Glomerular Diseases In Pediatrics

Glomerular Diseases In Pediatrics. Glomerular diseases Tubulointerstitial Vascular disease.
Dec 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Glomerular Diseases
In Pediatrics

• Glomerular diseases • Tubulointerstitial • Vascular disease

Glomerular Diseases
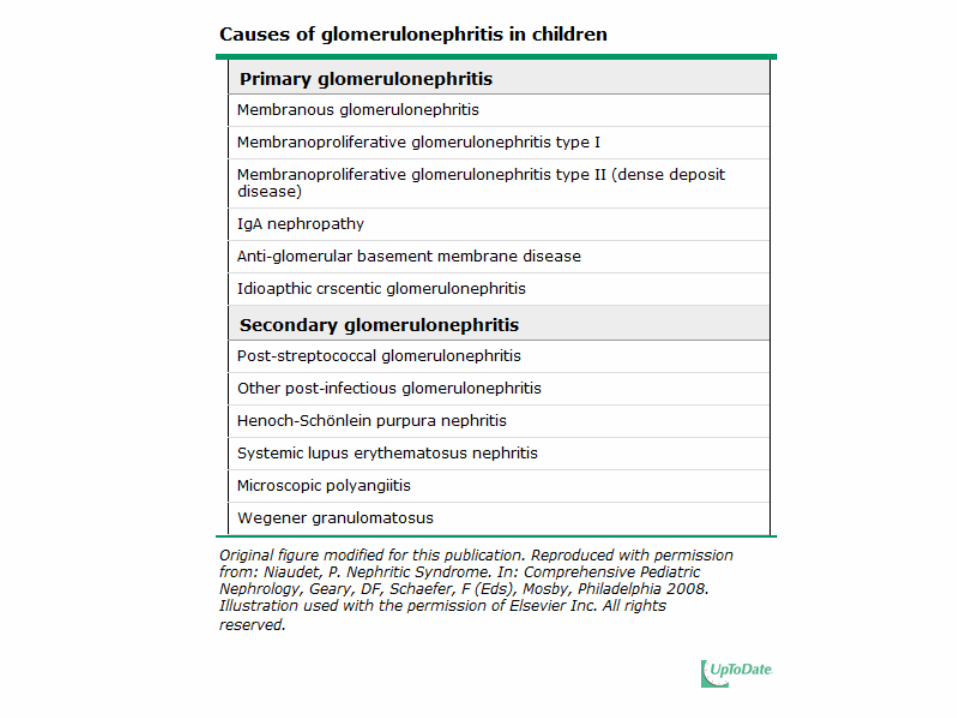
• Primary (renal disease alone) • Secondary (due to systemic autoimmune
disorders, vasculitis, or infection, drugs)

CLINICAL PATTERNS OF GLOMERULAR DISEASE
• Many causes of glomerular disease.• Urine sediment and the degree of proteinuria:
• Two clinical patterns:• Nephrotic • Nephritic

Nephritic Pattern
Active urine sediment:• Hematuria: Presence of RBC (Some acanthocytes)• Occasionally WBC• ± RBC cast • ± mixed cellular casts (Granular , RBC and other cellular casts)• variable degrees of proteinuria, ranging from normal protein
excretion to the nephrotic range (ie, both nephritic and nephrotic).
• Acanthocytes are considered virtually diagnostic of glomerular hematuria



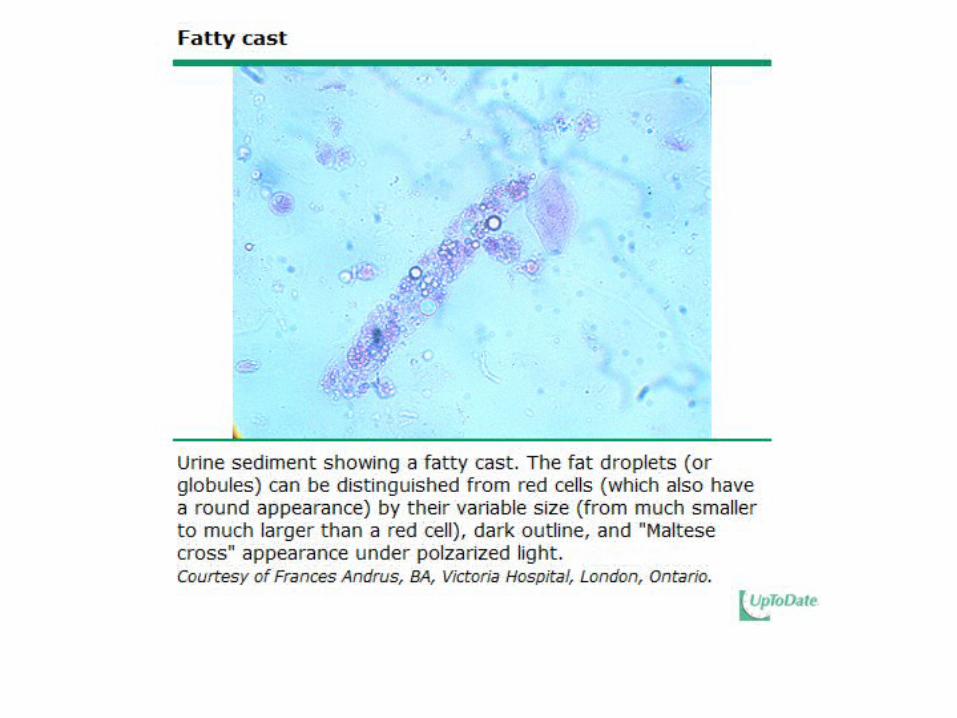
Nephrotic Pattern
• Proteinuria that is usually above 3.5 g/day • lipiduria• fatty casts • but few cells or few casts. • Some microscopic hematuria• Red cell casts are usually not seen (when
present, may result from a concurrent glomerulonephritis as has been described in diabetic nephropathy.)

INITIAL EVALUATION• Clinical features
• Urinalysis and urinary protein
• Renal function
• Patients with Glomerulonephritis
• Patients with Nephrotic Syndrome
Classification of Glumelular Diseases
• Mild glomerulonephritis• Moderate to severe
glomerulonephritis• Nephrotic syndrome
without a nephritic sediment

Mild glomerulonephritis
• Mild glomerulonephritis is defined as a nephritic sediment in patients who have a normal or near normal GFR and do not have the nephrotic syndrome.
• Less than 15 years • 15 to 40 years • Greater than 40 years


Moderate to severe glomerulonephritis
• Moderate to severe glomerulonephritis is defined as a nephritic sediment in patients who have a reduced GFR and/or nephrotic syndrome.
• Less than 15 years • 15 to 40 • Greater than 40 years


Nephrotic syndrome without a nephritic sediment
• Patients with nephrotic syndrome without a nephritic sediment do not have red cell casts but may have mild hematuria.
• Less than 15 • 15 to 40 years • Greater than 40 years


Clinical Features• Glomerulonephritis • edema, • hypertension, • reddish brown to brown
colored urine, • and a rising serum
creatinine.
• Nephrotic syndrome
• usually present only with edema.
• In severe cases:• anasarca with ascites, • and respiratory distress
caused by pleural effusions.

Diagnosis
• When approaching a patient with apparent glomerular disease,
• the urinalysis, urinary patterns (nephrotic and nephritic)• the degree of proteinuria• the estimated GFR• and patient age • help to identify the most likely causes; allow the
differential diagnosis to be substantially narrowed • However, confirmation by renal biopsy is usually
required.

Nephrotic Syndrome

Nephrotic Syndrome
• 4 clinical features, but the first two are used diagnostically: • Nephrotic range proteinuria — Urinary protein excretion
greater than 50 mg/kg per day
• Hypoalbuminemia — Serum albumin concentration less than 3 g/dL (30 g/L)
• Edema
• Hyperlipidemia

Nephrotic Syndrome…
• Nephrotic syndrome in children is classified into three categories:
• Primary nephrotic syndrome, which refers to nephrotic syndrome in the absence of an identifiable systemic disease
• Secondary nephrotic syndrome, which refers to nephrotic syndrome in the presence of an identifiable systemic disease.
• Congenital and infantile nephrotic syndrome.

Nephrotic Syndrome…
• Idiopathic nephrotic syndrome • The most common form of childhood
nephrotic syndrome:
• Representing more than 90 % of cases between 1 -10 years of age
• and 50 % >10 years of age.

Nephrotic Syndrome…• Minimal change disease (MCD) is the most commonly seen
histopathology of childhood nephrotic syndrome; renal biopsy:
• Minimal change disease (MCD) — 77 percent• Membranoproliferative glomerulonephritis (MPGN) — 8 percent• Focal segmental glomerulosclerosis (FSGS) — 7 percent• Proliferative glomerulonephritis — 2 percent• Mesangial proliferation — 2 percent• Focal and global glomerulosclerosis — 2 percent• Membranous glomerulonephropathy — 2 percent

Nephrotic Syndrome…
Treatment:
• Major Treatment• Treatment of Complications

Nephrotic Syndrome…
• The vast majority of patients with MCD (>90 percent) respond to steroid therapy.
• MCD can be clinically differentiated from those with other causes of nephrotic syndrome.

• Clinical findings at presentation accurately differentiated children with MCD from those with other glomerular pathology:
• Age younger than six years of age• Absence of hypertension• Absence of hematuria • Normal complement levels• Normal renal function
• Based upon these observations, an initial trial of steroid therapy is generally administered to children who are likely to have MCD based upon clinical diagnosis, thereby avoiding renal biopsy.
• Steroid-responsive nephrotic syndrome:• The majority (>90%) of children with idiopathic nephrotic syndrome are
steroid-responsive (also referred to as steroid-sensitive nephrotic syndrome).
• In these patients, the most likely histologic lesion is MCD, although some patients with FSGS will also respond to steroid therapy. Patients who are steroid-responsive have a favorable long-term outcome with a very low risk of chronic renal disease.
• Steroid-resistant nephrotic syndrome :• Approximately 20 percent of all children with idiopathic nephrotic
syndrome will not respond to steroid therapy. The response rate is better in younger children, who are much more likely to have MCD. (Renal biopsy)
• Time to response
• Most patients who respond to steroid therapy will do so within the first four weeks of therapy

• Initial therapy: Initial prednisone therapy of 2 mg/kg per day for six weeks, followed by alternate day prednisone of 1.5 mg/kg for an additional six weeks.
• First relapse/Infrequent relapse: Prednisone therapy of 2 mg/kg per day until the urine protein tests are negative or trace for three consecutive days, followed by alternate day prednisone of 1.5 mg/kg for four weeks.
• Frequent relapses: oral cyclophosphamide, cyclosporine, and mycophenolate mofetil
• Steroid-dependent disease• Steroid-resistant disease

Symptomatic management of nephrotic syndrome in children
Complications• Edema• Hypercoagulability • Hypoalbuminemia• Increased risk of infections• Hyperlipidemia• Hypertension

EDEMA• Edema increases gradually and becomes detectable
when fluid retention exceeds 3 to 5 percent of body weight.
• Typically, periorbital edema is noted first and is often misdiagnosed as a manifestation of allergy.
• The edema can become generalized and massive (anasarca) resulting in peripheral edema, ascites, umbilical or inguinal hernias, scrotal or vulva swelling, and/or pleural effusions.


EDEMA…
• Salt restriction • Diuretics• Because of the potential for serious complications,
diuretic management should be supervised by a nephrologist who has expertise in treating children with NS.
• Furosemide and albumin — Patients with anasarca (generalized and massive edema) may be treated with furosemide (1 to 2 mg/kg per dose) in combination with albumin (0.5 to 1 g/kg infused over four hours).

EDEMA…
• Despite the marked increase in extracellular fluid volume, some children with nephrotic syndrome, primarily those with MCD, present with or develop signs of a decrease in effective circulating volume, such as tachycardia, peripheral vasoconstriction, oliguria, decreased glomerular filtration rate, elevation of plasma renin aldosterone, and norepinephrine.
• In such children, a further insult such as diuretic therapy, sepsis, or diarrhea can lead to hypotension and rarely shock.

EDEMA…
• Albumin raises the intravascular oncotic pressure and thereby protects the intravascular compartment against volume contraction.
• Albumin infusion also increases protein-binding of furosemide, which improves the rate of delivery to the kidney resulting in increased renal salt excretion.

EDEMA…
• Fluid restriction
• Although there is debate on the role of fluid restriction, initial restriction of fluid intake to an equivalent volume of the patient's insensible losses plus his/her urine output will result in stabilizing the patient's weight without further accumulation of edema.

Hypercoagulability • Nephrotic patients with severe hypoalbuminemia are at risk for thromboembolic
complications.
• Preventative measures include mobilization, avoidance of hemoconcentration resulting from hypovolemia, and early treatment of sepsis or volume depletion.
• Most clinicians do not give prophylactic warfarin therapy initially.
• However, a few will initially treat high-risk patients with albumin concentration of less than 2 g/dL (20 g/L), a fibrinogen level of more than 6 g/L, or an antithrombin III level less than 70 percent of normal.
• Alternatively, high-risk patients can be treated with low-dose aspirin or dipyridamole, although there are no controlled trials that demonstrate their efficacy in thrombus prevention in children with NS.

Hypercoagulability…
• Heparin is given if thrombi do occur. However, the dose necessary to obtain a therapeutic effect is often greater than normal because of decreased antithrombin III, a cofactor required for heparin activity.
• In patients with previous thromboembolic complications, start treatment anticoagulation therapy if the patient remains nephrotic, which places them at continued risk for thrombosis.

Infections
• Bacterial — Nephrotic children are at increased risk of developing infection (eg, peritonitis, pneumonia, and sepsis) due to encapsulated bacteria, in part due to reduced serum concentrations of immunoglobulin, decreased cellular immunity, and the administration of immunosuppressive therapy. The most common agent is streptococcus pneumoniae followed by Escherichia coli.
• Varicella

Hyperlipidemia• Persistent hyperlipidemia is a risk factor for atherosclerosis and may play a
role in the progression of chronic renal failure.
• The lipid abnormalities induced by the NS reverse with remission.
• The optimal treatment of hyperlipidemia in children with persistent NS is unknown.
• In children with NS, statin therapy based on limited short-term observational data is effective and safe in reducing total and LDL cholesterol, and triglyceride levels.
• Nevertheless, statins should be used with caution until controlled studies are performed.

Hyperlipidemia…
• Based on evidence as well as data on the benefit of statin therapy in children with familial hypercholesterolemia,
• Treat children who remain persistently nephrotic and have hyperlipidemia with statin therapy.
• LDL apheresis with steroid therapy has been proposed in patients with hyperlipidemia and refractory nephritic syndrome.

Hypertension• Children with NS and persistent hypertension are more likely to have
chronic kidney disease with poor outcome.
• As a result, in patients with hypertension, ACE or ARBs are the preferred anti-hypertensive agents because of their potential additive antiproteinuric benefit and ability to slow progression of renal impairment.
• The maximal anti-proteinuric effect is observed after four weeks ;
• the antiproteinuric effect can be increased by low salt diet and/or diuretics .
• Other antihypertensive agents that have been used in children with NS include beta-blockers and calcium channel blockers.

Glomerulonephritis

INTRODUCTION
• Glomerulonephritis (GN) generally presents as a constellation of findings that includes hematuria, edema, and often hypertension.
• GN is caused by a number of disorders that are
all characterized by glomerular injury + inflammation.
• In some cases, GN may progress to renal failure.

ETIOLOGIC CLASSIFICATION
• Because the differential diagnosis for GN is broad, using a classification schema is helpful to narrow the causes of childhood GN in a systematic manner. The etiology of glomerulonephritis can be classified by the following methods:
• Clinical presentation• Histopathology
• The preferred etiologic approach is to use the clinical presentation schema because the histopathologic method requires a biopsy sample.

Classification of glomerulonephritis
• Acute glomerulonephritis• Rapidly progressive
glomerulonephritis• Recurrent macroscopic
hematuria• Chronic glomerulonephritis

Acute GN
Acute glomerulonephritis (GN) typically presents as:
Sudden onset of hematuria (either gross or
microscopic) ± proteinuria, decreased GFR, and retention of sodium and water, which usually results in an elevated blood
pressure and edema.

• In children, the most common cause of acute GN is poststreptococcal GN.
• Acute nephritis also has been associated with other infectious agents .
• Other causes of acute GN include secondary GN (eg, Henoch-Schönlein purpura [HSP], nephritis associated with subacute bacterial endocarditis, and shunt nephritis.



Poststreptococcal glomerulonephritis in children

Poststreptococcal glomerulonephritis (PSGN)
• Caused by prior infection with specific nephritogenic strains of group A beta-hemolytic streptococcus.

Prognosis
• PSGN is associated with a variable decline in GFR that is detected by a rise in serum creatinine. Acute renal failure requiring dialysis is uncommon.
• The prognosis is generally favorable, especially in children, but in some cases, the long-term prognosis is not benign.

Clinical Manifestations• Clinical presentation of PSGN varies from asymptomatic,
microscopic hematuria to the full-blown acute nephritic syndrome, characterized by red to brown urine, proteinuria (which can reach the nephrotic range), edema, hypertension, and acute kidney injury.
• There is usually an antecedent history of a group A beta-hemolytic streptococcal (GAS) skin or throat infection.
• The latent period between GAS infection and PSGN is dependent upon the site of infection: between one and three weeks following GAS pharyngitis and between three and six weeks following GAS skin infection.

Clinical Manifestations…• The following symptoms are the most common presenting signs in children:
• Edema — Generalized edema is present in about two-thirds of patients due to sodium and water retention. In severe cases, fluid overload leads to respiratory distress due to pulmonary edema.
• Gross hematuria — Gross hematuria is present in about 30 to 50 percent of patients. The urine looks smoky, and tea or coca cola-colored.
• Hypertension — Hypertension is present in 50 to 90 percent of patients and varies from mild to severe. It is primarily caused by fluid retention. Hypertensive encephalopathy was an uncommon but serious complication. These patients require emergent intervention.
• Subclinical cases of PSGN are primarily characterized by microscopic hematuria. Such patients were often detected during epidemics.

Laboratory findings
• DIAGNOSIS — PSGN is usually diagnosed based upon clinical findings of acute nephritis and demonstration of a recent group A beta-hemolytic streptococcal (GAS) infection.
• The clinical findings of acute nephritis include hematuria with or without red blood cell casts, variable degrees of proteinuria, edema, and hypertension.
• Documentation of a recent GAS infection includes either a positive throat or skin culture or serologic tests (eg, ASO or streptozyme test).

MANAGEMENT • There is no specific therapy for PSGN. There is no evidence that aggressive
immunosuppressive therapy has a beneficial effect in patients with rapidly progressive crescentic disease. However, patients with more than 30 percent crescents on renal biopsy are often treated with methylprednisolone pulses.
• Management is supportive and is focused on treating the clinical manifestations of the disease, particularly complications due to volume overload. These include hypertension and, less commonly, pulmonary edema. General measures include sodium and water restriction and loop diuretics.
• Loop diuretics generally provide a prompt diuresis with reduction of blood pressure and edema. In our practice, intravenous furosemide is given at an initial dose of 1 mg/kg (maximum 40 mg).

COURSE
• Resolution of the clinical manifestations of PSGN is generally quite rapid.
• A diuresis typically begins within one week,
• and the serum creatinine returns to the previous baseline by three to four weeks.
COURSE…
• The urinary abnormalities disappear at differing rates.
• Hematuria usually resolves within three to six months.
• Proteinuria also falls during recovery, but at a much slower rate.
• A mild increase in protein excretion is still present in 15 percent at 3 years, and 2 percent at 7 to 10 years.

COURSE…
• In severe cases with nephrotic range proteinuria, this degree of proteinuria may persist for six months or more, long after the hematuria has disappeared.
• Patients first seen at this late stage are often thought to have one of the causes of the idiopathic nephrotic syndrome (eg, membranous nephropathy, focal segmental glomerulosclerosis, or minimal change disease).

Recurrence
• Recurrent episodes of PSGN are rare .
• This may be due to the long-term persistence of antibodies to nephritis-associated streptococcal antigen.

THANK YOU
Related Documents











