Governing Body Meeting Agenda Tuesday, 01 September 2015, 14.30 – 17.15 Hall Two, Osmani Centre, 58 Underwood Road, London, E1 5AW 1 General Business Action required Presenter Enc. Time Page 1.1 Welcome, Introductions and Apologies - Sam Everington Verbal 14.30 (10 mins) - 1.2 Declarations of Interest - 1.3 Chair’s Report To note A 5 1.4 Chief Officer’s Report Jane Milligan 1.5 Minutes and Matters Arising of the Meeting Held July 7 2015 To approve Sam Everington B 14.40 (5 mins) 13 1.6 Members’ Story To note - - 14.45 (10 mins) - 2 Performance and Operations 2.1 Board Assurance Framework 2015/16 To note Jane Milligan C 14.55 (5 mins) 25 2.2 Finance and Activity • 2.2.1 Finance Report Month 4 • 2.2.2 Activity Report To note Henry Black Lee Eborall D E 15.00 (15 mins) 49 63 2.3 Performance and Quality Report To note Archna Mathur F 15.15 (15 mins) 71 2.4 Barts Health – RLH CQC Compliance Plan and Improvement Plan For information Karen Breen G 15.30 (30 mins) 85 2.5 Healthwatch – Rate Our Service Update For information Dianne Barham H 16.00 (15 mins) 115 5 minute break 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Governing Body Meeting Agenda
Tuesday, 01 September 2015, 14.30 – 17.15
Hall Two, Osmani Centre, 58 Underwood Road, London, E1 5AW
1 General Business
Action required Presenter Enc. Time Page
1.1 Welcome, Introductions and Apologies
-
Sam Everington
Verbal 14.30
(10 mins)
-
1.2 Declarations of Interest -
1.3 Chair’s Report To note A 5
1.4 Chief Officer’s Report Jane Milligan
1.5 Minutes and Matters Arising of the Meeting Held July 7 2015
To approve
Sam Everington B
14.40 (5 mins)
13
1.6 Members’ Story
To note - - 14.45
(10 mins) -
2 Performance and Operations
2.1 Board Assurance Framework 2015/16 To note Jane Milligan C
14.55 (5 mins)
25
2.2
Finance and Activity • 2.2.1 Finance Report
Month 4
• 2.2.2 Activity Report
To note
Henry Black
Lee Eborall
D
E
15.00 (15 mins)
49
63
2.3 Performance and Quality Report
To note Archna Mathur F
15.15 (15 mins)
71
2.4 Barts Health – RLH CQC Compliance Plan and Improvement Plan
For information Karen Breen G
15.30 (30 mins)
85
2.5 Healthwatch – Rate Our Service Update
For information
Dianne Barham H
16.00 (15 mins)
115
5 minute break
1

3 Commissioning and Strategy
3.1 Tower Hamlets Partnership – Community Plan 2015 To approve Kevin
Kewin I
16.20 (15 mins)
123
3.2 Operating Plan 2015/16
For information
Josh Potter / Dr
Somen Banerjee
J 16.35
(15 mins) 161
3.3 Public Health Update For information
Dr Somen Banerjee
K 16.50
(10 mins) 173
3.4 Audit Committee – Annual Report to the Governing Body 2014/15
For information
Mariette Davis
L 17.00
(5 mins) 183
4 For Information
4.1 Audit Committee Summary
To note
Mariette Davis M
17.05
(5 mins)
203
4.2 Finance, Performance and Quality Committee Summary
Jane Milligan
N 205
4.3 Locality Board Summary O 207
4.4 Executive Committee Summary P 209
4.5 Transformation and Innovation Committee Summary Maggie
Buckell
Q 211
4.6 Primary Care Commissioning Committee Summary R 213
5 Other Business Items
6 Questions from the Public 17.10
All questions received 48 hours before the meeting in will be recorded in the minutes of the meeting. If you are asking a question at the meeting please use the sign in sheet in the public area of the meeting. You will be asked for your name and the agenda item number your question refers to. You will be expected to retain a copy of your question. Questions that are asked verbally at the meeting will only be answered if an accurate answer can be provided. Otherwise, the question will be taken on notice and will be answered at the next meeting. Please email [email protected] for more information.
7 Date of Next Meeting
Meeting in public Nov 3rd 2015 – 2.30pm Room 205, Professional Development Centre, 229 Bethnal Green Road, London E2 6AB
2
Public information sheet Attendance at meetings The public are welcome to attend the Governing Body meeting of NHS Tower Hamlets CCG
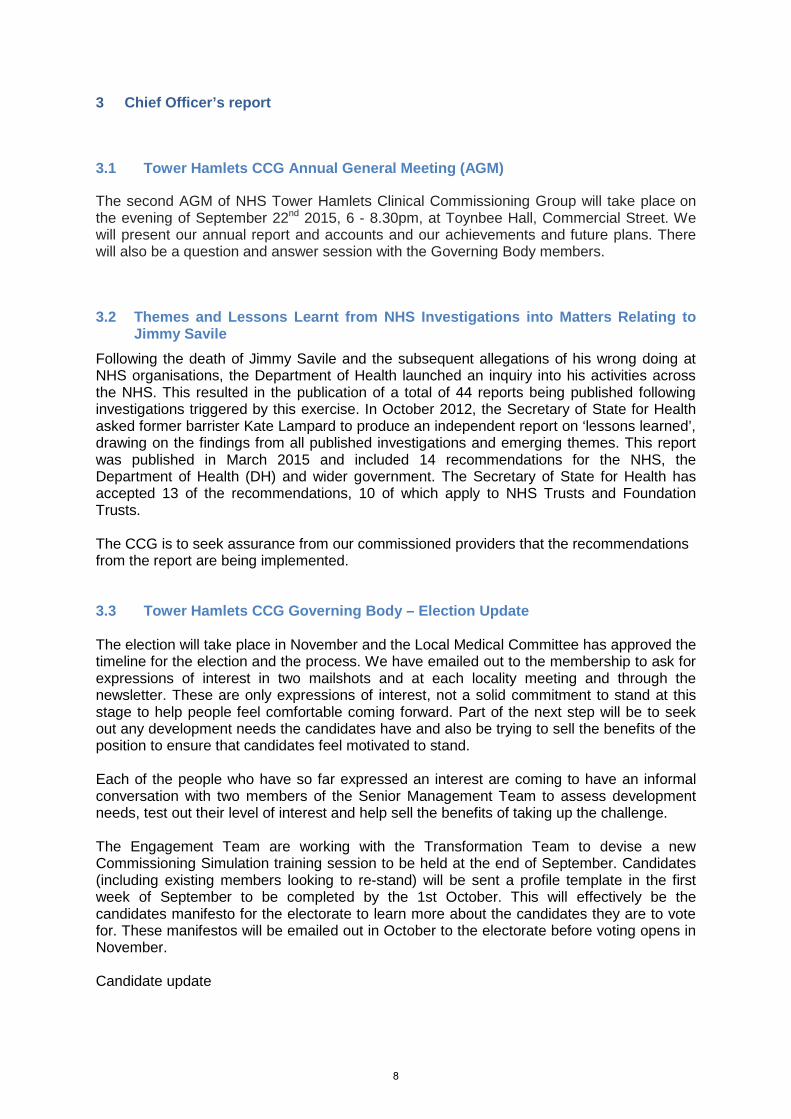
Getting to the Osmani Centre
Getting here by road: From the A11 – Whitechapel Road, turn down Vallance Road and then take the second left. The Osmani Centre is located on the corner.
Getting here by bus 25, 67, 149, 254, 388
Getting here by Underground Whitechapel - District, Circle, Hammersmith and City and Overground Lines.
Electronic agenda, reports and minutes Copies of agenda, reports and minutes for CCG meetings can be found on our website 5 working days before the meeting: http://www.towerhamletsccg.nhs.uk/News-and-publications/board-papers.htm
Disabled access and special requirements The main entrance is suitable for wheelchair users. Documents can be made available in large print, Brail or audio version. For further information, contact [email protected].
Questions from the public The Governing Body welcomes questions from the public.
In advance of the meeting At the meeting All questions received 48 hours before the meeting in will be answered and recorded in the meeting. Please email [email protected] with your question.
If you are asking a question at the meeting please use the sign in sheet in the public area of the meeting. You will be asked for your name, your question and the agenda item number your question refers to.
Please note: No photography or recording without permission and please switch all
electronic devices to silent mode whilst in the meeting.
3

4

Chair’s and Chief Officer’s Report
1 Purpose
The Chair’s and Chief Officer’s report will highlight items of interest to Governing Body members and the public. The Governing Body is invited to note this report and pursue any points of clarification or interest.
2 Chair’s report
2.1 Primary Care Funding in Tower Hamlets NHS Tower Hamlets Clinical Commissioning Group (CCG) is pleased to announce that an agreement has been reached with NHS England for a local solution that recognises the needs of the population and the workload of practices by using the flexibilities provided to us as a delegated commissioner of primary care. The locally commissioned solution will operate for a two year period effective from the 1st April 2015.
2.2 Tower Hamlets Primary Care Strategy
The Primary Care Strategy is currently in development and will be supported by a thorough engagement period from now until December. The Primary Care strategy will be co-produced with primary care professionals, the public and patients. The strategy will look to transform the way in which primary care is commissioned and delivered in Tower Hamlets by ensuring primary care empowers patients to self-care, proactively supports patients with complex long term conditions, and is accessible to those that need accessible and timely care. The strategy will consider the workforce, estates and informatics requirements to deliver a new model of care. There will be a strong emphasis on the wider determinants of health, reviewing how primary care can best support those with non-medical needs. Finally, a key component of the strategy will be the ways in which we commission and contract with primary care in the future, we will look to simplify the existing complex nature of primary care contracts and review the footprint within which we commission (network, locality, borough).
We will be issuing a primary care survey very shortly, on behalf of the CCG, the GP Care Group and the LMC. The survey will act as both a ‘mood test’ for professionals working in general practice, as well as exploring the appetite for transformation locally.
Enclosure A
5

2.3 Prime Minister’s Challenge Fund
Liane FitzGerald has started as programme support for the Tower Hamlets Prime Minister’s Challenge Fund programme. The virtual hub operational process has been agreed. A successful business process design session was held with the south-west locality hub in July and aiming for a September opening date for south-west and virtual hubs with the remainder to follow in October. The evaluation specification has been completed and will be going out to advert in the near future.
2.4 John Wardell Steps Down
On behalf of all staff at Tower Hamlets CCG, we wish John Wardell (Deputy Chief Officer) a fond farewell and best wishes as he takes up the position as Accountable officer at NHS Nene Clinical Commissioning Group.
We welcome Richard Quinton to the interim Director of Commissioning role. Richard has relatively recently finished with us as the interim director of contracting for Barts Health. As part of the interim arrangements Richard will be supporting the Primary care team and programme and Vanguard. He will also be picking up Royal London Hospital performance and the 111 programme.
2.5 John Atherton Appointed Acting Director of Commissioning NHS NCEL
Following Paul Bennett’s recent move to the Trust Development Authority, John Atherton will take up the role of Acting Director of Commissioning Operations for NCEL with immediate effect.
John’s appointment will ensure that NHS England can continue to work effectively with CCGs across NCEL in the interim while the recruitment process is underway to source a substantive replacement.
2.6 LBTH Changes
We welcome Will Tuckley as Chief Executive and Head of Paid Service of Tower Hamlets and the CCG looks forward to working closely together to drive improvements in health and social care for the local population of Tower Hamlets.
Robert McCulloch-Graham, Corporate Director of Education, Social Care, has stepped down from his post in the Council.
Luke Addams, Acting Director Adult Services, will replace Robert on the Tower Hamlets CCG Governing Body.
An interim appointment has been made to the position of Director of Children’s Services. This role will be covered by Debbie Jones. Debbie is highly experienced with substantial experience at Corporate Director level in Children’s Services in a number of local authorities.
6

2.7 John Bacon Appointed as Chair of Barts Health NHS Trust.
The NHS Trust Development Authority has confirmed the appointment of John Bacon as Chair of Barts Health NHS Trust. John, who has over 30 years' experience working in the NHS at regional and national level, took up post on August 1 2015. He will also continue as Chair of Community Health Partnerships, an independent company wholly owned by the Department of Health which works with NHS bodies to plan and utilise the community-based estate more efficiently. John was previously Chair of Sussex Partnership NHS Foundation Trust for seven years. He has also held a series of senior roles at regional level and at the Department of Health, where he was Director of Service Delivery from 2003 to 2006 with responsibility for the performance of the NHS in England and had oversight of finance, capital investment, education, training and relations with the private sector. John intends to move forward with the permanent appointment to the executive CEO and non-executive roles.
2.8 Professor Jo Martin Appointed as Interim Chief Medical Officer for Barts Health
Professor Jo Martin has been appointed as Interim Chief Medical Officer for Barts Health and assumed the post on 20 July. Jo, who has many years of experience of working for Barts Health, was previously the Trust's Director of Academic Health Sciences, leading on education and research, and also holds the position of National Clinical Director of Pathology for NHS England. She is a practicing Consultant Histopathologist and Professor of Pathology at Queen Mary University of London.
7
3 Chief Officer’s report
3.1 Tower Hamlets CCG Annual General Meeting (AGM)
The second AGM of NHS Tower Hamlets Clinical Commissioning Group will take place on the evening of September 22nd 2015, 6 - 8.30pm, at Toynbee Hall, Commercial Street. We will present our annual report and accounts and our achievements and future plans. There will also be a question and answer session with the Governing Body members.
3.2 Themes and Lessons Learnt from NHS Investigations into Matters Relating to Jimmy Savile
Following the death of Jimmy Savile and the subsequent allegations of his wrong doing at NHS organisations, the Department of Health launched an inquiry into his activities across the NHS. This resulted in the publication of a total of 44 reports being published following investigations triggered by this exercise. In October 2012, the Secretary of State for Health asked former barrister Kate Lampard to produce an independent report on ‘lessons learned’, drawing on the findings from all published investigations and emerging themes. This report was published in March 2015 and included 14 recommendations for the NHS, the Department of Health (DH) and wider government. The Secretary of State for Health has accepted 13 of the recommendations, 10 of which apply to NHS Trusts and Foundation Trusts. The CCG is to seek assurance from our commissioned providers that the recommendations from the report are being implemented. 3.3 Tower Hamlets CCG Governing Body – Election Update The election will take place in November and the Local Medical Committee has approved the timeline for the election and the process. We have emailed out to the membership to ask for expressions of interest in two mailshots and at each locality meeting and through the newsletter. These are only expressions of interest, not a solid commitment to stand at this stage to help people feel comfortable coming forward. Part of the next step will be to seek out any development needs the candidates have and also be trying to sell the benefits of the position to ensure that candidates feel motivated to stand. Each of the people who have so far expressed an interest are coming to have an informal conversation with two members of the Senior Management Team to assess development needs, test out their level of interest and help sell the benefits of taking up the challenge. The Engagement Team are working with the Transformation Team to devise a new Commissioning Simulation training session to be held at the end of September. Candidates (including existing members looking to re-stand) will be sent a profile template in the first week of September to be completed by the 1st October. This will effectively be the candidates manifesto for the electorate to learn more about the candidates they are to vote for. These manifestos will be emailed out in October to the electorate before voting opens in November. Candidate update
8
Commissioning Network 2 (post to be vacated by Haroon Rashid) – One GP has expressed an interest in standing. Commissioning Network 4 (post to be vacated by Martha Leigh) – No interested parties so far from this Network. Commissioning Network 6 (post currently held by Sam Everington) – Sam re-standing and no other interested parties so far. Commissioning Network 8 (post currently held by Shah Ali) – Shah re-standing and no other interested parties so far. We also have 1 GP from Network 7 who has expressed an interest in standing. As we are losing one partner and one salaried GP we need to make sure that we have the same roles stand to fit in with the quorum in the constitution (which states we must have 5 partners and 2 salaried GPs on the Governing Body). Practice Nurse Katherine Gerrans has recently left and we have had three expressions of interest so far for the post of Practice Nurse. 3.4 Care Homes Training Pilot The CCG Open Doors team and the Community Education Provider Network (CEPN) developed a pilot project last year to develop some training for residential care home staff as part of our CEPN policy of identifying educational needs which cross the traditional health and social care boundaries. Diane Gould and Michele Leworthy delivered workshops to 78 non clinical care staff from 3 local care homes. They designed the programme to enhance their understanding of common chronic conditions that the staff will encounter every day given the incidence of diabetes, heart disease, COPD and asthma amongst the elderly in Tower Hamlets. They also taught the staff about skin and how to spot the danger signs of pressure sores. The practical hands-on training was evaluated by an independent specialist and was found to be extremely effective and very well received by the staff and their managers. Most importantly, the staff made real changes to the care of residents following the training and there is evidence of ambulance call outs being avoided. We hope it will also help staff to work General Practice teams more effectively. The evaluation and a short video of staff talking about the training can be found on http://clemw5.wix.com/cepn (Learn more about care homes section) where there is a lovely video of staff and the teachers talking about their experiences. The project is now funded by the CCG and will continue with further training to staff in other homes. For more information or to let us know if there is a care home near you that would benefit from this training please contact [email protected]
3.5 Primary Care Facilitator Appointed to Support Tower Hamlets Practices with the Early Diagnosis of Cancer
The CCG is pleased to announce that Cancer Research UK, in partnership with the Transforming Cancer Services Team, London and with the full support of Tower Hamlets CCG, are now able to offer a valuable resource in the form of a Primary Care Facilitator to support Tower Hamlets GPs and practice teams with the early diagnosis of cancer.
9

Practice Profiles, which are produced by the National Cancer Intelligence Network are available to every General Practice in England were refreshed in March 2015.
3.6 New £15million Scheme to Give Patients Pharmacist Support in GP Surgeries
A new £15m scheme to fund, recruit and employ clinical pharmacists in GP surgeries has been launched by NHS England Chief Executive, Simon Stevens. The three year initiative, which will go live this year, will give patients the additional support of an expert pharmacist in their GP surgery. Examples of the benefits patients can expect include extra help to manage long-term conditions, specific advice for those with multiple medications and better access to health checks. The pharmacists will be employed directly by the general practice to help patients, while also easing GP workload and improving communication between general practice, hospitals and community pharmacists. The scheme will focus on areas of greatest need where GPs are under greatest pressure, and aims to build on the success of GP practices already employing pharmacists in patient-facing roles. The announcement is an important part of the New Deal for General Practice outlined by the NHS Five Year Forward View, and is the result of close collaborative work with Royal College of General Practice, the BMA’s General Practice Committee, the Royal Pharmaceutical Society and Health Education England.
Tower Hamlets CCG intends to further explore this initiative as another potential solution to address the increasing primary care workload pressures.
3.7 Barts Health: Leadership Operating Model
Barts Health is developing its quality improvement plan – Safe and Compassionate - in response to the findings of the Care Quality Commission’s (CQC) inspections. They are determined to make the necessary improvements for patients and are now finalising this improvement plan through further discussions with our staff and our partners.
Focus is given to both caring for patients today and how care can be best provided in the future. These are distinct challenges which require different leadership approaches.
The Trust is beginning to introduce a new management operating model, which will strengthen the leadership teams at each of its hospitals, helping improve the operational delivery and responsiveness to day-to-day issues. This model is in addition to the Managing Director posts that were immediately established following the CQC findings. Introducing these leadership teams will mean that there will be clear accountabilities for service delivery and for transformation at service, hospital and at corporate levels. It will mean that staff and stakeholders will know who to go to get things done at each hospital and staff will be clearer about what is expected of them, with a clear line of sight from their ward or department to the hospital leadership team. There will also be more rapid decision making to resolve quality, safety and performance issues in a timely way.
10
At the same time, the new model will retain all the strategic advantages of the Clinical Academic Groups (CAGs), enabling the CAGs to concentrate on clinical strategy and transformation and the development of clinical and professional standards across our sites.
3.8 Sam Everington Appointed Vice President of the BMA and receives fellowship from Queen Mary University of London Sir Sam Everington, Chair of Tower Hamlets CCG, has been appointed Vice President of the British Medical Association (BMA). His appointment is in acknowledgement of all the hard and innovative work Sam does to improve health care services. With over 153,000 members, Sam’s work with the BMA will enable him to continue to champion best practice and drive improvements in primary care services. Sam has also been awarded a Fellowship from Queen Mary University of London. Sam was awarded this honour because of the significant service he has given to the local community. This recognition is a great honour for Sam, for the NHS, and for the wider community of Tower Hamlets.
3.9 Freedom of Information Act Requests
In June and July 2015, a total of 39 FOI requests were closed for the CCG, of which 100 % were answered within the statutory 20 working days.
The majority of requests were from the media, individuals and private companies.
The nature of the requests have been very varied, for example IVF, mental health spending, CCG procurements and prescribing schemes.
End
11

12

Minutes of the NHS Tower Hamlets Clinical Commissioning Group Governing Body Meeting (Part 1)
Tuesday, 07 July 2015, 14.30 – 17.15
Room 205, Professional Development Centre,
229 Bethnal Green Road E2 6AB
1 General Business
1.1 Welcome, introductions and apologies
1.1.1 Present
Name Role Organisation Jane Milligan Chief Officer NHS THCCG John Wardell Deputy Chief Officer NHS THCCG Dr Sam Everington Chair – LAP 6 representative – Bromley By Bow Practice NHS THCCG Mr Tan Vandal Secondary Care Specialist Doctor NHS THCCG Henry Black Chief Finance Officer NHS THCCG Dr Judith Littlejohns LAP 1 representative – The Mission Practice NHS THCCG Dr Martha Leigh LAP 4 representative – Wapping Practice NHS THCCG Dr Haroon Rashid LAP 2 representative – Albion Practice NHS THCCG Dr Osman Bhatti LAP 7 representative – Chrisp Street Practice NHS THCCG Dr Victoria Tzortziou-Brown
LAP 3 representative - Principal Clinical Lead – All Saints Practice NHS THCCG
Virginia Patania Practice Manager representative NHS THCCG Dr Isabel Hodkinson LAP 5 representative - Principal Clinical Lead - The
Tredegar Practice NHS THCCG
Maggie Buckell Registered Nurse NHS THCCG Abigail Knight Acting Associate Director of Public Health LBTH
1.1.2 In attendance
Name Role Organisation Archna Mathur Director of Quality and Performance NHS THCCG Justin Phillips Governance and Risk Manager NHS THCCG Ellie Hobart Deputy Director of OD and Engagement NHS THCCG Charlotte Fry Commissioning Support Director NEL CSU Lee Eborall Director of Acute Contract Management NEL CSU
1.1.3 Apologies
Name Role Organisation Cate Boyle Vice Chair - Lay Member (Patient and Public
Engagement) NHS THCCG
Mariette Davis Lay Member (Governance) NHS THCCG Dr Shah Ali LAP 8 representative – Barkantine Practice NHS THCCG Dr Somen Banerjee Interim Director of Public Health LBTH
Enclosure B
13
Robert McCulloch-Graham
Corporate Director LBTH
1.1.5 Welcome
Dr Sam Everington welcomed members and attendees to the Governing Body meeting part I. Apologies were received for: Cate Boyle, Mariette Davis, Dr Shah Ali, Dr Somen Banerjee and Robert McCulloch-Graham.
1.2 Declaration of Interests
Dr Sam Everington asked Members for any declarations of interest. No declarations of interest were noted for Part I of the meeting.
The complete register of interests is published on the NHS Tower Hamlets Clinical Commissioning Group’s website: http://www.towerhamletsccg.nhs.uk/about/conflict-of-interest-register.htm or is available from the Governance and Risk Manager: [email protected]
1.3 Questions from the Public
Questions from the public were received prior to the Governing Body meeting and were addressed at the meeting by Dr Sam Everington, John Wardell and Henry Black:
1. Given the large losses our surgeries expect over the next seven years, how does the CCG plan to secure the long-term future of all our GP practices and the services they provide?
“We have done a lot of work already develop a longer term plan that addressed the sustainability of primary care and we will be working with primary care and patients to further refine and co-create a strategy that we can roll out over the next two to five years. This long term strategy will need a completely new approach to delivering care with primary care taking on a bigger role in the future so we can build on the success we have had over the last four years. With the development of the various programmes in Tower Hamlets we have a fantastic opportunity for care to be provided at a greater scale. The long term future for primary care is an exciting one, with much transformational change required to ensure its sustainability, but we have an absolute commitment to deliver it.”
2. What contingency plans does the CCG have in place in case any of the large practices close – given that any closure would have a major impact on all the surrounding practices?
“At this stage we are not anticipating a large scale practice closure and we will be doing everything we can to stop this happening. However, in reality practices are ‘’small businesses” and as such they may make the decision to close or a partner may decide to move on for a whole variety of reasons’. In this unlikely event we would work with the practice and NHS England to manage any closure in an appropriate way and to ensure a safe transition. We are very lucky in Tower Hamlets having such a strong and resilient system, with primary care networks and a culture of support that crosses organisational boundaries.”
14

3. Given the very real possibility that some of the worst-hit practices (for example, the Limehouse Practice in Gill Street) face closure within months if nothing changes, what will the CCG do in the extremely short term to protect these practices?
“We are working very closely with NHS England and as a result of these discussions we are close to agreeing a series of measures to support those practices in most need. The financial support being offered will be under strict criteria which will not just look at the amount of money any practice is losing but the overall impact on that practice’s viability, which will vary between practices. It is important to understand this doesn’t necessarily mean that all practices who have lost the minimum practice income guarantee would qualify for support if they don’t meet the essential criteria. It is worth stating again that we are not expecting any closures and all our focus at the moment is on identifying a solution that can bridge the gap between now and the implementation of our primary care strategy.”
4. Given that the emergency funding for Jubilee Street and Albion Health (the latter still being finalised) is for only two or possibly three years, what will the CCG do to protect these practices when the funding runs out?
“The government is currently planning to introduce a new practice funding formula from April 2017 to replace the Carr-Hill formula which has been shown not to adequately compensate for deprivation. This is why the package we are currently discussing with NHS England covers the next 2 to 3 years. We are playing an active role in the way the new formula is developed and in the meantime, the other piece of work we are doing locally to cover the medium term will help practices get the most out of their existing resources and optimise their efficiency.
Tower Hamlets Clinical Commissioning Group is wholeheartedly committed to supporting general practice and ensuring a sustainable future for primary care in Tower Hamlets. As a clinical commissioning group we are acutely aware that the future of effective and sustainable health services, which can meet the challenges of the 21st century, is dependent upon having dynamic and vibrant primary care provision. That is why primary care is a key focus of our strategic planning for the next 5 years and why we will do our utmost to support the practices that are delivering high quality services to Tower Hamlets residents.”
1.4 Chair’s report
Dr Sam Everington presented the Chair’s report. The following highlights were reported:
- Care Quality Commission Inspection Reports for Barts Health NHS Trust
- Prime Minister’s Challenge Fund
- Tower Hamlets Integrated Provider Partnership (THIPP)
Members noted the Chair’s report.
1.5 Chief Officer’s report
Jane Milligan presented the item. The following highlights were reported:
15
- One Year Cancer Survival Rate
- Annual General Meeting
Members noted the Chief Officers report.
1.6 Minutes and matters arising of the meeting held May 5th 2015
1.6.1 Minutes
The minutes for the Governing Body May 5th 2015 part I were approved as an accurate record of the meeting.
1.6.2 Matters arising
The matters arising were reviewed with outstanding actions carried forward.
1.7 Patient Story
Abul Miah, a local patient with Duchenne Muscular Dystrophy told his story on the experience of Barts Health Trust services as a patient receiving last years of life care. He is a triplet who sadly lost his siblings in 2009 to the same condition. He has since made an informed choice to seek healthcare from an alternative provider, otherwise managing his care in his own home with carers and family support. Abul speaks of the importance of joined-up, holistic care and ‘being treated like a person’ who is fully informed throughout the journey of healthcare.
In the same video, Abu Mumin shares his experience of losing his mother who also received end of life care. Spiritual/cultural sensitivity and strong engagement with staff through to the community are key messages to providers and commissioners to improve the experience of both patients and carers affected by Last Years of Life care. Abu has since initiated Eden Care, a local charity supporting people through the last years of their or their loved ones lives.
2 Performance and Operations
2.1 Performance and Quality report
Archna Mathur presented the Performance and Quality Report and highlighted that the coversheet provided a comprehensive review. The key areas to note were:
Archna highlighted that the CCG is in the process of issuing a contract performance notice (CPN) as a contractual lever relating to the Trust’s ongoing position on the Cancer, RTT and A&E standards and that also the CCG are awaiting the Trust’s responses on their remedial action plans (RAPs).
The Trust achieved the Cancer 2 week wait (2ww) standard for March with performance of 95.9%. As compared to February, where the 2ww was achieved for the first time since April 2014, performance RLH site dipped in March to 92.9%. The dip in 2ww performance at the RLH site is again due to speciality level underperformance, colorectal, head and neck, lung and urology. 62 Day performance was 81.9% for March an improvement from 75.6% in February against an 85% target which is in line with trajectory. 31 day from decision to 1st
16
Treatment was achieved for March at 97.66%. All other 31 standards were met at Trust level.
A&E: Barts Health has failed to achieve on the all types 95% standard for Q1 at 89.30%. Year to date performance into 201516 is also fragile with overall performance at 85.57% and RLH performance 82.96% for all types.
Referral to Treatment (RTT): Barts Health continues to underperform against the national waiting time standards at speciality level. The Trust are currently not reporting on RTT although monitoring via the CCGs/TDA continues.
The following points were raised in discussion:
Mr Tan Vandal expressed that he had continued anxiety relating to the cancer and non-cancer targets and that they were not really moving in any positive position. He queried if this was as a result of lack of understanding, ability or capacity. Archna Mathur stated that the CQC had also picked up the issue of the inability to meet national standards and Jane Milligan expressed that she thought the issues were due to capability and capacity.
Jane Milligan queried that given the new site level governance structures if the CCG needed to reconsider how we interface with the Trust ie does there need to be a change in CQRM membership. Archna Mathur explained that the CQRM’s ToR are inclusive and that going forward, consideration of attendance has been applied to ensure the right level of clinical engagement as per the CQRM forward planner.
Members noted the item.
2.2 Royal London Hospital – CQC Update
Dr Simon Harrod, a consultant anaesthetist, introduced himself as the newly appointed Chief Medical Officer of the Royal London Hospital (RLH), Barts Health. He opened up the meeting to questions relating to the RLH CQC action plan and improvement plan.
Mr Tan Vandal asked how the RLH intends to develop engagement between management and clinicians and additionally with primary care practitioners to ensure the CQC action plan is realised and to drive the overall delivery of good quality care. Dr Simon Harrod stated that historically there had been a suspicion of a lack of communication and transparency between clinicians and managers but that going forward that this would not be the case now that the right people had been recruited to the right posts. He highlighted the good work that is being achieved as part of the Stepping into the Future programme and that staff across a range of disciplines were getting together to drive this forward. It was also noted that the new interim Chief Executive did not want management consultants to design the programme of improvement but would use the expertise from the ‘shop floor’ such as nursing staff.
Maggie Buckell requested further clarification on the safer staffing level work and the Trust’s recruitment strategy including the work plan to address the issues of staff low morale. Dr Simon Harrod explained that staff morale varies considerably between the different services and sites and he highlighted work was being developed to address this; affordability of living on central London; new ways of working to be child and family friendly; ways of reducing agency staff spend; ways of increasing permanent staff numbers on education programmes and that work needed to be done to address the shortfall of junior doctor recruitment.
17

Dr Isabel Hodkinson stated that she is concerned with the underpinning informatics as a key enabler to the improvement plan. Dr Simon Harrod agreed that IT systems were outdated and not fit for purpose and that the interim Chief Executive was looking into the possibility of separate funding to update the IT infrastructure to address the ongoing problems.
Dr Victoria Tzortziou-Brown explained that there is a tendency for organisation in crisis to be very introspective and there is a need for a system wide approach such as that employed by the Integrated Care Programme where a portfolio of providers work collaboratively to come up with solutions. Dr Simon Harrod stated that the Barts Health are very committed to work with all the relevant agencies to drive improvement and that additionally more patients were needed to be part of this process.
Dr Martha Leigh asked how Barts Health will ensure a bottom up patient-centred approach to improvement delivery. Dr Simon Harrod stated that the Trust is committed to a programme of solution engagement encouraging clinicians, non-medical staff and patients to attend. Simon explained that historically some problems could be attributed to the on-going changes in team structures and that the recent site specific operational management should now hopefully free up capacity within the Clinical Academic Groups.
Jane Milligan queried how the Trust will be providing the CCG with the necessary assurance relating to the RLH CQC action and improvement plan and where the CQRMs fit into this process. Dr Simon Harrod stated that the CQC action plans and improvement plans were nearing being signed off and will be shared. It is important that CQRMs going forward will address CQC themes but build on these to be better.
CQC Action Plan and RLH Improvement Plan to be circulated to the Governing Body.
Jane Milligan, Sam Everington and Abigail Knight left the meeting to attend a Local Authority meeting. John Wardell chaired the remainder of the meeting. The meeting was still quorate.
2.3 Finance and Activity
2.3.1 Finance report month 2
Henry Black presented the month 2 Finance Report. The key areas to note:
As at the end of May (Month 2), the CCG is on plan to deliver its targeted surplus of £11.7m, however, at this early stage in the year the Month 2 Finance report is subject to a number of caveats regarding availability and accuracy of data and therefore should be read and interpreted in this context.
The CCG have been required to submit our operating plan to deliver a surplus of £11.7m, which is higher than the minimum 1% business rules. This is a result of a request from NHSE to increase our surplus by an additional £2.3m, however we still have sufficient resource to meet all of our recurrent and non-recurrent identified expenditure plans and this does not represent a risk to delivery of any of our statutory duties.
In 15/16 Tower Hamlets CCG has been able to secure £4.5m of the previous year’s surplus for use in 2015/16.
18
2.3.2 Activity report month 2
Lee Eborall presented the month 2 activity report. The following highlights were reported:
The CCG is forecasting a Year End Surplus of £11.7m which is in line with its financial plan for 2015/2016. The main components being: Barts £0.3 million overspend, non-acute has reported a £0.5 million overspend, corporate has reported a £0.2 million overspend and minor overspends and underspends across the SLA Portfolio.
The following points were raised in discussion:
Dr Isabel Hodkinson queried as per the figures outlined in the primary care co-commissioning budget report, if money was lost from practices and not from the local health economy. Henry Black explained that work was underway to better understand the primary care co-commissioning budget data provided by NHS England and he will update at a future Governing Body meeting.
Members noted the item.
2.4 Board Assurance Framework
Archna Mathur presented the Board Assurance Framework 2015/16 version 1 to the Governing Body explaining that the framework had been updated to reflect changes in programmes of work in the CCG. It was requested that Governing Body members familiarise themselves with those risks that link with their work streams and that where they sit on committees, that they ensure that appropriate controls are developed for the high level organisational risks.
Virginia Patania and Dr Isabel Hodkinson thought that the Board Assurance Framework should detail the high level informatics and urgent care risks. Archna Mathur requested that the risks are forwarded to Justin Phillips for discussion at a future SMT meeting.
Members noted the item.
Break
3 Commissioning and Strategy
3.1 Medicines Management Annual Report 2014/15
Moira Coughlan presented Medicines Management Annual Report 2014/15 to the Governing Body. The key areas to note were:
The Primary care prescribing spend for 14/15 is £29,028,613 against an allocated budget of £29,018,743 (an overspend of £9,870). This has been achieved against an increase in the total number of patients of 4.1% and an increase in the number of prescription items by 4.8%. The drugs element of the prescribing drugs budget is forecast to have grown by 3.8% in the last 12 months. There were significant increases in Category M prices in Q3 and 4.
Delivery of Commissioning Strategic plans: The team has been able to over-deliver on both scriptswitch savings and reducing the prescribing of ‘specials’ medicines, and have managed to reduce growth in two elements of oral nutritional prescribing.
19

Innovations: In a joint initiative between Barts Health NHS Trust and Tower Hamlets Medicines management team, asthma reviews were undertaken by specialist pharmacists in GP practices, to improve management of asthma in accordance to national guidelines and standards of care. Other innovation include developing a new electronic Tower Hamlets formulary which is a one stop electronic tool that incorporates both up-to-date National information and localised formulary decisions to support our clinicians.
Engagement: The TH MMT has had excellent engagement with clinical and non- clinical practice staff at education events and at practice and network levels. The team received positive feedback from these events. Patient engagement has always been considered vital in understanding the needs and improving outcomes for patients. The TH MMT has also started work on engaging with patients on areas such as asthma and will continue to develop this and extend into areas such as waste and nutrition.
Acute work. The TH MMT raised a significant number of High Cost Drugs challenges. £507,950 of these challenges were accepted for 2014/15. The team also reviewed Individual Funding Requests and Tickbox forms applications.
Restructure of the Medicines Committee The creation of Barts Health by merging 3 hospital sites in East London created the need for a review of how medicines decisions are made across the 3 local CCGs. Towards the end of 2014/15 TH, Newham and Waltham Forest agreed to work together to develop a WEL Medicines Committee. The focus of this group is to review the impact of medicines in primary care.
The following points were raised in discussion:
Dr Osman Bhatti queried if there was a good uptake of EPS across the membership as there are still many ongoing issues. Dr Isabel Hodkinson stated that practices should resist request from pharmacists for paper prescriptions and refer them to the CSU IT team.
Virginia Patania highlighted the recent article in Pulse regarding the £15 million fund for practices to pilot practice pharmacists and thought this would be a good area for Tower Hamlets to explore given the current difficulty with GP recruitment. Moira Coulghlan stated that she would be happy to support any applications for funding. John Wardell stated that this complemented the Integrated Care work, integrating pharmacists into the wider team.
Members noted the item.
3.2 Transformation and Innovation Committee Update
Maggie Buckell presented the Transformation and Innovation Committee Update. The key areas to note:
Digital Mental Health
The Digital Mental Wellbeing Pilot Project aims to set up an online platform to provide 24 hour mental health peer support in London. THCCG has agreed in principle to act as the lead commissioner for the service with 33 London CCG’s and 32 Local Authorities committing to funding £33k.
Darzi Fellow Business Case
The business case outlines the rationale for requesting £35k funding for the appointment of a Darzi Fellow in 2015/16. The key essence of the Darzi Fellow role includes:
20

- lead on engagement of professions and bridge communication between service users and providers in integrated care, in particular Integrated Personalised Commissioning (IPC)
- lead on the culture change required to deliver CCG’s agenda on personalisation as part of IPC. The learning from the can be broadened to wider IC work.
Finance fed back that there are sufficient funds to pay the £35K in 15/16. An agreement in principle was presented on the basis that the CCG could have input in the recruiting process. The Deanery has since confirmed that the CCG will be able to lead interviews and select the suitable candidate.
Barts Biosensor Project
Barts Health requests £470k (10% of total investment) from the CCG to support the trial of a new innovative technology that has the potential to transform productivity and patient pathways. Barts reported that analysis indicates a minimum potential net cost savings to Barts Health of £6million on a full year basis once rolled out if successful. However, the committee agreed that although the technology is impressive, there are concerns that it will not deliver the outcomes as indicated. It was suggested that Barts target trials in 3 to 4 specific areas and provide clinical re-assurance that patients would be discharged earlier with the device. The following points were raised in discussion: Virginia Patania queried why the social prescribing proposal was not approved by TIC. It was explained that the proposal was deemed to be too expensive but the CCG was committed to go back and look at how this could work in the future.
Josh Potter to circulate social prescribing brief to the Governing Body members.
Members noted the item.
4 For information
4.1 Audit Committee Summary
No further comments were raised. Members noted the item.
4.2 Finance, Performance and Quality Committee Summary
No further comments were raised. Members noted the item.
4.3 Equality and Diversity Committee Summary
No further comments were raised. Members noted the item
4.4 Executive Committee Summary
No further comments were raised. Members noted the item.
5 Questions from the public
No further questions were raised.
21

6 Any other business
No additional items were raised by members.
End
22

Matters arising
Action reference Action Lead Due
Date Update
July#1
CQC Action Plan and RLH Improvement Plan to be circulated to the Governing Body. JP Aug 2015
RLH CQC action plan and improvement plan on Governing Body agenda for September.
July#2
Josh Potter to circulate social prescribing TIC brief to the Governing Body members.
JoP Aug 2015
A business case went to the Integrated Care Board to introduce a borough wide social prescriber, and was approved. This will now go to the TIC in September for approval.
Jan#2
Scorecard to be discussed at future SMT with view to update metrics.
JP TBC
Discussed at SMT 2/2/15 – to be discussed after the NHSE CCG assurance scorecard is developed.
23

24

Governing Body Meeting Enclosure
Date of meeting September 1st 2015 C
Agenda item 2.1
Title of report: Board Assurance Framework
Author(s): Justin Phillips – Governance and Risk Manager – NHS Tower Hamlets CCG
Presented by: Sponsor (if different): For further information
Jane Milligan – Chief Officer - NHS Tower Hamlets CCG
Executive summary
The Board Assurance Framework lists the risks that could prevent the achievement of the CCG’s 5 corporate objectives.
This is the second iteration of the BAF 2015/16. No risk ratings were adjusted in this iteration. The following risks were updated:
- Risk 1.1: Failure to ensure effective systems and processes are in place to monitor, challenge and support Barts Health NHS Trust delivery of NHS Constitution targets and CQC action plan could result in the increased likelihood of poor quality, poor patient experience, delivery of poor clinical outcomes and the trust remaining in special measures in the longer term.
Changes to the governance architecture both internally in Barts Health and externally with partners ie TDA and NHSE ensures robust oversight and assurance of compliance with CQC action plans and site improvement plans. Controls have been updated as a result of the changes:
-Joint monthly site specific CQRMs / TDA oversight and assurance – process feeding into monthly trust level oversight and assurance led by TDA.
-Monthly extended contract review group (CRG) ensures greater contractual leverage whilst maintaining detailed performance management of RTT and cancer.
- Risk 1.2: Ineffective Governing Body succession planning could result in lack of senior clinical leadership experience which would impact on the ability to commission high quality health and social care services
Governing Body succession planning has been incorporated into the organisation plan of the developing strategic commissioning priorities programme.
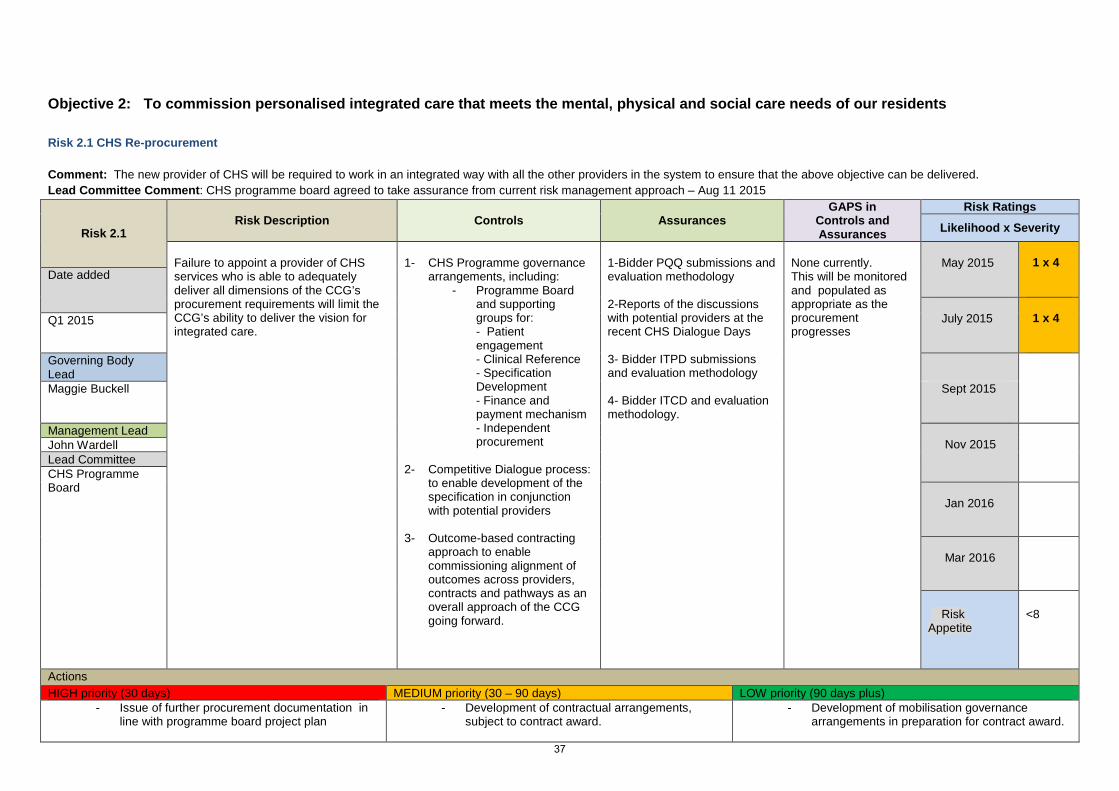
- Risk 2.1: Failure to appoint a provider of CHS services who is able to adequately deliver all dimensions of the CCG’s procurement requirements will limit the CCG’s ability to deliver the vision for
25
integrated care.
Additional assurance: Bidder ITCD and evaluation methodology.
- Risk 3.2: Poor quality Barts Health activity data could result in the CCG being incorrectly invoiced which could impact on the running costs in the longer term.
Month 2-4 data much improved but still occurrences of misattributions. Work in place with Trust to address issues including ongoing challenges by the Acute Contracting Team.
- Risk 3.6: Failure to deliver on the Operating Plan, including QIPP would result in: a negative financial impact on the CCG, lost opportunity to produce and deliver increased outcomes for the sickest people in Tower Hamlets and a negative impact on the reputation of the CCG.
Data from Prescribing Monthly Profiles which are used to calculate estimated forecast out-turns for 2015/16 prescriptions has estimated a prescribing forecast overspend of c£800k.
Action added: Prescribing Forecast overspend of c£800k to be investigated by CSU prescribing team to ascertain whether this is recoverable.
Recommendation
Information Approval To note Decision
The Board Assurance Framework is presented to the Governing Body to note the risks and make any comments on the risks within it.
Conflicts of Interest There are no declared interests affecting this report.
Key issues • The BAF is presented to Governing Body Members to provide oversight of risks to the achievement of the CCG objectives.
• This assists Governing Body Members to identify and prioritise risks, to evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively and economically.
• It is important that the Governing Body continue to make effective use of the BAF in 2015/16.
Report history This version of the BAF will be discussed at the Audit Committee on September 15 2015.
Patient and Public involvement
The BAF is a public document and provides assurance to all external stakeholders.
Link to the Board Assurance Framework
The BAF is an essential document in providing evidence of THCCG's system of internal control. It aims to provide the Chief Officer with sufficient assurance to be able to sign off the annual governance
26

statement of the CCG at the end of the financial year.
Impact on Equality and Diversity
The CCG has selected E&D as a Corporate Objective:
To promote equality both as an employer and a commissioner of health care services
Resource requirements There are no additional resources required.
Next steps The next round of risk reviews will commence during September – October 2015.
The Audit Committee will receive and review the BAF at each of its meetings. It will choose significant risks, on a rotational basis and subject them to “deep dive” reviews of risks, controls and assurances to ensure that the controls and assurances as recorded on the BAF are operating in practice.
In this way the Audit Committee will look to provide assurance to the Governing Body that the BAF is valid and suitable for the Governing Body’s requirements.
27

28

Board Assurance Framework
2015/16
Document information
Version Version 2 Dates covered July – Aug 2015 Next review Sept – Oct 2015 Author(s) Justin Phillips – Governance and Risk Manager
29
Corporate Objectives 2015/16
Our corporate objectives relate to the CCG in its entirety, providing the organisation with a clear direction for commissioning intentions and supporting the development of more detailed programme, team and personal objectives. The corporate objectives reflect our direction of travel as well as our obligation to fulfil our statutory duties. The objectives will be used to develop our approach to risk management, inform programme priorities and provide a framework for performance management.
1. To commission high quality health and social care services that are accessible, provide good treatment and achieve good patient outcomes
2. To commission personalised integrated care that meets the mental, physical and social care needs of our residents
3. To contribute towards a financially sustainable and responsive health and care economy, delivering value for money and innovation
4. To support local people and stakeholders to have a greater influence on services we commission and develop a responsive and learning commissioning organisation
5. To promote equality both as an employer and a commissioner of health care services
30
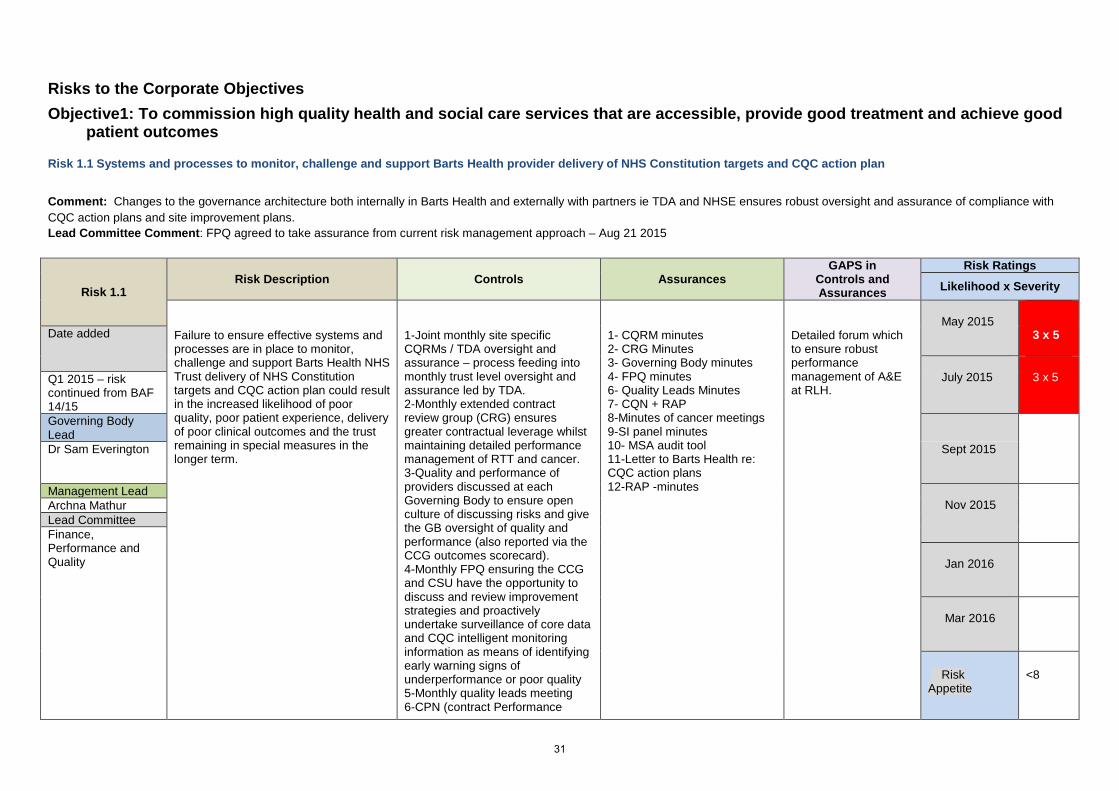
Risks to the Corporate Objectives Objective1: To commission high quality health and social care services that are accessible, provide good treatment and achieve good
patient outcomes
Risk 1.1 Systems and processes to monitor, challenge and support Barts Health provider delivery of NHS Constitution targets and CQC action plan
Comment: Changes to the governance architecture both internally in Barts Health and externally with partners ie TDA and NHSE ensures robust oversight and assurance of compliance with CQC action plans and site improvement plans. Lead Committee Comment: FPQ agreed to take assurance from current risk management approach – Aug 21 2015
Risk 1.1 Risk Description Controls
Assurances
GAPS in Controls and Assurances
Risk Ratings
Likelihood x Severity
Failure to ensure effective systems and processes are in place to monitor, challenge and support Barts Health NHS Trust delivery of NHS Constitution targets and CQC action plan could result in the increased likelihood of poor quality, poor patient experience, delivery of poor clinical outcomes and the trust remaining in special measures in the longer term.
1-Joint monthly site specific CQRMs / TDA oversight and assurance – process feeding into monthly trust level oversight and assurance led by TDA. 2-Monthly extended contract review group (CRG) ensures greater contractual leverage whilst maintaining detailed performance management of RTT and cancer. 3-Quality and performance of providers discussed at each Governing Body to ensure open culture of discussing risks and give the GB oversight of quality and performance (also reported via the CCG outcomes scorecard). 4-Monthly FPQ ensuring the CCG and CSU have the opportunity to discuss and review improvement strategies and proactively undertake surveillance of core data and CQC intelligent monitoring information as means of identifying early warning signs of underperformance or poor quality 5-Monthly quality leads meeting 6-CPN (contract Performance
1- CQRM minutes 2- CRG Minutes 3- Governing Body minutes 4- FPQ minutes 6- Quality Leads Minutes 7- CQN + RAP 8-Minutes of cancer meetings 9-SI panel minutes 10- MSA audit tool 11-Letter to Barts Health re: CQC action plans 12-RAP -minutes
Detailed forum which to ensure robust performance management of A&E at RLH.
May 2015
3 x 5
Date added
July 2015
3 x 5
Q1 2015 – risk continued from BAF 14/15 Governing Body Lead
Dr Sam Everington Sept 2015
Management Lead Nov 2015
Archna Mathur Lead Committee Finance, Performance and Quality
Jan 2016
Mar 2016
Risk Appetite
<8
31

Notice) –issued A&E, RTT, Cancer and Diagnostics performance 7- Bi-weekly deep dives into each challenged cancer tumour groups to understand root causes of failure, and trajectories for improvement. 8-Dedicated review across WELCCGs of the Barts Health, CSU, CCG serious incidents (SI) process to expedite closure of overdue cases. 9- Mixed Sex Accommodation (MSA) Audit 11-Attendance to the Quality Surveillance Group to share and gain intelligence on Barts Health with Healthwatch and fellow commissioners. 12- Remedial Action Plans (RAPs)
Actions HIGH priority (30 days) MEDIUM priority (30 – 90 days) LOW priority (90 days plus)
- RLH and MEH CQRM and oversight and assurance - Implementation of new governance architecture and processes
32

Risk 1.2: Governing Body Succession planning Comment: Governing Body succession planning has been incorporated into the organisation plan of the developing strategic commissioning priorities programme. The Governing Body practice representatives are elected from the membership with term of office – 2- 4 years (with eligibility to stand for 6 years). Lead Committee Comment: TBC
Risk 1.2 Risk Description Controls
Assurances
GAPS in Controls and Assurances
Risk Ratings
Likelihood x Severity
Ineffective Governing Body succession planning could result in lack of senior clinical leadership experience which would impact on the ability to commission high quality health and social care services
1- Staggered election process (half the Governing Body elected every 2 years) 2- Continuous Organisational Development programme 3- Governing Body induction process which includes coaching and peer support 4-Organisational strategy developed for staff, GB members, clinical leads which is inclusive of training needs analysis, induction, mandatory training and ‘Lunch and learn’ sessions. 5-CCG Constitution in place creating a structure for delivery of statutory functions. 6-Policy structure ensures policies clear identify any training, E&D and PPE requirements are. 7-ET and SMT oversight of OD delivery. 8- Management lead for OD identified within organisational structure.
1-CCG Constitution – Election process 2- OD strategy 3-OD agendas / papers / plan 4- Governing Body Induction Schedule 5-Staff PDPs. 6-Appraisals and objective setting 7-CCG Constitution and governance structure 8-ET and SMT action log and minutes 9-Agendas, papers and notes
Clinical leadership and succession plan
May 2015
2 x 4
Date added
July 2015
2 x 4
Q1 2015
Governing Body Lead
Jane Milligan Sept 2015
Management Lead Nov 2015
Ellie Hobart Lead Committee Executive Committee
Jan 2016
Mar 2016
Risk Appetite
<8
Actions HIGH priority (30 days) MEDIUM priority (30 – 90 days) LOW priority (90 days plus)
33

Clinical leadership and succession plan
Risk 1.3: Primary Care Commissioning Comment: In Tower Hamlets we submitted proposals related to delegated commissioning as we felt that this would provide us with the greater opportunity to shape the way in which primary care develops. Delegated commissioning offers an opportunity for CCGs to assume full responsibility for commissioning general practice services. Our intention is to act collaboratively across Waltham Forest, Tower Hamlets and Newham (WEL) and work towards the aims set out in the Strategic Commissioning Framework for Primary Care Transformation in London. Lead Committee Comment: TBC
Risk 1.3 Risk Description Controls
Assurances
GAPS in Controls and Assurances
Risk Ratings
Likelihood x Severity
Inadequate staff resources from NHS England to cover the requirements supporting delegated authority could impact on the ability to deliver the Primary Care strategy and appropriately manage the delegated responsibilities given to the CCG from NHSE.
1- NHSE Core contracting staff to remain as a central team for year one. Review of tasks vs roles in year one in preparation for greater devolution of staffing in year 2. 2- Tower Hamlets Primary Care Team 3- WEL Co-Commissioning Group
Local approach to staffing by setting up a new Primary Care Team in the CCG with an emphasis on supporting WEL wide staffing for economies of scale. 1 – Primary Care organogram 2- Memorandum of Understanding
Local Work Plan Local Primary Care Strategy TST Primary Care Work Plan
May 2015
2 x 4
Date added
July 2015
2 x 4
Q1 2015
Governing Body Lead
Maggie Buckell
Sept 2015
Management Lead Nov 2015
John Wardell Lead Committee Primary Care Committee
Jan 2016
Mar 2016
Risk Appetite
<8
Actions HIGH priority (30 days) MEDIUM priority (30 – 90 days) LOW priority (90 days plus)
- Mobilisation of Co-commissioning work plan including contract reviews
- Co-creation and mobilisation of Primary Care
- Development and mobilisation of Co-Commissioning work plan and Primary Care Strategy Implementation in year 2.
34
Strategy
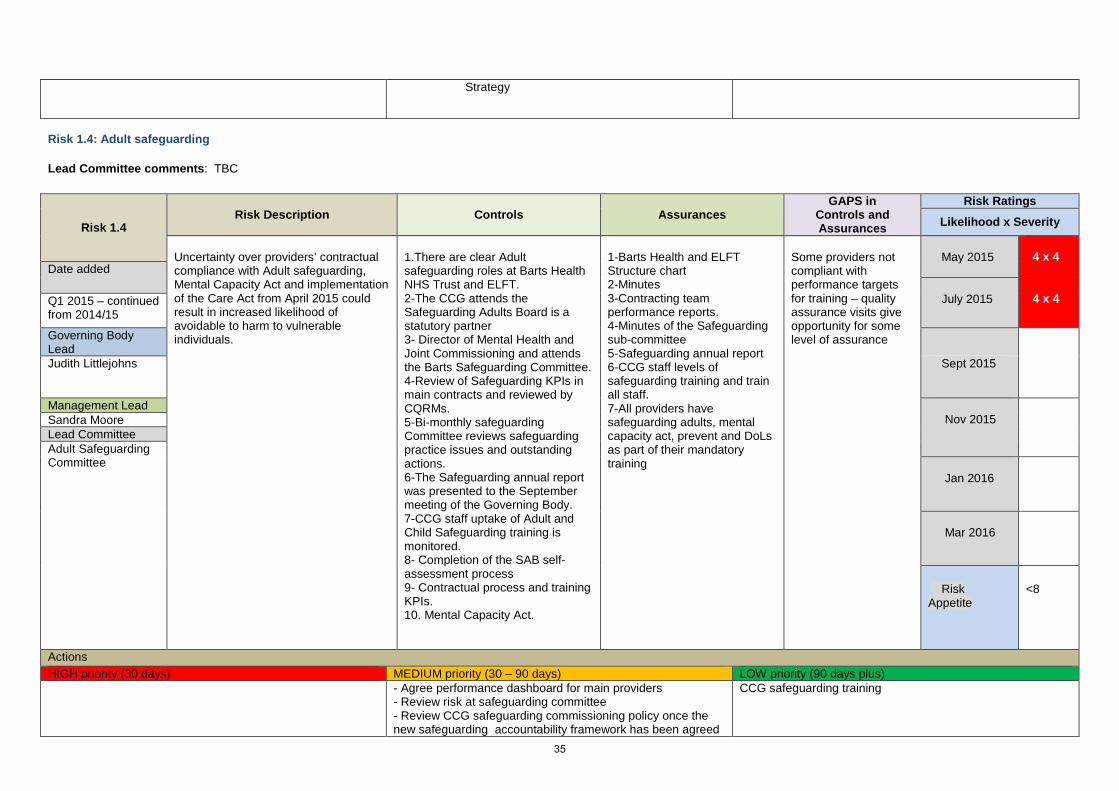
Risk 1.4: Adult safeguarding Lead Committee comments: TBC
Risk 1.4 Risk Description Controls
Assurances
GAPS in Controls and Assurances
Risk Ratings
Likelihood x Severity
Uncertainty over providers’ contractual compliance with Adult safeguarding, Mental Capacity Act and implementation of the Care Act from April 2015 could result in increased likelihood of avoidable to harm to vulnerable individuals.
1.There are clear Adult safeguarding roles at Barts Health NHS Trust and ELFT. 2-The CCG attends the Safeguarding Adults Board is a statutory partner 3- Director of Mental Health and Joint Commissioning and attends the Barts Safeguarding Committee. 4-Review of Safeguarding KPIs in main contracts and reviewed by CQRMs. 5-Bi-monthly safeguarding Committee reviews safeguarding practice issues and outstanding actions. 6-The Safeguarding annual report was presented to the September meeting of the Governing Body. 7-CCG staff uptake of Adult and Child Safeguarding training is monitored. 8- Completion of the SAB self-assessment process 9- Contractual process and training KPIs. 10. Mental Capacity Act.
1-Barts Health and ELFT Structure chart 2-Minutes 3-Contracting team performance reports. 4-Minutes of the Safeguarding sub-committee 5-Safeguarding annual report 6-CCG staff levels of safeguarding training and train all staff. 7-All providers have safeguarding adults, mental capacity act, prevent and DoLs as part of their mandatory training
Some providers not compliant with performance targets for training – quality assurance visits give opportunity for some level of assurance
May 2015
4 x 4 Date added
July 2015
4 x 4 Q1 2015 – continued
from 2014/15
Governing Body Lead
Judith Littlejohns Sept 2015
Management Lead Nov 2015
Sandra Moore Lead Committee Adult Safeguarding Committee
Jan 2016
Mar 2016
Risk Appetite
<8
Actions HIGH priority (30 days) MEDIUM priority (30 – 90 days) LOW priority (90 days plus) - Agree performance dashboard for main providers
- Review risk at safeguarding committee - Review CCG safeguarding commissioning policy once the new safeguarding accountability framework has been agreed
CCG safeguarding training
35

- Assess CCG compliance with new accountability framework
36
Objective 2: To commission personalised integrated care that meets the mental, physical and social care needs of our residents
Risk 2.1 CHS Re-procurement Comment: The new provider of CHS will be required to work in an integrated way with all the other providers in the system to ensure that the above objective can be delivered. Lead Committee Comment: CHS programme board agreed to take assurance from current risk management approach – Aug 11 2015
Risk 2.1 Risk Description Controls
Assurances
GAPS in Controls and Assurances
Risk Ratings
Likelihood x Severity
Failure to appoint a provider of CHS services who is able to adequately deliver all dimensions of the CCG’s procurement requirements will limit the CCG’s ability to deliver the vision for integrated care.
1- CHS Programme governance
arrangements, including: - Programme Board
and supporting groups for: - Patient engagement - Clinical Reference - Specification Development - Finance and payment mechanism - Independent procurement
2- Competitive Dialogue process: to enable development of the specification in conjunction with potential providers
3- Outcome-based contracting
approach to enable commissioning alignment of outcomes across providers, contracts and pathways as an overall approach of the CCG going forward.
1-Bidder PQQ submissions and evaluation methodology 2-Reports of the discussions with potential providers at the recent CHS Dialogue Days 3- Bidder ITPD submissions and evaluation methodology 4- Bidder ITCD and evaluation methodology.
None currently. This will be monitored and populated as appropriate as the procurement progresses
May 2015
1 x 4
Date added
July 2015
1 x 4
Q1 2015
Governing Body Lead
Maggie Buckell Sept 2015
Management Lead Nov 2015
John Wardell Lead Committee CHS Programme Board
Jan 2016
Mar 2016
Risk Appetite
<8
Actions HIGH priority (30 days) MEDIUM priority (30 – 90 days) LOW priority (90 days plus)
- Issue of further procurement documentation in line with programme board project plan
- Development of contractual arrangements, subject to contract award.
- Development of mobilisation governance arrangements in preparation for contract award.
37
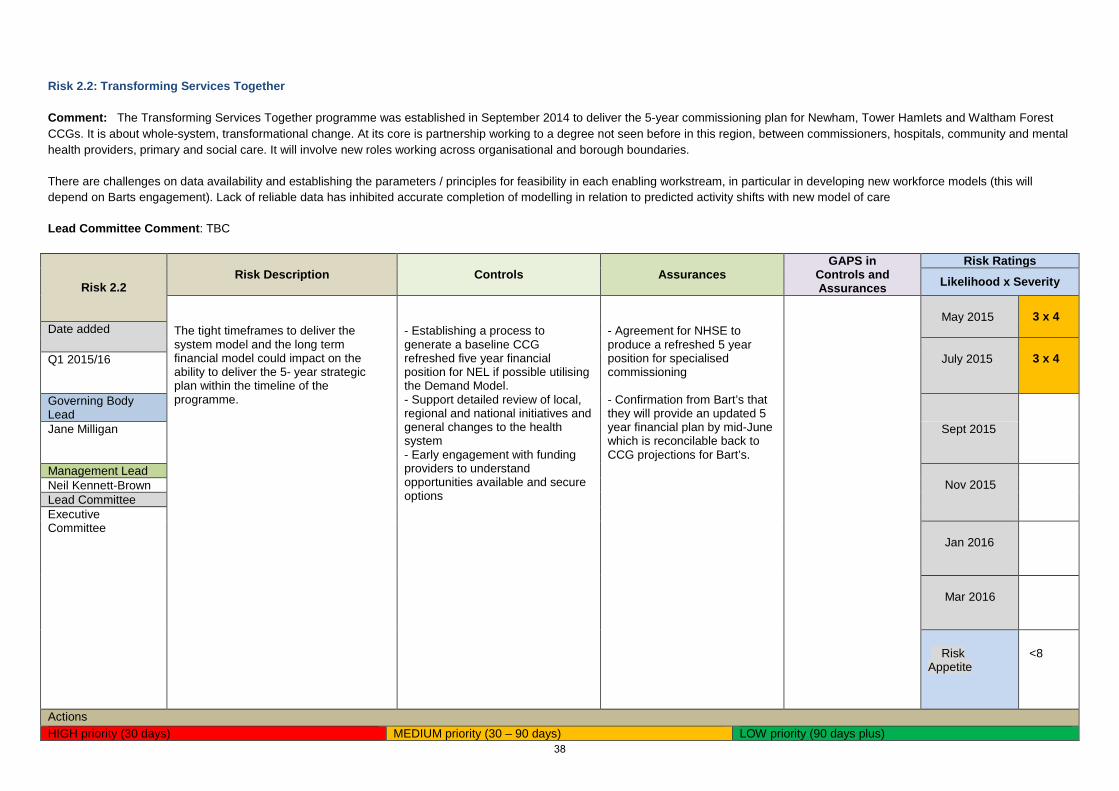
Risk 2.2: Transforming Services Together Comment: The Transforming Services Together programme was established in September 2014 to deliver the 5-year commissioning plan for Newham, Tower Hamlets and Waltham Forest CCGs. It is about whole-system, transformational change. At its core is partnership working to a degree not seen before in this region, between commissioners, hospitals, community and mental health providers, primary and social care. It will involve new roles working across organisational and borough boundaries. There are challenges on data availability and establishing the parameters / principles for feasibility in each enabling workstream, in particular in developing new workforce models (this will depend on Barts engagement). Lack of reliable data has inhibited accurate completion of modelling in relation to predicted activity shifts with new model of care Lead Committee Comment: TBC
Risk 2.2 Risk Description Controls
Assurances
GAPS in Controls and Assurances
Risk Ratings
Likelihood x Severity
The tight timeframes to deliver the system model and the long term financial model could impact on the ability to deliver the 5- year strategic plan within the timeline of the programme.
- Establishing a process to generate a baseline CCG refreshed five year financial position for NEL if possible utilising the Demand Model. - Support detailed review of local, regional and national initiatives and general changes to the health system - Early engagement with funding providers to understand opportunities available and secure options
- Agreement for NHSE to produce a refreshed 5 year position for specialised commissioning - Confirmation from Bart’s that they will provide an updated 5 year financial plan by mid-June which is reconcilable back to CCG projections for Bart’s.
May 2015
3 x 4
Date added July 2015
3 x 4
Q1 2015/16
Governing Body Lead
Jane Milligan Sept 2015
Management Lead Nov 2015
Neil Kennett-Brown Lead Committee Executive Committee
Jan 2016
Mar 2016
Risk Appetite
<8
Actions HIGH priority (30 days) MEDIUM priority (30 – 90 days) LOW priority (90 days plus)
38
Objective 3: To contribute towards a financially sustainable and responsive health and care economy, delivering value for money and innovation
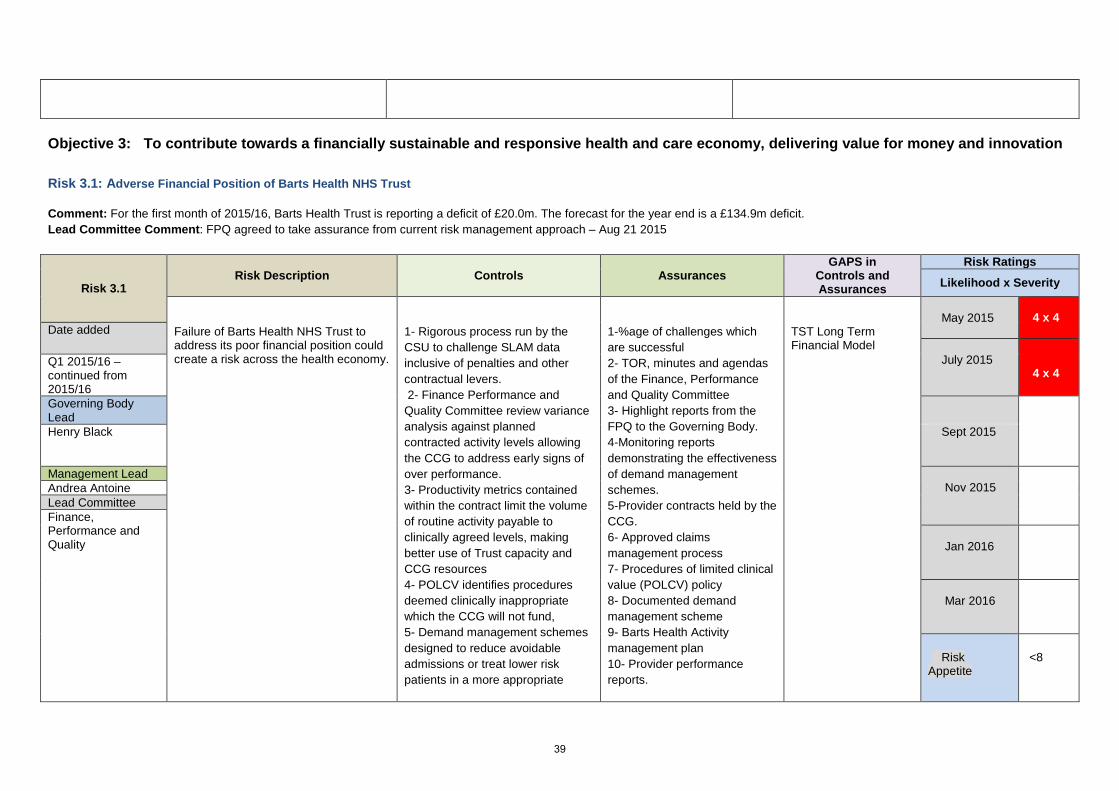
Risk 3.1: Adverse Financial Position of Barts Health NHS Trust Comment: For the first month of 2015/16, Barts Health Trust is reporting a deficit of £20.0m. The forecast for the year end is a £134.9m deficit. Lead Committee Comment: FPQ agreed to take assurance from current risk management approach – Aug 21 2015
Risk 3.1 Risk Description Controls
Assurances
GAPS in Controls and Assurances
Risk Ratings
Likelihood x Severity
Failure of Barts Health NHS Trust to address its poor financial position could create a risk across the health economy.
1- Rigorous process run by the CSU to challenge SLAM data inclusive of penalties and other contractual levers. 2- Finance Performance and Quality Committee review variance analysis against planned contracted activity levels allowing the CCG to address early signs of over performance. 3- Productivity metrics contained within the contract limit the volume of routine activity payable to clinically agreed levels, making better use of Trust capacity and CCG resources 4- POLCV identifies procedures deemed clinically inappropriate which the CCG will not fund, 5- Demand management schemes designed to reduce avoidable admissions or treat lower risk patients in a more appropriate
1-%age of challenges which are successful 2- TOR, minutes and agendas of the Finance, Performance and Quality Committee 3- Highlight reports from the FPQ to the Governing Body. 4-Monitoring reports demonstrating the effectiveness of demand management schemes. 5-Provider contracts held by the CCG. 6- Approved claims management process 7- Procedures of limited clinical value (POLCV) policy 8- Documented demand management scheme 9- Barts Health Activity management plan 10- Provider performance reports.
TST Long Term Financial Model
May 2015
4 x 4
Date added July 2015
4 x 4
Q1 2015/16 – continued from 2015/16 Governing Body Lead
Henry Black Sept 2015
Management Lead Nov 2015
Andrea Antoine Lead Committee Finance, Performance and Quality
Jan 2016
Mar 2016
Risk Appetite
<8
39

setting 6- Activity management plan within the provider contract requires Barts Health to explain and justify any unplanned increases in activity over agreed tolerance levels. 7- Transforming Services Together (TST) programme – Arrangement between WEL and Barts to bridge financial gap
11 -Audit report and TOR of scope of Barts Health internal review. (Remedial action reports from the Provider reviewed by the CCG 12- TOR and minutes of Commissioning NIS activity management plan 13- TST long-term financial management group minutes 14- TST - Governing Body Reports
Actions HIGH priority (30 days) MEDIUM priority (30 – 90 days) LOW priority (90 days plus) - TST work streams – further work to review financial models
for TST work streams.
40
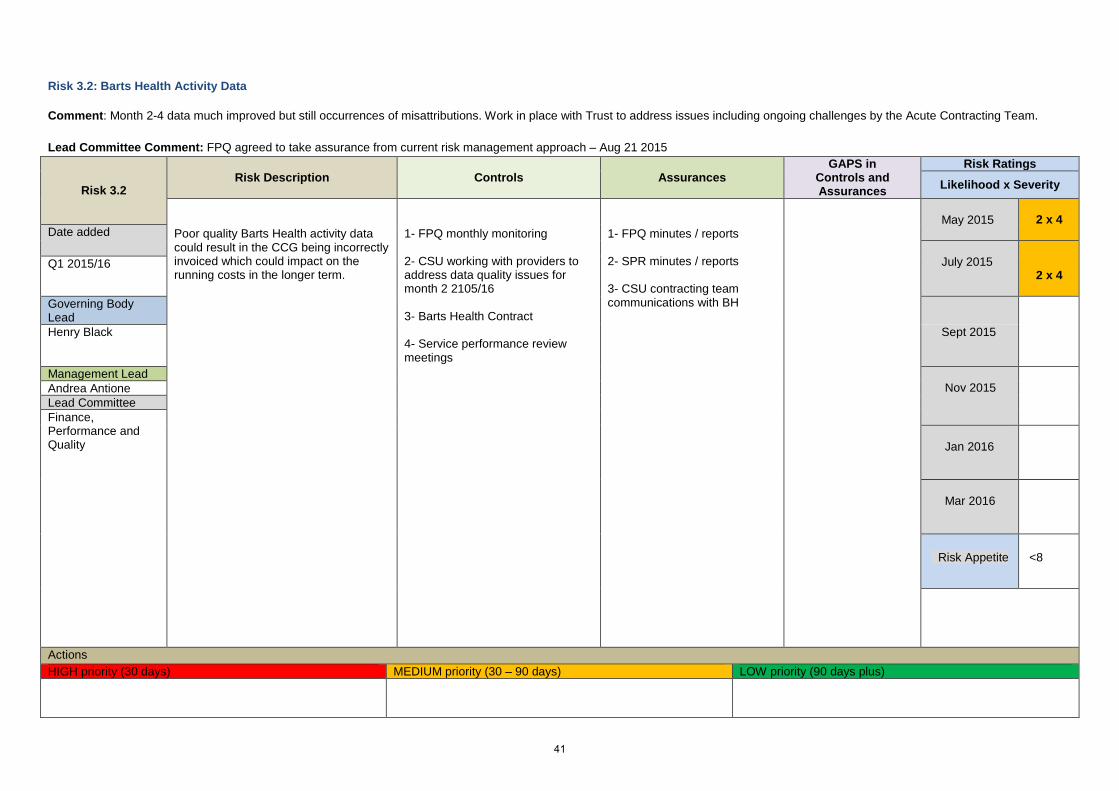
Risk 3.2: Barts Health Activity Data Comment: Month 2-4 data much improved but still occurrences of misattributions. Work in place with Trust to address issues including ongoing challenges by the Acute Contracting Team. Lead Committee Comment: FPQ agreed to take assurance from current risk management approach – Aug 21 2015
Risk 3.2 Risk Description Controls
Assurances
GAPS in Controls and Assurances
Risk Ratings
Likelihood x Severity
Poor quality Barts Health activity data could result in the CCG being incorrectly invoiced which could impact on the running costs in the longer term.
1- FPQ monthly monitoring 2- CSU working with providers to address data quality issues for month 2 2105/16 3- Barts Health Contract 4- Service performance review meetings
1- FPQ minutes / reports 2- SPR minutes / reports 3- CSU contracting team communications with BH
May 2015
2 x 4
Date added July 2015
2 x 4
Q1 2015/16
Governing Body Lead
Henry Black Sept 2015
Management Lead Nov 2015
Andrea Antione Lead Committee Finance, Performance and Quality
Jan 2016
Mar 2016
Risk Appetite <8
Actions HIGH priority (30 days) MEDIUM priority (30 – 90 days) LOW priority (90 days plus)
41

Risk 3.3: Continuing Care Comment: Risk of increased pressure on the Continuing Care budget as demand for complex packages increases. As technology and life expectancy increase, demand for continuing care packages is expected to rise in the coming years Lead Committee Comment: FPQ agreed to take assurance from current risk management approach – Aug 21 2015
Risk 3.3 Risk Description Controls
Assurances
GAPS in Controls and Assurances
Risk Ratings
Likelihood x Severity
Failure to effectively plan for the potential increase in demand in continuing care could result in a negative impact on the CCG’s running costs.
1- Robust controls in place to assess eligibility 2- Regular review to ensure all care packages are up to date and appropriate and any change in individuals’ circumstance is appropriately monitored and reflected in the revised package. 3- Development of integrated personal commissioning with Local Authority
1- Full documented records for each case, including the minutes of assessment panels 2- Process of continual review is recorded, monitored and reported to CCG 3- Broadcare database kept live and updated for all cases
There is no control which can be applied to the CCG’s contribution to the CHC risk pool. This is a national requirement and CCGs are statutorily responsible
May 2015
3 x 4
Date added July 2015
3 x 4
Q1 2015/16
Governing Body Lead
Henry Black Sept 2015
Management Lead Nov 2015
Andrea Antoine Lead Committee Finance, Performance and Quality
Jan 2016
Mar 2016
Risk Appetite <8
Actions HIGH priority (30 days) MEDIUM priority (30 – 90 days) LOW priority (90 days plus)
42

Risk 3.4: Financial challenges of Primary Care Co-commissioning
Comment: The CCG has agreed on full delegation of Primary Care Services from NHSE which is to be funded by allocation cost. Several concerns have been identified: - Uncertainty if allocation is sufficient - Financial reports from NHS England are high level with insufficient detail - Adjustments to allocations; not sure what they are and uncertain if allocations factored in growth - QIPP applied to allocation but no information relating to how this can be delivered and little opportunity for QIPP within GMS contracts
Lead Committee Comment: FPQ agreed to take assurance from current risk management approach – Aug 21 2015
Risk 3.4 Risk Description Controls
Assurances
GAPS in Controls and Assurances
Risk Ratings
Likelihood x Severity
Failure to understand primary care cost pressures and effectively plan the allocation could have a negative impact on the CCG’s running costs.
1- Monthly monitoring at Primary Care Committee
2- Monthly monitoring at FPQ 3 – Local financial reporting and forecasting based on NHS England information
1- Primary Care Committee minutes and reports 2- FPQ minutes and reports
This will be monitored and developed as appropriate as the new structures and resources are put in to place
May 2015
3 x 4
Date added July 2015
3 x 4
Q1 2015
Governing Body Lead
Henry Black
Sept 2015
Management Lead Nov 2015
Andrea Antoine
Lead Committee Finance, Performance and Quality
Jan 2016
Mar 2016
Risk Appetite
<8
Actions HIGH priority (30 days) MEDIUM priority (30 – 90 days) LOW priority (90 days plus)
- Review of allocation to date to check if on target with NHSE assumption
- Financial Planning aligned with re-structure
43

- Design of forward work plan
Risk 3.5: Running Costs Allocation
Comment: For 2015/16 there has been a £580k allocation reduction alongside 10 new CCG posts. This puts a pressure on reserves and has a potential impact on the CCG’s capacity as the admin cost threshold has been reached. Lead Committee Comment: FPQ agreed to take assurance from current risk management approach – Aug 21 2015
Risk 3.5 Risk Description Controls
Assurances
GAPS in Controls and Assurances
Risk Ratings
Likelihood x Severity
With the reduction in the allocation and the expanding workforce of the CCG, failure to develop workforce and programme financial plans could result in a negative impact on the CCG’s running costs.
1- Delays in recruitment of permanent staff 2- Monthly monitoring by FPQ 3- SMT management of resources
4- Efficiencies within each of the management budgets
1- FPQ reports and minutes
May 2015
3 x 4
Date added July 2015
3 x 4
Q1 2015/16
Governing Body Lead
Henry Black Sept 2015
Management Lead Nov 2015
Andrea Antione Lead Committee Finance, Performance and Quality
Jan 2016
Mar 2016
Risk Appetite
<8
44

Actions HIGH priority (30 days) MEDIUM priority (30 – 90 days) LOW priority (90 days plus)
Risk 3.6: Delivery of the Operating Plan, including QIPP Comment: Data from Prescribing Monthly Profiles which are used to calculate estimated forecast out-turns for 2015/16 prescriptions has estimated a prescribing forecast overspend of c£800k. - The QIPP proposals 2015/16 are projected to produce £7,935k of recurrent savings to the CCG from April 2015. Lead Committee Comment: TIC agreed to take assurance from current risk management approach – Aug 11 2015
Risk 3.6 Risk Description Controls
Assurances
GAPS in Controls and Assurances
Risk Ratings
Likelihood x Severity
Failure to deliver on the Operating Plan, including QIPP would result in: • a negative financial impact on the CCG. • Lost opportunity to produce and deliver increased outcomes for the sickest people in Tower Hamlets. • A negative impact on the reputation of the CCG.
1-Provider Productivity Programme is co-ordinated across WELC to ensure delivery at scale. 2-Plans are scrutinised and approved the TIC and Governing Body through a methodical process. 3-Very detailed HRGs exist for where the savings will be made. 4-Re-investment into services is determined by the return of savings e.g. Barts Health NHS Trust recruitment is based on savings. 5-QIPP programme management process 6-Monthly monitoring meetings to ensure programme boards are on track; off track programmes are discussed at the TIC. 7-All Programme Boards have a management and Governing Body lead with additional subject matter experts brought in as and when required.
1- TOR, minutes and
agendas of the Programme Boards, TIC, FPQ and Governing Body
2- HRGs
May 2015
3 x 4 Date added
July 2015
3 x 4
Q1 2015
Governing Body Lead
John Wardell Sept 2015
Management Lead Nov 2015
Josh Potter Lead Committee Transformation and Innovation Committee
Jan 2016
Mar 2016
Risk <8
45

Appetite
Actions HIGH priority (30 days) MEDIUM priority (30 – 90 days) LOW priority (90 days plus) Prescribing Forecast overspend of c£800k to be investigated by CSU prescribing team to ascertain whether this is recoverable
46
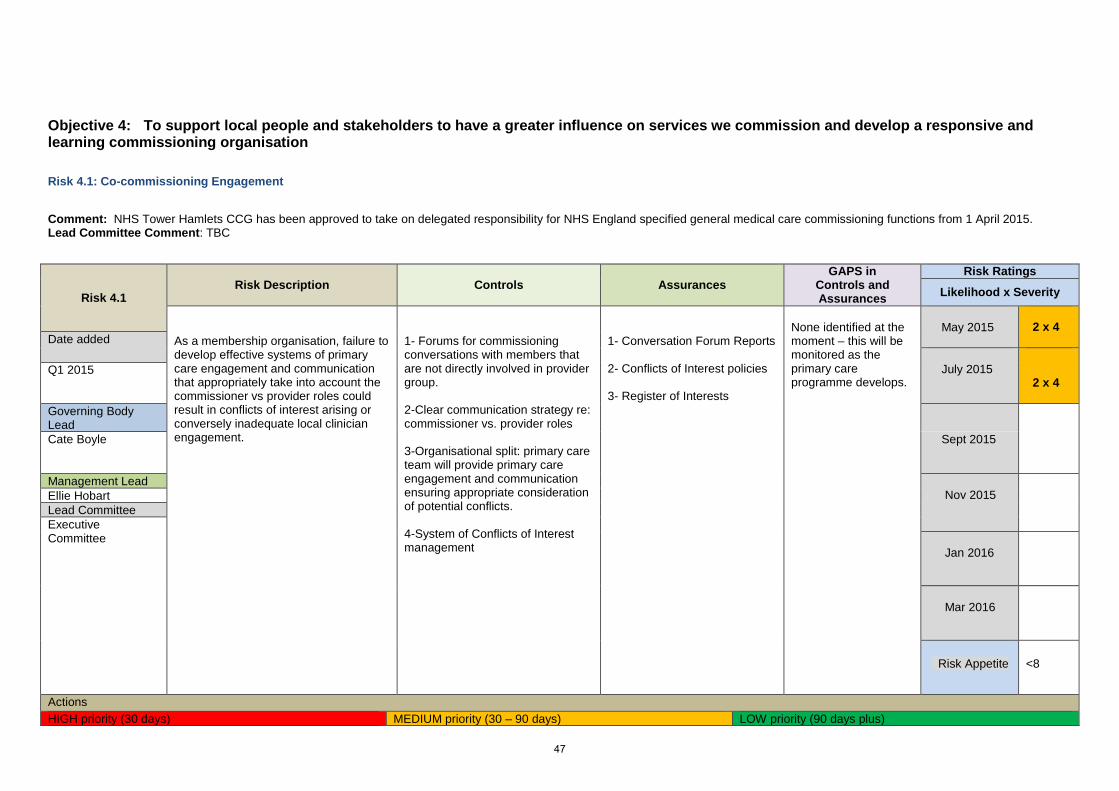
Objective 4: To support local people and stakeholders to have a greater influence on services we commission and develop a responsive and learning commissioning organisation
Risk 4.1: Co-commissioning Engagement
Comment: NHS Tower Hamlets CCG has been approved to take on delegated responsibility for NHS England specified general medical care commissioning functions from 1 April 2015. Lead Committee Comment: TBC
Risk 4.1 Risk Description Controls
Assurances
GAPS in Controls and Assurances
Risk Ratings
Likelihood x Severity
As a membership organisation, failure to develop effective systems of primary care engagement and communication that appropriately take into account the commissioner vs provider roles could result in conflicts of interest arising or conversely inadequate local clinician engagement.
1- Forums for commissioning conversations with members that are not directly involved in provider group. 2-Clear communication strategy re: commissioner vs. provider roles 3-Organisational split: primary care team will provide primary care engagement and communication ensuring appropriate consideration of potential conflicts. 4-System of Conflicts of Interest management
1- Conversation Forum Reports 2- Conflicts of Interest policies 3- Register of Interests
None identified at the moment – this will be monitored as the primary care programme develops.
May 2015
2 x 4 Date added
July 2015
2 x 4
Q1 2015
Governing Body Lead
Cate Boyle Sept 2015
Management Lead Nov 2015
Ellie Hobart Lead Committee Executive Committee
Jan 2016
Mar 2016
Risk Appetite <8
Actions HIGH priority (30 days) MEDIUM priority (30 – 90 days) LOW priority (90 days plus)
47

Objective 5: To promote equality both as an employer and a commissioner of health care services
There are no perceived current high level risks to this corporate objective.
48

Governing Body Meeting Enclosure
Date of meeting September 1st 2015 D
Agenda item 2.2.1
Title of report: Month 4 Finance report – 2015/16
Author(s): Henry Black – Chief Finance Officer Andrea Antoine – Deputy Chief Finance Officer
Presented by: Sponsor (if different): For further information
Henry Black – Chief Finance Officer – NHS Tower Hamlets CCG
Andrea Antoine – Deputy Chief Finance Officer [email protected] - 020 3688 2510
Executive summary
The month 2 report provides the Governing Body with the financial position of the CCG as at 31st July 2015 and consists of the following:
- Executive Summary,
- Key risks and issues,
- Revenue Financial Position,
- Statement of Financial Position,
- Cash Position and forecast and
- Payment Performance Measures position.
Recommendation
Information Approval To note Decision
To note the content of the report, and discuss any actions required
Key issues • 15/16 Drawdown of Surplus • Acute provider overperformance position at Month 4 • Continuing Healthcare position at Month 4 • Prescribing Position at Month 4 • Primary care Co-Commissioning position at Month 4
Conflicts of Interest There are no identified conflicts of interests.
Report history Finance, Quality & Performance (FPQ) meetings (CCG)- Information obtained at this meeting helps inform this Board report
Patient and Public N/A
49

involvement
Link to the Board Assurance Framework
Addresses several corporate objectives, those around finance, ensures the governance body is sighted on key finance and performance targets:
Strategic Objective 3: Creating a thriving and stable health and social care economy
Strategic objective 4: Delivering against our statutory duties.
Impact on Equality and Diversity
N/A
Resource requirements None
Next steps Action and next steps for each area identified is covered in the report.
50

Month 4 Finance Report – 2015/16
Executive Summary
This report provides an update on the financial position for the CCG at Month 4 (July 2015) and a forecast for the year. At month 4 the CCG is reporting a year to date surplus of £3.9m and forecasting a full year surplus of £11.7m, in line with the CCG’s Financial Plan. However, commissioning reserves are required to offset pressures on contract activity, particularly in the acute sector, continuing health care, prescribing and co-commissioning, in order to achieve the targeted position.
At this stage in the year the Month 4 finance report is subject to a number of caveats regarding availability and accuracy of data and therefore should be read and interpreted in this context.
Key Risks and Issues The main financial risks facing the CCG can be summarised as follows:
1. Re-submission of Operating Plan. THCCG have been required to submit our operating plan to deliver a surplus of £11.7m, which is higher than the minimum 1% business rules. This is a result of a request from NHSE to increase our surplus by an additional £2.3m, however we still have sufficient resource to meet all of our recurrent and non-recurrent identified expenditure plans and this does not represent a risk to delivery of any of our statutory duties.
2. Contract Performance Notices to Barts Health. The WEL CCGs issued Barts Health
with 4 contract performance notices in June 2015. Agreement has made to sign off the remedial action plans for RLH, and WX A&E, however further work is required on Newham A&E, RTT, diagnostics and Cancer.
3. 15/16 Drawdown on Surplus. In 15/16 Tower Hamlets CCG has been able to secure £4.5m of the previous year’s surplus for use in 2015/16. The table below shows the amount of drawdown Tower Hamlet CCG has secured for 2015/16 and how these non-recurrent funds will be used in 2015/16 – for which NHSE has approved our business case.
51

4. Contract finalisation: a. Barts Health – the contract has been agreed and signed at £137.6m b. CHS – the contract has been agreed and signed at £40.3m c. ELFT – the contract has been agreed and signed at £36.4m d. A number of associate contracts are still being negotiated with the providers,
these are as follows; Guys & St Thomas’, Kings College, Royal Free, UCL & Barnet and Chase Farm. These contracts are managed through lead commissioner arrangements by other London CCGs and the NELCSU contracts support team provide liaison.
5. Primary Care Co-Commissioning. These budgets transferred to the CCG in Month 2.
At month 4 we are reporting a year to date overspend of £209k with a full year forecast overspend position of £628k. The full year forecast outturn position is based on projecting forward the spend to date, with the variance based on NHSE assumption of including a QIPP within primary care of £578k. There are very limited plans at a London level to achieve this and no definitive delivery has been reported form any of these plans to achieve this QIPP.
6. Prescribing. At month 4 Prescribing is reporting a year to date over spend of £288k
with a full year forecast overspend position of £864k. This is based on using the NHS
THCCG Drawdown 2015/16 £000's £000'sTST Business Case Approval granted 2,500.0CHC Liability 2014/15 Underspend 800.0Sub-total 3,300.0
2014/15 Investment cfwd- Used to increase Surplus in 2014/15 3,500.0Less increase in 2015/16 Surplus (2,243.0)Sub -total - 2014/15 Investments cfwd 1,257.0
Total Drawdown 4,557.0
THCCG Co-Commissioning Delegated Budgets Less Qipp Total BudgetDescription £'000's £'000's £'000'sGeneral Practice - APMS 9,393 (182) 9,211General Practice - GMS 14,011 (286) 13,725General Practice - PMS 5,391 (110) 5,281QIPP (578) 578 0Enhanced Services 1,581 0 1,581QOF 2,488 0 2,488Premises Cost Reimbursement 7,555 0 7,555Other Premises Cost 56 0 56Dispensing/Prescribing Drs 141 0 141Other GP Services (includes Occ health) 680 0 680Grand Total 40,717 (0) 40,717
52

Business Services new profiles on projecting expected expenditure levels. Prescribing costs in April and May this year is 5.8% higher than the same time last year. The CSU are currently reviewing the reasons for the increases, areas to address to reduce this increase as well as try to identify areas of where potential savings can be made to reduce the overspend position.
Revenue Resource Allocation The CCG’s Revenue Resource Allocation for 2015/16 is £410.7m. In month 4 the CCG received another Prime Minister Challenge Fund allocation, this is a pass-through allocation that will be used to fund the APMS contract with the GP Care Group – total allocations received to date is £3.5m.
Included within the allocation is £6.7m for the Better Care Fund to which Tower Hamlets CCG are the hosts. The total budget for BCF is £19m which is included within the financial position is broken down as per the table below
Tower Hamlets CCG - 2015/2016 Revenue Resource Limit at Month 4
M3 Opening RRL
In Month movements
Closing M4 RRL
2015/16 Revenue Resource Limit £000's £000's £000'sProgramme Baseline Allocation (335,940) (335,940)BCF (6,714) (6,714)Non-Recurrent - Previous Year's Surplus \ (Deficit) C'fwd (16,257) (16,257)CCG Running Cost Allocation on Constrained Population Size (6,178) (6,178)2014/2015 Recurrent Post Allocation Transfers (221) (221)ETO/DTR Funding (826) (826)Primary Care Co-Commissioning (40,717) (40,717)London Transformation Fund 504 504Vanguard: MCP - Tower Hamlets (150) (150)PMCF - Pro-active, Accessible and Coordinated: Transforming General Practice in TOWER HAMLETS (1,519) (1,519)GPIT (755) (755)GPIT - Transition Funding (147) (147)PMCF - Pro-active, Accessible and Coordinated: Transforming General Practice in TOWER HAMLETS (1,803) (1,803)Waiting l ist validation and improving operational processes (10) (10)Total Resource Limit (408,920) (1,813) (410,733)
BCF BUDGET2015/16£'000'S
RAID 2,106MENTAL HEALTH RECOVERY COLLEGE 110INTEGRATED CARE INCENTIVE SCHEME 1,021INTEGRATED COMMUNITY HEALTH TEAM 7,3367 DAY WORKING AT SOCIAL WORK TEAM ROYAL LONDON HOSPITAL 8667 DAY HOSPITAL DISCHARGE 1,200REABLEMENT AND REHABILITATION 2,350INDEPENDENT LIVING 1,212STRATEGIC DEVELOPMENT 852ENABLERS 198RESERVES 1,800TOTAL 19,052
BETTER CARE FUND
53

Revenue Financial Position
The CCG’s summary revenue financial position is summarised below.
Tower Hamlets CCG - 2015/16 Financial Position at Month 4
Annual Budget £’000
YTD Budget £’000
YTD Actual £’000
YTD (Under)/Ove
rspend £’000
Forecast Actual £’000
Forecast (Under)/Ove
rspend £’000
DelegatedIn Sector Acute Trusts 141,337 47,112 47,344 232 142,032 695Out of Sector Acute Trusts 16,431 5,477 6,015 538 18,088 1,657Other Acute 12,871 4,290 4,283 (8) 13,215 344Subtotal Acute 170,640 56,880 57,641 761 173,335 2,696
Mental Health 42,536 14,179 14,162 (17) 42,485 (51)Community Health 42,334 14,111 14,119 7 42,356 22Other Non Acute 19,496 6,878 7,140 262 20,282 786Subtotal Non Acute 104,366 35,168 35,421 253 105,124 758
Prescribing 30,239 10,080 10,368 288 31,103 864Primary Care Co-Commissioning 40,717 13,572 13,782 209 41,345 628Prime Ministers Challenge Fund 3,472 1,157 1,157 0 3,472 0Other Primary Care Services 10,537 3,512 3,509 (4) 10,526 (11)Subtotal Primary Care 84,964 28,321 28,815 494 86,445 1,481
Operational Resilience 3,000 1,000 1,000 0 3,000 0
Better Care Fund 8,478 2,826 2,826 0 8,478 0
RTT 3,400 1,133 1,133 0 3,400 0
Reserves 8,947 2,982 1,451 (1,531) 3,904 (5,043)
TOTAL CSU 383,795 128,311 128,287 (24) 383,687 (108)
Corporate 15,238 5,079 5,103 24 15,346 108TOTAL CORPORATE 15,238 5,079 5,103 24 15,346 108
GRAND TOTAL 399,032 133,390 133,390 0 399,033 0IN YEAR RESOURCE LIMIT (394,476) (131,872) (131,872) 0 (394,476) 0IN YEAR (SURPLUS)/DEFECIT 4,556 1,518 1,519 0 4,556 0PRIOR YEAR SURPLUS (16,257) (5,419) (5,419) 0 (16,257) 0TOTAL (SURPLUS)/DEFICIT (11,701) (3,901) (3,900) 0 (11,701) 0
54
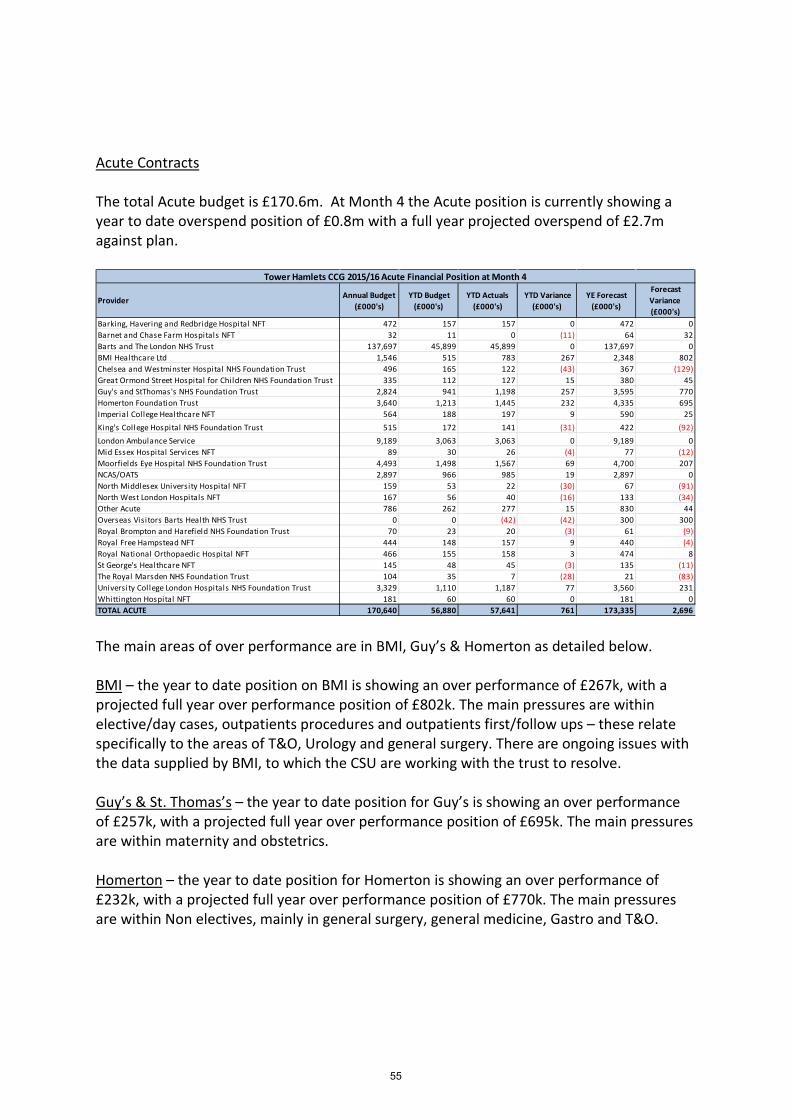
Acute Contracts The total Acute budget is £170.6m. At Month 4 the Acute position is currently showing a year to date overspend position of £0.8m with a full year projected overspend of £2.7m against plan.
The main areas of over performance are in BMI, Guy’s & Homerton as detailed below. BMI – the year to date position on BMI is showing an over performance of £267k, with a projected full year over performance position of £802k. The main pressures are within elective/day cases, outpatients procedures and outpatients first/follow ups – these relate specifically to the areas of T&O, Urology and general surgery. There are ongoing issues with the data supplied by BMI, to which the CSU are working with the trust to resolve. Guy’s & St. Thomas’s – the year to date position for Guy’s is showing an over performance of £257k, with a projected full year over performance position of £695k. The main pressures are within maternity and obstetrics. Homerton – the year to date position for Homerton is showing an over performance of £232k, with a projected full year over performance position of £770k. The main pressures are within Non electives, mainly in general surgery, general medicine, Gastro and T&O.
Provider Annual Budget (£000's)
YTD Budget (£000's)
YTD Actuals (£000's)
YTD Variance (£000's)
YE Forecast (£000's)
Forecast Variance (£000's)
Barking, Havering and Redbridge Hospital NFT 472 157 157 0 472 0Barnet and Chase Farm Hospitals NFT 32 11 0 (11) 64 32Barts and The London NHS Trust 137,697 45,899 45,899 0 137,697 0BMI Healthcare Ltd 1,546 515 783 267 2,348 802Chelsea and Westminster Hospital NHS Foundation Trust 496 165 122 (43) 367 (129)Great Ormond Street Hospital for Children NHS Foundation Trust 335 112 127 15 380 45Guy's and StThomas's NHS Foundation Trust 2,824 941 1,198 257 3,595 770Homerton Foundation Trust 3,640 1,213 1,445 232 4,335 695Imperial College Healthcare NFT 564 188 197 9 590 25King's College Hospital NHS Foundation Trust 515 172 141 (31) 422 (92)London Ambulance Service 9,189 3,063 3,063 0 9,189 0Mid Essex Hospital Services NFT 89 30 26 (4) 77 (12)Moorfields Eye Hospital NHS Foundation Trust 4,493 1,498 1,567 69 4,700 207NCAS/OATS 2,897 966 985 19 2,897 0North Middlesex University Hospital NFT 159 53 22 (30) 67 (91)North West London Hospitals NFT 167 56 40 (16) 133 (34)Other Acute 786 262 277 15 830 44Overseas Visitors Barts Health NHS Trust 0 0 (42) (42) 300 300Royal Brompton and Harefield NHS Foundation Trust 70 23 20 (3) 61 (9)Royal Free Hampstead NFT 444 148 157 9 440 (4)Royal National Orthopaedic Hospital NFT 466 155 158 3 474 8St George's Healthcare NFT 145 48 45 (3) 135 (11)The Royal Marsden NHS Foundation Trust 104 35 7 (28) 21 (83)University College London Hospitals NHS Foundation Trust 3,329 1,110 1,187 77 3,560 231Whittington Hospital NFT 181 60 60 0 181 0TOTAL ACUTE 170,640 56,880 57,641 761 173,335 2,696
Tower Hamlets CCG 2015/16 Acute Financial Position at Month 4
55

Healthcare Provision A summary analysis of the year to date and the forecast for healthcare provision budgets are shown below.
At month 4 the Healthcare Provision has a year to date overspend position of £746k with a projected full year overspend position of £2.2m. The main drivers of this position relate to overspends in Continuing Healthcare, Prescribing and primary care co-commissioning. Both Prescribing and primary care commissioning have already been reported within the executive summary of this report, which leaves the Continuing Healthcare overspend to explain further. Continuing Health Care - the year to date position on CHC is showing an overspend of £224k, with a projected full year over performance position of £673k. This is mainly caused by significant increases in fast tracked patients. The CCG has asked for a deep dive exercise to be conducted as we are concerned with how the forecasts for these fast tracked patients have been constructed.
Area
Annual Budget (£000s)
YTD Budget (£000's)
YTD Actual (£000's)
YTD Variance (£000's)
YE Forecast (£000's)
Forecast Variance (£000's)
Community Health 42,334 14,111 14,119 7 42,356 22Continuing Care 14,166 5,101 5,326 224 14,839 673Mental Health 42,536 14,179 14,162 (17) 42,485 (51)Other 8,730 2,910 2,948 38 8,843 114Prescribing 30,239 10,080 10,368 288 31,103 864Primary Care Co-Commissioning 40,717 13,572 13,782 209 41,345 628Prime Ministers Challenge Fund 3,472 1,157 1,157 0 3,472 0Other Primary Care Services 10,537 3,512 3,509 (4) 10,526 (11)Healthcare Provision Financial Position 192,730 64,623 65,369 746 194,969 2,239
Tower Hamlets CCG 2015/16 - Healthcare Provision Financial Position at Month 4
56

Corporate Costs The CCG’s corporate costs are made up of two different sources of funding; Administration costs, also known as Running Costs Allowance (RCA) and programme costs. At month 4 the CCG is on plan to spend within its running costs allowance of £6.2m, for this financial year. The programme costs are projecting a slight overspend of £108k at month 4 – mainly related to programme management costs. The forecast overspend is based on current costs projected forward, and it is expected that a recovery plan will bring the budget back into balance by the end of the year.
This budget will be continued to be monitored on a monthly basis, together with ongoing budget holder meetings, with all movements (increases and/or decreases) to the corporate budgets as a whole, being approved by the CCG’s SMT. QIPP The Tower Hamlets QIPP plan for 2015/16 has a total gross value of around £8.5m – this includes £0.5m primary care co-commissioning Qipp savings, which brings the net Qipp savings to £7.2m. At month 4 the CCG is projecting a year to date under achievement of £1m with a full year under achievement of £1.7m. Mainly related to delayed delivery of planned care design schemes and the urgent care recharging project as well as prescribing cost pressures and Primary Care Co-commissioning Qipp schemes not yet identified, as indicated earlier in this
Department
Annual Budget (£000s)
YTD Budget (£000's)
YTD Actual (£000's)
YTD Variance (£000's)
YE Forecast (£000's)
Forecast Variance (£000's)
ADMIN PROJECTS 0 0 3 3 0 0ADMINISTRATION & BUSINESS SUPPORT 201 67 98 31 198 (3)BUSINESS DEVELOPMENT 656 219 182 (36) 624 (32)CEO/ BOARD OFFICE 311 104 94 (10) 311 (1)CHAIR AND NON EXECS 404 135 167 32 428 24COMMISSIONING 115 38 112 74 148 33COMMUNICATIONS & PR 299 100 88 (12) 300 1CORPORATE COSTS & SERVICES 2,869 956 943 (14) 2,869 0EDUCATION AND TRAINING 0 0 3 3 0 0ESTATES AND FACILITIES (1) (0) (11) (10) (1) 0FINANCE 635 212 182 (30) 653 18PRIMARY CARE SUPPORT 346 115 23 (93) 252 (95)QUALITY ASSURANCE 72 24 24 0 126 54STRATEGY & DEVELOPMENT 270 90 152 62 271 1Sub-total Running Costs Allowance 6,178 2,059 2,059 0 6,178 (0)
Programme Projects 9,060 3,020 3,044 24 9,168 108Sub-total Other Corporate Costs 9,060 3,020 3,044 24 9,168 108
Total Corporate Financial Position 15,238 5,079 5,103 24 15,346 108
Tower Hamlets CCG -2015/2016 Corporate Financial Position at Month 4
57

report. These adverse variances were slightly offset by greater than expected gains in integrated care and provider productivity.
The Qipp will continue to be monitored on a monthly basis and reported within this report each month. Recommendations The Governing Body is asked to note the contents of this report, the risks highlighted and the management action undertaken to mitigate these risks.
Tower Hamlets CCG - QIPP Tracker 2015-16Reporting Period: July 2015 (M4) FULL YEAR
Work stream Scheme Title & Description YTD Plan
YTD Actual
YTDVariance
Full Year Savings
Full YearInvestment
Full Year Net Plan
Full Year Forecast
Full Year Variance
Bridge project (virtual ward) £21 £21 (£1) £63 £0 £63 £63 £0
Decommissioning of children's 0-5 NIS £21 £37 £16 £112 £0 £112 £112 £0
Integrated Care £375 £614 £239 £1,500 £0 £1,500 £1,841 £341Reduction in Self Care Budget £72 £96 £24 £288 £0 £288 £288 £0Orion (£30) (£40) (£10) £0 (£120) (£120) (£120) £0VOICES survey (£8) (£10) (£3) £0 (£30) (£30) (£30) £0RAID £153 £203 £51 £610 £0 £610 £610 £0Epilepsy telephone service (pending result on 14/15 pilot if completed)
£16 £21 £5 £63 £0 £63 £63 £0
Liver function testing £23 £31 £8 £91 £0 £91 £91 £0
ELFT EPC (£23) (£30) (£8) £0 (£91) (£91) (£91) £0ELFT EPC NR funding to support mobilisation (£33) (£43) (£11) £0 (£130) (£130) (£130) £0CAMHS waiting times (£48) (£64) (£16) £0 (£191) (£191) (£191) £0CAMHS conduct disorder (£38) (£50) (£13) £0 (£150) (£150) (£150) £0Early intervention in psychosis compliance (£58) (£78) (£19) £0 (£233) (£233) (£233) £0ELFT memory clinic waiting times (£49) (£66) (£16) £0 (£197) (£197) (£197) £0ELFT secondary care talking therapies waiting times
(£20) (£27) (£7) £0 (£80) (£80) (£80) £0
EPC £23 £30 £8 £91 £0 £91 £91 £0Square Smile £24 £32 £8 £95 £0 £95 £95 £0S117 £75 £100 £25 £300 £0 £300 £300 £0
Other Lapsing of Health Guides Service £33 £33 (£1) £100 £0 £100 £100 £0
Provider productivity £166 £267 £102 £497 £0 £497 £903 £406
Gastro redesign, including Calprotectin £295 £63 (£232) £997 (£112) £885 £133 (£752)
Barts Renal Proposal £64 £0 (£64) £193 £0 £193 £193 £0
Prescribing - Assumed Growth in Operating Plan
£865 £0 (£865) £2,596 £0 £2,596 £1,731 (£865)
Scriptswitch £7 £7 £0 £20 £0 £20 £20 £0
Resp meds optimisation (adults and children) £7 £7 £0 £20 £0 £20 £20 £0
Out of borough patient recharging for Tower Hamlets Walk In Centre activity
£89 £0 (£89) £268 £0 £268 £0 (£268)
Social marketing campaign £10 £11 £1 £30 £0 £30 £30 £0
Other List-Based Services (APMS incl.) £61 £0 (£61) £182 £0 £182 £0 (£182)General Practice - GMS £95 £0 (£95) £286 £0 £286 £0 (£286)
General Practice - PMS £37 £0 (£37) £110 £0 £110 £0 (£110)
£2,225 £1,164 -£1,061 £8,512 -£1,334 £7,178 £5,462 -£1,716
Prescribing
Urgent Care
PrimaryCare Co-Comm
Long Term Conditions
Mental Health
Planned Care
Children &Young People
Integrated Care
58
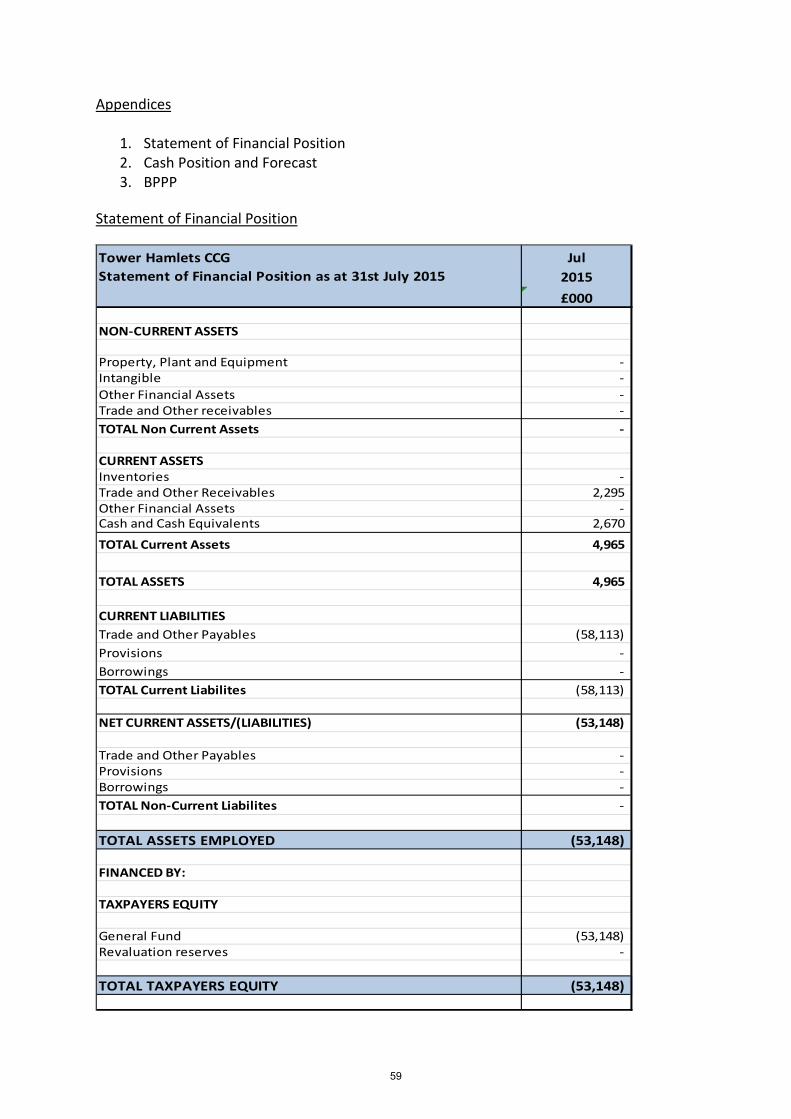
Appendices
1. Statement of Financial Position 2. Cash Position and Forecast 3. BPPP
Statement of Financial Position
Tower Hamlets CCG JulStatement of Financial Position as at 31st July 2015 2015
£000
NON-CURRENT ASSETS
Property, Plant and Equipment - Intangible - Other Financial Assets - Trade and Other receivables - TOTAL Non Current Assets -
CURRENT ASSETSInventories - Trade and Other Receivables 2,295 Other Financial Assets - Cash and Cash Equivalents 2,670
TOTAL Current Assets 4,965
TOTAL ASSETS 4,965
CURRENT LIABILITIESTrade and Other Payables (58,113) Provisions - Borrowings - TOTAL Current Liabilites (58,113)
NET CURRENT ASSETS/(LIABILITIES) (53,148)
Trade and Other Payables - Provisions - Borrowings - TOTAL Non-Current Liabilites -
TOTAL ASSETS EMPLOYED (53,148)
FINANCED BY:
TAXPAYERS EQUITY
General Fund (53,148) Revaluation reserves - TOTAL TAXPAYERS EQUITY (53,148)
59

Cash Position and Forecast
April May June July August September October November December January February March2015 2015 2015 2015 2015 2015 2015 2015 2015 2016 2016 2016
Actual Actual Actual Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast
RECEIPTS
Balance bfwd 228,443 55,246 2,565,182 305,035 3,152,612 222,612 299,612 296,612 58,612 219,612 309,612 213,612
NCB Drawdown 27,335,000 26,335,000 26,000,000 23,325,000 26,100,000 29,779,000 29,079,000 29,079,000 30,279,000 29,279,000 28,779,000 30,778,557
Other 492,135 208,257 413,499 3,450,761 22,000 152,000 22,000 37,000 136,000 265,000 29,000 895,000
PCS Payments Reimbursements - - - - - - - - - - - -
VAT 45,276 57,220 58,790 12,976 25,000 25,000 25,000 25,000 25,000 25,000 25,000 25,000
TOTAL 28,100,854 26,655,723 29,037,471 27,093,772 29,299,612 30,178,612 29,425,612 29,437,612 30,498,612 29,788,612 29,142,612 31,912,169
PAYMENTS
Creditors NHS 20,739,286 22,176,590 25,341,696 19,282,876 23,221,000 23,000,000 24,500,000 24,500,000 24,500,000 25,000,000 24,500,000 25,999,557
Creditors BACS 7,021,881 1,633,944 2,847,164 3,990,829 5,579,000 6,600,000 4,350,000 4,600,000 5,500,000 4,200,000 4,150,000 5,483,612
Creditors CHAPS - 644 260,532 333,793 - - - - - - - -
Salary CHAPS - - - 795 - - - - - - - -
Cleared Payable Orders 871 5,740 14,655 71,250 - - - - - - - -
Salaries & Wages 147,253 146,777 144,744 140,725 147,000 147,000 147,000 147,000 147,000 147,000 147,000 147,000
Pensions 43,641 44,024 45,047 43,397 45,000 45,000 45,000 45,000 45,000 45,000 45,000 45,000
Tax & NI 91,046 82,764 78,537 75,875 85,000 87,000 87,000 87,000 87,000 87,000 87,000 87,000
Standing Orders/Direct Debits 1,559 - - 1,559 - - - - - - - -
Foreign Payments - - - - - - - - - - - -
Other 72 59 61 62 - - - - - - - -
TOTAL 28,045,608 24,090,541 28,732,435 23,941,160 29,077,000 29,879,000 29,129,000 29,379,000 30,279,000 29,479,000 28,929,000 31,762,169
BALANCE CFWD 55,246 2,565,182 305,035 3,152,612 222,612 299,612 296,612 58,612 219,612 309,612 213,612 150,000
Tower Hamlets CCG Cashflow position as at 31st July 2015
60

BPPP
Number Value Number Value£'000 £'000
Non-NHS Creditors
Total Bills paid in the year 548 4,341 1,881 16,012
Total Bills paid within target 517 4,167 1,705 14,934
Percentage of Bills paid within target 94.3% 96.0% 90.6% 93.3%
NHS Creditors
Total Bills paid in the year 360 19,268 983 89,348
Total Bills paid within target 324 19,834 812 87,770
Percentage of Bills paid within target 90.0% 102.9% 82.6% 98.2%
All Creditors
Total Bills paid in the year 908 23,610 2,864 105,360
Total Bills paid within target 841 24,001 2,517 102,704
Percentage of Bills paid within target 92.6% 101.7% 87.9% 97.5%
Comparison with prior Year Performance (2014/15) Number Value Number Value
Percentage of Bills paid within target - Non NHS 94.1% 93.9% 92.6% 88.6%
Percentage of Bills paid within target - NHS 53.0% 99.4% 81.7% 98.0%
Tower Hamlets CCGPayment Performance MeasurePosition as at 31st July 2015
CumulativeJul-15
61
62

Governing Body Meeting Enclosure
Date of meeting September 1st 2015 E
Agenda item 2.2.2
Title of report: Tower Hamlets Finance & Activity Summary Report
Author(s): Lee Eborall – Director of Acute Contract Management, CSU Deane Kennett – Assistant Director of Contracting, CSU
Presented by: For further information
Lee Eborall – Director of Acute Contract Management, CSU Deane Kennett – Assistant Director of Contracting, CSU – [email protected]
Executive summary
The report provides a high level overview of finance and activity across Tower Hamlets for the month of July 2015 (based on June 2015 activity data). The report highlights the key issues, current performance, key actions and a delivery RAG rating for major providers providing healthcare services in Tower Hamlets.
Recommendation
Information Approval To note Decision
To note the content of the report, and discuss any actions required.
Conflicts of Interest N/A
Key issues • The CCG is forecasting a Year End Surplus of £11.7m which is in line with its financial plan for 2015/2016.
• Main components being:
• Acute has reported a £2.7m overspend.
• Non Acute has reported a £2.2m overspend.
• Corporate has reported a £0.1m overspend.
• With minor overspends and underspends across the SLA Portfolio.
• The attribution of HEMS activity to CCGs and development of Service Specification for in year contract Variation.
• 111 re-procurement programme and renegotiation of the cost per call.
Report history Information presented at the CCG Finance & Activity meetings informs this Board report
63

Patient and Public involvement
N/A
Link to the Board Assurance Framework
• This paper affects Strategic Objectives 3: Creating a thriving and stable health and social care economy
• The PbR (payment by result) basis of the Barts Health contract represents the main risk in conjunction with the disaggregation of NHS England (including Specialist Commissioned Group) commissioned activity.
Impact on Equality and Diversity
N/A
Resource requirements
N/A
Next steps Action and next steps for each area identified is covered in the report. Main areas of work include: Acute
• CSU to pursue challenge with Barts Health on increase in emergency excess bed days experienced in June, believed to be as a result of a data recording error.
• The CSU to issue a formal letter to Barts Health requesting an audit be undertaken at the Whipps Cross site, following large spends in Rheumatology drugs.
• CSU to negotiate reduction in the Barts Health’s automatic 17% management fee applied to patient journeys.
• CSU to continue to manage compliance with Barts Health’s Contract Performance Notices as part of the Contract Management process.
64
Finance & Activity Summary Report Tower Hamlets CCG
September 2015
65

Fina
nce
& A
ctiv
ity
CCG Finance Performance, M4 2015/16 Action Am
ber
Forecasted Year End position: £11.7m surplus
Key Messages The CCG is forecasting a Year End Surplus of £11.7m which is in line with its financial plan for 2015/2016. Acute has reported an Overspend of £2.7m
The main drivers for the overspend being BMI, Guys and Homerton with a £0.8m, £0.8m and £0.7m reported position. The main pressures continue to be, Maternity at Guy’s, Emergency activity at Homerton, and Elective and Day Case work at BMI, areas over spending are T&O, Urology and General Surgery, which is to be expected as Barts are failing to achieve RTT targets in these specialties, with GPs having been asked to refer elsewhere as a result. Non Acute has reported a £2.2m Overspend
The main drivers for this are Continuing Care which is reporting a £0.7m overspend, Primary Care Co-Commissioning which is due to overspends of £0.2m posted and advised by NHS England, for the YTD position it was considered prudent to forecast this out, thus showing the £0.6m overspend, and Prescribing which is reporting a £0.9m overspend. Corporate has reported a £0.1m Overspend The forecasted overspend relates to non Running Cost Allowance Programme costs which need to be identified and allocated to the relevant programme budgets. The CCG finance team expect this to be resolved by M5.
Tower Hamlets Finance & Activity Headlines: September 2015
Month 4 Financial Position based on Month 3 Activity data Annual Budget £’000
YTD Budget £’000
YTD Actual £’000
YTD (Under)/Overspe
nd £’000
Forecast Actual £’000
Forecast (Under)/Overspe
nd £’000
DelegatedIn Sector Acute Trusts 141,337 47,112 47,344 232 142,032 695Out of Sector Acute Trusts 16,431 5,477 6,015 538 18,088 1,657Other Acute 12,871 4,290 4,283 (8) 13,215 344Subtotal Acute 170,640 56,880 57,641 761 173,335 2,696
Mental Health 42,536 14,179 14,162 (17) 42,485 (51)Community Health 42,334 14,111 14,119 7 42,356 22Other Non Acute 19,496 6,878 7,140 262 20,282 786Subtotal Non Acute 104,366 35,168 35,421 253 105,124 758
Prescribing 30,239 10,080 10,368 288 31,103 864Primary Care Co-Commissioning 40,717 13,572 13,782 209 41,345 628Prime Ministers Challenge Fund 3,472 1,157 1,157 0 3,472 0Other Primary Care Services 10,537 3,512 3,509 (4) 10,526 (11)Subtotal Primary Care 84,964 28,321 28,815 494 86,445 1,481
Operational Resilience 3,000 1,000 1,000 0 3,000 0
Better Care Fund 8,478 2,826 2,826 0 8,478 0
RTT 3,400 1,133 1,133 0 3,400 0
Reserves 8,947 2,982 1,451 (1,531) 3,904 (5,043)
TOTAL CSU 383,795 128,311 128,287 (24) 383,687 (108)
Corporate 15,238 5,079 5,103 24 15,346 108TOTAL CORPORATE 15,238 5,079 5,103 24 15,346 108
GRAND TOTAL 399,032 133,390 133,390 0 399,033 0IN YEAR RESOURCE LIMIT (394,476) (131,872) (131,872) 0 (394,476) 0IN YEAR (SURPLUS)/DEFECIT 4,556 1,518 1,519 0 4,556 0PRIOR YEAR SURPLUS (16,257) (5,419) (5,419) 0 (16,257) 0TOTAL (SURPLUS)/DEFICIT (11,701) (3,901) (3,900) 0 (11,701) 0
66
Fina
nce
& A
ctiv
ity
Tower Hamlets Finance & Activity Headlines: September 2015
Executive Summary
Ambe
r
Barts Health (Acute) • The M3 YTD position for Barts Health is showing break even, however a number of adjustments have been made to arrive at this
position including, CQUIN (£789k), Emergency Readmissions rebate (-£571k), Productivity Metrics (-£226k), and Automated and Manual Claim Adjustments (-£538k). The most significant of these claims is in Patient Transport of -£418k whereby negotiations are underway to reduce the Trust’s automatic 17% management fee applied to patient journeys.
• The three WEL CCGs issued 4 Contract Performance Notices (CPNs) in June. CCGs have agreed to sign-off the Remedial Action Plans (RAPs) for Royal London Hospital and Whipps Cross A&E, but further work is required for Newham A&E, RTT, Cancer and Diagnostics.
• There has been an increase in emergency excess bed days in June however, this has been challenged as it is believed to be a data recording error.
• The CSU is continuing to investigate the large spend in Rheumatology drugs and will be issuing a formal letter to the Trust to undertake an audit at Whipps Cross site (where most of the increase has been noted). Mental Health
• The ELFT Mental Health Provider continues to meet the majority of contractual requirements. • The Adult DNA rate continues to exceed the 10% threshold at 14.2% in June, an action plan is in place to support recovery.
Community Health Services • A Contract Variation re-allocating £630k residing within the CHS contract, to Health Visiting has been signed by Barts Health. • Feedback on Business cases (OOH, Continence and Wheelchair Services) has been provided with further information requested
from the services involved. • Overall DNA rates remain comfortably below threshold (7.5%) at 6.0%, however there are still breaches within some services. The
CCG, CSU and the provider continue to work together to understand underlying causes and solutions.
Continuing Healthcare • There is a year end forecasted overspend of £671k at month 4. The number of Fast Track (last months of life) patients increased
with corresponding increase in projected cost. The increase in Fast Tracks is in line with the National Data set showing an increase in death rates.
• The CHC team are working on making more cost effective LD and Fast Track packages, the impact of which should be evident over the forthcoming months. 67

Fina
nce
& A
ctiv
ity
Helicopter Emergency Medical Service (HEMS) Key Messages
Summary of Service Dispatch • The helicopter can be dispatched anywhere within the M25 according
to a set protocol of accident types via the specific request of the London Ambulance Service (LAS), Metropolitan Police or London Fire and Rescue.
• Following a patient assessment at the scene, the HEMS doctors will determine the most appropriate hospital for further treatment. A patient can be taken to any multi-disciplinary hospital in London via helicopter or road, depending on the nature of their injuries. In certain cases, patients will be transferred to hospitals with specialist units, such as the neurosurgical unit at the Royal London.
Activity and Finance • CCGs are only charged for activity in which a patient is brought back to
the helipad at RLH site from the accident scene. The majority of the service’s activity is through the use of Response Cars, which make up approximately 60-80%. Patients without NHS numbers are checked for their residency, and this identifies the attributable CCG. If no residency is determined then the patient will be attributed to Tower Hamlets CCG as the host CCG of the Helipad potentially resulting in a disproportionate amount of activity being attributed to Tower Hamlets CCG. The CSU are investigating with the Trust as to the rigour involved in obtaining the necessary patient information in order to attribute the correct CCG.
• The CSU is working to agree a HEMS service specification for inclusion in the 2015/16 contract via Contract Variation. As part of this work the CSU are exploring the possibility and impact of, moving to a payment model based upon the geographic location of the incident rather than where the patient is registered with a GP; in line with how Ambulance Service activity is attributed.
• Figs. 1, shows HEMs spend over the last fifteen months. Activity from the first three months of 2014/15 was erroneous, with Barts allocating virtually all activity to Tower Hamlets (this was rectified as part of the Q1 14/15 reconciliation). Recording of data has significantly improved, showing a more even spread of spend across the twelve CCGs.
• Figure 2 shows Q1 NEL CCGs and Other CCGs activity. To note year to date NEL CCG activity represents 38% of total chargeable helicopter trips, with Tower Hamlets CCG representing 14%.
Tower Hamlets Finance & Activity Headlines: September 2015
Fig. 1 HEMS Spend – NEL CCGs
Fig. 2 HEMS Activity Split - Q1 2015/16
68
Fina
nce
& A
ctiv
ity
ELC 111 Key Messages ELC 111 Re-procurement Programme • Following national directive regarding the commissioning of an integrated urgent care access, treatment and clinical advice service a 7
CCG workshop (ELC, BHR and WF), was held on 31 July. Agreement was reached in principle for a 7 CCG procurement process with the recognition that further work must now be completed to enable a go / no go decision, including to:
• Scope the project • Identify the risks / benefits of a 7 CCG approach • Enable each CCG to assess and agree their position against the emerging national specification • Outline the governance arrangements for the 7 CCG collaboration (including the role and remit of the NEL Urgent and
Emergency Care Network in the process of being established).
• Following the initial meeting on 31 July, bi-weekly teleconferences are being held to delegate the above work, to inform a paper for discussion at the next face to face meeting towards end of Aug / early September (date TBC).
Activity and Finance • The FOT for July is £465k per CCG based on actuals for Q1 (call volumes and achievement against KPIs) and projected costs for Q2, Q3
and Q4. It is however, important to highlight that following financial review across the ELC and ONEL 111 services, PELC are seeking to renegotiate the cost per call as of the 1st of September. This request remains under discussion across the ELC CCGs (led by Jane Milligan, SRO ELC 111) and is subject to further scrutiny regarding the financial analysis completed, the underlying reasons / root cause of the financial pressures, as well as to provide assurance regarding the viability and future of the service.
Tower Hamlets Finance & Activity Headlines: September 2015
69

70
Governing Body Meeting Enclosure
Date of meeting September 1st 2015 F
Agenda item 2.3
Title of report: Performance and Quality Report
Author(s): Archna Mathur - Director Quality & Performance (CCG) CSU Performance team
Presented by: For further information
Archna Mathur – Director Quality & Performance – THCCG Archna Mathur – Director Quality & Performance THCCG [email protected] (020 3688 2528)
Executive summary
This paper provides a high level overview of quality and performance across Tower Hamlets reported for the month of May and June where data is available.The report highlights the key issues, current performance against key performance indicators and key actions taken by providers and Tower Hamlets CCG in managing the performance for the main providers of acute, community and mental healthcare in Tower Hamlets.
Recommendation
Information Approval To note Decision
The Governing Body is asked to note the contents of the report, particularly in relation to the Board Assurance Framework.
Key issues Cancer Waiting Times: The Trust achieved the 2ww standard for June with performance of 96.7%. This is an improvement on both April and May where the 2WW target was not achieved. • 2ww performance for RLH site is not available however
usingTower Hamlets CCG as a proxy measure demonstrates underperformance at 91.8%
• 62 Day performance increased from the May position of 73.4% to 77.2% for June.
• The Trust have been issued with a Contract Performance Notice (CPN) due to insufficient demonstration of plans to rectify the internal operational issues to achieve both the 2ww and 62 day standards. The Trust had submitted an action plan that did not provide sufficient assurance and hence an updated plan has been requested that more effectively addresses the gaps i.e.
- Specialty level detail for those challenged specialties with a link to the specialty level demand and capacity plans with underpinning trajectories for sustainable delivery for 2ww and 62 day performance.
71

• Speciality deep dives have been conducted for urology, head and neck, gynae and lung. Challenges for head and neck are in management of inappropriate consultant upgrades to the 2ww clinic ar RLH whilst 62 performance is meeting the target. For Gynae, there are very small numbers of breaches each month (0.5-1) which amonget small numbers of referrals, result in significant underperformance.
• All 31 day standards have been achieved at Trust level.
Referral to Treatment (RTT): Barts Health continues to underperform against the national waiting time standards at speciality level. The Trust are currently not reporting on RTT although monitoring via the CCGs/TDA continues.
• The Trust have been issues with a CPN for each of the national waiting time standards:
- Percentage of admitted Service Users starting treatment within a maximum of 18 weeks from Referral
- Percentage of non-admitted Service Users starting treatment within a maximum of 18 weeks from Referral
- Percentage of Service Users on incomplete RTT pathways (yet to start treatment) waiting no more than 18 weeks from Referral
- Zero tolerance RTT waits over 52 weeks for incomplete pathways
• Of current concern is the increasing numbers of patients waiting over 52 weeks and the Trust process for managing potential clinical harm.
• Performance against the trajectory for completing the incomplete backlog is in line with trajectory.
A&E: The RLH site continues to be challenged in delivering the 95% standard and a CPN has been issued for non compliance with this standard also.
• A trajectory for delivery has been produced supported by a robust action plan which the CCG will monitor delivery of on a bi-weekly basis. The trajectory demonstrates compliance with the 95% standard by Q4 201516 but with a non-compliant position for the financial year overall.
• The RLH site team are focussed on delivery of key work streams: - Majors light - Reducing patient journey time - AAU model of care - Improving discharge - LOS reduction
• Latest A&E position versus trajectory (w/e 19th August) is 88.84% vs trajectory of 91.72%
SI (Serious Incidents): Barts Health has 2 overdue SIs since June compared to 4 for May.
SIs for ELFT: there are 6 overdue SIs for June (a reduction from 12 in May), of which 4 relate to mental health and 2 to community health services
Never Events (Barts Health): As of the end of June Barts health have
72
declared 5 never events
Never Events for (ELFT) : Zero never events were reported June.
Mixed Sex Accommodation: There were 20 published breaches at Barts Health in June 2015. Of these, 17 were at The Royal London, 2 at Newham and 1 at Whipps Cross. There is a noticeable reduction in the number of MSA breaches from the same period last year. The Trust report the majority of breaches relate to step down from critical care linked to patient flow and bed availability.
• It is noted in the Emergency Care and Patient Flow improvement plan workstream is key to driving improvements.
• This will be monitored as part of the RLH CQRM/Oversight and Assurance Committee.
HCAI (HealthCare Associated Infection) – the year to date total for Cdiff infections at Barts Health is 14 versus full year threshold of 82. This is under the year to date threshold of 29 cases.
• There are currently no cases of C-diff due to lapses in care. • The MRSA figure for Barts Health is 3 cases which is unchanged
from the previous report.
Quality Assurance visits: Latest Quality Assurance visit undertaken was to ward 10E – care of the elderly at the RLH. The key observations from this ward were that staffing levels required improvement and the ward needs to recruit to full establishment to ensure patient safety. Some members of staff were found to also lack compassion. More positively, most patients were aware of their plans for discharge.
Special Measures: The new governance systems are taking effect with the first RLH/Oversight and Assurance meeting taking place on the 26th August. The focus of this meeting was on gaining assurance on progress against the compliance actions. Further detailed key lines of enquiry were in relation to audit results for the WHO surgical checklist application and assurance on systematic process for VTE prophylaxis. Going forward the aim will be to review progress on the improvement plans for each of the 6 improvement workstreams, where possible on real evidence of improvement. The workstreams are:
• Safe and Effective Care • Workforce • Outpatients and medical records • Emergency pathway and patient flow • Compassionate Care and patient experience • Leadership and OD
Trust Oversight and Assurance (TOAG): This Trust level assurance forum has met twice with the Trust to review improvement plan progress from a Trust level. The decision has been made that CQRMs for the Barts site will be picked up by NHSE in their capacity as specialised commissioners. The Barts site CQRM is yet to be
73
scheduled by NHSE.
Conflicts of Interest There are no identified conflicts of interest.
Report history Information presented at the CCG Performance & Quality meetings informs this Governing Body report.
Patient and Public involvement
The Friends and Family Test (FFT) provides patient feedback to improve service provision as well as NHS Choices providing patient comments on services.
Link to the Board Assurance Framework
This paper affects all of the risks under Strategic Objective 2: Systems and processes to monitor challenge and support provider delivery of the NHS Constitution targets.
Impact on Equality and Diversity
Monitoring and actively improving the performance and quality of service provision will have a benifical impact for all patients in Tower Hamlets.
Resource requirements N/A
Next steps Action and next steps for each area identified is covered in the report.
74

Tower Hamlets CCG Month 3 2015/16
Monthly Acute Performance, Serious Incidents & Quality Report
75
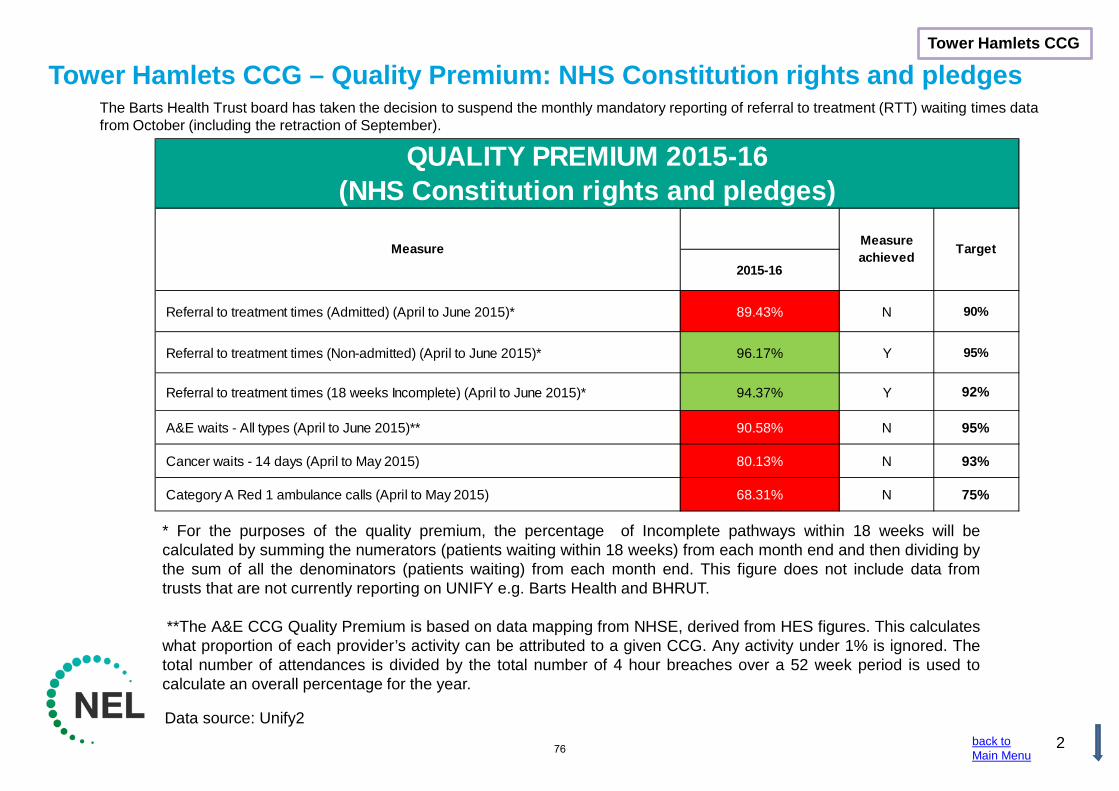
Tower Hamlets CCG – Quality Premium: NHS Constitution rights and pledges
Data source: Unify2
Tower Hamlets CCG
2
The Barts Health Trust board has taken the decision to suspend the monthly mandatory reporting of referral to treatment (RTT) waiting times data from October (including the retraction of September).
* For the purposes of the quality premium, the percentage of Incomplete pathways within 18 weeks will be calculated by summing the numerators (patients waiting within 18 weeks) from each month end and then dividing by the sum of all the denominators (patients waiting) from each month end. This figure does not include data from trusts that are not currently reporting on UNIFY e.g. Barts Health and BHRUT. **The A&E CCG Quality Premium is based on data mapping from NHSE, derived from HES figures. This calculates what proportion of each provider’s activity can be attributed to a given CCG. Any activity under 1% is ignored. The total number of attendances is divided by the total number of 4 hour breaches over a 52 week period is used to calculate an overall percentage for the year.
back to Main Menu
2015-16
Referral to treatment times (Admitted) (April to June 2015)* 89.43% N 90%
Referral to treatment times (Non-admitted) (April to June 2015)* 96.17% Y 95%
Referral to treatment times (18 weeks Incomplete) (April to June 2015)* 94.37% Y 92%
A&E waits - All types (April to June 2015)** 90.58% N 95%
Cancer waits - 14 days (April to May 2015) 80.13% N 93%
Category A Red 1 ambulance calls (April to May 2015) 68.31% N 75%
QUALITY PREMIUM 2015-16(NHS Constitution rights and pledges)
Measure Measure achieved Target
76
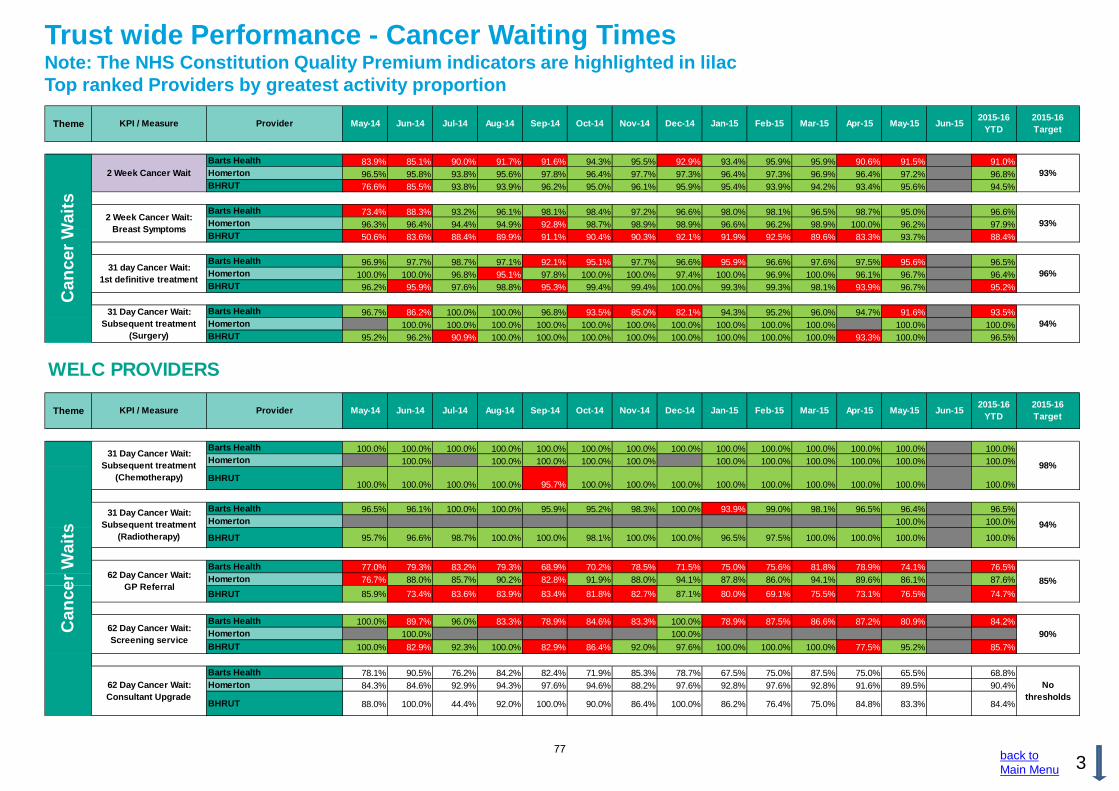
back to Main Menu 3
Trust wide Performance - Cancer Waiting Times Note: The NHS Constitution Quality Premium indicators are highlighted in lilac Top ranked Providers by greatest activity proportion
Barts Health 83.9% 85.1% 90.0% 91.7% 91.6% 94.3% 95.5% 92.9% 93.4% 95.9% 95.9% 90.6% 91.5% 91.0%Homerton 96.5% 95.8% 93.8% 95.6% 97.8% 96.4% 97.7% 97.3% 96.4% 97.3% 96.9% 96.4% 97.2% 96.8%BHRUT 76.6% 85.5% 93.8% 93.9% 96.2% 95.0% 96.1% 95.9% 95.4% 93.9% 94.2% 93.4% 95.6% 94.5%
Barts Health 73.4% 88.3% 93.2% 96.1% 98.1% 98.4% 97.2% 96.6% 98.0% 98.1% 96.5% 98.7% 95.0% 96.6%Homerton 96.3% 96.4% 94.4% 94.9% 92.8% 98.7% 98.9% 98.9% 96.6% 96.2% 98.9% 100.0% 96.2% 97.9%BHRUT 50.6% 83.6% 88.4% 89.9% 91.1% 90.4% 90.3% 92.1% 91.9% 92.5% 89.6% 83.3% 93.7% 88.4%
Barts Health 96.9% 97.7% 98.7% 97.1% 92.1% 95.1% 97.7% 96.6% 95.9% 96.6% 97.6% 97.5% 95.6% 96.5%Homerton 100.0% 100.0% 96.8% 95.1% 97.8% 100.0% 100.0% 97.4% 100.0% 96.9% 100.0% 96.1% 96.7% 96.4%BHRUT 96.2% 95.9% 97.6% 98.8% 95.3% 99.4% 99.4% 100.0% 99.3% 99.3% 98.1% 93.9% 96.7% 95.2%
Barts Health 96.7% 86.2% 100.0% 100.0% 96.8% 93.5% 85.0% 82.1% 94.3% 95.2% 96.0% 94.7% 91.6% 93.5%Homerton 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%BHRUT 95.2% 96.2% 90.9% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 93.3% 100.0% 96.5%
WELC PROVIDERS
Barts Health 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%Homerton 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
BHRUT100.0% 100.0% 100.0% 100.0% 95.7% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
Barts Health 96.5% 96.1% 100.0% 100.0% 95.9% 95.2% 98.3% 100.0% 93.9% 99.0% 98.1% 96.5% 96.4% 96.5%Homerton 100.0% 100.0%
BHRUT 95.7% 96.6% 98.7% 100.0% 100.0% 98.1% 100.0% 100.0% 96.5% 97.5% 100.0% 100.0% 100.0% 100.0%
Barts Health 77.0% 79.3% 83.2% 79.3% 68.9% 70.2% 78.5% 71.5% 75.0% 75.6% 81.8% 78.9% 74.1% 76.5%Homerton 76.7% 88.0% 85.7% 90.2% 82.8% 91.9% 88.0% 94.1% 87.8% 86.0% 94.1% 89.6% 86.1% 87.6%BHRUT 85.9% 73.4% 83.6% 83.9% 83.4% 81.8% 82.7% 87.1% 80.0% 69.1% 75.5% 73.1% 76.5% 74.7%
Barts Health 100.0% 89.7% 96.0% 83.3% 78.9% 84.6% 83.3% 100.0% 78.9% 87.5% 86.6% 87.2% 80.9% 84.2%Homerton 100.0% 100.0%BHRUT 100.0% 82.9% 92.3% 100.0% 82.9% 86.4% 92.0% 97.6% 100.0% 100.0% 100.0% 77.5% 95.2% 85.7%
Barts Health 78.1% 90.5% 76.2% 84.2% 82.4% 71.9% 85.3% 78.7% 67.5% 75.0% 87.5% 75.0% 65.5% 68.8%Homerton 84.3% 84.6% 92.9% 94.3% 97.6% 94.6% 88.2% 97.6% 92.8% 97.6% 92.8% 91.6% 89.5% 90.4%
BHRUT 88.0% 100.0% 44.4% 92.0% 100.0% 90.0% 86.4% 100.0% 86.2% 76.4% 75.0% 84.8% 83.3% 84.4%
Theme KPI / Measure Provider May-14 Jun-14 Mar-15 Apr-15 May-15 Jun-15Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14
Can
cer W
aits
2 Week Cancer Wait
2 Week Cancer Wait:Breast Symptoms
31 day Cancer Wait:1st definitive treatment
Jan-15 Feb-15
31 Day Cancer Wait: Subsequent treatment
(Surgery)
Theme KPI / Measure Provider May-14 Jun-14 Mar-15 Apr-15 May-15 Jun-15Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14
Can
cer W
aits
31 Day Cancer Wait: Subsequent treatment
(Chemotherapy)
31 Day Cancer Wait: Subsequent treatment
(Radiotherapy)
62 Day Cancer Wait: GP Referral
Jan-15 Feb-15
62 Day Cancer Wait: Screening service
62 Day Cancer Wait: Consultant Upgrade
98%
2015-16YTD
2015-16YTD
2015-16 Target
93%
93%
96%
94%
2015-16 Target
94%
85%
90%
No thresholds
77
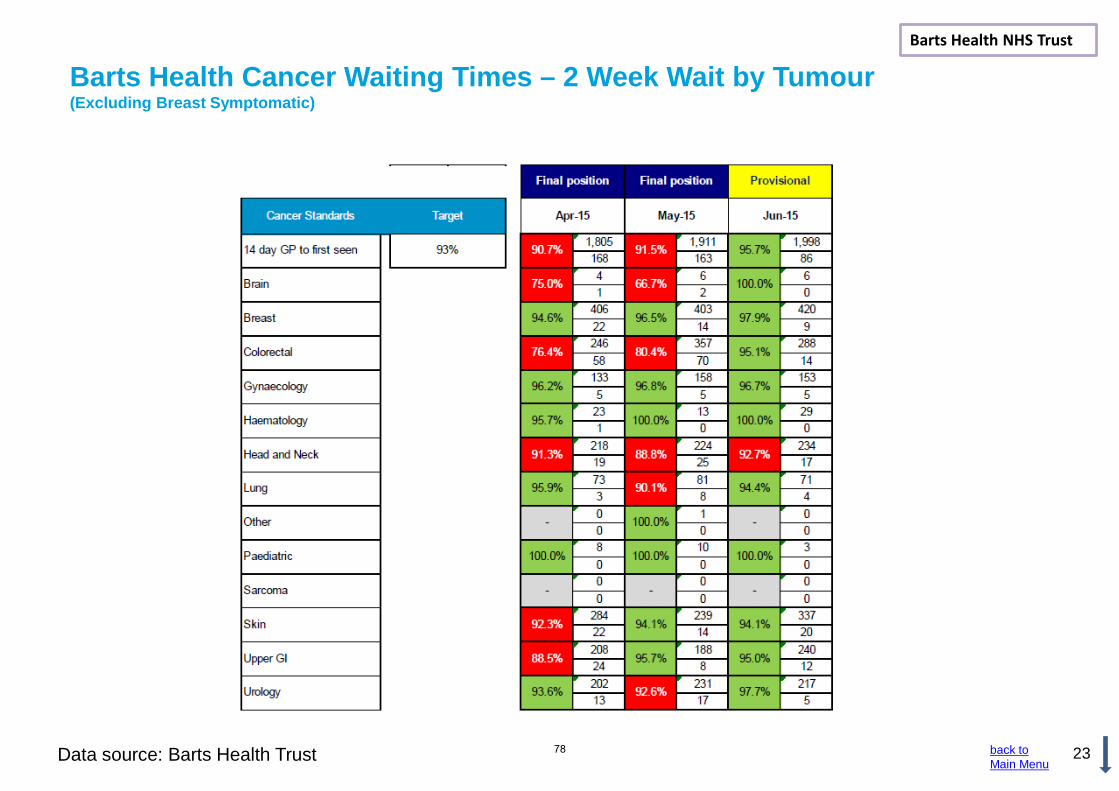
23
Barts Health Cancer Waiting Times – 2 Week Wait by Tumour (Excluding Breast Symptomatic)
Data source: Barts Health Trust
Barts Health NHS Trust
back to Main Menu
78
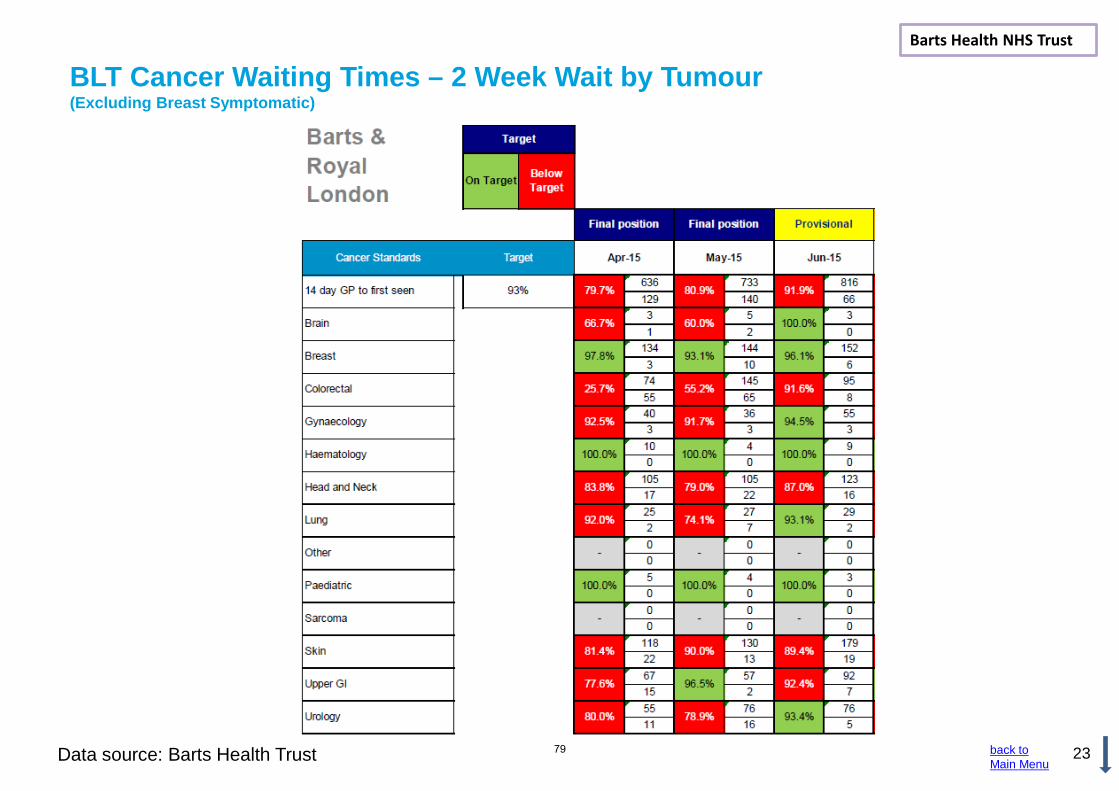
23
BLT Cancer Waiting Times – 2 Week Wait by Tumour (Excluding Breast Symptomatic)
Data source: Barts Health Trust
Barts Health NHS Trust
back to Main Menu
79

Data source: Barts Health Trust 22
Cancer Waiting Times – 62 day GP referral Barts Health Barts Health NHS Trust
back to Main Menu
There is the possibility of variation in data between that published on the national cancer waiting times database and that released by the trust. This may be caused by cases that are on the trust’s system but were either not uploaded to the national system before the deadline or uploaded under legacy sites which will be rejected by the Exeter system. Late uploads will be captured in the quarterly reports which often show a small amount of "churn".
80

23
BLT Cancer Waiting Times – 62 day Wait by Tumour
Data source: Barts Health Trust
Barts Health NHS Trust
back to Main Menu
81

back to Main Menu
8
Trust wide Performance – A&E and Ambulance Note: The NHS Constitution Quality Premium indicators are highlighted in lilac. Top ranked Providers shown by greatest activity proportion.
Royal London Hospital 89.8% 90.2% 93.4% 92.7% 92.2% 89.7% 83.4% 81.7% 83.6% 83.5% 82.8% 81.1% 84.9% 85.4% 83.6%Newham 96.8% 97.7% 97.0% 94.1% 95.2% 94.5% 93.1% 87.8% 94.0% 93.6% 94.4% 94.6% 95.5% 95.9% 95.3%Whipps Cross 86.7% 88.3% 91.3% 88.5% 90.7% 88.0% 84.9% 67.7% 73.2% 81.4% 74.9% 80.2% 83.6% 84.7% 82.7%Homerton 95.4% 96.0% 94.8% 96.1% 95.6% 96.0% 94.9% 95.1% 96.0% 93.5% 96.3% 94.8% 96.3% 95.6% 95.5%Queens Hospital 77.7% 76.5% 83.9% 78.1% 79.4% 73.6% 80.4% 76.3% 77.1% 89.8% 89.9% 89.3% 91.8% 92.7% 91.1%King George Hospital 89.5% 91.1% 91.4% 88.6% 89.4% 85.1% 77.5% 75.0% 86.3% 86.3% 90.0% 93.8% 94.2% 95.0% 94.3%Barts Health 90.5% 91.4% 93.6% 91.7% 92.4% 90.3% 86.2% 78.9% 82.9% 85.3% 83.1% 84.1% 87.1% 87.8% 86.2%BHRUT 81.5% 81.3% 86.3% 81.5% 82.7% 77.4% 79.4% 73.3% 80.0% 91.3% 90.0% 90.7% 92.6% 93.5% 92.1%
Royal London Hospital 91.2% 91.7% 94.5% 93.8% 93.4% 91.3% 85.9% 84.3% 85.6% 86.0% 85.4% 83.7% 86.8% 87.3% 85.8%Newham 98.0% 98.5% 98.1% 96.2% 96.9% 96.3% 95.4% 92.5% 95.9% 95.4% 95.2% 96.0% 95.9% 95.6% 95.8%Whipps Cross 91.6% 92.6% 94.4% 92.6% 93.8% 92.3% 90.1% 79.5% 83.0% 88.1% 83.2% 86.9% 88.5% 89.5% 88.2%Homerton 95.4% 96.0% 94.8% 96.1% 95.6% 96.0% 94.9% 95.1% 96.0% 93.5% 96.3% 94.8% 96.3% 95.6% 95.5%Queens Hospital 78.6% 77.4% 84.5% 79.1% 80.2% 74.6% 81.1% 77.2% 77.9% 90.1% 90.3% 89.7% 92.0% 93.0% 91.4%King George Hospital 93.1% 93.9% 94.4% 92.5% 92.9% 89.8% 85.2% 83.9% 90.9% 90.9% 93.3% 95.8% 96.1% 96.5% 96.1%Barts Health 93.4% 94.0% 95.5% 94.1% 94.6% 93.1% 90.2% 85.2% 87.9% 89.5% 87.6% 88.5% 90.1% 90.5% 89.6%BHRUT 84.5% 84.2% 88.5% 84.5% 85.4% 80.9% 82.7% 77.8% 83.0% 92.6% 91.5% 92.1% 93.7% 94.4% 93.3%
Homerton 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0Barts Health 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0
BHRUT 0 0 0 0 0 0 0 15 30 0 0 1 0 0 1
Homerton 0 0 0 0 0 0 0 0 0 0 0 0 0 0Barts Health 0 0 0 0 0 0 0 0 0 0 0 0 0 0BHRUT 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Category A calls resulting in emergency response arriving within 8 mins
(RED 1)
London Ambulance Service NHS Trust 73.0% 70.1% 70.4% 68.7% 62.0% 64.1% 64.3% 59.3% 68.6% 67.1% 62.7% 69.4% 67.0% 68.3% 75%
Category A calls resulting in emergency response arriving within 8 mins
(RED 2)
London Ambulance Service NHS Trust 69.1% 64.2% 60.7% 61.9% 54.1% 57.5% 55.0% 47.7% 59.9% 58.7% 59.1% 64.7% 66.5% 65.6% 75%
Category A calls resulting in emergency response arriving within 19 mins
London Ambulance Service NHS Trust 95.8% 94.5% 93.4% 93.9% 90.5% 91.5% 89.2% 84.7% 91.3% 91.8% 92.2% 94.1% 94.5% 94.3% 95%
Theme KPI / Measure Provider May-14 Jun-14 Apr-15 May-15 Jun-15Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14
Acc
iden
t & E
mer
genc
y an
dA
mbu
lanc
e C
alls
and
Han
dove
r
A&E Type I Performance
A&E All Types Performance
Jan-15 Feb-15 Mar-15
No of waits from decision to admit to admission
(Trolley waits - over 12 hours)
Urgent cancelled operations 2nd time
95%
95%
0
0
2015-16YTD
2015-16 Target
82
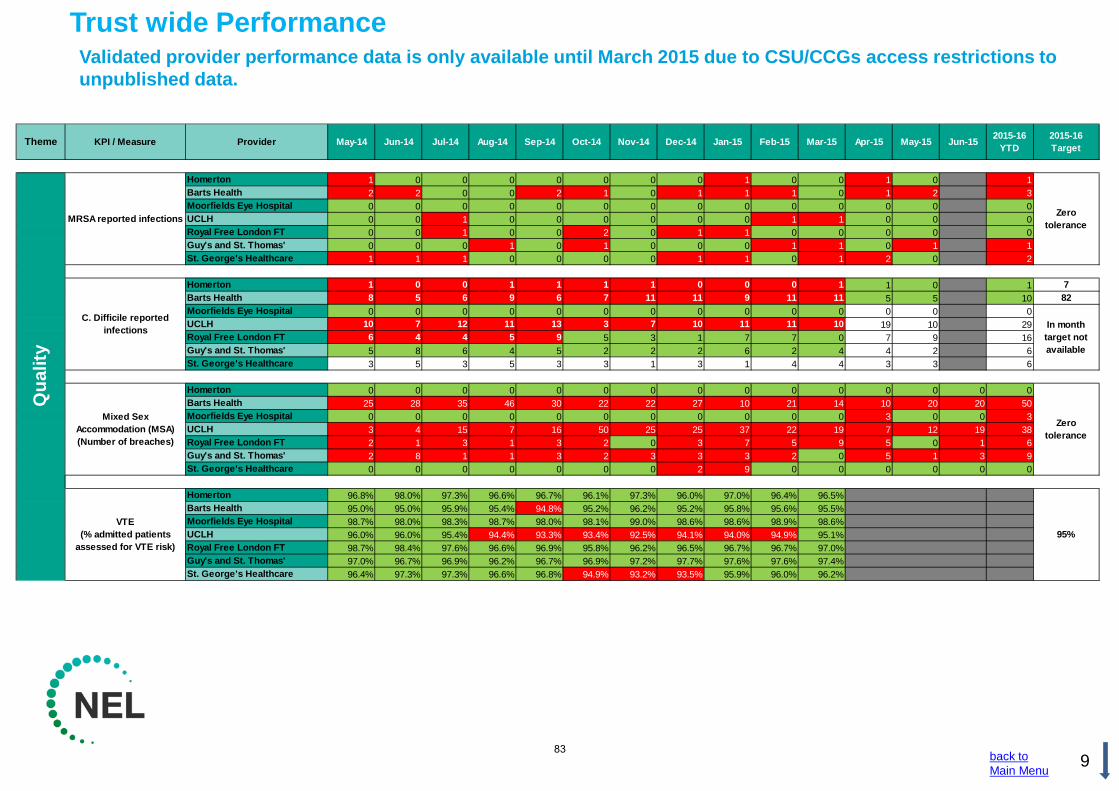
back to Main Menu
9
Trust wide Performance Validated provider performance data is only available until March 2015 due to CSU/CCGs access restrictions to unpublished data.
Homerton 1 0 0 0 0 0 0 0 1 0 0 1 0 1Barts Health 2 2 0 0 2 1 0 1 1 1 0 1 2 3Moorfields Eye Hospital 0 0 0 0 0 0 0 0 0 0 0 0 0 0UCLH 0 0 1 0 0 0 0 0 0 1 1 0 0 0Royal Free London FT 0 0 1 0 0 2 0 1 1 0 0 0 0 0Guy's and St. Thomas' 0 0 0 1 0 1 0 0 0 1 1 0 1 1St. George's Healthcare 1 1 1 0 0 0 0 1 1 0 1 2 0 2
Homerton 1 0 0 1 1 1 1 0 0 0 1 1 0 1 7Barts Health 8 5 6 9 6 7 11 11 9 11 11 5 5 10 82Moorfields Eye Hospital 0 0 0 0 0 0 0 0 0 0 0 0 0 0UCLH 10 7 12 11 13 3 7 10 11 11 10 19 10 29Royal Free London FT 6 4 4 5 9 5 3 1 7 7 0 7 9 16Guy's and St. Thomas' 5 8 6 4 5 2 2 2 6 2 4 4 2 6St. George's Healthcare 3 5 3 5 3 3 1 3 1 4 4 3 3 6
Homerton 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0Barts Health 25 28 35 46 30 22 22 27 10 21 14 10 20 20 50Moorfields Eye Hospital 0 0 0 0 0 0 0 0 0 0 0 3 0 0 3UCLH 3 4 15 7 16 50 25 25 37 22 19 7 12 19 38Royal Free London FT 2 1 3 1 3 2 0 3 7 5 9 5 0 1 6Guy's and St. Thomas' 2 8 1 1 3 2 3 3 3 2 0 5 1 3 9St. George's Healthcare 0 0 0 0 0 0 0 2 9 0 0 0 0 0 0
Homerton 96.8% 98.0% 97.3% 96.6% 96.7% 96.1% 97.3% 96.0% 97.0% 96.4% 96.5%Barts Health 95.0% 95.0% 95.9% 95.4% 94.8% 95.2% 96.2% 95.2% 95.8% 95.6% 95.5%Moorfields Eye Hospital 98.7% 98.0% 98.3% 98.7% 98.0% 98.1% 99.0% 98.6% 98.6% 98.9% 98.6%UCLH 96.0% 96.0% 95.4% 94.4% 93.3% 93.4% 92.5% 94.1% 94.0% 94.9% 95.1%Royal Free London FT 98.7% 98.4% 97.6% 96.6% 96.9% 95.8% 96.2% 96.5% 96.7% 96.7% 97.0%Guy's and St. Thomas' 97.0% 96.7% 96.9% 96.2% 96.7% 96.9% 97.2% 97.7% 97.6% 97.6% 97.4%St. George's Healthcare 96.4% 97.3% 97.3% 96.6% 96.8% 94.9% 93.2% 93.5% 95.9% 96.0% 96.2%
May-14Theme KPI / Measure Provider Jun-14 Mar-15 Apr-15Oct-14 Nov-14 Dec-14
Qua
lity
Sep-14 Jun-15Jul-14 May-15Aug-14 Jan-15 Feb-15 2015-16YTD
MRSA reported infections
C. Difficile reported infections
Mixed Sex Accommodation (MSA) (Number of breaches)
VTE(% admitted patients
assessed for VTE risk)
2015-16 Target
Zero tolerance
Zero tolerance
95%
In month target not available
83
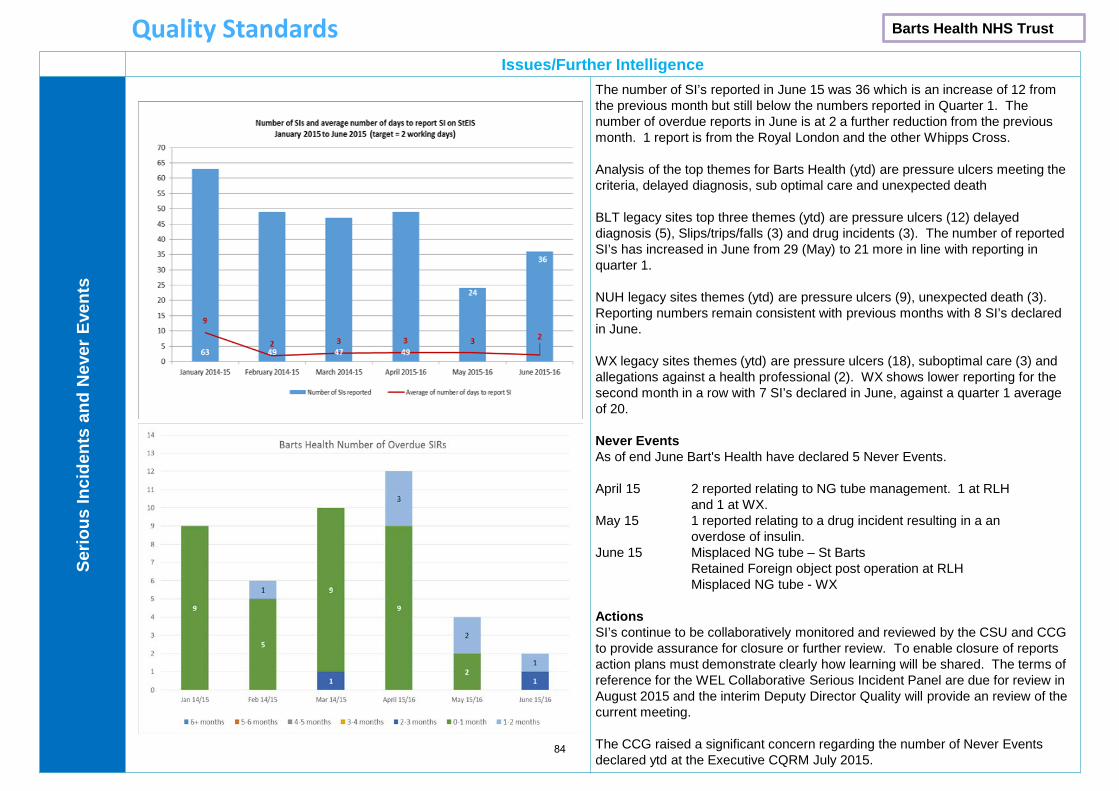
Issues/Further Intelligence Se
rious
Inci
dent
s an
d N
ever
Eve
nts
The number of SI’s reported in June 15 was 36 which is an increase of 12 from the previous month but still below the numbers reported in Quarter 1. The number of overdue reports in June is at 2 a further reduction from the previous month. 1 report is from the Royal London and the other Whipps Cross. Analysis of the top themes for Barts Health (ytd) are pressure ulcers meeting the criteria, delayed diagnosis, sub optimal care and unexpected death BLT legacy sites top three themes (ytd) are pressure ulcers (12) delayed diagnosis (5), Slips/trips/falls (3) and drug incidents (3). The number of reported SI’s has increased in June from 29 (May) to 21 more in line with reporting in quarter 1. NUH legacy sites themes (ytd) are pressure ulcers (9), unexpected death (3). Reporting numbers remain consistent with previous months with 8 SI’s declared in June. WX legacy sites themes (ytd) are pressure ulcers (18), suboptimal care (3) and allegations against a health professional (2). WX shows lower reporting for the second month in a row with 7 SI’s declared in June, against a quarter 1 average of 20. Never Events As of end June Bart's Health have declared 5 Never Events. April 15 2 reported relating to NG tube management. 1 at RLH and 1 at WX. May 15 1 reported relating to a drug incident resulting in a an overdose of insulin. June 15 Misplaced NG tube – St Barts Retained Foreign object post operation at RLH Misplaced NG tube - WX Actions SI’s continue to be collaboratively monitored and reviewed by the CSU and CCG to provide assurance for closure or further review. To enable closure of reports action plans must demonstrate clearly how learning will be shared. The terms of reference for the WEL Collaborative Serious Incident Panel are due for review in August 2015 and the interim Deputy Director Quality will provide an review of the current meeting. The CCG raised a significant concern regarding the number of Never Events declared ytd at the Executive CQRM July 2015.
Quality Standards Barts Health NHS Trust
84

Governing Body Meeting Enclosure
Date of meeting September 1st 2015 G, H
Agenda item 2.4
Title of report: Barts Health – RLH CQC Compliance Action Plan and Improvement Plan
Author(s): Karen Breen – Managing Director - RLH
Presented by: Sponsor (if different): For further information
Karen Breen – Managing Director - RLH Archna Mathur – Director Quality & Performance THCCG [email protected] (020 3688 2528)
Executive summary
This paper provides a brief overview of the RLH Improvement Programme and CQC compliance action plan.
The report highlights: the improvement workstreams and governance, leadership and organisational development, safe and effective care, workforce and complassionate care and patient experience.
Recommendation
Information Approval To note Decision
The Governing Body is asked to note the contents of the report especially in relation to the BAF risk 1.1: Failure to ensure effective systems and processes are in place to monitor, challenge and support Barts Health NHS Trust delivery of NHS Constitution targets and CQC action plan could result in the increased likelihood of poor quality, poor patient experience, delivery of poor clinical outcomes and the trust remaining in special measures in the longer term.
Key issues The CQC inspection (January 2015, published May 2015) rated the Royal London Hospital (RLH) overall as inadequate and Barts Health NHS Trust has been placed in special measures.
Conflicts of Interest There are no identified conflicts of interests.
Report history This is the first time these reports have been presented to the Tower Hamlets CCG Governing Body.
Patient and Public involvement
N/A
Link to the Board Assurance Framework
This paper affects all of the risks under Strategic Objective 1: Systems and processes to monitor challenge and support provider delivery of the NHS Constitution targets.
85
Impact on Equality and Diversity
N/A
Resource requirements None
Next steps As outlined in the reports.
86

Clinical Improvement programme at the RL hospital – our progress & focus on quality.
26th August 2015 CQRM Update
Oversight and Assurance
87

Introduction
• The Barts Health Quality Improvement Plan is not just a response to the Care Quality Commission’s (CQC) Inspection report of May 2015; it also includes the actions that staff feel are necessary to provide the communities we serve with safe, effective, compassionate and high quality care.
• The Programme and structure was considered at the Trust Board in August 2015
• Teams initial focus has been on addressing the CQC compliance actions and immediate concerns.
• Whilst continuing to support on-going actions, the workstreams are focusing on developing detailed milestone plans, resourcing plans and KPI improvement trajectories to ensure achievement of all objectives set per workstream to achieve safe, effective, compassionate and high quality care.
88

Regulation 19 - complaints − There was limited learning form complaints. − In some service complaints were not dealt with appropriately or
promptly.
Regulation 13 - Management of medicines RLH − There was no policy or guidance on the consistent use of opioids
which put patients at risk of drug errors or misprescribing when doctors moved between wards and failed to appreciate that the drugs had different potencies when administered by different methods; Ensure there is a policy on the consistent use of opioids.
Regulation 16 Safety, availability and suitability of equipment
− Suitable arrangements were not always in place to ensure enough of the correct equipment was readily available in theatres, in particular for children; Ensure there is enough surgical equipment for children.
Regulation 9 - Care & welfare of people who use services
− Patients’ needs were not always assessed and their care were not always planned or delivered to meet their needs.
− Ensure safety is a sufficient priority in all services. − Address the capacity issues across the hospital. − Ensure audits carried out to identify areas for improvements &
implementation monitored. − Ensure all policies are based on current and best practice guidelines. − Urgently improve security in maternity services. − Ensure staff carry out and document assessments of patient's needs
to ensure the planning & delivery of care meets their needs − Take definitive action to reduce the RTT & ensure accurate reporting. − Reduce number of cancelled procedures & operations. − Reduce patient waiting times in OP clinics.
The CQC report found weaknesses in each of our core values Regulation 22 - Staffing
− There were not enough staff across all staff groups and staff levels to provide safe care and treatment for patients.
− Ensure all services are well-led. − Take further action to improve and address the perceived culture of
bullying and harassment. − Ensure there are sufficient numbers of suitably qualified, skilled and
experienced medical staff to meet the needs of patients. In particular in maternity and children's services.
− Ensure there are sufficient numbers of suitably qualified, skilled and experienced nursing staff to meet the needs of patients. Staffing levels must meet RCN staffing guidelines and Core Standards for ICU
− Ensure the induction process for agency staff working in ACCU is consistent and monitored.
− Ensure all staff have an understanding of their responsibilities under the Mental Capacity Act (2005) and Deprivation of Liberty Safeguards. Staff in Urgent and emergency services clearly understood their role however other services were not clear.
− Ensure that all relevant ward staff receive training specific to managing patients at the EOL
Regulation 20 - Records
− Accurate records in relation to the care and treatment of patients were not kept.
− Nursing documentation was inconsistent and inaccurate. Ensure nursing records are completed fully and accurately to ensure patient safety.
− The WHO Surgical Safety Checklist were not always fully completed − Ensure the do not attempt cardio-pulmonary resuscitation (DNA CPR)
form and the new DNA CPR policy are clear and in keeping with any recent ruling or guidance; The DNACPR documents were not always fully completed
Caring
Well-led
Effective
Safe
Responsive
Regulation 10 Assessing and monitoring the quality of service provider − Patients were not protected against the risks of inappropriate or unsafe care by
the means of an effective operation of systems to regularly assess and monitor the quality of the service or identify assess and manage risks
− Ensure performance dashboards and information are reliable and service specific. Senior staff must have the information they need to have oversight of the services they lead.
− Address the lack of data specific to services at the hospital. − Ensure governance & risk management processes are robust and embedded
throughout RLH − Ensure incidents are investigated promptly and the learning from incidents,
complaints and never events is shared across services. 89
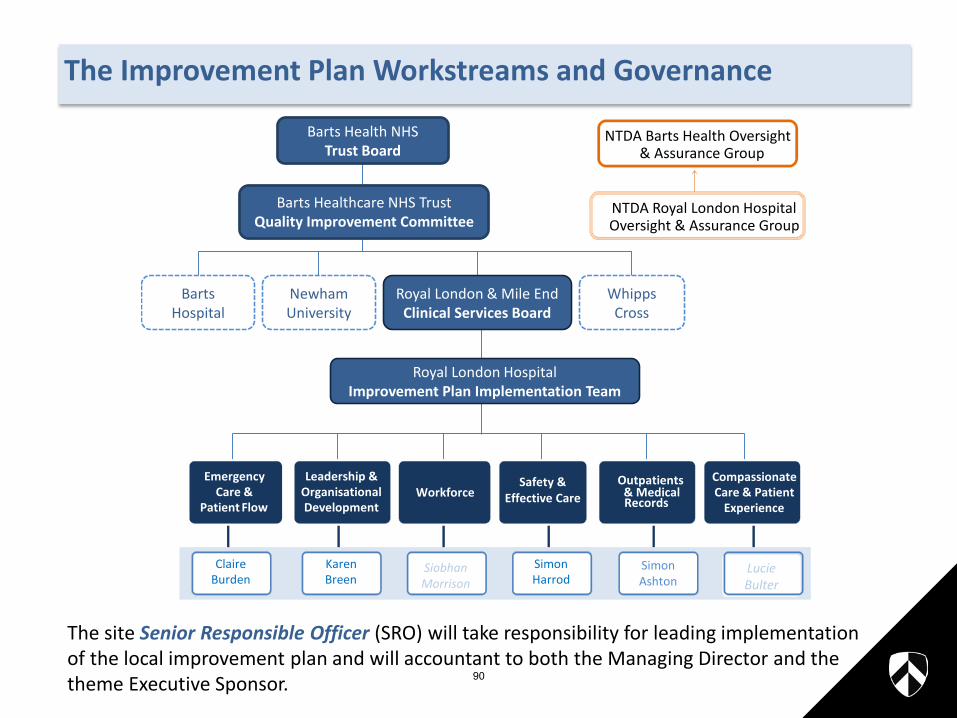
The Improvement Plan Workstreams and Governance
The site Senior Responsible Officer (SRO) will take responsibility for leading implementation of the local improvement plan and will accountant to both the Managing Director and the theme Executive Sponsor.
Newham University
Barts Hospital
Whipps Cross
Barts Health NHS Trust Board
Royal London & Mile End Clinical Services Board
Royal London Hospital Improvement Plan Implementation Team
Barts Healthcare NHS Trust Quality Improvement Committee
Emergency Care &
Patient Flow
Leadership & OrganisationalDevelopment
WorkforceSafety &
Effective CareOutpatients
& Medical Records
Compassionate Care & Patient
Experience
Claire Burden
Karen Breen
Simon Harrod
Simon Ashton
Lucie Bulter
Siobhan Morrison
NTDA Barts Health Oversight & Assurance Group
NTDA Royal London Hospital Oversight & Assurance Group
90

Leadership and Organisational Development SRO: Karen Breen
Patients forum & Expert Patients
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Immediate response to CQC compliance actions • There was no compliance actions that directly relate to this workstream however
leadership is implicit in the improvements the organisation is required to achieve Wider workstream objectives to address CQC Must Dos: • Establish a site based leadership team dedicated to RLH site • Introduce a leadership operating model that provides sufficient and consistent
leadership on site • Clearly define CAG and site responsibilities supported by reporting meetings to
ensure quality and safety and efficient running of the site have the required focus and sustainability
• Establish and embed performance dashboards to equip leaders with management information
• Each service line to have an strategy and annual business plan that is well communicated with clear roles and responsibilities
• Supporting Leaders and their teams to deliver Culture Change - including the development of the Trust approach to identifying and tackling culture
Progress: • Managing Director and Site Medical Director in place from June 15 • Trust wide leadership operating model reviewed and agreed in August. Full
transition to new site based leadership model in place from 1st September • Trust-wide Strategy and CAG function confirmed to ensure Trust-wide learning and
best practice shared • RLH performance dashboards established
Spans of Control
Leadership Development
Site based Structures
Information & Performance Effective Staff engagement
Leadership & Organisational Development
91

Leadership and Organisational Development SRO: Karen Breen
Patients forum & Expert Patients
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Progress (continued) • Values based recruitment training delivered for all new recruitment at Band 8A
and above including medical consultants • Completed General Manager Development Programme to be expanded in the new
Leadership Operating Model • Renal culture change diagnostic and improvement programme on-going • ‘Speak in Confidence’ being used by staff to escalate concerns through to
Executive for appropriate action • Small scale workshop on talent management and difficult conversations Next steps: • Transition to new leadership operating model management structure post 1st
September and embed the performance and accountability framework • Development of service line and improvement programme dashboard to ensure
clinical leaders are equipped with management information • Commence site based communications plan to all staff
Spans of Control
Leadership Development
Site based Structures
Information & Performance Effective Staff engagement
Leadership & Organisational Development
92

Emergency Care and Patient Flow SRO: Claire Burden
Patients forum & Expert Patients
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Required action Our response Progress Next steps Suitable arrangements were not always in place to ensure enough of the correct equipment was readily available in theatres, in particular for children.
Review of baseline equipment to be undertaken within Paediatric Theatres Business cases developed for identified items requiring capital investment Review all broken equipment and agree schedule of repair/ replacement Review sterilisation cycle times with Synergy to address any delays
Business cases & procurement processes initiated April-June 15 and a s a result most, but not all, kit has been purchased and in place from June 15. Remaining items have business cases completed and the Theatre Manager is working with the Capital Team to confirm funding. Review of repairs outstanding completed – replacement kit to be purchased to enable sets to return to use Quarantine systems and audits in place and reviewed weekly with Synergy weekly. Synergy has extended working hours which is also improving the turnaround of kit.
Approval of remaining kit and getting this kit into circulation Monitor and quantify the impact on cancellations and staff experience
Immediate response to CQC compliance actions
93

Emergency Care and Patient Flow SRO: Claire Burden
Patients forum & Expert Patients
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Wider workstream objectives to address CQC Must Dos: • Building on existing work to achieve improvements in ED processes to allow
achievement of the 4 hour standard • Establish and embed ambulatory care models on all sites • Internal standards to allow for acute surgical and acute medical units to run with <48hr
LOS • Implement best practice ward flow and discharge processes to support a reduction in
ALOS • Ensure the trauma capacity is sufficient for the demands of trauma, emergency
orthopaedics and emergency neurosurgery at RLH • Develop a Trust wide approach to reporting when a patient is ready to be discharged
but is still in hospital.
Progress: • Introduced the site management early warning tools (SMEWS) to keep RLH safe • Internal challenge standards set for ED and RLH site team • Reduced total journey time for admitted patients by 1hr 6 minutes • Increased bed availability at 08:30 from 6 to 20 beds on average • Reduced non-elective LOS by 1 day over last 4 months • Realigned care of the elderly to a single floor of the RLH (wards 14E/F) with no negative
impact to patient experience to improve consultant availability to patients • RLH priorities established for next 6 months with medical sponsorship and timelines for delivery and resourcing plan confirmed. See attached example • Establishing a RLH site team culture that is open and responsive;
as fed back by RLH staff and reported by ECIST (29th July 2015)
Theatre Programme
Pre - Op Assessment
Enhanced Recovery
Criteria led discharge
Complex Pt. Pathways
ED Improvement
Admission Avoidance
AAU/SAU Flow
Trauma & complex care
Complex Discharge
Specialist Paediatrics
Maternity Care
Emergency Care & Patient
Flow
94

Emergency Care and Patient Flow SRO: Claire Burden
Patients forum & Expert Patients
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Next steps: • Ambulatory care to start 2nd November • New Acute Physician 7 day model to start 2nd November • Trauma/Neuro/Ortho bed reconfiguration planned by October 15 • ED redesign of emergency assessment (first 60 mins) • Detailed planning for surgical acute model launch end November
Risks to delivery: • The continuous improvement required in the delivery of the RLH constitutional
standards whilst delivering significant operational and organisational change • Notably the ED, Cancer and RTT standards as winter pressures start
• System delivery of demand management • Delivering the Trust wide ICT programme • Recruitment timeline of November 2015 for new operating models • Backfilling posts for RLH staff to lead change • Procurement of monitoring equipment to enable the delivery of the clinical
reconfiguration • Sufficient programme and project support; inclusive of informatics from September 2015
Theatre Programme
Pre - Op Assessment
Enhanced Recovery
Criteria led discharge
Complex Pt. Pathways
ED Improvement
Admission Avoidance
AAU/SAU Flow
Trauma & complex care
Complex Discharge
Specialist Paediatrics
Maternity Care
Emergency Care & Patient
Flow
95

Monitoring and evaluation (examples) Weekly challenge & review sessions the Hospital Director and ED clinicians
Admitted patients
Non-admitted patients
96

Safe and Effective Care SRO: Simon Harrod
Patients forum & Expert Patients
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Required action Our response Progress Next steps Patients were not protected against the risks of inappropriate or unsafe care by the means of an effective operation of systems to regularly assess and monitor the quality of the service or identify assess and manage risks
Medical devices groups to determine appropriate strategy for the supplier for high volume and low value equipment in a timey manner relative to the lifespan of the devices Integration of ward accreditation data with IPR Sporadic checks of resuscitation trolleys are routinely allocated to 2 nurses on duty and are checked and signed for daily. If used over the 24 hour period, trolley is re-filled , re-checked and re-signed. Ward Managers to apply principles of quality improvement cycles to support staff at ward level to make local changes and apply improvements based on local data derived from incidents/complaints from their areas.
Project Manager assigned to work ward accreditation. Existing metrics challenged and new metrics confirmed. Ward based dashboard created and pilot 6 first metrics in September on medical wards Resus Training Officer attends daily safety huddle reporting any cardiac arrest activity in the previous 24 hrs highlighting any learning and shortfalls in equipment First 3 cohorts of ‘Leading a Care Environment ‘have completed their workshops and this included safety seminars and master clases using incidents and complaints to inform their ward based improvement. PDSA cycles introduced as an improvement tool during SITF i.e. currently undertaking a PDSA cycle of evening shift senior nurse supporting the wards during this critical handover period Datix User Group started in August with the purpose of improving reporting, improving staff access to Datix and report generation for local learning
Quality metrics from Ward to Board by in October 2015. Dashboard will form part of the new site based performance review documents Audit of resus equipment and trolley readiness by Resus Training Officer. A review on cardiac arrests audit forms to identify where equipment failures may have had an impact on the outcome . To ensure all Band 7s on site have attended the ‘Leading a Care Environment’ workshops Next Datix User Group will focus on the actions module to enable local leaders to update their action taken and provide evidence
Immediate response to CQC compliance actions (1)
97

Safe and Effective Care SRO: Simon Harrod
Patients forum & Expert Patients
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Required action Our response Progress Next steps There was no policy or guidance on the consistent use of opioids which put patients at risk of drug errors or misprescribing when doctors moved between wards and failed to appreciate that the drugs had different potencies when administered by different methods. Ensure there is a policy on the consistent use of opioids.
Stat & Mandatory Training and management of medicines training database to be compiled on a local level and entered on shared Trust wide database. Produce trust wide guideline for 1) acute pain management; and 2) pain management in end of life. Implement and audit adherence Produce a harmonised guideline for PCA, implement and audit Provide a single chart to inform conversion between opiates & implement.
Stat & Mandatory training is set up and current compliance is 66% Acute medicine policy and the PCA guidelines agreed at the Joint Prescribing Committee and published on the Intranet Pain management in end of life policy drafted Single chart reviewed and deemed appropriate. Further review scheduled for next few months
Targeted work with staff groups to improve Stat and Mandatory training compliance Briefing and communications on the Acute medicine policy and PCA guidelines Approval of Pain management in end of life policy and dissemination
98

Safe and Effective Care SRO: Simon Harrod
Patients forum & Expert Patients
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Required action Our response Progress Next steps Accurate records in relation to the care and treatment of patients were not kept.
The documentation standards revisited with consultant medical staff to ensure they meet required standards. Review all documentation that records patients' care and treatment to ensure that it has been standardised. Director of Nursing with medical director and lead for AHP will review tools in use and access to records. Ensure that senior staff audit records on at least a monthly basis
Trust induction included supporting junior doctors in the use of power chart for medical documentation Trust wide review of nursing documentation and Whipps Cross are piloting new structure. In August, RLH site Senior Nurses have been attending bed side handover and challenging documentation standards. Early implementers of paper light recording now includes critical care and neurosciences. Chief Clinical Information Officer working with site based team on further roll out plan. Clinical support app launched by the Chief Medical Officer to support clinical care Detailed audit tool written.
Await the outcome of Whipps Cross pilot and implement recommendations Further paper light recording areas to be identified Audit of clinical notes by nursing and medical teams. Enhance audit programme going forward.
Urgent improve security in the maternity services
Review security to ward areas and execute recommendations Amend and implement changes to visiting policy to allow maximum of 2 adults visitors per bedside at one time Increase visibility and presence of ward clerk
A security review has taken place and new protocol for practice For Royal London the central lift new swipe work has commenced and is a 3 phase approach to completion to ensure fire regulations maintained – completion end August.. Baby Tagging – cross site review and costing completed for implementation
8th floor – business plan to increase to 24hr reception cover to be considered 6th floor reception review – recruiting for 24hr cover Decision of implementation of Baby Tagging 99

Safe and Effective Care SRO: Simon Harrod
Patients forum & Expert Patients
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Wider workstream objectives to address CQC Must Dos: • Establish The Royal London Governance structure in the new leadership model • Achieve a culture of reporting incidents and demonstrating that concerns have been
listened to and acted upon • Greater staff understanding of incidents, the lessons learned and their part to play in
improvements • Improved response times to patients with complaints • Embedding safety tools on site to enhance patient safety • Improved recording in medical records of patient care plans • Compliance to national standards and protocols set for WHO checklist, DNACPR. • Achievement of quality standards set in national and local CQUIN
Progress: • WHO checklist part of daily practice and compliance is audited • Safety thermometer in place on all wards • Safer staffing model reviewed daily from the RLH site office • Daily 11:15am safety huddles in place • CQUIN Q1 achieved 82% compliance and detailed plans in place for Q2-4 • Project team planning session on 24th August Next steps: • Map existing and future governance arrangements for the site within the new site
Leadership Operating Model including existing weekly SI meetings • Complaints and SIs to be loaded into consultant PREP to develop reflective practice and learning • Formation of detailed plans to carry out remaining recommendations on ‘Must Dos’ with newly formed working group
Safety thermometer
Quality forum
Learning from SI’s
Complaints
CQUIN
Safety & Effective Care
100
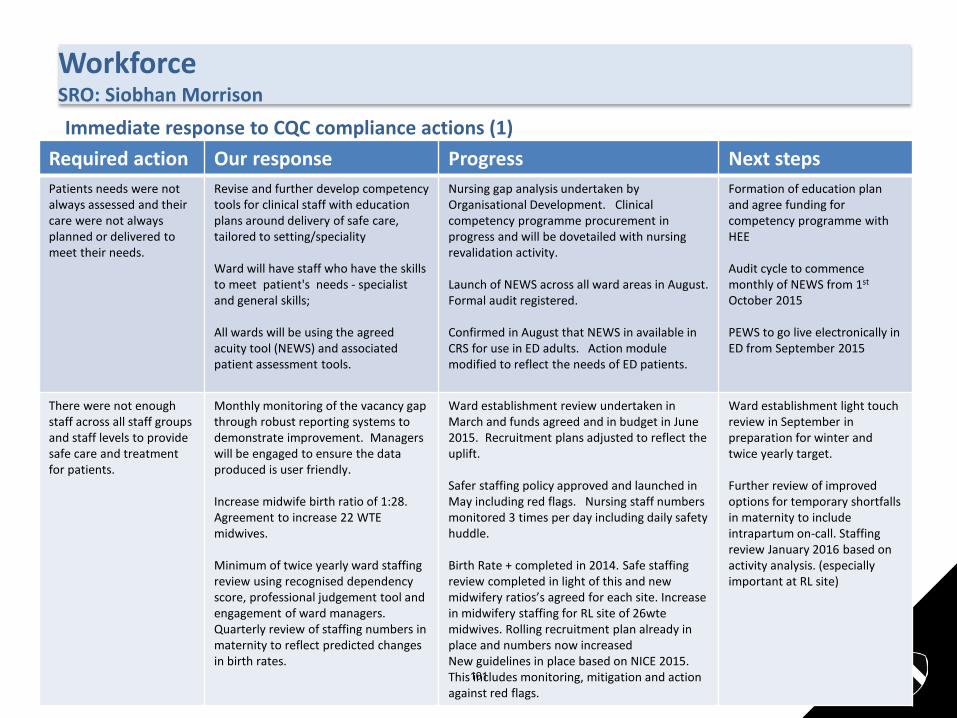
Workforce SRO: Siobhan Morrison
Patients forum & Expert Patients
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Required action Our response Progress Next steps Patients needs were not always assessed and their care were not always planned or delivered to meet their needs.
Revise and further develop competency tools for clinical staff with education plans around delivery of safe care, tailored to setting/speciality Ward will have staff who have the skills to meet patient's needs - specialist and general skills; All wards will be using the agreed acuity tool (NEWS) and associated patient assessment tools.
Nursing gap analysis undertaken by Organisational Development. Clinical competency programme procurement in progress and will be dovetailed with nursing revalidation activity. Launch of NEWS across all ward areas in August. Formal audit registered. Confirmed in August that NEWS in available in CRS for use in ED adults. Action module modified to reflect the needs of ED patients.
Formation of education plan and agree funding for competency programme with HEE Audit cycle to commence monthly of NEWS from 1st October 2015 PEWS to go live electronically in ED from September 2015
There were not enough staff across all staff groups and staff levels to provide safe care and treatment for patients.
Monthly monitoring of the vacancy gap through robust reporting systems to demonstrate improvement. Managers will be engaged to ensure the data produced is user friendly. Increase midwife birth ratio of 1:28. Agreement to increase 22 WTE midwives. Minimum of twice yearly ward staffing review using recognised dependency score, professional judgement tool and engagement of ward managers. Quarterly review of staffing numbers in maternity to reflect predicted changes in birth rates.
Ward establishment review undertaken in March and funds agreed and in budget in June 2015. Recruitment plans adjusted to reflect the uplift. Safer staffing policy approved and launched in May including red flags. Nursing staff numbers monitored 3 times per day including daily safety huddle. Birth Rate + completed in 2014. Safe staffing review completed in light of this and new midwifery ratios’s agreed for each site. Increase in midwifery staffing for RL site of 26wte midwives. Rolling recruitment plan already in place and numbers now increased New guidelines in place based on NICE 2015. This includes monitoring, mitigation and action against red flags.
Ward establishment light touch review in September in preparation for winter and twice yearly target. Further review of improved options for temporary shortfalls in maternity to include intrapartum on-call. Staffing review January 2016 based on activity analysis. (especially important at RL site)
Immediate response to CQC compliance actions (1)
101

Workforce SRO: Siobhan Morrison
Patients forum & Expert Patients
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Required action Our response Progress Next steps There were not enough staff across all staff groups and staff levels to provide safe care and treatment for patients (Continued)
Medical models reviewed against college guidance as part of team objective setting and job planning. Minimum of once a day dependency scoring on each ward. Paediatrics will introduce an acuity tool appropriate to the needs of children and young people. Clear model for escalation developed and made available to all staff in safer staffing returns and use of safety huddles to reallocate staff Wide circulation of the Trusts safer staffing policy including team briefings, posters and leaflets Achieve a 95% substantive fill rate by February 2017 recognising the current recruitment and retention rates. Work with Bank Partners to increase the supply of staff available for temporary shifts Optimal use of electronic rostering
Nursing staff numbers monitored 3 times per day including daily safety huddle. Planned and actual staffing for nursing published on the safety boards at the entrance to the ward and checked daily by Senior Nurses Sourced quotes of 2 commercial products to provide a paediatric acuity tool Safer staffing policy in place. Information circulated in safety huddles and disseminated to ward teams. Posters and leaflets agreed Vacancy analysis complete and top 9 areas of vacancy identified. One-stop-shop recruitment days in planning Approached universities for newly qualified staff Electronic rostering templates updated with new shift profiles further to ward establishment review changes. Weekly assurance meetings include 10 golden rules of rostering and are monitored weekly with Associate Directors of Nursing for ECAM. To be transitioned to site based in September
Creation of ward based notice boards with Safer Staffing information and leaflets available Procure an appropriate paediatric acuity tool Confirmation of recruitment strategies for the top 9 vacancy areas to be confirmed in September. One-stop-shop recruitment days for medical and surgical ward vacancies Program developed for return to practice, open day in September
102
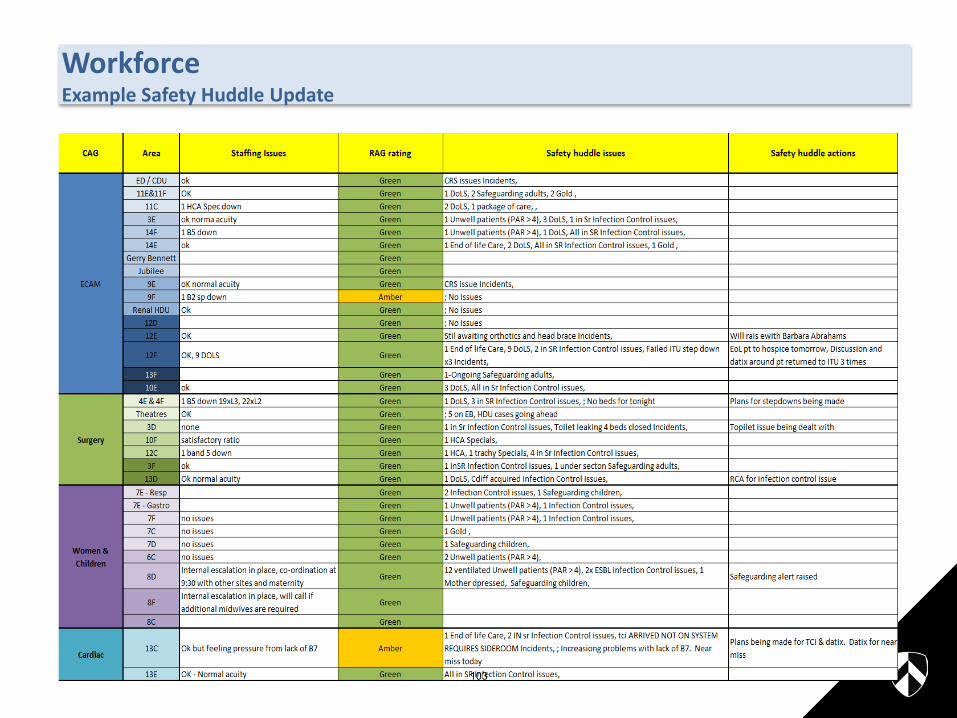
Workforce Example Safety Huddle Update
103

Workforce SRO: Siobhan Morrison
Patients forum & Expert Patients
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate
Experience
Family & Patient Centred Care
Wider workstream objectives to address CQC Must Dos: • Achieve a 95% fill rate across all our clinical areas • Develop recruitment strategies for the top 9 wards / departments with the highest level
of vacancies • Hold one-stop-shop recruitment days for medical and surgical ward vacancies • Maximise our use of staffing hours to ensure optimal use and staff know what shifts
they are working 8 weeks in advance • Retaining our staff but being clear on how their role fits in the organisation, offering
development and training opportunities and reflecting on feedback from Staff Surveys • Embedding a local and trust wide induction for new starters and agency workers caring
for our patients • Ensure bank rates of pay are comparable to other London NHS Trusts
Progress: • Analysis of high vacancy areas completed and top 9 areas of focus identified • Senior team undertaken visits to top 3 temporary staffing usage areas to support
recovery • Pilot elevated bank rate for ED in August and September • Fortnightly site based meetings with Bank Partners started Next steps: • Site based leadership recruitment strategies for top 9 areas to be developed in
September • One-stop-shop recruitment days to start in October • Focus sessions with nursing leaders on improving staff retention • Progress made on publication of rotas 8 weeks in advance for all ward areas
Roles & Resp. Review
Recruit to Retain plan
New Role Development Staff training/ Competencies
Drive ‘95
Workforce Capacity & Capability
104
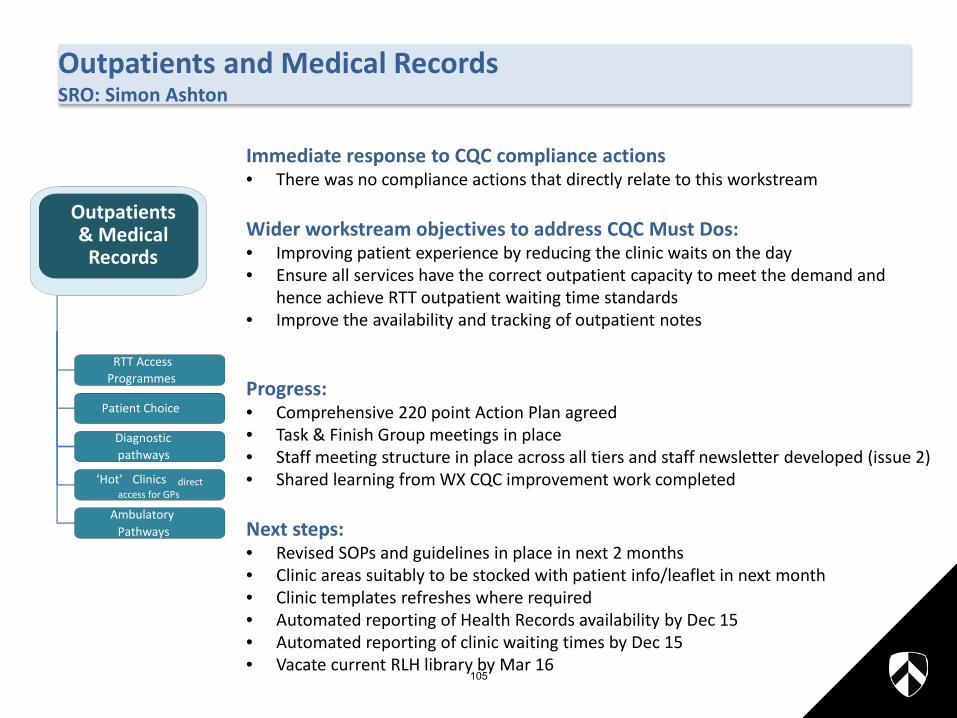
Outpatients and Medical Records SRO: Simon Ashton
Patients forum & Expert Patients
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Immediate response to CQC compliance actions • There was no compliance actions that directly relate to this workstream Wider workstream objectives to address CQC Must Dos: • Improving patient experience by reducing the clinic waits on the day • Ensure all services have the correct outpatient capacity to meet the demand and
hence achieve RTT outpatient waiting time standards • Improve the availability and tracking of outpatient notes Progress: • Comprehensive 220 point Action Plan agreed • Task & Finish Group meetings in place • Staff meeting structure in place across all tiers and staff newsletter developed (issue 2) • Shared learning from WX CQC improvement work completed Next steps: • Revised SOPs and guidelines in place in next 2 months • Clinic areas suitably to be stocked with patient info/leaflet in next month • Clinic templates refreshes where required • Automated reporting of Health Records availability by Dec 15 • Automated reporting of clinic waiting times by Dec 15 • Vacate current RLH library by Mar 16
RTT Access Programmes
Patient Choice
Diagnostic pathways
‘Hot’ Clinics direct access for GPs
Ambulatory Pathways
Outpatients & Medical
Records
105
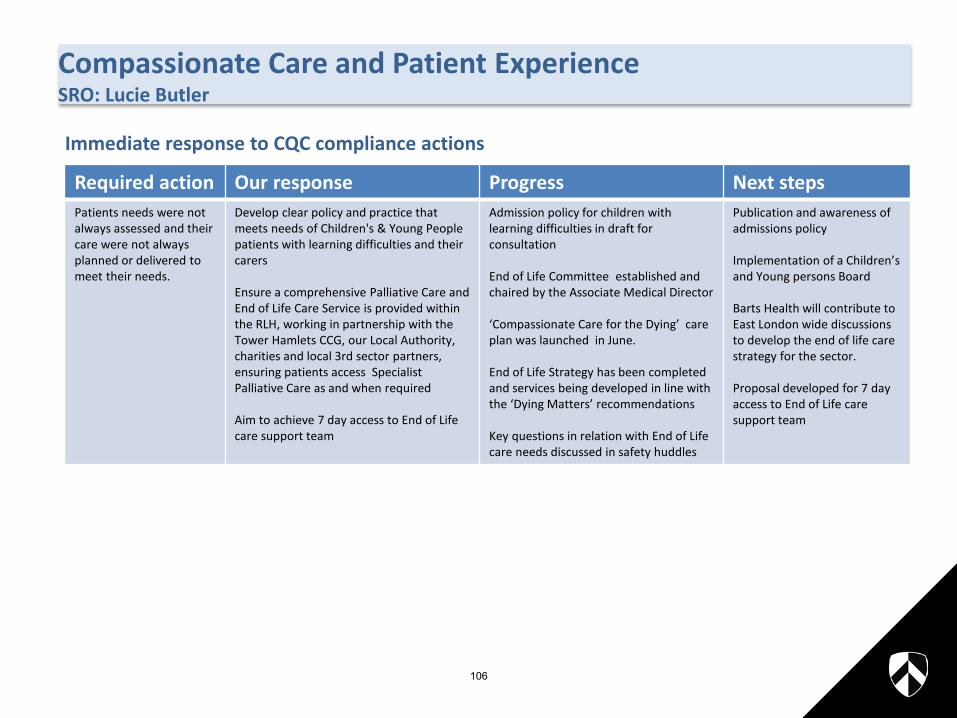
Compassionate Care and Patient Experience SRO: Lucie Butler
Patients forum & Expert Patients
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Required action Our response Progress Next steps Patients needs were not always assessed and their care were not always planned or delivered to meet their needs.
Develop clear policy and practice that meets needs of Children's & Young People patients with learning difficulties and their carers Ensure a comprehensive Palliative Care and End of Life Care Service is provided within the RLH, working in partnership with the Tower Hamlets CCG, our Local Authority, charities and local 3rd sector partners, ensuring patients access Specialist Palliative Care as and when required Aim to achieve 7 day access to End of Life care support team
Admission policy for children with learning difficulties in draft for consultation End of Life Committee established and chaired by the Associate Medical Director ‘Compassionate Care for the Dying’ care plan was launched in June. End of Life Strategy has been completed and services being developed in line with the ‘Dying Matters’ recommendations Key questions in relation with End of Life care needs discussed in safety huddles
Publication and awareness of admissions policy Implementation of a Children’s and Young persons Board Barts Health will contribute to East London wide discussions to develop the end of life care strategy for the sector. Proposal developed for 7 day access to End of Life care support team
Immediate response to CQC compliance actions
106
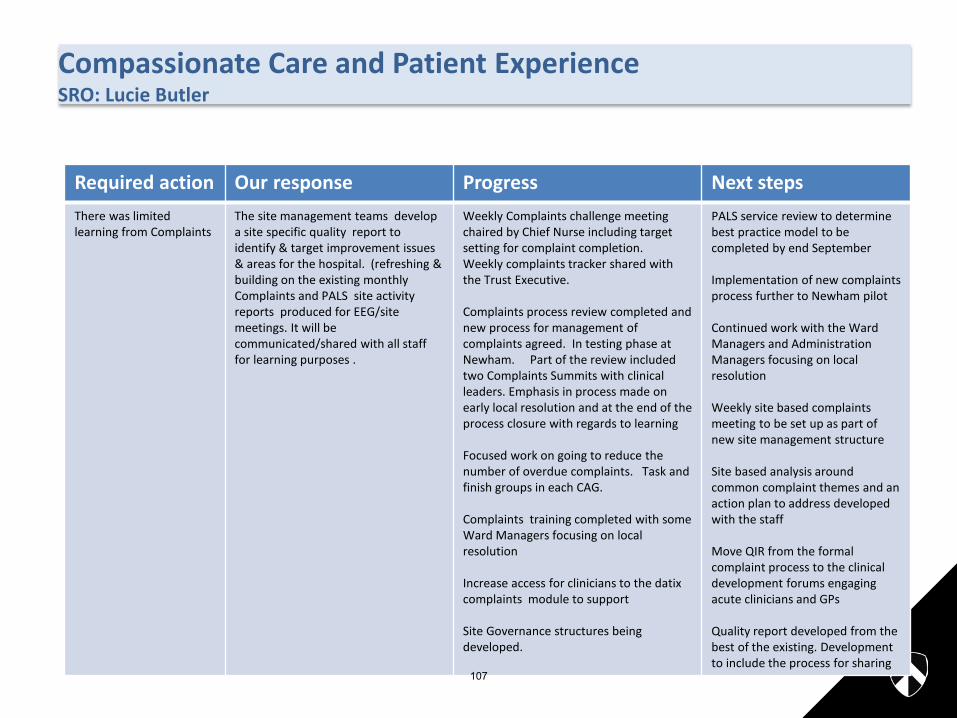
Compassionate Care and Patient Experience SRO: Lucie Butler
Patients forum & Expert Patients
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Required action Our response Progress Next steps There was limited learning from Complaints
The site management teams develop a site specific quality report to identify & target improvement issues & areas for the hospital. (refreshing & building on the existing monthly Complaints and PALS site activity reports produced for EEG/site meetings. It will be communicated/shared with all staff for learning purposes .
Weekly Complaints challenge meeting chaired by Chief Nurse including target setting for complaint completion. Weekly complaints tracker shared with the Trust Executive. Complaints process review completed and new process for management of complaints agreed. In testing phase at Newham. Part of the review included two Complaints Summits with clinical leaders. Emphasis in process made on early local resolution and at the end of the process closure with regards to learning Focused work on going to reduce the number of overdue complaints. Task and finish groups in each CAG. Complaints training completed with some Ward Managers focusing on local resolution Increase access for clinicians to the datix complaints module to support Site Governance structures being developed.
PALS service review to determine best practice model to be completed by end September Implementation of new complaints process further to Newham pilot Continued work with the Ward Managers and Administration Managers focusing on local resolution Weekly site based complaints meeting to be set up as part of new site management structure Site based analysis around common complaint themes and an action plan to address developed with the staff Move QIR from the formal complaint process to the clinical development forums engaging acute clinicians and GPs Quality report developed from the best of the existing. Development to include the process for sharing
107

Compassionate Care & Patient Experience SRO: Lucie Butler
Patients forum & Expert Patients
Compassion in Care team
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Wider workstream objectives to address CQC Must Dos: • Develop clinical leaders as role models for our values and behaviours • Create of culture of continuous improvement and empowering staff to
innovate and improve practice • Make clear links to quality, safety and effectiveness by building on safety
huddles and ward accreditation • Encourage and support staff to raise concerns and confidently challenge any
breaches of compassionate care • To renew and revitalise our relationship with patients, carers and patient
groups to ensure their voice is heard and contributes to the development of our care services. Responding to concerns in a timely respectful manner.
• Ensure patients have the right care, hydration and nutrition. Progress: • Compassion in Care group formed. TOR reference developed. Work groups
and leads identified. • Competency of ward leader defined with clear guidelines • Safety huddles for the site undertaken daily with wide MDT membership
agenda includes ward based risks, staffing, EOLc, Patients at risk of deterioration and those subject to DoLs
• Nutrition and Hydration action plan developed and activity monitored • Dementia friends workshops held on site. Volunteers trained to support care
in patients living with dementia • Audit tool for in depth assessment of fundamentals of care developed. • Successful Renal services joint patient and clinician development day. 108

Compassionate Care & Patient Experience SRO: Lucie Butler
Patients forum & Expert Patients
Compassion in Care team
Learning from complaints
Patient Champions For high risk groups
Education & involvement
Compassionate Care & Patient
Experience
Family & Patient Centred Care
Next steps: • Nutrition Link nurse program. Roll out of revised MUST score November
2015. • Revision of clinical Friday program to support workstream activity • Stocktake of existing patient forums and patient engagement activity-
consider a ‘network approach’ in speciality areas • Identification and development of ward based MCA and DoLs
champions
109
110

Site Compliance Reference number
Theme Compliance action raised by CQQ Outcome needed to address compliance action
Objective to address the concern raised Action(s) required to reach objective Executive lead Timescale for completion
RLH Regulation 9 Compassionate care
Patients were not always assessed and their care was not always planned or delivered to meet their needs using agreed patient assessment/ dependency scoring tools.
All clinical staff will be competent in the assessment of patient needs.
Each ward will have staff who have the skills to meet patients' needs.
Improved staff education and training ensures care is planned and delivered to meet patient needs.
Undertake a baseline assessment of the skills and knowledge of the nursing staff on all wards to identify gaps in competence/training. All clinical areas will have completed a skill mix review to include associated analysis to ensure support roles are clearly articulated.
Based on the outcome of the assessment and review, an education plan will be developed and resources identified to put it into place.
Minimum of twice a day dependency scoring to be introduced on each ward. Clear model for escalation of shortfalls evident in safer staffing returns. Senior Site team to relocate staff across the site.
Chief Nurse Jan-16
RLH Regulation 10 Safety Patients were not protected against the risks of inappropriate or unsafe care by the means of an effective operation of systems to regularly assess and monitor the quality of the service or identify assess and manage risks.
Staff have the knowledge and skills necessary to improve patient safety and understand their role both locally and corporately.
There are robust risk management systems in place to identify, address and report risks as they arise.Immediate risks to patient safety are escalated as necessary and reported to the Managing Director when overdue.
Line managers work with and actively support staff at ward/departmental level to make improvements in practice which reduce risk within the setting.
Integrated quality and performance report including data to assess and monitor quality of service and identify risks. To be shared with ward managers and senior staff responsible for leading the service
Evidence of completion of appropriate assessment and risk management checklists.
Each clinical service will be required to hold a risk register to be reviewed in line with policy. All services to have a risk management meeting.
All staff will be trained on appropriate identification, reporting and escaltaioin of risks.
Local risk meetings/ safety huddles will be introduced.
There will be a site quality and safety meeting which will provide overview and assurance of risk management systems and share the learning from incidents.
Issues on the site will be examined and action taken to support CAGs in remedying problems.
Chief Medical Officer
Mar-16
111
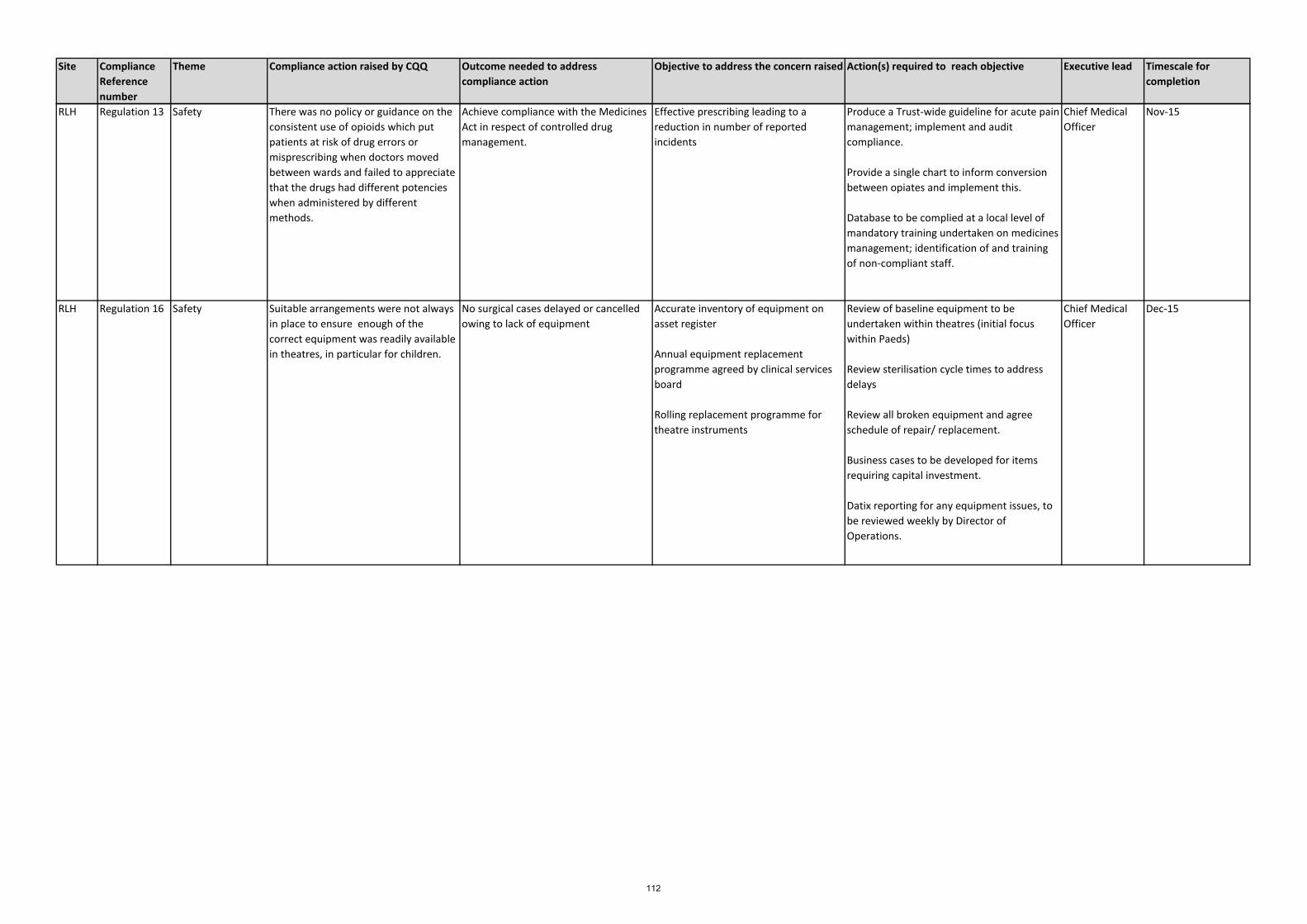
Site Compliance Reference number
Theme Compliance action raised by CQQ Outcome needed to address compliance action
Objective to address the concern raised Action(s) required to reach objective Executive lead Timescale for completion
RLH Regulation 13 Safety There was no policy or guidance on the consistent use of opioids which put patients at risk of drug errors or misprescribing when doctors moved between wards and failed to appreciate that the drugs had different potencies when administered by different methods.
Achieve compliance with the Medicines Act in respect of controlled drug management.
Effective prescribing leading to a reduction in number of reported incidents
Produce a Trust-wide guideline for acute pain management; implement and audit compliance.
Provide a single chart to inform conversion between opiates and implement this.
Database to be complied at a local level of mandatory training undertaken on medicines management; identification of and training of non-compliant staff.
Chief Medical Officer
Nov-15
RLH Regulation 16 Safety Suitable arrangements were not always in place to ensure enough of the correct equipment was readily available in theatres, in particular for children.
No surgical cases delayed or cancelled owing to lack of equipment
Accurate inventory of equipment on asset register
Annual equipment replacement programme agreed by clinical services board
Rolling replacement programme for theatre instruments
Review of baseline equipment to be undertaken within theatres (initial focus within Paeds)
Review sterilisation cycle times to address delays
Review all broken equipment and agree schedule of repair/ replacement.
Business cases to be developed for items requiring capital investment.
Datix reporting for any equipment issues, to be reviewed weekly by Director of Operations.
Chief Medical Officer
Dec-15
112

Site Compliance Reference number
Theme Compliance action raised by CQQ Outcome needed to address compliance action
Objective to address the concern raised Action(s) required to reach objective Executive lead Timescale for completion
RLH Regulation 19 Compassionate care
There was limited learning form complaints and in some service complaints were not dealt with appropriately or promptly.
Clinical teams use information and insight from complaints to improve outcomes and experience of care.
Updated complaints process to be agreed with managing directors.
Themes reported to the managing director and escalated to service leads where necessary.
Each service to management complaint investigation responses within agreed timelines.
Complaints data demonstrates improvement in terms of cycle time. Fewer complaints re-opened.
Training of staff in complaints management
Develop a site specific quality report to identify and target improvements. It will be communicated to all staff for learning purposes.
Patient forums to be established with support from PALS and external agencies.
Audits to be undertaken on complain responses to ensure the quality is of an acceptable standard and lessons learnt are taken from complaints.
Target compliance monitoring within services, with turnaround reported to the Managing Director and Senior Leadership Team monthly.
Chief Nurse Dec-16
RLH Regulation 20 Safety Accurate records in relation to the care and treatment of patients were not kept. Nursing documentation was inconsistent and inaccurate; the WHO Surgical Safety Checklist and the Do Not Attempt Cardio-Pulmonary Resuscitation (DNACRP) were not always fully completed.
Nursing documentation will meet NMC standard and areas of improvement will be identified. All adult wards at RLH will use standardised documentation.
Patient records clearly record the decision DNACPR. Records demonstrate that the decision is reviewed should the patient's condition change. Records show patient / relative has been given the opportunity to inform the decision.
All wards use consistent approved nursing assessment recording tools (including those on EPR) while a project is developed to deliver standardised documentation across the Trust.
Medical Staff record keeping demonstrates improvement in line with GMC best practice; Monthly audit of health records demonstrates compliance.
Audit demonstrates compliance with the WHO checklist.
Monthly audit of CPR attempts confirms compliance with DNACPR.
DNACPR policy is consistent with recognised best practice. DNACPR forms are designed to be readily identifiable in the patient record.
Review of all inpatient nursing documentation, led by DoN with Senior nurse/matron weekly review on wards
Monthly audit of health records. Documentation standards will be revisited with consultant medical staff to ensure they meet required standards.
Delivery of compliant WHO strategy /framework.
DNACPR policy to be approved by policy group and signed off by Trust board. Staff training included in annual Stat.Mand. Training programme with compliance monitored by clinical standards committee.
Training of medical staff on accurate record keeping - work with other education providers to refresh training and education programmes.
Review induction process for medical and nursing staff to ensure they are alerted to the importance of accurate and timely record keeping
Chief Medical Officer
Chief Nurse
Mar-16
113

Site Compliance Reference number
Theme Compliance action raised by CQQ Outcome needed to address compliance action
Objective to address the concern raised Action(s) required to reach objective Executive lead Timescale for completion
RLH Regulation 22 Workforce There were not enough staff across all staff groups and staff levels to provide safe care and treatment for patients.
Staffing meets the needs of the patients.
Pulse surveys indication improved staff satisfaction.
Transition to the new operating model with staffing levels matched to the organisational model.
Vacancy numbers are known. Size of recruitment challenge is understood. Monthly monitoring of vacancy gap through robust reporting.
Develop a future operating model and transition plan for the design, recruitment and communication with relevant education organisations.
Work towards a midwife: birth ratio to 1:28. Quarterly review of staffing numbers in maternity to reflect predicted changes in birth rates.
Minimum of twice yearly ward staffing review.
Medical models to be reviewed against college guidance as part of objective setting.
Temporary staff reduced to <10%.
Using best available guidance of staffing ratios, a gap analysis to be undertaken to risk assess shortfalls. Vacancy numbers to be identified. Each service line will undertake a reconciliation of vacant positions to form a site based recruitment strategy.
Development of retention plans to ensure services can address demand for skilled clinical and support staff.
Team briefing on safer staffing policy. Safer staffing posters to be made visible to the public.
Monthly assurance meetings will be chaired by the Director of HR and OD.
The Board will received a monthly safer staffing report.
All new staff automatically enrolled onto the staff bank. Staff bank to meet with local leaders to identify hard to fill areas for targeted recruitment.
Director of Human Resources
Mar-16
114
Governing Body Meeting Enclosure
Date of meeting September 1st 2015 I
Agenda item 2.5
Title of report: Healthwatch – Rate Our Service Update
Author(s): Dianne Barham, Chief Executive, Healthwatch Tower Hamlets
Presented by: Sponsor (if different): For further information
Dianne Barham, Chief Executive, Healthwatch Tower Hamlets
Dianne Barham, Chief Executive, Healthwatch Tower Hamlets
Executive summary
The presentation provides a new dashboard of patient and user experience of health services in Tower Hamlets
• We are able to analyse comments according to providers, commissioners and themes.
• All of the comments include a 5 star rating. Those which are gathered directly online or through Healthwatch outreach are visible on the website, are themed and have a positive, negative or neutral sentiment.
• We are also able to include data from NHS Choices, Patient Opinion and the relevant Barts complaints and PALS data.
• The system allows us to undertake the friends and family test and to collect basic equalities data.
• providers and commissioners have the ability to respond to comments
• Healthwatch moderate all comments before they go live on the site.
Recommendation
Information Approval To note Decision
Conflicts of Interest None
Key issues The system is still being tested and we are not totally confident of the accuracy at this point. However the data is starting to show us that patients perceptions of:
• the Royal London Hospital are generally very positive • A&E are positive but that the system is confusing and that they
do not feel involved in decision making • the quality of staff and the information that they provide is
improving
115
• discharge can feel poorly planned with long delays
Report history The development of the Healthwatch Tower Hamlets feedback and rating system was part funded by the THCGG in 2013/14. All though the online rating system has been operating for six months this is the first time we have been able to include other sources such as Healthwatch's own outreach together with NHS Choices and PALS and complaints data.
Patient and Public involvement
The report was produced from feedback from patients and the public. Please see sources for more detail. Members of the public can review feedback on providers and leave their own comments in response. A quarterly summary report is available on the Healthwatch Tower Hamlets website.
Link to the Board Assurance Framework
This report links to corporate objective 4 of the BAF: To support local people and stakeholders to have a greater influence on services we commission and develop a responsive and learning commissioning organisation.
Impact on Equality and Diversity
The system has only recently added the capacity to record equalities data. We will be updating data retrospectively where possible and this will enable us to compare experiences from across key equalities groups.
Resource requirements Outline the resources required to implement this recommendation.
Next steps We would like to discuss with the CCG how the informatics could be further tailored in order for themes and data to have a greater impact on quality assurance and commissioning decisions.
We are very keen to expand feedback from a wider range of sources and are working with social services as to how we encourage greater user feedback through provider contracts.
Information will be shared across commissioners and providers through the Health and Wellbeing Board Communications and Engagement Group.
116
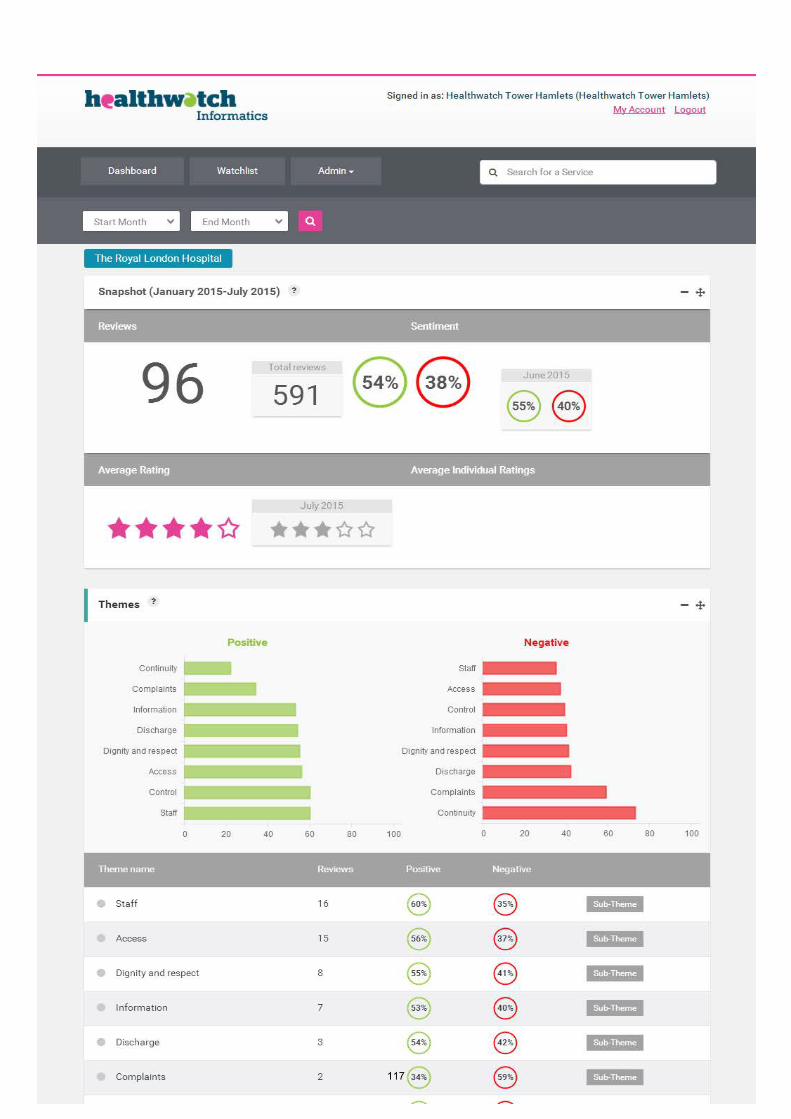
117

118

‘Stepping into the Future’ patient feedback summary 119 comments were collected from patients in: A&E (45), Discharge Lounge (39), AAU (18), and reception (17). They were collected between 13 July and 20 July including a Saturday and up until 7pm. We found a general improvement in patient experience at the Royal London Hospital. Patients were generally more positive about the quality of staff and communication.
I came in through reception, and we are now in the cubicles. It only took 5 minutes to be seen, so I was very impressed especially as I thought we would have to be waiting here for hours. When I last came to A&E it was in the old London Hospital, and I literally had to wait for about 6 hours. This all seems very clean. The doctor seems very attentive and caring and I really feel like I matter. I’m now just waiting for the doctor to return to let me know what happens next. The nurse I saw had a huge smile on her face and was very funny
A&E Patients were generally positive about the new system.
“Came through A&E via cab from work. Saw a nurse, emergency assistant, doctor and specialist all when I was I was in A&E. Whole process has been good- best experience. Used to go to Newham General and the experiences are completely different. Staff have all been polite, asking if I’m ok. Two different specialists I saw reassured me and made me feel as though I was going to be ok. They listened to me and spoke to me. Waiting time to be seen when I got to A&E has been ok, I always get seen quickly because of my asthma. Quality of care up here has been good- surprisingly shocked at how good it’s been. I hate feeling like a patient but I have enjoyed my experience so far. Rather than referring me the doctor said I should stay to sort out my problem so I’m happy with that.” “Came in through A&E because I was feeling ill. I spoke to reception, sat down and waited but I didn’t have to wait for long because I then saw a nurse, then a doctor and then a consultant had a scan and then I was transferred up here. So far it’s been good. I was expecting to be waiting for hours but I wasn’t. The staff are pretty good here and in A&E”
However many patients did not understand the system and found it complex and confusing.
“The system through A&E does seem a bit complicated though. I’ve been waiting to go to a ward and have been sent to about 2-3 different places before. I understand it is to try and make the system easier with less congestion. But it all seems quite counterproductive- can’t they just tell me to wait in one place and then when the bed in the ward is ready send me
119

there. The doctors and nurses are all very polite when I do see them though and are often very apologetic for any waiting times. Suggestion is don’t keep on moving the patients around” “Came here with my friend because he had chest pains whilst we were at work. We walked in at 11am to reception and sat for 30 minutes. We saw a nurse for 5 mins then came through to this bit; she said emergency assessment to see a consultant. We have seen someone but nothing much has been explained about tests he has done. This isn’t nice because there isn’t any explanation behind the tests they are doing and no results have been given. Feels like doctors are the only ones who need to know what’s happening but the patient doesn't. If they tell you what they are doing that can help reassure you. The process has also been slow moving, in terms for moving from one place to the next. You wait in one place only to be told to wait again which is tedious. A&E “Came straight here from holiday, arrived couple of hours ago off the plane. I have a head injury and I have been told I need an operation. I saw a navigator first, then a nurse and I was brought through to here. It’s a little confusing being here because I’ve spoken to 4 people and that doesn’t include a doctor, just feels as if I’m being transferred from person to person. I’m told to wait but I’m not given any indication of how long. Just feels as though the whole experience could be better explained. I mean did you just see that, I have a bandage on my head and that nurse just came and told me to take it off. What’s that about? My dad is worried as well now, it’s really worrying. How can she come and tell me to take a bandage off. I don’t know what is happening. It’s confusing. They should have a piece of paper for patients to explain the process coming through A&E. If they can’t do that then at least something on the walls. Other than that staff have been good apart from that nurse telling me to take my own bandage off.” “Although the communication was very good and I was told everything. I sometimes feel I am told once the decision has been made and I don’t often have a say.” “The staff are pretty good here and in A&E but some people need to be more aware of people with varying disabilities. In my case I’m blind and people gesturing to me to come forward is silly because I can’t see but it is a two way street. I still shouldn’t have to tell people I’m blind as my cane should be a dead giveaway. The only thing they can improve on is more awareness of people with disabilities. Other than that it has been fine and doctors have been engaging with me all the way through.”
Other suggestions and concerns covered:
• Not being checked as often as they would’ve liked by doctors in A&E and AAU.
• Not being offered pain relief in A&E while they wait. • Not being offering food if there is a long wait in A&E. Family members not
knowing where they can buy food. Inappropriate use of A&E
120
“I saw the nurse and they told me I would have to wait. They said before the wait time was 2.5 hours but it’s gone down now. I was going to come to the hospital anyway to see my grandma because she is here at the moment but my foot was hurting me so I thought I might as well come to hospital for myself.”
Discharge Still some long waits in the discharge lounge for medication and for transport.
Waiting a long time for my medication after being discharged, cold in the discharge lounge, waiting for transport. Put more reading material in the discharge lounge. Asked if I wanted tea something to eat. I have recently come from Newham Hospital, I was very happy with the care but felt it was all very abrupt and they just wanted to tick me off like a checklist. At 3am this morning I was transferred to the London- I’m not entirely sure why I had to be transferred at 3am instead of at 9am. It disrupted my sleep and when I asked why they just said it was easier to do it now. I feel it was juts easier for them and not for me. I’m here for anti-coagulant therapy- been here since 2nd June on and off. Transport is late and not arriving on time- an hour late. There aren’t enough wheelchairs. Busy during the summer. Patient transport waiting times need to improve.
Problems with discharge
“Son speaking for mum: She was meant to be discharged yesterday but the new medicine she was prescribed has been delayed and so she can’t go home. They said more time is needed to prepare her medicine. Personally, I feel the communication between the GP and the hospital isn’t that great and it’s impacting on her health. Our GP is very poor to be honest (our GP is xxx). Medicine side of things, I don’t feel like she is improving and there hasn’t been a review of her medicine whether it’s here or at the GP. She had a neurology appointment 6 months ago but they still haven’t done a brain scan. She was told she would have one and GP would refer her but nothing has been done. Feels as though everyone is playing pass the parcel with my mum. In that time she has been to A&E 8 times. During this stay, she has asked repeatedly for something for her chronic insomnia but nothing has been given. We asked for her to be given vitamin injections but they are refusing saying that she needs this to be referred from the GP. I think that hospitals need to look at their abilities instead of referring patients back to the GP- Process between the GP hospital also needs to be better” “In general, the staff do not spend enough time with patients. No one has discussed discharge with me yet - I might be staying here for longer. . . . Comment from son: My father was here before and his discharge could have been better. He wasn’t feeling well so we went to the GP after he was discharged and we were told to come back because he was passing blood. He shouldn’t have been discharged in the first place.”
There were also negative comments about:
• night nurses in some wards
121
• the fracture clinic • signposting and directions to wards and within the lifts. • insufficient staff “I also feel that they are understaffed- I just feel there
aren’t enough doctors and nurses around. The care they give when I do see them is fantastic and I have nothing to complain about but it’s just getting to see them- especially the doctors, If I request to see a doctor- while my dressing is being done they can never get one to see me so a senior nurse will just come. They should also pay the nurses more money- they do a fantastic job!”
122

Governing Body Meeting Enclosure
Date of meeting September 1st 2015 J
Agenda item 3.1
Title of report: Tower Hamlets Partnership – Community Plan 2015
Author(s): Mark Cairns, Senior Strategy, Policy and Performance Officer, Tower Hamlets Council
Presented by:
Sponsor (if different): For further information
Kevin Kewin, Strategy, Policy and Performance Service Manager, Tower Hamlets Council
Kevin Kewin, Strategy, Policy and Performance Service Manager, Tower Hamlets Council, 020 7364 4075, [email protected]
Mark Cairns, Senior Strategy, Policy and Performance Officer, Tower Hamlets Council, 020 7364 2260, [email protected]
Executive summary
• This report provides the Governing Body with an overview of the new proposed Tower Hamlets Community Plan.
• The Community Plan sets out the long-term vision and priorities for Tower Hamlets. The Strategy is developed and owned by the Tower Hamlets Partnership, led by Tower Hamlets Council.
• The previous Community Plan ran from 2011 to 2014, and the new Plan is intended to last to 2019.
Recommendation
Information Approval To note Decision
The Governing Body are asked to review and approve the Tower Hamlets Partnership – Community Plan 2015.
Conflicts of Interest N/A
Key issues Whilst the statutory duty for local strategic partnerships to publish sustainable community strategies has ceased, the Tower Hamlets Partnership believes there is value in continuing to strategically coordinate its work. The Community Plan therefore provides the long-term vision for the borough, articulating local aspirations, needs and priorities. As the high-level partnership strategy, it informs all other strategies and delivery plans of the Partnership.
123
It outlines how the Partnership will work together to improve the lives of all those who live and work in the borough. The Plan continues the existing focus on tackling poverty and social exclusion in Tower Hamlets, as well as the overarching theme of One Tower Hamlets, emphasising equality, cohesion and community leadership.
The proposed themes for 2015 are:
• A great place to live • A fair and prosperous community • A safe and cohesive community, and • A healthy and supportive community.
The only difference from the themes in the previous Community Plan is the amendment of the second goal to include the word ‘fair’. This change has been made to embed the recommendations of the Fairness Commission within the Community Plan. This was also echoed in the views of consultees that in promoting and supporting prosperity across the borough, we need to ensure that local residents and existing communities do not get left behind, and can benefit from growth. A cross-cutting One Tower Hamlets theme has also been retained, reflecting the importance of equality, cohesion and community leadership in our vision for the borough. Over the next four years, our focus will be on fairness and ensuring that no community is left behind; on empowering our communities and making them resilient, by building their engagement and capacity to lead; and on tackling inequality through healthy living and employment. However, alongside the existing strategies and structures in place to achieve the vision for the borough, partners were keen that the Community Plan adds value to these. It therefore identifies a set of four additional cross-cutting partnership priorities, focusing on issues which cross more than one Community Plan theme or are faced by a broad range of partners. The aim is to enable partners to accelerate progress by focusing their efforts jointly around specific shared goals, and thereby making the most of shrinking public sector resources. The priorities agreed by the Partnership are as follows:
Priority 1: Empowering residents and building resilience
We will enable residents to better support themselves and each other, so that partners can maximise their impact with limited resources. This encompasses involving residents in the design and delivery of services, building capacity in the voluntary and community sector, and early intervention and prevention. Crucial to this is making it easier for all groups to engage with public sector organisations, both as citizens and as service-users.
Priority 2: Promoting healthier lives
While life expectancy is increasing, we must address inequalities in
124
health both within the borough, and between Tower Hamlets and the rest of the country. This will involve tackling the wider determinants of health, our environment, and promoting prevention and early intervention so that conditions do not deteriorate and require more intensive interventions later. This will require all partners to understand the impact they can have on residents’ health, and to take a role in improving it. As part of this, we will also need to improve the evidence upon which we base our activities and interventions.
Priority 3: Increasing employment Employment is up in Tower Hamlets, but we continue to have some of the lowest rates in the country, especially among women and some ethnic minority groups. This is crucial, as employment is a major factor in wellbeing and life chances for residents. With many unemployed residents needing support to become ready for work, all partners can play a role, engaging them in activities, programmes or learning. These can be built into healthcare pathways, for example. We will work to address the affordability and accessibility of childcare, a major barrier for many parents highlighted by the Fairness Commission. We also need to engage more local employers through our networks and supply chains, and use our own practices as employers to tackle unemployment.
Priority 4: Responding to population growth
Our population is forecast to rise from around 272,000 to 320,000 by 2022 (and further beyond this) with growth driven mainly by an increase in the number of young working professionals. This is putting increasing pressure on local services and infrastructure, including the supply of affordable housing. Our residents aged 85 and older are also growing in number, which increases demand for adult social care services. Therefore partners will focus on developing a Local Plan which considers how we can manage growth and ensure sufficient infrastructure to meet local needs. We will further need to use data more effectively, to learn more about the nature of our changing population.
The Plan has been developed through a working group of staff from across partners, including Ellie Hobart from the CCG. The broader consultative process undergone by the drafts of the Plan is set out in a subsequent section. Since the election of the new Mayor in June, the Plan has been reviewed to align with some of his key priorities voted for by local people. It will be approved by the council’s Executive, the CCG Governing Body, and the Tower Hamlets Partnership Executive. The Partnership Executive will also receive progress reports.
Report history Previous drafts of the Community Plan have been circulated for review within the CCG by Ellie Hobart.
Patient and Public Preparation for the new Community Plan began in summer 2014 and, as required by the Best Value Statutory Guidance, consultation was
125

involvement undertaken by the council with representatives of council tax payers, those who use or are likely to use services provided by the council and its partners, and those appearing to have an interest in the area. This included initial discussions with the general public, the council’s Community Champion Coordinators (who facilitate Community Ward Forums), representatives of communities of interest, and service user groups. Following this, a draft of the Plan was put out to public consultation, and representatives of community and voluntary sector organisations also contributed to the development of the collaborative action projects for the new cross-cutting priorities. These elements of consultation, along with others, are expanded upon below. Starting with the Borough Profile as the evidence base for the Plan, council officers requested input on suitable themes and priorities from a wide range of stakeholders to help shape the Plan from its most formative stage, including: • Community Plan Delivery Groups (CPDGs) • Representatives of the third sector (through both the Third Sector Advisory Board and the Tower Hamlets CVS) • Faith representatives, through the Interfaith Forum • Community representative groups (such as HealthWatch, the Youth Council, and Local Voices) • Service user groups (such as the Learning Disabilities Service User group) • Partnership groups (such as the Mental Health Partnership Group) • Council staff forums (including the LGBT and BAME forums) • Partner organisations (including Tower Hamlets Clinical Commissioning Group) • Community Champion Coordinators, and • Members of the public (through Community Ward Forums, and stalls set up in markets around the borough). Feedback indicated the need for the Community Plan to build on, rather than replace, existing arrangements. In response to this consultation feedback, the existing Community Plan themes, which are embedded and aligned to our delivery structure, have been retained. Following the initial work to develop the themes and priorities in the Plan, councillors’ views were canvassed through a seminar and the Overview and Scrutiny Committee, which offered useful feedback. A draft version of the Community Plan was put out to consultation on the council’s website, with the survey asking residents’ views on the clarity of the Plan’s purpose, the current commitments and proposed cross-cutting priorities, and the areas of focus for equality, cohesion and community leadership, as well as for any comments. This ran for 21 days from 27th February to 20th March 2015, with the link publicised externally via the council’s homepage, and with a press release, as well as being tweeted from the Council’s main Twitter account and featured in East End Life. Partner groups and stakeholders previously
126
involved in developing the priorities were also invited to take part. Overall, respondents felt the Plan was clear about its purpose, and agreed with the current partnership commitments, cross-cutting priorities and areas of focus for equality, cohesion and community leadership. Comments from respondents expressed views about areas requiring greater emphasis, and these have been taken into account in producing the draft appended to this report. A Collaborative Action Day was also held, focusing on how partners could bring their resources and expertise together to tackle the four cross-cutting priorities identified in the draft Community Plan. The event was well-attended, with representatives from partners across all sectors, and a set of collaborative action projects for each cross-cutting priority has been developed as a result of this.
Link to the Board Assurance Framework
The proposed Community Plan 2015 encompasses all of the BAF corporate objectives 2015/16.
Impact on Equality and Diversity
The One Tower Hamlets theme focuses on reducing inequality and promoting cohesion. The priorities identified above reinforce this, for example: • A focus on fairness and ensuring that no community is left behind will be key in maintaining cohesion within the borough; and • A focus on health inequality and employment will enable us to tackle some of the key issues which militate against equality. In addition, it is proposed that programmes of work for partners explicitly include a focus on particular disadvantaged groups, as identified through a Borough Equality Analysis. This analysis has been updated and used to inform the development of initial proposals and ensure that in finalising the plan and accompanying action plans we show due regard to the requirements of particular equality groups and those with protected characteristics. For example, this Analysis identifies the need to strengthen intergenerational cohesion, which is a key dimension of one of our collaborative action projects to respond to population growth. Another project seeks to address the affordability of childcare, which should help more working age women into employment. Our current partnership plans also aim to address issues identified in the Analysis, such as tackling our high levels of childhood obesity, reducing violence against women and girls, increasing the numbers of disabled residents in employment, and providing more homes to meet the needs of disabled people. The shortage of social housing in Tower Hamlets has a disproportionate impact on families from Muslim and black and minority ethnic communities, and so this is a key focus of the partnership under the theme of “a great place to live”. We have also identified as a key enabler the need to understand and plan around needs of a changing population, given the pace of change and growth in our community, which should explicitly consider how we can project and respond to the needs of new communities.
127

Resource requirements As outlined in the report.
Next steps The collaborative action projects identified within the Community Plan form the basis of discussions for developing a robust action plan to deliver on the cross-cutting priorities.
128

2015Community Plan
Tower Hamlets Partnership
129

02 Tower Hamlets Partnership Community Plan 2015
Foreword
In this new Community Plan, the Tower HamletsPartnership articulates its vision for the borough,and how we will work together with residents torealise it. I believe it is important for us to put theconcerns of local people first, and maintain andimprove the services we secure for them, fromschools and housing to street-cleaning.
Though much of the development work for thisCommunity Plan took place before my election inJune 2015, I am committed to working with thepartnership and pursuing shared objectives.Rather than begin the Plan again from scratchafter so much has gone into its production, as apartnership we have agreed that it should remainlargely unchanged for the time being, though aswe move forward, it is likely that there will besome changes in emphasis and in some priorities.
For example, while we have increased thenumbers of homes meeting the technicaldefinition of “affordable”, in reality many of theseremain out of reach for those on low or evenmoderate incomes, and we must tackle thisserious challenge to our existing communities.We will also need to give greater emphasis tohelping people overcome low skills, low incomesand high unemployment. And in our role leadingthe community, we must further enhanceunderstanding and cohesion betweengenerations and between communities, andmaximise our consultation, engagement andoutreach with residents and stakeholders.
This Community Plan, then, is not set in stone. Itwill evolve as we develop our plans to achieve ourvision for the borough, and as we review otherkey partnership strategies like the CommunitySafety Plan, the Health and Wellbeing Plan, andthe Children and Families Plan, amongst others.
Together as partners, we will serve everyone inour community, and ensure that their interestsare served to achieve the vision of a TowerHamlets of which we can all be proud.
John BiggsMayor of Tower HamletsChair of Tower Hamlets Partnership
130

Tower Hamlets Partnership Community Plan 2015 03
About Tower HamletsTower Hamlets is a fast paced, fast growing andchanging borough. Its economy is thriving, moreand more people want to live here, and large-scale and ambitious regeneration andinfrastructure projects continue to bring freshopportunities. The population is diverse, butthere are many active communities who get onwell together, with a thriving community andvoluntary sector. Community facilities such asIdea Stores and leisure facilities are well-loved andwell-used. The borough has seen unprecedentededucational success, opening up moreopportunities to the young people comingthrough our schools, and employment rates arerising.
Despite all this change and success, TowerHamlets still has challenges to face. Too manyresidents have significant health problems. Highhousing costs and low incomes mean that homes
are unaffordable for many. Too many residentsare not in work and struggle to make ends meet,especially as reforms erode the welfare state andcosts of living rise. One of the biggest challengesthe borough faces is ensuring that the benefits ofgrowth and prosperity reach all parts of ourcommunity, with a fairer distribution of wealthand income across Tower Hamlets.
Along with this, the economic climate remainsextremely challenging, despite some recentpositive signs. Reduction of the national deficitwill continue under the current government, andthis will involve further deep public spendingcuts. At the same time, as this plan sets out, thedemand on services is increasing. A growing andageing population means that, for example,Tower Hamlets Council will need to save £91mover the four years from 2015-16 to 2018-19. Allpartners need to think carefully about the mosteffective way of using their resources, enablingresidents to support themselves and each other,and reducing their need for traditional services.
The 2015 Community PlanIn developing a Community Plan for 2015onwards, partners have emphasised the need forsomething which builds on and complements ourexisting partnership work, rather than replacingit. For this reason the existing Community Planthemes that partners have organised themselvesaround for some years now have been retained.They set out our ambition to make the borough:
X A great place to liveX A fair and prosperous communityX A safe and cohesive communityX A healthy and supportive community.
Introduction
131

A key change is from ‘a prosperous community’to ‘a fair and prosperous community’. All partnerswanted to reflect the contribution of the TowerHamlets Fairness Commission to the debateabout economic growth and fair outcomes forlocal people, and use the new Community Planto drive forward the recommendations of theCommission. Our consultation with residentsemphasised that the community wants to seeeveryone benefiting from economic growth andprosperity, with a fair distribution of resourcesand opportunities across the community, notgrowth at any cost.
This plan sets out recent achievements, currentchallenges and commitments, in relation to thefour Community Plan themes. Partnershipworking to pursue these priorities is wellembedded and overseen by a range ofpartnership bodies. To build on and complementthis work, this plan sets out proposed cross-cutting partnership priorities for the four yearsfrom 2015. Using this plan, partners will worktogether to harness the efforts of all partners andaccelerate progress in these four important areas.
04 Tower Hamlets Partnership Community Plan 2015132

Tower Hamlets Partnership Community Plan 2015 05
Achievements so farMore homes, better homesX The council and its housing provider partners
secured 8000 homes with rents meeting theGovernment's criteria for affordabilitybetween 2004 and 2013.
X Tower Hamlets is consistently one of the topperforming London boroughs for delivery ofaffordable homes, and many of these arefamily-sized, meaning that we have been ableto rehouse 4800 overcrowded families overthe last four years.
X As of April 2015, 78% of our social rentedhousing had achieved the Decent Homesstandard.
X Tower Hamlets has recently received anaward for having the highest number ofsustainable homes of any local area, and in2012 Tower Hamlets Energy CommunityPower was launched, giving residents adviceand information about saving money byswitching energy supplier.
Thriving community spacesX Tower Hamlets has over 232 hectares of open
space and residents who use local parks andopen spaces are consistently satisfied withthem. In 2013 eight local parks received theGovernment’s Green Flag Award, and in both2012 and 2014 Victoria Park won the GreenFlag ‘People’s Choice’ Award, and candeservedly be called the nation’s favouritepark.
X The borough’s Idea Stores and libraries haveover two million visits a year, and Idea StoreWhitechapel is the busiest in central London.These deliver over 900 courses and make amillion loans annually, winning awards fortheir website, English language and adultlearning provision. In 2013 a brand new IdeaStore opened at Watney Market with 320,000visitors in its first 10 months.
X Ahead of the Olympics, the boroughdelivered award-winning public realmimprovements in Hackney Wick and FishIsland, on the fringe of the Olympic Park.Wehave also substantially renewed the OceanEstate.
X We are continuing with development in ourLocal Plan and Core Strategy, withregeneration plans underway at BlackwallReach, in Bromley-by-Bow and in Poplar. OurWhitechapel masterplan will harness theeconomic benefits of Crossrail, and delivernew homes and community facilities by 2025.We will also develop plans for thetransformation of South Quay.
A great place to liveTower Hamlets will be a placewhere people live in qualityaffordable housing, locatedin clean and safeneighbourhoods served bywell-connected and easy toaccess services andcommunity facilities
133

06 Tower Hamlets Partnership Community Plan 2015
X Implementation of the new CommunityInfrastructure Levy, a non-negotiable levy charged on most new development, willmean that developers who benefit frombuilding housing in the borough will alsocontribute to developing and extending thenecessary infrastructure to support populationgrowth.
X We are keeping our streets cleaner than inprevious years, with significant reductions inlitter, graffiti and fly-posting. The council’sinnovative new app, Find It Fix It Love It,helps residents to instantly tell the councilabout issues that need to be fixed or clearedup.
The challenges we faceA fast growing populationTower Hamlets has experienced the fastestgrowing population in the country in recentyears, growing almost 30% between the 2001and 2011 Census. This growth has continued,with the population rising from 254,000 in 2011to 272,000 in 2013, and projected to rise to320,000 by 2022 and to over 350,000 by 2033.
Tower Hamlets is the third most denselypopulated borough in London, and the daytimepopulation increases by about 60%, rising to428,000. Around 107,000 commuters head towork in Canary Wharf each day, and major touristattractions like the Tower of London draw in over4 million visitors each year.
This scale of growth will impact across allorganisations and services, and responding to it istherefore one of the cross-cutting priorities whichwe will be addressing together over the life of thisCommunity Plan. We need to heed residents’concerns about the impact on existingcommunities of the large numbers of high valuehigh-rise homes being built, including onfacilities, quality of life, and on the cohesivenesswhich has long been a strength of the borough.These views will be considered in thedevelopment of our new Local Plan.
Housing pressuresLondon as a whole has seen unprecedentedincreases in house prices and rents, driven bysignificant overseas investment. As highlighted bythe Fairness Commission, market rates now bearlittle relation to the income of most residents. Thevery high price of property in Tower Hamlets,combined with rising rents, welfare reform,reductions in public funding and restrictions inborrowing for affordable homes, make ensuringsufficient affordable homes for residents one ofthe biggest challenges we face. Homes that meetthe Government’s definition of ‘affordable’ canstill be out of reach to many local people,
134

Tower Hamlets Partnership Community Plan 2015 07
including those on low and middle incomes, andaffordability is one of the biggest reasons forpeople planning to move out of the borough.
There is enormous pressure on social housing,with over 20,000 families on the housing waitinglist. Just under 40% of existing tenants in bothcouncil and other social housing want to movehome, with the majority of these wishing toremain within the borough. In particular there isa shortage of suitable family housing, and weknow that this has a disproportionate impact onblack and minority ethnic and Muslim families.There are also shortages in the number ofwheelchair accessible homes for disabled peopleon the housing register.
Homelessness is getting harder to prevent, andovercrowding continues to be a problem. 16% ofhouseholds have too few bedrooms, rising to22% in the social rented sector, and over 42% ofpeople planning to move want to do so becausetheir current home is too small. These issuesdisproportionately affect black and minorityethnic households. Nonetheless, the councilcontinues to re-house overcrowded families, witha target of 1000 families every year andovercrowded households are given high priorityon the housing waiting list.
The housing landscape in Tower Hamlets haschanged significantly over the last 30 years, withlarge swathes of the borough regenerated. Therehas been huge growth in the private rentedsector and many residents are understandablyconcerned about the quality of homes, theinsecurity of tenancies in this sector and theimpact that large numbers of privately rentedproperties have on estates and communities, aswell as high rents. The council has thereforecommitted to pursuing a landlord registryscheme for Tower Hamlets with the aim ofimproving the quality of accommodation, havingmore influence over landlords in this sector, andtaking action against those who exploit tenantsunfairly.
We also recognise that improving housing shouldgo hand in hand with other activities to improvethe wellbeing and life chances of our residents,which is overwhelmingly affected by having ajob. Increasing employment is another of ourcross-cutting priorities, and we will build this intoour development and housing activity, with allpartners aiming to engage unemployed residentsin activity that will help them towards work.
Taking pride in the local environment,making best use of community assetsWe have reduced litter, graffiti and fly-tipping.However, public satisfaction with the cleanlinessof the local environment is not as high as wewould like, and we want to understand andaddress the reasons for that. We also want toencourage and enable residents to recycle more,to catch up to rates in the rest of London.
We know that having quality community facilitiesand delivering great services is really important toresidents. Now, more than ever, the boroughmust make the best use of its assets, particularlybuildings, making sure they are being well usedby the community as well as generating value formoney. With population growth puttingincreasing pressure on these communityresources, and public sector funding cuts make itharder to maintain and invest in them, thecouncil and its partners must find innovative waysto utilise spaces, and to generate revenue andinvestment in local services and facilities.
135

08 Tower Hamlets Partnership Community Plan 2015
Current partnershipcommitmentsThere are a number of clear partnership prioritieswhich are all contributing to making TowerHamlets a great place to live, summarised below.These are captured by a range of strategicdocuments on housing and strategic planningand delivered by multiple partners. In addition,the Fairness Commission made a number ofchallenging recommendations on housing.
Build more affordable homes for localpeople and improve the quality ofexisting homes
X Build more affordable homes which meet theneeds of all residents
X Develop new models of long-term investmentin social housing
X Provide more homes to meet the needs ofdisabled people
X Improve the standard of private rentedaccommodation
X Keep all our council housing up to the DecentHomes standard
Deliver key regeneration projectsaround the borough
X Develop a new Local Plan to manage growthand development in the borough
X Begin the regeneration of Whitechapel byrealising the Whitechapel Vision Masterplan
X Continue the regeneration of Poplar includingprojects at Poplar Baths, Chrisp Street,Burdett, Aberfeldy and Bow Bridge
X Develop a Masterplan for South QuayX Continue development of Blackwall Reach
Reduce overcrowding and under-occupation
X Provide access to the right housing options atthe right time
Prevent people from becominghomeless, but support those who do
X Promote multi-agency working, earlyintervention and building resilience
Create good quality community spacesand facilities
X Ensure the implementation of the newCommunity Infrastructure Charging Schedulefor Tower Hamlets, whilst continuing tocollect the London Mayor’s CIL.
X Develop new libraries, youth and leisurefacilities
X Invest in parks and increase the number andquality of play spaces for children
Making Tower Hamlets ‘greener’
X Tackle air pollution by cutting CO2 emissions X Increase the recycling rateX Improve road safetyX Invest in cycling
136
Tower Hamlets Partnership Community Plan 2015 09
Achievements so farA thriving economyX The employment rate is improving and is now
the highest it has been for more than 10years, narrowing the gap with the rest ofLondon. The number of residents claimingJobseekers Allowance is reducing in line withLondon, and the rate of child poverty hasfallen significantly in the last 4 years.Regeneration programmes will fuel economicgrowth so that by 2030 there are likely to bearound 100,000 more jobs than at present.
Educational successX Tower Hamlets continues to experience
significant improvements in educationattainment and the borough’s schools havebeen identified as amongst the best urbanschools in the world. GCSE results are nowconsistently above the national average, andat A Level the gap between Tower Hamletsand London has significantly narrowed,particularly for girls.
X More working age residents now have somekind of qualification, with 44% at degreelevel, which is above the London average.
X Local partners have worked successfully inrecent years to reduce the number of 16-18year-olds who are not in education,employment or training.
X The council has introduced Education Awardsfor post-16 students and Higher EducationAwards to help students with the costs ofuniversity, and to offset the effect of changesto Government financial support for students.
A commitment to fairnessX In 2012 the Tower Hamlets Fairness
Commission brought together independentlocal community leaders and external thinkersto engage residents, local stakeholders,businesses and experts in a debate aboutgrowth, economic inequality and increasingausterity. Their recommendations aimed topromote fairness and equality in employment,housing and money. In 2014, one year onfrom the publication of their report, theFairness Commissioners expressed that theywere proud and impressed with what hadbeen achieved by local partners.
A fair and prosperouscommunityTower Hamlets will be a placewhere everyone, regardless oftheir background andcircumstances, has theaspiration and opportunityto achieve their full potential
137

10 Tower Hamlets Partnership Community Plan 2015
The challenges we faceHigh and persistent unemploymentDespite the buoyant economy and a risingemployment rate, Tower Hamlets continues tohave high and persistent levels of unemployment,particularly amongst women and amongstBangladeshi and Somali residents. Over 12,000people claim out of work benefits because ofillness or disability, 6.2% of the working agepopulation. Increasing employment is a cross-cutting priority for this Community Plan, and weneed to make sure that the broadest possiblecoalition of organisations is assembled to worktowards raising skills and incomes, and gettingmore people into work, with partners buildingthese into every aspect of their activity, includingas employers.
Continuing to narrow the gap ineducational attainmentAlthough we have made great gains, there isfurther progress to make for our young people.Post-16 results have started to improve but weare still slightly below the London average in
terms of performance. Early years attainment alsocontinues to be a challenge, with some of thelowest results in London. Despite overall success,there are variations in GCSE results for someethnic groups, with White British young peopleachieving below our targets.
Population growth means continued increases indemand for school places - by 2023, there will bethe need for an additional 7,500 primary placesand 4,500 secondary places. More free schoolsare opening, and there is continued pressurefrom Government for schools to switch toacademy status. Tower Hamlets passionatelybelieves that its schools are stronger workingtogether, and with the local authority, to pursueever greater educational attainment and fulfil theaspirations of local young people.
Alongside improving attainment, we believe thatschools can also play a crucial role in developingemployment skills in young people and helpingthem access careers support.
Helping everyone benefit from growthDespite the optimistic economic outlook for theborough, we know that many local people arestill concerned about the cost of living andmaking ends meet. Tower Hamlets is the thirdmost deprived area in the country. While levels ofchild poverty have decreased significantly inrecent years, they remain the highest in London,affecting 39% of local children. 1 in 5 householdshas an annual income of less than £15,000, andover half have an income of less than £30,000. Atthe other end of the scale, 15% of Tower Hamletshouseholds have an income of more than£60,000 per year.
Although there has been a fall in the number ofpeople claiming Jobseeker’s Allowance, moreTower Hamlets residents claim benefits than onaverage in London, with in-work poverty asignificant concern. About one third of housingbenefit claimants are in paid work.
138
Tower Hamlets Partnership Community Plan 2015 11
As a result of the Fairness Commission’srecommendations, one of the growing areas ofpartnership working in Tower Hamlets is reducingthe cost of living for families on low incomes bypromoting digital and financial inclusion. This isnecessary to help tackle the “poverty premium”that these families suffer from as consumers, dueto lacking internet access and bank accounts.
Welfare reformWelfare reform poses one of the biggestchallenges to the partnership, in terms of theeconomic wellbeing of residents as well as thefinancial impact on the council and housingproviders. Partners need to work together tounderstand and demonstrate its impact on localpeople, as well as supporting residents throughthe changes. The government’s welfare reformshave disproportionately affected local residentswith over 700 households subject to the benefitcap and a further 2300 losing income because ofthe Spare Room Subsidy. Locally commissionedresearch estimates that by 2015 the cumulativeimpact of all welfare reforms will mean thathouseholds claiming benefits will be £1670 peryear, or £32 per week, worse off. These impactswill affect over 40,000 households, over half willbe households where someone is in work.
The introduction of Universal Credit, and thetransition from Disability Living Allowance toPersonal Independence Payments has alreadybegun. Improving digital and financial inclusionare issues particularly relevant to these changes,as benefit claims become online by default andmonthly payments are made directly to residents.In terms of the services which support peopleinto work and to progress, feedback suggeststhey are still too disconnected and not focusedenough on the needs of individuals. We knowthat employment at living wage levels is the onlysustainable way to mitigate the impact of welfarereform. A commitment has therefore been madeto create more integrated employment services.This will be pursued by a range of partners tocreate a holistic response to residents in need ofsome extra help – not just in terms of
employment services, but housing and welfareadvice, health and wellbeing, family support,English and maths skills, financial and digitalinclusion and childcare. This partnershipapproach will be essential as we move towardsthe next phase of welfare reform: the nationalroll-out of Universal Credit.
Connecting businesses with theircommunityIn its report, the Fairness Commission advocatedmuch stronger links between locally-basedbusinesses and Tower Hamlets residents, throughemployment opportunities, work experience foryoung people, contract opportunities for localSMEs, and a better matching of corporate socialresponsibility activities with local needs. Goingforward, this will be driven by a new BusinessCharter for Tower Hamlets, which will bringtogether businesses with local public andvoluntary sector agencies encouraging everyoneto ‘buy local, employ local, support local’.
Creating healthy high streetsHealthy high streets and town centres are anessential part of a thriving local economy andhave been the subject of numerous reviews at alocal, regional and national level, including theindependent review by Mary Portas. Residentsand businesses alike want to see a range of shopsand other businesses which meet the needs andexpectations of a broad range of residents andoffer a range of jobs for local people, in apleasant and safe environment where retail spaceis occupied, and quality and healthy food isavailable to buy. At the same time, they want theproliferation of gambling outlets, fast foodtakeaways and payday lenders on local highstreets kept in check. The council has onlyrecently gained limited powers to directlyinfluence this, and we have begun work toconsider what ‘healthy high streets’ mean inTower Hamlets and how we can achieve thesetogether.
139
12 Tower Hamlets Partnership Community Plan 2015
Current partnershipcommitmentsPartnership priorities and activities in pursuit of aprosperous community are captured by theEnterprise and Employment Strategies, the workof the Economic Task Force, the welfare reformtask group, the Financial Inclusive Tower HamletsPartnership and the Children and Families Board.
Enable children and young people toachieve their full potential
X Provide free school meals for all primaryschool children in the borough
X Keep pushing our GCSE and A-Level resultsabove the national average
X Increase aspiration and educationalachievement post-16 and on to university
X Expand our schools and increase the numberof school places
X Deliver ambitious targets for expansion ofaffordable childcare provision
Better support residents throughwelfare reform, and into work, throughan integrated employment and supportservice for Tower Hamlets
X Reimagine local employment services so theywork better for local people
X Enable disabled residents and those withphysical and mental health conditions towork
X Become an online, more digitally inclusiveborough
Help reduce the costs of living anderadicate the ‘premium’ faced by manyresidents
X Promote financial inclusion through theFinancial Inclusive Tower Hamlets Partnership
X Continue to help residents reduce theirenergy bills with the Tower Hamlets EnergyCo-op
X Support the development of the credit unionand a Community Banking Partnership forTower Hamlets
Develop the skills of residents
X Generate more apprenticeships, traineeshipsand other opportunities for young people
X Develop skills provision for adults needing tore-enter the labour market or upskill
X Increase the number of employmentopportunities for disabled residents
Develop a new Business Charter, andencourage businesses to ‘employ local,supply local and support local’
X Support small and start-up businesses bydeveloping low-cost work space and creatingbusiness start-up grants.
X Encourage more businesses to pay theLondon Living Wage
X Develop a healthy high streets strategy
Build strong community leadership andsocial capital through a thrivingvoluntary and community sector
X VCS shape strategy and services and co-produce local services
X VCS resilience and financial sustainability X Monitor, evaluate and demonstrate impact
140

Tower Hamlets Partnership Community Plan 2015 13
Achievements so farFalling crime rates overallX In 2013/14, total notifiable offences had
dropped by over a third from their peak in2002/03, despite the dramatic growth inpopulation over that time. Personal robberyand residential burglary in particular havereduced, and crime rates in Tower Hamletsare better than in some of our neighbouringboroughs.
A strong sense of community cohesionX The vast majority of residents (78%) think
that people from different backgrounds geton well together, up from 69% in 2009.
X Our well-developed and responsive approachto cohesion and tension is recognised byexternal bodies, and we have effectivelyresisted organised attempts to divide ourcommunities. This is complemented by awell-established Prevent Programme, led bythe council in collaboration with a number oflocal partners.
X Working with students, their parents and thewider community, our schools promotetolerance and empathy between differentgroups, so students understand and reject allforms of unacceptable influence.
X Tower Hamlets is recognised as an exemplarof equality practice, and the council wasrecently assessed as Excellent against the LGAEquality Framework for Local Government.
The challenges we faceAddressing fear of crimeAs we have reduced crime levels, fear of crimehas also fallen considerably. Nonetheless, thisremains the top personal concern of residents.There are strong links between drug dependencyand acquisitive crime, and between alcohol abuseand anti-social behaviour and violence. We knowthat tackling problem drinking and drug use iskey to reducing these related crimes andreducing resident fear of crime further.
There are a small number of gangs operating inparticular geographical areas of Tower Hamletswhich are responsible for a significant proportionof youth violence and drug dealing. Thesecontribute to fears about community safety forlocal residents.
A safe and cohesivecommunityTower Hamlets will be a saferplace where people feel safer,get on better together anddifference is not seen as athreat, but a core strength ofthe borough
141

14 Tower Hamlets Partnership Community Plan 2015
Protecting vulnerable groupsThe partnership has recently developed a newstrategic approach to tackling violence againstwomen and girls, recognising the range ofagencies involved in this work and the need forstrong partnership working. Last year there was a20% increase in reported domestic violenceincidents, which may be due to an increase inreporting rather than actual incidents, and clearlyvalidates the priority placed on this area of work.
During our consultation process, people withlearning disabilities in particular said personalsafety was a key priority for them, as well asincreased awareness and understanding oflearning disabilities amongst those working inpublic services.
Current partnershipcommitmentsPartnership priorities under this theme are agreedand pursued through the Community SafetyPartnership Board, as set out in the CommunitySafety Partnership Plan.
Reduce acquisitive crime and anti-socialbehaviour by tackling problem drinkingand drug use
X Increase the number of THEOs and createjoint task forces between the police andcouncil to target hotspots
X Tackle drugs and alcohol misuseX Create safer streets by maintaining our local
police presence and improve lighting X Address fear of crime and public confidence
in the Police and other law enforcementservices
Limit local gangs and the impact theyhave on youth violence and fear ofcrime
X Implement our Ending Groups, Gangs andSerious Youth Violence Strategy, to tacklegangs and serious youth violence
Strengthen partnership work to reducedomestic violence and violence againstwomen and girls
X Increase investment in victim support andencourage reporting
Promote community cohesion
X Establish an ‘Every Voice Matters’ strategyX Continue to deliver a Preventing Violent
Extremism programmeX Increase the number of hate crime reporting
sites
Find solutions to increase cycling safetyon busy roads
142

Tower Hamlets Partnership Community Plan 2015 15
Achievements so farImprovements in healthy livingX We have worked to improve the
circumstances and surroundings which affectresidents’ health. For example, we haveincreased and improved green spaces,increased the availability of healthy food,reduced the availability of counterfeittobacco, alcohol and drugs, widened accessto sexual health services, and ensured thatpeople are informed and empowered to leadhealthy lives.
X In early years, more babies are breast feeding,childhood immunisation rates are amongstthe highest in the country (having risen frombelow the national average), and teenagepregnancy rates have fallen.
X More than 11,000 residents have beensupported to stop smoking over the last fouryears.
X We have made dramatic progress inmonitoring and controlling blood pressure forpeople with diabetes and coronary heartdisease (CHD), with amongst the best rates oftesting in England.
X Our performance has improved fromamongst the worst in the country to amongstthe best in prescribing for high blood,pressure, the proportion of those with CHDsuffering from high blood pressure, and theproportion dying from CHD.
X Tower Hamlets Clinical Commissioning Groupwas ranked as the best in England in2013/14.
X We now have the best rate in England foridentifying and measuring respiratorydiseases, having previously been in the lowest20%. This is crucial in enabling these diseasesto be properly diagnosed and managed.
X We have a dedicated Mental Health Strategysetting out how partners will work togetherto improve outcomes for people with mentalhealth problems. We have a new primary caremental health service, and we arestrengthening those services for mothers andbabies, as well as improving the partnershipapproach to working with children and youngpeople with a mental health problem. Ourservices to help people stop smoking and dealwith obesity have specific provision for thosewith serious mental illness, and we haveestablished a psychiatric liaison service at theRoyal London Hospital for those attendingA&E or requiring inpatient care.
X Progress has been made with dementiadiagnosis, with Tower Hamlets now havingthe second highest diagnosis rate in London.We have a range of services for people withdementia and their carers, including specificclinical support to care homes and four“dementia cafes” running each month,including two specifically for Bangladeshiresidents.
A healthy andsupportive communityTower Hamlets will be a placewhere people are supportedto live healthier, moreindependent lives and the riskof harm and neglect tovulnerable children andadults is reduced
143

16 Tower Hamlets Partnership Community Plan 2015
X We have also awarded grants to user-ledgroups to help them provide peer support toothers suffering mental health problems. OurHealth and Wellbeing Board was the first inthe UK to sign the Time to Change Pledge tostamp out mental health stigma anddiscrimination as a partnership.
X NHS Tower Hamlets Clinical CommissioningGroup has been recognised by Britain’s mostprestigious health sector awards for itssuccesses as an organisation, and inimproving care through technology.
Improving social care and integrating itwith health services X Tower Hamlets remains the only area in the
country to provide free, non-means testedhomecare, and local surveys show that thequality of life for users of adult social careservices is improving, with more residentshaving greater control over their package ofsupport.
X Children’s social care services are also workingwell, and both safeguarding and Looked AfterChildren services have been rated as good by
Ofsted. We have also kept the time between achild entering care and moving in with anadoptive family relatively low.
X Local services are putting people in control oftheir health and wellbeing, personalising careand supporting the self-management ofconditions and the promotion ofindependence. This will build resilience andindependence in individuals and families - across-cutting priority for the Community Plan.
X Tower Hamlets is part of an integrated careprogramme for north east London givenpioneer status by the Department of Health.Through this, we are ensuring that social careand health services are provided seamlessly,irrespective of the provider. We also now havemental health professionals working inintegrated health and social care teams forpeople who have multiple health needs.
The challenges we facePersistent health inequalitiesReducing the inequalities in health and wellbeingexperienced by so many Tower Hamlets residentsis one of the biggest challenges facing theborough. Although life expectancy has risen overthe last decade it continues to be lower than theLondon and national averages, and significanthealth inequalities persist. We know that peoplein Tower Hamlets tend to become ill at an earlierage and this is reflected in the ‘healthy lifeexpectancy’ figure which is significantly lowerthan the national averages. 13.5% of residentshave a disability which limits their daily activities,and Tower Hamlets has a higher number ofresidents with a severe disability compared withLondon and England, despite our relatively youngpopulation. Tower Hamlets has some of thehighest death rates due to cancer, cardiovasculardisease and chronic lung disease in the country,as well as the highest infection rates of HIV,tuberculosis and sexually transmitted infections.
144
Tower Hamlets Partnership Community Plan 2015 17
Ensuring good mental health andwellbeingGood mental health and wellbeing isfundamental to life outcomes and quality of life.Tower Hamlets has a high prevalence of riskfactors that can contribute to the development ofmental health problems in individuals, forexample long term unemployment,homelessness, and harmful alcohol use.
Tower Hamlets has a very high prevalence ofmental health problems. We have the fourthhighest proportion of people with depression inLondon, the fourth highest incidence of firstepisode psychosis, and the highest incidence ofpsychosis in east London, according to GPregisters. In total there are approximately 30,000adults estimated to have symptoms of a commonmental health problem in the borough, andbetween 3,400 and 15,000 children at any onetime are likely to be in touch with professionalsdue to concerns about their mental health.
The impact of mental health problems onindividuals, families and communities can beprofound. Mental illness has the same effect onlife-expectancy as smoking, and a greater effectthan obesity. Amongst people in work, mentalillness accounts for nearly half of all absenteeism;and amongst people out of work, almost half areon incapacity benefit on account of a mentalhealth problem.
A focus on health across the life course– from birth to deathMaternal health – before, during and afterpregnancy – and the first few years of a child’s lifeare a critical period for a child’s longer termhealth and wellbeing. Infant mortality in TowerHamlets is not significantly different to the rest ofLondon, but more babies are born with a lowbirth weight. This is not surprising given thecorrelation between birth weight anddeprivation. In terms of behaviours which affectthe health of a baby, 4% of mothers smokeduring pregnancy, but this rises to 16% amongst
white mothers. However there are good levels ofbreastfeeding, significantly higher than thenational averages, and immunisation take up forunder 5s is amongst the highest in the country.Unfortunately, Tower Hamlets has some of thehighest levels of child obesity in the country, with13% of children in Reception year obese,increasing to 25% by Year 6.
The health of older people in Tower Hamletsneeds particular focus. A survey of residentsshowed that more older people in Tower Hamletsare limited in their day-to-day activities comparedwith the average for London and England. 80%of over 80s have at least one chronic condition,and 35% have at least three at the same time. Westrongly suspect dementia is underdiagnosed,and Tower Hamlets has the second highest strokemortality rate in London. 50% of older peoplelive below the poverty line and a high proportionlive alone.
There is therefore significant concern aboutloneliness and isolation of many older residents,and the effect that has on their health.Furthermore, only 10% of older people consumethe recommended level of fruit and vegetablesand only 20% get the recommended amount ofexercise.
145

18 Tower Hamlets Partnership Community Plan 2015
Challenges to healthy living in Tower HamletsWe know that there are higher levels of ‘lifestylerisk factors’ in Tower Hamlets compared toelsewhere. There are higher levels of tobacco use,unhealthy diet, physical inactivity, problemdrinking amongst those who drink alcohol, riskysexual behaviours and drug use. These can bemade worse by the environment we live in. Forexample, there are 42 junk food outlets persecondary school in Tower Hamlets.
The spectrum of factors influencing the health ofour population is broad, and so we need allpartners to take a part in improving this acrossthe full range of their work. For this reason,healthier lives is a cross-cutting priority which wewill be focusing on over the next four years.
High numbers of carersUnpaid carers provide essential and highly-valuedsupport for family members, neighbours andfriends with needs. The 2011 Census identifiedthat in Tower Hamlets, 7.6% of our residents arein this position. Of those, 43% provide more than20 hours of care a week, and a quarter provide
over 50 hours a week – much higher than theLondon and England averages. 3% are youngcarers, 29% are aged 50 and over, and 9% areaged 65 and over.
The Care Act will increase the responsibilities oflocal agencies in relation to carers, ensuring theyare given more support and encouraged not toneglect their own health and wellbeing.
Continued structural change andfinancial pressures in the healtheconomyThere have been significant changes to the NHS,with responsibility for commissioning most localhealth services shifting to Clinical CommissioningGroups comprised of local GPs and other healthprofessionals. In the wake of this, theestablishment of the Health and Wellbeing Board,and the development of the Health andWellbeing Strategy, has enabled local partners towork better together to address healthinequalities and consider much more seriouslyhow we can embed health considerations in allaspects of policy. Change will continue over thenext few years with the implementation of theCare Act and the continuing shift towardsintegration between health and social careservices. Whilst all of this can createopportunities, it also presents a huge challenge inensuring the efficiency and effectiveness of localhealth services. Financial pressures on healthservices are significant, with NHS and social careservices facing continued demand pressures andno real increase in funding.
146

Tower Hamlets Partnership Community Plan 2015 19
Current partnershipcommitmentsEnsuring the residents of Tower Hamlets arehealthy and well supported is the responsibility ofthe Health and Wellbeing Board, a statutorypartnership body, as well as the Children andFamilies Partnership Board. Their priorities arecaptured by the Health and Wellbeing Strategyand Children and Families Plan.
Ensure a healthy start for every child
X Promote maternal health and people’sexperiences of maternity services
X Reduce infant mortality and promote infanthealth
X Ensure that all children are physically,emotionally, behaviourally and cognitivelyready for school
Empower people to live healthy livestogether
X Tackle obesity and promote physical activityX Reduce the prevalence of tobacco use and
substance misuseX Promote good sexual health
Promote good mental health andwellbeing
X Build resilience, mental health and wellbeingfor all
X Provide high quality treatment and supportX Support people to live well with a mental
health problem
Early identification and person-centredcare for people with disabilities, long-term conditions and cancer
X Create better care at home to help residentsstay out of hospital
X Embed promotion of healthy lives into healthand social care pathways through ‘EveryContact Counts’ programme
X Increase early awareness of symptoms ofcancer, and reduce delays in cancer pathways
Integration of health and social care toprovide joined-up and person-centredsupport
X Work together to support people'sindependence and help them live safely intheir own homes where possible
X Work with the local voluntary and communitysector to take individuals' wider needs andcircumstances into account
X Explore joint health and social care personalbudgets
Influence the wider social andenvironmental determinants of health
X Limit the impact of ‘unhealthy’ businesses onour high streets
X Tackle loneliness and reduce isolationamongst older residents
Safeguard children through focus onsexual exploitation, harmful practices,children with disabilities andimplementing a new neglect strategy.
Working with neighbouring boroughsto ensure safe, sustainable and high-quality health services
X Improve the health of our residents and helpthem take control of their own health
X Provide more co-ordinated health, social andmental health care
X Prepare for our growing and ageingpopulation
147

The Community Plan Your Borough Your Voiceconsultation has done much to generate debate,raise awareness and develop local partnerships.From late summer 2014, we carried out a widerange of exercises to canvass the views ofresidents and other stakeholders in the boroughon what we should prioritise in this Plan. Localpeople of all ages and backgrounds cametogether to talk about the issues that matter tothem.
We asked residents at Community Ward Forumsto feed in their views, and held an event forCommunity Champion Coordinators. However, itwas also important to talk with residents who arenot engaged on a regular basis with the councilor its partners, and so special events were held at
markets across the borough, as well as at Asda onthe Isle of Dogs. We met with representatives of awide range of service user groups, third sectororganisations and interest groups. Members ofthe partnership also discussed the Plan atmeetings of their themed Delivery Groups, as didthe council's Overview and Scrutiny Committeeat its first meeting in 2015.
Alongside the above, a web-based survey wasundertaken which was publicised online, in EastEnd Life and at the above events. We also heldtwo full-day in-depth events with residents,looking at service priorities in detail.
What we’ve heard
20 Tower Hamlets Partnership Community Plan 2015148

Tower Hamlets Partnership Community Plan 2015 21
Housing for allResidents are worried about the affordability ofhomes being developed in the borough, withmany households on low wages feeling that theyare beyond the reach of most people who wantto live in Tower Hamlets. Suitable housingoptions that meet the needs of people withlearning disabilities, mobility issues or mentalhealth problems are specific challenges.
Residents want the partnership to secure thecontinued existence of mixed communitiesthrough supporting a range of affordable housingchoices that reflect the people who live andaspire to reside in the borough. They also wantless development of high value housing whichpromotes gentrification and creates a divide,leaving certain communities behind.
Residents also highlighted the importance ofissues such as drugs misuse and anti-socialbehaviour which can blight individual andcommunity life on estates, and emphasised howgood housing and good living conditions isfundamental to wellbeing and cohesion.
Equality of opportunityand when managingausterity
The importance of ensuring that public sectorfunding is distributed fairly across groups wasraised by local communities. Residents feel thatincreased transparency in decisions over publicsavings should be a crucial aspect of the council’sand partnership’s commitment to fairness. Localpeople also highlighted the issue of fairness whenattempting to address the negative impacts ofpopulation growth within the borough. Oneresident said, “Community Champions are agood example of how to get involved in localaction and setting priorities.” Residentshighlighted that public services should recognisethe time and effort of people that save publicmoney, such as carers and volunteers, and shouldhelp empower and enable these individuals tocontinue making a difference to people’s lives.For example, a resident told us: "I like the idea ofgiving more small grants for faith and charitygroups involved with young people which buildon the good work being done in thecommunity.” To this end, local groups want towork more closely with the partnership tofundraise from external sources and maximiseinward investment in the borough. Residents alsoview culturally specific services as key to tacklingproblems amongst some communities who arewary of the authorities, such as addressing thestigma associated with domestic violence.
Local people want the partnership to be mindfulof the rising costs of living which may prompthouseholds to turn towards, and becomedependent on, unhealthy safety nets such as loansharks. Residents want to live longer and leadbetter lives, and understand the importance ofwider environmental factors such as healthyeating which can impact on this. They wanthealthy food available at affordable prices.
149

22 Tower Hamlets Partnership Community Plan 2015
Enterprising TowerHamlets and improvingresilience
Residents highlighted the importance of supportto secure sustainable employment including toaddress gaps in knowledge around how to accessjobs, soft skills and networks, especially sinceemployment is closely linked to welfare reforms.They feel greater investment and support tailoredfor disabled people to access the job market isrequired. Many community and voluntary groupsunderscore the fact that the financial servicessector is not the only provider of jobs in theborough, and that the opportunities offered byother types of business in the borough should bemaximised for local people. There is also concernthat low aspirations amongst some within theborough’s population remain unchallenged andthat education should continue to play a pivotalrole in breaking the cycle of poverty and raisingambitions. Residents told us: “By working withcommunities you increased our local skills and
confidence and a sense of pride starts to growwhere people become positive about theirfuture.” A lack of childcare provision, specificallyaffordable childcare to enable parents to work is apressing concern for local residents whichprovides a significant barrier to work, particularlyfor single parents.
There was anxiety amongst consultees about thehigh and persistent levels of in-work poverty inTower Hamlets. This is why they want the LondonLiving Wage to be adopted borough-wide byemployers to help ensure a fairer society.Residents care about helping people managetheir money as this is important to helphouseholds out of debt and into saving – theprovision of expert advice to solve deep-seatedfinancial or housing problems is important.
Cleaner, safer Tower Hamlets
The value of the borough’s public realm as thespace in which public life takes place washighlighted. It helps to deliver far reaching social,economic and environmental benefits. Takingpride in the local environment means thatresidents want the council to act more punitivelyon people who litter, fly tip or do not recycle.They also want to see a reduction in the numberof cars on the roads and a reduction in speedingon residential streets which poses a threat tosafety.
Concerns about the impact on quality of life ofanti-social behaviour and drug use were aparticular theme of resident feedback. Manyliving on estates wanted to see more action takenby partners to address these issues, and forcommunities to be given support to addressthem.
150

Tower Hamlets Partnership Community Plan 2015 23
We have reviewed our achievements, currentchallenges and existing priorities, in relation tothe four Community Plan themes. Partnershipworking to pursue these priorities is wellembedded and overseen by a range ofpartnership bodies – our Community PlanDelivery Groups – including the Health andWellbeing Board, the Economic Taskforce, theChildren and Families Partnership Board, theCommunity Safety Partnership Board and theTower Hamlets Housing Forum. Each of thesebodies has a clear set of priorities, action plansand a network of sub-groups which drive forwardpartnership work in their area.
In developing a Community Plan for 2015onwards, partners have emphasised the need forsomething which builds on and complements ourexisting partnership work, rather than replacingit. For this reason the Community Plan themeshave been retained. The only change is the aimof a ‘fair and prosperous community’. All partnerswanted to reflect the contribution of the FairnessCommission to the debate about economicgrowth in Tower Hamlets, and emphasise thatthe community wants to see everyone benefitingfrom economic growth and prosperity, with a fairdistribution of resources and opportunities acrossthe community, not growth at any cost.
To be more than a summary of ongoing work,the Community Plan needs a purpose of its own.In developing this plan we therefore looked atareas of work that don’t fit neatly into the workprogramme of one of the existing CommunityPlan Delivery Groups or strategies, and atchallenges which have been resistant toimprovement in the past. Partners want to usethis new plan to accelerate progress and harnessthe efforts of all partners around a few key sharedgoals, thereby adding value to existing work.Partners considered a range of areas andchallenges which met these criteria, anddeveloped a set of high level and cross-cuttingpriorities which will be the focus of collaborativepartnership action for the lifetime of this plan. Itis the intention that these priorities will galvaniseand motivate partners, strengthening anddeepening our focus in these areas and making areal difference locally. The four key prioritiesagreed are set out in the remainder of this Plan.More detailed delivery plans will be developed foreach of the agreed collaborative action projects.
Working bettertogetherCross-cutting partnership priorities for 2015 onwards
151

24 Tower Hamlets Partnership Community Plan 2015
The following diagram illustrates the close relationship between these priorities and current partnershipwork, as well as the One Tower Hamlets vision, and how these elements work together to form theCommunity Plan.
Community Plan
Community Planthemes:
X A great place to liveX A fair and prosperous
communityX A safe and cohesive
communityX A healthy and
supportive community
One Tower Hamletsprinciples:
X EqualityX CohesionX Community leadership
Cross-cutting priorities:
X Empowering residents andbuilding resilience
X Promoting healthier livesX Increasing employmentX Responding to population
growth
152

Tower Hamlets Partnership Community Plan 2015 25
Priority 1:Empowering residentsand building resilience
We know that partnership organisations need todo everything in their power to enable residentsto support themselves in all aspects of their lives.This is especially true in a context of significantlyreducing public sector resources. The moreresilient our communities and the better residentscan support themselves and each other, the morepartner organisations can do with the resourceswe have. We recognise that the nature of someservices in the past has sometimes led to peoplebecoming too dependent on them, which is notgood for that person, the community nor theservice overall.
By making this a cross-cutting priority in the2015 Community Plan, we can bring partnerstogether to consider all opportunities to createmore engaged and resilient communities. Thiswill be through a better understanding of whenand how residents can be involved in designingand delivering public services and how we cansupport this fully. We already have a dynamicvoluntary and community sector, but we need toall come together to develop a collective approach and build capacity in that sectorfurther. This may involve helping voluntary sectororganisations run as efficiently as possible,maximise the use of their assets and engage morewith the private sector. Co-production is animportant element of this, and we will ensurethat this is a key part of commissioningundertaken by partners. The Council’s renewedMainstream Grants Process for 2015-18 is seekingto embed these principles, and it is proposedthere will be a theme particularly focused ongreater community engagement and resilience.
An important way which we know builds theresilience of individuals and families is a focus onearly intervention and prevention. We willcontinue to work with children, young people
and their families to understand and improvetheir wellbeing, before they reach crisis point.
In social care, we are investing in technology andintegration of services which will reduce thenumbers of people being admitted to hospitaland delay their need for care. We are also rollingout personal budgets across health and socialcare. We have identified that some groups areparticularly isolated from their communities andthat work to tackle loneliness and isolation canbuild resilience, improve wellbeing and reducedemand for higher cost health and careprovision.
There are also opportunities for communities tocontribute to and influence service provision anddecisions - for example, Healthwatch representsresidents in sitting on the borough’s Health andWellbeing Board, and ward forums offer people achance to influence their local services. We willalso be developing a health and wellbeing surveyof residents, and training people to research andfeedback residents’ perceptions on health issuesand local services.
We recognise that it is more difficult for somegroups to engage with public sectororganisations, and so we support a range offorums to help bridge the gap. The council iscommitted to developing a range a forums tohear the voice of often excluded communitiesand ensure that ‘every voice matters’. To do this,we will be formalising funding for these, andeach will have a councillor to act as its“champion”. These forums will also be holdingopen events to raise their profile and reach out totheir communities, so that they are asrepresentative as possible.
Partners are also committed, through the multi-agency Digital Inclusion Strategy recently agreedby the council’s cabinet, to facilitating access tothe internet for residents, including providing wi-fi in key locations, and giving them the skills tobe able to use it. This can empower residents in avariety of ways, from enabling financial inclusion
153

26 Tower Hamlets Partnership Community Plan 2015
(online banking offers accessible and instant toolsfor money management), to allowing them tohave their say in consultations (which areincreasingly online, as part of the government’s“digital by default” agenda).
Within the context of this range of ongoing work,it is proposed that the Partnership focus on thefollowing collaborative action projects for the lifeof this Community Plan:
X Addressing loneliness and isolation through apartnership-wide action plan.
X Engaging all partners in the delivery of theTower Hamlets Digital Inclusion Strategy tomake Tower Hamlets a digitally inclusiveborough. This will include provision of freeWi-Fi in our public spaces, and we willinvestigate the provision of Wi-Fi or fibre-optic internet in social housing blocks.Support through digital skills training andchampions will also be increased.
X Developing a strategy to enhance communityengagement. We will review the CommunityChampions model and also look at otherways of engaging with the community andpartners, and in the design and delivery oflocal services. This will include meetings inthe community, active engagement withexisting groups and the encouragement ofactive community groups in areas, and forsectors, where this is limited.
X Enabling individuals and communityorganisations to apply for funding to helpreduce the energy use and carbon emissionsin their area, as well as to provide otherbenefits.
To measure progress towards buildingresilience we will develop a set of outcomemeasures relating to the above activity.
Priority 2:Promoting healthier lives
In line with national trends, life expectancy inTower Hamlets has been improving year on year.However, health inequalities between TowerHamlets and the rest of the country remain highand there are also significant health inequalitieswithin the borough that closely correlate withlevels of socioeconomic deprivation.
Tackling health inequalities requires a wholesystem approach recognising the importance ofwider determinants of health (e.g. income,employment, education), healthy environments,(e.g. housing, physical environment), strongcommunities and integrated services promotingprevention and early intervention. This approachalso recognises that behaviours impacting onhealth, such as diet, physical activity andsmoking, are strongly influenced by theenvironments that people live in. Understandingthe most effective ways of utilising our resourcesto change those environments requires robustand reliable evidence, and so we will add to thedata on which we base our activity.
We will put health and wellbeing at the heart ofeverything we do across the partnership. Bymaking healthy lives a partnership priority we aimto build on existing work and develop a borough-wide focus on healthy living, with all partnersconsidering their role and impact on improvinghealth and wellbeing in the borough. Forexample, we are seeking to make the wholeborough a car no-idling zone. We will also reducethe numbers of people killed and seriously injuredon our roads by imposing a speed limit of 20mphon residential streets across the borough.
In primary schools, Tower Hamlets is leading theway in supporting health and wellbeing. Thisincludes offering nutritious free school meals toall pupils and by equipping staff to addressemotional and mental health issues. As agreed bythe Health and Wellbeing Board in its Healthy
154

Tower Hamlets Partnership Community Plan 2015 27
Lives action plan for 2015/16, the HealthySchools programme is being expanded to take insexual health and relationship issues, as well asdrugs, alcohol and tobacco use. We are alsodeveloping a health offer to young people whichwill be available through our youth centres.
In its action plan, the Health and Wellbeing Boardhas also committed to make drugs and alcoholservices for all residents more joined-up, and toincrease screening for sexually transmittedinfections and improve diagnosis of Hepatitis Band C cases. To complement this, we will alsoincrease the uptake of contraception.
We aim to better harness the power of localpeople and peer support. We are developing acommunity-led pilot programme to identifywhere older residents are suffering from isolationand loneliness, as evidence suggests this has veryreal implications for their health and wellbeing. Ineach of the three neighbourhoods participating,we will develop networks of local people tounderstand and take action to tackle loneliness.More broadly, the community will lead aprogramme to tackle poor mental health, raisingawareness of this issue and helping to identifythose at risk, as well as helping those in need ofsupport to access it.
We will seek new ways to achieve theenvironmental and behavioural change neededto improve health and wellbeing, bringing astrong partnership focus to making progressagainst issues where this has been challenging.On childhood obesity, for example, the HealthyLives action plan sets out that we will helpchildren and families manage their weight, andincrease access to healthy food that is alsoaffordable. We will also make walking an easierand more attractive option for getting around theborough, and the Play Streets initiative will makeit easier for young people to enjoy sport andphysical activity in their local areas.
Within the context of this range of ongoing work,it is proposed that the Partnership focus on thefollowing collaborative action projects for the lifeof this Community Plan:
X Delivering a cross-Partnership campaign to‘get Tower Hamlets more active’, which willinclude a focus on:X encouraging walking and cycling X enhanced use of parks, sport and leisure
facilitiesX improving road safetyX supporting people with disabilities to be
more active.
X Establishing a campaign for healthy food,focusing on:X tackling fast food prevalenceX increasing options for accessing healthy
food.
To measure progress towards promotinghealthier lives we will develop a set ofoutcome measures relating to the aboveactivity.
Priority 3:Increasing employment
Employment rates have improved dramatically inTower Hamlets and across east London, but theborough still has some of the lowest rates ofemployment in the country, particularly amongstwomen and some minority ethnic groups. Weknow that unemployment due to ill health,especially mental ill health, is a huge issue and asignificant challenge for the partnership. Whilstthere are many local partners doing a lot of workto help more residents into work, employmentunderpins wellbeing and life chances to such anextent that there is real benefit from bringing abroader range of organisations together on thisagenda.
155
28 Tower Hamlets Partnership Community Plan 2015
There are a large number of Tower Hamletsresidents who have low skills, have not workedfor some time and are a long way from being‘job-ready’. All partners can play a role, makingevery contact count, engaging the unemployedresidents they work with in some form of activity,programme or learning – encouraging andsupporting them to move a step closer to work.For example, the council, Tower Hamlets College,Jobcentre Plus and other partners are alreadyworking together to prepare residents with arange of relevant skills and support to help themcompete in the local job market.
Young people can now access progressionsupport, including specialist careers guidancewhere necessary, in our youth centres; andcareers advisers help those on the PositiveActivities for Young People programme plan theirnext steps. We need to continue to embedemployment skills and careers guidance into workwith young people and their families in schools.
We also need to build employment activities intohealthcare pathways and in particular intorecovery from mental ill health.
Training should be a viable and attractive optionfor residents who can benefit from it. Forexample, the council, schools and the NationalApprenticeship Service plan to work together tocreate more local apprenticeships.
An identified barrier to work for many families isaffordable and accessible childcare. This issuewas identified by the Fairness Commission, andfurther work is needed to progress this. Flexibilityof working hours to accommodate working hourswas also raised in the course of the publicconsultation.
We also plan to engage more local employersthrough our networks and supply chains, andbring a stronger employment focus toregeneration, development and housingactivities. Partners can also play a significant role
in increasing employment through their activitiesincluding their own recruitment and employmentpractices.
This priority will also require us to engage andreach out to businesses more, successfullyengaging them in a range of agendas whichmeet the needs of their business as well as thoseof the local community, through our newBusiness Charter, “Tower Hamlets Works”.
As a partnership, we recognise that we can makethe greatest impact on increasing employmentby working together, pooling our resources andintegrating our services. For this reason, we willbring together all employment advisory servicesinto one community hub, along with otherrelevant support and outreach. This will alsofacilitate the sharing of information aboutavailable jobs, acknowledged by partners ascrucial in providing employment support.
Within the context of this range of ongoing work,it is proposed that the Partnership focus on thefollowing collaborative action projects for the lifeof this Community Plan:
X Delivering a cross-Partnership IntegratedEmployment service that addresses broaderneeds which can act as a barrier toemployment (eg skills, housing, health,money management, welfare reform advice).We will do this by piloting services intoWhitechapel and Chrisp Street Idea Stores,introducing a triage-like first contact systemwith a view to delivering this model morewidely across a range of appropriatelocations.
X Developing a new approach to improving thelocal childcare offer and making it moreaffordable.
To measure progress towards increasingemployment we will develop a set of outcomemeasures relating to the above activity.
156

Tower Hamlets Partnership Community Plan 2015 29
Priority 4:Responding topopulation growth
Tower Hamlets has experienced the fastestgrowing population in the country in recentyears, and this fast-paced growth is expected tocontinue. The current population of 272,000 isexpected to rise to 320,000 by 2022 and to over350,000 by 2033. As the population is growingits profile is changing – much of the growth isdriven by an increase in the number of youngworking professionals. Tower Hamlets has thehighest proportion of residents aged 21-28 ofanywhere in London, and the lowest proportionof residents aged 40 and over.
Although Tower Hamlets has a low number ofolder residents compared to other boroughs,their number will increase over the coming years,particularly the number of residents aged 85 andolder. The growth in the number of much olderresidents will put increasing pressure on servicesfor that age group, particularly adult social careservices. We need joint approaches to developinginfrastructure and managing service demand,working together to ensure effective use oflimited resources.
Tower Hamlets has long been a very diverseborough and is currently the 16th most diverselocal authority area in the country, with 43% ofresidents born outside the UK, 90 languagesspoken and a high level of population churn.This growing and changing population putsincreasing pressure on local services andinfrastructure. It is fuelled by the building of newprivate homes, which does not relieve theenormous pressures on affordable housing. Weaim to secure new affordable homes over thenext four years, while ensuring that the impact ofnew development on communities is taken intoaccount in the new Local Plan. These will bedelivered with around 30% of these having three
or more bedrooms for larger families. These willbe delivered by a combination of the council andhousing associations, as well as by privatedevelopers contributing as a result of planningagreements.
An increasing proportion of residents are living inTower Hamlets’ growing private rented sector(PRS). There will be a strong focus on improvingconditions in the PRS, including a landlordregistration scheme, with action taken againstlandlords who exploit their tenants unfairly.
As partners we need to ensure that we maintainquality of life in a borough which is growing andchanging so quickly. This includes a planned andcoordinated approach to delivering infrastructurethat meets the needs of new and existingresidents, workers and visitors. To this end, weare planning for more health facilities, includingGP surgeries, as well as new primary andsecondary school places. We are also planning toimprove green spaces, transport connections,community facilities and other elements of theborough's infrastructure. Existing fundingmechanisms such as the CommunityInfrastructure Levy and Section 106 will be usedto secure and deliver some of the infrastructureneeded. We are additionally seeking otherfunding mechanisms and opportunities to deliverthe necessary infrastructure.
Our Whitechapel Vision illustrates how we wantdevelopment to progress in Tower Hamlets, asalong with new homes, this will lead to thecreation of new public spaces by 2023. Localemployment and affordable workspacedevelopment will be integral to the regenerationof the area.
The above will form part of a new Local Plan,which will be prepared to respond to thechallenges of growth in our borough, and willinclude planning policies to manage newdevelopment. These policies will ensure that theright types of development are permitted in the
157

30 Tower Hamlets Partnership Community Plan 2015
right locations, and that growth is supported byappropriate services and infrastructure. The LocalPlan will be prepared in consultation with ourcommunity.
It is important that we fully understand thenature of our changing population, including theparticular needs of new or smaller communities.This will involve obtaining and using dataeffectively, including exploring a single point ofregistration for local residents.
Within the context of this range of ongoing work,it is proposed that the Partnership focus on thefollowing collaborative action projects for the lifeof this Community Plan:
X Developing a new Local Plan to managecurrent and future levels of growth anddevelopment. This will include working todeliver sufficient infrastructure, such as schoolplaces, GP surgeries, green spaces, transportconnections, and community facilitiesamongst others.
X Reviewing the Partnership’s approach tocohesion, including for new and smallercommunities, for example the Somalicommunity. This will also have anintergenerational dimension.
X Incorporating within regeneration – includingat Whitechapel – projects which bridgecommunities and promote cohesion.
X Understanding our changing communities,including through a renewed partnershipapproach to data use.
To measure progress towards responding topopulation growth we will develop a set ofoutcome measures relating to the aboveactivity.
EnablersIn addition, there are some different ways ofworking which will enable partners to have agreater impact on these proposed priority areas.Partners will work together to understand andrespond to financial interdependencies across thepartnership. This is crucial as there is increasingpressure on all public sector organisations toreduce costs and do more with less. There is stillmuch potential to explore sharing of services andassets across the partnership. This could meansharing buildings or services or people. We wantto make sure local services are more integrated,reducing inefficiencies and making it much easierfor residents to navigate between services. Key tothis will be understanding population growth andthe impact it is having on our communities andthe new communities being created, as well asour ability to deliver services.
158

The One Tower Hamlets vision has underpinnedour Community Plan and our Partnership for thelast seven years. The vision is to reduceinequality, promote community cohesion andenable community engagement and leadershipby giving people the tools and support toimprove their lives.
The One Tower Hamlets vision is of a boroughwhere everyone has an equal stake and status;where people have the same opportunities astheir neighbours; and where people have acommitment and a responsibility to contribute tothe well-being of their communities. TowerHamlets is a place of immense opportunity, butpoverty and inequality can stop local peopleachieving their full potential.
Existing plans and strategies seek to ensure thatwe tackle this inequality in all we do. Partnerorganisations are making the promotion ofequality an integral factor in the design anddelivery of their services, alongside dedicatedinitiatives to directly address inequality due toage, disability, gender, ethnicity, sexualorientation or region and belief.
One Tower Hamlets also means bringing differentparts of the community together, encouragingpositive relationships and tackling divisionsbetween communities. 78% of residents agreethat people from different backgrounds get onwell together, and we have worked with peoplefrom across the borough’s diverse communities ina unified response to those who seek to divide us.For example, in response to an EDLdemonstration, partners supported and took partin a very successful solidarity march, includingcommunity and faith leaders, young people,residents, the Police, the council and other localorganisations. A third element of our approach has been
focused on providing strong leadership, involvingpeople and giving them the tools and support toimprove their lives. The number of people whobelieve that they can influence decisions affectingtheir local area is increasing, and CommunityChampion Coordinators play a vital role insupporting local communities. The FairnessCommission brought together people from awide range of sectors including big business,public services and small community groups tocome up with ideas on making Tower Hamlets afairer place, which we are now implementing.
These principles remain at the heart of the way inwhich we will seek to deliver the Community Planpriorities. In particular we will drive this through:
X A focus on fairness and ensuring that nocommunity is left behind which is key tomaintaining cohesion across the borough
X A focus on empowerment and resilience thatwill ensure that communities are engagedand capacity is built for communityleadership
X A focus on healthy living and employmentthat will enable us to tackle some of the keybarriers to equality, and to focus particularlyon more disadvantaged parts of thecommunity.
Making One Tower Hamlets a reality will alsomean redoubling our efforts to inform andengage local people and make every voice count.This will include looking again at the structures ofthe Partnership which communicate with andengage people at a neighbourhood and wardlevel.
Tower Hamlets Partnership Community Plan 2015 31
One Tower Hamlets
159

Delivering thepriorities
Tower Hamlets Partnership Community Plan 2015 32
Our next steps will be to develop a set of activities focused around the proposed Community Planpriorities. The aim will be to consult with all partners and through a joint action planning session, agreea set of commitments which will enable us to progress the cross-cutting priorities agreed. This will takeexisting partnership strategies as a starting point but seek to enhance and accelerate these.
160
Governing Body Meeting Enclosure
Date of meeting September 1st 2015 K
Agenda item 3.2
Title of report: Operating Plan and Commissioning Strategy
Author(s): Josh Potter – Deputy Director of Commissioning and Transformation – NHS Tower Hamlets CCG
Presented by: Sponsor (if different): For further information
Josh Potter – Deputy Director of Commissioning and Transformation – NHS Tower Hamlets CCG
John Wardell – Deputy Chief Officer – NHS Tower Hamlets CCG
Josh Potter – Deputy Director of Commissioning and Transformation – NHS Tower Hamlets CCG – [email protected] 0203 6882518
Executive summary
This paper outlines the CCG’s approach to:
- Operating Plan for 2016/17
- Commissioning Intentions and QIPP for 2016/17
- Development of strategic commissioning programmes
Recommendation
Information Approval To note X Decision
The Governing Body are asked to NOTE the paper, and agree to maintain their engagement in this work as it develops.
Conflicts of Interest Whilst this paper is not seeking approval it should be noted that:
- Commissioning intentions will have a direct impact on the services provided by all main providers, including Barts Health, who some members of the Governing Body carry out clinical sessions for, and in General Practice, both as part of pathway redesign work, but also following delegation of co-commissioning.
Key issues Each year the CCG are required to review and develop their plans in line with the annual commissioning cycle, commissioning intentions, and assurance and delivery under the NHS Operating Framework. Over the last 3 years Tower Hamlets CCG has delivered ambitious and successful plans and this paper discusses how we will build on this delivery as we enter autumn and planning for 2016/17 and beyond.
161

Report history NA
Patient and Public involvement
The Commissioning schemes outlined above are the result of developed existing strategies within the CCG and are therefore supported by a significant amount of engagement activity to build our community intelligence and understanding of issues within the system. These engagement activities have included:
• VCS Health & Wellbeing Forum • Patient & Public Newsletter • Network Locality meetings • Community Intelligence Bursary Programme • Health Conversation Events • Maternity Service Liaison Committee
From September, using the AGM and Big Conversation Events, the CCG will develop this engagement on our strategic programmes, and delivery of commissioning plans for 16/17 and beyond. This will culminate in a refreshed CCG prospectus in April/May 2016.
Link to the Board Assurance Framework
A robust operating plan, commissioning intentions and QIPP gives the CCG and NHSE assurance on the following:
Risk 1.1 Systems and processes to monitor, challenge and support Barts Health provider delivery of NHS Constitution targets and CQC action plan
Risk 3.6: Delivery of the Operating Plan, including QIPP
Impact on Equality and Diversity
Strategy within the current CCG prospectus was subject to an EQIA on initial development. This will be reviewed and refreshed, in light of the CCG’s new Equality and Diversity Strategy
Resource requirements TBC
Next steps Continue to develop strategic commissioning programmes.
Continue to develop commissioning intentions and QIPP.
Submission of business cases to Transformation and Innovation Committee.
Await and respond to NHS Operating Framework for 2016/17.
162
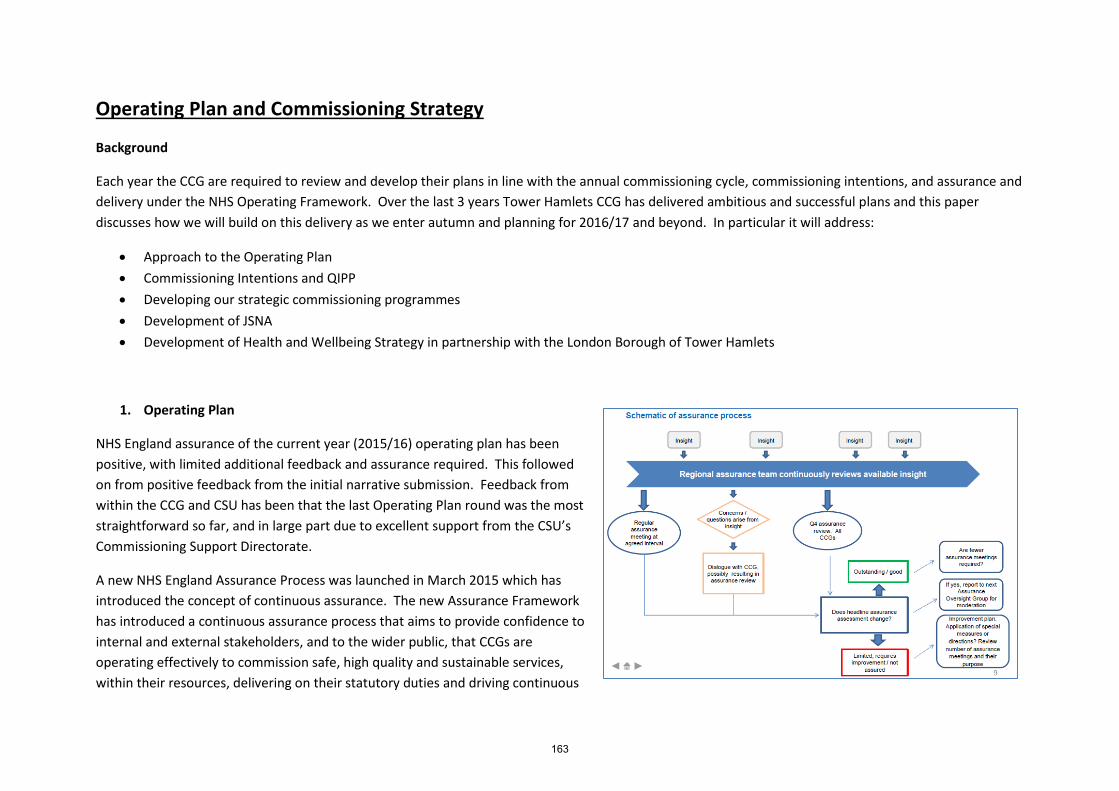
Operating Plan and Commissioning Strategy
Background
Each year the CCG are required to review and develop their plans in line with the annual commissioning cycle, commissioning intentions, and assurance and delivery under the NHS Operating Framework. Over the last 3 years Tower Hamlets CCG has delivered ambitious and successful plans and this paper discusses how we will build on this delivery as we enter autumn and planning for 2016/17 and beyond. In particular it will address:
• Approach to the Operating Plan • Commissioning Intentions and QIPP • Developing our strategic commissioning programmes • Development of JSNA • Development of Health and Wellbeing Strategy in partnership with the London Borough of Tower Hamlets
1. Operating Plan
NHS England assurance of the current year (2015/16) operating plan has been positive, with limited additional feedback and assurance required. This followed on from positive feedback from the initial narrative submission. Feedback from within the CCG and CSU has been that the last Operating Plan round was the most straightforward so far, and in large part due to excellent support from the CSU’s Commissioning Support Directorate.
A new NHS England Assurance Process was launched in March 2015 which has introduced the concept of continuous assurance. The new Assurance Framework has introduced a continuous assurance process that aims to provide confidence to internal and external stakeholders, and to the wider public, that CCGs are operating effectively to commission safe, high quality and sustainable services, within their resources, delivering on their statutory duties and driving continuous
163

improvement in the quality of services and outcomes achieved for patients.
The continuous approach replaces the previous requirement for an assurance meeting to be held each quarter. It introduces a more risk-based approach which differentiates high performing CCGs, those whose performance gives cause for concern, and those in between. It will help to identify emerging patterns of poor performance or any areas of potential risk, with less reliance on meetings and fixed points. All CCGs will be subject to a full assessment at the fourth quarter of the financial year to review performance against the five components of the assurance framework.
The domains against which CCGs are to be assured are:
• Well led organisation • Delegated functions • Finance • Performance • Planning (short and long term)
The exact timetable and requirements of the operating framework is usually released by NHSE England in December. The coordination of the operating plan will be overseen by the Deputy Director of Commissioning, with the support of the CSU’s Commissioning Support Directorate, and associated planning and analytics teams. The Governing Body are asked to note this, and agree to support the process, and review submissions as and when required.
2. QIPP and Commissioning Intentions
In line with the CCG prospectus, 2015/16 is the third year of Commissioning Intentions and QIPP of the CCG as an independent entity. The CCG’s Commissioning Team has continued to develop strategy and delivery, under the auspices of Governing Body leadership, and will seek to deliver the following service changes in 2016/17:
Programme Description Estimated
Savings
Planned Care
• New pathway redesign following procurement exercises in MSK and Pain, and Dermatology • Incorporation of previously community based activity into acute service provision in gastroenterology and
urology • Ensuring that Tower Hamlets realises the full benefits of redesign undertaken in 2015/16 in
gastroenterology straight-to-test, and community calprotectin testing
£2.5m-£3m
164

• Evaluation and wider roll-out of innovative renal pathway redesign • Continued focus on greater provider productivity • Exploration of other areas of opportunity such as sleep apnoea pathways and ophthalmology
Integrated Care
• Introduction of discharge to assess pathway for people with continuing healthcare needs, reducing length of stay and improving care package quality
• Review of clinical care and response to those living in residential homes • Undertake specialist palliative care review • Continue to realise the benefits of the integrated care service model • Develop recommendations for greater falls prevention • Roll out of social prescribing • Review of joint funded reablement services under the Better Care Fund • Re-procurement of vascular self-management programme • Post-evaluation roll-out of self-management programmes • Mental Health support for patients in the moderate risk cohort • TB early detection and new arrivals checks • Continued development of personalisation
£500k - £1.5m
Urgent Care
• Walk in Centre Review • Streaming optimisation • 111 Re-procurement
£0-£500k
Children • Evaluation and roll-out for the Bridge Project (Children’s virtual ward) • Pathway changes as a result of Barts Health Review
£500k - £1m
CHS • Procurement Efficiency £3m
Cancer
• Incorporating "cancer as LTC" guidance into Integrated Care • Gastro redesign (straight to test – see planned care) • Work with WELC CCGs on Early Detection and Patient Experience Cancer Board Priorities
TBC
Prescribing • Various improvement programmes e.g. scriptswitch, eBNF etc c£1m
Mental Health
RAID shift of funding to Barts TBC Continued delivery of the Tower Hamlets Mental Health Strategy
Other Vol Sec and NIS Contract Deflators c£200k Total £7.7m – £10.2m
165

As in previous years, commissioners will continue to develop and refine these schemes, with business cases going to the Transformation and Innovation Committee between November and January. The Governing Body will be asked to approve the final set of schemes in February 2016. The Governing Body are asked to note the above, and commit to reviewing and ratifying the recommendations of the Transformation and Innovation Committee.
3. Developing Strategic Commissioning Programmes
In October 2014 the Governing Body tasked the Senior Management Team to undertake a piece of work to identify and develop key strategic programmes that should shape the CCG’s agenda over the next 5-10 years. These programmes should deliver the CCG’s corporate objectives, and be in response to known current intelligence gathered from patient and public engagement, health intelligence and financial, performance and quality indicators. In order to carry this out, the Governing Body approved a partnership between Tower Hamlets CCG, McKinsey and Carnall Farrar to a) work with the Governing Body and partners to define these programmes in terms of vision, scope and outcomes, b) develop clear long term delivery plans for these programmes and c) provide expert input into the delivery of these schemes, including supporting a clear and robust organisational and leadership development strategy. This partnership has been in place since April 2015 and will be in place for a period of 18-24 months.
To date the partnership has undertaken:
• Diagnostic phase, exploring population health needs, review of policy and performance, forward look at opportunities and threats
• Interviews with wide range of stakeholders both internal and external
• Capability assessment including all levels of staff, identifying areas of strength on which to build, and areas for further development
• Number of Governing Body OD sessions to define priority programmes, and agree on scope and scale
Next steps are to spend 6 weeks between mid August and end of September in developing clear and final visions, scopes and objectives for each of the 10 work streams above. Delivery of programmes will commence from October 2015 onwards. Each programme will have a Governing Body and Senior
166

Management team lead, who will be responsible for the development of the work programme, and the delivery of objectives. The Governing Body are asked to note progress of this piece of work, and continue to proactively engage with its development over the coming months.
Engagement
The Commissioning schemes outlined above are the result of developed existing strategies within the CCG and are therefore supported by a significant amount of engagement activity to build our community intelligence and understanding of issues within the system. These engagement activities have included:
• VCS Health & Wellbeing Forum • Patient & Public Newsletter • Network Locality meetings • Community Intelligence Bursary Programme • Health Conversation Events • Maternity Service Liaison Committee
From September, using the AGM and Big Conversation Events, the CCG will develop this engagement on our strategic programmes, and delivery of commissioning plans for 16/17 and beyond. This will culminate in a refreshed CCG prospectus in April/May 2016.
4. Development of the Joint Strategic Needs Assessment (JSNA)
The JSNA Reference Group has Revisited its role, to now ensure that a range of stakeholders have the opportunity to input into the scope of new JSNAs and to ensure that recommendations are taken forward by the most relevant partnership working group. Its priority for this year is to work more closely with the Engagement and Communication Group to promote the role of community intelligence in strategic programmes. The refreshed JSNA Summary document is now available online. The JSNA programme for 2015/16 has been agreed as:
167
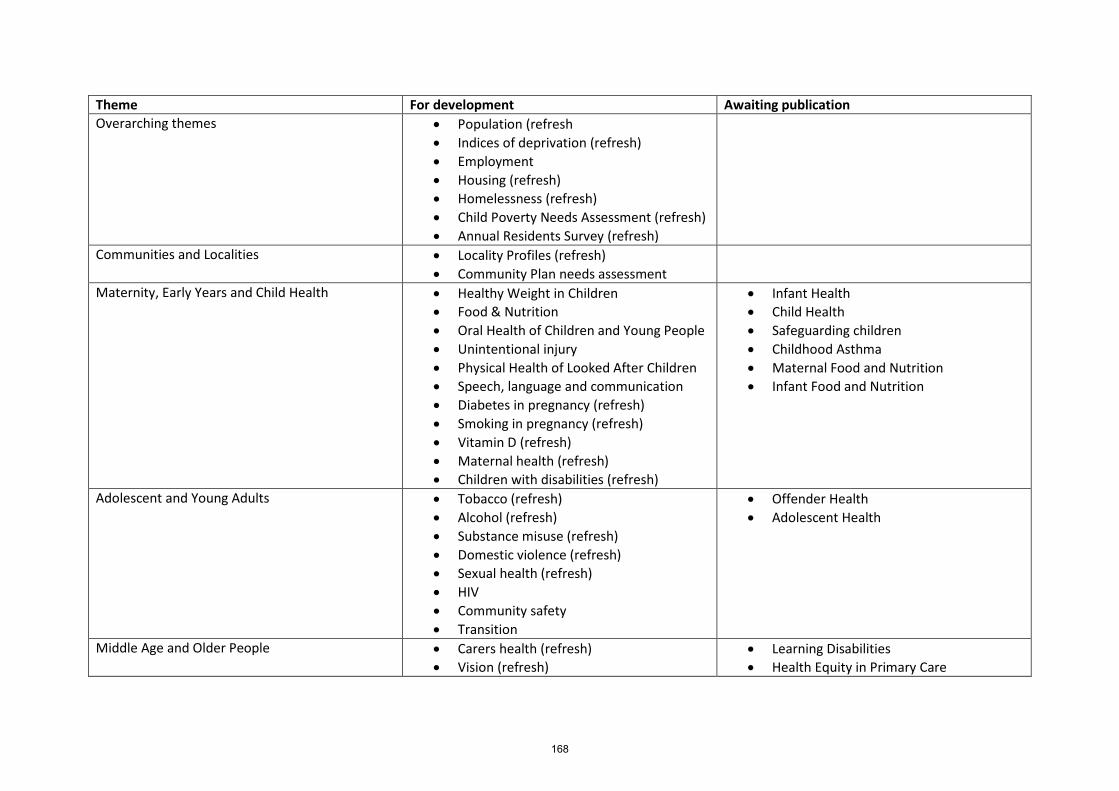
Theme For development Awaiting publication Overarching themes • Population (refresh
• Indices of deprivation (refresh) • Employment • Housing (refresh) • Homelessness (refresh) • Child Poverty Needs Assessment (refresh) • Annual Residents Survey (refresh)
Communities and Localities • Locality Profiles (refresh) • Community Plan needs assessment
Maternity, Early Years and Child Health • Healthy Weight in Children • Food & Nutrition • Oral Health of Children and Young People • Unintentional injury • Physical Health of Looked After Children • Speech, language and communication • Diabetes in pregnancy (refresh) • Smoking in pregnancy (refresh) • Vitamin D (refresh) • Maternal health (refresh) • Children with disabilities (refresh)
• Infant Health • Child Health • Safeguarding children • Childhood Asthma • Maternal Food and Nutrition • Infant Food and Nutrition
Adolescent and Young Adults • Tobacco (refresh) • Alcohol (refresh) • Substance misuse (refresh) • Domestic violence (refresh) • Sexual health (refresh) • HIV • Community safety • Transition
• Offender Health • Adolescent Health
Middle Age and Older People • Carers health (refresh) • Vision (refresh)
• Learning Disabilities • Health Equity in Primary Care
168
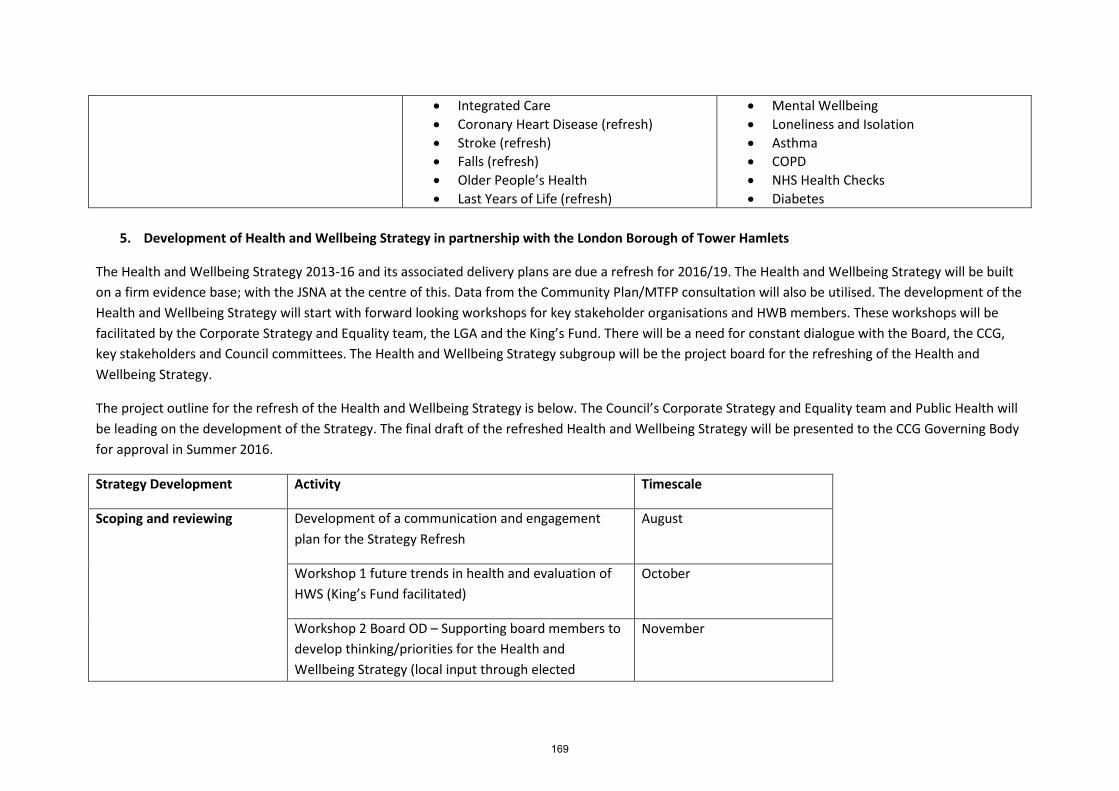
• Integrated Care • Coronary Heart Disease (refresh) • Stroke (refresh) • Falls (refresh) • Older People’s Health • Last Years of Life (refresh)
• Mental Wellbeing • Loneliness and Isolation • Asthma • COPD • NHS Health Checks • Diabetes
5. Development of Health and Wellbeing Strategy in partnership with the London Borough of Tower Hamlets
The Health and Wellbeing Strategy 2013-16 and its associated delivery plans are due a refresh for 2016/19. The Health and Wellbeing Strategy will be built on a firm evidence base; with the JSNA at the centre of this. Data from the Community Plan/MTFP consultation will also be utilised. The development of the Health and Wellbeing Strategy will start with forward looking workshops for key stakeholder organisations and HWB members. These workshops will be facilitated by the Corporate Strategy and Equality team, the LGA and the King’s Fund. There will be a need for constant dialogue with the Board, the CCG, key stakeholders and Council committees. The Health and Wellbeing Strategy subgroup will be the project board for the refreshing of the Health and Wellbeing Strategy.
The project outline for the refresh of the Health and Wellbeing Strategy is below. The Council’s Corporate Strategy and Equality team and Public Health will be leading on the development of the Strategy. The final draft of the refreshed Health and Wellbeing Strategy will be presented to the CCG Governing Body for approval in Summer 2016.
Strategy Development Activity Timescale
Scoping and reviewing Development of a communication and engagement plan for the Strategy Refresh
August
Workshop 1 future trends in health and evaluation of HWS (King’s Fund facilitated)
October
Workshop 2 Board OD – Supporting board members to develop thinking/priorities for the Health and Wellbeing Strategy (local input through elected
November
169

members and LGA facilitated)
Engaging with key stakeholders on their current priorities and strategies (CCG, CVS, and Healthwatch etc.)
September
Framework and emerging priorities
Priority mapping September - October
Gap analysis of stakeholder strategies and priorities September - October
Resident engagement programme to capture their views on health and their priorities
September – October
Review of needs analysis and other material September - October
Draft framework and emerging priorities papers taken to the HWS subgroup
October
Consultation on the draft framework with stakeholders, residents, Healthwatch and the Community Plan Delivery Groups
October/November
Amended framework and emerging priorities paper taken to the HWS subgroup
November
Framework and emerging priorities paper taken to the HWB
November
Priority development Templates completed by sub-group on agreement of the new priorities
November
Engage community plan delivery groups on the wider November - January
170
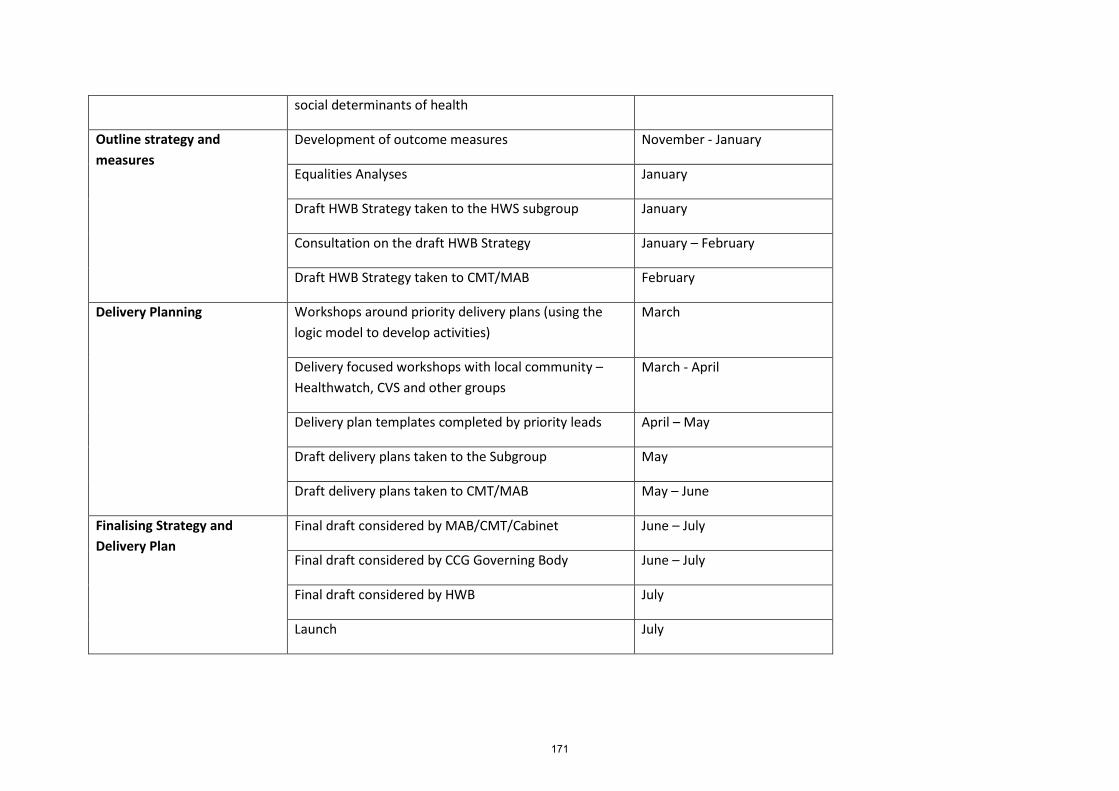
social determinants of health
Outline strategy and measures
Development of outcome measures November - January
Equalities Analyses January
Draft HWB Strategy taken to the HWS subgroup January
Consultation on the draft HWB Strategy January – February
Draft HWB Strategy taken to CMT/MAB February
Delivery Planning Workshops around priority delivery plans (using the logic model to develop activities)
March
Delivery focused workshops with local community – Healthwatch, CVS and other groups
March - April
Delivery plan templates completed by priority leads April – May
Draft delivery plans taken to the Subgroup May
Draft delivery plans taken to CMT/MAB May – June
Finalising Strategy and Delivery Plan
Final draft considered by MAB/CMT/Cabinet June – July
Final draft considered by CCG Governing Body June – July
Final draft considered by HWB July
Launch July
171
172

Governing Body Meeting Enclosure
Date of meeting September 1st 2015 L
Agenda item 3.3
Title of report: Public Health Report
Author(s): Dr Somen Banerjee – Director of Public Health
Presented by: Sponsor (if different): For further information:
Dr Somen Banerjee – Director of Public Health Dr Somen Banerjee – Director of Public Health – Tower Hamlets Local Authority
Executive summary
This briefing provides an overview of the Public Health in the council and summarises their aspirations, functions, organisational structure, resources and priorities.
Recommendation
Information Approval To note Decision
The Governing Body members are asked to note the contents of the report.
Conflicts of Interest There are no identified conflicts of interests.
Report history This is the first time this reports has been presented to the Tower Hamlets CCG Governing Body.
Patient and Public involvement
N/A
Link to the Board Assurance Framework
N/A
Impact on Equality and Diversity
N/A
Resource requirements As outlined in the report.
Next steps As outlined in the report.
173

174

Public Health in TH Council: Function, Form, Resources, Priorities15/16 Author: Somen Banerjee, Director of Public Health Report to: CCG Governing Body Meeting Date: 1st September, 2015 Contact: [email protected] _____________________________________________________________
1. Purpose: 1.1 This briefing provides an overview of the Public Health in the council and
summarises our aspirations, functions, organisational structure, resources and priorities.
2. What are the aims of Public Health? 2.1 The high level aspiration of Public Health for more people in the borough to live
healthy, fulfilling lives.
2.2 We frame this aspiration around people and place.
2.3 ‘Healthy place’ is an aspiration around more people living in healthy environments, protected from environmental harms and supported by strong community/family networks with easy access to high quality services.
2.4 ‘Healthy people’ is an aspiration around more people valuing their health, having the foundations for good physical and mental health and wellbeing and protected from health harms .
2.5 Based on opportunities for promoting health and wellbeing and informed by an understanding of patterns of disease through life, ‘Healthy people’ is framed around a life course model:
• pre-birth and early years • childhood and adolescence • young adulthood • middle age • later years
3. What is the function of the Public Health in the council? 3.1 The role of the public health department in the council and the rationale for its move
from the NHS is summarised in the following quote from the public health white paper which sets out the vison for local government leadership of public health:
175

‘Building on local government’s long and proud history of public health leadership, our vision is for local authorities to use their new responsibilities to put health and wellbeing at the heart of everything they do, thereby helping people to lead healthier lives, both mentally and physically’1 3.2 The core role of public health in the council is to work across the whole council and
with partners to deliver on the aspirations around Healthy Place and Healthy People. This in turn requires that the council puts ‘health and wellbeing at the heart of everything they do’.
3.3 In working across the council and with partners, the public health department has six functionsthat cross cut Healthy Place and Healthy People. These are:
• Public Health intelligence and insight (what are the health needs and assets?) • Strategy (what are the priorities for action and how do we mobilise our partners?) • Partnership and engagement (who do we work with and how?) • Commissioning and Delivery (what are we doing?) • Evaluation (how well are we doing?) • Research and innovation (how do we move forward where evidence is limited?)p
3.4 The public health work plan is framed as follows: Table 1 Summary framework of public health workplan Healthy
environments and communities, health promoting services
Healthy prebirth, early years, childhood, adolescence and families
Healthy early adulthood, middle age and later years
Insight Leading the Joint Strategic Needs assessment process providing insight into health needs in the borough, assessing the extent to which they are being met, reviewing the evidence base around health improvement, understanding local assets supporting health and making recommendations for change
Strategy Leading and supporting strategic partnerships for health improvement and protection – working with the corporate centre around shaping and implementing the Health and Wellbeing strategy and other strategies
Engagement Engaging and mobilising around public health issues in the borough with a wide ranges of partners eg public, NHS, council, voluntary sector, housing, business, academic, regional/national bodies
Delivery Using the Public Health Grant to commissioning programmes to improve population health both with external providers and within the council. Working with officers across the council and NHS to support their delivery around health and wellbeing outcomes
Evaluation Assessing the extent to which services delivered through the Public Health Grant and other sources are delivering against health and wellbeing outcomes and identifying how outcomes might be improved
Research and Working with academic partners and others to deepen our
1 Healthy Lives, Healthy People – June 2011
176
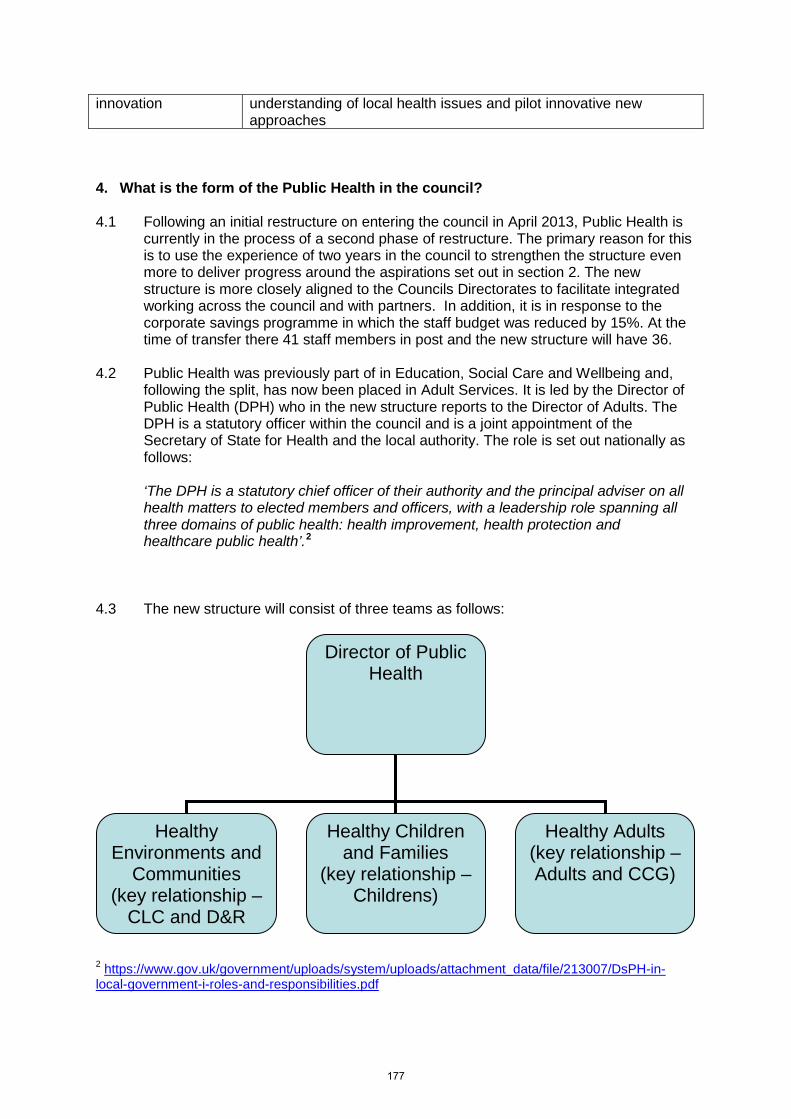
innovation understanding of local health issues and pilot innovative new approaches
4. What is the form of the Public Health in the council? 4.1 Following an initial restructure on entering the council in April 2013, Public Health is
currently in the process of a second phase of restructure. The primary reason for this is to use the experience of two years in the council to strengthen the structure even more to deliver progress around the aspirations set out in section 2. The new structure is more closely aligned to the Councils Directorates to facilitate integrated working across the council and with partners. In addition, it is in response to the corporate savings programme in which the staff budget was reduced by 15%. At the time of transfer there 41 staff members in post and the new structure will have 36.
4.2 Public Health was previously part of in Education, Social Care and Wellbeing and, following the split, has now been placed in Adult Services. It is led by the Director of Public Health (DPH) who in the new structure reports to the Director of Adults. The DPH is a statutory officer within the council and is a joint appointment of the Secretary of State for Health and the local authority. The role is set out nationally as follows:
‘The DPH is a statutory chief officer of their authority and the principal adviser on all health matters to elected members and officers, with a leadership role spanning all three domains of public health: health improvement, health protection and healthcare public health’.2 4.3 The new structure will consist of three teams as follows:
2 https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213007/DsPH-in-local-government-i-roles-and-responsibilities.pdf
Director of Public Health
Healthy Environments and
Communities (key relationship –
CLC and D&R
Healthy Children and Families
(key relationship – Childrens)
Healthy Adults (key relationship – Adults and CCG)
177

4.3 A Consultant in Public Health leads each team. Eligibility to be a Consultant in Public
Health requires professional registration on the GMC or UKPHR register and accreditation by the Faculty of Public Health following demonstration of competency against a national standards framework.
4.4 Each team consists of a number of public health heads, managers and officers. Job descriptions are generic but include the specific aspirations that each team member has responsibility for, which can be amended in response to changes in strategic priorties. All professional public health staff are expected to have the full competencies required at their level so that they can take on a new portfolio of work if required. The job descriptions are structured around the key public health functions of public health intelligence, strategy, partnerships and engagement, delivery, evaluation and research and innovation. Public Health heads and managers are required to have a post graduate qualification (usually at masters level) in public health or a related subject or to be able to demonstrate equivalent competencies
4.5 Progress against the public health aspirations (see table 2, section 5) requires working at all levels across the council as the work of every directorate in the council impacts significantly on health and wellbeing. It also requires working closely with partners outside the council. For this reason, the public health department has developed a hub and spoke model of work across the council and with partners
4.6 This is reflected in public health representation on senior level decision-making groups including Adults, Children’s and CLC DMTs, the Clinical Commissioning Group Governing Body and Partnership Boards including the Community Safety Partnership, LSCB and Children and Families Partnership Board. In addition, the DPH is the lead officer for the Health and Wellbeing Board and Health Scrutiny. Senior public health staff members also have lead roles at sector, London and national levels.
4.5 The restructure is an evolution from the previous structure and aims to:
• Clarify focus on public health strategy and aspirations • Align teams more tightly around aspirations • Align job descriptions to aspirations • Develop a structure within the new, reduced budget envelope • Enable recruitment to permanent post • Further strengthen integration across council and with partners • Further strengthen the establishment of public health networks across sectors • Reduce health inequalities and improve the health and well being of local
residents. 5. What are the financial resources of Public Health and how are they used? 5.1 The Public Health Grant for 14/15 was £32,261,000 and there was no increase in
15/16. Tower Hamlets has one of the the highest allocations in London and this reflects historical allocations due to prioritisation of public health programmes when public health was in the Primary Care Trust (PCT) and the high level of need in the Borough.
5.2 In addition, from October 2015 the council will take over responsibility for 0-5
services (Health Visiting and Family Nursing Partnership) with a full year allocation of
178

£7,710,000. This represents an expansion of the workforce and is a significant opportunity to improve the current and future wellbeing of 0-5 year olds. Evidence Indicates that these years are the most critical for long term health and wellbeing and offer the greatest opportunities to mitigate the impact of inequalities.
5.3 As part of the savings programme for 15/16, public health identified £3.8 million savings from its budget to accommodate expenditure of £1m children centre funding and £2.8m ongoing funding of free school meals. 5.4 The Chancellor recently announced an in in-year cut of £200m nationally local
authority public health budgets and the implications for Tower Hamlets will be clearer following the current consultation.
5.5 The main types of expenditure of the grant are on staffing (£2.4m), external
commissioning of public health programmes - mainly from the NHS and voluntary organisations (£15m) and ‘internal’ commissioning of services within the council - mainly within Children’s services and CLC (£5m – check this figure in context of children’s centres and free school meals). In addition, £8.7m of the public grant is used to commission drugs and alcohol through the Drugs and Alcohol Action Team in CLC (this includes council staff and external commissioning).
5.6 Table 2 overleaf summarises how funds within the PH grant are used to impact on outcomes linked to the public health aspirations.
179

Table 2 Public Health Grant expenditure in Tower Hamlets - Programme budgets Public health aspirations Main areas of PH grant expenditure
(bold = high spend areas) Maternity and early years
More parents: • enjoying good health and wellbeing More 0-5 year olds: • laying foundations for lifelong physical
and mental wellbeing o early attachment o healthy early nutrition o development through play o good oral health o fully immunised
• free from health harms o impacts of tobacco, alcohol,
drugs o neglect or abuse
Parents and infant wellbeing (£110k) Breast feeding (£471k) Early years accreditation (£50k) Active play (£54k) Healthy start vitamins (£44k) Fluoride varnish (£150k) Family Nurse Partnership and Health Visiting (from October 2015 – £7.7m)
Childhood and adolescence
More children and adolescents: • practicing and embedding habits for
lifelong physical and mental wellbeing o foundations for mental wellbeing o life skills for fulfilling relationships o regular physical activity o healthy eating o good oral health
• free from health harms o tobacco, alcohol, drugs o neglect or abuse
Free school meals (£2.8m) School nursing (£1.6m) Child and family weight management (£430k) Healthy Lives – schools (£188k) Mindfulness in schools (£43k) Peer education – smoking (£71k) Integrated sexual health (£600k) Substance misuse (£240k) Teenage pregnancy (£92k) Peer led SRE (£95k)
Adults More adults: • living healthily
o maintaining mental wellbeing o regular physical activity o healthy eating o good sexual wellbeing
• free from health harms o tobacco, alcohol, drugs, risky sex o neglect or abuse
• aware of and taking action on o risk of health conditions o symptoms of health conditions
Mental wellbeing awareness (£139k) Weight management (£826k) Health checks (£207k) Integrated sexual health (£1.4m) Genitourinary medicine (£4.3m) Tobacco – specialist (£420k) Tobacco – universal (£440k) Drugs and alcohol (£8.6m) Cancer early awareness (£96k) Domestic violence (£65k)
Environment and communities
More people: • living in healthy environments
o Safe and health enhancing o Supporting physical activity,
healthy eating • living in healthy communities
o Strong networks supporting healthy lives
• accessing high quality services o Integrated, prevention orientated,
accessible, high quality • whose health is supported by good
income, education, housing and employment
Health trainers (£1.1m) Making every contact count (£30k) Food for health awards (£72k) Tobacco/alcohol enforcement (£263k) Can do community (£70k) Social isolation pilots (£120k) ESOL health literacy (£58k) Community gardeners (£50k) Healthy housing (£35k) Health outreach workers (funding tbc)
180

6. What are the priorities for 2015/16? 6.1 The 2015/16 priorities for public health are aligned to those set out in the Health and
Wellbeing Strategy Action Plan 2015/16. These are set below based on the public health workstreams around insight, strategy, delivery, evaluation
6.2 Insight priorities
• To conduct a health and wellbeing survey of the borough • To develop a programme of participatory research (using researchers from
the community to provide insight into public health issues in the borough) • To embed new methods into the JSNA process: health impact assessment,
asset mapping and analysis of datasets that integrate health and social care 6.3 Strategy priorities
• To provide public health input to shape the new health and wellbeing strategy
for 2016/17 • To lead the health elements of the Community Plan around physical activity
and healthy food access • To provide the health and wellbeing input into spatial planning (the Local
Development Framework) • To integrate health into the integrated employment hub (being developed
through the economic taskforce) • To provide public health input to the CCG through the Memorandum of
Understanding • To provide public health input into the refresh of the Children and Families
Plan
6.4 Delivery priorities
• To develop and procure a new model for health visiting services • To implement the new model for school nursing • To reverse trends in oral in 5 year olds • To strengthen the public health impact of children’s centres and other early
years settings • To reduce demand for sexual health services by promoting safer sex and
improving treatment of STIs • To recommission drugs and alcohol services (led by CLC) • To work with Public Health England to address areas of concern around
screening and immunisation • To implement the public health elements of the Care Act around prevention
6.4 Evaluation and research priorities
• To evaluate tobacco cessation services • To review the paediatric dental pathway • To conduct community led pilots on
o Mental health awareness o Loneliness o Social prescribing o Coproduction (WELL London) o Healthy weight in primary school chilidren
181

6.5 These priorities are monitored through corporate oversight of the Health and Wellbeing Strategy 7. Conclusions Public Health came to the council with a strong track record of delivery and reputation. In the two years that it has been in the council it continues to build on this foundation and there have been fantastic opportunities for working across the whole council and it has established working relations with every directorate in the council. The restructure aims to further embed and focus this way of working and to support the council in the delivery of its duty under the Health and Social Care Act to improve the health of the population by ‘putting health and wellbeing at the heart of everything it does’.
182
Governing Body Meeting Enclosure
Date of meeting September 1st 2015 M
Agenda item 3.4
Title of report: Annual Report 2014/15 from the Audit Committee to the Governing Body
Author(s): Mariette Davis – Governing Body – Lay Member for Governance Justin Phillips – Governance and Risk Manager
Presented by: Sponsor (if different): For further information
Mariette Davis – Governing Body – Lay Member for Governance Justin Phillips – Governance and Risk Manager [email protected]
Executive summary
This paper provides a summary of the work carried out by the Audit Committee during the year 2014/15 under each of the key duties of the Committee, as set out in the terms of reference.
The Audit Committee’s role is to seek assurance that financial reporting and internal control principles are applied and to maintain an appropriate relationship with the organisation’s auditors, both internal and external. The Audit Committee offers scrutiny and advice to the Governing Body, about the reliability and robustness of the CCG’s processes of internal control.
Recommendation
Information Approval To note Decision
The Governing Body is asked to note the contents of the report.
Conflicts of Interest There are no identified conflicts of interests.
Report history This is the first time this report has been presented to the Tower Hamlets CCG Governing Body.
Patient and Public involvement
N/A
Link to the Board Assurance Framework
The Audit Committe reviews the Board Assurance Framework (BAF) at all Audit Committee meetings to ensure the establishment and maintenance of an effective system of integrated governance, risk management and internal control across the whole of the CCG’s activities.
183
Impact on Equality and Diversity
N/A
Resource requirements None
Next steps As outlined in the reports.
184
Annual Report 2014/15 from the Audit Committee to the Governing Body
Introduction
The Audit Committee (“The Committee”) is established under Governing Body delegation in accordance with the NHS Tower Hamlets CCG (“The CCG” ) Constitution. The Terms of Reference applicable to the Committee during the period covered by this report (1 April 2014 to 31 May 2015) are based upon the NHS Audit Committee Handbook (second edition) published in 2011 and are included at (Appendix A). The Terms of Reference have recently been updated by the Committee to reflect best practice as set out in the 2014 version of the NHS Audit Committee Handbook, which was published earlier this year. These updated Terms of Reference (which are subject to the approval of the CCG) are included at Appendix B
Membership
The Committee membership was as follows during the period covered.
Members
Name Role
Mariette Davis Lay Member for Governance and Chair Catherine Boyle Lay Member of Patient and Public Engagement Mr Tan Vandal Secondary Care Specialist
In attendance
Name Role Organisation
Andrea Antoine Deputy Director Finance NHS Tower Hamlets CCG Archna Mathur Director of Quality and Performance NHS Tower Hamlets CCG Henry Black Chief Finance Officer NHS Tower Hamlets CCG Dilani Russell Head of Financial Management NHS Tower Hamlets CCG Justin Phillips Governance and Risk Manager NHS Tower Hamlets CCG Richard Hewes Audit Manager KPMG Neil Thomas Partner KPMG John Keogan Local Counter Fraud Specialist Baker Tilly Business Services Limited John Elbake Internal Auditor Baker Tilly Business Services Limited Nick Atkinson Partner Baker Tilly Business Services Limited
A new member of the Committee is currently being sought as Catherine Boyle has expressed a wish to step down because of capacity constraints. The new member should ideally be a Governing Body member. I am waiting to receive the draft job specification for the new member from the Chief Officer of the CCG. It is important that the new member has an overview of the activities of the CCG in order that
185
that he or she can play the active and challenging role required by the Committee. As we enter Autumn, the recruitment of the new member is now becoming pressing.
Meeting schedule
The Committee met on the following dates and was quorate at each meeting:
• May 13th 2014 • June 2nd 2014 • September 8th 2014 • November 3rd 2014 • January 5th 2015 • March 23rd 2015 • May 19th 2015 • May 26th 2015
Review of the effectiveness and impact of the Audit Committee
The Committee has been active during the year in carrying out its duty in providing the Governing Body with assurance (or not) that effective control arrangements are in place. Specifically, the Committee has:
• Reviewed the Annual Financial Statements, the Annual Report (including the Annual Governance Statement) and recommended that the Governing Body should approve the Financial Statements.
• Reviewed and monitored the external auditors’ independence and objectivity and the effectiveness of the external audit process.
• Overseen a programme of internal audit work on systems and processes of integrated governance and risk management to provide assurance that internal controls and risk systems are in place and are working in practice.
• Reviewed arrangements in place for the management of conflicts of interest and suggested changes to the arrangements and CCG’s policy to strengthen them. The Committee was specifically active in reviewing our conflict of interest management arrangements for primary care co commissioning.
• Reviewed procurement processes generally and the CHS procurement process specifically and suggested changes to the process to enhance evidence of the highest standards of governance.
• Reviewed the CCG’s Constitution, including the standing orders, prime financial policies and scheme of delegation, and has suggested improvements to the content and format.
• Reviewed the Board Assurance Framework and Risk Management Strategy and influenced the drafting and ongoing development of these. Oversaw the carrying out of a deep dive into two risks in the Board Assurance Framework to provide assurance that the Board Assurance Framework reflected an accurate and reliable summary of the controls and assurances which were operating in practice. Continued to encourage the Governing Body to engage with the Board Assurance Framework process and to recommend that the Board Assurance Framework be presented by the Chief Officer and be considered at every meeting of the Governing Body high up on the agenda.
• Reported during the year to the Governing Body, in writing, on all matters considered significant by the Audit Committee.
186

• Reviewed our own terms of reference (see Appendix B for updated Terms of Reference, subject to CCG approval).
• The Audit Committee will shortly review its own effectiveness by undertaking a self-assessment in quarter three of 2015/16. The Committee is open to learning from experience and the input of others.
Principal review areas
A summary of the work carried out during the year under each of the key duties of the Committee, as set out in the terms of reference, is set out below.
Governance, risk management and internal control
The Committee reviewed relevant disclosure statements, in particular the Annual Governance Statement together with the Head of Internal Audit Opinion, external audit opinion and other appropriate independent assurances and considered that the Annual Governance Statement was consistent with the Committee’s view on the CCG’s system of internal control. Accordingly the Committee supported the Annual Governance Statement 2014/15, signed by the Accountable Officer in May.
The Committee has regularly reviewed the Board Assurance Framework (BAF). It believes that the BAF and its use by the CCG is continually improving and developing and is fit for purpose.
The Committee has reviewed and made recommendations regarding the Community Health Services (CHS) re-procurement programme governance, including: the governance structure, decision making authority, procurement route, reporting arrangements and proposals to manage conflicts of interest in line with the agreed quoracy arrangements in line with Constitution. The Committee has also reviewed the governance for phase II of the programme and will continue to request update papers and review the procurement process and the management of potential conflicts for the duration of the procurement.
In preparation for fully delegated primary care co-commissioning, the Audit Committee reviewed and oversaw the amendments to the Conflicts of Interest policy and the Constitution to ensure that they incorporated the NHS England guidance Managing Conflicts of Interest: Statutory Guidance for CCGs – Dec 2014. The Committee also reviewed and made recommendations relating to CCG delegated primary care co-commissioning, including: governance structures, committee terms of reference, committee scheme of delegations and the memorandum of understanding. Going forward, to ensure that the CCG has appropriate and robust conflicts of interest management processes, the Committee has requested the following reviews to be carried out by the Internal Auditors over the next few months:
• Assessment of the suitability of the Conflicts of Interest Policy and associated processes, consistency with best practice and how these are being applied in procurement decisions.
• Review of the governance arrangements in place to take forward the new responsibilities regarding primary care commissioning, as well as any existing contracts. This will also include an assessment of how contracts are awarded, review of the transparency of the procurement processes where work is awarded to the new GP Care Group and considerations of how Value for Money is obtained.
• Contract management assessment work to determine whether the amounts paid to the GP Care Group and to other primary care providers can be supported by demonstration of successful outcomes in line with agreed contracts. Authorisation and payment processes will be assessed.
The CCG has applied to NHS England for variation to the CCG Constitution twice during 2014/15. The Committee has reviewed and made recommendations relating to all the proposed Constitutional amendments.
187

The Committee has reviewed the CCG’s procurement governance to ensure procurement decisions are made with due regard to the Procurement, Patient Choice and Competition Regulations (2013) published by the Department of Health. The Committee has considered potential amendments suggested by the CFO to the delegation limits to expedite and support effective decision making. The Committee has suggested that these amendments be considered by the FPQ committee before being submitted to the Governing Body for approval.
The Committee has reviewed the governance of committees of the Governing Body; it periodically reviews the minutes of other Committees of the Governing Body.
The Committee has prepared a written ‘Key Messages report’ for the Governing Body after each of its meetings throughout the 14 Month period.
Internal Audit and Counter Fraud
Throughout the year the Committee has worked effectively with internal audit to monitor the CCG’s internal control processes. The Committee has in year:
• Reviewed and approved the internal audit strategy, and more detailed programme of internal audit work covering systems and functions within the CCG including reviews of new CCG work streams such as primary care co-commissioning.
• Reviewed and monitored the work of the Commissioning Support Unit (CSU) Assurance Group; comprising members (mainly the CFOs) from each CCG serviced by the North East London CSU to provide and manage the assurance process on those CCG functions outsourced to the CSU.
• Reviewed and approved the internal audit strategy and more detailed audit programme of internal audit work to be carried out on CSU systems.
• Reviewed internal audit reports throughout the year covering both internal audit work carried out on the CCG and on the CSU and considered their findings and recommendations. Ensured that management responded appropriately to the internal audit findings and followed up the implementation of recommendations.
• Reviewed and considered the work of the CSU Assurance Committee
• Reviewed the Annual Summary Report from the Internal Auditors and the Head of Internal Audit Opinion. The Audit Committee is assured that management within the CCG have responded to the internal audit reviews in an appropriate manner and that the Head of Internal Audit Opinion and the Annual Governance Statement reflect the evidence obtained. The Internal Auditors, Baker Tilly, provided the following Head of Internal Audit Opinion for 2014/15: “Based on the work undertaken in 2014-15, significant assurance can be given that there is a generally sound system of internal control, designed to meet the organisation’s objectives, and that controls are generally being applied consistently. During the year the Internal Audit did not issue any audit reports with a conclusion of limited assurance or no assurance.”
• Reviewed and approved the counter fraud plan for the year and considered reports covering counter fraud work carried out by the Local Counter Fraud Service on our behalf. During the year the Committee consistently raised a concern that there was no pro-active counter fraud work carried out at the CSU. We will continue to monitor this area.
External Audit The Committee reviewed and agreed external auditor’s annual plan.
The Committee has reviewed and discussed with the external auditors their work and reports prepared by them on the audit of the Statutory Financial Statements of the CCG.
188

Management
The Committee has continually challenged the assurance process when appropriate and has requested and received assurance from CCG management and other sources throughout the year.
This process has included calling managers to account when considered necessary to obtain relevant assurance.
The Committee has worked closely with the Accountable Officer, the Chief Financial Officer, the Director of Quality and Performance and the Governance and Risk Manager to ensure that the assurance mechanism within the CCG is effective.
Financial reporting
The Committee reviewed the CCG’s Annual Financial Statements with the external auditors on May 26th 2015, before submission to the Governing Body and had no significant matters to draw to the attention of the Governing Body on the financial statements. The Audit Committee recommended to the Governing Body that the Financial Statements should be approved by the Governing Body.
Conclusion
The Committee is of the opinion that this Annual Report is consistent with the Annual Governance Statement, Head of Internal Audit Opinion and the external audit review and there are no matters that the Committee is aware of that have not been disclosed appropriately to the Governing Body throughout the year.
Mariette Davis
Audit Committee Chair
Date: 31 July 2015
189
Appendix A: Audit Committee Terms of Reference
- Introduction
The requirement for Clinical Commissioning Groups (CCGs) to establish an Audit Committee is included in the Health and Social Care Act 2012. The Governing Body established this Committee of the Governing Body in its Constitution. Its role is to seek assurance that financial reporting and internal control principles are applied and to maintain an appropriate relationship with the organisation’s auditors, both internal and external. The Audit Committee offers scrutiny and advice to the Governing Body, about the reliability and robustness of the CCG’s processes of internal control.
- Aims and objectives
The duties of the Committee fall into the following main categories:
Governance, risk management and internal control
The Committee shall review the establishment and maintenance of an effective system of integrated governance, risk management and internal control across the whole of the CCG’s activities, that supports the achievement of the organisation’s objectives;
In particular, the Committee will review the adequacy and effectiveness of:
• All risk and control related disclosure statements (in particular the Annual Governance Statement ) together with any accompanying Head of Internal Audit statement, external audit opinion or other appropriate independent assurances, prior to endorsement by the Governing Body.
• The underlying assurance processes that indicate the degree of achievement of strategic objectives, the effectiveness of the management of principal risks and the appropriateness of the above disclosure statements.
• The policies for ensuring compliance with relevant regulatory, legal and code of conduct requirements and related reporting and self-certification.
• The policies and procedures for all work related to fraud and corruption.
The Committee will review any incident of fraud, corruption or possible breach of ethical standards, conflicts of interest or legal or statutory requirements that has been brought to its attention and could have a significant impact on the CCG’s financial accounts or reputation.
The Committee will note waivers or breaches to the Prime Financial Policies or standing orders which have been signed by the Chief Finance Officer or Chief Officer.
In carrying out this work the Committee will primarily utilise the work of internal audit, external audit and other assurance functions, but will not be limited to these sources. It will also seek reports and assurances from executives and managers as appropriate, concentrating on the over-arching systems of integrated governance, risk management and internal control, together with indicators of their effectiveness.
This will be evidenced through the Committee’s use of an effective Assurance Framework to guide its work and that of the audit and assurance functions that report to it.
190

Internal audit
The Committee shall ensure that there is an effective internal audit function established by management, that meets Public Sector Internal Audit Standards and provides appropriate independent assurance to the Audit Committee, Chief Officer and the Governing Body;
This will be achieved by:
• Consideration of the provision of the internal audit service, the cost of the audit and any questions of resignation and dismissal.
• Review and approval of the internal audit strategy, operational plan and more detailed programme of work, ensuring that this is consistent with the audit needs of the organisation as identified in the Assurance Framework.
• Considering the major findings of internal audit work (and management’s response), and ensuring co-ordination between the internal and external auditors to optimise audit resources.
• Ensuring that the internal audit function is adequately resourced and has appropriate standing within the organisation
• An annual review of the effectiveness of internal audit.
External audit
The Committee shall review the work and findings of the appointed external auditors and consider the implications of, and management’s responses to, their work.
This will be achieved by:
• Consideration of the appointment and performance of the external auditors, as far as the rules governing the appointment permit.
• Discussion and agreement with the external auditors, before the audit commences, of the nature and scope of the audit as set out in the annual plan, and ensuring co-ordination, as appropriate, with other external auditors in the local health economy.
• Discussion with the external auditors of their local evaluation of audit risks and assessment of the CCG and associated impact on the audit fee.
• Review of all external audit reports, including the report to those charged with governance, agreement of the annual audit letter before submission to the Governing Body and any work undertaken outside the annual audit plan, together with the appropriateness of management responses.
Other Assurance Functions
The Committee shall review the findings of other significant assurance functions, both internal and external to the organisation, and considering the implications for the governance of the CCG;
These will include, but will not be limited to, any reviews by Department of Health arm’s length bodies or regulators/inspectors (for example, the Care Quality Commission, NHS Litigation Authority, etc.) and
191
professional bodies with responsibility for the performance of staff or functions (for example, Royal Colleges, accreditation bodies, etc.)
In addition, the Committee will review the work of other committees within the organisation whose work can provide relevant assurance to the Audit Committee’s own scope of work. In particular, this will include the Finance Performance and Quality Committee
Counter fraud
The Committee shall satisfy itself that the organisation has adequate arrangements in place for countering fraud and shall review the outcomes of counter fraud work.
Management
The Committee shall request and review reports and positive assurances from directors and managers on the overall arrangements for governance, risk management and internal control.
The Committee may also request specific reports from individual functions within the organisation as they may be appropriate to the overall arrangements
In particular, a separate record of matters discussed during suspension of standing orders shall be kept. These records shall be made available to the Governing Body’s Audit Committee for review of the reasonableness of the decision to suspend standing orders.
Financial Reporting
The Audit Committee shall monitor the integrity of the financial statements of the CCG and any formal announcements relating to the CCG’s financial performance.
The Committee should ensure that the systems for financial reporting to the Governing Body including those of budgetary control are subject to review as to completeness and accuracy of the information provided to the Governing Body.
The Audit Committee shall review the annual report and financial statements before submission to the Governing Body, focusing particularly on:
• The wording in the Annual Governance Statement and other disclosures relevant to the terms of reference of the Committee
• Changes in, and compliance with, accounting policies, practices and estimation techniques
• Unadjusted mis-statements in the financial statements
• Significant judgements in preparation of the financial statements
• Significant adjustments resulting from the audit
• Letter of representation
• Qualitative aspects of financial reporting.
192

Authority
The Committee is authorised by the Governing Body to investigate any activity within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. The Committee is authorised by the Governing Body to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary.
Membership
Members
To maintain its independent assurance and scrutiny role, the committee will be made up of Lay Members of the CCG Governing Body:
• Lay Member – lead for Governance – Chair
• Lay Member - lead for Patient and Public Engagement
• Registered Nurse or Secondary Care Consultant
The Chair shall have recognised professional accountancy qualification
Attendance
The Chief Finance Officer and appropriate internal and external audit representatives shall normally attend meetings.
At least once a year the Committee should meet privately with the external and internal auditors.
The Chief Officer should be invited to attend and should discuss at least annually with the Audit Committee the process for assurance that supports the Annual Governance Statement or she should also attend when the Committee considers the draft internal audit plan and the annual accounts.
All other responsible executives can be invited to attend, particularly when the Committee is discussing areas of risk or operation that are the responsibility of that executive.
Note
The CCG chair of the Governing Body will not be a member of the Audit Committee to ensure appropriate scrutiny by the Committee.
Quorum
The Audit Committee will be considered quorate when 2 out of the three members are present. In the event of members not being able to attend the meeting will be rescheduled within 2 working weeks.
Frequency
The Committee will meet at least quarterly at appropriate intervals in the financial reporting and audit cycle and otherwise as required. The Chair can call a meeting of the Committee as and when required with at least three weeks’ notice.
193
Outside of the meeting the Chair will maintain a dialogue with the Chief Finance Officer
Reporting / Accountability
As a committee of the Governing Body, the committee shall produce a report of the key issues discussed to the Governing Body on its proceedings after each meeting on all matters within its duties and responsibilities.
The committee shall make whatever recommendations to the Governing Body as it deems appropriate on any area within its remit
The Committee shall produce an Annual Report to the Governing Body of its activities.
Secretary Support
The Committee shall be supported administratively by the Governance and Risk Manager, whose duties in this respect will include:
• Agreement of agendas and forward planner with Chair and attendees and collation of papers
• Taking the minutes
• Keeping a record of matters arising and issues to be carried forward
• Advising the Committee on pertinent issues/areas
• Enabling the development and training of Committee members
• Maintaining a record of all Audit Committee documentation .All Committee papers and minutes will be stored on the CCG I drive under a separate file called Audit Committee.
The meeting is not open to the public.
Management of conflicts of interest
• If any member has an interest, pecuniary or otherwise, in any matter and is present at the meeting at which the matter is under discussion, he/she will declare that interest as early as possible and shall not participate in the discussions.
• The Chair will have the power to request that member to withdraw until consideration of the conflicted item has been completed
• If the Chair has a conflict then an alternative Chairperson will be nominated from the membership of the committee by the other members
Review of Terms of Reference
The Committee terms of reference will be reviewed every 2 years unless required sooner.#
194
Appendix B: Audit Committee Terms of Reference – Updated 2015
Introduction
The requirement for Clinical Commissioning Groups (CCGs) to establish an Audit Committee is included in the Health and Social Care Act 2012. The Governing Body established this Committee of the Governing Body in its Constitution. The Committee is a non-Executive Committee of the Governing Body and has no executive powers, other than those specifically delegated in this Terms of Reference. Its role is to seek assurance that financial reporting and internal control principles are applied and to maintain an appropriate relationship with the organisation’s auditors, both internal and external. The Audit Committee offers scrutiny and advice to the Governing Body, about the reliability and robustness of the CCG’s processes of internal control.
Membership
The members shall be appointed by the Governing Body, and to maintain its independent assurance and scrutiny role, the Committee will be made up of Lay Members of the CCG Governing Body. A quorum shall be two of the three independent members. One of the members shall be appointed Chair of the Committee by the Governing Body. The Chair of the organisation shall not be a member of the Committee. Current members are:
• Lay Member – lead for Governance – Chair
• Lay Member - lead for Patient and Public Engagement
• Registered Nurse or Secondary Care Consultant
The Chair shall have recognised professional accountancy qualification.
Attendance at meetings
The Chief Finance Officer and appropriate internal and external audit representatives shall normally attend meetings.
The Counter Fraud Specialist shall attend at least two committee meetings a year.
The Accountable Officer should be invited to attend meetings and should discuss at least annually with the Audit Committee the process for assurance that supports the Annual Governance Statement. He or she should also attend when the Committee considers the Annual Governance statement and the Annual Report and Accounts.
Other executive directors/managers should be invited to attend, particularly when the Committee is discussing areas of risk or operation that are the responsibility of that director/manager.
Representatives from other organisations (for example NHS Protect) and other individuals may be invited to attend on occasion.
The organisation’s secretary (or governance lead) shall be secretary to the Committee and shall attend to take minutes of the meeting and provide appropriate support to the chair and the Committee members.
195

At least once a year the Committee shall meet privately with the internal and external auditors.
Meetings are not open to the public.
Access
The Head of Internal Audit, representative of external audit and counter fraud specialist have a right of direct access to the Chair of the Committee.
Frequency of meetings
The Committee will consider the frequency and timing of meetings needed to allow it to discharge all of its responsibilities. The Committee will meet at least quarterly at appropriate intervals in the financial reporting and audit cycle and otherwise as required. The Chair can call a meeting of the Committee as and when required with at least three weeks’ notice.
The Governing Body, Accountable Officer, external auditors or Head of Internal Audit may request an additional meeting of they consider one is necessary.
Outside of the meeting the Chair will maintain a dialogue with the Chief Finance Officer
Authority
The Committee is authorised by the Governing Body to investigate any activity within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. The Committee is authorised by the Governing Body to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary.
Responsibilities
The duties/responsibilities of the Committee fall into the following main categories:
Governance, risk management and internal control
The Committee shall review the establishment and maintenance of an effective system of integrated governance, risk management and internal control across the whole of the CCG’s activities, that supports the achievement of the organisation’s objectives;
In particular, the Committee will review the adequacy and effectiveness of:
• All risk and control related disclosure statements (in particular the Annual Governance Statement ) together with any accompanying Head of Internal Audit Opinion, external audit opinion or other appropriate independent assurances, prior to submission to the Governing Body.
• The underlying assurance processes that indicate the degree of achievement of strategic objectives, the effectiveness of the management of principal risks and the appropriateness of the above disclosure statements.
• The policies for ensuring compliance with relevant regulatory, legal and code of conduct requirements and related reporting and self-certification.
196

• The policies and procedures for all work related to fraud and corruption as required by NHS Protect.
The Committee will review any incident of fraud, corruption or possible breach of ethical standards, conflicts of interest or legal or statutory requirements that has been brought to its attention and could have a significant impact on the CCG’s financial accounts or reputation.
The Committee will note waivers or breaches to the Prime Financial Policies or standing orders which have been approved by the Chief Finance Officer or Chief Officer.
In carrying out this work the Committee will primarily utilise the work of internal audit, external audit and other assurance functions, but will not be limited to these sources. It will also seek reports and assurances from executives and managers as appropriate, concentrating on the over-arching systems of integrated governance, risk management and internal control, together with indicators of their effectiveness.
This will be evidenced through the Committee’s use of an effective assurance framework to guide its work and that of the audit and assurance functions that report to it.
As part of its integrated approach, the Committee will have effective relationships with other key committees (for example the Finance, Performance and Quality committee) so that it understands processes and linkages.
Internal audit
The Committee shall ensure that there is an effective internal audit function established by management that meets Public Sector Internal Audit Standards 2013 and provides appropriate independent assurance to the Audit Committee, Chief Officer and the Governing Body. This will be achieved by:
• Consideration of the provision of the internal audit service, the cost of the audit and any questions of resignation and dismissal.
• Review and approval of the internal audit plan and the more detailed programme of work, ensuring that this is consistent with the audit needs of the organisation as identified in the Assurance Framework.
• Considering the major findings of internal audit work (and management’s response), and ensuring co-ordination between the internal and external auditors to optimise audit resources.
• Ensuring that the internal audit function is adequately resourced and has appropriate standing within the organisation
External audit
The Committee shall review and monitor the external auditors’ independence and objectivity and the effectiveness of the audit process. In particular, the Committee will review the work and findings of the external auditors and consider the implications and management’s responses to their work. This will be achieved by:
• Considering of the appointment and performance of the external auditors, as far as the rules governing the appointment permit.
197
• Discussing and agreeing with the external auditors, before the audit commences, the nature and scope of the audit as set out in the annual plan.
• Discussing with the external auditors their evaluation of audit risks and assessment of the CCG and associated impact on the audit fee.
• Reviewing all external audit reports, including the report to those charged with governance (before submission to the Governing Body) and any work undertaken outside the annual audit plan, together with the appropriateness of management responses.
Other Assurance Functions
The Committee shall review the findings of other significant assurance functions, both internal and external to the organisation, and consider the implications for the governance of the CCG.
These will include, but will not be limited to, any reviews by Department of Health arm’s length bodies or regulators/inspectors (for example, the Care Quality Commission, NHS Litigation Authority, etc.) and professional bodies with responsibility for the performance of staff or functions (for example, Royal Colleges, accreditation bodies, etc.)
In addition, the Committee will review the work of other committees within the organisation whose work can provide relevant assurance to the Audit Committee’s own scope of work. In particular, this will include the Finance Performance and Quality Committee
Counter fraud
The Committee shall satisfy itself that the organisation has adequate arrangements in place for counter fraud and security that meets NHS Protect standards and shall review the outcomes of counter fraud work in these areas.
Management
The Committee shall request and review reports and positive assurances from directors and managers on the overall arrangements for governance, risk management and internal control.
The Committee may also request specific reports from individual functions within the organisation as they may be appropriate to the overall arrangements
In particular, a separate record of matters discussed during suspension of standing orders shall be kept. These records shall be made available to the Governing Body’s Audit Committee for review of the reasonableness of the decision to suspend standing orders.
Financial Reporting
The Audit Committee shall monitor the integrity of the financial statements of the CCG and any formal announcements relating to the CCG’s financial performance.
The Committee should ensure that the systems for financial reporting to the Governing Body including those of budgetary control are subject to review as to completeness and accuracy of the information provided to the Governing Body.
198

The Audit Committee shall review the annual report and financial statements before submission to the Governing Body, focusing particularly on:
• The wording in the Annual Governance Statement and other disclosures relevant to the terms of reference of the Committee • Changes in, and compliance with, accounting policies, practices and estimation techniques • Unadjusted mis-statements in the financial statements • Significant judgements in preparation of the financial statements • Significant adjustments resulting from the audit • Letter of representation • Qualitative aspects of financial reporting. • Explanation of significant variances Whistle blowing
The Committee shall review the effectiveness of the arrangements in place for allowing staff to raise ( in confidence) concerns about possible improprieties in financial, clinical or safety matters and ensure that any such concerns are investigated proportionately and independently.
Reporting / Accountability
The Committee shall report to the Governing Body on how it discharges its responsibilities.
The minutes of the Committee’s meetings shall be formally recorded by the secretary and made available for the Governing Body to review. The Chair of the Committee shall deliver a summary written report of the key issues discussed to the Governing Body on its proceedings after each meeting on all matters within its duties and responsibilities.
The committee shall make whatever recommendations to the Governing Body as it deems appropriate on any area within its remit
The Committee shall produce an Annual Report to the Governing Body of its work.
Administrative support
The Committee shall be supported administratively by the Governance and Risk Manager, whose duties in this respect will include:
• Agreement of agendas and forward planner with Chair and attendees and collation and circulation of papers in good time • Taking the minutes and helping the Chair prepare reports to the Governing Body • Keeping a record of matters arising and issues to be carried forward • Ensuring that action points are taken forward between meetings • Arranging meetings for the Chair, for example, with the internal or external auditors or local counter fraud specialists • Advising the Committee on pertinent issues/areas of interest/policy developments • Ensuring that Committee members receive the development and training they need • Maintaining a record of all Audit Committee documentation .All Committee papers and minutes will be stored on the CCG I drive under a separate file called Audit Committee. • Maintaining records of members’ appointments and renewal dates etc.
Management of conflicts of interest
199

If any member has an interest, pecuniary or otherwise, in any matter and is present at the meeting at which the matter is under discussion, he/she will declare that interest as early as possible and shall not participate in the discussions.
The Chair will have the power to request that member to withdraw until consideration of the conflicted item has been completed
If the Chair has a conflict then an alternative Chairperson will be nominated from the membership of the committee by the other members
Review of Terms of Reference
The Committee terms of reference will be reviewed every 2 years unless required sooner.
Last reviewed 21 July 2015
200

End
201

202

Item # Title Presenter Author Enc.
4.1 Audit Committee Mariette Davis Justin Phillips / Mariette Davis
N
Update and key achievements Audit Committee meeting July 21st 2015 - Key issues report from the Audit Committee to the Governing Body Constitution The Committee reviewed the Constitution including the scheme of reservation and delegation, the standing orders and the prime financial policies and suggested amendments (mainly for clarification and consistency) for processing at the next NHSE window for Constitutional amendments in December.
BAF
The Committee reviewed and discussed the Board Assurance Framework. It recommended going forward that the BAF should be reviewed, contributed to and monitored at quarterly at Executive Team meetings in order to ensure the Framework which comes to the Audit Committee and the Governing Body is as robust as possible.
External Audit
We received the Annual Audit Letter from KPMG; this describes work carried out in relation to 2014/15 annual report and accounts. This is now published on the CCG website.
Internal Audit
The Committee received internal audit progress reports in relation to work carried out on both CCG systems and also CSU systems. The Audit Committee noted that the Service Auditor recommendations (on CSU systems) need to be followed up at the CSU Assurance Group.
The Committee considered the membership of the CSU Assurance Group, which had not been uniformly attended across all CCGs who are members. The Audit Committee requested that an effectiveness review of this group be carried out.
Waivers of Standing Orders
Waivers of standing orders were reviewed and discussed.
Draft Annual Report of the Audit Committee to the Governing Body and review and update to the TOR of the Audit Committee
The draft Annual Report of the Committee to the Governing Body was received. It was
203
agreed that it, together with revised TOR for the committee would be agreed by e-mail.
Procurement
The Committee reviewed the procurement process paper it had requested from the finance team and suggested that this went to the FPQ for discussion prior to the Governing Body for approval.
204

Item # Title Presenter Author Enc.
4.2 Finance, Performance and Quality Committee
Jane Milligan Shanaz Islam O
Update and key achievements
Part 1: Quality and Performance
• Board Assurance Framework
The committee reviewed the finance and performance related BAF risks and were assured by the current risk management systems.
• Performance and Quality Report
The Committee reviewed the Performance and Quality report and existing escalations on red areas for Barts Health
o A&E/RTT/Cancer (updated RTT) o Serious Incidents/Never Events o HCAI – C Diff Lapses in care Q1 o Safeguarding Training Level 3 RLH o FFT – A/E response rates
• Feedback on Trust Oversight and Assurance Group (TOAG) led by NTDA
Archna Mathur updated the committee on the recent RLH & MEH Trust & Oversight Committee and CQRM.
• GP FFT
A paper was presented to the Committee which highlighted the GP Family and Friends data for June 2015.
• National Confidential Inquiry into Suicide and Homicide by People with Mental Illness
A review is being conducted on Suicide Prevention with THCCG and PHE and it was agreed that a further report to FPQ will be required once the recommendations are known.
• Kate Lampard’s Report March 2015
The committee discussed Kate Lampard’s Report - March 2015: Themes and lessons learnt from NHS investigations into matters relating to Jimmy Savile. The CCG will need to get assurance that the recommendations from the report are being implemented within our Providers.
205
• QA Visit: 10E, Elderly Care, RLH
The report on RLH 10E was presented and highlighted areas of good practice and areas for improvement.
• Safeguarding Update - Children
The Committee reflected on the processes to monitor the safeguarding dashboard and also discussed the pending NHSE assurance deep dive on safeguarding.
Part 2: Finance and Activity
The Committee reviewed the Finance & Activity report. The highlights of this are reported in the F&A report to the Governing Body. Particular discussion points included:
• Authorisation Limits
The Committee reviewed the proposed authorisation limits for TIC, SMT and Exec Team and recommended the GB to approve these.
• Finance and Activity
The Committee reviewed the overall financial position and the acute position.
• QIPP
The Committee received a verbal update on the QIPP position.
206

Locality Board Chairs Summary
Item # Title Presenter Author Enc.
4.3 Locality Chairs Board Jane Milligan Radha Gurung P
Update and key issues The Locality Chairs Board met on 28 July 2015 where a number of items were discussed including: Locality Chairs update The Locality Chairs reported on-going issues with Barts Health performance and highlighted some specific concerns faced by their localities which included: Choose and Book: some clinics such as ENT, Endocrine and paediatrics are not available on CAB. This has been fed back to the CCG as there have been similar incidents across all localities. LAS: Some patients in SE locality are being taken to Newham instead of the RLH because of a post-code divert being temporarily put in place at the RLH because of capacity pressures. CCG to ensure that this does not become business as usual as going out of the borough can be inconvenient for a patient who is receiving regular treatment in Tower Hamlets. The focus has to be on the needs of the patient. A specific case of a Cancer patient was highlighted, which will be brought to a future CQRM meeting as a case study. Adolescent services: There have been difficulties with referring patients to adolescent services as there is no clearly defined cut-off age for adults and children. Psychology and Mental Health services are particularly affected. Podiatry clinic: It has been reported that the podiatry clinic is understaffed, which has meant that patients often don’t receive their appointments on time even when appointments are available, due to delays in processing the referrals. Barts Health, CQC & Special Measures The CQC report and special measures were discussed at length and what that would mean for Barts Health going forward. It was reported that there will be leadership changes at Barts Health, with site specific leadership structures being put in place. Once appointed, the Medical Director, Chief Executive and Chief Nurse from the Royal London Hospital will be invited to a Network Leads meeting. The CCG, together with NHSE, TDA and Barts Health have been focusing on the implementation of the Compliance Action Plan as recommended by the CQC. The CCG has issued Barts Health with contractual performance notices on A&E, RTT, Cancer and Diagnostics, all of which have been signed off apart from Cancer. CCG will be monitoring these closely and there will be penalties if target is not achieved. Quality Assurance visits The CCG quality team regularly undertakes these visits to get a real-time view of what is happening in the wards by talking directly to staff and patients. The CCG is keen to get the
207
membership involved in these visits. The schedule will be sent to locality chairs and discussed at locality meetings. Primary Care strategy Governance arrangements are being put in place around managing conflicts of interest. The Primary Care Committee have begun to meet but have are yet to meet in public. The ToR will be taken to the Governing Body meeting in January in 2016 for final approval.
Agreed actions
• It was agreed that the case study on a Cancer patient from SE locality who was taken to Newham by the LAS will be brought to a future CQRM meeting.
• Once appointed, the Medical Director, Chief Executive and Chief Nurse from the Royal London Hospital will be invited to a Network Leads meeting.
• Discuss involvement of membership in the Quality Assurance visits at the locality meetings.
208

Executive Committee Summary
Item # Title Presenter Author Enc.
4.4 Executive Committee
Jane Milligan Tracey Price Q
Update and key issues The Executive Committee meeting was held on 20th August 2015 where the following key items were discussed: Tower Hamlets Leadership Board There was a proposal for establishing a Leadership Board for Tower Hamlets which aims to bring together both local providers and commissioners with the overarching aim of developing a shared vision, strategy and shared delivery plans for health and social care, using whole-system governance structures to do so. Suggested membership included representatives from the CCG, LBTH, ELFT, RLH and GP Care Group, Vanguard and PM Challenge Fund. MiDoS A overview was given on MiDoS which is a suite of applications designed to assist patients, call handlers and urgent care clinicians both in the field and based in Call Centres to find the most appropriate care pathway for their patient by searching the NHS Pathways Directory of Service (DoS), using clinical terms and demographic data relating to the patient in their care. The system is currently being trialled by the London Ambulance Service and will be piloted across five Local Authorities. It was agreed that CSU would link in with Somen Banerjee, Louise Phillips and Bill Jenks regarding taking forward in Tower Hamlets. POLCV Policy The POLCV policy was reviewed and approved by the Executive Committee. Assurance Framework NHS England has a statutory duty to make an annual assessment of each CCG’s performance. It meets this duty through its CCG Assurance Framework. The new Assurance Framework has introduced a continuous assurance process that aims to provide confidence to internal and external stakeholders, and to the wider public, that CCGs are operating effectively to commission safe, high quality and sustainable services, within their resources, delivering on their statutory duties and driving continuous improvement in the quality of services and outcomes achieved for patients. As part of the annual assessment, the CCG is required to assess itself and give a rating which is then reviewed by NHS England and an assurance category rating is given. Infrastructure Levy A discussion took place regarding the expenditure of funds from the infrastructure levy. Tower Hamlets CCG Annual General Meeting The AGM will be held on the 22nd September 2015 at Toynbee Hall.
209

Agreed actions
• Workshop with key stakeholders to be arranged to discuss the establishment of the Leadership Board.
• Jonathon Baker agreed to link in with Somen Banerjee, Louise Phillips and Bill Jenks regarding taking forward MiDoS.
210

Transformation and Innovation Committee Summary
Item # Title Presenter Author Enc.
4.5 TIC Summary
Jane Milligan Amanda Hutchinson
R
Update and key issues The Transformation and Innovation Committee (TIC) meets monthly and oversees the development and delivery of commissioning strategy.
QIPP 15/16 and 16/17
In August’s meeting Josh Potter gave a presentation on the 15/16 QIPP plan and 16/17 QIPP forecast.
Targeted Mental Health Service for Young People Business Case
The business case outlines the rationale for a request of £228k to invest in a new targeted mental health service for young people in Tower Hamlets aged 14 to 21. The service aims to deliver:
- Mental health promotion and awareness to existing young people’s out-of-school projects (with digital options) to engage and support young people where they are
- Therapeutic individual and group interventions at an early stage - Partnership working with, and referral to, other targeted and specialist young people’s mental
health services where interventions require a higher level of mental health skills
Through a procurement exercise, a provider will be commissioned to work with local organisations to engage young people, deliver interventions and develop partnerships.
Business case was agreed in principle- subject to confirmation that the £228k being requested is correct as outlined in the 2015/16 commissioning intentions.
211

212

Item # Title Presenter Author Enc.
4.6 Primary Care Committee Maggie Buckell Jenny Cooke S
Update and key achievements Performance and Operations
Decommissioning of Administration of Zoladex Injection under NHSE DES for minor Surgery
• The committee agreed for the Primary Care Team alongside Medicines Management to review the approach to Zoladex administration locally.
Funding arrangements for general practice impacted by GMS contract changes
• The committee noted an update on arrangements that were being put in place to support local practices that had been impacted by recent GMS contract changes
Portsoken Health Centre Services
• The committee noted the report describing the re-provision of services and contract at changes at Portsoken Practice from provision by the city Wellbeing Practice to AT Medic, effective from 1 April 2015.
TH CCG Performance and Quality Framework and Activity and Finance Report
• The committee noted progress toward the development of a performance, quality and outcomes framework that was being developed for primary care commissioning
Appointment of Primary Care Team
• The committee noted the recent appointments to the primary care team
Commissioning & Strategy
Emerging Primary Care Strategy (PCS)
• The committee reviewed progress on the development of the primary care strategy and the plans for engagement over the coming months.
• The committee approved the process for their on-going input into the strategy development alongside the engagement cycle. This would include each chapter going to the committee twice, once for discussion and then secondly for approval.
Primary Care Committee Organisational Development
Reflections on Away Day
• The committee noted their reflections of the away day and discussed on-going OD needs.
213

214
Related Documents











