Greater Manchester EUR Policy Statement on: Functional Electrical Stimulation (FES) for Foot Drop GM Ref: GM036 Version: 2.5 (18 December 2019)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Greater Manchester EUR Policy Statement on:
Functional Electrical Stimulation (FES) for Foot Drop GM Ref: GM036 Version: 2.5 (18 December 2019)
GM FES for Foot Drop Policy v2.5 FINAL Page 2 of 23
Commissioning Statement
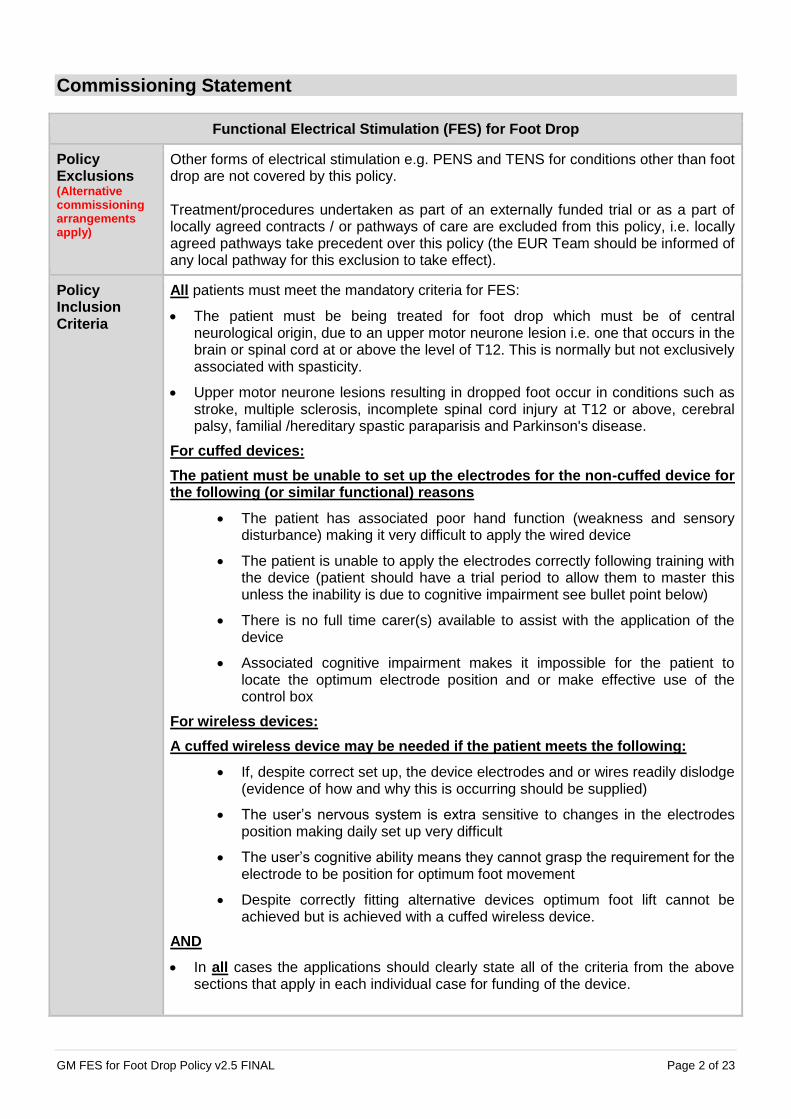
Functional Electrical Stimulation (FES) for Foot Drop
Policy Exclusions (Alternative commissioning arrangements apply)
Other forms of electrical stimulation e.g. PENS and TENS for conditions other than foot drop are not covered by this policy. Treatment/procedures undertaken as part of an externally funded trial or as a part of locally agreed contracts / or pathways of care are excluded from this policy, i.e. locally agreed pathways take precedent over this policy (the EUR Team should be informed of any local pathway for this exclusion to take effect).
Policy Inclusion Criteria
All patients must meet the mandatory criteria for FES:
The patient must be being treated for foot drop which must be of central neurological origin, due to an upper motor neurone lesion i.e. one that occurs in the brain or spinal cord at or above the level of T12. This is normally but not exclusively associated with spasticity.
Upper motor neurone lesions resulting in dropped foot occur in conditions such as stroke, multiple sclerosis, incomplete spinal cord injury at T12 or above, cerebral palsy, familial /hereditary spastic paraparisis and Parkinson's disease.
For cuffed devices:
The patient must be unable to set up the electrodes for the non-cuffed device for the following (or similar functional) reasons
The patient has associated poor hand function (weakness and sensory disturbance) making it very difficult to apply the wired device
The patient is unable to apply the electrodes correctly following training with the device (patient should have a trial period to allow them to master this unless the inability is due to cognitive impairment see bullet point below)
There is no full time carer(s) available to assist with the application of the device
Associated cognitive impairment makes it impossible for the patient to locate the optimum electrode position and or make effective use of the control box
For wireless devices:
A cuffed wireless device may be needed if the patient meets the following:
If, despite correct set up, the device electrodes and or wires readily dislodge (evidence of how and why this is occurring should be supplied)
The user’s nervous system is extra sensitive to changes in the electrodes position making daily set up very difficult
The user’s cognitive ability means they cannot grasp the requirement for the electrode to be position for optimum foot movement
Despite correctly fitting alternative devices optimum foot lift cannot be achieved but is achieved with a cuffed wireless device.
AND
In all cases the applications should clearly state all of the criteria from the above sections that apply in each individual case for funding of the device.

GM FES for Foot Drop Policy v2.5 FINAL Page 3 of 23
Funding Mechanism
Wired: Individual prior approval provided the patient meets the above criteria. Requests should be submitted with all relevant supporting evidence, which must be provided with the request. Cuffed / Wireless: Individual prior approval via Clinical Triage provided the patient meets the above criteria. Requests should be submitted with all relevant supporting evidence, which must be provided with the request.
Clinical Exceptionality
Clinicians can submit an Individual Funding Request (IFR) outside of this guidance if they feel there is a good case for exceptionality. More information on determining clinical exceptionality can be found in the Greater Manchester (GM) Effective Use of Resources (EUR) Operational Policy. Link to GM EUR Operational Policy
Best Practice Guidelines
All providers are expected to follow best practice guidelines (where available) in the management of these conditions.
GM FES for Foot Drop Policy v2.5 FINAL Page 4 of 23
Contents Commissioning Statement ........................................................................................................................ 2
Policy Statement ...................................................................................................................................... 5
Equality & Equity Statement ..................................................................................................................... 5
Governance Arrangements ....................................................................................................................... 5
Aims and Objectives ................................................................................................................................. 5
Rationale behind the policy statement ...................................................................................................... 6
Treatment / Procedure .............................................................................................................................. 6
Epidemiology and Need ........................................................................................................................... 6
Adherence to NICE Guidance .................................................................................................................. 7
Audit Requirements .................................................................................................................................. 7
Date of Review ......................................................................................................................................... 7
Glossary ................................................................................................................................................... 7
References ............................................................................................................................................... 8
Governance Approvals ............................................................................................................................. 8
Appendix 1 – Evidence Review ................................................................................................................ 9
Appendix 2 – Diagnostic and Procedure Codes ...................................................................................... 21
Appendix 3 – Version History ................................................................................................................. 22
GM FES for Foot Drop Policy v2.5 FINAL Page 5 of 23
Policy Statement The GM Effective Use of Resources (EUR) Policy Team, in conjunction with the GM EUR Steering Group, have developed this policy on behalf of Clinical Commissioning Groups (CCGs) within Greater Manchester, who will commission treatments/procedures in accordance with the criteria outlined in this document. In creating this policy the GM EUR Steering Group has reviewed this clinical condition and the options for its treatment. It has considered the place of this treatment in current clinical practice, whether scientific research has shown the treatment to be of benefit to patients, (including how any benefit is balanced against possible risks) and whether its use represents the best use of NHS resources. This policy document outlines the arrangements for funding of this treatment for the population of Greater Manchester. This policy follows the principles set out in the ethical framework that govern the commissioning of NHS healthcare and those policies dealing with the approach to experimental treatments and processes for the management of individual funding requests (IFR).
Equality & Equity Statement CCGs have a duty to have regard to the need to reduce health inequalities in access to health services and health outcomes achieved, as enshrined in the Health and Social Care Act 2012. CCGs are committed to ensuring equality of access and non-discrimination, irrespective of age, gender, disability (including learning disability), gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion or belief, gender or sexual orientation. In carrying out its functions, CCGs will have due regard to the different needs of protected characteristic groups, in line with the Equality Act 2010. This document is compliant with the NHS Constitution and the Human Rights Act 1998. This applies to all activities for which they are responsible, including policy development, review and implementation. In developing policy the GM EUR Policy Team will ensure that equity is considered as well as equality. Equity means providing greater resource for those groups of the population with greater needs without disadvantage to any vulnerable group. The Equality Act 2010 states that we must treat disabled people as more equal than any other protected characteristic group. This is because their ‘starting point’ is considered to be further back than any other group. This will be reflected in CCGs evidencing taking ‘due regard’ for fair access to healthcare information, services and premises. An Equality Analysis has been carried out on the policy. For more information about the Equality Analysis, please contact [email protected].
Governance Arrangements The Greater Manchester Joint Commissioning Board has given delegated authority to the Greater Manchester Directors of Commissioning and Directors of Finance to approve GM EUR treatment policies for implementation. Further details of the governance arrangements can be found in the GM EUR Operational Policy.
Aims and Objectives This policy document aims to ensure equity, consistency and clarity in the commissioning of treatments/procedures by CCGs in Greater Manchester by:
reducing the variation in access to treatments/procedures.
GM FES for Foot Drop Policy v2.5 FINAL Page 6 of 23
ensuring that treatments/procedures are commissioned where there is acceptable evidence of clinical benefit and cost-effectiveness.
reducing unacceptable variation in the commissioning of treatments/procedures across Greater Manchester.
promoting the cost-effective use of healthcare resources.
Rationale behind the policy statement Although the evidence base is relatively weak there is evidence to suggest that FES is a cost effective intervention for foot drop of central neurological origin. To ensure that the resource available to fund this intervention is targeted to the group that will gain the most benefit FES is routinely commissioned for this group only. All other uses of FES will be commissioned as part of a local pathway of care where appropriate or as part of a trial as appropriate and subject to local arrangements for trials and studies.
Treatment / Procedure FES has a number of applications, not all of which have a sound body of evidence to support their routine use. This policy aims to target the resource available for this intervention to those patients where there is evidence that they will benefit the most from the intervention. Functional Electrical Stimulation (FES) is a treatment using small electrical charges to improve mobility in a number of conditions. There is a reasonable body of evidence and it is recognised as cost effective for foot drop of central neurological and of upper motor neurone origin – it is used mostly for foot drop following stroke or in Multiple Sclerosis. Dropped foot
Dropped foot occurs when damage to nerve pathways means someone experiences weakness or poor coordination in their leg or ankle which affects the way that they walk. Dropped foot leads to a way of walking that requires more effort and uses more energy. The foot may drag along the ground or the toes hang down when walking, which makes the individual more vulnerable to tripping and falling. People may alter the way that they walk to compensate, commonly lifting their leg higher. In time, this can lead to further problems such as pain in the hips or lower back, a tightening of muscles and poor balance. Devices
Several different FES devices are available. Each has a control box, about the size of a pack of cards, which is either worn on the leg or at the waist. The devices apply impulses through electrodes attached to the skin. A version is also available that uses a surgically implanted nerve stimulator. These work by replacing the stimulation normally received from the brain to the muscles controlling the position of the foot resulting in a basic but useful movement. The device is activated by a pressure sensitive switch in the shoe. When the foot is lifted, an impulse is applied causing the foot to tilt to the correct angle. When the foot is placed on the ground again, pressure is reapplied to the switch and the impulse ceases.
Epidemiology and Need Foot drop of central neurological origin is most commonly due to Stroke or Multiple Sclerosis (MS). There are approximately 152,000 strokes in the UK every year, foot drop is a common sequelae of strokes.
GM FES for Foot Drop Policy v2.5 FINAL Page 7 of 23
A study of the UKGP database estimated that 126,669 people were living with MS in the UK in 2010 (203.4 per 100,000 population) and that 6,003 new cases were diagnosed that year (9.64 per 100 000/year). There is an increasing population living longer with MS, which has important implications for resource allocation for MS in the UK2.
Adherence to NICE Guidance This policy adheres to the guidance in NICE IPG278: Functional electrical stimulation for drop foot of central neurological origin.
Audit Requirements There is currently no national database. Service providers will be expected to collect and provide audit data on request.
Date of Review Five years from the date of the last review, unless new evidence or technology is available sooner. The evidence base for the policy will be reviewed and any recommendations within the policy will be checked against any new evidence. Any operational issues will also be considered at this time. All available additional data on outcomes will be included in the review and the policy updated accordingly. The policy will be continued, amended or withdrawn subject to the outcome of that review.
Glossary
Term Meaning
Central neurological Pertaining to the part of the nervous system consisting of the brain and spinal cord.
Cerebral Palsy A condition marked by impaired muscle coordination (spastic paralysis) and/or other disabilities, typically caused by damage to the brain before or at birth.
Familial hereditary spastic paraparisis
A group of inherited disorders that cause weakness and stiffness of the leg muscles, which gradually gets worse over time.
IPG Interventional Procedure Guidance
Multiple Sclerosis A progressive disease involving damage to the sheaths of nerve cells in the brain and spinal cord, whose symptoms may include numbness, impairment of speech and of muscular coordination, blurred vision, and severe fatigue.
NICE National Institute for Health and Care Excellence
Parkinson's disease. A progressive disease of the nervous system marked by tremor, muscular rigidity, and slow, imprecise movement, chiefly affecting middle-aged and elderly people. It is associated with degeneration of the basal ganglia of the brain and a deficiency of the neurotransmitter dopamine.
Sequelae A condition which is the consequence of a previous disease or injury.
Stroke A stroke is the sudden death of brain cells in a localized area due to inadequate bloodflow.

GM FES for Foot Drop Policy v2.5 FINAL Page 8 of 23
T12 or above Thoracic vertebrae 12 or above.
Upper motor neurone Neurons that originate either in the motor region of the cerebral cortex or in the brain stem and carry motor information down to the lower motor neurons (motor stimuli are those that result in movement).
References
1. Greater Manchester Effective Use of Resources Operational Policy
2. Incidence and prevalence of multiple sclerosis in the UK 1990–2010: a descriptive study in the General Practice Research Database, I.S. MacKenzie et al, J Neurol Neurosurg Psychiatry doi:10.1136/jnnp-2013-305450
Governance Approvals
Name Date Approved
Greater Manchester Effective Use of Resources Steering Group 08/07/2015
Greater Manchester Chief Finance Officers / Greater Manchester Directors of Commissioning
28/04/2016
Greater Manchester Association Governing Group 03/05/2016
Bolton Clinical Commissioning Group 01/06/2016
Bury Clinical Commissioning Group 27/05/2016
Heywood, Middleton & Rochdale Clinical Commissioning Group 15/07/2016
Central Manchester Clinical Commissioning Group 02/07/2016
North Manchester Clinical Commissioning Group 07/07/2016
Oldham Clinical Commissioning Group 03/05/2016
Salford Clinical Commissioning Group 03/05/2016
South Manchester Clinical Commissioning Group 03/07/2016
Stockport Clinical Commissioning Group 03/05/2016
Tameside & Glossop Clinical Commissioning Group 22/06/2016
Trafford Clinical Commissioning Group 17/05/2016
Wigan Borough Clinical Commissioning Group 01/06/2016
GM FES for Foot Drop Policy v2.5 FINAL Page 9 of 23
Appendix 1 – Evidence Review
Functional Electrical Stimulation (FES) for Foot Drop GM036
Search Strategy The following databases are routinely searched: NICE Clinical Guidance and full website search; NHS Evidence and NICE CKS; SIGN; Cochrane; York; BMJ Clinical Evidence; and the relevant Royal College websites. A Medline / Open Athens search is undertaken where indicated and a general google search for key terms may also be undertaken. The results from these and any other sources are included in the table below. If nothing is found on a particular website it will not appear in the table below:
Database Result
NICE IPG 278: Functional electrical stimulation for drop foot of central neurological origin
NHS Evidence and NICE CKS
CRD (York) reviews – cited below
SIGN SIGN 119: Management of patients with stroke: identification and management of dysphagia – cited reviews already listed so not cited here
Cochrane Nil additional
York (CRD) Surface-applied functional electrical stimulation for orthotic and therapeutic treatment of drop-foot after stroke: a systematic review, Roche A, o Laighin G, Coote S
The long-term cost-effectiveness of the use of Functional Electrical Stimulation for the correction of dropped foot due to upper motor neuron lesion, Taylor P, Humphreys L, Swain I
Health and fitness benefits of functional electrical stimulation-evoked leg exercise for spinal cord-injured individuals: a position review, Hamzaid NA, Davis GM
Functional electrical stimulation in the treatment of patients with chronic heart failure: a meta-analysis of randomized controlled trials, Sbruzzi G, Ribeiro RA, Schaan BD, Signori LU, Silva AM, Irigoyen MC, Plentz RD
General Search (Google)
Multiple self-help and provider websites – not cited here
Medline / Open Athens Not done as multiple reviews including NICE available
Other NWCSU Evidence Review: Functional electrical stimulation bicycle for patients with spinal cord injury, Date: November 2014
NWCSU Evidence Review: Functional electrical stimulation for the treatment of cauda equine pain, Date: June 2014
NWCSU Evidence Review: Functional electrical stimulation (FES) for the upper limb, Date: 21 October 2014
Stockport CCG Evidence Review: Functional electrical stimulation (FES) for the treatment of arm muscle paralysis, Date: February 2013

GM FES for Foot Drop Policy v2.5 FINAL Page 10 of 23
Summary of the evidence There is limited evidence for the cost effectiveness of FES for foot drop of central neurological origin that suggests it is a cost effective way of managing this condition. NICE also recommends further study.
The evidence
Levels of evidence
Level 1 Meta-analyses, systematic reviews of randomised controlled trials
Level 2 Randomised controlled trials
Level 3 Case-control or cohort studies
Level 4 Non-analytic studies e.g. case reports, case series
Level 5 Expert opinion
1. LEVEL 1: NICE IPG
NICE IPG 278: Functional electrical stimulation for drop foot of central neurological origin, Issued: January 2009
Guidance
a. Current evidence on the safety and efficacy (in terms of improving gait) of functional electrical stimulation (FES) for drop foot of central neurological origin appears adequate to support the use of this procedure provided that normal arrangements are in place for clinical governance, consent and audit.
b. Patient selection for implantable FES for drop foot of central neurological origin should involve a multidisciplinary team specialising in rehabilitation.
2. LEVEL 1: CRD REVIEW
Surface-applied functional electrical stimulation for orthotic and therapeutic treatment of drop-foot after stroke: a systematic review, Roche A, o Laighin G, Coote S
CRD summary: The review concluded that functional electrical stimulation can have a positive orthotic effect in patients who were in the chronic stage of stroke recovery. In light of the possibility of relevant studies being missed and the moderate or high risk of bias in nearly all included studies, the reliability of the authors' conclusions remains uncertain.
Authors' objectives: To evaluate the evidence for orthotic and therapeutic effects of surface functional electrical stimulation for the correction of drop-foot after stroke.
Searching: MEDLINE, EMBASE, CINAHL, AMED, Science Direct and Cochrane Central Register of Controlled Trials (CENTRAL) were searched for studies in English published between 1990 and June 2008. Search terms were reported. Reference lists of retrieved articles were searched.
Study selection: Studies of functional electrical stimulation for correction of drop-foot after adult stroke were eligible for inclusion. Studies that solely used implantable electrodes were excluded, as were studies that did not stimulate the lower limb/common peroneal nerve or tibialis anterior muscle.
Most populations were (at least partly) chronic cerebrovascular accident patients. Modes and durations of treatment varied. Comparator group treatments, where they existed, varied and included physiotherapy, botulinum toxin injections, electromechanical gait trainer and different applications of functional electrical stimulation. Several studies used functional electrical stimulation with a co-intervention. Studies assessed more than 30 different outcomes; the most common was a measure of walking.
Two reviewers independently selected studies for inclusion. Disagreements were resolved by consensus.
GM FES for Foot Drop Policy v2.5 FINAL Page 11 of 23
Assessment of study quality: Studies were quality assessed according to the presence of bias in relation to the following criteria (from Guidelines for Cochrane Reviewers): selection of participants; performance of care providers; detection of outcomes; and participant attrition. Studies were given an overall risk of bias (low risk when all criteria were met, moderate risk when one or more criteria were partly met or high risk when one or more criteria were not met).
The authors did not state how many reviewers performed the quality assessment.
Data extraction: The authors did not state how many reviewers performed the data extraction.
Methods of synthesis: A narrative synthesis was performed, grouped by study design or type of intervention.
Results of the review: Thirty studies were included in the review (n=1,159). Studies incorporated a range of study designs. Sample sizes ranged from one to 291 patients (25 studies had a sample size of fewer than 50 patients). Eleven studies had a high risk of bias, five were moderate-high, 12 were moderate and one was low.
Four before-and-after studies reported some orthotic effect using differing stimulators and two studies reported a therapeutic effect. Three studies (two of which had control groups) suggested that functional electrical stimulation may have been better than conventional therapy alone and that a combination of both interventions was more effective than either. No definitive conclusions could be drawn regarding the four studies of functional electrical stimulation with physiotherapy versus physiotherapy alone. Two small studies suggested that botulinum toxin injections followed by three days of functional electrical stimulation may have been more effective than botulinum toxin injections alone. Four studies of functional electrical stimulation and an electromechanical gait trainer with partial body weight support suggested combined therapy may be more effective than over-ground training in both the early and chronic stages of rehabilitation.
Authors' conclusions: Functional electrical stimulation can have a positive orthotic effect, particularly for gait speed and physiological cost index, in patients who were in the chronic stage of stroke recovery (although evidence for a therapeutic effect was less conclusive).
CRD commentary: The review addressed a clear question and was supported by broad inclusion criteria. Although several electronic databases were searched, the restriction to searching only for published studies in English from 1990 onwards (for purposes of practicality) meant that some relevant studies may have been missed. Suitable methods were employed to reduce risks of reviewer error and bias when selecting studies for inclusion; the authors did not report on whether such methods were used for the processes of data extraction and study quality assessment. Sufficient study details were provided, although the presence of statistical significance was inconsistently reported between studies. The narrative synthesis was somewhat difficult to follow and interpret as a very broad range of study designs and outcomes were reported. Study quality was assessed and used in interpreting the results of the review.
Considering that most studies were small, that all studies except one had a moderate or high risk of bias and that some relevant studies may have been missed during the searches, the reliability of the authors' conclusions remains uncertain. 3. LEVEL N/A: COST EFFECTIVENESS REVIEW
The long-term cost-effectiveness of the use of Functional Electrical Stimulation for the correction of dropped foot due to upper motor neuron lesion, Taylor P, Humphreys L, Swain I
CRD Summary: The objective was to assess the long-term cost-effectiveness of functional electrical stimulation (FES) for the correction of dropped foot due to damage to the upper motor neurone. The authors concluded that FES was cost effective. The validity of the data was unclear, due to limitations in the study methods and a lack of detail in the reporting. The results are uncertain and should be considered with these limitations in mind.
Type of economic evaluation: Cost-effectiveness analysis, cost-utility analysis
Study objective: The objective was to assess the long-term cost-effectiveness of functional electrical stimulation (FES) for the correction of dropped foot due to damage to the upper motor neurone.
GM FES for Foot Drop Policy v2.5 FINAL Page 12 of 23
Interventions: FES was applied to the common peroneal nerve, producing dorsiflexion and eversion, timed to the swing phase of gait, using a heal switch. The comparator was no such stimulation.
Location/setting: UK/secondary care.
METHODS
Analytical approach: A retrospective review of medical records was conducted to assess the long-term costs and benefits of FES. Follow-up assessments were conducted for as long as the device was used (mean 4.9 years). The perspective was not stated.
Effectiveness data: The key effectiveness outcome was the change in 10 metre walking speed. This was from the retrospective review of the records of 126 patients who were referred for treatment by a general practitioner or medical consultant. Patients began treatment in 1999 and were suffering from stroke, multiple sclerosis, spinal cord injury, cerebral palsy, or unspecified conditions. Four comparisons were used: the initial orthotic effect (with FES, end versus start of first day); the total orthotic effect (with FES, follow-up versus start); the training effect (without FES, follow-up versus start); and continuing orthotic effect (with versus without FES, at follow-up). Walking speed was measured at six, 18 and 42 weeks, and then every six or 12 months for as long as the device was used. The clinical utility of the change in walking speed was measured as the number of patients who changed functional walking category in the first 16.5 months of treatment (last point at which data were available for all patients).
Monetary benefit and utility valuations: An estimate of the utility gain associated with FES per year was derived from an economic report produced by the UK's Purchasing and Supply Agency, in 2010. The gain was calculated by translating the proportion of FES users crossing key walking speed thresholds to changes in the Health Utilities Index (HUI3). This calculation took account of the number of FES users with reduced utility due to skin reaction to the electrodes.
Measure of benefit: The health benefit was measured by increased walking speed and quality-adjusted life-years (QALYs).
Cost data: The costs were calculated using hospital tariffs, for each clinic assessment. These included all device, consumables and clinical costs. They were reported in 2012 UK £.
Analysis of uncertainty: The variation in estimates was presented as standard deviations and 95% confidence intervals.
Results: The effects were only reported for stroke and multiple sclerosis patients, as there were insufficient data for the other patients.
Continuing orthotic effect: at the end of the observation period, stroke patients walked 0.08 metres per second (m/s) faster with FES than without it (p<0.001); multiple sclerosis patients walked 0.06m/s faster (p=0.001). Training effect: without FES, stroke patients walked 0.11m/s faster than at the start (p<0.001); multiple sclerosis patients walked 0.05m/s slower. Total orthotic effect: with FES at any time point compared with no FES at the start, stroke patients increased their walking speed by 0.18m/s (p<0.001), and multiple sclerosis patients increased speed by 0.02m/s (p<0.001).
Over 16.5 months, 42 patients (38%) improved their functional walking category using FES.
The total mean cost per patient was £3,130 (SD 1,830) for stroke patients, and £3,095 (SD 1,490) for all patients. The mean QALY gain was 0.041, which was assumed to be the same for all patients. The mean cost per QALY was £15,268 for stroke patients, and £15,406 for all patients.
Authors' conclusions: The authors concluded that FES was cost-effective.
CRD COMMENTARY
Interventions: The intervention was clearly stated. A limited description was given, with details reported in another publication. It was unclear if no stimulation was the standard practice; and if other treatments should have been considered. Appropriate comparators are crucial in determining cost-effectiveness.
Effectiveness/benefits: The effectiveness measures were from a before-and-after study; an observational design with known risks of bias. No attempts to deal with any bias were reported. The authors considered improvements over time without FES (the training effect), but they suggested that the outcomes without FES were expected to improve as a result of using FES in general (a spill lover effect). So this result would not reflect the change in outcomes for a patient who never received the intervention. The effectiveness outcomes are uncertain. Limited details of the methods used to derive the utility were reported; the validity of the values used is unclear. The same utility gain was used for all patients, regardless of the cause of dropped foot.

GM FES for Foot Drop Policy v2.5 FINAL Page 13 of 23
Costs: The cost estimates were clearly reported and appear to have been appropriate. The costs seem to represent a health service provider (UK NHS) perspective, but this was not explicitly reported. No discounting was applied to the cost or benefit outcomes. Assuming that the costs and benefits were only accrued whilst using the device, and it was used for less than two years, discounting was not necessary. For long-term use, discounting would be relevant.
Analysis and results: The results of the analysis were clearly reported. Interpreting the cost per QALY results as cost-effectiveness ratios assumes that there was no cost and no benefit associated with the comparator. This is unlikely to reflect standard practice, where alternative interventions accrue costs and benefits, which would alter the cost-effectiveness results. No analysis of parameter uncertainty was conducted, so it was unclear how sensitive the results were to uncertainties in the cost and benefit estimates.
Concluding remarks: The validity of the data was unclear, due to limitations in the study methods and a lack of detail in the reporting. The results are uncertain and should be considered with these imitations in mind. 4. LEVEL 1: CRD REVIEW
Health and fitness benefits of functional electrical stimulation-evoked leg exercise for spinal cord-injured individuals: a position review, Hamzaid NA, Davis GM
CRD summary: This review concluded that across a variety of outcome domains functional electrical stimulation-evoked leg exercise promoted certain health and fitness benefits for people with spinal cord injury. Poor reporting of the review process, inclusion of small studies of unknown quality and the possibility of language and publication biases suggests that these conclusions should be treated with caution.
Authors' objectives: To investigate whether functional electrical stimulation (FES)-evoked leg exercise promoted health and fitness benefits in people with spinal cord injury.
Searching: MEDLINE, MEDLINE Daily Update, PREMEDLINE, OLDMEDLINE, SPORTDiscus, Web of Science (dates spanned 1830 to 31st July 2008) and The Cochrane Library and Cochrane Database of Systematic Reviews were searched. Search terms were reported. FES-specific annual international conference archives with known peer-review criteria were searched for published studies. Any language was included, provided an English abstract that described clear categorical outcomes was available.
Study selection: Studies of FES or functional neuromuscular stimulation (FNS) exercise of lower limbs of neurologically disabled people that evaluated health and fitness outcomes were eligible for inclusion. The term exercise referred mainly to predominantly lower limb physical training activities. Movements that may have involved concurrent upper extremity exercise were not excluded. Studies conducted on functional applications of FES (use of FES for daily activities without exercise training for health and fitness only) or technological developments (control approaches, analyses of FES stimulation parameters and controller performance, simulation and modelling studies or research into the technological domain without intention of describing possible physiological benefits) were included if secondary health and fitness were described. Randomised and non-randomised trials and other controlled studies were eligible for inclusion.
Included studies were of a variety of FES interventions. The most common involved FES cycling and some included arm cranking. Duration of included studies appeared to vary from one day to 11 months. Lesion level of patients varied between studies.
It appeared that more than one reviewer performed study selection.
Assessment of study quality: No formal validity assessment was described, but some aspects of study quality were described (whether the study was controlled, randomisation and how patients were allocated to treatment).
The authors did not state how many reviewers assessed study validity.
Data extraction: Outcomes that related to skeletal muscle morphology and biochemistry, cardiovascular and haemodynamic responses, metabolic responses and aerobic fitness changes, bone mineral density and stiffness, functional changes of exercise capacity and psychosocial outlook were extracted.
The authors did not state how many reviewers extracted data.

GM FES for Foot Drop Policy v2.5 FINAL Page 14 of 23
Methods of synthesis: The studies were pooled in a narrative synthesis grouped by domains of skeletal muscle morphology and biochemistry.
Results of the review: Thirty-two studies (reported in 33 papers) were included in the review (n= 644; range four to 90 patients). One study was a randomised controlled trial (RCT) (n=26) and 31 were randomised or controlled studies (n=618).
Positive changes to skeletal muscle morphology and biochemistry in adherents to FES training were reported in one RCT and five randomised or controlled studies. Seven out of nine randomised or controlled studies reported increased aerobic fitness or positive metabolic responses with FES-induced exercise training. Seven randomised or controlled studies showed positive changes in indicators of functional exercise capacity with FES-induced training. One controlled study reported positive effects of FES-induced exercise on depression levels. Changes to heart rate and blood pressure responses were inconsistent during FES-evoked muscle contractions in six controlled or randomised studies. One out of five controlled or randomised studies reported positive effects of FES on bone mineral density; the other studies were equivocal.
Authors' conclusions: Available data suggested that FES-evoked leg exercise promoted certain health and fitness benefits for people with spinal cord injury across a variety of outcome domains.
CRD commentary: The research question was supported by inclusion criteria for participants, intervention and outcomes; there were none for study design, which may have led to subjective decisions when selecting studies for inclusion. The authors did not report attempts to identify unpublished studies and inclusion was restricted to papers with English abstracts, so publication and language biases could not be ruled out. The review process was not described, so any steps taken to reduce the possibility of reviewer error and bias were unknown. Few aspects of study quality were assessed and so reliability of primary studies was unknown. Participant numbers in included studies were low. Study designs were unclear and few participant details were reported. Narrative synthesis appeared appropriate considering heterogeneity in study designs, interventions and outcomes. Poor reporting of the review process, inclusion of small studies of unknown quality and the possibility of language and publication biases suggests that the authors' conclusions should be treated with caution. 5. LEVEL 1: CRD REVIEW
Functional electrical stimulation in the treatment of patients with chronic heart failure: a meta-analysis of randomized controlled trials, Sbruzzi G, Ribeiro RA, Schaan BD, Signori LU, Silva AM, Irigoyen MC, Plentz RD
CRD summary: This review concluded that functional electrical stimulation may be an alternative therapy for people with chronic heart failure who were unable to perform conventional aerobic exercise. Data came from small studies of low methodological quality. Further research was needed. Given the available data and as they included a need for further research, the conclusions are suitably conservative.
Authors' objectives: To assess the effects of functional electrical stimulation in people with chronic heart failure.
Searching: MEDLINE, LILACS, PEDro and The Cochrane Library were searched from inception to January 2009. Search terms were reported. No language restrictions were applied.
Study selection: Randomised controlled trials (RCTs) that assessed the effects of functional electrical stimulation (FES) in people with chronic heart failure (New York Heart Association Class II, III or IV) were eligible for inclusion. Studies needed to have a follow-up of at least five weeks. The comparator could be conventional aerobic exercise training or control (same regime as the treatment group, but where the intensity of stimulation did not lead to visible or palpable contractions). Application of FES had to be in the quadriceps femoral muscle. Study objectives had to include assessments of peak oxygen consumption (VO2), six-minute walk test or muscle strength. Studies that failed to provide a reliable definition of chronic heart failure were excluded.
Most participants were men. Mean age ranged from 53 years to 63 years. All participants were on optimal medical therapy for heart failure. FES treatment programmes ranged from 30 to 240 minutes daily (five to seven days per week) for 25 days to 10 weeks.
Reviewers made an initial selection of studies that could possibly be eligible. Full texts were evaluated by two reviewers independently. Disagreements were resolved by consensus.
GM FES for Foot Drop Policy v2.5 FINAL Page 15 of 23
Assessment of study quality: Quality was assessed independently by two reviewers using items such as concealment of allocation, intention-to-treat analysis, baseline comparability, outcomes assessment blinding and description of losses to follow-up and exclusions. Quality was summarised using PEDro and Jadad scales.
Data extraction: Data were extracted to enable calculation of mean changes between baseline and end of treatment, and subsequent mean differences in changes, between treatment and comparison groups.
Two reviewers independently extracted data. Authors were contacted for further information.
Methods of synthesis: Pooled weighted mean differences (WMD) were calculated using a fixed-effect model. Heterogeneity was assessed using Cochran's Q test and I2 statistic. Where insufficient data were available, narrative results were provided. Sensitivity analyses were undertaken based on quality factors. Analysis was redone using a random-effects model.
Results of the review: Seven RCTs (224 participants) were included. Study size ranged from 24 to 46 participants. Five trials (168 participants) used conventional aerobic exercise as comparator and two trials (56 participants) used a control treatment
The quality of most studies was poor: on the Jadad scale one scored 3, four scored 2 and two scored 1 (out of a maximum of five); on the PEDro score two studies scored 6, two scored 5, two scored 4 and one scored 2 (out of a maximum of 10).
Compared to conventional aerobic exercise, FES was associated with less favourable change in peak VO2 (-0.74mL/kg per minute, 95% CI -1.38 to -0.10, I2-0%; five trials). There was no difference in muscle strength (two trials). A small increase in six-minute walk test was neither statistically nor clinically significant (I2=41%, five trials).
Compared to control treatment, FES was associated with an increase in VO2 (2.78mL/kg per minute, 95% CI 1.44 to 4.13, I2=52%; two trials). Two trials reported that there was a statistically significant change in the six-minute walk test with FES, but not with the control treatments. No data were available for muscle strength.
The overall low quality of trials precluded planned sensitivity analyses. Use of random-effects models gave results similar to those in the main analyses (data not presented).
PEDro: A scale to measure the quality of reports of randomised controlled trials indexed on PEDro, the Physiotherapy Evidence Database.
The Jadad scale assesses the quality of published clinical trials based methods relevant to random assignment, double blinding, and the flow of patients. There are 7 items. The last 2 attract a negative score, which means that the range of possible scores is 0 (bad) to 5 (good):
Authors' conclusions: FES may be an alternative to conventional aerobic exercise training for those people who are unable to perform these types of exercise; data came from small studies of low methodological quality and further research is needed.
CRD commentary: The aims of this review were clearly stated in terms of the inclusion criteria. The search covered a number of relevant sources. There were no language restrictions, which reduced the risk of language bias. It was unclear whether non published trials were eligible, and it may be that publication bias affected the review. The methods of study selection, data extraction and quality assessment aimed at reducing reviewer error or bias. The quality of included studies was assessed. The methods of synthesis appeared appropriate. Heterogeneity was assessed, but evident heterogeneity in some outcomes was not investigated.
As the authors commented, available data came from small studies of generally low quality. Their conclusions, which include a need for further research, are suitably conservative. 6. LEVEL N/A: RAPID APPRAISAL
NWCSU Evidence Review: Functional electrical stimulation bicycle for patients with spinal cord injury, Date: November 2014, Full review available on request from: [email protected]
Spinal cord injury - prevalence
It is estimated that 40,000 people in the UK are affected by SCI (BMJ Best Practice). The majority of them will have incomplete SCI. Men and younger people are more at risk (with road traffic accidents being a major cause), although falls in older people also constitute a substantial risk.

GM FES for Foot Drop Policy v2.5 FINAL Page 16 of 23
FES bicycle
FES applies a current to paralysed muscles to stimulate movement, despite a loss of voluntary muscle control. NWCSU has undertaken previous evidence reviews of FES for upper and lower limbs. The requested FES bicycle (RT300 from Cyclone) stimulates a cycling movement and can be used from a wheelchair; this particular machine also has an upper torso device which can be used for arm cycling (without FES). FES in SCI is primarily seen as a tool to counteract the deleterious effects of SCI.(1)
Context
Southport and Ormskirk NHS trust is home to the Regional Spinal Injuries Centre. The Centre has one FES bike for inpatients only. On enquiring from the requestor, she is aware that two other patients who have asked for CCG funding, have received funding for FES bikes at home from the Regional Centre (see email exchange in the case file).
The Cyclone (supplier) website mentions ‘Community Cycling Centres’ which have FES bikes. The nearest to Greater Manchester seems to be a private physiotherapy clinic in Rotherham. The clinic provides physiotherapist assessments, and persons deemed suitable to exercise on the FES bike can do so for £40/hour.
Search question parameters
Population = People with spinal cord injuries
Intervention = FES cycle
Comparator: none required
Outcomes: Overall health (including quality of life); any changes in health outcomes; clinical benefit.
Search Strategy
("FES" OR "functional electr* stimulation") AND ("bike" OR "cycling" OR "bicycle" OR "cycle" OR "RT300") AND (spinal OR SCI)
Excluded
Studies on patients with other conditions, including stroke; urinary function as outcome; short-term laboratory-based outcomes (e.g. blood parameters, muscle response during exercise only, i.e. without follow-up); single case reports; studies where it was not clear that FES cycling was involved; dosing studies (i.e. comparing different strengths of FES cycling without a no-FES comparison group).
Limitations
This rapid review relies mainly on information from published abstracts. Due to the large number of low-level studies identified, not all, but most, are represented in the results tables below. However, other studies reviewed show similar results.
Search results
Database Result
NHS Evidence 20 records
Cochrane Library 30 records
York CRD 13 records
BMJ Clinical Evidence Not searched
BMJ Best Practice Not searched
Medline / EMBASE / CINAHL / AMED 219 records
Summary of the evidence
A large number of relevant low-level studies (mostly case series) were identified, but few studies of higher level, with relatively small sample sizes. The main outcomes reported were cardiovascular measures, bone mineral density, muscle strength/volume, and general fitness. Several systematic reviews have been identified, but many of them are not limited to FES cycling, and they too rely on the same limited evidence base. Their conclusions suggest that FES cycling can

GM FES for Foot Drop Policy v2.5 FINAL Page 17 of 23
provide some benefits in terms of (cardiovascular) fitness, bone mineral density, oxygen uptake, and muscle strength, and a potential to reduce secondary complications. Hybrid (i.e. arm and leg) exercise seems to confer greater benefit than leg exercise alone. Conclusions need to be interpreted very cautiously in the light of the quality of underlying evidence. 7. LEVEL N/A: RAPID APPRAISAL
NWCSU Evidence Review: Functional electrical stimulation for the treatment of cauda equine pain, Date: June 2014, Full review available on request from: [email protected]
Functional electrical stimulation: A technique that uses electrical currents to activate nerves innervating extremities affected by paralysis resulting from spinal cord injury, head injury, stroke and other neurological disorders.
Cauda Equina syndrome (CAS): A serious neurological condition affecting the bundle of nerve roots at the lower end of the spinal cord. It is due to a nerve compression that an acute loss of function of the lumbar plexus occurs which stops the sensation and movement. The syndrome is characterized by dull pain in the lower back and upper buttocks and a lack of feeling in the buttocks, genitalia and thigh, together with the disturbance of bowel and bladder function. Cauda equina syndrome occurs in approximately 2% of cases of herniated lumbar discs.
Percutaneous electrical nerve stimulation: An enhanced and newer type of pain management therapy that makes use of very thin needles (much like those in acupuncture) that are inserted in the lower back by the chiropractor. Small, battery-powered TENS units also are available for use at home, work, or other activities.
Search Strategy
A search was made for FES and pain (and cauda equine)
Database Result
NICE Nil for FES and pain but an IPG for PENS was found – cited below for info
CG88 – not cited here as does not cover FES for CAS
NHS Evidence All papers relating to FES were for foot drop
SIGN Guidance for foot drop in stroke patients only – not cited
Cochrane Electrical stimulation for preventing and treating post-stroke shoulder pain, Price CIM, Pandyan AD, Published Online: 8 October 2008
General Search (Google)
Papers relating to foot drop and shoulder pain only
Medline / Open Athens Open Athens Ovid on line search returned no results
Open Athens search of all BMJ journals returned no results
Provider and associated website
Provider assessment pathway and Odstock medical information booklet – neither includes cauda equine syndrome as a condition for the use of FES
Summary of the evidence
There is no evidence available for the use of FES in pain associated with cauda equine syndrome. Most of the evidence related to its use in foot drop of central neurological origin and in neuropathic shoulder pain post stroke (the evidence for which is limited – a review is cited below for information on FES and pain relief but does not directly relate to the requested use of the therapy).
PENS (Percutaneous Electrical Nerve Stimulation) has been assessed by NICE for use in pain relief – guidance cited below for info – but should be used by specialist in pain management.
GM FES for Foot Drop Policy v2.5 FINAL Page 18 of 23
The Salisbury Centre (Odstock medical base) suggest its use in spinal compression above T12 – cauda equine syndrome is associated with lumbar disc herniation.
This treatment does not appear to be indicated for this condition – other forms of electrical stimulation e.g. PENS/TENS may be suitable but this condition is not specifically covered by the NICE IPG for back pain which recommends not using TENS as a therapy for low back pain. 8. LEVEL N/A: RAPID APPRAISAL
NWCSU Evidence Review: Functional electrical stimulation (FES) for the upper limb, Date: 21 October 2014, Full review available on request from: [email protected]
What is it?
Functional electrical stimulation: A technique that uses electrical impulses to activate nerves innervating extremities affected by paralysis resulting from spinal cord injury, head injury, stroke and other neurological disorders. Electrodes are usually placed on the skin close to the nerve supplying the muscle, and leads connect the electrodes to a stimulator producing the impulses.
Search Strategy
Search terms used were “Functional electrical stimulation” OR “FES”) AND (“arm” OR “upper” OR “shoulder”). For the search of the Medline, Embase, and AMED and CINAHL databases, the publication year was restricted to 2013 onwards, as there is a 2013 review from Stockport PCT available.
Only studies reporting on the effectiveness of FES in upper limb conditions were included. Studies aimed at improving cardiovascular function or bone density were excluded, as were studies of implanted prostheses, and brain-machine interface systems.
Database Result
NHS Evidence SIGN Brain Injury Rehabilitation in Adults Guidelines 2013
SIGN Management of Patients with Stroke Guidelines 2010
Treating patients with hemiplegic shoulder pain, Snels et al 2002 (Review)
Electrical stimulation for preventing and treating post-stroke shoulder pain, Price at al 2000 (Cochrane review)
SIGN Nothing additional to the above
Cochrane Nothing additional to the above
York Nothing additional to the above
BMJ Best Practice Not searched
Medline / Embase / AMED / CINAHL
Publication year 2013 onwards; applicable results included in results table below.
Summary of the evidence
There is little additional evidence to the 2013 review by Stockport PCT; nearly all the 2013 and 2014 studies identified in bibliographic databases are on stroke patients (see table). Trials are small, they use varied approaches to FES, or other treatments in combination with FES, and varied outcome parameters. Limited evidence suggests that FES may be effective for some outcomes relating to upper limb function in this patient group.
No recent studies of FES to upper limbs of patients with brain injury have been identified.
Limitations
This is a rapid review, limited to reviewing English-language abstracts of published studies.
GM FES for Foot Drop Policy v2.5 FINAL Page 19 of 23
9. LEVEL N/A: RAPID APPRAISAL Stockport CCG Evidence Review: Functional electrical stimulation (FES) for the treatment of arm muscle paralysis, Date: February 2013, Full review available on request from: [email protected]
SUMMARY OF THE EVIDENCE
Please note that this is not a comprehensive systematic review. Information has been extracted from abstracts only and no critical appraisal of the papers included has been undertaken.
FES of the upper limb for the purposes of exercising a patient with a spinal cord injury to improve cardiovascular function or bone density has not been included in this evidence summary.
NICE has not issued guidance on the use of FES for the treatment of arm muscle paralysis.
The use of FES of the upper limb has been studied for a number of indications.
Shoulder pain in stroke patients
One Cochrane review was found that concluded that there was not enough evidence to confirm or refute the benefit of surface applied electrical stimulation for the prevention or treatment of post-stroke shoulder pain.
Shoulder subluxation in stroke patients
Three RCTs were identified; two of which supported the use of FES to reduce shoulder subluxation in stroke patients. The third RCT supported the use of FES to reduce shoulder subluxation in stroke patients where the subluxation was of short duration but not where it had been present for some time.
Implanted FES for shoulder movement in patients post-stroke and patients with spinal cord injury
One case series was identified that supported the use of FES via implanted electrodes to improve shoulder movement in patients who had had a stroke or spinal cord injury.
Implanted electrode FES for arm function in patients with spinal cord injury
Seven case series were identified that investigated the use of FES via implanted electrodes for arm function in patients with spinal cord injury. The case series investigated the use of FES for different arm functions, for example one used FES for elbow movement, another for shoulder movement and others for hand function. All the series supported the use of implanted electrode FES for patients with a cervical spinal cord injury.
Surface applied FES for hand function in acute stroke patients
Six RCTs were identified; four supported the addition of FES to conventional therapy to improve hand function in patients who had recently had a stroke, whereas two did not. One case series was identified that supported the addition of FES to conventional therapy for acute stroke patients.
Surface applied FES for hand function in patients post-stroke
Eight RCTs were identified. One RCT supported the use of FES to improve hand function when there was still good residual function in the hand function. Four RCTs supported the additional of FES to conventional therapy to improve hand function in patients who had had a stroke; one of these RCTs compared real FES to sham FES. Two RCTs supported the use of FES to improve hand function in patients post-stroke when compared to no treatment. One RCT found no additional benefit with FES when used with an upper limb exerciser for this group of patients.
Three case control trials were found. One supported the use of surface applied FES for improving hand function in patients who had had a stroke whereas two studies did not support its use.
Fourteen case series were found; 13 supported the use of surface applied FES for improving hand function in patients who had had a stroke whereas one did not support its use.
Surface applied FES for hand function in patients post-stroke treated with botulinum toxin
One RCT was identified that did not support the use of FES to improve hand function in stroke patients treated with a botulinum toxin injection. One case report was identified that did support the use of FES improve hand function in stroke patients treated with a botulinum toxin injection.
Surface applied FES for hand function in patients with spinal cord injury
Two RCTs were identified; one supported the use of surface applied FES to improve hand function in patients with cervical spinal cord injury whilst the other did not. One case control study was identified
GM FES for Foot Drop Policy v2.5 FINAL Page 20 of 23
that found no benefit to hand function with either conventional physiotherapy or the addition of FES to conventional physiotherapy. One case series and one case report were identified that supported the use of surface applied FES to improve hand function in patients with cervical spinal cord injury.
Respiration controlled upper limb FES in patients with spinal cord injury
One case report was identified that supported the use of respiration controlled upper limb FES to improve arm function in patients with cervical spinal cord injury.
Surface applied FES for hand function in patients with Erb’s palsy
One RCT was identified that supported the use of surface applied FES to improve hand function in patients with Erb’s palsy (a paralysis of the arm caused by injury to the arm's main nerves)
Surface applied FES for hand function in patients with cerebral palsy
One RCT was identified that supported the addition of FES to botulinum toxin injections to improve hand function in children with cerebral palsy. One case series was identified that supported the use of surface applied FES to improve hand function in patients with cerebral palsy.
POLICY RECOMMENDATION
Most of the studies were in stroke patients and the FES was used alongside physio- and/or occupational-therapy. The evidence may support a stroke therapy service wishing to utilise FES but does not support FES being purchased for individual patients to use long-term at home.
Evidence for patients with spinal cord injury is less robust than for stroke patients and the benefit a patient would gain from FES probably varies depending on the residual arm function.
Evidence for the use of upper limb FES in other conditions is probably inadequate to support its use.
The recommendation based on the evidence would be not to commission upper limb FES for an individual patient.
GM FES for Foot Drop Policy v2.5 FINAL Page 21 of 23
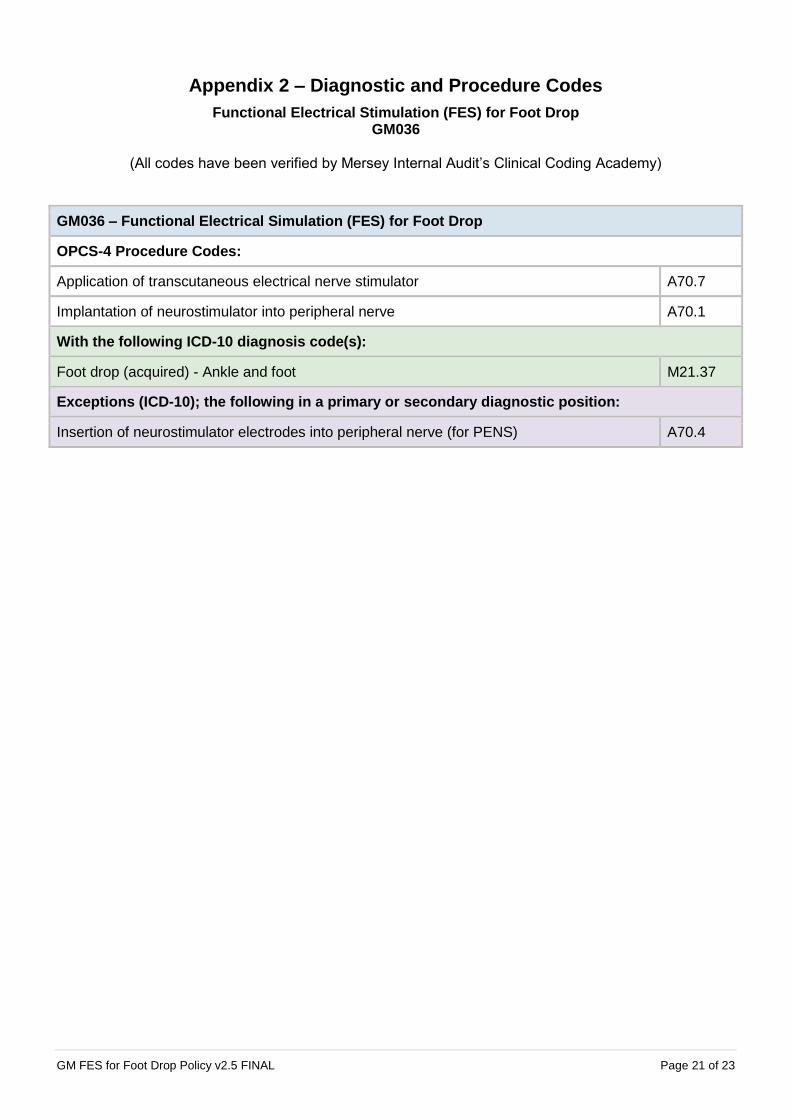
Appendix 2 – Diagnostic and Procedure Codes
Functional Electrical Stimulation (FES) for Foot Drop GM036
(All codes have been verified by Mersey Internal Audit’s Clinical Coding Academy)
GM036 – Functional Electrical Simulation (FES) for Foot Drop
OPCS-4 Procedure Codes:
Application of transcutaneous electrical nerve stimulator A70.7
Implantation of neurostimulator into peripheral nerve A70.1
With the following ICD-10 diagnosis code(s):
Foot drop (acquired) - Ankle and foot M21.37
Exceptions (ICD-10); the following in a primary or secondary diagnostic position:
Insertion of neurostimulator electrodes into peripheral nerve (for PENS) A70.4

GM FES for Foot Drop Policy v2.5 FINAL Page 22 of 23
Appendix 3 – Version History
Functional Electrical Stimulation (FES) for Foot Drop GM036
The latest version of this policy can be found here GM Functional Electrical Stimulation (FES) for Foot Drop policy
Version Date Summary of Changes
0.1 07/01/2014 Initial draft
0.2 26/01/2015 Amendments made after GM EUR Steering Group on 21/01/2015:
Section 4 – Criteria for Commissioning: Sentence added re. wireless FES devices and mention of criteria for this in Appendix 2
Section 9 – Mechanism for Funding: Amended to prior approval if meet mandatory criteria for wired FES with all other applications assessed by clinical triage
Appendix 2 added – Consideration of applications for wireless devices
1.0 20/07/2015 Amendments made after GM EUR Steering Group on 8th July 2015:
Title of policy amended to read ‘Functional Electrical Stimulation (FES) for foot drop’.
All reference to oropharyngeal dysphagia removed from the policy.
Subject to the above amendments being made the GM EUR Steering Group approved the policy to go through the governance process.
1.1 20/01/2016 Following GM EUR Steering Group on 20/01/2016 the wording for date of review changed to read as follows: ‘One year from the date of approval by Greater Manchester Association Governing Group thereafter at a date agreed by the Greater Manchester EUR Steering Group (unless stated this will be every 2 years).’
15/03/2016 Policy updated to Greater Manchester Shared Services template and references to North West Commissioning Support Unit changed to Greater Manchester Shared Services.
2.0 17/05/2017 GM EUR Steering Group reviewed the policy and agreed that no changes were necessary as no new evidence had been found. The group agreed that the policy would be reviewed again in 5 years unless new evidence or technology is available sooner.
Date of Review: Section amended to state: 'Five years from the date of the last review, unless new evidence or technology is available sooner. The evidence base for the policy will be reviewed and any recommendations within the policy will be checked against any new evidence. Any operational issues will also be considered at this time. All available additional data on outcomes will be included in the review and the policy updated accordingly. The policy will be continued, amended or withdrawn subject to the outcome of that review.'
2.1 06/06/2018 Appendix 3: Added Procedure and Diagnostic coding for policy
2.2 25/01/2019 Branding changed to reflect change of service from Greater Manchester Shared Services to Greater Manchester Health and Care Commissioning.
Links updated as documents have all moved to a new EUR web address.
Commissioning Statement: o ‘(Alternative commissioning arrangements apply)’ added after Policy
Exclusions

GM FES for Foot Drop Policy v2.5 FINAL Page 23 of 23
o ‘Best Practice Guideline’ section added
2.3 23/04/2019 Appendix 2 - Wireless FES Devices – Final bullet point below removed:- If a cuffed device is required the application must contain the results of a minimum 3 month trial of the device with clear measurement before and after use of the cuffed device to allow the individual case to be assessed for long term funding of the device.
2.4 01/08/2019 Clinical Exceptionality Section updated to read: Clinicians can submit an Individual Funding Request (IFR) outside of this guidance if they feel there is a good case for exceptionality. More information on determining clinical exceptionality can be found in the Greater Manchester (GM) Effective Use of Resources (EUR) Operational Policy. Link to GM EUR Operational Policy
2.5 18/12/2019 Appendix 2 – Wireless FES Devices - Removed and is now incorporated in the Commissioning Statement under the Policy Inclusion Criteria. Subsequent Appendices renumbered.
Related Documents











