Principles of Growth and Development Life is a dynamic, changing process. Human life proceeds in stages from infancy to adulthood to senescence. Humans spend one-third of their lives in preparation for the latter two-thirds. An extended stage of immaturity follows as the human passes through intancy, childhood and adolescence, before achieving the capacity for independent function. Although defined as separate physicological processes, they cannot be separated in nature; cells increase in size and number as they differentiate. All human beings share the same mechanisms of growth and development and proceed through the same stages of life. The rate of maturation and the final outcome are widely variable because of the expensive and diverse influences on each individual. Growth may be defined as a physiological process by which the organism assimilates or transforms essential, nonliving nutrients into living protoplasm. Growth involves the incorporation of new materials. Development is defined as a physiological process by which the individual progresses from an undifferentiated state to a highly organized and functional capacity. Development implies an increase in skill and in complexity of function. As growth is measured in pounds and inches, development is measured in abilities. Patterns of Growth and Development: The genetic code determines the rate of the growth and development of the various body parts, which occur in synchrony with overall growth and development. For example, at birth the lower limbs of the infant are less well developed than the upper limbs. The ratio of lower

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 1/32
Principles of Growth and Development
Life is a dynamic, changing process. Human life proceeds in stages
from infancy to adulthood to senescence. Humans spend one-third of
their lives in preparation for the latter two-thirds. An extended stage of
immaturity follows as the human passes through intancy, childhood and
adolescence, before achieving the capacity for independent function.
Although defined as separate physicological processes, they cannot be
separated in nature; cells increase in size and number as they
differentiate.
All human beings share the same mechanisms of growth and
development and proceed through the same stages of life. The rate of
maturation and the final outcome are widely variable because of the
expensive and diverse influences on each individual. Growth may be
defined as a physiological process by which the organism assimilates or
transforms essential, nonliving nutrients into living protoplasm. Growth
involves the incorporation of new materials.
Development is defined as a physiological process by which the
individual progresses from an undifferentiated state to a highly organized
and functional capacity. Development implies an increase in skill and in
complexity of function. As growth is measured in pounds and inches,
development is measured in abilities.
Patterns of Growth and Development:
The genetic code determines the rate of the growth and
development of the various body parts, which occur in synchrony with
overall growth and development. For example, at birth the lower limbs of
the infant are less well developed than the upper limbs. The ratio of lower

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 2/32
limb length to total height is 1:3 in the adult the ratio of lower limb length
is 1:3. In the adult the ratio of lower limb length to total height is 1:2.
During the prenatal and postnatal periods, growth and development
follow a cephalocaudal pattern, that is development proceeds from head
(cephalo) to toe (caudal). The head matures before the neck, the neck
before the chest, the chest before the pelvis, and so on.
The cephalocaudal and proximodistal patients of growth and
development are evident in the motor development of the infant. He rolls
over before he can sit; his arm and chest development enable thismaneuver. As his trunk and legs develop.

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 3/32
Stages of Growth and Development:
The human life span can be divided into two distinct biological
periods, prenatal and postnatal. The prenatal period includes three stagethe ovum, embryo, and fetus. Postnatal life begins with birth and
proceeds through the neonatal period, infancy, childhood, adolescence,
adulthood, and sensescence. The progression from one stage to the next is
dependent upon completion of the previous stage.
Prenatal Period:
The most rapid growth and development in the human life cycle
occurs in the prenatal period. During the embryonic period, the formation
of organs occurs rapidly. In the early fetal period the fetus's length
increases rapidly. During the last trimester, the fetus makes rapid gains
the weight.
Neonatal Life:
The neonatal period is defined as the first month of life. The first
24 hours of life comprise the most significant time of this period, as the
neonate must take the transition from an intrauterine to atmospheric
environment. Infant mortality is highest during this transition.

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 4/32
Table 3-1. Stages in the Life Cycle
Period Approximate Age on Stage Some Characteristics
Embryonic First trimester of prenatallife
Rapid differentiation;establishment of systemsand organs
Early fetal Second trimester of prenatal life.
Accelerated growth;elaboration of structures;early functionalactivities
Late fetal Third trimester of prenatallife
Rapid increase in bodymass; completion of
preparation for postnatallife
Parturient Period of labor anddelivery
Risk of trauma andanoxia; cessation of
placental function
Neonatal andearly infancy
First month of postnatallife
Postnatal adjustments incirculation; initiation of respiration and other functions.
Middle infancy 1 mo to 1 yr Rapid growth andmaturation; maturationof functions, especiallyof nervous system
Late infancy 1 to 2 yr Decelerating growth;Progress in waling andother voluntary motor activities, and in controlof excretory functions.
Preschool 2 to 6 yr Slow growth; increased physical activity; further coordination of functions and motor mechanisms; rapidlearning.
School Girls : 6 to 10 yr Boys : 6 to 12 yr
Steady growth;developing skills andintellectual processes
Prepubertal (late Girls 10 to 12 yr Accelerating growth;

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 5/32
school or earlyadolescent)
Boys : 12 to 14 yr rapid weight gain; earlyadolescent endocrineand sex organ changes
Pubrtal
(adolescence proper)
Girls : 12 to 14 yr
Boys : 14 to 16 yr
Maturation of secondary
sex characteristics;
Postpubertal Girls : 14 to 18 yr Boys 16 to 20 yr
Maximum postnatalgrowth increase;decelerating andterminal growth; rapidmuscle growth andincreased skills; rapidgrowth and maturing
functions of sex organs;need for self-relianceand independence.
Infancy:
Infancy is a period of rapid growth and development. During the
first three months of life, the infant gains an average of tow pound per
month; be five months of age, the birth weight has doubled. The infantalso grows rapidly in height. By the end of the first year the infant's
length is 50 percent greater than at birth. During this period, the infant
brain grows more rapidly than the whole body and attains nearly adult
size by two years age.
Childhood:
The preschool years (age 2 to 6) and the school years (age 6 to 12)
represents a period of relatively slow growth. The annual increment in
weight averages approximately 5 lb until the ninth or tenth birthday. The
height increment during the school years is approximately 2 in each year.
During this period, the child's social world expands as he enters school.
Adolescence:

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 6/32
The adolescent period comprises the years in which the child
"grows up," It is a period of profound changes in physical , mental and
emotional development. The period is marked by an accelerated gain in
weight and height.
Adulthood and Aging:
The adult years are a period of competency and ability. Unlike the
development stages, the adult years do not have a sequence of precisely
timed physiological events. This is also true of the aging years from 65
years until death.
Hormonal influence on growth and development:
The growth and development of an individual is influenced by four
major sources of hormones: the central nervous system, and the thyroid,
adrenal, and gonadal glands. Although the hormones have different
chemical structures and are produced by different organs, they all
influence growth and development by stimulating protein synthesis.
It is hypothesized that each hormone has its major effect on growthand development at a particular period of life.
Growth Hormone:
Growth hormone is secreted by the anterior portion of the pituitary
gland in response to growth hormone releasing factor, which is produced
by the hypothalamus; under the influence of various stimuli, the
hypothalamus controls the anterior pituitary and, thereby, the release of growth hormone. Thus, the pituitary is an intermediary gland.
Growth hormone is chiefly influential in protein synthesis. At the
cellular level, growth hormone stimulates increased transport of amino
acids into cells and increased incorporation of amino acids into protein.
The role of growth hormone in the prenatal period has not been
clearly delineated. The influence of growth hormone brings about an
increase in the child’s height and weight, changes in skeletal proportions

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 7/32
and head and face contours, dental development, and ossification of the
long bones.
Thyroid Hormones:
Thyroxine (T4) and triidothyrodine (T3) are the major thyroid
hormones and are secreted by the thyroid gland. Their release is regulated
by the hypothalamus and the pituitary gland. The thyroid hormones exert
their influence by stimulating protein synthesis.
In contrast to growth hormone, thyroid hormones have a great
influence on fetal and neonatal growth. In the absence of thyroid
hormones during this period, there is a lack of brain growth, probably in
both cell number and cell size.
Androgens:
An increase in androgens is felt to be responsible for most of the
growth and development that takes place during adolescence. The
androgens exert their influence like growth hormone and thyroid
hormone, i.e. by stimulating protein synthesis. They are responsible for overall growth and skeletal and muscular maturation.
Testosterone is the principal androgen produced by the testes.
Dehydroepiandrosterone is the principal androgen produced by the
adrenal cortex. The androgens and estrogens are responsible for sexual
maturation during adolescence.
Heredity and Environment:The human organism experiences a lengthy period of growth and
development, influenced by internal factors (those that are intrinsic of the
individual, i.e., genetic potential) and external factors (those that are
outside of the individuals, i.e., environmental influences). As has been
said, the final outcome of growth and development is a result of the
dynamic interplay of genetic potential and environmental factors.

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 8/32
Genetic Potential :
The information stored in the genes exerts a tremendous influence
on the individual’s maturation. Genetic factors affect the individual’s rate
of growth, the time of the onset of the adolescent growth spurt, and the
final size and shape of the body.
Genetic factors play a leading part in the growth difference
between males and females. Boys and girls have different patterns of
growth and development, and an obvious difference in final outcome.
Girls mature more rapidly than boys throughout the developmental
years. Adolescence begins sooner for girls, and they attain sexual
maturity and maximum height approximately two year earlier than boys.
Girls begin their growth spurt at approximately age 10 to 11 years and
will have reached adult height by about 16 years. Boys begin their growth
spurt at age 12 to 13 years and do not each adult stature until 18 years of
age. Genetic factors are also influential in the differences seen in different
ethnic groups.Environmental Factors:
The environment supplies the external factors that make growth
and development possible. Environmental factors include temperature,
nutrition, drugs, infections, radiation, and so on. These external factors
are influential throughout the life span.
The impact of an environmental factor on growth and developmentis dependent on the characteristics, intensity, duration, and timing of the
factors. The organism as a whole, and specific organs, is particularly
susceptible to environmental factors during specific stages called critical
periods.
The central nervous system is very susceptible to environmental
factors during the fetal period.

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 9/32
Skeletal Growth:
Skeletal growth is commonly taken as an index of overall growth
and development. Height, a reflection of an individual’s skeletal growth,
is a common clinical measure. Bone age may also be used as a clinic
measurement of physiological maturity.
Bone is a specialized tissue that supports the body and protects
vital organs. The human skeleton exits first in the form of connective
tissue, then cartilage, and finally bone. The adult skeleton is composed of
bone with no remnants of the original membranous skeleton. The closure
of the fontanelles in infancy demonstrates this progression from
connective tissue to bone in skeletal development.
During childhood, cartilage is found throughout the skeleton. The
length of the skeleton grows by dint of the proliferation of cartilage. The
cartilage changes to bone by the process of ossification. It is through the
two processes of cartilage proliferation and ossification that the bones
grow.Cartilage is produced in the metaphyses of bones and in the
cartilage plate. Ossification proceeds from the epiphysis (end) of the
bone, which contains the ossification centers.
Skeletal growth and development involves the continual growth of
ossification centers; skeletal maturation is initiated by the appearance of
ossification centers and is terminated when these centers are fused. Theindividual has approximately 400 ossification centers at birth, ad twice as
many by maturation. New ossification centers appear according to a
regular schedule. The growth of new ossification centers is under
hormonal control; growth hormone seems to have the most influence on
the growth of new ossification centers.

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 10/32
The stages of bone growth occur at regular intervals that vary little
between individuals. This relative uniformity permits the use of bone age
measurement as a reliable index of maturation.
Skull Growth
The skull is large at birth because of the relatively large size of the
brain. After birth, the skull continues to grow in order to accommodate
the very rapid further growth of the brain. In the first two years of life, the
skull’s capacity grows from 400ml to 950ml and its circumference
increases from about 33cm to 47cm.
At birth, the bones that comprise the cranial vault are separated bygaps filled with fibrous connective tissue; the gaps allows the bones to
slide over each other to some extent as the neonate passes through the
mother’s narrow birth canal.
As ossification of the fibrous connective tissue proceeds, the
individual bones come into contact with each other along a series of
fibrous joints known as sutures. It is at the sutures that skull growth takes place. Skull growth will continue until after puberty, accommodating the
growing brain. After skull growth stops, the sutures will be obliterated by
their ossification and fusing together .
ASSESSMENT OF GROWTH AND DEVELOPMENT
All measurements should be made in a room with adequate
lighting, comfortable temperature, and a firm, level floor. Childrenshould wear only minimal light-weight clothing or none at all.Shoes should not be worn.
Length:
During the first two years of life, the child's length must bemeasured while the child is in the recumbent position.
Arecumbent-length measuring table is required to obtain a obtain a
measurement (see Figure 3-5). Two persons are needed, one tohold the infant's head in contact with the headboard, and one to

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 11/32
bring the movable footboard firmly against the child's heels. Toposition the feet so that the soles are directed vertically against thefootboard, gentle traction may be applied to the legs. Recumbentmeasurement should be recorded to the nearest 0.1 cm.
The child should face forward, with heels together, back as straightas possible, and with heels, buttocks, and the upper part of theback touching the wall. The measurement should be recorded tothe nearest 0.1 cm.
Weight:
The child should be weighed while wearing a minimal amount of clothing, if any. Infants should be weighed on an infant scale
having a capacity of approximately 15kg. the accuracy of thescales should be checked and adjusted approximately three timesa month, and each time the scales are moved. The infant shouldbe placed centrally on the scale and the older child should standcentrally on the platform.
Erohjy djpi;f nr trvptfrf yp yjr mrstrdy 0.1kg.
Head circumference
Head circumference is measured until the child is 2 years old. Itshould be measured with a flexible narrow-width tape. Tle tapeshould be placed on the infant's head so as to obtain the maximalfrontal-occipital circumference. The head circumference should berecorded to the nearest 0.1cm.
The pattern of the growth of the cranium is very different from theof the body; its groth is nearly completed by 6 years of age, sogrowth evaluation is most relevant in infancy and early childhood.
The method for interpretation of head circumference on the growthgrid is identical to that for interpretation of height and weight. Ameasurement outside the normal range does not absolutelyindicate cranial abnormality; rather, it is the rate of growth thatmust be evaluated.
Bone Age
Another clinical tool that assists the clinician in evaluating thechild's progress toward maturity is bone age assessment.
Age can be helpful in interpreting the atypical chil's growth.

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 12/32
The progress of bone growth can be recorded by x-ray. Theappearance of the centers of ossification can be noted becausetheir calcium content makes them radiopaque. The sequence of bong growth is similar in every person.
That individual variations caused by genetic differences mayaccount for atypical maturation, that cannot be reconciled with anorm.
The clinical purpose of bonge age assessment is to identify thelevel of skeletal maturation. This information assists the examiner in making adecision concerning the child with abnormal growth byallowing a comparison with norms for the same chronological age.
Growth Grids
The national center for health statistics (NCHS) has developed agrowth grid that is commonly used in clinical practice. It is basedon a distance curve. The distance curve shows the height, weight,and head circumference of a child at various age.
The standards for each age are derived from measurements of alarge number of children of the specific age. An average (mean)and a rang (fifth through ninety-fifth percentiles) for each height,
weight, and head circumference have been determined for eachage. Ideally, every child's growth should be evaluated in relation tonorms established for children of the same sex, ethnic group, andsocioeconomic status.
The rationale for the use of growth grids is that children followpredicatable patterns of growth and development. The individualchild's measurements are interpreted in relation to the expectednorms for other children of the same age, sex, and ethnic group.
Achild whose measurements falls outside the normal range issuspected of having disease, although disease should not beregarded as the definite cause of atypical measurements.
Asingle measurement determines the size of a child, whereasseveral measurements must be made in order to evaluate thechild's growth.
Two important points should be kept in mind in comparing a child's
growth to a standardized grid. First, the curve derived from a largegroup of children naturally obscures the individual patterns of each

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 13/32
child in the original sample population and with be a smooth curvewith no dramatic peaks; many children with show peaks in thecourse of normal growth. Second, height is a more stable indicator then weight. Weight is more influenced by environmental factors
and may fluctuate more than height. Weight is still a reliablemeasurement but may be more difficult to interpret, especially ininfancy (Falkner, 1962).
Developmental Screening
As was said earlier, humans, unlike other animals, do not inherit arepertoire of instinctive behaviours but must learn behavior; theprolonged period of immaturity enables humans to benefit fromtheir experiences for optimal learning. Behavior is divided nito five
areas; gross motor, fine motor, language, personal social, andadaptive behavior.
Gross motor behavior includes the control of the head, trunk, andextremities. Fine motor behavior is the control of the movements of the vingers. The acquisition of motor control reflects the integrity of the child's neurological system.
Language behavior includes the production of single or combinedwords, and the ability to comprehend speech.
Wide variations exist in personalsocial behavior, since it isdependent on the child's interaction with his or her environmentand culture.
Adaptive behavior is significant because it stems from intellectualpotential. Adaptive behavior indicates the child's ability to solveproblems. It includes the use of motor abilities, to execute practicalsolutions and the use of past experience in the solution of new
problems.Developmental screening, like screening of physical growth, is anintegral part of pediatric health care. A development assessment isa clinical estimate of the developmental progress made in eacharea of behavior.
It must be kept in mind that developmental screening tests are notintelligence tests.
Developmental screening is also used to identify mentally retardedchildren.

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 14/32
Another area of significant clinical use of developmental screeningis its use to educate parents about their child's development. Anticipated developmental changes that the child will undergo canbe delineated for parents. This information can assist parents in
adjusting to their continually changing child. It can also assistparents to adjust the child's environment for optimal support andstimulation of his or her development.
Denver Developmental Screening Test
The Denver developmental screening test (DDST) is widely usedin clinical practice and is a typical screening instrument. The axiomunderlying the DDST is the development follows predicatedpatterns common to all, and that the child who does not follow the
expected pattern is more likely that the typical child to havedisease.
The rest consists of 105 tasks selected from existing infant andpreschool scales. The testWas first administered to a large group of infants and children inDenver, Colorado; the sample population of he children waschosen to match the sociocultural and economic status of Denver'soverall population, and is therefore not necessarily representative
of population of other parts of the United states. The ages at which25, 50, 75, and 90 percent of the subjects passed the items werecalculated for the entire sample (Frankenburg and Campbell,1975).Children between 2 weeks and 6 years old are tested on only 20 or so simple tasks by means of a few basic testing materials. Theitems are arranged in order of difficulty and are divided into four major behavioral areas: personal-social, fine motor adaptive,language, and gross motor.The DDST is a useful clinic tool because of its use an age range inestablishing the norms, which allows for a wider variation individualpatterns. Also, the heterogeneity of the original test population,from which the criteria were derived, allows for variations inchildren of different cultural and socioeconomic backgrounds(Frankenburg and Campbell, 1975).
SUMMARY
Humans are born immature. On the path to independent function,
they progress through the predictable stages of infancy, childhood,and adolescence. The physiological processes of growth and

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 15/32
development are responsible for the changes in body size andcomposition and in abilities that the individual undergoes beforeattaining adulthood.Growth and development begin at the cellular level and advance
under the influence of both the individual's genetic potential andenvironmental influences.Hormones influence growth and development by stimulatingprotein synthesis. The degree of influence of the individualhormones varies during the different stage of growth anddevelopment.The assessment of growth and development is an integral part of pediatric health care. However, the examiner must keep in mindthat individual variations caused by genetic and environmental
differences may cause the child to deviate from the norm.
ASSESSMENT AND MANAGEMENTOF THE HEALTHY CHILD
The nurse practitioner exercises professional judgments andaccepts responsibility for the delivery of primary health care. Mutual trustand collaboration among health care providers and families form the
bases for effective delivery of quality care. Incorporated in thisframework of care are the concepts of prevention, health promotion, and
health maintenance. Teaching and counseling are strongly emphasized.

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 16/32
Part one provides information necessary to maintain and promotethe health of the child from birth through adolescence and to assess and tomanage specific common concerns and conditions of the healthy child.
CHILD HEALTH ASSESSMENT
The Provision of pediatric primary care requires mastery of theknowledge and skills of data gathering, namely, the history and the
physical examination, as well as the ability.
It is often the key to solving many presenting concerns and inhelping formulate a diagnosis. Mastery in the art of interviewing requiresthe ability to weave observation and communication skills into theaccurate picture of a situation. In addition, it provides an excellent
opportunity to learn about the family and health.Clients and the nurse practitioner come to interviews with their
own agendas of concerns and with their own ideas of possible solutions.A useful question to ask the client is : What do you think I can do for youtoday? It is essential to use open-ended, nonjudgmental questions, toavoid the use of technical language, and to be aware of personal biases.The nurse practitioner must be keenly sensitive to client's real problems.The nurse practitioner might discover that a client presenting with acomplaint of "noisy breathing" is really worried about sudden infantdeath syndrome (SIDA) because the neighbor's infant recently diedsuddenly.
CLIENT – NURSE PRACTITIONER RELATIONSHIPS
The inclusion and active participation of clients in their care areimportant aspects of delivering primary care. Continuity of care by thenurse practitioner establishes a therapeutic relation with the family.
1. Personalize the interactions by introducing yourself to thechild and parent by name and addressing them by their names.
2.Use language that is clearly understood.
3.Consider the situation form the client's perspective.
4.Focus on parental needs as wells as those of the child.
5.Reinforce the ideas of the parents as appropriate and encouragethem to develop their own plans of action.
6-Provide information as appropriate
7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 17/32
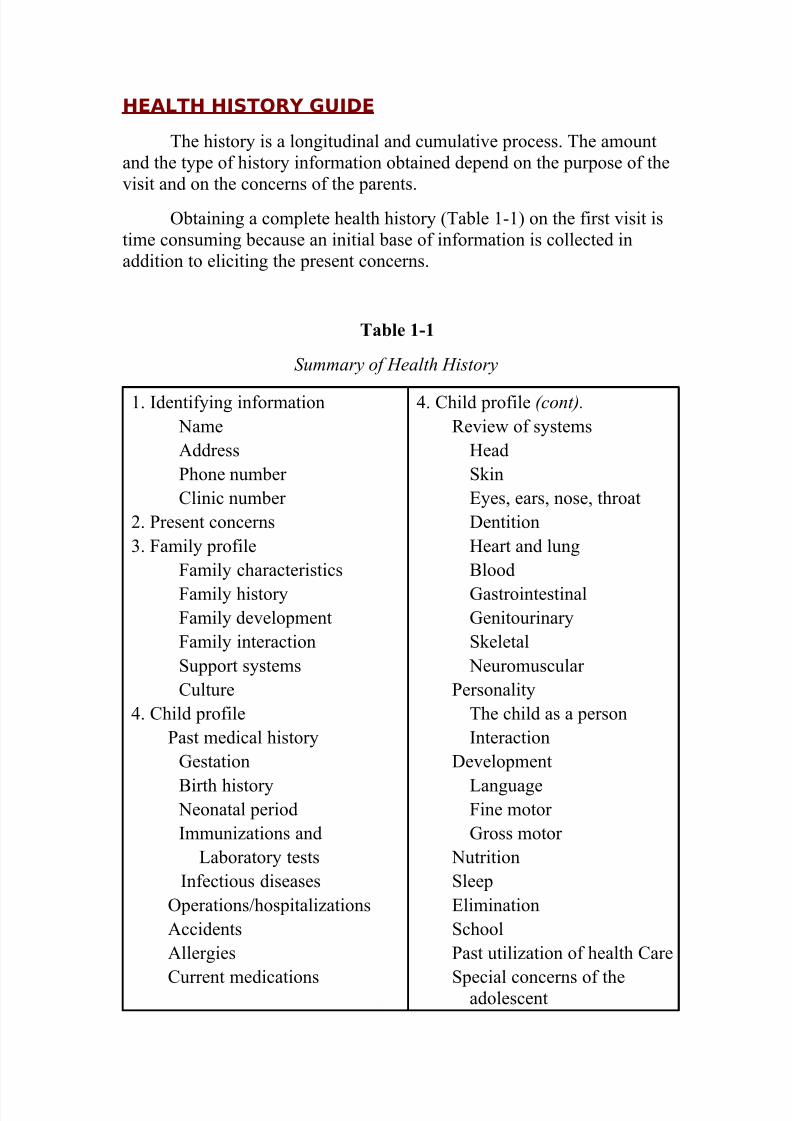
HEALTH HISTORY GUIDE
The history is a longitudinal and cumulative process. The amountand the type of history information obtained depend on the purpose of thevisit and on the concerns of the parents.
Obtaining a complete health history (Table 1-1) on the first visit istime consuming because an initial base of information is collected inaddition to eliciting the present concerns.
Table 1-1
Summary of Health History
1. Identifying information NameAddressPhone number Clinic number
2. Present concerns3. Family profile
Family characteristics
Family historyFamily developmentFamily interactionSupport systemsCulture
4. Child profilePast medical history
Gestation
Birth history Neonatal periodImmunizations and
Laboratory testsInfectious diseases
Operations/hospitalizationsAccidentsAllergies
Current medications
4. Child profile (cont).
Review of systemsHeadSkinEyes, ears, nose, throatDentitionHeart and lungBlood
GastrointestinalGenitourinarySkeletal
Neuromuscular Personality
The child as a personInteraction
Development
LanguageFine motor Gross motor
NutritionSleepEliminationSchoolPast utilization of health Care
Special concerns of theadolescent

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 18/32
24 – hour history
Present Concerns:
Elicit the chief concerns of the visit and obtain a detailed history of each
one. Indicate how each concern affects the child's ability to function (eat,
sleep, play) as appropriate.
Remember:
A parent or child's first stated concerns may not be the primary reason for
the visit. In eliciting the concerns of the parent, the parent and the child
are allowed to tell their story from their own perspectives.
An opening question might be:
What has been concerning you about your child? What brings you here
this particular day? What worries you most and why? What do you think
would be helpful? What ideas do you have about the cause of the
problem? What did you hope I could do for you today? What questions
do you have?
Family Profile:
Obtain information that provides an overall picture of the family's
strengths and vulnerabilities, dynamics, and patterns of coping.
FAMILY CHARACTERISTICS:
Inquire about demographic information socioeconomic status and
physical environment. Sample questions include:
Who else shares your household?
Do you live in an apartment or a house?
What kind of work do you do? Your spouse?
What year of school did you complete?
FAMILY HISTORY:

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 19/32
How would you describe your own health?
Are there any serious illnesses in the family such as convulsions,
diabetes, heart disease, hypertension, mental problems, or tuberculosis?
Is this your first pregnancy?
Does anyone in the family have a lot of problems?
FAMILY DEVELOPMENT:
Identify the stage of family development using the structure of the family
and the age of the oldest child as guideposts.
Helpful questions are:
How many children do you have?What is the age of the oldest child?
Can you describe what happened when your child first went to school?
Have you ever experienced financial difficulties? If so, how did you
handle the situation?
FAMILY INTERCTION:
Questions include:
How do you and your spouse settle arguments?
What do you argue about?
Do you feel you have enough support?
If not, how do you manage?
Do you have a favorite child? Does your spouse?
How do the children get along with each other?
Suggested questions are:
How do you manage?
Who and what are sources of support for you? For your child?
How do you react to all these pressures?
How does your child react?
What do you do when things get rough?

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 20/32
Do you ever have time for yourself? Are there extended family or close
adult relationships in your life?
CULTURE:
Obtain information that will increase sensitivity and understanding about
the family's cultural background, beliefs, practices, food preferences,
eating habits, concepts of health and illness healer and folk medicine,
sensitivity to personal problems, and experience with preventive health
care. Consider the following important factors in assessing the culture of
an emigrant family: country of origin receiving country (similarities and
differences of receiving country and country of origin, ecology language,skin color, style of dress.
Useful questions are:
What were the reasons for deciding to leave the country of origin?
Why did the family choose to immigrate to this country? How long has
the family been in this country? Is the family willing to learn a new
language or skill?What stresses are the family facing as a result of their emigration? How
is the present culture different?
What cultural differences does the family find most distressing?
Child Profile:
Obtain information that provides a picture of the child's strengths and
vulnerabilities, roadblocks and frustrations, and style of coping with problems.
PAST MEDICAL HISTORY:
Obtain information that establishes the relationship of gestational and
perinatal events and past health problems to the child's present state of
health.
Gestation Questions to ask include:
In what month did you start prenatal care?

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 21/32
How was your health during the pregnancy?
Were there any unusual stresses during the pregnancy? Was this a
planned pregnancy? Illnesses? Accidents? X-rays? Special diets?
Hospitalizations? Medications? How many months did the pregnancy
last? How much alcohol was ingested each day? Did you smoke during
your pregnancy?
Birth History:
Health Care of the Infant.
Questions to ask include:
How many hours was the labor?Was any anesthesia used?
What type of delivery was it (breech, cesarean section, vaginal?)
Was the birth of the baby unusual?
What was the baby's condition at birth?
Did the baby have any trouble breathing?
Was the baby's color yellow?What was the birth weight?
Was baby delivered at home?
Neonatal Period :
Assessment of the Newborn.
Questions to ask are:
Did the baby have any problems in the nursery? Was the baby's color ever yellowish or blue? Did the baby have any problems with feedings?
When did the baby go home? Did the mother and baby go home together?
What was the baby's weight at discharge? Did the baby have any illnesses
or problems in the first month of life?
Immunizations and Laboratory Tests:
Questions to ask are:
Has the baby received any baby shots? At what age?

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 22/32
Did the child have any reactions to the immunizations? If yes, can you
describe them?
Has the child ever had a tuberculin test?
What was the reaction?
Has the child had any other skin tests?
Infectious Diseases:
Questions to ask include: Has the child had chickenpox? Measles?
Mumps? Has the child had any streptococcal infections?
Operation/Hospitalizations:
Questions to ask include:
Has the child ever had any operations?
If yes, for what reasons?
How is the child now?
Has the child ever spent any time in the hospital?
For what reasons? Is the problem resolved?
Accidents/Safety:Questions to ask include:
Has the child ever had an accident?
Can you describe what occurred?
What safety measures do you use at home?
Allergies:
Questions to ask include:
Is the child allergic to any foods?
If yes, what types of food?
What is the reaction? Has the child had any reactions to insect bites,
medications, immunizations?

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 23/32
C u rrent Medications:
What medications do you give your child regularly? Is your child
receiving any medications for any illnesses?
Review of Systems:
Record problems not previously identified according to the baby part or
system. List the symptoms, treatments, and known sequelae:.
SKIN, EYES, EARS, NOSE, AND THROAT, DENTITION, HEART
AND LUNG, BLOOD, GASTROINTESTINAL,GENITOURINARY,
SKELETAL, NEUROMUSCULAR,
PERSONALITY
Elicit descriptions of the child's personality (activity, attention span,
intensity of reactions, adaptability, strengths, sensitivities, fears, crying
patterns) and independence (eating, separation, self-care,)
Questions to ask include:
How would you describe your child?
How does your child spend the day?How would you describe your child's ability to handle new situations?
Does your child withdraw of actively participate?
Is your child easily frustrated?
Can you describe his/her behavior?
What does he/she do when you leave?
What activities does he/she engage in outside of the home?
Interaction:
Can you leave the children alone in a room together? How would you
describe the older child's behavior toward the baby? When was the first
time you had to discipline your child? Does your child have playmates?
Language:
Questions to ask include:

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 24/32
Can you understand your child?
Does your child repeat words?
Does your child stutter?
How does your child let you know that he or she wants something?
Fine Motor:
Elicit information about manual dexterity, drawing, dressing, tying, and
writing.
Questions to ask include:
Does your child scribble?
Can your child use pencil?Can your child tie shoe laces? Button clothes?
Does your child have difficulty writing school assignments?
Gross Motor:
Questions to ask include:
What does your child do for fun?
Does your child have any difficulty walking? Running? How old wasyour child when she used a tricycle?
NUTRIRION:
Questions to ask include:
How would you describe your child's appetite (good, poor)? What is the
feeding schedule?
What kind of milk does your child drink?What solids does the child eat and in what quantities?
Is the child taking any vitamins?
SLEEP:
Questions to ask are:
Do you think your child is getting enough sleep?
How many hours of sleep in a 24-hour period?
Does your child take naps during the day?

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 25/32
How long are they?
Does the child awaken at night? If yes, how often?
Does the child have any nightmares or night terrors?
PHYSICAL EXAMINATION:
A skillful physical examination is done with aminimum of trauma tochild . It done with sensitivity to child behavior ,Activity level , and response , and take advantage of opportunities such ascrying by quickly looking into mouth.
There are four basic techniques : auscultation , palpation , percussion andopservation ( inspection : is the most important one. (
SUMMARY OF PHYSICAL EXAMINATION :
Measerement and vital signs. General condition.
Skin.Head:
Face ,eyes , ears , nose , mouth and throat Neck . Heart.
Abdomen.Genitalia.Skeletal.
Neuromuscular .
Measerement and vital signs. Obtain the following measurement : height , weight , headcircumference , temperature , respiration rate and blood pressure.
Approximal Height and Weight
At birth : Weight (w) in lb = 7 lb 6 oz (7.35 lb. (Form 3 to 12 month : (w) = age (mo) + 11From 1 to 6 year : (w) = (age yr * 5 ) + 17From 6 to 12year : (w) = (age yr * 7 ) + 5At birth : length = 20 in
At one year : length =30 inFrom 2 to 14 years : length = (age yr *2.5 ) + 30.
Head circumference in term infant

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 26/32
General condition:.
Note appearance (alert , happy , sick , distressed, pain(
Activity level (lethargic , playful , active , tired ) development andbehavior in relation to age and state of nutrition.
Skin:
Inspect color ( jaundice , pallor , cyanosis ) , hai r (texture , location ,amount , disteribtion ) , scalp (oily ,dry ) ,nails ( clpbbing , unusualmarking ) and lesion ( color , type , location , shape , size ) . Palpate
for tempreture (hot , cold ) ,texture ( edema ,rough ,moist , clammy. (NOTE:
1-Fingernails are replaced every 5.5 month.
2 – Toenails are replaced every 18 monthHead:
Inspect and palpate for shap , size ,symmetry (paralysis , weaknesses) .Fontanels ( measurements , tension , intracranial pressure ICP ) ,lesions ,position , movement and dilation of vein
Face:
Inspect for size , shape , symmetry , position of eyes , nose , mouth inrelation to each other , cleft , dimples ,paralysis , mandibular size
,swelling and palpate for sinus tenderness.
Eyes:
HC increment Period
month = 6 cm ./ 2cmmonth = 3 cm ./ 1cmmonth = 3 cm ./ .5cm
First 3 month4to 6 month6to 12month
12cm First year

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 27/32
Observe external eye for shap , symmetry , placement , lids ( position ,swelling , redness , edems , discharge , symmetry ) , cornea ( cloudiness ,ulceration ) , iris pigmentation and pupil ( color , size , symmetry ,
roudness , reaction of light and accommodation. (
Ears:Inspect the pinna ( shape , size , malformation , nodules , lesion ,swelling , tenderness ) , canal ( patency , discharge , narrowing , redness ,
pain foreign bodies) and tympanic membrane ( short process, umbo ,long process
Light reflex , color , foreign bodies.(Nose :
Inspect external nose for shap ( straight ) and nares (symmetry ,obstruction , discharge(
Inspect internal nose for color of mucosa ( pale , boggy , redness. (Mouth:Inspect lip (symmetry , paralysis , fullness , thinness, pallor , color ) ,mucosa bleeding , gum ( bleeding , discoloration , swelling ), dentition
( number , malocculation , discoloration) , tongue ( color , movement ,size ) , mandibular size , and salivary gland (parotid , submandibular ,
sublingual. (Throat:
Inspect color of mucosa and tonsils ( exudate, inflammation , size , color ) , voic ( pitch , hoarseness , stridor , grunting ), cry ( shrill , high-
pitched , whiny , weak ( ,Neck :
Position ( torticollis , opisthotonos ) , control , rang of motion ,
symmetry , stiffness , webbing .
Palpate for cysts, sternocleidomastoid muscle masses ( shape , size ,location , mobility ) , and thyroid ( size , tenderness , texture ,
nodules(Chest and lung:
Inspect for color (cynosis ) ,repirations ( quality , depth , effort , rate ,
rhythem) , chest , size , symmetry , shape ( pectus excavatum , barrelchest , slope. (
Auscultate for breath sound ( presence or absence , intensity , quality ,duration ) and abnormal chest sound (rales , rhonchi , wheezes. (
Percuss for dullness and lung size .
NOTE:
1-ratio of respiration to pulse should be 1:4.2-short periods of apnea can be normal in newborns.
Heart:
Observe activity level .Inspect color ( pallor , cynosis. (

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 28/32
Palpate for the point of maximal impulse ( PMI,( Pulse ( femoral , radial ) , and presence of thrill or heaves.
Auscultate heart sound ( S1 , S2 , rate , rhythem(NOTE:
*The kay to auscultation is to listen to one heartsound at a time:1-aortic valve is best heard sound in the second right intercostals space.2- pulmonic valve is best heard sound in the second left intercostals space
3-tricuspid valve is best heard sound in the fifth right intercostal spacenear the sternum.
4-mitral valve is best heart sound in the fifth left intercostals space near midclavicular line.
5-S1 is louder at the apex.
6-S2 is louder at the base. 7- bell of stethoscope detect low – frequency sound.8-diaphragm of stethoscope detect high– frequency sound.
Abdomen:Check size , shape , and symmetry .
Inspect protuberance , lesions , umbilicus (color , hernia , nodules ,fistulas , discharge ) , distention.
Auscultate bowel sounds ( peristalsis , tympanitic , dull , absent. (Palpate for softness , rigidity , pain , tenderness , masses
Palpate liver , spleen , bladder and kidney .
Percuss for liver edge , tympancy and shifting dullness.Femal genitalia:Inspect external genitia for color , labia (minora, majora.(Inspect vagina and cervix .
Palpate the uterus.Male genitalia:
Inspect external genitia for penis (size , gland , shape. (Urethra ( ulceration , position of meatus ) , scrotum (hydrocele , hernia(Palpate testes , epididymis , and spermatic cord .
Skeletal :Observe gait ( opposing arm and leg swing ,normal heel to toe gait ) . gross deformities , posture ,and symmetry .
Examine spine and back ( body alignment , curvature , rigidity ,tenderness , lesion ) , joints ( rang of motion , tightness , edema ,tenderness , redness ) , hips (abduction , internal rotation ) , knee
( length , symmetry,controur ) , forefoot ( abduction ) , fingers and toes (numbers , space ,
length , webbing , clubbing. (
Neuromuscular:

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 29/32
Observe mental status ( orientation , alartness ) ,motor development ,
muscle tone ( strength , symmetry , spasticity ) , cerebellar function
( gait , posture ) , sensory ( light touch on the limb(

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 30/32

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 31/32
*Growth and Development*Physical and assessment
Of children
: *
1. -2. -3. -4. -5. -6. -7. -8. -9. -

7/29/2019 Growth and Development Assess ment 1
http://slidepdf.com/reader/full/growth-and-development-assess-ment-1 32/32
Related Documents











