RBGO Gynecology & Obstetrics ISSN 0100-7203 eISSN 1806-9339 Revista Brasileira de Ginecologia e Obstetrícia Number 12 • Volume 43 • Pages 885–994 • December 2021

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
RBGO Gynecology & Obstetrics
ISSN 0100-7203eISSN 1806-9339
Revista Brasileira de Ginecologia e Obstetrícia Number 12 • Volume 43 • Pages 885–994 • December 2021

RBGO Gynecology and ObstetricsRevista Brasileira de Ginecologia e Obstetrícia
ISSN 0100-7203
Editor in Chief
Marcos Felipe Silva de Sá Universidade de São Paulo, Ribeirão Preto, SP, Brazil
Former Editors
Jean Claude NahoumRio de Janeiro, RJ (1979–1989)
Clarice do Amaral FerreiraRio de Janeiro, RJ (1989–1994)
Sérgio Pereira da CunhaRibeirão Preto, SP (1994–1997)
Jurandyr Moreira de AndradeRibeirão Preto, SP, Brazil (1997–2015)
Associated Editors
Agnaldo Lopes da Silva FilhoUniversidade Federal de Minas Gerais,Belo Horizonte, MG, Brazil
Alessandra Cristina MarcolinUniversidade de São Paulo,Ribeirão Preto, SP, Brazil
Ana Katherine da Silveira GonçalvesUniversidade Federal do Rio Grande doNorte, Natal, RN, Brazil
Andréa da Rocha TristãoUniversidade Estadual Paulista“Júlio de Mesquite Filho”, Botucatu, SP, Brazil
Angélica Nogueira RodriguesUniversidade Federal de Minas Gerais, Belo Horizonte, MG, Brazil
Antonio Rodrigues Braga NetoUniversidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brazil
Conrado Milani CoutinhoUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Corintio Mariani NetoUniversidade Cidade de São Paulo, São Paulo, SP, Brazil
Cristina Laguna Benetti PintoUniversidade Estadual de Campinas, Campinas, SP, Brazil
Daniel Guimarães TiezziUniversidade de São Paulo,Ribeirão Preto, SP, Brazil
Diama Bhadra Andrade Peixoto do ValeUniversidade Estadual de Campinas, Campinas, SP, Brazil
Eddie Fernando Candido MurtaUniversidade Federal do Triângulo Mineiro, Uberaba, MG, Brazil
Edward Araujo JúniorUniversidade Federal de São Paulo,São Paulo, SP, Brazil
Elaine Christine Dantas MoisésUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Eliana Aguiar Petri NahasUniversidade Estadual Paulista“Júlio de Mesquita Filho”, Botucatu, SP, Brazil
Fernanda Garanhani de Castro SuritaUniversidade Estadual de Campinas, Campinas, SP, Brazil
Fernando Marcos dos ReisUniversidade Federal de Minas Gerais,Belo Horizonte, MG, Brazil
Gabriel Costa OsananUniversidade Federal de Minas Gerais, Belo Horizonte, MG, Brazil
Gustavo Salata RomãoUniversidade de Ribeirão Preto, Ribeirão Preto, SP, Brazil
Helena von Eye CorletaUniversidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
Helmer HerrenUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Ilza Maria Urbano Monteiro Universidade Estadual de Campinas, Campinas, SP, Brazil
José Carlos PeraçoliUniversidade Estadual Paulista “Júlio de Mesquita Filho”, Botucatu, SP, Brazil
José Geraldo Lopes RamosUniversidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
José Guilherme CecattiUniversidade Estadual de Campinas, Campinas, SP, Brazil
José Maria Soares JúniorUniversidade de São Paulo, São Paulo, SP, Brazil
Julio Cesar Rosa e SilvaUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Lucia Alves da Silva LaraUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Lucia Helena Simões da Costa PaivaUniversidade Estadual de Campinas, Campinas, SP, Brazil
Luiz Carlos ZeferinoUniversidade Estadual de Campinas,Campinas, SP, Brazil
Luiz Gustavo Oliveira BritoUniversidade de São Paulo, Campinas, SP, Brazil
Marcos Nakamura PereiraInstituto Fernandes Figueira, Rio de Janeiro, RJ, Brazil
Maria Celeste Osório WenderUniversidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
Maria Laura Costa do NascimentoUniversidade Estadual de Campinas, Campinas, SP, Brazil
Melânia Maria Ramos de AmorimUniversidade Federal de Campina Grande, Campina Grande, PB, Brazil
Mila de Moura Behar Pontremoli Salcedo Universidade Federal de Ciências da Saúde de Porto Alegre, Porto Alegre, RS, Brazil
Omero Benedicto Poli NetoUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Patrícia El BeituneUniversidade Federal de Ciências da Saúde de Porto Alegre, RS, Brazil
Paula Andrea de Albuquerque Salles NavarroUniversidade de São Paulo,Ribeirão Preto, SP, Brazil
Renato Moretti-MarquesHospital Israelita Albert Einstein, São Paulo, SP, Brazil
Ricardo Carvalho CavalliUniversidade de São Paulo,Ribeirão Preto, SP, Brazil
Ricardo Mello MarinhoFaculdade Ciências Médicas de MinasGerais, Belo Horizonte, MG, Brazil
Rosana Maria dos ReisUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Rossana Pulcineli Vieira FranciscoUniversidade de São Paulo, São Paulo, SP, Brazil
Rosiane MattarUniversidade Federal de São Paulo, São Paulo, SP, Brazil
Rodrigo de Aquino CastroUniversidade Federal de São Paulo,São Paulo, SP, Brazil
Rogério Bonassi MachadoFaculdade de Medicina de Jundiaí, Jundiaí, SP, Brazil
Silvana Maria QuintanaUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Sophie Françoise Mauricette DerchainUniversidade Estadual de Campinas,Campinas, SP, Brazil
Alex Sandro Rolland de SouzaInstituto de Medicina Integral Prof. Fernando Figueira, Recife, PE, Brazil
Ana Carolina Japur de Sá Rosa e SilvaUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Aurélio Antônio Ribeiro da CostaUniversidade de Pernambuco, Recife, PE, Brazil
Belmiro Gonçalves PereiraUniversidade Estadual de Campinas, Campinas, SP, Brazil
Carlos Augusto Alencar JuniorUniversidade Federal do Ceará, Fortaleza, CE, Brazil
Carlos GrandiUniversidad de Buenos Aires, Buenos Aires, Argentina
Cesar Cabello dos SantosUniversidade Estadual de Campinas, Campinas, SP, Brazil
Délio Marques CondeHospital Materno Infantil de Goiânia, Goiânia, GO, Brazil
Dick OepkesUniversity of Leiden, Leiden, The Netherlands
Dino Roberto Soares de LorenziUniversidade de Caxias do Sul, Caxias do Sul, RS, Brazil
Diogo de Matos Graça Ayres de CamposUniversidade do Porto, Porto, Portugal
Eduardo Pandolfi PassosUniversidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
Edmund Chada BaracatUniversidade de São Paulo, São Paulo, SP, Brazil
Eliana Martorano AmaralUniversidade Estadual de Campinas, Campinas, SP, Brazil
Francisco Edson Lucena FeitosaUniversidade Federal do Ceará, Fortaleza, CE, Brazil
George CondousNepean Hospital in West Sydney, Sidney, Australia
Giuseppe RizzoUniversità degli Studi di Roma“Tor Vergata”, Roma, Italy
Gutemberg Leão de Almeida FilhoUniversidade Federal do Rio de Janeiro,Rio de Janeiro, RJ, Brazil
Iracema de Mattos Paranhos CalderonUniversidade Estadual Paulista“Júlio de Mesquita Filho”, Botucatu, SP, Brazil
João Luiz Pinto e SilvaUniversidade Estadual de Campinas, Campinas, SP, Brazil
João Sabino Lahorgue da Cunha FilhoUniversidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
José Carlos PeraçoliUniversidade Estadual Paulista “Júlio de Mesquita Filho”, Botucatu, SP, Brazil
José Juvenal LinharesUniversidade Federal do Ceará, Campus de Sobral, Fortaleza, CE, Brazil
Joshua VogelDepartment of Reproductive Health and Research, World Health Organization, Geneva, Switzerland
Juvenal Soares Dias-da-CostaUniversidade Federal de Pelotas, Pelotas, RS, Brazil
Laudelino Marques LopesUniversity of Western Ontario, London, Ontario, Canada
Luciano Marcondes Machado NardozzaUniversidade Federal de São Paulo, São Paulo, SP, Brazil
Luis Otávio Zanatta SarianUniversidade Estadual de Campinas, Campinas, SP, Brazil
Luiz Claudio Santos ThulerInstituto Nacional do Câncer, Rio de Janeiro, RJ, Brazil
Luiz Henrique GebrimUniversidade Federal de São Paulo, São Paulo, SP, Brazil
Manoel J. B. Castello Girão, Universidade Federal de São Paulo, São Paulo, SP, Brazil
Marcelo ZugaibUniversidade de São Paulo, São Paulo, SP, Brazil
Marcos Desidério RicciUniversidade de São Paulo, São Paulo, SP, Brazil
Maria de Lourdes BrizotUniversidade de São Paulo, São Paulo, SP, Brazil
Marilza Vieira Cunha RudgeUniversidade Estadual Paulista “Júlio de Mesquita Filho”, Botucatu, SP, Brazil
Newton Sergio de CarvalhoUniversidade Federal do Paraná, Curitiba, PR, Brazil
Nuno Henrique Malhoa Migueis ClodeFaculdade de Medicina de Lisboa, Lisboa, Portugal
Olímpio Barbosa Moraes FilhoUniversidade de Pernambuco, Recife, PE, Brazil
Paulo Roberto Nassar de CarvalhoInstituto Fernandes Figueira-Fiocruz, Rio de Janeiro, RJ, Brazil
Renato Augusto Moreira de SáUniversidade Federal Fluminense, Niterói, RJ, Brazil
Rintaro MoriNational Center for Child Health and Development, Tokyo, Japan
Roberto Eduardo BittarUniversidade de São Paulo, São Paulo, SP, Brazil
Rosane Ribeiro Figueiredo AlvesUniversidade Federal de Goiás, Goiânia, GO, Brazil
Roseli Mieko Yamamoto NomuraUniversidade Federal de São Paulo, São Paulo, SP, Brazil
Rossana Pulcinelli Vieira FranciscoUniversidade de São Paulo, São Paulo, SP, Brazil
Ruff o de Freitas JuniorUniversidade Federal de Goiás, Goiânia, GO, Brazil
Sabas Carlos VieiraUniversidade Federal do Piauí, Teresina, PI, Brazil
Sebastião Freitas de MedeirosUniversidade Federal do Mato Grosso, Cuiabá, MT, Brazil
Selmo GeberUniversidade Federal de Minas Gerais, Belo Horizonte, MG, Brazil
Silvia DaherUniversidade Federal de São Paulo, São Paulo, SP, Brazil
Shaun Patrick BrenneckeUniversity of Melbourne Parkville, Victoria, Australia
Técia Maria de Oliveira MaranhãoUniversidade Federal do Rio Grande do Norte, Natal, RN, Brazil
Toshiyuki HataUniversity Graduate School of Medicine, Kagawa, Japan
Valéria Cristina SandrimUniversidade Estadual Paulista “Júlio de Mesquita Filho”, Botucatu, SP, Brazil
Wellington de Paula MartinsUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Editorial Offi ce
Bruno Henrique Sena Ferreira
Editorial Production
Thieme Medical Publishers
Editorial Board

Federação Brasileira das Associações de Ginecologia e ObstetríciaBrazilian Federation of Gynecology and Obstetrics Associations
ISSN 0100-7203
Society Board (2020–2024)
PresidentAgnaldo Lopes da Silva Filho (MG)
Administrative Director Sérgio Podgaec (SP)
Scientifi c Director César Eduardo Fernandes (SP)
Financial DirectorOlímpio B. de Moraes Filho (PE)
Professional Status DefenceMaria Celeste Osório Wender (RS)
Vice-president of North RegionRicardo de Almeida Quintairos (PA)
Vice-president of Northeast Region Carlos Augusto Pires C. Lino (BA)
Vice-president of Middle West Region Marta Franco Finotti (GO)
Vice-president of Southeast Region Marcelo Zugaib (SP)
Vice-president of South Region Almir Antônio Urbanetz (PR)
Presidency and Executive Staff
Av. Brigadeiro Luís Antônio, 3421 - Sala 903 - Jardim Paulista, São Paulo, SP, BrazilCEP: 01401-001Phone.: (+55 11) [email protected]
RBGO Editorial Offi ce
editorial.offi [email protected]

RBGO Gynecology and ObstetricsRevista Brasileira de Ginecologia e Obstetrícia
Volume 43, Number 12/2021
online www.thieme-connect.com/products
Editorial
885 HPV Vaccination and Screening with High-Performance Test: Brazilian EvidenceJulio Cesar Teixeira and Cecilia Maria Roteli-Martins
Original Articles
Obstetrics
887 IgG Avidity in Samples Collected on Filter Paper: Importance of The Early Diagnosis of Congenital ToxoplasmosisJéssica Yonara de Souza, Taynara Cristina Gomes, Hanstter Hallison Alves Rezende, Heloisa Ribeiro Storchilo, Patrícia Giffron Rodrigues, and Ana Maria de Castro
High Risk Pregnancy /Preeclampsia
894 Preeclampsia and Gestational Hypertension: Biochemical and Antioxidant Features in Vitro Might Help Understand Diff erent OutcomesVictoria Elizabeth Galvão, Ricardo Carvalho Cavalli, and Valeria Cristina Sandrim
904 Uterine Artery Pulsatility Index as a Preeclampsia Predictor in the 3 Trimesters in Women with Singleton PregnanciesYuly Natalia Guzmán, Montserrat Uriel, Alexandra Porras Ramírez, and Ximena Carolina Romero
Image
911 Diagnosing Septate Uterus Using Three-Dimensional Ultrasound Using Three Diff erent Classifi cations: An Interobserver and Intraobserver Agreement StudyCarla Peixoto, Maite Castro, Isabel Carriles, Maria de Arriba, Victoria Lapresa, and Juan Luis Alcazar
Endometriosis
919 Overview of the Eff ect of Complementary Medicine on Treating or Mitigating the Risk of EndometriosisFiroozeh Mirzaee and Atefeh Ahmadi
Lower Genital Tract Diseases
926 School-based HPV Vaccination: The Challenges in a Brazilian InitiativeJulio Cesar Teixeira, Mariana Silva Castro Vianna, Diama Bhadra Vale, Daniella Moretti Arbore, Thais Helena Wilmers Perini, Tulio Jose Tomass Couto, Jose Pedroso Neto, and Luiz Carlos Zeferino
Covid-19
932 Increased Risk for Maternal Anxiety during the COVID-19 Outbreak in Brazil among Pregnant Women without ComorbiditiesRoseli Mieko Yamamoto Nomura, Ana Carla Franco Ubinha, Isabela de Paula Tavares, Maria Laura Costa, Maria Lucia da Rocha Opperman, Marianna Facchinetti Brock, Alberto Trapani Jr., Lia Cruz Vaz da Costa Damásio, Nadia Stella Viegas Reis, Vera Therezinha Medeiros Borges, Alberto Carlos Moreno Zaconeta, Ana Cristina Pinheiro Fernandes de Araujo, and Rodrigo Ruano
Thieme Revinter Publicações Ltda

RBGO Gynecology and Obstetrics Volume 43, Number 12/2021
Review Articles
940 Analysis of the Role of Female Hormones During Infection by COVID-19David Balbino Pascoal, Isabela Macêdo de Araujo, Lorenna Peixoto Lopes, Cristiane Monteiro da Cruz
949 Clinical and Obstetric Aspects of Pregnant Women with COVID-19: A Systematic ReviewSarah Nilkece Mesquita Araújo Nogueira Bastos, Bárbara Louise Freire Barbosa, Larisse Giselle Barbosa Cruz, Rayza Pereira de Souza, Simone Santos e Silva Melo, and Caroline Camargo Bandeira da Silveira Luz
961 Intermittent versus Continuous Catheterization and Diff erences in the Evolution of Labor: Systematic Review and Meta-analysisInês Reis, Sara Cunha, Matilde Martins, Luísa Sousa, Adérito Seixas, and Cátia Rasteiro
968 The Eff ect of Aromatherapy Alone or in Combination with Massage on Dysmenorrhea: A Systematic Review and Meta-analysisMona Najaf Najafi, Neshat Najaf Najafi, Farzaneh Rashidi Fakari, Somayeh Moeindarbary, Fatemeh Abdi, Zeinab Sadat Hoseini, and Masumeh Ghazanfarpour
Case Reports
980 High-Grade Transformation in Adenoid Cystic Carcinoma of the Bartholin Gland: Case ReportAline Evangelista Santiago, Nicky Teunissen, Bernardo Ferreira de Paula Ricardo, Eduardo Batista Cândido, Rafaela de Souza Furtado, and Agnaldo Lopes da Silva Filho
985 Antenatal Diagnosis of Parapagus Conjoined Twins: 3D Virtual and 3D Physical ModelsPedro Castro, Heron Werner, Ana Paula Matos, Gerson Ribeiro, Jorge Lopes, and Edward Araujo Júnior
Febrasgo Statement
988 Use of androgens at diff erent stages of life: reproductive periodAndrea Prestes Nácul, Gabriela Pravatta Rezende, Daniela Angerame Yela Gomes, Técia Maranhão, Laura Olinda Bregieiro Fernandes Costa, Fernando Marcos dos Reis, Gustavo Arantes Rosa Maciel, Lia Cruz Vaz da Costa Damásio, Ana Carolina Japur de Sá Rosa e Silva, Vinicius Medina Lopes, Maria Cândida Baracat,Gustavo Mafaldo Soares, José Maria Soares Junior, and Cristina Laguna Benetti-Pinto

Some of the product names, patents, and registered designs referred to in this publication are in fact registered trade marks or proprietary names even though specifi c reference to this fact is not always made in the text. Therefore, the appearance of a name without designation as proprietary is not to be construed as a representation by the Publisher that it is in the public domain.
All rights, including the rights of publication, distribution, and sales, as well as the right to translation, are reserved. No part of this work covered by the copyrights hereon may be reproduced or copied in any form or by any means—graphic, electronic, or mechanical, including photocopying, recording, taping, or information and retrieval systems—without written permission of the Publisher.
Important Note: Medical knowledge is ever-changing. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy may be required. The authors and editors of the material here-in have consulted sources believed to be reliable in their efforts to provide information that is complete and in accord with the standards accepted at the time of publication. However, in view of the possibility of human er-ror by the authors, editors, or publisher of the work herein, or changes in
medical knowledge, neither the authors, editors, or publisher, nor any other party who has been involved in the preparation of this work, warrants that the information contained here in is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from use of such information. Because of rapid advances in the medical sciences, independent verification of diagnoses and drug dosages should be made. Readers are encouraged to confirm the information con-tained herein with other sources. For example, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this publi-cation is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs.
Although all advertising material is expected to conform to ethical (medical) standards, inclusion in this journal does not constitute a guar-antee or endorsement of the quality or value of such product or of claims made by its manufacturer.
© 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved. RBGO Gynecology and Obstetrics/Revista Brasileiro de Ginecologia e Obstetrícia is published monthly by Thieme-Revinter Publicações Ltda., Rua do Matoso, 170, Rio de Janeiro 20270-135, Brazil.
Editorial comments should be sent to [email protected]. Articles may be submitted to this journal on an open-access basis. For further informa-tion, please send an e-mail to [email protected]. The content of this journal is available online at www.thieme-connect.com/products. Visit our Web site at www.thieme.com and the direct link to this journal at www.thieme.com/rbgo.
Revista Brasileiro de Ginecologia e Obstetrícia is an official publication of the Federação Brasileira das Associações de Ginecologia e Obstetrícia (Brazilian Federation of Association of Gynecology and Obstetrics, Febrasgo), It is listed in Isi - Web of Science, Web of Knowledge (Emerging), MEDLINE /PubMed, Index Medicus, Scopus (Sci Verse), SCImago, SciELO (Scientific Electronic Library Online), LILACS (Literatura Latino-Americana e do Caribe em Ciências da Saúde, Index Medicus Latino Americano), and Portal de Periódicos Capes (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior). Thieme Medical Publishers is a member of the CrossRef initiative.
ISSN 0100-7203
Complementary material is available online at www.rbgo.org.br.
Cover design: © ThiemeCover image source: © Thieme

Editorial
HPV Vaccination and Screening with High-Performance Test:Brazilian EvidenceJulio Cesar Teixeira1 Cecilia Maria Roteli-Martins2
1Universidade Estadual de Campinas, Campinas, SP, Brasil2 Faculdade de Medicina do ABC, Santo André, SP, Brasil
Rev Bras Ginecol Obstet 2021;43(12):885–886.
Brazil has a critical issue on women’s health to solve: onewoman dies every 90minutes due to cervical cancer witha mean age of 45 years.1 Considered eradicable cancer,there are two established strategies to control it: vacci-nation against HPV and periodic screening for detectionof precancerous lesions. The Brazilian public health sys-tem offers both, free of charge, although this is notenough.
Vaccination to Prevent HPV Infection andCancer
HPV vaccines were globally licensed from 2007–2008 andsome Brazilian researchers gave an important contributionto this achievement. Australia, the United Kingdom, Canada,and Sweden, started soon a wide vaccination action reach-ing large and sustainable coverage in preadolescent andadolescent girls. Their results were presented in recentpublications demonstrating the impact over cervical high-grade precursor lesions and cancer incidence, making itpossible to project the expected ’elimination’ of thiscancer.2–5
How was the Winner Strategy? The Answeris School-Based HPV Vaccination
Several other countries, including some consideredmiddle or low-income, are following the same strate-gy to provide HPV vaccination through schools.Brazil, a continental country with great regionaldifferences, has two main characteristics: the tradi-tion of vaccination with high popular acceptance anda network of elementary-level schools, most of themunder municipal administration. Furthermore, theNational Immunization Program itself demonstratedin 2014, the same winning strategy and achieved real-life success with 100% coverage for Dose-1.6
Why was this Strategy not Continued?
There was probably a lack of central coordination over thevarious administrative facets involved. Opposing it, anyBrazilian municipality can use your regulated autonomy toovercome several of these obstacles. In this issue of RBGO“School-based HPV vaccination: the challenges in a Brazilianinitiative,” Teixeira et al.7 reported the first results of aBrazilian city initiative based on a demonstration study totest this hypothesis: school-based HPV vaccination canincrease coverage?
The program started in 2018 and increased three timesthe Dose-1 coverage in the first year, although had sufferedfrom unexpected obstacles. The authors reported theseissues and the strategies applied to overcome them. It shouldbe noted that the problems were not related to safetyconcerns or acceptance by parents or by education profes-sionals. Even with great interest from local health managersto achieve high coverage vaccination, the program cannotachieve the initial goals, yet. Taking advantage of the mo-ment to disclose partial results and considering data fromthe period before the pandemic, some strategies adopted inthe program are worth highlighting and can be replicated:
1. School-based vaccination for girls and boys aged 9–10years: nullifying any discussion about gender and promptaccess to a high proportion of all children registered in aMunicipal school (level ’Fundamental 1’). The city has 87%of all children in this situation.
2. Yearly dose schedule: vaccination once a year facilitatesthe organization of the health care system to supplyvaccination teams to cover all schools. The Dose-2 ofthe current HPV vaccines has been indicated in six to12 months intervals, and the risk of interval infection forthis early age can be considered insignificant. In addition,studies had demonstrated that the 1-Dose schedule al-ready achieved significant protection.8
Address for correspondenceJulio Cesar Teixeira, PhD, MD,Cidade Universitária Zeferino Vaz,13083-970, Barão Geraldo,Campinas, SP, Brasil(e-mail: [email protected]).
DOI https://doi.org/10.1055/s-0041-1740953.ISSN 0100-7203.
© 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rightsreserved.This is an open access article published by Thieme under the terms of the
Creative Commons Attribution License, permitting unrestricted use,
distribution, and reproduction so long as the original work is properly cited.
(https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda., Rua do Matoso 170, Rio deJaneiro, RJ, CEP 20270-135, Brazil
THIEME
Editorial 885

After someunexpected situations limiting the program, thelast strategy to ensure the school-based vaccination activitywas the passing of a Municipal Law, which determines theavailability of a comprehensive structure for school-basedvaccination, independent of other competing requests.
Moving to a High-Performance ScreeningTesting
The same research team, coordinate another demonstrationstudy to replace the traditional cytological screening for aDNA-HPV test screening, ongoing in the same Brazilian city.Recently, a pivotal cost-effectiveness analysis was published,demonstrating the economic viability of the DNA-HPV testingimplementation,with the potential to save resources from thepublic health perspective.9 Subsequently, an analysis of theprogram’s early results, still without pandemic interference,has just beenpublished.10The researcherspointed to the greatpotential to save resources and lives when the DNA-HPVtesting was applied in a screening with higher coverage, anda higher proportion of the womenwith abnormal tests evalu-ated and followed the guidelines. There were demonstratedsignificant additional cervical cancer cases detected, most ofthemwere prevalent cases, but with an incredible two-thirdsproportion of cancer in microinvasive stage, highly curablewith more accessible procedures. The prompt impact of orga-nizing the screening program with a high-performance testresulted in anticipating the diagnoses of cervical cancer in10 years and at early-stage.
In conclusion, the available Brazilian scientific evidence,includingdatabasedon real-life, represents to all researchers inthis field a kind of mission accomplished. Now, the baton goesover to the next, people who have decision-making on healthactions. Our activity, as a medical association, and togetherwith organized society, is to make this information reach thepeople who decide and to demand them for effective actions.
Conflicts to InterestNone to declare.
References1 Ministério da Saúde. Instituto Nacional de Câncer Jose Alencar
Gomes da Silva. [Estimate 2020: cancer incidence in Brazil]
[Internet]. Rio de Janeiro: INCA; 2019 [cited 2021 Jun 22].Available from: https://www.inca.gov.br/sites/ufu.sti.inca.-local/files//media/document//estimativa-2020-incidencia-de-cancer-no-brasil.pdf. Portuguese
2 Garland SM, Cornall AM, Brotherton JML, Wark JD, Malloy MJ,Tabrizi SNVACCINE studygroup. Final analysis of a studyassessinggenital human papillomavirus genoprevalence in young Austra-lian women, following eight years of a national vaccinationprogram. Vaccine. 2018;36(23):3221–3230. Doi: 10.1016/j.vac-cine.2018.04.080
3 Falcaro M, Castañon A, Ndlela B, et al. The effects of the nationalHPV vaccination programme in England, UK, on cervical cancerand grade 3 cervical intraepithelial neoplasia incidence: a regis-ter-based observational study. Lancet. 2021;398(10316):2084-–2092 10.1016/S0140-6736(21)02178-4 [ahead of print]
4 Drolet M, Bénard É, Pérez N, Brisson MHPV Vaccination ImpactStudy Group. Population-level impact and herd effects followingthe introduction of human papillomavirus vaccination pro-grammes: updated systematic review and meta-analysis. Lancet.2019;394(10197):497–509. Doi: 10.1016/S0140-6736(19)30298-3
5 Lei J, Ploner A, Elfström KM, et al. HPV vaccination and the risk ofinvasive cervical cancer. N Engl J Med. 2020;383(14):1340–1348.Doi: 10.1056/NEJMoa1917338
6 Ministério da Saúde. SI-PNI - Sistema de Informação do ProgramaNacional de Imunizações. Coberturas vacinais – HPV Quadriva-lente - Sexo feminino de 11 a 14 anos por idade e dose -Total Brasil– 2014 [Internet]. Brasília (DF): Ministério da Saúde; 2014 [cited2020 Mar 12]. Available from: http://pni.datasus.gov.-br/consulta_hpv_14_C01.php
7 Teixeira JC, Vianna MS, Vale DB, et al. School-based HPV vaccina-tion: the challenges in a Brazilian initiative. Rev Bras GinecolObstet. 2021;43(12):923–931. Doi: 10.1055/s-0041-1740279
8 Kreimer AR, Struyf F, Del Rosario-Raymundo MR, et al; Costa RicaVaccine Trial Study Group Authors PATRICIA StudyGroup AuthorsHPV PATRICIA Principal Investigators/Co-Principal InvestigatorCollaborators GSK Vaccines Clinical Study Support Group. Efficacyof fewer than three doses of an HPV-16/18 AS04-adjuvantedvaccine: combined analysis of data from the Costa Rica Vaccineand PATRICIA Trials. Lancet Oncol. 2015;16(07):775–786. Doi:10.1016/S1470-2045(15)00047-9
9 Vale DB, SilvaMT, Discacciati MG, Polegatto I, Teixeira JC, ZeferinoLC. Is the HPV-test more cost-effective than cytology in cervicalcancer screening? An economic analysis from a middle-incomecountry. PLoS One. 2021;16(05):e0251688. Doi: 10.1371/journal.pone.0251688
10 Teixeira JC, Vale DB, Campos CS, Bragança JF, Discacciati MG,Zeferino LC. Organization of cervical cancer screening withDNA�HPV testing impact on early�stage cancer detection: apopulation�based demonstration study in a Brazilian city. LancetReg Health Am. 2022;5:100084. Doi: 10.1016/j.lana.2021.100084
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
HPV Vaccination and Screening with High-Performance Test Teixeira, Martins886
IgG Avidity in Samples Collected on Filter Paper:Importance of The Early Diagnosis of CongenitalToxoplasmosis
Avidez de IgG em amostras coletadas em papel filtro:Importância no diagnóstico precoce da toxoplasmosecongênitaJéssica Yonara de Souza1 Taynara Cristina Gomes1 Hanstter Hallison Alves Rezende1
Heloisa Ribeiro Storchilo1 Patrícia Giffron Rodrigues1 Ana Maria de Castro1
1Universidade Federal de Goiás, Goiânia, GO, Brazil
Rev Bras Ginecol Obstet 2021;43(12):887–893.
Address for correspondence Jéssica Yonara de Souza, 235th Street,Setor Universitário, 74605-050, Goiânia, State of Goiás, Brazil(e-mail: [email protected]).
Keywords
► toxoplasmosis► IgG avidity► filter paper► neonatal screening► pregnancy
Abstract Objective The purpose of the present study is to standardize and evaluate the use ofthe immunoglobulin G (IgG) antibody avidity test on blood samples from newbornscollected on filter paper to perform the heel test aiming at its implementation inongoing programs.Methods Blood samples from newborns were collected on filter paper simultaneous-ly with the heel prick test. All samples were subjected to immunoglobulin M IgM andIgG enzyme-linked immunosorbent assays (ELISA). Peripheral blood was collectedagain in the traditional way and on filter paper from newborns with high IgG levels (33).Three types of techniques were performed, the standard for measuring IgG in serum,adapted for filter paper and the technique of IgG avidity in serum and on filter paper.The results of the avidity test were classified according to the Rahbari protocol.Results Among the 177 samples, 17 were collected in duplicate from the same child,1 of peripheral blood and 1 on filter paper. In this analysis, 1 (5.88%) of the 17 samplescollected in duplicate also exhibited low IgG avidity, suggesting congenital infection. Inaddition, the results obtained from serum and filter paper were in agreement, that is,16 (94.12%) samples presented high avidity, with 100% agreement between the resultsobtained from serum and from filter paper.Conclusion The results of the present study indicate that the avidity test may beanother valuable method for the diagnosis of congenital toxoplasmosis in newborns.
receivedNovember 22, 2020accepted after revisionOctober 13, 2021
DOI https://doi.org/10.1055/s-0041-1740272.ISSN 0100-7203.
© 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rightsreserved.This is an open access article published by Thieme under the terms of the
Creative Commons Attribution License, permitting unrestricted use,
distribution, and reproduction so long as the original work is properly cited.
(https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda., Rua do Matoso 170, Rio deJaneiro, RJ, CEP 20270-135, Brazil
THIEME
Original Article 887

Introduction
Congenital toxoplasmosis is an infectious disease caused bythe transplacental transfer of Toxoplasma gondii tachyzoitesfrom the primary infection of the mother, by reinfection, orby resurgence of a previous infection, and is particularlyrelevant because of the damage inflicted on the developingfetus.1
Toxoplasmosis is one of the most harmful diseases for thefetus, particularly when the mother becomes infected in the1st 2 trimesters of pregnancy.2 Studies in Brazil have revealeda prevalence of congenital toxoplasmosis of between 3 and20 per 10,000 live births.3–6 Approximately 80% of verticallyinfected children show no symptoms at birth, but laterexhibit signs of the disease, mainly with ocular, motor, andcentral nervous system involvement.7,8
The importance of diagnosing active infection by T. gondiiduring pregnancy and of confirming congenital transmissionin newborns (NBs) cannot be overstated, because it allows forthe adoption of measures of primary and secondary care,minimizing serious impairments caused by congenitaltransmission.9
In the routine laboratory tests offered by the BrazilianUnified Health System (SUS, in the Portuguese acronym),toxoplasmosis is diagnosed by means of serological testsbased on the detection of specific antibodies of the classes ofimmunoglobulin M (IgM) and immunoglobulin G (IgG),mainly by means of the enzyme-linked immunosorbentassay (ELISA) method.10 However, assistance provided topregnant women during prenatal care is still not satisfactory.Pregnant women often have access to exams only in the last
month of pregnancy, when prenatal tests are performed inprograms that use filter paper for serological screening. Thissituation is one of the main factors that limit the control andthe prevention of infection, of confirmation of risk, and ofcongenital transmission.11
The diagnosis of toxoplasmosis is complex, and monitor-ing the NBs ofmothers infectedwith T. gondii, confirming theinfection, and providing early treatment, are crucial for theprognosis of the newborn.12 The literature recommends theIgG avidity test because it is a fast and inexpensive technique,and is an auxiliary method for optimization of the diagnosisof recent infection, and, therefore, of congenital toxoplasmo-sis. This recommendation favors the implementation of thistechnique in public health programs, especially in Brazil,where the incidence of congenital toxoplasmosis is high.
The infection is usually confirmed by laboratory tests thatidentify the parasite or by the presence of specific antibodiesthat do not cross the placental barrier (IgA, IgM or IgE) in theblood of the patient.13 Immunoglobulin G, which is a markerof chronic infection and crosses the transplacental barrier, isstill not used as a marker of congenital infection. However,when IgG levels in NBs differ frommaternal levels, they maysuggest infection.14
The functional affinity of IgG antibodies for antigens is lowin the primary antigen response and increases when theimmune system reachesmaturity.15 The IgG antibodyaviditytest analyzes the binding affinity of the antigen-antibody(AG-AB) complex. The AG-AB bond is easily dissociated in theacute phase of the disease because the synthesis of anti-bodies is recent. This is why IgG has low avidity for antigens,which are considered to be of low avidity (< 30%, depending
Resumo Objetivo O objetivo do presente estudo é padronizar e avaliar a utilização do teste deavidez de anticorpos imunoglobulina G (IgG) em amostras de sangue de recém-nascidos (RNs) coletadas em papel filtro para a realização do teste do pezinho visando aimplementação nos programas já vigentes.Métodos Foram coletadas amostras de sangue de recém-nascidos em papel filtrosimultaneamente ao teste do pezinho. Em todas as amostras, foram realizados ostestes imunoenzimáticos (ELISA) imunoglobulina M (IgM) e IgG. Dos RNs que apre-sentaram altos índices de IgG (33), foi novamente coletado sangue periférico da formatradicional e em papel filtro. Foram realizadas técnicas padrão para a dosagem de IgGem soro, adaptadas para papel filtro, e a técnica de avidez de IgG em soro e em papelfiltro. Os valores obtidos para o teste de avidez foram classificados de acordo com oprotocolo de Rahbari.Resultados Dentre as 177 recoletas, em 17 amostras foi realizada a coleta simultâneade sangue periférico e papel filtro da mesma criança. Nesta análise, 1 (5,88%) das 17amostras coletadas em duplicata obteve também baixa avidez de IgG, sugerindoinfecção congênita da criança, e houve concordância entre os resultados obtidos emsoro e em papel filtro: 16 (94,12%) das amostras apresentaram alta avidez, comconcordância de 100% entre os resultados obtidos em soro e em papel filtro.Conclusão Os dados do presente trabalho evidenciam que o teste de avidez poderáser mais um método valioso a ser utilizado no diagnóstico da toxoplasmose congênitaem RNs.
Palavras-chave
► toxoplasmose► avidez de IgG► papel filtro► triagem neonatal► gravidez
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
IgG Avidity in Samples Collected on Filter Paper Souza et al.888

on what kits and protocols are used). On the other hand, AG-AB complexes are difficult to dissociate in the chronic phase,exhibiting high IgG avidity, that is, late synthesis of anti-bodies considered to have high avidity.16
Therefore, the purpose of the present study was to stan-dardize and assess the use of the IgG antibody avidity test onblood samples fromNBs in order to optimize it and employ itin existing programs that use filter paper to collect blood forthe neonatal heel prick test.
Methods
The present research project was submitted to the Brazilianonline system for human subject research proposals, Plata-forma Brasil, and was accepted under the Protocol No.943,441 on February 11, 2015. Blood samples were collectedbetween April 2016 and February 2017 at the maternitywards of the Hospital das Clínicas da Universidade Federal deGoiás (HC-UFG, in the Portuguese acronym) and of theHospital e Maternidade Dona Iris (HDMI, in the Portugueseacronym), both in the municipality of Goiânia, state of Goiás,Brazil, and at thematernitywardof the Cais Nova Era (CNE, inthe Portuguese acronym) in Aparecida de Goiânia, state ofGoiás, Brazil. These maternity wards were chosen for conve-nience, and the patients came from the public health net-work of Goiânia, state of Goiás, Brazil.
The samples were collected on filter paper at the sametime as the heel prick test was applied, upon the consent ofthe person responsible for the NB. The blood was collectedfrom the lateral plantar region of the NB onWathman Grade1 filter paper, with the NB held in the burping position to
ensure good blood circulation in the feet. After the circlesmarked on the filter paper were filled with blood, the paperswere tagged and placed on horizontal shelves to dry for �3hours at room temperature, between 15 and 20°C, avoidingcontact with other samples. The dry biological samples werethen sent to the Laboratory for Parasite-Host RelationshipStudies at the Universidade Federal de Goiás (LAERPH-UFG,in the Portuguese acronym).
All samples were subjected to IgM and IgG ELISA usingQuibasa-Bioclin kits.
Newborns presenting higher IgG levels than the averagelevel of patients tested in the LAERPH routine, that is,patients with a level � 3, served as a risk criterion forcongenital infection. A new peripheral blood sample wascollected from these infants, drawn in the traditionalmannerand on filter paper, within a period of up to 3 months afterthe 1st blood sample collection, for confirmation and com-parison of the serology on filter paper and for the IgG aviditytest of the infant.
Avidity was evaluated using the protocol of Rahbariet al.,17 with some adaptations for filter paper, as describedin detail in Chart 1.
Two plates, A and B, were used simultaneously to deter-mine the reactivity. The serum samples were diluted 1:200and 100μl were added per well. After incubation, plate Awaswashed 5 times with sample buffer from the Bioclin com-mercial kits (Quibasa Química Básica Ltda), while plate Bwaswashed 3 times with sample buffer containing 6 Molar urea.The plates were then treated according to the instructions ofthe manufacturer. To validate the technique and standardizethe use of 5-mm filter paper discs, tests were carried out
Chart 1 ELISA technique (immunoenzymatic assay) according to the protocol of the manufacturer of the Quibasa-Bioclin kit, atechnique adapted for IgG avidity, and standardized in house with changes for the use of samples collected on filter paper
Standard technique tomeasure serum IgG levels
Technique adapted to measure IgG levelson filter paper
Technique to determine IgG avidity inserum and on filter paper
100 μl of sample diluentþ5 μl of sample Perforation with specific 5mm diameterperforatorþ 10 μl of sample diluent
Serum: 100 μl of sample diluentþ5 μl ofsampleFilter paper: 100 μl of samplediluentþone 5mm diameter filter paperdisc
Incubation for 30minutes at 37°C Incubation for 30minutes at 37°C Incubation for 30minutes at 37°C
First wash with 300 μl of washing solutionpreviously prepared according to themanufacturer’s instructions
Removal of filter papers and first wash with300 μl of washing solution previouslyprepared according to the manufacturer’sinstructions
First wash with 300 μl of previouslyprepared solution of 6M Urea
Addition of 100 μl of conjugate
Incubation for 30minutes at 37°C
Second wash with 300 μl of washing solution previouslyprepared according to the manufacturer’s instructions
Addition of 50 μl of substrate A and 50 μl of substrate B
Incubation for 10minutes at 37°C
Addition of 50 μl of stop solution
Reading on filters at 450nm and 630nm
Abbreviations: IgG, Immunoglobulin G.Source: Rahbari et al.17
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
IgG Avidity in Samples Collected on Filter Paper Souza et al. 889

concomitantly using the samples collected on filter paperusing the Virion Serion commercial kit for filter paper andthe Quibasa-Bioclin commercial kits used in our study. Afterthe readings and technical validations, the cutoff of eachplate and the indices of each sample were calculated todetermine IgG and IgM. The percentage of IgG avidity wascalculated based on the following formula: AI¼Abs (Uþ ) /Abs (U-) x 100,1 where the result of absorbance of wellswashedwith PBS-urea (Uþ ) was divided by the absorbancesof wells washed with PBS (U-) and then multiplied by 100.17
The values obtained in the avidity test were classifiedaccording to the protocol proposed by Rahbari et al.,17 andpatientswith avidity values� 30%were considered as havinglow IgG avidity.
Results
A total of 1,277 whole blood samples were collected on filterpaper from 3- to 7-day-old NBs in thematernity wards of theHC-UFG, the HMDI, and the CNE. The ELISA test detected thepresence of anti-T. gondii IgG antibodies in 44.4% (567/1,277)of the analyzed samples. Of the 567 blood samples collectedon filter paper that were reactive to IgG, 57.67% (327/567)presented an absorbance value�3.0 and were considered atrisk in the present study. Following the proposed methodol-ogy, the mothers of infants whose blood samples on filterpaper showed ELISA titers�3were contacted and peripheralblood samples were collected from their babies before theywere 3 months old (►Table 1).
1. Comparison of the results of blood on filter paper andperipheral blood
A total of 177 pairs of samples were collected, and theresults of 167 (94.36%) peripheral blood samples from NBswere in agreement with those obtained in the heel prick teston filter paper. However, 10 (5.64%) peripheral blood sam-ples showed results that were inconsistent with thoseobtained on filter paper.
2. Comparison of serology in samples collected simulta-neously of peripheral blood of infants and their mothers
All the 177 pairs of recollections (mothers and children)performed showed negative results for IgM. Regarding IgG,167 pairs (94,36%) of samples from both mother and child
were detected with the presence of anti-T gondii IgGantibodies.
3. High IgG avidity – filter paper versus peripheral blood
The 167 samples from babies that remained IgG-positiveafter 3 months were subjected to the IgG avidity test todetermine the binding strength of this immunoglobulinwiththe epitope, in order to ascertain if the infectionwas a recentor past infection of the mother. Among these 167 samples,163 (97.60%) showedhigh avidity of antibodies, and 4 (2.40%)of the samples showed lowavidity of IgG antibodies, which isindicative of a recent infection. Congenital infectionwas thenconfirmed in 50% of the samples from infants with low IgGantibody avidity by the Western Blot method. For infantswith high IgG avidity, thefindingmust be confirmed byothermethods. Among the 167 samples collected in duplicate, 17samples were randomly collected from peripheral blood andfilter paper simultaneously from the same infant. In thisanalysis, 1 (5.88%) of the 17 samples collected in duplicatealso showed low IgG avidity, suggesting congenital infectionof the infant, and the results obtained in serum and in filterpaper were in agreement. Sixteen (94.12%) of the samplesshowed high avidity, with 100% agreement between theresults obtained in serum and in filter paper, as shownin ►Table 2.17
Discussion
The clinical diagnosis of toxoplasmosis is complex, andsometimes inaccurate, as most pregnant women are asymp-tomatic. Moreover, when they do present symptoms, thesemay be mistaken for other infectious agents, such as Cyto-megalovirus, Herpes simplex virus (HSV-1 or HSV-2), Rubellavirus, HIV, Epstein Barr, Treponema pallidum, Listeria mono-cytogenes, Borrelia burgdorferi (Lyme disease), and Trypano-soma cruzi (Chagas disease).18
According to data presented by the Association of Parentsand Friends of Disabled Children (APAE, in the Portugueseacronym) in Goiânia, state of Goiás, Brazil, from 2003 to2013, 9,247,974 prenatal screening tests were performed onmothers in their 1st trimester of pregnancy, but only 653,562pregnant women underwent prenatal tests in the 3rd trimes-ter. In other words, � 93% of mothers did not undergo therecommended toxoplasmosis screening test during
Table 1 Comparison of Immunoglobulin G anti-Toxoplasma gondii, obtained by the ELISA test on serum samples from children andtheir respective mothers collected 3 months after birth
Results Mother Child
Absolute number % Absolute number %
Reagent (IgM) 0 0 0 0
Reagent (IgG) 167 94.36 167 94.36
Reactive mother and non-reactive child (IgG) 5 2.82 5 2.82
Non-reactive mother and child (IgG) 5 2,82 5 2,82
Total samples 177 100 177 100
Abbreviations: IgG, immunoglobulin G; IgM, immunoglobulin M.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
IgG Avidity in Samples Collected on Filter Paper Souza et al.890

pregnancy, although this is the third most frequent diseasediagnosed among the 24 tests performed during prenatalcare on a total of 27,924 pregnant women with confirmedinfections, while hepatitis B and syphilis rank in firstand second place, respectively.19
Neonatal infection is usually asymptomatic, and whenidentified, may present clinical signs similar to erythroblas-tosis fetalis and to certain degenerative diseases. The clinicalexamination only suggests the possibility of this etiology,even when toxoplasmosis is symptomatic.20
Most studies, including those by Buffolano et al.21 andCañedo-Solares et al.,22 focus on the predictive value of theIgG avidity test in pregnant women, demonstrating theimportance of this test in the diagnosis during the acutephase of the infection, with 100% sensitivity and 92.7%specificity.23,24 However, few studies in the literature fo-cused on the use of avidity in the blood of NBs, and observedlow IgG avidity values in infected NBs.25
The focus of the present studywas tomeasure and analyzethe levels of IgG and test the IgG avidity in peripheral bloodfrom NBs, following the aforementioned criteria. However,based on our findings and on the promising potential of thismethod in the early diagnosis of congenital toxoplasmosis,the possibility of validating an IgG avidity technique on filter
paper would be highly relevant, given its remarkable contri-bution to the primary care system for NBs, such as in the heelprick test, for example.
Brazil’s National Neonatal Screening Program (PNTN, inthe Portuguese acronym), known as the “Heel Prick Test”,was created and implemented by the Ministry of Healthunder Directive MG/MS No. 822/01,26 and is aimed at theearly detection of disorders and diseases in NBs to ensure theappropriate intervention and potentiation of treatment.Almost 3 million children are born each year in Brazil, andthe coverage of NB screening varies according to the state.Nevertheless, in 2017 (the most recent data), the nationalcoverage of the heel prick test reached 85.8%, demonstratingthe strong support of this program by the population.27
The clearly greater adherence to the heel prick test than toprenatal testing of the mother underscores the bias againstthe prenatal program. Hence, to compensate for this lack, theIgG avidity test on filter paper can be of great value as part ofthe methodological approaches carried out in the heel pricktest.
Detection of low-avidity IgG as early as in the heel pricktest of NBs may streamline the diagnosis of congenitalinfection. According to Fonseca et al.,23 NBs exposed to T.gondii show elevated serum IgM and IgG levels, and whentheir IgG shows low avidity, they exhibit more severe symp-toms of congenital toxoplasmosis. The aforementionedauthors observed that high IgG avidity in NBs probablyindicates a lower risk of infection by T. gondii.28
The 10 discordant samples reported in item 1 of theResults section can be explained by the 61.1 to 99.3%sensitivity rate of the ELISA test and by the timeframe ofthe 2nd blood collection, which, in some cases, was 3months.Despite this slight divergence, the use of serology on samplescollected on filter paper has already been standardized and iswidely used, and the technique is considered highly efficientand reproducible.29–32
As for the 4 samples that presented low IgG antibodyavidity described under item 2 of the Results section, andconsidering that IgG crosses the placental barrier, this anti-bodymay have been passed on to the fetus during pregnancy.However, this does not diminish its relevance, since it mayindicate primarymaternal infection, with a considerable riskof vertical transmission. This situation may indicate a recentinfection or even a current production of low avidity IgG bythe NB, which in both cases is extremely important for thediagnosis and earliest possible treatment.33,34
The fact that not all samples with high IgG concentrationswere collected in duplicate was due to the difficulty incommunicating with the parents of the infants and to theirlack of interest in allowing a second blood collection, as theinfants were apparently asymptomatic. It should be notedthat the lack of communication is one of the major problemsin the diagnosis of congenital toxoplasmosis, as NBs are oftenborn asymptomatic and only present sequelae months oreven years after their birth.30,35–37
Our data reveal that screening infants with high IgG titers,allied to avidity testing, can contribute to the tracking andearly diagnosis of postnatal toxoplasmosis.
Table 2 Comparison of anti-Toxoplasma gondii IgG avidityvalues obtained by ELISA using Quibasa-Bioclin kits adaptedfor IgG avidity in serum samples and adapted in house forsamples in filter paper, collected simultaneously 3months afterbirth
Samples IgG avidityserum
IgG avidityfilter paper
IgG serum(ELISAindex)
IgG filterpaper(ELISAindex)
Patient 1 26% 26% 3.52 3.31
Patient2 52% 56% 2.94 2.75
Patient3 48% 43% 2.65 2.37
Patient4 89% 89% 2.04 1.47
Patient5 61% 87% 1.51 1.71
Patient6 56% 73% 2.0 2.02
Patient7 87% 86% 1.27 0.99
Patient8 95% 77% 16.70 17.21
Patient9 76% 84% 1.24 1.56
Patient10 77% 88% 3.72 2.59
Patient11 81% 91% 5.13 4.60
Patient12 86% 73% 3.44 4.53
Patient13 52% 55% 3.86 3.54
Patient14 72% 81% 2.25 2.18
Patient15 94% 92% 1.88 1.83
Patient16 53% 99% 4.72 2.17
Patient17 52% 55% 3.86 3.54
Abbreviations: ELISA, enzyme-linked immunosorbent assay; IgG, Im-munoglobulin G.Source: Rahbari et al.17
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
IgG Avidity in Samples Collected on Filter Paper Souza et al. 891

Conclusion
The IgG avidity test proved to be efficient because it enabledthe detection of patients with low avidity in 2.4% of theanalyzed samples, contributing to the early identification ofcongenital toxoplasmosis in 50% of these samples, subse-quently confirmed by Western Blot tests. Screening fortoxoplasmosis in NBs with high IgG titers, allied with aviditytesting, can be performed on filter paper and easily includedin the current heel prick test. Thus, it can contribute totracking and early diagnosis, since congenital toxoplasmosisis difficult to diagnose and depends on several factors,particularly on those pertaining to the age of the fetuswhen infection set in, and on the absence of symptoms ininfected infants, which makes their identification even moredifficult. The data reported here indicate that the avidity testmay be another valuable method for the diagnosis of con-genital toxoplasmosis inNBs. Thismethod is inexpensive andeasy to implement on blood samples that present highconcentrations of IgG detected in the heel prick test, thebasic test of the postnatal program, offered nationwide bythe SUS.
ContributionsAll authors participated in the concept and design of thestudy, analysis and interpretation of data, in the draft orrevision of the manuscript, and they have approved themanuscript as submitted. All authors are responsible forthe reported research.
Conflict of InterestsThe authors have no conflict of interests to declare.
AcknowledgementsWe would like to thank the management and the staff ofthe Hospital Maternidade Dona Íris (HMDI, in the Portu-guese acronym), the Hospital das Clínicas da UniversidadeFederal de Goiás (HC-UFG, in the Portuguese acronym),and the Nova Era Center for Comprehensive Health Care(CNE/CAIS, in the Portuguese acronym) for the partner-ship developed throughout the present study. We alsothank all the patients who participated in the presentstudy and the financial support, public call N° 12/2013 -Programa Pesquisa para o SUS: Gestão Compartilhada emSaúde – PPSUS/GO – FAPEG.
References1 Teimouri A, Mohtasebi S, Kazemirad E, Keshavarz H. Role of
Toxoplasma gondii IgG avidity testing in discriminating betweenacute and chronic toxoplasmosis in pregnancy. J Clin Microbiol.2020;58(09):e00505–e00520. Doi: 10.1128/JCM.00505-20
2 Cruz AM, Araújo AM, Fit SS, Vieira LC, Felix LC, Sousa DS, et al.Incidência e delineamento epidemiológico de gestantes comtoxoplasmose, em uma unidade de referência de Santarém-Pará. Livro de Resumos da Feira de Trabalhos Acadêmicos eCientíficos–Fetac; Nov 2014; Santarém, PA.
3 Bahia-Oliveira LM, Jones JL, Azevedo-Silva J, Alves CC, Oréfice F,Addiss DG. Highly endemic, waterborne toxoplasmosis in north
Rio de Janeiro state, Brazil. Emerg Infect Dis. 2003;9(01):55–62.Doi: 10.3201/eid0901.020160
4 Neto EC, Anele E, Rubim R, Brites A, Schulte J, Becker D, et al. Highprevalence of congenital toxoplasmosis in Brazil estimated in a 3-year prospective neonatal screening study. Int J Epidemiol. 2000;29(05):941–947. Doi: 10.1093/ije/29.5.941
5 Lago EG, Carvalho RL, Silva VB, Fiori RM. Screening for Toxoplasmagondii antibodies in 2,513 consecutive parturient women andevaluation of newborn infants at risk for congenital toxoplasmo-sis. Sci Med (Porto Alegre). 2009;19(01):27–34. oai:doaj.org/article:ca7185a278114cd1925d5ba6f2301bef
6 Carvalheiro CG, Mussi-Pinhata MM, Yamamoto AY, De Souza CB,Maciel LM. Incidence of congenital toxoplasmosis estimated byneonatal screening: relevance of diagnostic confirmation inasymptomatic newborn infants. Epidemiol Infect. 2005;133(03):485–491. Doi: 10.1017/s095026880400353x
7 Wilson CB, Remington JS, Stagno S, Reynolds DW. Development ofadverse sequelae in children born with subclinical congenitalToxoplasma infection. Pediatrics. 1980;66(05):767–774
8 Soares JAS, Caldeira AP. Congenital toxoplasmosis: the challengeof early diagnosis of a complex and neglected disease. Rev SocBras Med Trop. 2019;52:e20180228. Doi: 10.1590/0037-8682-0228-2018
9 Amendoeira MR, Millar PR. Congenital toxoplasmosis: the impor-tance of implementing clinical practice guidelines. The LancetRegional Health – Americas. 2021;23:15–24. https://doi.org/10.1016/j.lana.2021.100023
10 Reis MM, Tessaro MM, d ’Azevedo PA. Perfil sorológico paratoxoplasmose em gestantes de um hospital público de PortoAlegre. Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(03):. Doi: 10.1590/s0100-72032006000300004
11 Gomes Filho C, Macedo Filho JV, Minuzzi AL, GomesMM, LuquettiAO. Detecção de doenças transmissíveis em gestantes no estadode Goiás: o teste da mamãe. Revista de Patologia Tropical/Journalof Tropical Pathology. 2016;45(04):369–386. https://doi.org/10.5216/rpt.v45i4.44610
12 Garnaud C, Fricker-Hidalgo H, Evengård B, Álvarez-Martínez MJ,Petersen E, Kortbeek LM, et al;under the auspices of the ESGCP ofESCMID. Toxoplasma gondii-specific IgG avidity testing in preg-nant women. Clin Microbiol Infect. 2020;26(09):1155–1160. Doi:10.1016/j.cmi.2020.04.014
13 Kheirandish F, Ezatpour B, Fallahi SH, Tarahi MJ, Hosseini P,Rouzbahani AK, et al. Toxoplasma serology status and risk ofmiscarriage, a case-control study among womenwith a history ofspontaneous abortion. Int J Fertil Steril. 2019;13(03):184–189.Doi: 10.22074/ijfs.2019.5740
14 Figueiró-Filho EA, Senefonte FR, Lopes AH,Morais OO, Souza JúniorVG, Maia TL, et al. [Frequency of HIV-1, rubella, syphilis, toxoplas-mosis, cytomegalovirus, simple herpes virus, hepatitis B, hepatitisC,ChagasdiseaseandHTLV I/II infection inpregnantwomenofStateof Mato Grosso do Sul]. Rev Soc Bras Med Trop. 2007;40(02):181–187. Doi: 10.1590/S0037-86822007000200007Portuguese.
15 Koppe JG, Loewer-Sieger DH, de Roever-Bonnet H. Results of 20-year follow-up of congenital toxoplasmosis. Lancet. 1986;1(8475):254–256. Doi: 10.1016/S0140-6736(86)90785-3
16 Montoya JG, Liesenfeld O. Toxoplasmosis. Lancet. 2004;363(9425):1965–1976. Doi: 10.1016/S0140-6736(04)16412-X
17 Rahbari AH, Keshavarz H, Shojaee S, Mohebali M, Rezaeian M. IgGavidity ELISA test for diagnosis of acute toxoplasmosis in humans.Korean J Parasitol. 2012;50(02):99–102. Doi: 10.3347/kjp.2012.50.2.99
18 Diniz EM. O diagnóstico da toxoplasmose na gestante e no recém-nascido [dissertation]. São Paulo: Faculdade de Medicina, Depar-tamento de Pediatria, Universidade de São Paulo. 2006;28:222–222
19 Storchilo HR. Triagem pelo teste do pezinho para diagnósticoprecoce da infecção congênita para toxoplasmose em três
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
IgG Avidity in Samples Collected on Filter Paper Souza et al.892
unidades de saúde pública da região metropolitana de Goiânia,Goiás [dissertação]. Goiânia: Universidade Federal de Goiás; 2016
20 Rey L. Parasitologia: parasitos e doençasparasitárias dohomemnasAméricas enaÁfrica. 2aed.Riode Janeiro:GuanabaraKoogan;1991
21 Buffolano W, Lappalainen M, Hedman L, Ciccimarra F, Del PezzoM, Rescaldani R, et al. Delayed maturation of IgG avidity incongenital toxoplasmosis. Eur J Clin Microbiol Infect Dis. 2004;23(11):825–830. Doi: 10.1007/s10096-004-1226-1
22 Cañedo-Solares I, Ortiz-Alegría LB, Figueroa-Damián R, Bustos-Bahena ML, González-Henkel H, Calderón-Segura E, et al. Toxo-plasmosis in pregnancy: determination of IgM, IgG and avidity infilter paper-embedded blood. J Perinatol. 2009;29(10):668–672.Doi: 10.1038/jp.2009.79
23 Fonseca ZC, Rodrigues IM,MeloNC, Avelar JB, CastroAM,AvelinoMM.IgG avidity test in congenital toxoplasmosis diagnoses in newbornspathogens. 2017;6(02):26. Doi: 10.3390/pathogens6020026
24 Candolfi E, Pastor R, Huber R, Filisetti D, Villard O. IgG avidity assayfirmsupthediagnosisofacutetoxoplasmosisonthefirstserumsamplein immunocompetent pregnant women. Diagn Microbiol Infect Dis.2007;58(01):83–88. Doi: 10.1016/j.diagmicrobio.2006.12.010
25 Fonseca FC, Rodrigues IM, Melo NC, Castro AN, Avelino MM.Importância do teste de avidez de IgG na toxoplasmose congênita.Revista de Patologia Tropical/Journal of Tropical Pathology. 2016;45(01):42–54. Doi: 10.5216/rpt.v45i1.40078
26 Ministério da Saúde. Portaria No. 822, de 6 de junho de 2001.Institui, no âmbito do Sistema Único de Saúde, o ProgramaNacional de Triagem Neonatal / PNTN [Internet]. 2001 [cited2020 Aug 12]. Available from: https://bvsms.saude.gov.br/bvs/saudelegis/gm/2001/prt0822_06_06_2001.html
27 Ministério da Saúde. Programa Nacional da Triagem Neonatal.Cobertura do Programa Nacional de Triagem Neonatal [Internet].Brasília (DF): Ministério da Saúde; 2018 [cited 2020 Aug 12].Available from: https://antigo.saude.gov.br/acoes-e-programas/programa-nacional-da-triagem-neonatal/indicadores-da-triagem-neonatal-no-brasil
28 Webster JP. Review of "Toxoplasmosis of animals and humans(Second Edition)" by J.P. Dubey Parasit Vectors. 2010;3(01):1–2.Doi: 10.1186/1756-3305-3-112
29 Dunn D, Wallon M, Peyron F, Petersen E, Peckham C, Gilbert R.Mother-to-child transmission of toxoplasmosis: risk estimates forclinical counselling. Lancet. 1999;353(9167):1829–1833. Doi:10.1016/S0140-6736(98)08220-8
30 Naessens A, Jenum PA, Pollak A, Decoster A, Lappalainen M,Villena I, et al. Diagnosis of congenital toxoplasmosis in theneonatal period: A multicenter evaluation. J Pediatr. 1999;135(06):714–719. Doi: 10.1016/S0022-3476(99)70090-9
31 Zhang K, Wang L, Lin G, Sun Y, Zhang R, Xie J, et al. Results of thenational external quality assessment for toxoplasmosis serologi-cal testing in China. PLoS One. 2015;10(06):e0130003. Doi:10.1371/journal.pone.0130003
32 Sartori AL, Minamisava R, Avelino MM, Martins CA. [Prenatalscreening for toxoplasmosis and factors associated with seropos-itivity of pregnant women in Goiânia, Goiás]. Rev Bras GinecolObstet. 2011;33(02):93–98. Doi: 10.1590/S0100-72032011000200007
33 Avelar JB, Rezende HH, Storchilo HR, Candido RR, Amaral WN,Avelino MM, Avelino MM, et al. Reativação da toxoplasmosedurante o oitavo mês de gestação. Revista Norte Mineira deEnfermagem. 2015;4(01):57–69
34 Avelar JBToxoplasmose crônica em gestantes. Avaliação da prev-alência, fatores de risco e acompanhamento de um grupo derecém-nascidos em Goiânia – Goiás [tese]. Goiânia: UniversidadeFederal de Goiás; 2013
35 Pena LT, Discacciati MG. Importância do teste de avidez daimunoglobulina G (IgG) antiToxoplasma gondii no diagnósticoda toxoplasmose em gestantes. Universidade de São Paulo:Revista do Instituto Adolfo Lutz. 2013;72(02):117–123. Doi:10.18241/0073-98552013721551
36 Deshpande PS, Kotresha D, Noordin R, Yunus MH, Saadatnia G,Golkar M, et al. IgG avidity Western blot using Toxoplasma gondiirGRA-7 cloned fromnucleotides 39-711 for serodiagnosis of acutetoxoplasmosis. Rev Inst Med Trop São Paulo. 2013;55(02):79–83.Doi: 10.1590/S0036-46652013000200003
37 Garcia MG, Ferreira EA, Oliveira FP. Análise da compreensão depais acerca do teste do pezinho. São Paulo: Journal of HumanGrowth and Development. 2007;17(01):1–12
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
IgG Avidity in Samples Collected on Filter Paper Souza et al. 893
Preeclampsia and Gestational Hypertension:Biochemical and Antioxidant Features in VitroMight Help Understand Different Outcomes
Pré-eclâmpsia e hipertensão gestacional: Fatoresbioquímicos e antioxidantes in vitro podem auxiliar noentendimento de resultados clínicos distintosVictoria Elizabeth Galvão1 Ricardo Carvalho Cavalli2 Valeria Cristina Sandrim1,3
1Department of Pharmacology, Instituto de Biociências, UniversidadeEstadual Paulista, Botucatu, SP, Brazil
2Department of Obstetrics and Gynecology, Faculdade de Medicina deRibeirão Preto, Universidade de São Paulo, Ribeirão Preto, SP, Brazil
3Center for Toxicological Assistance, Instituto de Biociências,Universidade Estadual Paulista, Botucatu, SP, Brazil
Rev Bras Ginecol Obstet 2021;43(12):894–903.
Address for correspondence Valeria Cristina Sandrim, PhD, Rua Prof.Dr. Antonio Celso Wagner Zanin - Jardim São Jose (Rubião Junior),18618-689, Botucatu, SP, Brazil (e-mail: [email protected]).
Keywords
► preeclampsia► potassium iodide► heme oxygenase-1► hypertension► endothelium
Abstract Objective Gestational hypertension (GH) is characterized by increased blood pressureafter the 20th gestational week; the presence of proteinuria and/or signs of end-organdamage indicate preeclampsia (PE). Heme oxygenase-1 (HO-1) is an antioxidant enzymewith an important role in maintaining endothelial function, and induction of HO-1 bycertain molecules shows potential in attenuating the condition’s effects over endothelialtissue. HO-1 production can also be stimulated by potassium iodide (KI). Therefore, weevaluated the effects of KI over HO-1 expression in human umbilical vein endothelial cells(HUVECs) incubated with plasma from women diagnosed with GH or PE.Methods Human umbilical vein endothelial cells were incubated with a pool ofplasma of healthy pregnant women (n¼ 12), pregnant women diagnosed with GH(n¼10) or preeclamptic women (n¼11) with or without the addition of KI for 24 hoursto evaluate its effect on this enzyme expression. Analysis of variance was performedfollowed by Dunnet’s test for multiple comparisons between groups only or betweengroups with addition of KI (p � 0.05).Results KI solution (1,000 µM) reduced HO-1 in the gestational hypertension group(p¼0.0018) and cytotoxicity in the preeclamptic group (p¼ 0.0143); treatment with KIreduced plasma cytotoxicity but did not affect the preeclamptic group’s HO-1 expression.Conclusion Our findings suggest that KI alleviates oxidative stress leading todecreased HO-1 expression; plasma from preeclamptic women did not induce theenzyme’s expression in HUVECs, and we hypothesize that this is possibly due toinhibitory post-transcriptional mechanisms in response to overexpression of thisenzyme during early pregnancy.
receivedAugust 31, 2020acceptedOctober 5, 2021
DOI https://doi.org/10.1055/s-0041-1740270.ISSN 0100-7203.
© 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rightsreserved.This is an open access article published by Thieme under the terms of the
Creative Commons Attribution License, permitting unrestricted use,
distribution, and reproduction so long as the original work is properly cited.
(https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda., Rua do Matoso 170, Rio deJaneiro, RJ, CEP 20270-135, Brazil
Original ArticleTHIEME
894

Introduction
Gestational hypertension (GH) is characterized by high bloodpressure after the 20th gestational week.1 Around 25% ofwomen diagnosedwith GH on averagewill eventually devel-op preeclampsia, presenting additional hematological ab-normalities and signs of end-organ damage such as edema,headaches, eyesight changes, difficulty breathing, and nau-sea.1,2 Preeclampsia (PE) is the major cause of maternaldeath in Latin America and the Caribbean region with aworldwide incidence of 5 to 10% of all pregnancies.3–5
These disorders’ exact causes are still unknown; riskfactors include obesity, nulliparity, and a family history forthese conditions.6 The most accepted hypothesis for thepathophysiology of preeclampsia consists of the “two-stagemodel,” in which it was proposed that an inadequate andinefficient placentation process early on in pregnancy leadsto an ischemic, defective organ that eventually secretesvasoactive molecules affecting the endothelium, leading tothe characteristic clinical signs and symptoms.7 When GHdoes not progress to PE, it usually displays an intermediatephenotype between normal pregnancy and PE, suggesting amore benign origin and presenting as less of a threat for bothmother and baby.8
Prooxidant, vasoconstricting, and antiangiogenic factorsare upregulated in this condition.9 The endotheliumresponds by increasing the expression of antioxidant
enzymes such as heme oxygenase-1 (HO-1), an inducibleenzyme expressed in many tissues that converts the hemegroup into carbon monoxide, bilirubin, and free iron, mole-cules with direct or indirect antioxidant and vasoactivefunctions.10,11 Heme oxygenase-1 has been implicated inthe pathogenesis of several diseases, including pregnancy-induced hypertension, and the induction of the enzyme hasbeen shown to improve markers for these conditions both invitro and in an in vivo model for PE.12–14
Beyond thewell-known role in thyroid hormones produc-tion, potassium iodide is crucial in pregnancy and alsoexhibits antioxidant and antiinflammatory properties;14
besides, it has been shown to be capable of increasing HO-1 expression in skin explants and cells exposed to ultravioletrays.15
Thus, the present study aimed to evaluate the effects ofplasma from women affected by GE and PE over humanumbilical vein endothelial cells (HUVECs) as well as theeffects of potassium iodide (KI) regarding cytotoxicity, anti-oxidant capacity, and HO-1 expression.
Methods
Source of Biological SamplesIn the present study, we used plasma samples from a previ-ous work aiming to compare clinical and laboratory
Resumo Objetivo A hipertensão gestacional (GH) é caracterizada pelo aumento da pressãosanguínea após a 20ª semana de gestação; a presença de proteinuria e/ou sinais dedanos a órgãos como rins, fígado e cérebro indicam pré-eclâmpsia (PE). A hemeoxigenase-1 (HO-1) é uma enzima antioxidante com um papel importante na manu-tenção da função endotelial, e a sua indução por certas moléculas se mostrapotencialmente benéfica frente à característica deletéria destas condições sobre oendotélio. Já foi demonstrado anteriormente que a produção de HO-1 pode serinduzida por iodeto de potássio (KI). Portanto, nós avaliamos os efeitos do KI sobrea citotoxicidade e expressão de HO-1 por células de veia de cordão umbilical humano(HUVECs) após incubação com o plasma de mulheres diagnosticadas com GH ou PE.Métodos Células de veia de cordão umbilical humano foram incubadas com pool deplasma de gestantes saudáveis (n¼12), gestantes com GH (n¼10) ou gestantes comPE (n¼11) com ou sem a adição de KI por 24 horas para avaliar a citotoxicidade atravésda dosagem de lactato desidrogenase e produção de HO-1 por ELISA. Foi realizadaANOVA seguida de teste de Dunnet para múltiplas comparações entre os gruposestudados, considerando significativos valores de p � 0,05.Resultados A solução de KI (1.000 µM) reduziu a produção de HO-1 no grupo GH(p¼0.0018) e a citotoxicidade no grupo PE (p¼0.0143); o tratamento com KI nãoafetou a produção de HO-1 por HUVECs incubadas com o plasma do grupo PE.Conclusão Nossos achados sugerem que o KI atenua os efeitos do plasma degestantes com GH ocasionando a diminuição da produção de HO-1; plasma do grupoPE não induziu a produção de HO-1 em HUVECs em comparação ao grupo saudável, enossa hipótese é a de que tal achado pode ser devido amecanismos pós-transcricionaisem resposta a uma superestimulação da produção de HO-1 nos estágios iniciais dagravidez.
Palavras-chave
► pré-eclâmpsia► iodeto de potássio► heme oxigenase-1► hipertensão► endotélio
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Preeclampsia and Gestational Hypertension Galvão et al. 895

characteristics, obstetric, and perinatal outcomes of patientswith PE or GH.16 A group of pregnant womenwere recruitedat the ambulatory clinic of the University Hospital of theFaculdade deMedicina de Ribeirão Preto. This previous studywas approved by the Institutional Review Board at RibeirãoPreto Medical School, Brazil (reference 4682/2006, approveddate June 20th, 2006) and was performed following theprinciples of the Declaration of Helsinki. All subjects gavewritten informed consent.
To avoid misdiagnosis of GH and PE, the 419 patientsenrolledwere diagnosed retrospectivelywith PE and GH. Thediagnosis criteria were used according to the AmericanCollege of Obstetricians and Gynecologists, and they were:systolic blood pressure above 140mmHg and diastolic bloodpressure above 90mmHg on two different occasions at least4 hours apart or systolic and diastolic blood pressure of160mmHg and 110mmHg respectively after the 20th gesta-tional week in women with previously normal blood pres-sure readings, plus proteinuria; in the absence of the latter,newly onset hypertension accompanied by symptoms andlaboratory findings such as neurological and visual im-pairment, pulmonary edema, thrombocytopenia, and im-paired liver and renal function were used to establish adiagnosis.1 High blood pressure (systolic � 140mmHg;diastolic � 90mmHg) after the 20th gestational week with-out proteinuria and/or the aforementioned symptoms andsigns was diagnosed as GH. The exclusion criteria were twinpregnancy, hemostatic abnormalities, chronic hypertension,diabetes mellitus, fetal abnormalities, cancer, and cardiovas-cular, autoimmune, renal, and hepatic diseases. All bloodsamples were obtained after the 30th gestational week.Venous maternal blood samples were collected in tubescontaining heparin, which were then centrifuged (1,000 gfor 3minutes). Plasma was collected, sampled in 1,000 μLtubes, and stored at �80°C prior to use. Due to the limitedplasma aliquots stocked and the small quantity needed toprepare the pool, we stipulated a minimum of 10 and amaximum of 15 samples per group.
Preparation of KI Solution and Redox TitrationPotassium iodide was purchased from Sigma-Aldrich Brazil(Catalogue number 221945–100G – Sigma-Aldrich BrazilLtda., Bauru, SP, Brazil). A KI solution was prepared bysolubilizing it in deionized water and for the redox titration;we used sodium thiosulfate, previously titrated with apotassium iodate solution as a primary standard. The stocksolution concentration was 58mM. For the experiments, wediluted that solution in growth culture to achieve a finalconcentration of 100 µM and 1,000 µM.
Human Umbilical Vein Endothelial Cell CultureHuman umbilical vein endothelial cells (ATCC, Virginia, USA;CRL-2873) were used for this in vitro model of hypertensivedisorders of pregnancy. Cells were cultivated in sterile25 cm2 flasks using growth medium (Gibco, CA, USA) sup-plementedwith fetal bovine serum 10% v/v (Gibco), 50μg/mlpenicillin, 50μg/ml streptomycin, and 0.5 μg/ml amphoteri-cin B (Gibco). For the experiments described ahead, cells
were detached from culture flask (Corning, Costar,Netherlands) using trypsin solution (Trypsin/EDTA 0.5/0.2mg/ml in phosphate-buffered saline, PBS) centrifuged at1,200 rpm for 10minutes, resuspended in growth mediumfree from fetal bovine serum containing antibiotic andantifungal solution and seeded on 96 well microplate(1.104 cells/well) overnight at 37°C, 5% CO2 tension, and95% humidity to ensure cell adhesion.
Incubation with Patients’ Samples Pools and KIPlasma samples from the healthy pregnancy (HP, n¼12), GH(n¼10), and PE (n¼11) groups were pooled bymixing equalvolumes of each patient’s plasma in 3 distinct 1,500 μL tubes(30 μL/patient). From the resulting volume, 240 μL of eachpool was diluted in growth medium free from fetal bovineserum (160 μL growth medium/well) using three Falcon15mL centrifuge tubes (Sigma-Aldrich, St. Louis, MO, USA).Cell culture supernatant was discarded, and 180 μL of thediluted pools were added to each well to achieve a 10% poolof plasma concentration per well. Then, 20 μL of KI solutionwas added to the wells, resulting in the final concentrationsof 10 µM, 50 µM, 100 µM, 500 µM, and 1,000µM, so the finalvolumewould be 200 μL per well. Only the 100 µM and 1,000µM final concentrations were selected due to their statisti-cally relevant results. Cells incubated with growth mediumand pool of plasma onlywere used as controls for each group,in which case the KI solution was not added, and the finalvolume was achieved by adding 20 μL of growth mediuminstead. After a 24-hour incubation period, the supernatantwas collected for posterior cytotoxicity, total antioxidantcapacity, and hHO-1 quantification assays.
Cytotoxicity AssayCytotoxicity was assessed bymeasuring the lactate dehydro-genase (LDH) activity using the Pierce LDH cytotoxicity assaykit — catalogue number 88954 (Thermo Fisher Scientific,Waltham, MA, USA). Lactate dehydrogenase can be detectedon cell culture supernatant when cell membrane integrity islost indicating cytotoxicity; after a 24-hour incubation peri-od with patients’ pool, 30 µL of supernatant were collectedand immediately transferred to another 96 well microplate,to which 30 µL of the substrate mix was added. After30minutes of incubation at room temperature while pro-tected from light, 30 µL of stop solution was added, and theabsorbance was read using 490nm wavelength, with anadditional 680nm reading for background signalelimination.
Total Antioxidant Capacity (TAC) and HO-1QuantificationTotal antioxidant capacity of culture supernatant wasassessed using the Ferric Reducing Antioxidant Power(FRAP) assay.17 The FRAP reagent was prepared by mixing50mL of 23mM acetate buffer (pH¼3.6), 5mL of 10mMtripyridyltriazine (TPTZ) solution, and 5mL 20mMFeCl3.6H2O. A total of 10µL of the supernatant sample wasadded to a 96-well microplate, to which 290 µL of FRAPreagent weremixed, and themicroplatewas incubated at 37°
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Preeclampsia and Gestational Hypertension Galvão et al.896

C for 4minutes. Absorbance was read at a 593nm wave-length. The standard solution was prepared using Fe2S-O4.7H2O, and the unit used was mM equivalent Fe2þ. TheHO-1 quantification assay Human Total HO-1/HMOX1 Duo-Set IC ELISA kit–catalogue number DYC3776 (R&D Systems,Inc., Minneapolis, MN, USA) was , and the experimentfollowedmanufacturer instructions. The 450 nmwavelengthwas used for readings.
Transmission Electron Microscopy (TEM)Cells were seeded in tissue culture 6 wells plate (500,000cells/well) overnight and incubatedwith HP, GH, and PE poolof plasma and with PE pool of plasma plus 1,000 µM of KI for24 hours. Cells were removed from the trypsin-EDTA solu-tion for a minute; the enzyme was neutralized with fetalbovine serum, and the cells were transferred to microtubesfor centrifugation (1,200 rpm, 10minutes). The supernatantwas then discarded, and the cell pellet was suspended inKarnovsky fixative for another centrifugation. The processwas repeated one more time before the cells were resus-pended in more fixative and delivered at the Electron Mi-croscopy Center of Universidade Estadual Paulista, Botucatucampus, for further processing.
Statistical AnalysisThe software used was GraphPad Prism 6 (GraphPad Soft-ware, San Diego, CA, USA). For statistical analysis of theclinical features of the patients enrolled, we used analysisof variance (ANOVA) followed by the Dunnet test for multiplecomparisons when variables obeyed normal distribution orKruskal-Wallis followed by the Dunn test for multiple com-parisons when at least one group followed a non-parametricdistribution. P-values are described in ►Table 1.
Cell culture results were analyzed using ANOVA followedby the Dunnet test for multiple comparisons, with statisti-cally significant p-values<0.05. We compared the effects ofplasma pool only over HUVECs in the three different groups
as well as the effect of adding KI to culture using each group’spool of plasma.
Ethical Approval and Consent of ParticipantsThe present study was approved by the Institutional ReviewBoard of the HCFMRP-USP (reference 4682/2006, approveddate June 20, 2006). All participants provided written in-formed consent.
Results
The clinical features of the patients from which plasmasamples were obtained are shown in ►Table 1. A total of41.6% of healthy pregnant patients and all patients from theother two studied groups had no children prior to the study.Non-parametric distribution was found when analyzingsystolic and diastolic blood pressure. No statistical differ-ences were found between groups regarding age or placentalweight; blood draws from preeclamptic patients were per-formed significantly earlier than the other two groups, andthe group’s average gestational week at delivery was signifi-cantly lower. Bodymass index (BMI) was significantly higherin the GH group only. Systolic blood pressure was higher inboth GH and PE groups, while diastolic blood pressure wassignificantly higher in the PE group only.
The GH group did not show higher lactate-dehydrogenaseactivity compared with the healthy pregnant group. Howev-er, plasma from the PE group was significantly more cyto-toxic (p¼0.0227,►Fig. 1A).When treatedwith thehighest KIconcentration, cytotoxicity in the PE group was significantlyreduced when compared with values from cell culture withPE plasma pool only (p¼0.0143, ►Fig. 3A).
Given the cytotoxicity results, we analyzed the cellularultrastructure. Cells incubatedwith PE plasma plus 1,000 μMKI had different visual aspects comparedwith cells incubatedwith GH or PE plasma only (►Fig. 2). There is mild vacuo-lization in the cytoplasm in these groups, but the overall
Table 1 Clinical characteristics of pregnant women and delivery conditions
Parameters HP GH PE p-value
N 12 10 11
Age (years) 22.3 (2.27) 21.3 (2.83) 21.6 (4.14) ns
GW sampling 37.3 (1.33) 38.7 (1.94) 31.5 (3.62)� �p< 0.0001
BMI sampling (kg/m2) 28.3 (2.28) 37.4 (7.78)� 28.9 (4.53) �p¼ 0.0006
SBP sampling (mmHg) 113.8 (10.69) 126 (10.50)� 136.2 (16.14)�� �p¼ 0.0310; ��p¼ 0.0011
DBP sampling (mmHg) 71.83 (8.96) 80.40 (9.96) 90 (10.00)� �p¼ 0.0001
Methyldopa (%) 0 100 90 (10/11) –
Nulliparous (%) 41.6 (5/12) 100 (10/10) 100 (11/11) –
GW delivery 39.5 (1.43) 40 (1.00) 34.5 (4.33)� �p¼ 0.0005
Placental weight (g) 536.8 (106.28) 613 (146.29) 408 (160.88) ns
Abbreviations: BMI, body mass index; DBP, diastolic blood pressure; GH, gestational hypertension; GW, gestational weeks; HP, healthy pregnant; PE,preeclamptic; SBP, systolic blood pressure.p values in comparison with the HP group.Data are shown as mean� (SD) or median (underlined)� (IQR).
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Preeclampsia and Gestational Hypertension Galvão et al. 897

images shown in D1 to D3 resemble the healthy pregnantgroup images supporting our cytotoxicity results.
Samples from cells incubatedwith PE plasma only showedhigher antioxidant capacity values when compared with theHP group (p¼0.0021, ►Fig. 1B). Supernatant from the HPand GH groups had increased antioxidant capacity when1,000 µM KI solution was used compared with untreatedgroups (p¼0.0006; p¼0.0025 respectively, ►Fig. 3B). Theantioxidant capacity of cells incubated with PE plasma plusKI did not change, even though there seems to be a tendencyto its increase.
The results of HO-1 dosages from the GH group (►Fig. 1C)showed increased expression of the enzyme compared withthe HP group (p¼0.074). Treatment with 100 µM KI inducedHO-1 expression in the HP group (p¼0.0065). The 1,000 µMtreatment reduced the enzyme expression of the GH groupwhen compared with results from cells incubated with thisgroup’s plasma pool only (p¼0.0018, ►Fig. 3C), but thepreeclamptic group’s HO-1 expression was not affectedwhatsoever by any concentration used.
Discussion
In the present work, we found that GH plasma did not alterlactate-dehydrogenase release or antioxidant capacity ofendothelial cells and that it induced HO-1 expression, whilethe opposite is seen in PE regarding the same parameters. It isremarkable, though, that KI reduced enzyme expression inthe GH group, as well as lactate-dehydrogenase release in thePE group. Contrary to expected, HO-1 levels in the lattergroup were the same as in the healthy group, while the GHgroup showed increased levels, as an evidence of a preservedantioxidant mechanism induced by GH patients’ plasma,which might explain the milder clinical features seenin ►Table 1. In the PE group, this mechanism seems to beabsent, even with increased total antioxidant capacityresults. Iodine as an antioxidant, probably in a direct wayby neutralizing oxidative species, as the treatment eitherreduced HO-1 expression or did not affect it whatsoever.
Both the GH and PE groups were already on methyldopatherapy at the time of sampling, whichmight explain the lack
Fig. 1 Cytotoxicity (A), total antioxidant capacity (B), and heme oxygenase-1 dosage (C) results. Human umbilical vein endothelial cells wereincubated with the three studied groups’ pool of plasma only. Healthy pregnant (HP) group’s results were considered baseline values andwere used as the control group for statistical analysis. Results are shown as mean� SEM of quadruplicate wells per assay. (�) p< 0.05. Thepreeclamptic group’s cytotoxicity and total antioxidant capacity results were significantly higher but showed the same capability of inducingheme oxygenase-1’s expression. Gestational hypertension pool induced increased enzyme expression significantly.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Preeclampsia and Gestational Hypertension Galvão et al.898

Fig. 2 Transmission electron microscopy images of endothelial cells incubated with pool of plasma from healthy pregnant women (A1-A3),women with gestational hypertension (B1-B3), and preeclamptic women (C1-C3). Magnification of 5µm, except for C3 (2 µm). D1 to D3 showcells incubated with preeclamptic plasma and 1,000 µM KI. Images are representative of one assay and were captured throughout the entirety ofthe microscope field.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Preeclampsia and Gestational Hypertension Galvão et al. 899

of statistical difference between the GH and HP groups’diastolic blood pressure values. Antihypertensive therapyoffered no benefit to women from the PE group as bothsystolic and diastolic blood pressure measurements weresignificantly higher than the one from the HP group. Indeed,lack of responsiveness to antihypertensive therapy in PEwomen is associated with worse outcomes, and there havebeen studies addressing this observation using pharmaco-dynamics tools to further understand which personalizedapproach could be beneficial for these patients.17,18
A previous study analyzed the oxidative stress markersand nitric oxide availability in the plasma of PE women andfound a higher total antioxidant capacity corroborating withwhat was found in this work, as well as lower carbonyl levels,a biomarker for protein oxidation. Lipid peroxidation mea-sured using the thiobarbituric acid reactive substances(TBARS) method was not different between groups, but itwas lower in the PE group when compared with the GHgroup, with nitrite levels significantly lower in both hyper-tensive groups.19 However, another study showed increasedlevels of 8-isoprostane and augmented oxidant stress in
plasma from PE patients, but also found increased totalantioxidant capacity, with no difference in vitamin E levels.20
A meta-analysis published in 2018 found increased plasmaoxidative stress markers in PE women, even though somestudies used in this analysis showed an increase in plasmacatalase and glutathione peroxidase,21 suggesting that, inpreeclampsia, the endogenous antioxidant defenses are in-deed upregulated in later pregnancy stages, but this com-pensatory mechanism does not seem to be enough tocounterbalance the systemic endothelial dysfunction causedby the disease. These observations support our results re-garding lactate dehydrogenase release, as an increased anti-oxidant capacity in the preeclamptic groupwas not followedby lower cytotoxicity results.
Lactate dehydrogenase activity was increased, comparedwith the HP group, when cells were incubated using PEplasma only, with similar HO-1 results, while the GH groupshowed elevated HO-1 levels compared with the healthygroup but with similar cytotoxicity results. This shows thecytoprotective effect of HO-1 in preserving cellular mem-brane integrity. Potassium iodide reduced lactate
Fig. 3 Cytotoxicity (A), total antioxidant capacity (B), and heme oxygenase-1 dosage (C) results. Human umbilical vein endothelial cells wereincubated with the three studied groups’ pool of plasma only (“pool”, used as control of each group) or pool of plasma from each group pluspotassium iodide in two different concentrations. Results are shown as mean� standard error of the mean (SEM) of quadruplicate wellsper assay. (�) p< 0.01. (��) p< 0.005. Treatment with 1,000 µM KI reduced significantly the preeclamptic group’s cytotoxicity and increasedtotal antioxidant capacity in the healthy pregnant and gestational hypertension groups. Potassium iodide induced heme oxygenase-1’sexpression in healthy pregnant but reduced it significantly in gestational hypertension; the preeclamptic group’s enzyme expression hasn’t beenaffected by treatment.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Preeclampsia and Gestational Hypertension Galvão et al.900

dehydrogenase activity in the PE and GH groups expressionof HO-1, which shows that plasma from the latter groupinduces the enzyme expression and, therefore, protectsendothelial cells, but with the addition of KI, endothelialcells responded by not increasing the enzyme expression.This effect might be due to the role of I- as a competitivesubstrate for oxidant enzymes such as myeloperoxidase,which were found to be elevated in cardiovascular diseaseas well as PE.22,23 I- can also react with reactive oxygenspecies (ROS) such as hydrogen peroxide forming water andmolecular iodine (I2), the latter being a stronger antioxidantthan KI.14,15 It has also been shown that peroxidases displaycatalytic activity in the presence of iodide, turning theminto effective catalases, thus reducing peroxides in sera invitro.24 Further research is needed to assess which directand indirect actions KI exerts to protect cell membranesfrom damage and, therefore, reduces cytotoxicity in vitro.
Our transmission electronmicroscopy images of endothelialcells showed slightly altered patterns in morphological struc-tures of diseased groups, with a noticeable increase in cyto-plasmatic vacuoles in the preeclamptic group; Focaccetti et al.25
demonstrated that endothelial cells subjected to longer treat-ments with low doses of antineoplastic agent 5-Fluorouracilexhibited a pattern associated with cellular distress, similar towhatwasseenhere. Preeclampticplasmapool inducedcells to afusiform morphology and abundant membrane projections,which is mostly seen in distressed glioma cells26; since theHP group showed a flat pattern with fewer cell projections, wemay assume that what is seen in the PE group display anabnormal morphology, compared to healthy pregnant, whichwas reversed by KI.
It has been demonstrated that PE women have highercirculating HO-1.10,27 However, incubation of HUVECswith PE plasma did not induce the enzyme’s expression,differently from what was seen in GH women. Previousstudies from our group found circulating levels of HO-1 tobe increased in the plasma of pregnant women who laterdeveloped preeclampsia with severe features comparedwith women who developed preeclampsia without severefeatures; moreover, the plasma of pregnant women wholater developed preeclampsia induced a 4-fold increase inthe expression of HO-1 by HUVECs.13,28 Another studyfrom our group showed a similar pattern when assessingendothelin-1, a potent vasoconstrictor found elevated inPE women’s plasma, as well as let-7 family micro ribonu-cleic acid (miRNA) targeting its transcripts.29 Plasmaendothelin-1 was found to be slightly increased beforethe onset of symptoms in the PE group and greatlyincreased after; circulating miRNA was increased in thePE group’s plasma but not in the HP group’s samples. Thein vitro results showed that the plasma of women wholater developed preeclampsia induced higher expression ofendothelin-1 in HUVEC’s before symptoms, but, after that,there was no difference between the HP and PE groups’endothelin-1 protein expression, followed by significantlyincreased miRNA targeting the protein’s transcripts.30 Theauthors concluded that protective posttranscriptional
mechanisms were developed in PE women to prevent theexpression of endothelin-1 in endothelial cells later on inpregnancy.
Despite the undeniable HO-1’s role in homeostasis, therehave been studies showing also the disadvantageous side ofthe chronic and/or overstimulation of this pathway in centralnervous system diseases, as well as lung disease and meta-bolic syndrome.31–34 It is possible that in PE women, theearly and intense stimulation of HO-1 expression might alsoinduce the development of posttranscriptional mechanismsto diminish its expression. Our data showed a better outcomein pregnant women with GH than in women with PE, whichsuggests that the severity of the condition might be associ-ated with the loss of HO-1 induction over endothelial cells.Further research is needed to evaluate possible miRNA thatcould be involved in this effect, and if they are absent in HPand GH cases.
Iodine is imperative for fertility and fetal and childdevelopment.35,36 In Brazil, mandatory iodization has im-proved the general iodine nutritional status and, yet, preg-nant women are still at risk for iodine deficiency37,38; atleast one study showed excessive iodine in the urine andbreast milk of pregnant and lactating Brazilian women.39
This is, most likely, due to the excessive amount of table saltconsumed in Brazil, on average, almost twice the recom-mended dose of 5 g/day, with almost 60% of the populationconsuming between 8 and 12 g/day.40 The form of iodineadded to salt in Brazil is potassium iodate, a much morestable form of iodine than KI, but it has been shown toincrease lipid peroxidation in porcine thyroid follicles indoses ranging from 2.5mM to 500mM, while KI did notexhibit these effects until a dose of 50mM was used41;potassium iodate, then, might not play the same role as KI inpreventing oxidative stress due to particular properties ofthis iodine form. Potassium iodide supplementation iniodine-deficient, overweight women led to a decrease inhypercholesterolemia,42 and a 300 μg dose KI/day wasshown to be harmless regarding thyroid hormones ineuthyroid subjects and even exerted modest anti-inflam-matory actions,43 showing that KI might be better toleratedand helpful in hypertensive disorders of pregnancy, as theseconditions share the common oxidative, proinflammatoryfeatures of cardiovascular disease, to which these women aspredisposed later in life.44,45
As of limitations found in the making of this researchwork, we highlight that the KI concentrations used herecould not possibly reproduce circulating plasma concentra-tions as these were found to be around 30μg/L;46 hence, ourresults express potential mechanisms only in an experimen-tal environment. We have not investigated whether theplasma of PE women contained known or novel miRNAtargeting HO-1 transcripts; therefore, the aforementionedhypothesis was not tested and is still to be further analyzed.Likewise, we have not analyzed endothelial cells from eitherhealthy or hypertensive pregnant women, which could alsoenlighten the differences in response to plasmamolecules inthe two studied groups.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Preeclampsia and Gestational Hypertension Galvão et al. 901

Conclusion
We conclude by highlighting the difference between GH andPE outcomes and effects over endothelial cells, an importantdistinction to be made when studying these conditions.Potassium iodide does have a protective effect over HUVECswhen incubated with the plasma of both hypertensivegroups that is independent of HO-1 activation, either bydirectly scavenging reactive species or by competing foroxidant enzymes as a substrate. Heme oxygenase-1 earlyoverexpression in preeclampsia may play a detrimental rolelater on pregnancy; therefore, possible posttranscriptionalmechanisms must be assessed to understand when thisenzyme activation is beneficial in each condition studied.Further research is needed to evaluate if iodine can affectthese parameters in vivo by reducing known biomarkers ofoxidative stress and cytotoxicity.
ContributorsAll of the authors contributed with the project and datainterpretation, the writing of the article, the criticalreview of the intellectual content, and with the finalapproval of the version to be published.
Conflict of interestsThe authors have no conflict of interests to declare.
AcknowledgmentsThis study was funded by grant #2015/20461–8, SãoPaulo Research Foundation (FAPESP); grant #2017/09140–0, São Paulo Research Foundation (FAPESPand The Brazilian National Council for Scientific andTechnological Development (CNPq).
References1 American College of Obstetricians. Gynecologists’ Task Force on
Hypertension in Pregnancy Hypertension in pregnancy. ObstetGynecol. 2013;122(05):1122–1131. Doi: 10.1097/01.AOG.0000437382.03963.88
2 Brown MA, Magee LA, Kenny LC, Karumanchi SA, McCarthy FP,Saito S, et al; International Society for the Study of Hypertensionin Pregnancy (ISSHP) Hypertensive disorders of pregnancy: ISSHPclassification, diagnosis, and management recommendations forinternational practice. Hypertension. 2018;72(01):24–43. Doi:10.1161/HYPERTENSIONAHA.117.10803
3 Sullivan SD, Umans JG, Ratner R. Hypertension complicatingdiabetic pregnancies: pathophysiology, management, and con-troversies. J Clin Hypertens (Greenwich). 2011;13(04):275–284.Doi: 10.1111/j.1751-7176.2011.00440.x
4 Roberts JM, Pearson G, Cutler J, Lindheimer MNHLBI WorkingGroup on Research on Hypertension During Pregnancy. Summaryof theNHLBIWorking Group on Research onHypertensionDuringPregnancy. Hypertension. 2003;41(03):437–445. Doi:10.1161/01.HYP.0000054981.03589.E9
5 Khan KS, Wojdyla D, Say L, Gülmezoglu AM, Van Look PF. WHOanalysis of causes of maternal death: a systematic review. Lancet.2006;367(9516):1066–1074. Doi: 10.1016/S0140-6736(06)68397-9
6 Hutcheon JA, Lisonkova S, Joseph KS. Epidemiology of pre-eclampsia and the other hypertensive disorders of pregnancy.
Best Pract Res Clin Obstet Gynaecol. 2011;25(04):391–403. Doi:10.1016/j.bpobgyn.2011.01.006
7 Roberts JM, Hubel CA. The two stage model of preeclampsia:variations on the theme. Placenta. 2009;30(Suppl A):S32–S37.Doi: 10.1016/j.placenta.2008.11.009
8 MyattL,RedmanCW,StaffAC,HanssonS,WilsonML,LaivuoriH,etal;Global Pregnancy CoLaboratory. Strategy for standardization ofpreeclampsia research study design. Hypertension. 2014;63(06):1293–1301. Doi: 10.1161/HYPERTENSIONAHA.113.02664
9 Granger JP, Alexander BT, Llinas MT, Bennett WA, Khalil RA.Pathophysiology of hypertension during preeclampsia linkingplacental ischemia with endothelial dysfunction. Hypertension.2001;38(3 Pt 2):718–722. Doi: 10.1161/01.hyp.38.3.718
10 Erdemli HK, Yıldırımlar P, Alper TY, Kocabaş R, Salis O, Bedir A.Increased serum heme oxygenase-1 levels as a diagnostic markerof oxidative stress in preeclampsia. Hypertens Pregnancy. 2014;33(04):488–497. Doi: 10.3109/10641955.2014.946613
11 Loboda A, Damulewicz M, Pyza E, Jozkowicz A, Dulak J. Role ofNrf2/HO-1 system in development, oxidative stress response anddiseases: an evolutionarily conserved mechanism. Cell Mol LifeSci. 2016;73(17):3221–3247. Doi: 10.1007/s00018-016-2223-0
12 George EM, Cockrell K, AranayM, Csongradi E, Stec DE, Granger JP.Induction of heme oxygenase 1 attenuates placental ischemia-induced hypertension. Hypertension. 2011;57(05):941–948. Doi:10.1161/HYPERTENSIONAHA.111.169755
13 Caldeira-Dias M, Montenegro MF, Bettiol H, Barbieri MA, CardosoVC, Cavalli RC, et al. Resveratrol improves endothelial cell markersimpaired by plasma incubation from women who subsequentlydevelop preeclampsia. Hypertens Res. 2019;42(08):1166–1174.Doi: 10.1038/s41440-019-0243-5
14 Aceves C, Anguiano B, Delgado G. The extrathyronine actions ofiodine as antioxidant, apoptotic, and differentiation factor invarious tissues. Thyroid. 2013;23(08):938–946. Doi: 10.1089/thy.2012.0579
15 Ben-YehudaGreenwaldM, Frušić-ZlotkinM, Soroka Y, Ben-SassonS, Bianco-Peled H, Kohen R. A novel role of topical iodine in skin:Activation of the Nrf2 pathway. Free Radic Biol Med. 2017;104:238–248. Doi: 10.1016/j.freeradbiomed.2017.01.011
16 Martinez NF, Filgueira GC, Machado JdeS, Dos Santos JE, SandrimVC, Duarte G, et al. [Clinical and laboratory characteristics ofpregnant womenwith preeclampsia versus gestational hyperten-sion]. Rev Bras Ginecol Obstet. 2014;36(10):461–466. Doi:10.1590/so100-720320140005029Portuguese.
17 Benzie IF, Strain JJ. The ferric reducing ability of plasma (FRAP) as ameasure of “antioxidant power”: the FRAP assay. Anal Biochem.1996;239(01):70–76. Doi: 10.1006/abio.1996.0292
18 Luizon MR, Palei AC, Cavalli RC, Sandrim VC. Pharmacogenetics inthe treatment of pre-eclampsia: current findings, challenges andperspectives. Pharmacogenomics. 2017;18(06):571–583. Doi:10.2217/pgs-2016-0198
19 Gomes HF, Palei AC, Machado JS, da Silva LM, Montenegro MF,Jordão AA, et al. Assessment of oxidative status markers and NObioavailability in hypertensive disorders of pregnancy. J HumHypertens. 2013;27(06):345–348. Doi: 10.1038/jhh.2012.58
20 Harsem NK, Braekke K, Staff AC. Augmented oxidative stress aswell as antioxidant capacity inmaternal circulation in preeclamp-sia. Eur J Obstet Gynecol Reprod Biol. 2006;128(1-2):209–215.Doi: 10.1016/j.ejogrb.2005.11.014
21 Taravati A, Tohidi F. Comprehensive analysis of oxidative stressmarkers and antioxidants status in preeclampsia. Taiwan J ObstetGynecol. 2018;57(06):779–790. Doi: 10.1016/j.tjog.2018.10.002
22 Gamon LF, Dieterich S, Ignasiak MT, Schrameyer V, Davies MJ.Iodide modulates protein damage induced by the inflammation-associated heme enzyme myeloperoxidase. Redox Biol. 2020;28:101331. Doi: 10.1016/j.redox.2019.101331
23 Gandley RE, Rohland J, Zhou Y, Shibata E, Harger GF, Rajakumar A,et al. Increasedmyeloperoxidase in the placenta and circulation of
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Preeclampsia and Gestational Hypertension Galvão et al.902

womenwith preeclampsia. Hypertension. 2008;52(02):387–393.Doi: 10.1161/HYPERTENSIONAHA.107.107532
24 Tatzber F, Griebenow S, Wonisch W, Winkler R. Dual method forthe determination of peroxidase activity and total peroxides-iodide leads to a significant increase of peroxidase activity inhuman sera. Anal Biochem. 2003;316(02):147–153. Doi:10.1016/s0003-2697(02)00652-8
25 Focaccetti C, Bruno A, Magnani E, Bartolini D, Principi E, DallaglioK, et al. Effects of 5-fluorouracil on morphology, cell cycle,proliferation, apoptosis, autophagy and ROS production in endo-thelial cells and cardiomyocytes. PLoS One. 2015;10(02):e0115686. Doi: 10.1371/journal.pone.0115686
26 Funchal C, Latini A, Jacques-Silva MC, et al. Morphological alter-ations and induction of oxidative stress in glial cells caused by thebranched-chain alpha-keto acids accumulating in maple syrupurine disease. Neurochem Int. 2006;49(07):640–650. Doi:10.1016/j.neuint.2006.05.007
27 Vitoratos N, Papakonstantinou K, Deliveliotou A, Economou E,Panoulis C, Hassiakos D, et al. Antepartum and postpartum serumheme oxygenase-1 levels in preeclamptic and normotensivepregnant women. In Vivo. 2011;25(03):445–450
28 Sandrim VC, Caldeira-Dias M, Bettiol H, Barbieri MA, Cardoso VC,Cavalli RC. Circulating heme oxygenase-1: not a predictor ofpreeclampsia but highly expressed in pregnant women whosubsequently develop severe preeclampsia. OxidMed Cell Longev.2018;2018:6035868. Doi: 10.1155/2018/6035868
29 Bernardi F, Constantino L, Machado R, Petronilho F, Dal-Pizzol F.Plasma nitric oxide, endothelin-1, arginase and superoxide dis-mutase in pre-eclamptic women. J Obstet Gynaecol Res. 2008;34(06):957–963. Doi: 10.1111/j.1447-0756.2008.00860.x
30 Caldeira-DiasM, LuizonMR, Deffune E, Tanus-Santos JE, Freire PP,Carvalho RF, et al. Preeclamptic plasma stimulates the expressionof miRNAs, leading to a decrease in endothelin-1 production inendothelial cells. Pregnancy Hypertens. 2018;12:75–81. Doi:10.1016/j.preghy.2018.03.001
31 Schipper HM, SongW, Tavitian A, Cressatti M. The sinister face ofheme oxygenase-1 in brain aging and disease. Prog Neurobiol.2019;172:40–70. Doi: 10.1016/j.pneurobio.2018.06.008
32 Jais A, Einwallner E, Sharif O, Gossens K, Lu TT, Soyal SM, et al.Heme oxygenase-1 drivesmetaflammation and insulin resistancein mouse and man. Cell. 2014;158(01):25–40. Doi: 10.1016/j.cell.2014.04.043
33 Raval CM, LeePJ. Hemeoxygenase-1 in lungdisease. CurrDrugTargets.2010;11(12):1532–1540. Doi: 10.2174/1389450111009011532
34 Song W, Kothari V, Velly AM, Cressatti M, Liberman A, GornitskyM, et al. Evaluation of salivary heme oxygenase-1 as a potentialbiomarker of early Parkinson’s disease. Mov Disord. 2018;33(04):583–591. Doi: 10.1002/mds.27328
35 Zimmermann MB. The importance of adequate iodine duringpregnancy and infancy. World Rev Nutr Diet. 2016;115:118–124. Doi: 10.1159/000442078
36 Mills JL, Buck Louis GM, Kannan K, Weck J, Wan Y, Maisog J, et al.Delayed conception in women with low-urinary iodine concen-trations: a population-based prospective cohort study. HumReprod. 2018;33(03):426–433. Doi: 10.1093/humrep/dex379
37 Mioto VCB, Monteiro ACCNG, de Camargo RYA, Borel AR, CatarinoRM, Kobayashi S, et al. High prevalence of iodine deficiency inpregnant women living in adequate iodine area. Endocr Connect.2018;7(05):762–767. Doi: 10.1530/EC-18-0131
38 Ferreira SM, Navarro AM, Magalhães PK, Maciel LM. Iodineinsufficiency in pregnant women from the State of São Paulo.Arq Bras Endocrinol Metabol. 2014;58(03):282–287. Doi:10.1590/0004-2730000002979
39 de Lima LF, Barbosa F Jr, Navarro AM. Excess iodinuria in infantsand its relation to the iodine in maternal milk. J Trace Elem MedBiol. 2013;27(03):221–225. Doi: 10.1016/j.jtemb.2013.01.003
40 Mill JG, Malta DC, Machado IE, Pate A, Pereira CA, Jaime PC, et al.Estimation of salt intake in the Brazilian population: resultsfrom the 2013 National Health Survey. Rev Bras Epidemiol.2019;22(22, Suppl 02)E190009–, 2. Doi: 10.1590/1980-549720190009.supl.2
41 Milczarek M, Stępniak J, Lewiński A, Karbownik-Lewińska M.Potassium iodide, but not potassium iodate, as a potential protec-tive agent against oxidative damage to membrane lipids in porcinethyroid. ThyroidRes. 2013;6(01):10. Doi: 10.1186/1756-6614-6-10
42 Herter-Aeberli I, CherkaouiM, El Ansari N, Rohner R, Stinca S, Chabaa L,et al. Iodine supplementation decreases hypercholesterolemia in io-dine-deficient, overweight women: a randomized controlled trial. JNutr. 2015;145(09):2067–2075. Doi: 10.3945/jn.115.213439
43 Soriguer F, Gutiérrez-Repiso C, Rubio-Martin E, Linares F, CardonaI, López-Ojeda J, et al. Iodine intakes of 100-300 μg/d do notmodify thyroid function and have modest anti-inflammatoryeffects. Br J Nutr. 2011;105(12):1783–1790. Doi: 10.1017/S0007114510005568
44 WangY, ShiD, ChenL. Lipidprofile andcytokines inhypertensionofpregnancy: A comparison of preeclampsia therapies. J Clin Hyper-tens (Greenwich). 2018;20(02):394–399. Doi: 10.1111/jch.13161
45 Brouwers L, van der Meiden-van Roest AJ, Savelkoul C, VogelvangTE, Lely AT, FranxA, et al. Recurrence of pre-eclampsia and the riskof future hypertension and cardiovascular disease: a systematicreview and meta-analysis. BJOG. 2018;125(13):1642–1654. Doi:10.1111/1471-0528.15394
46 Allain P, Mauras Y, Dougé C, Jaunault L, Delaporte T, Beaugrand C.Determination of iodine and bromine in plasma and urine byinductively coupled plasma mass spectrometry. Analyst (Lond).1990;115(06):813–815. Doi: 10.1039/an9901500813
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Preeclampsia and Gestational Hypertension Galvão et al. 903

Uterine Artery Pulsatility Index as a Pre-eclampsia Predictor in the 3 Trimesters inWomen with Singleton Pregnancies
Índice de pulsatilidade da artéria uterina como preditorde pré-eclâmpsia nos 3 trimestres em mulheres comgestações únicasYuly Natalia Guzmán1 Montserrat Uriel2 Alexandra Porras Ramírez 3 Ximena Carolina Romero4
1Universidad El Bosque, El Bosque Research Group of Maternal FetalMedicine and Gynecology, Bogotá, Colombia
2Universidad El Bosque, El Bosque Research Group of Maternal FetalMedicine and Gynecology, Ecodiagnóstico El Bosque SAS, Los CobosMedical Center, Bogotá, Colombia
3Universidad El Bosque, Research Group Community Medicine andCollective Health, Los Cobos Medical Center, Bogotá, Colombia
4Universidad El Bosque, El Bosque Research Group of Maternal FetalMedicine and Gynecology, Ecodiagnóstico El Bosque SAS, Los CobosMedical Center, Bogotá, Colombia
Rev Bras Ginecol Obstet 2021;43(12):904–910.
Address for correspondence Professor Ximena Romero Infante, MD.EspMFM, Av. Carrera 9 # 131a-02. Ecodiagnóstico El Bosque S. A. S,Calle 134 # 7B – 83. Bogotá, Colombia(e-mail: [email protected]).
Keywords
► uterine arterydoppler
► preeclampsia;pregnancy
► perinatal care► screening
Abstract Objective To evaluate the mean uterine artery pulsatility index (UtAPI) in eachtrimester of pregnancy as a predictor of early or late pre-eclampsia (PE) in Colombianpregnant women.Methods The UtAPI wasmeasured in singleton pregnancies in each trimester. Uterineartery pulsatility index as predictor of PE was evaluated by odds ratio (OR), receiveroperating characteristic (ROC) curves, and Kaplan-Meier diagram.Results Analysis in the 1st and 3rd trimester showed that abnormal UtAPI wasassociated with early PE (OR: 5.99: 95% confidence interval [CI]: 1.64–21.13; andOR: 10.32; 95%CI: 2.75–42.49, respectively). Sensitivity and specificity were 71.4 and79.6%, respectively, for developing PE (area under the curve [AUC]: 0.922). The Kaplan-Meier curve showed that a UtAPI of 0.76 (95%CI: 0.58–1.0) in the 1st trimester wasassociated with early PE, and a UtAPI of 0.73 (95%CI: 0.55–0.97) in the 3rd trimester wasassociated with late PE.Conclusion Uterine arteries proved to be a useful predictor tool in the 1st and 3rd
trimesters for early PE and in the 3rd trimester for late PE in a pregnant population withhigh prevalence of PE.
receivedNovember 28, 2020accepted after revisionOctober 13, 2021
DOI https://doi.org/10.1055/s-0041-1740273.ISSN 0100-7203.
© 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rightsreserved.This is an open access article published by Thieme under the terms of the
Creative Commons Attribution License, permitting unrestricted use,
distribution, and reproduction so long as the original work is properly cited.
(https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda., Rua do Matoso 170, Rio deJaneiro, RJ, CEP 20270-135, Brazil
Original ArticleTHIEME
904

Introduction
Pre-eclampsia (PE) is a disease with a high percentage ofmaternal and perinatal complications and continues to beone of the main causes of maternal death worldwide.1–4
Several methods have been studied to classify low- andhigh-risk populations; in recent years, early screening hasbeen increasingly performed in an attempt to reduce PEprevalence throughspecificpharmacological interventions.4–6
Several research groups, such as the National Institute forHealth and Care Excellence (NICE), the American College ofObstetricians and Gynecologists (ACOG), and the Fetal Medi-cine Foundation (FMF), have analyzed screeningmethods forPE inwhich different parameters regardingmaternal history,clinical symptoms, laboratory results, and biophysical vari-ables are evaluated. One of the biophysical measures is themean uterine artery pulsatility index (UtAPI).7,8
The pathophysiology of PE has been explained by severaltheories. Themost accepted etiology in recent years is that PEis a pathology secondary to an altered placental develop-ment,manifested by the increase in theflow resistance of theuterine arteries.1,8–11 These alterations have been observedin the 1st, 2nd, and 3rd trimesters of the pregnancies thatdevelop PE.12,13 Furthermore, uterine arteries were com-pared using Doppler in each trimester for predicting late PE;as a result, late PE can be best predicted during the 3rd
trimester.13,14A systematic reviewhas described that the 2nd
trimester is the best time to predict overall PE.15 Moreover,relevant international studies have evaluated the distribu-tion of UtAPI in different populations during the course ofpregnancy.1,7,16–18 In Latin America, there are no compara-ble studies that provide information about these valuesthroughout the pregnancy or their association with PE.
Pre-eclampsia is classified as early and late, being differ-entiated by gestational age at onset. In early PE cases, thepresentation is before 34 gestational weeks (GWs).10,19 This
period is frequently associated with various unfortunateevents, such as severe PE, eclampsia, hemolysis, elevatedliver enzymes, and low platelet count (HELLP) syndrome,maternal death, admission to obstetric intensive care unit(ICU), admission to neonatal ICU, low birthweight, andperinatal death.3
According to information dated from 2014, hypertensivedisorders are the second leading cause of death in pregnantwomen in the Latin American and Caribbean population.2,20
In Bogotá, Colombia, PE is the leading cause of maternaldeath, according to the Department of National Statistics –
Data Bases of 2017.21 Thus, early screening for hypertensivedisorder is crucial to optimize or develop clinical strategiesand public interest to reduce PE cases. Unfortunately, in theColombian population, no information about specific char-acteristics of uterine artery Doppler study during the threetrimesters of pregnancy is available.
The present study aimed mainly to evaluate the meanUtAPImeasured in each trimester of pregnancy as a predictorof early or late PE in a sample of Colombian pregnant women.
Methods
The data for the present study were derived from a databaseof 566 pregnant women>14 years old with singleton preg-nancies assessed 2 two hospitals in the city of Bogotá,Colombia, from a prospective study inwhich predictive testsof PE were analyzed in Colombian pregnant women in theperiod between October 2014 and March 2018. For thepresent work, pregnancies with major fetal malformations,chromosomopathies, and those under threat of miscarriagewere excluded. During the 1st visit, between 11þ0 and13þ6 GWs, a clinical history regarding the sociodemo-graphic and clinical characteristics of the patients wasobtained. Doppler study of the uterine arteries was per-formed in the 1st trimester between 11þ0 and 13þ6 GWs,
Resumo Objetivo Avaliar o índice médio de pulsatilidade da artéria uterina (UtAPI) em cadatrimestre da gravidez como preditor de pré-eclâmpsia (PE) precoce ou tardia emgestantes colombianas.Métodos O UtAPI foi medido em gestações únicas em cada trimestre. O UtAPI comopreditor de PE foi avaliado por odds ratio (OR), curvas receiver operating characteristic(ROC) e diagrama de Kaplan-Meier.Resultados A análise no 1° e 3° trimestres mostrou que um UtAPI anormal foiassociado com PE inicial (OR: 5,99; intervalo de confiança [IC] 95%: 1,64–21,13; OR:10,32; IC95%: 2,75–42,49, respectivamente). A sensibilidade e a especificidade foramde 71,4 e 79,6%, respectivamente, para o desenvolvimento de PE (area under the curve[AUC]: 0,922). A curva de Kaplan-Meier mostrou que um UtAPI de 0,76 (IC95%: 0,58–1,0) no 1° trimestre foi associado com PE precoce, e que um UtAPI de 0,73 (IC95%:0,55–0,97) no 3° trimestre foi associado com PE tardia.Conclusão As artérias uterinas mostraram ser uma ferramenta preditora útil no 1° e3° trimestres para PE inicial e no 3° trimestre para PE tardia em uma população degestantes com alta prevalência de PE.
Palavras-chave
► doppler da artériauterina
► pré-eclâmpsia;gravidez
► cuidado perinatal► triagem
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Uterine Artery Pulsatility Index in Women with Singleton Pregnancies Guzmán et al. 905

in the 2nd trimester between 18þ0 and 24þ0 GWs, and inthe 3rd trimester between 28þ0 to 34þ0 GWs. Gestationalage was determined by measuring the fetal crown–rumplength from 11þ0 GWs to 13þ0 GWs.
Regarding the characteristics of the patients, the follow-ing demographic variables are included:maternal age, ethnicorigin, and socioeconomic level (classified as high, middle,and low). The following clinical variables were also consid-ered: medical history of chronic hypertension, pregesta-tional diabetes, obesity defined as body mass index (BMI)� 30 Kg/m2, systemic lupus erythematosus, antiphospholi-pid antibody syndrome, personal and family history of PE,parity (nulliparity versus non-nulliparity), smoking habitduring pregnancy, maternal BMI, gestational age at thetime of PE diagnosis, and gestational age at the end ofpregnancy.
Doppler ultrasound examinations were performed trans-abdominally. Uterine artery pulsatility index measuringtechniques were used according to the guidelines by Khalilet al.22. At 11þ0 to 13þ6 GWs, a midsagittal section of theuterus was obtained, and the cervical canal and internalcervical oswere identified. Subsequently, the transducer wasgently tilted from side to side, and color flow mapping wasused to identify each uterine artery measurements weretaken before the uterine artery branches into the arcuatearteries.22–24
At 18þ0 to 24þ6 GWs and at 28þ0 to 34þ0 GWs, thetransducer was placed longitudinally in the iliac fossa,parallel to the iliac crest and to the uterine wall. Then, colorDoppler was used to identify each uterine artery at theapparent crossover with the external iliac arteries. Afterthe identification of each uterine artery, pulsed-wave Dopp-ler was used, with the sampling gate set at between 2 and3mmto cover thewhole vessel. Carewas taken to ensure thatthe angle of insonation was<30° and that the peak systolicvelocity was>60 cm/s, so that the uterine artery, rather thanthe arcuate artery, was examined. When three similar wave-forms were obtained consecutively, the pulsatility index wasmeasured and the mean UtAPI of the left and right arterieswas calculated.22,23 The presence or absence of a diastolicnotch was not considered in the present study. The meanUtAPI was analyzed qualitatively according to the normalityand abnormality criteria described by Gómez et al.17 in theirstudy, which was developed in a Spanish population, usingthe 95th percentile; hence, UtAPI values above this rangewere considered abnormal. All Doppler studies were per-formed by sonographers who had received the Certificate ofCompetence in Doppler of the FMF.
Patients were diagnosed with PE according to the 2013diagnostic criteria of hypertension in pregnancy.25–28 Inaddition, the gestational age at the onset of PE was consid-ered; PE was classified as early PE when it starts before 34GWs and as late PE when it starts after this gestationalage.10,19
Informed consent was obtained from all patients. Thepresent study was approved by the ethical committees ofeach participating hospital. In addition, the ethical principlesfor human research from the Helsinki Declaration and the
Colombian resolution 8430 of 1993 were considered in thepresent study, and it was classified as an investigation withminimum risk.29
Absolute and relative frequencies were performed withtheir respective confidence intervals (CIs) to describe thecharacteristics of the patients. Comparisons of groups wereanalyzed by the student t-test, theMann-WhitneyU test, andthe Fisher test, considering p<0.05 to stablish statisticaldifferences. To find the possible associations between uter-ine pulsatility in each trimester and the development of PE,the odds ratio (OR) was calculated. Receiver operating char-acteristic (ROC) curves and the area under the curve (AUC)were made to calculate the sensitivity and specificity ofUtAPI in order to determine the risk of developing PE.Kaplan-Meier probability diagrams were calculated to eval-uate the probability of developing PE (early and late) relatedwith gestational age in the upper and lower quintile of theUtAPI.
Results
The present study included 527 pregnant women who metthe inclusion criteria, out of a total of 566 women who werestudied. The average agewas 27.4 years old, and 97.3% of theparticipants were of mixed race. Furthermore, 96.9% of thesewomen were from middle and low socioeconomic levels.Sociodemographic characteristics and pathological historyof the study population are summarized in ►Table 1, as wellas the comparation between groups.
In the present study, 42women (7.9%) had PE, of whom34(6.4%) had late PE and 8 (1.5%) had early PE. The averagegestational age at the moment of diagnosis of early and latePE was 30þ1 GWs (21þ0 to 33þ0 GWs) and 37þ1 GWs(34þ0 to 40þ4 GWs), respectively. In the 1st trimester,12.9% (68) of the pregnant women had an UtAPI>95th
percentile. The mayor ratio of patients with UtAPI>95th
percentile in the 1st trimester was obtained in the groupof patients who developed early PE, 5 patients of the 8(62.5%). In the 2nd trimester, 14 women did not attend theultrasound appointment, but, of the new total of patientswho attended to the 2nd appointment, 9.6% (51) had abnor-mal UtAPI. Besides, the group that developed early PEshowed the highest ratio of patients with UtAPI>95th per-centile (5 patients of the 8 who developed early PE). Finally,in the 3rd trimester, 20 womenwere lost to follow-up. Of thepatients evaluated in the 3rd trimester, 12.7% (67) of womenwhowere in the 3rd trimester of gestation had a UtAPI>95thpercentile; the highest percentage of patients with UtAPI>95th percentile was in the group of early PE (75%)(6 patients of the 8 that developed early PE). The analysisof the ORs showed a positive association between abnormalUtAPI in the 1st trimester and the development of early PE(OR: 5.9; 95%CI: 1.64–1.13), with statistically significantdifferences. An association between having UtAPI>95th
percentile in the 3rd trimester and early PE (OR: 10.32;95%CI: 2.75-42.49) was found, as shown in ►Table 2.
Receiver operating characteristic curves were made toevaluate the ability to discriminate the likelihood of
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Uterine Artery Pulsatility Index in Women with Singleton Pregnancies Guzmán et al.906

developing PE. The ROC shows the importance of the UtAPI inthe 1st and the 2nd trimester, so that the model achieves aprediction of 92.2% of the risk of developing PE, with asensitivity and a specificity of 71.4 and 79.6%, respectively,by using all the characteristics described in►Figure 1. At the1st and 2nd trimesters, the sensitivity of the UtAPI was 20%of each one.
The analysis of the Kaplan-Meier probability diagramdemonstrated the relationship between the upper quintileof the UtAPI 0.76 (95%CI: 0.58–1.0) in the 1st trimester andthe development of early PE, with statistically significantresults. The risk of late PE for the upper quintile of UtAPI 0.73(95%CI: 0.55–0.97) in the 3rd trimester was statisticallysignificant. The Kaplan-Meier cumulative risk of PE is shownin ►Figure 2.
Discussion
According to thefindings of the present, PEwas found in 7.9%of the participants, suggesting that the Colombian popula-
tion has a higher incidence of PE than the world population(between 5 and 7%), with a high percentage of maternal andperinatal complications.30–32 Additionally, in relation to PEonset, 34 (6.4%) pregnant women had late PE and 8 (1.5%)had early PE onset.
Considering the elevated incidence of this hypertensivedisease, it is important to have knowledge about its probableetiology. The increase in the flow resistance of the uterinearteries is one of the bases of the pathophysiology of PE, asreferenced by O’Gorman et al.12 These alterations could beshown by Doppler changes in uterine arteries in each tri-mester or in all trimesters; consequently these variationshave been observed in the 1st,7 the 2nd,33 and the 3rd
trimesters.11,33 Other researches, as Mula et al.,13 haveexamined Doppler changes of the uterine artery in alltrimesters, as our study, in which women were evaluatedby trimester attending their routine care. In the presentstudy, abnormal UtAPI was found in all 3 trimesters ofpregnancy in 16.6% of the pregnant women with PE.
In this context, Doppler changes found in uterine arteriesby trimester are consistent with other research. In 2016,Arrue et al.34 concluded that patients with an abnormalUtAPI in the 3rd trimester had a higher rate of PE and adverseperinatal outcomes independent of UtAPI values in the 1st
and 2nd trimesters of pregnancy. In 2013, Jamal et al.33 foundthat an elevated UtAPI in the 2nd and 3rd trimesters ofpregnancy was associated with a higher risk of adversepregnancy outcomes, such as PE, intrauterine growth restric-tion (IUGR), intrauterine fetal death, and preterm delivery,than in the 1st trimester. Notably, in the present study,abnormal UtAPI in the 1st and 3rd trimesters was associatedwith early PE, with a statistically significant difference. Theearly PE association in the 3rd trimester was higher than inthe 1st trimester, conforming to the abovementioned studiesinwhich an abnormal UtAPI in the 3rd trimester had a greaterrisk of developing adverse outcomes, such as PE.
Table 1 Sociodemographic and clinical characteristics
Sociodemographic characteristics/pathological history
Pregnant womenincluded (n¼527)
Without PE(n¼ 485)
Early PE (n¼8) Late PE (n¼34) p-value
Median age, years old median (IQR) 27.0 (14–44) 27.8 (14–44) 27.9 (17–38) 30.4 (15–42) 0.062�
BMI in Kg/m2 (IQR) 24.6 (16.7–40.5) 26.6 (17.9–400) 29.0 (18.5–39.8) 28.3 (19.3–35.5) 0.429��
Gestational age at deliveryin weeks (IQR)
39.0 (28.2–43.1) 37.5 (29.3–43.1) 35.5 (30.4–40.4) 37.5 (36–40.4) 0.721��
Obesity % 47 (8.9) 39 (8.0) 2 (25.0) 6 (17.6) 0.043���
Pregestational diabetes % 3 (0.56) 2 (0.4) 1 (12.5) 0 –
CH % 14 (2.6) 6 (1.2) 5 (62.5) 3 (8.8) 0.399���
SLE % 2 (0.38) 1 (0.2) 0 1 (2.9) –
APS % 1 (0.19) 0 1 (12.5) 0 –
Smoking habit % 47 (8.9) 40 (8.2) 3 (37.5) 4 (11.7) 0.04���
Nulliparity % 203 (38.5) 191 (39.3) 3 (37.5) 9 (26.4) 0.002���
Abbreviation: APS, antiphospholipid antibody syndrome; BMI, body mass index; CH, chronic hypertension; IQR, interquartile range; PE, pre-eclampsia; SLE, systemic lupus erythematosus.�Mann-Whitney U test; ��Student’s t-test; ��� Fisher test.
Table 2 Bivariate analysis (OR) of abnormal UtAPI anddeveloping or not PE
Without PE Early PE Late PE
UtAPI> 95th
percentileby trimester
OR (95%CI) OR (95%CI) OR (95%CI)
First 1.01 (0.98–1.23) 5.99(1.64–21.13)� 0.46 (0.07–1.73)
Second 0.98 (0.75–2.36) 4.74 (0.94–19.66) 1.98 (0.64–5.21)
Third 1.10 (0.45–1.87) 10.32 (2.75–42.49)� 1.65 (0.59–4.05)
Abbreviations: CI, confidence interval; OR, odds ratio; PE, pre-eclamp-sia; UtAPI, uterine artery pulsatility index.�Statistically significant between groups.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Uterine Artery Pulsatility Index in Women with Singleton Pregnancies Guzmán et al. 907

Likewise, regarding the 2nd trimester, a systematic reviewand meta-analysis by Cnossen et al.15 has found a higherprediction of PE and IUGR when UtAPI was>95th percentilealone or combined with notching in the 2nd trimester whencompared with abnormal UtAPI in 1st and 3rd trimesters. In2013, 2,410 pregnant women were evaluated to determinethe biological interaction between uterine artery Dopplerand blood pressure in the 2nd trimester for the developmentof early and late PE.35 In this study, Takahashi et al.35 found acumulative risk of early PE in women with both abnormalUtAPI and elevated blood pressure, which is in contrast withthe present study, in which the association was not statisti-cally significant in the 2nd trimester.
Additionally, in 2019, Mula et al.13 evaluated the predic-tion of late PE bymeasuring the UtAPI in each trimester; theyfound that UtAPImeasurement in the 3rd trimester wasmore
sensitive (78%) and specific (82%) than in the 2 othertrimesters (AUC: 0.86). In the present study, according toROC curves (AUC: 0.922), the sensitivity and specificity todetermine the risk of developing PE were 71.4 and 79.6%,respectively.
Focusing on PE predictor tools, similarly, screening meth-ods for PE with evaluation of different parameters, such asmaternal history, clinical, laboratories, and biophysical var-iables (such as UtAPI, evaluated in the present study), wereanalyzed. Andrietti et al.,14 who demonstrated that thecombined measurement of UtAPI, mean arterial pressure(MAP), and serum placental growth factor in the 1st and/or2nd trimesters did not improve the prediction of early PEcompared with screening in the 3rd trimester. In the presentstudy, more cases of late PE were identified by UtAPImeasurements in the 3rd trimester.14 In general, amongthe biophysical measures, UtAPI has become one of themost useful parameters for PE screening since it is moreavailable than measurements of placental proteins, whichare not accessible for the entire population as part of theirhealth insurance plan, as it happens in Colombia.
Consequently, UtAPI measurement has been evaluatedwith inconsistent results between researches, with the pres-ent study being one of the few that analyzed the prognosticability in each trimester of pregnancy in the same group ofwomen, and these results show in which trimester themeasurement of uterine arteries was more efficient toimprove the PE screening rate in a country with a highincidence of PE. The main limitations of the present studywere that we incurred a random error because of the smallsample size. Furthermore, a selection bias was observed,given that the patients included in the present study corre-sponded to a specific population of Bogotá.
Fig. 1 Receiver operating characteristic curve.
Fig. 2 Kaplan–Meier probability diagram of early and late pre-eclampsia and their relationship with gestational age and the upperand lower quintiles of uterine artery pulsatility index.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Uterine Artery Pulsatility Index in Women with Singleton Pregnancies Guzmán et al.908

Conclusion
In conclusion, the measurement of the UtAPI in the 1st and3rd trimesters of pregnancymay be a useful technique for thescreening of early PE and, in 3rd trimester, for late PE.However, in the present study, the result of this predictortool was limited by the sample size. Hence, further studiesare necessary to validate the predictive and prognosticability of UtAPI in each trimester regarding PE in the Colom-bian population in isolation and in combination with otherPE predictors.
ContributorsAll the authors contributed with the project and datainterpretation, the writing of the article, the criticalreview of the intellectual content, and with the finalapproval of the version to be published.
Conflict of InterestsThe authors have no conflict of interests to declare.
AcknowledgmentsThe authors would like to thank the following institu-tions: Ecodiagnóstico El Bosque Unit Centre, Clinica ElBosque, South West Health Services Unit – HospitalOccidente de Kennedy, and Universidad El Bosque fortheir contribution in the present study.
References1 Tayyar A, Guerra L, Wright A, Wright D, Nicolaides KH. Uterine
artery pulsatility index in the three trimesters of pregnancy:effects of maternal characteristics and medical history. Ultra-sound Obstet Gynecol. 2015;45(06):689–697. Doi: 10.1002/uog.14789
2 Say L, Chou D, Gemmill A, Tunçalp Ö, Moller A-B, Daniels J, et al.Global causes of maternal death: a WHO systematic analysis.Lancet Glob Health. 2014;2(06):e323–e333. Doi: 10.1016/S2214-109X(14)70227-X
3 Guzmán-Yara YN, Parra-Amaya E, Javela-Rugeles JD, Barrios-Torres JC, Montalvo-Arce C, Perdomo-Sandoval HL. Expectantmanagement in non-severe pre-eclampsia obstetric and perinataloutcomes in a high complexity hospital in Neiva (Colombia). RevColomb Obstet Ginecol. 2018;69(03):160–168. Doi: 10.18597/rcog.3075
4 Wright D, Akolekar R, Syngelaki A, Poon LC, Nicolaides KH. Acompeting risks model in early screening for preeclampsia. FetalDiagn Ther. 2012;32(03):171–178. Doi: 10.1159/000338470
5 Rolnik DL, Wright D, Poon LCY, Syngelaki A, O’Gorman N, de PacoMatallana C, et al. ASPRE trial: performance of screening forpreterm pre-eclampsia. Ultrasound Obstet Gynecol. 2017;50(04):492–495. Doi: 10.1002/uog.18816
6 Yücel B, Gedikbasi A, Dündar O, Olgac Y, Y�ld�r�m D, Y�ld�r�m G,et al. The utility of first trimester uterine arteryDoppler, placentalvolume and PAPP-A levels alone and in combination to predictpreeclampsia. Pregnancy Hypertens. 2016;6(04):269–273. Doi:10.1016/j.preghy.2016.04.007
7 O’Gorman N, Wright D, Poon LC, Rolnik DL, Syngelaki A, deAlvarado M, et al. Multicenter screening for pre-eclampsia bymaternal factors and biomarkers at 11-13 weeks’ gestation:comparison with NICE guidelines and ACOG recommendations.Ultrasound Obstet Gynecol. 2017;49(06):756–760. Doi: 10.1002/uog.17455
8 Gestational hypertension and preeclampsia. ACOG Practice Bul-letin No. 222. Obstet Gynecol. 2020;135(06):e237–e260. Doi:10.1097/AOG.0000000000003891
9 Mazhar K, Bhatti F, Maraj H. Pre-eclampsia. InnovAiT.. 2014;7(01):14–24. Doi: 10.1177/1755738013499318
10 Orabona R, Donzelli CM, Falchetti M, Santoro A, Valcamonico A,Frusca T. Placental histological patterns and uterine artery Dopp-ler velocimetry in pregnancies complicated by early or late pre-eclampsia. Ultrasound Obstet Gynecol. 2016;47(05):580–585.Doi: 10.1002/uog.15799
11 Valiño N, Giunta G, Gallo DM, Akolekar R, Nicolaides KH. Uterineartery pulsatility index at 30-34 weeks’ gestation in the predic-tion of adverse perinatal outcome. Ultrasound Obstet Gynecol.2016;47(03):308–315. Doi: 10.1002/uog.14898
12 O’Gorman N, Tampakoudis G, Wright A, Wright D, Nicolaides KH.Uterine artery pulsatility index at 12, 22, 32 and 36 weeks’gestation in screening for pre-eclampsia. Ultrasound ObstetGynecol. 2016;47(05):565–572. Doi: 10.1002/uog.15819
13 Mula R, Meler E, Albaiges G, Rodriguez I. Strategies for theprediction of late preeclampsia. J Matern Fetal Neonatal Med.2019;32(22):3729–3733. Doi: 10.1080/14767058.2018.1471592
14 Andrietti S, Carlucci S, Wright A, Wright D, Nicolaides KH. Repeatmeasurements of uterine artery pulsatility index, mean arterialpressure and serum placental growth factor at 12, 22 and32 weeks in prediction of pre-eclampsia. Ultrasound ObstetGynecol. 2017;50(02):221–227. Doi: 10.1002/uog.17403
15 Cnossen JS, Morris RK, ter Riet G, Mol BWJ, van der Post JAM,Coomarasamy A, et al. Use of uterine artery Doppler ultrasonog-raphy to predict pre-eclampsia and intrauterine growth restric-tion: a systematic review and bivariable meta-analysis. CMAJ.2008;178(06):701–711. Doi: 10.1503/cmaj.070430
16 Poon LC, Karagiannis G, Leal A, Romero XC, Nicolaides KH.Hypertensive disorders in pregnancy: screening by uterine arteryDoppler imaging and blood pressure at 11-13 weeks. UltrasoundObstet Gynecol. 2009;34(05):497–502. Doi: 10.1002/uog.7439
17 Gómez O, Figueras F, Fernández S, Bennasar M, Martínez JM,Puerto B, et al. Reference ranges for uterine artery mean pulsa-tility index at 11-41 weeks of gestation. Ultrasound ObstetGynecol. 2008;32(02):128–132. Doi: 10.1002/uog.5315
18 Shwarzman P, Waintraub AY, Frieger M, Bashiri A, Mazor M,Hershkovitz R. Third-trimester abnormal uterine artery Dopplerfindings are associated with adverse pregnancy outcomes. JUltrasound Med. 2013;32(12):2107–2113. Doi: 10.7863/ul-tra.32.12.2107
19 Sibai BM. Management of late preterm and early-term pregnan-cies complicated by mild gestational hypertension/pre-eclamp-sia. Semin Perinatol. 2011;35(05):292–296. Doi: 10.1053/j.semperi.2011.05.010
20 Romero XC, Gutiérrez AM, Rojas NA, Ramírez A, Aldana J, EslavaM, et al. Incidencia de los trastornos hipertensivos en el embarazo,y características clínico-demográficas en tres instituciones enBogotá, D.C., Colombia. Investig Segur Soc Salud.. 2018;20(02):21–30
21 Organización Panamericana de la Salud. Indicadores de salud:aspectos conceptuales y operativos [Internet]. Washington (DC):OPS; 2018 [cited 2020 Jul 12]. Available from: https://www.ministeriodesalud.go.cr/index.php/vigilancia-de-la-salud/indi-cadores-de-salud-boletines/4072-indicadores-de-salud-aspec-tos-conceptuales-y-operativos-2018/file
22 Khalil A, Nicolaides KH. How to record uterine artery Doppler inthe first trimester. Ultrasound Obstet Gynecol. 2013;42(04):478–479. Doi: 10.1002/uog.12366
23 Bhide A, Acharya G, Bilardo CM, Brezinka C Cafici D, Hernandez-Andrade E, et al. ISUOG practice guidelines: use of Dopplerultrasonography in obstetrics. Ultrasound Obstet Gynecol.2013;41(02):233–239. Doi: 10.1002/uog.12371
24 Plasencia W, Maiz N, Poon L, Yu C, Nicolaides KH. Uterine arteryDoppler at 11 þ 0 to 13 þ 6 weeks and 21 þ 0 to 24 þ 6 weeks in
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Uterine Artery Pulsatility Index in Women with Singleton Pregnancies Guzmán et al. 909

the prediction of pre-eclampsia. Ultrasound Obstet Gynecol.2008;32(02):138–146. Doi: 10.1002/uog.5402
25 Bibbins-Domingo K, Grossman DC, Curry SJ, Curry SJ, Barry MJ,Davidson KW, et al; US Preventive Services Task Force. Screeningfor Preeclampsia: US Preventive Services Task Force Recommen-dation Statement. JAMA. 2017;317(16):1661–1667. Doi:10.1001/jama.2017.3439
26 Task Force on Hypertension in Pregnancy. Hypertension in preg-nancy. Washington (DC): American College of Obstetricians andGynecologists; 2013
27 Henderson JT, Thompson JH, Burda BU, Cantor A. Preeclampsiascreening: evidence report and systematic review for the USPreventive Services Task Force. JAMA. 2017;317(16):1668-–1683. Doi: 10.1001/jama.2016.18315
28 American College of Obstetricians and Gynecologists’ Committeeon Practice Bulletins—Obstetrics. ACOG Practice Bulletin No. 203:chronic hypertension in pregnancy. Obstet Gynecol. 2019;133(01):e26–e50. Doi: 10.1097/AOG.0000000000003020
29 World Medical Association. Declaration of Helsinki: ethical prin-ciples for medical research involving human subjects [Internet].2018 [cited 2020 Jan 23]. Available from: https://www.wma.-net/polices-post/wma-declaration-of-helsinki-ethical-princi-ples-for-medical-research-involving-human-subjects/
30 Uriel M, Romero XC. Reality of preeclampsia in Colombian preg-nant women. Open Access J Gynecol.. 2016;1(01):000105
31 Abalos E, Cuesta C, Grosso AL, Chou D, Say L. Global and regionalestimates of preeclampsia and eclampsia: a systematic review.Eur J Obstet Gynecol Reprod Biol. 2013;170(01):1–7. Doi:10.1016/j.ejogrb.2013.05.005
32 Rana S, Lemoine E, Granger JP, Karumanchi SA. Preeclampsia:pathophysiology, challenges, and perspectives. Circ Res. 2019;124(07):1094–1112. Doi: 10.1161/CIRCRESAHA.118.313276
33 Jamal A, Abbasalizadeh F, Vafaei H, Marsoosi V, Eslamian L.Multicenter screening for adverse pregnancyoutcomes by uterineartery Doppler in the second and third trimester of pregnancy.Med Ultrason. 2013;15(02):95–100. Doi: 10.11152/mu.2013.2066.152.aj1fa2
34 Arrue M, García M, Rodriguez-Bengoa MT, Landa JM, Urbieta L,MaitzeguiM, et al. Do low-risk nulliparouswomenwith abnormaluterine artery Doppler in the third trimester have poorer perina-tal outcomes? A longitudinal prospective study on uterine arteryDoppler in low-risk nulliparous women and correlation withpregnancy outcomes. J Matern Fetal Neonatal Med. 2017;30(07):877–880. Doi: 10.1080/14767058.2016.1190822
35 Takahashi K, Ohkuchi A, Suzuki H, Usui R, Kuwata T, Shirasuna K,et al. Biophysical interaction between blood pressure and uterineartery Doppler for the occurrence of early-onset preeclampsia: Aprospective cohort study. Pregnancy Hypertens. 2013;3(04):270–277. Doi: 10.1016/j.preghy.2013.07.006
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Uterine Artery Pulsatility Index in Women with Singleton Pregnancies Guzmán et al.910

Diagnosing Septate Uterus Using Three-Dimensional Ultrasound Using Three DifferentClassifications: An Interobserver andIntraobserver Agreement Study
Diagnóstico de útero septado com ecografiatridimensional usando três classificações diferentes: Umestudo de concordância interobservador eintraobservadorCarla Peixoto1,2 Maite Castro3 Isabel Carriles4 Maria de Arriba5 Victoria Lapresa6
Juan Luis Alcazar4
1Department of Obstetrics and Gynecology, Centro Hospitalar SãoJoão, Porto, Portugal
2Faculty of Medicine, University of Porto, Porto, Portugal3Centro de Infertilidad y Reproduccion Humana, Barcelona, Spain4Department of Obstetrics and Gynecology, Clínica Universidad deNavarra, University of Navarra, Pamplona, Spain
5Department of Obstetrics and Gynecology, University andPolytechnic Hospital La Fe, Valencia, Spain
6Department of Obstetrics and Gynecology, University Hospital,Salamanca, Spain
Rev Bras Ginecol Obstet 2021;43(12):911–918.
Address for correspondence Carla Peixoto, MD, Alameda Prof.Hernâni Monteiro, 4200-319, Porto, Portugal(e-mail: [email protected]).
Keywords
► uterus► ultrasonography► congenital anomaly
Abstract Objective Currently, there are up to three different classifications for diagnosingseptate uterus. The interobserver agreement among them has been poorly assessed.Objective To assess the interobserver agreement of nonexpert sonographers forclassifying septate uterus using the European Society of Human Reproduction andEmbryology/European Society for Gynaecological Endoscopy (ESHRE/ESGE), AmericanSociety for Reproductive Medicine (ASRM), and Congenital Uterine Malformations byExperts (CUME) classifications.Methods A total of 50 three-dimensional (3D) volumes of a nonconsecutive series ofwomen with suspected uterine malformation were used. Two nonexpert examinersevaluated a single 3D volume of the uterus of each woman, blinded to each other. Thefollowing measurements were performed: indentation depth, indentation angle,uterine fundal wall thickness, external fundal indentation, and indentation-to-wall-thickness (I:WT) ratio. Each observer had to assign a diagnosis in each case, according
receivedAugust 7, 2020acceptedOctober 13, 2021
DOI https://doi.org/10.1055/s-0041-1740271.ISSN 0100-7203.
© 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rightsreserved.This is an open access article published by Thieme under the terms of the
Creative Commons Attribution License, permitting unrestricted use,
distribution, and reproduction so long as the original work is properly cited.
(https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda., Rua do Matoso 170, Rio deJaneiro, RJ, CEP 20270-135, Brazil
THIEME
Original Article 911

to the three classification systems (ESHRE/ESGE, ASRM, and CUME). The interobserveragreement regarding the ESHRE/ESGE, ASRM, and CUME classifications was assessedusing the Cohen weighted kappa index (k). Agreement regarding the three classifica-tions (ASRM versus ESHRE/ESGE, ASRM versus CUME, ESHRE/ESGE versus CUME) wasalso assessed.Results The interobserver agreement between the 2 nonexpert examiners was goodfor the ESHRE/ESGE (k¼ 0.74; 95% confidence interval [CI]: 0.55–0.92) and very goodfor the ASRM and CUME classification systems (k¼ 0.95; 95%CI: 0.86–1.00; andk¼ 0.91; 95%CI: 0.79–1.00, respectively). Agreement between the ESHRE/ESGE andASRM classifications was moderate for both examiners. Agreement between theESHRE/ESGE and CUME classifications was moderate for examiner 1 and good forexaminer 2. Agreement between the ASRM and CUME classifications was good for bothexaminers.Conclusion The three classifications have good (ESHRE/ESGE) or very good (ASRMand CUME) interobserver agreement. Agreement between the ASRM and CUMEclassifications was higher than that for the ESHRE/ESGE and ASRM and ESHRE/ESGEand CUME classifications.
Resumo Objetivo Atualmente, existem até três classificações diferentes para o diagnóstico deútero septado. A concordância interobservador entre eles tem sido pouco avaliada.Objetivo Avaliar a concordância interobservador de ecografistas não especialistaspara classificar úteros septados usando as classificações European Society of HumanReproduction and Embryology/European Society for Gynaecological Endoscopy(ESHRE/ESGE, na sigla em inglês), American Society for Reproductive Medicine(ASRM, na sigla em inglês) e Congenital Uterine Malformations by Experts (CUME,na sigla em inglês).Métodos Foramutilizados 50 volumes tridimensionais (3D) deumasérie não consecutivade mulheres com suspeita de malformação uterina. Dois examinadores não especialistasavaliaram umúnico volume 3D do útero de cadamulher,mutuamente cegos. As seguintesmedidas foram aferidas: profundidade de indentação, ângulo de indentação, espessura daparede do fundo uterino, indentação externa do fundo e relação entre indentação e aespessura da parede (I:WT, na sigla em inglês). Cada observador teve que atribuir umdiagnóstico em cada caso, de acordo com os três sistemas de classificação (ESHRE/ESGE,ASRM e CUME). A concordância interobservador em relação às classificações ESHRE/ESGE,ASRM e CUME foi avaliada usando o índice kappa ponderado de Cohen (k). A concordânciaem relação às três classificações (ASRM versus ESHRE/ESGE, ASRM versus CUME e ESHRE/ESGE versus CUME) também foi avaliada.Resultados A concordância interobservador entre os 2 examinadores não especia-listas foi boa para a classificação ESHRE/ESGE (k¼0,74, intervalo de confiança [IC] 95%:0,55–0,92) e muito boa para os sistemas de classificação ASRM e CUME (k¼0,95; IC95%: 0,86–1,00; e k¼ 0,91; IC95%: 0,79–1,00, respectivamente). A concordância entreas classificações ESHRE/ESGE e ASRM foi moderada para ambos os examinadores. Aconcordância entre as classificações ESHRE/ESGE e CUME foi moderada para oexaminador 1 e boa para o examinador 2. A concordância entre as classificaçõesASRM e CUME foi boa para ambos os examinadores.Conclusão As três classificações apresentam concordância interobservador boa(ESHRE/ESGE) ou muito boa (ASRM e CUME). A concordância entre as classificaçõesASRM e CUME foi maior do que entre as classificações ESHRE/ESGE e ASRM eESHRE/ESGE e CUME.
Palavras-chave
► útero► ecografia► anomalia congênita
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Diagnosing Septate Uterus Using Three-Dimensional Ultrasound Peixoto et al.912

Introduction
Congenital uterine malformations were described for thefirst time in 1800s and, since then, several classificationsystems have been developed for describing different typesof uterine and cervical/vaginal anomalies,1 whose incidencehas been reported as of between 0.2 and 0.4% in the generalpopulation and of between 3 and 13% in infertile patients.2–7
Classically, septate uterus has been associated with poorreproductive and obstetric outcomes, and surgical metroplastyis advocated in these cases, with the aim of improving theseoutcomes.8–11 Notwithstanding, evidence that this surgery isbeneficial is rather arguable.12 Differently from septate uterus,arcuate/normal andbicornuate uteri donot require surgery.8–11
However, from the beginning, there was some difficulty in theclassification of uterine malformations, mainly due to thediscrepancy between the diagnostic criteria and the diagnostictechniquesused.13Toovercomethese limitations, three-dimen-sional (3D) ultrasound has been proposed as the gold standardtechnique to classify uterine malformations, as it seems to bebetter to evaluate the level of distortion of the uterine fundus,and also to reduce the interobserver variability.14,15
The European Society of Human Reproduction andEmbryology/European Society for Gynaecological Endoscopy(ESHRE/ESGE) and the American Society for ReproductiveMedicine (ASRM)havebothpublished their recommendationson how to classify uterine anomalies, using the coronal planeof the uterus. The ESHRE/ESGE classification suggests using anindentation-to-wall-thickness (I:WT) ratio>50% for diagnos-ing a septate uterus and an external fundal indentation>50%to diagnose a bicornuate uterus.13,16 The ASRM classificationconsiders auterusasseptatewhen there isbothan indentationdepth>15mm and an indentation angle<90°; anormal/arcuate uterus when there is both an indentationdepth<10mm and an indentation angle>90°; and a bicorn-uate uterus when the external fundal indentation is>10mm.According to this classification, some cases could not beclassified as septate or not-septate (falling in the so-calledgray zone).8 Although both classifications have very objectivecriteria, they do not coincide, which means that a highpercentage of uteri classified as septate by the ESHRE/ESGEclassification are classified as arcuate/normal by the ASRMclassification.17–20More recently, a group of experts (Congen-ital Uterine Malformations by Experts [CUME]) proposed newcriteria for diagnosing a septate uterus: indentation depth �10mm, indentation angle<140°, and I:WT>110%.18
The main objective of the present study was to assess theinterobserver agreement of nonexpert sonographers in clas-sifying septate uteri using the ESHRE/ESGE, ASRM, andCUME classifications in each case. Secondly, we also aimedto compare the agreement for each examiner for diagnosingseptate uterus between the three different classifications(ESHRE/ESGE, ASRM, and CUME).
Methods
The present study was a single-center retrospective analysisof patients with suspicion of congenital uterine malforma-
tion who underwent transvaginal ultrasound at the Depart-ment of Obstetrics andGynecology of the Clínica Universidadde Navarra, Pamplona, Spain. Due to the study design and tothe anonymization of the 3D volumes, formal approval by theInstitutional Review Board from the Clínica Universidad deNavarra was waived. However, all women had given oralinformed consent to acquire and use their 3D datasets for thepresent research. The present study was performed at theClínica Universidad de Navarra between September andOctober 2018.
The inclusion criterion was: women with suspecteduterine malformation in infertility setting who underwent3D uterine evaluation. The exclusion criteria were: diagno-sis of bicornuate or didelfis uterus or poor-quality 3Dvolume.
An expert examiner (Alcazar J. L.) randomly selected casesfrom the hospital database. Two nonexpert examiners (Peix-oto C. and Castro M) evaluated a single 3D volume of theuterus of each woman. All 3D datasets had been acquired byone expert examiner (Alcazar J. L.) using either a Voluson 730Expert or Voluson E8 machines (GE Healthcare, Chicago, IL,USA).
The nonexpert examiners had basic training on ultra-sound in gynecology, with no special focus on uterinemalformations, but both were undergoing a training pro-gram for ultrasound assessment of congenital uterine anom-alies. Before the study, the nonexpert examiners took a short(2 hours) theoretical training session focused on theESHRE/ESGE, ASRM and CUME classifications. Additionally,they read the original papers in which the criteria to classifyuterine malformations were described.8,13,18 They were alsotrained to use the 4D View Ultrasound software (GE Health-care, Chicago, IL, USA).
The two observers manipulated the uterine 3D volumes,blinded to each other. After obtaining the coronal plane andusing the Volume Contrast Imaging (VCI) function accordingto the CUME recommendations,18 they performed the fol-lowing measurements: indentation depth, indentation an-gle, uterine fundal wall thickness, external fundalindentation, and I:WT ratio. Each observer had to assign adiagnosis (normal/arcuate, septate) in each case, accordingto the three classification systems (ESHRE/ESGE, ASRM, andCUME) (►Fig. 1).
Arbitrarily, to avoid cases from falling in the grey zone,we decided the following: for the ASRM classification, incase that only one criterion was present, the case wasconsidered as normal. For the CUME classification, theuterus was considered as septate if at least two criteriawere present.
The examiners were also instructed not to discuss theirimpressions among themselves or with the expert after theassessment. We did not set a maximum time for performingevaluations of the 3D volumes.
The interobserver agreement between the two nonexpertexaminers regarding the ESHRE/ESGE, ASRM, and CUMEclassifications was assessed using the Cohenweighted kappaindex (k) with 95% confidence intervals (CIs) and percentageof agreement.21
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Diagnosing Septate Uterus Using Three-Dimensional Ultrasound Peixoto et al. 913

We also assessed the interobserver agreement for the twononexpert examiners regarding the three classifications(ASRM versus ESHRE/ESGE, ASRM versus CUME, andESHRE/ESGE versus CUME).
The kappa value was interpreted regarding thereporting of the reliability/strength of agreement as fol-lows: poor<0.20; fair¼0.21 to 0.40; moderate¼0.41to 0.60; good¼0.61 to 0.80; and very good¼0.81to 1.00.22
Statistical calculations were done using GraphPad soft-ware (GraphPad Software, Inc., San Diego, CA, USA). Samplesize calculation was not performed.
Results
Forty-seven 3D volumes of women were included in thepresent study. This number was chosen arbitrarily. Theinterobserver agreement between the two nonexpert exam-iners for classifying uterine malformations is shown in►Tables 1, 2 and 3. Overall, it was good for the ESHRE/ESGE (k¼0.74; 95%CI: 0.55–0.92) classification (►Table 1)and very good for the ASRM and CUME classifications(k¼0.96; 95%CI: 0.88–1.00; and k¼0.91; 95%CI: 0.79–1.00, respectively) (►Tables 2 and 3).
The agreement between the different classificationssystems is shown in ►Tables 4,5,6,7,8,9. When comparingthe agreement for classifying uterine anomalies betweenthe ESHRE/ESGE and ASRM classifications, we observed thatit was moderate for both examiners (►Tables 4 and 5). Wealso observed that 14 cases were classified as septate by theESHRE/ESGE classification and as normal/arcuate by theASRM classification by both examiners. For both examiners,9 of these cases were classified as normal/arcuate (64.3%)and 5 as septate (35.7%) when using the CUMEclassification.
The agreement between the ESHRE/ESGE and CUMEclassifications was moderate for examiner 1 and good forexaminer 2 (►Tables 6 and 7). Finally, the agreement be-tween the ASRM and CUME classifications was good for bothexaminers (►Tables 8 and 9).
Discussion
As far as we know, this is the first study to assess theinterobserver agreement of the three existing classificationsystems to describe normal, arcuate, and septate uterus. Wehave shown that the evaluation of 3D volumes of uteri isreproducible among nonexpert examiners.
Fig. 1 A case of a septate uterus according to the ESHRE/ESGEclassification (I:WT¼ 52%) (A), but normal/arcuate according to theASRM (indentation: 0.63 cm, angle: 130°) (B) and to the CUME(indentation: 0.63 cm, angle: 130°, I:WT: 52%) classifications (C).
Table 1 Interobserver agreement for nonexpert examiners for classifying uterine congenital anomalies using the ESHRE/ESGEclassification
ESHRE/ESGE
Examiner 1
Examiner 2 Normal/arcuate Septate Bicornuate Weighted Kappa(95% CI)
Agreement(%)
Normal/arcuate 16 3 – 0.74(0.55–0.92)
86%
Septate 3 25 –
Bicornuate – 1 2
Abbreviations: CI, confidence interval; ESHRE, European Society of Human Reproduction and Embryology; ESGE, European Society forGynaecological Endoscopy.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Diagnosing Septate Uterus Using Three-Dimensional Ultrasound Peixoto et al.914
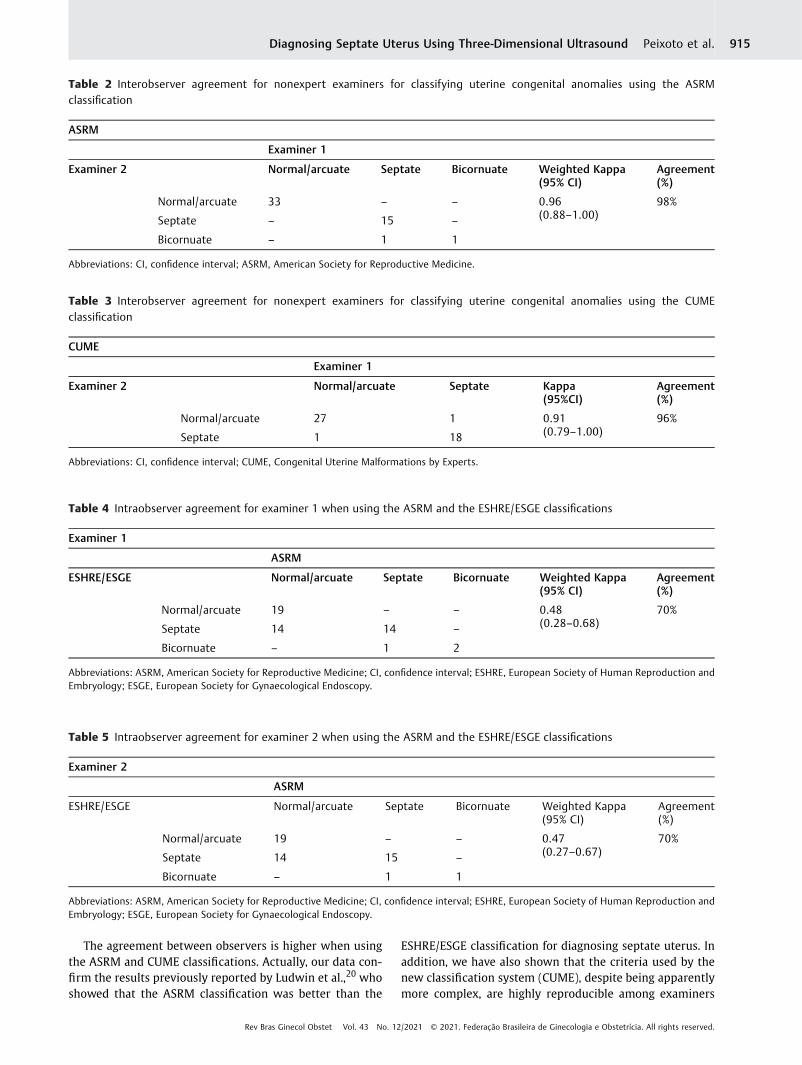
The agreement between observers is higher when usingthe ASRM and CUME classifications. Actually, our data con-firm the results previously reported by Ludwin et al.,20 whoshowed that the ASRM classification was better than the
ESHRE/ESGE classification for diagnosing septate uterus. Inaddition, we have also shown that the criteria used by thenew classification system (CUME), despite being apparentlymore complex, are highly reproducible among examiners
Table 2 Interobserver agreement for nonexpert examiners for classifying uterine congenital anomalies using the ASRMclassification
ASRM
Examiner 1
Examiner 2 Normal/arcuate Septate Bicornuate Weighted Kappa(95% CI)
Agreement(%)
Normal/arcuate 33 – – 0.96(0.88–1.00)
98%
Septate – 15 –
Bicornuate – 1 1
Abbreviations: CI, confidence interval; ASRM, American Society for Reproductive Medicine.
Table 3 Interobserver agreement for nonexpert examiners for classifying uterine congenital anomalies using the CUMEclassification
CUME
Examiner 1
Examiner 2 Normal/arcuate Septate Kappa(95%CI)
Agreement(%)
Normal/arcuate 27 1 0.91(0.79–1.00)
96%
Septate 1 18
Abbreviations: CI, confidence interval; CUME, Congenital Uterine Malformations by Experts.
Table 4 Intraobserver agreement for examiner 1 when using the ASRM and the ESHRE/ESGE classifications
Examiner 1
ASRM
ESHRE/ESGE Normal/arcuate Septate Bicornuate Weighted Kappa(95% CI)
Agreement(%)
Normal/arcuate 19 – – 0.48(0.28–0.68)
70%
Septate 14 14 –
Bicornuate – 1 2
Abbreviations: ASRM, American Society for Reproductive Medicine; CI, confidence interval; ESHRE, European Society of Human Reproduction andEmbryology; ESGE, European Society for Gynaecological Endoscopy.
Table 5 Intraobserver agreement for examiner 2 when using the ASRM and the ESHRE/ESGE classifications
Examiner 2
ASRM
ESHRE/ESGE Normal/arcuate Septate Bicornuate Weighted Kappa(95% CI)
Agreement(%)
Normal/arcuate 19 – – 0.47(0.27–0.67)
70%
Septate 14 15 –
Bicornuate – 1 1
Abbreviations: ASRM, American Society for Reproductive Medicine; CI, confidence interval; ESHRE, European Society of Human Reproduction andEmbryology; ESGE, European Society for Gynaecological Endoscopy.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Diagnosing Septate Uterus Using Three-Dimensional Ultrasound Peixoto et al. 915

(k¼0.91). This is an important finding, given that thisnew classification has not yet been validated after itspublication.
In our study, the agreement between the ESHRE/ESGE andASRMcriteriawasmoderate. Thisfinding is in linewith thoseof previous studies18,20 and raises concern regarding the useof the ESHRE/ESGE classification, since its use could lead toan overdiagnosis of septate uterus and to a potential increaseof surgical corrections.17 This is relevant since recent evi-dence suggests no benefit in obstetrical outcomes withsurgery.23 Our data also support the results published by
the CUME group,18 given that we demonstrated that, incomparison with CUME criteria, the ESHRE/ESGE classifica-tion overestimates the number of septate uteri. Overall, theagreement between the CUME and the ESHRE/ESGE and theASRM classifications was good, but it was slightly betterbetween the CUME and ASRM classifications than betweenthe CUME and ESHRE/ESGE classifications.
An interesting question is related to the fact that if theESHRE/ESGE classification would use the I:IþWT ratio,instead of the I:WT ratio, the rate of septate uterus wouldbe similar to CUME classification.
Table 6 Intraobserver agreement for examiner 1 when using the CUME and the ESHRE/ESGE classifications
Examiner 1
ESHRE/ESGE
CUME Normal/arcuate Septate Kappa(95%CI)
Agreement(%)
Normal/arcuate 18 10 0.59(0.39–0.80)
79%
Septate – 19
Abbreviations: CI, confidence interval; CUME, Congenital Uterine Malformations by Experts; ESHRE, European Society of Human Reproduction andEmbryology; ESGE, European Society for Gynaecological Endoscopy.
Table 7 Intraobserver agreement for examiner 2 when using the CUME and the ESHRE/ESGE classifications
Examiner 2
ESHRE/ESGE
CUME Normal/arcuate Septate Kappa(95%CI)
Agreement(%)
Normal/arcuate 19 9 0.63(0.43–0.83)
81%
Septate – 19
Abbreviations: CI, confidence interval; CUME, Congenital Uterine Malformations by Experts; ESHRE, European Society of Human Reproduction andEmbryology; ESGE, European Society for Gynaecological Endoscopy.
Table 8 Intraobserver agreement for examiner 1 when using the CUME and the ASRM classifications
Examiner 1
ASRM
CUME Normal/arcuate Septate Kappa(95%CI)
Agreement(%)
Normal/arcuate 28 – 0.77(0.58–0.96)
89%
Septate 5 14
Abbreviations: ASRM, American Society for Reproductive Medicine; CI, confidence interval. CUME, Congenital Uterine Malformations by Experts.
Table 9 Intraobserver agreement for examiner 2 when using the CUME and the ASRM classifications
Examiner 2
ASRM
CUME Normal/arcuate Septate Kappa(95%CI)
Agreement(%)
Normal/arcuate 28 – 0.77(0.58–0.96)
89%
Septate 5 14
Abbreviations: ASRM, American Society for Reproductive Medicine; CI, confidence interval; CUME, Congenital Uterine Malformations by Experts.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Diagnosing Septate Uterus Using Three-Dimensional Ultrasound Peixoto et al.916

The strengths of the present study are its design and theuse of an optimal diagnostic method (3D ultrasonography)for diagnosing uterine anomalies.6,24 The participation ofnonexpert examiners could be seen as a potential strength,since it allows the evaluation of the reproducibility of thedifferent classifications in “everyday practice.”
However, certainly, our study design can be also consid-ered as a limitation, since the sources of variability regardingthe real-time ultrasound and 3D volume acquisition werenot taken to account, since the two observers have usedpreviously acquired 3D datasets, which may overestimatethe reproducibility of the measurements.
As stated above, our study has limitations. One limitationof the present study is that the examiners had to manipulatethe 3D volumes by rotation in all 3 orthogonal planes. Thismanipulation has an inherent variability between observ-ers,18,20 as the same uterus might provide different imagesdepending on the angle at which the coronal plane isobtained. Other possible limitations of the present studyare the small number of cases analyzed and the high qualityof 3D volumes, which may have contributed to a lowernumber of “discrepant” cases. One final limitation thatmust be mentioned is that we arbitrarily decided to assumethat there were no gray-zone cases, since the uteri wereclassified as septate only when both criteria of the ASRMclassification or at least two criteria of the CUME classifica-tion were present. It is clear that this point could bias theresults, since, somehow, we forced providing a diagnosis inall cases, which is not true in the case of the ASRMclassification.
Despite these limitations, we consider that ourfindings may have clinical relevance and should promptfurther studies to determine which classification shouldbe used.
Conclusion
In general, the three classifications have good (ESHRE/ESGE)or very good (ASRM, CUME) interobserver agreement, whichmakes them all good methods to classify congenital uterineanomalies. However, agreement between the ASRM and theCUME classifications was higher than that for the ESHRE-ESGE and the ASRM and for the ESHRE/ESGE and the CUMEclassifications.
Conflict of interestsThe authors have no conflict of interests to declare.
References1 Doerr W. [Jean Cruveilhier, Carl v. Rokitansky, Rudolf Virchow.
Fundamente der Pathologie, Gedanken aus Anlass der hunderstenJährung von Rokitanskys Todestag]. Virchows Arch A Pathol AnatHistol. 1978;378(01):1–16. Doi: 10.1007/BF00427181 German.
2 Nahum GG. Uterine anomalies. How common are they, and whatis their distribution among subtypes? J ReprodMed. 1998;43(10):877–887
3 Chan YY, Jayaprakasan K, Zamora J, Thornton JG, Raine-Fenning N,Coomarasamy A. The prevalence of congenital uterine anomalies
in unselected and high-risk populations: a systematic review.Hum Reprod Update. 2011;17(06):761–771. Doi: 10.1093/humupd/dmr028
4 Byrne J, Nussbaum-Blask A, Taylor WS, Rubin A, Hill M, O’DonnellR, et al. Prevalence of Müllerian duct anomalies detected atultrasound. Am J Med Genet. 2000;94(01):9–12. Doi:10.1002/1096-8628(20000904)94:1<9:aid-ajmg3>3.0.co;2-h
5 Acién P. Incidence of Müllerian defects in fertile and infertilewomen. Hum Reprod. 1997;12(07):1372–1376. Doi: 10.1093/oxfordjournals.humrep.a019588
6 Saravelos SH, Cocksedge KA, Li TC. Prevalence and diagnosis ofcongenital uterine anomalies in women with reproductive fail-ure: a critical appraisal. Hum Reprod Update. 2008;14(05):415–429. Doi: 10.1093/humupd/dmn018
7 Oppelt P, von Have M, Paulsen M, Strissel PL, Strick R, Brucker S,et al. Female genital malformations and their associated abnor-malities. Fertil Steril. 2007;87(02):335–342. Doi: 10.1016/j.fertn-stert.2006.07.1501
8 Practice Committee of the American Society for ReproductiveMedicine. Electronic address: [email protected] Practice Commit-tee of the American Society for Reproductive Medicine. Uterineseptum: a guideline. Fertil Steril. 2016;106(03):530–540. Doi:10.1016/j.fertnstert.2016.05.014
9 Valle RF, Ekpo GE. Hysteroscopic metroplasty for the septateuterus: review and meta-analysis. J Minim Invasive Gynecol.2013;20(01):22–42. Doi: 10.1016/j.jmig.2012.09.010
10 Kowalik CR, Goddijn M, Emanuel MH, Bongers MY, Spinder T, deKruif JH, et al. Metroplasty versus expectant management forwomen with recurrent miscarriage and a septate uterus.Cochrane Database Syst Rev. 2011;(06):CD008576. Doi:10.1002/14651858.CD008576.pub3
11 Rikken JF, Kowalik CR, Emanuel MH, Mol BWJ, Van der Veen F, vanWely M, et al. Septum resection for women of reproductive agewith a septate uterus. Cochrane Database Syst Rev. 2017;1(01):CD008576. Doi: 10.1002/14651858.CD008576.pub4
12 Rikken JFW, Verhorstert KWJ, Emanuel MH, Bongers MY, SpinderT, Kuchenbecker WKH, et al. Septum resection in women with aseptate uterus: a cohort study. Hum Reprod. 2020;35(07):1578-–1588. Doi: 10.1093/humrep/dez284
13 Grimbizis GF, Di Spiezio Sardo A, Saravelos SH, Gordts S, Exa-coustos C, Van Schoubroek D, et al. The Thessaloniki ESHRE/ESGEconsensus on diagnosis of female genital anomalies. Hum Reprod.2016;31(01):2–7. Doi: 10.1093/humrep/dev264
14 Salim R, Woelfer B, Backos M, Regan L, Jurkovic D. Reproducibilityof three-dimensional ultrasound diagnosis of congenital uterineanomalies. Ultrasound Obstet Gynecol. 2003;21(06):578–582.Doi: 10.1002/uog.127
15 Ludwin A, Ludwin I, Banas T, Knafel A, Miedzyblocki M, Basta A.Diagnostic accuracy of sonohysterography, hysterosalpingogra-phy and diagnostic hysteroscopy in diagnosis of arcuate, septateand bicornuate uterus. J Obstet Gynaecol Res. 2011;37(03):178–186. Doi: 10.1111/j.1447-0756.2010.01304.x
16 Grimbizis GF, Gordts S, Di Spiezio Sardo A, Brukcer S, De Angelis C,GergoletM, et al. The ESHRE/ESGE consensus on the classificationof female genital tract congenital anomalies. Hum Reprod. 2013;28(08):2032–2044. Doi: 10.1093/humrep/det098
17 Knez J, Saridogan E, Van Den Bosch T, Mavrelos D, Ambler G,Jurkovic D. ESHRE/ESGE female genital tract anomalies classifica-tion system-the potential impact of discarding arcuate uterus onclinical practice. Hum Reprod. 2018;33(04):600–606. Doi:10.1093/humrep/dey043
18 Ludwin A, Martins WP, Nastri CO, Ludwin I, Coelho Neto MA,Leitão VM, et al. Congenital Uterine Malformation by Experts(CUME): better criteria for distinguishing betweennormal/arcuate and septate uterus? Ultrasound Obstet Gynecol.2018;51(01):101–109. Doi: 10.1002/uog.18923
19 Ludwin A, Ludwin I. Comparison of the ESHRE-ESGE and ASRMclassifications of Müllerian duct anomalies in everyday practice.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Diagnosing Septate Uterus Using Three-Dimensional Ultrasound Peixoto et al. 917

Hum Reprod. 2015;30(03):569–580. Doi: 10.1093/humrep/-deu344
20 Ludwin A, Ludwin I, KudlaM, Kottner J. Reliability of the EuropeanSociety of Human Reproduction and Embryology/European Soci-ety for Gynaecological Endoscopy and American Society forReproductive Medicine classification systems for congenital uter-ine anomalies detected using three-dimensional ultrasonogra-phy. Fertil Steril. 2015;104(03):688–97.e8. Doi: 10.1016/j.fertnstert.2015.06.019
21 Kundel HL, Polansky M. Measurement of observer agreement. Radi-ology. 2003;228(02):303–308. Doi: 10.1148/radiol.2282011860
22 Brennan P, Silman A. Statistical methods for assessing observervariability in clinical measures. BMJ. 1992;304(6840):1491-–1494. Doi: 10.1136/bmj.304.6840.1491
23 National Institute for Health and Care Excellence (NICE) Hystero-scopicmetroplasty of a uterine septum for recurrent miscarriage:interventional procedures guidance. Lyon: NICE; 2015
24 Berger A, Batzer F, Lev-Toaff A, Berry-Roberts C. Diagnosticimaging modalities for Müllerian anomalies: the case for a newgold standard. J Minim Invasive Gynecol. 2014;21(03):335–345.Doi: 10.1016/j.jmig.2013.10.014
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Diagnosing Septate Uterus Using Three-Dimensional Ultrasound Peixoto et al.918

Overview of the Effect of Complementary Medicine onTreating or Mitigating the Risk of Endometriosis
Visão geral do efeito da medicina complementar notratamento ou mitigação do risco de endometrioseFiroozeh Mirzaee1 Atefeh Ahmadi2
1Nursing Research Center, DepartmentofMidwifery, Razi Faculty ofNursingand Midwifery, Kerman Univeresity of Medical Sciences, Kerman, Iran
2Nursing Research Center, Department of Counselling in Midwifery,Razi Faculty of Nursing and Midwifery, Kerman University of MedicalSciences, Kerman, Iran
Rev Bras Ginecol Obstet 2021;43(12):919–925.
Address for correspondence Atefeh Ahmadi, M.D, PhD, Assistantprof., 2nd Floor, Building No. 1, Medical University Campus, Haft-BaghHighway, Kerman, Iran (e-mail: [email protected]).
Keywords
► complementarymedicine
► endometriosis► overview
Abstract Objective Endometriosis is a hormone-dependent chronic inflammatory disease withsymptoms such as pelvic pain, which affect the physical, emotional, and social health ofwomen in reproductive age. The current overview article aims to explore the effect ofcomplementary medicine on the treatment or in mitigating the risk of endometriosis.Methods This is an overview article done in Iran. Two separate researchers systemat-ically searched 3 databases (Medline, Scopus, and Cochrane Central Register Trials)until September 2020. The methodological quality of each study was assessed usingthe assessment of multiple systematic reviews (AMSTAR) tool.Results The results of two reviews suggested that physical activity, tobacco smoking,diet, coffee and caffeine intake had no effect on mitigating the risk of endometriosis orimproving its treatment, but acupuncture successfully reduced pain and relatedmarker (serum CA-125) levels.Conclusion As endometriosis is an annoying disease with many complications and ishard to diagnose and treat, related studies in complementary medicine can helppatients with endometriosis. Based on the relevant literature review, among thecomplementary medicine available for the treatment or to mitigate the risk ofendometriosis, only acupuncture seems to alleviate the pain of endometriosis.
Palavras-chave
► medicinacomplementar
► endometriose► visão geral
Resumo Objetivo A endometriose é uma doença inflamatória crônica hormono-dependentecom sintomas como dores pélvicas, que afetam a saúde física, emocional e social demulheres em idade reprodutiva. O presente artigo de visão geral tem como objetivoexplorar o efeito damedicina complementar no tratamento ou namitigação do risco deendometriose.Métodos Trata-se de um artigo de visão geral feito no Irã. Dois pesquisadoresseparados pesquisaram sistematicamente 3 bancos de dados (Medline, Scopus e
receivedDecember 6, 2020acceptedJuly 22, 2021
DOI https://doi.org/10.1055/s-0041-1735156.ISSN 0100-7203.
© 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rightsreserved.This is an open access article published by Thieme under the terms of the
Creative Commons Attribution License, permitting unrestricted use,
distribution, and reproduction so long as the original work is properly cited.
(https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda., Rua do Matoso 170, Rio deJaneiro, RJ, CEP 20270-135, Brazil
THIEME
Original Article 919

Introduction
Endometriosis is a disease with an estimated incidence ofbetween 6 and 10% in women in reproductive age, � 176million women worldwide.1,2 Endometriosis is a hormone-dependent chronic inflammatory disease with symptomslike pelvic pain, which affect the physical, emotional, andsocial health of women in the reproductive age.3,4 It has beenshown that several pathogeneses including menstrual, ge-netic, and environmental factors as well as lifestyle play apivotal role in the development of the disease.3,4
The symptoms associated with painful endometriosisinclude dysmenorrhea, nonmenstrual pelvic pain, and pain-ful deep intercourse, which may affect women’s quality oflife, work, social relationships and sexual function withdeleterious implications for the life of these patients andtheir relationships.5,6Despite the highmorbidity and health-care costs associated with this condition, the exact cause ofendometriosis remains unknown, although many theorieshave been developed about the pathophysiological causes ofthis condition. The risk factors for this condition are largelyunidentified.
The existing offered treatments as various pharmacologi-cal and surgical therapies7 are not completely effective. Mostof them are prescribed for pain suppression and reduction orreversion of lesions in women suffering from the disease.Some related mechanisms are based on blocking the secre-tion of estrogen from the ovaries. Oral contraceptives, pro-gestin, danazol, and gonadotropin-releasing hormoneagonists (GnRH-a) are used for the treatment of endometri-osis, to relieve short-term symptoms.8 However, these treat-ments may have considerable side effects, such asmenopausal and female climacteric states (2021 ICD-10-CM Diagnosis Code N95.1), such as hot flushes and fatigue.
In addition, danazol can cause androgenic changes, suchas acne and weight gain. Previous studies have showed itsrole in increasing low-density lipoprotein (LDL) cholesterollevels and its conceivable association with ovarian cancer.Gonadotropin-releasing hormone agonists generally de-crease estrogen levels more than danazol, and their meno-pausal related side effects, such as insomnia, hot flushes, low
libido, and vaginal dryness are more severe. Low estrogenlevels can also lead to serious osteoporosis. The long-termadverse effects of add-back regimes, which use small quan-tities of progesterone and estrogen, have not yet beencompletely explored. Patients using progestin treatmentsuffermore frombloating, acne, spotting, andfluid retention.Progestin may affect the level of high-density lipoproteins(HDL) in the blood, possibly increasing the risk of cardiovas-cular side effects, such as thrombosis.7,8
The role of complementary medicine and the develop-ment of endometriosis have received growing attention,which is largely due to the physiological and pathologicalprocesses related to the disease, including inflammation,estrogen activity, menstrual cycles, organochlorines, andthe metabolism of prostaglandin.9 There are several system-atic reviews and meta-analyses on the effect of complemen-tary medicine such as exercise, drinking diet andacupuncture on the endometriosis. In addition, the relation-ship between tobacco smoking and drinking coffee withendometriosis have been investigated. Therefore, there is aneed for simultaneous analysis of several reviews to offer in-depth information to clinicians, policymakers, patients, andresearchers. The purpose of the present overview article is todemonstrate the effect of complementary medicine on en-dometriosis in reproductive age.
Methods
Six meta-analyses were assessed to identify those thatevaluated the effect of complementary medicine on thetreatment of endometriosis. Two independent authors dida systematic search of 3 databases (Medline, Scopus, andCochrane Central Register Trials) until September 2020. TheMedical Subject Headings (MESH) keywords searched inEnglish were exercise, tobacco, coffee, diet, complementarymedicine, acupuncture, and endometriosis. The inclusioncriteria were: (1) population (women with endometriosis),(2) intervention (all complementary medicine), (3) results(the effect of complementary medicine on treating or miti-gating the risk of endometriosis), and (5) methods (meta-analysis). Duplicate papers were excluded. We also reviewed
Cochrane Central Register Trials) até setembro de 2020. A qualidade metodológica decada estudo foi avaliada usando a ferramenta avaliação da qualidade dos relatos derevisão sistemática (AMSTAR, na sigla em inglês).Resultados Os resultados de duas revisões sugeriram que atividade física, tabagismo,dieta, consumo de café e cafeína não tiveram efeito na redução do risco deendometriose ou na melhoria do tratamento, mas a acupuntura reduziu com sucessoa dor e os níveis de marcadores relacionados (CA-125 sérico).Conclusão Como a endometriose é uma doença incômoda, com muitas complica-ções e de difícil diagnóstico e tratamento, estudos relacionados em medicinacomplementar podem ajudar pacientes com endometriose. Com base na revisão daliteratura relevante, entre os medicamentos complementares disponíveis para otratamento ou risco de endometriose, apenas a acupuntura parece aliviar a dor daendometriose.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Complementary Medicine on Treating or Mitigating the Risk of Endometriosis Mirzaee, Ahmadi920

the references and bibliographies of all studies tofind furtherrelated studies. The references listed in the reviews, meta-analyses and articles were also manually searched to broad-en the scope of the search. The authors who searched thedatabases and other sources also assessed the quality of the
studies and data extraction (►Table 1). Before making a finaldecision, disagreements were settled by consensus. Themethodological quality of systematic reviews was alsoassessed using the 11-item assessment of multiple system-atic reviews (AMSTAR) tool developed by Oxman et al.10
Table 1 Characteristics of the six studies included in the present overview
Authors Year Type ofreview
Age range(years old)
Type of intervention Samplesize
Conclusion
Xu et al.6 2017 Meta- analysis 13–52 Acupuncture, shamacupuncture, Westernmedicine, traditional chinesemedicine
591 Acupuncture reduced pain andhad a positive effect onperipheral blood CA-125 levels
Chiaffarinoet al.14
2014 Meta- analysis 15–65 Coffee and caffeine intake 1,407 There was no evidence on theassociation betweencoffee/caffeine intake and therisk of endometriosis
Miraet al.9
2018 Meta- analysis 13–50 Acupuncture, exercise,electrotherapy, and yoga
385 All studies were inconclusive inaffirming benefits, butdemonstrated a positive trendin the treatment ofendometriosis symptoms
Hoorsanet al.13
2017 Meta- analysis Reproductiveage
Calcium intake, milk, eggsbacon, red meat
72,662 Calcium, milk, eggs, bacon, andredmeat intake increase the riskof endometriosis
Ricciet al.
2016 Meta-analysis Reproductiveage
Endometriosis women physicalactivity
79,55 Physical activity does notreduce the risk of endometriosis
Braviet al.11
2014 Meta- analysis 15–56 Tobacco smoking 13,129 No evidence on the associationbetween tobacco smoking andthe risk of endometriosis
The study population of all of the studies was composed of women with endometriosis
Table 2 Assessment of themethodological quality of systematic reviews according to criteria set by the Center for Evidence-BasedManagement
AMSTAR items
References Year 1� 2† 3‡ 4§ 5j 6¶ 7�� 8†† 9‡‡ 10§§ 11jj 12¶¶
Xu et al.6 2017 Yes Yes No No Yes Yes Yes Yes Yes Yes Yes Yes
Chiaffarino et al.13 2014 Yes Yes Yes No Yes No Yes Yes Yes Yes Yes Yes
Mira et al.9 2018 Yes Yes Yes No Yes Yes Yes Yes Yes Yes Yes Yes
Hoorsan et al.13 2017 Yes Yes Yes No Yes Yes Yes Yes Yes Yes Yes Yes
Ricci et al.12 2016 Yes Yes Yes No Yes Yes Yes Yes Yes Yes Yes Yes
Bravi et al.11 2014 Yes Yes Yes No Yes Yes Yes Yes Yes Yes Yes Yes
Abbreviation: AMSTAR, Assessment of Multiple Systematic Reviews.�1: Did the study address a clearly focused question?†2: Was a comprehensive literature search conducted using relevant research databases (e.g., ABI/INFORM, Business Source Premier, PsycINFO, Webof Science, etc.)‡3: Is the search systematic and reproducible (e.g., were searched information sources listed, were search terms provided)?§4: Has publication bias been prevented as far as possible (e.g., were attempts made at collecting unpublished data)?j5: Are the inclusion and exclusion criteria clearly defined (e.g., population, outcomes of interest, study design)?¶6: Was the methodological quality of each study assessed using predetermined quality criteria?��7: Are the key features (population, sample size, study design, outcome measures, effect sizes, limitations) of the included studies described?††8: Has the meta-analysis been conducted correctly?‡‡9: Were the results similar from study to study?§§10: Is the effect size practically relevant?jj11: How precise is the estimate of the effect? Were confidence intervals given?¶¶12: Can the results be applied to your organization?
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Complementary Medicine on Treating or Mitigating the Risk of Endometriosis Mirzaee, Ahmadi 921

(►Table 2). Each item was scored on a 3-point Likert scale(yes, no, and cannot answer). A predesigned form validatedby the research team members was utilized to extract thestudy data, including the type of review, year of publication,first author, study populations, sample size, and mainoutcomes.
Results
►Fig. 1 shows the process of selecting reviews for the over-view. As can be seen, six meta-analyses were included in theoverview, as listed in ►Table 1. It should be noted that somearticles focused on reducing the symptoms of endometriosisand others focused on reducing the risk of endometriosis.
Physical Activity and EndometriosisSix case-control and 3 cohort studies included 3,355 cases ofrecent physical activities, and 4,600 cases were related to pastphysical activities. The summary odds ratio (OR) for endome-triosis according to thephysical activity levelwas calculatedbythe random-effect model (0.85) [95% confidence interval [CI]:0.67–1.07] for recent versus lack of physical activities. Com-pared with lack of recent physical activities, ORs for low andmoderate/high physical activities were 1.00 (95%CI: 0.68–1.28) and 0.75 (95%CI: 0.53–1.07), respectively. It is oftensuggested that physical activity can mitigate the risk of endo-metriosis, but this hypothesis is not supported by the present
meta-analysis. Further research is warranted to lend credit toour findings regarding the benefits of exercise at molecularand endocrine levels, or the effect of related confoundingmechanisms such as study design, choice of controls, andphysical activity on pain improvement.
Tobacco Smoking and EndometriosisIn the present paper, summary estimates of the relative risk(RR) are made using the random effect model, and heteroge-neity studies are assessed by χ2 test and quantified by I2statistics. As compared to never-smokers, the summary RRwere 0.96 (95% CI 0.86 to 1.08) for ever smokers, 0.95 (95% CI0.81 to 1.11) for former smokers, 0.92 (95% CI 0.82 to 1.04) forcurrent smokers, 0.87 (95% CI 0.70 to 1.07) for moderatesmokers and 0.93 (95% CI 0.69 to 1.26) for heavy smokers.The present meta-analysis provided no evidence for theassociation between tobacco smoking and the risk of endo-metriosis. The results are constant considering ever, former,current, moderate and heavy smokers, and across the type ofendometriosis and study design.11
Diet and EndometriosisThe present systematic review and meta-analysis of studiessuggested that the intake of calcium (OR: 0.99) (95%CI: 0.83–1.18), milk (OR: 0.90) (95%CI: 0.65–1.23), eggs (OR: 1.01)(95%CI: 0.81–1.28), bacon (OR: 1.26) (95%CI: 0.60–2.65), andred meat (OR: 1.26) (95%CI: 0.73–2.18), increase the risk of
Fig. 1 Search strategy of the study.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Complementary Medicine on Treating or Mitigating the Risk of Endometriosis Mirzaee, Ahmadi922

endometriosis. The evidence highlights the prevention im-pact of dietary components on the risk of endometriosis.Furthermore,more studies are required to explore the role ofdiet and nutritional elements in the incidence and progres-sion of endometriosis.13
Complementary Treatments and EndometriosisThe complementary interventions considered in the presentstudy were acupuncture, exercise, electrotherapy, and yoga.Although, these studies showed effects for the treatment ofendometriosis symptoms but all of them yielded inconclu-sive outcomes. A meta-analysis of acupuncture indicated itsbenefits in pain reduction compared with placebo(p¼0.007). Several complementary treatments have beenused to relieve the symptoms of endometriosis, but onlyacupuncture has demonstrated a significant improvement inoutcomes. Nonetheless, other approaches have also beensuccessful in relieving symptoms. This calls for further effortsto design controlled studies that back up their applicability.9
Effect of Coffee and Caffeine Intake on EndometriosisIn the present paper, 8 (6 case-control and 2 cohort) studies,including a total of 1,407 women with endometriosis, werereviewed. The summary relative risks for the intake versusnonintake of caffeine (1.26) (95%:CI: 0.95–1.66) and coffee(1.13) (95%CI: 0.46–2.76) was obtained. The overall guesswas 1.18 (95% CI 0.92–1.49). Moreover, the summary relativerisks was 1.09 (95%CI: 0.84–1.42) and 1.09 (95%CI: 0.89–1.33) for high and low caffeine intake, respectively, asopposed to nonintake. The present meta-analysis providedno evidence for the association between coffee/caffeineintake and the risk of endometriosis. Therefore, thecoffee/caffeine intake, as currently used in diet, does notpose a health risk.14
Effect of Acupuncture on EndometriosisOut of 10 studies reviewed, only 1 pilot study had used aplacebo control and blinding. The rest had utilized variouscontrols (medications and herbs), for which blinding wasimpossible. The sample size was small in all studies, rangingfrom 8 to 36 patients per arm. The mean difference (MD) inthe pain reduction (preminus postinterventional pain levelmeasured on a 0�10-point scale) between the acupunctureand control group was 1.36 (95% confidence intervals [CI] ¼1.01-1.72, p < 0.0001). Acupuncture had a positive effect onperipheral blood CA-125 levels, compared with the controlgroup (MD ¼ 5.9, 95% CI ¼ 1.56-10.25, p ¼ 0.008). Similarly,acupuncture had a positive effect on clinical effective rate,when compared with the control groups (odds ratio ¼ 2.07;95% CI ¼ 1.24-3.44, p ¼ 0.005). Few randomized, blindedclinical trials have addressed the efficacy of acupuncture intreating endometriosis-related pain. However, current stud-ies suggest that acupuncture mitigates pain and serumCA-125 levels, regardless of the type of control interventionused. To corroborate these findings, additional blindedstudies with suitable controls and suitable sample sizesare needed.6
Discussion
In the present study, six systematic reviews and meta-analyses studying the effects of complementary medicineon endometriosis treatment were reviewed. It is hypothe-sized that physical activity can increase the levels of sexhormone binding globulin (SHBG), which decreases bioavail-able estrogens.15,16 Steady physical activity also reducesinsulin resistance and hyperinsulinemia. Hyperinsulinemiamay increase the concentration of estrogens by decreasingthe concentration of SHBG and elevating the concentration ofinsulin-like growth factor-1 (IGF-1), which can stimulateendometrial cell proliferation by dwindling concentrationsof insulin-like growth factor binding protein 1 (IGFBP-1).15
Finally, regular physical activity seems to have protectiveeffects on inflammatory processes and oxidative stress, as itraises systemic levels of anti-inflammatory cytokines.16
However, the meta-analyses reviewed in the present studydo not conclusively support this hypothesis.
The results of the present study provided no evidence forthe association between tobacco smoking and the risk ofendometriosis. Since endometriosis is an estrogen-dependentdisorder, the inverse association between smoking and endo-metriosis reported in some studies is normally attributed tothe antiestrogenic effect of tobacco smoking.17 Some authorshave suggested that estradiol can modify the mediators ofimmune system molecules or those involved in tissue celladhesion and invasion.18
Literature review in this study clarified the need for deeperinsights into the impact of dietary components on the endome-triosis. What is confirmed about diet is that risk of developingendometriosis drops by greater consumption of fish. In addi-tion, the results of this meta-analysis demonstrated that milk,calcium, and vitamin D have no effect on the risk of developingendometriosis, increase low-fat dairy products, reduce the riskof endometriosis and also increase the levels of 25- hydroxyl-vitamin D3. Also, dairy products reduce the risk of endometri-osis.19 This study indicates the positive effect of these foods onrisk mitigation, though none of these results were statisticallysignificant. The results do not support the association betweencoffee/caffeine intake and the risk of endometriosis. It has beensuggested that, in women, caffeine influences the hepaticproduction of SHBG and elicits subsequent reductions in bio-available testosterone.20 Other studies have demonstrated theroleofcaffeine in inhibitingaromatase, akeyenzymemediatingthe conversion of androgens to estrogens.21
Several complementary treatments have been proposedto alleviate the symptoms of endometriosis, but only acu-puncture has been able to produce significant positive out-comes.13 Acupuncture decreases pain and serum CA-125levels and improves endometriosis by various mechanisms.It seems that this complementary medicine reduces pain byraising pain thresholds in humans.22 It improves the releaseof neuro-hormonal factors, including adenosine, γ-amino-butyric acid, opioid peptide, acetylcholine, nitric oxide,noradrenaline, and dopamine.23,24 In addition, acupuncturesuppresses serum estradiol levels.25 Therefore, it may
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Complementary Medicine on Treating or Mitigating the Risk of Endometriosis Mirzaee, Ahmadi 923

constrain the growth of ectopic endometrium and relievepain. The last mechanism fosters the capacity of the immunesystem to remove malignant cells more actively by strength-ening the ability of natural killer (NK) cells to kill cancercells.26 More specifically, acupuncture stimulation increasesthe cytotoxicity of NK cells by promoting crosstalk betweenthe neurotransmitter network and the immune system.Mediated by nitric oxide, β-endorphins, and cytokines,27
this crosstalk is anchored by opioid and NK cell receptors.The findings of the present overview should be inter-
preted with caution because most of the studies has notreported or explained their randomization technique, drop-out rate, and attrition rate, no use of intention to treat,blinding method, sequence generation, and sample sizeestimation method. It is strongly recommended that futureresearch adopts consort criteria to provide high qualityresults for improving systematic reviews andmeta-analyses.
Conclusion
The present study suggests that, among different comple-mentary medicines like acupuncture, exercise, electrothera-py, and yoga for the treatment of endometriosis, onlyacupuncture is effective in alleviating endometriosis pain.Furthermore, some types of nutritional elements seem toincrease the risk of endometriosis. Physical activity does notreduce the risk of endometrioses, and there is no associationbetween tobacco smoking and the risk of endometriosis.
ContributionsAll authors were involved in the design and interpretationof the analyses, contributed to the writing of the manu-script, read, and approved the final manuscript.
Conflict of InterestsThe authors have no conflict of interests to declare.
References1 Rogers PA, Adamson GD, Al-Jefout M, Becker CM, D’Hooghe TM,
Dunselman GAJ, et al; WES/WERF Consortium for Research Priori-ties in Endometriosis. Researchpriorities for endometriosis. ReprodSci. 2017;24(02):202–226. Doi: 10.1177/1933719116654991
2 Mirzaee F, Ahmadi A, Zangiabadi Z, Mirzaee M. The Effectivenessof Psycho-Educational and Cognitive-Behavioral Counseling onFemale Sexual Dysfunction. Revista Brasileira de Ginecologia eObstetrícia. 2020;42:333–9
3 Parazzini F, Viganò P, CandianiM, Fedele L. Diet and endometriosisrisk: a literature review. Reprod Biomed Online. 2013;26(04):323–336. Doi: 10.1016/j.rbmo.2012.12.011
4 Berek JS. Berek & Novak’s gynecology. 15th ed. Philadelphia:Wolters Kluwer Health/Lippincott Williams and Wilkins; 2012
5 Callahan TL, Caughey AB. Blueprints obstetrics and gynecology.Baltimore: Lippincott Williams & Wilkins; 2013
6 Sesti F, Pietropolli A, Capozzolo T, Broccoli P, Pierangeli S, BolleaMR, et al. Hormonal suppression treatment or dietary therapyversus placebo in the control of painful symptoms after conser-vative surgery for endometriosis stage III-IV. A randomizedcomparative trial. Fertil Steril. 2007;88(06):1541–1547. Doi:10.1016/j.fertnstert.2007.01.053
7 Xu Y, ZhaoW, Li T, Zhao Y, Bu H, Song S. Effects of acupuncture forthe treatment of endometriosis-related pain: A systematic reviewand meta-analysis. PLoS One. 2017;12(10):e0186616. Doi:10.1371/journal.pone.0186616
8 Ilhan M, Gürağaç Dereli FT, Akkol EK. Novel drug targets withtraditional herbal medicines for overcoming endometriosis. CurrDrug Deliv. 2019;16(05):386–399. Doi: 10.2174/1567201816666181227112421
9 Mira TAA, Buen MM, Borges MG, Yela DA, Benetti-Pinto CL.Systematic review and meta-analysis of complementary treat-ments for women with symptomatic endometriosis. Int J Gynae-col Obstet. 2018;143(01):2–9. Doi: 10.1002/ijgo.12576
10 Oxman AD, Schünemann HJ, Fretheim A. Improving the use ofresearch evidence in guideline development: 8. Synthesis andpresentation of evidence. Health Res Policy Syst. 2006;4:20. Doi:10.1186/1478-4505-4-20
11 Bravi F, Parazzini F, Cipriani S, Chiaffarino F, Ricci E, Chiantera V,et al. Tobacco smoking and risk of endometriosis: a systematicreview and meta-analysis. BMJ Open. 2014;4(12):e006325. Doi:10.1136/bmjopen-2014-006325
12 Ricci E, Viganò P, Cipriani S, Chiaffarino F, Bianchi S, Rebonato G,et al. Physical activity and endometriosis risk in women withinfertility or pain: systematic review and meta-analysis. Medi-cine. 2016;95(40)
13 Hoorsan H, Mirmiran P, Chaichian S, Moradi Y, Akhlaghdoust M,Hoorsan R, et al. Diet and risk of endometriosis: a systematicreview andmeta-analysis study. Iran Red CrescentMed J. 2017;19(09):e41248
14 Chiaffarino F, Bravi F, Cipriani S, Parazzini F, Ricci E, Viganò, et al.Coffee and caffeine intake and risk of endometriosis: a meta-analysis. Eur J Nutr. 2014;53(07):1573–1579. Doi: 10.1007/s00394-014-0662-7
15 Friberg E, Wallin A, Wolk A. Sucrose, high-sugar foods, and risk ofendometrial cancer–a population-based cohort study. CancerEpidemiol Biomarkers Prev. 2011;20(09):1831–1837. Doi:10.1158/1055-9965.EPI-11-0402
16 Wu MH, Shoji Y, Chuang PC, Tsai SJ. Endometriosis: diseasepathophysiology and the role of prostaglandins. Expert Rev MolMed. 2007;9(02):1–20. Doi: 10.1017/S146239940700021X
17 Baron JA, La Vecchia C, Levi F. The antiestrogenic effect of cigarettesmoking inwomen. Am J Obstet Gynecol. 1990;162(02):502–514.Doi: 10.1016/0002-9378(90)90420-c
18 Boucher A, Mourad W, Mailloux J, Lemay A, Akoum A. Ovarianhormones modulate monocyte chemotactic protein-1 expressionin endometrial cells of women with endometriosis. Mol HumReprod. 2000;6(07):618–626. Doi: 10.1093/molehr/6.7.618
19 Harris HR, Chavarro JE,Malspeis S,WillettWC,Missmer SA. Dairy-food, calcium, magnesium, and vitamin D intake and endometri-osis: a prospective cohort study. Am J Epidemiol. 2013;177(05):420–430. Doi: 10.1093/aje/kws247
20 Kotsopoulos J, Eliassen AH, Missmer SA, Hankinson SE, TworogerSS. Relationship between caffeine intake and plasma sex hormoneconcentrations in premenopausal and postmenopausal women.Cancer. 2009;115(12):2765–2774. Doi: 10.1002/cncr.24328
21 Wedick NM, Mantzoros CS, Ding EL, Brennan AM, Rosner B, RimmEB, et al. The effects of caffeinated and decaffeinated coffee on sexhormone-binding globulin and endogenous sex hormone levels: arandomized controlled trial. Nutr J. 2012;11:86. Doi: 10.1186/1475-2891-11-86
22 Mirzaee F, Hasaroeih FE, Mirzaee M, Ghazanfarpour M. Compar-ing the effect of acupressure with or without ice in LI-4 point onlabour pain and anxiety levels during labour: a randomisedcontrolled trial. Journal of Obstetrics and Gynaecology. 2021;41(03):395–400
23 Staud R, Price DD. Mechanisms of acupuncture analgesia forclinical and experimental pain. Expert Rev Neurother. 2006;6(05):661–667. Doi: 10.1586/14737175.6.5.661
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Complementary Medicine on Treating or Mitigating the Risk of Endometriosis Mirzaee, Ahmadi924

24 Saeedi Z, Alidoosti K, Mirzaee F, Ahmadi A, Dahesh T. The effect ofcombination of psychological counseling and acupressure train-ing with couple therapy approach on nausea and vomiting inpregnancy. The Iranian Journal of Obstetrics, Gynecology andInfertility. 2019;21(11):71–79
25 Ma J, Yun-guang H, Zhang DH. [Effects of acupuncture on bonemetabolism and serum estradiol level in ovariectomy-inducedosteoporosis rats]. Zhen Ci Yan Jiu. 2008;33(04):235–239
26 Johnston MF, Ortiz Sánchez E, Vujanovic NL, Li W. Acupuncturemay stimulate anticancer immunity via activation of naturalkiller cells. Evid Based Complement Alternat Med. 2011;2011:481625. Doi: 10.1093/ecam/nep236
27 Hui KK, Hui EK, Johnston MF. The potential of a person-centeredapproach in caring for patients with cancer: a perspective fromthe UCLA center for East-West medicine. Integr Cancer Ther.2006;5(01):56–62. Doi: 10.1177/1534735405286109
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Complementary Medicine on Treating or Mitigating the Risk of Endometriosis Mirzaee, Ahmadi 925

School-based HPV Vaccination: The Challengesin a Brazilian Initiative
Vacinação contra o HPV em base escolar: Os desafios deuma iniciativa brasileiraJulio Cesar Teixeira1 Mariana Silva Castro Vianna2 Diama Bhadra Vale1
Daniella Moretti Arbore1 Thais Helena Wilmers Perini2 Tulio Jose Tomass Couto2
Jose Pedroso Neto2 Luiz Carlos Zeferino1
1Department of Obstetrics and Gynecology, Faculty of MedicalSciences, Universidade Estadual de Campinas, Campinas, SP, Brazil
2 Epidemiological Surveillance and Women Health Secretariat,Administration of the City of Indaiatuba – Mayor’s Office,Indaiatuba, SP, Brazil
Rev Bras Ginecol Obstet 2021;43(12):926–931.
Address for correspondence Julio Cesar Teixeira, PhD, MD, RuaAlexander Fleming, 101, 13083-881, Cidade Universitária, Campinas,SP, Brazil (e-mail: [email protected]; [email protected]).
Keywords
► humanpapillomavirus
► HPV vaccine► adolescents► schools► vaccination
Abstract Objective The present study assesses the implementation and the impact after2 years of a school-based human papillomavirus (HPV) vaccination program in a Braziliancity.Methods A prospective study assessing the implementation of the program, offeringquadrivalent HPV vaccine in two annual doses to girls and boys aged from 9 to 10 yearsold. The program was started in the city of Indaiatuba, state of São Paulo, Brazil, in2018, and had authorization from the National Immunization Program. The number ofHPV vaccine first doses applied and the coverage in 2018 was calculated and comparedto the year 2017. There were described events that have influenced the results.Results The program invited 4,878 children through schools (87.1% of the targetpopulation), and 7.5% refused vaccination. Several concurrent events required orcompeted for health professionals of the vaccination teams. The coverage of the firstdose (between 9 and 10 years old) was 16.1% in 2017 and increased to 50.5% in 2018(p<0.0001). The first dose in all ages increased 78% in 2018 compared with 2017(6,636/3,733). Competing demands over the program continued in 2019, and the firstdose coverage dropped (26.9%). For 2020, a municipal law instituted school-basedvaccination and the creation of dedicated teams for vaccination, and these strategiesare waiting to be tested.Conclusion School-based annual HPV vaccination in children between 9 and 10 yearsold was feasible and increased vaccination coverage, regardless of gender, although theprogram was vulnerable to competing events.
receivedSeptember 19, 2021acceptedNovember 3, 2021
DOI https://doi.org/10.1055/s-0041-1740279.ISSN 0100-7203.
© 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rightsreserved.This is an open access article published by Thieme under the terms of the
Creative Commons Attribution License, permitting unrestricted use,
distribution, and reproduction so long as the original work is properly cited.
(https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda., Rua do Matoso 170, Rio deJaneiro, RJ, CEP 20270-135, Brazil
Original ArticleTHIEME
926

Introduction
Human papillomavirus (HPV) infection is a necessary condi-tion for the development of cervical cancer, and HPV vacci-nation prevents up to 90% of this cancer.1 Screening andvaccination combined are the main strategies towards theeradication of cervical cancer.2–5
TheWorld Health Organization (WHO) has recommendedHPV vaccination since 2009, starting at the age of between 9and 10 years old, preferably for girls.6
The first population program with HPV vaccinationstarted in Australia (2007) and reached a high and sustainedcoverage reporting a continuous drop in the incidence ofcervical cancer precursor lesions.2 The National Immuniza-tion Program (PNI, in the Portuguese acronym) in Braziloffers the quadrivalent HPV vaccine (HPV 6/11/16/18)through the Brazilian Unified Health System (SUS, in thePortuguese acronym) since 2014. The target are girls from 9to 14 years old, but since 2017 boys from 11 to 14 years oldwere also included. In the 1st year (2014), the strategy wasschool-based and 5.3 million first doses were applied (cov-erage of 108%). In the second dose, after a 6-month interval,3.2 million doses were applied (coverage of 64.8%).7 In thefollowing year (2015), the strategy changed from school-based to be offered at primary health care facilities, and thePNI reported a significant drop in vaccination coverage:between 50 and 61% in the first dose and between 22 and38% in the second dose.8,9
In Indaiatuba, state of São Paulo, Brazil, a school-basedHPV vaccine programwas planned to increase coverage. The
present article describes the rationale, design, implementa-tion, and results of the 1st 2 years of the program. Severalunexpected competing events prevented the full develop-ment of the strategy. The present article is a critical report ofthe challenges to be overcome in a real-world setting of amiddle-income country.
Methods
This is a prospective study with the objective of evaluatingthe interventions of a school-based HPV vaccination pro-gram aiming to increase coverage in preadolescents andadolescents. In Brazil, the PNI offers HPV vaccine in a two-dose schedule (at a 6-month interval) to girls from 9 to14 years old and to boys from 11 to 14 years old in primaryhealth care facilities. Indaiatuba, in the state of São Paulo,Brazil, is an urban city with a population of 240,000 inhab-itants and a high (0.79) human development index.10 Themunicipality launched the school-based program in 2018.The program used the quadrivalent HPV vaccine provided bythe PNI (Ministry of Health). The premises and objectives ofthe program were as follows:
1. Strategy: School-based. In Indaiatuba,>80% of childrenare students in municipal public schools. The robustpublic health and educational framework enabled design-ing the strategy.
2. Targeted population: The target population were girlsand boys between 9 and 10 years old. The estimatedpopulation in 2018 was of 5,600 children from 9 to10
Resumo Objetivo O presente estudo avalia a implantação de um programa de vacinaçãocontra o papilomavírus humano (HPV) em escolas de uma cidade brasileira e o impactoapós 2 anos.Métodos Estudo prospectivo para avaliar a implementação do programa, oferecendoa vacina quadrivalente contra o HPV em duas doses anuais, para meninas e meninos de9 a 10 anos. O programa foi autorizado pelo Programa Nacional de Imunizações nacidade de Indaiatuba, estado de São Paulo, Brasil, e teve início em 2018. A coberturaanual da primeira dose foi comparada ao ano de 2017, e os eventos que influenciaramos resultados foram descritos.Resultados O programa convidou 4.878 crianças por meio das escolas (87,1% dapopulação-alvo) e 7,5% recusou a vacinação. Vários eventos concorrentes exigiram oucompetiram pelos profissionais de saúde das equipes de vacinação. A cobertura daprimeira dose (9 a 10 anos) foi de 16,1% em 2017 e aumentou para 50,5% em 2018(p<0,0001). A primeira dose em todas as idades aumentou 78% em 2018 emcomparação com 2017 (6.636/3.733). As demandas concorrentes sobre o programacontinuaram em 2019, e a cobertura da primeira dose caiu (26,9%). Para 2020, uma leimunicipal instituiu a vacinação nas escolas e a criação de equipes dedicadas àvacinação, e estas estratégias aguardam para ser testadas.Conclusão A vacinação anual contra o HPV em base escolar nas idades de 9 a 10 anosfoi viável e aumentou a cobertura vacinal, independentemente do gênero, embora oprograma fosse vulnerável a eventos concorrentes.
Palavras-chave
► papilomavírushumano
► vacina contra HPV► adolescentes► escolas► vacinação
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
School-based HPV Vaccination Teixeira et al. 927

years old and of 11,300 children from 11 to 14 years old.11
The program designers choose to unify the ages of thetarget girls and boys to facilitate the logistics of theprocess. The PNI authorized this change, with the condi-tion that a a surveillance research project were conductedin parallel. The research project was approved by theEthics Committee of the University of Campinas (CAAE87358318.2.0000.5404).
3. Vaccination schedule: Two annual doses were planned.The first dose was at 9 years old and the second dose at10 years old. The PNI also authorized this change. Theprogram expected a transition period for those who hadalready received the first dose at 10 years old. The leafletof the manufacturer indicates a 12-month vaccinationinterval (0, 6, and 12 months) from 9 to 15 years old, andthis recommendation is adopted by some representativeAmerican guidelines.12
4. Time for vaccination: The program designers definedMarch as the preferred month for immunization since, inBrazil, it is the first month of the academic year. No othercompeting seasonal vaccination campaign happens dur-ing this period. There was also the possibility of integrat-ing the events of ‘Lilac March’, the month of action forcervical cancer awareness and prevention.
The study protocol considered was planned for the years2017, 2018, and 2019. Data were obtained from the PNIinformation system, an official recording platform of theBrazilian Ministry of Health.13 The variables were thenumber of doses administered per month (first or seconddose), by age, and by gender. The program’s impact wasassessed by calculating the annual coverage. The numeratorwas the number of doses, and the denominator was theofficial estimated population for the year, age, and gender.The results related to the years 2018 and 2019 werecompared with 2017, just before the program started. Thestatistical analysis was done by the chi-squared test, with5% of significance. The implementation steps and results ofthe program were correlated with competing externalevents.
Results
Preparatory Phase (Year 1, February to August 2018)The program planners supported by the research team pre-sented the design of the program to the health and educationauthorities. Seminars about HPV infection, cervical cancerprevention, and immunization safetywere presented to stake-holders, such as teachers and other education personnel.According to the Brazilian legislation for the vaccination ofchildren, vaccines on the PNI list do not need authorizationfrom parents or guardians. If the choice is to not vaccinate, aTermofRefusalmust besigned.Of the target population, 4,878children were invited (87.1%), and the Term of Refusal waspresented by parents or guardians of 366 children (7.5%).
The vaccination that was scheduled to start earlier, due tosome external events, was postponed to start only inSeptember 2018:
1) The outbreak of yellow fever. It happened in March,displacing immunization team workers to the urgentvaccination against it. Considering the seasonal vaccina-tion against influenza in April and May, the beginning ofHPV vaccination was planned for June, just before thewinter school break.2) National truckers strike. In May, a national truckdriver strike began, with significant logistical reper-cussions for health supplies. The beginning ofthe vaccination was then rescheduled for August, afterthe school break.3) Measles recrudescence in Brazil. In August, unexpectedmeasles outbreaks were reported in Brazil, triggered bythe Latin America immigration crisis, and the PNIlaunched a national vaccination campaign, replacing theimmunization teams.4) Finally, the HPV vaccination program was started inSeptember, although there was an expectation of compe-tition for human resources due to the ’Pink OctoberCampaign’ of breast cancer awareness.
Vaccination Phase (Year 1, September toNovember 2018)Vaccination against HPV in schools was concentrated be-tween September to November. The first dose was given to2,830 children from 9 to 10 years old, 3 times more than in2017 (n¼904) for the same age range. The coverage of thefirst dose (children from 9 to 10 years old) in 2017 and 2018was, respectively, 16.1 and 50.5% (p<0.0001). At older ages(12 to 14 years old), the number of first dosesgivenwas lowerin 2018 than in 2017 (►Figure 1). The first dose vaccinationin all ages increased 78% in 2018 compared with 2017(6,636/3,733). It wasmore concentrated between Septemberand November (ratio¼5.12) when compared with the othermonths (ratio¼1.20) (►Figure 2).
There were no significant questions raised from parents,guardians, or the society. There were no adverse eventsconsistently reported in the period and no serious adverseevents were reported.
Vaccination in 2019 (Year 2)The vaccination against yellow fever, influenza, and measlesdisplaced the immunization health teams throughout the1st semester of 2019. In September, the vaccination cam-paign in schools resumed, with an evident reduction ofinterest by all involved. The results were poor, with asignificant drop in the number of first doses given tochildren from 9 to 10 years old (n¼1508; 26.9% coverage)(►Figure 3).
Reassessment of the Vaccination ProgramFollowing the poor results obtained in 2019, aMunicipal Lawwas approved on November 20th, instituting the ’Week ofHPV vaccination’ during the "Lilac March" (Law no.7255/2019).14 The objective was to protect the initiative ofthe HPV vaccination in schools from unexpected events oreven unscheduled vaccinations against other diseases.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
School-based HPV Vaccination Teixeira et al.928

Vaccination in 2020 (Year 3)Considering the obligation by law for City managers toprovide vaccination teams dedicated to immunizationagainst HPV, the work in schools was planned forMarch 2020. In February 2020, there was a recommenda-tion from the PNI to move the influenza vaccination to anearlier date, to March, due to the imminent COVID-19pandemic. Despite the efforts to keep the schedule, theCOVID-19 pandemic arrived, scared the populations, andschool activities were suspended in March. In 2020, mostimmunization programs were interrupted across thecountry.
Program for 2021 (Year 4)There is a commitment by the publicmanagers to achieve thegoals proposed by the municipal program, including thevaccination in March 2021, with dedicated teams. However,the COVID-19 pandemic persists and worsens. No presentialschool activities are planned by now. COVID-19 vaccinationhas started in January in Brazil, and there is an urgent need tostart the seasonal vaccination against influenza before thewinter season.
Discussion
School-based HPV vaccination through a municipal programhas proven to be feasible and can increase vaccine coverage.In contrast, the execution of the program presented vulner-abilities due to unexpected events competing for the activi-ties of the immunization team.
In the 1st year of the program, even facing several adver-sities, the age range from 9 to 10 years old achieved 50.5% ofcoverage with the first dose, a significant increase comparedwith only 16.1% in 2017. When considering the age rangefrom 12 to 14 years old that was not included in the program,thefirst doseswerekept at low levels. The increased coverageobserved in the months of execution of the program com-pared with the other months and with 2017 indicates thepotential success of school-based vaccination.
Countries with high and sustained vaccine coverage, suchas Australia, Canada, Sweden, and Malaysia, opted for theschool-based strategy.2,4,5,15 Some of them already demon-strate a progressive effect in the diagnosis of cervical cancer
Fig. 1. Considering the target ages of the PNI (9 to 14 years old), the first dose of HPV vaccine was given to 4,304 children in 2018 and to 2,974children in 2017 (Ratio 2018-2017¼ 1.45). The difference was due to the higher vaccination rate in the age range between 9 and 10 years old(�Ratio 2018-2017¼ 3.1).
Fig. 2. Distribution of the first dose of HPV vaccine applied accordingto the months of vaccination (school-based vaccination took placefrom September to November 2018; green bars). Ratio 2018/2017:September-November¼ 5.12; Other months¼ 1.20.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
School-based HPV Vaccination Teixeira et al. 929

precursor lesions, reporting a decreasing incidence.2,5 In2020, a Swedish population assessment demonstrated asubstantial reduction in the incidence of cervical cancer invaccinated women compared to unvaccinated women, espe-cially when vaccinating before 17 years old, with a decreaseof 88%.5
In 2014, the incredible mark of 5.3 million first doses(coverageof108.7%)was reached in the1st yearof theBrazilianprogram of HPV vaccination by the school-based strategy.The second dose coverage, 6 months later, dropped to64.8%.7 This variation in rates is attributed to the media effectraised about safety issues. Supporting global affirmative com-munication, the World Health Organization (WHO) attests tothe safety of the HPV vaccines. Higher levels of antibodies arereported in preadolescents or youngest adolescents, and someprotection is expected after the first dose.16 A 12-monthinterval for the second dose is recommended, and the risk offailure or of exposure to HPVat these ages is very low, close to1% in 10-year-old Brazilian girls.17–20
The difficulty of the parents in taking adolescents to bevaccinated in Health Care Units during business hours maybe the main obstacle and needs to be overcome. This issue isenough to explain the poor results achieved for other ages(from 12 to 14 years old). Therefore, vaccination in schoolsseems to be the solution.
The school-based strategy used was successful, althoughit presented points of weakness, some of which were un-foreseen. The following aspects need to be highlighted: theavailability of >80% of children under the tutelage andsurveillance of municipal schools; the unification of thetarget ages for girls and boys; and the annual vaccination
schedule. All these strategies are possible to be reproducedacross the country.
The program, however, showed its vulnerability to un-foreseen situations, mainly due to the lack of a dedicatedteam for immunization. The attempt for the approval of theMunicipal Law by the end of 2019 needs to be tested. It mayhelp to define the human resources to the school-basedstrategy, reducing the risk of unexpected events.
The COVID-19 pandemic in the year 2020 resulted in noconsistent presential school activity, and the vaccinationwasnot carried out. In 2021, with the evident burden andlongevity of the COVID-19 pandemic, it is necessary toemphasize that other healthcare actions should not besuspended or postponed but planned to be carried outconcurrently. HPV vaccination is essential for the WHO toachieve its goal of accelerating the eradication of cervicalcancer through the vaccination of 90% of girls up to 15 yearsold by 2030.21
Conclusion
The school-based HPV vaccination in an organized programsignificantly increased vaccination coverage in the age rangefrom 9 to 10 years old, regardless of gender, but showingvulnerability to unpredictable or competing events. Thecreation of dedicated teams prioritizing the execution ofthe vaccination program is crucial to achieving high cover-age. rates.
Conflict of InterestsThe authors have no conflict of interests to declare.
Fig. 3. Distribution of Dose1 and Dose 2 of the HPV vaccine administered and coverage by year and age group. School-based vaccination from2018 at the age range between 9 and 10 years old (yo).
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
School-based HPV Vaccination Teixeira et al.930

AcknowledgementsWe acknowledge the participation of the Indaiatuba’shealth managers staff Rita C. J. Vaz, and Maria de FatimaX. S. Maia, whose participationwas crucial in the planningand implementation of the immunization program. Wethank the Brazilian National Immunization Program andthe Immunization Division of the Epidemiological Sur-veillance Center, state of São Paulo, for assisting in theimplementation of the proposed program. Arbore D. M.was granted a scholarship from FAPESP (2020-05103-6).
References1 Bogani G, Taverna F, Lombardo C, Signorelli M, Chiappa V, Casarin I,
et al. Potential impact of introducing a nonavalent HPV vaccination.Int J Gynaecol Obstet. 2018;142(03):338–342. Doi: 10.1002/ijgo.12546
2 Patel C, Brotherton JM, Pillsbury A, Jayasinghe S, Donovan B,Macartney K, et al. The impact of 10 years of humanpapillomavirus(HPV) vaccination in Australia: what additional disease burdenwillanonavalent vaccineprevent?EuroSurveill. 2018;23(41):1700737.Doi: 10.2807/1560-7917.ES.2018.23.41.1700737
3 Hall MT, Simms KT, Lew JB, Smith MA, Brotherton JMI, Saville M,et al. The projected timeframe until cervical cancer elimination inAustralia: a modelling study. Lancet Public Health. 2019;4(01):e19–e27. Doi: 10.1016/S2468-2667(18)30183-X
4 Brisson M, Kim JJ, Canfell K, Drolet M, Gingras G, Burger EA, et al.Impact of HPV vaccination and cervical screening on cervicalcancer elimination: a comparative modelling analysis in 78 low-income and lower-middle-income countries. Lancet. 2020;395(10224):575–590. Doi: 10.1016/S0140-6736(20)30068-4
5 Lei J, Ploner A, Elfström KM, Wang J, Roth A, Fang F, et al. HPVVaccination and the risk of invasive cervical cancer. N Engl J Med.2020;383(14):1340–1348. Doi: 10.1056/NEJMoa1917338
6 World Health Organization. Human papillomavirus vaccines.WHO position paper. Wkly Epidemiol Rec. 2009;84(15):118–131
7 Ministério da Saúde do Brasil SI-PNI - Sistema de Informação doPrograma Nacional de Imunizações. Coberturas vacinais - HPVQuadrivalente - Sexo feminino de 11 a 14 anos por idade e dose -Total Brasil – 2014 [Internet]. Brasília (DF): Ministério da Saúde;2014 [cited 2020 Mar 12]. Available from: http://pni.datasus.gov.br/consulta_hpv_14_C01.php
8 Ministério da Saúde SI-PNI - Sistema de Informação do ProgramaNacional de Imunizações. Coberturas vacinais - HPV Quadriva-lente - Sexo feminino de 09 a 12 anos por idade e dose - Total SãoPaulo – 2015 [Internet]. Brasília (DF): Ministério da Saúde; 2015[cited 2020 Mar 29]. Available from: http://pni.datasus.gov.-br/consulta_hpv_15_C24_Estado.php?uf¼SP
9 Ministério da Saúde. Ministério da Saúde convoca 10 milhões deadolescentes para vacinação de HPV e meningite [Internet]. 2018[cited 2020Mar 29]. Available from: https://portalarquivos2.saude.gov.br/images/pdf/2018/marco/13/Campanha-HPV-2018.pdf
10 Atlas of Human Development in Brazil. The Municipal HumanDevelopment Index (MHDI): Indaiatuba (SP) [Internet]. 2017 [cited2021Mar29].Availablefrom:http://www.atlasbrasil.org.br/consulta
11 Fundação Sistema Estadual de Análise de Dados (SEADE) [Internet].São Paulo: Fundação SEADE; 2017 [cited 2017 Oct 28]. Availablefrom: http://produtos.seade.gov.br/produtos/projpop/index.php
12 Meites E, Szilagyi PG, Chesson HW, Unger ER, Romero JR, Marko-witz LE. Human papillomavirus vaccination for adults: updatedrecommendations of the Advisory Committee on ImmunizationPractices MMWR. MMWR Morb Mortal Wkly Rep. 2019;68(32):698–702. Doi: 10.15585/mmwr.mm6832a3
13 Ministério da Saúde do Brasil. SI-PNI - Sistema de Informação doPrograma Nacional de Imunizações. Coberturas vacinais - HPVQuadrivalente – Por sexo, idade e dose – Indaituba (SP). Acessorestrito a gestores cadastrados [Internet]. Brasília (DF):Ministérioda Saúde; 2020 [cited 2020 Mar 12]. Available from: http://sipni.datasus.gov.br/si-pni-web/faces/inicio.jsf
14 Prefeitura do Município de Indaiatuba. Secretaria Municipal dosNegócios Jurídicos. Departamento de Técnica Legislativa. Lei No.7.255, 20 Novembro 2019 [Internet]. Fica instituída no municípiode Indaiatuba a "Semana de Vacinação contra o HPV", a serrealizada no mês de março de cada ano, durante as ações deprevenção do câncer de colo do útero do "Março Lilás", visandoimunizar e orientar a população sobre os danos causados peladoença. Indaiatuba; 2019 [cited 2020 Mar 12]. Available from:https://sapl.indaiatuba.sp.leg.br/pysc/download_norma_pysc?cod_norma¼6329&texto_original¼1
15 Muhamad NA, Buang SN, Jaafar S, Jais R, Tan PS, Mustapha N, et al.Achieving high uptake of human papillomavirus vaccination inMalaysia through school-based vaccination programme. BMCPublic Health. 2018;18(01):1402. Doi: 10.1186/s12889-018-6316-6
16 DobsonSR,McNeil S,DionneM,DawarM,OgilvieG,KrajdenM,et al.Immunogenicity of 2 doses of HPV vaccine in younger adolescentsvs3doses inyoungwomen:a randomizedclinical trial. JAMA.2013;309(17):1793–1802. Doi: 10.1001/jama.2013.1625
17 Meites E, Kempe A, Markowitz LE. Use of a 2-dose schedule forhuman papillomavirus vaccination — updated recommendationsof the Advisory Committee on Immunization Practices. MMWRMorb Mortal Wkly Rep. 2016;65(49):1405–1408. Doi: 10.15585/mmwr.mm6549a5
18 Gonçalves H, Machado EC, Soares AL, et al. Início da vida sexualentre adolescentes (10 a 14 anos) e comportamentos em saúde.Rev Bras Epidemiol. 2015;18(01):1–18. Doi: 10.1590/1980-5497201500010003
19 Malta DC, Silva MA, Mello FC, Monteiro RA, Porto DL, VasconcelosLM, et al. Saúde sexual dos adolescentes segundo a PesquisaNacional de Saúde dos Escolares. Rev Bras Epidemiol. 2011;14(Suppl 1):147–156. Doi: 10.1590/S1415-790X2011000500015
20 World Health Organization. Safety update of HPV vaccines. WklyEpidemiol Rec. 2017;92(28):398–401 Available from https://apps.who.int/iris/bitstream/handle/10665/255870/WER9228.pdf cited 2019 May 4 [Internet]
21 World Health Organization. Launch of the global strategy toaccelerate the elimination of cervical cancer [Internet]. 2020[cited 2021 Mar 29]. Available from: https://www.who.-int/news-room/events/detail/2020/11/17/default-calendar/-launch-of-the-global-strategy-to-accelerate-the-elimination-of-cervical-cancer
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
School-based HPV Vaccination Teixeira et al. 931

Increased Risk for Maternal Anxiety during theCOVID-19 Outbreak in Brazil among PregnantWomen without Comorbidities
Aumento do risco de ansiedade materna durante o surto deCOVID-19 no Brasil entre gestantes sem comorbidadesRoseli Mieko Yamamoto Nomura1 Ana Carla Franco Ubinha1 Isabela de Paula Tavares1
Maria Laura Costa2 Maria Lucia da Rocha Opperman3 Marianna Facchinetti Brock4
Alberto Trapani Jr.5 Lia Cruz Vaz da Costa Damásio6 Nadia Stella Viegas Reis7
Vera Therezinha Medeiros Borges8 Alberto Carlos Moreno Zaconeta9
Ana Cristina Pinheiro Fernandes de Araujo10 Rodrigo Ruano11
1Department of Obstetrics, Escola Paulista de Medicina,Universidade Federal de São Paulo, São Paulo, SP, Brazil
2Department of Obstetrics and Gynecology, Universidade deCampinas, Campinas, SP, Brazil
3Department of Gynecology and Obstetrics, Hospital de Clínicas,Faculdade de Medicina, Universidade Federal do Rio Grande do Sul,Porto Alegre, RS, Brazil
4Department of Obstetrics and Gynecology, University of AmazonasState, Manaus, AM, Brazil
5Women’s Health Care Unit, Hospital Universitário, UniversidadeFederal de Santa Catarina, Florianópolis, SC, Brazil
6Department of Gynecology and Obstetrics, Universidade Federaldo Piaui, Teresina, PI, Brazil
7Department of Gynecology and Obstetrics, Hospital Universitário daFaculdade de Medicina Maria Aparecida Pedrossian, UniversidadeFederal do Mato Grosso do Sul, Campo Grande, MS, Brazil
Rev Bras Ginecol Obstet 2021;43(12):932–939.
Address for correspondence Roseli Nomura, MD, PhD, Rua Napoleãode Barros 875, 04024002, São Paulo, SP, Brazil(e-mail: [email protected]).
8Department Obstetrics and Gynecology, Faculdade de Medicina deBotucatu, Universidade Estadual Paulista, Botucatu, SP, Brazil
9Department ofGynecology andObstetrics, Faculty ofMedicine, HospitalUniversitário de Brasília, Universidade de Brasília, Brasília, DF, Brazil
10Department of Gynecology and Obstetrics, Maternidade Januário Cicco,Universidade Federal do Rio Grande do Norte, Natal, RN, Brazil
11Maternal-Fetal Medicine Division, Department of Obstetrics andGynecology, Mayo Clinic College of Medicine, Rochester, MN,United States
Keywords
► pregnancy► maternal anxiety► childbirth► postpartum► questionnaires► breastfeeding► coronavirus disease
2019► pandemic
Abstract Objective To studymaternal anxiety in pregnant womenwithout comorbidities in thecontext of the COVID-19 outbreak in Brazil and to study maternal knowledge andconcerns about the pandemic.Methods This is a secondary analysis from a national multicenter cross-sectionalstudy performed in 10 cities, from June to August, 2020, in Brazil. Interviewedpostpartum women, without medical or obstetrical comorbidities, were included inthe present subanalysis. A structured questionnaire and the Beck Anxiety Inventory(BAI) were applied.Results Out of the 1,662 women, 763 (45.9%) met the criteria for the current analysisand 16.1% presentedwithmoderate and 11.5%with severematernal anxiety. Moderateor severe maternal anxiety was associated with high school education (odds ratio
receivedJuly 2, 2021acceptedOctober 1, 2021
DOI https://doi.org/10.1055/s-0041-1740234.ISSN 0100-7203.
© 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rightsreserved.This is an open access article published by Thieme under the terms of the
Creative Commons Attribution License, permitting unrestricted use,
distribution, and reproduction so long as the original work is properly cited.
(https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda., Rua do Matoso 170, Rio deJaneiro, RJ, CEP 20270-135, Brazil
Original ArticleTHIEME
932

Introduction
Coronavirus disease 2019 (COVID-19) is a respiratory infectioncaused by the SARS-CoV-2 coronavirus, which is potentiallyserious andhighly transmissible.1Thefirst casewas identified inDecember 2019 in the city of Wuhan, China,2 and the infectionquickly reachedglobalproportionsandwasdeclaredapandemicby the World Health Organization (WHO) on March 11, 2020.3
In Brazil, the first case of COVID-19 was detected onFebruary 26, 2020, in São Paulo, and due to the rapid growthin the number of occurrences in Brazil, on May 22 the WHOdeclared South America as the epicenter of the pandemic.Brazil is among the countries with the highest number ofcases and deaths from COVID-19. The mortality of hospital-ized patients is high even in those<60 years old, mainly dueto regional disparities and delays within the health system.4
[OR]:1.58; 95% confidence interval [CI]:1.04–2.40). The protective factor was cohab-iting with a partner (OR: 0.46; 95%CI: 0.29–0.73). There was a positive correlationbetween the total BAI score and receiving information about care in the pandemic(rpartial 0.15; p<0.001); concern about vertical transmission of COVID-19 (rpartial 0.10;p¼0.01); receiving information about breastfeeding (rpartial 0.08; p¼ 0.03); concernsabout prenatal care (rpartial 0.10; p¼0.01), and concerns about the baby contractingCOVID-19 (rpartial 0.11; p¼0.004). The correlation was negative in the followingaspects: self-confidence in protecting from COVID-19 (rpartial 0.08; p¼0.04), havinglearned (rpartial 0.09; p¼ 0.01) and self-confidence in breastfeeding (rpartial 0.22;p<0.001) in the context of the pandemic.Conclusion The anxiety of pregnant women without medical or obstetrical comor-bidities was associated to high school educational level and not living with a partnerduring the COVID-19 pandemic. Self-confidence in protecting against COVID-19 andknowledge about breastfeeding care during the pandemic reduced maternal anxiety.
Resumo Objetivo Estudar a ansiedade materna em gestantes sem comorbidades no contextodo surto de COVID-19 no Brasil e estudar o conhecimento e as preocupações maternassobre a pandemia.Métodos Trata-se de análise secundária de um estudo transversal multicêntriconacional realizado em 10 cidades, de junho a agosto de 2020, no Brasil. Mulheresno pós-parto entrevistadas, sem comorbidadesmédicas ou obstétricas, foram incluídasnesta subanálise. Foram aplicados um questionário estruturado e o Inventário deAnsiedade de Beck (BAI, na sigla em inglês).Resultados Das 1.662 mulheres, 763 (45,9%) atenderam aos critérios da análise atuale 16,1% apresentaram ansiedade materna moderada e 11,5% ansiedade maternagrave. A ansiedade materna moderada ou grave foi associada à escolaridade no ensinomédio (odds ratio [OR]: 1,58; intervalo de confiança [IC] 95%: 1,04–2,40). O fatorprotetor foi coabitar com companheiro (OR: 0,46; IC95%: 0,29–0,73). Houve correla-ção positiva entre a pontuação total do BAI e o recebimento de informações sobrecuidados na pandemia (rparcial 0,15; p<0,001); preocupação com a transmissãovertical de COVID-19 (rparcial 0,10; p¼0,01); receber informações sobre amamentação(rparcial 0,08; p¼0,03); preocupações sobre cuidados pré-natais (rparcial 0,10; p¼0,01)e preocupações sobre o bebê contrair COVID-19 (rparcial 0,11; p¼0,004). A correlaçãofoi negativa com os seguintes aspectos: ter autoconfiança para se proteger (rparcial0,08; p¼0,04), aprender (rparcial 0,09; p¼0,01) e ter autoconfiança para amamentar(rparcial 0,22; p< 0,001) no contexto da pandemia.Conclusão A ansiedade de gestantes sem comorbidades médicas ou obstétricasesteve associada à escolaridade no ensino médio e não morar com companheirodurante a pandemia de COVID-19. A autoconfiança na proteção contra COVID-19 e oconhecimento sobre os cuidados com a amamentação durante a pandemia reduzirama ansiedade materna.
Palavras-chave
► gravidez► ansiedade materna► parto► pós-parto► questionários► amamentação► infecção por coronavírus
2019► pandemia
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Maternal Anxiety during the COVID-19 Nomura et al. 933

Since the beginning of the pandemic, it has been observedthat the elderly and people with comorbidities are vulnera-ble to the severe form of COVID-19.1 However, other groupshave been associated with an increased severity of thedisease, including pregnant and postpartum women. Evenamong healthy pregnant women without disease or anyidentified previous medical morbidity, COVID-19 can prog-ress to severe maternal morbidity and maternal death. InBrazil, COVID-19 has been associated with increased mater-nal deaths, with a substantial proportion of these deathsoccurring without intensive care or respiratory support,suggesting delays in the provision of health care. Takemotoet al.5 found a case fatality rate of 12.7% among women withsevere acute respiratory syndrome due to COVID-19 duringpregnancy and the postpartum period, using the nationalsurveillance system data on severe respiratory diseases.
In this critical scenario, a national online survey applied tothe Brazilian population during the pandemic found a highprevalence of depression (61%) and anxiety (44%).6 Pregnantwomen may be vulnerable to anxiety due to increasedconcerns about childbirth and the risks of vertical transmis-sion. The effects of maternal infection on the fetus and on thenewborn are a source of concern and insecurity,7 sinceCOVID-19 during pregnancy is associated with an increasedrisk of adverse maternal and perinatal outcomes.8
Results from the main study showed the impact of theCOVID-19 pandemic on maternal anxiety in Brazil.9 Ourstudy found moderate or severe anxiety in 23.4% of thewomen at the end of pregnancy. The present secondaryanalysis addressed a subgroup of interviewed women whohad no comorbidity in pregnancy and childbirth. The aimwas to verify the presence of maternal anxiety in pregnantwomen without medical or obstetrical comorbidities in thecontext of the COVID-19 outbreak and to analyze the associ-ation with maternal knowledge and concerns about thepandemic.
Methods
A multicenter cross-sectional survey design including twoquestionnaires was performed with data collected in 10cities in Brazil. This is a secondary data analysis from a largerstudy on anxiety during pregnancy. The study protocol wasapproved by the Brazilian National Ethics Committee –
CONEP (CAAE N° 31190120.6.1001.5505) and by each localResearch Ethics Committee where the data was collected. Awritten informed consent form was signed by all includedparticipants.
Women who delivered in the 10 public university hospi-tals were recruited from June 1, 2020, to August 31, 2020.Enrolment took place for a period of 60 consecutive days ateach center. All hospitals were linked to a federal or statepublic university located in 10 cities: Manaus, state ofAmazonas, Natal, state of Rio Grande do Norte, Teresina,state of Piaui, São Paulo, state of São Paulo, Campinas, state ofSão Paulo, Botucatu, state of São Paulo, Florianópolis, state ofSanta Catarina, Porto Alegre, state of Rio Grande do Sul,Campo Grande, state of Mato Grosso do Sul, and Brasília,
Federal District. Each university hospital had a local coordi-nator and trained medical residents who were involved inapplying the questionnaires.
For the present analysis, we considered postpartumwomen without medical or obstetrical comorbidities>18 years old; childbirth birth>36 weeks of gestation; singleand alive newborn without malformations; no clinical sus-picion or current diagnosis of COVID-19; absence of psychi-atric or mental disorder; and in good clinical condition. Thewomenwere interviewed after childbirth and beforehospitaldischarge. They were asked to complete a sociodemographicquestionnaire with questions that included maternal age,parity, educational level, marital status, habits (smoking andconsumption of alcohol and illicit drugs), companionshipduring labor, gestational age at birth, mode of delivery,birthweight, 5-minute Apgar score, history of COVID-19during pregnancy, and history of COVID-19 in the family.
A face-to-face interview was conducted using a question-naire with statements addressing their knowledge and con-cerns about the COVID-19 pandemic, including informationreceived on prenatal care and instructions for childbirth andthe postpartum, including breastfeeding. This questionnairecomprised four domains: general knowledge and preventivecare (4 items), prenatal concerns (4 items), cautions and fearsduring childbirth (5 items), care and concerns about thenewborn (5 items). Each item received a 5-point Likertresponse ranging from 1 to 5 (strongly disagree, partiallyagree, indifferent, partially agree, and fully agree). Thisquestionnaire was specifically designed for the presentstudy.
The Beck Anxiety Inventory (BAI) was used to measurematernal anxiety. The questions were answered followinginstructions to report symptoms of the last 7 days beforedelivery. The BAI consists of a 21-item self-reported ques-tionnaire for assessing anxiety level. Each item describes acommon symptom of anxiety and is rated on a 4-point Likertscale ranging from 0 (not at all) to 3 (severe). The respondentwas asked to rate each symptom and then the total score wascalculated (0–63). A high overall score indicates a high levelof anxiety. Anxiety levels are defined according to the totalscore as follows:minimal anxiety (0–7), mild anxiety (8–15),moderate anxiety (16–25), and severe anxiety (26–63).10 Avalidated Brazilian Portuguese version of the BAI was used inthe present study.11
Data were analyzed using MedCalc Statistical Softwareversion 19.5.3 (MedCalc Software Ltd, Ostend, Belgium).Descriptive statistics are presented as mean and standarddeviation (SD), median (IQR), or frequency and percentage(%). The associations of categorical variables with binaryoutcomes were analyzed using the chi-squared test or theFisher exact test when appropriate. The Mann-Whitney Utest was applied to continuous variableswith nonparametricdistribution. The analyses were adjusted using logistic re-gression for potential confounders:maternal age, nulliparity,race, educational level, marital status, religious belief, smok-ing, alcohol consumption, and geographical location. Corre-lation analysis was performed by the Spearman rank test andmultiple regression with enter procedure was used to
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Maternal Anxiety during the COVID-19 Nomura et al.934
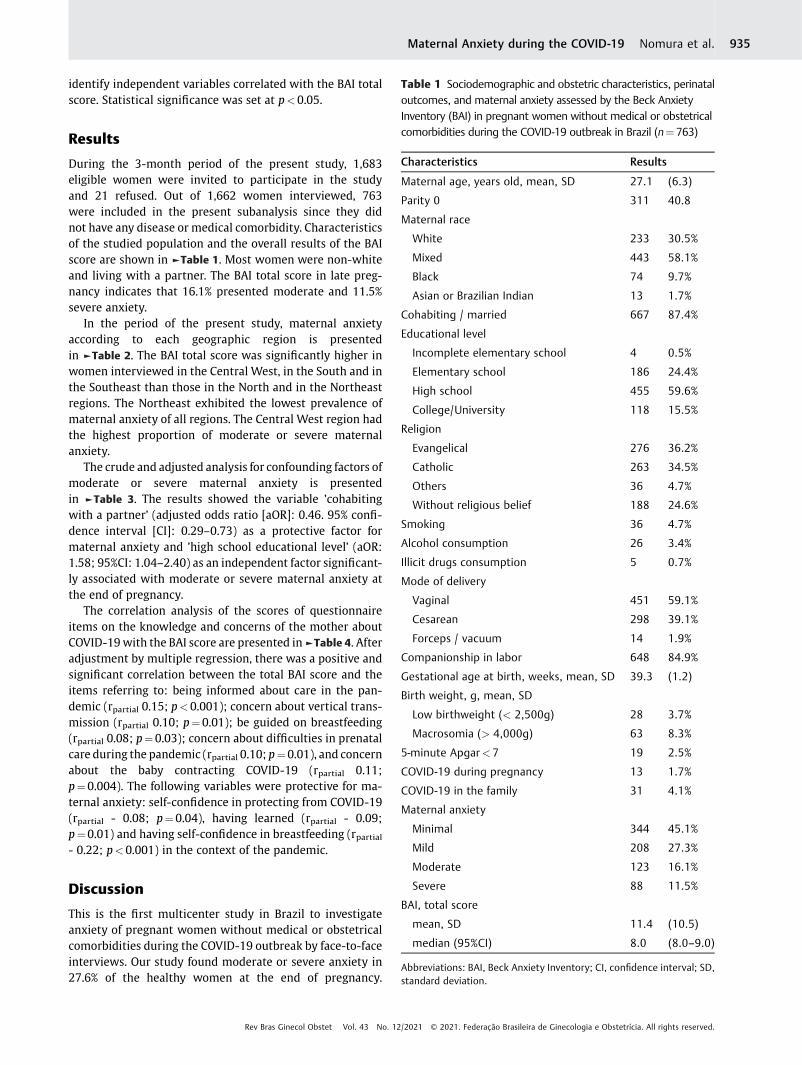
identify independent variables correlated with the BAI totalscore. Statistical significance was set at p<0.05.
Results
During the 3-month period of the present study, 1,683eligible women were invited to participate in the studyand 21 refused. Out of 1,662 women interviewed, 763were included in the present subanalysis since they didnot have any disease or medical comorbidity. Characteristicsof the studied population and the overall results of the BAIscore are shown in ►Table 1. Most women were non-whiteand living with a partner. The BAI total score in late preg-nancy indicates that 16.1% presented moderate and 11.5%severe anxiety.
In the period of the present study, maternal anxietyaccording to each geographic region is presentedin ►Table 2. The BAI total score was significantly higher inwomen interviewed in the Central West, in the South and inthe Southeast than those in the North and in the Northeastregions. The Northeast exhibited the lowest prevalence ofmaternal anxiety of all regions. The Central West region hadthe highest proportion of moderate or severe maternalanxiety.
The crude and adjusted analysis for confounding factors ofmoderate or severe maternal anxiety is presentedin ►Table 3. The results showed the variable ’cohabitingwith a partner’ (adjusted odds ratio [aOR]: 0.46. 95% confi-dence interval [CI]: 0.29–0.73) as a protective factor formaternal anxiety and ’high school educational level’ (aOR:1.58; 95%CI: 1.04–2.40) as an independent factor significant-ly associated with moderate or severe maternal anxiety atthe end of pregnancy.
The correlation analysis of the scores of questionnaireitems on the knowledge and concerns of the mother aboutCOVID-19with the BAI score are presented in►Table 4. Afteradjustment by multiple regression, there was a positive andsignificant correlation between the total BAI score and theitems referring to: being informed about care in the pan-demic (rpartial 0.15; p<0.001); concern about vertical trans-mission (rpartial 0.10; p¼0.01); be guided on breastfeeding(rpartial 0.08; p¼0.03); concern about difficulties in prenatalcare during the pandemic (rpartial 0.10; p¼0.01), and concernabout the baby contracting COVID-19 (rpartial 0.11;p¼0.004). The following variables were protective for ma-ternal anxiety: self-confidence in protecting from COVID-19(rpartial - 0.08; p¼0.04), having learned (rpartial - 0.09;p¼0.01) and having self-confidence in breastfeeding (rpartial- 0.22; p<0.001) in the context of the pandemic.
Discussion
This is the first multicenter study in Brazil to investigateanxiety of pregnant women without medical or obstetricalcomorbidities during the COVID-19 outbreak by face-to-faceinterviews. Our study found moderate or severe anxiety in27.6% of the healthy women at the end of pregnancy.
Table 1 Sociodemographic and obstetric characteristics, perinataloutcomes, and maternal anxiety assessed by the Beck AnxietyInventory (BAI) in pregnant women without medical or obstetricalcomorbidities during the COVID-19 outbreak in Brazil (n¼ 763)
Characteristics Results
Maternal age, years old, mean, SD 27.1 (6.3)
Parity 0 311 40.8
Maternal race
White 233 30.5%
Mixed 443 58.1%
Black 74 9.7%
Asian or Brazilian Indian 13 1.7%
Cohabiting / married 667 87.4%
Educational level
Incomplete elementary school 4 0.5%
Elementary school 186 24.4%
High school 455 59.6%
College/University 118 15.5%
Religion
Evangelical 276 36.2%
Catholic 263 34.5%
Others 36 4.7%
Without religious belief 188 24.6%
Smoking 36 4.7%
Alcohol consumption 26 3.4%
Illicit drugs consumption 5 0.7%
Mode of delivery
Vaginal 451 59.1%
Cesarean 298 39.1%
Forceps / vacuum 14 1.9%
Companionship in labor 648 84.9%
Gestational age at birth, weeks, mean, SD 39.3 (1.2)
Birth weight, g, mean, SD
Low birthweight (< 2,500g) 28 3.7%
Macrosomia (> 4,000g) 63 8.3%
5-minute Apgar<7 19 2.5%
COVID-19 during pregnancy 13 1.7%
COVID-19 in the family 31 4.1%
Maternal anxiety
Minimal 344 45.1%
Mild 208 27.3%
Moderate 123 16.1%
Severe 88 11.5%
BAI, total score
mean, SD 11.4 (10.5)
median (95%CI) 8.0 (8.0–9.0)
Abbreviations: BAI, Beck Anxiety Inventory; CI, confidence interval; SD,standard deviation.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Maternal Anxiety during the COVID-19 Nomura et al. 935

Table 3 Characteristics of women and geographic region in Brazil according tomoderate or severematernal anxiety as assessed bythe Beck Anxiety Inventory during the COVID-19 outbreak
Characteristic Maternal anxiety
Minimum or mild Moderate orsevere (n¼ 211)
p-valuea aOR (95%CI)b p-valueb
(n¼552)
Age, years old, median, AVR 26 (385.9) 26 (371.7) 0.426 – 0.896
Parity 0 212 (38.4) 99 (46.9) 0.032 – 0.133
Maternal race
White 154 (27.9) 79 (37.4) 33.9 0.011c – 0.137
Nonwhite 398 (72.1) 132 (62.6) 24.9
Cohabiting / married 495 (89.7) 172 (81.5) 0.002 0.46 (0.29–0.73) 0.001
Educational level
High school 305 (55.3) 140 (66.4) 0.007 1.58 (1.04–2.40) 0.030
College/University 89 (16.1) 29 (24.6) 0.484 – 0.985
No religious belief 136 (24.6) 52 (24.6) 0.998 – 0.430
Smoking 21 (3.8) 15 (7.1) 0.054 – 0.154
Alcohol consumption 17 (3.1) 9 (4.3) 0.420 – 0.290
COVID-19 during pregnancy 8 (1.4) 5 (2.4) 0.380 – 0.433
COVID-19 in the family 20 (3.6) 11 (5.2) 0.320 – 0.473
Geographic location
Central West 104 (18.8) 46 (21.8) – – –
North 125 (22.6) 36 (17.1) 0.125 – 0.139
Northeast 86 (15.6) 20 (9.5) 0.048 – 0,064
South 123 (22.3) 58 (27.5) 0.881 – 0.910
Southeast 114 (20.7) 51 (24.2) 0.940 – 0.821
Abbreviations: aOR: adjusted odds ratio; AVR: average rank; CI: confidence interval.Data are presented as median (average rank) or number (percentage); aChi-squared test; b Logistic regression to identify independent variables;cWhite versus nonwhite; d Black versus. nonblack.
Table 2 Maternal anxiety of pregnant women without medical or obstetrical comorbidities according to geographic regionsduring the COVID-19 outbreak in Brazil
Total Geographic region
Central West North Northeast South Southeast
(n¼ 150) (n¼161) (n¼ 106) (n¼ 181) (n¼165)
Maternal anxiety (BAI)
Minimal (0–7) 344 (45,1%) 63 (42.0) 82 (50.9) 61 (57.5) 75 (41.4) 63 (38.2)
Mild (8–15) 208 (27,3%) 41 (27.3) 43 (26.7) 25 (23.6) 48 (26.5) 51 (30.9)
Moderate (16–25) 123 (16,1%) 29 (19.3) 20 (12.4) 12 (11.3) 34 (18.8) 28 (17.0)
Severe (26–63) 88 (11,5%) 17 (11.3) 16 (9.9) 8 (7.5) 24 (13.3) 23 (13.9)
BAI score
Mean (SD) 11.4 (10.5) 12.1 (10.4) 10.2 (11.6) 8.4 (8.4) 12.4 (10.7) 12.6 (10.3)
Median (95%CI)� 8.0 (8.0–9.0) 10.0 (7.5–11.5) 5.0 (4.6–9.0) 7.0 (5.0–8.0) 10.0 (8.0–12.0) 10.0 (8.0–12.0)
Abbreviations: BAI, Beck Anxiety Inventory; CI, confidence interval; SD, standard deviation.�Kruskal-Wallis test p <0.001. Post-hoc analysis (Conover): Central West different from North and Northeast, p< 0.05; North different from CentralWest, South, and Southeast, p< 0.05; Northeast different from Central West, South, and Southeast, p< 0.05; South different from North andNortheast, p< 0.05; Southeast different from North and Northeast, p< 0.05.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Maternal Anxiety during the COVID-19 Nomura et al.936

Moderate or severe maternal anxiety was associated withhigh school educational level and not living with a partner.Womenwhowere better informed during the pandemic andwho demonstrated concerns about prenatal care, verticaltransmission, or about the baby contracting COVID-19 pre-sented increasedmaternal anxiety evaluated by the BAI totalscore. Self-confidence in protecting against COVID-19 andknowledge about breastfeeding care during the pandemicreduced maternal anxiety.
The COVID-19 pandemic has led to adverse mental healthconsequences in the general population.12 Multiple COVID-19-related factors should be considered, such as perceivedrisk and concerns about infection, full and partial lockdowns,and social restriction measures.13 Studies have examinedgeneral anxiety related toworries about the self and the babyduring COVID-19 pandemic.9,14,15 Matvienko-Sikar et al.16
found significant decreases in the perceived social supportfrom all sources by pregnant women during the COVID-19pandemic, and a nonsignificant increase in stress. Our studyfound that anxiety was decreased in those living with a
partner, which is an important factor of social support in ourculture.
Several patient groups were found to be more vulnerableto COVID-19 during the pandemic, and pregnant women areat a higher risk of death in Brazil.17Maternal and fetal effects,as well as the best management of COVID-19 in pregnancy,have not been completely elucidated.18 These uncertaintiesand changes may be the main aspects related to maternalanxiety during the pandemic.
Women are less concerned about their own health; nev-ertheless, many of them were significantly anxious. InWuhan, China, the COVID-19 outbreak increased the anxietyof pregnant women and affected their decision-makingregarding prenatal care schedules or timing of childbirth,mode of delivery, and infant feeding.19 Wu et al.20 reporteddepressive symptoms in 29.6% of pregnant women after thedeclaration of an epidemic. In Belgium, an online surveyduring the lockdown period revealed that 14% of pregnantand breastfeeding womenmet the criteria for high anxiety.21
Interventions targetingmaternal stress and isolation, such as
Table 4 Rank correlation analysis between maternal knowledge and concern items scores and Beck Anxiety Inventory total score
Questionnaire items Rho p-valuea Coefficient Standarderror
t p-valueb rpartial
Knowledge and preventive care – –
I am afraid about getting COVID-19. �0.033 0.367 �0.409 0.323 �1.27 0.206 �0.046
I know the signs and symptoms of COVID-19. �0.033 0.364 �0.410 0.307 �1.34 0.182 �0.049
I received information about care in the pandemic. 0.104 0.004 1.350 0.334 4.05 <0.001 0.147
I feel confident in protecting myself from COVID-19. �0.073 0.043 �0.630 0.298 �2.11 0.035 �0.077
Prenatal concerns
I was worried about COVID-19 affecting my baby duringpregnancy.
0.074 0.040 1.059 0.382 2.77 0.006 0.101
I was instructed on caring for the newborn. 0.025 0.495 �0.362 0.313 �1.16 0.247 �0.043
I was guided on breastfeeding during COVID-19. 0.093 0.010 0.630 0.288 2.18 0.029 0.080
I was worried about prenatal difficulties. 0.067 0.063 0.796 0.300 2.65 0.008 0.097
Cautions and fears during childbirth
I received guidance on childbirth care due to COVID-19. 0.031 0.395 0.134 0.237 0.56 0.573 0.021
My companion was afraid of COVID-19 at delivery. 0.076 0.036 0.171 0.253 0.68 0.499 0.025
I was worried about giving birth at the hospital. �0.020 0.582 �0.107 0.283 �0.38 0.706 �0.014
I was afraid to be without a companion at childbirth. 0.030 0.412 0.181 0.319 0.57 0.572 0.021
I was worried that childbirth care might be compromiseddue to COVID-19.
�0.030 0.406 �0.113 0.272 �0.42 0.678 �0.015
Care and concerns about the newborn
I learned how to breastfeed due to COVID-19. �0.050 0.164 �0.614 0.245 �2.51 0.012 �0.092
I feel confident to breastfeed despite COVID-19. �0.161 <0.001 �2.369 0.382 �6.20 <0.001 �0.222
I am worried about having COVID-19. 0.009 0.798 �0.637 0.360 �1.77 0.077 �0.065
I am worried that my baby has COVID-19. 0.011 0.757 �0.321 0.301 �1.07 0.287 �0.039
I am worried about my baby having COVID-19 after birth. 0.093 0.010 1.208 0.413 2.92 0.004 0.107
(Constant) – – 13.166 – – – –
aSpearman correlation; b Multiple regression with enter procedure to identify independent variables.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Maternal Anxiety during the COVID-19 Nomura et al. 937

effective communication and psychological support, shouldbe offered to decrease these mental health effects.
In the present study, data were collected from all geo-graphic regions in Brazil during the same period. Maternalanxiety was more prevalent and more severe in the CentralWest and in the South regions during the studied period. Atthat time, COVID-19 was receding in the North and in theNortheast and increasing in the South and in the CentralWest. This may have influenced the prevalence of maternalanxiety. The notifications of increased numbers of deathscould potentially impact maternal mental health, and therisk of anxiety disorders may have increased as a result. Liuet al.19 found that more women felt anxious in Wuhan thanin Chongqing, because the first city was more affected byCOVID-19. Brazil has great disparities among regions, notonly in COVID-19 mortality cases, but in other healthindicators and in social, cultural, and economiccharacteristics.
Another source of concern is not being able to reach theprenatal care appointments. Even though uninterruptedprenatal care was provided during the pandemic, the fre-quency of appointments diminished, and the same occurredwith exams and ultrasounds. The uncertainty about the besttreatment and clinical management of patients with COVID-19may also affect themind of pregnant women.22 Uncertainprognosis, social restrictions, economic financial losses, de-cline in quality of life, and conflicting messages from gov-ernment authorities are additional stressors and, possibly,trigger mental health crises.
An online survey in Belgium revealed higher levels ofoverall anxiety among pregnant women, 8.4% of whom hadmoderate and 5.2% had severe anxiety.21 We found 16.1%cases of moderate anxiety and 11.5% cases of severe anxiety.These differences may be related to the fact that we con-ducted face-to-face, not online, interviews,. We also foundthat high school educational level and not living with apartner were associated with higher scores on the totalBAI, indicating that social support should be improvedduring antenatal care. It is important for women to haveadequate support, which includes health care workers andcompanions during labor and childbirth, to improve theirmental well-being. Specific interventions that aim to reduceCOVID-19 stress may help to reduce overall stress levels inpregnant women during the pandemic.23
The strength of the present study lies in the inclusion of 10cities in all geographic regions in Brazil, most of which arestate capitals. Additionally, the women were interviewedface-to-face, not through online forms or phone calls. All theinterviews were performed by trained doctors who wereavailable to answer questions and minimize concerns. Ourstudy has the limitation of including only women fromreceiving care from the public sector in university hospitals.Another limitation is that the emergence of COVID-19 wasdifferent in each geographic region, which present organiza-tional differences in health systems in cities, and this mayhave influenced the quality of health care.
Conclusion
Anxiety of pregnant women without medical or obstetricalcomorbidities was related to high school educational leveland not livingwith a partner during the COVID-19 pandemic.Womenwhowere better informed during the pandemic andwho demonstrated concerns about prenatal care, verticaltransmission, or about the baby contracting COVID-19 pre-sented increased maternal anxiety. Self-confidence in pro-tecting against COVID-19 and knowledge aboutbreastfeeding care during the pandemic reduced maternalanxiety.
ContributionsAll authors contributed equally to the present paper;namely, to the conception and design, data collection oranalysis, and interpretation of data, writing of the article,and review of the intellectual content. Therefore, allauthors approved the final version to be published.
Conflict of InterestsThe authors have no conflict of interests to declare.
AcknowledgmentsMembers of the Brazilian Anxiety during PregnancyStudy group for COVID-19: Mariane Albuquerque Reis,Maria Teresa da Costa Urbano, Gabriela Vaz Cursino,Louise Beni Staudt de Siqueira, Gabriela Effting Crema,Mariana Schmidt Vieira, Roxana Knobel, Julia de Gas-peri, Giordanna de Bacco, Vanessa Krebs Genro, JorgeRoberto Di Tommaso Leão, Wendel Schramm Petrucio,Aida Pinto Fernandes, Juliana Borba Gomes, MônicaBarbosa Santos, Emanuela Silva Reis, Renan MassaoNakamura, Douglas Garcia da Silva, Marcela PeresCapela Pereira, Tainá Vieira Nilson, Renata Melo Cam-pos, Rafaela Cardoso Ribeiro de Barros, Giovana Copola,Eduardo Minoru Nomura, Rafaela Buchalla Bosco, Bibi-ana Pereira Finoketti.
References1 World Health Organization. Current outbreak of Coronavirus
(COVID-19) disease [Internet]. 2021 [cited 2021 Aug 3]. Availablefrom: https://www.who.int/health-topics/coronavirus#tab¼tab_1
2 Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al. Earlytransmission dynamics in Wuhan, China, of Novel Coronavirus-infected pneumonia. N Engl J Med. 2020;382(13):1199–1207.Doi: 10.1056/NEJMoa2001316
3 World Health Organization. WHO Director-General’s openingremarks at the media briefing on COVID-19 [Internet]. 2020 [cited2021 Aug 3]. Available from: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020
4 Ranzani OT, Bastos LSL, Gelli JGM, Marchesi JF, Baião F, HamacherS, et al. Characterisation of the first 250,000 hospital admissionsfor COVID-19 in Brazil: a retrospective analysis of nationwidedata. Lancet Respir Med. 2021;9(04):407–418. Doi: 10.1016/S2213-2600(20)30560-9
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Maternal Anxiety during the COVID-19 Nomura et al.938

5 Takemoto M, Menezes MO, Andreucci CB, Knobel R, Sousa L, KatzL, et al; Brazilian Group for Studies of COVID-19 and Pregnancy.Clinical characteristics and risk factors for mortality in obstetricpatients with severe COVID-19 in Brazil: a surveillance databaseanalysis. BJOG. 2020;127(13):1618–1626. Doi: 10.1111/1471-0528.16470
6 Campos JADB,Martins BG, Campos LA,Marôco J, Saadiq RA, RuanoR. Early psychological impact of the COVID-19 pandemic in Brazil:a national survey. J Clin Med. 2020;9(09):2976. Doi: 10.3390/jcm9092976
7 Preis H, Mahaffey B, Heiselman C, Lobel M. Pandemic-relatedpregnancy stress and anxiety among women pregnant during thecoronavirus disease 2019 pandemic. Am J Obstet Gynecol MFM.2020;2(03):100155. Doi: 10.1016/j.ajogmf.2020.100155
8 Brandt JS, Hill J, Reddy A, Schuster M, Patrick HS, Rosen T, et al.Epidemiology of coronavirus disease 2019 in pregnancy: riskfactors and associations with adverse maternal and neonataloutcomes. Am J Obstet Gynecol. 2021;224(04):389.e1–389.e9.Doi: 10.1016/j.ajog.2020.09.043
9 Nomura R, Tavares I, Ubinha AC, Costa ML, Opperman ML, BrockM, et al; BrAPS-Covid Brazilian Anxiety During Pregnancy StudyGroup In Covid-. Impact of the COVID-19 pandemic on maternalanxiety in Brazil. J Clin Med. 2021;10(04):620. Doi: 10.3390/jcm10040620
10 BeckAT, EpsteinN, BrownG, Steer RA. An inventory formeasuringclinical anxiety: psychometric properties. J Consult Clin Psychol.1988;56(06):893–897. Doi: 10.1037//0022-006x.56.6.893
11 Cunha JA. Manual da versão em português das Escalas Beck: BDI,BAI, BHS e BSI. São Paulo: Casa do Psicólogo; 2001
12 Yassa M, Birol P, Yirmibes C, Usta C, Haydar A, Yassa A, et al. Near-term pregnant women’s attitude toward, concern about andknowledge of the COVID-19 pandemic. J Matern Fetal NeonatalMed. 2020;33(22):3827–3834. Doi: 10.1080/14767058.2020.1763947
13 Matvienko-Sikar K, Meedya S, Ravaldi C. Perinatal mental healthduring the COVID-19 pandemic. Women Birth. 2020;33(04):309–310. Doi: 10.1016/j.wombi.2020.04.006
14 Durankuş F, Aksu E. Effects of the COVID-19 pandemic on anxietyand depressive symptoms in pregnant women: a preliminarystudy. J Matern Fetal Neonatal Med. 2020 May 18:1-7. doi:10.1080/14767058.2020.1763946. Epub ahead of print.
15 Taubman-Ben-Ari O, Chasson M, Abu Sharkia S, Weiss E. Distressand anxiety associated with COVID-19 among Jewish and Arabpregnant women in Israel. J Reprod Infant Psychol. 2020;38(03):340–348. Doi: 10.1080/02646838.2020.1786037
16 Matvienko-Sikar K, Pope J, Cremin A, Carr H, Leitao S, Olander EK,et al. Differences in levels of stress, social support, health behav-iours, and stress-reduction strategies for women pregnant beforeand during the COVID-19 pandemic, and based on phases ofpandemic restrictions, in Ireland. Women Birth. 2021;34(05):447–454. Doi: 10.1016/j.wombi.2020.10.010
17 Scheler CA, Discacciati MG, Vale DB, Lajos GJ, Surita F, Teixeira JC.Mortality in pregnancy and the postpartum period in womenwith severe acute respiratory distress syndrome related toCOVID-19 in Brazil, 2020. Int J Gynaecol Obstet. 2021;155(03):475–482. Doi: 10.1002/ijgo.13804
18 Narang K, Ibirogba ER, Elrefaei A, Trad ATA, Theiler R, Nomura R,et al. SARS-CoV-2 in pregnancy: a comprehensive summary ofcurrent guidelines. J Clin Med. 2020;9(05):1521. Doi: 10.3390/jcm9051521
19 Liu X, Chen M, Wang Y, Sun L, Zhang J, Shi Y, et al. Prenatal anxietyand obstetric decisions among pregnant women in Wuhan andChongqing during the COVID-19 outbreak: a cross-sectional study.BJOG. 2020;127(10):1229–1240. Doi: 10.1111/1471-0528.16381
20 WuY, Zhang C, Liu H, Duan C, Li C, Fan J, et al. Perinatal depressiveand anxiety symptoms of pregnant women during the coronavi-rus disease 2019 outbreak in China. Am J Obstet Gynecol. 2020;223(02):240.e1–240.e9. Doi: 10.1016/j.ajog.2020.05.009
21 Ceulemans M, Hompes T, Foulon V. Mental health status ofpregnant and breastfeeding women during the COVID-19 pan-demic: A call for action. Int J Gynaecol Obstet. 2020;151(01):146–147. Doi: 10.1002/ijgo.13295
22 Karavadra B, Stockl A, Prosser-Snelling E, Simpson P, Morris E.Women’s perceptions of COVID-19 and their healthcare experi-ences: a qualitative thematic analysis of a national survey ofpregnant women in the United Kingdom. BMC Pregnancy Child-birth. 2020;20(01):600. Doi: 10.1186/s12884-020-03283-2
23 Zilver SJM, Broekman BFP, Hendrix YMGA, de Leeuw RA, MentzelSV, van Pampus MF, et al. Stress, anxiety and depression in 1466pregnant women during and before the COVID-19 pandemic: aDutch cohort study. J Psychosom Obstet Gynaecol. 2021;42(02):108–114. Doi: 10.1080/0167482X.2021.1907338
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Maternal Anxiety during the COVID-19 Nomura et al. 939

Analysis of the Role of Female Hormones DuringInfection by COVID-19
Análise do papel dos hormônios femininos durante ainfecção por COVID-19David Balbino Pascoal1 Isabela Macêdo de Araujo1 Lorenna Peixoto Lopes2,3
Cristiane Monteiro da Cruz1,3
1Department of Medicine, Centro Universitário Cesmac, Maceió, AL, Brazil2Department of Gynecology and Obstetrics, Universidade Federal deAlagoas, Maceió, AL, Brazil
3Department of Medicine, UNIT University Center, Maceió, AL, Brazil
Rev Bras Ginecol Obstet 2021;43(12):940–948.
Address for correspondence Cristiane Monteiro da Cruz, PhD, CentroUniversitário Cesmac, Maceió, AL, Brazil (e-mail: [email protected]).
Keywords
► woman► hormones► coronavirus► thrombosis► contraception
Abstract Womenhavemetabolic, immunological, andgenetic variables that ensuremoreprotectionfrom coronavirus infection. However, the indication of treatment for several pathologiesand contraception is determined by hormones that have adverse effects and raise doubtsabout their use during the COVID-19 pandemic. Therefore, the present study searcheswomen specificities and the relation between female sexual hormones and COVID-19, andreports the main recommendations in this background. To this end, a review of theliterature was conducted in the main databases, auxiliary data sources, and officialwebsites. Therefore, considering the hypercoagulability status of COVID-19, the debateabout the use of contraceptives due to the relative riskof thromboembolic effects that theyimpose arises. However, the current available evidence, as well as the recommendations ofmain health organs around the world, demonstrate that the use of hormonal contra-ceptives must be maintained during the pandemic.
Palavras-chave
► mulher► hormônios► coronavírus► trombose► contracepção
Resumo Asmulheres possuemvariáveismetabólicas, imunológicas e genéticas que conferemmaiorproteção à infecção pelo coronavírus. Todavia, a indicação de tratamento para certaspatologias e para a contracepção é determinada por hormônios que possuem efeitosadversos e levantam dúvidas quanto ao seu uso durante a pandemia da COVID-19. Destaforma, o presente estudo busca investigar as especificidades da mulher e a relação doshormônios sexuais femininos com a COVID-19, assim como relatar as principais recomen-dações neste contexto. Para isso, realizou-se uma revisão da literatura nas principais basesde dados, fontes auxiliares de dados e sites oficiais. Portanto, considerando o estadohipercoagulável da COVID-19, surge o debate quanto à utilização de contraceptivos peloseu risco relativo de efeitos tromboembólicos. No entanto, as atuais evidências disponíveis,assim como as recomendações dos principais órgãos de saúde do mundo, demonstraramque o uso de contraceptivos hormonais deve ser mantido durante a pandemia.
receivedOctober 12, 2020acceptedAugust 31, 2021
DOI https://doi.org/10.1055/s-0041-1740208.ISSN 0100-7203.
© 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rightsreserved.This is an open access article published by Thieme under the terms of the
Creative Commons Attribution License, permitting unrestricted use,
distribution, and reproduction so long as the original work is properly cited.
(https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda., Rua do Matoso 170, Rio deJaneiro, RJ, CEP 20270-135, Brazil
Review ArticleTHIEME
940

Introduction
Coronavirus is a disease with high transmissibility andmortality, with 15,785,641 confirmed cases around theworld accumulated until July and, in Brazil, a total of2,343,366 cases according to the World Health Organization(WHO).1 The infection defies science to find therapeuticalternatives to its containment and cure. It is known thatsome specific conditions are analyzed as determining factorsto the high morbimortality of patients. Among these, epide-miological data demonstrated that women show less cases ofinfection by the virus and a lower mortality rate.2
Thereby, some of the factors that can influence in thedifferences between genders are determined by metabolic,genetic, and immunological variables, and studies demon-strate that these mechanisms provide more protection towomen.3 However, the main features in the treatment ofpathologies or in contraception must be critically analyzedwhen facing the pandemic. After all, with social isolation,health services have their attendance adapted to a reality ofsocial isolation, which does not allow integral monitoring tothe needs of women.4 In addition, the indication of treat-ment for some pathologies and contraception are deter-mined by hormones that have side effects and raise doubtsabout the right use when facing COVID-19.5 Consequently,the present study aims at investigating the main variables offemales, such as the relation between female sexual hor-mones and COVID-19, as well as at reporting alternatives forthe rational use of contraceptives in the pandemicbackground.
Methods
The present study consisted of a literature review thatperformed searches in the Medline (by PubMed), BibliotecaVirtual em Saúde (BVS, in the Portuguese acronym), GoogleScholar, ScienceDirect, and Cochrane Library and ClinicalTrials databases. In addition, other auxiliaries and officialWeb sites were consulted: Opengray, Agência Nacional deVigilância Sanitária (ANVISA, in the Portuguese acronym),Federação Brasileira das Associações de Ginecologia e Obste-trícia (FEBRASGO, in the Portuguese acronym), FédérationInternationale de Gynécologie et d’Obstétrique (FIGO) andWHO. The studies were tracked, systematically, according tothe strategy of population, intervention, comparison, andoutcomes (PICO), by the use of theMESH descriptorswomen,girl, contraceptive, hormone replacement, estrogen, progester-one, COVID-19, coronavirus, SARS-CoV-2, thrombosis andcoagulation. The present study was performed during themonth of July and included articles published since 2016.Due the heterogeneity of the studies, there was no quantita-tive analysis of the results.
Biological Differences between GendersWomen are less susceptible to SARS-CoV-2 infection andhave lower morbimortality rates, which are determinedby hormonal and chromosomal specificities that ensureincreased protection to them. Therefore, with theworldwide
dissemination of the disease, epidemiologic data showedthat males are more affected and have increased chances ofdeveloping the severe stage of the disease.5 It is known thatbehavioral factors, such as precarious health care and smok-ing, aswell as the presence of comorbid conditions, influencein the differences between genders and, consequently, in theseverity of the disease. Furthermore, it was observed thatbiological features, including chromosomes and sexual hor-mones, contribute to the increased risk of poor prognosis ofthe patient.3 Therefore, the genetic aspects linked to the Xchromosome and the female steroids hormones activitypositively modulate both innate and adaptive immunity,ensuring a more efficient, stronger, and extended responseto women.6–8 It is believed that this advantage of females isdue to the influence of estrogen levels and to the presence oftwo polymorphic X chromosomes.6,9
Genetic and Molecular AspectsThe genetic differences between genders, given by the extraX chromosome, ensures an increased variety of proteins andcellular population to females.6 In the COVID-19 background,it is known that the angiotensin 2 converting enzyme (ACE2)gene is located in the X chromosome, exerting a significantrole on the maintenance of arterial pressure and regulationof fluids, which reduces the risk of possible pulmonarydamages.3,10 Besides that, genes coded by this chromosomealso positively regulate the immunological function by risingTCD4 cells, antibodies, and Toll-like receptors (TLR3, TLR4 eTLR7).10 The TLR7 has the capacity of escaping from theinactivation of the X chromosome, increasing its expressionin female immune cells.3 Therefore, it is able to detect simpletape RNA, proper of the infection by SARS-CoV-2 and, then,reduce viral titers.10 It is also known that the FOXP3 gene ispresent in the X chromosome, modulating the function ofregulating T-cells (Treg).11
Hormonal AspectsHormones are chemical messengers that interact with recep-tors from different cells, leading to biochemical reactions thatlead to specific biological responses.12Therefore, 17β-estradiolexerts a reducing effect on the expression of ACE2 in the lungs,regardless of the chromosomal complement.10 Furthermore,the protection of women is due to the connection to itsreceptor, inducing the production and transduction of signsof cytokines.9,13 Estrogen levels influence the type of immuneresponse, since low doses activate Th1 response with therelease of proinflammatory cytokines (interleukin-1 [IL-1],IL-6, and TNF) –while higher doses result in their suppression,increasing Th2 response and humoral immunity. Besides, thishormone induces the expression of TLR4 on the surface ofmacrophages. Concomitantly, progesterone has anti-inflam-matoryeffects,with the transformation of Th1 response toTh2,along with the increase of the release of IL-4, IL-5 and IL-10. Inaddition, it increases the number of Treg cells and decreaseslevels of circulating Th17, and it may also antagonize TLR andNF-κB pathways.14
In the study by Suba,5 it was demonstrated that femalemice are less susceptible to SARS-CoV infection. Male mice
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Analysis of the Role of Female Hormones During Infection by COVID-19 Pascoal et al. 941

presented a viral titer considerably higher, in addition tointense inflammatory response, adding mortality risk to thisgender. It is worth pointing out that female mice infected bythe respiratory virus and submitted to ovariectomy or totreatment with estrogen receptors (ERs) antagonists hadtheir morbimortality rate increased, which shows theimportance of the role of estradiol on the activation of ERsfor protection against the virus.
The impacts of estrogen on the regulation of the immunesystemdepends on the concentration of thehormone, aswellas on its distribution, its density, and on different types ofERs present in immunological cells. It is known that women’simmune responses can vary with different concentrations ofestrogen during the menstrual cycle and that the capacity oftheir immunological response is substantially reducedwhenthey reach menopause, since estrogen is now replaced byestrone, which presents lower action capability.10,14 There-fore, menstrual regularity represents a major impact for theprotection against COVID-19.9
Regulation of Immunological ResponseFemales present a higher quantity of immunoglobulin G(IgG) antibodies in the beginning of the infection by SARS-CoV-2, as well as womenwho present with the severe type ofthe disease. Hence, it is observed that an increased percent-age of IgG in female patients provides more protectionagainst the evolution to the severe type of the disease orto death.15
Estrogen positively acts on the superior and inferior air-ways. In the nasal cavity, it has the capability of optimizing thelocal innate immune response, besides stimulating the reac-tivity of the mucosa, increasing the production of antiviralsubstances, such as electrolytes, mucins, lactoferrin, oligosac-charides, immunoglobulins A and G, and hyaluronic acid. Thelatter is also stimulatedbyhormone in theoral cavity, ensuringbetter oral hydration. Besides that, the increase in the produc-tion of antiviral agents also happens in the lungs, beingsustained by the effect of progesterone, which helps in thepulmonary repair by the release of amphiregulin.16
Estrogen receptors are classified as types α or β, which areexpressed in the immune system cells in different ways, sinceERα ishighlyexpressed inT-lymphocytesandERβ inB-cells.7,14
It is also known that ERs are expressed in innate immunecells, such as neutrophils, macrophages, and monocytes. Thus,estrogen-activated ERs regulate the development of immunecells, positively modulating the innate and adaptativeresponses.5
Fromthe activationof ERs in innate cells, there is the releaseof proinflammatory cytokines (IL-12, tumor necrosis factor-α[TNFα]) andof a chemokine (CCL2).17These are responsible forstimulating the expression of aromatase that promotes theconversion of androgen into estrogens, which potentiates thefemale immune response. The activation of ERα in T-cellspromotes the release of interferon types I and III (IFN), anessential factor for the inhibition of viral replication.5,9
Dendritic cells are also influenced by estradiol signaling viaERα, which are responsible for the increase of the number ofcells during inflammation.9
Themain dendritic cells involved in antiviral response areplasmocytoids (pDCs), which are responsible for producingmore IFN I when compared with males.5,9 The pDCs, whenstimulated by TLR7, present higher levels of IFN 5 regulatorfactor (IRF-5) and higher production of IFNα, which isimportant against the virus.3,14 It is worth noting that anexperiment with female mice demonstrated that the regu-lation of the transcription of IRF5 is controlled by thesignaling of ERα.14
At the end of the viral infection, the activation of ERα byhigh levels of estradiol stimulates a type 2 response of innateimmune cells (ILC2), myeloid cells, and alveolar macro-phages (AMs).7 These, in turn, have the ability of producingantiviral mediators, IFN I chemokines that recruit monocytesto the lungs.5,16 Thus, estrogen reduces the release of proin-flammatory cytokines in monocytes and macrophages,improves the expression of annexin-1 of neutrophilswithoutincreasing their activation, in addition to delaying apoptosisof neutrophils, attenuating viral hyperinflation and favoringtissue repair.9 ►Fig. 1 describes the immunological mecha-nism regulated by estrogen in the face of the infection byrespiratory virus, as well as the process of restoration of thelungs.
In a study conducted by Channappanavar et al.,8 it wasobserved that 72 hours after SARS-CoV infection, the levels ofchemokines (CCL-2 and CXCL-1) and of proinflammatorycytokines (IL-6) remained the same or even increased in thelungs of male mice, when compared with females. Thisexperiment was reinforced by Suba,5 who demonstratedthat high concentrations of estrogen in female mice, afterthe same period of the previous study, reduced the cytokinesstorm caused by SARS-CoV, while the high levels of inflam-matory in male mice lasted longer.
Therefore, the effects of female sex hormones on themodulation of molecular, biochemical, and immunologicalmechanisms in viral infection are evident. Nevertheless, tworesearch are in progress at ClinicalTrials and, based on theseeffects, they seek therapeutic alternatives to COVID-19through estrogen and progesterone.18,19
Given the evidence described, the genetic, molecular,hormonal, and immunological differences of women areperceptible, providing, therefore some advantage to femalesin the face of various infections. These differential character-istics are described in ►Fig. 2.
COVID-19 and Thromboembolic Events
Within pathophysiology, the SARS-CoV-2 virus is responsi-ble for damaging effects that, after the binding of the virus tothe receptors in lung pneumocytes, can reach other organs ofthe human body due to its affinity with ACE2 receptorsECA2.20 Therefore, besides causing a decline on respiratoryfunction, COVID-19 causes systemic effects that worsen themorbimortality of infected patients.21
Themain systemic complications are based in coagulationabnormalities suggestive of hematological pathologies suchas thrombotic microangiopathy or disseminated intravascu-lar coagulation (DIC) in severe patients. In this context,
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Analysis of the Role of Female Hormones During Infection by COVID-19 Pascoal et al.942
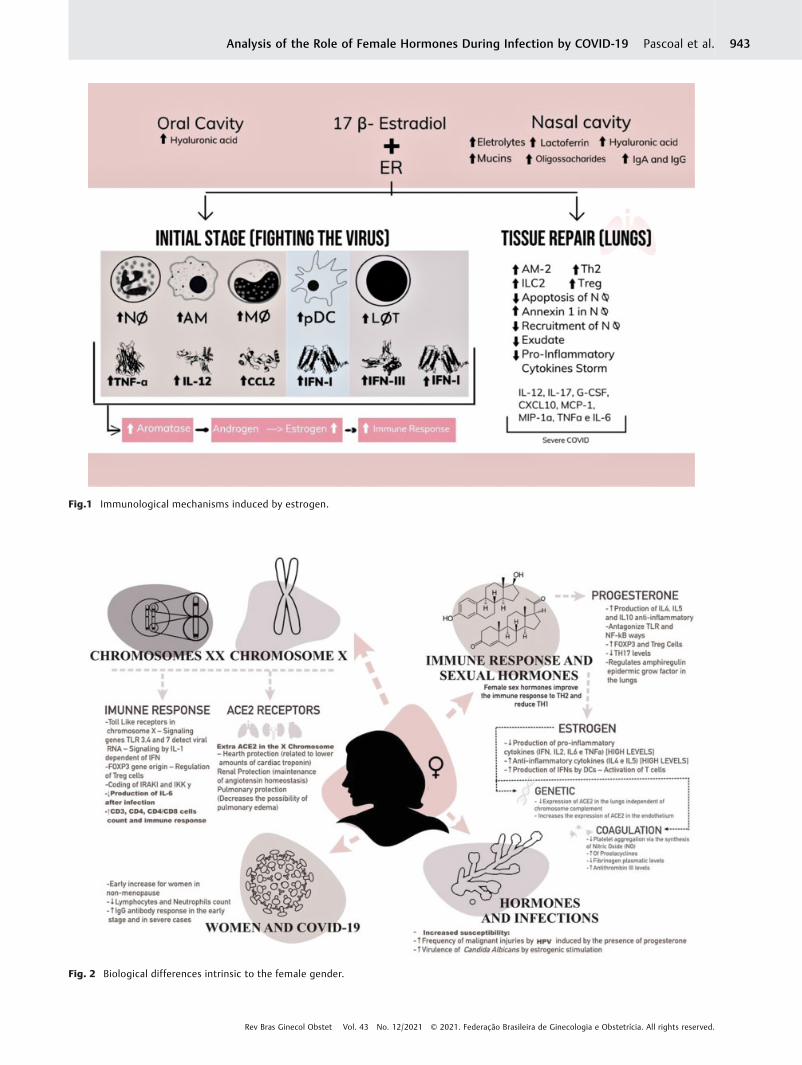
Fig.1 Immunological mechanisms induced by estrogen.
Fig. 2 Biological differences intrinsic to the female gender.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Analysis of the Role of Female Hormones During Infection by COVID-19 Pascoal et al. 943

venous thromboembolism (VTE) and arterial thromboem-bolism (ATE) have been frequently observed in intensive careunits (ICUs).2 According to Klok et al.,22 40% of ICU patientswith COVID-19 presented thromboembolic complications.
The vascular endothelium presents lesions due to cyto-pathic damage caused by the virus and to inflammationcaused by its generation of an endothelial dysfunction.23 Inaddition, lesions in endothelial cells result in the release ofplasminogen activators, which are the explanation for a highconcentration of D-dimer and fibrin in severe patients withCOVID-19.2,23 In the study by Guan et al.,24 46% of critical illpatients showed higher levels of D-dimer.
Autopsies of these patients revealed fundamental anato-mopathological aspects for the elucidation of the character-istics of viral activity. The detection of microthrombi in thelumen of pulmonary vessels could be better elucidated byimmunohistochemical analysis, which revealed a high plate-let production per CD61þ megakaryocytes.25 In the study, itwas found that the increase in the number of platelets wasdue to the activation of the complement system observed bythe deposition of complement system protein subtypes inthemicrovasculature,26 explaining the relationship betweencoagulopathy and immune response to COVID19.27
Hypercoagulability is determined, mainly, by the increaseof prothrombotic factors in critically ill patients.23 Together,the increase in the concentration of proinflammatory cyto-kines such as TNF-a and of interleukins such as IL-1, IL-6, andIL-10 may induce the expression of tissue factor in mononu-clear cells and, consequently, activate the coagulation chainand the generation of thrombin.2 Furthermore, a study hasshown that, in critically ill patients, an increase of platelet-monocytes aggregates – inducers of tissue factor expression– occurred, and this event was also related to an increase inmarkers such as fibrinogen and D-dimer.28
Critically ill patients with COVID-19 are hospitalized and,therefore, have movement limitations that alter their hemo-dynamics andfit theVirchow triad. Therefore, thevenousstasisdeterminedby the immobilizationof thesepatients is stronglyaggravating for the genesis of thrombotic events.23 Moreover,special situations with potential dysfunctions in coagulationshould be considered; after all, pregnant women, for example,have a physiological state of hypercoagulability.29
Women’s Health, Family Planning andCOVID-19
Medical services, including thoseofGynecologyandObstetrics,were strongly shaken and had to adapt to a new context withobstacles in providing care due the COVID-19 pandemic.However, it is vital that services aimed at women’s healthsuch as reproductivehealth and contraception bemaintained.4
According to official recommendations, these services shouldinstitute continued care, offering unrestricted access to treat-ment for clinical and pathological conditions and familyplanning.30,31
It is noticeable that no matter how there is no evidence ofworsening in pregnant patients with SARS-CoV-2 or ofvertical transmission, the possible intercurrences arising
from the pregnancy process thatmay requiremore advancedmedical care are concerns in this panorama. After all, giventhe severity and the speed of the spread of the virus, almostall hospital care flows were directed to these patients.Therefore, when possible, it is recommended to postponepregnancies.32
Thus, contraceptives are primordialwithin this premise ofmaintaining sociodemographic levels.4 However, accordingto Riley et al.,33 during the pandemic, therewas a decrease of� 10% in contraceptive use in 132 countries from low- andmiddle-income countries. This represents a shortage ofcontraception for 48,6 million women and, consequently,� 15million unwanted pregnancies. This can be explained bythe difficulty of access to these methods,34 but also by thehypothesis that contraceptives, due to their thromboembolicrisk,5 have a synergistic effect in the view of the thromboticpathophysiology of COVID-19.2,22,23
Hormonal Therapy and ThromboembolicRisk
Evidence determines that endogenous estrogen has a protec-tive effect regarding COVID-19.5,9,10 However, SARS-CoV-2has evolved beyond the understandable point of previousexperiences and challenges theories that suggest vascularprotection. As much as this effect has been documented,exogenous estrogen can increase the activation of coagulationfactors, increasing the thrombotic risk.35,36 In this view, oralcontraceptives with estrogen are excellent drugs in terms ofpregnancy prevention; however, in certain cases, they havedetermined unpredictable thromboembolic complicationssuch asmesenteric vein thrombosis,37VTE,38 stroke, and acutemyocardium infarction.5
As with contraception, menopausal hormone replace-ment therapy also needs to be evaluated, since womenwho use it have a 2.9 times greater risk of presentingthromboembolic events than those who do not.39 Similarly,despite its low incidence, the risk of thromboembolismduring fertilization procedures is similar that in pregnantwomen, which is 10 times higher than that in young womenof reproductive age.23
Hormonal Formulations and ThromboticRisk
The use of contraceptives is a thromboembolic risk factor forwomen susceptible to developing hemolytic diseases.40
However, even though the risk of hemostatic disorders is 4times higher in contraceptive users, the absolute riskremains low and is lower than the risk associated withpregnancy.41 Nevertheless, at � 35 years of age, the risk ofthrombosis in womenwho use contraceptives is the same asthat in pregnant women.40
In the contraceptive formula, estrogen fits as the ethologicagent for hemostatic disfunctions. According to Gialerakiet al.,42 the risk of thrombosis is double in women who takepills containing high doses of estrogen. Regarding the type ofestrogen, the formulations with estradiol (E2) are relatively
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Analysis of the Role of Female Hormones During Infection by COVID-19 Pascoal et al.944

better than those with ethinyl estradiol (EE).43 Similarly,estrogens administrated vaginally in low doses were notrelated to an increased risk of developing thrombosis.39
Regarding progestogens, there is a global consensus that,except for medroxyprogesterone acetate deposit, there is nosignificant association between the isolated use of progestinand increased VTE prevalence. Even in high doses of Levo-nogestrel or ulipristal – present in the formulation of emer-gency pills, isolated, are also not associated with vascularevents.40,44
Regarding combined oral contraceptives (COC), the risk ofdevelopingVTE ismuchhigher if comparedwithother isolatedformulations. This risk dependent on the dose of EE togetherwith gestodene, desogestrel, cyproterone acetate or drospir-enone (3rd and 4th generation progestins). All of these arebeneficial but are similar in terms of VTE risk and are �between 50 and 80% more likely than Levonogestrel.40,42,45
This fact is evidenced by the studies presented in Chart 1.46–50
Chart 1 describes five cohorts46–50 that evaluated thetypes of estrogen and progestogen – as well their combina-tion – and the relative risk of thrombotic events withindistinct multivariate analyses. The analysis of the studiesmentioned in Chart 1 may have limitations due to do notconsider the dosage, do not control all factors of confusionand different study methodologies.
Therefore, in relation to thromboembolic complications,Levonogestrel and the lowest possible dose of EE are associ-atedwith a lower risk of VTE (if only the risk is taken into theaccount), especially in novice users. After all, thromboem-bolic complications attributed to the use of hormones aregreater at between 6 and 12 months of initial use.42
Thromboembolic Physiopathology ofContraceptives
The thrombotic physiology of these formulations stems fromseveral complex multifactorial disorders with no definedcausal factor. Thrombotic events depend on congenital andacquired conditions ruled as themain risk factors amongusersof hormonal contraception, such as acquired conditions suchas surgery, pregnancy, age, smoking etc., and congenital alter-ations such as gene mutations related to coagulation factors(Leiden factor V gene, prothrombin gene, FGG etc.).45 In thecohort carried out by Dulicek et al.51 in users of hormonalcontraceptionwho had thrombotic events, 44% of the patientsthat had VTE had thrombophilia and, in the group of patientswho had arterial effects (CVA), 50% were smokers.
Thus, epidemiologically, the use of contraceptives is associ-atedwith increased levelsoffibrinogen,prothrombin,D-dimer,plasminogen tissue activator, plasminogen, and coagulation
Chart 1 Cohorts of relative risks of thrombotic events in different contraceptive formulations
Authors Contraceptive formula Thrombotic event Multivariate analysis (relative risk)
Laliberté et al.50 Transdermal estradiol VTE 0.67
Oral estradiol VTE
Larivée et al.47 Drospirenone ATE 0.89
Levonorgestrel ATE 1
Weill et al.48 Ethinyl estradiol (20 µg) PE 0.75
STROKE 0.82
AMI 0.56
Levonorgestrel PE 1
STROKE 1
AMI 1
Desogestrel PE 2.16
STROKE 0.96
AMI 1.01
Gestodene PE 1.63
STROKE 0.96
AMI 0.49
Ethinyl estradiol (20 µg)þ Levonogestrel PE 0.74
Ethynil estradiol (20 µg)þDesogestrel PE 0.75
Ethynil estradiol (20 µg)þGestondene PE 0.94
Hugon-Rodin et al.49 Desogestrel VTE 1.4
Cyproterone VTE 1.71
Drospirenone VTE 1.99
Dinger et al.46 Levonogestrel VTE 0.5
Abbreviations: AMI, acute myocardium infarction; ATE, arterial thromboembolism; PE, pulmonary embolism; VTE, venous thromboembolism.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Analysis of the Role of Female Hormones During Infection by COVID-19 Pascoal et al. 945
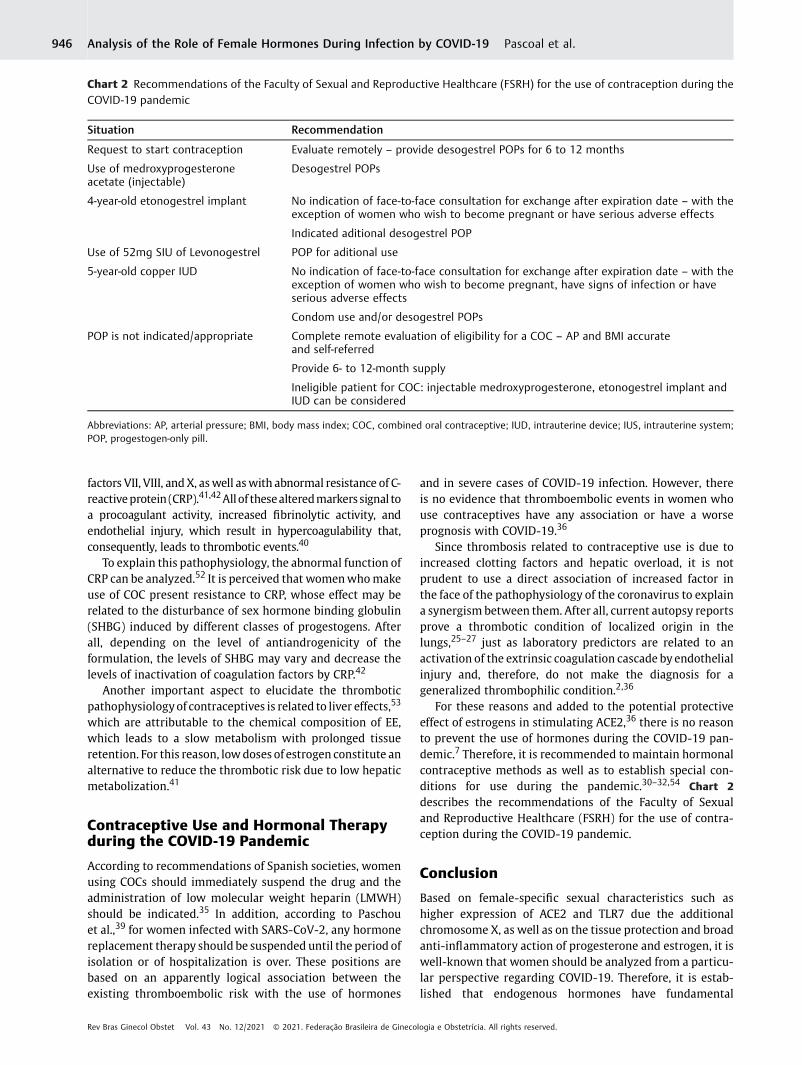
factors VII, VIII, andX, aswell aswith abnormal resistance of C-reactiveprotein (CRP).41,42Allof thesealteredmarkerssignal toa procoagulant activity, increased fibrinolytic activity, andendothelial injury, which result in hypercoagulability that,consequently, leads to thrombotic events.40
To explain this pathophysiology, the abnormal function ofCRP can be analyzed.52 It is perceived that womenwhomakeuse of COC present resistance to CRP, whose effect may berelated to the disturbance of sex hormone binding globulin(SHBG) induced by different classes of progestogens. Afterall, depending on the level of antiandrogenicity of theformulation, the levels of SHBG may vary and decrease thelevels of inactivation of coagulation factors by CRP.42
Another important aspect to elucidate the thromboticpathophysiologyof contraceptives is related to liver effects,53
which are attributable to the chemical composition of EE,which leads to a slow metabolism with prolonged tissueretention. For this reason, lowdoses of estrogen constitute analternative to reduce the thrombotic risk due to low hepaticmetabolization.41
Contraceptive Use and Hormonal Therapyduring the COVID-19 Pandemic
According to recommendations of Spanish societies, womenusing COCs should immediately suspend the drug and theadministration of low molecular weight heparin (LMWH)should be indicated.35 In addition, according to Paschouet al.,39 for women infected with SARS-CoV-2, any hormonereplacement therapy should be suspended until the period ofisolation or of hospitalization is over. These positions arebased on an apparently logical association between theexisting thromboembolic risk with the use of hormones
and in severe cases of COVID-19 infection. However, thereis no evidence that thromboembolic events in women whouse contraceptives have any association or have a worseprognosis with COVID-19.36
Since thrombosis related to contraceptive use is due toincreased clotting factors and hepatic overload, it is notprudent to use a direct association of increased factor inthe face of the pathophysiology of the coronavirus to explaina synergism between them. After all, current autopsy reportsprove a thrombotic condition of localized origin in thelungs,25–27 just as laboratory predictors are related to anactivation of the extrinsic coagulation cascade by endothelialinjury and, therefore, do not make the diagnosis for ageneralized thrombophilic condition.2,36
For these reasons and added to the potential protectiveeffect of estrogens in stimulating ACE2,36 there is no reasonto prevent the use of hormones during the COVID-19 pan-demic.7 Therefore, it is recommended to maintain hormonalcontraceptive methods as well as to establish special con-ditions for use during the pandemic.30–32,54 Chart 2
describes the recommendations of the Faculty of Sexualand Reproductive Healthcare (FSRH) for the use of contra-ception during the COVID-19 pandemic.
Conclusion
Based on female-specific sexual characteristics such ashigher expression of ACE2 and TLR7 due the additionalchromosome X, as well as on the tissue protection and broadanti-inflammatory action of progesterone and estrogen, it iswell-known that women should be analyzed from a particu-lar perspective regarding COVID-19. Therefore, it is estab-lished that endogenous hormones have fundamental
Chart 2 Recommendations of the Faculty of Sexual and Reproductive Healthcare (FSRH) for the use of contraception during theCOVID-19 pandemic
Situation Recommendation
Request to start contraception Evaluate remotely – provide desogestrel POPs for 6 to 12 months
Use of medroxyprogesteroneacetate (injectable)
Desogestrel POPs
4-year-old etonogestrel implant No indication of face-to-face consultation for exchange after expiration date – with theexception of women who wish to become pregnant or have serious adverse effects
Indicated aditional desogestrel POP
Use of 52mg SIU of Levonogestrel POP for aditional use
5-year-old copper IUD No indication of face-to-face consultation for exchange after expiration date – with theexception of women who wish to become pregnant, have signs of infection or haveserious adverse effects
Condom use and/or desogestrel POPs
POP is not indicated/appropriate Complete remote evaluation of eligibility for a COC – AP and BMI accurateand self-referred
Provide 6- to 12-month supply
Ineligible patient for COC: injectable medroxyprogesterone, etonogestrel implant andIUD can be considered
Abbreviations: AP, arterial pressure; BMI, body mass index; COC, combined oral contraceptive; IUD, intrauterine device; IUS, intrauterine system;POP, progestogen-only pill.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Analysis of the Role of Female Hormones During Infection by COVID-19 Pascoal et al.946

characteristics that determine a better prognosis for women,as demonstrated in epidemiological studies. However, due tothe broad necessity of hormonal treatments for the manage-ment of pathologies as well as for contraception, the use oftherapies with exogenous hormones, in the context ofCOVID-19 infection, was put under discussion. Based oncurrent evidence, as well as on the recommendations ofthe main health agencies of the world, the use of hormonalcontraceptives should be maintained during the currentpandemic context. Even so, it is highlighted that someformulations with 2nd generation progestogens (Levonoges-trel), despite having a greater androgenic effect, are the bestalternatives for patients with increased risk for thrombosis.
Conflict of InterestsThe authors have no conflict of interests to declare.
References1 World Health Organization. Coronavirus disease (COVID-19) out-
break situation [Internet]. 2020 [cited 2020 Sep 10]. Availablefrom: https://www.who.int/emergencies/diseases/novel-coronavi-rus-2019
2 Levi M, Thachil J, Iba T, Levy JH. Coagulation abnormalities andthrombosis in patients with COVID-19. Lancet Haematol. 2020;7(06):e438–e440. Doi: 10.1016/S2352-3026(20)3014(20)30145-9
3 Scully EP, Haverfield J, Ursin RL, Tannenbaum C, Klein SL. Consid-ering how biological sex impacts immune responses and COVID-19 outcomes. Nat Rev Immunol. 2020;20(07):442–447. Doi:10.1038/s41577-020-0348-8
4 Weinberger M, Hayes B, White J, Skibiak J. Doing things different-ly: what it would take to ensure continued access to contracep-tion during COVID-19. Glob Health Sci Pract. 2020;8(02):169–175. Doi: 10.9745/GHSP-D-20-00171
5 Suba Z. Prevention and therapy of COVID-19 via exogenousestrogen treatment for both male and female patients. J PharmPharm Sci. 2020;23(01):75–85. Doi: 10.18433/jpps31069
6 Strope JD, Chau CH, Figg WD. Are sex discordant outcomes inCOVID-19 related to sex hormones? Semin Oncol. 2020;47(05):335–340. Doi: 10.1053/j.seminoncol.2020.06.002
7 Grandi G, Facchinetti F, Bitzer J. The gendered impact of corona-virus disease (COVID-19): do estrogens play a role? Eur J Contra-cept Reprod Health Care. 2020;25(03):233–234. Doi:10.1080/13625187.2020.1766017
8 Channappanavar R, Fett C, Mack M, Ten Eyck PP, Meyerholz DK,Perlman S. Sex-based differences in susceptibility to severe acuterespiratory syndrome coronavirus infection. J Immunol. 2017;198(10):4046–4053. Doi: 10.4049/jimmunol.1601896
9 Breithaupt-Faloppa AC, Correia CJ, Prado CM, Stilhano RS, Ure-shino RP, Moreira LFP. 17β-Estradiol, a potential ally to alleviateSARS-CoV-2 infection. Clinics (São Paulo). 2020;75:e1980. Doi:10.6061/clinics/2020/e1980
10 Li Y, Jerkic M, Slutsky AS, Zhang H. Molecular mechanisms of sexbias differences in COVID-19 mortality. Crit Care. 2020;24(01):405. Doi: 10.1186/s13054-020-03118-8
11 Rozenberg S, Vandromme J, Martin C. Are we equal in adversity?Does Covid-19 affect women and men differently?. Maturitas.2020;138:62–68. Doi: 10.1016/j.maturitas.2020.05.009
12 Bonan C, Teixeira LA, Nakano AR. Absorção e metabolização doshormônios sexuais e sua transformação em tecnologias contracepti-vas:percursosdopensamentomédiconoBrasil. CiêncSaúdeColetiva.2017;22(01):107–16. Doi: 10.1590/1413-81232017221.26532016
13 Stelzig KE, Canepa-Escaro F, Schiliro M, Berdnikovs S, Prakash YS,Chiarella SE. Estrogen regulates the expression of SARS-CoV-2receptor ACE2 in differentiated airway epithelial cells. Am J
Physiol Lung Cell Mol Physiol. 2020;318(06):L1280–L1281. Doi:10.1152/ajplung.00153.2020
14 Klein SL, Flanagan KL. Sex differences in immune responses. NatRev Immunol. 2016;16(10):626–638. Doi: 10.1038/nri.2016.90
15 Zeng F, Dai C, Cai P, Wang J, Xu L, Li J, et al. A comparison study ofSARS-CoV-2 IgG antibody between male and female COVID-19patients: A possible reason underlying different outcome be-tween sex. J Med Virol. 2020;92(10):2050–2054. Doi: 10.1002/jmv.25989
16 Di Stadio A, Della Volpe A, Ralli M, Ricci G. Gender differences inCOVID-19 infection. The estrogen effect on upper and lowerairways. Can it help to figure out a treatment? Eur Rev MedPharmacol Sci. 2020;24(10):5195–5196. Doi: 10.26355/eur-rev_202005_21298
17 Cutolo M, Smith V, Paolino S. Understanding immune effects ofoestrogens to explain the reduced morbidity and mortality infemale versus male COVID-19 patients. Comparisons with auto-immunity and vaccination. Clin Exp Rheumatol. 2020;38(03):383–386
18 Nachman S. Estrogen patch for COVID-19 symptoms [Internet].New YorkStony Brook University2020 [cited 2020 Sep 15].NCT04359329. Available from: https://clinicaltrials.gov/ct2/show/NCT04359329
19 Ghandehari S. Progesterone for the treatment of COVID-19 inhospitalized men [Internet]. Los AngelesCedars Sinai MedicalCenter2020 [cited 2020 Sep 15]. NCT04365127. Available from:https://clinicaltrials.gov/ct2/show/NCT04365127
20 Zhao Y, Zhao Z, Wang Y, Zhou Y, Ma Y, Zuo W. Single-Cell RNAExpression Profiling of ACE2, the Receptor of SARS-CoV-2. Am JRespir Crit Care Med. 2020;202(05):756–759. Doi: 10.1164/rccm.202001-0179LE
21 Bhatraju PK, Ghassemieh BJ, Nichols M, Kim R, Jerome KR, NallaAK, et al. Covid-19 in critically Ill patients in the Seattle Region -Case series. N Engl J Med. 2020;382(21):2012–2022. Doi:10.1056/NEJMoa2004500
22 Klok FA, Kruip MJHA, van der Meer NJM, Arbous MS, GommersDAMPJ, Kant KM, et al. Incidence of thrombotic complications incritically ill ICU patients with COVID-19. Thromb Res. 2020;191:145–147. Doi: 10.1016/j.thromres.2020.04.013
23 Fabregues F, Peñarrubia J. Assisted reproduction and thrombo-embolic risk in the COVID-19 pandemic. Reprod Biomed Online.2020;41(03):361–364. Doi: 10.1016/j.rbmo.2020.06.013
24 GuanWJ, Ni ZY, Hu Y, LiangWH, Ou CQ, He JX, et al; ChinaMedicalTreatment Expert Group for Covid-19. Clinical Characteristics ofCoronavirus Disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. Doi: 10.1056/NEJMoa2002032
25 Carsana L, Sonzogni A, Nasr A, Rossi RS, Pellegrinelli A, Zerbi P,et al. Pulmonary post-mortem findings in a series of COVID-19cases from northern Italy: a two-centre descriptive study. LancetInfect Dis. 2020;20(10):1135–1140. Doi: 10.1016/S1473-3099(20)30434-5
26 Magro C, Mulvey JJ, Berlin D, Nuovo G, Salvatore S, Harp J, et al.Complement associated microvascular injury and thrombosis inthe pathogenesis of severe COVID-19 infection: A report of fivecases. Transl Res. 2020;220:1–13. Doi: 10.1016/j.trsl.2020.04.007
27 Menter T, Haslbauer JD, Nienhold R, Savic S, Hopfer H, Deigen-desch N, et al. Postmortem examination of COVID-19 patientsreveals diffuse alveolar damage with severe capillary congestionand variegated findings in lungs and other organs suggestingvascular dysfunction. Histopathology. 2020;77(02):198–209.Doi: 10.1111/his.14134
28 Hottz ED, Azevedo-Quintanilha IG, Palhinha L, Teixeira L, BarretoEA, Pão CRR, et al. Platelet activation and platelet-monocyteaggregates formation trigger tissue factor expression in severeCOVID-19 patients. Blood. 2020;136(11):1330–1341. Doi:10.1182/blood.2020007252
29 Vlachodimitropoulou Koumoutsea E, Vivanti AJ, Shehata N, Bena-chi A, Le Gouez A, Desconclois C, et al. COVID-19 and acute
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Analysis of the Role of Female Hormones During Infection by COVID-19 Pascoal et al. 947

coagulopathy in pregnancy. J Thromb Haemost. 2020;18(07):1648–1652. Doi: 10.1111/jth.14856
30 International Federation of Gynecology and Obstetrics (FIGO)COVID-19 contraception and family planning [Internet]. 2020[cited 2020 Jul 12]. Available from: https://www.figo.org/covid-19-contraception-family-planning
31 World Health Organization. Anticoncepção / Planejamento famil-iar e COVID-19 [Internet]. 2020 [cited 2020 Jul 15]. Availablefrom: https://www.who.int/reproductivehealth/publications/emer-gencies/WHO-COVID-Q-and-A-contraception-por.pdf?ua=1
32 Federação Brasileira das Associações de Ginecologia e ObstetríciaComissão Nacional de Anticoncepção Anticoncepção durante apandemia por COVID-19 [Internet]. 2020 [cited 2020 Set 10].Available from: https://www.febrasgo.org.br/pt/covid19/item/1002-anticoncepcao-durante-a-pandemia-por-covid-19
33 Riley T, Sully E, Ahmed Z, Biddlecom A. Estimates of the potentialimpact of the COVID-19 pandemic on sexual and reproductivehealth in low- and middle-income countries. Int Perspect SexReprod Health. 2020;46:73–76. Doi: 10.1363/46e9020
34 Faculty of Sexual and Reproductive Healthcare. FSRH CEU clinicaladvice to support provision of effective contraception during theCOVID-19 outbreak [Internet]. 2020 [cited 2020 Set 10]. Availablefrom:https://www.fsrh.org/documents/fsrh-ceu-clinical-advice-to-support-provision-of-effective/
35 Ramírez I, De la Viuda E, Baquedano L, Coronado P, Llaneza P,Mendoza N, et al. The thromboembolic risk in covid-19 womenunder hormonal treatment group. Maturitas. 2020;138:78–79.Doi: 10.1016/j.maturitas.2020.05.021
36 Cagnacci A, Bonaccorsi G, Gambacciani Mboard of the ItalianMenopause Society. Reflections and recommendations on theCOVID-19 pandemic: Should hormone therapy be discontinued?Maturitas. 2020;138:76–77. Doi: 10.1016/j.maturitas.2020.05.022
37 Rawla P, Pradeep Raj J, Thandra KC, Bandaru SS. Superior mesen-teric vein thrombosis in a patient on oral contraceptive pills.Gastroenterol Res. 2017;10(06):380–382. Doi: 10.14740/gr903w
38 Sueta D, Akahoshi R, Okamura Y, Kojima S, Ikemoto T, YamamotoE, et al. Venous Thromboembolism Due to Oral ContraceptiveIntake and Spending Nights in a Vehicle -A Case from the 2016Kumamoto Earthquakes. Intern Med. 2017;56(04):409–412. Doi:10.2169/internalmedicine.56.7785
39 Paschou SA, Goulis DG, Lambrinoudaki I, Papanas N. Menopausalhormone therapy for womenwith obesity in the era of COVID-19.Case Rep Womens Health. 2020;27:e00233. Doi: 10.1016/j.crwh.2020.e00233
40 Plu-Bureau G, Sabbagh E, Hugon-Rodin J. [Hormonal contracep-tion and vascular risk: CNGOF Contraception Guidelines]. GynécolObstét Fertil Sénol. 2018;46(12):823–833. Doi: 10.1016/j.gofs.2018.10.007
41 Sitruk-WareR.Hormonalcontraceptionand thrombosis. Fertil Steril.2016;106(06):1289–1294. Doi: 10.1016/j.fertnstert.2016.08.039
42 Gialeraki A, Valsami S, Pittaras T, Panayiotakopoulos G, Politou M.Oral contraceptives and HRT risk of thrombosis. Clin Appl ThrombHemost. 2018;24(02):217–225. Doi: 10.1177/1076029616683802
43 Fruzzetti F, Cagnacci A. Venous thrombosis and hormonal contracep-tion: what’s new with estradiol-based hormonal contraceptives?OpenAccess JContracept.2018;9:75–79.Doi:10.2147/OAJC.S179673
44 Rott H. Birth control pills and thrombotic risks: differences ofcontraception methods with and without estrogen. Hamostaseo-logie. 2019;39(01):42–48. Doi: 10.1055/s-0039-1677806
45 McDaid A, Logette E, Buchillier V, Muriset M, Suchon P, Pache TD,et al. Risk prediction of developing venous thrombosis in com-bined oral contraceptive users. PLoS One. 2017;12(07):e0182041.Doi: 10.1371/journal.pone.0182041
46 Dinger J, Do Minh T, Heinemann K. Impact of estrogen type oncardiovascular safetyof combinedoral contraceptives. Contraception.2016;94(04):328–339. Doi: 10.1016/j.contraception.2016.06.010
47 Larivée N, Suissa S, Eberg M, Joseph L, EisenbergMJ, Abenhaim HA,et al. Drospirenone-containing combined oral contraceptives andthe risk of arterial thrombosis: a population-based nested case-control study. BJOG. 2017;124(11):1672–1679. Doi: 10.1111/1471-0528.14358
48 Weill A, Dalichampt M, Raguideau F, Ricordeau P, Blotière P-O,Rudant J, et al. Low dose oestrogen combined oral contraceptionand risk of pulmonary embolism, stroke, and myocardial infarc-tion in five million French women: cohort study. BMJ. 2016;353:i2002. Doi: 10.1136/bmj.i2002
49 Hugon-Rodin J, Horellou MH, Conard J, Gompel A, Plu-Bureau G.Type of combined contraceptives, Factor V Leiden mutation andrisk of venous thromboembolism. Thromb Haemost. 2018;118(05):922–928. Doi: 10.1055/s-0038-1641152
50 Laliberté F, Dea K, DuhMS, Kahler KH, Rolli M, Lefebvre P. Does theroute of administration for estrogen hormone therapy impact therisk of venous thromboembolism? Estradiol transdermal systemversus oral estrogen-only hormone therapy.Menopause. 2018;25(11):1297–1305. Doi: 10.1097/GME.0000000000001232
51 Dulicek P, Ivanova E, Kostal M, Sadilek P, Beranek M, Zak P, et al.Analysis of risk factors of stroke and venous thromboembolism infemales with oral contraceptives use. Clin Appl Thromb Hemost.2018;24(05):797–802. Doi: 10.1177/1076029617727857
52 Liaw PC. Mediators of disseminated intravascular coagulation:molecular mechanisms. Blood. 2017;130(Suppl 1):SCI-2. Doi:10.1182/blood.V130.Suppl_1.SCI-2.SCI-2
53 Mahmood IH, Jaber IM. Effects of hormonal contraceptives onserum glucose, lipid profile and some liver function test. Iraqi JPharm.. 2014;14(01):1–6. Doi: 10.33899/iphr.2019.161187
54 Ministério da Saúde. Secretaria de Atenção Primária à Saúde NotaTécnica No. 10/2020-COSMU/CGCIVI/DAPES/SAPS/MS. Recomen-dações para as consultas ambulatoriais de saúde da mulherdurante a pandemia da COVID19 [Internet]. 2020 [cited 2020Jul 21]. Available from: http://docs.bvsalud.org/biblioref/2020/05/1095680/notatecnica102020cosmucgcividapessapsms.pdf
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Analysis of the Role of Female Hormones During Infection by COVID-19 Pascoal et al.948

Clinical and Obstetric Aspects of PregnantWomen with COVID-19: A Systematic Review
Aspectos clínicos e obstétricos de gestantes comCOVID-19: Uma revisão sistemáticaSarah Nilkece Mesquita Araújo Nogueira Bastos1 Bárbara Louise Freire Barbosa1
Larisse Giselle Barbosa Cruz1 Rayza Pereira de Souza2 Simone Santos e Silva Melo1
Caroline Camargo Bandeira da Silveira Luz1
1Departamento de Medicina, Universidade Federal do Delta doParnaíba, Parnaíba, PI, Brazil
2Departamento de Medicina, Faculdade Uninassau, Parnaíba, PI, Brazil
Rev Bras Ginecol Obstet 2021;43(12):949–960.
Address for correspondence Sarah Nilkece Mesquita Araújo NogueiraBastos, Doutora em Enfermagem, Avenida São Sebastião, 2819,64001-020, Parnaíba, PI, Brazil (e-mail: [email protected]).
Keywords
► pregnancy► coronavirus
infections► severe acute
respiratory syndrome► SARS virus► betacoronavirus
Abstract Objective To analyze the clinical and obstetric aspects of pregnant women withCOVID-19.Methods A systematic literature review in the MEDLINE/PubMed, LILACS, SCIELO, andCNKI databases was performed from March to May 2020, with the descriptors:Pregnancy; 2019-nCov; Coronavirus; SARS-Cov-2, Covid-19. Of those chosen were originaltitles, without language and period restriction and that addressed pregnant womenwith a clinical and/or laboratory diagnosis of COVID-19. Revisions, editorials, andduplicate titles were excluded. The Newcastle-Ottawa (NOS) and Murad et al. scaleswere used to assess the quality of the studies.Results We included 34 articles with 412 pregnant women infected with severe acuterespiratory syndrome (SARS-Cov-2), with an average age of 27.5 years of age and 36.0gestational weeks. The most common symptom was fever (205 [49.7%]), and 89(21.6%) pregnant women progressed to severe viral pneumonia. Laboratory testsshowed an increase in C-reactive protein (154 [37.8%]), and radiological tests showedpneumonia with peripheral ground-glass pattern (172 [51.4%]). Emergency cesareandelivery was indicated for most pregnant women, and the most common gestationalcomplication was premature rupture of ovarian membranes (14 [3.4%;]). We detected2 (0.5%) neonatal deaths, 2 (0.5%) stillbirths, and 1 (0.2%) maternal death.Conclusion Pregnant women with COVID-19 presented a clinical picture similar tothat of non-infected pregnant women, with few obstetric or neonatal repercussions.There was a greater indication of cesarean deliveries before the disease aggravated,and there was no evidence of vertical transmission of the infection.
receivedMay 25, 2020acceptedMarch 5, 2021
DOI https://doi.org/10.1055/s-0041-1733913.ISSN 0100-7203.
© 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rightsreserved.This is an open access article published by Thieme under the terms of the
Creative Commons Attribution License, permitting unrestricted use,
distribution, and reproduction so long as the original work is properly cited.
(https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda., Rua do Matoso 170, Rio deJaneiro, RJ, CEP 20270-135, Brazil
THIEME
Review Article 949

Introduction
At the end of December 2019, inWuhan, capital of the Hubeiprovince, located in China, there was an outbreak by a virusthat suddenly worried the authorities, due to their lack ofknowledge and the rapid spread of the virus to othercountries. The virus, belonging to the coronavirus family,was named severe acute respiratory syndrome (SARS-CoV2),and the illness caused by it was called coronavirus disease2019 (COVID-19). This virus causes a highly transmissibleinfectious disease that can entail mild symptoms, such as drycough, fever, odynophagia, or even severe acute respiratorysyndrome.1,2
Given the accelerated spread of the virus among coun-tries, in March 2020, the World health Organization (WHO)declared a status of pandemic, and the beginning of the needfor measures of social distance, with the purpose of avoidingthe crowding of people and containing the spread of suchinfection. Data for the month of June 2020 already highlightmore than 10 million confirmed COVID-19 cases worldwideand � 500 thousand deaths.3,4
Nevertheless, based on the information referring to theother aforementioned coronaviruses, SARS-CoV and middleeast respiratory syndrome coronavirus (MERS-CoV), wenoted a higher incidence of abortions, growth restriction,preterm births, and fetal death. In addition, these viruses inpregnant women determined a high number of complica-tions, such as hospitalization in intensive care units (ICU), theneed for assisted ventilation, renal failure, and death.3
These complications are erroneously explained by theunderstanding of pregnancy as a condition of immunosup-
pression, which is a misconception, since pregnancy repre-sents a peculiar immune condition that ismodulated, but notsuppressed. The correct concept allows caregivers and policymakers to make valid recommendations for the treatment ofpregnant women during pandemics. Accordingly, in thisCOVID-19 pandemic, health care professionals need to un-derstand the spectrum of presentations and outcomes ofCOVID-19 infection during pregnancy and childbirth.5
Systematic reviews5–8 published recently demonstratedgood obstetric results for pregnant women with COVID-19;however, there are still gaps on the influence of infection onthe choice of life of delivery, fetal and neonatal repercussions,as well as the possibility of vertical transmission. This study,therefore, aims to contemplate these points still little dis-cussed and strengthen the knowledge about the behavior ofthe virus during pregnancy and perinatal. Furthermore, itaims to concentrate the best evidence, since most of thepublished works are case reports/series, in Chinese, whichmakes it difficult to homogenize information and summarizeperinatal results in pregnant women with COVID-19.
Thus, a systematic literature review was performed toanalyze the clinical and obstetric aspects of COVID-19 inpregnant women.
Methods
This is a systematic literature review developed in accordancewith the PreferredReporting Items for SystematicReviewsandMeta-Analyses (PRISMA) recommendation.9 The study proto-col and reviewwere not registeredwith PROSPERO due to theneed for urgent information. We sought to answer research
Resumo Objetivo Analisar os aspectos clínicos e obstétricos de gestantes com COVID-19.Métodos Revisão sistemática da literatura nas bases: MEDLINE/PubMed, LILACS,SCIELO e CNKI, realizada de março a maio de 2020, com os descritores Pregnancy;2019-nCov; Coronavirus; SARS-Cov-2, Covid-19. Elegeram-se títulos originais, sem res-trição de idioma e período e que abordassem gestantes com diagnóstico clínico e/oulaboratorial de COVID-19. Excluíram-se revisões, editoriais, títulos duplicados. Asescalas de Newcastle-Ottawa (NOS, na sigla em inglês) e a de Murad et al. foramutilizadas para avaliar a qualidade dos estudos.Resultados Foram incluídos 34 artigos com 412 gestantes infectadas pela síndromerespiratória aguda grave (SARS-Cov, na sigla em inglês) com idade média de 27,5 anos emédia de36,0 semanasgestacionais.O sintomamais incidente foi a febre (49,7%;205). e 89(21,6%) gestantes evoluírampara pneumonia viral grave. Os exames laboratoriais demons-traram aumento da proteína C reativa (37,8%; 154) e os radiológicos mostraram pneumo-nia com padrão em vidro fosco periférico (51,4%; 172). O parto cesáreo de emergência foiindicado para a maior parte das gestantes, e a complicação gestacional mais comum foi aruptura prematura de membranas ovulares (3,4%; 14). Foram detectados 2 (0,5%) mortesneonatais, 2 (0,5%) natimortos, e 1 (0,2%) morte materna.Conclusão Gestantes com doença coronavírus (COVID-19, na sigla em inglês apresenta-ram quadro clínico semelhante a gestantes não infectadas, com poucas repercussõesobstétricas ou neonatais. Houve uma maior indicação de partos cesáreos antes doagravamentodadoençaenãoseobservaramevidênciasdetransmissãoverticalda infecção.
Palavras-chave
► gravidez► infecções por
coronavírus► síndrome
respiratória agudagrave
► vírus da SARS► betacoronavírus
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Clinical and Obstetric Aspects of Pregnant Women with COVID-19 Bastos et al.950

questions: “What are the clinical and obstetric repercussionsin pregnant women infected with SARS-Cov-2?”
The search strategy was held in the following electronicbibliographic databases: Medical Literature and Retrieval Sys-tem online (MEDLINE / PubMed); Latin American and Carib-bean Literature on Health Sciences (LILACS); ScientificElectronic Library Online (SCIELO); Chinese National Knowl-edge Infrastructure (CNKI). In addition,we considered second-ary research and gray bases in the pertinent literature in othersources, such as Google Scholar and OPENGREY. The referencesection of the included studies was manually searched foradditional relevant studies.
The search strategy included only key terms, according to apreestablished acronym of PICO (Population/Intervention/-Comparison/Outcome). The search strategy that combinesmedical subject headings (MeSH) terms and free text wordsthat will be used in MEDLINE (PubMed) and adjusted to otherelectronic databases, in the followingmanner: PregnantWom-en AND (coronavirus OR coronavirus OR COVID-19 OR 2019-nCoVOR SARS-CoV-2) AND Pregnancy. The strategy details arepresented in ►Table 1.
The eligibility criteria included complete original prima-ry studies, available online in the selected databases andpublished in any languages, with no time frame, thataddressed pregnant women with a clinical and/or laborato-ry diagnosis of COVID-19. All primary designs were consid-ered, including case reports and case series. Given theinfancy of the pandemic, urgent need of guidance, andlimited higher quality information available on the topic,this was deemed reasonable. The exclusion criteria wereliterature reviews, editorials, or studies in which it was notpossible to identify a relationship with the theme andduplicates in the databases as well as unreported maternalor perinatal results.
In the databases, we defined a peer search with specificdescriptors, from March to April 2020. The search for dataended on May 13th, 2020. The selection was made in pairs,
with three authors, who independently selected the titles ofthe articles and then proceeded to read all abstracts. Thosewho complied with the study object were read in full. Weconsidered original articles whose theme was related topregnant womenwith COVID-19, regardless of the employeddiagnostic technique. After selecting the articles, we heldconsensus meetings to confirm the equality of the selectedarticles. If there was disagreement, a fourth author wasinvited to give his/her opinion.
After agreement with the selected studies, we used a formdeveloped by the authors to manually extract the followingdata:
- Variables related to the studies: authorship, year, coun-try, method, population, and sample;
- Maternal variables: age, gestational age, signs, and symp-toms of the pregnant womanwith COVID-19, radiologicaland laboratory manifestations, gestational repercussions(delivery, obstetric complications), complications andclinical outcomes (respiratory failure, maternalmortality);
- Perinatal variables: perinatal complications (fetal distress,low birth weight, prematurity), vertical transmission ofCOVID-19, perinatal mortality.
The primary outcomes were to identify obstetric repercus-sions, such as delivery route, gestational complications, sever-ity of SARS-Cov-2 infection, and mortality; the fetalrepercussions were complications such as fetal distress, fetalandneonatalmortality, andvertical transmissionofCOVID-19.The severity was assessed based on pregnant women whodeveloped severe pneumonia or severe acute respiratorysyndrome (SARS), requiring oxygen supply.
The quality of the studies was based on checking interna-tional guidelines. For case studies, we used the tool proposedbyMurad et al. (2018),10 composed of four domains: selection,verification, causality, and communication. According to therecommendation, we made a general judgment about themethodological quality based on the questions consideredmore critical in the specific clinical setting. The quality wasconsidered either satisfactory or unsatisfactory, with satisfac-tory being when at least 1 item from each domain of theinstrument was met. We used the Newcastle-Ottawa Scale(NOS)11 for cohort studies in the cases ofobservational studies.The NOS uses a star system (0–9) to assess the selected studiesin 3 domains: selection (0–4), comparability (0–2), and results(0–3). Higher scores represent better quality. and then, weconsidered: strong evidence (6–9 points), moderate evidence(4–5 points), and limited evidence (< 4 points).
The studieswere presented and synthesized in tableswithexposure of the most relevant data, and the treatment ofthese tables was performed in the Microsoft Office Excelsoftware (Microsoft Corp., Redmond,WA, USA), to determinethe percentage of incidence of the variables.
Results
From the total of 267 identified articles, 102 were eliminatedbecause they were duplicated in the databases. One hundred
Table 1 Search strategy, according to PICO
PICO MEANING DESCRIPTORS
Population (P): Pregnant womenof any age
((“Pregnant Women”[MeSH Terms]))
Intervention (I): COVID-19infection
((“coronavirus”[MeSH Terms] OR“coronavirus”[All Fields])OR (“COVID-19”[All Fields]OR “2019-nCoV”[All Fields]OR “SARS-CoV-2”[All Fields]).
Comparison (C): Non-pregnantwomen
Not applicable
Outcomes (O): COVID-19interference inthe pregnancy
((“Pregnancy”[MeSH Terms]))
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Clinical and Obstetric Aspects of Pregnant Women with COVID-19 Bastos et al. 951

and sixty-five titles and abstracts were read, and, of these, 56manuscripts were chosen to be read in full. After eliminatingthose that did notmeet the object of the study, 34 studieswereselected for analysis, according to the flowchart (►Fig. 1).
As for the method, most studies were 1 or multiple casereports (23; 67.6%) and observational (11; 32,4%), withclinical and epidemiological characterization of pregnantwomen with COVID-19. The quality of the studies is dis-played in ►supplementary tables S1 and S2. In►supplementary table S1, we represented the quality ofthe studies of one or multiple cases, according to the toolof Murad et al. (2018),10 in which we observed a satisfactoryquality in all studies. ►Table 2 shows the quality of thestudies, according to the NOS scale. Quality scores rangedfrom 6 to 9 points, which denotes studies with strongevidence (Supplementary tables S1 and S2).
Description of the Study Findings
To compose the systematic review, we included 34 articles,all published in 2020, mainly produced in China (61.7%; 21)available in the PubMed/MEDLINE databases (►Table 2).
Altogether, 412 infected pregnant women, with an aver-age age of 27.5 years and who were mostly in the 3rd
trimester of pregnancy, with an average of 36.0 gestationalweeks, were assessed in the studies. All pregnant womenwere diagnosed with COVID-19 through the reversetranscription polymerase chain reaction (RT-PCR) method.The most frequent signs and symptoms were fever (205[49.7%]) dyspnea (130 [31.5%]), cough (109 [26.5%]), fatigue(34 [8.2%]), myalgia (29 [7.0%]), chest pain (23 [5.5%]),diarrhea (20 [4.8%]) and odynophagia (15 [3.6%])(►Table 2).
Fig. 1 Flowchart of PRISMA selection.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Clinical and Obstetric Aspects of Pregnant Women with COVID-19 Bastos et al.952

Table
2Cha
racterizationof
theselected
stud
ieson
COVID
-19in
preg
nant
wom
en.B
razil,20
20
Art
Autho
r/ye
ar/co
untry;
NDiagn
ostic
metho
dMaternal
age
Trim
ester
averag
eGA
Mainsign
san
dsymptoms
Radiologica
l/labo
ratory
man
ifestations
Maternal/gestational/fetal
repercu
ssions
1Xiong
etal.(202
0)12;
China
1RT
-PCR
(25)
2nd(26GW)
38°C
feve
r,dryco
ugh
,an
dtrem
orRa
diolog
ical:p
ulmon
aryop
acity
Labo
ratory:ne
utrophilia
andlymph
ocytope
nia
Witho
utrepe
rcussion
s
2Li
etal.(202
0)15;
China
16RT
-PCR
(31,5)26–
373r
d(35GW)
Fever(4;25.0%
)Ra
diolog
ical:b
ilateralp
neu
mon
ia43
.75%
(7)an
dun
ilateralp
neum
onia
50%(8)
Labo
ratory:leuk
open
iaan
dne
utrophilia
14(87.5%
)Cesarea
nde
liveries
3(18.75
%)P
remature
births,of
which
:2(66.67
%)
prem
atureruptureof
ovarianmem
bran
es(RPM
O)
and1(33.3%
)blee
ding
2(12.5%
)fetald
istress
3Chen
etal.(202
0)27;
China
5RT
-PCR
(28)
25–3
13r
d(39GW)
Fever(after
delivery)
anddryco
ugh(2;40.0%
)Ra
diolog
ical:b
ilateralp
neum
onia60
%(3)a
nd40
%(2)un
ilateral
Labo
ratory:inc
reased
CRP(4;8
0.0%
)an
dalka
line
phosph
ates
(4;80
.0%);leuk
open
ia40
%(2)
2(40.0%
)Cesarea
nde
liveries
4Yu
etal.(202
0)13;
China
7RT
-PCR
(32)
29–3
43r
d(39GW)
Fever(86%
;6),co
ugh,
dysp
nea,an
ddiarrhea
(14%
;1,e
ach)
Radiolog
ical:8
6%(6)b
ilateralp
neu
mon
iaan
d14
%(1)un
ilateral
Labo
ratory:ne
utrophilia
(71%
;5),lymph
open
ia(71%
;5),thrombo
cytope
nia(29%
;2)
and
elev
ationof
D-dim
er(100
%;7),a
lanine
aminotrans
ferase
(29%
;2)
andCRP(100
%;7)
Infected
NB36
hafterde
livery
5Ka
nget
al.(20
20)16;
China
1RT
-PCR
303r
d(35GW).
Cou
ghRa
diolog
ical:p
neum
onia
andbilateralp
leural
effusion
Labo
ratory:Withou
tch
ange
s
Emerge
ncy
cesarean
delivery
Fetalb
radycardia
6Liuet
al.(202
0)45;
China
15RT
-PCR
32 (23–
40)
1stto
3rd
(12to
38GW).
Fever(86.6%
;13
);Cou
gh(60.0%
;9);
fatigu
e(26.7%
;4);myalgia
(20.0%
;3);dy
s-pn
ea,od
ynop
hagia,
anddiarrhea
(6.6%;1,
each
)
Radiolog
ical:g
roun
d-glass
opac
ityan
dlate
pul-
mon
aryco
nsolidations
Labo
ratory:lympho
cytope
nia(80.0%
;12
)an
dincrea
sedva
lueof
C-reac
tive
protein(66.6%
;10
)
10(66.6%
)cesarean
deliv
eries
3(20.0%
)prem
aturebirths
7Chen
etal.(202
0)14;
China
9RT
-PCR
30 (26–
40)
3rd(37GW)
Fever(77.7%
;7);Cou
gh(44.4%
;4);
myalgia
(33.3%
;3);od
ynop
hagia
andmalaise
(22.2%
;2,
each
)
Radiolog
ical:g
roun
d-glass
opac
ity(88.8%
;8)
Labo
ratory:lympho
cytope
nia(55.5%
;5),
elev
ationof
aminotransferases(33.3%
;3)an
dC-reac
tive
protein-PC
R(66.6%
;6)
9(100
.0%)cesarean
deliveries
4(44.4%
)ne
wbo
rnsha
dbirthweight
less
than
2500
g1(11.1%
)PR
OM
8Liuet
al.(202
0)17;
China
13RT
-PCR
29 (22–
36)
2pa
tien
tsin
the2n
d(26GW);
11pa
tien
tsin
the3r
d(35GW)
Feveran
dfatigu
e(10;
77%);
Dyspne
a(3;23
%)
NR
10(77%
)cesarean
deliv
eries,
5(38.4%
)of
which
wereem
erge
ncy
6(46%
)prem
aturebirth
3(23%
)fetald
istress.
1(7.6%)PR
OM
1(7.6%)stillborn
1(7.6%)maternal
multipleorga
ndy
sfun
ction
synd
rome(M
ODS)
9Li
etal.(202
0)18;
China
1RT
-PCR
303r
d(35GW)
Dry
coug
h,fever,an
ddy
spnea
Radiolog
ical:b
ilateralirreg
ular
pulm
ona
ryinfiltrates
Labo
ratory:slightly
abno
rmal.
Emerge
ncy
cesarean
delivery
Fetalb
rady
cardia
10Chen
etal.(202
0)19;
China
3RT
-PCR
29,6
(23–
34)
3rd(36.6GW)
Preor
postnatalfeve
r(10
0%,3
)and
chestp
ain
(33.3%
;1).
Radiolog
ical:b
ilateralg
roun
d-glassop
acitiesan
dbron
chiectasis(100
%,3)
Labo
ratory:sign
ificant
increa
sein
CRP(100
%,3)
3(100
.0%)cesarean
deliveries
1(33.3%
)prem
aturebirth
1(33.3%
)prem
atureplacen
tald
isplace
men
t1(33.3%
)placen
taprev
ia1(33.3%
)NBwithLB
W
11Zh
anget
al.(202
0)20;
China
16RT
-PCR
29 (24–
34)
3rd(38GW)
Cou
gh;C
hestpa
in;dy
spne
a,an
ddiarrhea
NR
16(100
%)em
ergen
cycesarean
section
3(18.7%
)prem
aturebirths
2(12.5%
)fetald
istress
3(18.7%
)ruptureof
mem
brane
s1(6.25%
)fetald
istressan
dfetalb
rady
cardia
1(6.25%
)seve
rematernal
pneu
monia (C
ontin
ued)
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Clinical and Obstetric Aspects of Pregnant Women with COVID-19 Bastos et al. 953
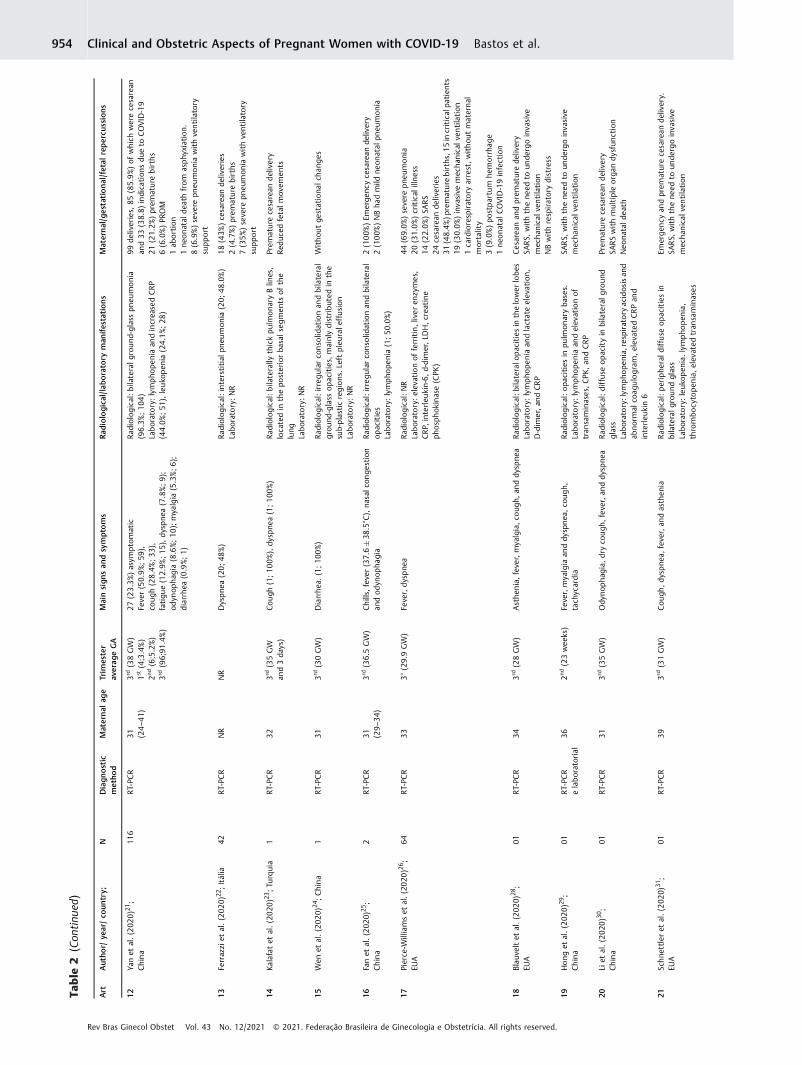
Table
2(Con
tinu
ed)
Art
Autho
r/ye
ar/co
untry;
NDiagn
ostic
metho
dMaternal
age
Trim
ester
averag
eGA
Mainsign
san
dsymptoms
Radiologica
l/labo
ratory
man
ifestations
Maternal/gestational/fetal
repercu
ssions
12Ya
net
al.(202
0)21;
China
116
RT-PCR
31 (24–
41)
3rd(38GW)
1st(4;3.4%)
2nd(6;5.2%)
3rd(96;91
.4%)
27(23.3%
)asym
ptom
atic
Fever(50.9%
;59
),co
ugh(28.4%
;33),
fatigu
e(12.9%
;15),dy
spne
a(7.8%;9
);od
ynop
hagia
(8.6%;10
);mya
lgia
(5.3%;6
);diarrhea
(0.9%;1)
Radiolog
ical:b
ilateralg
roun
d-glasspn
eumon
ia(96.3%
;10
4)Labo
ratory:lympho
peniaan
dincrea
sedCRP
(44.0%
;51
),leuk
open
ia(24.1%
;28
)
99de
liveries,
85(85.9%
)of
which
werece
sarean
and33
(38.8)
indication
sdu
eto
COVID
-19
21(21.2%
)prem
aturebirths
6(6.0%)PR
OM
1ab
ortion
1ne
ona
tald
eath
from
asphy
xiation.
8(6.9%)seve
repn
eumon
iawithventilatory
supp
ort
13Fe
rrazzi
etal.(202
0)22;Itália
42RT
-PCR
NR
NR
Dyspne
a(20;
48%)
Radiolog
ical:interstitial
pneu
mon
ia(20;
48.0%)
Labo
ratory:NR
18(43%
)cesarean
deliv
eries
2(4.7%)prem
aturebirths
7(35%
)severe
pneu
mon
iawithventila
tory
supp
ort
14Ka
lafatet
al.(20
20)23;Tu
rquia
1RT
-PCR
323r
d(35GW
and3da
ys)
Cou
gh(1;10
0%),dy
spne
a(1;10
0%)
Radiolog
ical:b
ilaterally
thickpu
lmon
aryBlin
es,
locatedin
thepo
steriorba
salseg
men
tsof
the
lung
Labo
ratory:NR
Prem
ature
cesarean
delivery
Reduc
edfetalm
ovem
ents
15Wen
etal.(202
0)24;China
1RT
-PCR
313r
d(30GW)
Diarrhe
a.(1;10
0%)
Radiolog
ical:irreg
ular
conso
lidationan
dbilateral
grou
nd-glass
opacities,
mainlydistributed
inthe
sub-plastic
regions.Left
pleu
rale
ffusion
Labo
ratory:NR
Witho
utge
stationa
lcha
nges
16Fanet
al.(202
0)25;
China
2RT
-PCR
31 (29–
34)
3rd(36.5GW)
Chills,
fever(37.6�38
.5°C),na
salc
onge
stion
andod
ynop
hagia
Radiolog
ical:irreg
ular
conso
lidationan
dbilateral
opacities
Labo
ratory:lympho
penia(1;5
0.0%
)
2(100
%)Em
ergen
cycesarean
deliv
ery
2(100
%)NBha
dmild
neon
atal
pneu
mon
ia
17Pierce
-Williamset
al.(20
20)26;
EUA
64RT
-PCR
333°
(29.9GW)
Fever,dy
spne
aRa
diolog
ical:N
RLabo
ratory:elev
ationof
ferritin,liver
enzymes,
CRP,
interleu
kin-6,
d-dimer,LD
H,crea
tine
phosph
okinase(CPK
)
44(69.0%
)severe
pneu
monia
20(31.0%
)critical
illne
ss14
(22.0%
)SA
RS24
cesarean
deliveries
31(48.4%
)premature
births
,15in
criticalpa
tien
ts19
(30.0%
)inva
sive
mec
hanicalv
entilation
1cardioresp
iratory
arrest,withou
tmaternal
mortality
3(9.0%)po
stpartum
hemorrhag
e1ne
ona
talC
OVID
-19infection
18Blau
veltet
al.(202
0)28;
EUA
01RT
-PCR
343r
d(28GW)
Asthe
nia,fev
er,myalgia,co
ugh,
anddy
spne
aRa
diolog
ical:b
ilateralo
pacitiesin
thelower
lobe
sLabo
ratory:lympho
peniaan
dlactateelev
ation,
D-dim
er,a
ndCRP
Cesarea
nan
dprem
aturede
livery
SARS,
withthene
edto
unde
rgoinva
sive
mec
hanical
ventilation
NBwithrespiratorydistress
19Hong
etal.(202
0)29;
China
01RT
-PCR
elabo
ratorial
362n
d(23wee
ks)
Fever,myalgia
anddy
spnea
,co
ugh,
tach
ycardia
Radiolog
ical:o
pacities
inpu
lmon
aryba
ses.
Labo
ratory:lympho
peniaan
delev
ationof
tran
saminases,CPK
,an
dCRP
SARS,
withthene
edto
unde
rgoinva
sive
mec
hanical
ventilation
20Li
etal.(202
0)30;
China
01RT
-PCR
313r
d(35GW)
Ody
nopha
gia,dryco
ugh
,fever,an
ddy
spne
aRa
diolog
ical:d
iffuse
opacityin
bilateralg
roun
dglass
Labo
ratory:lym
pho
penia,resp
iratory
acidos
isan
dab
norm
alco
agulogram
,eleva
tedCRPan
dinterleu
kin6
Prem
ature
cesarean
delivery
SARSwithmultipleorga
ndy
sfun
ction
Neo
natald
eath
21Schne
ttleret
al.(202
0)31;
EUA
01RT
-PCR
393r
d(31GW)
Cou
gh,d
yspne
a,fever,an
dasthen
iaRa
diolog
ical:p
eriphe
rald
iffuse
opacitiesin
bilateralg
roun
dglass
Labo
ratory:leuk
open
ia.lympho
penia,
thrombo
cytope
nia,
elev
ated
tran
saminases
Emerge
ncy
andprem
aturecesarean
deliv
ery.
SARS,
withthene
edto
unde
rgoinva
sive
mec
hanical
ventilation
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Clinical and Obstetric Aspects of Pregnant Women with COVID-19 Bastos et al.954

Table
2(Con
tinu
ed)
Art
Autho
r/ye
ar/co
untry;
NDiagn
ostic
metho
dMaternal
age
Trim
ester
averag
eGA
Mainsign
san
dsymptoms
Radiologica
l/labo
ratory
man
ifestations
Maternal/gestational/fetal
repercu
ssions
22Wuet
al.(202
0)32;China
08RT
-PCR
29 (26–
35)
3rd(38GW)
Feveron
admission(1;12.5%
),an
dfeverin
the
postpartum
period
(3;3
7.5%
)Ra
diolog
ical:p
eriphe
rald
iffuse
opacitiesin
bilateralg
roun
dglass(6;75
.0%)
Labo
ratory:leu
kocytosis(6;7
5.0%
);lympho
penia
(5;62
.5%),elev
ationof
D-dim
ersan
dcrea
tine
kina
se(CK)an
dcrea
tine
kina
se-M
B(CK-MB)
in4
(50.0%
)in
thepo
stpartum
period
6(75.0%
)Cesarea
nde
livery
1fetald
istress
23Pe
nget
al.(20
20)33;China
01RT
-PCR
253r
d(35SG
)Fe
ver,fatigu
ean
ddy
spne
aRa
diolog
ical:p
eriphe
rald
iffuse
opacitiesin
bilateralg
roun
d-glasspa
ttern
Labo
ratory:NR
Emerge
ncy
cesarean
andprem
aturede
livery
Fetald
istress
24Breslin
etal.(202
0)34;
EUA
43RT
-PCR
27 (20–
39)
3rd(37SG
)Cou
gh(19;
65.6%);
feve
r(14;
48.3%);
myalgia
(11;
37.9%).
head
ache
(8;27
.6%);
dysp
nea(7;24
.1%);
chestpa
in(5;1
7.2%
)
Radiolog
ical:p
eriphe
rald
iffuse
opacitiesin
bilat-
eral
grou
nd-glass
pattern(1;2
.32%
)Labo
ratory:NR
Cesarea
nde
livery(8;4
4.4%
)Prem
ature
birth(4;13
.8%)
1PR
OM
2(4.6%)seve
rematerna
lpneu
mon
ia1ne
wbo
rnwithrespiratorydistress
25Ka
ramie
tal.(20
20)35;
Irã
01RT
-PCR
273r
d(30SG
)Dyspne
a,feve
r,co
ugh
,myalgia,an
dtach
ypne
aRa
diolog
ical:b
ilaterald
iffuse
periphe
ral
grou
nd-glass
opacitiesan
dpleu
rale
ffusion
Labo
ratory:leuk
open
ia,thrombo
cytope
nia,
elev
ated
CRP,
lactic
dehy
droge
nase
(LDH)
Echo
cardiogram:sev
eresystolic
dysfun
ction
righ
t
Materna
ldea
thfrom
severe
acuteresp
iratory
synd
rome(SARS)
andMODS;
stillbo
rn
26Iqbaet
al.(202
0)36;
EUA
01RT
-PCR
343r
d(39GW)
Fever,co
ugh,
chills,
andmyalgia
Radiolog
ical:d
iffuse
pulm
onaryop
acities
Labo
ratory:lympho
penia
NR
27Xia
etal.(20
20)37;
China
01RT
-PCR
273r
d(36GW)
Fever,co
ugh,
drop
inox
ygen
saturation
(92%
)Ra
diolog
ical:b
ilaterald
iffuse
periphe
ralg
roun
d-
glassop
acities
Labo
ratory:ne
utrophilia
,lym
phop
enia,a
nd
elev
ated
CRP
Cesarea
nde
livery
Fetald
istress
28Bu
onsensoet
al.(20
20)38;Itália
07RT
-PCR
403r
d(36GW)
Cou
ghRa
diolog
ical:d
iffuse
interstitial
lung
disease
Labo
ratory:NR
2(28.5%
)Cesarea
nde
livery
1Prem
atureBirth
1Abortion
2Neo
natalC
OVID
-19infections
29Qianc
henget
al.(202
0)39;C
hina
28RT
-PCR
30 (18–
41)
3rd(38GW)
Fever(5;17
.9%),
asthen
ia(1;3
.6%),co
ugh
(7;25
%),
dysp
nea(2;7.1%
),ab
dominal
pain
(5;17
.9%)
Radiolog
ical:b
ilateralp
eriphe
rald
iffuse
grou
nd-glass
opacities(26;
92.9%)
Labo
ratory:Leuk
ocytosis(10;
35.7%),increa
sed
CRP(17;
68.0%),lympho
penia(8;28
.6)
17(60.0%
)Cesarea
nde
livery
1(4.3%)Prem
aturebirth
4(14.2%
)Induc
edab
ortion
2(7.1%)Se
vere
pneu
mon
ia
30Lyra
etal.(20
20)40;
Portug
al01
RT-PCR
353r
d(39GW)
Cou
ghNR
Cesarea
nde
livery
31Ke
llyet
al.(202
0)41;E
UA
01RT
-PCR
�3r
d(33GW)
Vom
iting,
coug
h,an
dtach
ycardia
Radiolog
ical:R
adiograp
hysh
owed
subs
egmen
tal
atelec
tasiswithou
tco
nso
lidation
Labo
ratory:lympho
peniaan
dmild
elev
ationof
liver
enzymes
Cesarea
nan
dprem
aturede
livery
1SA
RS,
withthene
edto
undergo
inva
sive
mec
hanical
ventilation
32Brow
neet
al.
(202
0)42;EU
A01
RT-PCRe
Serological
(IgG
/IgM
)
332n
d(23GW)
Fever,co
ugh,
andmyalgia
Radiolog
ical:N
RLabo
ratory:leuk
ocytosis
Prem
ature
cesarean
delivery
33Indraccolo(202
0)43;Itália
01RT
-PCR
NR
3rd(32GW)
Cou
gh,e
piga
stricpa
in,an
dch
estpa
inNR
NR
(Con
tinue
d)
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Clinical and Obstetric Aspects of Pregnant Women with COVID-19 Bastos et al. 955

Among themost common findings in laboratory tests, wefound elevated C-reactive protein (CRP) (154 [37.8%]), lym-phopenia (84 [20.3%]), leukopenia (58 [14.2%]) and neutro-philia (23 [5.5%]). In the assessment by computerizedtomography (CT) or chest X-ray, 51.4% (212) of the pregnantwomen presented a characteristic image of viral pneumoniawith ground-glass pattern, with 172 (51.5%) having bilateralpulmonary involvement (►Table 2).
Among the main gestational complications, we foundpremature birth (76 [18.4%]), abortion (4 [1.0%]), andpremature rupture of ovarian membranes (PROM) (14[3.4%]). Severe maternal pneumonia took place in 89(21.6%) of the pregnant women, with 1 (0.2%) maternaldeath being recorded. With regard to fetal repercussions,we detected 2 (0.5%) stillbirths, 2 neonatal deaths (0.5%), 11cases of fetal distress (2.7%), 3 cases of fetal bradycardia(0.7%). And 4 cases of low birth weight (LBW) (1.0%), and 4cases of neonatal COVID infection (1.0%) (►Table 2).
Discussion
Coronaviruses are a large class of viruses, among which thenewly discovered SARS-Cov-2 is the 7th coronavirus currentlyknown due to its capacity of infecting human beings. Thedisease caused by it, COVID-19, has become a challengingthreat to public health worldwide; and when it comes topregnant women, data on the outcomes of the disease are stilllimited.12
We analyzed 34 studies involving 412 infected pregnantwomen. Thesepaperswereall fromthecurrent year, and therewasapredominanceofChineseproductions,probablybecauseitwas the region initiallymost affectedby thediseaseand that,for this reason, gathered early evidence about the affectedpatients. The findings mainly highlighted young women whowere in the third trimester of pregnancy. This is a relevant fact,since the results of thepresent studycannot be extrapolated topregnant women with virus infection in the first or secondtrimester of pregnancy.13,14
Pregnant women presented a clinical course similar tonon-pregnant adult women.12,14–26 The current data onCOVID-19 infection suggests that pregnant women experi-ence similar or even lower rates of serious illness comparedwith non-pregnant women; however, additional data areneeded, and it is crucial to determine the peculiar factors inpregnant women who predict a more severe course of thisdisease, with to the goal of guiding the clinical management,as well as the ideal time of delivery.26
The most frequent signs and symptoms were fever,dyspnea, cough, and fatigue, respectively.8–10 We shouldunderline that asymptomatic pregnant women weredetected in the predelivery period and that they presentedsymptoms such as fever after delivery.19–32 A total of 89pregnant women evolved with severe viral pneumoniaand/or SARS, and 24 required invasive ventilatorysupport.17,26,28–41 We noted clinical pictures of multipleorgan dysfunction and reversed cardiorespiratory arrest;26
however, there was only one report of maternal deathrelated to COVID-19.35 The data indicate that 95% of theTa
ble
2(Con
tinu
ed)
Art
Autho
r/ye
ar/co
untry;
NDiagn
ostic
metho
dMaternal
age
Trim
ester
averag
eGA
Mainsign
san
dsymptoms
Radiologica
l/labo
ratory
man
ifestations
Maternal/gestational/fetal
repercu
ssions
34Lu
etal.(20
20)44;China
01RT
-PCR
223r
d(38GW)
Asymptomatic
Radiolog
ical:b
ilateralp
leurale
ffusion
Labo
ratory:hy
perproteine
mia,elev
ated
tran
saminases
andLD
H
Cesarea
nde
livery
Total
N 412
Diagno
stic
method
RTC-PC
R(412
;100
%)
Ave
rageag
e27
.5GA
36.0
Symptom
sFe
ver(49.7%
;20
5);
dysp
nea(31.5%
;13
0);
coug
h(26.5%
;109
),fatigu
e(8.2%;34
);myalgia
(7.0%;29
);ch
estpa
in(5.5%;23
),diarrhea
(4.8%;20
);od
ynop
hagia
(3.6%;15
)
Mainradiologica
lfind
ings
Pneu
mon
ia/groun
d-glasspa
ttern(51.4%
;212
),51
.5%(172
)of
which
werebilateral
Mainlabo
ratory
findings
Increa
sedCRP(37.8%
;154
);lymph
open
ia(20.3%
;84);
leuk
open
ia(14.2%
;58
);ne
utrophilia
(5.5%;2
3);
Maternal
andGestaciona
lrep
ercu
ssions
Cesarea
nde
livery(36.2%
;14
9);prem
aturebirth
(18.4%;76
);ab
ortion
(1.0%;4);
PROM
(3.4%;1
4);h
emorrhag
e(1.0%;4
);placen
tal
abruption(0.2%;1);p
prev
ia(0.2%;1
);seve
rematerna
lpneu
mon
ia(21.6%
;89);m
aterna
ldea
th(0.2%;1);
Fetalrepercu
ssions
Stillbo
rn(0.5%;2
);ne
onatal
death(0.5%;2
);fetal
distress
(2.7%;11
);fetalb
radycardia(0.7%;3
);LB
W(1.0%;4
);ne
onatal
COVID
infection(1.0%;4
)
Abbrev
iation
s:CRP,
C-reac
tive
protein;
GA,ge
stationa
lage
;GW,ge
stationa
lwee
k;LB
W,low
birthweight;NB,
newbo
rn;NR,no
trepo
rted
;PR
OM,prem
atureruptureof
ovarianmem
bran
es;RT
-PCR,reve
rse
tran
scriptionpo
lymerasech
ainreac
tion;
SARS,
seve
reacute
resp
iratorysynd
rome.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Clinical and Obstetric Aspects of Pregnant Women with COVID-19 Bastos et al.956

women who need intubation will do so 20 days after theonset of symptoms.26
We can notice that most respiratory symptoms found inthe studies were mild; however, pregnant women withcomorbidities, such as preeclampsia, can have worse out-comes, since pneumonia can aggravate pulmonary edemaand reduce oxygen saturation.11,28 This is because pregnantwomen have a higher oxygen consumption, with an increaseof 10 to 20%, changes in hormonal levels and decreased lungvolumes, caused by an increase in the size of the uterusduring pregnancy, as well as edema of the respiratory tractmucosa, which can cause a faster clinical deterioration andmake pregnant women more susceptible to respiratorypathogens and severe pneumonia, because they are in a stateof adaptive immunity.13,14,42
Nevertheless, we should consider the high number ofasymptomatic pregnant women in all studies and/or withatypical symptoms, which emphasizes the need to improvethe investigation of COVID-19 upon admission, as well as thestrengthening of infection control measures.15,21,43,44
Among the most common laboratory changes, we foundincreased CRP, lymphopenia, and leukopenia. It is recom-mended that, in addition to the RT-PCR test as the goldstandard for the diagnosis of COVID-19-related pneumonia,laboratory tests and a comprehensive assessment of themedical history of the patient, epidemiological exposureand symptoms are accomplished.14
The radiologicalfindings,mainly bychest CT, demonstratedpulmonary opacities with peripheral ground-glass patternwith bilateral pulmonary involvement, suggestive of viralpneumonia. In most cases, the tomographic images obtainedbefore and after delivery did not show signs of aggravatedpneumonia, indicating that pregnancy and childbirth do notseem to aggravate the course of the tomographic character-istics.45 Given the difficulty and delay in RT-PCR tests, low-dose chest CT, or even the use of chest ultrasound,23maybe aneffectivemethod to screen forCOVID-19-relatedpneumonia inpregnant women in the third trimester.15 In critical areas,radiological findings consistent with COVID-19 infection mayemerge before the results of RT-PCR.23
Regarding the gestational repercussions, we noted agreater indication of emergency cesarean deliveries forinfected pregnant women, many of these involving preterminfants. It is important to emphasize that the uncertaintyabout the risk of vertical transmission through vaginaldelivery or early delivery before the disease aggravationwere the main reasons for the recommendation of cesareansections.14 In these cases of emergency cesarean sections,maternal clinic should be assessed, giving preference tospinal anesthesia, to reduce the impact on the respiratorycirculation of the mother and her baby. If the infectedpregnant woman is critical, general anesthesia is recom-mended for tracheal intubation.16,37
Management of expectant support of the pregnant wom-an is reasonable for most42; however, for women over 34gestational weeks and with associated risk factors, cesareandelivery can be indicated early before the onset of the criticalillness.26 As for the event of severe maternal infection,
delivery should be postponed until pulmonary stability isachieved, unless the pregnancy has reached its term.31 Astudy demonstrated that pregnant women with COVID-19presented a higher factor indicating cesarean delivery due tomuscle fatigue and uterine contraction (1.3�0.6) than thecontrol group without infection [(0.5�0.7)] (p-value¼0.001). Pregnant women with COVID-19 are in an infectedand hypoxic state with greater inflammatory factors, in-creased uterine contractility and a higher risk of postpartumhemorrhage. The indication of termination of pregnancydepends on the status of the illness, but terminating it earlymay improve maternal lung function.26
The studies were not in agreement regarding the rela-tionship between COVID-19 and preterm births. A retrospec-tive study of data analysis of 116 pregnant women did notfind association among the gestational infection by SARS-Cov-2, the increase in premature births, and the risk ofabortion.21 Nevertheless, other studies corroborate thatthere is a higher incidence of premature births in confirmedcases of COVID-19, when compared with non-infected preg-nant women,15,42 and that the need for the accomplishmentof this procedure is greater in women with critical infection,to whom the indication is given, mainly, by maternal status,and not fetal.26,28
The most common gestational complication was thePROM15,17; however, in the studies, it was not possible toclarify the direct relationship between this complication andthe SARS-Cov-2 infection. Nevertheless, it is known thatinflammatory reactions caused by infection by the viruscan impair the development and the function of the placenta,especially in blood vessels, resulting in adverse outcomes inpregnancy.19
Regarding fetal manifestations, deliveries resulting intwo stillborn8,14 and two neonatal deaths21,30 weredetected, as well as cases of respiratory distress,28 fetaldistress,15,17,20,32,37 with fetal bradycardia16,19,20 andLBW.14,19 Severe SARS-Cov-2 infection can change the fetalintrauterine environment, and the inflammatory stormcaused by the infection triggers a systemic immune re-sponse that can also attack fetal organs.30 Despite thisfrequency of complications, most studies have shown thatNBs from infected mothers do not present significant differ-ences in the main indicators of neonatal complicationswhen compared with NBs from non-infected mothers.15
We did not find occurrence of vertical transmission ofCOVID-19.19,25,33,38,39,44 Tests with an oropharynx samplefrom 2 NBs were positive with 36hours and 48hours afterbirth,13,26 and 2 other NBs were positive two weeks later.38
Surveys investigating SARS-CoV-2 in maternal serum, pla-centa, umbilical cord, amniotic fluid, vaginal swabs, andbreast milk were negative in the nucleic acid test in allstudies that cited them, which precludes vertical intrauter-ine transmission. Premature neonates may be at particularrisk of perinatal COVID-19 infection, since the active transferof protective maternal immunoglobulins does not reach itspeak before 28 to 30 weeks of life, besides the immatureintegrity of the skin of NBs, which may be a risk factor forperinatal transmission.28
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Clinical and Obstetric Aspects of Pregnant Women with COVID-19 Bastos et al. 957

With regard to breastfeeding, as it is a recent infection,there is currently insufficient evidence to support thepresence of SARS-CoV-2 in breast milk; however, breast-feeding by infected mothers, in part of the studies, is notrecommended, according to the experience related toSARS.20,25,27 Nevertheless, an Italian consensus eases thisindication by admitting that COVID-19-positive motherswith mild or asymptomatic symptoms can breastfeed whilewearing a surgical mask.22 And those infected and symp-tomatic should be separated from their NBs, but they canperform weaning to provide their children with breastmilk.34
Four systematic reviews currently published on COVID-19and pregnant women5–8 were composed of 9, 6, 24, and 33studies, the majority of which were case series. Until themoment of completing this search in databases, this system-atic review is the one that addressed the largest number ofstudies and the largest sample of pregnant women infectedwith SARS-Cov-2.
The present systematic review demonstrated a low ma-ternal mortality rate, as well as a reduced incidence ofcomplications, such as SARS, concluding that COVID-19-positive pregnant women have fewer symptoms than thegeneral population and that this infection is not associatedwith poor perinatal results.5–8 One concern, however, wasrelated to the high rate of premature delivery by cesareansection in these women.6
This review considers the results of the aforementionedresearch when concluding that the maternal, fetal, andneonatal outcomes in COVID-19 were, in most studies,positive. And it brings new knowledge to the fact thatpregnant women can remain asymptomatic or when theyhave symptoms, fever is their main one, accompanied by theelevated serum CRP and that cesarean delivery is a recurrentoutcome in this type of infection. The absence of verticaltransmission was reinforced; however, neonatal COVID-19infection was demonstrated, which serves to reinforce theneed for infection control measures at the time of delivery.
Nevertheless, we should underline that the average age of27.5 years of women in this study reveals that, as in thegeneral epidemiological panorama of the disease, youngpeople are less prone to COVID-19 complications and thisfactor may be responsible for the reduced number of nega-tive outcomes, which can, consequently, undermine a possi-ble protective factor provided by pregnancy.
We should also underline that the findings of thissystematic review predominantly bring characteristics ofeastern, Chinese, and North American women, which pre-vents further generalization of the data, due to phenotypic,cultural, and structural differences in health services. Ac-cordingly, more studies are needed to assess the profile ofpregnant women from other countries with a high inci-dence of the disease, such as Brazil, with a view to compar-ing the findings.
The present review has limitations, because, as a result ofthe COVID-19 pandemic, new studies are published daily,and it listed works until May 13th, 2020. Moreover, theanalyzed studies, since they are mostly with case study
methods, add up to a small sample of pregnant womenand, in addition, despite presenting satisfactory quality,according to the assessment tools, they consist of studieswith lowevidence. Nevertheless, we believe that the tenden-cy toward the manifestation of symptoms in pregnant wom-en infectedwith SARS-CoV-2 does not differmuch fromwhatwas exposed in the results.
Furthermore, the findings of the current study character-ized women in the third trimester of pregnancy, and it is notpossible to generalize such considerations to pregnant wom-en in the first and second trimesters. Therefore, there is aneed for studies that focus on this viral infection in earliergestational periods.
Conclusion
The course of infection in pregnant womenwith SARS-Cov-2is similar to the one in non-infected pregnant women. Wedid not find occurrence of vertical transmission of COVID-19.The main symptom presented by pregnant women withCOVID-19 was fever; however, most of the patients wereasymptomatic. Themost common laboratory changewas theincrease in CRP, and the radiologicalfindingswere peripheralpulmonary opacities with ground-glass pattern. There was agreater indication of emergency cesarean deliveries forinfected pregnant women, many of these involving preterminfants; however, studies have not shown consensus on therisk of prematurity associatedwith COVID-19. Themain fetalmanifestations were fetal distress, with reduced fetal heartrate, but not directly related to SARS-Cov-2. Mortality con-sisted of two stillborn, two neonatal deaths, and one mater-nal death.
Conflict of InterestsThe authors have no conflict of interests to declare.
References1 Singhal T. A Review of Coronavirus Disease-2019 (COVID-19).
Indian J Pediatr. 2020;87(04):281–286. Doi: 10.1007/s12098-020-03263-6
2 Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospital-ized patients with 2019 novel coronavirus–infected pneumoniain Wuhan, China. JAMA. 2020;323(11):1061–1069. Doi: 10.1001/jama.2020.1585
3 Ramalho C. [COVID-19 in pregnancy, what do we know?] ActaObstet Ginecol Port [Internet] 2020 [cited 2020 May 6];14(1):6–7.Available from: lng¼pt. Portuguese.http://www.scielo.mec.pt/scielo.php?script¼sci_arttext&pid¼S1646-58302020000100001&
4 Johns Hopkins University & Medicine Coronavirus Resource Cen-ter. COVID-19 Dashboard by the Center for Systems Science andEngineering (CSSE) [Internet]. 2020 [cited 2020 May 6]. Availablefrom: https://coronavirus.jhu.edu/map.html
5 Elshafeey F, Magdi R, Hindi N, et al. A systematic scoping reviewofCOVID-19 during pregnancy and childbirth. Int J Gynaecol Obstet.2020;150(01):47–52. Doi: 10.1002/ijgo.13182
6 Smith V, Seo D, Warty R, et al. Maternal and neonatal out-comes associated with COVID-19 infection: A systematic review.PLoS One. 2020;15(06):e0234187. Doi: 10.1371/journal.pone.0234187
7 Juan J, Gil MM, Rong Z, Zhang Y, Yang H, Poon LC. Effect ofcoronavirus disease 2019 (COVID-19) on maternal, perinatal
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Clinical and Obstetric Aspects of Pregnant Women with COVID-19 Bastos et al.958

and neonatal outcome: systematic review. Ultrasound ObstetGynecol. 2020;56(01):15–27. Doi: 10.1002/uog.22088
8 Della Gatta AN, Rizzo R, Pilu G, Simonazzi G. Coronavirus disease2019 during pregnancy: a systematic review of reported cases.Am J Obstet Gynecol. 2020;223(01):36–41. Doi: 10.1016/j.ajog.2020.04.013
9 Moher D, Liberati A, Tetzlaff J, Altman DGPRISMA Group. Pre-ferred reporting items for systematic reviews andmeta-analyses:the PRISMA statement. PLoS Med. 2009;6(07):e1000097. Doi:10.1371/journal.pmed.1000097
10 Murad MH, Sultan S, Haffar S, Bazerbachi F. Methodologicalquality and synthesis of case series and case reports. BMJ EvidBased Med. 2018;23(02):60–63. Doi: 10.1136/bmjebm-2017-110853
11 Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale(NOS) for assessing the quality of nonrandomised studies inmeta-analyses [Internet]. 2000 [cited 2020 May 6]. Availablefrom: http://www.ohri.ca/programs/clinical_epidemiology/ox-ford.asp
12 Xiong X, Wei H, Zhang Z, et al. Vaginal delivery report of a healthyneonate born to a convalescent mother with COVID–19. J MedVirol. 2020;92(09):1657–1659. Doi: 10.1002/jmv.25857
13 Yu N, Li W, Kang Q, et al. Clinical features and obstetric andneonatal outcomes of pregnant patients with COVID-19 inWuhan, China: a retrospective, single-centre, descriptive study.Lancet Infect Dis. 2020;20(05):559–564. Doi: 10.1016/S1473-3099(20)30176-6
14 Chen H, Guo J, Wang C, et al. Clinical characteristics and intra-uterine vertical transmission potential of COVID-19 infection innine pregnant women: a retrospective review of medical records.Lancet. 2020;395(10226):809–815. Doi: 10.1016/S0140-6736(20)30360-3
15 Li N, Han L, Peng M, et al. Maternal and neonatal outcomes ofpregnant womenwith COVID-19 pneumonia: a case-control study.Clin Infect Dis. 2020;71(16):2035–2041. Doi: 10.1093/cid/ciaa352
16 Kang X, Zhang R, He H, et al. [Anesthesia management in cesareansection for a patient with coronavirus disease 2019]. Zhejiang DaXue Xue Bao Yi Xue Ban. 2020;49(01):249–252
17 Liu Y, Chen H, Tang K, Guo Y. Withdrawn: Clinical manifestationsand outcome of SARS-CoV-2 infection during pregnancy. J Infect.2020;•••:S0163-4453(20)30109-2. Doi: 10.1016/j.jinf.2020.02.028[ahead of print]
18 Li Y, Zhao R, Zheng S, et al. Lack of vertical transmission of severeacute respiratory syndrome coronavirus 2, China. Emerg InfectDis. 2020;26(06):1335–1336. Doi: 10.3201/eid2606.200287
19 Chen S, Huang B, Luo DJ, et al. [Pregnancy with new coronavirusinfection: clinical characteristics and placental pathological anal-ysis of three cases]. Zhonghua Bing Li Xue Za Zhi. 2020;49(05):418–423. Doi: 10.3760/cma.j.cn112151-20200225-00138
20 Zhang L, Jiang Y,WeiM, et al. [Analysis of the pregnancy outcomesin pregnant womenwith COVID-19 in Hubei Province]. ZhonghuaFu Chan Ke Za Zhi. 2020;55(03):166–171
21 Yan J, Guo J, Fan C, et al. Coronavirus disease 2019 in pregnantwomen: a report based on 116 cases. Am J Obstet Gynecol. 2020;223(01):111.e1–111.e14. Doi: 10.1016/j.ajog.2020.04.014
22 Ferrazzi EM, Frigerio L, Cetin I, et al. COVID-19 Obstetrics TaskForce, Lombardy, Italy: Executive management summary andshort report of outcome. Int J Gynaecol Obstet. 2020;149(03):377–378. Doi: 10.1002/ijgo.13162
23 Kalafat E, Yaprak E, Cinar G, et al. Lung ultrasound and computedtomographic findings in pregnant woman with COVID-19. Ultra-sound Obstet Gynecol. 2020;55(06):835–837. Doi: 10.1002/uog.22034
24 Wen R, Sun Y, Xing QS. A patient with SARS-CoV-2 infectionduring pregnancy in Qingdao, China. J Microbiol Immunol Infect.2020;53(03):499–500. Doi: 10.1016/j.jmii.2020.03.004
25 Fan C, Lei D, Fang C, et al. Perinatal Transmission of 2019Coronavirus Disease-Associated Severe Acute Respiratory Syn-drome Coronavirus 2: ShouldWeWorry? Clin Infect Dis. 2021;72(05):862–864. Doi: 10.1093/cid/ciaa226
26 Pierce-Williams RAM, Burd J, Felder L, et al. Clinical course ofsevere and critical coronavirus disease 2019 in hospitalizedpregnancies: a United States cohort study. Am J Obstet GynecolMFM. 2020;2(03):100134. Doi: 10.1016/j.ajogmf.2020.100134
27 Chen S, Liao E, Cao D, Gao Y, Sun G, Shao Y. Clinical analysis ofpregnant womenwith 2019 novel coronavirus pneumonia. J MedVirol. 2020;92(09):1556–1561. Doi: 10.1002/jmv.25789
28 Blauvelt CA, Chiu C, Donovan AL, et al. Acute respiratory distresssyndrome in a preterm pregnant patient with Coronavirus Dis-ease 2019 (COVID-19). Obstet Gynecol. 2020;136(01):46–51. Doi:10.1097/AOG.0000000000003949
29 Hong L, Smith N, Keerthy M, et al. Severe COVID-19 infection inpregnancy requiring intubationwithout preterm delivery: A casereport. Case RepWomens Health. 2020;27:e00217. Doi: 10.1016/j.crwh.2020.e00217
30 Li J, Wang Y, Zeng Y, et al. Critically ill pregnant patient withCOVID-19 and neonatal death within two hours of birth. Int JGynaecol Obstet. 2020;150(01):126–128. Doi: 10.1002/ijgo.13189
31 Schnettler WT, Al Ahwel Y, Suhag A. Severe acute respiratorydistress syndromeincoronavirusdisease2019-infectedpregnancy:obstetric and intensive care considerations. Am J Obstet GynecolMFM. 2020;2(03):100120. Doi: 10.1016/j.ajogmf.2020.100120
32 Wu C, Yang W, Wu X, et al. Clinical manifestation and laboratorycharacteristics of SARS-CoV-2 infection in pregnant women.Virol Sin. 2020;35(03):305–310. Doi: 10.1007/s12250-020-00227-0
33 Peng Z, Wang J, Mo Y, et al. Unlikely SARS-CoV-2 verticaltransmission from mother to child: A case report. J Infect PublicHealth. 2020;13(05):818–820. Doi: 10.1016/j.jiph.2020.04.004
34 Breslin N, Baptiste C, Gyamfi-Bannerman C, et al. Coronavirusdisease 2019 infection among asymptomatic and symptomaticpregnant women: two weeks of confirmed presentations to anaffiliated pair of New York City hospitals. Am J Obstet GynecolMFM. 2020;2(02):100118. Doi: 10.1016/j.ajogmf.2020.100118
35 Karami P, Naghavi M, Feyzi A, et al. WITHDRAWN: Mortalityof a pregnant patient diagnosed with COVID-19: A casereport with clinical, radiological, and histopathological findings.Travel Med Infect Dis. 2020;101665:101665. Doi: 10.1016/j.tmaid.2020.101665 [ahead of print]
36 Iqbal SN, Overcash R, Mokhtari N, et al. An UncomplicatedDelivery in a Patient with Covid-19 in the United States. N EnglJ Med. 2020;382(16):e34. Doi: 10.1056/NEJMc2007605
37 Xia H, Zhao S, Wu Z, Luo H, Zhou C, Chen X. Emergency Caesareandelivery in a patient with confirmed COVID-19 under spinalanaesthesia. Br J Anaesth. 2020;124(05):e216–e218. Doi:10.1016/j.bja.2020.02.016
38 Buonsenso D, Costa S, Sanguinetti M, et al. Neonatal Late OnsetInfection with Severe Acute Respiratory Syndrome Coronavirus 2.Am J Perinatol. 2020;37(08):869–872. Doi: 10.1055/s-0040-1710541
39 Qiancheng X, Jian S, Lingling P, et al; sixth batch of Anhui medicalteam aiding Wuhan for COVID-19. Coronavirus disease 2019 inpregnancy. Int J Infect Dis. 2020;95:376–383. Doi: 10.1016/j.ijid.2020.04.065
40 Lyra J, Valente R, Rosário M, Guimarães M. Cesarean section in apregnant womanwith COVID-19: first case in Portugal. Acta MedPort. 2020;33(06):429–431. Doi: 10.20344/amp.13883
41 Kelly JC, Dombrowksi M, O’Neil-Callahan M, Kernberg AS, FrolovaAI, Stout MJ. False-negative testing for severe acute respiratorysyndrome coronavirus 2: consideration in obstetrical care. Am JObstet Gynecol MFM. 2020;2(03):100130. Doi: 10.1016/j.ajogmf.2020.100130
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Clinical and Obstetric Aspects of Pregnant Women with COVID-19 Bastos et al. 959

42 Browne PC, Linfert JB, Perez-Jorge E. Successful treatment ofpreterm labor in association with acute COVID-19 infection.Am J Perinatol. 2020;37(08):866–868. Doi: 10.1055/s-0040-1709993
43 Indraccolo U. A pregnant woman and the SARS-CoV-2 infection:how are barriers easily crossed? Recenti ProgMed. 2020;111(04):259–260. Doi: 10.1701/3347.33190
44 LuD, Sang L, Du S, Li T, Chang Y, YangXA. Asymptomatic COVID-19infection in late pregnancy indicated no vertical transmission. JMed Virol. 2020;92(09):1660–1664. Doi: 10.1002/jmv.25927
45 Liu D, Li L, Wu X, et al. Pregnancy and perinatal outcomes ofwomen with coronavirus disease (COVID-19) pneumonia: apreliminary analysis. AJR Am J Roentgenol. 2020;215(01):127–132. Doi: 10.2214/AJR.20.23072
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Clinical and Obstetric Aspects of Pregnant Women with COVID-19 Bastos et al.960

Intermittent versus Continuous Catheterizationand Differences in the Evolution of Labor:Systematic Review and Meta-analysis
Cateterismo intermitente versus contínuo e diferençasna evolução do trabalho de parto: Revisão sistemática emeta-análiseInês Reis1 Sara Cunha1 Matilde Martins1 Luísa Sousa1 Adérito Seixas2,3 Cátia Rasteiro1,4
1Serviço de Ginecologia e Obstetrícia do Centro Hospitalar de Entre oDouro e Vouga, Santa Maria da Feira, Portugal
2Escola Superior de Saúde, Fundação Fernando Pessoa, Porto, Portugal3 LABIOMEP, INEGI-LAETA, Faculty of Sports, University of Porto,Porto, Portugal
4Faculdade de Ciências da Saúde, Universidade da Beira Interior,Covilhã, Portugal
Rev Bras Ginecol Obstet 2021;43(12):961–967.
Address for correspondence Inês Reis, Specialist in Gynecology andObstetrics, Rua Dr. Cândido de Pinho, 4520-211, Santa Maria da Feira,Portugal (e-mail: [email protected]).
Keywords
► labor► urinary catheter► bladder drainage► transurethral catheter
Abstract Objective To evaluate the differences between bladder emptying options (permanentcatheterization and intermittent bladder emptying/spontaneous urination) regarding theeffects on labor length, need of operative vaginal deliveries, and cesarean section rate.Data Sources The search was conducted in MEDLINE, Scopus, Web of Science, andThe Cochrane Central Register of Controlled Trials databases.Selection of Studies The survey returned 964 studies. A total of 719 studies wereevaluated by title and abstract, of which 4 were selected for inclusion.Data Collection All references were inserted in the Rayyan QCRI tool (Rayyan SystemsInc., Cambridge, MA, USA). The full text of the selected articles was obtained so wecould later decide whether or not to include them in this systematic review.Data Synthesis No differences were found in the number of instrumented deliveriesor in cesarean section rate between groups.Conclusions After evaluating the studies performed on the topic, we concluded thatthere is no clear advantage to either method, although continuous catheterization wasassociated with a greater occurrence of eutocic births. In the remaining outcomes,there were no differences between catheterization types.
receivedNovember 24, 2020acceptedSeptember 8, 2021
DOI https://doi.org/10.1055/s-0041-1740209.ISSN 0100-7203.
© 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rightsreserved.This is an open access article published by Thieme under the terms of the
Creative Commons Attribution License, permitting unrestricted use,
distribution, and reproduction so long as the original work is properly cited.
(https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda., Rua do Matoso 170, Rio deJaneiro, RJ, CEP 20270-135, Brazil
THIEME
Review Article 961

Introduction
In parturients under neuraxial analgesia, the reduced per-ception of a full bladder and the inability to void can lead tourinary retention. These aspects, together with fluid therapyand the duration of labor, make bladder emptying a necessi-ty. There is no consensus in the literature, or in the practice ofdelivery rooms, whether intermittent bladder emptying orcontinuous catheterization during neuraxial analgesia anduntil delivery is more appropriate. Therefore, the aim of thepresent study is to summarize and critically evaluate theevidence concerning the different bladder emptying options(permanent catheterization and intermittent bladderemptying/spontaneous urination) in terms of their effectson labor length, need of operative vaginal deliveries, andcesarean section rate.1–8
Childbirth, as a fundamental moment in a woman’s life,has been a popular subject of research over the past decades,with the introduction of methods and options that allowwomen to experience a less traumatic and painful experi-ence, promoting the well-being of women and fetuses.Neuraxial analgesia is considered an integral part of normallabor, being the most effective and safe analgesia option(Petitprez et al., 2020).5
Classically, neuraxial analgesia has been associated withan increase of cesarean section rates and operative vaginaldeliveries, as well as with a longer duration of labor(referred in several protocols as an additional 1 hour inthe 2nd stage of labor period). However, recent reviews,validated in guidelines, demonstrate that this is not the case(American College of Obstetricians and Gynecologists[ACOG], 2019).1
Methods
This review was reported based on the Preferred ReportingItems for Systematic Reviews and Meta-Analysis (PRISMA)recommendations.
Randomized controlled studies in humans that includedwomen in labor (induced or spontaneous) with neuraxialanalgesia in which continuous versus intermittent cathe-terization were compared were considered for inclusion iffocusing on the effects in labor length, type of delivery, andcesarean section rate. No publication date restrictions weredefined. Articles published in Portuguese, English, French,Spanish, and Italian were considered.
Continuous catheterization was defined as permanentcatheterization from the time of neuraxial analgesia untilthe 2nd stage of labor. Intermittent catheterizationwas considered as the introduction of a urinary catheterto empty the bladder, with immediate removal afteremptying.
Neuraxial analgesia included epidural, combined (spinal-epidural), and spinal techniques.
The duration of labor was defined as the time fromneuraxial analgesia to the end of the second stage of deliveryand was counted in hours.
The type of delivery was classified as eutocic, operativevaginal delivery (vacuum or forceps extraction), and cesare-an section.
The electronic search was conducted inMEDLINE, Scopus,Web of Science, and The Cochrane Central Register of Con-trolled Trials databases using the following search string(labor OR delivery OR parturition OR childbirth) AND
Resumo Objetivo Avaliar as diferenças entre as opções de esvaziamento vesical (cateterismopermanente e esvaziamento vesical intermitente/micção espontânea) em relação aosefeitos na duração do trabalho de parto, necessidade de partos vaginais operatórios etaxa de cesárea.Fontes de Dados A pesquisa foi realizada nas bases de dados MEDLINE, Scopus, Webof Science, e The Cochrane Central Register of Controlled Trials.Seleção de Estudos A pesquisa retornou 964 estudos. Um total de 719 estudos foramavaliados por título e resumo, dos quais 4 foram selecionados para inclusão.Coleta de Dados Todas as referências foram inseridas na ferramenta Rayyan QCRI(Rayyan Systems Inc., Cambridge, MA, EUA). O texto completo dos artigos selecionadosfoi obtido para posterior decisão de incluí-los nesta revisão sistemática.Síntese dos Dados Não foram encontradas diferenças no número de partos instru-mentados ou na taxa de cesariana entre os grupos.Conclusões Após avaliação dos estudos realizados sobre o tema, concluímos que nãohávantagem clara de qualquer um dosmétodos, embora o cateterismo contínuo tenhasido associado à maior ocorrência de partos eutócicos. Nos demais desfechos, nãohouve diferenças entre os tipos de cateterismo.
Palavras-chave
► trabalho► cateter urinário► drenagem da bexiga► cateter transuretral
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Intermittent vs Continuous Catheterization and Differences in the Evolution of Labor Reis et al.962

(urethral catheter� OR urinary catheter� OR bladder drainageOR transurethral catheter�).
In addition, a secondary search was conducted on thereference list of included articles to identify other possiblerelevant studies.
The keywords used were based on the Patient, Interven-tion, Comparison, and Outcome (PICO) strategy, focusing onwomen in labor with neuroaxis analgesia (participants) whoneeded bladder emptying (intervention), with a comparisonbetween permanent and intermittent catheterization (com-parison) to assess duration labor, type of delivery, and rate ofcesarean sections (outcomes).
All identified references through database and referencescreening (identification) were exported to the Rayyan QCRItool (Rayyan Systems Inc., Cambridge, MA, USA), and dupli-cate results were removed. Initially, articles were selected bytitle and abstract (screening). Subsequently, the full text ofthe selected articles was analyzed for eligibility (eligibility),and all relevant studies were included in the systematicreview. All steps were performed individually by two inde-pendent reviewers, and disagreements were resolved byconsensus. The same authors were responsible for extractingdata from the articles included in the review. Data related tostudy identification, study design, demographic data, follow-up time, intervention, and data related to childbirth andpostpartum were extracted.
Two reviewers used the Cochrane tool to analyze the riskof bias in randomized trials (RoB2).
Data extracted by both researchers were inputted in theRevMan software, version 5.3 (The Cochrane Collaboration,London, UK). Heterogeneity was assessed from a methodo-logical (methodology of the studies), clinical (clinical char-acteristics of the sample), and statistical (calculation of theI2value) perspective. Given the methodological and clinicalheterogeneity of the studies, the random-effects meta-anal-ysis model (REMA) was used to calculate the meta-analyticalmeasures. The decision of whether to report the meta-analysis or not was made depending on the value of I2.
Results
The survey returned a total of 964 studies. After removingduplicate records, 719 studies were evaluated by title andabstract, of which 4were selected for full-text reading. Sevenhundred and fifteen studies were excluded because of studydesign (they were not randomized controlled trials), partici-pant selection (they did not evaluate women in labor),variables analysis (they did not compare continuous versusintermittent catheterization), focus/language of the study(they did not focus on the effects on labor or were written inlanguages other than Portuguese, English, French, Spanish, orItalian). All full texts assessed for eligibility were selected forinclusion. The selection process is outlined in ►Fig. 1.
The description of the articles is summarized in ►Fig. 2.The analysis of methodological quality of the included stud-ies was generally good but revealed some weaknesses. Theanalysis performed with the RoB2 tool is summarizedin ►Fig. 2.
To calculate the meta-analytical measure of the durationof the 2nd stage of labor, 2 studies were included (Evronet al., 2008, and Suleiman et al., 2017).4,7 One of the works(Rivard et al., 2012)6 was not included because it did notspecify the duration of the 2nd stage, and the other because itdid not present the standard deviation for the reported laborduration averages (Wilson et al., 2015).8 Heterogeneity washigh (I2¼85%) and, in this sense, the meta-analytical mea-sure for this outcome was not reported. The duration of thefirst stage of labor was not evaluated due to the omission ofthese data by most authors.
Eutocic Delivery
In assessing the likelihood of eutocic delivery, three studieswere included. Only Wilson et al. (2015)8 did not differenti-ate eutocic deliveries from operative vaginal deliveries. Inthis outcome, heterogeneity was low I2¼0. The meta-ana-lytical measure favored continuous catheterization (OR¼1.56 [1.04, 2.34]; p¼0.03). The forest plot of this outcomeis shown in ►Fig. 3.
No differenceswere found in the number of instrumenteddeliveries between intermittent and continuous catheteri-zation (OR¼0.69 [0.33, 1.43]; p¼0.32), as shown in ►Fig. 4.
No differences were found in cesarean section rate be-tween interventions. In this outcome, the results of the 4studies were include in the meta-analysis. Heterogeneitywas moderate I2¼59%. The meta-analytical measure foundno differences between catheterization methods (OR¼1.25[0.63, 2.50]; p¼0.06). The forest plot is representedin ►Fig. 5 (►Table 1).
Discussion
The purpose of the present review was to assess differencesin outcomes related to childbirth between the options avail-able to prevent urinary retention. After evaluating the exist-ing studies and their limitations, the results seem to suggestthat both options may be valid.
The risk of bias is globally low. In all studies, randomiza-tionwas valid, and the allocationwas concealedwith opaqueenvelopes. Although the groups were different in one of thestudies (Evron et al., 2008),4 the randomization method wasclear, and the differences between groups were described,making it clear that it was random.
There was only one study that changed the initial inter-vention plan. In this study, at the end of the 2nd need forcatheter emptying, the pregnant woman was permanentlycuffed, and this happened in 14 of the 55 pregnant womenallocated to the intermittent catheterization arm (Wilsonet al., 2015).8
There is no suggestion of missing data in relation to thestudied outcomes.
Heterogeneity was high (I2¼85%), and, as such, it was notconsidered appropriate to report the meta-analytical mea-sure as statistical heterogeneity would make its interpreta-tion unfeasible. Sensitivity analysis not possible either asonly 2 studies were included in the outcome analysis.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Intermittent vs Continuous Catheterization and Differences in the Evolution of Labor Reis et al. 963

Wilson et al. (2015)8 and Suleiman et al. (2017)7 found nodifferences in the duration of the 2nd stage of labor, as didRivard et al. (2012)6 in the duration of labor (the latter notspecifying the criteria used to start the time counting in laboror differentiating the time of the second stage of labor)between the catheterization types. However, Evron et al.(2008)4 reported a longer duration of the second stage oflabor in the group with permanent catheterization. In thisgroup, there was also a greater need to use anesthetics, andlower mobility, according to the Bromage scale. One possibleexplanation is related to the fact that the women in thisgroup had a higher body mass index (BMI), which impliesthat they needed a greater amount of anesthetic and, conse-quently, had a greater degree of motor block. Moreover, the
Fig. 1 PRISMA flow diagram of the selection process.
Fig. 2 Summary of the risk of bias analysis of the studies included inthe review.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Intermittent vs Continuous Catheterization and Differences in the Evolution of Labor Reis et al.964

management of the 2nd phase of labor can have a culturalinfluence, conditioning the obtained data.
Evronet al. (2008),4Rivard et al. (2012),6 andSuleimanet al.(2017)7 foundnodifferences in the type ofdeliveryandWilsonet al. (2015)8 did not differentiate operative vaginal deliveriesfrom eutocic deliveries between catheterization types.
The fact that there were more eutocic deliveries in thegroup of women with intermittent catheterization suggeststhat in scenarios in which this type of methodology ispossible, it should be instituted. However, the preferenceof users and professionals, which must be an importantfactor in the decision, and the limited human resourcesexisting in many delivery rooms can be an obstacle to theirimplementation.
None of the authors reported differences in cesareansection rates, with the exception of except Wilson et al.(2015),8 who, in their work, described a lower rate of
cesarean section in the group with intermittent catheteriza-tion. However, they present no explanation for this finding(although the group size could help to explain). Consideringall studies, the type of catheterization does not seem toinfluence the rate of cesarean sections.
In the present review, risks of infectionwere not assessed.Only one study evaluated the preference of professionals,which is a factor that can affect the practices in the deliveryrooms.
None of the included studies analyzed the women’spreference for any of the methods, which would be animportant factor in decision-making considering the lackof clear advantages of either approach.
Despite the use of four databases considered to be refer-ence in the scientific area of obstetrics, whose scope is high,the use of additional databases could lead to the inclusion ofmore studies.
Fig. 4 Forest plot of the comparison regarding the occurrence of instrumented delivery in women with intermittent and continuouscatheterization.
Fig. 3 Forest plot of the comparison regarding the occurrence of eutocic delivery in women with intermittent and continuous catheterization.
Fig. 5 Forest plot of the comparison regarding the occurrence of cesarean section in women with intermittent and continuous catheterization.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Intermittent vs Continuous Catheterization and Differences in the Evolution of Labor Reis et al. 965

Table
1Su
mmarytableof
theinclud
edstud
iesin
thereview
withmainfind
ings
Author,Ye
arSa
mplech
arac
teriza
tion
Interven
tion
protoc
ol
Rated
outco
mes
Resu
lts
Evron,
2008
(Evron
etal.,20
08)4
n¼20
9(IC10
9;CC10
0)IC
group
:25�4years;
164�6cm
;74
�11
kg;4
0�2wee
ks;3
�1cm
whe
nep
idural;1
05�19
6minuteof
mem
bran
erupture;
55%withox
ytoc
icacceleration;
newbo
rnswith3,14
0�45
0gr
CCgrou
p:26
�4years;
164�6cm
;78
�13
kg;4
0�2wee
ks;3
�1cm
whe
nep
idural;1
05�20
3minutes
ofmem
bran
erupture;
67%withox
ytoc
icacceleration;
newbo
rnswith3,12
9�46
0gr
ICgroup
:clin
ical
evalua
tionforthe
diag
nosisof
urinaryretentionev
ery
90minutes;ifurinaryretentionis
suspec
ted-a
ttem
pted
spon
tane
ousurinationan
dblad
der
emptying
ifne
cessary
CCgroup
:catheterizationafter
neuroa
xisan
alge
sia
Prim
aryou
tcom
es:2
ndstag
eof
labo
rleng
th;an
esthetic
dose
Seco
ndaryou
tcom
es:
postpartum
urinaryretention;
postpartum
urinaryinfection
2ndstag
eof
labo
rlong
erin
the
CCgrou
p(105
�72
minute,)
compa
redwiththeIC
group
(75�52
minute).
Greater
useof
anesthetic
inthe
CCgroup
inthefirstan
dseco
ndstag
esof
labo
r.Be
tter
mob
ility
acco
rdingto
the
Brom
agescalein
theIC
group
Rivard,20
12(Rivardet
al.,20
12)6
n¼13
8(IC66
;CC72
)IC
group
:28
.7years;
2prev
ious
preg
nanc
ies,
38wee
ksan
d2da
ys,6
0%sp
ontane
ous
deliveries
CCgroup
:27.6years;2prev
ious
preg
nanc
ies,
38wee
ksan
d2da
ys,5
0%sp
ontane
ous
deliveries
After
determ
iningthene
edfor
blad
derem
ptying
ICgrou
p:Blad
derem
ptying
bycatheter
every2–
4ho
urs
CCgroup
:catheterizationun
til
expu
lsionpe
riod
Prim
aryou
tcom
e:timeinterval
untild
elivery
Seco
ndaryou
tcom
es:n
ursing
team
preferen
ce;c
osts;d
elivery
mod
e
Nosign
ificant
differen
cesin
duration
oflabor
orco
st.
Nursing
team
preferen
cefor
continuo
uscatheterization
Wilson
,20
15(W
ilson
etal.,20
15)8
n¼12
3(IC68
;CC55
)IC
group
:26.16
�4.76
years;
39.74�1.06
wee
ks;4
.69�1.33
cmwith91
.41%
whe
nep
idural;3
0.99
%of
indu
cedbirths
;43
.66%
withox
ytoc
icacceleration
;ne
wbo
rnswith
3,44
5�45
3.73
grCCgrou
p:25
.87�4.66
years;
39.77�1.22
wee
ks;4
.52�1.35
cmwith88
.23%
whe
nep
idural;3
4.62
%of
indu
cedbirths
;46
.15%
withox
ytoc
icacceleration
;ne
wbo
rnswith
3,48
6�44
5.08
gr
ICgrou
p:pe
riod
icev
alua
tion
(maxim
umof
6in
6ho
urs)
and
attempted
spon
tane
ous
urination
andinterm
ittent
blad
derem
ptying
whe
neve
rthisisno
tpo
ssible
(con
tinu
oustube
placem
enta
fter
2catheterizations
)CCgroup
:catheterizationafter
neuraxiala
nalgesia
Outco
mes
Durationof
the2n
dstag
eof
labo
r,incide
nceof
UTI
Nodifferen
cesrega
rdingthe
duration
ofthe2n
dstag
eof
labo
r.Highe
rrate
ofce
sarean
sections
intheCCgroup
Suleim
an,20
17(Suleiman
etal.,20
17)7
n¼18
4(IC¼
94;CC¼90
)IC
grou
p:27
.9�4.5years;BM
I23.9�4.9Kg
/m2;
39.3
�1.3wee
ks;3.4�1.1cm
whe
nep
idural;5
8.5%
ofindu
cedbirths
;ne
wbo
rns
with33
10.2
�42
3.1gr
CCgroup
:27.0�4.6years;BM
I23.8�4.9Kg
/m2;
39.5
�1.3wee
ks;3
.3�1.2cm
whe
nep
idural;6
0%of
indu
cedbirths
;ne
wbo
rns
with3,26
4.7�44
2.2gr
After
epidural
andinab
ility
tosp
ontane
ouslyurinate
ICgrou
p:ev
alua
tionev
ery2ho
urs
orwhe
nne
cessarywithblad
der
emptying
ifun
able
tourinateor
incase
ofurinaryretention
CCgrou
p:catheterizationup
tothe
2ndstag
eof
labo
r
Prim
aryou
tcom
e:Durationof
the2n
dstag
eof
labor
Seco
ndaryou
tcom
es:t
ypeof
delivery,
durationof
the3rd
stag
eof
labo
r,po
stpa
rtum
hemorrha
ge,u
rina
ryretention,
bacteriuria,
Apga
rscore,
umbilic
alartery
pH
Nodifferen
cesforinclud
edou
tcom
es.
Abbrev
iation
s:BM
I,bo
dymassinde
x;CC,co
ntinuo
uscatheterization;
IC,interm
ittent
catheterization;
UTI,urinarytrac
tinfection.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Intermittent vs Continuous Catheterization and Differences in the Evolution of Labor Reis et al.966

Conclusion
Neuraxial analgesia is associated with a higher urinaryretention rate, in some cases, leading to the need for bladderemptying. Urinary retention can produce a mass effect andhinder the descent of the fetal presentation. Catheterizationduring labor after neuraxial analgesia is not a consensualpractice in delivery rooms, and current clinical recommen-dations do not favor any of the catheterization types (Ameri-can Society of Anesthesiologists, 2015).2 The preference andavailability of professionals, as well as the preference and theexpectation of the parturient, must be considered whendeciding whether to carry out the catheterization intermit-tently or continuously. After reviewing the literature andcritically evaluating the four studies performed on the topic,we concluded that there is no clear advantage to eithermethod. However, due to the sample size and the identifiedbias, the results must be interpreted carefully. Thus, duringlabor and in low-risk women under neuraxial analgesia, bothcontinuous catheterization and emptying seem to be validoptions, although continuous catheterizationwas associatedwith a greater occurrence of eutocic births. In the remainingoutcomes, there were no differences between catheteriza-tion types.
ContributorsAll authors participated in the concept and design of thestudy, as well as in the analysis and interpretation of data,and draft or revision of the manuscript; they have alsoapproved the manuscript as submitted. All authors areresponsible for the research.
Conflict of InterestsThe authors have no conflict of interests to declare.
References1 American College of Obstetricians and Gynecologists’ Committee
on Practice Bulletins—Obstetrics. ACOG Practice Bulletin No. 209:obstetric analgesia and anesthesia. Obstet Gynecol. 2019;133(03):e208–e225. Doi: 10.1097/AOG.0000000000003132
2 American Society of Anesthesiologists. Practice Guidelines forObstetric Anesthesia: An Updated Report by the American Societyof Anesthesiologists Task Force on Obstetric Anesthesia and theSociety for Obstetric Anesthesia and Perinatology. Anesthesiology.2016;124(02):270–300. Doi: 10.1097/ALN.0000000000000935
3 Cunningham FG, Leveno KJ, Bloom SL, Spong CY, Dashe JS, Hoff-man BL, et al. Williams obstetrics. 24th ed. New York: McGrawHill; 2014
4 Evron S, Dimitrochenko V, Khazin V, Sherman A, Sadan O, BoazM,et al. The effect of intermittent versus continuous bladder cathe-terization on labor duration and postpartum urinary retentionand infection: a randomized trial. J Clin Anesth. 2008;20(08):567–572. Doi: 10.1016/j.jclinane.2008.06.009
5 Petitprez K, Guillaume S, Mattuizzi A, Arnal M, Artzner F, BernardC, et al. Accouchement normal : accompagnement de la physi-ologie et interventions médicales. Recommandations de la HauteAutorité de Santé (HAS) avec la collaboration du Collège Nationaldes Gynécologues Obstétriciens Français (CNGOF) et du CollègeNational des Sages-Femmes de France (CNSF) – Texte des recom-mandations (texte court). Gynécol Obstét Fertil Sénol. 2020;48(12):873–882. Doi: 10.1016/j.gofs.2020.09.013
6 Rivard C, AwadM, LiebermannM, DeJongM, Massey SM, SinacoreJ, et al. Bladder drainage during labor: a randomized controlledtrial. J Obstet Gynaecol Res. 2012;38(08):1046–1051. Doi:10.1111/j.1447-0756.2011.01837.x
7 Suleiman A,Mruwat-Rabah S, Garmi G, Dagilayske D, Zelichover T,Salim R. Effect of intermittent versus continuous bladder cathe-terization on duration of the second stage of labor amongnulliparous women with an epidural: a randomized controlledtrial. Int Urogynecol J Pelvic Floor Dysfunct. 2018;29(05):691–696. Doi: 10.1007/s00192-017-3357-9
8 Wilson BL, Passante T, Rauschenbach D, Yang R, Wong B. Bladdermanagement with epidural anesthesia during labor: a random-ized controlled trial. MCN Am J Matern Child Nurs. 2015;40(04):234–242, quiz E17–E18. Doi: 10.1097/NMC.0000000000000156
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Intermittent vs Continuous Catheterization and Differences in the Evolution of Labor Reis et al. 967
The Effect of Aromatherapy Alone or inCombination with Massage on Dysmenorrhea: ASystematic Review and Meta-analysis
O efeito da aromaterapia sozinha ou em combinaçãocom massagem na dismenorreia: Uma revisãosistemática e meta-análiseMona Najaf Najafi1 Neshat Najaf Najafi2 Farzaneh Rashidi Fakari3 Somayeh Moeindarbary4
Fatemeh Abdi5 Zeinab Sadat Hoseini6 Masumeh Ghazanfarpour7
1Clinical Research Development Unit, Mashhad University of MedicalSciences, Imam Reza Hospital, Mashhad, Iran
2Clinical Research Development Unit, Mashhad University of MedicalSciences, Imam Reza Hospital, Mashhad, Iran
3Department of Midwifery and Reproductive Health, School of Medicine,North Khorasan University of Medical Sciences, Bojnurd, Iran
4Department of Obstetrics and Gynecology, Neonatal and MaternalResearch Center, Mashhad University of Medical Sciences, Mashhad, Iran
5School of Nursing and Midwifery, Alborz University of MedicalSciences, Karaj, Iran
6Faculty of Medicine, Islamic Azad University of Mashhad, Mashhad,Iran
7Student Research Committee, Kerman University of MedicalSciences, Kerman, Iran
Rev Bras Ginecol Obstet 2021;43(12):968–979.
Address for correspondence Masumeh Ghazanfarpour, PhD,Kerman, Kerman Province, Iran(e-mail: [email protected]).
Keywords
► dysmenorrhea► herbal medicine► aroma oil► aromatherapy
Abstract Objective The aim of the present systematic review meta-analysis is to assess theeffect of olfactory stimulation on reducing dysmenorrhea.Methods Systematic search was conducted in several databases, such as PubMed,Web of Science, Cochrane, and Scopus, to identify relevant research up to October 26,2019. The identified studies were evaluated based on a modified Jadad scale. Theintervention involves aromatherapy alone or in combination with essential oils. Therewas no restriction for the control group such as a placebo group or other commontreatments. The Comprehensive Meta-Analysis Version 2 (Bio stat, Englewood, NJ, USA)was used for meta-analysis. Cochran’s Q and I2 tests were utilized.Results The findings of ourmeta-analysis, which contained 13 trials (15 data), showedthat dysmenorrhea decreased significantly in the group receiving aromatherapy withherbal compared with the control group (standardized mean difference [SMD]¼ -0.795; 95% confidence interval [CI]: -0.922 to- 0.667; 17 trials O<0.001); heterogene-ity; I2¼19.47%; p¼ 0.236). In addition, four studies with insufficient data were not
receivedDecember 5, 2020acceptedSeptember 3, 2021
DOI https://doi.org/10.1055/s-0041-1740210.ISSN 0100-7203.
© 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rightsreserved.This is an open access article published by Thieme under the terms of the
Creative Commons Attribution License, permitting unrestricted use,
distribution, and reproduction so long as the original work is properly cited.
(https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda., Rua do Matoso 170, Rio deJaneiro, RJ, CEP 20270-135, Brazil
Review ArticleTHIEME
968

Introduction
Menstrual pain, a common complaint expressed by � 25 to97% of women, can influence the quality of life in wom-en.1,2 Dysmenorrhea refers to painful menstruation asso-ciated with several adverse effects, including nausea andvomiting, back pain, fatigue, and abdominal cramps.3 Theseverest pain is experienced in the first day of menstrua-tion, and it takes a downward turn in the remaining days.Moreover, the pelvic pain associated with menstrual cycleis caused by the secondary dysmenorrhea coupled withpelvic discomforts, which is common during reproductiveage and ovulation. Dysmenorrhea is reported to be themost prevalent cause of absenteeism in female studentsand employees.4
The incidence of dysmenorrhea is reported to be between28 and 71.7%, but these figures vary worldwide.5
The primary causes of dysmenorrhea are uterine con-traction, vasoconstriction, inflammation, and the releaseof inflammatory mediators. Diminished progesterone lev-el in the late luteal phase leads to the activation ofcyclooxygenase and the biosynthesis of prostaglandin.Elevated prostaglandin production increases uterinetone and contractions, followed by dysmenorrhea.6 It
has been shown that dysmenorrhea is a major diseaseaffecting physical, social, and psychological parametersincluding social, emotional, and mental health.7 Dysme-norrhea may interfere with sports activities, disruptcommunication with family and friends, and lower thequality of life.8,9
Drug therapy is commonly used for the management ofdysmenorrhea, especially anti-inflammatory agents, and isthe first line in the treatment of primary dysmenorrhea.Nevertheless, these drugs present documented unwantedcomplications, including drowsiness, headache and dyspep-sia,10 nausea, vomiting, rashes, nervous disorders, emotion-al disturbances, bleeding tendency, metabolic disorders,and many more, including cancers and death.11 Anothertherapeutic regimen for dysmenorrhea involves the use ofhormonal agents, such as oral contraceptive.12 By reducingprostaglandins, these agents have a soothing effect ondysmenorrhea. Also, hormonal therapy is recommendedwhen treatment with non-steroidal antiinflammatorydrugs is ineffective or when contraceptive methods arepreferred.13 Despite the effect of these agents on painreduction, irregular bleeding is a major factor that provokeswomen’s dissatisfaction with hormonal treatment.14 Otherside effects of this therapy include headache, nausea, mood
included in our meta-analysis. The results of all studies suggested that aromatherapywith herbal medicine group compared with control group is effective.Conclusion Aromatherapy with herbal medicine decreased dysmenorrhea. Thistreatment was particularly effective when aroma oil was combined with massage orwhen a mixture of aroma oil was used for the treatment of dysmenorrhea.
Resumo Objetivo O objetivo desta revisão sistemática-metanálise é avaliar o efeito daestimulação olfatória na redução da dismenorreia.Métodos Pesquisa sistemática foi realizada em várias bases de dados, como PubMed,Web of Science, Cochrane e Scopus para identificar pesquisas relevantes até 26 deoutubro de 2019. Os estudos identificados foram avaliados com base em uma escala deJadadmodificada. A intervenção envolve aromaterapia sozinha ou em combinação comóleos essenciais. Não houve restrição para o grupo de controle, como um grupo deplacebo ou outros tratamentos comuns. O Comprehensive Meta-Analysis Version 2 (Biostat, Englewood, NJ, EUA) foi usado para meta-análise. Os testes Q e I2 de Cochranforam utilizados.Resultados Os resultados da nossa meta-análise, que continha 13 ensaios (15 dados),mostraram que a dismenorreia diminuiu significativamente no grupo que recebeuaromaterapia com ervas em comparação com o grupo de controle (diferença médiapadronizada [DMP]¼ -0,795; intervalo de confiança [IC] de 95%: -0,922 a- 0,667; 17ensaios O<0,001); heterogeneidade; I2¼19,47%; p¼0,236). Além disso, quatroestudos com dados insuficientes não foram incluídos em nossa meta-análise. Osresultados de todos os estudos sugeriram que a aromaterapia com o grupo defitoterápicos em comparação com o grupo de controle é eficaz.Conclusão A aromaterapia com fitoterapia diminuiu a dismenorreia. Este tratamentofoi particularmente eficaz quando o óleo aromático foi combinado com massagem ouquando uma mistura de óleo aromático foi usada para o tratamento da dismenorreia.
Palavras-chave
► dismenorreia► fitoterapia► óleo de aroma► aromaterapia
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
The Effect of Aromatherapy with Massage on Dysmenorrhea Najaf Najafi et al. 969

changes, and weight gain.13 Medicinal plants have receivedgrowing attention for the attenuation of dysmenorrhea,particularly due to the reluctance of young women tohormonal drug administration, the complications of chem-ical medications, and the high cost of raw materials.15
However, most of these treatments cannot be administeredby nurses, and routine drugs exhibit adverse effects orproduce short-term effects.16 Despite the effectives of thesedrugs in alleviating premenstrual syndrome, women be-lieve that these symptoms can be managed without usingany drug or prefer using traditional and alternative techni-ques.17 There are various complementary and alternativemedicine (CAM) methods used for menstrual pain relief,such as behavioral interventions, acupuncture, herbal med-icine, transcutaneous electrical nerve stimulation (TENS),omega-3 fatty acids, vitamin pills,18 and aromatherapy. As asafe therapeutic technique, aromatherapy relies on plant-based essential oils (Buckle, 2001),19 including melissa,lavender, and eucalyptus.
Many clinical studies assessed the effect of aromather-apy on dysmenorrhea. Three studies showed a significantreduction of pain in patients receiving rose essential oil incomparison with a control group.3,20,21 Studies showedthat lavender was effective both as monotherapy10,15,22
and in combination with another oil.23–26 Peppermint,27
rosemary,22 and geranium essential oils28 have shown tobe effective in clinical studies. Pervious meta-analyseshave illustrated the effectiveness of aromatherapy as acomplementary method in reducing dysmenorrhea.29,30
According to the results of a meta-analysis, the use ofessential oil in combination with massage was moreeffective than the control group. However, the study didnot clarify whether a mixture of aroma oils or a single oilproduced greater efficacy. Recently, new trials with a well-designed methodology have been published; therefore, itis necessary to update the meta-analysis. The aim of thepresent systematic review and meta-analysis is to assessthe effect of olfactory stimulation in the treatment ofdysmenorrhea.
Methods
A comprehensive systematic search without any languagerestriction was conducted in several databases such asPubMed, Web of Science, Cochrane, and Scopus using thefollwing keywords: (dysmenorrhea) OR (menstrual cramp)OR (menstrual pain�) OR (pain�, menstrual) OR (painfulmenstruation�) OR (menstruation�, painful)) AND (aroma-therapy) OR (Aroma�) OR (aromatic therapy) OR (fragrance)OR (fragrant oil�) OR (scent) OR (massage therapy) OR (medi-cal massage) OR (massage). The relevant studies were inves-tigated up to October 26, 2019. All terms were searched inthe title, abstract, and key words of the articles. In addition,the bibliography of the selected articles was manuallysearched to identify other relevant studies missed in theelectronic search. Gray literature was not included in thepresent review.
We examined clinical trials on girls and women of child-bearing age (18–45 years old) who experienced menstrualpain. The intervention had to involve aromatherapy alone orcombined with essential oils in the form of inhalation ormassage. There was no restriction regarding the controlgroup; therefore, no treatment, a placebo group, or othercommon treatments for dysmenorrheawere considered. Theseverity of pain should be assessed by a valid self-reportedinstrument, such as a numerical rating scale (NRS) or visualanalog scale (VAS).
The databases were searched by two independentresearchers, and duplicate papers or papers that did notmeet the inclusion criteria were excluded. The selectionprocess is shown in ►Fig. 1. Observational studies,reviews, letter to the editor and case reports were exclud-ed. Additionally, publications written in a languageother than English were also excluded. Three Englishabstracts (full texts were available in Farsi) wereexplored.20,21,23,28,31–48
Two authors assessed the quality of the selected studiesaccording to the Modified Jadad Scale for Randomized Con-trolled Trials. This assessment tool comprises eight specificitems, including a description of randomization, appropriaterandomization method, blinding description, appropriateblinding method, description of withdrawals and dropouts,description of inclusion and exclusion criteria, description ofadverse effects, assessment method, and the description ofstatistical analysis. The scores range from 0 to 8, with higherscores indicating a higher quality. A score below 4 indicateslow quality.
The data was extracted by two researchers. Any disagree-ments were settled through consensus and arbitration of athird person.
The selected studies were reviewed, and the followingdata was extracted by two authors: first author’s name, yearof study, place of study, type of study design, participants, theage of participants, intervention and control groups, thenumber of participants in the intervention andcontrol/placebo groups, duration of study, sample dropoutrate (%), measurement method, minimal primary dysmenor-rhea for inclusion in the study, and the primary outcome. Theprimary outcome was pain, which was measured by VASscore, numerical rating scales, or other validatedinstruments.
In the present study, the Comprehensive Meta-AnalysisVersion 2 software (Bio stat, Englewood, NJ, USA) was usedfor the meta-analysis. We used Cochran’s Q and I2 tests toevaluate heterogeneity and homogeneity, respectively. If thetest result of Cochran’s Q was p<0.05, the heterogeneity ofstudies was confirmed. Moreover, I2 values of 25%, 50%, or75% exhibited low, moderate, or high heterogeneity, respec-tively. If heterogeneity was confirmed, we used the randomeffects model for the analysis. To present treatment effects,we used a forest plot that demonstrated the effect size, and aconfidence interval of 95%. The Begg rank correlation and theEgger intercept tests were employed to evaluate publicationbias. We examined a funnel plot for checking publication
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
The Effect of Aromatherapy with Massage on Dysmenorrhea Najaf Najafi et al.970
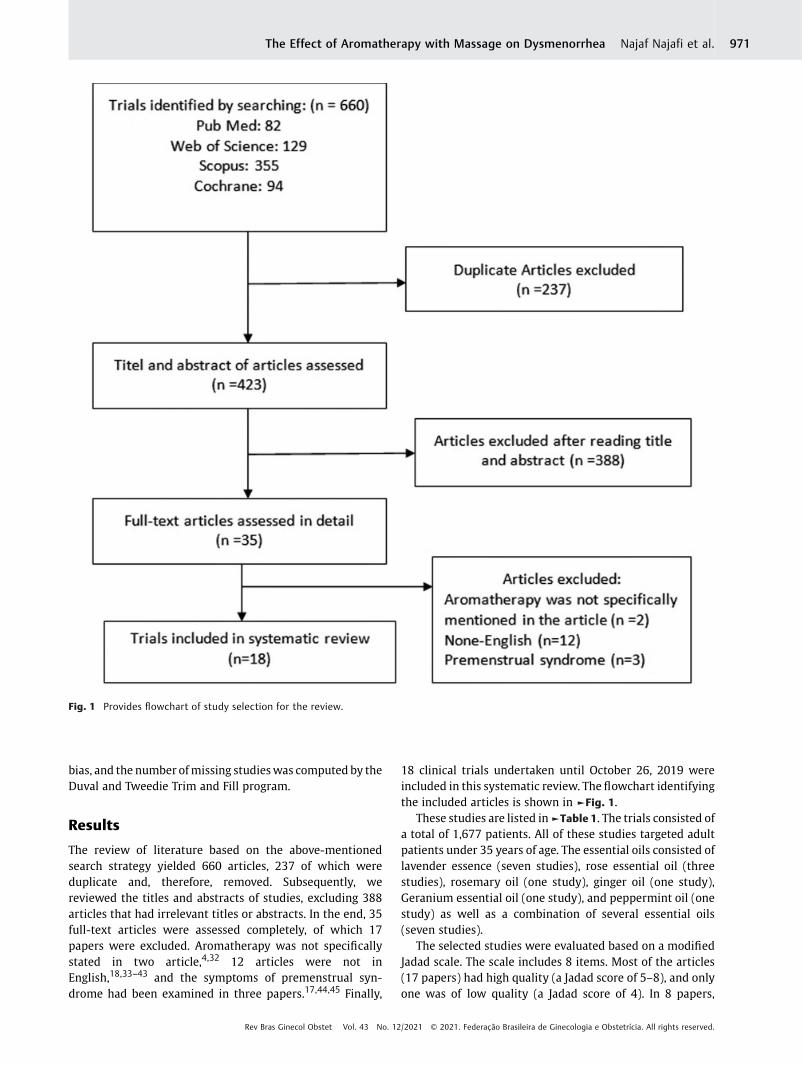
bias, and the number ofmissing studieswas computed by theDuval and Tweedie Trim and Fill program.
Results
The review of literature based on the above-mentionedsearch strategy yielded 660 articles, 237 of which wereduplicate and, therefore, removed. Subsequently, wereviewed the titles and abstracts of studies, excluding 388articles that had irrelevant titles or abstracts. In the end, 35full-text articles were assessed completely, of which 17papers were excluded. Aromatherapy was not specificallystated in two article,4,32 12 articles were not inEnglish,18,33–43 and the symptoms of premenstrual syn-drome had been examined in three papers.17,44,45 Finally,
18 clinical trials undertaken until October 26, 2019 wereincluded in this systematic review. The flowchart identifyingthe included articles is shown in ►Fig. 1.
These studies are listed in►Table 1. The trials consisted ofa total of 1,677 patients. All of these studies targeted adultpatients under 35 years of age. The essential oils consisted oflavender essence (seven studies), rose essential oil (threestudies), rosemary oil (one study), ginger oil (one study),Geranium essential oil (one study), and peppermint oil (onestudy) as well as a combination of several essential oils(seven studies).
The selected studies were evaluated based on a modifiedJadad scale. The scale includes 8 items. Most of the articles(17 papers) had high quality (a Jadad score of 5–8), and onlyone was of low quality (a Jadad score of 4). In 8 papers,
Fig. 1 Provides flowchart of study selection for the review.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
The Effect of Aromatherapy with Massage on Dysmenorrhea Najaf Najafi et al. 971

suitable randomization methods were described, andpatients were blind to the randomization in 14 studies.The rate of withdrawals and dropouts had been reportedin all studies, whereas the assessment of adverse effects wasonly discussed in 11 articles. The statistical methods andinclusion criteria were adequately described in all RCTs. Thequality assessment of the selected articles is depictedin ►Table 1. A comprehensive list of the selected studies’characteristics is outlined in ►Table 2.
The standardized mean difference (SMD) of dysmenor-rhea change was -0.904 (95% confidence interval CI: -1.023to- 0.786;16 trials, p<0.001) (►Fig. 2). However, the het-erogeneity of the included studies was moderate(I2¼60.43%) and significant (p¼0.003). To detect the poten-tial source of this heterogeneity, sensitivity analyseswere performed, with the results indicating that heteroge-neity was mainly caused by inclusion of Nikjou et al.’s48
study. The removal of this study caused a slight decreasein (SMD¼ -0.795; 95% CI: -0.922 to- 0.667; 15 trials), but the
heterogeneity reached acceptable level (p¼0.236; I2¼19%)(►Fig. 3). The results of ourmeta-analysis of 15 trials showedthat dysmenorrhea dropped significantly in the group ofaromatherapy with herbal medicine compared with theplacebo. The subgroup involved the type of treatment (acombination of aromaoils versus a single type of oil, and botharoma and massage versus aroma alone). The results of theanalysis of the lavender subgroup indicate higher effective-ness in the intervention than in the control group (p<0.001)(►Table 3). The results of subgroup analysis revealed thatpatients receiving a combination ofmassageþ aromatherapyreported greater pain relief than those receiving aromather-apy alone (p<0.001). The two groups were not significantlydifferent in the subgroup analysis comparing a mixture ofaroma oils and a single oil (p¼0.34).
Four studies with insufficient data were not included inour meta-analysis. The results of three studies1,16,27 arepresented as medians and interquartile ranges, and onestudy as graded severity of dysmenorrhea (mild, moderate,
Table 1 The quality assessment of the selected articles
Registration code Randomizationmention
Randomsequencegeneration
Blinding ofparticipantsandpersonnel
Blinding ofoutcomeassessment
Description ofwithdrawalsand dropouts
Cleardescriptionof theinclusionand exclusioncriteria
Descriptionof the methodused to assessadverse effects
The methodof statisticalanalysis
Totalscore
Apay et al.(2012)22
� 1 0 1 0 1 1 1 1 6
Amiri Farahaniet al. (2012)24
IRCT138902153869N13869 1 0 1 0 1 1 1 1 6
Ataollahi et al.(2015)21
IRCT201311216807N10 1 1 1 1 1 1 1 1 8
Azima et al.(2015)10
IRCT2013022611945N2 1 1 0 1 1 1 0 1 6
Bakhtshirinet al. (2015)15
� 1 0 1 1 1 1 0 1 6
Beiranvandet al. (2015)31
IRCT201310297697N2 1 1 1 1 1 1 0 1 7
Davari et al.(2014)23
� 1 0 1 1 1 1 1 1 7
Raisi Dehkordiet al. (2014)47
IRCT201105086412N1 1 1 1 1 1 1 1 1 8
Kim et al.(2011)18
� 0 0 0 0 1 1 1 1 4
Marzouk et al.(2013)25
� 1 1 1 1 1 1 1 1 8
Ou et al. (2012)26 � 1 1 1 1 1 1 0 1 7
Uysal et al.(2016)3
� 1 1 0 0 1 1 0 1 5
Hur et al. (2012)1 � 0 0 0 0 1 1 1 1 4
Nikjou et al.(2016)48
IRCT201470616252N2 1 1 1 1 1 1 1 1 8
Rizk (2013)27 � 1 0 1 0 1 1 0 1 5
Sadeghi Aval Shahret al. (2015)20
� 1 0 1 0 1 1 1 1 6
Sajjadi et al.(2018)28
IRCT2017013132329N1 1 0 1 1 1 1 0 1 6
Han et al.(2006)16
� 1 0 1 0 1 1 1 1 6
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
The Effect of Aromatherapy with Massage on Dysmenorrhea Najaf Najafi et al.972
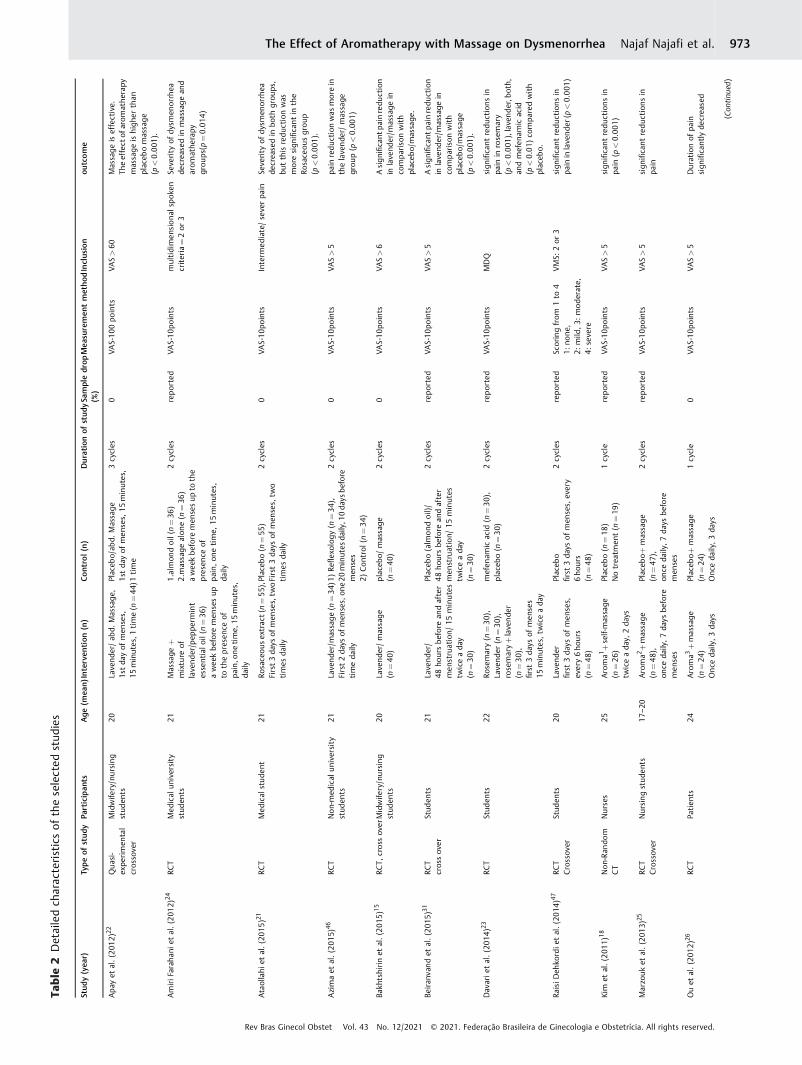
Table
2Detailedch
arac
teristicsof
theselected
stud
ies
Stud
y(yea
r)Typeof
study
Participan
tsAge
(mea
n)Interven
tion
(n)
Control(n)
Duration
ofstudy
Sampledrop
(%)
Mea
suremen
tmethod
Inclus
ion
outcome
Apay
etal.(201
2)22
Qua
si-
expe
rimen
tal
cros
sove
r
Midwife
ry/nursing
stud
ents
20Lavend
er/ab
d.Massage,
1stda
yof
men
ses,
15minutes,1
time(n
¼44
)Placeb
o/ab
d.Massage
1stda
yof
men
ses,
15minutes,
1time
3cycles
0VA
S-100
points
VAS>60
Massageiseffective.
Theeffect
ofarom
athe
rapy
massageishighe
rthan
placeb
omassage
(p<0.00
1).
AmiriFarah
anie
tal.(201
2)24
RCT
Med
ical
university
stud
ents
21Massage
þmixture
oflavend
er/pep
perm
int
essentialo
il(n
¼36
)awee
kbe
fore
men
sesup
tothepresen
ceof
pain,o
netime,
15minutes,
daily
1.almon
doil(n¼36
)2.massagealon
e(n
¼36
)awee
kbe
fore
men
sesup
tothe
presen
ceof
pain,on
etime,
15minutes,
daily
2cycles
repo
rted
VAS-10p
oints
multidimen
siona
lspok
encriteria¼2or
3Se
verity
ofdy
smen
orrhea
decrea
sedin
massagean
darom
athe
rapy
grou
ps(p
¼0.01
4)
Ataollahi
etal.(20
15)21
RCT
Med
ical
stud
ent
21Ro
sace
ous
extrac
t(n¼55
),First3da
ysof
men
ses,tw
otimes
daily
Placeb
o(n
¼55
)First3da
ysof
men
ses,
two
times
daily
2cycles
0VA
S-10p
oints
Interm
ediate/severpa
inSe
verity
ofdy
smen
orrhea
decrea
sedin
both
grou
ps,
butthisredu
ctionwas
moresign
ificant
inthe
Rosace
ousgroup
(p<0.00
1).
Azimaet
al.(201
5)46
RCT
Non-med
ical
university
stud
ents
21Lavend
er/m
assage(n
¼34
)First2da
ysof
men
ses,on
etimeda
ily
1)Re
flexolog
y(n
¼34
),20
minutes
daily,1
0da
ysbe
fore
men
ses
2)Con
trol
(n¼34
)
2cycles
0VA
S-10p
oints
VAS>5
pain
reduc
tion
was
morein
thelavende
r/massage
grou
p(p
<0.00
1)
Bakh
tshirinet
al.(201
5)15
RCT,
cros
sov
erMidwife
ry/nursing
stud
ents
20Lavend
er/massage
(n¼40
)placeb
o/massage
(n¼40
)2cycles
0VA
S-10p
oints
VAS>6
Asignificant
pain
redu
ction
inlave
nder/m
assagein
compa
riso
nwith
placeb
o/massage
.
Beiran
vandet
al.(201
5)31
RCT
cros
sov
erStud
ents
21Lavend
er/
48ho
ursbe
fore
andafter
men
struation/15
minutes
twiceada
y(n
¼30
)
Placeb
o(alm
ondoil)/
48ho
ursbe
fore
andafter
men
struation/
15minutes
twiceada
y(n
¼30
)
2cycles
repo
rted
VAS-10p
oints
VAS>5
Asignificant
pain
redu
ction
inlave
nder/m
assagein
compa
riso
nwith
placeb
o/massage
(p<0.00
1).
Dav
arie
tal.(20
14)23
RCT
Stud
ents
22Ro
semary(n
¼30
),Lavend
er(n
¼30
),rosemaryþlavende
r(n
¼30
),first3da
ysof
men
ses
15minutes,tw
iceada
y
mefen
amic
acid
(n¼30
),placeb
o(n
¼30
)2cycles
repo
rted
VAS-10p
oints
MDQ
sign
ificant
redu
ctionsin
pain
inrosemary
(p<0.00
1),lav
ende
r,bo
th,
andmefen
amic
acid
(p<0.01
)co
mpa
redwith
placeb
o.
RaisiD
ehko
rdie
tal.(20
14)47
RCT
Crossov
erStud
ents
20Lavend
erfirst3da
ysof
men
ses,
every6ho
urs
(n¼48
)
Placeb
ofirst3da
ysof
men
ses,
every
6ho
urs
(n¼48
)
2cycles
repo
rted
Scoringfrom
1to
41:
none
,2:
mild
,3:
mod
erate,
4:severe
VMS:
2or
3sign
ificant
redu
ctionsin
pain
inlavende
r(p<0.00
1)
Kim
etal.(201
1)18
Non-Ran
dom
CT
Nurses
25Aroma1þself-massage
(n¼26
)tw
iceada
y,2da
ys
Placeb
o(n
¼18
)Notrea
tmen
t(n
¼19
)1cycle
repo
rted
VAS-10p
oints
VAS>5
sign
ificant
redu
ctionsin
pain
(p<0.00
1)
Marzouket
al.(201
3)25
RCT
Crossov
erNursing
stud
ents
17–2
0Aroma2þmassage
(n¼48
),on
ceda
ily,7da
ysbe
fore
men
ses
Placeb
oþmassage
(n¼47
),on
ceda
ily,7
days
before
men
ses
2cycles
repo
rted
VAS-10p
oints
VAS>5
sign
ificant
redu
ctionsin
pain
Ouet
al.(201
2)26
RCT
Patien
ts24
Aroma3
þmassage
(n¼24
)Once
daily,3
days
Placeb
oþmassage
(n¼24
)Onc
eda
ily,3da
ys
1cycle
0VA
S-10p
oints
VAS>5
Durationof
pain
sign
ificantly
decrea
sed
(Con
tinue
d)
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
The Effect of Aromatherapy with Massage on Dysmenorrhea Najaf Najafi et al. 973

Table
2(Con
tinu
ed)
Stud
y(yea
r)Typeof
study
Participan
tsAge
(mea
n)Interven
tion
(n)
Control(n)
Duration
ofstudy
Sampledrop
(%)
Mea
suremen
tmethod
Inclus
ion
outcome
Uysal
etal.(201
6)3
RCT
Patien
tsad
mittedto
the
emerge
ncyun
it21
rose
essential
oilþ
diclofen
ac,75
mg
ampu
le(n
¼52
)
Placeb
oþdiclofen
ac,7
5mg
ampu
le(n
¼53
)co
ntinu
ously
sprayev
ery
10minutes
repo
rted
VAS-10p
oints
VAS>5
sign
ificant
redu
ctionsin
pain
after30
minute
(p¼0.01
9)
Hur
etal.(20
12)1
RCT
Highscho
olstude
nts
?Aroma4
þmassage
(n¼32
)acetam
inop
hen(n
¼32
)1cycle
repo
rted
VAS-10p
oints
VAS>5
sign
ificant
redu
ctionsin
pain
after24
hour
(p<0.00
1)
Nikjouet
al.(20
16)48
RCT
Triple
blind
Stud
ents
19–2
9Lavend
er(n
¼10
0)on
ceada
y,30
minutes,3
days
Placeb
o(n
¼10
0)on
ceada
y,30
minutes,3da
ys2cycles
0VA
S-10p
oints
Intolerable,
limitsac
tivities
exclud
esign
ificant
redu
ctionsin
pain
(p<0.00
1)
Rizk
(201
3)27
RCT
Nursing
stud
ents
17–2
1Pe
ppermintoilþ
massage
(n¼40
)ging
eroilþ
massage
(n¼40
),on
ceda
ily,15
minutes,
5da
ysbe
fore
men
ses
Placeb
oþmassage(n
¼40
)2cycles
repo
rted
VAS-10p
oints
Mode
rate
orsevere
dysm
enorrhea
Sign
ificant
redu
ctionsin
severity
ofpa
inin
Int.
grou
ps.
Sade
ghi
Ava
lSha
hret
al.(20
15)20RC
TStud
ents
18–3
5Ro
seessentialo
il(n
¼25
)on thefirstda
yof
men
ses,
15minutes
almon
doilþ
massage
(n¼25
)massage
(n¼25
)2Cy
cles
repo
rted
VAS-10p
oints
VAS>5
Sign
ificant
redu
ctionsof
pain
inrose
essential
oil
compa
riso
nto
massage
only
(p<0.00
1)or
almon
doilþ
massage
(p<0.05
)
Sajja
diet
al.(201
8)28
RCT
Stud
ents
18–3
5Geran
ium
essentialo
il(n
¼30
)on
thefirstda
yof
men
ses,
15minutes
1)Alm
ondoil(n¼30
)2)
Notrea
tmen
t(n
¼30
)2cycles
repo
rted
VAS-10p
oints
VAS>5
Sign
ificant
redu
ctionin
Geran
ium
essentialo
ilgrou
pco
mpa
riso
nto
othe
rs(p
<0.00
1).
Han
etal.(200
6)16
RCT
Stud
ents
20Aromathe
rapy
5þmassage
(n¼25
)15
minutes
onthefirstda
yof
men
ses
1)Alm
ondoilþ
massage
(n¼20
)2)
Notrea
tmen
t(n
¼22
)
2cycles
0VA
S-10p
oints
VAS>6
Theseverity
was
sign
ificantly
lower
inthe
arom
athe
rapy
group
than
intheothe
rtw
ogrou
ps
Abbrev
iation
s:MDQ,moo
ddiso
rder
question
naire;
RCT,
rand
omized
controltrial;VMS,
verbal
multi-dim
ension
alscoringsystem
.1Aroma:
otto
(Rosada
mascena
),clarysage
(Salviasclarea),rose
geranium
(Pelargo
nium
graveo
lens),an
dging
er(Zingiberofficinale)
inalmon
d,jojoba,
andev
eningprim
rose
oil.
2Aroma:
cinn
amon
,clov
e,rose,a
ndlave
nder
inaba
seof
almon
doil.
3Aroma:
lave
nder,clarysage,
andmarjoram
oils,in
jojobacrea
m.
4Aroma:
clarysage
,marjoram,cinn
amon
,ging
er,an
dge
ranium
inalmond
oil.
5Aroma:
lave
nder
(Lavan
dula
officinalis),clarysage
(Salviasclarea),an
drose
(Rosacentifo
lia)in
almon
doil.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
The Effect of Aromatherapy with Massage on Dysmenorrhea Najaf Najafi et al.974

and severe).47 Han et al.16 drew a comparison between theeffect of almond oilþmassage and placebo with no treat-ment (n¼22). Regression aromatherapywas associatedwithsignificant changes in the severity of dysmenorrhea (firstday: β¼ 0.31, p¼0.02; second day: β¼ 0.33, p¼0.006)compared with the control and placebo groups.16 Huret al.1 compared the effect of aroma (including clary sage,marjoram, cinnamon, ginger, and geranium in almond oil)
þmassage (n¼32) to that of a control group using acetamin-ophen (n¼32). Regression aromatherapy was strongly asso-ciated with a decrease in the severity of dysmenorrhea (β ¼�3.07, 95% CI�3.83 to�2.29, t¼�8.00, P<0.001). In a 2013study by Rizk,27 the effects of both peppermint oilþmassage(n¼40) and ginger oilþmassage (n¼40) were comparedwith placebo, with the findings suggesting a significantreduction in the severity of pain. According to Raisi Dehkordi
Fig. 2 Aromatherapy effect on the severity of dysmenorrhea based on the random effects model.
Fig. 3 Aromatherapy effect on the severity of dysmenorrhea based on the random effects model after removal of one study which causedheterogeneity.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
The Effect of Aromatherapy with Massage on Dysmenorrhea Najaf Najafi et al. 975

et al.,47 the ordinal logistic regression indicated that aroma-therapywas significantly effective in relieving dysmenorrheasymptoms (p<0.001).
Discussion
In this questionable pain relief mechanism, aromatherapyhas been proven to influence the olfactory-hippocampalpathway, which stimulates the putative and gamma-ami-nobutyric acid (GABA)ergic neurons (such as cholinergicneurons), regulates the release of acetylcholine, orchanges the feeling of pain. The olfactory receptors canbe triggered by essential oil inhalation, which transmitssignals to the brain and induces a composition of memory,thought, and emotion. Subsequently, it leads to the secre-tion of some internal chemicals such as endorphin andenkephalin, which can alleviate anxiety and pain,respectively.3
The identified major compounds of rose oil are β-citro-nellol (14.5–47.5%), nonadecane (10.5–40.5%), geraniol (5.5–18%), and nerol and kaempferol. Rose oil has many thera-peutic applications, including anticonvulsant, and analgesicand hypnotic effects.49 Three studies assessed the effect ofrose oil on dysmenorrhea. In the study of Ataollahi et al.,21
the severity of dysmenorrhea in medical students fell signif-icantly in the rosaceous group compared with the placebogroup. In the research, by Uysal et al.,3 rose essential oilþdiclofenac was more effective in pain relief after 30minutescompared with placeboþdiclofenac. Sadeghi Aval Shahret al.20 reported a significant pain relief in the rose essentialoil group compared with the massage only and the almondoilþmassage groups. The essential oil of the geranium plantcontains geraniol, citronellol, terpineol, and alcohols, whichhave anticancer, antimicrobial, antiinflammatory, analgesic,and antioxidant effects.50 Sajjadi et al.28 found a significantpain relief in patients receiving geranium essential oil incomparisonwith almond oil. Themechanism of pain relief indysmenorrhea may be related to the analgesic effect ofgeranium.
Rizk27 compared the effect of peppermint oilþmassagewith that of placebo, with their results suggesting a signifi-cant reduction in the severity of pain in the peppermintoilþmassage group.
Peppermint oil has antispasmodic,51–53 analgesic,54 anti-inflammatory, and antimicrobial effect,55 and it can inhibitprostaglandin F2α.56,57
The bioactive compounds of Rosmarinus officinalis oilsignificantly decreased the expression of IL-1β and TNF-αand inhibited COX-2 expression.58 Davari et al. (2014)23
reported a significant pain relief in the rosemary groupcompared with the placebo group.
Some aromatherapy textbooks suggest that two or moreoils should be combined to achieve a synergic effect.18,22
Consistent with this hypothesis, our meta-analysis revealedthat a mixture of aroma oil was more effective than a singlearoma oil.
Our meta-analysis shows that a combined use of botharomatherapy and massage is more effectiveness than aro-matherapy alone. There is no detailed information on how torelieve pain by massage. The gate control theory of pain isone of the most influential theories which is according to infact so that dorsal spinal horn cells acts like a gate whichinhibits or facilitates transmission from the body to the brainon according to the diameters of the active peripheral fibers.There are three types of nerve fibers, A, B and C, based on theconduction velocity and the axonal diameter. The massagesignals are rapidly transmitted via the sheathed A fiber,whereas pain signals are slowly transmitted via theunsheathed C fibers. The massage transfers these signalsrapidly, developing pressure signals that subsequently closethe pain signal gate.
According to the gate control theory, such signals encoun-ter “nerve gates” on the spinal cord and should be cleared viathese gates to travel to the brain. Other benefits of massageinclude the relaxation of contracted muscles, reduction ofstress, and enhancement of lymph and blood circulation.10
The effect of lavender on diminishing pain can be attributedto its sedative, antidepressant, antispasmodic, antiflatulent
Table 3 Subgroup analyses of the effect of aromatherapy in dysmenorrhea
Variable Number of RCTs Sample size(treatment/control)
Test ofheterogeneity
P-value Fixed¼ effect model
P I2(%) SMD (95% CI)
Types of treatment
Massageþ aromatherapy 9 540 0.7 0% < 0.001 -0.915 (-1.09 to -0.73)
Aromatherapy alone 9 729 0.13 34% < 0.001 -0.741 (-0.89 to -0.58)
Test for subgroup difference p<0.001
Types of treatment
A mixture of aroma oils 7 452 0.410 3% < 0.001 -0.865 (-1.01 to -0.715)
Single oil 11 817 0.273 20% < 0.001 -0.75 (-0.97 to -0.53)
Test for subgroup difference p¼0.34
Abbreviations: CI, confidence interval; SMD, standardized mean difference.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
The Effect of Aromatherapy with Massage on Dysmenorrhea Najaf Najafi et al.976

impact. It can also be used to treat infertility, infection,anxiety, fever, and stress.48
Our meta-analysis, in keeping with pervious meta-analy-ses, illustrated that aromatherapy oil in combination withmassage displayed a greater effectiveness comparedwith thecontrol group.30 According to the results of Sut and Kahyao-glu-Sut’s29 meta–analysis, RCTs decreased the risk of biassignificantly in comparison with the placebo group.
The present meta-analysis has several limitations thatneed to be addressed. First, the power of our meta-analysisdeclined in various subgroups. Secondly, plants may havedifferent therapeutic powers depending on the country orregion in which the plants are harvested.25 The absorptionand metabolism of some herbs vary in different individuals.The effectiveness of herbal medicine in the treatment ofdysmenorrhea may depend on the pathological source ofdysmenorrhea.48 Third, different massage methods andtechniques, and factors such as massage site and pain severi-ty may have influenced our meta-analysis. The severity ofdysmenorrhea reported in each study before treatment wasdifferent. For example, Ataollahi et al.21 and Apay et al.22
reported a mean severity of 4.98 and 82. This may be due toseveral reasons. Thehighest level ofmenstrual pain appearedon the first day of menstruation and then subsided.18 It hasalso been suggested that the perception and tolerance of painmay be influenced by various factors such as culture, society,and lifestyle.15 Lastly, in some studies, the subjects werestudents residing in a dormitory. It may be difficult toprovide suitable conditions for the application of aromather-apy in a dormitory.
Conclusion
Aromatherapy with herbal medicine was found to alleviatedysmenorrhea. Also, a combination of oil and massage had agreater effect compared with the control group. Aromather-apy is recommended to women suffering from dysmenor-rhea, especially towomenwho are reluctant to use hormonaldrugs or concerned about the complications or high costs ofchemicalmedications and, therefore, prefer herbalmedicine.However, due to heterogeneity of studies, weak methodolo-gies, and short-term follow-ups, the findings should beinterpreted with caution.
Conflict of InterestsThe authors have no conflict of interests to declare.
References1 Hur MH, Lee MS, Seong KY, Lee MK. Aromatherapy massage on
the abdomen for alleviating menstrual pain in high school girls: apreliminary controlled clinical study. Evid Based ComplementAlternat Med. 2012;2012:187163. Doi: 10.1155/2012/187163
2 Habibi N, Huang MS, Gan WY, Zulida R, Safavi SM. Prevalence ofprimary dysmenorrhea and factors associated with its intensityamong undergraduate students: a cross-sectional study. PainManag Nurs. 2015;16(06):855–861. Doi: 10.1016/j.pmn.2015.07.001
3 Uysal M, Doğru HY, Sapmaz E, Tas U, Çakmak B, Ozsoy AZ, et al.Investigating the effect of rose essential oil in patients withprimary dysmenorrhea. Complement Ther Clin Pract. 2016;24:45–49. Doi: 10.1016/j.ctcp.2016.05.002
4 Salmalian H, Saghebi R, Moghadamnia AA, Bijani A, Faramarzi M,Amiri FN, et al. Comparative effect of thymus vulgaris andibuprofen on primary dysmenorrhea: A triple-blind clinicalstudy. Caspian J Intern Med. 2014;5(02):82–88
5 Unsal A, Ayranci U, Tozun M, Arslan G, Calik E. Prevalence ofdysmenorrhea and its effect on quality of life among a group offemale university students. Ups J Med Sci. 2010;115(02):138–145. Doi: 10.3109/03009730903457218
6 De Sanctis V, Soliman A, Bernasconi S, Bianchin L, Bona G, BozzolaM, et al. Primary dysmenorrhea in adolescents: prevalence,impact and recent knowledge. Pediatr Endocrinol Rev. 2015;13(02):512–520
7 Shewte MK, Sirpurkar MS. Dysmenorrhoea and quality of lifeamong medical and nursing students: a cross-sectional study.Natl J Community Med. 2016;7(06):474–479
8 Al-Jefout M, Seham AF, Jameel H, Randa AQ, Ola AM, Oday AM,et al. Dysmenorrhea: prevalence and impact on quality of lifeamong young adult Jordanian females. J Pediatr Adolesc Gynecol.2015;28(03):173–185. Doi: 10.1016/j.jpag.2014.07.005
9 Emem EA, Hassan HE. Correlation between quality of life anddysmenorrhea among nursing schools students. Int J Nurs Sci.2017;7(06):123–132
10 Azima S, Bakhshayesh HR, Mousavi S, Ashrafizaveh A. Com-parison of the effects of reflexology and massage therapy onprimary dysmenorrheal. Biomed Res (Aligarh). 2015;26(03):471–476
11 Hakim A, Ghufran A, Nasreen J. Evaluation of anti-inflammatoryactivity of the pods of Iklil-ul-Malik (Astragalus hamosus Linn.).Indian J Nat Prod Resour. 2010;1(01):34–37
12 Zahradnik HP, Hanjalic-Beck A, Groth K. Nonsteroidal anti-inflam-matory drugs and hormonal contraceptives for pain relief fromdysmenorrhea: a review. Contraception. 2010;81(03):185–196.Doi: 10.1016/j.contraception.2009.09.014
13 Singh N, Rai S. Primary dysmenorrhoea. Indian Obstet Gynaecol.2017;7(02):38–45
14 Zigler RE, McNicholas C. Unscheduled vaginal bleeding withprogestin-only contraceptive use. Am J Obstet Gynecol. 2017;216(05):443–450. Doi: 10.1016/j.ajog.2016.12.008
15 Bakhtshirin F, Abedi S, YusefiZoj P, Razmjooee D. The effect ofaromatherapy massage with lavender oil on severity of primarydysmenorrhea in Arsanjan students. Iran J Nurs Midwifery Res.2015;20(01):156–160
16 Han SH, Hur MH, Buckle J, Choi J, Lee MS. Effect of aromatherapyon symptoms of dysmenorrhea in college students: A randomizedplacebo-controlled clinical trial. J Altern ComplementMed. 2006;12(06):535–541. Doi: 10.1089/acm.2006.12.535
17 Uzunçakmak T, Ayaz Alkaya S. Effect of aromatherapy on copingwith premenstrual syndrome: A randomized controlled trial.Complement Ther Med. 2018;36:63–67. Doi: 10.1016/j.ctim.2017.11.022
18 Kim YJ, Lee MS, Yang YS, Hur MH. Self-aromatherapy massage ofthe abdomen for the reduction of menstrual pain and anxietyduringmenstruation in nurses: a placebo-controlled clinical trial.Eur J Integr Med. 2011;3(03):e165–e168. Doi: 10.1016/j.eujim.2011.08.007
19 Buckle J. The role of aromatherapy in nursing care. Nurs Clin NorthAm. 2001;36(01):57–72
20 Sadeghi Aval Shahr H, SaadatM, KheirkhahM, Saadat E. The effectof self-aromatherapy massage of the abdomen on the primarydysmenorrhoea. J Obstet Gynaecol. 2015;35(04):382–385. Doi:10.3109/01443615.2014.958449
21 Ataollahi M, Akbari SA, Mojab F, Roshanaie G. Effects of aroma-therapy by Rosaceous on the severity and systemic symptoms of
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
The Effect of Aromatherapy with Massage on Dysmenorrhea Najaf Najafi et al. 977

primary dysmenorrhea. Adv Nurs Midwifery.. 2015;25(89):59–67
22 Apay SE, Arslan S, Akpinar RB, Celebioglu A. Effect of aroma-therapy massage on dysmenorrhea in Turkish students. PainManag Nurs. 2012;13(04):236–240. Doi: 10.1016/j.pmn.2010.04.002
23 Davari M, Reihani M, Khoshrang N. The aromatherapy effect ofrosemary and lavander on primary dysmenorrhea: a clinicalcontrolled trial. Majallah-i Danishkadah-i Pizishki-i Isfahan.2014;32(290):929–937
24 Amiri Farahani L, Heidari T, Roozbahani N, Attarha M, AkbariTorkestaniN, Bekhradi R, et al. Effect of aromatherapy on painseverity in primary dysmenorrhea. J Arak Univ Med Sci. 2012;15(04):1–9
25 Marzouk TM, El-Nemer AM, Baraka HN. The effect of aromather-apy abdominal massage on alleviating menstrual pain in nursingstudents: a prospective randomized cross-over study. Evid BasedComplement Alternat Med. 2013;2013:742421. Doi:10.1155/2013/742421
26 Ou MC, Hsu TF, Lai AC, Lin YT, Lin CC. Pain relief assessment byaromatic essential oil massage on outpatients with primarydysmenorrhea: a randomized, double-blind clinical trial. J ObstetGynaecol Res. 2012;38(05):817–822. Doi: 10.1111/j.1447-0756.2011.01802.x
27 Rizk SA. Effect of aromatherapy abdominal massage using pep-permint versus ginger oils on primary dysmenorrhea amongadolescent girls. J Am Sci. 2013;9(11):497–505
28 Sajjadi M, Bahri N, Abavisani M. Aromatherapy massage withgeranium essence for pain reduction of primary dysmenorrhea: adouble blind clinical trial. Majallah-i Zanan, Mamai va Nazai-iIran. 2018;20(12):50–57. Doi: 10.22038/ijogi.2017.10430
29 Sut N, Kahyaoglu-Sut H. Effect of aromatherapy massage on painin primary dysmenorrhea: A meta-analysis. Complement TherClin Pract. 2017;27:5–10. Doi: 10.1016/j.ctcp.2017.01.001
30 Song JA, Lee MK, Min E, Kim ME, Fike G, Hur MH. Effects ofaromatherapy on dysmenorrhea: A systematic review and meta-analysis. Int J Nurs Stud. 2018;84:1–11. Doi: 10.1016/j.ijnur-stu.2018.01.016
31 Beiranvand S, Hosseinabadi R, Anbari K, Pirdadeh Beiranvand S,Asti P. The effect of lavender aromatherapy massage on severityand symptoms of primary dysmenorrheal. ComplementMed J FacNurs Midwifery. 2015;5(01):1028–1041
32 Khorshidi N, Ostad SN, Mosaddegh M, Soodi M. Clinical effects offennel essential oil on primary dysmenorrhea. Iran J Pharm Res.2010;2(02):89–93
33 Chen Y, Shang GD, Fu GB. [Effect of massage on hemodynamicsparameters of uterine artery and serum prostaglandin in treatingpatients with primary dysmenorrhea]. Zhongguo Zhong Xi Yi JieHe Za Zhi. 2011;31(10):1355–1358
34 Cheon JA, Lim MH. Effect of aromatherapy using nutmeg, fenneland marjoram on menstruation cramps and dysmenorrhea. JKorean Soc Cosmetol. 2013;19(06):1138–1147
35 Choi EH. Comparison of effects lavender abdominal massage andinhalation on dysmenorrhea, pain, anxiety and depression. JKorean Acad Fundam Nurs. 2009;16(03):300–306
36 Han SH, Ro YJ, Hur MH. Effects of aromatherapy on menstrualcramps and dysmenorrhea in college student woman: a blindrandomized clinical trial. J Korean Acad Adult Nurs. 2001;13(03):420–430
37 Hyun J, Hur M. [Effect of aromatherapy on the menstrual pain incadet women]. J Mil. Nurs Res. 2004;22(01):64–87Korean.
38 Iravani M. Clinical effects of Zataria multiflora essential oil onprimary dysmenorrhea. Faslnamah-i Giyahan-i Daruyi. 2009;8(30):54–60
39 Kim HK, Kim HG, Cheong YS, Park EW, Yoo SM. [The effect ofaromatherapy on dysmenorrhea from high school girls]. J KoreanAcad. Fam Med. 2001;22(06):922–929Korean.
40 Kim NY, Kim CS, Kim YS. Effect that aromatherapy gets inwoman’s period pains. J Korean Soc Cosmetology. 2008;14(02):378–383
41 Lee HJ, Lee YS, Shin HY, et al. [Comparative analysis on the effectsof abdominal massage using aroma oil and ordinary oil on nurses’dysmenorrhea and painfulmenstruation]. J Korean. Clin Nurs Res.2006;11(02):121–133Korean.
42 Lee YM. Effects of aroma-foot-reflexology on premenstrualsyndrome, dysmenorrhea and lower abdominal skin tempera-ture of nursing students. Korean J Adult Nurs. 2011;23(05):472–481
43 Seo JY, Kim MY. The effects of aromatherapy on dysmenorrhea,menstrual pain, anxiety, and depression in nursing students.Korean J Adult Nurs. 2008;20(05):756–764
44 Heydari N, Abootalebi M, Jamalimoghadam N, Kasraeian M,Emamghoreishi M, Akbarzadeh M. Investigation of the effect ofaromatherapy with Citrus aurantium blossom essential oil onpremenstrual syndrome in university students: A clinical trialstudy. Complement Ther Clin Pract. 2018;32:1–5. Doi: 10.1016/j.ctcp.2018.04.006
45 MatsumotoT, Asakura H, Hayashi T. Does lavender aromatherapyalleviate premenstrual emotional symptoms?: a randomizedcrossover trial Biopsychosoc Med. 2013;7(01):12. Doi:10.1186/1751-0759-7-12
46 Azima S, Bakhshayesh HR, Kaviani M, Abbasnia K, Sayadi M.Comparison of the effect of massage therapy and isometricexercises on primary dysmenorrhea: a randomized controlledclinical trial. J Pediatr Adolesc Gynecol. 2015;28(06):486–491.Doi: 10.1016/j.jpag.2015.02.003
47 Raisi Dehkordi Z, Hosseini Baharanchi FS, Bekhradi R. Effect oflavender inhalation on the symptoms of primary dysmenorrheaand the amount of menstrual bleeding: A randomized clinicaltrial. Complement Ther Med. 2014;22(02):212–219. Doi:10.1016/j.ctim.2013.12.011
48 Nikjou R, Kazemzadeh R, Rostamnegad M, Moshfegi S, Karimol-lahi M, Salehi H. The effect of lavender aromatherapy on the painseverity of primary dysmenorrhea: a triple-blind randomizedclinical trial. Ann Med Health Sci Res. 2016;6(04):211–215. Doi:10.4103/amhsr.amhsr_527_14
49 Boskabady MH, Shafei MN, Saberi Z, Amini S. Pharmacologicaleffects of rosa damascena. Iran J Basic Med Sci. 2011;14(04):295–307
50 Gazerani A, Sarchahi Z, Hosseini SS, Abavisani M. The effect ofinhalation aromatherapy of geranium on pain and physiologicalindices after appendectomy: a double-blind randomized clinicaltrial. Int J Surg Open. 2021;28:44–49. Doi: 10.1016/j.ijso.2020.12.004
51 Zielińska A. Pain in irritable bowel syndrome. In: Fichna J,editors. A comprehensive overview of irritable bowel syndrome:clinical and basic science aspects. Amsterdam: Elsevier; 2020:145–66
52 Skalicka-Woźniak K, Walasek M. Preparative separation of men-thol and pulegone from peppermint oil (Mentha piperita L.) byhigh-performance counter-current chromatography. PhytochemLett. 2014;10:xciv–xcviii. Doi: 10.1016/j.phytol.2014.06.007
53 Shavakhi A, Ardestani SK, Taki M, Goli M, Keshteli AH. Premed-ication with peppermint oil capsules in colonoscopy: a doubleblind placebo-controlled randomized trial study. Acta Gastro-enterol Belg. 2012;75(03):349–353
54 Özmen T, Doğan H, Güneş Gencer GY. Effect of classic massagewith peppermint oil on muscle soreness and muscle strengthduring recovery from exercise. J Sports Perform Res. 2020;11(02):103–111. Doi: 10.17155/omuspd.606247
55 Pannuti CM,Mattos JP, Ranoya PN, Jesus AM, LotufoRF, Romito GA.Clinical effect of a herbal dentifrice on the control of plaque andgingivitis: a double-blind study. Pesqui Odontol Bras. 2003;17(04):314–318. Doi: 10.1590/s1517-74912003000400004
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
The Effect of Aromatherapy with Massage on Dysmenorrhea Najaf Najafi et al.978

56 Ibaadillah AA, Samtyaningsih D. Effect of peppermint tea ondismenorrhoe in midwifery students of diii study program stikesMaharani Malang. J Nurs Care Biomol. 2017;2(01):6–9. Doi:10.32700/jnc.v2i1.23
57 Masoumi SZ, Asl HR, Poorolajal J, Panah MH, Oliaei SR. Evaluationof mint efficacy regarding dysmenorrhea in comparison withmefenamic acid: A double blinded randomized crossover study.
Iran J Nurs Midwifery Res. 2016;21(04):363–367. Doi:10.4103/1735-9066.185574
58 Mengoni ES, Vichera G, Rigano LA, Rodriguez-Puebla ML, GallianoSR, Cafferata EE, et al. Suppression of COX-2, IL-1β and TNF-αexpression and leukocyte infiltration in inflamed skin by bioac-tive compounds from Rosmarinus officinalis L. Fitoterapia. 2011;82(03):414–421. Doi: 10.1016/j.fitote.2010.11.023
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
The Effect of Aromatherapy with Massage on Dysmenorrhea Najaf Najafi et al. 979

High-Grade Transformation in Adenoid CysticCarcinoma of the Bartholin Gland: Case Report
Transformação de alto grau em carcinoma adenoidecístico de glândula de Bartholin: relato de casoAline Evangelista Santiago1 Nicky Teunissen2 Bernardo Ferreira de Paula Ricardo3
Eduardo Batista Cândido2,4 Rafaela de Souza Furtado2 Agnaldo Lopes da Silva Filho1,2,4
1Gynecology Department, Universidade Estadual Paulista “Júlio deMesquita Filho”, Botucatu, SP, Brazil
2Gynecology Department, Univeridade Federal de Minas Gerais, BeloHorizonte, MG, Brazil
3Pathology Department, Hospital MaterDei, Belo Horizonte, MG, Brazil4Gynecology Department, Hospital MaterDei, Belo Horizonte, MG, Brazil
Rev Bras Ginecol Obstet 2021;43(12):980–984.
Address for correspondence Agnaldo Lopes da Silva Filho, PhD,Avenida Professor Alfredo Balena 190, 30130-100, Belo Horizonte,MG, Brazil (e-mail: [email protected]).
Keywords
► adenoid cysticcarcinoma
► Bartholin gland► gynecology► oncology► vulvar neoplasms
Abstract Introduction In the present study, we report a case of primary adenoid cysticcarcinoma (ACC) of the Bartholin glandwith high-grade transformation (HGT). Adenoidcystic carcinoma of the Bartholin gland is a rare tumor and HGT has only been reportedin head and neck tumors.Case Report A 77-year-old woman with a non-ulcerated vulvar lesion on the topogra-phy of the right Bartholin gland. The patient was submitted to tumor resectionfollowed by V–Y island flap and adjuvant radiotherapy. The histopathological exami-nation revealed primary ACC of the Bartholin gland, with areas of HGT and extensiveperineural invasion. The immunohistochemical study with p53 showed a diffuse andstrong positive reaction in areas with HGT. After 24 months of follow-up, the patientpresented distant metastases and died, despite having undergone to chemotherapy.Conclusion As far asweknow, this case is thefirst description in the literature ofHGT inACCof the Bartholin gland, and HGT appears to be associated with tumor aggressiveness.
Palavras-chave
► carcinoma adenoidecístico
► glândula de Bartholin► ginecologia► oncologia► neoplasias vulvares
Resumo Introdução Este estudo relata o caso de umcarcinoma adenoide cístico (CAC) de glândulade Bartholin com transformação de alto grau. O CAC de glândula de Bartholin é um tumorraro, e sua transformação de alto grau é relatada somente em tumores de cabeça e pescoço.Relato de caso Paciente de 77 anos de idade, do sexo feminino, com lesão vulvar nãoulcerada na topografia da glândula de Bartholin direita. A paciente foi submetida aressecção do tumor e realização de retalho em V-Y, seguidas de radioterapia adjuvante.O exame histopatológico revelou CAC primário de glândula de Bartholin, com áreas detransformação de alto grau e invasão perineural. O estudo imunohistoquímico comp53mostrou reação positiva difusa e intensa em áreas com transformação de alto grau.
receivedJuly 29, 2020accepted after revisionAugust 30, 2021
DOI https://doi.org/10.1055/s-0041-1736301.ISSN 0100-7203.
© 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rightsreserved.This is an open access article published by Thieme under the terms of the
Creative Commons Attribution License, permitting unrestricted use,
distribution, and reproduction so long as the original work is properly cited.
(https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda., Rua do Matoso 170, Rio deJaneiro, RJ, CEP 20270-135, Brazil
Case ReportTHIEME
980

Introduction
Primary adenoid cystic carcinoma (ACC) of the Bartholingland is a rare tumor first described in 1859.1 It correspondsto approximately 0.001% of all gynecological malignanciesand to 2% to 7% of vulvar malignant tumors. Tumors of theBartholin glands may have different histological forms, butapproximately 80% consist of squamous-cell carcinomas andadenocarcinomas.2–4 The diagnosis of Bartholin gland canceris usually late, because it has a nonspecific clinical presenta-tion and differential diagnosis with Bartholin gland cyst andBartolinitis. As a consequence, it is often discovered at anadvanced stage, with a risk of lymph node (inguinal andpelvic) or general (pulmonary and bone) metastases.4
The present article is the report of a rare case of ACC withhigh-grade transformation (HGT-ACC), which has only beenreported in carcinomas in other regions, such as thehead andneck. To our knowledge, this is the first reported case ofHGT-ACC of the Bartholin gland.
Case Report
A 77-year-old woman, nulliparous, postmenopausal but notundergoing hormonal therapy, with a history of infertilityand resection of an ovarian cyst in 1966. In October 2016, thepatient presented a non-ulcerated vulvar lesion of 5 cm indiameter on the topographyof the right Bartholin gland,withapparent deep-layer infiltration without associated inguinallymph node enlargement. Magnetic resonance imaging(MRI) and positron emission tomography-computed tomog-raphy (PET-CT) were performed, which showed a tumormeasuring 4.0�2.7�3.8 cm on the topography of the rightBartholin gland topography, involving the distal third of theright labia majora of the vulva, the lower third of the vagina,and the distal urethra, with vulvar uptake with a standard-ized uptake value (SUV) of 11.22, without metastatic disease,lymph node involvement, or invasion of the mesorectalfascia and pelvic floor musculature. A biopsy of the lesionrevealed a high-grade undifferentiated carcinoma in a limit-ed material with no recognizable morphology of ACC.
Tumor resectionwas performed under general anesthesiaand spinal anesthesia. In the perioperative period, tumorinvasion of the right ischioanal fossa was evidenced, withinvolvement of the levator ani muscle, extending up to thebladder, but without bladder invasion. Extended local exci-sion of the tumor was performed with macroscopically freemargins, without lymphadenectomy. At the end of theprocedure, no gross macroscopic lesions were observed(►Fig. 1). The intraoperative analysis of a frozen section
showed tumor-free surgical margins. We used the V-Y ad-vancement flap from the medial thigh for vulvar reconstruc-tion. Uponmacroscopic inspection of the resected specimen,we established that the lesion was a solid mass measuring5.0�4.0�3.0 cm, showing ulcerated tumor lesion measur-ing 4.0�3.5 cm, and distant 0.2 cm from the lowest margin.
The microscopic analysis of the histopathological exami-nation revealed a primary ACC of the Bartholin gland, withareas of high-grade morphology, extensive perineural inva-sion, and presence of angiolymphatic emboli (►Fig. 2). Theareas with conventional ACC had a morphological aspectranging from tubular and cribriform areas to solid areas, andsome transition areas composed of well-differentiated com-ponents with HGTwere observed (►Fig. 2E). The high-gradecomponents were predominantly composed of solid archi-tecture (71%) and highly atypical pleomorphic nuclei with ahigh number of mitoses. The immunohistochemical studywith p53 showed a diffuse and strong positive reaction inHGT areas, and some tubular and cribriform areas alsostained positively for p53 (►Fig. 3). In both the well-differ-entiated component and the HGT-ACC, P63 positivity wasobserved. The deep and circumferential margins of thesurgical piece had no signs of neoplasia.
Thepatient receivedadjuvant treatmentwithexternal pelvicradiotherapy. Intensity-modulated radiation therapy (IMRT)was indicated and the dose was 45 Gy divided into 25 fractionsof 1.8 Gy over the right inguinal region and the tumor bed. Inaddition, another boost of 14.4Gywasperformed, divided into 8fractions of 1.8Gy, reaching a total dose of 59.4Gy in the tumorbed, including theurethra. Thepatientpresentedgoodtoleranceto the treatment, evolving only to dermatitis and moderate
Fig. 1. Surgical specimen (A) and immediate postoperative view ofthe reconstructed vulva with a V-Y island flap (B).
Após 24meses de seguimento, a paciente apresentoumetástases à distância e faleceu,apesar de ter sido submetida a quimioterapia.Conclusão Pelo que sabemos, este caso é a primeira descrição na literatura detransformação de alto grau em CAC de glândula de Bartholin, e a transformação de altograu parece estar associada à agressividade do tumor.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
High-Grade Transformation in Adenoid Cystic Carcinoma of the Bartholin Gland Santiago et al. 981

dysuria (according to the scale of the Radiation Therapy Oncol-ogy Group [RTOG]), and remained in clinical follow-up for 24months, with no signs of relapse.
After the follow-up period, the patient remained asymp-tomatic, but presented signs of recurrence of the disease onPET-CT, with the presence of surgical-site hypermetabolism(SUV: 3.81) and bilateral pulmonary nodules (SUV: 3.35).Cisplatin and 5-fluorouracil (5-FU) chemotherapy was initiat-ed. However, the patient died during treatment due to diseaseprogression. Death occurred 36 months after the diagnosis.
Discussion
Slow growth, high rate of local recurrence, perineural inva-sion, and usual late onset of distant metastases are knowncharacteristics of ACC.5,6 It is found mainly in the glandular
tissues of the head and neck, especially in the salivary glands.However, in other tissues, such as in the breast and uterinecervix, ACC can also be detected, and displays the samebehavior as salivary gland carcinoma.5,7 Histologically,ACCs are characterized by three different growth patterns:tubular, cribriform, and solid growth. The number of solidsegments seems to be the most important prognostic factorfor adverse events.8 A study9 on ACC in the salivary glandsshowed that distant metastases occurred in 73% of thepatients with a solid growth pattern, compared to 17% ofcases with tubular growth pattern, and 8% with cribriformgrowth pattern. In the case herein reported, we observedpercentages of distribution of growth patterns similar tothose reported in the literature, with a predominance of thesolid pattern.
A rare phenomenon not reported in the traditional ACCclassification is the undifferentiation or HGT. The firstdescription of this phenomenon in a case of ACC wasmade in 1999.10 High-grade transformation is defined asthe abrupt change of a well-differentiated tumor intoundifferentiated morphology that does not have the origi-nal histological characteristics, making high-grade mor-phological areas usually well demarcated. However, insome cases, it is possible to identify a transition zone fora more typical morphology with cribriform and tubularareas, with frequent perineural invasion.8 Although noteasily identified, some transition areas, composed of well-differentiated components with HGT, were observed in themicroscopic analysis of the tumor of the case hereinreported (►Fig. 2E).
The histological features present in HGT areas are thick-ening or irregularity of the nuclear membranes, prominentcentral nucleoli, necrosis, and microcalcifications. In addi-tion, some features are considered major criteria, such asincrease in nuclear size, confluent solid nodules, incompleteand focally absent luminal cell layers, increased Ki-67labeling, fibrocellular desmoplastic stroma, micropapillary,squamous areas, and overexpression of p53.11 In the pres-ent case, although the electron microscopic findings of suchtumors revealed that the nuclear membranes were notthickened, such findings appear on hematoxylin-eosin(H&E) staining.
With the use of immunohistochemistry, specific tumorcharacteristics can be observed to distinguish well-differ-entiated areas of ACC from HGT-ACC. The p63 tumormarker, a myoepithelial marker, is present in well-differen-tiated ACC and absent or focally absent in HGT- ACC.11,12 Inthe case herein reported, p63 positivity was observed inboth the well-differentiated component and the HGT-ACC.Another marker that can be used for this identification is Ki-67, most expressed in areas with HGT.12 In addition tothese, some studies have shown that p53 genes haveincreased expression in the high-grade component, al-though other studies show that this marker may alsohave increased expression in well-differentiatedACC.8,10–12 There is evidence that overexpression of thep53 gene in well-differentiated ACC is accompanied by aworse prognosis. Thus, changes in the p53 gene may be
Fig. 2. Microscopic features of the case herein reported. Histologicevaluation of primary adenoid cystic carcinoma of the Bartholingland, with areas of high-grade morphology and extensive perineuralinvasion (hematoxylin-eosin, magnification �100). (A) Area with well-differentiated tumor component; (B,C,D) areas with high-gradetransformation; (E) transition area composed of well-differentiatedcomponents with high-grade transformation.
Fig. 3. Immunohistochemical evaluation of primary adenoid cysticcarcinoma of the Bartholin gland, with areas of high-grademorphology (magnification �100). (A) Difuse positivity of p53;(B) p53 positivity in the well-differentiated component; (C)Immunostaining for p63 in the well-differentiated component;(D) p63 in the high-grade component; (E) pan cytokeratin AE1/AE.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
High-Grade Transformation in Adenoid Cystic Carcinoma of the Bartholin Gland Santiago et al.982

associated with the appearance of undifferentiated tumorcells, characterizing a marker of poor prognosis.13,14 In thecase herein reported, a diffuse positivity was observed forp53 in the well-differentiated component, which may havecontributed to the poor outcome.
To differentiate between HGT-ACC and solid ACC, in addi-tion to the immunohistochemical characteristics, some cellu-lar characteristics can be evaluated. Nuclear increase,irregularities and necrosis of chromatin appear to be morepronounced in HGT-ACC. In addition, confluent sheets, fibro-cellular desmoplastic stroma, necrosis, and highmitotic activ-ity are also found in HGT-ACC. In cases inwhich the transitionfrom well-differentiated ACC to HGT-ACC is not as abrupt asdescribed in most cases, some characteristics can be found inboth HGT-ACC and solid ACC, such as pleomorphism, mitoticactivity, and focal necrosis.12 In the present case, the micro-scopic analysis of the histopathological examination of tumorrecurrence identified solid areas with pleomorphic areaswithhigh mitotic index.
HGT-ACC is a variant of ACC with a more aggressivebehavior, with a high probability for the development ofrecurrences and metastases.11,15 A study11 on subjects withhead and neck HGT-ACC showed that approximately 57% ofthese patients developed lymph node metastases, comparedto 5% to 25% of those with well-differentiated ACC. Inaddition, this study11 indicated that 81% of the patientsreported in the literature with HGT-ACC had recurrence ofthe disease. Of these 81%, 56.3% presented local recurrence,57.9% presented lymph node metastasis, and 47.1% werediagnosed with distant metastases.11 The most common siteof metastasis is the lung.2 The patient described in thepresent study presented both local recurrence and distantmetastasis at the most common site.
Since ACC is a rare tumor and there are no prospective andrandomized controlled trials on it, the treatment is notconsensual,4 but surgical resection is the preferred treat-ment. It can be performed with wide local excisions, hemi-vulvectomy, simple vulvectomy, and radical vulvectomywith and without inguinal and/or femoral lymphadenecto-my. In patients with deep local infiltration, positive inci-sional margin or recurrence, adjuvant radiotherapy orchemotherapy can be performed.2,3 The patient herein de-scribed underwent extended local excision of the tumorfollowed by adjuvant radiotherapy as the primary treatment,and chemotherapy after tumor recurrence. Considering thelack of consensus on treatment recommendations for Bar-tholin gland carcinomas and negative PET-CT for lymph nodeinvolvement, we chose not to perform lymphadenectomy.When we compare our case to a series of cases of Bartholingland carcinomas described in the literature,7 we observecoincident recurrence sites (the vulva and lung). However,the patient in the case herein presented was older whencompared to the average age observed in the literature(72 years against 57 years), and the follow-up was shorterin our case (36 months against 41.9 months) than in in thecase series mentioned.7 This shorter follow-up was due tothe patient’s death.
Conclusion
We reported a case of a 77-year-old woman with a primaryACC of the Bartholin gland, with areas of high-grade mor-phology, extensive perineural invasion, and presence ofangiolymphatic emboli. To our knowledge, this is the firstcase of HGT reported in ACC of the Bartholin gland. Ourpatient was treated with extended local excision of thetumor,with freemargins, followed byadjuvant radiotherapy.After 24 months of follow-up, the patient presented distantmetastases, and the outcome was death, despite the chemo-therapy received, reinforcing the aggressiveness of the tumorand probably of the HGT. A rare tumor, ACC of the Bartholingland has no established diagnostic methods or definedtreatment standards. Further research is needed to improvethe understanding of the incidence and prognosis ofHGT-ACC in gynecological tumors, including those of theBartholin glands.
Conflict of InterestsThe authors have no conflict of interests to declare.
References1 Cameron JM. Tumours of salivary tissue. J Clin Pathol. 1961;14
(03):232–245. Doi: 10.1136/jcp.14.3.2322 Chang Y, Wu W, Chen H. Adenoid cystic carcinoma of the
Bartholin’s gland: a case report and literature review. J IntMed Res. 2020;48(02):300060519863540. Doi: 10.1177/0300060519863540
3 Lo CCW, Leow JBY, Naing K, Jaaback K, Thachil T. Naing k, JaabackK, Thachil T. Adenoid cystic carcinoma of the Bartholin’s gland: adiagnostic dilemma. Case Rep Obstet Gynecol. 2019;2019:1784949. Doi: 10.1155/2019/1784949
4 Chraibi Z, Hebert T, Body G, Arbion F, Ouldamer L. [Bartholin’sgland carcinoma]. Gynécol Obstét Fertil. 2014;42(7-8):540-54210.1016/j.gyobfe.2014.05.008 French.
5 Momeni M, Korotkaya Y, Carrasco G, Prasad-Hayes M. Adenoidcystic carcinoma of Bartholin’s gland: case report. Acta Med Iran.2016;54(12):820–822
6 Hsu ST,Wang RC, Lu CH, Ke YM, Chen YT, ChouMM, et al. Report oftwo cases of adenoid cystic carcinoma of Bartholin’s gland andreview of literature. Taiwan J Obstet Gynecol. 2013;52(01):113–116. Doi: 10.1016/j.tjog.2012.10.005
7 Bhalwal AB, Nick AM, Dos Reis R, Chen CL, Munsell MF, Ram-alingam P, et al. Carcinoma of the Bartholin gland: a review of 33cases. Int J Gynecol Cancer. 2016;26(04):785–789. Doi: 10.1097/IGC.0000000000000656
8 Nagao T. “Dedifferentiation” and high-grade transformation insalivary gland carcinomas. Head Neck Pathol. 2013;7(Suppl 1):S37–S47. Doi: 10.1007/s12105-013-0458-8
9 BhayaniMK, YenerM, El-Naggar A, GardenA,Hanna EY,Weber RS,et al. Prognosis and risk factors for early-stage adenoid cysticcarcinoma of the major salivary glands. Cancer. 2012;118(11):2872–2878. Doi: 10.1002/cncr.26549
10 Cheuk W, Chan JK, Ngan RK. Dedifferentiation in adenoid cysticcarcinoma of salivary gland: an uncommon complication associ-atedwith an accelerated clinical course. Am J Surg Pathol. 1999;23(04):465–472. Doi: 10.1097/00000478-199904000-00012
11 Seethala RR, Hunt JL, Baloch ZW, Livolsi VA, Leon Barnes E.Adenoid cystic carcinoma with high-grade transformation: areport of 11 cases and a review of the literature. Am J Surg Pathol.2007;31(11):1683–1694. Doi: 10.1097/PAS.0b013e3180dc928c
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
High-Grade Transformation in Adenoid Cystic Carcinoma of the Bartholin Gland Santiago et al. 983

12 Costa AF, Altemani A, Hermsen M. Current concepts ondedifferentiation/high-grade transformation in salivary glandtumors. Pathol Res Int. 2011;2011:325965. Doi: 10.4061/2011/325965
13 ChauY,HongyoT,AozasaK,ChanJK.Dedifferentiationofadenoidcysticcarcinoma: report of a case implicating p53 gene mutation. HumPathol. 2001;32(12):1403–1407. Doi: 10.1053/hupa.2001.28966
14 Li Q, Huang P, Zheng C, Wang J, Ge M. Prognostic significance ofp53 immunohistochemical expression in adenoid cystic carcino-ma of the salivary glands: a meta-analysis. Oncotarget. 2017;8(17):29458–29473. Doi: 10.18632/oncotarget.15297
15 Dahlin DC, Beabout JW. Dedifferentiation of low-grade chondro-sarcomas. Cancer. 1971;28(02):461–466. Doi: 10.1002/1097-0142(197108)28:2<461:aid-cncr2820280227>3.0.co;2-u
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
High-Grade Transformation in Adenoid Cystic Carcinoma of the Bartholin Gland Santiago et al.984

Antenatal Diagnosis of Parapagus ConjoinedTwins: 3D Virtual and 3D Physical Models
Diagnóstico antenatal de gêmeos unidos parapagus:Modelos 3D virtuais e físicosPedro Castro1 Heron Werner1 Ana Paula Matos1 Gerson Ribeiro1,2 Jorge Lopes2
Edward Araujo Júnior3,4
1Department of Fetal Medicine, Clínica de Diagnóstico por Imagem,Rio de Janeiro, RJ, Brazil
2Department of Arts and Design, Pontifícia Universidade Católica, Riode Janeiro, RJ, Brazil
3Department of Obstetrics, Escola Paulista de Medicina, UniversidadeFederal de São Paulo, São Paulo, SP, Brazil
4Medical course, Universidade Municipal de São Caetano do Sul,Campus Bela Vista, São Paulo, SP, Brazil
Rev Bras Ginecol Obstet 2021;43(12):985–987.
Address for correspondence Edward Araujo Júnior, PhD, RuaBotucatu, 740, 04023-062, Vila Clementino, São Paulo, SP, Brazil(e-mail: [email protected]).
Keywords
► conjoined twins► magnetic resonance
imaging► three-dimensional
models
Abstract Conjoined twins (CTs) are a rare complication from monochorionic and monoamniotictwin pregnancies. We describe the use of 3D technologies, including 3D virtual and 3Dphysical models on prenatal evaluation of one parapagus CT. A 16-year-old G1P0womanwas referred for fetal magnetic resonance imaging (MRI) anatomical evaluationof a CT at 28 weeks of gestation. 3D images of the fetal surface were generated by thesoftware during the examination for spatial comprehension of the relationshipbetween the fetal parts. The pair of CTs died at the 32nd week of gestation, afew hours after cesarean section. 3D technologies are an important tool for parentalcounseling and preparation of themultidisciplinary care team for delivery and neonatalassistance and possible surgical planning for postnatal separation in CTs cases.
Palavras-chave
► gêmeos unidos► ressonância
magnética► modelos
tridimensionais
Resumo Gêmeos unidos (GUs) são uma complicação rara de gestações gemelares monocoriô-nicas e monoamnióticas. Descrevemos o uso de tecnologias 3D, incluindo modelos 3Dvirtuais e físicos, na avaliação pré-natal de GU parapagus. Mulher de 16 anos, G1P0, foiencaminhada para avaliação anatômica por ressonância magnética (RM) fetal de GUcom 28 semanas de gestação. Imagens 3D da superfície fetal foram geradas pelosoftware durante o exame para compreensão espacial da relação entre as partes fetais.O par de GUs morreu na 32ª semana de gestação, poucas horas após a cesariana. Astecnologias 3D são uma importante ferramenta de aconselhamento dos pais e depreparação da equipe multiprofissional para o parto e a assistência neonatal, além depossível planejamento cirúrgico para separação pós-natal em casos de GUs.
receivedNovember 29, 2020acceptedOctober 4, 2021
DOI https://doi.org/10.1055/s-0041-1739297.ISSN 0100-7203.
© 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rightsreserved.This is an open access article published by Thieme under the terms of the
Creative Commons Attribution License, permitting unrestricted use,
distribution, and reproduction so long as the original work is properly cited.
(https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda., Rua do Matoso 170, Rio deJaneiro, RJ, CEP 20270-135, Brazil
THIEME
Case Report 985

Introduction
Conjoined twins (CTs) are a rare complication from mono-chorionic and monoamniotic twin pregnancies with anincidence ranging from 1:50,000 to 1:100,000 live births.1
Conjoined twin pregnancies are surrounded by great com-motion and prompt disposition of multidisciplinary groupsfor the care and reception of the pair during pregnancy,delivery, and postnatal life. However, the singularity of theanatomy of CTs can increase the risk of fetal and neonataldemise. Of CTs deliveries, 46% are live born, 26% are stillborn,and 27% are terminated.2 The exact number of fetal demiseson the first half of pregnancy is unknown. This high rate ofmortality is extended to the postnatal period: the commonpresence of cardiac malformations and new circumstancesthat this singular anatomy is exposed to after birth increasesthe risk of death of the CTs. This also increases the risk ofneonatal demise of one of the CT, requiring urgent surgicalseparation.3 Recognizing anatomical singularities is crucialin the prenatal assessment and postnatal assistance of theCTs. For this, prenatal and postnatal imaging studies arefundamental. In the past decades, 3D virtual and 3D physicalmodels (3DPMs) have been described as emerging technolo-gies for the assistance of CTs and parental counseling. Thepresent study aimed at describing the antenatal use of 3Dimaging technologies in the assessment of one pair of CTs.
Case Report
A 16-year-old G1P0 woman was referred for fetal magneticresonance imaging (MRI) anatomical evaluation of CTs at 28weeks of gestation. Fetal magnetic resonance imaging (MRI)demonstrated a dicephalic parapagus CT. The thorax wasfused, and the heart, aorta, and liver were shared. However,therewere twovertebral spines, both fused in the lumbosacralregion. One fetus had a massive occipital encephalocele, dis-torting the cranium. This type of CT was considered lethal,because of one single shared heart and aorta associated withcentral nervous system malformations. The abdomen pre-sentedacysticmass,hypointenseat theT2-weightedsequenceand isointense at the T1-weighted sequence. Isotropic imageswere also obtained. 3D images of the fetal surface weregenerated by the software (of the MRI machine) during theexamination for spatial comprehension of the relationshipbetween the fetal parts. Digital Imaging and Communicationsin Medicine (DICOM) images were exported for posteriorprocessingusing thesoftware3DSlicer v4.11.10 (Birmingham,United Kingdom). Fetal images were generated for parentalcounseling and neonatal care programming. Standard TriangleLanguage (STL) files were generated, and a 3D Physical model(3DPM) was generated (Ultimaker 3 Extended; Utrecht,Netherlands; printingmaterial: PolylacticAcid (PLA); support:Polyvinyl Alcohol [PVA]). At the 32nd week, a prematurerupture of membranes anticipated the delivery. A cesareansectionwas performed, and the pair died after a fewhours dueto cardiopulmonary complications (►Figure 1). The neonatol-ogy team was informed of the lethal condition and onlyventilatory support was offered.
Discussion
Conjoined twins are a rare occurrence, with an incidenceranging from 1/2,800 in India to 1/200,000 live births in theUSA.4 The anatomical classification is based on the site offusion, and a standardized nomenclature was suggested bySpencer in 1996.5 The site of fusion may be associated to themortality rate. Thoracopagus has amortality rate of 80%, dueto the presence of severe cardiopulmonary abnormalities,while omphalopagus may have a mortality rate of 20%.6 Theanatomical presentation of the CTs is extremely variable, andeach CT has a singular anatomy. This singular anatomy leadsto the association of multiple major malformations, whichare present inmore than one-quarter of cases and contributeto the high neonatal mortality rate:>60% will not surviveafter birth.6 Of these, deaths occur on the 1st 24 hours in 68%of the cases andwithin 48 hours in 88% of the cases.7 To aid inthe care of CTs, imaging studies are fundamental, beforebirth, for parental counseling, individualized prenatal care,and delivery preparation of themultidisciplinary specializedcare and, postnatally, for clinical evaluation of the anatomy incases in which separation is not indicated and in case ofsurgical separation to provide accurate information for theparents and multidisciplinary care. Recently, many techno-logical advances are being applied and customized toimprove the comprehension of the singular anatomy ofCTs, including 3D imaging, virtual reality, and 3DPM print-ing.8 The formation of a 3D image is the first step afterimaging acquisition. The presence of multiple contrastsallows the proper segmentation of the anatomy to be stud-ied. The complex anatomy of CTs requires the presence of a
Fig. 1 Parapagus, at 28 weeks of gestation. They share the thorax andabdomen and had two spines, and one of the fetuses presented animportant encephalocele. (A) Magnetic resonance imaging was per-formed during the pregnancy. This image was used for the 3D virtualreconstruction (B) and 3D physical model printing (C) for parentalcounseling. (D) Postnatal image of the fetuses.
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Antenatal Diagnosis of Parapagus Conjoined Twins Castro et al.986

multidisciplinary care team to orient the segmentation of thecomputer-aided 3D volumes, which can be used for thedesign of skin and soft tissue flaps, and to calculate theamount of volume necessary in the tissue expander forproper closure of the area of attachment of the CTs.9 The3DPMwas established during the 1980s, when the patent ofa stereolithographic apparatus was registered. The poorresults of imaging and computer processing delayed theprogress of the technology until the current century. Thefirst description of CT using 3DPM was reported in 2000,when magnetic resonance images of a thoracopagus CTwereused for prenatal planning and to provide information to themultidisciplinary care specialist after birth, when surgicalseparation was immediately required.10 The 3DPMs areuseful for surgical guidance, providing spatial relationshipbetween tissues and organs, and may provide anatomicaldetails that are not visible in 2D images.11 Vascular connec-tion identification is one of the key factors for the success ofthe surgical separation of craniopagus CTs. There are manycases reporting the use of 3DPMs in the postnatal care ofcraniopagus CTs. 3DPMs can provide the physical character-istics and in real scale the relationship between the vessels,the skull, and the brain.12 From the surgical planning ofcraniotomy, cranial defects are reconstructed, cranial graftswere designed, and the use of tissue expander and itsplacement for posterior cranial coverage were pro-grammed.13 The postprocessing of the stereolithographicfiles andmaterial of good quality are the determinant factorsfor a high-quality 3DPM.14 In this case, the 3Dmodels helpedwith the parental comprehension of the fetal malformation,with a spatial perception that cannot be obtained by tradi-tional 2D ultrasound. For the neonatology team, the 3Dreconstruction helped the neonatal assistance, includingthe ventilatory support. 3D models can also help on thecomprehension of the difficulties (anatomy of organs andvessels) of a possible fetal separation by the pediatric surgeryteam.
Conclusion
In conclusion, 3D technologies can be useful in the prenatalevaluation of CTs and are an important tool for parentalcounseling and possible postnatal surgical separationplanning.
Conflict of InterestsThe authors have no conflict of interests to declare.
References1 Mian A, Gabra NI, Sharma T, Topale N, Gielecki J, Tubbs RS, et al.
Conjoined twins: From conception to separation, a review. ClinAnat. 2017;30(03):385–396. Doi: 10.1002/ca.22839
2 Frawley G. Conjoined twins in 2020 - state of the art and futuredirections. Curr Opin Anaesthesiol. 2020;33(03):381–387. Doi:10.1097/ACO.0000000000000864
3 Teixeira Castro P, Werner H, Matos AP, Daltro P, Araujo Júnior E.Symmetric and ventrally conjoined twins: prenatal evaluation byultrasound and magnetic resonance imaging and postnatal out-comes. J Matern Fetal Neonatal Med. 2021;34(12):1955–1962.Doi: 10.1080/14767058.2019.1651282
4 Mutchinick OM, Luna-Muñoz L, Amar E, Bakker MK, Clementi M,Cocchi G, et al. Conjoined twins: a worldwide collaborativeepidemiological study of the International Clearinghouse forBirth Defects Surveillance and Research. Am JMed Genet C SeminMed Genet. 2011;157C(04):274–287. Doi: 10.1002/ajmg.c.30321
5 Spencer R. Anatomic description of conjoined twins: a plea forstandardized terminology. J Pediatr Surg. 1996;31(07):941–944.Doi: 10.1016/s0022-3468(96)90417-0
6 Tannuri AC, Batatinha JA, Velhote MC, Tannuri U. Conjoinedtwins: twenty years’ experience at a reference center in Brazil.Clinics (São Paulo). 2013;68(03):371–377. Doi: 10.6061/clinics/2013(03)oa14
7 Willobee BA, Mulder M, Perez EA, Hogan AR, Brady A-C, Sola JE,Thorson CM, et al. Predictors of in-hospital mortality in newbornconjoined twins. Surgery. 2019;166(05):854–860. Doi: 10.1016/j.surg.2019.06.028
8 Goldman-Yassen AE, Goodrich JT, Miller TS, Farinhas JM. Preoper-ative evaluation of craniopagus twins: anatomy, imaging techni-ques, and surgical management. AJNR Am J Neuroradiol. 2020;41(06):951–959. Doi: 10.3174/ajnr.A6571
9 Wood BC, Sher SR, Mitchell BJ, Oh AK, Rogers GF, Boyajian MJ.Conjoined twin separation: integration of three-dimensionalmodeling for optimization of surgical planning. J CraniofacSurg. 2017;28(01):4–10. Doi: 10.1097/SCS.0000000000003412
10 Norwitz ER, Hoyte LP, Jenkins KJ, van der Velde ME, Ratiu P,Rodriguez-Thompson D, et al. Separation of conjoined twins withthe twin reversed-arterial-perfusion sequence after prenatalplanning with three-dimensional modeling. N Engl J Med.2000;343(06):399–402. Doi: 10.1056/NEJM200008103430604
11 Mathew RP, Francis S, Basti RS, Suresh HB, Rajarathnam A, CunhaPD, et al. Conjoined twins - role of imaging and recent advances. JUltrason. 2017;17(71):259–266. Doi: 10.15557/JoU.2017.0038
12 Swift DM,Weprin B, Sklar F, Sacco D, Salyer K, Genecov D, BarcelloR, et al. Total vertex craniopagus with crossed venous drainage:case report of successful surgical separation. Childs Nerv Syst.2004;20(8-9):607–617. Doi: 10.1007/s00381-004-1011-6
13 Heuer GG, Madsen PJ, Flanders TM, Kennedy BC, Storm PB,Taylor JA. Separation of craniopagus twins by a multidisciplinaryteam. N Engl J Med. 2019;380(04):358–364. Doi: 10.1056/NEJMoa1805132
14 Mehollin-Ray AR. Prenatal and postnatal radiologic evaluation ofconjoined twins. Semin Perinatol. 2018;42(06):369–380. Doi:10.1053/j.semperi.2018.07.015
Rev Bras Ginecol Obstet Vol. 43 No. 12/2021 © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Antenatal Diagnosis of Parapagus Conjoined Twins Castro et al. 987

988 FEBRASGO POSITION STATEMENT © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Key points• Althoughthereareseveralsituationsthatcanpotentiallyleadtolowerandrogenlevels,untilnowisnotdefined
asyndromeorbiochemicalcriteriatodiagnoseandrogendeficiencyinwomen.Benefitsofandrogentherapyin these situations are controversial.
• Girlswithdelayedpubertymanifestingprimarilyasa lackofdevelopmentofsecondarysexcharactersandprimaryamenorrheamaybedeficientinsexhormoneproduction,includingandrogenproductiondeficiency.
• Duetosurgicalmenopauseandprematureovarianfailure,androgenlevelsmaybereducedcomparedtoage-matched normal controls.
• Youngwomenwithhypopituitarism,anorexianervosa,andadrenalinsufficiencymayhavelowerserumandro-gen levels.
• Theuseofandrogensandanabolicsteroidsforaestheticpurposeshasincreasedconsiderablyduetoissuesrelatedtothecultofthebodyandbeauty.However,thisisassociatedwithundesirableandpotentiallyirrevers-ibleaestheticmanifestations,inadditiontoanincreaseinmorbidity.
Recommendations• Thereisnoevidencefortheuseofandrogentherapyinadolescentwomen,evenincasesofhypogonadism
duetoovarian(prematureovarianfailure)orcentralcauses.• Thereisnoevidenceforroutineandrogentherapyinadultwomenwithhypopituitarism,hypogonadotropic
hypogonadism,adrenalinsufficiencyandanorexianervosa.• Androgentherapy,preferablybythetransdermalroute,maybeconsideredforwomenwithprematureovar-
ianinsufficiency(POI)orsurgicalmenopausecomplainingoffemalesexualdysfunction(FSD),inadditiontoestrogen therapy.
• Theuseofandrogensandanabolicsteroidsforaestheticpurposesisnotrecommended.• Themeasurementoftotaltestosteroneorthecalculationofthefreeandrogenindexcanbeusedtocontrol
androgen replacement in women, but the available laboratory techniques do not present adequate sensitivity. Although the mass spectrometry technique has greater sensitivity, it is costly, which limits the use in clinical practice.
FEBRASGO POSITION STATEMENTUse of androgens at different stages of life: reproductive periodNumber 11 - December 2021DOI: https://doi.org/10.1055/s-0041-1740610
The National Specialty Commission on Gynecology Endocrinology of the Brazilian Federation of Gynecology and Obstetrics Associations (FEBRASGO) endorses to this document. The content production is based on scientific studies on a thematic proposal and the findings presented contribute to clinical practice.
BackgroundInthefemalesex,androgenisproducedbytheovariesand adrenals and by peripheral conversion. Circulating testosterone levels play an important role in musculo-skeletalandcardiovascularhealthandsexualfunction(SF).(1)Someauthorshavetriedtodefineanandrogendeficiency syndrome inwomenwith symptoms suchas low libido and global decrease in desire, fantasiesand arousal, in addition to fatigue and decreased
wellbeing.(2) However, several international entities,such as the Endocrine Society, the American College of Obstetricians and Gynecologists (ACOG), theAmericanSociety forReproductiveMedicine (ASRM),theEuropeanSocietyofEndocrinology (ESE)and theInternationalMenopauseSociety(IMS), throughtheirrecommendations for clinical practice, took a standagainsttheclinicalandlaboratorydiagnosisofandro-gendeficiencygiven the lackofuniformity inclinical

Nácul AP, Rezende GP, Gomes DA, Maranhão T, Costa LO, Reis FM, et al.
989 FEBRASGO POSITION STATEMENT © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
criteriaandthelackofstandardizationofserumtes-tosterone levels in women according to age group.(3) Consideringthedifficultyofdiagnosis,thetreatmentby androgen replacement in climacteric women has morewidespread indication in the presence of FSD,although other situations can potentially lead to lower androgen levels in premenopausal women and raise doubtsabouttheneedforreplacement.(3,4) These sit-uationsinclude,forexample,theuseofandrogenstomaintain bone mass and prevent osteoporosis, POI, hypopituitarismandadrenalinsufficiency.
This document will be divided into two parts, in which we will review current evidence of indicationsandcontraindicationsfortheuseofandrogens indif-ferentsituationsinawoman’slife–duringtherepro-ductiveperiod(partI)andduringtheclimactericperi-od(partII).
In women, is there an indication of androgen dosage for the diagnosis of androgen deficiency?The most commonly dosed androgen in women is testosterone. In premenopausal women, testoster-onelevelsdonotvarysignificantlywithcyclephaseand there is amodest increase during the peak ofluteinizinghormone (LH) inovulatorycycles.(5) This hormone circulates in the body in three ways: bound to sex hormone binding globulin – SHBG (66%),boundtoalbumin(33%)and in free form(1%).Thefree formand the albumin-bound formare consid-eredtheactive formsof testosterone.(6) Several sit-uations can increase SHBG levels, leading to a de-crease in the free fractionof testosterone. In thesecases,themeasurementoffreetestosteroneorthecalculationofthefreeandrogenindexaremoresuit-ableforevaluatingcirculatingtestosteroneinitsbio-logicallyactiveform.(7)
Themostwidely used tests formeasuring tes-tosterone such as immunometric assays and radio-immunoassay, had limitations, with low accuracy for detecting physiologically low levels in women.Currently, the liquid chromatography-mass spec-trometryassayhasgreatersensitivityfortestosteronemeasurement, so it is considered the gold standard test.(7,8)However,thehighercostandlowavailabili-tyof thismethod togetherwith theneed forhigh-ly specialized personnel limit its use. Testosteronemeasurement results should be carefully analyzedbecauseserumlevelsdonotreflectconcentrationintarget tissues nor the individual variability in the sen-sitivityofperipheralreceptors.(9) In addition, clinical effectsalsodependonconversionoftestosteronebyaromataseandby5α-reductaseintoestroneanddi-hydrotestosterone, respectively.(10) There is no indi-cationforthedosageofdihydrotestosterone.
Although there is an association between serum androgen levels with sexual desire, its low level inwomen does not reliably predict clinical symptoms. Furthermore, testosterone levels are not independent predictorsofSFinwomen.Thus,thereisnobiochemi-caldiagnosticcriteriontodiagnoseandrogendeficien-cy in women.(3)
First part: use of androgens in the reproductive periodIs there evidence for the use of androgens during adolescence?Inadolescence,theactivationofthehypothalamus-pi-tuitary-ovarianaxisstimulatestheproductionofovari-anhormones,especiallyestrogens,responsibleforthethelarche, pubarche and menarche in girls. In parallel, this activation also increases circulating testosterone levels, which, during adolescence and reproductive years, are produced in an equivalent way by theca cells andtheadrenalcortexataconcentrationofapproxi-mately 300 mcg per day.(11,12) Serum androgen levels are higher during adolescence, with a progressive de-creaseaftertheageof25years.(13)Inthisphaseoflife,theyplayanimportantroleinnormalpubertyandskel-etal growth.
Inadolescence,skeletalgrowthandbonemassgain are influenced by estrogens and androgens,with an important interaction between androgens, growthhormone(GH)andinsulin-likegrowthfactor(IGF-1).(14,15) Androgenic deficiencies can result indelayedpuberty,manifestedmainlybytheabsenceofdevelopmentofsecondarysexualcharacteristicsand primary amenorrhea, with hormone replace-ment being the first choice of treatment. The useofestrogenichormonetherapy(HT)inadolescentsdiagnosedwith hypogonadism is validated for pu-bertal stimulation, cardiovascular protection, and prevention of osteoporosis.(14-17) However, the useofandrogens inthisperiodof life isonlyvalidatedformale delayed puberty to promote growth andgain in muscle mass. There is not strong enough ev-idence to support its administration in adolescent women.
Although previous studieswith different andro-gen therapy regimens in this age group in women withTurnersyndromeandpan-hypopituitarismhaveshown some positive results such as bone and muscle mass gain and improved quality of life, they do notpresentenoughevidencetorecommenditsuseinfe-male adolescents.(18-20)
Therefore,thereisnorecommendationfortheuseof androgenic therapy in adolescent girls in any for-mulationorrouteofadministrationduetothelackofevidencetoconfirmitsefficacyandsafety inthisagegroup.

Use of androgens at different stages of life: reproductive period
990 FEBRASGO POSITION STATEMENT © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
When is the use of androgens indicated during the reproductive period?Premature ovarian insufficiency and surgical menopausePremature ovarian insufficiency and surgical meno-pause are two situations in which there is a reduction in androgen levels compared to women with pre-servedgonadal functionof the sameage,aswell asin comparison to women with natural menopause.(21) Theadditionofandrogens inHT inwomenwithPOIdoesnotseemstosignificantlyimprovequalityoflife,self-esteemormood.TheadditionoftestosteronetoHT,althoughwithlimitedevidence,doesnotseemtoaddbenefitstobonemasseither.Ontheotherhand,it also does not seem to increase adverse events or effects such as skin changes, hirsutism, acneor fre-quency ofwaxing.(22) Premenopausal women under-goingbilateraloophorectomyusuallypresentsexualdysfunctionsrelatedtolowhormonelevels.Evidencedemonstrates an improvement in SF with the addi-tionof testosterone toHT in thesecases,preferablyby transdermal route with minimal or mild adverse effects. However, the long-term effects are still un-clear.(23-25) Although in Brazil, there are no productsapprovedbyregulatoryagenciesfortheprescriptionof testosterone, the use ofmanipulated products isaccepted, highlighting thedifficulty of dose control.Testosterone1%formulated inahighabsorptiongel(egPentravan)canbeprescribedfortransdermaluseatadoseof0.5gofgelperdayforthreetosixmonths.Asasuggestion,theprescriptionoftestosterone5mgpermLinameasuringbottlecontaining30mLofgelwithareleaseof1mLperdayisrecommended.Thisdose canbe individualizedwith a variationbetween1and5mg.Dosetestosteronebeforestartingtreat-ment,afterthreetosixweeksofuseandforaslongasthe treatment lasts to avoid supraphysiological plas-malevelsandmonitortheonsetofclinicalsignsofhy-perandrogenism, because the clinical response does not always correlate with plasma testosterone levels. If there is improvement, reinforcetothepatientthelackofevidence regardingefficacyandsafety inuseformorethan24months.(23)
HypopituitarismHypopituitarismoftenincludeshypogonadotropichy-pogonadism and centrally-caused adrenal insufficien-cy, with a deficient production of androgens by thetwomajorsources–ovariesandadrenals.Astudythatevaluatedtheuseof300mcgtestosteronepatchesforone year in 51 women with hypopituitarism showed an increase in bone mass in the hip and radius and in mus-cle mass, as well as improvement in mood and SF in this groupofwomen.(24)Ifandrogentherapyisconsideredforwomenwithhypopituitarism,follow-upshouldbe
doneinthesamewayasforwomenwithFSD,althoughthelong-termsafetyisunknownandthereisnoformalrecommendationforthisreplacement.(3,25)
Adrenal insufficiencyWomenwithadrenalinsufficiencyhavelowerlevelsofdehydroepiandrosterone(DHEA)anditssulfatedform(SDHEA).Manywomenwithprimary and secondaryadrenal insufficiency present deterioration in theirgeneral health status despite glucocorticoid and min-eralocorticoid replacement.(26) Although some stud-ies demonstrate that DHEA replacement improvesdepressionandanxietyscores, feelingsofwellbeing,libidoandSF,asystematic reviewandmeta-analysisshowed onlymodest improvement in quality of lifeand depression scores. Dehydroepiandrosterone is a dietary supplement without regulatory control and robust evidence to indicate its routine use in adrenal insufficiency.(27) In practice, androgen replacement withDHEAissometimesusedforwomenwithsymp-toms of androgen deficiency and low plasma levelsofDHEA,withstartingdosesbetween25and50mgdailyforaperiodofthreetosixmonthsanddosead-justments according to circulating DHEA levels andclinical symptoms. In the absence of a satisfactorytherapeutic result or in the presence of adverse ef-fects,therapyshouldbesuspended.(28)
Anorexia nervosaWomen with anorexia nervosa have lower total andfreetestosteronelevelsthanwomenwithoutthiscon-dition.(29) Free testosterone levels have a positive cor-relationwith bodymass index (BMI) and spinal bonemineral density and a negative correlation with depres-sion levels in these women.(30) Although studies have shownhigherboneformationmarkerswiththeuseoftestosterone patches, this increase did not reflect inan increase in bone mass.(29,30) Although there may be an increaseof leanmass, theuseoftestosteronecaneven lead to a decrease in BMI.(31) Testosterone replace-mentalsodidnotshowpositiveeffectsondepressionandanxietyindices.(31) Thus, testosterone replacement should not be recommended for the prevention ofbone mass loss, weight gain and emotional disorders associatedwithanorexianervosa.
What can we say about the use of anabolic androgens for aesthetic/recreational purposes?Thecurrentexaggeratedcultofthebodyandaesthet-ic beauty has made many people seek quick resultsthrough substance abusewith the promise of betterbody image andphysical performance.Among thesesubstancesareandrogenicanabolic steroids (AAS),(32) including testosterone and its synthetic derivatives. Androgenic anabolic steroids are typically given in sup-

Nácul AP, Rezende GP, Gomes DA, Maranhão T, Costa LO, Reis FM, et al.
991 FEBRASGO POSITION STATEMENT © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
raphysiologicaldosesforperiodscalledcycles,orusedcontinuously with constant or varying doses. These substancesareefficientinpromotingincreaseinmus-clesizeandstrength,inthesearchforanidealizedbodyimage,asaresultofculturalstimulior,forsome,asaresultofbodydysmorphicdisorders.(33)
Empirical evidence suggested that AAS were used primarily by top-level competitive athletes and espe-cially weightlifters, bodybuilders, and track athletes.Currently, AAS are widely used not only by athletes in-volved in recreational and minor league sports, but also bynon-athletes.(34)
In Brazil, gestrinone, previously used for thetreatment of endometriosis and discontinued be-cause of its androgenic side effects, is now beingmarketedagainintheformofanimplantandcalled“beautychip”,givenapossibleaestheticeffect(re-duction of body fat and promotion of lean massgain). There are no studies evaluating gestrinonefor improved libidoor leanmassgain,aswellas itslong-termeffects,suchaspossiblecarcinogenicriskorsecondaryinfertility.Thisproductisnotapprovedfor use by theNationalHealth SurveillanceAgency(Anvisa), and the Federal Council of Medicine onlyrecommendstheuseofhormonalimplantsformed-icalpurposes,giventhe lackofanyevidenceofthepromisedaestheticbenefits.
UsersmayassociatedifferentAAS,aswellaswithother potentially anabolic products such as GH andinsulinforbetterresults,althoughwithanincreaseinandrogenicandmetaboliceffects.(35)
In women, the most frequent alterations at-tributed to AAS abuse are menstrual irregularities (late menarche, oligomenorrhea, secondary amen-orrhea),dysmenorrhea,anovulation,acne,alopecia,clitoris hypertrophy, libido alterations, breast tissue atrophyanduterineatrophy,manyofwhichareper-manent.(36)Inadolescents,itcancauseearlyskeletalmaturationwithclosureofthebonyepiphyses,shortstature and accelerated puberty, leading to dysmor-phic growth. The use of AAS has been associatedwithanumberofmedicalandpsychologicalsideef-fects,includingmentalhealthandcognitivefunctiondisorders, metabolic and endocrine disorders, and cardiovascular pathology.(37,38)
Therefore,wedonotrecommendtheuseofAASforaestheticpurposes.Thisuseisillegal,cancausead-diction,andnumerousharmfulsideeffects.
Is there an indication for the use of androgens in users of combined oral contraceptives (COCs)?TheeffectsofCOCsonSFremaincontroversial.Inor-der to improve SF, some authors have proposed the concomitantuseofandrogens,especiallyDHEA.Theexchangeofethinylestradiol for17β-estradiol isalso
suggested,withalowerelevationofSHBGandahigh-er indexoffreeandrogens.However,thereis lackofevidenceontheimpactofCOCsonSF,andonthefactthatthisdysfunction iscausedbya reduction inan-drogenic activity.(39)
Final considerationsThere is limitedevidenceon theuseof androgens inwomen during the age compatible with the reproduc-tiveperiod,indicatingtheiruseinsituationsofbilateraloophorectomy and premature ovarian insufficiency.Thereisalackofevidencetosupportotherindications.Theuseofandrogensforaestheticpurposesshouldnotbe recommended.
References1. Davis SR. Androgen therapy in women, beyond libido. Climacteric.
2013;16 Suppl 1:18-24. doi: 10.3109/13697137.2013.8017362. Barrett-Connor E, Young R, Notelovitz M, Sullivan J, Wiita
B, Yang HM, et al. A two-year, double-blind comparison of estrogen-androgen and conjugated estrogens in surgically menopausal women. Effects on bone mineral density, symptoms and lipid profiles. J Reprod Med. 1999;44(12):1012-20.
3. Wierman ME, Arlt W, Basson R, Davis SR, Miller KK, Murad MH, et al. Androgen therapy in women: a reappraisal: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2014;99(10):3489-510. doi: 10.1210/jc.2014-2260
4. Bolour S, Braunstein G. Testosterone therapy in women: a review. Int J Impot Res. 2005;17(5):399-408. doi: 10.1038/sj.ijir.3901334
5. Bui HN, Sluss PM, Blincko S, Knol DL, Blankenstein MA, Heijboer AC. Dynamics of serum testosterone during the menstrual cycle evaluated by daily measurements with an ID-LC-MS/MS method and a 2nd generation automated immunoassay. Steroids. 2013;78(1):96-101. doi: 10.1016/j.steroids.2012.10.010
6. Rosner W, Hryb DJ, Khan MS, Nakhla AM, Romas NA. Sex hormone-binding globulin mediates steroid hormone signal transduction at the plasma membrane. J Steroid Biochem Mol Biol. 1999;69(1-6):481-5. doi: 10.1016/s0960-0760(99)00070-9
7. Vesper HW, Botelho JC. Standardization of testosterone measurements in humans. J Steroid Biochem Mol Biol. 2010;121(3-5):513-9. doi: 10.1016/j.jsbmb.2010.03.032
8. Goodman N, Guay A, Dandona P, Dhindsa S, Faiman C, Cunningham GR, et al. American association of clinical endocrinologists and American college of endocrinology position statement on the association of testosterone and cardiovascular risk. Endocr Pract. 2015;21(9):1066-73. doi: 10.4158/EP14434.PS
9. Simpson ER. Aromatization of androgens in women: current concepts and findings. Fertil Steril. 2002;77 Suppl 4:S6-10. doi: 10.1016/s0015-0282(02)02984-9
10. Davis SR, Davison SL, Donath S, Bell RJ. Circulating androgen levels and self-reported sexual function in women. JAMA. 2005;294(1):91-6. doi: 10.1001/jama.294.1.91
11. Sawyer SM, Azzopardi PS, Wickremarathne D, Patton GC. The age of adolescence. Lancet Child Adolesc Health. 2018;2(3):223-8. doi: 10.1016/S2352-4642(18)30022-1

Use of androgens at different stages of life: reproductive period
992 FEBRASGO POSITION STATEMENT © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
12. Rothman MS, Carlson NE, Xu M, Wang C, Swerdloff R, Lee P, et al. Reexamination of testosterone, dihydrotestosterone, estradiol and estrone levels across the menstrual cycle and in postmenopausal women measured by liquid chromatography-tandem mass spectrometry. Steroids. 2011;76(1-2):177-82. doi: 10.1016/j.steroids.2010.10.010
13. Longcope C. Adrenal and gonadal androgen secretion in normal females. Clin Endocrinol Metab. 1986;15(2):213-28. doi: 10.1016/s0300-595x(86)80021-4
14. Zumoff B, Strain GW, Miller LK, Rosner W. Twenty-four-hour mean plasma testosterone concentration declines with age in normal premenopausal women. J Clin Endocrinol Metab. 1995;80(4):1429-30. doi: 10.1210/jcem.80.4.7714119
15. Weiss RV, Hohl A, Athayde A, Pardini D, Gomes L, Oliveira M, et al. Testosterone therapy for women with low sexual desire: a position statement from the Brazilian society of endocrinology and metabolism. Arch Endocrinol Metab. 2019;63(3):190-8. doi: 10.20945/2359-3997000000152
16. Vanderschueren D, Vandenput L, Boonen S. Reversing sex steroid deficiency and optimizing skeletal development in the adolescent with gonadal failure. Endocr Dev. 2005;8:150-65. doi: 10.1159/000084100
17. Mason KA, Schoelwer MJ, Rogol AD. Androgens during infancy, childhood, and adolescence: physiology and use in clinical practice. Endocr Rev. 2020;41(3):bnaa003. doi: 10.1210/endrev/bnaa003
18. Zuckerman-Levin N, Frolova-Bishara T, Militianu D, Levin M, Aharon-Peretz J, Hochberg Z. Androgen replacement therapy in turner syndrome: a pilot study. J Clin Endocrinol Metab. 2009;94(12):4820-7. doi: 10.1210/jc.2009-0514
19. Rosenfeld RG, France J, Attie KM, Brasel JA, Burstein S, Cara JF, et al. Six-year results of a randomized, prospective trial of human growth hormone and oxandrolone in Turner syndrome. J Pediatr. 1992;121(1):49-55. doi: 10.1016/s0022-3476(05)82540-5
20. Bilger M, Speraw S, LaFranchi SH, Hanna CE. Androgen replacement in adolescents and young women with hypopituitarism. J Pediatr Endocrinol Metab. 2005;18(4):355-62. doi: 10.1515/jpem.2005.18.4.355
21. Janse F, Tanahatoe SJ, Eijkemans MJ, Fauser BC. Testosterone concentrations, using different assays, in different types of ovarian insufficiency: a systematic review and meta-analysis. Hum Reprod Update. 2012;18(4):405-19. doi: 10.1093/humupd/dms013
22. Webber L, Anderson RA, Davies M, Janse F, Vermeulen N. HRT for women with premature ovarian insufficiency: a comprehensive review. Hum Reprod Open. 2017;2017(2):hox007. doi: 10.1093/hropen/hox007
23. Vegunta S, Kling JM, Kapoor E. Androgen therapy in women. J Womens Health. 2020;29(1):57-64. doi: 10.1089/jwh.2018.7494
24. Miller KK, Biller BM, Beauregard C, Lipman JG, Jones J, Schoenfeld D, et al. Effects of testosterone replacement in androgen-deficient women with hypopituitarism: a randomized, double-blind, placebo-controlled study. J Clin Endocrinol Metab. 2006;91(5):1683-90. doi: 10.1210/jc.2005-2596
25. Miller KK, Lawson EA, Mathur V, Wexler TL, Meenaghan E, Misra M, et al. Androgens in women with anorexia nervosa and normal-weight women with hypothalamic amenorrhea. J Clin Endocrinol Metab. 2007;92(4):1334-9. doi: 10.1210/jc.2006-2501
26. Hahner S, Loeffler M, Fassnacht M, Weismann D, Koschker AC, Quinkler M, et al. Impaired subjective health status in 256 patients with adrenal insufficiency on standard therapy based on cross-sectional analysis. J Clin Endocrinol Metab. 2007;92(10):3912-22. doi: 10.1210/jc.2007-0685
27. Alkatib AA, Cosma M, Elamin MB, Erickson D, Swiglo BA, Erwin PJ, et al. A systematic review and meta-analysis of randomized placebo-controlled trials of DHEA treatment effects on quality of life in women with adrenal insufficiency. J Clin Endocrinol Metab. 2009;94(10):3676-81. doi: 10.1210/jc.2009-0672
28. Castinetti F, Guignat L, Bouvattier C, Samara-Boustani D, Reznik Y. Group 4: replacement therapy for adrenal insufficiency. Ann Endocrinol (Paris). 2017;78(6):525-34. doi: 10.1016/j.ando.2017.10.007
29. Miller KK, Meenaghan E, Lawson EA, Misra M, Gleysteen S, Schoenfeld D, et al. Effects of risedronate and low-dose transdermal testosterone on bone mineral density in women with anorexia nervosa: a randomized, placebo-controlled study. J Clin Endocrinol Metab. 2011;96(7):2081-8. doi: 10.1210/jc.2011-0380
30. Miller KK, Grieco KA, Klibanski A. Testosterone administration in women with anorexia nervosa. J Clin Endocrinol Metab. 2005;90(3):1428-33. doi: 10.1210/jc.2004-1181
31. Kimball A, Schorr M, Meenaghan E, Bachmann KN, Eddy KT, Misra M, et al. A randomized placebo-controlled trial of low-dose testosterone therapy in women with anorexia nervosa. J Clin Endocrinol Metab. 2019;104(10):4347-55. doi: 10.1210/jc.2019-00828
32. Hanley Santos G, Coomber R. The risk environment of anabolic-androgenic steroid users in the UK: examining motivations, practices and accounts of use. Int J Drug Policy. 2017;40:35-43. doi: 10.1016/j.drugpo.2016.11.005
33. Kicman AT. Pharmacology of anabolic steroids. Br J Pharmacol. 2008;154(3):502-21. doi: 10.1038/bjp.2008.165
34. Sagoe D, Molde H, Andreassen CS, Torsheim T, Pallesen S. The global epidemiology of anabolic-androgenic steroid use: a meta-analysis and meta-regression analysis. Ann Epidemiol. 2014;24(5):383-98. doi: 10.1016/j.annepidem.2014.01.009
35. Anderson LJ, Tamayose JM, Garcia JM. Use of growth hormone, IGF-I, and insulin for anabolic purpose: pharmacological basis, methods of detection, and adverse effects. Mol Cell Endocrinol. 2018;464:65-74. doi: 10.1016/j.mce.2017.06.010
36. Nieschlag E, Vorona E. Mechanisms in endocrinology: medical consequences of doping with anabolic androgenic steroids: effects on reproductive functions. Eur J Endocrinol. 2015;173(2):R47-58. doi: 10.1530/EJE-15-0080
37. Gruber AJ, Pope HG Jr. Psychiatric and medical effects of anabolic-androgenic steroid use in women. Psychother Psychosom. 2000;69(1):19-26. doi: 10.1159/000012362
38. Rasmussen JJ, Schou M, Selmer C, Johansen ML, Gustafsson F, Frystyk J, et al. Insulin sensitivity in relation to fat distribution and plasma adipocytokines among abusers of anabolic androgenic steroids. Clin Endocrinol (Oxf). 2017;87(3):249-56. doi: 10.1111/cen.13372
39. de Castro Coelho F, Barros C. The potential of hormonal contraception to influence female sexuality. Int J Reprod Med. 2019;2019:9701384. doi: 10.1155/2019/9701384

Nácul AP, Rezende GP, Gomes DA, Maranhão T, Costa LO, Reis FM, et al.
993 FEBRASGO POSITION STATEMENT © 2021. Federação Brasileira de Ginecologia e Obstetrícia. All rights reserved.
Andrea Prestes Nácul1 1 - Unidade de Reprodução Humana, Hospital Fêmina, Grupo Hospitalar Conceição, Porto Alegre,RS, Brazil.
Gabriela Pravatta Rezende2 2 - Universidade Estadual de Campinas, Campinas, SP, Brazil.
Daniela Angerame Yela Gomes3 3 - Universidade Estadual de Campinas, Campinas, SP, Brazil.
Técia Maranhão4 4 - Universidade Federal do Rio Grande do Norte, Natal, RN, Brazil.
Laura Olinda Bregieiro Fernandes Costa5 5 - Universidade de Pernambuco, Recife, PE, Brazil
Fernando Marcos dos Reis6 6 - Universidade Federal de Minas Gerais, Belo Horizonte, MG, Brazil.
Gustavo Arantes Rosa Maciel7 7 - Faculdade de Medicina, Universidade de São Paulo, São Paulo, SP, Brazil.
Lia Cruz Vaz da Costa Damásio8 8 - Universidade Federal do Piauí, Teresina, PI, Brazil.
Ana Carolina Japur de Sá Rosa e Silva9
9 - Faculdade de Medicina de Ribeirão Preto, Ribeirão Preto, SP, Brazil
Vinicius Medina Lopes10 10 - Universidade de Brasília, Brasília DF, Brazil
Maria Cândida Baracat11 11 - Faculdade de Medicina, Universidade de São Paulo, São Pau-lo, SP, Brazil.
Gustavo Mafaldo Soares12 12 - Universidade Federal do Rio Grande do Norte, Natal, RN, Brazil.
José Maria Soares Junior13 13 - Faculdade de Medicina, Universidade de São Paulo, São Pau-lo, SP, Brazil.
Cristina Laguna Benetti-Pinto14 14 - Universidade Estadual de Campinas, Campinas, SP, Brazil.
Conflicts of interest: none to declare.
National Specialty Commission on Gynecology Endocrinology of the Brazilian Federation of Gynecology and Obstetrics Associations (FEBRASGO)
President: Cristina Laguna Benetti Pinto
Vice-President: Ana Carolina Japur de Sá Rosa e Silva
Secretary: José Maria Soares Júnior
Members:Andrea Prestes NáculDaniela Angerame YelaFernando Marcos dos ReisGabriela Pravatta RezendeGustavo Arantes Rosa MacielGustavo Mafaldo SoaresLaura Olinda Rezende Bregieiro CostaLia Cruz Vaz da Costa DamásioMaria Candida Pinheiro Baracat RezendeSebastião Freitas de MedeirosTecia Maria de Oliveira MaranhãoVinicius Medina Lopes


Instructions to AuthorsScope and policyAll content of the journal, except where otherwise noted, is licensed under a Creative Commons License.
The material submitted for analysis cannot be simultaneously submitted for publication in other journals or previously published. In the selection of man-uscripts for publication, are evaluated the originality, relevance of the theme, quality of the methodology used, and adequacy to the editorial standards adopted by the journal. The published material becomes intellectual prop-erty of the Brazilian Journal of Gynecology and Obstetrics and Febrasgo.
Manuscripts evaluation
The manuscripts submitted to the journal are received by the Editorial Offi ce that checks the mandatory documentation and examines if the edi-torial norms contained in the Instructions to Authors have been fulfi lled. If the process is in compliance, the manuscript is sent to the Editor-in-Chief, who will make a merit evaluation of the material. If the Editor-in-Chief concludes the work is in favorable scientifi c and technical conditions, the manuscript is forwarded to the Associate Editors, who will designate re-viewers (double mind process) to evaluate it. Then, the reviewers’ opin-ions and editor’s instructions are sent to authors to inform them about changes to be made. Then, the authors resubmit the text with the sug-gested changes within the requested deadline. When resubmitting the manuscript, the requested corrections should be highlighted in yellow. In cases of disagreement with the suggestions, observations should be included in the comments balloons. Be assertive and punctual with the inquiry, and support the hypothesis with references.
IMPORTANT! Authors must comply with the deadlines, since non-attend-ance will result in delay of manuscript publication or even archiving of the process. At any point in the process of analysis and editing of the text, the authors may request the process suspension and withdrawal of the manuscript, except when it is accepted for publication. The concepts and statements contained in the articles are of the authors’ responsibility.
Preparing a manuscript for submission
Mandatory submission documents
When submitting a manuscript to RBGO, attach the documents listed below on the ScholarOne submission platform. Note that not attach-ing the documents will result in cancellation of the submitted process. Mandatory documentation for online submission:
• Authorization of copyright transfer signed by all authors (scanned and attached as supplementary document) Model;
• In accordance with chapter XII.2 of Res. CNS 466/2012, in Brazil, research involving human subjects needs to inform the registration number referring to the Certifi cate of Ethical Assessment (CAAE) or the approval number of the research (CEP/CONEP) in the Ethics Committee. International manuscripts must present local ethical documentation to proceed with the submission process;
• Cover Letter: written to justify the publication. The authors should be identifi ed, together with the title of the team that intends to pub-lish, origin institution of the authors and intention of publication;
• Title page;
• Manuscript.
Title Page
• Title of the manuscript in English with a maximum of 18 words;
• Authors' full name without abbreviations and Orcid ID;
• Corresponding author (full name, professional mailing address and contact email);
• Institutional affi liation of each author. Example: Faculty of Medicine, University of São Paulo, Ribeirão Preto, SP, Brazil;
• Confl icts of interest: authors should report any potential confl icts of interest whether political, economic, of resources for research execution or intellectual property;
• Acknowledgements: restricted to people and institutions that contrib-uted to research development in a relevant way. Any fi nancial support provided by development agencies or private companies should be men-tioned in the section Acknowledgments. For Brazilian authors, RBGO re-quests the citation of CNPq, Capes, FAPESP and other fi nancing agencies, together with the number of research process or granted scholarships.
• Contributions: according to the criteria for scientifi c authorship of the International Committee of Medical Journal Editors (ICMJE), authorship credit must be based on three conditions met in full: 1. Substantial contributions to conception and design, data collection or analysis, and interpretation of data; 2. Writing of the article or critical review of the in-tellectual content; and 3. Final approval of the version to be published.
ManuscriptInstructions to Authors
The Brazilian Journal of Gynecology and Obstetrics publishes the follow-ing categories of manuscripts:
Original Articles, complete prospective, experimental or retrospec-tive studies. Manuscripts containing original clinical or experimental research results have priority for publication.
Case Reports, of great interest and well documented from the clinical and laboratorial point of view. In the letter of referral, authors should in-dicate new or unexpected aspects in relation to already published cases. The text of Introduction and Discussion sections should be based on an updated bibliographic review.
Review Articles, including comprehensive reviews, meta-analysis or systematic reviews. Spontaneous contributions are accepted. The meth-ods and procedures adopted for obtaining the text should be described, and based on recent references, including the current year. As this sub-ject is still subject to controversy, the review should discuss the trends and lines of research under way. In addition to the text of the review, there should be an abstract and conclusions. See the ‘Instructions to Authors’ section for information on the text body and title page;
Letters to the Editor, dealing with editorial matters or not, but presenting relevant information to readers. Letters can be summarized by the editor, but maintaining the main points. In case of criticism to published works, the letter is sent to the authors so their reply can be published simultaneously;
Editorial, only at the publisher’s invitation.
Title
When writing a scientifi c article, the researcher should focus on the manuscript title, which is the business card of any publication. It should be elaborated very carefully, and preferably written only after the article fi nalization. A good title adequately describes the manuscript content. Generally it is not a phrase, because it does not contain the subject, only verbs and arranged objects. Titles rarely contain abbreviations, chemical formulas, adjectives, names of cities, among others. The title of manu-scripts submitted to RBGO must contain a maximum of 18 words.
Abstract
The abstract should provide the context or basis for the study, establish the objectives, basic procedures, main outcomes and key fi ndings. It should emphasize new and important aspects of the study or observa-tions. Since the abstract is the only substantive part of the article in-dexed in many electronic databases, authors should ensure it refl ects the article content in an accurate and highlighted manner. Do not use abbreviations, symbols and references in the abstract. In case of original articles from clinical trials, authors must inform the registration number at the end of the text.

Informational abstract of structured type of original articles
Abstracts of original articles submitted to RBGO must be structured in four sections and contain a maximum of 250 words:
Objective: What was done; the question posed by the investigator.
Methods: How it was done; the method, including the material used to achieve the objective.
Results: What was found, the main fi ndings and, if necessary, the sec-ondary fi ndings.
Conclusion: The conclusions; the answer to the question asked.
Informational abstract of structured type of systematic review articles
Among the included items are the review objective to the question asked, data source, procedures for selecting the studies and data collec-tion, the results and conclusions. The abstracts of systematic review ar-ticles submitted to RBGO must be structured in six sections and contain a maximum of 250 words:
Objective: Declare the main purpose of the article.
Data sources: Describe the data sources examined, including the date, indexing terms, and limitations.
Selection of studies: Specify the number of studies reviewed and the criteria used in their selection.
Data collection: Summarize the conduct used for data extraction and how it was used.
Data synthesis: State the main results of the review and the methods used to obtain them.
Conclusions: Indicate the main conclusions and their clinical usefulness.
Informational abstract of unstructured type of review articles, except systematic reviews and case studies
It shall contain the substance of the article, covering the purpose, method, results and conclusions or recommendations. It exposes enough details so readers can decide on the convenience of reading the full text (Limit of words: 150).
Keywords
The keywords of a scientifi c paper indicate the thematic content of the text they represent. The main objectives of the aforementioned terms are the thematic content identifi cation, indexing of the work in databases, and rapid location and retrieval of contents. The keyword systems used by RBGO are DeCS (Health Sciences Descriptors - Lilacs Indexer) and MeSH (Medical Subject Headings - MEDLINE-PubMed Indexer). Please choose fi ve descriptors that represent your work on these platforms.
Manuscript body (Manuscripts submitted to RBGO must have a maximum of 4000 words. Note that tables, charts and fi gures in the Results section and References are not counted).
Introduction
The Introduction section of a scientific article has the purpose of in-forming what was researched and the reason for the investigation. This part of the article prepares the reader to understand the investigation and justification of its realization. The content informed in this sec-tion should provide context or basis for the study (i.e. the nature of the problem and its importance); state the specific purpose, research objective, or hypothesis tested in the study or observation. The study objective usually has a more precise focus when formulated as a ques-tion. Both the primary and secondary objectives should be clear, and any analyzes in a pre-specified subgroup should be described; provide strictly relevant references only and do not include data or conclusions of the work being reported.
MethodsAccording to the Houaiss dictionary, Methods “is an organized, logical and systematic process of research”. The method comprises the ma-terial and procedures adopted in the research in order to respond to the central research question. Structure the Methods section of RBGO starting with the study design; research scenario (place and period in
which it was performed); sample of participants; data collection; in-tervention to be evaluated (if any) and the alternative intervention; statistical methods used and the ethical aspects of the study. When thinking about the writing of the study design, refl ect if it is appropri-ate to achieve the research objective, if the data analysis refl ects the design, and if what was expected with use of the design was achieved to research the theme. Following, the guidelines used in clinical or epi-demiological research that should be included in the section Methods of manuscripts sent to RBGO:
Types of study (adapted from Pereira, 2014*):
Case Report (Case study): In-depth investigation of a situation in which one or a few people are included (usually up to ten);
Case series: A set of patients (for example, more than ten people) with the same diagnosis or undergoing the same intervention. In general, these are consecutive series of patients seen in a hospital or other health institu-tion for a certain period. There is no internal control group formed simul-taneously. The comparison is made with external controls. The name of external or historical control is given to the group used to compare the results, but that was not constituted at the same time within the study: for example, the case series is compared with patients from previous years.
Transversal (or Cross-sectional) study: Investigation to determine prevalence; examine the relationship between events (exposure, dis-ease, and other variables of interest) at any given time. Cause and eff ect data are collected simultaneously: for example, the case series is com-pared with patients from previous years.
Case-control study: Particular form of etiological investigation of ret-rospective approach in which the search of causes starts from the ef-fects. Groups of individuals, respectively with and without a particular health problem are compared in relation to past exposures in order to test the hypothesis that exposure to certain risk factors is the contrib-uting cause of the disease. For example, individuals affl icted with low back pain are compared with an equal number of individuals (control group) of the same sex and age, but without low back pain.
Cohort study: Particular form of investigation of etiological factors in which the search of eff ects starts from the cause; therefore, the oppo-site of case-control studies. A group of people is identifi ed, and perti-nent information on the exposure of interest is collected, so the group can be monitored over time, checking those who do not develop the disease in focus, and if the prior exposure is related to occurrence of disease. For example, smokers are compared to nonsmoker controls; the incidence of bladder cancer is determined for each group.
Randomized study: This has the connotation of an experimental study to evaluate an intervention hence the synonym of intervention study. Can be performed in a clinical setting; sometimes referred to simply as clini-cal trial or clinical study. It is also conducted at the community level. In clinical trials, participants are randomly assigned to form groups called study (experimental) and control (or testimony), whether submitted or not to an intervention (for example, a drug or vaccine). Participants are monitored to verify the occurrence of outcome of interest. This way, the relationship between intervention and eff ect is examined under controlled observation conditions, usually with double-blind evaluation. In the case of a randomized study, inform the number of the Brazilian Registry of Clinical Trials (REBEC) and/or the number of the International Clinical Trials Registration Platform (ICTRP/OMS) on the title page.
Ecological study: Research performed with statistics: the unit of observa-tion and analysis is not constituted of individuals, but of groups of individuals hence the synonyms: study of groups, aggregates, clusters, statistics or com-munity. For example, research on the variation of mortality coeffi cients for diseases of the vascular system and per capita consumption of wine among European countries.
Systematic Review and Meta-analysis: Type of review in which there is a clearly formulated question, explicit methods are used to critically iden-tify, select and evaluate relevant research, and also to collect and analyze data from the studies included in the review. There is use of strategies to

limit bias in the localization, selection, critical evaluation and synthesis of relevant studies on a given topic. Meta-analysis may or may not be part of the systematic review. Meta-analysis is the review of two or more stud-ies to obtain a global, quantitative estimate of the question or hypothesis investigated; and employs statistical methods to combine the results of the studies used in the review.
Source: *Pereira MG. Artigos Científi cos – Como redigir, publicar e avaliar. Rio de Janeiro: Guanabara-Koogan; 2014.
Script for statistical review of original scientifi c papers
Study objective: Is the study objective suffi ciently described, including pre-established hypotheses?
Design: Is the design appropriate to achieve the proposed objective?
Characteristics of the sample: Is there a satisfactory report on the selection of people for inclusion in the study? Has a satisfactory rate of responses (valid cases) been achieved? If participants were followed up, was it long and complete enough? If there was a pairing (eg. of cas-es and controls), is it appropriate? How did you deal with missing data?
Data Collection (measurement of results): Were the measurement methods detailed for each variable of interest? Is there a description of comparability of the measurement methods used in the groups? Was there consideration of the validity and reproducibility of the methods used?
Sample size: Has adequate information on sample size calculation been provided? Is the logic used to determine the study size described, includ-ing practical and statistical considerations?
Statistical Methods: Was the statistical test used for each comparison informed? Indicate if the assumptions for use of the test were followed. Was there information about the methods used for any other analysis? For example, subgroup analysis and sensitivity analysis. Are the main results accompanied by accuracy of the estimate? Inform the p value and confi dence interval. Was the alpha level informed? Indicate the al-pha level below which the results are statistically signifi cant. Was the beta error informed? Or indicate the statistical power of the sample. Has the adjustment been made to the main confounding factors? Were the reasons that explained the inclusion of some and the exclusion of oth-ers described? Is the diff erence found statistically signifi cant? Make sure there are suffi cient analyzes to show the statistically signifi cant diff er-ence is not due to any bias (eg. lack of comparability between groups or distortion in data collection). If the diff erence found is signifi cant, is it also relevant? Specify the clinically important minimal diff erence. Make clear the distinction between statistically relevant diff erence and relevant clinical diff erence. Is it a one- or two-tailed test? Provide this information if appropriate. What statistical program is used? Inform the reference where to fi nd it, and the version used.
Abstract: Does the abstract contain the proper article synthesis?
Recommendation on the article: Is the article in acceptable statistical stand-ard for publication? If not, can the article be accepted after proper review?
Source: *Pereira MG. Artigos Científi cos – Como redigir, publicar e avaliar. Rio de Janeiro: Guanabara-Koogan; 2014.
IMPORTANT!
RBGO joined the initiative of the International Committee of Medical Journal Editors (ICMJE) and the EQUATOR Network, which are aimed to improve the presentation of research results. Check the following international guides:
Randomized clinical trial: http://www.consort-statement.org/downloads/consort-statement
Systematic reviews and meta-analysis: http://www.scielo.br/pdf/ress/v24n2/2237-9622-ress-24-02-00335.pdf
Observational studies in epidemiology: strobe-statement.org/fi lead-min/Strobe/uploads/checklists/STROBE_checklist_v4_combined.pdf
Qualitative studies: http://intqhc.oxfordjournals.org/content/19/6/349.long
Results
The purpose of the Results section is to show the study fi ndings. It is the original data obtained and synthesized by the author with the aim to answer the question that motivated the investigation. For the writing of the section,
present the results in logical sequence in the text, tables and illustrations, fi rst mentioning the most important fi ndings. Do not repeat all information of the tables or illustrations in the text. Emphasize or summarize only important ob-servations. Additional or supplementary materials and technical details may be placed in an appendix where they will be accessible without interrupting the fl ow of the text. Alternatively, this information may be published only in the electronic version of the Journal. When data are summarized in the results section, provide numerical results not only in derived values (eg. percentages),but also in absolute values from which the derivatives were calculated, and specify the statistical methods used for their analysis. Use only the tables and fi gures necessary to explain the argument of the work and evaluate its foun-dation. When scientifi cally appropriate, include data analysis with variables such as age and sex. Do not exceed the maximum limit of fi ve tables, fi ve charts or fi ve fi gures. Tables, charts and/or fi gures should be included in the body of the manuscript and do not count the requested limit of 4000 words.
ATTENTION!
In Case Studies, the Methods and Results sections should be replaced by the term Case Description.
Discussion
In the Discussion section, emphasize the new and important aspects of the study and the conclusions derived therefrom. Do not repeat details of data or other information presented in the introduction or results sections. For experimental studies, it is useful to begin the discussion by briefly summarizing the main findings, comparing and contrasting the results with other relevant studies, stating the limita-tions of the study, and exploring the implications of the findings for future research and clinical practice. Avoid claiming precedence and referring to incomplete studies. Do not discuss data not directly related to the results of the presented study. Propose new hypotheses when justifiable, but qualify them clearly as such. In the last paragraph of the Discussion section, cite which information of your work contributes relatively to advancement of knowledge.
Conclusion
The Conclusion section has the function of relating the conclusions to the objectives of the study, but authors should avoid unfounded statements and conclusions not adequately supported by data. In particular, authors should avoid making statements about economic benefi ts and costs unless their original includes economic analysis and appropriate data.
References
A study is based on the results of other research that preceded it. Once published, it becomes support for future work on the subject. In the report of their research, authors state the references of prior works consulted that they deem pertinent to inform readers, hence the im-portance of choosing good References. Properly chosen references lend credibility to the report. They are a source for convincing readers of the validity of facts and arguments presented.
Attention! For manuscripts submitted to RBGO, authors should num-ber the references in order of entry into the manuscript and use those numbers for text citations. Avoid excessive references by selecting the most relevant for each statement and giving preference to the most recent work. Do not use hard-to-reach quotations, such as abstracts of papers presented at congresses, theses or restricted publications (non-indexed). Seek to cite the primary and conventional references (ar-ticles in scientifi c journals and textbooks). Do not use references such as ‘unpublished observations’ and ‘personal communication’. Authors’ publications (self-citation) should be used only if there is a clear need and relationship with the topic. In this case, include in bibliographical references only original works published in regular journals (do not cite chapters or revisions). The number of references should be 35, in ex-ception review articles. Authors are responsible for the accuracy of data contained in the references.
Please check the Vancouver Citation Style to format your references.

*The Instructions to Authors of this journal were elaborated based in the literary work Artigos Científi cos: Como redigir, publicar e avaliar de Maurício Gomes Pereira, Editora Guanabara Koogan, 2014.
Submission of papers
The articles must, necessarily, be submitted electronically, accord-ing to the instructions posted on the site: http://mc04.manuscript-central.com/rbgo-scieloThere is no fee for submission and review articles.
Revista Brasileira de Ginecologia e ObstetríciaAddress: Brigadeiro Luiz Antonio Avenue, 3421, 01401-001, 903 room, Jardim Paulista, São Paulo, SP, Brazil. Phone: + 55 11 5573.4919 E-mail: editorial.offi [email protected] Home Page: https://www.thieme.com/rbgo
Related Documents











