response to infectious disease environments for direct patient care, contact with blood or body fluids, prolonged close interaction (less than three feet), and contact with deceased individuals. This policy guidance addresses gaps in DoD capabilities to plan and manage the risks to DoD HCP operating in infectious disease environments during public health emergencies and other incidents and operations, such as pandemic influenza (PI) and Ebola virus disease (EVD) outbreaks. This policy guidance supersedes and expands on the Assistant Secretary of Defense for Health Affairs memorandum, "Personal Protective Equipment for Department of Defense Military Treatment Facility Healthcare Workers Assessing or Caring for Ebola Virus Disease Patients and Others Possibly Exposed to Ebola Virus," dated November 7, 2014. The DoD HCP should refer to the Deputy Secretary of Defense memorandum, "Termination of Operation United Assistance and Maintaining Certain DoD Ebola Virus Disease-related Guidance and Authorities," dated August 10, 2015. To mitigate risks to DoD HCP operating in infectious disease environments, this policy guidance establishes a PPE framework to expand the scope of current PPE guidance beyond PI and EVD medical responses to a wider range of infectious diseases. This guidance broadly addresses planning assumptions and PPE selection. The PPE framework is based on the U.S. Centers for Disease Control and Prevention Healthcare Infection Control Practices Advisory Committee (CDC/HICPAC) "2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings" 1 and it is the intent that the DoD will meet or exceed the recommended practices outlined in this guideline. The framework consists of two parts: 1) four PPE levels for infectious diseases, each corresponding to a category of precautions defined by characteristics of agent colonization or infection and modes of transmission, and patient condition (Attachment 1, Table 1) and 2) a list of PPE options designated for each PPE level to protect body parts of concern and limit exposure pathways 1 https://www.cdc.gov/infectioncontroVpdf/guidelines/isolation-guideiines.pdf

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
OFFICE OF THE ASSISTANT SECRETARY OF DEFENSE
1200 DEFENSE PENTAGON WASHINGTON, DC 20301-1200
SEP 2 5 2018
HEALTH AFFAIRS
MEMORANDUM FOR ASSISTANT SECRETARY OF THE ARMY (MANPOWER AND RESERVE AFFAIRS)
ASSISTANT SECRETARY OF THE NAVY (MANPOWER AND RESERVE AFFAIRS)
ASSISTANT SECRETARY OF THE AIR FORCE (MANPOWER AND RESERVE AFFAIRS)
DIRECTOR, JOINT STAFF DIRECTOR, DEFENSE HEALTH AGENCY
SUBJECT: Personal Protective Equipment Policy Guidance for Healthcare Personnel with Potential for Exposure to Infectious Agents
This memorandum provides policy guidance to Department ofDefense (DoD) healthcare personnel (HCP) concerning how to more efficiently organize and stockpile personal protective equipment (PPE), and select protective clothing and equipment in response to infectious disease environments for direct patient care, contact with blood or body fluids, prolonged close interaction (less than three feet), and contact with deceased individuals. This policy guidance addresses gaps in DoD capabilities to plan and manage the risks to DoD HCP operating in infectious disease environments during public health emergencies and other incidents and operations, such as pandemic influenza (PI) and Ebola virus disease (EVD) outbreaks. This policy guidance supersedes and expands on the Assistant Secretary ofDefense for Health Affairs memorandum, "Personal Protective Equipment for Department ofDefense Military Treatment Facility Healthcare Workers Assessing or Caring for Ebola Virus Disease Patients and Others Possibly Exposed to Ebola Virus," dated November 7, 2014. The DoD HCP should refer to the Deputy Secretary of Defense memorandum, "Termination ofOperation United Assistance and Maintaining Certain DoD Ebola Virus Disease-related Guidance and Authorities," dated August 10, 2015.
To mitigate risks to DoD HCP operating in infectious disease environments, this policy guidance establishes a PPE framework to expand the scope of current PPE guidance beyond PI and EVD medical responses to a wider range of infectious diseases. This guidance broadly addresses planning assumptions and PPE selection. The PPE framework is based on the U.S. Centers for Disease Control and Prevention Healthcare Infection Control Practices Advisory Committee (CDC/HICP AC) "2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings"1 and it is the intent that the DoD will meet or exceed the recommended practices outlined in this guideline. The framework consists of two parts: 1) four PPE levels for infectious diseases, each corresponding to a category of precautions defined by characteristics ofagent colonization or infection and modes of transmission, and patient condition (Attachment 1, Table 1) and 2) a list of PPE options designated for each PPE level to protect body parts ofconcern and limit exposure pathways
1 https://www.cdc.gov/infectioncontroVpdf/guidelines/isolation-guideiines.pdf
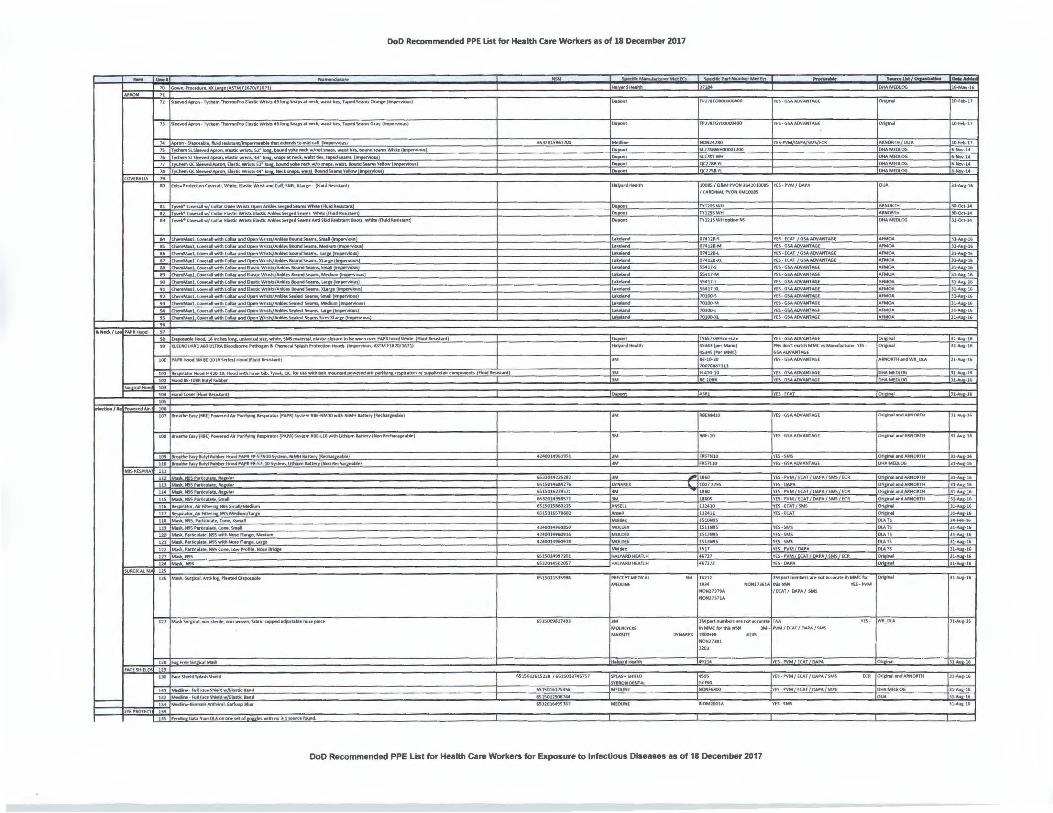
(Attachment 1, Table 2). Aligned with this framework is a complete list of approved specific DoD PPE items for HCP (Attachment 2). The protection offered by the recommended PPE levels ranges, in general, from least to most protective (Level I to IV) based on various exposure and disease variables.
The DoD components must determine the required quantities of PPE items across the PPE levels and develop training and logistical arrangements consistent with Attachments 1 and 2. These actions will ensure smooth expansion of PPE guidance from individual diseases to broader categorization by precautions that will provide acquisition efficiencies across the Military Health System.
Military medical treatment facilities will apply PPE in the context of comprehensive infection prevention and control programs. To do so, program administrators will conduct hazard vulnerability analyses, apply other needed prevention and control measures (such as engineering controls and safe work practices as well as other administrative controls), apply the appropriate types of precautions, and undergo the associated PPE selection process for infectious agent exposure prevention and control, as the hazards in each workplace environment can be unique and they must be evaluated and controlled accordingly.
Additional policy and guidance will be provided as needed to enable comprehensive, responsive, and effective infectious agent exposure prevention and control for DoD personnel and other beneficiaries. My point of contact for this action is Ms. Elizabeth Fudge. Ms. Fudge
may be reached at (703) 681-8295 or elizaheth.r ~mai ~
Tom McCaffery Principal Deputy Assistant Secretary of
Defense (Health Affairs)
Attachments: as stated
cc: Surgeon General of the Army Surgeon General of the Navy Surgeon General of the Air Force Joint Staff Surgeon
2

Attachment 1: PPE Levels and Options.
Below is a brief description of varying levels of PPE ensembles to protect HCP. Tables 1 and 2 provide additional information on the PPE levels and PPE options, respectively.
Level I PPE and the other related measures that compose standard precautions ( e.g., safe injection practices and respiratory hygiene/cough etiquette) apply to all patients regardless of documented or suspected infection status. This level ofPPE may provide sufficient protection to HCP from possible transmissible infectious disease due to patient encounters with those documented or suspected ofhaving certain contagious diseases (e.g., common cold and seasonal influenza) or those with non-contagious diseases (e.g., anthrax and tularemia). Patient presentation and condition even in cases ofnon-contagious disease may warrant the use ofhigher levels ofPPE and associated measures under this framework. For example, when considering anthrax, initial patient presentation without proper decontamination or excessive drainage of lesions will influence the level ofPPE selected. This level ofPPE may also be used for other zoonotic or plant diseases as a way to contain the spread and thus control the associated economic loss. Levels II, III, and IV PPE build on Level I to increase protection against different modes oftransmission.
Levels II and III PPE recommendations focus on contact and droplet modes of transmission, respectively. Level II PPE protects against direct and indirect transmission of infectious agents via interaction with the patient or their environment. Level III PPE is intended to prevent transmission ofinfectious agents spread through close contact of the mucous membranes or respiratory tract with respiratory secretions.
Level IV PPE offers respiratory protection to its users and when combined with PPE from the other levels protects all routes of entry into the human body, i.e., contact, inhalation, and ingestion. Level IV PPE is suitable for diseases with undetermined modes of transmission or due to suspected deliberate release until transmission is characterized sufficiently to inform control measures. In cases where patients are affected by diseases that are highly contagious; have high case-fatality risks; or may result in severe, persistent, recurrent, or irreversible morbidity, use of Level IV PPE and other infectious disease prevention and control measures should be considered to protect HCP and other patients.
Across all levels ofPPE consideration should be given to medical procedures that may aerosolize particles and create inhalation hazards requiring the use of a respirator not a surgical mask. For example, if a patient with a viral hemorrhagic fever is undergoing intubation, suction, or other medical procedures that can aerosolize the virus, HCP should use Level IV PPE and use other elements of airborne precautions. All PPE must be used under applicable Occupational Safety and Health Act requirements and standards, including the Bloodborne Pathogens {Title 29 Code ofFederal Regulations (CFR) 1910.1030); Personal Protective Equipment, general requirements (29 CFR 1910.132); and Respiratory Protection (29 CPR 1910.134) standards and other requirements under this Act.
Other factors to consider in the use ofappropriate precautions are the availability of medical products, e.g., vaccines and therapeutic regimens and related adjunctive measures. In

addition, vaccination status ofHCP may need to be considered when determining those who have patient interactions.
Table 1. PPE Levels, Applicability or Mode of Transmission, and Example Infections and Conditions1
PPE Levels Applicability or Mode of Transmission
Example Infections and Conditions
Level I (Standard Precautions) Universal Precautions and Body Substance Isolation Applicable for all patient encounters.
Anthrax, tularemia, ricin and some contagious disease (e.g., common cold and seasonal influenza)
Level II (Contact Precautions) Contact Generalized and progressive vaccinia
Level III (Droplet Precautions) Droplet Viral hemorrhagic fevers and pneumonic plague
Level IV (Airborne Precautions)
Airborne
.
Novel influenza, SARS, pulmonary or laryngeal tuberculosis, smallpox, EVD due to suspected deliberate release with undetermined modes of transmission, EVD undergoing aerosolizing activities ( e.g., childbirth, dialysis, etc.)
Notes: 1. Examples of infections and conditions may require multiple types ofprecautions to account for multiple modes of transmission. The example infections and conditions are listed according to the highest Level ofPPE required as associated with the types ofprecautions recommended in the CDC/HICP AC guidelines.
Table 2. PPE Options
rrypes Of
PPE !Protected Body nazards Parts Protected
Level IV !Level III !Level II !Level I
!Against
~ontact Coverall Suits1 Body ' Blood/Body X
lFluids) ~ontact
Gowns Body Blood/Body X X X xz Fluids) Contact
Aprons Body Blood/Body X Fluids) Contact
Scrubs, Top Body Blood/Body X X X X Fluids) -
Contact Scrubs, Bottom Body Blood/Body X X X X
Fluids)
2

X
X
X
X
X
X
X
X
X
x2
x2
X X X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
x2
Sh 11:·
Bool Covers Foot
Notes: 1. Coverall suits are acceptable although not an ideal alternative to gowns and aprons. The ease of donning and doffing of gowns and aprons make them preferred options for body protection, considering the risk of cross-contamination is low when the donning and doffing of PPE is simple. In cases of viral hemorrhagic fevers (e.g., EVD) impermeable garments are required and gowns must extend to at least mid-calf; impermeable coveralls are required any time whole-body decontamination will be applied as part of doffing procedures. 2. Use of these items may be required even when using Standard Precautions depending on type of patient interaction and the anticipated exposure. 3. Examples of respirators that may meet the requirements for respiratory protection include the following: National Institute for Occupational Safety and Health-certified filtering facepiece
3

respirators with appropriate filter type ( e.g., N95) or half-mask elastomeric air purifying respirators (APRs), loose-fitting powered air purifying respirators (P APRs), full facepiece elastomeric APRs, and helmet/hood P APRs. All elastomeric APRs must use the appropriate filters, cartridges, or canisters for the hazards in the workplace. P APRs as a complete unit include cartridges or canisters, a charger, breathing tube, and batteries. Respirator use requires compliance with the Respiratory Protection standard to include medical evaluations and initial and annual fit testing for tight-fitting respirators as well as training and maintenance requirements. Respirator selection must account for the workplace hazards, assigned protection factors, and user factors. Examples of factors to consider in the healthcare setting include the need for sterile fields as it relates to exhalation valves and first receivers managing patients exposed to unknown substances. For more information on respirator selection and other PPE selection in the healthcare setting see the following references: https://www.osha.gov/Publications/0SHA3767.pdf, https://www.osha.gov/Publications/osha3249.pdf, and https://www .osha.gov/Publications/OSHA _pandemic _health.pdf 4. Glove selection should account for the material and thickness ofgloves in the context of the specific needs of the workplace. Double gloves must be used in cases ofviral hemorrhagic fevers (e.g., EVD); at a minimum, outer gloves should have extended cuffs.
4
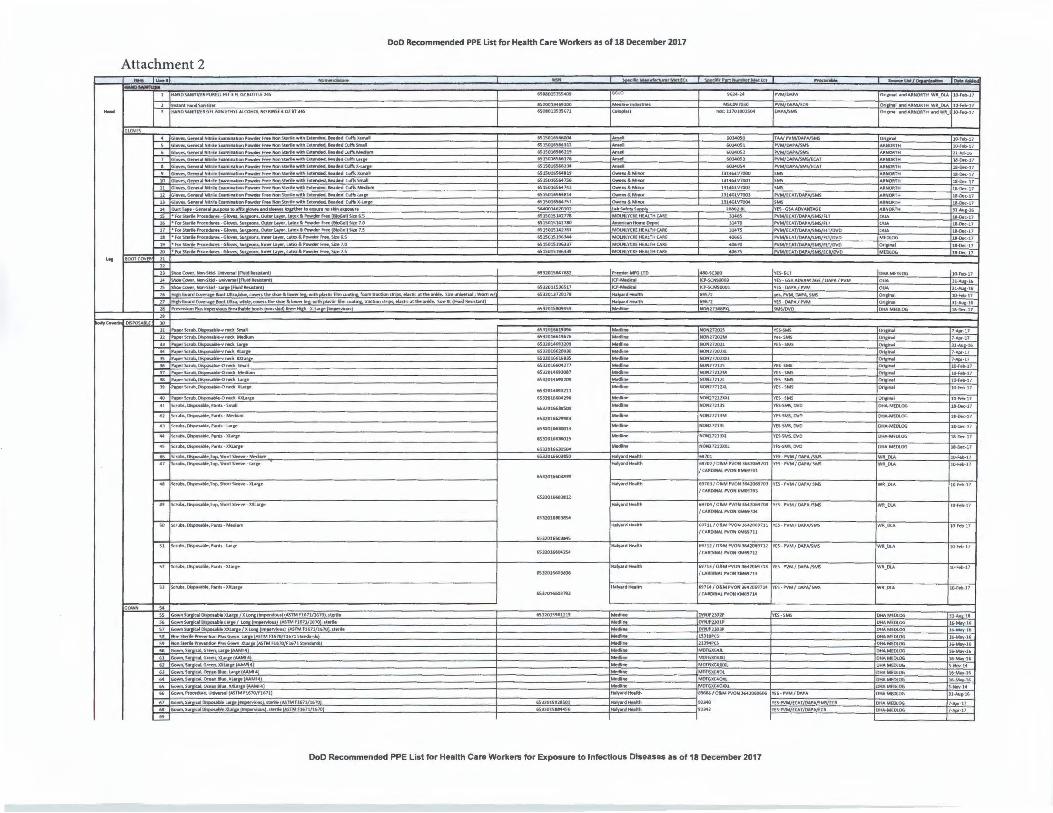
DoD Recommended PPE list for Health Care Workers as of 18 December 2017
Attachment 2 ...
--GLOVES
1 HAND~ITlllllPUAHLFSTJ~LOZIOTTL(l4S
HANOSAHITIZO.GU ~ £fH't'l ALCOHOL ,+Cl JIIMSE 4 OZ IT MS
11 Glciwt,GenerM Nitr.. EuminltionP-du F...eHonS~ilewithbtended, IQad Clll'h Mld11111
1l ~Genii'.! Nitrff EUl!linltian Powdff frM Mon StiN"ilit wittl httnded, a.-d Cliff\ ll-t.M"H
14 o...f1T--C..1"111'111 Mto•ffill1low1ilftdWftWStll) taffllulfel'ID~HIIO!illft
15 " forSCMlaProcecbe - Glows Sw rons,OU11tf 1..11~~6.l'owMFr• ~ Sli:.6.S 16 °fQrS.,.Proce...H -~SUrleDM.Oilfffl..,a'.LIIIIM·l'ow-kM 8loGrl Sitt7.0
19 " forS1trd,ProceMft·Glov.s.s« _,.llnrWfl.ll_.,lffl~ll'owdtrfr",Sire7.0
20 •f<JJSltfi'-Proce..H - Sit, ...a,.hWl..llftf,t..lb&'"-... frw Sln7.S
6SCa01J5lS671
,uso1,SMlu
l61S0l6S..11i
iS1S01,S66U4
,S1S01'5',1t7S7
~u,10101
'51S015141771 6Sl50151427IO
651501514271:1
651S01S1'6l37
65150151%3]9
-..... ...... .....
MOl.NlYCl£HEA1TH C.U.(
M191'1o:.nlimNI~
MOlNI.Y(I(( HEAi.TH CAIi[
MOl.YCQ HEALTH CAllf MOlNLYCl(( HCAI.THCAll[
MOI.HtYUEHf.AllHCAAE
nck: 11701DD2S04
6034051
JJt46l V7001
13146LV7002
U146LV700l
13J4GlV7004
2UOJ.M
""'31470
...,. """
--
.... ""'
""' VES -6!>AAOlf.-.HTA6E
fLT NM/lCAT/OAP,A/SMS/ff.T
l'VM/ECAT/OAr'/SMS/A.T/fNO
rvM [CAT OAP ECRIOVO
_ On inlll .....,,,
A.IINOJITH
,\~TH ....,.,, "IINOATH
OUA
OW\
MEDI.OG
OrilHlil
MEDI.OG
10-~17
tl-Oec-17
ll-CIK-17
1&-0..C-11
1&-DK-17
ll-DK-17
la.tllK-17 11-....•-1'
1&-0rec-11 11-DK-17
ll-DK-17
l.l-DK-17
ll-(»(-17 U,. IOOTCOVEII J1
2S Shm[O-,Nan-Skid- 1.Mp Rwd~ 26 Gu11rd"-t111•klDIUltni,.llllue,c-rtdwstlOelilowe'le1,watt,p11111icfitmco1tin&,fmmtrlll:Uon,tr.,.. Me'llic11tthellr'lkle. Slauniwfw,l ; WO,nw/
27 Hiffl61W"d(Cl¥ffllff8oolUllr11. ~.c-•tht~llawerlH.- withplMIK:Nffl lrlltbm1triM, .tnticatdw~. Siz•ll HutdllMtllnl)
21 Pfewndon'11alll'CIN'rioll11fulhalHbooblnon11QdlknffHilh · ll:-IMlh
"
,sno1s..1682
6Sl2011S1'S17
6Sl20U720171
6S320l5IO!MS9
PfMli« MRi lTO
icr-Mltdic.11 ··.......--1Cr-SCM50001
mn
NOfU7J41PJCl
Yl"S-ECT
YES-Gs.t.ADVAHTN.,E/DAf'A P'VM
Y[S - OArA / PVM
'!'e1,l'VM, DloVA.SMS
YlS - OUA/ NM
DHAM[llt.OG 1(1.-fm.17
.U-All-16
31-Aua-H,
10-Fft.17
ll-Au -1,
Jl -Scrub. ~.YnKkl#lh '5J2014MJJOI fMdllne N0Nl720U YES-SMS O..imnll Jl-All•-16 .M ,a_,.sc,uD, -Yl*k JU.lit• 6Sl20166200JO ,..,.. NON1720ZXL O..i in11 7-Aflr-17
JS r_,.Strllti,~-vnKkl(J(uJU 65U016'1w.JS ~ NON27202XJIL O..mNI 7-Apr-17
36 ,_,SU... -0 ,-ct SnwoM f6320l"OU77 Medline OntJAII 10-hlt-1)
J7 Scrub, -0,-• Mir4trn '5J2014MlOl7 JMdi!,e NOfill272t1M Yts-SMS Ot1DNI 10-f.M>.17
JI r1~Si:Tub.~nKk l«&• 6SllOMiHZDt ,_... NOM27112l YIS•SMS Olisinal JO-f8-17
it r11pnStr...~,-fi;J(lMe,c 6Sl20J.4MJltl MNlira N0Nl7212XI. YES•SMS Ori,;n.l l(H«.-17
r~Scrvti,DllfloUble-O!Wd llXlM&• 6U20JMD0M
41 Scnlbs,Oi~. ,11nb- SINII &Sll0166J05a>
xna.~-,.,., ·MNtum nno1"2HaJ
~.~,,.nb-Llfp
'icrutn., Oi~,Top,!ihortSlonw - lCLlr1e
SO sc,utK,D'f'0Hble, Pu11:s-Mit•u,,,
SI 5crubs, Dkpowble, P.Mlh - Lai-1•
" X1Mn:/11:1 ...... ,--......Kj{ASTMf1671/1670 ,sterilll'
56 Go1wnSur l•e/L rwMIS)IASTMH611/Ui70,,t«illl'
S7CiownSWP'-IIIDispo,,..ablR)OUMl• / K ~)lASTMfl671/1670L,terH '5,3 N!,n~"ff"-.1i,on'1u1C.-.. La,ru ASlMf1'70/H671S-.ndolrdt
St NonM«hr..ieventionP1u1Gown ll:lMie(A5lM H670/H671Slllndack
60 Go!wn,Sul'Rt.111,Grll,eft,lilr • AAMl4
61 GoWf\.SWtiul.64-eM,IUM 4
,2 6own.S..IICllf.6'-1,)(Xl.-p(~4
63 Gown,.Surmal.OtHnlli»,lMtt MM14
6' GOWf\S..,OQl,OteM ...., 11:1..-ff AAMl4
6S ~S111N..11.0te-,M1111,JUCLM• 4
66 Gown. '1ondule, I.Wwn.ll (ASTM n,70/f1671)
Gown,.SurlDUll!ltspol,Kll•lMH "ousLst«a ASTMf1'71/1'7'0
61 6-n,.S...R<al~lC1•f!''-).slll'f!l.tA\TMFl6JU1670
....!!...
'51201'6GU
'5J20166l00lt
ISJJ01ff038M
6Sl201660)7'2
6SJJOJ!i'MiU1'
---
----
Y(S - SMS
foK>frtl72JJS
NON27J:l3M YE5-SMS,OVD
VCs-sMS, OVD
,,,., 6'702/0&Ml'VONM~701 't'U • P'VM/ONA/SM§ / (AltDINAI. l'VON ICM69701
6970J/OIMP'VONJ6006'70J YU -PVM/ DNA/SM!i
J CAlt.DINAt.l'YONICMi!IJOJ
i'JJ04/01,Ml'\'0NJ6420'9704 YES - ,VM/ CWA/5M§
/ CAllOINAI. l'VDN KMW704
'97 11/0&MPIION.lfi.41(16'711 Yf5- NM/ ONA/SM5
/CA1tDINA1.NO.. ICMM711
H 7U/ OliMl'\'ONJ6420697U YlS-l"VM/Dit.l'A/SMS
/ CAltDINAI.. NON ll:MM712
ff7 U /OAMPVOHJ5420697 U vtS-l'VM / DloVA/5MS / CAllDIHAI.PVONICt.169713
M 7 M/06M,VON36420M114 Yl5 - PVM / CWA/S1.fl.
/ CAAOINAl !'VON ICMH714
OHA-M(OI.OG 11-0.C-17
DHA-MlOlOG
a -DK-17
DKA-M(OI.OG 11-DK-H
10-Fs-17
10-feo-17
Wll_OI.A
Wlt_OI.A
10-Feb---17
Wll_OlA
OY"Nlf'2302' YU·~ DHAMEOLOG 31·/l.u -16
CNNJf'lJOtr DHA MEDI.OG 16-Mll-,,•16
DVNJ'2J03' DUA M(Ol.00 u,-Mly-16 19310,CS DHAM(Ol()(j 16-Mly-1'
M01Gll:C4Jt DHAMEOlOG l6-Mlv·l6
Ml1TGll:C4JXl OHAMtOlOG 16-Mllv-16
MDfGIIC4JIOCl OHAMEDLOG S-frb,-14
MOTGll:C40l OHA MUllOG 16-Mrt·l6 M01GICC4011:l OMA MEOLOG 15-Mav-16
MOTGll:C40IOCL DHA M(llt.OG S-Noll-14
M606/0liMl'VON36410M606 n S-,vM/ 0,,,A DHAMEtllOG Jl·"-&·1~
l::YE;;-, .::::..,:::..,,:fCA::,T:,IW=.,,-=......=::a<:----+O:::HAc,Mc;f,c1',c06,-----f,,--...,.:...Jc-7 ~ "''" '12)41
DoD Recommended PPE List for Health Care Workers for Exposure to Infectious Diseases as of 18 December 2017
--DoD Recommended PPE List for Health Care Workers as of 18 December 2017
_!!,,of
70 \Gowft.Pfoudw,p, )Ol~,..~ _~1610/fl671_
1l fSIHWd·an·l-,.:hemThefffiDjii.o(IKticWfft1s49klt'IIWS&.Cnedi.w•S:11iH, T.-,d!ie_Or_,.{~)
7J fY--Apon-t,,dltmTtlennoPJv°ti.t.ticWd1,lsU'°'!ISl»pt.CAKk,w..sttiel, T ...S-.6n,y\i,np.fViouJ)
74 ~~--'----~-;;;i;blnti~rnHhk-1hMffllfMl.tofflilkalfj~)
7a JT'l'Chem0C~Apon,D.s~-Neck,,..,wan.~ lound§e_Y._
~_!ALL!__l ~
IO lutr•P1oe.ct1onc-.i1. 'Mllta. O.nKWllst&ndCuft,S'4)(l...-S~· (Ruld~)
a1 (rpn•~dwJ__~~Wf~s_9,anlftl____!!~SUm.wtwtit(flllldk-1¥1t ,2 trwn•cowH~~ C...., f1Mtkwmb0.111t~S.,.... s-m1 v.twtcfnwid11au1«o1
1-pet•-C-•l w/CollarEluticWrn11~k~~,,edSNmi AntiSlicl~.ntlllots WWlitlAuid~tl
M _JChemMul, c.-.itwithC,:,llir and..Qe!_nWri1h/ANdn 8ollndSeawn1, ~
as dwmMut.eo....r.!lwithCollM'...!~WrisliJJin/Jid,nkundS.-..,_._ I 15 a-nMu.l.~allwithCollilrMld~Writb/AnklesltlwwS..m1, lMtt
u Cha'IMl• l ,C-•llwilhccii&.,ilnd n Wr~h/AM!eslo&,ndS.-.ltlM, lm1 U ~LC-.alwi1hCollw..td[l•lil.'M'Db/'1tffJelllounds.M1S.)fflMI-..,-
11'9 o.mMu:1, Corftf*'! with coli.r Mid Eltitic Wrlsb/Ar*1~ IDl,nd SN11'ti, -clum !IO ClwfflMHl,C-.ilwilhColw.ndEl.-bo:WTitb/Artift loundSefflll, lM
•1 ~1,eo;;;-.i1witheoll&r~lk.WJtlD/AN!lft IDwndS.-.Xllr
!tl Owt,,Mu1,C-allwi1hCollArifld WrilbJAinklet,St,aledSe.111K,Smllllm1
Ci-.M.ul,C-.ilwithC.... ilnd()ptfl'Wmh/NWIM'!fSNld Sew, Mtdiuni !""Pf!IW) ~LCowflll'Mtt! Cdw-,o,,.nWtisbf.WO.S~ kiltm.UI'
!tS !ChemMaalJ...C-~wi1h(olll,1ilnd(pnWthbJ~SNled SNIMSiJHltl•p,. • Nect..l ,,.,.11.Hooct .,
-
'NI On:poytffHood,Jl1nc:hn IDWll.!tu:e,wtoitR,~1N.~i.i,tla.c,cdolureli:>loe_.-,,--;;;;;,~Whi.(Auidi.w~tn
99 ICLEEJ&iUAADMOUl11tA.llk»dbor1WPllthopn&C~~,rotecttunHDodt (~ASTMF1670/IU1J
100 1,Al'lt HoodlM IE-10(11Serlft) Hood (Fluid llflistllnt)
·-- ..._.H420-l0,_!~Mlhinner~.T,.-.ot,,._ 1>1ewlft!Mtl ,nounbdpowerect11iii purif'/W'CrftfNl"1l0tlor su1
lOl _~lf-lOIIII~~
~(~~~
~/ ,-..dAit• 106
107 lrNlheEaiy(ll:8()1'-edM l'W~ l'lftf-111Df (PA'1\)~m IIIIE-HMlO•ith NiMH ltttery(JledwrfNblt!
108 l1ruit,;Cl/iy (ll!ll) ,-;,s-Ai, l'w~ 11tsp1r11iDf (l'APRISyi,lem IIIHlO'#ith LlttNri lttt~ (NDn IIKhllr••~I
1()9 l lrulheEt:1y~~Hood,Anfll--57Nl0Splem,NiMHlllttffyj~Nbw:
lrN..f.¥y~!!_btierHood ,Al'II ffl-S7ll0 System, UINwll Alttny (Non Aechllr1HDle
NtS,•tKullllt,11,>.r.ul1r MI/K,N9S,1111icvMW,llel\,lltt
~~~1iculate,lle1UW
11S j Mllll,.N!tS,•IKulilll',Sntll
::: 1:::::::::.::~~ 111_JMM._N!tS-;-hrtir.ulffl,C-~
11,J Mnk.N95Plr1icvlite±C-. SIMN llO}Mffl.P•lkMWte,Hts 'Mth~Rq.,., Meilllffl
Mnl!,, ,,,,1.:\NW, N'5 with~Rqt, IMI"'
.H!JMAk,. '•~INl:t, _~ ~ .-~,ro~Now llrte41<1
m fMBl!.N!tS
"' SUIIGICAi""wl"'iis
_rm_
12' )MHl.Surtk~.Mti·IIJ&,,-at.,C,Di'fMl'lble
121·1~wr,1ul,nan-•tKile,nor1-1•011,in,fabrlcQ!Pptd1dju,.talMl'ID~plece
128 i t'ul ~ftS.-&Q! Mask
I JO (k<tSIM!dspri,~111
......... • kll ~-- Shield w/lLKtic -.cl
Fl I "',- -...·~--a,.,,•""'1----4---~. .,., .."'--l. MtdllrR·~Anth,,,,aLUrloopaw
EVEPIIOTECT 134
Olliffl,,..,_PV<onCNW~ofColllnwilh~J-1-tt!fuwnd,_
-ri!iJ201SK1700
1"'-11\eSKtlnl
4__!40014961951
651S014"4l.,.
6!15016:li.Sll
&SJ2014 lHS71
6S1S01Sl60l1S
~
4l40CJt4,60!lll
iSlSOl0,1201
~
651501153S•a
651soo,ano1n
6SlS0ll61S228 (iS1SOU 746757
6S150ll!kle744
, s J20t649SM7
MM._!!:f.turerMnK, llcP_!!!NllffiOlr ~Ea ._..... Hllprd .......h
,,...,,
,,...,,
-~ .!!!fee!,,...,,-Hll','ardHNlth
-....... ,t,.bland
~...... ~
i..i.1an,:1
~ ~ ~....... ~ ~ ;;;;; .........
.....,.dlifflth
... ANS[U
-;;;ii
••><00<
'"'"""...... HAt.YARDHfATLH
~
1'11:f<Cl"l"MEDK.Al
"'"""'
MOlNl,.TCICE
h•aff·-..d~h
jVI.ASHSHIHO 1SYl!.QNOFNTAI.
MEDUME
"""'"'
T'178TGYll0000400
Sll718Wl«IOOOllOD
!Sl271TWH
~l788Vl
ICX:lMYL
Y(S-GSAA.OIIANTAG(
YES•P'VM/DA1'4/SM~Clt
1CX>n / O&Ml'VON3'42010015 (YES - PVM / CWA / CAAOIHAL l'VON ICM1008S
lY12SSWH
ITYlUSWHaptionNS
,074128-5
:074128-M
~ 074Ul-n
5S4t7-S ™11-M ~ SS411-JU
~ 10100-M
~ 70100-~
Ives - [CAT 1 6S.AAINNfTAGE
YCS - 6!.AAINAHTAG[
YU • fCAT /GSAAINAKIA.GE
YES - 6SAACNAHTMi(
V(S ·GS,O,lN'IJfU,G[
lvo - GS.AAINAHTM>E
YES • GS.AACNAHTA.li(
VES•GSAADVANTM>l
YES· GSA Wv'AHTMiE
!ns -GSAAINNITAGF
YES~SAAOV~lM>(
DHAMEDl06
Oncillill
Ori~
ARMOII.THlOUA
OHAMEDlOG
~ ~
l>HAMEOlOG
AfMOA
i= 4FMOA ~ i= i= IAF~
i= ~
TY'57SWtwl+sile 4534] (pstMtn,)
4SJ45(~MMCJ
1:::.,~===vt~fct.n, Y[S· 1::: 100101N17ll3
~
11:lf.NMlO
-'l.!!60 [ h~7_2295
'-'"" lll410
l]Mll lS10MtS
~ltN9S
1SUN9S
1Sl7
'46121
~z
16~AINAl'fTMiE
Y£~SA AOJAHT~!
YES - GSAACNNffAGE
lns - 651.AINUffM>E
[~5 - GSAACWANTAGE
YES_• PVM / (CAT / OAPA. ( SM5/ ~CII
~... YES ·~M / ~ °"-P~~/ ~ 11
V£S- l'VM / £CA1 ( °"'A./5W1S/[CR 1V[S • (CAf/ SMS
VlS• [ CAT
YES -~MS
lns-SMS _'!!S • l'VM / OAPA.
YES - PYM/ f CAf /DAPAJSMS/ECft
YlS - 0,.PA
ARl'K>ltf Hlll'ldWfl_ OU.
DHAMfDl06
DHAMEOl~
~
10.i,-.a!M>dAIIN<HITM
Ori&inal ilndAAHOfl.TH
DHAM[OlOG
~IWMIARNDIIIH
Ori1iNI ilnd AIINOftTH
Ori&IMI .r"1AIINOATH
Or1pultndAIIN()fl.Tlt
~ Or_lpnal
~TS
"""' oum
"""' ~ Ori~
15112
""H0NH]79A
' lM ,.rtINmotft •e ml tt<.-<ll:'f In~for --io,~ NOH173'lA,thisMoM l'ES - "YM
1/ECAT / DA,A/ SMS
NOH17J71A
)Mp.rtnumtiers«tnDIIICCUflle,TM in MMC ltirthisNSN JM . l'VM / [CAT / OAPA / U..S
D'l'JWlfK 11800<-Nl 4235
YES · lw._ou.
NON27la1
""' "''.!14 On.1.lnal
4SOS 1YES•,VM / EUT/ i».,A / SMS [CII f Otlain!il andAftfilOflfH
NOHfSJOO YES- ,VM / ECAT / D4'AL5MS ""'"""-OG
""""""' YES·SMS
l'-MIV·!i
lO-fel>-11
10.fd>-17
10-~17
&..Nolf. 1'f
~ ~
ll·Ali&· l li
»Ott-14 l0-0!:M4 JH)U-14
U ·Au1-lli
]1-AuJ·lli
l l-Auc-1'
ll·Au,-1,
Jl·Ar.lJ· l6 ·u-.-u1 -1, 11-1,u1:_1,
~ l1·AuJ·1'
lH,111·1' Jl·A<il&· U•
31:All&:!6
111...;,-1,
ll· A<.1&·16
ll-A111·1'
11........• lf;
lt-A111·1'
ll-M.1-1'
11-Aua-1'
ll·Au&·U,
ll-Auf'. l ' 31-All,· 16
U ·All&· lli
ll-A.111-1,
.n-~16 3l·Au1·1'
n--Aua·te
~ Jt·Au1· t•
l1-Allt·16
]l-A<.11·16
Jl~·!'
,lt-Ar.11-16
ll-Au,-1,
31-Aul:!,e ll.........·16
DoD Recommended PPE List for Health Care Workers for Exposure to Infectious Diseases as of 18 December 2017
Related Documents











