Governance of purchasing arrangements in Estonia Triin Habicht Head of Department of Health System Development Ministry of Social Affairs OECD Joint Network on Fiscal Sustainability of Health Expenditure 4-5.02.2016 Paris

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Governance of purchasing arrangements in Estonia
Triin Habicht Head of Department of Health System Development
Ministry of Social Affairs
OECD Joint Network on Fiscal Sustainability of Health Expenditure
4-5.02.2016 Paris
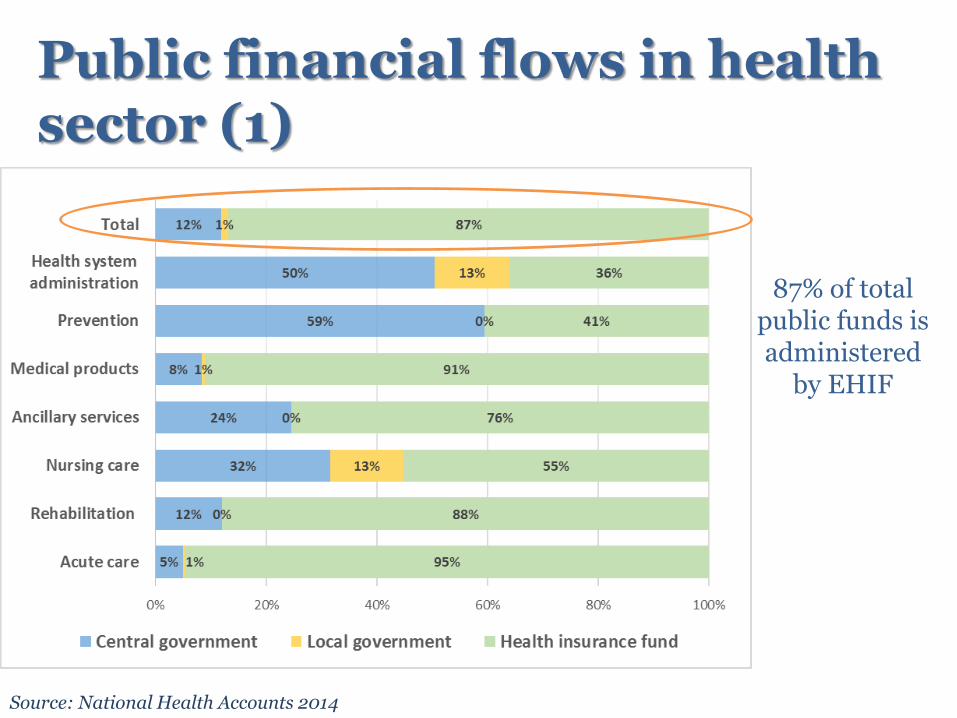
Public financial flows in health sector (1)
Source: National Health Accounts 2014
87% of total public funds is administered
by EHIF
State budget
MoSA
National Institute for
Health Development
Health Board
EHIF
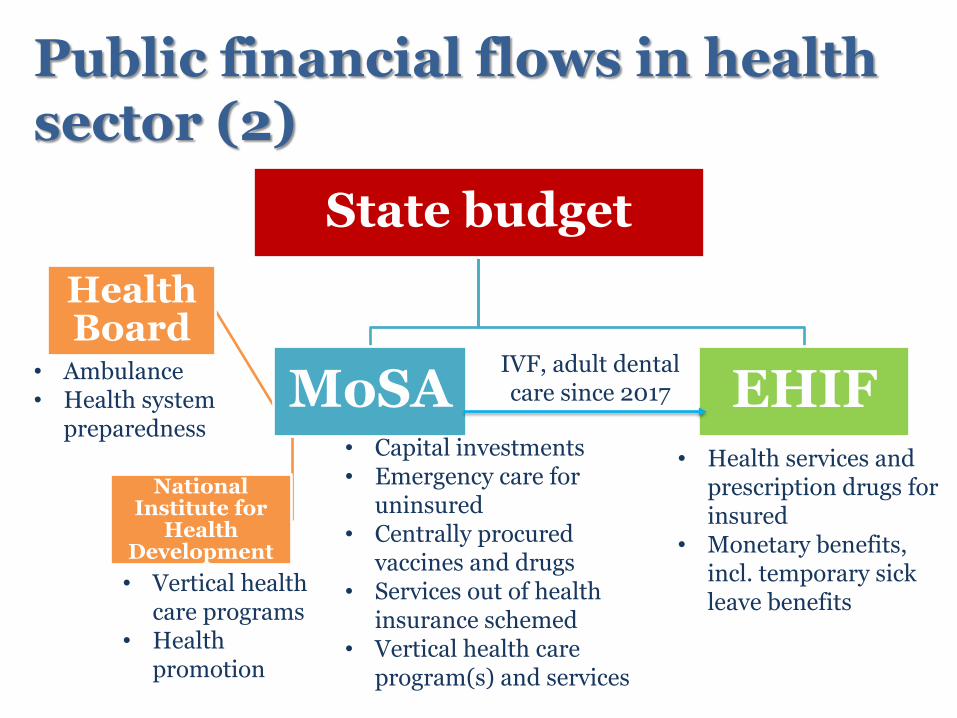
Public financial flows in health sector (2)
• Vertical health care programs
• Health promotion
• Ambulance • Health system
preparedness • Capital investments • Emergency care for
uninsured • Centrally procured
vaccines and drugs • Services out of health
insurance schemed • Vertical health care
program(s) and services
IVF, adult dental care since 2017
• Health services and prescription drugs for insured
• Monetary benefits, incl. temporary sick leave benefits

4
Evolution of the organization of health insurance
First sickness funds in 1913
Re-established regional non-competing sickness funds in 1991/92 (22 in total)
Central sickness fund to coordinate regional funds in 1994
Estonian Health Insurance Fund in 2001, Currently with 4 regional departments

5
Legal status of the EHIF
• EHIF operates as public independent legal entity – Founded in the public interest by separate act – General public service regulation does not apply to
EHIF, e.g. applies private sector labor codes
• EHIF is fully liable for its obligations with all its assets
• Tripartite supervisory board with 15 members
– 5 state (incl. Minister of Health and Labor, Minister of Finance), 5 employer and 5 beneficiaries representatives
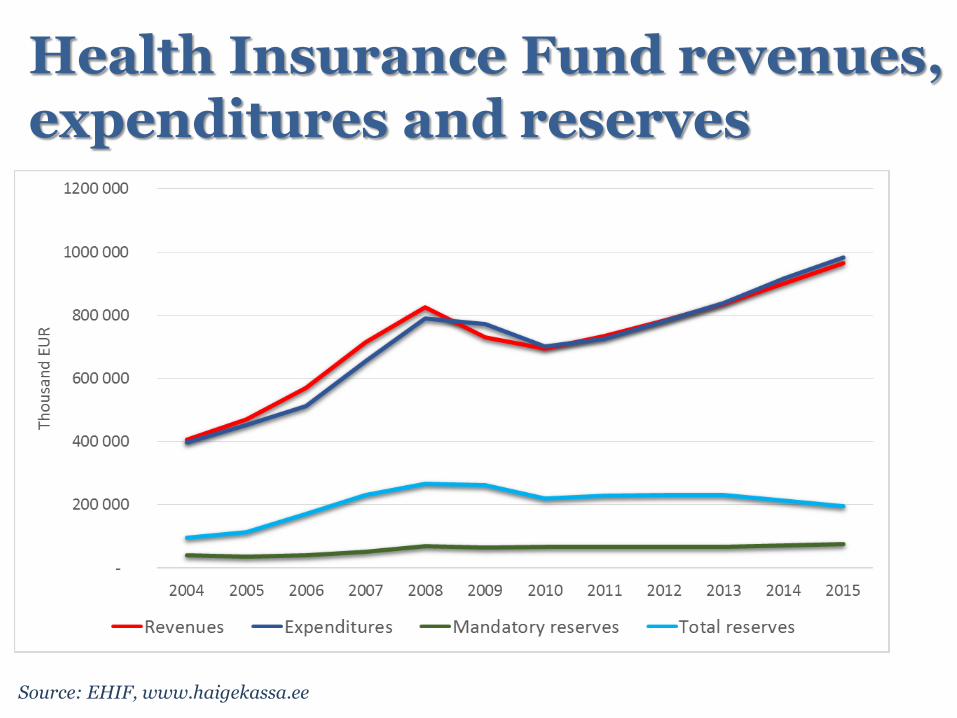
Health Insurance Fund revenues, expenditures and reserves
Source: EHIF, www.haigekassa.ee

The puzzle of public health funds (1)
• Health insurance revenue base is explicitly determined which gives incentive to optimize within the budget and to set explicit limits on the health insurance obligations
• Additional earmarked funds to health insurance to serve political priorities (e.g. IVF, dental care program)
– Broadening revenue base has been an issue since 2005 but no changes
• Changing role of health insurance reserves
The puzzle of public health funds (2)
• Other allocations from the state budget have to compete with priorities within MoSA as well as at Government level
– Explicit areas as ambulance and emergency care for uninsured are easy to protect
– Vertical public(?) health programs are easy to confuse with health insurance
– „Fixing the problems“ money
• External sources (e.g. EU funds) still play important role

Out of pocket payments in health sector
Source: National Health Accounts 2014
24% of total health funds
are out of pocket
payments
Summing up... • Majority of public funds is pooled to the EHIF
– Stable health insurance system and strong institutional design
• Still, existing fragmentation may lead to inefficiencies
− Differences in rules and power of purchasing
− Incentives to focus on „your own piece“ but not patient needs
− Not always clear who is responsible for what
• Program based funding rises the question of ownership and sustainability
• Easy to claim that there are unfunded mandates (....but this is the only way to increase the health sector funds)
• Who governs private out of pocket expenditures?

THANK YOU FOR YOUR ATTENTION!
Related Documents











