Global Health Governance : A Search for Meaning Tikki Pang Research Policy & Cooperation WHO, Geneva, Switzerland ST Lee Lecture, Sydney, July 16, 2009

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Global Health Governance :A Search for Meaning
Tikki PangResearch Policy & Cooperation
WHO, Geneva, Switzerland
ST Lee Lecture, Sydney, July 16, 2009
Global Health• An area of study, research and practice that
places a priority on improving health and achieving equity in health for all people worldwide
• Emphasizes trans-national health issues, determinants and solutions
• Inter- and multi-disciplinary collaboration within and beyond health sciences
• A synthesis of population-based prevention and individual-level clinical care
Koplan, Lancet 2009, 373, 1993-95
Global health governance (GHG)
Defined as the formal and informal institutions, norms and processes which govern or directly influence global health policy and outcomes

• Current global health challenges
• Landscape of global health governance-can it deal with the challenges?
• Recent developments-thoughts for the future
UN Millennium DevelopmentGoals (MDG's) (2000-2015)

NewInfluenza A(H1N1)

>1000 deaths20,000 cases
Threat of regional spread
As of June 6, 2009
4,300 deaths
100,000 cases
CFR : 4.3%
Czech Rep.
The b
oundaries an
d n
ames sh
own an
d th
e desig
natio
ns u
sed on
this
map
do n
ot im
ply th
e expressio
n of an
y opin
ion
whatso
ever on th
e part of th
e WH
O con
cernin
g th
e legal statu
s ofan
y country, territo
ry, city or area o
r of its au
thorities, o
r concern
ing th
e delim
itatio
n of its fro
ntiers o
r boundaries. D
otted
lines on
map
s represen
t approxim
ate bord
er lines fo
r which
there m
ay not yet b
e full a
greem
ent.
WH
O 2
005. A
ll rights reserved
Ecuador
Georgia
Argentina
Bangladesh
Germany
Rep of Korea
Armenia
Russian Fed.
South Africa
Portugal
Latvia
Mexico
Peru
USA
Brazil
UK
Sweden
Thailand
Chile
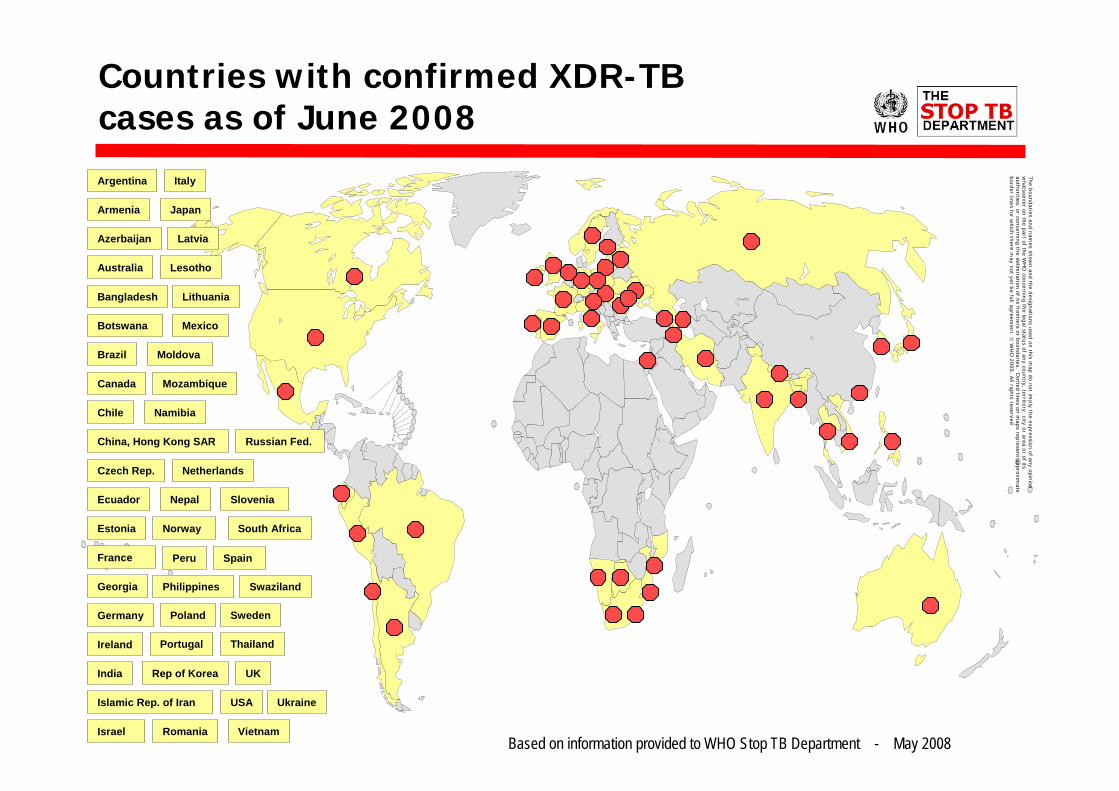
Based on information provided to WHO Stop TB Department - May 2008
Spain
China, Hong Kong SAR
France
Japan
Norway
Canada
Italy
Netherlands
Estonia
Lithuania
Ireland
RomaniaIsrael
Azerbaijan
Poland
Slovenia
India
Australia
Mozambique
Vietnam
Ukraine
Moldova
Philippines
Botswana
Nepal
Islamic Rep. of Iran
Lesotho
Swaziland
Namibia
Countries with confirmed XDR-TB cases as of June 2008
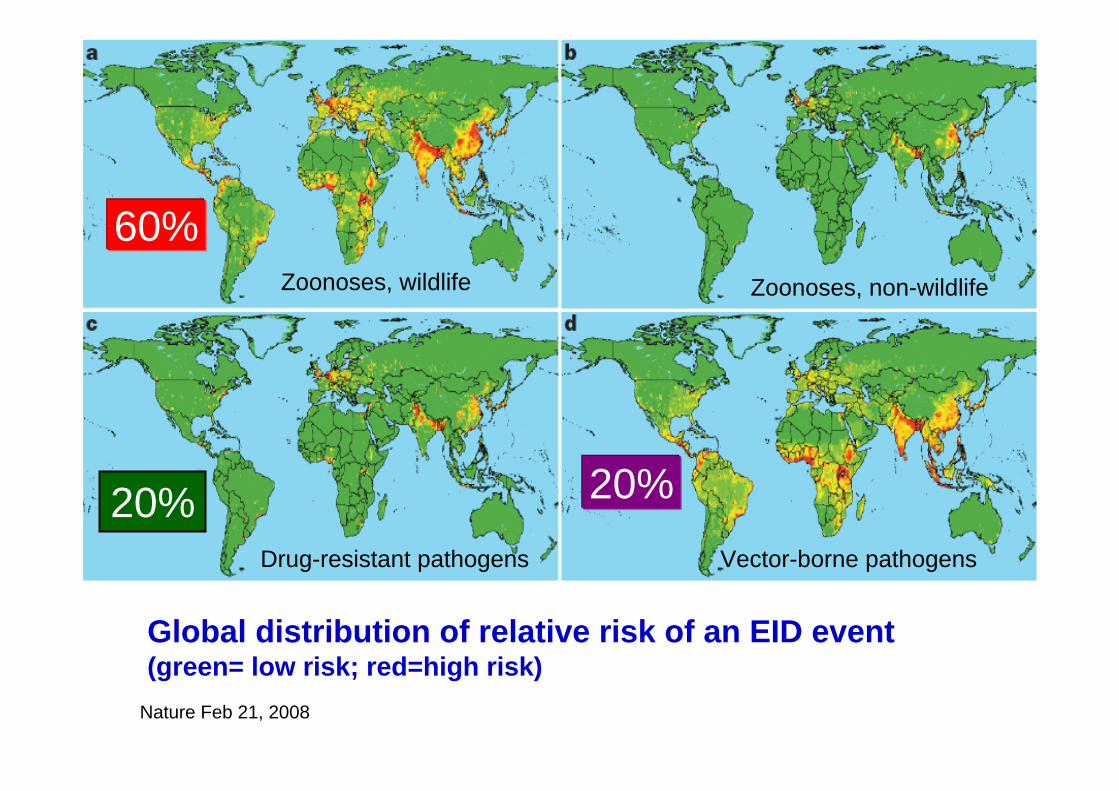
Nature Feb 21, 2008
Global distribution of relative risk of an EID event(green= low risk; red=high risk)
Zoonoses, wildlife Zoonoses, non-wildlife
Drug-resistant pathogens Vector-borne pathogens
60%
20%20%
Between 1975-20041,556 new drugs weredeveloped….
Only 21 (1.3%) were for tropical diseases of thedeveloping world
Chirac & Tourelle; Lancet 2006, May 12, pp. 1560-61
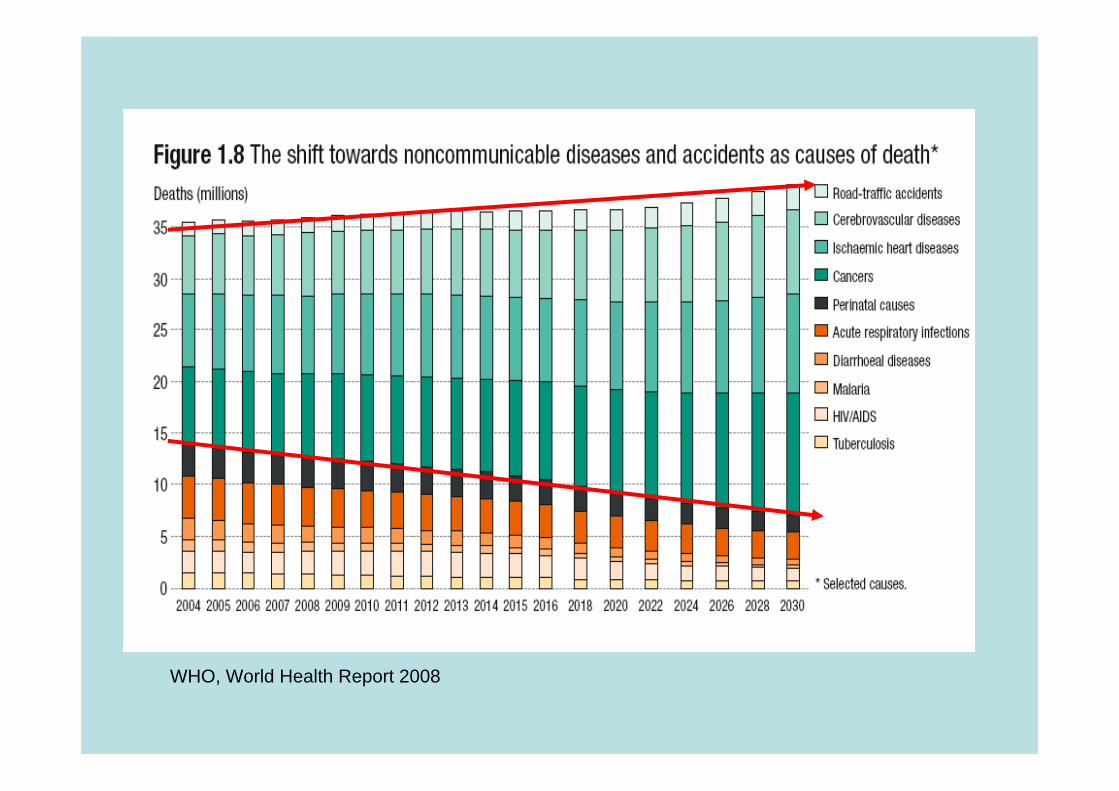
WHO, World Health Report 2008

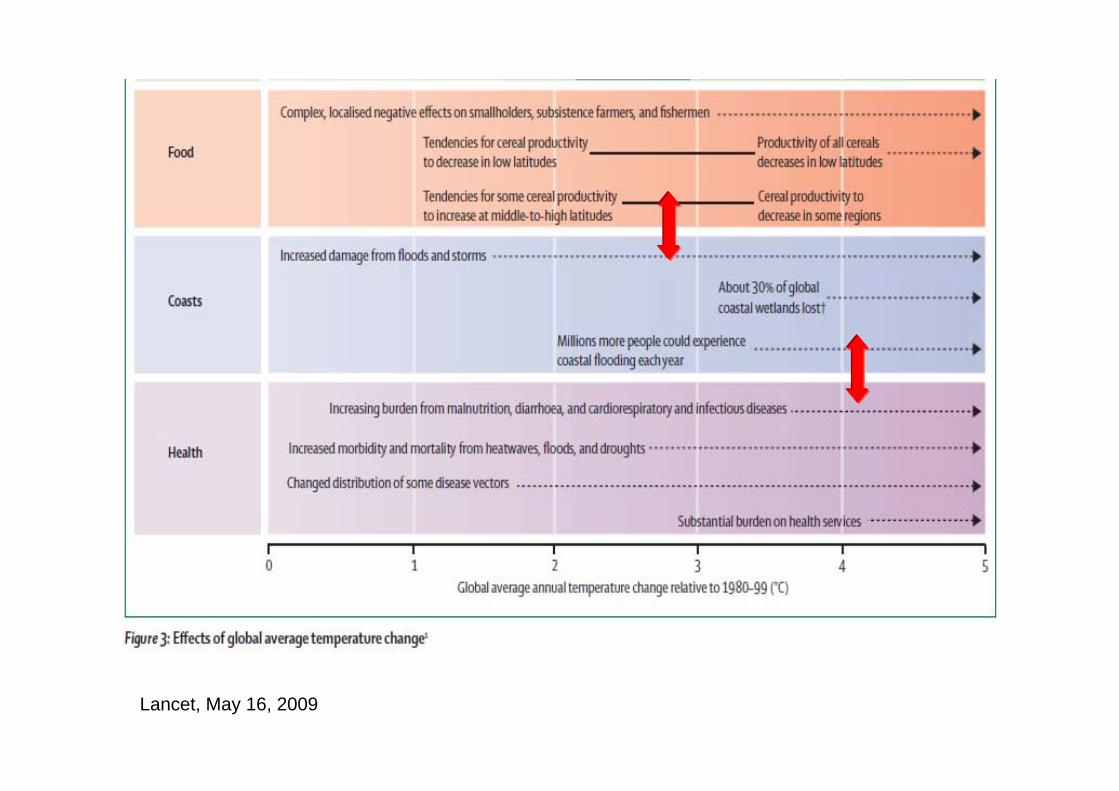
Lancet, May 16, 2009
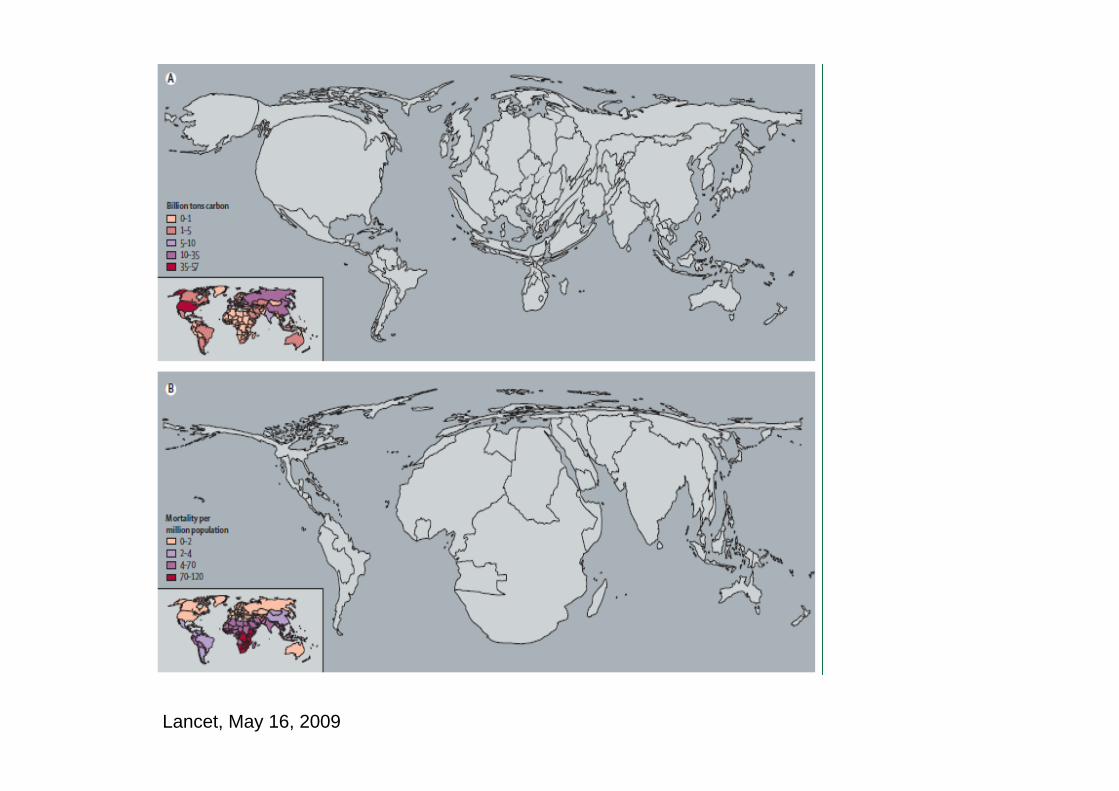
Lancet, May 16, 2009

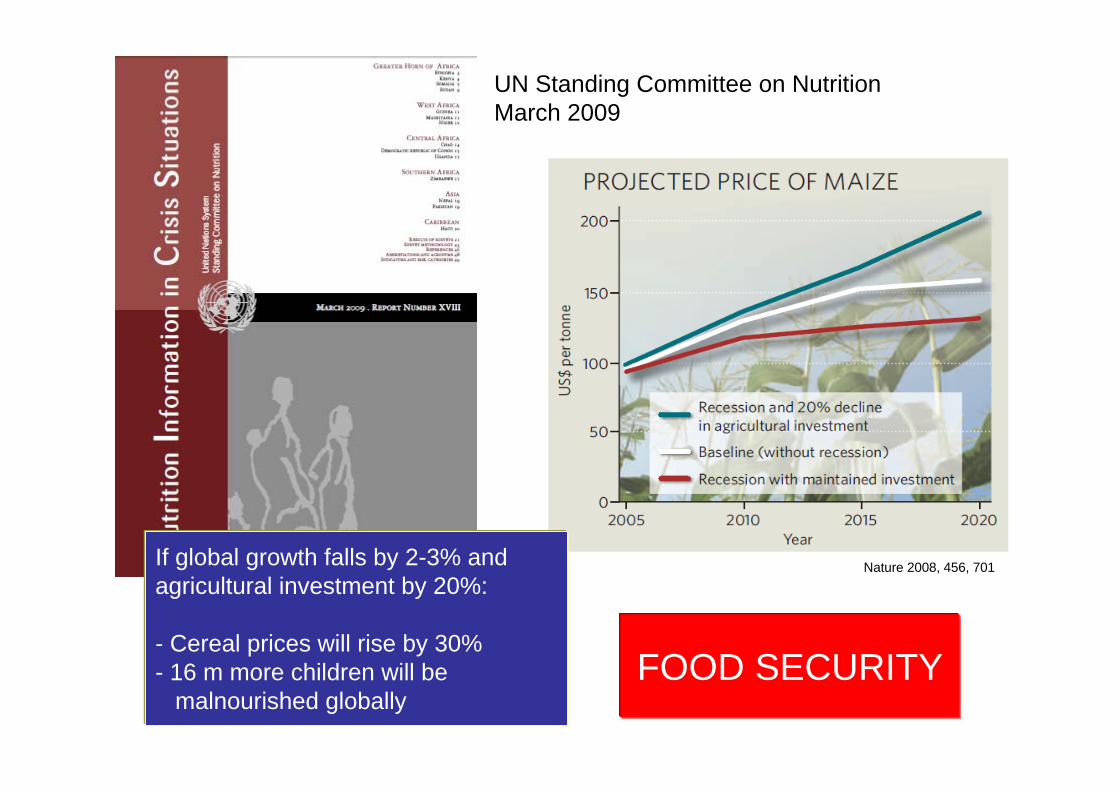
UN Standing Committee on NutritionMarch 2009
If global growth falls by 2-3% andagricultural investment by 20%:
- Cereal prices will rise by 30%- 16 m more children will be
malnourished globally
Nature 2008, 456, 701
FOOD SECURITY
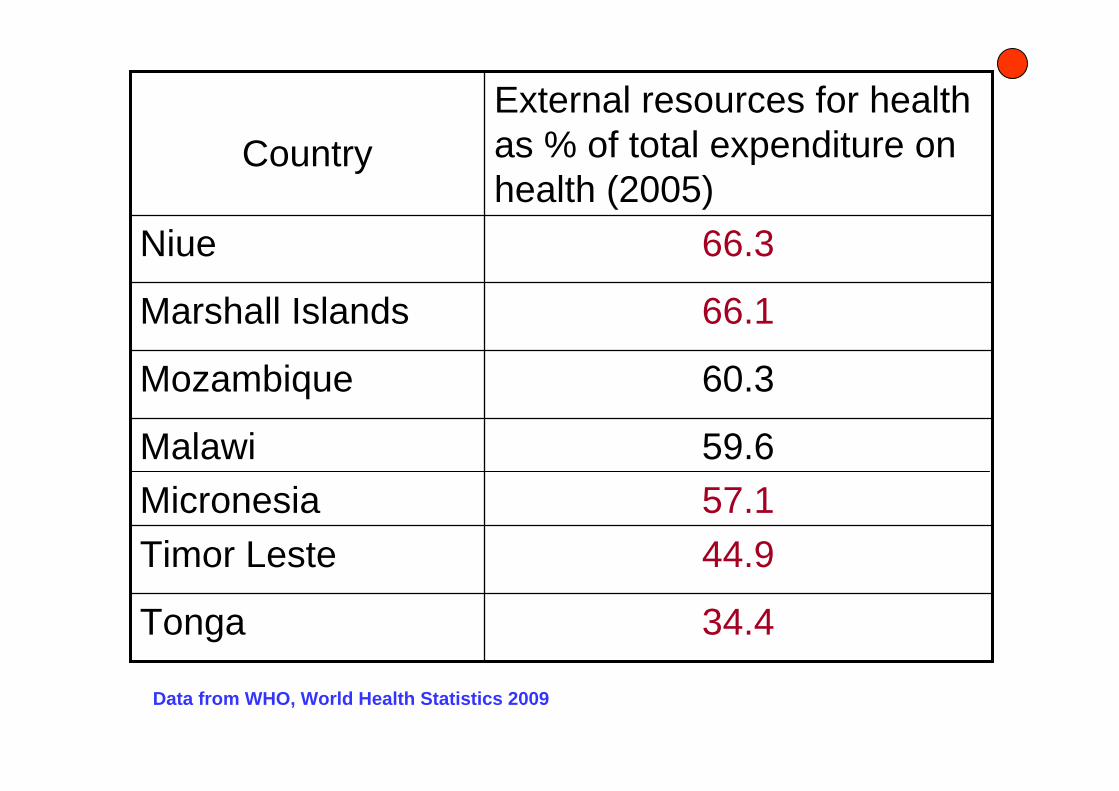
34.4Tonga
44.9Timor Leste
59.657.1
MalawiMicronesia
60.3Mozambique
66.1Marshall Islands
66.3Niue
External resources for health as % of total expenditure on health (2005)
Country
Data from WHO, World Health Statistics 2009

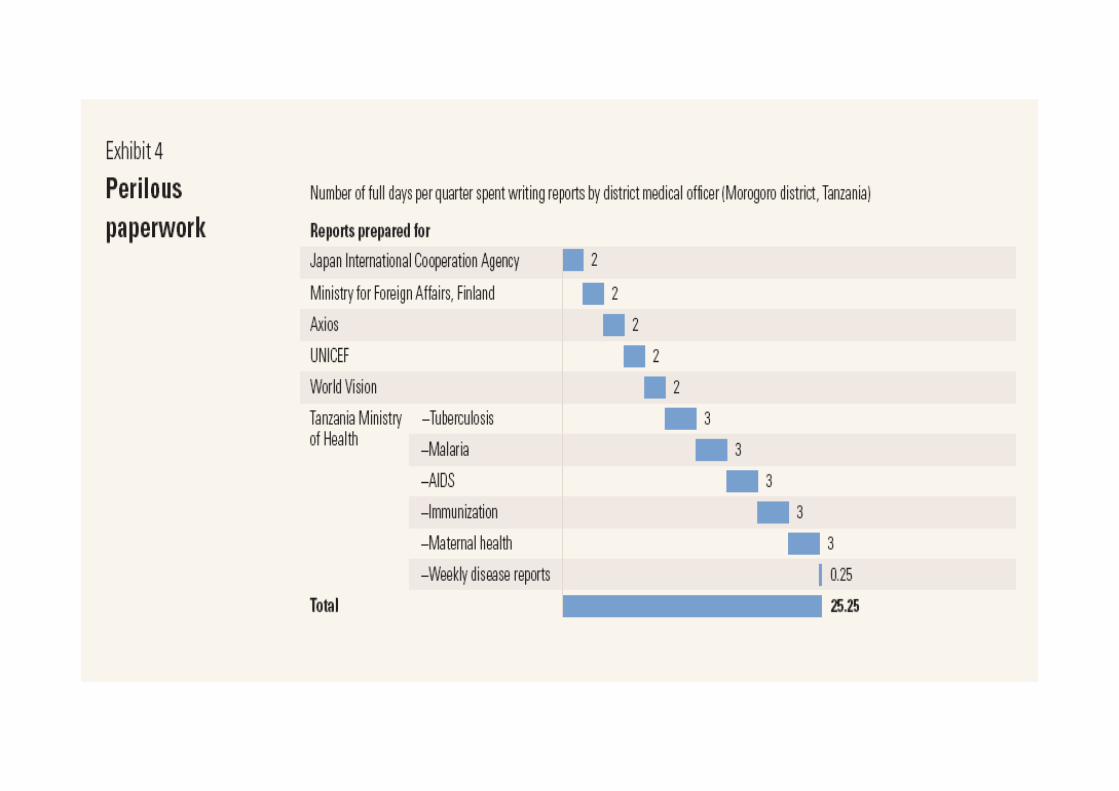
Many health caredelivery systems in the developingworld are in aprecarious state
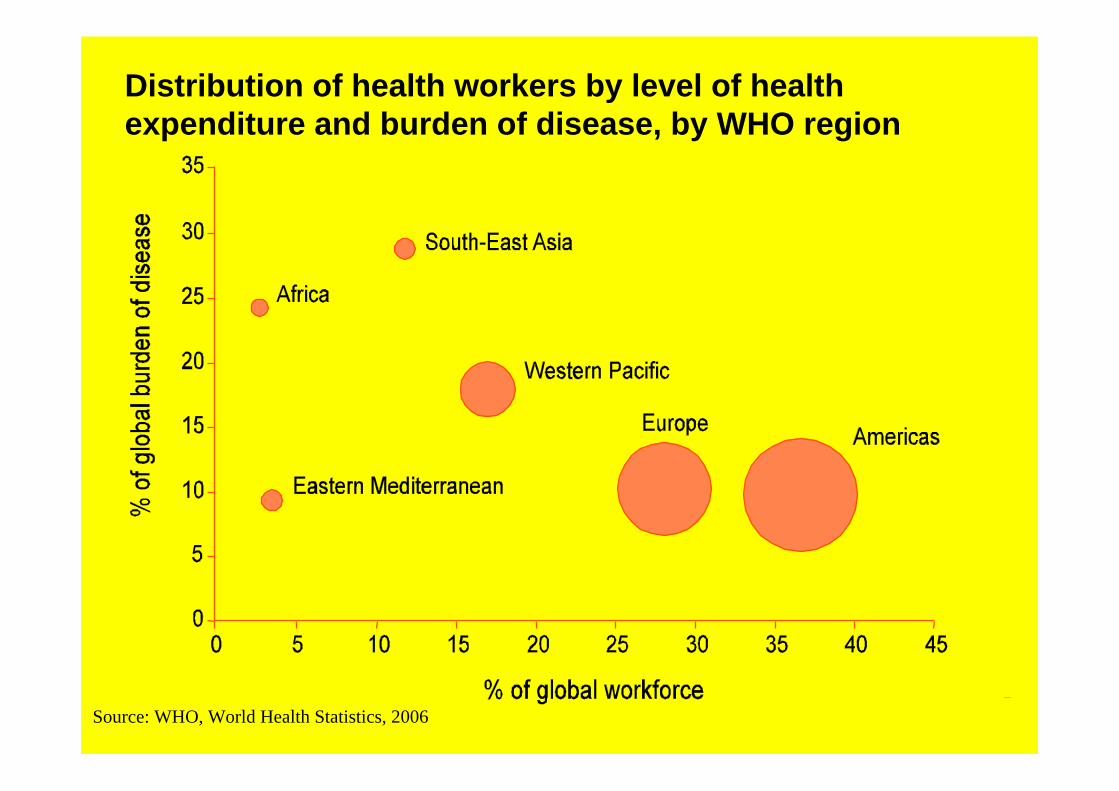
Distribution of health workers by level of healthexpenditure and burden of disease, by WHO region
Source: WHO, World Health Statistics, 2006
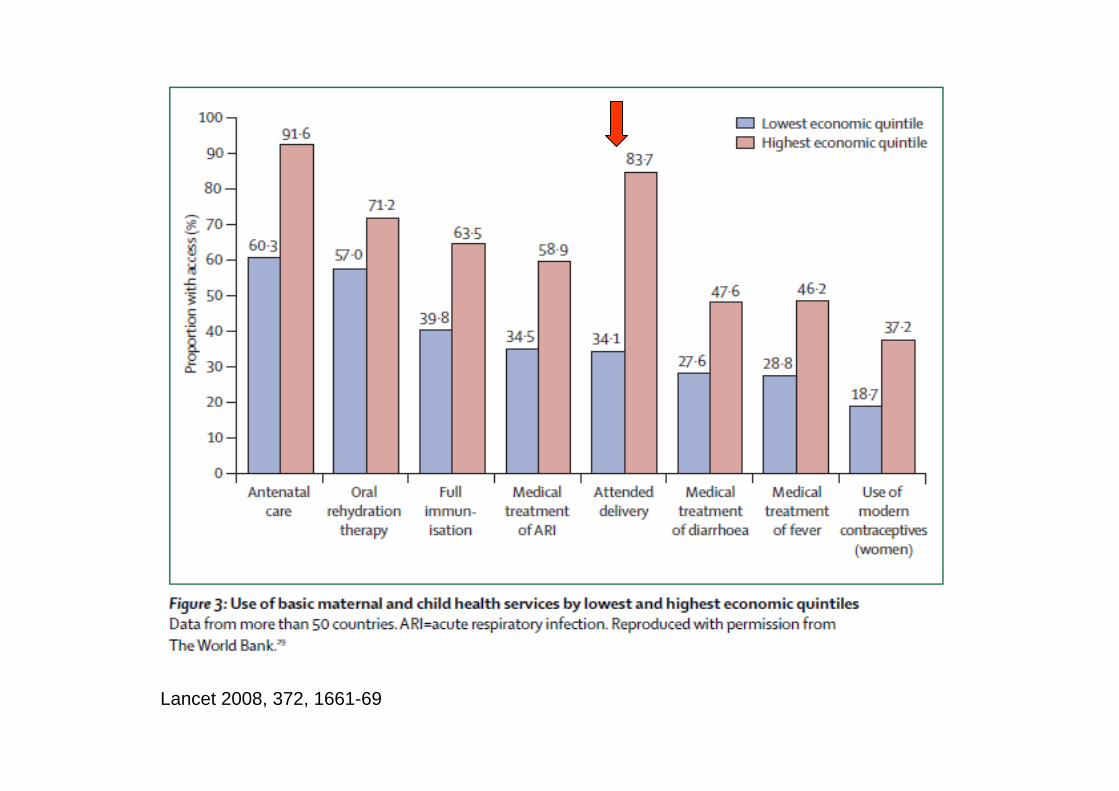
Lancet 2008, 372, 1661-69
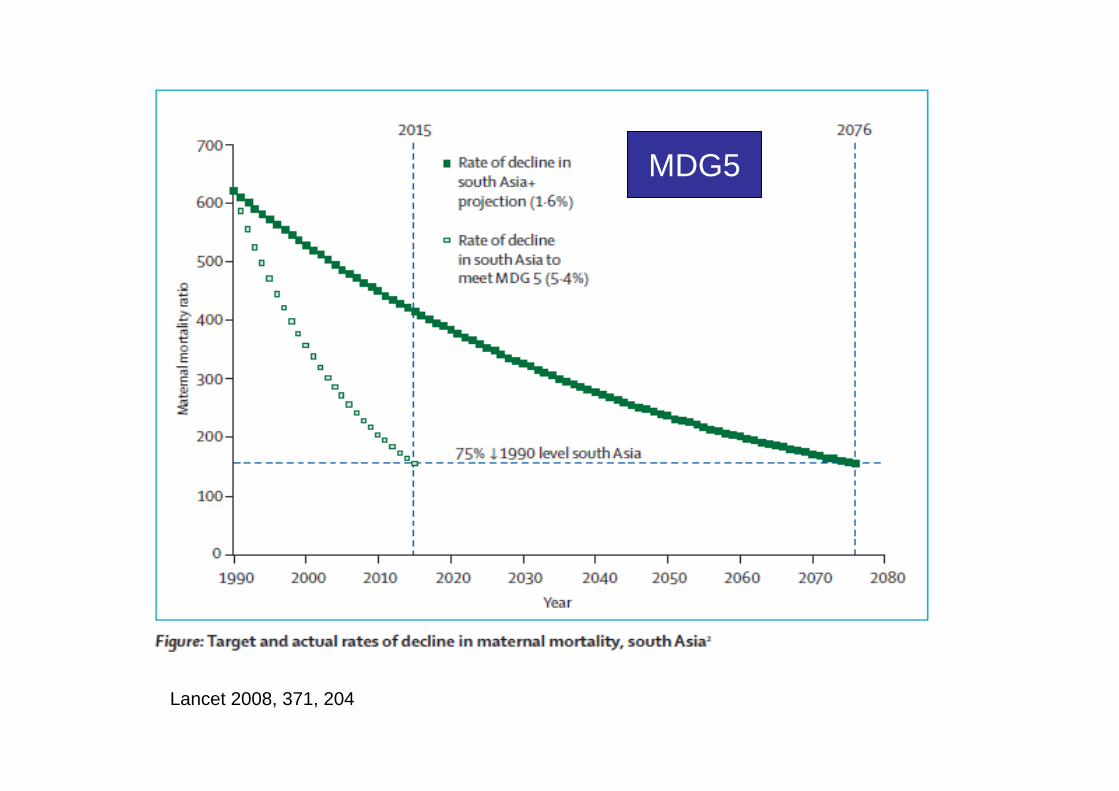
Lancet 2008, 371, 204
MDG5

Global health challenges• Impact of financial crisis & globalization• Multiple, diverse, emerging and inter-
sectoral health threats• Failures in delivery & access to both
existing and needed interventions• Gaps and inequities continue• Fragile health systems unable to
achieve MDG targets
The elephant inthe room is…"get the healthsystem in goodshape…"
What is the elephant in the room?What is the dead moose under the carpet?Even Blind Freddy could see it!Sticks out like a country dunny!
WHO Commission on SocialDeterminants of Health
World Health Report 2008:Primary Health Care-Now MoreThan Ever
2008 Highlights great health inequities caused by the social determinants of health
Equity strongly influenced bythe way health systems areorganized and financed
Champions primary health care(PHC) as a model for a healthsystem that acts on the underlying social, political & economic causes of ill health
Dr Margaret Chan,WHO Director-General,Sept 9, 2008Address to 61st Regional Committee SEARO
"Health systems will not naturally gravitate towards equity and unprecedented leadership inglobal health governance is needed"

• Current global health challenges
• Landscape of global health governance-can it deal with the challenges?
• Recent developments-thoughts for the future

(Slide courtesy of Ian Smith, WHO)
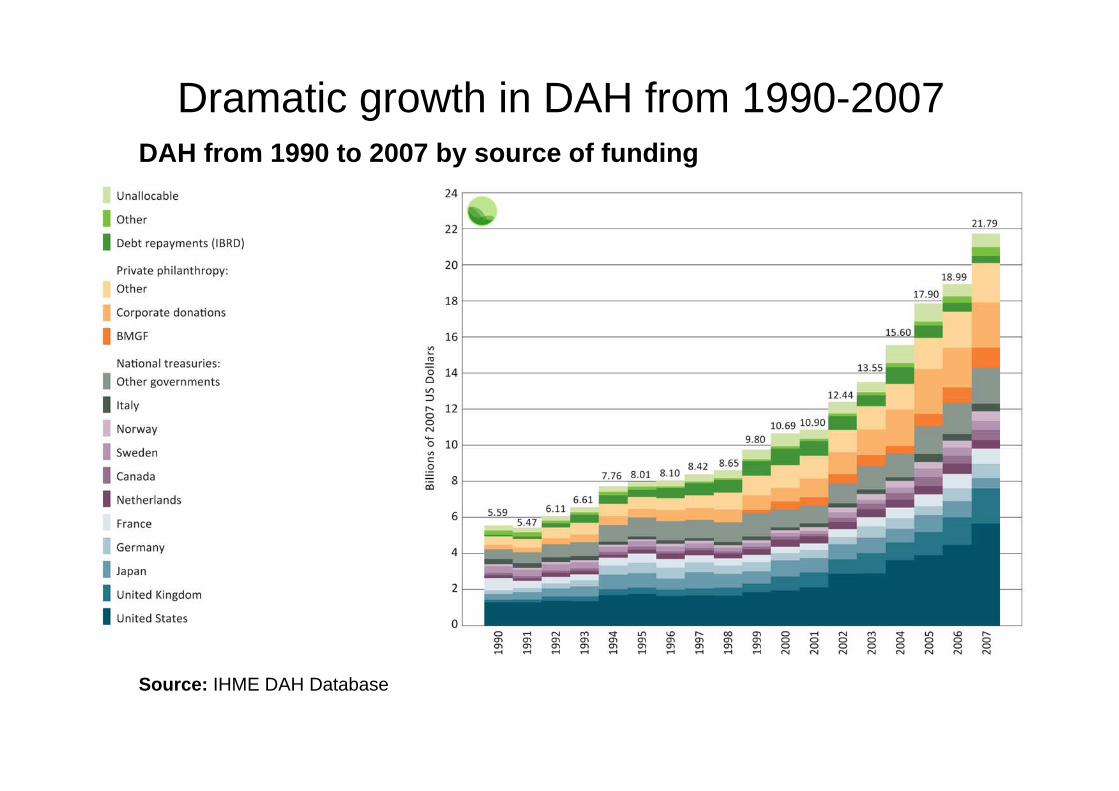
Dramatic growth in DAH from 1990-2007
Source: IHME DAH Database
DAH from 1990 to 2007 by source of funding
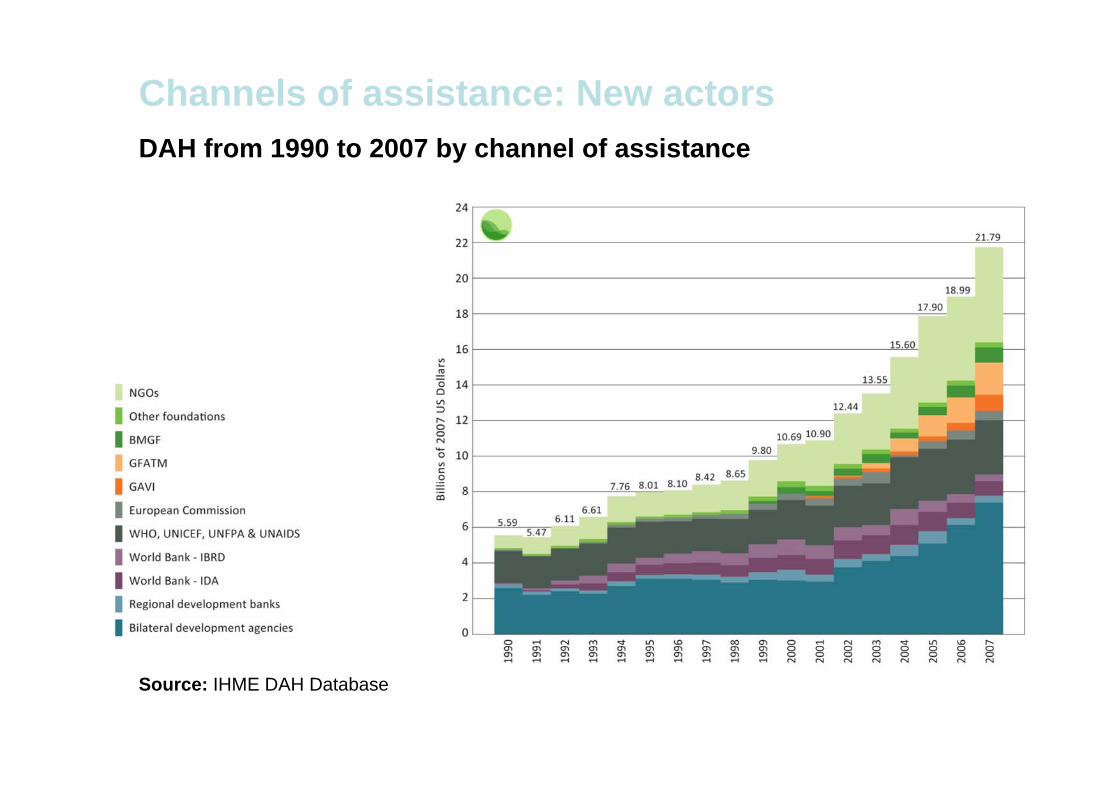
DAH from 1990 to 2007 by channel of assistance
Source: IHME DAH Database
Channels of assistance: New actors

Nature May 28, 2009
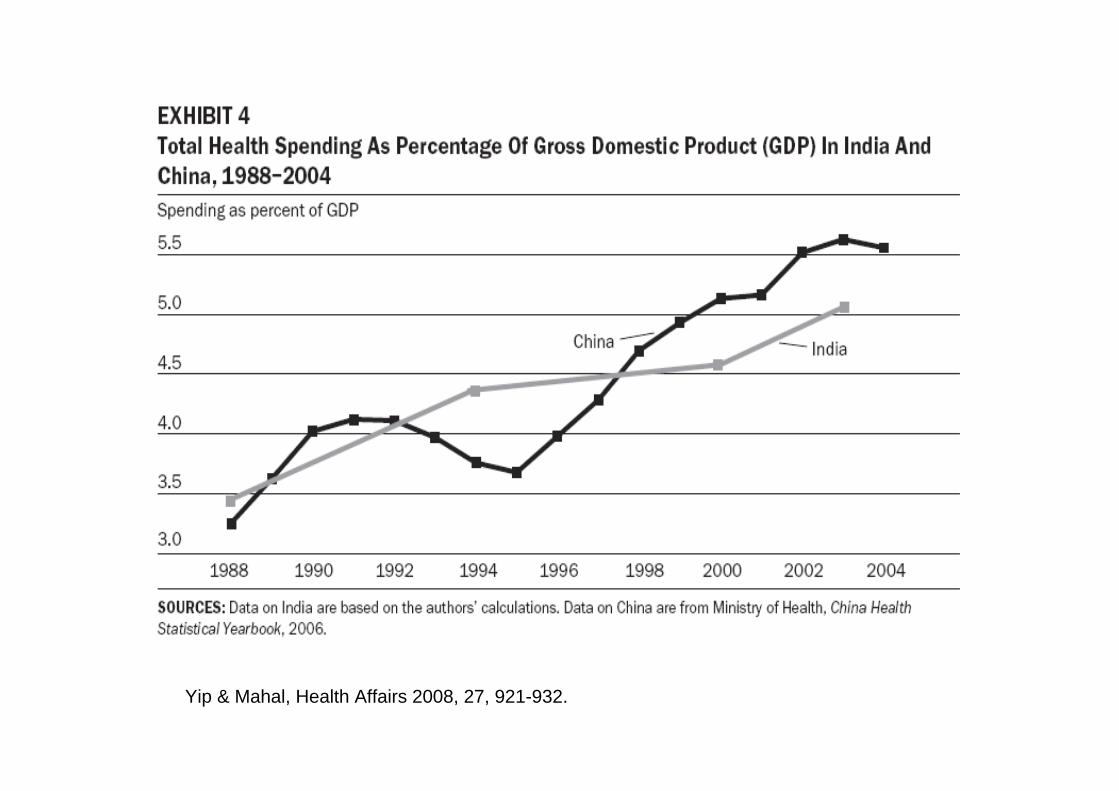
Yip & Mahal, Health Affairs 2008, 27, 921-932.
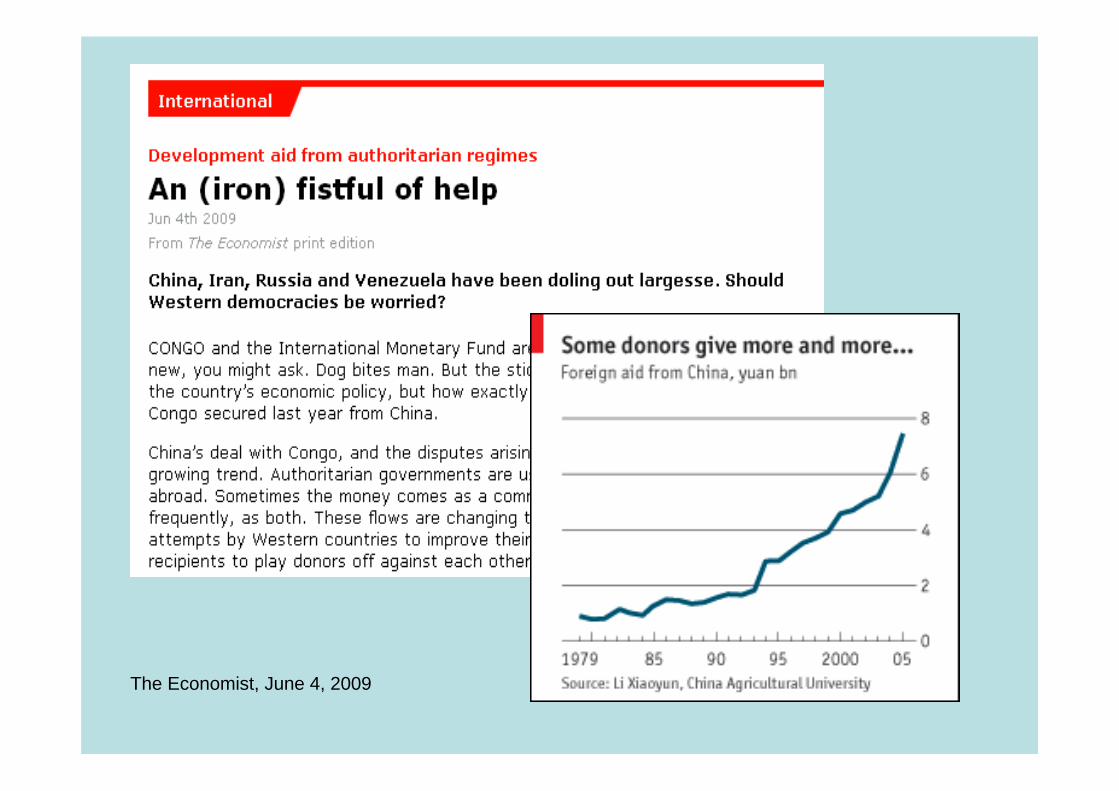
The Economist, June 4, 2009
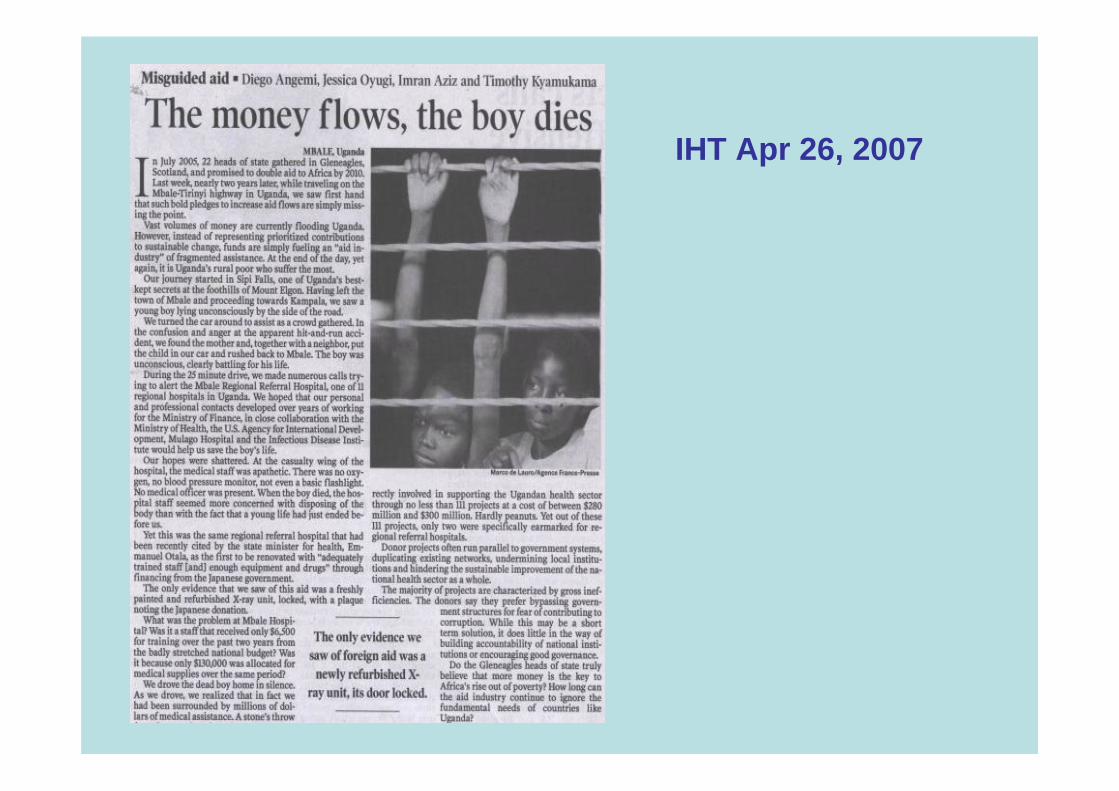
IHT Apr 26, 2007
Babatunde Osotimehin,Minister of Health of Nigeria,Ministerial Review of IHPP+Geneva, Feb 4, 2009
"When I asked for a briefing on malaria, I was given a briefing by funding streams…………..I asked myself: Is WHO dealing with a different strain of malariato the Global Fund??"
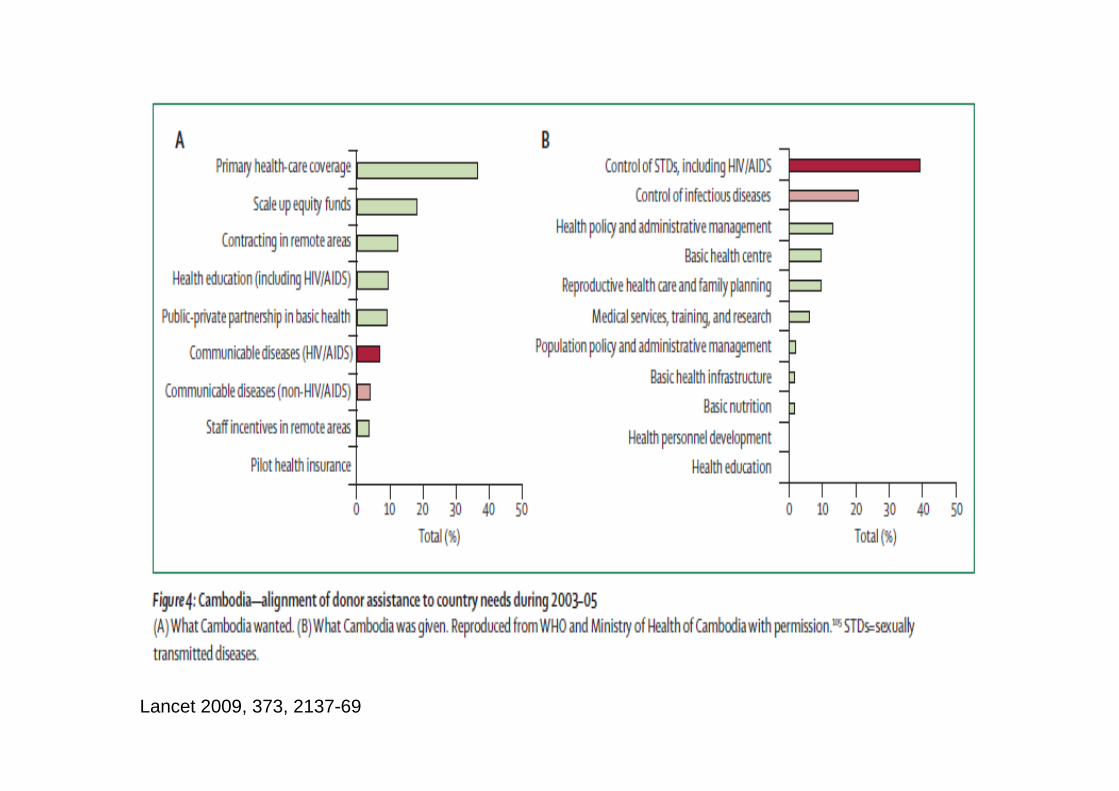
Lancet 2009, 373, 2137-69
Global health governance
• Multiple, diverse players• Fragmentation, lack of coordination• Top down, donor driven, negative impact on
countries with fragile health systems• Plenty of money…• …but imbalance in allocation to "big" diseases
(vertical) but not to health system strengthening (horizontal)
• Lack of evaluation, accountability-sustainability?

Research Programme
PlayersModels

Major Players• International organizations (WHO, UNAIDS,
UNICEF, World Bank)• Multilateral entities (G8, G20, G24)• Multilateral initiatives (GFATM, GAVI)• Bilateral initiatives (PEPFAR)• Philanthropies (Gates, Carso)• Global public-private partnerships• Private sector-industry• Civil society

Models & Mechanisms• Market-driven, global PPP's-GPG• Global Health Innovation Systems• Cross-sectoral "global action networks"• Trans-governmental platforms• Global Agenda Councils (WEF)• European Council on Global Health• Framework Convention on Global Health• "World Development Organization"
Global Health Law
Features & Challenges
• Features: mission, key participants, sources, structure, moral foundations
• Challenges to be overcome for global health law to be effective:State-centricity in the international legal systemSkewed priority settingFlawed implementation and complianceFragmentation, duplication, poor coordination
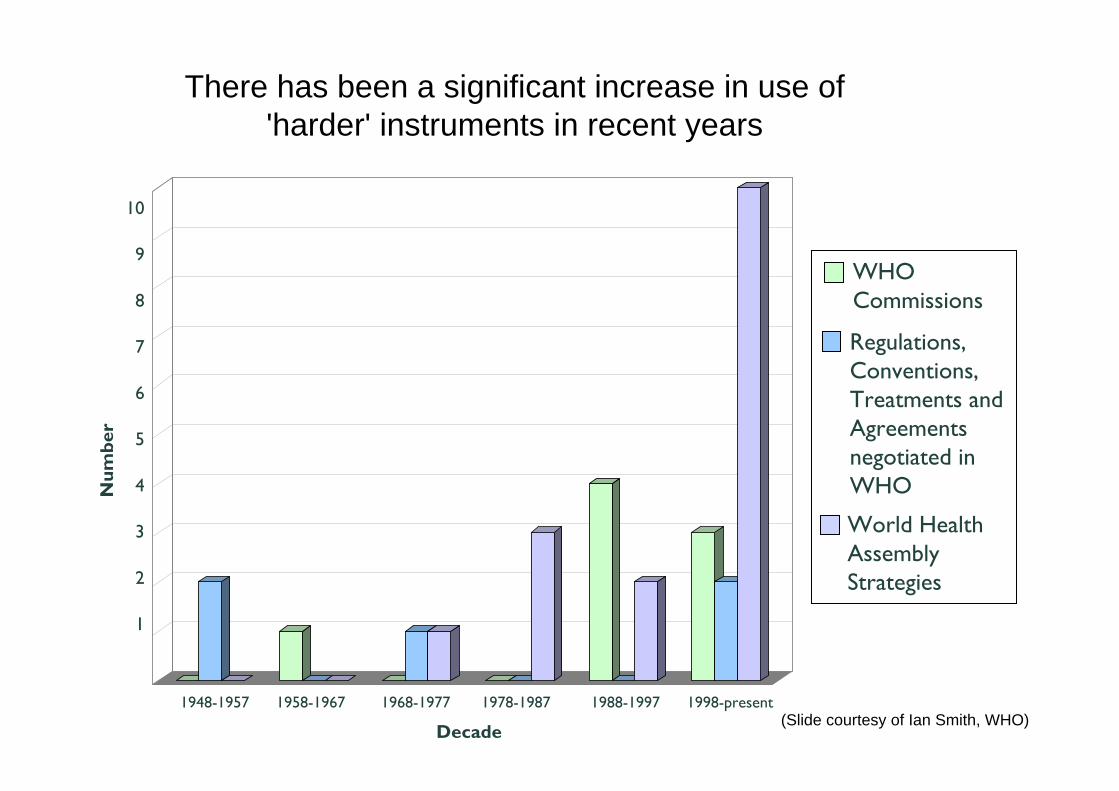
WHO Commissions
Regulations, Conventions, Treatments and Agreements negotiated in WHO
World Health Assembly Strategies
1948-1957 1958-1967 1968-1977 1978-1987 1988-1997 1998-present
Decade
Number
10
9
8
7
6
5
4
3
2
1
There has been a significant increase in use of 'harder' instruments in recent years
(Slide courtesy of Ian Smith, WHO)
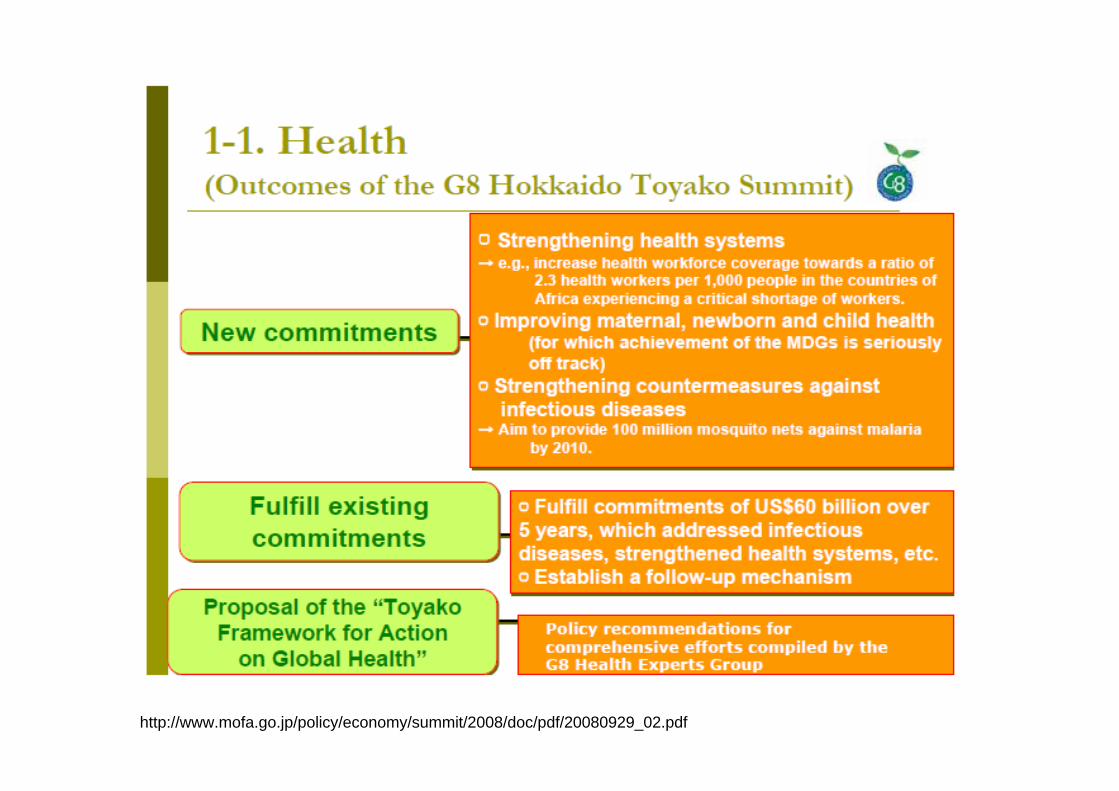
http://www.mofa.go.jp/policy/economy/summit/2008/doc/pdf/20080929_02.pdf

CHALLENGES FOR WHOINTERNAL FACTORS
biomedical vs social medicine approaches debate between vertical and horizontal approaches inadequate resources (zero real/nominal growth) unclear priorities among multitude of programmes weak leadership and accusations of waste & corruption
EXTERNAL FACTORS
declining commitment to multilateral action/UN after end of Cold War
primacy of international financial institutions (World Bank) political pressure exerted by powerful member states and
corporate interests growing calls for social justice amid accelerating economic
globalisation(Slide courtesy of Kelley Lee)
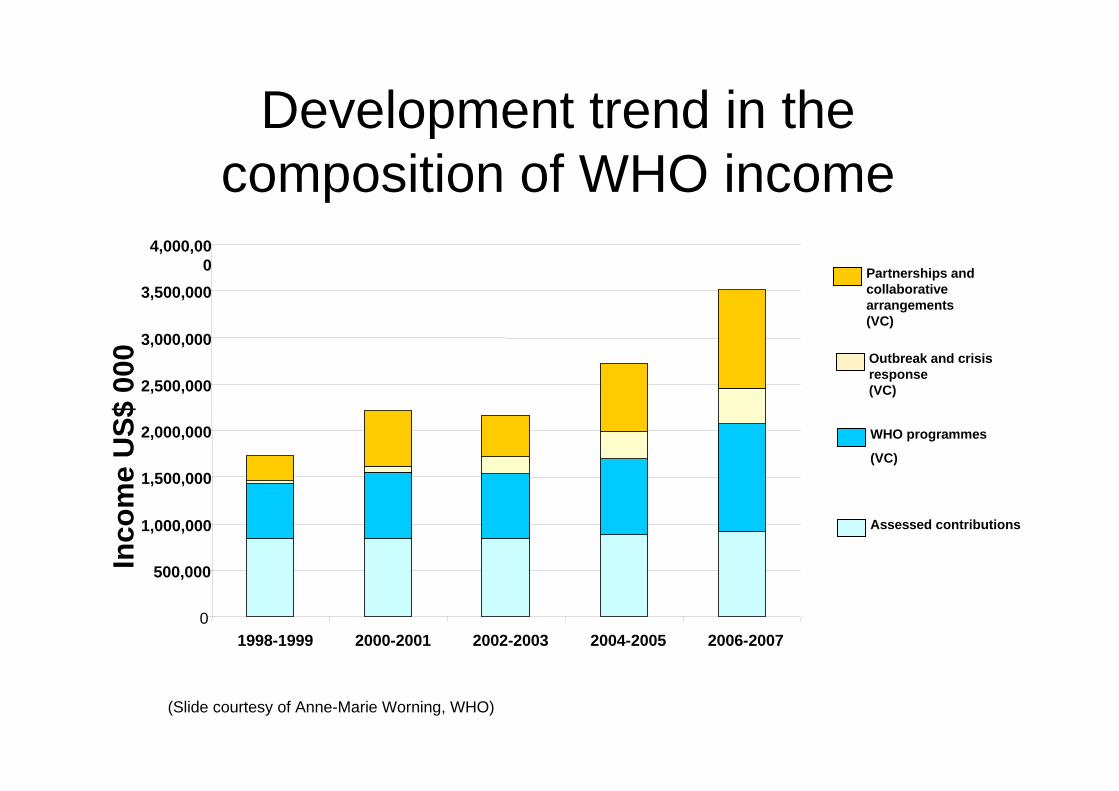
Development trend in the composition of WHO income
Partnerships and collaborative arrangements (VC)
Outbreak and crisis response (VC)
WHO programmes
(VC)
Assessed contributions
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
3,500,000
4,000,000
1998-1999 2000-2001 2002-2003 2004-2005 2006-2007
Inco
me
US$
000
(Slide courtesy of Anne-Marie Worning, WHO)
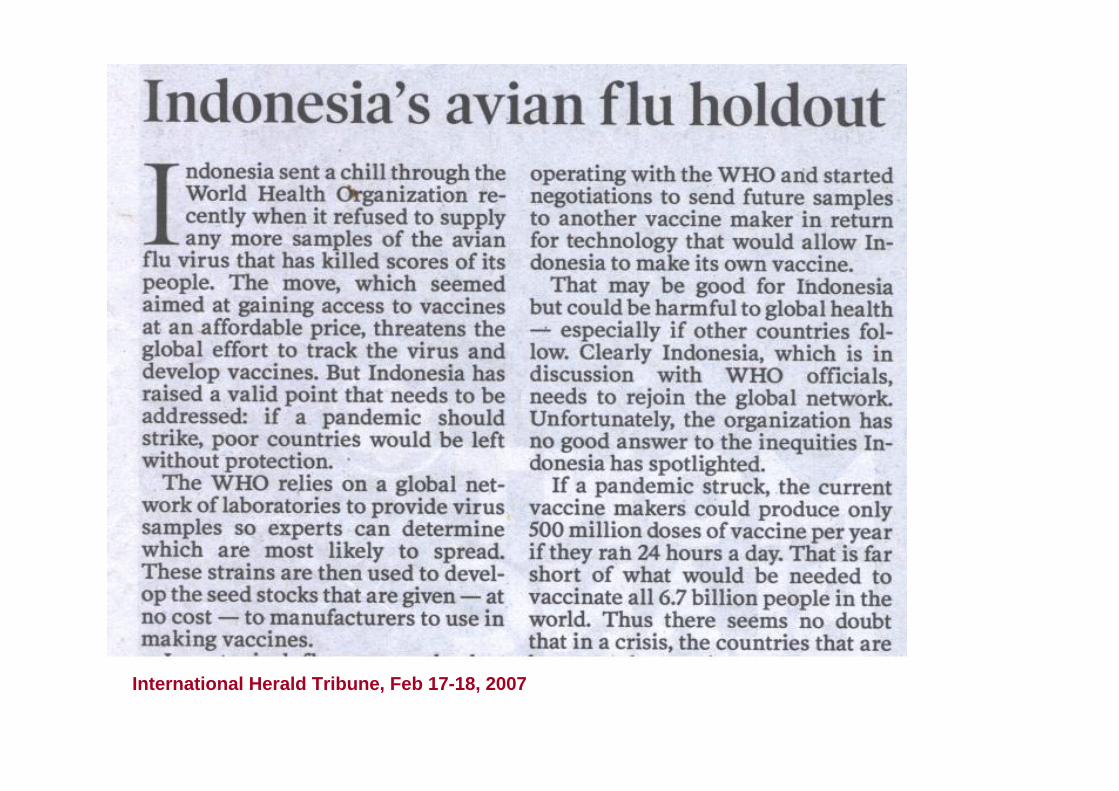
International Herald Tribune, Feb 17-18, 2007

WHO: Comparative Advantages
• Normative function• Direct reach into ministries of health• Independence, impartiality, neutral
broker, convenor & coordinator• Political legitimacy & credibility• Global reach• Gives a voice to, and champions the
health of poor people
"The only organization with thepolitical credibility to compel cooperative thinking is the WHO"
Laurie Garrett"The challenge of global health"Foreign Affairs 2007, 86, 4-38
"…the need for a strong, well-funded, and politicallysupported WHO has become a much sharper andconvincing argument today than for many years"Richard Horton, June 20, 2009
IOM Report 2009The US Commitment to Global Health:Recommendations for the Public and Private Sectors

• Current global health challenges
• Landscape of global health governance-can it deal with the challenges?
• Recent developments-thoughts for the future
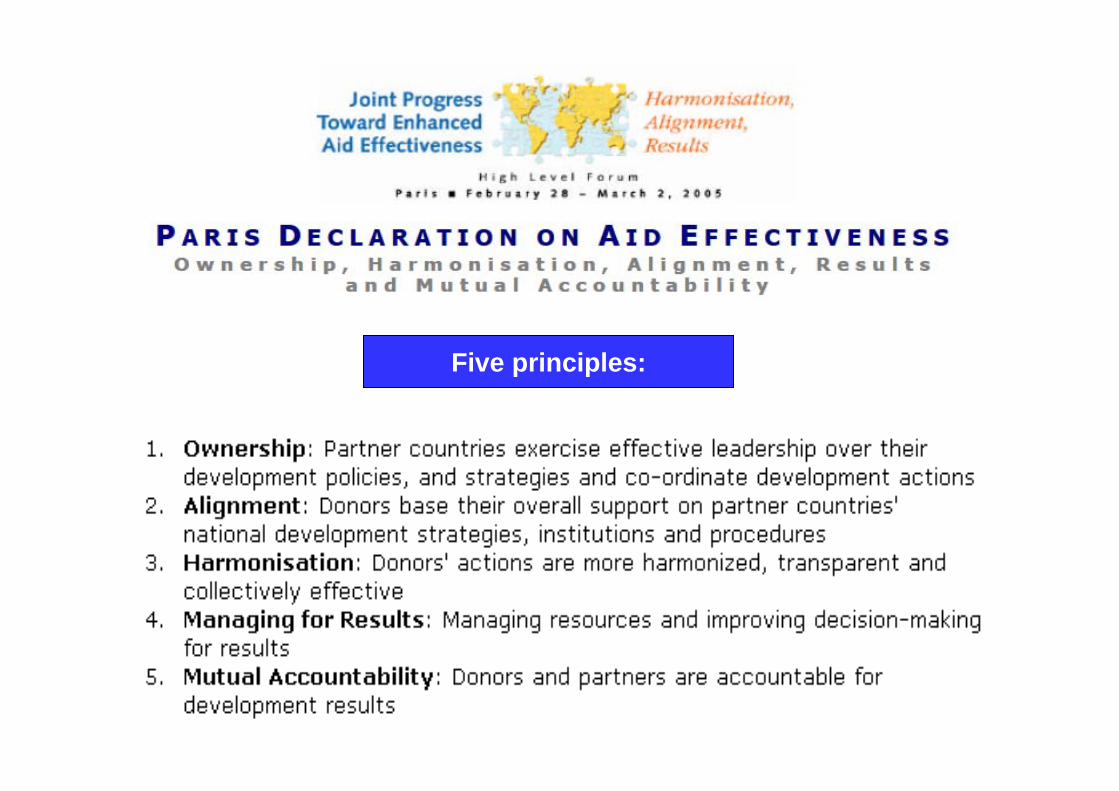
Five principles:

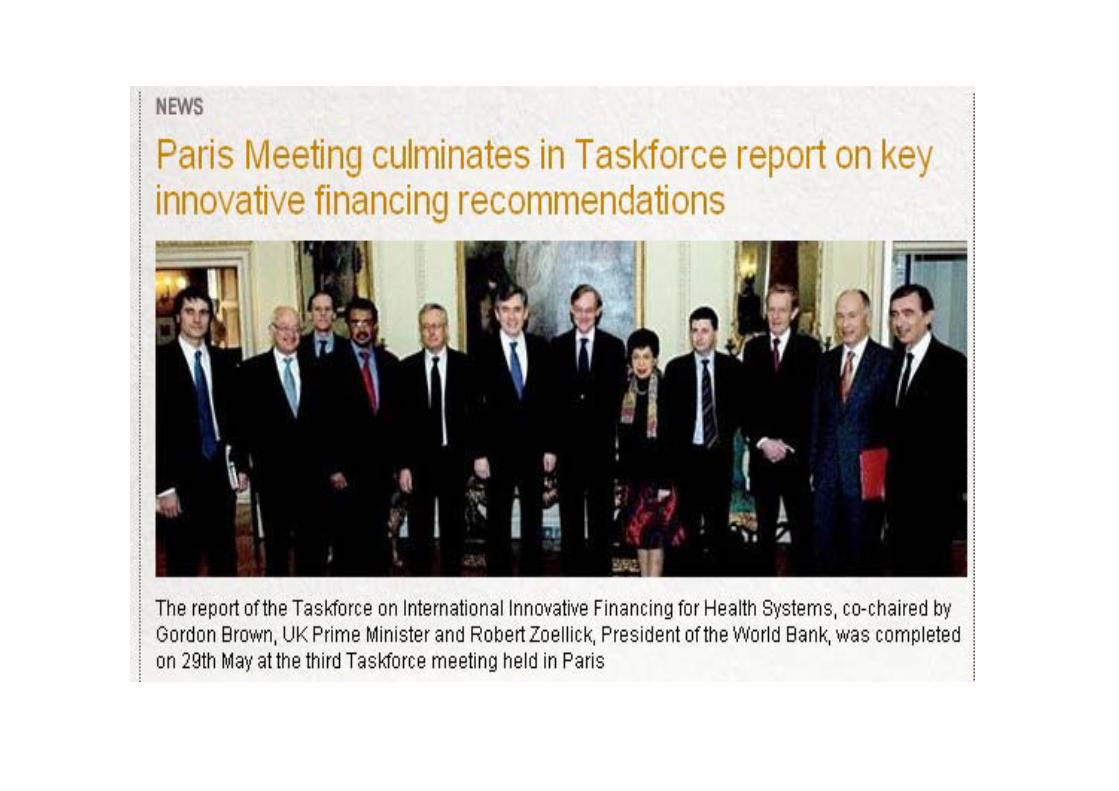
Main recommendations• Expand mandatory solidarity levy on airline
tickets • Explore feasibility of new voluntary solidarity
contribution schemes (e.g. levies on tobacco and currency transactions)
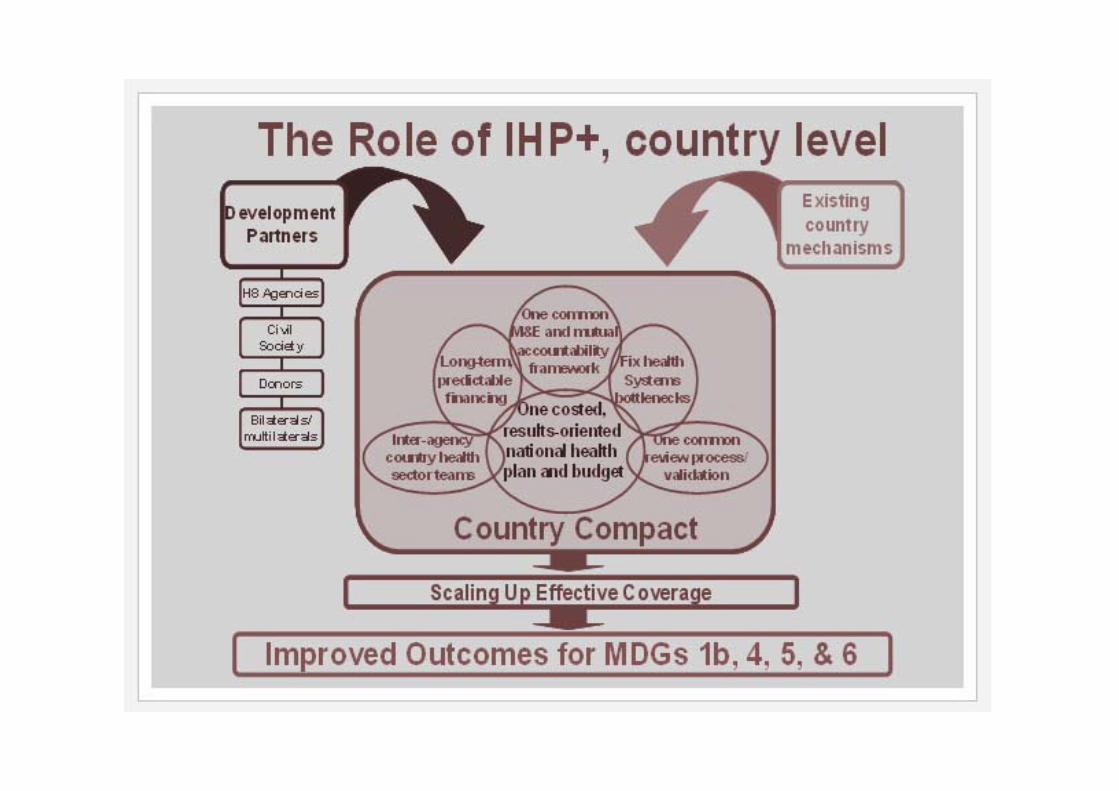
• Expansion of IFFIm and Debt2Health• Build and maintain effective health systems• Align resources with a comprehensive national
health strategy/plan• Sustainable domestic financing

"The Government will also fulfill its election commitment for a debt to health swapwith Indonesia through this Budget. Australia will cancel debt owed by Indonesiain parallel with Government of Indonesia investment in programs combating Tuberculosis".
Leading Innovative Financing for Equity (LIFE)
I-8 Group for MDGs (LIFE)
1. IFFIm-GAVI2. UNITAID3. Advance Market Commitment for Vaccines
(AMC)4. Debt2Health (GFATM)5. (PRODUCT) RED6. Responsible Social Investment Initiative of
French Agency for Development (AFD)7. Revenues form the Carbon Market8. Millennium Foundation for Innovative Finance
for Health
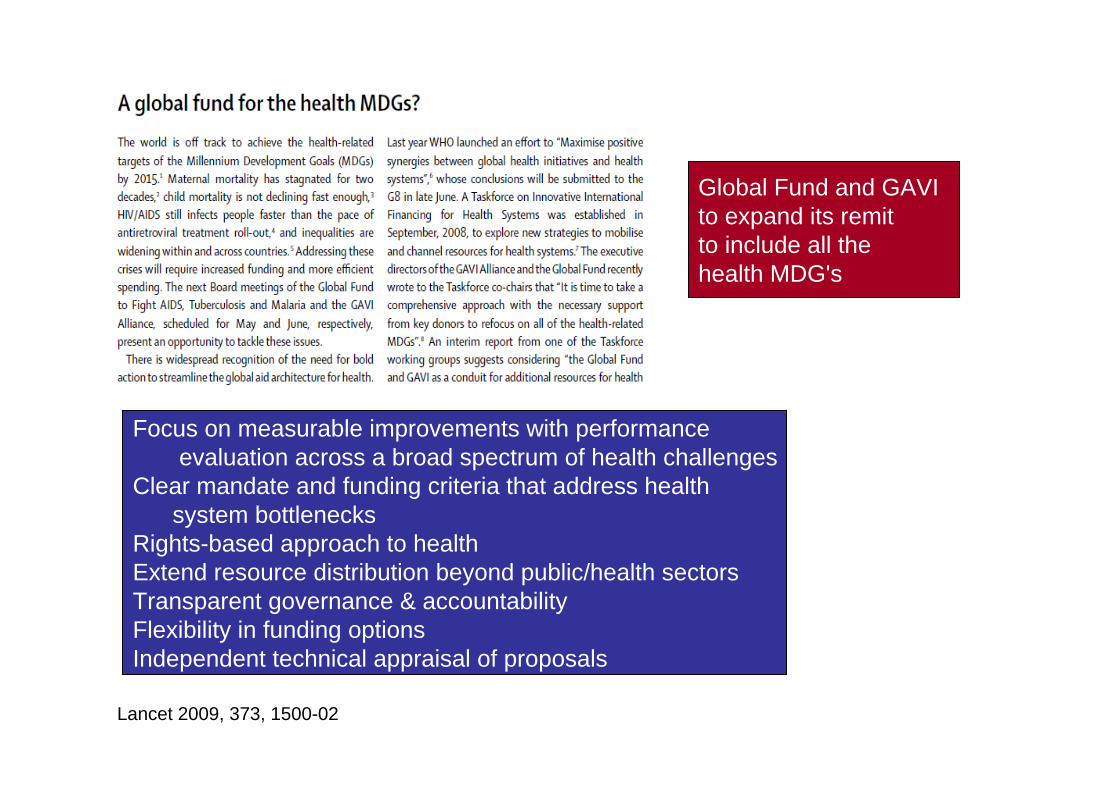
Lancet 2009, 373, 1500-02
Focus on measurable improvements with performance evaluation across a broad spectrum of health challenges
Clear mandate and funding criteria that address healthsystem bottlenecks
Rights-based approach to healthExtend resource distribution beyond public/health sectorsTransparent governance & accountabilityFlexibility in funding optionsIndependent technical appraisal of proposals
Global Fund and GAVIto expand its remitto include all thehealth MDG's
Diagonal approach toGlobal Fund financing
Globalization and Health 2008, 4:6
Diagonal financing aims for disease-specific resultsthrough improved health systems
Some thoughts forthe future……..

Seven effective habits of future governance
• Trans-sectoral, integrated view• Inclusive, embrace diversity• Define roles, substantive norms & values• Accountability & transparency• Information & evidence - harness ICT,
promote research on governance (towards evidence-informed governance)
• Balancing act

Balancing act between…….
• National and global governance• Formal and informal mechanisms• Market forces and social justice/equity• Specific diseases and systems strengthening• Legitimacy/democracy/participation and
effectiveness• Ideas/theories and implementation - the need
to "make it work"• Learning from past successes/failures and the
need for innovation on future governance
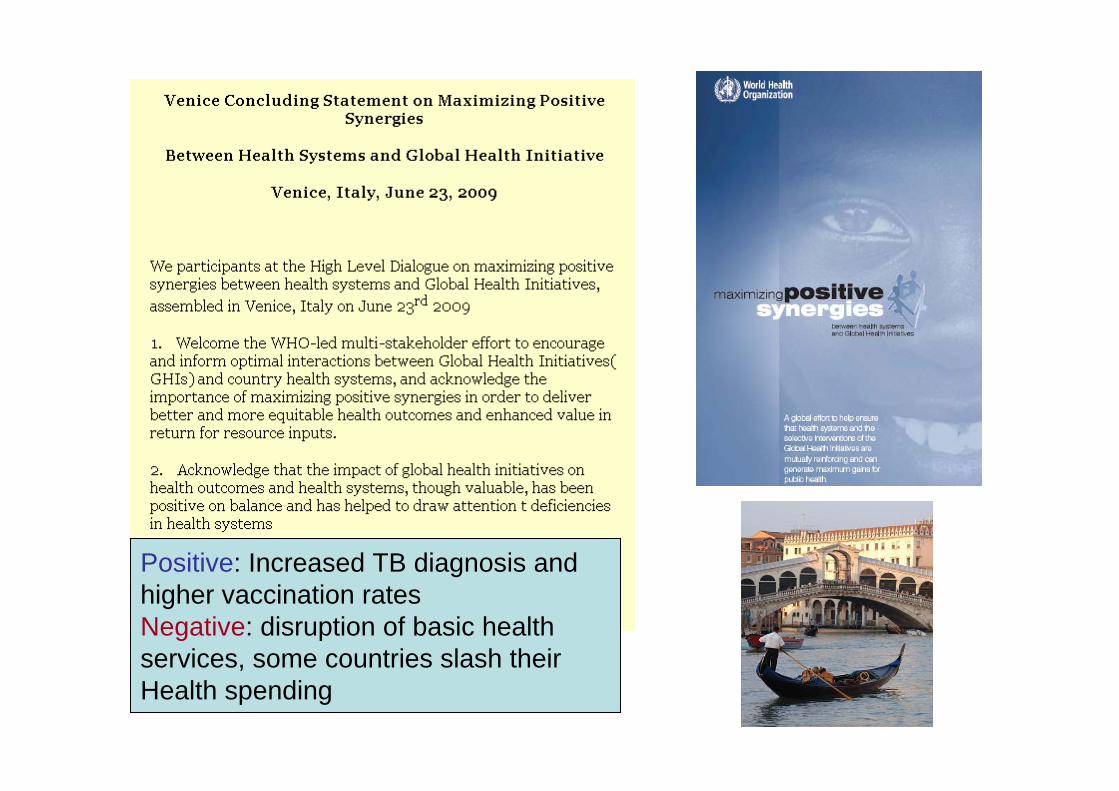
Positive: Increased TB diagnosis and higher vaccination ratesNegative: disruption of basic healthservices, some countries slash theirHealth spending
Seven effective habits of future governance
• Trans-sectoral, integrated view• Inclusive, embrace diversity• Define roles, substantive norms & values• Accountability & transparency• Information & evidence - harness ICT,
promote research on governance (towards evidence-informed governance)
• Balancing act• Focus more on the "why" and less on the
"how"
• "Focus on the problem not on 'architecture', structures or sacred notions of sovereignty" (Inge Kaul)
• "Global governance must be purpose-driven" (Strobe Talbott)
• "Global governance is actually global problem solving" (Sanjeev Khagram)
S.T. Lee Project on Global Governance Conference,Singapore, Dec 4-6, 2008
Meaning of GHG?
Ask not how health can shape governance,but ask what governance can do for health
Meaning of GHG?
Ask not how health can shape governance,but ask what governance can do for health systemstrengthening in thedeveloping countries
"He who has a why to live canbear with almost any how…"
Viktor FranklMan's Search for MeaningRider, London, 2004
Thank you
Related Documents











