INFECTIOUS ARTHRITIS 0889-857>(/98 $8.00 + .OO GONOCOCCAL ARTHRITIS Elena Cucurull, MD, and Luis R. Espinoza, MD Neisseria gonorrhoem infects humans exclusively and can colonize diverse mucosal surfaces and produce local and disseminated infections with potentially serious sequelae. Gonorrhea is the most frequently reported communicable disease in the United States, and disseminated gonococcal infection (DGI) remains the most common cause of acute septic arthritis in young sexually active adults. EPIDEMIOLOGY The prevalence of gonococcal infections and overall gonococcal morbidity is greater in developing countries than in North America and Western Europe.2In 1975, the number of reported cases of gonorrhea in the United States reached an all-time high of 468 per 100,000 population. Since then, the incidence has decreased gradually, and the most recent data available from the Centers for Disease Control and Prevention (CDC)lZ show that in 1995 the rate was 149.5 cases per 100,000 popula- tion (Fig. 1). That figure is approaching the Healthy People 2000 national objective of 100 cases per 100,000 population. In 1995, the incidence of gonorrhea decreased nationwide except in the southern states, which continued to have higher rates than did other regions of the country. The incidence of gonorrhea also decreased in large cities for both sexes and for all racial and ethnic groups.I2The reduction in the number of cases seems to be related to the changes in sexual behavior that have occurred since the beginning of the HIV epidemic. In 1995, the male-to- female ratio was almost 1:1.12 The peak incidence and prevalence of From the Section of Rheumatology, Louisiana State University Medical Center, New Orleans, Louisiana RHEUMATIC DISEASE CLINICS OF NORTH AMERICA VOLUME 24 NUMBER 2 - MAY 1998 305

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

INFECTIOUS ARTHRITIS 0889-857>(/98 $8.00 + .OO
GONOCOCCAL ARTHRITIS
Elena Cucurull, MD, and Luis R. Espinoza, MD
Neisseria gonorrhoem infects humans exclusively and can colonize diverse mucosal surfaces and produce local and disseminated infections with potentially serious sequelae. Gonorrhea is the most frequently reported communicable disease in the United States, and disseminated gonococcal infection (DGI) remains the most common cause of acute septic arthritis in young sexually active adults.
EPIDEMIOLOGY
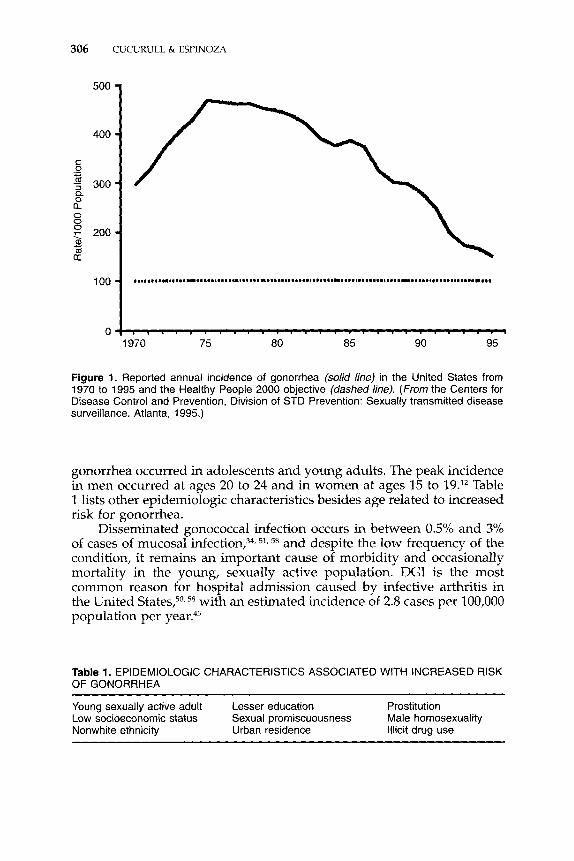
The prevalence of gonococcal infections and overall gonococcal morbidity is greater in developing countries than in North America and Western Europe.2 In 1975, the number of reported cases of gonorrhea in the United States reached an all-time high of 468 per 100,000 population. Since then, the incidence has decreased gradually, and the most recent data available from the Centers for Disease Control and Prevention (CDC)lZ show that in 1995 the rate was 149.5 cases per 100,000 popula- tion (Fig. 1). That figure is approaching the Healthy People 2000 national objective of 100 cases per 100,000 population. In 1995, the incidence of gonorrhea decreased nationwide except in the southern states, which continued to have higher rates than did other regions of the country. The incidence of gonorrhea also decreased in large cities for both sexes and for all racial and ethnic groups.I2 The reduction in the number of cases seems to be related to the changes in sexual behavior that have occurred since the beginning of the HIV epidemic. In 1995, the male-to- female ratio was almost 1:1.12 The peak incidence and prevalence of
From the Section of Rheumatology, Louisiana State University Medical Center, New Orleans, Louisiana
RHEUMATIC DISEASE CLINICS OF NORTH AMERICA
VOLUME 24 NUMBER 2 - MAY 1998 305
306 CUCURULL & ESPINOZA
500
400
C 0 .- u 4 300 n 0
0 0 0
0)
a
y 200
2 I
100
0 1970 75 80 85 90 95
Figure 1. Reported annual incidence of gonorrhea (solid line) in the United States from 1970 to 1995 and the Healthy People 2000 objective (dashed line). (From the Centers for Disease Control and Prevention, Division of STD Prevention: Sexually transmitted disease surveillance. Atlanta, 1995.)
gonorrhea occurred in adolescents and young adults. The peak incidence in men occurred at ages 20 to 24 and in women at ages 15 to 19.12 Table 1 lists other epidemiologic characteristics besides age related to increased risk for gonorrhea.
Disseminated gonococcal infection occurs in between 0.5% and 3% of cases of mucosal infecti0n,3~, 51, 58 and despite the low frequency of the condition, it remains an important cause of morbidity and occasionally mortality in the young, sexually active population. DGI is the most common reason for hospital admission caused by infective arthritis in the United States,5°,58 with an estimated incidence of 2.8 cases per 100,000 population per ~ e a r . 4 ~
Table 1. EPIDEMIOLOGIC CHARACTERISTICS ASSOCIATED WITH INCREASED RISK OF GONORRHEA
Young sexually active adult Lesser education Prostitution Low socioeconomic status Sexual promiscuousness Male homosexuality Nonwhite ethnicity Urban residence Illicit drug use
GONOCOCCAL ARTHRITIS 307
PATHOGENESIS
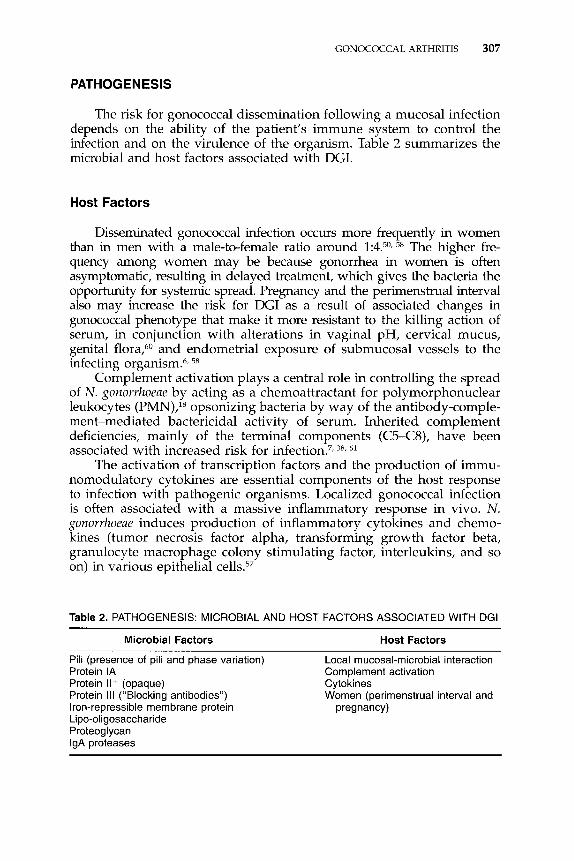
The risk for gonococcal dissemination following a mucosal infection depends on the ability of the patient’s immune system to control the infection and on the virulence of the organism. Table 2 summarizes the microbial and host factors associated with DGI.
Host Factors
Disseminated gonococcal mfection occurs more frequently in women than in men with a male-to-female ratio around 1:4.50, 58 The higher fre- quency among women may be because gonorrhea in women is often asymptomatic, resulting in delayed treatment, which gives the bacteria the opportunity for systemic spread. Pregnancy and the perimenstrual interval also may increase the risk for DGI as a result of associated changes in gonococcal phenotype that make it more resistant to the killing action of serum, in conjunction with alterations in vaginal pH, cervical mucus, genital flora:” and endometrial exposure of submucosal vessels to the infecting organism.6, 58
Complement activation plays a central role in controlling the spread of N. gonorrhoeae by acting as a chemoattractant for polymorphonuclear leukocytes (PMN),18 opsonizing bacteria by way of the antibody-comple- ment-mediated bactericidal activity of serum. Inherited complement deficiencies, mainly of the terminal components (C5-C8), have been associated with increased risk for infe~tion.~, 38, 61
The activation of transcription factors and the production of immu- nomodulatory cytokines are essential components of the host response to infection with pathogenic organisms. Localized gonococcal infection is often associated with a massive inflammatory response in vivo. N. gonorrhoeae induces production of inflammatory cytokines and chemo- kines (tumor necrosis factor alpha, transforming growth factor beta, granulocyte macrophage colony stimulating factor, interleukins, and so on) in various epithelial cells.57
Table 2. PATHOGENESIS: MICROBIAL AND HOST FACTORS ASSOCIATED WITH DGI
Microbial Factors Host Factors
Pili (presence of pili and phase variation) Protein IA Complement activation Protein Il+ (opaque) Cytokines Protein 111 (“Blocking antibodies”) Iron-repressible membrane protein pregnancy) Lipo-oligosaccharide Proteoglycan IgA proteases
Local mucosal-microbial interaction
Women (perimenstrual interval and

308 CUCURULL & ESPINOZA
Microbial Factors
Microbial factors related to the pathogenesis of infection are mainly cell-surface structures that are also potential immunogens for gonococcal vaccines. Modifications in any of these structures result in different serotypes, some of which are more likely to be invasive than others.
Pili
The first step in infection, attachment of the gonococcus to host epithelial cells, is mediated in part by pili, long, hair-like protein fila- ments on the bacterial cell surface. Each pilus is formed by the specific association of thousands of pili protein subunits and apparently minor amounts of pilus-associated proteins. The pili protein varies in sequence with serotype and consists of approximately 160 amino acids. Antigeni- cally, the pili molecule contains homologous (amino-terminal) and highly variable (carboxy-terminal) regions. The pilus expressed by a single gonococcal strain is able to undergo two variations: antigenic variation, in which strains shift the antigenic type of their pilus (P+a -+ Pep), and phase variation, in which strains switch between P+ and P-, that is, the presence or absence of p i l u ~ . ~ ~ , 65 These variations can occur during natural infection, which may also help gonococci avoid host defenses6, 31, 79 The genetic mechanisms responsible for phase variation seem to involve chromosomal rearrangements that result in modification of the carboxy-terminal part of the pili.16
Pili are a major virulence factor; thus, loss of pili from the gonococ- cal cell surface correlates with reduced v i r~ lence .~~ Pili, probably in conjunction with outer membrane proteins, such as opacity (Opa) pro- tein~:~ and pilus-associated proteins, such as PilC,6z facilitate gonococcal attachment to a variety of human cells, including spermatozoa, erythro- cytes, buccal epithelial cells, neutrophils, vaginal epithelial cells, and amniotic cells.lh Pili also help impede phagocytosis by PMN and mono- nuclear celk3
Outer-Membrane Proteins
Protein I is the principal protein on the outer membrane, accounting for about 60% of the surface? Protein I is antigenically conserved within a strain and is expressed by a particular strain in either of two structur- ally different forms, type IA (P.IA) or type IB (P.IB).39 Protein I functions as a porin, providing aqueous anion channels through the hydrophobic gonococcal membranes4 An interesting characteristic of this protein is that it can translocate from the gonococcal outer membrane into the cytoplasmic membrane of the eukaryotic cells while maintaining its voltage conducting This property may explain protein 1’s role in the pathogenesis of gonococcal infection. For example, when this interaction occurs with human neutrophils, a transient change in the membrane potential and inhibition of the host cell granulae exocytosis
GONOCOCCAL ARTHRITIS 309
Protein I is also able to bind the intracellular regulator calmodu- lin. The possible transfer of protein I with its channel-inserting and calmodulin-binding activity promotes endocytosis of the organism by the infected epithelial cells.76 As the predominant outer-membrane pro- tein and a genetically stable characteristic of gonococci, protein I has been used for classification of N. gonorrhoem serotypes and investigated as the vaccine antigen of the gonococcus.
Protein 11, also called opacity protein, is a group of outer-membrane proteins whose presence or absence is also associated with changes in gonococcal colony morphology. Colonies containing protein I1 appear opaque, whereas colonies lacking protein I1 are transparent. Protein I1 participates in gonococcal adhesion to host cells, including PMN, and in the resistance to the bactericidal activity of normal human serum.6, 28
These proteins are the primary mediators of interactions between N. gonorrhoem and PMN. Gonococci that lack protein I1 in their outer membrane may have an impaired chemotactic response and are associ- ated with DGI. Protein I1 may undergo phase and antigenic variation. An individual strain of N. gonorrhoem can express at least six different variants. This ability may facilitate evasion of host defenses by the gonococcus and enhance adaptation to different environment^.^^
Protein I11 is an antigenically preserved protein that is present in all pathogenic Neisseria. It is not as well known as proteins I and 11, but it also participates in pathogenesis, inducing generation of blocking antibodies that reduce serum bactericidal activity.5y, 65
Other potentially important membrane antigens include the H-8 antigen and the iron-repressible membrane proteins, but their role in pathogenesis is still unknown. Gonococci grown under conditions of relative iron deprivation produce increased concentrations of iron-re- pressible proteins. This may take part in the attachment and invasion steps of the infection, either because iron promotes adherence of N. gonorrhoem to eukaryotic cells or because it boosts production of other proteins that are important in adherence.32
Lipo-oligosaccharide
Gonococcal lipo-oligosaccharide (LOS) is comprised of lipid A and a core of oligosaccharide.28 Differing from the lipopolysaccharide (LPS) of most gram-negative bacteria, LOS lacks the repeating 0 side chain6 LOS has marked endotoxic activity and accounts for the severity of gonococcal infections. Some components of LOS are also related to the resistance to serum bactericidal
Proteoglycan
Between the inner cytoplasmic membrane and the outer membrane there is a proteoglycan layer that may contribute to the inflammatory response in gonococcal infection. Gonococcal proteoglycan fragments can cause complement consumption in vitro and have been detected in
310 CUCURULL & ESPINOZA
synovial fluid of patients with gonococcal arthritis-dermatitis syn- drome. l9
1gA Proteases
ism against the action of the IgA present in mucosal surfaces.55 Pathogenic Neisseria produce IgA proteases that protect the organ-
ANIMAL MODELS OF GONOCOCCAL ARTHRITIS
There is some controversy about the pathogenesis of articular involvement in DGI. The arthritis present in the arthritis-dermatitis syndrome has been attributed to immune mechanisms in part because of the failure to culture N. gonorrhoem from symptomatic sites. The fact that this arthritis does not respond to corticosteroids but responds so well to antibiotic treatment, however, weighs against the immune-medi- ated theory? Another theory is that N. gonorrhoem disseminates to the joint and skin but can only be recovered in early phases; thus, the arthritis is likely caused by an aseptic inflammatory response.z2
Goldenberg et a P developed an interesting animal model with rabbits to study the pathophysiology of gonococcal arthritis. Their re- sults showed that injection of lo8 N. gonorrhoeae organisms into the knee produced acute and chronic synovitis despite the fact that the bacteria could not be recovered from the animal’s synovial fluid 48 hours later and that most cultures were sterile within 2 hours. Moreover, to test the hypothesis that gonococcal cell-wall components may be important in this sterile synovitis, they injected penicillin-killed N. gonorrhoem and gonococcal LPS. The synovitis produced with this second experiment was indistinguishable from that following injection of viable organisms. These results suggest that sterile microbial antigenic components may play a role in the pathophysiology of gonococcal arthritis.
GONOCOCCAL TYPING AND CLINICAL CORRELATION
Gonococcal typing is an important tool for studying epidemiology and clinical manifestations and for directing vaccine development. Di- verse methods have been employed to classify N. gonorrhoem, but the most widely used are auxotyping and serotypingM N. gonorrhoem auxo- types are designated on the basis of the nutrients required by that isolate for growth. Serovars are based on outer-membrane antigenic variation and designated on the basis of their patterns of reactivity with a panel of monoclonal antibodie~.~~
Several studies have been conducted to determine the features of the strains that produced DGL5, 8, lo, 27* 58, 63 These showed that the domi- nance of N. gonorrhoem isolates from DGI patients belongs to the trans-
GONOCOCCAL ARTHRITIS 311
parent phenotype, which means they lack protein 11. They are also resistant to the complement-mediated bactericidal activity of normal human sera and are unusually sensitive to in vitro killing by penicillin G, although strains with high-level penicillin resistance caused by chro- mosomal mutation are capable of causing DGI.37, 67 It is known that serum resistance and penicillin sensitivity correlate with gonococcal strains characterized by nutritional requirements for arginine, hypoxan- thine, and uracil (AHU strains), and with the P.IA serotype.
Epidemiologic studies are useful in understanding why the preva- lence of DGI is higher in some geographic regions than in others.36 Gonococci vary from region to region with respect to the prevalence of PIA serotypes, and this variation affects the prevalence of DGI, as, for example, multicenter 63 of DGI isolates from different cities in the United States illustrate. In Seattle and Denver, isolates were found to be predominantly AHU strains (76% and 85%, respectively), whereas in Boston and Atlanta, AHU gonococci comprised only 58% and 34%, respectively. When protein I serotyping was used, investigators found the dominant association of P.IA on DGI prevalence. Most AHU gono- cocci belong to P.IA serogroups, and in cities in which gonococci isolated from DGI patients were not AHU strains, most isolates from DGI pa- tients were nonetheless P.IA strains.*O In those multicenter studies, 40% of isolates from patients with uncomplicated gonorrhea belonged to P.IA serogroups, as opposed to 84% of patients with DGI.'j3 Gonococcal serovars containing P.IA seem to be less common in the United Kingdom than in the United States.36 Variations in the clinical presentation of DGI also may reflect infection with different subtypes of N. g~norrhoeae .~~
CLINICAL FEATURES
The classic clinical triad in DGI is dermatitis, tenosynovitis, and migratory polyarthritis. Despite changes in the incidence of gonorrhoeae, gonococcal phenotype, and susceptiblity to antibiotics, the clinical mani- festations of DGI have not changed over the past decade.78 Underlying conditions seem to be more cornm0n,4~ but response to antibiotic therapy and eventual outcome remain excellent.
Following a genitourinary, rectal, or pharyngeal mucosal infection, which is asymptomatic in most the disseminated disease can present with two clinical pictures. One reflects a bacteremic infection and is also known as arthritis-dermatitis syndrome; the other is a local- ized septic arthritis. Some investigators have suggested that these clinical pictures reveal different stages in the evolution of DGI because blood cultures are almost never positive concurrent with positive synovial fluid cultures. Thus, an initial bacteremic stage, associated with fever, skin rash, and tenosynovitis, is followed by localization of the infection within the joint^.^^,^" Around 60% of patients present with the bacteremic picture, whereas the remainder present with suppurative arthritis.58
Asymmetric polyarthralgia, which may be migratory, is the most
312 CUCURULL & ESPINOZA
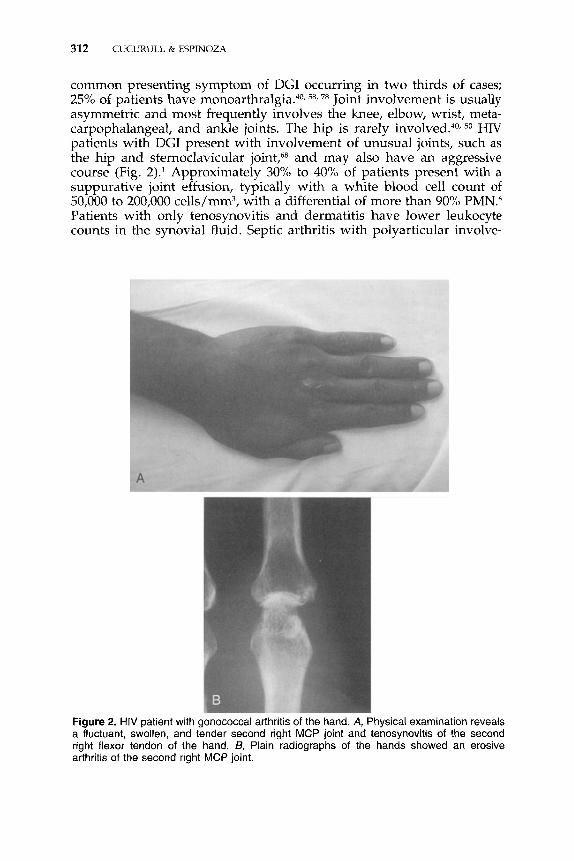
common presenting symptom of DGI occurring in two thirds of cases; 25% of patients have m~noarthralgia.~", 58, 78 Joint involvement is usually asymmetric and most frequently involves the knee, elbow, wrist, meta- carpophalangeal, and ankle joints. The hip is rarely 50 HIV patients with DGI present with involvement of unusual joints, such as the hip and sternoclavicular joint,68 and may also have an aggressive course (Fig. 2).l Approximately 30% to 40% of patients present with a suppurative joint effusion, typically with a white blood cell count of 50,000 to 200,000 cells/mm3, with a differential of more than 90% PMN.6 Patients with only tenosynovitis and dermatitis have lower leukocyte counts in the synovial fluid. Septic arthritis with polyarticular involve-
Figure 2. HIV patient with gonococcal arthritis of the hand. A, Physical examination reveals a fluctuant, swollen, and tender second right MCP joint and tenosynovitis of the second right flexor tendon of the hand. B, Plain radiographs of the hands showed an erosive arthritis of the second right MCP joint.
GONOCOCCAL ARTHRITIS 313
ment is the most common manifestation of gonococcemia in the neonatal period.25
Dermatitis is seen in two thirds of cases58 comprising a painless, nonpruritic skin rash that is usually maculopapular, pustular, necrotic, or vesicular on an erythematous base. Infrequently, hemorrhagic skin lesions, erythema nodosum, urticaria, and erythema multiforme have been described. Typically, the rash occurs below the neck, involving the torso, limbs, palms, and soles but sparing the scalp, face, and The skin lesions are often seen in various stages of development and typically resolve over 4 to 5 days without residual scarring. New lesions may appear even after antibiotic therapy has begun. Cutaneous vasculi- tis has been reported as the sole manifestation of the disease.52
Tenosynovitis also is present in two thirds of the patients with DGI,58 typically occurring in the hands and fingers, although the tendons around the small and large joints of the lower limbs also can be af- fe~ted.~O Distribution is usually asymmetric and involves more than one joint.
Systemic infection with N. gonovrhoeae generally produces fairly mild constitutional symptoms, with fever rarely reaching 39°C.
In a series of patients studied by Wise et a1,78 significant underlying conditions were identified in 11 of 41 patients (27%), including parenteral drug use, systemic lupus erythematosus, malignant neoplasm, diabetes mellitus, and HIV infection. The characteristics that identified those patients who required longer inpatient treatment included elevated erythrocyte sedimentation rate (ESR) on admission, positive synovial fluid culture results, and the presence of underlying conditions.
Rare manifestations of DGI comprise peri~arditisl~, 77; endocarditis, most commonly affecting the aortic valve73; perihepatitis (Fitz- Hugh-Curtis syndrome); pyomyo~itis~~; ~steomyelitis~~; and meningitis. The frequency of these complications has decreased dramatically in the era of antibiotics. Involvement of the meninges, heart valves, and bone occurs in 1% to 3% of patients with DGI.
DIFFERENTIAL DIAGNOSIS
Although several diseases mimic the clinical picture of DGI, clinical clues facilitate differentiation. For example, nongonococcal septic arthri- tis is usually monoarticular and affects the very young and the very old, the immunocompromised, and patients with prior joint damage; dermatitis and tenosynovitis are rarely present. Reiter’s syndrome, which is less common in women, presents with the triad of urethritis, conjunctivitis, and arthritis; onset is subacute, without fever, and arthritis involves the axial skeleton. Hyperkeratotic skin lesions in palms and soles are typical. Rheumatic fever follows a streptococcal infection, is associated with high fever, marked systemic illness, and a characteristic rash. It also responds well to salicylates or nonsteroidal anti-inflamma- tory drugs. The rash associated with secondary syphilis typically affects
314 CUCURULL & ESPINOZA
palms and soles. Hepatitis and bacterial endocarditis also have to be ruled out in a patient with arthritis and skin lesions.22, 64
DIAGNOSIS
Laboratory Tests
The most frequent laboratory findings in patients with DGI are mild leukocytosis and elevated ESR. Peripheral blood leukocytosis is present in approximately one half of the patients, with a mean leukocyte c o m P
58 of 10,500 to 12,500 cells/mm3. Although most patients have an elevated ESR,2* only one half have an ESR higher than 50 mm/h. Anemia and abnormal liver function also may be detected but are usually mild and t ran~ient .~~
Culture
A positive culture confirms the diagnosis of DGI and is not only crucial to the diagnosis but allows determination of drug susceptibility. Patients with DGI can be classified on the basis of their culture results into proven, probable, and possible DGI.22 Patients with positive cultures from blood, synovial fluid, skin lesions, or other sterile sources, such as spinal and pericardial fluid, are considered to have proven DGI; how- ever, this occurs in less than 50% of cases. Patients with the clinical features of DGI, positive cultures from primary mucosal sites and nega- tive cultures from sterile sites, are considered to have probable DGI. Patients with the typical clinical syndrome and the expected response to therapy but with negative cultures for N. gonorrhoeue are referred to as having possible DGI.
N. gonorrhoeae is cultured from synovial fluid in only about 50% of purulent joints and from 25% to 30% of all patients with DGI. This contrasts with the high yield of the culture and Gram’s stain at sites of primary mucosal infection in which the organism is recovered in most infected samples. More than 80% of cultures obtained from primary mucosal sites or from a sexual partner are positive. Typically, cervical cultures are positive in approximately 90% of women, urethral cultures in 50% to 75% of men, pharyngeal cultures in 20%, and rectal cultures in 15%. Blood cultures detect N. gonorrhoeae in only 20% to 30% of DGI patients, and cultures from skin detect infection in less than 5% of
Nevertheless, when DGI is suspected, culture samples must be obtained from all possible sites, including blood, synovial fluid, skin lesions, endocervix, urethra, rectum, and pharynx. Patients’ sexual con- tacts should be encouraged to seek evaluation and culture. To improve the culture yield, samples must be plated immediately. Joint fluid and other specimens from sterile sites must be inoculated on chocolate agar, but for samples from the genitourinary tract, rectum, and pharynx,
GONOCOCCAL ARTHRITIS 315
Thayer-Martin or modified New York media, which contain antibiotics, should be used.
Other Diagnostic Methods
Serologic tests have been developed to detect antibodies to N. gunor- rhoeae or its components using complement fixation, immunoprecipita- tion, latex agglutination, enzyme-linked immunoabsorbance, and so on. Most of them have sensitivities of less than 70% and specificities of less than SOYO, however, for patients with uncomplicated gonorrhea. In asymptomatic populations, serologic tests have a lower degree of sensi- tivity than do cultures, and in settings with a low prevalence of gonor- rhea, the specificities of these test methods may be unsatisfactory and thus not useful for screening, case finding, or diagnosis.35
Recent advances in molecular biology have allowed development of sensitive diagnostic assays, such as polymerase chain reaction (PCR) and ligase chain reaction (LCR), based on detection of specific nucleic acid sequences in clinical specimens. These tests are so sensitive that they allow the use of samples in which the number of microorganisms fall below the detection limits of more traditional assays. Recent studies have shown that PCR and LCR can detect N. gonorrhoeae in urogenital samples (male urethral, female cervical, and first-void urine specimens [FVU]) with high sensitivity and specificity compared with culture^.^, 33, 66 Because 50% of women infected with N. gonorrhoeae are asymptom- atic, the noninvasive nature of FVU collection provides a substantial advantage over the labor-intense and time-consuming procedures for obtaining urogenital swabs. Until antibiotic resistance can be tested by nucleic acid technologies, however, LCR or PCR are not likely to replace culture for routine testing.
Polymerase chain reaction allows identification of N. gonorrhoeae in synovial even when the culture is negative. It is not clear whether positive PCR results represent live organisms and inadequate culture technique or dead organisms and a reactive arthropathy. Liebling et a148 analyzed 41 culture-negative synovial fluid samples from 10 patients with clinical gonococcal arthritis and 27 controls, including 11 patients with Reiter’s syndrome. N. gonorrhoeae was detected in 11 of 14 samples obtained from patients with culture-negative clinical gonococcal arthritis but in none of the 11 samples from Reiter’s syndrome patients and only in one of 16 controls. The specificity of the technique was 96.4%, with a sensitivity of 78.6%. The rate of false-positive results was 3.6%. PCR was helpful in differentiating N. gonorrhoeae arthritis from acute Reiter ’s syndrome, which frequently has similar demographics and clinical presentation, and is one of the principal entities in the differential diagnosis of DGI.
316 CUCURULL & ESPINOZA
TREATMENT
Antimicrobial Resistance
N. gonorrhoeae has developed two mechanisms of antimicrobial resis- tance, chromosomal mutation and the acquisition of plasm id^."^ Two types of chromosomal resistance have been described. The first is caused in single-step mutation to high-level resistance. The second involves mutations at several chromosomal loci, and the combination of muta- tions determines the level and pattern of resistance. The acquisition of plasmids is a result of the interaction between genetic factors and the environmental selective effect.49 These mechanisms either decrease per- meability of the gonococcal membrane to antimicrobial agents, decrease affinity of the penicillin-binding proteins for beta-lactam antibiotics, or increase the concentration of penicillin-binding proteins.I6
Factors contributing to development and changes in prevalence of antibiotic-resistant gonococci within communities are complex and may vary from area to area. A number of studies have described outbreaks of antibiotic-resistant gonorrhea from overseas travelers and spread by high-frequency transmitters, such as prostitutes. Factors contributing to the more gradual evolution of chromosomally mediated antibiotic resistance are less clear; however, self-administered antibiotics may play a role in selecting for resistant gonococci.2"* 72
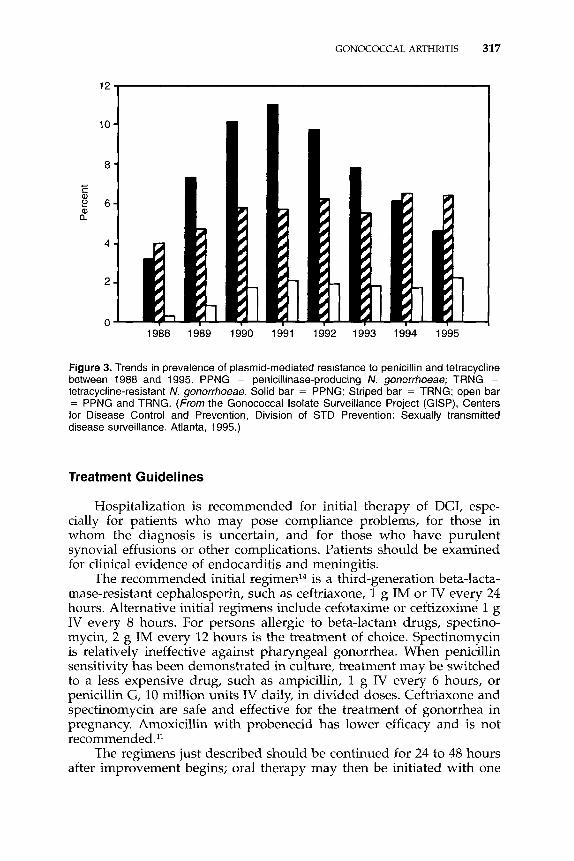
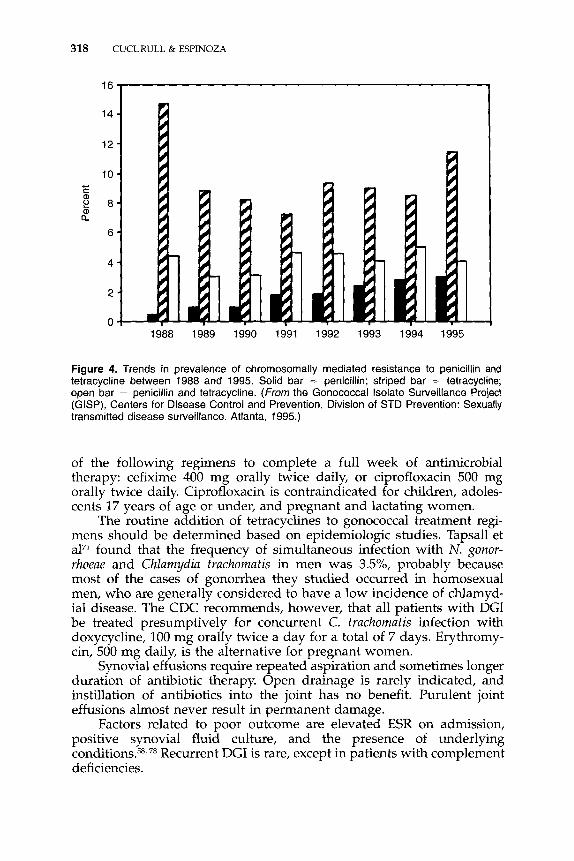
Antimicrobial resistance remains an important consideration in the treatment of gonorrhea. Data from the CDCl2 in 1995 revealed that overall, 31.6% of isolates collected by the Gonococcal Isolate Surveillance Project (GISP) were resistant to penicillin, tetracycline, or both. Between 1991 and 1995, the percentage of GISP isolates that were penicillinase- producing N. gonorrkoeae declined from 13.1% to 6.8% (Fig. 3). In con- trast, isolates with chromosomally mediated resistance to penicillin in- creased from 6.4% in 1991 to 7.0% in 1995 (Fig. 4). Chromosomally mediated tetracycline resistance increased from 13.5% in 1994 to 15.4% in 1995 after several years of stability (Fig. 4). Until now, all isolates were highly susceptible to broad-spectrum cephalosporins. Sporadic cases of spectinomycin-resistant gonorrhea have been reported, but such strains remain rare in the United States.35 Epidemiologic studies in different countries43, 74 show similar resistance patterns worldwide.
The GISP first identified resistance to ciprofloxacin in 1991, and isolates with decreased susceptibility to ciprofloxacin increased from 0.4% in 1991 to 1.3% in 1994.20 Importation of a fluoroquinolone-resistant strain with subsequent therapy failure and endemic transmission of a fluoroquinolone-resistant strain were documented for the first time13 in the United States in 1995. Since then, more literature has appeared.23, 2')
Resistance to fluoroquinolones is related to mutation in DNA gyrase subunit A (GyrA), a well-known mechanism of bacterial quinolone re~istance.'~, 70 Reduced susceptibility and resistance to ciprofloxacin cor- relate with reduced susceptibility and resistance to other fluoroquinolone antibiotics.
GONOCOCCAL ARTHRITIS 317
I
10 -
8 -
c c a al II 2 6 -
4 -
2-
0 1988 1989 1990 1991 1992 1993 1994 1995
Figure 3. Trends in prevalence of plasmid-mediated resistance to penicillin and tetracycline between 1988 and 1995. PPNG = penicillinase-producing N. gonorrhoeae; TRNG = tetracycline-resistant N. gonorrhoeae. Solid bar = PPNG; Striped bar = TRNG; open bar = PPNG and TRNG. (From the Gonococcal Isolate Surveillance Project (GISP), Centers for Disease Control and Prevention, Division of STD Prevention: Sexually transmitted disease surveillance. Atlanta, 1995.)
Treatment Guidelines
Hospitalization is recommended for initial therapy of DGI, espe- cially for patients who may pose compliance problems, for those in whom the diagnosis is uncertain, and for those who have purulent synovial effusions or other complications. Patients should be examined for clinical evidence of endocarditis and meningitis.
The recommended initial regimen14 is a third-generation beta-lacta- mase-resistant cephalosporin, such as ceftriaxone, 1 g IM or IV every 24 hours. Alternative initial regimens include cefotaxime or ceftizoxime 1 g IV every 8 hours. For persons allergic to beta-lactam drugs, spectino- mycin, 2 g IM every 12 hours is the treatment of choice. Spectinomycin is relatively ineffective against pharyngeal gonorrhea. When penicillin sensitivity has been demonstrated in culture, treatment may be switched to a less expensive drug, such as ampicillin, 1 g IV every 6 hours, or penicillin G, 10 million units IV daily, in divided doses. Ceftriaxone and spectinomycin are safe and effective for the treatment of gonorrhea in pregnancy. Amoxicillin with probenecid has lower efficacy and is not recommended."
The regimens just described should be continued for 24 to 48 hours after improvement begins; oral therapy may then be initiated with one
318 CUCURULL & ESPINOZA
16 I
14 -
12 - 10 -
2 8 -
6 -
4 -
2 -
c f a,
a, a
1988 1989 1990 1991 1992 1993 1994 1995
Figure 4. Trends in prevalence of chromosomally mediated resistance to penicillin and tetracycline between 1988 and 1995. Solid bar = penicillin; striped bar = tetracycline; open bar = penicillin and tetracycline. (From the Gonococcal Isolate Surveillance Project (GISP), Centers for Disease Control and Prevention, Division of STD Prevention: Sexually transmitted disease surveillance. Atlanta, 1995.)
of the following regimens to complete a full week of antimicrobial therapy: cefixime 400 mg orally twice daily, or ciprofloxacin 500 mg orally twice daily. Ciprofloxacin is contraindicated for children, adoles- cents 17 years of age or under, and pregnant and lactating women.
The routine addition of tetracyclines to gonococcal treatment regi- mens should be determined based on epidemiologic studies. Tapsall et al7I found that the frequency of simultaneous infection with N. gonor- rhoeae and Chlamydia fruchomafis in men was 3.5%, probably because most of the cases of gonorrhea they studied occurred in homosexual men, who are generally considered to have a low incidence of chlamyd- ial disease. The CDC recommends, however, that all patients with DGI be treated presumptively for concurrent C. frachomafis infection with doxycycline, 100 mg orally twice a day for a total of 7 days. Erythromy- cin, 500 mg daily, is the alternative for pregnant women.
Synovial effusions require repeated aspiration and sometimes longer duration of antibiotic therapy. Open drainage is rarely indicated, and instillation of antibiotics into the joint has no benefit. Purulent joint effusions almost never result in permanent damage.
Factors related to poor outcome are elevated ESR on admission, positive synovial fluid culture, and the presence of underlying conditions.58r78 Recurrent DGI is rare, except in patients with complement deficiencies.
GONOCOCCAL ARTHRITIS 319
Repeat cultures to ensure resolution of infection are recommended for all patients with gonorrhea% and should be performed at least 5 days following the last dose of antibiotics. All known infected sites should be recultured.
SUM MARY
Disseminated gonococcal infection is the most common systemic complication of acute gonorrhea and occurs in 0.5% to 3.0% of patients with untreated mucosal infection. It is also the most common cause of septic arthritis in patients less than 30 years of age. Fortunately, the incidence of gonorrhea is decreasing dramatically in the United States and Western Europe, although it is still high in developing countries. Increasing resistance to antibiotics requires continuous surveillance of antimicrobial susceptibilities to determine the efficacy of current thera- peutic measures.
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
Anaya JM, Joseph J, Scopelitis E, et al: Disseminated gonococcal infection and human immunodeficiency virus. Clin Exp Rheumatol 12:688, 1994 Aral SO, Holmes K K Epidemiology of sexually transmitted disease. In Holmes KK, M t d h PA, Sparling PF, et a1 (eds): Sexuallv Transmitted Diseases. New York, McGraw- Hill, 1984, p-126 Blake M. Swanson 1: Studies on eonococcus infection: IX. In vitro decreased association " of piliated gonococci with mouse peritoneal macrophages. Infect Immun 11:1402, 1975 Blake MS, Gotschlich EC: Gonococcal membrane proteins: Speculation on their role in pathogenesis. Prog Allergy 33:298, 1983 Bohnhoff M, Morello JA, Lener S A Auxotypes, penicillin susceptibility and serogroups of Neisseria gonorrhoeae from disseminated and uncomplicated infections. J Infect Dis 154:225, 1986 Britigan BE, Cohen MS, Sparling PF: Gonococcal infections: A model of molecular pathogenesis. N Engl J Med 312:1683, 1985 Brooks GF, Israel KS, Petersen BH: Bactericidal and opsonic activity against Neisseria gonorrhoeae in sera from patients with disseminated gonococcal infection. J Infect Dis 134:450, 1976 Brunham RC, Plummer F, Slaney L, et al: Correlation of auxotype and protein I type with expression of disease due to Neisseriu gonorrhoene. J Infect Dis 152:339, 1985 Buimer M, van Doornum GJJ, Ching S, et al: Detection of Chlamydia trachomatis and Neisseria gonorrhoeae by ligase chain reaction-based assays with clinical specimens from various sites: Implications for diagnostic testing and screening. J Clin Microbiol 34:2395, 1996 Cannon JG, Buchanan TM, Sparling PF: Confirmation of association of protein 1 serotype of Neisseria gonorrhoeae with ability to cause disseminated infection. Infect Immun 40:816, 1983 Cavenee MR, Farris JR, Spalding TR, et al: Treatment of gonorrhea in pregnancy. Obstet Gynecol 81:33, 1993 Centers for Disease Control and Prevention, Division of STD prevention: Sexually transmitted disease surveillance. http:/ /wonder.cdc.gov/wonder/STD/Title3600.html, Atlanta, 1995
320 CUCURULL & ESPINOZA
13. Centers for Disease Control and Prevention: Fluoroquinolone resistance in Neisseria
14. Centers for Disease Control and Prevention: 1993 Sexually transmitted diseases treat-
15. Coe MD, Hamer DH, Levy CS, et a1 Gonococcal pericarditis with tamponade in a
16. Dallabeta G, Hook EW 111: Gonococcal infections. Infect Dis Clin North Am 1:25, 1987 17. Deguchi T, Yasuda M, Nakano M, et al: Rapid detection of point mutations of the
Neisseria gonorrhoeae gyrA gene associated with decreased susceptibilities to quino- lones. J Clin Microbiol 34:2255, 1996
18. Densen P, MacKeen LA, Clark RA: Dissemination of gonococcal infection is associated with delayed stimulation of complement-dependent neutrophil chemotaxis in vitro. Infec Immun 38:563, 1982
19. Fleming TJ, Wallsmith DE, Rosenthal RS: Arthropathic properties of gonococcal pepti- doglycan fragments: Implications for the pathogenesis of disseminated gonococcal disease. Infect Immun 52:600, 1986
20. Fox KK, Knapp JS, Holmes KK, et al: Antimicrobial resistance in Neisseria gonorrhoeae in the United States, 1988-1994 The emergence of decreased susceptibility to the fluoroquinolones. J Infect Dis 1751396, 1997
21. Goldenberg DL, Reed JI, Rice PA. Arthritis in rabbits induced by killed Neisseria gonorrhoeae and gonococcal lipopolysaccharide. J Rheumatol 11:3, 1984
22. Goldenberg DL: Gonococcal arthritis. In Espinoza LR, Goldenberg DL, Arnett FC, et a1 (eds): Infections in the rheumatic diseases: A comprehensive review of microbial relations to rheumatic disorders. Orlando, Grune and Stratton, 1988, p 43
23. Gordon SM, Carlyn CJ, Doyle LJ, et al: The emergence of Neisseria gonorrhoeae with decreased susceptibility to ciprofloxacin in Cleveland, Ohio: Epidemiology and risk factors. Ann Intern Med 125:465, 1996
24. Gregg CR, Melly MA, Hellerguist GG, et al: Toxic activity of purified lipopolysaccha- ride of Neisseriu gonorrhoem for human fallopian tube mucosa. J Infect Dis 143:432, 1985
25. Gutman LT, Wilfert CM: Gonococcal diseases in infants and children. In Holmes KK, MQrdh PA, Sparling PF, et a1 (eds): Sexually Transmitted Diseases. New York, McGraw- Hill, 1990, p 803
26. Haines KA, Yeh L, Blake MS, et al: Protein I, a translocable ion channel from Neisseria gonorrhoeae, selectively inhibits exocytosis from human neutrophils without inhibiting 0,--generation. J Biol Chem 263:945, 1988
27. Handsfield HH, Knapp SS, Diehr PK, et a1 Correlation of auxotype and penicillin susceptibility of Neisseriu gonorrhoeae with sexual preference and clinical manifestations of gonorrhea. Sex Transm Dis 71, 1980
28. Hansfield HH: Neisseriu gonorrhoeae. In Mandell GL, Douglas RG, Bennett JE (eds): Principles and Practice of Infectious Diseases, ed 3. New York, Churchill Livingstone, 1990, p 1613
29. Harnett N, Brown S, Riley G, et al: Analysis of Neisseria gonorrhoeae in Ontario, Canada, with decreased susceptibility to quinolones by pulsed-field gel electrophoresis, auxotyping, serotyping and plasmid content. J Med Microbiol 46:383, 1997
30. Haugh PJ, Levy CS, Hoff-Sullivan E, et al: Pyomyositis as the sole manifestation of disseminated gonococcal infection: Case report and review. Clin Infect Dis 22:861, 1996
31. Heckels JE: Molecular studies on the pathogenesis of gonorrhoea. J Med Microbiol 18:293, 1984
32. Heine RP, Elkins C, Wyrich PB, et al: Transferrin increases adherence of iron-deprived Neisseria gonorrhoeae to human endometrial cells. Am J Obstet Gynecol 174659, 1996
33. Herrmann B, Nystrom T, Wessel H: Detection of Neisseria gonorrhoeae from air-dried genital samples by single-tube nested PCR. J Clin Microbiol 34:2548, 1996
34. Holmes KK, Counts GW, Beaty H N Disseminated gonococcal infection. Ann Intern Med 74:979, 1971
35. Hook EW, Handsfield HH: Gonococcal infections in the adult. In Holmes KK, MBrdh PA, Sparling PF, et a1 (eds): Sexually Transmitted Diseases. New York, McGraw-Hill, 1990, p 149
gonorrhoeae-Colorado and Washington. Morb Mortal Wkly Rep 44:761, 1995
ment guidelines. Morb Mortal Wkly Rep 42(No RR-14):1993
patient with systemic lupus erythematosus. Arthritis Rheum 331438, 1990
GONOCOCCAL ARTHRITIS 321
36. Hook EW: Septic gonococcal arthritis is much more common in the United States than in the United Kingdom. Br J Rheumatol29:283, 1990
37. Hoosen AA, Mody GM, Goga IE, et al: Prominence of penicillinase-producing strains of Neisseriu gonorrhoeue in gonococcal arthritis, experience in Durban, South Africa. Br J Rheumatol 33240, 1994
38. Joiner KA, Warren KA, Brown EJ, et al: Studies on the mechanism of bacterial resistance to complement-mediated killing: IV. C5b-9 forms high molecular weight complexes with bacterial outer membrane constituents on serum-resistant but not on serum- sensitive Neisseria gonorrhoeue. J Immunol 131:144, 1983
39. Judd RC: Protein I Structure, function and genetics. Clin Microbiol Rev 2:S41, 1989 40. Keiser H, Ruben FL, Wolinsky E, et al: Clinical forms of gonococcal arthritis. N Engl J
Med 279:234, 1968 41. Knapp JS, Thomsberry C, Schoolnik GA, et a1 Cooperative study group: Phenotypic
and epidemiologic correlates of auxotype in Neisseriu gonorrhoeue. J Infect Dis 132:160, 1978
42. Knapp JS, Tam MR, Nowinski RC, et al: Serological classification on Neisseriu gonorr- hoeue with use of monoclonal antibodies to gonococcal outer membrane protein I. J Infect Dis 150:44, 1984
43. Knapp JS, Mesola VP, Neal SW, et a1 Molecular epidemiology in 1994 of Neisseriu gonorrhoeue in Manila and Cebu City, Republic of the Philippines. Sex Transm Dis 24:1, 1997
44. Knapp JS, Wongba C, Limpakarnjanarat K, et al: Antimicrobial susceptibilities of strains of Neisseria gonorrhoeue in Bangkok, Thailand: 1994-1995. Sex Transm Dis 24:142, 1997
45. Koss PG: Disseminated gonococcal infection. Cleve Clin Q 52:161, 1985 46. Larribe M, Taha MK, Topilko A, et al: Control of Neisseriu gonorrhoeae pilin gene
expression by environmental factors: Involvement of the pilA/pilB regulatory genes. Microbiol 143:1757, 1997
47. Lewis DA, Pollock LM, Randell J, et al: Acute gonococcal arthritis: An unusual host and pathogen combination. J Clin Pathol48:86, 1995
48. Liebling MR, Arkfeld DG, Michelini GA, et al: Identification of Neisseriu gonorrhoeue in synovial fluid using the polymerase chain reaction. Arthritis Rheum 37702, 1994
49. Lind I: Antimicrobial resistance in Neisseriu gonorrhoeue. Clin Infect Dis 24(suppl):93, 1997
50. Manshady BM, Thompson GR, Weiss JJ: Septic arthritis in a general hospital, 1966- 1977. J Rheumatol 7:523, 1980
51. Masi AT, Eisenstein BI: Disseminated gonococcal infection (DGI) and gonococcal arthri- tis (GCA): 11. Clinical manifestations, diagnosis, complications, treatment, and preven- tion. Semin Arthritis Rheum 10:173, 1981
52. Mastrolonardo M, Loconsole F, Conte A, et al: Cutaneous vasculitis as the sole manifes- tation of disseminated gonococcal infection: Case report. Genitourin Med 70:130, 1994
53. Mauro A, Blake MS, Labarca: Voltage gating conductance in lipid bilayers induced by porins from outer membrane of Neisseriu gonorrhoeae. Proc Natl Acad Sci U S A 85:1071, 1988
54. Meyer TF, van Putten JPM: Genetic mechanisms and biological implications of phase variation in pathogenic Neisseria. Clin Microbiol Rev 2:S139, 1989
55. Mulks MH, Knapp J S Immunoglobulin A1 protease types of Neisseria gonorrhoeue and their relationship to auxotype and serovar. Infect Immun 55:931, 1987
56. Muralidhar B, Rumore PM, Steinman C H Use of the polymerase chain reaction to study arthritis due to Neisseria gonorrhoeae. Arthritis Rheum 37710, 1994
57. Naumann M, Wepler S, Bartsch C, et al: Neisseria gonorrhoeae epithelial cell interaction leads to the activation of the transcription factors nuclear factor kB and activator Protein 1 and the induction of inflammatory cytokines. J Exp Med 186:247, 1997
58. OBrien JP, Goldenberg DL, Rice PA: Disseminated gonococcal infection: A prospective analysis of 49 patients and a review of pathophysiology and immune mechanisms. Medicine 62:395, 1983
59. Rice PA, Kasper DL: Characterization of serum resistance of Neisseriu gonorrhoeue that
322 CUCURULL & ESPINOZA
disseminate: Roles of blocking antibody and gonococcal outer membrane proteins. J Clin Invest 70:157, 1982
60. Ross JDC: Systemic gonococcal infection. Genitourin Med 72:404, 1996 61. Ross SC, Densen P: Complement deficiency states and infection. Medicine 63:243,1984 62. Rude1 T, Scheuerpflug I, Meyer TF: Neisseria PilC protein identified as type-IV pilus
tip-located adhesin. Nature 373:357, 1995 63. Sandstrom EG, Knapp JS, Reller LB, et al: Serogrouping of Neisseriu gonorrhoeue:
Correlation of serogroup with disseminated gonococcal infection. Sex Trans Dis 11:77, 1984
64. Scopelitis E, Martinez-Osuna P: Gonococcal arthritis. Rheum Dis Clin North Am 19:363, 1993
65. Sparling PF: Biology of Neisseriu gonorrhoeue. In Holmes KK, MBrdh PA, Sparling PF, et a1 (eds): Sexually Transmitted Diseases. New York, McGraw-Hill, 1990, p 131
66. Stary A, Ching SF, Teodorowicz L, et a1 Comparison of ligase chain reaction and culture for detection of Neisseriu gonorrhoeue in genital and extragenital specimens. J Clin Microbiol 35239, 1997
67. Stewart K, Carlson M, Segal AM, et a1 Gonococcal arthritis caused by penicillinase- producing strains of Neisseriu gonorrhoeue. Arthritis Rheum 34:245, 1991
68. Strongin IS, Kale SA, Raymond MK, et al: An unusual presentation of gonococcal arthritis in an HIV-positive patient. Ann Rheum Dis 50:572, 1991
69. Swanson J, Robins K, Barrera 0, et al: Gonococcal pilin variants in experimental gonorrhea. J Exp Med 165:1344, 1987
70. Tanaka M, Otsuki M, Nishino T, et al: Mutation in DNA gyrase of norfloxacin-resistant clinical isolates of Neisseriu gonorrhoeue. Genitourin Med 72:295, 1996
71. Tapsall JW, Kinchington M: The frequency of co-infection with Neisseriu gonorvhoeae and Chlamydia truchornutis in men and women in eastern Sydney. Pathology 28:84, 1996
72. The Gonococcal Isolate Surveillance Project: National Surveillance of antimicrobial resistance in Neisseriu gonorrhoeae. JAMA 264:1413, 1990
73. Thompson EC, Brantley D: Gonococcal endocarditis. J Natl Med Assoc 88:353, 1996 74. Van Dyck E, Crabbe F, Nzila N, et al: Increasing resistance of Neisseriu gonorrhoeue in
West and Central Africa: Consequences on therapy of gonococcal infection. Sex Transm Dis 24:32, 1997
75. Waldbeser LS, Ajioka RS, Merz AJ, et al: The opuH locus of Neisseriu gonorrhoeue MS11- A is involved in epithelial cell invasion. Mold Microbiol 13919, 1994
76. Wee1 JFL, Hopman CTP, van Putten JPM: Bacterial entry and intracellular processing of Neisseria gonorrhoeae in epithelial cells: Immunomorphological evidence for alter- ations in the major outer membrane protein P.IB. J Exp Med 174705, 1991
77. Wilson J, Zaman AG, Simmons AV Gonococcal arthritis complicated by acute pericar- ditis and pericardial effusion. Br Heart J 63:134, 1990
78. Wise CM, Morris CR, Wasilauskas BL, et al: Gonococcal arthritis in an era of increasing penicillin resistance. Arch Intern Med 154:2690, 1994
79. Zak K, Diaz JL, Jackson D, et al: Antigenic variation during infection with Neisseriu gonorvhoeue: Detection of antibodies to surface proteins in sera of patients with gonor- rhea. J Infect Dis 149:166, 1984
Address reprint requests to Luis R. Espinoza, MD
Department of Medicine Section of Rheumatology
LSU Medical Center 1542 Tulane Avenue
New Orleans, LA 70112-2822
Related Documents











