GUIDELINES FOR THE MANAGEMENT OF ADULTS WITH COMMUNITY ACQUIRED PNEUMONIA (CAP) BY Ibrahim Al Sharabi from the guidelines of AMERICAN THORACIC SOCIETY

Guidelines for the management of adults with community acquired pneumonia
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

GUIDELINES FOR THE MANAGEMENT
OF ADULTS WITH COMMUNITY
ACQUIRED PNEUMONIA(CAP)
BYIbrahim Al Sharabifrom the guidelines
ofAMERICAN THORACIC SOCIETY

INTRODUCTION
• CAP remains a common and serious illness, in spite of the availability of potent new antimicrobials and effective vaccines.
• Sixth leading cause of death and number one infectious death in USA
• Up to 5.6 million cases of community-acquired pneumonia occur annually, and as many as 1.1 million of these require hospitalization.
• The annual cost of treatment was $9.7 billion (1994) ; 92 % inpatient therapy
• Among patients with CAP who require hospitalization, the mortality rate averages 12% overall, but increases in specific populations, such as those with bacteremia(30%of all CAP cases), and those from nursing home settings, and approaches 40% in those who are most ill and who require admission to the ICU.

DEFINITION AND CLASSIFICATION
- Pneumonia means inflammation of the lung substances.
- It can be classified as follow
Primary and secondary
Community-acquired and hospital acquired
Typical and atypical

CLINICAL FEATURES
Presenting symptoms
• Sudden onset of rigors
• Fever, pleuritic chest pain, and cough productive of purulent sputum 80 %
• Chest pain 30 % • Chills 40 - 50 %• Rigors 15 %
• Most individuals seek medical care within six days
Physical examination
• Fever 80 %
• Respiratory rate > 24 /minute 45 - 70 %
• Tachycardia
• Audible rales
• Evidence of consolidation 30 - 35 %

BOTH THE EPIDEMIOLOGY AND TREATMENT OF PNEUMONIA HAVE
UNDERGONE CHANGES.
• Pathogen not defined in as many as 50 % patients even with extensive diagnostic testing
• S. pneumoniae is the leading cause of CAP
• H. influenzae ( type B), S. aureus, and gram (-) bacteria each account for 3 to 10 %
• Staph aureus CAP is usually seen in the elderly and as post-influenza pneumonia
• P. aeruginosa causes CAP in neutropenia, cystic fibrosis, HIV infection & bronchiectasis
• N. meningitidis, M. catarrhalis & S. pyogenes can occasionally cause CAP
• Anaerobic organisms are implicated in aspiration pneumonia and lung abscess

• MRSA, M. tuberculosis, and certain viral agents are common in nursing-home patients
• Increasingly common in elderly and those with comorbid illnesses like COPD, DM, CHF, chronic liver disease and others
• Parallel to the improvement in our antibiotic armamentarium, bacterial resistance mechanisms have evolved
• Changing resistance patterns among pathogens commonly causing CAP:
S.pneumonia increasing resistance to tetracyclines and penicillens.
H.influenzae 30% resistance to penicillens. Moraxella catarrhalis 90% resistance to penicillens.
• Newly identified and previously unrecognized organisms are emerging (Atypical pneumonia):
Chlamydia pneumoniae 15% of CAP. Mycoplasma pneumoniae 20% of CAP. Legionella pneumophila 5% of CAP.

DIAGNOSTIC TESTING

Chest radiograph to :
Establish the presence of pneumonia.
Evaluate the severity.
Identify coexisting conditions like pleural effusion and bronchial obstruction.
Identify other diseases as T-B or lung abscesses.• Arterial blood gas analysis• CBC count• Chemistry profile, including renal and LFTs and electrolytes (Na,
glucose, and creatinine)• HIV serology (15 - 54 yrs )• Blood culture x 2

IDENTIFY A SPECIFIC ETIOLOGIC DIAGNOSIS
Sputum Gram stain and culture +/- AFB stain & culture and/or Legionella test (culture, DFA stain & urine antigen)
Sputum culture.
Serological testing .
Analysis of pleural fluid (if present) white blood cell, count and differential; protein, glucose, LDH, and pH; Gram's stain and acid-fast stain; and culture for bacteria, fungi, and mycobacteria
However in up to half of all CAP cases a specific etiology can not be identified even in the presence of extensive diagnostic testing .

GRAM'S STAIN OF EXPECTORATED GRAM'S STAIN OF EXPECTORATED SPUTUMSPUTUM
• Sensitivity and specificity vary widely depending on the criteria used to define a "positive” stain
• > 25 neutrophils and < 5 squamous epithelial cells per low power field
• No studies correlate data from sputum Gram stain and culture to cultures of alveolar material in large numbers of patients with CAP
• Cytologic screening criteria not evaluated for Legionella, mycobacteria or viral infections
• Direct staining of sputum may be diagnostic for Mycobacterium sp., endemic fungi, Legionella sp. (DFA stain) & P. carinii

PATIENT STRATIFICATION
We divided patients into four groups on the basis of place of therapy (outpatient, hospital ward, or intensive care unit); the presence of coexisting cardiopulmonary disease (COPD, CHF); and the presence of modifying factors that increase the risk of infection with specific pathogens as seen below

MODIFYING FACTORS
Penicillin-resistant and drug-resistant pneumococci Age > 65 yr β-Lactam therapy within the past 3 mo Alcoholism Immune-suppressive illness (including therapy with corticosteroids) Multiple medical comorbidities Enteric gram-negatives Residence in a nursing home Underlying cardiopulmonary disease Multiple medical comorbidities Recent antibiotic therapyPseudomonas aeruginosa Structural lung disease (bronchiectasis) Corticosteroid therapy (> 10 mg of prednisone per day) Broad-spectrum antibiotic therapy for >7 d in the past month Malnutrition

USING THESE FACTORS, THE FOUR PATIENT GROUPS WERE DEFINED AS THE
FOLLOWING

I - OUTPATIENTS WITH NO HISTORY OF CARDIOPULMONARY DISEASE, AND NO MODIFYING
FACTORS
ORGANISMS
Streptococcus pneumoniaeMycoplasma pneumoniaeChlamydia pneumoniae (alone or
as mixed infection)Hemophilus influenzaeRespiratory virusesMiscellaneous Legionella spp. Mycobacterium tuberculosis Endemic fungi
THERAPY
Advanced generation macrolide:
Clarithromycin (KLACID )
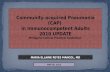
II- OUTPATIENTS WITH CARDIOPULMONARY DISEASE (CHF OR COPD) AND/OR OTHER MODIFYING FACTORS (RISK FACTORS FOR DRSP OR GRAM-NEGATIVE BACTERIA)
ORGANISMS
Streptococcus pneumoniae(including DRSP)
Mycoplasma pneumoniae
Chlamydia pneumoniae
Mixed infection
(bacteria plus atypical pathogen or virus)
Hemophilus influenzae
Enteric gram-negatives
Respiratory viruses
Miscellaneous
Moraxella catarrhalis, Legionella spp.,
aspiration (anaerobes), Mycobacterium
tuberculosis, endemic fungi
THERAPY
β-Lactam (oral cefpodoxime,cefuroxime ,
high-dose amoxicillin,amoxicillin/clavulanate;
or parenteral ceftriaxone followed by oral cefpodoxime)
plusAdvanced generation macrolide:
Clarithromycin (KLACID ) or
Antipneumococcal fluoroquinolone (used alone)

III. INPATIENTS, NOT ADMITTED TO THE ICU, WHO HAVE THE FOLLOWING
a. Cardiopulmonary disease, and/or other modifying factors (including being from a nursing home)
ORGANISMS
Streptococcus pneumoniae (Including DRSP)
Hemophilus influenzae
Mycoplasma pneumoniae
Chlamdia pneumoniae
Mixed infection
(bacteria plus atypical pathogen)
Enteric gram-negatives
Aspiration (anaerobes)
Viruses
Legionella spp.
Miscellaneous
M. tuberculosis, endemic fungi,
P. carinii
THERAPY
I.V β -lactam (cefotaxime, ceftriaxone,
ampicillin/sulbactam, high-dose ampicillin)
plus
I.V or oral macrolide
(KLACID)
or
I.V antipneumococcal
fluoroquinolone
alone

b. No cardiopulmonary disease, and no other modifying factors
ORGANISMS
S. pneumoniaeH. influenzaeM. pneumoniaeC. pneumoniaeMixed infection (bacteriaplus atypical pathogen)VirusesLegionella spp.Miscellaneous M. tuberculosis, endemic fungi, P. carinii
THERAPY
I.V. clarithromycin(KLACID I.V) alone
If macrolide allergic or intolerant
Doxycycline
and a β-lactam
or
An antipneumococcal
Fluoroquinolone alone

IV. ICU-ADMITTED PATIENTS WHO HAVE THE FOLLOWING :a. No risks for Pseudomonas aeruginosa
ORGANISMS
Streptococcus pneumoniae (including DRSP)Legionella spp. Hemophilus influenzaeEnteric gram-negative bacilli Staphylococcus aureus Mycoplasma pneumoniaeRespiratory virusesMiscellaneous Chlamydia pneumoniae,M tuberculosis, endemic fungi
THERAPY
I.V β-lactam (cefotaxime,ceftriaxone) .
plus I.V macrolide (KLACID)

b. Risks for Pseudomonas aeruginosa
ORGANISMS
P. aeruginosa(22%)
THERAPYSelected I.V antipseudomonal β-lactam
(cefepime, imipenem, meropenem, piperacillin/
tazobactam) plus
I.V antipseudomonal quinolone (ciprofloxacin)or
Selected IV antipseudomonal β -lactam (cefepime, imipenem, meropenem, piperacillin/
tazobactam) plus
I.V aminoglycosideplus either
IV macrolide (KLACID)or I.V nonpseudomonal fluoroquinolone

DECISION TO HOSPITALIZE
• 1. Age over 65 yr1. Age over 65 yr
• 2. Presence of coexisting illnesses or other findings2. Presence of coexisting illnesses or other findings– a. COPD, bronchiectasis, cystic fibrosis – b. Diabetes mellitus – c. Chronic renal failure – d. Congestive heart failure– e. Chronic liver disease of any etiology– f. Previous hospitalization within 1 yr – g. Suspicion of aspiration (gastric or oropharyngeal secretions) – h. Altered mental status– i. Postsplenectomy state – j. Chronic alcohol abuse or malnutrition
DECISION TO HOSPITALIZE
• 3. Physical findings3. Physical findings
– a. Respiratory rate > 30 breaths/min
– b. DBP 60 mmHg or a SBP 90 mmHg
– c. Temperature >38.3º C (101º F)
– d. Extrapulmonary sites of disease e.g, presence of septic arthritis,
meningitis, etc.
– e. Confusion and/or decreased level of consciousness

DECISION TO HOSPITALIZE• 4. Laboratory findings4. Laboratory findings
• a. WBC <4,000/mcL or >30,000/mcL or an ANC below 1,000/mcL
• b. Pao2 <60 mmHg or Paco2 of >50 mmHg on room air.
• c. Need for mechanical ventilation.
• d. Serum creatinine >1.2 mg/dl or BUN >20 mg/dl (>7 mmol/L)
• e. Unfavorable chest radiographic findings:- more than one lobe involvement - presence of a cavity- rapid radiographic spread z- pleural
effusion
• f. Hct of <30 % or hemoglobin <9 g/dl
• g. Evidence of sepsis or organ dysfunction as manifested by a metabolic acidosis, an increased PT, an increased PTT, decreased platelets, fibrin split products > 1:40
• 5. Social considerations5. Social considerations

COMPLICATIONS
• Risk factors include older age, preexisting lung disease, immunodeficiency or
AIDS
• Potential complications include parapneumonic effusion, empyema, necrotizing pneumonia, and lung abscess
• Parapneumonic effusions caused by PRP are associated with younger age (approximately two years) and a nearly universal incidence of bacteremia but do not result in poorer outcome than susceptible strains
• Bacteremia with subsequent seeding of other foci is seen in 25% of cases and represents the most significant complication. Bacteremic patients were more likely to die during the first week of illness. Splenectomized patients have an increased risk of overwhelming sepsis
• Abscesses are usually culture-positive and rapidly responsive to drainage
• Necrotizing pneumonia is culture-negative and responds adversely to interventional therapy

COMPLICATIONS

DURATION OF THERAPY
The presence of coexisting illness and/or bacteremia, the severity of illness at the onset of antibiotic therapy, and the subsequent hospital course should be considered in
determining the duration of antibiotic therapy.
S. pneumoniae pneumonia, and other bacterial infections, should be treated for 7 to 10 d
M. pneumoniae C. pneumoniae
10-14 d
Legionnaire’s disease 10-14 d
Patients chronically treated with corticosteroids with CAP 14 d or longer

RESPONSE TO THERAPY
On the basis of the clinical response to therapy, patients may be categorized into three groups
I- Patients with early clinical response should be considered for rapid switch to oral therapy, followed by prompt hospital discharge.
II- Patients with lack of clinical response which should be defined at Day 3 of hospitalization
III- Patients with clinical deterioration, which can occur as early as after 24–48 h of therapy
in the second and third categories need an evaluation of host and pathogen factors, along with a reevaluation of the initial diagnosis and a search for complications of pneumonia and pneumonia therapy.

SWITCH TO ORAL THERAPY
Patients should be switched to oral therapy if they meet four criteria
Improvement in cough and dyspnea.
Fever(<100°F) ) on two occasions 8 h apart.
Functioning gastrointestinal tract with adequate oral intake.

HOSPITAL DISCHARGE
In the absence of any unstable coexisting illnesses, or other life-threatening complications, the patient should be discharged home the same day that clinical stability occurs and oral therapy is initiated. In-hospital observation on oral therapy is not necessary, and only adds to cost and length of stay, without any measurable clinical benefit

EVALUATING THE NONRESPONDING PATIENT
Bronchoscopy is usually not needed, and patience is necessary to observe the full course of radiographic clearing of community-acquired pneumonia . However, bronchoscopy should be considered in patients below the age of 55 yr, who have multilobar disease and are nonsmokers. If bronchoscopy is performed, the goal is to identify unusual organisms or drug-resistant pathogens, but the clinician could also obtain this information by collecting lower respiratory tract secretions
(sputum or endotracheal aspirate) for culture. Cultures should be sent to evaluate for drug-resistant and unusual pathogens, including tuberculosis.

EVALUATING THE NONRESPONDING PATIENT
In addition to sampling lower respiratory tract secretions, other tests should be considered. Computed tomography may reveal unsuspected collections of pleural fluid, multiple lung nodules, or cavitation within a lung infiltrate. Lung scanning, spiral CT scanning, and/or pulmonary angiography should be considered if the patient is at risk for pulmonary embolus with infarction. While the routine use of serologic testing is not useful in the initial evaluation of patients with community-acquired pneumonia, serologic tests for Legionella sp., Myco-plasma pneumoniae, viral agents, endemic fungi, and other unusual pathogens should be considered at this point.

EVALUATING THE NONRESPONDING PATIENT
• Legionella urinary antigen testing should also be considered. This test is positive in more than half of all patients with proven Legionellapneumophila infection, and more than 80% of patients with Legionella pneumophila serogroup 1 infection (81, 82).
• If this extensive diagnostic evaluation has not been useful, and if the patient is seriously ill, open lung biopsy of an involved area of lung should be considered.

TREATMENT OF COMMUNITY-AQUIRED PNEUMONIA KEY POINTS
• CAP is frequently a mixed infection of typical and atypical bacteria.
• The clinical features of CAP can not be reliably used to identify the causative agent of pneumonia with adequate sensitivity and specifity .therefore empiric therapy is usually required.
• The initial side of care decision is perhaps the single most important clinical decision made by physicians during the entire course of CAP.

TREATMENT OF COMMUNITY-AQUIRED PNEUMONIA KEY POINTS
• When multiple risk factors co-exist, intensely supervised care should be strongly considered.
• A significant number of treatment failures have been documented for S. pneumoniae resistant to many drugs. Be prepared for possible treatment failure.

TREATMENT OF COMMUNITY-AQUIRED PNEUMONIA KEY POINTS
• Viral and pneumococcal infections predominant in the under age 5 population. Above age 5, atypicals begin to dominate with increasing age, but S. pneumoniae still represent 25-35% of the cases.
• In order to minimize the development of resistant to this valuable agents, antipneumococcal fluoroquinolones should not be used in patients under the age of 18 and should be avoided in adults when alternatives exists.

WHY KLACID XL ?
• Erythromycin was introduced in 1952 and has remained the prototype of the macrolides.
• The limitations of erythromycin include variable absorption, instability in gastric acid, poor tissues penetration, short elimination half life, GI irritation, and a narrow spectrum of activity.
• Modifications of the macrolide structure are designed to improve the chemical, biological and pharmacokinetic properties of erythromycin.
• Clarithromycin (KLACID) is a14-membered macrolide known as 6-O-methyl-erythromycin which overcomes all of the above limitations.

PERFECT SPECTRUM
• KLACID XL covers almost the whole spectrum of important pathogens in RTIs (Typical as S.pneumoniae ,H.influenzae, moraxella catarrhalis, S.aureus and atypical as C.pneumoniae,M.pneumoniae,L.pneumophila) with bactericidal activities. Therefore KLACID XL is the ideal antibiotic to be used empirically in the treatment of CAP.

Balanced distribution
• Pneumonia caused by pneumococci leads to bacteremia in about 30% of the patients. Only with sufficient serum antibiotic levels the circulating micro-organisms can be eliminated


Concentration of different antibiotics in serum ,soft tissues and macrophages
Antibiotic Serum level Extracellular levels
Conc. in macrophages
clarithromycin + + + + + +
Roxithromycin + + + +
Azithromycin + + + + + +
Β-lactams + + + + ▬

EXCELLENT SAFETY PROFILE
0
0.02
0.04
0.06
0.08
0.1
0.12
0.14
0.16
6% 15%
KLACID
Amoxicillin/clavulanate
• Significantly less GI upset than amoxicillin/clavulanate

EXCELLENT PATIENT COMPLIANCE
• KLACID XL improves patients compliance so reducing the risk of resistance
00.10.20.30.40.50.60.7
0.80.9
1
OD TID

NO FOOD INTERACTION
• Misadministration rate
00.10.20.30.40.50.60.70.8
0.91
0% 89% 94%
KLACID
Azithromycin
Roxythromycin
Related Documents