British Journal of Neurosurgery (1994) 8, 667-679 ORIGINAL ARTICLE Growing skull fractures: classification and management NAIM-UR-RAHMAN, ZAIN AL ABEDEEN B. JAMJOOM, ABDEL HAKIM B. J A M J O O M & W A L E E D R . M U R S H I D Division of Neurosurgery, College of Medicine, King Saud University & King Khalid University Hospital, P.O. Box 2925, Riyadh 11461, Saudi Arabia Abstract Seven patients with growing skull fractures treated between 1983 and 1993 are described. These growing fractures constituted 1.6% of all the cases of skull fractures seen during the period (a total of 449 cases). Based on aetiopathogertesis, computed tomography (CT) appearances, operative findings and management strategies required, three main types of growing skull fractures were recognised. In type I (n 3) a leptomcningcal cyst, in type II in = 3) damaged and gliotic brain, and in type III (n = 2) a porencephalic cyst extended through the skull defect into the subgalcal space. A combination of type I and type III co-existed in one patient. Initial head injury and neurological deficit were judged to be mild to moderate in all the seven cases. Continued growth of skull fractures correlated closely to the increasing neurological deficit in five cases. In two patients natural arrest of fracture growth at 5 and 7 months after trauma was accompanied by arrest in progress of neurological deficit. Available surgical options are discussed and general guidelines for the management are given. Key words: Trauma, lepzomeningeal cyst, porencephalic cyst, meningocele spuria, progressive neurological deficit, skull fracture Introduction Linear or non-linear skull fractures in chil- dren that enlarge with time are termed grow- ing skull fractures. 1 Although these lesions are much more common in children, 2 and 90% occur under the age of 3 years; 3 the process may occur following a skull fracture in an adult. 2,4,5 The incidence of 'growth' as a de- layed complication of skull fracture is rare and occurred in only 0.6% of the cases in one large series, 6 It is important to realize that the lesion expands not only between the fracture edges, but also intracranially and, thus, may cause atrophy of underlying cerebral tissue with re- sulting progressive neurological deficit; 7 as was seen in most of our cases. Because of the diverse clinical, radiological (CT) and operat- ive findings and variable temporal course, there is controversy concerning the terminol- ogy, aetiopathogenesis and management of growing skull fractures. 3 ' 6,8 Classification of the growing skull fractures into three types (Fig. 1) suggested here was found to be help- ful in explaining these diversities and planning the treatment. Similarly, based on the clinical presentation and temporal course, two forms of the growing skull fractures could be dis- tinguished. An active form with evidence of raised intracranial pressure (ICP), mass effect on CT, progressive separation of bone edges with a tense bulge between them; and an ar- 667

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
British Journal of Neurosurgery ( 1994) 8, 6 6 7 - 6 7 9
ORIGINAL ARTICLE
Growing skull fractures: classification and management
N A I M - U R - R A H M A N , Z A I N A L A B E D E E N B . J A M J O O M , A B D E L H A K I M B .
J A M J O O M & W A L E E D R . M U R S H I D
Division of Neurosurgery, College of Medicine, King Saud University & King Khalid University
Hospital, P.O. Box 2925, Riyadh 11461, Saudi Arabia
A b s t r a c t Seven patients with growing skull fractures treated between 1983 and 1993 are described. These growing fractures constituted 1.6% of all the cases of skull fractures seen during the period (a total of 449 cases). Based on aetiopathogertesis, computed tomography (CT) appearances, operative findings and management strategies required, three main types of growing skull fractures were recognised. In type I (n 3) a leptomcningcal cyst, in type II in = 3) damaged and gliotic brain, and in type III (n = 2) a porencephalic cyst extended through the skull defect into the subgalcal space. A combination of type I and type III co-existed in one patient. Initial head injury and neurological deficit were judged to be mild to moderate in all the seven cases. Continued growth of skull fractures correlated closely to the increasing neurological deficit in five cases. In two patients natural arrest of fracture growth at 5 and 7 months after trauma was accompanied by arrest in progress of neurological deficit. Available surgical options are discussed and general guidelines for the management are given.
Key w o r d s : Trauma, lepzomeningeal cyst, porencephalic cyst, meningocele spuria, progressive neurological deficit, skull
fracture
Introduction
Linear or non- l inea r skull fractures in chil
d r e n tha t enlarge wi th t ime are t e r m e d g row
ing skull f rac tures . 1 A l t h o u g h these lesions are
m u c h m o r e c o m m o n i n ch i ld ren , 2 and 9 0 %
occur u n d e r the age of 3 yea r s ; 3 the p rocess
m a y occur following a skull f racture in an
a d u l t . 2 , 4 , 5 T h e inc idence of ' g rowth ' as a de
layed compl ica t ion of skull fracture is rare a n d
occu r r ed in only 0 . 6 % of the cases in o n e large
ser ies , 6 I t is i m p o r t a n t to realize tha t t he lesion
e x p a n d s n o t only b e t w e e n the fracture edges ,
b u t also intracranial ly a n d , t h u s , m a y cause
a t rophy of unde r ly ing cerebral t issue wi th r e
sul t ing progress ive neurological deficit; 7 as was
seen in m o s t of our cases. Because of the
diverse clinical, radiological ( C T ) a n d ope ra t
ive f ind ings a n d variable t e m p o r a l course ,
there i s cont roversy conce rn ing the t e rmino l
ogy, ae t iopa thogenes is and m a n a g e m e n t of
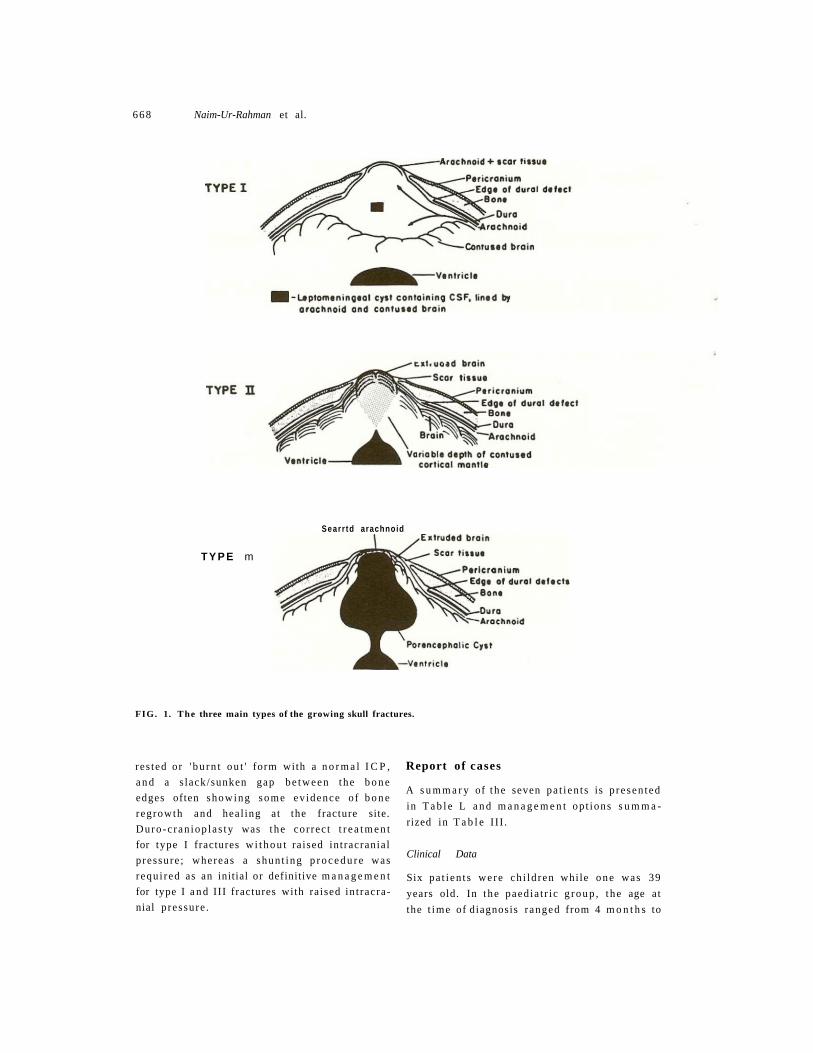
g rowing skull f r a c tu r e s . 3 ' 6 , 8 Classification of
t he growing skull fractures into t h r ee types
(Fig . 1) sugges ted he re was found to be he lp
ful in explaining these diversit ies a n d p l a n n i n g
the t r e a t m e n t . Similarly, based on the clinical
p resen ta t ion a n d t e m p o r a l cour se , two forms
of the growing skull f ractures could be dis
t inguished. An active form wi th evidence of
raised int racranial p ressure ( I C P ) , mass effect
on C T , progressive separa t ion o f b o n e edges
wi th a tense bu lge b e t w e e n t h e m ; and an a r -
667
668 Naim-Ur-Rahman et al.
Searr td arachnoid
T Y P E m
FIG. 1. The three main types of the growing skull fractures.
res ted or ' b u r n t o u t ' form with a n o r m a l I C P ,
a n d a s lack/sunken gap be tween the b o n e
edges often showing some ev idence of b o n e
regrowth and heal ing at the fracture site.
Duro -c ran iop las ty was t he cor rec t t r e a t m e n t
for type I fractures w i t h o u t ra ised int racranial
p ressure ; whereas a shun t ing p r o c e d u r e was
requ i red as an initial or definitive m a n a g e m e n t
for type I a n d III fractures with ra ised in t racra
nial p ressure .
Report of cases
A s u m m a r y of t he seven pa t i en t s is p re sen ted
in T a b l e L a n d m a n a g e m e n t op t ions s u m m a
rized in T a b l e I I I .
Clinical Data
Six pa t i en t s were ch i ld ren while o n e was 39
years old. In t he paed ia t r i c g r o u p , t he age at
the t ime of diagnosis r anged from 4 m o n t h s to

Growing skull fractures 669
6 years (mean : 2 4 , 6 m o n t h s ) . Six pa t i en t s
were female a n d o n e ma le . T h e interval be
tween the his tory o f h e a d injury a n d diagnosis
of growing skull f racture r a n g e d from 2
m o n t h s to 1 year ( m e a n : 7 m o n t h s ) . L o c a t i o n
of t he skull f racture was par ie ta l in th ree
pa t i en t s , f rontoparietal in one , occipi topar ie ta l
in one , and occipital in t he r ema in ing two
chi ldren.
T w o chi ldren (cases 1 and 2) h a d exper i
enced p e r m a n e n t remiss ions after a per iod of
active fracture g rowth . T h e r ema in ing f ive
showed evidence of ra ised int racranial press
u r e a n d m o r e or less progress ive neurological
deficits. Five chi ldren p r e s e n t e d wi th swelling
in the region of t he fracture site, while in two
(cases 1 and 7 ) , t he a rea b e t w e e n the gaping
b o n e edges was slack and depressed . Seizures
a n d h e m ip a re sis were the nex t c o m m o n
presen t ing s y m p t o m s a n d occu r r ed in four
pa t ien t s . Bl indness or progressive visual
de te r iora t ion was p resen t in two ch i ld ren with
occipital fractures, whi le r e t a rda t ion was seen
in o n e child.
Radiological evaluation
Plain r ad iographs o f t he skull a n d CT were
pe r fo rmed on all pa t i en t s . Skull r ad iographs
correctly d e m o n s t r a t e d the locat ion a n d ex ten t
of separa t ion of b o n y edges at the fracture site.
Extens ive b o n y resorp t ion wi th widely gaping
everted fracture m a r g i n s , seen in three chil
d r e n , corre la ted well with t he size of the u n
derlying cyst a n d b ra in d a m a g e on a CT scan.
C T clearly d e m o n s t r a t e d t he b o n y defect ,
the n a t u r e of in t racrania l c o n t e n t s he rn ia t ing
t h r o u g h it ( l ep tomeningea l cyst = 3, con tused
cerebral t issue = 3, po rencepha l i c cyst -2);
a n d the ex ten t of the under ly ing int racranial
lesion. T h u s , a l ep tomen ingea l cyst wi th C S F
densi ty was seen in three pa t i en t s , extensive
low densi ty areas of b ra in d a m a g e a n d en-
cephalomalac ia in three pa t ien ts a n d p o r e n
cephal ic cysts c o m m u n i c a t i n g wi th di la ted
ventr icles in two chi ldren.
Operative findings
Five of the seven pa t i en t s u n d e r w e n t surgery.
O n e child (case 4) h a d a vent r icu lopcr i tonea l
s h u n t for tense po rencepha l i c cyst a n d di la ted
ventr icles . In t he r ema in ing four chi ldren t he
defect was repa i red by durop las ty us ing fascia
lata or per icrania l graft, a n d an acrylic c ran io-
plasty. Of these four ch i ldren w h o u n d e r
w e n t c ran io tomies a t t he fracture sites, two
(cases 2 a n d 4) s h o w e d that the scalp and
p e r i c r a n i u m were densely adhe ren t to the
unde r ly ing conges ted , gliotic a n d he rn ia t ed
bra in . T h e d u r a was totally absen t u n d e r the
cranial defect. M o r e or less extensive n ibbl ing
of t he marg ins of b o n e defect was requ i red to
f ind a reasonab le dura l edge . Dissect ion and
elevation of the scalp f lap from the unde r ly ing
conges ted gliotic bra in was t ed ious a n d ac
c o m p a n i e d by m u c h bleeding. In case 5 , oper
a t ion was pe r fo rmed for a large tense occipital
swelling t h r o u g h a growing fracture of the
skull. E levat ion of a large occipital scalp flap
revealed a po rencepha l i c cyst on the right side
and a l ep tomeningea l cyst overlying a con
gested a n d softened left occipital lobe . T h e
occipital cyst was aspi ra ted and an acrylic
cranioplas ty carr ied ou t . Duroc ran iop la s ty was
s t ra ightforward in the seventh case.
Surgical results
C o m p l e t e reso lu t ion of t he ra ised in t racrania l
p res su re , extracranial swelling a n d progress ive
c losure of skull defect was ob t a ined in t he
child w h o u n d e r w e n t s h u n t surgery (case 3) .
Fo l l ow-up at 3 a n d 6 m o n t h s has s h o w n re
duc t i on in t he size of cranial defect with evi
d e n c e of b o n e r eg rowth a t t he fracture site.
C o m p l e t e obl i te ra t ion of t he cranial defect was
achieved in t h r ee ou t of four pa t i en t s w h o
u n d e r w e n t duro-c ran iop las ty ( m e a n follow-
u p : 4 years) . In t he four th pa t i en t , t he acrylic
plate loosened a n d bu lged 2 years after
surgery. Reope ra t i on was refused. All the f ive
pa t ien ts who u n d e r w e n t surgery recovered
wi thou t any increase in t he pre-exis t ing n e u r o
logical deficits and definite i m p r o v e m e n t was
r eco rded in four pa t i en t s .
Case 1. T h i s 3 0 - m o n r h - o l d girl was well unt i l
10 m o n t h s before admiss ion w h e n she was
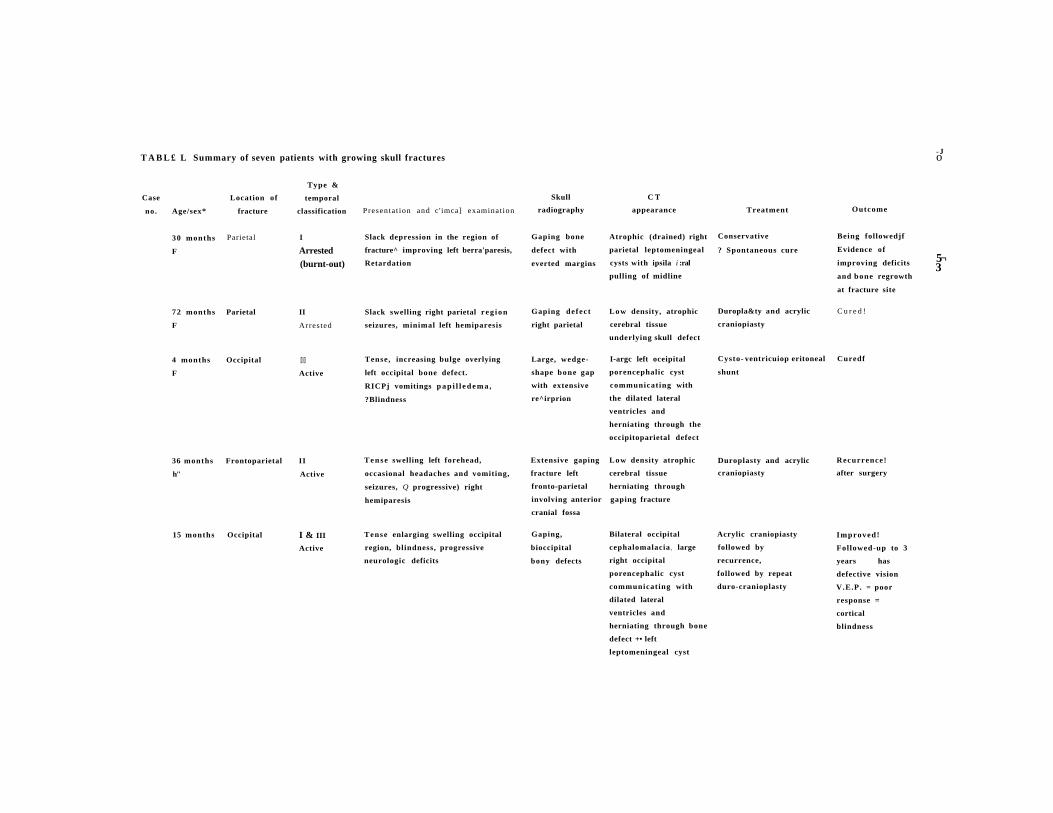
T A B L £ L Summary of seven patients with growing skull fractures - J o
Case
no. Age/sex*
Location of
fracture
Type &
temporal
classification Presentat ion and c'imca] examination
Skull
radiography
C T
appearance Treatment Outcome
5¬ 3
30 months
F
72 months
F
4 months
F
Parietal
Parietal
Occipital
15 months Occipital
I
Arrested (burnt-out)
II
Arrested
[|]
Active
36 months Frontoparietal II
h" Active
I & III
Active
Slack depression in the region of
fracture^ improving left berra'paresis,
Retardation
Slack swelling right parietal r eg ion
seizures, minimal left hemiparesis
Tense, increasing bulge overlying
left occipital bone defect.
RICPj vomitings p a p i l l e d e m a ,
?Blindness
T e n s e swelling left forehead,
occasional headaches and vomiting,
seizures, Q progressive) right
hemiparesis
Tense enlarging swelling occipital
region, blindness, progressive
neurologic deficits
Gaping bone
defect with
everted margins
Gaping defect
right parietal
Large, wedge-
shape bone gap
with extensive
re^irprion
Atrophic (drained) right
parietal leptomeningeal
cysts with ipsila i :ral
pulling of midline
Low density, atrophic
cerebral tissue
underlying skull defect
I-argc left oceipital
porencephalic cyst
communicating with
the dilated lateral
ventricles and
herniating through the
occipitoparietal defect
Extensive gaping
fracture left
fronto-parietal
involving anterior gaping fracture
cranial fossa
Low density atrophic
cerebral tissue
herniating through
Gaping,
bioccipital
bony defects
Conservative
? Spontaneous cure
Duropla&ty and acrylic
craniopiasty
Cysto- ventricuiop eritoneal
shunt
Bilateral occipital
cephalomalacia ? large
right occipital
porencephalic cyst
communicating with
dilated lateral
ventricles and
herniating through bone
defect +• left
leptomeningeal cyst
Duroplasty and acrylic
craniopiasty
Acrylic craniopiasty
followed by
recurrence,
followed by repeat
duro-cranioplasty
Being followedjf
Evidence of
improving deficits
and bone regrowth
at fracture site
C u r e d !
Curedf
Recurrence!
after surgery
Improved!
Followed-up to 3
years has
defective vision
V.E.P. = poor
response =
cortical
blindness
672 Naim-Ur-Rahman et al.
T A B L E II. Management options
Growing skull fracture
With normal 1CP
With raised 1CP
Tense porencephalic cyst with
hydrocephalus
Ventri c ulo peritoneal shunt
I I I
I
Tense leptomcningcal
cyst
Cysto-peritoneal
shunt
I
I
Duro-cranioplasry
t rea ted for h e a d injury with a fracture of t he
skull. Over t he nex t 5 m o n t h s the child devel
o p e d bu lg ing of t he scalp in t he right par ie ta l
region which b e c a m e progressively larger.
T h i s was a c c o m p a n i e d by progress ive left
h e m ip ares is, h e a d a c h e , vomi t ing and oc
casional seizures. Five m o n t h s p r io r to ad
mission the m o t h e r no t i ced a s p o n t a n e o u s
i m p r o v e m e n t in chi ld 's cond i t ion . T h e scalp
bulge b e c a m e softer t h e n rapidly d i sappea red
leaving a depressed gap be tween the b o n e
edges . T h i s was a c c o m p a n i e d by reso lu t ion of
h e a d a c h e a n d vomi t ing , a n d i m p r o v e m e n t in
t he left-sided weakness . T h e chi ld was admi t
ted to t he neurosurg ica l un i t wi th the chief
compla in t s of a soft gap on r ight s ide of head ,
seizures and res idual left hemipares i s . E x a m i n
at ion revealed a par ie ta l b o n y defect wi th a
slack depress ion , in an alert girl walking inde
penden t ly . Neuro log ica l examina t ion showed
min imal left hemipares is with pyramida l signs
a n d mi ld re ta rda t ion . Skull r ad iographs on
admiss ion showed a gaping r ight par ie ta l frac
tu re wi th ever ted saucer ized marg ins . C T
(Fig. 2) showed a l ep tomeningea l cyst u n d e r
lying the cranial defect and c o m m u n i c a t i n g
freely wi th t he pc r imesencepha l i c cistern. As
there was evidence of regrowth of b o n e edges
(Fig, 2) a long with c o n t i n u e d i m p r o v e m e n t in
h e r neurological s ta tus , i t was dec ided to o b
serve. At 3 - m o n t h fol low-up the b o n e gap had
n a r r o w e d .
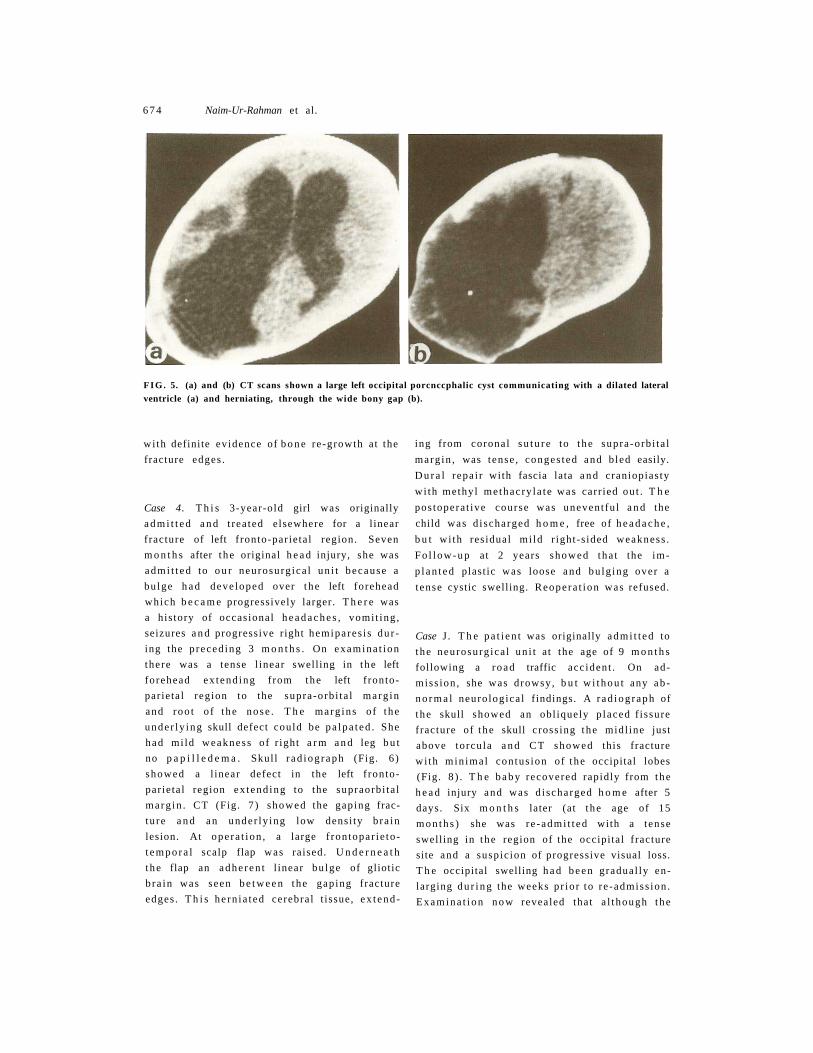
Case 2. T h i s 6-year-old girl p re sen ted wi th
seizures and a 'soft a r ea ' over t he r ight par ie ta l
region, no t i ced for the last 4 years . A h e a d
injury h a d occur red w h e n the child was 10
m o n t h s old. O n e year after t he head injury t he
pa ren t s no t i ced a soft, gradually increas ing
bu lge in the right par ie ta l region which g radu
ally 'flattened* in t ime leaving a 'soft a rea ' .
T h e r e was no his tory of h e a d a c h e or vomit ing .
E x a m i n a t i o n revealed an alert , b r igh t child. A
skull defect in t he r ight par ie ta l region m e a s u r
ing a b o u t 4 cm and covered by slack scalp
cou ld be felt. Neuro log ica l examina t i on re
vealed m i n i m a l left hemipares is with brisk ten
d o n jerks. T h e r e was n o p a p i l l e d e m a . Skull
r ad iograph (Fig. 3) showed a gap ing fracture
in r ight par ie ta l region. CT (Fig. 4) s h o w e d a
low densi ty lesion of the unde r ly ing bra in with
slight d i la ta t ion a n d ipsilateral 'pul l ing ' of the
right lateral ventr icle . At ope ra t ion , a large,
Growing skull fractures 673
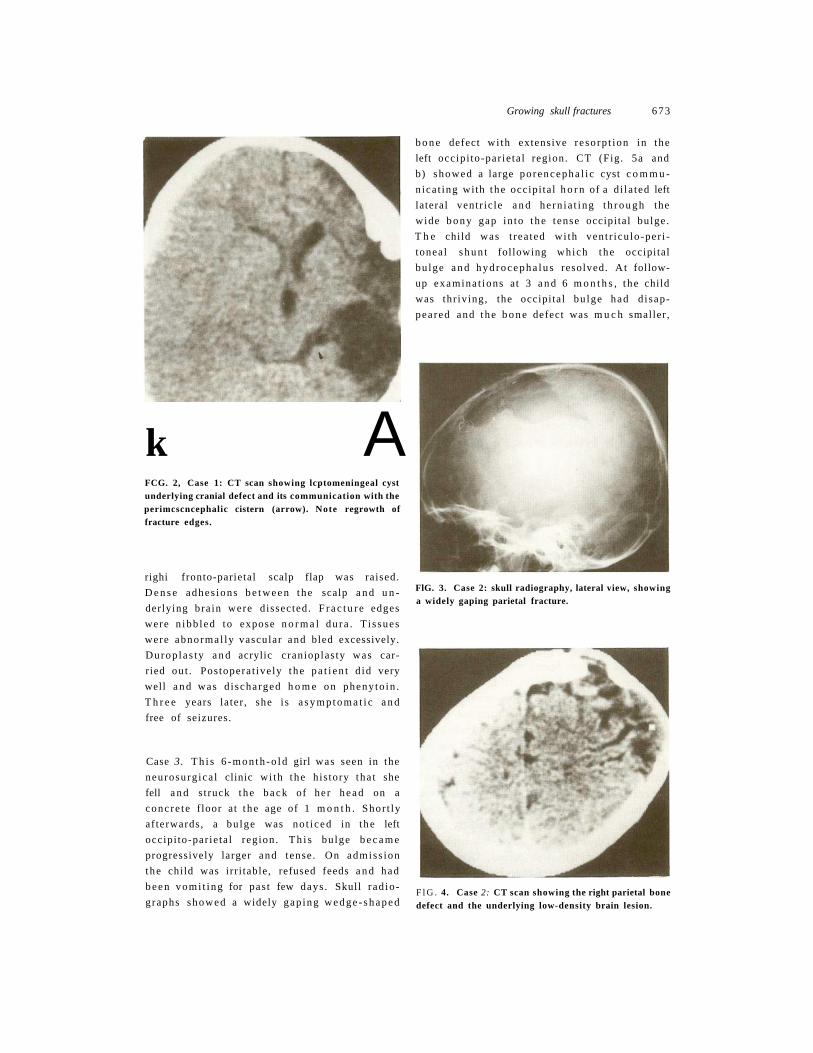
k A FCG. 2, Case 1: CT scan showing lcptomeningeal cyst underlying cranial defect and its communication with the perimcscncephalic cistern (arrow). Note regrowth of fracture edges.
righi fronto-parietal scalp flap was raised.
D e n s e adhes ions b e t w e e n the scalp a n d u n
derlying bra in were dissected. F r a c t u r e edges
were n ibb led to expose n o r m a l du r a . T i s sues
were abnormal ly vascular and bled excessively.
Durop la s ty a n d acrylic cranioplas ty was car
ried ou t . Pos topera t ive ly t he p a t i e n t d id very
well a n d was d i scharged h o m e on pheny to in .
T h r e e years la ter , she i s a s y m p t o m a t i c a n d
free of seizures.
Case 3. T h i s 6 - m o n t h - o l d girl was seen in the
neurosurg ica l clinic wi th t he his tory tha t she
fell a n d s t ruck the b a c k of her h e a d on a
conc re t e f loor at t he age of 1 m o n t h . Shor t ly
af terwards , a bu lge was no t i ced in t he left
occipi to-par ie ta l region . T h i s bu lge b e c a m e
progressively larger and tense . On admiss ion
the child was irr i table, refused feeds a n d had
b e e n vomi t ing for pas t few days . Skull r ad io
graphs showed a widely gap ing w e d g e - s h a p e d
b o n e defect wi th extensive resorp t ion in the
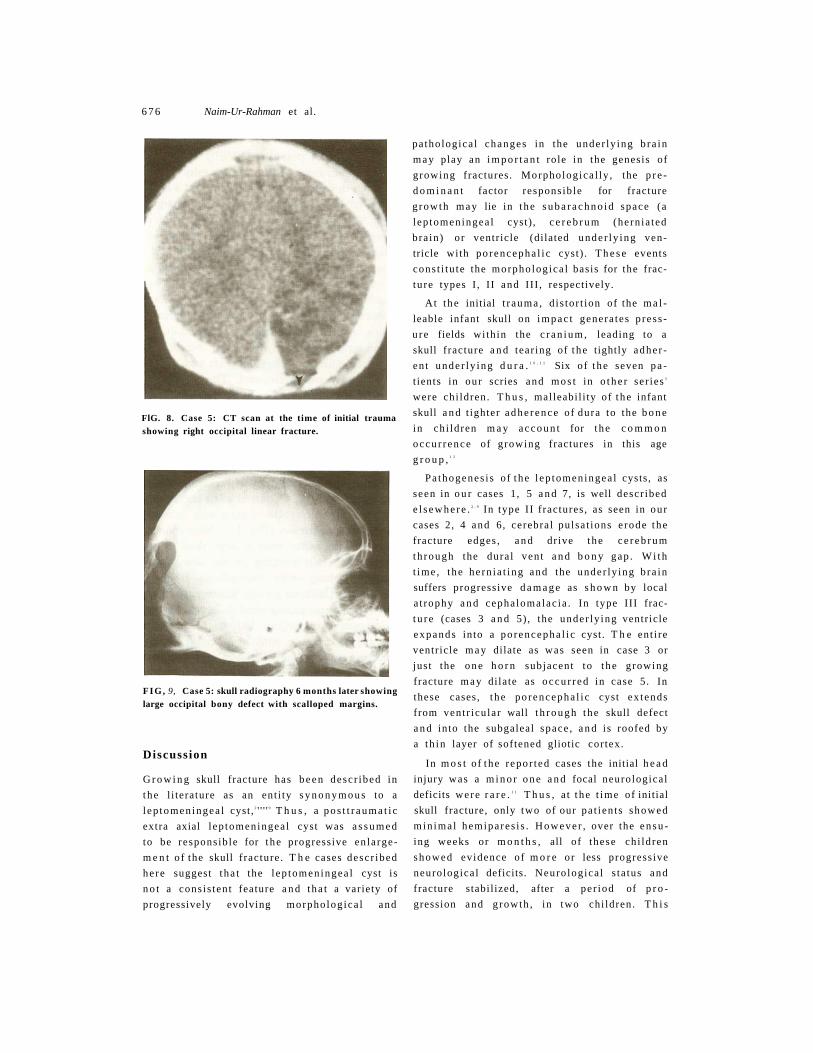
left occipi to-par ie ta l region. CT (Fig. 5a and
b) showed a large po rencepha l i c cyst c o m m u
nica t ing with t he occipi ta l h o r n of a d i la ted left
lateral ventr ic le a n d he rn ia t ing t h r o u g h the
wide b o n y gap in to t he tense occipital bulge .
T h e child was t rea ted wi th vent r icu lo-per i -
toneal s h u n t following which the occipital
bu lge a n d h y d r o c e p h a l u s resolved. At follow-
up examina t ions at 3 a n d 6 m o n t h s , t he child
was thr iving, the occipital bu lge had d i sap
peared and the b o n e defect was m u c h smaller ,
FlG. 3. Case 2: skull radiography, lateral view, showing a widely gaping parietal fracture.
F l G . 4. Case 2: CT scan showing the right parietal bone defect and the underlying low-density brain lesion.
6 7 4 Naim-Ur-Rahman et al.
F I G . 5. (a) and (b) CT scans shown a large left occipital ventricle (a) and herniating, through the wide bony gap
with definite evidence of b o n e re -growth at the
fracture edges .
Case 4. T h i s 3-year-old girl was originally
a d m i t t e d a n d t rea ted elsewhere for a l inear
fracture of left f ronto-par ie ta l region. Seven
m o n t h s after t he original h e a d injury, she was
admi t t ed to o u r neurosurg ica l un i t because a
bu lge h a d deve loped over t he left forehead
which b e c a m e progressively larger. T h e r e was
a his tory of occasional h e a d a c h e s , vomi t ing ,
seizures a n d progressive right hemipares i s du r
ing the p reced ing 3 m o n t h s . On examina t ion
there was a tense l inear swelling in t he left
forehead ex tend ing f rom the left f ronto
par ie ta l region to the supra-orb i ta l marg in
and roo t o f t he nose . T h e marg ins o f t he
unde r ly ing skull defect could be pa lpa t ed . She
had mi ld weakness o f r ight a r m a n d leg b u t
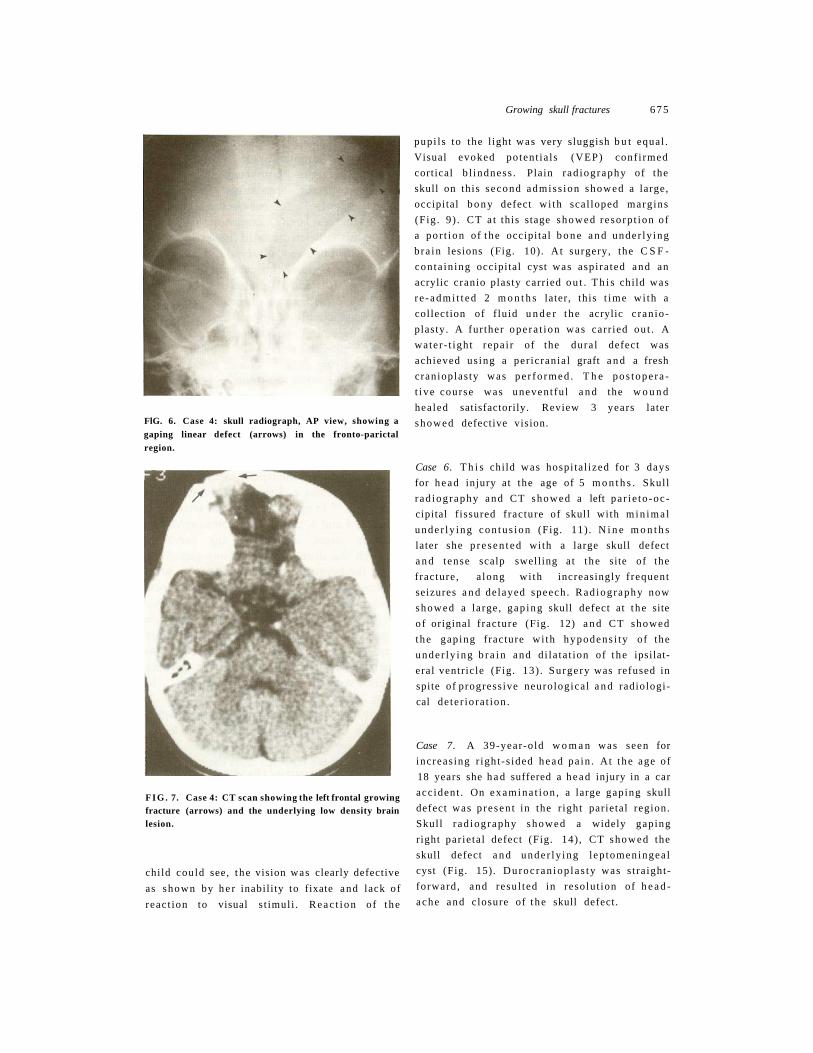
no p a p i l l e d e m a . Skull r a d i o g r a p h (Fig. 6)
showed a l inear defect in the left f ronto
par ie ta l region ex tend ing to the supraorbi ta l
marg in . CT (Fig. 7 ) showed the gaping frac
tu re a n d an under ly ing low densi ty b ra in
lesion. At ope ra t ion , a large f ron topar ie to-
t e m p o r a l scalp flap was raised. U n d e r n e a t h
t he flap an adhe ren t l inear bu lge of gliotic
b ra in was seen b e t w e e n the gaping fracture
edges . T h i s he rn ia t ed cerebral t issue, e x t e n d -
porcnccphalic cyst communicating with a dilated lateral (b).
ing from coronal s u t u r e to t he supra-orb i ta l
marg in , was tense , conges ted and b led easily.
D u r a l repa i r with fascia lata a n d craniopias ty
wi th methyl me thac ry la te was carr ied ou t . T h e
pos topera t ive course was unevent fu l a n d the
child was d i scharged h o m e , free of h e a d a c h e ,
b u t wi th res idual mi ld r ight-s ided weakness .
F o l l o w - u p at 2 years showed tha t the im
p l a n t e d plast ic was loose and bu lg ing over a
tense cystic swelling. Reopera t ion was refused.
Case J . T h e p a t i e n t was originally admi t t ed to
t he neurosurg ica l un i t at the age of 9 m o n t h s
following a r o ad traffic acc ident . On ad
miss ion , she was drowsy, b u t w i t h o u t any a b
n o r m a l neuro logica l findings. A r a d i o g r a p h of
t he skull showed an obl iquely p laced f issure
fracture of t he skull cross ing the midl ine just
above torcula a n d C T showed this fracture
wi th min ima l con tus ion of t he occipital lobes
(Fig. 8 ) . T h e b a b y recovered rapidly from the
h e a d injury and was d i scharged h o m e after 5
days. Six m o n t h s later (at t he age of 15
m o n t h s ) she was r e -admi t t ed with a tense
swelling in t he region of the occipital f racture
site and a suspic ion of progressive visual loss.
T h e occipital swelling h a d b e e n gradual ly en
larging d u r i n g the weeks p r io r to re -admiss ion .
Examina t i on n o w revealed that a l though the
Growing skull fractures 675
FlG. 6. Case 4: skull radiograph, AP view, showing a gaping linear defect (arrows) in the fronto-parictal region.
F I G . 7. Case 4: CT scan showing the left frontal growing fracture (arrows) and the underlying low density brain lesion.
child could see, t he vision was clearly defective
as shown by h e r inabili ty to fixate and lack of
reac t ion to visual s t imuli . R e a c t i o n of t he
pupi l s to the l ight was very sluggish b u t equal .
Visual evoked potent ia ls (VEP) conf i rmed
cortical b l indness . Plain r ad iography of the
skull on this second admiss ion showed a large,
occipital b o n y defect wi th scal loped margins
(Fig . 9) . CT a t this stage showed resorp t ion of
a po r t ion of t he occipital b o n e a n d under ly ing
b ra in lesions (Fig. 10). At surgery, the C S F -
conta in ing occipital cyst was aspi ra ted and an
acrylic cranio plasty carried o u t . T h i s child was
r e - admi t t ed 2 m o n t h s later, this t ime wi th a
collection of f luid u n d e r t he acrylic c ran io-
plasty. A fur ther ope ra t ion was carr ied ou t . A
water - t igh t repa i r of the dura l defect was
achieved us ing a per icrania l graft a n d a fresh
cranioplas ty was pe r fo rmed . T h e pos tope ra
t i ve course was unevent fu l a n d the w o u n d
healed satisfactorily. Review 3 years later
showed defective vision.
Case 6. T h i s child was hospi ta l ized for 3 days
for h e a d injury at the age of 5 m o n t h s . Skull
r ad iography and CT showed a left pa r i e to -oc -
cipital f issured fracture of skull with m i n i m a l
unde r ly ing con tus ion (Fig. 11) . N i n e m o n t h s
later she p r e s e n t e d with a large skull defect
a n d tense scalp swelling at t he site of the
fracture , a long wi th increasingly f requent
seizures a n d delayed speech . Rad iography now
showed a large, gap ing skull defect at t he site
o f original f racture (Fig. 12) a n d CT showed
the gaping fracture wi th hypodens i ty of the
unde r ly ing b r a i n and d i la ta t ion of t he ipsilat-
eral ventr icle (Fig. 13) . Surgery was refused in
spite of progress ive neurological a n d radiologi
cal de te r iora t ion .
Case 7. A 39-year-old w o m a n was seen for
increas ing r ight -s ided h e a d pa in . At t he age of
18 years she h a d suffered a h e a d injury in a car
acc ident . On examina t ion , a large gaping skull
defect was p resen t in the r ight parietal region.
Skull r ad iography showed a widely gaping
right par ie ta l defect (Fig. 14) , CT showed the
skull defect a n d unde r ly ing lep tomeningea l
cyst (Fig. 15). Duroc ran iop la s ty was s t ra ight
forward, and resul ted in resolut ion of h e a d
ache and closure of t he skull defect.
6 7 6 Naim-Ur-Rahman et al.
FlG. 8. Case 5: CT scan at the time of initial trauma showing right occipital linear fracture.
F I G , 9, Case 5: skull radiography 6 months later showing large occipital bony defect with scalloped margins.
Discussion
G r o w i n g skull fracture has b e e n descr ibed in
t he l i terature as an ent i ty s y n o n y m o u s to a
l ep tomeningea l cyst, 2 ' ' ' ' 9 T h u s , a p o s t t r a u m a t i c
extra axial l ep tomeningea l cyst was a s s u m e d
to be responsib le for t he progressive en la rge
m e n t o f the skull f racture . T h e cases descr ibed
he re suggest t ha t the l ep tomeningea l cyst is
n o t a cons is ten t feature a n d tha t a variety of
progressively evolving morpholog ica l and
pa thologica l changes in the under ly ing b ra in
m a y play an i m p o r t a n t role in the genesis of
growing fractures. Morphologica l ly , the p r e
d o m i n a n t factor responsib le for fracture
g rowth m a y lie in t he s u b a r a c h n o i d space (a
l ep tomeningea l cyst) , c e r e b r u m (hern ia ted
bra in) or ventr icle (dilated unde r ly ing ven
tricle with po rencepha l i c cyst) . T h e s e events
cons t i tu te the morpholog ica l basis for the frac
tu re types I , I I and III , respectively.
At t he initial t r auma , d is tor t ion of the m a l
leable infant skull on i m p a c t genera tes p ress
u r e fields wi th in the c r a n i u m , leading to a
skull f racture a n d tear ing of t he tightly adhe r
en t unde r ly ing d u r a . 1 0 , 1 1 Six o f t he seven p a
t ients in our scries and m o s t in o t h e r ser ies 3
were chi ldren. T h u s , malleabi l i ty of t he infant
skull a n d t ighter a d h e r e n c e of dura to the b o n e
in ch i ldren m a y a c c o u n t for t he c o m m o n
occu r r ence of growing fractures in this age
g r o u p , 1 2
Pa thogenes i s of t he l ep tomeningea l cysts, as
seen in o u r cases 1, 5 a n d 7, is well descr ibed
e l s e w h e r e . 2 , 9 In type II f ractures , as seen in our
cases 2, 4 and 6, cerebral pulsa t ions e rode t he
fracture edges , a n d drive t he c e r e b r u m
th rough the dura l vent a n d b o n y gap . W i t h
t ime , t he he rn ia t ing and the under ly ing b ra in
suffers progressive d a m a g e as s h o w n by local
a t rophy a n d cepha lomalac ia . In type III frac
t u r e (cases 3 a n d 5) , the under ly ing ventricle
expands into a po rencepha l i c cyst. T h e ent i re
ventr icle m a y dilate as was seen in case 3 or
jus t the o n e h o r n subjacent to t he growing
fracture m a y dilate as occu r r ed in case 5. In
these cases, t he po rencepha l i c cyst ex tends
from vent r icular wall t h r o u g h the skull defect
a n d into the subgaleal space , a n d is roofed by
a t h in layer of softened gliotic cor tex.
In m o s t of t he repor ted cases the initial h e a d
injury was a m i n o r o n e a n d focal neurological
deficits were r a r e . 1 1 T h u s , a t t he t ime of initial
skull fracture, only two of our pa t ien ts showed
min imal hemipares i s . Howeve r , over the e n s u
ing weeks or m o n t h s , all of these ch i ldren
showed evidence of m o r e or less progress ive
neurological deficits. Neuro logica l s ta tus and
fracture stabil ized, after a per iod of p r o
gression and g rowth , in two chi ldren. T h i s
Growing skull fractures 611
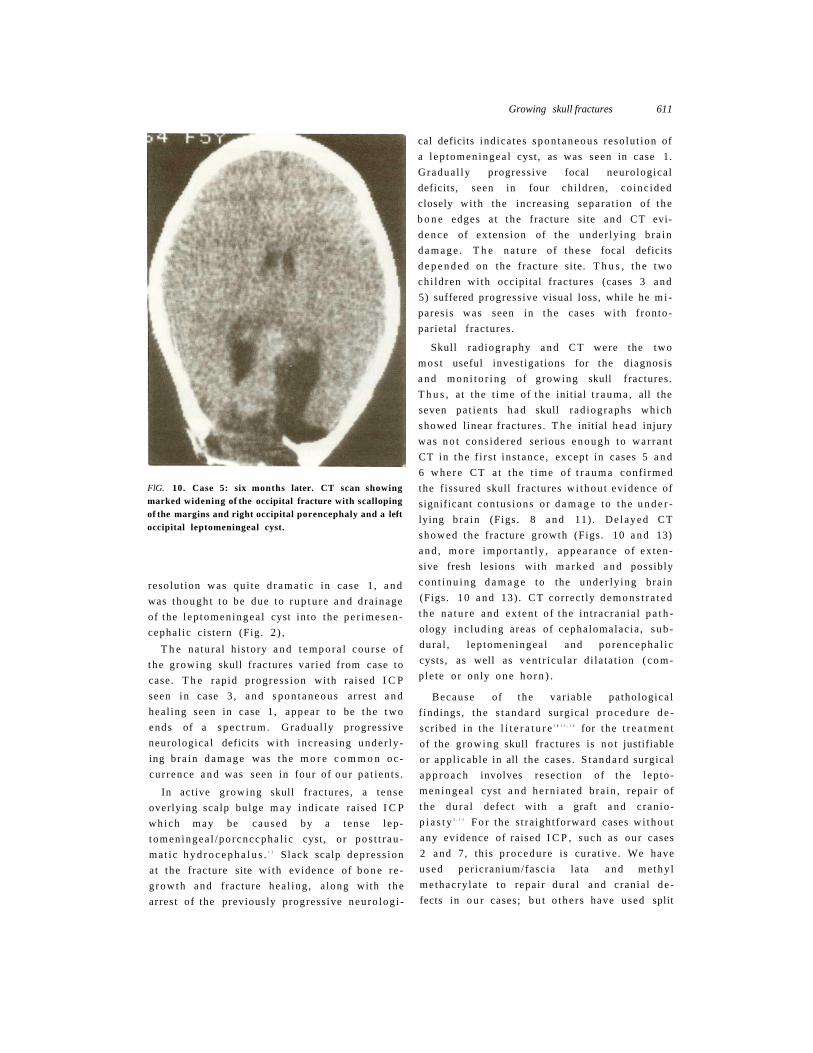
FlG. 10. Case 5: six months later. CT scan showing marked widening of the occipital fracture with scalloping of the margins and right occipital porencephaly and a left occipital leptomeningeal cyst.
resolut ion was qui te d r a m a t i c in case 1 , a n d
was t h o u g h t to be due to r u p t u r e a n d dra inage
of the l ep tomeningea l cyst into the pe r imesen -
cephal ic cistern (Fig. 2 ) ,
T h e na tura l his tory a n d t e m p o r a l course o f
t he growing skull fractures var ied from case to
case. T h e rapid progress ion with ra ised I C P
seen in case 3 , a n d s p o n t a n e o u s arrest a n d
heal ing seen in case 1, appear to be t he t w o
ends of a s p e c t r u m . Gradua l ly progress ive
neurological deficits wi th increas ing unde r ly
ing b ra in d a m a g e was t he m o r e c o m m o n o c
cur rence a n d was seen in four of o u r pa t ien t s .
In active growing skull f ractures , a t ense
overlying scalp bulge m a y indicate raised I C P
wh ich m a y be caused by a tense l ep-
tomen ingea l /po rcnccpha l i c cyst, o r pos t t r au
ma t i c h y d r o c e p h a l u s . 1 3 Slack scalp depress ion
at the fracture site wi th evidence of b o n e r e -
g rowth and fracture hea l ing , a long with t he
arrest of the previously progress ive neuro log i
cal deficits ind ica tes s p o n t a n e o u s reso lu t ion of
a l ep tomeningea l cyst, as was seen in case 1.
Gradua l ly progressive focal neurological
deficits, seen in four chi ldren , co inc ided
closely wi th the increasing separa t ion of t he
b o n e edges a t t he fracture site and CT evi
d e n c e of ex tens ion of the under ly ing b ra in
d a m a g e . T h e n a t u r e o f these focal deficits
d e p e n d e d on the fracture site. T h u s , t he two
chi ldren wi th occipital f ractures (cases 3 and
5) suffered progressive visual loss, while he mi -
paresis was seen in t he cases wi th f ronto
parietal fractures.
Skull rad iography a n d C T were the two
m o s t useful invest igat ions for the diagnosis
a n d m o n i t o r i n g of growing skull fractures.
T h u s , a t the t ime of t he initial t r a u m a , all the
seven pa t i en t s h a d skull r ad iographs which
showed l inear fractures. T h e initial h e a d injury
was n o t cons idered serious e n o u g h to war ran t
CT in t he f i r s t ins tance , except in cases 5 a n d
6 w h e r e CT a t t he t ime of t r a u m a conf i rmed
the f issured skull fractures w i thou t evidence of
significant con tus ions o r d a m a g e to t he u n d e r
lying b ra in (Figs. 8 a n d 11) . De l ayed CT
showed the fracture growth (Figs. 10 a n d 13)
a n d , m o r e impor tan t ly , appea rance o f ex ten
sive fresh lesions with m a r k e d a n d possibly
c o n t i n u i n g d a m a g e to the under ly ing bra in
(Figs. 10 a n d 13) . CT correct ly d e m o n s t r a t e d
t he n a t u r e and ex ten t o f t he in t racrania l p a t h
ology inc lud ing areas of cephalomalac ia , s u b
dura l , l ep tomeningea l and po rencepha l i c
cysts, as well as vent r icular d i la ta t ion ( c o m
ple te o r only o n e h o r n ) .
Because of t he var iable pathological
f indings, t he s t anda rd surgical p r o c e d u r e d e
scribed in t he l i t e r a t u r e 2 ' 1 1 , 1 4 for t he t r e a t m e n t
of the g rowing skull fractures is n o t justifiable
or appl icable in all the cases. S t a n d a r d surgical
a p p r o a c h involves resect ion of t he l ep to
men ingea l cyst a n d he rn ia t ed b ra in , repa i r of
t he du ra l defect with a graft a n d c ran io
p i a s t y 2 , 1 1 F o r the s t ra ightforward cases wi thou t
any evidence of raised I C P , such as our cases
2 and 7, this p r o c e d u r e is cura t ive . We have
u s e d per icranium/fascia lata a n d me thy l
methacry la te to repair du ra l and crania l de
fects in o u r cases; b u t o the r s have used split
6 7 8 Naim-Ur-Rahman et al.
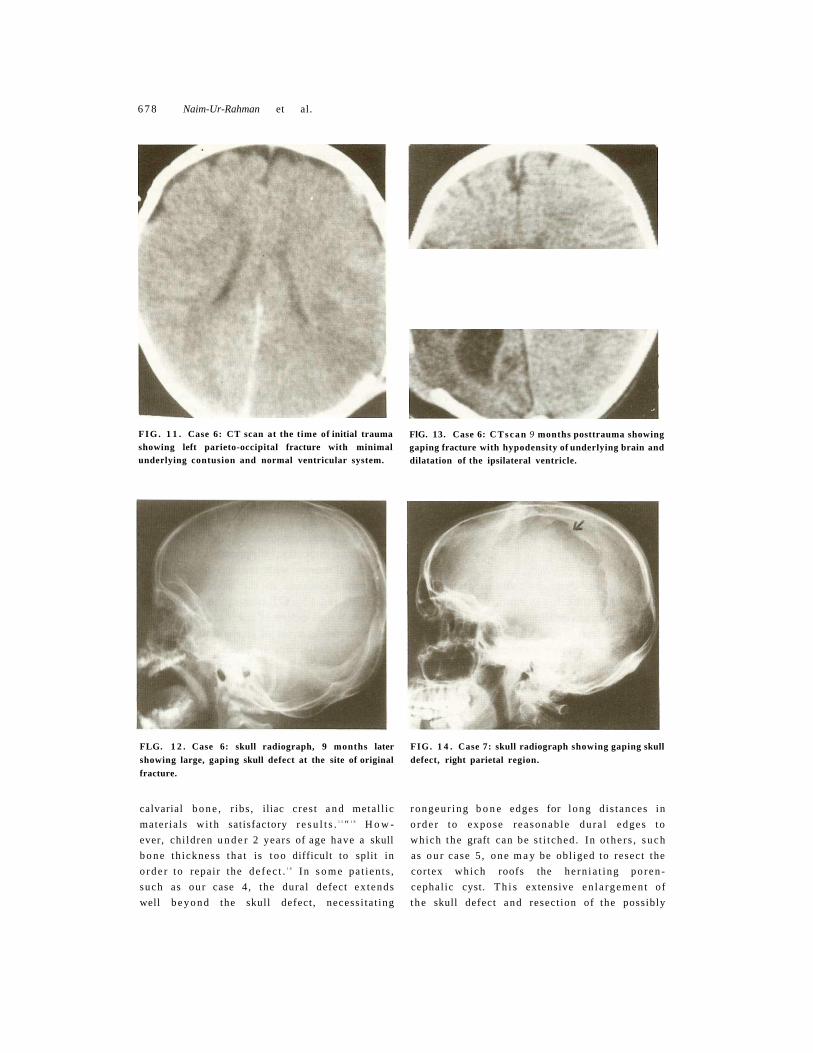
F I G . 1 1 . Case 6: CT scan at the time of initial trauma showing left parieto-occipital fracture with minimal underlying contusion and normal ventricular system.
FLG. 1 2 . Case 6: skull radiograph, 9 months later showing large, gaping skull defect at the site of original fracture.
calvarial b o n e , r ibs , iliac cres t a n d metal l ic
mater ia ls wi th satisfactory r e s u l t s . 1 5 " 1 8 H o w
ever, chi ldren u n d e r 2 years of age have a skull
b o n e th ickness tha t is t oo difficult to split in
o r d e r to repair the de fec t . 1 8 In s o m e pa t ien ts ,
such as our case 4, the dural defect ex tends
well b e y o n d the skull defect , necess i ta t ing
FlG. 13. Case 6: C T s c a n 9 months posttrauma showing gaping fracture with hypodensity of underlying brain and dilatation of the ipsilateral ventricle.
FIG. 1 4 . Case 7: skull radiograph showing gaping skull defect, right parietal region.
rongeur ing b o n e edges for long d is tances in
o r d e r to expose reasonab le du ra l edges to
which the graft can be s t i tched. In o the r s , s u c h
as o u r case 5 , o n e m a y be obl iged to resect the
cortex which roofs the he rn ia t ing po ren
cephal ic cyst. T h i s extensive en l a rgemen t of
t he skull defect and resect ion of the possibly

Growing skull fractures 6 7 9
FlG. 15. Case 7: CT scan showing right parietal skull defect overlying a leptomeningeal cyst.
funct ional a n d viable areas of t he infant b ra in
appear to be s o m e w h a t excessive. In these
c i r cums tances , t he modif ied m e t h o d for r e
pa i r ing this defect , as desc r ibed by Hal l iday et
al.,"* seems m o r e app rop r i a t e . T h i s t e chn ique
involves mobi l iz ing the p e r i c r a n i u m c i r cum-
fercntially a r o u n d the edges of the bone defect
a n d reflecting i t over the site of t he dura l
defect to provide t issue for r epa i r , 1
In g rowing skull f ractures associa ted wi th
ra ised I C P , s h u n t surgery shou ld be con
s idered as an initial or al ternative p r o c e d u r e ,
as i t m a y resul t in reso lu t ion of ra ised I C P ,
d i sappea rance of scalp swellings a n d regrowth
of b o n e edges a t t he fracture s i t e ; 1 3 as illus
t ra ted by case 3.
R e c u r r e n c e after surgical repair in two of
o u r pa t ien ts and o the r r epor ted c a s e s 1 3 co r re
lated with failure to secure water t igh t du ra l
c losure or failure to address the raised I C P .
Because of the k n o w n risk of fracture
g rowth a long wi th t he f requent ly progressive
n a t u r e o f b ra in d a m a g e a n d neurological
deficits, ch i ldren with l inear skull fractures
shou ld be examined clinically 2 - 3 m o n t h s
later to check for ev idence of growing fracture .
If a scalp bu lge or gaping b o n e defect is found ,
rad iography and C T shou ld b e repea ted . I f
g rowing skull fracture is conf i rmed, surgical
repair should be advised.
Address for correspondence: Professor N a i m - U r -
R a h m a n , Divis ion of N e u r o s u r g e r y , Col lege of
M e d i c i n e , K i n g S a u d Univers i ty & K i n g
K h a l i d Univers i ty Hosp i t a l , P O B o x 2 9 2 5 ,
Riyadh 1 1 4 6 1 , Saudi Arabia .
References
1 Scarff T B , Fine M, Growing skull fractures of childhood. In: Wilkins R H , Rengachary SS cds. Neurosurgery, Vol. 2. N e w York: McGraw Hill, 1985; 1627-8 .
2 Long D M , Kieffer SA, Chou S N . Leptomeningeal cyst. In: Youmans JR ed. Neurological surgery, Vol. 5. Philadelphia: WB Saunders, 1982; 3245¬ 50.
3 Lende R, Erickson T. Growing skull fractures of childhood. J Neurosurg 1961; 18:479-89 .
4 Soule A, Whitcomb B. Extensive erosion of the base of the skull from a leptomeningeal cyst. Report of a case. Arch Neurol Psychiat 1946; 55:382-7 ,
5 Halliday AL, Chapman PH, Heros RC. Leptomeningeal cyst resulting from adulthood trauma: case report. Neurosurgery 1990; 26 :150-3 .
6 Ramamurthi B, Kalyanaraman S. Rationale fot surgery in growing fractures of the skull. J Neurosurg 1970; 32:427-30 .
7 Chorobski J, Davis L, Cyst formation of skull. Gynecol Obstet 1934; 58 :12 -31 .
8 Stein E M , Tenner MS: Enlargement of skull fractures in childhood due to cerebral herniation. Arch Neurol 1972; 2 6 : 1 3 7 ^ 3 .
9 Tavcras JM, Wood EH. Leptomeningeal cyst. Diagnostic neuroradiology. Baltimore: Williams & Wilkins, 1976: 2(IV): 1055-9 .
10 Ommaya AK, Grubb RL, Naumann RA, Coup and counter-coup injury: observations on the mechanics of visible brain injuries in the rhesus monkey. J Neurosurg 1971; 35:503-632 ,
11 Bruce DA. Growing skull fracture: special considerations of the pediatric age group. In: Cooper PR cd. Head injury. Baltimore: Williams & Wilkins, 1982; 318 -19 .
12 Rahimizadeh A, Haddadian K. Bilateral traumatic leptomeningeal cysts. Neurosurgery 1986; 18:385¬ 7,
13 Sharma RR, Chandy MJ. Shunt surgery in growing skull fractures: report of two cases. Br J Neurosurg 1991; 5:93-8 .
14 McLaurin R, McLennan J. Diagnosis and treatment of head injury in children; In: Youmans JR ed. Neurological surgery, Vol. 4. Philadelphia: W B Saunders, 1982; 2 0 9 7 - 9 .
15 Guyuron B, Shafrom M, Columbi B. Management of extensive and different cranial defects. J Neurosurg 1988; 69 :210-12 .
16 Timmons RL. Cranial defects and their repair. In: Youmans JR ed. Neurological surgery. Philadelphia: W B Saunders, 1982; 2228-50 .
17 Malis LI. Titanium mesh and acrylic cranioplasty. Neurosurgery 1989; 25:351-5 .
18 Posnick JC, Goldstein JA, Armstrong D, Rutka JT. Reconstruction of skull defects in children and adolescents by the use of fixed cranial bone grafts: Ijmg-term results. Neurosurgery 1993; 32 :785-91 .
Related Documents




![Head 2 - newbooks-services.deria [4]. The incidence of skull fractures in children that present at the emergency department for a skull trauma ranges from 2% to 20% [5]. Most frequently](https://static.cupdf.com/doc/110x72/60e17dd88fe17338c62c2d1e/head-2-newbooks-ria-4-the-incidence-of-skull-fractures-in-children-that-present.jpg)






