CLINICAL MICROBIOLOGY REVIEWS, July 2009, p. 484–492 Vol. 22, No. 3 0893-8512/09/$08.000 doi:10.1128/CMR.00003-09 Copyright © 2009, American Society for Microbiology. All Rights Reserved. Gnathostomiasis, Another Emerging Imported Disease Joanna S. Herman 1 * and Peter L. Chiodini 1,2 Department of Clinical Parasitology, Hospital for Tropical Diseases, 3rd Floor, Mortimer Market, Capper Street, London WC1E 6JB, United Kingdom, 1 and London School of Hygiene and Tropical Medicine, London, United Kingdom 2 INTRODUCTION .......................................................................................................................................................484 EPIDEMIOLOGY .......................................................................................................................................................484 LIFE CYCLE AND MORPHOLOGY ......................................................................................................................485 CLINICAL FEATURES .............................................................................................................................................486 Cutaneous Gnathostomiasis ..................................................................................................................................487 Visceral Disease ......................................................................................................................................................488 Pulmonary manifestations .................................................................................................................................488 Gastrointestinal manifestations ........................................................................................................................488 Genitourinary manifestations ...........................................................................................................................488 Ocular ...................................................................................................................................................................488 Auricular manifestations ...................................................................................................................................488 CNS manifestations ............................................................................................................................................488 DIAGNOSIS ................................................................................................................................................................489 TREATMENT ..............................................................................................................................................................490 PREVENTION.............................................................................................................................................................491 ACKNOWLEDGMENTS ...........................................................................................................................................491 REFERENCES ............................................................................................................................................................491 INTRODUCTION International travel to the tropics has dramatically increased over the past few decades, with a subsequent and significant increase in the number of patients presenting with tropical diseases in countries where such infections are not endemic. It is estimated that 50 million residents of industrialized coun- tries travel annually to such areas (42, 44), which brings expo- sure to a broad range of pathogens rarely, if ever, encountered at home. These may vary from short-lived, easily detected and treatable infections (e.g., gastrointestinal infections) to more exotic infections such as filarial and helminthic infections (e.g., loiasis, stronglyoidiasis, and schistosomiasis). Such infections may be seen rarely by physicians in temperate climates, and therefore diagnosis can prove elusive if these infections are not considered. Travelers are becoming ever more adventurous in choice of country, pursuit of remoteness and immersion in local culture, which will frequently include eating all local delicacies (e.g., ceviche or “drunken crab”) without consider- ation of what organisms they might be harboring. Migration has also increased substantially over the past few decades, with people from the tropics and subtropics settling in the West, and many come harboring parasites of which they are unaware. Gnathostomiasis is a parasitic infection caused by the third- stage larvae of the helminths Gnathostoma spp., which are seen mostly in tropical and subtropical regions. It is a food-borne zoonosis and is endemic in areas where people eat raw fresh- water fish or shellfish, especially Thailand and other parts of Southeast Asia, Japan, and increasingly Latin America, partic- ularly Mexico. Previously, the disease was rarely seen outside areas of endemicity; however, over the past decade, the num- ber of cases seen in countries where it is not endemic has increased. Few clinicians outside areas of endemicity are fa- miliar with the disease, and therefore diagnosis is often missed or prolonged, with potentially serious consequences. The clas- sic triad of intermittent migratory swellings, eosinophilia, and a history of travel to Southeast Asia or other areas of ende- micity should alert physicians to the possible diagnosis. Vis- ceral disease is more serious than the cutaneous manifestations and, in the case of central nervous system (CNS) disease, may be fatal. This article describes the epidemiology, life cycle, clinical features, diagnostic tools, treatment, and prevention of this disease. EPIDEMIOLOGY Gnathostoma was first discovered in the stomach wall of a tiger that died at London Zoo in 1836 (35) and was first described in humans in 1889 in Thailand by G. M. R. Levinson (cited in references 5 and 24). The next case was not described until 1934, and shortly after, its life cycle was elucidated (37). The foci of endemicity have been predominantly in Japan and Southeast Asia, particularly Thailand, but the disease is also endemic in Cambodia, Laos, Myanmar, Indonesia, Phil- ippines, and Malaysia (Fig. 1). Cases have also been reported in China, Sri Lanka, and India (41). In more recent years it has become an increasing problem in Central and South America, particularly in Mexico (due to the consumption of ceviche [raw fish marinated in lime]) (12, 39), and also in Guatemala, Peru, and Ecuador (14, 23). There have also reports of cases in Myanmar, Zambia, and, most recently, Botswana (6, 16, 17). * Corresponding author. Mailing address: Department of Clinical Parasitology, Hospital for Tropical Diseases, 3rd Floor, Mortimer Market, Capper Street, London WC1E 6JB, United Kingdom. Phone: 020 7387 4411, ext. 5418. Fax: 020 7383 0041. E-mail: joherman @doctors.org.uk. 484 Downloaded from https://journals.asm.org/journal/cmr on 22 January 2022 by 2806:109f:10:2ccb:f878:ad63:e7c5:5087.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CLINICAL MICROBIOLOGY REVIEWS, July 2009, p. 484–492 Vol. 22, No. 30893-8512/09/$08.00�0 doi:10.1128/CMR.00003-09Copyright © 2009, American Society for Microbiology. All Rights Reserved.
Gnathostomiasis, Another Emerging Imported DiseaseJoanna S. Herman1* and Peter L. Chiodini1,2
Department of Clinical Parasitology, Hospital for Tropical Diseases, 3rd Floor, Mortimer Market, Capper Street, London WC1E 6JB,United Kingdom,1 and London School of Hygiene and Tropical Medicine, London, United Kingdom2
INTRODUCTION .......................................................................................................................................................484EPIDEMIOLOGY.......................................................................................................................................................484LIFE CYCLE AND MORPHOLOGY ......................................................................................................................485CLINICAL FEATURES .............................................................................................................................................486
Cutaneous Gnathostomiasis..................................................................................................................................487Visceral Disease ......................................................................................................................................................488
Pulmonary manifestations .................................................................................................................................488Gastrointestinal manifestations........................................................................................................................488Genitourinary manifestations ...........................................................................................................................488Ocular...................................................................................................................................................................488Auricular manifestations ...................................................................................................................................488CNS manifestations ............................................................................................................................................488
DIAGNOSIS ................................................................................................................................................................489TREATMENT..............................................................................................................................................................490PREVENTION.............................................................................................................................................................491ACKNOWLEDGMENTS ...........................................................................................................................................491REFERENCES ............................................................................................................................................................491
INTRODUCTION
International travel to the tropics has dramatically increasedover the past few decades, with a subsequent and significantincrease in the number of patients presenting with tropicaldiseases in countries where such infections are not endemic. Itis estimated that 50 million residents of industrialized coun-tries travel annually to such areas (42, 44), which brings expo-sure to a broad range of pathogens rarely, if ever, encounteredat home. These may vary from short-lived, easily detected andtreatable infections (e.g., gastrointestinal infections) to moreexotic infections such as filarial and helminthic infections (e.g.,loiasis, stronglyoidiasis, and schistosomiasis). Such infectionsmay be seen rarely by physicians in temperate climates, andtherefore diagnosis can prove elusive if these infections are notconsidered. Travelers are becoming ever more adventurous inchoice of country, pursuit of remoteness and immersion inlocal culture, which will frequently include eating all localdelicacies (e.g., ceviche or “drunken crab”) without consider-ation of what organisms they might be harboring. Migrationhas also increased substantially over the past few decades, withpeople from the tropics and subtropics settling in the West,and many come harboring parasites of which they are unaware.
Gnathostomiasis is a parasitic infection caused by the third-stage larvae of the helminths Gnathostoma spp., which are seenmostly in tropical and subtropical regions. It is a food-bornezoonosis and is endemic in areas where people eat raw fresh-water fish or shellfish, especially Thailand and other parts of
Southeast Asia, Japan, and increasingly Latin America, partic-ularly Mexico. Previously, the disease was rarely seen outsideareas of endemicity; however, over the past decade, the num-ber of cases seen in countries where it is not endemic hasincreased. Few clinicians outside areas of endemicity are fa-miliar with the disease, and therefore diagnosis is often missedor prolonged, with potentially serious consequences. The clas-sic triad of intermittent migratory swellings, eosinophilia, anda history of travel to Southeast Asia or other areas of ende-micity should alert physicians to the possible diagnosis. Vis-ceral disease is more serious than the cutaneous manifestationsand, in the case of central nervous system (CNS) disease, maybe fatal.
This article describes the epidemiology, life cycle, clinicalfeatures, diagnostic tools, treatment, and prevention of thisdisease.
EPIDEMIOLOGY
Gnathostoma was first discovered in the stomach wall of atiger that died at London Zoo in 1836 (35) and was firstdescribed in humans in 1889 in Thailand by G. M. R. Levinson(cited in references 5 and 24). The next case was not describeduntil 1934, and shortly after, its life cycle was elucidated (37).
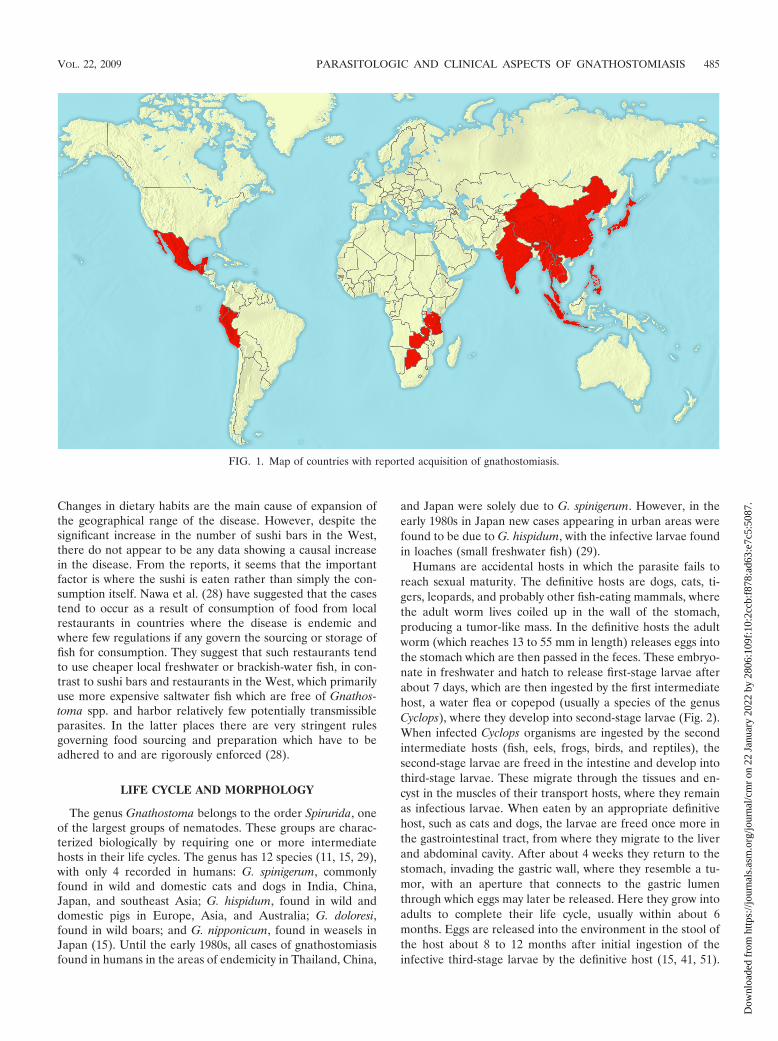
The foci of endemicity have been predominantly in Japanand Southeast Asia, particularly Thailand, but the disease isalso endemic in Cambodia, Laos, Myanmar, Indonesia, Phil-ippines, and Malaysia (Fig. 1). Cases have also been reportedin China, Sri Lanka, and India (41). In more recent years it hasbecome an increasing problem in Central and South America,particularly in Mexico (due to the consumption of ceviche [rawfish marinated in lime]) (12, 39), and also in Guatemala, Peru,and Ecuador (14, 23). There have also reports of cases inMyanmar, Zambia, and, most recently, Botswana (6, 16, 17).
* Corresponding author. Mailing address: Department of ClinicalParasitology, Hospital for Tropical Diseases, 3rd Floor, MortimerMarket, Capper Street, London WC1E 6JB, United Kingdom. Phone:020 7387 4411, ext. 5418. Fax: 020 7383 0041. E-mail: [email protected].
484
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/c
mr
on 2
2 Ja
nuar
y 20
22 b
y 28
06:1
09f:
10:2
ccb:
f878
:ad6
3:e7
c5:5
087.
Changes in dietary habits are the main cause of expansion ofthe geographical range of the disease. However, despite thesignificant increase in the number of sushi bars in the West,there do not appear to be any data showing a causal increasein the disease. From the reports, it seems that the importantfactor is where the sushi is eaten rather than simply the con-sumption itself. Nawa et al. (28) have suggested that the casestend to occur as a result of consumption of food from localrestaurants in countries where the disease is endemic andwhere few regulations if any govern the sourcing or storage offish for consumption. They suggest that such restaurants tendto use cheaper local freshwater or brackish-water fish, in con-trast to sushi bars and restaurants in the West, which primarilyuse more expensive saltwater fish which are free of Gnathos-toma spp. and harbor relatively few potentially transmissibleparasites. In the latter places there are very stringent rulesgoverning food sourcing and preparation which have to beadhered to and are rigorously enforced (28).
LIFE CYCLE AND MORPHOLOGY
The genus Gnathostoma belongs to the order Spirurida, oneof the largest groups of nematodes. These groups are charac-terized biologically by requiring one or more intermediatehosts in their life cycles. The genus has 12 species (11, 15, 29),with only 4 recorded in humans: G. spinigerum, commonlyfound in wild and domestic cats and dogs in India, China,Japan, and southeast Asia; G. hispidum, found in wild anddomestic pigs in Europe, Asia, and Australia; G. doloresi,found in wild boars; and G. nipponicum, found in weasels inJapan (15). Until the early 1980s, all cases of gnathostomiasisfound in humans in the areas of endemicity in Thailand, China,
and Japan were solely due to G. spinigerum. However, in theearly 1980s in Japan new cases appearing in urban areas werefound to be due to G. hispidum, with the infective larvae foundin loaches (small freshwater fish) (29).
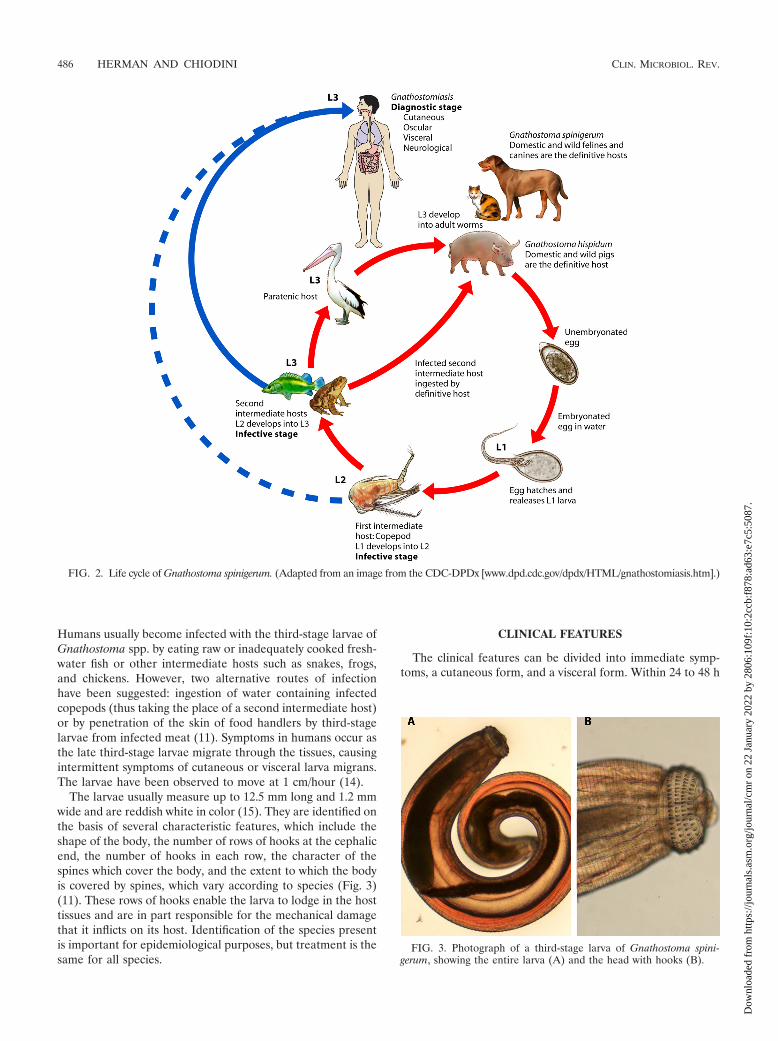
Humans are accidental hosts in which the parasite fails toreach sexual maturity. The definitive hosts are dogs, cats, ti-gers, leopards, and probably other fish-eating mammals, wherethe adult worm lives coiled up in the wall of the stomach,producing a tumor-like mass. In the definitive hosts the adultworm (which reaches 13 to 55 mm in length) releases eggs intothe stomach which are then passed in the feces. These embryo-nate in freshwater and hatch to release first-stage larvae afterabout 7 days, which are then ingested by the first intermediatehost, a water flea or copepod (usually a species of the genusCyclops), where they develop into second-stage larvae (Fig. 2).When infected Cyclops organisms are ingested by the secondintermediate hosts (fish, eels, frogs, birds, and reptiles), thesecond-stage larvae are freed in the intestine and develop intothird-stage larvae. These migrate through the tissues and en-cyst in the muscles of their transport hosts, where they remainas infectious larvae. When eaten by an appropriate definitivehost, such as cats and dogs, the larvae are freed once more inthe gastrointestinal tract, from where they migrate to the liverand abdominal cavity. After about 4 weeks they return to thestomach, invading the gastric wall, where they resemble a tu-mor, with an aperture that connects to the gastric lumenthrough which eggs may later be released. Here they grow intoadults to complete their life cycle, usually within about 6months. Eggs are released into the environment in the stool ofthe host about 8 to 12 months after initial ingestion of theinfective third-stage larvae by the definitive host (15, 41, 51).
FIG. 1. Map of countries with reported acquisition of gnathostomiasis.
VOL. 22, 2009 PARASITOLOGIC AND CLINICAL ASPECTS OF GNATHOSTOMIASIS 485
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/c
mr
on 2
2 Ja
nuar
y 20
22 b
y 28
06:1
09f:
10:2
ccb:
f878
:ad6
3:e7
c5:5
087.
Humans usually become infected with the third-stage larvae ofGnathostoma spp. by eating raw or inadequately cooked fresh-water fish or other intermediate hosts such as snakes, frogs,and chickens. However, two alternative routes of infectionhave been suggested: ingestion of water containing infectedcopepods (thus taking the place of a second intermediate host)or by penetration of the skin of food handlers by third-stagelarvae from infected meat (11). Symptoms in humans occur asthe late third-stage larvae migrate through the tissues, causingintermittent symptoms of cutaneous or visceral larva migrans.The larvae have been observed to move at 1 cm/hour (14).
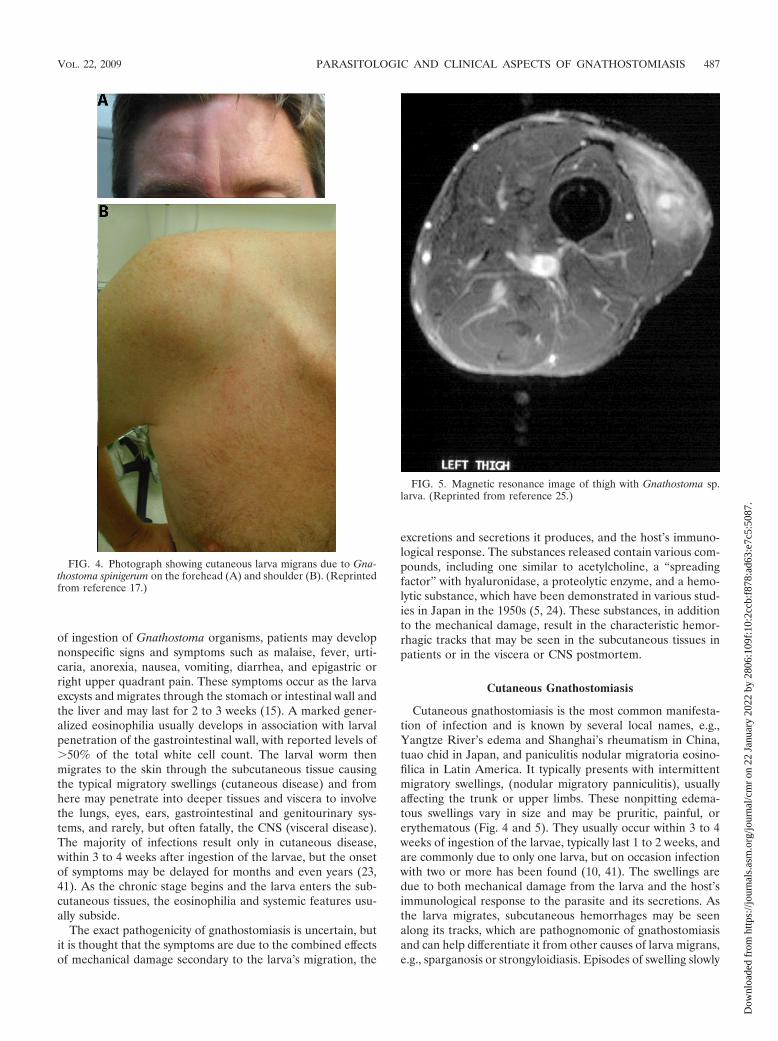
The larvae usually measure up to 12.5 mm long and 1.2 mmwide and are reddish white in color (15). They are identified onthe basis of several characteristic features, which include theshape of the body, the number of rows of hooks at the cephalicend, the number of hooks in each row, the character of thespines which cover the body, and the extent to which the bodyis covered by spines, which vary according to species (Fig. 3)(11). These rows of hooks enable the larva to lodge in the hosttissues and are in part responsible for the mechanical damagethat it inflicts on its host. Identification of the species presentis important for epidemiological purposes, but treatment is thesame for all species.
CLINICAL FEATURES
The clinical features can be divided into immediate symp-toms, a cutaneous form, and a visceral form. Within 24 to 48 h
FIG. 2. Life cycle of Gnathostoma spinigerum. (Adapted from an image from the CDC-DPDx [www.dpd.cdc.gov/dpdx/HTML/gnathostomiasis.htm].)
FIG. 3. Photograph of a third-stage larva of Gnathostoma spini-gerum, showing the entire larva (A) and the head with hooks (B).
486 HERMAN AND CHIODINI CLIN. MICROBIOL. REV.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/c
mr
on 2
2 Ja
nuar
y 20
22 b
y 28
06:1
09f:
10:2
ccb:
f878
:ad6
3:e7
c5:5
087.
of ingestion of Gnathostoma organisms, patients may developnonspecific signs and symptoms such as malaise, fever, urti-caria, anorexia, nausea, vomiting, diarrhea, and epigastric orright upper quadrant pain. These symptoms occur as the larvaexcysts and migrates through the stomach or intestinal wall andthe liver and may last for 2 to 3 weeks (15). A marked gener-alized eosinophilia usually develops in association with larvalpenetration of the gastrointestinal wall, with reported levels of�50% of the total white cell count. The larval worm thenmigrates to the skin through the subcutaneous tissue causingthe typical migratory swellings (cutaneous disease) and fromhere may penetrate into deeper tissues and viscera to involvethe lungs, eyes, ears, gastrointestinal and genitourinary sys-tems, and rarely, but often fatally, the CNS (visceral disease).The majority of infections result only in cutaneous disease,within 3 to 4 weeks after ingestion of the larvae, but the onsetof symptoms may be delayed for months and even years (23,41). As the chronic stage begins and the larva enters the sub-cutaneous tissues, the eosinophilia and systemic features usu-ally subside.
The exact pathogenicity of gnathostomiasis is uncertain, butit is thought that the symptoms are due to the combined effectsof mechanical damage secondary to the larva’s migration, the
excretions and secretions it produces, and the host’s immuno-logical response. The substances released contain various com-pounds, including one similar to acetylcholine, a “spreadingfactor” with hyaluronidase, a proteolytic enzyme, and a hemo-lytic substance, which have been demonstrated in various stud-ies in Japan in the 1950s (5, 24). These substances, in additionto the mechanical damage, result in the characteristic hemor-rhagic tracks that may be seen in the subcutaneous tissues inpatients or in the viscera or CNS postmortem.
Cutaneous Gnathostomiasis
Cutaneous gnathostomiasis is the most common manifesta-tion of infection and is known by several local names, e.g.,Yangtze River’s edema and Shanghai’s rheumatism in China,tuao chid in Japan, and paniculitis nodular migratoria eosino-filica in Latin America. It typically presents with intermittentmigratory swellings, (nodular migratory panniculitis), usuallyaffecting the trunk or upper limbs. These nonpitting edema-tous swellings vary in size and may be pruritic, painful, orerythematous (Fig. 4 and 5). They usually occur within 3 to 4weeks of ingestion of the larvae, typically last 1 to 2 weeks, andare commonly due to only one larva, but on occasion infectionwith two or more has been found (10, 41). The swellings aredue to both mechanical damage from the larva and the host’simmunological response to the parasite and its secretions. Asthe larva migrates, subcutaneous hemorrhages may be seenalong its tracks, which are pathognomonic of gnathostomiasisand can help differentiate it from other causes of larva migrans,e.g., sparganosis or strongyloidiasis. Episodes of swelling slowly
FIG. 4. Photograph showing cutaneous larva migrans due to Gna-thostoma spinigerum on the forehead (A) and shoulder (B). (Reprintedfrom reference 17.)
FIG. 5. Magnetic resonance image of thigh with Gnathostoma sp.larva. (Reprinted from reference 25.)
VOL. 22, 2009 PARASITOLOGIC AND CLINICAL ASPECTS OF GNATHOSTOMIASIS 487
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/c
mr
on 2
2 Ja
nuar
y 20
22 b
y 28
06:1
09f:
10:2
ccb:
f878
:ad6
3:e7
c5:5
087.

become less intense and shorter in duration, but in untreatedpatients symptoms may recur intermittently for up to 10 to 12years.
Other, less common manifestations of cutaneous gnathosto-miasis include a creeping eruption (which may be confusedwith cutaneous larva migrans), a skin abscess, or a nodule,which tend to occur when the larva is migrating more super-ficially (41). In these cases the larva can often be excised.Spontaneous extrusion of a larva from the subcutaneous tis-sues has also been described. If the migratory lesions are onthe face, there is a serious risk of CNS or ocular invasion.
Visceral Disease
The Gnathostoma larva is highly invasive and motile andtherefore can produce an extremely wide range of symptomsaffecting virtually any part of the body. In noncerebral diseasethe larvae may continue to cause intermittent symptoms untilthey die after about 12 years, if left untreated.
Pulmonary manifestations. Pulmonary symptoms that havebeen attributed to infection with Gnathostoma spp. includecough, pleuritic chest pain, heamoptysis, lobar consolidation orcollapse, pleural effusions, and pneumo- or hydropneumotho-rax (13, 27, 36, 41). In some cases expectoration of the larvahas led to resolution of the symptoms. Most patients have hadan accompanying eosinophilia, with a reported range of 30 to72%, and when a pleural effusion has been present it has beeneosinophilic in nature (41). Therefore, a triad of eosinophilia,subcutaneous swellings, and unexplained eosinophilic pleuraleffusion with a history of appropriate exposure risk should alertthe physician to a diagnosis of gnathostomiasis (15).
Gastrointestinal manifestations. Gastrointestinal manifes-tations are less common in humans but may present as sharpabdominal pains as the larva migrates through the liver andspleen or as a chronic mass in the right lower quadrant. Lesscommonly, there may be acute right iliac fossa pain with fevermimicking acute appendicitis or intestinal obstruction. Infec-tion has also been found as an incidental (and asymptomatic)finding at surgery for a different problem. Radiologically thefindings are of a thickened bowel wall with narrowing of thelumen (15). Histologically the lesions found at surgery areconsistent with eosinophilic granulomas, but macroscopicallythey resemble neoplastic lesions, which has led to inappropri-ate radical surgery. This can be avoided only by considerationof possible parasitic infection in the preoperative work-up ofsuch patients.
Genitourinary manifestations. Involvement of the genitouri-nary tract is uncommon, but hematuria and the passage of thelarva in the urine have been reported. Other symptoms attrib-uted to Gnathostoma spp. include profuse vaginal bleeding,cervicitis, balanitis, an adnexal mass, and hematospermia (15,36, 41).
Ocular. The eye is the only organ in which the larva may bevisualized, and therefore there are many more literature re-ports of ocular involvement than of involvement of other or-gans (15). Eye involvement has led to symptoms of uveitis(usually anterior), iritis, intraocular hemorrhage, glaucoma,retinal scarring, and detachment. The larva is usually be foundin the anterior chamber and may be recovered intact, but thereare a few reports of intravitreal localization (3, 4). The pres-
ence of eosinophilia is less likely in ocular disease because theeye is a privileged site, and it is usually mild if elevated at all(41).
Auricular manifestations. Various reports have described awide variety of manifestations, which include mastoiditis, sen-sorineural hearing loss, and extrusion of the larva from theexternal auditory canal, the soft palate, the cheek, the tip oftongue, and the tympanic membrane (15, 41).
CNS manifestations. Although gnathostomiasis was de-scribed in the 19th century, CNS involvement was proven onlyin the latter half of the 20th century, with the postmortemfinding of a gnathostoma larva in the cervical cord of a patientwith eosinophilic encephalomyelitis in 1967 (9). In the subse-quent year the parasite was found on the surface of the cere-bral hemisphere and attached to the choroid plexus of thelateral ventricle in two patients with fatal meningoencephalitis.There have been several case series of CNS disease, which hasincreased understanding of the pathophysiology (5, 38). Com-pared to other forms of disease, the CNS form of the infectioncarries the highest mortality, with reported rates of 8 to 25%,and 30% of survivors having long-term sequelae (5, 38, 41).However, these data are from the era before the use of al-bendazole and ivermectin.
The main features of CNS involvement are a radiculomyeli-tis, radiculomyeloencephalitis, eosinophilic meningitis, andsubarachnoid hemorrhage. The hallmark symptoms are anacute onset of excruciating radicular pain and/or headache(subarachnoid hemorrhage or eosinophilic meningitis), withsubsequent paralysis of the extremities and/or cranial nervepalsies. The typical clinical picture can be explained by themigratory pathway of the parasite, which gains entry to thespinal cord along nerve roots (cranial, cervical, thoracic, orlumbar), causing intense radicular pain (or headache in thecase of cranial nerve or cervical root involvement) which usu-ally lasts from 1 to 5 days (5). This initial pain is typicallyfollowed by a degree of paralysis ranging from weakness tocomplete paralysis of one to four limbs (the most commonbeing paraplegia of lower limbs) as the parasite ascends thespinal cord to the brain. Urinary retention is usual with radiculo-myelitis and radiculomyeloencephalitis. Cranial nerve palsiestend to occur after the onset of paralysis, and if multiple theysignify a poor prognosis. Cerebral involvement is usually indi-cated by a depressed consciousness level or coma, but inter-estingly, mental confusion does not tend to occur (5, 38).
In some cases different CNS symptoms may occur, or cur-rent ones may reappear after a quiescent period due to furthermigration of the larva to another location within the CNS. Thismost commonly occurs within the first 2 weeks of the onset ofthe initial neurological deficit but may be seen as early as 6 hor as late as 1 month.
The pathogenicity in the CNS is thought to be the same asthat elsewhere in the body, with direct mechanical injury caus-ing the most damage due to tearing with or without destructionof the nerve tissue and its vascular structures, as well as in-flammation and destruction of tissue due to toxin production.The hallmark signs of gnathostomiasis are hemorrhagic tracts,which have been well documented throughout the spinal cordand cerebral tissue postmortem (5, 24). Death occurs if vitalstructures in the brain stem are invaded, which may occurwithin 4 to 31 days following the onset of CNS symptoms, or if
488 HERMAN AND CHIODINI CLIN. MICROBIOL. REV.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/c
mr
on 2
2 Ja
nuar
y 20
22 b
y 28
06:1
09f:
10:2
ccb:
f878
:ad6
3:e7
c5:5
087.

the larva burrows through a cerebral arteriole, resulting inmassive subarachnoid hemorrhage (5). In Thailand 6% of sub-arachnoid hemorrhages in adults and 18% of those in childrenare due to gnathostomiasis (50).
The main differential diagnosis of CNS disease due to Gna-thostoma is infection with Angiostrongylus catonensis, anotherhighly prevalent parasite in southeast Asia. This may producea similar eosinophilic meningoencephalitis, but the acute nerveroot pain, signs of spinal cord compression, and hemorrhagicor xanthochromic spinal fluid seen in gnathostomiasis are ab-sent with Angiostrongylus infection (38). The Gnathostomalarva is more invasive than that of Angiostrongylus and there-fore produces more frequent focal neurological signs. In con-trast, the Angiostrongylus larva, which is considerably smaller(120 �m wide and 12 mm long) and usually multiple, morecommonly causes a meningoencephalitis, and although neuro-tropic, it is rarely fatal (21).
DIAGNOSIS
The triad of eosinophilia, migratory lesions, and obviousexposure risk are highly suggestive of the diagnosis of gnatho-stomiasis. Exposure risk must include residence in or travel toan area of endemicity and consumption of food that potentiallycontains the larval form of the parasite (raw or undercookedfish [in particular swamp eels, catfish, sleeper perch, bream,Nile tilapia, butterfish, loaches, or snake-headed fish], frogs,chickens, cats, or dogs). Clinically, the main differential diag-noses includes angiostrongyliasis, trichinosis, and cutaneouslarva migrans.
Before the advent of serology, the diagnosis was more oftenmade by the isolation of the larvae from the lesions theycaused, but this is often difficult in migratory skin lesions, isclearly not practical for visceral disease, and is no longer re-quired (Fig. 6).
Eosinophilia is frequently present during initial worm mi-
gration (as previously discussed), particularly in the skin orsubcutaneous tissues, but is not always present at other times,and its absence should not exclude the diagnosis. Eosinophiliaof the cerebrospinal fluid (CSF) is also highly supportive ofCNS disease, with reported levels of 5 to 94% and a total CSFwhite cell count of up to 500/mm3 (range, 20 to 1420/mm3),but may also be found with several other parasites, e.g.,Angiostrongylus cantonensis, Toxocara canis, Strongyloides ster-coralis, Ascaris lumbricoides, Paragonimus westermani, Fasciolahepatica, and Trichinella spiralis and with schistosomiasis,neurocystercercosis, and other infections such as coccidiodo-mycosis and aspergillus infection (5, 21). Noninfectious condi-tions involving the CNS should also be considered (e.g., lym-phoma, particularly Hodgkin’s) (40).
In the 1960s skin tests using intradermal injection of G.spinigerum antigen were developed in Japan, but these werelater shown to lack adequate sensitivity and specificity (26, 48).Scientists in Japan then went on to be the first to develop aserological test for the diagnosis, using crude somatic extract ofadult Gnathostoma doloresi worms found locally (23). How-ever, this was hampered by cross-reactivity with other locallyfound parasites, including Paragonimus westermani, Toxocaracanis, Anisakis, and Fasciola hepatica. Later it was found thatthis was a problem particular to the G. doloresi antigen butcould be overcome if the G. spinigerum antigen was used in-stead (1, 48).
Tests were improved by using antigen from the third-stagelarvae (L3) of G. spinigerum instead of the adult worm, butcross-reactivity remained a problem with other parasitic infec-tions. Furthermore, the L3 antigen was found to be highlycomplex, with over 20 components, some of which reacted withthe sera of healthy controls (32). Tapchaisri and colleaguesfound that a specific L3 antigen with a molecular mass of 24kDa had the greatest specificity and reacted only with gnatho-stomiasis sera and not with those from other parasitic infec-
FIG. 6. (A) Hematoxylin- and eosin-stained cross-section of a Gnathostoma organism taken from a subcutaneous nodule above the right breastof a patient, showing the esophagus. Note the presence of cuticular spines (arrow). (B) Another hematoxylin- and eosin-stained cross-section ofa Gnathostoma organism, taken from the same specimen as for panel A, showing the intestinal cells and characteristic large lateral chords (LC).(Panel A is from Diagnostix Pathology Laboratories LTD and the CDC-DPDx and panel B is from the CDC-DPDx [www.dpd.cdc.gov/dpdx/HTML/gnathostomiasis.htm].)
VOL. 22, 2009 PARASITOLOGIC AND CLINICAL ASPECTS OF GNATHOSTOMIASIS 489
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/c
mr
on 2
2 Ja
nuar
y 20
22 b
y 28
06:1
09f:
10:2
ccb:
f878
:ad6
3:e7
c5:5
087.

tions (49). This subsequently formed the basis of the immuno-blot and future trials on serodiagnosis (20).
An enzyme-linked immunosorbent assay (ELISA) for L3immunoglobulin G (IgG) antibody was also developed, but thesensitivity was poor, ranging from 59 to 87%, with a specificityof 79 to 96% (1, 22, 46). Nuchprayoon and colleagues thenshowed that by using IgG subclasses rather than total IgG, thesensitivity and specificity of the ELISA could be improved.This had been shown previously to improve the diagnosis forother parasitic infections such as ascariasis, leishmaniasis, andfilariasis (33). Their study showed that IgG2 had the leastcross-reactivity (particularly with Angiostrongylus, the main dif-ferential diagnosis) and had a specificity of 88% and positivepredictive value of 93%, whereas IgG1 had the highest sensi-tivity (98%) and negative predictive value (94%). With theexception of IgG2, cross-reactivity was found with An-giostrongylus cantonensis, hookworm, Strongyloides stercoralis,and Opisthorchis viverrini. They concluded that IgG1 antibodyshould be used as a screening test for those with presumptivegnathostomiasis and that IgG2 antibody could be used to con-firm the diagnosis. A further extensive retrospective study ofparasitic and nonparasitic diseases carried out over 7 yearsconfirmed these findings of a lack of cross-reactivity (P. De-kumyoy, personal communication).
Currently a number of serological tests are available for thediagnosis of gnathostomiasis. The most widely used in Europeis an immunoblot to detect the specific 24-kDa band consid-ered diagnostic of gnathostomiasis. This is carried out at var-ious places, with the United Kingdom serology being sent tothe Hospital for Tropical Diseases, Mahidol University,Bangkok, Thailand. The Swiss Tropical Institute (Basel, Swit-zerland), also performs serological testing. However, currentlythere are no commercial reagents available.
Specific mention should be made of the diagnosis of CNSdisease. The CSF typically shows an eosinophilia, with elevatedopening pressure and protein level. The use of CSF serology isnot routine, and there are no published data on its utility in thiscontext. Magnetic resonance imaging has also been useful indemonstrating the migratory lesions within the spinal cord (7,43). The parasite produces high-signal intensity on T2 weight-ing and contrast enhancement on T1 weighting, which if staticcould be attributed to various vascular, neoplastic, inflamma-tory, or infectious causes. However, the migratory nature ofsuch lesions would be consistent with the well-documentedpathway of the Gnathostoma larva. Multiple sclerosis wouldalso produce intermittent lesions on magnetic resonance im-aging, but this can be excluded by the absence of CSF oligo-clonal bands.
TREATMENT
For many years there was no effective treatment for gnatho-stomiasis, and surgical excision of the larvae remained the onlyeffective management. Various drugs were tried both in animalmodels and in humans without success, including thiabenda-zole, praziquantel, metronidazole, diethylcarbamazine, andquinine (18).
However, studies with albendazole in animal models werepromising, and a trial by Kraivichian et al. in 1992 (n � 112)confirmed its efficacy in humans, with cure rates of �90% at a
dose of 400 mg twice a day for 21 days (18, 30). Albendazole isa broad-spectrum benzmidazole antihelminthic which hasproven efficacy against intestinal helminths and also extraint-estinal helminthic infections such as opisthorchiasis, hydatiddisease, and cutaneous larva migrans. The principal mode ofaction for albendazole is by its inhibitory effect on tubulinpolymerization, with resultant loss of cytoplasmic microtu-bules. The loss of these impairs glucose uptake, with subse-quent depletion of the organism’s glycogen stores resulting inimmobilization and death. Albendazole is poorly absorbedfrom the gastrointestinal tract (although it is absorbed betterthan mebendazole) and is rapidly converted in the liver to itsactive primary metabolite, albendazole sulfoxide, prior toreaching the systemic circulation. Oral bioavailability appearsto be enhanced when albendazole is coadministered with afatty meal (2). The drug has been found to be safe and rela-tively well tolerated, with the main side effects being nausea,dizziness, headache, and occasionally abnormal liver functiontests and a transient leukopenia. Additionally, albendazole ap-pears to stimulate the outward migration of the larva, thusmaking it more accessible and possibly amenable to excision(19, 47). The reason for this migration is unknown, but it tendsto occur 7 to 14 days after commencing treatment.
Ivermectin has also been investigated for use in the treat-ment of gnathostomiasis, and it seems that its efficacy is similarto that reported for albendazole (30). Ivermectin binds selec-tively with high affinity to glutamate-gated chloride ion chan-nels which occur in invertebrate nerve and muscle cells. Thisleads to an increase in the permeability of the cell membraneto chloride ions with hyperpolarization of the nerve or musclecell, resulting in paralysis and death of the parasite (34). Iver-mectin may also interact with other ligand-gated chloride chan-nels, such as those gated by the neurotransmitter gamma-aminobutyric acid. It is metabolized in the liver and has fewside effects, the main one being dizziness, and is thereforegenerally well tolerated. Ivermectin has been shown to beeffective as either a stat dose of 0.2 mg/kg or as doses of 0.2mg/kg on two consecutive days, and therefore adherence is nota problem (31). The studies involving ivermectin have hadfairly small sample sizes (n � 17 to 21), and therefore itsevaluation with a larger prospective study is needed. Of note isthat a potential issue of flaring of disease was found in a studyby Kraivichian et al., which showed that those in the ivermectingroup experienced an exacerbation of cutaneous symptomscompared with those in the albendazole group (19). This couldtheoretically be a serious problem for visceral disease, in par-ticular ocular and CNS disease, although no such occurrenceshave been reported. This raises the issue of steroid use, whichfor neurocystercercosis is used to prevent inflammation in siteswhich could potentially be hazardous. Theoretically this ratio-nale for use could be applied to CNS or ocular gnathostomi-asis; however, data are limited, and the only study to examinethis (n � 162) showed no definite benefit in those who receivedoral or intravenous steroid treatment (38).
Initial treatment is not always successful, and second coursesof treatment have been needed in some cases. Either albenda-zole or ivermectin may be used in sequence in such patients,and both have been used with successful outcomes for initialtreatment failures (8, 25). However in regions of endemicity itmay be difficult to differentiate between treatment failure and
490 HERMAN AND CHIODINI CLIN. MICROBIOL. REV.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/c
mr
on 2
2 Ja
nuar
y 20
22 b
y 28
06:1
09f:
10:2
ccb:
f878
:ad6
3:e7
c5:5
087.

reinfection. A recent series reported by Strady et al., con-ducted with returning travelers outside areas of endemicity,indicated that initial relapse occurred up to 7 months aftertreatment, and the maximum period between two relapses was15 months, with the latter occurring in one patient with CNSdisease (45). A pragmatic approach would be that if the patientwas asymptomatic after 12 months of treatment, this would besufficient evidence of cure, particularly if supported by a res-olution of any eosinophilia and a decrease in ELISA levels. Inthe event of relapse, a new 12-month follow-up period shouldbe commenced.
Future trials would be useful to investigate the use of com-bined treatment with both albendazole and ivermectin and todetermine whether relapse rates are lower with combinationdrugs than with monotherapy.
PREVENTION
Eradication of the organism is unlikely given its global dis-tribution and expanding culinary tastes for exotic foods in theWest. Therefore, control will be achieved only through educa-tion campaigns to raise public awareness (22). Adequate cook-ing is the best way to ensure that the larvae are killed, althoughfreezing infected meat to �20°C for 3 to 5 days is also effective.However, the common practice in Mexico of marinating freshfish in lime juice is ineffective, and the organism has beenfound to be viable even after 5 days of immersion in lime juice(39). Public health education is essential to change the eatinghabits of people in areas with high levels of endemicity, andtravelers need to be aware of the potential consequences ofeating local delicacies. The large variety and wide distributionof animals that are intermediate hosts make it impossible toeliminate the parasite, and therefore appropriate cookingmethods and avoidance of raw or undercooked freshwater fishare the only measures that can be taken. However, while trav-elers continue to seek the exotic and remote, gnathostomiasiswill be seen with increasing frequency in the West and otherregions where it is not endemic, and it should be consideredanother emerging imported disease of which physicians shouldbe aware.
ACKNOWLEDGMENTS
We thank Paron Dekumyoy for helpful discussion and Julie Watsonand Patricia Lowe for use of photographic images.
Peter Chiodini is supported by the UCL Hospitals ComprehensiveBiomedical Research Centre Infection Theme.
REFERENCES
1. Anantaphruti, M. T. 1989. ELISA for diagnosis of gnathostomiasis usingantigens from Gnathostoma doloresi and G. spinigerum. Southeast Asian J.Trop. Med. Public Health 20:297–304.
2. Barrowman, M. M., S. E. Marriner, and J. A. Bogan. 1984. The binding andsubsequent inhibition of tubulin polymerization in Ascaris suum (in vitro) bybenzimidazole anthelmintics. Biochem. Pharmacol. 33:3037–3040.
3. Bhattacharjee, H., D. Das, and J. Medhi. 2007. Intravitreal gnathostomiasisand review of literature. Retina 27:67–73.
4. Biswas, J., L. Gopal, T. Sharma, and S. S. Badrinath. 1994. IntraocularGnathostoma spinigerum. Clinicopathologic study of two cases with reviewof literature. Retina 14:438–444.
5. Boongird, P., P. Phuapradit, N. Siridej, T. Chirachariyavej, S. Chuahirun,and A. Vejjajiva. 1977. Neurological manifestations of gnathostomiasis J.Neurol. Sci. 31:279–291.
6. Chai, J. Y., E. T. Han, E. H. Shin, J. H. Park, J. P. Chu, M. Hirota, F.Nakamura-Uchiyama, and Y. Nawa. 2003. An outbreak of gnathostomiasisamong Korean emigrants in Myanmar. Am. J. Trop. Med. Hyg. 69:67–73.
7. Chandenier, J., J. Husson, S. Canaple, C. Gondry-Jouet, P. Dekumyoy, M.Danis, G. Riveau, C. Hennequin, A. Rosa, and C. P. Raccurt. 2001. Medul-lary gnathostomiasis in a white patient: use of immunodiagnosis and mag-netic resonance imaging. Clin. Infect. Dis. 32:E154–E157.
8. Chappuis, F., T. Farinelli, and L. Loutan. 2001. Ivermectin treatment of atraveler who returned from Peru with cutaneous gnathostomiasis. Clin. In-fect. Dis. 33:E17–E19.
9. Chitanondh, H., and L. Rosen. 1967. Fatal eosinophilic encephalomyelitiscaused by the nematode Gnathostoma spinigerum. Am. J. Trop. Med. Hyg.16:638–645.
10. Daengsvang, S. 1949. Human gnathostomiasis in Siam with reference to themethod of prevention. J. Parasitol. 35:116–121.
11. Daengsvang, S. 1981. Gnathostomiasis in Southeast Asia. Southeast Asian J.Trop. Med. Public Health. 12:319–332.
12. Diaz-Camacho, S. P., M. Zazueta-Ramos, E. Ponce-Torrecillas, I. Osuna-Ramirez, R. Castro-Velasquez, A. Flores-Gaxiola, J. Baquera Heredia, K.Willms, H. Akahane, K. Ogata, and Y. Nawa. 1998. Clinical manifestationsand immunodiagnosis of gnathostomasis in Culican, Mexico. Am. J. Trop.Med. Hyg. 59:908–915.
13. Dow, C., P. L. Chiodini, A. J. Haines, and S. M. Michelson. 1988. Humangnathostomiasis. J. Infect. 17:147–149.
14. Feinstein, R. J., and J. Rodriguez-Valdes. 1984. Gnathostomiasis or larvamigrans profundus. J. Am. Acad. Dermatol. 11:738–740.
15. Guitierrez, Y. 2000. Diagnostic pathology of parasitic infections with clinicalcorrelations, 2nd ed. Oxford University Press, Oxford, United Kingdom.
16. Hale, D. C., L. Blumberg, and J. Frean. 2003. Case report: gnathostomiasisin two travellers to Zambia. Am. J. Trop. Med. Hyg. 68:707–709.
17. Herman, J. S., E. Wall, C. Van Tulleken, P. Godfrey-Faussett, R. L. Bailey,and P. L. Chiodini. 2009. Emergence of gnathostomiasis in Botswana inBritish tourists. Emerg. Infect. Dis. 15:594–597.
18. Kraivichian, P., M. Kulkumthorn, P. Yingyourd, P. Akarabovorn, and C. C.Paireepai. 1992. Albendazole for the treatment of human gnathostomiasis.Trans. R. Soc. Trop. Med. Hyg. 86:418–421.
19. Kraivichian, K., S. Nuchprayoon, P. Sitichalernchai, W. Chaicumpa, and S.Yentakam. 2004. Treatment of cutaneous gnathostomiasis with ivermectin.Am. J. Trop. Med. Hyg. 71:623–628.
20. Laummaunwai, P., K. Sawanyawisuth, P. M. Intapan, V. Chotmongkol, C.Wongkham, and W. Maleewong. 2007. Evaluation of human IgG class andsubclass antibodies to a 24 kDa antigenic component of Gnathostoma spini-gerum for the serodiagnosis of gnathostomiasis. Parasitol. Res. 101:703–708.
21. Lucas, S., J. Bell, and L. Chimelli. 2008. Chapter 19, p. 1476–1477. In S.Love, D. N. Louis, and D. W. Ellison (ed.), Greenfield’s neuropathology, 8thed. Oxford University Press, Oxford, United Kingdom.
22. Maleewong, W., N. Morakote, W. Thamasonthi, K. Charuchinda, S. Tesana,and C. Khamboonruang. 1988. Serodiagnosis of human gnathostomiasis.Southeast Asian J. Trop. Med. Public Health 19:201–205.
23. McCarthy, J., and T. A. Moore. 2000. Emerging helminth zoonoses Int. J.Parasitol. 30:1351–1360.
24. Miyazaki, I. 1960. On the genus Gnathostoma and human gnathostomiasis,with special reference to Japan. Exp. Parasitol. 9:338–370.
25. Moore, D. A., J. McCroddan, P. Dekumyoy, and P. L. Chiodini. 2003. Gna-thostomiasis: an emerging imported disease. Emerg. Infect. Dis. 9:647–650.
26. Morisita, T., M. Kobayashi, K. Nagase, H. Iwanga, and M. Sumi. 1969.Nonspecificity of intradermal test with Gnathostoma antigen. Jpn. J. Parasi-tol. 18:120.
27. Nagler, A., S. Pollack, G. Hassoun, H. Kerner, D. Barzilai, and J. Lengy.1983. Human pleuropulmonary gnathostomiasis: a case report from Israel.Isr. J. Med. Sci. 19:834–837.
28. Nawa, Y., C. Hatz, and J. Blum. 2005. 22 Sushi delights and parasites: the riskof fishborne and foodborne parasitic zoonoses in Asia. Clin. Infect. Dis.41:1297–1303.
29. Nawa, Y. 1991. Historical review and current status of gnathostomiasis inAsia. Southeast Asian J. Trop. Med. Public Health 22(Suppl.):217–219.
30. Nontasut, P., V. Bussaratid, S. Chullawichit, N. Charoensook, and K.Visetsuk. 2000. Comparison of ivermectin and albendazole treatment forgnathostomiasis. Southeast Asian J. Trop. Med. Public Health 31:374–377.
31. Nontasut, P., B. A. Claesson, P. Dekumyoy, W. Pakdee, and S. Chullawichit.2005. Double-dose ivermectin vs albendazole for the treatment of gnathos-tomiasis. Southeast Asian J. Trop. Med. Public Health. 36:650–652.
32. Nopparatana, C., P. Tapchaisri, P. Setasubun, W. Chaicumpa, and P.Dekumyoy. 1988. Antibody responses in human gnathostomiasis. SoutheastAsian J. Trop. Med. Public Health 19:219–224.
33. Nuchprayoon, S., V. Sanprasert, M. Suntravat, K. Kraivichian, and W.Saksirisampant. 2003. Study of specific IgG subclass antibodies for diagnosisof Gnathostoma spinigerum. Parasitol. Res. 91:137–143.
34. Ottesen, E. A., and W. C. Campbell. 1994. Ivermectin in human medicine. J.Antimicrob. Chemother. 34:195–203.
35. Owen, R. 1836. Gnathostoma spinigerum n.sp. Proc. Zool. Soc. (London)4:123–126.
36. Parola, P., G. Bordmann, P. Brouqui, and J. Delmont. 2004. Eosinophilicpleural effusion in gnathostomiasis Emerg. Infect. Dis. 10:1690–1691.
VOL. 22, 2009 PARASITOLOGIC AND CLINICAL ASPECTS OF GNATHOSTOMIASIS 491
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/c
mr
on 2
2 Ja
nuar
y 20
22 b
y 28
06:1
09f:
10:2
ccb:
f878
:ad6
3:e7
c5:5
087.

37. Prommas, C., and S. Daensgsvang. 1936. Further report of a study of the thelife cycle of Gnathostoma spinigerum. J. Parasitol. 22:180–186.
38. Punyagupta, S., T. Bunnag, and P. Juttijudata. 1990. Eosinophilic meningitisin Thailand. Clinical and epidemiological characteristics of 162 patients withmyeloencephalitis probably caused by Gnathostoma spinigerum. J. Neurol.Sci. 96:241–256.
39. Rojas-Molina, N., S. Pedraza-Sanchez, B. Torres-Bibiano, H. Meza-Mar-tinez, and A. Escobar-Guiterrez. 1999. Gnathostomiasis, an emerging food-bourne zoonotic disease in Acapulco, Mexico. Emerg. Infect. Dis. 5:264–266.
40. Roper, A. H., and R. H. Brown (ed.). 2005. Adams and Victors principles inneurology, 8th ed. McGraw-Hill, Columbus, OH.
41. Rusnak, J. M., and D. R. Lucey. 1993. Clinical gnathostomiasis: case reportand review of the English-language literature Clin. Infect. Dis. 16:33–50.
42. Ryan, E. T., M. E. Wilson, and K. C. Kain. 2002. Illness after internationaltravel. N. Engl. J. Med. 347:505–516.
43. Sawanyawisuth, K., S. Tiamkao, J. Kanpittaya, P. Dekumyoy, and S. Jitpi-molmard. 2004. MR imaging findings in cerebrospinal gnathostomiasis.Am. J. Neuroradiol. 25:446–449.
44. Steffen, R., C. deBarnardis, and A. Banos. 2003. Travel epidemiology—aglobal perspective. Int. J. Antimicob Agents 21:89–95.
45. Strady, C., P. Dekumyoy, M. Clement-Rigolet, M. Danis, F. Bricaire, and E.
Caumes. 2009. Long-term follow-up of imported gnathostomiasis shows fre-quent treatment failure. Am. J. Trop. Med. Hyg. 80:33–35.
46. Suntharasamai, P., V. Desakorn, S. Migasena, D. Bunnag, and T. Harina-suta. 1985. ELISA for immunodiagnosis of human gnathostomiasis. South-east Asian J. Trop. Med. Public Health 16:274–279.
47. Suntharasamai, P., M. Riganti, S. Chittamas, and V. Desakorn. 1992.Albendazole stimulatesoutward migration of Gnathostoma spinigerum tothe dermis in man. Southeast Asian J. Trop. Med. Public Health 23:716–722.
48. Tada, I., K. Kasashima, K. Nishimuta, and M. Miyahara. 1966. Intradermalreaction with Gnathostoma spinigerum antigen. Jpn. J. Parasitol. 15:256.
49. Tapchaisri, P., C. Nopparatana, W. Chaicumpa, and P. Setasuban. 1991.Specific antigen of Gnathostoma spinigerum for immunodiagnosis of humangnathostomiasis. Int. J. Parasitol. 21:315–319.
50. Visudhiphan, P., S. Chiemchanya, and R. Somburanasim. 1980. Causes ofspontaneous sub-arachnoid haemorrhage in Thai infants and children.J. Neurosurg. 53:185–187.
51. Yoshimura, K. 1998. Chapter 34, p. 651–659. In L. Collier, A. Balows, and M.Sussman (ed.), Topley and Wilson’s microbiology and microbial infections,9th ed. Hodder Arnold, London, United Kingdom.
Joanna Herman is a specialist registrar inInfectious Diseases and Tropical Medicineat the Hospital for Tropical Diseases, Lon-don. She has an M.Sc. in CommunicableDisease Epidemiology from The LondonSchool of Hygiene and Tropical Medicine.She has previously undertaken research inhuman immunodeficiency virus medicine.Her current research interest is in clinicalparasitology.
Peter L. Chiodini read Zoology at King’sCollege London and earned his Ph.D. inParasitology at the Wellcome ResearchLaboratories. He then studied Medicine inLondon before undergoing specialist train-ing in Communicable Diseases. He is Con-sultant Parasitologist at the Hospital forTropical Diseases, Honorary Professor atthe London School of Hygiene & TropicalMedicine, and Director of the UK HealthProtection Agency (HPA) Malaria Refer-ence Laboratory and the HPA Parasitology Reference Laboratory. Hisresearch interests include new diagnostic methods for parasitic infec-tions, malaria, and hydatid disease.
492 HERMAN AND CHIODINI CLIN. MICROBIOL. REV.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/c
mr
on 2
2 Ja
nuar
y 20
22 b
y 28
06:1
09f:
10:2
ccb:
f878
:ad6
3:e7
c5:5
087.
Related Documents











