Gram Stain, Culture, and Histopathology in IE • CID 2003:36 (15 March) • 697 MAJOR ARTICLE Gram Stain, Culture, and Histopathological Examination Findings for Heart Valves Removed because of Infective Endocarditis Arthur J. Morris, 1 Dragana Drinkovic, 1 Sudha Pottumarthy, 1 Marianne G. Strickett, 1 Donald MacCulloch, 1 Neil Lambie, 2 and Alan R. Kerr 3 Departments of 1 Microbiology, 2 Pathology, and 3 Cardiothoracic Surgery, Green Lane Hospital, Auckland, New Zealand Retrospective chart review was undertaken for 480 patients who underwent a total of 506 valve replacements or repair procedures for infective endocarditis. The influence of preoperative antimicrobial treatment on culture, Gram stain, and histopathological examination findings for resected valve specimens was examined. When valves were removed before the end of treatment, organisms were seen on the Gram stain of ground valve material performed in the microbiology laboratory and on Gram-stained histopathological sections in 231 (81%) of 285 and 140 (67%) of 208 specimens, respectively ( ). Gram-positive cocci were either P p .0007 cultured from or observed in excised valve tissue in 42 (67%) of 63 episodes involving negative preoperative blood cultures. Positive Gram stain results for microbiological specimens should be reintroduced into the definite pathological criteria for infective endocarditis. When deciding on how long to continue antimicrobial therapy after valve replacement for endocarditis, valve culture results should be the only laboratory finding taken into account, because it takes months for dead bacteria to be removed from sterile vegetations. Most cases of bacterial endocarditis can be cured by antimicrobial treatment alone. When infection causes valve dysfunction, prompt valve replacement is required for optimal outcome [1–3]. Valve replacement is also indicated when infection has not been controlled by antimicrobial treatment or when recurrent emboliza- tion occurs [1–4]. In these situations, surgery improves outcome, and delays in surgery (e.g., in an attempt to sterilize the valve) are associated with increased mor- bidity and mortality [1–3, 5–10]. After valve replacement is performed for active bac- terial endocarditis, there is no consensus on how long Received 10 September 2002; accepted 21 November 2002; electronically published 4 March 2003. Financial support: The Auckland Infectious Disease Education and Research Trust. Reprints or correspondence: Dr. Arthur J. Morris, Microbiology Laboratory, Auckland City Hospital, Auckland 1003, New Zealand ([email protected]). Clinical Infectious Diseases 2003; 36:697–704 2003 by the Infectious Diseases Society of America. All rights reserved. 1058-4838/2003/3606-0004$15.00 to continue antimicrobial treatment [1]. Although some researchers have given consideration to surgical findings and culture, Gram stain, or histopathological examination findings [3, 4, 7, 10–13], others administer treatment for a standard period after valve replacement [5, 14–21]. No previous study has systematically ex- amined the influence of preoperative antimicrobial treatment on the culture, Gram stain, and histopath- ological findings for resected valves. Previous reports have used different pathological cri- teria to define endocarditis with respect to the Gram staining of resected tissue performed in the microbi- ology laboratory [22–25]. We have undertaken a ret- rospective review of all patients who underwent valve replacement for infective endocarditis and have re- corded the results of valve cultures, Gram stains of valve specimens performed in the microbiology laboratory, and histopathological examinations (Gram stains and determination of the presence of acute inflammation). Our first objective was to describe the evolution of these findings while patients received antimicrobial treatment Downloaded from https://academic.oup.com/cid/article/36/6/697/318163 by guest on 30 June 2022

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Gram Stain, Culture, and Histopathology in IE • CID 2003:36 (15 March) • 697
M A J O R A R T I C L E
Gram Stain, Culture, and HistopathologicalExamination Findings for Heart ValvesRemoved because of Infective Endocarditis
Arthur J. Morris,1 Dragana Drinkovic,1 Sudha Pottumarthy,1 Marianne G. Strickett,1 Donald MacCulloch,1
Neil Lambie,2 and Alan R. Kerr3
Departments of 1Microbiology, 2Pathology, and 3Cardiothoracic Surgery, Green Lane Hospital, Auckland, New Zealand
Retrospective chart review was undertaken for 480 patients who underwent a total of 506 valve replacements
or repair procedures for infective endocarditis. The influence of preoperative antimicrobial treatment on
culture, Gram stain, and histopathological examination findings for resected valve specimens was examined.
When valves were removed before the end of treatment, organisms were seen on the Gram stain of ground
valve material performed in the microbiology laboratory and on Gram-stained histopathological sections in
231 (81%) of 285 and 140 (67%) of 208 specimens, respectively ( ). Gram-positive cocci were eitherP p .0007
cultured from or observed in excised valve tissue in 42 (67%) of 63 episodes involving negative preoperative
blood cultures. Positive Gram stain results for microbiological specimens should be reintroduced into the
definite pathological criteria for infective endocarditis. When deciding on how long to continue antimicrobial
therapy after valve replacement for endocarditis, valve culture results should be the only laboratory finding
taken into account, because it takes months for dead bacteria to be removed from sterile vegetations.
Most cases of bacterial endocarditis can be cured by
antimicrobial treatment alone. When infection causes
valve dysfunction, prompt valve replacement is required
for optimal outcome [1–3]. Valve replacement is also
indicated when infection has not been controlled by
antimicrobial treatment or when recurrent emboliza-
tion occurs [1–4]. In these situations, surgery improves
outcome, and delays in surgery (e.g., in an attempt to
sterilize the valve) are associated with increased mor-
bidity and mortality [1–3, 5–10].
After valve replacement is performed for active bac-
terial endocarditis, there is no consensus on how long
Received 10 September 2002; accepted 21 November 2002; electronicallypublished 4 March 2003.
Financial support: The Auckland Infectious Disease Education and ResearchTrust.
Reprints or correspondence: Dr. Arthur J. Morris, Microbiology Laboratory,Auckland City Hospital, Auckland 1003, New Zealand ([email protected]).
Clinical Infectious Diseases 2003; 36:697–704� 2003 by the Infectious Diseases Society of America. All rights reserved.1058-4838/2003/3606-0004$15.00
to continue antimicrobial treatment [1]. Although
some researchers have given consideration to surgical
findings and culture, Gram stain, or histopathological
examination findings [3, 4, 7, 10–13], others administer
treatment for a standard period after valve replacement
[5, 14–21]. No previous study has systematically ex-
amined the influence of preoperative antimicrobial
treatment on the culture, Gram stain, and histopath-
ological findings for resected valves.
Previous reports have used different pathological cri-
teria to define endocarditis with respect to the Gram
staining of resected tissue performed in the microbi-
ology laboratory [22–25]. We have undertaken a ret-
rospective review of all patients who underwent valve
replacement for infective endocarditis and have re-
corded the results of valve cultures, Gram stains of valve
specimens performed in the microbiology laboratory,
and histopathological examinations (Gram stains and
determination of the presence of acute inflammation).
Our first objective was to describe the evolution of these
findings while patients received antimicrobial treatment
Dow
nloaded from https://academ
ic.oup.com/cid/article/36/6/697/318163 by guest on 30 June 2022

698 • CID 2003:36 (15 March) • Morris et al.
for endocarditis. Our second objective was to compare the
findings for the Gram-stained specimens examined in the mi-
crobiology laboratory (hereafter referred to as “microbiology
Gram stains”) with the findings for Gram-stained histopath-
ological sections (hereafter referred to as “histopathology Gram
stains”) in this series of patients.
PATIENTS AND METHODS
Patient population. Green Lane Hospital (Auckland, New
Zealand) has a large cardiothoracic surgical unit serving ∼1
million people, and local hospitals refer 17%–25% of their
patients with endocarditis to Green Lane Hospital for surgical
treatment [26, 27]. All patients who undergo valve replacement
surgery have a known or possible cause for valve dysfunction
entered into a computer database. All patients who underwent
valve replacement surgery from September 1963 through De-
cember 1999 and who had a diagnosis of endocarditis recorded
in the database had their charts reviewed. All relevant infor-
mation was recorded for each patient, including the following
data: number of blood culture sets performed, number of pos-
itive blood culture sets, organism or organisms isolated, du-
ration of antibiotic treatment before surgery, operation find-
ings, and the results of microbiological (culture and Gram stain
findings) and histopathological (Gram stain findings and char-
acteristics of the inflammatory cell infiltrate) examinations for
the resected valve.
Valve replacement was considered to have occurred during
active endocarditis if the patient had not completed a standard
antimicrobial therapy (SAT) regimen. For viridans streptococci,
enterococci, and staphylococci, the recommendations of Wilson
et al. [28] were used to define SAT. When these recommen-
dations specified 4–6 weeks as the duration of treatment, 4
weeks was regarded as being SAT. For prosthetic valve endo-
carditis, 6 weeks was regarded as SAT, except for allografts, for
which 4 weeks was regarded as SAT. For other organisms on
native valves, 4 weeks was regarded as being SAT. Timing of
surgery was analyzed according to the proportion of SAT that
had been completed at the time of the operation. This approach
was taken because a given duration of treatment in days does
not convey sufficient meaning. For example, 14 days of peni-
cillin treatment for an episode of penicillin-susceptible viridans
streptococcal endocarditis would represent completed treat-
ment for a native valve if penicillin was combined with an
appropriate aminoglycoside, but as only one-half of a treatment
course if it was given as monotherapy, and as only one-third
of the recommended course if endocarditis involved a pros-
thetic valve. By analyzing treatment as the proportion of SAT
completed, the organism, valve type, and treatment regimen
could all be taken into consideration [28].
Days of receipt of parenteral antimicrobial treatment with
�1 active antibiotic were counted. Oral agents taken alone were
not counted in the duration of treatment. The duration was
determined from the start of appropriate treatment, not from
when diagnosis of endocarditis was made.
Definitions. The modified Duke criteria [24] were used
to define cases of endocarditis, with the additional criterion of
a positive microbiology Gram stain being included in the def-
inite pathological criteria for endocarditis. Patients who had
negative preoperation blood culture results but who underwent
valve replacement surgery while receiving antibiotic treatment
were considered to have blood culture–negative endocarditis,
regardless of the findings of Gram stain, culture, or histopath-
ological examination of samples of the valves removed or re-
sected at the time of surgery. Patients for whom endocarditis
was not suspected before the operation (i.e., the patient did
not have fever and no blood samples were obtained for culture)
but who were discovered at the time of surgery to have infected
valves were deemed to have incubating endocarditis.
Acute inflammation in histopathology sections was defined
as the presence of polymorphonuclear leukocytes (PMLs) in
the inflammatory cell infiltrate. Chronic inflammation was de-
fined as an inflammatory cell infiltrate (e.g., histiocytes and
lymphocytes) without PMLs being present.
Laboratory procedures. Resected valve specimens were
sent for Gram staining and culturing in sterile containers with-
out additives. After macroscopic examination, vegetations and
material that appeared to be infected were removed and ground
in 0.5 mL of trypticase-soy broth with a 15-mL tapered tissue
grinder. Gram stains of the ground material were made. Blood
and chocolate agar media were inoculated, examined regularly,
and discarded after 7 days’ incubation. Four liquid media (20
mL each) were inoculated: Sabouraud dextrose broth; biphasic
brain-heart infusion broth with a nutrient agar scope, with
4%–10% added CO2; hypertonic blood culture medium con-
taining 10% sucrose; and anaerobic thioglycollate broth. Me-
chanical valves were placed in anaerobic thioglycollate broth.
Inoculated broths were incubated at 35�C and inspected daily.
Routine subcultures were performed after 7 days onto Colum-
bia agar that contained 5% defibrinated sheep RBCs. Plates
were aerobically and anaerobically incubated for 48 h before
discarding.
The Gram stain finding for ground valve material was re-
ported without waiting for the findings of culture or histo-
pathological examination. Isolates recovered from surgical spec-
imens were compared with available preoperative blood culture
isolates. Obvious plate or broth culture contaminants were ig-
nored and were not taken to indicate a positive culture (e.g.,
1 of 4 broths with a coagulase-negative Staphylococcus species
that had a susceptibility profile different from that of the blood
culture isolate).
For histopathological examination, specimens were placed in
Dow
nloaded from https://academ
ic.oup.com/cid/article/36/6/697/318163 by guest on 30 June 2022

Gram Stain, Culture, and Histopathology in IE • CID 2003:36 (15 March) • 699
Table 1. Etiologies of 506 episodes of infective endocarditis inpatients who underwent valve surgery.
FindingNo. (%) ofepisodes
OrganismStaphylococci
All 181 (36)Staphylococcus aureus 114 (23)Staphylococcus epidermidis 56 (11)Other staphylococcia 11 (2)
Streptococci 177 (35)Viridans streptococci 56 (11)Streptococcus sanguis 43 (8)Streptococcus mitis 17 (3)Streptococcus bovis 12 (2)Streptococcus anginosus 10 (2)Otherb 39 (8)
Enterococcus speciesc 31 (6)Abiotrophia species 11 (2)Corynebacterium speciesd 12 (2)Other gram-positive organismse 7HACEK group organismsf 16 (3)Other gram-negative organismsg 15 (3)Fungih 7
Culture-negative cases 51 (10)Gram-positive cocci present 32 (6)Acute inflammation in histopathological specimen 10 (2)Definite endocarditisi 1Possible endocarditisi 8
NOTE. Two patients had polymicrobial endocarditis with 2 isolates presentin multiple preoperative blood cultures: a viridans Streptococcus species and anEnterococcus species; and S. epidermidis and a b-hemolytic Streptococcus spe-cies. One patient with incubating endocarditis with gram-positive cocci presentin a Gram-stained histopathological specimen is included in the culture-negativegroup. Thirteen of the blood culture–negative cases (table 3) had positive valvecultures and are included with the respective organisms, as are 9 of 10 casesof incubating endocarditis that had positive valve cultures. HACEK, Haemophilus,Actinobacillus, Cardiobacterium, Eikenella, and Kingella species.
a S. capitis (2 episodes), S. warneri (2), S. cohnii (1), and nonspeciatedcoagulase-negative staphylococci (6).
b S. mutans (8 episodes), Group G Streptococcus species (6), S. pneumon-iae (4), S. agalactiae (4), S. pyogenes (5), S. oralis (3), S. salivarius (2), S. mitior(1), and nonspeciated streptococci (6).
c E. faecalis (24 episodes), E. faecium (1), E. durans (1), and nonspeciatedenterococci (5).
d C. jeikeium (6 episodes), C. pseudodiphtheriticum (3), C. diphtheriae (1),and nonspeciated corynebacteria (2).
e Dermobacter hominis (1 episode), Gemella morbillorum (1), Lactobacilluscasei (1), Listeria monocytogenes (1), nonspeciated lactobacilli (2), and a non-speciated aerobic sporing bacillus (1).
f Haemophilus species: H. parainfluenzae (3 episodes), H. influenzae (2), H.paraphrophilus (2), and H. aphrophilus (1); Actinobacillus actinomycetemcom-itans (1), Cardiobacterium hominis (2), Eikenella corrodens (1), Kingella kingae(2), and Kingella denitrificians (2).
g Serratia marcescens (2 episodes), Pseudomonas aeruginosa (2), Pseu-domonas alcaligenes (1), Brucella abortus (1), Citrobacter diversus (1), Esch-erichia coli (1), Flavobacterium species (1), Klebsiella pneumoniae (1), Neisseriamucosa (1), Neisseria pharyngis (1), Salmonella species (1), Stenotrophomonasmaltophilia (1), and a nonspeciated, nonlactose fermenting gram-negative ba-cillus (1).
h Aspergillus fumigatus (2 episodes); Candida species: C. albicans (3), C.glabrata (1), C. parapsilosis (1).
i For clinical criteria, see [24].
formalin and sent to the histopathology laboratory for routine
processing and hematoxylin-eosin and Gram staining. Histo-
pathological findings were reported by the pathologist assigned
to the case. No special reporting protocol was in place to pro-
vide a standardized report, but when endocarditis is mentioned
on the laboratory request form, it is standard practice for the
histopathology report to specifically state the presence or ab-
sence of organisms and to describe the composition of the
inflammatory cell infiltrate. In a limited number of cases in
which the histopathology report lacked sufficient detail, one of
us would reread the slides. Histopathological findings were re-
corded as organisms present irrespective of the inflammatory
cell infiltrate, acute inflammation without organisms, chronic
inflammation without organisms, or other findings (e.g., fi-
brosis or valve thickening).
Blood culture methods. Cultures of blood samples ob-
tained from patients suspected of having endocarditis were in-
cubated for 14 days until mid-1994, when the duration was
reduced to our current practice of 10 days’ incubation. Manual
blood culture methods were in use until mid-1986, when the
BACTEC system (Becton Dickinson) was introduced. This was
replaced by the BacT/Alert system (Organon Tecknika) in early
1995.
Statistical analysis. Analysis was performed with use of
the x2 test for tables. was considered to be sta-2 � 2 P ! .05
tistically significant.
RESULTS
Patients. There were 480 patients who underwent 506 op-
erations for treatment of infective endocarditis. Twenty patients
underwent 2 valve replacements and 3 patients underwent 3
valve replacements for treatment of endocarditis. Of the 480
patients, men predominated (71%). Only 5 patients were
known injection drug users. Aortic valves were the most com-
monly infected valves, either alone (277 [58%]) or in combi-
nation with other valves (27 [8%]). One hundred ninety-three
patients (40%) had undergone previous valve surgery, and 55
(11%) had experienced a previous episode of endocarditis.
Inclusion criteria for endocarditis. A total of 424 (84%)
of 506 episodes met our pathological criteria for endocarditis:
153 (30%) had positive valve culture results, 230 (45%) had
organisms present in either the microbiology or histopathology
Gram stain, and 41 (8%) did not have organisms seen or grown
but had acute inflammation in sections obtained for histo-
pathological examination [24]. Of the 82 remaining episodes,
20 and 62 met the Duke clinical criteria for definite and possible
endocarditis, respectively [24].
Etiology of endocarditis. The etiologies of the 506 episodes
of endocarditis are shown in table 1. Episodes of blood cul-
ture–negative endocarditis that had positive valve culture results
Dow
nloaded from https://academ
ic.oup.com/cid/article/36/6/697/318163 by guest on 30 June 2022

700 • CID 2003:36 (15 March) • Morris et al.
Table 2. Gram stain, culture, and histopathological findings for 506 episodes of infective endocarditis that required removal orresection of heart valves.
VariableNo. of
episodes
Microbiological findings Histopathological findings
No. ofpositive Gramstain results/
total no.of samplesstained (%)
No. ofpositive
culture results/total no. ofcultures (%)
No. ofsamples with
organismspresent/no.
examined (%)
No. ofsamples withno organisms
found but acuteinflammationpresenta/no.
examined (%)
Proportion of standard duration antibiotic treatmentcompleted at time of operation
�25% 106 88/100 (88) 76/106 (72) 51/63 (81) 9/63 (14)
26%–50% 113 85/101 (84) 40/108 (37) 50/70 (71) 17/70 (24)
51%–75% 57 37/50 (74) 7/54 (13) 21/39 (54) 12/39 (31)
76%–100% 41 21/34 (62) 2/38 (5) 18/36 (50) 11/36 (31)
1100% but still receiving treatment 61 28/43 (65) 5/53 (9) 29/53 (55) 11/53 (21)
Patient stopped treatment
�1 month before operation 22 7/15 (47) 0/19 (0) 9/20 (45) 4/20 (20)
11 month but !6 months before operation 33 4/18 (22) 1/22 (5) 6/25 (24) 9/25 (36)
Negative blood cultureb 63 31/52 (60) 13/60 (22) 26/48 (54) 11/48 (23)
Incubating endocarditis presentc 10 7/8 (88) 9/9 (100) 4/6 (67) 2/6 (33)
a Presence of polymorphonuclear leukocytes in the inflammatory cell infiltrate.b One or more negative preoperative blood cultures.c Endocarditis was not suspected before the patient underwent surgery (i.e., the patient did not have fever and blood samples were not obtained preoperatively
for culture). See table 4.
( ) are recorded alongside the respective organisms, asn p 13
are the 9 episodes of incubating endocarditis that had positive
valve culture results. Patients with blood culture–negative en-
docarditis who had negative valve culture results ( ) aren p 50
recorded as having cases of culture-negative endocarditis and
are grouped according to the histopathological and clinical cri-
teria for endocarditis. One patient with incubating endocarditis
who did not have valve culture performed is included with the
culture-negative cases because gram-positive cocci were present
in histopathology Gram stains.
Findings of culture, Gram stain, and histopathological ex-
aminations. The results of culture, microbiology Gram stain,
histopathology Gram stain, and examination for the presence
of acute inflammation in patients with negative histopathology
Gram stain results are listed in table 2. Valves were seldom
culture positive after receipt of �50% of SAT, but microbiology
Gram stain findings were positive for 160% of patients who
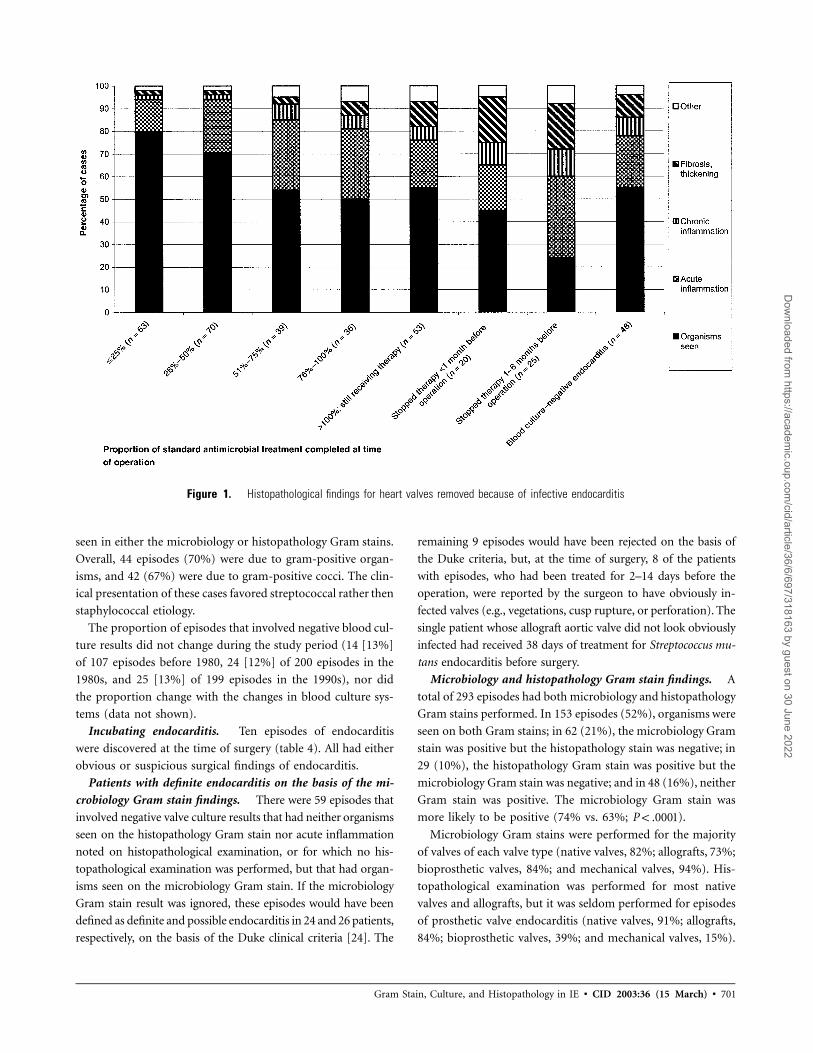
were still receiving antibiotic treatment. Nonviable bacteria per-
sist for weeks to months in sterilized vegetations, and acute
inflammation may persist for weeks to months after microbi-
ological cure (table 2 and figure 1). Chronic inflammation (i.e.,
inflammation without PMLs) made up a small but increasing
proportion of the histopathological findings late into and �6
months after completion of SAT (figure 1).
Five (9%) of 53 valves from patients who were still receiving
treatment but who had completed SAT were culture positive
(table 3). One additional valve was also culture positive (patient
6; table 3). This patient had completed 4 weeks of combination
therapy with ampicillin and netilmicin for Enterococcus faecalis
native aortic valve endocarditis. Three weeks later, he received
ampicillin prophylaxis for a colonoscopy. At the time of surgery,
12 days after undergoing colonoscopy, an obviously infected
(as determined macroscopically), culture-positive aortic valve
was removed.
Blood culture–negative episodes. There were 63 episodes
of suspected endocarditis that involved negative blood cultures.
For the 44 episodes in which the number of negative blood
culture results was recorded, the median number of blood cul-
tures was 4, and, for 20 episodes, there were �5 negative blood
culture results. Twenty-three patients (37%) were receiving or
had recently received antibiotic treatment at the time that blood
samples were obtained for culture, and 4 (17%) of the 23 had
positive valve culture results.
Thirteen (21%) of 63 episodes that involved negative blood
culture results had positive valve culture results. The isolates
were all gram positive: Staphylococcus aureus ( ), coagu-n p 1
lase-negative staphylococci ( ), Corynebacterium jeikeiumn p 6
( ), viridans streptococci ( ), and Abiotrophia defec-n p 2 n p 3
tiva ( ). Only the latter can be regarded as a fastidiousn p 1
organism. A further 31 episodes (49%) had gram-positive cocci
Dow
nloaded from https://academ
ic.oup.com/cid/article/36/6/697/318163 by guest on 30 June 2022
Gram Stain, Culture, and Histopathology in IE • CID 2003:36 (15 March) • 701
Figure 1. Histopathological findings for heart valves removed because of infective endocarditis
seen in either the microbiology or histopathology Gram stains.
Overall, 44 episodes (70%) were due to gram-positive organ-
isms, and 42 (67%) were due to gram-positive cocci. The clin-
ical presentation of these cases favored streptococcal rather then
staphylococcal etiology.
The proportion of episodes that involved negative blood cul-
ture results did not change during the study period (14 [13%]
of 107 episodes before 1980, 24 [12%] of 200 episodes in the
1980s, and 25 [13%] of 199 episodes in the 1990s), nor did
the proportion change with the changes in blood culture sys-
tems (data not shown).
Incubating endocarditis. Ten episodes of endocarditis
were discovered at the time of surgery (table 4). All had either
obvious or suspicious surgical findings of endocarditis.
Patients with definite endocarditis on the basis of the mi-
crobiology Gram stain findings. There were 59 episodes that
involved negative valve culture results that had neither organisms
seen on the histopathology Gram stain nor acute inflammation
noted on histopathological examination, or for which no his-
topathological examination was performed, but that had organ-
isms seen on the microbiology Gram stain. If the microbiology
Gram stain result was ignored, these episodes would have been
defined as definite and possible endocarditis in 24 and 26 patients,
respectively, on the basis of the Duke clinical criteria [24]. The
remaining 9 episodes would have been rejected on the basis of
the Duke criteria, but, at the time of surgery, 8 of the patients
with episodes, who had been treated for 2–14 days before the
operation, were reported by the surgeon to have obviously in-
fected valves (e.g., vegetations, cusp rupture, or perforation). The
single patient whose allograft aortic valve did not look obviously
infected had received 38 days of treatment for Streptococcus mu-
tans endocarditis before surgery.
Microbiology and histopathology Gram stain findings. A
total of 293 episodes had both microbiology and histopathology
Gram stains performed. In 153 episodes (52%), organisms were
seen on both Gram stains; in 62 (21%), the microbiology Gram
stain was positive but the histopathology stain was negative; in
29 (10%), the histopathology Gram stain was positive but the
microbiology Gram stain was negative; and in 48 (16%), neither
Gram stain was positive. The microbiology Gram stain was
more likely to be positive (74% vs. 63%; ).P ! .0001
Microbiology Gram stains were performed for the majority
of valves of each valve type (native valves, 82%; allografts, 73%;
bioprosthetic valves, 84%; and mechanical valves, 94%). His-
topathological examination was performed for most native
valves and allografts, but it was seldom performed for episodes
of prosthetic valve endocarditis (native valves, 91%; allografts,
84%; bioprosthetic valves, 39%; and mechanical valves, 15%).
Dow
nloaded from https://academ
ic.oup.com/cid/article/36/6/697/318163 by guest on 30 June 2022

702 • CID 2003:36 (15 March) • Morris et al.
Table 3. Characteristics of culture-positive patients who completed standard-duration antibiotic treatment.
Patient Infected valve(s)Treatment
(duration, days)
Microbiological findings
Culture findings
Findings ofhistopathological
examinationSurgical Gram stain
1 Aortic mitral, native Combination penicillinand gentamicin (20)
Para-aortic abscess Gram-positive cocci Streptococcussanguisa
Both valves with PMLinfiltration and gram-positive cocci
2 Aortic, biopros-thetic (Hancock)
b-Lactam agents (43;�19 in combinationwith gentamicin)
Large vegetation ex-tending to orifice ofright coronary artery
Gram-positive cocci Staphylococcusepidermidisb
Not done
3 Aortic, native Doxycycline andrifampicin (43)
Nodular thickened valve,granulations extend-ing into annulus
Not done Brucella abortus Fibrosis, calcification, andlymphocytic infiltration;no PMLs
4 Aortic, allograft Amphotericin (32) Vegetations Not done Candida albicans Vegetations with PMLsand pseudohyphae
5 Aortic mitral,mechanical
Amphotericin (52) anditraconazole (39;total therapy, 56)
Vegetations extensivepannus
Septate, branchinghyphae
Aspergillusfumigatus
Septate branchinghyphae
6 Aortic, native Ampicillin and netil-micin (28)c
Vegetations Gram-positive cocci Enterococcusfaecalis
Vegetations with PMLs;no organisms seen
NOTE. PML, polymorphonuclear leukocyte.a MIC of penicillin, 0.03 mg/L. The MIC was determined for the blood culture isolate; it was not determined for the valve culture isolate.b Endocarditis due to penicillin-susceptible S. epidermidis 33 months after native aortic valve replacement with Hancock bioprosthetic valve.c Five-week gap between completion of treatment and surgery.
DISCUSSION
The first objective in this study was to report the evolution of
culture and Gram stain findings during treatment for infective
endocarditis. In this series, organisms were seen in most epi-
sodes that involved operation during antimicrobial treatment
but recovered in an ever-decreasing proportion of patients as
treatment progressed. There are few previous data on Gram
stain and culture findings for valves resected for endocarditis
[20, 29–34]. Furthermore, when authors do comment on the
detection of organisms, it is unclear whether they are referring
to the microbiology Gram stain, the histopathology Gram stain,
or both.
Past reviewers have differed in their interpretation of the
disparity between Gram stain and culture results. The opinion
of Jung et al. [35] was that this “proves that conversion of
blood cultures from positive to negative results does not nec-
essarily mean that the organism was eradicated from the in-
volved valve” (p. 512). Manhas et al. [21] concluded, “This
suggests that even when a full course of antibiotic therapy
has not been given, the valve was rendered sterile in a number
of patients” (p. 745). We agree with Manhas et al. [21] and
believe that seeing organisms on Gram stains of ground valve
material or by histopathological examination does not mean
that viable organisms are present. Culture results should be
the index of whether the surgery has been performed in an
infected field, because it may take months for dead bacteria
in a vegetation to be removed by phagocytosis and/or bacterial
cell lysis (table 2).
The second objective of this study was to report the micro-
biology Gram stain findings for resected valves. We are unsure
why positive microbiology Gram stain results are omitted in
the Duke criteria as definitive pathological evidence of endo-
carditis [23, 24]. It may have been because microbiology Gram
stain was thought to be insufficiently sensitive or specific or
because the Duke endocarditis database did not have enough
microbiology Gram stain findings stored to allow adequate
analysis. If the latter were the case, this study removes any data
deficit. If it were the former, we have shown that the micro-
biology Gram stain performs as well, if not better, than the
histopathology Gram stain. As for any concern over the spec-
ificity of microbiology Gram stain, we believe this to be a the-
oretical consideration only. Microbiology technologists are
skilled microscopists and regularly examine Gram-stained
smears of tissue specimens. In our experience, there is such an
abundance of organisms in cases of streptococcal endocarditis
that it only takes examination of a few microscopic fields for
organisms to be unambiguously identified. Although staphy-
lococci can have variable size and staining characteristics, es-
pecially later in a course of antimicrobial therapy, a confident
assessment can be made in most instances. So, although the
original Duke article stated that “our … pathologic criteria are
essentially similar to those used in the definite category of von
Reyn, except for some minor improvements in wording” [23,
p. 202], we suggest that the rewording is not an improvement
because it dropped a positive microbiology Gram stain result
from being considered sufficient for the pathological definition
of endocarditis. We agree with the Beth Israel and St. Thomas
pathological definitions for endocarditis, which include micro-
biology Gram stain results [22, 25]. We suggest that future
modifications of the Duke criteria take our results into account.
Dow
nloaded from https://academ
ic.oup.com/cid/article/36/6/697/318163 by guest on 30 June 2022

Gram Stain, Culture, and Histopathology in IE • CID 2003:36 (15 March) • 703
Table 4. Causes of incubating endocarditis discovered during valve replacement surgery for valve failure.
Patient Infected valve
Microbiological findings
Culture findings Histopathological findingsSurgical Gram stain
1 Aortic, native Cusp destruction withragged edges
Not done Enterococcus faecalis Fibrinous nodules with PML infiltration; noorganisms seen
2 Aortic, allograft Vegetations NOS Streptococcus mitis Vegetations with PMLs and chronicinflammatory cell infiltration; noorganisms seen
3 Aortic, native Thickened soft valve Gram-positive cocci Streptococcus anginosus Vegetations with PMLs and gram-positive cocci
4 Mitral, mechanical Clot on suture line Gram-positive cocci Staphylococcus epidermidis Not done
5 Mitral, mechanical Partial dehiscence,fibrinous deposits
Gram-positive cocci S. epidermidis Not done
6 Aortic, allograft Vegetations Gram-positive bacilli Corynebacterium species No report in notes; slides and blocks not found
7 Aortic, allograft Vegetations Gram-positive bacilli Corynebacterium species Not done
8 Aortic, allograft Vegetations Not done Not done Vegetation with PML infiltration and gram-positivecocci
9 Aortic, mechanical Partial dehiscence ofsewing ring
Gram-positive bacilli Corynebacterium species Chronic inflammatory cells and gram-positive bacilli
10 Aortic, allograft Vegetations Gram-positive cocci Streptococcus oralis Vegetations with PML infiltration and gram-positivecocci
NOTE. Endocarditis was not suspected before the patient underwent surgery (i.e., the patient did not have fever and no blood samples were obtained forculture). PML, polymorphonuclear leukocyte.
This is of particular relevance for prosthetic valve endocarditis,
for which material for histopathological examination is infre-
quently available.
We also suggest a change to the wording of the histopath-
ological definition of endocarditis. The currently worded Duke
criteria for pathological lesions include “vegetation or intra-
cardiac abscess confirmed by histologic examination showing
active endocarditis” [24, p. 636]. We believe this wording is
ambiguous because “active endocarditis” has been used pre-
viously to describe when surgery has been performed before
the end of antibiotic treatment or for when the valve culture
result is positive [1, 4, 34]. By “active endocarditis,” we believe
that the authors meant the presence of acute inflammatory cells
(i.e., PMLs) in the inflammatory cell infiltrate of the valve,
vegetation, or abscess wall tissue. We suggest that the word
“active” be removed and a phrase indicating the presence of
acute inflammatory cells in the vegetation or tissue be used to
define histopathological findings establishing endocarditis in
lesions when bacteria are not seen.
There were 5 instances in which valves were culture positive
when the patient was still receiving antibiotic treatment but
had completed SAT (table 3). It was rare, however, for com-
monly encountered organisms (i.e., staphylococci and strep-
tococci) to be recovered from valve cultures after SAT had been
completed, a finding that provides support for commonly fol-
lowed treatment guidelines [28].
Our results for patients with negative blood cultures are sim-
ilar to those of Pesanti and Smith [36] in their series of 52
cases of endocarditis with negative blood culture results. In
their series, 25 patients had valvular tissue specimens obtained
for culture and Gram stain for organisms; 9 (36%) had or-
ganisms both seen and grown, and a further 6 (24%) had
organisms seen but not cultured [36]. Overall, 10 patients
(40%) had culture or Gram stain evidence of gram-positive
cocci. We saw or grew gram-positive cocci for 42 (67%) of 63
patients who had blood culture–negative endocarditis. In a
more recent study that described 32 patients with �3 negative
blood culture results, the valve culture result was positive for
6 (19%), and, for 5 (83%) of these patients, fastidious organ-
isms (i.e., nutritionally variant streptococci and a Haemophilus
species) were recovered [37]. Only one of our isolates, A. de-
fectiva, can be regarded as fastidious. Our results support the
notion that initial treatment for blood culture–negative cases
can be based on the assumption that the majority of the or-
ganisms responsible are the same as those found in cases with
positive blood cultures.
To our knowledge, this study is the first to have reported a
series of cases of incubating endocarditis. We use this term
because we believe that these cases would have eventually be-
come clinically evident. It seems highly improbable that they
would have resolved spontaneously. Isolated episodes of in-
cubating endocarditis have been reported previously [4, 22, 38].
In conclusion, this report provides insight into the evolving
culture findings, Gram stain findings, and inflammation status
of heart valves before, during, and shortly after completing
treatment for infective endocarditis. We suggest that the mi-
crobiology Gram stain should be reinstated into the patholog-
ical criteria for definite endocarditis. Finally, we do not believe
positive Gram stain results for microbiological or histopatho-
logical specimens of resected valves necessarily indicate an in-
Dow
nloaded from https://academ
ic.oup.com/cid/article/36/6/697/318163 by guest on 30 June 2022

704 • CID 2003:36 (15 March) • Morris et al.
fected surgical field because of the considerable time delay be-
tween vegetation sterilization and disappearance of organisms.
References
1. Dinubile M. Surgery in active endocarditis. Ann Intern Med 1982; 96:650–9.
2. Vlessis AA, Khaki A, Grunkemeier GL, Li H-H, Starr A. Risk, diagnosisand management of prosthetic valve endocarditis: a review. J HeartValve Dis 1997; 6:443–65.
3. Moon MR, Stinson EB, Miller DC. Surgical treatment of endocarditis.Prog Cardiovasc Dis 1997; 40:239–64.
4. Stinson E. Surgical treatment of infective endocarditis. Prog CardiovascDis 1979; 22:145–68.
5. Wilson W, Danielson G, Guiliani E, Washington J II, Jaumin P, GeraciJ. Cardiac valve replacement in congestive heart failure due to infectiveendocarditis. Mayo Clin Proc 1979; 54:223–6.
6. Boyd A, Spencer F, Isom W, et al. Infective endocarditis: an analysisof 54 surgically treated patients. J Thorac Cardiovasc Surg 1977; 73:23–30.
7. Richardson J, Karp R, Kirklin J, Dismukes W. Treatment of infectiveendocarditis: a 10-year comparative analysis. Circulation 1978; 58:589–97.
8. Young J, Welton D, Raizner A, et al. Surgery in active infective en-docarditis. Cardiovasc Surg 1979; 60:77–81.
9. Mills J, Utley J, Abbott J. Heart failure in infective endocarditis: pre-disposing factors, course and treatment. Chest 1974; 66:151–7.
10. Croft C, Woodward W, Elliott A, Commerford P, Bernard C, Beck W.Analysis of surgical versus medical therapy in active complicated nativevalve infective endocarditis. Am J Cardiol 1983; 51:1650–5.
11. Sethia B, Reece I, Forrester A, Davidson K. The surgical managementof extravalvular aortic root infection. Ann Thorac Surg 1984; 37:484–7.
12. David T, Bos J, Christakis G, Brofman P, Wong D, Feindel C. Heartvalve operations in patients with active infective endocarditis. AnnThorac Surg 1990; 49:701–5.
13. Kay P, Oldershaw P, Dawkins K, Lennox S, Paneth M. The results ofsurgery for active endocarditis of the native aortic valve. J CardiovascSurg (Torino) 1984; 25:321–7.
14. Pringle T, Webb S, Khan M, O’Kane H, Cleland J, Adgey J. Clinical,echocardiographic and operative findings in active infective endocar-ditis. Br Heart J 1982; 48:529–37.
15. Anker E, Thaulow E, Forfang K, Rostad H. Surgical treatment of bac-terial endocarditis: a review and follow-up of 36 patients. Acta MedScand 1981; 209:285–8.
16. Symbas P, Vlasis S, Zacharopoulos L, Lutz J. Acute endocarditis: surgicaltreatment of aortic regurgitation and aortico-left ventricular discon-tinuity. J Thorac Cardiovasc Surg 1982; 84:291–6.
17. de Costa Lins R, Soares D, Van Berg L, et al. Surgical treatment ofactive valvular infective endocarditis. Scand J Thorac Cardiovasc Surg1988; 22:43–5.
18. Sweeney M, Reul G Jr, Cooley D, et al. Comparison of bioprostheticand mechanical valve replacement for active endocarditis. J ThoracCardiovasc Surg 1985; 90:676–80.
19. Ergin M, Raissi S, Follis F, Lansman S, Griepp R. Annular destruction
in acute bacterial endocarditis: surgical techniques to meet the chal-lenge. J Thorac Cardiovasc Surg 1989; 97:755–63.
20. Soyer R, Redonnet M, Bessou J, Mutel P, Hubscher C, Letac B. Valvereplacement in acute valve endocarditis. Thorac Cardiovasc Surg1986; 34:149–52.
21. Manhas D, Mohri H, Hessel E, Merendina K. Experience with surgicalmanagement of primary infective endocarditis: a collected review. AmHeart J 1972; 84:738–47.
22. von Reyn CF, Levy BS, Arbeit RD, Friedland G, Crumpacker CS. In-fective endocarditis: an analysis based on strict case definitions. AnnIntern Med 1981; 94:505–18.
23. Durack DT, Lukes AS, Bright DK. New criteria for diagnosis of infectiveendocarditis: utilization of specific echocardiographic findings. DukeEndocarditis Service. Am J Med 1994; 96:200–9.
24. Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Dukecriteria for the diagnosis of infective endocarditis. Clin Infect Dis2000; 30:633–8.
25. Lamas CC, Eykyn SJ. Suggested modifications to the Duke criteria forthe clinical diagnosis of native valve and prosthetic valve endocarditis:analysis of 118 pathologically proven cases. Clin Infect Dis 1997; 25:713–9.
26. Wells AU, Fowler CC, Ellis-Pegler RB, Luke R, Hannan S, Sharpe DN.Endocarditis in a general hospital in Auckland, New Zealand. Q J Med1990; 76:753–62.
27. Peat EB, Lang SDR. Infective endocarditis in a racially mixed com-munity: a 10 year review of 78 cases. N Z Med J 1989; 102:33–6.
28. Wilson WR, Karchmer AW, Dajani AS, et al. Antibiotic treatment ofadults with infective endocarditis due to streptococci, enterococci,staphylococci, and HACEK microorganisms. JAMA 1995; 274:1706–11.
29. Utley J, Mills J, Hutchinson J, Edmunds L, Sanderson R, Roe B. Valvereplacement for bacterial and fungal endocarditis: a report of six cases.Am Surgeon 1964; 30:766–9.
30. Wilson W, Danielson G, Guiliani E, Washington J II, Jaumin P, GeraciJ. Valve replacement in patients with active infective endocarditis. Cir-culation 1978; 58:585–8.
31. Tuna I, Orszulak T, Schaff H, Danielson G. Results of homograft aorticvalve replacement for active endocarditis. Ann Thorac Surg 1990; 49:619–24.
32. Becker R, Frishman W, Frater R. Surgery for mitral valve endocarditis.Chest 1979; 75:314–9.
33. Kinsley R, Colsen P, Bakst A. Emergency valve replacement for primaryinfective endocarditis. S Afr Med J 1978; 53:86–8.
34. Blumberg EA, Robbins N, Adimora A, Lowy FD. Persistent fever inassociation with infective endocarditis. Clin Infect Dis 1992; 15:983–90.
35. Jung J, Saab S, Almond C. The case for early surgical treatment of left-sided primary infective endocarditis: a collective review. J Thorac Car-diovasc Surg 1975; 70:509–18.
36. Pesanti EL, Smith IM. Infective endocarditis with negative blood cul-tures an analysis of 52 cases. Am J Med 1979; 66:43–50.
37. Kupferwasser LI, Darius H, Muller AM, et al. Diagnosis of culturenegative endocarditis: the role of the Duke criteria and the impact oftransesophageal echocardiology. Am Heart J 2001; 142:146–52.
38. Chuard C, Antley CM, Reller LB. Clinical utility of cardiac valve Gramstain and culture in patients undergoing native valve replacement. ArchPathol Lab Med 1998; 122:412–5.
Dow
nloaded from https://academ
ic.oup.com/cid/article/36/6/697/318163 by guest on 30 June 2022
academic.oup.com/cid of 1 4
Please excuse the presence of this and the following test pages, which have been
added to a small number of article PDFs for a limited time as part of our process of
continual development and improvement.
academic.oup.com/cid
Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do academic.oup.com/cid of 2 4
eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. academic.oup.com/cid of 3 4
Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum. Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat. Duis aute irure dolor in reprehenderit in voluptate velit esse cillum dolore eu fugiat nulla pariatur. Excepteur sint occaecat cupidatat non proident, sunt in culpa qui officia deserunt mollit anim id est laborum.
academic.oup.com/cid of 4 4
Related Documents











