Guidelines for Integrated Care (Psychiatric & Medical) In the Community Module I: Diabetes and Glucose Monitoring

Guidelines for Integrated Care (Psychiatric & Medical) In the Community Module I: Diabetes and Glucose Monitoring.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Guidelines for Integrated Care (Psychiatric & Medical)
In the Community
Module I: Diabetes and Glucose Monitoring
ObjectivesAt the completion of Module I (Parts A and B),
participants will be able to:
Appreciate the need for integrated care in the mental health community to prevent premature deaths and increased disability from Diabetes Mellitus (DM) types I and II
Basic knowledge of DM (abnormal amounts of sugar in the blood)
Know the risk factors associated with DM

Objectives Identify patients with mental illness who have DM/risk
factors
Understand the concept of stages of change needed for appropriate interventions including use of tools for self-care, education and referral
Help those who are at risk for/diagnosed with DM in your caseload adequately communicate with their healthcare team for optimal care

Key Concept: Circulatory System

Controlling Blood Sugar: Balancing Act
Module I Part A:Importance of Integrated
Care
FactPeople with mental illness have a reduced life
expectancyThey die at least 20 years younger than the general
population from treatable physical Illnesses (such as DM)

Multi-State Study Mortality Data: Years of Potential Life Lost
Compared to the general population, persons with major mental illness typically lose 25 to 30 years of normal life span
Year AZ MO OK RI TX UT VA (IP
only) 1997 26.3 25.1 28.5 1998 27.3 25.1 28.8 29.3 15.5 1999 32.2 26.8 26.3 29.3 26.9 14.0 2000 31.8 27.9 24.9 13.5
(Colton CW, Manderscheid RW. Prev Chronic Dis [serial online] 2006 Apr [date cited]. Available from: URL:http://www.cdc.gov/pcd/issues/2006/apr/05_0180.htm)

Ohio Named 10th Fattest State: Persons with mental illness die even earlier in
Ohio

Severe Mental Illness (SMI) Morbidity and Mortality
Suicide and injury account for about 30-40% of excess mortality
60% of premature deaths in persons with schizophrenia are due to preventable (and costly) medical conditions with 20+ years of life lost
(URL:http://www.cdc.gov/pcd/issues/2006/apr/05_0180.htm)

Physical Health Care for People with SMI is Poor
The CATIE (Clinical Antipsychotic Trials in Intervention Effectiveness) study investigators found that at the beginning of the study, participants had the following medical conditions:
88.0% had high cholesterol (dyslipidemia) 62.4 % had high blood pressure (hypertension) 30.2% had diabetes
And they were not being treated!
(Nasrallah HA, et al. Schizophr Res. 2006;86:15-22)

Metabolic Syndrome

What is Metabolic Syndrome?Metabolic syndrome is a group of conditions/factors
that when present in an individual significantly increase risks of heart disease and other acute and chronic medical conditions, including DM

What is Metabolic Syndrome?Abdominal obesity: waist circumference >40 inches in men and
>35 inches in womenAbnormal amount of fats in the blood (dyslipidemia):
High levels of LDL “bad” cholesterol that promotes build up of “plaque” in the arteries
Low levels of HDL “good” cholesterol that helps reduce the build up of plaque
High blood pressureTendency to form blood clots (prothrombotic state) Inability of the body to use insulin and blood sugar (blood
glucose) so blood glucose levels rise above normal DM

National Cholesterol Education Program: Diagnostic Criteria for
Metabolic SyndromeThree or more of the following:• Waist Circumference:
> 40 inches in men > 35 inches in women
• Triglyceride level>=150 mg/dl
• HDL “Good” Cholestero <40 mg/dl in men <50 mg/dl in women
• BP >=135/85
• Fasting (8-10 hours) blood glucose >=100 mg/dl

What is Glucose? A source of energy needed by the body for all of its
functions (digestion, movement, thinking, etc.)
There is a range of blood glucose that is optimal for these bodily functions: 60-110 mg/dl Before meals less than 115 mg/dl Before bedtime less than 120 mg/dl
Glucose level is controlled by insulin that is secreted by the pancreas

Effects of Some Psychotropic Medications
Weight gain/obesity
Insulin resistance by impacting insulin receptor or post-receptor function abnormally high blood sugars and DM
Abnormal amounts of fat in blood (dyslipidemia)
Antipsychotic medications are associated with 2X the risk of sudden cardiac death
(Correll.MD et al, “Cardiometabolic Risk of Second-Generation Antipsychotic Medications During First-Time Use in Children and Adolescents”, JAMA, Oct., 2009)
(Ray et al, NEJM, Jan., 2009*)
Why is Diabetes Mellitus (DM) so important?
A common form of Metabolic Syndrome
Ranked as the 7th leading cause of death in the US
Estimated to affect 1 in 15 persons in the US
Persons with mental illness have a greater incidence of DM than the general population
Why is DM so Important?Untreated or mistreated DM can have severe
consequences in both the person’s mental and physical conditions
Mental Health clients have: 60-70% chance of suffering from mild to severe nerve
damage 65% chance of dying from heart disease or stroke increased chance of amputation, kidney failure and
adult blindness
Source: www.diabetes.org

What is DM?A chronic disease in which the body’s level of sugar
(glucose level in the blood) is not sufficiently regulated
In Type I DM, the body’s pancreas is not able to produce the needed level of insulin or any insulin at all resulting in a build up of sugar (glucose) in the blood
In type II DM, the body’s blood sugar (glucose) builds up because the body’s cells are not able to utilize insulin to metabolize its blood sugar
Risk Factors for Developing DMSedentary life style
Smoking
Nutritional intake
High BMI
Poverty
Genetic vulnerability

Risk Factors for Developing DMSide effects of medications (including some new-
generation anti-psychotics and anti-depressants)
History of Abuse (physical abuse: 26%-54, unwanted sexual touching:16%, forced sexual experience: 34%-69%)
Pregnancy
Diagnosis of Schizophrenia or Bi-polar disorder
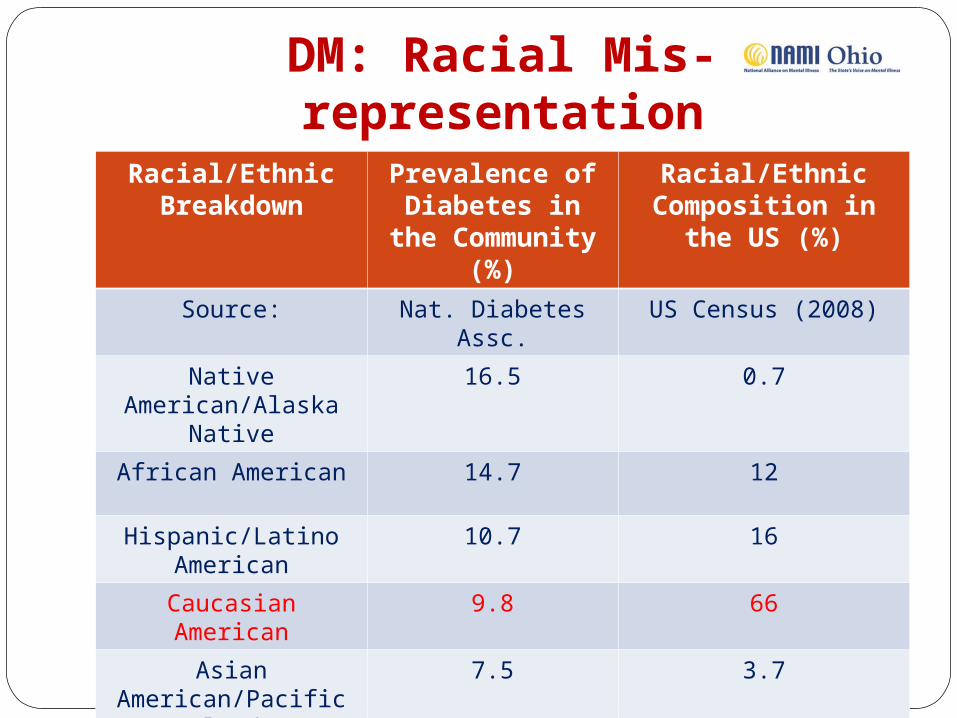
DM: Racial Mis-representationRacial/Ethnic
BreakdownPrevalence of
Diabetes in the Community (%)
Racial/Ethnic Composition in the US
(%)
Source: Nat. Diabetes Assc. US Census (2008)
Native American/Alaska Native
16.5 0.7
African American 14.7 12
Hispanic/Latino American
10.7 16
Caucasian American 9.8 66
Asian American/Pacific Islander
7.5 3.7

Importance of ‘at-risk’ ClientsBefore people develop type II DM, they almost always have
"pre-diabetes” (blood glucose levels that are higher than normal but not yet high enough to be diagnosed as diabetes)
There are 57 million people in the United States who have pre-diabetes.
Recent research has shown that some long-term damage to the body, especially the heart and circulatory system, may already be occurring during pre-diabetes

How can DM be Prevented or Managed?Life style changes and self-monitoring:
Sedentary life style exercise regularly
Smoking decrease/stop smoking
Nutritional intake regulation of dietary intake
High BMI monitor weight and waist circumference
Poverty referrals, resources, benefits
How can DM be Prevented or Managed?
Life style changes and self-monitoring:
Side effects of medications (some new-generation anti-psychotics and anti-depressants) switching medications, lower doses
Diagnosis of Schizophrenia or Bi-polar disorder optimal treatment
Possibly testing blood sugar level 1-8x daily
Taking oral glucose lowering medication or insulin injections

Module I Part B:Implementing Guidelines for
Diabetes within Community-Based Mental Health Services

Together we can make a difference!

Trans-disciplinary approachManagement of co-occurring conditions needs to be
team based
The team includes the client and family members (where appropriate or possible)
Implementation of the guidelines discussed below to be coordinated between disciplines and specialties
Guidelines preferably provided/coordinated in one location of care, if possible

Role of Mental Health ProfessionalsMonitor and Assess (integrated treatment begins with the
clinicians awareness) for risk factors/current DM Initial assessment questions/observations of client Medical records Current medications
Monitor and Assess for DM related risk factors of certain psychotropic medications Weight gain:
• Zyprexa (olanzapine), • Clozaril (clozapine), • Seroquel (quetiapine), • Risperdal (risperidone), • Depakote (valproic acid), • Lithium (lithobid), • Elavil (amitriptyline), • Remeron (mirtazipine)

Role of Mental Health ProfessionalsMonitor and Assess signs and symptoms of DM
Educate on DM and blood sugar monitoring
Encourage individuals to take more responsibility for their own health

Role of Mental Health ProfessionalsRemind yourself and your clients that small steps can yield
big results
Listen attentively to your clients and assist them in developing their own healthy living plans
Develop and Implement a healthy living plan: diet, exercise, smoking, alcohol, self-help groups, supportive relationships, medication management
Refer to primary care providers, specialists (podiatry, endocrinology, nutrition, etc.), home health, and support/education groups
Coordinate care between supports systems named above as well as with family and friends

Stages of Change
Pre-contemplation: Not yet acknowledging that there is a problem behavior that needs to be changed
Contemplation: Acknowledging that there is a problem but not yet ready or sure of wanting to make a change
Preparation/Determination: Getting ready to change
Action/Willpower: Changing behavior
Maintenance: Maintaining the behavior change
Initial Questions and ObservationsFor clients without a current diagnosis of DM but are at
increased risk:
Is this person obese?
Is there a family history of DM?
What is the client’s ethnicity?
Is there a family history of physical/sexual abuse?

Initial Questions and ObservationsFor clients without a current diagnosis of DM but are at
increased risk:
Is their diet heavy in fats and salt?
Does the client have high blood pressure?
Does the client have a sedentary lifestyle?
Is the client on medications with known side effect of weight gain?
Diagnosis of Schizophrenia, Bi-Polar Disorder, or Depression?
Initial Questions and Observations For clients with a current diagnosis of DM:
What do you know about your diagnosis?
Do you know the signs and symptoms of low and high blood sugar?
Do you see a PCP about the sugar in your blood?
Describe what you do to help control your diabetes each day?

Initial Questions and Observations For clients with a current diagnosis of DM:
Who tests your blood sugar?
If you test your own blood sugar, do you: Do you have a glucose meter?
Do you have test strips?
Do you keep a record of your blood sugar is and the time you tested it?
Do you understand what you need to do if your blood sugar is high or low?

Common DM Related TestsThree different tests the healthcare provider can use to
determine whether a person is pre-diabetic:
The A1C test
The fasting plasma glucose test (FPG) abnormal blood glucose level indicates impaired fasting glucose (IFG)
Oral glucose tolerance test (OGTT) abnormal blood glucose level indicates impaired glucose tolerance (IGT)
IFG and IGT are both also known as pre-diabetes

What Type I DM signs/symptoms to observe for?
Symptoms of Type I DM:
Unusual thirst
Extreme hunger
Unusual weight loss
Extreme fatigue and irritability
Fruity breath (ketones)

What Type II DM signs/symptoms to observe for?
Symptoms of Type II DM:
Any of the type I symptoms
Frequent infections
Blurred vision
Cuts/bruises that are slow to heal
Tingling/numbness in the hands/feet
Recurring skin, gum, or bladder infections
* Often people with type II DM have no symptoms
High Blood Sugar (Hyperglycemia) Skipping or forgetting insulin or oral glucose-lowering
medicine
Eating too much carbohydrates
Eating too much food and having too may calories
Infection
Illness
Increased stress
Decreased activity or exercising less than usual
Overly strenuous physical activity
Early Signs of HyperglycemiaIncreased thirst/hunger
Headaches
Difficulty concentrating
Blurred vision
Frequent urination
Fatigue (weak, tired feeling)
Weight loss

Prolonged Signs of Hyperglycemia Skin infection
Slow healing cuts or sores
Decreased field of vision
Nerve damage causing painful, cold, or insensitive feet
Loss of hair in lower extremities
Erectile dysfunction
Stomach or intestinal problems such as vomiting, diarrhea, or constipation

Urgent Hyperglycemia Conditions Urgent signs:
Seizures Hallucinations Confusion Disorientation Coma
Two specific types of hyperglycemic conditions:
1. Ketoacidosis: primarily type I DM, dangerously high levels of ketone acids in the blood
2. Hyperglycemic Hyperosmolar Nonketotic Syndrome (HHNS): primarily type II DM, usually brought on by illness or infection

Urgent Hyperglycemia Conditions
Urgent signs: Seizures Hallucinations Confusion, Disorientation, and Coma
Two specific types of hyperglycemic conditions: Ketoacidosis: primarily type I DM, dangerously high levels
of ketone acids in the blood Hyperglycemic Hyperosmolar Nonketotic Syndrome
(HHNS): primarily type II DM, usually brought on by illness or infection

Low Blood Sugar (Hypoglycemia)Blood glucose below normal levels
Can happen suddenly
Usually mild
Can be treated quickly and easily by eating or drinking a small amount of glucose-rich food:
Sugary candy
Banana
Peanut butter
Crackers

Signs of HypoglycemiaHunger
Shakiness
Nervousness
Sweating
Dizziness or light-headedness
Signs of HypoglycemiaCONFUSION and AGITATION/Combativeness
Difficulty speaking
Anxiety
Weakness
If severe/untreated: seizures, coma, and death
Hypoglycemia During SleepSigns include:
Crying out or having nightmares
Finding pajamas or sheets damp from perspiration
Feeling tired, irritable, or confused after waking up

Chronic uncontrolled DM Complications Complications of Diabetes are found in all body
systems: Eyes Peripheral nervous system Blood vessels Heart
EyesPersons with diabetes are at risk for eye diseases that
can lead to blindness
Blurred vision can be a safety issue
Regular check-up are needed at least once a year—check when reviewing care plan

Peripheral Nerve PainDM nerve pain has been described by some patients as
constant or that it comes and goes
Everyday things (bed sheets, socks) may cause pain
Words clients used to describe this pain: Aching Burning Numbness Shooting Pain Stabbing Throbbing Tingling
Blood Vessels: Skin and CirculationDM impairs the ability of the body to heal – feet are especially
affectedEncourage the client to perform skin assessment Inspect between the toes, bottom of the feet, and the heels
for: Broken skin Sores Blisters Areas of increased warmth or redness Changes in calluses
If your client presents with these conditions, please inform your medical staff before infection takes hold
Podiatrist referral/linkage for toe nail cutting/foot care

Kidneys and HeartChanges in blood pressure may indicate kidney damage
Refer to appropriate health care provider for routine lab tests/treatment
Heart attacks/failure are the major cause of death for persons with DM

What can I eat if I have diabetes?Eat lots of vegetables and fruit
Eat non-starchy vegetables such as spinach, carrots, broccoli or green beans with meals
Choose whole grain foods over processed grain products.
Try brown rice with stir-fry or whole wheat spaghetti with pasta sauce
Avoid foods high in fat (e.g. foods fried in oil or fat)
Choose liquid oils for cooking instead of solid fats (high in saturated and trans fats)

What can I eat if I have diabetes?Include dried beans (like kidney or pinto beans) and
lentils
Include fish in your meals 2-3 times a week
Choose lean meats like cuts of beef and pork that end in "loin" such as pork loin and sirloin
Remove the skin from chicken and turkey.
Choose non-fat dairy products such as skim milk, non-fat yogurt and non-fat cheese
If you're trying to lose weight, watch your portion sizes
ExerciseAnything that gets you moving, such as walking,
dancing, or working in the yard
Increases muscle/bone strength, flexibility, and endurance needed for daily activities
Helps the client feel and look better
Lowers blood glucose, blood pressure, and cholesterol
Reduces risk for heart disease and stroke
For optimal weight loss regimen, a combination of physical activity and wise food choices can help reach and maintain target weight
Glucose MetersThings to know about glucose meters:
Meters are vital to keeping track of day-to-day blood glucose levels
They're accurate, but improper use or faulty materials can cause incorrect readings
Many kinds of meters are available
Meters are relatively inexpensive—however test strips are expensive

Glucose MetersExperts testing meters in the lab setting found them accurate
and precise. But meter mistakes most often come from the person doing the blood checks.
For good results you need to do each step correctly.
Other things that can cause a meter to give a poor reading: Dirty meter Meter or strip that's not at room temperature Outdated test strip Meter not calibrated (set up for) the current box of test strips Blood drop that is too small
Client should ask their health care team to check their skills at least once a year

Supports and Referrals Interventions focused on prevention and information/activities:
The internet: local groups, message boards, education, statistics, podcasts, self-assessment of risk factors www.cdc.gov/diabetes American Diabetes Association: www.diabetes.org CDC BMI chart:
http://www.cdc.gov/healthyweight/assessing/bmi/
Referral/Linkage with RN, PCP, Specialty Providers (podiatrist, endocrinologist, ophthalmologist, dentist, nutritionist, etc.), local diabetes groups, Home health

CASE STUDIES

Case Study 1James is a 45 year old African American male with a
diagnosis of schizophrenia. He has stopped taking his medication since he was laid off six months ago. He currently has no insurance and has not applied for SSI or SSDI. He is 5’9” and 196lbs. He noted some weight gain (15 pounds) over the past few months from inactivity.
Recently, at a health fair, he had his blood sugar checked and he was told it was 187. His blood pressure was 140/92. He was told to follow up with a primary health care provider, but he states he isn’t sure where to go because of his lack of health insurance.

Case Study 1What are some of the risk factors James has for
diabetes?
How might a case manager follow-up with the psychiatric health care provider?
What other types of linkages/resources would be helpful for James?
What kind of education could you do with James?
Where would you document this information?

Case Study 2Mary Beth is a 37 year old Caucasian female who has a
diagnosis of schizoaffective disorder. She has been taking Geodon, Depakote, and Prozac. Through her medical health care provider, she is prescribed Glucophage (metformin), an oral medication to control her diabetes.
Her primary healthcare provider has her checking her blood sugar at least once a day. Lately it has been in the low 200s. She states she has been under a lot of stress lately since her son was incarcerated and hasn’t been sticking to her dietary plan. She also notices she has put on a few pounds.

Case Study 2 What are important assessment questions for Mary Beth?
What are some symptoms of high blood sugar that you could look for in Mary Beth?
What are some of the risk factors that predispose Mary Beth for diabetes?
What are some of the medications to watch out for that have a higher risk of leading to weight gain and diabetes?
How might a case manager follow-up with the psychiatric health care provider and primary care provider?
If Mary Beth was having trouble using her blood glucose machine, who should she see to learn how to use it correctly?

Case Study 3 Larry is a 48 year old Chinese American with a psychiatric diagnosis of
paranoid schizophrenia. He was recently diagnosed with end stage renal disease as a complication of his diabetes. Larry’s blood glucose readings ranged between 60 to 300 depending on when it is taken. His registered nurse, Susan, goes to Larry’s apartment to assess his psychiatric and medical condition and to administer his medications everyday.
When Andy, Larry’s case manager visited him, Larry appeared very anxious. He was pacing in his apartment and appeared irritable. Larry has a frown on his face and was cursing under his breath. He began to use profane language and asked if his plane reservations have been made and if his clothes were packed. Larry’s skin appeared sweaty and clammy, he was belligerent, and he slurred his speech more than he usual. After a few minutes of pacing his apartment, he threw his television remote control at his window and yelled at Andy, telling him to “get the f@#k out of my house!!!” Andy was confused as he felt that they had always had a positive working relationship.

Case Study 3What should Andy do at that moment?
What are some possible explanations for Larry’s behavior?
When Andy returns to his agency, what should he communicate to his treatment team?
Whose expertise should he seek to formulate a treatment plan?
What should be the team’s action steps in response to Larry’s outburst?

Questions?

Evaluation. Please take a moment to give me
feedback!
Thanks!!
Related Documents











