H 2 WHOA - 6 to 8 glasses of water an hour How water can distinguish physiological from pathological uptake in the GIT on PET/CT scans Melanie Crowthe

H2 WHOA
Jun 14, 2015
The use of water as a negative contrast agent in PET/CT to help distinguish physiological from pathological FDG uptake
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

H2WHOA - 6 to 8 glasses of water an hour
How water can distinguish physiological from pathological uptake in the GIT on
PET/CT scans
Melanie Crowther
Overview• Pathological vs Physiological FDG uptake on PET• Gastric uptake of FDG• Gastric distention to evaluate pathology vs
physiology• Unexpected findings in the bowel during PET/CT• 6-8 glasses of water an hour - moving things along
in the small bowel• Delaying tactics - the usefulness of a repeat study
to evaluate focal colon uptake of FDG

Pathological vs Physiological FDG uptake on PET
• Pathological - gastro-oesophageal junction and cardia, fundus, proximal body of stomach
• Physiological - colon (patient is a Type II diabetic on Metformin - Metformin significantly increases FDG uptake in the colon, and to a lesser extent in small intestine8)
• Physiological - bladder
• Physiological - laryngeal activity

?Gastric uptake of FDG• Physiological
misregistration• Initial image -
accentuated FDG activity at distal stomach/proximal duodenum
• Misregistered due to an extremely large breath hold
• Delayed image - no significant uptake in stomach/duodenum/liver

Gastric uptake of FDG• FDG gastric uptake can be
unrelated to malignant findings;
• Inflammatory disease• Physiological emptying
(peristalsis)• Visceral thickening• Gastric wall contraction
can increase FDG uptake, especially for a remnant stomach, increasing the percentage of false-positive results10
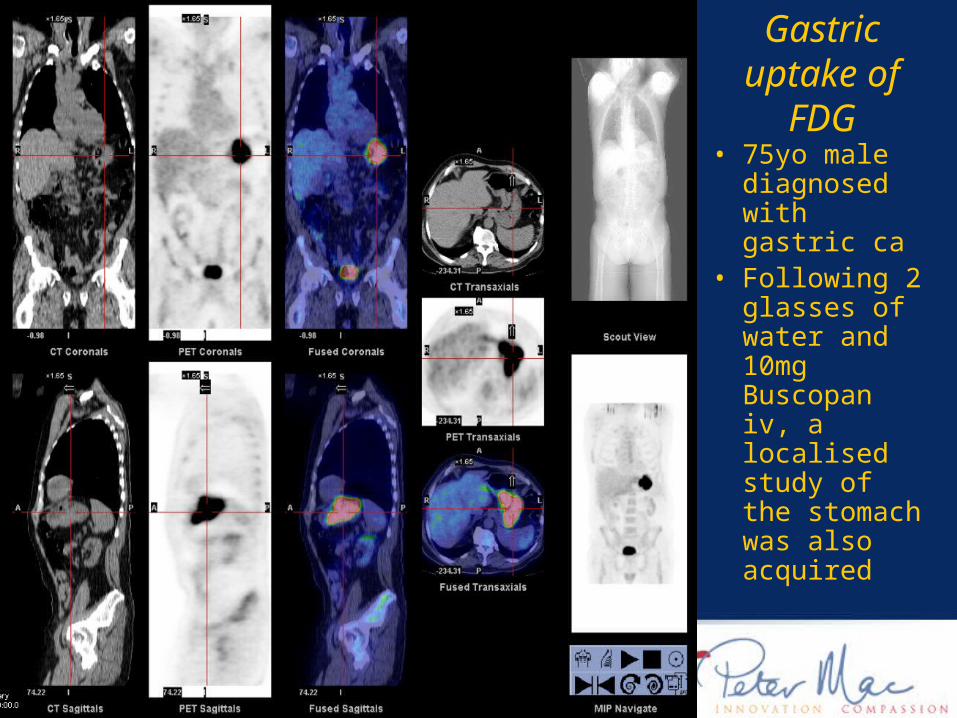
• 75yo male diagnosed with gastric ca
• Following 2 glasses of water and 10mg Buscopan iv, a localised study of the stomach was also acquired
Gastric uptake of FDG
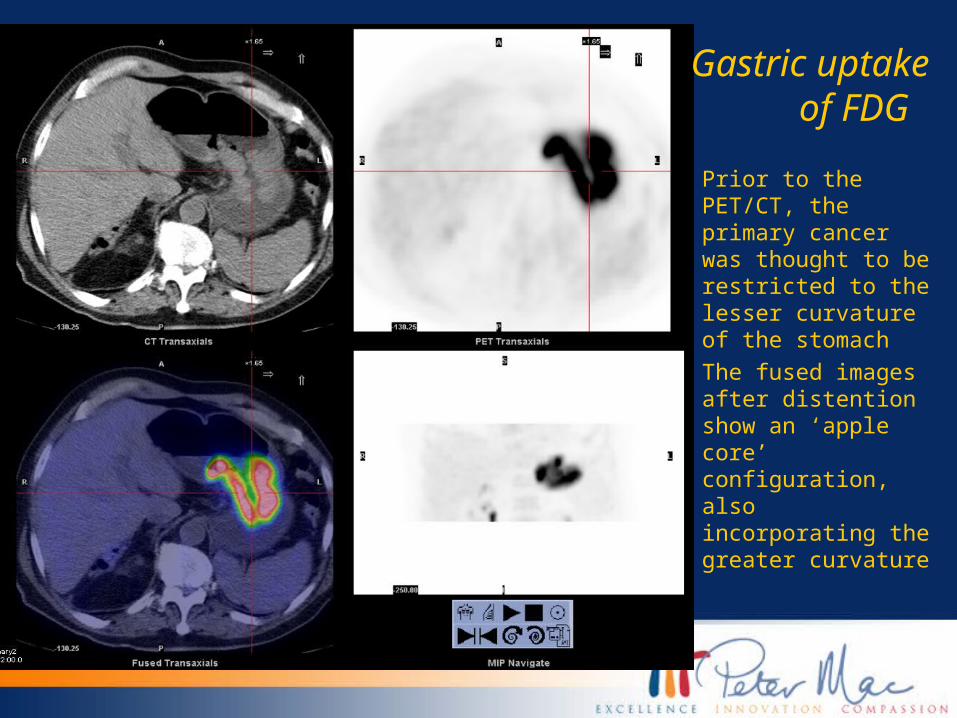
• Prior to the PET/CT, the primary cancer was thought to be restricted to the lesser curvature of the stomach
• The fused images after distention show an ‘apple core’ configuration, also incorporating the greater curvature
Gastric uptake of FDG
Gastric uptake of FDG
• Originally, our department policy for patients with primary gastric ca was to perform a WB PET/CT scan first, and if necessary, acquire a static of the stomach following administration of 10mg Buscopan iv
• Buscopan is an anti-spasmodic, the effects of which are most pronounced on the smooth muscle of the GIT wall. Since FDG uptake would reflect glucose utilisation in peristalsis, an anti-peristaltic agent should reduce extraneous FDG uptake7
• The radiologist-trained Nuclear Medicine specialists began prescribing 2 glasses of water and iv Buscopan on these type of referrals
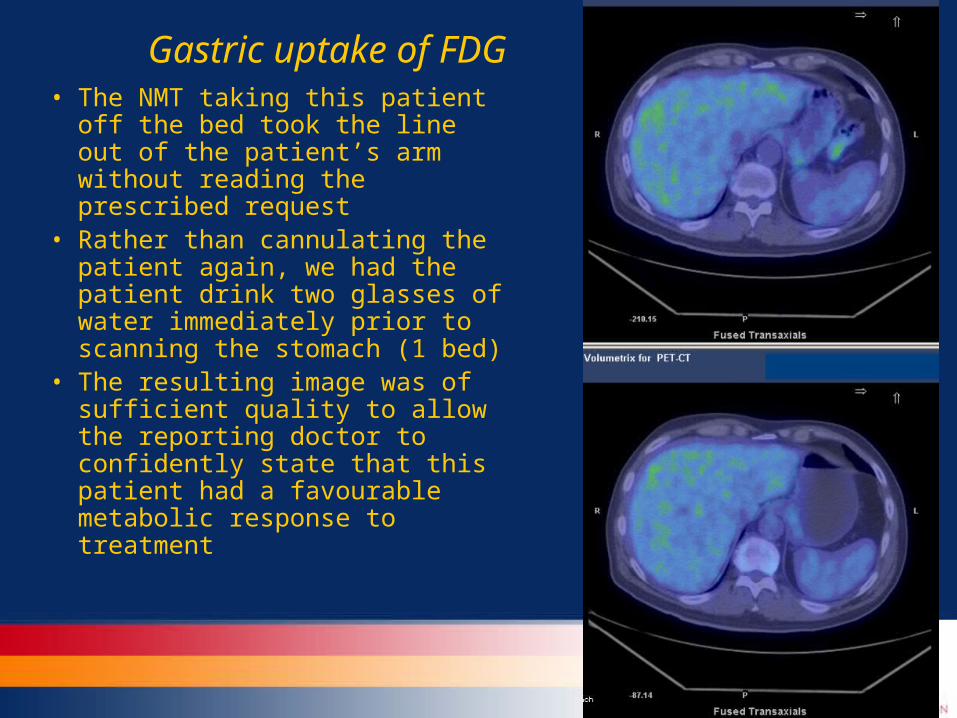
Gastric uptake of FDG• The NMT taking this patient off
the bed took the line out of the patient’s arm without reading the prescribed request
• Rather than cannulating the patient again, we had the patient drink two glasses of water immediately prior to scanning the stomach (1 bed)
• The resulting image was of sufficient quality to allow the reporting doctor to confidently state that this patient had a favourable metabolic response to treatment

Gastric distention to evaluate pathology vs physiology • FDG PET under
fasting conditions can be limited in the evaluation of gastric malignancies because of the high level of physiologic uptake in the contracted stomach32,30
• Water, contrast, milk and food have all been suggested aids to distend the stomach10,30,32-33

Gastric distention to evaluate pathology vs physiology
• The radiologists continued to prescribe the requests of patients with primary gastric ca, or other cancers with gastric involvement, with the addendum ‘possible stomach static - 2-3 glasses water to be given orally on bed’
• By October last year, we were routinely giving 3-4 glasses water on the bed before we began any scanning for these same patients
• Imperiale - focal FDG uptake mimicking malignant gastric localisation & Chamroonrat - malignant lesions mimicking gastric uptake on FDG PET5,10

Same patient we saw earlier with the apple core lesion.6 months later and post chemo-radiation

Materials and Methods-stomach
• A retrospective review of the >5000 PET/CT reports from 1 April 2008-20 April 2009 at PMCC was performed, searching for the words ‘delayed’, ‘static’ and ‘water’
• 20 patients, 23 stomach statics (11 pre/post H2O, 12 H2O before WB scanning)
• Between 2-4 glasses of water were administered immediately before acquisition (1 elderly pt could only manage 1 glass)

Materials and Methods
PET/CT Scan Acquisition - • Patients were fasted for at least 6 hours• All patients had blood glucose levels below 10.0 mmol/L• Injection of approximately 4.2MBq/kg (Discovery/Stellar),
approximately 3.17MBq/kg (Biograph) of 18F-FDG• ~60 minute uptake period• GE Discovery PET/CT (4 slice) 2D, 5mins/bed, GE Stellar
PET/CT (8 slice) 2D 5mins/bed, 3D 2-31/2mins/bed, Siemens Biograph PET/CT (64 slice) 3D 3mins/bed
• Images processed on GE Xeleris or Siemens True D workstation
Materials and Methods
Interpretation and analysis of images -• Studies were analysed by a Radiologist/Nuclear Medicine
Specialist and a Nuclear Medicine Physician independently
• Both reporters were given the patient’s clinical notes supplied on the referrals
• Visual analysis only was applied - 3 questions were asked1. Was water useful as a negative contrast agent?2. Did an appropriate amount and timing of water
administration assist in evaluating a specific region?3. Did a large ‘bolus’ of water allow distinction between
physiological and pathological FDG uptake in the GIT?
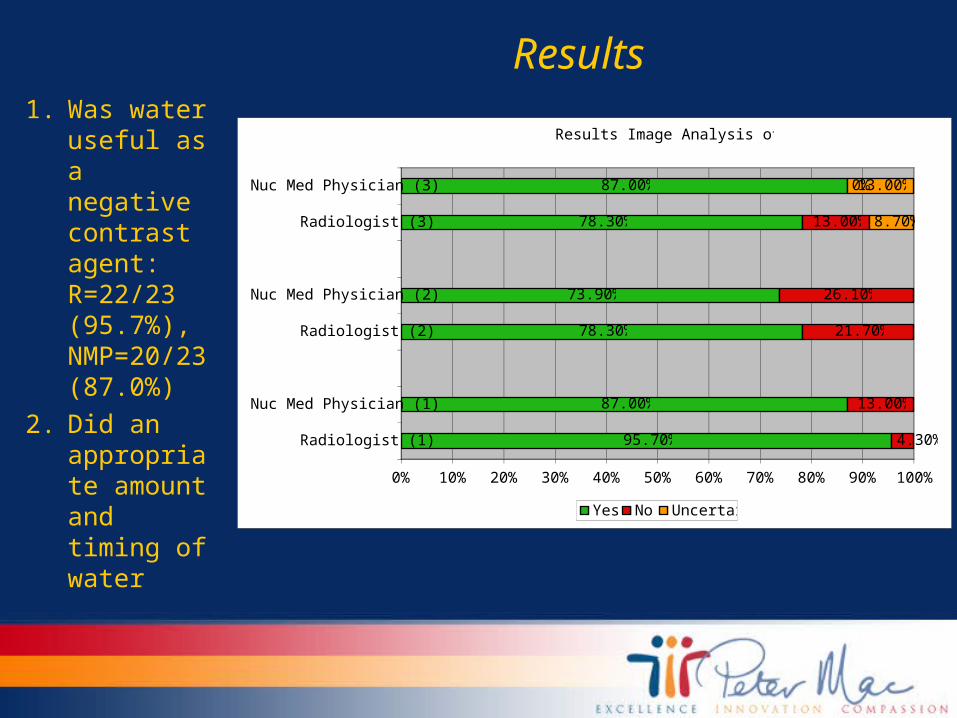
Results1. Was water
useful as a negative contrast agent: R=22/23 (95.7%), NMP=20/23 (87.0%)
2. Did an appropriate amount and timing of water
Results Image Analysis of Stomach
95.70%
87.00%
78.30%
73.90%
78.30%
87.00%
4.30%
13.00%
21.70%
26.10%
13.00%
0%
8.70%
13.00%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Radiologist (1)
Nuc Med Physician (1)
Radiologist (2)
Nuc Med Physician (2)
Radiologist (3)
Nuc Med Physician (3)
Yes No Uncertain
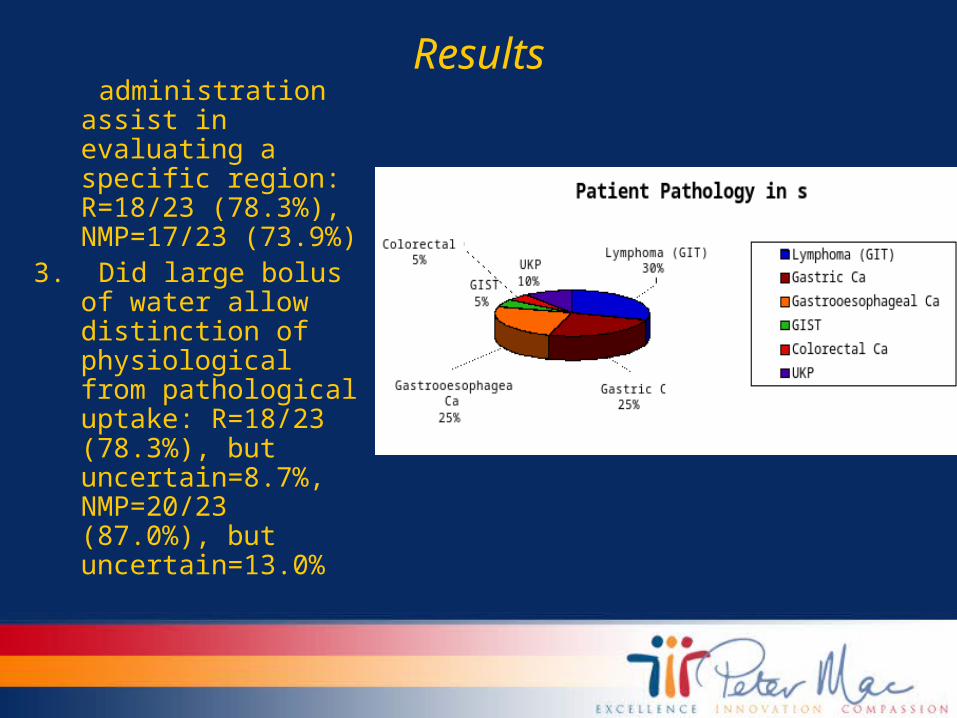
Results administration assist in
evaluating a specific region: R=18/23 (78.3%), NMP=17/23 (73.9%)
3. Did large bolus of water allow distinction of physiological from pathological uptake: R=18/23 (78.3%), but uncertain=8.7%, NMP=20/23 (87.0%), but uncertain=13.0%
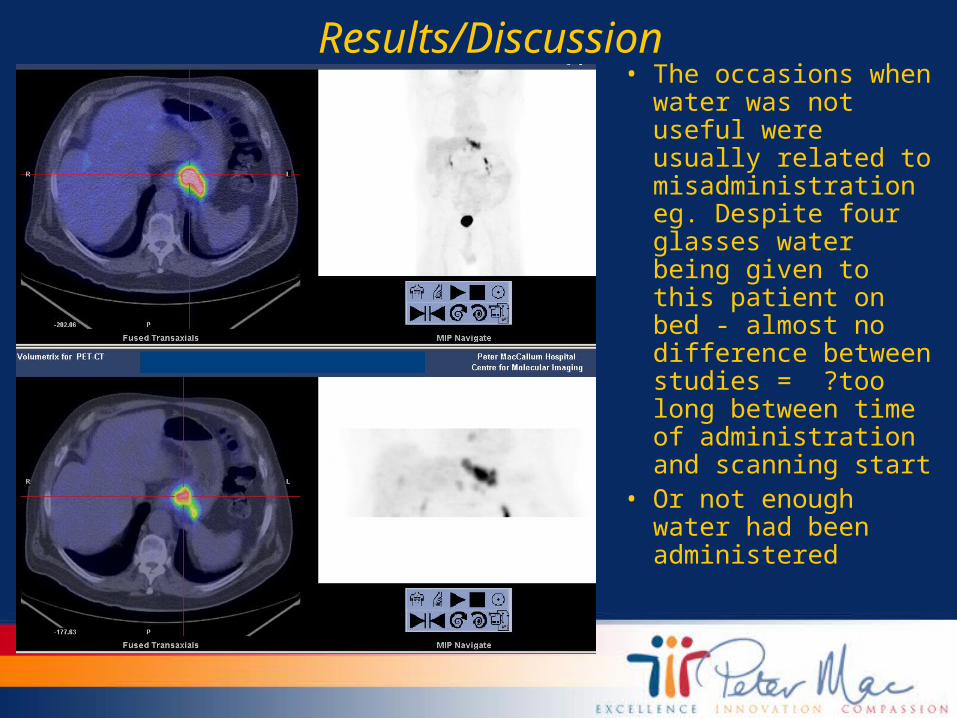
Results/Discussion• The occasions when
water was not useful were usually related to misadministration eg. Despite four glasses water being given to this patient on bed - almost no difference between studies = ?too long between time of administration and scanning start
• Or not enough water had been administered
Methods and Materials-small & large bowel
• A retrospective review of the >5000 PET/CT at PMCC reports from 1 April 2008-20 April 2009 was performed, searching for the words ‘delayed’, ‘static’ and ‘water’
• 9 patients were further evaluated with a delayed static (46-114 minutes after first PET scan)
• Between 6-8 glasses of water were administered after the first scan before a delayed static over the region of interest was acquired (1-2 beds)
Results
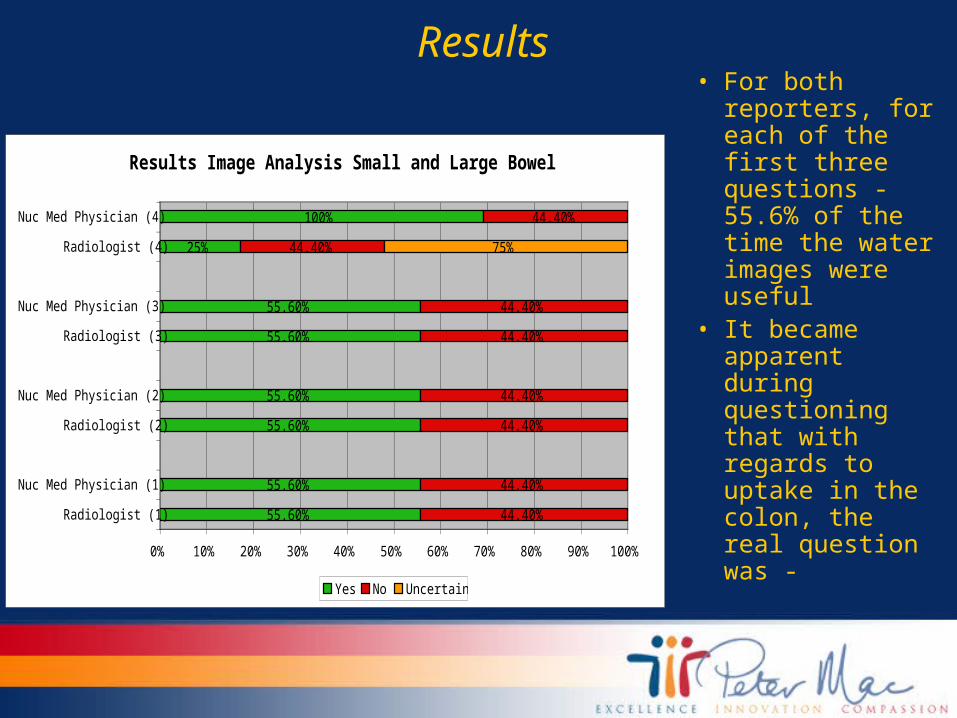
Results Image Analysis Small and Large Bowel
55.60%
55.60%
55.60%
55.60%
55.60%
55.60%
25%
100%
44.40%
44.40%
44.40%
44.40%
44.40%
44.40%
44.40%
44.40%
75%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Radiologist (1)
Nuc Med Physician (1)
Radiologist (2)
Nuc Med Physician (2)
Radiologist (3)
Nuc Med Physician (3)
Radiologist (4)
Nuc Med Physician (4)
Yes No Uncertain
• For both reporters, for each of the first three questions - 55.6% of the time the water images were useful
• It became apparent during questioning that with regards to uptake in the colon, the real question was -

Results• Did a delayed study allow the doctors to distinguish
between physiological and pathological uptake in the colon?
• The Nuclear Medicine Physician agreed that this technique was useful every time
• The Radiologist was uncertain, although this had more to do with all of the patients we found demonstrating FDG avidity in the colon on both early and delayed imaging, rather than having any examples of FDG avid colonic uptake disappearing over time
• Both doctors agreed unanimously that water was extremely useful in distinguishing physiological from pathological uptake in the small bowel
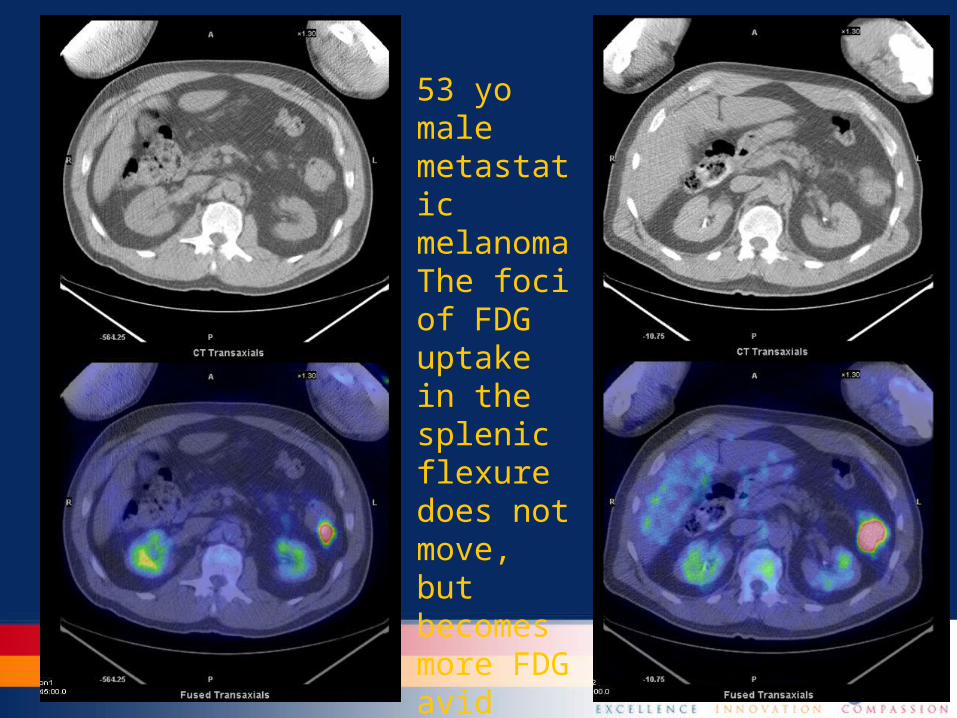
53 yo male metastatic melanoma The foci of FDG uptake in the splenic flexure does not move, but becomes more FDG avid

• In PET scanning, uptake in the gastrointestinal tract (GIT) is variable. Normal stomach, small intestine and colon may demonstrate increased FDG uptake due to a combination of factors.
• Physiologic tracer activity has been attributed to uptake by smooth muscles (mainly in the bowel), swallowed secretions, constipation, contraction and intraluminal concentration or metabolically active mucosa7,8,10,24,28

60yo female diagnosed with NHLThe tubular area of increased radiotracer activity in the right iliac fossa can only be determined as appearing in the small bowel on the fused CT images (sp. sagittal & axial views

6-8 glasses of water an hour
• Hybrid PET/CT cameras allow coregistration of simultaneously acquired PET and CT scans, which is particularly helpful in the abdomen and pelvis. PET/CT provides significantly improved localisation of abnormal or unexpected FDG findings compared with PET or CT alone
• Although PET/CT can help localise a focus of FDG uptake, physiological uptake in the GIT cannot be excluded with certainty. In this regard, PET/CT is not helpful in differentiating focal physiological bowel uptake from large or small bowel malignancies. This limit of sensitivity, in part, can be attributed to a lack of bowel distention
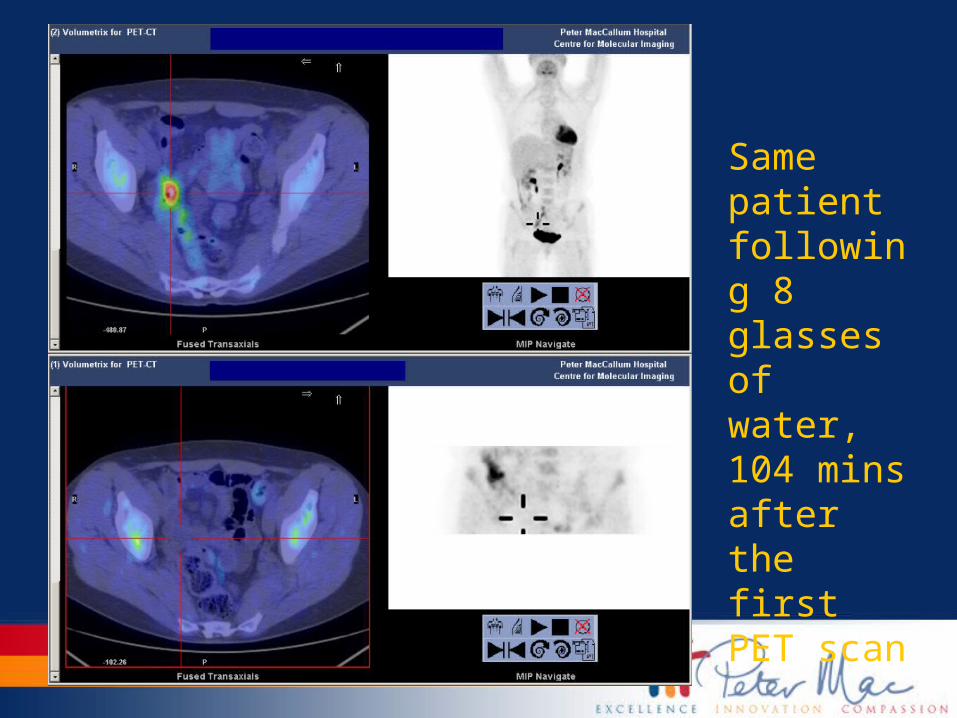
Same patient following 8 glasses of water, 104 mins after the first PET scan

• In the evaluation of bowel disease on PET/CT, orally administered contrast material is helpful for bowel distention.
• However, the use of high-density barium-based contrast agents can cause overestimation of PET activity
• High-density barium-based oral contrast material will attenuate more CT x-rays, with energies of 70-140 keV, than 511 keV photons
• This can lead to an overestimation in PET activity of up to 20% in regions where barium-based oral contrast material is present, and more pronounced overestimation may occur with both a) delayed passage of oral contrast material, and b) rapid transit of oral contrast medium, with areas previously demonstrating high attenuation now being clear
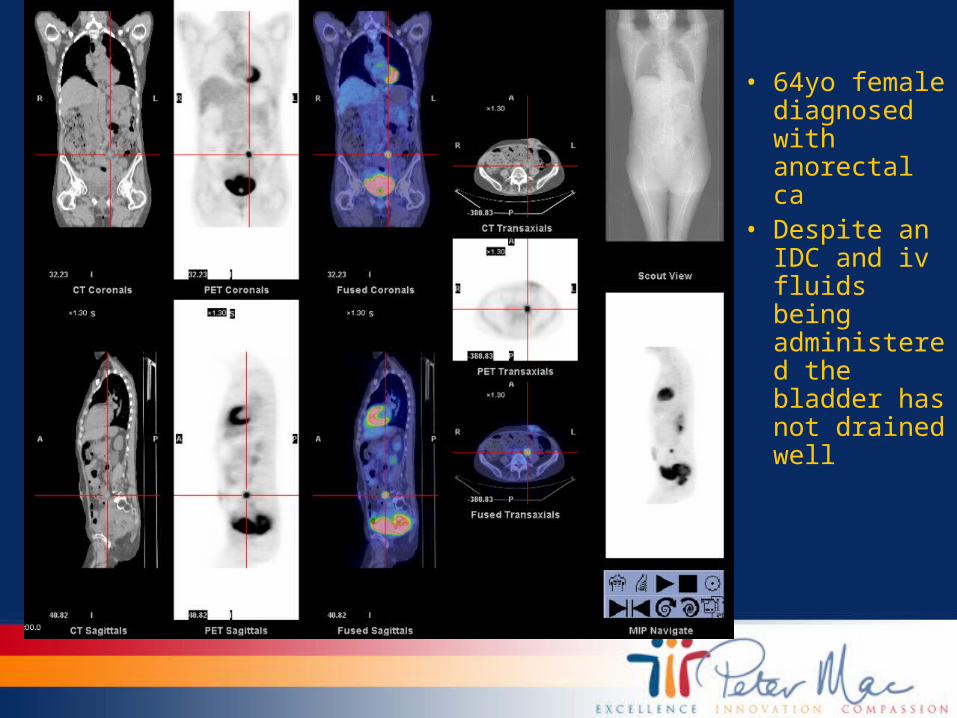
• 64yo female diagnosed with anorectal ca
• Despite an IDC and iv fluids being administered the bladder has not drained well
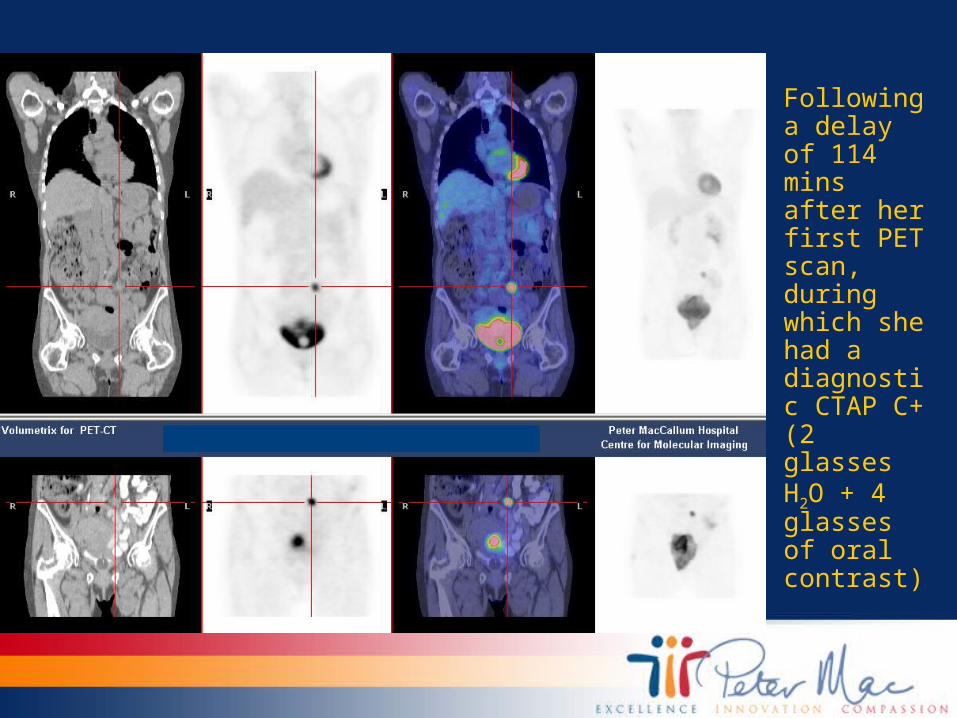
• Following a delay of 114 mins after her first PET scan, during which she had a diagnostic CTAP C+ (2 glasses H2O + 4 glasses of oral contrast)
• Oral contrast can cause focal or diffuse increased FDG uptake, which may be induced not only from the high CT density of oral contrast but also by an accelerated physiological reaction of the large bowel23
• Negative oral contrast material causes bowel distention without increasing CT attenuation, avoiding the potential issues with attenuation artifact that can be seen with high-density barium-based oral contrast material
• With increased bowel distention, disease affecting the bowel wall can be better assessed
6-8 glasses of water an hour
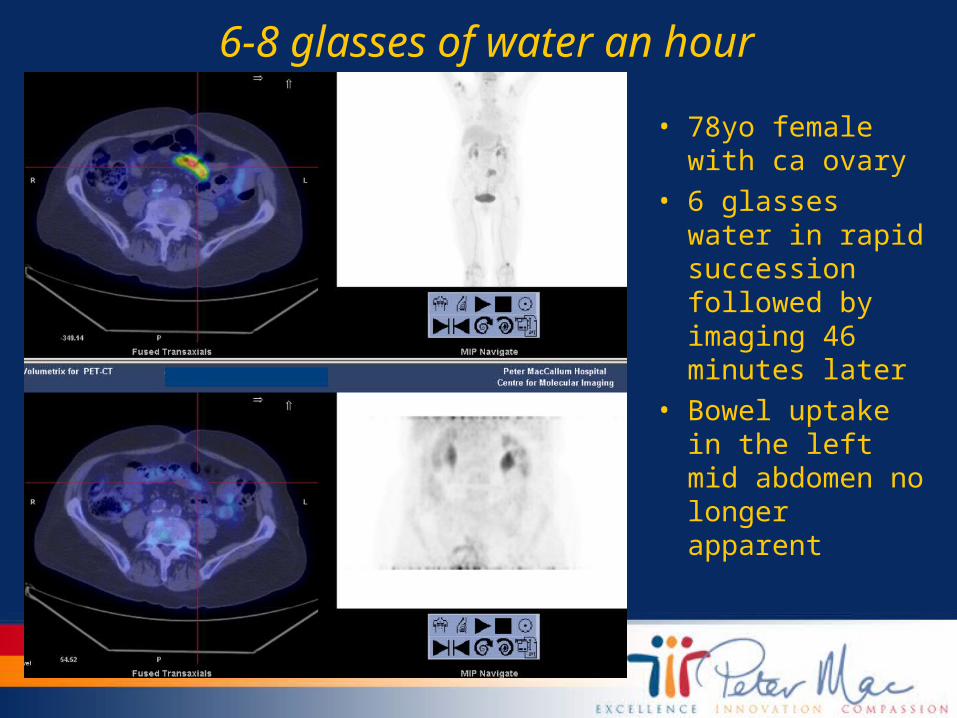
• 78yo female with ca ovary
• 6 glasses water in rapid succession followed by imaging 46 minutes later
• Bowel uptake in the left mid abdomen no longer apparent

• Side effects of using mannitol-based negative oral contrast include watery diarrhoea
• A recent study compared a combined mannitol and locust bean gum-based contrast agent with mannitol and water alone
• The same study argues that the patients who received the mannitol and locust bean gum-based contrast agent did not experience the brisk diuresis that can follow the ingestion of large amounts of water
• Diuresis in PET = good!

• A number of large studies have looked at the detection of clinically unexpected, ie abnormal unexpected hypermetabolism, in a location that did not conform to a usual distribution of metastases given the primary tumour for which the PET scan was requested1,9,11-12,19-
20,27,34
• These studies used further imaging to follow up the abnormalities found and on average ~75% of these abnormalities had subsequent tissue confirmation
• The literature suggests that of histopathologically confirmed abnormalities, in 60-75% of the time these are either malignant or pre-malignant
Delaying tactics - evaluating focal colon uptake of FDG
• In all of these published studies, the GIT vies with the thyroid as claiming the greatest percentage of unexpected abnormalities found on FDG PET
• Several studies (Lee, Tatlidil, Yasuda, Zhuang) have focussed on PET imaging identifying unexpected foci of FDG hypermetabolism in the colon alone
Delaying tactics - evaluating focal colon uptake of FDG
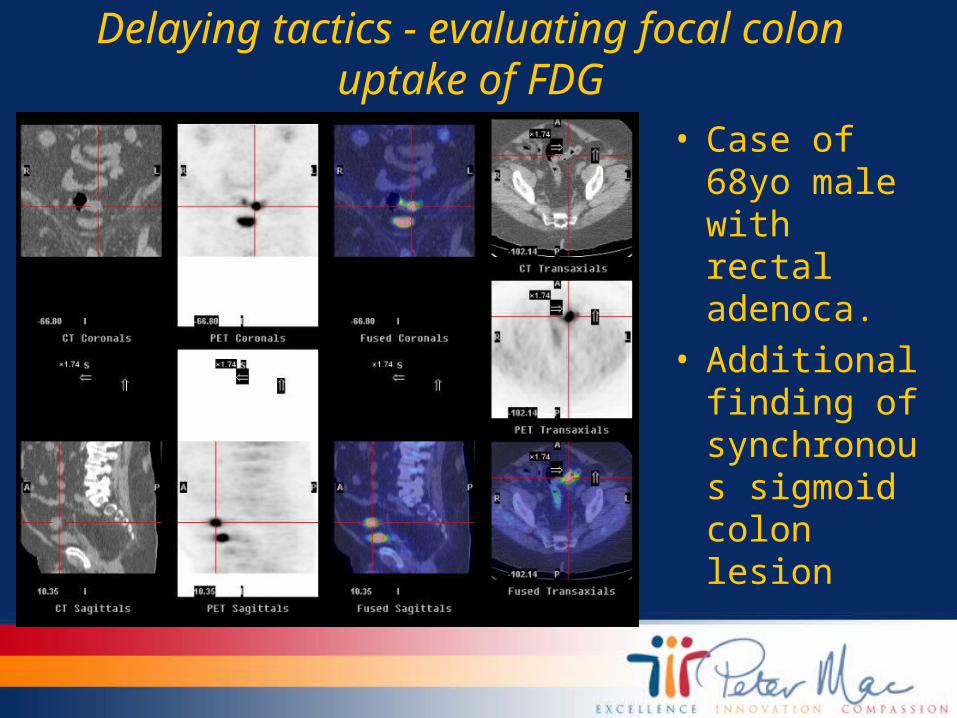
• Case of 68yo male with rectal adenoca.
• Additional finding of synchronous sigmoid colon lesion

Conclusions• Water as a
negative contrast agent in the stomach, gastro-oesophageal junction and to a lesser degree, the small bowel is very useful

Conclusions• Moving things along in the
small bowel• It is the distention of the
bowel with a rapid influx or ‘bolus’ of water that allows a simple, cost-effective way of improving the diagnostic accuracy of FDG PET in patients with disease in the small bowel

Conclusions• A delayed
study of the colon may be useful in eliminating any doubt as to whether FDG uptake is pathological or physiological

References
1.Agress H, & Cooper BZ. Detection of Clinically Unexpected Malignant and Premalignant Tumors with Whole-body FDG PET: Histopathological Comparison. Radiology. 2004;230:417-422.
2.Antoch G, Freudenberg L, Beyer T, et al. To Enhance or Not to Enhance? 18F-FDG and CT Contrast Agents in Dual-Modality 18F-FDG PET/CT. J Nucl Med. 2004;45: 56S-65S
3.Bar-Shalom, R. Normal and Abnormal Patterns of 18F-Fluorodeoxyglucose PET/CT in Lymphoma. Radiol Clin North Amer. 2007;45(4):677-688R.
4.Basu S & Nair N. Intense F-18 FDG Uptake in the Stomach Wall in Follicular Gastritis in Zollinger-Ellison Syndrome. Clin Nuc Med. 2007;32(2): 150-151.
5.Chamroonrat W, Zhuang H, Houseni M, et al. Malignant Lesions can Mimic Gastric Uptake on FDG PET. Clin Nucl Med. 2006;31: 37-38.
6.Chun H, Kim C, Krynckyi B, et al. The Usefulness of a Repeat Study for Differentiating between Bowel Activity and Local Tumour Recurrence on FDG PET Scans. Clin Nucl Med. 2003;28: 672-673.
7.Emmott J, Sanghera B, Chambers J, et al. The Effects of N-butylscopolamine on Bowel Uptake: an 18F-FDG PET Study. Nucl Med Comm. 2008;29: 11-16.
8.Gontier E, Fourme E, Wartski M, et al. High and Typical 18F-FDG Bowel Uptake in Patients Treated with Metformin. Eur J Nucl Med Imaging 2008;35: 95-99.
9.Gutman F, Alberini J, Wartski M, et al. Incidental Colonic Focal Lesions Detected by FDG PET/CT. AJR. 2005;185: 495-500.

References10.Imperiale A, Cimarelli S, Ben Sellem D, et al. Focal F-18 FDG Uptake Mimicking Malignant
Gastric Localizations Disappearing after Water Ingestion on PET/CT Images. Clin Nucl Med. 2006;31: 835-837.
11.Ishimori T, Pavni P, & Wahl R. Detection of Unexpected Additional Primary Malignancies with PET/CT. J Nucl Med. 2005;46(5):752-757.
12.Israel O, Yefremov N, Bar-Shalom R, et al. PET/CT Detection of Unexpected Gastrointestinal Foci of 18F-FDG Uptake: Incidence, Localization Patterns, and Clinical Significance. J Nucl Med. 2005;46(5):758-762.
13.Kaida H, Ishibashi M, Nakamura M, et al. Early Gastric Cancer and Early Colon Cancer Detected Simultaneously by PET Cancer Screening Incidentally. Ann Nucl Med. 2006;20(4): 317-320.
14.Kamel E, Thumshirn M, Truninger K, et al. Significance of Incidental 18F-FDG Accumulations in the Gastrointestinal Tract in PET/CT: Correlation with Endoscopic and Histopathologic Results. J Nucl Med. 2004;45: 1804-1810.
15.Kao P, Chou Y & Hsieh K. Focal FDG Uptake in the Gastric Contents: a PET/CT Misregistration Artifact due to Vesicant Ue and Water Loading. Clin Nucl Med. 2008;33: 231-233.
16.Kostakoglu L, Hardoff R, Mirtcheva R, et al. PET-CT Fusion Imaging in Differentiating Physiologic from Pathologic FDG Uptake. RadioGraphics. 2004;24:1411-1431.
17.Lee J, Hartnett G, Hughes B, et al. Nucl Med Comm. 2009;0: 1-5.18.Lee S, Tan T, Poon A, et al. Role of Low-dose, Noncontrast Computed Tomography from
Integrated Positron Emission Tomography/Computed Tomography in Evaluating Incidental 2-Deoxy-2[F-18]fluoro-D-glucose-avid Colon Lesions. Mol Imaging Biol. 2008;10: 48-53.
References
19.Metser U, Miller E, Lerman H, et al. Benign Nonphysiologic Lesions with Increased 18F-FDG Uptake on PET/CT: Characterization and Incidence. AJR. 2007;189.
20.Modi D, Fulham M, Mohamed A, et al. Intraluminal FDG Uptake in a Rectal Polyp Detected with PET CT: Identification of an Unsuspected Synchronous Primary Bowel Tumor. Clin Nucl Med. 2005;30: 180-181.
21.Mukai K, Ishida Y, Okajima K, et al. Usefulness of Preoperative FDG-PET for detection of Gastric Cancer. Gastric Cancer. 2006;9: 192-196.
22.Qureshy A, Kubota K, Iwata R, et al. Localization and Reduction of FDG Intestinal Uptake: Tissue Distribution and Autoradiography Study. Nucl Med Comm. 2002;23(4): 388.
23.Otsuka H, Graham M, Kubo A, et al. The Effect of Oral Contrast on Large Bowel Acyivity in FDG-PET/CT. Ann Nucl Med. 2005;19(2): 101-108.
24.Prabhakar HB, Sahani DV, Fischman AJ, et al. Bowel Hot Spots at PET-CT. RadioGraphics. 2007; 27(1): 145-159.
25.Phongkitkarun S, Varavithya V, Kazama T, et al. Lymphomatous involvement of Gastrintestinal Tract: Evaluation by Positron Emission Tomography with 18F-Fluorodeoxyglucose. World J Gastroenterol. 2005;11(46): 7284-7289.
26.Radan L, Fischer D, Bar-Shalom R, et al. FDG Avidity and PET/CT Patterns in Primary Gastric Lymphoma. Eur J Nucl Mol Imaging. 2008;35: 1424-1430.

References
27.Singh NK, Cook GJR, Lewington VJ, & Chua SC. PET/CT Assessment of Clinically Unsuspected, Incidental FDG-avid Lesions in Oncological Patients. Imaging. 2008; 20(3):159-168.
28.Tatlidil R, Jadvar H, Bading JR, et al. Incidental Colonic Fluoroglucose Uptake: Correlation with Colonoscopic and Histopathologic Findings. Radiology. 2002;224:783-787.
29.Watanabe N, Hayashi S, Kato H, et al. FDG-PET Imaging in Duodenal Cancer. Ann Nucl Med. 2004;18(4):351-353.
30.Yun M, Choi H, Yoo E, et al. The Role of Gastric Distentiopn in Differentiating Recurrent Tumour from Physiologic Uptake in the Remnant Stomach on 18F-FDG PET. J Nucl Med. 2005;46: 953-957.
31.Zhang Y, Xiu Y, Zhuang H, et al. Follow-up FDG PET in the Evaluation of Unexplained Focal Activity in the Abdomen. Clin Nucl Med. 2008;33(1): 19-22.
32.Zhu Z, Li F, Mao Y, et al. Improving Evaluation of Primary Gastric Malignancies by Distending the Stomach with Milk Immediately Before 18F-FDG PET Scanning. J Nucl Med Technol. 2008;36: 25-29.
33.Zhu Z, Li F & Zhuang H. Gastric Distention by Ingesting Food is Useful in the Evaluation of Primary Gastric Cancer by FDG PET. Clin Nucl Med. 2007;32(2): 106-109.
34.Zhuang H, Hickeson M, Chacko T, et al. Incidental Detection of Colon Cancer by FDG Positron Emission Tomography in Patients Examined for Pulmonary Nodules. Clin Nucl Med. 2002;27(9): 628-632.
Related Documents











